
Abstract
There has been enormous advancement in the field of shoulder surgery since its initial establishment as a subspecialty. This is due in large part to the numerous contributions made by clinicians who came before us. This review of eponyms in shoulder surgery provides the opportunity to honor our predecessors and their contributions as well as promote the correct use of eponyms going forward.
Introduction
The field of shoulder surgery has advanced rapidly in the past 30 years, with the discovery of new pathology, and the development of new techniques to diagnose and treat patients. We owe much of this evolution to the pioneers of the shoulder, such as Codman, Latarjet, Neer, Bigliani, and Jobe to name a few, who through their contributions laid the foundation for future progress and for the future generation of shoulder surgeons to stand even taller on their shoulders. 1
The earliest evidence of recognition for focused study and discussion regarding the complexity of the shoulder traces back more than 80 years. In 1935, during the third annual meeting of the American Academy of Orthopedic Surgeons, a symposium entitled, “Symposium on the Shoulder,” was held and moderated by Dr Ernest A Codman. 2 However, it would be nearly 50 years before the establishment by Dr Charles S Neer of the American Shoulder and Elbow Surgeons (ASES) society in 1982. 3 By the mid-1980s, the field was expanding quickly. Arthroplasty had become established by institutions such as the New York Orthopedic Hospital (NYOH) as a reliable treatment for shoulder osteoarthritis. 4 Arthroscopy was becoming a fast growing technique for the treatment of athletes as well as many shoulder and elbow pathologies.5,6,7 There was an expanding focus for understanding the biomechanics and rehabilitation of the throwing shoulder. 8 This all served to accelerate advancement in the field to where we are today with shoulder surgeons pushing the boundaries of what can be done with minimally invasive arthroscopy and the development of the reverse shoulder arthroplasty.
Throughout this period of advancement and going forward, similar to all fields of medicine, we have sought to honor the wisdom, knowledge, and experience of past physicians. Oftentimes, influential concepts, techniques, or pathology are attached to an eponym to honor the surgeon and their contribution. The word eponym is of Greek origin, derived from eponymos, and roughly translates into “to name after.” Eponym represents the name of a disease, structure, operation, or procedure, often derived from the name of the person who often but not always discovered it first. There are those that staunchly argue against the use of eponyms, claiming they lack descriptive value, have redundancy with multiple eponyms associated with a single entity, and often contain multiple inaccuracies.9,10 However, eponyms continue to be prevalent in orthopedics and correlate with a steadfast premise of medicine to remember those who came before.
The purpose of this article is to review commonly used eponyms in shoulder surgery. This review provides the reader with knowledge regarding both the background of the surgeon and the original description of the eponym with hopes of giving interesting insight into history and promoting correct use of these shoulder eponyms.
Lesions
Bankart Lesions
Dr Arthur Sydney Blundell Bankart (1897–1951) was born in Exeter, United Kingdom, in 1897. He is known primarily for his description of anterior shoulder instability and its operative management. He received his primary education from The Rugby School and Trinity College. He went to Cambridge and earned his medical degree from Guy’s Hospital in 1906. 11 Bankart completed his surgical fellowship in 1909, becoming a Fellow of the Royal College of Surgeons while working as Registrar at The Royal National Orthopaedic Hospital. One year later, he completed his Masters of Surgery degree. In 1911, he began working at multiple hospitals providing services in orthopedic surgery, neurosurgery, and pediatric surgery.12,13 During World War I, he worked with Dr Robert Jones, a prominent orthopedic surgeon of the time, at the Shepherd’s Bush Military Orthopaedic Hospital. He also served his country during World War II.
