
Abstract
Objective
To investigate the relationship between air concentrations of fine particulate matter <2.5 µm in diameter (PM2.5) and ischaemic attacks in high-risk elderly patients (aged ≥60 years).
Methods
This retrospective data analysis study extracted clinical data from an electronic medical chart system and environmental air quality data from the Ministry of the Environment Atmospheric Environmental Regional Observation System. Patients were stratified into four groups according to whether or not they had type 2 diabetes mellitus (T2DM) and/or an ischaemic attack (i.e. cerebral infarctions and myocardial infarctions) during the 2-year study period. Analysis of the combined clinical and environmental data produced the odds ratio for the likelihood of experiencing an ischaemic attack.
Results
Clinical data were collected from 94 647 patients. On days when the air temperature was ≥25℃ and PM2.5 concentration was ≥20µg/m3, an ischaemic attack was more likely to occur in the T2DM group than in the group without T2DM. An ischaemic attack was more likely to occur 2 days after an increase in the PM2.5 concentration compared with the same day as and 3–6 days after the increase.
Conclusion
The results of this study confirmed an association between PM2.5 and ischaemic attacks in high-risk patients.
Introduction
In guidelines regarding the relationships between air pollutants and health hazards, the World Health Organization (WHO) has reported associations not only with mortality rates, in the form of all-cause deaths and cardiovascular disease deaths, but also with hospital admissions, emergency examinations, the occurrence of ischaemic events, and a variety of symptoms, including arrhythmia, cardiovascular events and heart rate fluctuations. 1 Large-scale cohort studies in the same field began to be performed in around 1980, primarily in the USA, 2 but the degree of interest has increased in recent years, and the research field has expanded to other countries.
A study conducted in 20 US cities investigated the possibility that short-term changes in atmospheric concentrations of particulate matter <2.5 µm in diameter (PM2.5) increase the risk of acute ischaemic stroke. 3 A review article described higher mortality rates in regions where the PM2.5 concentration was high compared with regions where it was not. 4 For example, the overall number of deaths in regions where the mean PM2.5 concentration was 20µg/m3 was approximately 1.1 times higher than in regions where it was 10µg/m3. 4 The authors of the review also reported an approximately 1.25 times higher number of deaths from lung cancer and an approximately 1.15 times higher number of deaths from cardiovascular disease in regions where mean PM2.5 concentration was 20µg/m3 compared with regions where it was 10µg/m3. 4 The main stroke centre in Boston, USA, carried out analysis of data from 1705 stroke cases during a 10-year period. It reported that the incidence of stroke increased by 34% 24 h after air pollution worsened from a ‘good’ level (according to the ambient air pollution standard set by the US Environmental Protection Agency) to a ‘moderate’ level. 5 Analysis of data from Ontario, Canada, showed that a short-term rise in PM2.5 in specific patient groups increased the possibility of ischaemic attacks. 6 Studies have been conducted in individual European countries, such as the UK and Germany,7,8 and also in Europe as a whole – as a broad target region. For example, the ‘Air Pollution and Health: A European Approach 2’ project showed that short-term exposure to air pollutants was related to mortality rates. 9 An analysis of data from 22 European cohort studies suggested the existence of associations between air pollutants and cardiovascular disease mortality rates. 10
Research has been undertaken in other world regions. A study conducted in Santiago, Chile, found a relationship between PM2.5 exposure and hospital admissions for stroke. 11 A case-crossover study using Taiwan as the target region identified an association between PM2.5 and ischaemic stroke. 12 In Japan, a survey covering 100 000 subjects that extended over a 15-year period was conducted in three prefectures (Miyagi, Aichi and Osaka). 13 It identified a significant increase in the risk of male lung cancer deaths associated with PM2.5 exposure. 13 A survey undertaken in five prefectures in western Japan demonstrated that short-term exposure to air pollution may increase the risk of death from haemorrhagic stroke and ischaemic stroke. 14 Other studies have also reported relationships between exposure to air pollutants, including PM2.5, and health hazards.15–17
A meta-analysis of data from 34 previously published studies found that the short-term risk of a heart attack increased as air pollution concentrations increased. 18 Another meta-analysis showed that fine particulate matter ≤10 µm (PM10) and PM2.5 concentrations increased the risk of stroke and heart attack. 19 A review article found that several groups, including elderly subjects, patients with diabetes mellitus and patients with coronary artery disease, appeared to be particularly sensitive to the harmful effects that resulted from exposure to particulate matter. 20 Strong relationships between myocardial infarction and/or stroke were found in nine of 14 studies related to PM10 and in two of five studies related to PM2.5. 21 Research, including in animal models, has also been conducted to investigate the health impacts of PM2.5 exposure and to determine the pathophysiological mechanisms that link air pollution and diseases such as type 2 diabetes mellitus (T2DM) and myocardial infarction.22–24
The objective of this study was to analyse the relationship between air PM2.5 concentrations and ischaemic attacks in elderly patients (≥60 years) with T2DM – a high-risk population for ischaemic attacks (i.e. cerebral infarctions and myocardial infarctions).
Patients and methods
Extraction and accumulation of data
This retrospective data analysis study extracted clinical data from the Mega-Oak electronic medical chart system (National Centre for Global Health and Medicine database, which holds information on patients, clinical laboratory tests, medications, disease names and all ordering data) and publicly released environmental data from the Ministry of the Environment Atmospheric Environmental Regional Observation System (Soramame-kun).
25
The clinical and environmental data were then integrated using a database and rendered anonymous using Standardized Structured Medical Information eXchange software version 2 (Consortium for SS-MIX Dissemination and Promotion, Kanagawa, Japan).
26
A flowchart of the data processing procedure is shown in Figure 1.
