
Abstract
Tenotomy of the subscapularis is commonly used for exposure at the time of anatomic total shoulder arthroplasty. Understanding the anatomy of the subscapularis and its footprint for insertion into the lesser tuberosity helps perform an adequate tenotomy. Incision of the tendon at the right level, release of the anterior capsule to restore excursion, a sound repair, and postoperative protection are important. Controversy remains regarding the relative advantages and disadvantages of tenotomy compared with alternatives, in particular osteotomy of the lesser tuberosity. Tenotomy has been associated with a higher rate of positive physical examination findings for subscapularis weakness and concerning tendon attenuation or rupture in some shoulders evaluated with ultrasound. However, patient-reported outcomes, objective measurement of strength in internal rotation, and revision and reoperation rates are identical with tenotomy and osteotomy. Tenotomy is particularly attractive in terms of simplicity, shorter operative time, and use in stemless shoulder arthroplasty. Failure of the tenotomy to heal leading to anterior instability can be salvaged surgically, but oftentimes requires revision to a reverse arthroplasty.
Introduction
Shoulder arthroplasty with implantation of anatomic components (anatomic total shoulder arthroplasty [TSA]) is most commonly performed through a deltopectoral approach.1,2 Although there is interest in the use of a cuff-sparing approach for anatomic TSA,3–5 most surgeons divide or detach the subscapularis off the humerus to expose the glenohumeral joint. Traditionally, subscapularis detachment has been performed through vertical division of the subscapularis tendon a few millimeters medial to the lesser tuberosity, that is, performing a tenotomy.2,6
In the previous decade, concerns were raised about the reliability of subscapularis tenotomy healing, with some authors reporting relatively high rates of postoperative subscapularis weakness 7 and incomplete tendon healing. 8 Osteotomy of the lesser tuberosity, 9 detachment of the subscapularis tendon off the bone (so-called subscapularis peel), 10 and alternative repair techniques 11 were introduced in an effort to outperform the healing rates of traditional subscapularis tenotomy in shoulder arthroplasty.
In my practice, I continue to perform anatomic TSA through a subscapularis tenotomy. In this article, I will review some anatomic considerations relevant for this portion of the exposure, my preferred surgical technique and postoperative management, as well the best available evidence to guide selection of any of these alternative techniques for management of the subscapularis at the time of anatomic TSA.
Anatomic Considerations
