
Abstract
Background:
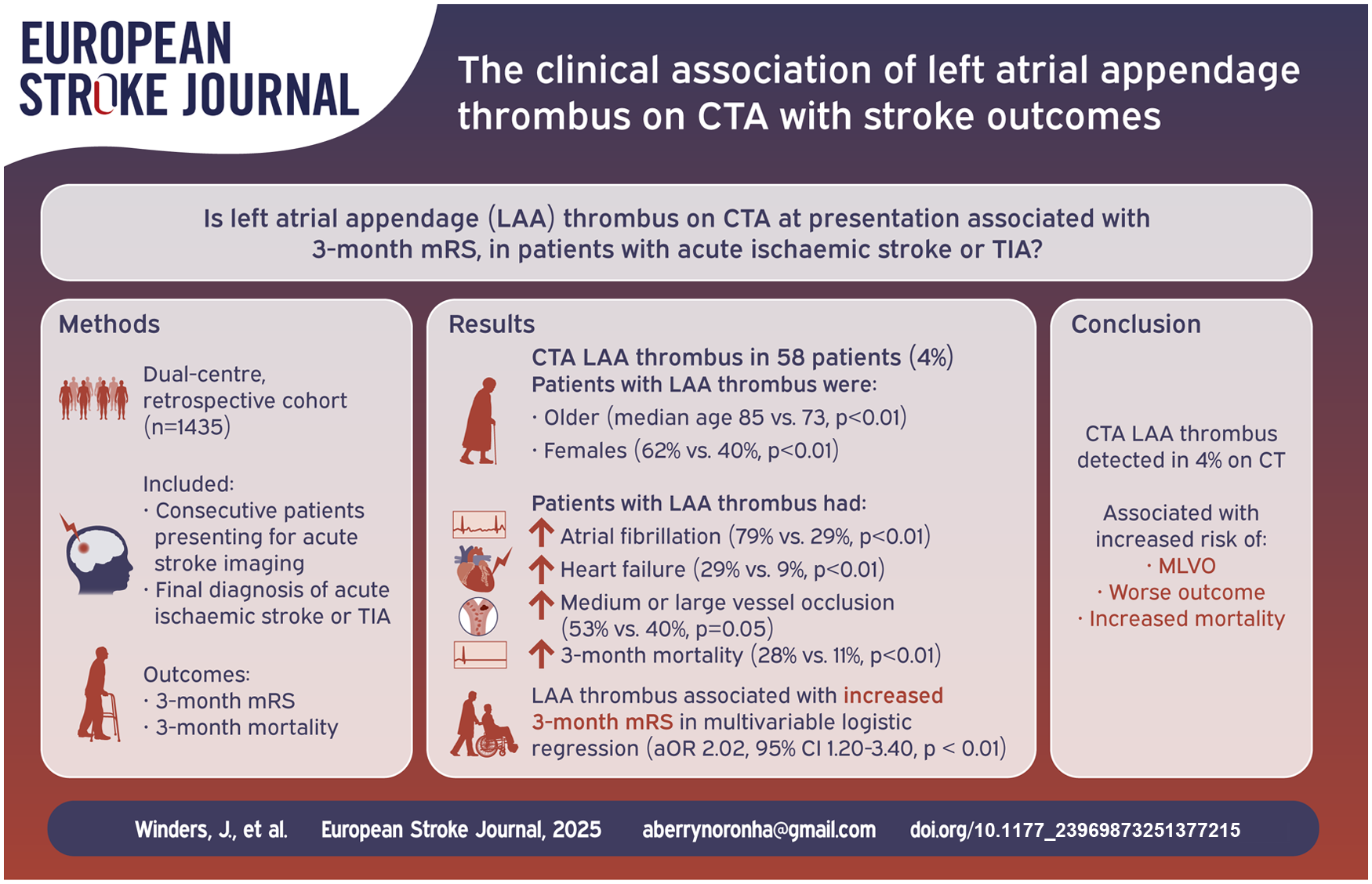
Left atrial appendage (LAA) thrombus is associated with atrial fibrillation (AF) and can be a marker of atrial cardiomyopathy. We determined the association between computed tomography angiography (CTA) identified LAA thrombus in patients presenting with acute ischaemic stroke or transient ischaemic attack (TIA), and 3-month outcome.
Methods:
We undertook a dual-centre, retrospective cohort study from New Zealand and Australia. All consecutive patients presenting with acute ischaemic stroke or TIA during the inclusion period who underwent acute stroke imaging were included. We analysed the association with CTA-LAA thrombus and 3-month outcome on modified Rankin Scale using multivariable logistic regression models adjusted for known predictors of outcome.
Results:
Of the 1435 patients included, 1304 (90.9%) had acute ischaemic stroke and 131 (9.1%) had TIA. 582 (41%) had confirmed intracranial medium or large vessel occlusion (MLVO), and 565 (40%) received reperfusion therapies. CTA-LAA thrombus was identified in 58 (4.0%) patients, and these patients were older (median age 85 (IQR 75–88) vs 73 (63–81), p < 0.01), more likely to be female (62% vs 40%, p < 0.01), had higher rates of AF (79% vs 29%, p < 0.01), heart failure (29% vs 9%, p < 0.01), MLVO (53% vs 40%, p = 0.05), and mortality at 3-months (28% vs 11%, p < 0.01). Adjusting for known predictors of poor outcome, LAA thrombus was independently associated with increased 3-month mRS score (OR: 2.02, 95% CI: 1.20–3.40, p < 0.01).
