
Abstract
Background:
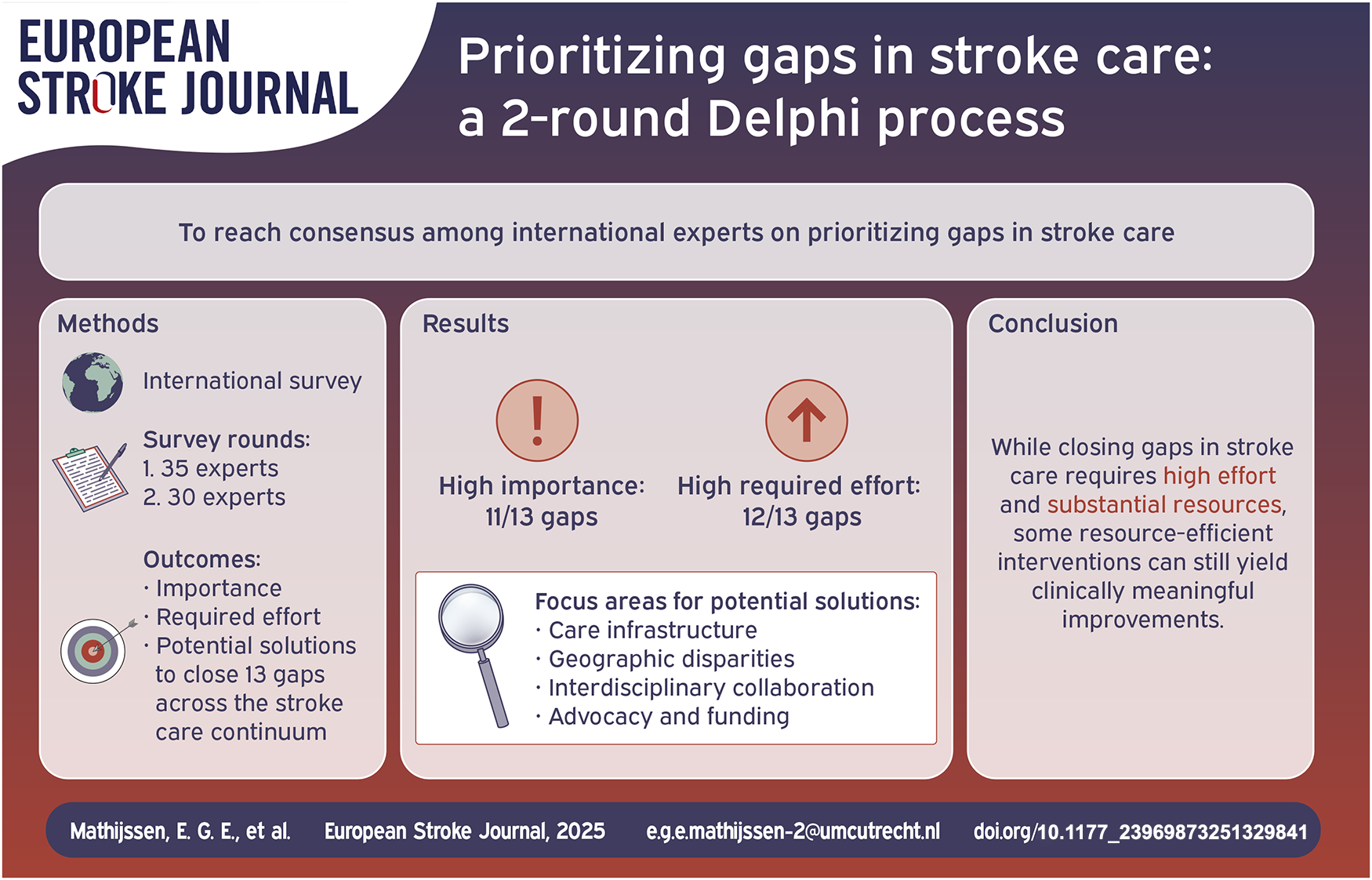
Despite international recognition of stroke as a significant health priority, discrepancies persist between the target values for stroke quality measures and the actual values that are achieved in clinical practice, referred to as gaps. This study aimed to reach consensus among international experts on prioritizing gaps in stroke care.
Methods:
A two-round Delphi process was conducted, surveying an international expert panel in the field of stroke care and cerebrovascular medicine, including patient representatives, healthcare professionals, researchers, policymakers, and medical directors. Experts scored the importance and required effort to close 13 gaps throughout the stroke care continuum and proposed potential solutions. Data were analyzed using descriptive statistics and qualitative analysis methods.
Results:
In the first and second Delphi rounds, 35 and 30 experts participated, respectively. Expert consensus was reached on the high importance of closing 11 out of 13 gaps. Two out of 13 gaps were considered moderately important to close, with expert consensus for one of these two gaps. Expert consensus indicated that only one gap, related to the prevention of complications after stroke, requires moderate effort to close, whereas the others were considered to require high effort to close. Key focus areas for potential solutions included: “Care infrastructure,” “Geographic disparities,” “Interdisciplinary collaboration,” and “Advocacy and funding.”
