SCIENTIFIC COMMUNICATION – ATHEROSCLEROSIS & STROKE
Abstract N°: 486
ASSOCIATIONS BETWEEN PLAQUE MORPHOLOGY AND STROKE MECHANISMS IN SYMPTOMATIC INTRACRANIAL ATHEROSCLEROTIC DISEASE
Xuan Tian*1, Yu Liu1, Shuang LI1, Yuying Liu1, Jill Abrigo2, Bonaventure Ym Ip1, Sze Ho MA1, Wt Lui1, Thomas Leung1, Xinyi Leng1
1The Chinese University of Hong Kong, Department of Medicine and Therapeutics, Hong Kong, China, 2The Chinese University of Hong Kong, Department of Imaging and Interventional Radiology, Hong Kong, China
On behalf of:
Background and aims: Intracranial atherosclerotic stenosis (ICAS) could cause an ischemic stroke via various mechanisms. We aimed to explore the associations between plaque morphology and stroke mechanisms in symptomatic ICAS.
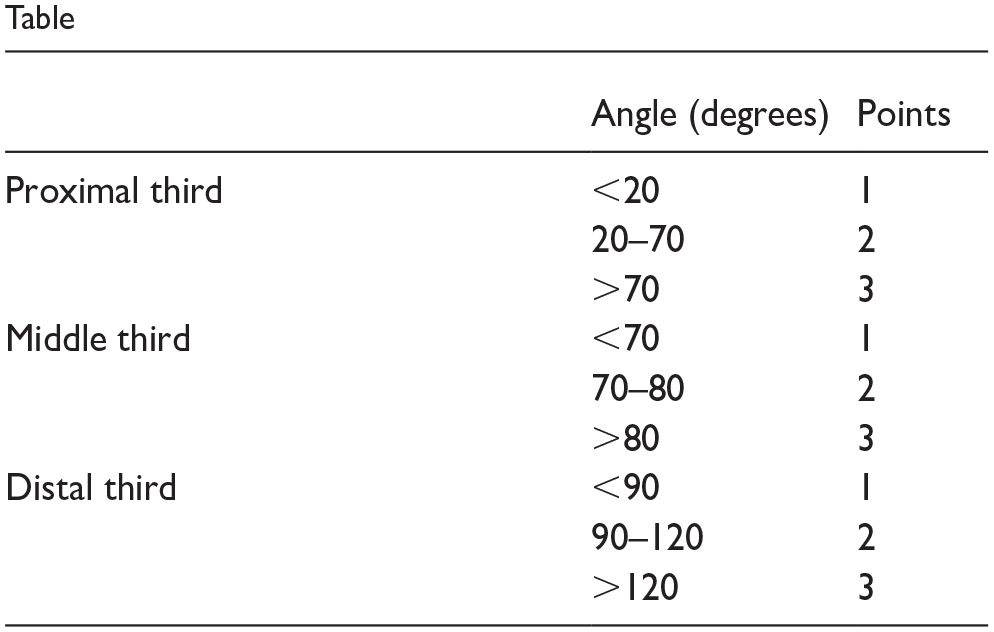
Methods: We prospectively enrolled patients with acute ischemic stroke due to high-grade ICAS (60%-99%) in anterior circulation identified in three-dimensional rotational angiography (3DRA). The probable stroke mechanisms were classified into parent artery atherosclerosis occluding penetrating artery (PAO), artery-to-artery embolism (AAE), hypoperfusion and mixed mechanisms. Plaque morphology was assessed in 3DRA, including luminal stenosis, plaque thickness/length, upstream shoulder angulation, plaque eccentricity, surface contour, longitudinal plaque distribution and presence of adjoining branch atheromatous disease. We compared these morphological parameters among patients with different stroke mechanisms.
Results: Among 145 patients (median age 62 years, 69.7% males), 23 (15.9%), 14 (9.7%), 58 (40.0%) and 50 (34.5%) respectively had isolated PAO, AAE, hypoperfusion and mixed mechanisms of AAE and hypoperfusion. Upstream shoulder angulation >45° was associated with presence of AAE (45.3% versus 17.4%, p=0.018), while none of the plaque morphology metrics was associated with presence of hypoperfusion. In multinomial logistic regression among those with a single stroke mechanism (n=95), upstream shoulder angulation was an independent predictor of isolated AAE, as a continuous (adjusted odds ratio 1.03, 95% confidence interval 1.00-1.06, p=0.030) or categorical variable (>45° versus ⩽45°, 8.61, 1.84-40.18, p=0.006), with isolated PAO as reference.
Conclusions: ICAS lesions with a steeper upstream plaque shoulder were more likely to cause an ischemic stroke via AAE. The mechanisms could be verified in rheological studies.
Disclosures of Interest: No
Abstract N°: 810
INTRACRANIAL ATHEROSCLEROTIC PLAQUES RISK STRATIFICATION: A RADIOMICS ANALYSIS
Elena Sagues Sese*1, Sebastian Sanchez2, Sricharan Veeturi3, Diego Ojeda1, Carlos Dier Melo1, Vicent Tutino3, Edgar Samaniego1
1University of Iowa Hospitals & Clinics, Neurology, Iowa City, United States, 2Yale University, Neurology, New Haven, United States, 3University at Buffalo (South Campus), Buffalo, United States
On behalf of:
Background and aims: High resolution vessel wall imaging (HR-VWI) enables accurate visualization of intracranial atherosclerotic plaques. Radiomics can be utilized as an objective quantification method of plaque appearance and shape. We aimed to analyze the radiomics features (RFs) obtained from 7T-HR-VWI to differentiate between culprit and non-culprit plaques in patients with intracranial atherosclerotic disease (ICAD).
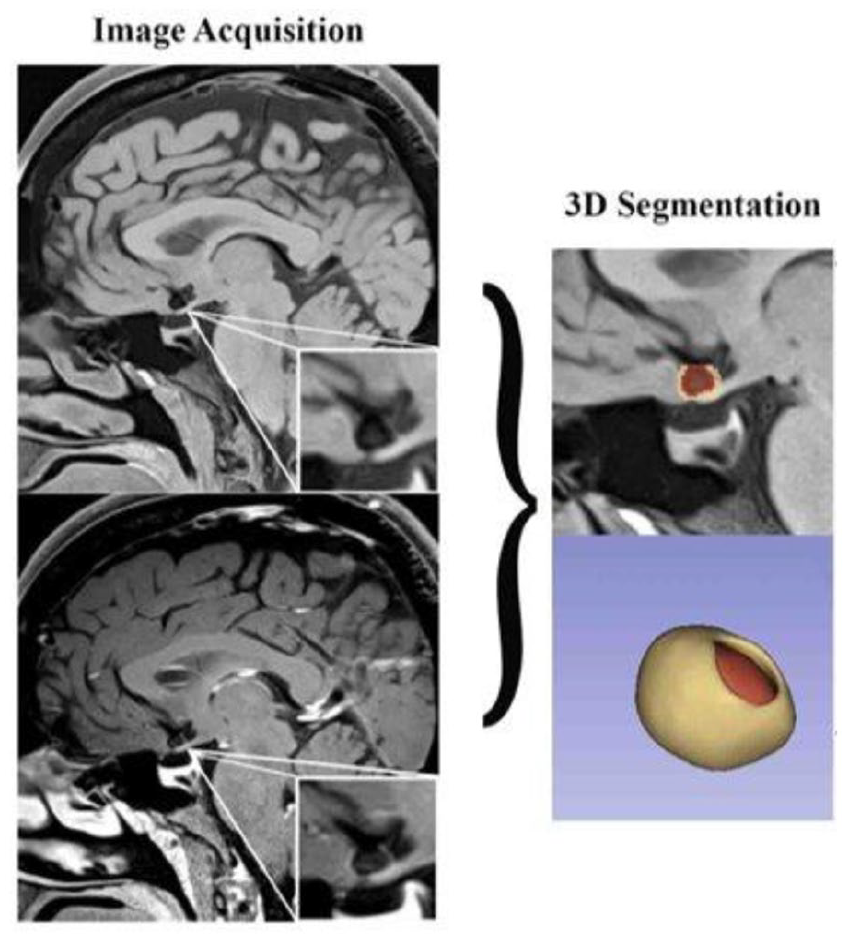
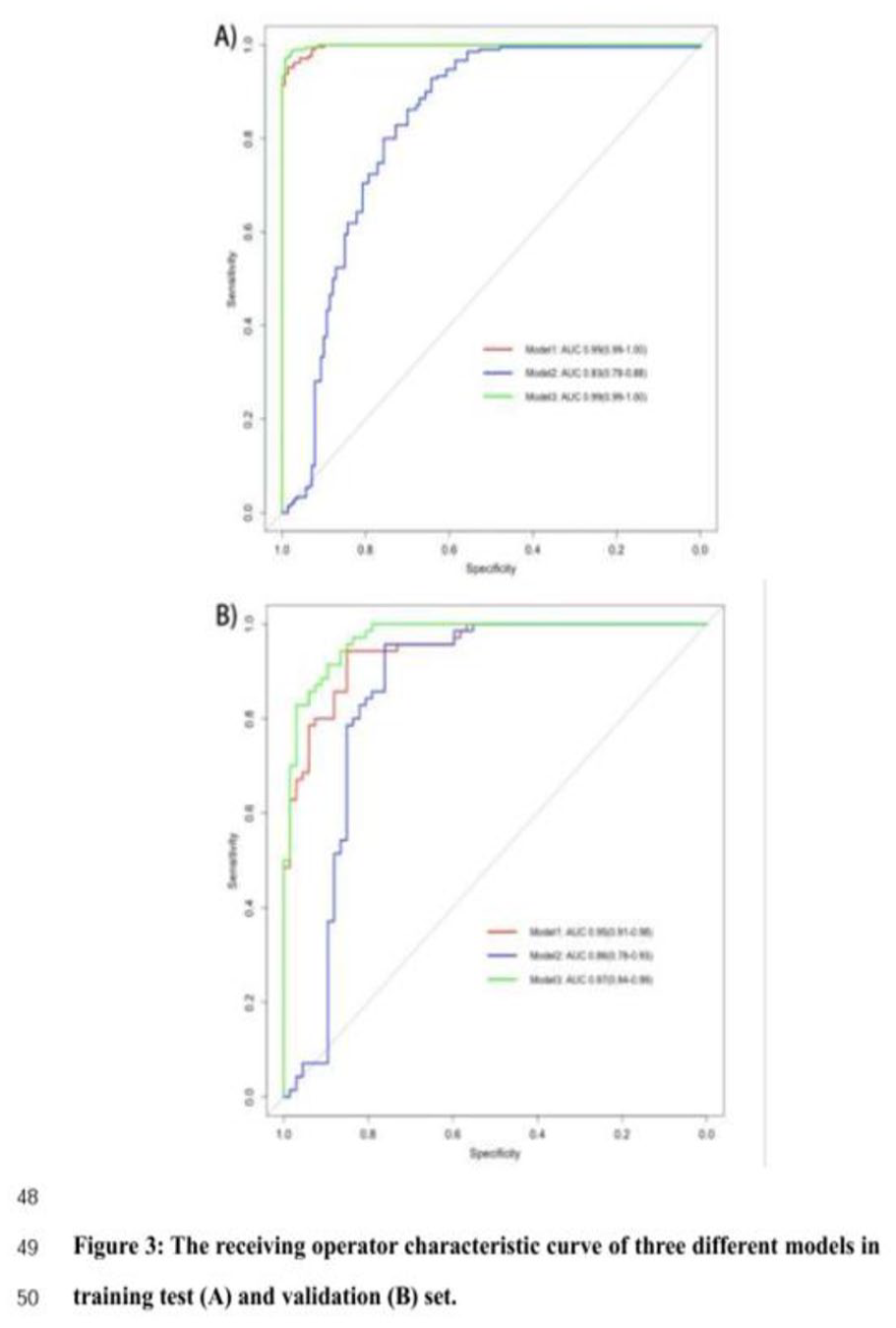
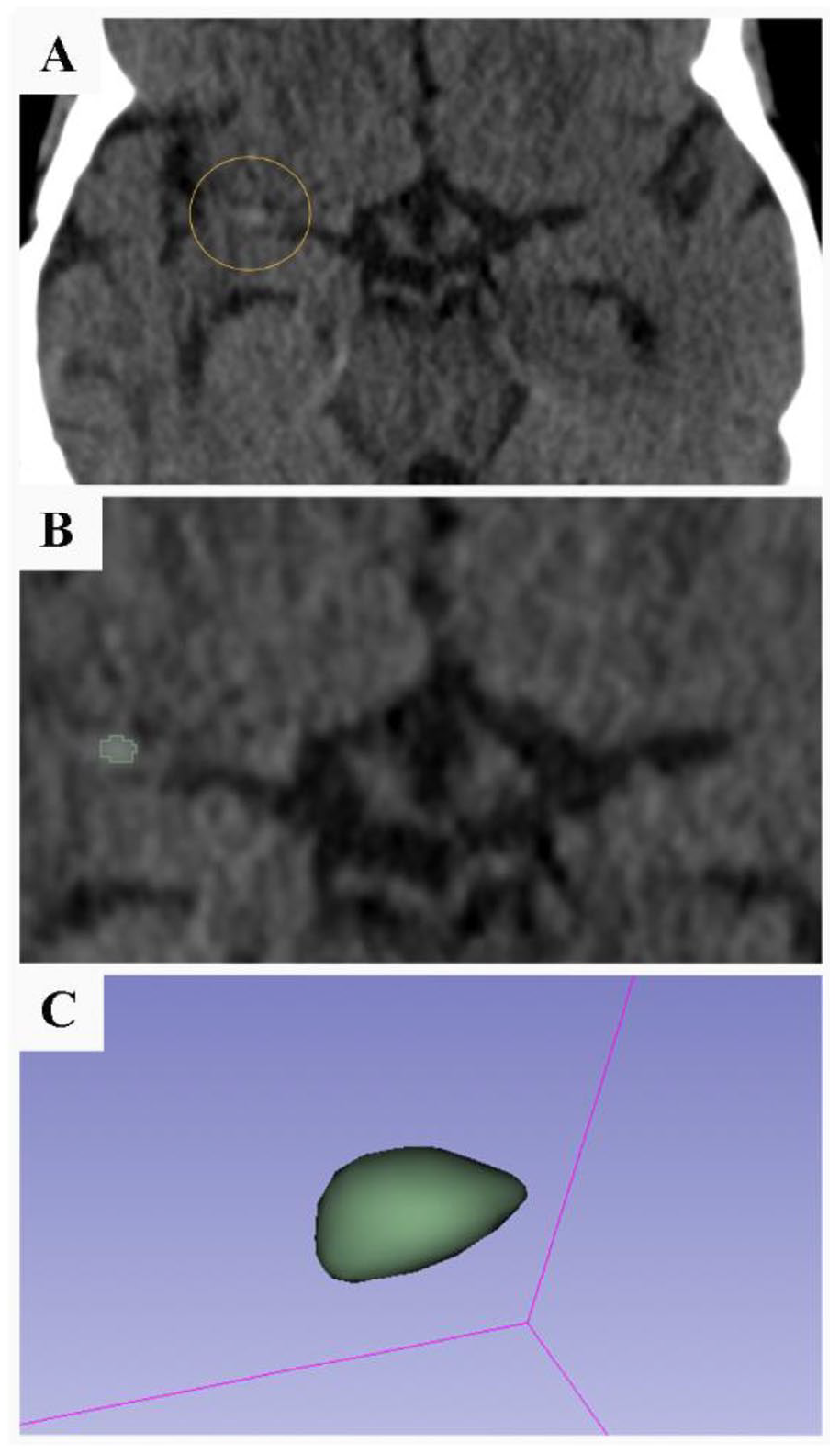
Methods: Patients with ICAD as stroke etiology undergoing HR-VWI were included in the study. Culprit plaques in the vascular territory of the stroke were identified. The degree of stenosis, area degree of stenosis and plaque burden were calculated. 3D segmentation of the plaque was performed, and RFs were extracted (Figure 1). We then evaluated multiple machine learning models to predict and identify culprit plaques (Figure 2).
Results: We included 33 patients with ICAD as the cause of stroke. Univariate analysis revealed 38 significantly different RFs between culprit and non-culprit plaques in pre-contrast MRI, 39 in post-contrast MRI and 25 RFs that were different between pre and post contrast MRIs (Figure 3). The random forest model achieved an accuracy rate of 81% (88% sensitivity and 75% specificity) in identifying culprit plaques in the independent testing dataset. This model successfully identified the culprit plaque in 7 out of 8 cases during the testing phase.
Conclusions: Radiomics is a promising tool for stratification of plaques in patients with ICAD.
A-D) Plaque visualization in 7T HR-VWI, segmentation and 3D reconstruction.
Flowchart of the data analysis.
Principal component analysis and mapping of representative RFs.
Disclosures of Interest: No
Abstract N°: 932
SYMPTOMATIC MIDDLE CEREBRAL ARTERY AND BASILAR ARTERY STENOSES: DIFFERENT PLAQUE MORPHOLOGY IN 3D ROTATIONAL ANGIOGRAPHY
Xinyi Leng*1, Bonaventure Ip1, Sze Ho MA1, Wai Ting Lui1, Florence Sy Fan1, Hing Lung Ip1, Simon Yu2, Wai Hong Thomas Leung1
1The Chinese University of Hong Kong, Department of Medicine and Therapeutics, 2The Chinese University of Hong Kong, Department of Imaging and Interventional Radiology
On behalf of:
Background and aims: The morphology of symptomatic atherosclerotic plaques may be different in the anterior and posterior circulations, which was investigated in this study.
Methods: We prospectively recruited adult patients with acute ischemic stroke or transient ischemic attack attributed to high-grade (60-99%), atherosclerotic stenosis in M1 middle cerebral artery (MCA-M1) or basilar artery (BA) as confirmed by three-dimensional rotational angiography (3DRA). We assessed the plaque morphology in 3DRA, including the percentage of luminal stenosis, non-ulcerative/ulcerative plaque surface contour, plaque thickness, length, eccentricity, upstream plaque shoulder angulation, longitudinal distribution of the maximal stenosis, and adjoining branch atheromatous disease (BAD). We compared patient characteristics and plaque morphology between those with MCA-M1 and BA plaques.
Results: Overall, 167 and 18 respectively having symptomatic MCA-M1 and BA plaques were analyzed. Age (medians 60 versus 62 years), male sex (64.6 versus 52.9%), history of common vascular risk factors and lab test results were similar between the two groups. Percentage of luminal stenosis (75 versus 81%), proportion of ulcerative plaques (13.8 versus 22.2%), upstream plaque shoulder angulation (32.1 versus 26.5 ˚), longitudinal distribution of the maximal stenosis, and presence of adjoining BAD (56.9 versus 66.7%) were similar between MCA-M1 and BA plaques. However, BA plaques were thicker (1.5 versus 1.3mm; p=0.031) and longer (16.5 versus 8.5mm; p<0.001), but less likely eccentric (66.7 versus 88.6%; p=0.010).
Conclusions: There were differences in the morphology of symptomatic atherosclerotic plaques in MCA and BA, independent of demographics and vascular risk factors. Different artery geometry and hemodynamics may underlie such differences.
Disclosures of Interest: No
Abstract N°: 1573
HIGHER INCIDENCE OF RETINAL ISCHEMIC PERIVASCULAR LESIONS IS ASSOCIATED WITH INCREASED CAROTID ARTERY STENOTIC DEGREE
Hang Wang*1, Le Cao1, William Robert Kwapong1, Yuying Yan1, Fayun Hu Fayun Hu1, Bo Wu1
1West China Hospital of Sichuan University
On behalf of:
Background and aims: Retinal ischemic perivascular lesions (RIPLs) have been reported as potential biomarkers for cardiovascular diseases and stroke. We aimed to investigate the incidence of RIPLs in carotid artery stenosis (CAS) patients and their association with neurological symptoms and stenotic degree. We also quantitatively compared the retinal microvasculature between eyes with and without RIPLs.
Methods: Patients with unilateral CAS or carotid artery occlusion confirmed by digital subtraction angiography (DSA) were recruited. Optical coherence tomography (OCT) was conducted for assessing the incidence of RIPLs and OCT angiography (OCTA) was used for evaluating microvascular density in superficial vascular complex (SVC) and deep vascular complex (DVC).
Results: Six hundred and one eyes from 336 CAS patients were included in data analysis (mean age, 62.31±10.52 years; male, 80.65%). Ipsilateral eyes had higher incidence of PRILs compared to contralateral eyes in CAS patients (39.67% vs 28.62%, OR 1.61, 95%CI [1.13-2.29], p = 0.005). CAS patients with cerebral infarction had a higher incidence of RIPLs compared to CAS patients without infarction (42.12% vs 29.39%, OR 1.75, 95%CI [1.23-2.50], p = 0.002). The incidence of RIPLs was positively associated with stenotic degree in CAS patients (p < 0.001). Eyes with RIPLs had lower SVC density (p = 0.013) compared to eyes without RIPLs.
Conclusions: RIPLs are anatomical markers of ischemia and are suggested to be associated with cerebral infarction and stenotic degree in CAS patients. OCT/OCTA is a noninvasive tool to detect retinal ischemic changes and quantitatively measure the retinal microvascular changes in CAS patients.
Disclosures of Interest:
No
Abstract N°: 1586
SOCIOECONOMIC POSITION (SEP) ACROSS THE LIFE COURSE AND VASCULAR AGEING IN MID-ADULTHOOD
1Menzies Institute for Medical Research, University of Tasmania, Hobart, Australia, 2University of Oxford, United Kingdom
On behalf of:
Background and aims: The cumulative impact of SEP across the life course on early vascular ageing, a risk factor for stroke, has not been investigated.
Methods: A cumulative SEP score was created from individual and area-level indicators in childhood (7-15 years), young (26-36 years) and middle (36-46 years) adulthood in the Australian Childhood Determinants of Adult Health study. Five trajectories were created for SEP: persistently advantaged, improving, inconsistent, declining and persistently disadvantaged. Vascular ageing outcomes included markers of arteriosclerosis (Young’s elastic modulus [YEM], carotid distensibility [CD], stiffness index [SI]) and atherosclerosis (carotid intima-media thickness (cIMT) and plaque) measured using carotid ultrasounds at middle age. Linear and log-binomial regression estimated the association between SEP and vascular ageing outcomes adjusted for demographic, lifestyle and health mediators in childhood, young and mid-adulthood.
Results: The analysis included 805 (YEM, CD and SI), 876 (cIMT) and 872 (plaques) participants. The proportion of people in trajectories was 26% in persistently advantaged, 20% in improving, 14% in changing, 17% in declining, and 22% in persistently disadvantaged. Compared to persistently high SEP category, persistently disadvantaged SEP was associated with higher (worse) YEM (β 0.07 95% CI 0.001, 0.14, p=0.04) and declining SEP with lower (worse) CD (β -0.07 95% CI -0.13 -0.001, p=0.04) when adjusted for only for childhood factors but were non-significant when adjusted for young and mid-adulthood factors.
Conclusions: Persistently disadvantaged and declining SEP across the life course was associated with small but significant early vascular ageing that was partly explained by concurrent unhealthier lifestyle behaviours.
Disclosures of Interest:
No
Abstract N°: 2676
NONINVASIVE IMAGING AND DETECTION OF CAROTID PLAQUE LIPID-RICH NECROTIC CORE AND FIBROUS CAP: A SYSTEMATIC REVIEW & DIAGNOSTIC ACCURACY META-ANALYSIS
David Pakizer*1, Patrick Taffé2, Jiří Kozel1, Jolanda Elmers3, Janusz Feber1,4, Patrik Michel5, David Skoloudik1, Gaia Sirimarco5,6
1Center for Health Research, Faculty of Medicine, University of Ostrava, Ostrava, Czech Republic, 2Center for Primary Care and Public Health, Division of Biostatistics, University of Lausanne, Lausanne, Switzerland, 3Medical Library, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland, 4Division of Nephrology, Department of Pediatrics, Children’s Hospital of Eastern Ontario, University of Ottawa, Ottawa, Canada, 5Stroke Center, Service of Neurology, Department of Clinical Neurosciences, Lausanne University Hospital, Lausanne, Switzerland, 6Neurology Unit, Department of Internal Medicine, Riviera Chablais Hospital, Rennaz, Switzerland
On behalf of:
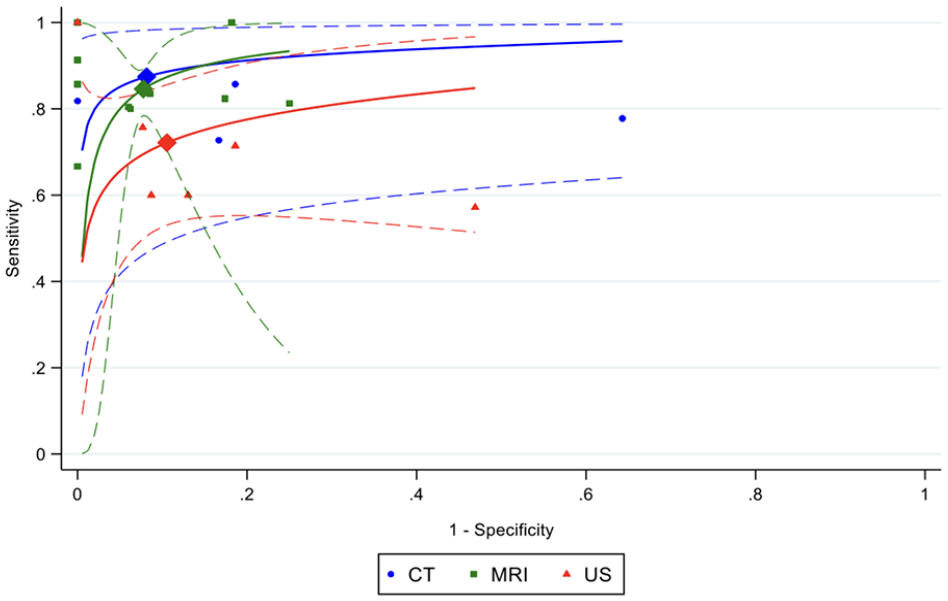
Background and aims: A large lipid-rich necrotic core (LRNC) with a thin overlying fibrous cap is associated with plaque rupture and the risk of a subsequent ipsilateral ischemic stroke. The study aimed to estimate the diagnostic accuracy of noninvasive imaging modalities (ultrasound [US],computed tomography [CT],magnetic resonance imaging [MRI]) to detect LRNC and fibrous cap status when compared to histology in patients with symptomatic and asymptomatic carotid plaques.
Methods: We searched Medline Ovid, Embase.com, Cochrane Library, and WoS Core (no search limitation used). We performed QUADAS-2 to assess the quality of studies and univariate and bivariate random-effect meta-analysis to analyze the results.
Results: We included 34 studies that investigated LRNC (5 CT/22 MRI/7 US studies) and 11 studies that investigated fibrous cap (4 intact/7 ruptured) using three different imaging techniques. In univariate meta-analysis, LRNC was visualized by all modalities with similar accuracy. MRI showed the highest accuracy (sensitivity 86% [95%CI:79-90], specificity 86% [95%CI:80-91], accuracy 86% [95%CI:81-89]), followed by CT (sensitivity 78% [95%CI:67-85], specificity 90% [95%CI:60-98], accuracy 84% [95%CI:72-91]) and US (sensitivity 75% [95%CI:60-86], specificity 85% [95%CI:72-92], accuracy 81% [95%CI:70-89]). Bivariate analysis showed no significant difference between these modalities in LRNC detection (Fig.1;p>0.5). Only MRI and US detected ruptured fibrous cap with the same accuracy (86%), MRI was superior in detecting an intact cap (accuracy 88% to 64%).
Conclusions: While MRI, CT and US showed similar high accuracy for detection of LRNC, only MRI can also assess the fibrous cap status with high accuracy.
Comparison of CT/MRI/US diagnostic accuracy in LRNC detection based on HSROC curves.
Disclosures of Interest: No
SCIENTIFIC COMMUNICATION – EPIDEMIOLOGY
Abstract N°: 132
DISEASE BURDEN OF ACUTE ISCHEMIC STROKE IN UNDERSERVED POPULATIONS ACROSS THE US IN 2022
Elizabeth Mearns1, Stacey Kowal1, Katherine Rosettie1, Barbara Purdon*1, Nikki Win1
1Genentech, Inc., South San Francisco, CA, United States
On behalf of:
Background and aims: In stroke care, race and ethnicity can influence whether patients receive treatment with thrombolysis or endovascular therapy. Our objective was to examine disparities in acute ischemic stroke (AIS) disease burden by sex, race and ethnicity in the US.
Methods: This secondary analysis of the Global Burden of Disease study included data on incidence and deaths (hereafter referred to as burden) in the US from 1 Jan 2022 to 31 Dec 2022. Age-standardized rates for burden measures per 100,000 (95% uncertainty interval) are presented.
Results: In 2022, the total US population AIS incidence was 79.4 (44.8–134.1), and deaths were 30.7 (22.4–42.8). Females had higher mortality (31.7 [21.8–46.6]) and males had higher incidence (84.2 [50.8–126.9]) compared with the total AIS population (Figure 1). Among both sexes, differences in AIS burden were observed by race and ethnicity. Incidence was highest for Black/African American (AA) individuals (104.9 [59.1–177.4]), followed by White (78.5 [44.0–133.5]), Hispanic/Latino (70.7 [38.5–123.0]), American Indian/Alaska Native (AI/AN) (62.1 [29.2–123.5]) and Asian/Pacific Islander (A/PAC) individuals (56.1 [30.1–99.5]) (Figure 2). Similarly, deaths were highest for Black/AA individuals (40.5 [26.9–56.1]), followed by White (30.7 [22.2–43.0]), Hispanic/Latino (26.9 [19.0–38.7]), AI/AN (23.8 [15.1–37.6]) and A/PAC individuals (21.6 [15.1–31.3]) (Figure 3).
Conclusions: Differences in AIS burden were observed by sex, race and ethnicity. Together, these results highlight possible barriers to equitable access to care and the need for tailored intervention.
Disclosures of Interest:
Yes Sponsored by F. Hoffmann-La Roche Ltd. Writing/editorial assistance provided by Nucleus Global. Disclosures: ES Mearns, S Kowal, KL Rosettie, B Purdon and N Win are employees and stockholders of F. Hoffmann-La Roche Ltd, N Win holds stock in Amgen.
Abstract N°: 257
NATIONAL INCIDENCE OF INTRACRANIAL HAEMORRHAGE RELATED HOSPITALISATIONS AND MORTALITY IN ENGLAND 2014-2019
Katherine Creeper*1,2, Andrew Stafford3, Allycia Macdonald4, Arvind Chandratheva5, Alexander Cohen6
1Sir Charles Gairdner Hospital, Nedlands, Australia, 2PathWest Nedlands, Nedlands, Australia, 3Curtin University, Bentley, Australia, 4Fiona Stanley Hospital, Murdoch, Australia, 5National Hospital for Neurology and Neurosurgery, Comprehensive Stroke Service, London, United Kingdom, 6Guy's and St Thomas' NHS Foundation Trust, London, United Kingdom
On behalf of:
Background and aims: Intracranial haemorrhage (ICrH) has the highest mortality compared to bleeding in other anatomical sites. However, few studies describe the national incidence of ICrH-related acute hospitalisations and mortality. We report the national burden and incidence of hospitalisation and mortality of ICrH and its subtypes.
Methods: A population-based review in England between 2014 and 2019 of acute admissions or deaths. Admission and mortality data were obtained from electronic databases (traumatic deaths data was unavailable). ICrH events were based on the International Statistical Classification of Diseases version 10 codes. Patients with an inherited or acquired coagulation or platelet disorder, and those who were not admitted were excluded. ICrH were subclassified by site, and either as traumatic or atraumatic.
Results: There was a total of 468,996 hospitalisations for ICrH, 280,003 (59.7%) were atraumatic and 188,993 (40.3%) were traumatic. 50,004 atraumatic ICrH-related deaths were recorded, of these deaths, 6943 were unclassified and 43,061 were subclassified. The mean annual incident rates (per 100,000 person years) were 141 for ICrH-related hospitalisations and 15.0 for atraumatic ICrH related mortality. 54.6% (n=256,130) of hospitalisations occurred in males (figure 1). Females had a higher mean annual atraumatic ICrH-related mortality (OR 2.33, p<0.05) (figure 2). 23.4% (n=109,770) of ICrH hospitalisations occurred in patients ⩾ 85 years (figure 3).
Conclusions: Around 60% of ICrH acute hospitalisations were atraumatic with males having a higher overall incidence. Females had a higher incidence of atraumatic ICrH-related mortality. Increasing age was associated with a higher incidence of hospitalisation and mortality.
Disclosures of Interest:
Yes Receives speaker honoraria from AstraZeneca
Abstract N°: 619
TWENTY-FIVE YEAR TIME TRENDS IN EPIDEMIOLOGY OF INTRACEREBRAL HAEMORRHAGE: RESULTS FROM THE ERLANGEN STROKE PROJECT
Viktoria Rücker*1, Felipe A. Montellano1,2, Kirsten Haas1, Michael Weingärtner3, Stefan Schwab4, Peter U. Heuschmann1,5,6,7, Peter Kolominsky-Rabas, Mba3
1Julius-Maximilian-University of Würzburg, Institute of Clinical Epidemiology and Biometry, Würzburg, Germany, 2University Hospital Würzburg, Department of Neurology, Würzburg, Germany, 3Friedrich-Alexander-University of Erlangen-Nürnberg, Erlangen Stroke Project, Interdisciplinary Centre for Health Technology Assessment (HTA) and Public Health, Erlangen, Germany, 4Universitätsklinikum Erlangen, Erlangen, Germany, 5University Hospital Würzburg, Institute for Medical Data Sciences, Würzburg, Würzburg, Germany, 6University and University Hospital Würzburg, Comprehensive Heart Failure Center, Würzburg, Germany, 7University Hospital Würzburg, Clinical Trial Unit, Würzburg, Germany
On behalf of:
Background and aims: Data on long-term time trends in epidemiology of intracerebral haemorrhage (ICH) are scarce. We investigated incidence, case fatality and recurrence over a 25-year period.
Methods: Data was collected within the Erlangen Stroke Project, a population-based stroke register in Germany covering a source population of 105,164 inhabitants (2010). Patients with incident ICH patients between 1998-2022 were analysed. Incidence rate ratio (IRR) with 95%-CI was compared between 2018-2022 and 1998-2002. 3-month, 1-year and 5-year case-fatality and recurrence rates were estimated with Kaplan-Meier estimates. Time trends in case-fatality and recurrence rates were investigated with Cox regression adjusted for age, sex and year of event.
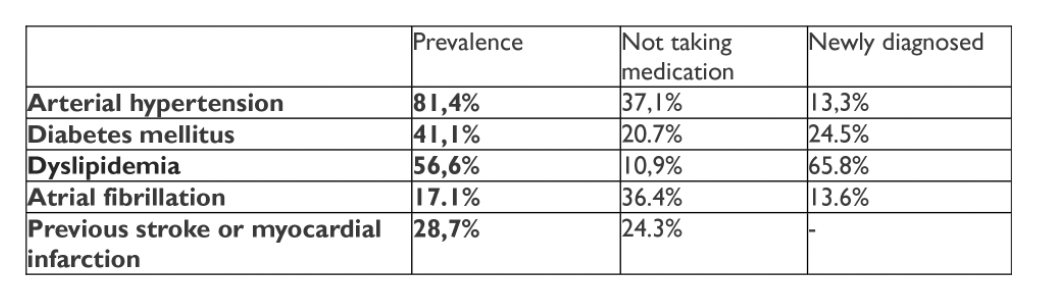
Results: 594 incident ICH patients were included (mean age 73 (SD 14) years, 51% females); of patients with complete information 75% had hypertension, 22% diabetes and 27% atrial fibrillation (AF). Overall, annual age standardized incidence was 24.6 per 100.000, decreasing from 27.6 within 1998-2002 to 19.8 per 100.000 within 2018-2022 (IRR 0.72 (95%-CI: 0.71-0.72)). Case-fatality rates at 3, 12, 60 months were: 32% (95% CI 28-36), 39% (95% CI 35-43), and 59% (95% CI 54-63). Recurrence rates at 3, 12, 60 months were: 2% (95% CI 1-4), 6% (95% CI 4-9), 19% (95% CI 14-23). Adjusted Cox regression revealed no significant time trends for case-fatality and recurrence. At 12-months of patients with AF at baseline, 21% were treated with oral anticoagulation, 8% had a recurrent stroke and 41% died.
Conclusions: Over 25-years of observation incidence of ICH decreased, but no substantial changes in ICH outcomes were found.
Disclosures of Interest:
No
Abstract N°: 703
RISK AND EPIDEMIOLOGY OF STROKE IN PATIENTS WITH MULTIPLE SCLEROSIS: A SYSTEMATIC REVIEW AND META-ANALYSIS
Maria Ioanna Stefanou*1, Vasileios Giannopapas2, Dimitrios Kitsos2, Maria Chondrogianni2, Aikaterini Theodorou2, Maria Kosmidou3, Elisavet Andreadou2, Ioannis Tzartos2, Sotirios Giannopoulos2, Georgios Tsivgoulis2
1National and Kapodistrian University of Athens, Second Department of Neurology, Athens, Greece, 2National and Kapodistrian University of Athens, 3University of Ioannina Greece
On behalf of:
Background and aims: There is a dearth of evidence regarding the risk of stroke in multiple sclerosis (MS). Here we sought to estimate the: (1) pooled prevalence of all-cause stroke, acute ischaemic stroke (AIS) and intracerebral haemorrhage (ICH) in patients with MS (PwMS); (2) relative risk for all-cause stroke, AIS and ICH in PwMS compared to the general population.
Methods: Systematic review and meta-analysis of registry-based and cohort studies.
Results: Thirteen observational studies comprising 146,381 PwMS were included. The pooled prevalence of all-cause stroke was 2.7% (95% confidence interval [CI]: 1.3-4.6%), with the relative risk of all-cause stroke being higher in PwMS compared to the general population (RR: 2.55; 95% CI: 1.97-3.29). Subgroup analyses per stroke-subtype revealed a pooled AIS and ICH prevalence of 2.1% (95% CI: 0.8-4.1%) and 0.6% (95% CI: 0.2-1.2%), respectively. Additionally, PwMS appear to harbor an increased risk for AIS (RR: 2.79; 95% CI: 2.27-3.41) and ICH (RR: 2.31; 95% CI: 1.04-5.11) compared to the general population. The pooled prevalence of cardiovascular risk factors in PwMS was 11.5% (95% CI: 2.9-24.7%) for dyslipidaemia, 18.2% (95% CI: 5.9-35.3%) for hypertension, and 5.4% (95% CI: 2.1-10.2%) for diabetes. In meta-regression, age was negatively associated with AIS risk (β=-.03, p=0.04), with a 1-year increase in age resulting in a significant 3% (95%CI: 0-5) attenuation of the risk of AIS.
Conclusions: MS is associated with an increased risk for ischaemic and haemorrhagic stroke. Implementation of targeted prevention strategies in PwMS is fundamental to reduce stroke burden and improve patient prognosis.
Disclosures of Interest: No
Abstract N°: 1171
RISK OF ISCHEMIC STROKE AND INTRACEREBRAL HEMORRHAGE IN WOMEN WITH MIGRAINE USING COMBINED HORMONAL CONTRACEPTIVES
Gasper Letnar1, Tom Skyhøj Olsen*2, Klaus Kaae Andersen1
1Omicron ApS, Copenhagen, Denmark, 2Bispebjerg University Hospital, Neurology, Copenhagen, Denmark
On behalf of:
Background and aims: Uncertainties remain regarding the stroke risk associated with combined hormonal contraceptives with ethinylestradiol (CHC) in women with migraine; the contraceptives most used. Limited evidence in a small number of studies suggest a 2-4-fold increase of ischemic stroke (IS) while studies on intracerebral hemorrhage (IH) are few and conflicting.
Methods: We followed all non-pregnant Danish women (18-49 years) 2003-2021. We registered IS and IH during use/non-use of CHC using the Danish Stroke Registry, the Danish Prescription Registry (DPR,) and other Danish high-quality registries with nation-wide coverage. In DPR we identified women with prescriptions for triptans defining these as having migraine. Hemorrhage due to aneurysms and vascular malformations were not included. Poisson regression models adjusting for age, ethnicity, education, calendar-year, and stroke risk factors were utilized.
Results: In total 1,735,306 non-pregnant women contributed 16,933,276 person-years (py) of observation. In women with migraine not using CHC (IS/HI events 585/47; 1,360,044 py) relative risk RR of IS/HI was 1.22 (CI 1.10; 1.36)/0.88 (CI 0.63; 1.22). In women with migraine using CHC (IS/HI events 151/5; 329,240 py) RR of IS/IH was 2.59 (CI 2.19; 3.06)/0.65 (CI 0.7; 1.57). Women without migraine not using CHC were used as reference.
Conclusions: In women of reproductive age (18-49 years), migraine was associated with increased risk of IS (RR 1.22) but not of IH. Use of CHC in women with migraine increased the risk of IS 2-fold while risk of IH was not affected.
Disclosures of Interest:
No
Abstract N°: 2505
ALTERNATIVE SCENARIOS FOR PROJECTED PREVALENCE OF STROKE AND POST-STROKE DEMENTIA TO 2046 IN IRELAND: A MODEL-BASED ANALYSIS
Eithne Sexton*1, Martin O'flaherty2, Anne Hickey1, David Williams1,3, Frances Horgan1, Chris Macey4, Suzanne Timmons5, Rónán Collins6, Kathleen Bennett1
1RCSI University of Medicine and Health Sciences, Dublin, Ireland, 2University of Liverpool, Liverpool, United Kingdom, 3Beaumont Hospital, Dublin, Ireland, 4Irish Heart Foundation, Dublin, Ireland, 5University College Cork, Cork, Ireland, 6Tallaght University Hospital, Ireland
On behalf of:
Background and aims: Understanding future population need is key for informing stroke service planning. This study aims to evaluate alternative scenarios for future trends in stroke age-specific incidence and case-fatality, and estimate impact on projected stroke and post-stroke dementia prevalence in Ireland.
Methods: We used a probabilistic Markov model to project and track incidence and prevalence of stroke and post-stroke dementia in the Irish population aged 40-89 years to 2046. Using systematic review and observational evidence, we extrapolated trends in stroke age-specific incidence and case-fatality from 1990-2019 to 2016-2046. We defined optimistic, realistic and pessimistic scenarios, including scenarios where trends decelerated over time.
Results: The stable (pessimistic) scenario indicates a projected 80,797 stroke survivors in 2046 (95% uncertainty interval, UI = 77,457-84,403) (22.7 per 1000 pop), an increase of 43% from 2022 to 2046. The most optimistic scenario would involve only a 3.7% increase from 2022 to 2046, to a projected 56,362 survivors. More realistic scenarios based on lower rates of incidence/case-fatality decline, or rates of decline slowing over time, imply an increase ranging between 23.2% and 25.7%.
The pessimistic scenario indicates a projected 16,103 with post-stroke dementia in 2046 (95% UI 14,133-18,202), an increase of 60% from 2022. In the most optimistic scenario, the increase would be 25.9%, with realistic scenarios implying an increase ranging between 42.4% and 47.3%.
Conclusions: Future stroke healthcare needs will vary substantially depending on epidemiological trends. Large increases in post-stroke dementia are projected across scenarios. Further work is needed to identify optimal policies to promote continuing decline in stroke incidence.
Disclosures of Interest:
No
SCIENTIFIC COMMUNICATION – CARDIOEMBOLISM & HEART-BRAIN INTERACTIONS
Abstract N°: 237
PRIOR ANTICOAGULATION IS LINKED TO A DECREASED RISK OF HAEMORRHAGIC TRANSFORMATION IN ACUTE STROKE
Gerrit M. Grosse*1,2,3, Anika Hüsing1, Andreas Stang1, Nils Kuklik1, Marcus Brinkmann1, Christoph Eschenfelder4, Christian Weimar1, Hans-Christoph Diener1
1Essen University Hospital, Essen, Germany, 2Hannover Medical School, Hannover, 3University Hopsital Basel, Basel, Switzerland, 4Human Pharma Germany, Boehringer Ingelheim Pharma GmbH & Co. KG, Ingelheim am Rhein, Germany
On behalf of: PRODAST investigators
Background and aims: Oral anticoagulation is highly effective in preventing ischaemic events in patients with atrial fibrillation (AF). Still, a considerable number of patients suffers an acute ischaemic stroke (AIS) or transient ischaemic attack (TIA) despite anticoagulation. In this study, we investigated the effects of antithrombotic regimens on stroke severity, volume and haemorrhagic transformation (HT).
Methods: This is a post-hoc analysis of the prospective, multicentre, observational, PRODAST study which was conducted in 86 stroke-units in Germany between July 2015 and November 2020. In 9,030 patients with AF who suffered AIS or TIA within 7 days before enrollment, we analysed the effects of oral anticoagulants in comparison to lack of prevalent antithrombotic treatment on clinical stroke severity, infarct size and risk for HT on initial brain imaging.
Results: 4,479 patients were on anticoagulation at the time of index event. Prevalence of vascular risk factors and age were not different from patients without antithrombotic treatment. After adjustment for confounders, patients with prior anticoagulation had less severe strokes (-2.5 NIHSS points, 95%CI: -2.8; -2.2) (Fig. 1), smaller infarct sizes (-23 mL, 95%CI: -44 mL; -2 mL) (Fig. 2) and a reduced odds for HT (5% vs 10%, odds ratio: 0.48, 95%CI: 0.40; 0.57) (Fig. 3) on initial brain imaging compared to patients without antithrombotic treatment. Antiplatelet therapy had no effect on endpoints compared to no antithrombotic pre-treatment.
Conclusions: Prior anticoagulation was not only associated with less severe stroke and smaller infarct size but also with a reduced risk of HT compared to no antithrombotic pretreatment.
Disclosures of Interest:
Yes The PRODAST study was funded by an unrestricted grant from Boehringer Ingelheim.
Abstract N°: 1353
LEFT ATRIAL DIVERTICULA DETECTED ON CARDIAC CT IN ACUTE ISCHEMIC STROKE PATIENTS ARE ASSOCIATED WITH STROKE RECURRENCE
Shan Sui Nio*1, Leon Rinkel1, Nerea Arrarte Terreros2, Henk Marquering2, Berto J Bouma3, Charles Majoie4, Yvo Roos1, Adrienne van Randen4, R. Nils Planken4, Jonathan Coutinho1
On behalf of: O.N. Cramer, Z.B. Özata, C.F.P. Beemsterboer, V. Guglielmi, S.M. Boekholdt, N.H.J. Lobé, L.F.M. Beenen
Background and aims: Left atrial diverticula (LAD) are focal outpouchings of the left atrial wall and may be a risk factor for ischemic stroke. We studied stroke recurrence in acute ischemic stroke (AIS) patients with LAD detected on acute cardiac CT.
Methods: We used data from a prospective cohort of AIS patients undergoing cardiac CT during the acute stroke imaging protocol. We compared ischemic stroke recurrence and functional outcome (modified Rankin Scale [mRS]) after 2-year follow-up between patients with and without LAD detected on acute cardiac CT. Cardiac radiologists systematically assessed presence of LAD, defined as left atrial wall outpouches with smooth contour.
Results: Of 447 patients, cardiac CT detected LAD in 132 (30%) patients. Age and sex ratio was similar between groups. There was no significant difference in history of ischemic stroke (LAD patients: 21% vs. patients without LAD: 17%, p=0.49), atrial fibrillation (11% vs. 19%, p=0.10), or baseline NIHSS-score (median 5 [IQR 2-14] vs. 5 [IQR 3-14], p=0.44). Ischemic stroke recurrence was more common in LAD patients (18/130 (14%) vs. 24/308 (8%), aHR 1.95, 95%CI 1.04-3.65). Functional outcome at 2 years was better in LAD patients (median mRS 2 [IQR 1-3] vs. 3 [IQR 1-6], acOR 0.67, 95%CI 0.45-0.99).
Conclusions: LAD were detected on acute cardiac CT in one third of AIS patients and these patients had a higher ischemic stroke recurrence, but a better functional outcome. LAD might be a novel risk factor for recurrent ischemic stroke, but larger prospective studies are required to draw firm conclusions.
Disclosures of Interest:
No
Abstract N°: 1451
STROKE TYPE AND SEVERITY IN THE LEFT ATRIAL APPENDAGE OCCLUSION DURING CARDIAC SURGERY TO PREVENT STROKE (LAAOS III) STUDY
Aristeidis Katsanos*1,2, Richard Whitlock2,3, Emilie Belley-Cote1,2, Katheryn Brady2, Angela Wang2, Abhilekh Srivastava1, Gregory Jacquin4, Luciana Catanese1, Ashkan Shoamanesh1,2, Mike Sharma1,2
1McMaster University, Department of Medicine, Hamilton, Canada, 2Population Health Research Institute, Hamilton, Canada, 3McMaster University, Division of Vascular Surgery, Hamilton, Canada, 4Centre hospitalier de l'Université de Montréal, Montreal, Canada
On behalf of: LAAOS III stroke group
Background and aims: The randomized LAAOS III trial demonstrated that patients with atrial fibrillation (AF) who underwent left atrial appendage occlusion (LAAO) during cardiac surgery had a lower risk of stroke than those who did not. We sought to characterize stroke subtype, mortality, and topography to assess the impact of LAAO on strokes of different mechanisms. We hypothesized that LAAO would preferentially reduce cardioembolic stroke.
Methods: LAAOS III randomly assigned 4811 patients with AF undergoing cardiac surgery for another indication to undergo LAAO or not. Ischemic/undetermined stroke or systemic embolism was the primary outcome. For the current analysis, adjudicators blinded to treatment allocation reviewed clinical records and imaging reports of all ischemic strokes that occurred in LAAOS III and classified them as cardioembolic if the acute infarct was not attributed to a competing mechanism by modified TOAST criteria, or if multiple acute infarcts in different vascular territories were present. We also classified infarcts as cortical and determined if infarcts were on multiple or single territories as additional factors associated with cardioembolic stroke.
Results: Fatal stroke was less likely in the LAAO group (HR=0.55, 95%CI:0.31-0.96), while perioperative ischemic or hemorrhagic stroke risk was similar. Suspected cardioembolism (43% vs. 58%) and cortical involvement (45% vs. 60%) on brain imaging was less common in participants who underwent LAAO. LAAO reduced the risks for cardioembolic stroke by 53% (HR=0.47,95%CI: 0.33-0.67) and cortical infarction by 49% (HR=0.51,95%CI:0.36-0.72).
Conclusions: LAAO decreases the risk for ischemic stroke related to cardioembolism and reduces stroke fatality without increasing the risks for perioperative or hemorrhagic cerebrovascular events.
Disclosures of Interest:
No
Abstract N°: 1758
THE ROLE OF NT-PROBNP FOR ATRIAL FIBRILLATION DETECTION AFTER ISCHEMIC STROKE: A TIME-DEPENDENT RELATIONSHIP
Isra Hatab*1, Markus Kneihsl1,2, Joan Montaner3,4,5, Katharina Spanaus6, Arnold von Eckardstein6, Alan Cameron7, Thomas Gattringer1,2, Urs Fischer8,9, Mira Katan8
1Medical University of Graz, Department of Neurology, Graz, Austria, 2Medical University of Graz, Division of Neuroradiology, Vascular and Interventional Radiology, Department of Radiology, Graz, Austria, 3Vall d’Hebron Institute of Research, Neurovascular Research Laboratory, Barcelona, Spain, 4Instituto de Biomedicina de Sevilla/Hospital Universitario Virgen del Rocío/Consejo Superior de Investigaciones Científicas/University of Seville, Stroke Research Program, Seville, Spain, 5Hospital Universitario Virgen Macarena, Department of Neurology, Seville, Spain, 6University Hospital of Zurich, University of Zurich, Institute of Clinical Chemistry, Zurich, Switzerland, 7University of Glasgow, School of Cardiovascular and Metabolic Health, Glasgow, United Kingdom, 8University Hospital Basel, University of Basel, Department of Neurology, Basel, Switzerland, 9Inselspital, University Hospital Bern, University of Bern, Department of Neurology, Bern, Switzerland
On behalf of: the BIOSIGNAL cohort study group and the Graz cryptogenic stroke study group
Background and aims: Atrial fibrillation detected after stroke (AFDAS) is a common ischemic stroke etiology, yet identification can be challenging. Easily accessible cardiac blood biomarkers such as n-terminal pro-brain natriuretic peptide (NT-proBNP) could guide diagnostic work-up, but clinical cutoff values and the time-dependent relationship between NT-proBNP and AFDAS are unclear.
Methods: This is a pooled data analysis of people included in the multicenter BIOSIGNAL (Biomarker Signature of Stroke Aetiology) cohort study and the Graz cryptogenic stroke study. AFDAS was defined as atrial fibrillation or flutter of ⩾30 seconds, diagnosed during the hospital stay and a one-year follow-up period. AFDAS was further categorized in in-hospital AFDAS versus AFDAS after hospitalisation.
Results: 374 (16%) of 2,292 people with ischemic stroke (median age: 74 years; 42% female), were diagnosed with AFDAS (268 during and 106 after hospitalisation; median duration of hospitalisation: 15 days, interquartile range: 10-19 days). While admission NT-proBNP levels were highly associated with in-hospital AFDAS in multivariable analyses (OR 5.2, CI 95% 3.9-7.1), no association was observed between admission NT-proBNP and AFDAS after hospitalisation (OR 1.3, CI 95% 0.9-2.0). The NT-proBNP cutoff of 505 pg/ml exhibited a relatively high diagnostic accuracy for in-hospital AFDAS (73%) and had a negative predictive value of 96%. No NT-proBNP cutoffs predicted AFDAS after hospitalisation, and 20% of these patients had normal NT-proBNP values at admission (<125 pg/ml).
Conclusions: An admission NT-proBNP cutoff of 505 pg/ml is an accurate discriminator for in-hospital AFDAS with a high negative predictive value of 96%. However, admission NT-proBNP does not predict AFDAS after hospitalization.
Disclosures of Interest: No
Abstract N°: 1868
PREDICTORS OF STROKE IN PATIENTS WITH RHEUMATIC HEART DISEASE-ASSOCIATED ATRIAL FIBRILLATION – RESULTS FROM THE INVICTUS TRIAL
Alexander P. Benz*1,2, Chinthanie Ramasundarahettige1, Ganesan Karthikeyan3, Mpiko Ntsekhe4, Sumathy Rangarajan1, Salim Yusuf1, Stuart Connolly1
1Population Health Research Institute, McMaster University, Hamilton, Canada, 2University Medical Center Mainz, Department of Cardiology, Mainz, Germany, 3All India Institute of Medical Sciences, New Delhi, India, 4University of Cape Town, Division of Cardiology, Faculty of Health Sciences, Cape Town, South Africa
On behalf of: The INVICTUS Investigators
Background and aims: Stratification of stroke risk in patients with atrial fibrillation (AF) has been based on data from individuals without rheumatic heart disease (RHD). This study aimed to determine risk factors for stroke in patients with RHD-associated AF receiving oral anticoagulation.
Methods: The INVICTUS trial randomized patients with AF and echocardiographically documented RHD to rivaroxaban or a vitamin K antagonist. Multivariable Cox regression models adjusted for randomized treatment were used to describe the association of clinical characteristics with stroke or systemic embolism during follow-up.
Results: A total of 4,451 patients with AF and RHD were included in the analysis (median age 50 years, 72.2% female and 14.6% with prior stroke). A total of 3,701 patients (83.1%) had mitral stenosis with a mitral valve area ⩽2.0 cm². Congestive heart failure was present in 1,708 patients (38.4%), and hypertension in 1,033 (23.2%). Few had diabetes mellitus (6.4%) or vascular disease (1.3%). During a mean follow-up of 3.1 years, 167 patients (3.8%) had a stroke or systemic embolism. In adjusted analyses, age (per 10-year increase, hazard ratio [HR] 1.23, 95% confidence interval [CI] 1.07-1.42), prior stroke, transient ischaemic attack or systemic embolism (HR 1.68, 95% CI 1.17-2.42), mitral stenosis (HR 1.94, 95% CI 1.12-3.35), diabetes (HR 1.80, 95% CI 1.10-2.94) and vascular disease (HR 3.73, 95% CI 1.71-8.13) were associated with stroke or systemic embolism.
Conclusions: In patients with RHD-associated AF receiving oral anticoagulation, advanced age, prior stroke, mitral stenosis, diabetes and vascular disease were associated with an increased risk of stroke.
Disclosures of Interest:
Yes Dr. Benz reports lecture fees from Bristol-Myers Squibb and AstraZeneca, and participation in an educational program supported by Boston Scientific (“Fellowship Herzrhythmus”).
Abstract N°: 3072
APIXABAN FOR STROKE PREVENTION IN PATIENTS WITH SUBCLINICAL ATRIAL FIBRILLATION AND PRIOR STROKE: INSIGHTS FROM THE ARTESIA TRIAL
Ashkan Shoamanesh*1, Thalia Field2, Shelagh Coutts3, Mike Sharma1, David Gladstone4, Rajibul Mian5, Christopher B. Granger6, Stuart Connolly7, Renato Lopes6, Jeff Healey7
1McMaster University / Population Health Research Institute, Hamilton, Canada, Medicine (Neurology), Hamilton, Canada, 2Vancouver Stroke Program, University of British Columbia, Neurology, Vancouver, Canada, 3Radiology and Community Health Sciences, University of Calgary, Clinical Neurosciences, Calgary, Canada, 4University of Toronto, Neurology, Toronto, Canada, 5Population Health Research Institute, Statistics, Hamilton, Canada, 6Duke University Medical Center, Cardiology, Durham, United States, 7McMaster University / Population Health Research Institute, Medicine (Cardiology), Hamilton, Canada
On behalf of: ARTESIA study investigators
Background and aims: In ARTESIA, apixaban reduced stroke or systemic embolism (stroke/SE) in patients with subclinical atrial fibrillation (SCAF), compared to aspirin. We studied its effect in the subgroup of patients with a history of stroke or transient ischemic attack (stroke/TIA).
Methods: ARTESIA is an international, double-blind trial that randomized patients with device-detected SCAF lasting 6 minutes to 24 hours to apixaban 5 mg twice daily or aspirin 81 mg daily. We performed an intention-to-treat analysis comparing rates of stroke/SE and ISTH major bleeding between participants with a history of stroke/TIA and those without.
Results: Of 4012 patients, 9% (n=346) had a history of stroke/TIA (175 with stroke and 171 with TIA). The annual rate of stroke/SE in patients with a history of stroke/TIA was lower with apixaban than aspirin (1.20% vs. 3.14%; HR 0.40; 95%CI 0.17-0.95). In those without prior stroke/TIA, rates were 0.74% and 1.07%, respectively (HR 0.69; 95%CI 0.48-1.00). The relative effect of treatment was not different according to a history of stroke/TIA (interaction p-value = 0.24). The annual rate of major bleeding in patients with a history of stroke/TIA was 2.26% on apixaban and 1.16% on aspirin (HR 1.94; 95%CI 0.77-4.87). Corresponding rates for patients without prior stroke/TIA were 1.46% and 1.12% (HR 1.30, 95%CI 0.95-1.77; interaction p-value = 0.42).
Conclusions: Patients with SCAF and a history of stroke/TIA receiving aspirin are at higher risk of stroke/SE. Apixaban significantly reduced this risk by an absolute margin that was nearly double that of the associated increased risk of major bleeding. (Clinicaltrials.gov. NCT01938248)
Disclosures of Interest:
No
Abstract N°: 3181
RISK SCORES AND BRAIN MRI MARKERS IN DISTINGUISHING ISCHEMIC FROM HEMORRHAGIC STROKE RISK AMONG ATRIAL FIBRILLATION PATIENTS: THE NEURO-AFIB STUDY
Edip Gurol*1, Alvin Das2, Elif Gokcal1, Kim Pena del Aguila1, Ofer Rotschild1, Avia Abramovitz Fouks1, Eric Smith3, Shadi Yaghi4
1Massachusetts General Hospital, Harvard Medical School, Neurology, 2BIDMC Neurology, Boston, United States, 3Calgary University, Neurology, Calgary, Canada, 4Brown Neurology, West Warwick, United States
On behalf of: The Neuro-AFib Study Group
Background and aims: Recent studies cast doubt on the accuracy of the most-commonly used risk scores in differentiating the risk of acute ischemic stroke (AIS) and intracerebral hemorrhage (ICH) among atrial fibrillation (AF) patients. We thus aimed to assess the value of risk scores and brain MRI markers to differentiate AIS and ICH risk in a large cohort of AF-related strokes.
Methods: Demographics, CHA2DS2-VASC and HAS-BLED scores, and ischemic/hemorrhagic brain MRI markers were compared between AF patients admitted with AIS and ICH to 15 stroke centers in the US between 1/2018-12/2019.
Results: Of 5694 stroke admissions with AF, 4826 (84.8%) had AIS and 868 (15.2%) ICH. Mean age was similar between groups while more ICH patients were male. Pre-index CHA2DS2-VASC (4.14+1.6 vs 4.22+1.6) and HAS-BLED (2.71+1.09 vs 2.68+1.13) were similar between groups. Cerebral microbleeds (CMB, 56% vs 33.5%), cortical superficial siderosis (cSS, 15% vs 9.4%), and moderate-to-severe leukoaraiosis (41% vs 33.4%) were more commonly found among ICH patients (all p<0.001). Chronic lacunar (43.5% vs 39.5%, p=0.03) and non-lacunar infarcts (29% vs 18%, p<0.001) were more common in AIS. In a multivariable logistic regression model, male sex, presence of CMBs, cSS, moderate-to-severe leukoaraiosis were associated with ICH, chronic non-lacunar infarcts with AIS (all p<0.005), while CHA2DS2-VASC (p=0.9) and HAS-BLED (p=0.9) were not related to the stroke type.
Conclusions: Our findings confirm the lack of specificity of CHA2DS2-VASC and HAS-BLED to categorize the risk of AIS vs ICH in AF patients. MRI markers should be incorporated into risk scores to select optimal stroke prevention methods in AF patients.
Disclosures of Interest:
Yes Research Grants to the Hospital only: AVID, Pfizer, Boston Scientific
SCIENTIFIC COMMUNICATION - DIAGNOSIS / INVESTIGATION OF STROKE ETIOLOGY AND PATHOPHYSIOLOGY
Abstract N°: 696
PREDICTION OF ISCHEMIC STROKE SUBTYPES BY MACHINE LEARNING: JAPAN STROKE DATA BANK
1National Cerebral and Cardiovascular, Department of Cerebrovascular Medicine, Suita, 2SoftBank Corp., Technology Unit, AI Strategy Office, Japan, 3National Cerebral and Cardiovascular, Department of Medical and Health Information Management, Suita, Japan
On behalf of: JSDB investigators
Background and aims: There are few reports of ischemic stroke subtype prediction by machine learning (ML), using large-scale stroke registry data. We aimed to analyze case data in the nation-wide stroke registry by ML algorithm and create a stroke subtype prediction formula using information that can be obtained early in hospitalization.
Methods: The Japan Stroke Data Bank (JSDB) is the largest acute stroke registry in Japan with individual data and have accumulated approximately 280,000 cases from more than 100 facilities nationwide over the past 24 years. Case data registered from 2016 to 2020 were analyzed by ML algorithm, Catboost, to predict cardioembolic stoke, atherothrombotic brain infarction, and lacunar infarction. Patients’ information that could be obtained early in the hospital visit, such as medical history, neurological symptoms, and brain image findings, and hospital information, including number of beds and certification of primary stroke center, was used.
Results: 46,344 patients (mean age 75.0±12.7 y.o, female 41.0%, median NIHSS 3 [1-9]) were included. The AUC of the prediction formula for cardioembolic stroke was 0.865, and important factors for prediction include anticoagulants before onset, heart rhythm, supratentorial cortical legion, level of consciousness, time from onset to hospital visit, age, use of the emergency system, and so on. In the same methods, the AUC for atherothrombotic brain infarction and lacunar infarction was 0.703 and 0.825 respectively.
Conclusions: ML analyses could predict ischemic stroke subtypes with high accuracy using information obtained early in the hospital visit.
Disclosures of Interest:
Yes Supported by grant from SoftBank Corp.
Abstract N°: 2165
CLINICAL IDENTIFICATION OF THE LATE ENDOVASCULAR STROKE CANDIDATE UP TO 24 HOURS INCLUDING LARGE CORE: THE FASTRAL SCORE
Edoardo Vancheri*1,2,3, Alexander Salerno1, Dimitris Lambrou1, Silvia Pistocchi4, Vincent Dunet4, Guillaume Saliou4, Fabrice Dami5, Patrik Michel1, Davide Strambo1
1Stroke Center, Neurology Service, Lausanne University Hospital and University of Lausanne, Department of Clinical Neurosciences, Lausanne, Switzerland, 2Neurology Unit, Policlinico “G. Rodolico-S. Marco”, Università Degli Studi di Catania, Dipartimento G.F. Ingrassia, Sezione di Neuroscienze, Catania, Italy, 3Stroke Unit, Department of Neurology, Hôpital Lariboisière, Paris, France, Department of Neurology, Paris, France, 4Neuroradiology Unit, Service of Diagnostic and Interventional Radiology, Lausanne University Hospital and University of Lausanne, Department of Medical Radiology, Lausanne, Switzerland, 5Emergency Department, Lausanne University Hospital and University of Lausanne, Emergency Department, Lausanne, Switzerland
On behalf of:
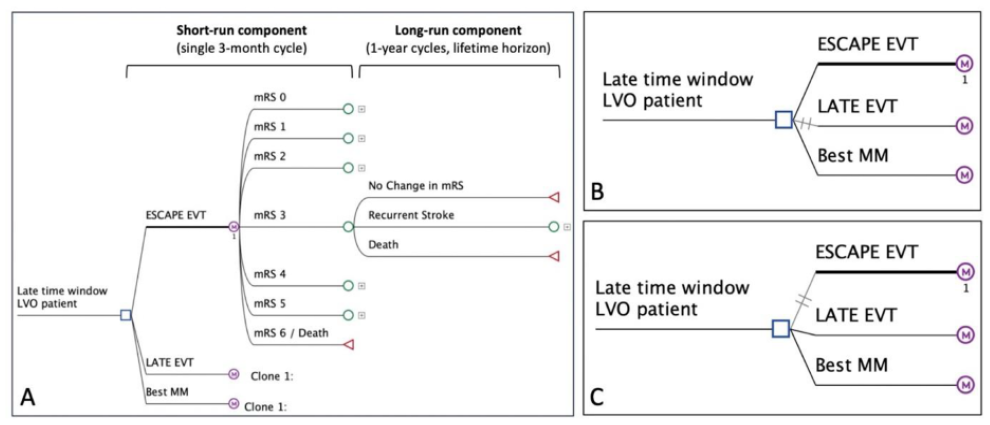
Background and aims: Recent evidence shows benefit of endovascular treatment (EVT) for acute ischemic stroke (AIS) with large vessel occlusion (LVO) up to 24hours, including large core patients. We aimed at identifying prehospital-available variables associated with updated EVT-eligibility in the early and late EVT windows, and at developing a score for the late window.
Methods: Using a large single-center registry, we retrospectively analysed premorbidly independent AIS with NIHSS⩾4 undergoing arterial imaging at our institution. We compared AIS fulfilling updated EVT-criteria (documented LVO and ASPECTS⩾3/pc-ASPECTS⩾6) with radiologically EVT-ineligible patients, both in the early (arrival 0-5hours) and late EVT-windows (arrival 5-23hours). Using multivariable binary regression analysis, we built and internally validated a late-window-score using 200-fold cross-validation. Area-under-the-receiver-operating-characteristics-curves (AUROC) were calculated.
Results: 2832/5660 consecutive AIS (median age 73years, 44% females) met the inclusion criteria. Among the 1935 in the early and 897 in the late phase, 39% and 31% fulfilled updated EVT-criteria, respectively. In the early phase, 9 variables were associated with EVT-eligibility (AUROC=77.9%). In the late phase, 7 variables were identified, resulting in the “FASTRAL-score” (see figure and graph; AUROC=75.6%, internal validation 75.1%). At sensitivity cut-offs of ⩾90% (⩽3points) and ⩾75% (⩽4points), the false-positive rates were 63% and 40%, respectively.
Conclusions: In a large cohort of AIS, we found that late EVT-eligibility from 6-24hours was associated with 7 variables available in the prehospital phase, partially different from the early phase. The FASTRAL-score for late patients might help with triage if validated externally in the prehospital phase.
Disclosures of Interest:
No
Abstract N°: 2996
RELATIONSHIP BETWEEN MICROEMBOLIC SIGNALS AND CAROTID PLAQUE CHARACTERISTICS
Inês Margarido*1,2, Joao Nuno Ramos3, João André Sousa4, iliana Igreja5, André Costa6, Cristina Duque7, Filipa Gonçalves8, Angelo Carneiro9, Luís Fontão10, Pedro Castro1,2
1Centro Hospitalar Universitário de São João, Neurology, Portugal, 2Faculty of Medicine, University of Porto, Clinical Neurosciences and Mental Health Department, Porto, Portugal, 3Centro Hospitalar de Vila Nova de Gaia / Espinho, Neuroradiology Diagnostic Unit, Portugal, 4Centro Hospitalar Universitário de Coimbra, Neurology, Portugal, 5Centro Hospitalar Universitário de Santo António, Neuroradiology, Portugal, 6Centro Hospitalar de Trás-os-Montes e Alto Douro, Neurology, Vila Real, Portugal, 7Unidade Local de Saúde de Matosinhos, Neurology, Matosinhos, Portugal, 8Hospital de Guimarães, Internal Medicine, Guimaraes, Portugal, 9Hospital de Braga, Neuroradiology, Braga, Portugal, 10Centro Hospitalar Entre-Douro e Vouga, Neurology, Santa Maria da Feira, Portugal
On behalf of:
Background and aims: literature is controversial regarding the association of microembolic signals(MES) and characteristics of carotid plaques. With this study we aimed to better understand this relationship.
Methods: multicentric retrospective study of patients with acute ischemic stroke due to anterior circulation large vessel occlusion, admitted for mechanical thrombectomy. Patients were included if monitored with transcranial-doppler within 7 days after stroke onset for detecting MES. Plaque features were assessed using admission CT-Angiography of the cervical arteries by two independent readers and averaged or determined after consensus. Analyses were performed with logistical regressions.
Results: data was available for 80 patients, corresponding to 160 carotid arteries. Concerning TOAST etiology: 10(12.50%) resulted from large-artery atherosclerosis, 46 (57.50%) cardioembolic due to atrial fibrillation (26 properly anticoagulated) and 24 (30.00%) of undetermined source. MES was positive in 24 patients (30%) and more prevalent in accordance with stenosis grade calculated through NASCET, being highest if >=70% (OR=13.40, CI95% 1.52–118.00, p=0.02). Carotid ulceration was significantly associated with MES (OR=3.66, CI95% 1.19–11.2, p=0.03). Floating thrombus was associated although not statistically significant with MES (OR=7.42, CI95% 0.75–73.10, p=0.08). Carotid thickness (>=3mm) but not extension or calcification pattern tended to be associated with MES (OR=1.97, CI95% 0.97–4.27, p=0.06). Apart from carotid axis, the aortic arch plaque ulceration was associated with MES (OR=5.27, CI95% 1.02–27.20, p=0.05).
Conclusions: MES have been associated with stroke recurrence. By supporting the association between some plaque characteristics and MES this study helps to better define which patients may be at risk of recurrence.
Disclosures of Interest:
No
Abstract N°: 3053
IMPACT OF INTRODUCTION OF STROKE AI DECISION-AID TOOL ON MECHANICAL THROMBECTOMY ACTIVITY IN ENGLAND
Kiruba Nagaratnam*1, Lauren Fensome2, Matthew Epton2, Gary Ford3,4, Tracey Marriott2, George Harston4,5, Neil Reeder6
1Royal Berkshire NHS Foundation Trust, Stroke Medicine, Reading, United Kingdom, 2Health Innovation Oxford and Thames Valley, Oxford, United Kingdom, 3University of Oxford, Radcliffe Department of Medicine, Oxford, United Kingdom, 4Oxford University Hospitals NHS Trust, Stroke Medicine, Oxford, United Kingdom, 5Brainomix Limited, Oxford, United Kingdom, 6Head and Heart Economics, London, United Kingdom
On behalf of:
Background and aims: Artificial Intelligence (AI) decision-aid tools have been widely adopted by primary and comprehensive stroke centres (PSCs and CSCs) in England but their impact on mechanical thrombectomy (MT) activity is unclear.
Methods: Using national stroke audit data from 71,642 patients in England, we compared MT activity in early adopters of e-Stroke (Brainomix, Oxford) as part of a systematic implementation programme (evaluation-cohort, n=26 centres) to other English stroke centres (comparator-cohort, n=73 centres). As some centres in the comparator-cohort independently adopted AI during the evaluation, MT rates were compared within periods defined by the proportion of the centres that had adopted AI (AI adoption-rate).
Results: The evaluation-cohort had a greater increase in MT than the comparator-cohort, 2.4% (2.1% to 4.5%) vs. 1.2% (1.7% to 2.9%)(p<0.001) and had a higher AI adoption rate by the end of the evaluation, 100% vs. 77%. The AI adoption rate had a positive effect on MT rates (p<0.0001) regardless of the cohort type (ANOVA,p=0.12). However, the impact of e-Stroke was significantly greater in the evaluation-cohort than comparator-cohort at adoption rates >25% (p<0.001, Figure.1).
MT activity increase was 2.1% in CSCs (4.3% to 6.4%, p=0.10) and 1.5% in PSCs (0.9% to 2.4%, p<0.0001) in evaluation-cohort.
Conclusions: Adoption of AI decision-aid tools was associated with increased MT activity, with significant impact of e-Stroke use on higher MT rate in the evaluation-cohort. The findings demonstrate the benefit of AI in stroke pathway. Collaborative models of care facilitated by systemic AI deployment could have contributed to the outcome observed in the evaluation-cohort.
Disclosures of Interest:
Yes Dr Kiruba Nagaratnam received lecture fees from Brainomix Limited and Dr George Haston is employed part-time by Brainomix limited
Abstract N°: 3279
PAIRED PLASMA-THROMBUS PROTEOMICS IDENTIFY KEY MECHANISMS AND MOLECULAR DRIVERS OF THROMBUS FORMATION
Teresa Wölfer*1, Yasin Eshraghi1, Walter Viegener1, Teresa Barth2, Martin Dichgans1, Jürgen Cox3, Axel Imhof2, Steffen Tiedt1
1Institute for Stroke and Dementia Research, LMU University hospital, LMU Munich, 2Protein Analysis Unit, Biomedical Center (BMC), Faculty of Medicine, Ludwig-Maximilians-University (LMU) Munich, 3Computational Systems Biochemistry, Max Planck Institute for Biochemistry, Martinsried, Germany
On behalf of:
Background and aims: The biology of human thrombosis is largely unexplored. Here, we adopted an unbiased approach integrating proteomics from stroke thrombi and matched plasma samples with immunohistochemistry and deep clinical phenotyping to identify key cellular and molecular determinants of thrombus formation and propagation.
Methods: We conducted proteomic profiling of thrombi and matched plasma samples from 250 patients with large-vessel-occlusion stroke using a semi-automated LC-MS workflow in data-independent-acquisition mode. Data were integrated with immunohistochemistry (H&E, MSB, anti-CD42b/-CD163/-MPO/-CD20), clinical phenotyping (eg, occlusion site, etiology, baseline inflammation), and a systematic review of previous stroke thrombi studies. We performed time-series clustering and knowledge-based differential dependency network analysis to identify key molecular drivers.
Results: 2,293 proteins were identified in thrombi, of which 696 have not been previously described. Thrombi from smaller vessels were compositionally more complex and tended to be more white (Fig.1). Across clinical traits, the number of significantly associated proteins was highest for vessel size (1050) and baseline immune cell counts (642-1613) while no single protein was associated with its corresponding plasma levels or etiology. Proteins more abundant in smaller-vessel thrombi linked to the immune system and coagulative pathways while proteins more abundant in larger-vessel thrombi, indicating a later stage of thrombus development, were of erythrocyte origin and linked to cellular stress. An integrated plasma-thrombus network analysis identified ITGA2B, PTPRJ, HRG, and VWF as key nodes with differential interaction partners between plasma and thrombus.
Conclusions: Using a paired plasma-thrombus proteomics approach, this study determined key stages of human thrombus development and identified molecular drivers of thrombus formation.
Disclosures of Interest:
No
SCIENTIFIC COMMUNICATION – SERVICE ORGANISATION
Abstract N°: 550
OPTIMIZING THE LOCATIONS OF THROMBECTOMY CENTRES AND THE PREHOSPITAL ACUTE TRANSFER OF PATIENTS GIVEN ECONOMIC CONSTRAINTS
Nicklas Ennab Vogel*1, Per Wester2,3, Tobias Andersson Granberg4, Lars-Åke Levin1
1Linköping University, Department of Health, Medicine and Caring Sciences, Linköping, Sweden, 2Umeå universitet, Sweden, 3Karolinska Institute, Department of Clinical Sciences, Stockholm, Sweden, 4Linköping University, Department of Science and Technology, Norrköping, Sweden
On behalf of:
Background and aims: Endovascular stroke therapy in the form of IV thrombolysis (IVT) and mechanical thrombectomy (MT) has become standard of care in eligible patients with acute ischaemic stroke (AIS) due to large vessel occlusion (LVO). Still, treatment with MT remains inaccessible and under-utilized across healthcare systems. Increasing the number of thrombectomy centres may alleviate these issues, as an expanded fleet of ambulance helicopters would too. Thus, this study aims to determine the most effective combination of optimally located ambulance helicopters and thrombectomy centres in economically constrained healthcare systems.
Methods: Based on anonymized patient-level register data (n=18793) from the Swedish Stroke Register, the Patient Register and emergency medical dispatchers stretching over a six-year study period (2012-2017), this nation-wide observational study combines operational research with the decision-analytical framework of cost-effectiveness modelling, to provide cost-effective solutions to the strategic decision problems of locating thrombectomy centres and ambulance helicopters optimally.
Results: The most cost-effective combination of optimally located thrombectomy centers and ambulance helicopters comprises of 11 thrombectomy centres and 14 ambulance helicopters, corresponding to densities of 1.05 and 1.34 per one million inhabitants, respectively. The solution yields an estimated annual INMB close to EUR 13.6 million in comparison with the current eight thrombectomy centers and no ambulance helicopter operability.
Conclusions: The most cost-effective combination of optimally located thrombectomy centers and ambulance helicopters brings about substantial health gains for patients with AIS due to LVO, compared with the current eight locations of thrombectomy centers in Sweden and no ambulance helicopters.
Disclosures of Interest:
No
Abstract N°: 1243
REGIONAL DISPARITY OF PREHOSPITAL DELAY IN ACUTE ISCHEMIC STROKE: THE KOREAN STROKE REGISTRY
Eung-Joon Lee*1, Keun-Hwa Jung1, Han-Yeong Jeong1
1Seoul National University Hospital, Neurology, Seoul, South Korea
On behalf of:
Background and aims: Late hospital arrival often keeps stroke patients from receiving recanalization therapy and is associated with poor outcomes. We used a nationwide acute stroke registry to investigate the trends and regional disparities in prehospital delay and analyze the significant factors associated with late arrivals.
Methods: Patients with acute ischemic stroke or transient ischemic attack between January 2012 and December 2021 were included. Prehospital delay was identified, and its regional disparity was evaluated using the Gini coefficient. Multivariate models were used to identify factors associated with prehospital delays of >4.5 h.
Results: Using the Korean Stroke Registry, 144,014 patients from 61 hospitals were included. The median prehospital delay was 460 min (interquartile range, 1,796), and only 36.8% of patients arrived at hospitals within 4.5 h. Long prehospital delays and high regional inequality (Gini coefficient > 0.3) persisted. After adjusting for confounders, age over 65 years old (adjusted odds ratio [aOR]=1.22; 95% confidence interval [CI], 1.18–1.27), female sex (aOR=1.09; 95%CI, 1.05–1.13), hypertension (aOR=1.12; 95%CI, 1.09-1.16), diabetes mellitus (aOR=1.38; 95%CI, 1.33-1.43), smoking (aOR=1.16, 95%CI, 1.12-1.21), premorbid disability (aOR=1.45; 95%CI, 1.37–1.52), and mild stroke severity (aOR=1.55; 95%CI, 1.50–1.61) were found to independently predict prehospital delays of >4.5 h.
Conclusions: Prehospital delays were still lengthy and had not improved with a high regional disparity in Korea. A deeper understanding of regional characteristics is required to overcome the inequalities, and further research is warranted to address the vulnerabilities identified.
Usage of reperfusion therapy and prehospital delay.
Regional disparity in prehospital delay.
Disclosures of Interest:
No
Abstract N°: 1992
STROKE TRANSPORT, TIME MANAGEMENT OF DRIP AND SHIP PATIENTS FOR MECHANICAL THROMBECTOMY
Anna Alegiani1, Tilman Lingner1, Amitis Pourian2, Bernd Eckert2, Till Illies2, Felix Butscheid3, Arno Reich4, Silke Wunderlich5, Gerhard F Hamann6, Joachim Röther*1
1Asklepios Klinik Altona, Neurology, Hamburg, 2Asklepios Klinik Altona, Neuroradiology, Hamburg, Germany, 3Buchholz in der Nordheide, Neurology, Buchholz in der Nordheide, Germany, 4Aachen, Neurology, Aachen, Germany, 5Munich, Neuroloy, Munich, Germany, 6Günzburg, Neurology, Günzburg, Germany
On behalf of: D. Tapias, T. Boeckh-Behrens, M. Vogel, B. Cheng, T. Ingwersen, G. Petzold, S.Theisen, J. Minnerup, L. Meyer, J.-H. Schäfer, L. Kellert, F. Schöberl, S. Gröschel, M. Ernst, N. Kunze-Szikszay, C. Nolte, K. Bollweg for the German Stroke Registry
Background and aims: Outcome of acute stroke treatment is time dependent (1). Many hospitals are organized in neurovascular networks (NVN) to facilitate optimal stroke treatment (2). Our project analyzed the time delay of secondary transportation of endovascular thrombectomy (EVT) patients from primary to tertiary stroke centers (drip-and-ship’ strategy) step-by-step.
Methods: The interhospital transportation times of all EVT patients that were admitted to the hospital from 2017-2022, were analyzed in different steps, starting with a retrospective analysis in our NVN. We then expanded the analysis in cooperation with hospitals of the German Stroke Registry (GSR) (3). The intervals analyzed started with the time of the diagnosis of stroke (CT Scan time) and ended with the arrival of the EVT patient in the thrombectomy center.
Results: Results of 215 local patients showed a mean transportation time of 128min. The longest delay with 67min was the time from CT Scan until the secondary transport was ordered (transfer notification order). In a second step we analyzed 898 patients from 11 tertiary stroke centers of the GSR (2022) and found similiar results with a mean transportation time of 141min and 62min for the organization of the secondary transportation.
Conclusions: The organization of the secondary transport is time consuming. In the next step we will start an intervention study with an focus hands-on training program to reduce the time until transfer notification order and the secondary transportation time.
References
Goyal et al. Lancet. 2016
Rother et al. Nervenarzt. 2020;91(10):902
Alegiani et al (2019). Int J Stroke. 14:372
Disclosures of Interest: No
Abstract N°: 2202
SIMULATING THE COST EFFECTIVENESS OF CONVERTING THE MELBOURNE MOBILE STROKE UNIT TO TELEMEDICINE
Lan Gao*1, Andrew Bivard2, Vignan Yogendrakumar2, Anna Balabanski2, Henry Zhao2, Stephen Davis2, Geoffrey A. Donnan2, Michael Valente2, Leonid Churilov2, Mark Parsons3
1Deakin University, Deakin Health Economics, Australia, 2University of Melbourne, Melbourne Brain Centre, Australia, 3The University of New South Wales, UNSW South Western Sydney Clinical School, Australia
On behalf of: Additional coauthors including Dr Skye Coote and Dr Angela Dos Santos
Background and aims: Mobile Stroke Units (MSU), a costly model of care, are able to accelerate timely access to treatment. We aimed to simulate cost-effectiveness of the Melbourne MSU by substituting the onboard neurologist with telestroke consultations.
Methods: The cost of telestroke services supporting the MSU was estimated using the hourly rate of a consultant neurologist and two teleconsultations per day over five-days-a-week of service throughout the year. Other costs of the MSU, healthcare cost offset due to MSU, and health outcomes (i.e., disability-adjusted life years, DALYs) were informed by the previous analysis. All costs were adjusted to 2022 values, and costs and DALYs were discounted at 5% annually. The incremental cost-effectiveness ratio (ICER) was calculated for telestroke-configured versus onboard MSU models over a 5-year time horizon. Using the cost-effectiveness threshold of AUD$50,000/DALY, the net monetary benefit of both MSU serviced models were estimated
Results: The costs of telestroke consultations compared with an onboard neurologist were $486,835 versus $1.44M resulting in total costs of $6.48M versus $7.43M for the two serviced models of the MSU over 5-years. When combined with the cost offset of $1.20M, net costs were $5.28M versus $6.23M. Based on 204 DALYs saved, the ICER was $25,924 or $30,587 per DALY saved in the Australian healthcare system. Net monetary benefit was $4.90M versus $3.95M for the telestroke-configured MSU and the neurologist-onboard MSU.
Conclusions: Configuring the MSU with telestroke was associated with improved cost-effectiveness and a greater monetary benefit to the healthcare system, supporting ongoing implementation and scale-up.
Disclosures of Interest:
No
Abstract N°: 2435
COMPARISON OF TREATMENT METRICS FOR HYPERACUTE TREATMENT OF INTRACEREBRAL HAEMORRHAGE AND ISCHEMIC STROKE
Bernhard Siepen*1,2, Janis Rauch1,2, Martina Göldlin1, Eva Bettschen1, Philipp Bücke1, Thomas Meinel1, Johannes Kaesmacher3, Simon Jung1, Werner Z'graggen1,4, David Seiffge1
1Department of Neurology, Inselspital Bern University Hospital, University of Bern, Bern, Switzerland, 2Graduate School for Health Sciences, University of Bern, Bern, Switzerland, 3University Institute of Diagnostic and Interventional Neuroradiology, Inselspital Bern University Hospital, University of Bern, Bern, Switzerland, 4Department of Neurosurgery, Inselspital Bern University Hospital, Bern, Bern, Switzerland
On behalf of:
Background and aims: Hyperacute treatment of both acute ischemic stroke (AIS) and intracerebral haemorrhage (ICH) is time-sensitive but knowledge about comparative performance is scarce. We compared door-to-needle times in patients with AIS and ICH directly admitted to a tertiary stroke-centre.
Methods: Single-centre retrospective cohort study (01/2018-08/2020) of consecutive patients directly admitted via code stroke with AIS or ICH. We compared door-to-needle times (AIS: intravenous thrombolysis [IVT] vs. ICH: start of blood pressure [BP] treatment and anticoagulation reversal) and used multivariable regression analyses to assess association with earlier treatment.
Results: We enrolled 1039 patients. Neither onset-to-admission (AIS: 128min vs. ICH: 130min; p=0.87) nor door-to-imaging time (AIS: 21min vs. ICH: 21min; p=1.00) differed between AIS and ICH patients. Among 871 AIS patients (age 76years; NIHSS 7, IQR 3-14), 353 (40.6%) received IVT. Among 168 ICH patients (age 74years; NIHSS 13, IQR8-21), 89 (53%) received BP treatment and 29 (17.3%) anticoagulation reversal. Door-to-needle time for IVT was significantly shorter (50min, IQR 38-70) compared to BP treatment (60min, IQR 36-81min; p=0.009) or anticoagulation reversal (58min, IQR 40-77min; p=0.019). In multivariable analysis, admission NIHSS was an independent predictor for earlier treatment for IVT (β, -1.2; 95%CI -1.8 to -0.6) and BP treatment (β, -1.5; 95%CI -2.7 to -0.4) but not for anticoagulation reversal.
Conclusions: In patients directly admitted via code stroke pre-notification, treatment times for BP treatment and anticoagulation reversal for ICH were significantly longer compared to IVT for AIS. Key time-based metrics for hyperacute treatment of ICH could be as fast as for AIS.
Disclosures of Interest:
No
SCIENTIFIC COMMUNICATION – RISK FACTORS, PRIMARY PREVENTION
Abstract N°: 674
THE IMPACT OF GENETIC POLYMORPHISMS ON DABIGATRAN LEVELS AND HEMORRHAGIC COMPLICATIONS IN ISCHEMIC STROKE PATIENTS
Anna Olserova*1, Silvia Kmetonyova1, Jaroslava Paulasova Schwabova1, Jansky Petr1, Katerina Benesova1, Martin Sramek1,2, Jan Macek3, Vaclav Matoska4, Ales Tomek1
1Motol University Hospital, Department of Neurology, 2nd Faculty of Medicine, Charles University, Prague, Czech Republic, 2Military University Hospital Prague, Department of Neurology, 3Pharmakl s.r.o., Prague, 4Hospital Na Homolce, Laboratory of molecular diagnostics
On behalf of:
Background and aims: Dabigatran is a direct thrombin inhibitor used to prevent strokes in individuals with non-valvular atrial fibrillation. The prodrug is absorbed by enteral P-glycoprotein (ABCB1) and then activated by hepatic and intestinal carboxylesterases (CES1) to produce active metabolites. Variations in dabigatran metabolism due to genetics may impact concentration levels and clinical outcomes. Our study assesses how polymorphisms in the CES1 (rs2244613) and ABCB1 (rs4148738) genes affect the cmin of dabigatran and its correlation with clinical outcomes.
Methods: Retrospective multicentric study of consecutive patients on dabigatran therapy. Examination of CES1 rs2244613 and ABCB1 rs4148738 polymorphisms, cmin 12 hours after administration, clinical follow-up (ischaemic stroke, clinically relevant haemorrhage, myocardial infarction, other thromboembolism, death).
Results: A total of 432 patients received treatment for an average of 19.78 months (SD of 20.165). 56.5% of the patients were male, and the average age was 67.56 years (SD of 14.7). The ABCB1 variant genotype was present in 67.8% of patients, 37.5% carried the CES1 polymorphism. Compared to wild-type patients, patients with the CES1 variant had significantly lower dabigatran plasma levels (with a mean difference of 16.986; 95% CI, 5.794 to 28.178 ng/mL, p = 0.003). We found a significant risk of major bleeding in patients carrying the ABCB1 rs4148738 allele (HR = 1.99, CI 95% 1.10 to 3.59, p = 0.024).
Conclusions: The CES1 variant genotype rs2244613 is linked with reduced cmin of dabigatran. Carriers of the ABCB1 rs4148738 polymorphism exhibit a tendency towards higher plasma levels, which leads to a significantly increased risk of bleeding.
Disclosures of Interest:
No
Abstract N°: 681
STROKE, MYOCARDIAL INFARCTION AND MORTALITY IN TYPE 2 DIABETES: A COMPARATIVE EFFECTIVENESS STUDY OF GLP-1RA, SGLT2I AND DPP-4I
Sidsel Hastrup*1, Jakob Nebeling Hedegaard2, Grethe Andersen1, Merete Osler3, Ida Kim Wium-Andersen3, Marie Kim Wium-Andersen3, Jorgen Rungby4, Søren Paaske Johnsen2
1Danish Stroke Centre, Department of Neurology, Aarhus University Hospital, 2Danish Center for Health Services Research, Aalborg University, 3Center for Clinical Research and Prevention, Bispebjerg and Frederiksberg Hospitals, Frederiksberg, Denmark, 4Steno Diabetes Center, Copenhagen
On behalf of:
Background and aims:
Cardiovascular outcome trials demonstrate that glucagon-like peptide-1 receptor agonists (GLP-1RA) and sodium–glucose cotransporter 2 inhibitors (SGLT2i) reduce the risk of major adverse cardio-vascular events in patients with type 2 diabetes (T2D), whereas dipeptidyl peptidase-4 inhibitors (DPP-4i) have not shown cardiovascular benefits. Comparative analyses of these newer glucose-lowering medications are lacking.
We investigated the risk of stroke (ischemic and hemorrhagic) amongst T2D patients, who were new users of GLP-1RA, SGLT2i and DPP-4i. Further, we investigated the risk of all-cause mortality and acute myocardial infarction.
Methods:
A nationwide population-based cohort study using high-quality national registries.
Study cohort: T2D without prior stroke from 2014-2020 in Denmark, who were new users of: GLP-1RA, SGLT2i or DPP-4i
Results were adjusted for age, sex, calendar year of initiation, socio-economic factors and co-morbidity.
Results:
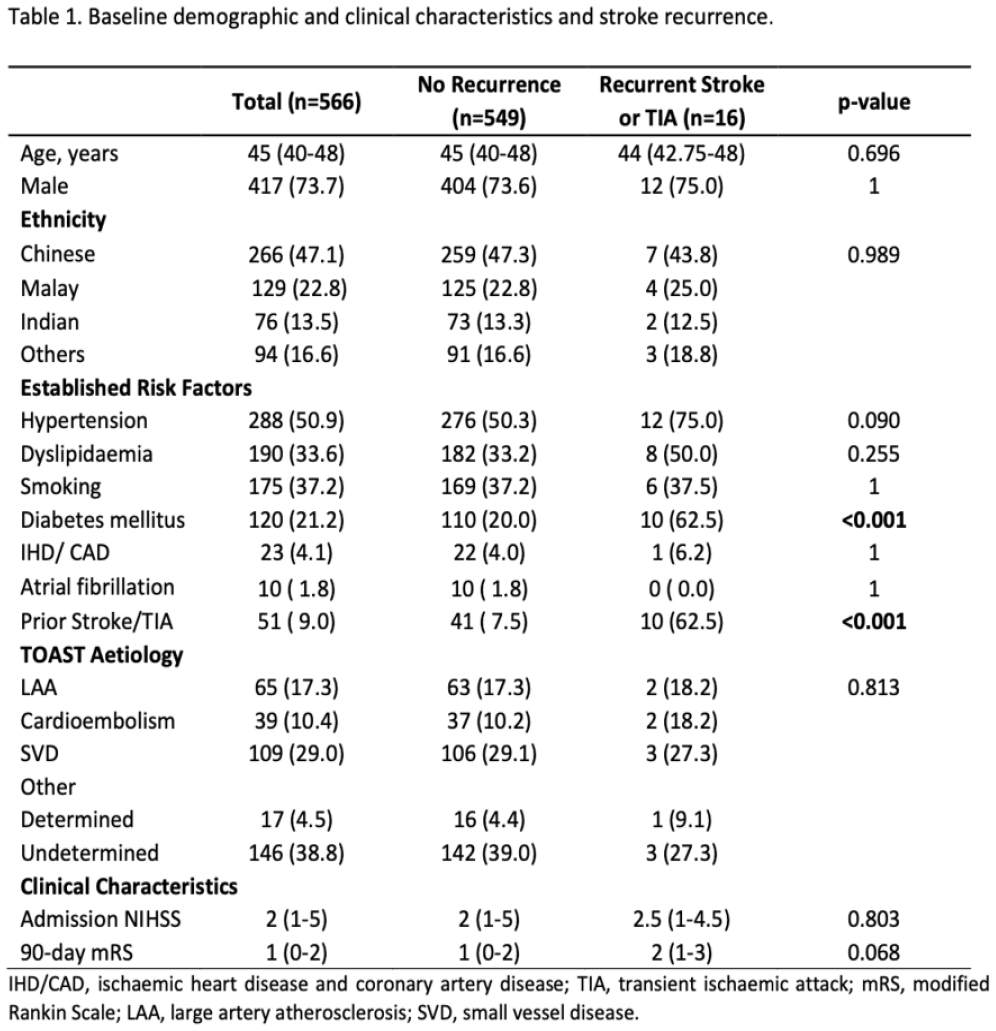
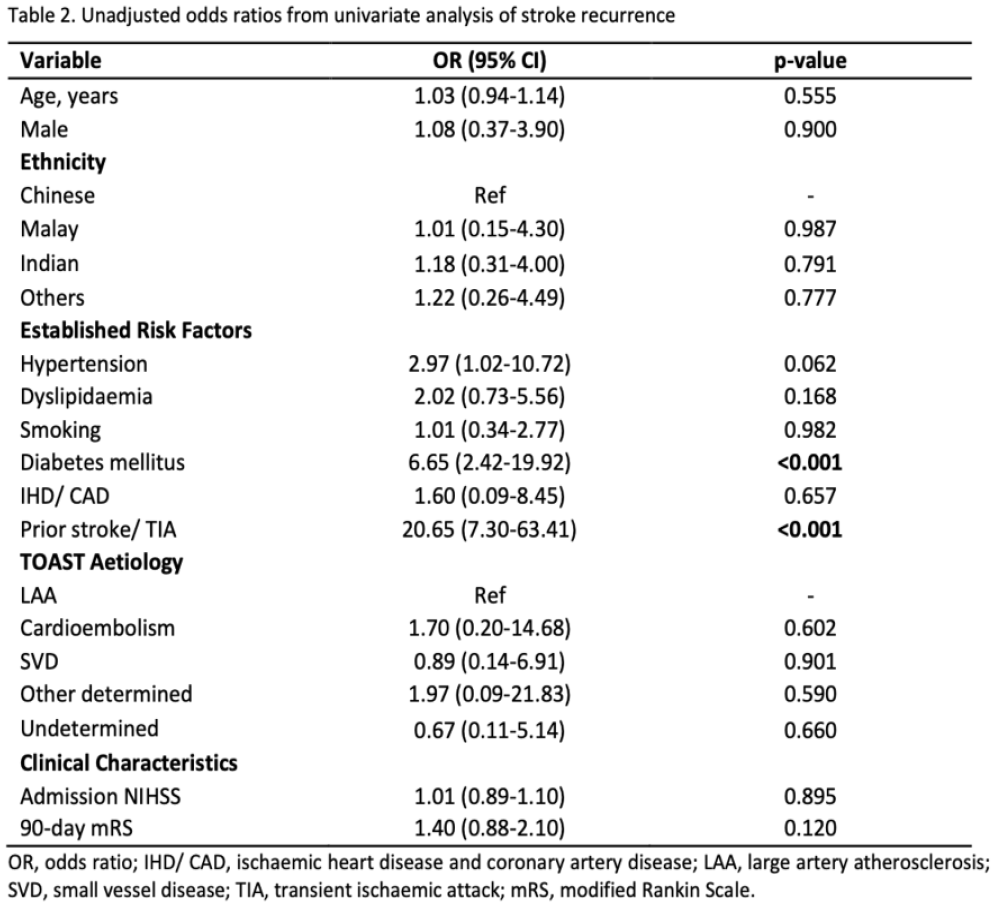
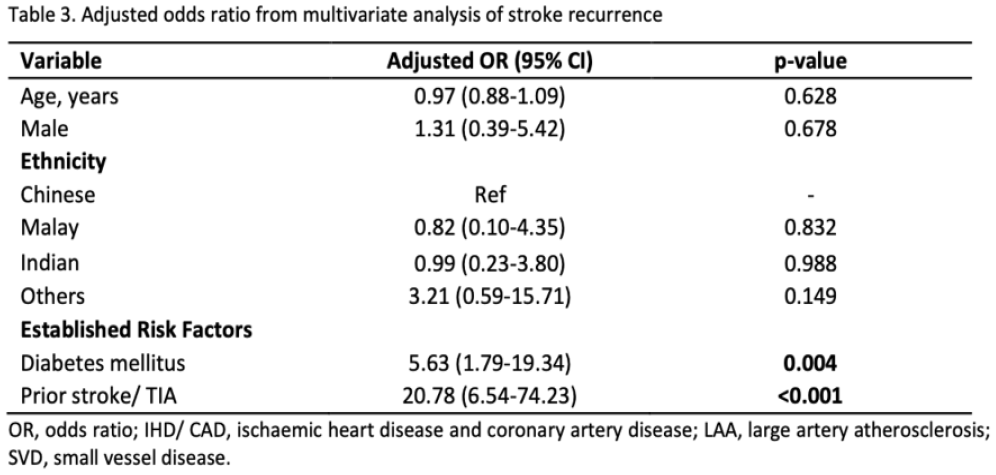
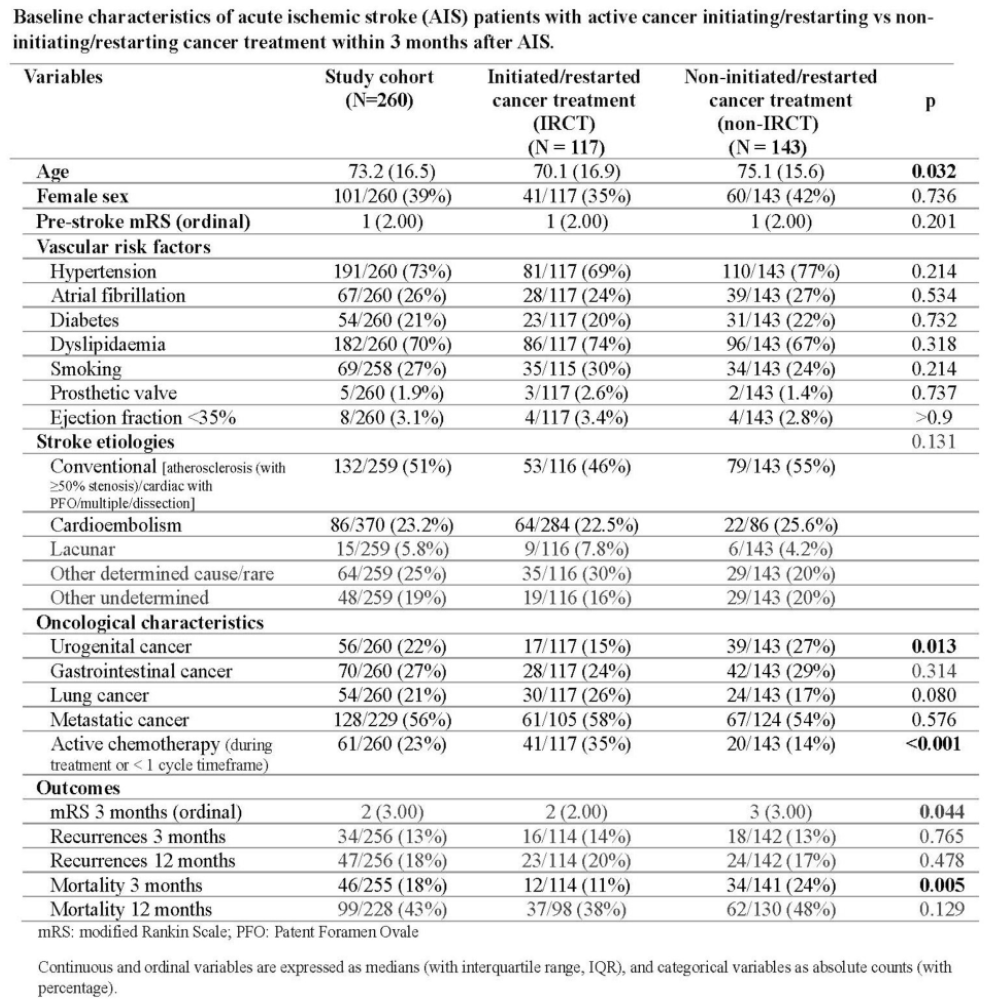
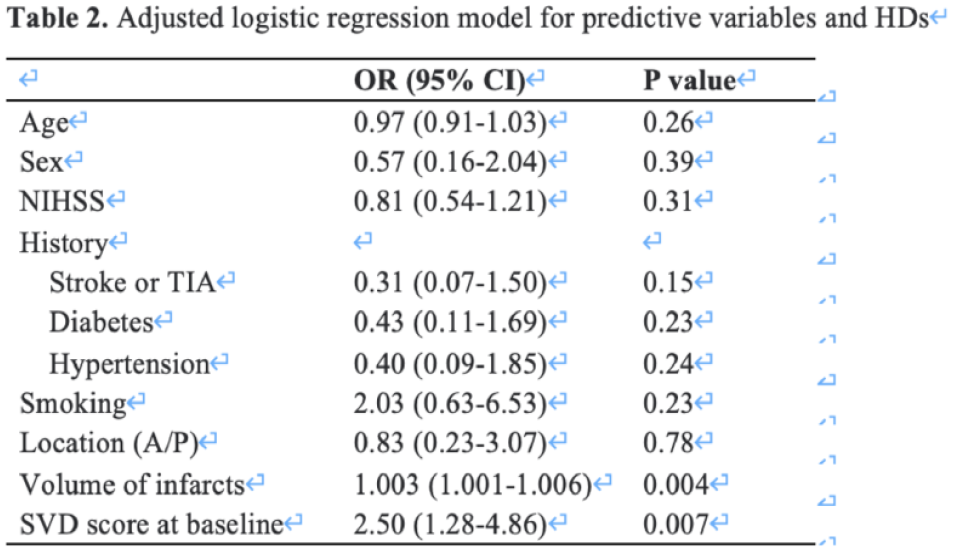
Baseline characteristics and results are presented in table 1 and table 2.
