
Abstract
Introduction:
Retroperitoneal lymphadenopathy represents a unique and infrequent complication within various malignancies. This case report exemplifies the intricate diagnostic challenges that arise when identifying nondilated obstructive nephropathy in the context of retroperitoneal lymphadenopathy due to diffuse large B-cell lymphoma (DLBCL), particularly when conventional imaging fails to reveal the hallmark feature of hydronephrosis.
Case description:
We present a 66-year-old male with relapsed chronic lymphocytic leukemia post-allogeneic stem cell transplantation. His direct admission to the hematology/oncology service was due to failure to thrive. Despite the absence of hydronephrosis on imaging, the patient developed volume overload and increased serum creatinine levels. An ultrasound unveiled mild bilateral collecting system dilation, while laboratory findings did not provide valuable insight into the underlying etiology. A Lasix renal scan confirmed split renal function with minimal bilateral excretion. High clinical suspicion resulted in an MRI scan showing interval enlargement of retroperitoneal lymph nodes and pelvicaliectasis, which prompted urological and interventional radiology involvement.
Conclusions:
This case underscores the complexity of diagnosing retroperitoneal lymphadenopathy and pelvicaliectasis, in DLBCL, particularly when hydronephrosis is absent on imaging. It emphasizes the significance of clinical acumen, collaboration among specialties, and the use of advanced imaging techniques. Timely recognition of nondilated obstructive nephropathy in the setting of retroperitoneal lymphadenopathy is pivotal for guiding appropriate management strategies and optimizing patient outcomes in the intricate clinical setting.
Keywords
Introduction
Acute kidney injury is a frequently encountered condition by nephrologists in clinical practice. The associated mortality rate with acute kidney injury is approximately 20%. Obstructive nephropathy stands out as one of the most prevalent reversible causes of acute kidney injury. While non-invasive renal ultrasound and CT scans are the preferred diagnostic tests, they may not definitively rule out obstruction in certain cases. Non-dilated obstructive nephropathy leading to acute kidney injury is a rare occurrence, accounting for approximately 5% of obstructive nephropathy cases. Given the absence of radiographic evidence showing dilation of the collecting system, clinicians are posed with a diagnostic challenge in these scenarios. 1
This maybe observed in pelvic malignancies, metastatic breast cancer, non-Hodgkin’s lymphoma, sarcoidosis, infections like tuberculosis, and other conditions resulting in chronic inflammation, fibrosis, and lymphadenopathy.2–4 Radiation treatment for testicular seminoma, colon and pancreatic cancer can rarely lead to secondary to retroperitoneal fibrosis.
Retroperitoneal lymphadenopathy and pelvicaliectasis represent intricate and uncommon complications due to the diagnostic challenges associated with identification especially in situations where the characteristic feature of hydronephrosis is not evident on imaging. Successfully identifying non-dilated obstructive nephropathy demands a heightened suspicion level and collaborative efforts among multiple specialties, including nephrology, urology, radiology, and oncology, to achieve early diagnosis and intervention. 1 A delay in recognizing this potentially reversible cause of acute kidney injury can ultimately lead to adverse events and poor patient outcomes.
