
Abstract
Background:
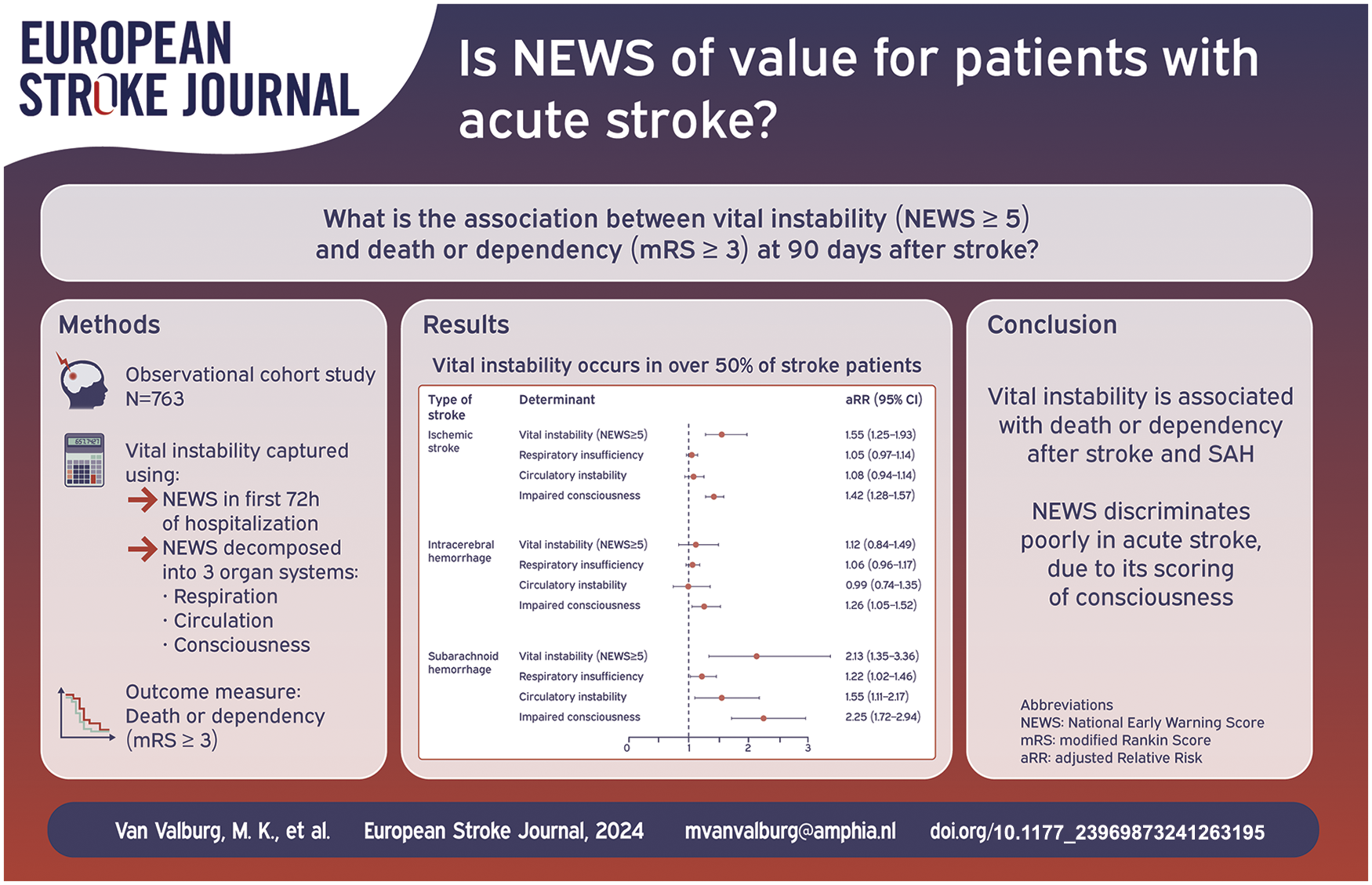
Patients with acute stroke are at risk of respiratory or circulatory compromise resulting in vital instability, which can be captured through the widely used aggregated National Early Warning Score (NEWS). We aimed to assess the relation between vital instability (defined as NEWS of five or higher) and death or dependency at 90 days after stroke.
Methods:
In this observational cohort study we studied 763 patients with ischaemic stroke (n = 400), intracerebral haemorrhage (ICH) (n = 146) or subarachnoid haemorrhage (SAH) (n = 217), hospitalized to a Dutch tertiary referral hospital from 1 January 2017 to 31 December 2018. We calculated NEWS for each 8 h time span during the first 72 h after hospitalization. We also decomposed NEWS into its three components respiration, circulation and consciousness. The primary outcome was death or dependency (modified Rankin Scale score ⩾3) at 90 days after stroke. The association of vital instability with functional dependency was examined using Poisson regression.
Results:
Two hundred and twenty-seven (58%) patients with ischaemic stroke, 101 (69%) with ICH and 142 (65%) with SAH had at least one episode of vital instability. In patients with ischaemic stroke or SAH, vital instability was associated after adjustment for confounders with death or dependency (adjusted relative risk 1.55 ((95% CI) 1.25–1.93 and 2.13 (1.35–3.36), respectively)). This was mainly driven by impaired consciousness, which was associated with death or dependency in all types of stroke. Respiratory insufficiency and circulatory instability were associated with death or dependency only in SAH.
Conclusion:
Vital instability in the first 72 h of hospitalization for ischaemic stroke or SAH is associated with death or dependency at 90 days. Impaired consciousness was the main driver of this relationship. NEWS may not be appropriate for patients with acute stroke, mainly due to the dichotomous manner in which the level of consciousness is classified, and modification of NEWS should be considered for these patients
Keywords
Introduction
Patients with acute stroke are at considerable risk of respiratory or circulatory complications.1,2 These may lead to vital instability: an undesirable patient status manifested by abnormal vital signs that may result in critical illness or death.3,4 Vital instability can be captured through an aggregated early warning score (EWS). An EWS is an aggregation of several vital signs and results in a composite sum score, in which weights are assigned to each vital sign according to the amount of deviation from normal physiology.5–9 Patients are characterized as ‘vitally unstable’ when a predefined threshold of an EWS is exceeded.5–7,9,10 Patients with vital instability often require evaluation by a rapid response team including anaesthesiologists or intensive care physicians.
