
Abstract
Introduction
As the revision number of shoulder arthroplasties increases, we focused on the difficulties of extracting or converting the humeral stem. The purpose of this multicentric study was to assess the outcomes and the radiographic results of a new, short, and convertible humeral stem (Aequalis Ascend™ Flex, Tornier SAS–Wright Medical Inc®, Bloomington, MN, USA), which could settle these complex revision problems.
Methods
Sixty-six primary shoulder replacements were enrolled with an average follow-up of 25.6 months (24–30.8 months). There were 24 reversed shoulder arthroplasty (RSA) and 42 anatomical shoulder arthroplasty. The functional outcomes were evaluated with the Constant-Murley score (CS) and the active range of motion. Humeral stems were radiologically analyzed at the last follow-up with special care to mechanical complications and bone resorption.
Results
The average CS improved from 30 preoperatively to 74 postoperatively (P < .0001) for anatomical shoulder replacements and from 21 to 63 (P < .0001) for RSA. The active anterior elevation and external rotation improved from 97° and 6° to 163° and 46°, respectively, for anatomical prosthesis (P < .0001) and from 79° and 10° to 139° and 28°, respectively, for RSA (P < .0001). No mechanical complication or loosening was reported. The comparison between postoperative and last follow-up X-rays showed a tendency to medial cortical bone thinning in some cases without any clinical relevance.
Conclusion
Two years follow-up of this short stem showed promising clinical and radiographic results without implant-related complication. Further X-rays study would be necessary.
Level of evidence: IV
Introduction
Shoulder arthroplasties, reversed (RSA) or anatomical (total shoulder arthroplasty [TSA]), are successfully used for treatment of glenohumeral disorders after nonoperative treatment failure. Significant improvements in range of motion, pain, and quality of life were mainly reported with durable efficiency.1–5 An increase of shoulder prosthesis implantations has been reported over the last years,6,7 which is inevitably associated with higher number of revision procedures.8,9
During revision surgeries, the humeral component, which is rarely the cause of the failure, frequently needs to be removed in order to allow glenoid exposure or to convert the prosthesis to RSA. 10 Removal of a well-fixed, cemented humeral component is challenging, with high risk of complications such as intraoperative fracture. 5 On the contrary, when a humeral loosening needs reoperation, the difficulty is mainly related to humeral bone-defect reconstruction. A new humeral stem must comply with these specifications: bone stock preservation, avoiding humeral loosening, and making the humeral revision easier. Recently, much attention has been paid to short, uncemented, and convertible stems, whose purpose is to preserve humeral bone stock. Several years will be necessary to estimate the potential advantage of this new short stem during revision or conversion surgery. The results of the preliminary generation of this new stem have already been reported, with high rate of radiolucencies. Proximal plasma spray was secondary associated to improve metaphyseal bone fixation.
The purpose of this multicentric study is to assess the preliminary clinical and radiological outcomes of this second generation, short, uncemented (with optional cementation), and convertible humeral stem with proximal metaphyseal plasma spray coating (Aequalis Ascend™ Flex, Tornier Inc®, Bloomington, MN, USA).
Method
Patient
This was an observational, retrospective, and multicenter study, including all the patients operated on between September 2012 and April 2013 for primary shoulder replacements, anatomical or reversed, using the Aequalis Ascend™ Flex (Tornier SAS–Wright Medical Inc®, Bloomington, MN, USA) in 2 specialized orthopedics centers. This study received the approval of the Institutional Review Board of the ethical committee of the Hopital Privé Jean Mermoz and the Centre orthopédique Santy (Study 2015—2).
Demographics Data of the Population.

Description of the Implant and Surgical Technique
The Aequalis Ascend™ Flex stem is a short humeral stem (66 mm–94 mm long) with proximal titanium plasma spray coating for metaphyseal press-fit fixation. Long (88 mm–120 mm) and short (66 mm–90 mm) stems were available for optional cementation with a polished surface finish. A universal female-taper connection on the humeral side provides convertibility from anatomic to reverse design and allows easier glenoid exposure in case of revision. Three different head shaft angles (noted A, B, and C) were offered: 127.5° (A), 132.5° (B), and 137.5° (C). For anatomical prosthesis, Angle A was used in 9 cases (21.4%), angle B in 18 cases (42.9%) and angle C in 15 cases (35.7%). Reverse prosthesis has an onlay design, using a reversed tray with low or high offset. Angle B was always used for RSA with a 12.5° angular asymmetric polyethylene insert to reach a 145° neck shaft angle.
