
Abstract
Objective:
Cold-induced transient myocardial ischemia has been described in patients with systemic sclerosis. The clinical impact of cold exposure in systemic sclerosis patients with acute cardiac conditions is unknown. We compared the seasonal variation of acute cardiac hospitalizations in patients with and without systemic sclerosis.
Methods:
We performed a retrospective cross-sectional study using the National Inpatient Sample from 2016 to 2019. The primary outcome was acute cardiac hospitalization primarily due to heart failure, acute myocardial infarction, or cardiac arrhythmias. We compared the proportion of acute cardiac hospitalizations in each season in patients with and without systemic sclerosis. We also performed a subgroup analysis by US geographic region (Northeast, Midwest, South, West).
Results:
There were a total of 10,118,002 acute cardiac hospitalizations over the 4-year study period. Compared to those without systemic sclerosis, patients with systemic sclerosis who were hospitalized for acute cardiac care were younger (mean age 67 ± 13 vs 70 ± 14 years, p < 0.01), a greater proportion were female (82% vs 45%, p < 0.01), and a smaller proportion were Caucasian (68% vs 71%, p < 0.01). There was a lesser proportion of traditional cardiovascular risk factors in systemic sclerosis compared to non-systemic sclerosis patients. There was no significant difference in the proportion of winter admissions between systemic sclerosis and non-systemic sclerosis patients for total acute cardiac hospitalizations (26.4% vs 25.9%, p = 0.51), heart failure (27.0% vs 26.5%, p = 0.64), acute myocardial infarction (26.9% vs 25.5%, p = 0.50), or arrhythmias (24.3% vs 25.0%, p = 0.68). The results were consistent across all four US geographic regions.
Conclusion:
Our study did not support that patients with systemic sclerosis had a disproportionally higher risk of acute cardiac hospitalization in winter compared to the general population. We found that systemic sclerosis patients hospitalized for acute cardiac care had a lower burden of traditional cardiovascular risk factors than their non-systemic sclerosis counterparts.
Introduction
Systemic sclerosis (SSc) is a systemic autoimmune rheumatic disease characterized by a complex interplay of fibrosis, vasculopathy, and immune dysregulation. SSc is associated with multiple cardiac manifestations, including heart failure, cardiac arrhythmias, and ischemic heart disease, which lead to significant morbidity and mortality.1,2
Microvascular dysfunction is a major feature of SSc with both vasospasm and structural alterations observed. 3 Raynaud’s phenomenon (RP) affects greater than 90% of patients with SSc and is characterized by cold-induced transient peripheral vasospasm. 4 A similar process of cold-induced transient myocardial ischemia has been described in SSc and is called “cardiac Raynaud phenomenon.” 5 Previous studies of the “cardiac Raynaud phenomenon” were based on imaging changes and were performed in SSc patients without cardiac symptoms;5–7 thus, the clinical impact of cold exposure in SSc patients with clinically diagnosed heart disease is unknown. Importantly, there is a significant seasonal variation of multiple acute cardiac diseases leading to hospitalizations, with a winter peak among the general population.8–10 However, it is unknown whether SSc patients in particular have a higher risk of acute cardiac hospitalizations during the winter months.
To address this knowledge gap, we compared the seasonal variation of acute cardiac hospitalizations in patients with and without SSc, with a particular focus on the winter season using a large US-based nationwide database.
Methods
Data source
We performed a retrospective, cross-sectional study using the National Inpatient Sample (NIS) database from 2016 to 2019. The NIS is the largest publicly available, all-payer inpatient database sponsored by the Healthcare Cost and Utilization Project (HCUP) and the Agency for Healthcare Research and Quality. It contains unweighted data from >7 million hospital stays each year. 11 Using a complex survey design with a stratified sampling of 95% of all hospital discharges in the United States, a weighted estimate can be calculated to represent >35 million hospitalizations nationally. 11 The NIS does not contain any patient identifiers, and the unit of analysis is the individual hospitalization, rather than the patient. 11 This study was approved by the Institutional Review Board (IRB) of Columbia University Irving Medical Center (IRB Protocol AAAU3511).
