
Abstract
Background
The complexity of total joint arthroplasty warrants significant patient counseling, and some surgeons are utilizing multimedia to aid in preoperative education. Our aim was to assess the effect of an educational video on patient understanding and satisfaction when supplementing a traditional office consultation for total shoulder arthroplasty.
Methods
This study was a surgeon-blinded, randomized control trial involving 60 consecutive patients undergoing primary total shoulder arthroplasty. Following a preoperative consultation by a single surgeon, patients were randomized in a 1:1 ratio to either a control or treatment group. All participants received a 9-question true-or-false test pertaining to basic shoulder arthroplasty knowledge. The treatment group subsequently viewed a 13-minute educational video explaining glenohumeral osteoarthritis, surgery, and postoperative expectations. At a second preoperative appointment, participants of both groups were asked to repeat the same test.
Results
Fifty-two patients were available for the second preoperative appointment. There was no difference in test scores between the video (7.84/9) and no video (7.89/9) groups (P = .75). All patients in the video group reported improved satisfaction and understanding.
Conclusion
Patients who watched an educational video supplementing a preoperative consultation for shoulder arthroplasty reported improved satisfaction but did not demonstrate increased understanding compared to those receiving a standard preoperative consultation.
Keywords
Introduction
Clear communication and education are essential for delivering quality patient care and ensuring patient satisfaction. The initial surgeon–patient consultation is important as a means of establishing trust in the surgeon and providing crucial information regarding the procedure. With the inherent complexity of joint arthroplasty, patients require significant counseling regarding their diagnosis, the basics of joint anatomy, the surgical experience, and postoperative expectations. These consultations provide an opportunity for shared decision-making, acquiring informed consent, and discussing potential risks and complications with patients.
There is growing evidence demonstrating a correlation between patient satisfaction and the degree to which patients feel adequately informed about their surgery. 1 Moreover, literature has shown that preoperative patient expectations can affect outcomes and patient satisfaction.2–4 Thus, it is crucial that surgeons attempt to maximize information retention and manage expectations preoperatively. However, patient recollection and retention of medical information have been shown to be unsatisfactory,5–7 despite the effort of surgeons to educate patients during preoperative consultations. To assist in providing adequate and accessible educational resources, some surgeons have created and published online videos detailing joint anatomy, the surgical experience, and, in some cases, video-recorded surgery. Evidence is mixed as to the appropriateness and effectiveness of educational videos to supplement traditional surgeon–patient interactions in joint arthroplasty.8–12
In line with efforts to reduce the cost of patient care, computer-based technology is being explored as a viable option in providing effective patient education. For example, in hip arthroplasty, a web-based computer program has successfully been developed for the purpose of providing additional patient education. 13 Among patients considering total knee arthroplasty, videos have been utilized to decrease decisional conflict 14 and address racial disparities in patient care. 9 Lin et al. demonstrated that educational videos significantly increased patients’ knowledge regarding their knee surgery. 9 Similarly, Hoppe et al. found that patients who watched a video prior to shoulder arthroscopy demonstrated greater knowledge than a nonvideo control group. 8 Hoppe et al. concluded that their educational video was an effective tool in preparing patients for the postoperative experience.
We are unaware of any literature addressing the applicability and appropriateness of utilizing an educational video to supplement the preoperative consultation in shoulder arthroplasty. Our objective was to assess the effect of an educational video on preoperative patient understanding and satisfaction when utilized as an adjunct to a standard office consultation for total shoulder arthroplasty. We hypothesized that the group of patients who watched an educational video in addition to a preoperative consultation would have improved satisfaction and understanding compared to a nonvideo control group.
