
Abstract
The revised Japan Stroke Society Guidelines for the Treatment of Stroke were published in Japanese in July 2021. In this article, the extracted recommendation statements are published. The revision keeps pace with the great progress in stroke control based on the recently enacted Basic Act on Stroke and Cardiovascular Disease in Japan. The guideline covers the following areas: primary prevention, general acute management of stroke, ischemic stroke and transient ischemic attack, intracerebral hemorrhage, subarachnoid hemorrhage, asymptomatic cerebrovascular disease, other cerebrovascular disease, and rehabilitation.
Keywords
Introduction
The Japan Stroke Society Guideline 2021 for the Treatment of Stroke is a totally revised version that is developed every 6 years, with two yearly updates in the intervening periods. The guidelines have been developed in conjunction with Japan Neurosurgical Society, the Japanese Society of Neurology, the Japanese Association of Rehabilitation Medicine, the Japanese Society of Neurological Therapeutics, the Japanese Society on Surgery for Cerebral Stroke, and the Japanese Society for Neuroendovascular Therapy. The guideline comprises 300 pages in Japanese. In this English version, recommendations of each topic are extracted and introduced. The guideline consists of seven chapters. Of these, the chapters for ischemic stroke, intracerebral hemorrhage (ICH), and subarachnoid hemorrhage are introduced in the main text and the other four chapters, as part of the full guideline, are presented in the supplemental material.
Method
The Committee for Stroke Guideline 2021, selected from the members of the Japan Stroke Society, developed the present guideline based on the literature searched for the guidelines up to the 2019 version (papers published up to December 2017) and additional papers published between January 2018 and December 2019. In the Committee, there was no distinction between those who reviewed the literature and those who wrote the recommendations.
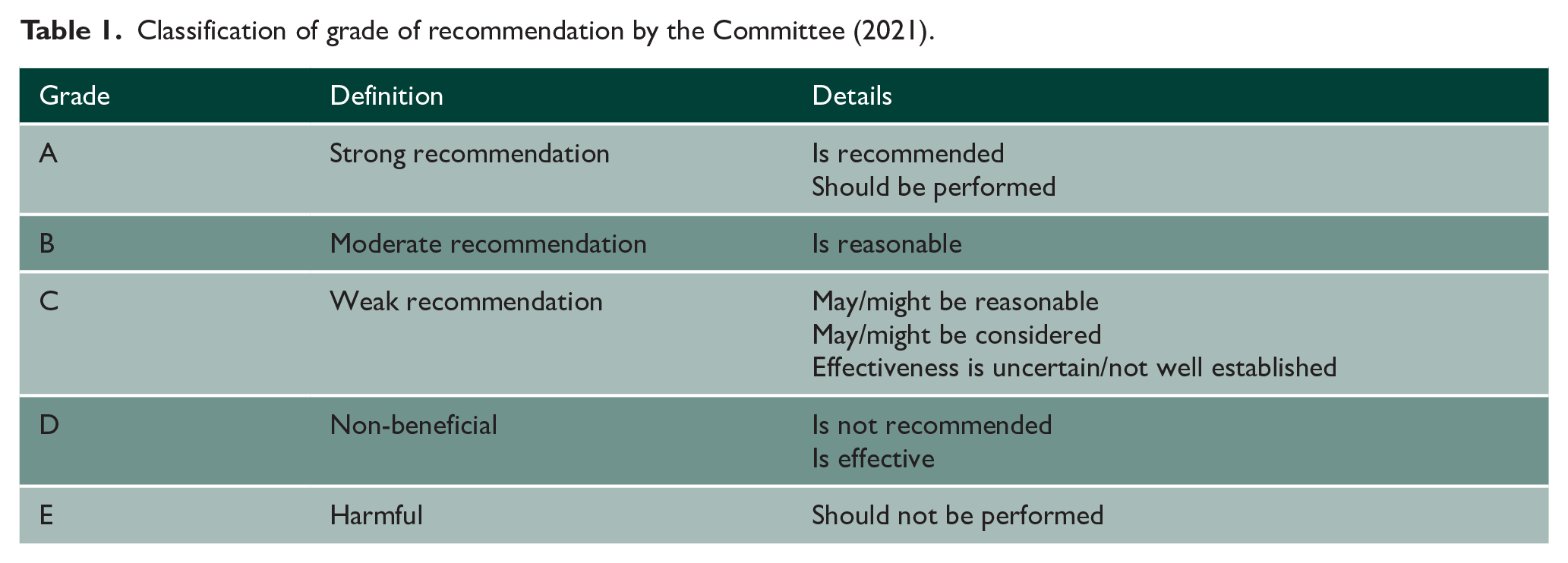
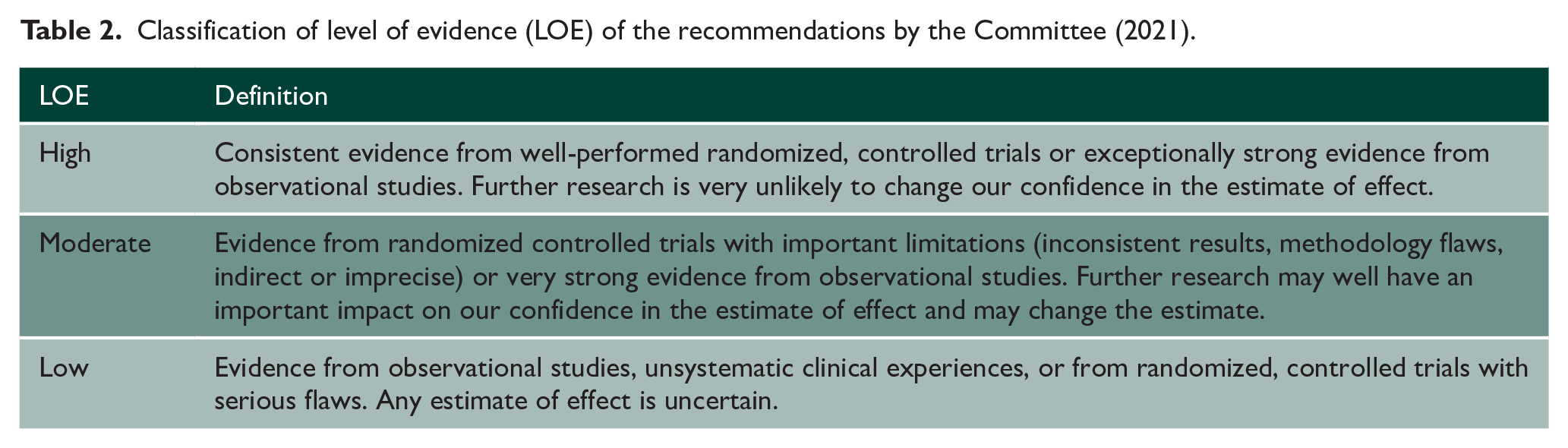
Taking into consideration the level of evidence, the balance between “benefit” and “harm” of the intervention, the influence of patient values and other factors, and the cost of the intervention and medical resources, the Committee members determined the grade of recommendations (Table 1). The level of bodies of evidence for the recommendations was determined by the Committee members after integrating the evidence of the relevant references (Table 2). Detailed explanation is described in “Level of Evidence and Grade of Recommendation” in the full article in the supplemental material.
