
Abstract
Introduction:
Limited data exist on cognitive performance and return to work after ischemic stroke, especially in patients under 50 years. We investigated whether cognitive performance in the subacute phase after ischemic stroke in young adults was associated with unemployment and the inability to retain their jobs among those who returned to work.
Patients and methods:
We conducted a multicenter prospective cohort study between 2013 and 2021, enrolling patients aged 18–49 years with first-ever ischemic stroke. Cognitive assessments were performed within 6 months following the index event, covering seven cognitive domains. We categorized patients with cognitive impairment (Z-score < −1.5 on a domain) and as no/mild or major vascular cognitive disorder (VCD; Z-score < −2.0 in one or more domains). Cognitive performance and other predefined characteristics were chosen to identify factors associated with unemployment and, among patients who returned to work, the inability to maintain employment.
Results:
Of 525 patients (median age 44.3 [IQR 38.0–47.4] years; 243 women [46.3%]); median follow-up of 6.6 [IQR 4.5–8.2] years), 426 patients (81.1%) returned to work. Sixty-five patients (15.3%) were unable to maintain employment. In multivariable logistic regression analysis, major VCD (OR = 2.0; 95% CI 1.3–3.0; p = 0.002) and cognitive impairment in processing speed (OR = 2.0; 95% CI 1.3–3.3; p = 0.004) were associated with unemployment, but not with the inability to maintain employment.
Discussion and conclusion:
In young patients after a first-ever ischemic stroke, major VCD and impaired processing speed in the subacute phase after stroke were independently associated with unemployment, but not with the inability to maintain employment.
Introduction
The incidence of stroke among young adults (aged 18–50 years) is increasing worldwide.1,2 Each year, over 2 million young adults experience a stroke globally. 1 Most young adults affected by a stroke are active participants of society, with demanding social lives, young families and busy (developing) careers. While most young stroke survivors have relatively mild strokes, measured with the National Institutes of Health Stroke Scale (NIHSS), 3 almost half of young adults experience cognitive impairment after stroke. 4 Moreover, they often experience other impairments, such as fatigue and mood disorders.5,6 These sequelae may result in unemployment, which has been shown to lead to lower levels of subjective well-being and life satisfaction. 7 In addition, not being able to return to work has a high socioeconomic impact. 8 Overall, about half to two-thirds of all working-age adults were able to return to work after their first stroke, although some studies report rates as high as 75%.9,10 In these studies, not only including young stroke patients (under 50 years), various factors were associated with return to work, such as age, sex, stroke subtype, etiology of ischemic stroke, aphasia, stroke severity, independence of daily living, depression, and type of work.9–11 While other factors, including education level, fatigue, and cardiovascular risk factors, may also be related, and therefore warrant further attention. 10 Besides that, cognitive impairment appeared to be negatively associated with return to work.9,10 However, previous studies on post-stroke cognition and return to work were performed in small samples, did not cover all major cognitive domains, had a short follow-up duration, or predominantly included patients over 50 years. These older patients are closer to their retirement and may have, as a result, a poorer return to work rate than younger stroke survivors. 9 Additionally, there are limited data on the ability of young stroke patients to retain their jobs after returning to work. Furthermore, it remains unclear whether difficulties to keep one’s job are associated with cognitive impairment.
The aim of this study was therefore to investigate (1) whether cognitive performance in the subacute phase after first-ever ischemic stroke in a large cohort of young patients was associated with unemployment median 6 years after stroke, and (2) the inability to maintain employment among patients who returned to work at least once during their follow-up.
Patients and methods
Patients and study design
This study is part of the “Observational Dutch Young Symptomatic StrokE studY”, a multicenter prospective cohort study examining risk factors and prognosis of stroke at young age.5,12 The present study included patients aged 18–49 years with a first-ever ischemic stroke with radiological evidence of cerebral ischemia, who underwent a cognitive assessment and had at least one follow-up moment with data on employment status. Patients were included between May 2013 and February 2021. Exclusion criteria were a history of stroke, retinal infarction, and cerebral venous sinus thrombosis. For this study, we also excluded patients who were not in paid employment or followed education/study prior to their stroke, and those who died during the follow-up before we could determine their employment status. Detailed information regarding data collection has been provided elsewhere. 12 This study involves human participants and was approved by the Medical Review Ethics Committee region Arnhem-Nijmegen approved the study (NL41531.091.12). We obtained written informed consent from all participants. If the patient was unable to provide informed consent, consent was provided by the patient’s legal representative.
Cognitive assessment
Patients underwent an extensive neuropsychological assessment within 6 months after stroke. We assessed the seven most relevant cognitive domains using multiple tests: episodic memory (3-trial version of the Rey Auditory Verbal Learning Test), processing speed (the written version of the Symbol-Digit Modalities Test, the abbreviated Stroop Color Word Test, parts I and II), visuoconstruction (Rey-Osterrieth Complex Figure – copy trial), executive functioning (Fluency test, Stroop interference score, Brixton Spatial Anticipation Test), visual neglect (Star Cancelation of the Behavioral Inattention Test), language deficits (Short Token test), attention and working memory (Digit Span subtest from the Wechsler Adult Intelligence Scale – Fourth Edition).
