
Abstract
Background
Mothers and their children demonstrate dyadic synchrony of hypothalamic–pituitary–adrenal (HPA) axis function, likely influenced by shared genetic or environmental factors. Although evidence has shown that chronic stress exposure has physiologic consequences for individuals—including on the HPA axis—minimal research has explored how unmet social needs such as food and housing instability may be associated with chronic stress and HPA axis synchrony in mother–child dyads.
Methods
We conducted a secondary analysis of data from 364 mother–child dyads with low-income recruited during a randomized trial conducted in an urban pediatric clinic. We used latent profile analysis (LPA) to identify subgroups based on naturally occurring patterns of within-dyad hair cortisol concentration (HCC). A logistic regression model predicted dyadic HCC profile membership as a function of summative count of survey-reported unmet social needs, controlling for demographic and health covariates.
Results
LPA of HCC data from dyads revealed a 2-profile model as the best fit. Comparisons of log HCC for mothers and children in each profile group resulted in significantly “higher dyadic HCC” versus “lower dyadic HCC” profiles (median log HCC for mothers: 4.64 vs 1.58; children: 5.92 vs 2.79, respectively; P < .001). In the fully adjusted model, each one-unit increase in number of unmet social needs predicted significantly higher odds of membership in the higher dyadic HCC profile when compared to the lower dyadic HCC profile (odds ratio = 1.13; 95% confidence interval [1.04-1.23]; P = .01).
Conclusion
Mother–child dyads experience synchronous patterns of physiologic stress, and an increasing number of unmet social needs is associated with a profile of higher dyadic HCC. Interventions aimed at decreasing family-level unmet social needs or maternal stress are, therefore, likely to affect pediatric stress and related health inequities; efforts to address pediatric stress similarly may affect maternal stress and related health inequities. Future research should explore the measures and methods needed to understand the impact of unmet social needs and stress on family dyads.
Introduction
Background
Individuals who experience persistent social adversity have a disproportionately higher risk of chronic disease and negative health outcomes.1,2 Such disparities are largely driven by structural factors, including discriminatory policies and the inequitable distribution of economic resources, which impact access to many medical and social services that support health in daily life. 1 Evidence is also mounting that experiences of social adversity may have physiologic consequences stemming from persistent and toxic levels of stress that compound inequities in chronic health conditions.3–5
Stress triggers activation of the hypothalamic–pituitary–adrenal (HPA) axis, which regulates glucocorticoids such as cortisol and other hormones that help the body cope or adapt in response to acute stressors. 5 Excessive or chronic cortisol activation, however, can stimulate persistent pathophysiologic processes such as alterations to energy metabolism and fat deposition, 6 disruptions to stress regulation, 7 or impaired function of the hippocampus and prefrontal cortex related to learning and mood regulation.8–10 Substantial evidence links stress from social adversity to elevated cortisol levels in children and adults,11,12 supporting the hypothesis that experiences of social adversity may contribute to prolonged and ultimately pathophysiologic stress responses.
Social needs are adverse social conditions associated with health outcomes and identified or prioritized by individuals—for example, food, housing, or employment needs.13,14 Existing research that links unmet social needs to stress in parents and children often has examined the impact of social adversity on physiologic stress at the individual level (effects on the parent or the child) rather than the dyadic level (effects on the parent–child dyad as a unit).15–18 However, several studies indicate that parents and children, particularly mothers and children, experience synchrony or attunement in cortisol regulation.19–23 This may be attributed to both physiologic factors such as genetics and prenatal programming, as well as behavioral or environmental processes such as shared environments and social interaction.22,24 Studies that focus on individual stress alone may underestimate the full extent of the adverse impacts of unmet social needs, given that a mother and child share a social environment and their responses to stress are interconnected.
The evaluation of HPA axis synchrony in parent–child dyads with shared exposures to persistent stressors requires special considerations related to measures and analysis. Hair cortisol concentration (HCC) has been historically used as an indicator of chronic physiologic stress.25,26 The average concentration of cortisol deposited in the hair corresponds to the slow rate of hair growth (ie, approximately 1 cm of hair represents a 1-month average of cortisol), and thus is thought to represent physiologic stress over a longer period.25,26 Few studies have investigated HPA axis synchrony using HCC in part because it cannot accurately indicate cortisol reactivity between dyad members that occurs in response to a specific or acute stressor, and it does not shed light on the sequencing of the stress response between members of the dyad. 27 However, these concerns are less salient in the context of persistent and multiple stressors such as those experienced by families with unmet social needs. The analysis of HCC may in fact be preferable in the context of unmet family social needs, where the outcomes of interest include the broader picture of synchrony in dyadic stress over time.
