
Abstract
Background
Limited evidence exists regarding the relative rates of glenoid loosening after total shoulder arthroplasty utilizing pegged or keeled cemented all-polyethylene glenoid components.
Methods
A systematic review of level I, II, and III studies comparing the development of radiolucent lines and glenoid failure after total shoulder arthroplasty with pegged or keeled glenoid components was conducted. Four articles were included in the final analysis with a total of 203 total shoulder arthroplasties comprising 107 pegged and 96 keeled glenoid components.
Results
Development of radiolucent lines was less likely with pegged glenoid components with a risk difference of −0.32 (95% CI −0.62, −0.03) favoring the pegged design. There was no statistically significant difference in the rate of radiographically at-risk glenoids, clinical glenoid failure, or the composite endpoint.
Conclusions
Although the development of radiolucent lines was less likely around pegged glenoid components, there was no significant difference in the rate of radiographic or clinical glenoid failure between pegged and keeled components. More high-quality studies are needed to determine the relative rates of glenoid loosening with pegged and keeled glenoid components.
Introduction
Total shoulder arthroplasty (TSA) is a reliable procedure for the treatment of end-stage glenohumeral arthritis, with 5-year implant survival rates of 95%. 1 Despite improved implant survival rates, glenoid loosening remains one of the leading causes of revision.1–4
A number of glenoid implant designs have sought to reduce the rate of glenoid loosening. Despite successful treatment of patients’ symptoms as reported by patient-reported outcomes measures, radiographic loosening continues to be a problem regardless of implant design. Pegged and keeled cemented all-polyethylene glenoid components are currently the most commonly used designs. However, there is insufficient evidence as to which design results in the lowest incidence of glenoid loosening.
The purpose of this systematic review was to determine whether pegged or keeled cemented all-polythethylene glenoid components differed with regard to the incidence of glenoid loosening. We hypothesized that no difference would exist in the published radiographic or clinical incidence of glenoid loosening after TSA with pegged versus keeled cemented all-polythylene glenoid components.
Methods
Pubmed, Cochrane, Ovid, and CINAHL (Cumulative Index to Nursing and Allied Health Literature) databases were searched using the terms “pegged AND keeled glenoid,” “glenoid component,” “pegged versus keeled,” “pegged glenoid,” and “keeled glenoid” in the manuscript title. There were 3294 citations identified at the time of search in July 2016. Upon review of the titles and abstract of these citations, 81 manuscripts were identified as relevant to this review and were subsequently retrieved for further analysis. Inclusion and exclusion criteria are given below.
Inclusion criteria:
English Language manuscript Comparison of pegged with keeled glenoid component Radiolucency evaluation Average follow-up of a minimum of 1 year Level of Evidence I, II, or III (prospective randomized trials, retrospective case-control study) Cemented all-polyethylene glenoid component
Exclusion criteria:
Less than 1 year follow-up No radiolucency evaluation Level of Evidence IV or V (case series, review articles) Animal studies and cadaveric studies Uncemented or metal-backed glenoid component
After application of the inclusion and exclusion criteria, 4 manuscripts were available for detailed review. Using methods previously described by Spindler et al., 5 a thorough evaluation of each manuscript assessing study design methodology, statistical approach, and sources of bias was performed. The primary outcome was glenoid component failure, defined as symptomatic glenoid component loosening requiring revision surgery or radiographic evidence of loosening termed “at risk” (Franklin grade 4 or 5). Evaluation for radiolucency and loosening was based on the Franklin grading system from Lazarus et al. 6 Shoulder-specific outcome measures (Constant and/or American Shoulder and Elbow Surgeons [ASES] shoulder score) were also analyzed. Data were assessed and extracted by 2 independent reviewers to ensure accuracy.
Statistical Methods
The results of each of the included studies were plotted as relative risks with corresponding 95% confidence intervals. A Mantel–Haenszel analysis using a random-effects model allowed for pooling of data from the included studies because data were found to be statistically heterogeneous. This methodology allowed for assessment of the risk difference between groups. Statistical tests for data heterogeneity for radiolucent lines, glenoids at risk, and glenoid failures (Chi-square test, I2, and Tau2) were employed from data of included studies. Differences between groups were assessed with use of the t test and significance was set at P ≤ .05.
