
Abstract
Objective:
The aim of this study was to investigate whether there are glenohumeral morphological differences between normal population, glenohumeral instability, and rotator cuff pathology.
Method:
In this study, shoulder magnetic resonance (MR) images of 150 patients were evaluated. Patients included in the study were studied in three groups of 50 individuals: patients with anterior shoulder instability in group 1, patients with rotator cuff tear in group 2, and control subjects without shoulder pathology in group 3.
Results:
There were statistically significant differences between groups in evaluations for glenoid version, glenoid coronal height, glenoid coronal diameter, humeral axial and coronal diameters, and coracohumeral interval distances. Significant differences were observed between groups 2 and 3 in glenoid axial diameter, glenoid coronal height, glenoid depth, humeral coronal diameter, and coracohumeral distances.
Conclusion:
The results obtained in this study suggest that glenoid version, glenoid coronal height and diameter, humeral diameter, and coracohumeral interval parameters in glenohumeral morphology-related parameters in patients with anterior instability are different from those of normal population and patients with rotator cuff pathology. In cases where there is a clinically difficult diagnosis, these radiological measurements will be helpful to clinicians in diagnosis and treatment planning, especially in cases of treatment-resistant cases.
Introduction
The shoulder joint is a very unstable joint because it is the most mobile joint in the body, and at the same time, it has unequal proportions of the glenoid surface areas compared with the humeral head in part. 1,2 The exact knowledge of the morphology of the surfaces forming the shoulder joint and the relationship between them is important in the diagnosis and treatment planning of conditions such as glenohumeral instability, labral and cuff pathologies.
Shoulder instability and rotator cuff injuries represent the most common causes of shoulder pain and dysfunction and often correlate with secondary glenohumeral osteoarthritis. 2 For this purpose, factors such as the glenoid version and inclinations have been investigated in a limited number of studies and some have been associated with glenohumeral instability. 3 –5 In these studies, glenoid size and version were calculated using computerized tomography, and gross measurements were made on the scapula in anatomical studies. 4,5
An imbalance of the head-glenoid size and the anterior glenoid tilt are the anatomical factors that favor instability. The etiology of anterior glenohumeral instability is multifactorial; however, there is also an anatomical predisposition for instability. 5 Current arthroscopic procedures showed similar success to open procedures, and the recurrence rate of instability after arthroscopic treatment ranged between 0 and 20%. 6,7 However, there is no study reporting the relationship between the size of the humerus, the version of the joint, and the joint surfaces with the glenoid.
Dynamic factors of the rotator cuff muscles and the static factors of the glenohumeral ligaments, the labrum, and the joint capsule play a role in glenohumeral joint stability. 8,9 Similarly, there are limited number of studies that focused on the possible association between the alignment of the humeral head in the glenoid fossa and the rotator cuff pathology.
The purpose of the present study was to analyze glenohumeral morphological parameters that may predispose shoulder pathologies such as anterior shoulder instability and rotator cuff injury. The hypothesis of the study is that the morphology of glenohumeral osseous and cartilaginous structures are significantly different from normal population in shoulder pathologies.
Materials and methods
After approval from the institutional review board, the examination and magnetic resonance (MR) records of 150 patients who were referred to our clinic with shoulder and neck circumference complaints were included retrospectively.
The width, length, version, and depth of the glenoid and labral glenoid in addition to humerus diameter and coracohumeral distance (CHD) were measured from sagittal, coronal, and axial MR sections, and correlations between these values for each group were investigated.
The MR scans, which had been randomly selected as 50 records being in each group, were evaluated in three separate groups. MR images of patients who underwent arthroscopic anterior capsulolabral plication for instability in group 1 (AI group) were evaluated. MR images of the patients who were arthroscopically treated because of rotator cuff tear in group 2 (RCT group) were evaluated. In the third group (N group), patients who had no shoulder complaints and who had completely normal findings on the MR images were evaluated.
Statistical analysis was performed using SPSS software (version 16.0; SPSS, Chicago, Illinois, USA). Data were analyzed using descriptive statistics (mean, standard deviation, median, frequency, percentage, minimum, and maximum). The Kruskal–Wallis test was used for the comparison of three or more groups without normal distribution, and the Mann–Whitney U test was performed to determine the difference between the groups.
