
Abstract
Introduction:
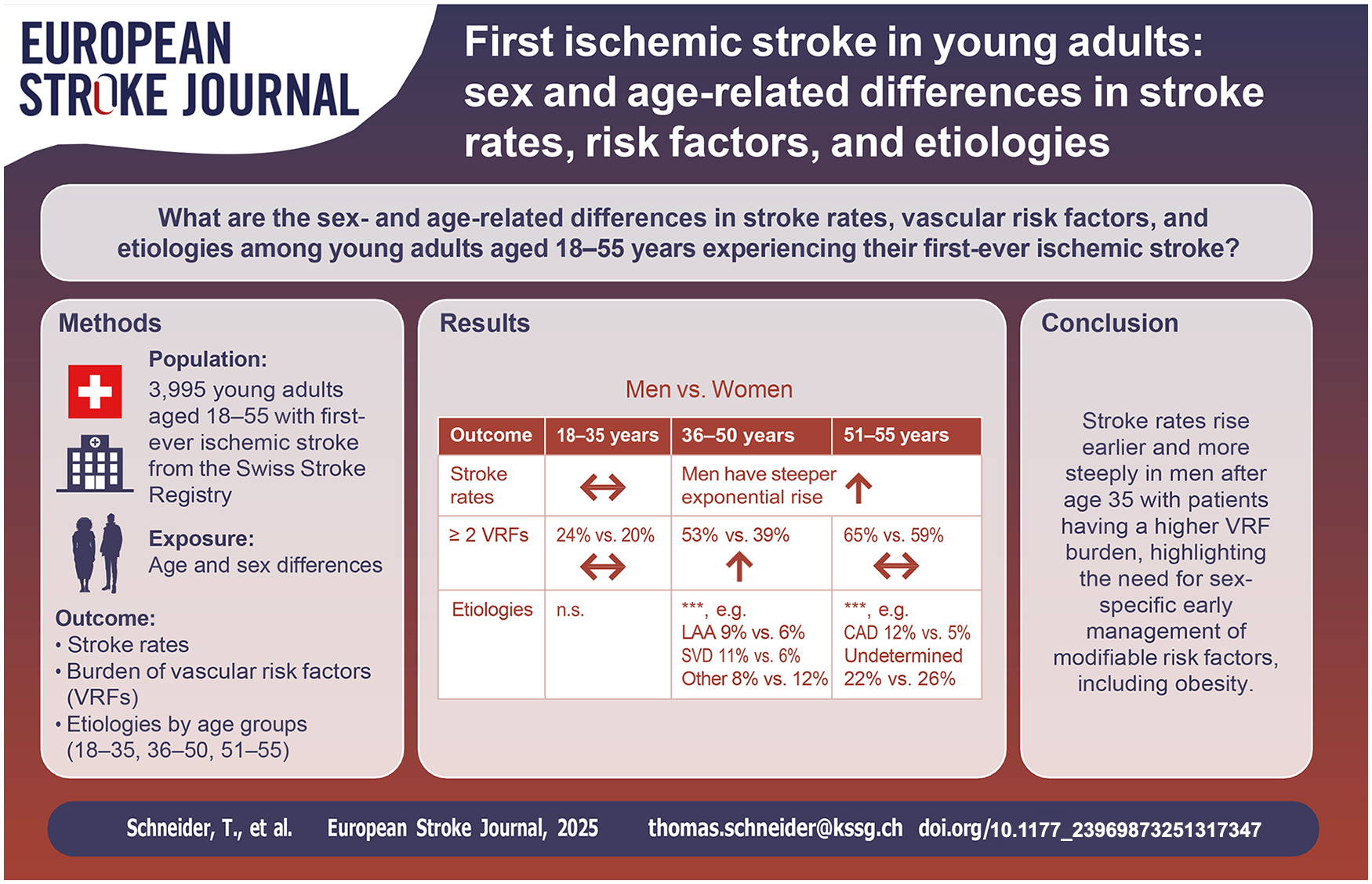
Sex differences in stroke incidence, vascular risk factors (VRFs), and etiologies among young adults remain underexplored, particularly regarding age-related patterns.
Patients and Methods:
We retrospectively analyzed young adults (18–55 years) with first-ever ischemic stroke treated at certified acute stroke units/centers between 2014 and 2022, using Swiss Stroke Registry data. Stroke rates (per 100,000 person-years), VRFs, and etiologies were assessed by age and sex.
Results:
Among 3,995 stroke patients, stroke rates were similar between sexes until age 35, after which men showed a more pronounced exponential increase. This rise was particularly notable in patients with elevated BMI and ⩾2 VRFs. The proportion of patients with ⩾2 VRFs rose with age (18–35: 22%; 36–50: 48%; 51–55: 63%). While no statistically significant differences in VRF profiles were observed between men and women aged 18–35, men accumulated VRFs about five years earlier than women, leading to a higher prevalence of multiple VRFs in men aged 36–50, with the gap narrowing in the 51–55 group. Stroke etiologies shifted with age: patent foramen ovale and cervical artery dissection predominated in younger patients, while large artery atherosclerosis, small vessel disease, and strokes of undetermined etiology increased with age, with notable sex differences.
Discussion and Conclusions:
This study highlights sex and age differences in ischemic stroke rates, VRFs, and etiologies among adults under 55 years. After 35, stroke rates rose more sharply in men, paralleling their higher VRF burden. These findings emphasize the importance of early management of VRFs—including overweight—to mitigate stroke risk.