The extraction and storage system used for the clinical and environmental data that were analysed in a Japanese study that examined the relationship between air concentrations of particulate matter <2.5 µm in diameter (PM2.5) and ischaemic attacks in elderly patients (aged ≥ 60 years) with and without T2DM. Database construction was achieved by extracting clinical data from the Mega-Oak electronic medical chart system and environmental data from the Ministry of the Environment Atmospheric Environmental Regional Observation System (Soramame-kun). The clinical and environmental data were then integrated and rendered anonymous using Standardized Structured Medical Information eXchange (SS-MIX) software.
Target data
Among the data obtained at the observation points of the Ministry of the Environment Atmospheric Environmental Regional Observation System (Soramame-kun), which are available to the public, PM2.5 concentration (daily means) and air temperature (daily means) data were collected for the 2-year period between 1 January 2011 and 31 December 2012 from the Tokyo Adachi-ku Ayase observation point – the closest observation point to the National Centre for Global Health and Medicine, Tokyo, Japan.
Clinical data were obtained by extracting data for patients aged ≥60 years (the age group in which ischaemic attacks are most common) from the insurance claim data of patients who were examined at the National Centre for Global Health and Medicine Hospital, Tokyo, Japan, during the designated 2-year period. From this information, data were then extracted for patients who had been examined in the hospital’s Department of Neurosurgery, Department of Emergency Medicine and Department of General Internal Medicine. There is evidence that because they eat a lot of fish, healthy Japanese people are at lower risk of heart disease than their healthy western counterparts;27,28 this study was therefore restricted to patients aged ≥60 years (i.e. high-risk patients). Data extracted and evaluated for each patient from the Mega-Oak electronic medical chart system were: age, sex, presence or absence of T2DM, date of an occurrence of an ischaemic attack and date of attendance at another clinical consultation. The dates of occurrence of ischaemic attacks consisted of a combination of the dates of occurrence of cerebral infarctions and myocardial infarctions, which were the main categories of ischaemic attacks analysed in this study.
The study protocol was approved by the Clinical Research and Ethics Committee of Aoki Hospital, Hakuseikai Healthcare Corporation, Honjo, Saitama Prefecture, Japan (no. 26-098). A notice in the hospital explained that the medical data spontaneously recorded during patient examinations would be used anonymously for an academic study. Each of the patients providing data also gave written informed consent at the initial consultation.
Statistical analyses
Counting schema and formula used for calculating odds ratios in a Japanese study examining the relationship between air concentrations of particulate matter <2.5 µm in diameter and ischaemic attacks in elderly patients (aged ≥60 years) with and without T2DM. a

Patients were divided into two groups: with type 2 diabetes mellitus (T2DM) or without T2DM. Odds ratios (ORs) were calculated after counting the examination data according to the air concentration of particulate matter <2.5 µm in diameter (PM2.5) (above or below the reference value) and whether they had T2DM. OR was calculated as (A/B)/(C/D).
Results
Basic demographic characteristics of four groups of Japanese patients aged ≥60 years with and without type 2 diabetes mellitus (T2DM) who did or did not experience an ischaemic attack during the 2-year study period and who were included in this analysis of the effects of air pollution with particulate matter <2.5 µm in diameter
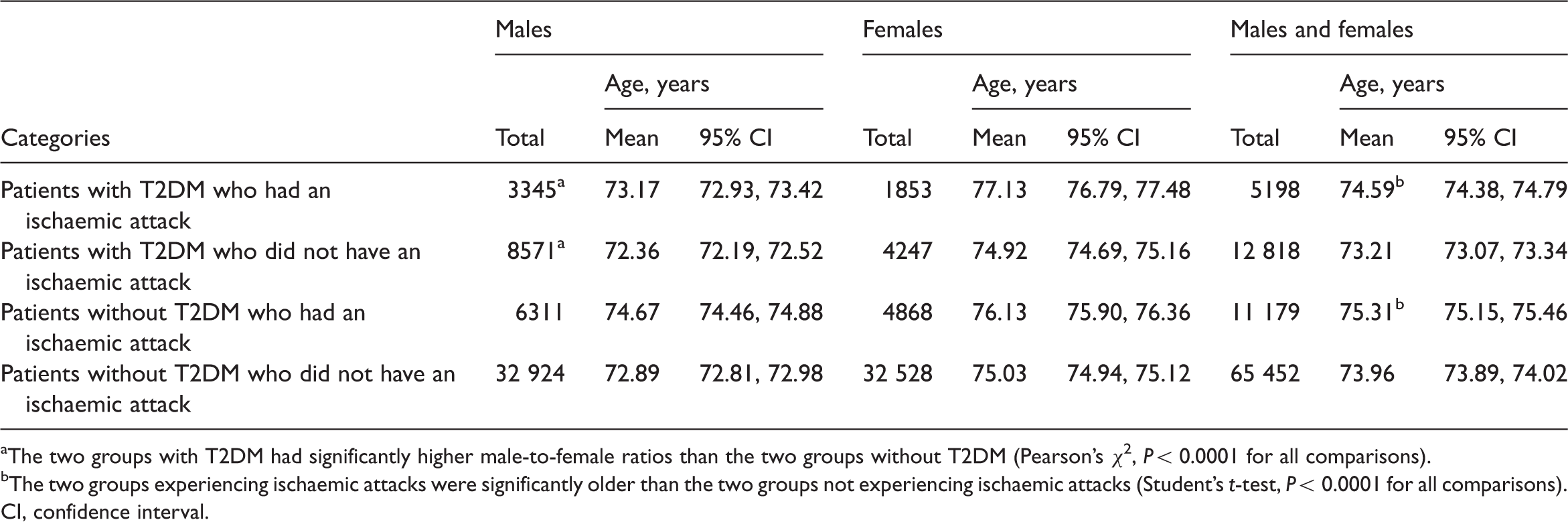
The two groups with T2DM had significantly higher male-to-female ratios than the two groups without T2DM (Pearson’s χ2, P < 0.0001 for all comparisons).
The two groups experiencing ischaemic attacks were significantly older than the two groups not experiencing ischaemic attacks (Student's t-test, P < 0.0001 for all comparisons).
CI, confidence interval.
