
Abstract
Introduction
Atrial fibrillation is an independent risk factor of thromboembolism. Women with atrial fibrillation are at a higher overall risk for stroke compared to men with atrial fibrillation. The aim of this study was to evaluate for sex differences in patients with acute stroke and atrial fibrillation, regarding risk factors, treatments received and outcomes.
Methods
Data were analyzed from the “Recurrence and Cerebral Bleeding in Patients with Acute Ischemic Stroke and Atrial Fibrillation” (RAF-study), a prospective, multicenter, international study including only patients with acute stroke and atrial fibrillation. Patients were followed up for 90 days. Disability was measured by the modified Rankin Scale (0–2 favorable outcome, 3–6 unfavorable outcome).
Results
Of the 1029 patients enrolled, 561 were women (54.5%) (p < 0.001) and younger (p < 0.001) compared to men. In patients with known atrial fibrillation, women were less likely to receive oral anticoagulants before index stroke (p = 0.026) and were less likely to receive anticoagulants after stroke (71.3% versus 78.4%, p = 0.01). There was no observed sex difference regarding the time of starting anticoagulant therapy between the two groups (6.4 ± 11.7 days for men versus 6.5 ± 12.4 days for women, p = 0.902). Men presented with more severe strokes at onset (mean NIHSS 9.2 ± 6.9 versus 8.1 ± 7.5, p < 0.001). Within 90 days, 46 (8.2%) recurrent ischemic events (stroke/TIA/systemic embolism) and 19 (3.4%) symptomatic cerebral bleedings were found in women compared to 30 (6.4%) and 18 (3.8%) in men (p = 0.28 and p = 0.74). At 90 days, 57.7% of women were disabled or deceased, compared to 41.1% of the men (p < 0.001). Multivariate analysis did not confirm this significance.
Conclusions
Women with atrial fibrillation were less likely to receive oral anticoagulants prior to and after stroke compared to men with atrial fibrillation, and when stroke occurred, regardless of the fact that in our study women were younger and with less severe stroke, outcomes did not differ between the sexes.
Keywords
Introduction
Strokes in atrial fibrillation (AF) patients are common and frequently devastating (70–80% of patients die or become disabled,1,2 yet these strokes are preventable with anticoagulant therapy: 64% reduction in the risk of stroke and 25% reduction in mortality. 3
Recent evidence shows that women are more frequently affected by AF compared to men, and have a higher associated risk for thromboembolic events.4–6 Therefore, female sex has been added as an independent risk-factor when calculating the CHA2DS2-VASc-score. 7 Despite of this increased risk, women with AF still tend to be less treated with anticoagulants.8,9
The “Early Recurrence and Cerebral Bleeding in Patients with Acute Ischemic Stroke and Atrial Fibrillation” (RAF) Study investigated for (1) the risk of recurrent ischemic event and severe bleeding; (2) the risk factors for recurrence and bleeding; and (3) the risks of recurrence and bleeding associated with anticoagulant therapy and its starting time after the acute stroke. 10 The results of this study have been recently published. 10
The aim of this study was to evaluate the sex-differences in patients with acute stroke and AF, regarding risk factors, treatments received and outcomes.
