
Abstract
Background
Numerous man-made and naturally occurring incidents cause human suffering, both psychologically and mentally. Such circumstances endanger people's emotional, physical, and social well-being if left untreated or if appropriate intervention is delayed. This trial examines the effectiveness of an Eye Movement Desensitization and Reprocessing (EMDR) intervention on improving the subjective well-being of patients with post-traumatic stress disorder (PTSD) in Jordan.
Methods
The current trial employed the quasi-experimental, interrupted time series design. This includes measuring the subjective well-being (SWB) three times: once before intervention (pre-test) and twice after the intervention (post-tests), including immediately and one-month follow-ups for both the intervention and control group. 70 patients (35 patients for each group) were recruited from a specialized psychiatric trauma healing center in Jordan. The primary outcome variable was measured using the World Health Organization- Five Well-Being Index (WHO-5).
Results
The statistical analysis of repeated measures using ANCOVA revealed significant differences across all time points within subjects [F (1, 56) = 5.18, p = .027]. The covariate effect was not controlled and showed statistically significant differences in the SWB across all time points in both interventional and control groups (between subjects) (F1,56 = 12.41,p = .001). There were no statistical differences in the total mean score of SWB correlated with sociodemographics and health-related factors.
Conclusion
The results suggest that EMDR may be an effective, pragmatic, and acceptable intervention for increasing SWB in patients with PTSD in Jordan. Findings support the continued investment in and adoption of EMDR among participants affected by trauma in the Arab World.
Keywords
Introduction
In recent years, psychological research has increasingly underscored positive mental health and human assets, shifting beyond a focus on dysfunction and psychopathology. This transition has been influenced, in part, by global organizations, such as the World Health Organization (WHO), which prioritizes the promotion of worldwide health. The WHO defines positive mental health as “a state of well-being in which the individual realizes his or her abilities, can cope with the normal stresses of life, can work productively and fruitfully, and can contribute to his or her community”. 1 This state of mental well-being has been associated with a plethora of positive outcomes, such as healthy aging and lifelong health, 2 flexible and creative thinking, 3 and good physical health. 4 Given such benefits, subjective well-being is deemed a psychological protective factor, enabling those with greater levels of SWB to cope more effectively with stressful circumstances and decreasing their vulnerability to the adverse effects of distress. 5 On the other hand, individuals with low SWB may be less equipped to manage distress, potentially leading to greater psychological dysfunction. 6
One such dysfunction that can significantly affect an individual's SWB is post-traumatic stress. In the aftermath of traumatic exposure, post-traumatic stress symptoms (PTSS), such as re-experiencing the traumatic event, alterations in cognition and mood, and being on guard or hypervigilant of one's environment may occur. 7 For those experiencing such symptoms, the ability to achieve psychological well-being or live with contentment and satisfaction can be significantly compromised. 8 Recently, PTSS was found to be negatively associated with psychological well-being. 8 Meanwhile, previous studies maintained that individuals with PTSS may engage in behaviors to avoid further harm, such as withdrawing from social connections that further diminish their SWB. 9 Moreover, disaster trauma was predicted to decrease social-psychological well-being via increased withdrawal from interpersonal contacts. 9 These findings underscore the vulnerability of individuals facing PTSS, not only to psychological dysfunction but also to decreased subjective well-being. As such, in the aftermath of a trauma, not only is PTSS a target for intervention, but so too is the preservation of psychological well-being.
Given that psychological well-being is often compromised in individuals with PTSS, interventions should target not only PTSS but also psychological well-being. In this context, we propose Eye Movement Desensitization and Reprocessing Therapy (EMDR) 10 as one such intervention that addresses both PTSS and the enhancement of psychological well-being. During EMDR therapy, patients are instructed to confront their trauma memory while engaging in bilateral stimulation, such as eye movements, which helps reduce the vividness of the memory and associated distress. EMDR has been found to effectively attenuate symptoms of PTSD.11–14 In addition, emerging research suggests that EMDR may also promote psychological well-being. 15 For instance, a prior study examining an EMDR-based online therapy group reported significant improvements in psychological well-being in a cohort of university students. 15 While such findings are promising, they have yet to be widely replicated. Furthermore, to our knowledge, no studies have examined the effects of EMDR on psychological well-being in individual therapy settings, as opposed to group therapy. Jordan has undergone notable advancements in its healthcare infrastructure, primarily fueled by demographic expansion, economic progression, and challenges stemming from internal conflicts as well as the substantial influx of refugees suffering from PTSD. 16 Currently, EMDR is being employed in Jordan to address PTSD. However, this methodology has not yet been substantiated through rigorous research within the Jordanian context. This indicates a significant gap in the empirical validation of using EMDR as a treatment approach, underscoring the urgent need for comprehensive studies to assess its effectiveness and support its implementation with solid evidence.
