
Abstract
Early childhood is an important developmental period, which lays the foundation for future learning, behaviour, physical and mental health and gene expression. The most vulnerable children in society are often referred to and receive services from the child welfare system because of a concern of abuse and neglect and/or a poor developmental trajectory. This paper presents an organizing framework for how the child welfare system, in concert with allied partners, can support interventions for young children and families by acknowledging its crucial role in improving their development and well-being. The framework is informed by research amassed from numerous disciplines, including child welfare, development, neuroscience, neurobiology and epigenetics. Although the notions of protection and well-being are central considerations in child welfare legislation in Ontario, Canada, the operationalization of wellbeing has proven challenging in child welfare practice, policy and research. The framework proposes ten key indicators and priorities for identifying and promoting optimal child development. Findings from the 2013 cycle of the Ontario Incidence Study of Reported Child Abuse and Neglect (OIS-2013), the only provincial source of aggregated child welfare investigation data, are presented to articulate the divide between the environmental context of a population of at-risk children and the conditions that both protect children and increase the likelihood that they will thrive in adulthood. This paper argues there are different points of entry and intervention across sectors and provides a foundation for further discussion on how to promote well-being for society's most vulnerable children.
Introduction
Background and Ontario Child Welfare Context
Optimal child development is the result of consistent, predictable, and stimulating interactions within nurturing relationships. 1 -3 When children experience maltreatment, it can contribute to poor physical, psychological, and behavioral outcomes. 4 -6 It is therefore recognized as a significant public health problem. 7,8 Infancy and early childhood are critical periods of development which lay the foundation for future learning, behavior, and physical and mental health. 1 Environmental factors and experiences during this developmentally sensitive period can permanently alter gene expression and function and can have devastating consequences on brain architecture, formation, and long-term development. 9 -11
A series of Canadian incidence studies of reported child abuse and neglect have helped to highlight the unique vulnerability, risks, and service needs of child welfare–involved young children and their families. 8,12 -16 When compared to older children, infants and young children (under the age of 5) are among the most likely to be investigated, 8,16 -18 to receive ongoing child welfare services following an investigation, 15,16 to be the subject of a court application, 15 and to experience an out-of-home placement. 15,16 These emerging trends converge on the importance of prioritizing and integrating the science of early childhood development into child welfare practice and policy contexts. 19
Not only are young children more likely to be in contact with the child welfare system and to receive intensive service responses, they are also disproportionately vulnerable to the developmental consequences of maltreatment and other adversities. The early years is a time of great opportunity and vulnerability as a result of the developing brain. 20,21 When compared to the general population, children reported for maltreatment have been found to have higher rates of developmental issues, 22 regardless of whether allegations investigated were substantiated. 23,24 At school entry, children have been involved with the child welfare system as infants have been found to have high levels of unmet mental health and educational needs. 22
There have been long-standing concerns noted in the extant literature with respect to the child welfare system’s inadequate response to the distinct developmental needs of infants and young children. 10,25 Developmental difficulties that emerge in early childhood are more difficult to address over time. 2 The benefit of services to young children and their families is dependent upon timely assessment and identification. 26 The importance of the child welfare system intervening early or collaborating with early intervention services that are readily available and accessible is supported by the science of early childhood development. The ever-expanding knowledge emerging from the social and biological sciences has not led to a significant policy response for child welfare–involved children in Ontario, Canada. 19 For instance, there is no comprehensive strategy with respect to the developmental screening, assessment, and monitoring of outcomes for young children involved with the Ontario child welfare system. 19 Moreover, the province does not have a child mental health strategy that specifically and explicitly focuses on the distinct needs of children under the age of 6. 27 Young children and families identified to the child welfare system for a concern of abuse or neglect present this system with an opportunity to contribute to ameliorating the impact of maltreatment by promoting their optimal development and well-being.
In Canada, child welfare services are governed by provincial and territorial legislation. 28 Prioritizing and enhancing the development of children involved with the child welfare system is consistent with child welfare statutes across Canada, including the province of Ontario which gives equal consideration to the notions of both protection and well-being. 29 The notion of protection focuses on the immediate safety of the child, whereas well-being focuses on the consequences of family dysfunction on child development. 29 Although well-being is a consideration central and equal to safety in Ontario’s child welfare legislation, 29 its operationalization and measurement have proven challenging in child welfare practice, policy, and research. Jones and colleagues 30 have posited that child well-being is more complex and difficult to operationalize and measure than child safety. There are also numerous and inconsistent definitions of child well-being within child welfare contexts in the literature. 30
Despite a decade of significant policy changes informed by Canadian incidence studies, surprisingly little is known about child welfare services provided to children and their impact on children’s service outcomes and developmental trajectories. 31 -33 These significant gaps in knowledge act as barriers to informed and responsive decision-making at both practice and policy levels. 31,32 The integration of evidence-based approaches is particularly challenging for the field given the complexity of the work, the lack of consensus and contradictions on the objectives of services, and the operationalization of child welfare’s dual mandate of safety and well-being. 33
Present Article
This article presents a framework for understanding and organizing how the child welfare system, in collaboration with allied partners, can support interventions with children and families that acknowledges this system’s crucial role in improving the well-being and development of vulnerable children. The organizing framework presented, the Human Development Top Ten, 34 proposes 10 key indicators and priorities for optimal child development. This framework reminds us that there are different points of entry and intervention across sectors. The framework is informed by literature amassed from various fields, including child welfare, development, neuroscience, neurobiology, and epigenetics. Findings from the 2013 cycle of the Ontario Incidence Study of Reported Child Abuse and Neglect (OIS-2013) 18 (the only provincial source of child welfare investigation data) are presented alongside the Human Development Top Ten indicators to contrast the adversities that child welfare–involved children experience with the Human Development Top Ten’s optimal circumstances. The purpose is to help inform priorities for better understanding and enhancing the development of children through research, practice, and policy in Ontario.