Conclusions:
While closing gaps in stroke care primarily requires high effort and substantial resources, targeted interventions in the identified key focus areas may provide feasible and clinically meaningful improvements.
Introduction
Stroke, the world’s second leading cause of death, 1 is internationally recognized as a significant health priority, 2 contributing to substantial morbidity and long-term disability.3,4 An alarming one in four people is at risk of experiencing a stroke in their lifetime. Moreover, the burden of stroke on already overstretched health systems has intensified in recent years due to ageing populations and an increasing prevalence of modifiable risk factors (e.g. hypertension, overweight, and smoking). 5
Clinical practice guidelines have been established by professional organizations worldwide to provide recommendations for evidence-based interventions regarding the prevention and treatment of stroke.6–11 However, the implementation and integration of these guidelines in clinical practice often encounters challenges due to resource constraints (e.g. workforce shortages, care infrastructure inequalities, and financial restrictions). 12 Consequently, there is considerable variability in the quality of stroke care both within and between countries.
Stroke registries are now widely implemented for quality monitoring and improvement.13–16 For example, the American Heart Association’s Get With The Guidelines – Stroke Program is one of the most extensive and enduring initiatives that registers data to promote consistent adherence to clinical practice guidelines. 13 Stroke registries use various quality measures (e.g. the proportion of stroke patients who received antithrombotic therapy within 2 days of symptom onset) to provide actionable information for health systems seeking to improve the quality of stroke care.16,17 However, persisting discrepancies between the target values for stroke quality measures and the actual values that are achieved in clinical practice, referred to as gaps, indicate quality issues that need to be addressed. 18
Given the resource constraints present within health systems, gaining a comprehensive understanding of and prioritizing the most pressing challenges in stroke care has significant potential to inform policymaking and resource allocation decisions. Therefore, this study aimed to reach consensus among international experts on prioritizing gaps in stroke care.
Methods
Study design
A Delphi process, based on the RAND/UCLA appropriateness method, 19 was conducted between October 2022 and January 2023 to reach consensus among international experts on prioritizing gaps in stroke care. This well-established method for reaching consensus among groups mitigates individual biases through iterative rounds of surveying. Its structured nature, combined with anonymized responses and controlled feedback, facilitates reliable results. 19 For this study, two iterations were chosen, as this number is generally sufficient to reach expert consensus, while minimizing sample fatigue. 20 This study was reported in accordance with the Guidance on Conducting and Reporting Delphi Studies checklist. 21
Expert panel
Experts were purposefully selected based on their extensive and notable academic and scholarly contributions (e.g. involvement in guidelines committees) in the field of stroke care and cerebrovascular medicine. They included patient representatives, healthcare professionals, researchers, policymakers, and medical directors. A diverse expert panel was sought in terms of geographic and clinical backgrounds. Initially, experts were selected from the following countries: United States (US), United Kingdom (UK), Ireland, Germany, Austria, Switzerland, France, Japan, and China. This initial selection was driven by practical considerations and ease of access to experts. Subsequently, experts from other countries were selected to increase the number of responses and ensure a more balanced representation of perspectives, contributing to the validity and generalizability of this study. The sample size was set at a minimum of 20 experts, a number that is generally sufficient for this type of research.19,22 Experts received an e-mail invitation and study information sheet, outlining the rationale and methods of this study (Supplementary file 1). They were informed that participation was voluntary and anonymous. Each expert was invited to participate in the second Delphi round, regardless of whether they had participated in the first Delphi round. This approach facilitates a diverse expert panel and reduces the risk of false consensus by mitigating the loss of non-random perspectives. 23
Data collection
Gaps were identified by reviewing (inter)national and regional quality improvement programs (e.g. the Action Plan for Stroke in Europe) and stroke registries that had published data in the preceding 5 years (Supplementary file 2). Publications were screened to identify gaps, which were then selected for surveying in this study through discussions within the coordinating research team (EM, ES, JR, and JT). In each Delphi round, experts received a survey to complete at their convenience within a four-week timeframe. Up to three e-mail reminders were sent to encourage completion. Additionally, experts were given the opportunity to be listed as co-authors on the current article, contingent on their compliance with the International Committee of Medical Journal Editors recommendations for authorship. The surveys were distributed via an email link, using the Castor electronic data capture system.