The current study attempts to bridge this empirical gap by investigating the effects of EMDR individual therapy on the subjective well-being of Jordanian patients presenting with moderate to severe PTSS. Building on previous findings, albeit limited, we hypothesize that, relative to a no-treatment control group, individuals who undergo an EMDR individual therapy intervention will experience significant increases in their subjective well-being immediately after the intervention period and one month later. The hypothesis of this trial is: There is a positive effect of using EMDR therapy on SWB level, immediately and one month after receiving three sessions, and when compared with the control group, controlling for specific socio-demographic and health-related factors among patients experiencing moderate to severe post-traumatic symptoms.
Method
Design
This trial utilized the quasi-experimental, interrupted time series design. The reason for choosing this design was that the sample size was inadequate to ensure control over a control group. And the intervention has been proposed voluntarily for the participants, therefore, there was little inerrability in making randomization and random assignment. The assigned center used an applied intervention is given this option. Although in terms of having a control group will enhance the comparison internal validity, however, one group design has been proposed to overcome obstacles related to the lack of control over control groups and the unavailability of subjects to meet the criteria for random assignment. The design includes measuring the study outcomes (subjective well-being) at three points of time: Once before intervention (pre-test) and twice after the intervention (post-tests): immediately and one-month follow-up for both the interventional and control groups. This design was suitable for examining the effectiveness of eye movement desensitization and reprocessing (EMDR) intervention on patients experiencing moderate to severe post-traumatic symptoms. In addition to recognizing the differences in socio-demographics and health-related factors that contribute to the effectiveness of using the EMDR therapeutics module.
Sampling and Setting
Participants were recruited from a specialized psychiatric trauma healing center that provides cognitive behavioral and psychological services for a population with traumatic experiences. The center was established in 2013, and its main aim is to promote the knowledge and abilities of the local community and provide psychological consultation, conducting EMDR therapy and other psychotherapy approaches, and run by trained and certified specialists and psychotherapists to meet current and future development challenges. The center provides psychological services through active participation, effective relationships with national and international organizations, and a wide connection with the local community. The physical structure of this center makes it appropriate for this study in that the center consists of many private, comfortable, and large therapeutic rooms that allow for effective interaction during the sessions, which is appropriate for conducting EMDR sessions.
The sample was recruited using a multi-strategic sampling technique. First, convenience sampling was used to recruit the participants, and then, a random assignment of the participants was made into control and interventional groups. Using the database of the target organization, patients diagnosed with PTSD and experiencing moderate to severe symptoms were approached and invited by the researcher to participate in the study. Patients who showed interest in participation were screened for eligibility. After completion of this study, the control group received the intervention.
Inclusion Criteria Included:
Patients diagnosed with PTSD and experiencing moderate to severe symptoms based on the initial screening (using PC-PTSD 5 is a screening tool for PTSD symptoms).
Aged 18 years and older,
Experiencing stressful life events in the last 6 months, such as the death of a family member, and suffering from moderate to severe symptoms, and no previous use of EMDR (using PC-PTSD 5 is a screening tool for PTSD symptoms). This part of the diagnostic criteria as per DMS-5 TR
Patients diagnosed with PTSD and experiencing mild symptoms based on the initial screening. Complain of acute cognitive or intellectual disability or mental retardation which may interfere with their ability to comprehend and answer the questions of the questionnaire. Eye disorders or visual impairment as documented by the medical record and physical examination. Because using EMDR among individuals with visual impairment as the desired treatment modality (for example, eye movements) is not applicable.
17
Sample Size
This trial included 70 participants. The sample was recruited according to symptom severity. Only those individuals endorsing A power analysis have performed using the G.Power program (version 3.0.10) 18 to estimate the minimum sample size to achieve a fully powered sample and to minimize errors in statistical tests. The minimum sample size needed was 62 participants, accounting for a medium effect size of 0.3, an alpha of 0.05 level of significance (two-tailed), power of 0.8, two groups, and three points of data collection. Considering 10% of the dropouts, 70 patients were recruited after screening for eligibility. The 70 patients were divided into two groups (35 patients in the interventional group and another 35 patients in the control group). The recruitment process was continued until the desired sample size was reached.
Data Collection Procedure
The data collection process started after the relevant ethics committees approved study procedures. All participants provided informed consent in compliance with the Institutional Review Boards. The researchers met the targeted center director. Then, the researchers explained the nature of the study, the purpose, the EMDR intervention, the implementation process, and required data, and all possible resources needed for the study.
The sample was recruited using a multi-strategic sampling technique. Initially, convenience sampling was employed to recruit the participants, and then random assignment was conducted to assign them to control and interventional groups. Using the accessible database and medical records of the target trauma healing center, the researcher approached and invited patients experiencing moderate to severe symptoms to participate in this trial. Patients who showed interest in participation were screened for eligibility.
Participants were administered a series of telephone-based questionnaires indexing the severity of PTSS and subjective well-being before random assignment to groups (T0), immediately following the third session of the EMDR therapeutics module (T1), and one month after the EMDR therapeutics module was completed (T2). The study took place over a total of 10 weeks. Participants assigned to the intervention group engaged in three weekly, 90-min individual EMDR therapy sessions conducted by a licensed and expert EMDR therapist. After T2, those participants in the control group were allowed to be involved in the three weekly, 90-min individual EMDR therapy sessions.
