
Abstract
Introduction
Primary reverse shoulder arthroplasty has been reported to provide good outcomes. The majority of designs utilize a large portion of the glenoid. Some studies have reported worrisome rates of notching and stress fractures of the acromion or scapular spine. The purpose of this study was to determine the outcome and complications of a bone-preserving reverse prosthesis with limited ingrowth glenoid surface paired with an onlay humeral component.
Materials and methods
Between 2014 and 2015, 96 reverse arthroplasties were implanted using a bone-preserving reverse with a 135° onlay humeral bearing. Six patients died. The remaining 87 patients (90 shoulders) were followed for 2 years or until revision. Mean age was 69.3 years. The underlying diagnosis was cuff tear arthropathy (13), irreparable cuff tear (39), osteoarthritis (32), and other (6). Shoulders were followed for 2 years or until revision surgery.
Results
Reverse shoulder arthroplasty resulted in significant improvements in pain, motion, and function. At most recent follow-up, 74 shoulders had no or mild pain. Elevation was 131° ± 31° and external rotation 46° ± 21°. The mean American Shoulder and Elbow Surgeons (ASES) score was 76. There were 4 reoperations for deep infection (2), periprosthetic fracture, and glenoid loosening. None of the remaining arthroplasties were loose. There was one stress fracture of the acromion and one of the spine of the scapula. No radiographic notching or dislocation was observed.
Discussion
Primary reverse arthroplasty using a bone-preserving glenoid component and an anatomic onlay humeral bearing provides satisfactory clinical outcomes with a very low rate of failure and complications.
Introduction
Reverse arthroplasty is considered the surgical procedure of choice for a number of shoulder conditions. Initially conceived for the management of rotator cuff tear arthropathy,1,2 the indications of reverse arthroplasty have been expanded to other diagnoses, including massive irreparable cuff tears, primary glenohumeral osteoarthritis with severe posterior subluxation, proximal humerus fractures, fracture sequelae, and others.3–6 A number of design features differ substantially among several of the reverse arthroplasty components available to date. Controversy remains regarding the ideal glenoid fixation method, reconstruction with a medialized or lateralized center of rotation, humeral versus glenoid lateralization, neck-shaft angle, and other parameters.7–11 Of particular concern is the “revisability” of failed reverse arthroplasty.12–14 This is particularly true with certain designs that utilize the majority of the glenoid vault at the time of primary surgery by replacing it with large pegs or cones.
Over the last 3 years, the lead author has used the Stryker ReUnion reverse shoulder arthroplasty implant (Stryker Corporation, Mahwah, NJ) in all primary reverse shoulder arthroplasties. This particular system combines a bone-preserving baseplate with a 135° neck-shaft angle humeral component proximally coated with hydroxyapatite and glenospheres of various sizes and thicknesses to provide both a more medial and a more lateral center of rotation options. The purpose of this study was to determine the clinical outcome, radiographic outcome, complications, and reoperations of primary reverse shoulder arthroplasty in a consecutive series of shoulders with a minimum follow-up time of at least 2 years.
Materials and Methods
Between May 2014 and December 2015, 96 consecutive primary reverse shoulder arthroplasties were performed by a single surgeon using the Stryker ReUnion reverse shoulder arthroplasty implant. Patients undergoing reverse arthroplasty for proximal humerus fracture were excluded. Six patients died prior to their 2-year follow-up evaluation with their implant in place. The remaining 90 shoulders formed the basis of this study.
Patients
Characteristics of the Shoulders Included in the Study.