Conclusions:
CTA-LAA thrombus detected during the acute stroke imaging protocol in patients with ischemic stroke or TIA is a predictor of worse outcome.
Background
A cardiac source of embolus accounts for approximately 30% of ischaemic strokes and is associated with a higher burden of disability and mortality compared to other causes of stroke. 1 One potential mechanism is thrombus formation in the left atrial appendage (LAA), as occurs in the presence of atrial fibrillation (AF) and atrial cardiomyopathy.2,3 Cardiac computed tomography (CT) is an imaging modality that has been adopted as part of routine hyperacute stroke imaging in several comprehensive stroke centres internationally, and may overcome issues with access to transthoracic echocardiography (TTE). It has been previously demonstrated that cardiac CT in hyperacute stroke has superior yield to TTE for identifying cardiac source of emboli. 4 In our previous study, CT angiography (CTA) LAA thrombus was present in 6.6% of patients with ischaemic stroke, and was associated with known or newly diagnosed AF. 5
The acute stroke pathway CT imaging sequences at Christchurch Hospital, Christchurch, New Zealand, and John Hunter Hospital, Newcastle, Australia (JHH), includes non-contrast CT, CT perfusion and CTA from the LAA to vertex. 6 This is a non-invasive method of detecting LAA thrombus,7 –13 which may serve as a marker of atrial cardiomyopathy, prolonging the scan by 30 s–2 min, without needing additional contrast. 5 The Christchurch and JHH protocols result in an estimated increased radiation of 1.2 and 3.7 mSv respectively. A recent randomised trial comparing standard acute stroke CTA imaging with extended CTA imaging 6 cm below the carina showed significantly higher rates of cardioaortic thrombus detection in the extended CTA group (8.8% vs 1.7%, p = 0.02) without compromising time to completion of imaging. 14 The presence of LAA thrombus may confer increased early recurrent ischaemic stroke risk, although there are no published studies addressing this as a primary outcome. LAA thrombus may also indicate undetected AF in patients without prior history of AF, enabling early anticoagulation and abrogate the need for resource-intensive cardiac rhythm monitoring. In patients with known AF, identification of LAA thrombus is also valuable as it may highlight compliance issues, or prompt consideration of change in treatment. The association between LAA thrombus detected with CTA at the time of acute stroke presentation and clinical outcome has not been fully explored. Our aim was to investigate this association, hypothesising that presence of CTA-LAA thrombus at the time of acute stroke imaging would be associated with higher morbidity and mortality.
Methods
We performed a retrospective analysis to investigate the association between CTA-LAA thrombus detected at time of initial cerebrovascular presentation with 3-month functional outcome.
Patients
We included all consecutive patients presenting to the emergency department with stroke-like symptoms who would have been potential candidates for acute thrombolysis or mechanical thrombectomy (MT). This typically included patients with potentially disabling deficit (Christchurch), or NIHSS ⩾ 4 (JHH). 15 all of whom underwent multimodal brain imaging (non-contrast CT, CT perfusion and CTA) and cardiac CT at two comprehensive stroke centres in New Zealand (Christchurch) and Australia (JHH) between September 2018 and December 2020, and November 2020 and August 2023, respectively. We excluded patients where the final diagnosis was not ischaemic stroke or transient ischaemic attack (TIA). Clinical data were extracted from comprehensive electronic clinical records and review of radiological imaging. We obtained clinical variables including baseline demographics, evidence of previous or current AF, reperfusion treatment, demographic risk factors and examined for presence of LAA thrombus, and medium or large vessel occlusion (MLVO). Three-month modified Rankin Scale (mRS) was determined from detailed electronic clinical records at 3-month follow up, as undertaken by the stroke rehabilitation team. MLVO was defined as CTA occlusion of the extracranial or intracranial internal carotid artery (ICA); anterior cerebral artery (ACA); first, second or third divisions of the middle cerebral artery (M1, M2 and M3 respectively); vertebral or basilar arteries. Ischaemic stroke was defined as an acute neurological deficit accompanied by evidence of acute ischaemia on imaging (CT or magnetic resonance imaging). TIA was defined as an acute neurological deficit lasting less than 24 h, with normal acute and follow-up imaging and no other explanation for the presentation. Recurrent ischaemic stroke was defined accordingly, with information recorded from hospital records. Recurrent embolic events included myocardial infarction or any diagnosis of thromboembolic events in hospital records.
Statistical analysis
Baseline demographics and risk factors were assessed using Shapiro–Wilk test for normality. These were then compared with p-values obtained using the Wilcoxon rank test, while binary variables were compared using the Chi-squared method. Where less than 10 values were present, Fisher’s exact test was used. To assess the association with LAA thrombus and 3-month outcome (mRS 0–6), we undertook a multivariable ordered logistic model adjusting for known predictors of poor outcome as fixed effects (age, premorbid mRS, NIHSS, MLVO, congestive heart failure, AF and treatment with MT or intravenous thrombolysis). A subgroup analysis was also undertaken on a cohort that excluded patients with TIAs. Statistical analysis was performed using RStudio 2023.03.0.
