
Abstract
Objective
To assess the prevalence of early minor and major complications (MMC) of reverse shoulder arthroplasty (RSA) according to the underlying pathology responsible for the surgical indication.
Methods
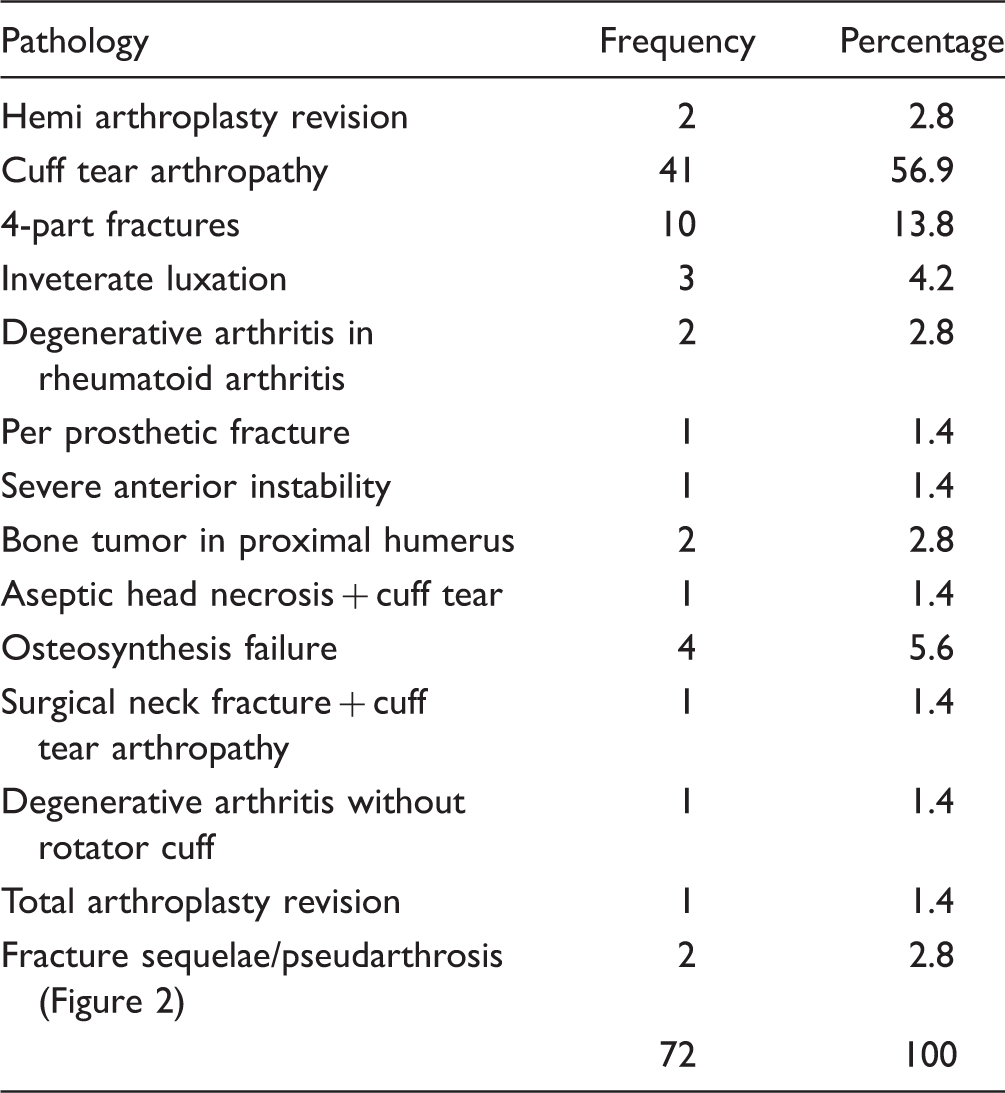
Between August 2009 and September 2015, 75 shoulders were submitted to RSA. Revision surgeries and patients with less than 2 months of follow-up were excluded. We analyzed 72 shoulders. The cuff tear arthropathy (CTA) represented 56.9% of cases and proximal humeral 4-part fractures (4PF) represented 13.8%. The index of MMC was analyzed according to the indication of basic pathology and the presence of rheumatoid arthritis, diabetes mellitus, and obesity.
