
Abstract
Introduction:
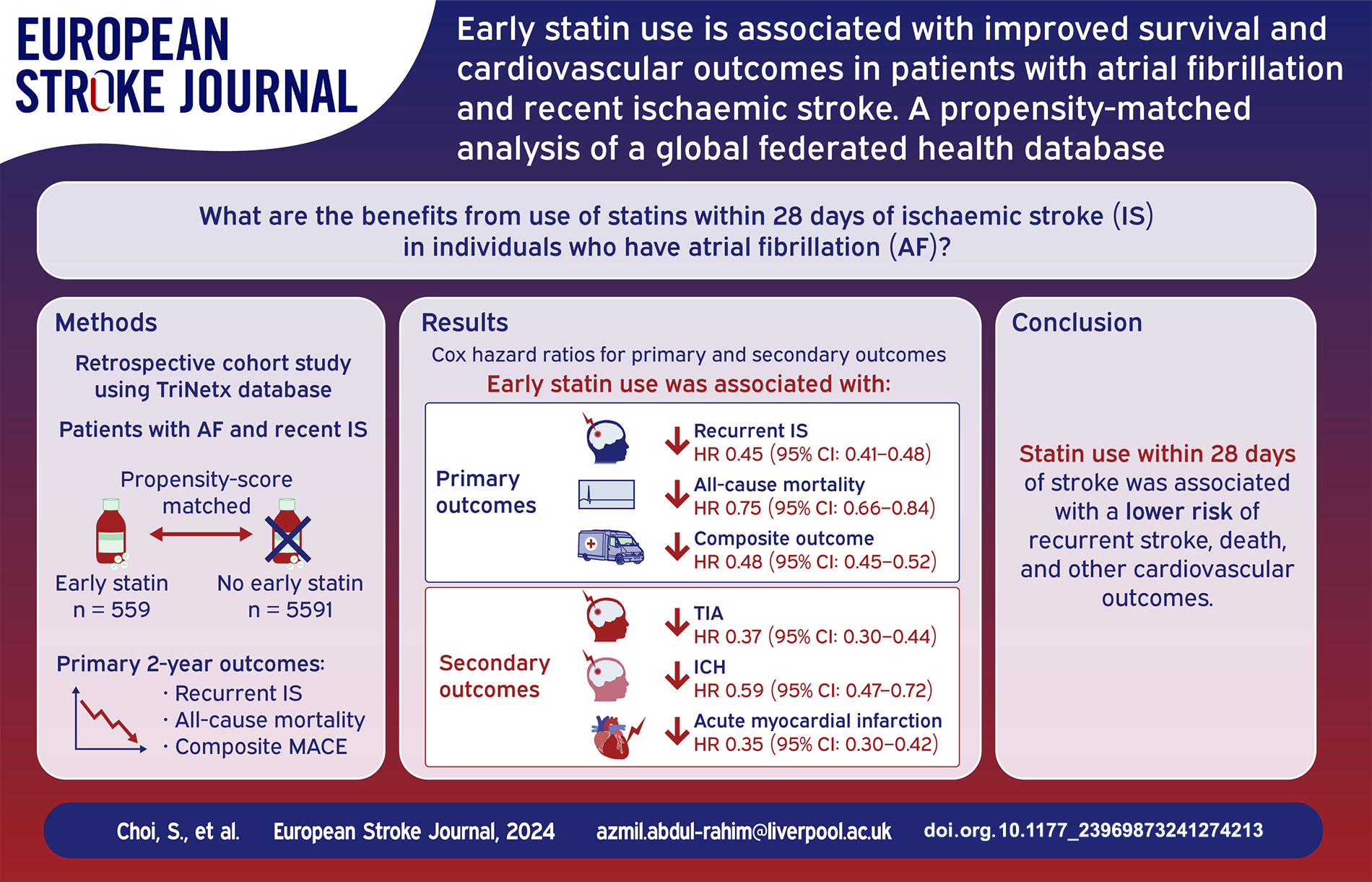
Statins reduce recurrent stroke and cardiovascular events in patients with non-cardioembolic stroke. The benefits of statins in patients with AF and recent IS remain unclear. We aimed to investigate the benefits of statins in patients with AF and recent IS.
Patients and methods:
This retrospective, cohort study was conducted using deidentified electronic medical records within TriNetX platform. Patients with AF and recent IS, who received statins within 28 days of their index stroke were propensity score-matched with those who did not. Patients were followed up for up to 2 years. Primary outcomes were the 2-year risk of recurrent IS, all-cause mortality and the composite outcome of all-cause mortality, recurrent IS, transient ischaemic attack (TIA), and acute myocardial infarction (MI). Secondary outcomes were the 2-year risk of TIA, intracranial haemorrhage (ICH), acute MI, and hospital readmission. Cox regression analyses were used to calculate hazard ratios (HRs) with 95% confidence intervals (95%CI).
Results:
Of 20,902 patients with AF and recent IS, 7500 (35.9%) received statins within 28 days of their stroke and 13,402 (64.1%) did not. 11,182 patients (mean age 73.7 ± 11.5; 5277 (47.2%) female) remained after propensity score matching. Patients who received early statins had significantly lower risk of recurrent IS (HR: 0.45, 95%CI: 0.41–0.48, p < 0.001), mortality (HR: 0.75, 95%CI: 0.66–0.84, p < 0.001), the composite outcome (HR: 0.48, 95%CI: 0.45–0.52, p < 0.001), TIA (HR: 0.37, 95%CI: 0.30–0.44, p < 0.001), ICH (HR: 0.59, 95%CI: 0.47–0.72, p < 0.001 ), acute MI (HR: 0.35, 95%CI: 0.30–0.42, p < 0.001) and hospital readmission (HR: 0.46, 95%CI: 0.42–0.50, <0.001). Beneficial effects of early statins were evident in the elderly, different ethnic groups, statin dose intensity, and AF subtypes, large vessel occlusion and embolic strokes and within the context of statin lipophilicity, optimal LDL-cholesterol levels, various cardiovascular comorbidities, treatment with intravenous thrombolysis or endovascular thrombectomy, and NIHSS 0–5 and NIHSS > 5 subgroups.
