
Abstract
Paul Klee (1879–1940), the 20th-century Swiss-German artist, suffered and died from complications of systemic sclerosis (SSc, scleroderma). This is the fifth in a series of clinical and historical vignettes wherein Klee’s cardiopulmonary symptoms are described with an emphasis on how progressive dyspnea impacted Klee’s life.
Caption: Dies ist jetzt mein Matterhorn [“This is now my Matterhorn”]
Dyspnea, the sensation of breathlessness, is often one of the earliest symptoms of systemic sclerosis (SSc, scleroderma), and so it appears to have been for Paul Klee (1879–1940), one of the most significant artists of the 20th century. Owing to the rising menace and assault on free artistic expression imposed by the third Reich, Klee departed Germany in late 1933 in the prime of his artistic career and having no known medical issues, returning to his homeland Switzerland. Two years later, in the summer of 1935, Klee fell ill.
The precise nature of Klee’s initial illness is unclear, but symptoms of profound fatigue, cough, and rash led to an initial diagnosis of “bronchitis with complications of the lungs and heart as a result of measles.” 1 Measles was later discounted as the cause of Klee’s presenting symptoms (the skin rash may have been a manifestation of a drug reaction) (p. 41). 2 By October of the same year, Klee’s physician noted “the heart was not functioning properly” (p. 39) and complete bed rest was prescribed. 2 The following month pneumonia with pleurisy was suspected. A chest X-ray was eventually obtained in April 1936, after which Klee’s wife Lily wrote “it was chronic double pneumonia.” Even today, patients with scleroderma and interstitial lung disease upon presentation to community emergency departments often mistakenly receive a diagnosis of “double pneumonia.” Lily later noted that “pleurisy and cardiac dilation had arisen” (p. 45). 2 Klee improved but never fully recovered. Dyspnea would become chronic and progressive.
Breathlessness, or dyspnea, is a frequent complaint of patients suffering from scleroderma (SSc), and dyspnea often is the first indication of lung or heart disease. The sensation of dyspnea arises from multiple sources of information including central, peripheral (chest wall and lung receptors), and chemoreceptor mechanisms. In a systemic disease like scleroderma, multiple different sources, sometimes in combination, can combine to produce the sensation of breathlessness.
When evaluating a scleroderma patient with a complaint of chronic dyspnea, three important etiologies are generally considered, keeping in mind that these are not mutually exclusive: (1) interstitial lung disease (SSc-ILD); (2) pulmonary arterial hypertension (SSc-PAH); and/or (3) cardiac disease, either primary scleroderma heart disease or heart disease secondary to systemic or pulmonary hypertension, aging, or other causes. In the early 20th century when Klee was struck ill, diagnostic tools were rudimentary compared to today’s wide array of testing. Chest X-rays were obtained infrequently and lacked both sensitivity and specificity. Klee’s initial chest X-ray obtained nearly a year after the onset of symptoms was reported to show “double pneumonia” (4), likely an interpretation of what now would be described as “interstitial lung disease.” A subsequent X-ray indicated that Klee’s pulmonary findings were indeed chronic. Lily wrote, “A few weeks ago he had another X-ray at the request of the doctors, who wanted it for their studies. His case is starting to arouse the interest of the Bern medical faculty” (p. 72). 2 It seems plausible that at least some of the chest X-ray findings of interest to the Bernese physicians were reflective of SSc-ILD.
