
Abstract
Background
Cardiovascular diseases (CVD) and depression are growing global health concerns as heart attack and stroke solely account for around 85% of total CVD deaths and 280 million ie, while 3.4% of the world's population have depression. A bi-directional relationship exists between depression and heart disease: about one-fourth of heart disease patients experience depression, and those with depression have a higher risk of developing heart disease compared to the general population. This study aims to examine the association between depression and heart attack as a dependent variable, focusing on demographic and behavioral correlates of individuals in Tennessee.
Methods
We performed a cross-sectional analysis using the 2022 Behavior Risk Factor Surveillance System (BRFSS) data for Tennessee (N = 5266). Our analytical approaches involved descriptive and multivariate analysis (logistic regression analysis) to assess the association between depression and heart attack in Tennessee. The primary dependent variable of interest was a self-reported lifetime heart attack and independent variables included self-reported lifetime depression, no exercise in the past 30 days, smoking status, race/ethnicity, gender, and age category.
Results
A total of 7.5% (N = 731) of participants reported lifetime heart attack and 27.8% (N = 828) of participants reported depression. Depression was found to be significantly associated with higher odds of a heart attack (AOR = 1.36; 95% CI, 1.06, 1.73), p < 0.001). Similarly, no exercise in the past 30 days (AOR = 1.74; 95% CI, 1.39, 2.20, p < 0.001) was also associated with higher odds of a heart attack. Furthermore, low income, current smoking status, and race/ethnicity were not found to be significantly associated with heart attack in our study.
Conclusion
This study reinforces the significant link between depression and heart attack while highlighting the complex interplay of demographic and behavioral factors influencing onset of cardiovascular diseases. The findings underscore the necessity for a comprehensive approach to cardiovascular health that integrates mental health considerations and addresses broader social determinants of health.
Background
Cardiovascular diseases (CVD) now account for almost one-half of the noncommunicable disease deaths worldwide. 1 CVD accounts for 19 million, ie, 32% of all deaths worldwide, among which 7.4 million of these are caused by coronary heart disease. An estimated 523 million people had some form of CVD in 2020, an absolute increase of 18.7% from 2010. 2 Heart attack, also known as myocardial infarction, is caused by plaque buildup in arteries, causing coronary circulation's failure to supply adequate blood to cardiac muscle and surrounding tissues. 3
Similarly, mental health disorders ranks among the most substantial causes of death worldwide and is one of the major contributors to the global burden of diseases.4,5 Depression is a highly prevalent mental health disorder worldwide. 4 Depression and heart attack each contribute significantly to the global disease burden.6–9 Furthermore, they share a bidirectional relationship, with depression serving as an independent risk factor for heart attack and heart attack, similarly increasing the risk of developing depression. 10 Depression is found to be three times more common among people after a heart attack compared to the general population. 7 In a cross-sectional study conducted among 388 hospitalized cardiac patients, 40% had clinically significant depression, and 78.4% had non-minimal depression. It was greater in women (83.1%) than men (72.9%). 11
One study found that post-myocardial infarction depression significantly increases mortality risk compared to individuals without post-MI depression, while chronic or recovered depression post-MI does not. 10 Depression is seen as highly prevalent in cardiac patients, among which 20–40% of patients later develop a chance of progression of coronary artery disease and other conditions eventually increasing the risk of mortality by 2 to 2.5 times. 12 A case-control study found that the patients with a first myocardial infarction exhibited higher rates of depression than matched controls but were less likely to receive antidepressant treatment. 12
Similarly, there is a strong association between female gender and depression. Depression is found to be 2–3 times more likely in women than men. 13 According to the National Institute of Mental Health, adult females (10.3%) experienced major depressive episodes compared to adult males (6.2%). 14 According to a CDC study, one in ten women in the US had symptoms that indicate they may have had a major depressive episode in the previous year, and 1 in 8 women experienced symptoms of depression after giving birth. 15
Similarly, a study examining the association between the poverty-to-income ratio (PIR) and depressive symptoms found that people with low PIR (1.30) and medium PIR (1.55) experienced a higher relative risk of having depressive symptoms. 16 A total of 15,674 people in Tennessee lost their lives in 2015 due to heart disease, which was almost 24% of all deaths in Tennessee in 2015. Tennessee recorded the seventh-highest heart disease rate and third-highest age-adjusted stroke in the United States in 2014. 17 In Tennessee 43.5% of adults were experiencing symptoms of anxiety or depression in 2021 among which 25.6% did not have access to counseling or therapy. 18 Similarly, rates of depression have been found to be significantlty higher in Tennessee in comparison to national averages. 19 A significant gap in the literature was found, as limited work has been conducted on assessing the association between heart attack and depression, particularly in Tennessee. This current study explores the relationship between heart attack and depression in Tennessee.