A deltopectoral approach was used for anatomical replacement with subscapularis tenotomy and transosseous suture repair. A biceps tenodesis was always performed. Both deltopectoral (20 shoulders, 83.3%) and anterosuperior (4 shoulders, 16.7%) approaches were used for reversed shoulder prosthesis according to the surgeon’s preferences.
On the humeral side, osteophytes were first resected before head cut at the anatomic neck with physiological retroversion. For RSA, a cutting guide of 132.5° was used to fit onto Angle B. The humeral canal was first sized using sounders; metaphyseal bone was then compacted and preserved by the use of compactors, progressively reaching the adapted size determined by the sounders and rotational stability. A surface planer ensured adequate contact between the stem and the humeral head or the reversed tray. All the anatomic stems were uncemented, whereas 8 RSA required a cemented stem (33.3%). Cementation was decided preoperatively for 6 patients (75%) and intraoperatively for 2 (25%), secondary to poor bone stock and low rotational stability. There were 5 long stems, all cemented.
The glenoid side was prepared as usual for a cemented, keeled implant in case of TSA and for uncemented sphere and baseplate in case of RSA. Bio-RSA was used for 18 of the 24 reverse designs (75%).
Method of Assessment
All the patients had a clinical evaluation preoperatively and at minimum a 2-year follow-up using the raw Constant-Murley score (CS), the subjective score value (SSV), and the active range of motion (ROM). Perioperative data (cementation or not, complications) and postoperative complications were reported. Radiological examination used standard radiographs in a strict anteroposterior view, defined by the visualization of the morse taper, and a Lamy profile view. Mechanical complications (implant loosening, disassembly, fracture, instability, and migration) were noted according to clinical and radiographic evaluation. Radiographic reading, measurements, and assessments were realized by a single independent examiner. Radiolucent lines (RLLs) around the stem and the glenoid component in postoperative and last follow-up X-rays were reported as well as their eventual progression. We used the RLL score for the glenoid component of TSA.
11
Scapular notching was reported for RSA such as described by Sirveaux et al.
4
The neck shaft angle (NSA) defined by the angle between the diaphyseal shaft and a perpendicular line to the reversed tray or humeral head was measured (Figure 1). This NSA was compared to the expected angle related to the chosen stem in order to evaluate misalignment. We defined a filling ratio to evaluate the stem size compared to the humeral diameter measured on the medial cortex 1 cm under the calcar-prosthesis junction, to be under the area of osteophyte resection. This filling ratio has been measured for all the patients on the immediate postoperative antero-posterior X-rays (Figure 2).
Neck Shaft Angle Measurement. Filling Ratio = Stem Diameter (S) / Humeral Diameter (H).

Statistical Analysis
Statistical analysis was performed using Statview© software (Optima, Mérignac, France). The parametric Student’s t test was used to compare quantitative values. We used the chi-square test to compare qualitative values with effective higher or equal than 5. The Fisher test was used for lower effective. A P value inferior to .05 was considered significant.
Results
Seven complications (10.6%) and 2 revisions (3.0%) were reported. Five minor complications concerned anatomical prosthesis: 3 calcar cracks without consequence on stability and integration of the stem, 1 hematoma without reoperation, and 1 unexplained painful shoulder. This last patient was reoperated for arthroscopic debridement, with a good functional outcome at the last follow-up (CS = 72). Two complications concerned RSA. There was 1 postoperative scapular spine fracture treated conservatively and 1 plexus palsy with shoulder stiffness secondary to an excessive arm lengthening. This patient was reoperated 1 month later for humeral shortening and cemented humeral stem reimplantation without difficulty to extract the primary stem. Nerve palsy regressed with good functional result at follow-up (CS = 70).
Preoperative and Postoperative CS and ROM of Anatomic Prosthesis.