Results
The evaluation was performed with a median of 11.5 months. Minor complications were found in 14 patients (19.4%) and major complications in 29 patients (40.3%). The statistical analysis was performed adding the contents of MMC—47.2%. In CTA patients, there were 43.9% (18/41) of MMC. In all other joint diseases, there were 51.6% (16/31) MMC. There was no statistical difference in the prevalence of MMC among the cases of CTA and the other diseases. There was a tendency, although not significant, of lower prevalence of MMC in cases of 4PF compared to CTA patients. Patients with rheumatoid arthritis and diabetes mellitus did not present with a higher prevalence of MMC, and obesity significantly increased the prevalence of MMC.
Conclusion
It was not possible to demonstrate a higher prevalence of MMC according to the pathology being treated. The presence of obesity significantly increased the prevalence of MMC. Rheumatoid arthritis and diabetes mellitus did not increase the prevalence of MMC.
Introduction
Reverse shoulder arthroplasty (RSA) was initially and mainly indicated in cases of rotator cuff arthropathy (cuff tear arthropathy, CTA) with pseudoparalysis of the upper limb.1,2
Over time, the experience of surgeons and the technology of the materials used, other pathologies of difficult treatment also have the indication of RSA, such as 4-part fractures (4PF) of the proximal third of the humerus in the elderly, tumors, failure, and sequelae of osteosynthesis or tendinous transfer, inveterate (locked) luxations, and revisions of other arthroplasties.1–4
However, along with promising results, there were high rates of minor and major complications (MMC). Minor complications are considered to be intra or postoperative events that do not compromise the final treatment outcome (eg, hematoma, suture dehiscence, phlebitis, heterotopic ossification, etc). Major complications are considered to be events that lead to compromising the final treatment outcome (eg, per prosthetic fractures, acromion fracture, infection, dislocation, neurological injury, aseptic loosening, etc).1,3,4–11
The main objective of this study is to verify the prevalence of RSA early MMC according to the underlying disease responsible for the surgical indication. The secondary objective will be to verify whether patients with comorbidities such as rheumatoid arthritis, diabetes mellitus, and obesity present a higher prevalence of complications.
Methods
During the period between August 2009 and September 2015, 75 shoulders (74 patients) attended at 2 different services of Orthopedic Residency were submitted to the RSA procedure. The patients of the study, at the time of their attendance, were informed and consented to the use of data from their medical records for scientific research. There was the release of the ethics committee from each of the institutions involved in the study. Both ethics committees of each institution involved in the study gave their approval.
For the purposes of analysis, primary surgeries and patients whose follow-up was over 2 months were included in order to avoid that early and compromising complications were excluded from the series.
The total number of shoulders operated for statistical analysis was 72.
The mean age of the patients enrolled in the study was 74.5 ± 7 years. There was a predominance of females (61 patients, 84.7%). There was a predominance of the right side between the operated cases (69.4%) and the dominant side was involved in 72.2% of the cases. At the time of admission, the height and weight of the patients were documented for the calculation of the body mass index (BMI).
Indications for RSA.

A, Preoperative X-ray anteroposterior view. B, Postoperative X-ray anteroposterior view.