Methods
Design
We used data from the 2022 Behavior Risk Factor Surveillance System (BRFSS) conducted by the Centers for Disease Control and Prevention. The BRFSS is a yearly collection of vital health related telephone survey data across the 50 states, the District of Columbia and the three U.S. territories. Participants for the survey were selected randomly by dialing on landlines and mobile phones and asked about health-related risk behaviors, utilization of health services and chronic diseases. The data is de-identified making it available for secondary analysis. This study included all individuals from the state of Tennessee (n = 5,266) that were available in the BRFSS dataset. Given that a de-identified data was used for this study and following the Federal Regulations Common Rule 45, Institutional Review Board (IRB) review was not required.
Primary Dependent Variable
The primary dependent variable of interest was self-report of lifetime heart attack.
Independent Variables
Depression, exercise in the past 30 days, smoking status, income, education, race, sex, and age were used as independent variables. Depression was based on participant self-report of lifetime depression. Exercise was based on self-report of exercise in the past 30 days, with no exercise representing 1, and any exercise representing 0. Sex was coded dichotomously for male and female. Smoking status was determined based on the survey question about the frequency of days respondents currently smoke, with 1 representing a current smoker and 0 representing a non-current smoker. Race/ethnicity was dummy coded into the following race groups: White-Non-Hispanic (referent), Black Non-Hispanic, Hispanic, Asian, and other race/ethnicity. Household income was coded binary as: <$35,000 per year, and ≥$35,000 per year. Similarly, education was coded binary as: did not complete high school and completed high school. Age was categorized into three groups, 18–34 (referent), 35–54, and 55 and older.
Data Analysis
Data cleaning and recoding of variables were conducted in SAS (version 9.4), with analyses performed in Stata Version 14 (Stata Corp LP, College Station, TX, USA). Descriptive statistics and prevalence for the sample are presented in Table 1. Logistic regression (Table 2) analysis was used to assess the association between depression and the dependent variable of self-reported lifetime heart attack and adjusted results were provided. Other covariates and controls that were included in the model include did not exercise in the past 30 days, low income, less than high school education, smoking status, race, sex, and age. All results were weighted using weights to adjust for the complex sampling design and provide population-based estimates.
Descriptive statistics and characteristic of sample (N = 5266).
