
Abstract
Ketamine, classical psychedelics and sleep deprivation are associated with rapid effects on depression. Interestingly, these interventions also have common psychotomimetic actions, mirroring aspects of psychosis such as an altered sense of self, perceptual distortions and distorted thinking. This raises the question whether these interventions might be acute antidepressants through the same mechanisms that underlie some of their psychotomimetic effects. That is, perhaps some symptoms of depression can be understood as occupying the opposite end of a spectrum where elements of psychosis can be found on the other side. This review aims at reviewing the evidence underlying a proposed continuum hypothesis of psychotomimetic rapid antidepressants, suggesting that a range of psychotomimetic interventions are also acute antidepressants as well as trying to explain these common features in a hierarchical predictive coding framework, where we hypothesise that these interventions share a common mechanism by increasing the flexibility of prior expectations. Neurobiological mechanisms at play and the role of different neuromodulatory systems affected by these interventions and their role in controlling the precision of prior expectations and new sensory evidence will be reviewed. The proposed hypothesis will also be discussed in relation to other existing theories of antidepressants. We also suggest a number of novel experiments to test the hypothesis and highlight research areas that could provide further insights, in the hope to better understand the acute antidepressant properties of these interventions.
Introduction
Depression is a world-wide leading cause of disability (World Health Organization, 2017). For both standard antidepressants, such as selective serotonin reuptake inhibitors (SSRIs), and psychological treatments, a significant treatment effect is generally only seen after weeks of treatment. Contrary, a number of less well-established treatments, including ketamine, psychedelics and sleep deprivation are shown to be associated with a rapid decrease in depressive symptoms (Bobo et al., 2016; Muttoni et al., 2019; Riemann et al., 2020).
One of the most popular theories for the neurocognitive effects of traditional antidepressants states that they target the affective biases commonly seen in depression (Beck et al., 1979). This negativity bias leads to a perception of the surrounding world in pessimistic terms, which eventually leads to a depressive worldview. By altering the affective bias, the depressive worldview becomes corrected over time (Harmer et al., 2009).
Cognitive inflexibility is a separate component of depression, believed to be an important treatment target (Rock et al., 2014; Solé et al., 2015). Cognitive flexibility is commonly defined as the ability to switch between different types of tasks or concepts (Diamond, 2013), but we here also refer to cognitive inflexibility as a broader inability to adjust one’s thinking from old situations to new situations. This aspect of depression likely interacts with the affective bias account described above, because in order to change a depressive worldview, a certain amount of flexibility in this worldview is required, such that expectations about negative and positive events can be corrected. Speculatively, this could indicate that traditional antidepressants potentially only affect cognitive inflexibility indirectly, which might contribute to the reason why they take multiple weeks to have their effect. This would be in line with the resource-allocation hypothesis by Park et al. (2018), which suggests that the ability of early changes in ‘cold’ cognition (e.g. executive functioning) to predict treatment response in depression is dependent on its association with ‘hot’ cognition, that is, cognitive-emotional functions.
Interestingly, ketamine, psychedelics and sleep deprivation have in common that they are acute antidepressants, as well as that they induce some of the symptoms of psychosis. These include in the case of ketamine distorted sense of self and thought, as well as experiences of dissociation (Krystal et al., 1994), whereas the effects of psychedelics are more perceptual but can also include experiences of distorted thinking (Gouzoulis-Mayfrank et al., 1998; Vollenweider and Kometer, 2010). Sleep deprivation causes progressively more severe symptoms of psychosis, starting with perceptual alterations initially, and distortions in thinking if sleep deprivation is maintained (Waters et al., 2018). However, there are also important differences between psychotic symptoms caused by ketamine, psychedelics and sleep deprivation, compared to clinical cases of psychosis, where the latter tends to involve more auditory hallucinations (Bauer et al., 2011), which are rare under the influence of ketamine and psychedelics. In contrast, psychedelics tend to affect the visual modalities more strongly, although distortions in self-awareness and thinking are present under higher doses as well (Leptourgos et al., 2020). Furthermore, clinical psychosis is often characterised by a lack of insight which is usually preserved under the influence of drugs (Leptourgos et al., 2020; Pomarol-Clotet et al., 2006). Interestingly, psychosis (in particular the early phases) has been commonly described to reflect an overly flexible brain (Fletcher and Frith, 2009; Sterzer et al., 2018). If cognitive inflexibility is indeed an important feature of depression, and psychotomimetic interventions increase cognitive flexibility, this raises the exciting possibility that psychotomimetics like ketamine, psychedelics and sleep deprivation have acute antidepressant effects precisely because of their ability to increase cognitive flexibility.