Dr Bankart (Figure 1), a man of many talents, was described as straightforward, yet shy and possessed great integrity. 12 He was the first surgeon in England to perform a lateral cordotomy for pain relief. 12 However, he is most well known for describing the common anteroinferior labral lesion associated with anterior shoulder dislocation and the surgical technique for its repair.12,13 The lesion is reported as “detachment of the glenoid ligament from the anterior margin of the glenoid cavity.” 14 The surgical technique for the repair of the lesion was first performed and described by Perthes in 1906, but it was Dr Bankart’s description in a 1938 journal article which gained considerable attention.14,15 Dr Bankart’s repair is centered around an anatomic reconstruction connecting the detached glenoid labrum to the joint capsule with a bony attachment to the anterior glenoid through drill holes and suture. In this technique, the subscapularis is not overlapped or shortened. Furthermore, Dr Bankart was a founding member of the British Orthopedic Association and continued serving the public and his country until his retirement in 1944.12,13 He died in 1951 at the age of 71, 11 but left a long lasting effect on the field of surgery. His name will always be remembered in the history of shoulder surgery.
Photograph of Arthur Sydney Blundell Bankart, MD.
Buford Complex
Dr Don Buford (1966–) grew up in Los Angeles, California (Figure 2). Besides academics, he was always interested in athletics, especially baseball. His abilities in baseball earned him a scholarship to attend Stanford University. After initially attending Stanford, Dr Buford transferred to the University of Southern California (USC) where he continued his baseball career and academic pursuits. After graduation from USC, he signed a professional contract with the Baltimore Orioles and enrolled at University of California, Los Angeles, medical school. Dr Buford spent 4 years with the Orioles organization. Of note, his father, Don Buford Sr, played for the Baltimore Orioles and was named to the Orioles’ Hall of Fame. 13 After graduating from medical school, Dr Buford completed his orthopedic residency training at the University of Texas Southwestern in Dallas. In 1999, he learned advanced arthroscopic techniques during his fellowship at the Southern California Orthopedic Institute. Currently, Dr Buford practices in the Dallas, TX area.

Photograph of Don Buford, MD.
Early in 1994, Dr Buford, along with his colleagues, conducted a review of arthroscopic shoulder anatomy paying specific attention to glenohumeral anatomy and the anatomy of the labroligamentous complex. During their review of the shoulder arthroscopic videos, they discovered a number of cases demonstrated a middle cord-like ligament and absent superior anterior labrum. They named this anatomical variant, “the Buford complex.” 14 In his initial paper, he found the incidence of the anatomical variant to be 1.5%. Clinically, Buford complex has been associated with higher rates of superior labrum anterior-posterior tears than the general population. 16 In addition, it can lead to severe painful restriction of rotation and elevation if mistakenly attached to the glenoid neck. Dr Buford in his review as well noted that 12% of patients had a sublabral foramina with 75% of those patients having a “‘ cord-like’ MGHL attached to anterior-superior labrum” and the remaining having a normal middle glenohumeral ligament. 17
Kim Lesion
The Kim lesion was first described by the Korean orthopedic surgeon Dr Seung-Ho Kim in 2004. He is currently a Chief of Shoulder Surgery at Madi Hospital in Seoul, Korea, and has served as Associate Professor of Orthopedic Surgery at Sungkuynkwan University. He has become well known outside of Korea as a result of his extensive publications in the American literature. Dr Kim is a member of various national and international Orthopedic societies. He is a member of the Korean Orthopedic Association, Korean Shoulder and Elbow Society, International Society of Arthroscopy, and honorary member of the American Orthopedic Society of Sports Medicine.
In 2004, Dr Kim described injury to the posterior inferior labrum and glenoid articular cartilage that is often concealed superficially through arthroscopic examination of 15 patients. He named this labral lesion a Kim Lesion. 18 He proposed the significance of the Kim lesion clinically is persistent posterior instability if the lesion is not addressed. The recommended steps are converting the concealed incomplete Kim lesion to a complete tear and repair with the posterior band of the inferior glenohumeral ligament. Dr Kim is also credited with first describing the Samsun Medical Center knot, often used for arthroscopic labral repair. 19
General/Miscellaneous
Bigliani Acromion Types
Dr Louis U Bigliani (Figure 3) is a distinguished orthopedic surgeon known for the extensive study of shoulder pathology. He received his primary education from Steven Academy in New Jersey from 1960 to 1964. He attended the College of Holy Cross in Massachusetts from 1964 to 1968 and played on the tennis team. After graduating from college, he received his medical degree from Stritch School of Medicine, Loyola University, in 1972. He spent internship year training in general surgery at Roosevelt Hospital, New York, then pursued further training in orthopedic surgery at NYOH/Columbia Presbyterian Hospital from 1974–1977. He was Dr Charles Neer’s first shoulder fellow in 1977–1978. He was a pioneer in describing the normal anatomical variants of the acromion. He described the anatomical morphology of acromion and divided it into 3 types namely Type I, Flat shaped; Type II, curved; and Type III, hooked morphology (Figure 4). 20 Dr Bigliani’s reported incidence rates were 17.1% for Type I, 42.9% for Type II, and 39.3% for Type 3.