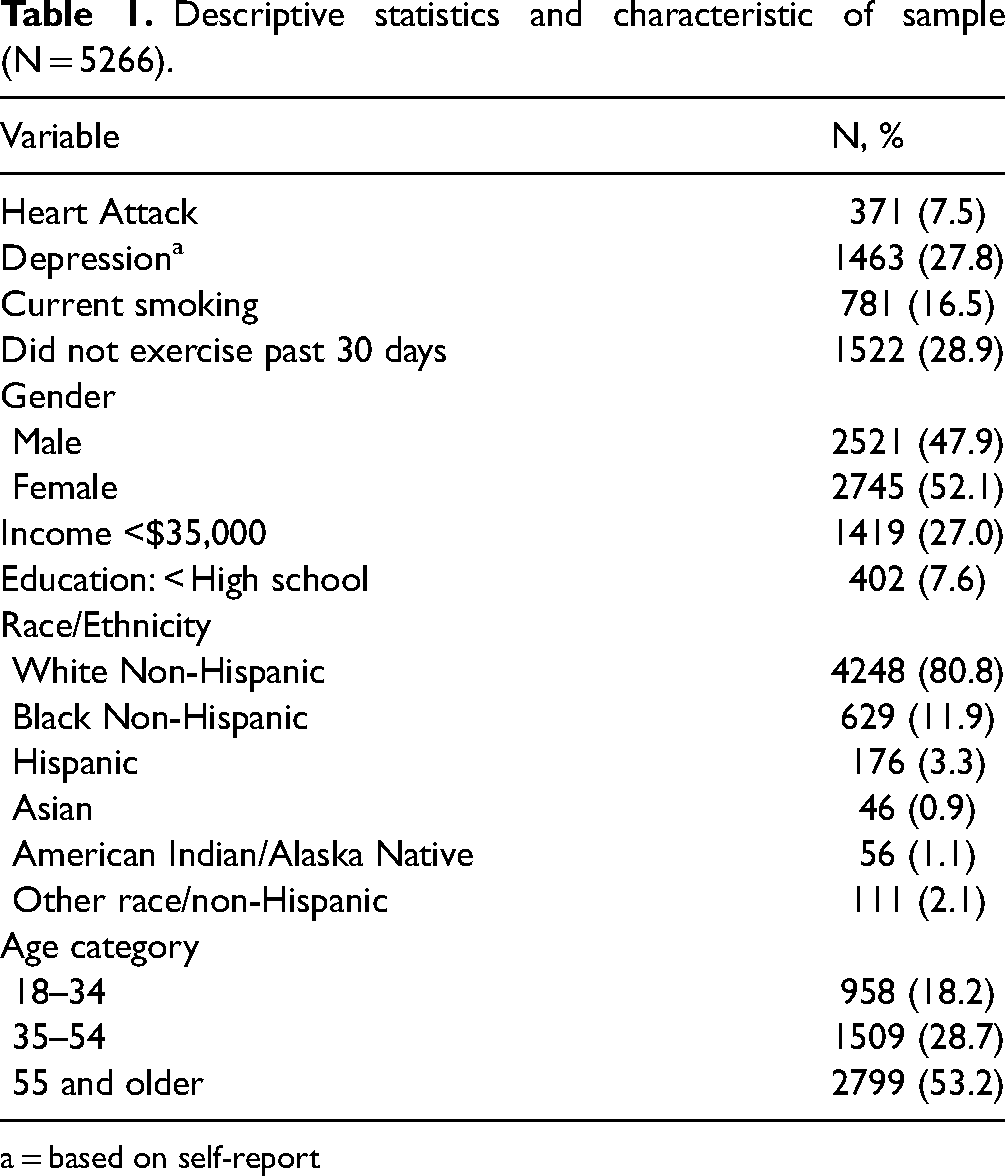
a = based on self-report
Logistic regression analysis between self-report of Depression and Heart Attacka as dependent variable.
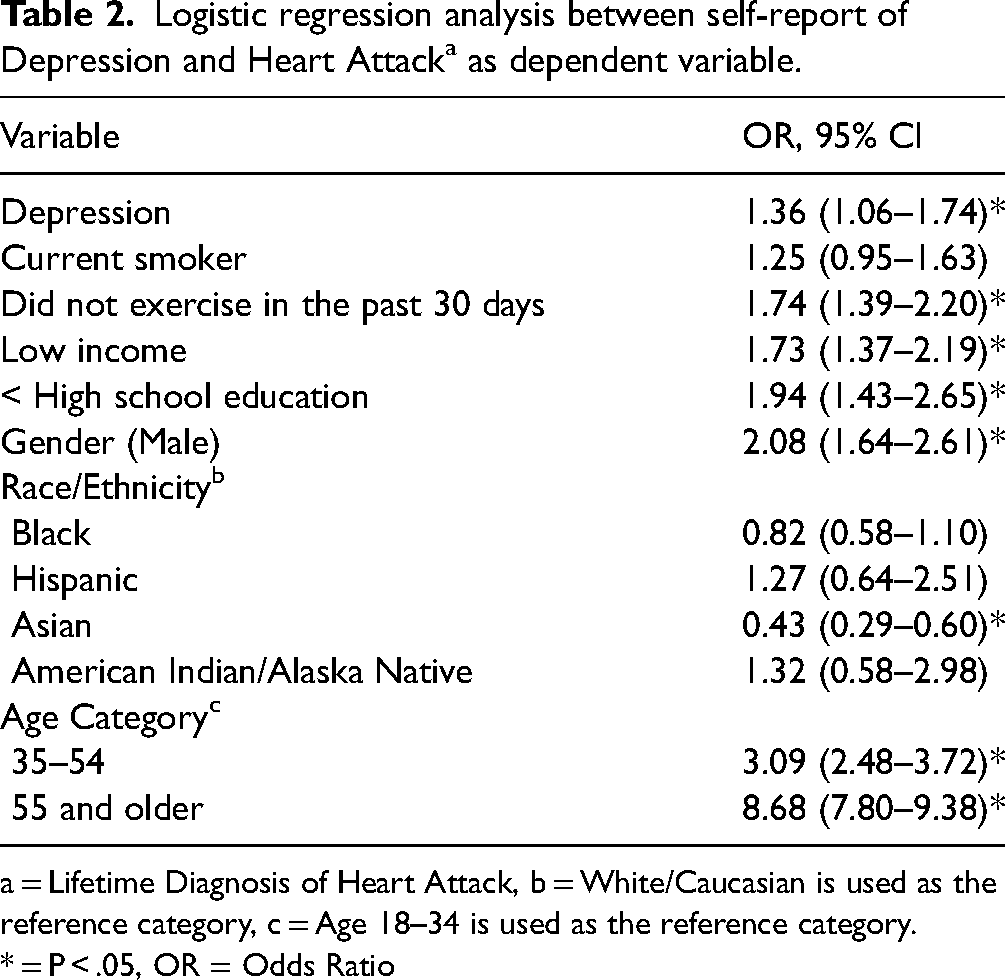
a = Lifetime Diagnosis of Heart Attack, b = White/Caucasian is used as the reference category, c = Age 18–34 is used as the reference category.
* = P < .05, OR = Odds Ratio
Results
Descriptive statistics were presented in Table 1. Overall, 7.5% (n = 371) of participants reported lifetime heart attack, while 27.8% (n = 1463) reported depression. The association between depression and heart attack as the dependent variable was presented in Table 2. Depression was significantly associated with heart attack (AOR = 1.36; 95% CI, 1.06, 1.73, p < 0.001). No exercise in the past 30 days (AOR = 1.74; 95% CI, 1.39, 2.20, p < 0.001) was also associated with higher odds of a heart attack.
Discussion
We investigated the relationship between depression and the dependent variable of lifetime heart attack, controlling for several demographic and behavioral factors, including age, race, sex, education, income, exercise habits, and smoking status. The results revealed a significant association between depression and an increased odds of heart attack, emphasizing the critical influence of mental health on cardiovascular outcomes.
Depression was found to be a significant factor for heart attack in our analysis, with those experiencing depression being approximately 36% more likely to suffer a heart attack compared to those without depression. This finding aligns with contemporary research that continues to affirm the strong link between depression and CVD.20–22 Furthermore, depression is often associated with poor health behaviors, such as physical inactivity, smoking, and poor adherence to medical treatments, which compound cardiovascular risk.23–25 Similarly, there are more study that shows depression to be often associated with premature CVD and suboptimal CVH (Cardiovascular Health). 6
