
Abstract
In the recent past, there has been a substantial push to increase the sanitation infrastructure in India to end open defecation and improve level of hygiene. The choice of the type of sanitation, however, depends on demographic, socio-economic, tenurial, cultural and sanitation surroundings, which not only impacts sanitation practices but also incidences of diseases. This paper empirically analyses the determinants of households’ choice of toilet facility and the relation between incidence of diseases and sanitation using National Sample Survey Office’s 76th round of the survey for 2018-19. The results indicate that the social, economic and cultural factors have significant impact on the households’ choices of a toilet. There is a preference for flush type toilets connected to a sewer among households with better socio-economic status. This research finds that the quality of microenvironment within which a household lives has a significant impact on the incidence of disease. The results imply that the interventions for improved sanitation need to be holistic, emphasising microenvironment improvement and providing better access to sanitation infrastructure and inculcating more hygienic behavioural practices.
Introduction
The relationship between water, sanitation and hygiene (WASH) practices and disease incidences is well studied globally (Zwane and Kremer, 2007; Spears et al., 2013; Hathi et al., 2017; Cetrulo et al., 2020; Cameron et al., 2021). The United Nations General Assembly declared the provision of safe drinking water and sanitation as a basic human right. The Sustainable Development Goal 6: ‘Ensure access to water and sanitation for all’, target 6.2 conveys the ambition in relation to sanitation services. The target states that ‘by 2030, (nations) achieve access to adequate and equitable sanitation and hygiene for all and end open defecation, paying special attention to the needs of women and girls and those in vulnerable situations’ (United Nations, 2015). The cause of diseases, such as diarrhoea, cholera, malaria, typhoid, hepatitis, is improper sanitation. The burden of these diseases is disproportionately skewed towards developing countries. For instance, diarrhoea constitutes nearly 57% of the disease burden internationally and is one of the leading causes of mortality in developing countries for children less than 5 years of age (Prüss-Ustün et al., 2014a; Hathi et al., 2017; Saroj et al., 2020). The lack of adequate sanitation infrastructure and practices is attributed to approximately 280,000 deaths in low and middle income countries (Prüss-Ustün et al., 2014a). Yet, inadequate access to sanitation continues to affect about 2.4 billion people in the world, with a third living in cities (Neira and Prüss-Ustün, 2016). The level of WASH access differs substantially between and within regions (Montgomery et al., 2009).
In India, about 800 million people do not have access to improved sanitation and nearly 600 million people practice open defecation (Saroj et al., 2020). National programs during the last four decades have focussed on developing sanitation infrastructure and instilling behavioural changes towards toilet use. The success of these programs is debatable. Most government initiatives have focussed on funding sanitation infrastructure improvement with little emphasis on educational programs to bring about behavioural changes (Novotný et al., 2018). Almost 15 percent of the Indian population defecate in the open. The problem is far more precarious in rural areas (WHO/UNICEF, 2015). For improved sanitation outcomes, the provision of infrastructure and behavioural practices need to be complemented, as noted in initiatives in Bangladesh (Rahman et al., 2021) and Jakarta (Sidabutar and Chotib, 2021).
The Constitution of India delegated the responsibility to plan and deliver WASH services to local governments (Gram Panchayats in rural and municipalities in urban areas). The central government formulates policies and guidelines for sanitation and provides financial and capacity building support to the state and local governments.
The earliest program to address open defecation in urban areas was the Integrated Low-Cost Sanitation Scheme, launched in 1980-81, which focussed on the construction of low-cost sanitation units. Sanitation became an important policy issue with the draft National Water Policy of 1987 laying targets for the provision of sanitation services in urban and rural areas. Earlier programs provided financial assistance to below poverty line households to construct toilets. However, the progress under these programs was slow as the prevalent household sanitation practices resulted in a low demand for toilets. A major shift in approach to sanitation occurred when The Employment of Manual Scavengers and Construction of Dry Latrines (Prohibition) Act was enacted in 1993, which sought to ban the practice of manual scavenging. The Act was important as it addressed the caste-based discrimination as the task of manual scavenging is carried out by households of ‘scheduled caste’, a social class within Hindu society in India. This Act was followed by Prohibition of Employment as Manual Scavengers and their Rehabilitation Act in 2013, which imposed targets on urban local bodies to replace dry latrines with community latrines to reduce manual scavenging. Other policies such as the National Health Policy, 2000 and Valmiki Ambedkar Awas Yojana (Housing policy), 2001 also emphasised the importance of sanitation. A large urban focussed infrastructure program, the Jawaharlal Nehru National Urban Renewal Mission (JnNURM) was launched in 2005 to provide basic services to the urban poor including improved housing, water and sanitation. The program supported infrastructure projects related to sanitation, sewerage and solid waste management. Sanitation gained significant importance when the country’s first National Urban Sanitation Policy was launched in 2008. A recent national government program, Swachh Bharat Mission (Clean India Mission) launched in 2014, focussed on solid and liquid waste management. The program aimed to make cities and villages ‘open defecation free (ODF)’ by 2019. A multidimensional approach that plugs the loopholes across the entire sanitation chain (including treatment, desludging, disposal practices and sustainable hygiene practices) was used for Swachh Bharat Mission (Novotný et al., 2018; Saroj et al., 2020). An important component of the program in rural areas included management of agricultural waste through conversion of these waste products to compost, bio-gas and bio-CHG. Behavioural change communication was an integral component of the program.
