
Abstract
Introduction:
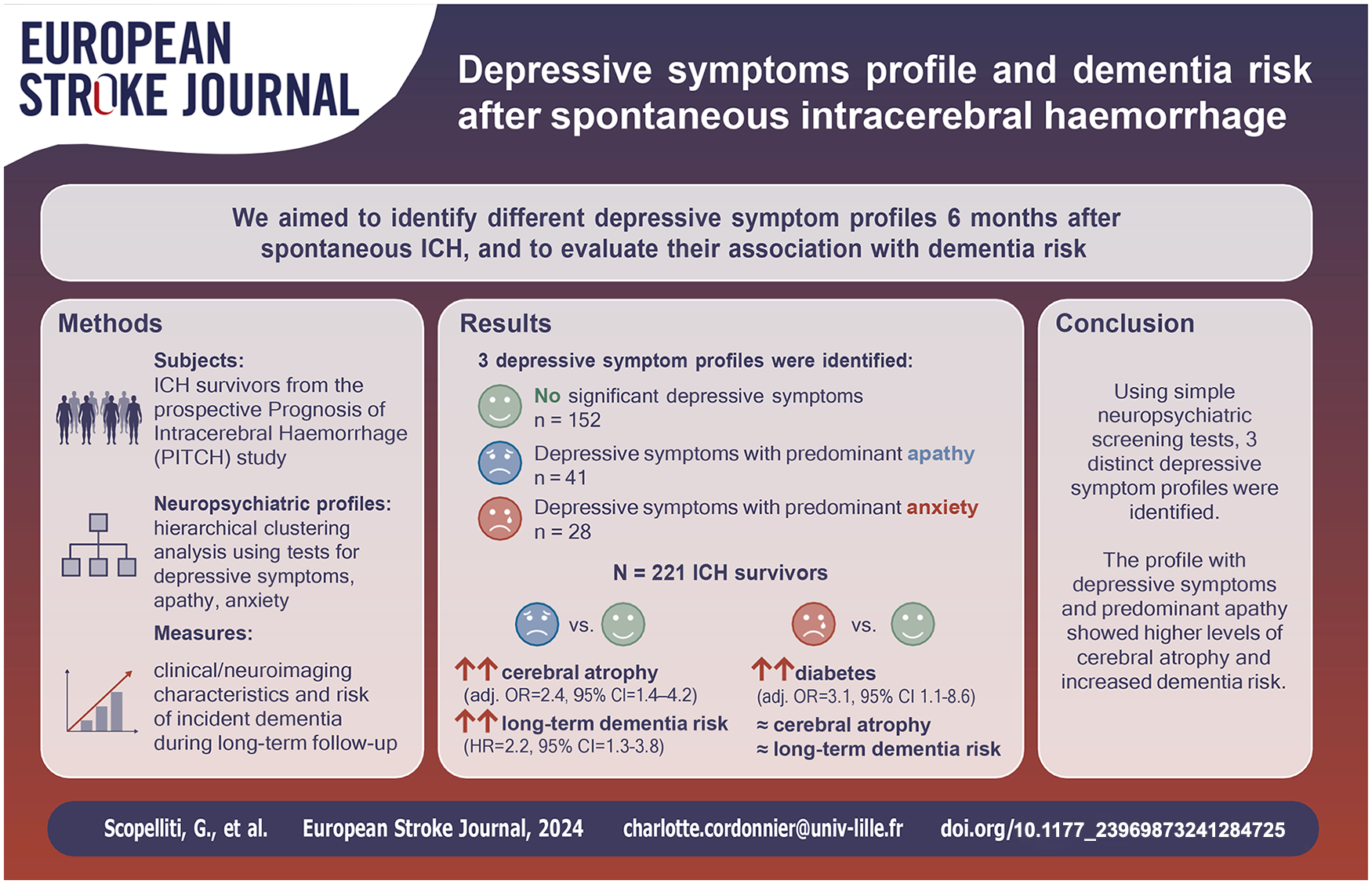
Depressive symptoms are commonly reported after spontaneous intracerebral haemorrhage (ICH) and frequently associated with cognitive decline. Using hierarchical clustering analysis (HCA), we aimed to identify different post-ICH depressive symptoms profiles and to evaluate their association with dementia risk.