Results
MR scans of 150 patients were included in the study. The patients of the three groups differed demographically (Table 1).
The distribution of descriptive characteristics of three groups.

SD: standard deviation.
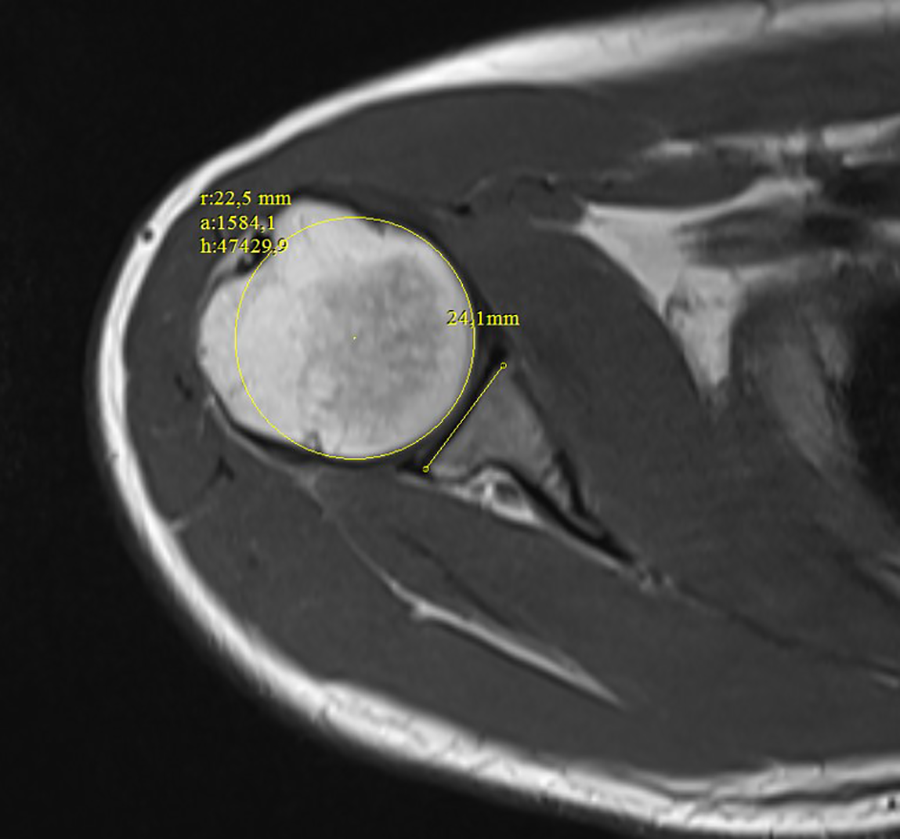
There were statistically significant differences between all three groups in terms of glenoid version (Figure 1), glenoid axial width and depth (Figure 2), glenoid coronal height (Figure 3), coronal diameters of glenoid and humerus (Figure 4), axial diameter of humerus (Figure 5), subacromial distance (SAD; Figure 6), and CHD (Table 2).