These programs resulted in increased toilet coverage in urban and rural India, but open defecation still persists. Purty and Vishwanathan (2020) report results from a randomised control trial in rural Bihar, which examined the impact of behavioural interventions to promote the use of toilets by households who already had a toilet in their house. Results indicated that while Swachh Bharat Mission has resulted in a significant shift towards the use of toilets, challenges associated with poor toilet design and disposal of faecal waste have hindered the progress with the consequence that open defecation continues.
The chain of sanitation infrastructure at the housing unit, community and city levels and motivation for their use is necessary for hygienic sanitation practice (Hueso et al., 2018). Previous research identifies lack of space within the house and non-availability of finances as major impediments to building toilets in India (Mehta et al., 2021). The premise of the Government programs has been to address the availability of toilets through bridging the financial gap. The lack of success with previous sanitation programmes has led to a push towards community led interventions, the focus of which has been to nudge more hygienic social norms, perception and attitudinal changes (Heijnen et al., 2015a). The household choice of the type of sanitation, however, depends on a range of socio-economic factors, the microenvironment and social, cultural norms as pointed out in the literature (Doron and Jeffrey, 2014; O’Reilly et al., 2017a).
Two aspects of sanitation have been examined in this paper – choice of private sanitation infrastructure and the linkage between hygiene of the microenvironment within which a household lives and health. The second aspect is important as it reflects the community level choices that affect health and hygiene. Local government infrastructure plays an important role. Using data from the 76th round of survey for the year 2018-19 from the National Sample Survey Office (NSSO), two questions are sought to be answered – (i) What factors contribute to the type of toilet that a household uses? and (ii) What is the impact of sanitation and a hygienic living environment on household health? The factors that have been examined include the demographic, socio-economic, housing and tenurial status, dwelling condition, sanitation and health microenvironment and the financial benefits that a household has received.
The rest of the paper is organised as follows. Section 2 discusses the extant literature. Section 3 sets out the empirical strategy for an analysis. Section 4 presents the results for assessing the impact of various factors on the choice of toilet and the impact of sanitation on incidence of diseases. Discussions and policy implications are presented in Section 5, followed by the conclusions in Section 6.
Literature review
Household choice of toilet to use is a complex decision that is affected by the availability of toilet infrastructure, socio-economic conditions and social norms. Jenkins and Scott (2007) find that factors affecting household toilet installation in Ghana depend on their satisfaction with existing defecating practices, motivations to improve sanitation, priority over competing household concerns and implementation related challenges. Examining motivations behind open defecation in Nepal, Bhatt et al. (2019) find that this choice is linked with personal preferences, and cultural and traditional norms with particular concerns for the privacy of women and girls in different communities. In their study on open defecation in rural India, Spears and Thorat (2019) find that the practice of open defecation was linked with the culture of purity, pollution, untouchability and caste. In another study on the factors contributing to open defecation in rural India, Doron and Jeffrey (2014) identified 11 factors that play a part in people’s acceptance of and access to controlled ways of dealing with human waste. These factors are class, caste, sociability, urban life, rural life, diversity, topography, technology, gender, education and crisis (Doron and Jeffrey, 2014). The role of caste in sanitation practices is underscored in a study by O’Reilly et al. (2017b) on three villages in South India where various sanitation improvement projects were attempted. They find that caste relations played a crucial role in the failed interventions by creating and reinforcing the sanitation practices by which caste groups distinguished themselves from each other at the village scale. Issues of cleaning toilets, access to subsidies, latrine design, and purity served to facilitate and limit the processes that enable unequal relationships of caste. Access and availability of toilets is an important consideration of sanitation practices but not the only consideration (Heijnen et al., 2015b). Poor quality and inappropriate toilet design under government sanitation schemes in rural areas has constrained the use of these toilets.
Corburn and Hildebrand (2015) find that inadequate, unsafe and unclean sanitation results in multiple and overlapping health, economic and social impacts that disproportionately impact women and girls living in informal urban settlements. Nallari (2015) argued that girls' lack of access to private toilets exposes them to health and social risks, the shame of being identified defecating in the open and withdrawal from educational institutions due to their lack of toilets. Augsburg and Rodríguez-Lesmes (2018), in their study on the impact of sanitation on child stunting in India, find that better sanitation coverage results in an increase in the height of children, and girls benefit more from an improved sanitation environment. Duflo et al. (2015) report that a community-level, infrastructure-based water and sanitation intervention in rural India resulted in a reduction of severe cases of diarrhoea. They emphasize that the complementarity in water and sanitation is required to have an impact on better health outcomes. Nagpal et al. (2021) found that the body mass index (BMI) of women living in slums was positively correlated with the use of private toilets.