The subscapularis muscle attaches to the proximal humerus at the lesser tuberosity. Understanding the dimensions and characteristics of the subscapularis attachment site is helpful when performing a subscapularis tenotomy or its alternatives (Figure 1). The footprint of the subscapularis is located at the lesser tuberosity and humeral neck, between the bicipital groove and the medial margin of the articular cartilage. The average width and length of the subscapularis footprint is approximately 2 cm by 4 cm (width varies from 15 to 25 mm, and length from 35 to 55 mm).12,13
The Footprint of the Subscapularis Attachment on the Proximal Humerus.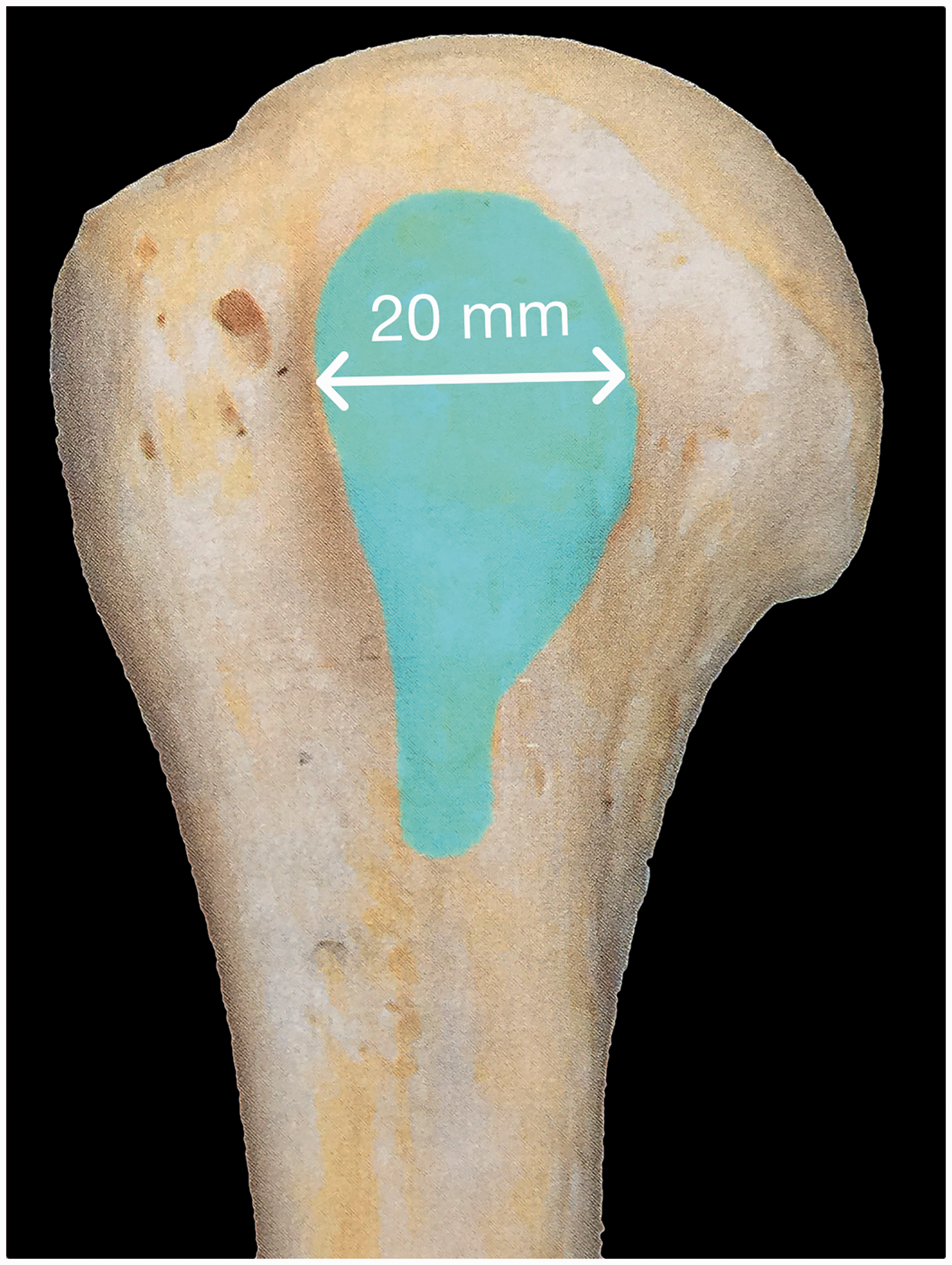
The shape of the subscapularis footprint is not rectangular: it is broad proximally (with a semicircular upper outline) and tapers distally, a shape similar to a comma sign. 13 Proximally, the subscapularis attaches very close to the articular margin (2–3 mm), whereas distally, the distance between the footprint and the articular cartilage is 17 to 18 mm.12,13 Proximally, the subscapularis attaches to the bone through tendon fibers, whereas the lower portion of the subscapularis attaches to the bone as muscle, with very short or no tendon fibers. The proximal to distal length of the tendinous portion of the subscapularis is approximately 2.5 cm (65% of the whole length of attachment). 13
Histologically, the subscapularis tendon fibers attach to the bone through a classic enthesis structure, transitioning into fibrocartilage and mineralized cartilage. It is important to remember that tendon to bone healing after experimental detachment does not result in the reestablishment of the original fibrocartilage enthesis with interfacing layers of fibrocartilage–calcified fibrocartilage, but ultimately results in a fibrous interface. 14
The capsule of the glenohumeral joint is intimately related to the subscapularis. 15 On the upper portion, the anterior capsule and subscapularis tendon are extremely difficult to separate, whereas there is a clear dissection plane between the lower subscapularis muscle fibers and the capsule. Proximal to the upper edge of the subscapularis, the boundaries of the interval region include the anterior capsule posteriorly and the coracohumeral ligament anteriorly.
Author’s Surgical Technique
Exposure for implantation of an anatomic TSA is achieved through a long deltopectoral approach. The cephalic vein is preserved and mobilized medially with the pectoralis major. The subdeltoid space is recreated and a deltoid retractor placed. The space between the conjoined tendon and the subscapularis is developed for medial retraction of the conjoined tendon. The arm is placed in approximately 45° of external rotation, and the following landmarks are identified: medial edge of the bicipital groove, coracoacromial ligament, and anterior humeral circumflex vessels (Figure 2(A), Table I).
