
Abstract

Keywords
Introduction
Calcaneal osteotomies play an important role in the correction of hindfoot deformities. Despite the use of various eponyms to denote them, the origins of the osteotomies have been less widely recognized over time. Further, with time there is a tendency for confusion and inaccurate use of these eponyms.
This current article will review the most commonly used eponyms for calcaneal osteotomies, defining the original procedures and delving into the historical background of the individuals who described them.
Eponyms Related to Hindfoot Valgus (Flatfoot) Deformity Correction
Hindfoot valgus is one of the main components of a flatfoot deformity. With advanced, symptomatic deformities, surgical intervention via osteotomies may be necessary. Although specific osteotomy techniques are often named after the surgeons who pioneered them, they share common goals. These procedures aim to realign the bones of the hindfoot, restore the collapsed arch, and enhance overall biomechanics, thereby mitigating pain and dysfunction. This section delineates the primary goals of osteotomies for the correction of hindfoot valgus while also exploring particular eponymous techniques.
Gleich Osteotomy
Dr Alfred Gleich played a pivotal role in the medical landscape during his tenure at the Billroth Clinic, an esteemed institution affiliated with the Organ of the Royal Society of Physicians in Vienna. His substantial contributions to the institution’s weekly journal significantly enriched the contemporary medical literature. In 1893, Gleich 14 showcased his innovative surgical technique for addressing flat feet in the “Archive for Clinical Surgery, Volume 46.”
Gleich’s procedure is characterized by an oblique osteotomy of the calcaneal tuberosity with plantar and thereby anterior displacement of the tuberosity (Figure 1). If a greater correction is required, a plantar closing wedge is resected. In addition, to correct hindfoot valgus, the tuberosity can also be translated medially (inward) based on the required deformity correction. An Achilles tenotomy should be performed before the osteotomy, allowing the tendon to heal in a lengthened position following the correction. 14 The Gleich osteotomy shifts heel ground contact medially, thus repositioning weight lateral to the center of gravity.33,40

Gleich osteotomy. Sagittal view of traditional plantar (forward) translation (A) and plantar closing wedge (B). Reproduced from Gleich. Arch Klin Chir. 1893. Figure out of copyright.
Koutsogiannis Osteotomy
Dr E. Koutsogiannis hails from Larissa, Greece, and has a notable background in orthopaedic surgery. Having gained valuable experience at Southmead Hospital in Bristol, England, Dr Koutsogiannis made a significant contribution to the field. In 1971, he published his innovative suggestion for calcaneal osteotomy in The Journal of Bone and Joint Surgery. 29 This proposal presented a variation from the original Gleich osteotomy with simple medial displacement of the calcaneal tuberosity.
The Koutsogiannis procedure involves making a lateral incision parallel to, and slightly behind and inferior to, the peroneal tendons. Care is taken to protect the sural nerve. After the osteotomy is opened, the periosteum is divided medially to enable the intended displacement. Long plantar ligament division may also be necessary for adequate displacement. The posterior calcaneal segment is then medially displaced until its border aligns with the sustentaculum tali, typically involving a displacement of one-third to half of the tuberosity width (Figure 2). 29 This osteotomy is commonly referred to as a medializing calcaneal osteotomy (MCO), and Koutsogiannis’s name is infrequently referenced.
