
Abstract
Background:
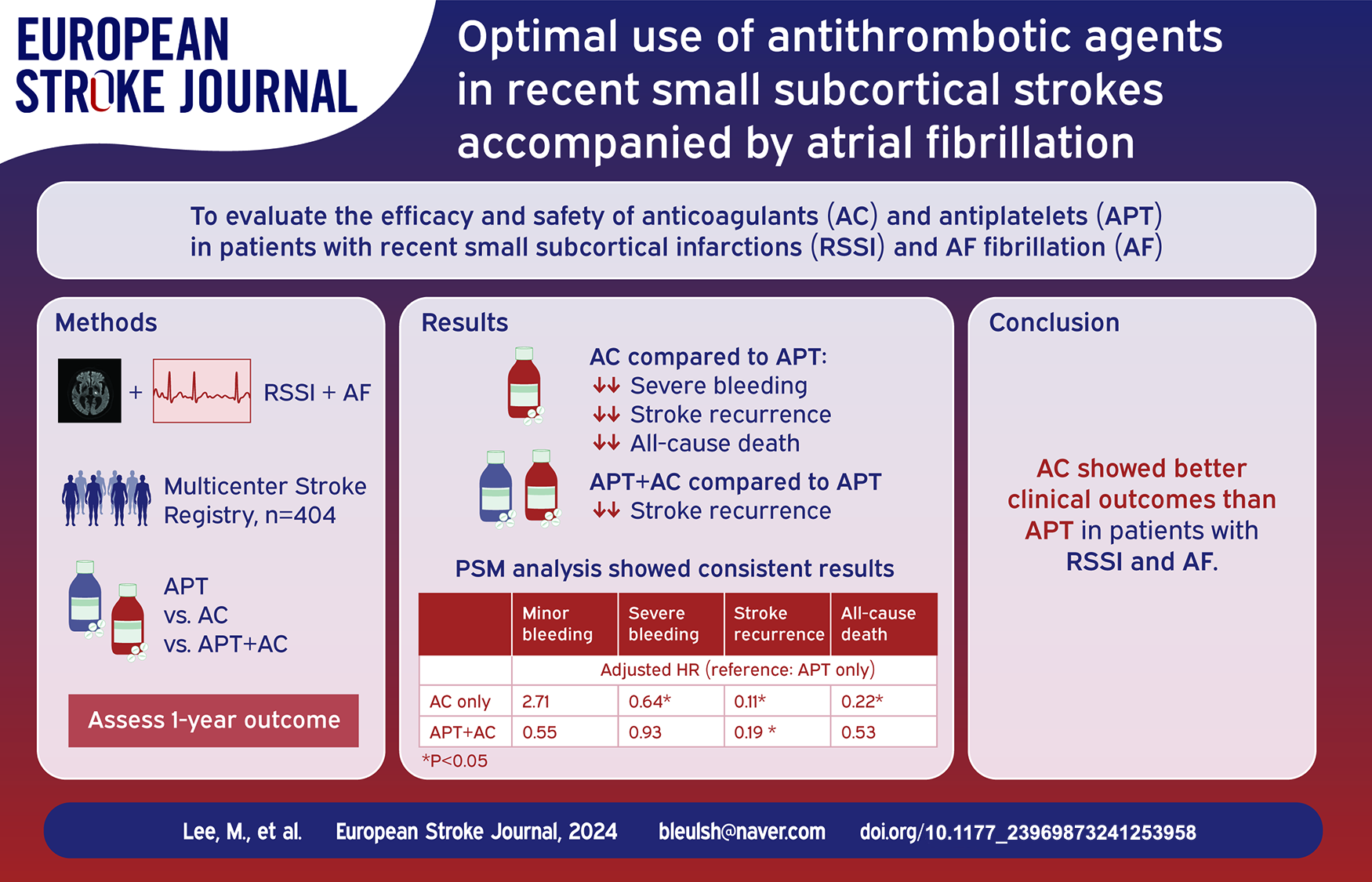
This study aimed to evaluate the efficacy and safety of anticoagulants (AC) and antiplatelets (APT) in patients with recent small subcortical infarctions (RSSI) and atrial fibrillation (AF).
Methods:
We utilized a prospective multicenter stroke registry database to identify patients with RSSI with a concurrent diagnosis of AF. Propensity score matching analysis was used to balance baseline differences among the AC-only, APT-only, and their combination groups. The main outcomes of interest were time to occurrence of minor and major bleeding, stroke recurrence, and all-cause mortality. Adjusted hazard ratios (aHRs) and 95% confidence intervals (CIs) for each outcome were calculated using the multivariable Cox proportional hazard regression analysis.
Results:
Of the 404 eligible patients, 28.2% received APT only, 53.0% received AC only, and 18.9% received a combination of both. Notable differences were observed between these groups in terms of the 1-year stroke recurrence (APT, 32.5%; AC, 5.6%; APT + AC, 9.2%) and all-cause mortality (APT, 21.9%; AC, 6.1%; APT + AC, 14.5%), whereas the rates of bleeding events were comparable. The multivariable analysis indicated a significant association of AC alone with reduced risks of severe bleeding, stroke recurrence, and all-cause mortality compared with APT alone (aHR 0.64, 95% CI 0.41–0.98; aHR 0.11, 95% CI 0.06–0.22; aHR 0.22, 95% CI 0.11–0.44, respectively). The combination group showed a reduced risk of stroke recurrence compared to APT alone (aHR 0.19, 95% CI 0.08–0.46). These findings remained consistent with the propensity score-matched analysis.
Conclusion:
AC showed better clinical outcomes than APT in patients with RSSI and AF. Additionally, combination therapy with AC and APT was associated with a lower risk of stroke recurrence than APT alone.