The lack of clinically meaningful cortisol level cutoffs that indicate psychological stress26,28–30 has traditionally made it difficult to categorize and compare patterns of lower or higher stress within dyads, regardless of the specimen used to measure cortisol (eg, hair, saliva, urine). Innovative methods such as latent mixture modeling, however, provide new opportunities to capture dyadic patterns even in the absence of established cutoffs. In this study, we applied these methods to improve our understanding of dyadic physiologic synchrony in the context of chronic stress exposure, with the overarching goal of informing dyadic interventions that might mitigate the health impacts of chronic stress for families at risk.
Study Aims and Hypotheses
Our study aims were 2-fold: (1) identify and describe naturally occurring subgroups (ie, profiles) of mother–child dyads based on patterns of within-dyad chronic physiologic stress (as indicated by HCC), and (2) examine associations between identified profiles and unmet social needs. We hypothesized that dyads with higher unmet social needs would be more likely to belong to profiles characterized by higher within-dyad physiologic stress.
Methods
Study Design and Sample
This was a secondary analysis of cross-sectional baseline data collected between 2016 and 2018 from an evaluation of a clinic-based social needs navigation program (SFGH Health Advocates Stage II [HAS-II] Study; NCT02746393). 31 The HAS-II Study enrolled a convenience sample of 622 English-speaking or Spanish-speaking parent–child dyads seeking care in a large federally qualified pediatric urgent care center housed in an academic medical center in San Francisco, California. Dyads were deemed eligible if they resided in the county of enrollment, including a child age 0 to 17 years, and a caregiver age 18 years or older who was English or Spanish-speaking and familiar with the child's household environment. 31 Children in foster care or presenting for child maltreatment evaluations were excluded, along with families who had already been enrolled in a similar social services navigation program within the previous 6 months. For this analysis, we limited the sample to the 364 dyads (59%) in which the parent identified as the child's mother and for whom there was no missing HCC data. The HAS-II Study was approved by the institutional review board of the University of California, San Francisco, and informed consent and assent were obtained per their approved study protocol. 31 All data were de-identified prior to our analysis and therefore exempt from review by the committee on human subjects’ research.
Data Collection
During the HAS-II study, mothers completed surveys to report sociodemographic and health characteristics for themselves, their child enrolled in the study, and their household. Surveys were administered in English or Spanish by a trained research assistant (RA), and either self-completed on an electronic tablet or conducted verbally and recorded by the RA to accommodate all levels of literacy. Additional details about the survey data collection process have been published elsewhere. 31
Measurement
Primary dependent variable: Chronic physiologic stress