Discussion and conclusion:
Patients with AF and recent IS, who received early statins, had a lower risk of recurrent stroke, death, and other cardiovascular outcomes including ICH, compared to those who did not.
Keywords
Introduction
Stroke is the third leading cause of death and disability worldwide. 1 Atrial fibrillation (AF) is a major cause of cardioembolic stroke present in up to 25% of all ischaemic strokes, which are often more severe or fatal.2,3 The recurrence of ischaemic stroke (IS) is high, up to 35% at 5 years and up to 50% at 10 years. 4 The risk of recurrent stroke in non-anticoagulated patients with AF and history of previous stroke is 2.5 fold higher, compared to anticoagulated patients, with an average rate of 10% yearly.5,6 This is particularly important given the multimorbidity burden associated with such patients,7,8 necessitating a holistic or integrated care approach to post-stroke management to mitigate clinical cardiovascular outcomes.9,10
Evidence for the beneficial effects of statin therapy in patients with a history of coronary heart disease (CHD) or at high risk of cardiovascular events is well documented.11,12 Moreover, the use of statins for prevention of recurrent strokes in non-AF related and non-cardioembolic IS patients without a history of CHD is well established.13–16 However, many major secondary prevention trials excluded patients with AF or patients who had cardioembolic strokes. In addition, whether the perceived higher risks of haemorrhagic strokes associated with statin use observed in some trials would extend to such patients, or would be influenced by stroke sub-type, is unknown. Thus, there remains a gap in evidence to support the role of early statin use in AF-related stroke. No specific recommendations on the use of statins for secondary prevention in cardioembolic stroke exists in clinical practice guidelines.
On the basis of current clinical evidence, many international stroke guidelines on the secondary prevention of stroke recommend intensive statin therapy for stroke patients with non-cardioembolic strokes or history of atherosclerotic disease, or those at very high-risk.17,18 The European Society of Cardiology (ESC) guidelines on management of dyslipidaemia and the European Stroke Organisation (ESO) guidelines on long-term secondary prevention after IS,19, 20 go even further. As patients with a history of IS are considered at very high risk of atherosclerotic cardiovascular disease, particularly recurrent IS, such patients should receive intensive lipid lowering therapy.19,20
Nevertheless, knowing whether or not to initiate statins in patients with AF and recent IS would help to clarify a familiar management conundrum. In this study, we aimed to investigate the effect of early statin therapy on clinical outcomes in patients with AF who have recently experienced an IS using a global federated research network.
Methods
Data source
The study used TriNetX, a global federated health research network containing electronic medical records (EMR) data provided by participating healthcare organisations (HCOs). HCOs are typically academic health centre-based healthcare systems or non-academic research-focused HCOs, and include hospitals, specialist physician practices, and primary care providers. Although HCOs are mainly within the United States, the network extends to 30 countries in North and South America, Europe, the Middle East, Africa, and the Asia-Pacific regions. 21 Data including demographics, encounters, diagnoses (using International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes), procedures, medications, laboratory results, and vital signs are accessible from 130 HCOs covering 170 million patients. 21
TriNetX is compliant with applicable regional data protection, security and privacy laws and regulations, such as the Health Insurance Portability and Accountability Act (HIPAA) in the United States, and the General Data Protection Regulation (GDPR) in Europe. 21 Participating HCOs in the TriNetX network provide EMR data in de-identified, pseudo-anonymised, or limited form. The identity of each HCO remains anonymous and the data they share through the TriNetX platform are attenuated to ensure that they do not include sufficient information to facilitate the determination of which HCO contributed specific information about a patient. To safeguard against the risk of patient reidentification, the TriNetX platform only uses aggregated counts and statistical summaries of de-identified information. As no patient identifiable information is received, studies using the TriNetX network do not require ethical approval or informed consent. Data is de-identified according to the de-identification standard defined in Section §164.514(a) of the HIPAA Privacy Rule. In the United States, the process by which data is de-identified has been attested to through a formal determination by a qualified expert as defined in Section §164.514(b)(1) of the HIPAA Privacy Rule. This formal determination by a qualified expert refreshed on December 2020.
Study design
This was a retrospective observational study using complete case, de-identified data from the TriNetX platform. The data used in this study was collected on 11th December, 2023 from the TriNetX Global Collaborative Network, which provided access to EMR from approximately 106 million patients aged 18 or over from over 110 healthcare organisations in up to 16 countries. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for observational studies (Supplemental Table S1).
Cohort
Patients aged 18 or over with AF or atrial flutter (ICD-10-CM code I48) and recent IS (ICD-10-CM code I63 (Cerebral infarction)) recorded in EMRs between 4th May 2008 and 3rd May 2018 were identified (Supplemental Table S2). At the time of the search, a total of 106 participating HCOs responded including HCOs returning data on the platform for patients who met the study inclusion criteria. The baseline index event date was the date that a patient was diagnosed with IS for the first time. Patients were treated as having received statin treatment during a time period, if the first recorded prescription or administration of statin occurred during that period. Patients were excluded from the study if they had received statin treatment within the year leading up to the date of the index stroke.
The cohort was divided into two groups using electronic health records: (i) individuals who received treatment with statins within 28 days of their index stroke; and (ii) individuals who did not receive statins within 28 days of their index stroke.