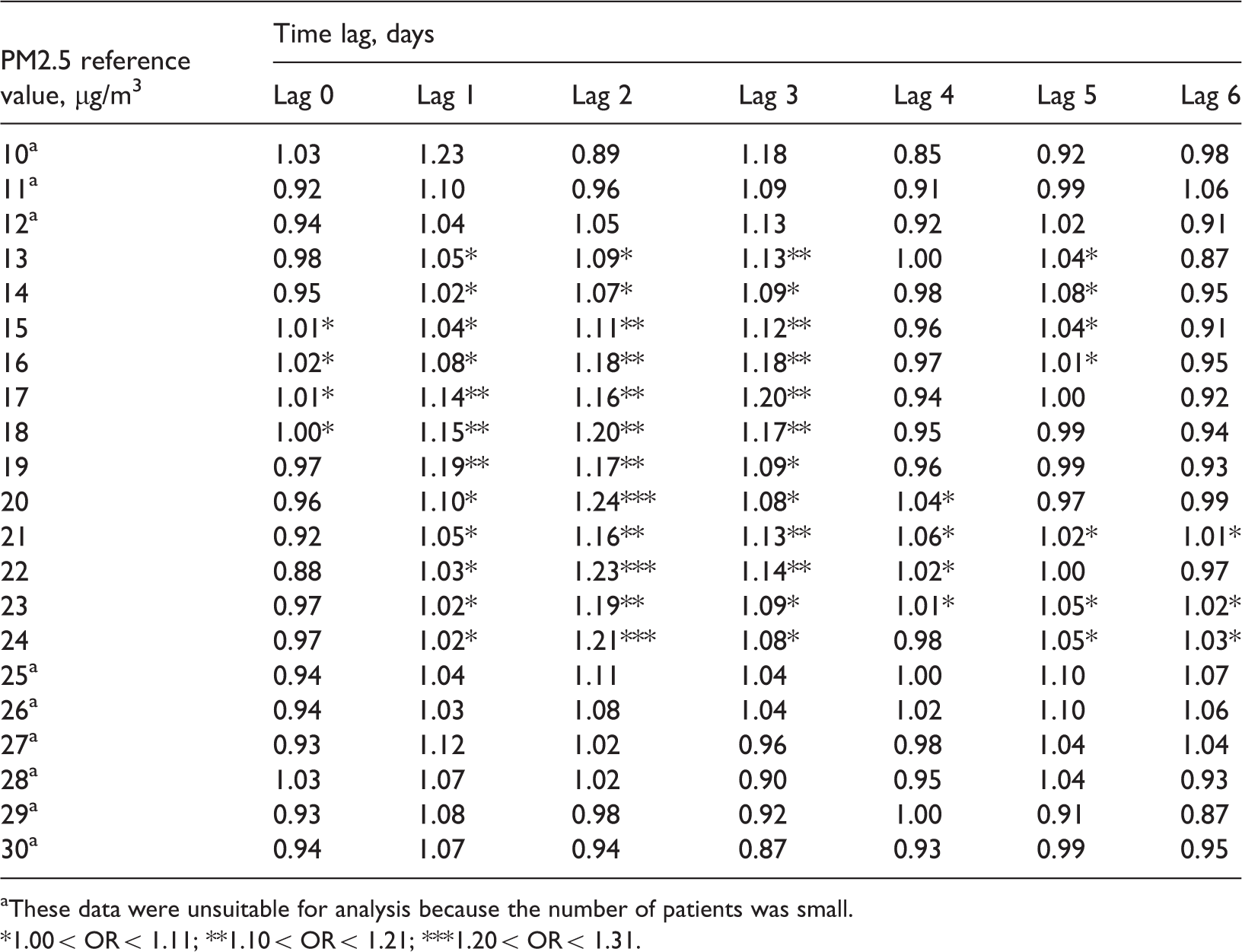
Results of the odds ratio (OR) analysis of the data set restricted to when the air temperature was ≥20℃ and patients had type 2 diabetes mellitus (T2DM) analysed according to the concentration of particulate matter <2.5 µm in diameter (PM2.5) and the time lag (in a Japanese study examining the relationship between air PM2.5 concentrations and ischaemic attacks in elderly patients [aged ≥ 60 years] with and without T2DM). There were no significant increases in ORs
These data were unsuitable for analysis because the number of patients was small.
1.00 < OR < 1.11.
Results of the odds ratio (OR) analysis of the data set restricted to when the air temperature was ≥20℃ and the patients did not have type 2 diabetes mellitus (T2DM) analysed according to the concentration of particulate matter <2.5 µm in diameter (PM2.5) and the time lag (in a Japanese study examining the relationship between air PM2.5 concentrations and ischaemic attacks in elderly patients [aged ≥ 60 years] with and without T2DM). There were no significant increases in ORs
These data were unsuitable for analysis because the number of patients was small.
1.00 < OR < 1.11.