EMDR Therapeutics Module
The EMDR therapy module was established by modifying the published clinical EMDR protocol (Shapiro, 2017), and eight EMDR therapeutic steps were accepted and approved. In the first phase, a complete assessment and history taking were conducted. This step consists of gathering the patient's history and specifying the traumatic experience that led to their present distressed status. In the second step, rapport and a therapeutic relationship between the therapist and patient were established, and the EMDR therapy module was described to patients. The patient also had the chance to ask questions regarding the EMDR therapy module throughout this step.
In the third step, the patient and the EMDR therapist reviewed the traumatic episodes that the patient had experienced throughout their life, as well as rated the subjective distress they felt when reliving these events on a scale of 1 to 10. Based on their SUDs, patients can select which traumatic event to highlight in succeeding EMDR sessions, named the target event. In the fourth step, the desensitization stage, the therapist used bilateral stimulation (BLS), in which the patient engaged in side-by-side eye movements, sounds, and taps, while concentrating on the traumatic incident. BLS consisted of 24 two-way arrangements using finger movements. Each arrangement continued for one second, and the patient and therapist were separated by one meter throughout the session. In the fifth step, the installation stage, patients were requested to imagine positive perceptions or thoughts they may associate with the target traumatic event, provided it was true.
In the sixth step, the body scan stage, after replacing the positive thought, patients were requested to imagine both the positive cognition and the target event in their mind while directing attention to their bodies and responding with BLS if needed. In the seventh step, the closure stage, the therapist helped the patient return to a state of comfort. In the final step, the reevaluation stage, the EMDR therapist and patient communicated about the newly discussed and recently processed target traumatic event. They confirmed that their distress over this experience is minimal while their positive cognition is significant. This phase also involved determining future treatment directions. The five-part EMDR Fidelity Rating Scale (EFRS) assesses compliance with the three-pronged protocol and eight-phase treatment method that are conventional in EMDR therapy.19,20 In addition, the EMDR therapist has a master's degree in Psychiatric Mental Health Nursing and is certified as an EMDR therapist by The EMDR International Association (EMDRIA™). In addition, the therapist has more than seven years of experience in conducting EMDR therapy.
Patients in the control group did not receive any EMDR therapeutic sessions. They completed study questionnaires before the intervention, immediately after the third EMDR therapy session in which the intervention group was involved, and one month after the EMDR therapy module.
Instruments
To ensure accessibility for all participants, an Arabic version of the validated study measures was used, aligning with the participants’ native language. 21 Self-report measures assessed the primary study variable, including SWB level. Instruments assessing participants’ sociodemographic and health-related factors were also administered. The validity is ensured through the three means—the statistical control. The second is environment control, in which the intervention and the therapist, the quality of the therapist, and the making of the package and the content are introduced.
Sociodemographic and Health-Related Questionnaire
Sociodemographic, lifestyle, and health-related variables were assessed by a researcher-developed questionnaire. This instrument collected information on participants’ age, sex, marital status, educational level, working status, monthly salary, smoking status, presence of chronic physical illness(es), history of mental illness(es), and receiving psychological intervention or psychiatric medications.
The World Health Organization- Five Well-Being Index
The World Health Organization-Five Well-Being Index21–23 was administered to assess participants’ subjective well-being. Participants were asked to indicate how frequently they experienced a series of five statements over the last two weeks. Example statements included, “I have felt cheerful and in good spirits” and “I have felt calm and relaxed.” Each item was rated 0 (at no time), 1 (some of the time), 2 (less than half of the time), 3 (more than half of the time), 4 (most of the time), and 5 (all of the time). Items were summed to obtain a total raw score ranging from 0 to 25. This raw score is then multiplied by 4 to calculate a final score ranging from 0 to 100, with higher scores indicating greater subjective well-being. Cronbach's alpha for the WHO-5 in the current study was 0.89, indicating high reliability.
PC-PTSD-5: Primary Care PTSD Screen for DSM-5
The presence of PTSS during the previous month was evaluated using the PC-PTSD-5 tool. A binary scale was used to rate the five items (0 = No, 1 = Yes). A greater severity of PTSS is reflected by higher scores on the PC-PTSD-5. The PC-PTSD-5 showed high internal consistency in the current study at T1 and T2 (α = 0.80). Except for the modified stem and the addition of a fifth item that measures guilt and blame related to trauma, the PC-PTSD-5 data are comparable to those of the PC-PTSD. In contrast to the Clinician-Administered PTSD Scale (CAPS; r = 0.83), a prior study on PC-PTSD showed good predictive validity and test-retest reliability (r = 0.83). 24
Data Analysis
Preliminary data screening and pre-processing were conducted before data analysis. The collected data was analyzed using SPSS version 26.0, IBM Corp, 2017. 25 A repeated measures ANOVA test was used to address our main question about group differences in SWB. Time (ie, T0, T1, and T2) was a constant within-subjects factor, while group (ie, interventional vs control) was a fixed between-subjects factor. The homogeneity of variances was examined using Levene's test. To examine the potential impact of sociodemographic and health-related variables on research results, a repeated measures ANCOVA test was used (age, sex, marital status, educational background, employment status, salary, smoking status, presence of chronic physical illness(es), history of mental illness(es), family history of mental illness, history of receiving psychological intervention, history of receiving psychiatric medication). The covariate has been used based on two approaches. First, the literature review supported the inter-relationship between these covariates and the expected outcomes. Second, because of the testing in the model, we use the testing before including them in the model, so the variables have been tested for possible effect on the model itself. Each model included sociodemographic and health-related factors as covariates, with time fixed within subjects and group fixed between subjects.
