
Abstract
A cardinal feature of Post-traumatic stress-related disorder (PTSD) is a paradoxical memory alteration including both intrusive emotional hypermnesia and declarative/contextual amnesia. Most preclinical, but also numerous clinical, studies focus almost exclusively on the emotional hypermnesia aiming at suppressing this recurrent and highly debilitating symptom either by reducing fear and anxiety or with the ethically questionable idea of a rather radical erasure of traumatic memory. Of very mixed efficacy, often associated with a resurgence of symptoms after a while, these approaches focus on PTSD-related symptom while neglecting the potential cause of this symptom: traumatic amnesia. Two of our preclinical studies have recently demonstrated that treating contextual amnesia durably prevents, and even treats, PTSD-related hypermnesia. Specifically, promoting the contextual memory of the trauma, either by a cognitivo-behavioral, optogenetic or pharmacological approach enhancing a hippocampus-dependent memory processing of the trauma normalizes the fear memory by inducing a long-lasting suppression of the erratic traumatic hypermnesia.
Despite a clear clinical picture of Post-traumatic stress disorder (PTSD), the psychobiological bases of this devastating stress-related disorder developed by 20 to 30% of victims of a traumatic life event experienced as a threat of injury or death, 1 are still poorly understood. Current treatments are mostly symptomatic, effective only for less than half of patients and include frequent side effects and residual symptoms, making this pathology a major medical challenge.
A key and very disabling symptom of PTSD is a recurrent, long-lasting and intrusive recollection of traumatic memories characterized by intense fear responses in safe situations (i.e. emotional hypermnesia). However, although often more discreet, a declarative amnesia for peritraumatic aspects such as the environment in which the traumatic event occurred completes the PTSD-related memory profile.2–5 Interestingly, some clinical studies have suggested that this contextual amnesia may constitute an etiological factor of PTSD-related hypermnesia: decontextualized, the traumatic memory would not be restricted to its context/place of origin and to its specific past time window; consequently, this pathological memory would be uncontrollable, and therefore prone to be automatically reactivated by any salient stimulus more or less linked to the trauma and in contexts that may be very different from the original traumatic context.
3
Using the first animal model that recapitulates the two memory components of PTSD (i.e. emotional hypermnesia and contextual amnesia),
9
we recently demonstrated that contextual amnesia is indeed responsible for the traumatic hypermnesia, and that promoting the hippocampus-dependent contextual memory of the trauma, either by a cognitivo-behavioral, optogenetic or pharmacological approach, durably suppresses this maladaptive hypermnesia, thus normalizing the memory of the traumatic event.
10
Contextual Amnesia as a Cause of Traumatic Hypermnesia: Cognitivo-Behavioral and Optogenetic Approaches
PTSD-like memory is induced in mice by the combination of contextual fear conditioning using a relatively high footshock intensity unpaired with a tone and post-training corticosterone (CORT) injection (2mg/kg, i.p.), the main stress hormone in rodents. While control (i.e. NaCl-injected) mice subsequently display a high conditioned fear to the context, which is the correct predictor of the shock, but not to the irrelevant (non-predictive) tone, CORT-injected mice identify the salient tone instead of the context as the predictor of the shock; thus, they display a PTSD-like memory attested by an abnormally high fear response to the tone (mimicking a pathological emotional hypermnesia) together with a reduced conditioned fear to the aversive context (mimicking contextual amnesia). 9
Combining this model with an optogenetic approach, we first showed that inhibition of the dorsal Cornu Ammonis-1 (dCA1) hippocampal sub-field during fear conditioning is sufficient to induce not only contextual amnesia but also the long-lasting emotional hypermnesia component of PTSD. Reciprocally, in traumatic condition, dCA1 activation not only promotes the contextual memorization of the trauma but also prevents the development of PTSD-like hypermnesia. 10 These findings demonstrate that amnesia for the traumatic context, which is due to hippocampal hypoactivity during the trauma, is causally involved in PTSD-like memory formation, and that promoting the contextual memory of the trauma through hippocampal activation can prevent this pathological process.
