
Abstract
A ‘Gram Panchayat (GP)’ is the lowest tier of self-government within the Panchayati Raj Institutions and is entrusted with critical responsibilities such as poverty alleviation, delivery of welfare measures, primary education, empowerment of marginalised communities, etc. Apart from these, GPs are also endowed with responsibilities with respect to the empowerment of women and welfare of children. The article proposes to develop a comprehensive framework that can help in analysing the underpinnings of what makes a GP child friendly. The framework is further extended to the overall governance of a GP as well. The institutional capability and governance of 10 GPs of Karnataka have been examined in detail using this framework.
Keywords
Introduction
Panchayat Raj Institutions (PRIs) were established in 1992 through the 73rd Constitutional Amendment Act. 1 This amendment contains provisions for the decentralisation of the administrative, fiscal and political structures in rural India. The decentralisation process involves the devolution of powers to PRIs at three levels: Gram Panchayat (GP) at the village level, Block Panchayat or Panchayat Samiti at the intermediate level and Zilla Panchayat at the district level. GP is the principal institution for local policymaking and rural service provision among the three levels of local governance.
In 1993, Karnataka became one of the earliest among all Indian states, to bring conformity legislation incorporating the provisions of the 73rd Constitutional Amendment Act in order to strengthen and streamline decentralised governance structures. In 2015, the Karnataka Panchayat Raj Act of 1993 was amended to the Karnataka Gram Swaraj and Panchayat Raj Act (1993) with the purpose of making local self-governance more vibrant (Gok, 2014). Meetings at the habitation and ward levels were made mandatory in addition to the Grama Sabha (GS). As the name of the Act suggests, the objective was to further the agenda of democratising the governance system of the country.
It has often been argued that the decentralisation of governance will lead to effective and equitable development at the grass root level (Maro, 1990; Tuner, 2000: p. 115; World Bank, 2000: p. 107) because the local elected representatives are more accessible and accountable to the local people. The local elected representatives are also better placed to provide services according to the electorate’s preference since they know their constituency better (Higgins, 1992: p. 3; Oates, 1999; Saito, 2008).
GPs are responsible for the overall development of the village and play a key role in providing basic services which are critical for the health and well-being of rural people such as providing drinking water, housing, sanitation facilities, street lighting, delivery of poverty alleviation measures, primary education, empowerment of marginalised communities, etc. Apart from these, GPs are also endowed with responsibilities with respect to the empowerment of women and the welfare of children. Moreover, democratic decentralisation in the states of Karnataka and Andhra Pradesh has been done on grounds that it increases the speed, quantity and quality of service delivery in India (Rajasekhar et al., 2018; Sangita, 2007). To be more effective, decentralisation reforms has to rely on (a) effective local authority and autonomy, (b) sufficient resources for localities, (c) effective institutions of collective action, and (d) open and accountable local political processes (Olowu & Wunsch, 2004).
However, the decentralisation efforts in the form of panchayat raj in India are not without their crises. Lack of own source revenues and insufficient autonomy over the funds largely incapacitate PRIs in being responsive to local needs (Babu, 2009). Many argue that the insufficient capacity of elected panchayat members has rendered the institution useless (Nanjunda, 2020; Rajni, 2021). Due to insufficient autonomy over funds, lack of proper devolution of functions and inadequate functionaries, the PRIs are devoid of any larger role in local governance beyond being an implementing organisation. Meaningful devolution of funds, functions and functionaries is necessary for successful PRIs (Mani, 2002).
GP level Institutions such as Schools, Anganwadis, Primary Health Centres, non-governmental organisations and other civil society organisations also play a significant role in the delivery of child-related services within the geographical boundaries of the GP. Given that the GP alone is not responsible for delivery of these services, their functioning overlaps with multiple actors at the local level. For ease of understanding in this article, the terminology ‘GP’ is the institution of local governance whereas ‘GPI’ refers to all the other institutions and ‘GP’ refers to the geographical entity that includes GP and GPIs within it.
In Karnataka, schools are run under the Department of Public Instruction, health services for children are provided under the Health Department, and early childhood development services are provided under the Department of Women and Child Development. These line departments have devised their own institutional structures to promote decentralised governance. Village-level committees such as the Bal Vikas Samiti (BVS) have been created to monitor Anganwadi centres, the Village Health Sanitation and Nutrition Committee (VHSNC) to oversee health and sanitation-related activities, and the School Development and Monitoring Committee (SDMC) for monitoring the activity of schools. These three critical institutions related to child-related service delivery often bypass the GP. This is argued to be weakening the panchayat raj system (Reddy, 2007; Vyasalu, 2003). The presence of multiple institutions working in silos towards service delivery also renders a situation where the role of GP is blurred in the overall developmental achievements of the GP (Singh, 1994). Added to this is the layer of various awards given to GPs to incentivise their performance even if GPIs are responsible for the same. Therefore, the need to unpack and delineate their contribution becomes important. This is also required to explore ways of working in such an environment and progressively empowering GPs.
