
Abstract
Background
Radiotherapy is widely used as an effective adjunctive treatment modality in conjunction with conservative surgery for breast cancer. Radiation-induced skeletal changes in the shoulder region have been reported in 1% to 3% of patients who have undergone this treatment modality. With treatment techniques improving life expectancy, there is an increasing number of patients undergoing shoulder arthroplasty surgery with a history of cancer radiation therapy. To our knowledge, there are no reports focusing on potential radiation-related pathologic fractures of the shoulder after shoulder arthroplasty.
Case report
We present a case of catastrophic failure of glenoid component fixation after reverse shoulder arthroplasty (RSA) in a patient with previous high-dose radiation to the breast and supraclavicular areas. In this patient, failure of ingrowth of the baseplate and incorporation of the glenoid bone graft lead to eventual component loosening and subsidence. In addition, insufficiency fractures of the scapular body and base of the scapular spine occurred, complicating the clinical situation. The likely cause of these complications stems from radiation-induced impaired bone metabolism directly limiting bone remodeling potential.
Conclusion
This is a rare complication following RSA but highlights a concern that must be considered prior to implantation of the prosthesis that requires bone ingrowth for fixation.
Introduction
Radiotherapy is widely used as an effective adjunctive treatment modality in conjunction with conservative surgery for breast cancer. 1 Radiation-induced skeletal changes in the shoulder region have been reported in 1% to 3% of patients who have undergone this treatment modality. 2 With treatment techniques improving life expectancy, there is an increasing number of patients undergoing shoulder arthroplasty surgery with a history of cancer radiation therapy. To our knowledge, there are no reports focusing on potential radiation-related shoulder pathologic fractures after shoulder arthroplasty. We present a case of pathologic scapula fractures and failure of glenoid component bony ingrowth following reverse shoulder arthroplasty (RSA) in a patient felt to be related to radiation-induced bony changes.
Case Report
This patient is a 72-year-old right hand-dominant female. She endorsed bilateral shoulder pain and decreasing range of motion over a 2-year period. At presentation, the right was more symptomatic than the left. Prior treatment included a combination of nonsteroidal anti-inflammatories and acetaminophen for discomfort. She had minimal pain relief from a previous image-guided glenohumeral joint injection. The patient had no history of shoulder trauma, cervical radiculopathy, or osteoporosis. She had a medical history of stage III breast carcinoma with positive lymph nodes and underwent a lumpectomy and radiation treatment on her right side approximately 8 years ago. The radiation therapy consisted of a protocol of a series focal radiation to 2 separate areas. For the breast area, the total radiation dose of 5000 cGy was performed in 25 cycles over a 34-day time frame. The collimator setting for the radiation field was 15 cm × 21 cm. For the supraclavicular area, the total radiation dose was 4600 cGY performed in 23 cycles over a 30-day time period. The collimator setting for the radiation field was 18 cm × 13 cm.
Physical examination demonstrated that scapular posture was normal and symmetric. Actively elevation of the right side was about 100°. Left side was slightly higher about 115°. External rotation on the right 20°, on the left 25°, neither with significant lag sign, but with some mild external rotation weakness on the right. She had mild abduction weakness on both sides. X-rays showed advanced glenohumeral osteoarthritis on both sides. Her heads were well located with no subluxation. There was significant glenohumeral medialization on both shoulders, much greater on the right than the left indicating significant glenoid central erosion (Figure 1(a) to (c)). There was no subluxation or signs of proximal humerus radiation necrosis at presentation. Prior ultrasound of bilateral shoulders showed no evidence of rotator cuff tear on either side.

AP (a), true AP (b), and axillary (c) views showing right humeral head flattening with patchy areas of humeral head sclerosis, severe secondary glenohumeral osteoarthritis with significant medialization. The humeral head was well located with no subluxation. AP: anteroposterior.
Based on the physical examination and radiology, a diagnosis of bilateral glenohumeral joint arthritis was made with associated glenoid bone loss. An outside computed tomography (CT) scan demonstrated moderate central glenoid bone loss and mild glenoid retroversion without significant posterior humeral subluxation. Given the presence of advanced osteoarthritis combined with limited glenoid bone stock, the patient was indicated for reverse total shoulder arthroplasty in her more symptomatic right shoulder.
