
Abstract
Background
Dislocation is a challenging complication after reverse shoulder arthroplasty (RSA). We sought to evaluate the outcome of nonoperative and operative management of the dislocation after primary and revision RSA.
Methods
Between 2006 and 2013, dislocation occurred in 12/1081 primary RSAs (1.1%) and 15/342 revision RSAs (4.4%). Seventeen (69%) shoulders dislocated within 3 months of surgery. Ten (68%) patients underwent revision RSA for prosthetic instability. Mean age was 69 years, and mean follow-up after index RSA was 4 years.
Results
Closed reduction and bracing achieved a stable shoulder in 60% (3/5 patients) after primary and 20% (1/5 patients) after revision RSA dislocation. Operative management achieved a stable shoulder in 88% (7/8 patients) of primary and 64% (7/11 patients) of revision RSAs (P = .40). Overall, 9 shoulders (33%) had persistent instability at the final follow-up: 2/12 (17%) primaries versus 7/15 (47%) revisions (P = .08). Preoperative prosthetic instability was the main risk factor for chronic instability in the revision cohort (P = .02). Worse functional outcomes were associated with the dislocation of a revision RSA (P = .02).
Conclusion
After primary RSA dislocations, closed reduction is successful in half, while revision surgery is successful in 85% of cases. Conversely, closed reduction of a dislocated revision RSA is rarely successful, while revision surgery is successful 65% of the time. Every attempt should be made to achieve stability at the time of primary and revision RSA, since reduction or revision surgery does not guarantee the restoring stability.
Keywords
Introduction
While traditionally designed as a salvage option, the use of the reverse prosthesis is increasing in the primary setting in the United States, with more than one-third of all primary shoulder arthroplasties utilizing a reverse shoulder arthroplasty (RSA) in 2011. 1 While early studies reported high complication rates with the use of reverse arthroplasty, 2 improvements in surgical technique and implant design have occurred3–8; recent studies report excellent clinical outcomes and survivorship free of revision of primary RSAs.2,9,10 Therefore, the indications for the reverse prosthesis continue to expand.11–18
One major biomechanical advantage of an RSA is the semiconstrained nature of the prosthesis and its ability to compensate for deficient dynamic and static shoulder stabilizers.3,5 However, while uncommon, postoperative prosthetic dislocation after RSA can occur, with an incidence ranging from 2.4% to 31%.2,4,5,13,19–23 Some studies suggest certain risk factors for the dislocation of a RSA, including subscapularis insufficiency, prior shoulder operations, RSA used in the revision setting, and component malposition.2,4,19–22
There is a paucity of literature on the treatment and outcomes of postoperative dislocation after primary and revision RSA dislocations. The goal of the current study was to characterize the incidence and nonoperative and operative treatment outcomes of primary and revision RSA dislocations. Further, we sought to identify risk factors for the success and failure of both nonoperative and operative management.
Patients and Methods
The study was initiated after the approval from our institutional board review (IRB#: 12-007498). Utilizing prospectively collected data from a single academic institutional registry, we retrospectively identified patients who sustained a dislocation of a primary or revision RSA performed at our institution between 1/1/2007 and 12/31/2013. Postoperative prosthetic dislocations were confirmed by the review of the medical records and imaging studies. All patients underwent primary or revision RSA by a fellowship-trained shoulder surgeon. Routine follow-up was performed at 3 months, 1 year, 2 years, 5 years, and every 5 years thereafter; patients not able to return for follow-up were requested to send radiographs and fill out patient questionnaires. We excluded patients for whom we were unable to obtain clinical or radiographic follow-up. Patients were followed until death, rerevision or reoperation, or until final clinical follow-up. The mean follow-up after the index RSA was 4 years (range, 2–9 years). We retrospectively collected patient demographics, surgical and implant details, complications including treatment modalities of each complications, and clinical outcomes.
Patients
The study group included 27 shoulders with a postoperative dislocation of a reverse prosthesis. This compromised 1.1% (12/1081) of all primary RSAs and 4.4% (15/342) of all revision RSAs performed at a single tertiary referral academic institution during the study period. For patients with a postoperative dislocation, mean patient age at RSA was 69 years (range, 48–89 years) and 12 patients (44%) were female. Mean body mass index was 28 kg/m2 (range 22–34 kg/m2). Mean follow-up was 4 years from index RSA (range, 2–9 years). Mean time for dislocation was 10 months (range, 1 month–4 years), with 17 (69%) patients dislocating within 3 months of the index RSA.
