
Abstract
Introduction:
Population-based knowledge of the characteristics of wake-up stroke and unknown-onset stroke is limited. We compared occurrence and characteristics of ischaemic and haemorrhagic wake-up stroke, unknown-onset stroke and known-onset stroke in a nationwide register-based study.
Patients and methods:
We included patients registered in the Norwegian Stroke Register from 2012 through 2019. Age, sex, risk factors, clinical characteristics, acute stroke treatment and discharge destination were compared according to stroke type and time of onset.
Results:
Of the 60,320 patients included, 11,451 (19%) had wake-up stroke, 11,098 (18.4%) had unknown time of onset and 37,771 (62.6%) had known symptom onset. The proportion of haemorrhagic stroke was lower among wake-up stroke patients (1107/11,451, 9.7%, 95% CI: 9.1–10.2) than for known-onset stroke (5230/37,771, 13.8%, 95% CI: 13.5–14.2) and for unknown-onset stroke (1850/11,098, 16.7%, 95% CI: 16.0–17.4). Mild stroke (NIHSS <5) was more frequent in ischaemic wake-up stroke (5364/8308, 64.6%, 95% CI: 63.5–65.5) than in known-onset (16,417/26,746, 61.4%, 95% CI: 60.8–62.0) and unknown-onset stroke (3242/5853, 55.4%, 95% CI: 54.1–56.7), while baseline characteristics were otherwise similar to known-onset stroke. Unknown-onset stroke patients were more often female, lived alone and had more severe strokes compared to wake-up stroke and known-onset stroke patients. Unknown-onset stroke patients were more often in need of community-based health care on discharge and had a higher in-hospital mortality.
Discussion and conclusions:
Ischaemic wake-up strokes shared baseline characteristics with known-onset strokes, but tended to be milder. Ischaemic unknown-onset stroke patients differed significantly from wake-up stroke, emphasising the importance of considering them as separate entities.
Keywords
Introduction
The reported percentage of wake-up stroke varies considerably in different studies, with numbers ranging from 10% to 30% of all strokes. 1 There is limited information on the relative proportion of wake-up strokes and strokes of otherwise unknown onset in the general population as both groups often are merged in the same category. Only few previous studies have presented data on known-onset stroke, wake-up stroke and unknown-onset stroke as separate entities,2,3 while others have used various combinations of stroke groups.1,4–6 This makes comparisons between studies challenging. Very little has been published on the occurrence of haemorrhagic wake-up stroke and unknown-onset stroke.6,7
Although both wake-up strokes and unknown-onset strokes have an undefined time of onset rendering them ineligible for intravenous thrombolytic therapy within the traditional 4.5-h time window, there is reason to suspect these two stroke-groups should be considered as separate entities. Previous studies have indicated that wake-up strokes share characteristics with strokes of known-onset, but may differ from unknown-onset strokes, supporting this notion.8,9
The population-based knowledge of the characteristics of wake-up stroke and unknown-onset stroke patients is limited. Most previous studies have been small and based on either single centre or regional registry data.1,3,4,8,10 We found only one large national register-based study from Austria comparing baseline characteristics in wake-up stroke and known-onset stroke. 11 Unknown-onset stroke was not included in this study. Existing knowledge is mainly based on studies of acute ischaemic stroke or all strokes combined. To the best of our knowledge, only one relatively small study on the characteristics of haemorrhagic wake-up stroke has been published. 12
In the present study, we aimed to describe the prevalence, baseline and clinical characteristics of ischaemic and haemorrhagic wake-up stroke, and to compare this to unknown-onset stroke and known-onset stroke, based on data from the nationwide Norwegian Stroke Register.