Surgery
The patient underwent reverse shoulder arthroplasty using a deltopectoral approach. Intraoperatively, the extreme medialization of the humeral head made dislocation somewhat difficult, but no coracoid osteotomy was necessary. Prior to humeral neck osteotomy, a 9-mm donut-shaped bone graft was harvested from the humeral head for implantation on the glenoid. The humeral head bone quality appeared normal. Glenoid exposure was routine. Although there was significant central and posterior erosion of the glenoid, there were no peripheral or cavitary bone defects. The glenoid baseplate was positioned in standard fashion in reference to the inferior glenoid rim. The glenoid was reamed medially to obtain roughly 50% to 60% glenoid baseplate support and expose inferior trabecular bone. The glenoid cortical plate was felt to be normal. Then, the donut-shaped graft was placed on the backside of a Zimmer trabecular metal base plate with a long (25 mm) central post and was impacted into position. Secure fixation was noted. Next, the base plate was affixed with 2 bicortical locking screws both having good purchase in the bone. The glenoid baseplate fixation was felt to be good intraoperatively. A 36-mm glenosphere was impacted onto the baseplate. The humeral implant was placed in an uncemented fashion at 20° of retroversion. The subscapularis was not repaired. Standard closure was performed.
Postoperative Course
The patient’s surgical wounds healed without complication over the next 2 weeks at which time physical therapy was initiated. The X-rays showed a well-positioned reverse shoulder arthroplasty (Figure 2(a) to (c)). She did well for the first 3 months noting fairly quick pain relief. At 3 months, active elevation improved to 150°, external rotation was 30°, and external rotation with abduction was 70°. She had significant external rotation weakness and a subtle lag sign. She could reach behind her back to the lateral iliac crest. She completed approximately 3 months of physical therapy.

First postoperation visit radiographs, AP (a), true AP (b), and axillary (c) views showing well-positioned reverse shoulder arthroplasty. AP: anteroposterior.
At 6 months postoperatively, the patient reported insidious onset of increasing shoulder pain and declining function. The patient had no acromial tenderness, but localized pain was noted with active elevation of 70° to 80°. Passive elevation was 120°. The deltoid was strong, but pain was noted with active elevation. A CT scan was performed showing a permeative appearance of right scapular body and a horizontally oriented pathologic scapular fracture just inferior to the scapular spine near the tip of the central glenoid post (Figure 3). A scapular punch biopsy was performed given the patient history and the radiologists interpretation of the CT scan, which was negative for metastatic carcinoma. As there were no signs of infection or metastatic disease, the patient was felt to have suffered from a pathologic fracture secondary to radiation. The patient was placed in a sling for 1 month and managed conservatively. The patients’ pain improved; however, limited active elevation persisted. Three months later radiographs demonstrated persistent scapular body nonunion with glenoid base plate and loosening and anterior subsidence (Figure 4(a) and (b)). Fortunately, the patient did not have much pain and we continued observation. She was able to regain active elevation of 90°.
