
Abstract
Introduction:
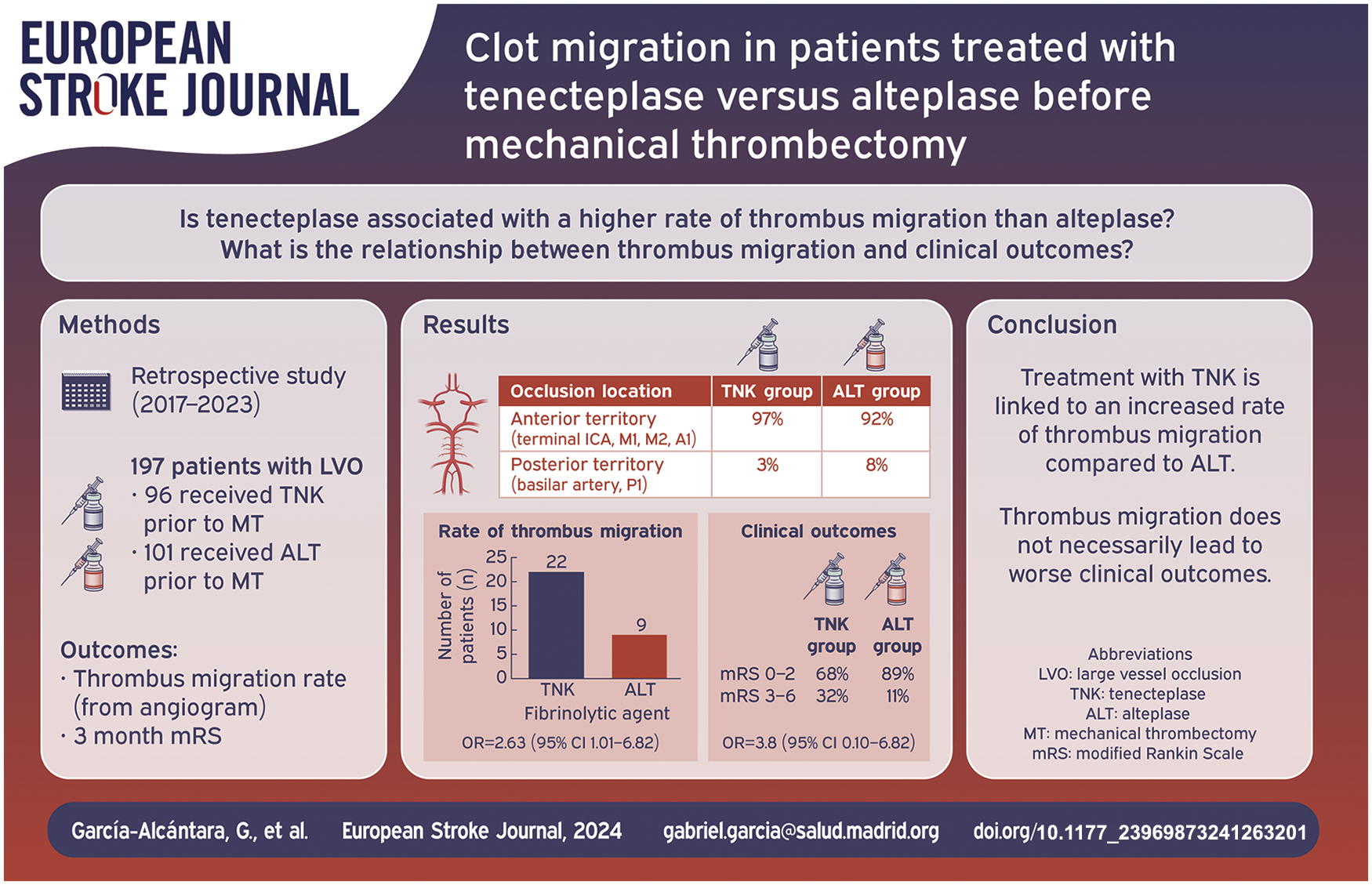
This study aimed to describe and analyze the rate of clot migration of vessel thrombosis to distal segments in patients with acute ischemic stroke (AIS) who received intravenous thrombolysis (IVT) with tenecteplase (TNK) and alteplase (ALT) before mechanical thrombectomy (MT). In addition, we aimed to determine the relationship between thrombus migration and functional prognosis.
Methods:
This study followed the STROBE reporting guidelines. We performed a retrospective analysis of a series of patients from November 2017 to April 2023 with an AIS with thrombosis on CT imaging, treated with IVT (TNK or ALT, split into two distinct groups) prior to mechanical thrombectomy.
Results:
Two hundred and fifty-six patients with large vessel occlusion (LVO) were included. Ninety-six had received TNK. One hundred and sixty had received ALT. Of the 96 TNK patients, 25 experienced either complete recanalization (n = 3) or thrombus migration (n = 22). Of the 160 ALT patients, 20 experienced either complete recanalization (n = 6) or thrombus migration (n = 14). The difference being statistically substantial for the thrombus migration rate (OR = 3.61, 95% confidence interval: 1.63; 7.98). Migration to an irretrievable very distal segment occurred in four (4%) patients with TNK and in three patients (2%) with ALT (p > 0.05). Thrombus migration was not significantly associated to a different functional prognosis, measured through Rankin scale after 3 months (OR = 0.44, 95% confidence interval: 0.17; 1.12).