Delphi round 1
The first survey commenced with a general introduction and instructions for completing the survey. Additionally, a general definition of gaps in stroke care was provided, namely “persisting discrepancies between the target values for stroke quality measures and the actual values that are achieved in clinical practice.” Four questions on demographic characteristics and 13 gaps, covering the domains of primary prevention (n = 1), emergency care (n = 2), (acute) in-hospital care (n = 6), secondary prevention (n = 1), rehabilitation (n = 1), community reintegration (n = 1), and organization of stroke care services (n = 1), were included. The survey was pre-tested by an independent researcher to assess the clarity of the questions and response options and identify potential technical issues. Supplementary file 3 includes the first survey. Experts were asked to score the importance and required effort to close gaps on a 9-point Likert scale. The importance of closing a gap was classified based on the median scores: low importance (median of 1, 2 or 3), moderate importance (median of 4, 5 or 6), and high importance (median of 7, 8 or 9). Similarly, the required effort of closing a gap was classified based on the median scores: low required effort (median of 1, 2 or 3), moderate required effort (median of 4, 5 or 6), and high required effort (median of 7, 8 or 9). Experts could elaborate on their scores in free-text fields. They had the opportunity to propose additional gaps and skip questions by selecting the “Not my area of expertise” checkbox. Interquartile ranges (IQRs) were calculated to determine the level of expert consensus, with an IQR ⩽ 2 pre-defined as expert consensus. The use of IQRs allowed for the identification of gaps where experts were most aligned in their scores, providing a robust measure of consensus in accordance with the RAND/UCLA appropriateness method. 19 Gaps with scores indicating high importance and low required effort were considered the prioritized targets for quality improvement in stroke care.
Delphi round 2
Experts received a summary of their responses to the first survey and were asked to consider their opinion in light of the group’s collective opinion. The second survey had practically the same design as the first survey but included only those gaps for which no expert consensus, that is, IQR > 2, was reached in the first Delphi round. Additionally, experts were explicitly asked to propose potential solutions.
Data analysis
Descriptive statistics were used to analyze and present the quantitative data. The analysis was performed with R Analytics Software. Qualitative data were reviewed and briefly summarized by one researcher (ES) and checked for accuracy by a second researcher (EM). Quotes were selected to illustrate the results.
Results
Expert panel
Thirty-five experts participated in the first Delphi round, representing a response rate of 14.9% (35/235). The second survey was completed by 30 experts (response rate 14.3%, 30/210). Twenty-five experts were not invited to participate in the second Delphi round for various reasons (e.g. invalid e-mail address). Demographic characteristics of the expert panel are shown in Table 1.
Demographic characteristics of the expert panel.
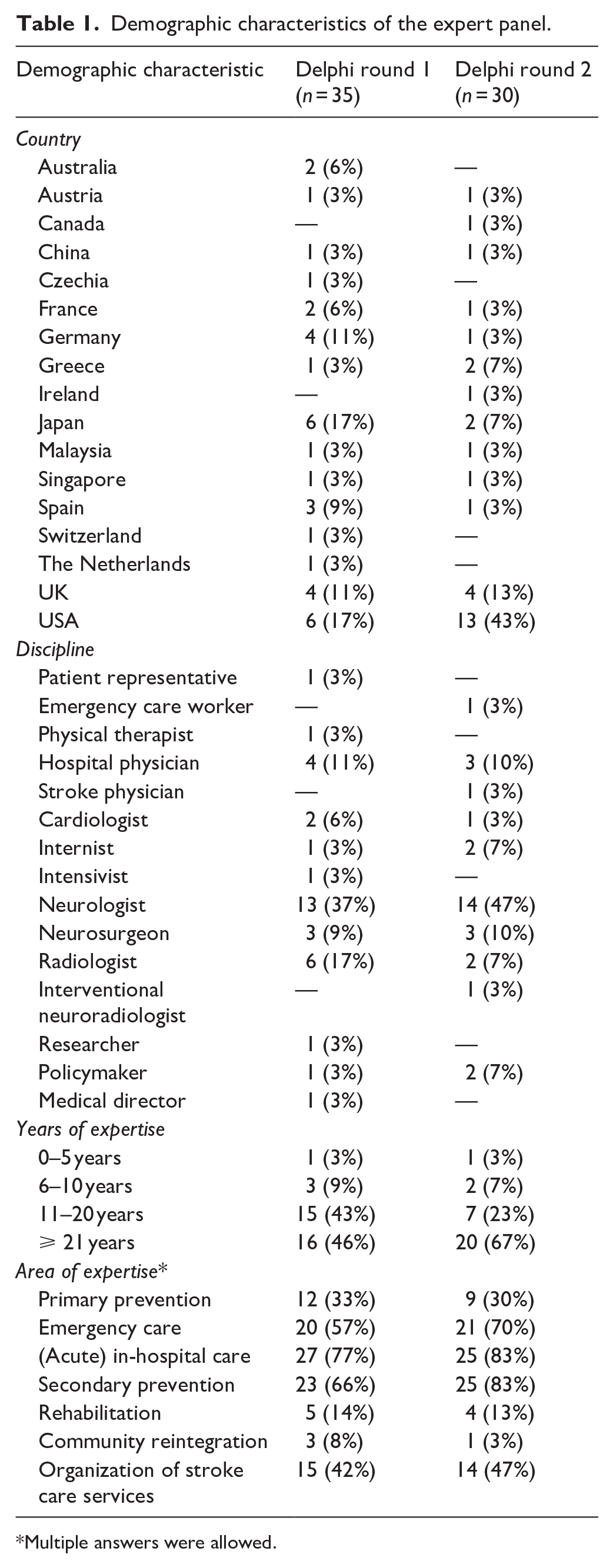
Multiple answers were allowed.