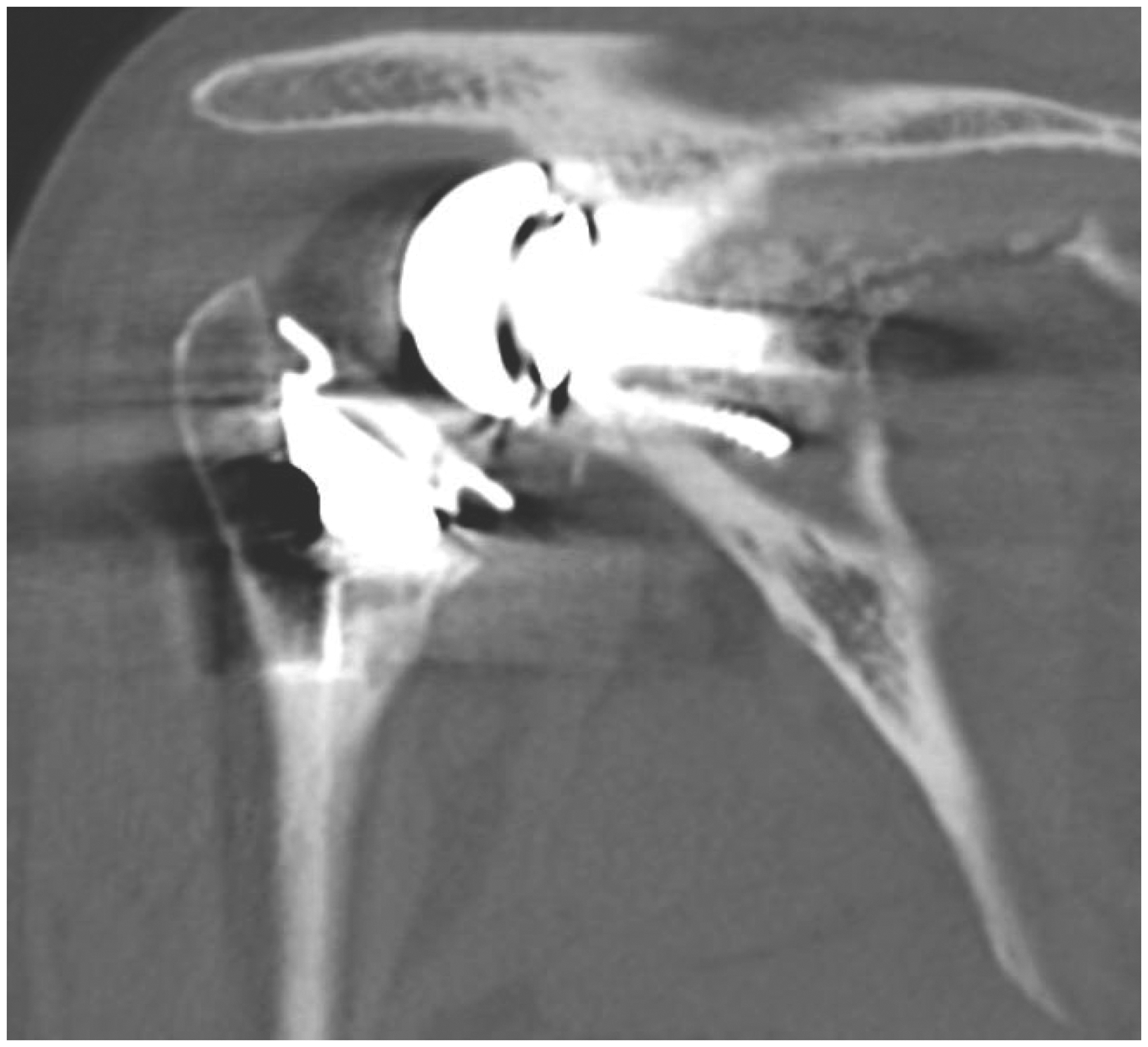
CT scan showing a pathologic fracture of the scapula just inferior to the scapular spine.

(a) Anteroposterior radiograph showing ununited scapular body fracture. (b) The axillary view showing glenosphere loosening and translating anteriorly.
At 14 months after surgery, her right shoulder developed increasing pain. Although the scapular body fracture was healed, X-rays showed a loose baseplate with progressive medialization and anterior anteverting of the baseplate in relation to the scapular body.
Over the next several months, her shoulder pain worsened and radiographs showed a new base of scapular spine fracture with shoulder dislocation (Figure 5(a) to (d)). At 21 months postoperatively, due to progressive destruction of the scapula, persistent pain, and new onset humeral implant dislocation, the decision was made to convert the reverse shoulder arthroplasty to a hemiarthroplasty (Figure 6(a) and (b)). No internal fixation or bone grafting to the scapula or glenoid was performed. Due to severe medialization from the glenoid bone loss, the humeral head, although anteriorly subluxated, was not grossly unstable, as it was contained by the coracoid process anteriorly.