As is often the case, Klee’s progressive dyspnea had a profound effect on his daily life. Even as a schoolboy, Klee loved to walk and hike in and around the Bernese Oberland, filling his sketchbooks with landscapes. Yet by the first year of his illness, while convalescing in Tarasp in the eastern Swiss Alps, Klee made note of his dyspnea: “At the top of the pass [elevation 2150 m] it was too high, I had to stand totally still while the others walked about . . .” going on to note, I breathe as deeply as I can. My shortage of breath depends on the paths, whether I’m walking uphill or on the flat . . . It also depends on the weather, yesterday during the Föhn [Alpine wind] it was not so good, but today it is better again. (p. 71)
2
Cardiac complications of scleroderma were not widely appreciated prior to the seminal paper by Soma Weiss et al. 3 , published 3 years following the death of Paul Klee. It seems that Klee may have had cardiac involvement early in the course of his disease, with pleurisy and cardiac dilation noted on the initial chest X-ray. An electrocardiogram (ECG) was obtained, but the results are not known. Lacking the sophisticated tools of today, for example, echocardiography, cardiac scintigraphy, magnetic resonance imaging (MRI), cardiac catheterization, and endomyocardial biopsy, one can only speculate that Klee’s heart condition was secondary to scleroderma involving the heart, that is, primary scleroderma heart disease, or secondary to other factors, for example, systemic or pulmonary hypertension.
By the summer of 1939, Klee’s friend Rolf Bürgi 4 noted the following: “Klee is ill, very ill. Leisurely strolls are strenuous for him, he is almost completely confined to his atelier. Even speaking is exhausting for him.” Hanni Bürgi (1880–1938) and her son Rolf (1906–1967) were intimately bound to the Klee family. Hanni accumulated the second largest collection of Klee’s pictures in the world. Rolf continued to add to the collection following his mother’s death. As one of Paul and Lily Klee’s closest friends and advisors, it was Rolf who made possible their escape from Nazi Germany and after Klee’s death administered his estate, saving it from liquidation and setting up the Paul Klee Foundation.
In his last year, Klee was largely confined to his modest three-room apartment on the second floor at Kistlerweg 6, Bern (Figure 1). Rolf Bürgi
4
wrote, From the balcony he could see the summit of the Jungfrau mountain. Now it’s the glow of the setting sun. He will no longer set his foot onto the mountain paths. One day my wife walks with him a small stretch on the street, just a few steps, but the Kistlerweg ascends slightly. The healthy Klee didn’t notice it. But now he is saying with a soft smile, Dies ist jetzt mein Matterhorn [This is now my Matterhorn].
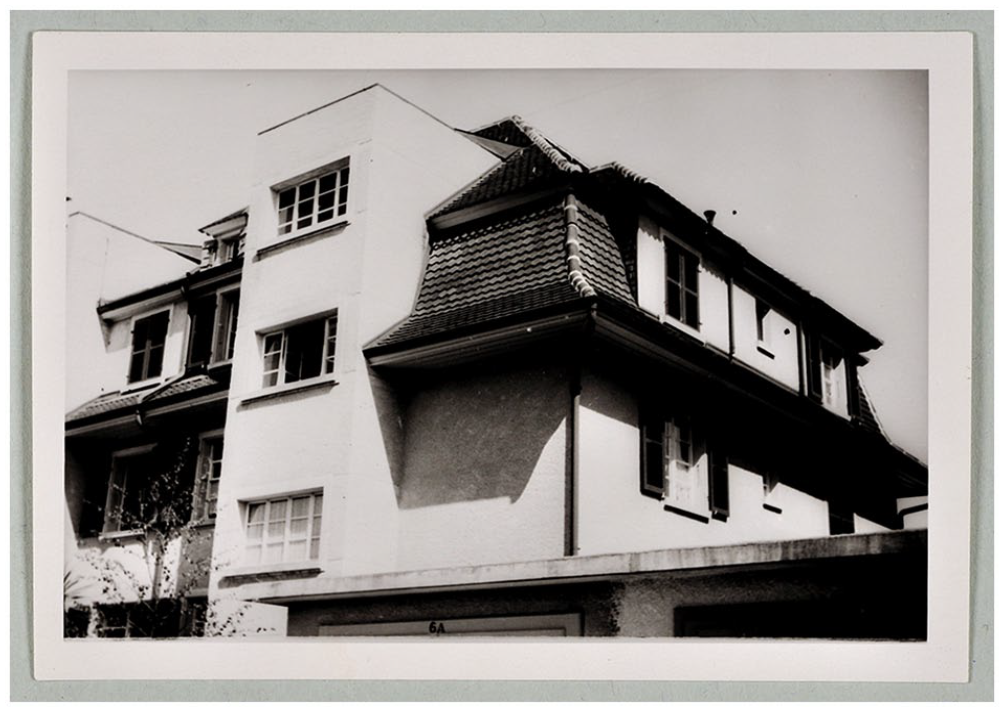
Residence of Paul and Lily Klee, Kistlerweg 6, Bern. On making the walk up to his apartment, Klee wryly noted, Dies ist jetzt mein Matterhorn [This is now my Matterhorn].