Conclusion:
The use of TNK over ALT as a fibrinolytic agent is associated with a higher thrombus migration rate. The migration of thrombi to distal segments, which are theoretically less accessible for mechanical thrombectomy, did not result in worse clinical outcomes.
Introduction
Ischemic stroke is one of the most important causes of disability in adults and its prevalence is expected to increase in the coming years. 1 More than 80% of all ischemic strokes are caused by brain arteries occlusion. 2 Since 1995, intravenous thrombolysis (IVT) has been used as the main reperfusion therapy after demonstrating an improvement in the prognosis of patients with ischemic stroke. 3 Current guidelines recommend two fibrinolytic agents for IVT: alteplase (ALT) and tenecteplase (TNK). 4
The available studies indicate that the sooner IVT is administered since the onset of stroke, the higher the probability of thrombus resolution. 5 In 2008, the EXTEND-IA TNK clinical trial proved that using TNK within the first 4.5 h after the onset of stroke is associated with a higher rate of thrombus recanalization than ALT. 6 Moreover, according to previous studies, IVT is associated with an increased rate of thrombus migration to more distal arterial segments. 7 Smaller clots, rich in erythrocytes, and shortest thrombus length have been demonstrated to be independent predictors of thrombus migration.8,9
Currently, it is unclear whether thrombus migration to more distal segments after IVT hinders retrieval during mechanical thrombectomy (MT) and affects patient prognosis. Previous studies have indicated that migration after IVT is associated with a lower complete recanalization rate and worse functional results after 3 months and there are scarce data regarding the effect of tenecteplase on thrombus migration.10–12
The objective of the study was to investigate and assess the incidence of vessel thrombus migration to distal segments in patients with acute ischemic stroke who received intravenous thrombolysis with tenecteplase or alteplase before undergoing mechanical thrombectomy and to determine whether there is a correlation between migration and the patient’s functional outcome.
Patients and methods
Study design
This study followed the STROBE reporting guidelines.
This was a retrospective observational study of a series of patients who were treated at a tertiary hospital (Stroke Center ESO Accredited), presented with acute ischemic stroke with vessel occlusion, and were treated with intravenous thrombolysis and mechanical thrombectomy.
The inclusion criteria were patients presenting with acute ischemic stroke with occlusion on computed tomographic angiography (CTA) from November 2017 to April 2023 who were treated with IVT (TNK or ALT, split into two different groups) and then underwent mechanical thrombectomy.
The Madrid region’s regional protocol for Mechanical Thrombectomy (MT) stipulates that all patients in the study were independent prior to treatment, with a score of <3 points on the modified Rankin Scale (mRS). 13
Patients treated with ALT from November 2017 to April 2023 were included in the study. Patients who received TNK at the beginning of its use at our hospital from November 2020 to April 2023 were selected.
The recommendations to perform mechanical thrombectomy and administer IVT did not differ between November 2017–October 2020 (ALT patients) and November 2020–April 2023 (TNK and ALT patients), according to the Madrid region’s regional stroke protocol. 13
The patients from the two groups (TNK or ALT) presented with an onset-needle time of <4.5 h, in cases of unknown onset stroke or between 4.5 and 9 h from the beginning of the symptoms, IVT was performed when perfusion CT was favorable (ischemic penumbra was defined as an area with >6 s of delayed arrival of contrast). 14
The exclusion criteria were as follows: (a) ischemic stroke without large-vessel thrombus; (b) ischemic stroke and large-vessel thrombus who were not eligible for reperfusion therapies; (c) patients with ischemic stroke and large-vessel thrombus treated with IVT without mechanical thrombectomy; and (d) mechanical thrombectomy performed at another hospital.
Data collection
The study obtained institutional review board approval, and the participants provided written consent after being informed. One of the authors (ACC) was granted unrestricted access to all study data and bore accountability for both its integrity and the analysis that was conducted.
The digital clinical histories of the patients from all groups were revised to gather demographic and clinical data. Demographic data collected included age and sex. Clinical data included baseline Modified Rankin Scale (mRS) scores, vascular risk factors (high blood pressure, dyslipidemia, diabetes, and smoking), previous ischemic heart disease, previous stroke/TIA, atrial fibrillation diagnosis (before or during admission), previous anticoagulant and antiplatelet treatment, glucose and platelet levels, and coagulation parameters (PT, INR, and aPTT) at admission.
In all patients initially evaluated in our hospital, multimodal CT was performed (baseline-cranial CT, supra-aortic vessels, and Circle of Willis CTA, as well as perfusion CT).
For patients who underwent IVT at a different hospital, multimodal CT was performed upon arrival at our center.
The on-duty neuroradiologists reported the site of occlusion from the angiogram and the resulting TICI grades to the neurologist. The final radiologic report was validated by a stroke neurologist.