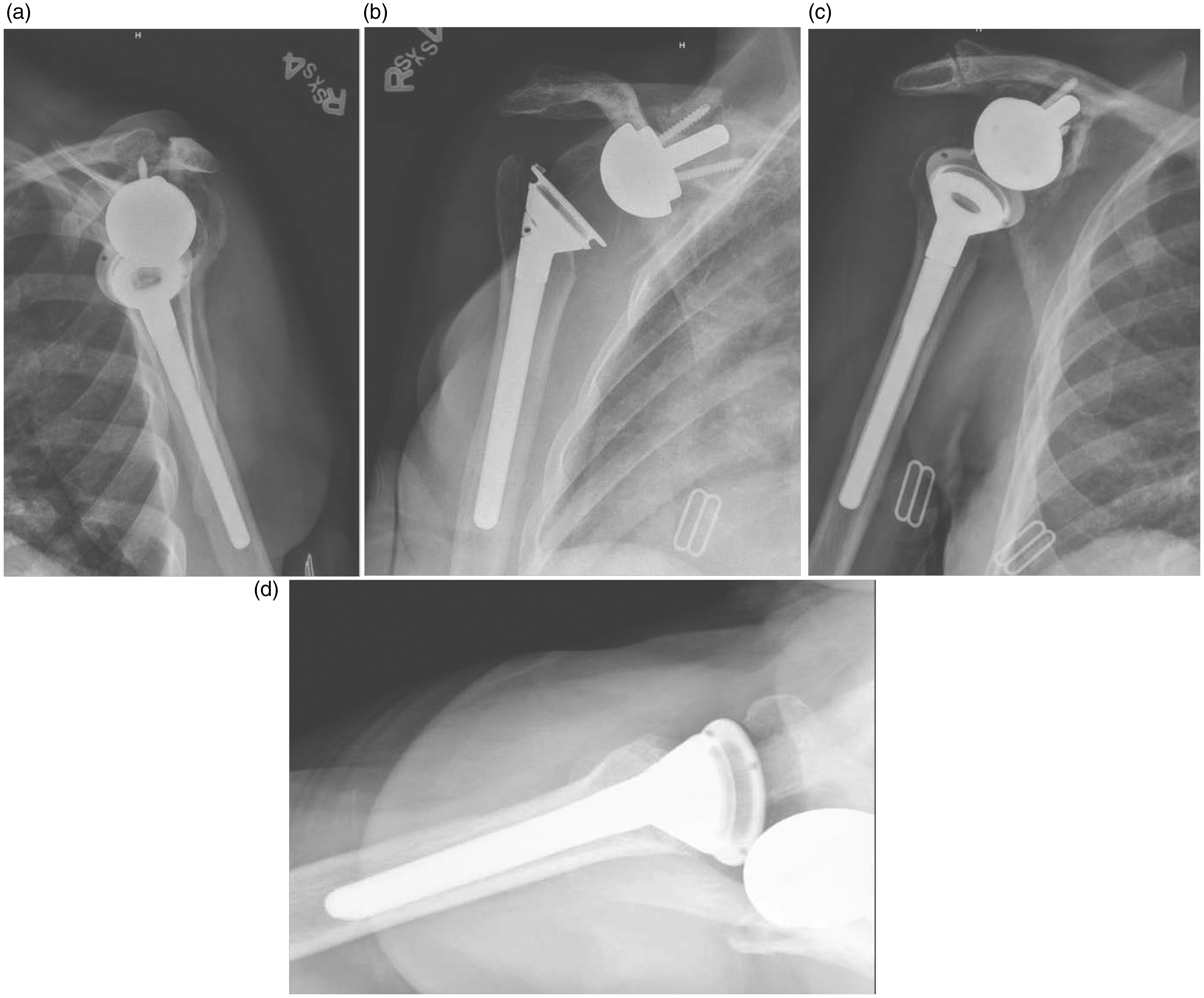
(a) and (b) True AP and Y views showing a new acromion base fracture; all of the 4 views showing progressive medialization and anterior anteverting of the baseplate, with subluxation. AP: anteroposterior.

(a) and (b) Revision hemiarthroplasty. The humerus is subluxated anteriorly, however, due to severe medialization remains contained under the coracoid process.