Classification of grade of recommendation by the Committee (2021).
Classification of level of evidence (LOE) of the recommendations by the Committee (2021).
Recommendations
Chapter 1. Primary prevention and acute management of stroke in general
(Refer the full version as the supplemental material)
Chapter 2. Ischemic stroke and transient ischemic attack
Acute ischemic stroke
Intravenous thrombolysis
Intravenous thrombolysis with recombinant tissue-type plasminogen activator (alteplase, 0.6 mg/kg) is recommended for patients with acute ischemic stroke who can be treated within 4.5 h of onset and for whom the indication has been carefully determined (Grade of recommendation: A, Level of evidence (LOE): High).
Intravenous thrombolysis should be initiated as quickly as possible (at least within 1 h of patient arrival; Grade A, LOE High).
If the onset time is unknown, intravenous thrombolysis may be considered for patients in whom ischemic changes on diffusion-weighted imaging are not evident on fluid-attenuated inversion recovery imaging (Grade C, LOE Moderate).
Intravenous recombinant tissue-type plasminogen activator other than alteplase is not recommended at present time because of the lack of sufficient evidence in Japan (Grade D, LOE Moderate).
(Clinical Question) Even in patients with mild ischemic stroke, intravenous thrombolysis may be reasonable after careful consideration of the indications (Grade C, LOE Moderate).
Intra-arterial revascularization
In patients with acute ischemic stroke—if they met all the following criteria: (a) acute occlusion of the internal carotid artery or the M1 segment of the middle cerebral artery, (b) modified Rankin Scale (mRS) score 0 or 1 before onset, (c) Alberta Stroke Program Early CT Score (ASPECTS) ⩾ 6 in computed tomography (CT) or diffusion-weighted imaging, (d) National Institutes of Health Stroke Scale (NIHSS) ⩾ 6, and (e) age ⩾ 18 years, in addition to medical therapy including intravenous thrombolysis with recombinant tissue-type plasminogen activator (alteplase)—mechanical thrombectomy using stent retriever or aspiration catheter within 6 h of onset (as soon as possible) is recommended (Grade A, LOE High).
In patients with ischemic stroke due to acute occlusion of the internal carotid artery or the M1 segment middle cerebral artery more than 6 h from the last known well time, after the judgment of indication based on neurological symptoms and quantitative evaluation of imaging, mechanical thrombectomy within 16 h of the last known well time is recommended (Grade A, LOE Moderate). In addition, the initiation of the same treatment within 16 to 24 h is reasonable (Grade B, LOE Moderate).
In patients with acute ischemic stroke due to large artery occlusion in the anterior circulation who have broad extent of ischemia with ASPECTS < 6, mild symptoms with NIHSS score < 6, occlusion of the M2 segment middle cerebral artery, or mRS score ⩾ 2 before the onset, mechanical thrombectomy within 6 h of onset may be reasonable (Grade C, LOE Low).
In patients with acute ischemic stroke due to the basilar artery occlusion, mechanical thrombectomy may be reasonable if the effectiveness is judged to outweigh the safety after careful consideration on a case-by-case basis (Grade C, LOE Low).
In patients with ischemic stroke due to acute occlusion of the internal carotid artery or the M1 segment or the proximal M2 segment middle cerebral artery, mechanical thrombectomy without intravenous thrombolysis within 4.5 h of onset may be considerable (Grade C, LOE Moderate).
In patients with ischemic stroke due to acute occlusion of the middle cerebral artery who have moderate to severe neurological symptoms and no or only minor ischemic changes on CT, selective local intra-arterial fibrinolysis within 6 h of onset is reasonable (Grade B, LOE High).
In patients with acute ischemic stroke due to severe stenosis or occlusion of the intracranial artery or extracranial carotid artery, the effectiveness of percutaneous transluminal angioplasty or stenting is not well established (Grade C, LOE Low).
Antiplatelet therapy
In patients with acute ischemic stroke in the early phase of onset (within 48 h), oral administration of aspirin 160 to 300 mg/day is recommended (Grade A, LOE High).
In patients with mild non-cardioembolic stroke in the early phase of onset up to the subacute phase (within 1 month as a rough indication), treatment with dual antiplatelet therapy (aspirin and clopidogrel) is recommended (Grade A, LOE High).