Case description
A 66-year-old male with a medical history of relapsed chronic lymphocytic leukemia, which progressed to diffuse B-cell lymphoma post-allogeneic stem cell transplantation who was recently started on epcoritamab, was directly admitted to the hematology/oncology service due to cough and failure to thrive. The initial workup yielded positive results for rhinovirus and parainfluenza virus from respiratory cultures. Urine cultures were positive for Escherichia coli and Enterococcus. Given his immunosuppressed state, antibiotic treatment with Zosyn was initiated. Initial vital signs included a blood pressure of 162/81 mmHg, a heart rate of 101 bpm, a respiratory rate of 24 bpm, oxygen saturation of 96% on room air, and a temperature of 99°F. Urinalysis upon admission indicated pyuria and hematuria. Urine sodium was measured at 23 mmol/L, and the fractional excretion of sodium was 0.7%, consistent with a prerenal etiology. He remained non-oliguric through the hospital course. Despite receiving 2 L of normal saline, there was no improvement in serum creatinine. Consequently, an Onconephrology consultation was sought due to acute kidney injury, with a serum creatinine of 3.83 mg/dL (baseline serum creatinine less than 1 mg/dL, reference range 0.6–1.3 mg/dL). Urine microscopy lacked sufficient evidence of muddy brown casts, granular casts, or dysmorphic RBCs. Cystatin C was 2.62 mg/L with eGFR of 21 mL/min/1.73 m2. An ultrasound revealed mild bilateral dilation of the collecting system, but no significant hydronephrosis (Figure 1). Following day upon examination, the patient exhibited signs of volume overload including crackles on lung auscultation and worsening lower extremity edema. His serum creatinine levels demonstrated a progressive upward trend over the next 3 days. Subsequently, a nuclear renogram with Lasix was performed, indicating split renal function yet minimal bilateral excretion, thereby providing insufficient insights into any potential obstruction. However, strong clinical suspicion for obstruction prompted a magnetic resonance imaging (MRI), revealing an increased size of retroperitoneal lymph nodes and pelvicaliectasis, with segmental visualization of the ureters without obvious obstruction (Figure 2). Further, Positron emission tomography–computed tomography (PET-CT) was notable for prominent fluorodeoxyglucose (FDG) uptake in the left external iliac node adjacent to mid-ureter and the right