Conclusions:
New users of GLP-1RA and SGLT2i in T2D-patients were associated with reduced risk of stroke and mortality in comparison with new users of DPP-4i. New users of GLP-1RA and DPP4-i were associated with reduced risk of myocardial infarction in comparison with new users of SGLT2i. A wider use of GLP-1RA and SGLT2i may be beneficial in terms of preventing stroke and mortality. To protect against both stroke and myocardial infarction GLP-1RA seems to be the best choice
Disclosures of Interest:
Yes The source of founding Novo Nordisk A/S had no influence on data collection, no data access and influence on interpretation of the results.
Abstract N°: 1198
RISK OF ISCHEMIC STROKE IN WOMEN USING COMBINED CONTRACEPTIVES WITH ETHINYLESTRADIOL
Gasper Letnar1, Tom Skyhøj Olsen*2, Klaus Kaae Andersen1
1Omicron ApS, Copenhagen, 2Bispebjerg University Hospital, Neurology, Copenhagen, Denmark
On behalf of:
Background and aims: Combined contraceptives with ethinylestradiol (CCE) are associated with increased risk for ischemic stroke (IS). It is still unclear, however, whether there is difference in risk of IS between CCEs containing 30-40 µg and <=20 µg ethinylestradiol (EE); currently the most used contraceptives. Likewise, there is no clarity on whether risk of IS when using 4th generation CCEs is different compared to using 2nd and 3rd generation CCEs.
Methods: In this Danish cohort study (2003-2021) we investigated risk of IS in women using CCEs when compared to non-users. We stratified between CCEs containing 30-40 µg and <=20 µg EE and use of 2nd, 3rd, and 4th generation CCEs. Poisson regression models adjusting for age, educational level, ethnicity, calendar-year, and stroke risk factors were utilized.
Results: In total 1,735,306 non-pregnant women contributed 16,933,276 person-years (py) of observation to the investigation.
Risk of IS in users of CCEs with 30-40 µg EE (599 events, RR 1.04 (CI 0.89; 1.23; 3,084,994 py) did not differ significantly from that of users of CCEs with <=20 µg EE (199 events, RR 1 (reference), 1,346,846 py).
Risk of IS in users of 4th generation CCEs (with drosperinone) was 31% lower (42 events, RR 0.69 (CI 0.49; 0.97), 390,192 py) than that of 2nd generation CCEs (with levonorgestrel) (241 events, RR 1 (reference), 1,478,701 py) and 3rd generation CCEs (with norgestimate, desogestrel, gestodene) (473 events, RR 1.10 (CI 0.92; 1.31), 2,279796 py).
Conclusions: Irrespective of content of EE, use of 4th generation CCEs are associated with the lowest risk of IS.
Disclosures of Interest:
No
Abstract N°: 1408
INCREASED STROKE RISK WITH LONGER DURATION HYPERTENSION
George Howard*1, Daniel Lackland2, Paul Muntner1, Timothy Plante3, Mary Cushman3, Brian Stamm4, Suzanne Judd1, Virginia Howard1
1University of Alabama at Birmingham, Birmingham, United States, 2Medical University of South Carolina, Charleston, United States, 3University of Vermont, Burlington, United States, 4University of Michigan, Ann Arbor, United States
On behalf of:
Background and aims: Much of the focus for reducing the stroke burden of hypertension has focused on management of blood pressure levels; however, little research has addressed the potential reduction in stroke risk by delaying the onset of hypertension.
Methods: Stroke-free participants from the REasons for Geographic And Racial Differences in Stroke (REGARDS) cohort were followed for incident stroke events. For those with hypertension, duration was categorized as ⩽5 years, 6-20 years and 21+ years. Differences in stroke risk were assessed after sequential adjustment for SBP and use of antihypertensive medication, demographic factors (age, race and sex), and cerebrovascular risk factors (diabetes, smoking, atrial fibrillation, left ventricular hypertrophy and heart disease).
Results: Participants (n=27,310, median age=64) were followed for a median of 12.4 years, during which 1,763 incident stroke events occurred. Compared to participants without hypertension, the risk of stroke increased across hypertension duration after each level of adjustment (see table).
Conclusions: Longer duration of hypertension was associated with a dose-dependent higher stroke risk, even at the same age and level of SBP. Delaying the onset of hypertension may reduce stroke risk.
Disclosures of Interest:
No
Abstract N°: 1692
VASCULAR RISK FACTORS IN CEREBRAL AMYLOID ANGIOPATHY: A COHORT STUDY IN HEREDITARY CAA AND A SYSTEMATIC REVIEW IN SPORADIC CAA
Sabine Voigt*1,2, Ingeborg Rasing1, Maaike van der Plas1, Sarah Khidir3, Emma Koemans1, Kanishk Kaushik1, Ellis van Etten1, Jan Schoones4, Erik van Zwet5, Marieke J.H. Wermer1,6
1Leiden University Medical Center, Neurology, Netherlands, 2Leiden University Medical Center, Radiology, Netherlands, 3Leiden University Medical Center, Rheumatology, Netherlands, 4Leiden University Medical Center, Directorate of Research Policy, Netherlands, 5Leiden University Medical Center, Department of Biomedical Data Sciences, Netherlands, 6University Medical Center Groningen, Neurology, Netherlands
On behalf of:
Background and aims: Cerebral amyloid angiopathy (CAA) is a major cause of ICH and vascular dementia. We investigated the prevalence of vascular risk factors and their effect on disease onset and disease course in Dutch-type hereditary (D-)CAA and sporadic CAA.
Methods: We performed a cohort study in D-CAA to investigate the association between vascular risk factors (hypertension, hypercholesterolemia, smoking and alcohol use) and age of ICH onset and recurrence with survival analyses. In addition, we performed a systematic review to assess the prevalence of vascular risk factors and their effect on clinical outcome in sporadic CAA. We created forest plots, calculated pooled estimates and reported heterogeneity and risk of bias.
Results: We included 70 participants with D-CAA (47% women, mean age 53y). Sixteen (23%) had hypertension, 15 (21%) hypercholesterolemia, 45 (64%) were smokers and 61 (87%) used alcohol. We found no clear effect of vascular risk factors on age of first ICH (log-rank hypertension: p=0.35, hypercholesterolemia: p=0.41, smoking: p=0.61 and alcohol use: p=0.55) or time until ICH recurrence (log-rank hypertension: p=0.71, hypercholesterolemia: p=0.20 and smoking: p=0.71). In the systematic review, the pooled prevalence estimate of hypertension was 62% (95%CI:59%-65%), dyslipidemia 78% (95%CI:71%-83%), diabetes 85% (95%CI:82%-88%) and smoking 78% (95%CI:73%-83%). Most studies showed no association between vascular risk factors and outcome. High quality studies focusing on vascular risk factors were lacking.
Conclusions: In patients with CAA the prevalence of vascular risk factors is high. Although this suggests an opportunity for prevention, we found no clear association between these risk factors and ICH onset and outcome.
Disclosures of Interest:
No
Abstract N°: 1782
POLYGENIC RESISTANCE TO BLOOD PRESSURE TREATMENT AND STROKE RISK
Shufan Huo*1, Cyprien Rivier1, Santiago Clocchiatti-Tuozzo1,2, Daniela Renedo1,3, Hongyu Zhao4, Adam de Havenon1, Kevin Sheth1, Guido Falcone1
1Yale University, Department of Neurology, New Haven, United States, 2Yale University, Department of Internal Medicine, New Haven, United States, 3Yale University, Department of Neurosurgery, New Haven, United States, 4Yale University, Department of Biostatistics, New Haven, United States
On behalf of:
Background and aims: Common genetic variation explains about 40% of inter-individual blood pressure (BP) variability, but its impact on BP treatment and its sequelae remains understudied. We investigated the impact of polygenic predisposition to hypertension (PPH) on BP treatment response and stroke risk in primary prevention.
Methods: We conducted a genetic association study using data from the All of Us Research Program. We included participants without prior stroke taking any BP medication. Subjects were categorized as having low, intermediate, or high PPH using percentiles (<20, 20-80, >80) of a polygenic risk score of 732 independent risk variants. Resistant hypertension was defined as systolic BP >140mmHg and stroke was ascertained using EHR data. We used multivariable logistic and Cox Proportional Hazards regressions to assess the relationship between PPH and both resistant hypertension and incident stroke and replicated all results in data from the UK Biobank.
Results: We included 106,333 participants (mean age 59, 59% female). Compared to low PPH, intermediate and high PPH were associated with 15% (OR 1.15, 95%CI 1.10-1.19) and 30% (OR 1.30, 95%CI 1.23-1.36) increase of resistant hypertension. Similarly, intermediate and high PPH were associated with 10% (HR 1.10, 95%CI 0.98-1.23) and 22% (HR 1.22, 95%CI 1.06-1.39) increased stroke hazard. These results were replicated in 102,252 participants (mean age 61, 47% female) from the UK Biobank.
Conclusions: Among participants on antihypertensive medication, increased PPH correlates with higher risk of resistant hypertension and stroke. Our findings support further research, including clinical trials, on personalized interventions targeting high-risk subjects.
Disclosures of Interest:
No
Abstract N°: 2046
A REGISTER-BASED STUDY ON ASSOCIATIONS BETWEEN STROKE MORTALITY AND RISK FACTORS INCLUDING SOCIAL DETERMINANTS OF HEALTH
Katharina Stibrant Sunnerhagen*1, Bilal El Nager1, Adam Viktorisson1, Malin Reinholdsson1
1University of Gothenburg, Clnical Neuroscience, Gothenburg, Sweden
On behalf of:
Background and aims: The aim is to investigate if there is an association between social determinants of health and stroke mortality in patients diagnosed with stroke in Gothenburg.
Methods: This is a register-based study with a longitudinal design based on retrospective data. Information on social determinants of health, comorbidities and stroke mortality is gathered from the local and national stroke registries, Statistics Sweden, and the National Patient Registry. Social determinants of health were defined as living area, country of birth, education, and income. Cox regression analysis was used.
Results: In the study population with 6901 patients, a higher education was associated with a 25.7% lower risk of death compared with primary education, high-income individuals had a 32.3% lower risk of death compared with low-income individuals. Living in a deprived area and country of birth did not show significant association with mortality. Lifestyle factors, including physical inactivity, diabetes, alcohol abuse, and atrial fibrillation, were associated with increased mortality risk. Analysis of the number of exposed social determinants of health factors revealed a significant trend, with individuals with one determinant having a 17.5% increased risk and those with two to four determinants having a 24.3% increased risk.
Conclusions: These findings highlight the cumulative impact of social determinants on post-stroke mortality and underscore the need for comprehensive interventions. While adjusting for other risk factors and comorbidities did not yield statistically significant associations, the overall analysis revealed significant links with both high and low educational and income attainment.
Disclosures of Interest:
No
SCIENTIFIC COMMUNICATION – IMAGING
Abstract N°: 770
THE BENEFIT OF FAVORABLE VENOUS OUTFLOW PROFILE IS MEDIATED THROUGH REDUCED MICROVASCULAR DYSFUNCTION IN ACUTE ISCHEMIC STROKE
1Huashan Hospital, Neurology, Shanghai, China, 2Seventh People's Hospital of Shanghai University of Traditional Chinese Medicine, Neurology, Shanghai, China, 3Yangpu Hospital, School of Medicine, Tongji University, Neurology, Shanghai, China
On behalf of:
Background and aims: Venous outflow (VO) is emerging as a marker of microvascular integrity in acute ischemic stroke. Using hemorrhagic transformation (HT) and infarct growth as mediators, we tested whether a favorable VO profile benefit functional outcome by reducing consequences of microvascular dysfunction.
Methods: Patients receiving thrombectomy in three comprehensive stroke centers due to acute anterior circulation occlusion were included. VO was assessed semi-quantitatively by the opacification of ipsilateral vein of Labbé, Trolard and superficial middle cerebral vein. HT was graded on follow-up CT. Infarct growth volume (IGV) was the difference of final infarct volume and baseline core volume. The association of VO and functional independence (90-day modified Rankin Scale ⩽2) was examined by logistic regression. Mediation analysis was performed among VO, HT or IGV, and functional outcome in patients with or without recanalization, respectively.
Results: In 242 patients analyzed, VO was strongly correlated with functional independence and VO⩾4 was defined favorable. In 175 patients recanalized, favorable VO was associated with a reduced risk of HT (OR=0.82, 95% CI 0.71–0.95, P=0.008), which accounted for 13.1% of the association between VO and favorable outcome. In 67 patients without recanalization, favorable VO was associated with decreased IGV (β=−0.07, 95% CI −0.11-−0.02, P=0.007). The association of favorable VO and functional independence was no longer significant (aOR=4.84, 95% CI 0.87-38.87, P=0.089) after including IGV in the model, suggesting a complete mediation.
Conclusions: In patients with acute large vessel occlusion, the clinical benefit of VO may be mediated through reduced microvascular dysfunction.
Disclosures of Interest: No
Abstract N°: 1579
PERFUSION ABNORMALITIES ON 24-HOUR PERFUSION IMAGING AMONG PATIENTS WITH COMPLETE MACROVASCULAR REPERFUSION
Adnan Mujanovic*1, Anick Imhof1, Christoph Kurmann1, Bettina Serallach1, Tomas Dobrocky1, Sara Pilgram-Pastor1, Eike Immo Piechowiak1, Jan Gralla1, Urs Fischer2, Johannes Kaesmacher1
1Inselspital, Department of Diagnostic and Interventional Neuroradiology, Bern, Switzerland, 2Universitätsspital Basel, Department of Neurology, Basel, Switzerland
On behalf of:
Background and aims: Potential reasons for achieving poor clinical outcome (modified Rankin scale, mRS>2) despite complete reperfusion (Thrombolysis in Cerebral Infarction, TICI3) has been contributed to microvascular reperfusion status. We aimed to evaluate different perfusion imaging patterns on the 24-hour follow-up perfusion imaging among TICI3 patients.
Methods: Single-institution’s stroke registry analysis for all stroke patients admitted 02/2015 – 12/2021. Macrovascular reperfusion status was graded on the expanded TICI (eTICI) scale. Microvascular reperfusion status was qualitatively evaluated within the area of infarct core on 24-hour follow-up CBV and CBF perfusion maps. All ratings were performed by a blinded core lab. Primary outcome was functional independence (mRS 0-2) and strong neurological improvement, defined as difference between National Institutes of Health Stroke Scale (NIHSS) score on discharge and admission ⩾8.
Results: Based on the microvascular reperfusion status, all eTICI3 patients (n=248) were grouped into one of the four clusters: 1) normoperfusion (no perfusion abnormalities; n=143/248); 2) hyperperfusion (hyperperfusion on both CBV and CBF maps; n=54/248); 3) hypoperfusion (hypoperfusion on both CBV and CBF maps; n=14/248) and 4) mixed cluster (discrepant ratings, e.g. hypoperfusion on CBV and hyperperfusion on CBF; n=37/248). Patients in the hypoperufsion cluster were less likely to achieve functional independence (aOR 0.3, 95%CI 0.1 – 0.8) or strong neurological improvement (aOR 0.1, 95%CI 0.03 – 0.4), while patients in the hyperperfusion cluster tended to have better overall outcome.
Conclusions: Around half of TICI3 patients experience perfusion abnormalities on the microvascular level. Microvascular hypoperfusion, despite complete macrovascular reperfusion, could partially explain poor prognosis among some TICI3 patients.
Disclosures of Interest:
No
Abstract N°: 1713
OXYGEN EXTRACTION FRACTION MAPPING ON ADMISSION MRI IN ISCHEMIC STROKE MAY PREDICT RECOVERY OF ISCHEMIC LESIONS AFTER THROMBECTOMY
Alexandre Bani-Sadr*1, Marc Hermier1, Charles De Bourguignon2, Laura Mechtouff2, Omer Eker1, Tae-Hee Cho2, Laurent Derex2, Norbert Nighoghossian2, Yves Berthezene1
1Hospices Civils de Lyon, Neuroradiology, Bron, France, 2Hospices Civils de Lyon, Neurology, Bron, France
On behalf of:
Background and aims: While dynamic-susceptibility contrast (DSC) perfusion MRI enables oxygen extraction fraction (OEF) mapping, the significance of DWI lesions with preserved OEF remains to be elucidated. This study investigated the relationship between the DWI lesions with increased OEF, as assessed at admission, and the evolution of these lesions in a cohort of patients treated with thrombectomy.
Methods: The HIBISCUS-STROKE cohort, a single-center observational study, prospectively recruited AIS patients post-MRI triage for thrombectomy, with a subsequent day 6 T2-FLAIR MRI. Admission DSC-MRIs were automatically post-processed to produce OEF maps. Volume changes were assessed by the absolute difference between the day 6 T2-FLAIR MRI and admission DWI assessments.
Results: Of the 321 cohort participants enrolled from 2016 to 2022, 135 were excluded due to incomplete neuroimaging protocol (n=135). The remaining 186 subjects constituted the study population (median age: 71 years, 55.4% of males, median NIHSS at admission: 14.0). Sixty-five had increased OEF within DWI lesions and 134 achieved recanalization. In non-recanalized patients, the volume changes from admission DWI to day 6 T2-FLAIR MRI did not vary according the OEF status (P=0.39). Conversely, those with DWI lesions with increased OEF achieving recanalization experencied a regression (median:-4.0mL, interquartile range (IQR): [-11.6,1.4] versus 4.8mL; IQR: [-1.4,17.9], P<0.0001). In these patients, multivariate analyses indicated that an increased OEF within DWI lesions was associated with a regression of DWI lesions (odds ratio: 0.68, 95% confidence interval: [0.49,0.87], P=0.008).
Conclusions: An increased OEF within DWI lesions was associated with the regression of DWI lesions in patients with successful thrombectomy.
Disclosures of Interest:
No
Abstract N°: 2049
GHOST PENUMBRA PATTERN IN ACUTE STROKE PATIENTS WITH LARGE-VESSEL OCCLUSION: DEFINITION AND PROGNOSTIC RELEVANCE
Mercedes de Lera Alfonso*1, Ana Isabel Calleja Sanz1, Elisa Cortijo Garcia1, Alicia Sierra Gómez1, Alirio Millan Urribarri2, Ignacio Eiros Bachiller2, Jorge Galván Fernández2, Miguel Arturo Schüller2, Mario Martínez-Galdámez2, Juan F. Arenillas1
1Hospital Clínico Universitario de Valladolid, Neurology. Stroke Unit., Valladolid, Spain, 2Hospital Clínico Universitario de Valladolid, Radiology, Valladolid, Spain
On behalf of: On behalf of the Stroke Program HCU Valladolid: Ramos Araque, ME; Reyes Muñoz, J; Gómez Vicente, B; Valle Peñacoba, G; Pérez Sánchez, I.
Background and aims: In acute ischemic stroke (AIS) patients with large vessel occlusion (LVO), the ‘ghost penumbra pattern’ (GPP) is characterized by non-contrast CT (NCCT) scan yielding a significantly larger core volume than the one depicted in processed CT perfusion (CTP) maps. We aimed to describe the frequency of GPP, the baseline factors associated with its presence, and its clinical and radiological impact.
Methods: Retrospective analysis of a prospectively collected sample of LVO-AIS patients successfully treated (full reperfusion) with EVT. NCCT-core volume was obtained manually. CTP-core volume was automatically provided by neuroimaging software. GPP was defined by a ratio NCCT-core / CTP-core > 1.5. We analyzed the prevalence of GPP and its pre-EVT associated factors, and studied its association with parenchymal hematoma (PH) risk and long-term functional outcome.
Results: From 06/2020 to 12/2021, 173 patients fulfilled all inclusion criteria, 90 (52%) were women, mean age 73 years, and median NIHSS 16. GP pattern was detected in 100 (58%) patients and was associated with better collateral circulation (OR 2.2 [1.3-3.4]; p<0.001) and with higher probability of the thrombus being located distally to the NNCT core (OR 0.2 [0.01-.098]; p<0.048). The risk of developing a PH at 24 hours was lower with GPP (OR=0.42 [0.19-0.92]; p=0.032). GPP did not affect functional outcome.
Conclusions: GPP was observed in half the patients and was associated with better collateral circulation and with the thrombus located distally to the NCCT-core, probably reflecting migration before EVT. GPP was associated with a benign safety profile as it predicted lower hemorrhagic risk.
Disclosures of Interest:
No
Abstract N°: 2211
CT OR MRI PROTOCOL FOR ACUTE STROKE REPERFUSION WITH EVT (COMPARE): AN INTERNATIONAL RETROSPECTIVE COHORT STUDY
Célina Ducroux*1, William Boisseau2, Robert Fahed1, Grant Stotts1, Julien Labreuche3, Maéva Kyheng3, Daniel Roy4, Bertrand Lapergue3, Alexandre Y. Poppe5
1The Ottawa Hospital Civic Campus, Neurology, Ottawa, Canada, 2Hospital Foundation Adolphe De Rothschild, Paris, France, 3Hospital Foch, Neurology, Suresnes, France, 4CHUM - Centre hospitalier de l'Université de Montréal, Radiology, Montréal, Canada, 5CHUM - Centre hospitalier de l'Université de Montréal, Neurology, Montréal, Canada
On behalf of: ETIS registry
Background and aims: Patients with an acute ischemic stroke (AIS) are selected to receive reperfusion therapy using either computed tomography (CT-CTA) or magnetic brain imaging (MRI). The aim of this study was to compare CT and MRI as the primary imaging modality for AIS patients undergoing EVT.
Methods: Data for AIS patients between January 2018 and January 2021 were extracted from two prospective multicenter EVT cohorts: the ETIS registry in France (MRI) and the OPTIMISE registry in Canada (CT). Demographics, procedural data and outcomes were collected. We assessed the association of qualifying imaging (CT vs. MRI) with time metrics, favorable 90-day functional outcomes and safety outcomes.
Results: From January 2018 to January 2021, 4059 patients selected by MRI and 1324 patients selected by CT were included in the study. Demographics were similar between the two groups. The median imaging-to-arterial puncture time was 37 minutes longer in the MRI group. Patients selected by CT had more favorable 90-day functional outcomes as compared to patients selected by MRI (48.5% vs 44.4%; adjusted OR (aOR), 1.54, 95%CI 1.31 to 1.80, p<0.001). In sub-group analyses, only “drip-and-ship” patients had better outcomes using CT. No significant difference was found regarding intracranial hemorrhage.
Conclusions: Patients with AIS undergoing EVT who were selected with MRI as opposed to CT had longer imaging-to-arterial-puncture delays and worse functional outcomes at 90 days. This difference was only found among patients transferred to an EVT center from a referring hospital.
Disclosures of Interest:
No
Abstract N°: 2359
GRAY MATTER ABNORMALITIES IN CEREBRAL SMALL VESSEL DISEASE: A MULTI-MODAL MRI STUDY
Marvin Petersen*1, Felix Nägele1, Maximilian Schell1, David Emskötter1, Götz Thomalla1, Bastian Cheng1
1University Medical Center Hamburg-Eppendorf, Neurology
On behalf of:
Background and aims: Cerebral small vessel disease (CSVD) raises the risk of cognitive impairment and dementia. While white matter changes due to CSVD are well-documented, its impact on the cerebral gray matter is less well understood.
Methods: We analyzed 2631 participants (43.9% women, average age 64.0) from the Hamburg City Health Study, employing multi-modal MRI to calculate a CSVD score by z-scoring and averaging the white matter hyperintensity load, Fazekas score, peak-width of skeletonized mean diffusivity, and perivascular spaces count. In a general linear model, we related this CSVD score to regional imaging measures of macrostructural and microstructural tissue integrity in the cortex, basal ganglia and hippocampus (adjusting for age, sex and education): thickness and volume, T1/T2-ratio, mean diffusivity, free-water and tissue fractional anisotropy. In a post-hoc analysis, we linked these imaging measures to cognitive test performances.
Results: Higher CSVD burden correlated with lower cortical thickness, higher subcortical volume and hippocampal thickness as well as abnormal gray matter T1/T2-ratio, mean diffusivity, free-water, and fractional anisotropy (figure 1). These abnormalities were evident in the anterior cingulate, insula, temporal lobe, and subcortical structures including the hippocampus. Furthermore, imaging markers in these regions were significantly associated with poorer performance in the Animal Naming, Trail Making Test A and B, and Multiple Choice Vocabulary Test (figure 2).
Conclusions: Our research shows that CSVD burden correlates with structural gray matter abnormalities linked to cognitive performance in the general population. These findings support the understanding of CSVD as a global brain disease, offering deeper insights into its pathophysiology.
Disclosures of Interest: No
Abstract N°: 2964
QUANTITATIVE OXYGEN METABOLISM MEASUREMENT WITH MRI OFFERS NEW READ-OUTS OF ACUTE AND POST-REPERFUSION SETTINGS
Lucie Chalet*1,2, Timothé Boutelier2, Christen Thomas3, Debatisse Justine4, Oceane Wateau5, Nicolas Costes6, Omer Eker7,8, Tae-Hee Cho1,9, Laura Mechtouff1,9, Emmanuelle Canet-Soulas1
1Univ. Claude Bernard Lyon 1, U1060 Cardiovascular Diseases, Metabolism, Diabetology and Nutrition Laboratory, Lyon, France, 2Olea Medical, La Ciotat, France, 3Univ. Grenoble Alpes, U1216 Grenoble Institute of Neuroscience, Grenoble, France, 4Univ. Claude Bernard Lyon 1, UMR5229 Institut des Sciences Cognitives Marc Jeannerod, Lyon, France, 5Cynbiose SAS, Marcy L'Etoile, France, 6Univ. Claude Bernard Lyon 1, CERMEP - imagerie du vivant, Lyon, France, 7Hospices Civils de Lyon, Neuroradiology Department, Lyon, France, 8INSA, UMR5220, U1294, CREATIS, Lyon, France, 9Hospices Civils de Lyon, Stroke Department, Lyon, France
On behalf of: All collaborators of the CYCLOPS and CMRO2 projects funded by the French National Research Agency (ANR-15-CE17-0020 and ANR-21-CE17-0028).
Background and aims: With the growing need for patient-tailored approaches in AIS management, oxygen metabolism imaging offers new perspectives to provide therapeutic target definitions as initially established with [15O]-PET imaging, now incompatible with clinical emergency settings. MRI represents an alternative to explore these historical parameters and the proposed pre-clinical AIS model with simultaneous PET-MRI is a key player in the validation of a quantitative approach in acute and sub-acute settings.
Methods: Pre-clinical PET-MRI data of 8 non-human primates in physiological, AIS, and reperfusion settings were evaluated. BOLD MRI acquisitions provided oxygen metabolism parameters mapping through a newly developed pipeline including magnetic field inhomogeneity (ΔB0) corrections, quantitative susceptibility mapping (QSM), and Bayesian deconvolution of perfusion signals (Fig1). Comparison of CBF, oxygen extraction fraction, and cerebral metabolic rate of oxygen to [15O]H2O and [15O]O2 PET scans enabled the validation of the MRI approach.
Results: Comparison of penumbra volumes between PET and MRI prior to registration showed a strong agreement for identical physiological thresholds (Fig2.A, B). However, quantitative evaluations of PET and MRI throughout brain regions demonstrated a proportional disagreement between physiological measurements highlighting the presence of ΔB0 and variations of susceptibility between brain regions (Fig2.C). Calculated ΔB0 maps outperformed MRI manufacturer acquisitions (Fig2.D) which, followed by QSM, provided enhanced oxygen mapping in sub-cortical, myelin-rich, and posterior brain territories. These new NHP-data corrective maps are paving the way for an answer to the quantitative measurement disagreement between the two methods.
Conclusions: We propose a key translational AIS model to validate quantitative brain oxygen metabolism measurement in pathophysiological clinical settings.
Disclosures of Interest:
Yes Lucie Chalet and Timothé Boutelier are employees of Olea Medical, a company developing software for stroke imaging processing.
Abstract N°: 3306
MR-PWI HYPERPERFUSION NOT HYPOPERFUSION OCCURS WITHIN THE DWI LESION AND SECONDARY GROWTH REGION FOLLOWING SUCCESSFUL EVT: REPERFUSE-NA1 STUDY RESULTS
Raneem Sheronick*1, George Tadros1, Akash Khaira1, Joachim Fladt2, Jen Guo1, Ryan Mctaggart3, Thalia Field4, Ruchir Shah5, Mayank Goyal1, Michael Hill1
1University of Calgary, 2University Hospital Basel, 3Rhode Island Medical Imaging, 4University of British Columbia, 5UT Erlanger Neurology
On behalf of: Richard Swartz6, Thalia Field7, Ruchir Shah8, Mayank Goyal9, Michael Hill2, Andrew Demchuk2, Michael Tymianski10,11, Christopher D’esterre2, Philip Barber
Background and aims: Mechanisms of early secondary infarct growth following successful recanalization remain largely misunderstood. We investigated whether post-treatment(MR-PWI can identify perfusion deficits that contribute to DWI lesion growth 24 hours after stroke onset.
Methods: This prospective multisite study(REPERFUSE-NA1) included patients with successful recanalization(mTICI2b-3) for anterior circulation LVOs. All patients underwent Dynamic susceptibility contrast enhanced(DSC) and DWI-MRIs <5 hours post-EVT (Day 1) and a follow-up DWI 24 hours post-EVT (Day 2). Relative Cerebral Blood flow(rCBF) was measured in the Day 1 DWI lesion, Day 2 DWI lesion and surrounding unaffected tissue, relative to the contralateral hemisphere.
Results: A total of 35 patients (mean age 65 years, SD=14, 48.57% female, median NIHSS 15(IQR= 9)) were included. The median DWI infarct lesion size increased from 5.65mL(IQR = 36.17) on Day 1 to 8.54 mL(20.14) on Day 2. Median rCBF in Day 1 DWI (early infarct) was 1.3(0.64), median rCBF in the Day 2 DWI(secondary infarct growth) was 1.11(0.66) and median rCBF in the unaffected tissue was 0.87(0.73). Significant differences in rCBF were observed between the Day 1 early infarct lesion, the Day 2 secondary growth region, and the unaffected tissue (p=0.000016). However, post-recanalization rCBF following EVT was not a statistically significant predictor of secondary DWI growth.
Conclusions: MR-PWI identified increased rCBF in both the Day 1 DWI lesion and the Day 2 secondary DWI growth region demonstrating that hyperperfusion and not hypoperfusion occurs in ischemic brain following successful recanalization. However, in this study, rCBF did not predict t the secondary DWI growth.
Disclosures of Interest:
No
SCIENTIFIC COMMUNICATION – SMALL VESSEL DISEASE
Abstract N°: 800
MESO-CORTICAL PATHWAY DAMAGE IN COGNITION, APATHY, GAIT DYSFUNCTION IN CEREBRAL SMALL VESSEL DISEASE
Hao Li*1, Mina Jacob1, Mengfei Cai1,2, Roy Kessels3,4,5, David Norris6, Marco Duering7,8, Frank-Erik De Leeuw1, Anil Tuladhar1
1Radboud University Medical Center, 2Guangdong Provincial People's Hospital, 3Radboud University, Donders Institute for Brain, Cognition and Behaviour, Centre for Cognition, 4Radboud University Medical Center, Department of Medical Psychology and Radboudumc Alzheimer Center, 5Vincent van Gogh Institute for Psychiatry, 6Radboud University, Donders Institute for Brain, Cognition and Behaviour, Centre for Cognitive Neuroimaging, 7Medical Image Analysis Center (MIAC AG) and Department of Biomedical Engineering, University of Basel, 8Institute for Stroke and Dementia Research (ISD), LMU University Hospital
On behalf of:
Background and aims: Cerebral small vessel disease (SVD) contributes to cognitive impairment, apathy, and gait dysfunction. The dopaminergic meso-cortical and meso-limbic pathways have been identified as key brain circuits for cognition, emotion, and motor functions. Here, we investigated the potential inter-relations between cognitive impairment, apathy, and gait dysfunction, with a specific focus on the effects of meso-cortical and meso-limbic pathways damage on these features in SVD.
Methods: We included SVD participants with MRI scans from the RUNDMC study. Comprehensive neurobehavioral assessments included processing speed, executive function, memory, apathy, and gait function (the time and steps in Timed Up and Go test). Using diffusion MRI, we reconstructed four tracts connecting ventral tegmental area (VTA) and the dorsolateral-prefrontal cortex (dlPFC), ventral-lateral PFC (vlPFC), medial-orbitofrontal cortex (mOFC) and nucleus accumbens (NAc) (Figure 1). The damage along these tracts was quantified using the free water (FW) fraction and FW-corrected mean diffusivity (MD-t).
Results: 227 SVD participants were included (mean age 74 years). Higher FW values of VTA-mOFC and VTA-vlPFC tracts were related to all clinical measures, independently of FW/MD-t beyond these tracts of interest. Principal component analysis showed strong inter-associations among all six clinical measures and identified a common component (Figure 2). Higher MD-t and FW values of VTA-mOFC and VTA-vlPFC tracts showed strongest associations with this common component.
Conclusions: Our study showed that cognitive impairment, apathy, and gait dysfunction in SVD are strongly inter-related and suggest meso-cortical pathways as a common neural basis underlying the three features in SVD.
Disclosures of Interest:
No
Abstract N°: 1041
CEREBRAL SMALL VESSEL DISEASE AS A MULTISYSTEM DISORDER – A PHENOME-WIDE ASSOCIATION STUDY OF CLINICAL PHENOTYPES IN UK BIOBANK
Angelina Kancheva*1, Donald Lyall2, Joanna Wardlaw3, Terence J Quinn1
1University of Glasgow, School of Cardiovascular and Metabolic Health, 2University of Glasgow, School of Health and Wellbeing, 3University of Edinburgh, Centre for Clinical Brain Sciences
On behalf of:
Background and aims: Cerebral small vessel disease (cSVD) is the most common pathology underlying vascular cognitive impairment. The importance of other clinical features is being recognised, including impaired gait and behavioural symptoms. Despite the increasing health burden of cSVD, the full spectrum of its clinical manifestations remains poorly understood.
Methods: We performed the first large-scale hypothesis-free phenome-wide association study (PheWas) to test for associations between presence of cSVD and multiple clinical phenotypes in a subset of UK Biobank (UKB) participants who underwent brain imaging. We used the PHESANT open-source phenome scan tool to perform PheWas. All associations were age at recruitment- and sex-adjusted, and corrected for multiple comparisons based on a conservative threshold of P<0.001.
Results: Our final PheWas analysis included 45,013 participants (mean age 54.97 years; 52.93% female). We corroborate many previously established associations with cSVD, including deleterious associations with higher body mass index, worse cognitive performance, depression and apathy, falls, vascular and heart problems, and a diagnosis of stroke. Additionally, we found associations with clinical features beyond classical cerebrovascular conditions, such as depression-related weight gain, chest pain when walking, insomnia, and hearing difficulties.
Conclusions: Our study demonstrates that the clinical profile of cSVD is more diverse than previously thought and includes presentations across multiple body systems. cSVD should be regarded as a multisystem disorder with a unique disease signature distinct from other progressive neurological conditions. To further advance our understanding of how cSVD manifests clinically, we need an integrated, holistic view of cSVD for policy and personalised healthcare.
Disclosures of Interest:
No
Abstract N°: 1646
PREVALENCE OF MONOGENIC GENE MUTATIONS IN TAIWAN-ASSOCIATED GENETIC AND NON-GENETIC SMALL VESSEL DISEASE (TAG-SVD) COHORT
1National Taiwan University Hospital, Department of Neurology, Taiwan, 2National Taiwan University Hospital, 3National Taiwan University, Graduate Institute of Medical Genomics and Proteomics, Taiwan
On behalf of:
Background and aims: The Taiwan-Associated Genetic and Non-genetic Small Vessel Disease (TAG-SVD) prospectively enrolled patients exhibiting clinical and/or neuroimaging features of cerebral small vessel disease (CSVD). The objective of this study is to delineate the current progress and baseline data of TAG-SVD.
Methods: All subjects enrolled in TAG-SVD underwent screening for the NOTCH3 R544C mutation. Those with negative R544C screening underwent NOTCH3 whole gene sequencing or next-generation sequencing using probes designed to target five candidate CSVD genes: NOTCH3, HTRA1, GLA, TREX1, and COL4A1. The TAG-SVD protocol involves a minimum 2-year follow-up assessing clinical features, neuroimaging, and outcomes.
Results: Currently, TAG-SVD comprises 1134 subjects with a mean age of 612±13.4 years and 57% being male. Among them, 663 (58.5%) had a history of stroke, and 230 (20.3%) exhibited cognitive impairment. Of the participants, 360 (31.7%) were identified with pathogenic or likely pathogenic monogenic mutations, including 325 with NOTCH3 R544C variant, 19 with NOTCH3 non-R544C sites, 9 with HTRA1 (heterozygous), 5 with TREX1, 1 with COL4A1, and 1 with GLA mutation. The functionality of all HTRA1 mutations was confirmed through standard in-vitro enzyme activity assays.
Conclusions: Monogenic mutations in patients with CSVD in Taiwan were not uncommon, particularly with a high prevalence of NOTCH3 R544C variant. TAG-SVD will further explore the clinical implications, long-term prognosis, and therapeutic strategies in genetic or non-genetic CSVD.
Disclosures of Interest:
No
Abstract N°: 1756
BRAIN STATE DYNAMICS PROVIDE A FUNCTIONAL LINK BETWEEN CEREBRAL SMALL VESSEL DISEASE AND VASCULAR COGNITIVE IMPAIRMENT
1University Medical Center Hamburg-Eppendorf, Neurology, Hamburg, Germany
On behalf of:
Background and aims: Cerebral small vessel disease (cSVD) predisposes to stroke and vascular cognitive impairment. However, our understanding of the mechanisms linking cSVD-associated brain damage to clinical deficits remains limited.
We hypothesized that white matter hyperintensities of presumed vascular origin (WMH) are associated with functional MRI-derived measures of brain state dynamics and that these measures are associated with executive dysfunction.
Methods: We analyzed demographic, imaging and behavioral data from the population-based Hamburg City Health Study. Using a prespecified analysis pipeline, we estimated brain states from structural and resting-state functional MRI. We used regression modelling to assess the associations between WMH volume and occupancy of DMN-related brain states, and between occupancy and trail making test scores. We varied brain parcellations and confound regression strategies to assess robustness of results.
Results: Analysing data from 1651 subjects, brain states characterized by activation or suppression of the DMN had a higher occupancy than non-DMN-related states. Every 5.1-fold increase in WMH volume was associated with a 0.94-fold reduction in the odds of occupying DMN-related brain states (P 5.01 × 10−8). Every 5% increase in time spent in DMN-related states was associated with a 0.98-fold reduction in the TMT-B time (P 0.0116). Findings were robust across brain parcellations and confound regression strategies.
Conclusions: We present results of a preregistered neuroimaging study of the association between cSVD, functional brain state dynamics and cognition. This contributes evidence for the clinical relevance of functional connectivity phenotypes underlying cognitive impairment in cSVD.
Disclosures of Interest:
No
Abstract N°: 1989
INCREASED WHITE MATTER MICROVESSEL DENSITY RELATIVE TO SEVERITY OF CEREBRAL SMALL VESSEL DISEASE SUGGESTS A COMPENSATORY RESPONSE
Johannes Reilly*1,2,3, Ivana Galinovic3
1Charité – Universitätsmedizin Berlin, Einstein Center for Neurosciences Berlin, Berlin, Germany, 2Charité - Universitätsmedizin Berlin, Department of Neurosurgery, Berlin, Germany, 3Charité - Universitätsmedizin Berlin, Center for Stroke Research Berlin, Berlin, Germany
On behalf of:
Background and aims: White matter hyperintensities (WMH) describe structural alterations of cerebral white matter and are thought to be caused by cerebral small vessel disease. Recent evidence suggests an active compensatory response of the brain to WMH-induced vascular injury. Individuals with high levels of WMH were found to have high levels of proangiogenic endothelial growth factor-D and epithelial progenitor cells in the plasma, and increased levels of proangiogenic placental growth factor in the cerebrospinal fluid. However, the structural effects of altered levels of angiogenic factors in individuals with WMH remain elusive.
Methods: Using magnetic resonance imaging-based vessel size imaging we investigated microvasculature in vivo in a clinical exploratory (N=88, mean age = 77.2) and replicative cohort (N=62, mean age= 65.0), as well as one young, healthy control group (N=9, mean age = 28.6).
Results: Here we show that microvessel density in white matter varies as a function of the severity of WMH. We found that the exploratory cohort had higher microvessel density in the centrum semiovale compared to controls (U=548.0, p<0.001). Relatedly, in both exploratory and replicative cohorts, there were significant positive correlations between microvessel density in the centrum semiovale and both Wahlund score (rs(70)=0.508, p<0.001; rs(54)=0.645, p<0.001) and age (rs(70)=0.449, p<0.001; rs(54)=0.540, p<0.001).
Conclusions: Our results suggest a complex relationship between areas of WMH and microvascular changes in occult white matter indicative of an active compensatory process. We are currently expanding these results with a more detailed investigation into the spatial extent of angiogenesis relative to WMH lesions.
Disclosures of Interest:
No
Abstract N°: 2644
ARTERIAL, VENOUS, AND CEREBROSPINAL FLUID FLOW AND PULSATILITY IN SPORADIC CEREBRAL SMALL VESSEL DISEASE: A LONGITUDINAL ANALYSIS
Alasdair Morgan1, Michael Stringer*1, Una Clancy1, Carmen Arteaga Reyes1, Maria Valdes-Hernandez1, Francesca Chappell1, Fergus Doubal1, Ian Marshall1, Michael Thrippleton1,2, Joanna Wardlaw1,2
1University of Edinburgh, Centre for Clinical Brain Sciences and UK Dementia Research Institute, Edinburgh, United Kingdom, 2University of Edinburgh, Edinburgh Imaging Facility (Royal Infirmary of Edinburgh), Edinburgh, United Kingdom
On behalf of: the Mild Stroke Study-3 study group
Background and aims: Total cerebral blood flow (tCBF) is lower and pulsatility index (PI) of arteries, veins and cerebrospinal fluid (CSF) altered in patients with higher cerebral small vessel disease (SVD) burden. How CBF and PI relate to SVD evolution is underexplored. We assessed flow and pulsatility in cerebral blood vessels and subarachnoid CSF to investigate associations with one-year SVD (white matter hyperintensity (WMH) and perivascular space (PVS) volumes) progression.
Methods: We recruited patients with mild stroke (Mild Stroke Study-3: ISRCTN 12113543). We acquired baseline and one-year 3T MRI to assess WMH, basal ganglia (BG) and centrum semiovale PVS volumes. At baseline, we measured arterial, venous and subarachnoid CSF flow/PI with phase-contrast MRI. We ran separate multivariable linear regressions between baseline or one-year WMH/PVS (outcome) and flow/pulsatility measure adjusting for age, sex and systolic blood pressure. In longitudinal analyses, we adjusted for baseline WMH/PVS volume.
Results: 205/210 patients (age:66.4±11.1y,67% male) had useable flow data. Patients with higher arterial PI had higher baseline WMH (B=0.260 log10(%WMH/intracranial volume)/unit PI,95% confidence interval (95%CI)=[0.077,0.442]) and BG PVS volumes (B=0.105 log10(%PVS/region volume)/unit PI,95%CI=[0.024,0.186]). However, baseline arterial PI did not differ with one-year WMH and PVS volume change (Fig.1, e.g. BG PVS:B=0.019 log10(%PVS/region volume)/unit PI,95%CI=[-0.039,0.076]). tCBF and CSF stroke volume were not generally related to baseline SVD severity or one-year progression.
Conclusions: We found higher arterial PI with higher baseline SVD burden (WMH and PVS volume), but not one-year progression. Higher WMH/PVS burden may therefore affect PI but not vice-versa, reflecting recent work, though confirmatory studies with longer follow-up duration are needed.
Disclosures of Interest:
No
Abstract N°: 2936
LINKING BLOOD PRESSURE VARIABILITY AND BRAIN HEALTH: CEREBRAL AMYLOID ANGIOPATHY-RELATED BRAIN INJURY AND COGNITIVE DECLINE
Lukas SVEIKATA*1,2, Maria Clara Zanon Zotin2, Dorothee Schoemaker2, Yuan MA3, Valentina Perosa2, Anthipa Chokesuwattanaskul2,4, Edip M. Gurol2, Frédéric Assal1, Steven Greenberg2, Anand Viswanathan2
1Hôpitaux Universitaires de Genève (HUG), Neurology Department, Genève, Switzerland, 2Massachusetts General Hospital, Harvard Medical School, Neurology Department, Boston, United States, 3Harvard T.H. Chan School of Public Health, Boston, United States, 4Faculty of Medicine, Chulalongkorn University, Thailand
On behalf of: J. Philip Kistler Stroke Research Center CAA Study Group, Andreas Charidimou, MD, PhD, Marco Duering, MD
Background and aims: To investigate the association between long-term blood pressure variability (BPV), brain injury, and cognitive decline in patients with mild cognitive symptoms and cerebral amyloid angiopathy (CAA).
Methods: Using a prospective memory clinic cohort, we enrolled 102 participants, of whom 52 with probable CAA. All underwent a 3.0 T research MRI at baseline and annual neuropsychological evaluation over 2 years, for which standardized z-scores were calculated. BPV was assessed using a coefficient of variation derived from serial outpatient BP measurements over five years. We measured the peak width of skeletonized mean diffusivity (PSMD) as a marker of white matter integrity, and other neuroimaging markers of CAA. Using regression models, we evaluated the association of BPV with microstructural brain injury and whether CAA modified this association. We also examined the association of BPV with subsequent cognitive decline
Results: Systolic BPV was dose-dependently associated with PSMD (estimate=0.22, 95% CI: 0.06, 0.39, p=0.010), independent of age, sex, mean BP, common vascular risk factors, brain atrophy, and CAA severity. The presence of probable CAA strengthened the association between BPV and PSMD (estimate=9.33, 95% CI: 1.32, 17.34, p for interaction = 0.023). Higher BPV correlated with greater ischemic injury (lobar lacunes and cortical cerebral microinfarcts) and a decline in global cognition and processing speed (estimate=-0.30, 95% CI: -0.55, -0.04, p=0.022).
Conclusions: Long-term BPV is significantly associated with altered white matter integrity, lobar lacunes, and cortical cerebral microinfarcts. Controlling BPV is a potential strategic approach to prevent cognitive decline, especially in early-stage CAA.
Disclosures of Interest:
No
SCIENTIFIC COMMUNICATION – HYPERACUTE MANAGEMENT
Abstract N°: 594
ENDOVASCULAR TREATMENT FOR ISOLATED CERVICAL INTERNAL CAROTID ARTERY OCCLUSION – ETIICA STUDY
João Pedro Marto*1,2, Christoph Riegler3,4, Pimrapat Gebert5,6, Tilman Reiff7, Marek Sykora8,9, Marcin Wiącek10, David Pakizer11, André Araújo12, Adrien Ter Schiphorst13, Christian Nolte3,4,6,14
1Hospital de Egas Moniz, Centro Hospitalar Lisboa Ocidental, Lisbon, Portugal, Neurology, Lisbon, Portugal, 2Lisbon Clinical Academic Center, NOVA Medical School, Universidade NOVA de Lisboa, Lisbon, Portugal, Lisbon, Portugal, 3Center for Stroke Research Berlin (CSB), Charité – Universitätsmedizin Berlin, Berlin, Germany, Berlin, Germany, 4Charité – Universitätsmedizin Berlin, Corporate member of Freie Universität Berlin and Humboldt Universität zu Berlin, Berlin, Germany, Neurology, Berlin, Germany, 5Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Institute of Biometry and Clinical Epidemiology, Germany, Berlin, Germany, 6Berlin Institute of Health at Charité –Universitätsmedizin Berlin, Germany, Berlin, Germany, 7Heidelberg University Hospital, Heidelberg, Germany, Neurology, Heidelberg, Germany, 8St. John’s Hospital, Vienna, Austria, Neurology, Vienna, Austria, 9Medical Faculty, Sigmund Freud University Vienna, Austria, Vienna, Austria, 10Institute of Medical Sciences, Medical College of Rzeszow University, Rzeszow, Poland, Neurology, Rzeszow, Poland, 11Faculty of Medicine, University of Ostrava, Ostrava, Czech Republic, Centre for Health Research, Ostrava, Czech Republic, 12Centro Hospitalar de Vila Nova de Gaia/Espinho, Gaia, Portugal, Neuroradiology, Gaia, Portugal, 13Centre Hospitalier Universitaire Gui de Chauliac, Montpellier, France, Neurology, Montpellier, France, 14Deutsches Zentrum für Herz-Kreislaufforschung DZHK, Berlin, Germany, Berlin, Germany
On behalf of: ETIICA study investigators
Background and aims: In patients with acute ischemic stroke and isolated cervical internal carotid artery occlusion (c-ICA-O), there is a lack of data regarding the benefits of endovascular treatment (EVT). We aimed to assess clinical outcomes and safety of EVT in patients with isolated c-ICA-O.
Methods: ETIICA is a multinational case-control study conducted at 42 sites in Europe and North America. Consecutive patients presenting with isolated c-ICA-O and within 24 hours of last-seen-well from January 2018 to December 2022 were included. We compared EVT to medical management (MM) combining inverse probability of treatment weighting with multivariable regression. The primary outcome was the 90-day modified Rankin Scale (mRS) ordinal shift. Symptomatic intracranial hemorrhage (sICH) and parenchymal hemorrhage were assessed as safety outcomes.
Results: Of 998 patients, 661 (66.2%) were male with mean age of 71.1±13.2 years. The median (interquartile range) NIHSS was 9 (3–17). Overall, 487 (48.8%) patients received EVT and 511 (51.2%) received MM. Intravenous thrombolysis was administered in 41.5% (EVT) and 28.2% (MM), respectively. There was no difference between EVT and MM groups in the 90-day mRS shift (aOR, 0.99 [95% CI, 0.75–1.31]). No patient (0%) had sICH in the MM group vs. 2.3% in the EVT group. Parenchymal hemorrhage was numerically higher in EVT patients (2.7% vs. 0.6%; aOR, 3.85 [95% CI, 0.98–15.23]).
Conclusions: In patients with isolated c-ICA-O, EVT was associated with similar odds of disability and higher numbers of intracranial bleeding compared with MM. Clinical trials in patients with isolated c-ICA-O are warranted.
Disclosures of Interest:
No
Abstract N°: 892
INFLUENCE OF STROKE SEVERITY AND OCCLUSION SITE ON ENDOVASCULAR THERAPY EFFECT FOR POSTERIOR CEREBRAL ARTERY OCCLUSION STROKES
Davide Strambo*1, Patrik Michel1, Thanh N. Nguyen2, Mohamad Abdalkader2, Muhammad M. Qureshi2, Silja Räty3, Martin Köhrmann4, Marta Olive Gadea5, Simon Nagel6,7, Daniel Strbian3
1Lausanne University Hospital, University of Lausanne, Switzerland, Neurology Service, Lausanne, Switzerland, 2Boston Medical Center, Boston University Chobanian and Avedisian School of Medicine, Boston, Massachusetts, USA, Department of Radiology and Neurology, United States, 3HUS, Helsinki, Finland, 4Essen University Hospital, Neurology, Essen, Germany, 5Vall d'Hebron University Hospital, Neurology, Barcelona, Spain, 6Klinikum Ludwigshafen: Klinik für Neurologischen, Ludwigshafen am Rhein, Germany, 7Heidelberg, Neurology, Heidelberg, Germany
On behalf of: PLATO study group
Background and aims: Acute ischemic stroke (AIS) with isolated posterior cerebral artery occlusion (iPCAO) lacks acute management evidence. We aimed to evaluate whether the association between endovascular treatment (EVT) and outcomes in iPCAO-AIS is modified by baseline stroke severity and arterial occlusion site.
Methods: Based on the international, multicenter, retrospective, case-control study of consecutive iPCAO-AIS (PLATO study, NCT0529163), we assessed the heterogeneity of EVT outcomes compared to medical management (MM) for iPCAO, according to stroke severity (NIHSS0-6vs.>6) and occlusion site (P1vs.P2), using multivariable regression models with interaction terms.
Results: Among 1,059 patients (median age 74 years, 43.7% women), 364 received EVT and 695 MM, including intravenous thrombolysis in 40%. Baseline stroke severity did not significantly modify the association of EVT with 3-month mRS distribution (pint=0.31), but did with functional independence (mRS0-2, pint=0.01), with a similar trend with excellent outcome (mRS0-1, pint=0.07). Specifically, EVT had a higher likelihood of these outcomes than MM in patients with baseline NIHSS>6 (mRS0-1: aOR=2.01,95%CI=1.22-3.31; mRS0-2: aOR = 1.64, 95% CI = 1.08-2.51), while those with NIHSS0-6 the difference was absent of in disfavor of EVT (mRS0-1: aOR=0.90,95%CI=0.49-1.64; mRS0-2: aOR = 0.55, 95% CI = 0.30-1.0). Arterial occlusion site did not significantly alter the association of EVT with outcomes compared to MM.
Conclusions: Baseline stroke severity, rather than the occlusion site, appears to be an important modifier of the association between EVT and outcomes in iPCAO. There were more favorable outcomes in EVT than MM in patients with NIHSS>6, whereas this difference was not observed in minor stroke. These observations might inform selection criteria in future randomized studies of EVT in iPCAO-AIS.
Disclosures of Interest:
No
Abstract N°: 1653
EDARAVONE DEXBORNEOL IN TREATMENT OF LARGE ARTERY ATHEROSCLEROSIS STROKE
1Beijing Tiantan Hospital, Capital Medical University, Department of Neurology, Beijing, China, 2Beijing Tiantan Hospital, Capital Medical University, China National Clinical Research Center for Neurological Diseases, Beijing, China, 3School of Public Health, Capital Medical University, Department of Epidemiology and Health Statistics, Beijing, China, 4Beijing Municipal Key Laboratory of Clinical Epidemiology, Beijing, China
On behalf of:
Background and aims: Evidenced by TASTE and TASTE-SL trials, both injectional and sublingual edaravone dexborneol improved the functional outcome on day90 after randomization in patients with acute ischemic stroke (AIS). The post-hoc analysis aimed at analyzing the effects of edaravone dexborneol in patients with large artery atherosclerosis (LAA) stroke.
Methods: Patients diagnosed as LAA stroke were included from the TASTE and TASTE-SL trial. The primary outcome was proportion of patients with modified Rankin Scale (mRS) score ⩽ 1 on day90 after randomization. The secondary outcomes were mRS score on day90 and the change of NIHSS score on day14. The safety endpoints were adverse events and serious adverse events within 90days.
Results: There were no significant differences in baseline characteristics between two groups (587 in edaravone dexborneol group, 589 in placebo group). Edaravone dexborneol group showed higher proportion of mRS score ⩽ 1 on day90 than placebo group (60.48% versus 51.44%; OR 1.44 [95% CI, 1.15–1.82]; P = 0.002).
There was a trend toward lower disability with edaravone dexborneol treatment based on the mRS score than with placebo ([OR 1.28 [95% CI, 1.03–1.56]; P = 0.023). No significant differences occurred between two groups in the NIHSS score from baseline to day14, P=0.562). The safety outcome indicated that two groups had similar incidences of AEs (541 [92.16%] versus 554 [94.06%], P=0.201) and SAEs (54 [9.20%] versus 54 [9.17%], P=0.985).
Conclusions: This analysis demonstrated that both injectional and sublingual edaravone dexborneol showed more favorable functional outcomes without increase in AEs in LAA stroke.
Disclosures of Interest:
No
Abstract N°: 2274
TIMING OF ANTIHYPERTENSIVE TREATMENT INITIATION IN ANTERIOR VERSUS POSTERIOR CIRCULATION ACUTE ISCHEMIC STROKE
1Beijing Tiantan Hospital Affiliated to Capital Medical University, Department of Neurology, Beijing, China, 2China National Clinical Research Center for Neurological Diseases, Beijing, China, 3School of Public Health, Suzhou Medical College of Soochow University, Department of Epidemiology, Suzhou, China, 4Tulane University School of Public Health and Tropical Medicine, Department of Epidemiology, New Orleans, United States, 5Tulane University Translational Science Institute, New Orleans, United States
On behalf of:
Background and aims: The China Antihypertensive Trial in Acute Ischemic Stroke II (CATIS-2) suggests that early antihypertensive treatment did not reduce the risk of dependency or death in patients with acute ischemic stroke (AIS), compared with delayed treatment. We aim to investigate whether infarct location modifies the effect of antihypertensive treatment timing on clinical outcomes among patients with AIS.
Methods: In the CATIS-2 trial, patients with AIS and elevated systolic blood pressure within 24-48 hours of symptoms onset were randomly assigned to receiving early (immediate) or delayed (starting on day 8) antihypertensive therapy. In this subgroup analysis, patients with positive diffusion-weighted imaging were included. Based on the hyperintense lesions on diffusion-weighted imaging, patients were categorized into anterior circulation infarct (ACI) and posterior circulation infarct (PCI) groups. The primary outcome was the combination of functional dependency or death (modified Rankin Scale score ⩾3) at 90 days.
Results: A total of 2463 patients were included in the current substudy, with 1551 (61.4%) ACI and 952 (38.7%) PCI. Among ACI patients, early antihypertensive treatment significantly increased the risk of primary outcome compared to delayed treatment (14.3% vs 10.4%; OR, 1.44; 95%CI, 1.06-1.97; P=.02); this finding was not observed in PCI patients (8.6% vs 8.0%; OR, 1.08; 95%CI, 0.68-1.72; P=.73).
Conclusions: In patients with ACI, early antihypertensive treatment was associated with an increased risk of functional dependency or death at 90 days compared to delayed antihypertensive treatment. Our study highlights the importance of tailored blood pressure management strategies according to the infarct location.
Disclosures of Interest:
No
Abstract N°: 2443
INTRAVENOUS THROMBOLYTIC IS ASSOCIATED WITH INCREASED FIRST PASS EFFECT IN THROMBECTOMY
Steven Bush*1,2, Peter Mitchell1,2, Bernard Yan1,2, Leonid Churilov2, Dominic Italiano2, Wenjie Zi3,4, Qingwu Yang3,4
1The Royal Melbourne Hospital, Parkville, Australia, 2The University of Melbourne, Parkville, Australia, 3Xinqiao Hospital, China, 4Army Medical University (Third Military Medical University), Neurology, Chongqing, China
On behalf of: Improving Reperfusion strategies in Ischemic Stroke (IRIS) collaboration
Background and aims: Six randomized controlled trials on bridging intravenous thrombolytic followed by endovascular thrombectomy compared to direct thrombectomy for large vessel occlusion stroke have produced varied results. First pass effect (FPE) is an independent predictor of favourable clinical outcome. However, it is unclear if intravenous thrombolytic increases the odds of FPE. We aimed to investigate the association between bridging thrombolytic and FPE. We hypothesised that bridging thrombolytic increases the likelihood of FPE.
Methods: Individual patient metanalysis of six randomized controlled trials (Improving Reperfusion strategies in Ischemic Stroke [IRIS]) was performed (n=2313). FPE was defined as successful reperfusion (TICI 2c to 3) after a single pass of thrombectomy procedure. Frequency of FPE was compared between bridging thrombolytic and direct thrombectomy groups after adjustment for onset-to-groin time and occlusion location and between-trial variance.
Results: FPE was achieved in 685 patients (29%). The median onset-to-groin time for FPE group was 169 mins (IQR: 125, 217) and for non-FPE group was 175 mins (IQR: 133, 228). Odds of FPE were decreased by 21% (OR = 0.79, 95% CI: 0.65, 0.95) in direct thrombectomy group compared with bridging thrombolytic group. Odds of a patient having an mRS score of 0-1 at 90 days increased by 106% by (OR = 2.06, 95% CI: 1.50, 2.82) with a successful first pass thrombectomy.
Conclusions: We showed that the likelihood of achieving first pass effect was significantly increased with bridging intravenous thrombolytic thrombectomy compared with direct thrombectomy, and this was associated with improved clinical outcome at 90 days
Disclosures of Interest:
No
Abstract N°: 2563
PATIENTS RANDOMIZED TO GLENZOCIMAB SUFFERED LESS HEMORRHAGIC TRANSFORMATION WITH GREATER BENEFIT IN LARGER BASELINE INFARCT CORE
Andrea Comenducci1, Adeline Meilhoc1, Yannick Plétan1, Sophie Binay1, Gilles Avenard1, Alistair Perry2, Olivier Joly2, George Harston2,3, Davide Carone*2,3,4
1Acticor Biotech, Paris, France, 2Brainomix Limited, United Kingdom, 3Oxford University Hospitals NHSFT, United Kingdom, 4University of Oxford, Radcliffe Department of Medicine, Oxford, United Kingdom
On behalf of:
Background and aims: ACTIMIS (NCT03803007) was a randomized phase 1b/2a clinical trial evaluating glenzocimab, a monoclonal antibody fragment targeting platelet receptor glycoprotein-VI in patients with acute ischemic stroke treated by thrombolysis or associated with mechanical thrombectomy (MT). Primary analysis demonstrated a reduction in intracranial hemorrhage occurrence and of stroke-related mortality. This sub-analysis used volumetric imaging biomarkers to assess glenzocimab efficacy.
Methods: In the phase 2a study, patients were randomized (1:1) with 1000mg glenzocimab or placebo. CT or MRI was acquired at baseline with CT at 24 hours for safety and efficacy analysis. Baseline and follow-up imaging were processed using AI core lab software (Brainomix, Oxford, UK). Automated output was reviewed for accuracy by an expert clinician (DC) blinded to treatment allocation.
Results: Follow-up imaging data were available from 104/106 patients (52 glenzocimab, 52 placebo) at 24 hours. There was significantly smaller volume of haemorrhagic transformation (HT) in the glenzocimab group at 24 hours compared to placebo (mean [SD]; 0.9mL [2.8] vs 13.59mL [46.16], P<0.05) and a trend towards smaller volume of ischemic injury in the glenzocimab group (32.3mL [58.2] vs 57.0 mL [104.6]). Multivariate regression modelling showed a significant interaction between baseline infarct core size and treatment arm (P=0.002), suggesting that the risk of bleeding associated with larger (upper tertile) baseline infarcts was reduced in patients treated with glenzocimab.
Conclusions: Glenzocimab reduced likelihood and volume of HT in patients undergoing recanalization treatment, with a greater effect in patients with larger cores. Glenzocimab is a promising adjunct for large core patients undergoing recanalization treatment.
Disclosures of Interest:
Yes Andrea Comenducci, Adeline Meilhoc, Yannick Plétan, Sophie Binay, Gilles Avenard are empoyed by Acticor Biotech. Alistair Perry, Olivier Joly, George Harston, and Davide Carone are employed and have share-options at Brainomix Limited
Abstract N°: 2734
SECONDARY ANALYSES FROM THE TIMELESS TRIAL
Gregory Albers*1, Ming Yang2, Christopher Streib3, Ashfaq Shuaib4, Minjee Kim5, Joseph Broderick6, Maarten Lansberg1, Barbara Purdon2
1Stanford Stroke Center, Department of Neurology and Neurological Sciences, Stanford University, Palo Alto, United States, 2Genentech, South San Francisco, United States, 3University of Minnesota, Department of Neurology, Minneapolis, United States, 4University of Alberta, Department of Medicine, Edmonton, Canada, 5Feinberg School of Medicine, Department of Neurology, Chicago, United States, 6UC Gardner Neuroscience Institute, Department of Neurology and Rehabilitation Medicine, Cincinnati, United States
On behalf of:
Background and aims: TIMELESS (NCT03785678) was a randomized, placebo-controlled trial (N=458) of tenecteplase (TNK) (0.25 mg/kg) in stroke patients 4.5-24 hours from last known well (LKW) with salvageable tissue on perfusion imaging (77% also received EVT). The study did not demonstrate benefit on 90-day ordinal mRS outcomes; Symptomatic ICH (SICH) did not differ: TNK, 3.2%; placebo, 2.3%.
Methods: Outcomes were assessed at 90 days and analyzed according to intention-to-treat principle, adjusted for baseline factors.
Results: The odds of the 90-day mRS ordinal shift was higher in TNK subjects with an M1 occlusion (n=227); OR (95% CI), 1.59 (1.00-2.52), P=0.051. EVT patients with TNK administered ⩽27 min prior to clot contact had a favorable response; OR (95% CI), 2.27 (1.15-4.54). TNK was associated with a reduction in infarct growth at 72-96 hours; median growth 12 ml (TNK) vs 16 ml (placebo), P=0.06 (most prominent with M1 occlusions; 12 ml vs 18 ml, nominal P=0.03). 173 of 458 (38%) study subjects had M2 occlusions. The 90-day mRS ordinal shift in M2s was similar between the TNK (n=89) versus placebo (n=84) arms; OR (95% CI), 0.76 (0.45-1.30). Time from LKW to randomization was longer among subjects with SICH/PH2; median, 15.3 hrs vs 12.5 hrs. SICH/PH2 was more common in ICA occlusion (8.7%) vs M1 or M2 (4.1% and 3.0%).
Conclusions: Future prospective studies evaluating tenecteplase in AIS patients with M1 occlusions may be beneficial. TNK effect on 90-day outcomes in M2 occlusions could not be established, further investigation is warranted.
Disclosures of Interest:
Yes G.W. Albers has served as a consultant for Genentech and iSchemaView and has equity in iSchemaView. The other authors also report COIs.
SCIENTIFIC COMMUNICATION – SAH, ANEURYSMS AND VASCULAR MALFORMATIONS
Abstract N°: 301
INTRACRANIAL ARTERIAL CALCIFICATION IN PATIENTS WITH UNRUPTURED AND RUPTURED INTRACRANIAL ANEURYSMS
Maarten Kamphuis*1,2, Laura van der Kamp2, Edwin Lette2, Gabriel J.E. Rinkel2, Mervyn Vergouwen2, Irene van der Schaaf1, Pim de Jong1, Ynte Ruigrok2
1UMC Utrecht, Department of Radiology, Utrecht, Netherlands, 2UMC Utrecht, Department of Neurology and Neurosurgery, Utrecht, Netherlands
On behalf of:
Background and aims: Arterial calcification is thought to protect against rupture of intracranial aneurysms, but studies in a representative population of intracranial aneurysm patients have not yet been performed. The aim was to compare the prevalence of aneurysm wall calcification and intracranial carotid artery calcification (ICAC) between patients with an unruptured intracranial aneurysm (UIA) and a ruptured intracranial aneurysm (RIA).
Methods: We matched 150 consecutive UIA patients to 150 RIA patients on age and sex. Aneurysm wall calcification and ICAC were quantified on non-contrast enhanced computed tomography images with the modified Agatston score. We compared the prevalence of aneurysm wall calcification, ICAC, and severe ICAC (defined as a modified Agatston score in the fourth quartile) between UIA and RIA patients using univariate and multivariate conditional logistic regression models adjusted for aneurysm characteristics and cardiovascular risk factors.
Results: Aneurysm wall calcification was more prevalent in UIA compared to RIA patients (OR 4.8, 95%CI:1.8–13), which persisted after adjustment (OR 6.1, 95%CI:1.9–20). ICAC prevalence did not differ between the two groups (OR 0.94, 95%CI:0.49–1.8). Severe ICAC was more prevalent in UIA patients (OR 1.9, 95%CI:1.1–3.5), but not after adjustment (1.1, 95%CI:0.5–2.5).
Conclusions: Aneurysm wall calcification but not ICAC was more prevalent in UIAs than in RIAs, which corresponds to the hypothesis that calcification may protect against aneurysmal rupture. Aneurysm wall calcification should be further assessed as a predictor of aneurysm stability in prospective cohort studies.
Disclosures of Interest:
No
Abstract N°: 315
PRESCRIBED DRUG USE AND ANEURYSMAL SUBARACHNOID HAEMORRHAGE INCIDENCE: A DRUG-WIDE ASSOCIATION STUDY
Jos Kanning*1, Shahab Abtahi2, Christian Schnier3, Olaf Klungel2, Mirjam Geerlings4, Ynte Ruigrok1
1UMC Utrecht, Utrecht, Netherlands, 2Utrecht University, Utrecht, Netherlands, 3University of Edinburgh, United Kingdom, 4Amsterdam UMC, locatie AMC, Amsterdam, Netherlands
On behalf of:
Background and aims: Invasive intracranial aneurysm therapies frequently pose greater risks than benefits, leaving the majority of aneurysms untreated. We conducted a drug-wide association study (DWAS) to look at commonly prescribed drugs for potential repurposing to reduce the risk of aneurysmal subarachnoid hemorrhage (aSAH).
Methods: We identified aSAH cases from 2000-2020 using International Classification of Diseases codes from the Secure Anonymised Information Linkage (SAIL) databank. Cases were matched with controls (9:1 ratio), focusing on drugs prescribed to over 2% of this population. We examined drug use within three timeframes relative to aSAH occurrence: current (within 3 months), recent (3-12 months), and past (>12 months), using logistic regression to analyze the data, adjusting for demographic factors, known risk factors, and healthcare usage.
Results: Among 4,879 aSAH cases (average age 61.4, 61.2% women) and 43,911 controls, nine out of 205 studied drugs showed significant associations with aSAH. We found similar trends for lisinopril and amlodipine, with a decreased aSAH risk for current use (lisinopril OR:0.63, amlodipine OR:0.82), and an increased aSAH risk for recent use (lisinopril OR:1.3, amlodipine OR:1.61). A decreased aSAH risk in current use was also found for simvastatin (OR:0.78), metformin (OR:0.58), and tamsulosin (OR:0.55). In contrast, an increased aSAH risk was found for current use of warfarin (OR:1.35), venlafaxine (OR:1.67), prochlorperazine (OR:2.15), and co-codamol (OR:1.31)
Conclusions: We found several drugs potentially influencing aSAH risk, with five showing potential protective effects. Further research is needed to confirm these findings and evaluate these drugs' effectiveness in aSAH prevention.
Disclosures of Interest:
No
Abstract N°: 1254
MULTIMODAL DETECTION OF DELAYED CEREBRAL ISCHAEMIA IN PATIENTS WITH ANEURYSMAL SUBARACHNOID HAEMORRHAGE
Andreas Ziebart*1, Hans-Georg Kesseler1, Andrea Weber1, Bernd Schmitz2, Christian Wirtz1, Thomas Kapapa1, Ralph König1, Andrej Pala1
1University Medical Center Ulm, Department of Neurosurgery, Günzburg, Germany, 2University Medical Center Ulm, Departement of Neuroradiology, Günzburg, Germany
On behalf of:
Background and aims: Delayed cerebral ischaemia (DCI) is a major determinant of poor neurological outcome in aneurysmal subarachnoid haemorrhage (aSAH). In addition to clinical examination, several different modalities have been used to monitor patients within the first two weeks after aSAH with equivocal positive predictive values described. We aimed to investigate the currently available methods and their association with DCI.
Methods: We enrolled patients with aSAH in a prospective observational study from March 2023 to January 2024. We used a dynamic infrared pupillometer for pupillometry measurements and daily transcranial Doppler (TCD), with a Neurological Pupil Index (NPi) of 0 to 2.9 and middle cerebral artery velocities >120 cm/s considered abnormal. CT angiography and CT perfusion were performed on suspicion of DCI or routinely on a weekly basis. Fisher's exact test was used to compare categorical variables.
Results: We analysed 41 patients with 194 paired pupillometry and TCD measurements and 59 CT scans. 18 patients developed DCI. Patients with DCI did not have abnormal NPi values. 83% had increased time to maximum and mean transit time on CT perfusion measurements (p<0.001), 56% had abnormal CT angiographic findings and 11% had increased TCD velocity measurements in the event of DCI. 62% of abnormal CT angiographic findings and 87% of increased TCD velocities were found in the absence of DCI.
Conclusions: Increased mean transit time and time to maximum on CT perfusion, but not TCD or decreased NPi, correlate with the occurrence of DCI. TCD and CT angiography show a significant rate of false positive predictions.
Disclosures of Interest:
No
Abstract N°: 1260
GADOLINIUM-ENHANCED ANEURYSM WALL IMAGING IN UNRUPTURED INTRACRANIAL ANEURYSMS – A LONG-TERM FOLLOW-UP STUDY
Laura van der Kamp*1, Maarten Kamphuis1, Olivier Naggara2, Thomas Le Tat3, Myriam Edjlali4, Gabriel J.E. Rinkel1, Gerard de Kort1, Jeruen Hendrikse1, Irene van der Schaaf1, Mervyn Vergouwen1
1UMC Utrecht, Utrecht, Netherlands, 2Hospital Sainte-Anne, Paris, France, 3Ambroise Paré Hospital, Boulogne-Billancourt, France, 4Laboratory Imaging Biomedical Cnrs Inserm - Sorbonne University, Paris, France
On behalf of:
Background and aims: In patients with an unruptured intracranial aneurysm (UIA), gadolinium enhancement of the aneurysm wall may predict short-term (1-year) aneurysm growth and rupture. We investigated whether aneurysm wall enhancement predicts aneurysm growth and rupture during a long-term follow-up period.
Methods: In this longitudinal study, individual patient data were obtained from two centers that performed aneurysm wall imaging and MRA in the years 2012-2016 in patients 18 years or older with ⩾ 1 untreated UIA. Patients without MRA, CTA, or rupture during follow-up were excluded. Using Royston-Parmar survival analysis, we calculated crude odds ratios with corresponding 95% confidence intervals of aneurysm wall enhancement for the prediction of aneurysm instability (defined as growth [⩾1 mm increase], morphologic change, or rupture), and adjusted for age and aneurysm size.
Results: We included 209 patients (146 (70%) female, median age 58 years) with 224 aneurysms, who had a median follow-up duration of 6.8 years (IQR 3.3-7.9 years). Instability occurred in 15/85 (18%) aneurysms with wall enhancement and in 13/139 (9%) aneurysms without wall enhancement (OR 3.0 [95%CI 1.3-6.8], aOR 3.1 [95%CI 1.1-8.3]).
Conclusions: Gadolinium enhancement of the aneurysm wall is an independent predictor of aneurysm instability during a long-term follow-up period. Our findings suggest that aneurysm wall imaging can improve risk prediction in patients with UIAs.
Funding:
This study was supported by a Clinical Established Investigator grant by the Dutch Heart Foundation (2018T076) to Dr M.D.I. Vergouwen, and by Bayer BV (investigator-initiated research, paid to institution).
Disclosures of Interest:
No
Abstract N°: 1438
DNA METHYLATION SIGNATURE OF ANEURYSMAL SUBARACHNOID HEMORRHAGE
Adrià Macias-Gómez*1, Joan Jimenez-Balado1, Isabel Fernández-Pérez1, Antoni Suárez-Pérez1, Marta Vallverdu-Prats1, Eva Giralt-Steinhauer1, Ana Rodríguez-Campello1, Angel Ois1, Jordi Jiménez-Conde1, Elisa Cuadrado-Godia1
1Hospital del Mar Research Institute – Pompeu Fabra University, Department of Neurology, Barcelona, Spain
On behalf of:
Background and aims: Aneurysmal subarachnoid hemorrhage (aSAH) entails a considerable rate of disability and mortality. Epigenetics might provide insight on the pathophysiology of aSAH, which nowadays is not fully understood. We aimed to compare the DNA methylation (DNAm) signature between aSAH and control subjects.
Methods: An epigenome-wide association study was conducted in 276 aSAH patients and 178 controls. DNAm was assessed with the EPIC Illumina chip (>850K CpG sites) in whole-blood samples. We identified differentially methylated positions (DMPs) at the CpG level using linear models adjusted for potential confounders (age, sex, smoking and vascular risk factors [VRF]). The analysis was repeated in a subset of the sample, paired by demographic and VRF via propensity score matching (191 cases and 62 controls).
Results: Median age of the sample was 56 years (49-63), observing no differences between cases and controls. Patients with aSAH were more often females (67% vs 51.7%) and had a higher prevalence of smoking (36.0% vs 9.0%). Control subjects had a higher prevalence of diabetes (36.6% vs 5.4%) and dyslipidemia (43.5% vs 20.3%). We observed that 6 CpGs were significant at the genome-wide level in the whole sample and matched subset: cg00493366, cg11330075, cg12385553, cg16267121, cg17307919, cg22311458 (p -value<5·10-8). Some of this CpGs were annotated to genes already associated with cerebral aneurysm such as MALAT1 (Figure-1).
Conclusions: Our findings support a role for epigenetic mechanisms in the pathogenesis of aSAH. However, further replication studies are needed.
Disclosures of Interest:
No
Abstract N°: 1774
CHICKEN OR THE EGG: A COHORT OF PATIENTS WITH BOTH DURAL ARTERIOVENOUS FISTULAS AND CEREBRAL VENOUS THROMBOSIS
Arshia Alimohammadi1, Ikreet Cheema1, Alexander Rebchuk1, Marco Marangoni1, Manraj Heran1, Thalia Field1, Lily Zhou*1
1The University of British Columbia, Medicine, Vancouver, Canada
On behalf of:
Background and aims: There is a known association between cerebral venous thrombosis (CVT) and dural arteriovenous fistulas (dAVF). However, the temporal and causal relationship between these entities is not well understood. We explored the time course of presentation, risk factors, radiologic features and treatment of patients diagnosed with both CVT and dAVF.
Methods: Patients with a diagnosis of CVT and dAVF between 2008-2018 were identified using free text search of hospital radiology reports and ICD-10 discharge codes. Patient demographics, diagnosis dates of CVT and dAVF, risk factors, clinical and radiological presentation details, management, and outcomes were extracted from electronic charts.
Results: There were 53 patients identified with a diagnosis of both CVT and dAVF (mean age 56, SD 17.6 years; 37.7% female). Most patients were diagnosed with dAVF and CVT at the same time (36/53, 68%) rather than symptomatic CVT followed by dAVF (13/53, 25%) or symptomatic dAVF followed by CVT (4/53, 7.6%). In those with dAVF after CVT, the median delay between diagnoses was 434 days (IQR 422). Those with symptomatic CVT before dAVF tended to have lower Borden class dAVF (Class 1/2/3: 53.9%/30.8%/15.4% vs. 25.0%/38.9%/36.1%) compared to those diagnosed with dAVF and CVT at the same time but this was not statistically significant (p=0.056).
Conclusions: Concurrent diagnosis of dAVF and CVT is the most common pattern of presentation in patients with both CVT and dAVF. In those with dAVF after CVT, the diagnoses may be separated by years and patients should be made aware of signs and symptoms for self-surveillance.
Disclosures of Interest:
No
Abstract N°: 2289
RISK FACTORS AND OUTCOMES OF ANEURYSM RUPTURE DURING TREATMENT IN PATIENTS WITH ANEURYSMAL SUBARACHNOID HAEMORRHAGE
Philippine B. van Wijngaarden*1, Mervyn D.I. Vergouwen1, Hieronymus D. Boogaarts2, Gabriel J.E. Rinkel1, Dagmar Verbaan3
1University Medical Centre Utrecht, Department of Neurology & Neurosurgery, 2Radboud University Nijmegen, Medical Faculty, Department of Neurosurgery, 3Amsterdam University Medical Centre, Department of Neurosurgery
On behalf of: the ULTRA Investigators
Background and aims: Intraprocedural aneurysm rupture (IPAR) is a feared complication during aneurysm treatment. We aimed to identify risk factors and outcomes of IPAR in patients with aneurysmal subarachnoid haemorrhage (aSAH) who underwent neurosurgical (NST) or endovascular (EVT) treatment.
Methods: We used data from aSAH patients included in the ULTRA trial (NCT02684812). We calculated proportions of IPAR, and risk ratios (RR) with 95% confidence intervals (CI) with Poisson regression to compare the risk of IPAR between NST and EVT, to determine risk factors for IPAR for both modalities separately, and to determine the risk of poor outcome and case-fatality in patients with IPAR compared to those without. For all analyses, we adjusted for variables statistically associated with the cRR.
Results: We included 699 patients. IPAR occurred in 38/171 (22%) of NST patients and in 28/528 (5%) of EVT patients (aRR 4.41;95%CI:4.51-7.02). The cRR of treatment <6h after aneurysm rupture versus >24h after rupture for IPAR was for NST 2.07 (95%CI:1.02-4.20) and for EVT 6.50 (95%CI:1.46-28.98). The aRR of IPAR for poor functional outcome was for the total cohort 1.25 (95%CI:1.00-1.55), for NST 1.42 (95%CI:1.12-1.81), and for EVT 1.08 (95%CI:0.72-1.63), and for case-fatality respectively 1.62 (95%CI:1.08-2.43), 1.63 (95%CI:0.91-2.93), and 1.54 (95%CI:0.83-2.87).
Conclusions: IPAR occurs more often during NST than during EVT, and in neurosurgically treated patients IPAR was associated with poor outcome. Aneurysm treatment within 6 hours after ictus was for both treatment modalities a risk factor for IPAR. Future studies should further investigate the relationship between treatment timing and IPAR.
Disclosures of Interest:
No
Abstract N°: 2536
LUMBAR PUNCTURE OR EXTERNAL VENTRICULAR DRAIN AS INITIAL TREATMENT FOR ACUTE HYDROCEPHALUS IN ANEURYSMAL SUBARACHNOID HAEMORRHAGE
Wenz Fabian*1, Tack Reinier2, Abdulazim Amr1, Van der Zwan Albert2, Vergouwen Mervyn2, Etminan Nima1, Rinkel Gabriel2
1Universitätsklinik Mannheim, Department of Neurosurgery, Mannheim, Germany, 2UMC Utrecht, Department of Neurology and Neurosurgery, Utrecht, Netherlands
On behalf of:
Background and aims: Acute hydrocephalus after aneurysmal subarachnoid haemorrhage (SAH) is typically treated by external ventricular drainage (EVD). Lumbar puncture (LP) may be an effective and less invasive alternative. We compared efficacy and safety of LP versus EVD as initial treatment.
Methods: We performed a two-centre cohort study comparing two different institutional approaches, with either LP or EVD as initial treatment. SAH patients treated within 72 hours for hydrocephalus, with GCS⩾7 and no contraindications for LP were included. We calculated odds ratios with adjustment (aOR) for baseline predictors to compare the rates of permanent ventriculoperitoneal shunts (VP-shunt), clinical and radiological complications, and unfavourable functional outcome (Glasgow Outcome Scale 1-3 at 3 months) between the two strategies.
Results: At one institution, 84 patients with acute hydrocephalus were initially treated with LP between 2007 and 2021, whereas at the other institution, 77 similar patients were initially treated with EVD between 2015 and 2021. Both groups had comparable initial clinical condition and extent of hydrocephalus. EVD could be avoided in 65 patients (77%) of the LP-group. A permanent VP-shunt was placed in 8 patients (10%) of the LP-group and 52 patients (68%) of the EVD-group (aOR=0.04; 95%CI=0.02-0.11). Complications occurred less frequent in the LP-group (LP-group=21%; EVD-group=38%; aOR=0.44; 95%CI=0.20-0.92) and there were no significant differences in unfavourable functional outcomes (LP-group=43%; EVD-group=52%; aOR=0.67; 95%CI=0.32-1.40).
Conclusions: LP is associated with lower rates of chronic hydrocephalus and need for VP-shunt, less complications and comparable clinical outcomes as EVD and should therefore be considered as initial treatment for acute hydrocephalus after SAH.
Disclosures of Interest:
No
SCIENTIFIC COMMUNICATION – PROGNOSIS AND OUTCOME AFTER STROKE
Abstract N°: 2235
FUNCTIONAL AND PATIENT-CENTERED OUTCOMES IN INTRACEREBAL AND INTRAVENTRICULAR HEMORRHAGE AFTER TRACHEOSTOMY AND GASTROSTOMY
Vishank Shah*1, Lourdes Carhuapoma2, Radhika Avadhani3, Julian Bösel1,4, Issam A. Awad5, Wendy Ziai1, Daniel F. Hanley3
1Johns Hopkins University School of Medicine, Neurology, Anesthesiology and Critical Care Medicine, Baltimore, United States, 2The Johns Hopkins Hospital, Neurocritical Care, Baltimore, United States, 3Johns Hopkins University School of Medicine, Brain Injury and Outcomes, Baltimore, United States, 4University Hospital Heidelberg, Neurology, Heidelberg, Germany, 5University of Chicago, Neurosurgery, Chicago, United States
On behalf of:
Background and aims: We described trajectories of long-term health-related quality-of-life (HRQOL), functional and cognitive outcomes in severe intracerebral and intraventricular hemorrhage (ICH/IVH) survivors receiving tracheostomy and/or percutaneous endoscopic gastrostomy (tracheostomy/PEG) in the acute-phase.
Methods: We conducted a longitudinal analysis of MISTIE-III and CLEAR-III trials. One-year trajectories of modified Rankin scale (mRS), European-QOL Visual Analog Scale (EQVAS), mini-mental status examination (MMSE) scores were assessed using mixed-effects linear regression in severe ICH/IVH patients receiving tracheostomy/PEG. Association of tracheostomy/PEG with 1-year mRS and EQVAS was assessed using multivariable regression and causal mediation analysis, adjusting for ICH-severity and demographics.
Results: Of 999 participants, 185(37%) severe-ICH (mean[SD] ICH-volume, 52.4[17.6]mL) and 219(44%) severe-IVH (IVH-volume, 31.4[20.7]mL) participants received tracheostomy/PEG. Median[IQR] day-30 mRS was 5[5-5]. By 1-year, 55% had >1-point improvement in mRS, 28% achieved good-outcome (mRS0-3), 9% achieved functional independence (mRS0-2) and 51% returned home. One-year mortality occurred in 24%, with no significant difference in Kaplan-Meier survival estimates in participants with and without tracheostomy/PEG. HRQOL was poor initially (median day-30 EQVAS=22[10-40]), but improved significantly over 1-year (β-slope[95%CI], 32[28-35]; p<0.001; 1-year EQVAS=65[50-80]), with time-trade-off health-utility index of 1.0 [0.7-1]. MMSE improved significantly over 1-year (β-co-efficient, 12[11-13] points), with 35% achieving normal cognition. In multivariable regression, tracheostomy/PEG was independently associated with poor 1-year functional-outcome, but not with lower 1-year EQVAS, and did not mediate associations of other covariates with EQVAS.
Conclusions: Severe ICH/IVH survivors receiving tracheostomy/PEG in the acute-phase had modest functional and cognitive recovery over 1-year, with ~30% achieving good functional-outcome, normal cognition and majority reporting an acceptable HRQOL.Tracheostomy/PEG may not influence long-term HRQOL
Disclosures of Interest:
Yes I received personal fees from Astra Zaneca (<1000$) for speaker bureau training
Abstract N°: 2330
DERIVATION AND EXTERNAL VALIDATION OF A TROPONIN T CUT-OFF TO IMPROVE RISK STRATIFICATION AFTER ACUTE ISCHEMIC STROKE OR TIA
Simon Hellwig*1,2,3, Valerian Altersberger4, Leo Bonati4,5, Henrik Gensicke4,6, Joachim Christian Fladt4, Matthias Endres1,2,3,7,8,9, Heinrich Audebert1,2, Christian Nolte1,2,3,7,8, Mira Katan4, Jan Scheitz1,2,3,7
1Department of Neurology, Charité - Universitätsmedizin Berlin, Berlin, Germany, 2Center for Stroke Research Berlin (CSB), Berlin, Germany, 3Berlin Institute of Health (BIH) at Charité - Universitätsmedizin Berlin, Berlin, Germany, 4Department of Neurology and Stroke Center, University Hospital Basel and University of Basel, Basel, Switzerland, 5Research Department, Reha Rheinfelden, Rheinfelden, Switzerland, 6Neurology and Neurorehabilitation, University Department of Geriatric Medicine Felix Platter, University of Basel, Basel, Switzerland, 7German Center for Cardiovascular Research (DZHK), Partner Site, Berlin, Germany, 8German Center for Neurodegenerative Diseases (DZNE), Partner Site, Berlin, Germany, 9NeuroCure Cluster of Excellence, Charité - Universitätsmedizin Berlin, Berlin, Germany
On behalf of:
Background and aims: High-sensitivity cardiac Troponin T (hs-cTnT) is associated with recurrent major cardiovascular events (MACE) after acute ischemic stroke (AIS) or TIA. We aimed to derive and validate an optimal hs-cTnT cut-off associated with event-free survival after AIS or TIA.
Methods: The derivation cohort comprised consecutive AIS or TIA patients admitted to a comprehensive stroke center in Basel, Switzerland between 2014-2020. The validation cohort consisted of patients prospectively enrolled in acute stroke studies at the Center for Stroke Research, Berlin, Germany between 2010-2023. The primary outcome was the occurrence of MACE at day 90. The cut-off with a negative predictive value (NPV) of >90% and the highest number of individuals correctly classified (CC) was considered optimal.
Results: The derivation cohort contributed 3,498 patients (median age 77 years, 43.2% female, 11.6% TIA, median hs-cTnT 15 ng/L), the validation cohort contributed 2,062 patients (median age 71 years, 38.1% female, 20.6% TIA, median hs-cTnT 12 ng/L). For derivation, hs-cTnT levels were associated with MACE at day 90 (n=585 [16.7%], adjusted odds ratio [aOR] for log10-transformed hs-cTnT 2.49 [95%CI 1.99-3.12]). The optimal hs-cTnT cut-off was 18 ng/L (NPV 90.2%, CC 2,248 [64.3%]). In the validation cohort, the derived hs-cTnT cut-off yielded a NPV of 96.7% (CC 1,570 [76.1%]).
Conclusions: A hs-cTnT cut-off at 18 ng/L predicted event-free survival 90 days after AIS or TIA in heterogeneous cohorts. This finding may be useful to guide clinical decision-making and inform intensity of clinical monitoring and the design of future stroke prevention trials and scores.
Disclosures of Interest:
No
Abstract N°: 2804
CHRONIC KIDNEY DISEASE PREDICTS STROKE SEVERITY, DISABILITY AND EARLY RECURRENCE: POPULATION-BASED COHORT STUDY
Dearbhla Kelly*1, Linxin LI1, Peter Rothwell1
1University of Oxford, Wolfson Centre for the Prevention of Stroke and Dementia, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
On behalf of: Oxford Vascular Study
Background and aims: Chronic kidney disease (CKD) increases the risk of cerebrovascular disease but impacts on stroke severity and recurrence risk are unclear. We aimed to determine these associations in a population-based study.
Methods: In a population-based study (Oxford Vascular Study), we studied initial stroke severity (NIHSS) and disability (modified Rankin scale; mRS) in relation to CKD (eGFR<60ml/min/1.73m2) in all patients presenting with TIA and stroke from 2002-2017 with follow-up for recurrent vascular events (stroke, myocardial infarction, and sudden cardiac death) to 2022. Associations were examined using ordinal or Cox regression models, adjusted for age, sex, and measured vascular risk factors, and stratified by TOAST subtype.
Results: Among 3178 patients (TIA=1167; ischaemic stroke=1802; intracerebral haemorrhage=209), 1267 (40%) had CKD. CKD was independently associated with ischaemic stroke vs TIA (adjusted OR=1.31, 95%CI=1.11-1.56; p=0.002) and with greater initial NIHSS (aOR=1.28, 1.04-1.46; p=0.018), driven mostly by eGFR<30 ml/min/1.73m2 (aOR=2.59, 1.44-4.66; p=0.001 for ischaemic stroke; aOR=4.06, 2.04-8.06; p<0.001 for NIHSS). Among patients with ischaemic stroke, CKD was also associated with higher one-month mRS (aOR/point=1.40, 1.13-1.74; p=0.002), again driven by eGFR<30 ml/min/1.73m2 (aOR=6.51, 3.04-13.97, p<0.001). Risk of early (<90 days) recurrent stroke was increased with CKD (aHR=1.60, 1.15-2.21; p=0.005), as was the long-term (0-15 years) risk of all vascular events (aHR=1.14, 1.05-1.46; p=0.01).
Conclusions: The association of CKD with event severity, early disability and recurrence risk suggests that there may be processes intrinsic to CKD leading to uniformly worse outcomes. Further research should determine whether CKD-specific treatments might improve outcomes.
Disclosures of Interest:
No
Abstract N°: 2838
GENOME-WIDE ASSOCIATION STUDY ON POST-STROKE MORTALITY REPORTS ASSOCIATION WITH UTS2B/CCDC50
Aniket Mishra*1, Yunfeng Huang2, Laura Ibañez3, Ellen Tsai2, Israel Fernandez Cadenas4, Boryana Stamova5, Carlos Cruchaga3, Sudha Seshadri6, Jin-Moo Lee7, Stéphanie Debette1
1University of Bordeaux, Inserm, Bordeaux Population Health Research Center, UMR 1219, Bordeaux, France, 2Biogen Pharmaceuticals Ltd, 3Washington University School of Medicine, Department of Psychiatry, St. Louis, United States, 4Biomedical Research Institute Sant Pau (IIB Sant Pau), Stroke Pharmacogenomics and Genetics Laboratory, Barcelona, Spain, 5University of California at Davis, Department of Neurology and MIND Institute, Sacramento, United States, 6UT Health Sciences Center, Glenn Biggs Institute for Alzheimer’s and Neurodegenerative Diseases, San Antonio, United States, 7Washington University School of Medicine, Department of Neurology, Saint Louis, United States
On behalf of: on behalf of the NeuroCHARGE consortium, the International Stroke Genetics Consortium and the GIGASTROKE consortium
Background and aims: Stroke is the second leading cause of death across the globe. Mortality rates within 30-days of stroke onset range between 13% and 35% in population-based cohorts. Genetic variants might influence stroke survival by modulating stroke severity and resilience to vascular brain injury.
Methods: Gathering prospective information on stroke incidence and death in ~1.5 million participants of population-based cohorts worldwide, we performed meta-analysis of genome-wide association studies on mortality within 30-days after 1st stoke incidence (N=5,272 fatal stroke cases). GWAS were performed under the additive model of genetic inheritance adjusting for age, sex, principal-components for population stratification, and if required family structure and/or study site.
Results: We identified association of common variants in the UTS2B/CCDC50 locus with fatal versus non-fatal any ischemic stroke GWAS model in Europeans. This association was successfully replicated in independent clinic-based samples on 90-days mortality after stroke incidence. The association at UTS2B/CCDC50 remained genome-wide significant after correcting for index event bias. The lead SNP at this locus is an eQTL of UTS2B and CCDC50 in blood, which is supported by differential gene expression analyses in independent clinical cohort.
Conclusions: We performed the largest GWAS on post-stroke mortality as a proxy for stroke severity using prospective information of ~1.5 million participants in different population-based cohorts. Our GWAS meta-analysis identified association of a novel, biologically relevant locus at UTS2B/CCDC50 with fatal vs non-fatal ischemic stroke.
Disclosures of Interest: No
Abstract N°: 2991
SYSTOLIC BLOOD PRESSURE REDUCTION STRATEGIES IN ACUTE ISCHEMIC STROKE FOLLOWING ENDOVASCULAR THROMBECTOMY: A SYSTEMATIC REVIEW AND META-ANALYSIS
Syed Gillani*1,2, Mohammed Maan Al-Salihi1,3, Ram Saha4, Mouhammad Jumaa5, Syed Zaidi5, Farhan Siddiq1,2, Camilo Gomez2, Mikael Mazighi6, Adnan Qureshi1,2
1Zeenat Qureshi Stroke Institute, 2University of Missouri, Department of neurology, Columbia, United States, 3University of Wisconsin-Madison, Madison, United States, 4Virginia Commonwealth University, Richmond, United States, 5The University of Toledo Health Science Campus, Department of neurology, Toledo, United States, 6Hospital Foundation Adolphe De Rothschild, Department of Interventional Neuroradiology, Paris, France
On behalf of:
Background and aims: There is no consensus on systolic blood pressure (SBP) target post-endovascular thrombectomy (EVT) in patients with acute ischemic stroke (AIS). This study intends to investigate the relationship between reducing SBP and clinical outcomes, to determine the therapeutic efficacy of moderate and intensive SBP reduction post EVT
Methods: A comprehensive search was conducted across five electronic databases to identify studies relevant to our analysis. Data from these studies were then analyzed using pooled relative risk (RR) along with their corresponding 95% confidence intervals (CI) for our categorical outcomes. Functional independence at 90 days post-EVT was defined as a mRS 0-2.