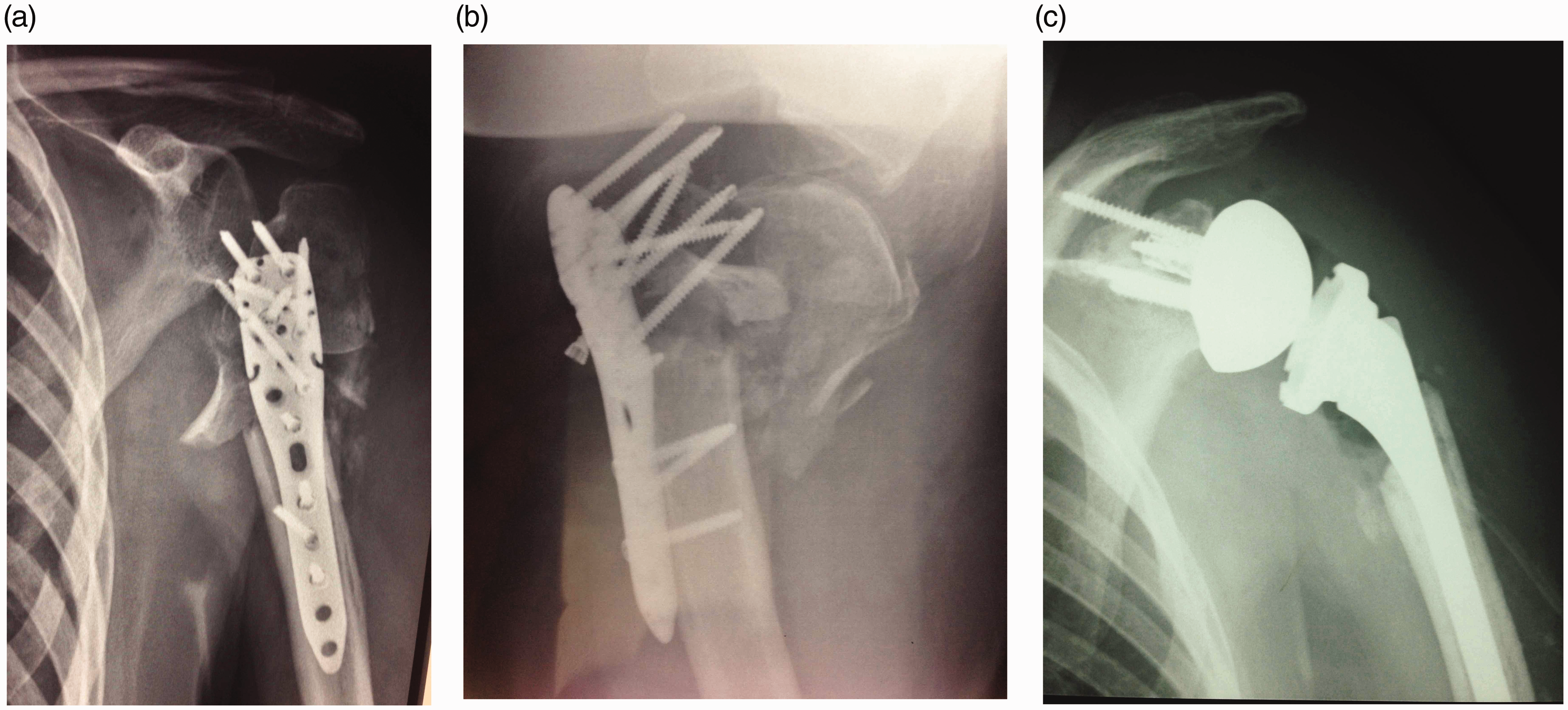
A, Preoperative X-ray anteroposterior view. B, Posterior view and postoperative X-ray anteroposterior view.
Two different surgeons, with specialization in shoulder surgery, operated the patients. The procedures were performed in the “beach chair” position and the surgical access used in 65 shoulders (90.2%) was the deltopectoral approach. In the other patients, the anterosuperior approach was used. In this study, 11 shoulders (15.2%) had previously undergone tendon cuff suture procedure.
The registered patent for the arthroplasties used in the procedures was Exactech brand products in 57 cases (79.1%), 9 Zimmer brand products, and 6 DePuy brand products. The humeral components were cemented in most cases, 52 shoulders (72.2%), and positioned with 10 degrees of retroversion in 32 shoulders (44.4%), being possible to perform the suture of the subscapular tendon, at the end of the procedure, in 39 cases (54.1%).
Glenoid reconstruction procedures with autologous graft removal of the humeral head (glenoplasty) were required in 6 shoulders (8.3%). The transfer of the tendons of the latissimus dorsi and teres major was performed for lateral rotators in 14 shoulders (19.4%).
The procedures had an average surgical time of 2 hours and 24 minutes, and there was a need for blood transfusion in 40.2% of the cases.
The variables used in the study were age, sex, disease responsible for surgical indication, the prevalence of MMC related to the procedure, and the presence of comorbidities such as rheumatoid arthritis, diabetes mellitus, and obesity (BMI > 30).
The data were analyzed by the IBM SPSS 22.0 statistical package (IBM Corporation 1989-2013). Where the data were normally distributed, they were expressed by the mean and standard deviation; when they were asymmetrical, the median and the interquartile range (IQ) were used. The chi-square test (Fisher’s exact test) and the prevalence ratio and their respective 95% confidence intervals (CI) were used to compare the proportions found. Statistical tests were bilateral, and P ≤ .05 was considered statistically significant.