A skilled vascular neurologist administered thrombolytic therapy. Patients treated with TNK received a 0.25 mg/kg dose (administered as a bolus), whereas those treated with ALT received a 0.9 mg/kg dose (10% as a bolus dose and the remaining 90% as an infusion). All mechanical thrombectomies were performed by an experienced interventional neuroradiologist with 20 years of experience.
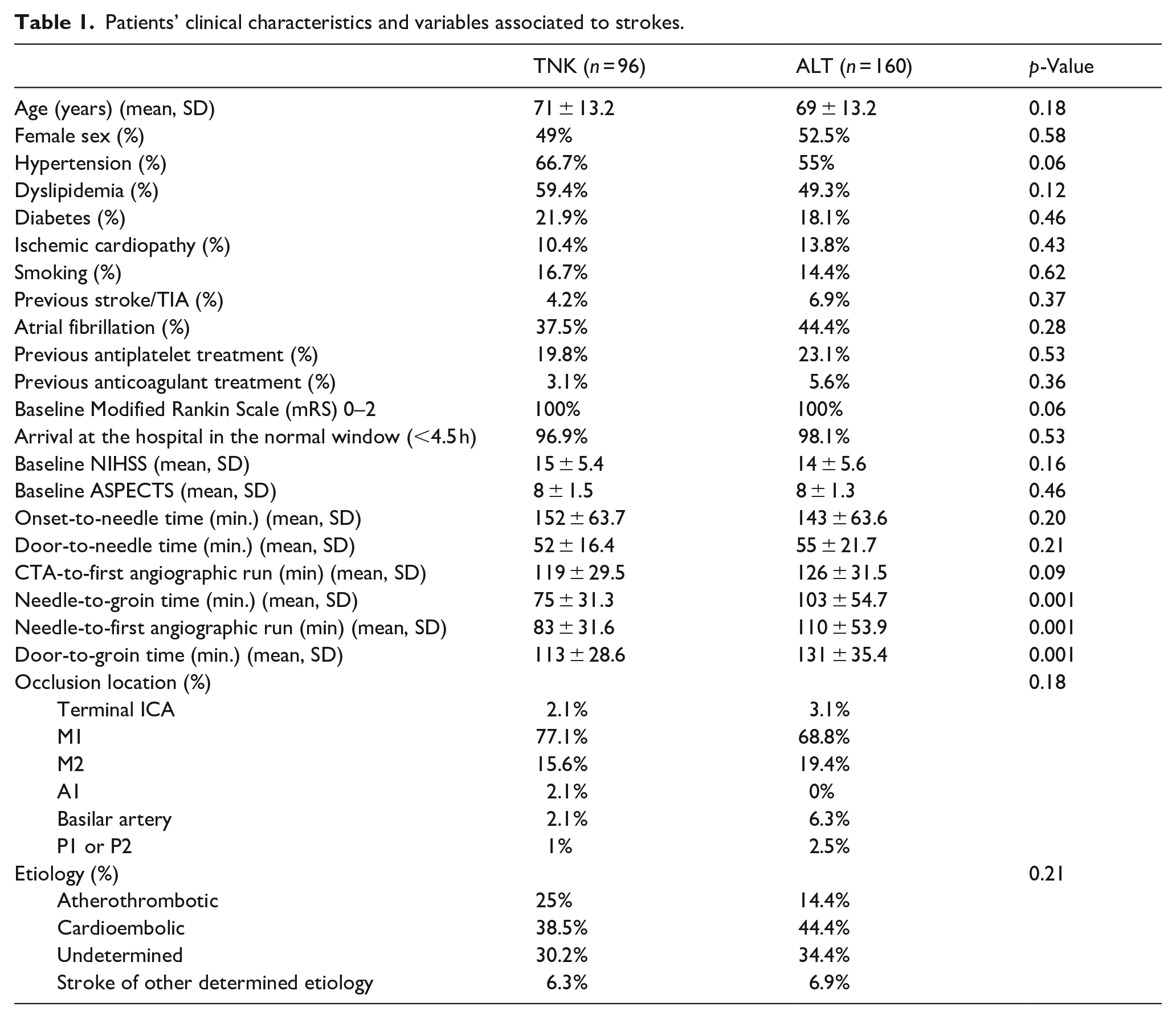
A range of clinical and radiological parameters, including baseline NIHSS scores upon arrival at the emergency room, were obtained from the AIS records of the patients: NIHSS score after IVT prior to MT; ASPECTS score on the baseline-cranial CT scan; thrombus location as identified on CTA (in terminal ICA, MCA segments; ACA segments, basilar artery, or PCA segments); high blood pressure within the first 24 h after IVT (defined as ⩾185/110 mmHg); whether the IVT was performed at our hospital or another facility; and time intervals such as onset-to-needle, door-to-needle, CTA-to-first angiographic run, needle-to-groin puncture, needle-to-first angiographic run, and door-to-groin puncture time (Table 1 for specific details).
Patients’ clinical characteristics and variables associated to strokes.
