
Abstract
Objective:
The objective of this study is to explore the role of adjunctive percutaneous revascularization of the hand in the management of patients with systemic sclerosis–associated refractory digital ischemia.
Methods:
We present our initial experience of using percutaneous upper extremity interventions to treat patients with systemic sclerosis and symptomatic Raynaud’s phenomenon who presented with either refractory digital ischemia or non-healing ulcers. We discuss patient characteristics, procedural findings, and short-term clinical outcomes of these interventions.
Results:
We performed 14 interventions in 6 patients with non-healing digital ulcers or refractory ischemia secondary to systemic sclerosis. Angioplasty was performed at or below the wrist in conjunction with intravenous prostaglandin therapy, started prior to or immediately after the revascularization procedure. All patients experienced symptomatic relief and demonstrated accelerated wound healing. Two patients required an additional procedure to treat recurrent ischemia (without new ulceration) in the treated digit. Three of the patients underwent multiple procedures during the study period to treat new ischemic lesions or Raynaud’s phenomenon symptoms, highlighting the progressive nature of the vascular occlusions in systemic sclerosis. There were no adverse events related to the interventions.
Conclusions:
Our retrospective analysis suggests that percutaneous revascularization in combination with vasodilator therapy in systemic sclerosis–associated digital ischemia is safe and can facilitate the healing of long-standing ulcers. Its role in the management of refractory digital ischemia in patients with systemic sclerosis should be explored further.
Introduction
Raynaud’s phenomenon (RP) is a condition characterized by an exaggerated vascular response to cold temperatures or stress resulting in cyanosis and pallor of the digits. 1 Almost all patients with systemic sclerosis (SSc) are affected by RP during the course of their disease, and the associated dysregulation of flow to the distal extremities may lead to chronic or recurrent digital ischemia and ulcers in severe cases. 2 Treatment options for RP include discontinuation of vasoconstrictive medications, avoidance of cold, physical warming techniques, and smoking cessation. Pharmacologic therapies include vasodilatory agents such as calcium channel blockers, phosphodiesterase (PDE) inhibitors, topical nitrates, and less conventional agents such as angiotensin receptor blockers and the serotonin reuptake inhibitor fluoxetine. 1 Refractory or progressive ischemia in SSc warrants the use of advanced therapies such as intravenous prostaglandin infusions, digital or regional blocks, and digital sympathectomy.1,3,4 However, these therapies may be poorly tolerated due to the adverse effects of systemic vasodilation. Furthermore, patients may develop refractory disease and disabling hand ischemia even if treatment is successfully delivered, making demarcation and amputation of the digit the most likely outcome. We have recently shown that percutaneous transluminal angioplasty in the cardiac catheterization lab may be a viable treatment option for selected SSc patients with refractory ulceration. 5
Digital ischemia in SSc develops as a result of stenoses or occlusions affecting the distal vasculature of the forearm and the hand. The etiology of vessel occlusion includes a combination of vasospasm, intimal hypertrophy, and in situ thrombosis. Many of these patients may be candidates for revascularization to facilitate wound healing, however, this is rarely considered to be a feasible option given the lack of data and technical expertise in this area. The current literature on revascularization of the hand in SSc is scant—while angioplasty has been discussed and recognized as a therapeutic alternative in selected patients, the technical aspects of the procedure and detailed patient outcomes have not been described. A prior study examining the utility of upper extremity diagnostic angiography briefly noted that angioplasty was attempted in this population with poor outcomes. 6 A more recent study described the use of angioplasty in combination with microvascular surgery in 178 patients with RP of all causes and digital ischemia; 29 of the patients in this cohort had a diagnosis of SSc. Periarterial digital sympathectomy was the most common procedure and adjunctive balloon angioplasty was performed in patients who had stenosis of either the radial or the ulnar artery. Angioplasty of any occluded arteries or vessels beyond the palmar arches was not attempted. The authors of the study reported clinical improvement in 75% of the patients treated with angioplasty for a proximal stenosis. 3
Our team has successfully performed a series of percutaneous interventions of the upper extremity—specifically, the distal vasculature of the hand—in a cohort of SSc patients presenting with refractory digital ischemia or non-healing digital ulcerations (DUs). All cases had been deemed non-responsive to conventional, pharmaceutical, and lifestyle therapies or presented with digital-threatening ischemia. In addition to an attempt at revascularization, patients also received intravenous prostaglandin infusion during the perioperative period. The clinical outcomes for these patients have been positive, yielding rapid restoration of blood flow and near-total reversal of digital ischemia and hand pain. Importantly, all patients were able to avoid digital amputation. To the best of our knowledge this represents one of the first documented series regarding limb salvage in scleroderma-induced hand ischemia using contemporary percutaneous revascularization techniques.