Results
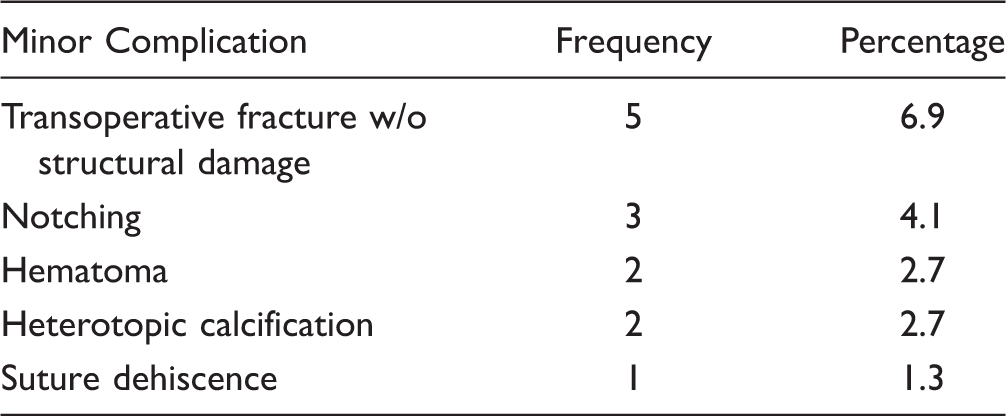
Minor Complications.
Major Complications.

A routine physical examination revealed the occurrence of transient and self-limited neuropraxia in the postoperative period of 13 patients (18.1%). All of them progressed satisfactorily in a maximum of 60 days.
The small sample size and consequently wide CI made statistical analysis possible only when the MMC found in the sample (47.2%) (95% CI: 35.7% to 58.8%) were simultaneously analyzed.
The initial analysis identified the prevalence of MMC among patients submitted to RSA by CTA to be 43.9% (18/41) and patients with other surgical indications to be 51.6% (16/31). No statistically significant difference was observed when the prevalence of MMC in these 2 groups was compared (P = .516).
The prevalence of MMC was compared between the 2 pathologies with the highest frequency of surgical indication (CTA with 41 cases and 4PF with 10 cases). There was a trend, however not significant, of a lower prevalence of MMC in cases of 4PF (P = .280).
There was no higher prevalence of MMC in patients with rheumatoid arthritis (P = .338) and diabetes mellitus (P = .898). However, when the data were analyzed in obese patients (BMI > 30), the prevalence of MMC increased significantly (P = .027).
Discussion
The RSA represents the main indication for CTA cases with pseudoparalysis of the upper limb as well as an option for the treatment of several severe shoulder pathologies. It is often used as a “last resource” in the choice of surgical treatment or as a salvage procedure after the failure of other previous treatments. The uncertainty of RSA survival makes its indication mainly for patients over 70 years of age. 7
The intentional anatomical alteration caused by RSA leads to the modification of shear forces and the activation of previously useless or almost obsolete muscle groups. The complexity of the cases and the anatomical alteration provoked in patients with advanced age and osteoporosis leads to an increase in the MMC index after performing this procedure. 7
The prevalence of MMC appears to be related to some extent with the RSA learning curve, so several authors analyzed it. Hasan et al.
12
verified, in their first 60 cases, that the initial 15 patients presented greater difficulty in gaining active anterior flexion, and there was also a higher rate of surgical reintervention 13.3% (8 patients) in which, 5 of these patients were among the first 15 cases. Groh and Groh,
13
analyzing their first 112 operated patients, verified 7% of complications and 5% of surgical reinterventions. Walch et al.
14
verified a decrease in the incidence of complications from 19% to 10.8% with an increase in the surgeon’s experience. There was also a decrease in the reinterventions rate from 7.5% to 5%. In our series, 8 patients required surgical reintervention (11.1%). In 4 patients reoperated by deep infection, 3 prostheses were removed and 1 patient obtained resolution of the infectious process. Two patients who evolved with dislocation of the shoulder reverse prosthesis were submitted to open reduction. The other 3 patients were operated on per prosthetic fracture at 10 months postoperatively (Figure 3), dissociation of the glenosphere from the metallic metaglena (Figure 4), and aseptic loosening of the prosthesis.