AIS etiology was classified according to the TOAST classification at discharge (Table 1).
The following diseases and conditions were considered causes of stroke of other determined etiologies: non-arteriosclerotic-non-inflammatory vasculopathy (spontaneous or traumatic arterial dissection, Moyamoya disease, fibromuscular dysplasia, and post-radiotherapy arteriopathy), non-arteriosclerotic-non-inflammatory vasculopathy from an infectious or immunological origin, arterial thrombophilia, and secondary hypercoagulable states.
As a safety variable, in both groups, the bleeding rate in the control CT scan 24 h after IVT was recorded using the Heidelberg Bleeding Classification.
In this study, the primary factor under evaluation was the thrombus migration rate on angiography after IVT in the TNK and ALT groups. The initial occlusion was identified as the thrombus’s most proximal location on the CTA. On the angiogram, occlusion was determined as the thrombus’s most proximal location on the first intracranial digital subtraction angiography. Thrombus migration was characterized as a change to a more distal occlusion on the angiogram compared to the initial occlusion on the CTA.
Our center’s neuroradiologist staff have identified the locations of retrievable clots in patients with thrombus migration since 2012, following a regional protocol shared by all stroke centers in the Madrid Region. 13 We determined that the internal carotid artery and the M1, M2, M3, A1, A2, P1, and P2 segments were the locations where the thrombus could be retrieved after one or more passes. Recanalization was defined as absence of arterial occlusion on angiography.
In all patients, we evaluated the success of recanalization using the Thrombolysis in Cerebral Infarction Scale (TICI). 15 A TICI score of 2b–2c was used to define successful recanalization, whereas a TICI score of 3 indicated complete recanalization.
The patient’s functional prognosis and mortality were measured using the modified Rankin Scale (mRS) after 3 months. Certified raters (ACC, RV, CM, ADF, SGM, and JM) assessed individually in person the mRS score. After 3 months, the patients were classified into two groups according to their modified Rankin Scale scores: functional independence (0–2 mRS) and functional dependence (⩾3 mRS).
Statistical analyses
The baseline characteristics and outcomes of the two groups are presented using descriptive statistics. Continuous variables with a normal distribution are expressed as mean ± standard deviation (SD), whereas those with a skewed distribution are described as medians with interquartile ranges (IQR). Categorical variables are presented as absolute and relative frequencies. Statistical comparisons between the two groups involved the chi-square test or Fisher ’s exact test for categorical variables and the Mann–Whitney U test or independent-sample t-test for continuous variables.
Subsequently, we performed propensity score matching (PSM) to address differences in the clot migration rate between the TNK and ALT groups, as well as to determine the effect of thrombus migration on the Rankin scale score. The propensity score, generated through a multivariable logistic regression model including covariates, such as age, clot location, onset-to-needle time, CTA-to-first angiographic run time, and thrombolytic agent (TNK or ALT), facilitated a 1:1 matching ratio of patients receiving TNK therapy to those receiving ALT therapy. The baseline NIHSS and modified Rankin Scale (mRS) scores were also included as covariates to determinate the effect of thrombus migration on the Rankin Scale score after 3 months.
Matching was performed without replacement, utilizing nearest neighbor matching and a caliper value of 0.2 SD logir propensity score. Standardized mean differences (SMD) in covariate means were calculated post-PSM to assess bias reduction. For this test, the impact of migration on the 3-month mRS and PS scores was assessed.
For both primary and secondary outcomes, odds ratios (OR) and the corresponding 95% confidence intervals (CI) were calculated for the PSM cohort. Additionally, sensitivity analyzes employing multivariable logistic regression models were conducted to assess the robustness of the results by adjusting for the same covariates and employing the inverse probability of treatment-weighting (IPTW) propensity score.
All data analyses were performed using Stata software version 18.1, and statistical significance was determined using a two-tailed p-value of <0.05.
Results
The mean age of the patients in the TNK and ALT groups was 71 ± 13.2 and 69 ± 13.2 years, respectively, and the mean baseline NIHSS score was 15 ± 5.4 in the TNK group and 14 ± 5.6 in the ALT group. The mean cranial-baseline CT ASPECTS score was 8 in both groups (±1.5 in the TNK group; ±1.3 in the ALT group). No statistically significant differences were observed in the clinical characteristics between the two groups (Table 1).
Of the 96 TNK-treated patients, 25 achieved complete recanalization (n = 3) or partial recanalization with thrombus migration (n = 22). In comparison, of the 160 ALT-treated patients, 20 achieved complete recanalization (n = 6) or partial recanalization with thrombus migration (n = 14). Patients who received TNK had a higher likelihood of recanalization (complete or with thrombus migration) (OR = 2.31, 95% confidence interval: 1.18; 4.5).
