
Abstract
Background
The subscapularis tendon is commonly released during shoulder arthroplasty, and its integrity and repair postoperatively have been shown important to help maximize patient function. However, diagnosing subscapular tendon failure can be difficult with magnetic resonance imaging secondary to metal artifact as well as very costly.
Purpose
The purpose of this study was to assess the utility of ultrasound imaging in evaluating subscapularis integrity at specific time points following shoulder arthroplasty, in a blinded fashion. Secondarily, we report on the correlation between the condition of the subscapularis and quality-of-life outcome measures.
Study Design
Prospective case series.
Methods
Ultrasounds were completed preoperatively and postoperatively at 1 week as well as at 1, 3, and 6 months. Each was read by a single musculoskeletal radiologist and categorized as “intact,” “torn,” or “unclear.” Clinical outcome was evaluated using the Western Ontario Osteoarthritis Shoulder (WOOS) index at these same time points.
Results
The final study group consisted of 35 procedures in 33 patients (19 females and 14 males, mean age 66 ± 9 years). Three patients had postoperative subscapularis failures that were confirmed in the operating room at the time of repair. Of 24 sonographs categorized as “unclear” in the postoperative period, the majority (n = 12, 50%) were taken at 1 week. Compared to preoperative scores, patients had lower WOOS scores at 1, 3, and 6 months postoperatively (P < .001). Correlation analysis did not reveal an association between the ultrasound readings and the WOOS scores postoperatively.
Conclusion
The utility of ultrasound examination of the subscapularis tendon following shoulder arthroplasty is limited by timing and may be most useful when used by the physician within clinical context. Significant improvement was noted in disease-specific quality-of-life scores regardless of the status of the subscapularis tendon as read on ultrasound.
Keywords
Introduction
The subscapularis tendon is commonly released during shoulder arthroplasty, and maintaining the integrity of the tendon throughout the postoperative period has been shown essential in maximizing patient function.1, 2 While the incidence of failure is not clearly established in the literature, reported rates range from 3% to 13%, with rates of revision as high as 5.8%.3,4 With repair options suboptimal, and failure identified late, this can lead to prosthesis failure. 5 Risk factors for failure include poor tissue quality, oversized prosthesis, insufficient repair, early postoperative trauma, or overly aggressive physical therapy.1, 6 – 9
Definitive postoperative subscapularis evaluation is unclear. The traditional abdominal compression test is considered unreliable following total shoulder arthroplasty (TSA), with a sensitivity and specificity of 25% and 73%, respectively.3, 10 Although magnetic resonance imaging (MRI) has a high resolution for soft tissue contrast, its use after shoulder arthroplasty has been limited due to metal artifact limitations. 11 Recent advents of metal suppressed MRI for shoulder arthroplasty have been shown to be useful but is costly and time-consuming.3, 11 -- 13 Ultrasound offers an ideal, noninvasive option that can be performed quickly in real time and has been shown useful when evaluating the postoperative total shoulder.4,14, 15 Furthermore, studies have suggested that sonography may detect tears where physical examination may not.3,16, 17
Additionally, the correlation between the integrity of the tendon and functional status is underreported in the literature.3,14,17, 18 One study has reported inferior functional scores in patients with abnormal postoperative ultrasounds of the subscapularis. 19 However, the study was in the setting of comparing surgical techniques to release the tendon (lesser tuberosity osteotomy vs peel back), and was not blinded.
The purpose of this study was to assess the utility of ultrasound imaging in evaluating subscapularis integrity at specific time points following shoulder arthroplasty when the reader is blinded. Secondarily, we report on the correlation between the condition of the reported subscapularis in relation to the patient’s quality-of-life outcome measures. The authors hypothesize that ultrasound imaging can reproducibly detect subscapularis failure in the acute period following shoulder arthroplasty.
