
Abstract
Introduction:
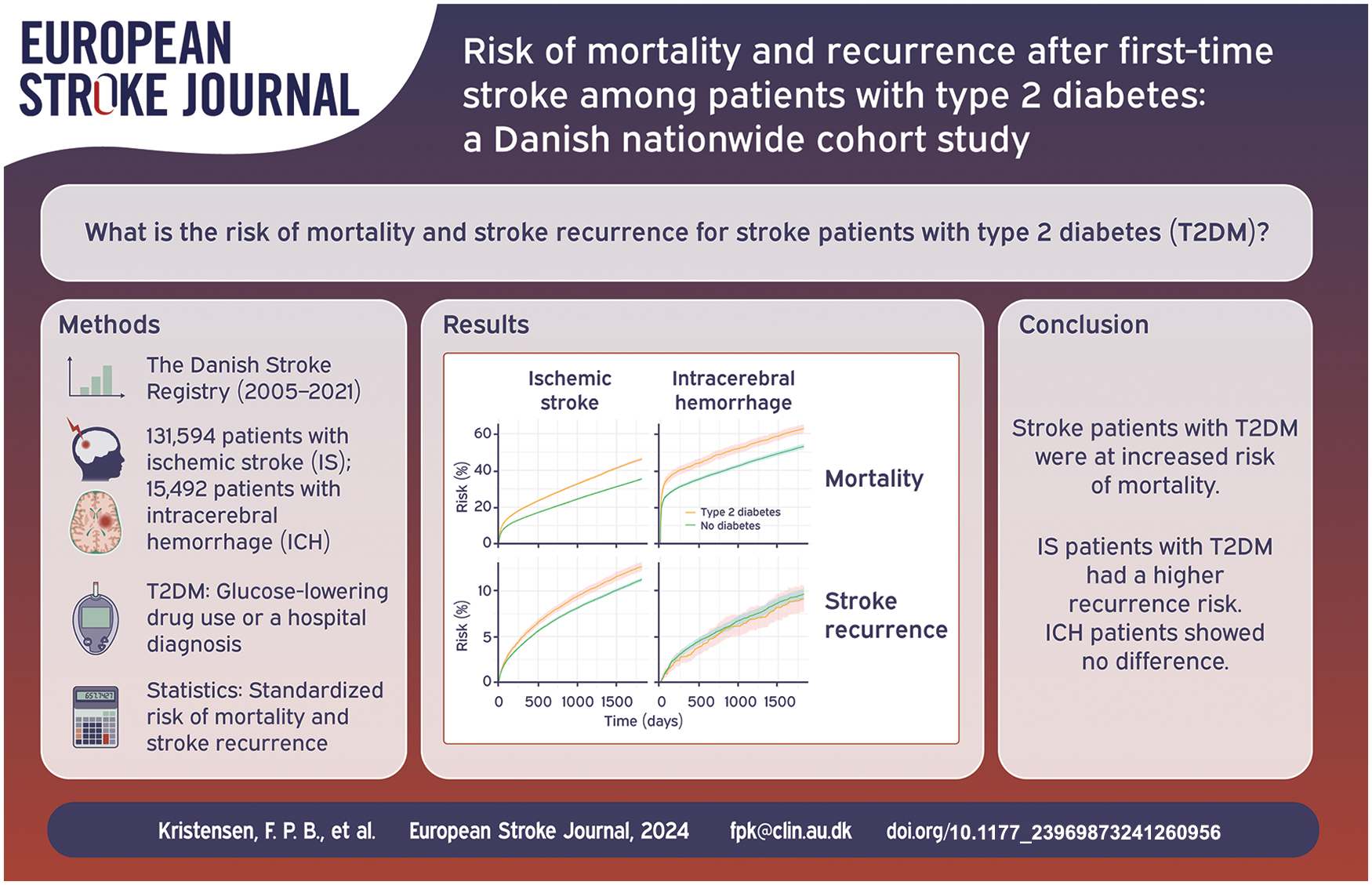
The prognosis for stroke patients with type 2 diabetes mellitus (T2DM) remains poorly understood. We examined the risk of mortality and stroke recurrence in stroke patients with T2DM and stroke patients without diabetes.
Patients and methods:
We conducted a population-based cohort study including all patients diagnosed with a first-time ischemic stroke (n = 131,594) or intracerebral hemorrhage (ICH, n = 15,492) in Denmark, 2005–2021. Patients with T2DM were identified using hospital diagnosis codes and glucose-lowering drug prescriptions. We calculated risks, risk differences, and risk ratios, standardized by age, sex, and calendar year of stroke admission.