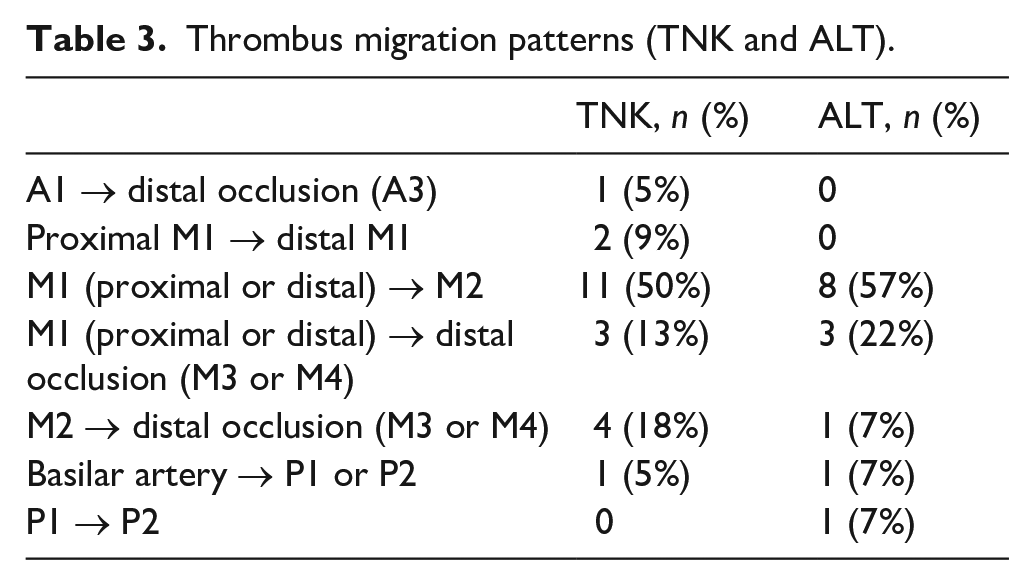
The reperfusion status achieved with thrombolysis (TNK vs ALT) is reported in Table 2. Table 3 provides a detailed overview of thrombus migration patterns (TNK and ALT).
Reperfusion status achieved with thrombolysis (TNK vs ALT).

Thrombus migration patterns (TNK and ALT).
After PSM, all variables showed standardized differences < 10%. Regarding the effect of the treatment on migration, 84 pairs were selected. After propensity score-matching, 84 patients were included in each group. Patients who received TNK had a higher probability of thrombus migration (OR = 3.61, 95% confidence interval: 1.63; 7.98) (Table 4).
Statistical analysis treatment (TNK or Alteplase) versus migration.
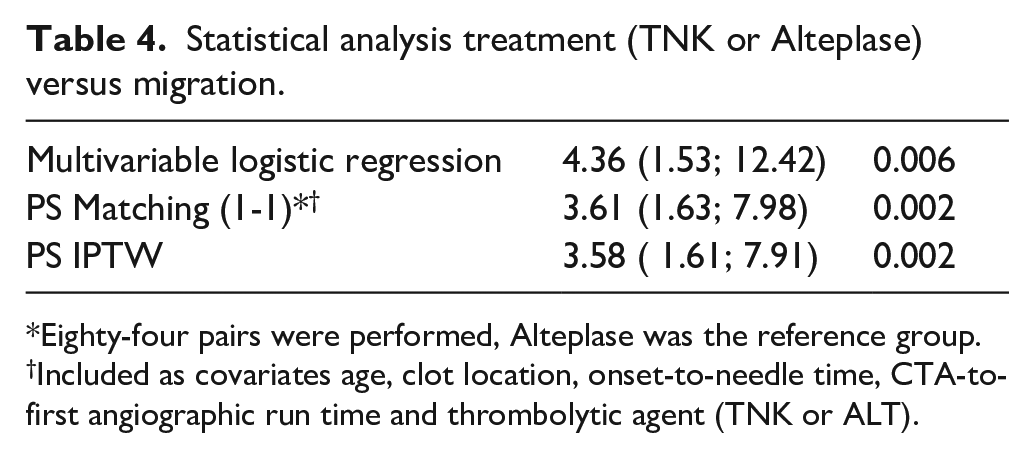
Eighty-four pairs were performed, Alteplase was the reference group.
Included as covariates age, clot location, onset-to-needle time, CTA-to-first angiographic run time and thrombolytic agent (TNK or ALT).
In patients without matching controls, 4 out of 22 migrations were recorded in the TNK group, compared to 9 out of 14 in the ALT group. The results from the IPTW propensity score and multivariable logistic regression analyses were consistent, suggesting a migration risk greater than 3 for TNK compared with ALT (Table 4).
In the TNK group, 78% (n = 17) of the 22 migrated thrombi were retrieved, and in the ALT group, 64% (n = 9) of the 14 migrated thrombi were successfully recovered. There were no significant differences in retrieval rates between the two groups. Successful or complete recanalization, was achieved in all patients with migrated thrombi on angiography, regardless of whether they received TNK or ALT, following mechanical thrombectomy.
There were no significant differences in the rates of successful reperfusion between patients with and without migrated thrombus (migration: 44.5% 2b–c TICI, 55.5% 3 TICI vs no migration: 29.1% 2b–c TICI, 65% 3 TICI).
