
Abstract
Background
Anatomic total shoulder arthroplasty is a viable treatment option for patients with glenohumeral arthritis and an intact rotator cuff with successful outcomes. However, one complication is rupture of the subscapularis tendon postoperatively. Controversy exists regarding the optimal technique of subscapularis tendon management. The purpose of the present article is to review subscapularis peel repair method.
Methods
The current literature on anatomic total shoulder arthroplasty and subscapularis peel was reviewed to determine the viability of the repair technique.
Results
Both biomechanical and clinical studies have demonstrated advantages and disadvantages of the subscapularis peel technique, most often by way of direct comparison with lesser tuberosity osteotomy, without consensus as to a superior repair method.
Discussion
The subscapularis peel repair in anatomic total shoulder arthroplasty when performed correctly may yield successful biomechanical and clinical outcomes for patients.
Introduction
Anatomic total shoulder arthroplasty is a viable treatment option for patients with glenohumeral arthritis with an intact rotator cuff. The procedure may confer pain relief, improved function, and increased quality of life scores.1–5 The prevalence of total shoulder arthroplasty procedures is increasing at a rate which is comparable to, or higher than, that for hip and knee arthroplasties. 6 Despite the success of the procedure, complications occur and vary. One infrequent but significant complication is rupture of the subscapularis tendon postoperatively. 7 This complication may result in inferior outcomes including pain, functional impairment, or anterior instability with symptomatic cases necessitating repeat surgery.8–10
Controversy exists regarding the optimal technique of subscapularis tendon mobilization and repair during anatomic total shoulder arthroplasty. Current techniques include subscapularis peel, subscapularis tenotomy, subscapularis split, and lesser tuberosity osteotomy.11–14 Subscapularis sparing techniques have also been described. 15 Regardless of technique, mobilization of the subscapularis is necessary for intraoperative visualization and correction of an internal rotation contracture when present. At this time, the American Academy of Orthopaedic Surgeons is unable to recommend for or against any single technique as all have their advantages and disadvantages. 1 The currently available review articles pertaining to subscapularis management in total shoulder arthroplasty briefly address the subscapluris peel technique, if at all.16,17 The purpose of the present article is to specifically review the subscapularis peel in anatomic total shoulder arthroplasty, including discussion of anatomy, surgical technique, biomechanical considerations, and clinical outcomes based on the currently available literature.
Anatomy
The subscapularis muscle originates on the anterior scapula in the subscapularis fossa. The upper 60% transitions into a tendinous portion inserting on the lesser tuberosity, while the lower 40% consists of a muscular portion inserting on the metaphysis of the proximal humerus. 18 The muscle is defined superiorly by the rotator interval and coracoid process, then inferiorly by the axillary nerve and posterior humeral circumflex vessels. The anterior humeral circumflex vessels separate the tendinous and muscular portions as described above. Innervation to the subscapularis is supplied by the upper and lower subscapular nerves (C5, C6, and C7 nerve root origin), which typically gain their origin from the posterior cord of the brachial plexus.
The primary function of the subscapularis muscle is internal rotation of the humerus. The secondary function is to act as a glenohumeral joint dynamic stabilizer by balancing the posterior muscles of the rotator cuff, constituting the anterior portion of the transverse force couple.19–22
Surgical Technique
The patient is positioned in the beach-chair position. As first described by Neer, a deltopectoral approach provides the best visualization of the subscapularis in open shoulder surgery. 23 The cephalic vein is mobilized medial or lateral based on surgeon preference. Release of the subdeltoid, subacromial, and subcoracoid spaces provides exposure to the subscapularis. A provisional tenodesis of biceps tendon to the pectoralis major tendon prevents retraction of the tendon and facilitates definitive tenodesis at the time of repair of the subscapularis peel. Coagulation of the anterior humeral circumflex vessels limits bleeding.