Introduction
Approximately one in seven ischemic strokes affects people under the age of 50, with stroke incidence rising among younger populations despite an overall decline in high-income countries.1,2
This rise is partly due to changing vascular risk factors, especially obesity and diabetes in adults aged 20 to 44. 3 Studies consistently show obesity raises stroke risk in young adults, largely mediated by hypertension and diabetes.4–6
Stroke etiologies specifically linked to traditional vascular risk factors (VRFs)—such as large artery atherosclerosis, small-vessel disease, and cardioembolism—remain relatively rare in young patients, with strokes of undetermined or other determined etiologies being more common.7,8 Recent data indicate an increased incidence of strokes in young adults, even in the absence of traditional VRFs, with non-traditional factors like migraine being significant risk contributors, particularly among those aged 18 to 34.9,10
Studies suggest that women are more frequently affected by stroke before age 30, with some research indicating a higher incidence in women up to age 44.8,11–14 In younger women, strokes are less often due to large artery atherosclerosis or small vessel disease and more frequently of undetermined or other etiologies,15,16 potentially associated with nontraditional risk factors like migraine. 10 As male stroke incidence rises sharply around age 44, the sex gap narrows, leaving it unclear whether men or women are more affected after age 35.17,18 Few studies have systematically examined sex differences in the distribution of vascular risk factors (VRFs) among young adults with acute ischemic stroke (AIS). A recent analysis from the Stroke Center of the University Hospital Inselspital Bern (2015–2018) found no significant differences in traditional VRFs between women and men but was limited by a small patient cohort. 14 In contrast, a single-center study from Peking Union Medical College Hospital reported that men had a higher burden of VRFs. 16 Similarly, an analysis utilizing data from the Swedish national stroke registry indicated that atrial fibrillation, diabetes, and antihypertensive use were more common in men, while smoking was more prevalent among women. 18 However, the latter study did not stratify findings by narrower age brackets, potentially obscuring nuanced patterns.
Overall, while sex differences in stroke incidence, etiologies, and VRFs among younger adults have been studied, large-scale studies with finer age stratification are needed to clarify these patterns.
In a nationwide Swiss cohort, we aimed to address sex- and age -related differences in stroke rates, traditional VRFs, and stroke etiologies among young adults (18–55 years) between 2014 and 2022.
Methods
Study design and cohort
This retrospective study used data from the Swiss Stroke Registry (SSR), a national prospective registry for quality assurance and multi-centric stroke research in Switzerland.19,20 The SSR collects standardized data on VRFs, presentation, diagnostics, treatment, and functional outcomes, including 3-month follow-ups for ischemic strokes treated at certified stroke centers and units in Switzerland (Supplemental Text Section S1). It employs a modified TOAST classification system (Trial of Org 10172 in Acute Stroke Treatment 21 ), categorizing ischemic stroke into five distinct subtypes: large artery atherosclerosis (LAA), cardioembolic, small vessel disease (SVD), stroke of other determined etiology, and stroke of undetermined etiology. Additionally, it captures specific etiologies like carotid artery dissection and patent foramen ovale (PFO), as well as cases with multiple possible etiologies.
This study included all consecutive first-ever, imaging-confirmed (diffusion restriction on MRI, and/or arterial occlusion on CT/MR angiography and/or perfusion deficit on CT/MR perfusion imaging) acute ischemic stroke patients aged 18–55, treated between January 2014 and September 2022.
We excluded patients with incomplete diagnostic workups, which we defined as requiring, at a minimum, extra- and intracranial cerebral artery assessments, ECG, and echocardiography, where stroke etiology remained undetermined, as well as stroke mimics, and those who declined research use of their data. A keyword review of “other determined stroke etiology” descriptions was conducted to enhance data quality. Cases labeled “embolic stroke of unknown etiology (ESUS)” were reclassified as “undetermined etiology.” Modified TOAST classifications were adjusted: hypertensive or microangiopathic cases were recoded to SVD, large artery dissections to cervical artery dissection (CAD), and PFO closure cases to PFO (only cause and <3 vascular risk factors). Patients with atrial fibrillation or mechanical prosthetic valves—high-risk cardioembolism sources per TOAST 21 —were reclassified as cardioembolism.
Age and sex-specific population count data, averaged over the years 2014 to 2022, were retrieved from the Swiss Federal Statistical Office. 22
This study was approved beforehand by the Ethics Committee Northwestern Switzerland (ID 2023-01248).
Study outcome measures
Primary outcomes of interest were the age- and sex specific rates of first-ever ischemic stroke per 100,000 person-years (py) by sex, stroke etiology, and BMI. Secondary outcomes were: (a) the prevalence of traditional VRFs (arterial hypertension [>140/90 mmHg repetitively], diabetes, dyslipidemia [treatment or LDL>2.6 mmol/L], smoking [actively or stopped <2 years ago], obesity [BMI ⩾ 30]) and (b) stroke etiology distribution across age groups. Supplemental Table S1 provides the number of observations for each variable.
Statistical analysis
All analyses were performed with RStudio version 4.3.0 23 (Supplementary Text Section S2). Missing values were discarded from analyses. Age- and sex-specific stroke rates per 100,000 py were calculated according to the formula detailed in Supplemental Text Section S3. Categorical variables are presented as counts with percentages (%), and continuous variables as medians with interquartile ranges (IQR). Group comparisons between age groups (18–35, 36–50, 51–55) and sex, stratified by age groups, were conducted using the Kruskal-Wallis rank-sum test (continuous variables) and the Pearson χ²-test (categorical variables).
