
Abstract
Keywords
Introduction
Total shoulder arthroplasty (TSA) is an effective procedure to offer pain relief and improved function to patients with a wide variety of shoulder pathology. 1 Utilization of primary shoulder arthroplasty has risen dramatically over the past several decades, with a 339% increase between 1993 and 2008. 2 Food and Drug Administration approval for the reverse TSA (rTSA) in 2003, along with expanded surgical indications for rTSA account for a significant proportion of this increase.2–5
In today’s economic climate, cost and utilization of health-care resources have become an important issue when considering providing appropriate patient care. Longer hospital inpatient admissions lead directly to an increase in health-care costs and optimizing length of stay (LOS) can decrease this cost burden. Many studies have investigated factors affecting LOS in patients undergoing TSA, including both patient and nonpatient specific factors.6–10 However, to our knowledge, no study to date has investigated the effect of which day of the week surgery is performed on a patient’s LOS after shoulder arthroplasty. Day of the week that surgery is performed may have the most significant impact on the LOS of patients being discharged to extended care facilities (ECFs) as this disposition requires the most coordination of care. Physicians, care managers, physical therapists, and insurance company personnel all play an integral role in discharging patients to an ECF.
The goal of this study is to analyze the LOS for patients undergoing primary anatomic or rTSA at a single institution by a single surgeon. Specifically, we look to investigate whether the day of the week of surgery effects the LOS, both in patients being discharged home and to an ECF. We hypothesize that patients undergoing surgery on Friday will have a longer LOS compared to those on Monday and Wednesday, due to the decreased resources available for discharging patients over the weekend. Considering the additional resources required for discharging patients to ECF compared to home, we expect this effect to be more significant in the ECF cohort. Understanding this effect could facilitate the goal of decreasing health-care costs by allowing surgeons to schedule patients appropriately.
Methods
Expedited institutional review board approval was obtained for this project. Inclusion criteria were patients undergoing primary TSA (reverse or anatomic), procedures performed by single surgeon, procedures performed on a normal operating room (OR) day (M, W, F) (ie, an elective procedure), and those who required inpatient admission. Revision surgery, outpatient surgery, and patients admitted through the emergency department were excluded. All cases performed by a single surgeon between June 2006 and December 2016 were identified. A combination of ICD-9 and ICD-10 billing codes were used to identify the cases: 81.80—Other Total Shoulder Replacement, 81.83—Shoulder Arthroplasty NEC, 81.88—Reverse Total Shoulder Arthroplasty, ORRKOJZ/ORRKOJ6/ORRKOJ7—Replacement of Left Shoulder Joint, and ORRJOJZ/ORRJOJ6/ORRJOJ7—Replacement of Right Shoulder Joint. Patients were further selected by inpatient status to exclude mislabeled outpatient procedures and patients admitted for complications through the emergency center. Preoperative diagnoses were further reviewed to exclude revision patients with a diagnosis of failed prior arthroplasty who fell under one of our selected billing codes. Each individual procedure was organized by their hospital account record number and duplicates were removed.
For each patient, data collection included: age, sex, day of surgery, preoperative diagnosis, LOS, and discharge disposition. Comorbidities that were collected were chronic obstructive pulmonary disease (COPD), congestive heart failure (CHF), renal failure, and diabetes, since these variables have been shown to impact LOS. 9 The primary outcome was LOS for surgery performed Monday, Wednesday, and Friday and LOS for each of those days stratified by those discharged home versus discharge to an ECF. Demographic data between the groups were used to identify any disparities.
Patient discharge disposition was determined by a multidisciplinary approach. Input from physical therapists, nurse discharge care coordinators, and surgeons was used to recommend the optimal patient disposition. Physical therapy recommendations are determined either on postoperative day (POD) 0 or 1, depending on the timing of the patient’s surgery. Ultimately, the patient and their family members have the final decision in their postdischarge care.