In patients with non-cardioembolic stroke within 48 h of onset, cilostazol 200 mg/day as single antiplatelet therapy or dual antiplatelet therapy with low-dose aspirin may be considered (Grade C, LOE Moderate).
In patients with non-cardioembolic stroke, ozagrel sodium 160 mg/day may be considered (Grade C, LOE Moderate).
Anticoagulation
In patients with non-cardioembolic and non-lacunar stroke within 48 h after onset, intravenous administration of argatroban (selective thrombin inhibitor) may be considered (Grade C, LOE Moderate).
In patients with acute ischemic stroke, the use of unfractionated heparin, low-molecular-weight heparin (unapproved in Japan), or heparinoid (not covered by Japanese Health Care Insurance System) may be considered (Grade C, LOE Moderate).
In patients with acute ischemic stroke who have non-valvular atrial fibrillation (NVAF), direct oral anticoagulant (DOAC) may be considered at an appropriate timing after considering the risk of hemorrhagic infarction (Grade C, LOE Low).
Medication for cerebral edema
In patients with acute major ischemic stroke due to cardioembolic stroke or atherothrombotic infarction and who have intracranial hypertension, intravenous hypertonic glycerol (10%) may be considered (Grade C, LOE Low).
In patients with acute ischemic stroke, mannitol (20%) may be considered (Grade C, LOE Low).
Neuroprotective agents
In patients with acute ischemic stroke, edaravone is reasonable (Grade B, LOE Moderate).
Hemodilution therapy
In patients with acute ischemic stroke, the effectiveness of plasma expander is not well established (Grade C, LOE High).
In patients with acute ischemic stroke, extracorporeal circulation is not recommended (Grade D, LOE Low).
Hyperbaric oxygen therapy
In patients with acute ischemic stroke, the effectiveness of hyperbaric oxygen therapy is not well established (Grade C, LOE Low).
Therapeutic hypothermia
In patients with acute ischemic stroke, therapeutic hypothermia is not recommended (Grade D, LOE Low).
Dyslipidemia
In patients with acute ischemic stroke, the start of HMG-CoA reductase inhibitor (statin) may be considered (Grade C, LOE Low).
In patients with acute ischemic stroke, who were using statin before stroke onset, discontinuation of oral statin is not recommended (Grade D, LOE Low).
Even in patients with acute ischemic stroke, who have undergone intravenous thrombolysis or intra-arterial revascularization, statin therapy may be considered (Grade C, LOE Low).
Regenerative therapy
In patients with acute ischemic stroke, neural regenerative therapy is not recommended (Grade D, LOE Low).
Decompressive craniectomy
In patients with unilateral hemispheric large infarct in the territory of the middle cerebral artery—if they met the following criteria: (a) 18 to 60 years, (b) NIHSS score exceeds 15, (c) NIHSS Item 1a score is ⩾1, (d) infarct in the territory of the middle cerebral artery occupies at least 50% in CT or the range of infarct exceeds 145 cm3 in diffusion-weighted image, and (e) within 48 h after onset—decompressive craniectomy with duraplasty is recommended (Grade A, LOE High).
In patients with infarct in the territory of the middle cerebral artery who are aged 60 years or older, meeting the criteria for indication of decompressive craniectomy except age, decompressive craniectomy may be considered (Grade C, LOE Moderate).
In patients with cerebellar infarction who have moderate consciousness disorder due to hydrocephalus, ventricular drainage may be considered (Grade C, LOE Low). In addition, in patients presenting severe consciousness disorder such as coma due to compression of the brain stem, posterior fossa decompression is reasonable (Grade B, LOE Low).
Other surgical therapy
In patients with acute ischemic stroke, urgent surgical therapy including carotid endarterectomy (CEA), bypass surgery, and surgical clot removal by craniotomy may be considered (Grade C, LOE Low).
Acute and chronic management of transient ischemic attack
In patients of suspected transient ischemic attack (TIA), evaluation of the mechanism as soon as possible after admission and immediate initiation of treatment for stroke prevention is recommended (Grade A, LOE High). The use of risk prediction score (e.g. ABCD2 score) is reasonable to predict risk of stroke and determine treatment strategy (Grade B, LOE Moderate).
In TIA patients within 48 h after onset, aspirin 160 to 300 mg/day is recommended for prevention of recurrence during the acute phase (Grade A, LOE High). In high-risk TIA patients with ABCD2 score ⩾ 4, dual antiplatelet therapy (aspirin and clopidogrel) limited to the acute phase is reasonable (Grade B, LOE High).
In patients with post-acute TIA, management in accordance with prevention of stroke for patients with ischemic stroke is recommended (Grade A, LOE Moderate).
Ischemic stroke in the chronic stage
Non-cardioembolic stroke—antiplatelet therapy
Administration of antiplatelet drugs is recommended for the prevention of recurrent non-cardioembolic stroke (Grade A, LOE High).
Antiplatelet drugs that are effective for the prevention of recurrent non-cardioembolic stroke (available in Japan) are aspirin 75 to 150 mg/day, clopidogrel 75 mg/day, and cilostazol 200 mg/day at present time (Grade A, LOE High), as well as ticlopidine 200 mg/day (Grade B, LOE Moderate).
Coadministration of aspirin and dipyridamole is not recommended in Japan (Grade D, LOE Moderate).
Long-term dual antiplatelet therapy is not recommended because it is not demonstrated to have a significant effect of stroke prevention compared to single antiplatelet therapy, but rather increases hemorrhagic complications (Grade D, LOE High). However, in patients with non-cardioembolic stroke who have stenosis/occlusion of a major extracranial or intracranial artery or two or more vascular risk factors, dual antiplatelet therapy including cilostazol is reasonable (Grade B, LOE Moderate).