Since 2011–2012, the Ministry of Panchayati Raj (MoPR), Government of India has been incentivising the best performing GPs recommended by the State Governments/Union Territories (UT) Administrations. These awards and assessment frameworks are supposedly aimed at incentivising GPs to implement government schemes effectively, better utilise the funds allocated, have a system of rigorous data collection and to ensure better coordination and collaboration between GPs and the GPIs (GP Level Institutions). Government of India Ministry of Panchayati Raj (2022), the Rural Development and Panchayat Raj (RDPR) Department, Government of Karnataka has constituted the Gandhi Gram Puraskar Award that is given to GPs in Karnataka by assessing the successful implementation of state and centrally sponsored schemes (related to drinking water, health and hygiene, women empowerment and sanitation) and efficiency of tax collection. Such incentivisation in combination with other efforts has shown some positive results. For instance, a study indicated that assessment and awards resulted in an improvement in child-friendly governance in Himachal Pradesh (Ganju & Ganju, 2015). Similarly, the introduction of best model villages awards under the Nirmal Puraskar Yojana brought competition among villages to achieve these awards and increased the overall performance (Brahmanandam, 2016). Guidelines for local governance assessment by the Swiss Agency of Development Corporation suggested that local governance assessments are critical for improving service delivery and deepening democratic processes and identifying institutional capacity gaps (Paul et al., 2012).
This article is based on research on one such award for the GPs that are child friendly. In 2019, the MoPR, Government of India, introduced the ‘Child-Friendly GP Award’ 2 under the Incentivisation of Panchayats Scheme to encourage child-friendly practices in GPs. The basic purpose of this award is to promote social development and to create a conducive environment for the overall development of children. This article first critiques the existing assessment framework of the award and then attempts to develop an alternative, more comprehensive framework for assessing the child-friendly governance of a GP. Subsequently, the framework is extended to also examine a GP’s overall governance. The article also presents the results of the assessment of ten GPs in Karnataka in terms of their child friendliness through application of this alternative framework followed by an examination of overall governance of these GPs. Finally, the article gauges whether there is a correlation between child friendliness and overall good governance of a GP.
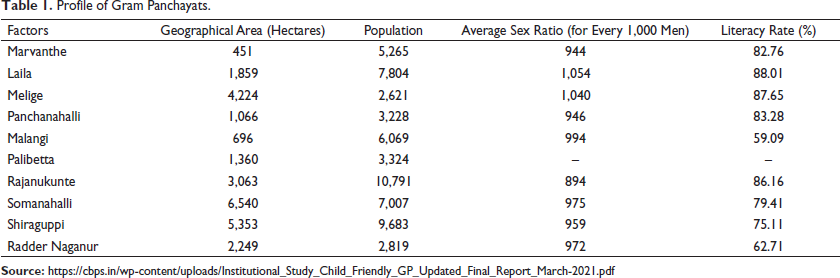
The 10 GPs selected for the study were identified as child friendly GPs by RDPR, and are spread across the five geographical divisions (Mumbai Karnataka, Central Karnataka, Coastal Karnataka, South Karnataka and Greater Bangalore region), of Karnataka. The 10 GPs are—Marvanthe and Laila (Coastal Karnataka), Melige and Panchanahalli (Central Karnataka), Malangi and Palibetta (South Karnataka), Rajanukunte and Somanahalli (Greater Bangalore region) and Shiraguppi and Radder Naganur (Mumbai Karnataka). A brief profile of these 10 GPs is given in Table 1. These 10 GPs undertook visible child-friendly initiatives as they were given prominence by the RDPR such as digital library or disbursing dolphin talking pens to anganwadi children. Child-friendly awards were also largely aligned with such child friendly initiatives by the GP.
The fact that these 10 GPs having already been identified as child friendly by RDPR provided an opportunity to clearly decipher the roles of GPs and GPIs in making the GP child friendly.
Profile of Gram Panchayats.
Existing Assessment Framework for Child-friendly GP
The existing awards and assessment framework of panchayats (MoPR, RDPR) rely heavily on outcome indicators. The incentivisation process fails in stimulating higher efficiency when it is too output/outcome oriented instead of giving substantial weight to efficiency in procedures (Lockwood & Porcelli, 2013). In achieving the said outcome, the existing assessment framework for child-friend GP does not differentiate between the roles of GP and GPIs.