The literature has also examined the appropriateness of ‘shared’ sanitation facilities as a viable option for household sanitation needs where exclusive toilet infrastructure is not possible for affordability reasons. The definition of ‘improved sanitation’ does not include use of sanitation infrastructure by more than one household for reasons such as inadequate cleanliness resulting in lower health benefits, inaccessibility during the night for women, and no clear, demonstrable advantage over exclusive use of the facilities (Fuller et al., 2014). However, community toilets or shared facilities are an attractive policy option for reaching a larger population in developing countries (Geruso and Spears, 2018). In India, approximately nine per cent of the population access shared toilet facilities, with much higher proportion in urban areas. Among the various determinants that influence the effectiveness of shared facilities, water availability is the most important (Bhardwaj et al., 2013). Less than 10% of Indian cities have sewerage networks connected to treatment plants resulting in septic tanks being a common toilet design, which are not de-sludged regularly (Mehta et al., 2019).
The lack of available information on the service levels across most of India has made it challenging to assess the impact of different government programs (Friedrich et al., 2020; Mehta et al., 2021).
This brief literature review highlights gaps in comprehensive understanding of the factors that determine toilet choices of households, which are embedded in empirical evidence. Factors such as socio-cultural norms, household affordability, housing conditions and government programs have been discussed individually but not together to enable assessment of their relative importance. The link between the microenvironment within which a household lives and its impact on health outcomes is also less investigated empirically.
Empirical strategy
There are two linked but not necessarily interdependent questions that have been examined in this paper: First, the type of toilet that a household uses and its determinants and the second, the impact of sanitation and a hygienic living environment on household health.
Method
To empirically analyse households’ choice of toilet type, an econometric estimation of the use of toilet function is conducted. The type of toilet used is categorised under four categories: 1= toilet with flush or pour flush to piped sewer; 2 = Septic tank/twin leach pit; 3 = single pit/ventilated improved pit latrine/pit latrine with slab/pit latrine without slab/open pit/composting latrine; and 4 = all other including open defecation. While the use of types 1, 2 and 3 implies private sanitation practices, type 4 refers to less private and open defecation.
The choice of toilet use will depend on the households’ socio-economic factors. The type of toilet use function is given by

For econometric specification, a multinomial logit model is adopted. For j alternatives, the probability function yields a multinomial logit model

The estimated multinomial logit model produces J-1 coefficients for each independent variable. The Jth alternative is the reference with which estimated coefficients are compared. In this paper, ‘Type 4 – Open defecation’ is considered as the baseline. Estimation of the multinomial logit model is conducted using a maximum likelihood estimation procedure.
The second question is answered by estimating a model where household sufferance from illness is explained as a function of sanitation conditions within the house and in the neighbourhood.
Information on illness that households suffered is limited to discrete ‘yes or no’ in our data, limiting the extent to which the relationship between illness and its causal factors could be analysed. However, it is possible to examine the prevalence of disease and sanitation conditions.
The empirical framework for analysis of the impact of sanitation and the microenvironment on health is presented below

The function can be rewritten as:
The dependent variable is defined as


Data
The data are from the 76th round of surveys conducted by the National Sample Survey Office (NSSO), Ministry of Statistics and Programme Implementation, India, for 2018-19. The sample size is 466,680 households covering all the states and union territories. The sample has 174,316 urban and 292,208 rural households. The NSSO survey captures various demographic, socio-economic, tenurial status, water-related source, accessibility and sufficiency data. Summary statistics are available in a Supplementary File. This paper estimates a single function for all households and the rural/urban difference is captured through a dummy variable. This implies that the slope coefficients for various determinants of the toilet choice variable are not different between urban and rural households. The intercept determines the difference between urban and rural households.
80% of households in the data own their houses and 83% live in independent houses. Only 42% of houses are of good quality. 57% of households indicate that they have access to daily water supply. On average, for 33% of months in a year, water availability is insufficient. An estimated 71% of rural households and 96% of urban households have access to a latrine. Half of the households use flush/pour-flush or a septic type of latrine. Merely 61% of rural and 92% of urban houses are connected to a drainage system. About 15% of households have accessed assistance from a government program to improve their toilet infrastructure.
Results
Choice of toilets
Results – preference of toilet type.