Photograph of Louis U Bigliani, MD.
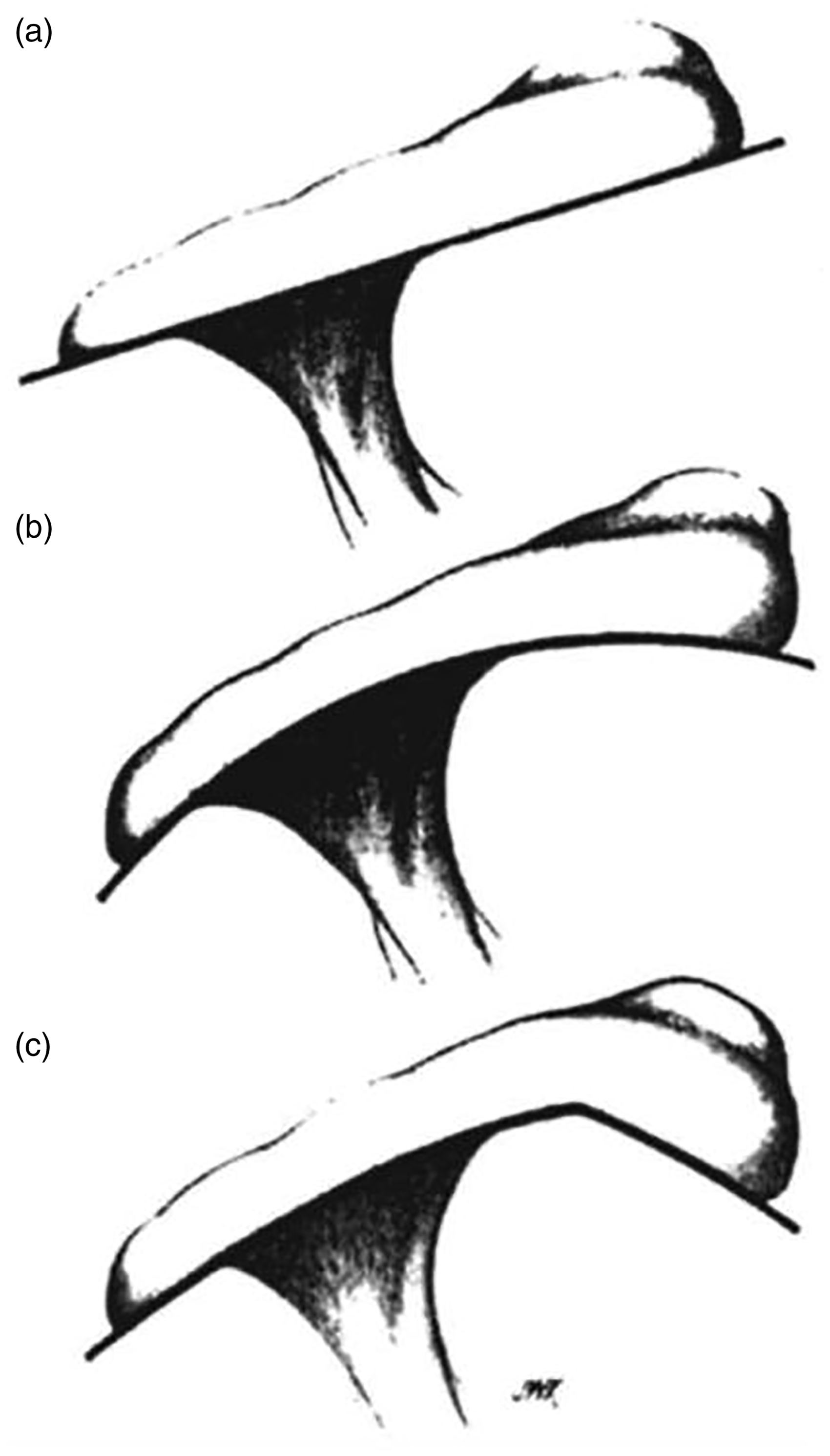
Image From Bigliani’s Original Article Defining Acromion Morphology: (A) Type I, (B) Type II, and (C) Type III. 20
The acromion morphologies reported by Dr Biglianai clinically have been correlated with the incidence of rotator cuff tears in these patients. Studies have linked Type III acromions with partial and full rotator cuff tears while the relationship with Type I and II is less clear. 21 Studies have shown a low interobserver reliability for acromial morphology putting into question the utility of this classification system. 22
Dr Bigliani is a founding member of the ASES. He has also served as Frank E. Stinchfield Professor and Chairman of Orthopedic Surgery at Columbia University Medical Center. In addition, he was selected as the President of the American Orthopedic Association in 2008. He is a member of multiple national and international orthopedic societies.