Methods
This is a single-center retrospective study of consecutive patients with SSc and RP who presented with refractory digital ischemia or non-healing DUs (>3 months or disabling RP symptoms >4 weeks on standard therapy) and underwent percutaneous revascularization between 1 January 2020 and 31 May 2021. DU was defined as any loss of continuity of skin epithelium. Demographic, clinical, and serologic data were obtained by review of electronic medical records. The presence or absence of pulmonary arterial hypertension was determined using echocardiography. The study received approval by our institutional review board (IRB Number HSC-MS-21-0539). A waiver of informed consent was obtained as only de-identified data is reported.
Results
A total of six patients underwent percutaneous intervention (15 procedures) for scleroderma-associated digital ischemia during the study period. Table 1 shows the demographics, clinical, and serologic characteristics of these patients. Most (83%) were female with an age range of 40–63 years. Notably, all patients had positive antinuclear antibodies (ANA) in a 1:1280 titer, five in a centromere pattern and one in a speckled pattern, and all patients fulfilled the 2013 American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) classification for SSc. Two patients had SSc sine skin sclerosis, three had limited cutaneous disease, and one had diffuse cutaneous SSc. Two of the patients had interstitial lung disease without hypoxia and none had established diagnosis or clinical suspicion of pulmonary arterial hypertension. Disease duration from onset of RP to time