To assess the impact of sex, VRFs, and elevated BMI (⩾25) on the increase of stroke rates with aging, we applied Quasi-Poisson regression models to stroke counts, accounting for potential overdispersion in the data. An offset of the natural logarithm of the population size was used to standardize rates (Supplementary Tables S5–S8). We transformed the model count predictions to stroke rates and visualized them alongside the observed stroke rates (Figure 2). Stroke rates were modeled as functions of:
(a) Age, sex, and their interaction.
(b) Age, sex, and the number of VRF, including all two-way and three-way interactions.
(c) Age, sex, and BMI category, with all two-way and three-way interactions.
(d) Age, sex, and stroke etiology, including all two-way and three-way interactions.
We used ordinal regression to analyze the number of cardiovascular risk factors across age and sex, employing the “polr” function from the MASS package. 24 Age, sex, and their interaction were included as predictors.
P values <0.05 were considered significant and 95% confidence intervals were reported. Our reporting adheres to the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines. 25
Results
Cohort characteristics across age groups
Among 8,158 individuals aged 18 to 55 with acute ischemic stroke (AIS), TIA, or mimics, 4,556 (55.8%) had first-ever AIS confirmed by imaging (Figure 1). After excluding 560 patients with incomplete diagnostics and reclassifications, 3,995 remained for analysis (median age: 48.2 [IQR: 41.5, 52.1] years, 66% male). Supplemental Table 1 contrasts the outlined factors between individuals aged 18–35 (n = 546), 35-50 (n = 2,122) and those aged 51–55 (n = 1,324), while Supplemental Table 2 compares these factors across 5-year age intervals. Supplemental Table 3 provides a comparison of characteristics between male and female patients, stratified by the trichotomized age groups. Supplemental Table 4 presents estimated stroke rates with 95% confidence intervals across 5-year age intervals.
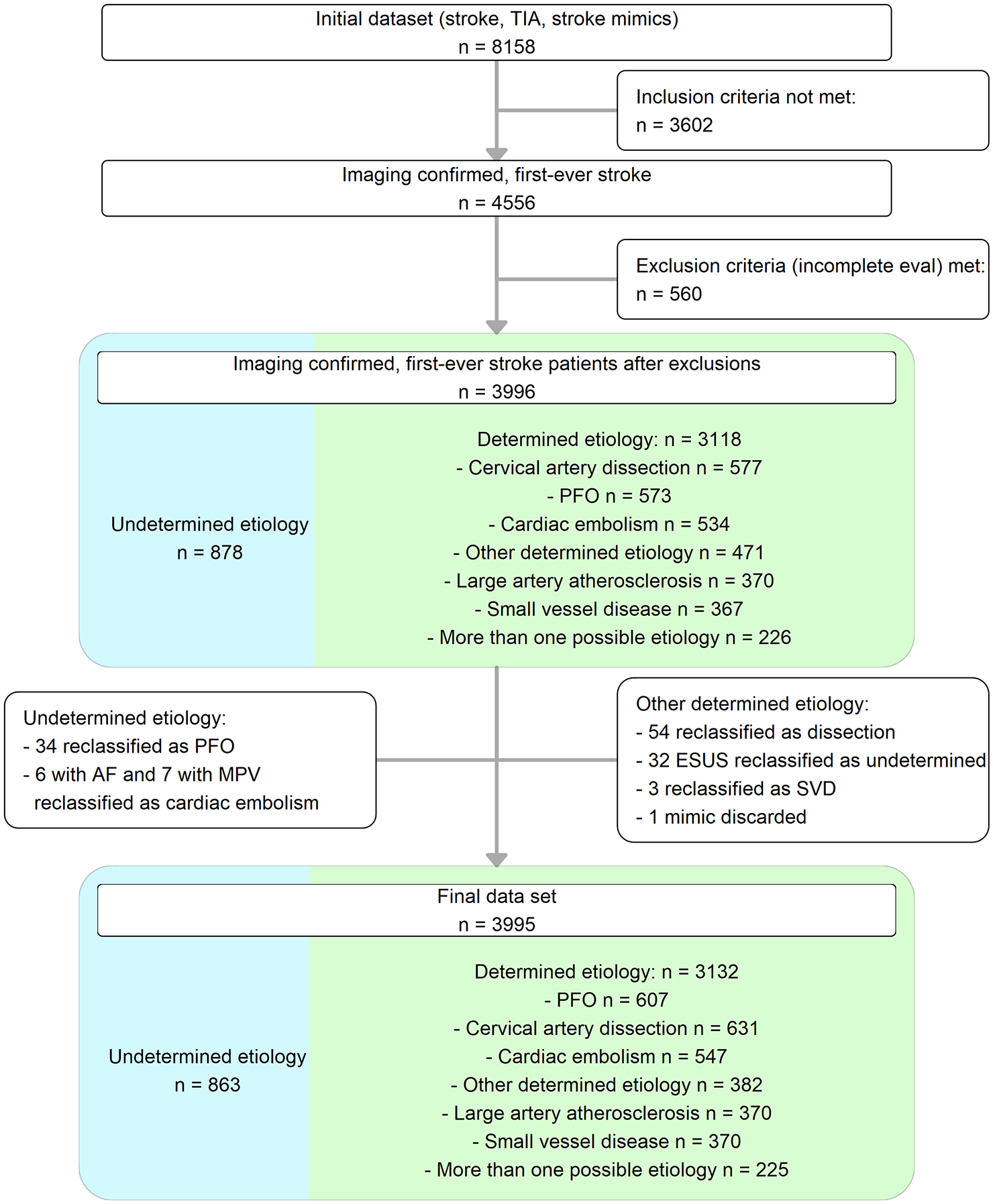
Patient flow chart.