Surgical Procedure
All procedures were performed under general anesthesia after preoperative placement of an interescalenic cathether for blockade of the brachial plexus prior to surgery and maintained over the following 24 h. All arthroplasties were implanted using a deltopectoral approach. The long head of the biceps was tenodesed to the conjoined tendon when intact. When present, the subscapularis was divided through tendon, and if possible repaired at the end of the procedure. The leading edge of the supraspinatus tendon was released when intact only if it interfered with implant relocation using the thinnest possible humeral bearing. An associated transfer of the latissimus dorsi and teres major was associated in 3 shoulders with lack of active external rotation preoperatively due to extension of cuff tearing to the teres minor. 15
Implants
The Stryker ReUnion reverse shoulder arthroplasty system consists of a platform humeral stem, baseplate, screws for glenoid fixation, glenosphere, and a modular humeral bearing with a metal base and a polyethylene liner (Figure 1, Table 2).
Components implanted at the time of reverse shoulder arthroplasty. Components Implanted in the Study.

The humeral component is designed with bone-preserving features, including a narrow anteroposterior cross-section. The cementless version is proximally textured and coated with hydroxyapatite. It achieves primary stability by a combination of distal line-to-line ream and fit, proximal underbroaching, and an extended metaphyseal flare. The neck-shaft angle of the humeral component is 135°. The cemented component is identical in geometry but has a surface roughness of approximately 40 Ra and no coating. The author prefers to use cementless fixation whenever possible; cement fixation was only used in 3 shoulders due to lack of adequate primary stability with cementless fixation.
The baseplate is 28 mm in diameter, curved, and back-coated with porous titanium (Tritanium™, Stryker). It has no intraosseous extension in the form of a coated central peg or cone in order to maximize bone preservation. It achieves fixation by the use of proprietary locking compression screw technology (Variax, Stryker). Briefly, each of the 5 holes of the baseplate has an internal titanium rib; the cobalt-chrome screws have the usual screw thread and an additional small thread in the screw head. As the small thread contacts the rib, it will compress the baseplate against bone and eventually deform and engage the rib, becoming a locking screw. This allows variable angle locking within an arc of 30°. The central screw is 6.5 mm in diameter, whereas the peripheral screws are 4.5 mm in diameter. An effort was made to place the glenoid baseplate flush with the inferior aspect of the glenoid. Bone graft was used on the glenoid side in one of the shoulders in this consecutive series of primary reverse arthroplasty.
The glenospheres are manufactured in 3 diameters (32 mm, 36 mm, and 40 mm). Each diameter option is manufactured with 2 mm of lateral offset or 6 mm of lateral offset. Each 36-mm component is manufactured without eccentricity (standard) or with 2 mm of eccentricity. Each 40 mm component is manufactured without eccentricity, with 2 mm of eccentricity or with 4 mm of eccentricity. The size of the glenosphere used was selected by the orthopedic surgeon performing the procedure based on the size of the patient; whenever possible, the largest diameter glenosphere was implanted.
The humeral bearing component is an onlay design. The humeral bearing thickness ranges between 8 mm and 22 mm. This thickness is the addition of the individual thicknesses of either a 4-mm or a 10-mm metal humeral tray with various thicknesses of polyethylene inserts. All inserts are made of ultra-high-molecular-weight highly cross-linked polyethylene, manufactured using proprietary X3 technology (Stryker). The thickness of the humeral bearing to be implanted was selected by the orthopedic surgeon performing the procedure in order to achieve the best possible balance between stability and soft-tissue tension.
Postoperative Management
After surgery, all shoulders were place in a shoulder immobilizer with a small abduction pillow (DonJoy Ultrasling, DJO Global, Vista, CA). Patients were instructed to perform active and active-assisted elbow, wrist, and hand motion on postoperative day 1. Shoulder therapy was initiated at the time of discontinuation of the shoulder immobilizer, 2 to 3 weeks after surgery. Patients performed active-assisted range of motion exercises at that time, adding isometrics at week 6 and elastic band strengthening at weeks 10 to 12.