Normative data from the Advanced Neuropsychological Diagnostics Infrastructure (ANDI), which includes data of 26,000 healthy individuals across all age groups were employed for most tests. This allowed fine-grained adjustment based on age, sex and education level. 13 For the written version of the Symbol-Digit Modalities Test, we used the normative data from the test’s manual (n = 1,307), 14 adjusted for age and education level. For the Star Cancelation Test, we used a cutoff value (<44) instead of Z-scores, to indicate cognitive impairment on the domain visuospatial neglect. 15 Further details regarding the collection and preparation of cognitive data can be found elsewhere.5,16
Cognitive impairment on a domain was defined as an age and education-adjusted composite Z-score of <−1.5.5,17 Criteria for vascular cognitive disorder (VCD) were based on the criteria of the International Society for Vascular Behavioral and Cognitive Disorders (VASCOG). We defined major VCD as a composite Z-score of <−2.0, in one or more cognitive domains. 18 All remaining patients were classified as no/mild VCD.
Return to work data
We collected follow-up data on return to work systematically through standardized, structured questionnaires by phone or by an online survey between November 2013 and February 2024. We classified patients as employed if they were working or studying at their last follow-up assessment. We defined unemployment as either (1) not having any paid employment in any capacity or studying during the follow-up period, or (2) having returned to work or study at least once during their follow-up, but not working or studying at the last follow-up assessment. The latter group was classified for the secondary analysis as unable to maintain employment. Due to the absence of an exact date of return to work, we used the dates of the follow-up moment for the moment of return to work. We gathered details of return to work from the first follow-up moment in which the patient reported having returned to work.
Other measurements
We scored level of education with a Dutch scoring system comprising seven categories 19 that align with the UNESCO international classification of education levels. 20 Lesion type was scored on available imaging data. Lesions were categorized as lacunar in the case of small subcortical infarcts, usually smaller than 20 mm. 21 We segmented all stroke lesions on MRI using ITK- SNAP, 22 registered them to a standard template using Advanced Normalization Tools (ANTs, v 2.1.0), 23 and calculated normalized lesion volumes using FSLstats. 24 At the time of the cognitive assessment, we assessed symptoms of depression using the Mini International Neuropsychiatric Interview (MINI) 25 and fatigue using the subscale Subjective Fatigue of the revised Checklist Individual Strength (CIS-20R). 26 We assessed functional outcome using the Barthel Index 27 at the follow-up moment when a patient returned to work, or, if a patient did not returned to work, the last available follow-up moment. Additionally, we evaluated the cause of stroke (based on modified Trial of ORG 10172 in Acute Stroke Treatment; TOAST)3,28 and severity at admission and discharge (National Institutes of Health Stroke Scale; NIHSS), 29 if necessary retrospectively, using a validated approach.30,31 We assessed the following cardiovascular factors associated with an increased risk of stroke systematically through medical files and a standardized questionnaire at time of index event: hypertension, dyslipidemia, diabetes, smoking, excess alcohol use, and obesity. 32
Statistical analysis
We compared baseline characteristics between patients who were employed (i.e. those who returned to work and were able to maintain employment) and those who were unemployed, using the independent t-test or Mann-Whitney U test for continuous variables and Pearson’s Chi-squared test/Fisher’s exact test for categorial variables. We performed univariate and multivariable logistic regression analyses to assess the associations between predefined factors based on literature (age, sex, education level, stroke severity, imaging characteristics, functional outcome, depressive symptoms, post-stoke fatigue, cognitive performance, stroke etiology, number of cardiovascular risk factors, and recurrent stroke)9–11 and unemployment. Next, we assessed the associations between the predefined factors and the inability to maintain employment, compared to the patients who were able to maintain work participation, using univariate and multivariable logistic regression. We performed multiple imputation to handle the missing data for the multivariable logistic regression models. The logistic regression models were fitted to each of the imputed datasets. We then pooled the results to obtain a single odds ratio (OR) with a 95% confidence interval (CI) for each predefined factor. We calculated McFadden’s pseudo R2 (R2McF) for each multivariable logistic regression model across all imputed datasets to assess model fit. We pooled the R2McF values from the imputed datasets to obtain a single R2McF per model. Since only 1 (0.2%) patient scored as cognitively impaired on the visual neglect domain, we excluded this domain from the regression analyses. Multivariable analyses were performed using associated factors with alpha set at 0.10 in the univariate analyses. To address multicollinearity, we created two different multivariable models: one including the VCD score as the indicator of cognitive performance (VCD model) and the other including the separate cognitive domains (cognitive domains model). For the NIHSS we selected the score at discharge as the measure of stroke severity, since patients often recover during admission. Lesion volume was missing in 60 (11.4%) patients. The fatigue severity scores were missing in 83 (15.8%) of the patients. These missing data points were not at random, as patients without fatigue score showed lower rates of return to (and stayed at) work (p = 0.013), higher NIHSS scores at discharge (p = 0.012), more frequent a poor outcomes on the Barthel Index (p = 0.019), more frequent depressive symptoms (p = 0.050), and more frequent major VCD (p = 0.009; Supplemental Table 1). Therefore, we developed separate multivariable regression models that include lesion volume and the fatigue severity score. Significance level was predefined at 0.05 (2-tailed). All statistical analyses were performed using R, version 4.1.3. 33
Results
Of the 1322 patients participating in the ODYSSEY study, 525 patients were included in this analysis (median age 44.3 [IQR 38.0–47.4] years; 243 women [46.3%]; Figure 1). Baseline characteristics, stratified by employment status, are described in Table 1. Median time to cognitive assessment was 85 (IQR 56–120) days. Median follow-up was 6.6 (IQR 4.5–8.2) years. Median NIHSS at admission was 2 (IQR 1–5) and at discharge 1 (IQR 0–2). In total, 426 (81.1%) patients returned to work at least once during their follow-up, and 361 (68.8%) patients were able to maintain work participation and were employed at their last follow-up assessment. The median time to the survey, when patients reported returning to work, was 1.3 (IQR 0.7–1.7) years. During the follow-up 45 patients (8.6%) experienced a recurrent stroke, all of which were ischemic. Additionally, 8 (1.5%) patients died, of whom 2 (0.4%) had returned to work before they died.