The subscapularis peel starts by incising the fascia over the biciptal groove and extending proximally through the rotator interval up to the base of the coracoid process. Cut the biceps tendon at the articular margin of the humeral head and excise the tendon down to the level of the tenodesis at the pectoralis major tendon. The subscapularis and muscle insertion is removed directly from the lesser tuberosity beginning at the medial border of the bicipital groove using scalpel or electrocautery. 11 This technique is distinguished from traditional subscapularis tenotomy, which divides the subscapularis tendon 1 cm medial to the bicipital groove, leaving a cuff of tendon for repair at the time of closure. 13 The tendon is separated from the bone along its entire length as defined by its superior and inferior margins. Sutures are placed in the tendon for later identification as well as for retraction purposes. The author’s preference is to release the anterior capsule with the subscapularis tendon. The subscapularis and anterior capsule are then carefully separated medially, if needed to address any internal rotation contracture. This technique leaves some of the lateral capsule attached to the tendon and improves the quality of the tissue for repair. The surgeon needs to carefully identify and protect the axillary nerve during the peel and contracture releases.
Repair of the subscapularis peel may be performed with degrees of variation dependent on the initial method of subscapularis mobilization and surgeon preference.11,24,25 The author’s preferred method entails creating bone tunnels directed from the anatomic neck of the humerus to the medial border of the bicipital groove. Heavy nonabsorbable suture is then passed through the tunnels and through the subscapularis tendon to complete the repair. Figures 1 through 4 are intraoperative images of a patient undergoing right shoulder arthroplasty with demonstrating repair using bone tunnels, nonabsorbable suture, and tenodesis of the biceps tendon in final repair. In situations of poor quality bone, tying the sutures over a mini plate placed on the lateral aspect of the greater tuberosity can prevent suture cutout. 11 Other repair methods utilize the humeral stem to augment the repair, using either specialty made components to incorporate suture or by circling the suture around the prosthesis prior to stem insertion. 26