The major benefit of a general EWS is that nurses and clinicians from different specialities ‘speak the same language’ when communicating about deteriorating patients. However, it can be questioned whether such a ‘one size fits all’ approach is appropriate when hospitalized patients differ in their reason for admission and medical history, and whether a single aggregated EWS score has the same meaning in different patient populations. 11
Several different EWS systems are in use, including the widely used National EWS (NEWS). 12 The major drawback of using NEWS for stroke patients is the dichotomous manner in which consciousness contributes to the NEWS. This binary approach (e.g. presence or absence of a maximum Glascow Coma Scale (GCS) sum score) is reasonable in patients with sepsis for example, but is an oversimplification of the clinical situation in many stroke patients. NEWS has been adapted earlier to subsets of hospitalized patients, for example in patients with chronic obstructive pulmonary disease.13–15 The updated NEWS2 Guidelines explicitly allow new adaptations.16,17 There is no NEWS variant specifically for patients with stroke.
We aimed to assess the usefulness of NEWS in patients with acute stroke. We therefore calculated the incidence of vital instability as defined by NEWS in the first 72 h of hospital admission for acute stroke, and assessed the association between vital instability and death or dependency at 90 days. Additionally, we decomposed the NEWS score into deterioration by organ system (respiration, circulation and consciousness) to assess the contribution of each component to this association. Because of differences in treatment, clinical course, and prognosis, the association was evaluated for each type of stroke separately (ischaemic stroke, intracerebral haemorrhage (ICH) or subarachnoid haemorrhage (SAH)).
Methods
Study design
This observational cohort study comprises all adult (18 years and older) patients in the prospective Utrecht Stroke Database18–20 with hospital admission to the comprehensive stroke centre at the University Medical Centre Utrecht, Utrecht, the Netherlands, because of acute stroke between January 1st, 2017 and December 31st, 2018. We only included patients with a first episode of acute stroke during the study period.
We included patients with ischaemic stroke, ICH or SAH, confirmed by neuroimaging, and excluded patients in case of hospitalization >48 h after stroke onset, hospital stay shorter than 24 h due to discharge or death, or withdrawal of all curative treatments within 24 h after admission.
Data collection
Patient characteristics including information on six comorbidities (hypertension, diabetes mellitus, peripheral vascular disease, history of malignancy, history of myocardial infarction and previous stroke), baseline stroke severity as measured with the National Institutes of Health Stroke Scale (NIHSS) 21 and functional status assessed with the modified Rankin Scale (mRS) 22 before and 90 days after stroke were collected.
Vital signs were acquired from the electronic medical records or from clinical bedside monitoring systems, in which case only actual values validated by the attending nurse were incorporated. The EWS system used to calculate vital instability in this study was the NEWS, developed by the Royal College of Physicians of London. 12 All seven vital signs incorporated in NEWS (i.e. consciousness, heart rate, systolic blood pressure, respiratory rate, oxygen saturation, supplemental oxygen use and temperature) and measured within 72 h after hospitalization were extracted. All vital sign values were aggregated into nine successive time spans of 8 h (i.e. one nurse shift) from the time of admission onwards.
According to the Institutional Review Board (IRB) of the University Medical Centre Utrecht, the study was not subject to the Medical Research Involving Human Subjects Act and therefore the necessity of informed consent was waived (IRB number 19-338/C). All procedures and reporting were performed in accordance with the STROBE statement (