Dependent variable = Type of toilet used by the household (1= Toilet with flush or pour flush to piped sewer; 2 = Septic tank/twin leach pit; 3 = single pit/ventilated improved pit latrine/pit latrine with slab/pit latrine without slab/open pit/composting latrine)
Base toilet category = 4 (open defecation)
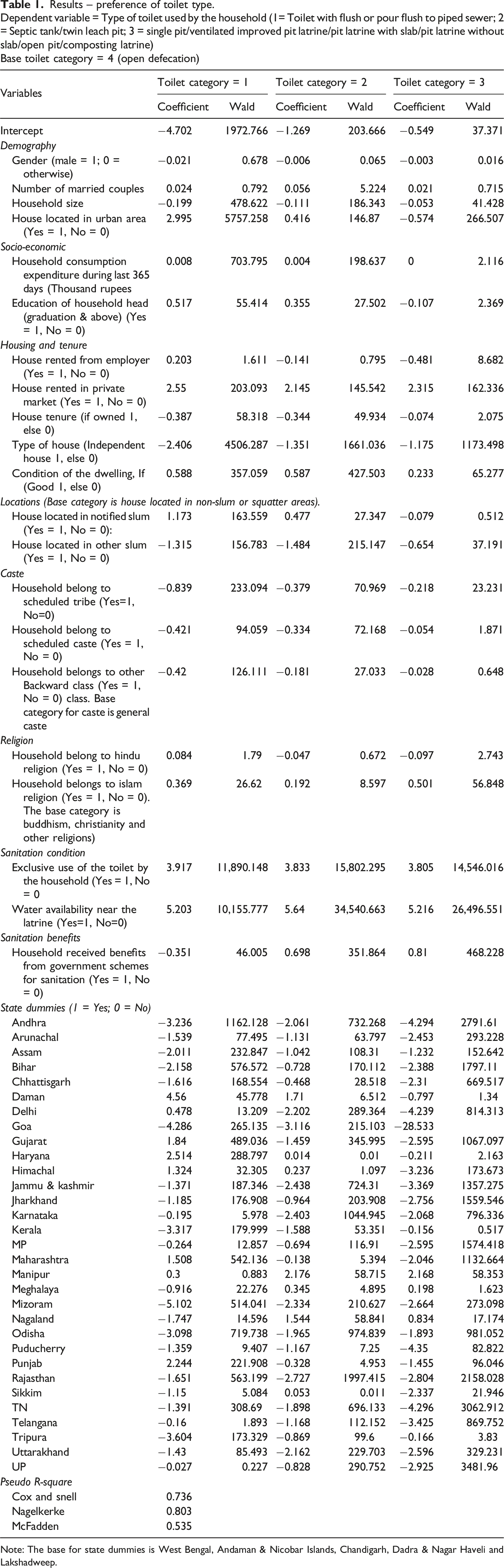
Note: The base for state dummies is West Bengal, Andaman & Nicobar Islands, Chandigarh, Dadra & Nagar Haveli and Lakshadweep.
An increase in household size negatively impacts the choice of private toilets, indicating that the larger the number of people residing in a dwelling unit, the more likely they will practice open defecation due to inadequate infrastructure to cater to all members of a household. Large households are affordability constrained, which limits their ability to spend on private toilet construction. The other reason is that the available space in a house for construction of private toilets is also limited as household size increases. For those households who have either a Category 1, 2 or 3 type of toilet, the larger households prefer a Category 3 type of toilet due to its lower cost rather than a toilet connected to piped sewer or double pit toilet. The number of married couples increases the probability of the choice of a Category 2 toilet, implying that the more the number of married people, the more likely the dwellers use a private toilet of some form. In India, where joint families comprising multi-generation members are still prevalent, as younger male members get married, the demand for private toilets increases for protecting the privacy of newly added female member to the households. Marriages also improve the financial position of households, who then can improve their housing amenities. The higher the education levels, the more likely the households have toilet usage, with Category 1 being the preferred choice. Educated households can appreciate the benefits of improved sanitation and the role that the private toilets have in reducing disease incidences. Income is positively associated with the type of toilet category. A wealthier household is less likely to practise open defecation. The coefficient for Category 1 for households is higher than Category 2 for affluent households as income affordability allows them to have better sanitation facilities. Households who have rented houses in the private market have some form of private toilet. In the rental market, households can demand better sanitation facilities. Households who have rented houses from their employers have toilets with piped sewers.
Homeowners and those staying in an independent house have a significant negative association with categories that reflect private toilets. This implies that, in general, the dwellers with their own houses/or those who stay in independent houses prefer to defecate outside their dwelling unit and that most houses are old and still not connected to a piped sewer system. The reasons for such behaviour, particularly in rural areas, are due to strong cultural connotations in India, as defecation is seen as a purification process and needs to be carried out far from the dwelling unit. The availability of space to build a toilet within a house and its additional cost burden are other deterrents to private toilet use. The coefficient for the condition of the dwelling unit has a positive coefficient, with that of Category 1 and 2 greater than the coefficient of Category 3. This implies that the better the quality of dwelling, the more likely are the households to use a toilet, and better-quality houses are likely to be connected to public sewers or a double pit toilet. The availability of a toilet and housing quality are also associated with the age of the house. Older houses are generally in poor condition and lack a private toilet facility. The households who stay in notified slums indicate having a positive association with the type of toilet. Notified slums are recognised through an Act or in a government gazette. Formal recognition results in increased availability of community toilets and emphasis on privacy and hygiene in notified slums through programs implemented by the government and non-governmental agencies. The results, however, contrast in the ‘other slums’. ‘Other slums’ are unrecognised settlements on encroached public or private land, usually without any formal access to water, power, or sanitation services. Non-recognition crowds these households out of any government program. Uncertainty of even ‘loose’ tenure limits households’ own investment in improved sanitation. The dwellers here are more likely to practice open defecation.