Introduction
Atrial fibrillation (AF)-related ischemic stroke is associated with a higher risk of stroke recurrence, disability, and mortality, compared to ischemic strokes from other etiologies. 1 Oral anticoagulants (AC) have been found to benefit patients with AF-related stroke by preventing recurrent ischemic stroke and systemic embolism. 2 Therefore, current guidelines recommend the use of oral AC over antiplatelet agents (APT) to prevent recurrent stroke in these patients. 3 However, it is important to highlight that ischemic strokes in AF patients can be non-cardioembolic, and few studies have suggested that oral anticoagulants may not be as helpful in preventing non-cardioembolic strokes. It is important to note that not all ischemic strokes in AF patients are of cardioembolic origin.4–7
Recent small subcortical infarcts (RSSI), previously known as lacunar stroke, account for approximately 25% of all ischemic strokes. 8 The majority of RSSI cases are attributed to cerebral small vessel disease (SVD), while up to 15% are accompanied by AF. 9 The current guidelines universally recommend oral AC for patients with AF who have a CHA2DS2-VASc score of 2 or higher. This scoring system automatically allocates two points for a history of stroke or transient ischemic attack, which applies to all stroke survivors, irrespective of the stroke’s etiology.10,11 Therefore, for secondary prevention, AC are recommended over APT for patients with any etiology of previous stroke who either have existing AF or develop it subsequently. This is significant because oral AC may not be as effective and may increase the risk of intracranial hemorrhage in patients with RSSI.12,13 In real-world practice, antithrombotic selection in these patients often deviates from the guidelines. This presents a clinical conundrum: patients qualify for AC therapy based on their AF and stroke histories; however, the pathology of small-vessel occlusion may necessitate a different treatment approach.
Therefore, this study aimed to compare the efficacy and safety of AC, APT, and their combination in patients with RSSI and AF. This study utilized data from a prospective multicenter stroke registry to determine the optimal antithrombotic strategy for this unique patient group.
Methods
Study population
Data were collected from the stroke registry databases of three university-affiliated hospitals – Hallym University Sacred Heart Hospital, Dongtan Sacred Heart Hospital, and Chuncheon Sacred Heart Hospital – between March 2013 and April 2022. The stroke registry used in this study was a component of the Clinical Research Collaboration for Stroke in Korea (CRCS-K) Registry.14,15 This registry is a nationwide multicenter prospective stroke database known for its comprehensive query capabilities and robust outcome adjudication system. This study focused on patients diagnosed with AF either before or after their index stroke. These strokes were specifically classified as RSSI according to the Standards for Reporting Vascular Changes on Neuroimaging-2 (STRIVE-2) criteria. 16 This definition presents neuroimaging evidence of a recent infarction that occurred within the territory of a penetrating artery, accompanied by characteristic imaging features and corresponding clinical symptoms. In this study, a maximal axial lesion diameter cutoff of 20 mm was applied; singular lesions exceeding 20 mm in size or any multiple lesions were not considered as RSSI. Two expert vascular neurologists (M. Lee and S.H. Lee) determined RSSI using diffusion-weighted imaging, achieving an excellent intraclass correlation coefficient of 0.932 (p < 0.001). Neuroimaging examples of RSSI are demonstrated in the Supplemental Figure 1. The study excluded patients who had a modified Rankin Scale score of 2 or higher before their stroke.
Data collection and variable definitions
Demographic, clinical, and laboratory data, as well as patient outcomes, were extracted from the participating hospitals’ web-based registry databases. The types of antithrombotic medication administered at discharge, including APT and AC, were documented. Patients were categorized into three groups based on their discharge medications. This study investigated the use of APT-only (single or dual antiplatelet agents), AC-only (novel oral anticoagulants or warfarin), and a combination of APT and AC in patients with AF. A history of AF was confirmed through patient and relative interviews and through a review of medical records, including post-hospitalization electrocardiography results.
Outcome measurement
Stroke coordinators and nurses at each center followed a multicenter institutional protocol to prospectively gather patient outcome data. This included collecting modified Rankin Scale scores, incidences of death, minor and major bleeding, and other vascular events, which were monitored at 3 months and 1-year post-stroke through telephone interviews and comprehensive electronic medical record reviews. The primary outcome measure was stroke recurrence (ischemic or hemorrhagic). Secondary outcomes assessed in this study included major bleeding, minor bleeding, and all-cause mortality. Major bleeding was defined as fatal bleeding, symptomatic bleeding in critical areas or organs (such as intracranial bleeding), bleeding causing a drop in hemoglobin levels of 2 mg/dL or more, or requiring a transfusion of two or more units of blood or red cells. Minor bleeding events were classified as clinically overt bleeds that did not meet the criteria for major bleeding. 17 The patients were monitored for 1 year following the index stroke.
Statistical analysis
To compare the demographic and clinical characteristics across the three antithrombotic groups (APT only, AC only, and the combination of APT + AC), Pearson’s chi-square test was utilized for categorical variables, while continuous variables were analyzed using either ANOVA or the Kruskal–Wallis test.
To evaluate the primary and secondary outcomes in the AC and APT + AC groups, we conducted a Cox proportional hazard regression analysis using the APT group as a reference. This analysis was adjusted for clinically plausible covariates or those with univariate p-values < 0.10. Both crude and adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. We used the Kaplan–Meier method to estimate event rates across the antithrombotic groups. Then the log-rank test was applied to determine the statistical significance of the rates between the groups.
We conducted a sensitivity analysis using propensity score matching (PSM) to create three cohorts derived from the total cohort: PSM cohort 1 (APT vs AC), PSM cohort 2 (APT vs APT + AC), and PSM cohort 3 (AC vs APT + AC). The propensity score for each patient using logistic regression was calculated. The score was based on the initial demographics, vascular risk factors, and baseline laboratory values and was defined as the probability of receiving APT, AC, or APT + AC. The cohorts were then matched in a 1:1 ratio using the nearest-neighbor method. Subsequent analysis of the two PSM cohorts involved the Cox proportional hazards regression to assess the effects of AC and APT + AC on the primary and secondary outcomes.