To mitigate the risk of time-related biases, the follow-up period started at the end of 28 days after the index stroke only in those who were alive at that date, and individuals were included in the study if they received either angiotensin converting enzyme inhibitors or angiotensin II inhibitors within 28 days of their index stroke.
Outcomes
Patients who received treatment with statins within 28 days of their index stroke were propensity score-matched with patients who did not, before comparing outcomes between the two groups. All patients were followed up for up to 2 years. Primary outcomes were the 2-year risk of recurrent IS (ICD-10-CM code I63), all-cause mortality and the composite outcome of recurrent IS, transient ischaemic attack (TIA) (ICD-10-CM code G45), acute myocardial infarction (MI) (ICD-10-CM code I21) and all-cause mortality (Supplemental Table S2). Secondary outcomes were the 2-year risk of TIA, intracranial haemorrhage (ICH) (ICD-10-CM code I61-I62), acute MI, and hospital readmission (Supplemental Table S2).
Statistical analysis
All statistical analyses were performed on the TriNetX online research platform. Baseline characteristics were compared using chi-squared tests for categorical variables and independent-sample t-tests for continuous variables. Propensity score matching was used to control the differences in the comparison cohorts. Cohort matching was performed for age at index stroke, gender, ethnicity, baseline comorbidities (hypertension, ischaemic heart diseases, peripheral vascular diseases, heart failure, lipid disorders, type 2 diabetes mellitus, chronic kidney disease, neoplasms, overweight and obesity, pulmonary heart disease, and obstructive sleep apnoea), and medications (β-blockers, diuretics, calcium channel blockers, angiotensin-converting enzyme inhibitors, angiotensin II inhibitors, prior use of antiplatelet agents or anticoagulants, insulin and oral hypoglycaemic agents) (Supplemental Table S2). Those variables were selected because they may influence the clinical outcomes.
TriNetX performs a 1:1 greedy nearest neighbour matching model with a calliper of 0.1 pooled standard deviations using logistic regression. Any baseline characteristic with a standardised mean difference between cohorts lower than 0.1 is considered well-matched. After propensity score matching, Cox-regression proportional hazard models were used to calculate hazard ratios with 95% confidence intervals to assess the association between treatment with statins within 28 days of an index stroke and the 2-year incidence of primary and secondary outcomes. The proportional hazards assumption was assessed using a scaled Schoenfeld residual-based approach. Differences in Kaplan-Meier curves between the group that received early statins and the group that did not were evaluated with the log-rank test. Patients were censored from the Kaplan-Meier analysis at the end of the follow-up period or on the day after the last entry in their record (if earlier). A patient having an outcome after their index stroke and on or before the date falling 28 days after their index stroke, was censored at the end of the 28-day period. To test the generalisability of our hypothesis, we conducted two sensitivity analyses to investigate the risk of the primary outcomes: (i) in older patients aged ⩾ 75 years; and (ii) without propensity score matching. We conducted subgroup analyses examining the effects of early statins across different ethnicities, statin dose intensities, low-density lipoprotein cholesterol (LDL-C) levels, and within the context of statin lipophilicity, large vessel occlusion and embolic strokes, different AF subtypes, patients with and without various comorbidities (hypertension, diabetes mellitus, dyslipidaemia and ischaemic heart disease (IHD)), stroke treated with intravenous thrombolysis (IVT) or endovascular thrombectomy (EVT) (Supplemental Table S2), and patients with NIHSS 0–5 or NIHSS > 5. All analyses were performed in the TriNetX platform which uses R’s survival package v3.2-3. No imputations were made for missing data. The level of statistical significance was set at p < 0.05.
Results
Cohort characteristics
We identified 20,902 individuals who met the study inclusion criteria. Of these, 7500 (35.9%) received statins within 28 days of their index stroke, and the remaining 13,402 (64.1%) did not receive statins within 28 days of their stroke. Supplemental Table S3 summarised the baseline characteristics of the two cohorts before and after propensity score matching, respectively.
Compared to patients who did not receive early statins, the group who received early statins had a statistically higher prevalence of white patients (69.8% vs 64.7%, p < 0.001), and a lower prevalence of Black or African American patients (10.7% vs 11.9%, p = 0.010) and female patients (46.6% vs 48.3%, p = 0.019). Statin users were less likely to suffer from major comorbidities, and were more likely to receive cardiovascular medications (such as betablockers, angiotensin-converting enzyme inhibitors, calcium channel inhibitors and diuretics), antiplatelet agents, anticoagulants, insulin and oral medications for diabetes.
After propensity score matching, a total of 11,182 well-matched patients remained (mean age 73.7 ± 11.5; 5277 (47.2%) female). Each group (n = 5591) was followed up for up to 2 years for the primary and secondary outcomes.
Primary outcomes: Recurrent IS, all–cause mortality, and the composite outcome
After propensity score matching, compared with patients who did not receive early statins following their index stroke, those that did receive early statins had a significantly lower risk of all primary outcomes. Early statin use was associated with a significantly lower risk of recurrent IS within 2 years (872 (15.6%) vs 2130 (38.1%); Hazard Ratio (HR): 0.45, 95% Confidence Interval (CI): 0.41–0.48, p < 0.001). The risk of all-cause mortality within 2 years was reduced (444 (8.0%) vs 793 (14.2%); HR: 0.75, 95%CI: 0.66–0.84, p < 0.001), as was the risk of the composite outcome (1375 (24.6%) vs 2945 (52.7%); HR: 0.48, 95%CI: 0.45–0.52, p < 0.001) in patients who received early statin therapy, compared with those who did not (Figure 1).