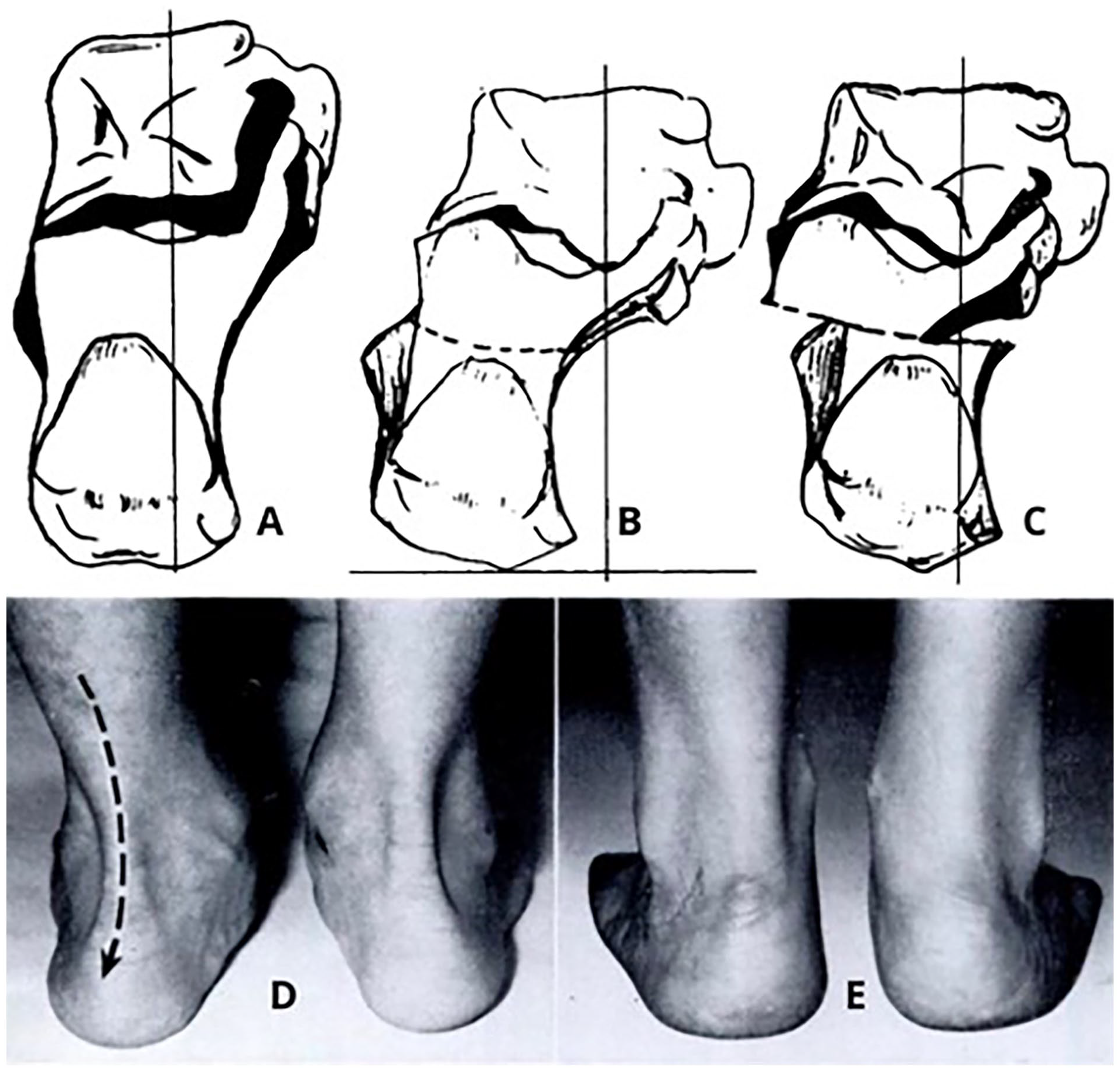
Koutsogiannis osteotomy. Foot’s weightbearing line and talus-calcaneus relationship from a posterosuperior viewpoint: (A) normal foot; (B) flatfoot; (C) surgical displacement; (D) preoperative valgus heels; (E) postoperative neutral heel position. Reproduced from Koutsogiannis, J Bone Joint Surg Br. 1971. Permission obtained from British Editorial Society of Bone & Joint Surgery.