Results: Our meta-analysis included eight studies with 2922 patients: 1376 patients were treated with intensive SBP reduction, 306 with moderate, and 1243 with standard SBP reduction. There was no difference in the risk of functional independence at 90 days post-EVT with both intensive-SBP reduction (target 120-140 mmHg, RR=1.05, 95% CI 0.82, 1.34, p = 0.72) and moderate-SBP reduction (>160 mm Hg) (RR= 0.95, 95% CI 0.69, 1.31, p = 0.76) compared with standard SBP reduction (>180 mm Hg). The risk of symptomatic intracranial hemorrhage (sICH) did not significantly differ between standard-SBP reduction and intensive-SBP reduction (RR = 0.93, 95% CI 0.66, 1.31, p = 0.36) or moderate-SBP reduction (0.72 (95% CI [0.28, 1.87], p = 0.50) groups, respectively. Intensive-SBP reduction significantly decreased the risk of hemicraniectomy.
Conclusions: We did not identify difference in functional independence at 90 days in AIS with either intensive-SBP reduction or moderate-SBP reduction compared with standard SBP reduction post-EVT.
Disclosures of Interest:
No
Abstract N°: 3084
MORE PRECISE: LONGITUDINAL PATIENT REPORTED OUTCOME MEASURES (PROMS) IN STROKE
Amber Corrigan*1, Ben Carter1, Astrid Verstraete2, Alexander Smith3, Anna Pennington3, Jonathan Hewitt3
1King's College London, United Kingdom, 2Stoke Mandeville Hospital, United Kingdom, 3Cardiff University, United Kingdom
On behalf of: More Precise study group
Background and aims: Post-stroke morbidity is a prevalent issue. The integration of Patient-Reported Outcome Measures (PROMs) may allow global impact on patients to be better measured. This study employed a stroke-specific PROM encompassing Mental Health (MH) and Physical Health (PH) domains. The primary objective was to examine the correlation between PROMs and clinical measures at 6-months
Methods: A multicentre prospective cohort study at 19 UK hospital sites. Data was considered immediately following stroke event, and at 3 and 6 months.The association between each PROM domain clinical measures were calculated using a multilevel multivariable linear model fitting the adjusted mean difference (aMD) at 6 months.
Results: At 6 months, symptoms of depression (PHQ-9, aMD=-0.45, CI -0.59, -0.32) and anxiety (GAD-7, aMD=-4.4, CI -0.59, -0.29) were associated with poorer mental health. Disability (MRS, aMD -1.91, CI -2.41, -1.47) was associated with diminished mental health. Patient-reported outcomes - poor walking (aMD=-3.86, CI -5.34, -2.38), needing help for toileting (aMD=-3.77, CI -5.15, -2.40), and requiring assistance with dressing (aMD=-4.75, CI -3.40, -6.10), were correlated with poorer mental health. All clinical measures were associated with poor physical health outcomes.
Conclusions: The longitudinal design, spanning across 6-months, enables a nuanced understanding of the evolving mental and physical health needs post-stroke. Importantly, the mental health morbidity was associated with all commonly measured clinical morbidity and appears to extend beyond what clinical measures can discern. PROMs may serve as a predictor of global morbidity based on its impact on the patient's quality of life rather than relying solely on only clinical descriptors and variables.
Disclosures of Interest:
No
Abstract N°: 3305
DEVELOPMENT AND EXTERNAL VALIDATION OF THE POSTERIOR CIRCULATION CLOT BURDEN SCORE (PC-CBS) IN A LARGE INTERNATIONAL COHORT
Alexander Salerno*1, Davide Strambo1, Dimitris Lambrou1, Guillaume Marie2, Gaia Sirimarco1, Vincent Dunet2, Guillaume Saliou2, Patrik Michel1
1Lausanne University Hospital and University of Lausanne, Stroke Center, Neurology Service, Department of Clinical Neurosciences, Lausanne, Switzerland, 2Lausanne University Hospital and University of Lausanne, Department of Diagnostic and Interventional Radiology, Lausanne, Switzerland
On behalf of: on behalf of the PC-CBS collaborators
Background and aims: Early evaluation and prompt treatment are key elements for the correct management of acute ischemic stroke (AIS). The early identification of an accurate prognosis currently lacks a tool able to correlate vascular patency status to long-term functional outcome for application across the entire PC, not limited solely to BAOs.
Methods: The posterior circulation clot burden score (PC-CBS) was an investigator-initiated, global, retrospective cohort study. Based on a multivariable ordinal logistic regression model able to predict a modified Rankin Scale of 3-to-6, we attributed integer points to relevant PC arterial segments and developed a prognostic model (Figure 1). Discriminative ability was described using Harrell’s C-statistic after undergoing 500-fold cross-validation. External validation was performed with data from 21 centers worldwide.
Results: The score was developed on 488 derivation patients (median age 71 (IQR:59-81), 36%female, NIHSS 6 (IQR:3-13)) and validated in 1057 patients globally (median age 72 (IQR:61-81), 40%female, NIHSS 8 (IQR:4-18)). The PC-CBS, a 10-point scale assessing the main PC arterial segments (Figure 1), demonstrated good prediction accuracy for the angiographic score alone (AUC=0.70) and was an independent prognostic predictor. Upon integrating additional clinical-radiological variables, we found very good metrics (Figure 2) (AUC=0.84). External validation confirmed these findings with an AUC=0.71 for the angiographic model and AUC=0.85 for the combined clinical-radiological model.
Conclusions: The PC-CBS stands as a valuable and externally validated prognostic tool for clinicians managing PC-AIS and providing information to families. It also promises potential as a stratification criterion in future clinical trials in posterior circulation acute revascularization therapies.
Disclosures of Interest:
No
SCIENTIFIC COMMUNICATION – CLINICAL TRIALS
Abstract N°: 755
TENECTEPLASE VERSUS ALTEPLASE IN CHINESE PATIENTS WITH ACUTE ISCHAEMIC STROKE (ORIGINAL): A MULTICENTRE RANDOMISED PHASE III STUDY
1Beijing Tiantan Hospital affiliated to Capital Medical University, Beijing, China, 2Linfen Central Hospital, Linfen, China, 3Hexigten Banner Mongolian Traditional Chinese Medicine Hospital, Chifeng, China, 4Xianyang Hospital of Yan’an University, Xianyang, China, 5Linyi People’s Hospital, Linyi, China, 6Zhejiang Provincial People’s Hospital, Hangzhou, China, 7Boehringer Ingelheim (China), Shanghai, China
On behalf of:
Background and aims: Tenecteplase is a bioengineered variant of alteplase with greater fibrin specificity and a longer half-life. The ORIGINAL study aimed to establish the non-inferiority of tenecteplase to alteplase in Chinese patients with acute ischaemic stroke (AIS) within 4.5 hours of symptom onset.
Methods: This multicentre, prospective, randomized, open-label, blinded-endpoint (PROBE), Phase III study was performed at 55 sites in China. Adults with AIS who were admitted within 4.5 hours of symptom onset and eligible for thrombolysis were assigned (1:1) to tenecteplase (0.25 mg/kg; Boehringer Ingelheim) or alteplase (0.9 mg/kg). The primary outcome was the proportion of patients with a favourable outcome (modified Rankin Scale [mRS] 0–1) at day 90. The prespecified non-inferiority risk ratio (RR) margin was 0.937.
Results: Between 14 July 2021 and 14 July 2023, 1489 patients were randomized and 1465 patients included in the full analysis set. Of these, 72.7% (532/732) in the tenecteplase group and 70.3% (515/733) in the alteplase group had a favourable outcome at day 90 (adjusted RR=1.0278, 95% CI 0.9678–1.0915; non-inferiority threshold met). Adjudicated symptomatic intracerebral haemorrhage events by the Third European Cooperative Acute Stroke Study (ECASS III) definition (both 1.2%, RR=1.005, P>0.05) and mortality at 90 days (4.6% vs 5.8%, RR=0.795, P>0.05) were comparable between the tenecteplase and alteplase groups.
Conclusions: In Chinese patients with AIS eligible for intravenous thrombolysis within 4.5 hours after stroke onset, tenecteplase was non-inferior to alteplase regarding a favourable outcome at day 90. Tenecteplase showed a similar safety profile to alteplase. ClinicalTrials.gov: NCT04915729.
Disclosures of Interest:
Yes None, except for MS and XL, who are employees of Boehringer Ingelheim (China).
Abstract N°: 2438
TWIN2WIN: A RANDOMIZED STUDY TO COMPARE THE EFFICACY OF FIRSTLINE DUAL VS SINGLE STENTRETRIEVER TECHNIQUE. PROCEDURAL OUTCOMES
Alejandro Tomasello1, Manuel Moreu2, Manuel Requena1, Lavinia Dinia3, Herbert Tejada Meza4, Marta Rubiera1, Magda Jablonska1, Judith Cendrero1, Tomas Carmona1, Marc Ribo*1
1Vall d'Hebron University Hospital, Barcelona, Spain, 2Hospital Clinico Universitario San Carlos, Madrid, Spain, 3Hospital de la Santa Creu i Sant Pau, Barcelona, Spain, 4Miguel Servet University Hospital, Zaragoza, Spain
On behalf of: Twin2win investigators: Alan Flores, David Hernandez, Marta de Dios, Francesco Diana, Alvaro garcia-Tornel, Marc Rodrigo, Federica Rizzo, Santiago Ortega-Gutierrez, Marta olive-Gadea
Background and aims: In endovascular treatment (EVT) of stroke, first pass recanalization (FPR) has shown to improve clinical outcome. The use of a dual stentretriever (DS) technique has been proposed as an effective rescue approach when standard techniques fail. We aim to investigate if primary DS is safe and leads to higher rates of FPR.
Methods: Twin2win (NCT05632458) is a prospective multicenter, randomized, open treatment and blinded adjudication endpoint study in which stroke patients undergoing EVT were randomized to receive firstline DS Vs single stentretriever (SS). Switching technique was allowed after first pass. The primary objective was to evaluate the rate of FPR (TICI 2c-3). Additional procedural outcomes are reported.
Results: From April 2022 to October 2023, 106 patients were included: SS:47.2% (n=50), DS:52.8% (n=56) with no baseline differences between groups.Occlusion locations were: TICA:34.9%, M1-MCA:57.5% and basilar:7.5%. Rate of FPR was: SS:24% Vs DS:49% (p<0.01).. Rate of final complete recanalization (TICI 2c-3) was: SS:72% Vs DS:70.6% (p=0.87).The mean number of passes was SS:2.1±1.3 VS DS:1.7±1 (p=0.08). In the SS arm 6 patients were switched to DS after a failed first pass. Rescue therapy (angioplasty/stenting/IA lytics) was needed in SS:14% DS:5.4% (p=0.12).Median procedural time was SS:37[27-60] minutes Vs DS:39[26-64] minutes (p=0.93). Rate of procedural complications was: SS:6% VS DS:8.9% (p=0.42) and symptomatic ICH occurred in SS:4.5% Vs DS 6.8% (p=0.5).
Conclusions: In stroke patients undergoing EVT, primary DS is safe and superior to SS in achieving FPR but not final recanalization. Implications on clinical outcomes should be studied in specifically designed trials
Disclosures of Interest:
No
Abstract N°: 2656
INTRAVENOUS THROMBOLYSIS BEFORE ENDOVASCULAR TREATMENT IN PATIENTS WITH CAROTID TANDEM LESIONS: MR CLEAN-NO IV RANDOMIZED CLINICAL TRIAL RESULTS
Fabiano Cavalcante*1, Carlos Rangkuti1, Manon Kappelhof1, Kilian Treurniet1,2, Theodora Van Elk3, Vincent Costalat4, Hester Lingsma5, Yvo Roos6, Charles Majoie1, Bart Emmer1
1Amsterdam University Medical Centers, University of Amsterdam, Amsterdam Neuroscience, Department of Radiology and Nuclear Medicine, Amsterdam, Netherlands, 2Haaglanden Medical Center, Department of Radiology, The Hague, Netherlands, 3University Medical Centre Groningen, Department of Neurology, Groningen, Netherlands, 4Centre Hospitalier Universitaire de Montpellier, Department of Radiology, Montpellier, France, 5Erasmus Medical Center, Department of Public Health, Rotterdam, Netherlands, 6Amsterdam University Medical Centers, University of Amsterdam, Amsterdam Neuroscience, Department of Neurology, Amsterdam, Netherlands
On behalf of: MR CLEAN-NO IV Investigators and CONTRAST collaboration
Background and aims: We assessed whether the presence of carotid tandem lesions modifies the effect of intravenous thrombolysis (IVT) prior to endovascular treatment (EVT) in patients with stroke presenting directly to centres capable of providing EVT.
Methods: The MR CLEAN-NO IV trial (trial registration number: ISRCTN80619088) randomised patients with acute ischaemic stroke due to anterior circulation large vessel occlusions to IVT plus EVT or EVT alone. This prespecified subgroup analysis assessed the effect heterogeneity of IVT plus EVT in patients with and without ipsilateral carotid tandem lesions on baseline cross-sectional imaging. The primary effect parameter was the adjusted common odds ratio (acOR) for a one-point shift lower on the modified Rankin Scale (mRS) at 3 months. Secondary outcomes included poor outcome (3 month mRS 5-6), 5-7 day National Institutes of Health Stroke Scale (NIHSS) score, any intracranial haemorrhage, and symptomatic intracranial haemorrhage.
Results: Carotid tandem lesions were present in 88/507 (17%) patients. A statistically significant interaction was observed for the primary outcome (pinteraction=0.03). Patients with tandem lesions had worse functional outcomes (acOR, 0.55; 95%CI 0.25-1.17) and patients without tandem lesions had better functional outcomes (acOR 1.46; 95% CI 1.03-2.07) with IVT plus EVT. Significant interactions in the same direction were observed for poor functional outcome (pinteraction<0.01) and 5-7 day NIHSS score (pinteraction=0.02).
Conclusions: The effect of IVT plus EVT versus EVT alone differs significantly in patients with and without carotid tandem lesions. Patients with tandem lesions showed no benefit and potential harm, while those without tandem lesions exhibited better functional outcomes with IVT plus EVT.
Disclosures of Interest: No
Abstract N°: 2679
ENDOVASCULAR THROMBECTOMY FOR LARGE ISCHEMIC STROKES WITH TANDEM LESIONS: A SECONDARY ANALYSIS OF THE SELECT2 TRIAL
Santiago Ortega-Gutierrez*1, Aaron Rodriguez-Calienes1, Malik Ghannam1, Milagros Galecio-Castillo1, Deep Pujara2, Faris Shaker3, Clark Sitton4, Bruce Campbell5, Edgar Samaniego1, Amrou Sarraj2
1University of Iowa Hospitals and Clinics, Department of Neurology, Iowa City, United States, 2Case Western Reserve University, Department of Neurosurgery, Cleveland, United States, 3The University Of Texas Health Science Center At Tyler: Emergency Room, Department of Neurosurgery, Tyler, United States, 4The University Of Texas Health Science Center At Tyler: Emergency Room, Department of Radiology and Neuroradiology, Tyler, United States, 5Royal Melbourne Hospital Car Park, Department of Neurology, Parkville, Australia
On behalf of:
Background and aims: We aimed to compare efficacy and safety outcomes in patients with tandem lesions (TLs) and large core infarcts treated with endovascular thrombectomy (EVT) vs. medical management (MM).
Methods: This is a secondary analysis of Endovascular Thrombectomy for Large Ischemic Strokes (SELECT2) trial. SELECT2 enrolled patients with large ischemic strokes according to ASPECTS 3-5 on computed tomography (CT) or ischemic core ⩾50 ml on CT perfusion imaging, and TLs with more 70% stenosis based on NASCET criteria were included in the analysis. Functional and safety outcomes were compared between patients receiving EVT vs. MM.
Results: Among 352 enrolled patients, a total of 100 (28%) exhibited TLs. Of those, 56 received EVT (median [IQR] age, 69 [59-76] years; 17 females [30.4%]) and 44 received MM (median [IQR] age, 66 [58-77] years; 16 females [36.4%]). Patients receiving EVT demonstrated significantly better functional outcomes (aGenOR=2.35;95%CI 1.56-3.54; p<0.001). (Figure 1). EVT led to improved mRS scores at 90 days across prespecified subgroups independent of age, baseline NIHSS, ischemic-core volume, and CT ASPECTS category (Figure 2). A sensitivity analysis by acute carotid artery stenting (CAS) approach showed no significant differences in terms of sICH (CAS:0% vs. non-CAS:2%, p=1.00) and petechial hemorrhage (CAS:85.7% vs. non-CAS:71.4%, p=0.66).
Conclusions: EVT was associated with better functional outcomes without significant safety concerns when compared to MM in patients with TLs and large ischemic stroke. This effect is independent on age, clinical severity and the core infarct volume at presentation. Further exploration in larger cohorts on the optimal cervical technique in this population is needed.
Disclosures of Interest:
No
SCIENTIFIC COMMUNICATION – REHABILITATION AND RECOVERY
Abstract N°: 299
SAEBOGLOVE THERAPY FOR UPPER LIMB DISABILITY AND SEVERE HAND IMPAIRMENT AFTER STROKE (THE SUSHI TRIAL)
Jen Alexander1, Patrycia Duklas1, Robert Heggie1, Frederike van Wijck2, Mark Barber3, Christine Mcalpine4, Terence J Quinn1, Felicity Boyce4, Olivia Wu1, Jesse Dawson*1
1University of Glasgow, United Kingdom, 2Glasgow Caledonian University, United Kingdom, 3NHS Lanarkshire, United Kingdom, 4NHS Greater Glasgow and Clyde, United Kingdom
On behalf of: Lisa Kidd, Alex McConnachie, Peter Langhorne, Teresa J Kimberley
Background and aims: Arm and hand weakness are common and disabling after stroke. We assessed the effect of self-directed therapy using a dynamic hand orthosis which offers digital extensor assistance to enable hand opening started between 7 and 60 days after stroke.
Methods: SUSHI was a pragmatic, multicentre, parallel-group, randomised controlled trial with blinded outcome assessment. Participants were randomised (1:1) basis to receive 6 weeks of individualised self-directed, repetitive, functional-based practice involving a SaeboGlove plus usual care, or usual care only. The primary outcome was change in Action Research Arm Test (ARAT) at 6 weeks after randomisation. All analysis are intention to treat.
Results: 78 participants were randomised (39 to SaeboGlove and 39 to usual care) from 6 study sites in the UK. At randomisation, mean age was 63 years (SD 13), 28 (36%) were female, 63 (81%) suffered ischaemic stroke, mean time from stroke 29 days (SD 15). Mean baseline ARAT score was 13.3 (SD 11.8).
The total ARAT score at 6 weeks increased by 23.8 points in the SaeboGlove group and by 15.8 points in the usual care group (adjusted between group difference 7.1 points, 95% CI 0.22 to 14, p=0.047). ARAT grasp, pinch and grip subscores were also significantly improved at 6 weeks. Secondary outcomes and cost effectiveness data are available.
Conclusions: Individualised self-directed, repetitive, functional-based practice involving a SaeboGlove, started between 7 and 60 days after stroke in people with hand and arm impairment, led to significant improvements in ARAT score at 6 weeks after randomisation.
Disclosures of Interest:
No
Abstract N°: 1341
EFFECTS OF 1-YEAR AEROBIC AND STRENGTH TRAINING ON COGNITIVE FUNCTIONING AFTER TIA OR MINOR STROKE:A RANDOMIZED CONTROLLED TRIAL
Inger Deijle*1, Ilse Jonkers2, Hooghiemstra Astrid M.3, Gwenda Engels1, Jos Twisk4, Henry Weinstein1, Sander van Schaik1, Renske M. Van den Berg-Vos1
1OLVG Location West, Neurology, Amsterdam, Netherlands, 2Woonzorggroep Samen, Department of Psychology, Schagen, Netherlands, 3VU University Medical Center, Alzheimer Center Amsterdam, Amsterdam, Netherlands, 4VU University Medical Center, Epidemiology and Data Science, Amsterdam, Netherlands
On behalf of:
Background and aims: Patients who have recently suffered a transient ischemic attack (TIA) or minor ischemic stroke are at increased risk of cognitive impairment. As an in-depth analysis of our primary study, in the present study, we aimed to investigate the effect of a 1-year exercise intervention on cognitive functioning up to 2 years post intervention.
Methods: In this secondary analysis of the MoveIT trial, we investigated the effect of an exercise intervention on cognitive functioning. Patients with a TIA or minor stroke were randomly allocated to an intervention group receiving the 1-year exercise intervention (n=60), or to usual care (n=59). Outcome measures were assessed at baseline and after 1 and 2 years. We measured cognition with neuropsychological tests on three domains: 1) executive functioning, 2) attention-psychomotor speed, and 3) memory. Linear mixed models were used for longitudinal data to determine the effect of the exercise intervention on cognitive functioning.
Results: We found that over the two years study period, corrected for age, sex, and educational level, the intervention group on average improved significantly more in executive functioning than the control group (β = 0.13; 95 % CI [0.02 to 0.25]; p = 0.03). No significant intervention effects were found on either memory or attention-psychomotor speed.
Conclusions: Our data show that a 1-year exercise intervention significantly improved executive functioning over time, compared to usual care. We recommend that health care professionals consider broadening standard secondary stroke prevention treatment in patients with TIA/minor stroke by adding exercise and physical activity.
Disclosures of Interest:
No
Abstract N°: 1565
IS MOBILE HEALTH-DELIVERED PHYSICAL ACTIVITY FEASIBLE AND ACCEPTABLE IN PEOPLE POST STROKE OR TRANSIENT ISCHAEMIC ATTACK?
David Moulaee Conradsson*1,2, Charlotte Thurston1, Hanna Lagerlund1, Sophia Humphries1, Lucian Bezuidenhout1, Sverker Johansson1,2
1KAROLINSKA INSTITUTET, Division of Physiotherapy, Department of Neurobiology, Care Sciences and Society, STOCKHOLM, Sweden, 2Karolinska University Hospital, Medical unit Occupational therapy & Physiotherapy, Theme Women’s Health and Allied Health Professional, Stockholm, Sweden
On behalf of:
Background and aims: Digital interventions, facilitated by a mobile application (mHealth), emerge as promising solutions to enhance engagement in long-term support for physical activity (PA). This study aimed to assess the feasibility and acceptability of mHealth support for PA post stroke or TIA.
Methods: In this parallel-group feasibility study (ClinicalTrials: NCT05111951), 116 adults with mild stroke/TIA were randomised to either i) mHealth-delivered supervised physical exercise and behavioural change techniques for PA or, ii) mHealth-delivered behaviour change techniques for PA only. Pre-defined progression criteria were developed to assess intervention feasibility (reach, adherence, safety, fidelity) and acceptability.
Results: Of 134 eligible participants, 116 (86%) were included in the trial of which 105 (90%) completed the 6-month intervention. The completion rate for outcomes at baseline was high; digital questionaries (98%), sensor-derived PA (86%), and blood pressure monitoring (92%). The participants, who resided in diverse regions of Sweden (see Figure 1), averaged 70 years of age (64% females, 70% with a history of stroke) and demonstrated a baseline PA level of 6405 steps/day. Approximately 1800 digital exercise sessions were conducted without any severe adverse events related to the intervention. A majority of the participants were satisfied with the mHealth technology (73%) and perceived the digital intervention as equivalent to in-person visits (77%).
Conclusions: Whilst the mHealth intervention appears feasible and acceptable, findings highlight certain areas for development, such as recruitment strategies to avoid selection bias of people with high levels of health literacy and PA.
Disclosures of Interest: No
Abstract N°: 2186
PREVALENCE AND PREDICTORS OF NON-MOTOR OUTCOMES 6 MONTHS AFTER STROKE: RESULTS FROM A HOSPITAL-BASED STROKE REGISTRY
Hatice Ozkan*1,2, Gareth Ambler3, John Mitchell4, Gargi Banerjee2,5, Carmen Barbato1, Simone Browning2, Alexander Leff2, Rob Simister1,2, David Werring1,2
1UCL Queen Square Institute of Neurology, London, UK, 2National Hospital for Neurology and Neurosurgery, University College London Hospitals NHS Foundation, Queen Square, London, 3Department of Statistical Science, University College London, Gower Street, London, UK, 4UCL Department of Epidemiology, 5MRC Prion Unit at UCL, Institute of Prion Diseases, London, UK
On behalf of:
Background and aims: Post stroke non-motor outcomes place a major burden on both patients and caregivers, but current understanding is limited. Our aims are to evaluate: the prevalence of adverse non-motor outcomes in single and multiple health domains; their baseline predictors; and the co-occurrence of adverse outcomes in different domains.
Methods: We obtained data from the Stroke Investigation Group in North and Central London (SIGNAL) registry based at the University College London (UCH) Comprehensive Stroke Service. We included adult patients diagnosed with acute stroke due to cerebral ischaemia or intracerebral haemorrhage (ICH) from January 2017 to January 2020. We evaluated non-motor outcomes across 13 health domains at 6-month follow-up.
Results: Follow-up was 92% complete for 3080 patients (2534 acute ischaemic stroke, 547 ICH). At 6 months, the most prevalent adverse non-motor outcomes were fatigue (57%), reduced social participation (55%), sleep disturbance (54%), and constipation (44%) (See Figure 1). Rates of ⩾1, ⩾2, ⩾3, ⩾4, and ⩾5 adverse non-motor outcomes were 75%, 51%, 49%, 40%, 26%, respectively. Common factors associated with adverse outcomes were ICH, NIHSS score>5 at admission, and previous stroke or TIA. Moderate correlations were found between fatigue and sleep disturbance (k=0.72), memory and thinking impairment and reduced ADL/IADL (k=0.68), communication problems and ADL/IADL (k=0.70).
Conclusions: Adverse non-motor outcomes are very common 6 months after stroke: fatigue, sleep disruption, and reduced social participation each affect over 50% of survivors, and one-quarter suffer from five adverse outcomes. Our findings support the need for targeted interventions to mitigate these adverse outcomes.
Disclosures of Interest:
No
Abstract N°: 2638
THE EFFECT OF INSTANT MESSAGE-DELIVERED COGNITIVE BEHAVIOURAL THERAPY (IMCBT) FOR STROKE CAREGIVERS’ PSYCHOLOGICAL SUPPORT
Jay Jung Jae Lee*1,2, Kui Kai Lau3, Esther Yuet Ying Lau4, Pui Hing Chau1, Mu-Hsing Ho1, Pim Cuijpers5, Man Ping Wang1
1The University of Hong Kong (HKU), School of Nursing, Hong Kong, 2The George Institute for Global Health, Global Brain Health, Barangaroo, Australia, 3The University of Hong Kong (HKU), Department of Medicine, Hong Kong, 4The Education University of Hong Kong (EdUHK), Department of Psychology, Hong Kong, 5Vrije Universiteit Amsterdam, Department of Clinical, Neuro and Developmental Psychology, Amsterdam, Netherlands
On behalf of:
Background and aims: Many stroke patients require long-term care, often relying on assistance from family caregivers within the community. Numerous stroke caregivers need psychological support to cope with caregiver stress. However, a significant proportion of these caregivers receive insufficient psychological support. If left unmanaged, this can lead to adverse health outcomes for both caregivers and care-recipients. This trial aimed to evaluate the effectiveness of instant message-delivered cognitive-behavioural therapy (imCBT) for providing psychological support to caregivers.
Methods: A randomised controlled trial was conducted with 256 stroke caregivers, who were randomly allocated to either the Intervention (n=128) or Control (n=128) group. The intervention group received imCBT via WhatsApp, accompanied by nurse-led real-time chat support for three months. Depression (PHQ-9; primary outcome), anxiety (GAD-7), stress (PSS-4), and loneliness (ULS-8) were measured at baseline, three, and six months. Intention-to-treat (ITT) analysis was employed to analyse the data. Generalised estimating equations were used to estimate the parameters and evaluate post-test differences between the groups.
Results: The participants' mean age was 51 years(SD=14.2), and 54.3% were male. A significant reduction in depressive symptoms was observed in the intervention group compared to the control group at the 6-month post-intervention (B = 2.771, SE = 0.473, p <.001). Additionally, post-intervention anxiety symptoms (B=2.261, SE=0.498, p<.001), stress (B=1.397, SE=0.308, p<.001), and loneliness (B=2.230, SE=0.504, p<.001) were significantly reduced in the intervention group compared to the control group.
Conclusions: This study demonstrated that imCBT is effective in improving the psychological well-being (depressive and anxiety symptoms, stress, and loneliness) of stroke caregivers.
Disclosures of Interest:
No
Abstract N°: 3261
CONCURRENT VALIDITY AND RESPONSIVENESS OF UPPER LIMB OUTCOEM AND SENSOR-BASED ARM USE WITHIN THE FIRST YEAR AFTER STROKE: A LONGITUDINAL COHORT STUDY
Johannes Pohl1,2,3, Geert Verheyden2, Jeremia Held4, Andreas Luft1,5, Chris Awai-Easthope3, Janne Veerbeek6
1University of Zurich, Neurology, Zürich, Switzerland, 2KU Leuven, Department of Rehabilitation Sciences, Leuven, Belgium, 3Data Analytics and Rehabilitation Technology (DART) Lab, Lake Lucerne Institute, Vitznau, Switzerland, Vitznau, Switzerland, 4Kliniken Valens, Rehaclinic Triemli, Zürich, 5cereneo, Ceneter for Neurology and Rehabiliation, Neurology, Weggis, Switzerland, 6Luzerner Kantonsspital, Neurocente, Lucerne, Switzerland
On behalf of:
Background and aims: Concurrent validity and responsiveness of upper limb outcome is essential to interpret motor recovery after stroke. Evaluating the associations between clinical upper limb measures and sensor-based arm use (AU) fosters an understanding of motor recovery. We aimed to investigate the measurement properties of comprehensive clinical outcome measures and sensor-based AU, excluding gait and non-functional upper limb movements.
Methods: In a prospective, longitudinal cohort study, impaired individuals were measured at days 3 (D3), 10 (D10), 28 (D28), 90 (D90), and 365 (D365) after first stroke. The Fugl-Meyer Assessment, Action Research Arm Test, Box & Block Test, and Motor Activity assessed upper limb functioning. Individuals wore five movement sensors (trunk, wrists, and ankles). Thirteen AU metrics were computed, including functional movements during non-walking bouts. Spearman correlations for each time point determined concurrent validity across outcomes. Responsiveness was examined by correlating patient-reported Global Rating of Perceived Change (GRPC) with observed change. Minimal important changes (MIC) were estimated by ROC curve analysis.
Results: Ninety-three individuals participated. Time points after D10 showed strong associations between capacity measures and AU metrics (rs: 0.73-0.94, p<0.01). Unilateral nonaffected AU had low-to-high negative associations (rs: 0.48-0.77). Responsiveness across outcomes was highest between D9-D28 with moderate-to-strong relations (rs: 0.60-0.73, p<0.01).
Eight MIC values were estimated for clinical measures and nine for AU metrics, showing moderate-to-good accuracies (66-87%).
Conclusions: We present reference values on concurrent validity and responsiveness of clinical upper limb measures and specified AU metrics across stroke recovery. Estimated MIC values can be used as a benchmark for clinical stroke rehabilitation.
Disclosures of Interest:
No
SCIENTIFIC COMMUNICATION – THROMBOLYSIS
Abstract N°: 536
ARTERIAL RECANALIZATION DURING INTER-HOSPITAL TRANSFER FOR THROMBECTOMY
Pierre Seners*1, Anke Wouters2, Adrien Ter Schiphorst3, Maarten Lansberg4, Greg Albers4
1Hôpital Fondation A. de Rothschild, Paris, France, 2KU Leuven, Neurology, Leuven, Belgium, 3CHU Gui de Chauliac, Neurology, Montpellier, France, 4Stanford Hospital, Stanford Stroke Center, Palo Alto, United States
On behalf of: CRISP-2 and Infarct-Growth investigators
Background and aims: We evaluated the incidence and predictors of arterial recanalization during inter-hospital transfer for thrombectomy, as well as the relationship between recanalization during transfer and clinical outcomes.
Methods: We analyzed data from two cohorts of acute stroke patients with an anterior circulation large vessel occlusion transferred for thrombectomy to a comprehensive center, regardless of whether thrombectomy was eventually attempted, with systematic arterial imaging at the referring hospital and upon comprehensive stroke center arrival. Inter-hospital recanalization was determined by comparison of the baseline and post-transfer arterial imaging, and was defined as revised Arterial Occlusive Lesion (rAOL) score 2b or 3.
Results: A total of 520 patients were included, of whom 111/520 (21%) experienced inter-hospital recanalization (partial recanalization [rAOL=2b] in 77% and complete [rAOL=3] in 23%). Pre-transfer variables independently associated with recanalization were intravenous thrombolysis (adjusted OR=6.8, 95%CI 3.8-11.3; P<0.001), more distal occlusions (P<0.001), and smaller clot burden (P<0.001). Recanalization during transfer was associated with less inter-hospital infarct growth and greater inter-hospital NIHSS score improvement, with greater benefit from complete vs partial recanalization (P for trend test <0.001). Recanalization was independently associated with reduced 3-month disability (adjusted common OR=2.5, 95%CI 1.7-3.8, P<0.001), with greater benefit from complete than partial recanalization.
Conclusions: Substantial rates of recanalization are observed during inter-hospital transfer for thrombectomy, with a strong association with favorable post-transfer and 3-month clinical outcomes, even for partial recanalization. Broadening thrombolysis indications in primary stroke centers and developing therapies that increase the rate of recanalization during transfer will likely improve clinical outcomes.
Disclosures of Interest:
No
Abstract N°: 746
TENECTEPLASE VERSUS ALTEPLASE IN THE TREATMENT OF ACUTE ISCHEMIC STROKE WITHIN 4.5 HOURS: A SYSTEMATIC REVIEW AND META-ANALYSIS
Lina Palaiodimou*1, Aristeidis Katsanos2, Guillaume Turc3,4,5,6, Peter Schellinger7, Aikaterini Theodorou1, Robin Lemmens8,9, Simona Saaco10, Apostolos Safouris1,11, Amrou Sarraj12, Georgios Tsivgoulis1
1National and Kapodistrian University of Athens, Second Department of Neurology, “Attikon” University Hospital, Athens, Greece, 2McMaster University/Population Health Research Institute, Department of Medicine (Neurology), Hamilton, Canada, 3GHU Paris Psychiatrie et Neurosciences, Department of Neurology, Paris, France, 4Université Paris Cité, Paris, France, 5INSERM U1266, Paris, France, 6FHU NeuroVasc, Paris, France, 7Ruhr-University Bochum, Department of Neurology and Neurogeriatrics, Johannes Wesling Klinikum Minden, Minden, Germany, 8University Hospitals Leuven, Department of Neurology, Leuven, Belgium, 9KU Leuven-University of Leuven, Department of Neurosciences Division of Experimental Neurology, Leuven, Belgium, 10University of L'Aquila, Department of Biotechnological and Applied Clinical Sciences, L'Aquila, Italy, 11Metropolitan Hospital, Stroke Unit, Piraeus, Greece, 12Case Western Reserve University - University Hospitals Cleveland Medical Center, Department of Neurology, Cleveland, United States
On behalf of:
Background and aims: The current European Stroke Organisation expedited recommendation on tenecteplase (TNK) for acute ischaemic stroke (AIS) advocates that TNK 0.25mg/kg can be used alternatively to alteplase for AIS of <4.5-hours duration. Since the publication of these guidelines, two additional randomized-controlled clinical trials (RCTs) have provided further insight.
Methods: We conducted an updated systematic review and meta-analysis including all available RCTs that investigated efficacy and safety of TNK 0.25mg/kg compared to alteplase for the treatment of AIS within 4.5-hours of onset. The primary outcome was defined as the excellent functional outcome at 3-months (modified Rankin Scale (mRS)-score 0-1), while good functional outcome (mRS-score 0-2), reduced disability at 3-months (⩾1-point reduction across all mRS-scores), symptomatic intracranial haemorrhage (sICH), and 3-month mortality were evaluated as secondary outcomes. Pooled estimates were calculated with random-effects model.
Results: Nine RCTs were included comprising a total of 2,719 patients treated with TNK vs 2,678 patients treated with alteplase. TNK was associated with higher likelihood of excellent functional outcome (RR 1.07; 95%CI:1.01-1.14; p=0.015; I2=0%) and reduced disability (common OR 1.10; 95%CI:1.00-1.22; p=0.049; I2=0%) compared to alteplase, while good functional outcome (RR 1.05; 95%CI:0.99-1.12; p=0.098; I2=36%) was similar between the groups. Regarding safety outcomes, similar rates of sICH (RR 1.10; 95%CI:0.78-1.56; p=0.574; I2=0%) and 3-month mortality (RR 0.97; 95%CI:0.81-1.15; p=0.709; I2=6%) were observed.
Conclusions: The updated meta-analysis confirms similar safety of TNK 0.25 mg/kg to alteplase, while, for the first time, marginal superiority of TNK is shown for excellent functional outcome and reduced disability at 3 months.
Disclosures of Interest:
No
Abstract N°: 1590
EFFECT OF INTRAVENOUS THROMBOLYTICS ON DELAYED REPERFUSION FOLLOWING INCOMPLETE MECHANICAL THROMBECTOMY
Adnan Mujanovic*1, Vignan Yogendrakumar2, Felix Ng2, Markus Kneihsl3, Thomas Gattringer3, Jan Gralla1, Timothy Kleinig4, Urs Fischer5, Bruce Campbell2, Johannes Kaesmacher1
1Inselspital, Department of Diagnostic and Interventional Neuroradiology, Bern, Switzerland, 2Melbourne Brain Centre, Department of Medicine and Neurology, Heidelberg, Australia, 3Medical University of Graz, Department of Neurology, Graz, Austria, 4Royal Adelaide Hospital, Department of Neurology, Adelaide, Australia, 5Universitätsspital Basel, Department of Neurology, Basel, Switzerland
On behalf of:
Background and aims: More than half of endovascularly treated ischemic stroke patients with incomplete reperfusion (expanded Thrombolysis in Cerebral Infarction, eTICI<3) show delayed reperfusion (DR) at 24h, which is associated with good outcomes. We aimed to investigate the association between intravenous thrombolysis (IVT) and DR occurrence.
Methods: Pooled individual-patient data from three randomized controlled trials (EXTEND-IA, EXTEND-IA TNK part 1 and 2) and two prospective stroke studies (University Hospitals Graz and Bern) were analyzed. Primary outcome was status on follow-up perfusion imaging, dichotomized as DR or persistent perfusion deficit. DR was defined as the absence of any focal perfusion deficit on follow-up perfusion imaging, despite incomplete reperfusion on the final angiography series. Only eTICI 2a-2c patients with available perfusion imaging on 24±12 hour follow-up were included in the analysis.
Results: Out of 830 patients (median age 74, 51% male, 63% IVT), 61% had DR. There was an independent association between DR and IVT (aOR 1.4, 95%CI 1.0 – 2.1), in addition to age, atrial fibrillation, number of device passes, collateral score and eTICI. In those who have received IVT (n=520), when adjusting for the aforementioned cofactors, there was an independent association between DR and time between start of IVT and end of the intervention (aOR 0.7, 95%CI 0.6 - 0.9, per hour increase).
Conclusions: Pre-treatment with IVT was associated with the occurrence of DR among <eTICI3 patients. Association between IVT and DR appears to be stronger if IVT is still running at the time point when the proximal vessel is recanalized, but distal emboli occur.
Disclosures of Interest:
No
Abstract N°: 1669
ACUTE STENTING WITH OR WITHOUT INTRAVENOUS THROMBOLYSIS IN STROKE PATIENTS WITH CAROTID TANDEM LESIONS
Fabiano Cavalcante*1, Kilian Treurniet1,2, Manon Kappelhof1, Johannes Kaesmacher3, Daan Nieboer4, Hester Lingsma4, Jan Gralla3, Urs Fischer5, Yvo Roos6, Charles Majoie1
1Amsterdam University Medical Centers, Department of Radiology and Nuclear Medicine, Amsterdam, Netherlands, 2Haaglanden Medical Center, Department of Radiology, The Hague, Netherlands, 3University Hospital of Bern, University of Bern, University Institute of Diagnostic and Interventional Neuroradiology, Bern, Switzerland, 4Erasmus Medical Center, Department of Public Health, Rotterdam, Netherlands, 5University Hospital of Bern, University of Bern, Stroke Research Center, Department of Neurology, Bern, Switzerland, 6Amsterdam University Medical Centers, Department of Neurology, Amsterdam, Netherlands
On behalf of: IRIS collaboration
Background and aims: Whether carotid tandem lesions in patients with acute ischaemic stroke undergoing endovascular treatment (EVT) should be treated at the time of the procedure remains unclear. Required antiplatelet regimen after stent placement might predispose haemorrhagic transformation when combined with intravenous thrombolysis (IVT). We assessed the effect of acute stenting during EVT, with and without IVT.
Methods: Individual participant data meta-analysis of six clinical trials randomising patients presenting directly to comprehensive stroke centres to IVT plus EVT versus EVT alone. All patients with carotid tandem lesions and available information on intraprocedural stent placement were included. The primary outcome was the 90-days modified Rankin Scale, analysed with mixed-effect ordinal regression models with random intercepts and slope for study. Inverse propensity of treatment-weighted (IPTW) analysis was used to account for indication bias. We assessed the heterogeneity of the effect of acute stenting between patients randomised to IVT plus EVT and EVT alone.
Results: A total of 329 patients with carotid tandem lesions were included, with 113 (34%) receiving acute stenting. Stenting during EVT was associated with better functional outcomes (acOR before IPTW: 1.60 [95%CI 1.03-2.47], acOR after IPTW: 1.66 [95%CI 1.08-2.54]). No effect heterogeneity was observed for patients receiving IVT plus EVT versus EVT alone (ratio of acORs: 1.08 [95%CI 0.56-2.09]; p-interaction = 0.809).
Conclusions: Our data suggest that in stroke patients eligible for EVT, acute stenting of carotid tandem lesions is associated with better functional outcomes. IVT did not adversely affect this association, and stenting appears safe in patients with prior IVT.
Disclosures of Interest:
No
Abstract N°: 1915
RUNNING ALTEPLASE INFUSION UPON RECANALIZATION WITH THROMBECTOMY: A SUBSTUDY OF THE IRIS META-ANALYSIS
Johannes Kaesmacher*1, Fabiano Cavalcante2, Manon Kappelhof3, Kilian Treurniet3, Urs Fischer4, Jan Gralla1, Peter Mitchell5, Yvo Roos2, Charles Majoie3, Iris Collaborators6
1University Hospital Bern, Neuroradiology, Bern, Switzerland, 2AMC Amsterdam, Neurology, Amsterdam, Netherlands, 3AMC Amsterdam, Radiology, Amsterdam, Netherlands, 4University Hosital Basel, Neurology, Basel, Switzerland, 5Royal Melbourne Hospital, University of Melbourne, Department of Radiology, Australia, 6IRIS Collaborators, IRIS Collaboration, Amsterdam, Netherlands
On behalf of: IRIS Collaborators
Background and aims: It has been suggested that patients undergoing endovascular treatment (EVT) may particularly benefit from intravenous thrombolytics (IVT) if the infusion is running at the time point of recanalization. We aim to test this hypothesis by studying whether the effect of IVT+EVT versus EVT alone is modified by whether the infusion of IVT was still running at the time point of recanalization.
Methods: Using IRIS individual participant data from six randomized-controlled trials, we assessed treatment effect heterogeneity of IVT before EVT vs. EVT alone in groups with running or finished IVT-infusion upon recanalization, defined as bolus-to-recanalization-time below or above 60min, using a test for interaction. Primary outcome was the rates of mRS 0-2 at 90 days. To address the fact that patients in whom IVT-infusion is still running at recanalization have faster procedures and better reperfusion scores we estimated/imputed IVT-infusion time for all patients (including the EVT-only group) based on baseline characteristics.
Results: In IVT+EVT-patients, running IVT-infusion upon recanalization with EVT was associated with higher rates of functional independence (64% vs 46%, aOR 1.44, 95%CI 1.02-2.03, Fig1). However, there was no significant treatment effect heterogeneity regarding the effect of IVT depending on whether IVT-infusion was still running at the timepoint of recanalization (Pinteraction=0.11, Fig2).
Conclusions: In patients randomized to EVT alone or IVT+EVT, there was no treatment effect heterogeneity concerning a running IVT infusion at the time point of recanalization. This analysis does not support previous data suggesting that circulating alteplase after proximal recanalization leads to better outcomes.
Disclosures of Interest:
Yes The IRIS Collaboration has been supported by Stryker, Boehringer-Ingelheim, AMC Amsterdam and Inselspital Bern.
Abstract N°: 1966
TENECTEPLASE THROMBOLYTIC THERAPY FOR ACUTE ISCHEMIC STROKE IN CHINA. A MULTI-CENTER REAL-WORLD STUDY
Ye Liu*1, Dan LI2, Guang Wu3, Xiao Yu Zhou4, Rong Bo Qu5, Xin Cheng1, Qiang Dong1
1Huashan Hospital, China, 2Keshiketeng Banner Traditional Chinese Medicine Mongolian Medicine Hospitalorem Ipsum, Mogolia, China, 3Nanshi Hospital of Nanyang, Nan Yang Shi, China, 4The NO.10 People's Hospital of Shanghai, China, 5Yantai Affliated Hosiptal of Binzhou Medical University, Yan Tai Shi, China
On behalf of: TTT-AIS CHINA collaborators
Background and aims: Tenecteplase (TNK) has the logistic advantage over alteplase in stroke thrombolytic therapy. The non-inferiority of TNK compared to alteplase was proved by two randomized controlled clinical trials but the evidence is lacking regarding the real-world effectiveness and safety in China.
Methods: We retrospectively collected data using alteplase or TNK for acute ischemic stroke (AIS) within 4.5 hours of onset between March 1, 2019, and October 1 2023 from 17 stroke centers in China. Patients receiving TNK were 1:1 matched with alteplase by propensity score matching (PSM). The primary outcome was the rates of patients with symptomatic intracranial hemorrhage (sICH) in the 72 hours after thrombolysis. Secondary outcomes include any intracranial hemorrhage, any systematic bleeding requiring blood transfusion, 90-day mRS score, and death within 90 days.
Results: After PSM, a total of 1049 tenecteplase-treated AIS patients (median age 66 years, 63.97% male, median National Institutes of Health Stroke Scale score =5, interquartile range 3-9, 8.77% received endovascular thrombectomy) were matched to 1047 patients treated with alteplase (Table 1). Patients treated with TNK had better 90-day functional outcome (OR: 1.37, 95% CI: 1.11-1.7, p=0.003) and less any intracranial hemorrhage (OR=0.5, 95% CI 0.3-0.83, p=0.006) compared to alteplase. No difference was found in the sICH (1.72% v.s.2.1%, OR: 0.81, 95% CI: 0.43-1.52, p=0.52), systematic bleeding (OR:1.99, 95% CI: 0.365-10.93, p=0.425) and death within 90 days (OR: 0.81, 95% CI: 0.57-1.14, p=0.23) (Table 2).
Conclusions: Thrombolysis with tenecteplase was associated with better 3-month functional outcomes compared to alteplase in AIS patients, with no increased risk of sICH.
Disclosures of Interest:
No
Abstract N°: 2291
INTRAVENOUS THROMBOLYSIS IN PATIENTS WITH RECENT DOAC INGESTION - A TARGET TRIAL ANALYSIS AFTER LIBERALISATION OF OUR GUIDELINES
Philipp Bücke*1, Simon Jung1, Johannes Kaesmacher2, Martina Göldlin1, Thomas Horvath1, Ulrike Prange1, Urs Fischer1, Marcel Arnold1, David Seiffge1, Thomas Meinel1
Background and aims: We aimed to report the safety and efficacy of off-label intravenous thrombolysis(IVT) after changing our internal guidelines allowing IVT for all patients with recent direct oral anticoagulant(DOACs) intake regardless of DOAC-activity, last-intake or reversal.
Methods: We utilized the target-trial methodology to emulate the hypothetical criteria of a randomized controlled trial in the prospective stroke registry of our comprehensive stroke center. We assessed safety and efficacy outcomes (symptomatic intracranial hemorrhage ECASS-II, asymptomatic Heidelberg classification, major bleeding, 90 day mortality, 90 day good functional outcome mRS0-2 or return to baseline mRS) of consecutive patients (06/2021-10/2023) with recent DOAC intake(<48h) otherwise qualifying for IVT using inverse-probability-weighted regression-adjustment comparing those with versus without IVT.
Results: 92 patients fulfilled the target-trial criteria (median age 81years, 46%female, median NIHSS8, 47%thrombectomy, no reversal agent use). IVT was given in 44/92(48%) patients at a median of 189min after symptom onset and with median DOAC-activity level of 81ng/ml(IQR 52-113, max.350 ng/ml, available in 36/44 patients,2/3 intake within 24h). Symptomatic intracranial hemorrhage occurred in 0/44 patients receiving IVT and 2/46 patients not receiving IVT. Adjusted difference +0.7%,95%CI -3.7%to+5.3%. Mortality rates at 3 months were comparable (adjusted difference with IVT-6.2%,95%CI -18.9%to+6.4%) and IVT patients were more likely to have good outcome or return to baseline mRS (adjusted difference +22.3%,95%CI 9.0to35.6%). There was no significant difference in major bleeding or asymptomatic intracranial hemorrhage
Conclusions: After liberalizing our approach to IVT regardless of recent DOAC intake, we did not experience any safety concerns. The association of IVT with better outcomes warrants prospective randomized studies.
SCIENTIFIC COMMUNICATION – CLINICAL PRACTICE, MANAGEMENT AND CARE
Abstract N°: 684
ANTIPLATELET THERAPY IN EMERGENT CAROTID STENTING AFTER INTRAVENOUS THROMBOLYSIS: A MULTICENTER RETROSPECTIVE MATCHED ANALYSIS
Francesca Colò*1, Andrea Alexandre2, Francesco Arba3, Luca Scarcia4, Anne Falcou5, Maria Ruggiero6, Mariangela Piano7, Andrea Zini8, Guido Bigliardi9, Aldobrando Broccolini1
1Agostino Gemelli University Policlinic, Neurology, Rome, Italy, 2Agostino Gemelli University Policlinic, Neuro-Radiology, Rome, Italy, 3Careggi University Hospital, Firenze, Italy, 4Henri-Mondor University Hospital, Créteil, France, 5Clinica ospedaliero-universitaria Policlinico Umberto I, Neurology, Roma, Italy, 6AUSL Romagna - Sede Cesena, Neurology, Cesena, Italy, 7Niguarda, Neurology, Milan, Italy, 8ospedale MAGGIORE bologna, Bologna, Italy, 9Modena, Modena, Italy
On behalf of:
Background and aims: Mechanical thrombectomy (MT) with emergent carotid stenting (eCAS) is beneficial in patients with tandem occlusion (TO). Our aim was to address safety and efficacy of different intra-procedural antiplatelet regimens in patients undergoing eCAS after intravenous thrombolysis (IVT) and define predictors of parenchymal hemorrhage (PH).
Methods: The databases of 17 European stroke centers were screened for consecutive patients with TO who received MT with eCAS. Intra-procedural antiplatelet therapy was categorized in: 1) low intensity regimen, 2) high intensity regimen, and 3) high intensity regimen followed by i.v. Glycoprotein IIb/IIIa inhibitors (GPI) infusion. Propensity score matching (PSM) was used to estimate differences in outcome between treatment groups. Outcome measure included the occurrence of PH type 2 and type 1 and the 90-day mRS score 0-2.
Results: 621 patients were collected, 48.5% received IVT. After PSM there was no significant difference between IVT and non-IVT patients under different antiplatelet regimens concerning rates of PH type 2 and type 1. Subgroup analysis showed increased rate of PH type 2 in IVT patients receiving high intensity regimen plus GPI maintenance, but without difference in clinical outcome. In multivariate analysis, presence of atrial fibrillation (OR 4.089, 95% CI 1.759-9.508), high intensity antiplatelet regimen with GPI maintenance (OR 2.364, 95% CI 1.086-5.147) and stent thrombosis (OR 2.631, 95% CI 1.160-5.970) were predictors of PH type 2.
Conclusions: Different intra-procedural antiplatelet regimens for eCAS are overall safe after IVT. Increased risk of PH type 2 is associated with use of intra-procedural GPI maintenance in IVT patients and presence of atrial fibrillation.
Disclosures of Interest:
No
Abstract N°: 1176
FACTOR XA INHIBITOR–ASSOCIATED INTRACRANIAL HAEMORRHAGE INCIDENCE AND OUTCOMES IN THE MULTICOUNTRY OBSERVATIONAL AXIOM STUDY
Alexander Cohen1, Robert Welch2, Jenneke Leentjens3, Ali Canbay4, Craig Coleman5, Satarupa Choudhuri6, Chaozer Er7, Chatree Chai-Adisaksopha8, Douglas Dover9, Jordy Gaspersz10
1Department of Haematological Medicine, Guys and St. Thomas’ Hospitals NHS Foundation Trust, King’s College, London, United Kingdom, 2University of Alberta and Mazankowski Alberta Heart Institute, Edmonton, AB, Canada, 3Radboud UMC, Nijmegen, Netherlands, 4Universitãtsklinikum Knappschaftskrankenhaus Bochum, Bochum, Germany, 5Department of Pharmacy Practice, University of Connecticut, Storrs, CT, United States, 6Northern Care Alliance NHS Foundation Trust, Salford, United Kingdom, 7Department of General Medicine, Woodlands Health, Singapore, 8Department of Internal Medicine, Chiang Mai University, Thailand, 9University of Alberta, Edmonton, AB, Canada, 10PHARMO Institute for Drug Outcomes Research, Utrecht, Netherlands
On behalf of: Lisa Smits, Jil Billy Mamza, He Gao, Ruiqi Zhang, Arsh K. Randhawa, Elena Babak, Wendy Beekman, Noortje Houthuizen, Felix Scherg, Katarina Kopke, Julia Winter, George Godfrey, Eddy Lang, Juan Arenillas, and AXIOM Research Group
Background and aims: Intracranial haemorrhage (ICH) is one of the most severe complications associated with use of anticoagulants, such as Factor Xa inhibitors (FXai), and may result in significant morbidity and mortality. The goal of this multicountry study was to explore the burden of ICH following initial FXai use.
Methods: This retrospective observational cohort study involved analysis of electronic health records from new FXai users in Canada, Germany, and the UK and followed ⩽10 years. Subjects with a FXai prescription for a therapeutic indication (eg, venous thromboembolism, atrial fibrillation [AF], non-mechanical cardiac-valve replacement) were included. Incidence rates of ICH associated with FXai use and select outcomes (mortality, cardiovascular [CV] outcomes) were assessed and reported per 100 person years (PYR) with 95% confidence intervals.
Results: For Canada, Germany, and the UK, respectively, 75,806; 141,711; and 240,357 new FXai users were included in this analysis. A total of 326 ICHs were reported in Canada, 636 in Germany, and 1,649 in the UK; 3-year incidence rates were 0.72, 0.54, and 0.50 per 100 PYR, respectively. The most common FXai indication among patients with ICH was AF (Table 1). During the first 3 months after ICH, the rate of all-cause mortality was high, at 292 per 100 PYR in Canada; 215 per 100 PYR in Germany; and 265 per 100 PYR in the UK (Table 2).
Conclusions: In this observational study, FXai-associated ICH incidence rates were relatively consistent across the 3 included countries, and rates of all-cause mortality were high during the first 3 months after ICH.
Disclosures of Interest:
Yes ATC: consultant for AbbVie, ACI Clinical, Alexion, AstraZeneca, Bayer, Boehringer-Ingelheim, Bristol-Myers Squibb, Cardinal Health, Centrix, Daiichi-Sankyo, EmstoPA Ltd, Janssen, Johnson & Johnson, Medscape, Sanofi Aventis, and Pfizer
Abstract N°: 1635
ASPIRATION VS. STENT RETRIEVER THROMBECTOMY IN BASILAR ARTERY OCCLUSION. AN ANALYSIS OF THE GERMAN STROKE REGISTRY
Johannes Wischmann*1, Hanna Zimmermann2, Linus Keidel1, Thomas Liebig2, Christian Nolte3,4,5,6, Lars Kellert1
1LMU University Hospital Munich, Department of Neurology, Munich, Germany, 2LMU University Hospital Munich, Institute of Neuroradiology, Munich, Germany, 3Charité - Universitätsmedizin Berlin, Department of Neurology, Berlin, Germany, 4Charité - Universitätsmedizin Berlin, Center for Stroke Research Berlin (CSB), Berlin, Germany, 5Charité - Universitätsmedizin Berlin, Berlin Institute of Health (BIH) at Charité, Berlin, Germany, 6Charité - Universitätsmedizin Berlin, German Center for Cardiovascular Research (DZHK), Partner Site, Berlin, Germany
On behalf of: German Stroke Registry-Endovascular Treatment (GSR-ET) Investigators
Background and aims: Endovascular treatment has become the standard care for acute basilar artery occlusion (BAO). Uncertainty persists regarding the optimal thrombectomy technique. We compared aspiration thrombectomy with stent retriever thrombectomy in BAO patients in a multi-center real-world patient population.
Methods: We analyzed data from the German Stroke Registry-Endovascular Treatment (GSR-ET). Patients with isolated BAO who underwent either aspiration or stent retriever thrombectomy were compared including propensity score matching. The primary outcome measure was the modified Rankin Scale (mRS) shift at 90 days. Secondary outcomes included symptomatic intracranial hemorrhage (sICH), procedure complications and metrics.
Results: Out of 13,082 patients in the GSR-ET, 387 patients (mean age 72.0±13.1 years; 45.0% female) fulfilled inclusion criteria. Thrombectomy technique was aspiration in 195 (50.4%) and stent retriever in 192 (49.6%) patients. Functional outcome did not differ between groups, neither before (common Odds Ratio [cOR] 0.94; 95% Confidence interval [CI] 0.64-1.38) nor after matching (cOR 1.37; 95% CI 0.90-2.09). There was no significant difference in sICH (2.6 vs. 5.5%; p=0.231; OR 0.46; 95% CI 0.14-1.47) but aspiration thrombectomy demonstrated less procedure related complications (4.6% vs. 12.5%; p=0.017), a shorter procedure duration (24 vs. 48 minutes; p=<0.001) and higher first pass recanalization rates (75.1% vs. 44.8%; p=<0.001).
Conclusions: This study adds to the growing evidence, that both aspiration and stent retriever thrombectomy are equally efficient in terms of functional outcome in BAO patients. However, procedure complications and metrics may favor aspiration over stent retriever thrombectomy.
Disclosures of Interest:
No
Abstract N°: 1876
PREDICTORS OF STROKE RECURRENCE IN PATIENTS TREATED WITH SHORT-TERM DAPT FOR MINOR STROKE OR TIA – DATA FROM THE READAPT STUDY
1University of L'Aquila, Department of Biotechnological and Applied Clinical Sciences, L'Aquila, Italy, 2Imperial College London, Department of Brain Sciences, London, United Kingdom, 3AUSL Romagna, Department of Neuroscience, Maurizio Bufalini Hospital, Cesena, Italy, 4Santa Corona Hospital, Department of Neurology, Pietra Ligure, Italy, 5Città di Castello Hospital, Department of Neurology, Città di Castello, Italy, 6University of Rome La Sapienza, Department of Human neurosciences, Rome, Italy
On behalf of: READAPT study group
Background and aims: Dual antiplatelet therapy (DAPT) is effective for preventing recurrent ischemic events in patients with minor ischemic stroke or high-risk transient ischemic attack. We aimed to analyze real-world data to identify predictors of such events in DAPT-treated patients.
Methods: The REAl-life study on short-term Dual Antiplatelet treatment in Patients with ischemic stroke or Transient ischemic attack (READAPT) study, conducted from February 2021 to February 2023, prospectively included patients with minor stroke or transient ischemic attack (TIA) receiving short-term dual antiplatelet treatment. We compared patient characteristics between those with and without a 90-day recurrence of ischemic events.
Results: Among 1920 enrolled patients (65.4% male, 97.8% Caucasian, median age 72 [Interquartile Range – IQR 62.79]), 69.9% had a minor stroke (median NIHSS 3 [IQR 2-4]) and 30.1% a TIA (median ABCD2 score 5 [IQR 4-5]). Over the 90-day follow-up, 3.3% experienced ischemic recurrence - 2.0% recurrent ischemic stroke (median NIHSS 4 [IQR 3-6.25]) and 1.4% recurrent TIA (median ABCD2 score 2 [IQR 1-3]). Patients with recurrent events, compared to those without, were less frequently treated with revascularization (7.8% vs. 17.3%, p=0.046), had lower utilization of prolonged ECG monitoring (71.8% vs. 83.8%, p=0.011) and brain MRI (56.2% vs. 68.9%, p=0.031), and lower compliance to DAPT (3.6% vs 9.3%, p=0.020). Cox regression analysis showed that female sex (HR=0.50, CI 0.28-0.91, p=0.023) and good DAPT compliance (HR=0.41, CI 0.18-0.96, p=0.040) are independent protective factor for ischemic recurrence.
Conclusions: Our data justify clinician to encourage strict adherence to DAPT especially in men, resulted at the highest risk of ischemic stroke recurrence.
Disclosures of Interest:
No
Abstract N°: 1937
IMPACT OF ANTICOAGULANT DISCONTINUATION ON OUTCOME IN ACUTE ISCHEMIC STROKE PATIENTS WITH ATRIAL FIBRILLATION
1Daejeon Eulji medical Center, Eulji University School of Medicine, Daejeon, South Korea, 2Korea University Guro Hospital, Neurology, Seoul, South Korea, 3Chonnam National University Hospital, Neurology, Gwangju, South Korea, 4Hallym University Sacred Heart Hospital, Neurology, Anyang, South Korea, 5Ulsan University Hospital, Ulsan University College of Medicine, Neurology, Ulsan, South Korea, 6Inje University Ilsan Paik Hospital, Neurology, Goyang, South Korea, 7Yeungnam University Medical Center, Neurology, Daegu, South Korea, 8Jeju National University Hospital, Neurology, Jeju, South Korea, 9Korea University College of Medicine, Biostatistics, Seoul, South Korea, 10Seoul National University Bundang Hospital, Neurology, Bundang, South Korea
On behalf of: the CRCS-K (Clinical Research Collaboration for Stroke in Korea) investigators
Background and aims:This study examines the frequency and consequences of anticoagulant discontinuation in acute ischemic stroke (AIS) patients with concurrent atrial fibrillation (AF).
Methods: We enrolled 2,431 AIS patients with AF across 15 hospitals from 2018 to 2021, all of whom were prescribed anticoagulants at discharge. Our prospective data collection involved information on prescribed anticoagulants, vascular events, bleeding episodes, and mortality for up to 3 years. We conducted a matched case-control study (1:3 ratio, matched by age, sex, and discharge modified Rankin Scale score) to assess the impact of temporary anticoagulant interruptions.
Results: The cohort, with an average age of 75 and 55% male, predominantly used non-vitamin K antagonist oral anticoagulants (NOACs) (92.6%) at discharge. Anticoagulant discontinuation rates were 9.5%, 20.2%, and 23.9% at 3 months, 1 year, and 2 years post-discharge, respectively. Discontinuation was associated with an increased risk of the composite outcome (recurrent stroke, myocardial infarction, and death) up to 1 year after the initial stroke (hazard ratio 1.54 [95% CI: 1.04-2.30], p=0.03), but not beyond 1 year. Temporary interruptions (412 episodes) were mainly due to medical procedures (48.3%) and bleeding (38.4%). Interruptions exceeding 5 days increased the risk of recurrent stroke by sevenfold compared to those lasting 4 days or less.
Conclusions: Discontinuation of anticoagulants in AIS patients with AF significantly increases the risk of recurrent stroke and mortality. Notably, interruptions exceeding 5 days are particularly risky, underscoring the critical need to minimize temporary discontinuations to optimize patient outcomes.
Disclosures of Interest:
Yes This study was supported by an Investigator Initiated Research fund from Bayer Korea.
Abstract N°: 2450
TIMING IS EVERYTHING: LARGE-SCALE MAPPING OF 55,380 POST-STROKE BLOOD DRAWS UNCOVERS 24-HOUR RHYTHMS OF ROUTINE LABORATORY TESTS
Orsalia Veloudiou*1, Michael Karg1, Vanessa Granja Burbano1, Steffen Tiedt1
1University Hospital Ludwig-Maximilians-University (LMU) Munich, Institute for Stroke and Dementia Research (ISD), Munich, Germany
On behalf of: Leducq Consortium International pour la Recherche Circadienne sur l’AVC Effects in Stroke (CIRCA), and for the German Stroke Registry (GSR) investigators.
Background and aims: Patients with acute stroke receive routine blood work-up to evaluate inflammation, metabolism, and peripheral organ function. Under physiological conditions, these are known to oscillate over a 24-hour period. Whether these 24-hour rhythms persist in patients with stroke is unknown but would be important for diagnostic interpretation.
Methods: We mapped levels of 51 routine blood tests including measures of inflammation, metabolism, and peripheral organ function to their time of day of sampling. Data were collected over the first week of stroke from 5,036 patients with large-vessel occlusion stroke (55,380 blood collections) at 17 German sites. We applied sinusoidal regression analysis to determine whether blood tests results showed 24-hour rhythms.
Results: 49 of 51 (96%) analyzed blood tests showed 24-hour rhythms on at least one day within the first week after stroke. 14 of these blood tests including CRP, white blood cell count, glucose, hemoglobin, sodium, potassium, and aPTT showed 24-hour rhythms at all seven days (Figure 1). Peak times differed considerably between blood tests and changed over time (Figures 1 and 2). For multiple tests including white blood cell count and glucose, sampling at specific times of the day was more likely to generate results outside the reference range (Figure 2).
Conclusions: The majority of routine blood tests show 24-hour rhythms in the first seven days after stroke. The time of day of blood sampling is a novel, previously unrecognized modulator of blood test results from stroke patients, necessitating consideration when interpreting results.
Disclosures of Interest:
No
Abstract N°: 2904
HEMORRHAGE RISK WITH COMBINATION OF ANTIPLATELETS AND ANTICOAGULANTS FOR SECONDARY STROKE PREVENTION IN: A CROSS-SECTIONAL COHORT STUDY
1The Johns Hopkins Hospital, Baltimore, United States, 2Arkansas, United States, 3University of Arkansas for Medical Sciences, United States, 4University of Arkansas for Medical Sciences, 5University Hospital Heidelberg, Heidelberg, Germany, 6Johns Hopkins University, Baltimore, United States
On behalf of:
Background and aims:We studied risk of hemorrhage in patients receiving combined antiplatelets and anticoagulants (AC) for secondary stroke prevention after acute ischemic stroke (AIS) in setting of atrial fibrillation (AF) and acute myocardial infarction (MI).
Methods: We retrospectively queried a cross-sectional cohort in the TriNetX health-research network, collecting real-time electronic health records’ data from >120 US centers. AIS patients with AF and concomitant acute MI were extracted. We compared the risk of intracerebral hemorrhage (ICH) and gastrointestinal bleeding (GIB) in patients receiving AC alone versus AC+ single antiplatelet (AC+1AP) versus AC+ dual antiplatelet (AC+2AP) therapy at 3 months, 12 months, and lifetime post-ictus, after propensity-score matching for demographics and vascular co-morbidities.
Results: Among 143,919 AIS patients with AF and MI (mean[SD] age: 75.8[12.3] years; 45%female), propensity-score matching yielded 8,706 patients each in AC vs. AC+1AP matched-cohorts, 8,684 patients in AC vs. AC+2AP matched-cohorts, and 47,104 patients in AC+1AP vs. AC+2AP matched-cohorts. Odds of ICH was not increased at 3-months or 12-months (1.13 [0.98-1.31]; p=0.08), but was significantly increased lifetime after combining >1 antiplatelet with AC (AC+1AP: 1.26[1.11-1.45]; AC+2AP: 1.47[1.30-1.67]; p<0.001). Combining >1 antiplatelet with AC significantly increased 3-month,12-month and lifetime odds for GIB. No difference in hemorrhage risk was noted between AC+1AP and AC+2AP.
Conclusions: Combining antiplatelets with AC for secondary stroke prevention in patients with AF and acute MI may carry a low short-term risk of ICH, but may significantly elevate this risk long-term, along with increased short- and long-term risk of GIB. Clinical trials evaluating their safety and efficacy are warranted.
Disclosures of Interest:
No
Abstract N°: 3297
ECONOMIC INEQUALITY PREDICTS ACCESS TO MECHANICAL THROMBECTOMY INDEPENDENT OF NATIONAL GDP: A REPORT FROM MISSION THROMBECTOMY (MT 2020-PLUS)
1HonorHealth Research and Innovation Institute, 2Ascension Health, 3State University of New York Upstate Medical University, 4University of Iowa Hospitals, 5Virginia Mason Medical Center, Seattle, United States, 6Sree Chitra Tirunal Institute for Medical Sciences & Technology, Thiruvananthapuram, India, 7Narayana Health, 8Barrow Neurological Institute, 9Westchester Medical Center, Valhalla, United States, 10University of Miami, Coral Gables, United States
On behalf of: Mission Thrombectomy
Background and aims: A country’s income level and financial resources invested in national healthcare are predictors of access to Mechanical Thrombectomy (MT). We conducted a worldwide survey of countries on six continents to study the impact of economic inequality on access to MT, the disparities between countries, and its determinants on a global scale.
Methods: Our survey was conducted in 75 countries through the Mission Thrombectomy 2020+ global network. MT Access (MTA) was defined as the proportion of estimated LVO patients receiving MT in a given region annually. Economic inequality was defined using the GINI index published by the World Bank in 2021. Univariable and multivariable analyses were used to find the factors associated with economic inequality and MT access.
Results: We analyzed 61 countries with a total of 875 responses. The median global MTA was 2.79% (0.70-11.74) and median GINI index was 37.9 (32.8-42.8). Countries with low MT access (0-5%) were associated with higher median GINI co-efficients (worse economic inequality) when compared with counties with higher MT access (Table1, Figure1). MT operator and center availability, lower GINI index (lower economic inequality), and developed pre-hospital stroke systems were independent predictors of higher MT access.
Conclusions: Economic inequality is a significant determinant of access to mechanical thrombectomy in a country. Further analysis is needed to identify factors associated with better MT access despite economic inequality.
Disclosures of Interest:
No
SCIENTIFIC COMMUNICATION – SECONDARY PREVENTION
Abstract N°: 406
RISK OF ISCHAEMIC AND HAEMORRHAGE EVENTS WITH ANTICOAGULATION EARLY AFTER STROKE - AN ANALYSIS FROM THE ELAN TRIAL
1National Cerebral and Cardiovascular Center, Department of Cerebrovascular Medicine, Suita, Japan, 2University of Bern, Clinical Trials Unit, Bern, Switzerland, 3Helsinki University Hospital, and University of Helsinki, Department of Neurology, Helsinki, Finland, 4Glan Clwyd Hospital, Department of Geriatric Medicine, Denbighshire, United Kingdom, 5Morriston Hospital, Swansea Bay University Health Board, Stroke Unit, Swansea, United Kingdom, 6National Cerebral and Cardiovascular Center, Department of Neurology, Suita, Japan, 7University Hospital Basel, University of Basel, Department of Neurology, Basel, Switzerland, 8Inselspital Bern University Hospital and University of Bern, Department of Neurology, Bern, Switzerland, 9Queen Elizabeth University Hospital, University of Glasgow, School of Cardiovascular and Metabolic Health, Glasgow, United Kingdom
On behalf of: The ELAN investigators
Background and aims: To investigate whether vascular risk factors and stroke severity influence rates of ischaemic and bleeding events and the effect of early DOAC initiation in people with ischaemic stroke and atrial fibrillation (AF).
Methods: We used data from the randomized ELAN trial (n=2013). Participants with ischaemic stroke and AF were randomised to early (<48 hours in minor/moderate, day 6-7 in major stroke) or late (day 3-4 in minor, day 6-7 in moderate, and day 12-14 in major stroke) DOAC initiation. The primary outcome was a composite of recurrent ischaemic stroke, systemic embolism, major extracranial bleeding, symptomatic intracranial hemorrhage, or vascular death within 30 days. Subgroup analyses were performed to assess the interaction between the effect of risk factors on outcomes and the treatment groups.
Results: The primary-outcome occurred in 29/1006 participants (2.9%) with early and 41/1007 (4.1%) with late initiation. On adjusted analysis, prior heart failure (OR 2.49, 95% CI 1.27-2.19) and NIHSS score (⩾10) (3.33, 2.02-5.49) were associated with the primary outcome. In addition, early-treatment (0.65, 0.43-0.99) and diastolic BP (⩾79mmHg) (1.66, 1.06-2.59) were associated with the composite outcome within 90 days. Early-treatment was associated with lower odds of the primary outcome in people with body weight <75 kg (0.44, 0.22-0.88) but not in with body weight ⩾75kg (1.24, 0.62-2.48) (p for interaction=0.040).
Conclusions: People with prior heart failure, severe strokes, and late DOAC initiation have an increased risk for the composite outcome. People with low body weight appear to have a beneficial effect from early DOAC initiation.
Disclosures of Interest:
Yes Honoraria from Bayer Yakuhin, Daiichi-Sankyo, BMS/Pfizer, and BMS/Janssen Pharmaceuticals, and research supports from Daiichi-Sankyo, and Nippon Boehringer Ingelheim, all of which are outside of the submitted work.
Abstract N°: 525
NON-TRADITIONAL LIPID PROFILES AND 1-YEAR VASCULAR OUTCOMES IN ISCHEMIC STROKE PATIENTS WITH PRIOR STATIN THERAPY
1Chonnam National University Hospital, Neurology, 2Cerebrovascular Center, Seoul National University Bundang Hospital, Neurology
On behalf of:
Background and aims: This study aimed to investigate the association between non-traditional lipid profiles and the risk of 1-year vascular events in patients who were already using statins at the time of stroke occurrence and had admission LDL-C <100 mg/dL.
Methods: This study was an analysis of a prospective, multicenter, nationwide registry of Clinical Research Center for Stroke-Korea (CRCS-K) registry. The subjects were non-cardioembolic stroke within 1 week of onset whose admission LDL-C was controlled to below 100mg/dL through statin pretreatment. Each non-traditional lipid profile was divided into four quartiles (Q1, Q2, Q3, Q4). Primary outcome within one year was a composite of recurrent stroke, myocardial infarction (MI) and all-cause of mortality. The secondary outcomes were consisted of each individual outcome.
Results: A total of 7028 patients were included in the analysis. Regarding the LDL/HDL ratio, when comparing to Q1 as a reference, the event rate increased as the ratio increased for Q4 (adjusted HR 1.48, 95% CI 1.19-1.83, p = 0.0004). LDL/HDL had linear correlations with primary outcome (p for overall effect = 0.0001, P for non-linear effect = 0.5882).
Conclusions: In patients whose LDL-C level is well controlled by statin treatment prior to index event, non-traditional lipid profiles can be regarded as the next focus for treatment. Particularly, higher quartiles of the LDL/HDL ratio were significantly associated with increasing the risk of 1-year composite vascular events, showing a linear correlation.
Disclosures of Interest:
No
Abstract N°: 1043
ANTITHROMBOTIC DRUGS FOR CAROTID ARTERY DISSECTION - UPDATE OF A COCHRANE SYSTEMATIC REVIEW
Philippe Lyrer1, Nikolaos S. Avramiotis*1, Fabian Schaub2, Sebastian Thilemann1, Stefan Engelter1,3
1Universitätsspital Basel, Department of Neurology and Stroke Center, Basel, Switzerland, 2Inselspital Bern, Department of Neurology, Bern, Switzerland, 3University Department of Geriatric Medicine Felix Platter, Neurology and Neurorehabilitation, Basel, Switzerland
On behalf of:
Background and aims: Extracranial internal carotid artery dissection (eICAD) is a leading cause of stroke in younger patients. In this Cochrane Review update we sought to determine the differences in functional outcome and occurrence of major adverse events between antiplatelets and anticoagulants in eICAD-patients.
Methods: Eligible studies were identified through Cochrane Stroke Group Trials Register, CENTRAL, MEDLINE and EMBASE and personal search up to June 2023. We included observational and experimental studies comparing anticoagulants with antiplatelets in eICAD-patients. Primary outcomes were death (all causes) and death or disability. Secondary outcomes were ischemic stroke (IS), symptomatic intracranial hemorrhage (SIH), and major extracranial hemorrhage (MEH) during the reported follow-up period.
Results: We identified 2 completed randomized and 6 new non-randomized studies for a total of 44 included studies. Comparing antiplatelets with anticoagulants there was a significant difference in the odds of death (OR 2.69, 95% CI 1.27 to 5.72) and of death or disability (OR 2.05, 95% CI 1.58 to 2.66) in favor of anticoagulants, across 42 studies (2624 patients) and 31 studies (1953 Patients) respectively. For the occurrence of IS there was a non-significand trend in favor of anticoagulants. In turn, there was a statistically significant difference in favor of antiplatelets concerning SIH. MEH occurred only in the anticoagulation group.
Conclusions: The evidence for antiplatelets as standard of care in eICAD is weak. Moreover, the argument for anticoagulation is reinforced, although the superiority of anticoagulation is still unproven. Individualized treatment decisions based on risk of ischemic stroke versus bleeding complications seem recommendable.
Disclosures of Interest:
No
Abstract N°: 1473
INCREASED RISK OF RECURRENT STROKE IN PATIENTS WITH IMPAIRED KIDNEY FUNCTION: A POOLED ANALYSIS OF INDIVIDUAL PATIENT DATA
Philip Nash*1, Gareth Ambler2, Jeremy Molad3, Einor Ben Assayag3, Kaori Miwa4, Natan Bornstein3, Masatoshi Koga4, David Wheeler5, Rob Simister1, David Werring1
1UCL Queen Square Institute of Neurology, Stroke Research Centre, London, United Kingdom, 2University College London, Department of Statistical Science, London, United Kingdom, 3Tel-Aviv University, Sackler Faculty of Medicine, Tel-Aviv, Israel, 4National Cerebral and Cardiovascular Center, Department of Cerebrovascular Medicine, Osaka, Japan, 5University College London, Department of Renal Medicine, London, United Kingdom
On behalf of: The Microbleeds International Collaborative Network
Background and aims: Associations of reduced kidney function (estimated glomerular filtration rate (eGFR)<60ml/min/1.73cm2) with recurrent stroke have scarcely been investigated. eGFR<60 might be associated with recurrent stroke, microbleed presence, distribution, and severity.
Methods: We used data from the Microbleeds International Collaborate Network to investigate associations of eGFR<60 with microbleed presence, distribution (strictly deep or infratentorial, strictly lobar and mixed distributions) and severity. We investigated whether eGFR <60 was associated with increased risk of recurrent ischaemic stroke (IS), intracranial haemorrhage (ICrH) and a composite of those two outcomes.
Results: 11,175 patients (mean age 70.7, 42% female) were included in the analysis, 2815 with eGFR<60. Compared to eGFR>60, eGFR<60 was independently associated with microbleed presence (aOR 1.14, 95% CI 1.03-1.26, Fig. 1), microbleed severity (aOR 1.17, 95% CI 1.06-1.29, Fig. 1), increased risk of a composite of IS and ICrH (aHR 1.33, 95% CI 1.14-1.56, Table 1, Fig. 2) and increased risk of IS (aHR 1.33, 95% CI 1.12-1.58). eGFR<60 was not associated with ICrH risk (aHR 1.07, 95% CI 0.70-1.60). Compared to having no microbleeds, eGFR was significantly lower in those with strictly lobar microbleeds (adjusted mean difference (aMD) -2.10 ml/min/1.73 cm2, 95% CI -3.39 to -0.81) and mixed microbleeds (aMD -2.42, 95% CI -3.70 to -1.15), but not strictly deep microbleeds (aMD -0.67, 95% CI -1.85 to 0.51).
Conclusions: Patients with reduced kidney function are at increased risk of recurrent stroke, and this might in part be related to cerebral small vessel disease. Further research is needed to investigate potential additional treatments for this high-risk group.
Disclosures of Interest:
No
Abstract N°: 1497
EARLY VERSUS LATER ANTICOAGULATION AFTER ISCHEMIC STROKE IN PEOPLE WITH ATRIAL FIBRILLATION AND HEMORRHAGIC TRANSFORMATION
Roman Rohner*1, Markus Kneihsl2,3,4, Martina Göldlin5, Thomas Meinel5, Arsany Hakim1, Mattia Branca6, Stefanie Abend5, Sabine Fenzl1, Jesse Dawson7, Urs Fischer4,5
1Inselspital Bern University Hospital and University of Bern, University Institute of Diagnostic and Interventional Neuroradiology, Bern, Switzerland, 2Medical University of Graz, Department of Neurology, Graz, Austria, 3Medical University of Graz, Division of Neuroradiology, Vascular and Interventional Radiology, Graz, Austria, 4University Hospital Basel, Department of Neurology, Basel, Switzerland, 5Inselspital Bern University Hospital and University of Bern, Department of Neurology, Bern, Switzerland, 6University of Bern, CTU Bern, Department of Clinical Research, Bern, Switzerland, 7Queen Elizabeth University Hospital, University of Glasgow, School of Cardiovascular and Metabolic Health, Glasgow, United Kingdom
On behalf of: the ELAN investigators
Background and aims: The presence of hemorrhagic transformation (HT) of acute ischemic stroke (IS) may increase bleeding risk with direct oral anticoagulants (DOAC). We aimed to assess whether presence of HT modifies estimated safety and efficacy of early versus late DOAC initiation in people with IS and atrial fibrillation (AF).
Methods: This is a post-hoc analysis of the international, multi-center, randomized controlled ELAN trial, which compared early versus late DOAC initiation in people with IS and AF. The primary outcome was recurrent IS, symptomatic intracranial hemorrhage (sICH), major extracranial bleeding, systemic embolism, or vascular death within 30 days. Secondary outcomes were the individual components, and 30- and 90-day functional outcome. We estimated outcomes based on HT on pre-randomization imaging (core-lab rating) using adjusted odds ratios (aOR) and risk differences (aRD) between treatment arms.
Results: Of 1918 included participants, 244 (12.5%) had HT, with an aOR for a poor 90-day prognosis (mRS 3-6) of 1.6 (95% CI 0.6-3.7). For the primary outcome, the aRD (early versus late treatment) was -2.1% (95% CI -7.8-3.5) in people with HT and -0.8 (95% CI -2.5-0.9) in people without. Numbers of sICH were identical in participants with early (HT-group: 0/129, 0%; Non-HT group: 2/846, 0.2%) versus late (HT-group: 0/115, 0%; Non-HT group: 2/865, 0.2%) DOAC initiation.
Conclusions: We found neither major treatment effect heterogeneity nor safety concerns between people with and without HT and IS who were randomized to early versus late DOAC initiation. In general, post-stroke outcome is worse in people with HT.
Disclosures of Interest:
No
SCIENTIFIC COMMUNICATION – INTRACEREBRAL HEMORRHAGE
Abstract N°: 507
MINIMALLY INVASIVE SURGERY IS ASSOCIATED WITH LOWER MORTALITY AFTER INTRACEREBRAL HEMORRHAGE IN A U.S NATIONAL REGISTRY
Santosh Murthy*1, Cenai Zhang1, Gregg Fonarow2, Lee Schwamm3, Deepak Bhatt4, Eric Smith5, Guido Falcone3, Wendy Ziai6, Hooman Kamel1, Kevin Sheth3
1Weill Cornell Medicine, Neurology, New York, United States, 2University of California Los Angeles, Cardiology, 3Yale University School of Medicine, 4Mount Sinai Hospital, 5University of Calgary, 6Johns Hopkins University
On behalf of:
Background and aims: The efficacy of minimally invasive surgery (MIS) in improving outcomes after intracerebral hemorrhage (ICH) remains uncertain, with inconsistent findings from randomized clinical trials. We therefore sought to evaluate the association of MIS with ICH outcomes in a real-world, nationally representative US cohort.
Methods: We performed a retrospective cohort study of patients with ICH in the Get With The Guidelines-Stroke registry, from 2011-2021. The exposure was MIS, defined as a composite of stereotactic and endoscopic surgical evacuation. The primary outcome was in-hospital mortality. Using overlap propensity matching, we matched patients who underwent MIS with medically managed patients on age, sex, race, NIH Stroke Scale, prior antithrombotic therapy, external ventricular drain use, and withdrawal of care. Logistic regression was used to study the relationship of surgery with mortality.
Results: Among 555,964 patients with ICH, MIS was performed in 703 patients of whom, 330 had stereotactic surgery and 373 had endoscopic surgery. The matched cohort included 485 patients in each group. In-hospital deaths occurred in 63 (13.0%) with MIS and 96 (19.8%) without surgery. In regression analyses, MIS was associated with lower in-hospital mortality (aOR, 0.51; 95% CI, 0.39-0.66, Table). Secondary analyses showed that both, stereotactic surgery (aOR, 0.36; CI, 0.23-0.56) and endoscopic surgery (aOR, 0.64; CI, 0.47-0.89) were independently associated with lower mortality. Similar results were noted in pre-specified subgroup analyses (Figure).
Conclusions: In a large diverse US cohort of ICH patients, MIS was associated with lower in-hospital mortality. Longer-term outcomes require further exploration to substantiate the full benefit of surgery after ICH.
Disclosures of Interest:
Yes Grant funding from the National Institutes of Health
Abstract N°: 1344
TIMING AND LOCATION OF RECURRENT INTRACEREBRAL HAEMORRHAGE - INDIVIDUAL PATIENT DATA ANALYSIS FROM 12 EUROPEAN COHORTS
Martina Goeldlin*1, Simon Fandler-Höfler2,3, David Gaist4, Jochen Sembill5, Espen Saxhaug Kristoffersen6, Alexandros Polymeris7, Nicolas Raposo8, David Werring2, Christian Nolte9, David Seiffge1
1Inselspital Bern University Hospital and University of Bern, Department of Neurology, Bern, Switzerland, 2UCL Queen Square Institute of Neurology, Department of Brain Repair & Rehabilitation, London, United Kingdom, 3Medical University of Graz, Department of Neurology, Austria, 4Odense University Hospital, Research Unit for Neurology, Odense, Denmark, 5University Hospital Erlangen, Department of Neurology, Erlangen, Germany, 6Akershus University Hospital, Department of Neurology, Norway, 7Universitätsspital Basel, Department of Neurology, Basel, Switzerland, 8Hospital Center University De Toulouse, Department of Neurology, Toulouse, France, 9Charité – Universitätsmedizin Berlin, Department of Neurology, Berlin Institute of Health and Center for Stroke Research Berlin, Berlin, Germany
On behalf of: European Intracerebral Haemorrhage Recurrence Alliance (EURECA)
Background and aims: Mechanisms underlying recurrent intracerebral haemorrhage (ICH) are poorly understood. We aimed to assess timing and location (adjacent [adjICH] vs remote to a previous ICH [remICH]) of recurrent ICH.
Methods: We performed an individual patient data analysis of patients with ⩾2 ICH from twelve European cohorts. Main outcomes were adjICH, defined by CHARTS location and side, and time to recurrence. We performed multivariable regression analysis. We defined probable cerebral amyloid angiopathy (CAA) by Boston 2.0 or simplified Edinburgh criteria.
Results: We included 567 patients with 1277 ICH (567 index and 701 recurrent ICH, range 2-7, median 2) over a median follow-up of 2.49 years (IQR 0.54-5.31). 274 patients (48.2%) had adjICH and 293 (51.8%) had remICH. Lobar ICH accounted for 328/394 recurrences (85.6%) in patients with adjICH versus 164/307 recurrences in patients with remICH (53.4%,p<0.001). CAA at index ICH was associated with adjICH (aOR 1.95, 95%-CI 1.18-3.24). Median time to recurrence was shorter in patients with adjICH (median 1.15 years, IQR 0.31-3.59 versus 2.34 years, IQR 0.66-5.15; p<0.001) and decreased with each additional event (figure 1). Among patients with CAA at any timepoint, 175/289 (60.6%) had adjICH and 114/289 (39.4%) had remICH. Median time to recurrence was 1.10 years (IQR 0.28-3.38) in adjICH versus 1.26 years (IQR 0.32-3.75) in remICH (p=0.22).
Conclusions: Half of recurrent ICH were adjacent to prior ICH. This phenomenon was associated with lobar ICH location and a diagnosis of CAA. These findings suggest regional disease burden and activity as a potentially modifiable treatment target in CAA.
Disclosures of Interest:
No
Abstract N°: 1699
MRI-BASED PREDICTION OF MACROVASCULAR CAUSES OF INTRACEREBRAL HEMORRHAGE: THE MACRO SCORE
Simon Fandler-Höfler*1,2, Gareth Ambler3, Martina Goeldlin4, Hatice Ozkan2, Philip Nash2, Christian Enzinger1, H Rolf Jäger25, David Seiffge4, Thomas Gattringer1,6, David J Werring2
1Medical University of Graz, Department of Neurology, Graz, Austria, 2UCL Queen Square Institute of Neurology, Stroke Research Centre, Department of Brain Repair & Rehabilitation, London, United Kingdom, 3University College London, Department of Statistical Science, London, United Kingdom, 4University Hospital Bern/Inselspital, Department of Neurology, Switzerland, 5UCL Queen Square Institute of Neurology, Neuroradiological Academic Unit, Department of Brain Repair & Rehabilitation, London, United Kingdom, 6Medical University of Graz, Division of Neuroradiology, Vascular and Interventional Radiology, Department of Radiology, Graz, Austria
On behalf of: MACRO score investigators
Background and aims: Although most spontaneous intracerebral haemorrhages (ICH) are caused by cerebral small vessel diseases (SVDs), a relevant minority are due to macrovascular causes. Rapid diagnosis has important therapeutic and prognostic implications but often requires digital subtraction angiography, an invasive procedure with potential complications. Previous risk stratification scores for macrovascular causes of ICH did not include MRI, which provides optimal sensitivity for markers of SVD.
Methods: We pooled data from two large observational study cohorts of consecutive patients with ICH with available MRI and angiography. Using lasso logistic regression, we built the MRI Assessment of the Causes of intRacerebral haemOrrhage (MACRO) score to assess the probability of a macrovascular cause. We performed internal validation using bootstrapping and external validation in an independent cohort.
Results: We included 1043 patients with ICH, 78 of which had a macrovascular cause (7.5%). The final score includes: age (0-39, 40-69, ⩾70); location of ICH (lobar, deep, infratentorial); and SVD markers on MRI (microbleeds, lacunes, cortical superficial siderosis, white matter hyperintensities). The MACRO score showed an optimism-adjusted c-statistic of 0.90 (95% CI 0.88-0.93), superior to existing CT-based scores (p<0.001). In external validation, the c-statistic was 0.87 (95% CI 0.80-0.94). A MACRO score ⩾6 (present in 59.5% of patients) indicated a very low risk of a macrovascular cause (0.2%), while a score ⩽2 indicated a high risk (48.9%).
Conclusions: The MRI-based MACRO score shows excellent performance in predicting the likelihood of macrovascular causes of spontaneous intracerebral hemorrhage, making it useful for guiding further investigations.
Disclosures of Interest:
No
Abstract N°: 1949
HEMATOMA EXPANSION IN WAKE-UP INTRACEREBRAL HEMORRHAGE
Tove Almqvist*1,2, Anna Falk Delagado1,3, Christina Sjöstrand1,4, Michael Mazya1,2
1Karolinska Institutet, Dep. of Clinical neuroscience, Sweden, 2Karolinska University Hospital, Dep. of Neurology, Sweden, 3Karolinska University hospital, Dep. of Neuroradiology, 4Danderyds hospital, Dep. of Neurology
On behalf of:
Background and aims: While understudied, wake-up intracerebral hemorrhage (WU-ICH) is not uncommon (8.8-20.3% of ICH patients). Uncertain onset time in WU-ICH may influence the risk of in-hospital hematoma expansion (HE) and potential effects of HE-preventive treatments. We aimed to evaluate HE and functional outcomes in WU-ICH compared to known-onset ICH.
Methods: We included ICH patients admitted to the Karolinska University Hospital 2016-22, comparing WU-ICH versus known-onset ICH regarding baseline characteristics, hematoma expansion, and functional outcomes. Patients with unknown, presumed awake onset were excluded.
Results: Of 763 patients, 147 (19%) had WU-ICH and 616 (81%) had known onset, median (IQR) last-known-well to hospital time 9.6 h (5.9-12.2 h) vs 1.3 h (0.9-2.0 h). WU-ICH patients more often had dementia (22/147 (15%) vs 32/616 (5%), p<0.001), oral anticoagulants (38/147 (26%) vs 98/616 (16%), p=0.005), and pre-stroke dependence (35/147 (24%) vs 93/616 (15%), p=0.01). Baseline ICH volume was 14 ml (6-35 ml) vs 13 ml (5-34 ml) and 22/76 (15%) vs 169/421 (27%) had CTA spot signs (p=0.002). Of patients with CT follow-up <72 h, HE occurred in 24/77 (31.2%) in WU-ICH, and 123/356 (34.6%) in known-onset ICH, p=0.57. Oral anticoagulants, dementia, antiplatelets, lower admission GCS, and pre-stroke independence were independently associated with HE, while WU onset was not. Unadjusted and adjusted analysis of 3-month mRS (Figure 1) showed no significant differences (median 4 vs 4), unadjusted p=0.35, adjusted common OR 0.93, p=0.78.
Conclusions: WU-ICH had similar risk of hematoma expansion and similar 3-month outcomes compared to known-onset ICH. Excluding WU-ICH from future trials targeting HE may be unwarranted.
Disclosures of Interest:
No
Abstract N°: 2508
DIAGNOSTIC VALUE OF FINGER-LIKE PROJECTIONS AND SUBARACHNOID HEMORRHAGE IN NEUROPATHOLOGICALLY-CONFIRMED CEREBRAL AMYLOID ANGIOPATHY IN LOBAR HEMATOMA
Alexandra Maury*1, Guillaume Turc1, Joseph Benzakoun2, Virginie Desestret3, Peggy Reiner4, Hassan Hosseini5, Pierre Seners6, Catherine Oppenheim2, Pascale Varlet7, Jean-Claude Baron1
1GHU Paris Psychiatrie et Neurosciences, Department of Neurology, Paris, France, 2GHU Paris Psychiatrie et Neurosciences, Department of Radiology, Paris, France, 3Hospital for Neurology and Neurosurgery Pierre Wertheimer, Department of Neurology, Bron, France, 4Lariboisière Hospital, Department of Neurology, Paris, France, 5Mondor Hospital, Department of Neurology, Créteil, France, 6Rothschild Foundation Hospital, Department of Neurology, Paris, France, 7GHU Paris Psychiatrie et Neurosciences, Department of Neuropathology, Paris, France
On behalf of:
Background and aims: Based on a post-mortem study, subarachnoid hemorrhage (SAH) adjacent to, and finger-like projections (FLP) of, the hematoma on acute-stage CT have recently been proposed as novel diagnostic markers to ‘rule-in’ CAA-related lobar ICH. We investigated the diagnostic value of these imaging markers in less severely affected patients.
Methods: We designed a retrospective (2002-2022) multi-center study (HEMALOB) of ⩾45 year-old no-clear-cause lobar ICH patients in whom acute-stage CT or MRI and neuropathological material (mainly hematoma evacuation) were available. Central reading (two raters, then consensus) of the imaging datasets and neuropathological material (including Aβ immunohistochemistry) was performed.
Results: We report findings from 86 patients (age: 64±9 years; men 42%; hematoma volume: 46.4±36 mL; early death in 15%). Neuropathological material included hematoma evacuation (n=69), biopsy (n=16) and autopsy (n=1). CAA was present in 38 (44%) patients, and FLP and SAH in 37 (43%) and 56 (66%) patients, respectively. Sensitivity and specificy (95%CIs) for the diagnosis of CAA were 0.61 (0.43-0.76) and 0.71 (0.43-0.76), and 0.89 (0.75-0.97) and 0.46 (0.31-0.91 for FLP and SAH, respectively. Corresponding values for the association of FLP and SAH were 0.57 (0.39, 0.73) and 0.79 (0.65, 0.90). Restricting the analysis to samples containing ⩾10 vessels (N=60; CAA prevalence: 55%) did not substantially change these results.
Conclusions: These findings suggest overall weaker diagnostic performance of FLP and SAH, particularly regarding the specificity of SAH+FLP, in this more representative lobar ICH population. Pending results from a larger sample, SAH however exhibited excellent sensitivity, suggesting potential clinical utility.
Disclosures of Interest:
No
Abstract N°: 2623
IMPACT OF DOAC PLASMA LEVELS ON HEMATOMA EXPANSION IN DOAC-ASSOCIATED INTRACEREBRAL HEMORRHAGE
Daniela Schoene*1, Simon Winzer1, Oliver Tiebel2, Daniel Kaiser3, Timo Siepmann1, Tareq Juratli4, Volker Puetz1, Kristian Barlinn1
1Department of Neurology, Faculty of Medicine and University Hospital Carl Gustav Carus, Technische Universität Dresden, Dresden, Germany, 2Institute of Clinical Chemistry, Faculty of Medicine and University Hospital Carl Gustav Carus, Technische Universität Dresden, Dresden, Germany, 3Institute of Neuroradiology, Faculty of Medicine and University Hospital Carl Gustav Carus, Technische Universität Dresden, Dresden, Germany, 4Department of Neurosurgery, Faculty of Medicine and University Hospital Carl Gustav Carus, Technische Universität Dresden, Dresden, Germany
On behalf of:
Background and aims: Pretreatment with direct oral anticoagulants (DOAC) increases risk of hematoma expansion (HE) in spontaneous intracerebral hemorrhage (ICH), yet the critical DOAC level is unknown. We explored the impact of DOAC levels on HE in DOAC-associated ICH.
Methods: We retrospectively analyzed patients with DOAC-associated ICH who had DOAC-calibrated anti-Xa/IIa activity levels measured upon admission. Patients were categorized by a <30ng/ml clinically established cutoff for subtherapeutic DOAC levels. HE was defined as ⩾35% increase in hematoma volume from admission to 24-72 hour CT scans, with symptomatic HE defined by a concurrent ⩾4 points increase in NIHSS. Multivariable logistic regression was used to assess associations between DOAC levels and HE, adjusting for baseline ICH volume, onset-to-imaging time, systolic blood pressure and reversal agent use.
Results: Of 2147 ICH patients admitted (01/2012-11/2023), 88 had DOAC-associated ICH with available DOAC levels (apixaban, n=36; rivaroxaban, n=30; edoxaban, n=17; dabigatran, n=4). Neither baseline (24.3±27.5 vs. 19.5±16.6 ml; p=0.6) nor follow-up ICH volumes (30.6±36.4 vs. 36.4±14.6 ml; p=0.6) levels differed between high and low DOAC levels. Rates of HE (15.4% vs. 22.2%; p=0.6) and symptomatic HE (7.7% vs. 11.1%; p=0.5) were also similar. DOAC cutoff level did not predict HE (aOR 0.7, 95%CI 0.1-4.5; p=0.7). Consistent results were observed when using a <50ng/ml DOAC cutoff and when only considering those who did not receive reversal therapy.
Conclusions: High baseline DOAC level was not associated with HE in DOAC-associated ICH irrespective of the selected cutoff value and whether reversal therapy was administered, warranting further study in larger cohorts.
Disclosures of Interest:
No
SCIENTIFIC COMMUNICATION – NEUROINTERVENTION
Abstract N°: 62
INTRA-ARTERIAL TENECTEPLASE AFTER EVT IN ACUTE POSTERIOR CIRCULATION ARTERIAL OCCLUSION-A MULTICENTER RANDOMIZED CONTROLLED TRIAL
1Department of Neurology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, 2the Zeenat Qureshi Stroke Institute and Department of Neurology, 3Department of Neurology, Boston Medical Center, Boston University School of Medicine, 4Department of Neurology and Comprehensive Stroke Center, David Geffen School of Medicine at UCLA, 5the UPMC Stroke Institute, Department of Neurology and Neurosurgery, University of Pittsburgh School of Medicine
On behalf of:
Background and aims: Data from trials investigating the effects and risks of intra-arterial thrombolysis after successful recanalization in patients presenting with large and medium vessel occlusion of the posterior circulation are limited.
Methods: ATTENTION-IA was an multicenter, prospective, randomized clinical trial at 31 centers in China. After achieving successful recanalization (expanded Thrombolysis In Cerebral Infarction (eTICI) 2b50-3) of an occlusion of the vertebral, basilar, or posterior cerebral artery, patients were randomized 1:1 to receive intra-arterial tenecteplase or standard of care. The primary effect parameter was a modified Rankin Score of 0–1 at day 90.