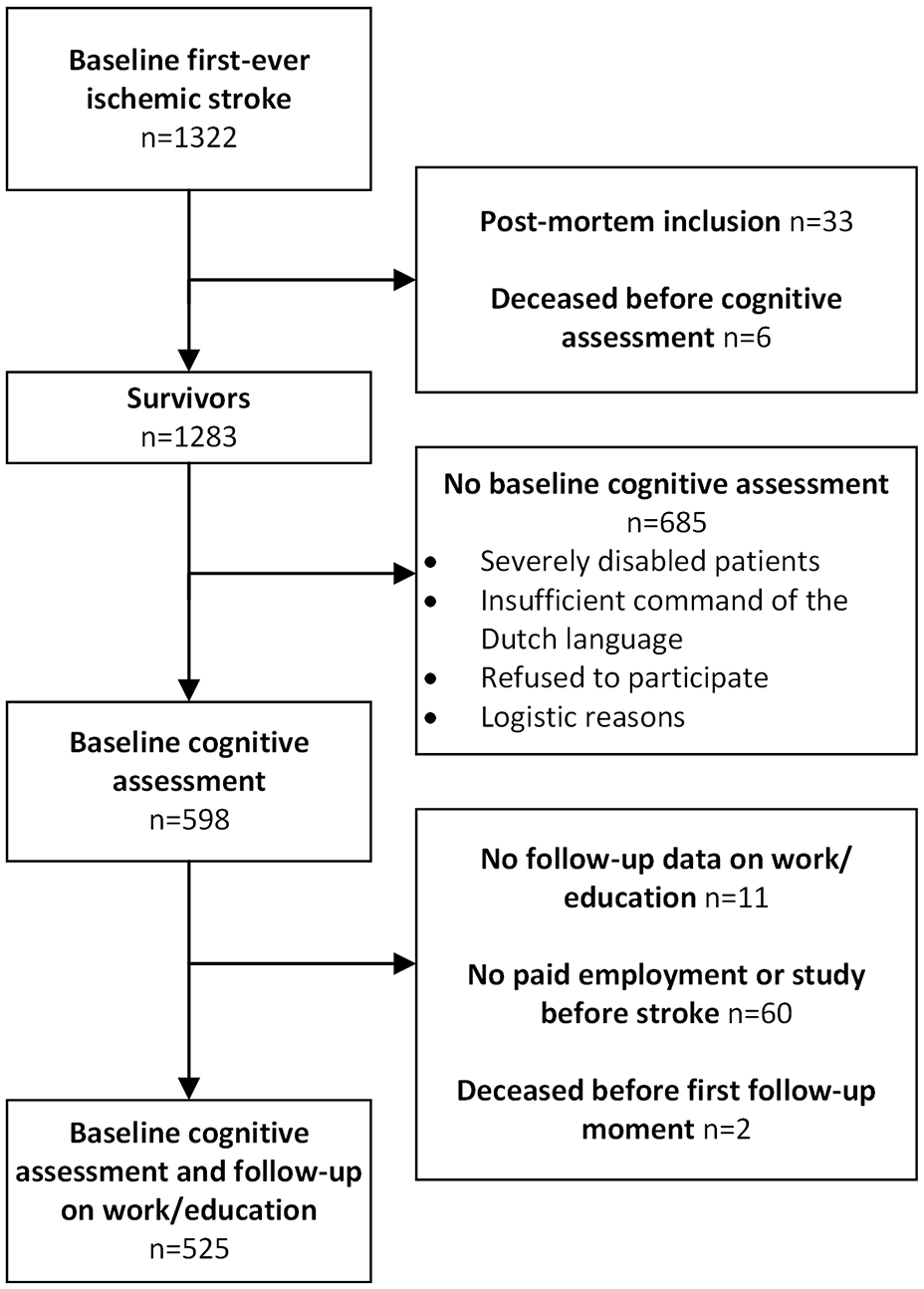
Flowchart of the study population.