Brain imaging protocol
The Christchurch imaging protocol consists of non-contrast CT brain, followed by CT perfusion and extended range CTA from the left atrium to the vertex. All patients were examined using either a 128-slice (SOMATOM Definition Flash, Siemens Healthcare, Erlangen, Germany) or 64-slice (GE VCT Lightspeed, GE Healthcare, Milwaukee, WI, USA) CT scanner. The JHH imaging protocol consisted of non-contrast CT brain, followed by CT perfusion, and then CTA from aortic arch to skull vertex after 5 min. CTA of the left atrium was performed at 30 s and 2 min. All patients were examined using a 384 (2 × 192) slice Dual Source CT scanner (SOMATOM Force, Siemens Healthcare, Erlangen, Germany or GE VCT Lightspeed, GE Healthcare, Milwaukee, WI, USA). CTA was not cardiac-gated at either site. See the Supplementary Appendix S1 for more detailed protocols.
Radiological analysis
CTA review was undertaken by independent radiology investigators at respective sites (AD and SS at Christchurch; CG, BC and SA at JHH) with images read by the clinical research team.
The following criteria for determining likely presence of LAA thrombus were used:
Positive: Filling defect not caused by motion artefact or atrial trabeculae that has Hounsfield units (HU) < 100 AND oval/rounded in shape with well-defined border (Figure 1).
Negative: LAA completely opacifies with contrast, except of changes that can be explained by motion artefact or atrial trabeculae (Figure 2).
Indeterminate: Not fulfilling criteria for positive or negative (Figure 3). This includes cases of slow-flow in the LAA.
Indeterminate results were reviewed with a second reader (AL at Christchurch, and SA radiologist with cardiac fellowship at JHH) and either resolved by mutual agreement or were recorded as indeterminate and excluded from the final analysis. This included cases of slow-flow to the LAA. Delayed phase CTA was used when available to clarify if necessary.
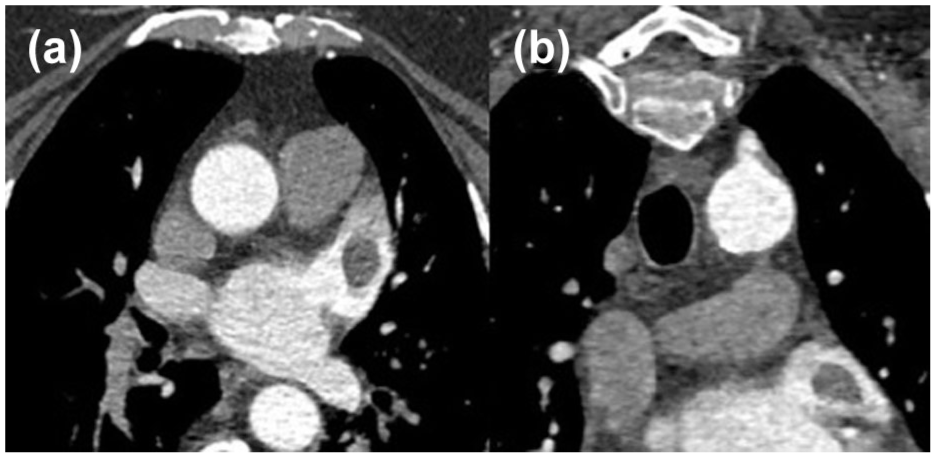
Positive CTA imaging demonstrating free-floating LAA thrombus on axial (a) and coronal (b) sequences.
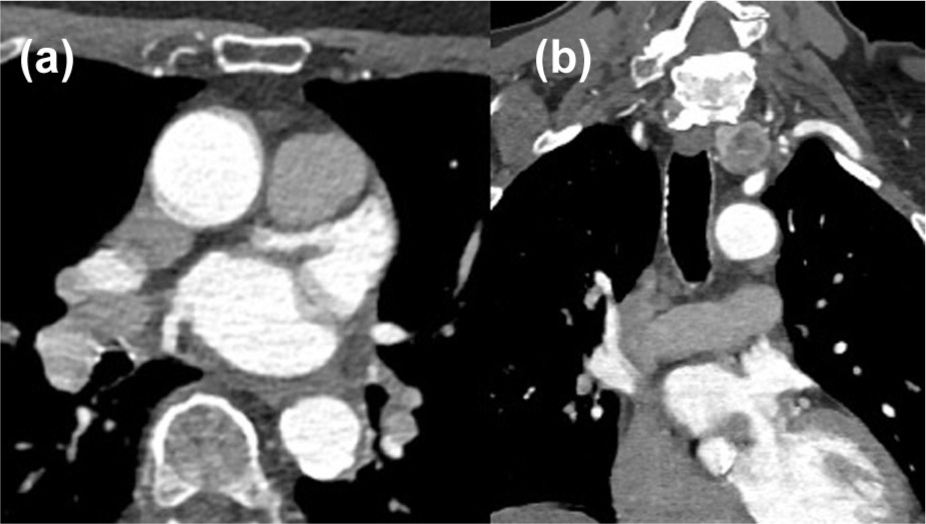
CTA imaging negative for LAA thrombus on axial (a) and coronal (b) sequences.