We observed a balanced sex distribution of stroke patients aged 18 to 35 (male 49%), but a marked shift toward male predominance in older age groups (36–50: 66%, 51–55: 72%, Supplemental Table S1, Figure 2(a)).
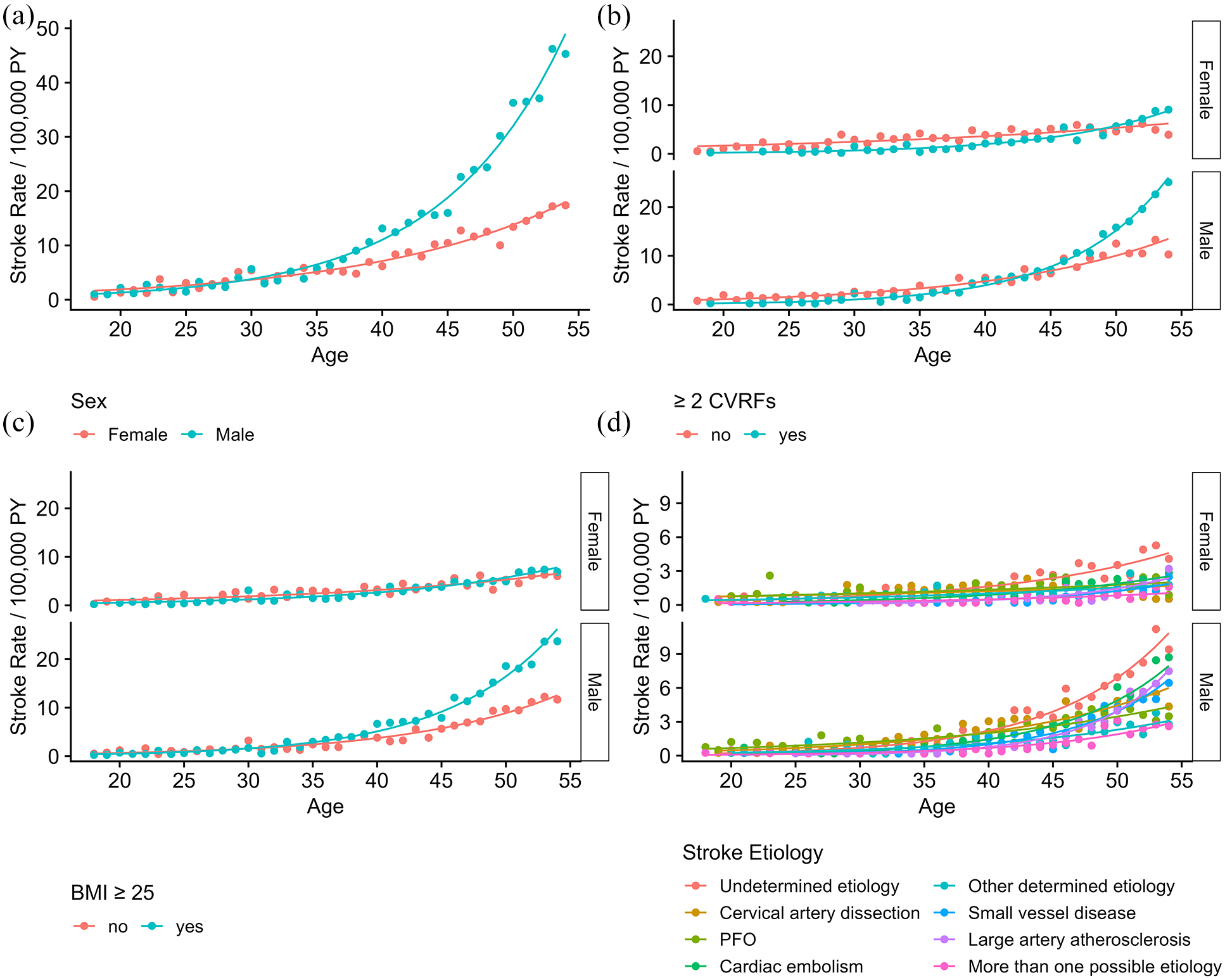
Age- and Sex-specific occurrence rates of first-ever ischemic stroke in Switzerland (2014-2022). Stroke rates per 100,000 person-years, stratified by sex and age (a), presence of ⩾ 2 vascular risk factors (VRFs) (b), BMI ⩾ 25 (c), and etiology (d). Data points represent observed rates; solid lines are fitted rates from Quasi-Poisson regression models adjusting for age, sex, their interactions, and additional interactions with etiology, number of risk factors, and BMI (Supplemental Tables 1–4).
