
Abstract
Purpose
To report a unique case of detritic synovitis with associated lytic lesion leading to pathologic fracture of the acromion and deltoid avulsion following total shoulder arthroplasty (TSA).
Methods
An institutional review board-approved retrospective case analysis was performed using Electronic Medical Records (EMR) sourced pathology and radiology results, clinic notes, and surgical reports.
Discussion
This is a previously unreported complication of TSA resulting from detritic synovitis, a destructive inflammatory reaction to polyethylene wear debris within an artificial joint. The differential diagnosis includes periprosthetic infection with osteomyelitis and metastatic disease. This patient presented with extensive osteolysis, pathologic fracture of the acromion and deltoid avulsion that was successfully treated with debridement and surgical repair of the deltoid.
Conclusion
As the prevalence of TSA rises, orthopedic surgeons should be aware of the possibility of detritic synovitis in patients who present with pain after shoulder arthroplasty with imaging studies demonstrating periarticular osteolysis.
Keywords
Introduction
Over the past 2 decades, the number of shoulder arthroplasty procedures performed has increased significantly. Between 1993 and 2007, the prevalence of total shoulder arthroplasty (TSA) increased 369%, with an annual increase of 9.4%.1 This trend is expected to continue. Complication rates following TSA have been found to range from 7% to 11%. 2 Commonly reported complications include periprosthetic fracture, infection, neurologic injury, joint instability, loosening of the glenoid component, osteolysis, and pathologic fracture. 3
Detritic synovitis is an inflammatory response of the synovium secondary to free floating intra-articular material including bone, metal, or polyethylene debris, which results in synovial ulceration, necrosis, and osteolysis.4–6 In comparison to periprosthetic osteolysis, defined as the resorption of bone and loss of calcium about a prosthetic joint implant, detritic synovitis causes much more extensive and widespread resorption of bone. 6 In advanced cases, extra-osseous and extra-articular synovial extension and soft tissue injury can also occur. The extensive osteolysis associated with detritic synovitis can lead to catastrophic implant loosening, pathologic fracture, as well as soft tissue injury. Detritic synovitis has been reported in the foot, hand, and hip arthroplasty literature since its first description in 1978.7–9 To date, only a theoretical discussion of detritic synovitis exists in the shoulder arthroplasty literature. 9 We report a unique case of detritic synovitis leading to pathologic fracture of the acromion with deltoid avulsion.
Case Description
A 79-year-old right hand dominant woman with a significant history of rheumatoid arthritis was treated with an anatomic total shoulder arthroplasty at an outside institution in April 2010. The patient did well postoperatively with reduction of pain and improvement in function.
She presented in September 2015 with debilitating left shoulder pain of 3 days duration that began after hearing an audible pop while raising her arm. There were no associated neurologic or constitutional symptoms.
On examination, swelling and ecchymosis of the left shoulder was noted. The left upper extremity was neurovascularly intact. Active range of motion included 70° forward flexion, 60° external rotation (arm at side), 70° external rotation in abduction, and internal rotation to the gluteal area. A positive lift off test, internal rotation lag sign, and a palpable defect in the lateral deltoid were present. Grashey AP and axillary radiographs of the shoulder revealed a total shoulder arthroplasty implant with an avulsion fracture and lytic lesion of the acromion (Figure 1). Further imaging studies including computed tomography with 3D reconstruction confirmed a lytic lesion and avulsion fracture of the acromion (Figure 2). No additional lytic lesions were visualized about the shoulder.

Grashey AP and axillary radiographs showing avulsion fracture secondary to lytic lesion within the acromion.

Computed tomography confirming osseous lesion to the acromion, multiple views.
Given the permeative nature of the lytic lesion, a fine needle aspirate of the area was performed, which was nondiagnostic. Subsequently, an incisional biopsy and culture of the lytic lesion revealed a benign inflammatory process consistent with detritic synovitis. A concomitant curettage of the acromion, synovectomy, and repair of the avulsed deltoid was performed.
Surgical Technique and Postoperative Course
The fracture site and deltoid were explored through a longitudinal incision centered over the lateral deltoid defect. There was substantial subdeltoid synovitis and bursitis. The abnormal appearing synovium presented as a hemorrhagic pannus in the glenohumeral joint that extended into the subacromial space through a rotator cuff defect. Multiple soft tissue samples of the synovial pannus and the acromial lesion were collected for pathologic examination. Intraoperative biopsies were consistent with extensive foreign body reaction, fibrosis, and synovial hyperplasia, which were attributed to polyethylene wear debris from the glenoid component (Figure 3). Fresh frozen pathology results showed less than 5 white blood cells per high-powered field and no evidence of acute inflammation. No evidence of malignancy or infection was found, and all cultures were negative. All abnormal appearing synovitis was sharply resected. The acromial lesion was debrided to healthy appearing bone. There were no other areas of osteolysis noted within the proximal humerus or glenoid. The avulsion fracture and deltoid were repaired with transosseous sutures to the remaining intact acromion. Additional pertinent intraoperative findings included a full thickness anterior superior rotator cuff tear (subscapularis, supraspinatus, and infraspinatus) that was found to be irreparable as well as focal anterior superior polyethylene wear of the glenoid component. There was no obvious instability of the glenoid or humeral components. Based on the patient’s medical comorbidities, limited functional needs, and directive to avoid an extensive procedure, it was elected not to remove the glenoid component or revise the arthroplasty to a reverse prosthesis. In this low-demand patient, the primary objective of surgery was to achieve an accurate diagnosis of the pathologic lesion and provide pain relief. A secondary goal was an improvement in shoulder function. The acromial pathology and deltoid defect were also concerning enough to the senior author that revision to a reverse TSA was not considered an ideal option.