In patients with history of ischemic stroke or TIA who undergo a procedure or minor surgery where bleeding is easily controlled (e.g. tooth extraction or cataract surgery), continuation of aspirin is recommended (Grade A, LOE Moderate). In addition, continuation of other antiplatelet drugs is reasonable (Grade B, LOE Low). In patients at high risk for thromboembolism who undergo gastrointestinal endoscopy with high risk of bleeding, replacement with aspirin or cilostazol may be considered (Grade C, LOE Low).
Non-cardioembolic stroke—CEA
In patients with symptomatic severe carotid artery stenosis (NASCET 70–99%), in addition to the best medical treatment including antiplatelet therapy, CEA by an operator at an institution experienced in surgery and perioperative management is recommended (Grade A, LOE High). In patients of severe stenosis with post stenotic collapsing (near occlusion), CEA may be also considered (Grade C, LOE Moderate).
In patients with symptomatic moderate carotid artery stenosis, in addition to the best medical treatment including antiplatelet therapy, CEA by an operator at an institution experienced in surgery and perioperative management is reasonable (Grade B, LOE High).
In elderly patients with carotid artery stenosis for whom carotid revascularization should be considered, CEA rather than carotid artery stenting (CAS) is reasonable (Grade B, LOE High).
In patients with symptomatic severe or moderate carotid artery stenosis, CEA early after the onset is reasonable (Grade B, LOE Moderate).
(Clinical Question) In patients with symptomatic mild carotid artery stenosis, who are refractory to medical therapy, and imaging examination indicates ulcer or unstable plaque, although its effectiveness is not well established, CEA may be reasonable (Grade C, LOE Low).
Non-cardioembolic stroke—endovascular treatment of carotid arteries
In patients with symptomatic severe carotid artery stenosis who have risk factors for CEA (cardiac disease, severe respiratory disease, contralateral carotid artery occlusion, contralateral recurrent laryngeal nerve palsy, history of irradiation or surgical approach for neck, restenosis after CEA), in addition to the best medical therapies including antiplatelet therapy, CAS by an operator at an institution experienced in surgery and perioperative management is reasonable (Grade B, LOE Moderate).
In patients with symptomatic severe carotid artery stenosis who have no risk factors for CEA, in addition to the best medical therapies including antiplatelet therapy, CAS by an operator experienced at an institution in surgery and perioperative management may be reasonable (Grade C, LOE Moderate).
Non-cardioembolic stroke—endovascular treatment of intracranial arteries
In patients with symptomatic stenosis of intracranial artery or extracranial vertebral artery, the effectiveness of percutaneous transluminal angioplasty or stenting is not well established (Grade C, LOE Moderate).
Non-cardioembolic stroke—extracranial-intracranial bypass
In patients with minor stroke or TIA due to symptomatic occlusion or stenosis of internal carotid artery or middle cerebral artery, after carefully considering its indication based on the timing of onset, age, mRS, and quantitative assessment of cerebral circulation, extracranial-intracranial bypass by an experienced operator with very few perioperative complications is reasonable (Grade B, LOE Moderate).
Cardioembolic stroke—anticoagulation
In patients with ischemic stroke or TIA and NVAF, anticoagulant therapy with a DOAC or warfarin for prevention of stroke recurrence is recommended (Grade A, LOE Moderate).
In patients younger than 70 years who undergo warfarin therapy for NVAF, prothrombin time-international normalized ratio (PT-INR) 2.0 to 3.0 is recommended (Grade A, LOE Moderate). In patients aged 70 years or older, PT-INR 1.6 to 2.6 is reasonable (Grade B, LOE Low).
In patients with ischemic stroke or TIA and NVAF who can be treated with DOACs, DOAC rather than warfarin is recommended (Grade A, LOE Moderate).
It is recommended to select a DOAC and adjust its dosage considering the renal function, age, body weight, and concomitant drugs (Grade A, LOE Low).
In patients with ischemic stroke or TIA after mechanical valve replacement, it is recommended to maintain PT-INR between 2.0 to 3.0 with warfarin (Grade A, LOE Moderate). DOAC should not be used (Grade E, LOE Moderate).
In patients with ischemic stroke or TIA who have rheumatic mitral stenosis and atrial fibrillation, it is recommended to maintain PT-INR between 2.0 to 3.0 with warfarin (Grade A, LOE Low).
In patients with ischemic stroke or TIA who have cardiomyopathy or heart failure and atrial fibrillation, anticoagulant therapy is recommended (Grade A, LOE Low).
In patients with ischemic stroke or TIA who undergo usual tooth extraction or gastrointestinal endoscopy, continuation of DOAC or warfarin (PT-INR within the therapeutic range) without withdrawal is reasonable (Grade B, LOE Low). If gastrointestinal endoscopy with high risk of bleeding is performed, continuation of warfarin (PT-INR within the therapeutic range) is reasonable. In patients with NVAF, it is also reasonable to consider temporal switching to DOAC. In patients using DOAC, it is reasonable to continue DOAC until the day before the procedure, discontinue it on the morning of the procedure, and then resume it on the morning after the procedure after confirming that there is no bleeding (Grade B, LOE Low).
Management of risk factors—hypertension
In patients who experience ischemic stroke or TIA, antihypertensive therapy for prevention of recurrence is recommended (Grade A, LOE High).
In patients who experience ischemic stroke or TIA, with bilateral severe carotid artery stenosis, occlusion of major intracranial artery, or without vascular assessment, a target value of <140/90 mm Hg for antihypertensive therapy is reasonable (Grade B, LOE Low).