In the following review, we will formulate the hypothesis that there is a shared mechanism that underlies the psychotomimetic properties and acute antidepressant effects of these treatments. First, we will describe the various acute antidepressants and their psychotomimetic features. We will subsequently review these treatments through the theoretical framework referred to as predictive coding theory (Friston, 2010; Spratling, 2017) which we suggest can help us understand why psychotomimetic interventions might be acute antidepressants. Finally, we will compare our suggested hypothesis with existing theories and make suggestions for future studies to test the validity of the hypothesis.
An overview of acute antidepressants with psychotomimetic effects
Ketamine
Ketamine is a non-competitive open channel N-methyl-D-aspartate (NMDA) antagonist, first synthesised in 1962 by Calvin Stevens at Parke-Davis Co and as an anaesthetic used in humans since 1965 (Gao et al., 2016; Mion, 2017). During the last two decades, sub-anaesthetic dosage of ketamine has repeatedly been shown to cause an acute antidepressant effect (Berman et al., 2000; Bobo et al., 2016; Kishimoto et al., 2016). The effect is seen within hours and peaking at 24 h after administration, with a decline during the following week (Bobo et al., 2016). A number of meta-analyses have investigated the efficacy in treatment showing overall large effect sizes for the acute effect (McGirr et al., 2015; Newport et al., 2015; Xu et al., 2016). Although the treatment is associated with some side-effects, including psychotomimetic symptoms, these generally resolve within hours after administration (Bobo et al., 2016).
Ketamine administration causes a burst in glutamate via inhibition of gamma-aminobutyric acid (GABA) interneurons, followed by a cascade involving stimulated AMPA receptors and activation of calcium channels leading to a release of brain-derived neurotrophic factor (BDNF) and mammalian target of rapamycin complex–1 (mTORC1) signalling, and in turn an increased synthesis of synapse proteins (Autry et al., 2011; Li et al., 2010; Moghaddam et al., 1997). The exact pathway that mediates the effect of ketamine on depressive symptoms is however not clear, even though an increase in synaptic plasticity has been suggested as one possible mechanism (Krystal et al., 2013; Monteggia et al., 2013).
As indicated above, ketamine is also associated with psychotomimetic effects, which has been shown both as side-effects in relation to anaesthesia (Bobo et al., 2016) and in experimental studies in healthy volunteers (Krystal et al., 1994; Malhotra et al., 1996). The latter has made it a useful model for psychosis (Corlett et al., 2007). Psychotomimetic effects are often manifested as alterations in perception, dissociations and hallucinations (Corlett et al., 2007, 2016; Krystal et al., 1994), but some studies have also emphasised the ability of ketamine to mimic the negative symptoms of schizophrenia including apathy and social withdrawal (Anis et al., 1983; Krystal et al., 1994).
Psychedelics
Classical psychedelics, that is, psychedelics that exert their effects through 5HT2a receptor agonism, have a long history of usage in spiritual practices, ranging as far back as 5700 years ago in native Mexican cultures (Bruhn et al., 2002). Psychedelics became popular in the West in the 1950s and 1960s, which was accompanied by a surge in research into the properties of the drug (Reiff et al., 2020). In the last decade, there has been an increasing interest in the use of classic psychedelics in treating individuals with treatment-resistant depression (Reiff et al., 2020). Psilocybin, ayahuasca and lysergic acid diethylamide (LSD) have been shown to reduce depressive symptoms and anxiety as single treatments, but more often in combination with psychotherapy (Carhart-Harris et al., 2016, 2018a; de Osório et al., 2015; Reiff et al., 2020).
Psychedelics exert their effects by increasing glutamatergic activity following activation of pyramidal neurons, primarily in layer 5 of the cortex (Aghajanian and Marek, 1996, 1999; Béïque et al., 2007). Initially this was believed to be due to activation of the presynaptic 5HT2a receptors (González-Maeso et al., 2007; Puig et al., 2003), but more recent studies have pointed to postsynaptic receptors (González-Maeso et al., 2007; Puig et al., 2003). This activation can subsequently lead to downstream effects on serotonergic and dopaminergic activity in the raphe nucleus and ventral tegmental area following activation of 5HT2a receptors in the medial prefrontal cortex (Vollenweider and Kometer, 2010). Indeed, following the intake of psilocybin, increases in dopamine levels in the striatum, which correlated to euphoria and depersonalisation, have been shown (Vollenweider et al., 1999). Speculatively, psychedelics have furthermore been suggested to cause neuroplastic adaptations that might underlie some of the therapeutic effects (Vollenweider and Kometer, 2010).