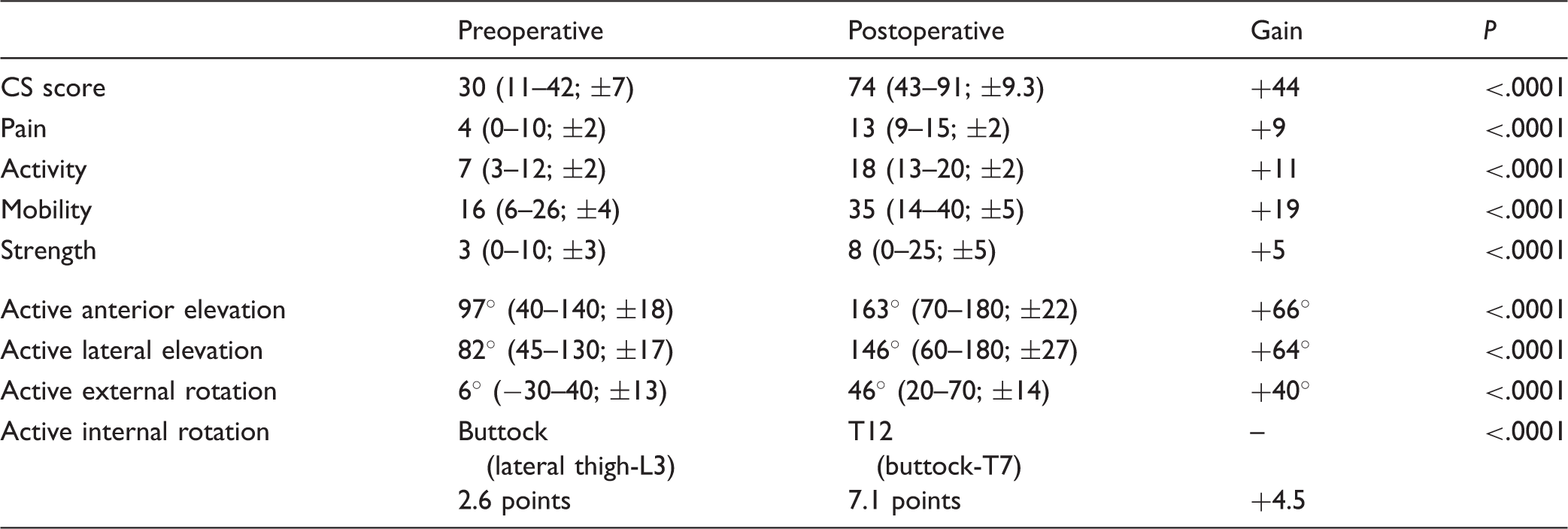
CS, Constant-Murley score; ROM, range of motion.
Preoperative and Postoperative CS and ROM of RSA.

CS, Constant-Murley score; ROM, range of motion; RSA, Reversed shoulder arthroplasties.
Incidence, Clinical Consequence, and Association With Stem Filling Ratio of Proximal Cortical Bone Resorption at 2-Year Follow-up.

Concerning the NSA, we reported a mean difference between expected and measured angles of 3.7° (1.5° varus to 11.5° valgus).
Discussion
The concept of a short uncemented stem is a new concept, half way between long cemented stems that remain the gold standard and stemless prosthesis. We reported promising clinical and radiological results at 2-year follow-up for this short uncemented and convertible stem.
Functional outcomes of TSA were satisfying and comparable to previous published studies,12–15 such as the multicentric study of Walch et al., 15 which reported the results of 320 long humeral cemented stems. Jost et al. 14 and Schnetzke et al. 16 published the results of two short uncemented stems and reported a mean active forward elevation of 142° and 157°, respectively, similar to our study.
The functional outcomes of RSA of the 2-year follow-up appeared to be comparable with the literature for CS and range of motion. Molé and Favard 17 , in a French multicentric study, found a mean CS of 62 using a standard cemented humeral stem. Teissier et al. 18 and Ballas and Béguin 19 , respectively, reported a mean active flexion of 143° and 140° using stemless reverse shoulder arthroplasty and a mean gain of 28 and 33 points on CS. The mean CS improved by 43.5 points for Atoun et al. 20 using a short and uncemented metaphyseal stem.
We did not observe any implant-related complication. The humeral components stability was good at the minimum 2-year follow-up for both anatomical replacements and RSA. No RLL around the stems was observed. Casagrande et al.