No differences were noted between the groups with respect to the occlusion sites on CTA. A total of 32 patients from the ALT group (20%) and two from the TNK group (2.1%) received IVT at a different hospital (“drip and ship”) (p < 0.05). In TNK group, two patients (2%) with thrombus migration were treated at a different hospital. In ALT group, four patients (2.5%) with thrombus migration were treated at a different hospital.
One hundred and fifty-seven ALT-treated patients (98.1%) and 93 TNK-treated patients (96.9%) arrived at the hospital in the normal window (<4.5 h). Three patients of in each group (ALT and TNK) arrived at the hospital after 4.5 h.
The mean onset-to-needle time of the TNK and ALT-treated patients was 152 ± 63.7 and 143 ± 63.6 min, respectively (p > 0.05). The mean time from qualifying CTA to time of first angiographic run was 119 ± 29.5 min in the TNK group and 126 ± 31.5 min in the ALT group (p > 0.05).
Significant variations (p < 0.05) were seen in the needle-to-groin time (75 min average ± 31.3 in the TNK group; 103 min average ± 54.7 in the ALT group), in the time from thrombolytic agent bolus (needle) to time of first angiographic run (83 min average ± 31.6 in the TNK group; 110 min average ± 53.9 in the ALT group), and in the door-to-groin time (113 min average ± 28.6 in the TNK group; 131 ± 35.4 in the ALT group).
No differences were found in the etiological diagnosis of stroke or other clinical variables related to stroke between the two groups (Table 1).
Regarding safety, no statistically significant differences were observed in the incidence of intracranial bleeding post-treatment between the TNK and ALT groups (p > 0.05). Intracranial bleeding occurred in 14 patients (14%) in the TNK group and 15 patients (9%) in the ALT group.
In patients with thrombus migration, 68% (n = 15) TNK-treated patients and 93% (n = 13) ALT-treated patients reached functional independence (0–2 mRS) after 3 months. Among those without migration, 57% (n = 42) TNK-treated patients and 56% (n = 82) ALT-treated patients achieved an 0–2 mRS score after 3 months. Figure 1 display 3 month modified Rankin scale score comparisons between migration and no migration groups with each treatment (TNK or ALT).
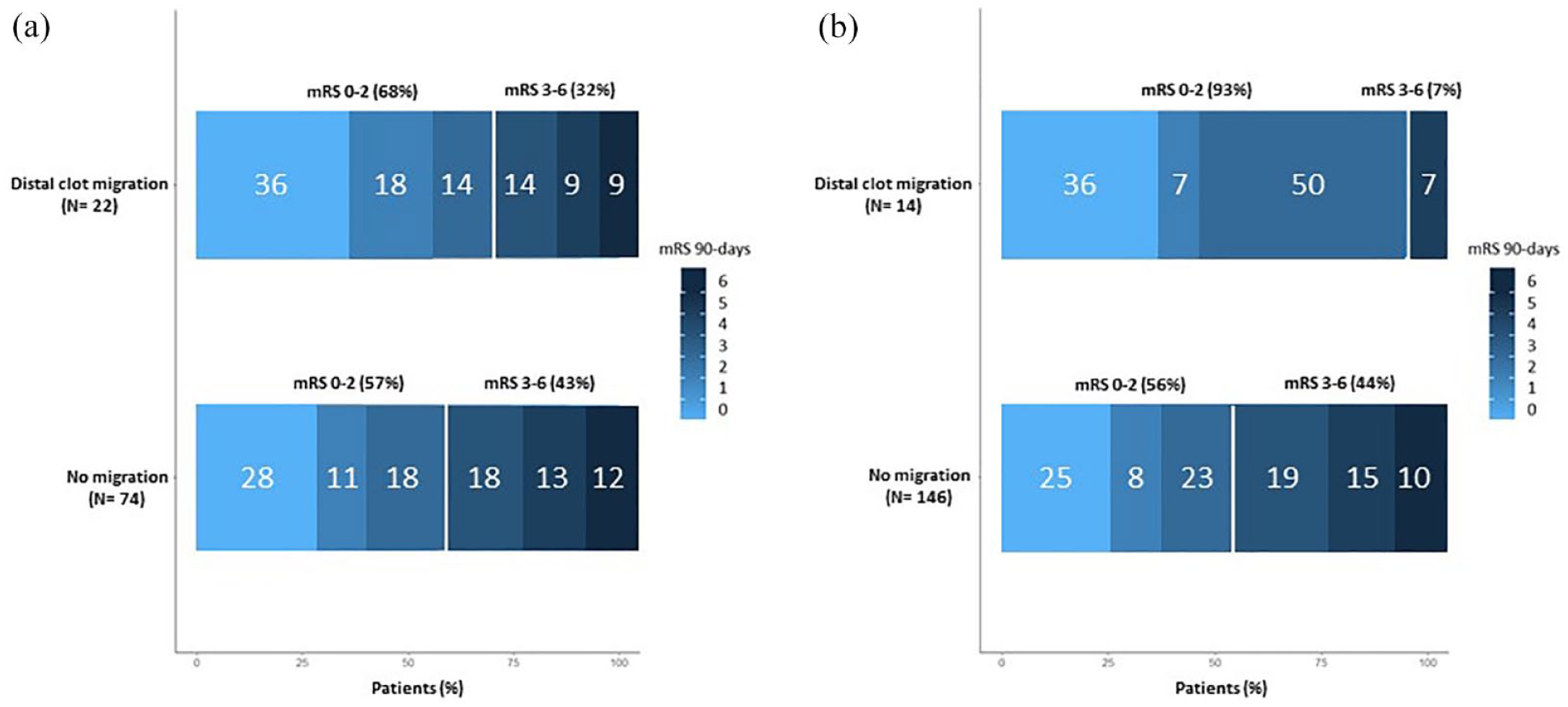
Modified Rankin Scale Scores at 90 days in TNK and Alteplase group.