Psychedelics induce pronounced changes in consciousness, including changes in perceptual experiences such as brightening of colours, synaesthesia, illusory patterns, or full-blown hallucinations and a sense of derealisation (Hoch et al., 1952; Leptourgos et al., 2020; Leuner and Holfeld, 1962). These experiences are not unlike the experiences sometimes described in the early stages of clinical psychosis, sometimes referred to as the prodromal period, where patients often experience a heightening of the senses, and an inability to dissociate the important from the unimportant (Bowers and Freedman, 1966; Chapman, 1966; Gouzoulis-Mayfrank et al., 1998).
Sleep deprivation
Sleep deprivation as an antidepressant treatment was first reported in 1818, by the German psychiatrist Johann Christian August Heinroth (Steinberg and Hegerl, 2014). In the mid-1960s, the antidepressant effects of sleep loss was suggested in a case study of a teacher whose depression eased after sleepless nights (Schulte, 1966) and the first trial of sleep deprivation for depression was published in 1971 (Pflug and Tölle, 1971). A meta-analysis published in 2017 combining 66 studies showed an overall response rate to sleep deprivation in depression of 45%–50% of patients (Boland et al., 2017). Notably, most studies of sleep deprivation as a treatment for depression have been performed with little experimental control, such as randomisation or blinded assessments. In most patients, the depressive symptoms, also, revert after sleep.
A number of putative mechanisms have been suggested to cause the antidepressant effect of sleep deprivation. Bunney and Bunney (2013) proposed that the effect is mediated via CLOCK gene transcription and a ‘reset’ of the circadian rhythm. Wolf and colleagues formulated a synaptic plasticity model theory which suggests that sleep deprivation enhances cortical synaptic strength and facilitates long-term potentiation, through homeostatically shifting the brain to a window of long-term potentiation inducibility (Wolf et al., 2015). A handful of studies investigated changes in neurotransmitters in association to therapeutic sleep deprivation, suggesting a possible role for serotonin (Lopez-Rodriguez et al., 2003; Salomon et al., 1994), dopamine (Benedetti et al., 1996, 2001; Ebert et al., 1994) or the glutamatergic system (Murck et al., 2009).
Analogous with ketamine and psychedelics, sleep deprivation is associated with psychotic symptoms, in healthy volunteers (Waters et al., 2018) but even more pronounced in patients with bipolar disorder (Lewis et al., 2017; Wehr et al., 1987). A recent review suggested that psychotic symptoms after sleep deprivation develop in an almost dose-dependent manner with perceptual distortions, anxiety, irritability, depersonalisation and temporal disorientation starting within 24–48 h of sleep loss, followed by complex hallucinations and disordered thinking after 48–90 h, and delusions after 72 h (Waters et al., 2018).
A theoretical framework to understand the link between psychosis and rapid antidepressants
The previous section described interventions that are both rapid antidepressants as well as psychotomimetic. In order to understand what kind of mechanisms underlie this phenomenon, we need to have a framework for how the brain forms a model of the world in the first place, such that we can start to see how changes in that model can lead to both depression-like symptoms and psychosis. The model we will use in this article is the hierarchical predictive coding model (Friston, 2009, 2010; Friston and Kiebel, 2009; Rao and Ballard, 1999; Spratling, 2008, 2010, 2017).
Predictive coding is a solution to how the brain forms a model of its environment on an algorithmic and neural level (Clark, 2015; Hohwy, 2013). Although various iterations of the hierarchical predictive coding model exist, they have in common the idea that the brain forms a hierarchical generative model of its environment where predictions are generated about the most likely causes of sensory information. These predictions are compared to new sensory input. When there is a mismatch between the two, a prediction error is generated that updates the brain’s predictions about the sensory input, which over time improves the brain’s model of its environment. Importantly, both predictions and sensory input are represented by probability distributions which have a mean and variance. The mean can be seen as the brain’s estimate of the belief whereas the variance is an estimate of how certain this belief is. This certainty is often referred to as the precision of sensory input (in the case of new evidence) or priors (in the case of predictions) and is used to weight the influence of higher-level beliefs versus lower-level evidence (Friston, 2009; Friston and Kiebel, 2009; Rao and Ballard, 1999). For example, a self-image might be stable (precise prior), and unchangeable in the light of evidence, or flexible and responsive to change (imprecise/flexible prior). Experimentally, it can be difficult to disambiguate whether a behavioural phenomenon is due to increased precision of sensory input or a flexibility of priors, as they tend to result in similar experiences (Haarsma et al., 2020c).