Results
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis
7
flow diagram is given in Figure 1. After initial search and screening, 81 articles were retrieved for detailed review. Eleven studies were excluded because they reported results of a metal-backed glenoid component. Twelve studies were excluded because they consisted of cadaveric or animal models. Four studies were excluded because results reported less than 1 year of clinical follow-up. Seventeen studies were excluded because they compared outcome of glenoid components other than pegged to keeled. An additional 33 studies were excluded because of study design, yielding 4 studies8–11 included in the final analysis (Table 1).
PRISMA flow-chart describing the inclusion and exclusion of studies for the present meta-analysis. Description of the Studies Included in the Current Systematic Review.

Edwards et al. 8 performed a prospective randomized trial comparing pegged to keeled glenoids in 53 patients with primary glenohumeral osteoarthritis. An a priori power analysis indicated a minimum of 18 patients was needed in each group. Twenty-six shoulders were randomized to the pegged group and 27 to the keeled group. Radiographs were obtained following surgery at postoperative day 7 and yearly thereafter. Radiolucency of the glenoid component was graded for pegged components as described by Lazarus et al. 6 and Franklin et al. 12 for keeled components. The authors reported 89% rate of follow-up (47 patients; 21 pegged, 26 keeled) at a mean of 26 months (range 12–38 months) postoperatively. The authors reported no significant difference in radiolucency of at least grade 2 in the immediate postoperative period. At final follow-up, keeled components demonstrated a higher rate of radiolucency of grade 2 or higher, 46% compared with 15% (P = .003). Two patients in the keeled group had glenoid failure requiring additional surgery. There were no failures in the pegged group.
Throckmorton et al. 10 performed a retrospective case-control study examining the results of pegged and keeled glenoid components in 100 shoulders (50 pegged and 50 keeled) at a mean follow-up of 51.3 months. At final follow-up, 13 pegged subjects had no radiolucent lines, 19 had lucency under the faceplate only, 12 with 1 column involvement, and no pegged components with 2 or 3 column involvement. There were 11 subjects with keeled components with no radiolucency, 22 with lucency under the baseplate only, 11 with 1 column involvement, 2 patients had 2 column involvement, and none with 3 column involvement. Six (12%) pegged and 4 (8%) keeled components were found to be radiographically at risk for clinically symptomatic loosening. This difference was not statistically significant (P = .74). The keeled group had a single case of symptomatic glenoid component loosening, which did not result in a revision surgery at the conclusion of the study. No shoulders in the pegged group were revised for glenoid loosening. At final follow-up, both pegged and keeled glenoid groups demonstrated clinically and statistically significant improvements in pain and range of motion However, there was no significant difference in the functionality and/or pain scores between groups. In the pegged population, the preoperative pain score was 4.6 and improved to 1.5 postoperatively. The preoperative forward flexion, external rotation, and internal rotation were 96.7°, 25.2°, and sacrum, respectively. These improved to 147°, 53.2°, and L1 postoperatively. For the keeled population, the preoperative pain score was 4.6 as well, and improved to 1.7 postoperatively. The preoperative forward flexion, external rotation, and internal rotation measurements were 103.7°, 28.8°, and L5, while the postoperative measurements were 150°, 58°, and L1, respectively.
Rahme et al. 9 performed a prospective randomized trial comparing pegged and keeled glenoid components in 26 TSAs, 14 pegged, and 12 keeled, with 2 years of follow-up. A priori power analysis was performed to estimate sample size and determined a minimum of 12 subjects per group were required to detect a significant difference in micromotion using radiosterometric analysis. The primary outcome was to measure glenoid component translation of at least 0.25 mm on radiostereometric evaluation. The study was not powered to detect differences in clinical outcomes or radiolucent lines. Clinical outcomes were assessed using the mean Constant–Murley score preoperatively and at the 2-year postoperative visit. The mean preoperative score for a pegged glenoid component was 25 points while the mean preoperative score for the keeled component was 22 points. These improved to a postoperative score of 70 points for both the pegged and keeled glenoid components (P < .0001). The authors also had the patients assign an average subjective shoulder value at the same time intervals. The results were that the pegged arthroplasties improved from 39 points to 80 points and the keeled components improved from 35 points to 80 points (P < .0001). These measures demonstrated both clinically and statistically significant improvement following surgery in both groups with no significant difference between groups.