Subscapularis Tenotomy. A, Landmarks. B, Palpation of the superior border of the subscapularis and interval region; identification of the bicipital groove. C, Planned incision 2.5 cm medial to the bicipital groove; the tendinous portion will measure approximately 25 mm before reaching the more muscular portion of the insertion. D, Upper two-thirds of the subscapularis tendon and capsule divided and tagged with suture. E, Subscapularis and capsule divided inferiorly in a lazy S fashion along the medial aspect of the humeral shaft past the humeral attachment of the inferior capsule. F, Inferior capsule released off the humeral neck.
Subscapularis Tenotomy and Capsular Incision
Incision of the subscapularis and arthrotomy can be conceptually divided into three portions: division of the interval, incision of the upper two-thirds of the subscapularis tendon and capsule, and division of the lower third of the subscapularis with release of the inferior capsule from the proximal humerus (Figure 2(B)).
Interval incision
Our preference is to divide the interval region horizontally at its lowest portion, just proximal to, and in line, with the upper edge of the subscapularis tendon. This landmark is easily identified by palpation (Figure 2(C)). There are two important reasons for performing the interval division as low as possible. First, a lower incision avoids inadvertent damage to the tendon of the long head of the biceps if preserved. Second, preservation of the connective tissue at the interval region, just anterior to the supraspinatus tendon, may contribute to prevention of anterosuperior escape if the subscapularis tenotomy failed to heal fully.
Tenotomy
The location of the vertical incision of the subscapularis tendon is paramount for a successful repair at the end of the procedure, the goal being to create tendon flaps on each side of the tenotomy that will hold sutures (Figure 2(D)). If the tenotomy is performed too lateral, or runs obliquely from medial to lateral, at the end of the procedure the lateral tendon stump will be insufficient for adequate repair. If the incision is too medial, it will be placed at the musculotendinous junction, providing poor suture fixation on the muscular side. The depth of the incision is to bone, so that the subscapularis and capsule at divided are the same level.
Since the width of the upper third of the subscapularis footprint is between 1.5 and 2 cm as measured from the medial lip of the bicipital groove, our preference is to divide the upper third of the tendon and underlying capsule to 2 to 2.5 cm medial to the medial edge of the bicipital groove. The will leave a 5 to 10 mm cuff of the lateral tendon stump for repair at the end of the procedure. The upper 2.5 cm of the tendon are divided vertically at this level. Subscapularis and capsule are tagged together with two sutures (Figure 2(E) to (G)).
Inferior subscapularis division and capsular release
The incision on the inferior third of the subscapularis and capsule follows the shape of a lazy S (Figure 2(H)). The incision is curved laterally toward the medial aspect of the proximal humeral diaphysis, and then continues distally along the humeral shaft to the superior edge of the latissimus dorsi. Care must be taken to coagulate or ligate the anterior recurrent circumflex humeral vessels prior to dividing them inadvertently.
Placement of a pointed lever retractor around the medial aspect of the humeral shaft just proximal to the latissimus dorsi provides visualization of the inferior capsule for release. Complete release of the inferior capsule off the humerus is facilitated by progressive external rotation and flexion of the shoulder (Figure 2(I) and (J)). The release continues past the equator of the humeral head. Performing an extensive inferior capsular release facilitates exposure: the arthrotomy is larger, and the inferior capsule does not prevent posterior translation of the humerus at the time of glenoid exposure. Ample release of the inferior capsule also provides the opportunity for improved elevation after shoulder arthroplasty, since the inferior capsule no longer tethers the proximal humerus.
Release of the Anterior Capsule
The anterior glenohumeral joint capsule is thickened and contracted in the majority of shoulders that undergo arthroplasty. Failure to release the anterior capsule has the potential to compromise external rotation after surgery. It can also increase the tension on the subscapularis tendon repair at the end of the procedure, which could contribute to lack of tendon healing. Some surgeons release the anterior capsule right after mobilizing the subscapularis. My preference is to perform the anterior release at the time of glenoid exposure (Figure 3).
Release of the Anterior Capsule. A, Schematic representation of the anterior capsular release. B, Superior glenohumeral ligament and coracohumeral ligament on the superior aspect of the subscapularis tendon. C, Release of the coracohumeral ligament. D, Release of the superior glenohumeral ligament. E, Superior release finalized. F, Anteroinferior capsular release. G, Medial release. H, Completed subscapularis release. SCT: subscapularis tendon.