Certain neurotransmitters are believed to play an important role in coding of the precision of sensory evidence, as well as the precision of prior expectations. For example, dopamine has been associated with coding the precision of prediction errors (Diederen et al., 2017; Haarsma et al., 2020a) as well as acetylcholine, which has been associated with increasing reliance on bottom-up information (Baldeweg et al., 2006; Moran et al., 2013). In contrast, the NMDA-receptors that ketamine binds to have been suggested to play a role in coding the precision of prior beliefs (Sterzer et al., 2018).
Relevant to the current theoretical perspective is that there are various ways in which learning about the world can go awry. First, there can be changes in the degree to which new information is given weight. For example, when negative information is given more weight when learning about our environment, a more negative worldview will emerge. This is what is known as an affective bias, which is thought to contribute to depression, and is suggested to be altered by SSRIs (Harmer et al., 2009). In contrast, the prior expectation can be given undue weight, such that it is inflexible to new changes. For example, in depression, one might expect negative events to be very likely to occur and positive events likely to be absent. When these expectations are overly precise, this could lead to a phenomenon of cognitive inflexibility, which is known to contribute to depression (Coifman and Summers, 2019; Leahy et al., 2012).
Psychosis and depression as disorders of precision
Psychosis
If the brain indeed forms a model of the world through a process of hierarchical inference, where precision of prior expectations, sensory input and prediction errors is key, erroneous models of the world can be the result of misallocation of precision, resulting in symptoms of hallucinations and delusions as commonly seen in psychosis. One of the earliest accounts suggested that strong prior expectations might be the cause of hallucinations and delusions (Stephan et al., 2006), whereas others suggested that psychosis can be understood as a case of weaker prior expectations resulting in overly precise prediction errors (Fletcher and Frith, 2009). More recent accounts aimed to reconcile these different accounts by suggesting that they might be differently related to state and trait symptoms (Adams et al., 2013) and the most recent reiteration of the hierarchical predictive coding model of psychosis suggested that psychosis can best be understood as a result of aberrant changes in precision in different levels of the cortical hierarchy through different stages of psychotic illness (Sterzer et al., 2018). Specifically, precision of prior expectations is suggested to be weakened in early perceptual processes perhaps more pronounced in the early stages of illness, whereas the precision of higher order learned beliefs becomes stronger and can start to dominate perception (Sterzer et al., 2018). Indeed, there are various lines of evidence supporting this view, demonstrating weakened perceptual priors in psychosis (Dima et al., 2010; Haarsma et al., 2020b; Schmack et al., 2013), as well as stronger learned priors (Cassidy et al., 2018; Haarsma et al., 2020b; Teufel et al., 2015; Valton et al., 2019).
Depression
There are multiple variations of the hierarchical predictive coding model of depression, which emphasise different features of depression and go into varying levels of detail. However, there is a high degree of overlap between the models, in the sense that they all involve an increased influence of prior expectations on cognitive as well as interoceptive processes. It has been argued that predictive coding models are particularly applicable to depression, as the core symptoms seem to be centred on expecting negative events to occur with high likelihood as well as positive events with low likelihood (Kube and Rozenkrantz, 2020). Understanding how these prior expectations can be altered therefore seems to be a crucial component of understanding the core mechanisms underlying depression and developing novel treatments (Kube and Rozenkrantz, 2020). Others have emphasised the importance of estimating uncertainty in predictive coding models, and that an inability to reduce uncertainty seems to be particularly related to anxiety and depressive symptoms, whereas reducing uncertainty is related to positive emotions (Clark et al., 2018). Another view puts the emphasis on aberrant interceptive predictions (Barrett et al., 2007). Here it is argued that there is a deficit in minimising prediction errors in the limbic system as a result of prolonged stress, which in time generates false interoceptive predictions about autonomic, metabolic and immunological requirements. In other words, these predictions generate false stress responses, effectively dysregulating the hypothalamic–pituitary–adrenal (HPA)-axis. Sickness behaviour and negative affect are subsequently used by the body to reduce energy expenditure, which overtime results in depression. Thus, depression is viewed here as a perturbation in energy regulation and interoceptive inference, that is, the prediction errors and associated precision (Barrett et al., 2016).