Age was identified as the most significantly associated factor of heart attack, with older individuals showing a higher prevalence of heart attack. This finding is consistent with the well-documented progression of cardiovascular risk with age due to factors such as the advancement of cardiac structural and functional modifications and other age-related vascular changes.9,26 Similarly, sex differences were also apparent, with males showing more than double the risk of heart attack compared to females. This finding is in line with recent research, which indicates that while men generally have a higher incidence of CVD, women often experience worse outcomes, partly due to delays in care and differences in symptom presentation. 27 Education and income levels were also significant covariates, with those lacking a high school education or with lower incomes showing a higher likelihood of suffering a heart attack. These results reflect the broader impact of social determinants of health, where lower socioeconomic status correlates with higher risks for adverse health outcomes, including heart disease. 28 Factors contributing to this relationship include limited access to healthcare, higher stress levels associated with financial insecurity, and poorer health literacy. 29 Smoking, a well-recognized associated factor for heart disease, showed a trend toward higher prevalence of heart disease, however, this association did not reach statistical significance in our analysis. This may be attributed to the overwhelming influence of other covariates, such as age and sex, which are dominant factors associated with heart attack risk.9,30
Our study also examined racial and ethnic disparities in heart attack risk. Interestingly, Black individuals had lower odds of experiencing a heart attack compared to their White counterparts, though this finding was not statistically significant. This result contrasts with much of the existing literature, which often reports higher rates of CVD among Non-Hispanic Black populations due to factors such as socioeconomic disparities, limited access to healthcare, and a higher prevalence of risk factors like hypertension and diabetes.31,32 This non-significant finding in our study suggests that more nuanced research is needed to explore the complex factors at play, including potential protective factors or sampling issues.