Of the 12 dislocated primary RSAs, the underlying diagnosis was cuff tear arthropathy in 10 shoulders (83%) and proximal humerus malunion in 2 shoulders (17%). None of the patients who underwent primary RSA had a history or examination findings consistent with prior glenohumeral instability. Previous prostheses in the revision RSA cohort included hemiarthroplasties (8 patients, 53%), total shoulder arthroplasties (3 patients, 20%), and RSAs (4 patients, 27%). Indications for revision RSA in the revision cohort included prosthetic instability (7 shoulders, 47%), hemiarthroplasty with tuberosity nonunion or resorption (2 shoulders, 13%), glenoid loosening (3 shoulders, 20%), second-stage reimplantation for deep periprosthetic joint infection (1 shoulder, 7%), and glenoid polyethylene wear of a Total Shoulder Arthroplasty (TSA) (1 shoulder, 7%). Ten shoulders (67%) in the revision RSA cohort had prior prosthetic dislocations or instability, and 7 shoulders (47%) required glenoid bone grafting of defects. Overall in the primary and revision cohort, 17 patients (69%) had either partial or complete subscapularis tendon repair at the closure.
Postoperative rehabilitation at our institution is standardized for the primary RSA but varies for the revision RSA. Shoulder immobilizers were used for 3 to 6 weeks. The range of motion exercises were advanced from passive, to active-assisted, then active, at 4- to 6-week intervals. Strengthening was introduced last.
Clinical Assessment
Clinical outcomes in the form of pain level and active shoulder range of motion were collected for all patients who were pre- and postoperatively and retrospectively reviewed. Both pre- and postoperative pain and active shoulder motion details were collected for all the patients. Pain levels were graded as none, mild, moderate, or severe.
Statistical Methods
Descriptive analyses and univariate statistics were analyzed for the current study. Preoperative and postoperative differences and risk factors for poor clinical outcomes and chronic instability were compared using the t tests for continuous variables and Fisher’s exact tests for categorical variables.
Results
Treatment of RSA Dislocations and Outcomes
Nonoperative management