In patients who experience ischemic stroke or TIA, without bilateral severe carotid artery stenosis and occlusion of major intracranial artery, who present with lacunar infarction, or undergoing antithrombotic therapy, as lower target value of blood pressure is favorable if possible, a target value of <130/80 mm Hg for antihypertensive therapy is reasonable (Grade B, LOE Moderate).
Management of risk factors—diabetes mellitus
In patients with chronic ischemic stroke, the effectiveness of blood glucose control for the prevention of stroke recurrence is not well established (Grade C, LOE Moderate).
Diabetes mellitus treatment with pioglitazone, an insulin sensitizer, for the prevention of stroke recurrence is reasonable (Grade B, LOE Moderate).
Management of risk factors—dyslipidemia
In patients with non-cardiogenic stroke or TIA, proactive administration of HMG-CoA reductase inhibitors (statins) for prevention of recurrent non-cardiogenic stroke or TIA is recommended (Grade A, LOE Moderate).
In patients with non-cardiogenic stroke or TIA, a target value of LDL-cholesterol <100 mg/dL for lipid control to prevent recurrence of non-cardiogenic stroke or TIA is reasonable (Grade B, LOE Moderate).
In patients with non-cardiogenic stroke or TIA and coronary artery disease, a target value of LDL-cholesterol <70 mg/dL for stroke prevention may be reasonable (Grade C, LOE Moderate).
In patients with ischemic stroke under lipid control with statin, coadministration of ethyl icosapentate product for prevention of stroke recurrence is reasonable (Grade B, LOE Low).
Management of risk factors—obesity and metabolic syndrome
Treatment of obesity and metabolic syndrome for prevention of stroke recurrence may be considerable (Grade C, LOE Low).
Cryptogenic stroke and embolic stroke of undetermined source—antithrombotic therapy
In patients with cryptogenic stroke or embolic stroke of undetermined source, antiplatelet therapy with aspirin is reasonable (Grade B, LOE Moderate).
In patients with cryptogenic stroke or embolic stroke of undetermined source, dabigatran and rivaroxaban are not recommended (Grade D, LOE Moderate).
In patients with cryptogenic stroke who do not have a history of hypertension or posterior circulation infarcts not involving the brainstem, warfarin may be considered (Grade C, LOE Low).
In patients with cryptogenic stroke and embolic stroke of undetermined source who have aortic atheromatous lesion, warfarin (PT-INR ⩾ 1.5) instead of aspirin may be considered (Grade C, LOE Low).
Paradoxical embolic stroke including cryptogenic stroke with patent foramen ovale (PFO)
In patients with paradoxical embolic stroke (definite or suspected), it is recommended to consider a policy for prevention of stroke recurrence based on reliable pathophysiological diagnosis by stroke specialist (Grade A, LOE Low). In addition, it is also recommended to decide treatment policy through a process of shared decision-making involving stroke specialist, cardiologist, and patients (Grade A, LOE Low).
In patients with embolic stroke of undetermined source suspected of involving PFO, either antiplatelet therapy or anticoagulation for prevention of stroke recurrence is reasonable (Grade B, LOE Moderate). In patients with venous thromboembolism, anticoagulant therapy is recommended (Grade A, LOE Low). Even in patients without venous thromboembolism, anticoagulant therapy rather than antiplatelet therapy may be considered (Grade C, LOE Moderate).
In patients younger than 60 years old with cryptogenic stroke suspected of involving PFO (including definitive paradoxical embolism), percutaneous PFO closure is reasonable (Grade B, LOE High). Especially, in patients with high-risk PFO (e.g. large shunt or atrial septal aneurysm), percutaneous PFO closure is recommended (Grade A, LOE High).
In patients aged 60 years or older with cryptogenic stroke suspected of involving PFO (including definitive paradoxical embolism), the effectiveness of percutaneous PFO closure is not well established (Grade C, LOE Low).
Continuation of antithrombotic therapy after percutaneous PFO closure is reasonable (Grade B, LOE Low).
In patients with paradoxical cerebral embolism due to pulmonary arteriovenous fistula, percutaneous closure of pulmonary arteriovenous fistula to prevent stroke recurrence is reasonable (Grade B, LOE Low).
Cerebral metabolism/circulation improving drug
In patients with sequela of ischemic stroke such as dizziness, ibudilast may be considered (Grade C, LOE Low).
Elevated hematocrit or fibrinogen level
In patients with ischemic stroke, treatment of elevated hematocrit level is not recommended (Grade D, LOE Low).
In patients with ischemic stroke, treatment of elevated fibrinogen level may be considered (Grade C, LOE Low).
Regenerative therapy
In patients with chronic ischemic stroke, neural regenerative therapy is not recommended (Grade D, LOE Low).
Chapter 3. Intracerebral hemorrhage
Prevention of ICH
In patients with hypertension, antihypertensive therapy for prevention of ICH is recommended (Grade A, LOE High).
It is reasonable to instruct heavy drinkers to reduce their alcohol consumption and smokers to quit smoking (Grade B, LOE Moderate).
In patients who require prophylactic treatment for thromboembolism, the selection of antithrombotic drugs considering the risk of ICH is reasonable (Grade B, LOE High).
Acute management for hypertensive ICH
Management of blood pressure
In patients with acute ICH, it is reasonable to lower elevated blood pressure to systolic blood pressure <140 mm Hg as early as possible and maintain this limit for 7 days (Grade B, LOE Moderate). Maintaining a lower systolic blood pressure limit of >110 mm Hg may be reasonable (Grade C, LOE Low).
Intensive antihypertensive therapy to reduce systolic blood pressure by >90 mm Hg is not recommended to avoid acute kidney injury (Grade D, LOE Moderate).
Continuous intravenous infusion of calcium antagonist or nitrate is reasonable as antihypertensive drugs for acute ICH (Grade B, LOE Low). The appropriate use of nicardipine among calcium antagonists may be reasonable (Grade C, LOE Low).