Delphi round 1
Experts scored the importance and required effort to close 13 gaps (Table 2). Eleven out of 13 gaps were considered highly important to close, with expert consensus for eight of these 11 gaps. Two out of 13 gaps were considered moderately important to close, without expert consensus for either. Eleven out of 13 gaps were considered to require high effort to close, with expert consensus for six of these 11 gaps. Two out of 13 gaps were considered to require moderate effort to close, with expert consensus for one of these two gaps. Notably, experts did not propose any additional gaps beyond those already included in the first survey or deemed relevant at an international level.
The results of Delphi round 1 and 2 (color coding: green/orange/red for high/moderate/low importance and green/orange/red for low/moderate/high required effort; an IQR in italics indicates no expert consensus).
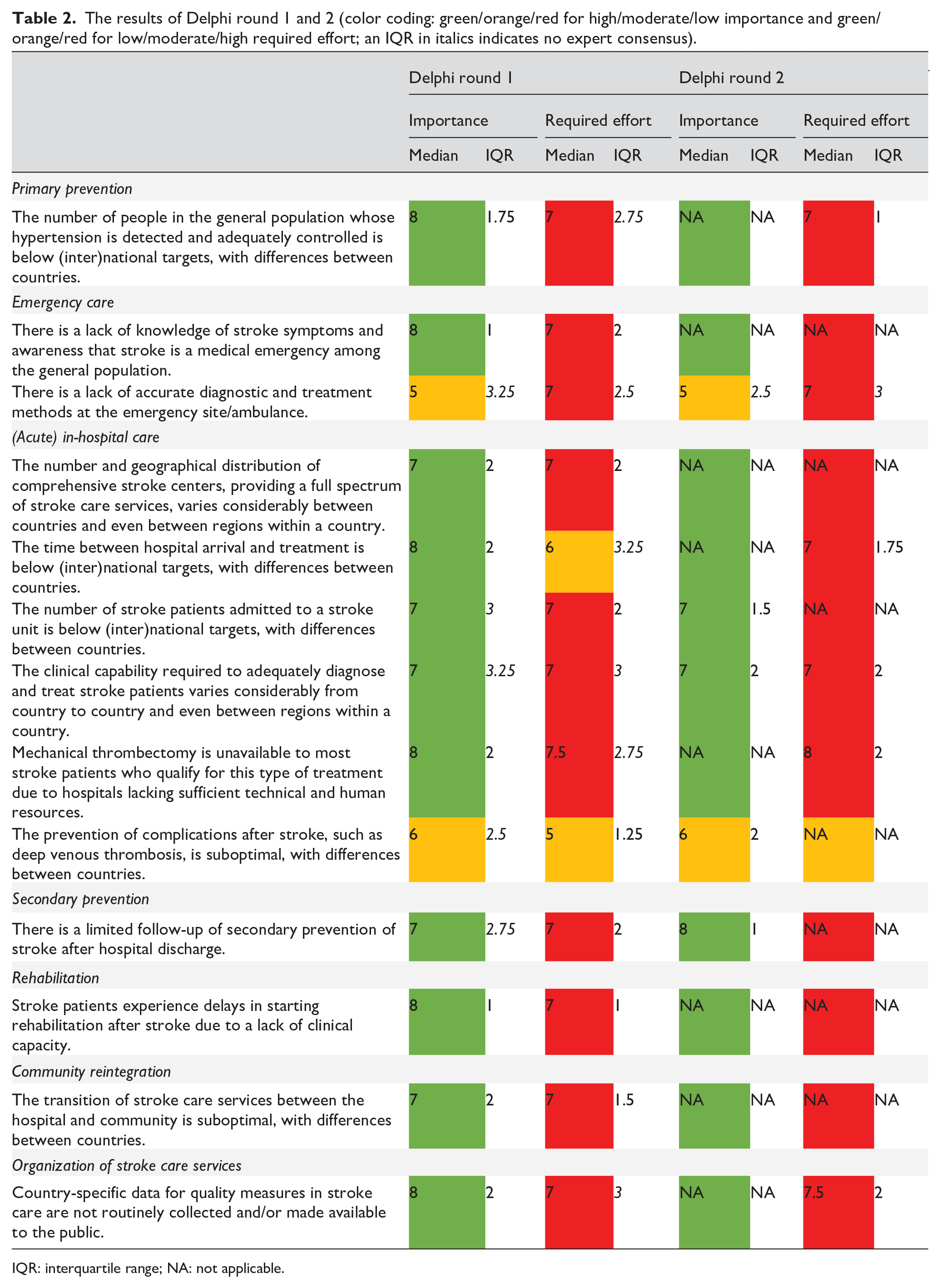
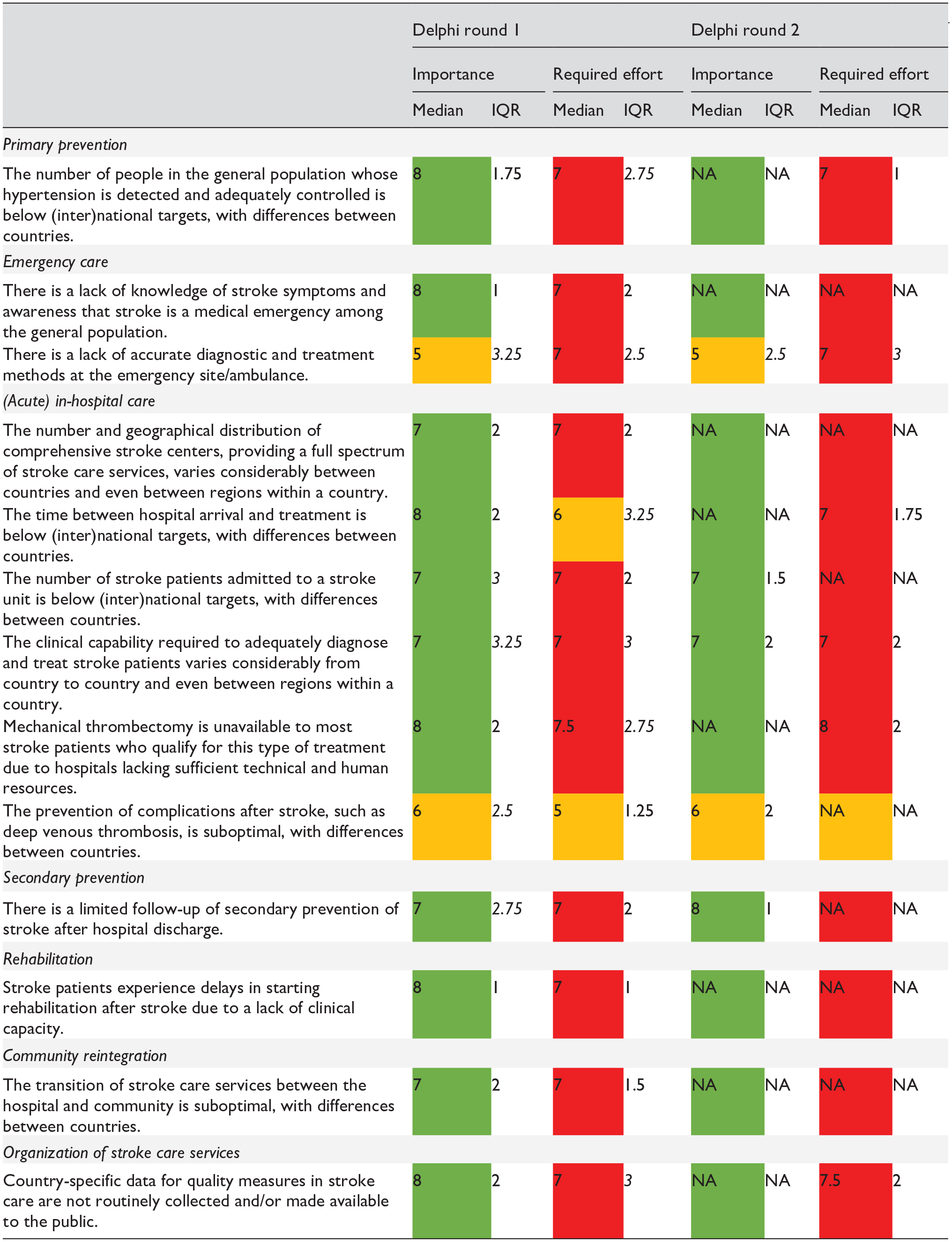
IQR: interquartile range; NA: not applicable.
Delphi round 2
Experts scored the importance to close five gaps for which no expert consensus, that is, IQR > 2, was reached in the first Delphi round (Table 2). Three out of five gaps were considered highly important to close, with expert consensus for all. Two out of five gaps were considered moderately important to close, with expert consensus for one of these two gaps. Furthermore, experts scored the required effort to close six gaps for which no expert consensus, that is, IQR > 2, was reached in the first Delphi round. All six gaps were considered to require high effort to close, with expert consensus for five of these six gaps. Supplementary file 4 includes boxplots, depicting the gaps surveyed in this study, with the median score, IQR, and experts’ individual scores for each gap.