Bioecological Theory of Human Development
This article is informed by a biopsychosocial orientation. The bioecological theory of human development posits that multiple nested factors and contexts shape child development and acknowledge the influence of biology. 10,35,36 Four related systems within which the child exists were proposed by Bronfenbrenner: the microsystem, the mesosystem, the exosystem, and the macrosystem. 10,35,36 The microsystem includes factors that are the most proximal to the child; the mesosystem incorporates interactions between elements within microsystems (people, settings, etc.); the exosystem represents contexts that indirectly affect a child’s well-being and development, such as the child welfare system; and the macrosystem considers culture, policy, and social contexts. 10,35,36
The science of early childhood development has helped to highlight what children need to thrive and how the child welfare system can help to optimize child development by mitigating the negative impact of early childhood maltreatment and other risks on development. 1,10 There are complex interactions between genes, the environment, and experiences that can negatively impact biological systems. 1,11,37,38 Prenatal and early childhood experiences can temporarily modify genes as well as permanently alter their expression. 11 Impairment to the organization and functioning of neurotransmitter systems in utero or in early childhood can disrupt development. 38 Adverse experiences can lead to changes in gene function and epigenetic modifications to developing organs, including the brain, that can be detrimental to physical and mental health outcomes. 11 There is evidence that some epigenetic modifications are transgenerational, emphasizing the need for early intervention. 11
Adverse experiences or stressors in the child’s immediate environment can cause repetitive activation and lowering of the threshold of the stress response system. Toxic stress is stress that is considered excessive, frequent, uncontrollable, and prolonged and it occurs in the absence of a responsive caregiver to buffer this stress. 3,39 Risk factors for toxic stress include chronic neglect, poverty, exposure to family violence, and caregiver depression. 3,39 One consequence of prolonged activation of the stress response system is the elevated cortisol levels, which can be toxic to developing brain architecture and increase the likelihood of stress-related physical illnesses and mental health challenges. 3,39 The most critical developmental protective factor for modulating stress responses and recovering from trauma is a young child’s relationship with a stable, responsive, and competent caregiver, 40,41 thus underscoring the primacy of the child–caregiver dyad for assessment and intervention. 42
A Framework for Prioritizing and Unifying Practice, Policy, and Research Efforts: The Human Development Top Ten 34 and the OIS
The Human Development Top Ten (Figure 1) is a list of indicators developed to understand the environmental conditions and actions that increase the likelihood that children will move through the life course on a positive trajectory. Beginning with the mother’s pregnancy, these 10 indicators follow children through the developmental stages of childhood. 34

The Human Development Top Ten.
Each of the 10 indicators is summarized below underscoring why they are important for promoting optimal development.
Mother experiences stress-free and toxin-free pregnancy
The human placenta works as a sensory organ that absorbs information from its maternal host environment, 43 and so the human fetus is sensitive to exposure to toxins and maternal stress hormones. 44,45 The barrier that inhibits chemicals in the blood from entering the brain is not formed in the developing fetus. 46 Therefore, a fetus’ brain is extremely vulnerable to toxins. There is a substantial body of literature that documents the negative, lifelong effects of fetal alcohol spectrum disorder. 47 -51 Fetal alcohol spectrum disorder is caused by exposure to alcohol in utero and can have effects in many domains of the child’s life including their cognitive, social, physical, and adaptive abilities. 48 Exposure to other toxins, including environmental chemicals, recreational drugs, and prescription medications, can have varied and severe effects on the child’s long-term physical and mental health. 46,52 -55 These toxins inhibit the brain’s development by affecting both the health of individual brain cells and their functions. 46 Additionally, when a woman is anxious, stressed, or depressed during pregnancy, she releases increased stress hormones. Exposure to this increased hormone level can lead to delayed fetal maturation, 43,56 impaired neurodevelopment and cognitive performance, 43,57,58 disrupted emotional regulation, and decreased brain volume in areas associated with learning and memory. 43,59 There is evidence that males and females respond differentially to changes in the concentration of maternal stress hormones (glucocorticoids), with the female placenta being more responsive to such changes than the male placenta. 43
Child is breastfed
A large body of research has found a correlation between breastfeeding and cognitive development in early childhood. 60,61 In a cohort study comparing language ability of children who were breastfed for different amounts of time, Whitehouse and colleagues 62 found that increased breastfeeding duration had a positive effect on language ability in children at 5 and 10 years of age. While several studies have pointed to confounding factors such as maternal education and intelligence as the reason for the correlation, breastfeeding is still strongly associated with cognitive development when controlling for these maternal factors. 61 Explanations for this correlation discuss the unique constituents of breast milk. 60,61 For example, studies have found that the docosahexaenoic acid in breast milk improves the visual acuity and verbal IQ of young children. 63,64 Despite the proven benefits of breastfeeding, exclusive breastfeeding until 6 months of age remains uncommon in many countries. 65
Child is free of injury and disease