Statistical Calculations
SPSS v.22 (IBM) was used for all statistical analyses. An independent samples t-test was used to compare age for patients discharged to home versus ECF and a chi-squared test to compare sex and comorbidities. We used the POD of discharge (1 through 8+) for statistical analysis and therefore treated this variable as ordinal data. Because of this and because the data were highly skewed, we chose to use nonparametric tests for this variable. A Mann–Whitney rank test was used to compare POD of discharge between discharge to home and ECF. Patients were then divided into groups based on the day of week of their surgery. A 1-way analysis of variance test was used to assess differences in age, and a chi-squared test was used to analyze the differences in sex and comorbidities. To compare POD of discharge, a Kruskal–Wallis H test was used with the Mann–Whitney rank test with a Bonferroni correction for pairwise comparisons. A P value less than .05 was considered significant for all tests.
Results
A total of 1784 cases were identified that fit the inclusion criteria. The mean age of the entire cohort was 69 ± 9 years and the average LOS was 2.9 ± 1.8 days. The group was 55.7% males.
Discharge Home Versus ECF
Most patients undergoing TSA were discharged home (86.1%). This group of patients had an even distribution of males (48.8%) and females (51.2%). However, of the patients who were discharged to an ECF, 83.5% were female versus 16.5% male. Patients being discharged to an ECF were also significantly older than those being discharged home (mean 75 ± 9 years vs 68 ± 9 years, P < .001), and had a significantly higher incidence of CHF (6.5% vs 2.9%, P = .005) and renal failure (2.0% vs 0.5%, P = .010), but no difference in diabetes (P = .139) or COPD (P = .809). Patients discharged to an ECF had a longer LOS (mean 4.3 ± 3.3 days vs 2.6 ± 1.3 days, P < .001). The percentage of patients discharged on each POD shows that the majority of patients discharged home left on POD 2, and those going to an ECF had the majority of discharges on POD 3 (Table 1).
Number of Patients Discharged on Each POD Based on Discharge Disposition.

Abbreviations: ECF, extended care facility; POD, postoperative day.
LOS by Surgery Day of Week
There were 711 patients (39.9%) who underwent surgery on Monday, 737 patients on Wednesday (41.3%), and 336 on Friday (18.8%). There was no significant difference in age (P = .523), distribution of males and females (P = .874), or incidence of diabetes (P = .537) or CHF (P = .097) between patients having surgery on each of these 3 days (Table 2). There was a difference in renal failure (P = .018) and COPD (P = .009). The overall mean LOS for all patients undergoing surgery on Monday was 2.9 ± 2.0 days, on Wednesday was 2.7 ± 1.7 days, and on Friday was 3.0 ± 1.9 days (P = .002). Post hoc analysis showed a significant difference in LOS between those who had surgery Wednesday versus Friday, with Friday having a longer LOS (P = .002). Surgery on Monday did not result in a significantly different LOS when compared to Wednesday or Friday.
Patient Demographics by Day of the Week of Surgery.

Abbreviations: CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease.
In addition, we broke the entire study period down and grouped patients into 2006 to 2009, 2010 to 2013, and 2014 to 2017. We then examined the differences in LOS between these time periods. There was a significant difference in LOS across these time periods (decreasing from 2006–2009 to 2014–2017 from a mean stay of 3.3 ± 1.5 days to a mean of 2.6 ± 1.6 days, P < .001). However, study period did not impact the significant difference between surgery day and LOS (P = .935).
LOS by Surgery Day of Week for Discharge Home Versus ECF
Day of surgery was found to have a more significant impact on LOS in patients being discharged to an ECF versus home. For patients discharged to an ECF, there was no significant difference in age (P = .266), sex (P = .993), diabetes (P = .095), CHF (P = .124), renal failure (P = .151), or COPD (P = .165) based on day of the week of surgery. There was a significant difference, however, in overall LOS, with surgery on Friday resulting in a significantly longer LOS (mean 4.8 ± 3.4 days) than both Monday (mean 4.2 ± 3.4 days, P = .028) and Wednesday (mean 4.1 ± 3.2 days, P = .010). Table 3 shows that patients undergoing surgery on Friday had a higher percentage of patients being discharged on POD 4 (29.8%) versus Monday (14.4%) and Wednesday (8.5%).
Postoperative Day of Discharge Based on Day of Surgery for Patients Discharged to an Extended Care Facility.