Expert consensus
The number of gaps for which expert consensus was reached increased between the first and second Delphi round. Expert consensus was reached on the high importance of closing 11 out of 13 gaps. Two out of 13 gaps were considered moderately important to close, with expert consensus for one of these two gaps. Seven gaps had a median importance score of 8, including: (1) the number of people in the general population whose hypertension is detected and adequately controlled is below (inter)national targets, with differences between countries; (2) there is a lack of knowledge of stroke symptoms and awareness that stroke is a medical emergency among the general population; (3) the time between hospital arrival and treatment is below (inter)national targets, with differences between countries; (4) mechanical thrombectomy is unavailable to most stroke patients who qualify for this type of treatment due to hospitals lacking sufficient technical and human resources; (5) there is a limited follow-up of secondary prevention of stroke after hospital discharge; (6) stroke patients experience delays in starting rehabilitation after stroke due to a lack of clinical capacity; and (7) country-specific data for quality measures in stroke care are not routinely collected and/or made available to the public. The others had a median importance score of ⩽ 7. Expert consensus indicated that only one gap, related to the prevention of complications after stroke, requires moderate effort to close, whereas the others were considered to require high effort to close.
Qualitative insights
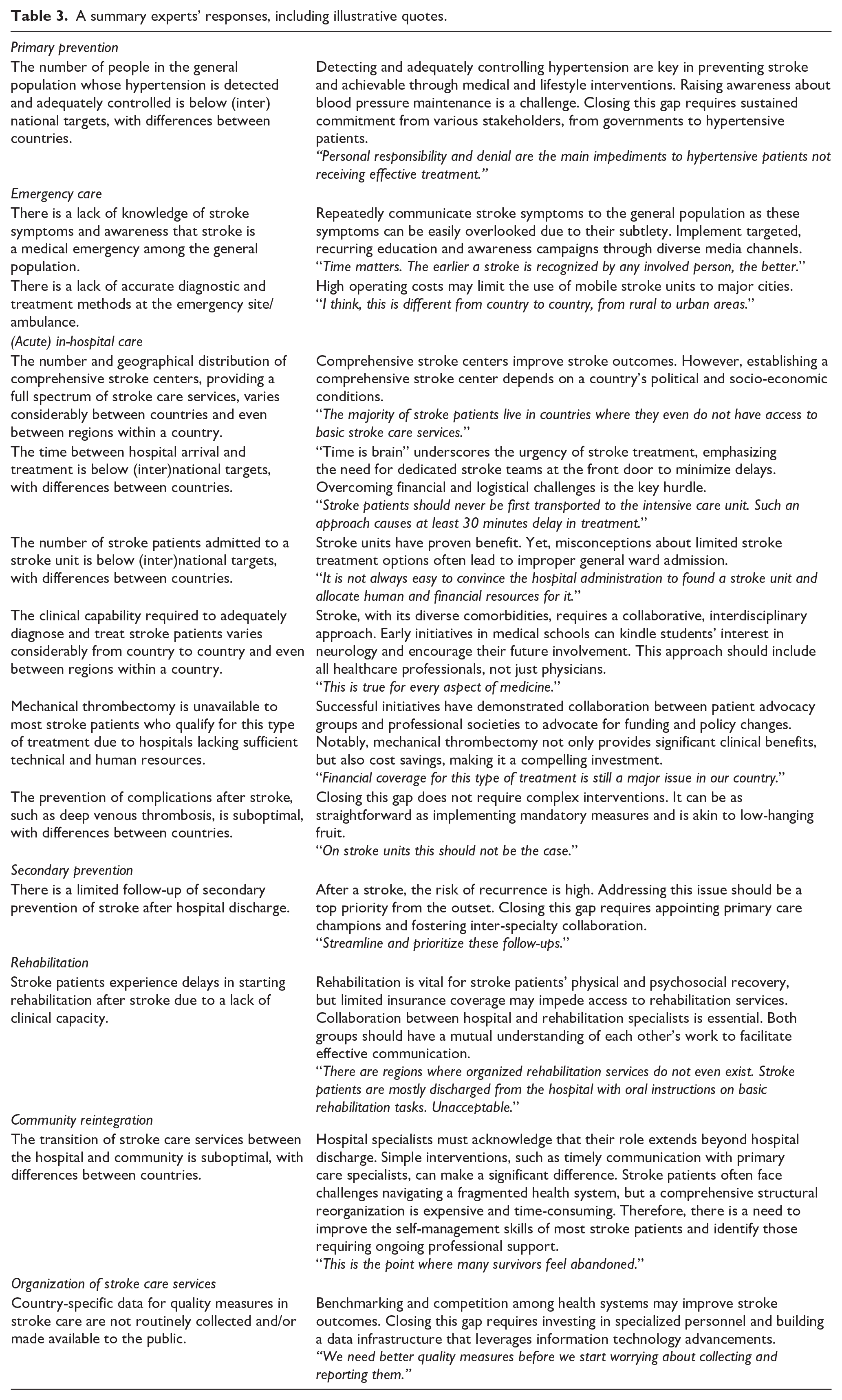
Experts’ responses in free-text fields provided additional insights into the nature of gaps, as well as potential solutions (Table 3). Categories were identified, recurring across various gaps throughout the stroke care continuum, including “Care infrastructure,” “Geographic disparities,” “Interdisciplinary collaboration,” and “Advocacy and funding.” These categories represent key focus areas for potential solutions.
A summary experts’ responses, including illustrative quotes.