Injury is a prominent cause of child and youth death and disability worldwide and is the leading cause of death for all Canadians between ages 1 and 44. 66 The vast majority of these accidents are preventable and accidental injuries are considered by many health authorities to be a public health concern. 67 There is evidence that boys are injured more frequently than girls starting at about 2 years of age. 66 This difference could be due to a variety of factors, including higher impulsivity and activity in boys as well as differential socialization. 66 Research shows that external causes of injury change with each stage of development. 67,68 For example, young children face specific risks of injury due to their psychological and physiological limitations negotiating environmental hazards. 68 Interventions to prevent injuries should, therefore, be adapted to fit each developmental stage. Infectious diseases, such as pneumonia and malaria, are also among the leading causes of death for children under 5 globally. 69 Prevention efforts like immunization programs have the potential to eliminate deaths from infectious diseases, such as polio, measles, and diphtheria. 69
Child is securely attached
Attachment theory posits that children’s relationships with primary caregivers directly impact children’s socioemotional development. 70 Modern attachment theory formulations underscore the influence of attachment to neurobiological systems associated with emotional processing and regulation. 10,71 Secure attachments help infants with emotional and physiological regulation in times of stress. 71 Caregiver sensitivity modulates children’s stress responses 72 and children who are not securely attached are more vulnerable to stressful stimulation because they lack attachment-related coping mechanisms. 73 This increased vulnerability to stress has the potential to create long-term challenges for children, as it can inhibit future emotional and social development 73 and contribute to the etiology of affective disorders, such as depression. 74 One study found sex differences in infants’ vulnerability to caretaking differences, assessed by mother–infant interactions during feeding and play. 75 Specifically, male infants were found to be more vulnerable to these changes than female infants. 75 Caregivers of insecurely attached children frequently exhibit challenges understanding their infants’ needs, 75 lack of emotional responsiveness, psychological unavailability, 75 low parenting efficacy, 76 and poor marital quality. 77
Child is exposed to language prenatally and during infancy
Language is essential to the cognitive and social development of children. 78 During early to late infancy, a child develops a complex system of language made up of an array of physical expressions, complex sentence structures, and thousands of words. 78 Although the ability to learn language is innate, children’s social environments are key to language acquisition. 79 For example, research shows that children from lower socioeconomic statuses (SESs) build their vocabularies at slower rates than children from higher SES due to reduced quantity, lexical richness, and sentence complexity of maternal speech. 80 Disparities in vocabulary have been found to appear at 18 months of age and are associated with family socioeconomic disadvantage and education. 81 Children who experience delays in language acquisition are at high risk for academic and mental health challenges later in the life course. 82,83
Child is engaged in play-based learning
Play is an integral and unique component of child development. 84 Evidence suggests that play contributes to cognitive development in the emotion, motivation, and reward regions of the brain 85 and has potential to reduce impulsivity. 86 Different types of play, including imaginative play, structured play, and rough and tumble play all help children to develop important skills. 87 Using their imaginations, children are able to explore abstract ideas and give new meanings to their concrete worlds. 84 This kind of play allows young children to more easily deal with the social process of working with abstract symbols, content knowledge, and thinking that preliteracy and prenumeracy demand. 84 Free play helps children to form appropriate higher-order generalizations 88 and rough and tumble play has been proven to promote physical health 89 and optimize brain organization. 86
Child is safe in a digital/social media context
In the twenty-first century, technology is an unavoidable aspect of children’s lives. The emerging literature on the impact of technology on early child development is concerned with very young children (under the age of 2) viewing television or screens. 90 Infants and toddlers are sensory learners who need to touch, taste, look at, listen to, and explore objects and have contact with people in their environments. 91,92 This is not possible for children when they are passively watching television or video programs. 92 Still, parents believe that educational media is important to children’s intellectual development, 93 and some studies have shown that certain television programs can encourage particular forms of play 94 and improve prelinguistic representational abilities. 95 Researchers consequently explain that if caregivers introduce children to television or video programs as a tool to encourage play, choice of appropriate program type according to content and age is essential. 92,96,97 Therefore, a safe digital context for infants and toddlers depends on caregiver presence and interactions with the child to encourage play-based learning. 92
Child is free from corporal punishment
Recent studies have demonstrated that physical punishment and physical abuse cause similar detrimental changes to the structure and organization of children’s brains. 98 Physical punishment has been proven to activate toxic stress, 98,99 disrupt the brain’s stress regulation mechanism, 100 alter the dopaminergic regions of the brain, 101 and reduce the brain’s gray matter—which is associated with intelligence. 102 As a result, physical punishment is linked to lower cognitive development, lower academic achievement, 103 increased antisocial behaviour, 104 and higher vulnerability to abuse of drugs and alcohol. 101 Children who have been physically punished demonstrate higher levels of mental health problems including depression, anxiety, and feelings of hopelessness during childhood and later in life. 105