The households belonging to scheduled castes (SC), scheduled tribes (ST) and other backward classes (OBC) have a negative association with private categories of toilets, with the coefficients smaller for the Category 1 type of toilet. This implies that the households belonging to marginalised social classes still resort to defecating in the open due to social discrimination. Social segregation of marginalised castes from other social classes forces them to live in areas that are poorly connected with sanitation facilities, particularly in rural areas. Mohanti and Dwivedi (2018) highlight that the caste system also has a visible presence in sanitation practices in urban areas even though these practices have been prohibited due to their social legitimacy, which are attributable to traditional caste divisions and practices. Scheduled caste households are disadvantaged in this sense (Doron and Jeffrey, 2014). Households belonging to the Islam religion are less likely to practise open defecation, as the variables indicate a positive association with private toilets. The coefficient for Category 1 is greater than that of Category 2, indicating that the preference is more for a flush type connected to a sewer system. Households belonging to the Hindu religion prefer category 1 toilets. However, the probability of choice of category 2 and 3 are lower than open defecation. After controlling for income, education, location and caste, this result indicates that behavioural practices associated with open defecation are linked with the notion of ‘purity’. Excreta in any form that is not removed immediately from the house is considered impure. Private toilet type 1 connected to a flushing or sewer system removes the excreta from the house immediately. Type 2 and 3 face the constraint that excreta are not removed till the tank or pit is desludged. Caste barriers, which require de-sludging activity to be carried out by members of a scheduled caste further pose constraints. Changes in the mindset to use private toilets other than category 1 would require efforts through behavioural change and educational programs.
The exclusive access to toilets is positively associated with the type of toilet, indicating that the households are less likely to defecate in the open when they have dedicated access to a toilet although there is no dominant preference for the type of private toilet. The households who have availed themselves of sanitation benefits under a government program seem more likely to build a category 3 toilet. Government programs for sanitation offer subsidies, and part of the cost of construction of toilets must be met by the household. A flush toilet or double pit toilet is expensive to build, and the government subsidy is inadequate to cover the cost. Category 3 is the choice of low-income households who are covered by government subsidies. These toilets are not as hygienic as Category 1 and 2 and result in slippage back to open defecation.
Most state variables indicate negative coefficients for both categories of toilets, painting a uniform pattern across the country. When the preference of the flush type of toilet connected to the public sewer is compared with open defecation (Category 1), Delhi, Gujarat, Maharashtra, Haryana, Punjab, Daman, Himachal Pradesh, Maharashtra and Manipur states have positive coefficients. There has been an active social marketing effort (a program called colloquially as ‘No toilet no bride’) in areas where discrimination against women is very high leading to an underlying demand for private toilets from women in these parts of the country (Stopnitzky, 2017). Southern states present a negative coefficient, indicating that the flush toilet is less preferred. This could be due to the caste and cultural factors prevalent strongly in these states. When the open defaecation is compared with the Category 2 and 3 type of toilets, only a few from the North Eastern part of the country (Manipur, Meghalaya, Nagaland) present a positive coefficient, indicating that preference for these types of toilets is more over open defecation.