Methods
The methods and results of the RAF-study have been published recently. 10 Briefly, RAF-study was performed between January 2012 and March 2014 and included 29 Stroke Units across Europe and Asia. All of the participating 29 Stroke Units provided standard stroke unit care and monitoring. 10
On admission, stroke severity was assessed using the National Institutes of Health Stroke Scale (NIHSS). All patients underwent cerebral computed tomography examination without contrast or cerebral magnetic resonance to exclude intracranial hemorrhage. Thrombolysis treatment was administered as per local standard protocol, when appropriate. All patients were monitored for blood pressure, temperature, glucose level, heart rate, and blood gases in the first days after stroke. The choice of anticoagulant treatment (low molecular weight heparin [LMWH] or oral anticoagulants), as well as the day of its initiation, was left to the discretion of the treating physicians. AF was classified as paroxysmal, persistent, or permanent. A second brain computed tomography scan or magnetic resonance was performed 24–72 h from stroke onset in all patients. Hemorrhagic transformation was defined as any degree of hyperdensity within the area of low attenuation and was classified as either hemorrhagic infarction or parenchymal hematoma.11,12 The sites and sizes of the qualifying infarcts were determined based on standard templates as small, medium, large anterior or large posterior infarctions.11,13,14 Data on known stroke risk factors and treatment were collected and reported in the main paper. 10 The CHA2DS2-VASc score before the index event was also calculated. The standard protocol also included a transthoracic echocardiography (TTE) during the hospital stay. Patients were followed up prospectively through face-to-face or telephone interviews. Study outcomes were (1) recurrent ischemic cerebrovascular events (stroke or TIA) and symptomatic systemic embolism; (2) symptomatic cerebral bleedings and major extracerebral bleeding at 90 days. The primary outcome was the composite of stroke, TIA, symptomatic systemic embolism, symptomatic