Child has access to cultural values and customs
The cultural environment and background of a child contributes a set of values, customs, shared assumptions, and ways of living that influence development through the life span. 106 Research has shown that culture provides a unique context for children’s development and structures their cognition. 107 For example, culture influences how caregivers respond to children’s emotions, which then structures how children communicate their emotions. 108 Effective interventions and supports must account for children’s cultural and ethnic backgrounds in order to effectively address the needs of diverse children. 106
Child is free from poverty
Poverty in the early years has been identified as being a particularly adverse developmental influence. 109 A growing body of research has found links between lower SES and compromised child development outcomes in various areas, including cognitive development, 110 -113 executive functioning, 114 school readiness, 115 and school performance. 116 Research has also demonstrated a correlation between child poverty and numerous other risk factors, such as behavioral difficulties, poor physical health, greater likelihood of adolescent pregnancy, and increased probability of drug and alcohol abuse. 111 Poverty has also been identified as a risk factor for neglect. 117 Interventions in the first 3 years of life can decrease the developmental gap between children from families with lower versus higher resources. 110 Poverty is believed to exert its greatest influence through the child–caregiver relationship, more specifically, through parental depression and its disruptive impact on parenting behaviors in low-income families. 109
Methodological Approach
The OIS-2013: Advancing Knowledge and Informing Practice and Policy in Ontario
This study used the 2013 cycle of the OIS-2013 18 to explore where child welfare–involved children fall on several key indicators or developmental constructs contained in the Human Development Top 10. 34 The findings from this study further articulate the divide between the environmental context of a population of at-risk children and the conditions that both protect children and increase the likelihood that they will thrive in adulthood. Canadian incidence studies, such as the OIS (carried out in 1993, 1998, 2003, 2008, and 2013), 17,18,118 -120 have been instrumental to advancing knowledge of child welfare services. The OIS is cyclical and is one of the longest running incidence studies in North America. The primary objective of the OIS is to collect information on the scope and characteristics of child abuse and neglect investigations in Ontario in the year the study takes place. 18 It is the only source of provincially aggregated child welfare data that describe the characteristics of children and families investigated by the Ontario child welfare system.
The OIS-2013 used a multistage sampling design to select a representative sample of 17 child welfare sites from 46 child welfare organizations in Ontario. Then cases opened in the 3-month period from October 1, 2013, to December 31, 2013, within these selected sites were sampled for inclusion. 18 Maltreatment-related investigations that met the criteria for inclusion in the OIS-2013 included situations in which there were concerns that a child may have already been abused or neglected (maltreatment investigations) as well as situations in which there was no specific concern about past maltreatment but where the risk of future maltreatment was being assessed (risk investigations). These procedures yielded a final sample of 5265 child maltreatment-related investigations. 18 For each of these investigations, investigating child welfare workers were asked to complete a standardized data collection instrument which captured information on investigation outcomes, forms and severity of maltreatment, and the characteristics of the children and families. 18 Weighted provincial annual estimates were derived based on these investigations. Please see the OIS Major Findings Report for a detailed description of weighting procedures. 18
Several items collected in the OIS-2013 can be used to operationalize development and well-being for child welfare–involved children. These items reflect information that an investigating child welfare worker would know at the end of their initial investigation and are specifically related to the characteristics of the alleged maltreatment, child, family, and household. 18
In order to document overrepresentation within and differential interactions with the child welfare system, the OIS-2013 asked about the child’s ethnoracial status. 18 Eighteen child functioning concerns were included in the study, some of which indicate inappropriate child development. Workers were asked to rate, for each child functioning concern, the degree to which this was a concern for the child using the following scale: confirmed, suspected, no, or unknown. 18 Workers were asked to indicate whether there was physical harm to the child over the course of the investigation and, in cases of substantiated maltreatment, whether there was emotional harm to the child as a result of the maltreatment. 18
The OIS-2013 also documented up to 9 caregiver risk factors. Workers were instructed to use the same scale used for measuring child functioning concerns (confirmed, suspected, no, unknown) when evaluating caregiver risk factors. 18 Corporal punishment is operationalized by asking whether caregivers used spanking in the last 6 months. 18 The OIS-2013 also collected information on the primary form of alleged maltreatment and organized maltreatment into 5 major typologies (physical abuse, sexual abuse, neglect, emotional maltreatment, and exposure to intimate partner violence). 18 One form of physical abuse, hit with hand, can also be used to indicate use of corporal punishment by the caregiver. The OIS-2013 collected information regarding the environment of the family and household. Questions about family moves, household hazards, the household running out of money, and the caregiver’s income source were captured as measures of socioeconomic disadvantage. 18 The University of Toronto provided ethical approval.