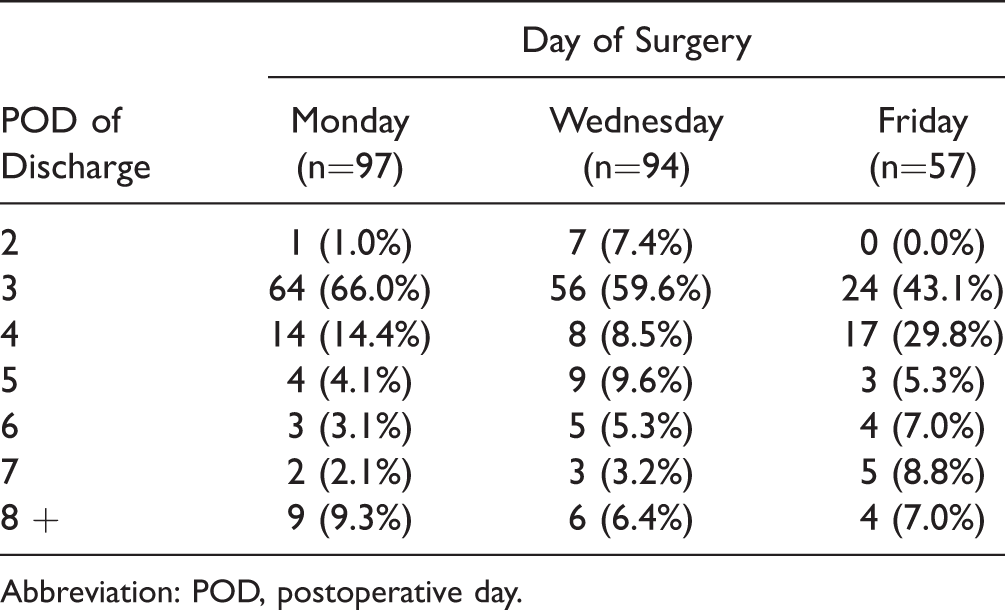
Abbreviation: POD, postoperative day.
For patients discharged home, the mean LOS was 2.7 ± 1.5 days for Monday, 2.5 ± 1.2 days for Wednesday and 2.6 ± 1.0 days for Friday (P = .038). Although there was a trend toward surgery on Wednesday resulting in a significantly shorter LOS, post hoc testing with an adjusted P value was .095, falling short of our significant alpha value.
Discussion
The results of this study confirm our hypothesis that the day of week of surgery does have a significant effect on LOS for patients undergoing primary TSA, with surgery on Friday resulting in the longest LOS. This effect was most evident in the subset of patients being discharged to an ECF in which a higher percentage of patients were discharged on POD 4 as compared to the other days. As health-care costs and utilization of resources become more important, it is useful to be aware of this trend to help optimize patient scheduling. The increased costs associated with a prolonged LOS are not negligible, especially added over several patients.
Despite the recent interest in decreasing LOS and even outpatient shoulder arthroplasty, there will always be a subset of patients for which an inpatient admission is necessary due to medical or social reasons. A significant percentage of these patients will not only require an inpatient admission, they will also require a discharge to an ECF. Thus, the findings of the present study are particularly relevant to this subset of patients. The cause of increased LOS for patients having surgery Friday, especially those being discharged to ECF, is likely multifactorial; however, we believe the biggest contributor is the decreased health-care personnel staffing over the weekend. In our facility, the number of care managers and physical therapists working over the weekend is significantly less than during a weekday. Therefore, these employees are often responsible for a greater number of patients, which can hinder the overall discharge planning process. In addition, it is likely that ECFs and insurance companies also have decreased staffing over the weekend. Because discharge to an ECF requires the coordination of all these parties, it is not surprising to find that delays occur over the weekend. In our study, patients requiring ECF who had surgery on Friday had on average nearly a full day increased LOS (mean 0.7 days more than Monday). This may indicate that little to no discharge planning occurs over the weekend, and that even on Monday, when hospitals, ECFs, and insurance companies are fully staffed, it is difficult to discharge Friday ECF patients. Patients discharged home after shoulder arthroplasty require much fewer resources. It is not surprising, therefore, that the LOS for this cohort of patients was not affected by surgical day of the week.