Results:
Following ischemic stroke, the 5-year standardized mortality was 46.1% for patients with T2DM and 35.4% for patients without diabetes (standardized risk difference: 10.7% [95% CI 9.9–11.6]; risk ratio: 1.3 [95% CI 1.3–1.3]). The 5-year risk of recurrence following ischemic stroke was 12.7% for patients with T2DM and 11.3% for those without diabetes (risk difference: 1.4% [95% CI 0.9–2.0]; risk ratio: 1.1 [95% CI 1.1–1.2]). Following ICH, the 5-year mortality was 62.8% for patients with T2DM and 53.0% for patients without diabetes (risk difference: 9.8% [95% CI 7.2–12.4)]; risk ratio: 1.2 [95% CI 1.1–1.2]). The 5-year risk of recurrence after ICH was 9.1% for patients with T2DM and 9.7% for patients without diabetes.
Discussion and conclusion:
Stroke patients with T2DM were at increased risk of mortality. The risk of stroke recurrence was slightly higher for ischemic stroke patients with T2DM than patients without diabetes, while no difference was observed among ICH patients.
Introduction
Type 2 diabetes mellitus (T2DM) is a major risk factor for both ischemic stroke and intracerebral hemorrhage (ICH).1,2 Over recent decades, stroke mortality has declined attributable to improved control of modifiable risk factors and improvements in acute stroke care, including the widespread adoption of reperfusion therapy.1,3,4 Still, survival after stroke for patients with T2DM is poorly understood and contemporary data are lacking.5–14
Survival after stroke may be shorter in patients with T2DM compared with those without diabetes, but evidence is mixed. Studies have reported either no difference6,7 or up to 1.5-fold increased mortality following ischemic stroke for patients with T2DM versus patients without diabetes.5,7–10,12,14 However, the majority of these studies were conducted before 2013 or based on selected single-hospital cohorts, limiting their generalizability.5,6,8–10,14 Furthermore, few have been able to characterize stroke patients with T2DM according to stroke severity, lifestyle behaviors, and comorbidities, or to examine mortality following ICH for patients with T2DM.8,11–13
Recurrent stroke is associated with increased mortality compared with first-time events. 15 It is uncertain whether the risk of stroke recurrence is higher in patients with T2DM than in those without diabetes.12,14,16–18 Existing studies have mainly focused on ischemic stroke, and have rarely reported on both the short-term and long-term risk.12,14,16–18 Contemporary data on short-term and long-term stroke recurrence risk are needed to provide a better understanding of the clinical course following stroke for patients with T2DM.
Our study aimed to (1) examine clinical characteristics of patients with T2DM and patients without diabetes at time of incident ischemic stroke or ICH; and (2) examine risks of mortality and stroke recurrence.
Methods
Data sources
We used data from the Danish Civil Registration System, the Danish Stroke Registry, the Danish National Patient Registry, the Danish Psychiatric Central Research Register, the Danish National Prescription Registry, and the two laboratory databases: the Clinical Laboratory Information System Research Database and the Register of Laboratory Results for Research (Supplemental Material). 19
Study cohort
We included 168,046 adults admitted to a Danish hospital with a first-time diagnosis of ischemic stroke or ICH between January 1, 2005 and November 30, 2021, as recorded in the Danish Stroke Registry. A validation of the Danish Stroke Registry showed that the positive predictive value and the sensitivity of stroke diagnoses were above 90%.20,21 We excluded patients who had a prior ischemic stroke or ICH recorded in the Danish National Patient Registry (n = 16,328 [9.7%]) and patients who immigrated to Denmark within 1 year before their stroke event (ensuring sufficient time to assess baseline characteristics (n = 2947 (2%)]).
Definition of patients with T2DM and patients without diabetes
Patients with T2DM were identified using the Danish National Patient Registry and the Danish National Prescription Registry. 19 Diabetes was defined as either an International Classification of Diseases, Tenth Revision hospital diagnosis of diabetes or a redeemed prescription for a glucose-lowering drug at any time before or on the day of stroke admission. A validation study reported a positive predictive value above 90% for identifying patients with any diabetes subtype based on hospital diagnosis codes or redeemed drug prescriptions. 22 We excluded patients with diabetes using insulin monotherapy because they likely represent patients with type 1 diabetes mellitus or Latent Autoimmune Diabetes in Adults (n = 1685 [7% of those with diabetes]). The remaining stroke patients with diabetes were categorized as having T2DM. Patients who did not meet any of the criteria for diabetes were defined as patients without diabetes.
All-cause mortality and stroke recurrence
We retrieved data on mortality from the Danish Civil Registration System. A recurrent stroke was defined as an ischemic stroke or an ICH occurring at least 24 h after the onset of a first-time stroke, as recorded in the Danish Stroke Registry, regardless of vascular territory. 15
Covariates
Covariate definitions are described in Supplemental Tables 1–4. We retrieved information about stroke severity, stroke treatment, lifestyle behaviors, BMI, socioeconomic determinants, routine clinical care biomarkers, comorbidities, and medication use. The two laboratory databases provided data on routine clinical care biomarkers for a geographical subcohort (60% of the study cohort) where hospital information systems are linked to the databases (Supplemental Table 5 describes proportion of missingness).23,24 Use of preventive cardiovascular drugs were assessed within 1 year before and up to 180 days after stroke admission because treatment with these drugs impacts the clinical course after stroke.