Other models focus on reward learning. Here depressed brains are characterised by a hierarchical structure of depressive beliefs, producing a consistent negative bias. This bias leads to oversampling the environment to confirm these negative expectations (Chekroud, 2015). In similar vein, depression has been argued to reflect impaired reward-approach behaviours, as a result of having prior beliefs reflecting positive outcomes being unlikely (Joffily and Coricelli, 2013). These views echo earlier affective bias accounts (Harmer et al., 2009), although these earlier accounts emphasise changes in the sensory input rather than prior predictions. Recently, a predictive coding perspective has integrated cognitive immunisation, the tendency to reappraise evidence that disconfirms negative views about oneself, with overgeneralisation of negative feedback (Kube and Rozenkrantz, 2020), suggesting that these can be understood as overly strong negative prior expectations suppressing positively valenced prediction errors and exaggerated signalling of negatively valenced prediction errors (Kube and Rozenkrantz, 2020).
Taken together, these models suggest that symptoms of depression can be understood as overly precise prior expectations. These can be valence-specific where an overly strong, negatively valenced prior can cast everything in a negative light, whereas priors regarding positively valenced events can be such that these are not to be expected, thereby blunting reward responses. This maps onto the cognitive inflexibility that plays an important role in depression (Davis and Nolen-Hoeksema, 2000; Houston et al., 2004; Joormann et al., 2011; Remijnse et al., 2009, 2013). That is, an overly precise prior is less resistant to change, and making the priors more flexible might therefore be of therapeutic value (Badcock et al., 2017; Barrett et al., 2016; Edwards and Koob, 2012).
Do psychotomimetics have antidepressant effects by decreasing precision of priors?
So far, we have described that sleep deprivation, classical psychedelics and ketamine have a tendency to induce symptoms of psychosis in healthy individuals, as well as acute antidepressant effects in depressed patients. Other examples of interventions that are both (acute) antidepressant as well as known to induce some psychosis-like symptoms are meditation and isolation-tanks, but these are not further discussed in this article (Feinstein et al., 2018; Heuschkel and Kuypers, 2020; Kjellgren et al., 2008; Kuijpers et al., 2007). It could be argued that this link between the tendencies for these interventions to induce psychotic-like phenomenon might be coincidental to the antidepressant effect. However, an alternative explanation might be that the mechanisms for these substances and interventions to induce psychosis and have rapid antidepressant effects are the same, through making the brain’s prior expectations more flexible and malleable to change. In predictive coding terms, this means that these interventions might loosen the brain’s prior beliefs, which can induce a state of psychosis in healthy individuals, whereas it might push an excessively rigid brain into a more normal state of flexibility, reducing depressive symptoms. We will onwards present arguments for this view, which we will refer to as the continuum hypothesis of psychotomimetic rapid antidepressants, summarised in Figure 1.
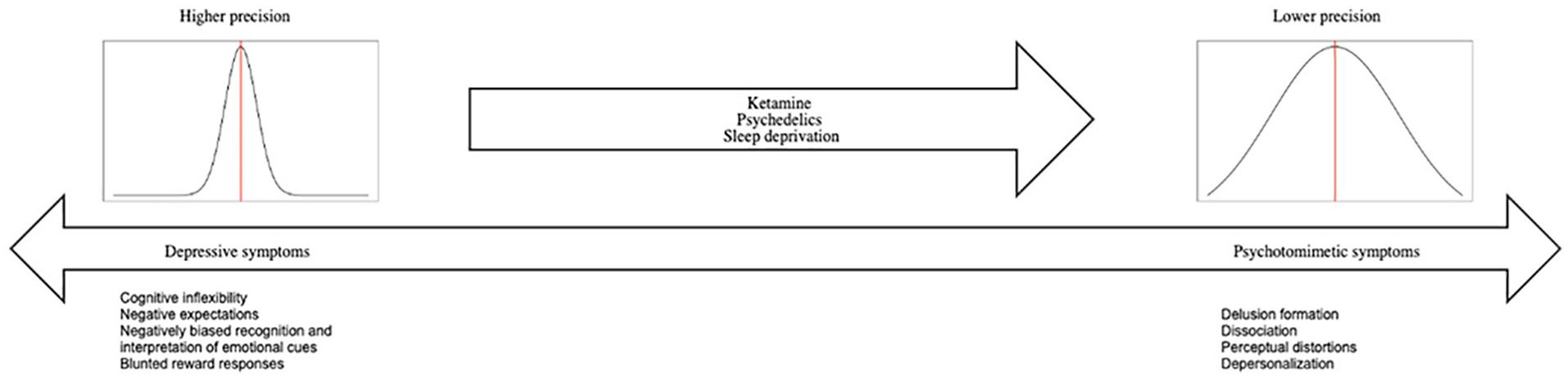
An overview of the continuum hypothesis of psychotomimetic rapid antidepressants.