Gleich-Koutsogiannis Osteotomy
The combined Gleich-Koutsogiannis technique involves a medial displacement osteotomy with translation of the posterior fragment forward, medially, and downward in an attempt to reestablish the normal calcaneal pitch angle. 18 This method incorporates a wedge resection, resulting in the distal end being displaced medially and plantarly, thereby transforming the triceps surae into an invertor rather than an evertor in the deformed foot.17,23,25,39 It combines the forward (downward) calcaneal displacement from Gleich’s technique with the medial displacement described by Koutsogiannis (Figure 3). 42
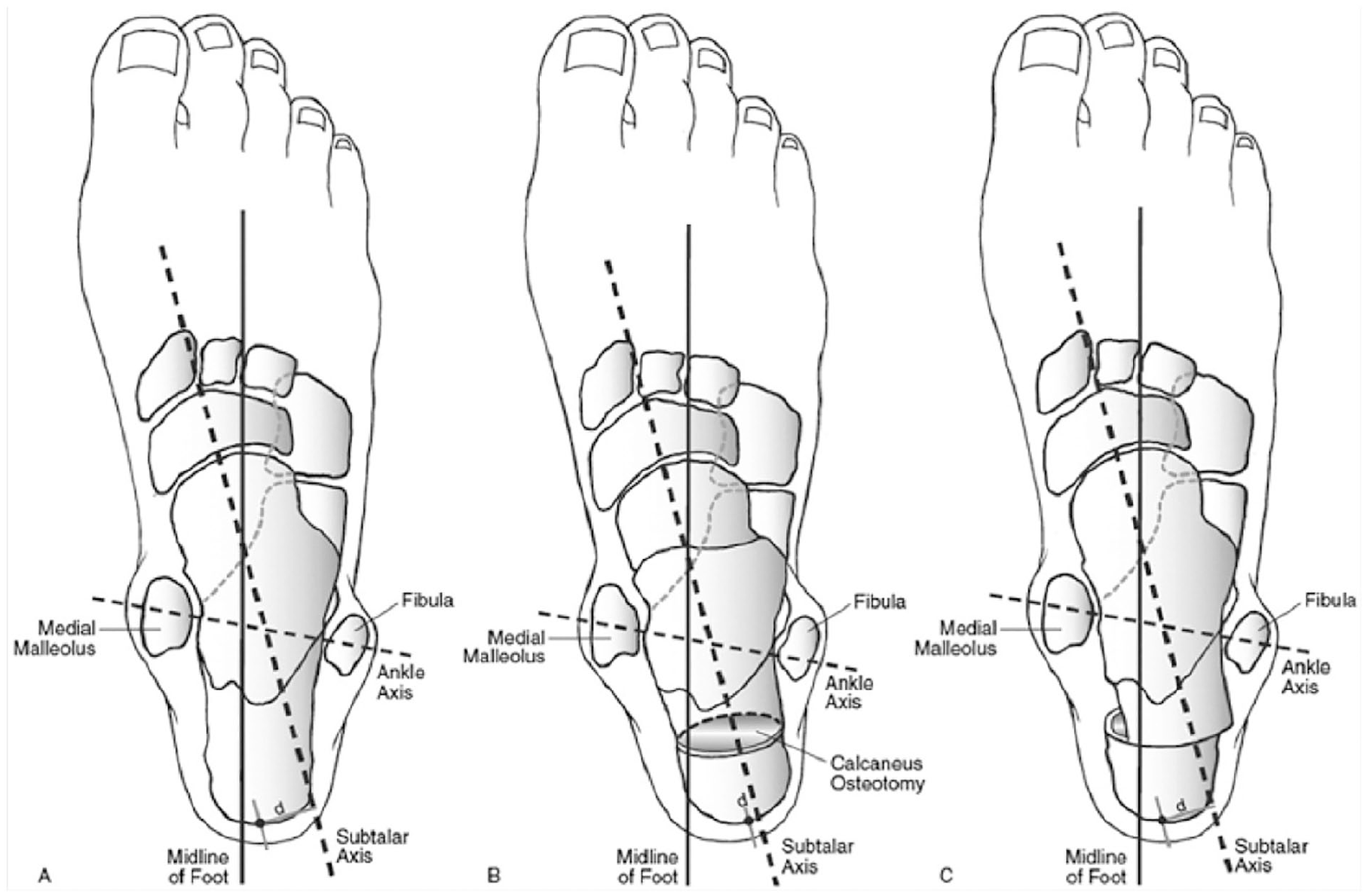
Gleich-Koutsogiannis osteotomy. Illustration of foot alignment and calcaneal osteotomy. (A) Preoperative valgus alignment showing the deviated subtalar axis. (B) Planned calcaneal osteotomy for realignment, with correction of the subtalar axis. (C) Postoperative alignment with the subtalar axis restored, achieving improved foot mechanics following the medial and anterior (plantar) calcaneal translation. Reproduced from Jastifer and Coughlin, Foot Ankle Spec. 2015. Permission obtained from SAGE Publications.