To our knowledge, this is the first study evaluating LOS based on day of surgery in a shoulder arthroplasty population. Similar studies, however, have been performed in the total hip and knee population, demonstrating comparable results. Lilly et al., in study from our institution, focused on total hip and knee patients discharged to an ECF and found that patients who had surgery on Thursday had a significantly longer LOS when compared to all other surgical days. 11 In addition, patients with Tuesday surgeries had a significantly shorter LOS when compared to Thursday or Friday. They recommended avoiding scheduling patients requiring discharge to an ECF late in the week. 11 In 2014, Muppavarapu et al. compared LOS for primary total joints patients undergoing surgery on Monday and Tuesday as compared to Thursday and Friday. 12 They found a significantly longer LOS for the Thursday and Friday group, which they also attributed to inconsistencies in weekend functionality and staffing. 12 Similarly, a 2016 study by Keswani et al. showed that total hip patients had a significantly longer LOS when surgery was done on a Thursday or Friday, or after 2 pm. 13 They proposed surgical scheduling and staffing modification as a potential method to reduce postoperative costs. 13
Although no studies in the setting of shoulder arthroplasty have evaluated the effect of day of surgery, multiple studies have been performed looking at other factors affecting LOS in this patient population. The largest of these studies, by Menendez et al., used a nationwide database of 40 869 patients and found that significant patient factors contributing to prolonged LOS were advanced age, female sex, CHF, renal failure, COPD, and diabetes. 9 They recommended promptly identifying higher risk patients to expedite discharge planning. 9 Other studies have corroborated these findings.6,8 Hospital-specific factors impacting LOS have also been examined, finding Medicaid insurance, low volume hospitals, and surgery in the south or northeast to contribute to extended LOS.8,9,14 All of the aforementioned patient and hospital specific factors should be accounted for along with the day of surgery when attempting to minimize LOS for shoulder arthroplasty patients. Along with attempts to minimize LOS, there is currently a nationwide trend toward performing outpatient total shoulder arthroplasties. Early studies have shown similar complication and readmission rates compared to inpatient procedures, seemingly making it a viable and cost-effective option in the appropriate patient population.15,16
Our study should be viewed in light of its weaknesses. First, it is a retrospective review, with no prospective or cohort matched patient populations. Second, the data came from a single surgeon in a single institution. Although this allowed us to control for different surgeon-specific variables, such as technique or perioperative pain management, it also brings into question the generalizability of our findings to other institutions. Furthermore, the senior author only operates on Monday, Wednesday, and Friday, and therefore, we were not able to compare LOS in surgeries performed Tuesday or Thursday. Third, the average LOS of our study population was 2.9 days, which is higher than the average found in most of the studies referenced earlier. This may be attributed to data collection dating back greater than 10 years, at a time when LOS was not a primary concern. Finally, comorbidities did vary between patients discharged home versus to an ECF. However, differences in LOS were seen between days within the ECF discharge group, and there were no differences in incidence of comorbidities across days in that group. In addition, we were unable to obtain surgical indication or BMI for all patients, which could also contribute to LOS.
With an aging population and a rapidly growing shoulder arthroplasty volume in the United States, the findings of this study are relevant as a certain percentage of shoulder arthroplasty candidates will remain better suited, due to patient and nonpatient factors, for an inpatient surgical experience followed by discharge to an ECF. Ideally, the day of the week surgery is performed should have no bearing on the discharge disposition of the patient. To control health-care costs, hospitals, ECFs, and third-party payers can use the findings of this study and others to justify increasing resources and staffing on the weekend to allow expeditious discharge of patients having surgery at the end of the week. Until then, we recommend patients likely to require discharge to an ECF should have surgery early in the week.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The senior author reports research support from Biomet and DJ Orthopaedics, IP Royalties from Smith and Nephew, consulting fees from Catalyst OrthoScience and Zimmer, and stock or stock options from Catalyst OrthoScience, Coracoid Solutions, and Hoolux Medical. The rest of the authors report no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.