of percutaneous intervention ranged from 3 to 9 years. Five out of the six patients were on a calcium channel blocker and PDE inhibitor at the time of the angioplasty; the sixth patient was newly diagnosed with SSc and was not on any medication for RP. All patients had DUs, dry gangrene, or severe RP at the time of presentation.
Demographics and clinical characteristics of patients.
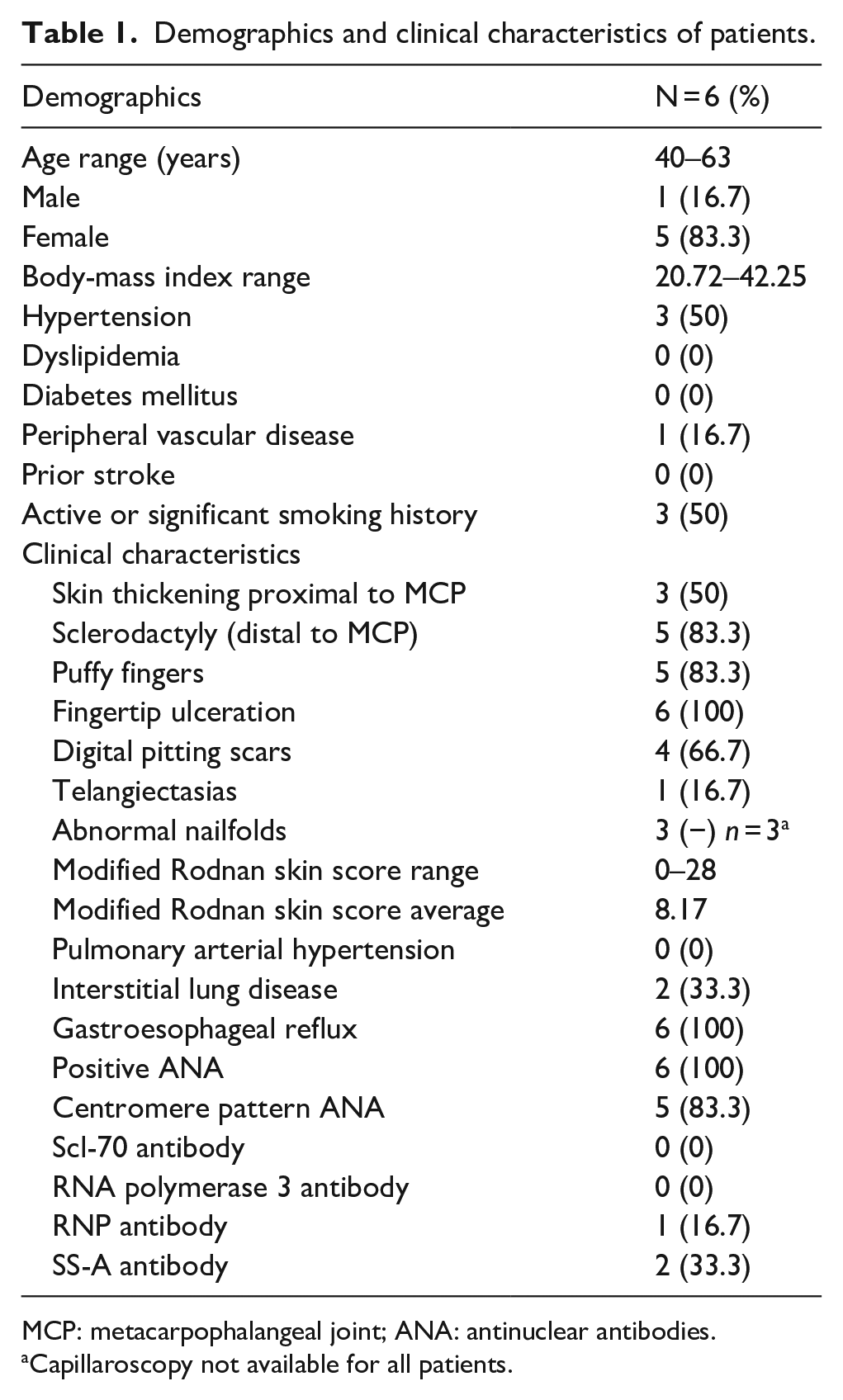
MCP: metacarpophalangeal joint; ANA: antinuclear antibodies.
Capillaroscopy not available for all patients.
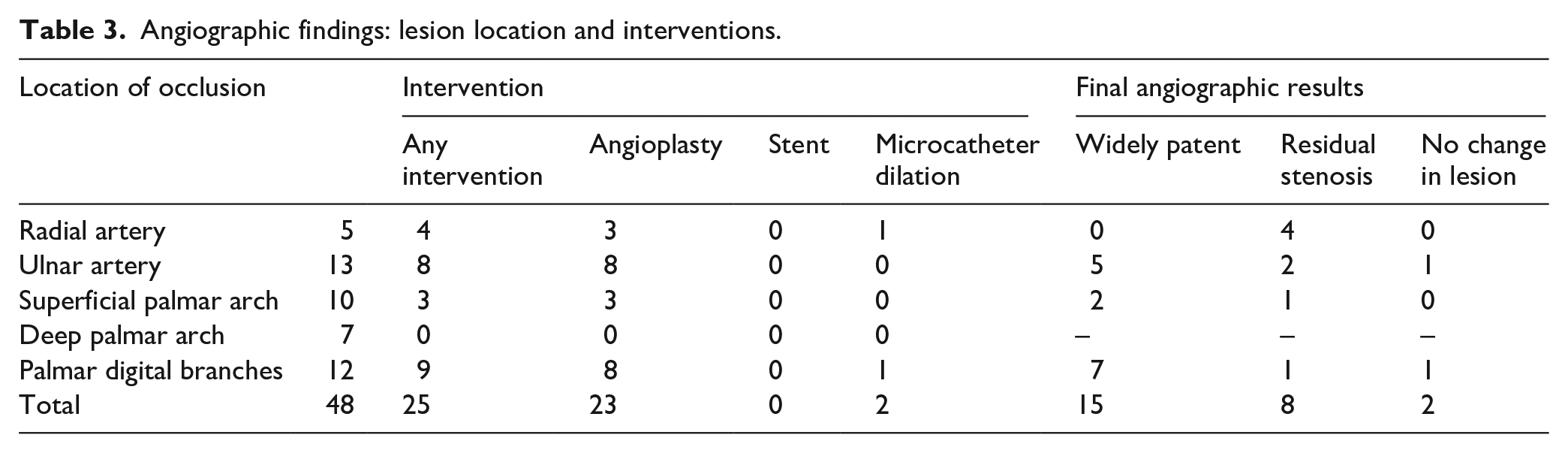
The six patients in the cohort underwent a total of 15 percutaneous angiograms to treat 10 different digits within the period. Four patients required multiple procedures: the most common indication was a new lesion in the same hand, often involving a different digit. Patient 1 was treated with four procedures for three unique lesions on separate digits of the same hand. Patient 2 underwent four procedures to treat ulcers or disabling RP (two occurrences each) in the same hand. Patient 3 had three procedures to treat both hands. Patient 5 had angiography of both upper extremities, but only one intervention was performed to treat the left hand. Plans to intervene upon the right hand in this patient were aborted due to abnormal vascular anatomy following a prior surgery (unrelated to the patient’s diagnosis of SSc) and our inability to advance catheters across the subclavian artery; this case was excluded from our final analysis (Table 2). Ulnar arterial occlusion (UAO) was the most common vascular finding in 13/14 percutaneous