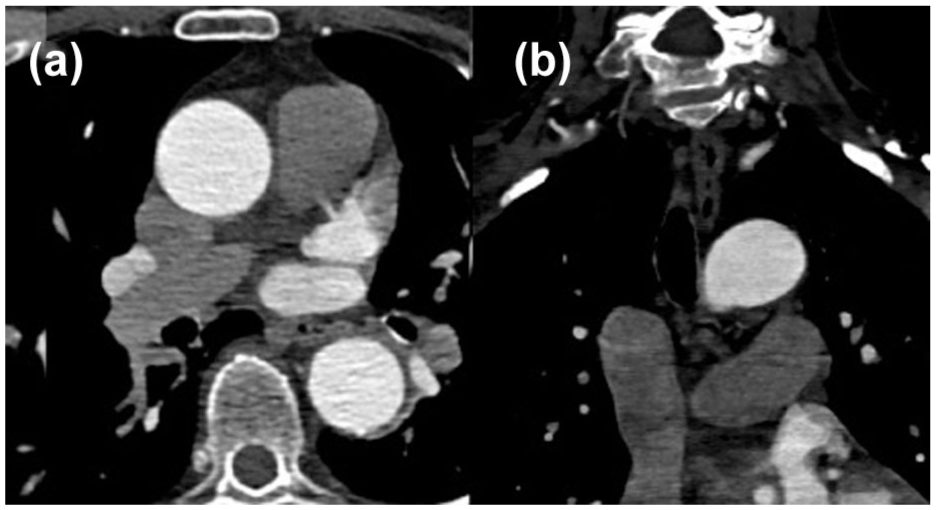
Indeterminate CTA imaging for LAA thrombus on axial (a) and coronal (b) sequences.
Ethics approval
For the Christchurch patients, data were taken from the Christchurch Stroke Registry study and have full approval from the National Health Disability Committee (application reference 17/CEN/84). For the JHH patients, data were retrieved from the International Stroke Perfusion Imaging Registry (INSPIRE), with ethics approval by the Hunter New England Local Health District Human Research Ethics Committee in accordance with Australian National Health and Medical Research Council guidelines (Reference No: 11/08/17/4.01).
Results
A total of 2016 patients presenting with stroke-like symptoms underwent multimodal brain imaging with hyperacute cardiac CT across the two sites