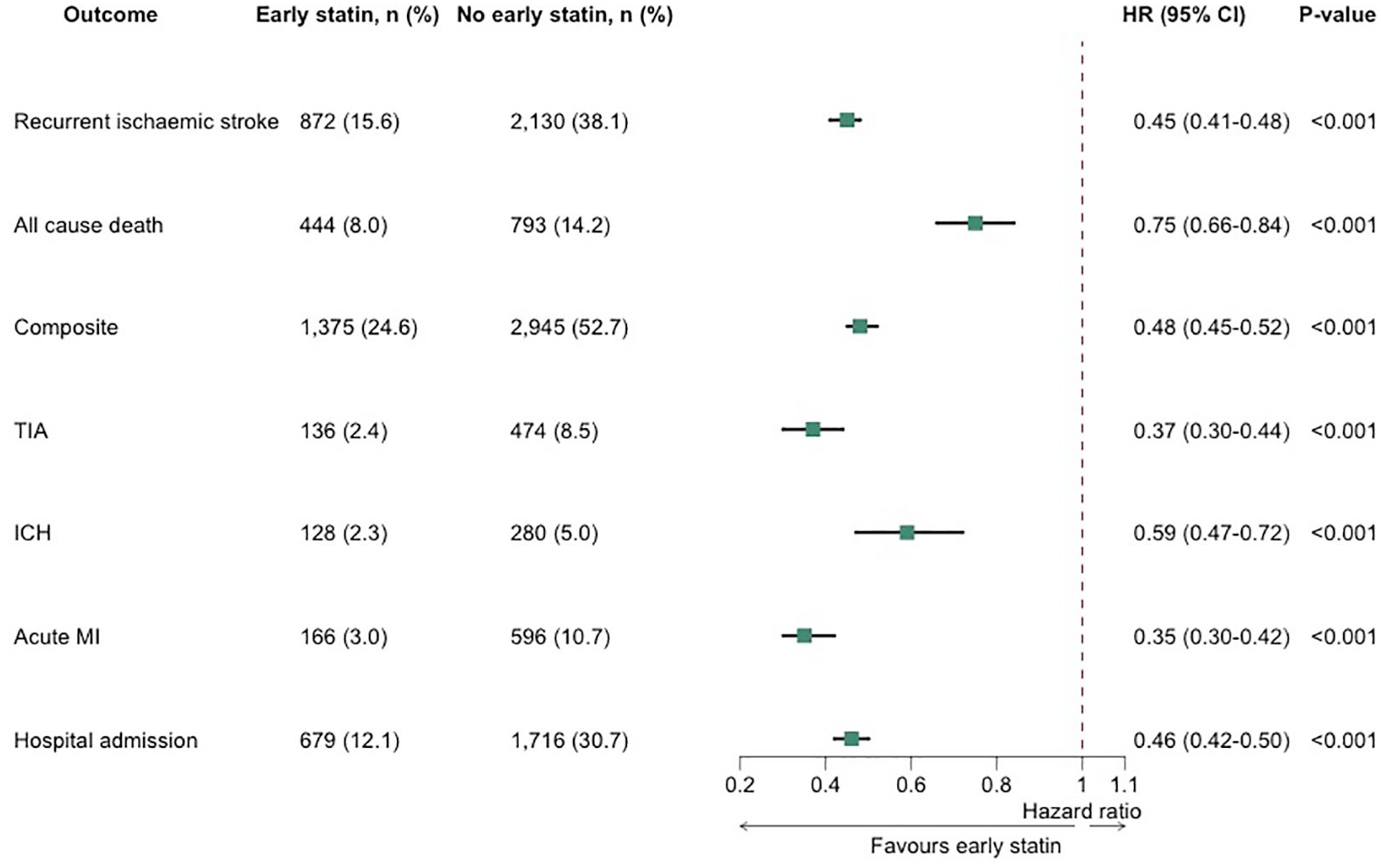
Cox regression analysis of primary and secondary outcomes. The Cox analysis is applied after propensity score matching.
Secondary outcomes
Patients who received early statins within 28 days of their index stroke had a significantly lower risk of the secondary outcomes, compared to patients who did not receive early statins. Early statin use was associated with a lower risk of TIA (136 (2.4%) vs 474 (8.5%); HR: 0.37, 95%CI: 0.30–0.44, p < 0.001), ICH (128 (2.3%) vs 280 (5.0%); HR: 0.59, 95%CI: 0.47–0.72, p < 0.001), acute MI (166 (3.0%) vs 596 (10.7%); HR: 0.35, 95%CI: 0.30–0.42, p < 0.001) and hospital readmission (679 (12.1%) vs 1716 (30.7%); HR: 0.46, 95%CI: 0.42–0.50, p < 0.001) (Figure 1).
Sensitivity analyses and subgroup analyses
We conducted sensitivity analyses without adjusting for the effects of propensity score matching and found that results were similar for the primary outcomes. Before propensity score matching, early statin use was associated with a lower risk of recurrent IS (1144 (15.2%) vs 5098 (38.0%); HR: 0.44, 95%CI: 0.41–0.47, p < 0.001), all-cause mortality (593 (7.9%) vs 2002 (14.9%); HR: 0.70, 95%CI: 0.64–0.77, p < 0.001), and the composite outcome (1819 (24.2%) vs 7023 (52.4%); HR: 0.48, 95%CI: 0.46–0.51, p < 0.001) after 2 years’ follow-up (Supplemental Figure S1).
