
Abstract
Introduction:
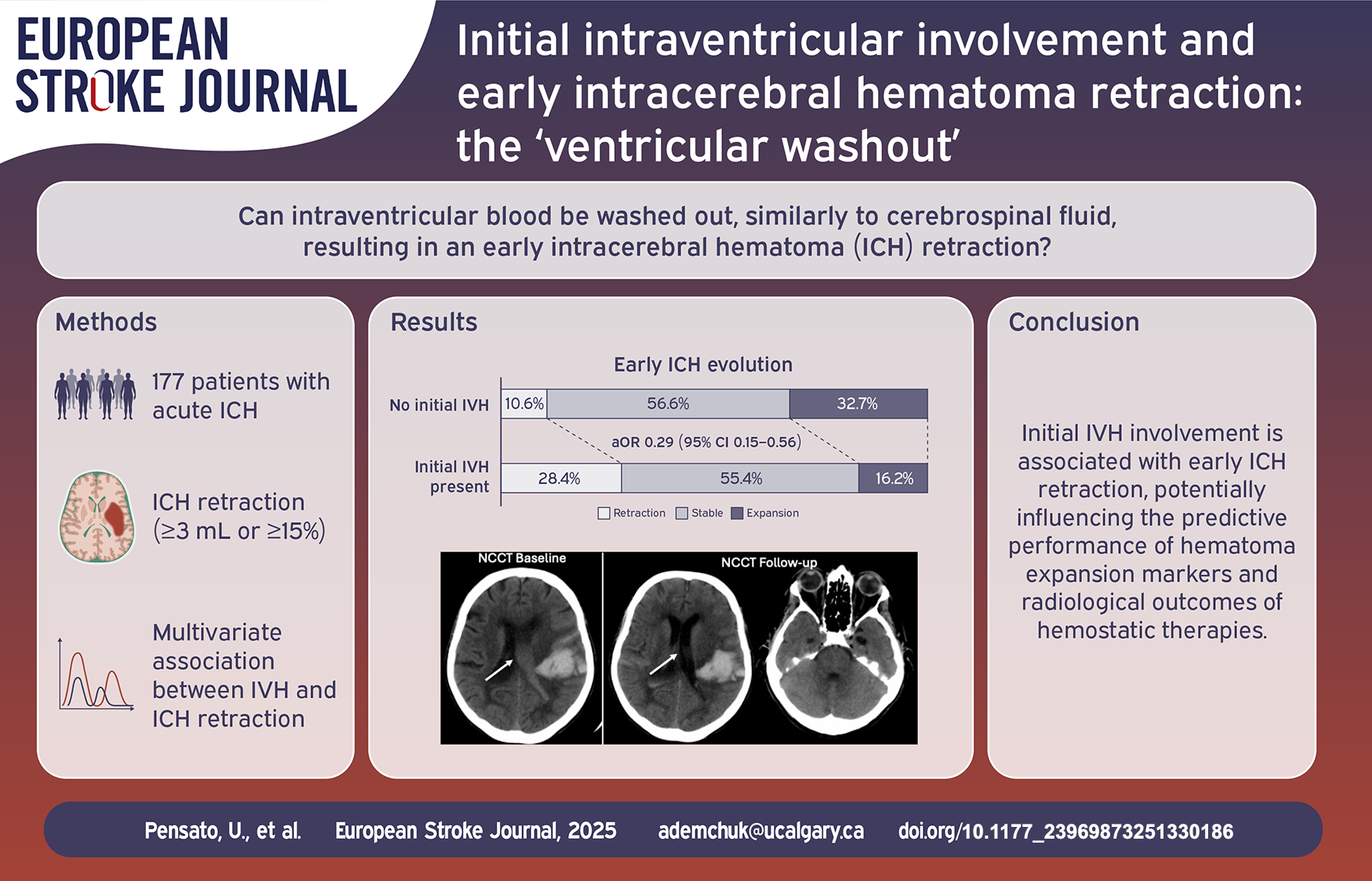
Intraventricular hematoma (IVH) occurs in approximately 40% of acute intracerebral hemorrhage (ICH) patients and is significantly associated with worse clinical outcomes. According to cerebrospinal fluid dynamics, some blood within the ventricles may circulate through the subarachnoid spaces, leading to its apparent “disappearance” on follow-up imaging. We aim to investigate the association between initial IVH involvement and significant early ICH retraction at follow-up imaging.