Second, we showed that once PTSD-like memory has been developed, recontextualizing the traumatic memory restores a normal fear memory. Specifically, reactivating the traumatic memory, through re-exposure to the salient tone (which has been abnormally strongly associated with the footshock) in the original traumatic context specifically restores a normal contextual memory of the trauma, while suppressing the abnormal emotional hypermnesia. In contrast, partial re-exposure to trauma-related cues, either to the tone alone (in a safe context), to the conditioning context alone, or to both the tone and the context but spaced out by 2 h, fails to cure the traumatic memory, which remains PTSD-like.
10
In PTSD patients, frequent reactivation of PTSD-related memory through flashbacks in safe contexts seems to contribute to the persistence of this pathological memory. We suggest that reactivation of traumatic memory in PTSD would be incomplete. More particularly, disconnected from a hippocampus-dependent memory representation, such incomplete (intrusive/uncontrolable) memory reactivation would strengthen the original memory trace.
3
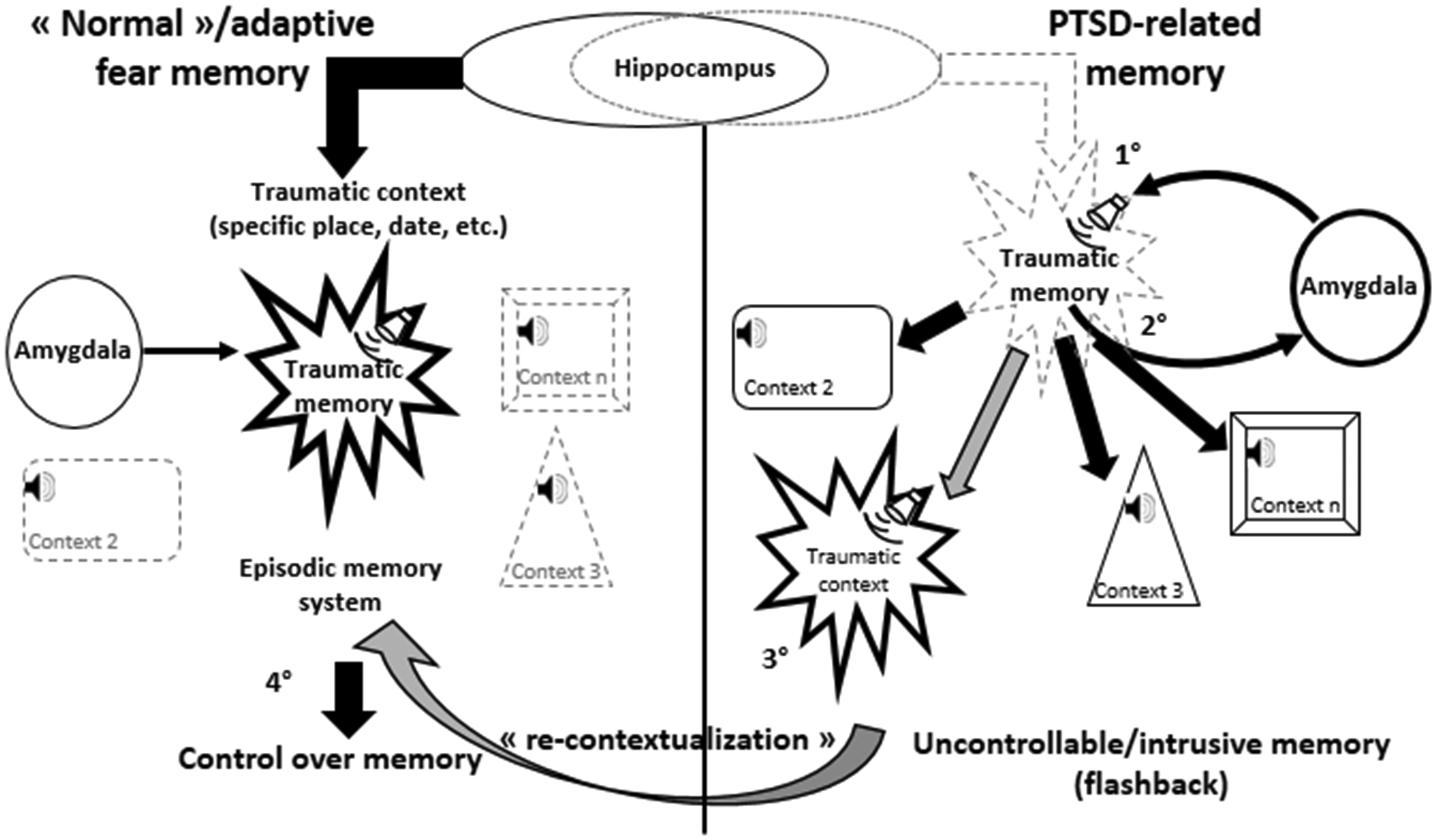
Proposed underlying mechanisms of normal vs. PTSD-like fear memory.
Preventing PTSD-Like Hypermnesia by Promoting Contextual Memory: A Pharmacological Approach
Using the same animal model, we also showed that acute administration of brexpiprazole (BREX, 0.3 mg/kg), a new antipsychotic drug with pro-cognitive effects in rodents, 7 days’ post-trauma, persistently prevents the expression of PTSD-like memory: enhancing (with superior efficacy when compared to diazepam, prazosin, and escitalopram) memory for the traumatic context, while blocking the expression of the maladaptive fear memory for a salient but irrelevant trauma-related tone. In addition, this treatment not only promotes the switch from PTSD-like to normal (contextual) fear memory, but also normalizes most of the alterations in the hippocampal-amygdalar network activation associated with PTSD-like memory. 11 These preclinical data indicate that BREX could represent a new pharmacological treatment of PTSD.