Results: Between Jan 24 2023, and Aug 24, 2024, 208 participants were randomly allocated to the tenecteplase group (n=104) or control group (n=104). At 3 months, 36 patients in the tenecteplase group (34.6%) and 27 in the control group (26.0%) achieved mRS 0-1 (adjusted risk ratio, 1.33; 95% confidence interval, 0.90 to 1.96; P=0.15). Mortality at 90 days was 27.9% in the tenecteplase group and 27.0% in the control group (adjusted risk ratio, 1.12; 95% CI, 0.73 to 1.71, p=0.61). Symptomatic intracranial hemorrhage occurred in 8 patients (5%) in the tenecteplase group and in 3 (3%) in the control group.
Conclusions: The results of this trial in patients with acute ischemic stroke indicate that intra-arterial tenecteplas after successful recanalization is not superior to standard treatment in patients with large and medium vessel occlusion of the posterior circulation.
Disclosures of Interest:
No
Abstract N°: 450
NONCONTRAST COMPUTED TOMOGRAPHY SELECTED THROMBECTOMY VERSUS MEDICAL MANAGEMENT FOR LATE-WINDOW ANTERIOR LARGE VESSEL OCCLUSION
Thanh N. Nguyen*1, Raul Nogueira2, Muhammad M. Qureshi3, Simon Nagel4, Jelle Demeestere5, João Pedro Marto6, Volker Puetz7, Anne Dusart8, Patrik Michel9, Daniel Strbian10
1Boston Medical Center, Neurology, Boston, United States, 2University of Pittsburgh Medical Center, Pittsburgh, United States, 3Boston Medical Center, Boston, United States, 4Klinkum Ludwigshafen, Ludwigshafen, Germany, 5UZ Leuven, Leuven, Belgium, 6Hospital Egas Moniz, Lisboa, Portugal, 7University Hospital Carl Gustav Carus Dresden, Dresden, Germany, 8Civil Hospital Marie Curie, Charleroi, Belgium, 9Lausanne University Hospital, Lausanne, Switzerland, 10, Helsinki, Finland
On behalf of: on behalf of the CLEAR study group
Background and aims: There is uncertainty whether patients with large vessel occlusion presenting in the 6-to-24-hour time window can be selected for EVT by noncontrast computed tomography (NCCT) and CTA for LVO detection. We evaluated the clinical outcomes of patients selected for EVT by NCCT compared with those who were medically managed in the extended time window.
Methods: This cohort study (NCT04096248) was conducted at 66 sites. Consecutive patients with proximal anterior LVO selected for EVT by NCCT or medically managed (MM) and within 6-24 hours of onset from January 2014 to May 2022 were included. The primary endpoint was 90-day ordinal mRS. Multivariable and inverse probability of treatment weighting (IPTW) were utilized.
Results: Of 5098 patients screened, 839 patients were included, with a median(IQR) age of 75(64-83). 616 patients were selected to EVT by NCCT(73.4%) and 223(26.6%) were MM. In IPTW analyses, there was a more favorable 90-day ordinal mRS in patients selected by NCCT to EVT versus MM (OR 1.99[95%CI 1.53-2.59]; P<0.001). There were higher rates of 90-day functional independence (mRS 0-2) in the EVT group (40.1% vs. 18.4%, OR 3.31[95%CI 2.11-5.20]; P<0.001). sICH was non-significantly higher in the EVT group (8.5% vs. 1.4%, OR 3.77[0.72-19.7], p=0.12), whereas mortality was lower (23.9% vs. 32.3%, OR 0.61[0.45-0.83], p=0.002).
Conclusions: In patients with anterior LVO in the extended window, there was a lower rate of disability and mortality in patients selected with NCCT and CTA to EVT compared with MM. These findings support use of NCCT to patient selection in the extended window.
Disclosures of Interest:
Yes Advisory board Idorsia, Brainomix; Research support Medtronic; Associate Editor Stroke
Abstract N°: 988
RELATION BETWEEN FIRST-LINE THROMBECTOMY TECHNIQUE AND OUTCOMES IN LATE-WINDOW STROKE PATIENTS; A MR CLEAN-LATE TRIAL SUB-STUDY
Robrecht Knapen*1,2, Susanne Olthuis3, Adriaan van Es4, Bart Emmer5, Wouter Schonewille6, Christiaan Van der Leij1, Wim Van Zwam1,2, Robert van Oostenbrugge2,3
1Maastricht UMC+, Radiology and Nuclear Medicine, Maastricht, Netherlands, 2Maastricht University, School for Cardiovascular Diseases, Maastricht, Netherlands, 3Maastricht UMC+, Neurology, Maastricht, Netherlands, 4Leiden University Medical Center (LUMC), Radiology, Leiden, Netherlands, 5Amsterdam University Medical Center, Radiology and Nuclear Medicine, Amsterdam, Netherlands, 6St. Antonius Hospital, Neurology, Nieuwegein, Netherlands
On behalf of: MR CLEAN LATE investigators
Background and aims: This study aimed to compare direct aspiration, stent retriever, and the combined thrombectomy technique on clinical, safety, and technical outcomes in late-window stroke patients included in the MR CLEAN-LATE trial.
Methods: This post-hoc analysis of the MR CLEAN-LATE trial included patients treated with direct aspiration, stent retriever, or combined thrombectomy technique as first-line approach. Primary outcome was the modified Rankin Scale (mRS) score at 90 days follow-up, and compared between the three groups with ordinal logistic regression analysis. Secondary outcomes included mortality at 90 days, total technique switches, procedure time, recanalization rate measured with the expanded thrombolysis in cerebral infarction (eTICI) score, and symptomatic intracranial hemorrhage (sICH). Predefined variables were used for adjustments.
Results: In the MR CLEAN-LATE trial 258 patients underwent endovascular treatment, 232 were included in our analyses. The mRS at 90 days did not differ (stent retriever versus direct aspiration: adjusted common [ac] OR1.35, 95%CI:0.73-2.50; stent retriever versus combined: acOR1.13, 95%CI:0.64-2.00; direct aspiration versus combined: acOR1.19, 95%CI:0.64-2.21). Direct aspiration thrombectomy was accompanied with more switches to another technique compared to the stent retriever (aOR:6.50, 95%CI:2.52-16.8) or combined group (aOR:4.67, 95%CI:1.80-12.1), and with higher sICH rates compared to the combined technique (13% versus 2.5%; aOR: 8.19, 95%CI:1.49-45.1). Mortality, procedure time, and eTICI did not differ.
Conclusions: Stent retriever, direct aspiration, or the combined thrombectomy technique as first-line approach showed no differences in clinical outcome in late-window stroke patients. Direct aspiration was accompanied with higher sICH rates and more switcher to another technique compared to the combined group.
Disclosures of Interest:
No
Abstract N°: 989
THE BENEFIT OF A COMPLETE OVER A SUCCESSFUL REPERFUSION DECREASES WITH TIME
Stefanos Foinitsis*1, Benjamin Maïer2, Mikael Mazighi3, Bertrand Lapergue4, Gaultier Marnat5, Igor Sibon5, Sébastien Richard6, Christophe Cognard7, Benjamin Gory6, Jean Marc Olivot7
1Aristotle University of Thessaloniki, Thessaloniki, Greece, 2Hospital Paris Saint-Joseph, Paris, France, 3Sorbonne Paris Nord University, Villetaneuse, France, 4Hospital Foch, Suresnes, France, 5University Hospital Bordeaux, Bordeaux, France, 6University of Lorraine, Nancy, France, 7Hospital Center University De Toulouse, Toulouse, France
On behalf of: ETIS Registry Investigators
Background and aims: Time from stroke onset to reperfusion (TSOR) is strongly associated with outcomes after endovascular treatment. A near-to-complete or complete reperfusion (modified Treatment in Cerebral Ischemia [mTICI] 2c–3) is associated with improved outcomes compared with a successful reperfusion (mTICI 2b). However, it is unknown whether this association remains stable as TSOR increases. Therefore, we sought to investigate the association between TSOR and outcomes according to the reperfusion status.
Methods: We analyzed data from the ETIS registry, a prospective, observational, multicentric study of acute ischemic stroke patients treated with endovascular treatment in 21 centers in France. We included patients with anterior occlusions (M1, internal carotid artery, tandem), with a known time of symptom onset. Outcomes were early neurological improvement at 24 hours and favorable outcome (mRS between 0 and 2) at 90 days.
Results: Overall, 4,444 patients were analyzed. Compared with a mTICI 2b, a mTICI 2c-3 at 1 hour was associated with higher mean marginal probabilities of early neurological improvement (25.6%, 95% CI 11.7–39.5, p = 0.0003) and favorable outcome (15.2%, 95% CI 3.0–27.4, p = 0.0143), and progressively declined with TSOR. The benefit of a mTICI 2c-3 over a mTICI 2b was no longer significant regarding the rates of early neurological improvement and favorable outcome after a TSOR of 414 and 344 minutes, respectively.
Conclusions: The prognostic value of a complete over a successful reperfusion progressively declined with time, and no difference regarding the rates of favorable outcome was observed between a complete and successful reperfusion beyond 5.7 hours.
Disclosures of Interest:
No
Abstract N°: 1458
COMPARISON OF ANESTHETIC STRATEGIES FOR ENDOVASCULAR THERAPY OF ISOLATED POSTERIOR CEREBRAL ARTERY OCCLUSION: A PLATO STUDY
Christian Herweh*1, Anne Berberich2, Muhammad M. Qureshi3, Davide Strambo4, Silja Räty5, Mohamad Abdalkader3, Marta Olive Gadea6, Marios Psychogios7, Joji B. Kuramatsu8, Simon Nagel2
1Heidelberg University Hospital, Neuroradiology, Heidelberg, 2Städtisches Klinikum Ludwigshafen, Neurology, Ludwigshafen am Rhein, Germany, 3Boston Medical Center, Radiology, Boston, United States, 4Lausanne University Hospital, Neurology, Lausanne, Switzerland, 5Helsinki University Hospital, Neurology, Helsinki, Finland, 6Hospital Universitario Vall d’Hebron, Neurology, Barcelona, Spain, 7Basel University Hospital, Radiology, Basel, Switzerland, 8University of Erlangen-Nuremberg, Neurology, Erlangen, Germany
On behalf of: PLATO study group
Background and aims: The optimal anesthetic strategy for endovascular therapy (EVT) of acute ischemic stroke (AIS) remains under debate. This study aimed to compare the clinical outcomes of patients with isolated posterior cerebral artery (PCA) occlusion stroke undergoing EVT using either local anesthesia with or without conscious sedation (non-GA) versus general anesthesia (GA).
Methods: Patients from the PLATO registry were analyzed regarding anesthetic strategy. The study compared non-GA with GA as an anesthetic procedure using multivariable logistic regression and inverse probability of weighting treatment methods (IPTW). The primary endpoint was the 90-day distribution of the ordinal modified Rankin Scale (mRS). Secondary outcomes included successful reperfusion, defined as eTICI 2b to 3. Safety endpoints consisted of symptomatic intracranial hemorrhage and mortality.
Results: A total of 376 patients with isolated PCA occlusion stroke underwent EVT treatment, of whom 193 (51%) had non-GA and 183 (49%) had GA. The IPTW analysis showed no difference between the GA and non-GA groups in terms of ordinal mRS shift analysis (odds ratio, OR 0.89 [95% CI 0.53-1.51], p=0.67) or functional independence (OR 0.84 [95% CI 0.50-1.39], p=0.49). There were greater odds for successful reperfusion with GA than LA+CS (OR 1.70, 95% CI 1.17-2.47, p=0.005). Safety outcomes were comparable in both groups.
Conclusions: In patients with isolated PCA occlusion stroke undergoing EVT, the 90-day functional and safety outcomes were similar between both anesthetic strategies. General anaesthesia was associated with higher recanalization rates compared to local anaesthesia with conscious sedation.
Disclosures of Interest:
No
Abstract N°: 1607
SAFETY AND EFFICACY OF ENDOVASCULAR TREATMENT FOR LARGE-CORE ISCHAEMIC STROKE: A SYSTEMATIC REVIEW AND META-ANALYSIS
Georgios Tsivgoulis*1, Lina Palaiodimou1, Apostolos Safouris1,2, Georgios Magoufis3,4, Robin Lemmens5,6, Else Charlotte Sandset7,8, Peter Schellinger9, Guillaume Turc10,11,12,13, Marios Psychogios14, Amrou Sarraj15
1National and Kapodistrian University of Athens, Second Department of Neurology, “Attikon” University Hospital, Athens, Greece, 2Metropolitan Hospital, Stroke Unit, Piraeus, Greece, 3National and Kapodistrian University of Athens, Interventional Radiology Department, “Attikon” University Hospital, Athens, Greece, 4Metropolitan Hospital, Neuroradiology Department, Piraeus, Greece, 5University Hospitals Leuven, Department of Neurology, Leuven, Belgium, 6KU Leuven-University of Leuven, Department of Neurosciences Division of Experimental Neurology, Leuven, Belgium, 7Oslo University Hospital, Stroke Unit, Department of Neurology, Oslo, Norway, 8The Norwegian Air Ambulance, Oslo, Norway, 9Ruhr-University Bochum, Department of Neurology and Neurogeriatrics, Johannes Wesling Klinikum Minden, Minden, Germany, 10GHU Paris Psychiatrie et Neurosciences, Department of Neurology, Paris, France, 11Université Paris Cité, Paris, France, 12INSERM U1266, Paris, France, 13FHU NeuroVasc, Paris, France, 14University Hospital of Basel, Department of Neuroradiology, Clinic of Radiology & Nuclear Medicine, Basel, Switzerland, 15Case Western Reserve University - University Hospitals Cleveland Medical Center, Department of Neurology, Cleveland, United States
On behalf of:
Background and aims: High-quality evidence on efficacy and safety of endovascular treatment (EVT) for large-core ischaemic stroke (AIS) has recently become available from several randomized-controlled clinical trials (RCTs).
Methods: We conducted an updated systematic review and meta-analysis including all available RCTs that investigated efficacy and safety of EVT in addition to best medical treatment (BMT) versus BMT alone for large-core AIS (defined by ASPECTS 0-5 or volumetric methods). The primary outcome was defined as the reduced disability at 3-months [⩾1-point reduction across all modified Rankin Scale (mRS)-scores]. Independent ambulation (mRS-score 0-3), good functional outcome (mRS-score 0-2), and excellent functional outcome (mRS-score 0-1), mortality at 3 months and symptomatic intracranial haemorrhage (sICH), were evaluated as secondary outcomes.
Results: Six RCTs were included comprising a total of 948 patients treated with EVT vs 939 patients treated with BMT. Compared with BMT, EVT was significantly associated with reduced disability (common OR 1.75; 95%CI:1.50- 2.05; I2=12%), independent ambulation [risk ratio (RR) 1.90; 95%CI:1.50-2.40; I2=51%], good functional outcome (RR 2.49; 95% CI:1.89-3.29; I2=7%) and excellent functional outcome (RR 2.57; 95%CI:1.68-3.95; I2=0%) at 3 months. Although rates of sICH (RR 1.70; 95%CI:1.09-2.65; I2=0%) were higher in the EVT group, 3-month mortality (RR 0.84; 95%CI:0.69-1.01; I2=52%) did not differ between the two groups.
Conclusions: EVT appears to be consistently associated with all efficacy outcomes, while additionally presenting a signal of reducing mortality, despite the higher rates of sICH compared to BMT.
Disclosures of Interest:
No
Abstract N°: 2071
EFFECT OF THROMBOLYSIS TYPE ON THE EFFICACY OF ASPIRATION VS STENT-RETRIEVER FIRST-LINE THROMBECTOMY: RESULTS FROM THE ACT TRIAL
Fouzi Bala*1,2, William Diprose2, Ibrahim Alhabli2, Nishita Singh3, Thalia Field4, Gary Hunter5, Michael Hill2, Richard Swartz6, Bijoy Menon2, Mohammed Almekhlafi2
1Tours University Hospital, Neuroradiology, Tours, France, 2University of Calgary, Clinical Neurosciences, Calgary, Canada, 3University of Manitoba, Canada, 4University of British Columbia, Vancouver, Canada, 5University of Saskatchewan, Canada, 6University of Sunnybrook, Toronto, Canada
On behalf of: The AcT Investigators
Background and aims: Intravenous (IV) tenecteplase is increasingly being used in lieu of alteplase before endovascular thrombectomy (EVT) for acute ischemic stroke. We sought to study the influence of IV tenecteplase versus alteplase on the efficacy of first-line thrombectomy strategy.
Methods: This is a secondary analysis of the Alteplase compared to Tenecteplase (AcT) trial. We included patients in whom a thrombectomy was attempted and the type of first-line strategy recorded. We compared first-line EVT strategy with stent-retriever to contact aspiration alone and evaluated its interaction with thrombolysis type. Outcomes were 90-day modified Rankin Scale 0-1 and 0-2, safety (mortality and symptomatic intracerebral hemorrhage) and angiographic outcomes (eTICI 2b-3 and eTICI 2c-3 on final angiography). Mixed-effect regression analyses with interaction terms were performed.
Results: Among 506 EVT patients in AcT, 435 were included: 222 (51.0%) received tenecteplase and 213 (49.0%) received alteplase. First line-line stent-retriever was used in 288 (66.2%) and aspiration in 147 (33.8%) patients. Final eTICI 2c-3 was achieved in 57.0%% in the stent-retriever vs 61.9%% in the aspiration first-line strategy (p=0.35).
There was a significant interaction between thrombolysis type and first-line EVT strategy for final eTICI 2c-3 (p=0.02). Tenecteplase was associated with higher odds of final eTICI 2c-3 in the aspiration subgroup (aOR 2.29, 95% CI 1.10-4.75), but not in the stent-retriever subgroup (aOR 0.63, 95% CI 0.38-1.04). No significant interaction was found for the other outcomes.
Conclusions: IV tenecteplase before EVT may enhance the efficacy of first-line aspiration, but it may have no effect on stent-retrievers.
Disclosures of Interest:
No
Abstract N°: 2631
RESCUE THERAPY FOR FAILED MECHANICAL THROMBECTOMY: ANALYSIS OF THE SOCIETY OF VASCULAR AND INTERVENTIONAL NEUROLOGY REGISTRY
Aaron Rodriguez-Calienes1, Fazeel Siddiqui2, Mahmoud H. Mohammaden3, Ameer Hassan4, Shahram Majidi5, James Siegler6, Sunil Sheth7, Italo Linfante8, Raul Nogueira9, Santiago Ortega-Gutierrez*1
1University of Iowa Hospitals and Clinics, Department of Neurology, Iowa City, United States, 2University of Michigan, Department of Neurosciences, Ann Arbor, United States, 3Grady Memorial Hospital, Marcus Stroke and Neuroscience Center, Atlanta, United States, 4The University of Texas Rio Grande Valley, Department of Neurology, Edinburg, United States, 5Icahn School of Medicine at Mount Sinai, Department of Neurosurgery, New York, United States, 6Cooper Medical School of Rowan University, Department of Neurology, Camden, United States, 7McGovern Medical School at UTHealth Houston, Department of Neurology, Houston, United States, 8Baptist Hospital of Miami: Carbot-Flores Elsy MD, 10.Department of Interventional Neuroradiology & Neuroendovascular Surgery, Miami, United States, 9University of Pittsburgh, Department of Neurology, Pittsburgh, United States
On behalf of:
Background and aims: We aimed to evaluate the association between rescue therapy (RT) and functional outcomes compared to medical management (MM) in patients presenting failed mechanical thrombectomy (MT) stratified by vascular territory.
Methods: This cross-sectional study utilized prospectively collected and maintained data from the Society of Vascular and Interventional Neurology (SVIN) Registry, spanning from 2011 to 2021. The cohort comprised patients with large-vessel occlusions (LVOs) with unsuccessful MT. The primary outcome was the shift in the degree of disability, as gauged by the mRS at 90 days. Additional outcomes included functional independence and independent ambulation (90-day mRS score of 0-2 and 0-3), symptomatic intracranial hemorrhage (sICH), and 90-day mortality.
Results: Of a total of 7,018 patients, 958 presented failed MT and were included in the analysis. The RT group comprised 407 (42.4%) patients, while the MM group consisted of 551 (57.5%) patients. After adjusting for confounders, the RT group showed a favorable shift in the overall 90-day mRS distribution (acOR=1.79; 95% CI 1.31-2.45; p<0.001) and higher rates of functional independence (RT:28.8% vs. MM:15.7%, aOR=1.96; 95%CI 1.02-3.14; p=0.04) compared to the MM group, lower rates of sICH (RT:3.8% vs. MM:9.1%, aOR=0.52; 95%CI 0.28-0.97;p=0.039) and 90-day mortality (RT:33.4% vs. MM:45.5%, aOR=0.52; 95%CI 0.35-0.77;p=0.001). These associations remained significant in the anterior circulation cohort (Figure).
Conclusions: Our findings advocate for the utilization of RT as a potential treatment strategy for cases of LVO resistant to conventional MT techniques. Prospective studies are warranted to validate these observations and optimize the endovascular approach for failed MT patients.
Disclosures of Interest:
No
SCIENTIFIC COMMUNICATION – SEX MATTERS
Abstract N°: 876
SEX DIFFERENCES IN FREQUENCY AND PROGNOSTIC SIGNIFICANCE OF CEREBRAL MICROBLEEDS IN STROKE
Simon Fandler-Höfler1, Sebastian Eppinger1, Gareth Ambler2, Philip Nash3, David Werring3, Thomas Gattringer*1
1Medical University of Graz, Neurology, Graz, Austria, 2University College London, Statistical Science, London, United Kingdom, 3UCL Queen Square Institute of Neurology, Stroke Research Centre, London, United Kingdom
On behalf of: Microbleeds International Collaborative Network
Background and aims:
Data on sex-related differences in cerebral small vessel disease (SVD) are scarce. In a large multinational stroke cohort, we investigated whether the frequency, distribution and prognostic associations of cerebral microbleeds (CMB) and other SVD markers on MRI differ between women and men.
Methods: In this pooled individual patient data analysis from the Microbleeds International Collaborative Network (MICON), we included patients from 38 prospective cohort studies who had an ischemic stroke or transient ischemic attack, available brain MRI and clinical follow-up of at least three months. We used multivariable random-effects logistic regression models and Cox regression to investigate sex differences in individual SVD markers, risk of recurrent cerebrovascular events and death.
Results: We investigated 20314 patients (mean age 70±13 years, 42% women), of whom 5649 (27.8%) had CMB. CMB were more frequent in men, consistent throughout different age groups, locations and in multivariable models (aOR for women 0.86, 95%-CI 0.80-0.92, p<0.001). Women had fewer lacunes (aOR 0.82, 95%-CI 0.74-0.90, p<0.001), but a higher rate of severe white matter hyperintensities (aOR 1.10, 95%-CI 1.01-1.20, p=0.04). 2419 patients (11.9%) died during a median follow-up of 1.4 years. CMB presence was associated with a higher risk of mortality in women (HR 1.15, 95%-CI 1.02-1.31), but not men (HR 0.95, 95%-CI 0.84-1.07, p-interaction=0.01). 1113 patients (5.5%) had recurrent ischemic stroke and 189 (0.9%) recurrent intracranial hemorrhage, with no sex differences (p>0.20).
Conclusions: With varying frequencies of individual SVD markers, there appear to be pathophysiological differences in manifestation and severity of SVD between women and men.
Disclosures of Interest:
No
Abstract N°: 1437
SEX DIFFERENCES IN ACUTE ISCHEMIC STROKE MULTIMORBIDITY: DATA FROM A NATIONWIDE CHILEAN DATABASE
Maria Ignacia Allende Echanez1, Marilaura Nuñez*1, Francisca Mccawley1,2, Paula Muñoz Venturelli1,3,4
1Centro de Estudios Clínicos, Facultad de Medicina Universidad del Desarrollo, Las Condes, Chile, 2Facultad de Ciencias de la Salud Blanquerna, Universitat Ramón Llull, Barcelona, Spain, 3Departamento de Neurología y Psiquiatría, Facultad de Medicina Clínica Alemana Universidad del Desarrollo, Vitacura, Chile, 4The George Institute for Global Health, Faculty of Medicine University of New South Wales, Sydney, Australia
On behalf of:
Background and aims: Multimorbidity in stroke pose a growing public health concern, and its complex sex influence remains understudied. Therefore, we aimed to analyze multimorbidity in acute ischemic stroke (AIS) patients with a sex-based approach.
Methods: Retrospective cohort analysis of the 2019 Chilean Diagnosis-Related Group database corresponding to 70% of all discharges of the national public health sector. AIS was defined as main diagnosis ICD-10 code (I63) and multimorbidity as the coexisting of ⩾2 comorbidities. Logistic regression, reported in odds ratio and 95% confidence intervals, was performed to evaluate the association of multimorbidity and sex with STATA v18.
Results: Among 1,048,575 hospital discharges, we identified 10,440 patients with AIS and 4,659 (44.63%) were women. Multimorbidity was present in 7,721 (73.96%) patients and the most common presentation in both sexes was the co-occurrence of diabetes and hypertension (women 10.05%[468/4,659]; men 9.27%[536/5,781]). There were no overall sex differences in multimorbidity prevalence (OR 1.09, 0.99-1.20 [P=0.05]), but stratification by age showed women had more multimorbidity in the 35-54 age range (1.28, 1.01-1.63 [P=0.04]). Further analysis identified different patterns of multimorbidity by sex, with women having higher prevalence of multimorbidity that involves depression (2.83, 2.26-3.55 [P<0.001]), while men had higher prevalence of multimorbidity that involves addictions (2.06, 1.82-2.33 [P<0.001]).
Conclusions: In this nationwide analysis, multimorbidity was more prevalent in women with AIS in the age range of 35-54 years, while specific patterns vary between sexes. Further research is warranted to elucidate the impact of multimorbidity in AIS outcomes.
Disclosures of Interest:
Yes PMV receives research grants from ANID Fondecyt Regular 1221837, Pfizer and Boehringer Ingelheim.
Abstract N°: 1529
SEX DIFFERENCES IN CLINICAL PRESENTATION OF WOMEN AND MEN EVALUATED AT A COMPREHENSIVE STROKE CENTER FOR SUSPECTED STROKE
Jordi Kühne Escolà*1, Bessime Bozkurt1, Woon Hyung Chae1, Lennart Milles1, Doreen Pommeranz1, Christoph Kleinschnitz1, Martin Köhrmann1, Benedikt Frank1
1University Hospital Essen, Department of Neurology and Center for Translational Neuro- and Behavioral Sciences (C-TNBS), Essen, Germany
On behalf of:
Background and aims: Understanding sex-specific differences in the clinical presentation of patients with suspected stroke is important to reduce sex disparities and improve care. We aimed to characterize presenting symptoms in women and men referred to our comprehensive stroke center for suspected stroke.
Methods: This was a retrospective analysis of consecutive patients with suspected stroke who were treated at the University Hospital Essen comprehensive stroke center between January 2017 and December 2021. Patient characteristics, symptoms and final diagnoses in women and men were compared.
Results: We included 6069 patients in our final analysis. Cerebrovascular disease (ischemic stroke, TIA or intracerebral haemorrhage) was diagnosed in 85.2% (2576/3022) of women and 88.0% (2681/3047) of men (p = 0.002). Impairments in level of consciousness (17.0% vs 14.6%, p = 0.012), orientation (42.5 vs. 36.4%, p < 0.001), completion of tasks (31.2% vs. 26.0%, p < 0.001) as well as gaze deviation (21.0% vs. 18.8%, p = 0.034), aphasia (31.4% vs. 27.7%, p < 0.001) and neglect (15.5% vs. 12.8%, p = 0.003) were more common in women. Women had a lower prevalence of limb ataxia (8.1% vs. 11.2%, p < 0.001) and dysarthria (44.0% vs. 46.8%, p = 0.030). Neglect and gaze deviation were independent positive predictors of cerebrovascular disease in women but not in men.
Conclusions: Despite an overlap of focal symptoms we observed significant sex differences in the clinical presentation of patients with suspected stroke. Cortical symptoms may be more common and have greater predictive value in women than in men.
1Institute of Medicin, Department of Molecular and Clinical Medicine, Gothenburg, Sweden, 2Skaraborg institute for Research and Development, Department of Health Sciences, Skövde, Sweden, 3Institute of Health and Care Sciences, Institute of Health and Care Sciences, Gothenburg, Sweden, 4Department of Cardiothoracic Surgery, Department of Cardiothoracic Surgery, Gothenburg, Sweden
On behalf of:
Background and aims: Mortality in stroke patients have declined but some studies have reported an increased mortality in younger individuals. Earlier studies have shown that in ages <65 years had 5-18% of stroke patients died within 28-30 day of the event. Few recent studies have investigated short-time survival in an unselected national stroke population. Therefore, we aimed to investigate short-term survival after stroke in younger men and women.
Methods: This prospective register study comprised 13385 patients aged 18-54 years hospitalized with a first-time stroke between 1 January 2011 and 31 December 2021 identified through Swedish National Inpatient Registry and linked to the Cause of Death Registry. Stroke was defined according to ICD-10 codes: I60-I64.
Results: Of 13 385 stroke cases the majority were men (61.9 %). Overall, the mean age was about 46 years. In total had 25% of patients’ hemorrhagic stroke. The most common comorbidity was hypertension with higher prevalence (39.3%) in men than women (29.9%) followed by diabetes, ischemic heart disease and atrial fibrillation: 6.2%, 6.1%, 6.0% and 5.6%, 4.1%, 3.2% in men and women respectively. At 28-day follow-up 6.0 % of men and 5.6% of women had died. In numbers almost twice as many men (n=495) as women (n=286) died.
Conclusions: Stroke incidence is higher in men than women and stroke mortality within the first 28 days affect men more. Comorbidities are common in younger with stroke and even more so in men. This result emphasizes the importance of primary prevention and optimized treatment of the young.
Disclosures of Interest:
No
Abstract N°: 2898
BRAIN HEALTH OUTCOMES IN SEXUAL AND GENDER MINORITY GROUPS
Shufan Huo*1, Cyprien Rivier1, Santiago Clocchiatti-Tuozzo1,2, Daniela Renedo1,3, N. Abimbola Sunmonu1, Adam de Havenon1, Kevin Sheth1, Guido Falcone1
1Yale University, Department of Neurology, New Haven, United States, 2Yale University, Department of Internal Medicine, New Haven, 3Yale University, Department of Neurosurgery, New Haven, United States
On behalf of:
Background and aims: Sexual and gender minority (SGM) groups are historically underrepresented in neurological research and their brain health disparities are largely unknown. We evaluated whether SGM persons are at higher risk of adverse brain health compared to cisgender heterosexual individuals.
Methods: We conducted a cross-sectional study in participants from the All of Us Research Program. We used baseline questionnaires to identify participants from sexual minorities (non-straight, e.g., gay, lesbian, bisexual) and gender minorities (gender identity different from birth-assigned sex). We divided gender minorities into diverse (e.g., non-binary) and transgender. The primary outcome was a composite of stroke, dementia, and late-life depression. Secondarily, we evaluated each subgroup and disease separately. We used multivariable logistic regression to assess the relationship between SGM groups and brain health outcomes.
Results: We included 393,041 participants (mean age 51, female birth-assigned sex 62%), of whom 39,632 (10%) belonged to SGM groups. Of these, 38,528 (10%) belonged to a sexual and 4,431 (1%) to a gender minority (2,212 [50%] diverse, 2,219 [50%] transgender). SGM individuals had 23% higher odds of the composite outcome (OR 1.23, 95%CI 1.17-1.29). These results persisted across all SGM subgroups (95%CI>1). Assessing individual diseases, all SGM groups had higher odds of late-life depression, all SGM except transgender persons had higher odds of dementia, and gender minorities had higher odds of stroke (full results see Figure).
Conclusions: In a large population study, SGM persons had higher odds of adverse brain health outcomes. Further research should explore causes of inequity to advance inclusive and diverse neurological care.
Disclosures of Interest:
No
Abstract N°: 3095
SEX DIFFERENCES REGARDING PATIENT CHARACTERISTICS AND MORTALITY AFTER INTRACEREBRAL HEMORRHAGE
Trine Apostolaki-Hansson*1, Christine Kremer1, Jesper Petersson1, Bo G. Norrving2, Teresa Ullberg1
1Skåne University Hospital Malmö/Lund, Department of Neurology, Malmö, Sweden, 2Skåne University Hospital Malmö/Lund, Department of Neurology, Lund, Sweden
On behalf of:
Background and aims: Compared to ischemic stroke, sex differences in patient outcome after intracerebral hemorrhage (ICH) is underreported. We aimed to determine sex differences in patient characteristics and mortality in a large unselected Swedish cohort.
Methods: In this study, data on 19906 patients with spontaneous ICH registered in the Swedish Stroke Register between 2012–2016 and 2018–2019 were used to compare sex differences in patient baseline characteristics and 90-day mortality. Multivariable Cox regression analysis, with adjustment for relevant confounders, was used to compare 90-day mortality between males and females.
Results: The crude 90-day mortality rate was 37.0% in females (3368/9104) and 32.1% in males (3464/10802). In multivariable analysis, the hazard ratio (HR) for death at 90-days following ICH in females was 0.90 (95%CI: 0.85–0.95). Patient factors associated with a higher death rate included age (HR=1.04;95%CI:1.03–1.04), pre-stroke dependency (HR=1.38;95%CI:1.30–1.47), atrial fibrillation (HR=1.11;95%CI:1.03-1.20), antiplatelet drugs (HR=1.17;95%CI:1.10–1.25), oral anticoagulant drugs (HR=1.29;95%CI:1.19–1.41), and more severe ICH based on the Reaction Level Scale score ((drowsy HR=3.61;95%CI:3.38–3.85)(comatose HR=12.55;95%CI:11.76–13.38)).
Conclusions: In this large observational study, female sex was independently associated with a lower 90-day mortality rate after ICH compared to males. Analyses are currently being undertaken to provide additional insights into these findings.
Disclosures of Interest:
No
SCIENTIFIC COMMUNICATION – COGNITION AND VASCULAR COGNITIVE IMPAIRMENT
Abstract N°: 1277
STRATEGIC WHITE MATTER HYPERINTENSITY LOCATIONS FOR POST-STROKE COGNITION: A MULTICENTER STUDY IN 1568 STROKE PATIENTS
Floor de Kort*1, Mirthe Coenen1, Matthijs Biesbroek1
1UMC Utrecht, Neurology, Netherlands
On behalf of: the Meta VCI Map consortium
Background and aims: White matter hyperintensities (WMH) are associated with cognitive functioning after stroke, but the role of WMH location in this association is unclear. We determined if WMH in strategic white matter tracts explains cognitive performance after stroke.
Methods: Individual patient data from 9 ischemic stroke cohorts with MRI were harmonized through the Meta VCI Map consortium (n=1568, 39.9% female, mean age 67.3 years, Figure shows prevalence maps of WMH and infarcts). The association between WMH volumes in strategic white matter tracts and domain-specific cognitive functioning (attention and executive functioning (AEF), information processing speed (IPS), language and verbal memory) was assessed using mixed linear models and lasso regression. We used a hypothesis-driven design, primarily addressing four white matter tracts known to be strategic in memory clinic patients: the left and right anterior thalamic radiation, forceps major and left inferior fronto-occipital fasciculus.
Results: Total WMH volume was strongly related to cognitive performance on all four cognitive domains. WMH volume in the left anterior thalamic radiation was significantly associated with cognitive performance on AEF (coefficient -0.175, p=0.007) and IPS (coefficient -0.197, p=0.006), and WMH volume in the forceps major with IPS (coefficient -0.132, p=0.014). These associations were independent of age, sex, education, and total infarct volume and stronger than total WMH volume.
Conclusions: These results show tract-specific relations between WMH volume and cognitive performance after ischemic stroke, independent of total WMH volume. This implies that the concept of strategic lesions for post-stroke cognitive impairment extends beyond acute infarcts and also involves pre-existing WMH.
Disclosures of Interest:
No
Abstract N°: 1390
WHITE MATTER INTEGRITY AND COGNITIVE PERFORMANCE IN YOUNG ISCHEMIC STROKE
Mijntje Schellekens*1,2, Hao LI1,2, Esther Boot1,2, Merel Ekker1,2, Jamie Verhoeven12, Anton Meijer3, Roy Kessels2,4,5, Frank-Erik De Leeuw1,2, Anil Tuladhar1,2
1Radboud University Medical Centre, Neurology, Nijmegen, 2Donders Institute for Brain, Cognition and Behaviour, Nijmegen, 3Radboud University Medical Centre, Radiology, Nijmegen, 4Vincent van Gogh Institute for Psychiatry, Venray, 5Radboud University Medical Centre, Department of Medical Psychology and Radboudumc Alzheimer Centre, Nijmegen
On behalf of:
Background and aims: A potential contributor of post-stroke cognitive impairment could be the reduced white matter integrity outside the initial stroke lesion. We aimed to investigate whether the integrity of the non-lesioned white matter tracts is associated with cognitive performance in the subacute phase after ischemic stroke in young adults.
Methods: Patients from the ODYSSEY study, aged 18-49 years, with a first-ever ischemic stroke, underwent 3T MRI and cognitive assessment, covering seven cognitive domains. We calculated the mean Fractional Anisotropy (FA), Mean Diffusivity (MD), and Free Water (FW) of white matter tracts excluding the stroke lesion using TractSeg. Patients were compared with a stroke-free control group. Major vascular cognitive disorder (VCD) was defined as a Z-score <−2.0 in one or more domains.
Results: Sixty-six patients, median age 40.3 years (IQR 31.3-46.2), underwent MRI (median one month post-stroke) and completed cognitive assessment (median three months post-stroke). Patients with major VCD had lower FA values in most tracts on the side of the lesion, compared to controls (n=23) [Cohen’s d (0.79; 1.72)]. No group differences were observed for MD and FW. Only processing speed performance was associated with FA values on the side of the lesion in most tracts [R2adj (0.19; 0.32)].
Conclusions: Lower white matter integrity, measured by FA, is associated with cognitive impairment after stroke at young age, particularly in the cognitive domain processing speed. The observed findings were limited to the side of the brain where the stroke occurred. Early white matter degeneration in the affected hemisphere may contribute to post-stroke cognitive impairment.
Disclosures of Interest:
Yes AT is a junior staff member of the Dutch Heart Foundation (grant number 2016T044). FEL is a Clinical established investigator of the Dutch Heart Foundation (2014 T060).
Abstract N°: 1486
SECONDARY STROKE PREVENTION AND LONG-TERM COGNITIVE FUNCTION: A POPULATION-BASED STUDY
1King’s College London, School of Population Health & Environmental Sciences, London, United Kingdom
On behalf of:
Background and aims: Limited data exist on the impact of secondary stroke prevention and on cognitive function after stroke. This study aims to investigate whether post-stroke care strategies protect cognitive function up to ten-year.
Methods: Data were collected between 1995 and 2018 from a population-based stroke register (n=6504). Multivariable Poisson regression models with robust standard errors and confounders were constructed to evaluate adjusted relative risks (aRRs) between cognitive impairment and different treatment strategies; before, at acute care or after stroke. Use multiple imputation to manage the missing data.
Results: The prevalence of cognitive impairment was 29% (confidence interval (CI) 26-32). 5-years after stroke, in ischemic stroke patients with a history of atrial fibrillation (AF), there was a reduced risk of cognitive impairment of 50% associated with antihypertensive (aRR:0.5, 0.27-0.91), 77% with statin (aRR:0.23, 0.06-0.91) and 82% with anticoagulant (aRR:0.18, CI 0.05-0.64). In ischemic stroke patients with no history of AF, the reduced risk was 26% (aRR:0.74, 0.57-0.95) with antihypertensive and 19% (aRR:0.81, 0.64-1.03) with statin. All these protective associations tend to diminish over time up to ten years after stroke. When clinically indicated, a combined treatment of these were strongly associated with a reduced risk of cognitive impairment. Small risk reduction was observed between cognitive impairment and acute stroke unit admission (aRR:0.96, 0.93-0.98).
Conclusions: Cognitive impairment may be altered by the treatment at acute care as well as secondary care especially with a combined treatments regime.
Disclosures of Interest:
No
Abstract N°: 2275
BLOCKING THE VCAM1-VLA4 AXIS PREVENTS COGNITIVE DECLINE IN A MOUSE MODEL OF INFARCT-INDUCED NEURODEGENERATION
Kristy Zera1, Karen Bradshaw1, Oliver Hahn1, Aulden Foltz1, Todd Peterson1, Hanadie Yousef1, Tony Wyss-Coray1, Marion Buckwalter*1
1Stanford University School Medicine, Neurology and Neurological Sciences, Stanford, United States
On behalf of:
Background and aims: Infarct-induced neurodegeneration occurs after stroke and is mediated by B lymphocytes. Vascular cell adhesion molecule 1 (VCAM1) facilitates immune cell diapedesis by binding very late antigen 4 (VLA4), and plasma levels are elevated after stroke in people and mice. We tested here whether chronic treatment with anti-VCAM1 or anti-VLA4 would reduce lymphocyte infiltration, prevent cognitive decline, and change immune or endothelial cell gene expression in the peri-stroke cortex.
Methods: Aged (10 month old) C57BL/6 male & female mice (N=9-10/group) underwent permanent middle cerebral artery occlusion and were dosed with anti-VCAM1, anti-VLA4, or control IgG every 3 days beginning 4 days after stroke for 10 weeks. Sham mice were dosed with IgG. Barnes maze and Novel object were performed at -1, 1 and 6 weeks relative to stroke, and single-cell RNA sequencing on immune and endothelial cells at 10 weeks.
Results: Blocking either VCAM1 or VLA4 reduced B cells 67% or 55%, respectively, compared to control IgG treated stroked mice, and prevented the development of a cognitive deficit in both Barnes maze and novel object by 6 weeks (See below). Single-cell sequencing demonstrated that most changes occurred in endothelial cells and not immune cells, and that anti-VCAM1 and anti-VLA4 stimulate heat shock protein expression and genes consistent with decreased inflammation and increased angiogenesis
Conclusions: Blocking either VCAM1 or VLA4 prevents infarct-induced neurodegeneration in aged mice and changes brain endothelial but not immune cell gene expression. Thus, the VCAM1-VLA4 axis is a promising and easily translatable target to prevent infarct-induced neurodegeneration.
Disclosures of Interest:
No
Abstract N°: 2403
ENHANCING COGNITIVE PERFORMANCE PREDICTION USING WHITE MATTER HYPERINTENSITY DISCONNECTIVITY: A LESION NETWORK MAPPING STUDY
Marvin Petersen*1, Bastian Cheng1
1University Medical Center Hamburg-Eppendorf
On behalf of: On behalf of the Meta VCI Map Consortium
Background and aims: White matter hyperintensities (WMH) are linked to cognitive impairment. However, WMH volume alone insufficiently explains the extent of cognitive deficits. We hypothesize that brain network disconnectivity measures, quantifying the disruptive effect of WMH on the connectome, enhance prediction of cognitive performance compared to volumetric WMH measures.
Methods: We analysed cross-sectional data of 3,485 patients from 10 memory clinic cohorts within the Meta VCI Map Consortium, using harmonized test results in 4 cognitive domains and WMH segmentations, in conjunction with normative connectome data. WMH segmentations were registered to standard space and integrated with existing normative connectome data. We employed functional and structural lesion network mapping (LNM) to quantify WMH disconnectivity across 480 atlas-based regions of interest (ROI). Ridge regression models (10-fold cross-validation, 10 repeats) were applied based on WMH volumes or LNM scores to predict cognitive performance (Pearson r of actual and predicted performance, adjusted for age, sex and education) (figure 1).
Results: LNM scores significantly improved the prediction of performances in three cognitive domains (attention and executive function, information processing speed, and verbal memory) compared to models based on WMH volume (figure 2a). ROI-level inferential statistics revealed an association between cognitive performance and disconnectivity in dorsal and ventral attention networks (figure 2b).
Conclusions: LNM scores, capturing WMH location and strategic impact on brain networks, significantly enhance the prediction of cognitive performance in memory clinic patients. Our findings highlight the role of network connectivity, particularly in attention-related brain regions, in understanding vascular cognitive impairment, advocating for the inclusion of network effects in diagnostic assessments.
Disclosures of Interest:
No
Abstract N°: 3006
RISK FACTOR ASSOCIATIONS WITH POST-STROKE DEMENTIA ARE MODULATED BY SMALL VESSEL DISEASE ON BASELINE BRAIN IMAGING
Sarah Pendlebury*1, Ramon Luengo-Fernandez1, Peter Rothwell1
1Wolfson Centre for Prevention of Stroke and Dementia, University of Oxford, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
On behalf of: Oxford Vascular Study
Background and aims: Studies of post-stroke dementia and its predictors do not generally consider dementia subtype despite known differences in risk factors. Small vessel disease identifies individuals at greater risk of vascular vs Alzheimer-type dementia. Its presence on brain imaging might therefore affect the risk factor associations for dementia after TIA and minor stroke.
Methods: In patients with TIA/minor stroke (NIHSS<3) ascertained from 2002-2012 in a population-based study (Oxford Vascular Study - OXVASC), 5-year post-event dementia (excluding pre-stroke dementia) was diagnosed using clinical/cognitive assessment, supplemented by medical records. Dementia risk factor associations were determined using multivariable Cox regression stratified by the presence of moderate/severe white matter disease (WMD) on baseline CT/MRI brain imaging.
Results: Among 1,369 patients (n=655 TIA, n=714 minor stroke, mean/SD age=72/13 years, 674 female) 364 (27%) had moderate/severe WMD. During 4,979 patient years of follow-up, 209 (15%) patients developed dementia. Age, and less education were associated with dementia irrespective of WMD, but NIHSS score (HR/point=1.55, 1.08-2.23, p=0.02) and prior systemic vascular disease (HR=3.12, 1.39-6.99, p=0.006) were associated with dementia only in those with WMD, whereas low baseline cognitive score (HR=4.63, 2.47-8.69, p<0.001), ApoE-∈4 homozygosity (HR=7.03, 1.85-26.8, p=0.004), and Charlson comorbidity index (HR/point=1.05, 1.01-1.08, p=0.005) were associated with dementia only in those without WMD.
Conclusions: In dementia occurring after TIA and minor stroke, the predictive value of risk factors is modulated by the presence of WMD, suggesting that risk models should be stratified accordingly, and that future studies of predictors should classify dementia subtype.
Disclosures of Interest:
No
SCIENTIFIC COMMUNICATION – RARE CAUSES, STROKE IN THE YOUNG
Abstract N°: 105
20-YEAR RISK OF RECURRENT ISCHEMIC STROKE AND MORTALITY AFTER EARLY-ONSET ISCHEMIC STROKE
Nicolas Martinez-Majander*1, Karoliina Aarnio1, Elena Haapaniemi1, Eeva Kokkola1, Jenna Broman1, Lauri Tulkki1, Turgut Tatlisumak1, Markku Kaste1, Jukka Putaala1
1Helsinki University Hospital, Department of Neurology, Helsinki, Finland
On behalf of:
Background and aims: Long-term outcome after young-onset ischemic stroke (IS) still remains understudied. We aimed to explore the cumulative 20-year risk of recurrent IS and all-cause death in our registry, stratified by gender and stroke etiology.
Methods: Patients aged 15-49 years with a first-ever IS occurring between 1994-2007 were included into the analysis. Cumulative 20-year risk for recurrent IS and all-cause death were analyzed with life tables and adjusted risks were based on Cox proportional hazard analyses adjusted for relevant comorbidities.
Results: A total of 970 patients were included (median age 46 years, interquartile range 43-48, 33% women), of which 155 (16.0%) had a recurrent IS and 261 (26.9%) died during the median follow-up time of 17.8 years. The 20-year cumulative risk for recurrent IS and death were 23.0% (95% confidence interval [CI] 18.1-28.0%) and 43% (37.2-48.8%) for men, and 16.0% (12.0-20.1%) and 31.0% (23.8-38.1%) for women. Compared to women, men had a non-significantly higher risk for IS (hazard ratio [HR] 1.1; 0.8-1.6) and death (HR 1.3; 95% CI 0.9-1.8). The cumulative risk for recurrent IS and death was highest in patients with small-vessel disease (SVD) (38.3%; 25.3-51.3% and 62.6%; 49.5-74.9%, respectively). Compared to stroke of undetermined cause, large-artery atherosclerosis carried a significantly higher risk for recurrent IS (HR 2.2; 1.2-4.0) and SVD for death (HR 2.0; 1.4-3.0).
Conclusions: Young IS patients have a high risk for recurrent IS and all-cause death especially when the index IS is caused by large-artery atherosclerosis or small-vessel disease.
Disclosures of Interest:
No
Abstract N°: 323
FUNCTIONAL OUTCOMES IN PRIMARY ANGIITIS OF THE CENTRAL NERVOUS SYSTEM: DEVELOPMENT OF A PREDICTIVE MODEL
Ahmad Nehme*1, Clothilde Isabel2, Jean Capron3, Caroline Arquizan4, Alexis Régent5, Benoît Guillon6, Nelly Dequatre Ponchelle7, Emmanuel Touzé1, Christian Pagnoux8, Hubert de Boysson9
1CHU de Caen-Normandie, Neurology, Caen, France, 2GHU Paris, Neurology, Paris, France, 3Hôpital Pitié-Salpêtrière, Neurology, Paris, France, 4CHU de Montpellier, Neurology, Montpellier, France, 5Hôpital Cochin, Internal Medicine, Paris, France, 6CHU de Nantes, Neurology, Nantes, France, 7CHU de Lille, Neurology, Lille, France, 8Mount Sinai Hospital, Vasculitis clinic, Toronto, Canada, 9CHU de Caen-Normandie, Internal Medicine, Caen, France
On behalf of: Cohort of Patients with PACNS study group
Background and aims: A model to predict functional independence in patients with primary angiitis of the central nervous system (PACNS) may help guide treatment decisions.
Methods: We conducted a multicenter, international cohort study of adults with PACNS. The primary endpoint was functional independence 12 months after the start of immunosuppressants, defined as a modified Rankin Score between 0 and 2. Baseline demographic, clinical and imaging characteristics independently associated with functional independence at 12 months were identified through multivariable analyses. Discrimination was assessed by AUC-ROC.
Results: Among the 201 patients included with PACNS, 63 (31%) were diagnosed based on a positive biopsy. At 12 months, 132 (66%) patients were functionally independent and 12 (6%) had died. In the multivariable model, variables predictive of functional independence at 12 months were presence of ⩾ 1 intracranial stenosis on CT- or MR-angiogram (aOR 3.00, 95% CI: 1.23-7.71, p=0.01), headache (aOR 2.51, 95% CI: 1.22-5.28, p<0.01), absence of an altered level of consciousness (aOR 0.09, 95% CI: 0.02-0.29, p<0.001), ⩾ 1 acute brain infarct (aOR 0.12, 95% CI: 0.04-0.31, p<0.001), and cognitive impairment (aOR 0.24, 95% CI: 0.11-0.51, p<0.01). A predictive model including these five variables showed good discrimination (AUC: 0.80, 95% CI: 0.74-0.87). The probability of functional independence did not vary between purely lymphocytic (n=23/36) and granulomatous or necrotizing PACNS (n=19/27; OR 0.75, 95% CI: 0.25-2.15, p=0.59).
Conclusions: Baseline clinical and imaging variables may predict 12-month functional independence in adults with PACNS. Validation of these results is required in other cohorts.
Predictive nomogram of 12-month functional independence in PACNS
Disclosures of Interest:
No
Abstract N°: 547
LONG-TERM RISK OF RECURRENT CERVICAL ARTERY DISSECTION AND STROKE AFTER PREGNANCY (LONG-RECAP STUDY)
Sandro Fischer*1,2, Josefin E. Kaufmann1,2, Alessandro Pezzini3, Stefan Engelter1,2, Christopher Traenka1,2
1University Hospital Basel, Department of Neurology, Basel, Switzerland, 2University Department of Geriatric Medicine FELIX PLATTER, Neurology and Neurorehabilitation, Basel, Switzerland, 3Department of Medicine and Surgery, University of Parma, Stroke Care Program, Department of Emergency, Parma University Hospital, Parma, Italy
On behalf of: LONG-RECAP study group
Background and aims: Cervical artery dissection (CeAD) is the leading cause of stroke in the young and uncertainties remain whether subsequent pregnancy increases the long-term risk of recurrent CeAD (re-CeAD) or delayed stroke.
Methods: Multicentric, observational, case-control study based on pooled individual patient data. Among women who had CeAD, we compared those who had subsequent pregnancies to those who did not. The primary endpoint was a composite of (i) re-CeAD, (ii) ischaemic stroke, (iii) haemorrhagic stroke, and (iv) death. Secondary endpoints included the individual components of the primary endpoint. We performed logistic regressions using the penalised likelihood method with adjustment for age.
Results: 1013/1149 (88.2%) women with prior CeAD were eligible for analysis, of whom 114 (11.3%) had at least one pregnancy during follow-up. During a median follow-up of 5.3 years (IQR 2.0-11.3), the primary endpoint occurred in 11/114 (9.6%, 8 re-CeADs, 2 ischaemic,1 haemorrhagic strokes) women in the pregnancy-group compared to 74/899 (8.2%) women in the non-pregnancy-group (ORadjusted 0.82, 95% CI 0.39-1.60). In the pregnancy group, 4/8 re-CeADs occurred in temporal relationship to pregnancy (all in the postpartum period). Adjusted ORs for secondary endpoints were 1.01 (95% CI 0.42-2.20) for re-CeAD, 0.62 (95% CI 0.12-2.09) for ischaemic stroke, 1.09 (95% CI 0.10-7.33) for haemorrhagic stroke and 1.56 (0.01-21.25) for death.
Conclusions: Our data do not suggest that pregnancy increases the risk of recurrent CeAD or delayed stroke in women who had had CeAD. These findings are important for the individual counselling of women with prior CeAD.
Disclosures of Interest:
Yes Stefan T. Engelter has received funding for this study from the Swiss Heart Foundation.
Abstract N°: 1236
SELF-PERCEIVED STRESS IS ASSOCIATED WITH CRYPTOGENIC ISCHEMIC STROKE IN THE YOUNG
Lauri Tulkki*1, Nicolas Martinez-Majander1, Ulrike Waje-Andreassen2, Ana Catarina Fonseca3, Patricia Martínez Sánchez4, Phillip Ferdinand5, Janika Korv6, Kristina Ryliskiene7, Alessandro Pezzini8, Jukka Putaala1
1Helsinki Unversity Hospital, Department of Neurology, Helsinki, Finland, 2Haukeland University Hospital, Department of Neurology, Bergen, Norway, 3Hospital de Santa Maria-CHLN, Department of Neurosciences and Mental Health (Neurology), Lisboa, Portugal, 4Hospital Universitario Torrecárdenas, Neurology, Almería, Spain, 5University Hospitals of North Midlands NHS Trust, Stroke Service, Stoke-on-Trent, United Kingdom, 6University of Tartu, Department of Neurology and Neurosurgery, Tartu, Estonia, 7Vilnius University, Centre of Neurology, Vilnius, Lithuania, 8University of Parma and Parma University Hospital, Department of Medicine and Surgery and Department of Emergency, Parma, Italy
On behalf of: SECRETO Collaborators
Background and aims: Recently, psychosocial stress has been suggested as one of the most important risk factors for ischemic stroke in young adults. We aimed to explore whether this association holds true also in young-onset cryptogenic ischemic stroke (CIS).
Methods: Consecutive 18-49-year-old patients with a recent CIS and age- (±5 years) and sex-matched stroke-free controls were enrolled. Self-perceived stress was assessed using the Perceived Stress Scale (PSS) in which patients responded based on the pre-stroke situation. Conditional logistic regression was used to assess the associations of PSS score (as a continuous and divided in tertiles) with CIS. Confounders included age, sex, low education, hypertension, hypercholesterolemia, diabetes, cardiovascular diseases, smoking, physical inactivity, unhealthy diet, obesity, and heavy alcohol use.
Results: In total, 420 patients (median age, 40.9 years [33.2-45.9]; 52.4% men) and 420 controls (41.1 years [33.4-46.0], 52.4% men) were included. Median PSS score was significantly higher in patients compared with controls (13 [7-18] vs 10 [7-15], p<0.001). In fully adjusted models, continuous PSS score associated with CIS in the entire sample (odds ratio, 1.05 per point; 95% confidence interval, 1.02-1.08), in women (1.07 per point; 1.02-1.11), and in participants aged 35-44 years (1.08 per point; 1.03-1.14). Similar associations emerged when PSS score was categorized in tertiles, suggesting an exposure-response effect (Figure).
Conclusions: Higher levels of perceived stress were associated with a greater likelihood of CIS in the young after intensive adjustment for well-documented stroke risk factors. This association appeared to apply especially to women and those aged 35-44 years.
Disclosures of Interest:
No
Abstract N°: 1634
INCIDENCE OF CEREBRAL VENOUS THROMBOSIS ACCORDING TO AGE AND SEX. A NATIONAL POPULATION-BASED EPIDEMIOLOGICAL STUDY
Eduardo Mariño*1, Jorge Rodriguez-Pardo1, Carlos Hervás Testal1, Ricardo Rigual1, Gerardo Ruiz-Ares1, Elena de Celis Ruiz1, Javier Diaz-Fuentes2, Blanca Fuentes1
1Neurology Department and Stroke Center. Hospital La Paz Institute for Health Research – IdiPAZ (La Paz University Hospital – Universidad Autónoma de Madrid, Madrid (Spain)), Neurology Department, Madrid, Spain, 2Alcala University. Institute of Telematic Engineering., Telematic Engineering, Alcalá de Henares, Madrid, Spain
On behalf of:
Background and aims: Cerebral venous thrombosis (CVT) accounts for less than 1% of all strokes. Recent studies have shown an increase in its incidence, yet with varying patterns across different age and sex subgroups. We aim to analyze the incidence of CVT in Spain from 2005 to 2021, examining year-on-year trends, demographic variations across age and sex, and associated mortality rates.
Methods: We conducted a population-based retrospective analysis of CVT cases from 2005 to 2021 using the Hospital Morbidity Registry provided by the Spanish National Institute of Statistics.
Results: Out of 76,793,382 hospital discharges, 7,625 were primarily diagnosed as CVT, mean age 54.6±21.9 years. Women represented 57.1% of CVT diagnoses. Global incidence of CVT declined from 2.03 in 2005 to 0.47 in 2017, followed by a sustained increase reaching 0.85 cases per 100,000 inhabitants in 2021. Incidence was consistently higher in women than men (2.15 vs 1.93 in 2005; 1.93 vs 0.73 in 2021). According to age, incidence was initially higher in > 50 than in 16-50 year-olds (4.22 vs 1.13) but also experienced a greater drop over time, finally being surpassed by the latter (0.87 vs 1.02 in 2021). The greatest increase in recent incidence was observed in 16-50 year-old women (0.47 to 0.99). Mortality during hospitalization fluctuated over time ranging between 1.3-5.3% in women and 0-4.5% in men.
Conclusions: CVT incidence trends in Spain behaved differently according to age and sex. Despite an overall decline in CVT incidence, we observed an increasing trend in the last years, especially in young women.
Disclosures of Interest:
No
Abstract N°: 1811
RISK FACTORS FOR ACUTE ISCHEMIC STROKE FOLLOWING CERVICAL ARTERY DISSECTION: INSIGHTS FROM THE STOP-CAD STUDY
Liqi Shu*1, Daniel Mandel1, Karen Furie1, Shadi Yaghi1
1Warren Alpert Medical School of Brown University, Neurology, Providence, United States
On behalf of: STOP-CAD investigators
Background and aims: Cervical artery dissection (CAD) accounts for up to 25% of strokes in the young adults. This study aims to identify predictors of subsequent acute ischemic stroke (AIS) in CAD.
Methods: We conducted a secondary analysis of the STOP-CAD study, a multicenter international retrospective study of non-traumatic CAD patients. The primary outcome was subsequent AIS within the follow-up period of 180 days. Patient characteristics were compared between those who developed with vs. without subsequent AIS. Stepwise Cox regression analyses including variables with p<0.1 and Lasso regression were utilized to identify significant predictors of AIS.
Results: The study included 4,023 patients (mean age of 47.4 years and 44.5% women). The ischemic stroke rate was 5.3% by 180 days. Predictors of AIS in stepwise Cox regression analyses were history of stroke (aHR 1.87, 95% CI 1.11-3.14, p=0.018), presence of acute infarct (aHR 2.18, 95% CI 1.55-3.07, p<0.001), presentation within 1 week from first dissection symptoms (aHR 1.47 95% CI 1.02-2.13, p = 0.04), and occlusive dissection (aHR 1.33 95% CI 1.00-1.76, p = 0.05). The Lasso regression confirmed that the presence of imaging infarction is the most robust predictor.
Conclusions: Certain clinical and imaging variables help risk stratify patients with cervical artery dissection. Further studies are warranted to confirm these associations and explore optimal therapeutic approaches in high-risk patients.
Disclosures of Interest:
No
Abstract N°: 2086
OUTCOMES AND COMORBIDITITIES ASSOCIATES WITH ATRIAL FIBRILLATON IN YOUNG STROKE PATIENTS: A NATIONWIDE ANALYSIS
Tania Garrido Hernández1, Laura Amaya-Pascasio*1, Patricia Martínez Sánchez1,2, Miguel Quesada López1
1Hospital Universitario Torrecárdenas, Neurología, ALMERIA, 2University of Almeria, Faculty of Health Sciences. CEINSA Health Research Centre., La Cañada de San Urbano Almería, Spain
On behalf of:
Background and aims: The knowledge about the prevalence of atrial fibrillation (AF) in young stroke patients, as well as its associated factors is scarce. Our objective is to analyze it.
Methods: Retrospective analysis of Spain's Nationwide Inpatient Sample (2016-2020) focused on ischemic stroke (IS) patients aged 18-50. Multivariate analyses were conducted to identify AF diagnosis factors.
Results: A total of 11,615 young IS patients were admitted to the Nationwide Inpatients Hospitals in Spain, of them 426 had AF (3.7%). AF patients were older (median of age [IQR], 45 [6], vs. 44 [7] years, p<0.001), had greater disabling symptoms, in-hospital complications, mortality rate, and were less often discharged to home (p< 0.001). The multivariate analyses showed that older age (OR 1.052, 95%CI 1.032- 1.073), obstructive sleep apnea (OSA) (OR 1.542, 95%CI 1.041-2.285), hyperthyroidism (OR 3.856, 95%CI 1.861-7.990), hypothyroidism (OR 1.590, 95%CI 1.004-2.518), valvular heart disease (OR 6.400, 95%CI 4.482-9.140) and heart failure (OR 2.909, 95%CI 1.765-4.794) were independently associated with higher probability of AF, whereas female gender (OR 0.653, 95%CI 0.520-0.819), diabetes mellitus (OR 0.520, 95%CI 0.364-0.744), smoking (OR 0.606, 95%CI 0.492-0.746) and patent foramen ovale (PFO) (OR 0.090, 95%CI 0.034-0.234) were independently associated with a lower probability of having AF.
Conclusions: Young individuals with AF face increased in-hospital complications and disabling strokes, linked to factors like older age, OSA, thyroid disorders, and heart disease. Interestingly, diabetes mellitus and smoking, typically linked to atherothrombotic stroke, correlate with a lower likelihood of AF diagnosis in this cohort.
Disclosures of Interest:
No
SCIENTIFIC COMMUNICATION – GENETICS, ‘OMICS AND BIOMARKERS
Abstract N°: 634
HTRA1 PROTEASE ACTIVITY AND CIRCULATING LEVELS INDEPENDENTLY PREDICT RISK OF ISCHEMIC STROKE AND CORONARY ARTERY DISEASE
Rainer Malik*1, Martin Dichgans1, Nathalie Beaufort1
1Institute for Stroke and Dementia Research, München, Germany
On behalf of:
Background and aims:HTRA1 has emerged as a major risk gene for stroke and cerebral small vessel disease with both rare and common variants contributing to disease risk. However, the precise mechanisms mediating this risk remain unknown as does the full spectrum of phenotypes associated with genetic variation in HTRA1 in the general population.
Methods: Applying gene burden tests and a family-history informed approach to whole-exome sequencing data from the UK Biobank we examined whether rare variation in HTRA1 associates with ischemic stroke. We further determined the activity profile of 76 mutations occurring in the UK Biobank by biochemical experiments.
Results: We show that rare variants in HTRA1 are linked to ischemic stroke in 425,338 European individuals from the UK Biobank with replication in 143,149 individuals from the Biobank Japan. We further show that rare variants causing loss of protease function in vitro associate with ischemic stroke, coronary artery disease, and skeletal traits. In addition, a common causal variant (rs2672592) modulating circulating HTRA1 mRNA and protein levels enhances the risk of ischemic stroke, small vessel stroke, and coronary artery disease while lowering the risk of migraine and age-related macular dystrophy in GWAS and UK Biobank data from > 2,000,000 individuals. There was no evidence of an interaction between genetically proxied HTRA1 activity and levels.
Conclusions: Our findings demonstrate a central role of HTRA1 for human disease including stroke and coronary artery disease and identify two independent mechanisms that might qualify as targets for future therapeutic interventions.
Disclosures of Interest:
No
Abstract N°: 972
BRAIN-DERIVED TAU FOR MONITORING BRAIN INJURY IN ACUTE ISCHEMIC STROKE: A PROSPECTIVE OBSERVATIONAL COHORT STUDY
Naomi Vlegels*1, Fernando Gonzalez-Ortiz2,3, Nicoló Knuth1, Thomas Liebig4, Marco Duering1,5, Paul Reidler6, Martin Dichgans1,7,8, Thomas Karikari2,9, Kaj Blennow2,3, Steffen Tiedt1
1Institute for Stroke and Dementia Research, LMU University Hospital, München, Germany, 2Department of Psychiatry and Neurochemistry, University of Gothenburg, Gothenburg, Sweden, 3Clinical Neurochemistry Laboratory, Sahlgrenska University Hospital, Mölndal, Sweden, 4Institute of Neuroradiology, LMU University Hospital, München, Germany, 5Medical Image Analysis Center (MIAC) and Department of Biomedical Engineering, University of Basel, Basel, Switzerland, 6Department of Radiology, LMU University Hospital, München, Germany, 7German Center of Neurodegenerative Diseases, München, Germany, 8Munich Cluster for Systems Neurology (SyNergy), München, Germany, 9Department of Psychiatry, University of Pittsburgh, Pittsburgh, United States
On behalf of:
Background and aims: Unlike most other organs, the brain lacks an early and accurate blood test for injury monitoring in clinical practice similar to troponins for the heart. Here, we explored the value of tau as a blood biomarker for neuronal injury to track infarct progression in patients with acute ischemic stroke (IS).
Methods: We conducted the prospective Precision Medicine in Stroke (PROMISE) study (NCT05815836) with longitudinal neuroimaging and serial blood sampling upon admission and at days 2, 3 and 7 in patients with acute IS (N=502) and stroke mimics (N=51). Using a single-molecule technology-based assay specifically capturing tau from the brain (BD-tau), we determined the temporal course of plasma BD-tau, its relation to imaging-derived metrics of brain injury, and its predictive value for functional outcome.
Results: Upon admission (median time-from-onset: 4.4h), BD-tau levels in IS patients correlated with ASPECTS (p<0.0001) and were predictive of final infarct volume (FIV, p<0.0001). From admission to day 2 (median time-from-onset: 22.7h), BD-tau increased in IS patients but not in stroke mimics and in relation to infarct progression (p<0.0001; Figure 1). At day 2, BD-tau was highly predictive of FIV (rho=0.59; p<0.0001) and showed superior value for predicting the 90-day mRS score compared with FIV (Figure 2). Trajectories of BD-tau across the first week captured secondary intracerebral hemorrhage and identified differences in brain injury in patients with complete vs incomplete recanalization (Figure 3).
Conclusions: This study identifies BD-tau as an early and accurate blood-based biomarker of brain injury in IS patients, with potentially broad applications in neurological diseases.
Disclosures of Interest:
No
Abstract N°: 1148
ORAL HEALTH AS A RISK FACTOR FOR SPONTANEOUS INTRACEREBRAL HEMORRHAGE:A MENDELIAN RANDOMIZATION ANALYSIS
Cyprien Rivier*1, Santiago Clocchiatti-Tuozzo1, Shufan Huo1, Daniela Renedo1, N. Abimbola Sunmonu1, Kevin Sheth1, Guido Falcone1
1Yale School of Medicine, New Haven, United States
On behalf of:
Background and aims: Poor oral health is a highly prevalent and modifiable risk factor that is associated with higher risk of cardiovascular disease, including ischemic stroke. However, the relationship between oral health and spontaneous intracerebral hemorrhage (ICH) has not been studied.
Methods: We conducted a two-sample Mendelian Randomization (MR) study using summary statistics from the largest genome-wide associations studies of oral health and ICH conducted to date. As genetic instruments (genetic risk variants for oral health), we identified 105 independent single nucleotide polymorphisms known to be associated with higher risk of caries, dentures and missing teeth at genome wide levels (p<5x10-8). The primary analysis employed summary statistics-based MR to assess the relationship between poor oral health and risk of ICH in any brain location. Secondary analyses evaluated deep and lobar ICH separately.
Results: The primary analysis using the inverse variance-weighted MR method showed that genetically-increased risk of poor oral health was associated with a higher risk of ICH (OR:3.01[1.43-6.33],p=0.003). Secondary analyses indicated a more potent association with deep ICH (OR:4.68[1.93-11.37],p<0.001), whereas no evidence of an association with lobar ICH was detected (OR:1.36[0.60 -3.08],p=0.45). Sensitivity analyses detected no horizontal pleiotropy in our findings (MR-PRESSO global test p-value>0.05).
Conclusions: Genetically-determined poor oral health is associated with an increased risk of ICH, particularly deep ICH. Because gene-disease associations are less prone to confounding, our results suggest that this association is causal. Because oral health is an easily modifiable process, it may be a promising target for very early interventions focused on mitigating the risk of hemorrhagic stroke.
Disclosures of Interest:
No
Abstract N°: 2087
EPIGENOME-WIDE ASSOCIATION STUDY IN THE EARLY STROKE OUTCOME
Natalia Cullell*1, Cristina Gallego-Fabrega2, Joan Jimenez-Balado3, Jara Cárcel-Márquez2, Elena Muiño Acuña2, Miquel Lledós2, Laia Llucia Carol2, Jordi Jimenez Conde3, Jerzy Krupinski1, Israel Fernandez Cadenas2
1Fundació Docència i Recerca MútuaTerrassa, 2Institut de Recerca Hospital de la Santa Creu i Sant Pau, 3Department of Neurology, Hospital del Mar; Neurovascular Research Group, IMIM (Institut Hospital del Mar d'Investigacions Mèdiques)
On behalf of:
Background and aims: Stroke outcome variability is influenced by genetics and epigenetics. Early neurological evolution, measured by the difference in NIHSS scores at baseline and 24 hours (∆NIHSS24), is linked to long-term stroke outcomes. While the ∆NIHSS24 genetic basis has been explored, the epigenetic modifications impact remains unexamined.
Methods: We conducted an Epigenome-wide Association Study(EWAS) involving 1166 incident stroke patients (322 in the discovery and 844 in the replication). DNA methylation was analysed using the Infinium HumanMethylation450 and EPIC BeadChip. In a three-step analysis—discovery, replication, and meta-analysis—we assessed DNA methylation associated with early improvement (∆NIHSS24 ⩾ 4)(Analysis1) and early worsening (∆NIHSS24 ⩽ -4)(Analysis2), with sex, age, smoking and rTPA as covariates.
Results: Among the 412,839 CpG-sites analysed in the discovery, a CpG-site in the 3'UTR of a gene in 5q33.3 exhibited differential methylation in patients with early favourable outcomes (p-value=5.5x10-7 in Analysis1). This finding was replicated (p-value=1x10-2) and linked to a gene previously associated with cholesterol, leukocyte levels, and post-stroke depression. In the meta-analysis from the analysis1, the CpG in 5q33.3 and a CpG in 1p33 (previously associated with stroke risk) were associated with the early favourable outcome (p-value=2.1x10-7 and 3.8x10-7, respectively). Six additional CpG-sites in 1p33 were also nominally associated (p-value < 0.05). In Analysis2 meta-analysis, a CpG-site in the 12q23.3 was significantly associated with early worsening (p-value= 8.9x10-7), in a gene associated with neutrophil count in GWAS.
Conclusions: This study unveils the involvement of DNA methylation in the neurological evolution during the acute stroke phase.
Disclosures of Interest:
No
Abstract N°: 2147
GENEVADER STUDY: GENOME-WIDE ASSOCIATION STUDY ON DELAYED CEREBRAL ISCHEMIA IN ANEURYSMAL SUBARACHNOID HEMORRHAGE
Joan Jiménez-Balado*1, Isabel Hostettler2, Ynte Ruigrok3, Mark Bakker3, Behnam Rezai Jahromi4, M Niemelä´s4, Sandrine Morel5, Philippe Bijlenga5, David Werring2, Elisa Cuadrado-Godia1
1Hospital del Mar, Barcelona, Spain, 2UCL Queen Square Institute of Neurology, United Kingdom, 3UMC Utrecht, Utrecht, Netherlands, 4University of Helsinki, Helsinki, Finland, 5University of Geneva, Geneva, Switzerland
On behalf of:
Background and aims: Delayed cerebral ischemia (DCI) is a key predictor of outcomes in aneurysmal subarachnoid hemorrhage (aSAH), yet its underlying mechanisms are not completely understood, with no genome-wide association studies conducted to date. This study aims to identify genetic variants associated with DCI and to compare with stroke etiologies using genetic correlations.
Methods: Multicentric cohort study within the ISGC in individuals of European ancestry. Discovery sample was composed of data from four centers (N=1078), while replication sample consisted in 801 patients from a fifth center. We conducted a Genome-Wide Association study following standard quality controls and adjusting for sex, age, the world federation of neurosurgeons grading scale (WFNS) and principal components. Heritability and genetic correlations with ischemic stroke were conducted using Linkage Disequilibrium Score (LDSC) Regression using data from the Gigastroke consortium.
Results: Prevalence of DCI in the whole cohort was 22.8%. Patients with DCI were more often females (73.8 vs 66.3%) and had a higher WFNS punctuation (WFNS4-5: 37.0% vs 19.3%). When we meta-analyzed the five cohorts, we found 12 loci suggestively significant (Figure-1, p-value<10-5), which require validation. A single variant, rs7636350, achieved genome-wide significance (p-value=4.9·10-8), which was annotated to COL6A6 gene. Patients with this variant showed an increased risk of DCI (Figure-2). Heritability was estimated to be 25%. Genetic correlation between DCI and ischemic stroke showed a significant correlation with large artery atherosclerosis etiology.
Conclusions: We conducted the first GWAS of DCI, identifying several locus. These findings warrant validation through further international, multicenter studies to deepen our understanding of DCI pathophysiology.
Disclosures of Interest:
No
Abstract N°: 2760
PROTEOGENOMICS IN CEREBROSPINAL FLUID AND PLASMA REVEALS NEW BIOLOGICAL FINGERPRINT OF CEREBRAL SMALL VESSEL DISEASE
Ilana Caro*1, Daniel Western2, Yukinori Okada3, Philip De Jager4, Marie-Gabrielle Duperron1, Muralidharan Sargurupremraj5, Sudha Seshadri5, David-Alexandre Trégouët1, Carlos Cruchaga2, Stéphanie Debette1,6
1University of Bordeaux, Bordeaux Population Health research center, Bordeaux, France, 2Washington University in St. Louis, St. Louis, United States, 3Osaka University, Department of Statistical Genetics, Graduate School of Medicine, Osaka, Japan, 4Columbia University Irving Medical Center, 4Center for Translational and Computational Neuroimmunology, Dpt. of Neurology, New York, United States, 5UT Health San Antonio - Glenn Biggs Institute for Alzheimer's & Neurodegenerative Diseases, San Antonio, United States, 6Bordeaux University Hospital, Department of Neurology, Institute for Neurodegenerative Diseases, Bordeaux, France
On behalf of: neuroCHARGE working group
Background and aims: Cerebral small vessel disease (cSVD) is a leading cause of stroke and dementia. Its underlying mechanisms remain elusive and specific mechanism-based drugs are lacking.
Methods: We integrated more than 2,800 CSF and 4,600 plasma pQTL, derived from the largest proteomic studies so far (SOMAscan 7k and 4k; in up to 35,559 individuals), and the two most prevalent MRI-markers of cSVD (MRI-cSVD, white matter hyperintensities and perivascular spaces burden; in up to 48,454 individuals) in a Mendelian Randomization (MR) framework to identify causal and druggable targets for cSVD. Identified association were followed-up using a multipronged approach: across fluids, proteomics platforms (Olink 3072, N=8,590) and lifespan (N=1,748), using both MR and individual-level data.
Results: We found 51 proteins associated with MRI-cSVD of which 46 in CSF and 9 in plasma. Among available significant CSF- and plasma-proteins, 32% and 31% replicated in cross-fluid and cross-platform follow-up, and 47% were associated with stroke and/or dementia at least at nominal significance. We found converging evidence that protein-cSVD associations are enriched in extracellular matrix and immune response pathways. Immunity-related proteins already showed association with MRI-cSVD already in young adults in their twenties. Furthermore, we provide genetic support for drug repositioning opportunities for cSVD, including compounds crossing the blood brain barrier.
Conclusions: Together, these findings provide a novel proteogenomic signature of cSVD and pave the way for novel therapeutic developments.
Disclosures of Interest:
No
Abstract N°: 3077
GENETICALLY PROXIED IL-18 INHIBITION AND RISK OF STROKE: A DRUG TARGET MENDELIAN RANDOMISATION STUDY
Stephen Brennan*1, Peter Kelly2,3,4, Sarah Gorey1,2,3, Pádraig Synnott5, Martin Dichgans6,7,8, Marios Georgakis6,9,10, Christina Jern11,12, Hugh Markus13, William Whiteley14,15, John Mccabe1,2,3
1Mater Misericordiae University Hospital, Department of Geriatric Medicine, Dublin, Ireland, 2Health Research Board Stroke Clinical Trials Network Ireland, Dublin, Ireland, 3School of Medicine, University College Dublin, Dublin, Ireland, 4Mater Misericordiae University Hospital, Department of Neurology, Dublin, Ireland, 5University of Galway, Health Research Board, Clinical Research Facility, Galway, Ireland, 6University Hospital, LMU Munich, Germany, Institute for Stroke and Dementia Research, Munich, Germany, 7German Center for Neurodegenerative Disease, Munich, Germany, 8Munich Cluster for Systems Neurology (SyNergy), Munich, Germany, 9Massachusetts General Hospital, Center for Genomic Medicine, Boston, United States, 10Broad Institute of Harvard and the Massachusetts Institute of Technology, Program in Medical and Population Genetics, Boston, United States, 11Sahlgrenska University Hospital, Department of Clinical Genetics and Genomics, Gothenburg, Sweden, 12University of Gothenburg, Department of Laboratory Medicine, Institute of Biomedicine, the Sahlgrenska Academy, Gothenburg, Sweden, 13University of Cambridge, Stroke Research Group, Department of Clinical Neuroscience, Cambridge, United Kingdom, 14University of Oxford, Nuffield Department of Population Health, Oxford, United Kingdom, 15University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
On behalf of:
Background and aims: Inflammation is a promising new target for prevention after stroke and elevated IL-18 is associated with an increased risk of cardiovascular events. This drug-target Mendelian Randomisation (MR) study aims to elucidate the on-target effects of pharmacological IL-18 inhibition on incident stroke. Furthermore, this study seeks to explore the effect of IL-18 inhibition on cardio-metabolic traits, cardiac structure and function, and identify potential adverse outcomes.
Methods: Three independent IL-18-lowering variants from around the IL18 locus were used in two-sample MR to assess the effect of genetically proxied IL-18 inhibition on the risk of stroke subtypes and cardiac magnetic resonance (CMR) measurements of cardiac structure and function in GIGASTROKE and UK Biobank.
Results: Leveraging data from 1,296,908 participants and following correction for multiple comparisons, lower genetically predicted IL-18 was associated with reduced odds of cardio-embolic stroke (OR 0.86, CI 0.81-0.91), but not other stroke subtypes (Figure 1). Furthermore, lower IL-18 was associated with reduced odds of atrial fibrillation (OR 0.94, CI 0.89-0.99), chronic kidney disease (OR 0.91, 0.85-0.97), and heart failure (OR 0.87, CI 0.77-0.98), as well as improvements in CMR traits, including left atrial volume (β -0.03, CI -0.06, -0.01). Lower IL-18 was associated with less autoimmune disease, a favourable cardio-metabolic profile, higher odds of lung cancer, but no association with infection.
Conclusions: Findings indicate that impaired IL-18 signalling is associated with a lower risk of cardio-embolic stroke, possibly mediated through prevention of cardiac re-modelling and atrial fibrillation. IL-18 is a potential target for anti-inflammatory therapy in stroke and cardiovascular disease.
Disclosures of Interest: No
Abstract N°: 3125
AN INTEGRATIVE POLYGENIC RISK SCORE FOR ALL-CAUSE DEMENTIA SHOWS POTENTIAL FOR RISK STRATIFICATION ACROSS POPULATION AND CLINICAL SETTINGS
1Université de Bordeaux, Gironde, Bordeaux, France, 2Iwate Medical University, Iwate, Morioka, Japan
On behalf of:
Background and aims: The vast majority of dementia cases in the population arise due to combined neurodegenerative – most commonly Alzheimer’s Disease (AD) - and vascular pathologies - frequently in the form of cerebral small vessel disease. An integrative polygenic risk scoring approach (iPRS) has potential to quantify the genetic burden of both these components and improve risk prediction.
Methods: We trained an iPRS for all-cause dementia (iPRS-DEM) in the Bordeaux-Montpellier subset of the 3C population-based cohort (age 65+; N = 2,039) accounting for the competing risk of death. Using Fine-Gray regression models, the iPRS-DEM was evaluated against APOE and AD-PRS in the Dijon subset of 3C (3C-Dijon, N = 3,702) and externally validated in Memento (N = 2,032), a French clinic-based cohort including patients with cognitive complaints without dementia at baseline.
Results: The iPRS-DEM was associated with incident dementia independent of age, sex, and APOE in 3C-Dijon (HRper1SD = 1.152, [95% CI 1.034 – 1.283]) and in Memento (HRper1SD = 1.254, [1.111 – 1.416]), and achieved a time-dependent AUC = 0.771 at 10-years in 3C-Dijon and AUC = 0.758 at 5-years in Memento. Combining iPRS-DEM and APOE revealed that those at highest genetic risk (APOE4+ & High iPRS-DEM) relative to the low risk group (APOE4- & Low iPRS-DEM) have increased dementia risk in 3C-Dijon (HR = 2.23 [1.64-3.03]) and Memento (HR = 5.76 [4.18-7.93]).
Conclusions: We provide suggestive evidence that beyond APOE and AD-PRS, the iPRS-DEM may be particularly well-suited for refining risk stratification and identifying those at highest dementia risk in both population-based and clinical settings.
Disclosures of Interest:
No
ESOC 2024 – Moderated Poster Abstracts
Moderated Poster - Acute Management – Day 1
Abstract N°: 1017
CLINICAL SEVERITY AND ENDOVASCULAR THERAPY OUTCOMES IN PATIENTS WITH LARGE INFARCTS: A POST HOC ANALYSIS OF THE ANGEL-ASPECT TRIAL
1Beijing Tiantan Hospital, Capital Medical University, Department of Neurology, Beijing, China, 2Beijing Tiantan Hospital, Capital Medical University, China National Clinical Research Center for Neurological Diseases, Beijing, China, 3Beijing Anzhen Hospital, Capital Medical University, Cerebrovascular Disease Department, Neurological Disease Center, Beijing, China
On behalf of:
Background and aims: Endovascular therapy (EVT) was effective for acute ischemic stroke (AIS) patients with large infarcts. It has also been reported to benefit AIS patients with severe neurological deficit, while in those with small-to-moderate infarctions. We aimed to investigate the efficacy of EVT versus medical management (MM) in patients with large infarcts stratified by clinical severity.
Methods: This was a post hoc analysis of the ANGEL-ASPECT, involving patients with acute anterior-circulation large vessel occlusion and large infarcts (ASPECTS 3-5 or infarct-core volume 70-100ml). They were randomly assigned to receive EVT and MM versus MM alone. Patients were dichotomized into 2 subgroups with moderate stroke and severe stroke respectively, based on baseline NIHSS score of < 20 or ⩾ 20. Primary outcome was the 90-day modified Rankin Scale (mRS).
Results: Among 455 patients enrolled, 347 (76%) had moderate stroke and 108 (24%) had severe stroke. A significant shift in the 90-days mRS distribution with EVT versus MM was observed (generalized OR, 1.66; 95% CI, 1.29 to 2.13; P < 0.001) in patients with moderate stroke, but not in those with severe stroke (P = 0.86). The treatment effect between two subgroups with different clinical severity was significant (P for interaction = 0.03).
Conclusions: In patients with large infarcts, EVT was associated with better functional outcomes than MM in those with moderate stroke, but not in those with severe stroke. The clinical severity should be considered when selecting patients with large infarcts for EVT. A pooled analysis of large-infarct trials is warranted to verify our findings.
Disclosures of Interest: No
Abstract N°: 2772
THE SECOND ALTEPLASE-TENECTEPLASE TRIAL EVALUATION FOR STROKE THROMBOLYSIS (ATTEST-2): MAJOR SUBGROUPS AND SECONDARY ENDPOINTS
Keith Muir*1, Gary Ford2, Ian Ford3, Joanna Wardlaw4, Alex Mcconnachie3, Nicola Greenlaw3, Grant Mair4, Nikola Sprigg5, Chris Price6, Mary Joan Macleod7
1University of Glasgow, School of Psychology & Neuroscience, Glasgow, United Kingdom, 2University of Oxford, 3University of Glasgow, 4University of Edinburgh, 5University of Nottingham, United Kingdom, 6Newcastle University, United Kingdom, 7University of Aberdeen, United Kingdom
On behalf of: ATTEST-2 Investigators
Background and aims: ATTEST-2 compared tenecteplase 0.25mg/kg to alteplase 0.9mg/kg among thrombolysis-eligible patients within 4.5h of stroke onset. For the primary endpoint of day 90 modified Rankin Scale (mRS) distribution, pre-specified non-inferiority margins were met. Data for major subgroups and secondary endpoints are described.
Methods: ATTEST-2 was a prospective, multicentre, parallel group open label trial with blinded end-point evaluation. Secondary endpoints included major early neurological improvement (NIHSS score of 0 or 1 or >8 point improvement), excellent (mRS 0-1) and independent (mRS 0-2) recovery, Barthel Index and health-related quality of life (EQ-5D) at day 90. Home time was an exploratory measure. Day 90 mRS distribution, excellent and independent recovery were analysed in subgroups of age, stroke severity, onset to treatment time, LVO presence, and those undergoing thrombectomy.
Results: Of 1858 randomised, 1776 received thrombolysis (885 allocated tenecteplase and 891 alteplase). Median NIHSS was 7. LVO was present in 18.7% and 12.4% underwent thrombectomy. Tenecteplase was non-inferior to alteplase by both mRS distribution and excellent recovery. There were no significant differences in early neurological recovery, day 90 EQ-5D or Barthel Index, home time, mortality, or SICH incidence. No treatment interaction with day 90 mRS distribution was seen by age group (⩽80 v >80y, p=0.85), stroke severity (by NIHSS, p=0.32), onset to treatment time (p=0.82), thrombectomy (p=0.77) or LVO presence (p=0.43).
Conclusions: Tenecteplase was non-inferior to alteplase among patients treated within 4.5h of symptom onset, but was not superior for any primary or secondary endpoint. Effects were consistent across all subgroups.
Disclosures of Interest: Yes ATTEST-2 tenectelase supplied by Boehringer Ingelheim. KM - Lecture fees and advisory board participation - Boehringer Ingelheim.
Abstract N°: 2938
ADMISSION SYSTOLIC BLOOD PRESSURE AND OUTCOMES AFTER ENDOVASCULAR TREATMENT IN ACUTE ISCHEMIC STROKE: A COHORT STUDY FROM THE EVA-TRISP COLLABORATION
Nabila Wali*1, Abris Mumcuoglu1, Mirjam Rachel Heldner2, Susanne Wegener3, Patrik Michel4, Sami Curtze5, Georg Kaegi6, Henrik Gensicke7,8, Stefan Engelter7,8, Paul Nederkoorn1
1Amsterdam UMC, University of Amsterdam, Department of Neurology, Amsterdam, Netherlands, 2Inselspital, Bern University Hospital and University of Bern, Department of Neurology, Bern, Switzerland, 3University Hospital Zurich and University of Zurich, Department of Neurology, Zurich, Switzerland, 4Lausanne University Hospital and University of Lausanne, Stroke Center, Neurology Service, Lausanne, Switzerland, 5University of Helsinki and Helsinki University Hospital, Department of Neurology, Helsinki, Finland, 6Kantonsspital St. Gallen, Department of Neurology, St. Gallen, Switzerland, 7University Department of Geriatric Medicine FELIX PLATTER, University of Basel, Department of Neurology and Neurorehabilitation, Basel, Switzerland, 8University Hospital Basel and University of Basel, Stroke Center and Department of Neurology, Basel, Switzerland
On behalf of: the EndoVAscular treatment and ThRombolysis for Ischemic Stroke Patients (EVA-TRISP) investigators.
Background and aims: Previous studies suggested that both low and high admission systolic blood pressure (aSBP) are associated with poor functional outcome after EVT. The aim of this study was to investigate the relation between aSBP and outcomes after EVT in a large international multicenter observational study.
Methods: In the EndoVAscular treatment and ThRombolysis for Ischemic Stroke Patients Registry (EVA-TRISP) the relation between sSBP and outcome was investigated. Main outcomes were functional outcome (modified Rankin Scale scores (mRS)) at 90 days, rate of successful reperfusion (eTICI scores between 2b-3), symptomatic intracranial haemorrhage (sICH) and 90-day mortality. The relation between aSBP and outcomes were studied using multivariable regression analysis.
Results: In total, 8981 EVT treated patients were included. The association of SBP with mRS score was J-shaped, with an inflection point at 150 mmHg. Within an aSBP range of 50 – 150mmHG, an increase in SBP was associated with lower odds of poor functional outcome (adjustedOR 0.92 (0.88-0.96)) and mortality (adjustedOR 0.84 (0.79-0.89)). Within an aSBP range of 150-270mmHG, an increase in SBP was only associated with higher odds of sICH (adjustedOR 1.08 (1.01-1.16)). In this cohort no association was found between aSBP and rate of successful reperfusion.
Conclusions: In EVT treated patients, low admission SBP was associated with poor functional outcome and mortality. High SBP was associated with higher rates of sICH. EVT was most effective in patients with an aSBP of approximately 150 mmHG.
Disclosures of Interest: No
Abstract N°: 1016
OUTCOMES OF BRIDGING INTRAVENOUS THROMBOLYSIS VS. ENDOVASCULAR THERAPY ALONE IN LATE-WINDOW ACUTE ISCHEMIC STROKE
Jelle Demeestere*1, Muhammad M. Qureshi2, Anke Wouters1, Daniel Strbian3, Simon Nagel4, Volker Puetz5, João Pedro Marto6, Raul Nogueira7, Robin Lemmens1, Thanh N. Nguyen2
1Leuven University Hospital, Neurology, Leuven, Belgium, 2Boston Medical Center, Boston, United States, 3Helsinki University Hospital, Finland, 4Klinikum Ludwigshafen, Neurology, Germany, 5University Hospital Carl Gustav Carus, Dresden, Germany, 6Hospital de Egas Moniz, Centro Hospitalar Lisboa Occidental, Lisboa, Portugal, 7University of Pittsburgh Medical Center, Pittsburgh, United States
On behalf of: CLEAR study investigators
Background and aims: Comparison between bridging intravenous thrombolysis (IVT) with direct endovascular therapy (EVT) in late-presenting acute ischemic stroke patients is lacking. We aimed to compare outcomes of bridging IVT in patients with anterior circulation large vessel occlusion (acLVO) who underwent EVT 6 to 24 hours after time-last-known-well (TLKW).
Methods: We included patients from the multicenter, retrospective CT for Late EndovasculAr Reperfusion (CLEAR) study. We used inverse probability of treatment weighting modeling adjusted for clinical and imaging confounders to compare functional outcomes, reperfusion success, symptomatic intracranial hemorrhage and mortality between EVT patients with and without prior IVT.
Results: We included 2749 EVT patients, of whom 549 received bridging IVT. Witnessed stroke onset and transfer rates were higher in the bridging IVT group (25% vs 12% and 77% vs 55% respectively, p for both < 0.0001), and TLKW to EVT time interval was shorter (median 560 min [IQR 432-791] vs. 724 min [IQR 544-912], p< 0.0001). After adjustment we found no difference in functional outcome at 3 months (adjusted common OR for mRS shift =1.03 [95%CI 0.89-1.19], Figure 1) or successful reperfusion (adjusted OR 1.19 [0.81-1.75], p=0.39). Bridging IVT was not associated with safety concerns (sICH: adjusted OR 0.75 [0.81-1.75], p=0.40; mortality: adjusted OR 1.14 [0.89-1.46]; p=0.31). Results remained unchanged when the analysis was limited to patients who received IVT > 6h after TLKW.
Conclusions: In patients with acLVO who underwent EVT 6 to 24 hours from TLKW, bridging IVT was not associated with differences in functional or safety outcomes compared to direct EVT.
Disclosures of Interest: No
Abstract N°: 1203
THE TREATMENT EFFECT OF TENECTEPLASE COMPARED TO ALTEPLASE ACROSS ASPECTS IN ACUTE ISCHEMIC STROKE: ANALYSIS FROM THE ACT TRIAL
Chitapa Kaveeta1,2, Ibrahim Alhabli3, Fouzi Bala1,4, Mackenzie Horn1, Faysal Benali1, Mohammed Almekhlafi1,3,5, Aravind Ganesh1,5, Bijoy Menon1,3,5, Nishita Singh*1,6
1Cumming School of Medicine, University of Calgary, Department of Clinical Neurosciences, Calgary, Canada, 2Faculty of Medicine Siriraj Hospital, Mahidol University, Department of Medicine, Neurology Division, Bangkok, Thailand, 3Cumming School of Medicine, University of Calgary, Department of Clinical Neurosciences and Radiology, Calgary, Canada, 4University Hospital of Tours, Diagnostic and Interventional Neuroradiology Department, TOURS, France, 5University of Calgary, Department of Community Health Sciences, Calgary, Canada, 6Rady Faculty of Health Sciences, University of Manitoba, Department of Internal Medicine, Neurology Division, Winnipeg, Canada
On behalf of: The AcT Trial Investigators
Background and aims: Early ischemic changes are commonly evaluated for acute stroke decision-making. We aimed to assess the association of early ischemic changes on clinical outcomes and whether it differs between intravenous tenecteplase versus Alteplase.
Methods: Data are from the Alteplase compared to Tenecteplase (AcT) trial. Early ischemic changes were assessed using the ASPECTS. Outcomes included modified Rankin scale (mRS) 0-1 at 90 days, 24-hour symptomatic intracerebral hemorrhage (sICH), and 90-day mortality rate. Mixed effects logistic regression was used to assess the association of ASPECTS [continuous and categorical (0-4 vs. 5-7 vs. 8-10)] with outcomes and if these associations were modified by thrombolytic type after adjusting for age, sex, and baseline stroke severity.
Results: Of the 1577 patients in the trial, 901 patients (56.3%) (median age 75 years [IQR 65-84], 50.8% females, median NIHSS 14 [IQR 17-19]) with suspected anterior circulation stroke were included. mRS 0-1 at 90d was achieved in 1/14 (0.3%), 43/160 (14.7%) and 252/726 (85.1%) in the ASPECTS 0-4, 5-7 and 8-10 groups respectively. Every 1-point decrease in ASPECTS was associated with 2.7% decrease in chances of mRS 0-1 (Fig.A) and 1.9% chances of increase in mortality at 90 days (Fig.B). Thrombolytic type did not modify this association between ASPECTS and 90-day mRS 0-1 (P interaction 0.75). There was no significant interaction by thrombolytic type with any other outcome.
Conclusions: Similar to prior studies, we found that every one-point increase in ASPECTS was associated with better clinical and safety outcomes. This effect did not differ between alteplase and tenecteplase.
Disclosures of Interest: No
Abstract N°: 2449
VALUE OF INTRAVENOUS THROMBOLYSIS IN ENDOVASCULAR TREATMENT DEPENDING ON THE OCCLUDED VESSEL: RESULTS OF SIX RCTS POOLED IN IRIS
Kentaro Suzuki*1, Toshiaki Otsuka2, Fabiano Cavalcante3, Jahannes Kaesmacher4, Jan Gralla4, Manon Kappelhof3, Yuji Matsumaru5, Charles Majoie3, Urs Fischer4, Kazumi Kimura1
1Nippon Medical School Hospital, Neurology, Japan, 2Nippon Medical School, Hygiene and Public health, Japan, 3Amsterdam university medical centers, Radiology and Nuclear medicine, 4University of Bern, Diagnostic and Interventional Neuroradiology, 5Tsukuba University hospital, Neurosurgery
On behalf of: IRIS
Background and aims: Intravenous thrombolysis (IVT) before endovascular treatment (EVT) for anterior circulation large-vessel occlusion (aLVO) stroke has not been shown to be non-inferior to EVT alone. We aimed to clarify whether the effect of IVT before EVT depends on the occluded vessel.
Methods: We included patients from individual participant data meta-analysis of six randomised clinical trials comparing IVT before EVT with direct EVT (the IRIS collaboration). The main outcome was the 90-days modified Rankin Scale (mRS), analysed with mixed-effect ordinal regression models with an interaction between occlusion and IVT before EVT vs. direct EVT. Secondary outcomes were the reperfusion rate defined as extended Thrombolysis in Cerebral Infarction ⩾ 2B and intracranial haemorrhage after EVT.
Results: A total of 2291 patients were eligible for analysis and divided to two groups (1137 assigned to EVT alone and 1154 assigned to IVT plus EVT). The median age was 71 [62-78] years, 56% were male, and Occluded vessels were ICA (n=623), M1 (n=1326), and M2 (n=342). The mRS distribution was similar between the two treatment arms for any occluded vessel. The reperfusion rate after EVT was higher in patients treated with IVT plus EVT for ICA (268 [91%] vs. 249 [81%], p<0.01), but not for M1 (p=0.10) and M2 occlusions (p=0.96), with significant effect heterogeneity (p-interaction<0.01). No significant differences were observed in the rate of any and symptomatic intracranial haemorrhage.
Conclusions: Clinical outcomes were not significantly different for IVT before EVT compared to EVT alone and this finding was consistent across occlusion location.
Disclosures of Interest: No
Abstract N°: 2694
SAFETY AND OUTCOMES OF DABIGATRAN REVERSAL WITH IDARUCIZUMAB PRIOR TO IVT TREATMENT IN PATIENTS WITH ACUTE ISCHEMIC STROKE: A SITS REGISTRY STUDY
Marius Matusevicius*1,2, Malin Säflund1, Maurizio Plocco3, Alberto Chiti4, Senta Frol5, André Peeters6, Tiago Holm-Moreira1,2, Niaz Ahmed1,2
1Karolinska Institute, Department of Clinical Neuroscience, Stockholm, Sweden, 2Karolinska Universitetssjukhuset, ME Neurologi, Stockholm, Sweden, 3Policlinico di Bari, Stroke Unit, Bari, Italy, 4Nuovo Ospedale Apuane, UOC Neurologia, Marina di Massa, Italy, 5University Medical Center Ljubljana, Department of Vascular Neurology, Ljubljana, Slovenia, 6Cliniques universitaires Saint-Luc (UCLouvain), Department of Neurology and Stroke Unit, Bruxelles, Belgium
On behalf of:
Background and aims: Intravenous thrombolysis (IVT) is contraindicated in patients with acute ischemic stroke (AIS) while on dabigatran or other oral anti-coagulant treatment (OAC). Idarucizumab completely reverses the effect of dabigatran within minutes, without increasing the risk of thromboembolism. Limited data exists on IVT treatment after dabigatran reversal with Idarucizumab (DRI). We aimed to investigate the safety and outcomes of IVT after DRI in AIS patients.
Methods: We collected data on IVT treated patients from the SITS International Stroke Thrombolysis Registry. The main outcome was safety as measured by any parenchymal hematoma (PH), symptomatic intracerebral hemorrhage (SICH) per SITS, and death within 3 months. The secondary outcome was functional independence as measured by modified Rankin Scale (mRS) 0-2 at 3 months. Propensity score matching (PSM) was used to compare DRI treated patients to patients without prior OAC.