HCC was used as an indicator of chronic physiologic stress in both members of the dyad (mother and child). In the HAS-II study, the RA collected hair samples of at least 3 cm length from the scalp of each participant. These samples were sent to an external laboratory for analysis using a liquid chromatography–mass spectrometry protocol which is detailed in a published supplement. 31 HCC data are in units of picogram per milligram (pg/mg). Although there is no consensus on cutoff values for HCC to date, increasing levels are widely considered a marker for a chronic physiologic stress response.25,26 Prior to analysis, HCC data were log-transformed to approximate a normal distribution, and outliers greater than 3 standard deviations from the mean (n = 6 observations) were excluded from the sample. 32
Primary independent variable: Count of unmet social needs
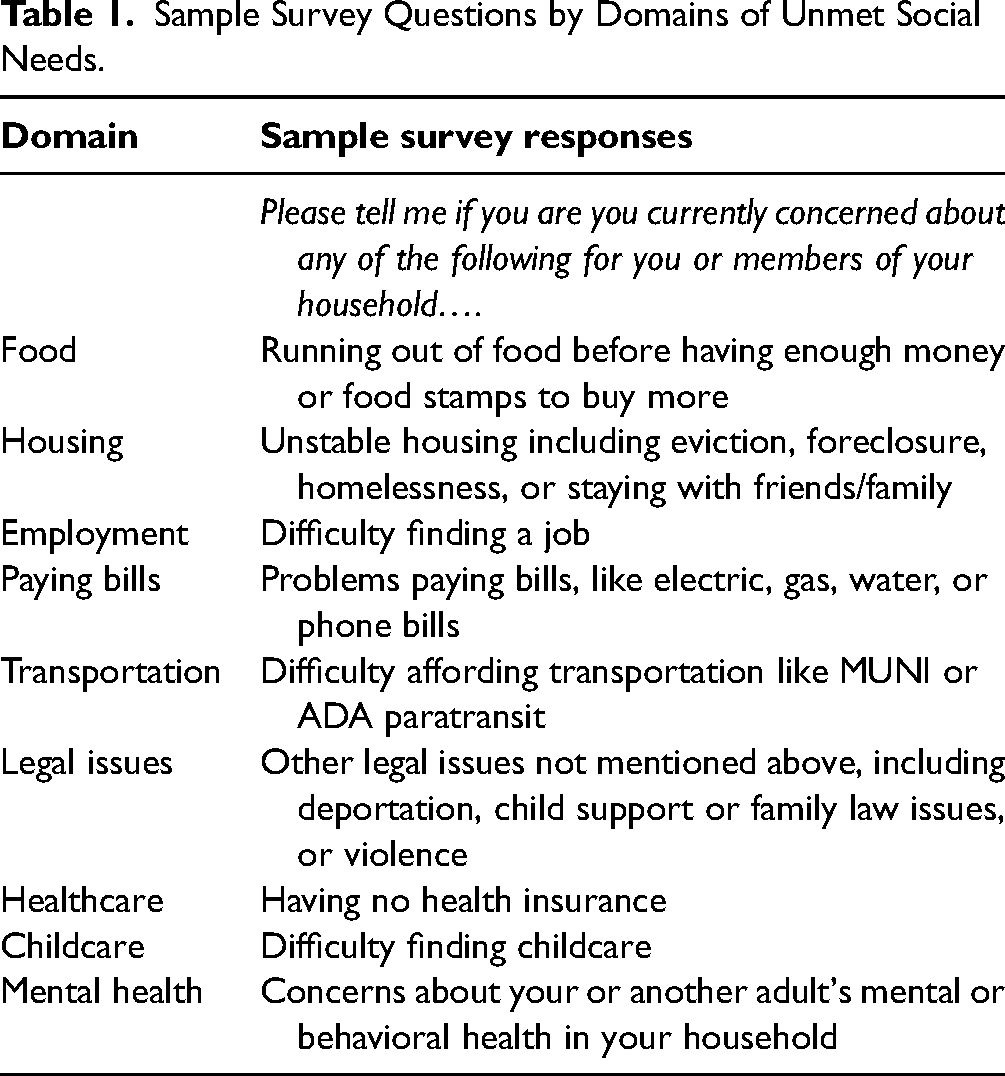
Self-reported unmet social needs were indicated by mothers’ responses to the statement: “Please tell me if you are currently concerned about any of the following for you or members of your household…”. Mothers were able to choose from a list of up to 18 social needs from 9 different domains, including food, housing, employment status, and various other social risk factors (see Table 1). The social needs survey was designed by the HAS-II study investigators based on a combination of survey tools and questions used in prior social needs research (eg, the Medical Advocacy Screening Questionnaire 33 ), and versions of it had been used in 2 prior studies.34,35 Count of unmet social needs was determined by summation of the total number of needs reported as a concern by the mother, and therefore, ranged from 0 to 18.
Sample Survey Questions by Domains of Unmet Social Needs.
Covariates
Covariates were selected based on potential confounding due to their influence on HCC through stress or other physiologic mechanisms. Demographic covariates include mother's age (18–24 years, 25–34 years, 35–44 years, and 45 years and older), child's age (0–5 years, 6–12 years, and 13–17 years), and child sex (male and female). Mothers’ self-reported race/ethnicity (Latinx; Black, non-Latinx; Asian or Pacific Islander, non-Latinx; White, non-Latinx; Multiracial or other) was also included as a proxy for exposure to racism or discrimination, which is associated with social risk 1 and physiologic stress.3,36,37
Covariates related to physical and mental health were also included. Mother's report of child global health status was measured with a single item from the National Survey of Children's Health that assessed child mental and physical health status on a 5-point scale from poor to excellent in response to the statement, “In general, would you say your child's health is…”31,38 Mothers self-reported their own physical health status on a 5-point scale from poor to excellent in response to the question, “In general, how would you rate your physical health?” taken from the Patient-Reported Outcomes Measurement Information System (PROMIS®) global physical health scale. 39 Mothers also reported on their mental health status via the Patient Health Questionnaire-8 survey of depressive symptoms (scores range 0-24, with higher scores indicating greater risk for depression), 40 and the Perceived Stress Scale-4 which measures perceived control over or ability to handle stress in the previous month (scores range 0-16, with higher scores indicating greater perceived stress).41,42 Ratings or scores for health measures were used as continuous variables in the models.