Ketamine
The evidence that supports the hypothesis that ketamine reduces precision of prior expectations mostly comes from psychosis research. In hierarchical predictive coding, the NMDA-receptor, on which ketamine acts, has been linked to coding the precision of prior expectations (Corlett et al., 2007, 2016). It is argued that ketamine alters inference by effectively making prior expectations more flexible and therefore more malleable by new experiences and that ketamine can induce symptoms of early psychosis through reducing the precision of prior expectations in otherwise healthy individuals. Neuroimaging studies have indeed shown aberrant prediction errors in the right inferior frontal cortex following ketamine infusion similar to what is seen in psychosis (Corlett et al., 2006). Furthermore, a sense of agency has been suggested to rely on suppression of prediction errors, which is likewise disturbed in both psychosis and after ketamine (Moore et al., 2011). Research on more higher-level learning and ketamine has demonstrated similar findings, in line with a reduced precision of prior expectations. For example, Vinckier et al. (2016) demonstrated that a single dose of ketamine changes the degree to which confidence modulates decision making, leading to a state of increased flexibility during learning. These effects on confidence were related to altered activity in the anterior cingulate cortex, which has previously been related to the therapeutic effects of ketamine on anhedonia (Lally et al., 2014, 2015; Morris et al., 2020). This suggests a potential link between cognitive flexibility and anhedonia that could be investigated in further research. Others (Weber et al., 2020) combined a roving mismatch paradigm with computational modelling, showing that prediction errors related to higher level statistics, that is, the volatility with which the probability of a mismatch could occur, were specifically perturbed. Coherently, using a similar computational model, other studies have found that there is an overestimation of volatility in schizophrenia (Deserno et al., 2020; Kaplan et al., 2016) and individuals at risk for psychosis (Cole et al., 2020).
Neurocognitive studies focusing on emotion processing after ketamine administration have shown reduced neural reactivity in the bilateral amygdalo-hippocampal complex during emotional stimulation (Scheidegger et al., 2016), a decrease in amygdala reactivity after ketamine for both positive and negative emotional face processing (Loureiro et al., 2020), and enhanced sensitivity for rewarded items accompanied by increased activity of reward-related brain regions in patients with depressive disorder (Sterpenich et al., 2019), findings that are not necessarily related to the brain becoming more flexible. Our continuum hypothesis of psychotomimetic rapid antidepressants suggests that ketamine’s rapid antidepressant effects are due to the substance’s ability to put the brain in a more flexible state. As mentioned above, cognitive inflexibility is an important part of depression, considered not to be a result of affective symptoms but representing a distinct sub-component of depression (Rock et al., 2014). Furthermore, cognitive deficits, including cognitive inflexibility, also predict treatment outcome and have been considered a treatment target (Rock et al., 2014; Solé et al., 2015). Interestingly, although ketamine has been found to impair cognitive functioning in healthy individuals on a wide range of tasks (Adler et al., 1998; Krystal et al., 2005; Malhotra et al., 1996), when given to individuals with depression, there are pro-cognitive effects found on simple processing speed tasks, as well as cognitive flexibility (Basso et al., 2020; Zheng et al., 2019). Other studies have also found differing effects of ketamine on depressive symptoms in healthy and patients with depression, showing increases in depression in healthy individuals following ketamine, whereas lowered depression was found in patients (Nugent et al., 2019). In summary, we suggest that ketamine reduces the precision of prior expectation during inference, and thereby reduces the cognitive biases, for example, cognitive inflexibility and overly precise negative and positive expectations, in depression.
Psychedelics
In similar fashion, psychedelics have long been suggested to make the mind more flexible. The most recent iteration of this model has been referred to as the REBUS model, which stands for relaxed beliefs under psychedelics (Carhart-Harris and Friston, 2019). The evidence in favour of this model primarily comes from experiments related to sensory preprocessing, that are reinterpreted in a predictive coding framework. For example, LSD reduces mismatch negativity responses (Timmermann et al., 2018), interpreted as reduced precision in prior expectations. Similarly, the Kanizsa illusion, which is believed to rely on top-down feedback from higher visual regions (Kok et al., 2016; Pak et al., 2020), is reduced under psilocybin (Kometer et al., 2011) and binocular rivalry is altered during the psychedelic state (Carter et al., 2005, 2007). Furthermore, pre-pulse inhibition is reduced under psychedelics (Quednow et al., 2012; Schmid et al., 2015) and increased bottom-up signalling from the parahippocampus to the visual cortex during music listening was observed after LSD (Kaelen et al., 2016).