Health and sanitation
Relationship of the microenvironment of sanitation to disease.
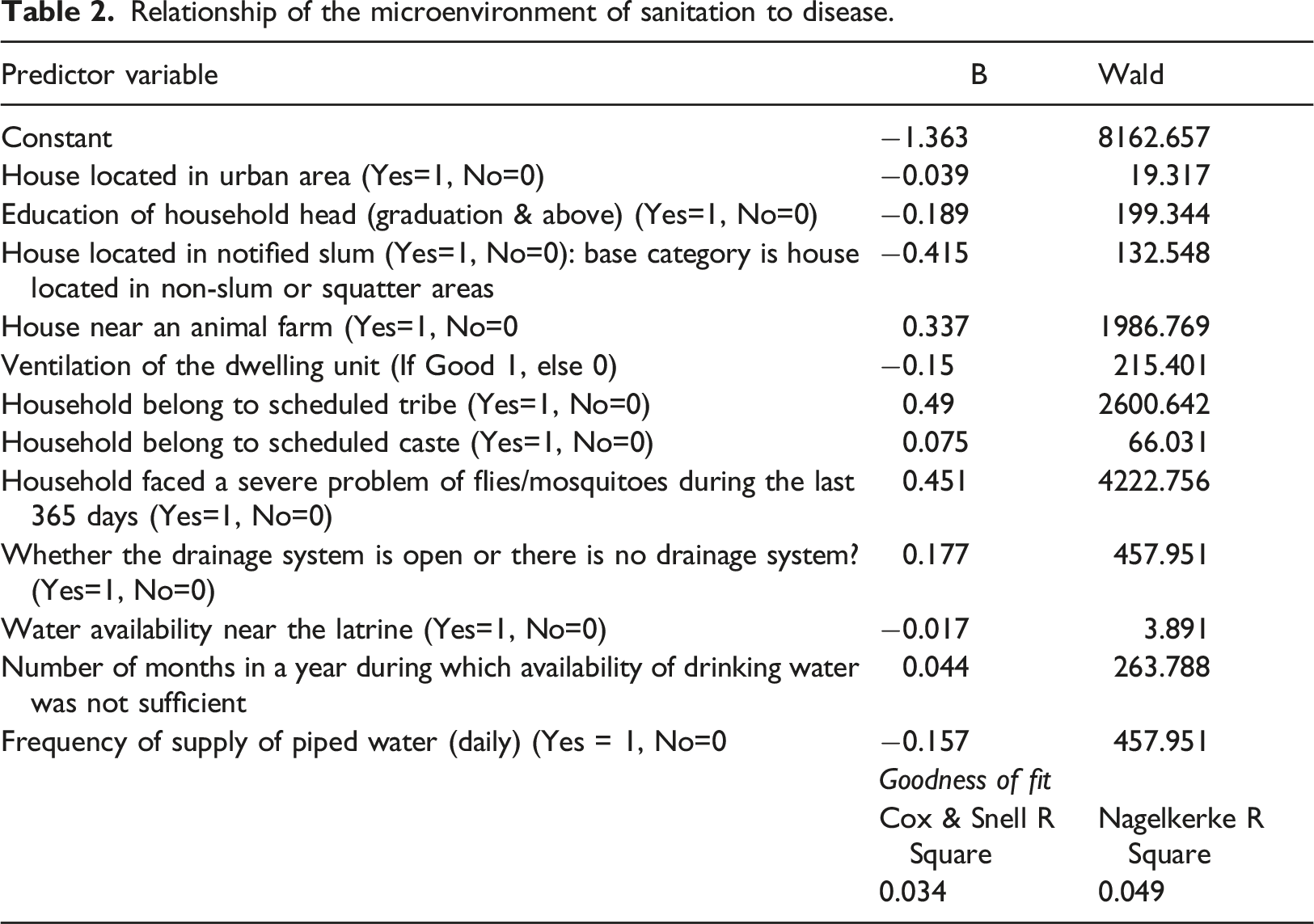
The results indicate that the prevalence of the diseases is expected to be lower in the urban areas. Urban locations have better access to hygienic surroundings, and greater interventions by the local municipal authorities. Households with better education qualification for its head are less likely to suffer from these diseases relative to those with less educated heads. The notified slums have a negative coefficient indicating that the dwellers of these settlements have a lesser incidence of diseases. This is due to their access to better sanitation facilities and other services being provided by the local governments.
The households with an animal farm near their dwelling unit have a higher prevalence of diseases (as indicated by the positive sign of the variable). Houses with better ventilation have a lesser incidence of diseases. The variables denoting scheduled tribes (ST) and scheduled castes (SC) have positive coefficients indicating that diseases are higher in these communities. This could be due to the relatively poor microenvironments within which they live and the practices of open defecation around their locations. The households that faced a severe problem of mosquitoes during the previous year of the survey have a higher incidence of diseases (with a positive coefficient). The variable denoting the availability of water near the toilet is negatively associated with the disease incidence, indicating that water availability leads to better hygiene and better health outcomes. The households having access to daily water have a negative association with disease incidence implying that water availability for all activities promotes hygiene. Similarly, the households that face insufficient water during the year have a positive coefficient, indicating that inadequate availability of water increases the disease incidence.
Taken together, all the microenvironment variables point towards a need for managing the surroundings better to have better health outcomes (Buttenheim, 2008; Prüss-Ustün et al., 2014b).
Discussions and policy implications
Households having a better socio-economic status or having a greater ability to spend have better access to toilet facilities (Osei et al., 2015; Adams, 2018). Households from poorer or underprivileged social classes struggle with access to flush toilets with sewer connections or even in access to double pit toilets.
Having access to a household toilet or even a facility that caters to a group (community toilet or a public toilet) could lead to the conclusion that the availability and access to sanitation infrastructure is adequate. However, such an approach may still suffer from the challenges of measurement and assessing the condition of the microenvironment around communal facilities (Park et al., 2016). The previous research indicates that open defecation is increasingly seen as an undesirable social norm, and households may not wish to state their practices (Barnard et al., 2013; Park et al., 2016). The consequent result will be an underestimate of the impact and need for interventions to promote better hygienic practices.
Mere availability or access to a sanitation facility does not lead to better hygienic practices and reduced incidence of diseases. A strong push towards using the toilets through behavioural interventions is necessary (Rahman et al., 2021). The policymakers can expand the survey instrument coverage to track the behavioural aspects in addition to the physical infrastructure status to get a higher-order understanding of the challenges and accordingly configure more targeted interventions (Park et al., 2016). Gender, marital status, size of households, education and socio-cultural norms play an important role in sanitation choices.