Rolf Bürgi 4 noted that Klee did not fear death: “He had experienced it anyhow in many ways spiritually, and in reality, and had even shaped it: Geister der Abgeschiedenen (‘Ghosts of the Departed’), Angelus norvus (New Angel), Engel im Werken (‘Angel at Work’), and Der Teufel jongliert (‘The Devil Juggles’).” Writing to Will Grohmann 1 , his biographer and longtime friend, Klee noted, “Naturally, I have not struck the tragic vein without some preparation. Several pictures have pointed the way with their message: The time has come.” Two such examples include a drawing entitled ein Kranker macht Pläne (A Sick Man Makes Plans) (Figure 2(a)) and a drawing entitled Kranker im Boot (Sick Man in a Boat) (Figure 2(b)). The latter drawing depicts a sick or dead faceless person lying in a boat steered by an oarsman, considered to be a representation of Klee’s death with the boat guided by Charon, the ferryman from Greek mythology who brought the dead across the River Styx into the Kingdom of Hades, the world of the dead.
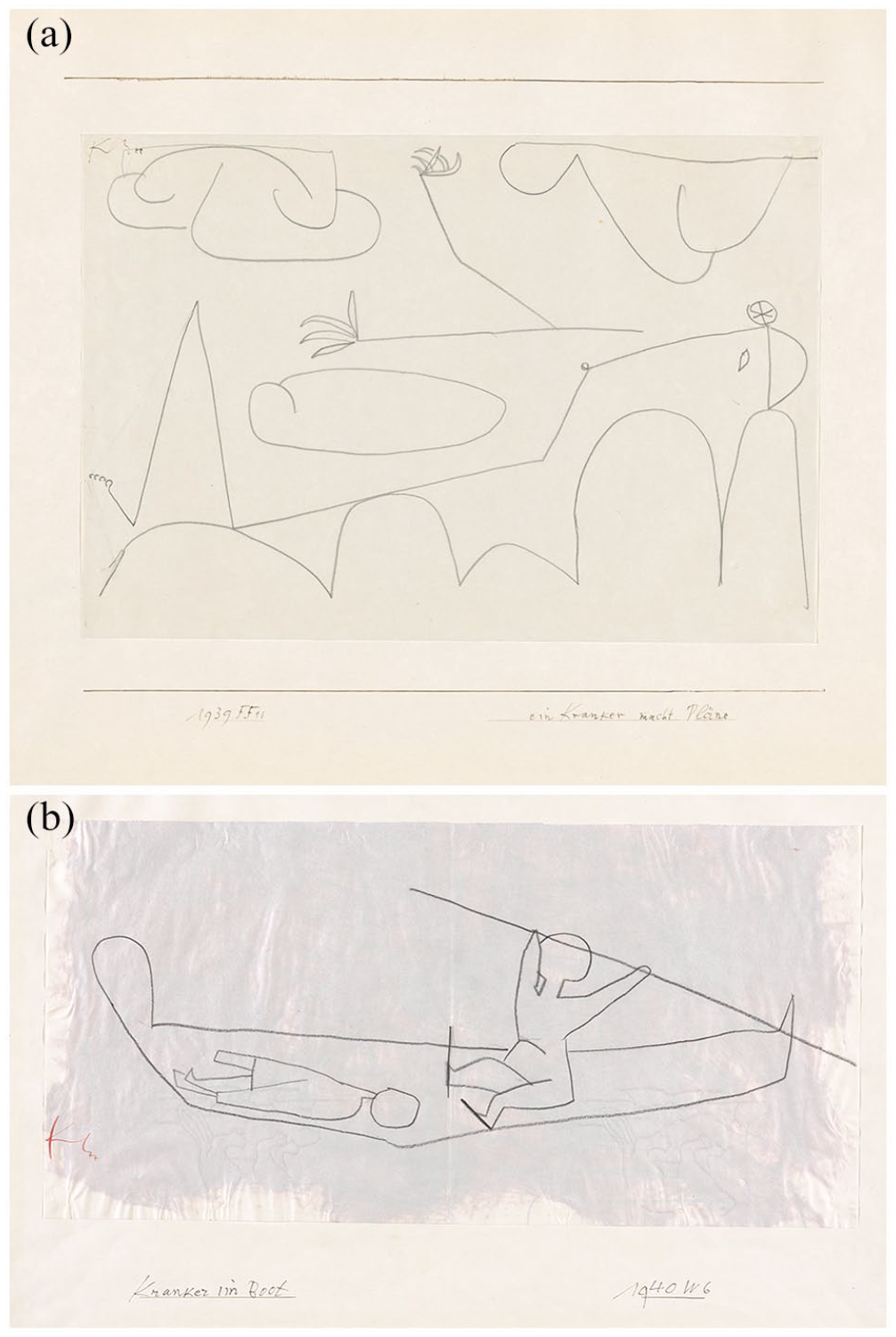
(a) ein Kranker macht Pläne (A Sick Man Makes Plans), pencil on paper on cardboard, 1939. (b) Kranker im Boot (Sick Man in a Boat), chalk on paper on cardboard, 1940.