As with ketamine, some studies explored emotional processing in relation to psychedelics. For example, Müller et al. found reduced reactivity of the left amygdala and the right medial prefrontal cortex relative to placebo during the presentation of fearful faces after LSD (Mueller et al., 2017), whereas Roseman et al. (2018) showed the opposite pattern with increased amygdala responses to both negative and positive stimuli after psilocybin. Whereas the former finding supports an effect more in line with a change in affective biases, the latter finding might be more easily explained as a valence nonspecific upregulation of the brain’s responses to both positive and negative stimuli, which could reflect a more flexible brain state. This is in line with what has recently been found in a behavioural study where the learning rates for both rewards and punishments were increased after taking LSD, which again is in line with a reduction in the precision of the brain’s prior expectations (Kanen et al., 2021). Future studies can use computational models to explore whether this is indeed explained by reductions in prior precision (see section ‘How does the continuum hypothesis fit with existing theoretical perspectives?’).
In summary, there is some indirect evidence that psychedelics reduce the precision of prior expectations in sensory processing, although studies focusing on cognition have been limited due to the difficulties of doing behavioural experiments with psychedelics, that is, participants becoming disengaged (Carhart-Harris et al., 2018b).
Sleep deprivation
Various studies have looked into the effects of sleep deprivation on cognition and emotion, usually conducted in healthy individuals focusing on impairments in attention, emotion processing and decision making (Killgore, 2010; Krause et al., 2017; Lowe et al., 2017). In healthy volunteers, the most prominent effects of sleep deprivation are an increase in sleepiness as well as decreased performance in attentional tasks in a dose-dependent manner (Lowe et al., 2017). Furthermore, sleep deprived healthy subjects make more risky decisions, assign greater weights to more recent rewards (Killgore et al., 2006; Olson et al., 2016), and show lower response inhibition and cognitive control (Acheson et al., 2007; Cedernaes et al., 2014; Demos et al., 2016). Subcortical reward‑related regions of the brain also seem to become hypersensitised by acute sleep deprivation (Gujar et al., 2011; Krause et al., 2017). However, evidence directly supporting the notion that prior expectations become more flexible following sleep deprivation is lacking. Hence, there is some evidence suggesting that sleep deprivation causes an increase in the AMPA–NMDA ratio (McDermott et al., 2006). It has been argued that prior expectations are realised top-down via NMDA and GABA signalling and mismatch between those priors and incoming information is signalled bottom-up via AMPA receptors (Corlett et al., 2016), which would in turn indicate that sleep deprivation would lead to a favouring of bottom-up signalling. It is however unclear whether these alterations might make depressed people more cognitively flexible or underlie the psychotomimetic effects of sleep deprivation.
How does the continuum hypothesis fit with existing theoretical perspectives?
In the previous section, we presented the continuum hypothesis of psychotomimetic rapid antidepressants and reviewed some evidence underlying the hypothesis. In this section, we will further discuss how this hypothesis can be tested on a clinical, behavioural and neural level.
First, our hypothesis predicts that the precision of prior expectations, of both negative and positive events, is reduced by the interventions described above. Although there is some indirect evidence supporting this, few studies have addressed how these interventions alter the precision of prior expectations regarding negative and positive events, and to what extent this underlies the acute antidepressant effects. Future studies could consequently use behavioural paradigms that allow the study of how precision of prior expectations change during inference, in healthy volunteers and more importantly in patients with depression. Reversal learning paradigms where expectations about negative and positive events are learned over time might be particularly useful for this purpose (Browning et al., 2015; Pulcu and Browning, 2017). For example, see Pulcu and Browning (2017) for a paradigm where an agent was required to respond adaptively to fluctuations in the volatility of both losses and rewards. It has been argued before that affective disorders might manifest themselves through altered signalling of different forms of uncertainty (Pulcu and Browning, 2019). We predict that ketamine, psychedelics and sleep deprivation could reduce the precision of prior expectations in such tasks, making the patient more receptive to upcoming rewards and losses and expect this to be related to the antidepressant effects. This again highlights the interesting parallel to clinical effects of ketamine on anhedonia and reward processing. Computational models that allow for the modelling of higher order prior expectations during inference could be especially suitable for these experiments (Iglesias et al., 2013; Mathys et al., 2011, 2014; Piray and Daw, 2020).
Second, we expect that effects of ketamine, psychedelics and sleep deprivation are separable from the effects of commonly used SSRIs, in that they to a larger extent directly alter the use of information that has already been acquired (i.e. priors and their precision) (Stuart et al., 2015). This would be in line with what others have suggested to be the effects of ketamine (Stuart et al., 2015), but in contrast with a hypotheses that suggest that ketamine works on the same mechanism as SSRIs but acts faster (Hales et al., 2017).