The reason for open defecation, despite having access to Category 2 or Category 3 type toilets, relates to the need for desludging and its cost (Mehta et al., 2019). Regular desludging is necessary for efficient performance of the Category 2 and 3 type toilets. The economic and social conditions of low-income households prohibit incurring such expenses. In a few Indian cities, it has been found that delinking a direct payment for sanitation services and combining this with statutory taxes like property tax substantially improves the compliance and consequent uplift of the surrounding environment (Mehta et al., 2019).
Another important result is that notified slums are better off than other locations in terms of sanitation infrastructure. It is important for the government programs to focus on rural areas and locations of households with low income or of marginalised castes in urban areas. A targeted and context specific approach would result in better outcomes.
The microenvironment is increasingly a factor that has an influence on better sanitation practices and health outcomes (Sidabutar and Chotib, 2021). Results confirm that various elements of the microenvironment impact health outcomes/disease incidence. Diseases can be reduced through better access to safe facilities and a microenvironment, as the exposure to the disease vectors can be restricted without trips for open defecation (Keiser et al., 2005). The severity of mosquito infestation also points to the lack of a hygienic microenvironment, including the presence of stagnant water, animal farms and related elements.
The management of the microenvironment suffers from the institutional structure that is prevalent in India. The government Water and Sewerage Boards, which typically manage the construction and operation of the sewerage and drainage services, do not explicitly assume responsibility for the microenvironments. The responsibility of the individual household toilet and the surrounding within the house is left to the dweller. The microenvironment surrounding the house is usually the responsibility of the local governments. An awareness of the ecosystem that seamlessly integrates the physical sanitation infrastructure, the behavioural changes required and the augmentation of the microenvironment is limited due to the institutional and governance structures (Centre for Policy Research, 2019). This also percolates to the components of the configuration of national and state government’s policies and financial schemes. Government programs appear to have assumed that the initial activity is to provide better access to low-cost sanitation infrastructure, and the associated health benefits can be realized in due course. The current discourse on the demand-led approach to sanitation through better community involvement (Novotný et al., 2018) is substantiated with the results pointing to disparity based on socio-economic conditions and the challenges in the microenvironment. A demand-led approach, however, has its limitation as it reduces the responsibility of the government in the provisioning of services.
The two major national government programs to improve the living conductions of households are (i) Pradhan Mantri Awas Yojana (Housing Policy) (MoHUA, 2021a) and (ii) Swacch Bharat Mission (MoHUA, 2021b). One of the components of the Housing Policy is beneficiary-led individual house construction, which provides eligible low-income households with a financial subsidy to improve their housing through the addition of a room, kitchen, toilet, bath or a combination of these. The Swacch Bharat Mission focuses on assistance for the construction of individual private or community toilets and community or city level improvement of solid and wet waste management systems. The Mission also has behavioural change program components. The effectiveness of these programs could be further enhanced by linking them together. Housing conditions and sanitation are interlinked, as results in this paper indicate. The means tested subsidy provided under the Housing Policy does not address the requirement of toilets adequately as low-income households who are usually constrained by the available liveable space would prefer to build a room or kitchen rather than a toilet. Building and using toilets also requires behavioural change, which has pushed the demand for these to be lower than the demand for a room or kitchen. The subsidy for the construction of a toilet under the Swacch Bharat Mission does not address the problem of the shortage of land or space for low-income households. The results in this paper also indicate the importance of ventilation within houses. The specific focus on the addition of rooms, a kitchen, bath and toilet in the Housing Policy limits other aspects through which the housing condition could be improved. The focus of programs to improve the toilet infrastructure needs to be widened from low-income households to lower-middle and middle-income households. Many of the ownership houses are old and are not in good condition. A rise in the income of households would lead first to improvements in the general condition of houses and then to toilet infrastructure. Open defecation is also a problem for other households. Incentivisation to change behaviour of other households would also be necessary.
Dwivedi (2021) identifies lack of participation of communities in program planning and implementation as a major hurdle for the success of sanitation programs. She states, ‘recognising the direct impact of improved sanitation on the lives of people, the role of communities, especially the most marginalised sections (including girls and women), in planning, implementing, and evaluating schemes holds utmost importance’ (Dwivedi, 2021).
Households living in non-notified slums suffer poor sanitation conditions. The Housing Policy and Swacch Bharat Mission need to include non-notified slums in their target for the improvement of sanitation conditions.
The availability of water (not just the access) has a substantial bearing on the behavioural practices of improved sanitation. As observed in the results, the incidence of diseases is lower with better access to water. The experience of an NGO managed public toilet reiterates the need to make continuous water availability, thereby reducing the impediments to maintaining the facilities and motivating households' usage (Balakrishnan and Khurshid, 2016). In their research, Dwivedi and Dasgupta (2020) find that ‘Given that usage and adequate maintenance of sanitation infrastructure is a learned and imbibed behaviour – a practice developed over time – it is crucial to aid this process through appropriate communication inputs that help generate awareness about the impact of poor containment, collection, transportation and treatment systems on the environment among all stakeholders’. Further they note that rigid personal boundaries in non-slum communities and limited time and avenues for community bonding and collective action have hampered the development of appropriate communication channels (Dwivedi and Dasgupta, 2020).