Methods
This was a prospective study examining the utility of ultrasound to examine the subscapularis tendon following shoulder arthroplasty. Our institution’s institutional review board provided approval (IRB#12-146-3). Study participants were recruited from the practice of 2 attending fellowship-trained Shoulder and Elbow Society member orthopedic surgeons. The study period was from January 2013 to January 2015. Inclusion criteria include ages 50 to 85 years, physical examination and imaging studies documenting osteoarthritis of the affected shoulder, failure of 6 months or more of conservative treatment, total shoulder and hemiarthroplasty procedures, and the ability to adhere to rehab protocol (Figure 1). Exclusion criteria included active joint infection, patients with significant comorbidities and unacceptable surgical risk, insufficient glenoid bone stock, deficient rotator cuff or rotator cuff arthropathy, those undergoing a reverse TSA, or those undergoing shoulder arthrodesis.
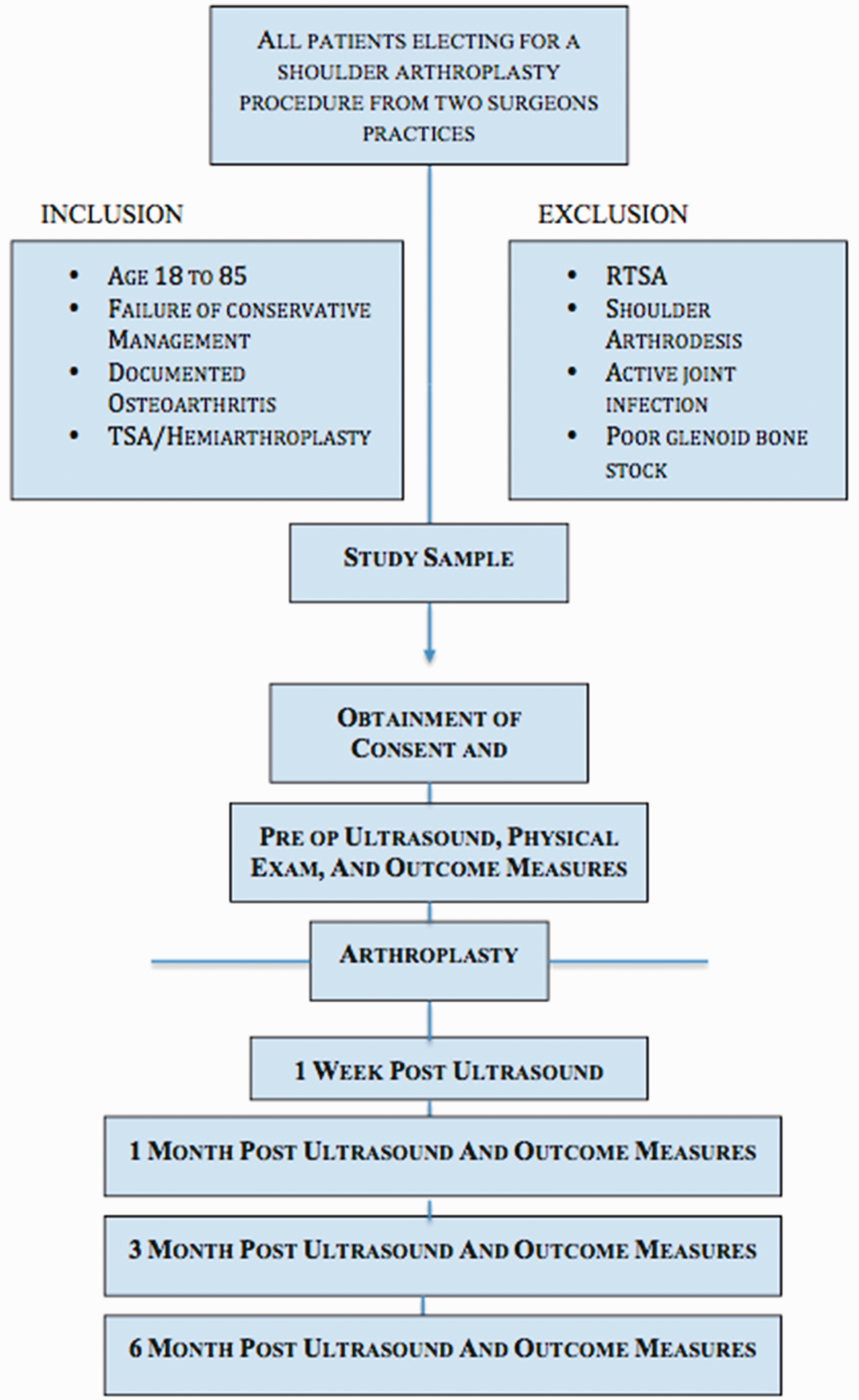
Demonstrates study algorithm and selection process. RTSA, reverse total shoulder arthroplasty; TSA, total shoulder arthroplasty.