Data Analysis
Summary statistics were used to describe the sociodemographic and health characteristics of the mothers and children in our sample. Initial Pearson correlations were examined between mother and child HCC and all variables to test broad associations. To accomplish our first aim, we used latent profile analysis (LPA) to determine whether distinct profiles of mother–child dyads could be identified based on naturally occurring patterns in their HCC, and if so, how many profiles were present. 43 With the dyad as the unit of analysis, latent profile models were sequentially estimated, beginning with a 2-profile model. We continued to estimate models adding one additional profile at a time until model fit began to deteriorate, resulting in 3 models with 2, 3, and 4 profiles, respectively. In each model, HCC values for mother and child were modeled as continuous indicator variables, and residual correlations of mother and child HCC values were included to adjust for dyadic nonindependence. Maximum likelihood estimation with robust standard errors was used in all models, and all were run using Mplus version 8.7 (Muthen & Muthen).
After the initial series of LPA models had been estimated, the same models were then reestimated to include adjustments for child age and biological sex. This was to account for the known effects of sex and age on HCC in children.44,45 Models with and without adjustment were equivalent: there were no substantive differences in model parameters or fit statistics, and dyads did not switch between identified profiles (all stayed within the same profiles identified in the original unadjusted models). As a result, the more parsimonious set of models (ie, without adjustments) went forward for formal evaluation and comparison of fit.
There are differing views on the optimal criteria for latent class or latent profile model selection, although most support the use of multiple metrics. 43 In alignment with previous work,46,47 we used the following criteria to evaluate and compare fit across models: (1) posterior probabilities for most likely profile assignment closest to 100%; (2) model convergence (entropy) closest to 1.0; (3) model is a significantly better fit for the data as compared to a model with k–1 (ie, one fewer) profiles (Lo–Mendell–Rubin and parametric bootstrapped likelihood ratio tests significant at P < .05); (4) lower Bayesian Information Criterion (BIC); and (5) no profile containing less than 5% of the sample. After selecting the best-fitting model, a new variable was created that indicated to which profile each dyad in the sample belonged. Features and key sample characteristics of identified profiles were then assessed (by Chi-square, t test, or Wilcoxon rank-sum tests, as appropriate) for clinically and theoretically meaningful differences.
To accomplish our second aim, we modeled the main outcome of the LPA analysis (ie, mother–child dyadic HCC profile membership) in relation to the unmet social needs composite. The final model included covariates showing a significant correlation with mother's HCC, child HCC, or unmet social needs at P = .10 or less using a Bonferroni-adjusted significance level (see Appendix). Logistic regression was used to predict dyadic HCC profile membership as a function of the summative count of unmet social needs, controlling for all demographic and health covariates. We used Stata version 17 for all descriptive and regression analyses.
Results
Sample Characteristics
Characteristics of the full sample are summarized in Table 2. Most mothers were between the ages of 25 and 44 years, 50% of children were under 5 years of age, and 56% were identified as female. Approximately 85% of mothers in the sample self-identified as Latinx, therefore, this was used as the reference group in later regression models. Mothers on average reported good physical health for themselves and their children, and low-to-moderate symptoms of depression or perceived stress. Median log HCC was higher in children than in mothers, as expected due to known age differences in cortisol levels. 48 Mother and child log HCC were moderately positively correlated (r = 0.51, P < .05; see Appendix).
Demographic and Health Characteristics of Mother–Child Dyads, by HCC Latent Profiles (n = 364).

Abbreviations: IQR, interquartile range; PHQ-8, Patient Health Questionnaire (8-item), higher score indicates greater risk for depression; PSS-4, Perceived Stress Scale (4-item), higher score indicates greater perceived stress; PROMIS, Patient-Reported Outcomes Measurement Information System, higher score indicates better physical health.
Median (IQR) presented to account for variables with positively skewed distribution of data.
Higher score indicates better overall health.
Significance at P < .05.
Identification of Profiles Based on Within-Dyad HCC Patterns
Table 3 presents the statistical metrics of fit and uncertainty we used to select our final LPA model. We found that the 2-profile model provided the best fit, given the high posterior probabilities and entropy in comparison to the other models, the significance of both Lo–Mendell–Rubin and parametric bootstrap likelihood ratio tests, and adequately sized subsamples within each profile. Differences in BIC across the 3 models were negligible. 43
Metrics of Fit and Uncertainty for Latent Profile Models of Dyadic HCC.a

Abbreviations: BIC, Bayesian Information Criterion; LMRT, Lo–Mendell–Rubin likelihood ratio test; PBLRT, parametric bootstrapped likelihood ratio test.