The interval tissue just anterior and posterior to the upper edge of the subscapularis is divided first while lateral traction is applied through the tagging sutures (Figure 3(B)). This includes fibers of the coracohumeral ligament (anteriorly) and superior glenohumeral ligament (posteriorly). A second incision is then placed along the inferior glenohumeral ligament, separating the anterior from the inferior capsule (Figure 3(C)). This radial capsulotomy is directed to the 5-o'clock position on the glenoid (right shoulder; 7-o'clock for the left shoulder). The third incision is performed along the lateral aspect of the anterior labrum, connecting the previous two incisions. Once these three incisions are performed, the anterior capsule no longer restricts lateral excursion of the subscapularis.
Some surgeons prefer to excise the anterior capsule. Our preference is to preserve the rectangle of anterior capsule on the posterior aspect of the subscapularis tendon. This capsular flap provides superior suture holding power compared to the subscapularis tendon alone at the time of repair, especially in patients with inflammatory arthritis or associated mild tendinopathy.
Subscapularis Repair and Effects of Passive Motion
Subscapularis Tenotomy in Anatomic TSA: Key Points.
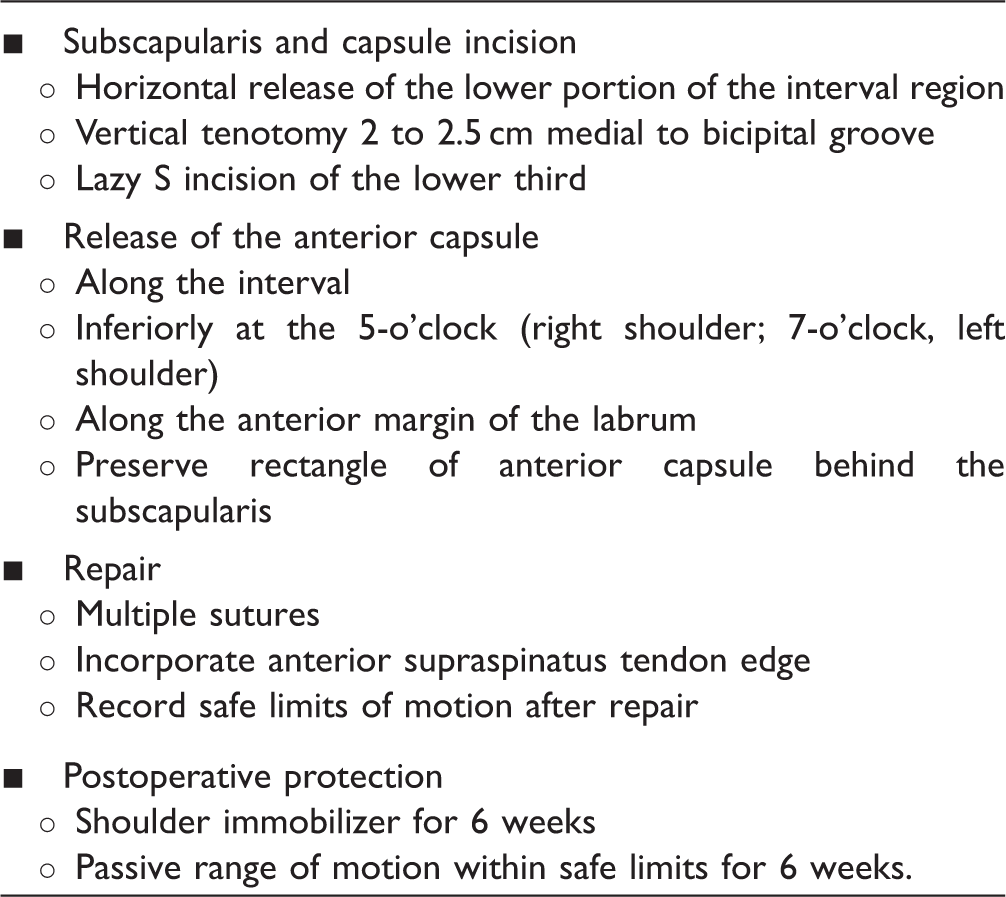
TSA: total shoulder arthroplasty.