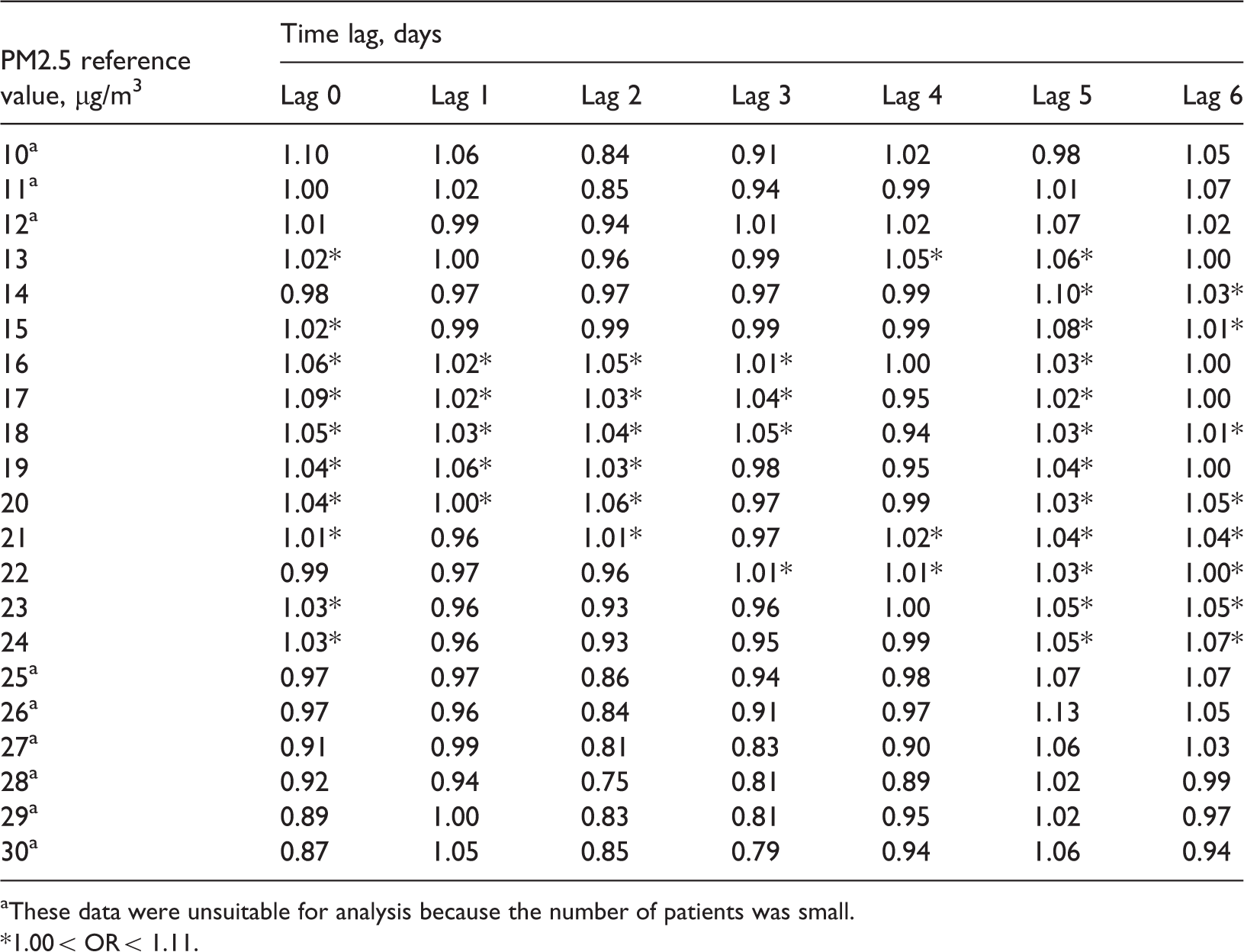
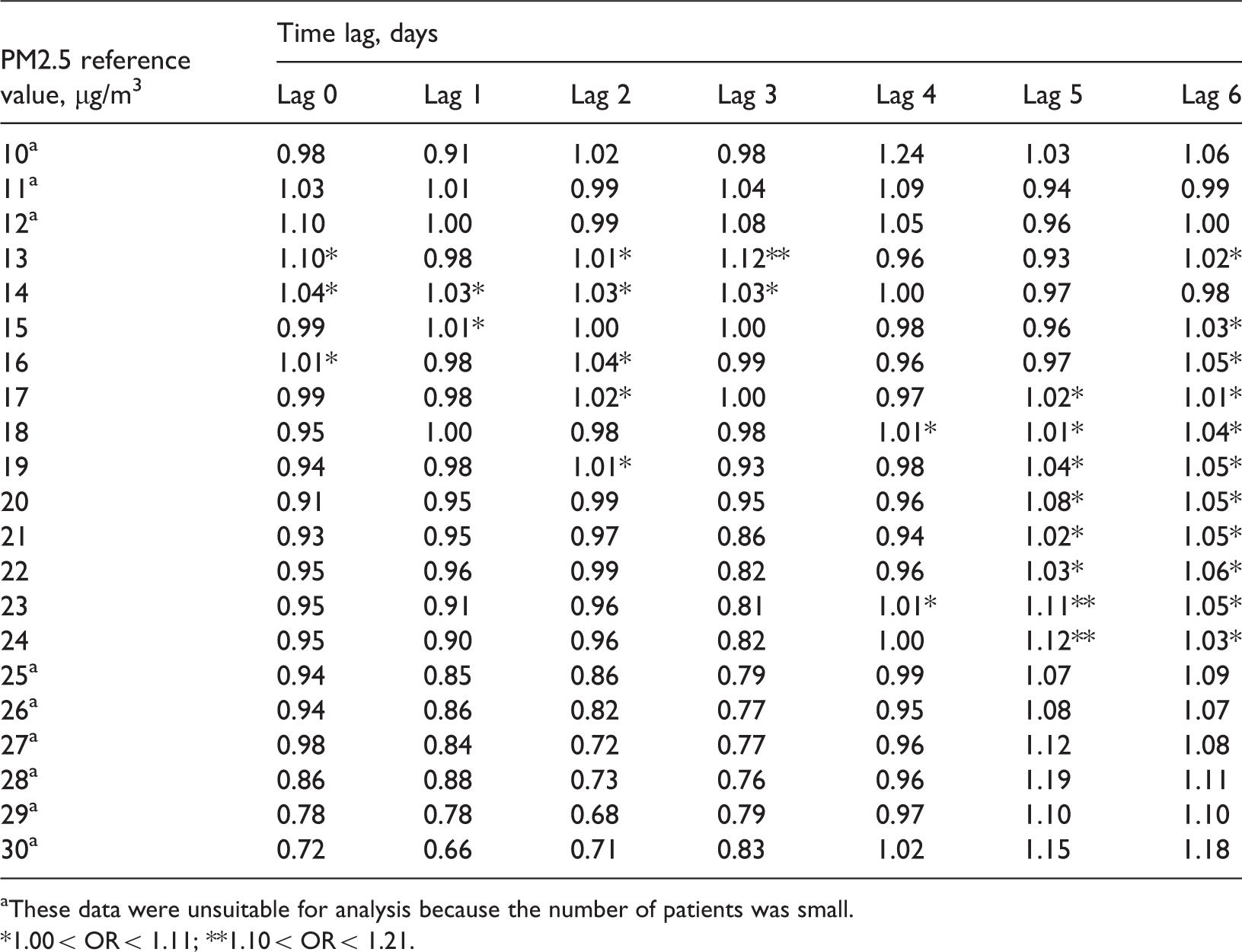
Results of the odds ratio (OR) analysis of the data set restricted to when the air temperature was ≥25℃ and the patients had type 2 diabetes mellitus (T2DM) analysed according to the concentration of particulate matter <2.5 µm in diameter (PM2.5) and the time lag (in a Japanese study examining the relationship between air PM2.5 concentrations and ischaemic attacks in elderly patients [aged ≥ 60 years] with and without T2DM). There was a tendency for the OR to be higher than the other analytical conditions – particularly when the time lag was 2 days, the values were higher in the 20–24 µg/m3 PM2.5 reference value range and ischaemic attacks were more likely to occur than under other conditions. At the PM2.5 reference value of 20µg/m3 and above, the OR 2 days after PM2.5 exposure was 1.24, which was significantly higher than the OR for the group without T2DM under the same conditions (see Table 6)
These data were unsuitable for analysis because the number of patients was small.