Right shoulder subscapularis peel repair intraoperative image demonstrating bone tunnels drilled from anatomic neck of the humerus to the medial border of the bicipital groove with nonabsorbable suture passed through the tunnels.

Right shoulder subscapularis peel repair intraoperative image demonstrating subscapularis tagged by suture being mobilized to its original footprint on the lesser tuberosity with previously passed nonabsorbable suture visible.
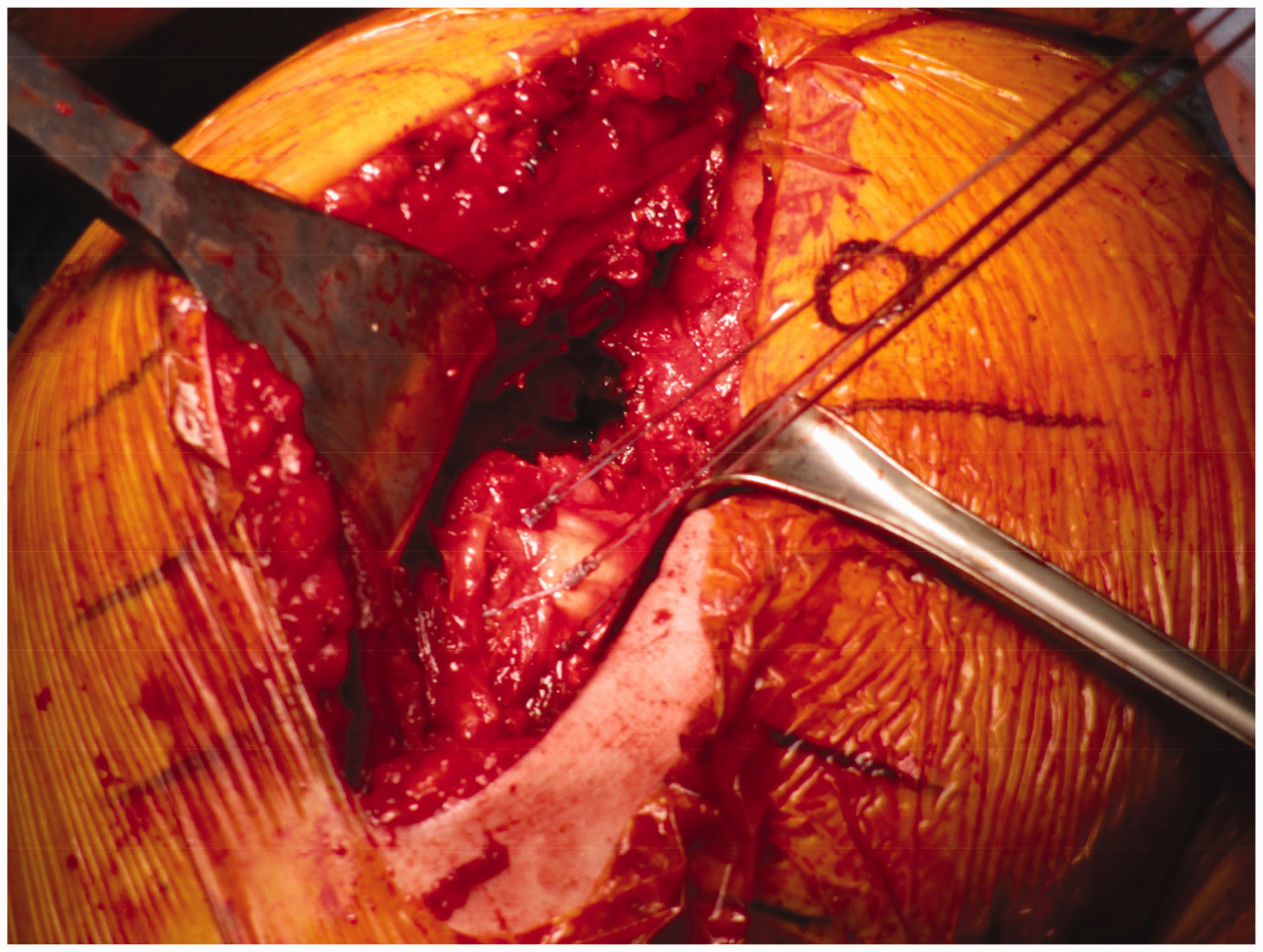
Right shoulder subscapularis peel repair intraoperative image demonstrating subscapularis peel repair using nonabsorbable suture which was previously passed through bone tunnels.

Right shoulder subscapularis peel repair intraoperative image demonstrating final subscapularis peel repair with additional biceps tenodesis performed using tails of nonabsorbable suture tied over subscapularis.
Biomechanical Studies
Although the literature has not consistently demonstrated any single superior subscapularis repair method, there are few biomechanical studies with data pertaining to subscapularis peel. Lederman et al. 27 performed a cadaveric study comparing subscapularis peel to lesser tuberosity osteotomy in 20 matched pairs of fresh frozen shoulders. Each cadaveric pair had an uncemented short-stemmed humeral prosthesis implanted, and the subscapularis repair was randomized for one cadaveric side to undergo subscapularis peel with a through-implant repair technique and the contralateral side to undergo lesser tuberosity osteotomy. Each specimen was then subjected to a hydraulic testing system cycling at 10 N to 100 N for 500 cycles and then pulled to failure. Displacement at the repair site was then measured. No significant differences were established between the 2 groups for displacement at 10 cycles, displacement at 500 cycles, load to failure, or ultimate stiffness. Limitations of the study include small numbers, limited number of cycles, and overall short-term nature due to cadaveric study design.
Van Thiel et al. 28 conducted another cadaveric study using 24 specimens comparing lesser tuberosity osteotomy, subscapularis peel, and subscapularis tenotomy. There were no significant differences in elongation amplitude, cyclic elongation, or failure testing for maximum load, mode of failure, or stiffness.