Evans Osteotomy
Dillwyn Evans (July 29, 1910–November 9, 1974) was born in Cardiff, United Kingdom. He intended originally to become an ear, nose, and throat surgeon, but after clinical exposure developed an interest in orthopaedic surgery. Evans earned his BSc in 1930 and MB in 1933, achieving FRCSE status in 1938. 7 Subsequently, he spent 2 years at the Robert Jones and Agnes Hunt Orthopaedic Hospital in Oswestry and was later appointed as an orthopaedic surgeon at the Prince of Wales Hospital, Cardiff, in 1938.4,7,8
A significant contributor to the field, Evans played a crucial role in advancing the treatment of relapsed clubfoot, with an operation named in his honor. Evans’s 12 work on hindfoot deformity was based on the concept, in his own words, “that whereas in the normal foot the medial and lateral columns are about equal, in talipes equinovarus the lateral column is longer and in the calcaneovalgus foot it is shorter than the medial.” Evans proposed equalizing the length of these columns as a vital requirement in treating both deformities. Following the publication of his influential clubfoot article, he visited Brazil twice as a visiting professor under the British Council, establishing a training program for Brazilians. Evans, as member of the British editorial board of The Journal of Bone and Joint Surgery, contributed actively to the field and spoke as a member of the British Orthopaedic Travelling Club.7,8
In 1961, Evans introduced a lateral column-lengthening procedure designed to preserve the calcaneocuboid joint. The technique involves making an incision over the lateral aspect of the calcaneus, running parallel to and just above the peroneal tendons, with meticulous care taken to avoid and protect the sural nerve. The anterior half of the calcaneus is then exposed, and the calcaneocuboid joint identified. Subsequently, the anterior aspect of the calcaneus is osteotomized with an osteotome. The osteotomy is located anterior to the peroneal tubercle and approximately 10-15 mm proximal to the calcaneocuboid joint. The cut surfaces are then gradually opened with a laminar spreader, and a cortical tibial autograft is inserted to maintain lengthening. 12
Hintermann Osteotomy
Dr Beat Hintermann, MD, is the distinguished Founder and Chair of the Center of Excellence for Foot and Ankle, at the Clinic for Orthopaedics and Traumatology at Kantonsspital Baselland in Switzerland, building on a career that spanned over 15 years as Chairman. 5 Dr Hintermann is acknowledged as an innovator in foot and ankle surgery, leading the adoption of new techniques and the conceptualization of innovative surgical instruments. His contributions included advancements in ankle arthroscopy, corrective osteotomies, hindfoot arthrodesis, and total ankle arthroplasty.19 -21,24,48,49
Hintermann’s lateral lengthening calcaneal osteotomy was described in 1999. 22 Hintermann proposed that this osteotomy focuses as close as possible on the talonavicular joint axis, which is thought to be the main center of rotation of the subtalar joint complex. 22 An oblique incision is made laterally on the hindfoot, avoiding the sural nerve’s dorsal cutaneous branch. A lateral opening wedge hindfoot osteotomy is created near the posterior facet’s anterior border. The medial longitudinal arch is restored as the spreader widens. A corticocancellous bone graft is harvested, fashioned, and placed in the osteotomy site. Stability is maintained by compression forces, often without internal fixation. If needed, a cortical screw is inserted distally through the cranial aspect of the graft into the posteromedial calcaneus (Figure 4).11,22,44

Hintermann osteotomy. Illustration of the biomechanical principles of the Hintermann osteotomy for hindfoot deformity correction. The left image shows preoperative alignment with a deviated mechanical axis (red dashed line) and malalignment angle (α), highlighting the subtalar joint deformity (blue circle). The right image depicts postoperative realignment, showing corrected mechanical axis and normalized angle (α), restoring proper load distribution across the subtalar joint. Reproduced from Brilhault, Orthopaedics & Traumatology: Surgery & Research. 2022. Figure out of copyright.