Baseline characteristics.
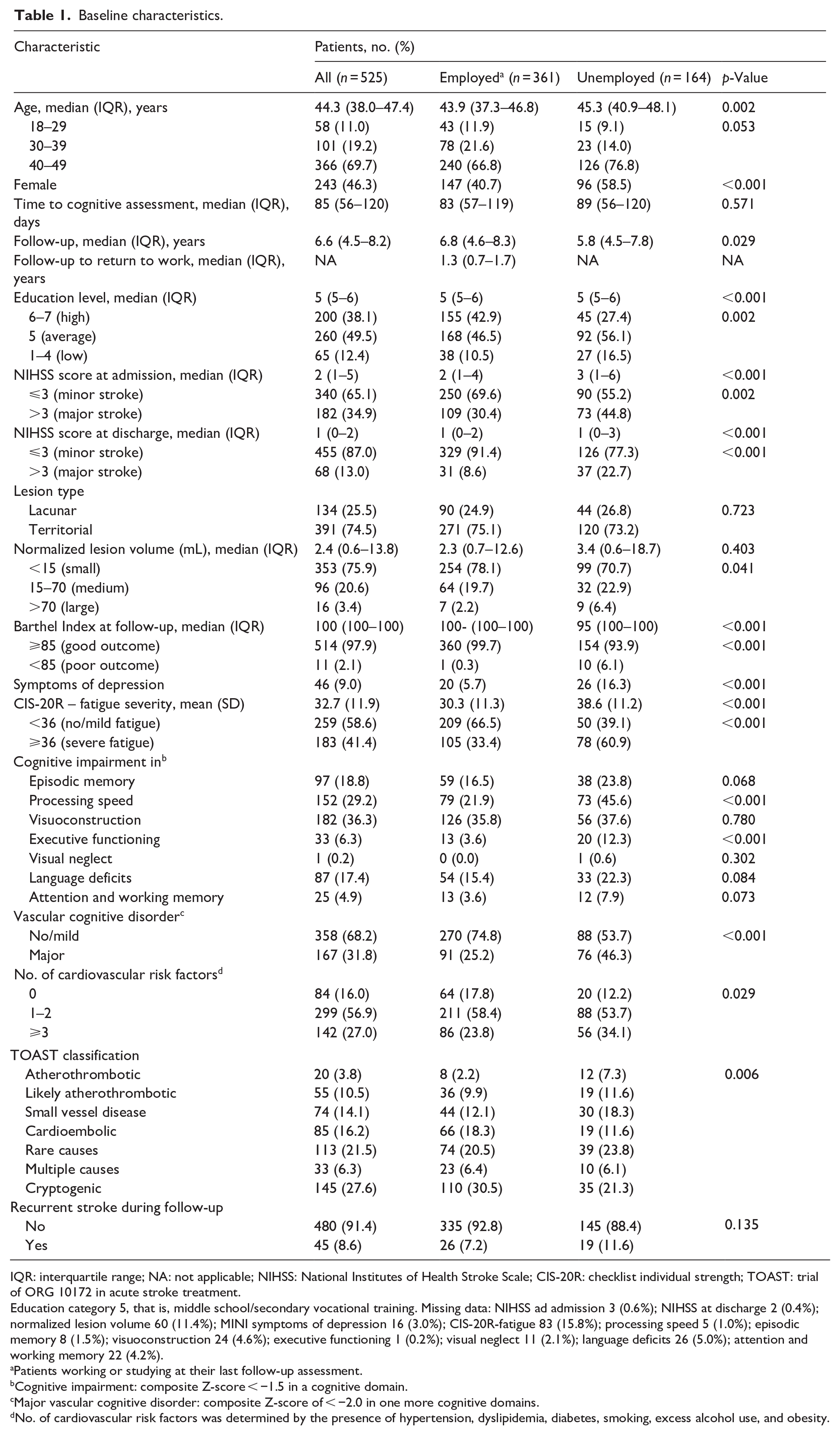
IQR: interquartile range; NA: not applicable; NIHSS: National Institutes of Health Stroke Scale; CIS-20R: checklist individual strength; TOAST: trial of ORG 10172 in acute stroke treatment.
Education category 5, that is, middle school/secondary vocational training. Missing data: NIHSS ad admission 3 (0.6%); NIHSS at discharge 2 (0.4%); normalized lesion volume 60 (11.4%); MINI symptoms of depression 16 (3.0%); CIS-20R-fatigue 83 (15.8%); processing speed 5 (1.0%); episodic memory 8 (1.5%); visuoconstruction 24 (4.6%); executive functioning 1 (0.2%); visual neglect 11 (2.1%); language deficits 26 (5.0%); attention and working memory 22 (4.2%).
Patients working or studying at their last follow-up assessment.
Cognitive impairment: composite Z-score < −1.5 in a cognitive domain.