Analytic sample
Our analytic sample consisted of hospitalizations of adult patients (age ⩾ 18 years) between 2016 and 2019. Diagnoses were identified using the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) codes. SSc was identified with ICD-10-CM primary or secondary diagnosis codes M34.xx. The use of ICD-10-CM code in identifying SSc has been validated with a positive predictive value of 82%–93%.12,13
Study outcomes
The primary outcome was the proportion of acute cardiac hospitalizations in the winter season. Acute cardiac hospitalizations included those with a principal discharge diagnosis of heart failure (HF), acute myocardial infarction (AMI), and arrhythmia. The secondary outcomes included clinically distinctive subtypes of the primary outcomes, including HF with or without coronary artery disease (CAD), ST-elevation MI (STEMI) or non-ST-elevation MI (NSTEMI), and tachyarrhythmias or atrioventricular (AV) block. Seasons were defined based on the meteorological classification of the Northern Hemisphere as: spring (March to May), summer (June to August), fall (September to November), and winter (December to February). The ICD-10-CM codes used to identify the outcomes are shown in Supplemental Table 1.
Statistical analysis
We used descriptive statistics to compare characteristics of acute cardiac hospitalizations between patients with and without SSc. Continuous variables are expressed as mean ± standard deviation (SD) and were compared using the Mann–Whitney test. Categorical variables are presented as frequencies and percentage and were compared using the chi-square test. The difference in proportions of acute cardiac hospitalizations in winter between SSc and non-SSc patients was assessed using the chi-square test.
We performed an exploratory analysis to examine the proportion of acute cardiac hospitalizations in winter in four geographic regions of the United States: Northeast, Midwest, South, and West, as classified by the HCUP. Because other systemic autoimmune rheumatic diseases that can involve the heart sometimes co-occur with SSc, we performed a sensitivity analysis to exclude patients with an ICD-10-CM code of systemic lupus erythematosus (M32.xx) and polymyositis and dermatomyositis (M33.xx). The ICD-10-CM codes do not differentiate between left-sided HF due to primary cardiomyopathy and right-sided HF due to pulmonary hypertension (PH); therefore, we performed a sensitivity analysis in patients with HF excluding those with PH.
All analyses were performed using survey-specific analysis methods and accounted for the NIS data set’s complex survey design, stratification, and clustering. 11 The variable “year” was included as a stratification variable in the analysis after combining the 3-year data set per HCUP recommendations. For missing values, the month of admission is absent in 0.06% of the hospitalizations. The principal discharge diagnosis is absent in 0.03% of the hospitalizations. Hospitalizations with these missing values were excluded from the analyses. Stata software (version 17, StataCorp, College Station, TX, USA) was used for statistical analyses.
Results
Baseline demographic and clinical characteristics
A total of 10,118,002 acute cardiac hospitalizations were identified over the 4-year study period; 13,200 (0.13%) of these hospitalizations occurred in patients with SSc. Compared to those without SSc, patients with SSc who were hospitalized for acute cardiac care were younger (67 ± 13 vs 70 ± 14 years, p < 0.01), a greater proportion were female (82% vs 45%, p < 0.01), and a smaller proportion were Caucasian (68% vs 71%, p < 0.01). In addition, compared to non-SSc patients, SSc patients were more frequently hospitalized for acute cardiac care in urban (93% vs 90%, p < 0.01) and teaching (73% vs 67%, p < 0.01) hospitals (Table 1).
Demographic and clinical characteristics of acute cardiac hospitalizations with and without systemic sclerosis.