Griend (or Vander Griend) osteotomy
Dr Robert Vander Griend, MD, obtained his medical degree from the University of Florida in 1978, followed by the completion of his residency in Orthopaedic Surgery at the same institution. 41 His commitment to advancing orthopaedic knowledge led him to pursue a fellowship in Trauma Research in Davos, Switzerland, and the Clinical Orthopaedic Society Travelling Fellowship, specializing in Foot and Ankle. Returning to the University of Florida in 1986, Dr Vander Griend joined the Department of Orthopaedics, where he has held various key roles such as the Chief of the Orthopaedic Oncology Division, Program Director of the Orthopaedic Residency Training Program, and Chief of the Foot and Ankle Service. 41 Vander Griend’s influence extends beyond his clinical roles, as evidenced by his authorship of more than 45 publications and his position as Senior Associate Editor for Foot & Ankle International.
The calcaneal osteotomy proposed by Vander Griend is characterized by correcting hindfoot valgus through medial translation of the distal calcaneal fragment. The procedure commences with an oblique lateral incision parallel and posterior to the peroneal tendons. This incision is strategically positioned in the internervous plane between the superficial peroneal nerve and the sural nerve. The distal vertical cut, positioned 8-10 mm from the calcaneal-cuboid joint, must traverse the dorsal half of the calcaneal neck to prevent dorsal displacement of the distal fragment—a potential concern with other lateral column lengthening techniques. Simultaneously, a plantarly directed proximal vertical cut is made at approximately the level of the peroneal tubercle. To finalize the “Z,” a longitudinal cut connects the distal and proximal limbs, completing the osteotomy. Holding the hindfoot secured, the forefoot is adducted using the medial aspect of the talonavicular joint as a fulcrum. This maneuver, combined with the application of a metal ruler, facilitates the mobilization of the osteotomy. Consequently, there is a medial rotation of the distal part of the “Z,” inducing an opening lateral wedge effect between 5 and 10 mm, as illustrated in Figure 5. 15

Griend osteotomy. Series of images demonstrating the osteotomy technique. (A) Initial osteotomy cut at the posterior calcaneus. (B) Lateral displacement of the posterior calcaneal fragment using an osteotome. The lower row shows various views post-osteotomy, emphasizing the corrected alignment of the hindfoot with improved positioning of the posterior fragment relative to the anterior calcaneus. Reproduced from Griend, Techniques in Foot & Ankle Surgery. 2008. Permission obtained from Wolters Kluwer Health.
Eponyms Related to Hindfoot Varus Deformity Correction
Hindfoot varus deformity entails an inward angulation of the heel bone, disrupting the natural alignment of the foot’s arch, particularly the medial longitudinal arch. This misalignment often results in functional impairments, including instability, pain, and compromised weight distribution. Corrective surgical strategies have evolved over time, with various techniques bearing the names of pioneering surgeons, encapsulated in eponyms. Through an exploration of these eponyms, this section aims to outline the primary objectives of osteotomies in correcting hindfoot varus deformity.
Dwyer Osteotomy
Frederick Charles Dwyer, born in 1907 in East London, South Africa, embarked on a distinguished medical journey that culminated in significant contributions to orthopaedic surgery. After graduating from the University of Cape Town in 1931, he initially practiced general medicine in Kimberley, South Africa, before pursuing advanced orthopaedic training in England. Completing his surgical training just before the onset of World War II, Dwyer played a pivotal role in the war effort, overseeing orthopaedic services at Wigan, England. 37 After the war, Dwyer’s career flourished with appointments at Alder Hey Children’s Hospital and Sefton General Hospital. As a former general practitioner, his keen interest in foot pathology became a focal point of his work. Notably, his calcaneal osteotomy emerged as a groundbreaking intervention for addressing talipes equinovarus and pes cavus.
Dwyer’s lateral closing wedge osteotomy, originally outlined in 1959, is commonly used to address mild cavovarus deformities. This procedure is conducted through a lateral hindfoot approach similar to the approach used by Hintermann and Griend. An 8- to 12-mm laterally based wedge of bone is excised from the lateral aspect of the calcaneal tuberosity. The orientation of the initial cut is perpendicular to the bisection of the tibia and to the longitudinal axis of the calcaneus, whereas the second cut, made posterior to the first, is advanced perpendicular to the lateral wall of the calcaneus. The osteotomy is then closed and stabilized without translation, reorienting the plantar, weightbearing aspect of the tuberosity into a more neutral or valgus position. Dwyer’s resection creates an isosceles-shaped triangular wedge (Figure 6). This technique proves advantageous in cases where there is excessive loading on the lateral edge of the heel due to a cavovarus foot. Despite necessitating a break in the medial cortex, this can be accomplished in a “greenstick” fashion. As such, the osteotomy does not mandate a complete corticotomy of the medial cortex with the saw blade, thereby minimizing the risk of potential injury to neurovascular structures.10,45

Dwyer osteotomy. The left panel shows guide wire placement and initial osteotomy cuts: the first perpendicular to the tibial axis and the second to a distal reference line. The central panel highlights the bone wedge (α°) to be removed to correct the deformity. The right panel illustrates the final calcaneal alignment post-osteotomy, with the wedge removed and the calcaneus repositioned to restore the proper mechanical axis. Dwyer, The Journal of Bone & Joint Surgery British Volume. 1959. Permission obtained from British Editorial Society of Bone & Joint Surgery.