Analytic Approach
For the purpose of this analysis, data collected during the 3-month-sampling period were weighted with annualization and regionalization weights in order to derive a representative sample of children who were identified to the child welfare system, and frequency counts were generated in order to identify the proportion of children who were categorized with a deficit when compared to an optimal environment. Bivariate analyses were conducted to examine differences between child sex and type of primary maltreatment investigated and child functioning concerns. Tests of significance were weighted with a sample weight.
Results
As shown in Table 1, risk factors for negative developmental outcomes are widespread in the child welfare population. For example, 37% of children investigated by child welfare authorities have at least one child functioning concern and 56% have a caregiver with at least one risk factor (see Table 1). Furthermore, household risk factors are present for between 4% and 12% of families in this population.
Ten indicators for optimal development and risk factors in an Ontario child welfare sample.
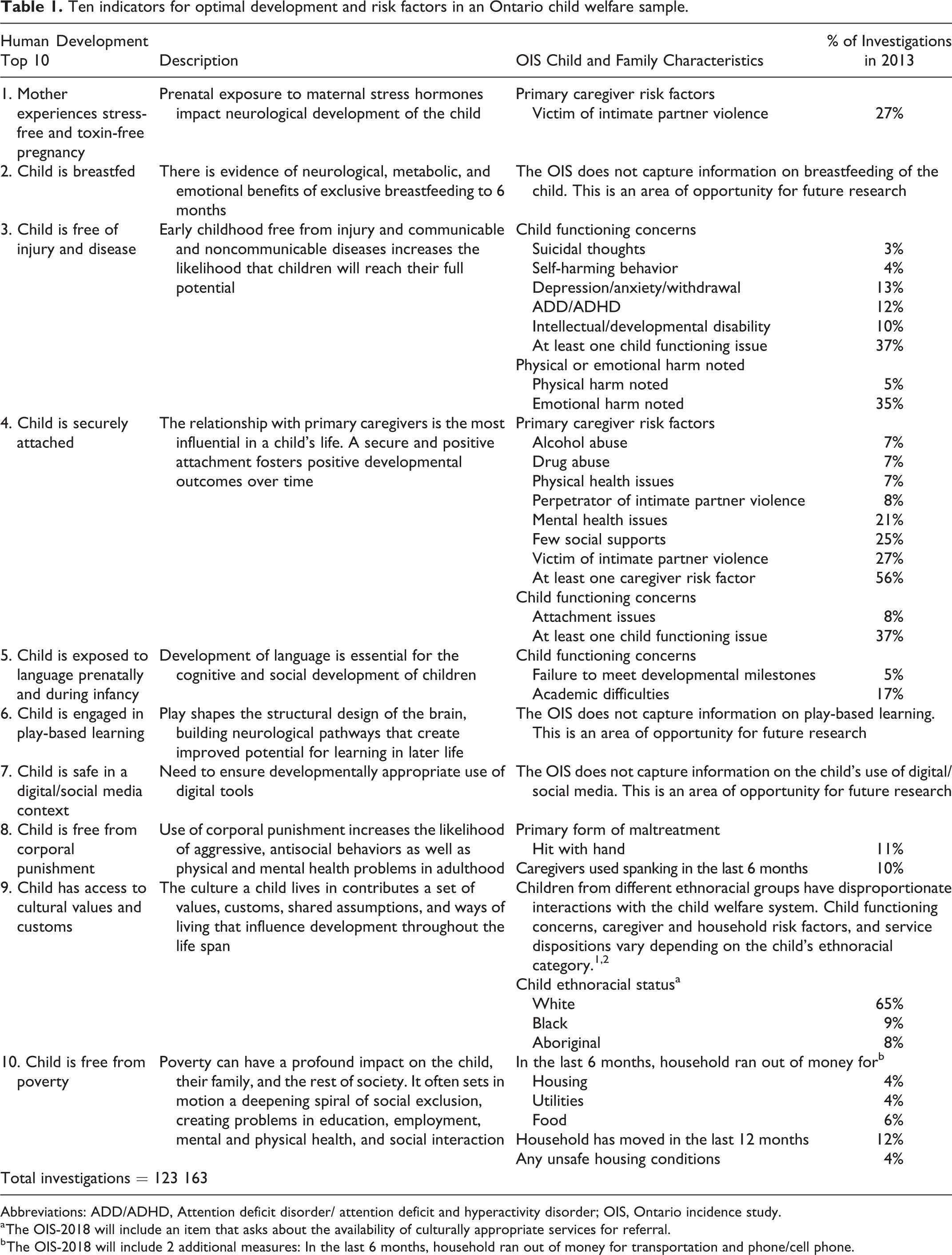
Abbreviations: ADD/ADHD, Attention deficit disorder/ attention deficit and hyperactivity disorder; OIS, Ontario incidence study.
a The OIS-2018 will include an item that asks about the availability of culturally appropriate services for referral.
b The OIS-2018 will include 2 additional measures: In the last 6 months, household ran out of money for transportation and phone/cell phone.