Methods:
We included consecutive patients from the prospective Prognosis of Intracerebral Haemorrhage (PITCH) study who survived 6 months after the ICH. We performed HCA using depressive symptoms severity (assessed using the Montgomery–Åsberg Depression Rating Scale (MADRS)), along with the presence of apathy and anxiety (screened using Neuropsychiatric Inventory questionnaire). Baseline clinical/neuroimaging characteristics and risk of incident dementia were compared between different profiles using univariate and multivariable models.
Results:
Of 265 six-month ICH survivors, 221 (83%) underwent neuropsychiatric screening (mean age 65.5 years; 57% male). Using HCA, 3 profiles were identified: (1) without significant depressive symptoms (n = 152; median MADRS score = 2 [IQR 0–4]); (2) depressive symptoms with predominant apathy (n = 41; median MADRS score = 15 [IQR 5–20], 68% with apathy); (3) depressive symptoms profile with predominant anxiety (n = 28; median MADRS score = 17 [IQR 9–25]; 100% with anxiety). Compared to patients without depressive symptoms, patients with depressive symptoms and predominant apathy (but not those with predominant anxiety) were more likely to have cerebral atrophy (OR = 2.4, 95% CI = 1.4–4.2) and had significantly higher long-term new-onset dementia risk (adjusted hazard ratio = 2.2, 95% CI = 1.3–3.8).
Conclusion:
Screening for apathy and anxiety on top of depressive symptoms might help identifying patients at risk for dementia. Future studies on treatment should account for different post-ICH depressive symptoms profiles that may impact on cognitive function.
Keywords
Introduction
Depressive symptoms have been increasingly recognized as one of the most reported unmet needs of stroke survivors, 1 and psychological disturbances are acknowledged among top research priorities to improve the outcome. 2 Thoroughly described among all stroke survivors,3,4 depressive symptoms are also commonly reported after spontaneous intracerebral haemorrhage (ICH). 5 Preliminary evidence suggests that post-ICH depressive symptoms might represent a spectrum of distinct neuropsychiatric disturbances, which vary in terms of clinical presentation, underlying cerebral pathology, and long-term prognosis.6–8
ICH survivors are also at high risk for cognitive decline, with roughly 1 in 3 patients developing dementia within 4 years after the index event. 9 Depressive symptoms and cognitive decline have been frequently described as entangled clinical entities in ICH survivors, and they are both associated with worse outcomes and long-term functional decline.6,10,11 In a prior study, we showed the potential utility of neuropsychiatric profiling for stratifying the risk of long term new-onset dementia in ICH survivors. 12 Even if different neuropsychiatric manifestations (including apathy and anxiety) frequently co-occur with depressive symptoms, no previous study has evaluated whether these manifestations could influence cognitive outcomes following ICH. In this view, it has been suggested that the presence of apathy could serve as an early indicator of cognitive impairment in stroke patients.13,14 Hence, we hypothesized that the presence of apathy and anxiety could be used to better characterize depressive symptoms of ICH survivors and predict the future risk of dementia.
In a prospective cohort of ICH survivors, using hierarchical clustering analysis (HCA), we aimed to identify different post-ICH depressive symptoms profiles, and to evaluate their association with the risk of incident new-onset dementia.