Modified Dwyer or Krackow Osteotomy
Kenneth A. Krackow, born in 1944 in Baltimore, is a distinguished figure in the field of orthopaedic surgery. His professional journey includes the successful completion of his medical degree from Duke University in 1971, as well as an internship in General Surgery and a residency in Orthopaedic Surgery at Johns Hopkins University, concluded in 1976. In 1992, Krackow joined the faculty at the University at Buffalo, ultimately leading the Department of Orthopaedics at Buffalo General Hospital. 27 Dr Krackow’s influential contributions extend to the realm of surgical innovation, including the development of an activity scale crucial for evaluating patient conditions pre- and postoperatively. Furthermore, his groundbreaking inventions include the first computerized total knee replacement apparatus and the widely recognized running locking Krackow suture, acknowledged by orthopaedic surgeons across the field.27,47
In 1985, Krackow et al introduced a novel method, modifying Dwyer’s osteotomy. Their article reported an initial lateral transverse cut located in the posterior aspect of the calcaneus and oriented perpendicular to the axis of the calcaneal pitch. A second oblique cut is then made on the posterior tuberosity fragment and oriented obliquely, allowing for wedge removal and subsequent closure. 30 Krackow’s technique deviates from the original Dwyer osteotomy, in which neither of the bony cuts was perpendicular to the longitudinal axis of the calcaneus. His technique results in a right-triangle–shaped resection (Figure 7). 31 This unique osteotomy also allowed for the additional lateralization of the calcaneal tuberosity fragment following the osteotomy to minimize the shortening that can occur in Dwyer’s original osteotomy. 16

Krackow osteotomy. The first bone model shows the initial lateral transverse cut at the posterior calcaneus, oriented perpendicular to the calcaneal pitch axis, and the oblique cut on the posterior tuberosity fragment, creating a right-triangle–shaped wedge for removal. The second image shows the final alignment post-osteotomy, with the calcaneus repositioned to correct malalignment. The third image shows the result when performed with additional displacement and shortening due to lateral translation. Kraus et al. Foot Ankle Int. 2014. Permission obtained from SAGE Publications.
Malerba Osteotomy
Dr Francesco Malerba, an orthopaedic surgeon associated with the Department of Ankle and Foot Surgery at Galeazzi Hospital in Milan, Italy, introduced an additional lateral closing wedge calcaneal osteotomy incorporating a Z-shaped osteotomy.1,13 Malerba and De Marchi 34 introduced the calcaneal lateral closing wedge Z-osteotomy in 2005. The procedure is performed through a lateral oblique incision, ensuring careful protection of the sural nerve and peroneal tendons. Using a saw, a Z-shaped osteotomy is executed with a distal inferior limb and proximal superior limb exiting posterior to the posterior facet. Pisani initially described the removal of a long horizontal subtalar bone slice, a technique later modified with the “Z” osteotomy by Malerba and De Marchi 34 to eliminate the risk of damaging the subtalar joint. A Scarf-type osteotomy of the calcaneus is then performed, which includes the removal of a horizontal bone wedge, 5-10 mm in width, depending on the required correction, and finally fixed with the use of a staple (Figure 8).