Materials and Methods
Sample Selection and Randomization
For this prospective study, institutional review board approval (protocol #688298) was obtained from New England Baptist Hospital. Informed consent was obtained during the initial consultation. Patients were eligible for the study if they elected to proceed with primary anatomic total shoulder arthroplasty for glenohumeral osteoarthritis during an initial consultation with a single, fellowship-trained surgeon (AJ). Exclusion criteria included patients eligible for reverse or revision shoulder arthroplasty, patients who had previously undergone shoulder arthroplasty on the contralateral side, and a diagnosis other than glenohumeral osteoarthritis such as rheumatoid arthritis, rotator cuff arthropathy, or humeral fracture. Participants were also required to speak and understand English—as the video was produced in English—and have access to a digital video disc (DVD) player to watch the video.
Based upon a power analysis (see Statistical Analysis section), a total of 60 patients were sought to be enrolled: 61 patients were asked to participate in the study, of which 1 declined. Thus, 60 consecutive patients were prospectively enrolled in the study between April and November 2015 following a standard preoperative consultation by a single, fellowship-trained shoulder surgeon. Participants were randomized in a 1:1 ratio into control and treatment groups. Surgeon-blinded randomization was carried out by a research assistant using sealed surgery packets (ie, “sealed envelope system”). Fifty-two patients who completed the initial questionnaire were available for the second preoperative appointment, with 25 patients comprising the treatment group and 27 patients in the control group. Eight patients (13%) did not attend the second visit due to cancellation, postponement of surgery, or other factors. Data were collected at an outpatient orthopedic surgery office.
Preoperative Consultation
True/False Questions for Comprehension and Information Retention.

Educational Video
The treatment group watched a 13-minute educational video following the consultation that offered visual and verbal information on glenohumeral osteoarthritis, risks and benefits of surgery, the surgical experience, and expectations for functional improvement postoperatively. The video was produced professionally and primarily featured the surgeon utilizing various visual aids such as an anatomically accurate shoulder model and prosthetic implant models. The video’s script was based on the information provided in the surgeon’s standard consultation and was designed to be easily understandable without excessive medical terminology. The video was distributed via DVD, and participants were asked to watch the DVD prior to their second appointment.
Additional Questions for Video Group at the Second Preoperative Appointment.

Statistical Analysis
Statistical analysis was performed by an experienced biostatistician using SAS 9.4 (SAS Institute, Cary, NC). A power analysis, adapted from the results of a prior study evaluating the effects of a preoperative educational video in shoulder arthroscopy by Hoppe et al., 8 was completed to estimate the appropriate sample size for this study. This analysis indicated that 25 subjects per group would be necessary to achieve over 80% power with a level of significance of α = 0.05. Therefore, it was suggested that approximately 30 subjects per group be enrolled. Responses from true/false questionnaires were graded from 0 (all incorrect answers) to 9 (all correct answers). The scores were normally distributed. Independent-samples t tests were subsequently performed to assess differences between the control and video group. Statistical tests were 2-sided with level of significance set at α = 0.05.
Results
Baseline Demographics and Patient
There were no significant differences between the 2 groups in sex (video group = 15 females; control group = 19 females; P = .29), mean age (video group = 69 ± 6 years; control group = 69 ± 9 years; P = .80), mean preoperative VAS pain (video group = 5.6 ± 2; control group = 6.0 ± 3; P = .57), or mean preoperative ASES score (video group = 38.1 ± 15; control group = 36.9 ± 22; P = .82). Highest achieved education level of the overall sample was 25% attended high school, 38% attended college for at least 2 years, 31% earned a postgraduate or professional degree, and 6% chose not to report.
Comparing Scores on True/False Questionnaires and Patient Outcomes
Comparison of True/False Scores as a Measurement of Comprehension.

Data presented as mean ± standard deviation.
Data presented as mean difference (95% confidence interval).
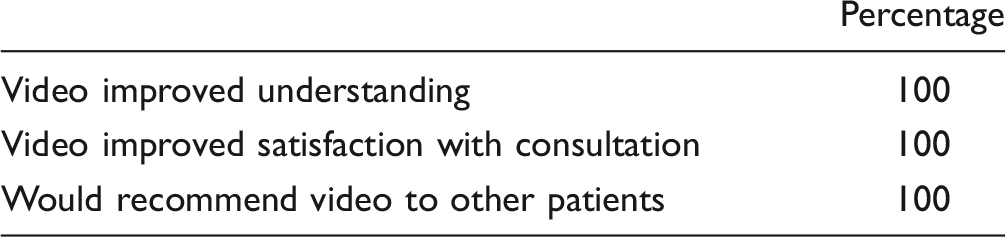
Video Group-Specific Responses.