Klee entered a sanitorium at Orsolina near Locarno on 10 May 1940, but by 8 June, his condition was so much worse that he was transferred to the Clinic of Sant’ Agnesse at Muralto. A heart specialist was called in from Zurich when Klee’s condition deteriorated, but by then, nothing else could be done. Klee died at 7:30 a.m. on 29 June 1940. His attending physician, Dr Hermann Bodmer, noted the cause of death: malattia di cuore (myocardite) (heart disease (myocarditis)) (Figure 3).
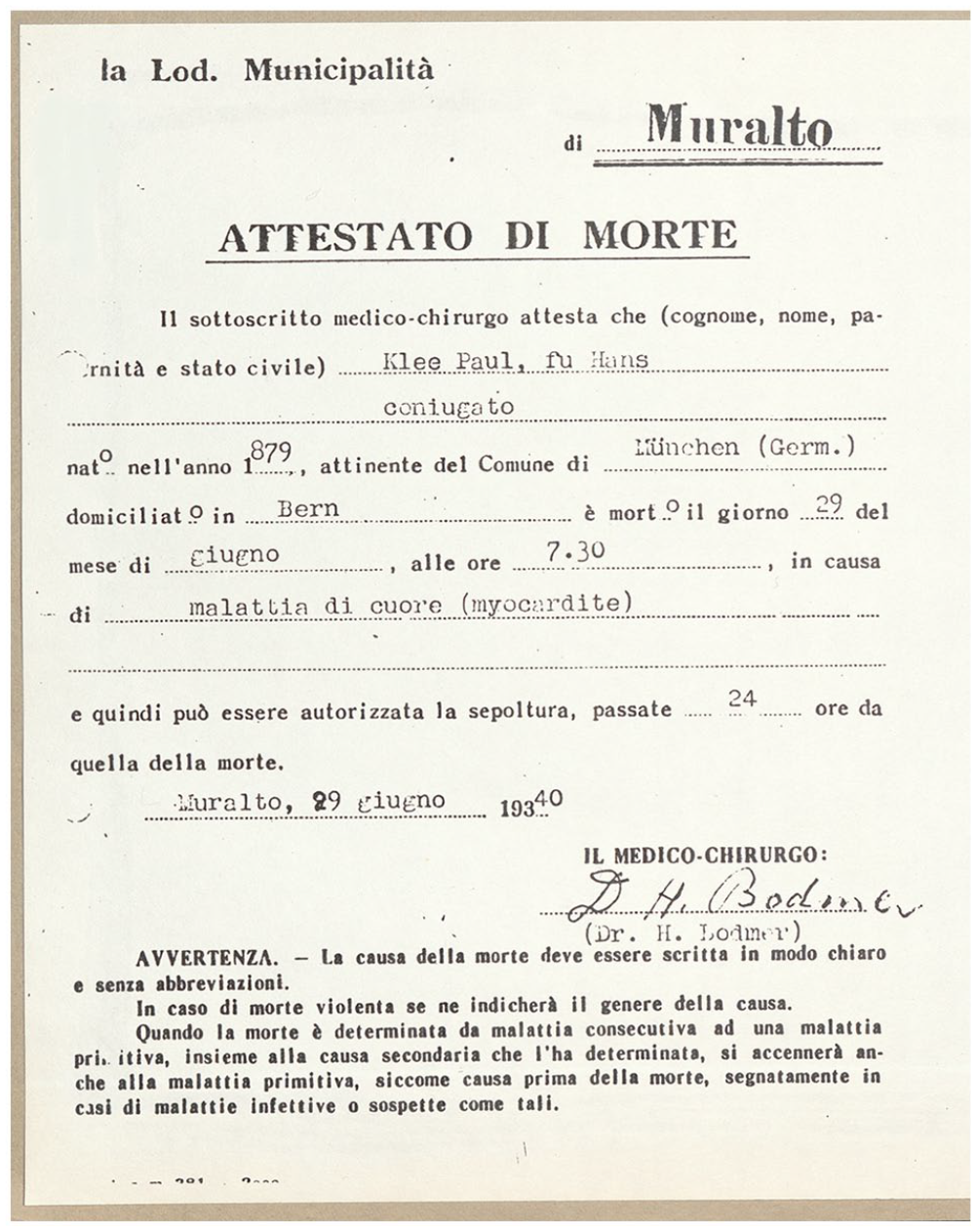
Certificate of death of Paul Klee, Muralto, 29 June 1940.
Both the diagnosis and the management of cardiopulmonary complications of scleroderma have advanced greatly since the days of Klee’s illness. With little or no understanding of the systemic nature of scleroderma and with no means to accurately assess heart and lung disease, Klee’s physicians faced significant limitations that also extended to the management of his disease. To no avail, treatment for Klee’s lung and heart disease included bed rest, theobromine, luminal, and possibly digitalis (p. 81). 2 In today’s world, a scleroderma patient with chronic dyspnea might be expected to undergo a battery of diagnostic tests to ascertain the potential cause(s). Treatment might include an ever increasing array of medications, devices and procedures, including immunosuppressive and anti-fibrotic agents, drugs to treat right-sided and left-sided heart disease, anti-arrhythmic agents, implantable cardio-defibrillators, and even, in some cases, organ transplantation. By extending the length and by preserving quality of life for our patients, we provide a great service for both patient and family. In doing so, we may also have an opportunity to enrich society by preserving the creative spirit so embodied by the artist and patient Paul Klee.
Footnotes
Acknowledgements
The author thanks Katrin Keller, Zentrum Paul Klee, for assistance in providing historical documentation and permission to reproduce photographs, and Alexander Awgulewitsch, PhD for translations.
Author’s note
The Editor/Editorial Board Member of JSRD is an author of this paper; therefore, the peer review process was managed by alternative members of the Board and the submitting Editor/Board member had no involvement in the decision-making process.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.