Surgical Technique
All surgeons utilized a standard deltopectoral approach with a subscapularis tenotomy. At the conclusion of the procedure, a soft tissue repair of the subscapularis tendon back to its native insertion is then performed utilizing five #2 Orthocord™ (Depuy Synthes, Raynham, MA) stitches in a Mason-Allen fashion. In the one instance, the peel technique was performed, and the tendon was repaired through transosseous tunnels with suture passage around the intramedullary component of the humeral stem.
The Tornier Aequalis Ascend (Bloomington, MN) was used for the majority of cases, Arthrex Universe II (Naples, FL) for 1 total shoulder, and Arthrosurface HemiCAP (Farnklin, MA) for the hemiarthroplasty procedures.
Postoperatively, a sling was utilized for 4 weeks. Active and active-assisted range of motion is started immediately, with active internal rotation avoided for 6 weeks, and strengthening begun after 12 weeks.
In addition to a preoperative ultrasound examination, all patients received a comprehensive physical examination and a plain radiographic shoulder series (true Anterior-Posteior [AP], supraspinatus outlet, and axillary views). Sonographs were obtained with a Sonosite M Turbo (Bothell, WA) with a 15-6 MHz linear transducer and depth varying between 2.2 and 4.0 cm based on patient body habitus. The ultrasound scans were performed by physicians and clinical personnel trained according to the standardized method described by Rutten et al. 20 This particular method was chosen, as the results are more generalizable and applicable to the orthopedic surgeon performing these sonographs in the clinical setting. This method includes 6 scanning positions that optimize visualization of the rotator cuff and surrounding tissue. For the subscapularis, the arm is positioned in external rotation with the elbow held against the trunk and flexed at 90°. The transducer is moved slightly medially and turned 90° counterclockwise to be parallel with the subscapularis tendon fibers then moved slowly up and down to image the tendon’s insertion. 20 In addition to still frames, video clips were taken, as the patient’s arm was externally rotated from midline in the position described above. All sonographs were coded to blind the reader to both patient identity and time point. Each scan was read by a single, board certified, fellowship-trained musculoskeletal radiologist and categorized as “intact,” “torn,” or “unclear.” Both partial and complete tears were categorized into the “tear” group, while an “unclear” examination was classified when the radiologist suspected a potential tear, but it was not clearly identifiable on ultrasound findings. The reviewer was blinded to group. Ultrasounds were performed both preoperatively and postoperatively at 1 week, 1, 3, and 6 months. Clinical outcome was evaluated using the Western Ontario Osteoarthritis Shoulder index (WOOS). Outcome measures were collected preoperatively and at 1, 3, and 6 months postoperatively.
Statistics
Given the exploratory nature of this study, an a priori power analysis was not performed. Descriptive statistics to characterize the group are reported using mean and standard deviation or proportion where appropriate. Pearson’s correlation coefficients were calculated to examine the relationship between ultrasound readings and WOOS scores at the 1-, 3-, and 6-month postoperative visits. Mixed-effect linear regression was used to explore changes in WOOS and domain scores over time with the ultrasound reading considered as a covariate. An alpha level of 0.05 was considered significant for all analyses. All statistics were performed using Stata 12 (StataCorp, 2011, Stata Statistical Software: Release 12. College Station, TX: StataCorp LP).