Patient Outcomes.
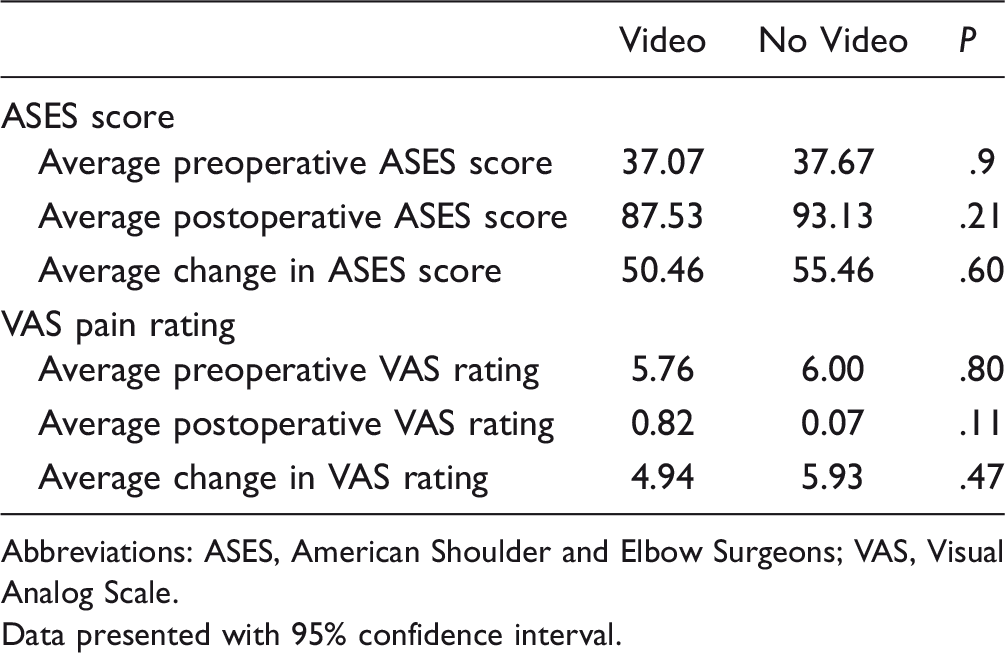
Abbreviations: ASES, American Shoulder and Elbow Surgeons; VAS, Visual Analog Scale.
Data presented with 95% confidence interval.
Discussion
Patients in the video group exhibited no difference when compared to the control group in information retention or knowledge of shoulder arthroplasty at the second preoperative consultation. However, the treatment group uniformly indicated that the video improved their understanding of shoulder arthroplasty and satisfaction with the preoperative consultation and that they would recommend the video to future shoulder arthroplasty patients. This statement provides insight as to the appropriateness of the intervention; regardless of whether the video had a measurable impact on patient understanding, it serves as a well-regarded resource that improves a patient’s perceived level of information as they undergo shoulder arthroplasty. Thus, the results of the current study demonstrate that our educational video did not objectively improve patient performance on the questionnaire of the information provided in the preoperative consultation but subjectively improved understanding and satisfaction with the consultation experience.
Despite these perceived improvements, the video group did not exhibit improved questionnaire scores compared to the control group at the second preoperative visit. Patient information retention and recall following surgical consultation have been shown to be poor.5–7,13 Crepeau et al. found that after a period of no more than 2 weeks, patients undergoing orthopedic surgery demonstrated a significant deterioration in recall and comprehension of preoperative information. 13 Given the patients in the treatment group were able to choose when to watch the video, it is possible the information was not retained over the full 6-week interim period between appointments, conferring a weakness to the current study. In addition, patients were not asked to record the date on which they watched the video and thus we were unable to determine whether time between the video and questionnaire had an effect on retention. Future investigation is recommended to explore the appropriate time frame to employ educational material relative to the actual surgical date to maximize patient information retention.