Bold font indicates characteristics of final model selection.
Comparison of sample characteristics by dyadic HCC profile
We then compared the characteristics of the 2 naturally occurring profiles of within-dyad HCC identified by our LPA model. Median mother and child log HCC levels were both significantly lower in one profile as compared to the other profile (Table 2). Specifically, the mother's log HCC levels were 1.58 (interquartile range [IQR] 1.15-2.12) in the first profile as compared to 4.64 (IQR 3.89-5.28) in the second profile (P < .001), and the child's median log HCC was 2.79 (IQR 1.79-4.15) in the first profile as compared to 5.92 (IQR 4.26-7.61) in the second profile (also P < .001). Since the naturally occurring patterns reflected in profile 1 as compared to profile 2 were generally characterized by significantly lower versus higher HCC levels for both members of the dyad, we chose to label them “lower dyadic HCC” and “higher dyadic HCC,” respectively (Figure 1).
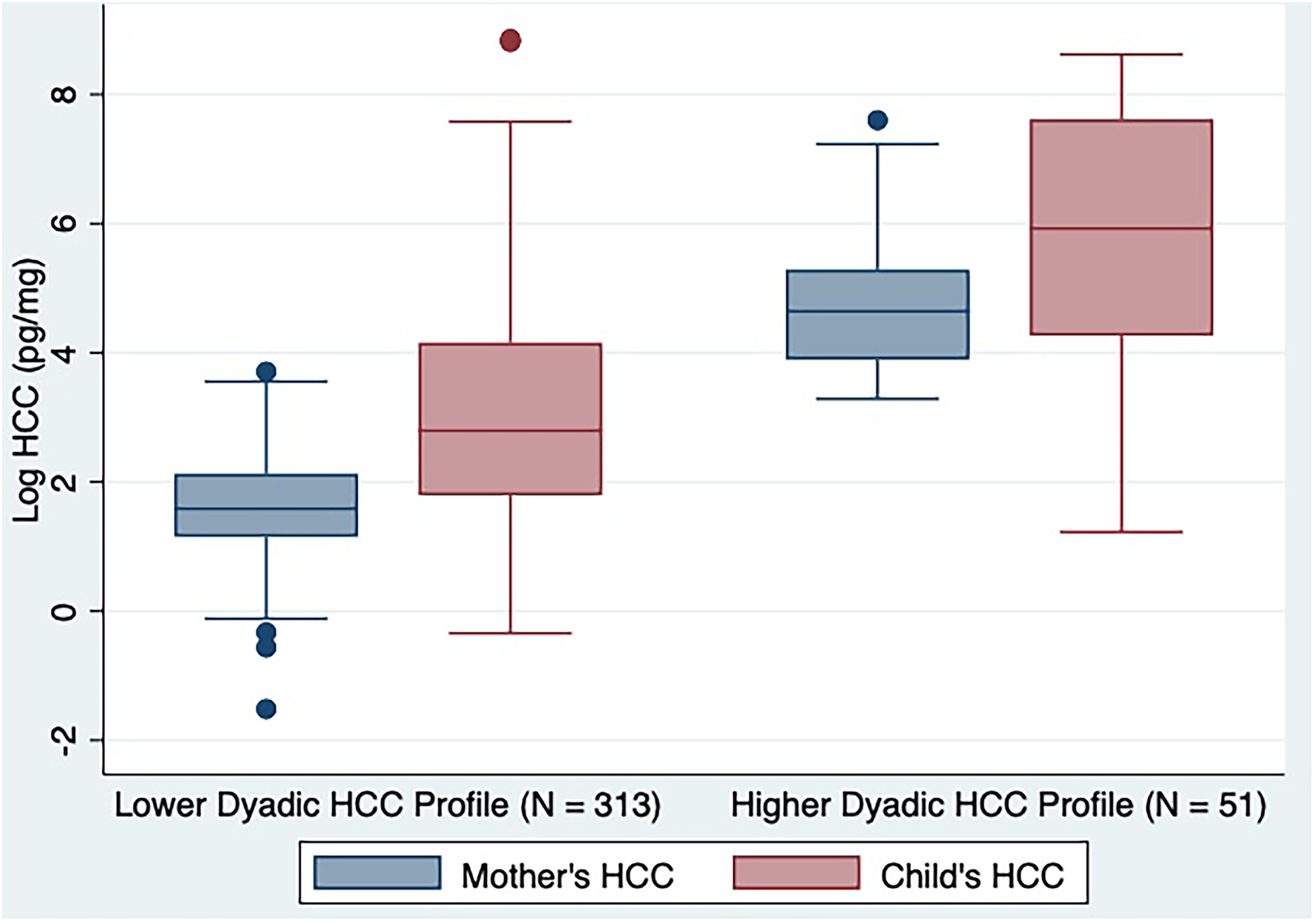
Boxplots of mother and child HCC, by latent profile membership.