Results
During the study period, there were 41 procedures in 39 patients. One patient cancelled surgery, and 1 went on to have a reverse TSA. Four patients withdrew at their first postoperative visit; reasons were refusal of ultrasound and time constraints. The final group consisted of 35 procedures in 33 patients (19 females and 14 males, mean age 66 ± 9 years). Patient demographics and WOOS scores are presented in Table 1. A total of 30 total shoulders and 5 hemiarthroplasty procedures (4 hemicaps, 1 standard) were included. Subscapularis tenotomy was performed in all cases with the exception of case in which a peel technique was utilized.
Patient Demographics and Clinical Outcome Scores.
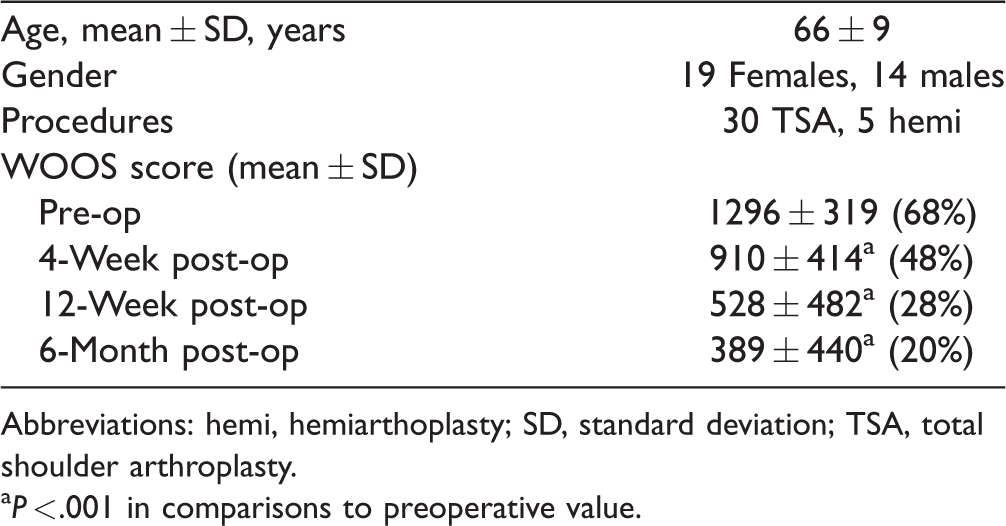
Abbreviations: hemi, hemiarthoplasty; SD, standard deviation; TSA, total shoulder arthroplasty.
aP < .001 in comparisons to preoperative value.
At the time of the procedure, all patients had an intact subscapularis. Interestingly, 2 preoperative scans were read as “torn,” and 11 were “unclear.” Ultrasound readings are presented in Table 2. The majority completed all study visits. At the 1-week visit, 4 patients were not available (31/35). At 1 month, 1 patient missed their study visit (34/35). At 12 weeks, 5 patients missed their study visit; 1 was revised at 8 weeks secondary to traumatic failure, 4 either did not show up or rescheduled their standard of care visit (30/35). At 6 months, 5 scans had not been performed; 2 patients were unable to stay to have the examination performed, 1 patient rescheduled, and 2 were lost to follow-up (30/35). Of the 24 postoperative sonographs categorized as “unclear,” the majority (n = 12, 50%) were taken at 1 week.
Ultrasound Subscapularis Interpretation at Interval Follow-Up.

Three TSA patients had postoperative subscapularis failures that were confirmed in the operating room at the time of repair. The first patient was doing well until their 6-month visit, when the patient began experiencing anterior instability. Upon repair, the subscapularis appeared highly attenuated. All ultrasound scans, including the 6-month study, were read as “intact” for this patient. The second patient experienced a fall 2 days prior to their 6-month visit. On repair, the subscapularis was noted to be edematous and attenuated. The 6-month scan was read as “torn.” The third patient experienced a traumatic event 2 months after surgery and was admitted for immediate repair. The surgeon who performed the repair noted a full thickness tear of the subscapularis tendon. Prior to this incident, the 1-month ultrasound was read as “torn.” No further data were collected on this patient. In addition, 3 other ultrasounds were read as “torn” at 6 months. While subscapularis intactness can only be definitively evaluated intraoperatively, all 3 of these patients were doing well clinically with full range of motion, good internal rotation strength, and no signs of instability.