cerebral bleeding, and major extracerebral bleeding. Disability and mortality at 90 days were also assessed using the modified Rankin Scale (mRS). Functional outcome was defined as either favorable (mRS 0–2) or unfavorable (mRS 3–6).
Statistical analysis
Continuous variables, as well as NIHSS score, were reported as mean ± SD, and categorical variables were reported as percentages. Pearson’s chi-square test was used to compare categorized proportions. A comparison of discrete variables was conducted using a non-parametric test (Mann–Whitney). Multivariate logistic regression was performed in order to investigate sex differences for dichotomous outcomes. Included variables were: age, vascular risk factors, NIHSS on admission, the type of AF, lesion size, antithrombotic treatment before and after stroke, previous use of statins. The decision concerning which variables to include and to adjust in the multivariable analysis was guided by either the presence of an a priori theoretical or biological relationship among the examined patient characteristics as well as primary endpoints. 15 A two-sided p < 0.05 was considered significant for all statistical tests. All statistical analyses were performed using software SPSS/PC Win package 20.0.
Results
Baseline characteristics of patients.
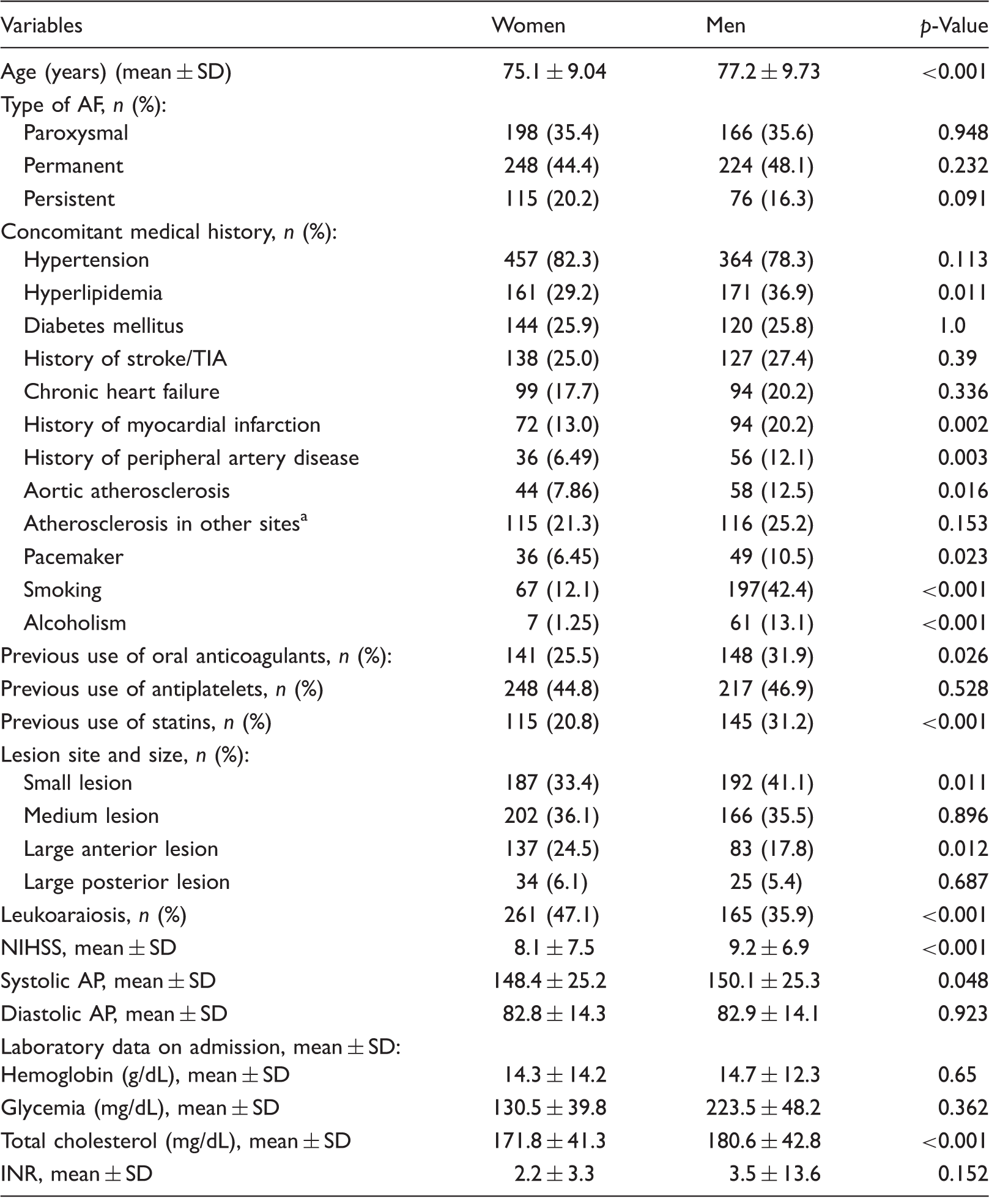
Presence of internal carotid/vertebral artery stenosis ≥50%. AF: atrial fibrillation; AP: arterial pressure; INR: International Normalized Ratios at admission for all patients; TIA: transient ischemic attack.
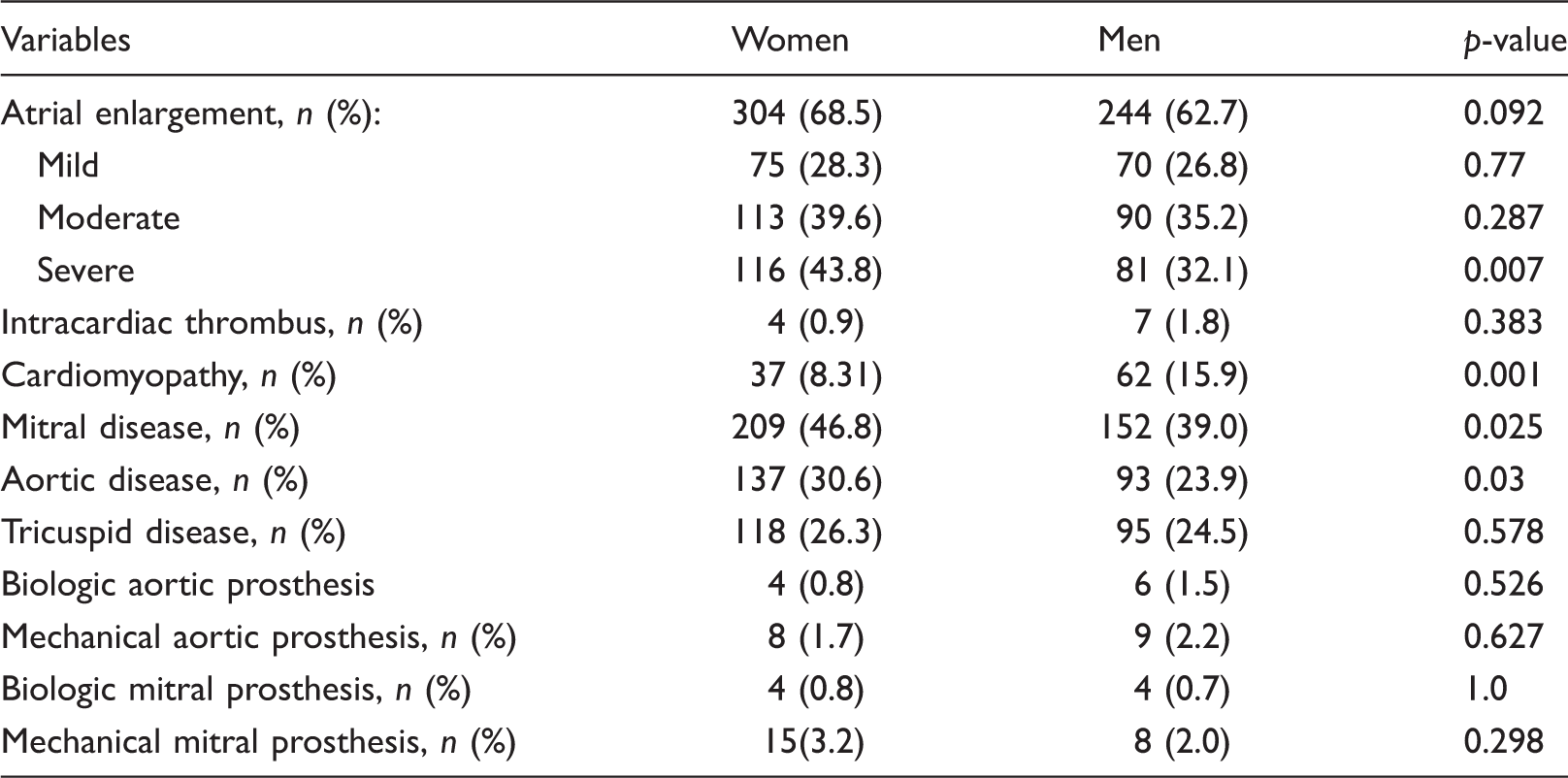
Findings on transthoracic echocardiography, performed in 843 patients.
Treatment of patients in the acute period of stroke and outcome effects at 90 days.
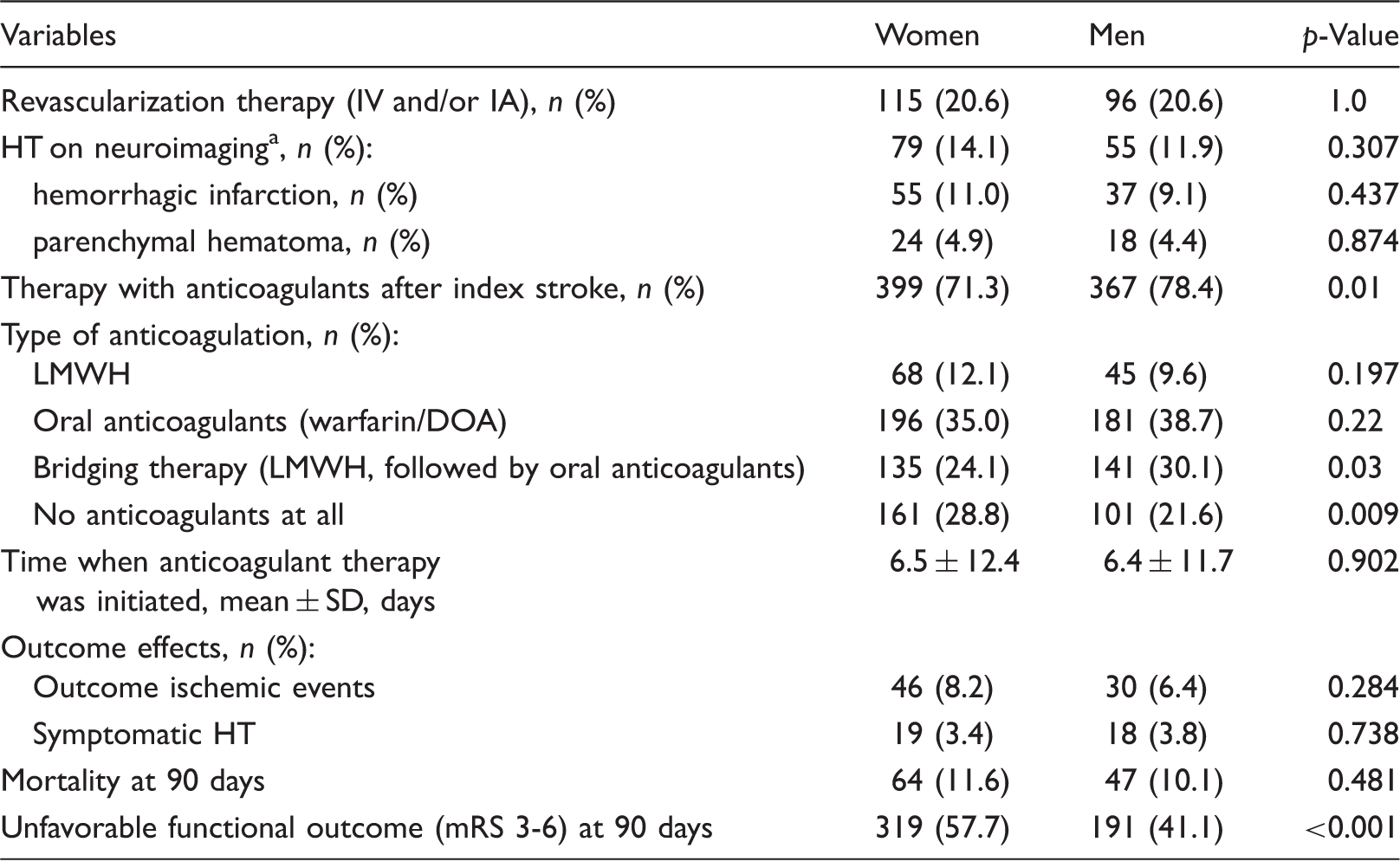
Neuroimaging performed after 24–72 h from stroke onset. DOA: direct oral anticoagulants; HT: hemorrhagic transformation (either hemorrhagic infarction or parenchymal hematoma); IA: intra-arterial revascularization therapy; IV: intravenous revascularization therapy; LMWH: low molecular weight heparin.
Multivariate logistic regression model for dichotomous outcomes.