All VRFs, including hypertension, hyperlipidemia, diabetes, smoking, and obesity, increased with age (Supplementary Table S1 and S2, Figure 3(a) and (b)). The proportions of stroke patients who had two or more VRFs (18–35: 22%, 36–50: 48%, 51–55: 63%, p < 0.001), atrial fibrillation (18–35: 1.1%, 36–50: 3.9%, 51–55: 7.0%, p < 0.001) and coronary heart disease (18–35: 0.7%, 36–50: 4.2%, 51–55: 7.3%, p < 0.001) significantly differed between age groups.
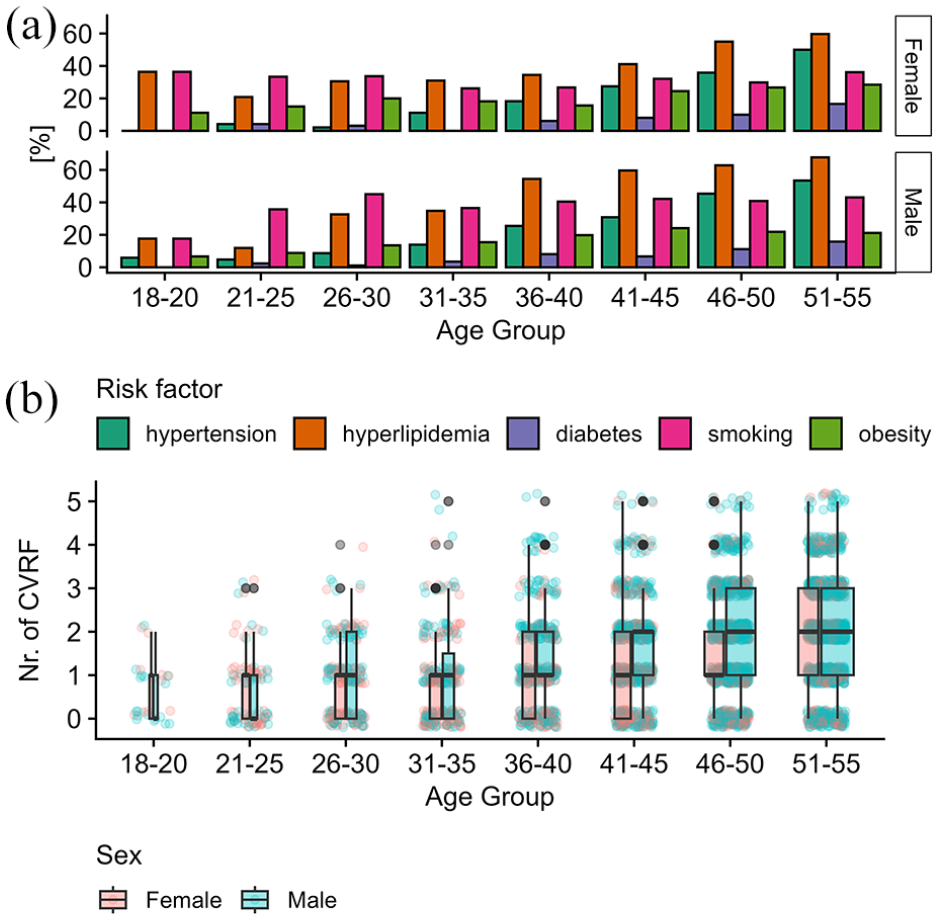
Vascular risk factors across age groups and sex: (a) percentage distribution of hypertension, hyperlipidemia, diabetes, smoking, and obesity across different age groups for both sexes and (b) Boxplot distribution of the number of cardiovascular risk factors by age group and sex.
The distribution of stroke etiologies showed marked differences across age groups (Figure 4(a)). PFO and CAD were the most frequent etiologies among younger age groups (18–35: PFO 27%, CAD 22%, undetermined etiology 18%), but their relative proportion decreased with age. Conversely, the rate of patients with undetermined etiology, cardiac embolism, SVD, and LAA increased in the older age group (51–55: PFO 9.5%, CAD 10%, undetermined etiology 23%, SVD 12%, LAA 15%).