psoas muscle adjacent to the kidney (Figure 3). These findings led to the involvement of urological specialists for decompression. An initial attempt to place bilateral ureteral stents was made, but it resulted in massive hematuria, leading to procedure discontinuation. Consultation with interventional radiologists was sought for the placement of percutaneous nephrostomy tubes. Unfortunately, during this period, the patient suffered from an acute coronary incident leading to a decline in his overall health and subsequent transition to hospice care.
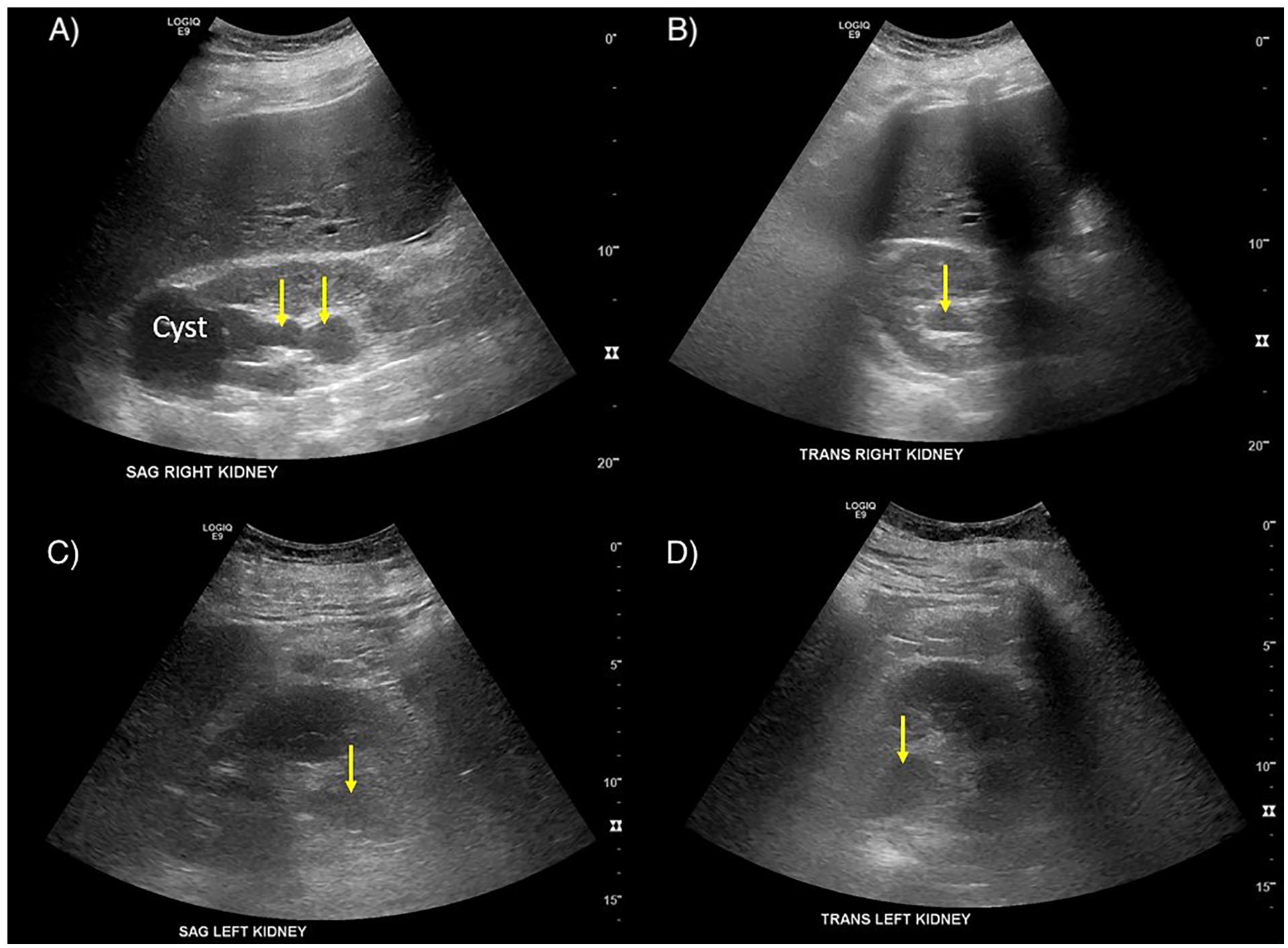
Kidney ultrasound images demonstrating mild dilation of the collecting system bilaterally (arrows).
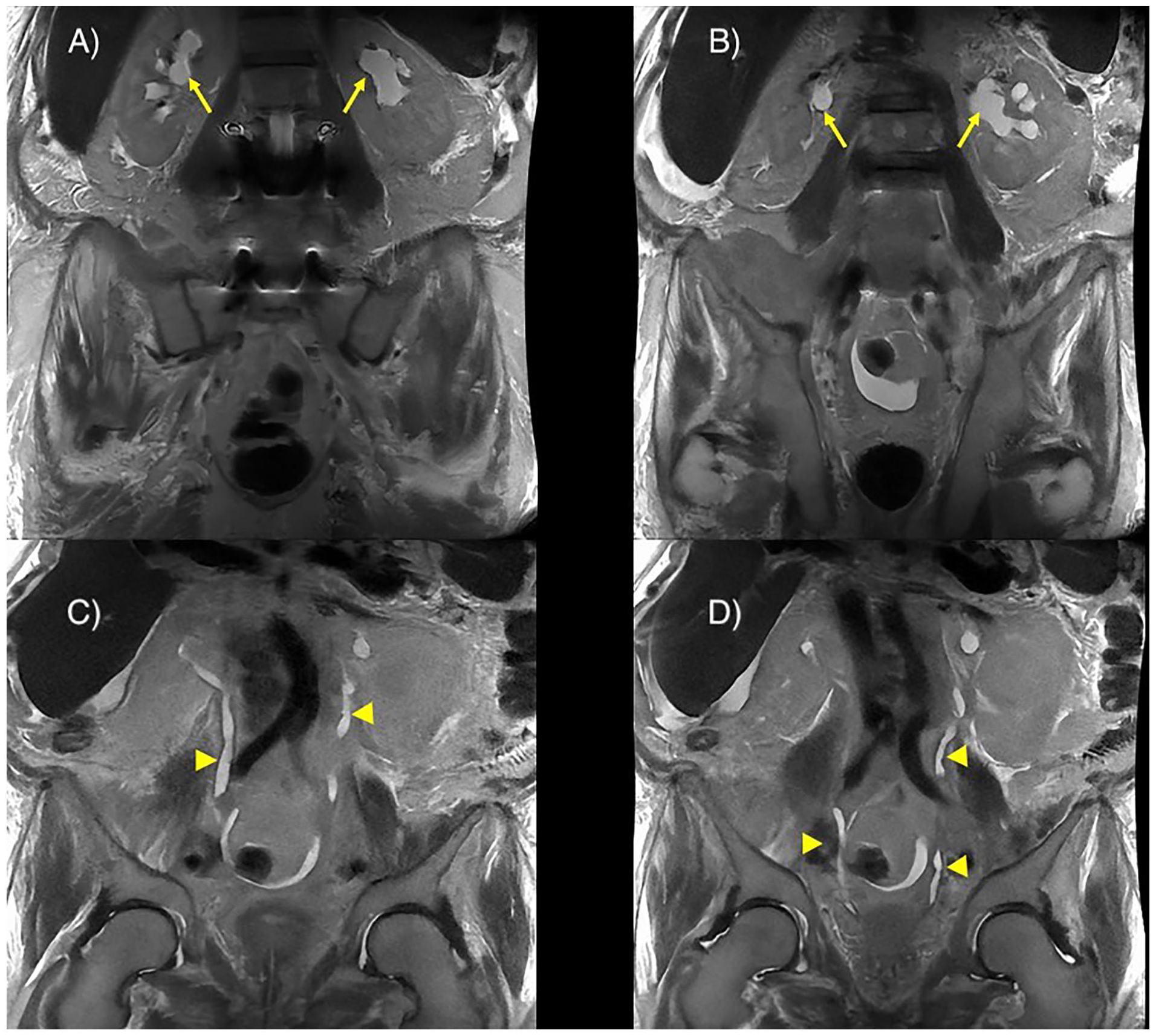
Magnetic resonance imaging (MRI) demonstrating (a and b) bilateral mild hydronephrosis that appears prominent than on the sonogram (arrows). (c and d) Segmental visualization of bilateral ureters (arrowheads).
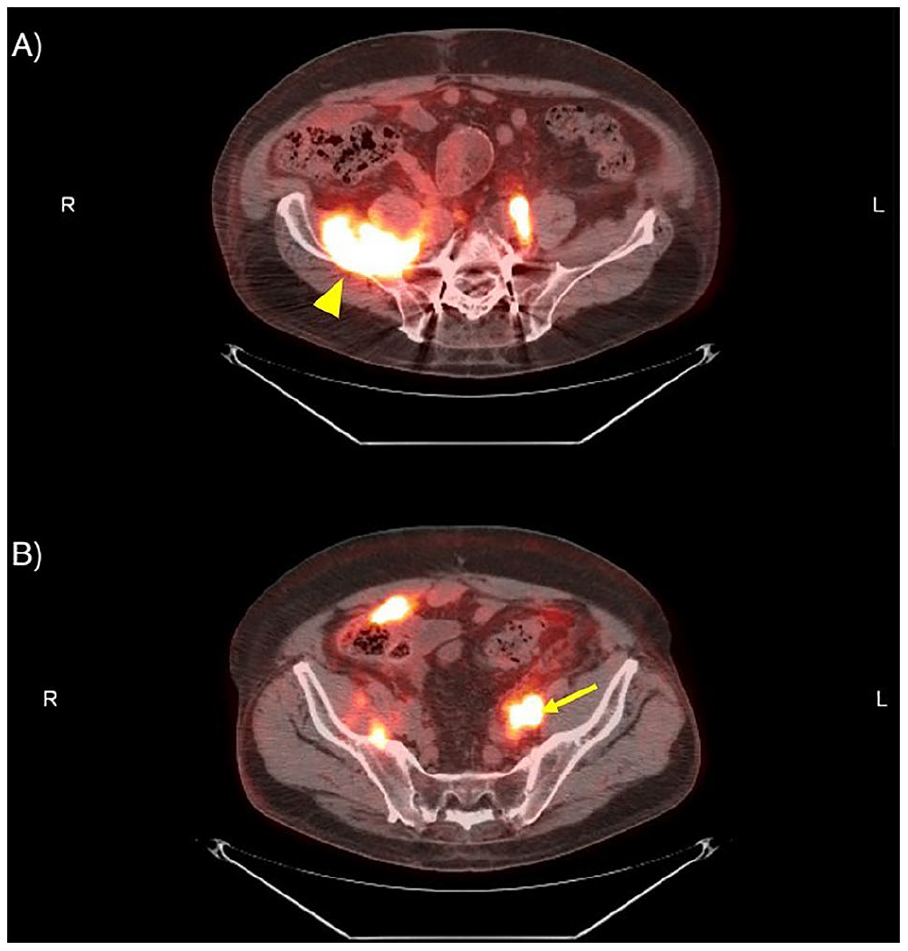
Positron emission tomography–computed tomography (PET-CT) demonstrating prominent fluorodeoxyglucose (FDG) uptake in the left external iliac node adjacent to mid-ureter (arrow) and the psoas muscle in the right perinephric area (arrowhead).