Definition of vital instability
Vital instability was defined as a NEWS score >5 at any point in time within the first 72 h after hospital admission.12,24 First, the validity of recorded vital signs was checked and artefacts were removed (
The NEWS scoring system.
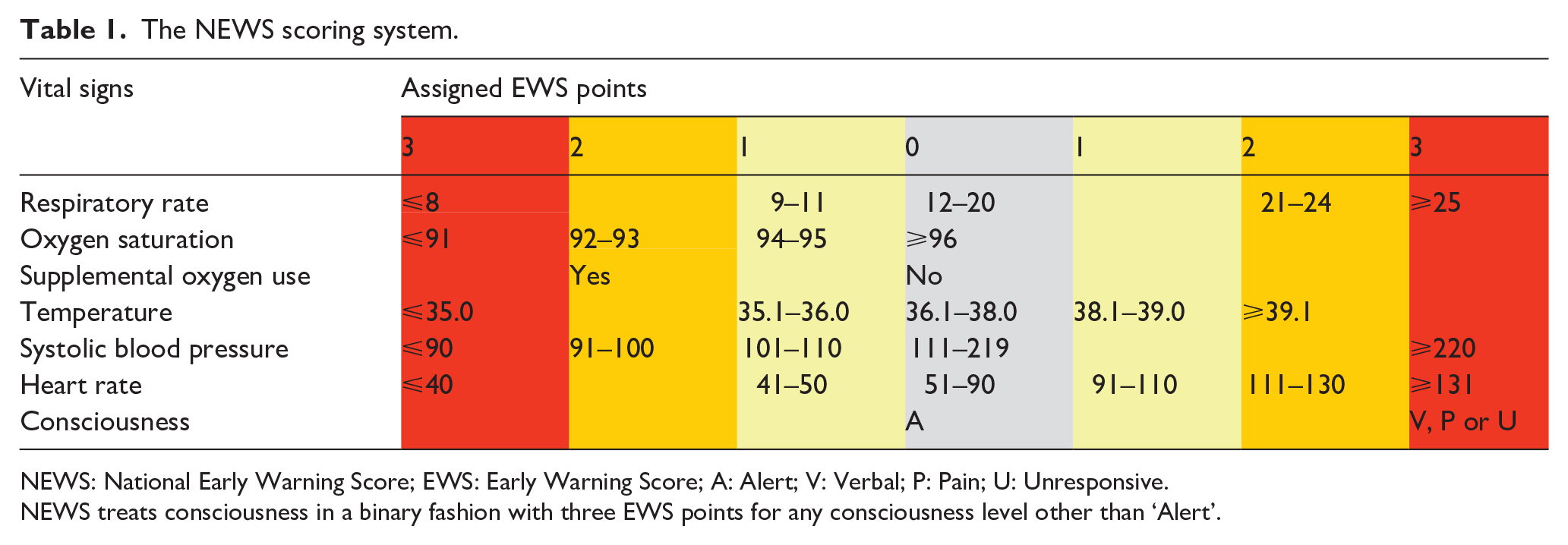
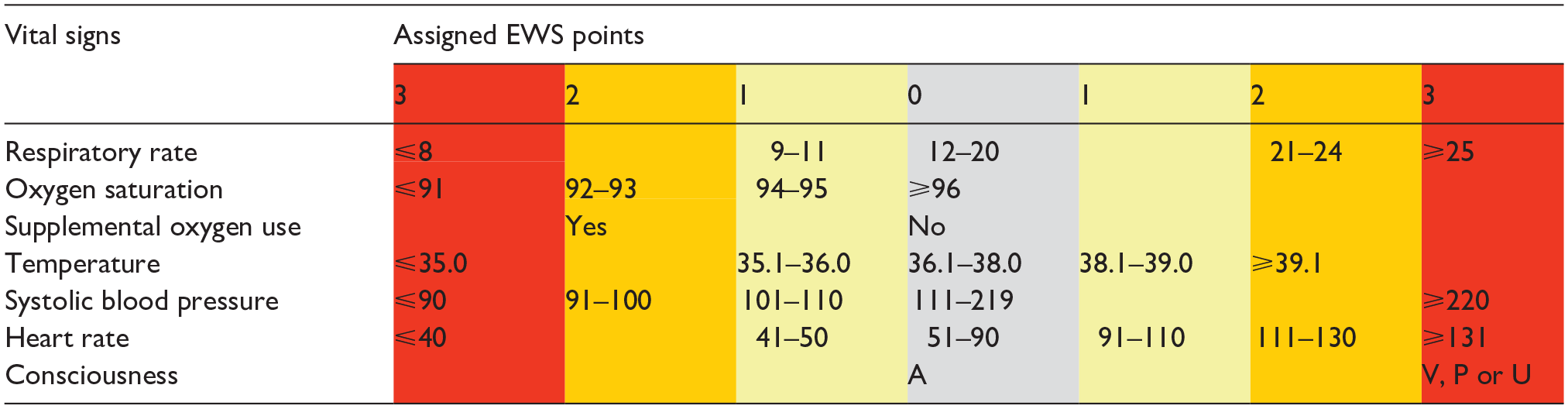
NEWS: National Early Warning Score; EWS: Early Warning Score; A: Alert; V: Verbal; P: Pain; U: Unresponsive.
NEWS treats consciousness in a binary fashion with three EWS points for any consciousness level other than ‘Alert’.
Deterioration by organ system
The total NEWS calculation per time span for each patient was also decomposed into deterioration by organ system: respiration, circulation and consciousness. EWS points assigned to each separate organ system were calculated per time span. The score for respiration was calculated using the EWS points for respiratory rate, oxygen saturation and supplemental oxygen use, leading to a value range of 0–8 EWS points. The score for circulation was calculated using the EWS points for heart rate and systolic blood pressure, leading to a value range of 0–6 EWS points.
The original NEWS definition treats consciousness in a binary fashion with 3 EWS points for any consciousness level other than ‘alert’, based on the nurse’s assessment of alertness, response to verbal command, response to pain and unconsciousness, also abbreviated as AVPU. 25 As stroke patients are assessed with the full Glasgow Coma Scale (GCS), we assigned 3 EWS points for any GCS score lower than 15, leading to a value for consciousness of 0 versus 3 EWS points. Consecutively, we calculated the mean EWS score of each component for each of the nine 8-h time spans. Deterioration per organ system (respiration, circulation and consciousness) was assessed as a continuous variable.
Outcome
The primary outcome was death or dependency, defined as an mRS score ⩾3 at 90 days after stroke. 26 The secondary outcome was death at 90 days.
Missing values
Missing values were handled using multiple imputation. When vital sign data from one 8 h time span were missing, they were first interpolated using the directly preceding or following measurement. If vital signs measurements remained missing, we conducted multiple imputation using the ‘mice’ library 27 in R, creating 30 imputation datasets. All analyses were conducted in the imputed datasets and subsequently, estimates were pooled using Rubin’s rule. 28
Statistical analysis
Statistical analyses were performed for each type of stroke separately (ischaemic stroke, ICH and SAH). The incidences of vital instability, death or dependency at 90 days, and 90-day mortality were calculated, as well as mean values of vital signs and deterioration per organ system. The numbers of time spans with vital instability were computed and consecutively the Kruskal-Wallis H test with posthoc testing was used to assess differences between the three type of stroke groups. We assessed whether the incidence of vital instability varied over time between the three type of stroke groups using a factorial repeated measure Analysis of Variances (ANOVA). Additionally, we classified vital instability as ‘early’ if this occurred in the first 24 h of admission (day 1) and as ‘late’ if this occurred between 24 and 72 h (day 2–3). Chi-Square (χ²) Test was used to assess if incidences of vital instability differed between early (day 1) and late periods (day 2–3) of time in each type of stroke.
The association of vital instability with death or dependency was examined using multivariable Poisson regression analysis. We used Poisson regression models with robust standard errors to present effect estimates as relative risks, since the rare-case assumption was not met. 29 All models were adjusted for the following predefined confounders: age, sex, the six above mentioned comorbidities, pre-stroke mRS score, and stroke severity assessed with the NIHSS (the latter not for patients with SAH). The Poisson regression analyses were repeated for 90-day mortality as secondary endpoint.