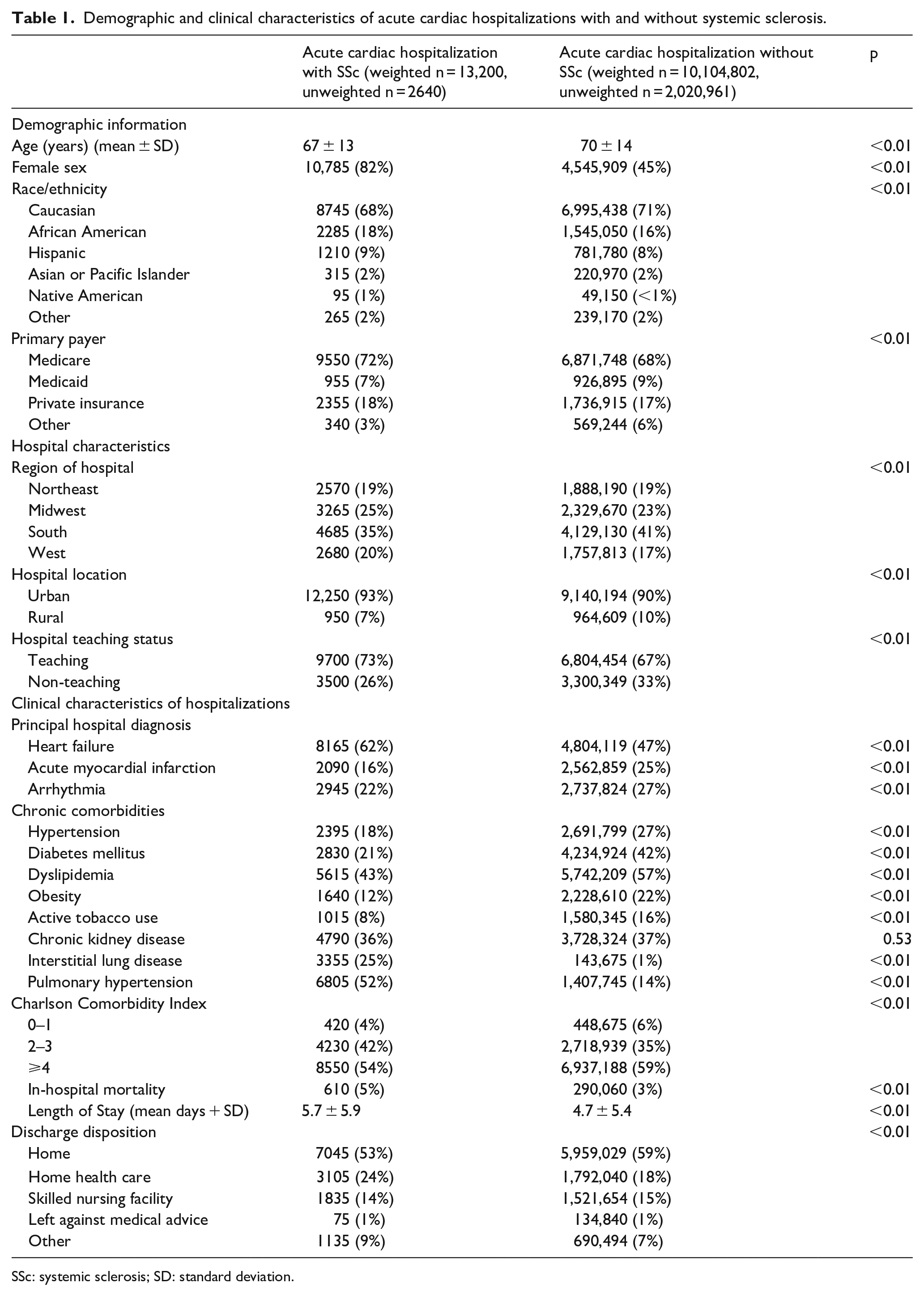
SSc: systemic sclerosis; SD: standard deviation.
A greater proportion of SSc than non-SSc acute cardiac hospitalizations were due to HF (62% vs 47%, p < 0.01). A smaller proportion of SSc than non-SSc patients hospitalized for acute cardiac care had traditional cardiovascular risk factors, including hypertension (18% vs 27%, p < 0.01), diabetes mellitus (21% vs 42%, p < 0.01), dyslipidemia (43% vs 57%, p < 0.01), and obesity (12% vs 22%, p < 0.01). In comparison, a greater proportion of hospitalized SSc patients than non-SSc patients had interstitial lung disease (25% vs 1%, p < 0.01) and pulmonary hypertension (52% vs 14%, p < 0.01). Regarding the overall comorbidity burden, a smaller proportion of hospitalized SSc patients than non-SSc patients had a Charlson Comorbidity Index (CCI) ⩾ 4. Overall, SSc patients hospitalized for acute cardiac conditions had higher in-hospital mortality (5% vs 3%, p < 0.01), greater length of stay (mean days 5.7 ± 5.9 vs 4.7 ± 5.4, p < 0.01), and more unfavorable discharge disposition (discharge home 53% vs 59%, while discharge with home health care 24% vs 18%, p < 0.01) (Table 1).