Statistical analyses were performed using the IBM SPSS version 21.0 (IBM Corporation, Armonk, NY, USA) and MoonBook and MatchIt software (R version 4.0.3; R Core Team 2020, R Foundation for Statistical Computing, Vienna, Austria).
Ethics approval
The local institutional review boards of all the participating centers approved the collection of clinical information for the CRCS-K registry. This study was also approved with a waiver of informed consent due to the use of anonymized data and minimal risk to the participants (IRB No. 2023-01-024).
Results
Patient demographics
Of the 9062 patients who suffered from acute ischemic stroke during the study period, 1891 (20.9%) had a documented history of AF diagnosed either before or after their index stroke. Among these patients, 404 (21.4%) were selected for this study as they exhibited accompanying symptoms, and their ischemic lesions were consistent with the RSSI according to the STRIVE-2 diagnostic criteria. All participants underwent transthoracic echocardiography and were confirmed to have non-valvular AF during their hospital stay. The distribution of patients according to treatment group was as follows: 28.2% (114/404) received APT only, 53.0% (214/404) received AC only, and 18.8% (76/404) received a combination of APT and AC. Among the 214 AC-only users, 171 (79.9%) were prescribed novel oral anticoagulants (NOACs). (Figure 1). Of 62 patients who received both APT and AC, 53 (85.5%) received NOACs.
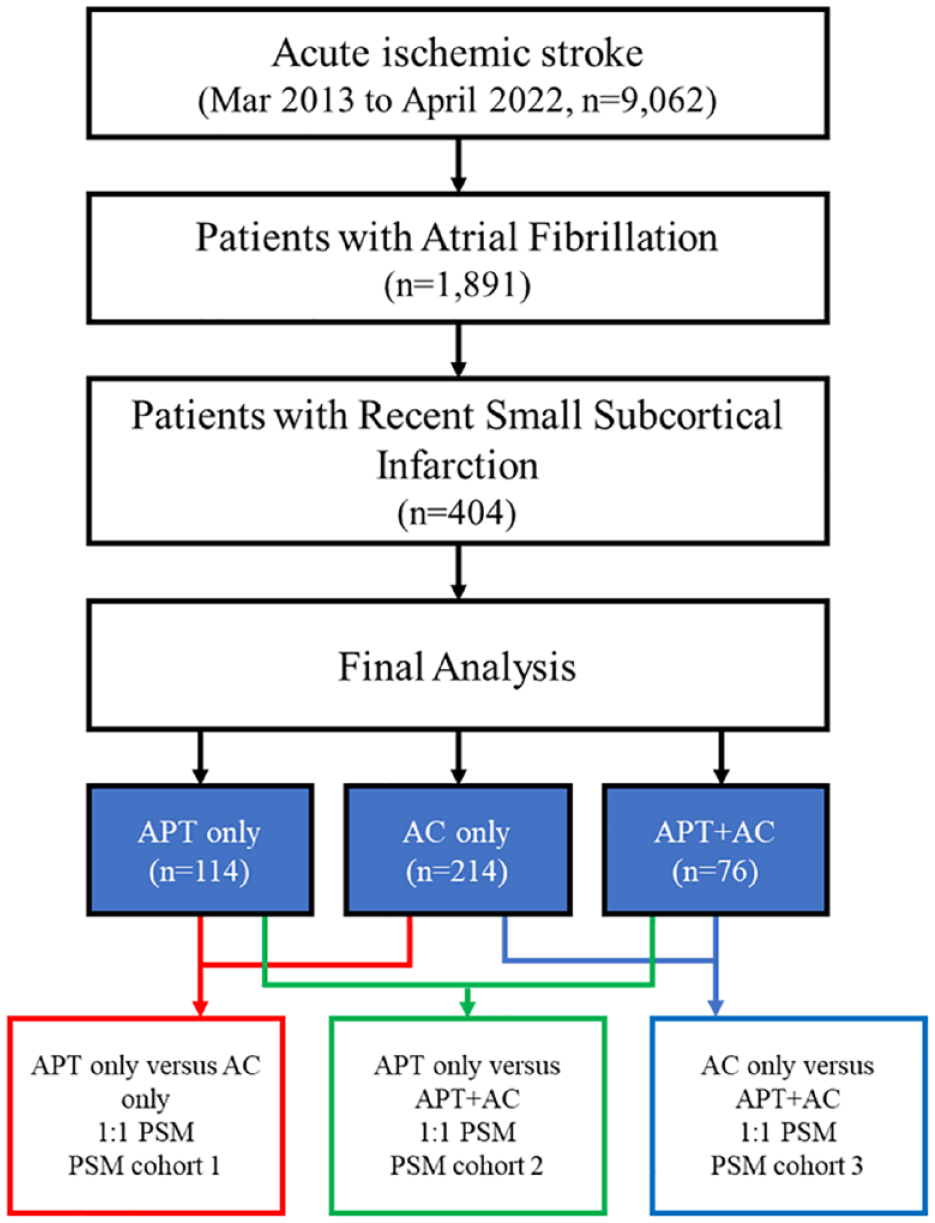
Flowchart of the study enrollment and the structure of the propensity score matching groups.
In our study population, the one-year rates for stroke recurrence and all-cause mortality were 13.9% and 12.4%, respectively. The APT + AC group had a higher prevalence of previous stroke or coronary heart disease when compared to the APT-only or AC-only groups in the univariate analysis. This group also had a greater history of antiplatelet use. However, there were no significant differences among the three groups in terms of initial stroke severity or most other clinical and laboratory parameters (Table 1). Regarding outcomes, the AC group had a significantly lower risk of stroke recurrence and all-cause mortality within one-year post-index stroke, whereas the APT-only group had the highest risk of both stroke recurrence and all-cause mortality. The cumulative incidence rates of minor and major bleeding did not significantly vary across the groups, although there was a numerical trend toward more frequent minor bleeding incidents in the AC-only group (Figure 2).