Statistical analyses
We performed separate analyses for patients with ischemic stroke and patients with ICH. We described patient characteristics for patients with T2DM and those without diabetes. For analyses of all-cause mortality, we followed patients from the admission date for incident stroke until all-cause mortality, emigration, or end of study period (December 31, 2021), whichever occurred first. For analyses of recurrence, we additionally followed patients until a recurrent stroke. We estimated standardized 30-day, 1-year, and 5-year absolute risks, risk differences, and risk ratios using the Kaplan-Meier estimator for mortality and the Aalen-Johansen estimator for stroke recurrence, considering death as a competing event. Based on standardized morbidity ratio weighting, 25 we employed a logistic regression model including information on age (cubic spline), sex, and calendar year of stroke admission (cubic spline) to calculate a propensity score representing the predicted probability of having T2DM. The included covariates had no missing values. Bootstrapping with replacement was used to obtain standard errors for calculating 95% confidence intervals (CIs).
We performed stratified analyses of the 5-year risk estimates of mortality and stroke recurrence in subgroups of age, sex, calendar year of stroke admission, time since first diabetes diagnosis, baseline HbA1c measurement in patients with T2DM, stroke severity, cohabitation, BMI, atrial fibrillation/flutter, hypertension, ischemic heart disease, heart failure, cancer, and chronic kidney disease. For each subgroup, propensity score weights were re-estimated.
Additional analyses – ischemic stroke and ICH
We performed two additional analyses. First, because the presence and magnitude of comorbidity may impact the risk of mortality and stroke recurrence, we calculated 30-day, 1-year, and 5-year risks after running the propensity score model including age, sex, and calendar year of stroke admission, BMI category, stroke severity category, hypertension, atrial fibrillation/flutter, ischemic heart disease, chronic kidney disease, and cancer. Second, to increase the completeness of our T2DM algorithm, we reran the main analysis after adding an HbA1c level ⩾48 mmol/mol as a criterion for the T2DM definition (in addition to hospital diagnosis codes and glucose-lowering drug therapy). Analyses were conducted using SAS and R studio.
Results
Characteristics of ischemic stroke patients
We included 131,594 patients with a first-time diagnosis of ischemic stroke, among whom 19,590 patients (14.9%) had T2DM. The median age was similar between patients with T2DM and those without diabetes (73 years in patients with T2DM vs 72 years in patients without diabetes) and the proportion of men was slightly higher among patients with T2DM (58.4% vs 52.9%) (Supplemental Table 6). Stroke severity in patients with T2DM was comparable to that in patients without diabetes (median Scandinavian Stroke Scale score: 50 vs 51). Compared with patients without diabetes, patients with T2DM were more often obese (BMI > 30 kg/m2: 32.2% vs 15.3%), were less likely to drink more than the recommended weekly alcohol intake (9.0% vs 11.3%), and were more often former smokers (33.3% vs 28.1%) (Supplemental Table 6).
Patients with T2DM had more comorbidities than those without diabetes. Accordingly, patients with T2DM more often used cardiovascular-related drugs before their ischemic stroke admission, including statins (53.98% vs 19.6%) and antihypertensive drugs (e.g. ACE inhibitors/ARBs: 31.0% vs 62.6%). During the 180-day period following ischemic stroke admission, patients with and patients without diabetes had a similar use of secondary preventive medications, except for antihypertensive drugs (e.g. ACE inhibitors/ARBs: 58.7% vs 40.2%) (Supplemental Table 7).
Risk of mortality and stroke recurrence following a first-time ischemic stroke
The 30-day standardized risk of mortality following a first-time ischemic stroke was 8.6% in patients with T2DM and 6.0% in those without diabetes (risk difference: 2.6% [95% CI 2.1–3.0]; risk ratio: 1.4 [95% CI 1.4–1.5]). During follow-up, the risk ratio remained nearly unchanged (1 year: 1.4 [95% CI 1.3–1.4]; 5 years: 1.3 [95% CI 1.3–1.3]) (Figure 1 and Table 1). In subgroup analyses of 5-year mortality risks, the risk difference increased with age until age 80, whereas the risk ratio diminished at older ages (e.g. patients < 50 years: risk ratio of 1.7 [95% CI 1.2–2.2]; patients ⩾ 80 years: risk ratio of 1.1 [95% CI 1.1–1.2]). Longer time since diabetes diagnosis, greater ischemic stroke severity, BMI < 25 kg/m2, and presence of comorbidities were associated with higher risk of 5-year mortality than in the main analysis but the risk differences and ratios were comparable with the main analysis (Supplemental Table 8).