Discussion
We present a case of catastrophic failure of glenoid component fixation after RSA in a patient with previous high-dose radiation to the breast and supraclavicular areas. In this patient, failure of ingrowth of the baseplate and incorporation of the glenoid bone graft lead to eventual component loosening and subsidence. In addition, insufficiency fractures of the scapular body and base of the scapular spine occurred, complicating the clinical situation. The likely cause of these complications stems from radiation-induced impaired bone metabolism directly limiting bone remodeling potential. This is a rare complication following RSA but highlights a concern that must be considered prior to implantation of the prosthesis that requires bone ingrowth for fixation.
Radiotherapy is being widely used as an effective locoregional treatment modality in conjunction with conservative surgery for breast cancer. 1 The dose of radiation varies considerably based on the several factors and often the orthopedic surgeon is unaware of the extent of an individual’s radiation treatment. Radiation therapy may cause changes in the skeletal system in a dose-dependent manner, 3 and radiation-induced skeletal changes in the shoulder region have been reported in 1% to 3% of patients after treatment. 2 The pathogenesis of radiation osteitis is a combination of direct cell injury and radiation-induced vascular injury. 4 Radiation-related late changes in mature bone include atrophy, osteoradionecrosis, pathologic fractures, and radiation-induced malignancies. 5 Sengupta and Prathap6 suggested that lack of normal dynamic osteoblastic activity was responsible for the thinning of the bone and the osteoporosis that may lead to pathologic fracture. They first described 3 cases of histologically proved radiation necrosis of the humeral head following treatment for breast cancer. With cancer treatments improving life expectancy, there are an increasing number of patients who receive arthroplasty surgery with a history of cancer radiation therapy. Jacobs et al. 7 demonstrated lack of acetabular component ingrowth and clinical failure in one-third of patients with a history of pelvic radiation following total hip arthroplasty. Currently, the dose-dependent effect of radiation treatment on bone remodeling potential is unknown. Certainly, higher doses of radiation delivered in larger fields can potentially have serious adverse effects on bone remodeling. Consideration should be entertained in planning orthopedic reconstructive in these patients in a case-by-case manner.
Our patient’s history is notable for having had a stage III breast cancer with positive lymph nodes. She, subsequently, underwent an experimental protocol for extensive radiation to the breast and supraclavicular area of the shoulder which likely had secondary effects to her scapula and glenoid. Although the shoulder implant used has a high bone ingrowth potential, failure of bony ingrowth was seen. This clinical situation was likely exacerbated by the use of a structural glenoid bone graft. In this case, successful component ingrowth is predicated on healing and incorporation of the bone graft given the lack of contact of the implant to the host glenoid. Unique to this case were the development of scapular body and scapular spine fractures that occurred following component loosening. This may have been predicted to some degree given the known effects of RSA on acromial and scapular spine bone stresses. 8 It is likely that the limited bone remodeling potential created by the radiation contributed to these fractures. In this case, the workup failed to demonstrate evidence of infection or local metastatic disease in the scapula. We do believe that these are important pathologies to consider in the differential diagnosis in this clinical situation.
The treatment of a patient with the constellation of complications such as this is challenging and further procedures are limited. The primary goals of treatment are to reduce pain and to prevent further destruction of the bone and salvage some degree of shoulder function. Some healing potential of the scapula was evident as the patient eventually healed her scapular body fracture. In this case, we chose to convert the RSA to a hemiarthroplasty and not to bone graft the glenoid or internally stabilize the scapular spine fracture given the poor bone healing/remodeling potential. Salvage of a failed RSA to a hemiarthroplasty has been described. Although pain relief can be expected, poor shoulder function is predictable. 9
Conclusion
To our knowledge, we present the first case of scapular pathological fracture and glenoid component loosening after reverse shoulder arthroplasty secondary to the effects of bony radiation. The treatment of shoulder periprosthetic pathologic fractures in patients undergoing previous local radiation warrants further investigation to determine to dose-dependent effects of radiation on component incorporation. Surgeons should recognize the variable dosing and localization of radiation treatment among patients and the subsequent potential adverse effects on bone remodeling.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jay Keener is a consultant for Arthrex, Shoulder Innovations, and Imascap and has received royalties from Shoulder Innovations and Imascap. The other authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Jay Keener has received research support from National Institutes of Health.