Methods:
Data are from the MCAHP (Multiphase CT Angiography Hematoma Prediction) Study, which included consecutive patients with acute ICH investigated with multimodal CT imaging. Patients who underwent surgery before follow-up imaging were excluded. IVH severity was assessed using the IVH score. The primary outcome was significant early ICH retraction, defined as volume decrease (⩾3 ml or ⩾15%) between the initial and follow-up scans. Secondary outcomes included early absolute and relative ICH decrease. Associations between outcomes and initial IVH involvement or IVH score were assessed with logistic regression adjusted for age, baseline NIHSS, initial ICH volume, and onset-to-CT time.
Results:
Overall, 177 ICH patients were included. The median age was 71 years (IQR = 59–80), 71 (40.1%) patients were female, and 64 (36.2%) presented with initial IVH involvement. Patients with initial IVH, compared to those without, had a larger initial ICH volume (28.5 ml [IQR = 12.7–52.5] vs. 18.9 ml [IQR = 8.1–30.6], p < 0.001) and different ICH location (deep = 54.7% vs 47.8%; lobar = 35.9% vs 46.0%; infratentorial = 7.3% vs 6.2%; p < 0.001). Early ICH retraction was observed in 33 (18.6%) patients: 21 (32.8%) with initial IVH and 10 (10.6%) without initial IVH. There was a significant association between early ICH retraction and initial IVH involvement (adjusted odds ratio [aOR] 4.02 [95% CI = 1.72–9.41]) and IVH score (aOR 1.14 [95% CI = 1.05–1.23] per 1-point increase). Similar results were observed for secondary outcomes.
Conclusion:
Initial IVH involvement is associated with early ICH retraction – “intraventricular washout.” This might result in an underestimation of hematoma expansion occurrence and severity in these patients, with potential implications when evaluating the predictive performance of hematoma expansion markers/scores and the radiological efficacy of hemostatic treatments.
Keywords
Introduction
Hemorrhagic stroke is a leading cause of death and disability worldwide. 1 Hematoma expansion (HE) – a significant increase in intracerebral hematoma (ICH) volume between baseline and follow-up imaging – represents the primary target for hyperacute management and a widely accepted radiological surrogate outcome for evaluating hyperacute treatment effectiveness. 2 The extension of the intraparenchymal hematoma (IPH) into the ventricular system occurs in approximately 40% of patients and is associated with poorer outcomes.3–5 Including blood within the ventricular system in the total ICH volume count improves the evaluation of HE occurrence and severity. 6
Physiologically, cerebrospinal fluid (CSF) circulates from the ventricles through the cranial and spinal subarachnoid spaces before being reabsorbed by the arachnoid villi and the glymphatic system.7,8 Because of these CSF dynamics, intraventricular hematomas (IVH) could get “washed out” of the ventricles and diluted in the subarachnoid spaces. As a result, some blood could seemingly “disappear” on follow-up imaging (Figure 1). This phenomenon can potentially result in underestimating HE occurrence and severity, with research implications.
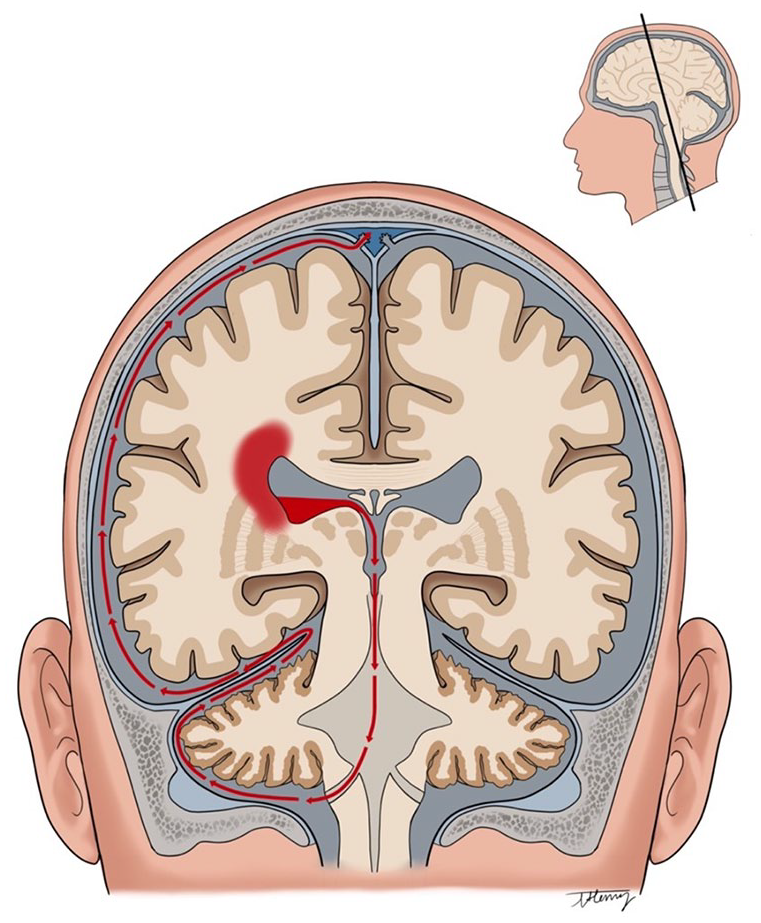
Illustration of the “ventricular washout” in intracerebral hemorrhage patients with initial intraventricular hematoma involvement. Blood circulates from the ventricles through the cranial and spinal subarachnoid spaces before being reabsorbed by the arachnoid villi and the glymphatic system.