Baseline characteristics and outcome events between antiplatelet only, anticoagulant only, and combination of antiplatelet and anticoagulant among patients with AF related ischemic stroke.
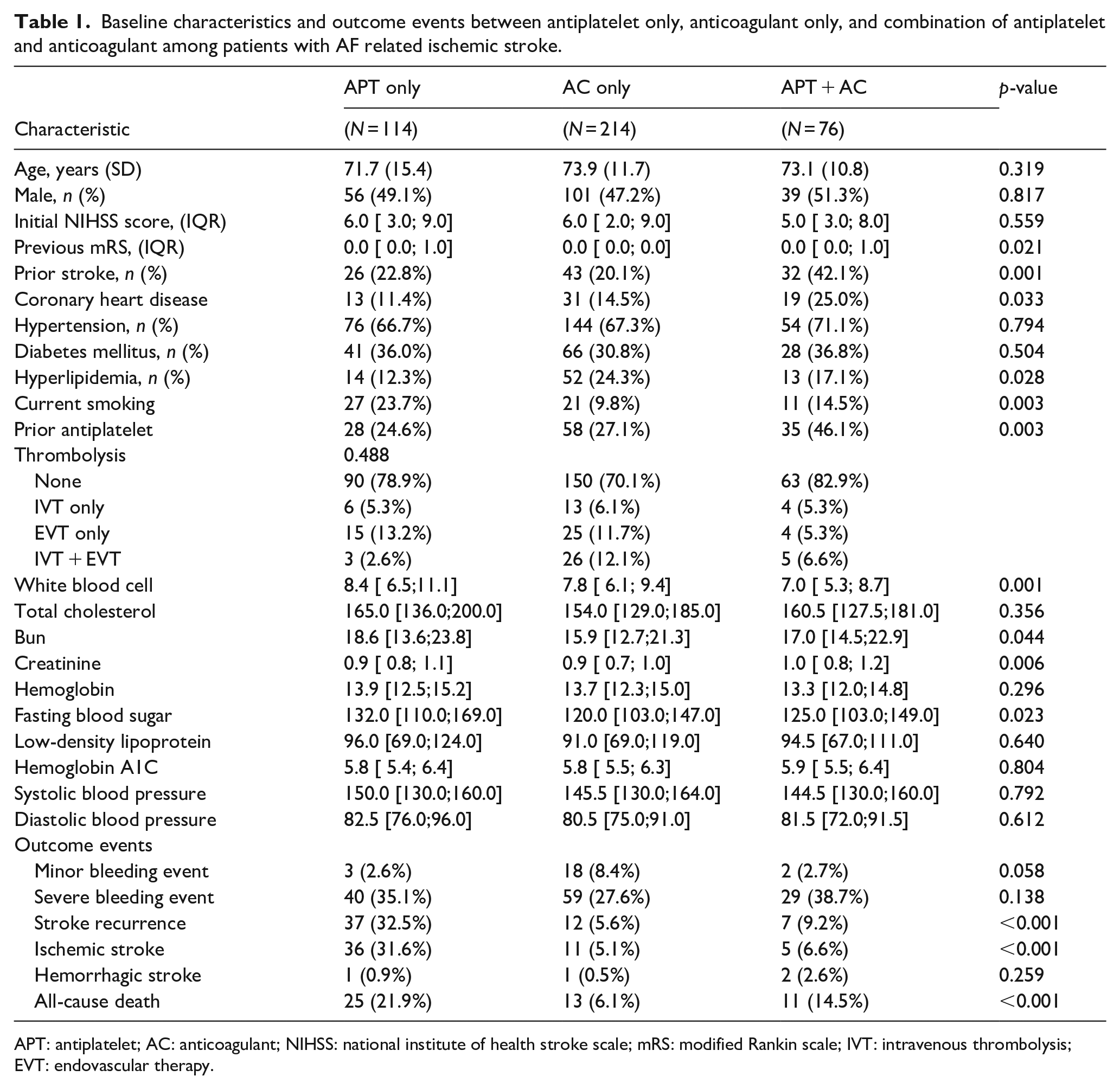
APT: antiplatelet; AC: anticoagulant; NIHSS: national institute of health stroke scale; mRS: modified Rankin scale; IVT: intravenous thrombolysis; EVT: endovascular therapy.