Materials and methods
The Norwegian Stroke Register is a nationwide quality register established in 2012. It is mandatory for all hospitals in Norway to report to the register data on all patients hospitalised with an acute stroke. 13 The register has excellent coverage and has been found to be adequately complete and correct to serve as a source of data for stroke research with a high reliability.14–16 The inclusion criteria are all acute strokes (ICD-10 codes I61, I63 and I64) hospitalised within 28 days of symptom onset. 13 The stroke diagnosis requires acute definitive focal neurological findings such as hemiparesis, aphasia, dysarthria, unilateral sensory disturbance, neglect, ataxia, diplopia or visual field defect. Isolated vertigo is only registered as a stroke when confirmed by imaging. Unconscious patients, where assessment of focal neurological deficits is difficult, are registered if imaging verifies stroke. Patients presenting with stroke in relation to traumatic injury, intracranial tumours or subarachnoid haemorrhage are not included in the Norwegian Stroke Register, nor are silent strokes. Data are not harvested from administrative data, but manually entered into the register by trained nurses and physicians, by use of a web-based form. The stroke diagnosis (ICD-10 code) is assigned by a physician, not a clinical coder.
For the present study, we included all ischaemic and haemorrhagic strokes admitted between April 1st 2012 and December 31st 2019 and registered in the Norwegian Stroke Register. Cases registered with the ICD-10 code I64; stroke not specified as haemorrhage or infarction, were excluded (n = 1004). Each case represents an acute stroke event, not a person, thus recurrent stroke beyond 7 days from the index stroke is classified as a new case. Three stroke groups were defined by time of stroke onset for comparison; wake-up stroke, known-onset stroke and unknown-onset stroke. One case was excluded due to missing information on time of onset.
Smoking habits were categorised as current/previous/never, with ‘previous’ being defined as smoking cessation >1 month prior to stroke. History of atrial fibrillation (confirmed by ECG), diabetes mellitus and previous myocardial infarction were categorised as yes/no. Information on previous stroke and/or previous transient ischaemic attack (TIA) was combined as previous cerebrovascular events (yes/no). Information on use of medication (yes/no) before stroke onset was available for statins, antiplatelets, oral anticoagulants and antihypertensive medication. Information on the use of antihypertensive medication prior to stroke was unavailable for the two first years (2012–2013) of the observation period. For all other variables, information was available for the 8-year study period. We further obtained information on living arrangements (alone, with someone or institution) prior to stroke and time from stroke onset to admission.
Stroke severity on admission to hospital was assessed by the National Institutes of Health Stroke Scale (NIHSS), and level of consciousness on admission. In 2012–2013, the NIHSS on admission registered can potentially be from any time point during the first 24 h upon admission. In 2014 this was changed to ensure the NIHSS on admission is strictly the admission scoring. NIHSS scores were categorised as mild (<5), moderate (5–15) and severe (>15). 17 Furthermore, we received information on use of thrombolytic treatment (yes/no).
The study was approved by the Regional Committee for Medical and Health Research Ethics (REC) and by the data protection officials at the Hospital of Southern Norway.
Statistical analysis
Data for continuous variables are presented as mean values with standard deviation (SD) or medians with interquartile range (IQR). Categorical variables are presented with absolute (n) and relative (%) frequencies.
The non-parametric test Kruskal-Wallis was used to compare means for duration of hospital stay as well as median NIHSS on admission across stroke subgroups due to non-normal distribution. The Oneway-ANOVA test was used to compare mean age across the three stroke groups. Pearson’s chi-square test was used to compare categorical variables across stroke groups. p-Values are reported as Bonferroni corrected values due to multiple comparisons, and values <0.05 were considered statistically significant.
Age and sex adjusted differences in baseline characteristics between stroke groups were assessed by multinomial logistic regression using known-onset stroke as reference group. Assumptions for the test were met. Analyses were done for each variable separately, with and without adjustment for age and sex. The odds ratios for death during hospital stay and for being discharged to an institution was compared by logistic regression analysis with adjustment for age, sex and pre-stroke living arrangements.
There is limited missing data. In most cases missing data represent either ‘not registered’ or ‘unknown’, the latter being the most prevalent of the two. Reported proportions for the various variables are based on known cases, unknown or not registered were not included in the further analyses. Missing values are <5% for all variables except ‘current smoking’, ‘use of antihypertensive drugs’ and ‘NIHSS on admission’, for which the percentage of missing values were 17.8%, 12.7% and 23.8% respectively (for more detail please see Supplemental materials).
Sensitivity analysis for the variable NIHSS on admission was performed. Descriptive and comparative analyses were performed including and excluding the first 2 years, and a similar distribution and results were found. Based on these results we chose to include information on NIHSS on admission for the whole observation period.