during the inclusion period. Of them, 523 patients were not ultimately diagnosed with a stroke or TIA; 58 patients had a non-diagnostic cardiac CT (due to movement artefacts or an indeterminate filling defect), and 96 had no 3-month outcome data available, leaving a total of 1339 included in this study (Figure 4). A final diagnosis of acute ischaemic stroke was diagnosed in 1304 (90.9%) patients, and 131 (9.1%) were diagnosed as TIA. The median age was 74 (IQR: 63–82) years, 589 (41%) were female sex, 582 (41%) had confirmed intracranial MLVO, and 565 (40%) received any type of hyperacute reperfusion therapy (Table 1).
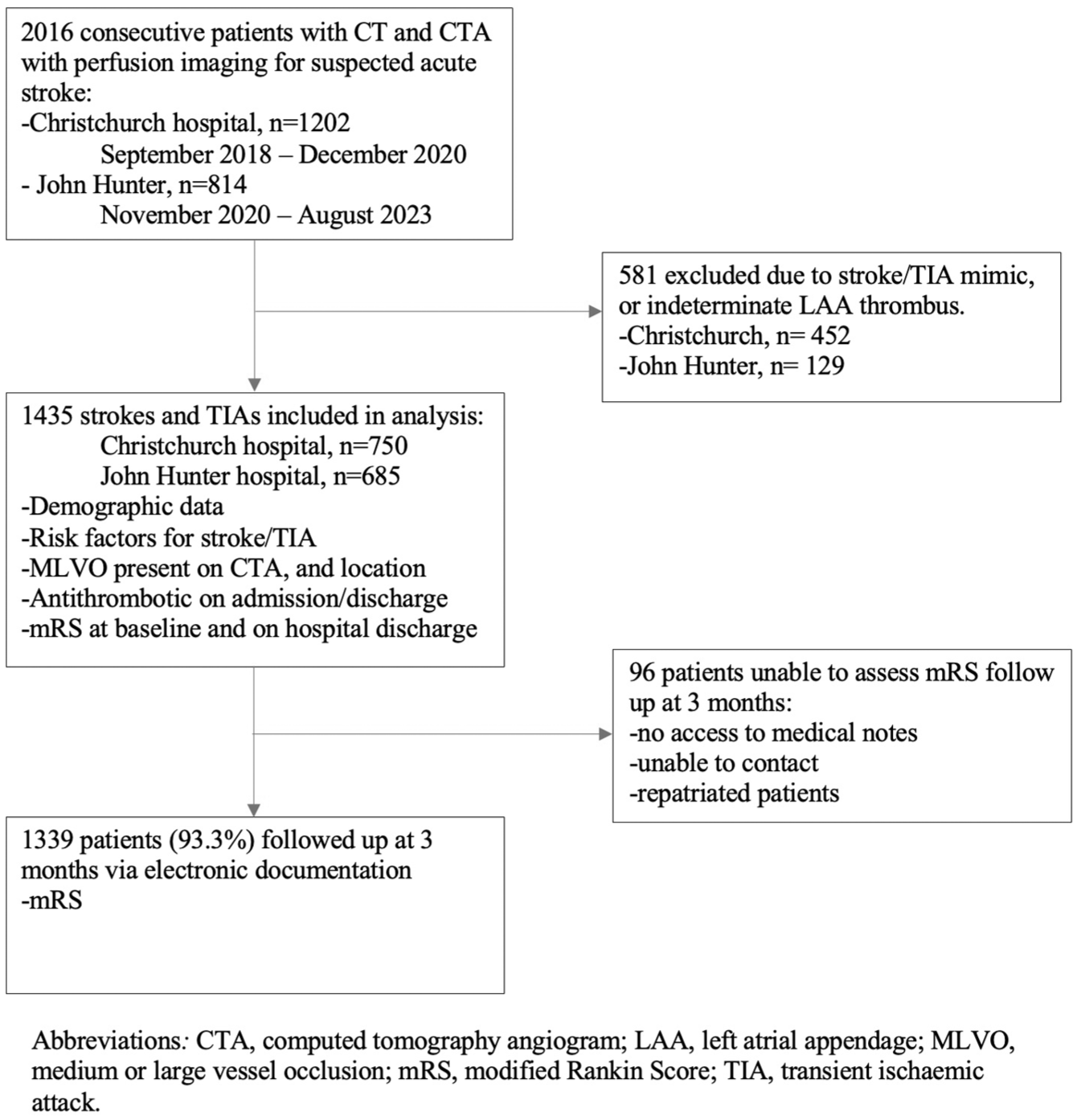
Flow diagram of patient recruitment to follow-up.
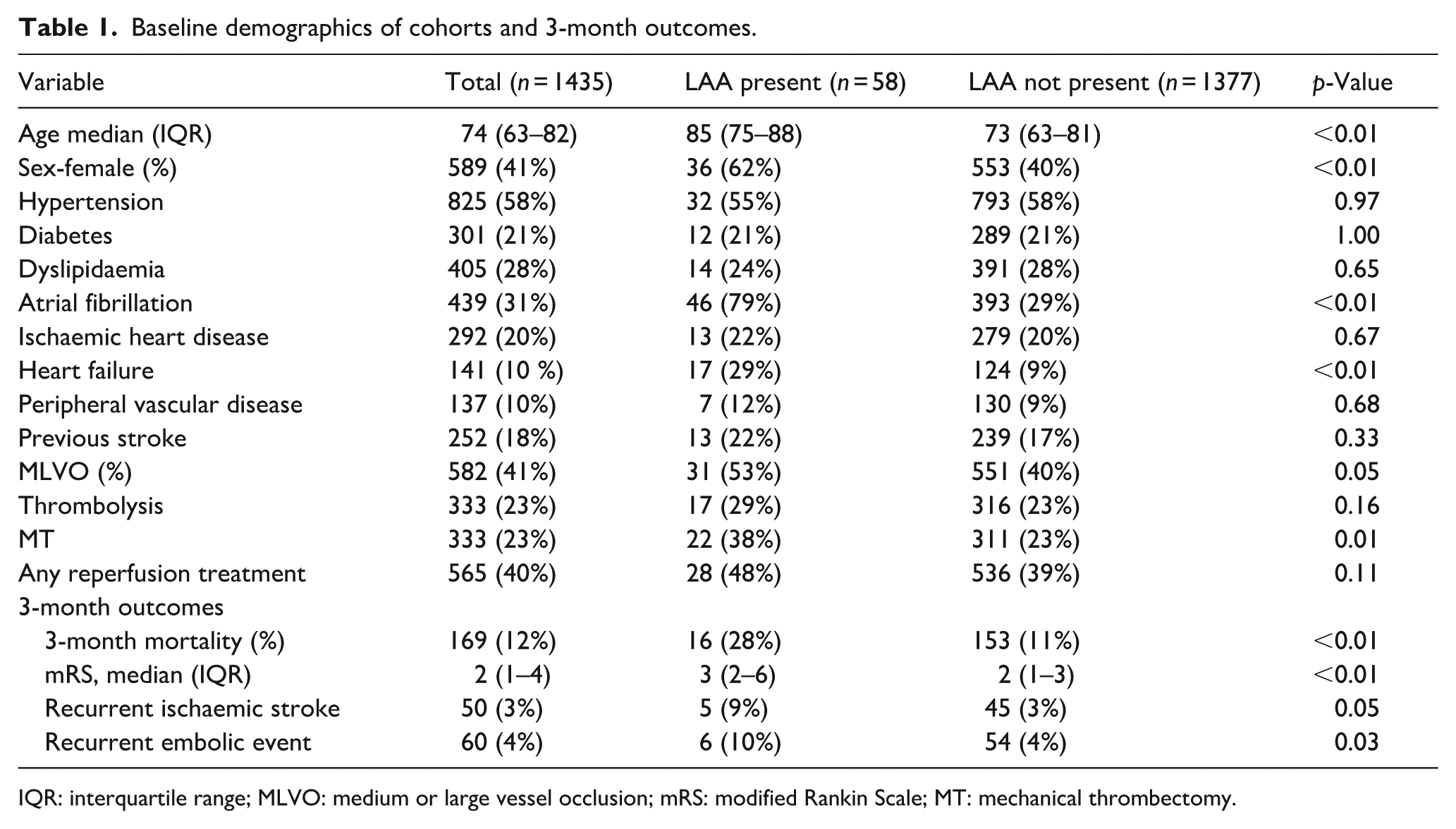
Baseline demographics of cohorts and 3-month outcomes.