Ethical Consideration
The first step in conducting this study was to obtain the Institutional Review Board (IRB) approval from the Scientific and Ethics Research Committee at the School of Nursing at the University of Jordan, which granted permission with a reference number of (2348/2023/1). Following this approval, approvals from the Ethics Committees of the accessible organization were then obtained, with a reference number (50/KCBS/2023). Permissions to approach the patients for data collection were also obtained from the administration of the selected center and the managers of the targeted departments to facilitate the process of data collection. Furthermore, all eligible patients were invited to participate, and those who expressed an interest in the study were approached and given relevant information about the study's purpose and significance, after which they were given consent to sign and approve their participation. Confidentiality and voluntary participation were assured and sustained.
Results
Sample Characteristics
During this trial, 70 participants from the intervention (n = 35) and control (n = 35) groups were assessed. The intervention group's mean age was 30 years (SD = 9.62), while the control group's average age was 30 years (SD = 7.92). In terms of sex, there were 18 (25.7%) males and 17 (24.3%) females in the intervention and control groups, respectively; 19 (27.1%) females and 16 (22.9%) males. Furthermore, the majority of the participants in the intervention group (n = 18) and the control group (n = 17) were single, with 13 (50%) in each group married. In terms of educational background, 10 (14.3%) of the participants in the intervention group and 11 (15.7%) in the control group had completed high school education, and 12 (17.1%) in the intervention group and 13 (18.6%) in the control group they held the first university degree. In terms of Employment Status, 13 (18.6%) of participants in the intervention group and 16 (21.4%) in the control group were employed and working full-time, whereas 12 (17.1%) in the intervention group and 10 (14.3%) in the control group were not currently employed. For more details, see Table 1, which presents participants’ sociodemographic characteristics.
Participants’ Sociodemographic Characteristics (N = 70).

M: mean, SD; standard deviation, N: number, %: percentage
This table represents the sociodemographic characteristics of the participants in both groups control and interventional.
Table 2 represents the participants’ daily lifestyles and health-related factors. In terms of smoking status, 15.7% (n = 11) in the intervention group and 21.4% (n = 15) in the control group are smokers, and 28.6% (n = 20) in the intervention group and 27.1% (n = 19) in the control group they are non-smokers. Additionally, 25.7% (n = 18) of the same in both groups reported a history of at least one chronic physical illness, and 21 (30%) in the intervention group and 10 (14.3%) had a positive family history of mental illnesses. In terms of engaging previously with other forms of psychotherapy, 25 (35.7%) were the same in each group. The participants reported that they had not received any type of psychotherapy previously. In addition, 9 (12.9%) in the intervention group and 11 (15.7%) in the control group revealed that they were now using psychiatric medications.
Participants’ Daily Lifestyles and Health-Related Factors (N = 70).

Hx: History, N: number, %: percentage. This table represents Daily Lifestyles and Health-Related Factors in both groups control and interventional.
Variables of the Study
Subjective Well-Being
When comparing the Subjective Well-being SWB of Participants in intervention and control groups, the statistical analysis showed that the overall mean score of SWB for all study participants (n = 70) at baseline (Before intervention T0) was 4.24 (SD = 2.63) ranging from (1 to 15). of them, 85.7% (n = 60) had scores ranging from (1 to 7) indicating the participants have had a low score in well-being.
To compare SWB among participants in both intervention and control groups, the independent samples t-test was conducted. At the first point of measurement, before conducting EMDR intervention, the overall mean score of SWB at baseline (T0) among participants in the intervention group was (4.51, SD = 2.77), and participants in the control group at baseline were (3.97, SD = 2.49). There was no significant mean difference between the two groups (t = 0.86, p = .93). The second point of measurement was immediately after conducting 3 sessions of EMDR intervention (TI), participants in the control group had a SWB mean score of 5.29 (SD = 2.62), ranging from 2 to 10, with 82.9% (n = 29) of participants having a very low score in SWB. The mean score of participants in the interventional group increased to 12.03 (SD = 4.04), ranging from 3 to 21, and the majority of participants had an SWB mean score of 71.51% (n = 25), ranging from 10 to 21, indicating improvement in their well-being score. These mean differences were significant (t = 8.29, P = .03), with participants in the interventional group and their SWB scores improved.