Major vascular cognitive disorder: composite Z-score of < −2.0 in one more cognitive domains.
No. of cardiovascular risk factors was determined by the presence of hypertension, dyslipidemia, diabetes, smoking, excess alcohol use, and obesity.
Factors associated with unemployment
In the multivariable logistic regression model including VCD, without lesion volume and the fatigue score (R2McF = 0.148), the risk of unemployment was higher for women (OR = 2.5; 95% CI 1.6–3.8; p < 0.001), patients with average (OR = 1.6; 95% CI 1.0–2.6; p = 0.043) or low (OR = 2.3; 95% CI 1.2–4.6; p = 0.015) education level, major stroke at discharge (OR = 2.9; 95% CI 1.6–5.4; p < 0.001), poor functional outcome (OR = 9.0; 95% CI 1.1–78.1; p = 0.045), depressive symptoms (OR = 3.2; 95% CI 1.6–6.3; p = < 0.001), major VCD (OR = 2.0; 95% CI 1.3–3.0; p = 0.002), atherothrombotic stroke (OR = 3.9; 95% CI 1.3–11.9; p = 0.015), small vessel disease as the cause of stroke (OR = 2.3; 95% CI 1.1–4.7; p = 0.022), and other rare cause of stroke (OR = 1.9; 95% CI 1.0–3.5; p = 0.039), compared with cryptogenic stroke (Table 2).
Factors associated with unemployment.
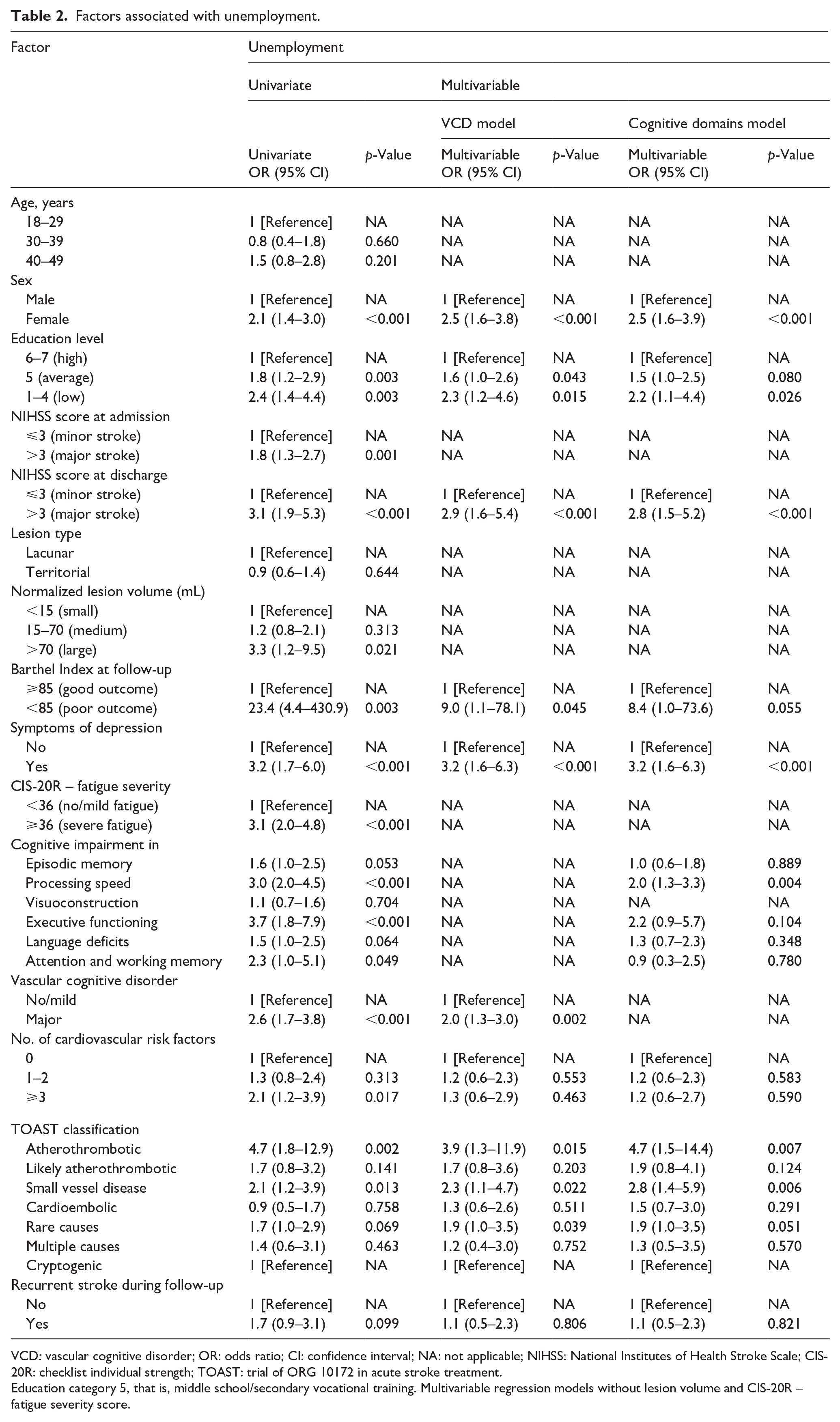
VCD: vascular cognitive disorder; OR: odds ratio; CI: confidence interval; NA: not applicable; NIHSS: National Institutes of Health Stroke Scale; CIS-20R: checklist individual strength; TOAST: trial of ORG 10172 in acute stroke treatment.