IQR: interquartile range; MLVO: medium or large vessel occlusion; mRS: modified Rankin Scale; MT: mechanical thrombectomy.
LAA thrombus was present in 58 (4.0%) of patients, all of whom had a final diagnosis of ischaemic stroke. In comparison to patients without LAA thrombus, patients with LAA thrombus were older (85 vs 73 years, p < 0.01), more likely to be female (62% vs 40%, p < 0.01), had a higher rate of AF (79% vs 29%, p < 0.01) and heart failure (29% vs 9.0%, p < 0.01). Rates of hypertension, diabetes, dyslipidaemia, ischaemic heart disease, peripheral vascular disease, thrombolysis and any reperfusion treatment were similar between groups, though patients with LAA thrombus had increased rate of MT (38% vs 23%, p = 0.01). Patients with LAA thrombus had a higher rate of MLVO (53% vs 40%) but this did not reach statistical significance (p = 0.05; Table 1).
Patients with a final diagnosis of ischaemic stroke or TIA and presence of LAA thrombus in the hyperacute cardiac CT imaging had increased 3-month mortality (28% vs 11%, p < 0.01) and worse functional outcome (3-month mRS score of 3 (2–6) vs 2 (1–3), p < 0.01).
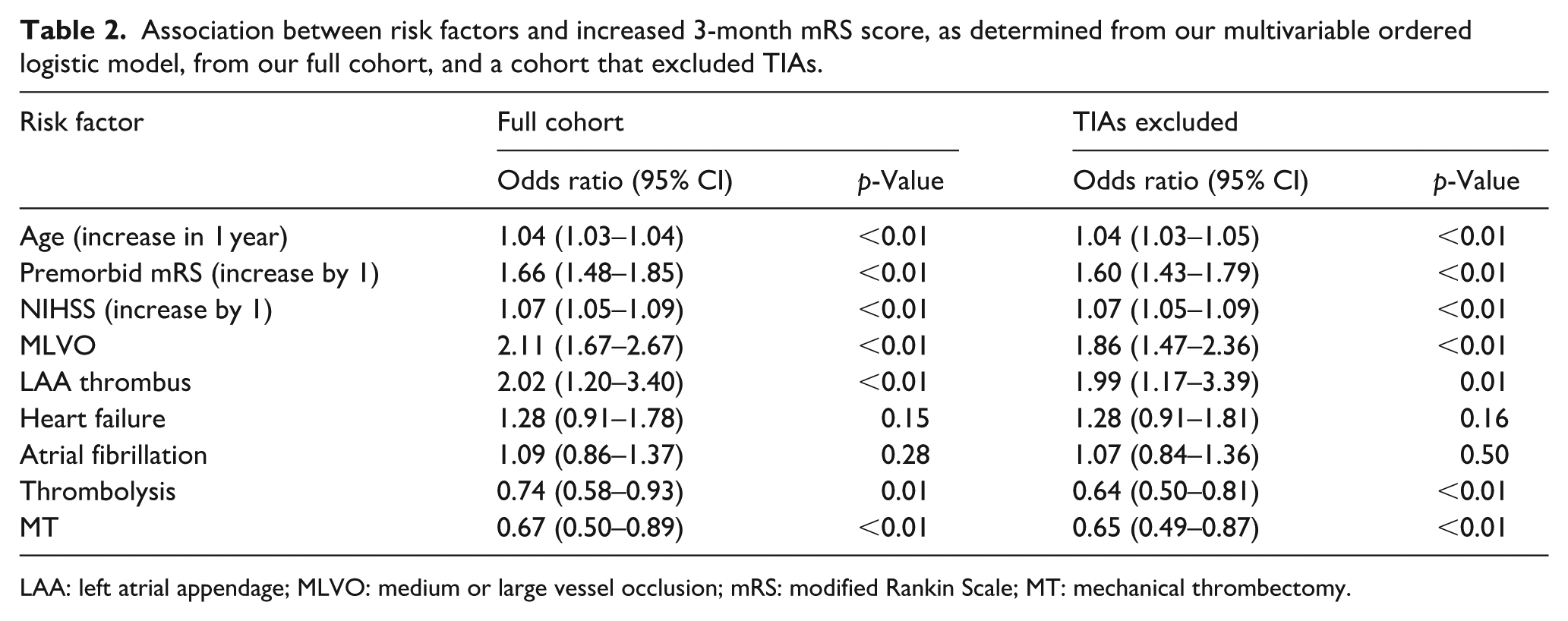
In our multivariable ordered logistic model adjusting for known predictors of poor outcome, LAA thrombus was associated with increased odds of morbidity, based on higher 3-month mRS scores (aOR: 2.01, 95% CI: 1.20–3.40, p = 0.01; Table 2). Other variables associated with increased morbidity in this model were age-increase by 1-year (1.04 (1.03–1.04), p < 0.01) and MLVO (2.11 (1.67–2.67), p < 0.01), while treatment with thrombolysis (0.74 (0.59–0.93), p = 0.01) and MT (0.67 (0.50–0.89), p < 0.01) were associated with reduced morbidity. These findings did not differ with exclusion of TIAs from the analysis.