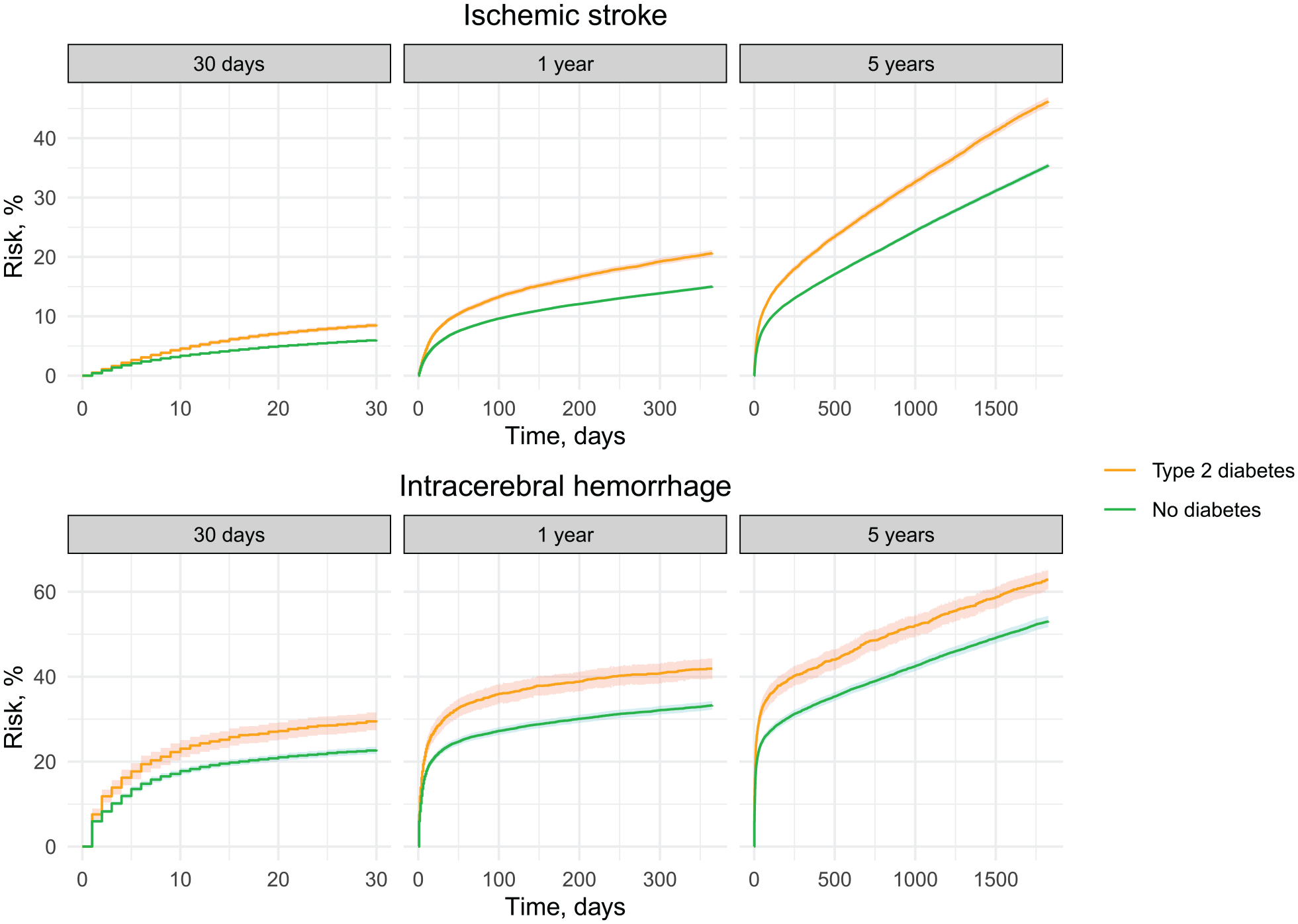
Standardized mortality following first-time stroke for patients with T2DM and patients without diabetes. The curves were standardized according to age, sex, and calendar year of stroke admission.
Standardized risks, risk differences, and risk ratios of mortality and stroke recurrence following first-time stroke.