Results: Among 182692 IVT treated patients, 126 received DRI. DRI patients were older (75 vs.70 years, p<0.01), had similar median baseline NIHSS (9 vs. 9, p=0.51), and longer onset to IVT time (180 vs. 150 min, p<0.01) compared to patients without prior OAC treatment (n=175066). After PSM analysis with a good balance at baseline, patients treated with DRI before IVT had similar results in all outcomes as compared to patients without prior OAC (any PH: 3 vs 7%, p=0.52; SICH: 1 vs 1%, p=1.00; Death: 26 vs 21%, p=0.67, functional independence: 50 vs 50%, p=1.00).
Conclusions: In our observational study with AIS patients, IVT treatment after DRI was safe and had similar outcomes to IVT without previous OAC.
Disclosures of Interest: No
Abstract N°: 502
ENDOVASCULAR THERAPY IN PATIENTS WITH ACUTE INTRACRANIAL NON-TERMINAL INTERNAL CAROTID ARTERY OCCLUSION (ICA-I)
Christoph Riegler*1,2, Mirjam Rachel Heldner3, Susanne Wegener4, Sami Curtze5, Paul Nederkoorn6, João Pedro Marto7, Simon Trüssel8, Henrik Gensicke8,9, Stefan Engelter8,9, Christian Nolte1,2
1Charité – Universitätsmedizin Berlin, Corporate member of Freie Universität Berlin and Humboldt Universität zu Berlin, Department of Neurology and Experimental Neurology, Campus Benjamin Franklin, Berlin, 2Center for Stroke Research Berlin, Department of Neurology and Experimental Neurology, Campus Benjamin Franklin, Berlin, 3Inselspital Bern, University Hospital and University of Bern, Department of Neurology, Bern, Switzerland, 4University Hospital Zürich and University of Zürich, Department of Neurology, Zürich, Switzerland, 5University of Helsinki and Helsinki University Hospital, Department of Neurology, Helsinki, Finland, 6Amsterdam UMC, University of Amsterdam, Amsterdam Neuroscience, Department of Neurology, Amsterdam, Netherlands, 7Hospital de Egas Moniz, Centro Hospitalar Lisboa Ocidental, Department of Neurology, Lisboa, Portugal, 8University Hospital Basel and University of Basel, Department of Neurology, Basel, Switzerland, 9University Department of Geriatric Medicine FELIX PLATTER, University of Basel, Basel, Neurology and Neurorehabilitation, Basel, Switzerland
On behalf of:
Background and aims: Acute intracranial occlusion of the internal carotid artery (ICA) can be distinguished into (a) occlusion of the terminal ICA (ICA-L/T) and (b) non-terminal intracranial ICA occlusion (ICA-I). While ICA-L/T occlusion patients were included in most trials on endovascular therapy (EVT), data on ICA-I occlusion is scarce. We assessed effectiveness and safety of EVT in ICA-I compared to ICA-L/T patients.
Methods: EVATRISP, a large multicenter cohort was searched for EVT-treated patients with intracranial ICA occlusion between 2014 and 2023. Patients were stratified differentiating ICA-I and ICA-L/T occlusion. We analyzed technical outcome (modified thrombolysis in cerebral infarction (mTICI) scale), functional outcome (modified Rankin scale [mRS] at three months) and rates of intracranial hemorrhage (ICH).
Results: Of 13,453 EVATRISP patients, 1825 (13.6%) had isolated intracranial ICA occlusion. ICA-occlusion pattern was ICA-I in 559 (4.2%) and ICA-L/T in 1266 (9.4%) patients. Age (years: 74 vs. 73), sex (female: 45.8% vs. 49.0%) and pre-stroke functional independency (pre-mRS⩽2: 89.9% vs. 92.2%) did not differ between groups. Stroke severity was lower in ICA-I patients (NIHSSadmission 14 [7-19] vs. 17 [13-21] points). EVT was similarly successful with respect to technical (mTICI2b/3: 76.1% (ICA-I) vs. 76.6% (ICA-L-/T); aOR 1.01 [0.76 – 1.35]) and functional outcome (mRS ordinal shift: aOR 1.01 [0.83 – 1.23]. Rates of ICH (18.9% vs. 34.5%; aOR 0.47 [0.36 – 0.62] and symptomatic ICH (4.7% vs. 7.3%; aOR 0.58 [0.35 – 0.97] were significantly lower in ICA-I patients.
Conclusions: EVT can be performed safely and similarly successful in patients with intracranial but non-terminal ICA occlusion as in patients with ICA-L/T occlusion.
Disclosures of Interest: No
Abstract N°: 2234
UNSUCCESSFUL RECANALIZATION VERSUS MEDICAL MANAGEMENT OF PATIENTS WITH LARGE ISCHEMIC CORE
1Beijing Tiantan Hospital, Capital Medical University, 2Boston Medical Center, 3Beijing Anzhen Hospital, Capital Medical University
On behalf of: Mengxing Wang, PhD, Hesham E. Masoud, MD, Alice Ma, MBBS, Xu Tong, MD, Gaoting Ma, MD, Xuan Sun, MD, Ligang Song, MD, Ning Ma, MD, Feng Gao MD, Dapeng Mo, MD, On belf of ANGEL-ASPECT study group
Background and aims: The outcomes of patients with large ischemic core who fail to recanalize with endovascular therapy (EVT) compared to medical management (MM) are uncertain. The objective was to evaluate the clinical and safety outcomes of patients who underwent EVT in patients with large ischemic core and unsuccessful recanalization.
Methods: This was a post-hoc analysis of the ANGEL-ASPECT randomized trial. Unsuccessful recanalization was defined as patients who underwent EVT with eTICI 0-2a. The primary endpoint was 90-day very poor outcome (mRS 5-6). Multivariable logistic regression was conducted controlling for ASPECTS, occlusion location, intravenous thrombolysis, and time to treatment.
Results: Of 455 patients, 225 were treated with MM. Of 230 treated with EVT, 43 (19%) patients had unsuccessful recanalization. There was no difference in 90-day very poor outcomes (39.5% vs. 40%, aOR 0.93, 95%CI 0.47-1.85, p=0.95), sICH (7.0% vs. 2.7%, aOR 2.81, 95%CI 0.6-13.29, p=0.19), or mortality (30% vs. 20%, aOR 1.65, 95%CI 0.89-3.06, p=0.11) between the unsuccessful EVT and MM groups, respectively. There were higher rates of ICH (55.8% vs. 17.3%, p<0.001), infarct-core volume growth (142.7ml vs. 90.5 ml, β=47.77, 95%CI 20.97-74.57ml, p<0.001), and decompressive craniectomy (18.6% vs. 3.6%, p<0.001) in the unsuccessful EVT versus MM group.
Conclusions: In a randomized trial of patients with large ischemic core undergoing EVT with unsuccessful recanalization, there was no difference in very poor outcomes, sICH or death versus medically managed patients. In the unsuccessful EVT group, there were higher rates of any ICH, volume of infarct-core growth, and decompressive craniectomy.
Disclosures of Interest: No
Abstract N°: 563
EFFECTIVENESS OF PROXIMAL BALLOON OCCLUSION VERSUS DISTAL FILTER FOR EMBOLIC PROTECTION DURING CAROTID ARTERY STENTING
Seung Young Chung*1, Jae Guk Kim2
1Daejeon Eulji Medical Center, Eulji University School of Medicine, Department of Neurosuregery, Daejeon, South Korea, 2Daejeon Eulji Medical Center, Eulji University School of Medicine, Department of Neurology, Daejeon, South Korea
On behalf of:
Background and aims: CAS is rapidly alternative to CEA and even more effective for high-risk cases. The main concern is preventing procedural embolus dislodgement and so preventative embolic protection devices (EPDs) have significantly improved prognosis.
Methods: This retrospective study included all 106 patients with symptomatic or asymptomatic ICA stenosis ⩾70% treated with CAS with either of 2 EPDs: distal filter protection device (DFP) or proximal balloon occlusion device (PBO). All underwent pre- and post DWI to detect new ischemic lesions. We compared clinical outcomes and postprocedural embolization rates in both.
Results: In 111 cases with CAS, DFP success rate was 98.4% and subsequent DWI revealed 249 new ischemic lesions in 81%. In contrast, PBO was 91.4% and 71 new ischemic lesions in 58%. No differences were observed in success rate. PBO resulted in lower new ischemic lesions (p=0.031). PBO also showed fewer total new ischemic lesions (p=0.002) and new ischemic lesions per patient (p=0.027). And in ⩾3 new ischemia, significantly lower rate in PBO (p=0.002). In the subtype of stent, there is no significant interaction effect between stent and EPDs and type of stent also did not affect the number of new ischemic lesions. Complications occurred in 1 for DFP and 3 for PBO but all improved.
Conclusions: The incidence of postprocedural ischemic lesions was lower in PBO than DFP. And the total number and new ischemic lesions per patient on DWI were also lower in PBO. So, as compared with DFP, PBO might be more effective in reducing cerebral embolism during CAS.
Disclosures of Interest: No
Moderated Poster – Clinical Trials – Day 1
Abstract N°: 1600
EFFECT OF EARLY ANTIHYPERTENSIVE TREATMENT IN ACUTE ISCHEMIC STROKE BY RENAL FUNCTION – A SUBGROUP ANALYSIS OF THE CATIS-2 TRIAL
1The Second Affiliated Hospital of Xi'an Jiaotong University, Department of Neurology, Xi'an, China, 2Beijing Tiantan Hospital, Capital Medical University, Department of Neurology, Beijing, China, 3Department of Medical Administration, Suzhou Industrial Park Medical and Health Management Center, Suzhou, China, 4Tulane University Translational Science Institute, New Orleans, United States
On behalf of: for the CATIS-2 Investigators
Background and aims: It is unclear whether antihypertensive treatment should be administrated individually by different renal function in acute ischemic stroke. We conducted a subgroup analysis of CATIS-2 trial to investigate the effect of early antihypertensive treatment in acute ischemic stroke by baseline renal function.
Methods: CATIS-2 trial was a randomized multicenter clinical trial comparing the effect of early antihypertensive treatment stared within 24-48 hours of stroke versus delayed treatment until day 8. In this subgroup analysis, the effect of early antihypertensive therapy on dependency or death at 90 days were assessed by different estimated glomerular filtration ratio (eGFR) values (<90 vs ⩾90 mL/min per 1.73 m2).
Results: 4685 patients were enrolled in final analysis, 1061 patients had impaired renal function (eGFR <90), 3624 patients had normal renal function (eGFR ⩾90). Among impaired renal function patients, early antihypertensive treatment significantly increased the risk of dependency or death at 90 days (61.6% vs 38.4%, OR 0.64, 95% CI 0.44-0.93, P=0.02). However, in patients with normal renal function, there was no significant difference (50.8% vs 49.2%, OR 0.94, 95% CI 0.76-1.17, P=0.63), P for interaction was 0.07.
Conclusions: In acute ischemic stroke patients with impaired renal function, early antihypertensive treatment was associated with an increased risk of functional dependency or death at 90 days.
Disclosures of Interest: No
Abstract N°: 2747
EFFICACY AND SAFETY OF APIXABAN IN THE TREATMENT OF CEREBRAL VENOUS SINUS THROMBOSIS: A MULTI-CENTRE STUDY
Naaem Simaan*1, Issa Metanis2, Asaf Honig2, Andrei Filioglo2, Ronen R Leker2, Jeremy Molad3
1Ziv Medical Center - Israel, Neurology - stroke unit, 2Hadassah medical center, 3Department of Neurology & Stroke, Tel-Aviv Sourasky Medical Center, Tel-Aviv, Israel.
On behalf of:
Background and aims: Information regarding the safety and efficacy of specific direct oral anticoagulants (DOAC) in the treatment of cerebral sinus and venous thrombosis (CSVT) is scarce. Apixaban is one of the most frequently-prescribed DOACs.
Therefore, we aimed to compare the safety and efficacy of Apixaban with those of vitamin k antagonists (VKA) in patients with CSVT
Methods: Prospective CSVT databases from seven academic medical centers were retrospectively analyzed. Patients treated with Apixaban were compared to those treated with VKA. Data on demographics, clinical presentations, risk factors, radiological and outcome parameters were studied
Results: Overall, 403 patients were included in the analysis. Of them, 48 (12%) were treated with Apixaban, and 355 (88%) were treated with VKA. Rates of coagulopathies were significantly higher in the VKA-treated patients but no other differences between the groups were found in baseline characteristics and underlying etiology. No significant differences were found between groups in efficacy or safety parameters including the rates of recanalization, favorable outcomes, one-year mortality, seizures, intracranial hemorrhage or CSVT recurrences
Conclusions: Our data suggests that Apixaban may be safe and effective for patients with CSVT. These results should be tested in prospective randomized clinical studies.
Disclosures of Interest: No
Abstract N°: 2761
A REAL-WORLD STUDY TO ASSESS THE EFFECTIVENESS OF EDARAVONE DEXBORNEOL IN ACUTE ISCHEMIC STROKE: BASELINE CHARACTERISTICS AND PRELIMINARY RESULTS
1Xuanwu Hospital, Capital Medical University, Department of Neurology, China, 2Xuanwu Hospital, Capital Medical University, Department of Evidence-Based Medicine
On behalf of:
Background and aims: Edaravone dexborneol is a novel brain cytoprotection agent by acting on multiple active targets of antioxidation and anti-inflammation. We report preliminary results from a prospective, two-arm, parallel, cohort study (EXPAND) assessing the effectiveness of Edaravone dexborneol in acute ischemic stroke (AIS).
Methods: The study was conducted at 72 hospitals in China between December 2022 to October 2023. Eligible patients were diagnosed as AIS, ⩾18 years, within 14 days of onset, modified Rankin Scale (mRS) score of 0-1 prior to onset. Patients were divided into exposed/unexposed group with a 2:1 ratio based on the use of Edaravone dexborneol. One of the efficacy endpoints was the change of National Instituted of Health Stroke Scale (NIHSS) score from baseline to discharge.
Results: A total of 4684 patients were recruited and divided to the exposed (n=3197) or the unexposed group (n=1487). The median baseline NIHSS score was higher in the exposed group compared with the unexposed group (4 [2-7] vs. 3 [1-6]). The rate of revascularization treatment was 39.30% and 31.29% in the exposed and unexposed group respectively. The NIHSS score changed from baseline to discharge was -2.26 (95% CI, -2.41 to -2.10) in the exposed group and -1.76 (95% CI, -1.99 to -1.52) in the unexposed group.
Conclusions: EXPAND is the first real-world study to elucidate the effectiveness and safety of edaravone dexbornel in AIS. The preliminary results show that Edaravone dexborneol might improve NIHSS score change with further data expected from this study.
Trial registration number: NCT05644223.
Disclosures of Interest: No
Abstract N°: 2209
EFFICACY OF ENDOVASCULAR THERAPY IN PATIENTS WITH LARGE INFARCT BY THE INTERHOSPITAL-TRANSFER STATUS
1Beijing Tiantan Hospital, Capital Medical University
On behalf of:
Background and aims: The benefit of endovascular therapy (EVT) has been proved in patients with large infarct, but it’s unknown whether the benefit would be affected by interhospital-transfer.
Methods: This was a subgroup analysis of the ANGEL-ASPECT randomized controlled trial. Patients with acute anterior-circulation large vessel occlusion (LVO) and large infarct, defined as an ASPECT score of 3-5 or an infarct-core volume of 70-100mL, were enrolled and randomly assigned to receive EVT or medical treatment (MM) alone. We dichotomized patients into direct and transfer subgroup, based on whether they were admitted directly to the comprehensive stroke center or transferred from a primary center. Primary outcome was the 90-day modified Rankin Scale (mRS) score.
Results: Among 455 patients enrolled, 210 (46.2%) and 245 (53.8%) were in the direct and transfer subgroup, respectively. Transfer patients had longer median onset-to-recanalization time than the direct ones (626 vs. 515mins, p=0.03), while there was no significant difference in the image-to-puncture time (155 vs. 161mins, p=0.30), or puncture-to-recanalization time (75 vs. 75mins, p=0.86) between the two subgroups. A significant ordinal shift of 90-day mRS towards a better functional outcome in EVT than MM was found in both the direct subgroup (generalized OR, 1.67; 95% CI,1.03-2.70; p=0.04) and the transfer subgroup (1.60; 1.02-2.50; 0.04). There was no significant interaction of the two subgroups over the treatment effect of EVT versus MM on the primary outcome (p=0.71).
Conclusions: In acute anterior-circulation LVO patients with large infarct, the benefit of EVT compared to MM did not vary by the interhospital transfer status.
Disclosures of Interest: No
Abstract N°: 2779
ADJUNCTIVE INTRA-ARTERIAL TENECTEPLASE VS STANDARD OF CARE FOLLOWING MECHANICAL THROMBECTOMY: ANALYSIS OF ALLY PILOT TRIAL
Hisham Alhajala1, Rahul Rao1, Mouhammad Jumaa1, Alicia C. Castonguay1, Richard Burgess1, Sunil Sheth2, Ashutosh Jadhav3, Diogo C. Haussen4, Osama Zaidat5, Syed Zaidi*1
1University of Toledo, Neurology, Toledo, United States, 2University Of Texas Medical School At Houston, Houston, United States, 3Barrow Neurological Institute, Phoenix, United States, 4Emory University Hospital, Atlanta, United States, 5Mercy Health - St. Vincent Medical Center Emergency Department, Toledo, United States
On behalf of:
Background and aims:The ALLY pilot study (clinicaltrials.gov identifier:NCT05172934) assessed the safety of intra-arterial tenecteplase (IA-TNK) in patients undergoing mechanical thrombectomy (MT) with post-treatment TICI 2b or 2c recanalization. In this study, we compare the outcomes of the ALLY patients with age matched control treated during the study period.
Methods: The ALLY inclusion criteria entailed stroke patients between 18-85 years with stroke due to intracranial ICA, MCA M1 or M2 occlusion who underwent mechanical thrombectomy and achieved TICI reperfusion of 2b/2C. These patients received at least one dose of 1.5 mg IA-TNK (max 4.5 mg). We compared ALLY patient outcomes to age-matched controls who also achieved TICI 2b/2c reperfusion. The control patients didn’t receive post MT lytic treamtent. Data abstracted includes demographics, treatment times/modalities, 24-hours and 90-days outcome. The study outcomes include rate of symptomatic ICH within 24hr and 90 days functional outcome.
Results: We compared the ALLY study patients who received adjunctive IA-TNK to 62 controls treated during the study period. The mean age was 66 and 68.7 for IA-TNK and control groups, respectively. Baseline characteristics including comorbidities, NIHSS, ASPECT score, and occlusion sites were comparable between the two groups. The 24-hour SICH rate (5% vs 8%) was comparable. At 90 days, 50% of ALLY group achieved functional independence (mRS 0-2) compared to 39.2% controls (p 0.4).
Conclusions: The ALLY pilot study results show that IA-TNK upto 4.5 mg following MT for residual clots is safe and may lead to improved clinical outcomes when compared to standard MT.
Disclosures of Interest: No
Abstract N°: 1013
TENECTEPLASE COMPARED TO ALTEPLASE IN THE EARLY WINDOW IN ACUTE ISCHAEMIC STROKE: META-ANALYSIS OF RANDOMISED CONTROLLED TRIALS
Ammad Mahmood*1, Keith Muir1
1University of Glasgow, School of Neuroscience and Psychology, Glasgow, United Kingdom
On behalf of:
Background and aims: Several trials have shown non-inferiority or superiority of tenecteplase 0.25mg/kg compared to alteplase 0.9mg/kg in acute ischaemic stroke (AIS) patients treated <4.5 hours from onset. We carried out a meta-analysis of published trial results.
Methods: Medline and EMBASE databases were searched for randomised controlled trials comparing intravenous tenecteplase 0.25mg/kg to alteplase 0.9mg/kg for AIS treated <4.5hrs from symptom onset. Data were collected on functional outcome measured by modified Rankin Scale (mRS), rate of symptomatic intracranial haemorrhage (sICH - as per individual trial definition) and mortality. Random-effects binary outcome meta-analysis was carried out.
Results: We identified 9 trials (including one presented but unpublished), totalling 5417 participants. Tenecteplase 0.25mg/kg was superior to alteplase 0.9mg/kg in achieving excellent outcome (mRS 0-1; OR 1.15 (1.03-1.28) p=0.01); but not functional independence (mRS 0-2; OR 1.19 (1.00-1.41) p=0.05). There was no significant difference between treatments with respect to mortality (OR 0.96 (0.78-1.18) p=0.70); or rate of sICH (OR 1.11(0.78-1.58) p=0.57). A sensitivity analysis excluding two trials using a tenecteplase bio-copy showed superiority of tenecteplase for functional independence (OR 1.29 (1.01-1.66) p=0.04); but not excellent outcome (OR 1.14 (1.00-1.30) p=0.05).
Conclusions: In meta-analysis of aggregate trial data, tenecteplase 0.25mg/kg was superior to alteplase in achieving mRS 0-1, exhibited a strong trend towards superiority for mRS 0-2, and did not significantly modify mortality or SICH incidence. Excluding trials of the tenecteplase bio-copy showed significant benefit for mRS 0-2 and trend for mRS 0-1.
Disclosures of Interest: Yes KM is Chief Investigator of ATTEST2 funded by the Stroke Association and British Heart Foundation and supported by Boehringer Ingelheim and UK CI for the TEMPO-2 trial supported by Canadian Institute of Health Research and British Heart Foundation
Moderated Poster – Diagnosis and Imaging – Day 1
Abstract N°: 505
IMPACT OF THROMBUS CHARACTERISTICS ON OUTCOME IN PATIENTS WITH BASILAR ARTERY OCCLUSION: A POST HOC ANALYSIS OF THE BASICS TRIAL
Martin Arndt*1, Kristian Barlinn1, Patrik Michel2, Lucianne Langezaal3, Fabrício Oliveira Lima4, Francisco Mont'alverne4, Wim Van Zwam5, Albert Yoo6, Wouter Schonewille3, Volker Puetz1
1University Hospital Carl Gustav Carus Dresden, Neurology, Dresden, Germany, 2Lausanne University Hospital, Neurology Service, Lausanne, Switzerland, 3St. Antonius Hospital, Department of Neurology, Nieuwegein, Netherlands, 4Fortaleza General Hospital, Neurointerventional Service, Brazil, 5Maastricht UMC+, Department of Radiology and Nuclear Medicine, Maastricht, Netherlands, 6Texas Stroke Institute, Department of Radiology, Dallas-Fort Worth, United States
On behalf of: BASICS study group
Background and aims: Endovascular therapy (EVT) is an effective treatment for patients with basilar artery occlusion (BAO). We assessed the impact of thrombus characteristics and extent as predictors of treatment response and outcome in the randomized BASICS trial.
Methods: We analyzed presence of hyperdense basilar sign, length of basilar thrombus and thrombus extent as determined with a novel semiquantitative 10-point basilar artery Clot-Burden-Score (BA-CBS, where 10 is best and 0 worst), based on review by imaging core lab. We utilized ROC-analysis to stratify cut-off values and performed multivariable analysis to test for an association of imaging parameters with favorable outcome (mRS 0-3).
Results: Among 282 patients with complete imaging data (median age 69 [IQR 60-76], NIHSS 22 [IQR 11-35], 226 IVT [80.1%], 145 EVT [51.4%]), median thrombus length was 9.5mm (IQR 5-17), median BA-CBS was 7 (IQR 5-8), and 135 patients (47.8%) had hyperdense basilar sign. In ROC-analysis, thrombus length >7.5mm (AUC 0.64; p=0.001) and BA-CBS >6.5 (AUC 0.62, p=0.001) were most discriminative for outcome. Multivariable analysis revealed that only thrombus length >7.5mm (OR 0.51, 95%CI 0.26-0.97), age (OR 0.97, 95%CI 0.95-1.00), baseline NIHSS (OR 0.91, 95%CI 0.89-0.94), and IVT (OR 2.61, 95%CI 1.07-6.37) were associated with favorable outcome, whereas EVT was not (OR 1.27, 95%CI 0.67-2.38). Hyperdense basilar sign and BA-CBS were not associated with favorable outcome in multivariable analysis.
Conclusions: Basilar artery thrombus length >7.5mm was associated with worse outcomes among patients in the BASICS trial. IVT appears to benefit patients even with extensive basilar artery thrombi.
Disclosures of Interest: No
Abstract N°: 753
PREDICTION OF THROMBECTOMY OUTCOMES USING PERFUSION PROFILE OF ELOQUENT BRAIN REGIONS: A MULTICENTER STUDY
Haipeng Li*1, Ho Ko1, Sangqi Pan1, Lt Lui2, Trista Hung1, Vincent Ct Mok1, Wai Hong Thomas Leung1, Hao Wang3, Yuan Che Fung3, Bonaventure Ym Ip1
1Division of Neurology, Department of Medicine and Therapeutics, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR, China, 2Department of Electrical Engineering, Faculty of Engineering, City University of Hong Kong, Hong Kong SAR, China, 3Department of Neurology, Linyi People’s Hospital, Linyi, Shandong Province, China
On behalf of: Chun Ngo Yau, Edward Hui, Xinyi Leng, Jill M. Abrigo, Bonnie Y. K. Lam, Rosa H. M. Chan
Background and aims: Pivotal endovascular thrombectomy (EVT) for acute large vessel occlusion (LVO) based on clinical-core and core-penumbra mismatch were suboptimal in predicting EVT outcomes. Hypothesizing that the perfusion status of eloquent brain regions is more crucial than the overall cerebrum in post-EVT prognostication, we aimed to determine EVT outcomes in patients with critical hypoperfusion in pre-specified eloquent brain regions.
Methods: In this multicentre retrospective study, we retrieved patients with acute middle cerebral artery or internal carotid artery occlusion who received CT perfusion (CTP) before EVT from 4 hospitals in Hong Kong and mainland China from 01/2020 to 08/2023, excluding patients with angiographic results of mTICI < 2b. Employing a custom-developed pipeline (Figure-1) with SVD and tensor-total-variation-regularization, along with SynthSeg2.0-based whole-brain segmentation, we automatically generated perfusion profiles for 34 brain regions, focusing on a priori set for regional analysis, including the primary-motor/sensory cortex, pallidum, sub-motor/sensory cortical-white-matter, internal capsule, etc. We assessed the association between the regional-infarct-core-fraction (regional infarct-core to regional volume ratio) and poor functional recovery (mRS > 4) using multivariate logistic regression adjusted for infarct-core volume, ASPECTS score, collateral score and onset-to-puncture time.
Results: Among 242 identified acute LVO patients, 68 (28.1%) had poor functional recovery despite successful EVT. Multivariate logistic regression revealed regional-infarct-core-fraction in primary-motor cortex (aOR=19.95, p=0.039), pallidum (aOR=9.46, p=0.05), and sub-motor cortical-white-matter (aOR=16.48, p=0.049) were associated with poor functional recovery independent of other control factors.
Conclusions: Automated processing of regional brain perfusion parameters is feasible with CTP scans. The eloquent brain regions may significantly improve the prognostic accuracy of successful EVT. (NCT05578300)
Disclosures of Interest: No
Abstract N°: 2688
THE DIAGNOSTIC YIELD OF ACUTE CARDIAC CT FOR DETECTION OF HIGH-RISK CARDIOEMBOLIC SOURCES IN ACUTE ISCHEMIC STROKE PATIENTS: A SYSTEMATIC REVIEW
Aletta Goedman*1, Shan Sui Nio1, Leon Rinkel1, R. Nils Planken2, Jonathan Coutinho1
Background and aims: Cardiac CT performed in the acute imaging protocol in ischemic stroke patients is a promising alternative to echocardiography for the detection of cardiac sources of embolism.
Methods: We conducted a systematic review, including literature on acute cardiac CT for the detection of high-risk cardioembolic sources. We included studies in which cardiac CT was performed as part of the acute stroke imaging protocol, and data on the detection of high-risk cardioembolic sources were reported. Outcomes of interest were the number of detected high-risk cardioembolic sources, the additional radiation exposure and administered contrast.
Results: We included fourteen studies (2016-2023), encompassing 2081 patients. This included two case-control and twelve cohort studies. All studies were single center. Cardiac CT identified 259 high-risk sources in 243/2081 (12%) patients. Cardiac thrombi were most often detected (230/259 (89%)) and were located in the left atrial appendage (177/230 (77%)), left ventricle (34/230 (15%)) and left atrium (6/230 (3%)). Among all patients, 512/2081 (25%) had known atrial fibrillation and cardiac CT detected a cardiac thrombus in 144/512 (28%) of these patients. Studies comparing echocardiography and cardiac CT found a higher proportion of high-risk sources on cardiac CT (60/164 (37%) vs. 104/164 (63%)). In eight studies, additional contrast was administered for the cardiac CT, and mean additional radiation exposure ranged from 0.91 millisievert (mSv) to 13.5 mSv.
Conclusions: Cardiac CT performed in the acute phase may have a higher diagnostic yield than echocardiography for the detection of high-risk cardioembolic sources, but larger, prospective, multi-center studies are warranted.
Disclosures of Interest: No
Abstract N°: 2822
PERFUSION VARIABLES PREDICT EARLY NEUROLOGICAL DETERIORATION IN MILD STROKE WITH LARGE VESSEL OCCLUSION OR SEVERE STENOSIS
1Huashan Hospital, Department of Neurology, National Center for Neurological Disorders, National Clinical Research Centre for Aging and Medicine, Shanghai, China
On behalf of:
Background and aims: Acute ischemic stroke (AIS) Patients with mild symptoms due to large vessel occlusion (LVO) or severe stenosis have risk of early neurological deterioration (END). This study aimed to identify the optimal imaging markers to predict the occurrence of END in this population.
Methods: This multicentric retrospective study included AIS patients between 2015 and 2023, presenting within 24 hours from last known well, with a baseline National Institutes of Health Stroke Scale score (NIHSS)⩽5 and anterior circulation LVO or severe stenosis. Patients who underwent endovascular treatment before END were excluded. END was defined as an increase of NIHSS⩾4 points within 72 hours without evidence of parenchymal hemorrhage.Clinical data and imaging parameters based on CTA and CTP within 24 hours from last known well were measured.
Results: 143 AIS patients with mild symptoms due to anterior circulation LVO or severe stenosis were included and END occurred in 18% of the participants. END was more frequently occurred among patients with internal carotid artery (ICA) occlusion/severe stenosis (53.8%). Severe hypoperfusion volume (volume of delay Time [DT] >6 seconds) on CTP were associated with END in univariable logistic regression and larger severe hypoperfusion volume is an independent predictor of END after adjusted baseline NIHSS and occlusion/stenosis sites (adjusted OR: 1.02, 95%CI:[1.00,1.04], P=0.026).
Conclusions: AIS patients with mild symptoms due to anterior circulation LVO/severe stenosis, experiencing END more frequently had ICA occlusion/severe stenosis and presented larger severe hypoperfusion volume. Moreover, larger severe hypoperfusion volume is an independent predictor of END.
Disclosures of Interest: No
Abstract N°: 3146
MULTICENTER STUDY ON THE FREQUENCY OF LARGE VESSEL OCCLUSION (LVO) IN PATIENTS WITH MINOR ISCHEMIC STROKE IN VALENCIAN COMMUNITY (SPAIN)
Pablo Ros-Arlanzón*1,2, Carlos Aledo-Sala1,2, Diego Corona-García1,2, Luis Moreno-Navarro1,2, Mònica Farrerons-Llopart1,2, Pau Mahiques-Ochoa1,2, Manuel Warnken-Miralles1,2, Raquel Hernández-Lorido1,2, Isabel Beltrán-Blasco1,2, Nicolas López-Hernández1,2
1General University Hospital of Alicante, Neurology, Alacant, Spain, 2Instituto de Investigación Sanitaria y Biomédica de Alicante (ISABIAL), Alicante (Alacant), Spain
On behalf of: CODICT Study Group: Elisa Gines-Murcia, Carlos Lapeña-López, Cristina Soriano, José Tembl Ferrairo
Background and aims: This study addresses the significant challenge in diagnosing and treating minor ischemic stroke, where controversies persist regarding the use of CT angiography and endovascular treatment (EVT). It aimed to ascertain LVO frequency in minor strokes, map LVO locations within the vascular tree, and evaluate patient management and the outcomes of therapeutic choices.
Methods: A multicenter registry analysis was conducted, involving three comprehensive stroke centers in Valencian Community (Spain) from 01/07/2020 to 30/11/2023. All patients with minor ischemic stroke (NIHSS ⩽ 5) underwent multimodal CT studies. LVO was defined as occlusion in the internal carotid, vertebral, basilar, middle cerebral artery (MCA) segments M1 and M2, anterior cerebral artery (ACA) segments A1 and A2, and posterior cerebral artery (PCA) segments P1 and P2.
Results: Out of 5474 Stroke Alerts during the study period, 919 patients experienced a minor ischemic stroke. 16.2% (n=149) of these cases showed a LVO on CT angiography. 44.3% of patients with minor stroke and LVO underwent EVT. The most frequently occluded vessel was the MCA in its M2 segment (n=55), followed by the M1 segment (n=54). However, the M1 segment was the most frequently treated by EVT (n=43), followed distantly by M2 (n=16).
Conclusions: This study emphasizes the necessity of multimodal CT scans for all Stroke Alert patients, irrespective of clinical severity. LVO changed clinical management for about half of the patients, underscoring the need for thorough evaluation and possible intervention in minor strokes, and affirming the value of advanced imaging in treatment planning.
Disclosures of Interest: No
Abstract N°: 1201
CT PERFUSION PATTERNS IN STROKE MIMIC DIAGNOSIS: IMPLICATIONS FOR INTRAVENOUS THROMBOLYSIS
Cristina Sanabria Gago*1, Esther Valiente1, Alicia Gonzalez-Martinez1, Sara Lozano Veiga1, Carmen Sánchez-Rodríguez1, Javier Collada Carrasco2, Celia Alonso2, Donna Zhan Chen2, Juan Vega3, Santiago Trillo Senin1
1Hospital de La Princesa, Neurology Department, Madrid, Spain, 2Hospital de La Princesa, Radiology Department, Madrid, Spain, 3Hospital de La Princesa, Interventional Neuroradiology Service, Madrid, Spain
On behalf of:
Background and aims: Perfusion CT (CTP) in stroke code (SC) can exclude ischemia in stroke mimics (SM), occasionally revealing distinctive alterations. The aim of this study is to identify specific patterns in CTP associated with specific etiologies of SM, and assess whether CTP results influence the administration of IV thrombolysis (IVT).
Methods: A retrospective single-center analysis of SC cases attended between January/2015-December/2021, involving evaluable CTP and a SM diagnosis. We examined the association between CTP patterns and the etiological subtypes of SM, as well as the correlation between CTP results and IVT administration.
Results: Out of 3814 SC cases, 15.8% were SM. 572 were finally included with assessable CTP. Mean age 65y(SD:18.29), with 48.3% women. Altered CTP was observed in 184 cases (32.2%), with seizures 105(57.1%), PRES 16(8.7%), status epilepticus(SE) 21(11.4%), and migraine 8(4.3%). Altered CTP was significantly associated with PRES (55.26%, p=0.01); SE(55.17%, p=0.002) and seizures (48.85%, p<0.001). Seizures were associated with a decreased flow (p=0.003) and increased time in TCP (p=0.001), focal non-vascular alteration (p<0.001), hemispheric (p=0.002), multifocal (p=0.030) and parietal lobe (71.31%, p<0.001) alteration. SE correlated with an increase in flow maps (0=0.029) and volume maps (p=0.030) in parietal area (85.71 %, p=0.024). PRES associated with time delay (p=0.042) and occipital area alteration(82.35 %, p=0.002). Among 231(40.4%) candidates for IVT, only 17(3%) received it, being more frequent with TCP altered (64.7%, p=0.002).
Conclusions: CTP reveals suggestive alterations of SM in 30% of cases. Identifiable patterns for etiologies include parietal involvement in seizures/SE and occipital alterations in PRES. CTP would contribute to avoid IVT in SM patients, especially when it indicates alterations.
Disclosures of Interest: No
Abstract N°: 2731
THREE-YEAR FOLLOW-UP IMAGING AND QUALITY OF LIFE EVALUATION AFTER ENDOVASCULAR TREATMENT FOR ACUTE ISCHEMIC STROKE PATIENTS
Praneeta R Konduri*1,2, Dimitrios Karkalousos1, Stefan Roosendaal2, Maarten Lahr3, Chi Nguyen3, Henk Marquering1,2, Charles Majoie2, Bart Emmer2, Luka Liebrand1, Matthan Caan1
1Amsterdam UMC - location University of Amsterdam, Biomedical Engineering and Physics, Amsterdam, Netherlands, 2Amsterdam UMC - location University of Amsterdam, Radiology and Nuclear Medicine, Amsterdam, Netherlands, 3University Medical Center Groningen, Epidemiology, Groningen, Netherlands
On behalf of: the MR CLEAN-NO IV Investigators
Background and aims: Long term (>36 months) changes within and remote to the 24-hour stroke lesion and their influence on Quality of Life (QoL) are understudied. We hypothesize that quantitative MRI metrics can detect differences between ipsi- and contra-lateral region-of-interests (ROIs) and that these are associated with long-term QoL.
Methods: In 62 patients from the MR CLEAN-NO IV trial, early stroke lesion was identified on standard MRI (DWI, FLAIR, SWI) 24 hours post-EVT. Twenty-four of these patients underwent a comprehensive 3T MRI protocol after 37 (IQR: 28-38) months to quantify long term white-matter microstructure damage (R-1 mapping, Fractional Anisotropy (FA)), iron deposition (R2*), and local volume changes within/remote to the early lesion relative to a contralateral ROI. NIHSS was derived at baseline. A combined QoL score was derived using the EQ5D5 questionnaire. Bayesian analysis was used to evaluate differences between ipsi- and contralateral ROIs (Bayes Factor(BF)<3:no/weak;BF>3:moderate;BF>10:strong evidence) and association between MRI and NIHSS/QoL-metrics.
Results: All patients had a lesion at 24-hours in line with their baseline occlusion and treatment characteristics. White matter microstructural degradation was observed in an ipsilateral ROI (ΔR1=-0.036±0.037, BF=2.7*102, ΔFA=0.011±0.074, BF=0.28). Increased iron deposition and lower ipsilateral basal ganglia volume were observed. Baseline NIHSS was associated with lower caudate and pallidum volume (BF=20,BF=4.4) and higher iron deposition in the pallidum (BF=6.7). Lower hippocampus volume and higher iron deposition were associated with QoL (BF=11, BF=5.5).
Conclusions: There is moderate-to-strong evidence for long term lateralized demyelination, iron deposition and atrophy within/remote from the early lesion affecting QoL.
Disclosures of Interest: Yes PK:co-founder, share holder-inSteps.HM:co-founder, shareholder-Nico.lab, Trianect, inSTeps.CM: funds from EU Commission, CVON/Dutch Heart Foundation, Stryker, TWIN Foundation, Health Evaluation Program Netherlands, shareholder-Nico.lab.MC:shareholder-Nico.lab.
Abstract N°: 1424
RISK OF STROKE ASSOCIATED WITH CEREBRAL MICROBLEEDS IN DIFFERENT SUBTYPES OF ISCHEMIC STROKE AND TIA
Annaelle Zietz*1,2, Yannie, Oi Yan Soo3, Vincent Ct Mok3, Winnie Chu4, Alexandros Polymeris1, David Seiffge5, Philip Nash6, David Werring6, Stefan Engelter1,2, Nils Peters1,2,7
1University Hospital Basel and University of Basel, Department of Neurology and Stroke Center, 2University Department of Geriatric Medicine Felix Platter, University of Basel, Neurology and Neurorehabilitation, 3Prince of Wales Hospital, The Chinese University of Hong Kong, Hong Kong, Division of Neurology, Department of Medicine and Therapeutics, 4The Chinese University of Hong Kong., Department of Imaging and Interventional Radiology, 5University Hospital Inselspital Bern, University of Bern, Department of Neurology, 6UCL Queen Square Institute of Neurology, London, UK, Stroke Research Centre, Department of Brain Repair and Rehabilitation, 7Klinik Hirslanden, Zürich, Switzerland, Stroke Center
On behalf of: MICON collaborators
Background and aims: In patients with ischemic stroke or TIA, cerebral microbleeds (CMBs) are associated with an increased risk of recurrent ischemic stroke (IS) and intracerebral hemorrhage (ICH). However, little is known about whether this risk varies among different stroke etiologies.
Methods: We performed a sub-analysis from the Microbleeds International Collaborative Network (MICON) pooled individual patient data cohort on patients with IS and available index etiology based on the TOAST classification. The primary outcome was the composite of IS or ICH during follow-up, the secondary outcome was the stroke subtype respectively. We used a Cox regression hazard model to compare the impact of CMBs in different stroke etiologies adjusted for potential confounders.
Results: We included 12133 patients with available TOAST classification. In cardioembolic stroke, CMBs were associated with the primary outcome (aHR [95%-CI] 1.49 [1.18-1.89], p = 0.001) and ICH (aHR 3.12 [1.62-5.99], p = 0.001), and weakly associated with IS (aHR 1.30 [0.99-1.72], p = 0.06). CMBs were associated with ICH but not IS in patients with undetermined (including competing) etiologies (aHR 8.59 [1.61-45.8], p = 0.012). In large-artery-arteriosclerosis, the presence of CMBs was not associated with the primary or secondary outcomes. In patients with lacunar stroke a high load of CMBs (⩾ 5 CMBs) – but not the presence of CMBs alone - was associated with the primary outcome (aHR 2.0 [1.19-3.36], p =0.008) and ICH (aHR 7.38 [2.07-26.2], p=0.002) - but not IS.
Conclusions: The prognostic impact of CMBs may vary according to the index stroke etiology.
Disclosures of Interest: No
Moderated Poster – Epidemiology + Sex and Gender – Day 1
Abstract N°: 1450
DIETARY APPROACHES TO STOP HYPERTENSION (DASH) DIET AND THE RISK OF ISCHEMIC STROKE; A CASE-CONTROL STUDY
1Paris 12 Val de Marne University, Créteil, France, 2American University of Beirut, Beirut, Lebanon, 3Lebanese University - Hadat Campus, Beirut, Lebanon, 4Nicosia, Nicosia, Cyprus, 5Henri-Mondor University Hospital, Créteil, France
On behalf of:
Background and aims: Hypertension is a major risk factor for ischemic stroke. An important strategy in controlling hypertension is through dietary modification. The present study evaluates the effect of Dietary Approaches to Stop Hypertension (DASH) diet on the risk of ischemic stroke.
Methods: A case-control study was carried out, including 214 ischemic stroke cases within the first 48 hours of diagnosis and 214 controls, divided equally into hospitalized and non-hospitalized participants. Controls were matched to cases based on age and gender. Sociodemographic characteristics were assessed, in addition to the concordance with DASH diet, which was measured using a preconstructed DASH diet index (ranging from 0 (lowest) to 11 (highest)). For stroke patients, Modified Rankin Score (mRS) was measured to assess disability.
Results: Smoking, hypertension, hyperlipidemia, atrial fibrillation and myocardial infarction were significantly associated to ischemic stroke (p<0.001). Higher concordance to DASH diet was correlated to lower rates of stroke, where cases scored 5.042 ± 1.486 compared to 6.654 ± 1.471 for controls (p<0.001). Eating more grains, vegetables, fruits, dairy products, nuts, seeds and beans, and lower fat, sweets and sodium were associated to lower rates of ischemic stroke (p<0.001), while meat, poultry and fish did not have any significant effect (p=0.46). Higher disability (higher mRS score) was also correlated to lower DASH diet abidance (p=0.038).
Conclusions: The relation between DASH diet and risk of stroke highlights the necessity for strict abidance to dietary restrictions, suggesting a protective role for DASH diet in stroke pathogenesis and prognosis.
Disclosures of Interest: No
Abstract N°: 2237
CLINICAL OUTCOMES OVER TIME IN PATIENTS WITH PRE-STROKE DISABILITY IN THE SITS REGISTRY: A PROSPECTIVE COHORT STUDY
Vanessa Ha1, Magnus Thorén2, Niaz Ahmed2, Charith Cooray2, Aravind Ganesh*1
1University of Calgary, Clinical Neurosciences, Calgary, Canada, 2Karolinska Institutet, Department of Clinical Neuroscience, Stockholm, Sweden
On behalf of:
Background and aims: There is a paucity of data on post-stroke outcomes in patients with pre-stroke disability (PSD). Our objective was to assess post-stroke outcomes between patients with and without PSD over time
Methods: We included patients who were enrolled in the SITS-International Stroke Treatment Registry between 2003-2021 and received IV thrombolysis with or without endovascular therapy. Patients with PSD had a pre-stroke mRS score ⩾2. Primary outcome was return to pre-stroke mRS at 3 months. We performed regression analyses adjusting for age, sex, year of stroke, stroke severity, and comorbidities. Time-trends were analyzed for each study year.
Results: The mean age of patients with PSD (n=21,414) was 76.88±11.8 years and without PSD (n=140,410) was 68.7±13.2 years. Patients with PSD were less likely to return to their pre-stroke mRS (aOR=0.65 [95% CI:0.62,0.69]) and have higher mortality [aOR=1.31 (95% CI:1.23,1.39)]. The odds of death improved over time but return to pre-stroke mRS did not change over time even when adjusted for acute stroke intervention and secondary prevention. There were no differences in the odds for symptomatic intracranial hemorrhage and NIHSS score at 24 hours and 7 days.
Conclusions: In this observational registry-based study, patients with PSD were less likely to return to their pre-stroke function at 3 months. This relationship did not change with time even when adjusted for acute stroke interventions and secondary prevention. They also have higher mortality although this improved over the study period. More research inclusive of patients with PSD and optimizing their functional outcome is needed.
Disclosures of Interest: No
Abstract N°: 3074
DECREASED LEVEL OF CONSCIOUSNESS IN ACUTE ISCHEMIC STROKE: PATIENT AND STROKE CHARACTERISTICS, LOCALISATION, REVASCULARISATION AND OUTCOME
1Lausanne University Hospital and University of Lausanne, Stroke Center, Neurology Service, Department of Clinical Neurosciences, Lausanne, Switzerland, 2Riviera-Chablais Hospital, Neurology Unit, Rennaz, Switzerland, 3Lausanne University Hospital and University of Lausanne, Diagnostic Neuroradiological Unit, Service of Diagnostic and Interventional Radiology, Department of Medical Radiology, Lausanne, Switzerland, 4Lausanne University Hospital and University of Lausanne, Interventional Neuroradiological Unit, Service of Diagnostic and Interventional Radiology, Department of Medical Radiology, Lausanne, Switzerland, 5Cantonal Hospital of Fribourg, Cardiology Service, Fribourg, Switzerland, 6University of Thessaly, Department of Medicine, Larissa, Greece, 7Lausanne University Hospital and University of Lausanne, Epilepsy/EEG Unit, Neurology Service, Department of Clinical Neurosciences, Lausanne, Switzerland
On behalf of:
Background and aims: Decreased level of consciousness (DLOC) at stroke onset is infrequent in acute ischemic stroke (AIS). We aimed to assess patient and stroke characteristics, revascularization rates, and long-term outcome in AIS patients presenting with acute DLOC.
Methods: We assessed all AIS from 1/2003-6/2021 admitted within 24hours to a single academic institution. DLOC was defined as it being described in the prehospital phase and/or being present on NIHSS-testing on arrival. Using logistic regression for multiple demographic, clinical, and biological variables, we compared patients with and without DLOC regarding baseline characteristics, anatomical stroke localisation, frequency of revascularization, favourable 3-month outcome (modified-Rankin-scale 0-2), and (Cox-regression) 12-month mortality.
Results: Among 6491 consecutive patients (median age=75 years, IQR:20; 44% female; median admission NIHSS=6, IQR:11), 778 (12%) had DLOC. The latter was independently associated with unwitnessed stroke onset, increased admission NIHSS, missing the stroke diagnosis, posterior circulation, right cerebral, and multiple territory involvements (all padj<0.05). Admission temperature showed a J-shaped, and systolic blood pressure a U-shaped association with DLOC. Strokes affecting the diencephalon and temporal lobes more frequently showed DLOC (Figure 1). Adjusted favourable 3-month outcome was less frequent (ORadj:0.54, 95%CI:0.43-0.69) and 12-months mortality higher in DLOC-patients (ORadj:1.35 (95%CI:1.16-1.56, Figure 2).
Conclusions: One out of eight patients have DLOC in the acute phase. These patients have a higher likelihood of unwitnessed stroke onset, their stroke being missed, and multi-territory localization. They most often involve diencephalon and temporal lobes. Long-term functional outcome and mortality with DLOC are worse, independently of other factors.
Disclosures of Interest: No
Abstract N°: 2155
TEMPORAL TRENDS OF ATRIAL FIBRILLATION IN 48,402 YOUNG STROKE PATIENTS: A NATIONWIDE COHORT STUDY
Tania Garrido Hernández1, Laura Amaya-Pascasio*1, Patricia Martínez Sánchez1,2, José María López Martín3, Adrián Aparicio Mota3, Juan Manuel García Torrecillas4
1Hospital Universitario Torrecárdenas, Neurología, ALMERIA, 2University of Almeria, Faculty of Health Sciences. CEINSA Health Research Centre, La Cañada de San Urbano Almería, Spain, 3Hospital Universitario Torrecárdenas, Department of Emergency Medicine, ALMERIA, 4Hospital Universitario Torrecárdenas, Biomedical Research Unit, ALMERIA
On behalf of:
Background and aims: To analyze the evolution of atrial fibrillation in ischemic stroke patients aged 18-50 during the period 2000-2020, conducting a time series analysis.
Methods: Retrospective time series analysis of Spain's Nationwide Inpatient Sample (2000-2020) focused on the evolution of AF in 48,402 IS patients aged 18-50. We employed standard deviation-mean graph analysis to identify the most suitable model, followed by behavioral pattern characterization through series decomposition. Validating the trend using the Mann-Kendall Test, we applied a linear regression to determine positivity or negativity. Furthermore, we verified the series’ stationarity using the Dickey-Fuller test. Due to series characteristics, the Holt Winters additive method was ultimately applied. To ensure the model’s validity, residuals underwent Ljung-Box and Shapiro-Wilk tests.
Results: We plotted the AF time series in young ischemic stroke patients, showing a randomly distributed cloud of points that stabilized in a decreasing trend (p=0.014). Furthermore, it is a stationary series over time (p=0.050). Fitting well to the Holt Winters additive method, we confirmed lack of correlation (p=0.470) and normality (p=0.413) in residuals. Finally, a 3-year forecast predicts a continued decrease in AF percentage from 2020 to 2023 (ME=-0.089, MAE=1.224).
Conclusions: The time series of atrial fibrillation (AF) in young stroke patients indicates a declining average incidence over the analyzed period with stable variability. This may signify improved health, effective preventive measures, or altered risk factors. Consideration of other variables is crucial for a comprehensive understanding of these patterns.
Disclosures of Interest: No
Abstract N°: 3265
LIFE’S ESSENTIAL 8 AND BRAIN HEALTH CLINICAL OUTCOMES IN MIDDLE-AGED ADULTS
Santiago Clocchiatti-Tuozzo*1, Cyprien Rivier1, Daniela Renedo1, Shufan Huo1, Victor Torres-Lopez1, Adam de Havenon1, Kevin Sheth1, Thomas Gill2, Guido Falcone1
1Yale University, Neurology, New Haven, United States, 2Yale University, Internal Medicine, New Haven, United States
On behalf of:
Background and aims: There is a strong connection between cardiovascular risk during middle-age and brain health later in life. The American Heart Association’s Life’s Essential 8 (LE8) constitute a validated tool that captures key determinants of cardiovascular health. We tested the hypothesis that worse LE8 profiles are associated with higher composite risk of the most important clinical endpoints related to brain health.
Methods: We conducted a two-stage prospective study using data from the UK Biobank (UKB) and All of Us (AoU). Participants with prior stroke, dementia, or late-life depression were excluded. The exposure was the LE8 score, comprised of eight components (blood pressure, glucose, cholesterol, body mass index, smoking, physical activity, diet, and sleep), organized in 3 categories (optimal, intermediate, and poor). The outcome was a composite of stroke, dementia, or late-life depression. We evaluated the associations via multivariable Cox proportional hazard models.
Results: After 5 years of follow-up, 3,539 (1.2%) of the 303,951 UKB participants (mean age 56, 52% female) and 378 (6.1%) of the 68,359 AoU participants (mean age 57, 60% female) sustained the composite outcome. In multivariable Cox proportional hazard models, there was a two-fold increase in the risk of the composite outcome for optimal vs. poor cardiovascular health in both cohorts: UKB:HR:2.01,95%CI:1.80–2.25,p<0.001 and AoU:2.02,95%CI:1.83–2.23,p<0.001).
Conclusions: Among middle-aged UKB and AoU participants, poorer cardiovascular health profiles were strongly associated with higher risks of developing a composite endpoint capturing the most important brain health related diseases. These findings support the utilization of this endpoint in brain health focused clinical trials.
Disclosures of Interest: No
Abstract N°: 630
PROGNOSTIC FACTORS FOR CLINICAL OUTCOMES IN INTRACEREBRAL HAEMORRHAGE SURVIVORS WITH ATRIAL FIBRILLATION - A SYSTEMATIC REVIEW
Viktoria Rücker*1, Steffi Hillmann1, Felipe A. Montellano1,2, Eleni Korompoki3,4, Virginia Cancelloni5, Marlene Steinwachs1,6, Roland Veltkamp3,7, Peter U. Heuschmann1,6,8,9
1Julius-Maximilians-Universität Würzburg, Institute of Clinical Epidemiology and Biometry, Würzburg, Germany, 2University Hospital Wuerzburg, Department of Neurology, Würzburg, Germany, 3Imperial College London, London, United Kingdom, 4National and Kapodistrian University of Athens Alexandra Hospital, Department of Clinical Therapeutics, Athens, Greece, 5Azienda Ospedaliera di Perugia, Perugia, Italy, 6University Hospital Würzburg, Institute for Medical Data Sciences, Würzburg, Würzburg, Germany, 7Alfried Krupp Krankenhaus, Department of Neurology, Essen, Germany, 8University and University Hospital Würzburg, Comprehensive Heart Failure Center, Würzburg, Germany, 9University Hospital Würzburg, Clinical Trial Unit, Würzburg, Germany
On behalf of: PRESTIGE-AF investigators
Background and aims: Accurate prediction of clinically relevant outcomes is essential to allow adequate clinical decision making in intracerebral haemorrhage (ICH) patients with atrial fibrillation (AF). A systematic review was conducted to identify prognostic factors for (1) functional outcome, (2) mortality, (3) ICH recurrence and (4) new ischaemic stroke in ICH survivors with AF.
Methods: We searched MEDLINE, EMBASE and The Cochrane Library from inception until 08/12/2023. We included studies reporting prognostic factors for pre-defined outcomes at least 3 months after index event in patients with ICH and >=80% AF. Pairs of independent reviewers assessed study eligibility, extracted data, and evaluated the methodological quality using the Quality In Prognosis Studies (QUIPS) risk of bias assessment tool.
Results: Of 1,380 abstracts screened, 88 were assessed full text, and six were included comprising 4,979 patients (mean age range 75.2-81.0 years). One study reported prognostic factors for functional outcome (NIHSS admission), four studies for mortality (age, previous stroke, stroke severity, ICH volume and location), and one study for ICH recurrence (no significant factors). Two studies reported only univariable prognostic factors on mortality and recurrence. Most studies (5/6) were at high risk of bias due to a lack of adjustment for relevant confounders, small sample size, and suboptimal model development.
Conclusions: There is a paucity of high-quality data on prognostic factors for ICH survivors with AF, undermining reliable clinical decision making for these patients. Adequately powered studies implementing best-practice modelling strategies are needed in this population.
PROSPERO-CRD42023492490
Funding
Analyses were partly funded within PRESTIGE-AF by EU’s Horizon2020 programme (No. 754517).
Disclosures of Interest: No
Abstract N°: 1848
DOMAIN-SPECIFIC PHYSICAL ACTIVITY AND STROKE: A 20-YEAR PROSPECTIVE POPULATION-BASED COHORT STUDY
Adam Viktorisson*1,2, Annie Palstam1,2, Fredrik Nyberg3, Christina Berg4, Lauren Lissner3, Katharina Stibrant Sunnerhagen1,2
1University of Gothenburg, Institute of Neuroscience and Physiology, Sahlgrenska Academy, Gothenburg, Sweden, 2Sahlgrenska University Hospital, Department of Rehabilitation medicine, Gothenburg, Sweden, 3University of Gothenburg, Institute of Medicine, Sahlgrenska Academy, Gothenburg, Sweden, 4University of Gothenburg, Department of Food and Nutrition, Gothenburg, Sweden
On behalf of:
Background and aims: Associations of domain-specific physical activity with stroke are uncertian. We investigate the relationships between leisure, work, transport, and household physical activity with stroke incidence and death or dependency in activities of daily living (ADL) three months after stroke.
Methods: This was a prospective population-based cohort study with a mean follow-up of 20.0 years.
A random sample of 3614 individuals from an urban-rural area covering western Sweden were examined in 2001 to 2004. Physical activity levels were self-reported. Follow-up for stroke incidence and mortality rates continued until December 31, 2022. Death and ADL dependency was assessed at three months after stroke.
Results: There were 269 stroke events, of which 120 were dead or ADL dependent three months after stroke. Intermediate and high levels of leisure-time physical activity were associated with a reduced incidence of stroke (adjusted hazard ratio [aHR] 0.61, 95% confidence interval [CI] 0.42-0.88, and aHR 0.59, 95% CI 0.38-0.93, respectively). An intermediate level of physical activity in transportation was associated with a decreased stroke risk (aHR 0.73, 95% CI 0.54-0.98), while high levels of leisure-time physical activity were associated with a reduced risk of post-stroke death or ADL dependency (adjusted odds ratio 0.37, 95% CI 0.18-0.79). Work and household physical activity did not significantly predict stroke incidence or outcomes.
Conclusions: This prospective population-based study suggests that leisure-time and transport-related physical activity levels are associated with reduced stroke incidence, and a high level of leisure-time physical activity is associated with a better post-stroke outcome at three months.
Disclosures of Interest: No
Abstract N°: 2533
DO SEX DIFFERENCES IN RATES OF CAROTID ENDARTERECTOMY IN PRACTICE OR IN PREVIOUS TRIALS INDICATE BIAS? A POPULATION-BASED STUDY
Ya Yuan Rachel Leung*1, Dominic Pj Howard1, Peter Rothwell1
1Centre for Prevention of Stroke and Dementia, Department of Clinical Neurosciences, University of Oxford, Oxford, United Kingdom
On behalf of: Oxford Vascular Study
Background and aims: It is argued that fewer women than men recruited into randomised trials of carotid endarterectomy (CEA) indicates inclusion bias, which potentially undermines external validity, and that similar bias might explain lower rates of CEA in women in routine clinical practice. We therefore compared sex ratios in incidence of symptomatic stenosis in a population-based study of all potentially eligible individuals with CEA rates in a national registry and with recruits to randomised trials.
Methods: We compared the age-specific sex-ratio of incident 50-99% symptomatic carotid stenosis in a population-based study (Oxford Vascular Study; OxVasc; 2002-2023) with that in a UK registry of all patients undergoing CEA for symptomatic stenosis (National Vascular Registry; NVR 2012-2022) and with recruits to previous randomised trials of CEA identified in a systematic review.
Results: Among 333 patients with potentially eligible symptomatic carotid stenosis in OxVasc, 112 (36.6%) were female (age-adjusted sex-ratio=0.49, 0.33-0.77, p<0.001), with a trend towards a higher proportion of women with increasing age (Figure 1). The sex-ratio and age-trends were similar both in the NVR UK CEA registry (Figure 2) and in the previous trials of CEA for symptomatic stenosis and for asymptomatic stenosis (Figure 3).
Conclusions: In our population-based study, the sex-ratio for incidence of symptomatic carotid stenosis was in line with both national UK rates of CEA in routine practice and with recruitment to previous randomised trials. Any sex-related bias in use of CEA for symptomatic stenosis in routine practice and in recruitment to previous trials must therefore be limited.
Disclosures of Interest: No
Abstract N°: 1122
LONG-TERM MORTALITY, RECOVERY, AND VOCATIONAL STATUS AFTER A MATERNAL STROKE – NATIONWIDE OBSERVATIONAL CASE-CONTROL STUDY
Liisa Verho*1,2, Karoliina Aarnio2, Minna Tikkanen3, Outi Äyräs1, Kirsi Rantanen2, Aino Korhonen2, Anna Richardt2, Hannele Laivuori4,5,6, Mika Gissler7,8, Petra Ijäs2
1Department of Obstetrics and Gynecology, University of Helsinki and Helsinki University Hospital, 2Department of Neurology, University of Helsinki and Helsinki University Hospital, 3Department of Obstetrics and Gynecology, University of Helsinki, 4Department of Obstetrics and Gynecology, Tampere University Hospital and Tampere University, 5Medical and Clinical Genetics, University of Helsinki and Helsinki University Hospital, 6Institute for Molecular Medicine Finland, Helsinki Institute of Life Science, University of Helsinki, 7Department of Knowledge Brokers, Finnish Institute for Health and Welfare, 8Region Stockholm, Academic Primary Health Care Centre and Karolinska Institutet
On behalf of:
Background and aims: Data on the long-term prognosis after a maternal stroke is limited. We aimed to examine the long-term mortality, recovery, vocational status and morbidity following maternal stroke.
Methods: In this register-based study with chart validation, we included all women with maternal stroke in Finland in 1987-2016 who survived the first year after the event (n=235). The recovery was assessed from charts by Modified Ranking Scale (mRS). Three controls were selected for each case (n=694). Deaths until 2016 and vocational status were obtained from Statistics Finland and data on morbidity, including stroke recurrence, from Hospital Discharge Register and charts.
Results: The median follow-up time was 11.8 years. Mortality during the follow-up was 3.0% among cases and 1.0% among controls (age adjusted odds ratio (OR) 3.0, 95% confidence interval (CI) 1.0-8.7) and concentrated on women with prior subarachnoid haemorrhage. At the end of the follow-up, 90.3% of the cases were independent in daily activities (mRS ⩽ 2). Fewer women with a maternal stroke (65.9%) were working in 2016 compared to controls (79.1%) (OR 0.5, 95% CI 0.4-0.7) and being retired was more common (18.2% vs 4.9%, OR 4.4, 95% CI 2.7-7.3). Stroke recurred in 14 (6.0%) of cases.
Conclusions: Despite having higher mortality, majority of maternal stroke survivors recovered well. The vocational status of the cases was inferior to the controls, but most women were working at the end of follow-up. Our study provides novel information on the prognosis after maternal stroke, essential in counselling and secondary prevention.
Disclosures of Interest: No
Moderated Poster – Genetics and Translational Medicine – Day 1
Abstract N°: 2462
IMMUNOTROMBOSIS AS A THERAPEUTIC TARGET: EFFECT OF DNASE-I IN EXPERIMENTAL ISCHEMIC STROKE
GAOHONG DI*1, Cristina Granados-Martinez1, Sandra Vazquez2, Blanca Díaz Benito1, Carolina Peña-Martinez3, Manuel Navarro1, Ana Moraga1, Jesus Pradillo1, M.Angeles Moro2, Ignacio Lizasoain1
1Complutense University of Madrid, Neurovascular Research Unit, Facultad de Medicina., 2Centro Nacional de Investigaciones Cardiovasculares Carlos III, 3Rey Juan Carlos University
On behalf of:
Background and aims: The occurrence of hemorrhagic transformation after stroke is a major concern. Neutrophils, that undergo circadian oscillations, play a key role in immunothrombosis by releasing neutrophil extracellular traps (NETs). Strategies aimed enhancing NETs clearance are expected to play a protective role in mitigating ischemic damage and improving responsiveness to tPA. In addition, modulation of circadian rhythms has been identified as a critical factor in this complex interplay.
Methods: Focal cerebral ischemia was induced by middle cerebral artery occlusion (MCAO) using a thromboembolic model in C57BL/6 mice and transgenic mice (TLR4loxP/Pf4-cre, PAD4-/-, DNase-/-, C57BL/6-Ly6g/Cre-tdTomato mice). Drugs included: aspirin, tPA, DNase-I. MCAO was performed at different "Zeitgebers" (ZT4-ZT7 and ZT13-ZT16) according to mouse circadian rhythm.
Results: First, we have demonstrated that DNase-I administration reduce infarct volume and improved neurological symptoms in ischemic stroke and, its addition to tPA treatment, increases the rate of successful arterial recanalization in reperfused animals regardless aspirin chronic administration. Moreover, during the resting phase (ZT4-ZT7), animals had larger infarcts associated with a decrease in the percentage of spontaneous reperfusion and an increase in the presence of NETs at this time, and the administration of DNase-I has a protective effect only when administered during this time.
Conclusions: Overall we have demonstrated the protective effect of DNase-I treatment single or coadministered with tPA after stroke during the resting phase. These results are crucial to be consider for the success of the actual clinical trials with DNase-I.
Disclosures of Interest: No
Abstract N°: 1475
PREDICTORS OF FAST AND SLOW PROGRESSORS: ANALYSIS FROM THE ITALIAN REGISTRY OF ENDOVASCULAR TREATMENT IN ACUTE STROKE (IRETAS)
Antonio Ciacciarelli*1, Ettore Nicolini1, Valentina Saia2, Giovanni Pracucci3, Salvatore Mangiafico4, Danilo Toni1
1Sapienza University of Rome, Emergency Department, Roma, Italy, 2Santa Corona Hospital, Pietra Ligure, Italy, 3University of Florence, Firenze, Italy, 4IRCCS Neuromed Mediterranean Neurological Institute, Pozzilli, Italy
On behalf of: IRETAS Group
Background and aims: acute ischemic stroke from large vessel occlusion can manifests with a large variability of initial core volume, often regardless of stroke onset time. We aim to identify prevalence and determinants of Fast and Slow progression of infarct growth.
Methods: Patients prospectively registered in the Italian Registry of Endovascular Treatment in Acute Stroke (IRETAS) across 45 centers from January 2011 to December 2021 were analyzed. Only patients with anterior circulation involvement and known stroke onset were included. Progressors were categorized as Fast, Slow, or nonFast-nonSlow based on onset-to-imaging time and ASPECT scores. Fast progressors: onset-to-imaging⩽6hs and ASPECTS⩽6, Slow progressors: onset-to-imaging>6hs and ASPECTS>6, nonFast-nonSlow progressors: onset-to-imaging⩽6hs and ASPECTS>6 or onset-to-imaging>6hrs and ASPECTS⩽6.
Results: Among 6811 patients Fast progressors were 570 (8.4%), Slow progressors 451 (6.6%) and nonFast-nonSlow progressors 5790 (85%). Predictors of Fast progressors included younger age (OR:0.991, CI:0.984-0.998), recent history of Stroke or TIA (OR:1.605, CI:1.088-2.368) and heart failure (OR:1.527, CI:1.120-2.082). Predictors of Slow progressors were male sex (OR:0.720, CI:0.582-0.892), and carotid stenosis > 70% (OR:1.704, CI:1.079-2.692). In the subset of patients with Careggi Collateral circulation score (CCS) in the analysis, poor CCS was directly related to Fast progressors (OR:2.485, CI:1.810-3.411, p-value<0.001) and inversely related to Slow progressors (OR:0.468, CI:0.330-0.664, p-value<0.001).
Conclusions: We identified the prevalence and the predictors of Fast and Slow Progressors in a large national stroke registry. Moreover, our results suggests that collaterals circulation may represent the clock of infarct expansion.
Disclosures of Interest: No
Abstract N°: 1747
ACTIVATION OF INTRAVASCULAR INNATE IMMUNE CELLS IN THE ISCHEMIC ARTERIAL BLOOD AFTER STROKE
Justine Münsterberg*1, Caspar Brekenfeld2, Marius Piepke1, Thomas Renne3, Bettina Clausen4, Eva Tolosa5, Tim Magnus1, Mathias Gelderblom1
1University Medical Center Hamburg Eppendorf, Department of Neurology, Hamburg, Germany, 2University Medical Center Hamburg Eppendorf, Department of Neuroradiology, Hamburg, Germany, 3University Medical Center Hamburg Eppendorf, Department of Clinical Chemistry, Hamburg, Germany, 4Institute of Molecular Medicine, University of Southern Denmark, Department of Neurobiology, Odense, Denmark, 5University Medical Center Hamburg Eppendorf, Department of Immunology, Hamburg, Germany
On behalf of:
Background and aims: Neuroinflammation contributes substantially to stroke pathophysiology. However, analyzing inflammatory pathways in human stroke is challenging. To overcome this limitation, we established a workflow for collection and immediate analysis of ischemic blood from the occluded middle cerebral artery in acute stroke patients.
Methods: Arterial blood from behind the thrombus (ischemic blood) and from the common carotid artery proximal to the thrombus were obtained during mechanical thrombectomy. Using flow cytometry and immunoassays we assessed inflammasome activation by measuring ASC-speck formation and the expression of pro-Interleukin-1 beta (IL-1beta) and IL-1beta, respectively. Furthermore, we analyzed neutrophil extracellular trap formation (NETosis). For analysis, values obtained in ischemic blood samples were normalized to their paired common carotid artery counterparts.
Results: Monocytes in the ischemic sample produce more pro-IL-1 after restimulation than those from the control carotid artery. In a complementary setting mimicking exposure to ATP, we find that more monocytes activated the inflammasome. In line with this, IL-1beta levels were elevated in the ischemic samples. Furthermore, the number of neutrophils was higher in ischemic samples, and we detected significantly increased levels of citrullinated histone H3 (CitH3) in ischemic plasma samples, indicating NETosis.
Conclusions: Taken together, our data suggest that the ischemic environment leads to activation of innate immune pathways already in the intravascular space. In particular, priming of the inflammasome in monocytes and release of NETs from invading neutrophils appear to contribute to the early excessive inflammation. Targeting these immune pathways in patients undergoing thrombectomy is therefore an exciting new option to attenuate the early detrimental immune response.
Disclosures of Interest: No
Abstract N°: 1275
POST-RECANALIZATION MICROTHROMBI-MEDIATED DYSFUNCTION OF THE BLOOD-BRAIN BARRIER
Igor Khalin*1,2, Antonia Wehn2,3, Eva Krestel2, Andrey Klymchenko4, Nikolaus Plesnila2,5
1Normandie University, Institute Blood and Brain @ Caen-Normandie, Caen, France, 2LMU University Hospital, Institute for Stroke and Dementia Research, Muenchen, Germany, 3LMU University Hospital, Department of Neurosurgery, Muenchen, Germany, 4Université de Strasbourg, Laboratoire de Biophotonique et Pharmacologie, Strasbourg, France, 5Munich Cluster of Systems Neurology, Muenchen, Germany
On behalf of:
Background and aims: Recanalization of large cerebral arteries by thrombectomy or thrombolysis does not necessarily prevent tissue infarction after ischemic stroke. The aim of the current study was to elucidate how the cerebral microcirculation is involved in this process.
Methods: Mice were subjected to filament middle-cerebral artery occlusion (fMCAo) or to a magnetic nanoparticle-based microvascular occlusion model (nano-stroke) and 30 nm superbright lipid nanodroplets (LNDs) were systematically administered to visualize the cerebral microcirculation for two hours by in vivo by 2-photon microscopy and thereafter ex vivo by confocal and correlative light-electron microscopy (CLEM).
Results: LNDs accumulate in cerebral microvessels with the ischemic penumbra indicating microthrombus formation (p=0.02 vs. sham). Already present and newly formed microthrombi were observed. The number of newly formed microthrombi increased by 300% 80 min after reperfusion. In 25% of cases microthrombi were associated with BBB disruption, while all BBB disruptions were associated with microthrombi. A gradual activation of microglia around microthrombi was observed. CLEM demonstrated accumulation of LNDs between erythrocytes and fibrine as well as LND extravasation at the site of microthrombi.
Conclusions: The occurrence of microvascular thrombosis in the penumbra after recanalization is associated with BBB leakage and inflammation. Further discovery of this process as well as targeting microthrombi with LNDs could emerge as a novel experimental approach to explore microvascular pathologies after cerebral ischemia and to develop novel therapeutic interventions.
Disclosures of Interest: No
Abstract N°: 843
EDARAVONE DEXBORNEOL AMELIORATES BRAIN DAMAGE BY REGULATING THE ACTIVATION OF ASTROCYTE IN MICE WITH ISCHEMIA AND REPERFUSION
Baoshan Qiu*1, Nan Wang1, Yimei Wang1, Yilong Wang1
1Beijing Tiantan Hospital, Capital Medical University, Neurology, Beijing
On behalf of:
Background and aims: Stroke is a leading cause of mortality and disability worldwide. However, the mechanism of acute ischemic stroke is complex, and there is currently a lack of effective neuroprotective therapeutic drugs. TASTE trial proved that edaravone dexborneol significantly improves outcomes in patients with acute ischemic stroke, yet the underlying mechanisms are not fully understood. Here, we aim to investigate the potential mechanisms of edaravone dexborneol in acute ischemic stroke.
Methods: We established a transient middle cerebral artery occlusion (tMCAO) mouse model of ischemic stroke to evaluate the neuroprotective effects of Edaravone dexborneol. We employed single-cell sequencing, immunostaining, cell oxygen-glucose deprivation (OGD) models, transcriptome sequencing, and western blot experiments to explore the molecular mechanisms underlying the neuroprotective effects of Edaravone dexborneol.
Results: Edaravone dexborneol was found to significantly reduce the infarct volume three days post-stroke and improve neurological function in animals at the same time point. Single-cell sequence data revealed a significant impact of Edaravone dexborneol on astrocytes post-stroke. Edaravone dexborneol upregulated neuroprotective pathways (vascular transport, synapse organization, modulation of chemical synaptic transmission) in astrocytes while downregulating inflammation-related pathways (response to cytokines, regulation of cellular response to stress, innate immune response). Further validation using immunofluorescence, cellular transcriptome sequencing, and western blot confirmed key target pathways regulated by edaravone dexborneol in astrocytes.
Conclusions: Our study demonstrates that Edaravone dexborneol’s pivotal role of astrocytic modulation for enhanced recovery, providing new evidence for edaravone dexborneol as a therapeutic intervention in acute ischemic stroke.
Disclosures of Interest: No
Abstract N°: 1673
EXPLORING THE PATHOPHYSIOLOGICAL ROLE OF CELLULAR SENESCENCE IN STROKE AND VASCULAR COGNITIVE IMPAIRMENT
1National Taiwan University Hospital, Department of Neurology, Taiwan
On behalf of:
Background and aims: The role of cell senescence in stroke and vascular cognitive impairment (VCI) remains largely unexplored. This study investigates the induction of cell senescence in vitro and in vivo in response to ischemia-reperfusion (IR) injury
Methods: Cultured cortical neurons, astrocytes, and BV2 microglia underwent oxygen-glucose deprivation/reperfusion (OGD/R, 0.5% O2 for 3 h, followed by recovery in a 5% CO2 incubator for 24 h). In vivo, adult male mice underwent the bilateral carotid artery stenosis (BCAS) procedure. Post-stroke human brain samples and non-stroke donor samples were obtained for further analysis
Results: OGD/R challenge in vitro led to a significant increase in senescence-associated beta-galactosidase (SA-ß-gal) staining in astrocytes and microglia, with a lesser impact on neurons. In BCAS mice, p21 expression significantly increased in brain tissues post-operation, including the double-positive p21/Iba1 and p21/NeuN cells. Immunohistochemistry in human brain tissue from stroke patients revealed increased p21-positive cells in the infarct region, in contrast to the scarcity observed in non-stroke donors. Senescent cells, known for inducing neighboring cell senescence and chronic inflammation through the senescence-associated secretory phenotype (SASP), were confirmed through BV2 cell-conditioned media/exosomes, which increased senescence and SASP upregulation in naïve BV2 cells. The senolytic cocktail dasatinib and quercetin (D+Q) selectively eliminated senescent BV2 cells, prompting further studies to explore senotherapeutic activity in BCAS mice
Conclusions: These preliminary findings propose cellular senescence in chronic ischemic injury and advocate targeting senescent cell and related SASP as potential therapeutic strategies for post-ischemic cognitive impairment
Disclosures of Interest: No
Abstract N°: 3109
LECTIN PATHWAY OF COMPLEMENT ACTIVATION IN A NON-HUMAN PRIMATE MODEL OF ISCHEMIC STROKE MIMICKING MECHANICAL THROMBECTOMY
1Université Lyon 1, CarMeN Laboratory, INSERM U1060 / INRA U1397, LYON, France, 2Hospices Civils de Lyon - HCL, Stroke Department, Lyon, France, 3Mario Negri Institute for Pharmacological Research, Department of Acute Brain and Cardiovascular Injury, Milano, Italy, 4Hospices Civils de Lyon - HCL, Neuroradiology Department, Lyon, France, 5Université Lyon 1, CREATIS, CNRS UMR 5220, INSERM U1044, LYON, France, 6CERMEP – Imagerie du Vivant, Lyon, France
On behalf of:
Background and aims: Rodent models have demonstrated the key pathogenic role of the lectin pathway (LP) of complement activation in brain ischemic injury. Here we assessed the LP activation and its association with stroke severity and outcome in a well-characterized model of stroke mimicking mechanical thrombectomy in non-human primates.
Methods: Transient middle cerebral artery occlusion was performed in Macaca fascicularis randomly allocated in cyclosporine A or placebo group. Neurological status was serially assessed. Lesion volumes and the blood-brain barrier permeability using quantitative transfer constant Ktrans ratio were assessed using a PET-MRI. Functional LP-specific C3 deposition assay was performed in plasma. Mannose binding lectin (MBL), MBL associated serine proteases-2 (MASP-2), C3b/iC3b and interleukin-6 were measured in plasma, cerebrospinal fluid and brain homogenates. MBL, MASP-2 and C3b/iC3b deposition and glycocalyx were detected by immunofluorescence and confocal analyses.
Results: Twenty-three subjects were included. C3b deposition on plasma collected late after recanalization was significantly decreased compared with baseline conditions. C3b/iC3b peaked at day 7 and this increase correlated with a more severe neurological deficit at day 1 and day 7, larger volumes of final lesion and lesion growth between occlusion and day-7 as well as a greater Ktrans ratio. C3b/iC3b, MBL and MASP-2 were present in microvascular thrombi at day-30.
Conclusions: Our results support that the LP is involved in microvascular thromboinflammation in a non-human primate model of stroke.
Immunofluorescence and confocal analysis. Microphotographs obtained in the ischemic area at day 30 (40x magnification).
Disclosures of Interest:
No
Abstract N°: 1413
EDARAVONE DEXBORNEOL ATTENUATES BLOOD-BRAIN BARRIER DISRUPTION AFTER RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR TREATMENT VIA REDUCING PDGF-CC
Pang Shu-Yan1, Chen Nai-He1, Sun Ying-Ying1, Zhu Hong-Jing1, Yang Yi1, Guo Zhen-Ni*1
1The First Hospital of Jilin University, Stroke Center, Department of Neurology, Changchun
On behalf of:
Background and aims: Intravenous thrombolysis is an established therapy for acute ischemic stroke (AIS) patients. However, recombinant tissue plasminogen activator (rt-PA) could aggravate blood-brain barrier (BBB) disruption, which remains a critical clinical problem. Our study aimed to assess whether Edaravone dexborneol (EDB), an effective agent in the treatment of AIS, could attenuate rt-PA-associated BBB disruption and explore the possible mechanism.
Methods: We used the rat embolic middle cerebral artery occlusion model followed by rt-PA thrombolysis and then performed with EDB or saline within 30 minutes. We measured brain infarction, neurological outcomes, BBB permeability, histopathological changes, brain injury markers (UCHL-1, NSE, GFAP, S100β) and tight junction proteins (claudin-5, occludin, ZO-1, laminin). Furthermore, the PDGF-CC/PDGFRα signaling in brain tissue, PDGF-CC rerum levels were also detected.
Results: Our results showed that EDB significantly reduced cerebral infarction, neurological deficits, and attenuated BBB injury and increased tight junction protein expression after stroke, even when rt-PA was administrated in a delayed therapeutic time window. Mechanistically, EDB significantly decreased PDGFRα activation in ischemic brain and reduced blood PDGF-CC levels. Simultaneously, intraventricular recombinant PDGF-CC supplementation abolished EDB protective effects on BBB integrity. Moreover, EDB reduced serum levels of brain injury markers significantly, which was also found in acute ischemic stroke patients treated with EDB in the clinical research part of this study.
Conclusions: Our study demonstrated that EDB can ameliorate rt-PA aggravated BBB disruption after stroke via reducing PDGF-CC/PDGFRα pathway, even when rt-PA was administrated beyond 4.5h, which could be potentially used to improve the safety and efficacy of delayed thrombolytic therapy.
Disclosures of Interest: No
Moderated Poster – Prevention – Day 1
Abstract N°: 723
ONCE- VERSUS TWICE-DAILY DIRECT ORAL ANTICOAGULANTS AFTER ISCHAEMIC STROKE IN ATRIAL FIBRILLATION – AN ELAN TRIAL ANALYSIS
Alexandros Polymeris*1, Masatoshi Koga2, Daniel Strbian3, Adhiyaman Vedamurthy4, Manju Krishnan5, Mattia Branca6, Thomas Meinel7, Martina Göldlin7, Jesse Dawson8, Urs Fischer1,7
1University Hospital Basel and University of Basel, Switzerland, Department of Neurology and Stroke Center, 2National Cerebral and Cardiovascular Center, Osaka, Japan, Department of Cerebrovascular Medicine, 3Helsinki University Hospital, Finland, Department of Neurology, 4Glan Clwyd Hospital, Betsi Cadwaladr University Local Health Board, Rhyl, United Kingdom, 5Morriston Hospital, Swansea Bay University Health Board, Swansea, United Kingdom, Stroke Unit, 6University of Bern, Bern, Switzerland, Clinical Trial Unit, 7Inselspital, Bern University Hospital and University of Bern, Switzerland, Department of Neurology, 8School of Cardiovascular and Metabolic Health, College of Medical, Veterinary & Life Sciences, Queen Elizabeth University Hospital, Glasgow, United Kingdom
On behalf of: ELAN Investigators
Background and aims: Twice-daily (BID) direct oral anticoagulant (DOAC) dosing may yield a better risk-benefit profile than once-daily (QD) dosing in atrial fibrillation (AF). We explored whether this was true in people with a recent AF-related ischaemic stroke in a post-hoc analysis of ELAN trial data.
Methods: ELAN (NCT03148457) randomized people with recent AF-related ischaemic stroke to early or delayed DOAC initiation. We compared rates of the primary outcome (recurrent ischaemic stroke, systemic embolism, symptomatic intracranial haemorrhage, major extracranial bleeding and vascular death) at 90 days in participants treated with QD or BID DOAC dosing regimens. Secondary 90-day outcomes were the individual primary outcome components, all-cause death, and functional outcome. We used logistic and cause-specific Cox proportional hazards regression, both in unadjusted and inverse-probability-of-treatment-weighted models to account for confounding. We calculated the net benefit of BID over QD DOAC by subtracting the weighted rate of excess bleeding events attributable to BID DOAC from the rate of excess ischaemic events prevented by BID DOAC.
Results: We analyzed data of 1987 participants (median age 77 years, 45% female), of whom 402 received QD (20%) and 1585 (80%) BID DOAC. The primary outcome occurred in 82 (4.3%) participants. There was no difference in the rate of the primary or any secondary outcomes between the DOAC dosing regimens (Figure 1). There was no evidence of a net benefit of BID over QD dosing (Figure 2).
Conclusions: The risk-benefit profile of QD and BID DOAC after an ischaemic stroke in people with atrial fibrillation does not seem to differ.
Disclosures of Interest: No
Abstract N°: 246
USE OF ANTIPLATELETS PRIOR TO ANTICOAGULANT INITIATION AFTER ISCHAEMIC STROKE IN ATRIAL FIBRILLATION – AN ELAN TRIAL ANALYSIS
Alexandros Polymeris*1, Masatoshi Koga2, Daniel Strbian3, Adhiyaman Vedamurthy4, Manju Krishnan5, Mattia Branca6, Thomas Horvath7, Martina Göldlin7, Jesse Dawson8, Urs Fischer1,7
1University Hospital Basel and University of Basel, 2National Cerebral and Cardiovascular Center, Osaka, Japan, Department of Cerebrovascular Medicine, 3Helsinki University Hospital, Finland, Department of Neurology, 4Glan Clwyd Hospital, Betsi Cadwaladr University Local Health Board, Rhyl, United Kingdom, 5Morriston Hospital, Swansea Bay University Health Board, Swansea, United Kingdom, Stroke Unit, 6University of Bern, Bern, Switzerland, Clinical Trial Unit, 7Inselspital, Bern University Hospital and University of Bern, Switzerland, Department of Neurology, 8School of Cardiovascular and Metabolic Health, College of Medical, Veterinary & Life Sciences, Queen Elizabeth University Hospital, Glasgow, United Kingdom
On behalf of: ELAN Investigators
Background and aims: Antiplatelets are often used before direct oral anticoagulant (DOAC) initiation in people with ischaemic stroke related to atrial fibrillation (AF). However, the relative risks and benefits of this approach are unclear.
Methods: In a post-hoc analysis of ELAN trial data (NCT03148457), we compared the risk of recurrent ischaemic stroke, systemic embolism, symptomatic intracranial haemorrhage (ICH), major extracranial bleeding and vascular death within 30 days (as a combined and as individual outcomes) in participants treated with and without antiplatelets prior to DOAC initiation after an AF-associated ischaemic stroke. We used logistic and cause-specific Cox proportional hazards regression, both in unadjusted and inverse-probability-of-treatment-weighted models to account for confounding. We calculated the net benefit of antiplatelet use by subtracting the weighted rate of excess bleeding events attributable to antiplatelets from the rate of excess ischaemic events prevented by antiplatelets.
Results: We analyzed data from 2013 participants (median age 77 years, 46% female), of whom 1090 (54%) received antiplatelets and 70 (3.5%) suffered the composite outcome. Antiplatelet use was not associated with the composite outcome (ORweighted 1.06 [95%-CI 0.66,1.72], HRweighted 1.06 [0.65,1.72]), but was associated with a lower risk of ischaemic stroke recurrence (ORweighted 0.58 [0.30,1.08], HRweighted 0.57 [0.30,1.10]), and a higher risk of major bleeding (ORweighted 1.76 [0.56, 6.63], HRweighted 1.88[0.56, 6.39]). Its net benefit was positive (+0.60 to +0.38 weighted events/100 patient-months for ICH-weights 1.5 to 3.1).
Conclusions: Following an AF-associated ischaemic stroke, use of antiplatelet therapy before DOAC introduction reduces recurrent ischaemic stroke risk but increases bleeding risk, leading to a small net benefit.
Disclosures of Interest: No
Abstract N°: 1317
MEDICAL MANAGEMENT +/- SURGERY FOR SYMPTOMATIC CEREBRAL CAVERNOUS MALFORMATION: A RANDOMISED OPEN PILOT TRIAL
Rustam Al-Shahi Salman*1,2
1The University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom, 2NHS Lothian, Departments of Clinical Neurosciences and Stroke Medicine, Edinburgh, United Kingdom
On behalf of: CARE PILOT TRIAL COLLABORATION
Background and aims: The top uncertainty for people with symptomatic cerebral cavernous malformation (CCM) is whether to have medical management and surgery (with neurosurgery or stereotactic radiosurgery) or medical management alone.
Methods: The CARE pilot trial (ISRCTN41647111) sought 60 people resident in the UK/Ireland with mental capacity and a symptomatic CCM. Computerised, web-based randomisation assigned participants (1:1) to CCM treatment with medical management and surgery or medical management alone, stratified by consensus about intended type of surgery before randomisation. Assignment was open to investigators, participants, and care givers, but not clinical outcome event adjudicators. The primary clinical outcome was intracranial haemorrhage or new persistent/progressive non-haemorrhagic focal neurological deficit due to CCM or surgery during at least 6 months of follow-up.
Results: At 28 (70%) of 40 sites, investigators screened 511 patients: 322 (63%) were eligible, 202 (63%) were approached, 96 (48%) were uncertain about whether to have surgery for a symptomatic CCM, and 72 participants (median age was 50·6y [38·6-59·2], 68 [94%] adults, 41 [57%] female, 66 [92%] white, 56 [78%] had prior ICH, and 28 [39%] had prior epileptic seizure) were randomly assigned to medical management and surgery (n=36; 12 to neurosurgical resection and 24 to stereotactic radiosurgery) or medical management alone (n=36). 67 participants completed follow-up (retention 93%) and adherence was 91%. The primary clinical outcome occurred in 2/33 assigned to medical management and surgery and 2/34 assigned to medical management alone (HR 0·99, 95%CI 0·14-7·03).
Conclusions: This pilot phase trial exceeded its recruitment target, but a definitive trial will require extensive international engagement.
Disclosures of Interest: Yes Funded by a grant from the UK National Institute for Health and Care Research, paid to The University of Edinburgh
Abstract N°: 1514
EARLY VERSUS LATER ANTICOAGULATION AFTER ISCHEMIC STROKE IN PEOPLE WITH ATRIAL FIBRILLATION AND COVERT BRAIN INFARCTS
Markus Kneihsl*1,2,3, Arsany Hakim4, Martina Göldlin5, Thomas Meinel5, Mattia Branca6, Sabine Fenzl4, Roman Rohner4, Stefanie Abend5, Jesse Dawson7, Urs Fischer3,5
1Medical University of Graz, Department of Neurology, Graz, Austria, 2Medical University of Graz, Division of Neuroradiology, Vascular and Interventional Radiology, Department of Radiology, Graz, Austria, 3University Hospital Basel, Department of Neurology, Basel, Switzerland, 4Inselspital Bern University Hospital and University of Bern, University Institute of Diagnostic and Interventional Neuroradiology, Bern, Switzerland, 5Inselspital Bern University Hospital and University of Bern, Department of Neurology, Bern, Switzerland, 6University of Bern, CTU Bern, Department of Clinical Research, Bern, Switzerland, 7Queen Elizabeth University Hospital, University of Glasgow, School of Cardiovascular and Metabolic Health, Glas, United Kingdom
On behalf of: the ELAN investigators
Background and aims: Covert brain infarcts (CBI) in people with first-ever ischemic stroke (IS) and atrial fibrillation (AF) are associated with an increased stroke recurrence risk. We aimed to assess whether the presence of CBI modifies the estimated safety and efficacy of early versus late direct oral anticoagulation (DOAC) initiation in IS people with AF.
Methods: This is a post-hoc analysis of the international, multi-center, randomized controlled ELAN trial, which compared early versus late initiation of DOACs in IS patients with AF. The primary outcome was the composite of recurrent IS, symptomatic intracranial hemorrhage, major extracranial bleeding, systemic embolism, or vascular death within 30 days; secondary outcomes were the individual components. We estimated outcomes based on the presence of CBI on pre-randomization imaging (core-lab rating) using risk differences between treatment arms.
Results: Of 784 included first-ever IS participants, 328 (41.8%) had CBI. The primary outcome occurred in 4/169 (2.4%; recurrent IS: 1/169) participants with CBI assigned to early versus 9/159 (5.9%; recurrent IS: 6/159) assigned to late treatment (adjusted risk difference, aRD: -3.7%, 95% CI: -8.2 to 0.7). Early DOAC initiation decreased IS recurrence risk in CBI participants (aRD: -3.7, 95% CI -7.2 to -0.2), but not in participants without CBI (aRD: 1.5, 95% CI -1.2 to 4.2).
Conclusions: First-ever IS people with AF and CBI may indicate a subgroup of IS people that particularly benefits from early DOAC initiation to prevent recurrent IS without increasing harm.
Disclosures of Interest: No
Abstract N°: 1163
DUAL ANTIPLATELET THERAPY AFTER MINOR STROKES OR HIGH-RISK TIA: EVIDENCE FROM THE AUSTRIAN STROKE REGISTRY
Stefan Krebs*1, Dominika Mikšová2, Michael Knoflach3, Thomas Gattringer4, Simon Fandler-Höfler4, Martha Marko5, Stefan Greisenegger5, Julia Ferrari1, Marek Sykora1
1Hospital St. John of God, Neurology, Vienna, Austria, 2Gesundheit Österreich GmbH, Vienna, Austria, 3Medical University of Innsbruck, Neurology, Innsbruck, Austria, 4Medical University of Graz, Neurology, Graz, Austria, 5Medical University of Vienna, Neurology, Vienna, Austria
On behalf of: Austrian Stroke Registry Collaboration
Background and aims: Three large, randomized studies demonstrated the benefit of dual antiplatelet therapy (DAPT) versus monotherapy in the first 3 weeks after minor stroke or high-risk transient ischemic attack (TIA), leading to its inclusion into the guidelines. The aim of this study was to evaluate the effects of DAPT versus monotherapy on recurrent events, intracerebral hemorrhages, and functional outcome (mRS) in patients with minor stroke or high-risk TIA in a real-life setting.
Methods: Patients with minor stroke (NIHSS <5) or high-risk TIA (ABCD2 score >4) of non-cardioembolic origin without large vessel occlusion or revascularization therapy (thrombolysis or thrombectomy) were extracted from a nationwide registry. Risk factors, etiology, admission stroke severity (NIHSS), mRS at 3 months, and mortality were extracted. Combined vascular endpoints (recurrent stroke, myocardial infarction, death), recurrent stroke, mRS 0-1 at 3 months, and symptomatic intracranial hemorrhages (SICH) were defined as endpoints.
Results: Between 2018 and 2022, 27.1% of 8579 patients received DAPT. These patients had significantly more risk factors and comorbidities. After adjustment for inequalities, DAPT was significantly associated with a lower occurrence of combined vascular events (aOR 0.55, 95% CI 0.35-0.87) and mRS 0-1 at 3 months (aOR 1.57, 95% CI 1.13-2.19), but neutral for recurrent stroke (aOR 1.01, 95% CI 0.48-2.13) or SICH (aOR 0.78, 95% CI 0.13-4.71). In subgroup analysis, DAPT was associated with fewer recurrent strokes/TIA in patients with small vessel disease etiology (aOR 0.44, 95% CI 0.21-0.96).
Conclusions: DAPT in real life setting appears to be safe and associated with fewer vascular events and better functional outcome
Disclosures of Interest: No
Abstract N°: 2553
INTENSITY OF STATIN THERAPY AFTER ISCHEMIC STROKE AND LONG-TERM OUTCOMES: A POPULATION-BASED COHORT STUDY
Jori Ruuskanen*1, Julia Åivo1, Ville Kytö2
1Neurocenter, Turku University Hospital and University of Turku, Neurology, Turku, Finland, 2Heart Center, Turku University Hospital and University of Turku, Turku, Finland
On behalf of:
Background and aims: Statins are essential component of secondary prevention after ischemic stroke (IS). However, statin intensity recommendations differ in guidelines, and there is a concern about intracerebral haemorrhage (ICH). We studied the long-term impacts of initial statin intensity after IS.
Methods: Consecutive patients in Finland who used statins early after IS (n=45,512) were retrospectively studied using national registries. Differences were adjusted using multivariable regression. The primary outcome was all-cause death within 12-year follow-up (median 5.9 years). Secondary outcomes were studied using competing risk analyses.
Results: High-intensity statin therapy was used by 16.0%, moderate-intensity by 73.8%, and low-intensity by 10.2%. Intensity of statin therapy remained constant during follow-up. Risk of death was lower with high-intensity vs. moderate-intensity (adj.HR 0.92; CI 0.87-0.97; NNT 32.0), with moderate-intensity vs. low-intensity (adj.HR 0.91; CI 0.87-0.95; NNT 27.5), and with high-intensity vs. low-intensity (adj.HR 0.83; CI 0.78-0.89; NNT 14.6) statin. Statin intensity was dose-dependently associated with lower probability of recurrent IS (p<0.0001) and cardiovascular death (p<0.0001). Occurrence of ICH was not associated with statin intensity (p=0.646).
Conclusions: Higher initial statin intensity after IS is associated with better long-term outcomes but not with risk of ICH. These results underline the importance of maximizing statin intensity early after IS.
Disclosures of Interest: No
Moderated Poster - Rehabilitation and Outcomes – Day 1
Abstract N°: 143
PHASE 3 STUDY TO EVALUATE THE EFFICACY AND SAFETY OF LIZTOX IN POST-STROKE UPPER LIMB SPASTICITY
Dong Hyun Ye*1, Min Ho Chun2, Yoon Ghil Park3, Nam-Jong Paik4, Shi-Uk Lee5, Seung Don Yoo6, Deog Young Kim7
1Asan medical center, Department of Rehabilitation Medicine, Seoul, South Korea, 2Asan medical center, Department of Rehabilitation Medicine, Seoul, 3Gangnam Severance Hospital, Department of Rehabilitation Medicine, South Korea, 4Seoul National University College of Medicine, Department of Rehabilitation Medicine, South Korea, 5SMG-SNU Boramae Medical Center, Department of Rehabilitation Medicine, South Korea, 6Kyung Hee University Hospital at Gangdong, Department of Rehabilitation Medicine, South Korea, 7Yonsei University College of Medicine, Department and Research Institute of Rehabilitation Medicine, South Korea
On behalf of:
Background and aims: Botulinum toxin type A (BTX-A) injection is a commonly used therapeutic intervention for upper limb spasticity in stroke patients.
Methods: This study was designed as a randomized, active drug-controlled, double-blind, multicenter, phase III clinical trial to evaluate the safety and efficacy of Liztox® in comparison to onabotulinum toxin A (Botox®) for individuals with post-stroke upper limb spasticity. The primary outcome was the alteration in wrist flexor muscle tone from the initial assessment to the fourth week, evaluated using the modified Ashworth scale (MAS). Secondary outcomes included MAS change for the wrist at weeks 8 and 12 from baseline, MAS change for finger and elbow flexors, Disability Assessment Scale (DAS), Subject’s Global Assessment (SGA), the Investigator’s Global Assessment (IGA), and Caregiver Burden Scale (CBS) at weeks 4, 8, and 12 from baseline.
Results: The MAS score for wrist flexor spasticity decreased by −1.14±0.59 in the Liztox® group and −1.22±0.59 in the Botox® group from baseline to week 4. The difference [97.5% confidence interval (CI)] between the test and control groups was 0.08 [-∞, 0.26], confirming non-inferiority of the test group compared to the control group. Furthermore, there were consistent improvements in the IGA, SGA, and CBS scores across all assessment intervals, with no statistically significant variances detected between the two groups. No safety-related concerns were reported during the study.
Conclusions: In conclusion, Liztox® injection proved to be a secure and efficacious intervention for managing upper extremity spasticity in post-stroke patients.
Disclosures of Interest: Yes This research was supported by Huons Biopharma, Republic of Korea.
Abstract N°: 3288
WEARABLE DEVICES FOR UPPER EXTREMITY REHABILITATION AFTER STROKE: A SYSTEMATIC REVIEW AND META-ANALYSIS OF RANDOMIZED CLINICAL TRIALS
Marianna Gerardo Hidalgo Santos Jorge Leite*1, Rafael Eduardo Streit2, Pedro Henrique Reginato2, Elizabet Taylor Weba3, Maria Galvão4, Vivian Gagliardi5,6
1Santa Marcelina School of Medicine, São Paulo, 2Federal University of Paraná, Curitiba, Brazil, 3State University of the Tocantins Region of Maranhão, Imperatriz, Brazil, 4Federal University of Piauí, Teresina, Brazil, 5Santa Casa de São Paulo, São Paulo, Brazil, 6Albert Einstein Israelite Hospital, São Paulo, Brazil
On behalf of:
Background and aims: In order to improve recovery of patients with motor impairment after stroke, new technologies and support devices have emerged. We performed a meta-analysis to assess the efficacy of wearable devices versus conventional physical therapy for Upper Extremity rehabilitation after stroke.
Methods: PubMed, Embase, and Cochrane databases were searched for randomized studies from inception to 28th December 2023. A random effects model was used for the data analysis. P-values < 0.05 were considered statistically significant. Review Manager 5.4.1 software was used for statistical analysis.