Early switching to oral antihypertensive drugs, if possible, may be reasonable (Grade C, LOE Low).
Hemostatic therapy
In patients with hypertensive ICH, administration of tranexamic acid may be considered (Grade C, LOE Moderate).
In patients of acute hypertensive ICH without abnormality in coagulation system and without antithrombotic therapy, blood products including coagulation factors should not be administered (Grade E, LOE High).
Management of brain edema and intracranial hypertension
In patients with acute ICH who have intracranial hypertension, intravenous hypertonic glycerol may be considered (Grade C, LOE Low).
In patients with progressive increase of intracranial pressure due to hematoma or edema, and with worsening of clinical findings associated with compression on surrounding tissues, intravenous administration of mannitol may be considered (Grade C, LOE Moderate).
In patients with acute ICH who had brain edema, administration of corticosteroid is not recommended (Grade D, LOE High).
In patients with intracranial hypertension due to acute ICH, it may be considerable to elevate head and upper body position by 30° (Grade C, LOE Low).
Management of chronic hypertensive ICH
Hypertension
In patients after hypertensive ICH, a target value of <130/80 mm Hg for antihypertensive therapy is reasonable as poor blood pressure control often causes recurrent ICH (Grade B, LOE Moderate).
In patients at high risk of ICH recurrence, more intensive antihypertensive therapy with a target value of <120/80 mm Hg may be reasonable (Grade C, LOE Low).
It is reasonable to consider complication of microbleeds, use of antithrombotic drugs, and age, to select patients at high risk of ICH recurrence (Grade B, LOE Moderate).
Surgical treatment for hypertensive ICH
Craniotomy and neuroendoscopic surgery
In patients with minor hemorrhage of hematoma volume <10 mL or mild neurological symptoms, regardless of location of hematoma, surgical treatment should not be performed (Grade E, LOE Moderate). In addition, in patients with deep coma (Japan Coma Scale 300), hematoma evacuation is not recommended (Grade D, LOE Low).
In patients with intracerebral or intraventricular hemorrhage who are considered for surgical treatment, neuroendoscopic surgery or stereotactic hematoma evacuation may be considered (Grade C, LOE Moderate).
Putaminal hemorrhage: In patients with moderate neurological symptoms, hematoma volume ⩾ 31 mL, and severe compression findings due to hematoma, hematoma evacuation may be considered (Grade C, LOE Moderate). In patients with consciousness disorder of about Japan Coma Scale 20 to 30, stereotactic hematoma evacuation is reasonable (Grade B, LOE Moderate), and craniotomy with hematoma evacuation or neuroendoscopic surgery may be also considered (Grade C, LOE Moderate).
Thalamic hemorrhage: Hematoma evacuation as treatment in acute phase is not recommended (Grade D, LOE Low).
Lobar hemorrhage: In patients with hematoma located at a depth of ⩽1 cm from brain surface, surgery may be considered (Grade C, LOE Moderate).
Cerebellar hemorrhage: In patients with hematoma of ⩾3 cm in the maximum diameter, and with worsening neurological symptoms, or in patients with obstructive hydrocephalus due to compression on brainstem by hematoma, hematoma evacuation is reasonable (Grade B, LOE Low).
Brainstem hemorrhage: hematoma evacuation in the acute phase is not recommended (Grade D, LOE Low).
In patients suspected of obstructive hydrocephalus due to intraventricular hemorrhage, ventricular drainage is reasonable (Grade B, LOE Moderate). Intraventricular administration of fibrinolytic drugs for hematoma evacuation may be also considered (Grade C, LOE Moderate).
Non-hypertensive ICH
Arteriovenous malformation
For unruptured cerebral arteriovenous malformation (AVM), medical therapy for symptoms may be considered rather than surgical intervention (Grade C, LOE Moderate). In some cases, intervention by surgical excision, endovascular embolization, or radiosurgery alone or by the combination thereof may be considered (Grade C, LOE Low).
Re-hemorrhage often occurs in cerebral AVM with hemorrhage. In such case, surgical excision, stereotactic radiosurgery, or endovascular embolization alone or by the combination thereof may be considered together with the treatment of acute ICH by taking the bleeding risk and surgical risk into consideration (Grade C, LOE Low).
If the risk of surgical excision is high and the lesion is small (⩽10 mL in volume or ⩽3 cm in maximum diameter), stereotactic radiosurgery may be considered (Grade C, LOE Low).
For Spetzler-Martin Grade I and II AVMs, surgical excision may be considered (Grade C, LOE Low). For Spetzler-Martin Grade III AVMs, surgical excision or a combination of endovascular embolization and subsequent surgical excision may be considered (Grade C, LOE Low). For Spetzler-Martin classification Grade IV and V AVMs, conservative therapy may be considered (Grade C, LOE Low).
For cerebral AVMs with convulsion, surgical excision and stereotactic radiosurgery may be considered to suppress epileptic seizure (Grade C, LOE Low).
Dural arteriovenous fistula (dAVF)
For asymptomatic dAVF without reflux to cortical veins in cerebral angiography, conservative observation with regular follow-up using MRI may be considered (Grade C, LOE Moderate).
For symptomatic dAVF or dAVF with reflux to cortical veins in cerebral angiography, active treatment with endovascular therapy, surgical excision, or stereotactic radiosurgery alone or a combination thereof may be considered depending on the site or hemodynamics (Grade C, LOE Moderate).
Although endovascular therapy is the first choice for the transverse/sigmoid sinus dAVF, combination with surgical excision and stereotactic radiosurgery may be considered if occlusion cannot be achieved (Grade C, LOE Low).