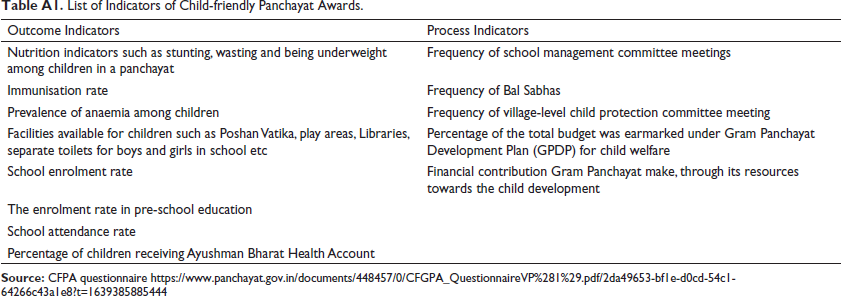
The GPs are awarded as Child-Friendly based on a combination of health- and education-related outcome indicators (for example, stunting, enrolment rate), indicators related to the functioning of institutions (frequency of SDMC meetings) and resource allocation for children (percentage of the total budget earmarked under GP Development Plan (GPDP) for children). Eight out of the 13 total indicators chosen for child-friendly GP awards are outcome indicators (Table A1) and the rest are process indicators.
GPs gave a lot of importance to visible child-friendly initiatives. They undertook these populist child-friendly initiatives as they are also given prominence by the RDPR. The diligence that GPs showed in constructing a digital library or disbursing dolphin talking pens to anganwadis children did not translate to maintaining child-related data or the effective functioning of child-related committees. Child-friendly initiatives undertaken by GPs were largely aligned with child-friendly awards. Though it is reasonable to assess a GP based on the performance of the child-related outcome indicators, it also leads to murky territories regarding how much of these achievements can be solely attributed to GP since GPIs also play a role in child-related service delivery with or without collaborating with the GP. Creating a comprehensive framework to assess GPs purely from the lens of institutional capacity and processes of governance becomes critical in this aspect
The Proposed Comprehensive Framework
The framework has been developed on the following four vital themes.
Functions of a GP
The Karnataka Gram Swaraj and Panchayat Raj Act, 2015 clearly enumerates the basic functions of a GP. Based on the 29 developmental subjects outlined in the eleventh schedule of the constitution, the obligatory functions of a GP along with department-specific duties are listed in Chapter IV, Section 58 (1A) 3 and Schedule 1 of the Act.
The basic functions of the GP as stated in the Act are leveraged into the framework related to child friendliness and overall governance. Along with obligatory functions such as ensuring universal enrolment of children in primary schools and achieving universal immunisation of children, other department specific functions are also included.
Similarly, the functions related to overall governance such as the management and monitoring of GP-level libraries and reading rooms, monitoring health facilities and health services at the GP-level and participation in the implementation and monitoring of WCD programmes are also included.
Institutional Processes of the GP
The institutional processes within a GP play a vital role in governance. GP has to constitute mandatory standing committees and sub-committees, 4 GS and ward sabhas 5 and meetings. 6 They include Panchayat Development Officer, elected members, department officials and citizens.
The standing committees focus on poverty alleviation programmes and are expected to prioritise the effective utilisation of funds based on the needs of the community. The Social Justice Standing Committee and the Women and Child Trafficking 7 and Prohibition of Child Marriage 8 Sub Committee are the two mandated standing committees with the welfare of children as one of their primary objectives. The GP conducts periodic general body meetings to discuss the implementation of various government schemes and other issues that fall within their jurisdiction. These general body meetings are also considered in the framework since child-friendly governance should also be part of these discussions. Apart from these, the Karnataka state government has also mandated GPs to conduct the Karnataka Development Programme (KDP) 9 meetings with line department officials to discuss civic, health, education and agricultural-related issues.
GPs were assessed based on whether these committees are formed, and if formed, whether the proceedings are systematically maintained, and if maintained, whether they proactively discussed the welfare of children. The interaction between the GP and GPIs was also assessed especially the role and influence of the GP member who is a part of these committees.
Financial Indicators
GP is responsible to prepare Action Plan, Budget Document 10 and take action on Audit Report. 11 These documents provide information related to scheme-wise utilisation of funds, collection of Own Source Revenue and cess payment. The action plan document prepared as part of the GPDP consolidates the funds available from various sources for GP to undertake developmental activities. The framework uses the percentage of resources earmarked for child-related services in the action plan as one of the indicators. The maintenance of registers required for audit along with budgets were used to assess the overall governance of GPs.
Citizen Participation
Citizen Participation in Governance helps to understand their role in various GP activities and in turn how the GP responds to needs of the citizens. The GPs have been made accountable to their citizens through GS, Jamabandi and Makkala Gram Sabha (MGS). 12 The GPs are required to organise these meetings to share information related to various schemes and welfare activities. Apart from this, GPs are expected to address the questions raised by citizens in these forums. The MGS is a platform for children to express their concerns and actively participate in the governance process. 13 The framework assessed the performance of these citizen forums as well.