angiograms (93%); palmar digital branch occlusion was the second most common feature seen in 12/14 angiograms (86%). Radial artery occlusion was diagnosed in 5/14 angiograms (36%). This high percentage was mostly driven by Patient 2 who presented with recurrent occlusions of both the ulnar and radial arteries in every procedure; notably, this patient had a significant smoking history and was taking immunosuppressants following liver transplantation. A total of 25 discrete occlusions were treated with either balloon angioplasty (23/25, 92%) or microcatheter dilation (2/25, 8%). Stents were not used because of the small caliber of the arteries (typically less than 2 mm), vessel tortuosity, or location of the treatment zone across the flexion axis at the wrist. Thrombolysis was not considered because all occlusions were deemed to be chronic (based on the duration of symptoms and difficulty in advancing wires within the vessel), and therefore unlikely to respond to thrombolytic agents. Our interventions restored complete or partial flow in 23 of the treated vessels (92%): 15/25 vessels were widely patent (<10% residual stenoses), 8/25 had mild or moderate (⩾10% to 70%) residual stenosis, and 2/25 vessels had no observable improvement in flow at the end of the procedure (Table 3).
Procedural and clinical outcomes following angioplasty in SSc patients with refractory RP.
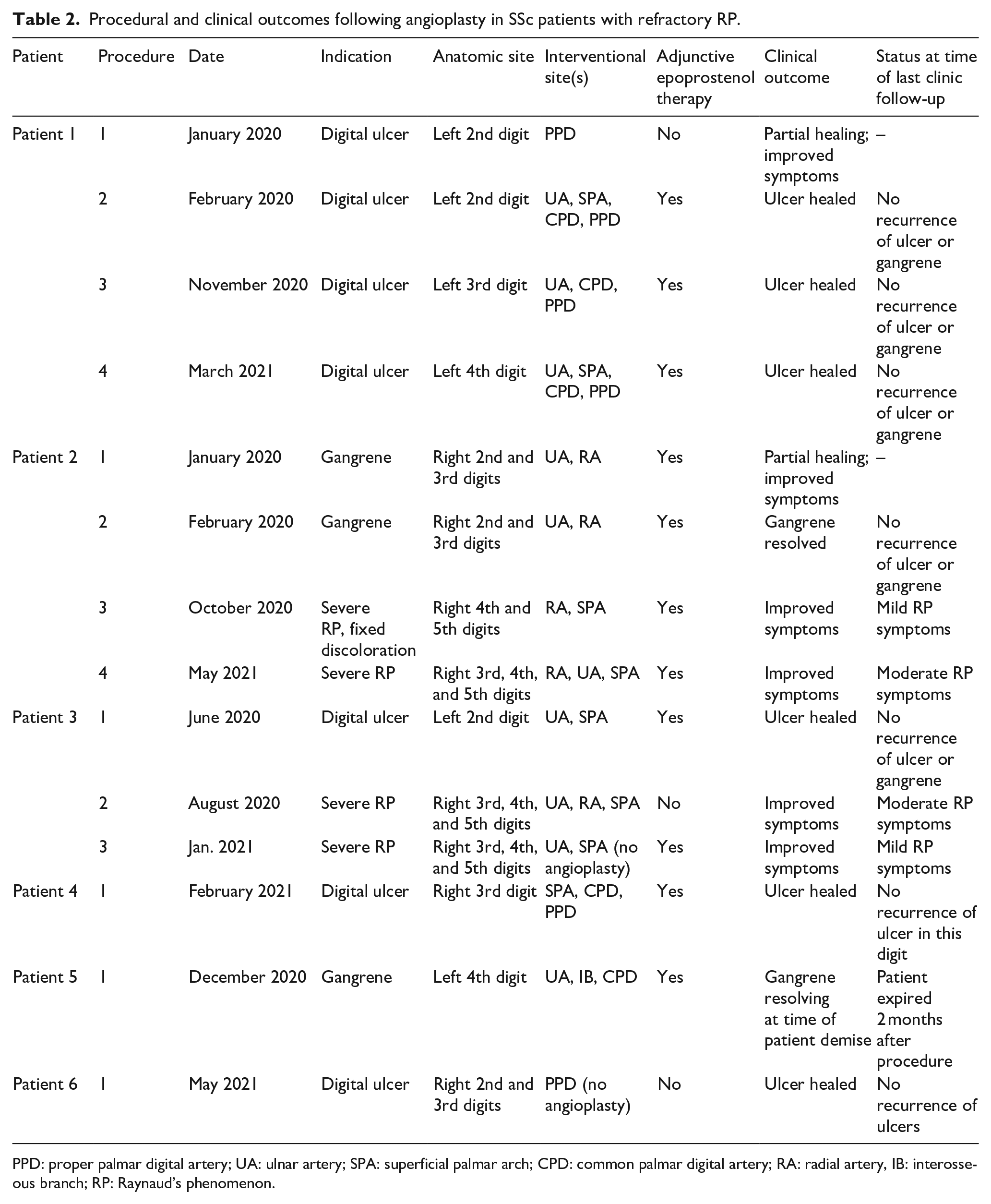
PPD: proper palmar digital artery; UA: ulnar artery; SPA: superficial palmar arch; CPD: common palmar digital artery; RA: radial artery, IB: interosseous branch; RP: Raynaud’s phenomenon.