For the cavernous sinus dAVF, endovascular embolization may be considered (Grade C, LOE Low).
For the dAVF at the anterior cranial fossa, tentorium, or craniocervical junction, surgical excision may be considered (Grade C, LOE Low). If surgical excision is difficult, a combination of surgical excision and endovascular therapy or endovascular therapy alone may be considered (Grade C, LOE Low).
Cavernous hemangioma
For asymptomatic solitary cavernous hemangioma, it is reasonable to perform conservative observation (Grade B, LOE Moderate). If it is located in a non-eloquent area enabling easy approach, surgical excision may be considered to prevent future hemorrhage (Grade C, LOE Low).
For symptomatic cavernous hemangioma (hemorrhage, poorly controlled convulsion, and progressive neurologic symptoms) where the lesion is located near the brain surface including the brain stem, surgical excision may be considered (Grade C, LOE Low).
For symptomatic cavernous hemangioma located in a surgically unresectable deep region including the brain stem, stereotactic radiosurgery may be considered with a low radiation dose to prevent re-hemorrhage (Grade C, LOE Moderate).
Developmental venous anomaly
Developmental venous anomaly is generally benign, and it is reasonable to follow up conservatively if asymptomatic (Grade B, LOE Low).
Other vascular malformations, such as cavernous hemangioma, may be complicated with symptomatic developmental venous anomaly including cases with hemorrhagic onset. In such cases, it is not recommended to surgically resect developmental venous anomaly responsible for normal venous reflux (Grade D, LOE Low).
Stereotactic radiosurgery is not recommended for developmental venous anomaly because of the low therapeutic effect and the high risk for complications (Grade D, LOE Low).
ICH associated with brain tumor
If severe visual disturbance/visual field defect, oculomotor nerve palsy, or consciousness disorder is noted due to pituitary apoplexy, it may be considerable to perform surgical excision (Grade C, LOE Low). It may be considerable to perform surgical excision in the early phase of onset (Grade C, LOE Low).
In ICH associated with metastatic brain tumor, surgical therapy may be considered if the tumor and hematoma cause the mass effect and the cancerous foci outside the brain are controlled (Grade C, LOE Low).
ICH associated with antithrombotic therapy
It is reasonable to administer prothrombin complex concentrate to patients with ICH taking a vitamin K antagonist (warfarin) with the PT-INR of ⩾2.0 (Grade B, LOE Moderate). In such cases, it is reasonable to administer vitamin K together to avoid a re-increase in PT-INR (Grade B, LOE Low).
It is reasonable to administer idarucizumab to patients with ICH taking a direct thrombin inhibitor (dabigatran; Grade B, LOE Low). Platelet transfusion is evenly not recommended for patients with ICH taking antiplatelet agents (Grade D, LOE Moderate).
Administration of protamine sulfate may be considered for patients with ICH during infusion of unfractionated heparin (Grade C, LOE Low).
For ICH during thrombolytic therapy, it may be considered to evaluate coagulation factor disorder and correct it with the use of appropriate blood product, and so on (Grade C, LOE Low).
Antithrombotic therapy should be basically discontinued to patients with ICH receiving antithrombotic therapy. If blood pressure is high, it may be considered to lower the systolic blood pressure to <140 mm Hg (Grade C, LOE Low).
It may be considered to inhibit absorption by oral activated charcoal or enhance diuretic excretion by fluid loading to patients with ICH shortly after the last dose of DOACs (Grade C, LOE Low).
After ICH, during antithrombotic medication, it is reasonable to resume the use of antithrombotic agents taking the re-hemorrhage risk into consideration (Grade B, LOE Moderate).
ICH associated with chronic kidney disease and end-stage renal disease
For acute ICH in patients with chronic kidney disease, it is reasonable to lower blood pressure intensively while paying attention to worsening of renal function due to excess reduction of blood pressure (Grade B, LOE Low).
For patients on hemodialysis, it may be considered to avoid hemodialysis during the initial 24 h after onset of ICH (Grade C, LOE Low). In addition, it may be considered to select peritoneal dialysis or continuous hemofiltration (and continuous hemodiafiltration) rather than hemodialysis and switch continuous hemofiltration through intermittent hemofiltration or continuous hemodiafiltration to maintain hemodialysis while observing the stabilization of neurologic symptoms (Grade C, LOE Low).
Nafamostat mesylate may be considered as an anticoagulant during hemodialysis, and it has a shorter half-life and a lower risk of hemorrhagic complications than unfractionated heparin (Grade C, LOE Low).
Chapter 4. Subarachnoid hemorrhage
Prevention of aneurysm rupture
To prevent the onset of subarachnoid hemorrhage, smoking cessation, blood pressure control, and alcohol savings or avoidance is recommended (Grade A, LOE Moderate).
Initial managements
In aneurysmal subarachnoid hemorrhage, rapid and appropriate diagnosis and treatment by specialists are recommended since delayed diagnosis leads to poor outcome (Grade A, LOE Low).
When noncontrast head CT cannot detect subarachnoid hemorrhage, MR imaging or lumbar puncture is reasonable (Grade B, LOE Moderate).
When the diagnosis of aneurysmal subarachnoid hemorrhage is made, it is reasonable to keep the patient at rest and avoid invasive tests or procedures immediately after onset to avoid rebleeding (Grade B, LOE Moderate).
It is reasonable to provide adequate pain relief and sedation to prevent rebleeding (Grade B, LOE Low). In mild- or moderate-grade cases, it is reasonable to lower the systolic blood pressure to <160 mm Hg (Grade B, LOE High).
In poor-grade cases, the maintenance of cerebral circulation is important, and it is reasonable to administer hyperosmotic diuretics and manage systemic circulation paying attention to cardiopulmonary complications (Grade B, LOE Low).