Next, we analysed the association of deterioration by organ system: (1) respiratory insufficiency, (2) circulatory instability and (3) impaired consciousness with death or dependency at 90 days. Since no cut-off values for deterioration per organ system are available, deterioration for each organ system (respiration, circulation and consciousness) was assessed as a continuous variable.
Finally, sensitivity analyses were performed for different definitions of vital instability: (A) multiple (⩾2 and ⩾3) instances of NEWS ⩾5 within 72 h after hospitalization and (B) different thresholds of NEWS other than ⩾5 (NEWS ⩾3, NEWS ⩾4, NEWS ⩾6 and NEWS ⩾7).
Effect estimates in all abovementioned analyses were expressed as adjusted risk ratios (aRR) with corresponding 95% confidence intervals (95% CI). A statistical analysis plan was written before analyses began. A two-sides p-value of 0.05 was considered statistically significant. Analyses were performed using R statistics, version 3.4.3 (R Foundation for Statistical Computing, Vienna, Austria) and IBM SPSS Statistics for Windows, version 26.0 (IBM Corp. Armonk, NY, USA).
Results
Of 1039 patients admitted for acute stroke during the study period, 763 were included in this study (Figure 1). Patient characteristics are shown in Table 2. Patients with ischaemic stroke were older and more often had comorbidities than patients with ICH or SAH. Patients with ICH had higher NIHSS scores (median [IQR] 11 [4–19]) than those with ischaemic stroke (7 [4–15]). Patients with SAH were more often female (70%), had the highest frequency of independent functional status pre-stroke (mRS 0–2 in 93%) and were more frequently admitted to the ICU (54%).
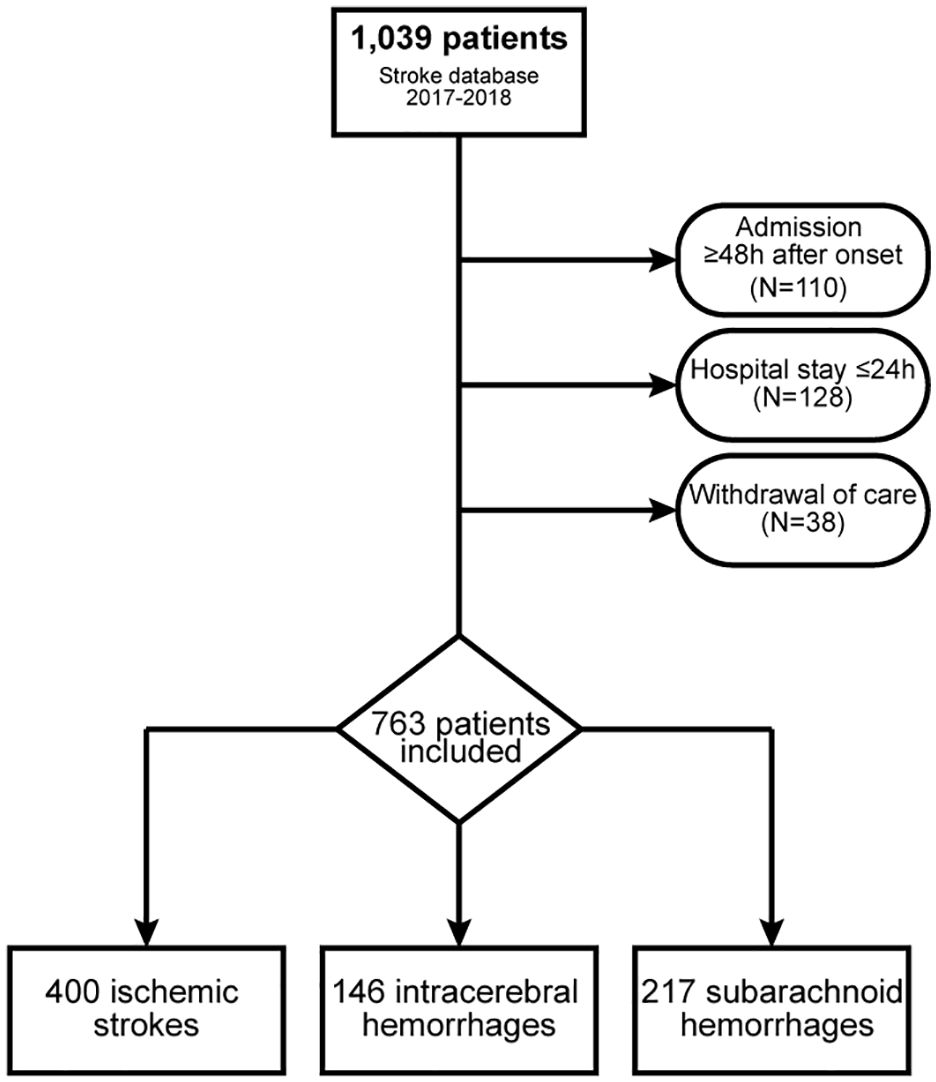
Patient flow chart.
Patient characteristics.