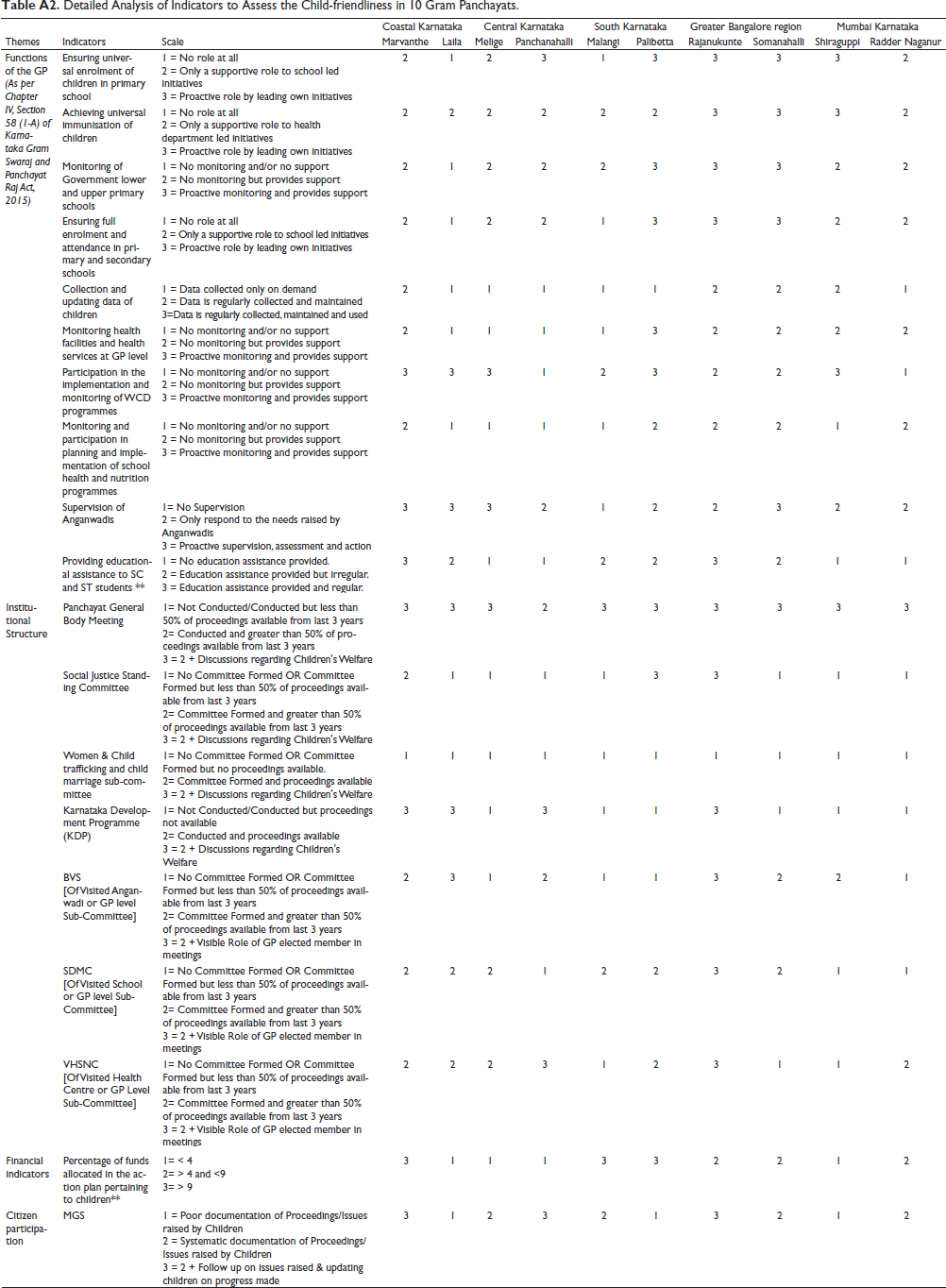
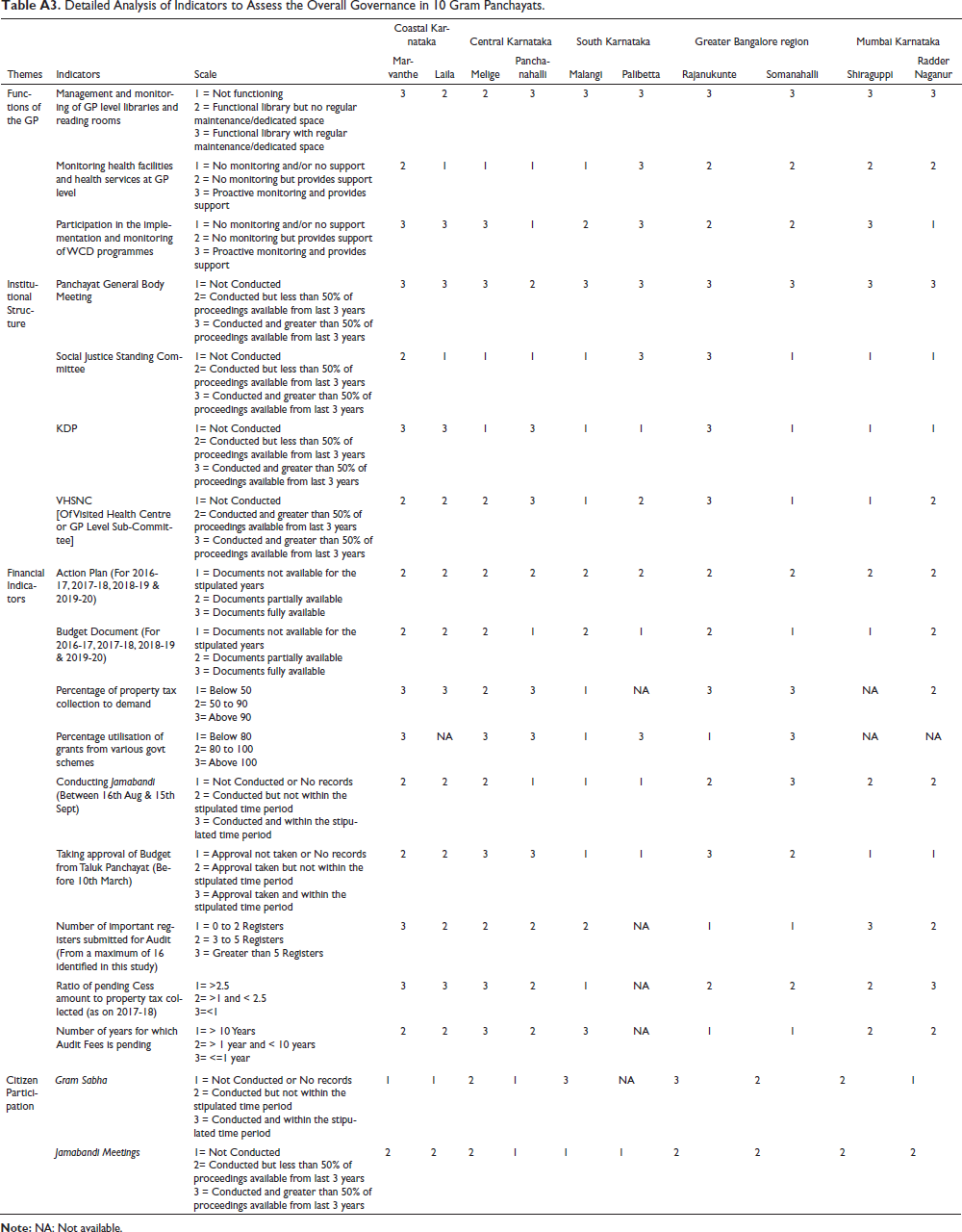
The four themes namely, functions of the GP, institutional processes, financial indicators and citizen participation are relevant to the framework for both child-friendly governance and overall governance. These four themes have been represented using 19 indicators for child-friendly governance and 18 indicators for overall governance (refer to Tables A2 and A3). Each indicator has been assessed at three levels.
For example, ensuring universal enrolment of children in primary schools is one of the obligatory functions of the GP. Instead of evaluating a GP based on the enrolment rate as in the case of existing awards framework (MoPR, RDPR), in the proposed comprehensive framework it was assessed at three levels (level 1-Has