Discussion
This study sought consensus among an international expert panel on prioritizing gaps in stroke care. Over two survey rounds, experts scored the importance and required effort to close 13 gaps. Our results highlight the complexity of gaps that significantly impact clinical practice but lack straightforward solutions, primarily due to the multifaceted nature of stroke and need for timely, multidisciplinary measures, alongside individual and systemic barriers. 24 This study shows that gaps exist throughout the stroke care continuum, rather than being confined to some isolated domains. Thus, there are diverse opportunities to improve the quality of stroke care, each with varying levels of impact and resource needs, all requiring targeted, evidence-based interventions.
The year 2015 marked a revolution in stroke care, with clinical trials demonstrating that endovascular therapy (EVT) is highly effective in treating ischemic stroke caused by large artery occlusion, especially when compared to conventional drug therapy alone.25–29 However, due to the relative recency of these break-through trials, many countries still lack a well-developed care infrastructure that facilitates timely access to EVT.30–32 Indeed, the translation of evidence into clinical practice is a slow and complex process, necessitating a thorough reevaluation of patient pathways and streamlined processes to reduce time to treatment. Our results highlight the vulnerability of transitions through patient pathways, with siloed working practices among healthcare professionals. Establishing multidisciplinary stroke teams, operating under standardized protocols for patient assessment, treatment, and follow-up, could foster a collaborative approach to clinical practice, ensuring a seamless transition of stroke patients from symptom onset to treatment and, ultimately, community reintegration.
As part of the core cluster of noncommunicable diseases (NCDs), quality improvement in stroke care contributes to the United Nations 2030 Agenda for Sustainable Development, aimed at reducing premature mortality from these diseases. 33 However, in 2021, only 3% of 135 countries globally allocated funds for stroke and other NCDs within their national health plans. 34 This lack of commitment highlights the challenge of implementing system-wide policy changes that require sustained investment and well-coordinated implementation strategies. Indeed, quality improvement in stroke care is an ongoing, context-specific process, rather than a fixed endeavor. To date, successful initiatives have shown that when stakeholders collaborate and leverage their collective voices to advocate for policy changes and secure funding, substantial progress is possible. 35 These initiatives often take a multicomponent approach, adopting a holistic perspective on stroke care that includes the active involvement of stroke patients. However, ensuring feasibility remains a major challenge. While closing gaps in stroke care primarily requires high effort and substantial resources, some resource-efficient interventions can still yield clinically meaningful improvements. For example, our results indicate that likely feasible interventions, such as mandatory clinical measures aimed at preventing complications after stroke, could prevent recurrent strokes and other vascular events, making a tangible impact on stroke care.
This study’s strengths include the extensive reach of the Delphi process, enabling participation from a geographically diverse expert panel. However, the predominance of experts from English-speaking, high-income countries, including the US and UK, introduces a potential bias. 36 While we achieved a sample size exceeding the required number, with experts from 16 countries across Asia, Europe, and North America, there was a notable lack of representation from regions such as Scandinavia, Eastern Europe, and low- and middle-income countries. This geographic imbalance may have skewed our results, as challenges faced by these underrepresented regions may differ from those represented in this study. Consequently, caution is warranted regarding the generalizability of our results, particularly to non-English-speaking and low- and middle-income countries. Additionally, most experts were neurologists, potentially skewing our results toward the perspective of this discipline. Future research should aim to complement this study with quantitative investigations that mitigate the potential geographical and disciplinary biases of this study. For example, large-scale, regional surveys could provide more nuanced insights, helping to identify context-specific challenges and priorities that vary by region. Furthermore, the response rates in this study can be considered relatively low. Although such response rates are common in this type of research, particularly when targeting busy, high-level experts, it is important to acknowledge that these rates may have constrained the comprehensiveness of perspectives. Despite this limitation, the purposive selection of experts ensured that they were capable of providing rich, in-depth insights. Moreover, the use of anonymized responses and controlled feedback helped mitigate groupthink and power imbalances, strengthening the methodological rigor of this study. 37
Conclusion
This study provides valuable insights into the prioritization of gaps in stroke care, encompassing both the importance and required effort to close 13 gaps throughout the stroke care continuum. Closing these gaps primarily requires high effort and substantial resources that may not always be available, especially in resource-limited settings. However, targeted interventions in the identified key focus areas (i.e. “Care infrastructure,” “Geographic disparities,” “Interdisciplinary collaboration,” and “Advocacy and funding”) may provide feasible and clinically meaningful improvements. Armed with the insights provided by this study, we urge governments and policymakers to consistently implement context-specific, evidence-based interventions to close gaps in stroke care, thereby contributing to international efforts to mitigate the impact of stroke.