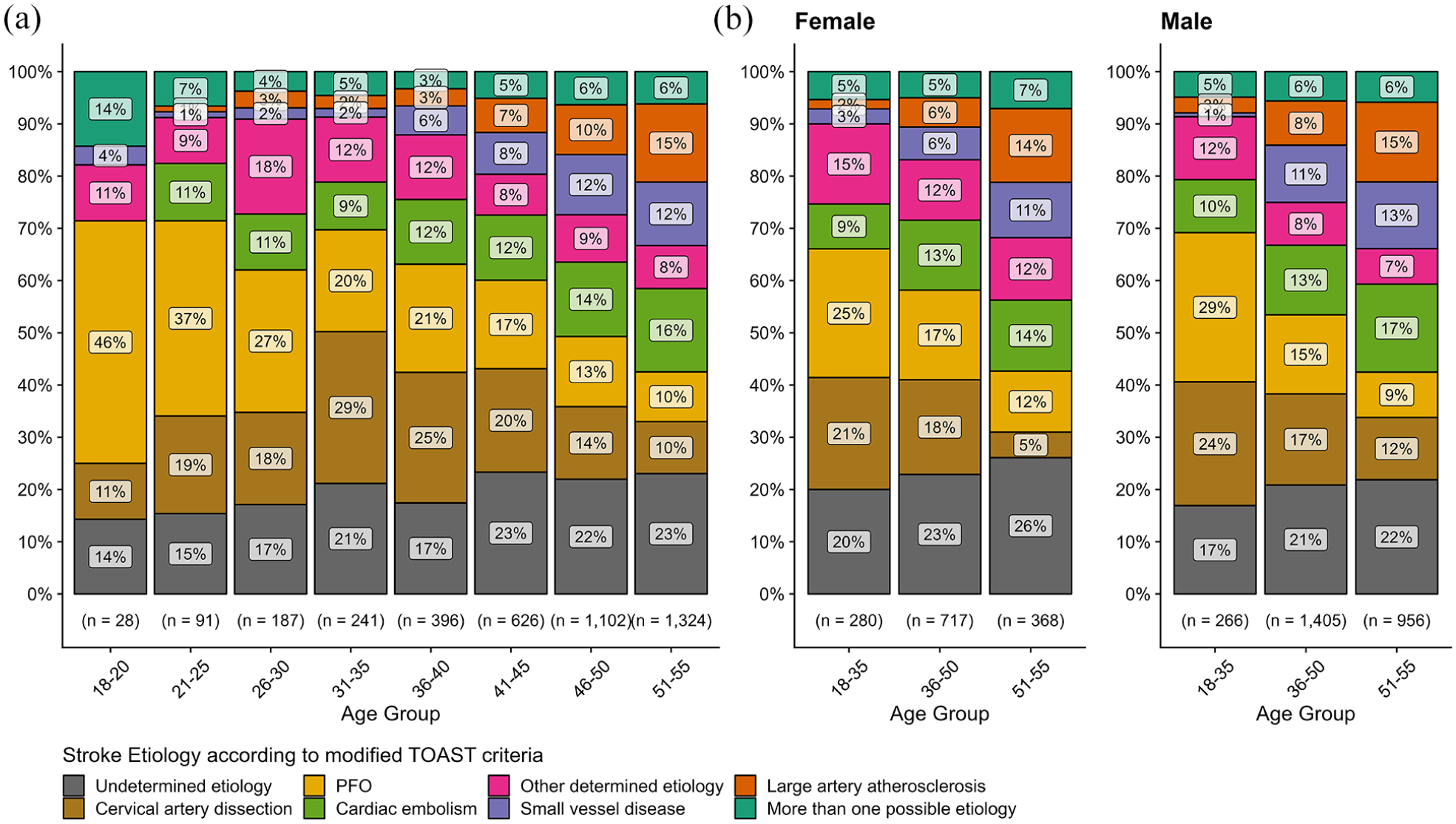
Distribution of Stroke Etiologies across age groups and sex. Percentage distribution of stroke etiologies across age groups (a) and in age groups 18–45 and 46–55 and segmented by sex (b).
Comparisons of women and men with AIS in age groups 18–35, 36–50, and 51–55
In the 18–35 group, men had a slightly higher BMI (23.8 vs 24.7, p = 0.048). However, there were no statistically significant differences in the prevalence of BMI ⩾ 25 (women: 39% vs men: 46%, p = 0.2) or obesity (women: 18% vs men: 13%, p = 0.2). In the 36–50 age group, the BMI gap widened significantly (women: 24.4 vs men: 26.1, p < 0.001), with a greater proportion of men having BMI ⩾ 25 (women: 48% vs men: 63%, p < 0.001); however, obesity rates were not statistically different between the sexes (women: 24% vs men: 22%, p = 0.5). This gap narrowed again in the 51–55 group (women: 26.2 vs men: 26.2, p = 0.2), though men still had higher rates of BMI ⩾ 25 (women: 55% vs men: 65%, p = 0.003), while obesity rates were significantly higher in women (28% vs 22%, p = 0.016).
In the 18–35 age group, there were no statistically significant differences between men and women with AIS in the prevalence of hypertension, hyperlipidemia, and smoking. However, there was a non-significant trend toward higher smoking rates in men (women: 30% vs men: 38%, p = 0.069). In the 36–50 age group, these risk factors became significantly more prevalent in men, and in the 51–55 group, only hyperlipidemia and smoking remained significantly higher in men (Supplemental Table S3). The proportion of patients with ⩾2 VRFs did not significantly differ between sexes in the 18–35 group (women: 20% vs men: 24%, p = 0.3) but were higher in men aged 36-50 (women: 39% vs. men: 53%, p < 0.001). By ages 51–55, the gap had narrowed (women: 59% vs. men: 65%, p = 0.058).
The distribution of stroke etiologies did not statistically differ between men and women with AIS in the 18-35 group (p = 0.4). However, significant differences were observed in the 36–50 and 51–55 age groups (both p < 0.001, Figure 4(b), Supplemental Table S3). In the 36–50 group, men had numerically higher rates of large artery atherosclerosis (LAA, women: 5.6% vs men: 8.5%) and small vessel disease (SVD, women: 6.3% vs men: 11%), while women had more strokes of undetermined (women: 23% vs men: 21%) or other determined etiologies (women: 12% vs men: 8.2%). In the 51–55 group, LAA (women: 14% vs men: 15%) and SVD (women: 11% vs men: 13%) rates were numerically similar between the sexes, but women had higher rates of undetermined (women: 26% vs men: 22%) and other determined etiologies (women: 12% vs men: 8.7%), and men had more strokes due to CAD (women: 4.9% vs men: 12%).