Discussion
Non-Hodgkin’s lymphomas represent a heterogeneous group of malignancies, with B-cell lymphomas comprising around 90% of cases. Extra nodal involvement is common in B-cell lymphomas, although direct lymphoma involvement of the urinary tract is rare. However, compressive effects from retroperitoneal lymphadenopathy often become evident later in the course. Non-dilated obstructive nephropathy due to retroperitoneal lymphadenopathy is an infrequent but significant complication observed across various malignancies, including hematologic neoplasms like diffuse large B-cell lymphoma. This case report provides a vivid illustration of the intricate diagnostic challenges faced in identifying non-dilated obstructive nephropathy, especially when the characteristic feature of hydronephrosis is absent on imaging. 5
Complete bilateral obstruction can lead to a rapid and irreversible decline in kidney function unless the obstruction is promptly alleviated. Therefore, a thorough and expedient investigation into the cause of obstruction is crucial. Maintaining a high index of suspicion in patients at risk for non-dilated obstructive nephropathy is paramount. 6 This includes those with known malignancy, infection, chronic inflammatory conditions, sarcoidosis, or unexplained acute kidney injury accompanied by a sudden, significant rise in serum creatinine. 2 These patients would benefit from conducting an extensive diagnostic workup to illicit the etiology behind their acute kidney decline. If the workup remains inconclusive and suspicion remains elevated, further invasive interventional procedures should be considered. Since non-dilated obstructive nephropathy is diagnosed based on clinical suspicion, integration of clinical findings of acute renal failure with no clear etiology along with imaging studies is recommended. The choice of imaging modality depends on the availability and severity of the suspected obstruction. Renal sonography, a widely used non-invasive modality, provides valuable information about the collecting system, renal parenchyma, kidney size, echogenicity, and cortical thickness, aiding clinicians in assessing potential kidney function recovery.7,8 However, it does not always identify early hydronephrosis.
Alternatively, CT-assisted radioisotope renography proves useful in acute obstructive nephropathy by demonstrating delayed cortical clearance. It is also worth mentioning that renal angiography is less commonly used due to its invasive nature, retrograde pyelography confirms and defines the diagnosis of obstruction. MR urography has been a test of choice in some cases where contrast exposure is a concern. PET scan is however not the diagnostic modality of choice. PET scan findings can be used in patients with malignancy related retroperitoneal lymphadenopathy to assist in diagnosis when imaging studies are inconclusive. In our case above, MRI findings along with new retroperitoneal lymphadenopathy findings from PET scan intensified our suspicion.