Codman Exercises
Dr Ernest A Codman (1869–1940) was born in Boston, Massachusetts (Figure 5). 23 He is remembered not only for his efforts in orthopedics and oncology but also for his contributions to anesthesiology, gastrointestinal surgery, and radiology. He was an ardent campaigner for the importance of clinical outcome measurement in medicine. 24 Dr Codman received both his undergraduate degree and medical degrees from Harvard University. He joined the Massachusetts General Hospital faculty after completing his clinical training in surgery. There he launched Morbidity and Mortality conferences. However, strained relations with other staff members led to his resignation from Harvard in 1914. He was always fervent in collecting and analyzing data in order to point out mistakes made by the surgeons, an idea not welcomed by elite surgeons at Massachusetts General Hospital. 24 Although the idea to improve quality care was first presented by British Physician Thomas Percival, it was Dr Codman who first implemented this in clinical practice. He developed his own private hospital “The End Result Hospital” where he formulated the outcome analysis from 1911 to 1916.23,25

Photograph of Ernest A Codman, MD. 23
In early 1920s, his efforts studying orthopedics gained considerable attention. 26 Most notably, he described Codman exercises for the purpose of recovering range of motion in the shoulder. A typical exercise involves forward leaning of the patient with the support of one arm and performing pendulum-like movements in the effected arm, which can reduce pain and increase joint mobility after shoulder pathology. 27 As well, in 1934, he published his landmark text “The shoulder: rupture of the supraspinatus tendon and other lesions in or about the subacromial bursa.” His text described a variety of topics including the normal anatomy of the shoulder, normal motions of the shoulder joint, rotator cuff tears, and neurologic injuries to name a few. 28 His name is also attached to the commonly used oncologic eponyms, Codman’s triangle and Codman’s tumor. 29 His prototypical ideas and contributions to clinical orthopedics and patient outcome follow-up laid solid basis for future medicine. He died of malignant melanoma at the age of 70. 29
Neer Proximal Humerus Fracture Classification and Impingement Sign
Dr Charles Sumner Neer (1917–2011) was born in Vinita, Oklahoma. He completed high school at Shattuck Military Academy and then went to Dartmouth College. After completing medical school at the University of the Pennsylvania, he continued his postgraduate training at NYOH/Columbia-Presbyterian. There, he had the chance to work with many influential personalities including Drs Harrison McLaughlin, Alan Smith, and Frank Stinchfield. Dr Neer was encouraged by Dr Stinchfield for his early interest in humeral fractures. 1 He worked around the world during World War II including Europe, Japan, and the Philippines. After completion of his residency in 1949, he became part of the NYOH/Columbia Orthopedic faculty. He went on to perform his first humeral head replacement for a complicated humeral head fracture in 1951. 30 He modernized and developed shoulder and elbow specialization. He often took initiative as a speaker for major shoulder and elbow conferences around the world. 3 He was appointed as the Chief of Adult Reconstructive Surgery in 1975. In 1976, his continuous efforts for the field of shoulder and elbow surgery culminated in the formation of the first Shoulder fellowship in the United States. 30
In 1970, Neer defined a classification for proximal humeral fractures based largely on fracture parts and displacement. His classification was based on the analysis of over 300 displaced fractures and dislocations of the proximal humerus. The major segments of the humerus were considered to be the articular surface, greater tuberosity, lesser tuberosity, and shaft. Segment displacement more than 45° or 1 cm was used to define a displaced fracture. As such, there are 4 major groupings, based on number of displaced parts. In cases of “1-part” fracture, fracture lines involve 1 to 4 parts without any displacement. A “2-part” fracture involves 1 part displaced from the other 3 parts. Criteria for a “3-part” fracture are that the fracture involves 2 parts displaced from the rest. Finally, a “4-part” fracture is defined as having 3 displaced parts.31,32,33