The lower dyadic HCC profile consisted of n = 313 dyads, and the higher dyadic HCC profile consisted of n = 51 dyads. Age and sex characteristics did not significantly differ between profiles. Dyads with mothers who identified as Latinx were significantly more likely to fall into the lower dyadic HCC profile (87.5% vs 66.7%), while the higher dyadic HCC profile was more likely to include participants who identified as Black, non-Latinx (15.7% vs 5.1%), Asian/Pacific Islander (7.8% vs 2.6%), and multiracial/other (5.9% vs 1.6%); those who identified as White, non-Latinx were equally likely to be in either profile (3.2% vs 3.9%; P = .002). Mothers’ reports of physical health, depression symptoms, or perceived stress were not significantly different between profiles. Dyads in the higher dyadic HCC profile were significantly more likely to report a greater median number of unmet social needs when compared to the lower HCC profile (5 vs 3, respectively; P = .001).
Associations Between Unmet Social Needs and Dyadic HCC Profiles
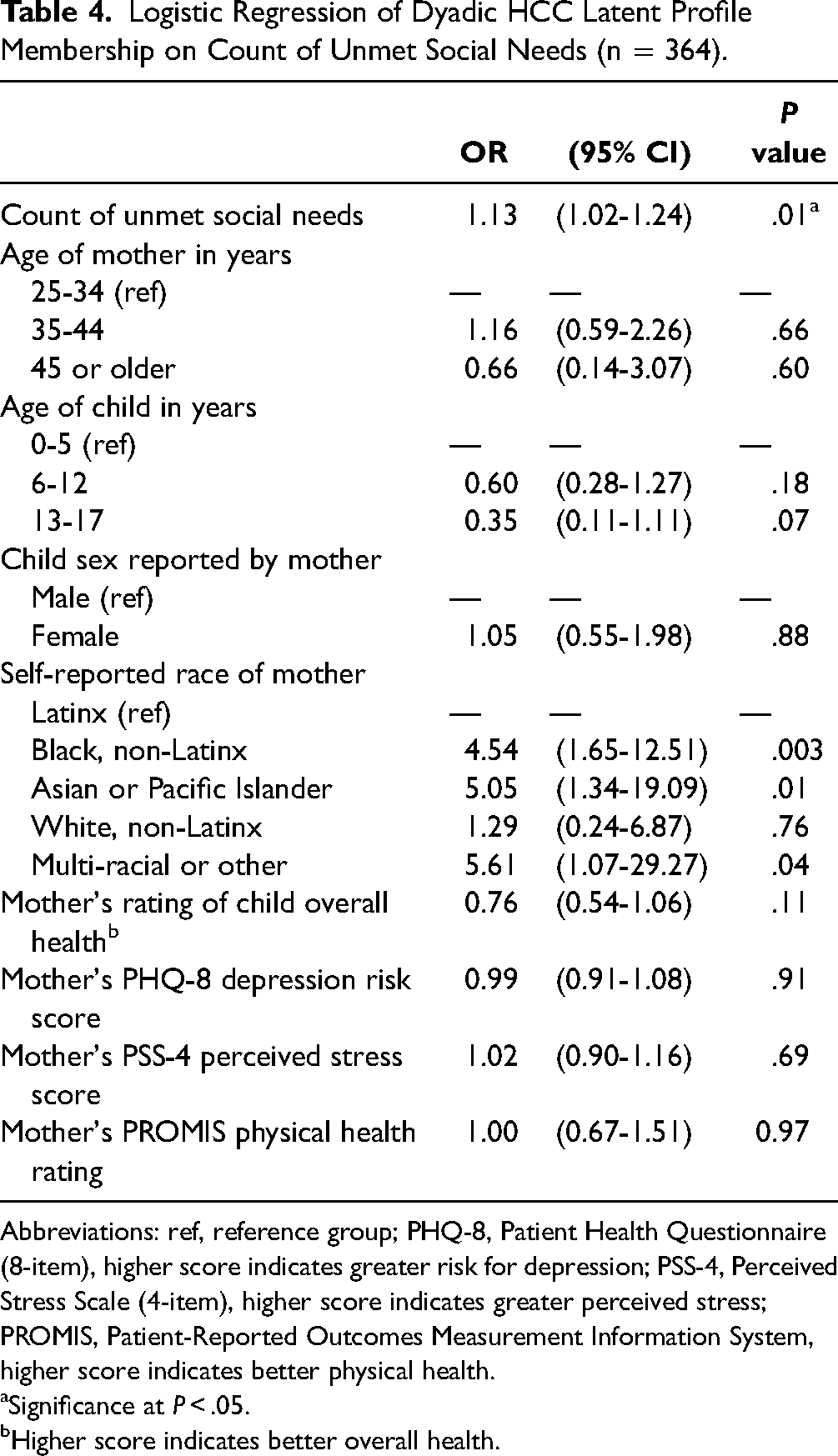
Table 4 presents the results of the logistic regression model. In the fully adjusted model, each one-unit increase in number of unmet social needs predicted significantly higher odds of membership in the higher dyadic HCC profile when compared to the lower dyadic HCC profile (odds ratio [OR] = 1.13; 95% confidence interval [CI] [1.04-1.23]; P = .01). In post hoc analyses, we examined whether any individual unmet social needs independently predicted profile membership but did not detect any significant associations in unadjusted or adjusted models (results not shown). Although race/ethnicity was a significant predictor in the models, the very small proportions of participants in non-Latinx racial/ethnic groups (<5% of the sample for most groups) and wide CIs led us to question the precision of these findings. In sensitivity analyses, excluding the race/ethnicity variable did not result in significant changes to the ORs or standard errors of other variables in the model. In effect modification analyses to test whether the association between unmet social needs and dyadic HCC was moderated by race/ethnicity, we noted no significant interactions to prompt further stratified analyses.