Methods
Patient selection
We included patients with spontaneous ICH enrolled in the ‘Prognosis of Intra-Cerebral Haemorrhage’ (PITCH) cohort from November 2004 to March 2009, 9 who were alive at 6 months and able to undergo neuropsychiatric assessment. Patients aged ⩾ 18 years, with evidence of parenchymal haemorrhage on their first CT scan were included. The enrolment criteria and the design of the prospective PITCH cohort have been extensively described in previous studies.9,15
Baseline clinical evaluations
At baseline, we collected demographic characteristics, vascular risk factors, history of stroke (ischaemic or haemorrhagic) as previously detailed.9,15 We defined the presence of pre-existing dementia in case of an Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE) score ⩾ 64.9,16 We used the National Institute of Health stroke scale (NIHSS) score to assess the severity of ICH symptoms at admission. 17 We used the modified Rankin Scale (mRS) scores based on clinical history and caregiver interviews to assess functional status before ICH. 18
Follow-up evaluation
Patients were invited to be followed-up at pre-specified time points (6 months and 1, 2, 3, 4.5, 6, 8, and 10 years after the index ICH), as previously detailed.9,19 The occurrence of new-onset dementia was assessed at each follow-up according to the National Institute on Ageing-Alzheimer’s Association criteria for all-cause dementia, as previously described.9,20 Patients (or their relatives, or family physician) were contacted by phone if they did not show up for the planned follow-up visit to ascertain whether they were alive or not.
Neuropsychiatric evaluation
The neuropsychiatric evaluation was performed by a stroke neurologist at 6–12 months (first available follow-up visit) after the index ICH, using the Montgomery–Åsberg Depression Rating Scale (MADRS) to evaluate the severity of depressive symptoms, and the Neuropsychiatric Inventory Questionnaire (NPI-Q) to ascertain the presence/absence of apathy and anxiety. MADRS is well-recognized screening tool for the detection of depressive symptoms in patients with stroke. 21 NPI-Q is an informant-based, self-administered battery encompassing 12 items (hallucinations, delusions, agitation, depression, anxiety, elation, apathy, disinhibition, irritability, aberrant motor behaviour, night-time behaviour, appetite change) that allows a quick evaluation of neuropsychiatric symptoms. 22 For each item, the informant was asked if the principal symptoms were absent or present; if present, severity (range 1–3) was recorded for each item.
Neuroimaging
All patients in the study were evaluated using CT scan at admission. We dichotomized ICH location into lobar and non-lobar, including in the latter also brainstem and cerebellar haemorrhages. 23 We calculated the ICH volume using the ABC/2 method. 24 All patients without contraindications underwent a 1.5 Tesla brain MRI a few days after the index ICH. The MRI protocol included at least fluid attenuated inversion recovery (FLAIR) and T2*-weighted gradient-echo (GRE) sequences (echo time: 228 ms, repetition time: 700 ms, flip angle: 25°, field of view: 250 mm, matrix: 352 × 224, slice thickness: 5 mm, and interslice gap: 1.5 mm).19,23 We recorded the presence of lacunes and cortical superficial siderosis (CSS), presence of cerebral microbleeds (CMB), white matter hyperintensities severity (Fazekas et al. 25 scale), according to STRIVE criteria. 26 We reported cerebral atrophy using a simplified version of a validated scale, with scores ranging 0–3.19,27 To minimize the impact of large brain lesions on our assessments, we focussed on the unaffected hemisphere for evaluating white matter hyperintensities and cerebral atrophy. Neuroradiologists blinded to clinical data conducted CT scan and MRI assessments.
Statistical analysis
Quantitative variables are expressed as means (standard deviation, SD) in case of normal distribution; otherwise, they are expressed as median values (interquartile range, IQR). Categorical variables are expressed as numbers (percentage). Normality of distributions was assessed using histograms and the Shapiro-Wilk test.
We performed a hierarchical clustering analysis (HCA) to classify patients in homogenous subgroups according to depressive symptoms, apathy and anxiety scores at 6 months (Supplemental Materials).
Baseline characteristics were compared between the three identified clusters using Chi-square tests for categorical variables and analysis of variance (ANOVA) for quantitative variables (or Kruskall-Wallis test in cases of non-normal distribution). To assess the variables associated with each of the three identified clusters, baseline characteristics that differed between the three clusters with p < 0.10 in univariate analyses were included into a multivariable multinomial logistic model with a forward-stepwise approach using a removal criterion of p > 0.05; multinomial odds ratio (OR) were derived from the model as effect sizes. The absence of collinearity between the candidate variables was checked by calculating the variance inflation factors (VIF).
Finally, in patients without pre-existing dementia, the cumulative incidence of dementia during follow-up was estimated using Kaplan-Meier methods and was compared between the three identified clusters by using a Cox proportional Hazard model adjusting for age as a pre-specified covariate. The proportional hazard assumption was evaluated by using the Schoenfeld residual plot.