Angiographic findings: lesion location and interventions.
All patients showed a favorable hemodynamic response to intervention at the completion of the procedure. This was assessed by bedside Allen’s test and capillary refill time immediately after the procedure and during the hospital stay. We also noted if the patient reported improvement of pain and the ability to flex and extend fingers without pain. At 1 month of follow-up, no patients had experienced any adverse events directly related to the procedure. All patients experienced accelerated healing of any digital ulceration and improvement in RP symptoms after the interventions. Patient 1 and Patient 2 had incomplete healing after their initial procedures and required a subsequent intervention to treat the same lesion. In all other cases, the follow-up interventions were performed to treat new lesions in different digits. Notably, there was no recurrence of ulceration after healing in the treated digits (Table 2).
Discussion
Patients with SSc and RP commonly present with symptoms related to digital ischemia. Manifestations of ischemia include pain, paresthesia, loss of function of the digit (and the hand), and in extreme cases, tissue loss and ulceration. Chronic digital ulceration is associated with significant morbidity related to pain and neuropathy, and can lead to loss of the digit. Patients with SSc who have experienced digital ischemia and ulceration once remain at high risk of recurrent gangrene, chronic infections of the hand, and amputation. Several strategies have been employed in the treatment of SSc-associated refractory digital ischemia; however, healing is often prolonged and many patients with advanced ischemia may fail to respond. In this observational study, we report the clinical characteristics and outcomes of patients who were treated with percutaneous intervention in addition to epoprostenol infusion for refractory DUs and gangrene (>3 months) or severe RP symptoms (>4 weeks) on optimal therapy in five patients and after a new diagnosis in one patient.
All patients in our study were found to have disruption of straight line flow to affected digits. Ulnar artery occlusion (UAO) was highly prevalent and was found in 13 out of 14 cases. This observation is in line with previous studies.3,7–9 In one case-controlled study, Frerix et al reported a 21.5% prevalence of UAO in a cohort of 79 SSc patients compared with none in a healthy control group. Patients with UAO had a higher risk of new or recurrent digital ulcers at follow-up, a finding that was also evident in our patient population. 8 Another study by Lescoat et al reported a prevalence of 37.3% of UAO among 76 patients. The authors reported a higher association between UAO and anticentromere antibody positivity, higher modified Rodnan skin scores, history of digital ulcers, and lower diffusing capacity of the lungs for carbon monoxide (DLCO) values, suggesting that UAO is a marker of vasculopathy severity in SSc. 7
It is notable that three (50%) of the six patients in our small cohort required multiple interventions within the study period, most commonly to treat new ischemic lesions in a different arterial territory. This observation underscores the progressive nature of this disease. Patents with symptomatic SSc frequently manifest vasculopathy of small to medium-sized vessels characterized by intimal proliferation and fibrosis, endothelial dysfunction, and smooth muscle activation. Activated smooth muscle cells demonstrate increased α2-adrenergic receptor expression and activity which underlies the exaggerated vasoconstrictive response to cold and stress in SSc patients. These smooth muscle cells are also known to differentiate into myofibroblasts which secrete collagen and extracellular matrix in the intimal layer of the vessels, further contributing to the vascular dysfunction. 10 The combination of these vasculopathic phenomena leads to impaired perfusion of the distal vascular bed in up to 50% of SSc patients, and can lead to profound digital ischemia. Our patients reported almost immediate improvement in pain and other subjective measures of hand ischemia (finger stiffness and paresthesia) after restoration of flow to the digit. More importantly, they noted accelerated wound healing in the days following the intervention and were thus able to avoid amputation of the digit. This observation supports the notion that chronic under-perfusion is major contributor to delayed wound healing in patients with advanced SSc, and revascularization can reverse this process by restoring flow to the ischemic vascular beds. Interestingly, percutaneous intervention did not prevent vascular reocclusion in the treated hand; however, this was not associated with recurrence of ulceration once the digit had healed completely.