Logistic Regression of Dyadic HCC Latent Profile Membership on Count of Unmet Social Needs (n = 364).
Abbreviations: ref, reference group; PHQ-8, Patient Health Questionnaire (8-item), higher score indicates greater risk for depression; PSS-4, Perceived Stress Scale (4-item), higher score indicates greater perceived stress; PROMIS, Patient-Reported Outcomes Measurement Information System, higher score indicates better physical health.
Significance at P < .05.
Higher score indicates better overall health.
Discussion
In this study of mother–child dyads with low income, we found that the number of unmet social needs is positively associated with membership in a higher HCC dyadic profile. This finding builds on prior work showing associations between unmet social needs and HCC in mothers and unmet social needs and HCC in children15,16,49 and now extends that work to show that unmet social needs also influence mothers and children as a dyadic unit. Across these studies, the growing evidence that unmet social needs affect physiology builds support for strategies to address economic disadvantage as a way to improve population health.2,3,12
The link between unmet social needs and dyadic physiologic stress has implications for clinical practice and health policy. The presence of latent profiles of higher and lower dyadic HCC in this sample supports emerging evidence that many children are physiologically attuned to their parent's stress levels, although the mechanisms for this attunement are likely multifactorial and reflective of a complex interaction of biologic and environmental factors.22,23,27 Prior studies of parent-child dyads have found that in the context of negative environmental factors, physiologic synchrony may be associated with greater physiologic stress and maladaptive patterns of self-regulation or relational patterns in the dyad.50,51 This could mean that clinical interventions for stress reduction in either parents or children may have mutual physiological benefits for both. From a policy perspective, this also underscores the potential physiologic and health benefits of targeting approaches that support both individual social needs and population-level social conditions.