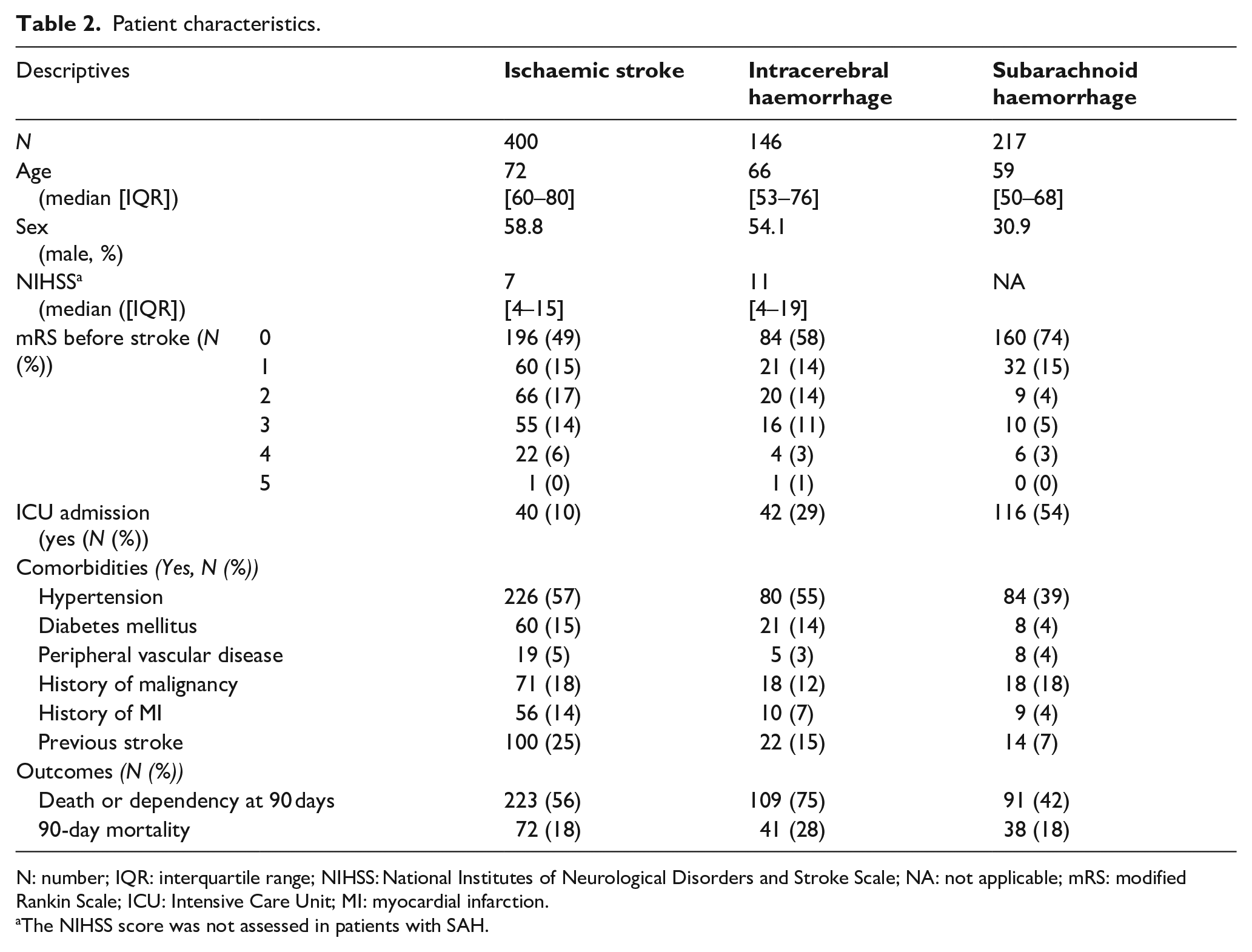
N: number; IQR: interquartile range; NIHSS: National Institutes of Neurological Disorders and Stroke Scale; NA: not applicable; mRS: modified Rankin Scale; ICU: Intensive Care Unit; MI: myocardial infarction.
The NIHSS score was not assessed in patients with SAH.
Vital instability
There have been recorded 770,076 valid vital signs measurements during the first 72 h of hospitalization. The distribution of missing data and the number of missing vital signs (5.3%) are shown in
Vital instability occurred in 232 (58%) patients with ischaemic stroke, 101 (69%) with ICH and 142 (65%) with SAH (Table 3). The number of time spans with vital instability varied between stroke types (Kruskal-Wallis H χ2(2)=27.9, p < 0.0001). Compared to patients with ischaemic stroke, patients with ICH or SAH were unstable during more time spans (both p < 0.001), but no difference was observed between patients with ICH and SAH (p = 0.68).
Vital signs and vital instability.
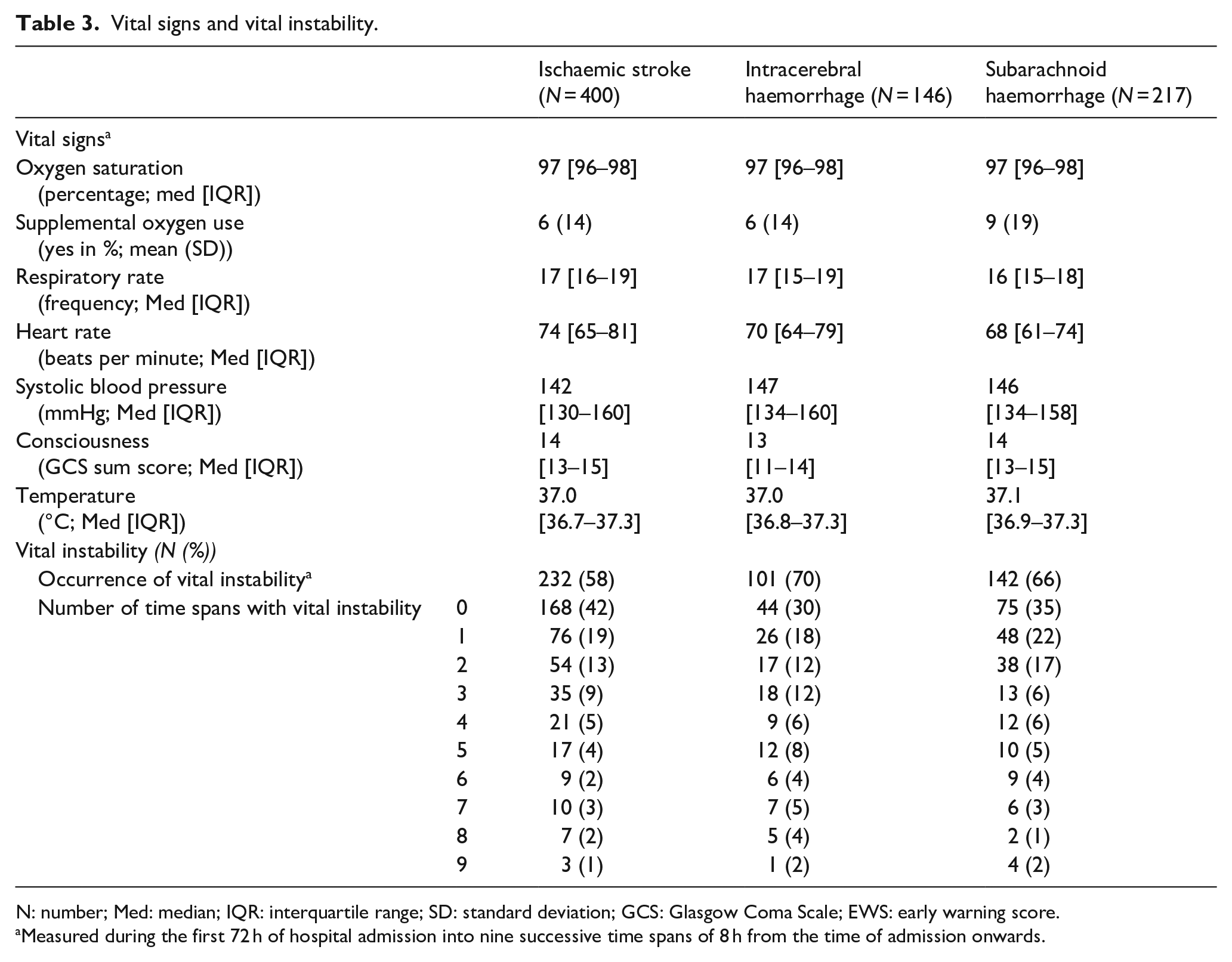