Primary maltreatment type (primary reason for investigation) and child functioning concerns were analyzed differentially by sex, as shown in Table 2. There were significant differences between maltreatment type and sex (χ2 = 29.990, df = 5, P < .001). For instance, males were more likely to be investigated for physical abuse when compared to females (22.3% vs 17.6%). Several differences emerged between child functioning concerns by sex. For instance, females were more likely to be identified as having concerns with depression/anxiety or withdrawal (14.8% vs 11.6%, χ2 = 12.336, df = 1, P < .001). In contrast, males were more likely to be identified as having difficulties with aggression (14.4% vs 6.7%, χ2 = 81.162, df = 1, P < .001).
Maltreatment type and child functioning characteristics in maltreatment-related investigations by gender.a
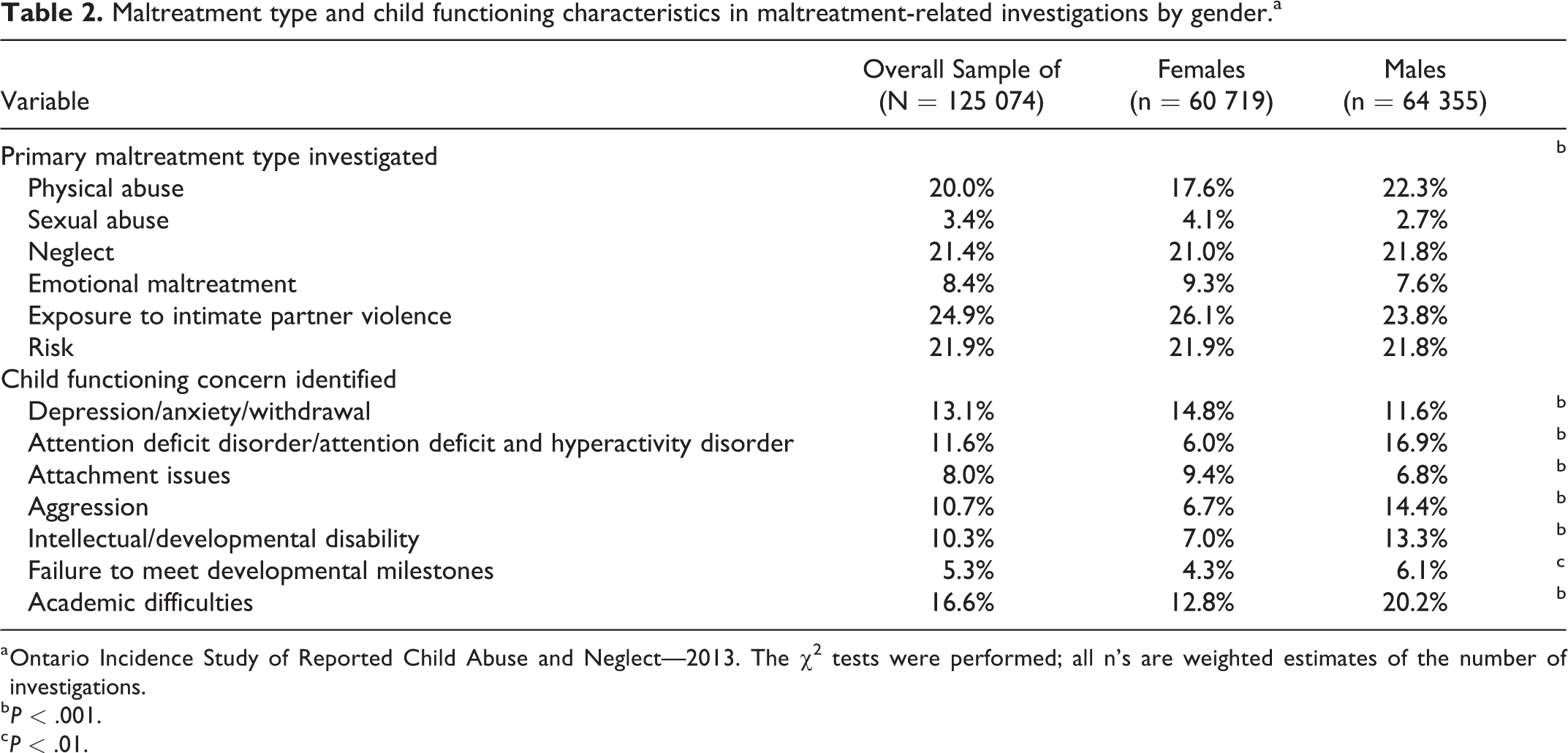
a Ontario Incidence Study of Reported Child Abuse and Neglect—2013. The χ2 tests were performed; all n’s are weighted estimates of the number of investigations.
b P < .001.
c P < .01.