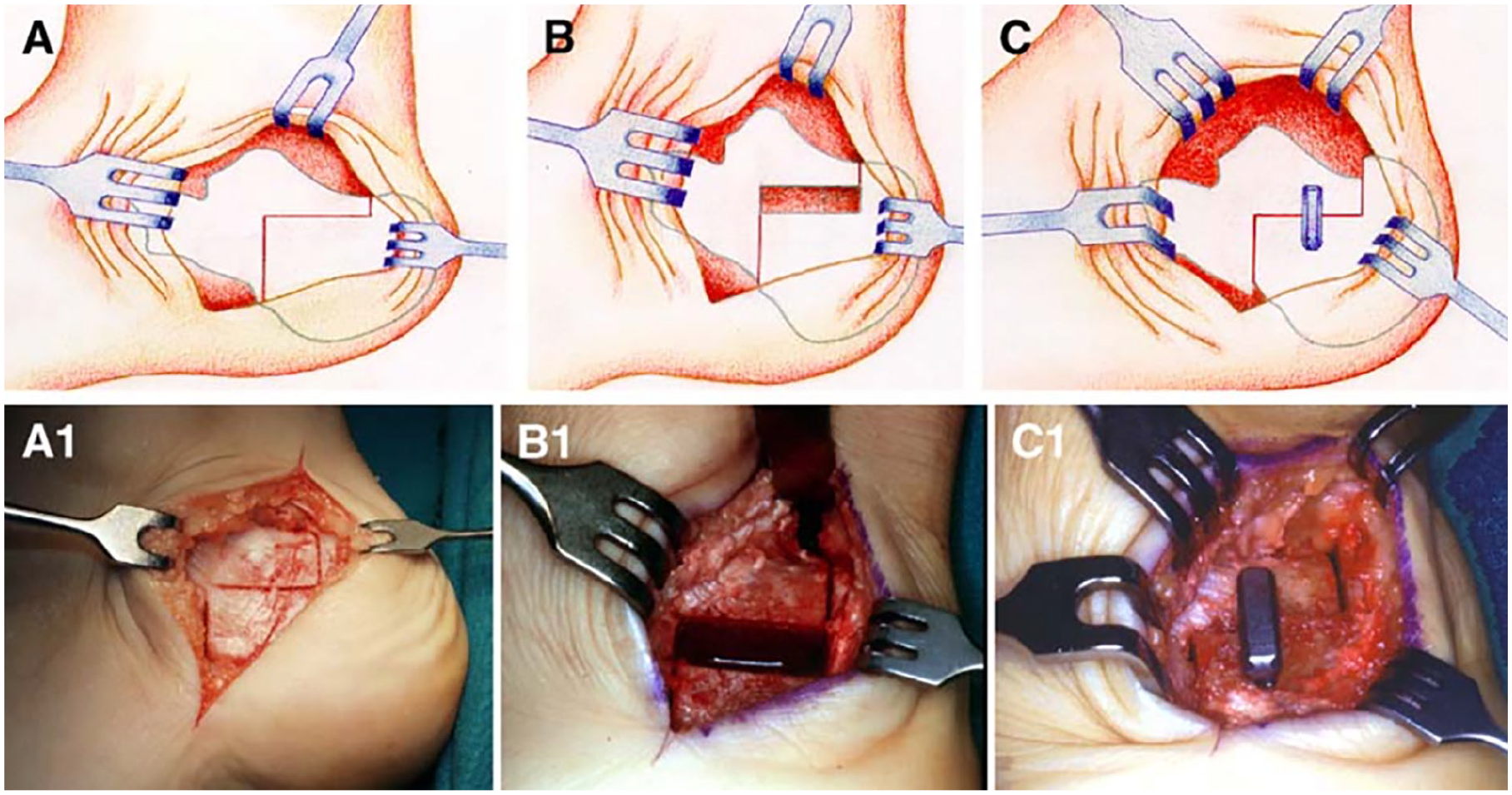
Malerba osteotomy. The top row (A-C) shows schematic drawings of the surgical steps: (A) planned osteotomy cut on the medial calcaneus, (B) bone wedge removal for correction, and (C) insertion of a bone graft or implant to maintain alignment. The bottom row (A1-C1) presents corresponding intraoperative images. Malerba and De Marchi, Foot and Ankle Clinics. 2005. Permission obtained from Elsevier.