N: number; Med: median; IQR: interquartile range; SD: standard deviation; GCS: Glasgow Coma Scale; EWS: early warning score.
Measured during the first 72 h of hospital admission into nine successive time spans of 8 h from the time of admission onwards.
Overall, the incidence of vital instability varied over time (F (2,567) = 445.54; p < 0.001), though this could not be attributed to the type of stroke (F = 1.37; p = 0.26). Contingency tables of the incidence of vital instability in each type of stroke are shown in
Death or dependency
In total, 223 patients (56%) with ischaemic stroke, 109 (75%) with ICH and 91 (42%) with SAH had died or were dependent at 90 days (Table 2). Figure 2 shows the mRS score at 90 days for each type of stroke in patients with and those without vital instability. After adjustment, vital instability was associated with death or dependency at 90 days in patients with ischaemic stroke or SAH, but not in patients with ICH (Figure 3).
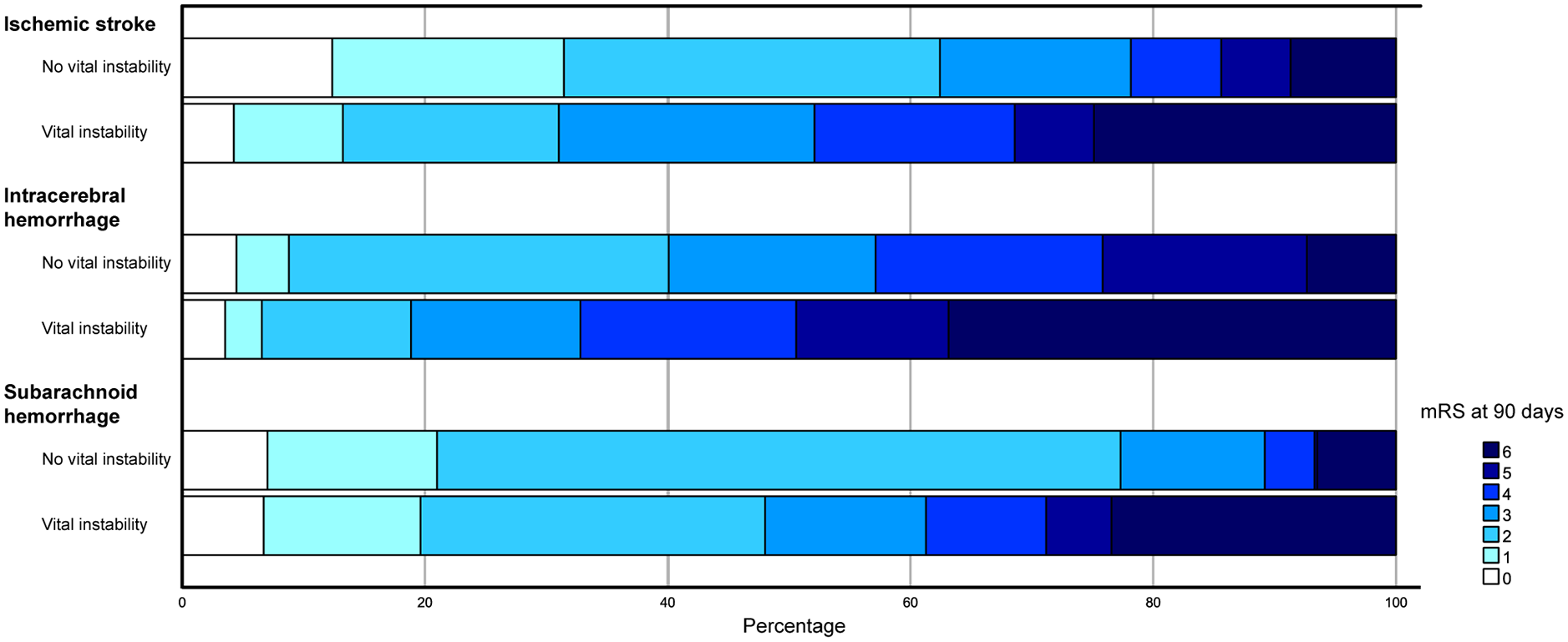
mRS score at 90 days in all types of stroke with and without vital instability.