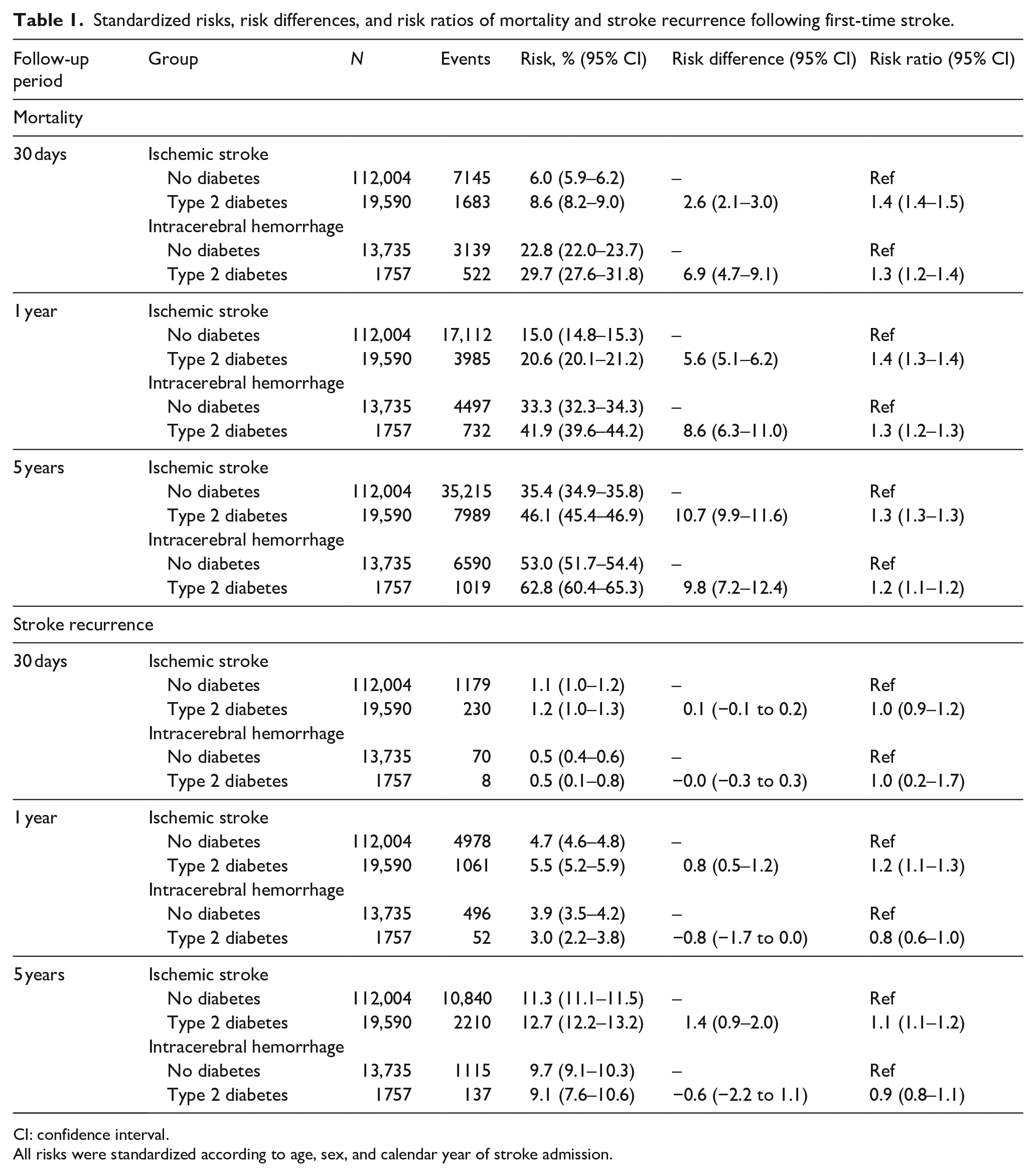
CI: confidence interval.
All risks were standardized according to age, sex, and calendar year of stroke admission.
The 30-day risk of stroke recurrence was low and similar for patients with T2DM (1.2%) and those without diabetes (1.1%) (Figure 2 and Table 1). The 5-year risk of stroke recurrence was 12.7% for patients with T2DM and 11.3% for patients without diabetes (risk difference: 1.4% [95% CI 0.9–2.0]; risk ratio: 1.1 [95% CI 1.1–1.2]). In age subgroups, the 5-year risk difference of recurrence was highest among ischemic stroke patients <50 years of age (risk difference: 4.7% [95% CI 1.9–7.5]; risk ratio: 1.5 [95% CI 1.2–1.9]) and lowest among patients aged ⩾80 years (risk difference −1.1% [95% CI −2.1 to −0.1]; risk ratio: 0.9 [95% CI 0.8–1.0]). Overall, no deviation in risk differences and ratios from the main analysis was found among patient subgroups (Supplemental Table 9).