This is the rationale for my repair technique. Nonabsorbable and absorbable sutures will both loosen up if the tendon fails to heal, so my preference is to use absorbable sutures, so that if infection were to occur, suture material does not need to be removed. If the tendon does not heal, use of nonabsorbable sutures will not provide any added benefit. The use of many sutures (one every 3–4 mm) will distribute the load across a larger number of fixation points (Figure 4).
16
Suture Repair of the Subscapularis Tenotomy.
Sutures between the anterior supraspinatus and the upper subscapularis function as a margin convergence rotator cuff repair, providing further security to the subscapularis repair through an intact supraspinatus. Although concerns have been raised over the possibility of limiting motion, (in particular external rotation) when closing the interval region, studies in cadaver have proven the superior strength of subscapularis repair when sutured to the supraspinatus tendon without detrimental effects on motion. 17 I tie the interval sutures with the arm in external rotation resting on a Mayo stand to further prevent overtightening of the interval region.
It may be easier to place the sutures between the upper subscapularis and the anterior supraspinatus prior to implantation of the humeral component. All interval sutures may be placed and tagged, but not tied until after the humeral component has been implanted and the joint has been relocated.
Occasionally, suture repair feels not secure enough, most of the times due to a very short stump on the lower half of the repair. In those circumstances, the repair may be reinforced passing sutures through bone, around the humeral component, through holes in the humeral component (selected designs), or through the tendon of the long head of the biceps if intact.
Once the repair has been finalized, the shoulder should be passively moved into external rotation and elevation to determine safe limits of range of motion during the first few weeks after surgery. These limits may be documented in the operative report and/or hospital summary to provide guidance to physical therapists and other members of the health care team.
Pits and Pitfalls
Consistent performance of a good subscapularis tenotomy is difficult. The most common mistakes include wrong placement of the vertical incision on the subscapularis (either too lateral or too medial), failure to release the anterior capsule to restore subscapularis excursion, and suboptimal repair of the subscapularis.
Postoperative Management
Our preference is to recommend use of a shoulder immobilizer for the first 6 weeks after surgery. On postoperative day 1, patients initiate passive range of motion exercises in elevation (in the scapular plane) and external rotation according to the limits established intraoperatively. Active assisted exercises are added at week 6, isometrics at week 8, and elastic band strengthening exercises at weeks 10 to 12. Stretching is added at weeks 8 to 10 for patients with residual stiffness.
Reported Outcomes and Best Available Evidence
Laboratory Studies
The majority of the studies performed in cadavers to determine cyclic displacement and/or load to failure have demonstrated better biomechanical performance of a lesser tuberosity osteotomy in comparison with a tenotomy. 18 However, some studies have shown superiority of tenotomy or no differences.11,19 A major concern with many of these studies is that the number of sutures used to repair the tenotomy in the cadaveric models was substantially less than what we use in clinical practice.
Clinical Testing of Subscapularis Function After Tenotomy
A number of studies have investigated strength in internal rotation and other tests for subscapularis integrity (lift-off test, belly-press test, and bear-hug test) after anatomic TSA performed though a tenotomy.6–8,20–23 Most of these studies have shown that a relatively large number of shoulders (30%–70%) have weakness in internal rotation at 1 and 2 years postoperatively. However, correlation between clinical tests of subscapularis integrity and concerning findings on imaging studies has been poor.8,23 Interestingly, although the number of shoulders with abnormal tests for subscapularis integrity is less in studies on lesser tuberosity osteotomy, these numbers are still substantial (10%–25%).9,24 One study has shown clinical evidence of subscapularis integrity in the majority of anatomic TSA performed through a tenotomy. 25
Imaging Evaluation of Subscapularis Tendon Healing
Most studies on healing rates of subscapularis tenotomy after anatomic TSA have used ultrasound evaluation. There are a number of potential problems with ultrasound evaluation of these shoulders: ultrasound is operator dependent and somewhat subjective, and the ultrasound aspect of a healed tenotomy is likely different than a subscapularis tendon that has never been violated, which may explain the low correlation between concerning ultrasound findings and clinical findings.8,23 Having said that, several studies have reported ultrasound evidence of tendon attenuation or rupture in a number of anatomic TSAs performed through a subscapularis tenotomy. The rates of concerning findings in comparative studies are summarized later.