The incidence of both stroke and AF increases with age. To evaluate the benefit of statins for secondary prevention of AF-related stroke in older patients, we conducted a sensitivity analysis for patients aged 75 years and over. We identified 15,840 patients aged ⩾ 75 years with AF and recent IS (mean age 78.8 ± 7.2, 52.1% female), 5762 (36.4%) of whom received early statins, and 10,078 (63.6%) of whom did not. After propensity score matching, there were 4313 well-matched individuals in each group. Supplemental Table S4 showed the baseline characteristics of individuals aged ⩾ 75 years before and after propensity score matching. Among patients aged ⩾ 75 years, early statin use was associated with a significantly reduced risk of all primary outcomes within 2 years. There was a lower risk of recurrent IS (581 (13.5%) vs 1552 (36.0%); HR: 0.41, 95%CI: 0.37–0.45, p < 0.001), all-cause mortality (376 (8.7%) vs 668 (15.5%); HR: 0.76, 95%CI: 0.67–0.86, p < 0.001), and the composite outcome (998 (23.1%) vs 2234 (51.8%); HR: 0.46, 95%CI: 0.43–0.50, p < 0.001)(Supplemental Figure S1).
Ethnicity
Patients falling within the white ethnic group who received early statins showed reductions in the risk of all primary outcomes, similar to the main analysis (Supplemental Figure S1). Patients in the Black or African American ethnic group who received early statins were associated with a lower risk of recurrent IS and of the composite outcome, compared to those who did not receive early statins. Due to the small size of that ethnic group, no statistical difference could be established in all-cause mortality between the early statin and no-early statin groups and the 95%CIs were wide (HR: 0.89, 95%CI: 0.62–1.29) (Supplemental Figure S1). Findings similar to those reported in the Black or African American ethnic group were observed in the Hispanic and Asian ethnic groups (Supplemental Figure S1).
Dose intensity of statin
We compared three subgroups comprising patients receiving (1) low-intensity statin, (2) moderate-intensity statin, and (3) high-intensity statin (in each case, as defined by the American College of Cardiology/American Heart Association Guideline on the Management of Blood Cholesterol). 22
After propensity score matching, compared to patients who did not receive early statins, patients in the high-intensity statin subgroup showed a lower risk of all primary outcomes, with a reduction in the risk of recurrent stroke (395 (18.9%) vs 788 (37.7%); HR: 0.57, 95%CI: 0.51–0.65, p < 0.001), all-cause mortality (155 (7.4%) vs 305 (14.6%); HR: 0.68, 95%CI: 0.56–0.82, p < 0.001), and the composite outcome (598 (28.6%) vs 1119 (53.5%); HR: 0.58, 95%CI: 0.53–0.64, p < 0.001). Patients in the low-intensity and moderate-intensity statin subgroups showed a reduction in the risk of recurrent stroke and the composite outcome; however, there was no difference in the risk of all-cause mortality between the no-early statin group and the low-intensity statin or moderate-intensity statin subgroups (Supplemental Figure S1).
Lipophilicity of statins
We analysed two subgroups including (1) patients receiving early statins regarded as relatively lipophilic (atorvastatin, simvastatin, fluvastatin, lovastatin, pitavastatin, and cerivastatin), and (2) patients receiving early statins regarded as relatively hydrophilic (pravastatin and rosuvastatin).
After propensity score matching, compared to patients who did not receive early statins, patients in each subgroup receiving either lipophilic or hydrophilic statins, had significantly lower risk of all primary outcomes (Supplemental Figure S1). There was a reduced risk of ICH in the lipophilic statin group when compared to the no-early statin group (HR 0.60, 95%CI: 0.49–0.74). This difference was not seen when comparing the hydrophilic statin group with the no-early statin group (HR 0.68, 95%CI: 0.45–1.04) (Supplemental Figure S1).
LDL-C level
Compared to patients with optimal LDL-C who did not receive early statins, the subgroup of patients with optimal LDL-C who did receive early statins had a lower risk of all three primary outcomes and a reduced risk of ICH (Supplemental Figure S1).
It is likely that due to the smaller number of individuals in the subgroups of patients who had higher recorded baseline LDL-C levels and/or more modest treatment targets prevailing at the time, we were unable to establish any association between early statin use and the risk of all-cause mortality in those subgroups (Supplemental Figure S1). As seen in Supplemental Figure S1, no statistical difference was found in the risk of all-cause mortality between the early statin and no-early statin groups within the subgroup of patients with baseline LDL-C 130–159. There was no difference in the event rates for all-cause mortality in the early statin group compared to the no-early statin group within the subgroup of patients with baseline LDL-C > 160 (Supplemental Figure S1).
Large vessel occlusion and embolic stroke
Two subgroup analyses of AF patients with recent large vessel occlusion (LVO) IS (ICD-10-CM code I63.5 (Cerebral infarction due to unspecified occlusion or stenosis of cerebral arteries)) and AF patients with recent embolic strokes (ICD-10-CM code I63.40 (Cerebral infarction due to embolism of unspecified cerebral artery)), demonstrated an association between early statin use and a lower risk of all primary outcomes after 2-year follow-up (Supplemental Figure S1).
AF subtype
We conducted two subgroup analyses of (1) patients with persistent and chronic AF (ICD-10-CM code 148.1 and 148.2) and recent IS and (2) patients with paroxysmal AF (ICD-10-CM code 148.0) and recent IS. After propensity score matching, the subgroup of patients with paroxysmal AF demonstrated an association between early statin use and a lower risk of all primary outcomes (Supplemental Figure S1).
A smaller subgroup of patients with persistent and chronic AF showed an association between early statin use and a reduced risk of recurrent IS (HR 0.59, 95%CI: 0.49–0.71) and the composite outcome (HR 0.64, 95%CI: 0.55–0.75) (Supplemental Figure S1). There was no significant difference between the early statin group and the no-early statin group with regards to the endpoint of all-cause mortality.