Results: A total of 14 studies with a cohort of 1,169 patients were included, of whom 587 underwent rehabilitation with the use of wearable devices. Statistical difference favoring the experimental group was found in Fugl-Meyer Upper Extremity Score (MD = 3.32; 95% CI = 1.38–5..26; p<0.01; I2=78%) and Jebsen-Taylor Hand Function Test (MD = 10.01; 95% CI 2.10–17.91; p=0.01; I2=53%). No significant differences were found regarding outcomes of Wolf Motor Function Score (MD = 1.78; 95% CI -1.53–5.09; p=0.29; I2=78%) and Motor Activity Log Amount of Use (MD = -0.10; 95% CI -0.53–0.33; p=0.64; I2=54%) and Quality of Movement (MD = -0.07; 95% CI -0.29–0.16; p=0.56; I2=0%).
Conclusions: In this meta-analysis of RCTs of patients recovering after stroke, wearable devices showed benefit in Fugl-Meyer scores and Jebsen-Taylor Hand Function Test compared to conventional physical therapy for Upper Extremity rehabilitation
Disclosures of Interest: No
Abstract N°: 2574
THE NEED FOR SPEED – WHY WALKING SPEED AFTER STROKE IS IMPORTANT FOR OPTIMISING FUNCTION AND WALKING PERFORMANCE
Hannah Jarvis*1, Philip Nagy1, Daniel Allen1, Ewan Dean1, James Smith1
1Lancaster University, Lancaster Medical School, Lancaster, United Kingdom
On behalf of:
Background and aims: Deriving a consensus on how gait is affected after a stroke is challenging. It is dependent on lesion size and shape, patient age, activity level and health status. No study has comprehensively quantified the spectrum of how a stroke affects biomechanical function, which parameters are clinically meaningful and can drive rehabilitation intervention. This study compared joint kinematics and kinetics of young stroke survivors who walk <0.79m/s (slow) or >0.80m/s (fast) compared to a healthy able-bodied and provides clinical recommendations for guiding the gait rehabilitation of stroke survivors.
Methods: Twenty-two young stroke survivors (18-55years) were recruited from 6 hospital sites. Participants were classified by walking speed as slow (<0.79) or fast (>0.80m/s) and joint kinematics and kinetics at the pelvis, hip, knee, and ankle were measured during walking on level ground at self-selected speed.
Results: Ten walking biomechanical parameters correlated to walking speed (ρ>0.550). Stroke survivors in the slow group walked with significantly greater (pelvic range of sagittal motion p<0.009), or reduced range (hip adduction and abduction p<0.011), peak angle (hip extension p<0.011), moment (hip flexion p<0.029) for the paretic limb, and significantly reduced moment (hip flexion p<0.040) for the non-paretic limb compared to the fast group and control.
Conclusions: We are the first to report how biomechanical function during walking is compromised in young stroke survivors classified by walking speed as slow (<0.79m/s) or fast (>0.80m/s) and propose these peak angle, range of motion and moment parameters be used to inform rehabilitation programmes to improve walking for stroke survivors.
Disclosures of Interest: No
Abstract N°: 1130
FACTORS ASSOCIATED WITH FATIGUE AMONG PEOPLE WHO HAVE RETURNED TO WORK AFTER STROKE: AN EXPLORATORY STUDY
Anna Norlander*1,2, Ingrid Lindgren1,2, Christina Brogårdh1,2
1Lund University, Department of Health Sciences, Lund, Sweden, 2Skåne University Hospital, Department of Neurology, Rehabilitation Medicine, Memory Disorders and Geriatrics, Lund, Sweden
On behalf of:
Background and aims: Fatigue is a common problem after stroke that can negatively affect work resumption among younger stroke survivors. Little is understood about how to effectively support people with fatigue to be able to continue working. Therefore, the aim of this study was to explore the associations between fatigue and a) personal and stroke-related characteristics, b) functional impairments and c) work-related factors among individuals who have returned to work after stroke.
Methods: The study comprises cross-sectional data from a comprehensive postal survey one year after stroke. Fatigue was evaluated using the Fatigue Severity Scale (FSS). Multivariable logistic regression models were created to explore factors associated with fatigue (dependent variable).
Results: In total, 87 working stroke survivors were included in the study (mean age 52 years, women 37 %). Fatigue (FSS total score ⩾4) was reported by 43% of the participants. Several factors representing all the investigated areas were associated with fatigue. In a final pooled regression model, self-perceived low cognitive functioning (p<0.001), low decision control at work (p=0.021) and high quantitative job demands (p=0.031) had the strongest independent effects on the odds for having fatigue.
Conclusions: Among people who were working one year after stroke, fatigue was associated with both personal and stroke-related characteristics as well as functional impairments and work-related factors. This highlights the complex nature of post-stroke fatigue and the need to also consider the work environment as part of fatigue management interventions.
Disclosures of Interest: No
Abstract N°: 2299
LONG-TERM PROGNOSIS FOR 5-YEARS IN PATIENTS WITH ANEURYSMAL SUBARACHNOID HEMORRHAGE: THE KOSCO STUDY
Ho Seok Lee*1, Dae Hyun Kim1, Yun-Hee Kim2, Won Hyuk Chang1
1Samsung medical center, Department of Physical and Rehabilitation Medicine, Center for Prevention and Rehabilitation, Heart Vascular Stroke Institute, South Korea, 2Sungkyunkwan University, School of Medicine, South Korea
On behalf of: KOSCO study group
Background and aims: Long-term prognosis including functional recovery patterns in patients with aneurysmal subarachnoid hemorrhage (aSAH) are still not well-known. The aim of this study was to investigate the 5-year prognosis and functional outcome of patients with aSAH.
Methods: We retrospectively analyzed data of patients with aSAH from the Korean Stroke Cohort for Functioning and Rehabilitation study (KOSCO), up to 5 years after the onset. Assessments were performed sequentially from 7 days to 5 years after onset. Prognosis, including death, was measured by the modified Rankin Scale (mRS). Good prognosis was defined as an mRS score of 0 or 1. In addition, sequential functional outcomes were assessed using the Functional Independence Measure (FIM) in aSAH survivors at 5 years after onset.
Results: A total of 338 patients were included in KOSCO data. Among survivors of aSAH at 7 days, the 5-year mortality rate was 8.3%. 77.2% of the 338 patients with aSAH showed a good outcome 5 years after onset. The distribution of mRS plateaued at 12 months after onset, with 74.4% having no significant disability and 18.5% having some disability (Fig.1). Age, initial aSAH severity and K-MMSE at 7 days were identified as significant independent predictors of good prognosis at 12 months after onset (p<0.001, Nagelkerke R2=0.582). In aSAH survivors at 5 years, FIM showed a significant improvement up to 4 years after onset (p<0.05, Fig.2).
Conclusions: These results demonstrate the long-term prognosis in patients with aSAH. These results may provide insight into appropriate management in terms of functional outcome.
Disclosures of Interest: Yes This work was funded by the Research Program funded by Korea Disease Control and Prevention Agency.
Abstract N°: 296
ROBOT-ASSISTED GAIT THERAPY USING THE LOKOMAT IN SUBACUTE PHASE OF ISCHEMIC STROKE–A FINAL ANALYSIS OF RCT
Ondrej Volny*1,2, Iva Fiedorova3,4, Tomas Adamec3,4, Irina Chmelová3,4, Adela Konde5, Pavla Hanzlíková6, Michal Bar1,2, Sarka Banikova3,4
1University Hospital Ostrava, Department of Neurology, Ostrava, Czech Republic, 2University Ostrava, Faculty of Medicine, Department of Clinical Neurosciences, Ostrava, Czech Republic, 3University Hospital Ostrava, Department of Rehabilitation and Sports Medicine, Ostrava, Czech Republic, 4University Ostrava, Faculty of Medicine, Department of Rehabilitation and Sports Medicine, Ostrava, Czech Republic, 5Technical University of Ostrava, Faculty of Electrical Engineering and Computer Science, Ostrava, Czech Republic, 6University Hospital Ostrava, Department of Radiodiagnostics, Ostrava, Czech Republic
On behalf of:
Background and aims: Robot-assisted gait training (RAGT) represents a modern concept of neurorehabilitation. Limited data exist on efficacy of RAGT in combination with conventional rehabilitation in subacute phase of stroke. This study aimed to determine the additive effect of protocol-defined RAGT on the Functional Ambulation Categories (FAC), walking, balance and selected anthropometric parameters.
Methods: This is a randomised control trial with 1:1 PROBE design (NCT04910217) comparing two groups: conventional rehabilitation and RAGT group. All participants received a protocol-defined conventional rehabilitation (15 sessions over 3 weeks). The RAGT group had additional RAGT using the Lokomat Pro FreeD (15 sessions over 3 weeks). All subjects were evaluated for Functional Ambulation Categories (FAC), modified Rankin Scale (mRS), 10-meter walk test (10MWT), Timed Up and Go (TUG), Berg Balance Scale (BBS) and anthropometric parameters (BMI, Skeletal Muscle mass, Sarcopenic Index) by assessors blinded to intervention.
Results: Two hundred and two patients were screened between June 1, 2020, and November 30, 2022; 43 were included (19 in RAGT and 24 in conventional group). Median time-to-randomization was 12 days (IQR: 11-16), median age was 66 years (IQR: 58-71). Both groups improved in FAC and mRS. RAGT group improved also in the BBS (p<0.001) and Sarcopenic index (p<0.001). The improvement by ³2 FAC points (p=0.044), TUG (p=0.026) and BBS (p=0.034) was significant only in the RAGT group.
Conclusions: The addition of RAGT to conventional rehabilitation demonstrated beneficial effects on improving gait, balance and muscle mass in the subacute phase of stroke. Supported by grant: MH CZ-DRO-FNOs/2020.
Disclosures of Interest: No
Abstract N°: 1223
EARLY MOBILITY TRAINING AFTER SEVERE INTRACEREBRAL HAEMORRHAGE. A PROTOCOL DEVELOPED BY AN INTERNATIONAL COLLABORATION (PEMTEAM)
Ramage Emily*1,2,3
1Florey Institute, Heidelberg, 2Western Health, St Albans, 3University of Melbourne, Parkville
On behalf of: Lipson-Smith R, Baggio J, Delcourt C, Dorsch S, Edmonds G, Gandhi D, Hiddleson M, Hindson M, Inche Mat L, Kavanagh H, Lin C, Lio T, Maso I, Miranda L, Mullens A, Parsons B, Silver B, Suttie L, Thilarajah S, Ullberg T, WanAsyraf WZ, Weir M Bernhardt J
Background and aims: Clinicians identify further guidance regarding early mobility after intracerebral haemorrhage (ICH) is needed. If early mobility training is too intensive after ICH it may negatively influence clinical outcomes in this population. Applying best evidence with expert judgment, we developed an early mobility training protocol for people after severe ICH
Methods: Expert clinicians, research and people with lived experience of stroke across 9 countries working in diverse setting utilised a Value Focused Thinking approach to develop the protocol through iterative workshops. A staged process was used to define the key objectives of the protocol and then the protocol which included a decision matrix.
Results: Twenty-five stroke experts (including researchers, people with lived experience, neurologists, nurses and physiotherapists) collaborated through Stage 1 and 2. Absence of deterioration, agitation, blood pressure, oxygen saturation, cerebral perfusion pressure monitoring, management of acute interventions and seizures, palliative status, plans for surgical intervention and time post-event were key considerations identified for determining clinical readiness to initiate early mobility training after ICH. These factors with parameters defined (where appropriate) were integrated into the decision matrix for early mobility training after stroke.
Conclusions: The living protocol for early mobility training after severe ICH has been developed with best evidence and patient and clinical expertise. It is intended to meet current demand. Monitoring of safety, effect and implementability of the protocol with refinement are the next steps to progressing research and practice.
Disclosures of Interest: No
Abstract N°: 1319
A PILOT STUDY OF LONG-TERM HIGH-DOSE TELEREHABILITATION AT HOME
Anna Knill*1, Spencer Arbuckle2, Gabriela Rozanski3, Jenna Tosto-Mancuso3, Anastasia Ford2, Louis Derungs2, Michelle Chan-Cortés2, David Putrino3, Meret Branscheidt4,5,6
1ETH Zürich, Rehabilitation Engineering Laboratory, Zürich, Switzerland, 2MindMaze, Lausanne, Switzerland, 3Icahn School of Medicine at Mount Sinai, Department of Rehabilitation and Human Performance, New York, United States, 4cereneo Hertenstein - center for Neurology & Rehabilitation, Weggis, Switzerland, 5ETH Zürich, Health Science and Technology, Zürich, Switzerland, 6Lake Lucerne Institute AG, Vitznau, Switzerland
On behalf of:
Background and aims: Stroke rehabilitation requires high-dose therapy to achieve enduring and meaningful improvements. Unfortunately, in real-world settings, only a fraction of the recommended therapy is typically delivered due to patient-related issues like motivation and time constraints, and resource limitations such as therapist availability and cost.
This study aims to connect evidence-based recommendations with practical implementation, offering outpatients a long-term (⩾3 months) asynchronous and constantly available therapy platform at home.
Methods: 17 chronic stroke patients participated in a 12-18 week high-dose rehabilitation plan. Therapy involved independent, asynchronous home-training utilizing the game-based digital therapy device MindMotion GO, complemented by synchronous telerehabilitation sessions 1-3 times a week. In-person functional and physiological assessments were conducted at the program's beginning and end.
Results: Patients demonstrated strong adherence of 74% (percentage of patients who completed ⩾60 minutes of Active Training Time (ATT) per week) to the program, regardless of age and impairment, with an average of 118 minutes ATT across 3 days/week for 19.5±2.9 weeks. Improvements of +6.4±5.1 points in the Fugl-Meyer UE (p<0.01) and +6.1±4.4 points in the Berg Balance Scale (p<0.01) demonstrate meaningful clinically important changes for the majority of patients. Despite varied initial impairment levels, patients were overall highly satisfied and 83% wished to continue.
Conclusions: This primarily asynchronous telerehabilitation shows that long-term high-dose training at home can be delivered with minimal therapist involvement and improve clinical outcomes. The program's effectiveness, demonstrated by strong adherence and satisfaction, expands therapy accessibility to more patients.
Disclosures of Interest: Yes Spencer A. Arbuckle is a consultant for Mind Maze; Anastasia E. Ford, Louis T. Derungs, and Michelle H. Chan-Cortés are full-time employees of MindMaze.
Abstract N°: 2595
SENSOR-DERIVED PHYSICAL ACTIVITY BEHAVIOR AMONGST PEOPLE POST STROKE/TRANSIENT ISCHAEMIC ATTACK
Lucian Bezuidenhout*1, David Moulaee Conradsson1
1Karolinska Institutet, Department of Neurobiology, Care Sciences and Society, Stockholm, Sweden
On behalf of:
Background and aims: Mild strokes are the most prevalent type, accounting for about 60% of all strokes. There are multiple contributing risk factors to secondary stroke/transient ischaemic attack (TIA) with increasing physical activity (PA), coupled with reducing sedentary time, being paramount for recurrent stroke prevention. This study aimed to 1) describe and compare sensor-derived PA between people post stroke/TIA with different ambulation and sedentary behavior profiles, and 2) determine factors associated with low levels of PA and prolonged sedentary time.
Methods: One hundred and thirteen participants post stroke/TIA with mild symptoms were included. For the first aim, independent t-tests were used to compare the PA outcomes between the two ambulation (i.e., low PA: ⩽5000 vs. high PA >5000 steps/day) and sitting (i.e., prolonged sitting: ⩾8 vs.reduced sitting: <8 hours/day) subgroups. For the second aim, multiple logistic regression models were performed to determine potential factors associated with physical inactivity and prolonged sitting.
Results: The results showed a significant difference in total daily steps (3094 vs. 8624, p<.001), walking time (45 min vs. 107 min, p<.001), and sitting time (606 min vs 515 min, p=.012) between the low and high PA active groups post stroke/TIA. Furthermore, using a walking aid was associated with physical inactivity, whereas contextual factors; living alone and living in rural areas, were associated with prolonged sitting time.
Conclusions: Even though the participants had mild strokes/TIA symptoms, the results showed a large variation in physical activity behavior. The results also gave insight into contextual factors that need to be considered in stroke rehabilitation.
Disclosures of Interest: No
Moderated Poster – SAH and ICH – Day 1
Abstract N°: 3153
INFLUENCE OF EARLY ANXIETY/DEPRESSION ON LONGITUDINAL TRAJECTORIES OF FUNCTIONAL, COGNITIVE AND QUALITY-OF-LIFE OUTCOMES AFTER SEVERE ICH
Lourdes Carhuapoma*1, Radhika Avadhani2, Issam A. Awad3, Daniel F. Hanley4, Wendy Ziai5, Vishank Shah5
1The Johns Hopkins Hospital, Anesthesia and Critical Care Medicine, Baltimore, United States, 2Brain Injury Outcomes at Johns Hopkins University, Department of Neurology, Baltimore, United States, 3UChicago Medicine, Chicago, United States, 4Brain Injury Outcomes at Johns Hopkins University, Baltimore, United States, 5The Johns Hopkins University School of Medicine, Baltimore, United States
On behalf of:
Background and aims: We assessed the impact of early anxiety/depression on longitudinal trajectories of functional, cognitive and quality-of-life (QoL) outcomes after severe intracerebral/intraventricular hemorrhage (ICH/IVH).
Methods: Using trial-data from CLEAR-III and MISTIE-III, participants were dichotomized by presence or absence of moderate-to-severe anxiety/depression on EuroQol-5D three-level descriptive system at day-30. Functional, cognitive and QoL outcome trajectories over 1-year were compared using mixed-effects linear regression, treating day-of-assessment as fixed effects and participants as random effects.
Results: Among 871 ICH/IVH survivors at day-30, (mean[SD] age 59.4[11.9] years, 57.5% male, median[IQR] modified Rankin scale (mRS) 5[4-5]), moderate-to-severe anxiety/depression was reported by 49% at day-30 and 44% at 1-year. Linear trajectory of mean mRS was steeper between day-30 and 1-year among participants without early anxiety/depression (b-slope, -1.0[-1.1 to -0.8]; p<0.001) versus those with anxiety/depression (b-slope, -0.7[-0.8 to -0.6];p<0.001). Fewer participants with early anxiety/depression were independent for activities of daily living (ADL) (Barthel Index>60) at 1-year (67% versus 79%; p=0.002). MMSE trajectories were steeper between day-30 and 1-year in participants reporting anxiety/depression (b-slope, 8.1 [7.4 to 8.9]; p<0.001) versus not (b-slope, 6.0 [5.1 to 6.9]; p<0.001); no significant difference in cognitive dysfunction at 1-year (36% versus 29%; p=0.11). A greater proportion of participants with early anxiety/depression reported problems with societal activities at 1-year compared to those without (287 [83%] versus 185 [68.5%]; p<0.001).
Conclusions: Early anxiety/depression was associated with slower functional recovery, with greater long-term dependence in ADL and societal function, in survivors of severe ICH/IVH. Early anxiety/depression may be a therapeutic target in ICH/IVH recovery.
Disclosures of Interest: No
Abstract N°: 260
RAPID PREHOSPITAL IDENTIFICATION OF INTRACRANIAL HEMORRHAGE IN PATIENTS WITH ACUTE COMA USING A GFAP POINT-OF-CARE DEVICE
Love-Preet Kalra*1, Sabina Zylyftari1, Stephan Barthelmes1, Sebastian Humm1, Kristaps Blums1, Andreas Heilgeist2, Stephan Meckel3, Hannsjoerg Baum4, Sebastian Luger1, Christian Foerch1
1RKH Klinikum Ludwigsburg, Neurology, Ludwigsburg, Germany, 2RKH Klinikum Ludwigsburg, Department of Anesthesiology, Intensive Care Medicine and Pain Medicine, Ludwigsburg, Germany, 3RKH Klinikum Ludwigsburg, Institute of Diagnostic and Interventional Neuroradiology, Ludwigsburg, Germany, 4Regional Clinics Holding GmbH RKH, Institute for Laboratory Medicine and Transfusion Medicine, Ludwigsburg, Germany
On behalf of:
Background and aims: Prehospital triage and treatment of patients with acute coma is challenging for rescue services, as the underlying pathologic conditions are highly heterogenous. Glial fibrillary acidic protein (GFAP) has been recently identified as a biomarker of intracerebral hemorrhage. The aim of this study was to test the diagnostic value of a GFAP point-of-care device to rapidly differentiate intracranial hemorrhage from other causes of acute coma in the prehospital phase.
Methods: Patients who were admitted to the emergency department due to acute coma (Glasgow Coma Scale scores between 3-8) were enrolled prospectively. Blood samples were collected in the prehospital phase. Plasma GFAP measurements were performed on the i-STAT Alinity® (Abbott) device (duration of analysis 15 min). The primary endpoint was the underlying etiology of coma (i.e., the final diagnosis at hospital discharge).
Results:143 patients were enrolled (mean age 65±20 years, 42.6% female). GFAP plasma concentrations were strongly elevated in patients with intracranial hemorrhage (n=51) compared to all other etiologies (3352 pg/mL [IQR 613-10001] vs. 43 pg/mL [IQR 29-91.25], p<0.001). When using an optimal cut-off value of 101 ng/mL, sensitivity for identifying intracranial hemorrhage was 94.1% (specificity 78.9%, positive predictive value 71.6%, negative predictive value 95.9%). In-hospital mortality was strongly associated with prehospital GFAP values.
Conclusions: Increased GFAP plasma values in patients with acute coma identify intracranial hemorrhage with high diagnostic accuracy. Prehospital GFAP measurements on a point-of-care platform allow rapid stratification according to the underlying cause of coma by rescue services. This could have major impact on triage and management of these critically ill patients.
Prehospital probability charts for acute coma patients. Bar charts showing the probability of an intracranial hemorrhage (A). In-hospital mortality rates correlated to GFAP plasma value ranges are visualized in graph B
Disclosures of Interest: Yes Prof. Foerch is patent holder of the following European and US patent (No. 03021571.9): “Use of GFAP for identification of intracerebral hemorrhage”
Abstract N°: 1298
FACTORS ASSOCIATED WITH HAEMATOMA CLEARANCE RATE IN INTRACEREBRAL HAEMORRHAGE AND THEIR ASSOCIATION WITH CLINICAL OUTCOMES
Gemma Lancaster*1, Kayode Ogungbenro2, Lilli Nelson3, Hitesh Mistry4, Daniel F. Hanley5, Adrian Parry-Jones6
1University of Manchester, Manchester, United Kingdom, 2University of Manchester, Division of Pharmacy and Optometry, Manchester, United Kingdom, 3Alfred Health, Melbourne, Australia, 4University of Manchester, Division of Pharmacy, Manchester, United Kingdom, 5Johns Hopkins University, Baltimore, United States, 6Northern Care Alliance & University of Manchester, Manchester Academic Health Science Centre, Geoffrey Jefferson Brain Research Centre, Manchester, United Kingdom
On behalf of:
Background and aims: Large haematoma volumes worsen outcomes after intracerebral haemorrhage (ICH) through mechanical damage and secondary injury. Accelerating endogenous haematoma clearance may be beneficial. We investigated factors associated with haematoma clearance and whether clearance rate is associated with clinical outcomes.
Methods: A biexponential model of ICH volumes from CT scans (days 3-7, day 30) from medical patients in MISTIE II&III (n=165) was used to estimate haematoma clearance rate k. Multiple linear regression tested factors for association with k, including initial ICH volume (V0), intraventricular haemorrhage (IVH), haematoma surface area:volume ratio (S:V), age, location, oedema volume, and white blood cells and platelets at diagnosis. Associations with the modified Rankin Scale (mRS) score at day 180 were investigated with logistic regression.
Results: IVH (β=-0.274, 95%CI:-0.428 to -0.121, p=<0.001), V0 (β=-0.287, 95%CI:-0.451 to -0.082, p=0.003), lobar location (vs. deep) (β=-0.213, 95%CI:-0.354 to -0.072, p=0.003) and S:V (β=0.247, 95%CI:0.081 to 0.413, p=0.004) were significant predictors of ln(k).
Age (OR:1.066; 95%CI:1.030 to 1.103; p<0.001), V0 (OR:1.055; 95%CI:1.018 to 1.093; p=0.003), GCS (OR:0.749; 95%CI:0.628 to 0.892; p=0.001) and location (OR:0.241; 95%CI:0.060 to 0.972; p=0.046) were significant predictors of mRS at day 180. ln(k) was associated with mRS in univariable analysis (OR:0.398; 95%CI:0.165 to 0.960; p<0.040), but not when adjusting for other known predictors (OR:2.246; 95%CI:0.552 to 9.146; p=0.259).
Conclusions: IVH, V0, location and S:V were predictors of clearance rate. Clearance rate was not independently associated with outcome. Further investigation in a larger dataset will also investigate evolution of inflammatory markers and additional radiological characteristics.
Disclosures of Interest: No
Abstract N°: 1368
TIME TRENDS IN INCIDENCE, CASE FATALITY AND FUNCTIONAL OUTCOME OF INTRACEREBRAL HAEMORRHAGE: SYSTEMATIC REVIEW AND META-ANALYSIS
Axel Wolsink*1,2, Maaike Cliteur1,2, Charlotte van Asch3, Jeroen Boogaarts4, Ruben Dammers5, Gerjon Hannink6, Catharina Jm Klijn1,2, Floris Schreuder1,2
1Radboud University Medical Center, Neurology, Nijmegen, Netherlands, 2Donders Centre for Cognitive Neuroimaging, Nijmegen, Netherlands, 3Stichting Epilepsie Instellingen Nederland (SEIN), Zwolle, Netherlands, 4Radboud University Medical Center, Neurosurgery, Nijmegen, Netherlands, 5Erasmus MC, Neurosurgery, Rotterdam, Netherlands, 6Radboud University Medical Center, Medical Imaging, Nijmegen, Netherlands
On behalf of:
Background and aims: Intracerebral haemorrhage (ICH) accounts for approximately 28% of all strokes worldwide and has a high case fatality and number of disability-adjusted life-years. In this systematic review, we aim to provide a comprehensive overview of the incidence, 1-month case fatality, and 12-month functional outcome of ICH over the last 15 years.
Methods: We systematically searched PubMed and Embase from 2008 to April 2023 for prospective population-based studies describing the incidence, case fatality, or functional outcome of first-ever ICH. We used random-effects meta-analyses to pool the overall crude incidence, the percentage of patients deceased within 1 month, and the percentage of patients with good functional outcome after 12 months (or 3 or 6 months if not available), as defined by the authors on the modified Rankin Scale. Time trends were assessed using a weighted linear meta-regression.
Results: For the preliminary results, we identified 65 eligible studies, describing 70 cohorts with 10,864 ICH patients. Of these, 53 cohorts reported on overall crude incidence, 42 on case fatality, and 11 on functional outcome. The preliminary crude incidence was 28.1 (95% CI 22.0-35.9) per 100,000 person-years. The 1-month case fatality was 34.7% (95% CI 31.1-38.5), whereas the percentage of patients with good functional outcome was 33.9% (95% CI 26.3-42.3). We found no time trends in incidence, 1-month case fatality or 12-month functional outcome in our study period.
Conclusions: Our preliminary results emphasise the need for better preventive and acute treatments of ICH. The final results are expected in March 2024.
This review is registered on PROSPERO (CRD42023413314).
Disclosures of Interest: No
Abstract N°: 2381
HAEMATOMA INTERLEUKIN-1 RECEPTOR ANTAGONIST AFTER INTRACEREBRAL HAEMORRHAGE IS ASSOCIATED WITH GOOD OUTCOME AT ONE YEAR
Adrian Parry-Jones*1, Blessing Nyakutsikwa2, Wendy Ziai3, Matthew Gittins4, Daniel F. Hanley3
1University of Manchester, Geoffrey Jefferson Brain Research Centre, Salford, United Kingdom, 2University of Manchester, School of Medical Sciences, Manchester, United Kingdom, 3Johns Hopkins University, Baltimore, United States, 4University of Manchester, School of Health Sciences, Manchester, United Kingdom
On behalf of: MISTIE-III Investigators
Background and aims: The interleukin(IL)-1, IL-6, C-reactive protein (CRP) pathway plays a key role in the immune response in ICH and the naturally occurring IL-1 receptor antagonist (IL-1Ra) represents a potential treatment. We tested for associations between patient outcomes and cytokine concentrations in haematoma aspirate samples from ICH patients enrolled in MISTIE-III.
Methods: INFLAME-ICH was a prospective observational sub-study nested in MISTIE III. Daily haematoma aspirate was collected following stereotactic aspiration and thrombolysis until drain removal and daily venous blood was collected from medical and surgical patients for cytokine measurements in a central laboratory. Multiple regression models compared log10-transformed haematoma cytokine concentrations to modified Rankin Scale (mRS) score at 1 year and oedema extension distance (OED) at day 5, adjusting for severity index and age. Correlations between haematoma cytokine and plasma cytokine concentrations were determined.
Results: 89 patients were recruited (47 surgical, 42 medical). Mean haematoma log10[IL-1Ra] (OR:5.92; 95%CI:1.08 to 32.54; n=38) and mean haematoma log10[IL-6] (OR:3.23; 95%CI:1.33 to 7.81; n=45) were independently associated with mRS 0-3 (vs. 4-6) at 1 year. Haematoma log10[IL-1Ra] was lower in lobar bleeds (vs. deep; β-coefficient: -0.81; 95%CI:-1.45 to -0.16) and was associated with higher OED (β-coefficient: 0.16; 95%CI:0.01 to 0.32). Higher haematoma log10[IL-1β] was associated with higher plasma log10[CRP] (β-coefficient: 21x10-6; 95%CI:4x10-6 to 38x10-6; n=117 paired samples).
Conclusions: Higher haematoma IL-1Ra concentrations are independently associated with good outcome at one year, supporting further investigation of IL-1Ra as a potential treatment for ICH. Plasma CRP may be an indicator of upstream IL-1β-mediated haematomal inflammation.
Disclosures of Interest: No
Abstract N°: 2185
PREHOSPITAL TREATMENT IN THE STOP-MSU TRIAL OF TRANEXAMIC ACID IN ICH
Henry Zhao*1,2, Nawaf Yassi1,2, Teddy Wu3,4, Leonid Churilov1,5, Vignan Yogendrakumar1,2, Henry MA6, David Anderson7, Bruce Campbell1,2, Geoffrey A. Donnan1,2, Stephen Davis1,2
1The Royal Melbourne Hospital, Department of Neurology, Australia, 2The University of Melbourne, Department of Medicine, Royal Melbourne Hospital, Australia, 3Christchurch Hospital, Department of Neurology, New Zealand, 4New Zealand Brain Research Institute, New Zealand, 5The University of Melbourne, Melbourne Medical School, Australia, 6Monash Health, Department of Neurology, Australia, 7Ambulance Victoria, Australia
On behalf of: STOP-MSU Investigators
Background and aims: The neutral STOP-MSU RCT of tranexamic acid in ICH was the first haemostatic trial to include recruitment on a Mobile Stroke Unit (MSU). We aimed to investigate time metrics, hematoma growth and outcomes for participants receiving prehospital treatment on the recruiting MSU.
Methods: We conducted a post-hoc analysis of the STOP-MSU trial assuming neutral treatment effect. We compared MSU-recruited to hospital-recruited patients for treatment time, haematoma growth (dichotomised 33%/6ml or absolute growth) and 90-day mRS. Outcomes were analysed as a binary logistic regression adjusted for baseline haematoma volume.
Results: Of n=201 trial patients, 44(21.9%) were recruited on MSU. MSU-patients were older (med 71.5 vs 65y,p=0.191) with fewer deep ICH location (77.3% vs 86.6%,p=0.156) but other demographics, including baseline severity, BP and glucose were similar. MSU-patients received treatment faster from onset (76min[IQR 67.5-100] vs 107min[IQR 97-118],p<0.001) and were treated more frequently ⩽60min from onset (OR 15.0[95%CI 3.0-75.1]). MSU patients had higher rates of haematoma growth on both dichotomised (52.3% vs 36.3%,aOR 2.0[95%CI 1.0-4.2],p=0.062) and absolute criteria (median 3.3ml[IQR 0.5-17.8] vs 0.8ml[IQR -0.8-6.5], mean 16.0ml[SD28.5] vs 7.0[SD15.4]). No differences were observed in 90-day outcomes for mRS 0-3/return-to-baseline (40.9% vs 52.2%,aOR 0.75[95%CI 0.33-1.71]) and mortality (25.0% vs 14.7%,aOR 1.3[95%CI 0.4-3.8].
Conclusions: MSU-recruited patients received treatment ~30mins faster and were 15-fold more likely to receive treatment ⩽60min from onset. This resulted in approximately two-fold increased odds of haematoma growth, while absolute growth exceeded that of prior haemostatic trials. Although tranexamic acid was not associated with benefit, MSU-facilitated prehospital recruitment is valuable for future ICH trials.
Disclosures of Interest: No
Abstract N°: 2921
IMPACT OF MINIMALLY INVASIVE SURGERY ON MIDLINE SHIFT AND EARLY MORTALITY IN LARGE SUPRATENTORIAL SPONTANEOUS ICH: POST HOC ANALYSIS OF MISTIE III
Wendy Ziai*1, Yunke LI1, Joshua Gruber2, Meghan Hildreth1, Issam A. Awad3, Daniel F. Hanley1
1The Johns Hopkins University School of Medicine, Baltimore, United States, 2Johns Hopkins Bloomberg School of Public Health, Baltimore, United States, 3The University of Chicago Pritzker School of Medicine, Chicago, United States
On behalf of: MISTIE-III Investigators
Background and aims: Minimally invasive surgery (MIS) for large supratentorial intracerebral hemorrhage (ICH) addresses primary brain injury through reduction of mass effect causing midline shift (MLS). We investigated associations between MIS, MLS and mortality in a large clinical trial.
Methods: Retrospective analysis of all 499 patients from the Minimally Invasive Surgery with intra-hematomal delivery of rtPA for large ICH Evacuation (MISTIE-III) trial. We assessed MLS at pineal gland (PG) and septum pellucidum (SP) on CT scans at diagnosis, end of treatment (EOT) and hospital discharge. Primary outcome was day 30 mortality. We performed multivariable logistic regression analyses adjusted for demographics, ICH characteristics and treatment.
Results: Participants had median age 62 years, 61% male, and median ICH volume 44 mL. Day 30 mortality was 12%. MLS on EOT CT in day 30 surgical survivors was significantly lower compared to medically treated survivors and non-survivors, respectively (PG: 1.87 vs 3.22 vs 3.85 mm; p<0.001, and SP: 2.78 vs 4.83 vs 6.70 mm; p <0.001). The odds of day 30 mortality were significantly increased per 1mm increase in MLS at both PG and SP (PG: odds ratio[OR], 1.22; 95% confidence interval[CI]: 1.06-1.41; SP: OR, 1.22; 95% CI, 1.10-1.36). Thresholds of MLS change <3mm (SP) and <5mm (PG) were associated with mortality reduction. Association of MIS with day 30 mortality was significantly mediated by change in SP MLS from diagnostic to EOT CT (natural direct effect[95%CI], -0.001[-0.08-0.08]; p=0.99; natural indirect effect[95%CI], -0.04[-0.08-0.003]; p=0.04).
Conclusions: Among ICH surgical candidates, reduction in MLS significantly mediated reduction in day 30 mortality with MIS.
Disclosures of Interest: No
Abstract N°: 2199
ASSOCIATION OF INTRACEREBRAL HEMORRHAGE SUBTYPE AND CEREBRAL MICROBLEEDS LOCATION IN PATIENTS WITH ISCHEMIC CEREBROVASCULAR EVENTS
Bonaventure YM Ip*1, Philip Nash2, Kui Kai Lau3, Joan Martí-Fàbregas4, Simon Jung5, Nils Peters6, Fethiye Dilek Orken7, Jonathan Best2, David Werring2, Yannie, Oi Yan Soo1
1The Chinese University of Hong Kong, Medicine and Therapeutics, Hong Kong, 2UCL Queen Square Institute of Neurology, Brain Repair and Rehabilitation, United Kingdom, 3University of Hong Kong, Medicine, Hong Kong, 4Biomedical Research Institute, Hospital de la Santa Creu i Sant Pau, Spain, 5University Hospital Inselspital Bern, Neurology, Switzerland, 6University Hospital Basel, Neurology and Stroke Centre, Switzerland, 7Istanbul Arel University, Neurology, Turkey
On behalf of: Duncan Wilson, Gareth Ambler, Gregory Lip, Houwei Du, Rolf Jager, Rustam Al-Shahi Salman, Heinrich Mattle, Leonidas D Panos, Martina B Goeldlin, Marwan El-Koussy, Urs Fischer, Franz Fazekas, Sebastian Eppinger, Simon Fanler-Hofler, Thomas Gattringer, Aad van der Lugt, Dianne H.K. van Dam-Nolen, Eline Kooi, Florian Dubost, Jeroen Hendrikse, Paul J. Nederkoorn, Werner Mess, Chris Karayiannis, Lee-Anne Slater, Thanh Phan, Velandai Srikanth, Ji-Hoe Heo, Tae-Jin Song, Young Dae Kim, Alejandro Martinez Domeno, Beatriz Gomez Anson, Luis Prats-Sánchez, Roger Collet, Hideo Hara, Jun Tanaka, Masaaki Yoshikawa, Masashi Nishihara, Shuhei Ikeda, Yusuke Yakushiji, Zeynep Tanriverdi, Eric E. Smith, Shelagh B. Coutts, Henry Mak, Kay Cheong Teo, Alexandros A Polymeris, Annaelle Zietz, David Seiffge, Philippe Lyrer, et al.
Background and aims: The role of cerebral microbleeds (CMBs) distribution in predicting deep and lobar intracerebral haemorrhage (ICH) is uncertain among patients with ischaemic stroke. This study aimed to determine the association of ICH subtype and CMBs distributions.
Methods:We performed a nested case-control study within the Microbleed International Collaboration Network that included patients with a history of ischemic stroke or transient ischemic attack. CMBs distribution was categorized into lobar, deep, mixed. Each case consisted of lobar ICH, deep ICH, or mixed ICH. Controls were matched by propensity scores based on age, sex, ethnicity, medical comorbidities, antithrombotic regimen, follow-up period, and CMBs burden. We determined the risk of ICH subtype with initial CMBs distributions by logistic regression.
Results: Over a median follow-up period of 15 months (IQR 4-26), we identified 64 patients with deep ICH, 33 with lobar ICH, and 4 with mixed ICH. We identified 449 matched controls from a total of 6342 patients under the MICON network. Lobar CMBs were associated with lobar ICH (aOR 3.79, 95%CI 1.51-9.52, p=0.005). Deep CMBs were associated with deep ICH (aOR 3.91, 95%CI 1.77-8.67, p=0.001) and lobar ICH (aOR 2.68, 95%CI 1.01-7.13, p=0.048). Mixed CMBs were associated with deep ICH (aOR 4.18, 95%CI 1.99-8.81, p<0.001).
Conclusions:The association between deep CMBs and lobar ICH provides evidence that a subset of lobar ICH could be related to hypertensive arteriopathy. Additional biomarkers such as cortical superficial siderosis are warranted to reliably differentiate between hypertensive arteriopathy and cerebral amyloid angiopathy to guide antihypertensive and antithrombotic therapy.
Disclosures of Interest: No
Moderated Poster – Small Vessel Disease and Cognition – Day 1
Abstract N°: 178
LONGITUDINAL ASSOCIATION OF CARDIOMETABOLIC MULTIMORBIDITY WITH DEMENTIA IN THE UK BIOBANK
Yang Zhao1,2, Wendy Wang2, Mark Woodward2,3, Craig Anderson2, John Chalmers2, Cheryl Carcel2, Lili Song1, Katie Harris*2
1The George Institute for Global Health, Beijing, China, 2The George Institute for Global Health, University of New South Wales, Sydney, Australia, 3The George Institute for Global Health, Imperial College, London, United Kingdom
On behalf of:
Background and aims: Multiple chronic diseases could have a lasting impact on cognitive function in later life through biological and socioeconomic pathways. The aim of this study was to determine associations of cardiometabolic multimorbidity (CMM) and dementia.
Methods: The UK Biobank is a large-scale prospective population-based cohort study of 500,000+ women and men aged 40 to 69 years recruited between 2006 and 2010. CMM was defined at baseline as presence of ⩾2 chronic cardiovascular and/or metabolic conditions: hypertension, hyperlipidaemia/dyslipidaemia, diabetes, hyperuricaemia, central obesity, heart disease, and stroke. Cox proportional hazards models were used to estimate hazard ratios (HR) with 95% confidence intervals (CI) of CMM and incident dementia, adjusting for sociodemographic factors.
Results: There were 7,129 (47.8% women) with incident dementia (median 12.7 years follow-up) in 480,462 UK Biobank participants without dementia at baseline.
There was a 30% higher risk of incident dementia with CMM (vs no CMM) similarly in women HR (95%CI) 1.31 (1.22, 1.41), and men 1.32 (1.22, 1.42). In subgroup analysis, CMM was associated with a higher risk of dementia in participants who were young (<60 years) and with greater socioeconomic disadvantage, and obesity. Of the seven cardiometabolic conditions, stroke (vs no stroke) was associated with twice the risk of dementia, similarly in women 1.98 (1.68, 2.08) and men 2.08 (1.84, 2.36).
Conclusions: CMM is associated with a higher risk of dementia, particularly in younger adults and those with low socioeconomic status and obesity. Timely identification of CMM and preventing disease accumulation might improve cognitive function and prevent dementia.
Disclosures of Interest: No
Abstract N°: 3239
LONG-TERM INCIDENCE OF DEMENTIA ASSOCIATED WITH TRANSIENT ISCHEMIC ATTACK: A LONGITUDINAL, MATCHED COHORT STUDY
Vasileios-Arsenios Lioutas*1,2, Gina Peloso2,3, Jose Rafael Romero2,4, Hugo Aparicio2,4, Mitzi Gonzales5, Dibya Himali2,4, Jayandra Himali2,6,7, Vasan Ramachandran2,6, Alexa Beiser2,3, Sudha Seshadri2,7
1Beth Israel Deaconess Medical Center, Boston, United States, 2Framingham Heart Study, Framingham, United States, 3Boston University, Biostatistics, Boston, United States, 4Boston University Medical Center, Neurology, Boston, United States, 5Cedars-Sinai, Jona Goldrich Center for Alzheimers and Memory Disorders, Los Angeles, United States, 6The University of Texas School of Public Health San Antonio, San Antonio, United States, 7Glenn Biggs Institute for Alzheimer's and Neurodegenerative Diseases, San Antonio, United States
On behalf of:
Background and aims: The association between transient ischemic attack (TIA) and dementia is incompletely characterized. Determining the cognitive sequalae of TIA is important as it can function as an early warning sign. We sought to determine the long-term incidence of post-TIA dementia and examined whether TIA prompts changes in vascular risk factor control.
Methods: Nested matched longitudinal cohort study within the Framingham Heart Study. Prospectively collected sample of non-demented TIA- free participants matched on age and sex (5:1) to participants with first incident TIA >60 years. Main outcome was the 20-year incidence of all-cause dementia.
Results: 297 participants with TIA, 141(47%) men, mean age 72.7±7.7 years were matched to 1485 TIA-free controls.TIA cases were significantly more likely to have hypertension, coronary heart disease and atrial fibrillation. Over 20 years of follow up, 57(19%) participants with TIA and 353(24%) controls developed dementia (HR 0.93, 95% CI (0.85-1.19), p=0.63). Adjusting for stroke and accounting for the competing risk of death did not alter this association. Participants with TIA were more likely to have a significant reduction in the frequency of smoking (18% to 11%, p=0.025), a significant increase in anticoagulant use from 3% to 18%, (p=0.0005), and a marginal increase in aspirin use (46% to 61%, p=0.052).
Conclusions: We found no significant difference in dementia incidence over a 20-year follow up period compared to matched TIA-free controls. Our findings suggest that TIA might act as forewarning, prompting treatment and behavioral shifts that mitigate cardiovascular risk and therefore might act preventatively for dementia
Disclosures of Interest: No
Abstract N°: 907
MAPPING THE LESION NEUROANATOMY OF POST-STROKE SENSORY HYPERSENSITIVITY: INSIGHTS FROM LESION-SYMPTOM AND CONNECTIVITY ANALYSIS
1KU Leuven, Brain and Cognition, Leuven, Belgium, 2Hospital East-Limbourgh, Department Psychology, Genk, Belgium, 3Centre for Translational Psychological Research (TRACE), Genk, Belgium, 4KU Leuven, Department of Neurosciences, Leuven, Belgium, 5University Hospitals Leuven, Department of Neurology, Leuven, Belgium, 6Hospital East-Limbourgh, Neurology, Genk, Belgium, 7Utrecht University, Experimental Psychology, Utrecht, Netherlands, 8University Medical Center Utrecht, Department of Neurology and Neurosurgery, Utrecht, Netherlands, 9RevArte Rehabilitation Hospital, Antwerp, Belgium, 10KU Leuven, Department of Movement Sciences, Leuven, Belgium
On behalf of:
Background and aims: Patients with acquired brain injuries, including stroke survivors, commonly report heightened sensory sensitivity following their injury, impacting functional outcomes. However, the precise neural mechanisms behind these symptoms remain unknown. Taking advantage of the visibility of focal stroke lesions through imaging, this study aimed to investigate the neural basis of post-stroke sensory hypersensitivity.
Methods: To pinpoint the specific lesion locations and white matter tracts associated with post-stroke sensory hypersensitivity, we used multivariate support vector regression lesion-symptom mapping and indirect structural disconnection mapping in a cohort of 103 first-ever subacute stroke survivors.
Results: Among the participants, 48% reported experiencing post-stroke sensory hypersensitivity across various sensory modalities. Our analyses revealed several neural structures implicated in post-stroke sensory hypersensitivity. These encompassed the basal ganglia, thalamus and insula in the grey matter, as well as the fronto-insular tract and uncinate fasciculus in the white matter.
Conclusions: Our analysis of post-stroke sensory hypersensitivity in a large stroke cohort sheds light on the neuroanatomical underpinnings of this phenomenon. Our findings highlight the involvement of specific brain regions and white matter tracts, advancing our understanding of the neural mechanisms contributing to and those at risk for developing post-stroke sensory hypersensitivity.
Disclosures of Interest: No
Abstract N°: 1759
HOW DO NURSES ASSESS AND MANAGE POST-STROKE COGNITIVE IMPAIRMENT IN A MIDDLE-INCOME COUNTRY. A MIXED-METHODS STUDY IN INDONESIA
Arina Nurfianti*1,2, Terence J Quinn3, Grigorios Kotronoulas1, Lisa Kidd4
1University of Glasgow, School of Medicine, Dentistry and Nursing, United Kingdom, 2Universitas Tanjungpura, School of Nursing, Indonesia, 3University of Glasgow, School of Cardiovascular and Metabolic Health, United Kingdom, 4Glasgow Caledonian University, School of Health and Life Sciences, United Kingdom
On behalf of:
Background and aims: The evidence-base for managing post-stroke cognitive impairment (PSCI) is increasing. However, guidance around the application of this evidence is limited for nursing practice particularly in low- and middle-income countries where the prevalence of stroke disabilities and the challenges are higher. This study aims to explore and understand nurses’ roles in assessing and managing PSCI in Indonesia.
Methods: The study employed mixed methods and involved nurses who worked in all stroke care setting in Indonesia. The quantitative study was a cross-sectional online survey identifying familiarity of stroke guidelines, assessment tools and PSCI management. The survey was distributed via Indonesian Neuroscience Nurses Association and Twitter. Quantitative data were analysed descriptively. The qualitative study involved one-to-one in-depth interviews and thematic analysis was used to analyse the data.
Results: We analysed 162 survey data and 17 interview data from nurses. Only 22.8% (36/158) of respondents routinely assessed PSCI. Just over 30% (49/152) of nurses reported having role in PSCI management, however more nurses claimed they used physical exercise (81.4%,127/156) or cognitive rehabilitation (29.5%, 46/156) interventions in PSCI management. Qualitative findings revealed cognitive assessment is primarily conducted by medical doctors; nurse’s emphasis on therapeutic communication; absence of rehabilitation nurse roles; and unequal nurse training of cognitive management.
Conclusions: Nursing practice for PSCI in Indonesia needs improvement. Education support through training programmes is a possible means to enhance the care quality for people living with PSCI. Addressing the issues and challenges is imperative to improve nurses’ roles in PSCI care and optimise patient outcomes.
Disclosures of Interest: No
Abstract N°: 3148
PARKINSONISM IN CEREBRAL SMALL VESSEL DISEASE IS RELATED TO DISRUPTION OF SPECIFIC WHITE MATTER TRACTS: A 14 YEAR FOLLOW-UP STUDY
Mina Jacob*1, Hao LI1, Mengfei Cai2, Mayra Bergkamp1, Rianne Esselink1, Marco Duering3, Frank-Erik De Leeuw4, Anil Tuladhar4
1Radboud University Medical Center, Department of Neurology; Radboud Institute for Medical research and Innovation and Donders Institute for Brain, Cognition and Behaviour. The Netherlands, Neurology, 2Department of Neurology, Guangdong Neuroscience Institute, Guangdong Provincial People's Hospital, Guangdong Academy of Medical Sciences, Southern Medical University, Guangzhou, China., Neurology, 3Medical Image Analysis Center (MIAC AG) and qbig, Department of Biomedical Engineering, University of Basel, Basel, Switzerland., Neurology, 4Radboud University Medical Center, Department of Neurology; Radboud Institute for Medical research and Innovation and Donders Institute for Brain, Cognition and Behaviour. The Netherlands
On behalf of:
Background and aims: Converging evidence suggest that small vessel disease (SVD) is associated with incidence and severity of Parkinsonism. However, a knowledge gap still exists regarding how SVD contributes to Parkinsonism, specifically, whether it occurs 1) by affecting strategic white matter tracts, or 2) as a result of widespread disruption of the white matter. We investigated the association between Parkinsonism and (progression of) Parkinsonian signs, and microstructural integrity of different white matter tracts.
Methods: This study is embedded within the RUNDMC-study, a longitudinal prospective cohort-study on sporadic SVD patients. Patients underwent motor tests in 2006, 2011, 2015, and in 2020. Parkinsonism screening was based on the UK-Brain-Bank-criteria, and Parkinsonian signs according to the Unified Parkinson's Disease Rating Scale (UPDRS). Imaging data from a standardized MRI-protocol in 2020 was used. We analyzed the white matter integrity (mean diffusivity) of 72 white mater tracts by using TractSeg, a convolutional neural network based white matter tract segmentation approach that is derived from diffusion-weighted MRI
Results: 228 patients were included. 18 (7.9%) participants had parkinsonism; median UPDRS-score of all patients was 6 (IQR 5-8). Of the 72 tracts, integrity of mainly the thalamic, thalamo-prefrontal, thalamo-premotor, striato-prefrontal, and striato-premotor tracts, were associated with prevalent Parkinsonism, severity of UPDRS-score, and 14-year progression of UPDRS-score (all P<0.0001; Table 1).
Conclusions: Parkinsonism in SVD might result from damage in specific strategic white matter tracts, rather than a widespread white matter disruption. This data aids in understanding the pathogenesis of vascular Parkinsonism. Future imaging studies in Parkinsonism should put more focus on the identified tracts.
Disclosures of Interest: No
Abstract N°: 322
CONTRIBUTION OF NOTCH3 R544C VARIANT AND HYPERTENSION IN CEREBRAL HEMORRHAGE AMONG CADASIL PATIENTS
Chihhao Chen*1, Ruiting Zhang2, Yu-Wen Cheng1, Sophie Tezenas Du Montcel3, Hugues Chabriat4, Sung-Chun Tang1
1National Taiwan University Hospital, Neurology, Taipei, Taiwan, 2The Second Affiliated Hospital of Zhejiang University, School of Medicine, Hangzhou, China, 3Sorbonne Université, Paris Brain Institute, Inria, AP-HP, Paris, France, 4Lariboisière Hospital AP-HP, Paris, France
On behalf of:
Background and aims: Intracerebral hemorrhage (ICH) in CADASIL has been frequently reported among CADASIL patients carrying certain NOTCH3 variant. We aimed to investigate the contributions of NOTCH3 variants and hypertension to ICH in CADASIL.
Methods: We enrolled patients from two independent CADASIL cohorts in France and Taiwan. Clinical history and neuroimaging features were recorded. Logistic regression and mediation analyses were used to investigate factors associated with ICH.
Results: Of 552 patients with CADASIL (440 from France and 112 from Taiwan), 34 had history of ICH. Patients with ICH were older (62.9±11.4 vs 53.4±12.3 years), had higher proportion of NOTCH3 R544C variant (79.4% vs 15.3%) and hypertension (85.3% vs 24.9%, all P<0.01). On neuroimaging, they had more cerebral microbleeds, worse cerebral atrophy, and more severe basal ganglia dilated perivascular space. NOTCH3 R544C variant (OR 9.9, 95% CI 3.8–25.6) and hypertension (7.9, 2.8–22.1) were each independently associated with ICH. Having both NOTCH3 R544C variant and hypertension carried a significantly higher risk of ICH (36.9% if both present, 7.3% if having NOTCH3 R544C variant only, 5.4% if having hypertension only, and 0.6% if both absent; Ptrend < 0.01); the attributable proportion due to the additive interaction effects was 67.1%. Finally, 49.9% of the effects of NOTCH3 R544C variant on the occurrence of ICH were mediated by hypertension.
Conclusions: Both NOTCH3 R544C variant and hypertension were independent risk factors for ICH in CADASIL patients, and the two factors may act additively. Our results reveal the potential heterogeneity of vascular pathology across different loci of NOTCH3 variants in CADASIL.
Disclosures of Interest: No
Abstract N°: 1310
PERIVASCULAR AND PARENCHYMAL BRAIN FLUID DIFFUSIVITY IN PATIENTS WITH A RECENT LACUNAR STROKE
Salvatore Rudilosso*1, Carlos Laredo2, Emma Muñoz-Moreno2, Angels Calvet2, Alejandro Rodríguez Vázquez1, Andres Girona1, Xabier Urra1, Maria Dels Angels Calderon3, Francisco Gil4, Angel Chamorro1
1Hospital Clínic de Barcelona, Neurology, Barcelona, Spain, 2Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain, 3Universitat de Barcelona, Barcelona, Spain, 4Hospital Universitari Sagrat Cor, Barcelona, Spain
On behalf of:
Background and aims: Fluid exchanges between perivascular spaces (PVS) and the interstitium might be involved in waste removal mechanisms in small vessel disease (SVD). We aimed to analyze brain fluid diffusivity measures and their relationship with PVS load and SVD severity in patients with lacunar stroke.
Methods: Transversal study of 50 consecutive patients admitted with a recent lacunar stroke. We collected clinical variables including a sleep quality questionnaire (PSQI score). The 3-Tesla MRI protocol included multishell-diffusion images to measure free water (FW) content in the extracellular space of normal-appearing white matter (NAWM) and basal ganglia (BG), and water diffusivity along the perivascular spaces (ALPS index). We calculated white matter hyperintensity / intracerebral volume ratio (WMH ratio) and PVS ratio in BG and WM regions using automatic segmentation algorithms. We counted lacunes and microbleeds, then we calculated a summary SVD score. We used linear regression models to assess the correlations in univariable and multivariable models including age, sex, history of hypertension, diabetes, and PSQI score.
Results: PVS load was associated with FW-NAWM and FW-BG in univariable (p<0.001) and multivariable models (p<0.02), but not with ALPS index. FW-NAWM did not correlate with ALPS index. Higher FW-NAWM was related to WMH ratio, lacunes and microbleeds count, and summary SVD in univariable models and remained significant (p=0.015) for WMH ratio in multivariable models.
Conclusions: The increased extracellular water in SVD suggests impaired brain fluid dynamics associated with PVS dilation, while perivenular fluid drainage dysfunction remained uncertain. Diffusivity measures as markers of waste removal function should be validated in further studies.
Disclosures of Interest: No
Abstract N°: 261
CEREBROVASCULAR REACTIVITY IN SPORADIC CEREBRAL SMALL VESSEL DISEASE: A LONGITUDINAL STUDY
Emilie Sleight1, Michael Stringer*1, Una Clancy1, Carmen Arteaga Reyes1, Daniela Jaime Garcia1, Maria Valdes-Hernandez1, Francesca Chappell1, Fergus Doubal1, Michael Thrippleton1,2, Joanna Wardlaw1,2
1University of Edinburgh, Centre for Clinical Brain Sciences and UK Dementia Research Institute, Edinburgh, United Kingdom, 2University of Edinburgh, Edinburgh Imaging Facility (Royal Infirmary of Edinburgh), Edinburgh
On behalf of: the Mild Stroke Study-3 study group
Background and aims: Patients with higher cerebral small vessel disease (SVD) burden have lower cerebrovascular reactivity (CVR). However, how CVR relates to SVD evolution is underexplored. We assessed associations between CVR and one-year progression in SVD features, cognition, stroke recurrence, incident infarcts, stroke severity and outcome.
Methods: We recruited patients with mild stroke (Mild Stroke Study-3: ISRCTN 12113543). We acquired baseline and one-year 3T brain MRI to assess quantitative SVD features using STRIVE-1 criteria, computational white matter hyperintensity (WMH) and perivascular space (PVS) volumes and, at baseline, CVR in subcortical grey (SGM), normal-appearing white matter (NAWM) and WMH. We assessed cognition, stroke severity and dependence using Montreal cognitive assessment, NIHSS and mRS. We recorded recurrent stroke/TIA diagnosis and new incident infarct visibility at one-year. We ran separate multivariable linear/logistic regressions between each one-year SVD feature or clinical/cognitive score as outcome adjusted for baseline value, age, sex and key vascular risk factors with CVR (independent variable).
Results: 163/208 patients (age:32.7-86.3y,Male:68%) had adequate baseline CVR data and one-year structural images. Patients with lower baseline CVR had increased WMH (e.g. NAWM:B=-1.14,95% confidence interval (95%CI)=[-2.13,-0.14]) and PVS (e.g. NAWM:B=-1.90,95%CI=[-3.21,-0.60]) volumes at one-year (Fig.1). We found no associations between CVR and one-year change in lacunes, microbleeds, brain volume, cognition, stroke severity or dependence. While patients with new stroke/TIA had lower CVR, these represented only 3% of the cohort.
Conclusions: Lower baseline CVR predicted SVD progression (WMH and PVS volume increase) over one-year. Further research is needed to determine whether reductions in CVR cause tissue damage linked to SVD or vice versa.
Disclosures of Interest: No
Abstract N°: 1948
SAFETY OF ENDOVASCULAR THERAPY IN ISCHEMIC STROKE PATIENTS ⩾ 90 YEARS – A COHORT STUDY FROM THE EVA-TRISP COLLABORATION
Jasmine Jost*1, Christian Nolte2, Guido Bigliardi3, Gian Marco De Marchis4, Sami Curtze5, Paul Nederkoorn6, Patrik Michel7, Susanne Wegener8, Mirjam Rachel Heldner9, Henrik Gensicke10
1University Hospital Basel, Neurology, Switzerland, 2Charité – Universitätsmedizin Berlin, Klinik und Hochschulambulanz für Neurologie, Germany, 3Modena University Hospital, Department of Neuroscience, Ospedale Civile di Baggiovara, Italy, 4Kantonsspital St. Gallen, Department of Neurology, Switzerland, 5University of Helsinki and Helsinki University Hospital, Neurology, Finland, 6Amsterdam UMC location University of Amsterdam, Neurology, Netherlands, 7Lausanne University Hospital and University of Lausanne, Neurology, Switzerland, 8University Hospital Zurich and University of Zurich, Neurology, Switzerland, 9Inselspital, Bern University Hospital and University of Bern, Neurology, Switzerland, 10University Department of Geriatric Medicine FELIX PLATTER and University of Basel, Neurology and Neurorehabilitation, Switzerland
On behalf of: EndoVAscular treatment and Thrombolysis for Ischemic Stroke Patients (EVA-TRISP) collaborators
Background and aims: Data on safety of endovascular therapy (EVT) in the very elderly are scarce. Using data from a large prospective EVT registry, we aimed at providing better evidence for EVT decision-making in patients aged 90 years and older.
Methods: This multicenter observational study from the EndoVAscular treatment and ThRombolysis for Ischemic Stroke Patients Registry (EVA-TRISP) compares patients ⩾90 years with those <90 years using multivariate logistic regression analysis and reporting odds ratios and 95% confidence intervals. Covariates were chosen by a step-down approach. Primary outcomes were occurrence of symptomatic intracranial hemorrhage (sICH, defined by ECASS-II-/III-criteria), poor functional outcome in survivors (defined by mRS 3-5 if pre-stroke mRS 0-2 and mRS 4-5 if pre-stroke mRS 3-5) and mortality at 3 months after stroke.
Results: Of 11’615 eligible patients, 746 were ⩾90 years old (6.4%). Patients ⩾90 years had higher median NIHSS on admission (16 vs. 14) and more often pre-stroke mRS 3-5 (33.5% vs. 7.8%). The probability of poor functional outcome (ORadjusted, 4.23 [2.73-6.55]; 60.8% vs. 38.5%) and death (ORadjusted, 3.37 [2.41-4.72]; 55.8% vs. 21.1%) was significantly higher in patients ⩾90 years. However, the probability of sICH did not differ significantly between both groups (ORadjusted, 1.17 [0.82-1.66]; 6.1% vs. 5.3%).
Conclusions: EVT-treated stroke patients aged 90 years and older had higher mortality and poor functional outcome rates compared to younger patients. However, the probability of sICH after EVT was not increased, indicating that EVT should not be refrained from all stroke patients in this age group.
Disclosures of Interest: No
Abstract N°: 411
PREDICTORS OF FUTILE RECANALIZATION IN NONAGENARIANS WITH MECHANICAL THROMBECTOMY: A MULTICENTRE OBSERVATIONAL STUDY
Lucio D'ANNA*1, Michele Romoli2, Liqun Zhang3, Mohamed Aggour3, Matteo Foschi4, Maria Ruggiero2, Kyriakos Lobotesis1, Giovanni Merlino5, Mariarosaria Valente5, Soma Banerjee1
1Imperial College London, United Kingdom, 2Maurizio Bufalini Hospital, Cesena, Italy, 3St George’s University Hospitals NHS Foundation Trust, United Kingdom, 4University of L'Aquila, L'Aquila, Italy, 5Università degli Studi di Udine, Udine, Italy
On behalf of: STUDY COLLABORATORS
Background and aims: There is a lack of data regarding patients aged 90 years or older undergoing mechanical thrombectomy and their predictors of futile recanalization. We sought to evaluate the predictors of futile recanalization in patients ³ 90 years with large vessel occlusion undergoing mechanical thrombectomy.
Methods: This multicentre observational study included patients ³ 90 years consecutively treated with mechanical thrombectomy in four thrombectomy capable centres between January 1st, 2016 and 30th March 2023. Futile recanalization was defined as large vessel occlusion patients experiencing a 90-day poor outcome (mRS 3–6) despite successful recanalization (mTICI⩾2b) after mechanical thrombectomy.
Results: Our cohort included 139 patients ³ 90 years with acute ischemic stroke due to anterior circulation large vessel occlusion treated with mechanical thrombectomy (FIGURE 1). 117 of 139 patients ³ 90 years who achieved successful recanalization were included in the analysis (76 female (64.9%)), of whom, 31 (26.49%) experienced effective recanalization and 86 (73.51%) experienced futile recanalization. Patients with futile recanalization had higher NIHSS on admission (p<0.001); they were less frequently treated with intravenous thrombolysis (p=0.048), had more often general anaesthesia (p = 0.011) and longer door to groin puncture delay (p=0.002). Multivariable regression analysis showed that use of intravenous thrombolysis was associated with reduced probability of futile reperfusion (FIGURE 2)
Conclusions: Our study suggests that mechanical thrombectomy with intravenous thrombolysis is associated with reduced probability of futile reperfusion in a multi-centre cohort of patients aged 90 years or older.
Disclosures of Interest: No
Abstract N°: 831
CLINICAL FRAILTY SCALE AS A PROGNOSTIC MARKER IN ELDERLY PATIENTS UNDERGOING MECHANICAL THROMBECTOMY FOR ACUTE ISCHAEMIC STROKE
Joshua Yeo*1, Volker Maus2, Sebastian Fischer2, Stefab Schob3, Davide Simonato4, Giacomo Cester5, Joseph D. Gabrieli5, Teddy Wu6, Benjamin Tan1, Leonard Yeo1
1National University Hospital (NUH) - Singapore, Singapore, Singapore, 2University Hospital Knappschaftskrankenhaus Bochum GmbH, Bochum, Germany, 3Martin-Luther-University Halle-Wittenberg, Halle (Saale), Germany, 4Nuffield Department of Population Health (NDPH), University of Oxford, United Kingdom, 5Padova University Hospital, Padova, Italy, 6New Zealand Brain Research Institute, Christchurch, New Zealand
On behalf of:
Background and aims: Endovascular therapy(EVT) is the standard of care for treatment of acute ischemic stroke. Our group aimed to study frailty based on the Clinical Frailty Scale(CFS) as a prognostic marker reflecting true biological age.
Methods: A multi-center retrospective study of 571 patients over the age of 70 who underwent EVT from 2017-2021 was performed. CFS was studied in addition to various clinico-radiological parameters that had been reported to affect functional outcomes. Univariate, multivariate and ordinal shift analysis was performed.
Results: Within our cohort, age, CFS, pre-admission mRS, NIHSS, ASPECTS and successful recanalisation were associated with 90-day functional independence(P<0.05) on multivariate analysis. Frailty demonstrated significance on ordinal shift analysis(OR 6.4, CI 4.2-9.8, p<0.001).
Conclusions: CFS is a relevant and important marker for post-stroke functional independence in patients over the age of 70.
Disclosures of Interest: No
Abstract N°: 2456
ENDOVASCULAR THROMBECTOMY IN ACUTE ISCHEMIC STROKE PATIENTS DEPENDENT ON THE DAILY HELP OF OTHERS BEFORE STROKE
Ines Piot*1, Paul Nederkoorn2, Christian Nolte3,4, Andrea Zini5, Georg Kaegi6, Sami Curtze7, Patrik Michel8, Susanne Wegener9, Marcel Arnold10, Henrik Gensicke11
1University Hospital Basel and University of Basel, Stroke Center and Department of Neurology, Basel, Switzerland, 2Amsterdam University Medical Centres, Department of Neurology, Amsterdam, Netherlands, 3Charité-Universitätsmedizin Berlin, Berlin Institute of Health, Berlin, Germany, 4Charité-Universitätsmedizin Berlin, Department of Neurology, Center for Stroke Research Berlin, Berlin, Germany, 5Maggiore Hospital, IRCCS Istituto Delle Scienze Neurologiche Di Bologna, Department of Neurology and Stroke Center, Bologna, Italy, 6Kantonsspital St. Gallen, Department of Neurology, St. Gallen, Switzerland, 7University of Helsinki and Helsinki University Hospital, Neurology, Helsinki, Finland, 8Lausanne University Hospital and University of Lausanne, Stroke Center, Neurology Service, Lausanne, Switzerland, 9University Hospital Zurich and University of Zurich, Department of Neurology, Zurich, Switzerland, 10Inselspital, Bern University Hospital and University of Bern, Department of Neurology and University Institute of Diagnostic and Interventional Neuroradiology, Bern, Switzerland, 11University Department of Geriatric Medicine FELIX PLATTER, University of Basel, Neurology and Neurorehabilitation, Basel, Switzerland
On behalf of: EVATRISP Collaboration
Background and aims: To compare outcome and bleeding complications in patients treated with endovascular thrombectomy (EVT) who could not live alone without help of another person before stroke (prestroke dependency) versus independent ones.
Methods: This prospective multicenter study from the EndoVAscular treatment and ThRombolysis for Ischemic Stroke Patients Registry (EVA-TRISP) compares poor functional outcome (mRS 3-6 in prestroke independent patients and mRS higher than the prestroke mRS in prestroke dependent patients) and death at 3-months, symptomatic intracranial haemorrhage (sICH) and successful recanalization (TICI score 2b/3) between prestroke dependent and independent patients. Prestroke dependency was defined by a modified Rankin Scale (mRS) score ⩾ 3 prior to stroke.
Results: Of 11409 patients, 1102 were prestroke dependent (9.7%). Prestroke dependent patients were older, more often women, had a higher NIHSS at onset and more cardiovascular risk factors. Poor outcome (68.5% vs 51%) and death (49.8% vs 20%) was more frequent in prestroke dependent patients. However, the frequency of sICH (4.8% vs 5.4%) and successful recanalization (76.9% vs 80%) were similar. After adjusting for covariates, the odds of poor outcome (OR=1.09 (95%-CI 0.92-1.29)), sICH (OR=0.86 (95%-CI 0.61-1.18)) and successful recanalization (OR=0.84 (95%-CI 0.70-1.00)) did not differ significantly between both groups. The odds for death remained higher in prestroke dependent patients (OR=2.22 (95%-CI 1.85 to 2.66)).
Conclusions: EVT in prestroke dependent patients was associated with increased odds for death but not for poor functional outcome, sICH and unsuccessful recanalization. Thus, EVT should not be withheld solely on the basis of prestroke dependency.
Disclosures of Interest: No
Abstract N°: 2708
PERFUSION DSA SEPARATING SUCCESSFUL REPERFUSION
Matthijs van der Sluijs*1, Ruisheng Su2, Sandra Cornelissen1, Bridget Schoon2,3, Rob van de Graaf1, Wim Van Zwam4, Jeannette Hofmeijer5, Aad van der Lugt1, Theo van Walsum1
1Erasmus University Medical Center, Radiology & Nuclear Medicine, Rotterdam, Netherlands, 2Erasmus University Medical Center, Rotterdam, Netherlands, 3Erasmus University Medical Center, Neurology, Rotterdam, Netherlands, 4Maastricht UMC+, Radiology, Maastricht, Netherlands, 5Rijnstate, Neurology, Arnhem, Netherlands
On behalf of: MRCLEAN Registry
Background and aims: The Thrombolysis in Cerebral Infarction (TICI) score is used to determine the reperfusion grade on digital subtraction angiography (DSA) after endovascular treatment (EVT) in acute ischemic stroke patients. Almost half of patients with successful reperfusion have poor clinical outcome. In addition to the large vessels, DSA also depicts the passage of contrast material in the brain parenchyma. We aim to study subtle differences in the DSA time intensity curves (TICs) that might differentiate between good and poor clinical outcome in patients who achieved successful reperfusion.
Methods: Patients from the MR CLEAN Registry with an ICA, M1 and M2 occlusion and successful reperfusion (eTICI ⩾2B) were selected. TICs were computed by deconvolution with the arterial input function obtained from the internal carotid artery. Four perfusion parameters were extracted from these TICs: cerebral blood volume (DSA-CBF), cerebral blood flow (DSA-CBF), time to maximum (DSA-Tmax) and mean transit time (DSA-MTT). The association between the TIC-parameters and the dichotomized modified Rankin scale at 90 days (0-2 mRS) was analyzed using logistic regression with adjustments for prognostic patient characteristics.
Results: In total, 95 patients were included. A lower DSA-MTT was significantly associated with better functional outcome (adjusted odds ratio, 3.1 [95%CI 1.1-9.2]). DSA-CBV, DSA-CBF and DSA-Tmax and were not significantly associated with mRS.
Conclusions: A lower DSA-MTT is associated with better functional outcome in patients with successful reperfusion. This perfusion parameter provides additional information about reperfusion status and could be used to differentiate between good and bad functional outcome.
Disclosures of Interest: No
Abstract N°: 2824
DOES THE ISCHEMIC CORE REALLY MATTER? AN UPDATED SYSTEMATIC REVIEW AND META-ANALYSIS OF LARGE CORE TRIALS AFTER TESLA, TENSION AND LASTE
Mahmoud Dibas1, Malik Ghannam1, Mohammad Almajali1, Milagros Galecio-Castillo1, Abdullah Al-Qudah2, Aaron Rodriguez-Calienes1, Albert Yoo3, Tudor Jovin4, Amrou Sarraj5, Santiago Ortega-Gutierrez*6
1University of Iowa Hospitals and Clinics, Department of Neurology, Iowa City, United States, 2UPMC Stroke Institute, Department of Neurology, University of Pittsburgh Medical Center, Pittsburgh, United States, 3Texas Stroke Institute, Dallas, United States, 4Cooper Neurological Institute, New Jersey, United States, 5University Hospitals Cleveland Medical Center, Department of Neurology, United States, 6University of Iowa Hospitals and Clinics, Department of Neurology, United States
On behalf of:
Background and aims: This study assesses the efficacy and safety of endovascular thrombectomy (EVT) for large core acute ischemic stroke (AIS) patients, stratifying the cohort by infarct core at presentation, using a comprehensive meta-analysis of aggregate data.
Methods: This study includes all randomized trials that compared EVT to medical management (MM) for large core AIS (ASPECTS⩽5 on non-contrast CT and/or core⩾50ml on CT-perfusion/MR). The primary outcome is the 90-day-modified-Rankin-Scale (mRS) shift analysis. Secondary outcomes include functional independence (mRS 0-2), independent ambulation (mRS 0-3), mortality, and symptomatic intracranial hemorrhage (sICH). Pooled odds ratios (OR) are calculated for shift mRS through the random-effects, while risk ratios (RR) are used for the other outcomes.
Results: Six trials with 1886 patients are included. The EVT group has a higher shift towards a lower mRS than MM (OR: 1.49, 95%CI: 1.24-1.79). EVT has higher rates of functional independence (19.5% vs. 7.5%, RR: 2.49, 95%CI: 1.92-3.24), independent ambulation (36.5% vs. 19.9%, RR: 1.91, 95%CI: 1.51-2.43) and sICH (5.5% vs. 3.2%, RR: 1.73, 95%CI: 1.01-2.95) compared to MM. The two groups have similar mortality rates (31.5% vs. 36.8%, RR: 0.86, 95%CI: 0.72-1.02). Importantly, EVT is consistently superior in the shift analysis to MM in patients with ASPECTS 3-5 (OR: 1.60, 95%CI: 1.10-2.32) and ASPECTS 0-2 (OR: 1.45, 95%CI: 1.17-1.80).
Conclusions: Our results confirm the efficacy of EVT for AIS with large core and suggest a consistent benefit across all ASPECTS categories, shifting the concept of core infarct as an absolute inclusion criterion in the LVO selection paradigm.
Disclosures of Interest: No
Abstract N°: 3165
ANESTHETIC APPROACHES DURING ENDOVASCULAR TREATMENT FOR ACUTE ISCHEMIC STROKE PATIENTS: A SYSTEMATIC REVIEW AND META-ANALYSIS
Faisal S. Alqahtani*1, Mohammed Almanna1, Mohamed Asiri1, Ziyad Alqahtani1, Mishari Alqahtani1, Ahmed Alkhiri2, Montaha Almatrafi2, Anfal Felimban2, Nuha Alharbi2, Dalia Alghamdi2
1King Saud bin Abdulaziz University for Health Sciences (KSAU-HS), College of Medicine, Riyadh, Saudi Arabia, 2King Saud bin Abdulaziz University For Health Sciences, Jeddah, Saudi Arabia
On behalf of:
Background and aims: The optimal choice of anesthetic approach during endovascular treatment (EVT) remains uncertain. This systematic review and meta-analysis aim to evaluate the safety and efficacy of general anesthesia (GA) and non-general anesthesia (non-GA) during EVT.
Methods: A systematic search for Randomized Controlled Trials (RCTs) in which stroke EVT patients were randomized to GA or non-GA was performed in PubMed, EMBASE, Scopus, Cochrane Library and clinicaltrials.gov up to November 2023. Outcomes were assessed using random-effects or fixed-effects.
Results: Eight RCTs were included. There is no significant difference between GA and non-GA in terms of the good functional outcomes, defined by a mRS score of 0-2,([RR]=1.09, 95% [CI]:0.95–1.24, p=0.23), mortality rates (RR=0.95, 95% CI:0.75–1.22, p=0.70), and NIHSS scores at 24 hours post-treatment ([SMD]= −0.01, 95% CI: −0.13 to 0.11, p= 0.89). However, the GA group had a higher rate of successful recanalization (RR= 1.13, 95% CI: 1.07–1.19, p < 0.0001), which is a critical factor for patient recovery. In terms of safety, we observed a higher risk of hypotension (RR= 1.87, 95% CI: 1.42–2.47, p < 0.00001) and ventilation-associated complications (RR= 1.43, 95% CI:1.07–1.90, p= 0.01) associated with GA. Conversely, the risk of symptomatic intracerebral hemorrhage did not differ significantly between the two groups (RR= 0.94, 95% CI: 0.74–1.26, p=0.68).
Conclusions: In conclusion, GA appears to have an advantage in terms of successful recanalization but comes with an increased risk of hypotension and ventilation-associated complications. These findings should be carefully considered when determining the anesthetic approach for EVT.
Disclosures of Interest: No
Abstract N°: 1640
EMERGENT CAROTID ARTERY STENTING DURING ENDOVASCULAR TREATMENT IN PATIENTS WITH ACUTE ISCHAEMIC STROKE
Garbiñe Ezcurra-Díaz*1, Pere Cardona2, Noelia Rodriguez-Villatoro3, Antonio Doncel-Moriano4, Belén Flores-Pina5, Georgina Laia Figueras-Aguirre6, Tomàs Xuclà-Ferrarons7, Isabel Fernandez Perez8, Mercè Salvat-Plana9, Pol Camps Renom1
1Hospital de la Santa Creu i Sant Pau, Neurology, Stroke Unit, Barcelona, Spain, 2Hospital Universitari de Bellvitge, Neurology, Stroke Unit, L'Hospitalet de Llobregat, Spain, 3Hospital Universitari Vall d'Hebron, Neurology, Stroke Unit, Barcelona, Spain, 4Hospital Clínic i Provincial de Barcelona, Neurology, Stroke Unit, Barcelona, Spain, 5Hospital Universitari Germans Trias i Pujol, Neurology, Stroke Unit, Badalona, Spain, 6Hospital Universitari Parc Taulí, Neurology, Stroke Unit, Sabadell, Spain, 7Hospital Universitari Doctor Josep Trueta, Neurology, Stroke Unit, Girona, Spain, 8Hospital del Mar, Neurology, Stroke Unit, Barcelona, Spain, 9Pla director de les malalties vasculars cerebrals. Agència de Qualitat i Avaluació Sanitàries de Catalunya (AQuAS), Barcelona, Spain
On behalf of: Francisco Purroy-García, Alan Flores, Joan Martí-Fàbregas, Anna Ramos-Pachón, Luis Prats-Sánchez, Alejandro Martínez-Domeño, Marina Guasch-Jimenez, Álvaro Lambea-Gil, Ana Aguilera-Simón and Cat-SCR Consortium
Background and aims: In patients with acute ischaemic stroke (AIS) due to tandem lesions (TL) or acute internal carotid artery (ICA) occlusion, the optimal management of the carotid lesion during endovascular treatment (EVT) is still controversial. We aimed to study functional and safety outcomes of emergent carotid artery stenting (CAS) during EVT, compared to differed or no carotid revascularization.
Methods: Retrospective multicentre study using a prospective population-based registry (CICAT) of patients with AIS undergoing EVT in Catalonia (Spain) between January 2017-March 2023. We included patients with acute ICA occlusion or TL (⩾70% ICA stenosis/occlusion + intracranial occlusion), and compared those who underwent emergent CAS vs. those who not. Patients with a non-atherosclerotic aetiology were excluded. The primary outcome was the shift on mRS score at three months of follow-up. Secondary outcomes were symptomatic intracranial haemorrhage (sICH) and death. Multivariable ordinal regression analysis was performed to test association between CAS and the primary outcome.
Results: We included 731 patients (mean age 69.2 [SD=12.7]; 221 [30.2%] women). CAS was performed in 295 (40.4%) of the patients. In a multivariable ordinal regression analysis (adjusted for age, baseline NIHSS, prior mRS, ASPECTS, previous thrombolysis, time from onset and final mTICI), CAS was independently associated with lower probability of 1-point mRS worsening (cOR=0.69, 95%CI 0.51-0.93; p=0.014) without significant differences on sICH rates (6.9% vs. 4.3%, p=0.123). Mortality was higher in non-CAS group, although it was no significant after adjustment.
Conclusions: In patients with AIS due to TL/acute ICA occlusion, emergent CAS was associated with better functional outcome without increasing the risk of sICH.
Disclosures of Interest: No
Abstract N°: 1807
INTRAVENOUS THROMBOLYSIS IN PATIENTS WITH CERVICAL ARTERY DISSECTION: A SECONDARY ANALYSIS OF THE STOP-CAD STUDY
Liqi Shu*1, Daniel Mandel1, Karen Furie1, Shadi Yaghi1
1Warren Alpert Medical School of Brown University, Neurology, Providence, United States
On behalf of: STOP-CAD investigators
Background and aims: Cervical artery dissection (CAD) contributes to 2% of ischemic strokes but up to 25% among young adults. This study evaluated the risks and benefits of acute thrombolysis in CAD-associated acute ischemic stroke (AIS).
Methods: A secondary analysis of the STOP-CAD study was conducted including patients with AIS. The primary outcome was 90-day modified Rankin Score (mRS) 0-2, and the secondary outcome was symptomatic intracranial hemorrhage (sICH). We built binary logistic regression models adjusting for age and NIHSS score to determine associations between IVT with the primary and secondary outcomes.
Results: The study included 2,613 patients; mean age was 47.8 years and 38.4% were women; 23.5 % received IVT. IVT was associated with improved 90-day mRS (adjusted odds ratio [aOR] 1.77, 95% CI 1.31-2.38, P<0.001) but increased odds of sICH (aOR 3.51, 95% CI 1.73-7.15, P=0.001).
Conclusions: In patients with CAD, IVT in patients with suspected stroke was associated improved functional outcome but increased sICH risk. Studies are needed to validate our findings.
Disclosures of Interest: No
Abstract N°: 2934
CEREBRAL VENOUS THROMBOSIS AND INTRACRANIAL HYPOTENSION: OUTCOME IN 40 PATIENTS
Emma Davila*1, Isabelle Crassard1,2, Caroline Roos1, Mikael Mazighi1,2,3,4, Peggy Reiner1,2
1Lariboisière Hospital AP-HP, Neurology, Paris, France, 2FHU Neurovasc, France, 3Université Paris Cité, Paris, France, 4INSERM 1144, Paris, France
On behalf of:
Background and aims: Cerebral venous thrombosis (CVT) is a recognized complication of Intracranial Hypotension (IH). Pathophysiology of CVT in this context is fairly well described but data are scarce concerning prognosis and treatment remain challenging. In this study, we aim to investigate characteristics and outcome of patients with CVT in the context of spontaneous or provoked IH.
Methods: We conducted a retrospective study among a prospective cohort of CVT patients at Lariboisière Hospital (2002-2022). Patients were included if they met ICHD-3 criteria for spontaneous or provoked IH after detailed investigation of clinical charts and imaging. Clinical, biological and MRI data were analysed, as well as, therapeutic strategy and prognosis.
Results: Among 512 patients diagnosed with CVT, 40 patients had IH. Mean age was 33.8 years and 32/40 (80%) were women. All patients had headaches, which were isolated in 23 cases (57.5%). Cortical vein thrombosis was present in 35 cases and isolated in 14 cases (35%), 5 patients (12.5%) had venous infarct associated. Twenty patients (50%) had spontaneous IH: they were older than patients with provoked IH, but otherwise did not differ for clinical, radiological features, therapeutic strategy, sinus recanalization or functional outcome. Modified Rankin Score at 3 month was ⩽1 for 87% of patients.
Conclusions: Patients with IH and CVT presented predominantly with favorable outcome with less parenchymal lesions than usually described in the literature. Spontaneous and provoked IH didn’t differ in terms of initial severity and prognosis. Of note cortical vein involvement was common.
Disclosures of Interest: No
Abstract N°: 1614
IMPLEMENTATION OF AN OPTIMISED TELE-MEDICINE PLATFORM FOR STROKE IN SOUTH AUSTRALIA IMPROVES PATIENT CARE
Craig Kurunawai*1, Chushuang Chen2, Andrew Bivard3, Mathew Willcourt1, Aaron Tan1, Jackson Harvey1, Jim Jannes1, Geoffrey A. Donnan3, Stephen Davis3, Timothy Kleinig1
1Royal Adelaide Hospital, Adelaide, Australia, 2University of Newcastle, Callaghan, Australia, 3The University of Melbourne, Parkville, Australia
On behalf of:
Background and aims: Thrombectomy is only offered in large cities, with limited access in regional centres. This makes the acute stroke care pathway for regional hospitals quite significant, and requires multi agency coordination for patient retrieval. We sought to optimise stroke care access in South Australian to improve patient access to thrombectomy.
Methods: We undertook an interventional historically controlled cohort study comparing acute stroke care metrics in the South Australian Tele-Stroke Service (SATS) during a 12-month control period with 12 months of deployment of the digital and education intervention in the 61 rural hospitals in South Australia, including Alice Springs in the Northern Territory. The study intervention considered of an education package provided to the regional hospitals, and the deployment of a centralised tele-stroke system ‘Zeus’ to provide treatment advice and organise patient transfers where needed.
Results: Over the 24-month study period there were 919 patient referrals with 449 consultations in the pre-deployment phase and 470 in the post-deployment phase. Demographic features in both epochs were similar. The post-deployment phase achived significantly shorter door-to-scan time (35minutes, IQR: 18, 70;vs.49 minutes, IQR:25,102, P<0.0001), faster door-to-thrombolysis time (58 minutes, IQR: 39,91, vs.83 minutes, IQR: 55,100, P=0.0324) and a higher portion of patients treated with thrombectomy (26, 5.8% vs. 54 11.5%, p=0.002).
Conclusions: An optimised implementation of a streamlined telehealth platform with ongoing education and feedback to referring sites was associated with improved stroke workflow metrics and higher thrombectomy rates in rural south Australia.
Disclosures of Interest: No
Moderated Poster - Clinical Trials – Day 2
Abstract N°: 2219
ASSOCIATION OF MISMATCH PROFILES AND CLINICAL OUTCOME FROM ENDOVASCULAR THERAPY IN LARGE INFARCT
Dapeng Sun*1, Xiaochuan Huo2, Thanh N. Nguyen3, Yue-Song Pan1, Xu Tong1, Ning MA1, Feng Gao1, Dapeng Mo1, Zhongrong Miao1
1Beijing Tiantan Hospital, Capital Medical University, 2Beijing Anzhen Hospital, Capital Medical University, 3Boston Medical Center
On behalf of: Raynald, MD, Mengxing Wang, PhD, Mohamad Abdalkader, MD, Hesham Masoud, MD, Raul G. Nogueira, MD, for the ANGEL-ASPECT study group
Background and aims: A mismatch profile on perfusion imaging has been pivotal in guiding selection of patients with large vessel occlusion without large infarct who benefit from endovascular treatment (EVT). We aimed to investigate whether patients with large infarct and perfusion mismatch is associated with EVT benefit.
Methods: Subgroup analysis of ANGEL-ASPECT. Mismatch ratio was defined as Tmax>6s cerebral volume/infarct-core volume and mismatch volume was defined as Tmax>6s volume minus infarct-core volume. We divided patients into mismatch ratio⩾1.2 and mismatch volume⩾10ml, and mismatch ratio⩾1.8 and mismatch volume⩾15ml groups. The primary outcome was the 90-day modified Rankin Scale score ordinal distribution. Safety outcomes were symptomatic intracranial hemorrhage and 90-day mortality.
Results: There were 425 patients included. In both mismatch ratio⩾1.2 and mismatch volume⩾10ml (mismatch+, n=395;mismatch-, n=31) and mismatch ratio⩾1.8 and mismatch volume⩾15ml groups (mismatch+, n=346; mismatch-, n=80), better 90-day mRS outcomes was found in the EVT compared to MM groups (4[2-5]vs.4[3-5], common odds ratio [cOR],1.9,95%CI1.3-2.7, P<.001;4[2-5]vs.4[3-5], cOR,1.9, 95%CI1.3-2.8, P<.001, respectively) but not in patients without mismatch ratio⩾1.2 and mismatch volume⩾10ml (5[3-6]vs.5[4-6],cOR,1.2,95%CI0.3-4.1, P=0.83) and mismatch ratio⩾1.8 and mismatch volume⩾15ml (4[3-6]vs.5[3-6],cOR,1.2,95%CI0.6-2.7, P=0.60). However, no interaction effect was found in both subgroups (P>0.10).
Conclusions: EVT may be associated with better outcomes than medical management (MM) in patients with mismatch profiles. However, there was no interaction effect of EVT compared with MM by the presence or absence of mismatch. A pooled analysis of large core trials stratified by mismatch is warranted.
Disclosures of Interest: No
Abstract N°: 575
TREATMENT OF CERVICAL ARTERY DISSECTION: AN INDIVIDUAL PATIENT DATA META-ANALYSIS OF THE CADISS AND TREAT-CAD RANDOMISED TRIALS
Josefin E. Kaufmann*1,2, Eric Harshfield3, Susanne Wegener4, Levi Christopher5, Marcel Arnold6, Philip Bath7, Stefan Engelter1,2, Christopher Kenan Traenka1,2, Hugh Markus3
1Universitätsspital Basel and University of Basel, Neurology and Stroke Center, Basel, Switzerland, 2Universitäre Altersmedizin FELIX PLATTER, Neurology and Neurorehabilitation, Basel, Switzerland, 3University of Cambridge, Stroke Research Group, Department of Clinical Neurosciences, Cambridge, United Kingdom, 4University Hospital of Zurich, and University of Zurich, Division of Vascular Neurology and Neurorehabilitation, Department of Neurology, Zurich, Switzerland, 5John Hunter Hospital and University of Newcastle, Faculty of Health and Medicine, Newcastle, Australia, 6University Hospital Bern and University Bern, Department of Neurology, Bern, Switzerland, 7University of Nottingham, Stroke Trials Unit, Mental Health & Clinical Neuroscience, Nottingham, United Kingdom
On behalf of: CADISS and TREAT-CAD investigators
Background and aims: Cervical artery dissection is the most common cause of stroke in the young. To date, there is no conclusive evidence on which antithrombotic therapy should be used to treat patients.
Methods: We performed a preplanned individual patient data meta-analysis on the two randomised controlled trials CADISS and TREAT-CAD (registered in PROSPERO CRD42023372742). The primary outcome was a composite of (i) any stroke, (ii) death, (iii) major bleeding (extra- or intracranial) at 90 days follow-up. The components of the composite outcome were also secondary outcomes. Subgroup analyses based on baseline characteristics with a putative impact on the outcome were performed. We performed logistic regression using the maximum penalized likelihood method including interaction in the subgroup analyses.
Results: 444 patients were included in the intention-to-treat (ITT) population and 370 patients in the per-protocol (PP) population. Baseline characteristics were balanced. There was a non-significant tendency for there to be fewer primary outcomes in those randomised to anticoagulation, 3/218 (1·4%), vs aspirin, 10/226 (4·4%), OR=0·33 (95% CI 0·08-1·05), p=0·061. In comparison with aspirin, anticoagulation was associated with fewer recurrent strokes, 1/218 (0·5%) vs 9/226 (4·0%), OR=0·16 (95% CI 0·02-0·69), p=0·012, and more bleeding events, 2 vs 0.
Conclusions: This IPD analysis of all currently available RCT data found no difference between anticoagulants and antiplatelets in preventing early recurrent events. However, the trend towards better outcomes with anticoagulants suggests that larger trials are required. These should include more modern forms of antithrombotic therapy, including direct oral anticoagulants (DOACS) and dual antiplatelet therapy.
Disclosures of Interest: Yes Individual funding of Josefin E. Kaufmann by the Goldschmidt-Jacobson Foundation.
Abstract N°: 1430
PHOSPHODIESTERASE4 INHIBITOR ROFLUMILAST TO IMPROVE COGNITION AFTER STROKE A DOUBLE-BLIND RANDOMIZED CONTROLLED PHASE 2 TRIAL
Jill Kerckhoffs*1, Ieke Winkens1, Arjan Blokland1
1Maastricht University Psychology Neurosciences Department (FPN), Neuropsychology & Psychopharmacology, Maastricht, Netherlands
On behalf of:
Background and aims: Effective pharmacological treatments for Post Stroke Cognitive Impairment (PSCI) currently remain elusive. Animal studies have shown improved cognition after phosphodiesterase type 4 (PDE4) inhibition in post-stroke models. Additionally, memory enhancing effects were already found after acute treatment with roflumilast (100 µg) in healthy elderly. The current study aimed to test whether 100 µg q.d. roflumilast (PDE4 inhibitor for the treatment of COPD) for three months, could improve cognition in PSCI patients.
Methods: In a double-blind randomized placebo-controlled phase 2 clinical trial, 100 participants (n=50 per group) were included and 97 participants completed the study, they were 41-70 years old; >1-year post-stroke; and screened for memory complaints (< normative score on Verbal Word Learning Task: VLT). The primary outcome was the delayed recall on the VLT. Secondary outcomes were other cognitive functions and the influence on daily life. A predefined prognostic covariate adjustment analysis was conducted by Cognivia, according to FDA guidelines, to identify therapeutic effects in a high-placebo effect population.
Results: The predefined prognostic covariate adjustment analysis, demonstrated a tendency for improved memory performance based on performance on the VLT and RBMT. No real safety or tolerability issues were detected. No clear effects were found for other cognitive or daily life measures. A follow-up after 3 months indicated no decline in memory performance, but showed more reported subjective memory problems.
Conclusions: The current proof of concept phase 2 trial demonstrates a tendency for a treatment effect of roflumilast (100 µg Q.d. for 3 months) on memory. These results encourage further studies.
Disclosures of Interest: Yes Arjan Blokland has a proprietary interest in the PDE 4 inhibitor roflumilast.
Abstract N°: 2305
INFLUENCE OF MULTIMORBIDITY ON FUNCTIONAL OUTCOME IN POST-EVT PATIENTS: POST HOC ANALYSIS OF THE ENCHANTED2/MT TRIAL
Xinwen Ren*1,2, Yang Zhao1,2, Craig Anderson1,2,3, Lili Song1,3
1The George Institute for Global Health, Beijing, China, 2The George Institute for Global Health, University of New South Wales, Sydney, China, 3Royal Prince Alfred Hospital, Neurology, Sydney, Australia
On behalf of:
Background and aims: Multimorbidity (MM) is increasingly common and predicts adverse outcomes, but its influence on recovery from acute ischaemic stroke (AIS) has not been well established. We assessed the relationship between MM and functional recovery in the second Enhanced Control of Hypertension and Thrombolysis Stroke Study (ENCHANTED2/MT).
Methods: Post hoc analysis of the ENCHANTED2/MT trial involving 816 AIS patients with successful reperfusion after endovascular thrombectomy (EVT) for any large-vessel occlusion (LVO) randomly allocated to more-intensive group (SBP target <120 mmHg) versus less-intensive (SBP target 140-180 mmHg) BP lowering. Associations of MM (⩾2 coexisting chronic diseases) and functional outcome (death and major disability [mRS 3-5]) at 90-days and SBP post-randomization to Day 7 were assessed in logistic regression and repeated-measure linear mixed models.
Results: Overall, 810 AIS patients (mean age 67 years, 38% female) were included. Significant association of MM and death (aOR 1.51, 95%CI 1.05-2.48; p=0.031) but not major disability (aOR 1.23, 95%CI 0.85-1.78; p=0.268). Patients with MM had higher SBP than those without (aMD 2.80, 95%CI 2.27-3.32; p<0.001).
Conclusions: MM increases the odds of death and is associated with higher SBP in AIS patients after successful EVT.
Disclosures of Interest: No
Abstract N°: 2771
NMDAR1-ABS-SEROSTATUS ASSOCIATED WITH WORSE OUTCOME IN DEPRESSION SCORE 6 MONTHS POST-STROKE: RESULTS FROM THE PHYS-STROKE CLINICAL TRIAL
Charlotte Pietrock*1,2, Konrad Neumann3, Kristin Rentzsch4, Winfried Stöcker4, Andreas Meisel1,2,5, Matthias Endres1,2,5,6,7,8, Alexander Nave1,2,6,7
1Department of Neurology with Experimental Neurology, Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Berlin, Germany, 2Centre for Stroke Research Berlin, Charité – Universitätsmedizin Berlin, Berlin, Germany, 3Institute of Biometry and Clinical Epidemiology, Charité – Universitätsmedizin Berlin, 4Institute of Experimental Immunology, EUROIMMUN AG, Lübeck, Germany, 5Neuroscience Clinical Research Centre, Charité – Universitätsmedizin Berlin, Berlin, Germany, 6Berlin Institute of Health, Berlin, Germany, 7German Center for Cardiovascular Research, partner site Berlin, Berlin, Germany, 8German Centre for Neurodegenerative Diseases, partner site Berlin, Berlin, Germany
On behalf of:
Background and aims: NMDAR1-abs (anti-N-Methyl-D-Aspartate receptor GluN1 antibodies) are associated with long-term outcome in various disorders. Our study aimed to investigate their long-term role in stroke.
Methods: 200 patients (41% female; age: 69 ± 12 years) with subacute ischemic or hemorrhagic stroke (median National Institutes of Health stroke scale (NIHSS): 8 (IQR: 5-12)) participated in the multicenter PHYS-STROKE clinical trial (Identifier: NCT01953549). Serum samples were collected at baseline (5-45 days post-stroke), post-intervention (4 weeks after baseline), and at three and six months after stroke. NMDAR1-abs (IgM, IgA, IgG) were measured in cell-based assays. Titers ⩾ 1:10 were considered seropositive. Outcome measures of interest were functional and neuropsychological scores (modified Rankin Score, Barthel-Index, Montréal Cognitive Assessment, Trail Making Test, Center for Epidemiologic Studies-Depression Score) at 6 months post-stroke.
Results: 109 patients (55%) received NMDAR1-abs analyses at all visits. NMDAR1-abs (IgM, IgA, and/or IgG) were detected in 14 of these patients (13%) at baseline, 13 patients (12%) post-intervention, 10 patients (9%) at three months and 12 patients (11%) at six months. Female sex (p=0.043) and a history of cerebrovascular disease (stroke and/or transient ischemic attack, p=0.029) were associated with seropositivity at baseline. NMDAR1-abs seropositivity at baseline was associated with a worse score in the Center for Epidemiologic Studies-Depression Score 6 months post-stroke (linear regression analysis: ß = 5.75[95% CI = 0.92 to 10.57] p=0.020). No significant associations were observed with other functional and neuropsychological scores.
Conclusions: Our findings suggest a possible association between NMDAR1-abs and depressive symptoms at 6 months after stroke.
Disclosures of Interest: No
Moderated Poster - Diagnosis and Imaging – Day 2
Abstract N°: 1005
DECODING STRUCTURAL CONNECTIVITY AFTER STROKE FOR CLINICAL USE: BYPASSING THE NEED FOR DIFFUSION TENSOR IMAGING
Franziska Hildesheim*1,2,3, Anja Ophey4, Anna Zumbansen5,6, Thomas Funck7, Keith Jamison8, Amy Kuceyeski8, Alexander Thiel1,2,3
1McGill University, Department of Neurology & Neurosurgery, Montreal, Canada, 2Lady Davis Institute for Medical Research, Jewish General Hospital, Montreal, Canada, 3Canadian Platform for Trials in Non-Invasive Brain Stimulation (CanStim), Montreal, Canada, 4Center for Neuropsychological Diagnostics and Intervention, University of Cologne, Department of Medical Psychology | Neuropsychology and Gender Studies, Cologne, Germany, 5School of Rehabilitation Sciences, University of Ottawa, Ottawa, Canada, 6Music and Health Research Institute, University of Ottawa, Ottawa, Canada, 7Forschungszentrum Jülich GmbH, Jülich, Germany, 8Weill Cornell Medical College, Department of Radiology, New York, United States
On behalf of:
Background and aims: Understanding connectome disruption is vital for predicting patient-specific functional recovery after stroke. Despite Diffusion Tensor Imaging (DTI) being the gold-standard for assessing structural connectivity, it is not routinely included in clinical imaging protocols. This study presents a model-based alternative approach for the evaluation of connectivity disruption, relying solely on routinely collected T1 images and bypassing the need for DTI data. The primary objective of this study is to demonstrate the clinial utility of this model-based approach by validating it against individual tractography results within a cohort of stroke patients.
Methods: Individual tractography was performed using DTI data from 23 subacute aphasic stroke patients (mean age: 65.00±10.03 years, 11 females). Tractograms were overlaid with manually outlined dilated lesionmasks to calculate Change in Connectivity (ChaCo) scores as estimates of structural connectivity disruption in 13 language-relevant grey matter regions. Results were compared to ChaCo scores obtained with the model-based approach (Network Modification/NeMo tool), which involves overlaying lesionmasks on a tractogram reference set of 420 healthy subjects.