Compared to preoperative scores, patients had lower WOOS scores at 1, 3, and 6 months postoperatively (P < .001). Domain scores decreased over time in all domains (Table 3). At 1 month, the largest improvements were seen in physical symptoms (23% improvement, P < .001) and emotions (23% improvement, P < .001), followed by lifestyle (17%, P < .001). Improvements in sports, recreation, and work were not statistically significant until 3 months (P < .001). The total WOOS scores decrease at each time point (P < .001). Interestingly, there was no statistically significant difference in WOOS scores between hemiarthroplasty and TSA at any time point.
Mean WOOS Scores at Interval Follow-Up.

Abbreviations: SD, standard deviation; WOOS, Western Ontario Osteoarthritis Shoulder.
The values of P are in reference to comparisons to preoperative value.
There was no correlation between the ultrasound readings and the WOOS scores postoperatively (R = −.292, P = .104 at 1 month; R = .003, P = .989 at 3 months; and R = .018, P = .928 at 6 months). The addition of the ultrasound reading to the mixed-effects regression was not statistically significant (1% difference in score in favor of the torn group, P = .886).
Discussion
The purpose of this study was to determine the utility of ultrasound in evaluating the subscapularis tendon in patients who have a TSA when evaluated in a blinded fashion. Using a blinded reader, the ultrasound readings were inconsistent and seem to be associated with a high false-positive rate. This differs from Savoie et al., who utilized ultrasound technique to evaluate subscapularis tendon postoperative after using a subscapularis-sparring approach technique.15 Their patients had clinical and ultrasonographic evidence of intact rotator cuff at a minimum 2-year follow-up. 15
Our data suggest a high false-positive rate for blinded evaluation of ultrasounds. Two false positives were confirmed in patients who were categorized as “torn” preoperatively, which were intact at the time of surgery. Postoperatively, several patients were classified as “torn” at some points and “intact” at subsequent time points. A computed tomography (CT) arthrogram or a metal suppression MRI unfortunately was not obtained postoperatively, and with the expectation of 1 known failure, patients with a reading of “torn” were doing well clinically without complaints of instability or physical examination findings consistent with subscapularis insufficiency.
The inconsistency in blinded ultrasound readings may be the result of several factors. Tendon to bone healing can take up to 12 weeks before reaching the later remodeling stages. During this time, it is possible that early “torn” scans are a consequence of edema around the insertion, creating hypoechogenicity that is mistaken for a tear. Also, the type of failure may play a role. The patient identified as “torn” had attenuation with edema due to a fall. Conversely, the patient with chronic attenuation was classified as “intact” on ultrasound. This suggests a limitation in the type of failure that ultrasound can identify. Acute failures with full or partial thickness tears, or those with considerable edema, for example, associated with trauma, are more likely to be identified than chronic attrition over time resulting in attenuated muscles.
Ultrasound may be more useful later in the postoperative period. The majority, 71% (n = 17) of “unclear” scans, appeared in the first and fourth-week visits. Furthermore, at the 1-week time point, the patient is appropriately immobilized, which limits the examiner’s ability to external rotate the shoulder diminishing the quality of sonograph. As patients heal and begin physical therapy at 6 weeks, this position is more obtainable. Given this lack of clarity with readings at 1 and 4 weeks, ultrasound alone may not be sufficient if subscapularis failure is suspected early in the postoperative course.