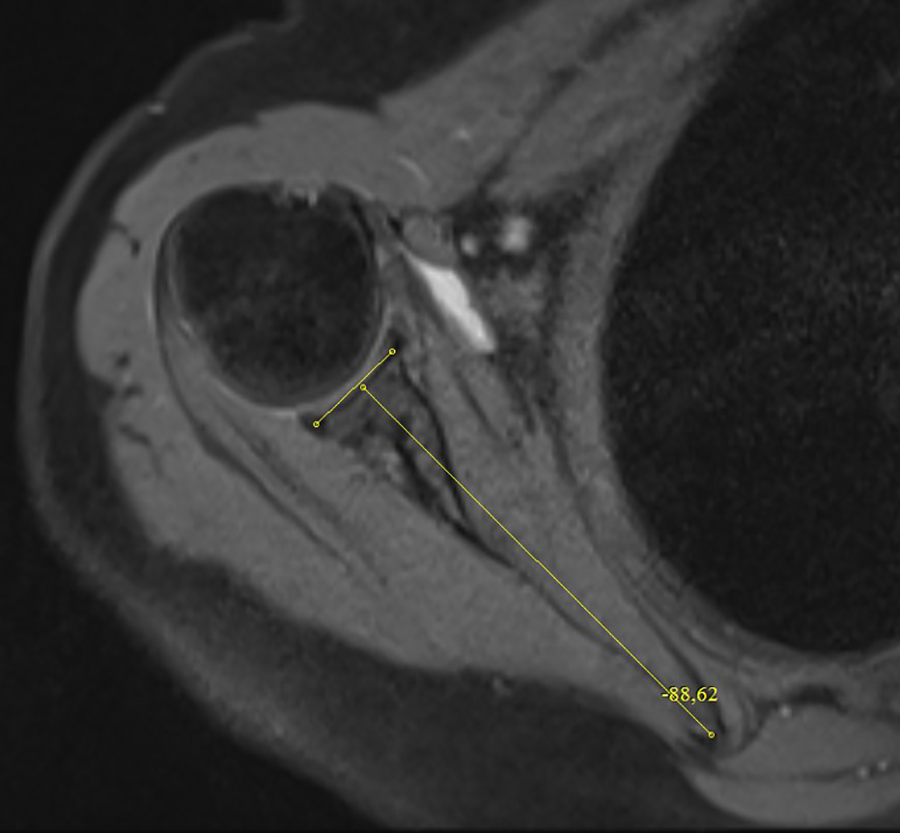
Measurement of glenoid version.

Measurement of glenoid axial width and depth.

Measurement of glenoid coronal height.

Measurement of coronal diameters of glenoid and humerus.
Measurement of axial diameter of humerus.
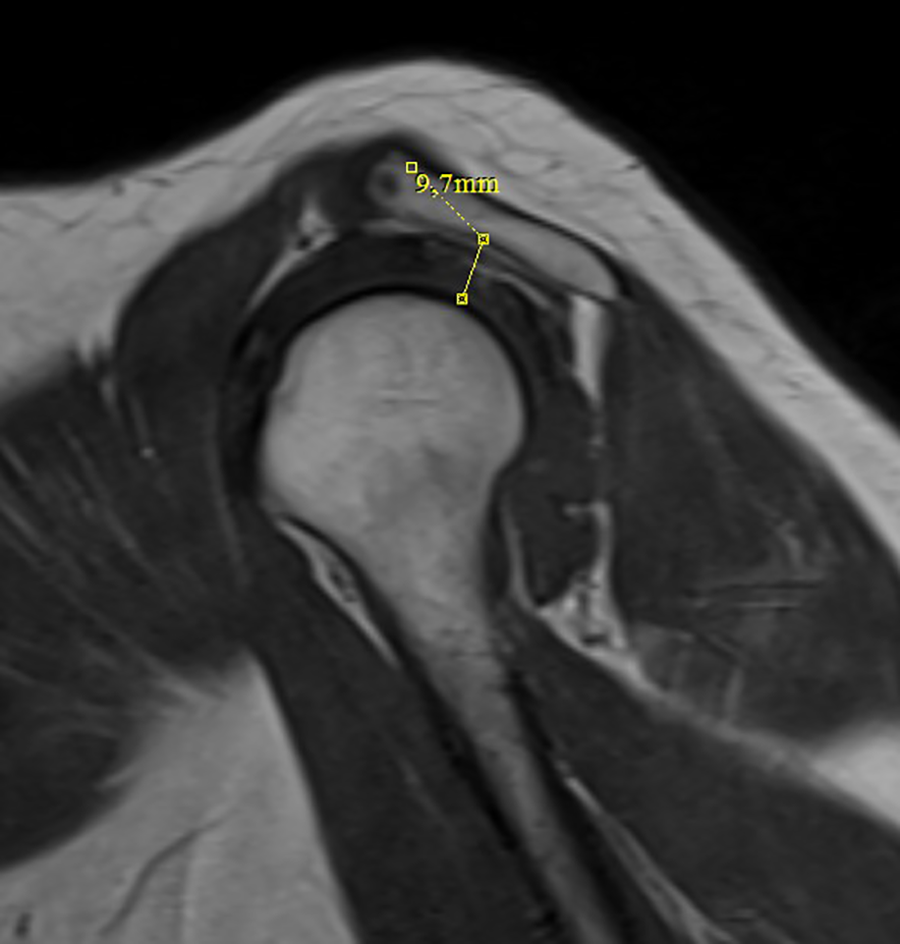
Measurement of subacromial distance.