As for the effect of thrombus migration on the Rankin scale score after 3 months, we did not observe any significant differences in the degree of functional dependency in either group (TNK or ALT) (OR = 0.44, 95% confidence interval: 0.17; 1.12) (Table 5).
Statistical analysis migration versus Rankin (0–2 vs 3–6).
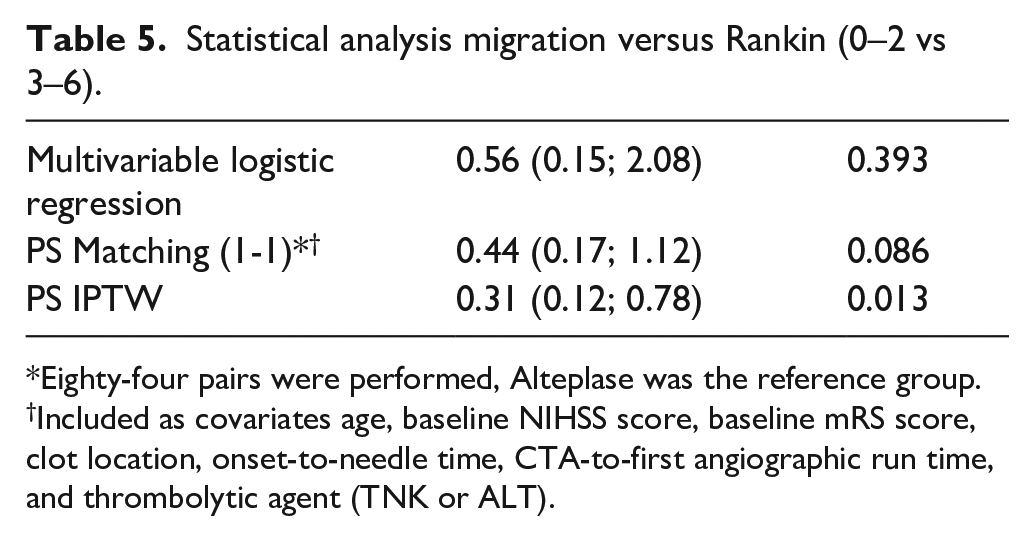
Eighty-four pairs were performed, Alteplase was the reference group.
Included as covariates age, baseline NIHSS score, baseline mRS score, clot location, onset-to-needle time, CTA-to-first angiographic run time, and thrombolytic agent (TNK or ALT).
Discussion
TNK therapy was associated with a higher thrombus migration rate than ALT therapy. Furthermore, recanalization, whether complete or partial, was more common in patients treated with TNK.
These results are consistent with those of a study by Yogendrakumar et al., 12 in which patients who received TNK experienced higher recanalization and thrombus migration rates. The rate of thrombus migration with ALT was similar to those reported in other studies. 16
Prior research has suggested that thrombus migration may increase the chance of the clot being inaccessible during MT due to its movement to distal segments. 17 In this study, most migrated thrombi were successfully retrieved during thrombectomy, with 78% in the TNK group and 64% in the ALT group, which is consistent with other studies’ findings. 18
Thrombus retrieval rates were comparable between the two groups. This suggests that TNK, unlike ALT, may not lead to thrombus migration to distal segments that are beyond retrieval.
Moreover, there were no differences in the successful reperfusion rates between patients with migrated thrombi treated with TNK or ALT and those without.
This study showed no disparity in the rate of complete recanalization with intravenous thrombolysis (IVT) between the TNK and ALT groups. Both groups included patients within a <4.5 h and 4.5–9 h window from symptom onset to the start of thrombolysis, contrasting with other studies that reported a higher recanalization rate with TNK when administered within the first 4.5 h after stroke symptoms begin.2,5
The frequency of IVT conducted at a different hospital was greater for ALT than for TNK. This correlates with the lower availability of TNK in some hospitals in the Madrid Region during the study period (our Stroke Center was the second in Madrid to adopt TNK for IVT).
The proportion of drip-and-ship patients with thrombus migration was similar in the TNK (2%) and ALT (2.5%) groups.
The onset-to-needle time was longer in the TNK group. This is likely explained by a lower proportion of drip-and-ship patients in the TNK group, than in the ALT group, which led to a shorter delay in the administration of IVT in this last group.