the GP played any role, level 2—if it has, is it limited to supporting school-led initiatives and level 3—has the GP taken proactive initiatives to ensure universal enrolment). All the other indicators were also unpacked and scored in a similar manner. The overall score was arrived at for each GP following a two-step process and a ranking was given based on it.
The first theme—Functions of a GP has 10 indicators under it. Each indicator is assessed based on a scale that ranged from level one to three. Thus, the maximum achievable score for any GP in this theme is 30. The total actual score calculated for Radder Naganur GP for the first theme was 17 (Table 2). Hence, the percentage score of Radder Naganur GP was:
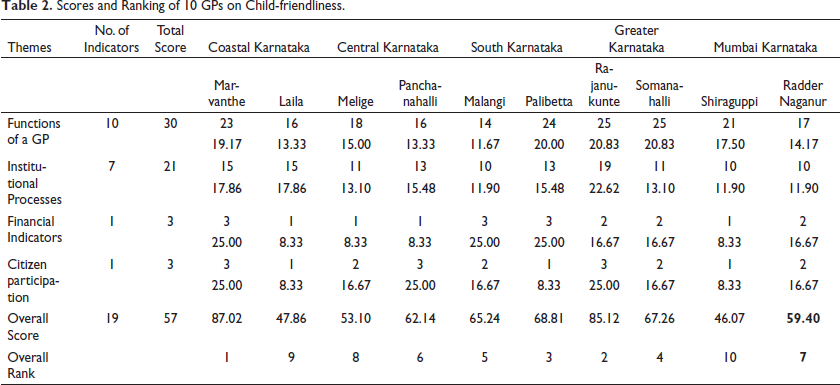
Scores and Ranking of 10 GPs on Child-friendliness.