A meta-analysis article released in Clinical Orthopaedics and Related Research evaluated both reliability and utility of Neer’s system. Although there is variability in the interobserver reliability of the system, the authors concluded that no other fracture classification is more reliable than the Neer system. In addition, it correlates well to complications and functional results that may occur after the treatment of the fracture. Therefore, it is a system useful for aiding in the treatment of proximal humerus fractures. 34
Neer also described the important diagnostic physical examination maneuver for rotator cuff impingement. It is performed by passively flexing the subject’s arm. The advent of pain in the anterior or anterolateral proximal arm shows rotator cuff impingement.33,35,36
In 1982, Dr Neer founded the ASES (Figure 6). He retired from the Columbia Orthopedic Department in 1990 and returned to Oklahoma with his family. Dr Neer is the primary author for 5 articles in the Orthopedic Top 100 most cited articles, more than any other author. 37 Clearly, his contributions have redefined the subspecialty of shoulder surgery.

Photograph of Charles S Neer, MD.
Physical Examination Maneuvers
Hawkins’ Test
Dr Richard J Hawkins (1942–) is a Canadian-born orthopedic surgeon who attended the University of Western Ontario for his Orthopedic residency. He received advanced training in shoulder, knee, and spine before returning to University of Western Ontario to become Professor of Orthopedics and Director of the Residency Program. In 1990, Dr Hawkins moved to Vail, Colorado, where along with his colleague Dr Richard Steadman, they founded a sports medicine-specific orthopedic practice, the Steadman-Hawkins Clinic.
Dr Hawkins is a founding member and Past President of the ASES (Figure 7). He has had numerous other leadership roles including Director of the Sports Medicine Council of Canada, Team Physician to Canada during the 1988 Olympics in Calgary, Consultant to the US Ski Team, Team Physician for the Colorado Rockies as well as the 1998 and 1999 Super Bowl Champion, Denver Broncos, and Professor of Orthopaedic Surgery at the Medical University of South Carolina. Dr Hawkins has extensive clinical and research experience with a primary interest in shoulder and elbow. In 2004, Dr Hawkins expanded his practice to South Carolina, where he is Program Director of the Carolinas Fellowship Program and Chairman of the Orthopaedic Research Foundation of the Carolinas. 38

Photograph of Richard J Hawkins, MD.
In 1980, Dr Hawkins and Dr Kennedy defined a test for assessment of subacromial impingement especially for athletes with repetitive overhead use of the arm. The test is performed with forward flexion of the upper extremity to 90° and forceful internal rotation effectively wedging the greater tuberosity against the anteroinferior surface of the acromion. 39 Reproduction of pain and resulting facial expression is positive for impingement. This test would later become the Hawkins-Kennedy test and now is more commonly referred to as the Hawkins Test. Dr Hawkins stated that this maneuver is the most reliable physical sign in establishing the diagnosis of impingement syndrome which may result in degeneration and tears of the rotator cuff over time. 39 In management of impingement syndrome, he recommends conservative therapy through the use of flexibility exercises; strengthening programs; as well as rest, ice, and anti-inflammatory agents. Dr Hawkins states that surgical decompression of coracoacromial ligament resection or anterior acromioplasty are less likely to be indicated.