21
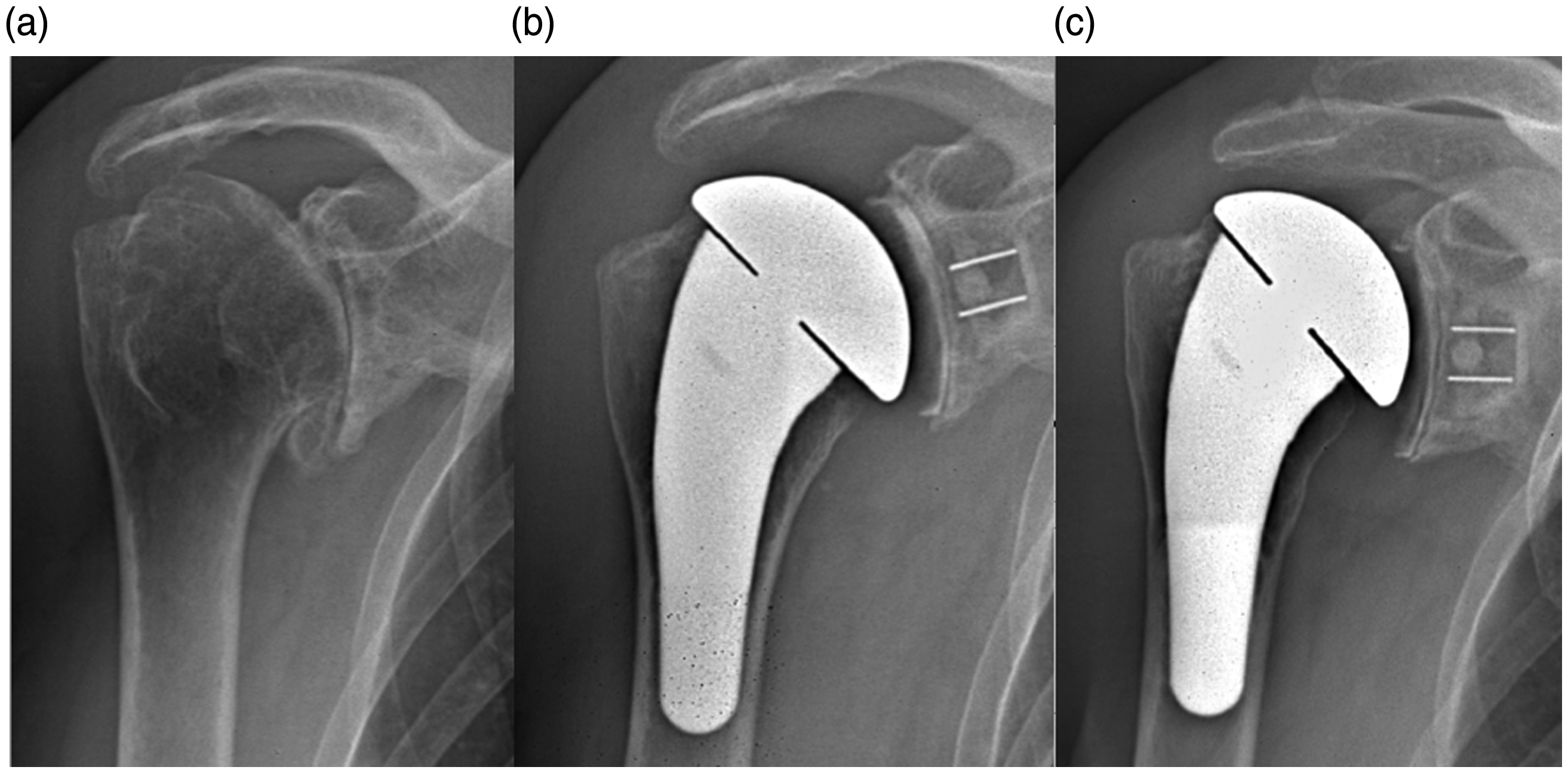
assessed the result of the first generation of this stem and reported 71% cases of radiolucencies around the stem, 10.9% stem loosening, and 8.7% stem at risk of loosening. The adjunction of proximal titanium plasma spray coating on this second-generation stem seems to improve stability and bone ingrowth. However, the radiographic analysis in our study reported a tendency to humeral proximal bone resorption in some cases (Figures 3 to 6). Published studies described bone resorption in shoulder arthroplasty using an uncemented stem.22,23 Schnetzke et al.
16
found 13.6% of slight stress shielding with TSA using a previous generation of the Aequalis Ascend™ stem. There was no clinical relevance or loosening associated with bone resorption, confirming the literature.16,24 Recently, Schnetzke et al.
25
published that the occurrence of bone adaptation was associated with high metaphyseal and diaphyseal filling ratios. The assessment of metaphyseal filling ratios in our study found an association between bone resorption and higher mean filling ratio. Moreover, we hypothesize, in our experience, that the bone mineral density may be the key factor of osteolysis, as described by Nagels;
22
with tendency to use higher stem size in case of poor bone quality. Complementary study will be necessary to explain these cases of bone resorption.