We aim to investigate the association between initial IVH involvement and early ICH retraction, defined as shrinkage of the ICH volume (IPH + IVH) from baseline to follow-up, in patients with acute ICH.
Materials and methods
Standard protocol approval, registrations, and patient consent
The ethics committee at the University of Calgary approved the study (approval protocol number: REB17-0573). In accordance with ethical guidelines, informed consent was waived for this study due to its retrospective nature. All procedures followed the latest version of the Declaration of Helsinki.
Patient sample and study design
Data used in this study derived from the MCAHP (Multiphase CT Angiography Hematoma Prediction) Study which included consecutive adult patients admitted to the Foothills Medical Centre in Calgary, Canada, between February 2012 and May 2020 with confirmed acute ICH.
The design and inclusion criteria of the study have been published elsewhere. 9 In brief, the study included all patients with (i) primary spontaneous intraparenchymal hemorrhage, (ii) baseline multimodal imaging (non-contrast CT plus multiphase CT angiography) performed within 12 h from symptom onset, (iii) follow-up imaging (CT or MRI) performed 12–72 h post-baseline, and (iv) no hematoma evacuation performed before follow-up imaging. Patients were managed with a bundle of care interventions according to local protocols and international guidelines. No standardized protocol was adopted for head positioning during the first 72 h following the onset of stroke symptoms.
For the current study, we excluded patients who received a surgical intervention to place an external ventricular drainage (EVD), as it can contribute to diminishing the ventricular component of the ICH. Moreover, we excluded patients with an initial ICH volume ⩽ 3 ml due to potential challenges and measurement errors in accurately estimating a volume reduction over time in such small hematomas.
Image acquisition and analysis
All patients underwent a comprehensive acute stroke imaging protocol, including NCCT and multiphase CTA, using Discovery CT 750HD or Revolution CT (GE Healthcare, Milwaukee, WI). Hematoma volumes at baseline (initial volume) and follow-up (final volume) were quantified using the semi-automatic segmentation software Quantomo (Cybertrial Inc, Calgary, Canada), which has been validated for accurate ICH volume analysis. 10 Both intraparenchymal and intraventricular components were included in the total ICH volume (ICH = IPH + IVH). Early ICH decrease was defined as the difference between initial (baseline) ICH volume and follow-up ICH volume. To maintain consistency and avoid negative ICH decrease results, cases where the follow-up ICH volume was larger than the initial volume were defined as having a 0 ml decrease.
Initial IVH involvement was defined as the presence of blood inside the ventricular system on the baseline NCCT. IVH severity was assessed using the modified Graeb Score 11 or IVH score 12 on the baseline NCCT. The IVH score ranges from 0 to 23 and assigns up to 3 points each for the right ventricle (RV) and left ventricle (LV) based on the extent of blood filling in the ventricles (1-point: up to one-third; 2-points: one to two-thirds; 3-point: most of the ventricle), 1-point for the presence of blood in third (III) ventricle, 1 point for the presence of blood in the fourth (IV) ventricle and 3 points for the presence of hydrocephalus. The total IVH score is calculated with the following formula:

Significant early ICH retraction (IPH + IVH) was defined as a hematoma volume decrease of at least 3 ml or 15% between the initial and follow-up volumes. These thresholds were selected based on the sole previous study addressing early hematoma retraction. 13 Hematoma volume changes were further evaluated both categorically and continuously. For the categorical classification, hematoma changes were defined as follows: (i) significant early hematoma retraction (a volume decrease of ⩾ 3 ml or ⩾ 15%), (ii) stable hematoma (a volume decrease of <3 ml or <15% and a volume increase <6 ml or <33%), and (iii) hematoma expansion (a volume increase of ⩾6 ml or ⩾33%). 2 For the continuous classification (early absolute and relative hematoma decrease), we assigned a value of 0 ml decrease in all cases where the follow-up ICH volume was larger than the initial volume to avoid reporting negative ICH decrease results.