Clinical and Radiographic Evaluation
At our Institution, all patients undergoing shoulder arthroplasty are enrolled in a Joint Registry database and followed prospectively. 16 Patients are invited to return for a follow-up visit 2, 5, and 10 years after surgery, and at 5-year intervals thereafter. Data collected before surgery and at each follow-up visit include pain, motion, strength, complications, reoperations, and American Shoulder and Elbow Surgeons (ASES) scores. Standardized radiographs, including anteroposterior radiographs in internal and external rotation as well as Y and axillary views, are obtained as well. Patients not able to return are evaluated with a validated mailed or telephone questionnaire and requested to send radiographs.
Pain was graded using a VAS and further categorized into no, mild, moderate, or severe. Motion was measured in degrees for elevation and external rotation and as the highest vertebral level reached by the thumb for internal rotation. Strength was graded using manual testing as normal (5), weak but able to resist the examiner (4), weak but able to resist gravity (3), contraction with no ability to resist gravity (2), or paralysis (1). Radiographs were evaluated for component position and fixation, notching, 17 calcifications or heterotopic ossification, and fractures of the acromion or spine of the scapula. 18
Statistical Analysis
Results are reported as mean and standard deviation (SD) for ordinal variables and as value frequency for categorical variables. Differences in pain, motion, strength, and ASES scores were compared using Student’s t tests. The statistical significance was established at a P value of <.05.
Results
Complications and Reoperations
There were a total of 4 reoperations for the whole study group (4.4%). Two shoulders developed a late hematogenous deep infection. In one of these shoulders, cultures were positive for Cutibacterium (Propionibacterium) acnes. After a successful 2-stage reimplantation, the shoulder visual analog scale (VAS) for pain was 0, and there was no evidence of recurrence of infection. Cultures in the second shoulder (in an upper extremity with lymphedema) were positive for Enterococcus faecalis. This shoulder recently underwent a resection arthroplasty and is planned for a reimplantation approximately 8 weeks after the resection.
Another patient fell and sustained a periprosthetic humeral fracture with subsidence of the humeral component. This shoulder was successfully revised to a cemented humeral component, with fixation of the associated fracture. At the time of the most recent follow-up, the shoulder VAS for pain was 0, and motion included elevation to 145° and external rotation to 40°.
A fourth shoulder with severe medial and posterior glenoid erosion was initially replaced using a reverse arthroplasty and structural bone grafting from the resected humeral head. The glenoid component was determined to be loose at follow-up, and the prosthesis was revised to a hemiarthroplasty. At most recent follow-up, 2.1 years after revision to a hemiarthroplasty, the shoulder VAS for pain was 1, and motion included elevation to 170, external rotation to 30, and internal rotation to the T10 vertebral level.
Other complications not requiring reoperation included stress fracture of the acromion (1), stress fracture of the spine of the scapula (1), and hematoma (2).
Clinical Outcome
Reverse shoulder arthroplasty was associated with substantial improvements in pain, motion, and function (Figure 2). Before surgery, 74 patients (86%) rated their shoulder pain as moderate or severe. At most recent follow-up, pain was rated as no or mild in 74 patients. Elevation improved from a mean (SD) of 98 ± 43 (range, 0–170) to 131 ± 31 (range, 50–180), external rotation from a mean (SD) of 34 ± 24 (range: −30 to 80) to 46 ± 21 (range, 0–90), and internal rotation from a mean of sacrum (range, T6 to trochanter) vertebral level to a mean of iliac crest (range, T10 to sacroiliac joint) vertebral level. At most recent follow-up, the mean ASES score was 77.2 points (range, 21–100). Using the Neer rating system, clinical results were excellent in 46 shoulders, satisfactory in 31 shoulders, and unsatisfactory in 9 shoulders (Neer rating was not available for 4 shoulders at most recent follow-up).
Range of motion in elevation (a), internal rotation (b), and external rotation (c) after reverse arthroplasty.