Interestingly, certain data strongly suggest that this beneficial effect of BREX might be, at least in part, mediated by a pharmacologically-induced enhancement of hippocampus-dependent cognitive processing, which could be based on its partial agonist activity at 5-HT1A receptors. Indeed, BREX was shown to fully reverse subchronic phencyclidine (PCP)-induced cognitive impairments in the hippocampus-dependent novel object recognition test, which is known to require episodic memory; a beneficial effect which was reduced by administration of a 5-HT1A antagonist.
13
In parallel, BREX was also shown to inhibit conditioned avoidance behavior, a response which is based on the simple conditioned association between a salient (e.g. tone) conditional stimulus and a footshock unconditional stimulus. This inhibitory effect, thought to be based on its D2 partial agonism,
13
Conclusion: Starting Point for a Translational Research Developing a New Therapeutic or Preventive Approach of PTSD
The demonstration that recovery from PTSD-like hypermnesia depends on recovery from contextual amnesia calls for promoting therapeutic approaches of PTSD centered on trauma contextualization and its underlying hippocampal mechanisms.
Clinical observations suggest that mental narrative of the event during the trauma would constitute a resilience factor to the development of PTSD. 12 In line with this suggestion, our findings suggest that the hippocampus-dependent connection (or reconnection) of the traumatic episode with its context (i.e. its specific place, date and sequence of events), therefore its integration into the episodic memory system, would promote a relativization of the trauma through narration, a necessary condition to keep (or regain) control over “traumatic” memory, thus preventing (or eliminating) flashbacks.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Institut National de la Santé et de la Recherche Médicale, Fondation pour la Recherche sur le Cerveau, Ministère de l’Enseignement supérieur et de la Recherche, University of Bordeaux and the Agence Nationale pour la Recherche Grant PTSDmemo (ANR-14-CE13-0026-01).