Example of TSA Without Proximal Bone Resorption: Man, 72 years old. A, Preoperative X-rays. B, Postoperative X-rays. C, 2-year follow-up X-rays. TSA, total shoulder arthroplasties. Example of TSA With Proximal Bone Resorption: Woman, 69 years old. A, Preoperative X-rays. B, Postoperative X-rays. C, 2-year follow-up X-rays. TSA, total shoulder arthroplasties. Example of RSA Without Proximal Bone Resorption: Woman, 72 years old. A, Preoperative X-rays. B, Postoperative X-rays. C, 2-year follow-up X-rays. RSA, reversed shoulder arthroplasties. Example of RSA With Proximal Bone Resorption: Woman, 70 years old. A, Preoperative X-rays. B, Postoperative X-rays. C, 2-year follow-up X-rays. RSA, reversed shoulder arthroplasties.


The actual increasing number of shoulder arthroplasties revisions8,9 is mainly related to the glenoid component.26,27 During glenoid revision procedure, well-fixed humeral stems are found in more than 80% and often need to be removed for glenoid exposure or prosthesis conversion with high risk of complications. 2 In our study, 1 patient needed stem removal, which could be performed easily thanks to the short stem design, without any loss of bone stock at the time of extraction.
Furthermore, short stem and stemless prosthesis are usable when the humeral shaft is not soundable such as sequelae of diaphyseal fracture or long humeral stem of elbow prosthesis. We choose a short stem to limit errors of humeral neck shaft angle, sometimes reported with stemless prosthesis, by centering the stem into the shaft, which is especially important for RSA.
Metaphyseal bone compaction and press-fit fixation also aim to preserve bone stock. The efficiency of the cementless stem has been already proven for anatomic shoulder prosthesis using long stem.18,28–30 Weusten et al. reported good survivorship of the humeral stem at 5-year follow-up without difference between cemented and uncemented stems. 31 Jost et al. reported good results of a short uncemented stem without mechanical complications at 29-month follow-up. 14 Promising midterm radiological results were found by Schnetzke et al. 16 without stem loosening at 31.2-month mean follow-up with a previous generation of the stem used in this study. Moreover, recent studies published good results of cementless fixation for RSA. Wiater et al. and King et al. found similar clinical and radiographic results between cemented and cementless humeral stem.32,33 Giuseffi et al. assessed the outcomes of 44 short uncemented stems for RSA with a mean follow-up of 27 months. They reported no radiological evidence of loosening in any patient. 23 All these studies agreed with our results, showing no humeral stem loosening or implant-related complication. However, in 8 cases, cemented stems (short or long) were used in our cohort. The decision to cement the stem was made during surgery for only 2 cases because of low bone quality. The optional cementation allowed by this stem could be a solution for all patients for whom rotatory stability cannot be obtained. Furthermore, we did not report any proximal cortical bone thinning with cemented stems.
The convertibility of the stem allows for avoidance of humeral component removal. Castagna et al., 34 Kany et al., 35 and Wieser et al. 36 evaluated the use of a convertible stem and reported less intraoperative blood loss and operative time, which are associated with fewer complications and revisions with the modular system than patients needing stem exchange to convert anatomic arthroplasty to RSA. Functional outcomes appeared to be good after revision without stem exchange in these studies. Convertibility of these stems implies an onlay design, the lateralizing effect of which changes the initial design of Grammont. However, Berhouet et al. evaluated the onlay design of RSA in a biomechanical study. 37 It appeared that humeral tray position had an effect on impingement by allowing the adjustment of the anteroposterior offset and lowering or lateralization of the humerus.
Our study had several limitations. The 2-year follow-up remains insufficient to assess long-term evolution of a stem. Longer follow-up appears necessary to evaluate these encouraging results and to analyze the convertibility. Further X-rays study will be necessary to assess proximal cortical bone thinning.
Conclusion
The second generation of this new, short, and convertible stem provides good functional results and stable fixation without mechanical failure at an intermediate follow-up. Proximal titanium plasma spray coating seems to improve bone ingrowth compared with the first generation stem.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Pr. Daniel Mole, Dr. Lionel Neyton, and Pr. François Sirveaux report personal fees from Tornier SAS–Wright Medical, during the conduct of the study; personal fees from Tornier SAS–Wright Medical, outside the submitted work. Dr. Arnaud Godeneche reports personal fees from Tornier SAS–Wright Medical, during the conduct of the study; personal fees from Tornier SAS–Wright Medical, personal fees from FH, outside the submitted work. Dr. Gilles Walch reports personal fees from Tornier SAS–Wright Medical, other from Imascap, during the conduct of the study; personal fees from Tornier SAS–Wright Medical, other from Imascap, outside the submitted work. The rest of the authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.