Radiographic Findings
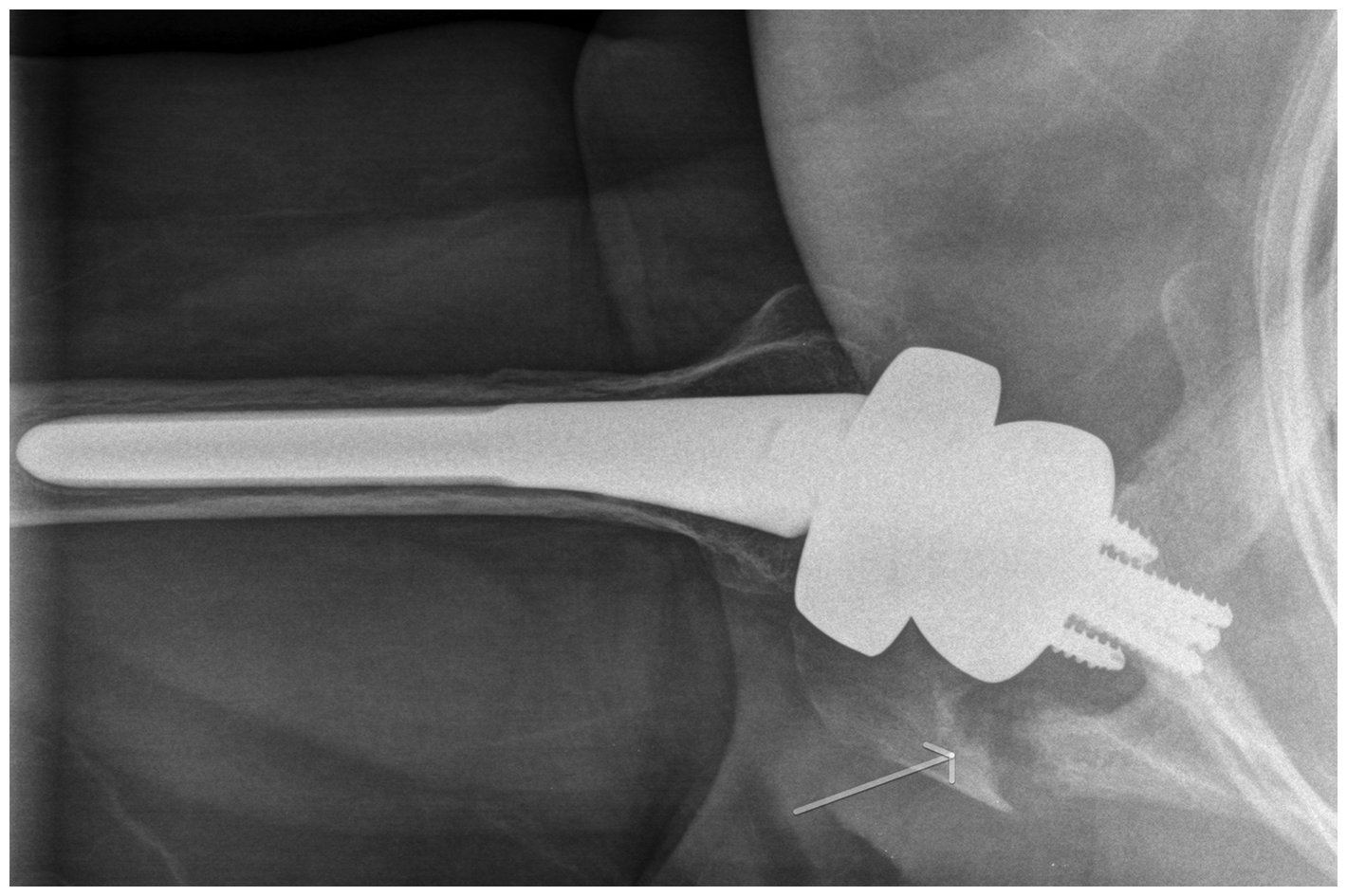
Excluding the 4 shoulders that required reoperation for infection, periprosthetic fracture, and glenoid loosening, no other shoulder had radiographic evidence of loosening of either the humeral component or the glenoid component (Figure 3). As noted earlier, stress fractures occurred in one shoulder at the acromion and in another shoulder at the spine of the scapula (Figure 4). Heterotopic ossification along the inferior margin of the glenoid rim was noted in 15 shoulders. No shoulder had radiographic evidence of notching.