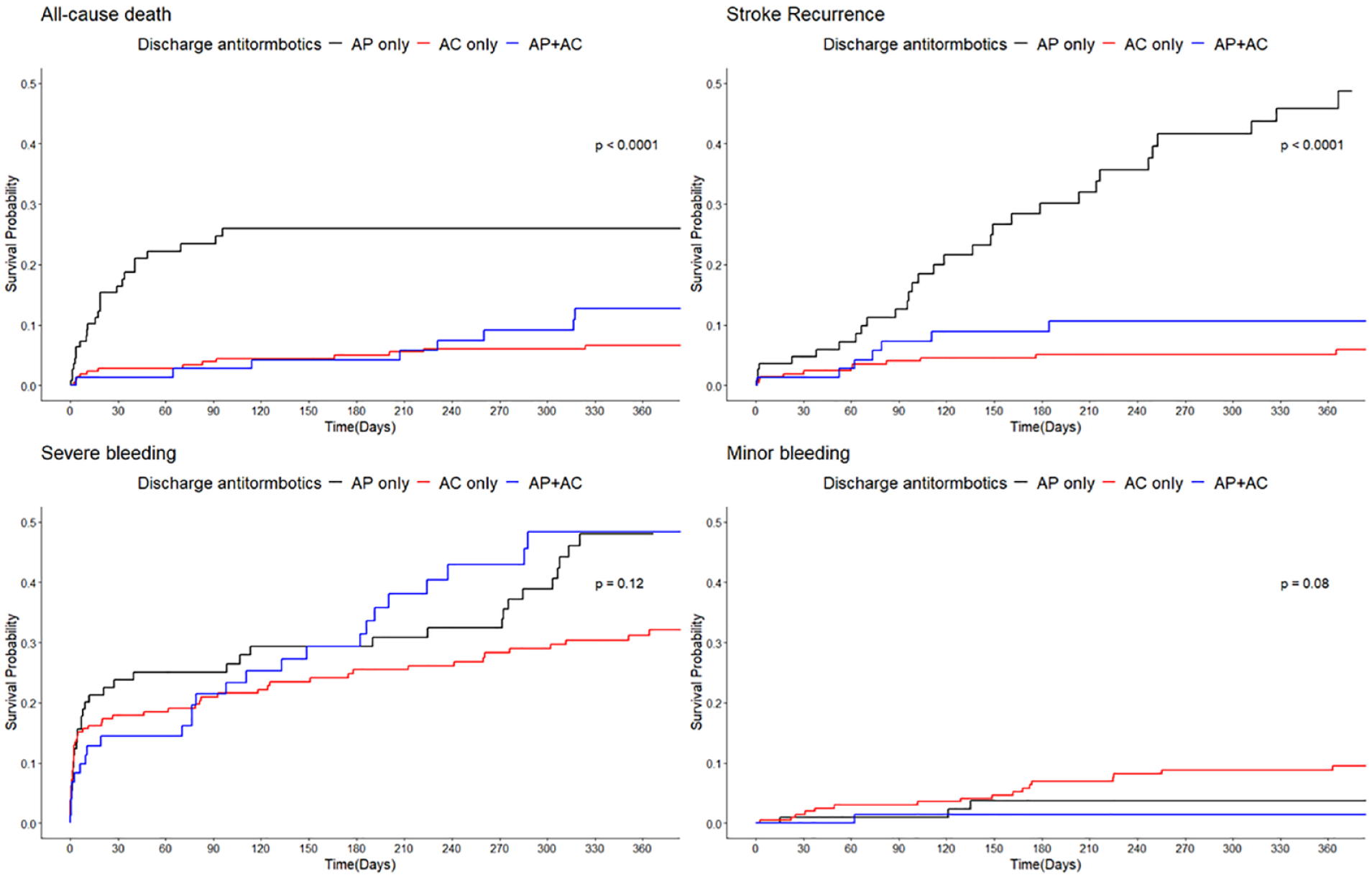
Kaplan–Meier curves for each outcome variable in the APT-only, AC-only, and APT + AC groups within the total cohort. p-values were derived from the log-rank test. APT: antiplatelet; AC: anticoagulant.
The multivariable analysis revealed that the AC-only group had a significantly lower risk of stroke recurrence in patients with AF who experienced RSSI than the APT-only group. This was supported by an adjusted hazard ratio (aHR) of 0.19 and a 95% confidence interval ranging from 0.08 to 0.46. Furthermore, the APT + AC group was also associated with a reduced risk of stroke recurrence compared to the APT-only group, with an aHR of 0.11 and a 95% CI of 0.06−0.22. Regarding secondary outcomes, the AC-only group was significantly associated with a reduced risk of severe bleeding and all-cause mortality; however, there was no significant reduction in the risk of minor bleeding. In contrast, the APT + AC group did not show a significant association with reduced risk of these secondary outcomes (Table 2).
Multivariable cox proportional-hazard regression analysis showing impact of antithrombotic on stroke outcomes using total cohort.
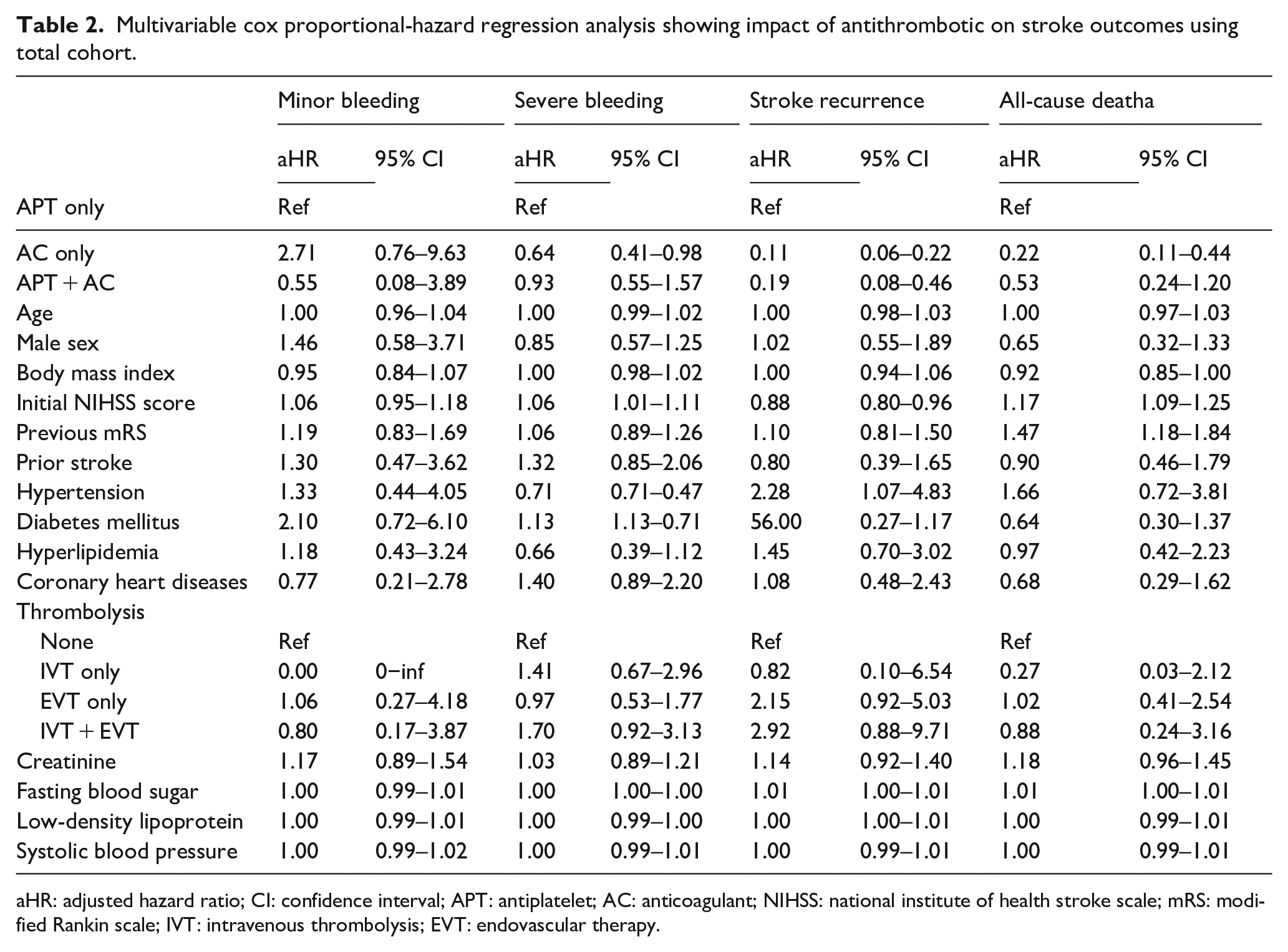
aHR: adjusted hazard ratio; CI: confidence interval; APT: antiplatelet; AC: anticoagulant; NIHSS: national institute of health stroke scale; mRS: modified Rankin scale; IVT: intravenous thrombolysis; EVT: endovascular therapy.