Analyses were conducted using IBM SPSS Statistics version 26.
Results
A total of 60,320 stroke cases were registered in the 8-year study period, 52,133 (86.4%) were ischaemic strokes and 8187 (13.6%) were haemorrhagic strokes. Overall, 11,451 (19%) patients had wake-up stroke, 11,098 (18.4%) unknown-onset stroke and 37,771 (62.6%) known-onset stroke.
The most frequent time of admission to hospital in all stroke patients was in the hours around noon, with a subsequent gradual decrease throughout the afternoon. The peak for hospital admission of wake-up stroke patients was around 11 am, while the peak for both known-onset stroke and unknown-onset stroke was reached around 1 pm (Figure 1).
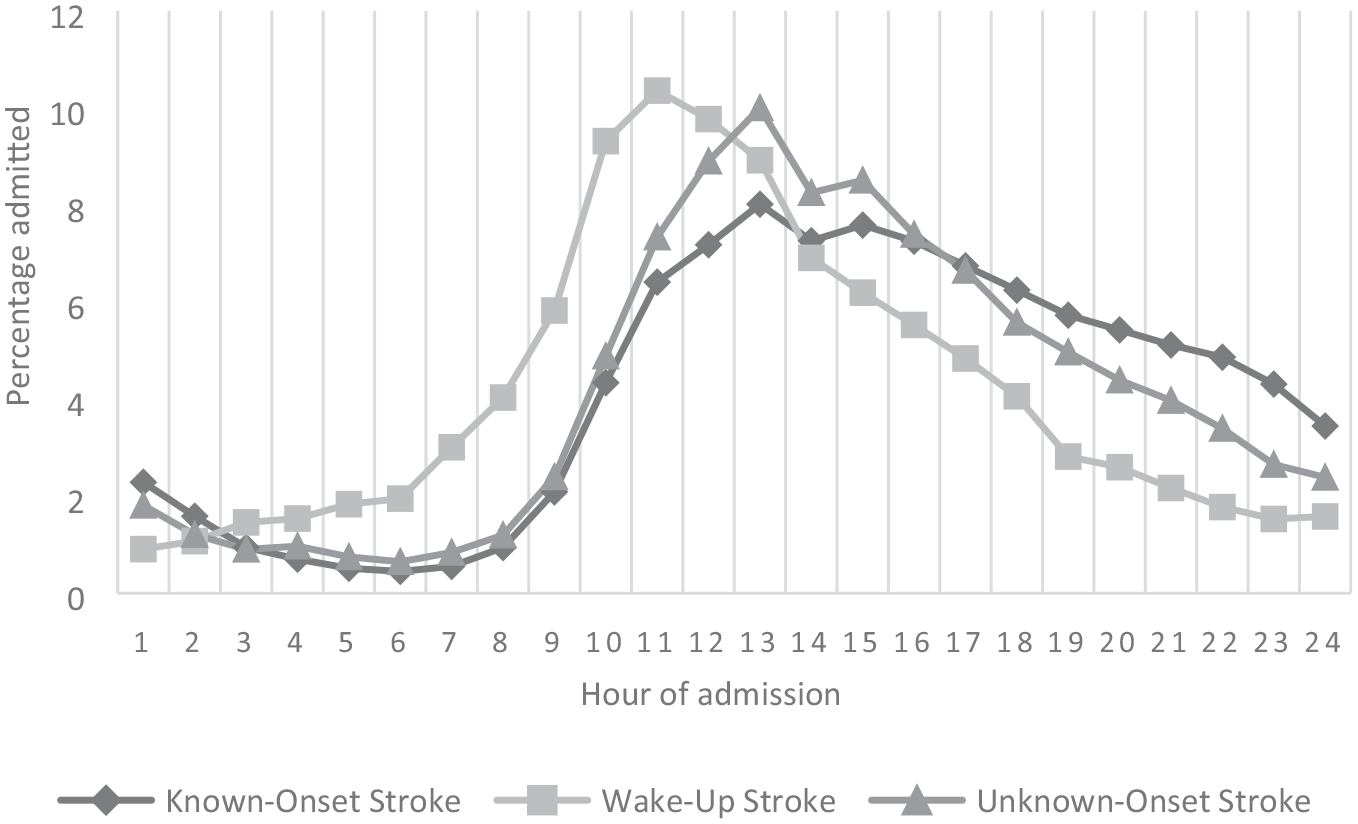
Hour of admission in known-onset, wake-up and unknown-onset strokes.