When no vascular abnormality is found on admission examination, it is reasonable to repeat the examination later with a certain interval (Grade B, LOE Low).
Treatments of ruptured aneurysms
Microsurgical repair with open surgery or endovascular treatment should be performed to prevent rebleeding from the ruptured aneurysms (Grade A, LOE Low).
It is reasonable to decide whether to treat the cerebral aneurysm with open surgery or endovascular treatment based on the overall findings of the patient and the cerebral aneurysm (Grade B, LOE Moderate).
It is reasonable to perform open surgery or endovascular treatment to prevent rebleeding within 72 h after the onset in World Federation of Neurosurgical Societies (WFNS) Grade I to III patients without any limitations of age, systemic complications, or difficulty of treatment (Grade B, LOE Moderate).
In patients with WFNS Grade IV, the adequacy of open surgery or endovascular treatment may be determined, considering the patient’s age and the location of the aneurysm (Grade C, LOE Low).
In patients with WFNS Grade V, open surgery or endovascular treatment may be considered when their neurological conditions improve after admission (Grade C, LOE Low).
Open surgery for ruptured aneurysms
Timing of open surgery
It is reasonable to perform open surgery within 72 h after the onset of subarachnoid hemorrhage (Grade B, LOE Moderate).
If the patient is admitted after 72 h of onset, open surgery may be performed after the delayed vasospasm period has passed (Grade C, LOE Low).
Procedures of open surgery
For microsurgical repair of aneurysms, neck clipping is recommended using specialized clips (Grade A, LOE Low).
In patients with unclippable aneurysms, it may be reasonable to perform aneurysm trapping or proximal parent artery occlusion with surgical revascularization as necessary (Grade C, LOE Low).
If any of the above treatments are not feasible to achieve, it is reasonable to perform aneurysm coating or wrapping to reinforce the aneurysm wall (Grade B, LOE Low).
Perioperative managements of open surgery
Induced hypotension during open surgery may reduce the risk of aneurysm rupture, but the effect of excessive hypotension is not well established (Grade C, LOE Low).
It is reasonable to avoid hyponatremia during perioperative period in acute phase of aneurysmal subarachnoid hemorrhage (Grade B, LOE Low). It may be reasonable to maintain circulating blood volume and serum protein concentration within the normal ranges (Grade C, LOE Low).
Endovascular treatment for ruptured aneurysms
Timing of endovascular treatment
It is reasonable to perform endovascular treatment as early as possible after the onset of subarachnoid hemorrhage (Grade B, LOE Moderate).
Procedures of endovascular treatment
It is reasonable to perform coil embolization when suitable based on the location, shape, and size of the aneurysm (Grade B, LOE Moderate).
It is reasonable to obtain highest possible obliteration rate using appropriate assisting measures (Grade B, LOE Moderate).
Perioperative managements of endovascular treatments
When ischemic complications are suspected after endovascular treatment is completed, it may be reasonable to promptly search for the cause and treat it (Grade C, LOE Moderate).
In chronic stage, it is reasonable to follow up for a long period by paying attention to the density of coil mass, the recanalization of aneurysms or obliterated arteries, and the regrowth of aneurysms (Grade B, LOE Moderate).
Conservative treatments
If surgical or endovascular treatment is not performed, it is recommended to prevent rebleeding with conservative treatment as much as possible (Grade A, LOE Low).
Prevention of vasospasm-induced delayed cerebral ischemia, managements of cardiopulmonary function and nutrition, and prevention of infection are recommended (Grade A, LOE Low).
In chronic stage, it is recommended to prevent hydrocephalus with suitable procedures (Grade A, LOE Low).
Treatment for delayed cerebral vasospasm
It is reasonable to remove subarachnoid clots with a cisternal drainage after open surgery (Grade B, LOE Moderate). Lumbar drainage or external ventricular drainage may be reasonable after endovascular treatment (Grade C, LOE Low).
Intravenous administration of fasudil or ozagrel sodium is reasonable to prevent delayed cerebral vasospasm (Grade B, LOE Low).
Triple H (hypervolemia, hemodilution, and hypertension) therapy may be considered to improve impaired cerebral hemodynamics (Grade C, LOE Low). Alternatively, hyperdynamic therapy may be considered to maintain normal circulating blood volume and enhance cardiac function (Grade C, LOE Low).
Endovascular treatments such as selective intra-arterial administration of vasodilators or percutaneous transluminal angioplasty may be considered (Grade C, LOE Moderate).
Chapter 5. Asymptomatic cerebrovascular disease
Chapter 6. Other cerebrovascular diseases
Chapter 7. Rehabilitation for subacute to chronic stroke
(Refer the full article as the supplemental material)
Supplemental Material
sj-docx-1-wso-10.1177_17474930221090347 – Supplemental material for Japan Stroke Society Guideline 2021 for the Treatment of Stroke
Supplemental material, sj-docx-1-wso-10.1177_17474930221090347 for Japan Stroke Society Guideline 2021 for the Treatment of Stroke by Susumu Miyamoto, Kuniaki Ogasawara, Satoshi Kuroda, Ryo Itabashi, Kazunori Toyoda, Yoshiaki Itoh, Yasuyuki Iguchi, Yoshiaki Shiokawa, Yasushi Takagi, Toshiho Ohtsuki, Hiroyuki Kinouchi, Yasushi Okada, Jun C Takahashi, Hiroyuki Nakase and Wataru Kakuda in International Journal of Stroke
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosures
All the authors completed the declaration of their conflicts of Interest (COIs) to the office of the Japan Stroke Society. COIs for all the authors are below the maximum amount for the inauguration of committee members of guidelines in the Japanese Association of Medical Sciences COI Management Guideline.
Supplemental material
Supplemental material for this article is available online.
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.