It is important to note that although some studies have reported 100% healing rates after lesser tuberosity osteotomy,26,27 there are a number of reports on nonunion of the lesser tuberosity osteotomy, occasionally leading to reoperation.28–30 Imaging evaluation of atrophy and fatty infiltration has not been performed in patients undergoing tenotomy. Atrophy and fatty infiltration have been reported after both osteotomy and peel.26,31
Electromyography
Armstrong et al. 20 performed an electromyographic (EMG) evaluation of 30 anatomic TSAs performed through a subscapularis tenotomy. At 1 year, 50% of the shoulders had an abnormal EMG. Interestingly, denervation and reinnervation changes were similar across all 4 rotator cuff muscles, suggesting that EMG changes are related to factors other than tenotomy (eg, traction neuropathy during exposure, interscalenic regional anesthesia).
Comparative Studies
Several published studies have compared the outcome of tenotomy with lesser tuberosity osteotomy. Scalise et al. 27 reported on a retrospective review of 35 anatomic TSAs performed using a tenotomy (15) or osteotomy (20). At 2 years, differences in Penn Shoulder Scores or strength in internal rotation were not significant. Ultrasound evaluation was concerning in 7 shoulders after tenotomy and 2 after osteotomy. Jandhyala et al. 32 performed a retrospective comparison of tenotomy (10 shoulders) versus osteotomy (26 shoulders). All outcome measures were similar in both groups, except for a better grade on the belly-press test in the osteotomy group. Buckley et al. 33 compared tenotomy (32 shoulders) versus osteotomy (28 shoulders) and found no differences on WOSI (Western Ontario Shoulder Instability), DASH (Disabilities of the Arm, Shoulder and Hand), or Constant scores or in belly-press or bear-hug test resistance. Ultrasound was concerning in 4 shoulders in the tenotomy group; these 4 shoulders had worse scores and inferior internal rotation strength. 33
The only prospective randomized study published to date has compared lesser tuberosity osteotomy with subscapularis peel, not tenotomy. 10 This study found no differences in clinical outcome or internal rotation strength. A subsequent publication on the same group of patients reported no differences in healing rates or fatty infiltration. 31 Louie et al. 34 published a systematic review of studies comparing subscapularis tenotomy and lesser tuberosity osteotomy. Tenotomy was associated with better active elevation, there were no other differences in other clinical outcomes, and complication rates were almost identical.
Summary of Best Available Evidence
Anatomic TSA performed through a subscapularis tenotomy provides satisfactory clinical outcomes in the majority of the patients. Subscapularis failure leading to anterior instability and reoperation is rare provided meticulous attention is paid to surgical technique and postoperative management. 35 However, a number of shoulders will not recover normal strength in internal rotation; will have positive bear-hug test, belly-press test, and/or lift-off test; and will also present concerning findings on ultrasound evaluation.
Subscapularis Tenotomy Versus Lesser Tuberosity Osteotomy: Relative Advantages.
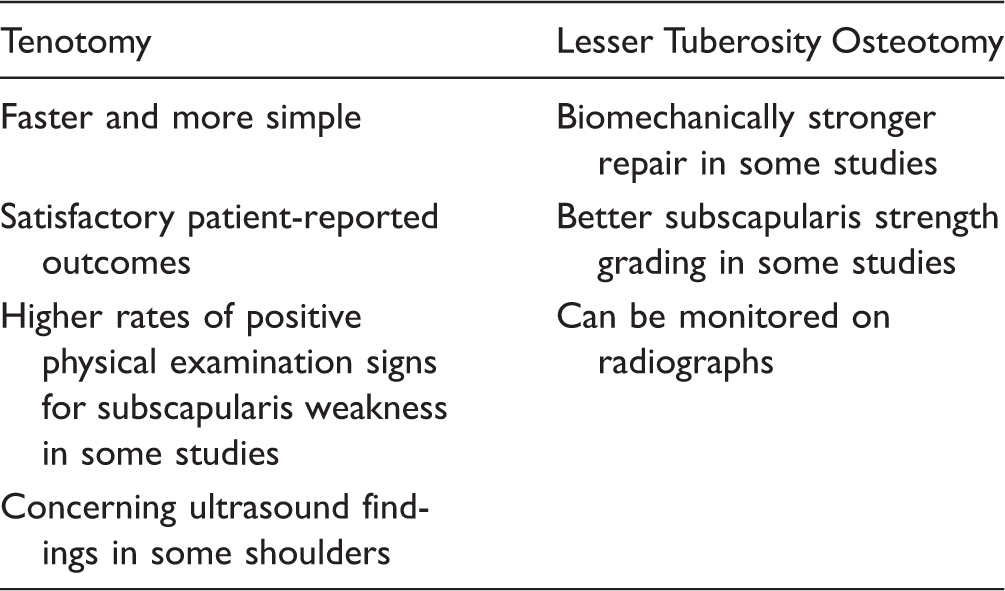
Based on this review of published studies, my interpretation of the literature is that the outcome of anatomic TSAs performed through a subscapularis tenotomy is not inferior compared to alternative techniques for subscapularis management, but abnormalities in strength testing and ultrasound studies will be present in a substantial number of shoulders postoperatively.