Results: Linear regression analyses revealed significant positive correlations for connectivity disruption scores obtained through the model-based vs. individual tractography-based approach across all 13 brain regions (mean discrepancy: 10±2%, mean slope coefficient: 1.07±0.17, R2 range: 0.84-0.96). Insula, angular and heschl gyrus demonstrated the lowest ChaCo score discrepancies.
Conclusions: The presented model-based approach provides a robust, DTI-independent alternative for assessing structural connectivity disruption, thereby enhancing accessibility and clinical feasibility of connectivity assessment in stroke patients. Integrating structural connectivity data into multivariate models holds promise for refining predictions of functional outcomes after stroke.
Disclosures of Interest: No
Abstract N°: 1286
TEMPORAL PATTERNS OF VESSEL WALL ABNORMALITIES IN YOUNG STROKE
Esther Boot*1, Anton Meijer2, Sjoert Pegge2, Sjan Teeselink1, Mijntje Schellekens1, Merel Ekker1, Jamie Verhoeven1, Frank-Erik De Leeuw1, Anil Tuladhar1
1Radboud University Medical Centre; Donders Institute for Brain, Cognition and Behaviour; Department of Neurology, Nijmegen; The Netherlands, 2Radboud University Medical Centre; Donders Institute for Brain, Cognition and Behaviour; Department of Radiology, Nijmegen; The Netherlands
On behalf of:
Background and aims: Causes of stroke in young adults differ from the older stroke population, and 25% remains cryptogenic. Approximately one-fourth of this demographic exhibit vessel wall (VW) abnormalities at baseline, however the temporal patterns of VW lesions remain unknown. We aimed to examine the temporal patterns of VW lesions on high-resolution 3T MRI (HR-MRI) in young stroke survivors.
Methods: This substudy of the ODYSSEY is a single-center prospective cohort study comprising participants aged 18-50, who experienced imaging proven cerebral stroke and underwent HR-MRI at baseline and follow-up. These scans were independently reviewed by two neuroradiologists blinded to clinical information.
Results: 75 participants (median age: 40.5 (32.1-46.2)) were included. Time between the HR-MRIs was 2.0 years (IQR 1.8-2.2). At baseline, 17 (23%) participants exhibited 35 VW lesions, mainly VW enhancement (VWE) (60%). During follow-up, eleven participants (15%) exhibited 22 lesions, mostly VWE (90.9%), comprising eleven persistent baseline lesions, eleven newly developed lesions, and 68.5% baseline lesions resolved (Figure 1). Sixteen participants developed new ischemia with four being symptomatic, of which one showed resolved VWE in the corresponding vascular territory. Of the asymptomatic participants, three exhibited VW lesions with various temporal patterns in the corresponding territory. Stroke etiology was not associated with temporal patterns, but atherothrombotic causes were more frequent in persistent lesions (p=0.08).
Conclusions: This study underscores the dynamic nature of VW lesions in young stroke survivors. Baseline lesions frequently resolved, while new ones appeared during follow-up, with underlying mechanisms and implications yet to be fully understood. Further research is needed to determine their clinical significance.
Disclosures of Interest: No
Abstract N°: 3150
STROKE LESION GROWTH IN THE LONG-TERM FOLLOW-UP AFTER ENDOVASCULAR THERAPY
Maria Berndt-Mück*1, Kathleen Bernkopf2, Johanna Härtl2, Moritz Hernandez Petzsche1, Claus Zimmer1,Christian Maegerlein1, Tobias Boeckh-Behrens2
1Klinkum rechts der Isar, TU Munich, Neuroradiology, München, 2Klinkum rechts der Isar, TU Munich, Neurology, München
On behalf of:
Background and aims: Clinical outcome of endovascular treated stroke is dependent on multiple variables, resulting in a large inter-individual variability. In this context, secondary stroke injury might be of relevance but has not been systematically investigated yet.
Aim of the study was to uncover secondary phenomenon in follow-up-imaging and identify possible underlying reasons.
Methods: In a prospective, longitudinal single-center study endovascular treated patients were included and followed-up after 3 to 12 months by clinical and imaging investigations. Stroke lesions were segmented, microstructural alterations were assessed by analyzing DTI-metrics and associations to clinical parameters were investigated.
Results: Within the cohort (n=81), 25 patients (31%) were identified with a lesion growth (LG) in the follow-up-imaging, either adjacent to primary stroke lesion (Fig.1) or distant (Fig.2). DTI-metrics show a partially reversible loss of microstructural integrity (Fig.3).
72% of the patients within the LG group can be identified with an underlying vascular pathology (vs. 39%, p<0.01), either with an acute carotid pathology and/or persisting stenosis in the follow-up.
None of the LG patients present with new clinical symptoms, but the LG-group shows a lower rate of neurological improvement (p<0.01) and higher follow-up-NIHSS-values (p=0.03).
Conclusions: The phenomenon of lesion growth in the follow-up with microstructural changes is newly described for a high proportion of endovascular treated stroke patients. Of note, the described lesions are predominantly localized in the white matter within the deep watershed zone. Underlying reasons for the secondary injury may be multifactorial, but the association to underlying vascular pathologies directs to a possible connection to disturbed vascular auto-regulation functions.
Disclosures of Interest: No
Abstract N°: 1620
BNP AND ECHOCARDIOGRAPHIC PARAMETERS AS PREDICTORS OF NEW ATRIAL FIBRILLATION DETECTION AFTER ACUTE ISCHEMIC STROKE
Giovanna De Marco1, Stefano Forlivesi1, Letizia Riva2, Maria Maddalena Viola1, Matteo Paolucci1, Luana Gentile1, Mauro Gentile1, Gianni Casella2, Rita Mancini3, Andrea Zini1
Background and aims: Early detection of atrial fibrillation (AF) after acute ischemic stroke (AIS) is crucial for identifying a cardioembolic etiology and starting an anticoagulant therapy. We aimed to investigate the role of brain natriuretic peptide (BNP) and echocardiographic parameters for the prediction of new AF detection in a large cohort of AIS patients.
Methods: We retrospectively included 2337 consecutive patients admitted for AIS to the Stroke Unit at the Maggiore Hospital (Bologna, Italy), from January 2018 to May 2023. Blood BNP levels were measured <48 hours from symptom onset. A specific BNP cut-off of 100 pg/ml was chosen to classify patients into high and low BNP levels. Clinical and echocardiographic variables were evaluated. Twelve-lead electrocardiography (ECG), continuous ECG monitoring, and loop recorder with external or implantable devices were used to detect new AF during the hospitalization and 3-month follow-up.
Results: New AF was detected in 424 (22%) among 1907 patients without previous-AF. In the multivariable analysis, high BNP levels (OR 3.99, 95%CI 2.71-5.88, p<0.001), left atrium enlargement (OR 2.90, 95%CI 2.01-4.17, p<0.001), pulmonary arterial hypertension (OR 2.39, 95%CI 1.04-5.48, p=0.039), higher baseline NIHSS (OR 1.05, 95%CI 1.03-1.07, p<0.001), and older age (OR 1.03, 95%CI 1.01-1.04, p<0.001) were independent predictors of new AF detection within 3 months of AIS. The BNP cut-off demonstrated 88% sensitivity and 52% specificity for detecting new AF.
Conclusions: BNP levels ³100 pg/ml <48 hours from AIS onset, left atrium enlargement, and pulmonary hypertension may be useful biomarkers for predicting new AF detection within 3 months.
Disclosures of Interest: No
Abstract N°: 2651
PREVALENCE OF RIGHT-LEFT SHUNT IN STROKE PATIENTS WITH CANCER
Philipp Bücke*1, Fabienne Steinauer1, Eric Buffle2, Babak Navi3, Ava Liberman3, Marcel Arnold1, Thomas Pabst4, Martin Berger4, Simon Jung1, Morin Beyeler1
1Inselspital, Bern University Hospital and University of Bern, Department of Neurology, Bern, Switzerland, 2Inselspital, Bern University Hospital and University of Bern, Department of Cardiology, Switzerland, 3Weill Cornell Medicine, Clinical and Translational Neuroscience Unit, Feil Family Brain and Mind Research Institute and Department of Neurology, New York City, United States, 4Inselspital, Bern University Hospital and University of Bern, Department of Medical Oncology, Bern, Switzerland
On behalf of:
Background and aims: Cancer is associated with an increased risk of acute ischemic stroke (AIS) and venous thromboembolism. The role of paradoxical embolization as a stroke etiology in AIS patients with cancer is controversial. Our study investigated the relationship between the presence of a right-left shunt (RLS) and cancer in AIS patients.
Methods: AIS patients hospitalized at our tertiary stroke center between January 2015 and December 2020 with available RLS status as detected on transesophageal echocardiography (TEE) were included. Active cancers (known at the time of stroke or newly diagnosed within one year after the index event) were retrospectively identified. The association between RLS and active cancer was assessed with multivariable logistic regression and inverse probability of treatment weighting to minimize the confounding effect of TEE indication.
Results: Among 2236 included AIS patients, 103 (4.6%) had active cancer, of whom 24 (23%) were diagnosed with RLS. A RLS was present in 774 out of the 2133 AIS patients without active cancer (36%). After adjustment and weighting, the absence of RLS was associated with active cancer (adjusted odds ratio 2.29, 95% confidence interval 1.14-4.58). The association became insignificant in patients younger than 60 years of age. No association was found between the presence of high-risk RLS (Risk of Paradoxical Embolism Score ⩾6) and cancer.
Conclusions: RLS was diagnosed less frequently in AIS patients with cancer compared to cancer-free patients, suggesting arterial and not venous origin of the thromboembolism in the AIS patients with cancer. Further studies need to confirm our findings and evaluate potential therapeutic implications.
Disclosures of Interest: No
Abstract N°: 1142
THE BIDIRECTIONAL RELATIONSHIP BETWEEN EPIGENETIC AGE AND BRAIN HEALTH EVENTS
Cyprien Rivier*1, Natalia Szejko2, Daniela Renedo1, Adam de Havenon1, Kevin Sheth1, Thomas Gill1, Guido Falcone1
1Yale School of Medicine, New Haven, United States, 2University of Calgary, Calgary, Canada
On behalf of:
Background and aims: It is increasingly recognized that chronological age provides an incomplete assessment of true biological age. Epigenetic clocks use DNA methylation data to estimate biological age more accurately.
Methods: We conducted a 3-stage study within the Health and Retirement Study (Figure). In 2016, participants provided blood samples and methylation and genomic data were generated. Epigenetic age was calculated as the average of thirteen epigenetic clocks that used different combinations of methylation data. Brain health events (BHe) was a composite of stroke, dementia and late-life depression. Stage 1 entailed testing for association between BHe prior to 2016 (exposure) and epigenetic age (outcome). Stage 2 entailed testing for association between epigenetic age (exposure) and BHe occurring after 2016 (outcome). Stage 3 entailed testing for causal associations using Mendelian Randomization (MR).
Results: Out of 4,018 participants with epigenomic data, 2,221(55%) had a history of a BHe before 2016. A history of BHe was associated with an older epigenetic age (beta:0.05;SE:0.01;p<0.01). Of the 3,047 study participants with available follow-up data, 1,018(33%) developed a BHe over a mean follow up of 4 years. Epigenetic age acceleration was associated with higher odds of BHe (OR:1.57[1.22-2.01]). Causal associations estimated via MR analyses confirmed both results.
Conclusions: A history of BHe was associated with epigenetic age acceleration and, conversely, epigenetic age acceleration was associated with higher risk of BHe. MR analyses suggest that these associations are causal. These results indicate that more nuanced strategies for ascertaining biological age are needed and point to epigenetic clocks as a promising tool for this purpose.
Disclosures of Interest: No
Abstract N°: 288
DISTINCTION BETWEEN ISCHEMIC STROKE AND TRANSIENT ISCHEMIC ATTACK BASED ON ADMISSION NON-CONTRAST CT USING DEEP LEARNING MODEL
Hyunho Mo*1, Brian Berghout2,3, Maarten Leening1,2,4, Mohammad Kamran Ikram2,3, Daniel Bos1,2, Bron Esther E.1
Background and aims: Patients experiencing focal neurological deficit typically undergo non-contrast CT (NCCT) imaging to distinguish hemorrhagic from ischemic stroke. NCCT could aid in distinguishing temporary from lasting symptoms, which may hold great consequences for clinical decision-making. We evaluated the performance of a deep-learning network in the classification of TIA and ischemic stroke on acute stroke NCCT, and visualized relevant cerebral areas that influenced its classification decisions.
Methods: Our study consisted of 740 patients; 442 (60%) were diagnosed with ischemic stroke and 298 (40%) had TIA. We implemented a convolutional neural network (CNN) to classify their NCCT into two classes. We obtained relevant areas by sliding a black occlusion patch across the image and recalculating the network output.
Results: The CNN was trained on 592 and tested on 148 out of 740 patients (stratified 80:20 split, this was iterated 10 times). The network showed a mean AUC of 0.61 [95% CI, 0.58-0.69] and mean accuracy of 0.59 [95% CI, 0.52-0.64] (Figure 1). The sensitivity for ischemic stroke diagnosis reached a mean of 0.75 [95% CI, 0.52-0.89], while the mean specificity was low, 0.35 [95% CI, 0.25-0.53] (Figure 2). Figure 3 shows visualization examples for ischemic stroke patients. The highlighted regions did not always include known imaging biomarkers of ischemia.
Conclusions: The sensitivity indicates that our CNN detects and exploits early ischemic signs on NCCT. The visualization results imply that brain NCCT may contain ischemic stroke-related imaging evidence that is currently overlooked or is impossible to pinpoint for the human eye.
Disclosures of Interest: No
Abstract N°: 750
ENHANCING OUTCOME PREDICTION OF INTRACEREBRAL HEMORRHAGE WITH DETAILED CLINICAL AND RADIOLOGICAL ANALYSIS USING MACHINE-LEARNING
Qinghua Hou1, Eunhye Yang2, Barbara Wong2, Kui Kai Lau3, Wing-Kei Ho2, Kay Cheong Teo*3
1Sun Yat-sen University, The seventh affiliated Hospital, department of Neurology, China, 2LKS Faculty of Medicine, The University of Hong Kong, School of Biomedical Sciences, Hong Kong, 3LKS Faculty of Medicine, The University of Hong Kong, Division of Neurology, Department of Medicine
On behalf of:
Background and aims: Effective treatment for intracerebral hemorrhage (ICH) has remained elusive. This may be partly due to outcome heterogeneity resulting from the variation in patient and hematoma characteristics, which confounds therapeutic effects. Better outcome prediction with more detailed clinical and radiological analyses may aid individualized treatment strategies in ICH. Using machine learning (ML), we investigated whether applying more detailed clinical and radiological characteristics will enhance outcome prediction in ICH.
Methods: We developed a random forest ML model for 6-month outcome prediction using 80% of data as training data from 533 ICH patients of the University of Hong Kong stroke registry, who presented from 2011-2018. The remaining 20% were used for validation. The 6-month outcome was categorized as good (mRS 0-2), poor (mRS 3-5), and death. The enhanced outcome prediction model consisted of additional characteristics, which include individual components of Glasgow Coma Scale (GCS), worse limb power, specific ICH location, laterality, and Graeb score; and was compared with a conventional model derived from components of the ICH score.
Results: The enhanced outcome prediction ML model has precision and recall rates of 78% and 88% for good outcome; 71% and 71% for poor; and 85% and 73% for death. Compared to the conventional model, the enhanced model had a significantly higher accuracy (78% vs. 68%, p=0.015). Using recursive feature elimination, the most predictive features identified included hematoma volume, age, limb power of the affected side, and individual components of the GCS.
Conclusions: ML analysis using detailed clinical and radiological characteristics can enhance outcome prediction in ICH.
Disclosures of Interest: No
Abstract N°: 2683
AGREEMENT OF ASPECTS GENERATED BY RAPIDAI AND BRAINOMIX WITH NEURORADIOLOGISTS ON NON-CONTRAST CT (NCCT) SCANS AFTER STROKE
1University of Chester, United Kingdom, 2Countess of Chester Hospital NHS Foundation Trust, United Kingdom
On behalf of:
Background and aims: The Alberta Stroke Programme Early CT Score (ASPECTs) is routinely utilised to identify early ischaemic changes following an acute stroke. Whilst a variety of artificial intelligence software programmes can generate an ASPECT score on NCCT, their agreement with one another and with neuroradiologists has not been extensively examined.
Methods: Between 2022 and 2023, consecutive NCCT scans from suspected hyperacute stroke patients at the Countess of Chester Hospital were analysed using RapidAI and Brainomix. An independent neuroradiologist, blind to these results, assigned ASPECTs scores. Agreement levels were evaluated using quadratic Kappa and corelation coefficient, based on the presence or absence of LVO.
Results:A total of 176 scans underwent evaluation. Agreement between neuroradiologists and Brainomix proved satisfactory, while agreement between neuroradiologists and RapidAI was deemed fair, as detailed in Table 1. In contrast to prior assertions by RapidAI, their agreement with neuroradiologists showed no improvement in cases involving an LVO. This observation is visually demonstrated by the heatmap presented in Figure 1.
Conclusions: The ASPECTs score generated by RapidAI demonstrated only modest agreement with the neuroradiologist’s interpretation, and its performance did not improve in the presence of an LVO. This highlights the necessity for further development and validation of these software programs on a larger dataset. Despite claiming to utilise machine learning, neither system exhibited the ability to autonomously learn from their errors. This underscores the ongoing requirement for advancements and enhancements to enhance the precision and reliability of their results.
Disclosures of Interest: No
Moderated Poster - Epidemiology + Sex and Gender – Day 2
Abstract N°: 543
SEX DIFFERENCES IN REHABILITATION INTENSITY PROVIDED AFTER STROKE IN ONTARIO, CANADA: A RETROSPECTIVE COHORT STUDY
Shannon MacDonald*1,2,3, Jamie Fleet4,5, Elizabeth Linkewich6,7, Jiming Fang3, Sue Peters8,9, Mark Bayley1,3,10
1University of Toronto, Division of Physical Medicine & Rehabilitation, Toronto, Canada, 2Hennick Bridgepoint Hospital, Sinai Health, Toronto, Canada, 3ICES, Toronto, Canada, 4Western University, Department of Physical Medicine and Rehabilitation, London, Canada, 5Parkwood Institute, St. Joseph’s Health Care London, London, Canada, 6University Hospital, London Health Sciences Centre, London, Canada, 7University of Toronto, Department of Occupational Science and Occupational Therapy, Toronto, Canada, 8Western University, School of Physical Therapy, London, Canada, 9Lawson Health Research Institute, St. Joseph's Health Care, London, Canada, 10KITE Research Institute, UHN-Toronto Rehabilitation Institute, Toronto, Canada
On behalf of:
Background and aims: Females have worse outcomes after stroke than males. Increased rehabilitation intensity (defined as the number of minutes per day of direct therapy provided to a patient divided by rehabilitation length of stay) is associated with improved patient outcomes. The aim of this study was to examine whether there are sex differences in the rehabilitation intensity provided after stroke in the inpatient rehabilitation setting.
Methods: This was a sub-analysis of a previously described retrospective cohort of acute stroke patients admitted to inpatient rehabilitation in Ontario, Canada between January 2017 and December 2021. Patient clinical and socio-demographic data were obtained and linked from several administrative databases. The association between sex and rehabilitation intensity was examined using regression analyses, stratified by age.
Results: A total of 5877 females and 6893 males were included. Mean (SD) rehabilitation intensity was 75.86 mins/day (29.69) for males and 73.33 mins/day (29.76) for females (p <.0001). After adjusting for baseline characteristics, sex differences (male vs female) varied by age category [Risk Difference (RD) (95% CI)]: <60 years [RD 3.34 (1.33 to 5.35), p=0.001], 60-79 years [RD 1.37 (0.21 to 2.53), p=0.02], and >= 80 years [RD 1.15 (-0.23 to 2.53), p = 0.10].
Conclusions: Males <80 years received greater rehabilitation intensity than females, although the absolute difference was small. Future research should explore possible reasons for this difference, including whether factors such as mood and pain, which are more prevalent in females, impact rehabilitation intensity after stroke.
Disclosures of Interest: No
Abstract N°: 813
IMPACT OF SEX ON THROMBECTOMY OUTCOMES IN ISCHEMIC STROKE: A PROPENSITY SCORE-MATCHED STUDY, SYSTEMATIC REVIEW AND META-ANALYSIS
Michele Romoli*1, Francesco Cordici1, Marco Longoni1, Aristeidis Katsanos2, Lina Palaiodimou3, Andrea Zini4, Maria Ruggiero1, Thanh N. Nguyen5, Georgios Tsivgoulis3, Lucio D'anna6
1BUFALINI HOSPITAL, NEUROSCIENCE, CESENA, Italy, 2McMaster University, Canada, 3Attikon University Hospital, Greece, 4IRCCS Istituto delle Scienze Neurologiche di Bologna, Neurologia e rete stroke metropolitana, Italy, 5Boston Medical Center, United States, 6Imperial College London NHS Trust, United Kingdom
On behalf of: Soma Banerjee, Kyriakos Lobotesis, Elvis Lafe
Background and aims: Women are underrepresented in stroke thrombectomy trials, and the impact of sex differences on the outcomes of thrombectomy(EVT) is unclear. Here we report a multicenter propensity matching (PSM) study defining sex-related differences in outcomes after EVT, and a meta-analysis to detail global trends.
Methods: We included patients with anterior circulation large vessel occlusion (LVO) consecutively treated with thrombectomy at two Centres (2016-2023; n=1121). PSM was implemented to control for demographic, CV risk factors and event.related features. Systematic review included all studies reporting EVT outcomes in anterior circulation LVO stroke, applying PSM to control for differences in confoounders across sex groups. MEDLINE, EMBASE and Cochrane CENTRAL were searched up to 15th August 2023. Pooled estimates calculated according to random-effect modelling meta-analysis and reported as odds ratio (OR) and standard confidence interval (95%CI). Outcomes were good functional outcome (mRS 0-2 at 90 days), and symptomatic intracranial hemorrhage (sICH), adjudicated according to ECASS II criteria.
Results: After matching, 698 patients (349 women vs 349 men) had similar cardiovascular risk factors, baseline features and treatment approach. No significant differences were found for good functional outcome (OR=0.89, 95%CI=0.66-1.2) and sICH (OR=1.00, 95%CI=0.44-2.26) in the cohort study by sex. Systematic review identified 3 studies (n=3706), all of high quality. No differences emerged in rates of good functional outcome (OR=1.00, 95%CI=0.79-1.21) or sICH (OR=0.85, 95%CI=0.60-1.19) depending on sex.
Conclusions: Women receiving EVT for anterior circulation LVO-related stroke have similar rates of good functional outcome and sICH compared to men. Equity in access to thrombectomy should be guaranteed.
Disclosures of Interest: No
Abstract N°: 2509
IS THE EFFECT OF SEX ON POST-THROMBECTOMY OUTCOMES IN ACUTE ISCHEMIC STROKE AGE-DEPENDENT? RESULTS FROM THE EVA-TRISP REGISTRY
Leon Rinkel*1, Johanna Ospel1, Nabila Wali1, Marcel Arnold1, Susanne Wegener1, Patrik Michel1, Stefan Engelter1, Henrik Gensicke1, Paul Nederkoorn1
1
On behalf of: the EndoVAscular treatment and ThRombolysis for Ischemic Stroke Patients (EVA-TRISP) investigators.
Background and aims: To assess sex differences in outcomes after endovascular treatment (EVT), and whether the effect of sex on post-EVT outcomes is age dependent.
Methods: We used data from EVA-TRISP, a pan-European registry of consecutive patients undergoing EVT. We compared women with men and assessed the interaction between age and sex. Primary outcome was the 90-day modified Rankin Scale score, analyzed with mixed model ordinal regression. We assessed age both as a continuous variable and dichotomized at the population median.
Results: In total, 12,915 patients were included (6,251 [48.4%] women and 6,664 [51.6%] men, median age 74 [IQR 64–82] years). Female patients were older (77 [IQR 67–84] vs 72 [IQR: 62–80], p<0.001) and less frequently treated with intravenous thrombolysis (2888 [46.2%] vs 3309 [49.7%], p<0.001). Female sex was associated with worse functional outcome in the unadjusted analysis (cOR: 1.22, 95%CI: 1.14–1.29) but not after adjusting for potential confounders (acOR 1.02, 95%CI 0.95–1.09). We observed no significant interaction between sex and age as a continuous variable (p=0.08), but found a significant interaction when dichotomizing age at 74 years (p=0.01). In patients younger than 74, women had significantly worse outcomes than men (acOR 1.10, 95%CI 1.003–1.20) while sex was not associated with outcome in older patients (acOR 0.93, 95%CI 0.85–1.02).
Conclusions: We did not find clear evidence that the effect of sex on post-EVT outcomes is modified by age when using age as continuous variable, but observed a worse outcome in women in the age group younger than 74.
Disclosures of Interest: No
Abstract N°: 3302
WORK ENVIRONMENT CHARACTERISTICS OF WOMEN STROKE CARE PROFESSIONALS IN LATIN AMERICA: A SURVEY-BASED DESCRIPTIVE STUDY
Julieta Rosales*1, Maria Paz Rodriguez2, Ana Claudia de Souza3, Florencia Brunet4
1Fleni, Buenos Aires, Argentina, 2Hospital Maciel, Montevideo, Uruguay, 3Moinhos de Vento Hospital, Brazil, 4Casmu 2, Montevideo, Uruguay
On behalf of: LUMNI ALATAC COMMITEE
Background and aims: Few studies have described the sex and gender disparities experienced by women stroke professionals in Latin America. Unconscious bias, traditional gender roles, manifestations of sexism, and the absence of clear policies and guidelines for inclusiveness are some examples of the barriers encountered. This study aimed to investigate the impact of sex and gender disparities in LATAM
Methods: An observational study using a multiple-choice online survey to examine work environments of women stroke professionals. Data was collected from September to November 2023. Three sections were included: personal data, marital status and maternity's career impact, and traditional gender roles in academic life. Descriptive analyses were conducted to calculate the sample's means and percentages.
Results: A total of 294 responses were obtained from 17 LATAM countries. Mean age 40±9 years, only 34% occupied leadership positions, and 50% had a woman as a leader. Forty-two percent were married, 55% had children, 50% responded that children have negatively impacted their academic career, and 72% were limited to attending academic meetings for this reason. Only 16% of the respondents hold a leadership position in a professional or scientific society, and 51% had a teaching activity at the university
Conclusions: Our survey unveiled the barriers encountered by women stroke professionals, concerning maternity and its negative effects on their work performance and career development. Furthermore, fewer leadership positions and unbalanced career opportunities were frequently reported. Through these data, our objective is to raise awareness of women's challenges and devise practical, region-specific strategies for mitigating these issues.
Disclosures of Interest: No
Abstract N°: 653
SEX DIFFERENCES IN PERCEIVED RESTRICTIONS IN SOCIAL ACTIVITY PARTICIPATION AMONG OLD AGE STROKE SURVIVORS
Chen Chen*1, Mathew Reeves2, Lynda Lisabeth1
1University of Michigan, Epidemiology, Ann Arbor, United States, 2Michigan State University, Epidemiology, East Lansing, United States
On behalf of:
Background and aims: Women experience more post-stroke physical activity limitations, but sex differences in social activity participation, an important patient-reported outcome for stroke recovery, is unclear.
Methods: Community dwelling incident stroke patients aged ⩾ 65 years were identified from US National Health Aging and Trends Study (2011-2021). Participants were asked whether in the last month their health or functioning restricted their participation including visiting friends/family; attending religious services; participating in clubs, classes, or other organized activities; and going out for enjoyment. Logistic regressions were used to assess sex differences in any participation restrictions across the four activities and restrictions in each activity without and with adjustment for potential confounders in Table 1, one at a time and simultaneously.
Results: Among 469 self-reported incident stroke patients, women were more likely to be older, less educated, widowed, and live alone (Table 1). In unadjusted analyses, women were significantly more likely to report any restrictions and restrictions in attending religious services (Table 2). Sex differences in these outcomes were attenuated but remained after individual adjustment for marital status, living arrangement, driving frequency, comorbidities, physical capacity, and activity limitations (data not shown). No significant sex differences were found after simultaneously including all these factors in models (Table 2).
Conclusions: Perceived social participation restriction was high among stroke survivors and more prevalent among women than men, potentially attributable to sex differences in social factors and prestroke health. Future interventions targeting at vulnerable groups, including socially isolated women and women with poorer health, should be considered.
Disclosures of Interest: No
Abstract N°: 177
SEX AND AGE DIFFERENCES IN THE PARTICIPATION IN STROKE STUDIES, A RETROSPECTIVE ANALYSIS
Kurt Mölgg*1,2, Michael Knoflach1,2, Anel Karisik1,2, Benjamin Dejakum1, Raimund Pechlaner1, Christian Boehme1, Lukas Mayer-Suess1, Stefan Kiechl1,2, Thomas Töll1, Silvia Komarek1
1Medizinische Universität Innsbruck, Department of Neurology, Innsbruck, Austria, 2VascAGE, Innsbruck, Austria
On behalf of: Neurovacular Study Group of the Department of Neurology
Background and aims: Women remain consistently underrepresented in stroke trials, particularly in those addressing secondary prevention, raising uncertainties about sex-related differences in treatment efficacy and safety. The cause for this sex-gap remains debated.
Methods: Our analysis includes the screening logs of the Department of Neurology (Medical University of Innsbruck, Austria) for stroke studies, exploring sex and age differences in the participation of three different secondary prevention trials, each varying in complexity and burden: OCEANIC-STROKE (ClinicalTrials.gov ID: NCT05686070), STROKE-CARD (ClinicalTrials.gov ID: NCT02156778), and STROKE-CARD Registry (ClinicalTrials.gov ID: NCT04582825) studies. Screening logs prospectively document information on admission date, age, sex, fulfilment of inclusion criteria and cause of non-participation of every patient with ischemic stroke or transient ischemic attack (TIA) admitted to our department.
Results: Since 2014, 4,513 TIA/stroke patients were documented in the screening logs and 1,437 were not included into the studies. Excluded women were significantly older than men and less likely to give their informed consent due to a more severe neurological or medical impairment, including cognitive impairment (27.3% women vs. 18.4% men), aphasia (12.4% women vs. 5.8%) and terminal care (16.6% women vs. 12.5% men). Overall, 23.5%, 40.4% and 38.7% women were included in the OCEANIC-STROKE, STROKE-CARD, and STROKE-CARD Registry studies.
Conclusions: Exclusion criteria varied across the studies, but a common trend emerged — women were older and more likely to be unable to provide informed consent due to neurological impairment or reduced general condition. Addressing these barriers is crucial for achieving equitable representation and obtaining meaningful insights in future stroke trials.
Disclosures of Interest: No
Abstract N°: 3221
GENDER AND AGE-RELATED DIFFERENCES IN CARDIOVASCULAR RISK FACTORS, STROKE ETIOLOGY AND OUTCOMES AMONG STROKE PATIENTS AGED 18-55 YEARS IN SWITZERLAND
Thomas Schneider*1, Tolga Dittrich1, Mira Katan2, Marcel Arnold3, Emmanuel Carrera4, Timo Kahles5, Leo Bonati6, Alexander Tarnutzer7, Krassen Nedeltchev5, Gian Marco De Marchis1
1Kantonsspital St.Gallen, Klinik für Neurologie, St. Gallen, Switzerland, 2Universitätsspital Basel, Klinik für Neurologie, Basel, Switzerland, 3Inselspital, Klinik für Neurologie, Bern, Switzerland, 4Hôpitaux Universitaires de Genève (HUG), Department of Neurology, Genève, Switzerland, 5KSA Kantonsspital Aarau, Klinik für Neurologie, Aarau, Switzerland, 6Reha Rheinfelden, Klinik für Neurologie, Rheinfelden, Switzerland, 7Kantonsspital Baden AG, Klinik für Neurologie, Baden, Switzerland
On behalf of: Swiss Stroke Registry Investigators
Background and aims: Stroke in young adults is an increasingly recognized health concern, yet gender and age-related disparities in occurrence rates, cardiovascular risk factors (CVRFs), and outcomes remain underexplored.
Methods: This study analyzed 3,978 young adults aged 18-55 who hospitalized in a Stroke Unit or Stroke Center with a first-ever stroke, utilizing Quasi-Poisson models to investigate gender-specific differences in stroke occurrence rates (calculated per 100,000 person-years), risk factors, etiologies, and functional outcomes.
Results: Stroke occurrence rates were similar in males and females until the mid-thirties, after which rates increased exponentially, more so in males. At the average age of 45.8, males had a 95% higher stroke occurrence rate than females. This disparity was reduced to 60% in males with fewer than two CVRFs and 43% in normal-weight males. Overweight or obese males had a 68% higher stroke occurrence rate than females. Additionally, the annual increase in stroke rates was more pronounced in patients with at least two CVRFs and those with a BMI ⩾ 25, regardless of gender. Stroke etiologies varied by age and gender, with a more pronounced shift in males. Functional outcomes deteriorated with age but remained similar between genders.
Conclusions: The study highlights significant gender disparities in stroke occurrence rates, influenced by CVRFs and BMI, with males at a higher risk, particularly as they age. These findings emphasize the need for gender-specific preventive strategies and interventions targeting modifiable risk factors in young adults to reduce stroke risk.
Stroke Occurrence Rates.
Cardiovascular Risk Factors.
Stroke Etiology and Outcomes.
Disclosures of Interest: No
Abstract N°: 2799
ETHNIC DIFFERENCES IN STROKE INCIDENCE, SUBTYPES, MANAGEMENT, AND OUTCOME IN THE UNITED KINGDOM: A SYSTEMATIC REVIEW
Joseph Kamtchum-Tatuene*1, Peter Rothwell1
1Centre for Prevention of Stroke and Dementia, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
On behalf of:
Background and aims: Whether stroke guidelines are applicable across ethnic groups is uncertain. We aimed to summarize UK data on ethnic differences in stroke incidence, presentation, management, and outcome.
Methods: We searched PubMed/Ovid-EMBASE for studies reporting ethnic differences in stroke incidence, presentation, management, and outcome in UK, published before July 31, 2023.
Results: Seventy-six reports were included (29 studies). UK-wide and metropolitan registry-based studies consistently reported a 24-53% higher incidence of stroke in Blacks vs Whites, but differences between Asians and Whites were less consistent. In London, stroke incidence declined from 1995-2010 in Whites (41.3%, 233.4 to 137.1/100 000, p<0.0001) but not in Blacks (13.7%, 310.1 to 267.5, p=0.36). Blacks were more likely than whites to have haemorrhagic stroke (13.3% vs 9.6%), lacunar stroke (aOR=2.60, 1.94-3.48), or stroke due to intracranial stenosis (aOR=3.27, 1.17-9.12), but less likely to have stroke due to cardioembolism (aOR=0.62, 0.39-0.97) or extracranial atherosclerosis (aOR=0.39, 0.26-0.58). Blacks were less likely to present within 3 hours of stroke onset (aOR=0.61, 0.42-0.90) or to receive thrombolysis (aOR=0.49, 0.26-0.95), but both Black Caribbeans (aHR=0.85, 0.74-0.98) and Black Africans (aHR=0.61, 049-0.77) had lower post-stroke mortality than Whites. Blacks were less likely than Whites to return to work (aOR=0.41, 0.19-0.88), possibly due partly to higher odds of poststroke cognitive impairment (aOR=1.91, 1.16-3.15).
Conclusions: There are ethnic differences in stroke incidence, presentation, management, and outcome in UK, which likely reflect, at least in part, differences in aetiological subtype of stroke. Future disparity studies should report subtype-specific data where possible.
Disclosures of Interest: No
Abstract N°: 1300
RESULTS FROM A NATIONWIDE ACUTE (ISCHEMIC) STROKE REGISTRY: THE DUTCH ACUTE STROKE AUDIT 2017-2022
Lotte J Stolze*1, Nabila Wali1, Laurien S Kuhrij2, M Irem Baharoglu3, Renske M Van den Berg1,4, Paul J Nederkoorn1
1Amsterdam University Medical Centers, Department of Neurology, Amsterdam, Netherlands, 2Leiden University Medical Center, Department of Biomedical Data Sciences, Leiden, Netherlands, 3Haaglanden Medical Center, Department of Neurology, The Hague, Netherlands, 4OLVG, Department of Neurology, Amsterdam, Netherlands
On behalf of: On behalf of the Clinical Audit Board of the Dutch Acute Stroke Audit
Background and aims: The Dutch Acute Stroke Audit (DASA) is the nationwide acute stroke registry in the Netherlands. This study aims to evaluate DASA’s results between 2017 and 2022.
Methods: All consecutive patients with an acute ischemic stroke (AIS) presenting in all Dutch hospitals between 2017 and 2022 were included. Results were studied per year, and in particular, trends in workflow times were assessed.
Results: A total of 186,889 AIS-patients were included, presented in 18 comprehensive and 52 primary stroke centers. They had a median age of 75 years, 47% were female, median National Institutes of Health Stroke Scale (NIHSS) score at presentation was 3, and median onset-to-door time was 148 minutes. Intravenous thrombolysis (IVT) was received by 21.0% of patients (2017: 21.0%; 2022: 22.1%). Median door-to-needle time increased from 24 minutes (IQR 18-33) in 2017 to 27 minutes (IQR 20-40) in 2022. The percentage of patients receiving endovascular thrombectomy (EVT) increased from 12.1% in 2017 to 21.7% in 2022. Median door-to-groin time decreased from 54 minutes (IQR 31-82) to 49 minutes (IQR 26-73). Patients being referred from a primary stroke center to an EVT-capable comprehensive stroke center had a median door-in-door-out time of 67 minutes.
Conclusions: The growing proportion of patients receiving EVT may reflect recent advancements in daily practice following several trials and did not cause increased door-to-groin times. The minor rise in door-to-needle time may be due to the more frequent use of perfusion imaging. The DASA will continue to monitor the implications of developments in acute stroke treatments in daily clinical practice.
Disclosures of Interest: No
Moderated Poster - Genetics and Translational Medicine – Day 2
Abstract N°: 2741
EXPERIMENTAL ISCHEMIC STROKE INDUCES LONG-TERM SUPPRESSION OF NEURONAL ACTIVITY IN THE CONTRALATERAL HEMISPHERE
Gian Marco Calandra*1, Alessio Ricci2, Susanna Valero2, Joshua James Shrouder2, Burcu Seker2, Severin Filser3, Jürgen Bernhagen2, Farida Hellal4, Nikolaus Plesnila2
1Institute for Stroke and Dementia Research (ISD), Munich, Germany, 2Institute for Stroke and Dementia Research (ISD), München, Germany, 3German Center for Neurodegenerative Diseases (DZNE), Light Microscope Facility, Bonn, Germany, 4Institute for Tissue Engineering and Regenerative Medicine (iTERM), Helmoltz Center, Neuherberg, Germany
On behalf of:
Background and aims: Following ischemic stroke white matter damage leads, among others, to impaired interhemispheric communication with subsequent symptoms in the contralateral hemisphere, termed diaschisis. The underlaying cellular mechanisms of diaschisis, however, are not well understood. Therefore, we investigated neuronal activity of the transcallosal network and in the contralateral hemisphere after stroke by long-term in vivo 2 photon microscopy
Methods: Mice carrying a genetically-encoded calcium sensor in excitatory cortical neurons (Thy1-GCaMP6s) received an injection with AAV-retro-CAG-tdTomato into the left barrel cortex, which retrogradely labeled transcallosal neurons projecting into the contralateral hemisphere. Thereafter, the left middle cerebral artery was occluded permanently to induce ischemic stroke. Basal and evoked neuronal activity (whisker stimulation) were assessed longitudinally before and up to three months after stroke using in vivo 2-photon imaging in the contralateral hemisphere.
Results: While the frequency of basal neuronal activity remained unchanged, the amplitude of the response was reduced by 10% starting two months after stroke. When activating neurons by whisker stimulation, the amplitude of neuronal responses was significantly reduced by 36% and accompanied by a substantial reduction in response kinetics (decay time: -66%, total time of the response: -60%).
Conclusions: In summary, our findings suggest that diaschisis occurring after ischemic stroke is caused by long-term suppression of neuronal activity in the contralateral hemisphere. The underlaying cellular mechanism may be a long-term maladaptive plasticity of the contralateral excitatory and inhibitory neuronal network. Our results may serve as a basis for developing targeted therapeutic interventions to enhance post-stroke rehabilitation.
Disclosures of Interest: No
Abstract N°: 245
IDENTIFYING NOVEL THERAPEUTIC TARGETS FOR ISCHEMIC STROKE WITH DIFFERENT ETIOLOGY
Shuang Li*1, Xuan Tian1, Yuying Liu1, Yu Liu1, Ziqi LI1, Xinyi Leng1, Thomas Leung1
1The Chinese University of Hong Kong, Department of Imaging and Interventional Radiology
On behalf of:
Background and aims: Ischemic stroke (IS) is prevalent worldwide, among which novel and effective therapeutic targets are urgently needed to improve the prognosis. Large artery atherosclerosis (LAA), cardioembolism (CE) and small vessel disease (SVD) are common causes of IS. Circulating proteins may be helpful in exploring new targets. We aimed to identify potential plasma proteins as the pharmacological targets in IS subtypes, using a Mendelian randomization (MR) methods.
Methods: Gene instruments in 734 plasma proteins were employed as causative connections with each subtype in MEGASTROKE consortium by MR, and further verified using ISGC consortium. Sensitivity analyses, including bidirectional MR, Steiger filtering and Bayesian colocalization, were conducted to confirm the causal associations, and retrieval of confounders. Protein-protein interaction (PPI) networks were plotted to reveal associations of identified targets and known drug target of IS medications.
Results: With the Bonferroni correction (p<0.05/738=6.78x10-5), LPA (OR=1.22, 95% CI=1.12-1.32, p=2.06x10-6), F11 (OR=1.21, 95% CI=1.11-1.32, p=1.40x10-5) and SPATA20 (OR=1.48, 95% CI=1.23-1.78, p=3.70x10-5) were primarily selected as the target for LAA-, CE- or SVD-caused IS. Similar results were also verified in ISGC consortium. In sensitivity analyses, no reverse casualty was found. Bayesian co-localization analyses indicated that they may respectively share the same variant with corresponding subtypes. In protein-protein interaction networks, LPA interacted with HMGCR, a target of atorvastatin.
Conclusions: Our results indicated that LPA, F11 and SPATA20 might respectively have causal effects on LAA-, CE- or SVD-caused IS, which were possible targets for corresponding IS subtypes.
Disclosures of Interest: No
Abstract N°: 2945
AN EXPANDED EPIGENOME-WIDE ASSOCIATION STUDY OF ISCHEMIC STROKE RISK REVEALS ENRICHMENT OF HYPOMETHYLATED GENES IN NEURONAL BIOLOGICAL PATHWAYS
Cristina Gallego-Fabrega*1, Joan Jiménez-Balado2, Natalia Cullell1, Jara Cárcel-Márquez1, Elena Muiño Acuña1, Miquel Lledós1, Ana Aguilera-Simón3, Joan Martí-Fàbregas3, Jordi Jimenez Conde2, Israel Fernandez Cadenas1
1Institut de Recerca Sant Pau (IR SANT PAU), Stroke Pharmacogenomics and Genetics Group, Barcelona, Spain, 2Hospital del Mar Research Institute, Neurovascular Research Group, Barcelona, Spain, 3Hospital de la Santa Creu I Sant Pau, Department of Neurology, Barcelona, Spain
On behalf of: L Llucià-Carol; J.M. Martin; S Alzate; L. Marine; P Villatoro; J. Krupinski; P. Delgado; J. Montaner
Background and aims: Previous studies suggest a role of epigenetic factors in stroke risk. Here, we seek to evaluate the largest DNA methylation (DNAm) cohort of stroke patients using an Epigenome Wide Association Study (EWAS).
Methods: Two hospital cohorts were combined to obtain the DNAm dataset of ischemic stroke (IS) patients, N=1,372. Individual level data of DNAm intensity values from Illumina EPIC beadchip were preprocessed and analyzed together from hospital 1 and 2 (N=1,019). Likewise, individual level data from Illuminan 450K beadchip were also preprocessed and analyzed together (N=353). Common CpG sites (CpGs) from both arrays (424,536 CpCs) were then meta-analyzed weighting by dataset sample size. Differentially methylated positions (DMPs) were obtained adjusting for sex, age, smoking and two principal components. Significance threshold was set at epigenome-wide level (p-val<2.4·10-07). Finally, a gene enrichment analysis on Gene Ontology pathways was conducted using the significant DMPs from the Meta-analysis.
Results: 15 DMPs in 12 loci were identified in the meta-analysis, being 13 of them nominally significant in both cohorts. Top signals include an intragenic region in chromosome 11 (p-val=8.02·10-14) and a locus in an intragenic region in chromosome 1 containing 3 DMPs (lead CpG, p-val=6.71·10-10). Results were enriched in neuron projection regeneration, response to axion injury and axon development pathways.
Conclusions: We observed an enrichment of hypomethylated genes in biological pathways related to neuronal function in IS patients compared to controls. Hinting a potential regulatory role of those genes in stroke risk must be further investigated.
Disclosures of Interest: No
Abstract N°: 129
MOLECULAR PROFILING OF MINOR STROKE USING PERIPHERAL BLOOD GENE EXPRESSION
1University of California at Davis, Department of Neurology, 2University of Alberta, Division of Neurology, 3University of Pennsylvania Medical Center, 4Stanford University Medical Center
On behalf of:
Background and aims: The peripheral immune system is involved in the response to stroke, being demonstrated in part from peripheral blood gene expression changes. We investigated the peripheral blood transcriptome in patients with transient neurologic symptoms lasting <24h with acute infarction on MRI (DWI+), referred to here as minor stroke, and how it differs from controls, including vascular risk factor-matched controls (VRFC) and stroke mimics.
Methods: Peripheral blood RNA of 90 minor ischemic stroke (blood collected at 15h average post ictus), and 169 controls (88 VRFC and 81 mimics) was sequenced using the Lexogen 3' QuantSeq FWD. Differentially expressed (DE) genes were identified using an Analysis of Covariance (ANCOVA) including diagnosis, age, sex, hypercholesterolemia, hypertension, diabetes mellitus, and recruitment site.
Results: 261 genes were DE in minor stroke versus controls (p < 0.05, fold-change >|1.2|). Of these, 106 genes were up-regulated and 165 down-regulated. They included 23 transcriptional regulators, 21 of which were down-regulated in minor stroke, including zinc-finger-proteins implicated in stroke. Interleukin-1 Family signaling, and several transcription, translation and transcript processing pathways were suppressed (Z<-2), while mitochondrial dysfunction was activated (Z=2.1) in minor stroke. DE genes were enriched in Natural Killer-cell specific genes (Benjamini-Hochberg p=2.4E-02).
Conclusions: The findings expand our knowledge of the minor stroke’s peripheral immune response which likely differs from major stroke because of differences in BBB compromise. The identified genes/pathways may guide the search for novel therapeutic targets and help develop a blood diagnostic where minor stroke could be diagnosed from these gene profiles without need for MRI.
Disclosures of Interest: No
Abstract N°: 1858
LONGITUDINAL MEASUREMENT OF SERUM NEUROFILAMENT LIGHT CHAIN IN PATIENTS WITH CADASIL
Jay Chol Choi*1, Jung Seok Lee1, So Young Yoon2, Joong-Goo Kim1, Chul-Hoo Kang2, Ji-Hoon Kang1
1Jeju National University College of Medicine, Department of Neurology, Jeju, South Korea, 2Jeju National University Hospital, Department of Neurology, Cheju, South Korea
On behalf of:
Background and aims: Serum neurofilament light chain (NfL) levels have been shown to be strongly associated with MRI markers of cerebral small vessel disease, cognitive deficits, and disability in cross-sectional studies of patients with cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL). This study aimed to investigate the longitudinal changes in serum NfL levels and their correlation with disease progression in patients with CADASIL.
Methods: We prospectively enrolled a group of CADASIL patients and assessed their clinical symptoms, cognitive function, brain MRI, and serum NfL levels at baseline and after a three-year follow-up. Global cognitive function was evaluated using the Seoul Neuropsychological Screening Battery dementia version (SNSB-D), with a maximum score of 300. We used linear mixed-effects models to investigate associations between changes in serum NfL levels and changes in cognitive function and MRI markers.
Results: At baseline, we examined 59 CADASIL patients between October 2018 and August 2019, and 51 patients completed the three-year follow-up, including clinical assessment, brain MRI, and serum NfL measurement. During the three-year follow-up, there was a significant increase in mean serum NfL levels (19.04 ± 1.90 pg/ml vs. 30.84 ± 3.41 pg/ml, P<0.001). Changes in serum NfL levels were also significantly associated with age, changes in SNSB-D score, and cortical thickness. After adjusting for age, changes in serum NfL levels could predict changes in cortical thickness (P <0.001) or SNSB-D score (P <0.001).
Conclusions: Longitudinal measurements of serum NfL could serve as a valuable blood biomarker for monitoring disease progression in patients with CADASIL.
Disclosures of Interest: No
Abstract N°: 375
DECIPHERING POTENTIAL GENETIC SIGNATURES IN YOUNG ISCHEMIC STROKE WITH FAMILIAL CLUSTERING THROUGH WHOLE EXOME SEQUENCING
1All India Institute of Medical Sciences, New Delhi, India, 2Institute of Genomics and Integrative Biology, New Delhi, India
On behalf of:
Background and aims: The global incidence of ischemic stroke in young adults, comprising 10-30% of cases aged 18-45 years, is on the rise. Whole Exome Sequencing (WES) emerges as a vital tool for identifying rare genetic variants and uncovering novel contributory genes which were never implicated in the neurological disorders.
Identify pathogenic determinants in early-onset ischemic stroke with familial clustering of stroke.
Methods: We conducted WES in 100 young ischemic stroke patients with the age range of 18-40 years. Total 459 controls were used for frequency and family-based segregation analysis. Identified 41 variations across 22 genes from intrafamily and interfamily analysis were further validated in unaffected family members. Confirmed variations were replicated in another cohort of 100 cases and 100 controls using mass array genotyping.
Results: Nineteen variations from 13 genes were identified, with 11 genes (HBB, vWF, HHIPL2, CUL9, KALRN, ZNF318, TGFB2, TTBK1, F13A1, CCND3, and RPL7L1) found in intra-family analysis and two genes (PDE4DIP and NOS2) in inter-family analysis. Among them, three genes (TTBK1, CUL9, and RPL7L1) are not previously associated with any neurological disorder. Notably, variations c.17_18del, p.P6fs in HBB and c.G2561A, p.R854Q in vWF were deemed pathogenic. Additionally, two loci, rs10482721 in TGFB2 and rs56320013 in KALRN, were replicated in another cohort of 100 cases and 100 controls.
Conclusions:TGFB2 and KALRN emerged as potential genetic signatures, offering valuable insights for further research and clinical implications.
Disclosures of Interest: No
Abstract N°: 1284
EPIGENETIC AGE ACCELERATION ASSOCIATES WITH AN INCREASED RISK OF CANCER AFTER STROKE IN LONG-TERM FOLLOW-UP
Antoni Suárez-Pérez*1, Angel Ois1,2, Adrià Macias-Gómez1,2, Marta Vallverdú-Prats1, Elisa Cuadrado-Godia1,1, Eva Giralt-Steinhauer1,2, Isabel Fernández-Pérez1,2, Daniel Guisado-Alonso1,2, Jordi Jiménez-Conde1,2, Joan Jiménez-Balado1
1Hospital del Mar Research Institute, Neurovascular Research Group, Barcelona, Spain, 2Hospital del Mar, Neurology, Barcelona, Spain
On behalf of:
Background and aims: Patients who have experienced a stroke exhibit an increased susceptibility to incident cancer, with both diseases sharing an age-dependent association. Our study seeks to investigate the potential influence of biological age (B-age) on this association, independently of chronological age (C-age).
Methods: We included stroke survivors from a prospective acute stroke registry (2005 to 2017) with a minimum of three-month follow-up and no prior cancer diagnosis. The study endpoint was the incidence of cancer and the follow-up was censored at ten years. DNA methylation data were obtained from whole blood samples obtained within the initial 24 hours after stroke onset. B-age was estimated using several epigenetic clocks (Hannum, Horvath, PhenoAge, Zhang and EPITOC). We then calculated the age acceleration (ageAcc) by regressing out the effect of C-age on the difference between B-age and C-age. We used Kaplan-Meier and Cox multivariate regression models to explore how cancer incidence was affected by ageAcc independently of confounding factors.
Results: We followed-up 632 patients over a median period of 4.61 years, finding that 73 individuals (11.6%) developed cancer. C-age (p=0.002), male sex (p=0.012), carotid atherosclerosis (p=0.023), and alcohol consumption (p=0.031) associated with incident cancer in the univariate analyses. The Cox multivariate analyses (HR [95% CI]) revealed that a higher ageAcc in Hannum (1.08 [1.04-1.13]), PhenoAge (1.03 [1.00-1.06]), Zhang BLUP (1.07 [1.01-1.14]), Zhang EN (1.09 [1.02-1.16]), and EPITOC (1.11 [1.01-1.22]) increased the risk of incidental cancer.
Conclusions: Our results suggest that stroke patients developing cancer are biologically older than those who do not.
Disclosures of Interest: No
Abstract N°: 1351
EXPLORING SUBCLINICAL BIOMARKERS OF ATHEROSCLEROSIS USING DEEP LEARNING ON UK BIOBANK DATA
Murad Omarov*1, Andreas Papadopoulos1, Saman Jorshery2,3, Rainer Malik1, Martin Dichgans1,4,5, Vineet Raghu3,6, Christopher Anderson2,3, Marios Georgakis1,2,3
1Institute for Stroke and Dementia Research, München, Germany, 2Broad Institute of MIT and Harvard, Cambridge, United States, 3Massachusetts General Hospital, Boston, United States, 4Munich Cluster for Systems Neurology (SyNergy), München, Germany, 5German Center for Neurodegenerative Diseases, Göttingen, Germany, 6Harvard Medical School, Boston, United States
On behalf of:
Background and aims: Atherosclerosis is the major condition underlying cardiovascular disease (CVD) and its most fatal complications. The presence of carotid plaques on carotid ultrasound is a well-known marker of subclinical atherosclerosis. The accumulation of extensive data on the presence of atherosclerotic plaques, along with deep phenotyping, is crucial to address the effectiveness of carotid ultrasound in routine clinical practice and to shed light on the biology of atherosclerosis development.
Methods: A deep-learning model was trained on 190 carotid ultrasound images with manually segmented plaques and applied to the carotid ultrasound images of 19,700 UK Biobank participants. Logistic and Cox regression were used to estimate the association of predicted phenotypes with conventional CVD risk factors and the risk of CVD events (252 events of stroke and myocardial infarction). A genome-wide association study (GWAS) on plaque presence was conducted using Regenie, followed by meta-analysis using METAL.
Results: Our plaque detection model achieved metrics of accuracy, sensitivity, and specificity of over 85% on a test set of 40 images (50% plaque prevalence). Both predicted presence and the number of plaques were associated with most CVD risk factors and with the future risk of CVD events in the population-scale sample. Meta-analysis of GWAS with the summary statistics from the CHARGE consortium revealed a new locus in the LPA gene significantly associated with the presence of plaques.
Conclusions: We have developed and applied an efficient plaque detection model to the UK Biobank data, which offers great potential for studying atherosclerosis at the population-scale level.
Disclosures of Interest: Yes
Moderated Poster – Prevention – Day 2
Abstract N°: 6
DUAL ANTIPLATELET THERAPIES IN MINOR NONDISABLING ACUTE ISCHEMIC STROKE: A NETWORK META-ANALYSIS
Andy Lim*1, Henry MA1, John Ly1, Shaloo Singhal1, Yuesong Pan2, Yongjun Wang2, S. Claiborne Johnston3, Thanh Phan1
1Monash University Clayton Campus, Stroke and Ageing Research Group, Clayton, Australia, 2Beijing Tiantan Hospital, Department of Neurology, China, 3University of California, San Francisco, San Francisco, United States
On behalf of:
Background and aims: Dual antiplatelet therapy (DAPT) appears to be an effective treatment option for minor (nondisabling) acute ischemic stroke. This conclusion is based on trials that include both transient ischemic attack (TIA) and minor stroke. Aim: to compare DAPT regimens specifically for minor stroke.
Methods: Literature search to November 2023 for trials testing DAPT within 24 hours of minor stroke (National Institutes of Health Stroke Scale score ⩽5). A Bayesian network meta-analysis was conducted using fixed-effects. A secondary analysis was performed for high-risk TIA alone.
Results: Five trials describing 28,148 patients were included (Figure 1), of whom 22,203 patients (78.9%) had a minor stroke (Figure 2). Of these, 13,995 (63.0%) were in DAPT arms and 8,208 (37.0%) in aspirin arms. Aspirin and ticagrelor had a 94% probability of being the most effective treatment in minor stroke (SUCRA 0.94) for the primary outcome. Both aspirin-ticagrelor (NNT 43, 95% CI 33-67) and aspirin-clopidogrel (NNT 61, 95% CI 41-142) were superior to aspirin alone in the prevention of recurrent ischemic stroke at 90 days. Both had higher rates of major hemorrhage than aspirin alone (NNH 357, 95% CI 135-2160 and NNH 415, 95% CI 148-4320 respectively), but neither had increased risk of hemorrhagic stroke nor death. For TIA, neither ticagrelor (SUCRA 0.60) nor clopidogrel (SUCRA 0.40) was optimum, but both were superior to aspirin.
Conclusions: DAPT with ticagrelor and aspirin has higher probability of being the superior treatment among patients with minor stroke. For patients with TIA, the superiority of ticagrelor-aspirin versus clopidogrel-aspirin was not demonstrated.
Disclosures of Interest: No
Abstract N°: 1096
EFFECTS OF DYADIC INTERVENTIONS ON HEALTHY DIETS IN PATIENTS WITH CARDIOVASCULAR DISEASES AND INFORMAL CAREGIVERS: A META-ANALYSIS
YONG YANG YAN*1, Yangxi Huang1, Man Ping Wang1, Kui Kai Lau2, Jung Jae Lee1
1The University of Hong Kong, School of Nursing, Hong Kong, China, 2The University of Hong Kong, Department of Medicine, Hong Kong, China
On behalf of:
Background and aims: Unhealthy diets contribute to cardiovascular diseases (CVDs). Although informal caregivers often assist CVD patients’ diets, the effectiveness remains understudied. This systematic review examined the effectiveness of dyadic interventions on promoting healthy diets among CVD patient-informal caregiver dyads.
Methods: : A literature search was conducted in PubMed, Cochrane Library, Embase, CINAHL, PsycINFO, and Web of Science, from inception to August 10, 2023. Randomised controlled trials promoting healthy diets within CVD patient-informal caregiver dyads and reporting relevant dietary adherence outcomes were included. Random and fixed effects meta-analyses were performed to assess the effectiveness.
Results: This review included 12 studies with 1199 CVD patients (mean age 61.6 years). Most caregivers were partners/spouses (76.29%) and female (75.84%). All studies were rated as having some concerns or high risk of bias. The interventions significantly reduced patients’ 24-hour urinary sodium at follow-up (mean difference [MD]=-628.73mg/24 hours, 95%CI=-970.09, -287.37) and improved the proportion of participants reducing salty food intake (odds ratio [OR]=2.07, 95%CI=1.25, 3.43), compared to the control group. The interventions also significantly improved patients’ self-efficacy (standardised mean difference [SMD]= 0.60, 95%CI=0.18, 1.02), heart disease knowledge at post-intervention (SMD=0.67, 95%CI=0.43, 0.90), perceived autonomy support (SMD=0.49, 95%CI=0.16, 0.83), but not dietary adherence score (SMD=1.27, 95%CI=-0.07, 2.61).
Conclusions: Dyadic interventions significantly improved patients’ sodium intake reduction, self-efficacy, heart disease knowledge, and perceived autonomy support, but not dietary adherence score. More high-quality trials with a wider dietary adherence measure are needed to strengthen the long-term effects on promoting healthy diets within CVD patient-informal caregiver dyads.
Disclosures of Interest: No
Abstract N°: 2794
HOW DOES PRIOR ANTIDIABETIC MEDICATION INFLUENCE SECONDARY PREVENTION AND CLINICAL OUTCOMES AFTER ISCHAEMIC STROKE?
Kadie-Ann Sterling*1, Melanie Turner1, Mary Joan Macleod2
1Institute of Applied Health Sciences, School of Medicine, Medical Sciences and Nutrition, Aberdeen, United Kingdom, 2Institute of Medical Sciences, School of Medicine, Medical Sciences and Nutrition, Aberdeen, United Kingdom
On behalf of:
Background and aims: Diabetes is associated with increased stroke risk and poorer clinical outcomes after stroke. This study aims to compare secondary prevention prescribing in patients taking and not taking antidiabetic medication (ADM) before stroke, and to examine the effect on all-cause mortality.
Methods: This national retrospective data-linkage study includes 47,087 first-ever ischaemic stroke patients admitted between January 2011 and December 2018 in acute care hospitals in Scotland. Secondary prevention prescribing and one-year mortality data were compared between patients taking and not taking ADM before their stroke using regression analysis.
Results: 7128 (15.1%) were prescribed ADM within three months prior to their stroke. They were younger (72.1 (±11.30) vs 72.8 (±13.7) years) and more likely to be male (56.0% vs 49.1%). At six months, antihypertensives (adjusted odds ratio (aOR), 2.67; 95% confidence interval (CI), 2.43 – 2.94), antiplatelets (aOR, 1.14; 95% CI, 1.04 – 1.24) and statins (aOR, 1.36; 95% CI, 1.22 – 1.51) were prescribed more frequently in the ADM group, while oral anticoagulants were less frequently prescribed (aOR, 0.92; 95% CI, 0.84 – 0.99). One-year all-cause mortality was significantly higher in the ADM group (adjusted hazard ratio, 1.52; 95% CI, 1.31 – 1.77).
Conclusions: Prior ADM prescribing is associated with higher use of secondary prevention medicines after stroke. However, all-cause mortality was higher in this group even after adjusting for available confounders. The impact of diabetes is likely to influence stroke outcomes more than the effect of secondary prevention medications. Unmeasured variables such as frailty, other comorbidities or complications associated with diabetes may also play a part.
Disclosures of Interest: No
Abstract N°: 210
OUTCOMES OF EARLY SHORT-DURATION DAPT IN MINOR ISCHEMIC STROKE DUE TO SMALL ARTERY OCCLUSION
1University of L'Aquila, Department Biotechnological and Applied Clinical Sciences, 2AUSL Romagna, Department of Neuroscience, Neurology Unit, Maurizio Bufalini Hospital, Cesena, Italy, 3Santa Corona Hospital, Department of Neurology, Pietra Ligure, Italy, 4University Hospital Santa Maria della Misericordia, Department of Internal and Cardiovascular Medicine - Stroke Unit, Perugia, Italy, 5Città di Castello Hospital, Department of Neurology, Città di Castello, Italy, 6University of Rome La Sapienza, Department of Human neurosciences, Rome, Italy
On behalf of: READAPT study group
Background and aims: There is unclear evidence of differences in the benefit of dual antiplatelet treatment (DAPT) in patients with stroke due to small artery occlusion (SAO) relative to other stroke subtypes. We aimed to evaluate the effectiveness and safety of early short-duration DAPT in patients with SAO-related minor ischemic stroke (SAO-MIS).
Methods: This is a prespecified subgroup analysis from a prospective multicentric real-world study (READAPT, NCT05476081). The analysis included patients with minor (NIHSS⩽5) non-cardioembolic ischemic stroke who started DAPT within 24h of index event. The primary efficacy outcome was a composite of new stroke and death due to vascular causes at 90-day. The primary safety outcome was moderate-to-severe bleeding at 90-day.
Results: We included 678 MIS, of whom 253 (37.3%) were due to SAO. SAO-MIS patients had significantly more hypertension, leukoaraiosis and prior lacunar infarcts at neuroimaging compared to non-SAO-MIS; the risk of primary efficacy outcome was extremely low and similar in both groups (2.1% versus 4.9%; p=0.037), while primary safety outcome was rare in both groups (0 versus 0.5%; p=0.718). Taking DAPT loading dose and having SAO etiology were independently associated with lower risk of primary efficacy outcome (HR 0.44, 95%CI 0.19-0.98; p=0.045 and HR 0.24, 95%CI 0.07-0.79; p=0.019, respectively).
Conclusions: Our results support the use of early short-term DAPT in patients with SAO-MIS for preventing early recurrences. DAPT appeared effective and extremely safe in terms of bleeding risk. Loading dose must be given to all patients since it is associated with even lower risk of recurrent events.
Disclosures of Interest: No
Abstract N°: 2090
ANTITROMBOTIC THERAPY IN PATIENTS UNDERGOING CAROTID ARTERY STENTING WITH CONCOMITANT ATRIAL FIBRILLATION
Manuel Medina-Rodriguez1,2, Antonio Cristobal Luque-Ambrosiani*1, Leire Ainz1,2, Pablo Baena Palomino1,2, Juan Antonio Cabezas Rodriguez1,2, Blanca Pardo-Galiana1,2, Elena Zapata Arriaza2,3, Asier de Albóniga-Chindurza2,3, Alejandro González2,3, Francisco Moniche Alvarez1,2
1Virgen del Rocío University Hospital, Stroke Unit. Department of Neurology, Sevilla, Spain, 2Ibis- Biomedicine Institute of Sevilla, Neurovascular Lab, Sevilla, Spain, 3Virgen del Rocío University Hospital, Interventional Neuroradiology, Sevilla, Spain
On behalf of:
Background and aims: Antithrombotic therapy strategy following carotid artery stenting (CAS) in patients with concomitant atrial fibrillation (AF) is not well established and triple antithrombotic therapy is associated with high risk of bleeding. Our aim was to explore a new regimen including a direct oral anticoagulant (DOAC) plus clopidogrel.
Methods: We designed a retrospective, observational single-center study including patients with AF following CAS during 2010-2023. We compared patients receiving oral anticoagulation plus dual antiplatelet therapy [triple-therapy-group] vs those receiving a DOAC plus clopidogrel [dual-therapy-group]. The safety outcome was major or clinically relevant nonmajor bleeding event and the efficacy outcome was thromboembolic events (in-stent thrombosis, myocardial infarction, stroke, systemic embolism) during follow-up (1 month).
Results: We included 102 patients, 50 assigned to triple-therapy-group and 52 to dual-therapy-group. The median age was 74 (IQ=69-80). CHAD2S2-VASc [5 (IQ=3.2-6) vs 4.75 (IQ=3-5.5), p=0.55] and HAS-BLED [4 (IQ=3-5) vs 4 (IQ=4-4), p=0.39] scores were similar in both groups. Emergent CAS was performed in 7 (14%) vs 15 (28.8%), p=0.06. The incidence of the safety outcome was 22% in triple-therapy-group as compared with 1.9% in the dual-therapy-group (hazard ratio, 0.079; 95% CI, 0.01-0.61, p=0.015) (Figure 1). The incidence of efficacy outcome was 0 in triple-therapy-group, as compared to 3.8% in dual-therapy-group (risk difference 3.8%, 95%CI, -2 – 9, p=0.49).
Conclusions: In patients with AF who underwent CAS, the risk of bleeding was lower among patients who received a DOAC plus clopidogrel than among those with triple therapy, without significant differences in the incidence of thromboembolic events.
Disclosures of Interest: No
Abstract N°: 2463
REPEATED CAROTID ARTERY SURGERY IN SWEDEN 2008-2017 – AN OBSERVATIONAL NATION-WIDE COHORT STUDY IN SWEDEN 2008-2017
Kimberley Hammar1, Louise Ziegler1, Magnus Jonsson2, Per Wester1,3, Annika Lundström*1
1Karolinska Institute, Clinical Sciences Danderyd Hospital, Stockholm, Sweden, 2Karolinska Institute, Molecular Medicine and Surgery, Stockholm, Sweden, 3Umeå University, Faculty of Medicine, Dept of Public Health and Clinical Medicine, Umeå, Sweden
On behalf of:
Background and aims: Outcome after surgery for carotid stenosis has improved, however a risk for new ischemic events and progression of atherosclerosis remains. The aim of this observational, nation-wide Swedish cohort study was to determine rates of repeated ipsi- and contralateral carotid surgery in patients with previous carotid intervention and to explore patient characteristics.
Methods: All patients with carotid surgery registered in the Swedish National Registry for Vascular Surgery (Swedvasc) 2008-2017 were screened for multiple operations. Indication for surgery and side of operation were retrieved. Swedvasc data was merged with Riksstroke, the national stroke register, to identify patients with stroke. Primary outcome was stroke after a second operation. Perioperative complications and all-cause mortality were secondary outcomes. For comparison of patient characteristics and outcomes, a group of age- and sex-matched controls 2:1 operated on only one side was established.
Results: In total 352 out of 8 676 patients (4.1%), had more than one carotid operation over a mean follow-up of 4.4 years, i e 0.9%/year. In 89% of cases, the second operation was on the contralateral side. A second operation was more common after primary surgery for asymptomatic as compared to symptomatic stenosis, 7.6% vs 3.6%. The indication for repeated surgery was asymptomatic stenosis in 52% of cases. Mean incidence of primary outcome stroke was 1.7%/year, which was not significantly higher than for matched controls, 1.4%/year.
Conclusions: Repeated carotid surgery is not uncommon. It generally concerns the contralateral carotid and is mainly performed without development of new ischemic symptoms.
Disclosures of Interest: No
Moderated Poster - Rehabilitation and Outcomes – Day 2
Abstract N°: 1113
IS CARDIORESPIRATORY FITNESS INDEPENDENTLY ASSOCIATED WITH FATIGUE IN PATIENTS WITH TRANSIENT ISCHEMIC ATTACK OR MINOR STROKE?
Inger Deijle*1, Erwin Van Wegen2, Renske M. Van den Berg-Vos1, Gert Kwakkel2
1OLVG Location West, Neurology, Amsterdam, Netherlands, 2VU University Medical Center, Rehabilitation and Development, Amsterdam Movement Sciences, Amsterdam, Netherlands
On behalf of:
Background and aims: Fatigue is a common complaint and a disabling symptom among patients following transient ischemic attack (TIA) or minor stroke. In patients with stroke, decreased cardiorespiratory fitness (CRF) is believed to be related to increased severity of post-stroke fatigue (PSF). However, this association between PSF and CRF in patients with TIA or minor stroke has been less investigated, and currently there is no proven treatment for PSF. We aimed to determine the association between PSF and CRF in patients with TIA or minor stroke and to find out whether this association was distorted by confounders.
Methods: A cross-sectional association study was conducted among a total of 119 patients with TIA or minor stroke. PSF was measured by the Fatigue Severity Scale (FSS) and CRF was quantified by maximal exercise capacity (V˙O2max).
Results: The FSS showed a significant association with V˙O2max (ß = −0.061, standard error (SE): 0.022; p = 0.007). This association was confounded by anxiety (ß = −0.044, SE: 0.020; p = 0.028) and depression (ß = −0.030, SE: 0.022; p = 0.177) as measured by the subscales of the Hospital Anxiety and Depression Scale (HADS). After controlling for HADS scores on depression and anxiety, the univariate relationship between V˙O2max and FSS was no longer significant.
Conclusions: These results suggest that the association between PSF and CRF in patients with TIA or minor stroke is weak and significantly confounded by the factors depression and anxiety.
Disclosures of Interest: No
Abstract N°: 3190
KNOWLEDGE AND UTILIZATION OF CLINICAL PRACTICE GUIDELINES FOR STROKE AMONG REHABILITATION PROFESSIONALS IN LMICS (REFORM STUDY)
1Christian Medical College & Hospital, Department of Neurology, Ludhaina, India, 2University of Leicester, Institute of Precision Health, Ulverscroft Eye Unit, Leicester, United Kingdom, 3Christian Medical College & Hospital, Department of Neurology & College of Physiotherapy, Ludhiana, India, 4Christian Medical College & Hospital, College of Physiotherapy, Ludhiana, India
On behalf of: GCSR collaborators
Background and aims: Stroke has consistently been the second leading cause of death and the third leading cause of disability in Low-and-Middle-Income-Countries (LMICs). The evidence base of stroke rehabilitation has grown in the past decade, however, its application in clinical practice is sub-optimal among LMICs. We aimed to explore the knowledge and utilization of the clinical practice guidelines (CPGs) among rehabilitation professionals in LMICs
Methods: A cross-sectional survey was undertaken to identify user knowledge and implementation of evidence-based CPGs. The validated questionnaire was shared to practicing rehabilitation therapists (physiotherapists and occupational therapists) working in LMICs using online modes (email, WhatsApp, etc) across national associations/bodies for rehabilitation using the snowballing technique.
Results: There were 155 respondents from 23 countries, which included 136 physiotherapists (88%) and 27 neurorehabilitation specialists. 51% had <5 years work experience, most worked in a hospital (62%) and a majority treated upto 5 patients a week (60%). About 50% said they didn’t have CPGs in their country or were not sure. Among those that were aware, a third each said the guidelines were national or hospital or both, that were adapted/adopted (70%) from another country, while the indigenous guidelines were derived from multiple sources. Barriers to implement CPGs included accessibility, awareness, motivation and resources. Training, quality supervision, infrastructure, networking and research were reported to help implement CPGs in addition to developing guidelines
Conclusions: There is a need to develop indegenous evidence-based National CPGs in LMICs. Its successful implementation would require creating awareness, training and rigorous implementation with quality controls.
Disclosures of Interest: No
Abstract N°: 169
TRENDS IN 90-DAYS CASE-FATALITY AND FUNCTIONAL OUTCOME AFTER FIRST-EVER STROKE IN SWEDEN 2010–2019
Conrad Drescher*1, Fredrik Buchwald1, Teresa Ullberg1, Mats Pihlsgård2, Bo G. Norrving1, Jesper Petersson1
1Lund University, Department of Clinical Sciences Lund and Skånes University Hospital, Malmö/Lund, Sweden, 2Lund University, Department of Clinical Sciences Malmö, Malmö/Lund, Sweden
On behalf of:
Background and aims: Stroke incidence in Sweden has decreased between 2010 and 2019. We analyzed national trends in case-fatality and functional outcome 90 days after stroke during the same period.
Methods: We included patients (⩾18 years) with first-ever stroke registered in the Swedish Stroke Register (Riksstroke) 2010 to 2019. Mortality data were obtained from the Swedish Causes of Death Register. Functional outcome data were based on the Riksstroke follow-up surveys at 90 days. Extrapolation was used for missing data on functional status in survey non-responders (15.2% of total cohort). Data were analyzed by stroke subtype and in 3 different time periods (2010–12, 2013–16 and 2017–19).
Results: Between 2010 and 2019, 176,154 cases of first-ever stroke were registered in Riksstroke; 87.3% were ischemic stroke (IS) and 12.7% were intracerebral hemorrhage (ICH). From 2010–2012 to 2017–2019, 90-days case-fatality in all strokes decreased from 15.9% to 14.7% (p<0.001). Case-fatality in IS decreased from 13.8% to 12.4% (p<0.001) and in ICH from 31.0% to 30.4% (p<0.001). Proportion of favorable functional outcome (mRS 0-2) after 90 days in all strokes increased from 47.7% to 51.1% (p<0.001). Whereas favorable outcome increased from 49.8% to 53.8% (p<0.001) in IS, there was a small decrease from 32.9% to 32.4% (p<0.001) in ICH.
Conclusions: We observed a decline in 90-days case-fatality and an increased proportion of patients with favorable functional outcome (mRS 0-2) 90 days after stroke in Sweden between 2010 and 2019. These results were mainly driven by positive trends in ischemic stroke patients.
Disclosures of Interest: No
Abstract N°: 2590
AN EXPLAINABLE CONVOLUTIONAL NEURAL NETWORK TO BETTER UNDERSTAND PREDICTED FUNCTIONAL OUTCOMES AFTER ACUTE ISCHEMIC STROKE
Hakim Baazaoui*1, Jonas Brändli2, Lisa Herzog3, Martin Hänsel1, Beate Sick2, Susanne Wegener1
1University Hospital Zurich, Department of Neurology, Zürich, Switzerland, 2Zurich University of Applied Sciences, Institute of Data Analysis and Process Design, Winterthur, Switzerland, 3University of Zurich, Zürich, Switzerland
On behalf of:
Background and aims: The reasoning of artificial intelligence models in stroke outcome prediction is often opaque. Therefore, we aimed to assess the performance of an explainable convolutional neural network (CNN) in predicting acute ischemic stroke (AIS) outcomes and infer patterns from its predictions.
Methods: We included 407 patients with AIS (n=304) or transient ischemic attack (TIA, n=103) treated at our stroke centre between 2014 and 2016. DWI images acquired 0-3 days after onset were input into a CNN to predict dichotomized 90-day modified Rankin Scale: 0-2 for favourable and 3-6 for unfavourable outcome. We applied gradient-weighted class activation mapping (Grad-CAM) to illustrate the importance of different brain regions for the predicted outcome.
Results: In a cross-validation experiment, an area under the receiver operating curve of 0.87 (95% CI: 0.81-0.91) was achieved for predicting functional outcome. Most patients with a predicted unfavourable outcome displayed bilateral frontal lobe Grad-CAM signals. In the subgroup of patients with frontal signals (n=84), an unfavourable outcome was predicted in 94.0% of cases, with a sensitivity of 89.7% and a specificity of 2.2%. Furthermore, the frontal signal subgroup was significantly older than the rest of the cohort (78.7±8.4 vs. 64.6±15.2 years, p<0.0001). This was also observed in TIA patients (81.7±5.7 years with frontal signal vs. 65.8±15.5 years for other TIA patients, p<0.0001).
Conclusions: The CNN highlighted regions unaffected by AIS, most notably the frontal lobes for unfavourable outcome, even in TIA patients without stroke lesions. Age-related frontal atrophy may have served as a proxy for worse outcomes.
Disclosures of Interest: No
Abstract N°: 1922
RECURRENT ISCHAEMIC EVENTS AFTER PATENT FORAMEN OVALE CLOSURE: A REAL-WORLD COHORT STUDY
Henrik Sørensen*1, Johanne Andersen Højbjerg2, Erik Lerkevang Grove3, Claus Ziegler Simonsen1
1Aarhus Universitetshospital, The Department of Neurology, Aarhus, Denmark, 2Aarhus Universitetshospital, Department of Clinical Biochemistry, Aarhus, Denmark, 3Aarhus Universitetshospital, The Department of Cardiolocal Medicine B, Aarhus, Denmark
On behalf of:
Background and aims: Patent foramen ovale (PFO) has been associated with paradoxical embolism and ischaemic stroke. PFO closure has been shown to reduce the risk of future ischaemic stroke and is increasingly used in clinical practise. We aimed to evaluate complications and outcomes in patients after PFO closure as well as the prevalence of thrombophilia as a possible contributor to post-closure complications.
Methods: Patients from the Central Denmark Region who underwent PFO closure between November 5, 2018, and May 12, 2023, following a stroke or transient ischaemic attack, were included. Data on patient demographics, risk factors, procedural details and post-intervention outcomes were collected from electronic medical records.
Results: PFO-closure was performed in 310 patients (median age: 49 years). During a median follow-up of 2.6 years (range 0.4-4.9, 814 total patient-years), recurrent ischaemic cerebrovascular events were observed in 8 patients (2.6%) translating into 0.98 recurrent strokes per 100 patient years. Recurrent stroke was more frequent in patients with hypertension (p= 0.039). New-onset atrial fibrillation was observed in 8.4% of patients within 45 days after the procedure. Other adverse effects were uncommon. Thrombophilia assessment in 45.5% of patients revealed positive results in 22 cases, with lupus anticoagulant identified in two of the nine patients with re-stroke.
Conclusions: Rates of recurrent stroke or transient ischaemic attack after PFO closure were low. Thrombophilia emerged as a potential contributing factor to complications. Patients with hypertension had a higher risk of recurrent stroke and antihypertensive treatment may therefore be important for prevention of recurrent stroke after PFO closure.
Disclosures of Interest: No
Abstract N°: 1624
PITFALLS IN BETWEEN-COUNTRY COMPARISONS OF OUTCOME AFTER ENDOVASCULAR THROMBECTOMY FOR ISCHEMIC STROKE BASED ON REGISTRY DATA
Paula Janssen*1, Jan Vinklarek2,3, Robert Mikulik3,4, Hester Lingsma5, Diederik Dippel1
1Erasmus MC University Medical Center Rotterdam, Neurology, Rotterdam, Netherlands, 2St Anne’s University Hospital, Neurology, Brno, Czech Republic, 3Faculty of Medicine at Masaryk University, Brno, Czech Republic, 4St Anne’s University Hospital, International Clinical Research Center, Brno, Czech Republic, 5Erasmus MC University Medical Center Rotterdam, Public Health, Rotterdam, Netherlands
On behalf of: MR CLEAN Registry investigators and the SITS-TBY Registry investigators from the Czech Republic.
Background and aims: Assessment of between-country variation in outcomes after endovascular thrombectomy (EVT) for ischemic stroke offers opportunities to improve quality of care, but interpretation may be challenging. To illustrate this, we compared functional outcomes between patients treated in the Czech Republic and the Netherlands.
Methods: We used nationwide registry data of stroke patients treated with EVT in both countries. Primary outcome was modified Rankin Scale (mRS) score at 90 days. We used multilevel ordinal regression with multiple imputation to analyze step by step the impact of missing data, differences in patient characteristics, time-to-groin puncture, and clustering of patients by center on the estimated between-country variation in outcome, expressed as common odds ratio (cOR).
Results: We included 4518 patients (3253 from the Netherlands; 1265 from the Czech Republic). Without imputation of missing mRS scores at 90 days (n=822, 18%) and without any adjustment, between-country variation was substantial (cOR of a more favorable outcome in the Czech Republic 1.48, 95% CI 1.27-1.73). Differences between the countries decreased after imputation of missing data (cOR 1.22, 95% CI 1.09-1.38), adjustment for patient characteristics (cOR 1.13, 95% CI 1.00-1.29), time to groin puncture (cOR 1.06, 95% CI 0.93-1.21), and were no longer present after finally adding clustering by center (cOR 0.99, 95% CI 0.78-1.26).
Conclusions: Thorough analysis shows that between-country variation in outcome after EVT may appear larger then it actually is. For a better interpretation of between-country comparisons, the methodology should be carefully considered and transparently reported, for example regarding handling of missing data and adjustment for potential confounders.
Disclosures of Interest: No
Abstract N°: 2196
PC-ASTRAL2: A CLINICAL-RADIOLOGICAL INTEGER SCORE PREDICTING FUNCTIONAL OUTCOME IN POSTERIOR CIRCULATION ACUTE ISCHEMIC STROKE
Anastasia Adamou1, Alexander Salerno*2, Davide Strambo2, Dimitris Lambrou2, Vincent Dunet3, George Ntaios1, Patrik Michel2
1University of Thessaly, Faculty of Medicine, Department of Internal Medicine, Larissa, Greece, 2Lausanne University Hospital and University of Lausanne, Stroke Center, Neurology Service, Department of Clinical Neurosciences, Lausanne, Switzerland, 3Lausanne University Hospital and University of Lausanne, Department of Diagnostic and Interventional Radiology, Lausanne, Switzerland
On behalf of: AA and AS contributed equally
Background and aims: Multiple prognostic instruments exist for general acute ischemic strokes (AIS), but none specifically for posterior circulation (PC) strokes. We aimed to develop a distinct PC prognostic AIS score.
Methods: This single-center, investigator-initiated, retrospective cohort study involved the development and internal validation of the PC-ASTRAL2 score, a new prognostic tool able to predict poor functional outcome at three months defined as a modified Rankin Scale (mRS) of 3 to 6. The study population included individuals with AIS attributable only to the PC, as determined by combined clinical and radiological information, regardless of stroke severity or arterial patency. Using binary regression models, weights for point attribution were assigned, and the model's discriminative ability was evaluated using Harrell’s C-statistic. A 500-fold cross-validation assessed the model's performance and optimization.
Results: The PC-ASTRAL2 score was derived from consecutive 1525 acute PC-AIS from the ASTRAL registry from 1/2003 to 4/2022. Model performance showed a C-statistic of 0.86 and an accuracy of 0.83. Variables were chosen based on univariate analyses and clinical rationale informing the scoring system (Figure 1). Internal validation with a 500-fold cross validation confirmed the model's robustness, with a C-statistic of 0.85 (CI:0.77-0.92) and an accuracy of 0.82 (CI:0.76-0.88).
Conclusions: The PC-ASTRAL2 is a tool that can accurately predict the level of disability of a patients 3 months after a PC stroke. Ongoing external validation aims to confirm the score's wider applicability and generalizability.
Disclosures of Interest: No
Abstract N°: 652
FACTORS ASSOCIATED WITH RETURN TO WORK IN A YOUNG SOUTHEAST ASIAN COHORT: A LOGISTIC REGRESSION ANALYSIS
Gabriel Kwok*1, Yao-Hao Teo2, Nicole Yeong2, Sarah Ming LI Tan3, Nur Hafizah Mohd Amin4, Maznah Marmin4, Fadhlina Hassan4, Leonard Yeo2,3, Aftab Ahmad4, Benjamin Tan2,3
1Barts and The London School of Medicine and Dentistry, Institute of Health Sciences Education, London, United Kingdom, 2Yong Loo Lin School of Medicine, Singapore, Singapore, 3National University Hospital (NUH) - Singapore, Division of Neurology, Department of Medicine, Singapore, Singapore, 4Ng Teng Fong General Hospital, Division of Neurology, Singapore, Singapore
On behalf of:
Background and aims: Ischaemic stroke (IS) has become increasingly common among young adults globally, leading to significant morbidity and disability during patients’ most productive years. Returning to work (RTW) is thus important for post-stroke rehabilitation.
Methods: We performed a retrospective cohort study of all consecutive IS patients aged 18-50 years admitted to 2 tertiary hospitals covering the entire Western region of the Singapore population from 2020-2022 (n=566). We performed univariate and multivariate logistic regression evaluating associations between demographic characteristics, cerebrovascular risk factors, TOAST aetiologies, 90-day modified Rankin Scale (mRS) score and 90-day RTW status.
Results: A total of 284 patients were included after removing those previously unemployed and lost-to-follow-up. In univariate analysis, large artery atherosclerosis (LAA) aetiology (OR 0.31, 95% CI 0.13-0.70, p=0.005), admission NIHSS scores (OR 0.73, 95% CI 0.66-0.79, p<0.001), 90-day mRS score (OR 0.28, 95% CI 0.19-0.40, p<0.001) and diabetes mellitus (OR 0.31, 95% CI 0.17-0.57, p<0.001) were significantly associated with inability to RTW. In multivariate regression analysis of baseline variables, these associations remained significant for LAA aetiology (aOR 0.29, 95% CI 0.10-0.84, p=0.02), admission NIHSS scores (aOR 0.73, 95% CI 0.65-0.80, p<0.001) and diabetes mellitus (aOR 0.35, 95% CI 0.15-0.81, p<0.001). Overall, 68.3% (194/284) of patients successfully RTW at 3 months, while 82.3% (223/273) achieved functional recovery (defined as a 90-day mRS score of 0-2).
Conclusions: Patients with LAA aetiology, higher admission NIHSS and diabetes mellitus are less likely to RTW. While lower 90-day mRS is significantly associated with RTW, many patients achieving functional recovery do not RTW.
Disclosures of Interest: No
Moderated Poster - SAH and ICH – Day 2
Abstract N°: 3205
APOE EPSILON 4 AND RISK OF INTRACRANIAL HEMORRHAGE IN ATRIAL FIBRILLATION PATIENTS ON APIXABAN
Santiago Clocchiatti-Tuozzo*1, Cyprien Rivier1, Shufan Huo1, Adam de Havenon1, Maximiliano Hawkes2, Lee Schwamm1, Emily Gilmore1, Kevin Sheth1, Thomas Gill3, Guido Falcone1
1Yale University, Neurology, New Haven, United States, 2Mayo Clinic, Neurology, Rochester, United States, 3Yale University, Internal Medicine, New Haven, United States
On behalf of:
Background and aims: The APOE-epsilon(ε) 4 variant is a known risk factor for intracranial hemorrhage (ICH) in patients with atrial fibrillation on warfarin. However, the role of this variant in atrial fibrillation patients on apixaban is unknown. We tested the hypothesis that APOE-ε4 leads to higher risk of ICH in this patient population.
Methods: We performed a prospective genetic association study within All of Us, a large cohort study in the United States. Participants were aged >50 years, had atrial fibrillation, were on apixaban, and had no prior ischemic stroke or ICH. Variants rs429358 and rs7412 were used to determine APOE genotype, which was modelled dominantly (one or two alleles vs. no alleles). The primary outcome was incident ICH, defined as any form of brain hemorrhage. We evaluated associations using multivariable Cox proportional hazard regressions.
Results: Of the 2,115 participants, 488 (23%) had at least one APOE-ε4 allele and 1,627 (77%) had none. Of these, 957 (45%) were female and 1,685 (80%) were of European ancestry. After a median follow-up of 2.9 years (interquartile range:1.7-3), 26 (1.13%) participants sustained an ICH. 14 (0.9%) of these were non-carriers and 12 (2.5%) were carriers (p-value:0.005). Multivariable Cox proportional hazards regressions showed that APOE-ε4 was significantly associated with a three-fold increase in the risk of ICH (HR:3.02;95%CI:1.37-6.67;p-value: 0.006).
Conclusions: Among atrial fibrillation patients on apixaban, APOE-ε4 was associated with a significantly increased risk of ICH. Additional research is needed to determine whether APOE-ε4 information can improve existing clinical tools that estimate a patient’s risk of ICH when on apixaban.
Disclosures of Interest: No
Abstract N°: 941
ADMISSION BLOOD GLUCOSE AND FUNCTIONAL OUTCOME IN NON-DIABETIC PATIENTS WITH INTRACEREBRAL HEMORRHAGE
Menglu Ouyang*1, Craig Anderson1, Lili Song2
1The George Institute for Global Health, Neurology, Sydney, Australia, 2The George Institute for Global Health China Office, Stroke, Beijing, China
On behalf of:
Background and aims: Control of hyperglycaemia is not routine in non-diabetic patients with acute intracerebral hemorrhage (ICH). As few studies have explored the relationship between blood glucose (BG) and long-term outcome, our study aimed to determine associations of BG and unfavourable functional outcome in ICH patients without diabetes.
Methods: Post-hoc analysis of INTERACT3, an international, multicentre, stepped-wedge cluster randomised controlled trial where baseline characteristics and BG were collected at hospital admission in ICH patients. Logistic regression models were used to determine associations of BG as continuous and categorical (<7.8, 7.8-10.0, and >10.0 mmol/L) exposures and 6-month functional outcome (mRS), adjusted for study design, patient, and management variables.
Results: Of 7036 patients, 6306 (89.6%) were non-diabetic (median BG 7.1 [IQR 6.0-8.5] mmol/L). Patients with high BG (>10 mmol/L) were more likely to be female, with greater neurological severity and hematoma volume, as compared to the other groups. Overall, there was no significant association between BG and functional outcome (aOR 1.01, 95% CI 0.98-1.04, p=0.64). However, higher BG increased the risk of death (aOR 1.08, 95% CI 1.04-1.12, p<0.0001); in those with BGL >10mmol/L, the odds of death increased by 50% (aOR 1.50, 95% CI 1.15-1.96, p=0.0019) compared to those with normal BG (<7.8mmol/L). No significant association for outcomes was evident for slightly high (7.8-10.0 mmol/L) and normal BGL (<7.8 mmol/L).
Conclusions: In non-diabetic patients with ICH, very high BG is associated with death over 6 months. Glycaemic control should be applied to non-diabetic patients with BGL >10.0 mmol/L.
Disclosures of Interest: No
Abstract N°: 931
PREDICTIVE ACCURACY OF PHYSICIANS’ ESTIMATES OF DEATH AND RECOVERY AFTER ACUTE INTRACEREBRAL HEMORRHAGE
Menglu Ouyang*1, Craig Anderson1, Lili Song2
1The George Institute for Global Health, Neurology, Sydney, Australia, 2The George Institute for Global Health China Office, Stroke, Beijing, China
On behalf of:
Background and aims: Accurate prediction of a patient’s prognosis is important for decision-making in intracerebral hemorrhage (ICH). We aimed to determine physician’s ability to predict survival, functional recovery, and quality of life in their patients with ICH.
Methods: Pre-specified secondary analysis of INTERACT3, an international, multicenter, stepped-wedge cluster randomized controlled trial. Clinician perspectives on prognosis were collected at hospital admission and Day 7 (or before discharge). Prognosis questions were the likelihood of survival at 48 hours and 6 months, and favorable functional outcome (recover walking and self-care) and quality of health (return to usual activities) at 6 months. Clinician prediction was compared with actual outcomes.
Results: Most of the clinicians completed the questions were neurosurgeons (75%) with a median of 8 working years. Of the 6305 randomized patients who survived 48 hours, 213 (3.4%) were predicted to die (positive predictive value [PPV] 0.99, 95% confidence interval [CI] 0.99-0.99). Of 5435 patients who survived 6 months, 209 (3.8%) were predicted to die (PPV 0.93, 95% CI 0.92-0.93). Predictions on favourable functional outcome (PPV 0.51, 95% CI 0.49-0.53) and satisfied quality of health (PPV 0.50, 95% CI 0.49-0.52) were poor. Patients who predicted survival at 48 hours were less likely to have withdrawn active care and decompressive surgery but more likely to receive physiotherapy
Conclusions: In ICH, a treating physician’s estimate of the likelihood a patient will survive 48 hours and 6 months is very good. However, their ability to predict the degree of functional recovery and quality of life is poor.
Disclosures of Interest: No
Abstract N°: 1092
THE RELATIONSHIP BETWEEN HAEMATOMA LOCATION AND VOLUME WITH OUTCOME: DATA FROM THE RIGHT-2 AND TICH-2 TRIALS
Kailash Krishnan*1,2, Zhe Kang Law3, Lisa Woodhouse4, Robert Dineen4, Chaamanti Menon1,2, Joanna Wardlaw5, Philip Bath1,2, Nikola Sprigg1,2
1Queen's Medical Centre, United Kingdom, 2University of Nottingham, Stroke Trials Unit, United Kingdom, 3Malaysia National University Kuala Lumpur Campus, Kuala Lumpur, Malaysia, 4University of Nottingham, United Kingdom, 5Western General Hospital, Centre of, United Kingdom
On behalf of:
Background and aims: Poor prognosis after acute intracerebral haemorrhage (ICH) is associated with ICH volume (ICHV) and location. However, it is unclear whether outcomes differ by thresholds of ICHV according to brain location. We examined these effects using data from the Rapid Intervention with Glyceryl Trinitrate in Hypertensive Stroke-2 Trial (RIGHT-2) and Tranexamic acid for hyperacute intracerebral haemorrhage (TICH-2) trial
Methods: Data from 1215 ICH participants recruited within 8 hours of ictus and randomised to sham/control were analysed. ICHV was measured using semi-automated segmentation. The threshold of ICHV, sensitivity and specificity which predict early death, acute neurological deterioration and death or disability (modified Rankin scale, mRS 4-6) at day 90 were determined using receiver operating characteristic curves. Logistic regression was used to assess whether each ICHV threshold according to brain location were associated with outcomes.
Results: 360 participants (29.6%) had supratentorial lobar, 772 (63.5%) had supratentorial deep and 83 (6.8%) had infratentorial ICH. The mean ICHV was 43.4 (SD 35.0)mL, 16.7 (18.8)mL and 8.4 (10.3)mL for supratentorial lobar, supratentorial deep and infratentorial ICH. ICHV threshold predictive of early death were >67.6mL (AUROC 0.84), >16.3mL (AUROC 0.77) and >5.5mL (AUROC 0.78) for supratentorial lobar, supratentorial deep and infratentorial ICH. Thresholds of >36.6mL (AUROC 0.79), >13.4mL (AUROC 0.74) and >5.2mL (AUROC 0.73) predicted acute neurological deterioration; >27.9mL (AUROC 0.78), >16.0mL (AUROC 0.76) and >2.5mL (AUROC 0.67) predicted day 90 death or disability.
Conclusions: Prognosis after ICH differs by volume according to brain location. This finding could inform trials testing potential treatments in ICH.
Disclosures of Interest: No
Abstract N°: 1191
HORMONAL CONTRACEPTION AND RISK OF INTRACEREBRAL HEMORRHAGE
Tom Skyhøj Olsen*1, Gasper Letnar2, Klaus Kaae Andersen2
1Bispebjerg University Hospital, Neurology, Copenhagen, Denmark, 2Omicron ApS, Copenhagen, Denmark
On behalf of:
Background and aims: Risk of intracerebral hemorrhage (IH) associated with use of hormonal contraception (HC) remains unclear. Studies dates to the 1990s, they do not distinguish between pill generations and results diverge. We studied risk IH associated with use of (HC) in the Danish female population 2003-2021.
Methods: We followed all non-pregnant women (18-49 years) registering IH during use/non-use of HC using Danish high-quality registries with nation-wide coverage. Hemorrhage due to aneurysms and vascular malformations were not included. Poisson regression models adjusting for age, ethnicity, education, calendar-year, and stroke risk factors were utilized.
Results: In total 1,735,306 non-pregnant women contributed 16,933,276 person-years (py) of observation. Mean age 29 years; 432 had HI.
Relative risk (RR) of IH in users of combined contraceptives with ethinylestradiol (CCE) (53 events, 4.488,768 py) and progesterone-only contraceptives (POC) (63 events, 2,216,889 py) was not increased and did not differ significantly from that of non-users (316 events, 10,251,433 py): CCE RR 0.86 (CI 0.63; 1.18), POC RR 0.95 (CI 0.72; 1.25), non-users RR 1 (reference).
RR of IH in users of 3rd generation CCE (norgestimate/desogestrel/gestodene) (31 events; 2,279,796 py), 4th generation CCE (drosperinone) (<4 events; 390,192 py) did not differ significantly from that of 2nd generation CCE-users (levonorgestrel) (20 events, 1,478,701 py): 3rd generation RR 0.99 (CI 0.51; 1.91), 4th generation RR 0.23 (CI 0.03; 1.73), 2nd generation RR 1 (reference). Risk of IH was not increased for plasters, implants, or vaginal rings.
Conclusions: Use of HC was not associated with increased risk of IH regardless of type and route of administration.
Disclosures of Interest: No
Abstract N°: 1980
LIFE EXPECTANCY IN PATIENTS WITH UNRUPTURED INTRACRANIAL ANEURYSMS – A SYSTEMATIC REVIEW AND META-ANALYSIS
Marina Heilig*1, Laura van der Kamp2, Margot van Genderen2, Svetlana Hetjens3, Mervyn Vergouwen2, Nima Etminan1, Gabriel Rinkel1,2
1University Hospital Mannheim, Department of Neurosurgery, Mannheim, 2UMC Utrecht Brain Center, Department of Neurology and Neurosurgery, Utrecht, 3Medical Faculty Mannheim, Department of Medical Statistics and Biomathematics, Mannheim
On behalf of:
Background and aims: Since life expectancy is a pivotal factor in deciding on preventive aneurysm treatment, we assessed mortality and risk of vascular diseases and cancer in patients with unruptured intracranial aneurysms.
Methods: After a systematic search of the literature on PubMed and EMBASE, we screened 3791 articles by title/abstract and 215 articles by full text. We included studies with a longitudinal study design and at least three months of follow-up, reporting on the occurrence of overall and non-aneurysm-related death, cancer, or vascular disease (not treatment- or aneurysm-related). We used linear regression models for data analysis and the Observational Study Quality Evaluation (OSQE) score to select studies for sensitivity analysis for high-quality studies.
Results: We included 58 studies with data on 61,949 patients and 64,535 unruptured intracranial aneurysms. Patients had a mean age at baseline of 60.4±5.6 years. 37% of patients underwent neurosurgical, 43% endovascular, and 20% no preventive aneurysm treatment. Follow-up data were available for 57,423 patients with a mean follow-up period of 4.9 ± 3 years. In total, 5.6% (95% CI, 5.4–5.8) of patients died during follow-up. In high-quality long-term studies, 12.9% (95% CI, 10.3–15.8) of patients died from non-aneurysm related causes, 4.5% (95% CI, 2.5–5.2) were diagnosed with vascular disease, and 7.3% (95% CI, 5.4–9.6) were diagnosed with cancer.
Conclusions: Five years after diagnosis, more than 20% of patients with an unruptured intracranial aneurysm will have died or been diagnosed with cancer or vascular disease. This proportion should be considered when balancing pros and cons of preventive treatment.