At the third point of measurement (TII), one-month follow-up post-EMDR intervention, the mean score of the SWB in the control group was 7.11 (SD = 2.75), ranging from 2 to 12, with almost 85.7% (n = 30) of participants having very low SWB scores. On the other hand, the mean score of SWB participants in the interventional group increased to 21.54 (SD = 1.82), ranging from 18 to 25. The analysis showed that there were significant mean differences between the two groups with (t = 25.87, P = .007), which indicates that the SWB scores among participants in the intervention group had significantly increased and improved than participants in the control group. See Table 3.
Subjective Well-Being Differences Between Interventional and Control Groups at all Points of Measurement.

M: mean, SD: standard deviation, P values ≤ 0.05
Bivariate Analysis
Repeated Measures Mixed ANOVA for the Subjective Well-Being
A Repeated Measures Mixed ANOVA test has been used to assess if SWB scores improved during and after the EMDR intervention.
Sphericity is the main assumption for using repeated measures mixed ANOVA, which indicates that all variances of the different points of measurements are essential to be homogenous. To investigate whether the sphericity assumption was violated, the Mauchly test was used; the results were not significant (Mauchly's W = .972, 2 (2) = 1.885, p = .390), as well as, the Greenhouse-Geisser value of .973 which indicated that the sample variance/covariance matrix did not deviate significantly from sphericity; however, since the Greenhouse-Geisser value was near 1.00, no correction was needed to the degrees of freedom that had been used to assess the significance of the F ratio.
The results of repeated measure ANOVA (see Table 4) showed that there were significant differences across the three times of measurement within the subject (F1, 68 = 827.32, p < .001). Also, the Time of Measurement * Group was significant (F1, 68 = 392.05, p < .001), and there were significant differences between groups (F1, 68 = 196.3, p < .001), indicating that there is a significant increase in SWB scores after EMDR sessions. This supports the hypothesis of the study that the EMDR intervention is effective and can be used successfully to improve the level of SWB among PTSD patients. The analysis also showed that there is a significant effect of EMDR sessions on the level of SWB (Wilk's Lambda = .076, (F2, 67 = 408.08, p = > .001). Additionally, the relevant effect size (partial η2) was 0.92, demonstrating that the EMDR sessions were responsible for most of the variance in SWB. The EMDR intervention was effective in improving the level of SWB among PTSD patients.
Overall Results of Repeated Measures Mixed ANOVA for the Subjective Well-Being Across Three Time Points Within-Subject and Between-Subject.
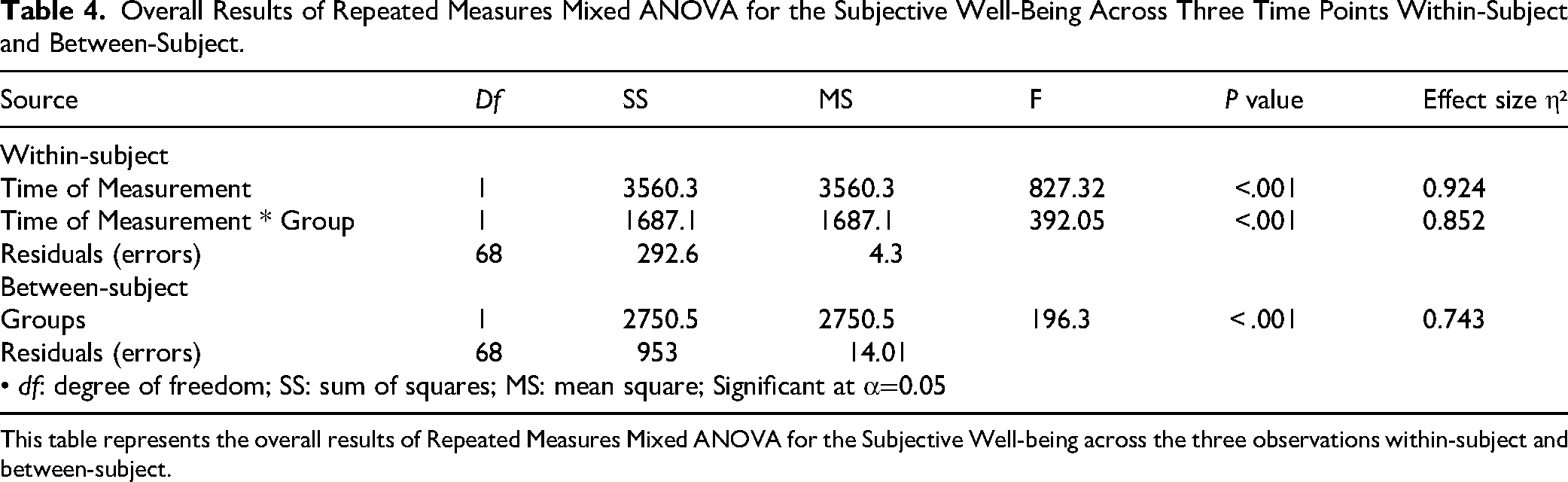
This table represents the overall results of Repeated Measures Mixed ANOVA for the Subjective Well-being across the three observations within-subject and between-subject.