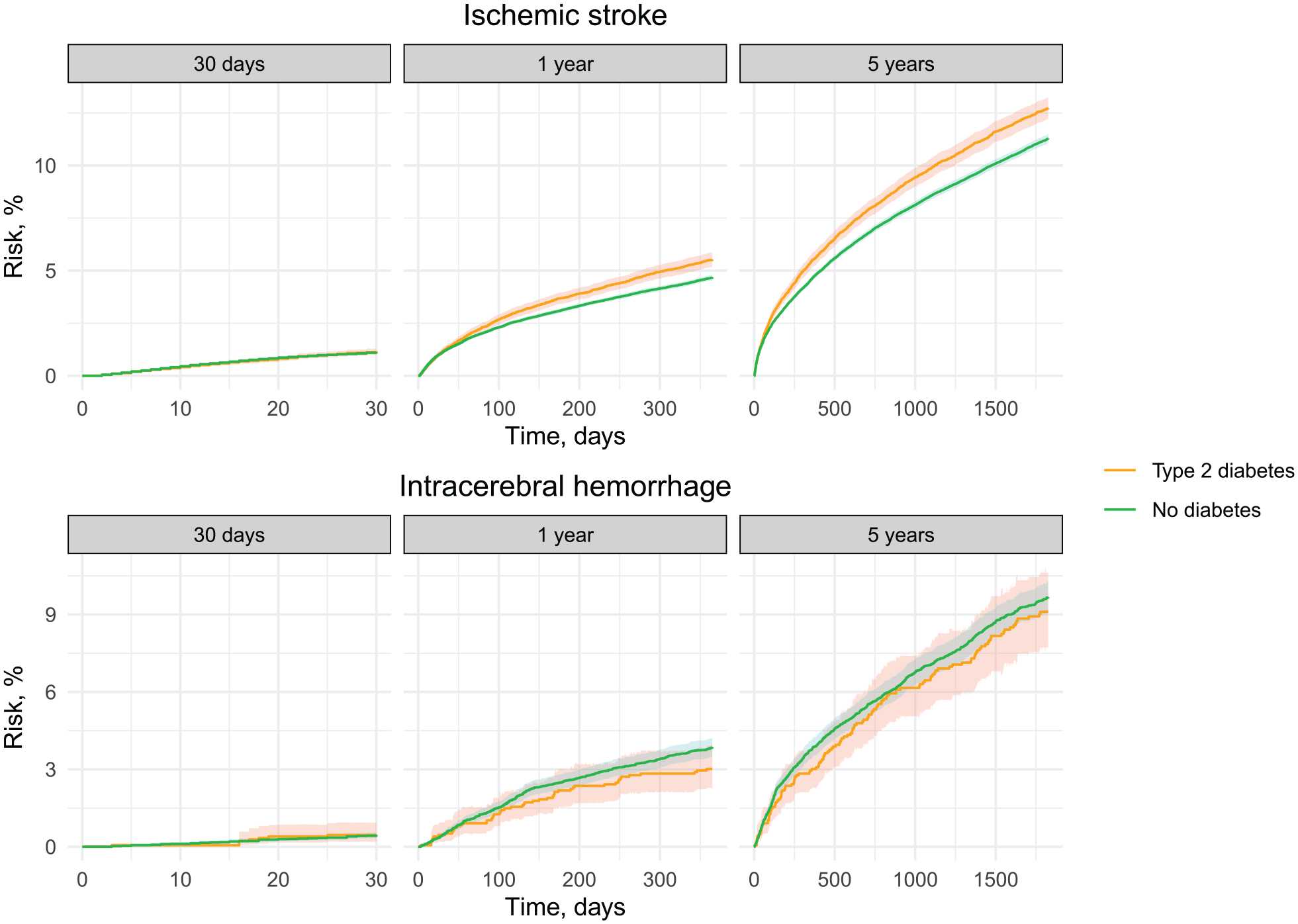
Standardized risk of recurrence following first-time stroke for patients with T2DM and patients without diabetes. The curves were standardized according to age, sex, and calendar year of stroke admission.
Characteristics of ICH patients
Among 15,492 patients with ICH, 1757 had T2DM (11.3%). The median age was 74 years both in patients with T2DM and in those without diabetes, and more men than women had T2DM (59.2% were men in the patients with T2DM vs 51.1% were men in patients without diabetes). The median stroke severity score was similar in the two groups (36 points). Among the ICH cohort, we observed distributions of characteristics similar to patients with ischemic stroke (Supplemental Tables 6 and 7).
Risk of mortality and stroke recurrence following a first-time ICH
The 30-day risk of mortality following a first-time ICH was 29.7% in patients with T2DM and 22.8% in those without diabetes (risk difference: 6.9% [95% CI 4.7–9.1]; risk ratio: 1.3 [95% CI 1.2–1.4]) (Figure 1 and Table 1). During follow-up, the 5-year mortality was 62.8% (95% CI 60.4–65.3) among patients with T2DM and 53.0% (95% CI 51.7–54.4) among those without diabetes (risk difference: 9.8% [95% CI 7.2–12.4]; risk ratio: 1.2 [95% CI 1.1–1.2]). As in patients with ischemic stroke, younger patients with T2DM had the highest mortality risk ratio compared to patients without diabetes (e.g. patients < 50 years: 2.4 [95% CI 1.5–3.3]; patients ⩾ 80 years: 1.1 [95% CI 1.0–1.1]). Presence of other comorbidities increased the risk of mortality in both patients with and those without diabetes, but with overall similar mortality risk differences and ratios in these subgroups compared with the main analysis (Supplemental Table 10).