Closed reduction and nonoperative management were attempted in 10 patients (37%), including 5 primary RSA dislocations and 5 revision dislocations. In the primary RSA dislocations, success of nonoperative management, defined as no recurrent instability or chronic dislocation, was achieved in 60% (3 of 5 patients). One patient who failed nonoperative management after sustaining a repeat dislocation ultimately required a revision surgery to increase the polyethylene thickness; the patient had a stable shoulder at the final follow-up with no subsequent dislocations. The other patient had a chronically dislocated RSA but was not deemed a candidate for further surgery secondary to advanced age and medical comorbidities. In the 5 dislocations of a revision RSA, nonoperative management was successful in 20% (1 of 5 patients). Three of these patients had chronically dislocated RSAs that were either not extremely painful (2 patients) or not deemed surgical candidates (one patient). One patient sustained another prosthetic dislocation and was revised to a lateralized component with an increased polyethylene thickness; the patient had a stable shoulder at the final follow-up (Figure 1).
Flowchart of patients as treated in this retrospective cohort of dislocations after primary or revision reverse shoulder arthroplasty (RSA) from 2006 to 2013. Success is defined by achieving a clinically and radiographically stable shoulder at the final follow-up.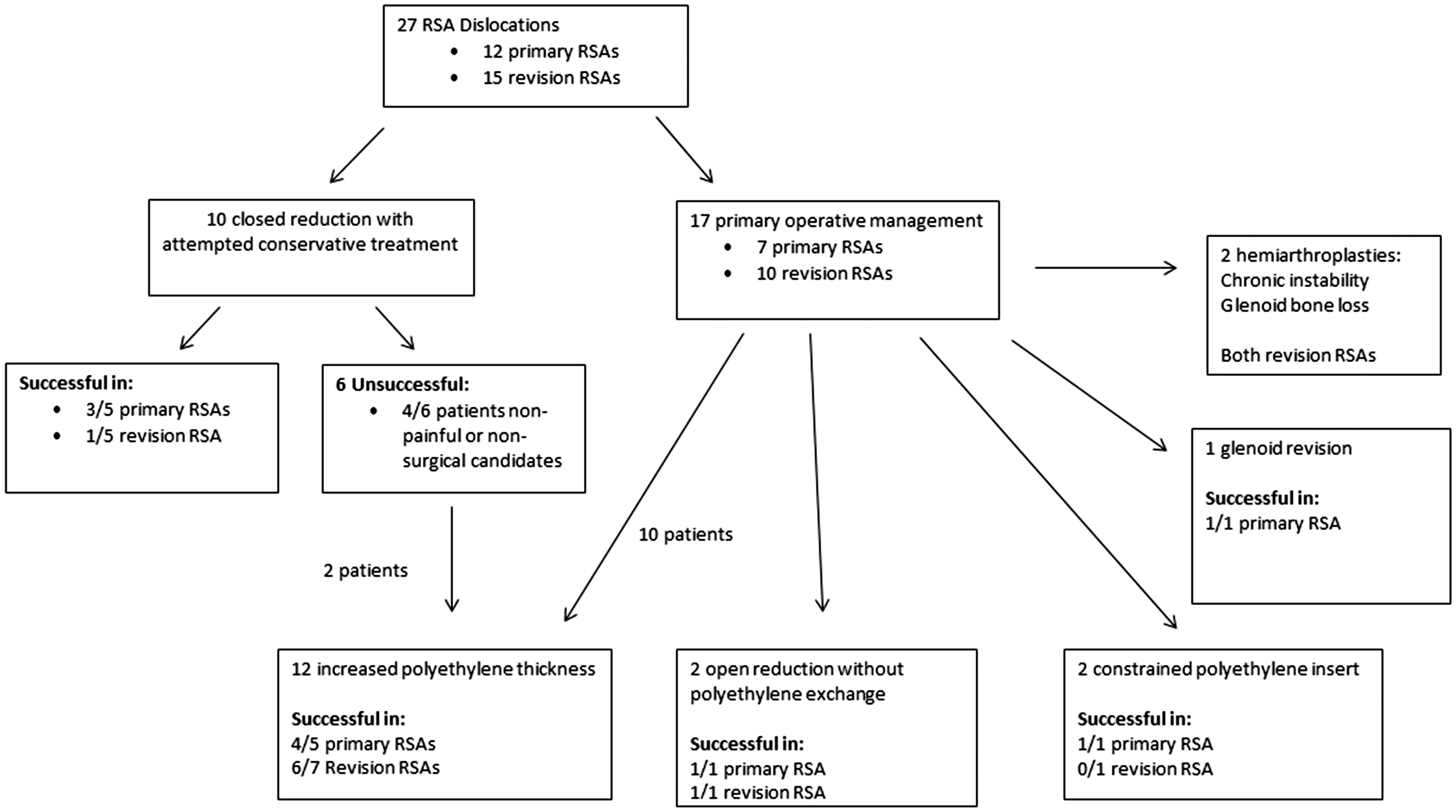
Surgical management
Ultimately, 19 patients underwent surgical management of a primary or revision RSA dislocation. Of the 8 patients with dislocated primary RSAs treated surgically, 4 of 5 patients achieved a stable shoulder with open reduction and upsizing of the polyethylene component (Figure 2). One patient required glenoid revision for malpositioning to achieve a stable shoulder. One patient underwent open reduction without component exchange and obtained a stable shoulder at the final follow-up. Finally, one patient underwent placement of a constrained polyethylene liner and achieved a stable shoulder at the final follow-up. Of the 11 patients with dislocated revision RSAs treated surgically, 6 of 7 patients achieved a stable shoulder with open reduction and upsizing of the polyethylene component. One patient underwent open reduction without component exchange to obtain a stable shoulder. One patient was revised to a more constrained insert but continued to sustain dislocations postoperatively. Finally, 2 patients with the dislocated revision RSAs underwent salvage conversion to hemiarthroplasties due to major glenoid bone loss and recurrent instability, with resultant chronic instability at the final follow-up. Overall, operative management was successful in 73% of patients (7 of 8 primary RSAs vs 7 of 11 revision RSAs, P = .4) (Figure 1).