Jobe’s Drop Arm Sign
Dr Frank Wilson Jobe (1925–2014) was born in Greensboro, North Carolina. He graduated from Collegedale Academy in Tennessee in 1943. He enlisted for military training at Camp Berkeley at the start of World War II. 40 He served admirably and was awarded with the Bronze Star Medal, Combat Medical Badge, and Glider Badge. 41 During the war years, he also joined the Southern Missionary College and then attended La Sierra University. He earned his medical degree at Loma Linda University Medical School in 1956. 40 He worked initially as a general practitioner. During this time, he developed a strong interest in Orthopedics, completing an orthopedic residency at Los Angeles County Hospital.42,43 In 1965, he teamed with Dr Robert Kerlan to develop a sports medicine focused orthopedic practice initially named “Southwestern Orthopedic Medical Group.” This would later become known as the Kerlan-Jobe Orthopaedic Clinic. Their innovative approaches to caring for athletes led their clinic to provide medical coverage for multiple professional sports team in Southern California, including the Los Angeles Dodgers, Los Angeles Rams, Los Angeles Lakers, Los Angeles Kings, and Anaheim Ducks. 44
Dr Jobe (Figure 8) 45 is likely best known for the surgical procedure he performed on pitcher Tommy John in 1974 to reconstruct his torn ulnar collateral ligament (UCL). 13 This surgical technique would be popularized in sports media and is most commonly referred to as “Tommy John” surgery. Prior to this technique for UCL reconstruction, a tear to this ligament was considered a career-ending lesion. Tommy John would remain on the field for a stunning 14 more seasons accumulating 288 wins, seventh highest total all-time for a left-handed pitcher. 43

Photograph of Frank W Jobe, MD.
In addition to the elbow, Dr Jobe had a passion for the shoulder. He developed 2 well known and useful physical examination maneuvers which carry his name. The Jobe’s drop test or empty can test is performed by having the patient actively elevate the arm in the scapular plane, with the arm extended and thumb pointing to the floor. The patient resists the examiner’s downward pressure on the arm.46,47 The test is positive with a sudden drop of the arm or pain. In addition, he described the relocation test for the detection of anterior shoulder instability. 48
Speed’s Test
James Spencer Speed (1890–1970) was born on July 30, 1890, in Rapid City, South Dakota. His family moved to Virginia where he spent his childhood. He attended the University of Virginia in 1912. He received his medical degree from John Hopkins University. After his internship from Jefferson Hospital and training at Union Protestant Infirmary, he served in World War I in the United States Army Medical Corps. After returning from war, he completed his residency at the Hospital for Women in Baltimore, Maryland.
He set up his own private practice until he met Dr Willis C Campbell who was an orthopedic surgeon in Memphis. After a few meetings, the 2 formed a team, and for the next 42 years, the 2 surgeons worked together. After the death of Dr Campbell in 1941, Dr Speed became the Chief of Orthopedic Services at the Campbell Clinic, Crippled Children’s Hospital, and the Hospital for Crippled Children. 49 He worked as the Chair of the Department of Orthopedic surgery at the University of Tennessee. He also served as President of American Orthopedic Association and board member of the American Board of Orthopaedic Surgery. He served as an editor for Journal of Bone and Joint Surgery, coauthored 2 editions of Campbell’s Operative Orthopaedics, and published 40 papers. 50
Dr Speed became best known for the physical examination maneuver, bearing his name, that evaluates the biceps tendon. The examination entails forward elevation of the shoulder, with the elbow extended and the hand supinated. In the case of biceps tendonitis, resisted pressure on the supinated hand produces pain in the bicipital groove. Of note, the test was not initially described by Speed himself, but rather by several of his colleagues. 51 However, his name became forever attached to the maneuver (see Figure 9).

Photograph of James S Speed, MD.