Supplemental Material
sj-docx-1-eso-10.1177_23969873251329841 – Supplemental material for Prioritizing gaps in stroke care: A two-round Delphi process
Supplemental material, sj-docx-1-eso-10.1177_23969873251329841 for Prioritizing gaps in stroke care: A two-round Delphi process by Elke GE Mathijssen, Jaap CA Trappenburg, Mark J Alberts, Angelique Balguid, Robert J Dempsey, Mayank Goyal, Bianca TA de Greef, Marjan J Hummel, Koji Iihara, Enrique C Leira, Winston Lim, Gregory YH Lip, Paolo Madeddu, Randolph S Marshall, Dominick JH McCabe, Ahmad S Muda, Dimitrios N Nikas, George Ntaios, Terence J Quinn, Marta Rubiera, Tatjana Rundek, Shashank Shekhar, Wen-Jun Tu, Pearl Vyas, Wim van Zwam, Johannes B Reitsma and Ewoud Schuit in European Stroke Journal
Supplemental Material
sj-docx-2-eso-10.1177_23969873251329841 – Supplemental material for Prioritizing gaps in stroke care: A two-round Delphi process
Supplemental material, sj-docx-2-eso-10.1177_23969873251329841 for Prioritizing gaps in stroke care: A two-round Delphi process by Elke GE Mathijssen, Jaap CA Trappenburg, Mark J Alberts, Angelique Balguid, Robert J Dempsey, Mayank Goyal, Bianca TA de Greef, Marjan J Hummel, Koji Iihara, Enrique C Leira, Winston Lim, Gregory YH Lip, Paolo Madeddu, Randolph S Marshall, Dominick JH McCabe, Ahmad S Muda, Dimitrios N Nikas, George Ntaios, Terence J Quinn, Marta Rubiera, Tatjana Rundek, Shashank Shekhar, Wen-Jun Tu, Pearl Vyas, Wim van Zwam, Johannes B Reitsma and Ewoud Schuit in European Stroke Journal
Supplemental Material
sj-docx-3-eso-10.1177_23969873251329841 – Supplemental material for Prioritizing gaps in stroke care: A two-round Delphi process
Supplemental material, sj-docx-3-eso-10.1177_23969873251329841 for Prioritizing gaps in stroke care: A two-round Delphi process by Elke GE Mathijssen, Jaap CA Trappenburg, Mark J Alberts, Angelique Balguid, Robert J Dempsey, Mayank Goyal, Bianca TA de Greef, Marjan J Hummel, Koji Iihara, Enrique C Leira, Winston Lim, Gregory YH Lip, Paolo Madeddu, Randolph S Marshall, Dominick JH McCabe, Ahmad S Muda, Dimitrios N Nikas, George Ntaios, Terence J Quinn, Marta Rubiera, Tatjana Rundek, Shashank Shekhar, Wen-Jun Tu, Pearl Vyas, Wim van Zwam, Johannes B Reitsma and Ewoud Schuit in European Stroke Journal
Supplemental Material
sj-docx-4-eso-10.1177_23969873251329841 – Supplemental material for Prioritizing gaps in stroke care: A two-round Delphi process
Supplemental material, sj-docx-4-eso-10.1177_23969873251329841 for Prioritizing gaps in stroke care: A two-round Delphi process by Elke GE Mathijssen, Jaap CA Trappenburg, Mark J Alberts, Angelique Balguid, Robert J Dempsey, Mayank Goyal, Bianca TA de Greef, Marjan J Hummel, Koji Iihara, Enrique C Leira, Winston Lim, Gregory YH Lip, Paolo Madeddu, Randolph S Marshall, Dominick JH McCabe, Ahmad S Muda, Dimitrios N Nikas, George Ntaios, Terence J Quinn, Marta Rubiera, Tatjana Rundek, Shashank Shekhar, Wen-Jun Tu, Pearl Vyas, Wim van Zwam, Johannes B Reitsma and Ewoud Schuit in European Stroke Journal
Footnotes
Acknowledgements
The authors would like to express their gratitude to Prof. Dr. Didier Leys, Prof. Dr. Tony Rudd, and other experts for their commitment in dedicating time to participate in the expert panel and providing valuable input for this study.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Prof. Dr. Dominick McCabe’s Vascular Neurology Research program is currently supported by grants from The Meath Foundation, Ireland; The Adelaide Health Foundation, Ireland; The Vascular Neurology Research Foundation Ireland; the Enterprise Ireland-Innovation Partnership Programme (co-funded by the European Regional Development Fund); and by unrestricted educational grant funding from Werfen, Spain; Sysmex UK/Siemens, Germany; SINNOWA Medical Science & Technology Co., China; and Acquis BI Technology Ltd., Ireland. The other authors report no competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by Philips Healthcare, Eindhoven, The Netherlands. The funder of this study had no role in study design, data collection, data analysis and interpretation, or writing the report.
Ethical approval
Ethical review by an accredited research ethics committee was not required for this study by Dutch law. Data handling adhered to the Dutch implementation act of the General Data Protection Regulation.
Informed consent
Digital informed consent was obtained from experts at each Delphi round.
Guarantor
Elke GE Mathijssen.
Contributorship
EM, ES, JR, and JT conceived the study. EM and ES collected and analyzed the data. EM wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
ORCID iDs
Data availability
The data collected and analyzed during this study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.