Postoperative radiograph obtained 2 years after reverse shoulder arthroplasty shows well-positioned and well-fixed components and no notching. Postoperative stress fracture of the spine of the scapula.
Discussion
Reverse shoulder arthroplasty has become the surgical procedure of choice for a number of conditions. Primary reverse arthroplasty is most commonly performed for cuff tear arthropathy, massive irreparable cuff tear, and primary osteoarthritis with severe posterior subluxation and bone loss.1,3,6,19,20
In general, reported outcomes of primary reverse shoulder arthroplasty using a variety of implants have been satisfactory. However, some implants have been reported to have a very high rate of progressive scapular bone loss17,21,22 or fractures of the acromion and the spine of the scapula.18,23 Due to the limited bone stock provided by the human glenoid, concerns have been raised about bone preservation at the time of primary reverse arthroplasty. However, the majority of implants used currently do utilize a major portion of the glenoid at the time of arthroplasty, leaving major defects when revision surgery becomes necessary.12,13 For these reasons, there is interest in the development of bone-preserving implants. However, the outcome of implants with more conservative ingrowth surfaces is largely unknown. The implant system reported in the current study is not unique in terms of using only screw fixation and no post; there is another implant in the market (DJO RSA, DJO Global, Vista CA) with similar features, although there is only one length for the central screw. 24
The results of our study seem to indicate that a modern bone-preserving reverse prosthesis may be utilized for primary arthroplasty with a very low mechanical failure rate and good clinical outcomes. In addition, implantation of a reverse prosthesis with a truly anatomic (135°) polyethylene inclination does translate in a very low rate of scapular notching at short-term follow-up. Finally, the rate of fractures of the acromion or spine of the scapula in this series was low for an implant that does lateralize on the humeral side based on the onlay design of the humeral bearing.
The results of our study compare favorably with those of other reverse arthroplasty implants in the primary setting. Multiple authors have reported on the outcome of reverse shoulder arthroplasty in a number of conditions, including cuff tear arthropathy, massive irreparable cuff tears, proximal humerus fractures, the sequels of trauma, and revision of a failed shoulder arthroplasty.25–29 Pain relief seems to be predictable, but less motion and worse complications are reported when reverse is used to salvage sequels of trauma or for revision shoulder arthroplasty surgery.6,30 Of note, the rate of notching has varied tremendously depending on the design features of the reverse prosthesis, being extremely high in designs with a medialized center of rotation and a valgus orientation of the polyethylene liner, and lowest with implants as the one described in this study.21,31–33 Stress fractures of the acromion and spine of the scapula remain of concern.18,23 Dislocation has become extremely uncommon in the primary setting with modern reverse arthroplasty designs.34,35
Our study has a number of limitations, including the short-term follow-up and the inclusion of patients operated on by only one surgeon. However, the majority of the shoulders had adequate clinical and radiographic follow-up, and complications and reoperations were well documented.
In summary, the results of this study seem to indicate that primary reverse arthroplasty using a bone-preserving glenoid component, an anatomic inclination angle for the polyethylene bearing, and an onlay humeral bearing design provides good clinical outcomes with a very low rate of mechanical failure, notching, stress fractures, and other complications. Longer follow-up is needed to determine whether this particular design continues to perform well at medium and long-term follow-up.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mayo Clinic and Dr Joaquin Sanchez-Sotelo receive consulting fees and royalties from Stryker Corporation for the design of shoulder arthroplasty implants and instruments.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.