Results and Discussion: Applying the Comprehensive Framework to Assess the Child Friendliness of 10 GPs
Marvanthe and Rajanukunte GPs scored the highest in child-friendly governance, ranking first and second, respectively (Table 2). While Rajanukunte performed better than Marvanthe in two themes—functions and institutional processes, Marvanthe’s significantly scored higher on financial indicators which led it to be placed above Rajanakunte. Shiraguppi and Laila ranked the lowest at tenth and ninth respectively, with a total score of less than 50. Even though these 10 GPs were identified as child-friendly by RDPR, our comprehensive framework assessed them to be at different levels and also helped identify specific areas of improvement for each of these 10 GPs. In the following section, the four themes are further analysed.
Thematic Analysis
Functions of a GP
Table A2 shows that only three out of 10 GPs have taken proactive measures in at least five out of the 10 listed functions related to children. Malangi and Radder Naganur GPs showed a reactive approach and have not played any role in discharging their functions as stipulated in the Act. Even the best-performing GPs in this theme—Rajanukunte and Somanahalli were taking proactive measures in only 50% of the functions related to children.
Many of these GPs performed poorly when it came to the collection and updating of data related to children, monitoring and participation in planning and implementation of school health and nutrition programmes. Six out of the 10 GPs did not maintain proper data and even in GPs where data was being collected, it was not being used in planning or monitoring child-related services. For example, in Shiraguppi GP the child-related data is collected and maintained systematically. However, this data wasn’t being used in governance at the GP level. Ensuring universal enrolment of children in primary school, and participation in the implementation and monitoring of WCD programmes are the only two functions where five GPs had played an active role.
Institutional Processes
The performance of standing committees related to children was pretty poor. Either they were not formed at all or their proceedings were not available in seven out of 10 GPs. Palibetta and Rajanukunte were the only two GPs that constituted the Social Justice Standing Committee and actively discussed the welfare of children. The Women & Child Trafficking and Child Marriage Sub-Committee was not formed in any of the 10 GPs. Even though the SDMCs were formed in all the schools, only in seven out of 10 GPs they were functional with more than 50% of proceedings available for the period 2016–2017 to 2019–2020. Only in one of the GPs, had an elected GP member played a prominent role in the SDMC meetings. The situation is not very different when it came to the BVS and the VHNSC. Laila and Rajanukunte were the only two GPs where elected members actively participated in the BVS. Panchanahalli and Rajanukunte were the only two GPs where elected members actively participated in the VHNSC. On the other hand, in Melige GP, the elected representative who is a member of the SDMC did not reside in the village and hence unavailable for SDMC activities. This negatively impacted the scores for this GP.
Financial Indicators
The average percentage of child-related allocations according to the action plan in the 10 GPs for the four years between 2016–2017 and 2019–2020 has been shown in Figure 1. Though allocations do not necessarily translate to actual expenditures, the framework used it to assess the intent of the GP in recognising the needs of children. The percentages were calculated by computing all the child-related allocations as a proportion of total allocation. The action plan also indicated that allocation of funds towards children’s welfare is largely limited to building infrastructure in schools and anganwadis such as building classrooms, boundary walls, drinking water facilities, playgrounds, and toilets. Expenditures on scholarships and on special initiatives for children such as digital libraries and transportation facilities were also included. Apart from the above allocations, the total allocation included all the work undertaken by the GP such as sanitation, water supply and roads.
Child-Related Allocation According to Action Plan.
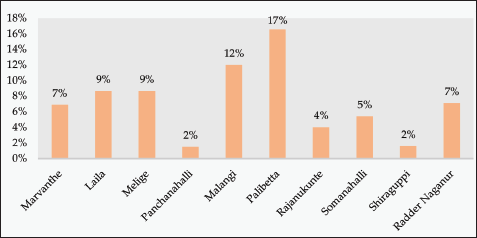
Palibetta recorded the highest average allocation of 17% to children across the four years. Palibetta and Malangi were the only two GPs that have invested more than 10% of their total funds for allocation for children. Shiraguppi and Panchanahalli allocated the least amount with less than 2% of the total fund for children.