1.00 < OR < 1.11; **1.10 < OR < 1.21; ***1.20 < OR < 1.31.
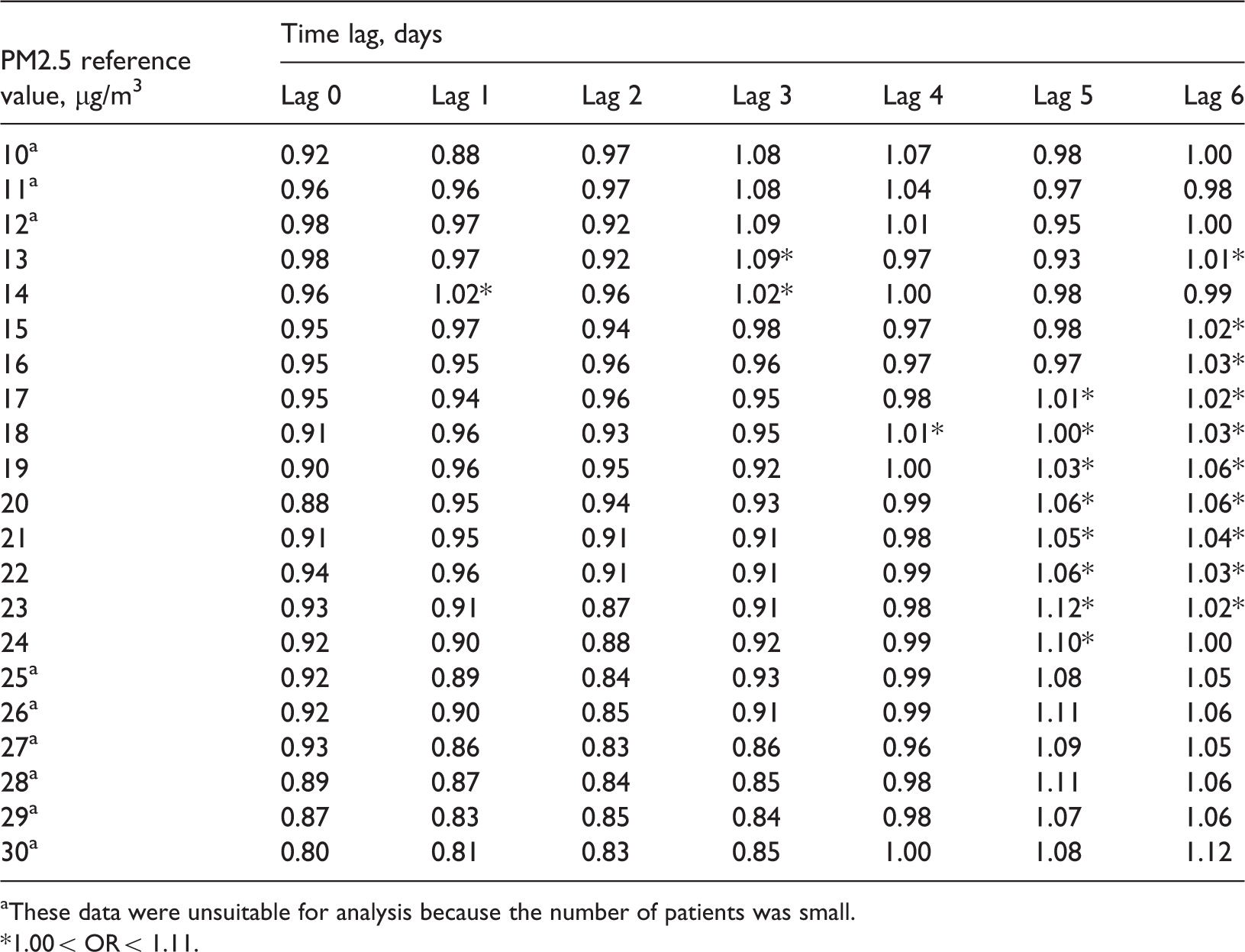
Results of the odds ratio (OR) analysis of the data set restricted to when the air temperature was ≥25℃ and the patients who did not have type 2 diabetes mellitus (T2DM) analysed according to the concentration of particulate matter <2.5 µm in diameter (PM2.5) and the time lag (in a Japanese study examining the relationship between air PM2.5 concentrations and ischaemic attacks in elderly patients [aged ≥ 60 years] with and without T2DM). There were no significant increases in ORs, and even 2 days after exposure to PM2.5 at the PM2.5 reference value of ≥20 µg/m3, there was no increase in OR, which was in contrast to the group with T2DM (see Table 5)
These data were unsuitable for analysis because the number of patients was small.