Yergason Test
Robert Moseley Yergason (1885–1949) was a preeminent surgeon known for his contribution to orthopedics, specifically in shoulder surgery. He is best remembered for his introduction of a clinical maneuver to test for biceps tendonitis. He was born in 1885 in Connecticut and attended Trinity College in 1908. He spent most years of his clinical practice in Saint Francis Hospital, Connecticut. Dr Yergason was also a great contributor to orthopedics both on the clinical side and academics. He was involved with the Hartford Medical Society, serving as its President in 1942, and also served as a benefactor to the Connecticut Historical Society. He was known to enjoy the outdoors and published an article in Field and Stream describing the way to set up an all-purpose tent. 52
In 1931, the Yergason test was first described in his publication in the Journal of Bone and Joint Surgery. 53 Initially referred to as the “Supinator Sign,” the examination maneuver would later be renamed after Yergason. The test is performed with resisted supination of the wrist with the arm flexed to 90°. If the patient experiences pain with this maneuver, the test is considered positive for possible biceps pathology such as partial tear or synovitis of the tendon sheath. In the initial article, Yergason describes the case report of a 45-year-old woman, suspected of having biceps synovitis due to handwashing a large amount of clothes. After recommending purchase of a washing machine, the patient had complete resolution of symptoms. 53
O’Brien Test
Stephen J. O’Brien (1955–) is a Professor of Orthopedic Surgery at Weil Cornell Medical College and Consultant Surgeon at the Hospital for Special Surgery (Figure 10). 54 He received his undergraduate degree from Harvard University in 1977 where he was a member of the baseball and football teams. After college, he went on to medical school at the School of Medicine, University of Virginia. He received his residency training from the Hospital for Special Surgery; he stayed for further advanced fellowship training in Sports Medicine. He would later pursue an MBA, graduating from the Columbia University Business School in 2000.

Photograph of Stephen J O’Brien, MD.
Dr O’Brien has been involved in research from the start of his career, with numerous book chapters and publications. His research interests have largely been focused on the shoulder and specifically biceps-labral disorders. 54 The active compression test, which would later become known as the O’Brien test, was introduced with his 1998 publication. The goal of this test was to elicit symptoms for superior labral pathology in hopes of differentiating it from acromioclavicular joint disorders. The test is performed by having the patient forward flex the arm to 90° with the elbow in full extension. Then, adduction of arm 10° with internal rotation so that the thumb points downward. Downward force is applied by the examiner with resistance from the patient. The palm is then fully supinated and same test is repeated. Pain experienced by subject during the first internal rotated position and elimination with the second position indicates a positive test. 55
Operative Procedures
Latarjet Procedure
Michel Latarjet (1913–1999) was born in Lyon, France. He was a surgeon and an anatomist. In 1954, he introduced the surgical technique for the treatment of unstable shoulders. He was the son of well-known surgeon, Dr Andre Latarjet. He played a critical role in the application of descriptive anatomy into clinical sciences. 56 He completed his medical degree in 1939. His professional studies and career were interrupted by World War II. He continued his training under the supervision of his father. At the young age of 33, he achieved the post of Professor, following the death of his father in 1946. Initially, this faculty position was more directed to anatomy and basic sciences, but gradually it was transitioned to a more clinical and surgical-oriented position. In the beginning of his clinical practice, he mostly spent time treating thoracic disease and managing general surgical patients. It was later in 1954, he performed his first coracoid transfer for the treatment of shoulder instability. This surgical technique would later become known as the Latarjet procedure. 57 The surgical technique transferred a large block of the coracoid process with the attached conjoint tendon to the anteroinferior portion of the glenoid. This placement of the coracoid worked to increase the glenoid depth as well as create soft tissue restraint with the sling effect of the conjoint tendon and repair of the capsule to the coracoacromial ligament. 58 He received multiple honors and served as Director in the National Academy of Surgery and the Academy of Lyon.