Grading hydronephrosis has always been a challenge. While there is no universally accepted system, the grading system developed by the society of fetal urology has been widely used in understanding and interpretation of fetal and adult hydronephrosis. Hydronephrosis is usually classified as mild, moderate, and severe in routine clinical practice. In mild cases, there is dilatation of renal pelvis but the pelvicalyceal pattern is retained and cortex is unaffected. In moderate cases, there is significant dilatation of the pelvicalyceal system with outpouching of the calyces sometimes referred to as “cauliflower” appearance, mild cortical thinning may be seen. In severe cases, there is significant dilatation of the pelvicalyceal system with loss of borders between the renal pelvis and calyces along with cortical thinning. 9
Despite the range of available imaging modalities, diagnosing non-dilated obstructive nephropathy remains notably complex due to its inconspicuous presentation and the absence of characteristic signs. The clinical manifestations of non-dilated obstructive nephropathy often overlap with those of acute tubular necrosis, potentially leading to a delayed recognition of the underlying renal obstruction. Patients may present with generalized fatigue, malaise, or varying degrees of renal dysfunction. Therefore, clinicians must maintain a heightened clinical suspicion when managing DLBCL patients exhibiting unexplained renal dysfunction.
In the case discussed above, the patient had relapsed DLBCL and had recently started epcoritamab treatment. Chemotherapy-related acute kidney injury was considered, although there is limited data on epcoritamab renal effects. There is insufficient data regarding the side effects of epcoritamab. The most common toxicity reported is cytokine release syndrome which was noted in 49.7% of patients from a recent multicenter trial, with 2.5% noted to have severe form. Our patient did not exhibit signs or symptoms or cytokine release syndrome
Initially, the working diagnosis considered sepsis-related acute kidney injury or acute tubular necrosis, along with the possibility of interstitial nephritis due to multiple antibiotics and chemotherapy. However, due to the rapid decline in kidney function and known risk factors, further investigation was pursued. An intriguing aspect of the case is that despite significant deterioration in kidney function, urine output was maintained, which can be misleading. In partial obstruction cases, angiotensin and AT-1 receptors often upregulate to sustain ureteric peristalsis.
There are absolute and relative indications for relieving obstruction in cancer patients. Absolute indications are sepsis from urinary tract infection and excruciating pelvic pain. Relieving obstruction in cases with Acute renal failure with end stage cancer patients should be weighed against the prognosis. In some cases, urinary diversion will help improve kidney function making them eligible for chemotherapy which might improve survival. For majority of cases, decompression and maintaining ureteral patency is mandatory as a palliative measure.
Options available are ureteral stent placement and percutaneous nephrostomy tube placement. Retrograde placement of Ureteral stent is the first choice by urologists for extrinsic ureteral compression by tumor. This might be the preferred option in patients with anticipated technical challenges for placement of nephrostomy tubes. The presence of coagulopathy is a relative contraindication to nephrostomy tube placement.
Placement of nephrostomy tube is the preferred modality in cervical, prostrate, colorectal. and bladder malignancies where attempting to identify ureteral orifices usually fails. In patients with peritoneal carcinomatosis and retroperitoneal fibrosis, there is anatomic distortion of the ureters which makes ureteral stent placement difficult. 10
In conclusion, diagnosing non-dilated obstructive neph-ropathy stemming from retroperitoneal lymphadenopathy in patients with malignancy presents considerable challenges due to its subtle presentation and the lack of hydronephrosis on imaging. Despite its high sensitivity (93%) and specificity (100%), ultrasound imaging of the kidneys might not definitively exclude obstruction, especially in cases with volume depletion or early hydronephrosis. Thus, clinical acumen, early utilization of advanced imaging techniques, and interdisciplinary collaboration are pivotal in navigating these complexities. Timely recognition and precise diagnosis of non-dilated obstructive nephropathy are critical for guiding optimal management strategies and enhancing patient outcomes in acute scenarios.
Footnotes
Acknowledgements
N/A.
Author contributions
SG and PH composed the manuscript. AH, WA, and PH provided the images, mentorship, and review of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors certify that they have NO affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or materials discussed in this manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
N/A.
Informed consent
Informed consent could not be obtained as a result of the patient’s demise.
Trial registration
N/A.
Guarantor
PH.