Modelling stroke rates by age, sex, vascular risk factors, and stroke etiologies
The first Quasi-Poisson model (Supplementary Table S6, Figure 2(a)) showed that stroke rates in women increased by 7% annually (age effect: SRR = 1.07, CI = [1.06, 1.07], p < 0.001) with an additional 4% annual increase in men (age x sex interaction: SRR = 1.04, CI = [1.03, 1.05], p < 0.001).
In the second model, incorporating age, sex, and the presence of ⩾2 VRFs (Supplemental Table S7, Figure 2(b)), stroke rates in women with fewer than two VRFs increased by 4% per year (age effect: SRR = 1.04, CI = [1.03, 1.05], p < 0.001), with an additional 4% increase in men (age x sex interaction: SRR = 1.04, CI [1.03, 1.05], p < 0.001). An additional 7% annual increase was observed in patients with ⩾2 VRFs compared to those with fewer (age x ⩾2 VRFs interaction: SRR = 1.07, CI [1.06, 1.09], p < 0.001), with a 45% higher rate in men with ⩾2 VRFs (male x ⩾2 VRFs interaction: SRR = 1.45, CI [1.25, 1.68], p < 0.001). No significant three-way interaction was found (age × male × ⩾2 VRFs: SRR = 0.99, CI [0.97, 1.01], p = 0.4).
The third model (Supplemental Table S5, Figure 2(c)) examined stroke rates by BMI. In women with BMI <25, stroke rates increased by 5% annually (SRR = 1.05, CI [1.04, 1.06], p < 0.001), with an additional 4% increase in men (age × sex interaction: SRR = 1.04, CI [1.02, 1.05], p < 0.001). Overweight women (BMI ⩾25) showed an additional 3% annual increase (age x BMI ⩾25 interaction: SRR = 1.03, CI [1.01, 1.04], p < 0.001), with no significant three-way interaction (age × sex × BMI ⩾25: SRR = 1.01, CI [0.99, 1.02], p = 0.6).
Finally, analysis by stroke etiology (Supplemental Table S8, Figure 2(d)) showed an 8% annual increase in undetermined etiology (reference) strokes in women (SRR = 1.08, CI [1.06, 1.09], p < 0.001), with an additional 4% increase in men (age x sex interaction: SRR = 1.04, CI [1.02, 1.06], p < 0.001). Significantly smaller increases were observed for CAD, PFO, and other determined etiologies, while LAA showed a higher increase. Sex-etiology interactions indicated higher stroke rates from SVD (male x SVD interaction: SRR = 1.63, CI [1.24, 2.16], p < 0.001) and CAD (male x CAD interaction: SRR = 1.37, CI [1.10, 1.72], p = 0.006) for men at the reference age of 45.8.
Ordinal regression analysis on the influence of age and sex on the number of vascular risk factors
Ordinal regression analysis (Supplemental Table S7) showed a significant association between age and the number of VRFs (Figure 3(c)). Each additional year of age increased the odds of having more VRFs 7% (age effect: OR = 1.07, CI [1.06, 1.08]). Men were more likely than women to have a higher number of VRFs at the mean reference age of 45.8 (male sex effect: OR = 1.40, CI = [1.24, 1.58]). However, the interaction between age and sex was not significant (male sex effect: OR = 1.00, CI = [0.99, 1.02], p = 0.7), suggesting that age influences VRFs similarly across sexes.
Discussion
Key findings include: (a) Stroke rates were similar until the mid-thirties, but men showed a significantly steeper increase after age 36, leading to male predominance. (b) The age-related rise in stroke cases was more pronounced in individuals with elevated BMI and those with ⩾2 VRFs, especially among men. (c) While no statistically significant differences in VRFs were observed between men and women aged 18–35, VRFs accumulated earlier in men, leading to a higher prevalence of multiple VRFs in men aged 36–50, with the gap narrowing by ages 51–55. (d) Stroke etiologies shifted with age, with increasing proportions of cases attributed to LAA, SVD, and cardioembolism, alongside sex differences in etiology distribution across age groups.