Not all biomechanical studies have data supporting the subscapularis peel, however. Ponce et al. 29 compared tendon to tendon repair, tendon to bone repair, and lesser tuberosity osteotomy repair. Mean displacement was significantly less in the lesser tuberosity osteotomy group (0.88 mm) compared to tendon to tendon repair (2.72 mm) and tendon to bone repair (2.11 mm). Mean load to failure was significantly greater in the lesser tuberosity group (738 N) compared to tendon to tendon repair (506 N) and tendon to bone repair (334 N). The study advocates for the strength of the lesser tuberosity osteotomy and encourages its use in total shoulder arthroplasty for achieving an overall successful outcome.
Furthermore, Ahmad et al. 30 compared tendon to bone repair and a combination technique of tendon to tendon with bone tunnels. The combined repair technique required significantly greater number of cycles to reach 1 mm, 3 mm, and 5 mm gaps compared with the tendon to bone technique. There was no significant difference in load to failure between the groups. Overall, the study demonstrated that subscapularis peel results in weaker strength of fixation under cyclic load and less contact area compared to the other method.
Clinical Outcomes
The literature contains prospective studies that support the subscapularis peel as a reliable method. Lapner et al. 11 performed a multicenter double-blind randomized controlled trial comparing subscapularis peel versus lesser tuberosity osteotomy during shoulder arthroplasty analyzing 73 patients total with 24 months of follow-up data. The primary outcome of the study was subscapularis strength assessed in the belly-press position by an electronic hand held dynomometer as an objective proxy for subscapularis repair healing. The study revealed mean subscapularis strength increased significantly in both groups compared to baseline; however, there was no significant difference in strength between the 2 groups at any time point. The secondary outcomes of the study were disease-specific quality of life and function as measured by the Western Ontario Osteoarthritis of the Shoulder Index and American Shoulder and Elbow Surgeons score. Both groups experienced improvement in secondary measures compared to baseline; however, once more there was no significant difference between the 2 groups. Furthermore, there were no reoperations for the treatment of subscapularis failure in either group. Limitations of the study include 17% rate of loss to follow-up, a significant difference in cohort mean ages despite randomization, inclusion of hemiarthroplasty and total shoulder arthroplasty, and use of belly-press test as an outcome measure.
Lapner et al. 12 in a subsequent analysis of the patients included in the previous multicenter double-blind randomized controlled trial compared healing rates and subscapularis fatty infiltration after subscapularis peel versus lesser tuberosity osteotomy during shoulder arthroplasty analyzing 79 patients with 12 months of follow-up data. The primary outcome of the study was to compare healing status at 12 months. The secondary outcomes included investigating the status of the subscapularis muscle based on Goutallier fatty infiltration grade, progression of fatty infiltration grade over time, as well as association between fatty infiltration grade and subscapularis strength. Computed tomography scans with 2-mm-thick slices were obtained for the patient population preoperatively and at 12 months after surgery. The subscapularis peel group experienced 100% healing of the tendon on follow-up imaging, while the lesser tuberosity osteotomy group experienced 95% bony healing; the difference was not statistically significant. Preoperative fatty infiltration grades were not different between the 2 groups at baseline, and at the follow-up computed tomography (CT) scan, fatty infiltration grade significantly increased in both groups. However, there was no significant difference between the 2 groups for fatty infiltration grade. The study analysis demonstrated a trend suggesting increased degree of fatty infiltration correlates with poorer subscapularis strength for both groups, without reaching statistical significance. Limitations of the study include a 12% rate of loss to follow-up, use of postoperative CT to assess healing status, as well as degree of fatty infiltration in both groups.
Gobezie et al. 26 performed a prospective analysis in a consecutive series of 60 total shoulder arthroplasties performed using subscapularis peel with a stem-based repair with a mean follow-up of 15 months examining functional outcomes and subscapularis healing. The results demonstrated subscapularis peel with stem-based repair leads to improved functional outcome scores, as well as reliable subscapularis healing based on ultrasound assessment with the tendon being healed in 91.7% of cases, attenuated in 5%, and torn in 3.3%. Postoperatively, the belly press test was positive in 6.7% of patients. Limitations of the study include lack of a comparison group, lack of comparison between preoperative and postoperative subscapularis strength, no radiographic evaluations, and inherent limitations of ultrasound.