Ischaemic stroke
Among the 52,133 with ischaemic stroke, 10,344 (19.8%) were wake-up stroke, 9248 (17.7%) unknown-onset stroke and 32,541 (62.4%) known-onset stroke.
Patients with unknown-onset stroke were on average 3 years older than patients with wake-up stroke and known-onset stroke, and a higher proportion were women and lived alone (Table 1). The proportion of patients with atrial fibrillation was higher in unknown-onset stroke patients and this remained statistically significant also after adjustment for age and sex (data not shown). Other cerebrovascular risk factors did not differ substantially between groups. Age- and sex-adjusted NIHSS >15, reduced level of consciousness on admission and longer hospitalisation were all more frequent in patients with unknown-onset stroke than in known-onset stroke and wake-up stroke. The multivariable-adjusted risk of death during hospital stay was significantly higher in ischaemic unknown-onset stroke both compared to known-onset stroke (OR 1.63, 95% CI: 1.48–1.79) and to wake-up stroke (OR 1.60, 95% CI: 1.42–1.82), as was the risk of discharge to an institution, with OR of 1.47 (95% CI: 1.40–1.55) and 1.37 (95% CI: 1.29–1.45) when compared to known-onset and wake-up stroke, respectively.
Baseline characteristics of known-onset, wake-up and unknown-onset ischaemic and haemorrhagic stroke cases.
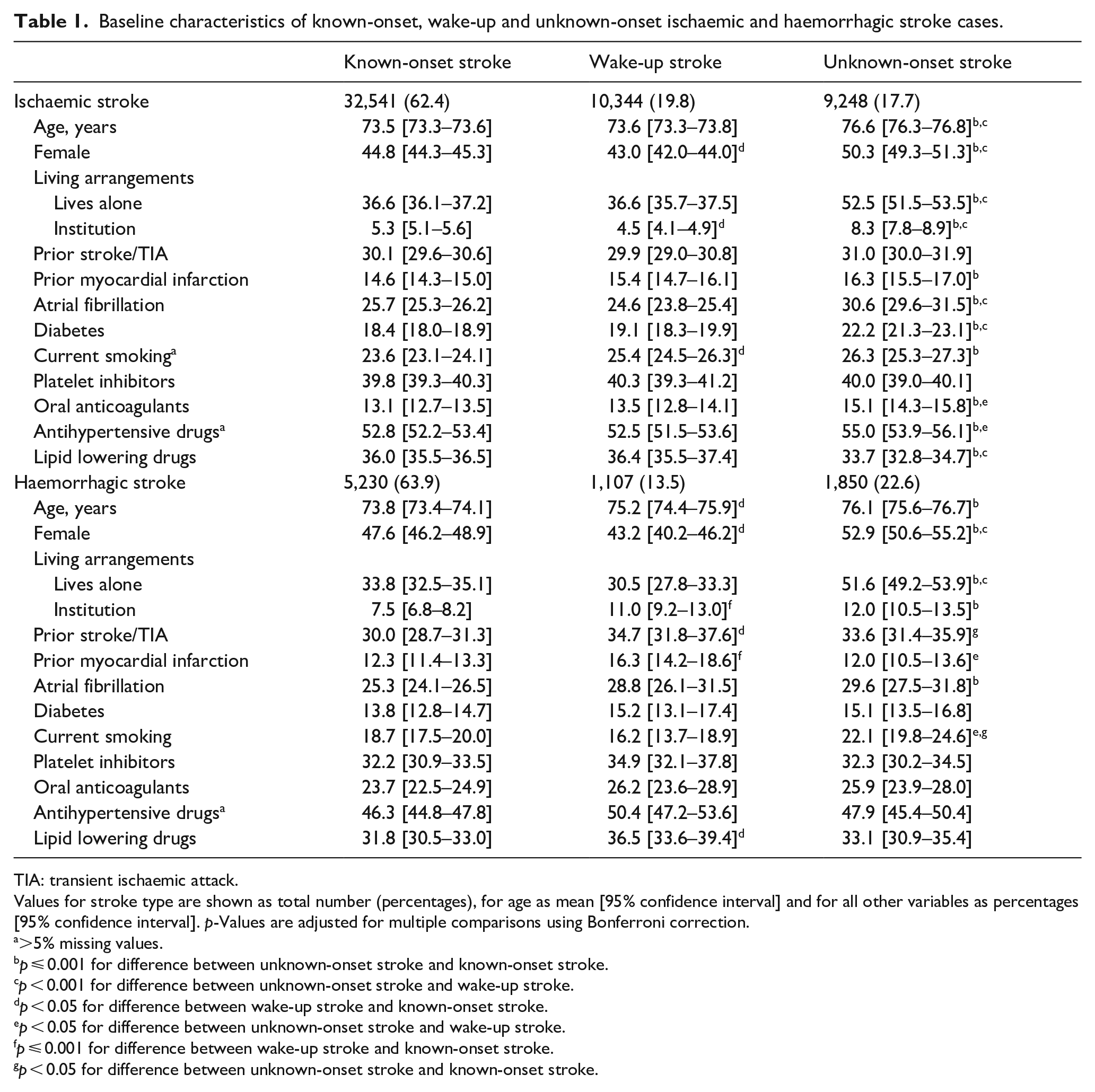
TIA: transient ischaemic attack.
Values for stroke type are shown as total number (percentages), for age as mean [95% confidence interval] and for all other variables as percentages [95% confidence interval]. p-Values are adjusted for multiple comparisons using Bonferroni correction.
>5% missing values.
p ⩽ 0.001 for difference between unknown-onset stroke and known-onset stroke.
p < 0.001 for difference between unknown-onset stroke and wake-up stroke.