As indicated in Table 4, the significant F test means differences or changes within the three points of measurement and between the groups. As the EMDR intervention took place after the baseline, the intervention showed a positive effect on increasing the level of SWB at Time I and Time II. See Figure 1.

SWB means scores across the three points of measurement without controlling for covariates. The blue column represents the interventional group, and the red column represents the control group. It seems from Figure 1 an improvement in SWB scores in the intervention group at the second and third points of measurement.
Testing the SWB mean differences among the intervention group across all points of measurement, a post-hoc pairwise comparison test was obtained by using the Bonferroni test to determine where the differences occurred. and the result showed significant differences between the baseline and each point of time (T0, T1, and T2) with (p = < .001).
Based on the result; there is a statistically significant difference (p = < .001) in the mean of SWB scores after three sessions of EMDR interventions at (T1) and the mean of SWB before the EMDR sessions compared with the baseline (T0) and the control group, as well as there is a statistically significant difference (p = <.001) in the mean of the SWB after one month follow up post three sessions of EMDR intervention (T2) and the mean of SWB before EMDR sessions compared with the baseline (T0) and the control group. Consequently, this means that the Psychological Well-being after EMDR interventions for patients experiencing moderate to severe symptoms of PTSD was increased significantly from the baseline in both measurement points (TI and TII). See Table 5.
Pairwise Comparison of Subjective Well-Being Means Differences Across all Times of Measurement in the Interventional Group (n = 35) and Control Group (n = 35).

SE: standard error, significance at p ≤ 0.05, T0: the time of baseline, T1: Immediately after the intervention, T2: one-month follow-up after the intervention. This table represents the Pairwise comparison of Subjective Well-being means differences across all times of measurement in the intervention group (N = 35) and the Control Group (n = 35).
Repeated Measures Mixed ANCOVA for Subjective Well-Being with Controlling for Specific Socio-Demographics and Health-Related Factors
A repeated measure mixed ANCOVA was used to examine the hypothesis, which states that “Exposing individuals diagnosed with Post-Traumatic Stress Disorder and experiencing moderate to severe symptoms after receiving three sessions of EMDR intervention will increase the SWB level with controlling for specific socio-demographic and health-related factors”.
The mean total scores of SWB increased gradually across all three points of time among PTSD patients in the interventional group, before EMDR intervention T0 (M 4.51, SD = 2.77) and continuing immediately after three sessions of EMDR intervention TI (M = 12.03, SD 4.04), with PTSD patients’ SWB increasing at one month of EMDR intervention TII (M = 21.54, SD 1.82).
After meeting the assumptions, a repeated measure analysis of covariance (ANCOVA) mixed design test was used to see if there were significant differences between dependent variables SWB at time T0, TI, and TII after controlling for particular socio-demographic and health-related factors.
The results of a repeated measure analysis of covariance (ANCOVA) mixed design test (including interaction) between dependent variable SWB at time 1(T0), time 2(TI), and time 3(TII) and covariance variables (specific socio-demographics and health-related factors: (age, sex, marital status, educational level, working status, monthly salary, smoking status, presence of chronic physical illness(es), history of mental illness(es), and receiving psychological intervention or psychiatric medications).
The null hypothesis was rejected since the overall result showed that there is a significant difference between the SWB at time 1(T0), time 2(T1), and time 3(T2). After controlling for specific socio-demographics and health-related factors within subjects [F1, 56 = 5.18, p = .027, partial η2 = 0.085], the value of η2 is a medium effect according to Cohen, 26 which indicates how much of the variance in the dependent variable is explained by the independent variable. Furthermore, the results of the final ANCOVA were that the covariate effect was not controlled and showed that there are statistically significant differences in the SWB across the three points of measurements in both interventional and control groups (between subjects) (F = 12.41, P = .001). There was no relationship between the SWB and socio-demographics and health-related factors. (see Table 6), there is a statistically significant difference in the F value after adjusting for the covariate. Finally, there are no statistical differences in the total mean score of SWB correlated with socio-demographics and health-related factors. Levene's test for homogeneity of variance was used and showed that no significant violation was found [ F1, 68= 2.66, P = .608]. See Figure 2.

SWB Means Scores Across the Three Points of Measurement While Controlling for Specific Socio-Demographic and Health-Related Factors. This Figure Represents SWB with Controlling for Specific Socio-Demographics and Health-Related Factors, and Across all Points of Measurement. the Blue Line Represents the Interventional Group, and the red Line Represents the Control Group. It Seems from Figure 2 an improvement in the SWB scores in the interventional group at the second and third points of measurement over time.