Association between risk factors and increased 3-month mRS score, as determined from our multivariable ordered logistic model, from our full cohort, and a cohort that excluded TIAs.
LAA: left atrial appendage; MLVO: medium or large vessel occlusion; mRS: modified Rankin Scale; MT: mechanical thrombectomy.
Discussion
In our study, the presence of CTA-LAA thrombus detected during acute stroke imaging was both independently associated with 3-month mortality and associated with increased 3-month mRS. Our results suggest CTA-LAA thrombus can be used as an important biomarker for risk and prognosis.
The independent association between LAA thrombus and increased 3-month mortality and morbidity substantiates preliminary findings from previous literature, where stroke patients with LAA thrombus have been shown to have more severe baseline stroke, a higher risk of cardiovascular death (RR: 5.52) and poor clinical outcome defined as mRS score of >3 (RR: 3.73).16,17 There are several possible mechanisms accounting for the increased morbidity in stroke patients with CTA-LAA thrombus. Firstly, the association in our study between CTA-LAA and MLVO suggests that these patients are more likely to have larger infarcts with more severe baseline strokes, translating to worse functional outcome or increased risk of mortality. Secondly, LAA thrombus could be a marker of underlying cardiac disease, which can contribute to poorer outcomes. Thirdly, patients with LAA thrombus are older; however we found this association independent of age. Importantly, our study demonstrates these associations in an acute stroke population not limited to patients with AF. The combination of increased morbidity and mortality outcomes suggests that CTA-LAA thrombus can be used as a radiological biomarker of clinical prognosis.
Our results contrast with those from a recent study of 370 acute stroke and TIA patients, where a higher mRS score in patients with CTA-LAA thrombus (3 (1–6) vs 2 (1–5), p = 0.11) was not statistically significantly. 8 This may be attributed to smaller sample size, with our results being further validated by inclusion of multiple centres, reducing bias. It is notable that this study found a higher rate of LAA thrombus (9%) than both our study (4%) and other similar studies (6.7%). 3 This higher rate could be attributable to differences in imaging techniques used, such as spectral CT reconstructions and iodine maps, potentially increasing diagnostic sensitivity compared to CTA. A change in protocol in our study resulted in 465 patients undergoing non-delayed imaging, which may have contributed to under-detection. It is also possible that non-uniformity in CTA protocols between centres and a retrospective design may have contributed to variability in our study results. Other differences include an older median patient age in our cohort (67 years vs 60), and a lower rate of intravenous thrombolysis in our study (23% vs 36%), though these would not necessarily explain the difference in association between LAA thrombus and outcome.
It is notable that the rate of LAA thrombus was different between our two sites (1.7% in JHH and 6.0% in Christchurch). This difference may be attributable to population differences between the cohorts, including a lower median age (73 (61–80) vs 75 (66–83)) and a higher rate of anticoagulation in the Australian cohort (16% vs 12.5%) despite a lower rate of AF (26% vs 35%) and lower rate of heart failure (8% vs 11%). This difference may also be influenced by differences in local protocols, with Christchurch using stroke severity as the threshold for undertaking hyperacute CT scan, which may selected for higher severity strokes. The lower rate of AF in the JHH cohort is likely the main contributing factor for the lower CTA LAA detection rate between the two groups.
The higher rates of recurrent ischaemic stroke and embolic events in patients with LAA thrombus is hypothesis generating. While this has been explored with transoesophageal echocardiography in non-stroke populations previously, an association between LAA thrombus and recurrent events has not been consistently demonstrated.16,18,19 Due to the low overall recurrent event numbers in our study, this should be considered exploratory and validated in larger, prospective studies.
Validating the use of CTA for left atrial or LAA thrombus identification was not an aim of this study, but CTA has the advantage of being non-invasive, and can be undertaken at the time of an acute stroke imaging protocol. In centres where transoesophageal echocardiogram is not commonly performed, LAA thrombi may not be identified in stroke patients which may lead to an incorrect diagnosis of embolic stroke of undetermined source (ESUS), or cryptogenic stroke. Recent ESUS trials20 –22 assessed the efficacy of oral anticoagulation for secondary stroke prevention in those classified as ESUS or cryptogenic stroke. These trials failed to show a clinical benefit of oral anticoagulation in secondary stroke prevention. The classification of ESUS or cryptogenic stroke in these trials did not include dedicated LAA imaging to investigate a cardioembolic source of stroke, thus potentially missing a biomarker for embolic stroke, which may have masked treatment benefit. Future studies could investigate enriched ESUS cohorts with LAA thrombus assessment to determine the benefit of prolonged cardiac monitoring or anticoagulation.