Cardiovascular comorbidities
The early and no-early statin groups were further stratified into subgroups by reference to certain cardiovascular comorbidities (hypertension, type 2 diabetes mellitus, dyslipidaemia and IHD). Some of our analyses for comorbidity positive subgroups were affected by reduced statistical power as a result of smaller sample sizes and, in some instances, smaller effect sizes (Supplemental Figure S1). We found that for all the comorbidity negative samples, early statin use, compared to no-early statin use, was associated with a reduced risk of all primary outcomes consistent with the main analysis (Supplemental Figure S1).
Specifically, compared with patients with hypertension who did not receive early statins following their index stroke, those who did receive early statins had a significantly lower risk of mortality and the primary composite endpoint, and a non-significant reduction in the risk of recurrent stroke (Supplemental Figure S1). Early statin use in patients with dyslipidaemia and in patients with IHD was associated with a lower risk of recurrent stroke and the primary composite endpoint, but there was no significant difference between the early statin and no-early statin groups with respect to the risk of mortality. In the subgroup of patients with type 2 diabetes mellitus, early statin use was associated with a non-significant reduction in the risk of all three primary outcomes (Supplemental Figure S1).
IVT and EVT
Early statin use in patients receiving either IVT or EVT for treatment of stroke was associated with a significantly lower risk of recurrent stroke and the primary composite outcome, when compared with no-early statin use. In this subgroup of patients given IVT or EVT, an association between early statin use and a reduction in the risk of all-cause mortality did not reach significance as a result of the smaller sample sizes (Supplemental Figure S1).
NIHSS scores
In the subgroup of patients who had NIHSS scores exceeding 5, patients receiving early statins had a significantly lower risk of all primary outcomes, as well as a reduction in the risk of ICH, compared to patients who did not receive early statins (Supplemental Figure S1). There was a lower risk of recurrent IS (HR: 0.72, 95%CI: 0.57–0.90, p = 0.004), all-cause mortality (HR: 0.65, 95%CI: 0.45–0.95, p = 0.027), the composite outcome (HR: 0.70, 95%CI: 0.57–0.86, p = 0.001) and ICH (HR: 0.50, 95%CI: 0.28–0.88, p = 0.014) (Supplemental Figure S1).
The analysis of the subgroup of patients who had NIHSS scores 0–5 showed an association between early statin use and a significantly reduced risk of recurrent stroke and the primary composite outcome. That analysis was insufficiently powered to draw any firm conclusions between early statin use and the risk of all-cause mortality or ICH.
Discussion
In this retrospective, propensity score matched analysis of 11,182 individuals with AF and recent IS who were followed up for up to 2 years, patients who received early statins within 28 days of their index stroke had a significantly lower risk of recurrent IS, mortality, ICH and other cardiovascular events compared to patients who did not. The present study adds to findings from previous studies, showing that the beneficial effects of early statins were still evident in relation to the elderly, across different ethnicities, and within the setting of varying statin dose intensity (low, moderate, and high), statin lipophilicity (vs hydrophilic), optimal LDL-C levels, LVO and embolic strokes, different AF subtypes, different cardiovascular comorbidity subgroups, treatment of stroke with IVT or EVT, and stroke severity (by reference to NIHSS scores >5 and ⩽5).
The observed benefits of early statin use in this cohort of AF patients with recent IS can be attributed to a reduction in both cerebrovascular and cardiovascular events. Hence, statins may also play an important role in the secondary prevention of AF-related stroke.
In contrast to suggestions from prior studies, the present study found an association between early statin use and a reduction of recurrent stroke, with no increase in haemorrhagic stroke or ICH. It also confirms findings in previous studies that statins may reduce mortality and future cardiovascular events in patients with AF and recent stroke.
The pathophysiological basis for the beneficial effect of statins in IS remains unclear and a direct relationship between LDL-C and IS has not been firmly established. Nevertheless, clinical evidence for the preventive effects of statins in patients with a history of CHD, and those at risk of cardiovascular disease is clear.11, 12,23–26 The Stroke Prevention and Aggressive Reduction in Cholesterol Levels (SPARCL) trial established that high dose atorvastatin is effective for the prevention of recurrent IS in patients without CHD. 13 However, the results in the SPARCL study (and many other stroke secondary prevention trials14–16) cannot be generalised to all strokes (including AF-related stroke) because they specifically excluded patients who had AF or other cardioembolic sources of stroke. Nevertheless, numerous observational studies have shown that statins may reduce stroke recurrence, as well as improve survival and functional outcome in acute IS patients.27–29 Although international practice guidelines follow the clinical evidence,17–20 the position on use of post-stroke statins specifically in AF-related strokes remains unclear. Furthermore, patients were included in the SPARCL trial if they had suffered a stroke or TIA within the previous 1–6 months. Accordingly, the routine use of statins in the acute phase of stroke is not supported by strong evidence from any randomised clinical trials. 30
Observational studies have shown that statin therapy is associated with reduced mortality and improved prognosis in IS patients with AF31,32 and patients with cardioembolic stroke,33,34 and a lower risk of future cardiovascular events in cardioembolic 34 and AF-related stroke patients.31,35 However, there is limited evidence from those studies of any link between statin therapy and reduction of stroke recurrence. A significant association was not established despite a strong trend in favour of the group discharged on statins in one study involving patients with AF-related stroke. 31 More recently, a small prospective cohort study 36 found that the use of statins may help to prevent stroke recurrence and improve functional outcomes in patients with cardioembolic stroke. In patients with embolic stroke of undetermined source, treatment with statins at discharge was associated with low rates of stroke recurrence, major adverse cardiovascular events and death. 37
As well as a reduction of recurrent stroke risk, the present study suggests that statins may have a beneficial effect on reducing ICH following IS. This is at odds with the SPARCL trial where the reduction of recurrent stroke risk was counterbalanced by a small increase in the incidence of haemorrhagic stroke. 13 Such trend for increased haemorrhagic stroke has been found in other studies 38 but not in the later Treat Stroke to Target clinical trial. 39 Although because of SPARCL, stroke practitioners are often reluctant to use statins following ICH, due to the uncertainty in the evidence, international guidelines have not imposed restrictions on the use of statins in such circumstances. 19 Indeed, the benefit of post-stroke statin therapy may outweigh its risks.