Conclusions
This study investigates the empirical choices of households in choosing different types of toilets using the data from the 76th round of survey by NSSO. The results indicate that the demographic, socio-economic factors, housing and tenurial status, the sanitation and the health related variables have a significant association with the choice of toilets (Park et al., 2016; Sinha et al., 2017; Friedrich et al., 2020). The better the social and economic position of the household, the choice of toilet gravitates towards flush toilets connected to a public sewer. There is a still substantial open defecation resulting from the socio-economic factors, and a microenvironment comprising the cleanliness of the immediate surroundings (Buttenheim, 2008) and the availability of water (Khatri and Vairavamoorthy, 2007). A poor microenvironment is linked with higher disease incidences.
While the coverage of households with toilet infrastructure has increased in India, the open defecation persists in rural areas and in locations of low-income households in urban areas. Inconsistent usage of toilets, lack of cleanliness and hygiene in and around the community toilets, and the lack of a water supply for toilets are some of the reasons for open defecation to persist. The analysis in this paper indicates that pit toilets are the predominant type provided under government programs. These may not be appropriate in areas prone to flooding or rocky areas where leaching may not be possible. Programs should be flexible to incorporate solutions that are context and site-specific.
Behaviours and socio-cultural norms have played a major role in the low usage of toilets. Although the recent programs have focussed on behavioural change, these have not been very successful (Bharat et al., 2020). The approach to Swacch Bharat Mission is top down with a focus on toilet construction. The focus of program implementation agencies has been on the construction of toilets rather than its use resulting in continuation of open defecation practices despite increasing sanitation coverage (Bharat et al., 2020). While the communities and community led organisations have been active in promoting behavioural change in some pockets, their participation in planning and resource allocation is still nascent. Seth and Jain (2021) argue that the involvement of the community in sanitation programs is necessary to instil behavioural change and use of toilets. The programs need to be inclusive (involving marginalised social classes and women) and must involve communities in the design and implementation of programs. Various programs that address sanitation need to be aligned for better outcomes.
The majority of villages lack a sewerage system, which poses challenges for faecal waste management. Site based waste containment systems depend on toilet technology and space availability, which can become a constraint for individual households, should they have to manage waste locally. Developing a faecal management service for an entire village depends on various demographic and economic factors for its viability. However, the social cost of not having a faecal management service is huge. It is, therefore, important that the focus of government programs should shift towards the development of a sewerage system rather than solely on individual toilet construction.
Women and girls are severely affected by the lack of sanitation facilities. In some states, women have been at the forefront of change through the demand for toilets in house. The policies would need to assign a prominent role for women in planning and implementation of sanitation programs. The role of women could also be envisaged in education related to behavioural management.
The sanitation strategy needs to go beyond toilet use to include the appropriate construction of toilets and the disposal of faecal matter. The programs that were launched in the country aimed to bring uniform financing and technical standards across different states. The components could be strengthened by augmenting the engagement of communities and addressing the whole of the sewage chain. As Purty and Vishwanathan (2020) argue, sanitation policy needs to factor in the inherent caste dynamics in faecal disposal, which assigns the task of faecal disposal to members of the scheduled caste. Changing this attitude would require regulatory and program-based intervention for active community engagement to battle social taboos, and socially inclusive campaigns advocating self-pit emptying, safe de-sludging and disposal practices.
This paper highlights the importance of the microenvironment in addition to the interventions that are infrastructure related in achieving a lower incidence of diseases. The institutional and governance structures prevalent in India emphasize the provision of water and support to construction of individual or public toilets. The recent focus has also been ramping up the education on behavioural aspects (Routray et al., 2015). However, the responsibility of managing the microenvironment is blurred between the individual household, community and the public governing body. The results from this paper reinforce the need for a more holistic approach of involving stakeholders at different levels to improve sanitation and reduce related disease incidence.
The move from open defecation to improved sanitation systems will need a holistic approach to address the infrastructure, behavioural and microenvironment improvements. The efforts of policymakers would need to shift the direction from infrastructure provision to simultaneously developing institutional and implementation structures that can support key components of the microenvironment. There is a need for better measurement metrics (Jenkins et al., 2014) that capture infrastructure provision, behavioural aspects and the microenvironment for greater awareness in managing the sanitation challenge. Water availability has been a sore point for expanding sanitation services, across the chain. The sewerage connectivity has typically lagged that of water and would need to be ramped up, particularly aimed at the marginalised sections. The regional, cultural and caste-based aspects need further investigation to provide pointers for how to build upon the gains achieved in the sanitation improvement. Alongside financial factors, social factors such as caste and religion are crucial predictors of households’ decision on the type of toilet. A close consideration of socio-economic differences is crucial to policy success on this sensitive matter (Doron and Jeffrey, 2014).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.