Outcomes
The primary outcome was early ICH retraction. Secondary outcomes included substantial early ICH retraction, defined as a hematoma volume decrease of at least 6 ml or 33% (mirroring the standard hematoma expansion definition), 2 and early absolute (in ml) and relative (in %) ICH decreases as continuous variables. Moreover, we evaluated the early ICH evolution (retraction, stable, expansion).
Statistical analysis
Continuous variables were presented as medians and interquartile ranges (IQR), while categorical variables were reported as counts and percentages. Baseline clinical and radiological features, as well as radiological outcomes, were compared between patients with and without IVH on baseline NCCT. Univariable comparisons were conducted using Fisher’s exact test for categorical variables and Wilcoxon rank-sum test for continuous variables.
Associations between initial IVH involvement and outcomes were assessed using logistic regression analyses (binary, ordinal, or linear as appropriate), and adjusted for age, baseline NIHSS, initial ICH volume, and onset-to-CT time. Effect size estimates from logistic regression analyses were reported as adjusted odds ratios (OR) or beta-coefficients with 95% confidence intervals (95% CI). The ORs reported in this study represent the odds of outcomes for having initial IVH extension, with no initial IVH extension as the reference category. Linear regression assumptions, and particularly the normal distribution of residuals, were assessed with PP-plots, QQ-plots, kernel density plots, and the Shapiro-Francia-Wilk text analyses.
Since the last detectable location of intraventricular blood on the head CT is supposed to be the fourth ventricle before it circulates into the subarachnoid spaces,7,8 as part of a sensitivity analysis, we assessed the association between initial blood in the fourth ventricle and outcomes, as well as between initial IVH score and outcomes.
All calculated p-values were two-tailed. Statistical significance was assumed at p < 0.05. The statistical analysis was performed with Stata (Version 18.0).
Results
Patient characteristics
Of 217 patients enrolled in the MCAHP study, six patients were excluded due to early placement of EVD, and 34 patients were excluded due to initial ICH volume < 3 ml (Supplemental Figure 1). Overall, 177 patients were included in the study sample, and their demographics and baseline characteristics are summarized in Table 1. The median age was 71 years (IQR = 59–80), 71 (40.1%) patients were female, 64 (36.2%) presented with initial IVH involvement, and 21 (11.9%) presented with initial blood in the IV ventricle.
Demographics and baseline features of patients with and without initial IVH involvement.

IVH: intraventricular hematoma; IQR: interquartile range; NIHSS: National Institution of Health Stroke Scale; GCS: Glasgow Coma Scale; ICH: intracerebral hemorrhage. Signicant p-values are marked in bold.
Data available for 165 patients.
Patients with initial IVH involvement, compared to those without, had a larger initial ICH volume (28.5 ml [IQR = 12.7–52.5] vs 18.9 ml [IQR = 8.1–30.6], p < 0.001) and different ICH location (deep = 54.7% vs 47.8%; lobar = 35.9% vs 46.0%; infratentorial = 7.3% vs 6.2%; p < 0.001). Other demographics and baseline characteristics were similar between the two groups (Table 1).
Similarly, patients with initial blood in the fourth ventricles, compared to those without, had a larger initial ICH volume (32.8 ml [IQR = 13.0–52.0] vs 21.4 ml [IQR = 8.9–35.0]), p = 0.041), and different ICH locations (deep = 57.1% vs 49.4%; lobar = 19.0% vs 45.5%; infratentorial 23.8% vs 5.1%; p < 0.001). Other demographics and baseline characteristics were similar between the two groups (Supplemental Table 1).
Association between initial IVH involvement and outcomes
Significant early ICH retraction (⩾3 ml or ⩾15%) was observed in 33 (18.6%) patients, substantial early ICH retraction (⩾6 ml or ⩾33%) in 12 (6.8%), ICH expansion 49 (27.7%), and no early ICH retraction or expansion in 95 (53.7%). The median early absolute ICH decrease was 0 ml (IQR = 0–1.2), and the median early relative ICH decrease was 0% (IQR = 0–7).