The 30-day risk of stroke recurrence was low following a first-time ICH (0.5% in both groups) (Figure 2 and Table 1). The 5-year risk of stroke recurrence was 9.1% for patients with T2DM and 9.7% for patients without diabetes (risk difference: −0.6% [95% CI −2.2 to 1.1]; risk ratio: 0.9 [95% CI 0.8–1.1]). In subgroup analyses, T2DM was often associated with a negative risk difference and a risk ratio below 1.0 for stroke recurrence compared with patients without diabetes (Supplemental Table 11).
Additional analyses
After further adjusting for baseline differences in BMI, stroke severity, and comorbidities, the risk differences and risk ratios for mortality and stroke recurrence diminished slightly, however, remained increased for patients with T2DM compared to those without diabetes across stroke subtypes (Supplemental Table 12). Defining patients with at least one HbA1c level ⩾ 48 mmol/mol as having T2DM yielded similar risk differences and risk ratios for mortality and stroke recurrence (Supplemental Table 13).
Discussion
Based on this cohort study of more than 150,000 first-time stroke patients, we here highlight three main findings. First, irrespective of stroke subtype, patients with T2DM were more often former smokers, obese, had a higher burden of comorbidities, and used preventive cardiovascular medications more often prior to the stroke admission compared with stroke patients without diabetes. Yet, stroke severity was similar between the two groups. Second, the risk of mortality was higher in stroke patients with T2DM than in those without diabetes, an association that was most pronounced in younger patients. Third, the risk of stroke recurrence was higher in patients with T2DM following ischemic stroke but not ICH when compared with patients without diabetes.
Our study extends the current literature with contemporary data on mortality among ischemic stroke patients with T2DM. Prior studies reported that diabetes was associated with an up to 1.5-fold increased risk of 30-day,5,7,9,10 1-year,7–9,14 and long-term mortality after ischemic stroke.6,12,14 This was also evident in our cohort. However, prior studies rarely reported T2DM-specific risk estimates and characterized stroke patients with T2DM in detail to provide an explanation for this increased mortality. Our results underscore that comorbidities – including chronic kidney disease, heart failure, and atrial fibrillation – are more common among stroke patients with T2DM. This combination of comorbidities and diabetes complications may potentially contribute to the poor prognosis, however, the association between T2DM and mortality after stroke persisted after adjusting for baseline differences in BMI, stroke severity, and comorbidities. This suggests that at least some deaths are attributed to T2DM itself beyond other clinically relevant factors.
The few prior studies examining ICH patients reported no difference in 30-days mortality for patients with T2DM compared with those without diabetes.8,11–13 In contrast to previous research focusing on short-term risks, our results indicate that 5-year mortality exceeds 50% after ICH, with an up to 10% increased mortality risk for patients with T2DM. This indicates that T2DM is a clinically relevant marker for mortality following ICH.
We found effect modification by age. On the relative scale, mortality risk ratios declined with age, whereas on the absolute scale, risk differences increased with age. While most studies of ischemic stroke either did not stratify on age,6,8,12 involved only patients aged ⩾65 years, 14 or used broad age categories (e.g. 35–74 and 75–94 years),5,10 our results are consistent with evidence from a few other ischemic stroke cohorts which found a similar worse prognosis for young stroke patients with T2DM.7,9 In contrast, no studies of ICH have stratified on age.8,11–13 A possible explanation for these age-dependent differences may be that T2DM debut at a young age is associated with a more aggressive natural history of diabetes disease. 26 Compared with young stroke patients without diabetes, patients with T2DM may have accumulated more risk factors before their stroke which increase their risk of dying after stroke.
We found that there were minor differences in the risk of stroke recurrence between patients with T2DM and those without diabetes. This contrasts with the results of previous studies. A meta-analysis of 27 studies focusing mainly on ischemic stroke with different length of follow-up reported that T2DM is associated with an increased risk of stroke recurrence (pooled hazard ratio: 1.50 [95% CI 1.36–1.65]). 16 The small difference found in our study may be explained by patients receiving similar hospital treatment after the initial stroke, in accordance with current guidelines. 27 Stroke guidelines recommend that virtually all patients should be treated with relevant cardioprotective drugs in addition to initiating lifestyle changes. 27
Although our study yielded low absolute risks of recurrence, preventing stroke recurrence in patients with T2DM remains important because recurrent stroke events are associated with higher mortality than first-time events. 15 Of note, our findings of a lower risk of recurrent stroke for patients with T2DM in some subgroups should be viewed in light of a higher mortality (e.g. from a more severe first-time stroke, chronic kidney disease, heart failure, or cancer) precluding recurrence. Accordingly, patients with a mild first-time stroke had the highest absolute risk of recurrence whom may have the greatest benefit of preventative initiatives.