Sensitivity analysis, which utilized PSM cohorts, assessed the effectiveness of the AC-only and APT + AC groups in terms of primary and secondary outcomes, comparing them to the APT-only group. Additionally, we compared the effectiveness of the AC-only and APT + AC groups. The demographic and clinical characteristics of each PSM cohort are presented in Supplemental Table 1. Regarding primary outcomes, the group treated only with AC showed a significantly lower risk of stroke recurrence, all-cause mortality, and severe bleeding in the PSM cohort than in the group treated only with APT. These findings are consistent with those of the primary analysis (Table 3 and Supplemental Tables 2–4). Similarly, the APT + AC group was associated with a lower risk of stroke recurrence; however, no significant differences were observed in the other outcomes, which is consistent with the results of the primary analysis. In the PSM 3 cohort, the APT + AC group showed a lower risk of minor bleeding compared to the AC-only group.
Multivariable analysis showing the impact of antithrombotic regimens on stroke outcome using propensity score matching cohorts.
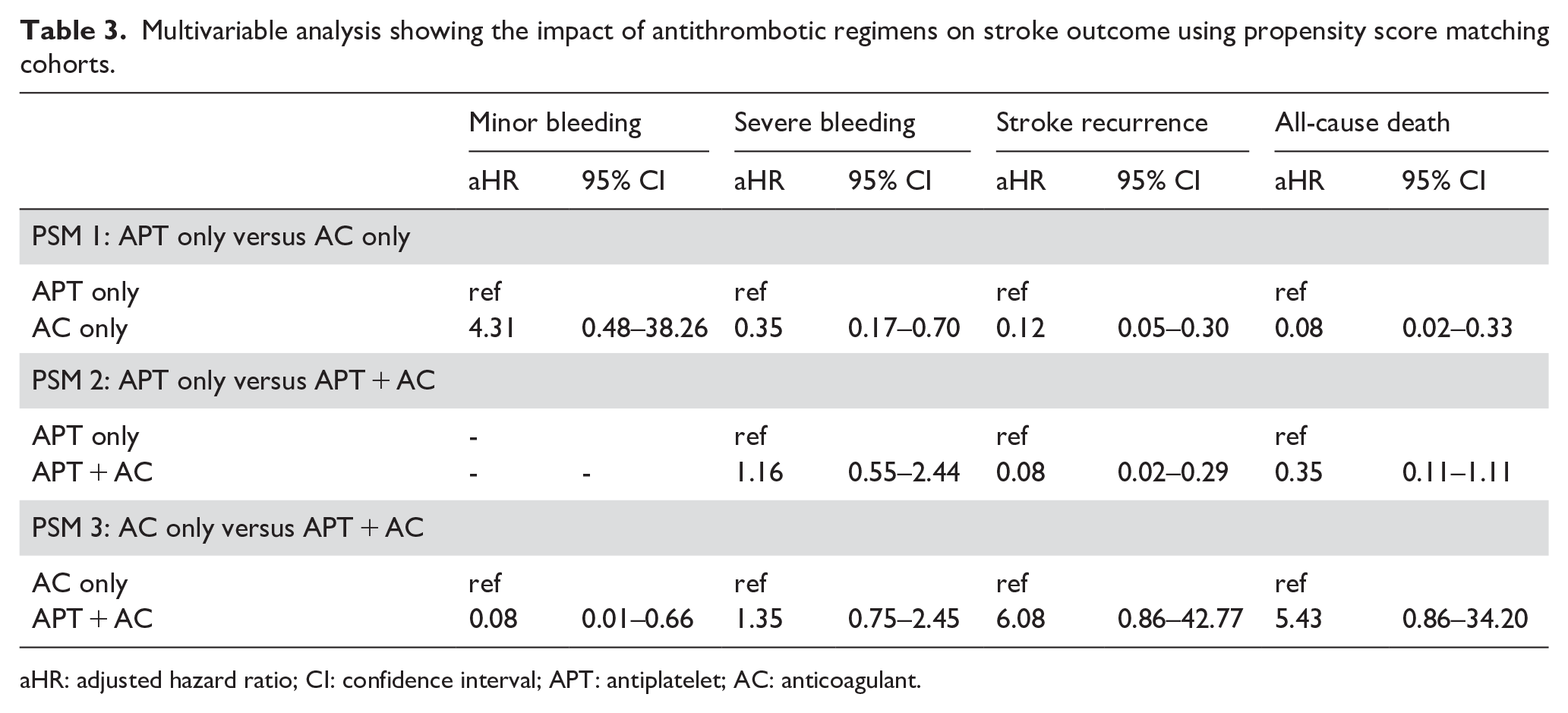
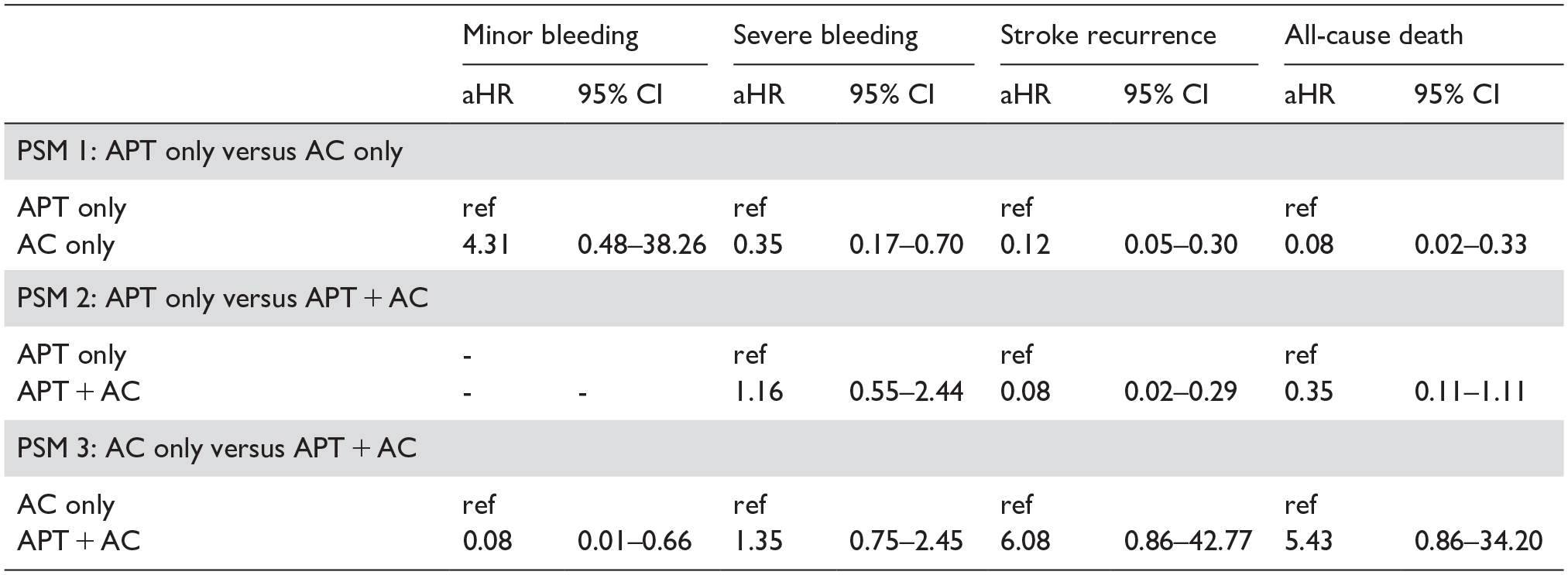
aHR: adjusted hazard ratio; CI: confidence interval; APT: antiplatelet; AC: anticoagulant.
Discussion
The main findings of this study are as follows: (1) 21.4% of stroke patients with AF had stroke lesions and symptoms consistent with RSSI; (2) the one-year stroke recurrence and all-cause mortality rates for the RSSI with AF population were 13.9% and 12.4%, respectively; (3) the use of AC demonstrated a lower incidence of stroke recurrence, major bleeding, and all-cause mortality compared to APT in patients with RSSI and AF; (4) the combination of AC + APT was more effective than APT alone in preventing stroke recurrence. These findings align with the current guidelines that recommend