There was a significant association between initial IVH involvement and significant early ICH retraction (adjusted OR 4.02 [95% CI = 1.72–9.41]) and substantial early ICH retraction (adjusted OR 7.94 [95% CI = 1.60–39.72]). There was a significant positive relationship between initial IVH involvement and early absolute ICH decrease (adjusted Beta-Coefficient 1.69 [95% CI = 0.69–2.69]) and early relative ICH decrease (adjusted Beta-Coefficient 0.07 [95% CI = 0.03–0.10]; Table 2). There was a significant association between initial IVH involvement and early ICH evolution: aOR 0.29 (95% CI = 0.15–0.56; Figure 2).
Association between initial IVH involvement and outcomes.

IVH: intraventricular hematoma; ICH: Intracerebral hematoma; CI: confidence intervals.
Adjusted for age, baseline NIHSS, baseline ICH volume, and onset-to-imaging time.
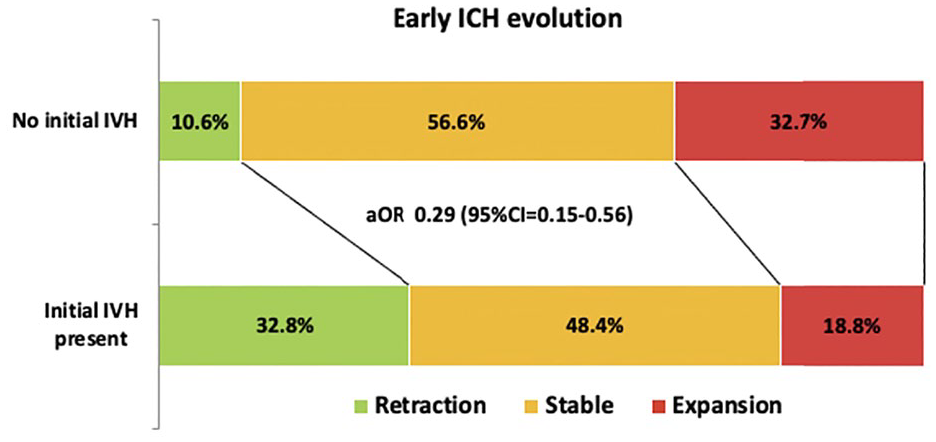
Distribution of early ICH evolution across patients with versus without initial IVH involvement.
An exemplary case of initial IVH associated with early ICH retraction is shown in Figure 3.
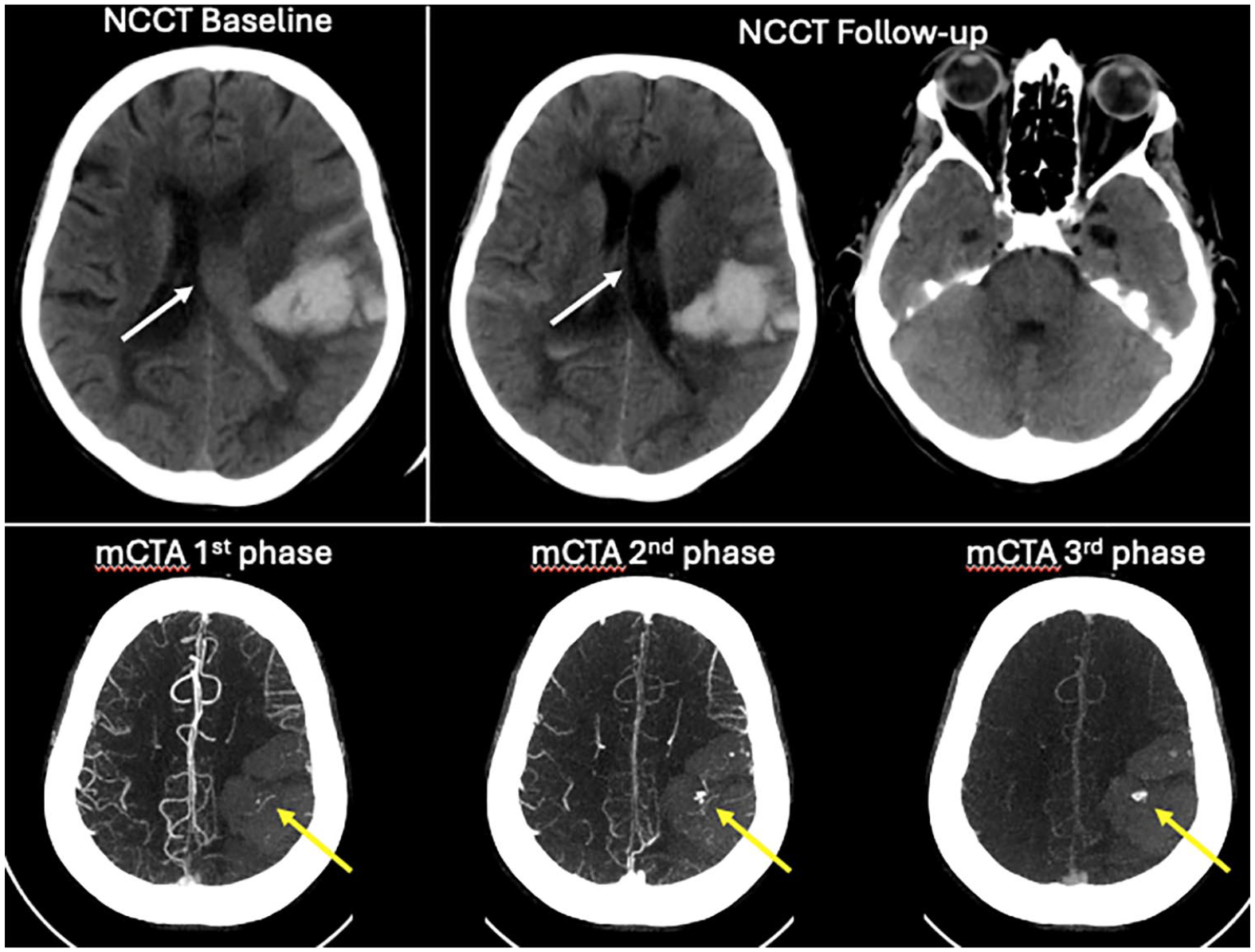
Exemplary case of “intraventricular washout phenomenon.”
Sensitivity analysis in patients with initial blood in the fourth ventricle