Radiographs were assessed for radiolucency grade immediately postoperatively as well as at 1 - and 2-year follow-up. There were no significant differences with regard to rate of radiolucency between groups (P = .429). At final follow-up, 9 of 12 (75%) keeled shoulders had some grade of radiolucency and 8 of 14 (57%) in the pegged group had some grade of radiolucency. No component had grade 4 or 5 lucency on final 2-year follow-up. There was no statistically significant difference found between groups with regard to motion of the glenoid component as measured by radiosterometric analysis at any time point. Also, there was no statistically significant difference observed in micromotion for the different grades of radiolucency. No patient underwent reoperation for glenoid loosening.
Trail and Nuttal 11 conducted a retrospective case-control study comparing shoulder arthroplasties in patients with rheumatoid arthritis. Their study included 105 shoulder operations: 65 humeral head replacements and 40 TSAs with at least 2 years follow-up. Of the 40 TSA procedures, 11 were a keeled glenoid design while the remaining 29 were pegged. Radiographic follow-up at 2 years was limited to only 32 of the original 40 patients (22 pegged, 10 keeled). Clinical outcomes assessed include range of motion, Constant–Murley score, and ASES shoulder score. When compared with the preoperative measurements, all 3 were significantly different (P = .001) at final follow-up, with the mean difference being 6 for pain, 30 for ASES score, and 20 for Constant–Murley score. At 2 years, presence of any radiolucency was less likely in the pegged group (36%) than in the keeled group (90%). One keeled glenoid was deemed at risk due to significant lucency. No pegged glenoid designs were deemed at risk. No glenoid component required revision at final follow-up.
In the current systematic review, outcomes of 203 TSAs were analyzed, 107 pegged and 96 keeled glenoid components. Three glenoid failures were reported, all from the keeled group. Additionally, 7 keeled and 6 pegged components were determined to be at risk (Franklin grade 4 or 5) for loosening based on radiolucent lines visualized on final radiographs. Shoulder-specific outcome measures were incompletely reported in the studies and could not systematically analyzed.
Presence of any radiolucent line was more common in keeled glenoid components with a risk difference of −0.32 (P < .05, CI −0.62, −0.03) favoring pegged components, as shown in Figure 2. There was significant heterogenetity among the studies with I2 = 82% (P = .0009) with regard to the development of radiolucent lines. There was no statistically significant difference in radiographically at-risk glenoids, glenoid failure, or the composite outcome as demonstrated in Figure 3. The event rate for at risk glenoids and glenoid failure was low across studies and the heterogeneity among the studies was very low (I2 = 0%).
Forest plot of radiolucent lines after TSA with pegged and keeled glenoid components. Forest plot of radiographically at-risk glenoids and glenoid failure after TSA with pegged and keeled glenoid components.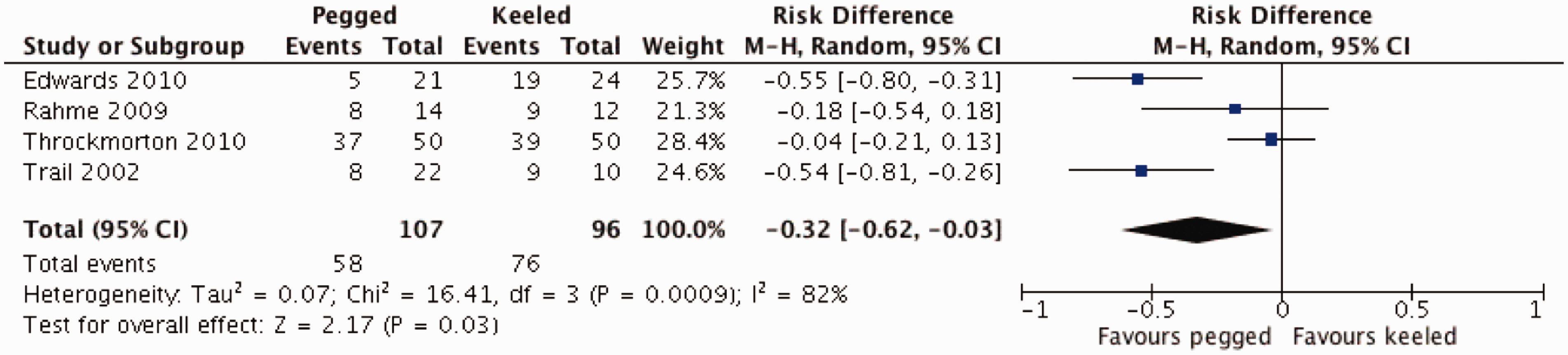

Discussion
The purpose of this systematic review was to compare the incidence of radiographic and clinical loosening of pegged and keeled cemented all-polythyelene TSA glenoid components. While there was evidence of an increased incidence of radiolucent lines after TSA with keeled designs, there was no statistically significant increased rate of radiographically at-risk glenoids or glenoid failure.