p < 0.05 for difference between wake-up stroke and known-onset stroke.
p < 0.05 for difference between unknown-onset stroke and wake-up stroke.
p ⩽ 0.001 for difference between wake-up stroke and known-onset stroke.
p < 0.05 for difference between unknown-onset stroke and known-onset stroke.
A higher proportion of wake-up stroke patients (64.6%) had mild strokes, defined as NIHSS <5 on admission compared to patients with known-onset stroke (61.4%) and unknown-onset stroke (55.4%). For all other baseline characteristics, wake-up stroke patients did not differ significantly from known-onset stroke patients (Table 1).
The proportion of cases treated with intravenous thrombolysis was, as expected, significantly lower among wake-up ischaemic stroke patients than in patients with known-onset stroke (7.6% vs 26.4%), and lowest among unknown-onset stroke (3.2%). Endovascular thrombectomy was performed in 3.6% of known-onset strokes, 2.5% of wake-up strokes and 1.2% of unknown-onset strokes.
Haemorrhagic stroke
Of the 8187 cases with haemorrhagic strokes in our study, 13.5% were wake-up stroke, 22.6% unknown-onset stroke and 63.9% known-onset stroke. The proportion of haemorrhagic stroke was lower in patients with wake-up stroke (9.5%) compared to patients with known-onset stroke (13.6%) and unknown-onset stroke (16.3%).
Overall, haemorrhagic strokes were more severe than ischaemic strokes with a higher proportion of cases presenting with NIHSS >15 (23.2% vs 17.0%). They had longer duration of hospitalisation (mean duration 8.2 (SD 9.8) vs 6.3 (7.0) days) and a substantially higher proportion of deaths during hospitalisation (24.6% vs 5.1%) (Table 2).
Clinical presentation, length of hospitalisation and death during hospitalisation in known-onset, unknown-onset and wake-up ischaemic and haemorrhagic stroke.