Previous evidence has shown that stroke mortality has declined over the past decade, but evidence focusing on patients with T2DM is lacking.1,3,4 We found a declining trend from 2005 to 2016 in 5-year risk of mortality across stroke subtypes, aligning with previous studies of a general stroke population. 15 Despite the decline in mortality, a mortality gap remained for patients with T2DM over the study period. Reducing mortality in stroke patients with T2DM would require early prevention of common T2DM complications before the stroke event and an increased focus on the interplay between comorbidities, social determinants, and lifestyle behaviors associated with T2DM and mortality. 28
Several limitations of our study must be emphasized. First, despite the high positive predictive value of hospital diagnosis codes and glucose-lowering drugs for identifying patients with diabetes, 22 the sensitivity of our algorithm for identifying T2DM is unknown. This may have led to a misclassification of some patients with another underlying pathophysiology, such as type 1 diabetes mellitus, as having T2DM. Furthermore, we were unable to identify patients with T2DM treated with lifestyle interventions. We expect such misclassification to have biased our estimates toward the null. Still, the results of our analysis including patients with an HbA1c > 48 mmol/mol as an eligibility criterion yielded similar results to those found in the main analysis. Second, subgroup analyses were limited to patients with complete data and we did not have information on exact blood pressure. Missing BMI measurements depended on the registration period, since registration of height and weight stopped in 2015. Missing laboratory measurements depended on the timing of linking hospital laboratory data to LABKA or RLRR. 23 In our study, 60% of the overall study cohort resided in a municipality with an established data linkage at the time of their first-time stroke, which may explain the large proportion of missingness for laboratory values. To examine the importance of this issue, we calculated risks in subgroups with missing data (e.g. missing values of HbA1c and BMI), and found risk estimates similar to those found in the main analysis. Third, we lacked detailed data on the underlying stroke etiology.
Conclusion
Our contemporary data show that stroke patients with T2DM differ in patient characteristics compared to those without diabetes in terms of smoking habits, obesity, comorbidity burden, and use of preventive medications. Further, stroke patients with T2DM appear to have a poorer prognosis, particularly following ischemic stroke. T2DM is a clinically relevant prognostic marker in patients with a first-time stroke.
Supplemental Material
sj-docx-1-eso-10.1177_23969873241260956 – Supplemental material for Risk of mortality and recurrence after first-time stroke among patients with type 2 diabetes: A Danish nationwide cohort study
Supplemental material, sj-docx-1-eso-10.1177_23969873241260956 for Risk of mortality and recurrence after first-time stroke among patients with type 2 diabetes: A Danish nationwide cohort study by Frederik Pagh Bredahl Kristensen, Helene Matilde Lundsgaard Svane, Kristina Laugesen, Sofie Kejlberg Al-Mashhadi, Diana Hedevang Christensen, Henrik Toft Sørensen and Nils Skajaa in European Stroke Journal
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DHC has received support from Novo Nordisk for attending the European Association for the Study of Diabetes (EASD) Annual Meeting 2023 in Hamburg. DHC is supported by a research grant from the Danish Diabetes and Endocrine Academy, which is funded by the Novo Nordisk Foundation, grant number NNF22SA0079901. NS reports receiving speaker honoraria from Pfizer outside the submitted work. N.S was affiliated with the Department of Clinical Epidemiology, Aarhus University and Aarhus University Hospital during the initiation of this study but is now an employee of Novo Nordisk A/S. Department of Clinical Epidemiology, Aarhus University, receives funding for other studies in the form of institutional research grants to (and administered by) Aarhus University. None of these studies has any relation to the present study. The other authors report no conflicts.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by a grant from the Danish Center of Population Medicine and a grant from Lundbeck (grant number R433-2023-1140).
Ethical approval
The study was approved by the Danish Health Data Authority (No 2016-051-000001/1502). According to Danish legislation, ethical committee approval is not needed for register-based studies.
Informed consent
Not required.
Guarantor
FPBK, NS
Contributorship
Conceptualization: FPBK, NS, KL, HTS. Data curation: HTS. Statistical analyses: HMLS. Writing - first draft: FPBK and NS. Guarantors: FPBK, NS. All authors contributed to the interpretation of data, to the drafting of the manuscript as well as critically revised the draft manuscript. All authors approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.