Result of Repeated Measures Mixed ANCOVA Concerning the Subjective Well-Being with Controlling for Specific Socio-Demographics and Health-Related Factors.
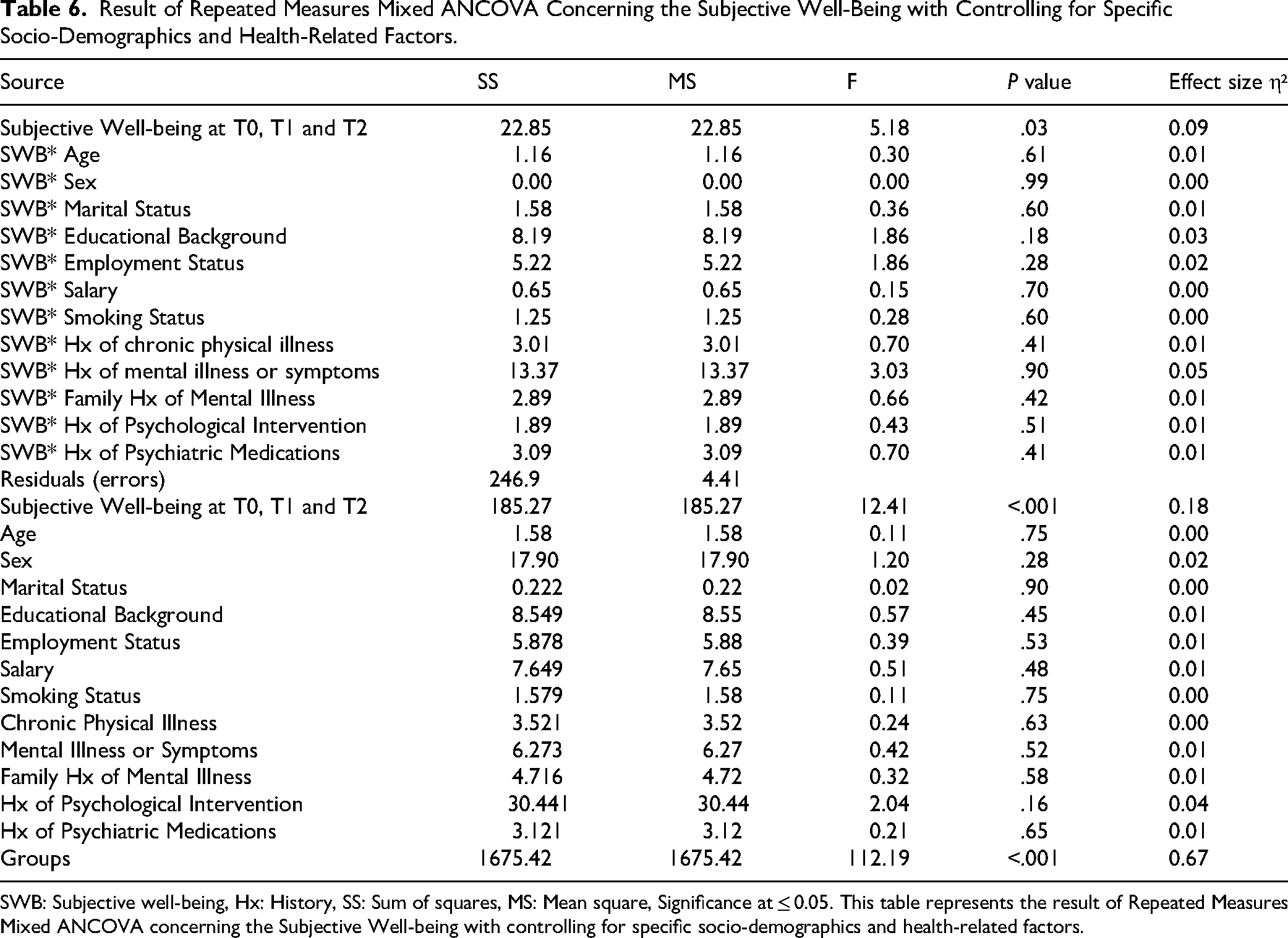
SWB: Subjective well-being, Hx: History, SS: Sum of squares, MS: Mean square, Significance at ≤ 0.05. This table represents the result of Repeated Measures Mixed ANCOVA concerning the Subjective Well-being with controlling for specific socio-demographics and health-related factors.