Statistical testing was conducted at the two-tailed α-level of 0.05. Data were analysed using the SAS software version 9.4 (SAS Institute, Cary, NC).
Results
Out of 560 patients with spontaneous ICH included in the PITCH cohort, 265 (47%) were alive 6 months later, 221 of whom (83%) were able to undergo depressive symptoms questionnaire and were included in the study (Figure 1); 125 were men (57%), mean age was 65.5 years (SD 14.1) Baseline characteristics of included patients (compared to those who did not undergo neuropsychiatric screening) are reported in Supplemental Table 1. Previous history of depression was present in 45 patients (20%), and 21 patients (10%) had a pre-ICH dementia.

Flowchart of patient inclusion.
Clustering
Using HCA, we identified 3 depressive symptoms profiles (Supplemental Table 2):
(1) no significant depressive symptoms (ND) – 152 patients (69%);
(2) depressive symptoms and predominant apathy (DAp) – 41 patients (19%);
(3) depressive symptoms and predominant anxiety (DAx) – 28 patients (13%).
Baseline variables associated with the three identified clusters
Baseline characteristics of patients according to their profile were reported in Table 1. Median age was 67 years (IQR 54–76) in the ND profile, 74 years (IQR 60–81) in the DAp profile, and 58 years (IQR 52–70) in the DAx profile (p = 0.005). The rate of pre-ICH depression was 14% in the ND profile, 27% in the DAp profile, and 46% in the DAx profile (p < 0.001). The prevalences of diabetes and excessive alcohol intake were also significantly different between the three profiles in univariate analyses (p = 0.024 and 0.039, respectively). Concerning the neuroimaging parameters, we found that cerebral atrophy score was significantly different between the three groups in univariate analysis (p = 0.029).
Comparison in baseline characteristics between neuropsychiatric profiles.

CMBs, cerebral microbleeds; CT, computed tomography; CSS, cortical superficial siderosis; ICH, intracerebral haemorrhage; IQR, interquartile range; MRI, magnetic resonance imaging; NIHSS, National Institutes of Health Stroke Scale; SD, standard deviation.
Values are expressed as number (%) unless otherwise indicated. Profile 1: without significant depressive symptoms (ND); profile 2: depressive symptoms with predominant apathy (DAp); profile 3: depressive symptoms with predominant anxiety (DAx).
p-Value was calculated using chi-square analysis for discrete variables and Kruskall-Wallis test for continuous variables.
After a forward selection, the selected multivariable model included diabetes, previous depression, baseline NIHSS score and cerebral atrophy score (Supplemental Table 3). Compared to the ND profile, the DAp profile and the DAx profile had higher rates of pre-ICH depression (respectively, OR = 3.2, 95% CI = 1.1–9.1, and OR = 5.2, 95% CI = 1.9–14.3). Patients in the DAx profile had higher rates of diabetes than patients of two other groups: compared to the ND profile, odds ratio (OR)= 3.1 (95% CI = 1.1–8.6); compared to DAp profile, OR = 4.6 (95% CI = 1.0–21.0). Compared to the ND profile, patients in the DAp profile had higher baseline NIHSS (OR = 1.09; 95% CI = 1.02–1.15), and cerebral atrophy scores (OR = 2.4, 95% CI = 1.4–4.2).
Long-term dementia risk
Twenty-one patients with pre-existing dementia were excluded. Figure 2 shows the cumulative incidence of dementia according to the depressive symptoms profile. The median follow-up time was 7.1 years (IQR 4.8–8.2). Dementia was diagnosed during follow-up in 41 patients in the ND profile (3-year cumulative incidence, 23.5%), in 35 patients in the DAp profile (3-year cumulative incidence, 53.9%), and in eight patients in the DAx profile (3-year cumulative incidence, 35.2%). After adjustment on age, the risk of dementia differed between the three cluster (p = 0.017), with a significant higher risk in DAp profile compared to the ND profile (hazard ratio [HR] 2.2, 95% CI = 1.3–3.8); the other two pairwise comparisons showed no significant difference, with an HR for DAp profile versus DAx profile of 1.40 (95% CI = 0.60–3.26) and an HR for DAx profile versus ND profile of 1.57 (95% CI = 0.73–3.38).