Citizen Participation
All 10 were regularly conducting MGS. However, in four out of the 10 GPs, the meeting proceedings were not systematically documented. Even in the six GPs where proceedings were documented, only three GPs followed up on the issues raised, thus indicating that the MGS has seen very limited success. Panchanahalli GP is a positive example of how an MGS can effectively facilitate children’s participation in governance. In Panchanahalli MGS is not a 1-day event but a year-long process. The process included an orientation session for the children before the MGS to facilitate them to effectively participate in the same apart from ensuring the participation of all key stakeholders, presenting a status update report on all the issues raised in the previous year’s MGS and sharing the latest child-related data of the GP. The GP authorities meticulously documented the MGS proceedings and rigorously tracked the progress made on issues raised by children. Shiraguppi GP gave a contrary picture wherein the MGS was used as a platform to create awareness among children about the importance of nutritious food, enrolling in schools & AWCs. The issues of child labour, security, sexual harassment, were discussed and the platform was not used for hearing the voice of children.
Results and Discussion: Applying the Comprehensive Framework to Assess the Overall Governance of 10 GPs
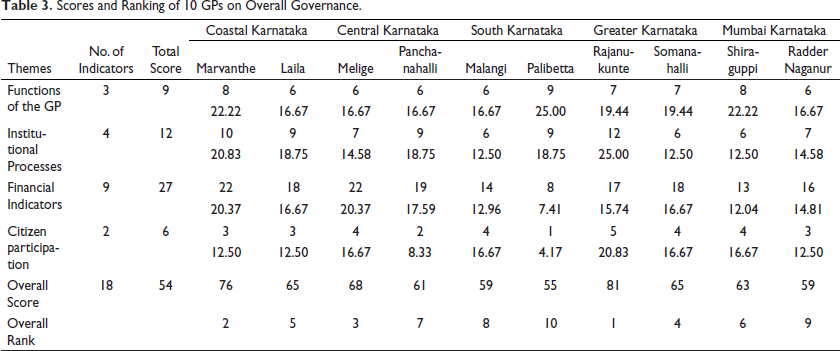
Rajanukunte (81) and Marvanthe (76) GPs have scored well in overall governance (Table 3). On the other hand, Radder Naganur and Palibetta GPs stood in ninth and tenth positions, respectively. Even though Rajanukunte and Marvanthe GPs have fared well in overall governance, they were less proactive when it came to financial indicators such as collection of property tax, utilisation of funds received under various schemes, conducting the Jamabandi meetings and seeking approval for the budget.
Scores and Ranking of 10 GPs on Overall Governance.
Thematic Analysis
Functions of a GP
Palibetta, Marvanthe and Shiraguppi GPs fared well in discharging their functions as stipulated in the Act. They were seen to be proactively managing and monitoring GPIs in implementing various welfare schemes. A majority of the remaining GPs have instead taken a reactive approach and expected the GPIs to highlight any issues or support that they may need from them.
Institutional Processes
Rajanukunte and Marvanthe GPs were effectively conducting the mandatory meetings as stipulated in the Act. General body meetings were conducted fairly regularly in all the 10 GPs. However, the proceedings of the meetings have been systematically maintained only in Rajanukunte and Palibetta GPs. Only three out of the 10 GPs had constituted the Social Justice Standing Committee. Palibetta and Rajanukunte were the only two GPs that had maintained more than 50% of the proceedings during the years 2016, 2017 and 2018. The KDP initiative, introduced to formalise the interaction between line departments and PRIs is also largely non-functional. In seven out of 10 GPs, KDP meetings were either not conducted or their meeting proceedings not properly documented. This suggested a gap between the GP and line departments that supervise the GPIs.
Financial Indicators
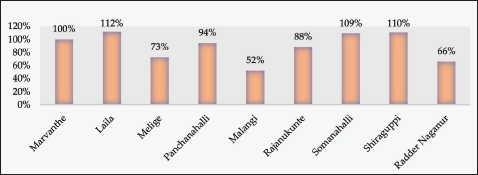
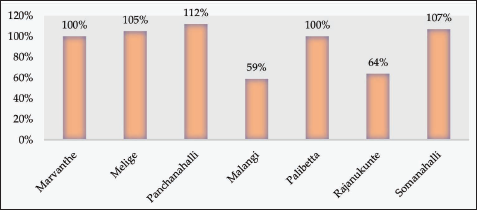
Half of the GPs had not prepared their budget documents for the 4 years from 2016–2017 to 2019–2020 while the remaining GPs shared budget documents for these four years which were largely incomplete. None of the 10 GPs were found to have conducted their Jamabandi meeting for the year 2017–2018 within the stipulated time period (between 16th August and 15th September of any given year). Additionally, half the GPs had not paid their audit fees while none of the 10 GPs maintained all the required registers and submitted them for the audit. Four out of the 10 GPs collected 100% and more of the property tax (Figure 2) against the demand. Malangi and Radder Naganur GPs were found to be collecting less than 70% of the property tax against the demand Five out of the 10 GPs fully utilised the funds received from various schemes 15 (Figure 3). Compared to other GPs, Malangi GP utilised only 59% of the scheme fund.