Education category 5, that is, middle school/secondary vocational training. Multivariable regression models without lesion volume and CIS-20R – fatigue severity score.
In the multivariable model including the cognitive domains, without lesion volume and the fatigue score (R2McF = 0.162), the risk of unemployment was higher for patients with cognitive impairment in processing speed (OR = 2.0; 95% CI 1.3–3.3; p = 0.004).
Cognitive impairment in executive functioning (OR = 3.7; 95% CI 1.8–7.9; p < 0.001) and in attention and working memory (OR = 2.3; 95% CI 1.0–5.1; p = 0.049) were associated with unemployment only in the univariate analysis.
In the multivariable model including VCD, with lesion volume and the fatigue score (R2McF = 0.180), the risk of unemployment was also higher for patients with severe fatigue (OR = 2.6; 95% CI 1.5–4.4; p < 0.001). In this model, average education level, functional outcome, and rare cause of stroke were no longer significant (Supplemental Table 2).
Inability to maintain employment
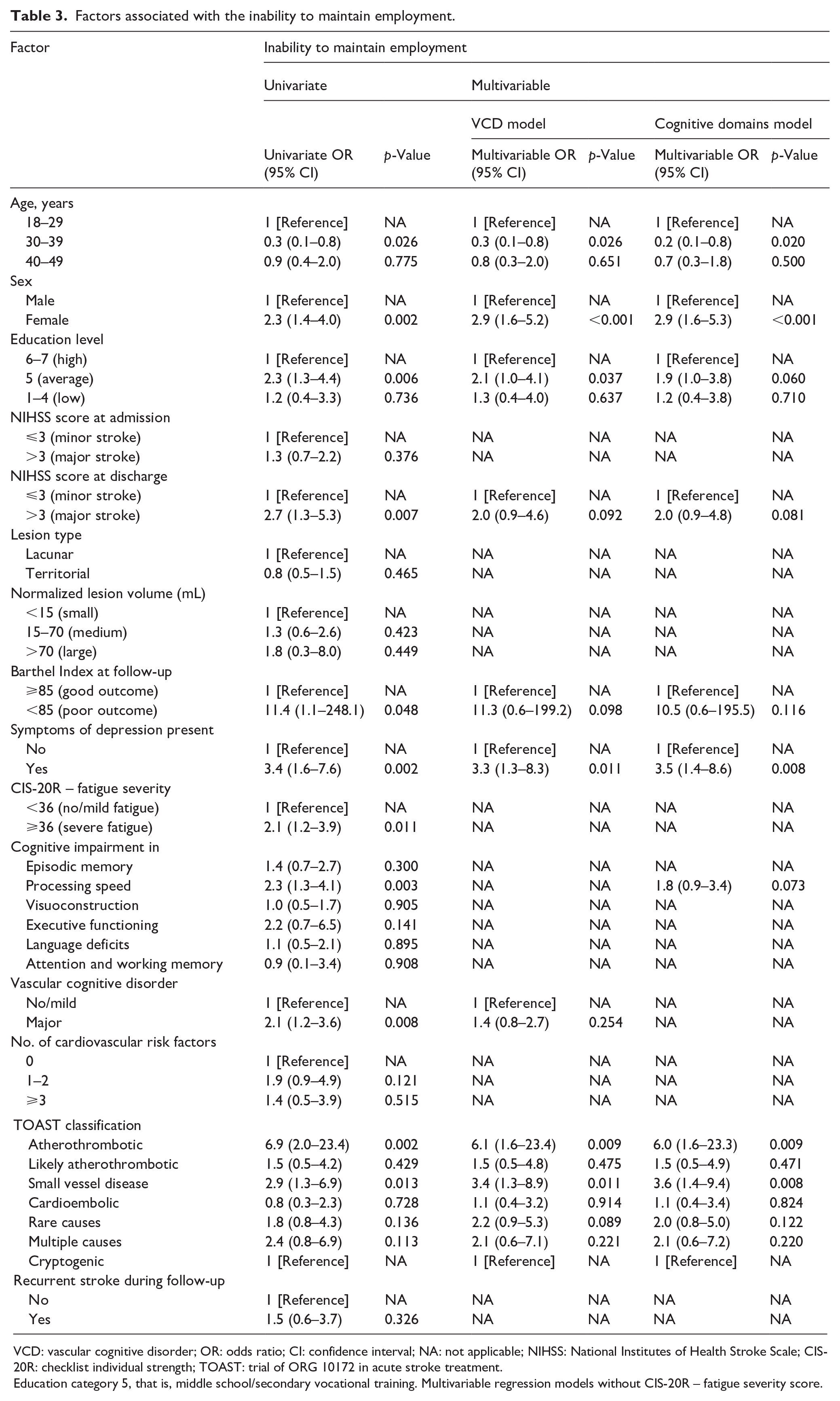
Of the 426 patients who returned to work, 380 (89.2%) initially returned to their same job. Sixty-five (15.3%) patients were unable to maintain employment. Cognitive impairment in processing speed (OR = 2.3; 95% CI 1.3–4.1; p = 0.003) and the presence of a major VCD (OR = 2.1; 95% CI 1.2–3.6; p = 0.008) were associated with the inability to maintain employment only in the univariate analysis (Table 3).