The findings of the current systematic review fit with the established literature that keeled glenoid components are more likely to develop radiolucencies than pegged components, but the development of radiolucent lines does not directly correlate with revision for glenoid failure. A systematic review by Papadonikalakis et al. 13 investigating the rate of radiolucency and glenoid loosening demonstrated that the mean annualized rate of asymptomatic radiolucent lines was 7.3% per year, 1.2% per year for symptomatic glenoid loosening, and 0.8% per year for revision for glenoid failure. The rate of asymptomatic radiolucent lines weakly correlated with the annualized rate of symptomatic glenoid loosening but was not correlated with revision for glenoid failure. Moreover, the authors found a 13.6% annualized rate of radiolucent line development with keeled components, compared with 8.3% per year for pegged components.
Other studies have investigated the presence of early radiolucent lines after TSA. As a part of a multicenter prospective study, Lazarus et al. 6 demonstrated that radiolucencies about the glenoid were common after TSA with both pegged and keeled components. Keeled components were more likely to demonstrate early radiolucencies and incomplete glenoid component seating. In a prospective randomized trial, Gartsman et al. 14 compared early glenoid radiolucencies between pegged and keeled components. The authors found higher rates of radiographic lucency immediately after surgery with keeled components, 39% versus 5%.
The strengths of the current study include the stringent inclusion criteria with regard to level of evidence and length of follow-up. Because the systematic review was limited to studies directly comparing pegged and keeled glenoids, 2 level one studies and 2 level three studies are included in the analysis. Case series without a comparison group were excluded. In addition, the mean follow-up for the included studies ranges from 2 to 5.1 years.
Weaknesses of the current systematic review include variable glenoid component designs, limited number of published studies in the literature, and lack of consistency with reported shoulder-specific outcome measures. Studies included used designs with minor variations and this review did not compare similar pegged glenoid component designs. Throckmorton et al. 10 and Rahme et al. 9 utilized a pegged component with 3 vertical in-line pegs. Edwards et al. 8 and Trail and Nuttall 11 used a pegged component with 1 central peg and 3 peripheral pegs. It is unknown whether peg design plays a significant role in implant stability.
Another limitation of our study includes evaluation of the clinical and functional outcomes between pegged and keeled glenoids. The 4 studies analyzed in this review used various functional assessments prohibiting the comparison between studies. Edwards et al. 8 did not conduct functionality assessments. Trail and Nuttall 11 reported significant postoperative improvement in range of motion measurements, Constant–Murley scores, and ASES scores, but did not delineate between pegged and keeled outcomes. Throckmorton et al. 10 assessed pain and range of motion measurements and found no clinically or statistically significant differences between pegged and keeled glenoids. Similarly, Rahme et al. 9 showed no significance between groups using the Constant–Murley mean score and the average subjective shoulder value (0%–100%) rating. Although we were unable to perform statistical analysis of the functionality assessments, of the studies that recorded them, all exhibited substantial improvement postoperatively. The 2 studies9,10 that directly compared clinical outcomes of pegged glenoids to keeled glenoids did not see a statistically significant difference between the designs. There is not enough data to conclude that both implants are equal in terms of functionality. Future studies evaluating the clinical outcomes associated with implants that display radiolucency versus implants without radioluceny is warranted to see if this radiographic evidence correlates to clinical evidence.
The paucity of comparative keeled and pegged outcomes data in the literature renders detecting differences between the 2 designs difficult. The rate of glenoid loosening may be different between the 2 groups but larger comparative studies will be needed investigate this further. The current systematic review did not compare shoulder specific outcome measures between the pegged and keeled glenoid designs because these validated outcome measures are incompletely reported in the included studies.
In conclusion, the current systematic review demonstrates that keeled glenoid components are more likely to develop radiolucent lines after TSA. There was, however, no difference in the rate of radiographically deemed “at risk” glenoids or revision for glenoid failure between pegged and keeled cemented all-polyethylene components. Further comparative studies are needed to assess the relative rates of glenoid loosening between pegged and keeled glenoid components as well as evaluate standardized clinical outcomes between the groups.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.