Seasonal variation of acute cardiac hospitalizations
The seasonal variation of acute cardiac hospitalizations in those with and without SSc is shown in Figure 1. There was no significant difference in the proportion of winter admissions between SSc and non-SSc patients for total acute cardiac hospitalizations (26.4% vs 25.9%, p = 0.51), HF (27.0% vs 26.5%, p = 0.64), AMI (26.9% vs 25.5%, p = 0.50), or arrhythmias (24.3% vs 25.0%, p = 0.68) (Table 2). There was also no significant difference in the proportion of winter admissions between SSc and non-SSc patients for HF with CAD (28.4% vs 26.5%, p = 0.25), HF without CAD (26.1% vs 26.6%, p = 0.69), STEMI (20.5% vs 25.3%, p = 0.29), NSTEMI (29.1% vs 25.5%, p = 0.15), tachyarrhythmia (24.5% vs 25.1%, p = 0.75), or AV block (21.8% vs 23.6%, p = 0.75) (Table 3 and Figure 2).
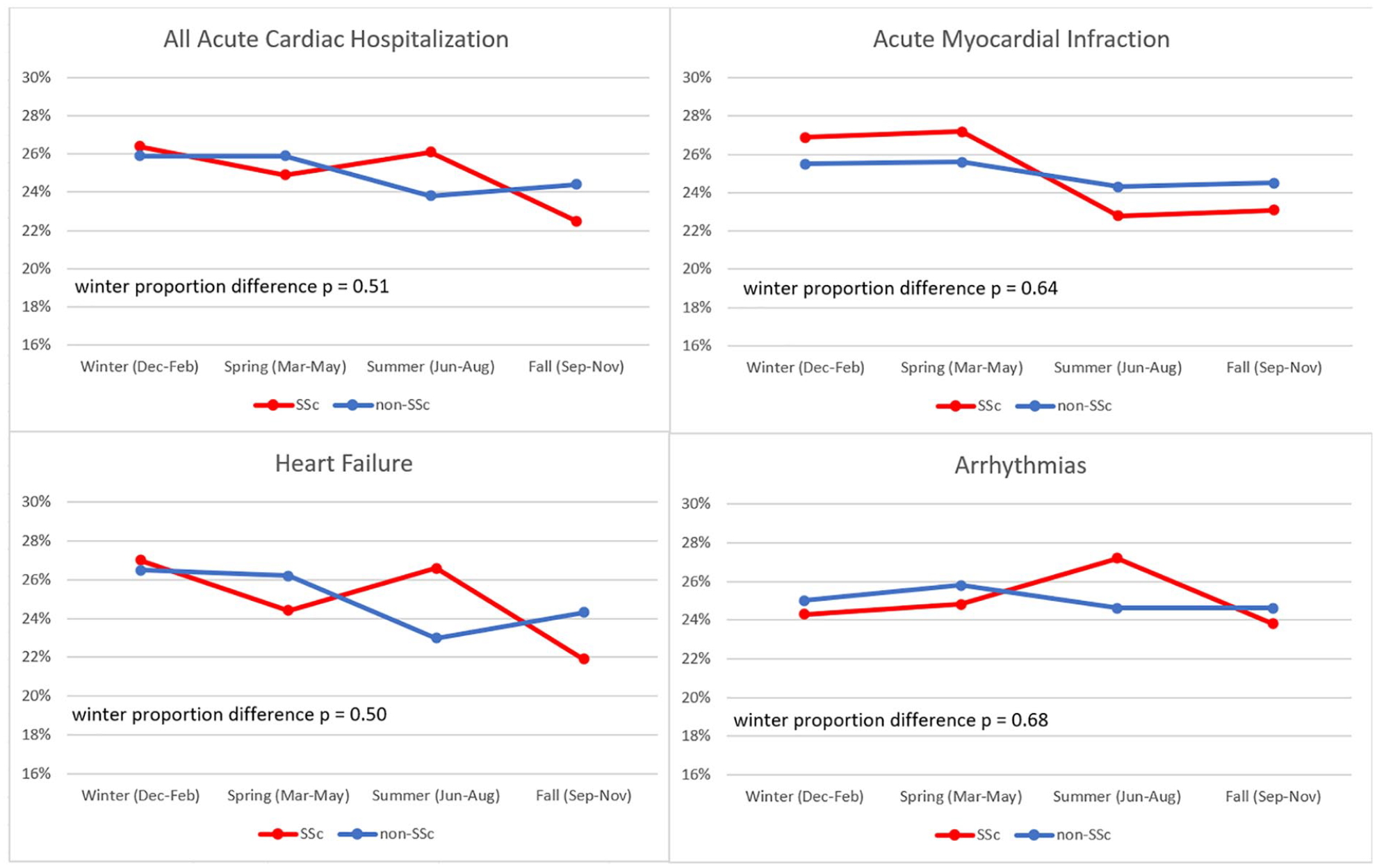
Seasonal variation of acute cardiac hospitalizations in patients with and without SSc.