A, Preoperative X-ray anteroposterior view. B, 75 days postoperative X-ray anteroposterior view with allograft integration. A, Preoperative X-ray anteroposterior view. B, Postoperative X-ray anteroposterior view.

The literature is vast regarding the index of minor and major complications found in RSA, with indexes varying from 10.8% to 69%.4,14–18 Farshad and Gerber 3 reported that the complications found in patients after RSA were about 4 times greater than the incidence of complications found in patients undergoing anatomic arthroplasties.
The literature also suggests that the expansion of RSA indications for resolution of other shoulder pathologies has also led to a higher rate of complications.18,19 Florschütz et al. 19 found that the rate of complications in anatomical and reverse arthroplasties of the shoulder was greater when there was previous surgery in the shoulder in question. This complication rate was particularly higher in patients with RSA.
Saltzman et al. 18 in their series found 25% of complications in primary RSA and 69% of complications in revision surgeries. In cases where RSA was used to treat sequelae of failure osteosynthesis of the proximal third of the humerus, Raiss et al. 5 found an unacceptable postoperative dislocation rate.
The indication of RSA for the treatment of 4PF in the elderly has presented promising results. 8 Reitman and Kerzhner 20 verified a 7.7% incidence of postoperative hematoma after RSA by fracture of the proximal third of the humerus. We verified 20% MMC in our RSA procedures by 4PF, without having found any postoperative hematoma. Our RSA patients with fractures of the proximal humerus had an average age of 81.3 years. Although the prevalence of MMC in our 4PF cases was less than in the cases of CTA, this difference was not considered significant.
The RSA indication for patients with osteoarthritis associated with rheumatoid arthritis increased from 0.4% in 2003 to 6.3% in 2007. 7 Pappou et al. 21 found a high rate of complications in these patients, and 9.52% were patients who developed infection and the need for reintervention was of the order of 14% in their series. Ekelund and Nyberg 22 found an RSA infection rate in patients with rheumatoid arthritis similar to that of the general population. Young et al. 23 verified 22.2% of transoperative and postoperative fractures in patients with rheumatoid arthritis. In our study, the prevalence of RSA MMC in patients with rheumatoid arthritis was similar to patients without this comorbidity.
Diabetes mellitus is known to increase the risk of postoperative complications, particularly the rate of infection. 24 Morris et al. 10 and Richards et al. 11 in their search for risk factors for infection following shoulder arthroplasties failed to demonstrate diabetes mellitus as an increased risk factor. Yian et al. 25 also did not identify diabetes mellitus as a risk factor for postoperative neuropathy in shoulder arthroplasties. We did not find in the literature articles that looked for the index of complications in general after RSA in diabetic patients. Our study did not find higher prevalence of MMC in this group of patients.
The literature is controversial regarding the increase in MMC index in obese patients submitted to shoulder arthroplasties. Linberg et al. 26 found a higher rate of complications (35%) in anatomical arthroplasties of the shoulder in patients with BMI > 30. The same was verified by Beck et al. 27 Pappou et al. 21 reported longer surgical time, greater blood loss, and higher hospital costs in morbidly obese patients (BMI > 40) submitted to RSA, although the MMC rate was similar to that of nonobese patients. In our study, we found statistically significant that patients with BMI > 30 had an increase in MMC prevalence after RSA.
We considered a possible bias in our study and the procedures were performed by 2 surgeons in 2 different services. Although the criteria for indication and selection of the patients were similar, the anesthetic and postoperative clinical staff was different. The fact of the literature does not point a “universal” hemoglobin threshold that could serve as a transfusion trigger, 28 the decision that involves the subjective evaluation of the anesthesiologist, the RSA patient profile that is, usually an elderly person, with less capacity for cardiac compensation, and the considerable postoperative dead space around RSA may be some possible reasons to the high rate of blood transfusion found in our series.
Conclusion
It was not possible to demonstrate a higher prevalence of early MMC according to the different diseases under treatment. The indication of RSA for the treatment of 4PF in the elderly showed a tendency to present a lower prevalence of MMC.
It was not possible to demonstrate a higher prevalence of MMC in the presence of rheumatoid arthritis or diabetes mellitus after RSA procedures.
Obesity with a BMI > 30 was responsible for the increase in the prevalence of MMC after RSA procedures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.