These features are most strikingly demonstrated by the clinical course of Patient 1. The patient initially presented with a non-healing ulcer of the left second fingertip and worsening RP symptoms in the left second and third digits (Figure 1(a) and (b)). She was found to have left UAO and severe stenosis of the first proper palmer digital artery by angiography. Our initial attempt to revascularize the occluded ulnar artery was unsuccessful. The patient underwent angioplasty (PTA) of the proper palmar digital artery via the radial artery. She reported immediate improvement in her RP symptoms; however, the ulcer at the second fingertip had only partially healed after 1 month. A second procedure was performed 8 weeks later, and the occluded ulnar artery was successfully revascularized with retrograde PTA (Figure 1(e)). The intervention was followed by completed healing of the second digit over the next 2 months (Figure 1(c) and (d)). Nine months later, the patient presented with new fingertip ulceration of the left third digit (Figure 2(a)). Angiography of the left hand showed occlusive restenosis of the ulnar artery and a new occlusion of the common and proper palmar digital arteries supplying the third digit. These vessels were successfully treated with PTA (Figure 2(b) and (c)). Four months after this repeat procedure, the ulcer at the left third fingertip had completely healed. However, 1 month later the patient developed new ulceration at the fourth left fingertip (Figure 2(d)). She underwent angiography after the ulcer failed to heal, and was treated with PTA of the ulnar artery, superficial palmar arch, common palmar digital artery and fourth digit proper palmar artery (Figure 2(e) and (f)). The ulcer healed completely over the subsequent 4 weeks, and all the fingers were intact without ulceration at 6 months (Figure 2(g) and (h)). Notably, the patient received epoprostenol with the second, third, and fourth interventions. This suggests that the combined therapeutic effect of angioplasty and epoprostenol is synergistic in promoting wound healing, and is not protective against the development of new ulcers at a later stage.