Seasonal variation of primary outcomes in hospitalizations with and without systemic sclerosis.
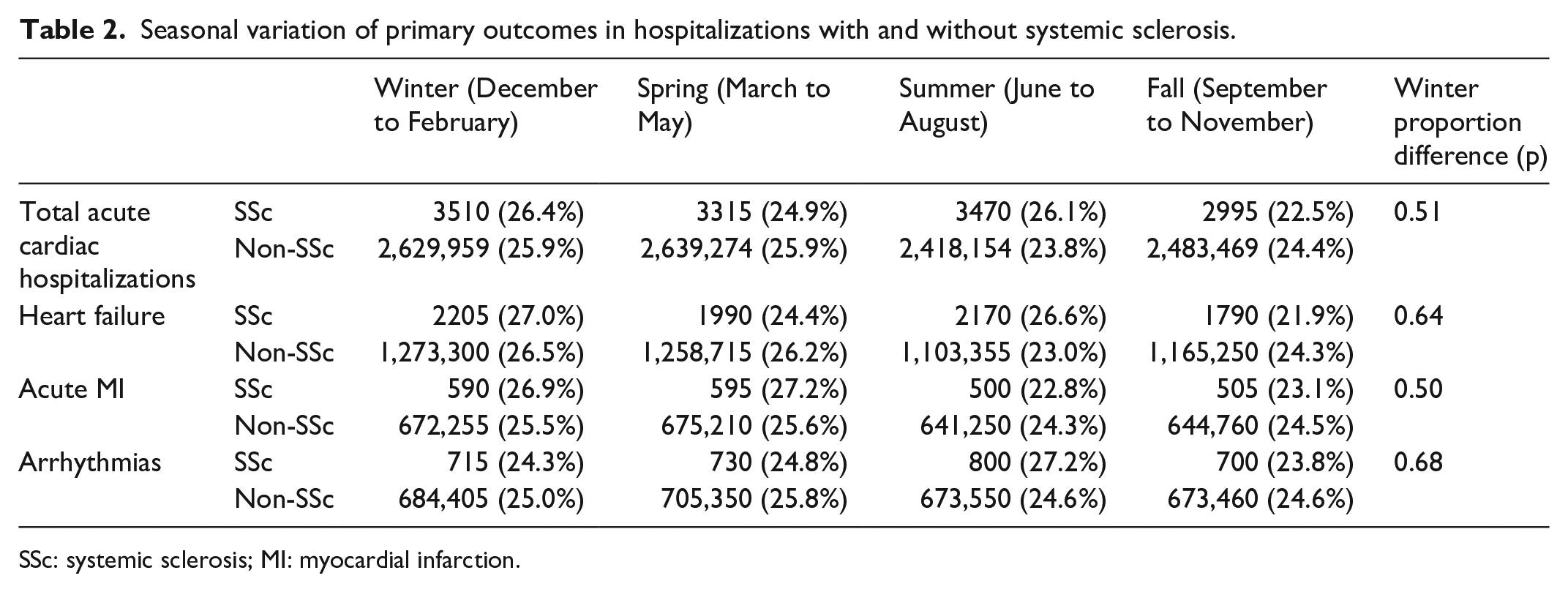
SSc: systemic sclerosis; MI: myocardial infarction.
Seasonal variation of secondary outcomes in hospitalizations with and without systemic sclerosis.