The odds ratio for Asian individuals was near zero, a result likely indicative of a statistical anomaly due to a small sample size. This finding should be interpreted with caution, as other studies have highlighted that Asian populations do have unique cardiovascular risk profiles that warrant further investigation.33,34 American Indian/Alaska Native (AI/AN) individuals displayed an elevated risk of heart attack, though this was not statistically significant. Previous research has consistently shown higher rates of CVD among AI/AN population, often linked to high prevalence of traditional risk factors such as diabetes and obesity.33,35 The lack of statistical significance in our study emphasizes the need for larger-scale studies to validate these associations.
These findings have significant public health implications, particularly concerning the prevention and management of heart attacks/cardiovascular disease, which can be fatal. The strong association between depression and heart attack underscores the importance of integrating mental health assessments into cardiovascular risk evaluations. Psychiatrists can effectively use approaches like cognitive-behavioral therapy (CBT) and interpersonal therapy (IPT) to tackle depressive symptoms and enhance patients’ coping mechanisms. When needed, they may prescribe antidepressants to help manage severe or ongoing depression, which can lead to improved heart health. Additionally, psychiatrists play a vital role in guiding patients toward healthier lifestyle choices, such as better nutrition, increased physical activity, and smoking cessation, all essential for both mental and cardiovascular wellness. They can also teach various stress-reduction techniques, including mindfulness practices, relaxation exercises, and biofeedback, to help alleviate the negative impacts of stress on mental and heart health. Interventions aimed at referring patients for psychiatric services and treating depression in individuals with cardiovascular risk factors could play a critical role in reducing the incidence of heart attacks. Moreover, the observed disparities based on race, sex, education, and income levels highlight the necessity for targeted public health interventions that address the social determinants of health. Efforts to reduce cardiovascular risk should prioritize vulnerable populations, especially those with lower socioeconomic status, to address the root causes of these disparities.
Our findings should be interpreted with caution, given the following limitations. First, the BRFSS survey demonstrated self-reported bias which is based on participant participation rather than screening individuals for heart disease or depression. Second, the survey used a pre-established database and pre-determined survey questions, limiting the ability to determine variables, and data is cross-sectional. Third, self-report of depression, implies that the individual has received care and treated in the medical system. These results may not include individuals who may be burdened with depression but have not been diagnosed or treated. Fourth, heart attack may be underreported, as some may be burdened with depressive systems, while suffering from a heart attack, without ever being diagnosed. For example, a silent myocardial infarction, also known as a silent heart attack. 36
In conclusion, this study reinforces the significant link between depression and heart attack while highlighting the complex interplay of demographic and behavioral factors influencing cardiovascular risk. This study highlights the critical need for psychiatric evaluations in patients at risk for cardiovascular disease, particularly those exhibiting symptoms of depression. Early identification and treatment of depressive disorders can significantly improve overall health outcomes and potentially reduce the incidence of heart attacks in vulnerable populations. The findings underscore the necessity for a comprehensive approach to cardiovascular health that integrates mental health considerations and addresses broader social determinants of health.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.