An 80-year-old female who underwent primary RSA for rotator cuff arthropathy that sustained an anterior dislocation (a) of the prosthesis 1 year after surgery. The patient was initially managed with closed reduction but had continued instability events. She was then treated with upsizing of the polyethylene component during a modular exchange. (b) An intraoperative photograph of the polyethylene insert showing damage to the anterior lip from chronic instability events. Her shoulder remains stable at 2 years after revision (c).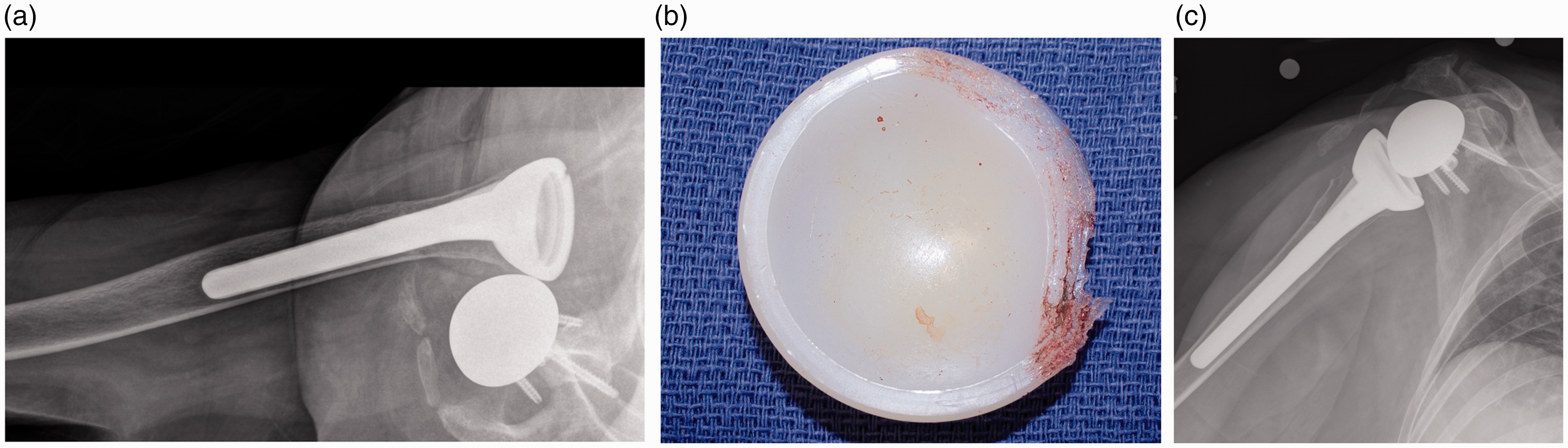
Risk Factors for Chronic Instability
Management, operatively or nonoperatively, was more successful in obtaining a stable shoulder at the final follow-up in patients with dislocations after primary compared to revision RSA (P = .08). Two patients (17%) after primary RSA and 7 patients (47%) after revision RSA had chronically unstable shoulders at the final clinical follow-up. With the numbers available, incompetency of the subscapularis at the closure was not a significant risk factor for persistent or chronic instability in our study for either primary or revision RSA dislocations. In the revision RSA cohort, 6 of 10 patients (60%) with preoperative instability had chronically unstable shoulders at the follow-up, compared to 1 of 5 patients without preoperative instability (P = .02). All 3 patients revised for glenoid loosening ultimately had chronic instability, compared to 4 of 12 patients (33%) revised for other indications (P = .006). Revision of a prior failed hemiarthroplasty was also a risk factor for persistent or chronic instability, with 4 of 5 (80%) patients with final prosthetic instability compared to 3 of 10 patients for other indications (P = .1).
Clinical Outcomes
In patients who had a stable shoulder prostheses at the final follow-up, 15 of 18 (83%) had pain scores of “none” or “mild.”Mean American Shoulder and Elbow Surgeon's shoulder score for these patients was 84 (range, 64–94). Mean elevation improved from 35° preoperatively to 104° postoperatively (P < .001) and mean external rotation improved from 12° preoperatively to 30° postoperatively (P < .001). Risk factors for worse range of motion after the treatment for an RSA dislocation included dislocation of a revision RSA (P = .02), preoperative instability (P = .006), and female gender (P = .02). Nine patients with unstable shoulders at the final follow-up had chronically dislocated shoulders or were revised to hemiarthroplasties with chronic prosthetic instability. Six of these nine patients (67%) had “moderate” pain levels with daily activities at the final follow-up.
Discussion
RSA is becoming increasingly utilized in primary and revision shoulder arthroplasty. 1 The design advantages of the reverse prosthesis, namely the semiconstrained nature and the combination of various degrees of lengthening and lateralization, allow it to be utilized in patients with substantial bony or soft tissue compromise. 3 However, despite the increased constraint and stability of the implant, dislocations of RSAs do occur and remain a challenging complication. The incidence of dislocation after RSA has been reported to range from 2.4% to 31%.2,13,19,20,22 The majority of studies published to date on this topic include small case series of patients.2,13,19,21–23 There is conflicting data on the optimal treatment and outcomes of prosthetic dislocations after primary or revision RSA. The goal of the current study was to report the incidence, as well as functional and stability outcomes, after nonoperative and operative treatment of prosthetic dislocations complicating primary and revision RSA and to identify risk factors for the success or failure of the treatment.