1.00 < OR < 1.11; **1.10 < OR < 1.21.
The combination of analytical conditions under which the OR was the highest (OR 1.24) was: patients with T2DM, PM2.5 concentration reference value 20µg/m3, mean air temperature ≥25℃ and a time lag of 2 days from exposure (Table 5). When the χ2-test was performed in relation to these conditions, the χ2-test value for the null hypothesis ‘When the PM2.5 concentration is ≥20µg/m3, there is no difference in incidence of ischaemic attacks from when the PM2.5 concentration is <20µg/m3’ was 5.63 (P = 0.018). Thus, the null hypothesis was rejected at a 5% significance level, thereby confirming that the PM2.5 concentration made a significant difference to the incidence of ischaemic attacks. When the χ2-test was performed in relation to patients without T2DM under the same analytical conditions, the χ2-test value was 6.04 and the difference was not significant (P = 0.865).
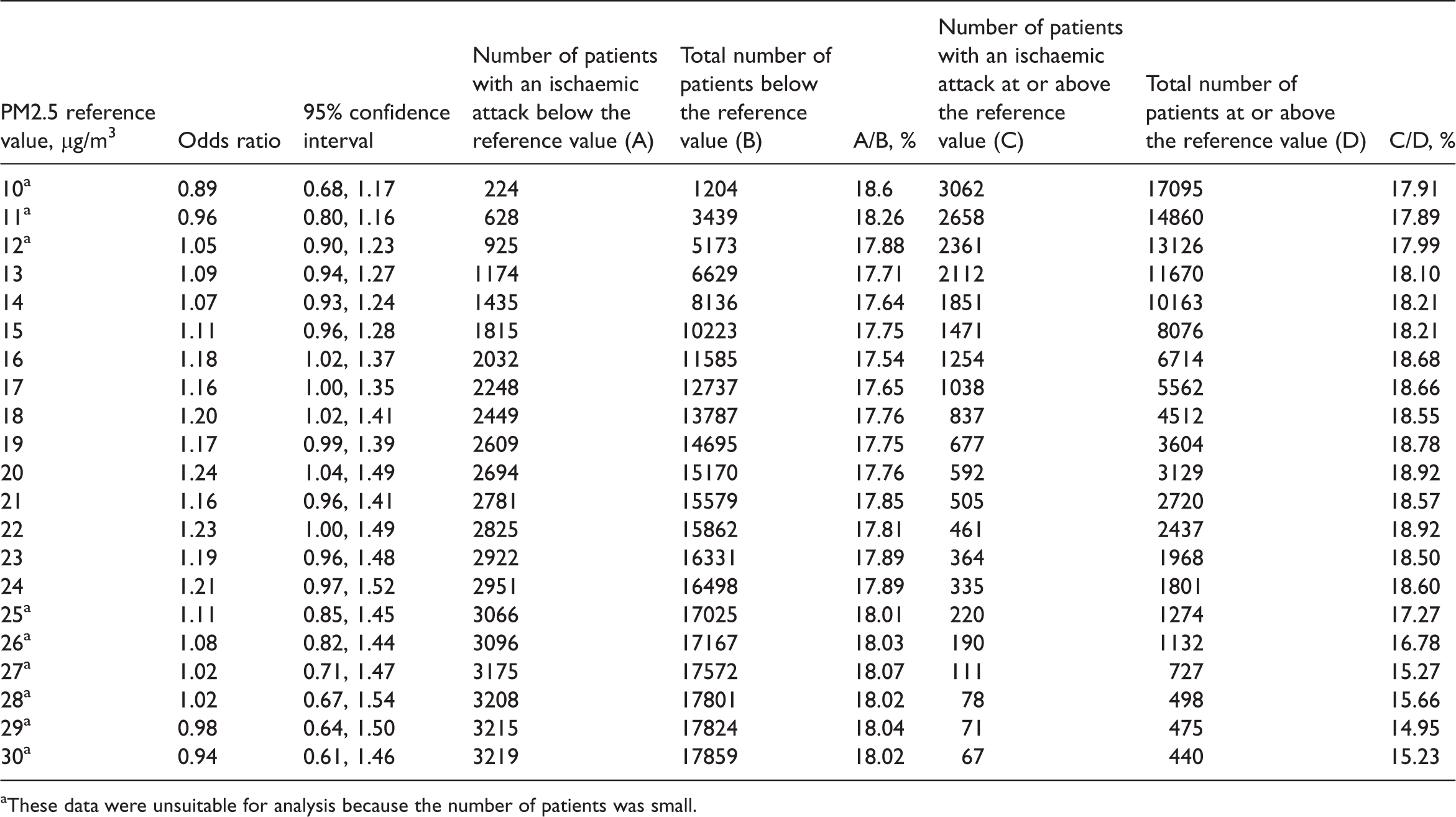
The following section describes the analysis of patients with T2DM aged ≥60 years exposed to a mean air temperature ≥25℃ with a time lag 2 days after exposure to PM2.5. Table 7 shows the details of the numbers of patients included in the OR and 95% confidence interval analyses of the occurrence of ischaemic attacks. These detailed data were used to review material for future tasks, including determining the advantages and limitations of the analytical methods that were used in this present study. The results in Table 7 demonstrate that the numbers of patients who had an ischaemic attack below the reference value and at or above the reference value were very small, and that the 95% confidence intervals widened as the patient numbers got smaller. Some sections of the data were unsuitable for analysis, as identified in Table 7. Figure 2 shows the changes in ORs according to the PM2.5 concentration reference values in the optimal range for the analysis without inclusion of the unsuitable data described previously in Table 5 (i.e. for 10–12 µg/m3 and 25–30 µg/m3). The ORs for the occurrence of ischaemic attacks on Day 2 after exposure showed that the occurrence of ischaemic attacks gradually increased at a mean PM2.5 concentration of 16 µg/m3 and peaked at 20 µg/m3; although the ORs varied widely, the high ORs tended to continue.