Needle-to-first angiographic run time was shorter for TNK. This might be related to the higher ease of administering TNK (prefilled syringe and bolus administration) compared with ALT, which requires continuous infusion for an hour. Furthermore, the lower proportion of drip-and-ship patients in the TNK group, probably contribute to the shorter delays in the needle-to-first angiographic run time.
Previous studies have indicated that the longer the time, the more likely it is for clot migration to occur. 19 The needle-to-first angiographic run time was lower in patients who received TNK; therefore, this finding supports the hypothesis that its use is associated with a higher rate of thrombus migration.
Although the incidence of intracranial bleeding in the control CT group was slightly higher with TNK (14%) than with ALT (9%), no significant differences in Rankin scores or 90-day mortality rates were observed between the groups. This is in line with recent publications, such as that of Marnat et al., 20 which describes a slight tendency toward bleeding with tenecteplase.
Concerning the clinical results, we did not find any association between thrombus migration and functional outcomes measured using mRS after 3 months (regardless of thrombus retrieval during MT). These results may be explained by the fact that most migrated thrombi were retrieved during MT (78% and 64% in the TNK and ALT groups, respectively). In addition, in all cases where retrieval was not possible due to migration to more distal segments (five patients in TNK and five in Alteplase), the reperfusion rate was successful (TICI 2b-c). Despite the non-significant differences, we observed a trend toward functional improvement after 90 days in patients with thrombus migration. Therefore, we considered it interesting to use a broader patient registry to verify our results.
This observation contrasts with the findings from Heitor C. Alves et al.′s study, which identified a positive correlation between thrombus migration and improved functional outcomes, and Kaesmacher et al.′s research, where thrombus migration correlated with poorer prognosis.6,10 The discrepancy may stem from the different criteria for defining thrombus migration. Our study, along with that of Heitor C. Alves et al., relied on direct evidence from angiograms, while Kaesmacher et al. utilized indirect evidence through perfusion deficits in the lenticulostriate artery territory.6,10
A noteworthy aspect of the study is the inclusion of a representative sample of patients with large vessel thrombus ischemic stroke who were treated with IVT (either TNK or ALT) and mechanical thrombectomy (MT). The uniformity of having all MTs conducted at the same hospital by experienced interventional neuroradiologists contributes to the consistency in CT evaluation, angiogram interpretation, and MT outcomes.
This study has some limitations. First, a retrospective design was used; therefore, some bias may have been present. We assumed a selection bias because all the patients included in the study were treated with MT after thrombolysis. This prevents us from establishing conclusions about the actual thrombus migration percentage with each fibrinolytic agent, because we do not know the migration rate in patients who have not undergone this procedure. Second, there were a greater proportion of drip-and-ship patients in the ALT group due to the lower availability of TNK in some hospitals in the Madrid region. However, the proportion of drip-and-ship patients with thrombus migration was similar in TNK and ALT groups. Third, the raters (GGA, ACC) were not blinded to the treatment and knew whether the patient had received TNK or Alteplase. Additionally, neurologists and interventional neuroradiologists were aware of the patient’s clinical presentation and the initial location of the thrombus on CT. Fourth, no significant differences were observed in the degree of functional dependency in patients who received TNK or ALT with migrated thrombi; therefore, we assume the possibility of a type II error due to the limited sample size. Further studies with larger sample sizes are necessary to verify these results. Finally, the choice of thrombolytic agent (TNK or ALT) was determined by the treating neurologist’s personal preference. The selection of TNK at our center could be attributed to its simple and rapid administration. Nevertheless, neurologists had the option of choosing between two treatments: TNK or ALT.
Conclusion
The use of TNK over ALT as a fibrinolytic agent is associated with a higher thrombus migration rate. The migration of thrombi to distal segments, which are theoretically less accessible for mechanical thrombectomy, did not result in worse clinical outcomes.
Supplemental Material
sj-docx-1-eso-10.1177_23969873241263201 – Supplemental material for Clot migration in patients treated with tenecteplase versus alteplase before mechanical thrombectomy
Supplemental material, sj-docx-1-eso-10.1177_23969873241263201 for Clot migration in patients treated with tenecteplase versus alteplase before mechanical thrombectomy by Gabriel García-Alcántara, Cristina Moreno-López, Rodrigo López-Rebolledo, Pablo Lorenzo-Barreto, Patricia Garay-Albízuri, Beatriz Martínez-García, Ana Llanes, Daniel Pérez-Gil, Juan Luis Chico, Rocío Vera-Lechuga, Sebastián García-Madrona, Consuelo Matute-Lozano, Alicia De Felipe-Mimbrera, Jaime Masjuan and Antonio Cruz-Culebras in European Stroke Journal
Footnotes
Acknowledgements
We would like to thank Alfonso Muriel García for his exceptional assistance in performing the statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.
Ethical approval
The Research ethics committee (CEI) of Ramón y Cajal University Hospital approved this study.
Guarantor
ACC.
Contributorship
GGA and ACC designed the study. GGA and ACC researched the literature. GGA acquired the data, did analysis statistical and wrote the first draft of the manuscript. ACC supervised the study. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.