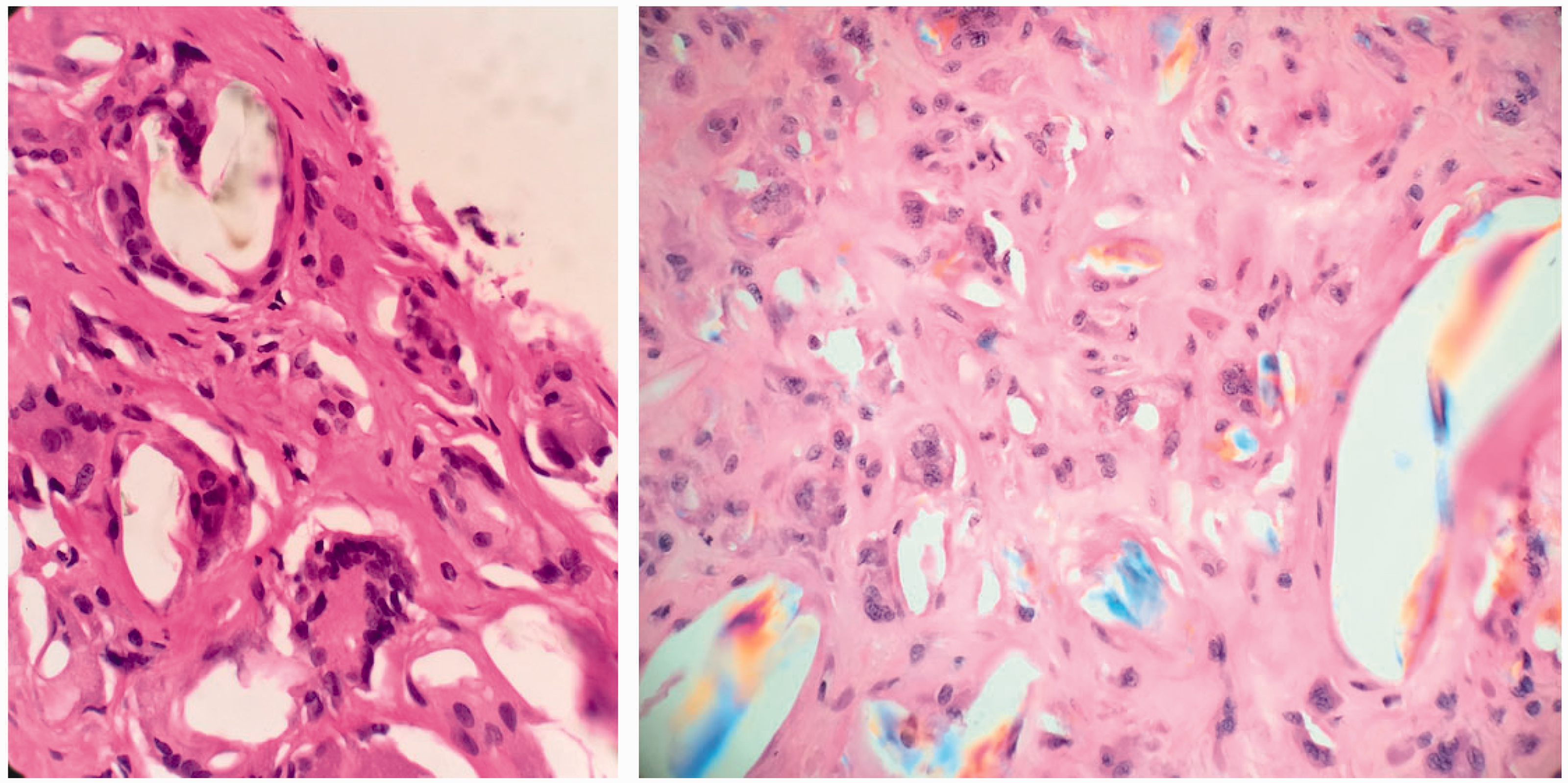
Histopathology showing significant multinucleated giant cell foreign body reaction (left), and microscopy under polarized light showing polyethylene wear debris within multinucleated giant cells (right).
The patient was placed in an abduction sling for 6 weeks postoperative and underwent an uncomplicated physical therapy program. The patient did well with complete pain relief postoperatively as well as improvement in strength and range of motion (Figure 4).