Changes in odds ratio (OR) of Japanese patients aged ≥ 60 years with type 2 diabetes mellitus experiencing an ischaemic attack 2 days after exposure at an air temperature of ≥25℃ according to the concentration of particulate matter <2.5 µm in diameter (PM2.5) reference values in the optimal analysis range. OR for the occurrence of an ischaemic attack on Day 2 after exposure gradually increased starting at a mean PM2.5 concentration of 16µg/m3; OR peaked at 20µg/m3. Although the ORs varied widely, the tendency for the OR values to be high continued Details of the number of patients included in the odds ratio (OR) and 95% confidence interval analysis of the data set restricted to when the air temperature was ≥25℃ and the patients had type 2 diabetes mellitus (T2DM) analysed according to the concentration of particulate matter <2.5 µm in diameter (PM2.5) and a time lag of 2 days from exposure (in a Japanese study examining the relationship between air PM2.5 concentrations and ischaemic attacks in elderly patients [aged ≥ 60 years] with and without T2DM) These data were unsuitable for analysis because the number of patients was small.
Discussion
Patients at high risk of ischaemic events, such as the elderly and those that have arrhythmias, are more vulnerable than healthy people to changes in the environment; they might therefore be more likely to manifest the effects of exposure to air pollutants, including PM2.5. Among existing research on high-risk patients, a study on myocardial infarct survivors in Israel showed a clear association between cumulative chronic exposure to PM2.5 and recurrence of a cardiovascular event after a first myocardial infarct; a strong possibility that increases in PM2.5 concentration act as a trigger in high-risk patients was suggested. 29 A study conducted in collaboration with the American Heart Association concluded that a strong association existed between short-term exposure to a high PM concentration and the acute cardiovascular mortality rate, and that the association was particularly strong in high-risk patients. 30 Moreover, they showed that even within the standard set by the US Environmental Protection Agency, there was an association between PM2.5 and the acute cardiovascular mortality rate. 30 The present study showed that when the PM2.5 concentration was ≥20µg/m3, ischaemic attacks were more likely to occur in high-risk patients aged ≥60 years who had T2DM compared with those without T2DM. In research investigating other environmental factors, a study conducted in Mexico City showed strong associations between changes in cardiac autonomic nerve control in ischaemic heart disease patients and exposure both to PM2.5 and carbon monoxide; 31 it will be necessary to assess the impact of carbon monoxide on ischaemic attacks in a high-risk group in future ongoing research in Japan. A Swedish study, which analysed the relationship between air pollution and the occurrence of ventricular arrhythmias in patients at high risk for ventricular arrhythmias, demonstrated that a worsening of air pollution could trigger an arrhythmia within 2 h. 32 In contrast, the present study of the occurrence of ischaemic attacks (i.e. cerebral infarction and myocardial infarction) demonstrated that there was a significant increase in the occurrence of attacks 2 days after exposure. The reason for this may be that thrombosis or embolism occurs against the background of circulatory failure after an arrhythmia develops, and there is a time lag before an ischaemic attack occurs. Research has shown a time lag of ≥1 day between an increase in PM2.5 concentration and the time an event such as a stroke occurred. 33 The same study reported that the number of deaths due to the occurrence of an event tended to increase after the PM2.5 concentration rose in comparison with the day before it rose; and that the events did not just occur on the day of the increase in PM2.5 concentration but sometimes occurred on and after the following day. 33 Moreover, events tended to be four-times more common during warm periods than cold periods. 33 The results of the present study also showed an association between warmer air temperatures of ≥25℃ and the occurrence of ischaemic attacks 2 days after PM2.5 exposure in patients with T2DM who were ≥60 years of age. A time series analysis of data collected at the National Taiwan University Hospital showed that during warm seasons, PM2.5 was associated with emergency room visits for ischaemic stroke by patients who were ≥65 years of age and by female patients. 34 In Japan, based on epidemiological findings related to the health of highly sensitive and vulnerable persons (e.g. those with a respiratory or cardiovascular disease, or diabetes), an expert committee on environmental standards for fine particulate matter stated the importance of assessing environmental standards to protect such individuals. 13 Thus, there is a strong likelihood of an association between warm weather and ischaemic attacks in high-risk patients, and further assessments (e.g. of the impact of ultraviolet rays in warm weather) and elucidation of the mechanisms responsible for the associations would be useful.
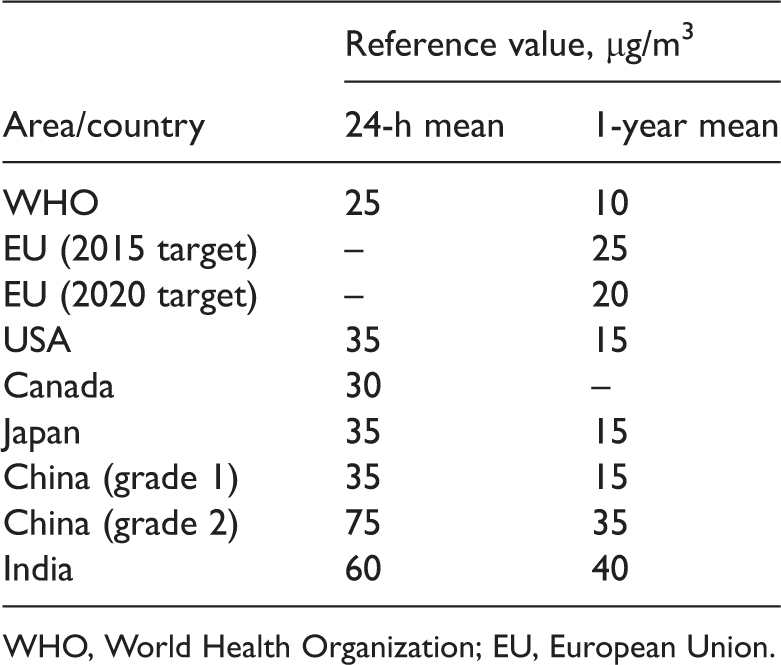
WHO, World Health Organization; EU, European Union.