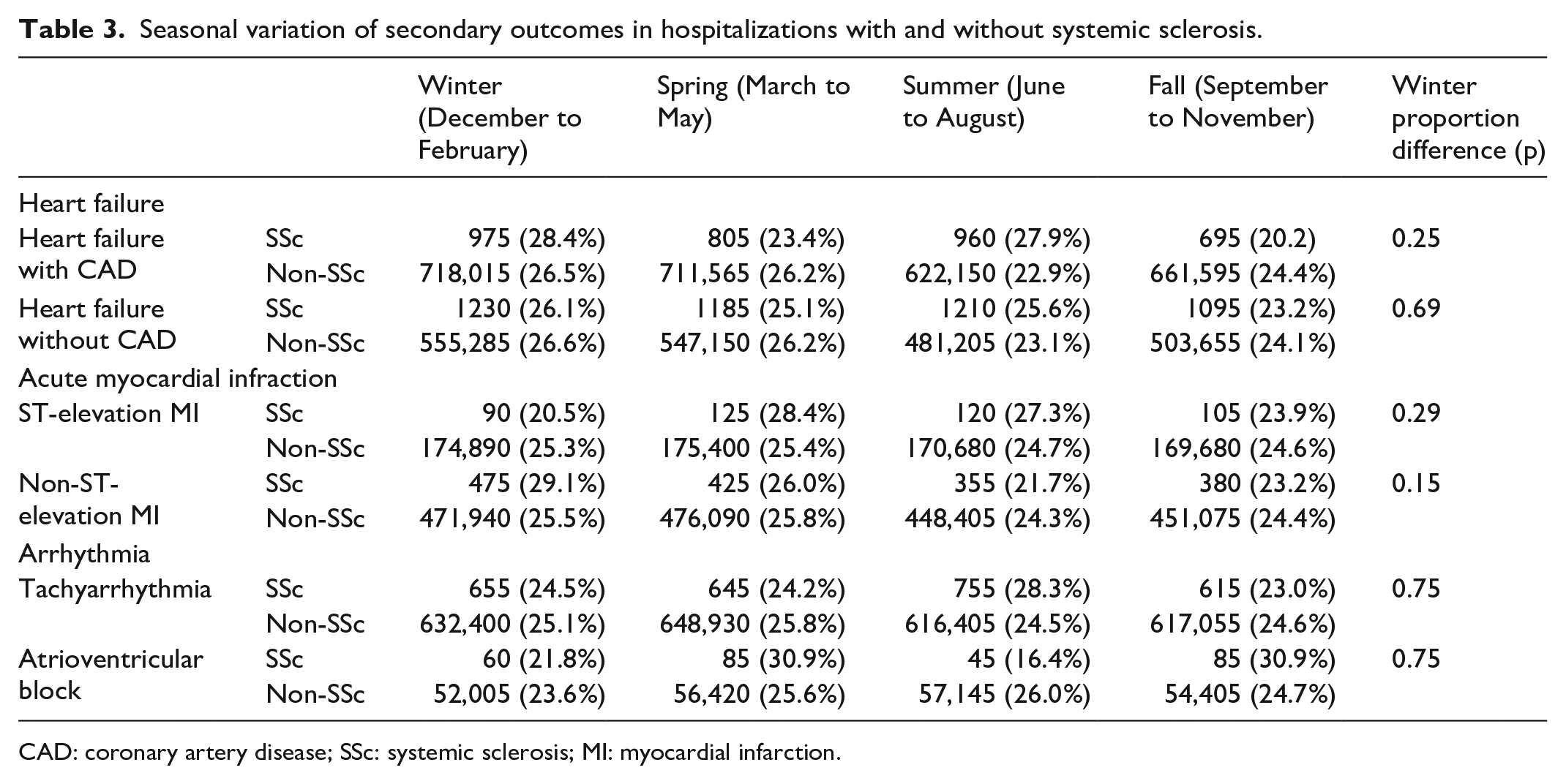
CAD: coronary artery disease; SSc: systemic sclerosis; MI: myocardial infarction.