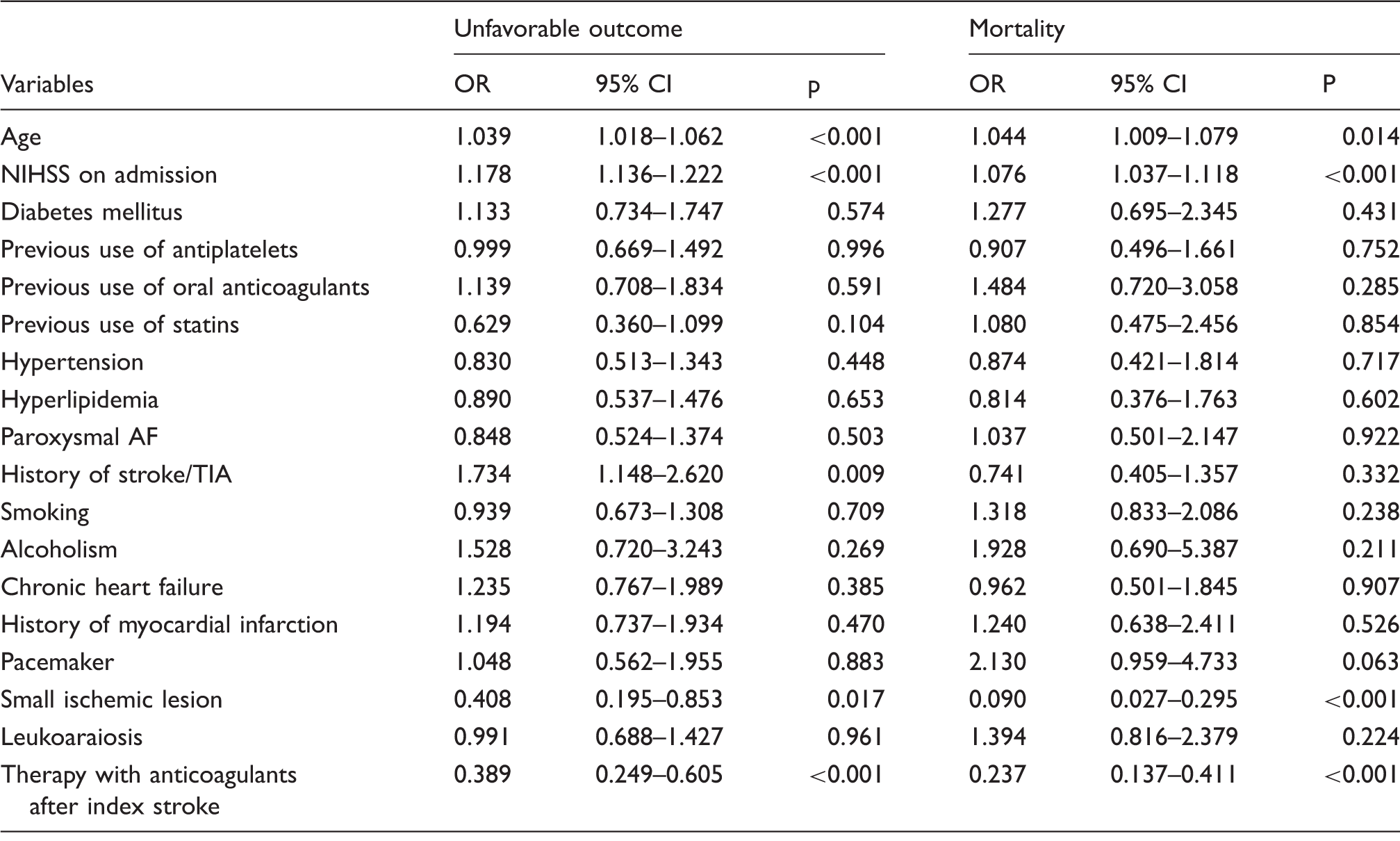
AF: atrial fibrillation; AP: arterial pressure; INR: International Normalized Ratios at admission for all patients; TIA: transient ischemic attack.
Regarding sex differences, East European Stroke Units had 71 patients: 33 women (46.5%) and 38 men (53.5%)) and other Stroke Units in Europe (900 patients: 492 women (54.7%) and 408 men (45.3%)). Comparing women and men from Eastern Europe, the former were older (mean age 79.9 ± 8.3 versus 71.2 ±11.8, respectively, p < 0.001) and had more severe strokes than men (mean NIHSS 10.0 ± 7.2 versus 5.8 ± 4.96, respectively, p = 0.006) (Supplementary Table 1). No differences in the rates of prescribing anticoagulants between women and men in East Europe before and after index stroke were observed. While, after index stroke, LMWHs were prescribed more often to women than men (66.7% versus 31.6%, p = 0.004) and much more often than oral anticoagulants in East Europe. There were no observed sex differences regarding the time of initiating anticoagulant therapy in East Europe: (3.95 ± 15.9 days for men versus 3.67 ± 7.5 days for women, p = 0.923). (Supplementary Table 2).