There was a significant association between initial blood in the fourth ventricle and significant early ICH retraction (adjusted OR 4.73 [95% CI = 1.58–14.20]) and substantial early ICH retraction (adjusted OR 5.58 [95% CI = 1.34–23.30]). There was a significant positive relationship between initial IVH involvement and early absolute ICH decrease (adjusted Beta-Coefficient 1.89 [95% CI = 0.34–3.44) and early relative ICH decrease (adjusted Beta-Coefficient 0.08 [95% CI = 0.02–0.13]; Table 3). There was a significant association between initial blood in the fourth ventricle and early ICH evolution: aOR 0.24 (95% CI = 0.09–0.65; Supplemental Figure 2).
Association between initial blood in the fourth ventricle and outcomes.

OR: odds ratio; CI: confidence intervals.
Adjusted for age, baseline NIHSS, baseline ICH volume, and onset-to-imaging time.
Sensitivity analysis for initial IVH score
Among patients with initial IVH involvement, the median initial IVH score was 9 (IQR = 6–13). There was a significant association between initial IVH score and significant early ICH retraction (adjusted OR 1.14 [95% CI = 1.05–1.23] per 1-point increase) and substantial early ICH retraction (adjusted OR 1.19 [95% CI = 1.06–1.33] per 1-point increase; Figure 4). There was a significant positive relationship between the initial IVH score and early absolute ICH decrease (adjusted Beta-Coefficient 0.17 [95% CI = 0.07–0.26] per 1-point increase) and early relative ICH decrease (adjusted Beta-Coefficient 0.01 [95% CI = 0.01–0.01] per 1-point increase). Results were similar when IVH extension was assessed with the modified Graeb Score (Supplemental Materials).