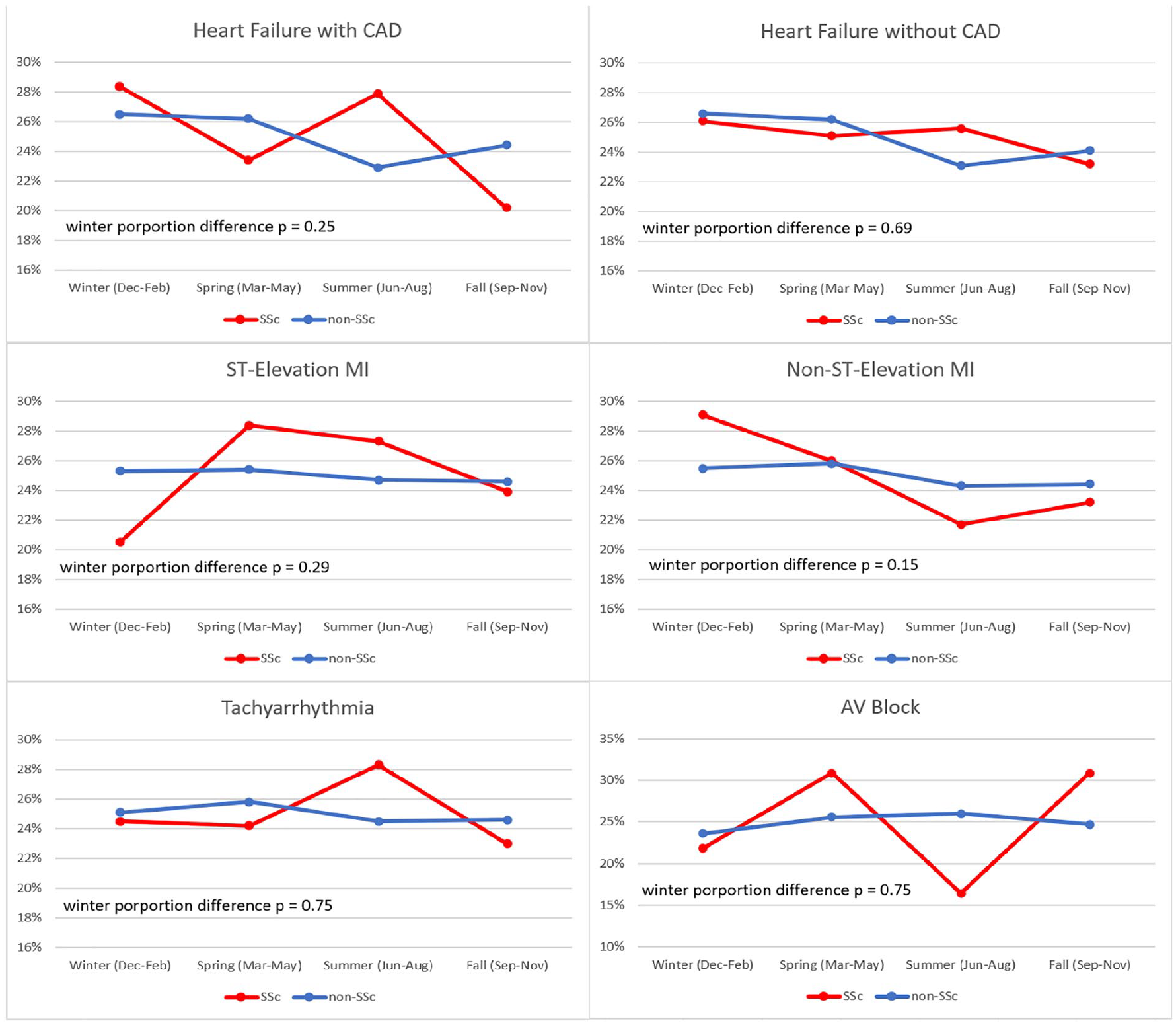
Seasonal variation of subcategories of acute cardiac hospitalizations in patients with and without SSc.
In the exploratory analysis, there was no significant difference in the proportion of acute cardiac hospitalizations in winter between SSc and non-SSc patients in any of the four US geographic regions (Supplemental Tables 1 and 2). The results of both sensitivity analyses were consistent with our main results (Supplemental Tables 3 and 4).
Discussion
In this large US-based nationwide observational study of hospitalized patients, we did not observe a greater risk of acute cardiac hospitalizations in winter in patients with SSc compared to those without SSc. Compared to patients without SSc, those with SSc who were hospitalized for acute cardiac conditions have unique demographic and clinical features. Patients with SSc were younger, a greater proportion were female and on Medicare, and a lower proportion were Caucasian. We found that SSc patients with acute cardiac hospitalizations had significantly fewer traditional cardiovascular risk factors than their non-SSc counterparts. This corroborates the results of a previous study which found that using scoring systems based on traditional cardiovascular risk factors dramatically underestimates cardiovascular risk in SSc. 14 These findings suggest that SSc may contribute to clinical heart disease, either in the form of scleroderma heart involvement or as an independent risk factor for CAD. CCI is a validated prognostic indicator for inpatient outcome prediction.15,16 However, even though a smaller proportion of SSc patients hospitalized for acute cardiac conditions had a CCI ⩾ 4, their outcomes were worse (i.e. higher mortality, longer length of stay, and worse discharge dispositions) than those without SSc.