Stroke rates remained low in both sexes until age 35, when men began to show a growing predominance. This contrasts with some earlier studies suggesting higher stroke incidence in women up to age 45,8,13,14 but aligns with other research reporting male preponderance after age 35–40. 11 Women-specific risk factors, such as pregnancy26,27 and oral contraceptive use, 28 may be less prominent in this analysis due to declining prescriptions of combined oral contraceptives29,30 and falling birth rates in Switzerland. 31 Notably, a recent report from the Bern Stroke Center found that 20% of women aged 16–35 with AIS were pregnant or in the puerperium. This may be offset by young men more frequently engaging in cardiovascular risk behaviors, such as heavy drinking and poor dietary habits. 32
We confirmed an exponential increase in stroke cases with age, extending Putaala et al.’s findings by showing greater increases in men and those with elevated BMI and multiple VRFs. 12 This is consistent with studies from Sweden and Finland, showing stroke occurs about 10 years earlier in men than women in the 40–69 group, and remains higher in men. 33
Our analysis revealed distinct sex-specific patterns in vascular risk factors (VRFs) across age groups, with the faster increase in stroke cases among men paralleled by an earlier accumulation of traditional VRFs. Among male stroke patients aged 36–50, 53% presented with ⩾2 VRFs compared to 39% of women (p < 0.001). In contrast, no significant sex differences in VRFs were observed in stroke patients aged 18–35, although there was a trend towards higher smoking rates in men. In the 36–50 age group, men had higher proportions of hypertension, hyperlipidemia, and smoking. By ages 51–55, no significant difference in hypertension rates was observed between the sexes; however men continued to have higher rates of hyperlipidemia and smoking, while women had higher rates of obesity. Diabetes prevalence showed no statistically significant differences across all age groups. While VRF accumulation increased similarly with age in both sexes, men had a higher intercept at the population mean reference age (45.8 years), suggesting that male stroke patients develop an equivalent number of VRFs approximately 5 years earlier than women (see Figure 3(c)). This aligns with findings from Denmark’s stroke registry, which reported a higher prevalence of hypertension and smoking in men up to age 50 and greater obesity in women. However, unlike our findings, the Danish study observed higher diabetes rates in men. 34 Notably, the pronounced exponential increase in stroke cases among men with elevated BMI supports the strong association between elevated BMI and stroke risk, driven by conditions such as hypertension and diabetes.3,4,6 While the gap in VRFs between men and women narrowed in the 51–55 age group, the difference in stroke rates continued to widen. This is consistent with prior reports, which noted the highest male preponderance in stroke cases in the 50–59 and 50–69 age groups, followed by a decline thereafter. 11
Stroke etiologies shifted by age and sex: PFO and CAD predominated in younger patients (18–35), while undetermined etiology, LAA, SVD, and cardioembolism increased from 36 to 50 onward. This trend continued and was more pronounced in the 51–55 age group, where strokes due to LAA, SVD, and cardioembolism became even more prevalent. The incidence of strokes related to SVD and LAA increased more markedly with advancing age compared to strokes of undetermined etiology. Men aged 36–50 exhibited higher rates of LAA and SVD, while women in this group had more strokes of undetermined and other determined etiologies. In the 51–55 age group, men showed higher rates of CAD and LAA, while women maintained higher rates of undetermined and other determined etiologies.
A recent analysis of the Utrecht Cardiovascular Cohort secondary prevention study demonstrated that sex modifies how VRFs affect stroke incidence: hypertension, smoking, and diabetes elevate stroke risk in women, while in men, risk is linked to hypertension, smoking, LDL cholesterol, and low activity. 35 Moreover, recent evidence showed that non-traditional risk factors, such as migraine and thrombophilia, played a significant role in stroke risk, particularly among younger women, whereas men were more frequently affected by strokes related to traditional risk factors like hypertension and smoking. 10
Strengths and limitations
Strengths include: (a) The use of comprehensive, consecutively collected data from all major Swiss hospitals certified for acute stroke treatment. (b) The large sample size and wide covered time frame that provides a robust basis for the assessment of age and sex-related differences. However, the sample size may still be insufficient to detect small differences in the subgroup of patients aged 18–35 and, to a lesser extent, in the 51–55 age group.
Limitations are: (a) The retrospective design, characterized by missing data on key variables like BMI, exclusion of potentially relevant factors such as pregnancy, and an inherent risk of residual confounding. (b) The SSR does not provide population-based data since several stroke units did not participate in the SSR at the start of the registry. Therefore, we cannot infer stroke incidence rates at population level. (c) The exclusion of patients with incomplete etiological workup and those presenting to a center contributing to the SSR could limit the generalizability of our findings. (d) Stroke rates were normalized using age- and sex-specific population data averaged over 2014–2022. However, as the Swiss Stroke Registry is not population-based and not all stroke centers contributed data from the beginning of the study period, the normalized stroke rates may be biased.
Conclusions
Our study highlights age and sex differences in stroke rates and VRF profiles. The steep increase in male stroke rates after age 35 underscores the importance of early, sex-specific interventions targeting modifiable risk factors.
Supplemental Material
sj-docx-1-eso-10.1177_23969873251317347 – Supplemental material for First ischemic stroke in young adults: Sex and age-related differences in stroke rates, risk factors, and etiologies
Supplemental material, sj-docx-1-eso-10.1177_23969873251317347 for First ischemic stroke in young adults: Sex and age-related differences in stroke rates, risk factors, and etiologies by Thomas R Schneider, Tolga D Dittrich, Timo Kahles, Mira Katan, Andreas R Luft, Marie-Luise Mono, Manuel Bolognese, Marcel Arnold, Mirjam Heldner, Patrik Michel, Elisabeth Dirren, Biljana Rodic, Carlo W Cereda, Nils Peters, Leo H Bonati, Susanne Renaud, Andrea M Humm, Friedrich Medlin, Sylvan Albert, Rolf Sturzenegger, Alexander A Tarnutzer, Philip Siebel, Markus Baumgärtner, Christian Berger, Pasquale Mordasini, Jochen Vehoff, Krassen Nedeltchev and Gian Marco De Marchis in European Stroke Journal
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
In accordance with Swiss legislation, enrollment in the Swiss Stroke Registry (SSR) is mandated for quality assurance measures. Patients are notified about the potential utilization for research with the provision that individuals who dissent to the use of their data are excluded from research projects.
Ethical approval
This study has received prior approval from the Ethics Committee Northwestern Switzerland (ID 2023-01248).
Contributorship
TRS, TDD and GMDM planned the work. TRS performed the analyses. TRS, TDD and GMDM drafted the manuscript. All authors interpreted the results and substantially contributed to the final manuscript.
Guarantor
Thomas R Schneider, MD
ORCID iDs
Data availability
Anonymized data and statistical code are available upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.