Factors associated with the inability to maintain employment.
VCD: vascular cognitive disorder; OR: odds ratio; CI: confidence interval; NA: not applicable; NIHSS: National Institutes of Health Stroke Scale; CIS-20R: checklist individual strength; TOAST: trial of ORG 10172 in acute stroke treatment.
Education category 5, that is, middle school/secondary vocational training. Multivariable regression models without CIS-20R – fatigue severity score.
In the multivariable model including VCD, without the fatigue severity score (R2McF = 0.162), this risk of the inability to maintain employment was higher for women (OR = 2.9; 95% CI 1.6–5.2; p < 0.001), for patients with average education level (OR = 2.1; 95% CI 1.0–4.1; p = 0.037), those with depressive symptoms (OR = 3.3; 95% CI 1.3–8.3; p = 0.011), atherothrombotic stroke (OR = 6.1; 95% CI 1.6–23.4; p = 0.009), and small vessel disease as the cause of stroke (OR = 3.4; 95% CI 1.3–8.9; p = 0.011), compared to patients with cryptogenic stroke. For patients aged 30–39 years, the risk of the inability maintain employment was lower (OR = 0.3; 95% CI 0.1–0.8; p = 0.026) compared to patients aged 18–29.
The multivariable model including VCD and with the fatigue severity score (R2McF = 0.171) is presented in Supplemental Table 3. Fatigue was not significantly associated with the inability to maintain employment.
Discussion
In this prospective cohort study of young ischemic stroke patients, we found that cognitive performance, measured by the presence of a major VCD in the subacute phase after stroke, was independently associated with unemployment 6 years post-stroke. Processing speed was the key cognitive domain affecting return to work. The presence of a major VCD and impaired processing speed were not independently associated with the inability to maintain employment.
In this cohort, 81% of the patients who were previously working or studying returned to work at least once after a median of 6 years after stroke, and 69% remained employed. This is a relatively high percentage of patients compared to earlier studies, reporting overall return to work proportions of 51% and 66%.9,10 Patients in most previous studies were closer to retirement age than those in our study, potentially resulting in a lower number of patients returning to work. Besides that, most patients in our study have had a relatively mild stroke (median NIHSS 2) and all were able to complete a cognitive assessment, potentially resulting in higher return to work rates.
Patients with a major VCD were twice as likely to be unemployed compared to patients with no or mild VCD. This was controlled for demographic and clinical factors, as well as depression and fatigue. Processing speed independently affected unemployment, whereas executive functioning and attention and working memory were associated with unemployment only in univariate analysis. This is line with other studies reporting that, next to independence in Activities of Daily Living (ADL), cognitive ability was the second most common factor influencing return to work and may be a limiting factor for those who have an otherwise good functional recovery. 9 However, cognitive disorders were evaluated using a variety of assessments and questionnaires in those studies. In studies focusing on specific cognitive domains, processing speed and executive functioning were associated with unemployment.34,35 However, sample sizes of previous studies were more than three times smaller,34,35 not all cognitive domains were assessed, 35 the assessments were conducted 7 years post-stroke, 35 or the follow-up period was limited to 6 months. 34 There were also studies that found no association between cognitive performance on specific cognitive domains and employment.36,37 However, these studies were not restricted to young stoke patients and had a follow-up duration that did not exceed 12 months.
Of the patients who returned to work at least once during their follow-up, 15% was unable to maintain employment. This highlights that a notable percentage of patients struggle to maintain employment after initially returning to work. It is noteworthy that patients in the 30–39 age group were more likely to stay employed after returning to work. Possible reasons include longer employment duration, more stable work contracts, and greater familial responsibilities, such as children relying on their income. Better guidance could potentially lead to higher rates of successful return to work. However, to date, limited data are available with evidence regarding the effectiveness of interventions to promote return to work. 38 Cognitive impairment in processing speed and the presence of a major VCD were univariately associated with the inability to maintain employment. However, these associations did not persist in multivariable analysis. Overall, processing speed seems to be the most important domain in relation to return to work and maintain employment, as it is crucial for maintaining productivity, adaptability, and effective communication in the workplace.
In line with other studies, we found a higher odds ratio of unemployment for women, patients with a low or average education level, those who experienced a major stroke, patients with a poor functional outcome, patients affected by a depression, those experiencing severe fatigue, and those with atherothrombotic stroke, small vessel disease, and other rare cause of stroke, compared with cryptogenic stroke.9–11 Our data suggest that less visible impairments, such as symptoms of a depression, severe fatigue, and cognitive impairment, also play an important role in unemployment in young stroke patients, besides motor impairment.