Our study failed to demonstrate a greater proportion of acute cardiac hospitalizations in SSc patients compared to non-SSc patients during the winter months. This finding is unexpected, given that previous studies have shown that SSc is associated with multiple cardiovascular manifestations, and pathological changes in coronary arteries can be triggered by cold exposure.17 –20 There are multiple potential explanations for this finding. First, the detrimental effect of cold exposure may be small in SSc heart disease and may therefore not translate into an acute cardiac event requiring hospitalization. There may be important differences between SSc patients with symptomatic heart disease leading to acute hospitalization and those with “cardiac RP.” For example, in studies of SSc patients with clinical symptoms of heart disease, multiple abnormal cardiac findings have been identified, including inflammation and fibrosis, all in a setting without cold exposures.21–24 These cardiac findings were different from those identified in SSc patients in the studies of “cardiac Raynaud phenomenon.”5–7 in which cold-induced reversible perfusion defects were demonstrated in SSc patients without chest symptoms. Thus, cold exposure may not play a significant role in acute exacerbation of cardiac disease in patients with SSc once the cardiac disease progresses to the symptomatic stage. Second, SSc patients with RP likely often avoid outdoor activities in cold weather, which could contribute to the similar proportion of acute cardiac winter exacerbations between SSc and non-SSc patients. 25 Finally, the deleterious effects of cold exposure on heart disease in SSc may be slowly progressive over time rather than acute in onset. For example, given that a high burden of cardiac involvement in SSc is asymptomatic, it is possible that repeated ischemia–reperfusion abnormalities due to cold exposures could be detrimental by leading to myocardial fibrosis in a chronic, progressive manner.26,27
There are some limitations of our study. We used ICD-10-CM codes to capture disease diagnosis, which has a risk of misclassification bias. We were also unable to ascertain whether the heart disease was primarily due to SSc or to other causes. In addition, we cannot exclude the possibility that the impact of the winter season on acute cardiac hospitalization in SSc has a smaller effect size than that which we were powered to detect. Finally, individual SSc characteristics such as SSc subtype (limited vs diffuse), SSc duration, autoantibodies, and treatment are unavailable in the NIS database. Notably, the absence of data regarding therapy is a significant limitation. Patients with SSc often undergo therapy with antiplatelet agents and vasodilators, treatments which have been shown to influence the outcomes of SSc heart disease. 28
There are, however, multiple strengths of our study. In this large data set of hospitalizations across the entire United States, we were able to evaluate different cardiac manifestations and perform subgroup analyses across different geographic regions and heart disease subtypes to confirm the robustness of our findings. Furthermore, our findings are generalizable across a large patient population.
In conclusion, this is the first study to investigate the clinical impact of the winter season on acute cardiac hospitalizations in SSc patients. We did not identify a higher risk of acute cardiac hospitalization in winter in patients with SSc compared to those without SSc. However, we found that SSc patients hospitalized for acute cardiac care had a lower burden of traditional cardiovascular risk factors and worse outcomes than their non-SSc counterparts.
Supplemental Material
sj-pdf-1-jso-10.1177_23971983231197268 – Supplemental material for Are there more acute cardiac hospitalizations in winter in patients with systemic sclerosis? An analysis from the National Inpatient Sample
Supplemental material, sj-pdf-1-jso-10.1177_23971983231197268 for Are there more acute cardiac hospitalizations in winter in patients with systemic sclerosis? An analysis from the National Inpatient Sample by Yiming Luo, Laura Ross, Jiayi Zheng and Elana J Bernstein in Journal of Scleroderma and Related Disorders
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Rheumatology Research Foundation Scientist Development Award (Dr Y.L.); the National Institute of Arthritis and Musculoskeletal and Skin Diseases (grant K23-AR-075112, Dr E.B.); the National Heart, Lung, and Blood Institute (grant R01-HL-164758, Dr E.J.B.); and the Department of Defense (grant W81XWH2210163, Dr E.J.B.).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.