Discussion
This article used a developmental framework in order to (1) operationalize the conditions that are likely to lead to optimal child development and (2) contrast this with the concerns for children and families that are documented during initial contact with the child welfare system. The article used a bioecological theory to assess the multiple systems that impinge on a child’s development in an effort to further articulate and define how this framework could be used to inform research, policy, and practice efforts in the service of vulnerable children. Environments that threaten or harm a child can lead to epigenetic modifications with adverse and long-term developmental consequences. 11 As revealed in the OIS-2013, children who have child welfare involvement struggle with emotional, behavioral, and developmental concerns (see Table 1). When these child functioning concerns are organized according to the Human Development Top 10, it becomes abundantly clear that the children who come into contact with the Ontario child welfare system are not developing in environments that facilitate them thriving. Contributing to these environments are both personal challenges these children face and their caregivers’ risk factors that impact their ability to parent (these include addictions, mental health concerns, and few social supports). All of these deficits usually take place in the context of extreme poverty (see Table 1).
Adapting the bioecological theory of human development, Figure 2 depicts the number of concerns that are present for a child welfare service population. Four levels, the individual (operationalized in the OIS-2013 as child functioning concerns), the microsystem (operationalized in the OIS-2013 as caregiver risk factors), the mesosystem (operationalized in the OIS-2013 as household risk factors), and the macrosystem (operationalized in the OIS-2013 as the social and political context), are considered. As suggested in Table 1, the child welfare population is at particular risk for poor development due to the presence of these risk factors. Furthermore, according to bioecological theory, these risk factors act in concert with each other to exacerbate their negative impacts on child welfare–involved children’s development and well-being. As shown in Figure 2, the scope of these risk factors spans from individual health concerns for the child or caregiver to governing laws and policies. Therefore, to appropriately target interventions to ameliorate these risk factors, interprofessional collaboration is needed. Health-care providers, social workers, education professionals, policy-makers, researchers, and other professionals need to come together to ensure that research, policy, and practice are informed by knowledge from different domains.
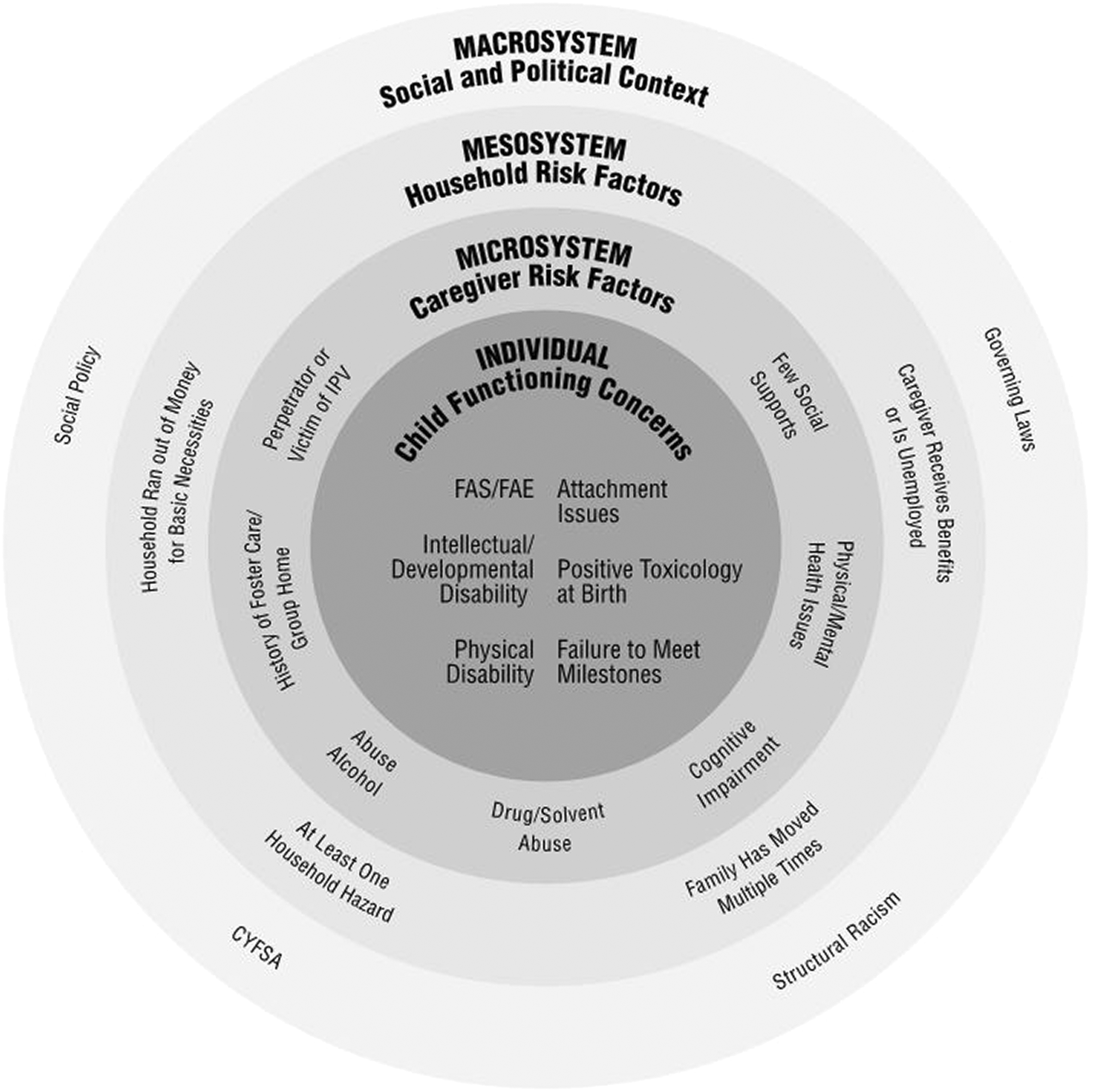
An adapted ecological model and risk factors present in a child welfare service population.