The 24-h mean environmental standard was set at 25µg/m3 by the WHO 1 and at 35µg/m3 in Japan. 39 According to the results of previous studies,1–24,29–40 it appears that the closer the reference value for stratification approaches these standards, the clearer the associations between PM2.5 concentrations and ischaemic attacks tend to become. In the present study, the ORs were highest when the PM2.5 concentration was 20µg/m3. However, when the reference value for the data used in this study was increased, the amount of data available to calculate the OR decreased; for example, when a level of ≥28 µg/m3 was used for the analysis, data for <10 days in the 2-year period qualified for inclusion in the analysis. It is therefore unlikely that further studies of whether ischaemic attacks are more common at higher reference values will be possible at the locations used in the present study. It would be useful, however, to accumulate more data for higher reference values in the future.
In terms of the reliability of the data used in this study, measurements made at the Adachi-ku Ayase observation point provided the environmental data and the National Centre for Global Health and Medicine Hospital provided the clinical data. Both sites are located within the 23-ward (ku) part of Tokyo, and the Adachi-ku Ayase observation point is the closest observation point to the hospital. Nevertheless, the distance between the two sites in a straight line is 12 km, and it is impossible to rule out the possibility of differences arising between the PM2.5 concentration around the hospital and the PM2.5 concentration at the Adachi-ku Ayase observation point. Moreover, in terms of geographical distribution of patients who attend the hospital, because the diseases targeted in the present study required emergency transportation to the hospital and a corresponding outpatient clinic examination, most of the patients lived within 20 km of the hospital; therefore, in this study there is a reliable link between geographical location, environmental data and health effects. However, when analysing data of other patients in the future, geographical distribution may be even more varied and the analysis more difficult. The time lag data revealed no significant difference between ORs of the groups with and those without T2DM on the day of the increase in PM2.5 concentration, but there was a significant difference between them 2 days later. Ischaemic attacks are pathological conditions that develop as a result of occlusion of an artery; and they occur as a result of an arterial occlusion by a thrombus based on an atherosclerotic lesion, or by embolization caused by an embolism that develops due to an arrhythmia. Particularly because the risk of thrombosis is higher in elderly versus young patients, the symptoms progress more slowly and in a stepwise manner than in embolism, which is more common in younger people; thus, the development of a time lag of at least several hours between the environmental exposure that acts as the trigger and the completion of the clinical pathology is inevitable. Because the length of time lag varies from disease to disease, improving the reliability of the linkage between the patient and environmental data in relation to other diseases will be a future challenge.
Even though this present study used data from a 2-year period, the PM2.5 concentration was ≥25µg/m3 on only 16.7% of the days, and it exceeded 35µg/m3, the reference value in Japan, on only 4.4% of the days. When the present study tried extracting data only on the days when the air temperature was high, even fewer data were available. Consequently, because there were so few days when both the PM2.5 concentration and air temperature were high, it will be necessary to increase the reliability of the results of the analysis by accumulating data continuously. Our study group has developed a tool for extracting and accumulating clinical and environmental data. Because the clinical data used in the present study had been input daily by physicians and nurses during routine clinical practice, and the environmental data used are publicly available, the introduction of the tool to extract and combine these data kept costs down, compared to costs involved with building a clinical database from the ground up. Continuous monitoring with this tool may be a good method of analysing associations between environmental factors and disease structure.
In the 13–24 µg/m3 PM2.5 concentration range, the numbers of patients were sufficient for analysis; at 20 µg/m3 in the high temperature range, the OR for the occurrence of ischaemic attacks in patients with T2DM was significantly higher than in patients without T2DM. In high-risk patients, even when the PM2.5 exposure concentration was below the environmental standard value, as shown by the changes in the ORs, the risk gradually increased starting at a PM2.5 concentration of ∼20 µg/m3, which suggests that it is impossible to rule out the possibility of an impact of low-concentration exposure on the occurrence of ischaemic attacks.
As for the methods used in this study, from the standpoint of searching for the lowest value at which air pollutants affect so-called low-concentration-exposure groups and the time lags in the occurrence of the ischaemic attacks, at present, when big data are formed based on extraction from electronic charts, it would seem that some parts of the methodology will be useful in other clinicoepidemiological studies. Nevertheless, even when there is a large number of patients, as in the present study, the reliability of the ORs decreased when the lowest and highest concentrations in the target period of the analysis were approached; the inability to make comparisons between them would seem to be a limitation of this method of analysis.
In the present study, the time lag of the occurrence of ischaemic attacks after PM2.5 exposure appeared to be ∼2 days, so research in the future will target a number of environmental factors, including other air pollutants and weather phenomena. After taking the numbers of patients and the mean values of 3-day changes in environmental factors into account and performing partial correlation analyses of each element, and then by eliminating duplicate environmental factors and performing a multiple regression analysis according to the items selected, future monitoring will calculate the degree to which PM2.5 and other environmental factors are related to ischaemic attacks and the extent of their individual contributions. Using PM2.5 and other environmental factors as parameters, future analyses will determine the seasonal fluctuations in their impact and search for methods of prevention.
In conclusion, this study constructed a database combining environmental and clinical data and then analysed the data for associations between ischaemic attacks and PM2.5 concentrations. Analyses showed that on days when air temperature was ≥25℃ and the PM2.5 concentration was ≥20µg/m3, ischaemic attacks were more likely to occur in elderly patients with T2DM than in those without T2DM. Ongoing, continuous monitoring of the clinical and environmental data will help to improve the accuracy of future evaluations of the associations between environmental factors and disease structure.
Footnotes
Acknowledgement
We thank Mr Yuichi Hirayama, information systems engineer, for providing advice and assistance on the tabulation method and spreadsheet calculations that were required for handling the large amounts of data generated by the study.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.