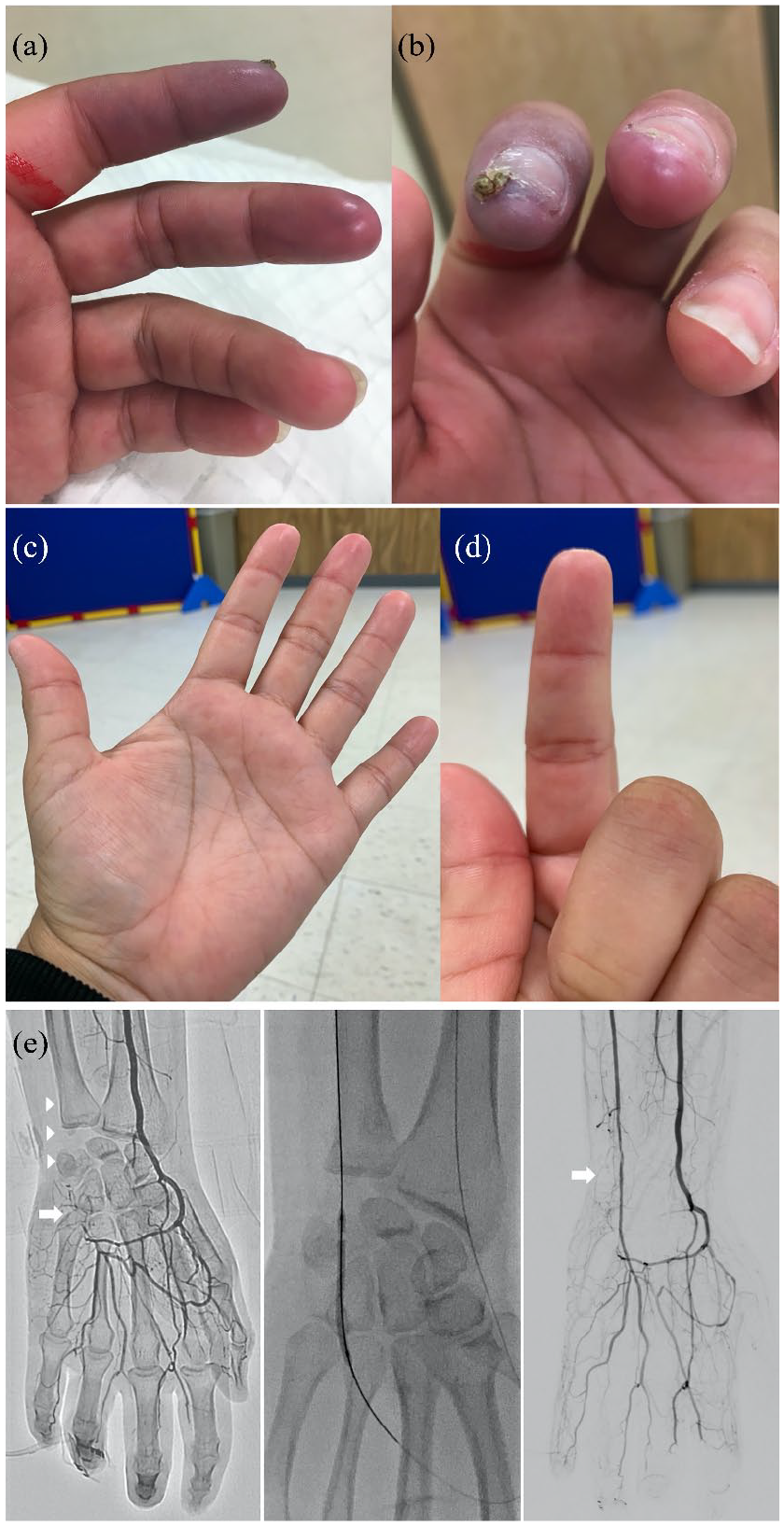
Left hand of Patient 1. (a) Impending skin necrosis at the tips of the second and third digits, prior to Procedure 1. (b) Occlusion of the left ulnar artery (arrowheads) and interrupted superficial and deep palmar arches (arrow). (c) and (d) Resolution of ischemia after Procedure 2. After percutaneous transluminal angioplasty of the ulnar occlusion (middle image), the final angiogram shows restoration of antegrade flow into the superficial and deep palmar arches through the patent ulnar artery (arrow).
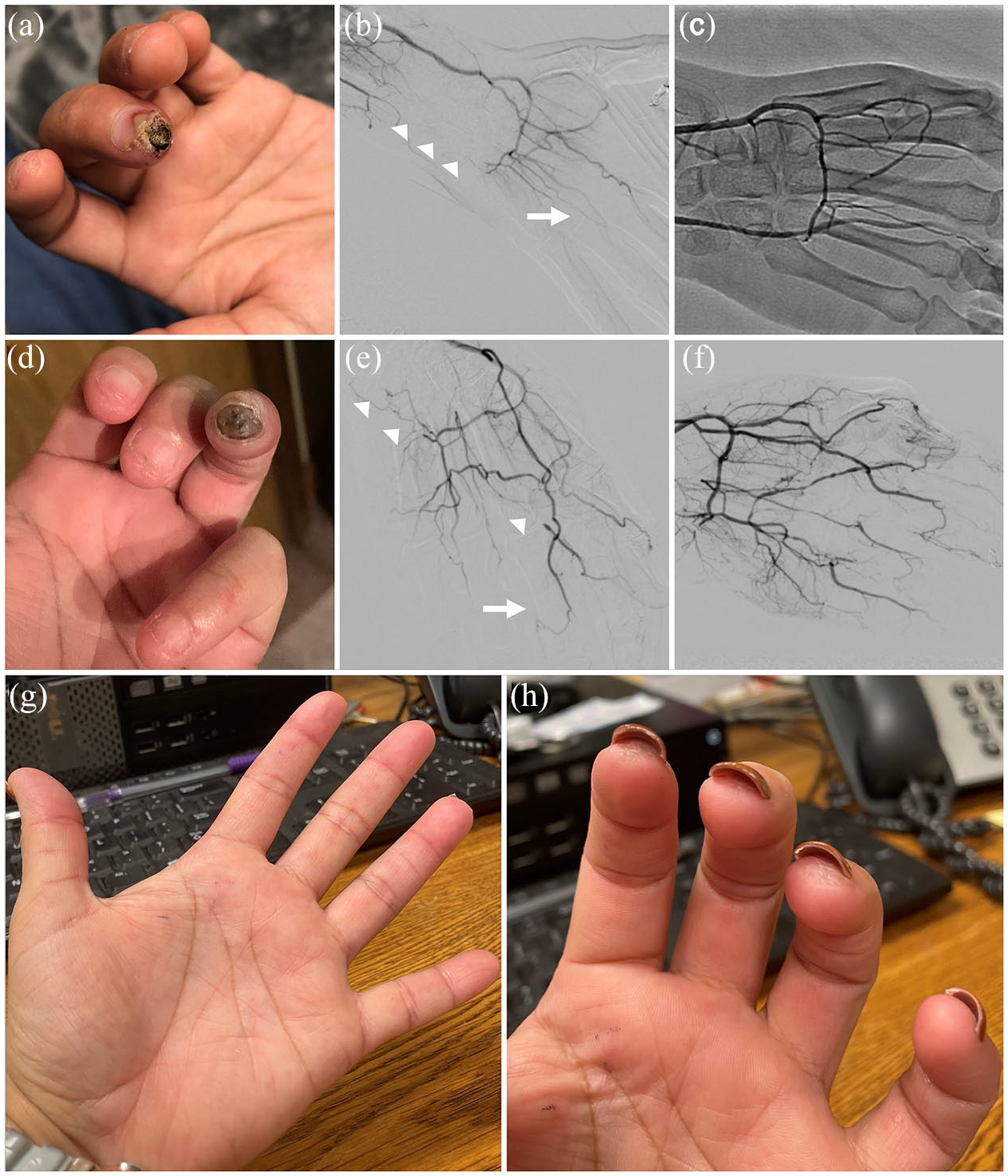
Left hand of Patient 1—clinical course following the initial intervention. The patient developed two new ulcers in the third (a) and fourth digits (d) at different time periods, and was treated percutaneously for both. The diagnostic angiograms (b and e) show areas of restenosis (arrowheads) and new occlusions (arrow). There is under-perfusion of all digits prior to and improved flow after angioplasty (c and f). (g) and (h) The patient’s hand at 6 months after the last intervention. All digits are intact and without ulceration. She continues to have moderate RP symptoms in cold weather.
Limitations of the current study
Our findings are limited due to a small sample size and retrospective nature of the study. Outcomes were reported based on the last clinical note, clinical images, and documented patient communications. The exact time to healing of DUs could not therefore be determined, although all patients reported improved symptoms and a subjective experience of accelerated healing after the procedure. Almost all patients received epoprostenol at the time of or immediately after angioplasty, therefore the relative contributions of revascularization versus epoprostenol in promoting wound healing cannot be determined. The protocol for the treatment of refractory digital ischemia in patients with SSc at our institution includes epoprostenol. Therefore, we felt it would be unethical to withhold epoprostenol in these patients given the fact that angioplasty of the hand for treatment of SSc is still “investigational.” Our study is hypothesis generating and highlights the possible role of percutaneous revascularization of ischemic digits in patients with SSs.