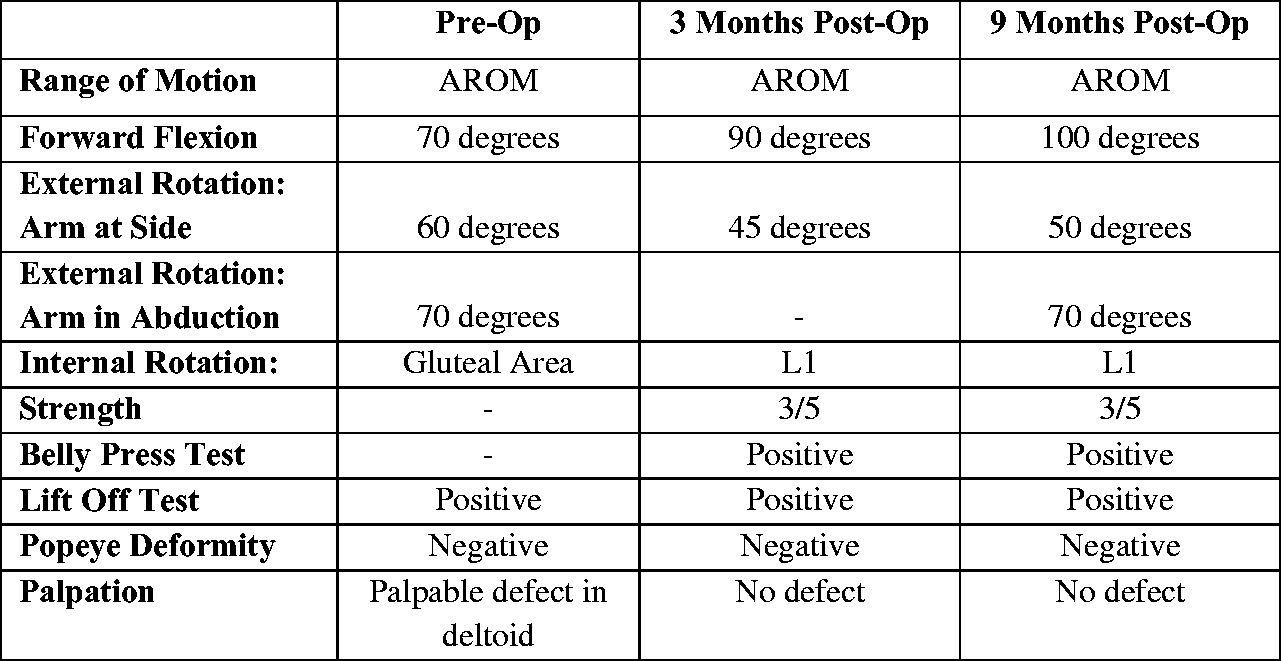
Comparison of patient’s pre- and postoperative shoulder function tests.
Discussion
We present a unique complication of total shoulder arthroplasty secondary to detritic synovitis resulting in a pathologic acromial fracture and deltoid avulsion. We hypothesize that the patient suffered a full thickness rotator cuff tear following the original TSA surgery. This is not uncommon in rheumatoid patients. The resulting mechanical dysfunction and joint imbalance consistent with the “rocking horse” theory led to the formation of extensive polyethylene wear debris. 10 Ultimately, this created a significant foreign body inflammatory reaction that was able to freely communicate between the glenohumeral and subacromial spaces, leading to osteolysis, acromial fracture, deltoid avulsion, and progressive rotator cuff tearing.
A patient presenting with soft tissue complications, mechanical loosening, or catastrophic failure after shoulder arthroplasty requires a comprehensive workup to determine the etiology. Infection must be considered even in the absence of traditional signs, symptoms, and laboratory findings associated with septic arthritis. Indolent infection from Propionibacterium acnes is a well-documented complication in patients who have undergone prior total shoulder arthroplasty. 11 Serum inflammatory markers and joint aspirates have high false-negative rates in this setting. 12
Similarly, workup of an osteolytic lesion requires a high level of suspicion for metastatic disease. The workup of a solitary osseous lesion, or multiple lesions, should be comprehensive, to rule out primary or secondary neoplasms. 13 Diagnostic needle biopsy or open biopsy is required. The incidence of metastases to bone from carcinoma is increasing as survivorship rates among cancer patients, particularly in the elderly population, continues to rise. 14
This is the first report of pathologic acromial fracture and deltoid avulsion secondary to detritic synovitis after shoulder arthroplasty. The extensive osteolysis and soft tissue injury present requires the surgeon to rule out infection and metastatic disease. The diagnosis of detritic synovitis requires tissue biopsy with comprehensive histopathologic analysis. In the setting of a painful shoulder arthroplasty with signs of osteolysis, tissue samples from involved areas will show polarizable material within giant cells.
Conclusion
In describing the constellation of osseous and soft tissue injury as a result of inflammation related to polyethylene debris in this patient, we demonstrate that the condition of detritic synovitis must be considered in the differential diagnosis for workup of a painful shoulder arthroplasty. This has important ramifications on surgical decision making, specifically in ruling out infection and metastatic disease. In addition to standard serologic and radiologic evaluation of patients, obtaining tissue for culture and pathologic evaluation is required in confirming the diagnosis of detritic synovitis and ruling out metastatic disease and infection.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.