Counter to the findings of the Lapner and Gobezie studies, Shafritz et al. 31 performed a retrospective study comparing patients with primary anatomic total shoulder arthroplasty performed with either subscapularis peel or lesser tuberosity osteotomy, which ultimately favored lesser tuberosity osteotomy. The study evaluated 90 procedures; 46 performed with subscapularis peel and 44 with lesser tuberosity osteotomy. Mean follow-up time period was 4.1 years. The primary outcome measure was performance of a lift-off test as described by Gerber, which can reliably diagnose clinically relevant subscapularis tendon rupture. 32 Secondary outcome measures included the Simple Shoulder Test and Disabilities of the Arm, Shoulder and Hand score, obtained preoperatively and at postoperative visits beginning at 6 months. The results demonstrated that in the subscapularis peel group, 69.6% had a normal lift-off test, while in the lesser tuberosity osteotomy group 91.0% had a normal lift-off test; however, the difference was statistically significant. 31 In multivariate logistic regression analysis, odds ratio estimates revealed that patients in the lesser tuberosity osteotomy group were 4.5 times more likely to demonstrate a normal lift-off test than those in the subscapularis peel group postoperatively. The authors suggest the difference among the groups may be explained by the lesser tuberosity osteotomy relying on bone-to-bone healing, rather than disrupting the bone-tendon interface. Limitations of the study include it being a retrospective cohort study, different surgical techniques employed, varying implants, the follow-up interval was different between groups, and assessment using the lift-off test which has known shortcomings.
Scalise et al. 33 performed a retrospective cohort study comparing clinical, radiographic, and ultrasonographic comparison of subscapularis tenotomy where the tendon was sharply elevated off its lesser tuberosity and lesser tuberosity osteotomy. Patients in the osteotomy group had better clinical outcome scores as measured by the Penn Shoulder Score. Using ultrasonography, in the subscapularis tenotomy group 7 of 15 tendons were abnormal, while only 2 of 20 tendons in the osteotomy group were attenuated. These results demonstrated a correlation between tendon appearance on ultrasound and improved outcomes. Limitations include its retrospective design, and again, inherent limitations of ultrasound.
Conclusion
During anatomic total shoulder arthroplasty, subscapularis tendon mobilization and repair is necessary for intraoperative visualization. Current techniques include subscapularis peel, subscapularis tenotomy, subscapularis split, and lesser tuberosity osteotomy.11–14 Officially, the American Academy of Orthopaedic Surgeons does not recommend any single technique. 1 The present article served to specifically review subscapularis peel in anatomic total shoulder arthroplasty based on the currently available literature. Both biomechanical and clinical studies have demonstrated advantages and disadvantages of the technique, most often by way of direct comparison with lesser tuberosity osteotomy. The authors of the only randomized control trial to study subscapularis peel demonstrated that subscapularis peel and lesser tuberosity osteotomy both increased subscapularis strength, improved disease-specific quality of life and function scores, without any reoperations. Studies with less rigorous design demonstrated a mix of results. In general, there is a paucity of well-done studies pertaining to subscapularis management in anatomic total shoulder arthroplasty, let alone focused studies addressing subscapularis peel. This review highlights that further research is needed if a superior repair technique is to be established. The authors of this review maintain that the subscapularis peel is a viable technique, and may be of special consideration in cases when it is desired to mobilize the tendon insertion point, such as when a significant internal rotation contracture is encountered. Furthermore, value of the technique may then be emphasized in cases of reverse total shoulder arthroplasty. Overall, the subscapularis peel in anatomic total shoulder arthroplasty can yield successful biomechanical and clinical outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declare the following potential conflicts of interest with respect to the research, authorship, and/or publication of the article: Royalties – Exactech, Zimmer Biomet.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.