Other Considerations
There are other factors that may incline the balance in favor or against subscapularis tenotomy and its alternatives, including complexity, cost, learning curve, and exposure for stemless prosthesis; these factors have not been analyzed scientifically to date. Lesser tuberosity osteotomy seems to add to the complexity and duration of the shoulder arthroplasty procedure. This may translate in more hesitation when allowing trainees to perform the exposure, as well as increased cost related to longer operating room time.
Osteotomizing the lesser tuberosity may translate in better glenoid exposure, since the bulk of the proximal humerus is decreased. However, removal of the cortical rim of the bone around the lesser tuberosity may facilitate crushing of the proximal humerus cancellous bone with posterior glenoid retractors. Finally, as stemless prostheses become more popular, surgeons may be hesitant about performing a lesser tuberosity osteotomy, since the bone stock in the metaphysis is extremely important for the primary stability of stemless humeral components.
Management of the Failed Subscapularis Tenotomy
The majority of shoulders with clinical evidence of subscapularis weakness compared to the opposite side need no additional treatment: positive subscapularis signs may be detected on physical examination, but most of this shoulder arthroplasties are pain free, provide excellent patient-reported outcomes, and do not translate in radiographic evidence of subluxation.
On the contrary, subscapularis failure may lead to anterior instability with or without frank dislocation. This will translate in worse patient-reported outcomes, with or without pain, as well as radiographic evidence of anterior subluxation or frank dislocation. If subscapularis failure is detected in the first few weeks after the index arthroplasty, consideration should be given to revision repair of the subscapularis tenotomy as soon as possible. My experience is that the tissues at the revision repair site are very frail, and augmentation with allograft tendon or commercially available patches may need to be considered.
For patients presenting later on with anterior instability after arthroplasty, revision repair, augmentation, and transfer of the pectoralis major have been associated with high failure rates,36,37 and most surgeons would be inclined to recommend revision to reverse shoulder arthroplasty instead.38,39
Summary and Future Directions
Adequate management of the subscapularis is extremely important when implanting an anatomic TSA. Tenotomy of the subscapularis is my preferred alternative. Care must be taken to incise the tendon in the right location, release the anterior capsule to gain excursion, and perform a secure repair. My preference is to repair the tenotomy with multiple interrupted sutures placed every 3 to 4 mm, to preserve a rectangular flap of capsule on the posterior aspect of the subscapularis to increase suture holding power, and to repair the upper edge of the subscapularis to the anterior border of the supraspinatus tendon.
Complete failure of tenotomy leading to anterior instability is relatively uncommon and may be salvaged with revision repair with or without augmentation or with revision to a reverse arthroplasty. However, weakness in internal rotation is common, and some patients do develop concerning ultrasound findings (tendon attenuation or rupture). Lesser tuberosity osteotomy seems to provide similar outcomes, except for better grades in belly-press and other subscapularis tests. Some authors have reported universal healing of the osteotomy, but there are several reports of nonunion as well. Osteotomy does not prevent weakness in internal rotation or fatty infiltration in some shoulders.
Subscapularis tenotomy seems to translate in shorter operative times, which may have cost implications. It is particularly attractive when considering implantation of a stemless humeral component, when every effort must be made to preserve the corticocancellous bone at the proximal humerus metaphysis.
Subscapularis tenotomy is the main reason for postoperative immobilization and protection of the shoulder after anatomic TSA. Taking into account the need for postoperative protection, the fact that a number of patients will have weakness in internal rotation and worrisome imaging findings, and the relatively marginal gain provide by an osteotomy of the lesser tuberosity, the need for easy to perform, reliable cuff-sparing approach remains.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Sanchez-Sotelo has implant designs and royalties with Stryker.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.