There were several strengths to our study. This one of the largest studies to focus on the relationship between LAA thrombus in patients presenting with acute stroke/TIA, and their clinical outcomes. We included all consecutive patients undergoing acute stroke imaging within the study timeframe. Inclusion of two centres improved the generalisability of our results at an international level. Finally, the availability of 3-month follow-up data was high (93.3%).
Our study also had limitations. Our patient cohort is selected based on centre-specific practices that determine selection for acute stroke imaging. In terms of imaging, CT was not cardiac-gated in either site during the study period. Furthermore, in Christchurch a change in protocol during the study period meant that the initial 465 patients underwent only non-delayed CTA, which may have reduced sensitivity of diagnosis of LAA thrombus. It is also recognised that the imaging protocols between the two sites, whilst similar, were not identical, with interpretation by separate radiologists, which may have impacted detection rates. Radiologists were not strictly blinded in this study, however the interpretation of LAA thrombus was in isolation to the overall CT imaging and clinical outcome, thus limiting risk for bias. Data collection was non-contemporaneous between the two sites, with Christchurch completing their recruitment a month after JHH started recruiting in 2020, but work-flow between the centres was similar. 23 The primary outcome, mRS, may be subject to inter-observer variability which may have impacted our results. This is perhaps further impacted through the retrospective collection from medical records, as well as influence of prior functional status (noting that 18% of our cohort had a previous stroke). Imaging beyond the LAA was not available in this study, thus some patients with alternate cardioembolic aetiologies (such as left ventricular thrombi) may not be identified. Known history of AF and new AF at presentation were not distinguished. Data on post-stroke antiplatelets and anticoagulant therapy were not available for all patients, thus limiting our analysis of recurrent ischaemic stroke or embolic events.
Conclusions
Our results suggest LAA thrombus identified on acute stroke CTA imaging has potential to be an easily obtainable and clinically meaningful prognostic biomarker of morbidity and mortality. The role of CTA-LAA thrombus in recurrent ischaemic stroke or embolic events needs to be investigated in future larger, prospective studies.
Supplemental Material
sj-docx-1-eso-10.1177_23969873251377215 – Supplemental material for The clinical association of left atrial appendage thrombus on CTA with functional outcome
Supplemental material, sj-docx-1-eso-10.1177_23969873251377215 for The clinical association of left atrial appendage thrombus on CTA with functional outcome by Joel Winders, Angelo Di Bartolo, Jamin Kim, Duncan Wilson, Sajith Senadeera, Yassar Alamri, John Fink, James Beharry, Mark W Parsons, Christopher Levi, Neil Spratt, Beng Lim Alvin Chew, Md Golam Hasnain, Ferdinand Miteff, Leon Rinkel, Shan Sui Nio, Sinan Al-Hadethi, Anthony Lim, Jonathan Coutinho, Carlos Garcia-Esperon, Teddy Y Wu and Alexander Berry-Noronha in European Stroke Journal
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Carlos Garcia-Esperon has received travel funding for travel for conferences from Boehringer Ingelheim and Bayer and speaker honoraria from Astra Zeneca, outside the submitted work. Alexander Berry-Noronha has received research funding from the Neurological Foundation of New Zealand, outside the submitted work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has received funding from the Greater Charitable Foundation (Australia), Heart and Stroke program (Hunter Medical Research Institute, Australia) and NSW Office for Health and Medical Research Cardiovascular Research Collaborative Grant. It is also supported by an Australian Government Research Training Program (RTP) Scholarship.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Guarantor
Alexander Berry-Noronha.
Contributorship
Joel Winders: data collection, data acquisition, drafting and revision. Angelo Di Bartolo: data collection, data acquisition, drafting and revision. Jamin Kim: data collection, data acquisition and revision. Duncan Wilson: study conception, data collection, drafting, data analysis and revision. Sajith Senadeera: data collection, data acquisition. Yassar Alamri: review of draft/revision. John Fink: review of draft/revision. James Beharry: data acquisition and review of draft/revision. Mark W Parsons: data acquisition and review of draft/revision. Christopher Levi: data acquisition and review of draft/revision. Neil Spratt: data acquisition and data collection, review of draft/revision. Beng Lim Alvin Chew: data acquisition, data collection, review of draft/revision. Md Golam Hasnain: data acquisition, data collection, review of draft/revision. Ferdinand Miteff: data acquisition, data collection, review of draft/revision. Leon Rinkel: data acquisition and review of draft/revision. Shan Sui Nio: data acquisition and review of draft/revision. Sinan Al-Hadethi: data acquisition, data collection, review of draft/revision. Anthony Lim: data acquisition, data collection, review of draft/revision. Jonathan Coutinho: data acquisition and review of draft/revision. Carlos Garcia-Esperon: study conception, data collection, drafting, conception of work and review of draft/revision. Teddy Y Wu: study conception, data collection, drafting, review of draft/revision. Alexander Berry-Noronha: conception of work, data acquisition, analysis, drafting and revision.
Data availability statement
Further data is available from the authors on request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.