In total shoulder arthroplasty, patient satisfaction has a greater correlation with subjective rather than objective outcome measures. 15 Further, there was no significant improvement in postoperative ASES score for patients who watched the video (Table 5). This suggests that the surgeon’s goals for surgical outcomes should be patient-centric rather than based on the functional measures. Considering the video cohort’s perceived improvement in understanding and satisfaction after viewing the video, the literature suggests that such an intervention may have positive effects on both patient-reported and functional outcomes.2–4,8 However, our study showed no correlation between the use of a preoperative educational video and improved postoperative outcomes. In addition, we did not request the control group to report on their satisfaction or understanding, which precludes a direct comparison between groups and is a significant weakness.
We also postulate that the educational video would have been more impactful on information retention if patients in the current study underwent a less thorough office consultation. Both groups returned high scores in the true/false questionnaires, indicating that the control group was well informed from the consultation alone. The initial surgeon consult lasts between 30 and 45 minutes, with ample time for a thorough explanation of the shoulder anatomy, surgical indications, risks and benefits of surgery, and postoperative expectations, as well as for patient questions. This extensive consultation may explain the high understanding of pertinent surgical concepts in both groups. For surgeons who typically give less-detailed consultations, a supplemental video may still be beneficial in improving patient understanding. In addition, it is possible that a ceiling effect arising from the high true/false scores of both groups (Table 3) impacted the ability of our questionnaire to adequately measure the effect of the video on comprehension. From a social perspective, more than two thirds of our overall sample reported having attended college or a postgraduate program. The advanced education level of our cohort may be another factor influencing the high average questionnaire scores.
The research on utilizing computer and multimedia services in shoulder arthroplasty is limited, but this topic has been explored in knee arthroplasty,9,11,14 hip arthroplasty,12,16 and shoulder arthroscopy. 8 Hoppe et al. sought to determine the effectiveness of an educational video as an adjunct to a standard presurgical consultation in patients undergoing shoulder arthroscopy. 8 This group concluded that an educational video improved retained knowledge when compared to a control group, a finding that was not reinforced by the current study. Moreover, Hoppe et al. found that their video was an effective educational tool for all stages of the surgical process. With regard to multimedia, it is difficult to compare findings between studies due to the inherent differences in the content and presentation of the videos. It is important to note that both our study and the study of Hoppe et al. found the video to be regarded positively, despite the lack of a measurable educational advantage demonstrated by the present study.
An inherent limitation of the current study is the difficulty in generalizing the results to the population at large. For example, if another surgeon produces an educational video for his or her patients, there is innate variability in content and presentation and thus the video may be more or less useful. The thoroughness, detail, and duration of the preoperative consultation may be a factor affecting the usefulness of an adjunctive educational video or other similar tool. It is possible that a thorough consultation might nullify the benefit of a video that covers similar material; we theorize that this contributed to the lack of improvement in questionnaire scores of the treatment group in the current study.
Our institution currently provides the educational video to all patients prior to total shoulder arthroplasty consultation. By watching the video before meeting with the surgeon, patients have an opportunity to hear the information and formulate questions to be addressed during the consultation. Given the complexity of shoulder arthroplasty and the amount of information the surgeon must convey to the patient, we find it beneficial to present the material twice. The video has been made available online as well; therefore, for patients who find it interesting, seek more knowledge, or would like to show their family and friends about the procedure, the video acts as resource that can be viewed from home.
Conclusion
A preoperative educational video provided as an adjunct to a standard preoperative office consultation for total shoulder arthroplasty does not improve patient understanding or information retention when compared to a traditional preoperative consultation. However, all patients who watched the video perceived improvements in understanding and satisfaction with the overall consultation.
Footnotes
Author Note
This investigation was performed at New England Baptist Hospital, Boston, MA.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Andrew Jawa has been a paid speaker and consultant for DJO Global.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.