Long-term risk of dementia according to depressive symptoms profile. Profile 1: no significant depressive symptoms (ND); profile 2: depressive symptoms with predominant apathy (DAp); profile 3: depressive symptoms with predominant anxiety (DAx).
Discussion
Using hierarchical clustering analysis in a prospective cohort of patients with spontaneous ICH, we identified three different post-ICH depressive symptoms profiles: a profile without significant depressive symptoms, a profile with depressive symptoms and predominant apathy, and a profile with depressive symptoms and predominant anxiety. Interestingly, these three profiles differed in terms of baseline clinical and neuroimaging characteristics. Patients with depressive symptoms and predominant apathy were at higher risk of developing dementia compared with patients without depressive symptoms, in an age-adjusted model. Overall, our data confirm the importance of characterizing the distinct neuropsychiatric profiles underlying depressive symptoms of ICH survivors, as they can inform on future risk of dementia.
Depressive symptoms are commonly reported after stroke, but various studies highlighted a relevant heterogeneity of presentation among stroke survivors.3,8,28 Anxiety and apathy have been frequently reported to be associated with depressive symptoms after stroke.14,29,30 Moreover, the presence of apathy has been linked to cognitive decline in patients with stroke.28,31 Based on these data, we hypothesized that the presence of apathy and anxiety might be used to better characterize depressive symptoms using hierarchical clustering analysis in patients with ICH: in fact, using this approach, we identified three different neuropsychiatric profiles that show distinct clinical and neuroimaging features. Characterization of depressive symptoms by the presence/absence of apathetic features might help stratifying the future risk of cognitive decline. 31 However, post-stroke apathy and depression, although closely related and often difficult to disentangle, likely represent two distinct clinical entities recognizing different neurobiological substrate and response to therapy.14,32 It has also been reported that initial symptoms of cognitive decline might be incorrectly interpreted as depression, especially in elders. 33 In this perspective, screening tools can help correctly identifying the different neuropsychiatric syndromes that may arise after ICH, and also discern pure affective depressive symptoms from apathetic syndromes, informing on the individual long-term cognitive risks.12,34
The clinical entity of mild behavioural impairment as a prodromal stage of different type of cognitive impairment has emerged in the recent years, mostly in the field of neurodegenerative diseases. 35 In our study, DAp patients – but not DAx patients – showed higher rates of cerebral atrophy compared to ND patients: this observation supports the existence of different neurobiological substrates underlying post-ICH depressive symptoms profiles. Furthermore, DAp patients showed higher dementia risk compared to ND patients, while DAx patients did not: in line with recent studies, our findings suggest a link between certain neuropsychiatric features, alterations in brain structure, and an increased risk of dementia.8,14,28,36 We did not observe a statistically significant difference in long-term dementia risk between DAp and DAx patients: as this finding might be due to the small number of events, our results need to be replicated in larger datasets. Apart from cerebral atrophy, other markers of cerebral small vessel disease (i.e. cerebral microbleeds, cortical superficial siderosis, white matter hyperintensities) were not associated with neuropsychiatric profiles in our ICH cohort: this finding was surprising, given the close relationship between SVD – particularly cerebral amyloid angiopathy – and poor cognitive outcomes. More studies on larger datasets are needed to ascertain the role of SVD subtypes in the expression of neuropsychiatric symptoms. Although age was accounted for in our analyses, the variable was not retained in the final model due to its association with cerebral atrophy; nevertheless, its potential influence on the relationship between cognitive and neuropsychiatric outcomes warrants consideration.