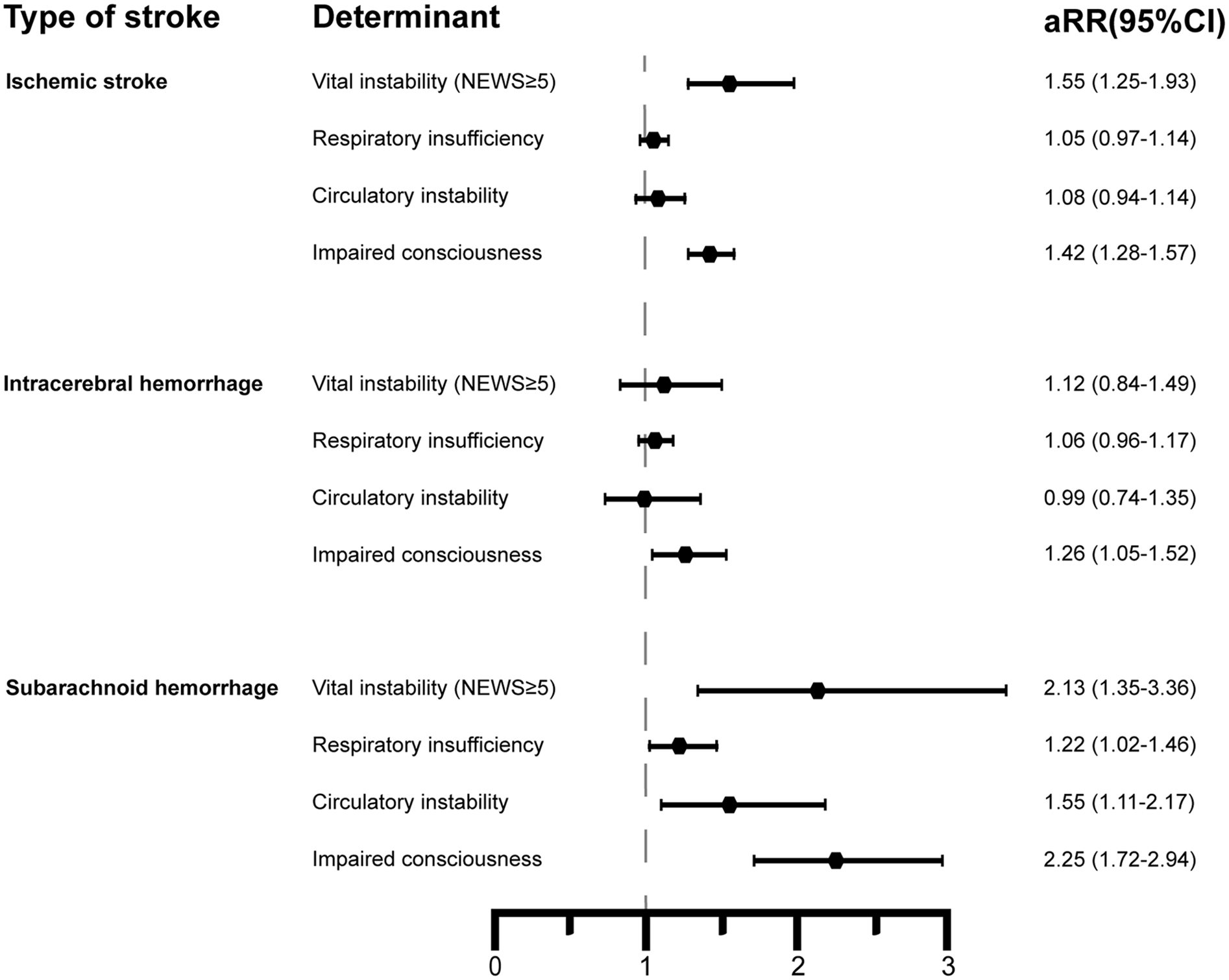
Association of vital instability and deterioration per organ system with death or dependency at 90 days after ischaemic stroke, intracerebral haemorrhage or subarachnoid haemorrhage.
90-day mortality
At 90 days, 72 patients (18%) with ischaemic stroke, 41 (28%) with ICH and 38 (18%) with SAH had died (Table 2). Vital instability was associated with mortality at 90 days in all types of stroke after adjustment (aRR (95% CI) 1.93 (1.11–3.35) in ischaemic stroke, 3.67 (1.12–12.01) in ICH and 2.81 (1.12–7.09) in SAH).
Deterioration by organ system
Mean EWS points assigned per organ system are shown in Table 3. In patients with ischaemic stroke or ICH, no association was found between respiratory insufficiency or circulatory instability and death or dependency at 90 days. In patients with SAH, both respiratory insufficiency and circulatory instability were associated after adjustment with death or dependency at 90 days. After adjustment, impaired consciousness was associated with death or dependency in all types of stroke (Figure 3).
Sensitivity analyses
Discussion
In this cohort study, vital instability defined as NEWS ⩾5 occurred in more than half of the patients during the first 72 h after hospitalization for acute stroke. After adjustment, the occurrence of vital instability was associated with death or dependency at 90 days in patients with ischaemic stroke or SAH and was associated after adjustment with death at 90 days in all types of stroke. Impaired consciousness was associated with death or dependency in all three types of stroke, and respiratory insufficiency and circulatory instability only in patients with SAH.
The incidence of vital instability among stroke patients in our study was higher than in previous studies, with an earlier reported incidence among stroke patients varying from 7% to 25%.30,31 Vital instability may have occurred more frequently in our study due to the definition of one or more episodes with NEWS ⩾5 within 72 h after hospitalization or by differences in study population. Current treatment guidelines on in-hospital general supportive care for patients with ischaemic stroke 32 or ICH 33 emphasize the stabilization of vital signs. However, this topic has received little attention, indicated by the small number of previous studies on vital instability in stroke patients. The present study demonstrates that vital instability as defined by NEWS ⩾5 in the first 72 h after hospital admission is associated with poor functional outcome after stroke, even after adjustment for age, comorbidities and stroke severity and therefore underlines the importance of preventing and treating vital instability as stated in the abovementioned guidelines.