Although previously published evidence has shown HPA axis synchrony in similar populations of mother–child dyads, the majority of studies have been conducted using laboratory-administered stressors and measured stress using salivary cortisol to reflect the acute stress response.20,21 In contrast, in this study we used HCC, which is a better estimate of chronic stress exposure experienced by families with unmet social needs. Additionally, though several studies have examined and shown correlations between mother and child HCC,52–58 in this study, we used LPA as a novel analytic alternative to deepen insights into dyadic synchrony in HCC. Our study is also one of few we know of to test whether mother–child HCC synchrony is significantly associated with social adversity.53,54
Our findings add to a large and growing body of evidence that clearly demonstrates that health inequities are driven by structural determinants, including programs, policies, and practices that shape health behaviors and access. 59 Environmental exposures such as neighborhood disadvantage have been linked to stress and HPA activity60,61 and can impact the health of multiple members of the household. The impact of the COVID-19 pandemic has significantly widened inequities in unmet social needs for communities with low income,62–64 and it is likely our findings underestimate the current state of need and stress in this population. Studies find that social care interventions can support health by improving access to services and resources related to food, housing, and employment. 65 Most current social care interventions involve assisting with or adjusting for each individual need—for example, a client who reports food insecurity may be referred to a local food pantry. Yet, while we found associations between count of unmet social needs and stress patterns within the dyad, our post hoc analysis did not reveal associations between HCC and individual unmet social needs, indicating the importance of the cumulative effect of unmet social needs on family health. Other studies have shown associations between cumulative social risk burden and decreased utilization of health services.66–68 Taken together, evidence suggests that in addition to domain-specific interventions, it may be beneficial for interventions targeting family stress to recognize the cumulative burden of unmet social needs and its potential impact on health care access and utilization.
Limitations
Findings from our study should be considered in the context of 5 limitations. First, in this secondary analysis, we were unable to account for unmeasured confounders that may also influence unmet social needs and physiologic stress, either independently or in relation to each other (eg, body mass index, 69 experiences of racism,3,70 immigration status 71 ). Second, while LPA is a promising approach for determining subgroups according to data patterns, class assignment is based on probabilities and therefore may lead to misclassification. 46 Third, the sample studied included treatment-seeking, mostly Latinx mothers and children with low income, which limits the generalizability of findings to other populations. Fourth, our findings should be interpreted with the understanding that HCC is only one indicator of physiologic stress. Sympathetic nervous system arousal does not necessarily reflect the same psychological state in each participant or each dyad member; it can also reflect social processes or relationship characteristics between the dyad that we could not account for in this study. 24 Finally, our investigation of cross-sectional HCC data limits our ability to infer causality from these findings or understand within-dyad temporal influences of one dyad member's physiological stress on the other member (ie, coregulation). 24 Additional studies using longitudinal dyadic HCC data are needed to better understand dyadic synchrony and coregulation in the context of chronic stress, and the effect of these on health outcomes.
Conclusion
In this study, we find that profiles of dyadic HCC can be identified to describe synchrony of long-term HPA axis function between mothers and their children with low income. Study findings confirm our hypothesis that dyads with more unmet social needs are more likely to belong to profiles characterized by higher physiologic stress. Physiologic synchrony in mother–child dyads may influence each member of the dyad's chronic stress experience. These findings underscore that there are likely to be intergenerational impacts of social care policies and other interventions that address structural drivers of unmet social needs.
Supplemental Material
sj-docx-1-css-10.1177_24705470231173768 - Supplemental material for Unmet Social Needs and Patterns of Hair Cortisol Concentration in Mother–Child Dyads
Supplemental material, sj-docx-1-css-10.1177_24705470231173768 for Unmet Social Needs and Patterns of Hair Cortisol Concentration in Mother–Child Dyads by Victoria F Keeton, Julie T Bidwell, Euclides José de Mendonça Filho, Patricia P Silveira, Danielle Hessler, Matthew S Pantell, Holly Wing, Erika M Brown, Bradley Iott and Laura M Gottlieb in Chronic Stress
Footnotes
Authors’ Note
This paper uses data from a previous RCT. After publication, deidentified participant data are available by request to researchers whose proposed use of the data has been approved. Requests can be made to holly.wing@ucsf.edu, and approval is at the discretion of the primary RCT research team, with signed data use agreement.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded in part by the Gordon and Betty Moore Foundation through GBMF4294 to the University of California, Davis Betty Irene Moore School of Nursing. The primary RCT whose data we analyzed was financially supported by the Lisa and John Pritzker Family Fund, and the JPB Foundation of New York through a grant to the JPB Research Network on Toxic Stress: A Project of the Center on the Developing Child at Harvard University. Dr Keeton is currently supported by a University of California, San Francisco, Preterm Birth Initiative transdisciplinary post-doctoral fellowship, funded by Marc and Lynne Benioff and a T32 training grant (1T32HD098057) from the National Institute of Child Health and Human Development.
Supplemental Material
Supplemental material for this article is available online.
Appendix
Bivariate Correlation Results Between Outcomes and Select Covariates.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.