Given that clinical benefits of statins have been established in patients at high risk of cardiovascular disease and those with a history of heart disease, the influence of statins in the present study on reducing future stroke does not seem incongruous. As in the present study, patients with AF, as well as patients with a history of stroke, represent a population at high risk of atherosclerotic disease who often have concomitant comorbidities such as hypertension, CHD, heart failure or diabetes mellitus. A proportion of recurrent strokes in the present study may have been attributable to atherosclerotic causes. Indeed, our findings suggest that statins may be beneficial for secondary prevention in patients with a history of IHD or dyslipidaemia, and possibly hypertension and type 2 diabetes mellitus as well. Our findings are aligned with the holistic or integrated care approach to AF management, including attention to comorbidities, and statins are clearly beneficial here.40,41 This is important given the multimorbidity, frailty and inappropriate polypharmacy seen in patients with AF, with implications for treatments and outcomes.42–44
The mean age at index date of 73.7 years in our study was representative of that seen in the general population. 45 However, the incidence of stroke and post-stroke major adverse outcomes is high in the elderly. 45 Our sensitivity analyses in patients aged 75 years and over showed consistent results for all primary outcomes. In addition, LVO IS are more likely to be associated with AF 46 and greater neurological deficits, and to contribute disproportionately to mortality and more severe functional outcomes after acute IS.47,48 Consistent with the main analysis, our data suggest that statins may be associated with improved survival and cardiovascular outcomes even in patients with AF and recent LVO IS. This notion was reinforced in this study by similar findings of an association between early statin use and a lower risk of all primary outcomes and ICH in patients with NIHSS > 5, and reduced cardiovascular risk in cases where IVT or EVT was given. Similar benefits to those seen in patients with AF and recent LVO IS were observed in patients with AF and recent embolic stroke.
When evaluating the effect of early statin use across different ethnic groups, we observed similar findings for the primary outcomes in the white ethnic group. In other ethnic groups studied (Black or African American, Hispanic, and Asian), we found an association between early statin use and reduced risk of recurrent IS and the composite outcome.
Stroke secondary prevention guidelines do not distinguish between AF subtype, and stroke risk is thought to be independent of AF subtype. Nevertheless, in IS patients, persistent AF is thought to be associated with a higher risk of recurrent IS49,50 and mortality 50 than paroxysmal AF. Our data suggest that early statin use may have secondary prevention benefits in IS patients with either non-paroxysmal or paroxysmal AF, with beneficial effects on mortality in IS patients with paroxysmal AF.
Whether statins act in stroke only by lowering serum cholesterol or through effects beyond lipid lowering (so-called ‘pleiotropic effects’) remains a subject of debate. In the literature, the positive results in cardiovascular disease from clinical trials of proprotein convertase subtilisin/kexin type-9 (PCSK9) inhibitors and ezetimibe strengthen the argument that statins act through lipid-lowering.51,52 PSCK9 inhibitors and ezetimibe are thought to act through lipid lowering, though the possible presence of other anti-thrombotic effects is emerging. 53 However, as the trials were conducted on statin-treated patients, the position is not free from doubt, and elsewhere, anti-inflammatory interventions that do not act through lipid lowering, have been shown to reduce recurrent events compared with placebo. 54
In the area of stroke, there is increasing evidence that statins act predominantly through lipid lowering.39,55–57 The link between lipids and stroke is not as strong as the association between cholesterol levels and coronary artery disease, and appears to vary by stroke subtype.58–60 The relationship seems strongest for atherosclerotic stroke subtypes, as supported by a recent meta-analysis of randomised clinical trials.59,61,62 Nevertheless, the effect of statins in AF-related stroke remains unclear with most studies failing to demonstrate an association between dyslipidaemia and embolic stroke.60,63–65
In the present study, low, moderate and high intensity statins all reduced the risk of future stroke in the early statin group, which might suggest that the effects of statins in AF-related stroke are not only commensurate with the degree of lipid lowering. We also found that the risk of all primary outcomes were reduced in the early statin group even in patients with optimal levels of LDL-C less than 100 mg/dl. This might suggest that statins may have effects beyond lipid-lowering.
The pleiotropic effects of statins66,67may extend to cardioprotective or neuroprotective effects that include changes in endothelial function, anti-inflammatory, anti-oxidant, and anti-thrombotic activities (including reduced platelet activation), angiogenesis, and promotion of plaque stability.58,67 Numerous experimental and animal models of stroke (including embolic stroke) support possible neuroprotective effects of statins.68–77
Although the finding of a lower 2-year risk of ICH in the early statin group in our study might be indirectly attributable to the non-lipid lowering properties of statins, a possible explanation could not be clearly derived in this study from the pleiotropic effects of statins. Also, statins can be classified according to their synthesis (natural or synthetic), or their hydrophilicity. Lipophilic statins can more readily cross cell membranes and the blood brain barrier, and are thought to have greater pleiotropic effects (including neuroprotective effects on the central nervous system). 78 In the present study, both lipophilic and hydrophilic statins reduced the risk of all primary outcomes in AF patients with recent IS. However, only lipophilic statins showed a significant reduction in the risk of ICH following stroke. Nevertheless, as the 95%CI for the hydrophilic group likely exceeds 1 due to the smaller cohort and incidence of ICH, no strong conclusions can be drawn from this study regarding whether or not lipophilic statins may have stronger pleiotropic effects.