Conclusion
The combined approach of percutaneous revascularization and vasodilatory therapy is safe and effective in improving symptoms and promoting wound healing in SSc patients with refractory digital ischemia who do not respond to or have failed standard therapies. Our novel therapeutic approach suggests that percutaneous revascularization of ulcerated digits is feasible in most patients, and may allow for restoration of flow to areas of chronic ischemia. We hope to expand on these data with a future prospective trial that will use standardized methods for digital ulcer assessment and mandate more uniform follow-up times and outcomes reporting. These additional studies will also help us define the role of adjunctive pharmacologic therapies. We hope that these techniques can be replicated in different centers so that we establish the reproducibility of our findings and better understand the role of percutaneous revascularization in preventing amputation and reversing tissue loss in patients with SSc and non-healing digital ischemia.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.A.A. serves as a consultant for Teleflex, Inc. M.D.M. has no conflicts of interest for the data presented in this manuscript. She is a Clinical Trial Investigator with Mitsubishi-Tanabe, Boehringer-Ingelheim, EICOS, Corbus, Prometheus and Horizon. She is also a member and on the Scientific Advisory Board for Mitsubishi-Tanabe and Boehringer-Ingelheim. She is a Grant reviewer for the Young Investigator Program for Actelion Pharma and is a conference speaker on autoantibodies for Medtelligence. The other authors have no conflicts of interest to declare; there are no other commercial sources for the work reported on in the manuscript, or any other financial interests that any of the authors may have, which could create a potential conflict of interest or the appearance of a conflict of interest regarding the work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of ethics and consent
Ethical approval was obtained by the site’s Institutional Review Board (IRB Number HSC-MS-21-0539).