Discussion
The findings of this trial suggest that PTSD patients who were exposed to EMDR showed significant improvement in their SWB across all periods of testing. It is noted, further, that the interventional group had a significantly lower mean difference in SWB scores than the control group immediately after the intervention and one month later. On the other hand, at time 2 (T2, immediately post-intervention), the interventional group also showed significantly greater increases in SWB levels compared to the control group. Furthermore, participants in the interventional group demonstrated a significant mean increase in post-test and one-month follow-up (time 3, T3) scores as compared to their baseline scores. In comparison, no significant increase was observed among participants in the control group at T2 and T3. These findings suggest that the EMDR intervention resulted in a considerable rise in SWB, with the intervention groups outperforming the control group. In other words, the intervention considerably improved SWB, relative to a no-treatment control, consistent with our hypothesis. The EMDR-related benefits observed herein may be attributable not only to the effectiveness of EMDR,27,28 but also to the fidelity of intervention delivery and participants’ compliance with intervention protocols. The participants in this study strictly adhered to the intervention protocol, which facilitated greater benefits and interact more effectively with the therapies. The benefits of EMDR observed herein are consistent with prior studies 29 reporting salutary effects of EMDR on participants’ SWB scores. In addition, the present study observed significant effects immediately following the intervention, which may suggest the feasibility of the EMDR intervention, which is well-established. Studies have consistently shown that EMDR is a safe, feasible, and effective intervention among individuals suffering from PTSD. 30 Despite its known feasibility and effectiveness, EMDR therapy has been relatively underutilized as a treatment for PTSD patients. In contrast, Kraiss et al (2022) 31 reported that psychological interventions play a significant role in promoting overall well-being.
Such results are also alarming to the psychotherapists aiming at using EMDR, which requires sustainable promoter sessions, and such an interventional approach requires sustainable promoter sessions and cannot be done once and ever all. Furthermore, Yilmaz Dinç and Sapmaz 15 conducted a clinical trial to evaluate the effectiveness of EMDR among individuals with trauma pictures. Their study finding revealed that EMDR intervention was not only effective in managing the severity of symptoms but was also proved to be effective in terms of resilience and well-being.
The current study also examined multiple sociodemographic and health-related characteristics, including age, sex, marital status, educational background, employment status, salary, smoking status, chronic illnesses, psychiatric history, positive family history of mental illnesses, psychological treatment, and psychiatric medications. Consistent with (Wright et al, 2024), the current study also found that, in the presence of such covariates, EMDR remained an effective treatment for improving SWB. 32
Finally, we found that no statistically significant associations between total SWB scores and participants’ sociodemographic or health-related characteristics. This finding is consistent with a prior study in the existing literature. Gielkens and colleagues 33 conducted a study in 2025 to assess the effectiveness of EMDR intervention among older patients with PTSD. Their results showed positive outcomes through improvement in well-being and quality of life scores among the EMDR group after intervention. On the other hand, existing literature typically describes only basic sociodemographic characteristics and does not account for diversity factors concerning EMD.4,35
Taken together, the findings observed in the current investigation suggest that EMDR is an effective and pragmatic intervention for increasing SWB in patients with moderate-to-severe symptoms of PTSD.
Strengths of the Trial
One of the strengths of this trial is that it is the first to investigate the effectiveness of EMDR intervention in Jordan. In addition, this study supports the assertions that the components of EMDR interventions are also effective among PTSD patients who experience moderate to severe symptoms of PTSD. This adds to the body of literature suggesting the benefits of EMDR on psychological health. The salutary effects of EMDR observed in this novel population point to the potential suitability of EMDR in an Arab country, such as Jordan.
Limitations of the Trial
While this study was conducted in a novel population and demonstrated salutary effects of EMDR, it is not without limitations. One such limitation is participant recruitment, which only took place in one setting. As such, our findings are not generalizable to the larger population of patients with PTSD in Jordan. Furthermore, PTSS was screened using a short, non-clinical measure. While this contributed to the pragmatic nature of testing, it may limit the replicability of participants’ symptom severity. Future studies may consider using a clinical-administered interview or a more robust measure of PTSD symptoms, like the PTSD Checklist for DSM-5 (PCL-5).
Implications for Mental Health Policy
The results of the current investigation have the potential to result in the continued adoption of EMDR as a psychological treatment for addressing PTSD symptoms in Jordan. In addition, study findings may offer further areas of concentration for policymakers and mental health organizations advocating for mental health amelioration in Jordan.
Conclusion
Overall, the current investigation showed the benefits of EMDR therapy for increasing SBW in a population of Jordanian patients with PTSD, relative to a no-treatment control. This study is the first to investigate EMDR in Jordan and to find beneficial effects of this treatment in this population. Such findings motivate increased investment in EMDR as an effective, practical, and acceptable treatment for targeting SWB in patients with PTSD in the Arab World.
Footnotes
List of Abbreviations
Ethics Approval and Consent to Participate
Prior to their involvement in the trial, all subjects provided written informed consent. The Institutional Review Board (IRB) and the research and ethics committee at the assigned community-based center approved this study, which has the reference number 50/KCBS/2023. All human research procedures were carried out under the moral standards of the committee responsible for human experimentation (institutional and national), as well as the Helsinki Declaration of 1964, as revised in 2009, and its amendments.
Competing interests
The authors declare that they have no competing interest
Author Contributions
RHH, AH: Conceptualization, methodology, formal analysis, validation, investigation, writing- original draft preparation, visualization, writing- reviewing and editing. MP, RH, YA, AA: Methodology, data collection, and RH, AA: writing-reviewing and editing the final manuscript. The authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Source(s) of Support/Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.