The results of our study seem to indicate that closed reduction is successful in over half of the dislocations complicating a primary RSA but is seldom successful in the dislocated revision RSAs. Surgical management of a dislocated primary RSA may be successful in 80% of the shoulders, whereas the success rate is only 50% for the dislocated revision RSA. Other risk factors for failure included prior hemiarthroplasty, prior periprosthetic instability, and prior glenoid component loosening.
Several recent studies on the incidence of prosthetic dislocation after primary or revision RSA have reported a 2%–3% dislocation rate19,22 similar to our study. The incidence of RSA dislocations was significantly higher after revision RSA (P = .004); while other studies report on prosthetic instability after both primary and revision RSA,19,22 few studies differentiate dislocations after primary or revision RSAs. Consistent with other reports, the majority of RSA dislocations occur within 3 months of index RSA but can occur years later.19,22,23
Recent reports of initial nonoperative treatment of the prosthetic dislocations have found similar results as the current study in success rates of closed reduction and bracing. Chalmers et al. 19 have reported a 44% (4 of 9 patients) success rate of nonoperative management of dislocations after primary RSA; Teusink et al. 23 have reported a 62% success rate. However, neither of these studies delineates the success rate differences between dislocations after primary versus revision RSA. In the current study, 60% (3 of 5) of patients with dislocations after primary RSA were successfully managed nonoperatively. Based on the current evidence, an initial trial of nonoperative management with closed reduction and bracing is reasonable to attempt after primary RSA. One of the five patients eventually underwent revision surgery for upsizing of his polyethylene insert and had a stable shoulder at follow-up (Figure 2). The remaining patients initially treated nonoperatively did develop chronic shoulder instability but were too frail to undergo further revision surgery. On the contrary, given the 20% success rate at treating dislocations of revision RSA nonoperatively, we are not inclined to consider nonoperative treatment of the dislocated revision RSA.
The main indications for operative management after dislocations of primary RSAs included an irreducible dislocation, failure to maintain reduction with nonoperative management, and individual surgeon and patient factors. Overall, operative management of dislocated primary RSAs, either as initial treatment or after failed nonoperative management, was highly successful with over 80% of patients obtaining a stable shoulder at the final follow-up (Figure 2). Chalmers et al. 19 have found a similar rate of success of treatment in a combined nonoperative and operative management approach at 82%. To our knowledge, there are little data specifically reporting on the nonoperative and operative management options of dislocations after revision RSA. Although operative management of revision RSA dislocations is not as successful as primary RSA dislocations, it was still able to achieve a stable shoulder in over half of the patients in this series. We recommend surgical management in all patients who are surgical candidates with prosthetic dislocations after revision RSA.
We acknowledge several limitations of the current study, most notably the inherent disadvantages of a retrospective study. While all patients experienced a dislocation after primary or revision RSA at a single institution, the initial treatment was not uniform and may have been affected by patient factors and surgeon bias. There are a relatively small number of patients in this series, given this is a relatively rare complication; however, to our knowledge, this is the largest report of RSA prosthetic dislocations in the literature. Finally, in patients who dislocated a revision RSA, we attempted to analyze risk factors, including preoperative indications for their index revision; while the numbers in this study include patients who experienced a dislocation, it is not a review of all patients undergoing revision surgery for that specific indication (ie, preoperative prosthetic instability).
Conclusion
Two-thirds of the dislocations complicating RSA occur within the first 3 months after surgery, more commonly after revision RSA. Closed reduction is successful in over half of the dislocations after primary RSA and unsuccessful in most dislocated revision RSAs. Revision surgery is successful in approximately 85% of the dislocations after primary RSA and over 50% after revision RSA. Female gender and a history of previous prosthetic instability in the revision setting are associated with worse outcomes. Every attempt should be made to achieve stability at the time of primary and revision RSA, since revision surgery is not guaranteed to restore stability.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Cofield/Royalties: Smith/Nephew, DJO; Dr. Sperling/Royalties: Biomet; Dr. Sanchez-Sotelo/Royalties: Stryker; The remaining authors declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.