anticoagulation for secondary prevention in stroke patients with AF, regardless of the specific cause of the initial stroke. This highlights the importance of adhering to these guidelines and challenging the occasional clinical inclination toward APT in RSSI cases with AF.
Our study found that 21.4% of the patients with AF-related stroke had an RSSI pattern, which is notably higher than the 8.7% reported in a previous Korean study conducted between 2008 and 2012. 18 This difference may be due to various factors including demographic changes and evolving treatment practices. The aging population and widespread use of oral anticoagulants in the general atrial fibrillation patient cohort over recent decades may contribute to the higher incidence of lacunar strokes than embolic strokes in patients with AF. Although this is a speculative interpretation, it highlights the dynamic nature of stroke patterns in relation to evolving patient demographics and treatment modalities.
In our study, the one-year stroke recurrence rate was higher than that of the small-vessel occlusion group (10.02%) but lower than that of the cardioembolic stroke group (14.78%), according to comparisons with statistics from the Korean Stroke Registry, which includes similar academic hospital-affiliated institutions from 2011 to 2019. Conversely, the one-year all-cause mortality rate was significantly higher than that of the small vessel occlusion group (1.97%) but lower than that of the cardioembolic stroke group (18.82%). This highlights the importance of the population with RSSI and AF, as they demonstrate vascular outcomes more similar to those seen in AF-related stroke rather than in SVD.