Bristow Procedure
Walter Rowley Bristow (1883–1947) was a British orthopedic surgeon. He trained at St. Thomas Hospital receiving a diploma in 1907 and graduated as Bachelor of Medicine, Bachelor of Surgery in 1908. 59 He continued his training as Fellow in the Royal College of Surgeons. As a student, he was always involved in athletic activities, playing on the soccer, tennis, and water polo teams. 59 He worked under the supervision of Sir George Makins, as House Surgeon in Trauma Surgery during his early career. With the outbreak of World War I, he was appointed to a military hospital in 1916. There he met Dr Robert Jones and started a long-lasting collaboration and friendship. 59
After the end of the war, he returned to St. Thomas to aide in development of the Orthopedic department. His growing reputation led to his later appointment at King Edward VII’s Convalescents Homes for Soldiers. 59 During his career, he served various leadership roles, including President of the Orthopaedic Section of the Royal Society of Medicine, Hunterian Professor of Royal College of Surgeons, and President of the British Orthopaedic Association. 59
He initially described his technique for transfer of the coracoid tip, in his 1958 article published in the Journal of Bone and Joint Surgery. 60 The method was unique in its nature, as it involved removal of just the coracoid tip allowing the remaining coracoid to stay in place and recreating stability mostly through the soft tissue sling created with the conjoint tendon. The eponym for his procedure is often used in conjunction with the Latarjet eponym when discussing coracoid transfer, but it is essential to understand the difference between the 2 procedures.
Weaver-Dunn Procedure
Dr James K Weaver (1929–) was born in 1929. He received his medical degree from the University of Colorado School of Medicine in Denver. He interned at the University of California, San Francisco, before returning to Colorado to complete his residency in orthopedics. After completion of residency, he spent several years in the military service at Elgin Air Force base before joining the faculty at the University of New Mexico. He would later serve as Department Chair during the late 1960s. 13
Harold K Dunn (1939–) grew up in New Mexico on a cattle ranch. He developed roping skills that would earn him a scholarship to Texas Christian University. 61 Dr Dunn then attended Baylor Medical School and stayed in Texas to complete his internship at Ben Taub General Hospital in Houston. He completed his residency at the University of New Mexico where he would meet and collaborate with Dr Weaver. In 1969, he joined the faculty of the University of Utah. Dr Dunn’s main academic interest included the areas of adult reconstruction and also spinal deformities. 62 He would later become Chairman at the University of Utah, a post he would hold for nearly 25 years (Figure 11).

Photograph of Harold K Dunn, MD. 61
Dr Weaver and Dr Dunn collaborated to develop a technique for acromioclavicular joint reconstruction, which they published in 1972 in the Journal of Bone and Joint Surgery. 63 Their surgical technique described resection of the distal 2 cm of the clavicle and transfer of the coracoacromial ligament. The coracoacromial ligament was passed through the clavicle and secured superiorly in an effort to restore the stabilizing effects of the torn coracoclavicular ligaments. 63 Recent biomechanical studies have demonstrated superior results with anatomic reconstruction of the coracoclavicular ligaments using allograft, and thus, this technique has fallen out of favor. 64
McLaughlin Procedure
Dr Harrison L McLaughlin (1906–1970) was a Canadian surgeon never technically trained as an orthopedic surgeon. In 1933, he graduated from Queen’s University Medical College going on to intern at Ottawa Civic Hospital. Following his internship, he became a resident at Presbyterian Hospital on the fracture service lead by William Darrach and Clay Ray Murray eventually becoming Chief of the Fracture Service after Dr Murray’s death. In addition, he was a clinical professor at the College of Physicians and Surgeons, Columbia University. He was the Chairman of the Trauma Committee of both the American College of Surgeons (1959–1964) and American Association for the Surgery of Trauma, becoming president of the latter in 1961. A major focus of his career was the management of shoulder problems. 65
Dr McLaughlin is notable for a procedure for the treatment of posterior shoulder dislocation that he first described in 1952 in the Journal of Bone and Joint Surgery. The McLaughlin procedure involved transfer of the subscapularis tendon from the lesser tuberosity to the reverse Hill-Sachs defect caused by the dislocation. Of note, he reported usage of this procedure, when the Hill-Sachs lesion was between 20% and 45% of the joint surface. 66 Since the release of this procedure, multiple studies have evaluated the success of Dr McLaughlin’s original description. Overall, the data have shown an improvement in success rate and clinical results when the lesser tuberosity is transferred along with the subscapularis.67,68 This has led to a modified form of the initial procedure described that continues to hold Dr McLaughlin’s name.
Conclusion
If I have seen further than others, it is by standing upon the shoulders of giants. (Isaac Newton)
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.