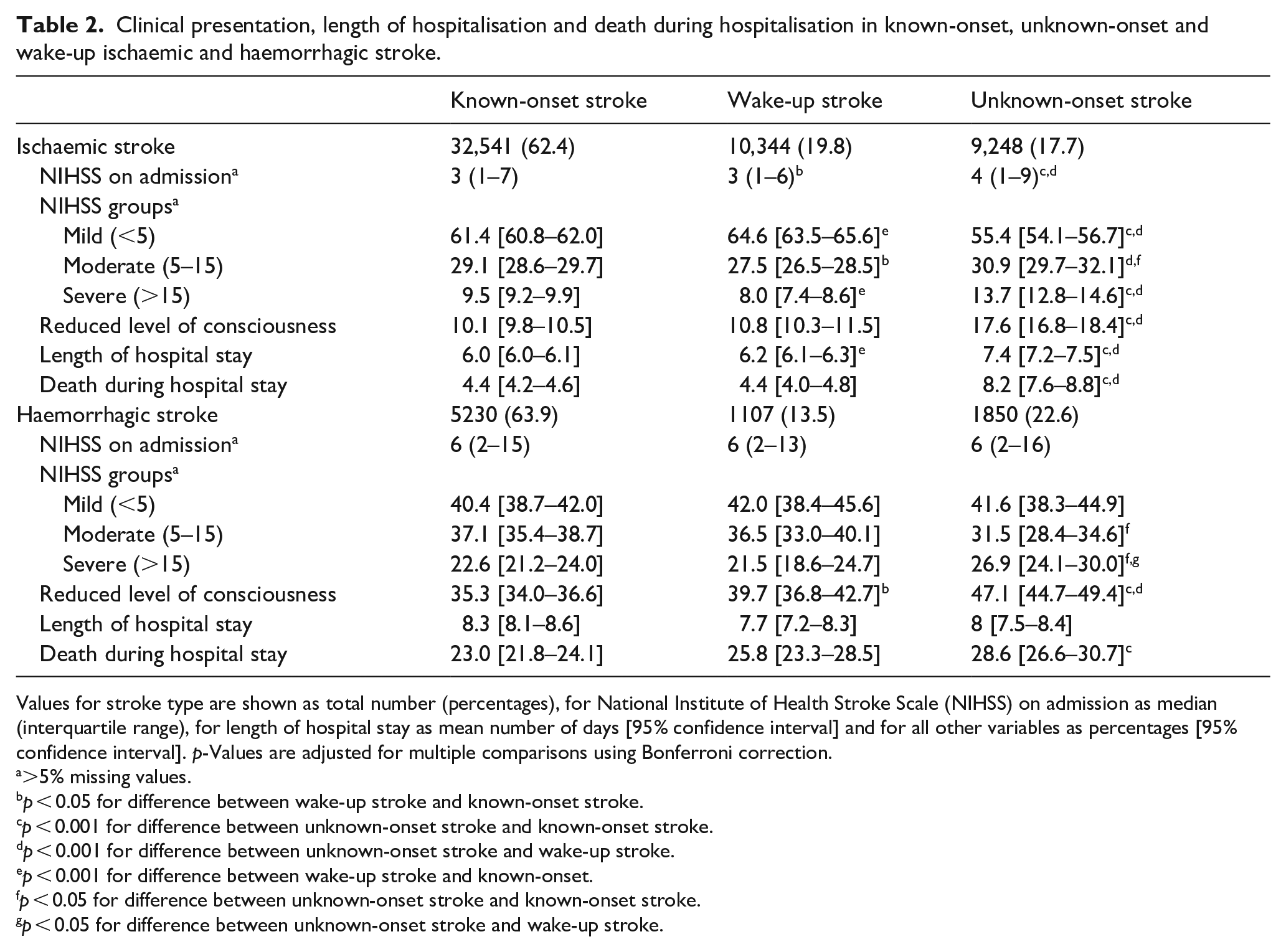
Values for stroke type are shown as total number (percentages), for National Institute of Health Stroke Scale (NIHSS) on admission as median (interquartile range), for length of hospital stay as mean number of days [95% confidence interval] and for all other variables as percentages [95% confidence interval]. p-Values are adjusted for multiple comparisons using Bonferroni correction.