Strengths and limitations
The main strengths of this study lie in the large size of the cohorts included in the analysis, and the use of propensity score matching to minimise the risk of bias from confounding.
Nevertheless, there were several limitations. Firstly, the retrospective nature of the study is more liable to error due to confounding and bias, and the observational nature cannot prove causality. Health care organisation EMR data are subject to entry errors and data gaps, and some diagnoses may be underreported, while outcomes which occurred outside the studies network may have not been captured. The recording of ICD codes in EMR may vary by factors including age, comorbidities, severity of illness, length of in-hospital stay, and in-hospital mortality. Further residual confounding may stem from influences such as geographical location, socioeconomic factors, and lifestyle factors including alcohol consumption and physical activity, which were not available. Although propensity score matching was used to adjust for many variables, it may not be able to control for and balance unmeasured confounders, such as disease severity and duration, resulting in possible residual confounding and bias.79,80 Furthermore, propensity score matching, when used in analyses of small sample sizes, may lead to biased estimations of treatment effect.81,82
Use of a Cox model for analysis did not allow for adjustment for competing risks. This may have resulted in bias and overestimation of disease outcomes. Data were not available for cardiovascular and non-cardiovascular causes of mortality. This may have resulted in the overestimation of the absolute risk of all-cause mortality over time.
Assessments of disability following stroke using the modified Rankin Scale (mRS) or the National Institutes of Health Stroke Scale (NIHSS) scores were often not available or insufficient. Accordingly, important information about patients’ stroke severity could not generally be determined from the available data, or used to support or strengthen further analyses (including sensitivity analyses). A degree of selection bias was likely present in the study because statins may not have been initiated in patients with severe neurological deficits and disabilities following stroke and those thought to have a poor prognosis. Added to that, selecting patients for enrolment to the study only if they were not taking statins during the year leading up to their index stroke may have enhanced such bias. It is possible that bias may have been introduced where there was a difference between the two cohorts being compared as regards their patients’ mean or median follow-up times (e.g. due to loss to follow-up). To minimise biases, the study used propensity score matching and statistical adjustments to account for potential confounders.
The proportion of patients receiving early statins who later discontinued them, or the proportion of patients in the no-treatment group who later received statins is not known. As data confirming the date when patients started taking statins were not available, patients may have been included in the study when prescribed statins within 28 days, but before actual use began. The study does not account for patients on combination therapy for dyslipidaemia, such as statin and ezetimibe. Data on underlying aetiologies of stroke were not available. Whether or not strokes were attributable to atherosclerosis, or embolic strokes resulted from emboli from the carotid arteries, aortic arch or left ventricle, could not be determined. Finally, the effect of long-term statin use was not investigated.
Conclusions
Patients with AF and recent IS, who received statins within 28 days of their index stroke, had a lower 2-year risk of recurrent stroke, death, future cardiovascular outcomes and ICH, compared to those who did not.
Supplemental Material
sj-docx-1-eso-10.1177_23969873241274213 – Supplemental material for Early statin use is associated with improved survival and cardiovascular outcomes in patients with atrial fibrillation and recent ischaemic stroke: A propensity-matched analysis of a global federated health database
Supplemental material, sj-docx-1-eso-10.1177_23969873241274213 for Early statin use is associated with improved survival and cardiovascular outcomes in patients with atrial fibrillation and recent ischaemic stroke: A propensity-matched analysis of a global federated health database by Sylvia E Choi, Tommaso Bucci, Jia-yi Huang, Kai-Hang Yiu, Christopher TW Tsang, Kui Kai Lau, Andrew Hill, Greg Irving, Gregory YH Lip and Azmil H Abdul-Rahim in European Stroke Journal
Footnotes
Acknowledgements
None
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SEC, TB, JH, KHY, CTWT, AH and GI report no conflicts of interest.
KKL received grants from Croucher Foundation, Research Fund Secretariat of the Food and Health Bureau, Innovation and Technology Bureau, Research Grants Council, Amgen, Boehringer Ingelheim, Eisai and Pfizer; and consultation fees from Amgen, Boehringer Ingelheim, Daiichi Sankyo and Sanofi, all outside the submitted work.
GYHL reports Consultant and speaker for BMS/Pfizer, Boehringer Ingelheim, Daiichi-Sankyo, Anthos. No fees are received personally. GYHL is a National Institute for Health and Care Research Senior Investigator and co-principal investigator of the AFFIRMO project on multimorbidity in AF, which has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement No 899871.
AHAR reports Member of the Editorial Board of Stroke and European Stroke Journal.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Data received from TriNetX is in de-identified form. As no patient identifiable information is received, studies using the TriNetX network do not require ethical approval or informed consent.
Informed consent
Participating healthcare organisations (HCOs) in the TriNetX network provide data from electronic medical records in de-identified, pseudo-anonymised, or limited form. To protect against the risk of patient reidentification, the TriNetX platform only uses aggregated counts and statistical summaries of de-identified information. As no patient identifiable information is received, studies using the TriNetX network do not require informed consent.
Guarantor
Dr Abdul-Rahim takes full responsibility for the article, including for the accuracy and appropriateness of the reference list.
Contributorship
All authors critically reviewed and contributed to the intellectual content of the manuscript. SC, TB, JH, KHY, GYHL, and AHAR were involved in the concept and design of the study. SC was involved in the acquisition and analysis of the data. SC wrote the first and subsequent drafts of the manuscript. All authors reviewed and edited the manuscript, and approved the final version of the manuscript.
Data availability
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.