The model presented in this article is suggested to provide a framework for how to understand how psychotomimetic rapid antidepressants can be further understood. There are however a number of potential caveats to our suggested model, and the model does not provide an explanation for how the different treatments should be understood at a molecular/neurochemical level. Whether the suggested model can be linked to work suggesting expression of genes/growth factors (Bunney and Bunney, 2013), functional connectivity (Bosch et al., 2013; Carhart-Harris et al., 2017; Scheidegger et al., 2012; Timmermann et al., 2018) and/or alteration in the immune system (Irwin et al., 2016; Loix et al., 2011) as mechanisms for the different treatment is also not known, and in fact these underlying mechanisms might differ between treatments.
Furthermore, even in terms of neurocognitive research, the continuum hypothesis of psychotomimetic rapid antidepressants needs to be tested against other possible theories. For example, we have suggested that the interventions described above alter the way negatively and positively valenced prior expectations shape inference. However, there are various other ways they could influence prior expectations, which are not limited to negatively or positively valenced information per se. Rather than influencing the expectations of valenced information, ketamine, as a well-known dissociative, might affect interoceptive signalling, which has been hypothesised to play an important role in depression (Barrett et al., 2016). Furthermore, rather than suggesting that these interventions decrease the effect of negative memories or experiences, our model suggests that the influence of both negative and positive expectations will be diminished by the interventions discussed, putting the brain in a more flexible state, allowing change to occur. In these more flexible brain states, we might paradoxically find that brain and behavioural responses to positive as well as negative outcomes can be upregulated (Kanen et al., 2021; Roseman et al., 2018). This might highlight the importance of combining these substances with, for example, psychological interventions.
Finally, we have made the case that psychedelics, ketamine and sleep deprivation are psychotomimetic, as well as acute antidepressants, and that this might relate to the ability to lower the precision of prior expectations. However, this is not to say that it is the psychotomimetic effects that are the key driving factor underlying the antidepressant effects. Instead, psychosis might be an excessive state of heightened cognitive flexibility. Indeed, some studies using ketamine have found no relationship between the psychotic-like effects ketamine induces and the therapeutic effects of the drug (Acevedo-Diaz et al., 2020), whereas others found the opposite pattern (Sos et al., 2013). Thus, it would be as possible that the psychosis and acute antidepressant model share that their explanation relies on flexibility of prior expectations, but does not necessarily entail that the state of psychosis is itself antidepressant. It should also be highlighted that depressive and psychotomimetic symptoms do not necessarily translate to specific diagnoses.
Keeping all the above-mentioned limitations in mind, the proposed hypothesis might still be informative when developing future treatments. For example, psychotomimetic side-effects of new treatments might in some cases be seen acceptable, at least at an early stage of development. Furthermore, incorporating the continuum hypothesis of psychotomimetic rapid antidepressants with existing theories, including affective bias, might provide a better understanding of how different treatments might interact. As, for example, the combination of fast-acting antidepressants with psychotherapy might lead to additive effects, since there may be greater adaptation to new information gained through therapy. Indeed, psychedelics, and to some extent ketamine, are often used in combination with psychotherapy, supporting this view (Carhart-Harris et al., 2016, 2018a; de Osório et al., 2015; Dore et al., 2019; Reiff et al., 2020).
Conclusion
In summary, we have reviewed various rapid antidepressants, primarily ketamine, classical psychedelics and sleep deprivation, that also have psychotomimetic properties. We furthermore suggest that this link between the tendency for rapid antidepressants to be psychotomimetic is not necessarily accidental, but instead might rely on their propensity to diminish the brain’s priors across different levels of the cortical hierarchy and we refer to this idea as the continuum hypothesis of psychotomimetic rapid antidepressants. In healthy individuals, this results in more weight being put on new information, that is, exaggerated bottom-up prediction errors, effectively causing an overly flexible state of mind and leading to psychotic symptoms. In patients with depression, increasing the flexibility of the brain’s prior expectations might, on the contrary, remediate the cognitive inflexibility characterising the disorder, in almost an immediate fashion.
Footnotes
Acknowledgements
We are grateful to the two anonymous reviewers for their constructive input on the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CJH is supported by the Oxford Health NIHR Biomedical Research Centre. ST is supported by the Swedish Brain Foundation.
CRediT author statement
Joost Haarsma contributed to the conceptualisation, methodology, visualisation, writing – original draft, and writing – review and editing. Catherine J Harmer contributed to the conceptualisation and writing – review and editing. Sandra Tamm contributed to the conceptualisation, methodology, visualisation, writing – original draft, and writing – review and editing.