>5% missing values.
p < 0.05 for difference between wake-up stroke and known-onset stroke.
p < 0.001 for difference between unknown-onset stroke and known-onset stroke.
p < 0.001 for difference between unknown-onset stroke and wake-up stroke.
p < 0.001 for difference between wake-up stroke and known-onset.
p < 0.05 for difference between unknown-onset stroke and known-onset stroke.
p < 0.05 for difference between unknown-onset stroke and wake-up stroke.
Patients with haemorrhagic wake-up stroke were on average older compared to known-onset haemorrhagic stroke patients (Table 1), but had similar stroke severity (Table 2). There were no significant differences between the known-onset, unknown-onset and wake-up haemorrhagic stroke groups regarding smoking habits, cardiovascular disease, diabetes, atrial fibrillation or use of medication (Table 1).
As for ischaemic stroke, patients with unknown-onset haemorrhagic stroke were more often female and lived alone (Table 1). Unknown-onset haemorrhagic strokes were more likely to present with NIHSS >15 (26.9% vs 22.6% in known-onset stroke and 21.5% in wake-up stroke), and to have a reduced level of consciousness on admission. The proportion who died during hospital stay was higher in unknown-onset haemorrhagic stroke compared to the other two stroke groups (Table 2). After adjustment for age, sex and pre-stroke living arrangements, the risk of death during hospital stay was higher in unknown-onset stroke (OR 1.24, 95% CI: 1.09–1.40) than in known-onset stroke, while the difference between wake-up stroke and unknown-onset stroke and between wake-up stroke and known-onset stroke were no longer statistically significant. Patients with unknown-onset haemorrhagic stroke were more likely to be discharged to an institution than the other two groups (26.2% vs 18.9% in known-onset stroke and 20.5% in wake-up stroke), however this was not significant after adjustment for age, sex and pre-stroke living arrangements, and was mainly explained by being institutionalised prior to the stroke.
Discussion
To our knowledge, this is the first nationwide study on the occurrence and characteristics of both acute ischaemic and haemorrhagic wake-up stroke and unknown-onset stroke. Our study using a large sample size with nationwide data confirms previous findings indicating that one in five strokes are wake-up strokes,1,18 while another fifth are unknown-onset strokes. 3 Ischaemic wake-up strokes tended to be milder compared to ischaemic known-onset strokes and ischaemic unknown-onset strokes, while baseline and clinical characteristics were otherwise similar to known-onset stroke. Furthermore, we found that unknown-onset strokes differed from strokes with known-onset and wake-up strokes concerning female predominance, older age, higher prevalence of atrial fibrillation, higher in-hospital mortality and higher likelihood of continued health care after discharge from hospital. Our results give support to the notion that wake-up strokes and unknown-onset strokes should be considered as separate entities.
Previous findings on comparison of stroke severity in wake-up stroke and known-onset stroke are inconsistent. Among 17,398 participants of the International Stroke Trial 3, a higher proportion of ischaemic wake-up stroke patients were fully conscious on admission, but had similar mean number of neurological deficits compared to patients with ischaemic known-onset strokes. 18 In a large register-based nationwide study from Austria with 107,895 patients, mean NIHSS on admission was four in wake-up strokes and three in known-onset strokes, while other baseline characteristics were similar in the two groups. 11 The registry-based study from Halifax, Canada found identical stroke severity score in wake-up and known-onset strokes. 2 In our study, ischaemic wake-up stroke tended to be milder than known-onset stroke while stroke severity in haemorrhagic wake-up stroke was similar to known-onset stroke. Most previous studies did not present results for ischaemic and haemorrhagic strokes separately.2,11 Little has been published regarding severity of haemorrhagic wake-up strokes. One previous publication from a single centre prospective registry study with 368 patients reported that haemorrhagic wake-up strokes were more severe than known-onset strokes. 12
The higher severity of unknown-onset stroke in our population is in line with previous findings of unknown-onset stroke being more severe on admission.3,19 This finding was consistent for both ischaemic and haemorrhagic stroke.
While circadian variations in cardiovascular risk factors20,21 are thought to precipitate the observed increase in ischaemic stroke in the morning and early hours of the day,22–24 unknown-onset stroke patients represent a different group who are more often unable to acknowledge and communicate their symptoms and seek medical help. This is further underscored by their older age, and higher proportion who live alone.