Modified Malerba or Knupp Osteotomy
Prof Markus Knupp functions as the chair of the foot and ankle unit at Kantonsspital Baselland and has contributed more than 100 scientific articles to the orthopaedic literature. Knupp et al 28 modified the Malerba Z-osteotomy in 2008 by introducing an additional translational component. In an anatomical model, they demonstrated that the Z-osteotomy with a lateral heel slide had greater effectiveness in lateralizing the center of force at the ankle compared with an isolated Z-osteotomy or heel slide osteotomy. 6
The osteotomy’s horizontal segment, around 2 cm long, parallels the plantar fascia. The anterior vertical cut is slightly anterior of the tuberosity. The posterior cut is strategically placed in the tuberosity’s posterior half (Figure 9). Care is taken not to extend it too far posteriorly to avoid Achilles tendon interference. Using an oscillating saw, the osteotomy is performed, and the wedge is extracted. A distracter, like a laminar spreader, may mobilize the osteotomy if needed. The tuberosity can then be laterally displaced, closing the gap. Optionally, lengthening the calcaneus involves posterior displacement of the tuberosity. 28

Knupp osteotomy. The top bone model shows the lateral view of the calcaneus after the osteotomy cut has been made, with a spacer in place to simulate the realignment. The bottom models provide anterior and posterior views, illustrating the repositioning of the calcaneus achieved through the osteotomy. Knupp et al. Techniques in Foot & Ankle Surgery. 2008. Permission obtained from Wolters Kluwer Health.
Eponyms Related to Achilles Tendinopathy Management
Achilles tendinopathy is characterized by the degeneration and pain of the Achilles tendon. An osteotomy may be used to address biomechanical factors contributing to the symptoms associated with this condition.
Zadek osteotomy
Zadek, 51 an accomplished American orthopaedic surgeon, is credited with first describing a pioneering osteotomy for the treatment of Haglund deformity and insertional Achilles tendinopathy. He obtained his medical degree in 1914 at Johns Hopkins Medical School and served in France during World War I. On his return, Dr Zadek established himself in New York at the Hospital for Joint Diseases, marking the continuation of his impactful career in orthopaedic surgery. 9
The Zadek 51 osteotomy was initially detailed in 1939. In this report, a calcaneal osteotomy was used to treat 3 female patients with recalcitrant “achillobursitis.” The procedure entailed a dorsal closing-wedge osteotomy anterior to the Achilles insertion (Figure 10). The osteotomy rotates the Haglund deformity and any insertional calcification anteriorly, thus relieving pressure and optimizing biomechanics. To this end, the osteotomy functionally lengthens the triceps surae, thus decreasing tension at the insertion. The Zadek osteotomy adds another tool to the foot and ankle surgeon’s arsenal in the treatment of Haglund deformity, avoiding tendon takedown and Haglund resection. 50

Zadek and Keck and Kelly osteotomies. (A) Zadek osteotomy involves a dorsal closing-wedge resection anterior to the Achilles to adjust the calcaneus-tibia angle, shown before and after the procedure. (B) Keck and Kelly osteotomy involves removing a posterior-superior dorsal closing wedge, with the arrow indicating the direction of correction. Zadek, The American Journal of Surgery. 1939; Keck and Kelly, The Journal of Bone and Joint Surgery. 1965. Permission obtained from Elsevier and Wolters Kluwer Health.
Zadek’s osteotomy may be performed using either open or minimally invasive techniques.32,35,36,43,46 It has recently been modified by Keck and Kelly, focusing more on directly reducing the bony prominence of the posterior-superior aspect of the calcaneus without significantly changing the posterior calcaneal angle (Figure 10).2,26,38,44
Conclusion
This review provides an overview of the historical context surrounding eponyms used to describe calcaneal osteotomies, highlighting the significant contributions of orthopaedic surgeons to the surgical management of foot deformities. By bridging the gap between the past and present, nuanced perspective hopefully enhances both appreciation and understanding of these procedures.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241300151 – Supplemental material for Standing on the Heels of Giants: A Historical Perspective of Eponyms for Calcaneal Osteotomies
Supplemental material, sj-pdf-1-fao-10.1177_24730114241300151 for Standing on the Heels of Giants: A Historical Perspective of Eponyms for Calcaneal Osteotomies by Thelma R. Jimenez Mosquea, Andrew S. Bi, Nina D. Fisher, Hugo A. Ubillus and Raymond J. Walls in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval was not sought for the present study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.