Child welfare professionals have been described as service brokers or gateways provider to services. 121,122 Child welfare–involved children and families are often referred to social services that exist in the community, and community supports can help to reduce social isolation, a risk factor for both maltreatment and poor development. 117,123 The social service system is part of the broader ecological context surrounding children and families. 124 For instance, early intervention services can promote children’s optimal development by enhancing child–caregiver relationships.
In comparison to other pediatric public health challenges, interventions in the area of child maltreatment lack robust evidence which limits the ability of research findings to help deliver effective services and to influence policy and practice. 125 -127 Interventions are often implemented based on their promising theoretical foundations and not on adequate evaluation. 126 In a review of all of the Canadian child protection outcome studies published between 1995 and 2005, only 10 peer-reviewed impact evaluations were found. 128 Greater acceptance in the child welfare community has been noted toward assessment methods and interventions that are based on empirical research that has been found to improve child and family outcomes. 125 Research-supported interventions can help guide child welfare workers in the selection of prevention and treatment programs that are likely to generate positive outcomes. Landers and colleagues 129 conducted a review of evidence-based interventions that were available to child welfare–involved parents of maltreated children aged 0 to 5 and found that randomized control trials (RCTs) made up only 26% of all included study designs. Additionally, the majority of studies reviewed were conducted in the United States (78%), whereas far less were conducted in Canada (16%). 129 Future research would benefit from additional RCTs to evaluate the overall effectiveness and impact of interventions, with a particular focus on interventions for parents of children under age 5 in child welfare 125,129 and within a Canadian context. In addition, some studies using Canadian incidence study data have explored sex differences with respect to decision-making and the findings are mixed. 12,16 Using data from Canadian incidence studies to explore sex differences is an important area for future research.
Sex-specific analysis highlights interesting differences in the primary type of maltreatment investigated and the child functioning concerns identified. The importance of exploring sex-specific differences from a transdisciplinary perspective is indicated as there is emerging research that suggests that there are sex differences in the vulnerability of various brain structures to maltreatment type. 130 There is also research that suggests that the impact of maltreatment on behavioral outcomes in children is impacted by sex. 131 Canadian studies on decision-making in child welfare are mixed with respect to the influence of child sex; however, a greater understanding of how the child welfare system responds is important given the emerging research from biological sciences. 12
The use of traditional child welfare service approaches and models for young children has been called into question given the rapidity of brain development and the unique developmental needs of children. 1,3,10,11 Traditional child welfare service responses place greater emphasis on acute safety concerns and investigating incidents of alleged maltreatment, as opposed to assessing the quality of the child–caregiver relationship or child development. 132,133 As a result of the potential biological consequences of adversity, it has been argued that the quality of the child–caregiver relationship and the assessment and planning of a child’s developmental and mental health needs should receive comparable attention to that afforded to child physical safety. 11 Child welfare service models in Ontario are not yet aligned with investigative trends that indicate a dramatic shift from immediate safety concerns to the long-term impact of family dysfunction. 134 Although other Canadian provinces have implemented differential response programs, wide-scale programs have yet to be implemented. 135
Jonson-Reid and Drake 136 note that indicators for child well-being are largely absent from administrative information data systems. The operationalization of well-being has been identified as a key barrier to the inclusion of indicators in data systems in the United States. 136 Jonson-Reid and Drake 136 suggest that well-being consists of 2 interrelated components—psychological/developmental and contextual; more specifically, the environmental context within which a child exists can help to support a child’s development and capacity for future success. As such, Jonson-Reid and Drake 136 propose that contextual well-being is an important element for operationalization and for inclusion in data systems. Contextual well-being is an important element to capture as it is aligned with best practice and is important for promoting optimal development.
Conclusion
The importance of articulating a framework for optimal child development especially for vulnerable children was the focus of this article. Children and families identified in the child welfare system present with a number of risk factors and the system’s ability to respond and ameliorate these conditions is limited by a lack of evidence-based interventions and resources. A bioecological orientation reminds us that prevention and intervention efforts that promote children’s well-being must be rooted in identifying and addressing specific risk factors and opportunities for resilience in multiple ecologies. Although most North American child welfare systems are authorized to respond to situations that threaten the development and well-being of a child, the focus of child welfare interventions is usually an immediate safety concern. A framework that operationalizes the environments that promote optimal child development can be used to inform research, policy, and practice across systems who work with children and their families.
Footnotes
Acknowledgments
The authors acknowledge the funding support of the Social Sciences and Humanities Research Council Canada Research Chair in Child Welfare (#950-231186).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Received funding support of the Social Sciences and Humanities Research Council Canada Research Chair in Child Welfare (#950-231186).