By decomposing the NEWS into its three components respiration, circulation and consciousness, we observed that ‘impaired consciousness’ was the main driver of the association between vital instability and functional outcome. This finding consequently fuels the question whether NEWS measures what it aims to measure in acute stroke patients, and which possible solutions can be considered. To our knowledge, this item analysis of NEWS into its three components has not been performed before.
From the perspective of any acutely ill patient, impaired consciousness is a sign of potentially serious clinical deterioration. In sepsis, new-onset confusion or disorientation is often interpreted as an expression of diminished brain function due to its underlying cause.34–36 Hence in NEWS, any GCS sum score lower than 15, results in the maximum score of 3 EWS points, a score comparable in magnitude to a respiratory rate of <8 or >25 per minute.
In most stroke patients, however, impaired consciousness is likely related to the primary brain injury. NEWS weights consciousness in a binary fashion and lacks granularity; it is either normal (no points) or abnormal (3 points). This contrasts sharply with the level of detail in the GCS score. Therefore, serial NEWS are unable to capture further deterioration in consciousness in patients with stroke and a GCS sum score <15, whereas deterioration in consciousness is a major reason for concern.
Another problem that makes NEWS less applicable in stroke patients, is that possibly high (false positive) alarm rate can be expected when general, hospital-wide NEWS thresholds are used as alerting criteria. When 3 NEWS points are assigned due to a GCS of 14 or lower, the NEWS threshold of 5 is reached more easily, while possibly there is no immediate reason for action. Such false positive alarms can reduce confidence in scoring systems as NEWS, both from users (mostly nurses on the wards) and responders (usually a rapid response team).
A possible solution could be to adjust NEWS by assigning points to any decrease in consciousness, proportional to the GCS score. This would add granularity to the consciousness component of NEWS in patients with primary brain injury. Additionally, since NEWS does not take aphasia into account, only Eye and Motor scores of the GCS could be considered combined with respiratory and haemodynamic measurements. Our suggestions might create a more applicable EWS for stroke patients without diverging too far from current scores to ensure that nurses and clinicians from several specialities still ‘speak the same language’ when communicating about deteriorating patients. All possible adjustments should, of course, be validated in further research.
Our study has several strengths. We have used a strict definition of vital instability using a literature-based threshold,12,24 which is easy to use and to reproduce. Importantly, we adjusted for potential confounders, including age, stroke severity and comorbidities, as these have previously been associated with poor outcomes after stroke. 37 Additionally, we performed sensitivity analyses by using alternative definitions of vital instability to test the robustness of our study results. As no norms have previously been published we used six different definitions to test this robustness.
Nonetheless, several limitations must be mentioned. As with all retrospective studies, there is a potential for residual confounding and missing data. Missing values, for example due to skipped measurements, were addressed using interpolation and multiple imputation. Second, we were not always sufficiently informed on the awareness of vital instability among nurses and clinicians, and on the application of corrective interventions based on the recognition of vital instability. The effectiveness of possible treatments to prevent or cure the underlying causes of vital instability could therefore not be incorporated. In the likely case that interventions did happen frequently, we probably have underestimated the relation between vital instability and functional outcome. Future research should incorporate the timing of vital instability after hospitalization, to facilitate timely initiation of corrective interventions, as we found that vital instability occurred more frequently on the second and third day of hospitalization than on the first day. Finally, the sample size of the ICH population was relatively small. We cannot exclude that the smaller size of the ICH subset was partially responsible for not observing a statistically significant association between vital instability and death or dependency as was observed in other types of stroke.
Conclusion
Vital instability in the first 72 h of hospitalization for ischaemic stroke or SAH is associated after adjustment for confounders with death or dependency at 90 days. This is largely driven by the dichotomous consciousness component of NEWS, resulting in high alert rates in patients with stroke. We question whether NEWS is of value in its current form for patients with acute stroke. Currently used NEWS thresholds may not be appropriate for patients with acute stroke and modification of NEWS should be considered for these patients. Possible solutions might be raising the NEWS alarm threshold, focussing on new changes in GCS or adjust EWS systems for stroke patients. Nonetheless, early recognition of vital instability may facilitate timely initiation of corrective interventions to prevent further harm and improve functional outcome in acute stroke patients.
Supplemental Material
sj-docx-1-eso-10.1177_23969873241263195 – Supplemental material for Is NEWS of value for patients with acute stroke?
Supplemental material, sj-docx-1-eso-10.1177_23969873241263195 for Is NEWS of value for patients with acute stroke? by Mariëlle K van Valburg, Lisette M Vernooij, Cornelis J Kalkman and H Bart van der Worp in European Stroke Journal
Footnotes
Acknowledgements
We would like to thank JLP Vromen, PhD and LS Ruijs, PDEng for their assistance in the data collection and JC de Jonge, MD for his contribution to the manuscript.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: HBvdW has received fees from Bayer and TargED for consultancy and grants from Stryker and the Dutch Heart Foundation (paid to the CONTRAST consortium) and the European Union, all paid to his institution. CJK received grant funding from the European Commission for a competitive precommercial procurement project (Nightingale, grant No. 727534) to facilitate industry to develop advanced wireless wearable monitoring systems.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was entirely funded by departmental resources. No external funding was obtained.
Ethical approval
According to the Institutional Review Board (IRB) of the University Medical Centre Utrecht, the study was not subject to the Medical Research Involving Human Subjects Act and therefore the necessity of informed consent was waived (IRB number 19-338/C) on 15 May 2019.
Guarantor
MKvV
Contributorship
MKvV, CJK and HBvdW designed the study. MKvV and LMV performed data collection, analysis & interpretation. MKvV collected the data and wrote the first draft of the manuscript. All authors reviews and edited the manuscript and approved the final version.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request and with permission of all authors of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.