The WOOS score improved throughout the postoperative period. With the exception of the sports, work, and recreation, statistically significant improvements were observed at 1, 3, and 6 months. The sports, work, and recreation domains improved at 3 and 6 months. The lack of improvement at 1 month is not surprising, given that patients are not expected to or encouraged to participate in these activities early in the postoperative period. The reading of the ultrasound at 1, 3, and 6 months was not correlated with the WOOS score. Additionally, incorporating the ultrasound reading into the mixed-effects regression did not result in a tangible effect (estimated 1% difference in WOOS score in favor of those read as “torn,” P = .948).
A strength of this study was the use of a single, fellowship-trained musculoskeletal radiologist blinded to all patient information and time point. Several studies have commented on the utility of ultrasound in visualizing tears, but all were read in a clinical setting and unblinded. Iannotti et al. reported on the accuracy of office-based ultrasonography in diagnosing rotator cuff tears. 17 The surgeon correctly diagnosed 88% of full-thickness rotator cuff tears, 70% of partial-thickness tears, and 80% of shoulders with normal tendons. 17 Farin et al. showed ultrasonography accurately diagnosed 82% of subscapularis tendon tears, 86% of full-thickness tears, and 67% of partial-thickness tears, concluding ultrasound can diagnose not only tears but also size of tears. 21 Sofka et al. describes the ability to assess muscle atrophy on ultrasound following shoulder arthroplasty, corresponding to diffuse increased echogenicity with associated decrease muscle bulk, and stating that sonography is a rapid and reliable method to assess the periprosthetic soft tissues of the shoulder. 22 In contrast, we found that blinding the interpreter to any patient identifiers and time point revealed a significant inconsistency in diagnosing integrity of the subscapularis. While ultrasound may be useful within a clinical context to confirm or refute a physician’s suspicions, in this study, the examination itself was not as reliable.
There were limitations to this study. First, a validation processing assessing accuracy of the reads was not performed by the ultrasound specialist prior to the study. A prior validation process may have helped identify a trend of false positives. A second potential limitation in this study is the quality of each scan, which is both technician and patient dependent. Studies have shown that sonographs taken by trained clinicians have a high sensitivity for detecting rotator cuff tears.8,23--25 Although all clinicians were trained appropriately, multiple clinicians performed scans in an attempt to gather data at each time point. While this may make the results more generalizable for those clinicians performing these scans in the clinical setting, operator experience could produce variability in sonograph quality and possibly hinder interpretation. The patient also influences the quality of each scan. The size of the shoulder and muscle mass changes the depth needed to observe the rotator cuff and, coincidently, the clarity of the image. Another limitation is the lack of physical examination provocative testing recorded postoperatively, which was initially avoided as part of the postoperative protocol. While classic subscapularis tests have been found to be unreliable following shoulder replacement, signs of anterior instability were further investigated radiographically or with CT arthrogram to determine whether surgical repair was needed. In addition, a larger sample size would have made the study more generalizable. However, we observed substantial inconsistency with the ultrasound readings suggesting that an examination alone is not sufficient to determine subscapularis insufficiency. Lastly, of the 3 patients who underwent a revision procedure to repair the subscapularis, 2 of these were classified by the surgeon as attenuated tears at time of repair. Interestingly enough, both were seen there at 6-month visit and resultantly underwent revision. One patient’s 6-month scan was read as “intact,” while the other as “torn.” Conceptually, the utility of ultrasound in part depends upon its ability to identify tears in patients such as these but failed to do so.
Conclusion
We did not find ultrasound to be a reliable method in determining subscapularis insufficiency when the reader was blinded to patient information. It has been shown to be reliable when done in the clinical setting.4,17,22, 26 The utility of ultrasound may improve after the first 4 weeks given the decreasing number of unclear readings and presumably fewer false positives at later time points. Additionally, ultrasound may be most useful when used by the physician within clinical context, as blinded images in isolation are associated with a high number of false positives and uncertainty. Finally, shoulder arthroplasty resulted in significant improvement in disease-specific quality-of-life scores regardless of the status of the subscapularis tendon as seen on ultrasound.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Augustus D. Mazzocca is a paid consultant for Arthrex Inc. as well as receives research laboratory support funding from Arthrex Inc.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.