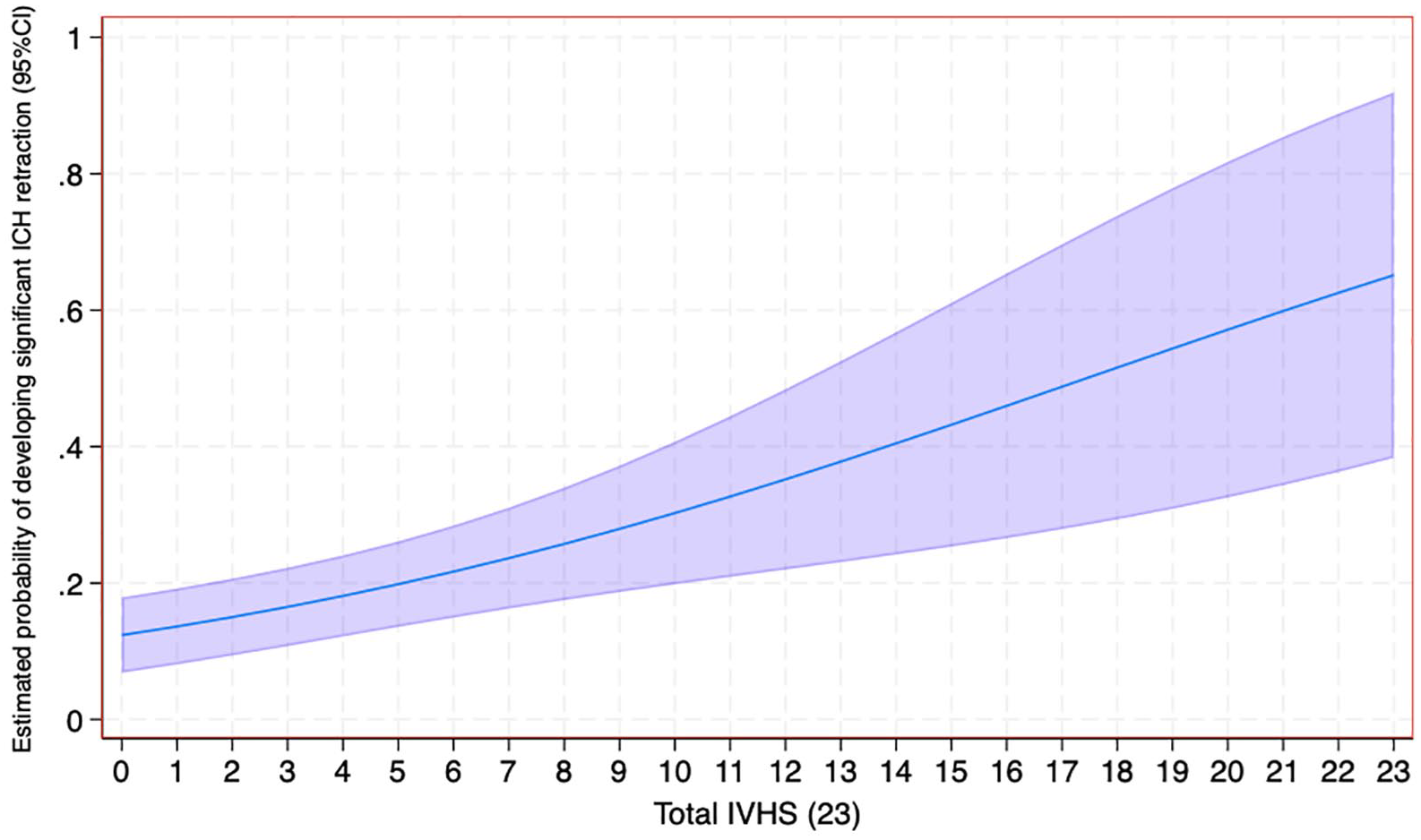
Association between total Intraventricular Hematoma (IVH) score and estimated probability of developing early significant ICH retraction (⩾3 ml or ⩾15%).
Association between functional outcomes and early ICH retraction
There were no differences in functional outcomes at 3-month between patients with versus those without early ICH retraction (Supplemental Materials).
Discussion
In our cohort, significant early ICH retraction, defined as shrinkage of the ICH volume (IPH + IVH) from baseline to follow-up, was observed in a small subset of patients (18.6%). Initial IVH involvement was associated with a fourfold increase in the probability of developing early ICH retraction. This robust association remained consistent across multiple secondary outcomes and in the sensitivity analysis.
Hematoma retraction is a physiological process in the evolution of ICH, typically occurring over several days to weeks as a result of hemostasis. 14 Therefore, while it is possible that patients with initial IVH may exhibit a different hemostatic profile than those without initial IVH, its impact on early hematoma retraction in our cohort is likely minimal. Conversely, early hematoma retraction occurrence suggests a rapid blood redistribution beyond the hematoma volume. CSF circulates from the ventricle to the cerebral and spinal subarachnoid spaces to be reabsorbed by the arachnoid villi and the glymphatic system, resulting in a complete turnover of the CSF approximately every 8 h. 7 One would assume that blood components within the ventricles in acute ICH may also follow this pathway, contributing to early ICH retraction. Our data support this hypothesis, indicating that the presence and severity of IVH involvement correlate with the degree of “apparent” early hematoma shrinkage – “ventricular washout” phenomenon.