Recent research has suggested that patients with AF-related stroke who initially present with lacunar stroke are more likely to experience recurrent strokes with a lacunar pattern than those who initially present with cardioembolic stroke. This trend appears to be consistent regardless of the antithrombotic strategy employed.19–21 These findings suggest that some patients with RSSI are more likely to develop pathologies related to small vessel occlusion, even in the presence of AF. In addition, a previous study indicated that long-term anticoagulation therapy may not necessarily decrease the risk of stroke recurrence in patients with lacunar stroke and AF. 19 Meanwhile, the use of AC in patients with RSSI and other small-vessel pathologies, including chronic microbleeds, may increase the risk of major bleeding. This increased bleeding risk, as highlighted in studies,12,13 can lead to a degree of reluctance among physicians when considering anticoagulant therapy for patients with both RSSI and AF. However, our study showed that AC is both safe and effective compared to APT alone, even after adjusting for covariates through both multivariable and PSM analyses. This finding is significant since it suggests that despite the potential risks associated with AC in patients with RSSI and small-vessel pathologies, the benefits of AC in reducing stroke recurrence and all-cause mortality outweigh these risks. Furthermore, the introduction of NOACs may have reduced the risk of intracranial bleeding compared to that in warfarin, which was predominantly used in earlier studies.22,23 This reinforces the beneficial effects of AC over APT observed in the present study. 19 However, the choice of antithrombotics was at the discretion of the treating physicians, suggesting that patients receiving APT rather than AC may have been deemed at higher risk of bleeding. Although there were no significant differences in demographics, initial stroke severity, prior use of AC or APT, initial hemoglobin levels, systolic blood pressure, and other known bleeding risk factors between the AC and APT groups, it is important to note that unmeasured confounders such as previous history of gastrointestinal bleeding, or neuroimaging features like chronic microbleeds or superficial siderosis were not fully accounted for. Despite using PSM analysis to reduce potential biases, unmeasured confounders still exist, which necessitates further studies.
Our study also found that patients who received a combination of APT and AC had better mortality outcomes than those who received APT alone. The rationale for prescribing both APT and AC could be linked to the patient’s previous medical history, such as a previous diagnosis of myocardial infarction, insertion of coronary or carotid stents, or cases where an initial antithrombotic regimen failed to prevent the first stroke. This observation was particularly noteworthy in this high-risk patient group. These data suggest that the combination of AC and APT is associated with a lower risk of mortality and presents a comparable risk of stroke recurrence or bleeding to that of the APT-only group.
This study provides valuable insights; however, it is important to acknowledge its limitations. First, as an observational study, it was subjected to inherent biases and the potential for unmeasured confounding factors. These limitations should be considered when applying the findings to a broader patient population. Second, the choice of antithrombotic therapy was at the discretion of the treating clinicians, leading to an unavoidable selection bias. Although antithrombotic selection often correlates with the initial severity of stroke, our study groups exhibited similar initial stroke severities. To mitigate this bias, we incorporated PSM into our secondary analyses. Finally, distinguishing whether the RSSI was due to small-vessel occlusion or cardioembolism was challenging, which might lead to misclassification bias.
In conclusion, our study provides evidence supporting the use of AC in patients with RSSI and AF, which is consistent with current stroke and AF management guidelines. This emphasizes the importance of following guideline-recommended AC therapy, regardless of the etiology of the index stroke, which appears to offer significant benefits in reducing stroke recurrence and mortality. Further research is required to explore the nuances of antithrombotic therapy in diverse patient populations and clinical scenarios, particularly in the context of RSSI and AF.
Supplemental Material
sj-docx-1-eso-10.1177_23969873241253958 – Supplemental material for Optimal use of antithrombotic agents in recent small subcortical strokes accompanied by atrial fibrillation
Supplemental material, sj-docx-1-eso-10.1177_23969873241253958 for Optimal use of antithrombotic agents in recent small subcortical strokes accompanied by atrial fibrillation by Minwoo Lee, Mi-Sun Oh, Kyung-Ho Yu, Chulho Kim, Jong-Hee Sohn, Hee-Jung Mo, Yerim Kim and Sang-Hwa Lee in European Stroke Journal
Supplemental Material
sj-png-2-eso-10.1177_23969873241253958 – Supplemental material for Optimal use of antithrombotic agents in recent small subcortical strokes accompanied by atrial fibrillation
Supplemental material, sj-png-2-eso-10.1177_23969873241253958 for Optimal use of antithrombotic agents in recent small subcortical strokes accompanied by atrial fibrillation by Minwoo Lee, Mi-Sun Oh, Kyung-Ho Yu, Chulho Kim, Jong-Hee Sohn, Hee-Jung Mo, Yerim Kim and Sang-Hwa Lee in European Stroke Journal
Footnotes
Acknowledgements
None
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Bio&Medical Technology Development Program of the National Research Foundation (NRF) funded by the Korean government (MSIT) (No. RS-2023-00223501) and by a grant from the Korea Health Technology R&D project of the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (HR21C0198).
Ethical approval
This study was approved by the institutional review board of Chunceon Sacred Heart Hospital (IRB number: 2023-01-024).
Informed consent
This study was approved with a waiver of informed consent due to the use of anonymized data and minimal risk to the participants.
Trial registration
Not applicable
Guarantor
SH Lee
Contributorship
M Lee and SH Lee were involved in conception, design and conduct of the study and the analysis and interpretation of the results. M Lee wrote the first draft of manuscript, MS Oh, KH Yu, C Kim, JH Sohn, HJ Mo, Y Kim revised manuscript. All authors edited, reviewed, and approved the final version of the manuscript. SH Lee are the guarantors of this work and as such had full access to all data in the study and takes responsibility for the integrity of data and the accuracy of the data analysis.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.