Discussion
This study found that women overall in Europe with AF were less likely to receive oral anticoagulants prior to and after stroke compared to men and regardless of the fact that women were significantly younger and with less severe stroke at onset; outcomes did not differ between the sexes. The RAF-study included more women (54.5%) than men, who were on average younger and had less severe stroke at onset compared to previous studies.16,17 Moreover, while previous studies had included patients with all types of stroke and with and without AF,16–18 the RAF-study included only ischemic stroke patients with AF. Furthermore, women more frequently had mitral disease and severe atrial enlargement. The latter fact has been reported by Gómez-Doblas, who has stating that women have more rheumatic aetiologies, while men tend to be more affected by ischemic or congenital aetiologies. 19 Rheumatic aetiologies have been correlated with a higher embolic risk of AF and an earlier onset of stroke. 20
In this study, women were less likely to receive oral anticoagulants before the index stroke, a finding in line with past population studies.8,9 Likewise, women were less likely to receive anticoagulation therapy for secondary prevention. This clear disparity in treatment delivery has also been documented by the Austrian Stroke Unit Registry. 18 This under-treatment for women has been hypothesized as being due to a lack of social support, as well as other concomitant diseases afflicting these patients, including cognitive decline, a higher burden of vascular brain disease, epilepsy and an increased risk of falls. 18 Furthermore, we also observed that women had a lower rate of statin use, despite an equal rate of atherosclerosis between the sexes.18,21
Even though men were older and had more severe stroke, the mortality and disability rates between the sexes were similar. The selection of patient cohorts could have influenced this, as only cardioembolic strokes were included, which could also explain the younger age of women at stroke onset.
Study limitations
This hospital-based clinical study was not randomized but based upon consecutively admitted patients fulfilling inclusion criteria.
Conclusions
The RAF-study observed that women regardless of lower NIHSS-score at admission and younger age, experienced the same outcomes as men with higher NIHSS at admission and older age. Moreover, this study also observed that women were less likely, compared to men, to have been prescribed anticoagulants before and after stroke.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M Paciaroni has received honoraria as a member of the speaker bureaus of Sanofi-Aventis, Boehringer Ingelheim, Bayer and Pfizer. G Agnelli has received honoraria as a member of the speaker bureaus of Boehringer Ingelheim and Bayer. C Becattini has received honoraria as a member of the speaker bureaus of Bristol Meyer Squibb and Bayer P Michel has received a Research Grant from the Swiss National Science Foundation and Swiss Heart Foundation; he has also received speaker fees from Bayer, Boehringer Ingelheim, Covidien, St. Jude Medical as well as received honoraria for an advisory relationship from Pierre-Fabre, Bayer, Bristol Meyer Squibb, Amgen, and Boehringer Ingelheim. J Putaala has received honoraria for lectures related to atrial fibrillation and anticoagulants for Orion Pharma, Bristol Meyer Squibb, Pfizer, Bayer, and Boehringer Ingelheim. T Tatlisumak received honoraria as consultant or advisory relationship by Lundbeck and Boehringer Ingelheim. G Tsivgoulis had research support by European Regional Development Fund, Project St. Anne's University Hospital, Brno, International Clinical Research Center (FNUSA-ICRC) (No. CZ.1.05/1.1.00/02.0123). D Toni has received honoraria as a member of speaker bureaus and as advisory board member for Boehringer Ingelheim and Bayer. The other authors report no conflicts.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the local hospital board.
Informed consent
not necessary as the study report on clinical practice.
Guarantor
KA.
Contributorship
All authors contributed equally.