The comparison of glenohumeral morphological parameters of three groups.
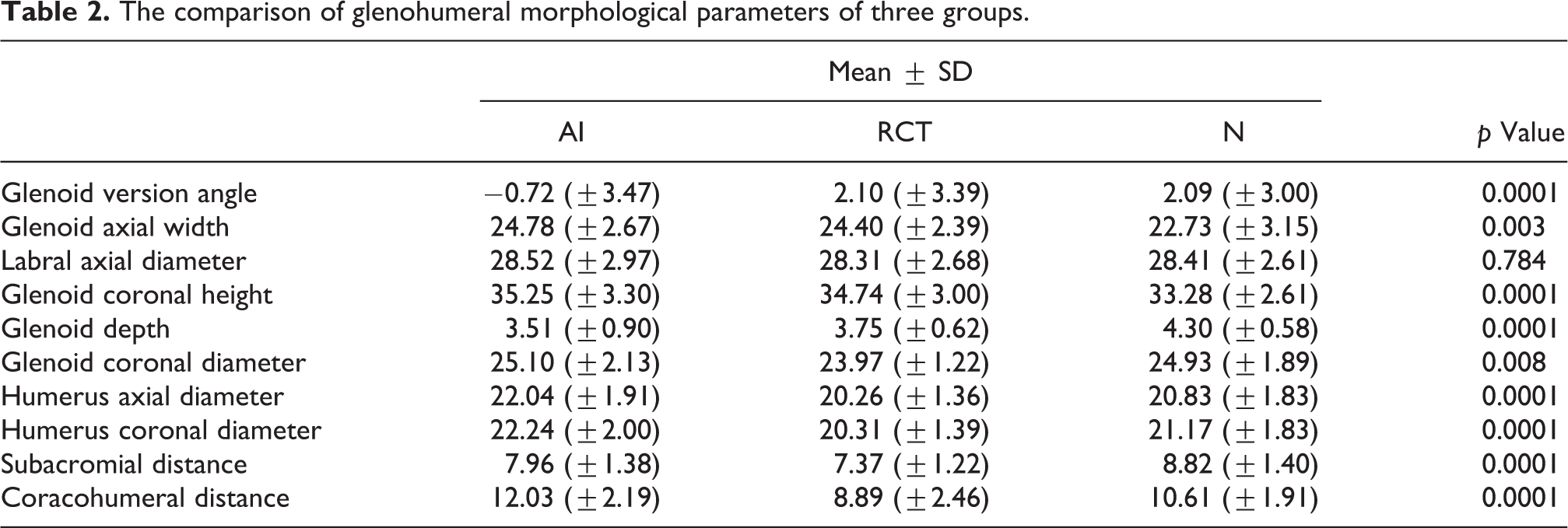
Significant differences were observed between the AI and RCT groups in terms of glenoid version, glenoid coronal height, glenoid coronal diameter, humeral axial and coronal diameters, and CHD (Table 3). However, there was no difference in glenoid axial width and SAD.
Statistical paired comparison of groups.

Statistical significance was found between the AI and N groups in terms of glenoid version, glenoid axial width, glenoid coronal height, glenoid depth, humeral axial and coronal diameters, SAD, and CHD (Table 3). However, glenoid coronal diameter was assessed to be similar.
The differences were statistically significant in glenoid axial width, glenoid coronal height, glenoid depth, glenoid coronal diameter, humeral coronal diameter, SAD, and CHD between the RCT and N groups (Table 3). No significant difference was observed in glenoid version and humeral axial diameter. On the other hand, labral diameters of all three groups were almost similar (Tables 2 and 3).
Discussion
Glenohumeral structure is important, because angular and morphological varieties of it can trigger pathological conditions similar to other joints. In the current study, the glenohumeral morphology has been investigated to find out whether any bony structural variety exists in anterior instability and cuff pathology that can predispose their present soft tissue pathologies.
Finding out the irregularities in the osseous architecture of the glenohumeral joint is critical for the treatment of glenohumeral instability and rotator cuff pathology. 10 –12 To our knowledge, no published research has investigated the structural properties of glenohumeral joint in comparison between normal population, rotator cuff tears, and anterior shoulder instabilities. In the current study, in addition to glenoid version, other parameters that might be potential risk factors for the defined shoulder pathologies had been assessed. These could be meaningful for evaluation and management of recurrent anterior instability and rotator cuff tear.