A previous study explored ICH retraction, defined as a hematoma decrease of at least 3 ml, in a cohort of 136 acute ICH patients. 13 In that study, hematoma retraction occurred in 4.6%, with initial IVH involvement as the only independent predictor. Contrary to the authors’ initial hypothesis, no significant association was observed between better clinical outcomes and ICH retraction. 13 This is in line with results from our study and with the association of ICH retraction with IVH involvement, which can lead to complications such as impaired CSF resorption with obstructive hydrocephalus and aseptic meningitis. 15
Our findings have research implications: initial IVH involvement may result in an underestimation of both the occurrence and severity of HE. This underestimation is particularly critical when assessing the predictive performance of hematoma expansion markers and scores.16,17 Moreover, since hematoma expansion is a widely adopted radiological outcome of clinical trials exploring hemostatic treatments, 2 this oversight could hamper the radiological efficacy of such therapies. Future studies should aim to validate our findings and define a corrective factor when evaluating hematoma expansion in patients with initial IVH, as no or minimal hematoma increase in patients with IVH, which current definitions fail to capture as hematoma expansion,2,18,19 may actually indicate an expansion. Accordingly, the proportion of HE was lower in patients with initial IVH extension in our cohort. Moreover, hematoma expansion markers and score should be evaluated separately in patients with and without initial IVH and anti-hematoma expansion trials should ensure a balanced representation of patients based on the presence of initial IVH involvement.
Our study has several limitations. First, we did not separately measure the volumes of intraparenchymal and intraventricular hematomas, limiting our ability to determine the relative contribution of each component to the hematoma volume decrease in follow-up. However, a recent study showed difficulties in volumetric analyses of intracranial hematomas by compartments, suggesting that total volume measurements may be more feasible and reliable. 20 Second, we did not investigate the extension of IVH at follow-up, which could also lead to an underestimation of the severity of the HE. 3 Third, we excluded patients with very small hematomas, which could have biased the patient sample toward sicker, more severely affected patients. Fourth, we excluded patients who underwent EVD placement before follow-up imaging. These patients likely experienced the most severe initial IVH involvement, 15 potentially introducing a selection bias in our cohort. Fifth, we have not assessed the potential contributing role of peri-hematoma edema. Finally, follow-up imaging timing and modality were not homogeneous in our study, which reflected clinical practice.
Conclusions
Initial IVH involvement is associated with a fourfold probability of showing significant early ICH retraction. This “intraventricular washout” may result in an underestimation of hematoma expansion occurrence and severity in these patients, with potential implications when evaluating the predictive performance of hematoma expansion markers/scores and the radiological efficacy of hemostatic treatments. Further studies are needed to validate our findings and better characterize the relationship between IVH involvement and ICH volume changes.
Supplemental Material
sj-docx-1-eso-10.1177_23969873251330186 – Supplemental material for Initial intraventricular involvement and early intracerebral hematoma retraction: The “ventricular washout”
Supplemental material, sj-docx-1-eso-10.1177_23969873251330186 for Initial intraventricular involvement and early intracerebral hematoma retraction: The “ventricular washout” by Umberto Pensato, Chitapa Kaveeta, Koji Tanaka, Johanna M Ospel, Mohamed A AlShamrani, MacKenzie Horn, Dar Dowlatshahi, Girish Kulkarni, Ericka Teleg, Abdulaziz Sulaiman Al Sultan, Linda Kasickova, Tomoyuki Ohara, Piyush Ojha, Sina Marzoughi, Bijoy K Menon, Mayank Goyal and Andrew M Demchuk in European Stroke Journal
Footnotes
Acknowledgements
We would like to thank Tyler Henry (Division of Neurology, Dalhousie University, Halifax, Canada) for his valuable contribution in designing ![]() . We would like to thank the following individuals, who are part of the MCAHP Stroke Group, for their contribution to the study: Ankur Banerjee, David Rodriguez-Luna, Sanchea Wasyliw, Kennedy Horn, Amy Bobyn, Anneliese Neweduk, Nishita Singh, Wu Qiu,
. We would like to thank the following individuals, who are part of the MCAHP Stroke Group, for their contribution to the study: Ankur Banerjee, David Rodriguez-Luna, Sanchea Wasyliw, Kennedy Horn, Amy Bobyn, Anneliese Neweduk, Nishita Singh, Wu Qiu,
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the ethics committee at the University of Calgary (Approval number: REB17-0573).
Informed consent
In accordance with ethical guidelines, informed consent was waived for this study due to its retrospective nature.
Guarantor
AMD
Contributorship
UP and AMD conceived the study. UP drafted the manuscript. All Authors contributed to data acquisition, reviewed and edited the manuscript, and approved the final version of the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.