Previous knowledge on the occurrence of haemorrhagic wake-up stroke is very limited. We found a lower proportion of haemorrhagic stroke in wake-up stroke compared to both known-onset stroke and unknown-onset stroke, which corroborates the findings of a registry-based study of 3890 patients from Halifax, Canada. 2 A link to lower night time blood pressure is a possibility. 25
Ischaemic wake-up stroke and unknown-onset stroke have both been considered ineligible for intravenous thrombolytic therapy within the traditional 4.5-h time window. Recent studies have shown that patients with wake up stroke and unknown-onset stroke may benefit from intravenous thrombolytic treatment when selected by advanced imaging methods such as MRI with DWI -FLAIR mismatch, or CT or MRI core/perfusion-mismatch.5,26,27 This has led to recent changes in guidelines.28,29 The rate of thrombolysis in wake-up stroke in our study was similar to that of the Austrian Stroke Unit Registry where approximately 7% received intravenous thrombolysis. 11 Although this may be high by international comparison, the similarities between wake-up strokes and known-onset strokes seen in our study may imply a larger potential for treatment benefit in patients with wake-up stroke and underscores the need for improved access to acute reperfusion therapies for this group.
Strengths of our study include the register-based design, which eliminates self-selection bias, the statutory obligation for all centres to report to the registry and the high coverage of the registry, enabling near complete nationwide data, as well as the large size ensuring high statistical power. Some limitations identified are the registration of stroke diagnosis and onset of stroke. Despite the high quality of the register there are still some incorrect registrations in terms of stroke diagnosis. We found 1.6% of cases were registered as unspecified stroke, however, most of these had in fact had either a CT or an MRI done and should thus be expected to be classified as either ischaemic stroke or haemorrhagic stroke. Furthermore, we have had to accept use of antihypertensives and statins as proxy variables for hypertension and hyperlipidaemia as this information is not available in the register. There is also some uncertainty regarding the registration of stroke onset in a small proportion of cases, however this is not likely to affect the results due to the large sample size.
Summary
In conclusion, wake-up stroke and unknown-onset stroke each account for approximately 20% of all strokes. Ischaemic wake-up strokes share baseline characteristics with known-onset strokes, but tend to be milder. Unknown-onset stroke patients have more severe strokes, are of older age and more often female, live alone, are less likely to be independent upon discharge, and have a higher in-hospital mortality. The proportion of haemorrhagic stroke is lower among wake-up stroke. This study highlights the need to consider the stroke subgroups known-onset stroke, wake-up stroke and unknown-onset stroke as separate entities.
Supplemental Material
sj-docx-1-eso-10.1177_23969873221089800 – Supplemental material for Wake-up stroke and unknown-onset stroke; occurrence and characteristics from the nationwide Norwegian Stroke Register
Supplemental material, sj-docx-1-eso-10.1177_23969873221089800 for Wake-up stroke and unknown-onset stroke; occurrence and characteristics from the nationwide Norwegian Stroke Register by Mary-Helen Søyland, Arnstein Tveiten, Agnethe Eltoft, Halvor Øygarden, Torunn Varmdal, Bent Indredavik and Ellisiv B Mathiesen in European Stroke Journal
Footnotes
Acknowledgements
The authors would like to thank Are Hugo Pripp, OCBE for statistical support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Søyland is supported by the South-Eastern Norway Regional Health Authority.
Ethical approval
Ethical approval for this study was obtained from the Regional Committee for Medical and Health Research Ethics (REC). Reference number 97084.
Informed consent
Informed consent was not sought for the present study because registration in the Norwegian Stroke Register is mandatory for all hospitals in Norway. Informed consent is therefore not needed.
Guarantor
MHS takes full responsibility for the article, including for the accuracy and appropriateness of the reference list.
Author contributions
MHS, AT, and EBM developed the protocol for the study. AT gained ethical and legal approvals. TV generated the dataset. MHS did the statistical analyses and drafted the manuscript. All authors reviewed, edited and approved the final version of the manuscript.
Trial registration
Not applicable because this is an observational study, not a clinical trial.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.