The finding that increasing CHD being a risk factor for anterior instability is interesting. With an increase of CHD, the coracohumeral ligament, coracobrachialis, and biceps short-head tendon are located further away from the glenohumeral joint which may affect their ability to stabilize the joint throughout a range of motion. In addition of this, coracoid along with its soft tissue attachments may behave as an anterior buttress to prevent humeral head displacement.
On the other hand, CHD is significantly decreased in rotator cuff tear patients. Similarly, narrower CHD had been seen in patients with degenerative subscapularis tendon tears. 13
Distinct acromial morphological characteristics were present in patients with degenerative rotator cuff tears. Shoulders with degenerative tears show a narrower subacromial space. 14 Additionally, in the current study, SAD was significantly decreased in both anterior instability and rotator cuff tear patients compared to normal population.
In the current study, findings are similar to that in anterior instability, the glenoid is retroverted, apparently wider transversely, longer longitudinally, and shallower in depth; head of the humerus is larger both transversely and longitudinally; CHD is increased, but SAD is narrowed. In rotator cuff tears, glenoid is anteverted, less obviously wider, higher, and shallower; glenoid coronal diameter is small; head of the humerus is small both transversely and longitudinally; CHD and SAD are both shortened.
Most of the studies about anterior shoulder instability and rotator cuff generally focus on the soft tissue problems; however, there are many different components including bony structures that could take part in instability or rupture in and around the joint. Griffith et al.’s study compared the accuracy of computed tomography (CT) in determining the presence and severity of glenoid bone loss in patients with shoulder dislocation. 15 They found that CT was more sensitive and specific. Although CT scan is highly sensitive for assessing osseous structures, magnetic resonance imaging (MRI) is the widely used method for evaluating articular soft tissue lesions preoperatively. In the current study, all measurements were done by MRI. With the help of MRI, it is possible to make bone morphometric measurements while seeking for soft tissue problems.
The relationship between glenoid version and anterior glenohumeral instability is well established and documented. Hohmann and Tetsworth found out in their study that both retroversion and inclination of glenoid are much increased in anterior instability patients compared with the control group. 16 Similarly, we found retroversion (−0.72 ± 3.47) only in AI patients. However, RCT (2.10 ± 3.39) and normal (2.09 ± 3.00) cases had anteversion of glenoid cavity, and there was no difference between them.
By the angular measurements of shoulder bone and joint, it is possible to determine potential population who are under risk. It was shown that excessive retroversion and flatness of the glenoid can predispose to posterior instability of shoulder. 17 Glenoid osteotomy is a successful operation for this condition, but the relatively high rate of degenerative has to be taken into account. Whether corrective osteotomies may be beneficial in treatment of recurrent anterior shoulder instability remains speculative at this stage and requires further research.
The present study has some limitations. One is that MR images were used for the determination of osseous morphology. The reason, why we preferred MRI, was that bony structures, bursa, and rotator cuff tendons of the shoulder all together could have been evaluated using MRI with no need for other imaging modalities. The other limitation is that there were no elbow images of patients. So this could have limited more accurate measurements in relation with elbow, humeral head, and glenoid version.
Appropriate preoperative imaging is essential for the detection and quantification of osseous abnormalities in shoulder pathologies. By doing so, it is possible to analyze preoperatively the glenohumeral structural morphology of the patient using MRI. In that way, this information may help to predict which cases have potential risk for instability and cuff tear because of their bony structure besides their soft tissue pathologies.
Conclusion
The results obtained in this study suggest that glenoid version, glenoid coronal height and diameter, humeral diameter, and coracohumeral interval parameters in glenohumeral morphology-related parameters in patients with anterior instability are different from those of normal population and patients with rotator cuff pathology. In cases where there is a clinically difficult diagnosis, these radiological measurements will be helpful to clinicians in diagnosis and treatment planning, especially in cases of treatment-resistant cases.
Footnotes
Authors’ note
No benefits in any form have been received or will be received from anybody or a commercial party related directly or indirectly to the subject of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.