Our study has several strengths. Firstly, this is a large prospective cohort of young adults who experienced a first-ever, radiologically confirmed ischemic stroke. Secondly, we used extensive neuropsychological testing, with limited missing data. Thirdly, we have a long follow-up period, making it likely that if patients returned to work, it is captured within this timeframe.
However, some study limitations need to be addressed. Firstly, the exact dates of return to work were not collected. At subsequent follow-up moments, we surveyed patients regarding their then-current employment status. The first follow-up assessment, conducted at a median of 1 year, may have contributed to the relatively long return to work intervals, as we used the date of the follow-up assessment as the return to work date. Additionally, for patients who had not returned to work at their first follow-up assessment, it remains unclear whether they were employed at any time between their stroke and the first follow-up moment. Secondly, we did not collect data on the percentage of hours worked compared to the original number of hours. Binary representation of work status may not fully capture nuances of patients who experience varying degrees of reduced work capacity. Thirdly, cognitive data were unavailable for patients who were unable or refused to participate, often due to severe stroke. Consequently, our study includes patients with relatively mild strokes. This could potentially lead to an overrepresentation of the number of patients returning to work, and likely leads to an underrepresentation of the effect of cognitive impairment. A shorter stroke-specific cognitive screening assessment 39 may be used in future research to get an estimate of the cognitive status of individuals unable to complete a full comprehensive assessment, providing a more accurate understanding of the relationship between cognitive impairment and return to work outcomes. Fourthly, the fatigue severity score is missing in almost 16% of our patients, and these missing data were not at random; patients without a fatigue score had poorer motor and cognitive performance. Since fatigue was a strong associated univariate factor, we analyzed its impact in a separate multivariable model after imputing the missing data. Fifthly, the prevalence of some factors (e.g. the Barthel Index) in the logistic regression was rare, making it harder to detect significant results or resulting in large confidence intervals. Finally, we did not have data on pre-stroke levels of stress and depression. These factors could influence return to work, with pre-stroke stress and depression potentially having a negative impact, possibly even independently of post-stroke depression.
In rehabilitation, return to work is an important goal for young stroke patients. The recognition of key drivers for the (in)ability to return to work and the subsequent development of cognitive rehabilitation programs may facilitate this process. 40 Future studies should focus on developing and improving methods to enhance cognitive function and accurately assess its effects on everyday activities. 40 Additionally, there is need for controlled studies to evaluate interventions to promote return to work. 38
Conclusion
In conclusion, in young patients after a first-ever stroke, cognitive performance in the subacute phase after stroke was independently associated with unemployment, but not the inability to maintain employment. Neuropsychological assessments or cognitive screenings may be considered in the young stroke population to obtain information regarding cognitive status, which may enable better predictions of return to work outcomes, and may be helpful facilitating successful return to work.
Supplemental Material
sj-docx-1-eso-10.1177_23969873251324400 – Supplemental material for Cognitive performance is associated with return to work after ischemic stroke in young adults: The ODYSSEY study
Supplemental material, sj-docx-1-eso-10.1177_23969873251324400 for Cognitive performance is associated with return to work after ischemic stroke in young adults: The ODYSSEY study by Mijntje MI Schellekens, Esther M Boot, Jamie I Verhoeven, Merel S Ekker, Esmée Verburgt, Maikel HM Immens, Anne Mertens, Mayte E van Alebeek, Paul JAM Brouwers, Renate M Arntz, Gert W van Dijk, Rob AR Gons, Inge WM van Uden, Tom den Heijer, Julia H van Tuijl, Karlijn F de Laat, Anouk GW van Norden, Sarah E Vermeer, Marian SG van Zagten, Robert J van Oostenbrugge, Marieke JH Wermer, Paul J Nederkoorn, Frank G van Rooij, Ido R van den Wijngaard, Paul LM de Kort, Frank-Erik de Leeuw, Roy PC Kessels and Anil M Tuladhar in European Stroke Journal
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AT is a junior staff member of the Dutch Heart Foundation (grant number 2016T044). FEL is a Clinical established investigator of the Dutch Heart Foundation (2014 T060). MW has received a VIDI grant (9171337) of the ZonMw/NWO and the Clinical established investigator Dutch Heart Foundation grant (2016T86).
Ethical approval
The Medical Review Ethics Committee region Arnhem-Nijmegen approved the study.
Informed consent
We obtained written informed consent from all participants.
Guarantor
MS
Contributorship
MS researched literature, did data analysis, wrote the first draft of the manuscript. RA, MA, FEL, RK were involved in protocol development. FEL gained ethical approval. MS, EB, JV, ME, FEL, AT were involved in patient recruitment. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
ORCID iDs
Data availability
Anonymized data not published within this article will be made available by request from any qualified investigator after permission of regulatory bodies and medical ethics committees. Anonymized R scripts will be made available by request from any qualified investigator.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.