Distinct depressive symptoms profiles recognize different predictors and associated factors. The DAx profile – but not DAp profile – was predicted by the presence of diabetes mellitus: while depression has been frequently observed in patients with diabetes, our findings suggest that diabetes might be associated only with certain subtypes of post-ICH depressive symptoms. Pre-ICH depression was more common in both DAp and DAx profiles compared to ND profile, with numerically higher rates in the DAx group. Moreover, DAx profile was not associated with any markers of brain damage, while more severe ICH symptoms and higher degree of cerebral atrophy were associated with the DAp profile. Our results suggest that, while the DAp profile might be driven by age-related changes prior to ICH (neurodegeneration and cerebral small vessel diseases, leading to higher dementia risk), 37 the DAx profile might depend more on pre-existent psychiatric conditions: the higher incidence of excessive alcohol intake in DAx patients, though not confirmed in multivariable analyses, might support this hypothesis.
Our study has limitations. The retrospective nature of our analysis on prospectively collected data from a single-centre cohort potentially might question the generalizability of our findings; however, the risk of recruitment bias should be minimized, since the characteristics of our cohort are similar to those of a population-based ICH study of the same country. 15 We acknowledge the limitation that cortical atrophy was evaluated through a validated visual scale rather than volumetric measurements. We recognize that the exclusion of the minority of patients who did not undergo neuropsychiatric screening, including those with severe aphasia who were unable to complete the questionnaire, may have constituted a bias in the interpretation of our findings. MADRS and NPI-Q are screening tools rather than comprehensive batteries, preventing to formulate accurate diagnoses. However, we showed that cluster analyses are helpful to recognize different depressive symptoms profiles and correctly identified the patients at high risk for dementia. We acknowledge that since the two subgroups were extrapolated from cluster analyses, a minority of patients did not show overt neuropsychiatric symptoms (i.e. apathy or anxiety) according to the NPI-q. Due to the multidimensional and overlapping nature of neuropsychiatric symptoms, the clusters represent predominant symptom profiles rather than mutually exclusive groups. We acknowledge the lack of comprehensive pre-ICH cognitive testing as a limitation, preventing to formulate conclusive diagnoses; nevertheless, we used the validated and reliable IQCODE to estimate prior cognitive status. We understand that apathy might, in some cases, be an early symptom of cognitive impairment that was previously unrecognized, rather than a predictor. Finally, due to the relatively small number of events, our cluster analysis-based prognostic model should be interpreted with caution: despite we prospectively collected long-term outcome data on many 6-month ICH survivors, further studies are needed to validate our findings. We acknowledge that, due to the limited number of events, we only adjusted for age in our analysis on long-term dementia risk, which may not account for all potential confounders.
In conclusion, our results derived from cluster analysis suggest the presence of distinct neuropsychiatric syndromes underlying post-ICH depressive symptoms. The presence of apathy and anxiety might reveal the expression of different depressive symptoms profiles, each one showing distinct clinical and imaging determinants and long-term cognitive risks.
Supplemental Material
sj-docx-1-eso-10.1177_23969873241284725 – Supplemental material for Depressive symptoms profile and dementia risk after spontaneous intracerebral haemorrhage
Supplemental material, sj-docx-1-eso-10.1177_23969873241284725 for Depressive symptoms profile and dementia risk after spontaneous intracerebral haemorrhage by Giuseppe Scopelliti, Maéva Kyheng, Barbara Casolla, Grégory Kuchcinski, Grégoire Boulouis, Solène Moulin, Julien Labreuche, Hilde Hénon, Marco Pasi and Charlotte Cordonnier in European Stroke Journal
Footnotes
Acknowledgements
Coauthors are members of the STROKELINK network.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study protocol was considered observational by the Internal Review Board of the Lille University Hospital that gave ethics approval for this study.
Informed consent
Patients (or their relatives, or primary caregiver) gave informed consent for the study.
Guarantor
CC.
Contributorship
GS designed and conceptualized the study, analysed, and interpreted all data, and drafted the manuscript. MP, HH, CC designed and conceptualized the study, analysed, and interpreted all data, drafted, and reviewed the manuscript. MK, JL performed statistical analyses, designed, and conceptualized the study, analysed, and interpreted all data, drafted, and reviewed the manuscript. BC, SM contributed to data collection and revised the manuscript. GB, GK contributed to data collection, analysed imaging data, and revised the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.