Citizen Participation
According to the Act every year GP has to conduct two GSs. GS discusses programmes at the village level for poverty alleviation, social and economic development, cultural preservation, empowerment of weaker sections of society, etc. The audit reports of GPs indicated that only two out of 10 had regularly conducted the GS meetings for the years 2016, 2017 and 2018. Many of the GPs had not submitted the records of Jamabandi proceedings during audit while three GPs had not even conducted the Jamabandi meetings.
Child-friendly Governance and Overall Governance of GP: Are they Related?
A comparative analysis was undertaken to understand the relation between the child-friendly governance and overall governance of GPs using a quadrant graph of 10 GPs (Figure 4).
Quadrant Graph of 10 GPs in Child-friendly Governance and Overall Governance Rankings.
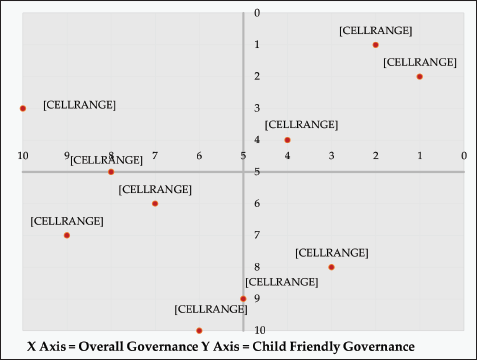
The first quadrant of the graph shows the GPs that have not performed well both in child-friendly governance and overall governance and the third quadrant indicate the GPs that have performed well in both. Rajanukunte and Marvanthe GPs ranked high not just in child-friendly governance but overall governance as well. Somanahalli is another GP though in the same quadrant has performed little less in both child-friendly governance and overall governance. On the other hand, Radder Naganur and Shiraguppi GPs were ranked low both in child-friendly governance and overall governance.
However, GPs like Melige and Palibetta have thrown some interesting contradictions. Melige GP ranked eighth in terms of being child-friendly but third in overall governance. Apart from maintaining child-related data, the GP has not performed well in any other child-friendly governance indicators, especially in allocating funds towards children’s welfare. However, it has been very systematic in financial processes, such as utilising grants for various schemes and regularly paying the cess thus resulting in a higher score on overall governance. Palibetta GP ranked third in terms of being child-friendly but was ranked lowest in overall governance. The GP had effectively discharged all mandatory functions as stipulated in the Act. It also prioritised fund allocation towards children’s welfare and had taken up initiatives such as providing transportation facilities for school-going children. However, it fared poorly when it came to maintenance of financial documents and utilisation of grants.
Summary and Conclusion
This article proposes a comprehensive framework that helps to examine the role of GP as an institution of local self-governance, with the aim of assessing their child-friendliness and overall governance. Applying the comprehensive framework to the 10 GPs suggested that while they were recognised as child-friendly by RDPR, do not necessarily perform well on holistic child-friendly governance.
The analysis using the comprehensive framework also revealed that there exists a tenuous relationship between the GP and GPIs. The existing framework of assessing child-friendly GPs does not distinguish the role and influence of GPs vis-a-vis GPIs. This also stems from a lack of proper delineation of responsibilities between GP and GPIs. Anganwadi workers and school authorities felt that the GP’s role in school and anganwadis should be limited to providing the required physical infrastructure. The limited role of GP elected members in SDMC, VHSNC and BVS, limited data sharing and the poor functioning of KDP all point towards a lack of fruitful interaction between GP and GPIs.
The proposed comprehensive framework revealed that current approach tends to prioritise visible initiatives to prioritise visible initiatives adjust the content above as the appendix should be after the conclusion section, (Prasad et al., 2020). is less holistic in nature, and focuses less on interaction between GPs and GPIs. Diligent data collection and reporting without using it for local decision making, or ritualistic conduct of MGS without following up on the issues raised by children indicated poor child friendly governance. This also indicated that child-friendly governance largely goes hand-in-hand with overall governance which could be attributed to the fact that child-friendly GPs are also the ones with good governance structures, promoting discussions and embracing the spirit of decentralisation.
Annexure A
List of Indicators of Child-friendly Panchayat Awards.
Detailed Analysis of Indicators to Assess the Child-friendliness in 10 Gram Panchayats.
Detailed Analysis of Indicators to Assess the Overall Governance in 10 Gram Panchayats.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.