Disclosures of Interest: No
Abstract N°: 170
CASE FATALITY AND FUNCTIONAL OUTCOME AFTER SPONTANEOUS SUBARACHNOID HAEMORRHAGE
Andreas Ziebart*1,2, Judith Dremel1, Svetlana Hetjens3, Dennis Nieuwkamp4, Francisca H.H. Linn5, Nima Etminan1, Gabriel Rinkel1
1Medical Faculty Mannheim, University of Heidelberg, Department of Neurosurgery, Mannheim, Germany, 2University Medical Center Ulm, Department of Neurosurgery, Ulm, Germany, 3Medical Faculty Mannheim, University of Heidelberg, Department of Medical Statistics and Biomathematics, Mannheim, 4Jeroen Bosch Hospital, Departement of Neurology, Hertogenbosch, Netherlands, 5Brain Center Rudolf Magnus, University Medical Center Utrecht, Department of Neurology and Neurosurgery, Utrecht, Netherlands
On behalf of:
Background and aims: A previous systematic review of population-based studies performed between 1973 and 2002 showed a decrease in case fatality for spontaneous subarachnoid haemorrhage, but included too few studies to assess changes in case morbidity. Since then, treatment has advanced, including the widespread availability of endovascular treatment. We updated the meta-analysis to assess whether case fatality has further decreased and functional outcome has improved.
Methods: We searched PubMed and Web of Science for reports of population-based studies to until May 2022 and used the same inclusion criteria as previously. We integrated the newly identified studies with previously included ones and assessed changes in case fatality and case morbidity using linear regression.
Results: After including 24 new studies with 827 patients, we analysed 60 study periods and 9542 patients. Overall, case fatality decreased by 0.3% (95% CI -0.7 to 0.1) per year. In a sensitivity analysis excluding studies that did not provide one-month outcome and outliers, the age and sex-adjusted decrease was 0·1% per year (95%CI:-0·9<->0·6%). The mean case fatality rate decreased from 47% in the 1970's to 35% in the 1990’s, and remained stable thereafter. In 15 studies, the proportion of patients living independently ranged between 31 and 83%, and increased by 0.2% per year (95%CI:-0.7<->1.1%).
Conclusions: From 1973 to 2017, the case-fatality rate of spontaneous subarachnoid haemorrhage decreased without significant regional differences, but remained stable over the last two decades. The data on time trend in functional outcomes were inconclusive and warrant further properly designed prospective population-based studies.
Disclosures of Interest: No
Moderated Poster - Small Vessel Disease and Cognition – Day 2
Abstract N°: 1184
ASSOCIATION OF TOTAL SMALL VESSEL DISEASE BURDEN WITH RENAL FUNCTION: AN ANALYSIS USING POOLED DATA FROM THE MICON COLLABORATION
Philip Nash*1, Jonathan Best1, Gareth Ambler2, David Wheeler3, Tae-Jin Song4, Rob Simister1, David Werring1
1UCL Queen Square Institute of Neurology, Stroke Research Centre, London, United Kingdom, 2University College London, Department of Statistical Science, London, United Kingdom, 3University College London, Department of Renal Medicine, London, United Kingdom, 4Ewha Womans University College of Medicine, Department of Neurology, Seoul, South Korea
On behalf of: The Microbleeds International Collaborative Network
Background and aims: Associations between renal function and total cerebral small vessel disease (SVD) burden are incompletely characterised. Renal hyperfiltration represents glomerular endothelial dysfunction, so could be associated with SVD as part of a multi-system disorder, as could impaired kidney function.
Methods: Participating centres from the Microbleed International Collaborative Network contributed data on estimated glomerular filtration rate (eGFR) and SVD burden. We investigated associations of SVD burden (using a validated 5-point ordinal scale) with eGFR, dividing the cohort into four groups as recommended by Kidney Disease International: eGFR ⩾105 (stage G1a, possible hyperfiltration), eGFR 60-105 (stages G1b-2); eGFR 30-60 (stages G3a-3b); and eGFR <30 (stages G4-5).
Results: 8 study centres provided data, contributing 5784 patients (mean age 70.4 ± 12.8, 42.2% female) to the analysis. The severity of SVD burden increased as eGFR decreased, and the eGFR >105 group had the least severe SVD. Median (IQR) SVD burden scores were 0 (0-1), 1 (0-2), 1 (0-2) and 2 (2-3) for stages G1a, G1b-2, G3a-3b G4-5 respectively (p<0.001, Fig. 1). The severities of all individual SVD biomarkers also increased as eGFR decreased (Fig. 2). SVD burden was independently associated with eGFR stage in an ordinal logistic regression model (e.g. adjusted OR 1.66 for stage G4-5, 95% CI 1.19-2.31, overall p<0.001, Table 1).
Conclusions: Impaired kidney function was independently associated with SVD burden in our study population, and there was a graded increase in SVD severity as eGFR decreased. Further longitudinal studies should be done to better characterise this relationship.
Disclosures of Interest: No
Abstract N°: 1261
EAST ASIAN-SPECIFIC NOTCH3 P.R75P MUTATION INDUCES PRO-HEMORRHAGIC CADASIL
1National Cerebral and Cardiovascular Center, Neurology, Suita, Japan, 2Asan Medical Center, University of Ulsan College of Medicine, Neurology, South Korea, 3National Cerebral and Cardiovascular Center, Advanced Medical Technologies, 4School of Medicine, Jeju National University, Neurology, South Korea, 5National Cerebral and Cardiovascular Center, Pathology, Japan, 6Graduate School of Medical Science, Kyoto Prefectural University of Medicine, Neurology, Japan
Background and aims: East Asian patients with cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) are more prone to cerebral bleeding than White individuals. We hypothesized that the East Asian-specific NOTCH3 p.R75P mutation confer the difference.
Methods: We retrospectively included the patients with CADASIL in Japanese and Korean cohorts. The association between the p.R75P mutation and symptomatic intracerebral hemorrhage (sICH) and multiple cerebral microbleeds (mCMB) (>5) was analyzed. The in silico predicted NOTCH3 extracellular domain (N3ECD) protein structures and the N3ECD immunostaining grades in skin vessels were compared between p.R75P and conventional cysteine-altering mutations.
Results: In the Japanese cohort (n=63; median age: 55 years; male: 56%), the p.R75P mutation was significantly correlated with sICH (adjusted relative risk [95% CI], 9.56 [2.45–37.31]), mCMB (3.00 [1.34–6.71]), and the absence of temporopolar lesions (4.91 [2.29–10.52]) after adjusting for backgrounds. The results were replicated in the Korean cohort (n=55; median age: 55 years; male: 51%) (13 with p.R75P mutation; sICH, 8.11 [1.83–35.89], mCMB, 1.90 [1.01–3.56], absence of temporopolar lesions, 2.32 [1.08–4.97]). The N3ECD structures in cysteine-altering mutations showed solvent-exposed free cysteine thiols, which are prone to direct aggregation; however, the structure due to the p.R75P mutation demonstrated a stereochemically incompatible proline residue, which could disturb correct disulfide bond formation, indirectly causing aggregation. The N3ECD immunostaining grades of skin vessels were lower in the p.R75P mutation than the cysteine-altering mutations.
Conclusions:NOTCH3 p.R75P mutation induces cerebral bleeding and milder temporopolar lesions with specific protein aggregation properties.
Disclosures of Interest: No
Abstract N°: 1959
GLYMPHATIC SYSTEM IS ASSOCIATED WITH CEREBROVASCULAR PULSATILITY IN PATIENTS WITH SMALL VESSEL DISEASE
Yu Tian*1, Yulu Shi1, Yilong Wang1
1beijing tiantan hospital, beijing, China
On behalf of:
Background and aims: Preclinical reports suggested paravascular cerebrospinal fluid and interstitial fluid Exchange may be driven by arterial pulsation. This study aimed to assess the relationships of glymphatic pathway with cerebral blood flow (CBF) and intracranial pulsatility in patients with cerebral small vessel disease(CSVD).
Methods: We recruited 76 patients with CSVD. We rated the severity of periventricular and deep WMH (PV-WMH and D-WMH) using the Fazekas scores. We estimated CBF and pulsatility in the main cerebral arteries and veins using phase-contrast MR. We measured glymphatic system using the diffusivity along perivascular spaces based on diffusion tensor imaging (DTI-ALPS index). We investigated the associations between flow, pulsatility and DTI-ALPS index using linear regression analyses as appropriate.
Results: The mean age was 59.17±11.57 years, and 51 (67.1%) participants were men. The mean DTI-ALPS index was 1.33 (IQR: 1.21, 1.44). After adjusting for age, sex and MAP, a resistance index (RI)(β 0.04, 95% CI 0.002,0.08, P=0.04) and pulsatility index (PI)(β 0.12, 95% CI 0.030.21, P=0.02) in left internal jugular veins was associated with left DTI-ALPS index, and PI in right transverse sinus was related to right (β 0.53, 95% CI 0.26,0.80, P<0.001) and mean(β 0.39, 95% CI 0.16,0.62, P=0.001) DTI-ALPS index. CBF were not associated with the DTI-ALPS index.
Conclusions: Our results support an independent association of glymphatic pathway with intracranial pulsatility rather than with global CBF, implying that intracranial pulsatility is a key driver of glymphatic pathway in patient with CSVD.
Disclosures of Interest: No
Abstract N°: 1737
MEDIATION EFFECT OF GLYMPHATIC SYSTEM IN ASSOCIATION BETWEEN LACUNES AND COGNITION
Yu Tian*1, Yilong Wang1
1beijing tiantan hospital, China
On behalf of:
Background and aims: This study aims to investigate the mediation effect of glymphatic system in association between lacunes and cognition in a community-based population.
Methods: This report included 2198 community-dwelling people aged 50–75 years who participated in the PolyvasculaR Evaluation for Cognitive Impairment and vaScular Events cohort. The diffusivity along perivascular spaces based on diffusion tensor imaging (DTI-ALPS index) was measured to assess glymphatic pathway. The definition of lacune was based on STRIVE criteria. The cognitive function was measued by Montreal Cognitive Assessment(MoCA). The associations between lacune, glymphatic pathway, and cognition was investigated by linear regression analysis.
Results: Among 2198 included participants, the mean age was 61.3±6.6 years, and 1013(46.1%) participants were men. The average DTI-ALPS index was 1.67±0.14. After adjusting for potential confounders, lacune was associated with sex, BMI, hypertension, hypercholesterolemia, stroke and anticoagulant drugs. Lacune was associated with other neuroimaging markers of small vessel disease, including white matter hyperintensity, perivascular spaces, cerebral microbleeds, and brain atrophy. Lacune was associated with glymphatic system as measured by DTI-ALPS index(β -0.16, 95% CI [-0.22, -0.09]), independent of vascular risk factors. Glymphatic pathway as evidenced by DTI-ALPS index explained 14.63% (95% CI, 1.60%-27.67%, P=0.03) of the relationship between lacune and cognitive impairment as estimated by MoCA scores.
Conclusions: Glymphatic system mediates less than 20% of the association between lacune and vascular cognitive impairment in a community-dwelling population, and provide a potential target for treatment and prevention of vascular dementia.
Disclosures of Interest: No
Abstract N°: 2050
DEEP MEDULLARY VEIN INTEGRITY ASSOCIATIONS WITH SMALL VESSEL DISEASE LOAD AND FLUID DIFFUSIVITY IN PATIENTS WITH LACUNAR STROKE
Carla Brenlla Lorenzo*1, Caterina Sozzi2, Andres Girona1, Emma Muñoz-Moreno1, Carlos Laredo1, Angels Calvet1, Alejandro Rodríguez Vázquez1, Xabier Urra1, Salvatore Rudilosso1, Angel Chamorro1
1Hospital Clínic de Barcelona, Neurology, Barcelona, Spain, 2University of Milan, Neurology, Milano, Italy
On behalf of:
Background and aims: The venous compartment might play a role in brain fluid dynamics in small vessel disease (SVD). We assessed whether deep medullary vein (DMV) integrity correlated to SVD severity and fluid clearance in patients with lacunar stroke.
Methods: In 50 consecutive patients with a recent lacunar stroke, we collected demographic, clinical and imaging data from 3T-MRI acquisitions. We assessed SVD markers (number of lacunes, microbleeds, white matter hyperintensity (WMH) ratio, perivascular space (PVS) ratio in basal ganglia and WM, and summary-SVD score), and diffusivity measures including mean diffusivity (MD), fractional anisotropy (FA), free water (FW) in normal-appearing white matter, and diffusivity along the perivascular spaces (ALPS index). To assess DMV integrity, we applied two visual scales according to their appearance on SWI (appearance-DMV, 0-18 range score) and count (count-DMV). After categorizing the cohort in quartiles according to DMV integrity, we assessed the correlations with SVD markers and diffusivity measures using multivariable ordinal regression analyses adjusting for age, sex, and other relevant variables in univariable analysis (p<0.2).
Results: In univariable analysis WMH ratio, PVS in basal ganglia, lacunes, summary-SVD score, and diffusivity measures except for ALPS index were associated with worse appearance-DMV or count-DMV scores. In the multivariable analysis, FW, MD, and FA were associated with appearance-DMV, while only FA remained significant for count-DMV.
Conclusions: In patients with lacunar stroke, although the results differed using different visual scales, DMV integrity seems to be related to an increase in extracellular water and microstructural WM damage, but not with a decreased fluid clearance along PVS.
Disclosures of Interest: No
Abstract N°: 1485
IN VIVO IMAGING OF GADOLINIUM-BASED CONTRAST AGENT LEAKAGE IN PATIENTS WITH CEREBRAL AMYLOID ANGIOPATHY
Hilde van den Brink*1, Mariel Kozberg1, Nazanin Makkinejad1, John Kirsch2, Whitney Freeze3, Anand Viswanathan1, Susanne van Veluw1
1Massachusetts General Hospital, Neurology, Boston, United States, 2Athinoula A. Martinos Center for Biomedical Imaging, Boston, United States, 3Leiden University Medical Center (LUMC), Leiden, Netherlands
On behalf of:
Background and aims: Blood-brain barrier (BBB) leakage is hypothesized to be an early step in the pathophysiology of cerebral amyloid angiopathy (CAA), possibly preceding haemorrhages. This study aims to measure BBB leakage in vivo in the parenchyma and at the level of the leptomeningeal blood vessels in patients with probable CAA without lobar intracerebral haemorrhage and non-CAA controls.
Methods: 14 participants with probable CAA without prior intracerebral haemorrhage (age 68±9 years, 57% female) and 7 non-CAA controls with mild cognitive impairment (CDR 0.5 or 1) (age 70±7 years, 29% female) were included. 3T-MRI included SWI, pre-and postcontrast T2-FLAIR and a Dynamic Contrast Enhanced (DCE) scan. Participants received a gadolinium-based contrast agent (0.2 mL/kg of Dotarem) during the DCE scan. DCE scans were analysed with ROCKETSHIP to quantify leakage from the plasma into the parenchyma. Leptomeningeal CSF enhancement was measured by multiple blinded raters by visually inspecting pre-contrast versus post-contrast T2-FLAIR scans (Figure 1).
Results: Preliminary analysis revealed greater whole-brain BBB leakage into the parenchyma in CAA compared to non-CAA controls (Figure 2). Focal CSF enhancements were seen in both patients and controls, while sulcal enhancement was only observed in patients (Table 1). Within patients, sulcal enhancement was associated with cortical superficial siderosis (β=0.65, p=0.006), but not with microbleed count (β=0.29, p=0.29).
Conclusions: These results suggest that BBB leakage into the parenchyma occurs in patients with probable CAA. Moreover, leakage from the leptomeningeal vessels may be indicative of cortical superficial siderosis formation, awaiting further analyses.
Disclosures of Interest: No
Abstract N°: 2932
CEREBRAL AMYLOID ANGIOPATHY WITH AND WITHOUT CORTICAL SIDEROSIS: CAN WE TALK ABOUT MICROBLEEDERS AND MACROBLEEDERS?
Mattia Losa*1, Pierumberto Mortola1, Andrea Donniaquio2, Federico Massa1, Luca Roccatagliata3, Ilaria Gandoglia4, Angelo Schenone1, Matteo Pardini1, Massimo Del Sette4
1University of Genoa, Department of Neuroscience, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health (DINOGMI), Genoa, Italy, 2Ospedali Galliera, Neurology, Italy, 3University of Genoa, Neuroradiology, Department of Health Sciences, Genoa, Italy, 4Ospedale Policlinico San Martino, Neurology, Genoa, Italy
On behalf of:
Background and aims: Cerebral amyloid angiopathy (CAA) is a cerebral small vessel disease (cSVD) associated with cognitive impairment and lobar hemorrhages. Some studies explored the existence of distinct subtypes in the CAA spectrum, differentiating patients with prominent hemorrhagic manifestations from those without it. Nevertheless, it is not clear whether and how CAA can be distinguished into phenotypes.
Methods: We enrolled 40 patients with probable CAA according to Boston Criteria 2.0 and we collected data from medical records and brain MRI scans. We applied validated visual scales to measure radiological markers of cSVD and atrophy (Scheltens and Koedam scale). Patients were divided in two groups, according to the presence of cortical superficial siderosis (no-cSS vs cSS-CAA). In a subgroup (20 patients), we analyzed core CSF biomarkers of neurodegeneration. Chi-square and t-test were performed between groups.
Results: No-cSS compared to cSS-CAA has more frequently cognitive onset (86%vs25%) compared to hemorrhagic/TFNE (14%vs75%-p=0,0006), higher prevalence of microbleeds (p=0,001), lower presence of lobar hemorrhages (6%vs65%-p=0,0001) and higher degree of medial temporal lobe atrophy (1,56±0.75vs1,00±0.74-p=0,027). In the CSF subgroup, cSS-CAA has lower level of Aβ40 compared to nocSS-CAA (6648±2360vs11.191±1946-p=0,001).
Conclusions: We highlighted how CAA with and without siderosis differs from a clinical, biological and radiological point of view, reinforcing the concept of the phenotypic spectrum of CAA. More studies are needed to confirm if we can identify a “cognitive-neurodegenerative CAA”, with higher prevalence of microbleeders, from “haemorrhagic CAA'', more prone to macrobleeding.
Disclosures of Interest: No
Abstract N°: 3051
USING SMALL VESSEL DISEASE ON ROUTINELY ACQUIRED BRAIN IMAGING AND ELECTRONIC PATIENT RECORDS IN “BIG DATA” STUDIES OF VASCULAR COGNITIVE IMPAIRMENT
Emma Colbourne1, Emily Boucher1, Sarah Pendlebury*1
1Wolfson Centre for Prevention of Stroke and Dementia, University of Oxford, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
On behalf of:
Background and aims: White matter changes (WMC) of vascular origin modify dementia risk factor associations including with non-vascular factors such as infection and delirium. To inform future “Big data” studies on vascular cognitive impairment, we determined frequency of brain scanning and rates of cognitive frailty in unselected older hospital patients
Methods: The Oxford Cognitive Comorbidity and Ageing Research Database (ORCHARD-EPR) includes real-world hospital electronic patient record (EPR) data from all older (>/=65 years) patients with unplanned hospital admission from the Oxfordshire region (n=660,000 population). ORCHARD-EPR includes diagnoses, comorbidities including dementia and delirium, 10-point Abbreviated-Mental-Test Score-AMTS, frailty, clinical observations, laboratory tests and long-term dementia outcomes. ORCHARD-EPR is linked to routinely acquired brain imaging. For this study, WMC was rated using the Age-Related WMC (ARWMC) and atrophy with the Global Cortical Atrophy (GCA) scale.
Results: Among 51,202 consecutive unplanned admissions (2017-2019, mean/SD age=82/7 years) cognitive frailty was present in 17,466 (34.5%, 95%CI 34.0-34.9): delirium=7,411 (14.6%), delirium+dementia=4,757 (9.4%), dementia=3,784 (7.5%), AMTS<8 without delirium/dementia=1,514 (3%). In a subset of 1100 consecutive patients, 668 patients had available brain imaging (CT=1056, MRI=242, both=198). WMC was mild in 58%, moderate in 38%, and severe in 3%. Moderate/severe atrophy was present in 87% (global) and 47% (temporal).
Conclusions: Over half of older hospital patients had brain imaging available with high rates of moderate/severe WMC and atrophy. Cognitive frailty, particularly delirium without dementia, was prevalent. These findings suggest that routinely acquired brain imaging can be used together with EPRs for dementia risk prediction in “Big Data” studies using real-world hospital data.
Disclosures of Interest: No
ESOC 2024 – Paper Poster Abstracts
Paper Poster - Acute Management
Abstract N°: 1465
THE ROLE OF SAE IN STROKE PATIENTS OF THE TENSION TRIAL
Moritz Link*1, Fabien Subtil2, Denis Angélique2, Martin Bendszus3, Götz Thomalla1
1University Medical Center Hamburg-Eppendorf, Hamburg, Germany, 2Service de Biostatistique, Hospices Civils de Lyon, Lyon, France; Université Claude Bernard Lyon 1, UMR 5558, CNRS, Villeurbanne, France, 3University Hospital Heidelberg, Heidelberg, Germany
On behalf of: TENSION investigators
Background and aims: Serious adverse events (SAEs) commonly impact outcomes and survival in stroke patients. This post hoc analysis of the TENSION trial investigated predictors of SAEs and their effects on clinical outcomes in stroke patients.
Methods: TENSION was a randomized trial comparing the safety and efficacy of thrombectomy versus medical care alone in stroke patients with extended lesions and time windows. We analyzed the frequency, types, and outcomes of SAEs. Group comparisons between patients with and without SAEs focused on markers of stroke severity, frailty, treatment effect, and clinical outcome. Multivariate logistic regression analysis was used to investigate predictors of SAEs and their impact on clinical outcomes.
Results: Among 253 patients, 159 (63%) experienced 260 SAEs. SAEs occurred in 70% of patients with medical care alone (88/125) versus 55% in the thrombectomy group (71/128, p=0.014). The median number of SAEs was 1 in both groups. Fatal SAEs comprised 64.9% in the medical care group and 55.4% in the thrombectomy group. Detailed analyses, including multivariate analysis of predictors and outcomes in patients with SAEs, will be presented in final at the conference.
Conclusions: Patients with extended stroke lesions experienced higher rates and more fatal SAEs with medical care alone compared to thrombectomy. Identifying patients at risk for SAEs could enhance the development of preventive treatment strategies for severe stroke patients.
Disclosures of Interest: No
Abstract N°: 327
THE EFFICACY OF EARLY HYPERTONIC SALINE IN THE OUTCOME OF ACUTE ISCHEMIC STROKE PATIENTS: A DOUBLE BLIND CLINICAL TRIAL
1Shahid-Beheshti University of Medical Sciences, Neurology Department & Stroke Unit, Tehran, Iran, 2Qom University of Medical Sciences, 3Zanjan University of Medical Sciences, 4Tabriz University of Medical Sciences
On behalf of:
Background and aims: After acute ischemic stroke (AIS), the expansion of the ischemic cascade and a large core of severe ischemia and consequent brain edema leads to early neurologic decline and the prognosis will be generally poor. The present study aimed to evaluate the effectiveness of early hypertonic saline administration on 3-month outcomes of moderate and severe ischemic strokes.
Methods: In a multi-center clinical trial study conducted in three stroke care unit centers during 2021-2022, 397 patients with severe AIS were randomly entered into two groups: 196 in the case group, received IV 5% hypertonic saline, and 201 in the control group, received normal saline for seven days. The patients were followed up for 90 days and were assessed on days 7 and 90. The measured outcomes of patients were mortality, NIHSS score, MRS score, and medication side effects.
Results: The mean age of patients was 67.64±12.735 and 69.54±12.946, whereas 107 and 102 males were enrolled in control and case groups respectively. In the base of similar first scores, the final mRS score at day 90 was scored as 4.89±1.152 and 4.65±1.199 for the control and case groups (P-value<0.05). However, the final NIHSS score at day 90 was significantly lower in the case group than in control patients (16.1±5.229 and 17.72±5.093; P-value<0.023, respectively). The investigation of complications and mortality of patients in the two groups showed non-significant differences.
Conclusions: Findings showed that early administration of IV hypertonic saline was associated with a better outcome and less complication at day 90, in the presence of non-significant complication.
Disclosures of Interest: No
Abstract N°: 2184
EFFECT OF EDARAVONE DEXBORNEOL ON HEMORRHAGIC TRANSFORMATION AFTER THROMBOLYTIC THERAPY IN ACUTE ISCHEMIC STROKE PATIENTS
1Huashan Hospital Fudan University, Department of neurology, Shanghai, China, 2Chenzhou First Peoples Hospital, Chenzhou, China, 3People’s Hospital of Leshan, Leshan, China, 4Anyang People's Hospital, Anyang, China, 5Huzhou Central Hospital, Hu Zhou, China, 6the Second Affiliated Hospital of Chongqing Medical University, Chongqing, China
On behalf of:
Background and aims: Hemorrhagic transformation (HT) is a serious complication in acute ischemic stroke (AIS) after intravenous thrombolytic therapy(IVT). Treatments for reducing the risk of HT are limited. This study aimed to explore whether edaravone dexborneol (ED) decreased the risk of HT and blood-brain barrier (BBB) disruption in AIS patients after IVT.
Methods: We did a multicenter, double-blind, randomized, placebo-controlled trial at 9 centers in China. Eligible patients were AIS patients aged 18-80 years, with a National Institute of Health stroke scale (NIHSS) score of 8-24, treated with thrombolytic within 4.5h of onset(ClinicalTrials.gov-NCT05035953). The participants were randomly assigned into ED group or placebo group. The proportion of HT at 36-48h and cumulative HT within 7 days were analyzed. MRI was performed and BBB disruption was evaluated by whether Gd-DTPA crossed BBB in FLAIR images at 36-48h.
Results: Between Oct. 30, 2021 and Aug. 16, 2023, 59 patients were included and randomly assigned to ED group (30 patients, aged 64.79±12.56) or placebo group (29 patients, aged 66.56±9.15). All the observed HT were asymptomatic intracranial hemorrhage. Patients in ED group had lower proportion of HT at 36-48h (28.57% vs 44%, p=0.2423), within 7 days (53.57% vs 64%, p=0.4418) and BBB disruption at 36-48h (25% vs 28%, p=0.8047).
Conclusions: In this small-sized exploratory study, ED showed a nonsignificant but tendency to reduce HT and BBB disruption. Larger studies are necessary to confirm these findings.
Disclosures of Interest: No
Abstract N°: 2175
ACT-GLOBAL_ENCHANTED3/MT: THIRD ENHANCED CONTROL OF HYPERTENTIOSN AND THROMBECTOMY STROKE STUDY
Xiaoying Chen*1, Bijoy Menon2, Lili Song1, Pengfei Yang3, Yongwei Zhang3, Tolulope Sajobi2, Andrew Demchuk2, Jianmin Liu3, Michael D Hill2, Craig Anderson1
1University of New South Wales, The George Institute for Global Health, 2University of Calgary, Cumming School of Medicine, 3Naval Medical University, Changhai Hospital
On behalf of: the ACT-GLOBAL_ENCHANTED3/MT Investigators
Background and aims: Several clinical trials have produced variable conclusions regarding the effects of intensive blood pressure (BP) lowering in post-EVT acute ischaemic stroke (AIS) patients. Although two trials indicate harm from very intensive target-based treatment (SBP <130 mmHg), the others neutral effects in the SBP range 140-160 mmHg. The ENCHANTED3/MT domain of the ACT-GLOBAL platform trial aims to test different approaches to the treatment of elevated SBP in post-EVT AIS patients to find an optimal BP management strategy.
Methods: ACT-GLOBAL is an international, multi-factorial, multi-arm, multi-stage, randomized, adaptive platform trial designed to simultaneously evaluate multiple treatments that may improve outcomes in AIS. One domain is ENCHANTED3/MT, to randomize (1:1:1) up to 1,800 patients with SBP ⩾150 mmHg post-EVT to conservative (no or minimal ↓5-10mmHg), moderate (↓10-20mmHg), or intensive (↓30-50mmHg) SBP. Primary outcome is modified Rankin scale (mRS) at 90 days analysed with utility-weighted mRS using a Bayesian hierarchical linear model. Adaptive analyses will be conducted 3-monthly with prespecified statistical triggers for superiority, inferiority and equivalence.
Results: The trial kicked off in April 2024 and will involve up to 150+ hospitals in 8+ countries over the next 2-years.
Conclusions: ENCHANTED3/MT will compare three BP lowering management strategies in post-EVT AIS patients with elevated SBP determine the best approach to improve functional outcome.
Disclosures of Interest: No
Abstract N°: 2653
DOES BIOLOGICAL SEX HAVE AN IMPACT ON OUTCOMES IN PATIENTS WITH EXTRACRANIAL CERVICAL ARTERY DISSECTIONS?
Naaem Simaan*1, Issa Metanis2, Yoel Schwartzmann2, Tamer Jubeh2, Asaf Honig2, Hamza Joubran2, Jad Magadlla2, Jose Cohen3, Ronen R Leker2
1Ziv Medical Center - Israel, Neurology - stroke unit, rama village, Israel, 2Hadassah medical center, Neurology - stroke unit, 3Hadassah medical center
On behalf of:
Background and aims: Cervical arterial dissections (CeAD) are a common cause of stroke in young adults of both biological sexes. Whether biological sex plays a role in the pathogenesis and outcome of CeAD remains unclear
Methods: Patients with CeAD were retrospectively identified from a large institutional database of stroke patients. Clinical, imaging, treatment and outcome parameters were compared between females and males. Multivariate logistic regression analyses were used to determine associations witho utcomes
Results: Overall, 154 patients were included (93 males, 60%). Males significantly more often smoked (39% vs 11%, p=0.002) and had a significantly higher prevalence of hyperlipidemia (19% vs. 7%, p=0.026), isolated traumatic neck injury (20% vs. 8%, p=0.041) and vessel occlusions (39% vs. 23%, p=0.027). Other risk factors and clinical attributes did not differ between the groups. No differences were observed between the groups regarding treatment strategies including administration of systemic thrombolysis or stent placements and the rates of recurrent stroke and recurrent dissections. Favorable outcomes and symptomatic intracranial hemorrhage rates were also similar on the univariate analyses and biological sex was not associated with outcomes on regression analyses
Conclusions: CeAD occurs more frequently in males, who were more likely to smoke and have traumatic neck injuries and vessel occlusions. However, biological sex was not associated with outcomes in patients with CeAD
Disclosures of Interest: No
Abstract N°: 3115
ACT-GLOBAL_ACT-WHEN: A RANDOMIZED, OPEN LABEL, BLINDED-ENDPOINT TRIAL TO OPTIMIZE THE USE OF INTRAVENOUS TENECTEPLASE IN ACUTE ISCHEMIC STROKE
Xiaoying Chen1, Dar Dowlatshahi2, Mohammed Almekhlafi3, Michael D Hill3, Andrew Demchuk3, Tolulope Sajobi3, Craig Anderson1, Bijoy Menon*3
1University of New South Wales, The George Institute for Global Health, 2University of Ottawa, Ottawa Hospital Research Institute, 3University of Calgary, Cumming School of Medicine
On behalf of: the ACT-GLOBAL_ACT-WHEN Investigators
Background and aims: Tenecteplase (TNK) is emerging as the global first choice intravenous thrombolytic (IVT) agent but there is uncertainty about its optimum dose and use in certain patient groups including those on DOACs and prior to EVT. The ACT-WHEN domain of the ACT-GLOBAL platform trial aims to determine the effectiveness of IVT-TNK standard-dose vs. low-dose vs. no TNK in patients with acute ischemic stroke where there is uncertainty over benefits and risks.
Methods: ACT-GLOBAL is an international, multi-factorial, multi-arm, multi-stage, randomized, adaptive platform trial designed to simultaneously evaluate multiple treatments that may improve outcomes in acute ischemic stroke patients. The ACT-WHEN domain will randomize up to 4,000 patients into either of 2-doses of TNK (0.25 mg/kg vs. 0.18 mg/kg) or no TNK. Stratification is based on EVT and DOAC status, creating four pre-defined strata. Primary outcome is modified Rankin scale (mRS) at 90 days analysed with utility-weighted mRS using a Bayesian hierarchical linear model. Adaptive analyses will be conducted every 400 patients enrolled with prespecified statistical triggers for superiority, inferiority, and lack-of-significant benefit.
Results: The trial kicked off in April 2024 and will involve up to 150+ hospitals in 8+ countries over the next 2-years.
Conclusions: The ACT-WHEN domain of ACT-GLOBAL will compare IVT-TNK use (Yes vs No) and dose (standard vs low) where evidence is lacking or insufficient. This large adaptive randomized study in the various patient conditions will increase physician confidence and potentially result in better and faster utilization of IVT-TNK, thus helping to improve patient outcomes.
Disclosures of Interest: No
Abstract N°: 1532
EFFECT OF TENECTEPLASE VERSUS ALTEPLASE ON FIRST-PASS REPERFUSION IN ENDOVASCULAR THROMBECTOMY: RESULTS FROM THE ACT TRIAL
William Diprose1, Fouzi Bala*2, Nishita Singh3, Ibrahim Alhabli1, Thalia Field4, Gary Hunter5, Michael Hill1, Richard Swartz6, Bijoy Menon1, Mohammed Almekhlafi1
1University of Calgary, Canada, 2University Hospital of Tours, France, 3University of Manitoba, Canada, 4University of British Columbia, Canada, 5University of Saskatchewan, Canada, 6University of Toronto, Canada
On behalf of: The AcT investigators
Background and aims: It is unknown whether thrombolysis with intravenous (IV) tenecteplase prior to endovascular thrombectomy (EVT) improves the chances of first-pass reperfusion (FPR) when compared to IV alteplase.
Methods: We investigated the effects of thrombolysis type (IV tenecteplase or IV alteplase) on FPR in EVT patients from the Alteplase compared to Tenecteplase (AcT) trial. Outcomes were expanded treatment in cerebral infarction (eTICI) score 2c-3 and eTICI 2b-3 after first pass (FPR and modified FPR respectively), number of passes, and final eTICI score. Mixed-effect regression analyses with interaction terms were performed.
Results: Among the 506 patients who underwent EVT in the AcT trial, 455 patients were included (230 [51.7%] women; median [IQR] age, 73 [63-81]). 226 (50.8%) received IV tenecteplase and 219 patients received IV alteplase (49.2%). FPR and modified FPR was achieved in 169 (38.0%) and 245 (55.1%) of patients respectively. FPR was achieved in 79 (35.0%) IV tenecteplase and 90 (41.1%) IV alteplase patients (P=0.20). Modified FPR was achieved in 123 (54.4%) IV tenecteplase and 122 (55.7%) IV alteplase patients (P=0.85). Median (IQR) number of passes was 2 (1-3) in the tenecteplase group and 1 (1-2) in the alteplase group (P=0.07). There was no difference in final eTICI 2c-3 scores. There were no significant interactions between sex, occlusion site, thrombus length, residual flow, clot burden score, hyperdense artery sign, or first-line thrombectomy technique with thrombolysis type on FPR.
Conclusions: Contrary to expectation, IV tenecteplase did not improve the chances of FPR when compared to IV alteplase.
Disclosures of Interest: No
Abstract N°: 1548
ONE-PASS TIROFIBAN IN MANAGEMENT OF ISCHAEMIC STROKE THROMBECTOMY IN CHINA (OPTIMISTIC)
Longting Lin1,2, Feifeng Liu1, Wenhuo Chen3, Yueqi Zhu4, Jianhong Yang5, Yanxin Zhao6, Feng Wang7, Leonid Churilov8, Mark Parsons2, Gang Li*1
1East Shanghai Hospital, School of Medicine, Tongji University, Shanghai, China, Department of Neurology, Shanghai, China, 2South Western Sydney Clinical Campuses, University of New South Wales, Sydney, NSW 2170, Australia., 3Zhangzhou Affiliated Hospital of Fujian Medical University, Zhangzhou, China, 4Shanghai Sixth People's Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, China, 5The First Affiliated Hospital of Ningbo University, Zhejiang, China, 6Central Hospital Affiliated to Shandong First Medical University, Jinan Hospital of Xuanwu Hospital, Capital Medical University, Jinan Central Hospital., Shandong, China, 7Seventh People's Hospital of Shanghai University of Traditional Chinese Medicine, Shanghai, China, 8The Royal Melbourne Hospital, University of Melbourne, Parkville, VIC, 3010, Australia
On behalf of: the OPTIMISTIC Investigators
Background and aims: Tirofiban is a potent inhibitor of Glycoprotein IIb/IIIa receptors often used as an adjunct to thrombectomy. Early trials of tirofiban in patients receiving thrombectomy produced conflicting results, and the best paradigm for tirofiban use remains unclear. There is evidence that tirofiban is safest if delivered intravenously prior to thrombectomy and is more effective in stroke due to atherosclerosis than cardioembolic stroke. OPTIMISTIC aimed to determine whether intravenous tirofiban delivered before thrombectomy increased the rate of first-pass recanalization without increasing the risk of symptomatic intracranial haemorrhage (sICH) in a Chinese population without evidence of cardioembolic aetiology.
Methods: Patients were randomized 1:1 to intervention group or control. Intervention group received bolus 10 micrograms/kg tirofiban followed by 24-hour infusion of 0.1 micrograms/kg/min. The control group did not receive intravenous or intraarterial antiplatelets before first thrombectomy attempt. The primary outcome was first-pass recanalization (mTICI⩾2b) without sICH. Results are presented as adjusted risk ratios (aRR) followed by [95% confidence intervals] and p-values.
Results: A total of 194 patients were included in the intention-to-treat analysis (99 intervention, 95 control). The intervention was associated with an increased likelihood of first-pass recanalization (aRR 1.29 [1.01-1.73], p=0.045) while none of the intervention patients suffered sICH (vs 6 controls, p<0.0001). The aRR for the composite primary outcome was 1.34 [1.04-1.73], p=0.025. In patients with residual post-thrombectomy stenosis (66-intervention, 69-control) the effect was greater (aRR 1.57 [1.17-2.11], p=0.003).
Conclusions: Intravenous tirofiban prior to thrombectomy is safe and increases first-pass recanalization, particularly stroke due to intracranial atherosclerosis.
Disclosures of Interest: No
Abstract N°: 1964
DABIGATRAN EXTEXILATE VERSUS WARFARIN IN CEREBRAL THROMBOSIS IN CHINESE PATIENTS (CHOICE-CVT): AN OPEN-LABEL, RANDOMIZED CONTROLLED TRIAL
1Xuanwu Hospital, Capital Medical University, Department of Emergency, Beijing, China, 2Xuanwu Hospital, Capital Medical University, Department of Neurology, Beijing, China, 3Beijing Fengtai You’anmen Hospital, Department of Neurology, Beijing, China, 4Xuanwu Hospital, Capital Medical University, Department of Neurosurgery, Beijing, China
On behalf of:
Background and aims: The efficacy and safety of dabigatran etexilate for Chinese patients with cerebral venous thrombosis (CVT) has not been well established.
Methods: This was an exploratory, single-center, randomized, open-label study in National Center for Neurological Disorders involving Chinese patients with CVT aged 18 to 80 years who were randomly assigned (1:1) to either dabigatran etexilate or warfarin arm. The oral anticoagulants were initiated at randomization. The primary efficacy and safety endpoints included number of patients with recurrent CVT and/or deep venous thrombosis (DVT) and clinical major bleeding within 180 days. Secondary efficacy endpoints included venous recanalization and change in papilledema at day 180. Secondary safety outcomes comprised death, clinical non-major bleeding, and any bleeding. The study registration number is NCT03930940.
Results: Between October 2017 and February 2023, a total of 89 patients were enrolled and randomly assigned to receive either dabigatran etexilate(n=44) or warfarin (n=45). At day 180, dabigatran etexilate group showed a comparable number of patients with recurrent CVT and/or DVT, clinical major bleeding, and clinical non-major bleeding but demonstrated a lower risk of any bleeding compared to warfarin group. Most patients in both groups achieved venous recanalization according to Modified Qureshi scale (27 [75%; 95%CI, 60.1-89.9] in dabigatran etexilate group vs. 34 [82.9%; 95%CI, 70.9-95.0] in warfarin group) and exhibited improvement in papilledema(35 [97.2%; 95%CI, 91.6-100.0] in dabigatran etexilate group vs. 37 [88.1%, 95%CI, 77.9-98.3] in warfarin group).
Conclusions: These findings regarding efficacy and safety support the consideration of dabigatran etexilate therapy as a viable treatment option for Chinese patients with CVT.
Disclosures of Interest: No
Abstract N°: 2221
PROGNOSTIC SIGNIFICANCE OF POST-EVT BLOOD GLUCOSE LEVEL: POST HOC ANALYSIS OF THE ENCHANTED2/MT TRIAL
Xinwen Ren*1,2, Yang Zhao1,2, Craig Anderson1,2,3, Lili Song1,2
1The George Institute for Global Health, Beijing, China, 2The George Institute for Global Health, University of New South Wales, Sydney, Australia, 3Royal Prince Alfred Hospital, Neurology, Sydney, Australia
On behalf of:
Background and aims: The relation between blood glucose (BG) level and complications of endovascular thrombectomy (EVT) for acute ischemic stroke (AIS) is unclear. We evaluated BG level and mortality, symptomatic intracerebral hemorrhage (sICH) and serious adverse events (SAEs) in participants of the second Enhanced Control of Hypertension and Thrombolysis Stroke Study (ENCHANTED2/MT).
Methods: ENCHANTED2/MT involved 816 ‘hypertensive’ post-EVT AIS patients who were randomly allocated to more-intensive (SBP target <120 mmHg) versus less-intensive (SBP target 140-180 mmHg) BP-lowering. Associations of baseline BG level on 90-day mortality, sICH and SAEs were assessed in logistic regression models.
Results: In 752 AIS patients (mean age 67 years, 38% female) with available BG data, higher BG level was significantly associated with mortality after adjustment for clinical variables (adjusted odds ratio [aOR] 1.12, 95%CI 1.05-1.20; p=0.001). The odds of sICH and SAEs increased in patients with higher BG level (aOR 1.18, 95%CI 1.08-1.28, p=0.0003 and aOR 1.12, 95%CI 1.06-1.19, p <0.0001, respectively).
Conclusions: Increased BG levels predict adverse in AIS patients after successful EVT.
Disclosures of Interest: No
Abstract N°: 1376
INTRAVENOUS TENECTEPLASE COMPARED WITH ALTEPLASE FOR AIS IN CANADA (ACT): BRIDGING THE GAP FROM ACADEMIA TO REGULATORY APPROVAL
Nuala Peter*1, Thierry Danays2, Alain Pages3, Brian Buck4, Nishita Singh5, Mohammed Almekhlafi6, Luciana Catanese7, Tolulope Sajobi8, Richard Swartz9, Bijoy Menon10
1Boehringer Ingelheim Pharma GmbH & Co. KG, Biometrics and Data Sciences, Biberach, Germany, 2TDC, Aix en Provence, France, 3Boehringer Ingelheim International, Ingelheim-am-Rhein, Germany, 4University of Alberta, Edmonton, Canada, 5Department of Internal Medicine- neurology division Rady Faculty of health sciences, University of Manitoba, Winnipeg, Canada, 6Cumming School of Medicine & The Hotchkiss Brain Institute, Calgary, Canada, 7McMaster University, Ontario, Canada, 8University of Calgary, Calgary, Canada, 9University of Toronto, Toronto, Canada, 10Cumming School of Medicine & The Hotchkiss Brain Institute, Department of Clinical Neurosciences, Radiology and Community Health Sciences, Calgary, Canada
On behalf of:
Background and aims: This extended re-analysis was aimed to customize the academic presentation of AcT trial results, to those expected by regulatory agencies, complying with International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) guidelines.
Methods: All aspects of efficacy and safety were investigated. For efficacy (Day90 mRS0-1, mRS ordinal), estimand components were tested in sensitivity analyses, adjusting for key prognostic factors, handling of missing data and checking proportional odds assumption. The constancy assumption behind the population (study) adjusted non-inferiority margin, accounting for the shift of patients treated earlier compared to historical meta-analysis (Emberson 2014) was assessed. For safety, various definitions of intracerebral haemorrhages were derived, time to death was investigated using Kaplan Meier curves.
Results: Regardless of which mRS0-1 sensitivity analysis implemented (Figure 1), non-inferiority to alteplase was demonstrated. The assumption of proportional odds was confirmed (Figure 2).The SITS-MOST definition of intracerebral hemorrhage most resembled historical meta-analysis, definitions revealed similar results. Time to death was similar between alteplase and tenecteplase (Figure 3).
Conclusions: The successful customisation and extended re-analysis of the AcT data, to meet regulatory requirements, confirmed robustness of results of the original manuscript (Lancet 2022). This study constituted a key piece of evidence in the submission, and ultimately regulatory approval of tenecteplase 25mg for the treatment of acute ischaemic stroke within 4.5 hours of onset.
Acknowledgements
The authors thank Gabriele Biegert, Dorothea Krieg, Ellen von der Heyde for programming support.
Results of Day90 mRS0-1 sensitivity analyses.
Cumulative mRS odds ratios across severity levels.
Time to death.
Disclosures of Interest: Yes Employee of Boehringer Ingelheim Pharma GmbH & Co. KG
Abstract N°: 1690
EFFICACY AND SAFETY OF MECHANICAL THROMBECTOMY IN CAROTID ARTERY DISSECTION
Marek Sykora*1,2, Sven Poli3, Michail Panagiotis Giannakakis4, Joshua Mbroh3, Hannes Deutschmann5, Michael Knoflach6, Jens Fiehler7, Tomas Dobrocky4, Urs Fischer4, Julia Ferrari1
1St. Johns Hospital, Neurology, Vienna, Austria, 2Sigmund Freud University Vienna, Wien, Austria, 3Eberhard Karls University of Tübingen, Tübingen, Germany, 4University of Bern, Bern, Switzerland, 5Medical University of Graz, Graz, Austria, 6Medizinische Universität Innsbruck, Innsbruck, Austria, 7University of Hamburg, Hamburg, Germany
On behalf of:
Background and aims: Patients with carotid artery dissection (CAD) stroke harboring large vessel occlusion (LVO) are often treated with mechanical thrombectomy (MT), however, data on clinical outcome of this specific subgroup are scarce. We aimed to compare MT to best medical treatment (BMT) or intravenous thrombolysis (IVT) in patients with anterior circulation stroke due to CAD with LVO.
Methods: Pooled data from the national Austrian, German and Swiss Stroke Registries were analyzed.
Results: Of 1023 patients (mean age 54 years, 72% males), 516 received MT (47.6% with IVT) and 507 received IVT only or BMT (IVT=161, BMT=346). Patients treated with MT had higher admission NIHSS scores as those treated with BMT (median 14 versus 3) or those with only IVT (median 3), all other characteristics were statistically equally distributed. After adjustment for baseline imbalances, MT was not associated with favorable functional outcome (mRS 0-2 at 3 months) as compared to BMT (aOR 1.04, CI 0.7-1.6). In subgroup analysis, MT in patients presenting with NIHSS 0-8 resulted in lower odds of mRS 0-2 at 3 months (aOR 0.4, CI 0.1-0.9) and in those presenting with NIHSS>8 in higher odds of mRS 0-2 at 3 months (aOR 2.6, CI 1.1-6.5) as compared to BMT.
Conclusions: In patients with admission NIHSSS ⩽ 8 due to a CAD with LVO, MT was associated with worse functional outcome as compared to BMT. Patients presenting with NIHSS > 8 seemed to benefit from MT. Further detailed results will be presented at the ESOC 2024.
Disclosures of Interest: No
Abstract N°: 933
INFARCT GROWTH RATE AND FUNCTIONAL INDEPENDENCE FOR LARGE INFARCT PATIENT WITH ENDOVASCULAR THROMBECTOMY
Ximing Nie1, Jie Chen1, Bernard Yan2, Yuesong Pan1, Meng-Xing Wang1, Bizhong Che3, Zhongrong Miao4, Liping Liu1,4
1Beijing Tiantan Hospital, Capital Medical University, Department of Neurology, Beijing, China, 2Royal Melbourne Hospital, The University of Melbourne, Melbourne Brain Centre, Melbourne, Australia, 3School of Public Health and Jiangsu Key Laboratory of Preventive and Translational Medicine for Geriatric Diseases, Suzhou Medical College of Soochow University, Department of Epidemiology, suzhou, China, 4Beijing Tiantan Hospital, Capital Medical University, Department of Interventional Neuroradiology, Beijing, China
On behalf of: ANGEL-ASPECT Study Group
Background and aims: How the pretreatment infarct growth rate (IGR) influence on the therapeutic efficacy of endovascular thrombectomy (EVT) in patients with large core infarcts remains unclear.
To evaluate the correlation between pretreatment IGR and the therapeutic benefits of EVT in large infarcts.
Methods: This study performed a post-hoc analysis of EVT in ANGEL-ASPECT trial. The primary outcome was the 90-day functional independence, defined as a modified Rankin Scale score of 0-2. The IGR was calculated as the quotient of infarct core volume and the time from stroke onset to image and were divided into three categories based on its relationship with functional independence.
Results: Among 455 patients, the mean age was 66 years (SD, 9.8), with 38.7% being women. IGR interacted the functional outomes between EVT and medical management (Figure 1-2). Patients were categorized into slow-progressing (IGR <5mL/h, n=148), intermediate-progressing (IGR 5-20 mL/h, n=221), and fast-progressing (IGR >20mL/h, n=86) groups. There was a significant interaction among IGR groups and treatment groups in odds of achieving functional independence (adjusted odds ratio, 10.23 [95% CI, 3.7-28.29] vs. 3.07 [95%CI, 1.41-6.71] vs. 1.45 [95%CI, 0.45-4.71], P for interaction =0.03). (Figure 3)
Conclusions: Patients with large infarcts who experience slower progression tend to derive greater benefits from EVT, but not those fast-progressing patients. Incorporating IGR assessment may help tailor EVT treatments for patients with large infarcts.
Effect of EVT on Functional Independence across Varying IGRs.
Locally Weighted Scatterplot Smoothing Regression of IGR with Functional Outcomes.
Distribution of 90-day mRS Score in IGR groups.
Disclosures of Interest: No
Abstract N°: 1267
INTRAVENOUS THROMBOLYSIS IN YOUNG ADULTS WITH ISCHEMIC STROKE: A COHORT STUDY FROM THE INTERNATIONAL TRISP COLLABORATION
Miranda Nybondas*1, Nicolas Martinez-Majander1, Sami Curtze1, Henrik Gensicke2, Peter A. Ringleb3, Patrik Michel4, Charlotte Cordonnier5, Christian Nolte6, Guido Bigliardi7, Paul Nederkoorn8
1Department of Neurology, University of Helsinki and Helsinki University Hospital, Helsinki, Finland, 2Stroke Center and Department of Neurology, University Hospital Basel and University of Basel, Basel, Switzerland, 3Department of Neurology, University Hospital Heidelberg, Heidelberg, Germany, 4Stroke Center, Neurology Service, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland, 5Univ. Lille, Inserm, CHU Lille Lille Neuroscience & Cognition, Lille, France, 6Charite University Hospital, Berlin, Germany, 7Stroke Unit, Department of Neuroscience, Modena University Hospital, Modena, Italy, 8Department of Neurology, Amsterdam UMC, University of Amsterdam, Amsterdam, Netherlands
On behalf of: TRISP collaborators
Background and aims: Previous observational data indicate that intravenous thrombolysis for acute ischemic stroke is safe in young adults, and that they have more favorable outcomes compared to older adults. Given the limited evidence on this topic, we aimed to provide more evidence on safety and clinical outcomes in such patients, using a large international thrombolysis registry.
Methods: We used data from the Thrombolysis in Ischemic Stroke Patients (TRISP) registry from 1998 to 2020. Using multivariable regression models, we compared thrombolysed young patients aged 18-49 years with those aged ⩾50 years with regards to the following outcomes: symptomatic intracranial hemorrhage (sICH) according to European Cooperative Acute Stroke Study II criteria, 3-months all-cause death, and good outcome in stroke survivors (modified Rankin Scale ⩽2).
Results: The 1,384/17,024 (8.1%) thrombolysed young adults in TRISP were more often male (59.7% vs 54.2%), had lower NIHSS score on admission, and had less cardiovascular risk factors except for smoking (41.7% vs 19.3%) when compared to older patients. The most common etiology in young adults was undetermined (41.3%), versus cardioembolism (36.7%) in patients ⩾50 years. When compared to thrombolysed patients aged ⩾50 years, a good functional outcome was more likely in young adults: 81.1% vs 56.1%, aOR 2.36 (1.94-2.87), whilst unfavorable outcome events were less likely: sICH 1.8% vs 4.6%, aOR 0.56 (0.33-0.97) and death 2.6% vs 14.2%, aOR 0.20 (0.10-0.41).
Conclusions: Intravenous thrombolysis in young adults has less risks and clinical outcomes are more favorable, when compared to older patients, even after multiple adjustments for confounding factors.
Disclosures of Interest: No
Abstract N°: 2161
MOBILE STROKE UNIT DISPATCH AND FUNCTIONAL OUTCOMES AFTER ACUTE STROKE IN BERLIN: B_PROUD-2.0 AND POOLED B_PROUD-1.0+2.0 RESULTS
Jessica L Rohmann*1,2, Marco Piccininni1,2, Martin Ebinger1,3, Joachim Weber1,4,5,6, Peter Harmel5, Ira Rohrpasser-Napierkowski4,5, Bruno-Marcel Mackert7, Andreas Hartmann8, Matthias Endres1,4,5,9,10, Heinrich Audebert1,4
1Charité - Universitätsmedizin Berlin, Center for Stroke Research Berlin, Berlin, Germany, 2Charité Universitätsmedizin Berlin, Institute of Public Health, Berlin, Germany, 3Medical Park Berlin (MPB) Humboldtmühle, Klinik für Neurologie, Berlin, Germany, 4Charité - Universitätsmedizin Berlin, Klinik und Hochschulambulanz für Neurologie, Berlin, Germany, 5Berlin Institute of Health at Charité – Universitätsmedizin Berlin, Berlin, Germany, 6German Centre for Cardiovascular Research (DZHK), partner site Berlin, Berlin, Germany, 7Vivantes Auguste-Viktoria-Klinikum, Klinik für Neurologie mit Stroke Unit, Berlin, Germany, 8Klinikum Frankfurt (Oder), Klinik für Neurologie, Frankfurt (Oder), Germany, 9NeuroCure Cluster of Excellence, Berlin, Germany, 10German Center for Neurodegenerative Diseases (DZNE), partner site Berlin, Berlin, Germany
On behalf of: The B_PROUD-2.0 Study Group (M Wendt, E Schwabauer, E Freitag, M Zuber, L Bernhardt, J Lange, H Erdur, J Behrens, R Ganeshan, L Schlemm, T Liman, I Lorenz-Meyer, A Hille, G Bohner, D G Nabavi, I Schmehl, A Ekkernkamp, G J Jungehuelsing)
Background and aims: Prehospital stroke management on Mobile Stroke Units (MSUs) shortens time from dispatch to intravenous thrombolysis (IVT) and improves functional outcomes. With time-dependent IVT effects, optimising MSU-related procedures may enhance MSU benefits.
Methods: Planned workflow modifications aimed at improving dispatch accuracy and streamlining processes. We evaluated process indicators and clinical outcomes in the nonrandomized, controlled B_PROUD-2.0 study (05/2019-01/2021, NCT03931616) in Berlin (Germany), in which MSUs were additionally dispatched whenever available. The primary population consisted of ischemic stroke/TIA patients with disabling neurological symptoms and no contraindications to reperfusion therapies. The primary and coprimary outcomes were 3-month modified Rankin Scale scores and a 3-tiered disability scale.
Results: The COVID-19 pandemic disrupted realisation of planned procedural improvements and a smaller-than-expected sample (planned N=1,500) resulted from time-limited funding (MSU group: 667 patients; non-MSU: 364). In B_PROUD-2.0, we found no statistically significant effect of MSU dispatch on the primary (common OR (cOR)=0.90, 95%CI:0.72-1.14) or coprimary (cOR=0.86, 95%CI:0.63-1.17) outcomes, despite substantially higher odds of IVT ⩽1h of dispatch in the MSU group (OR=10.15, 95%CI:7.10-14.51). In pooled analyses of the B_PROUD-1.0+2.0 primary populations (n=2,666), we found a beneficial effect of MSU dispatch on both primary (cOR=0.80, 95%CI:0.67-0.96) and coprimary (cOR=0.79, 95%CI:0.64-0.97) outcomes. The average effect across all stroke/TIA patients (including those with treatment contraindications) was also favourable (n=4,336; primary cOR=0.85, 95%CI:0.75-0.95; coprimary cOR=0.86, 95%CI:0.75-0.99).
Conclusions: No statistically significant differences in functional outcomes were observed in the underpowered B_PROUD-2.0 study, while statistically significant beneficial effects consistent with prior work were found when considering both B_PROUD periods.
Disclosures of Interest: Yes M.En. reports fees paid to the Charité from Covidien and funding from the Deutsche Forschungsgemeinschaft (DFG) for B_PROUD 2.0. H.A. reports receiving personal fees from Boehringer Ingelheim, Roche and Novo Nordisk.
Paper Poster – Atherosclerosis
Abstract N°: 195
INVERSE ASSOCIATION BETWEEN FAT INTAKE AND STROKE
Juanying Zhen*1, Bernard Man Yung Cheung1,2,3, Chao LI1,2
1The University of Hong Kong (HKU), Department of Medicine, School of Clinical Medicine, Hong Kong, China, 2The University of Hong Kong (HKU), State Key Laboratory of Pharmaceutical Biotechnology, Hong Kong, China, 3The University of Hong Kong (HKU), Institute of Cardiovascular Science and Medicine, Hong Kong, China
On behalf of:
Background and aims: Diet is an important target for primary prevention of stroke. Health effects of dietary fats have been extensively studied for decades. Evidence on the relationship between dietary fat intake and stroke is still controversial. We aimed to investigate the relationship of stroke with fats, including total fat, saturated fatty acids (SFA), monounsaturated fatty acids (MUFA) and polyunsaturated fatty acids (PUFA).
Methods: We analysed data on 27,673 participants, representing 206,611,970 American citizens aged 20 years and older, who had valid data on dietary fat intake and stroke from the National Health and Nutrition Examination Survey 2007-2018. Age, sex, race/ethnicity, body mass index, diabetes, hypertension, hypercholesterolemia, smoking, alcohol consumption and physical activity were adjusted in the multivariable models.
Results: 3.8% (n=1054) of participants had a previous diagnosis of stroke. In the multivariable models, stroke was inversely associated with supplement use of total fat (OR=0.88, 95%CI=0.79-0.99, P=0.035), SFA (OR=0.46, 95%CI=0.23-0.90) and MUFA (OR=0.08, 95%CI=0.02-0.37, P=0.002). There was an inverse association between stroke and PUFA intake (from foods: OR=0.89, 95%CI=0.78-0.999, P=0.049; from supplements: OR=0.44, 95%CI=0.27-0.72, P=0.001). Among 19 specific fatty acids, higher octadecadienoic acid (18:2) intake from foods was associated with lower risk of stroke (OR=0.99, 95%CI=0.97-1.00, P=0.043).
Conclusions: In this large-scale nationally-representative study, stroke is inversely associated with fat intake from supplements and PUFA intake from foods. Higher octadecadienoic acid (18:2) intake from foods is associated with lower risk of stroke. Our findings suggest that increasing fat intake from supplements and PUFA intake from foods have beneficial effects on stroke prevention.
Disclosures of Interest: No
Abstract N°: 562
IDENTIFYING PREDICTIVE MRI MARKERS IN THE TRANSITION OF LOW-GRADE CAROTID STENOSIS
1Kurashiki Central Hospital, Neurosurgery, Kurashiki, Japan
On behalf of:
Background and aims: Carotid artery stenosis is a major contributor to cerebrovascular events, with a critical transition from asymptomatic to symptomatic phases. This retrospective study explores intraplaque hemorrhage and plaque characteristic changes as predictors for this progression, focusing on low-grade carotid stenosis. We hypothesize that MRI features, specifically changes in plaque signal intensity and volume, indicate a shift from asymptomatic to symptomatic stenosis.
Methods: We retrospectively analyzed 30 cases of symptomatic low-grade carotid stenosis (<50%) from a database of 123 patients, focusing on pre-symptomatic carotid MRI data. Relative plaque signal intensity (rSI) and high-intensity plaque volume were measured and compared between asymptomatic and symptomatic periods.
Results: Analysis revealed a significant increase in mean rSI, rising from 1.32±0.32 in the asymptomatic phase to 1.69±0.25 during the symptomatic phase (p<0.001). Additionally, plaque volume showed a notable increase, from an average of 296.4±362.7 mm³ in the asymptomatic period to 717.5±554.9 mm³ at the onset of symptoms (p<0.001).
Conclusions: The study demonstrates that increases in rSI and plaque volume are closely associated with the progression from asymptomatic to symptomatic stages in low-grade carotid stenosis. These MRI parameters potentially play a crucial role in identifying patients at an increased risk of symptomatic progression.
Disclosures of Interest: No
Abstract N°: 1452
ASSOCIATION OF TRIGLYCERIDE-GLUCOSE INDEX AND ASYMPTOMATIC INTRACRANIAL STENOSIS IN THE NORTHERN MANHATTAN STUDY (NOMAS)
Edgar Lopez-Navarro*1, Kevin Strobino1, Farid Khasiyev2, Mitchell Elkind3, Tatjana Rundek4, Jose Gutierrez1
1Columbia University Irving Medical Center, Department of Neurology, New York, United States, 2Saint Louis University, Department of Neurology, 3Columbia University, 4University of Miami Miller School of Medicine, Department of Neurology
On behalf of:
Background and aims: Intracranial atherosclerotic stenosis (ICAS) contributes to 10% of strokes in the USA. Insulin resistance and diabetes elevate atherosclerotic risk. A higher TyG index, a surrogate for insulin resistance, is linked to asymptomatic ICAS and stroke risk in Asians. The study investigates the TyG index in a multi-ethnic US population.
Methods: We investigated the ICAS and TyG index relationship in this stroke-free cohort. Participants had time-of-flight MRA. We rated the degree of luminal stenosis as follows: 0 = no stenosis, 1 = <50% stenosis, 2 = 50-69%, 3 = ⩾70%, and 4 = flow gap. ICAS was defined with a score of ⩾1. Participants had fasting plasma levels of glucose and triglycerides. The TyG index was calculated as ln [Fasting triglyceride (mg/dl)xFasting glucose (mg/dl)]/2.
Results: Out of 1,149 participants, 44% had ICAS. In univariate analysis, TyG index was associated with ICAS (OR 1.38, 95% CI 1.13-1.69). After adjusting for age, sex, race/ethnicity, and vascular risk factors, the association between TyG index and ICAS did not change (model 1: OR 1.41, 95% CI 1.14-1.74; model 2: OR 1.29, 95% CI 1.03-1.62). Considering ICAS ⩾50% (ICAS score ⩾2 in at least one artery), the association between ICAS and TyG index was insignificant (OR 1.10, 95% CI 0.72-1.66).
Conclusions: TyG index was associated with the presence of ICAS but not with ICAS >50%. These findings highlight the potential of TyG index as a marker of ICAS in a multi-ethnic US population and underscore the relevance of metabolic factors in cerebrovascular health.
Disclosures of Interest: No
Abstract N°: 1568
OUTCOMES IN PATIENTS WITH INTRACRANIAL ATHEROSCLEROSIS (ICAS): RESULTS FROM THE ALTEPLASE COMPARED TO TENECTEPLASE (ACT) TRIAL
Vivian Fu1, Fouzi Bala*1,2, Bijoy K. Menon1, Nishita Singh3, Shelagh Coutts1, Luciana Catanese4, Richard Swartz5, Dar Dowlatshahi6, Gary Hunter7, Mohammed Almekhlafi1
1University of Calgary, Calgary, Canada, 2University Hospital of Tours, Tours, France, 3University of Manitoba, Winnipeg, Canada, 4Hamilton Health Sciences Centre and McMaster University, Hamilton, Canada, 5Sunnybrook Health Sciences Centre and the University of Toronto, Toronto, Canada, 6University of Ottawa, Ottawa, Canada, 7University of Saskatchewan, Saskatoon, Canada
On behalf of: the AcT trial investigators
Background and aims: Intracranial atherosclerosis (ICAS) is a common cause of stroke worldwide. We assessed the prevalence and impact of ICAS in the Canadian AcT trial.
Methods: This post-hoc analysis of AcT divided patients into 3 subgroups based on the ICAS presence (⩾ 50% stenosis) and relevance: non-ICAS, ICAS in the stroke territory (ICAS-stroke), ICAS outside the stroke territory (any ICAS). Outcomes were 90-day modified Rankin Scale (mRS) 0-1 and 0-2, mortality, symptomatic intracerebral haemorrhage (sICH), and angiographic reperfusion (eTICI 2b-3) on final images. Multivariable regression analyses assessed the association between ICAS and outcomes.
Results: ICAS was seen in 373/1558 patients (23.9%): 102/373 (27.3%) were ICAS-stroke and 271/373 (72.6%) any ICAS. The ICAS-stroke and any ICAS had lower likelihood of 90-day mRS 0-1 (risk ratio [RR] 0.66 95%CI 0.50-0.90, and RR 0.69 95%CI 0.52-0.90) and mRS 0 – 2 (RR 0.74 95%CI 0.63-0.87, and RR 0.72 95%CI 0.63-0.82) compared with non-ICAS. Any ICAS had lowest SICH rate (0.7% vs. 1.9% ICAS-stroke vs. 3.9% non-ICAS) but highest mortality (24% vs. 15.0% ICAS-stroke vs. 13.4% non-ICAS). Final eTICI 2b-3 rates were lowest in ICAS-stroke (66.7% vs. 71.4% any ICAS vs. 85.1% non-ICAS). No interaction between thrombolytic agent and ICAS was seen for all outcomes.
Conclusions: ICAS in the same or different stroke territories is present in almost a quarter of stroke patients eligible for thrombolysis. ICAS patients were more likely to have poorer functional and angiographic outcomes compared with patients without ICAS.
Disclosures of Interest: No
Abstract N°: 2654
ASSOCIATION BETWEEN INFLAMMATION AND CLINICAL OUTCOME IN PATIENTS WITH ATHEROSCLEROTIC DISEASE UNDERGOING EVT FOR AIS
Yan Wang*1, Sven Luijten2, Daniel Bos2, Inge Mulder3, Manon Kappelhof4, Willeke Westendorp1, Bart Emmer4, Diederik van de Beek1, Jonathan Coutinho1
1Amsterdam UMC, Neurology, Amsterdam, Netherlands, 2Erasmus Medical Center, Radiology and Nuclear Medicine, Rotterdam, Netherlands, 3Amsterdam UMC, Biomedical Engineering and Physics, Amsterdam, Netherlands, 4Amsterdam UMC, Radiology and Nuclear Medicine, Amsterdam, Netherlands
On behalf of: MR CLEAN Registry Investigators
Background and aims: Intracranial atherosclerotic disease (ICAD) is a distinct cause of large vessel occlusion (LVO) stroke and these patients often respond poorly to endovascular treatment (EVT). There is a potential association between systemic markers of inflammation, such as C-Reactive Protein (CRP), and atherosclerotic events. We hypothesized that elevated CRP levels are associated with poor outcome and stroke recurrence, especially in patients with ICAD-LVO.
Methods: We used data from the MR CLEAN Registry (2014-2017) with LVO stroke due to ICAD, extracranial atherosclerotic disease (ECAD) and atrial fibrillation (AF). ICAD was defined as the presence of the predominant intimal subtype of calcification in the internal carotid artery, ICA-terminus or middle cerebral artery [M1] on NCCT. ECAD was identified as an atherosclerotic stenosis ⩾50% at the carotid bifurcation. Baseline CRP was used as marker of systemic inflammation. Patients with missing CRP, incomplete imaging, and other causes of LVO were excluded.
Results: We included 1024 patients of whom 294 had ICAD, 172 ECAD and 558 AF. ICAD patients were younger (ICAD 69 years, ECAD 74 years, AF 78 years, p<0.001) and more often male (63%-55%-46%, p<0.001). Median NIHSS score did not differ between groups (15-16-15, p=0.285). Median baseline CRP levels were lower in the ICAD group (3.20mg/L-4.00mg/L-5.70mg/L, p<0.001). Higher baseline CRP level correlated with worse clinical outcome at 3 months in the ICAD (r=0.139, p=0.017) and AF patients (r=0.159, p<0.001), but not in ECAD patients (r=0.124, p=0.106) (Figure 1).
Conclusions: Higher CRP levels on admission are associated with poor outcomes among patients with ICAD-LVO.
Disclosures of Interest: No
Abstract N°: 2250
DIFFERENTIAL GENE PROFILES IN HUMAN ARTERY SMCS: INSIGHTS INTO ATHEROSCLEROSIS
Hyungseok Kim*1, Jongtae Park1, Sujin Lee2
1Chonnam National University Medical School, Department of Forensic Medicine, 2Chonnam National University Hospital, Biomedical Researsh Instisute
On behalf of:
Background and aims: Human cerebral artery smooth muscle cells (SMCs) differ significantly from coronary artery SMCs, suggesting unique roles in atherosclerosis. This study examines the gene expression differences between these two types of muscle cell layers.
Methods: We collected vascular smooth muscle layers from the middle cerebral artery (MCA) and left anterior descending coronary artery (LAD) post-mortem from the same individual. Using cDNA microarray, we conducted a comparative analysis, supported by KEGG and Gene Ontology. We validated significant gene groups with qRT-PCR and compared genes associated with vascular plasticity.
Results: Our analysis identified 341 differentially expressed genes between cerebral and coronary artery-derived vSMCs. In cerebral artery vSMCs, 256 genes were upregulated and 85 downregulated. These vSMCs exhibited higher expression in genes related to angiogenesis, extracellular matrix, cell migration, neurogenesis, and inflammation. The top 13 upregulated genes, including ApoD, Desmin, Claudin-11, and Netrin-1, are linked to atherosclerosis, inflammatory cell migration, and retinal metabolism. MCA-expressed genes correlated with type 2 diabetes and hypertension, key atherosclerosis risk factors. Cerebral vSMCs also showed higher expression of contractile marker genes and regulators Oct4 and Klf4.
Conclusions: The study reveals distinct gene expression profiles between human cerebral and coronary artery SMCs. These findings offer insights into arterial function differentiation and atherosclerosis susceptibility, potentially guiding future vascular disease diagnostics and therapies..
Disclosures of Interest: No
Abstract N°: 2292
HIGH WALL SHEAR STRESS IS RELATED TO COMPLICATED CAROTID ARTERY PLAQUES IN CAROTID STENOSIS
Christoph Strecker*1, Tobias Saam2, Axel Krafft3, Markus Hüllebrand4, Ute Ludwig3, Anja Hennemuth4, Jürgen Hennig3, Andreas Harloff1
1University Hospital Freiburg, Neurology and Neurophysiology, Freiburg, Germany, 2Die Radiologie, Rosenheim, Germany, 3University Hospital Freiburg, Medical Physics, Freiburg, Germany, 4Charité-Universitätsmedizin Berlin, Institute for Imaging Science and Computational Modelling in Cardiovascular Medicine, Berlin, Germany
On behalf of:
Background and aims: Complicated carotid artery plaques (cCAPs) are associated with ischemic stroke and stroke recurrence and local hemodynamics seem to play a relevant role for their development. Thus, we investigated the influence of 4D flow-MRI derived wall shear stress (WSS) and oscillatory shear stress (OSI) on the presence of cCAPs in patients with internal carotid artery (ICA) stenosis.
Methods: 39 patients (49 carotid arteries) with a 10-50% stenosis of the ICA were included in this analysis. Plaque composition was determined according to the modified American Heart Association classification of lesions by 3T-MRI. We determined WSS (minimum, mean and maximum) and OSI by 4D flow-MRI at different locations (proximal, center, distal). We studied the association of each hemodynamic parameter with the presence cCAPs by logistic regression analysis adjusted for age, sex and wall thickness.
Results: 11 of 49 ICA-stenoses showed a cCAP. No difference of WSS and OSI was detected at the beginning of the stenosis between complicated and stable plaques, while in cCAPs WSS was significantly higher in the stenosis center and distal. In stable plaques, OSI was significantly higher in the stenosis center. Logistic regression analysis revealed a significant association for WSSmean (OR 1.97, 95%-CI 1.14-3.39, p=0.015) and for WSSmax (OR 1.84; 95%-CI 1.10-3.08; p=0.020), but not for WSSmin and OSI with the presence of cCAPs.
Conclusions: Higher wall shear stress was associated with the presence of cCAPs indicating a potential interrelation. Our results provide further evidence for the influence of high WSS in the pathophysiology of cCAPs.
Disclosures of Interest: No
Abstract N°: 2635
TYPES OF INTRACRANIAL CAROTID ARTERIOSCLEROSIS ARE ASSOCIATED WITH STROKE AND VASCULAR DEATH IN PATIENT WITH RENAL IMPAIRMENT
Bo-Ching Lee*1, Tai-Shuan Lai2
1NTUH (National Taiwan University Hospital), Medical Imaging, Taiwan, 2NTUH (National Taiwan University Hospital), Nephrology, Taiwan
On behalf of:
Background and aims: This cohort study aimed to investigate the prevalence of different morphological subtypes of intracranial carotid arteriosclerosis and evaluate their respective impacts on stroke risk in chronic kidney disease (CKD) patients.
Methods: Utilizing data from the National Taiwan University Hospital's pre-end-stage renal disease care database, we enrolled 2,622 CKD patients with available non-contrast brain CT scans (mean age 70.2, 58.4% men) between 2006 and 2020. We classified intracranial carotid calcification into intimal, internal elastic lamina (IEL), and mixed subtypes. Multivariable Cox regression was employed to analyze associations between each subtype, incident stroke, and death.
Results: Among 2,622 patients, 2,470 (94.2%) had calcifications classifiable as intimal (n=719, 27.4%), IEL (n=1,642, 62.6%), or mixed (n=109, 4.2%) subtypes, with the mixed subtype subsequently excluded. Multivariable analysis revealed that both intimal and IEL subtypes were associated with age, diabetes, and renal function (P<0.05). Over a median follow-up of 3.2 years, IEL subtypes exhibited a higher risk of ischemic stroke (adjusted hazard ratio [HR] [95% CI]: 2.1 [1.3-3.4], P=0.003) and vascular death (adjusted HR [95% CI]: 2.0 [1.4-3.0], P<0.001), compared to those without calcification. Furthermore, the IEL subtype displayed a higher risk of ischemic stroke (adjusted HR [95% CI]: 1.5 [1.1-2.1], P=0.021) and vascular death (adjusted HR [95% CI]: 1.6 [1.3-2.1], P<0.001) compared to the intimal subtype.
Conclusions: In CKD patients, calcification of the IEL was the predominant subtype of intracranial arteriosclerosis, associated with age, diabetes, and renal function, and it carried a worse prognosis than those without calcification or with intimal subtype.
Disclosures of Interest: No
Abstract N°: 2667
RELATIONSHIP BETWEEN FIBROBLAST GROWTH FACTOR IN PLASMA AND CAROTID PLAQUE NEOVASCULARIZATION
1University of Oslo (UIO), Institute of Clinical Medicine, Oslo, Norway, 2Oslo University Hospital (OUS) Rikshospitalet, Department of Neurology, Oslo, Norway, 3Oslo University Hospital (OUS) Rikshospitalet, Department of Cardiothoracic Surgery, Oslo, Norway, 4Oslo universitetssykehus HF, Rikshospitalet, Research Institute of Internal Medicine (RIIM), Oslo, Norway, 5Oslo universitetssykehus HF, Rikshospitalet, Section of Clinical Immunology and Infectious Diseases, Norway
On behalf of:
Background and aims: Unstable atherosclerotic carotid plaques with intraplaque neovascularization (IPN) carry a substantial risk for ischemic stroke. Conventional ultrasound methods fall short in detecting IPN, where superb microvascular imaging (SMI) has emerged as a promising tool for both visualizing and quantification. High levels of fibroblast growth factor 23 (FGF-23) have, in observational studies, been suggested as related to cardiovascular morbidity and mortality. The association of FGF -23 to atherosclerotic carotid plaque instability remains relatively unexplored.
Methods: A cohort of twenty-nine patients with ⩾50% atherosclerotic carotid stenosis underwent conventional carotid ultrasound, SMI, and blood tests, including measurement of FGF-23 in plasma. Nineteen patients were characterized as symptomatic and ten as asymptomatic.
Results: Our major findings were: i) Higher FGF-23 levels were strongly correlated with increased SMI-assessed IPN. ii) Neo-vessel count recorded by quantitative SMI was positively correlated to increased FGF-23 levels, but not with FGF-21 and basic FGF levels. (iii) In contrast, traditional risk factors for plaque instability exhibited no noteworthy associations with SMI-assessed IPN or with FGF-23 levels.
Conclusions: This study underscores the potential of FGF-23 as a valuable marker for neovascularization and atherosclerotic carotid plaque instability as a risk factor for ischemic stroke. Further research involving larger cohorts and prospective data is necessary to understand FGF-23's role in this context comprehensively.
Disclosures of Interest: No
Abstract N°: 1683
DISTINCT LIPID PROFILES OF RADIATION-INDUCED CAROTID PLAQUES REVEALED BY UPLC-QTOF-MS AND DESI– MSI
Xiao Zhang*1,2, Liqun Jiao1
1Xuanwu Hospital, Capital Medical University, Department of Neurosurgery, Beijing, China, 2University of Oxford, Sir William Dunn School of Pathology, Oxford, United Kingdom
On behalf of:
Background and aims: Radiotherapy is a standard treatment for head and neck tumors that significantly increases patients’ long-term survival rates. However, late cerebrovascular complications, especially carotid artery stenosis (CAS), have gained increasing attention. Investigation of biomarkers of radiation-induced CAS may help to elucidate the mechanism by which radiation induces damage to blood vessels and identify possible preventive measures against such damage.
Methods: In this study, we used lipidomics strategy to characterize the lipids present in 8 radiation-induced carotid plaques (RICPs) and 12 atherosclerotic carotid plaques (ASCPs). We also used desorption electrospray ionization–mass spectrometry imaging (DESI–MSI) to map the spatial distribution of the screened lipids from 2 RICPs samples and 2 ASCPs samples
Results: The results showed that 31 metabolites in RICPs were significantly higher than that in ASCPs, 24 of which were triglycerides (TGs). We used four machine learning models to select potential indicators from the 31 metabolites. Six TGs [TG(17:2/17:2/18:0), TG(17:1/17:2/18:0), TG(17:0/17:2/18:0), TG (17:2/17:2/20:0), TG(17:1/17:2/20:0), TG(15:0/22:0/22:2)] were found to be the potential markers for distinguishing RICPs and ASCPs (AUC = 0.83). The DESI–MSI results suggested that the 6 TGs were localized in the collagen fiber regions and confirmed the differences of these TGs between the two kinds of plaques.
Conclusions: The 6 TGs primarily localized in the collagen fiber regions of plaques are likely to be potential indicators for the differentiation of RICPs from ASCPs which may have implications in the mechanisms and possible preventive measures against RICPs.
Disclosures of Interest: No
Abstract N°: 2946
CORRELATION OF PLAQUE FEATURES WITH INFARCT PATTERNS IN ATHEROSCLEROTIC CAROTID ARTERY DISEASE
Nour El Houda Sguiar Lhamdani*1, Khattab Hajar1, Kamal Haddouali1, Salma Bellakhdar1, Hicham El Otmani1, Bouchera El Moutawakil1, Mohammed Abdoh Rafai1
1CHU Ibn Rochd, Hassan II University, Neurology and Clinical Physiological Explorations Department, Casablanca, Morocco
On behalf of:
Background and aims: Carotid artery (CA) atherosclerosis is a major cause of ischemic stroke. Certain characteristics of the CA plaque, known as high risk features, have a 3 times higher incidence of ipsilateral ischemic events than stable plaques. Our aim is to explore the relationship between plaque features and ischemic infarction patterns.
Methods: Symptomatic patients with CA atherosclerotic plaques were prospectively recruited. Patients with total CA occlusion were excluded. Infarct patterns were analyzed on diffusion weighted imaging and divided into: cortical (CI), deep perforator (DI), border zone: superficial (SBI) or deep (DBI), territorial (TI) and mixed infarcts. CA Plaques were explored on CT angiography of supra-aortic arteries and their different features and distribution were recorded. Infarct patterns and CA plaque features were compared using the Chi-square test.
Results: 26 patients (62.8 ± 11.9 years, 16 men) were included. CA plaques with low degree of stenosis (less than 50%) often induced CI (41%), while those with high degree of stenosis (more than 70%) were more responsible of CI + SBI (50%). Calcified plaques were more commonly associated with CI (55.6%). Hypodense and ulcerated plaques resulted frequently in CI + SBI (50% and 66.7% respectively). Embolic infarcts were significantly associated with contralateral carotid stenosis (p=0.05).
Conclusions: In this study, high risk CA plaque features including hypodense and ulcerated plaques are more associated with multiple infarcts (CI + SBI). These findings may suggest possible pathophysiological correlations and need to be confirmed by larger-scale studies.
Disclosures of Interest: No
Abstract N°: 98
CAROTID ARTERY STENTING INFLUENCES THE RETINA AND CHOROID
Le Cao*1, Hang Wang1, William Robert Kwapong1, Bo Wu1
1West China Hospital, Sichuan University, Neurology, China
On behalf of:
Background and aims: Carotid artery stenting improved blood flow and perfusion of the ophthalmic artery and cerebral vessels in patients with carotid artery stenosis. We explored the impact of carotid artery stenting on the retina and choroid.
Methods: Patients with unilateral carotid stenosis and underwent stenting were included. Optical coherence tomography (OCT)/ OCT angiography (OCTA) examination was conducted before stenting, 4 days after stenting and 3 months after stenting. The retinal nerve fiber layer (RNFL), ganglion cell-inner plexiform layer (GCIPL), choroidal vascular volume (CVV), Choroidal vascular index (CVI), superficial vascular complex (SVC) and deep vascular complex (DVC) were measured on OCT/OCTA images.
Results: The final analysis included 160 patients with 303 eyes. 4 days after stenting, RNFL thickness increased in overall eyes and contralateral eyes (both p < 0.05). GCIPL thickness decreased in overall eyes, ipsilateral and contralateral eyes (all p < 0.05). A significant increase was seen in SVC density in all eyes and ipsilateral eyes (both p < 0.05) while a significant increase was seen in CVV in overall eyes, ipsilateral eyes and contralateral eyes (all p < 0.05). 3 months after stenting, significant decrease was seen in GCIPL thickness ipsilateral and contralateral eyes (all p < 0.001).
Conclusions: Thicker RNFL and thinner GCIPL, increased SVC density, and increased CVV were shown after stenting. OCT/OCTA measurements may have potential to detect retinal and choroidal changes after stenting. Future research on the long-term effectiveness of stenting on the retina and choroid will be guided by these findings.
Disclosures of Interest: No
Abstract N°: 277
ASSOCIATING INTRACRANIAL ATHEROSCLEROSIS WITH WHITE MATTER DISEASE IN MIDDLE-AGED AND OLDER COMMUNITY-DWELLING ADULTS
1The Hong Kong Polytechnic University, Department of Health Technology and Informatics, HONG KONG, Hong Kong, 2Shanghai General Hospital, Department of Neurology, Shang Hai, China, 3The Second Affiliated Hospital of Guangzhou University of Chinese Medicine, Department of Brain Function, Guang Zhou, China, 4The Hong Kong Polytechnic University, Department of Biomedical Engineering, HONG KONG, Hong Kong
On behalf of:
Background and aims: Intracranial Atherosclerosis (ICAS) is a major cause of ischemic stroke worldwide and shares some common risk factors with white matter disease (WMD). However, the relationship between ICAS and WMD remains unclear. We aimed to investigate the relationship between ICAS identified by high resolution magnetic resonance and white matter hyperintensity (WMH).
Methods: Consecutive 162 participants (mean age, 64.06±6.3; male, n= 77) were recruited. The prevalence, severity, and plaque characteristics (eccentricity, thickening patterns, and surface morphology) identified in middle cerebral artery (MCA), vertebral artery (VA) and basilar artery (BA) were analysed. Multivariate logistic regression analysis was performed to investigate the. associations between ICAS and WMH severity.
Results: A total of 145 lesions were detected in 60% subjects, including MCAs (60/324,), VAs (56/306), and BAs (29/162), respectively. WMH was detected in 94% of subjects, with 54.3% having mild WMH, 37% having moderate WMH, and 2.5% having severe WMH. Subjects with intracranial arterial stenosis had a higher prevalence of moderate to severe WMH (p-value = 0.03). Univariate analysis showed that the severity of WMH correlated with irregular surface (p = 0.047) or diffuse pattern (p = 0.040), respectively. In binary logistic regression found a positive correlation between the severity of WMH and the degree of stenosis (OR 1.94, 95% CI 1.14 – 3.30, p=0.014), irregular plaque surface (OR 2.04, 95% CI 1.00 – 4.16, p=0.049), and diffuse pattern of intracranial atherosclerotic lesions (OR 1.57, 95% 1.07 – 2.31, p= 0.020).
Conclusions: This study investigated the possible correlation between intracranial large artery disease and cerebral small vessel disease.
Disclosures of Interest: No
Abstract N°: 488
ASSOCIATIONS OF ICA BIFURCATION GEOMETRY, MCA GEOMETRY AND PLAQUE LOCATION IN SYMPTOMATIC ATHEROSCLEROTIC MCA STENOSIS
Yu Liu*1, Shuang LI1, Linfang Lan2, Xuan Tian1, Yuying Liu1, Ziqi LI1, Haipeng Liu3, Bonaventure Ym Ip1, Thomas Leung1, Xinyi Leng1
1The Chinese University of Hong Kong, Department of Medicine and Therapeutics, Hong Kong, Hong Kong, 2First Affiliated Hospital of Sun Yat-sen University, Department of Neurology, Guangzhou, China, 3Coventry University, Research Centre for Intelligent Healthcare, Coventry, United Kingdom
On behalf of:
Background and aims: The geometry of terminal internal carotid artery (ICA) bifurcation may affect the geometry of middle cerebral artery (MCA) trunk, and they may jointly influence plaque characteristics in MCA, which was investigated in this study.
Methods: Patients with an ischemic stroke or transient ischemic attack due to atherosclerotic MCA-M1 stenosis were recruited. MCA-M1 were defined as ventrally- or dorsally-oriented in axial images and superiorly- or inferiorly-oriented in coronal images of CT angiography. The plaque location was defined as in the proximal and distal halves of MCA-M1. Geometric characteristics at terminal ICA bifurcation and MCA-M1 were assessed, e.g., diameter of arteries, angles between arteries, and diameter ratio of proximal and distal MCA-M1. Associations of these parameters were analyzed with univariate and multivariate logistic regression.
Results: Among 132 patients (median age 62 years; 70.5% males), a larger diameter of MCA-M1 origin (adjusted odds ratio [aOR]: 9.089, 95% confidential interval [CI]: 1.149-72.035, p=0.036) and a smaller diameter of terminal MCA-M1 (0.078, 0.007-0.838, p=0.035) were associated with dorsally- versus ventrally-oriented MCA-M1, independent of patients’ characteristics. A larger angle between ICA and MCA-M1 (1.025, 1.004-1.046, p=0.022) was independently associated with superiorly- versus inferiorly-oriented MCA-M1. A larger diameter of MCA-M1 origin (9.622, 2.849-32.492, p<0.001) and dorsally-oriented MCA-M1 (11.950, 3.563-40.086, p<0.001) were independently associated with distal versus proximal MCA-M1 plaque.
Conclusions: The geometry of terminal ICA bifurcation may affect MCA trunk orientation, and these two may jointly influence the plaque location in MCA trunk. The findings may help predict atherosclerosis in MCA.
Disclosures of Interest: No
Paper Poster - Cardioembolism & Heart-Brain Interactions
Abstract N°: 2339
BRAIN NATRIURETIC PEPTIDES CORRELATE WITH CEREBRAL BLOOD FLOW IN HEALTHY STUDY POPULATION
Maximilian Schell*1, Marvin Petersen1, Felix Nägele1, Bastian Cheng1, Götz Thomalla1, Tanja Zeller2, Raphael Twerenbold2, Märit Jensen1
1University Medical Center Hamburg-Eppendorf, Department of Neurology, Hamburg, Germany, 2University Medical Center Hamburg-Eppendorf, University Center of Cardiovascular Science, University Heart and Vascular Center Hamburg, Clinic for Cardiology, Hamburg, Germany
On behalf of:
Background and aims: Blood-based cardiac biomarkers of hemodynamic stress (natriuretic peptides, e.g., MR-proANP, NT-proBNP) and myocardial injury (cardiac troponin) are associated with structural brain changes. Alterations in cerebral perfusion resulting from cardiac disease may provide an explanation for this association. To test this hypothesis, we analyzed cardiac biomarkers and perfusion MRI data from 832 participants in the Hamburg City Health Study.
Methods: Cerebral blood flow (CBF) was computed based on arterial spin labeling (ASL) MRI and measured within 400 cortical and 16 subcortical regions, defined by Schaefer and Melbourne Subcortex Atlas, respectively. We employed partial least squares correlation (PLS), enabling to model multivariate relationships within a single statistical model, to relate circulating ardiac biomarkers and regional CBF measures, adjusting for demographic and cardiovascular risk factors.
Results: PLS revealed one significant latent variable (p = 0.036, figure 1A) explaining 90.6% of shared variance between regional CBF and circulating cardiac biomarkers. The latent variable linked lower NT-proBNP as indicated by a negative loading (-0.085, 95%-CI -0.139 – -0.022, figure 1B) to higher CBF in specific cortical and subcortical regions as shown by a positive bootstrap ratio (figure 1C, 1D). MR-proANP and troponin showed no significant association (figure 1B).
Conclusions: Our analysis reveals a principal axis of interindividual variation showing an association of higher NT-proBNP with lower CBF. These findings support the hypothesis that reduced cardiac output, captured by elevated NT-proBNP, is associated with altered cerebral blood flow which may be one of the key mechanisms of long-term structural brain damage in cardiac disease.
Disclosures of Interest: No
Abstract N°: 2895
LONG-TERM OUTCOMES OF PATIENTS ENROLLED IN THE POST-EMBOLIC RHYTHM DETECTION WITH IMPLANTABLE VS EXTERNAL MONITORING (PER-DIEM) TRIAL
Thao Nguyen1, Sona Ohanyan*1, Erik Youngson2, Jillian Stang2, Mahesh Kate1, Bijoy Menon3, Russell Quinn4, Derek Exner4, Michael Hill3, Brian Buck1
1University of Alberta, Division of Neurology, Department of Medicine, Edmonton, Canada, 2Alberta Health Services, Edmonton, Canada, 3University of Calgary, Department of Clinical Neurosciences, Calgary, Canada, 4Libin Cardiovascular Institute, University of Calgary, Calgary, Canada
On behalf of: PERDIEM Study Group: K Butcher, S Gulamhusein, M Siddiqui, S Coutts, T Jeerakathil, EE Smith, K Khan, PA Barber, G Jickling, L Reyes, S Save, P Fairall, L Piquette, N Kamal, DS Chew, AM Demchuk, A Shuaib
Background and aims: Prolonged ECG monitoring with implantable loop recorders (ILR) increases atrial fibrillation (AF) detected after stroke compared to less intensive monitoring strategies. There however remains uncertainty about the clinical significance of low-burden ILR-detected AF. This study uses administrative data to evaluate AF rates and clinical outcomes in PER-DIEM trial participants up to 7 years after enrolment.
Methods: PER-DIEM randomized (1:1) stroke patients without AF to prolonged ECG monitoring for 12 months (ILR) vs 30 days (ELR) between May 2015-Nov 2017. Participants were linked with administrative databases to retrospectively identify encounters to December 2022 with a diagnosis of AF, stroke, MI, systemic embolism, and/or cardiovascular death. Outcomes were compared between groups as randomized using the Kaplan-Meier method and Cox proportional hazards model.
Results: 300 patients were included: median (IQR) age, 64.1years (56.1-73.7); 121(40%) female, median follow-up 69.6 months (42.7-78.8). Beyond 12 months, new AF was diagnosed in 16 ILR patients and 15 ELR patients (Figure1) resulting in an overall AF incidence of 26.0% and 14.7%, respectively (log-rank,p=0.0072). Of the patients with AF, oral anticoagulants were initiated in 95% and 91% in the ILR and ELR group respectively. Recurrent stroke occurred in 18 ILR-assigned patients (12%) and 24 ELR-assigned (16%) patients (Figure 2; HR=0.75;95%CI,0.45-1.3); this and other cardiovascular outcomes were not significantly different between device groups (Table1).
Conclusions: AF rates remained higher in ILR-assigned PER-DIEM participants up to 7 years after enrolment. There were no significant differences between groups in stroke and other clinical outcomes; however, the study was not powered for these endpoints.
Disclosures of Interest: Yes Dr Buck reported nonfinancial support from Medtronic and grants from Alberta Innovates.
Abstract N°: 473
MAPPING THE INTERPLAY OF ATRIAL FIBRILLATION, BRAIN STRUCTURE AND COGNITIVE DYSFUNCTION
Marvin Petersen*1, Céleste Chevalier1, Felix Nägele1, Thies Ingwersen1, Renate Schnabel1, Paulus Kirchhof1, Eckhard Schlemm1, Bastian Cheng1, Götz Thomalla1, Märit Jensen1
1University Medical Center Hamburg-Eppendorf
On behalf of:
Background and aims: Atrial fibrillation (AF) is associated with an elevated risk of cognitive impairment and dementia. The investigation of the cognitive sequelae and alterations of brain structure linked to AF is crucial to help address ensuing health care needs.
Methods: In this study, we conducted a comprehensive neuropsychological and neuroimaging analysis of 1335 stroke-free individuals with AF (30% women, average age 69.1 years) and compared them with 2683 demographically and cardiovascular risk-matched controls (31% women, average age 69.1 years). Primary study outcomes were neuropsychological test scores and advanced magnetic resonance imaging (MRI) measures of gray matter morphology, gray and white matter microstructure, and white matter hyperintensity (WMH) load (figure 1).
Results: Our analysis revealed that individuals with AF exhibited deficits in executive function, processing speed, and reasoning, accompanied by lower cortical thickness, elevated extracellular free-water content, and white matter abnormalities, indicative of small vessel pathology (table 1). Notably, brain structural differences statistically mediated the relationship between AF and cognitive performance (figure 2).
Conclusions: By integrating a multimodal analysis approach with extensive clinical and MRI data, our study highlights small vessel pathology as a possible unifying link between AF, cognitive impairment and abnormal brain structure. These insights can inform diagnostic approaches and motivate the ongoing implementation of effective therapeutic strategies.
Investigated neuroimaging markers.
Mediation analysis.
Disclosures of Interest: Yes PK reports holding patent WO2015140571 on atrial fibrillation therapy, licensed to the University of Birmingham, and patent WO2016012783 on markers for atrial fibrillation, licensed to the University of Birmingham.
Abstract N°: 828
HIGHER STROKE RECURRENCE RISK IN AF KNOWN BEFORE STROKE OCCURRENCE COMPARED TO ECG-DIAGNOSED AF POST-STROKE
Alonso Alvarado Bolanos1, Sebastian Fridman2, Diana Ayan3, Facundo Lodol3, Lauren Mai2, Alexander Khaw2, Lorraine Fleming3, Chrysi Bogiatzi2, Jennifer Mandzia2, Luciano Sposato*2,3
Background and aims: Ischemic stroke (IS) risk in patients with atrial fibrillation (AF) detected post-stroke is not uniform. AF newly-detected on 12-lead ECGs post-stroke has a 5-fold higher IS recurrence risk relative to AF newly captured on 14-day Holter. Given the high IS recurrence risk of ECG-detected AF, we hypothesized that ECG-detected AF has a similar IS recurrence rate to AF known before stroke occurrence (known AF–KAF), which is also generally ECG-detected. We compared IS recurrence risks of ECG-detected and KAF.
Methods: Retrospective observational cohort study of IS/TIA patients with ECG-detected AF and KAF. Cox proportional-hazards models adjusted for event type (IS/TIA), CHA2DS2-VASc score, anticoagulation, dyslipidemia and left atrial volume index (LAVI) were used to calculate adjusted hazard ratios (aHR) for IS recurrence during follow-up (primary outcome). Safety outcomes were major bleeding and all-cause death.
Results: We included 623 patients (IS, 78.8%; TIA 21.2%), 236 with ECG-detected AF and 387 with KAF. IS, dyslipidemia, type 2 diabetes mellitus, heart failure and previous IS were more frequent, and CHA2DS2-VASc score and LAVI were higher in KAF. 77.7% of the cohort received anticoagulants post-stroke/TIA. At 20.0 [3.0-35.0] months of follow-up, KAF was associated with a higher risk of IS recurrence (aHR 2.23: 95% CI 1.09-4.54; p=0.027), with no differences in safety outcomes.
Conclusions: IS recurrence risk was higher in KAF relative to ECG-detected AF, suggesting that a risk gradient exists in IS/TIA patients with AF after an ischemic event, largely influenced by timing of diagnosis, diagnostic modality, and AF burden.
Disclosures of Interest: Yes Speaker honoraria. Medtronic, Pfizer, Boehringer Ingelheim.
Abstract N°: 1010
SMALL VESSEL DISEASE BURDEN IN ISCHAEMIC STROKE PATIENTS WITH CARDIAC DYSFUNCTION. THE PROSPECTIVE SICFAIL COHORT STUDY
Felipe Andrés Montellano*1,2, Christoph Vollmuth2, Marius Vogt3, Kathrin Ungethüm1, Victoria Rücker1, Caroline Morbach4,5, Mirko Pham3, Stefan Störck4,5, Karl Georg Häusler2, Peter Heuschmann1
1Julius-Maximilians-Universität Würzburg, Institute of Clinical Epidemiology and Biometry, Würzburg, Germany, 2University Hospital Würzburg, Department of Neurology, Würzburg, Germany, 3University Hospital Würzburg, Department of Neuroradiology, Würzburg, Germany, 4University Hospital Würzburg, Comprehensive Heart Failure Center, Department of Epidemiology and Clinical Research, Würzburg, Germany, 5University Hospital Würzburg, Department of Internal Medicine I, Würzburg, Germany
On behalf of: SICFAIL study group
Background and aims: Cardiac dysfunction is an independent risk factor for acute ischaemic stroke (AIS) and is associated with poor outcome after AIS. Whether this association is mediated by cerebral small vessel disease (cSVD) is unknown. We investigated whether cSVD burden in patients with AIS differs depending on the presence/absence of cardiac dysfunction
Methods: Data was collected within the Stroke Induced Cardiac FAILure (SICFAIL) study. AIS patients underwent detailed cardiac phenotyping including medical history, clinical examination, brain imaging, blood sampling, and standardized echocardiography by expert sonographers. Systolic and diastolic cardiac dysfunction were defined according to current guidelines. We used the chi-square test to compare the prevalence of white matter hyperintensities (WMH; Fazekas scale ranging from 0-3 with higher scores representing increasing severity) and cerebral microbleeds.
Results: Overall, 459 patients were included: median age 71 years (quartiles 61-71); admission NIHSS score 3 points (1.5-5); 64% men. The prevalence of WMH severity did not differ (p=0.7) among AIS patients with and without systolic dysfunction (Fazekas scale 0:14%/1:38%/2:26%/3:22% vs. 17%/45%/21%/17%). Severe WMH (Fazekas 3) was more prevalent in patients with diastolic dysfunction yet normal systolic function compared to those without (4%/43%21%/32% vs 21%/45%/21%/12%, p<0.001). Microbleeds were more frequent among patients with systolic dysfunction (43% vs. 21%; p=0.012) or diastolic dysfunction (18% vs. 7%; p<0.001) when compared to individuals without the respective cardiac dysfunction.
Conclusions: Considering the detected burden of cSVD among patients with AIS and cardiac dysfunction, future strategies aiming towards improving outcomes in this population should also address cSVD as a contributing factor.
Trial registration number-DRKS00011615
Disclosures of Interest: No
Abstract N°: 1145
BLOOD-BASED BIOMARKERS AS PREDICTORS OF BRAIN ATROPHY IN PATIENTS WITH ATRIAL FIBRILLATION
Ludvig Dahlheim*1, Alexandros Polymeris2, Rebecca Paladini1, Michael Coslovsky1,3, Giorgio Moschovitis4, David Conen5, Stefan Osswald1, Michael Kühne1, Tim Sinnecker2,6, Leo Bonati2,7
1Cardiovascular Research Institute Basel, Departement of Cardiology, University Hospital Basel, Basel, Switzerland, 2Department of Neurology and Stroke Center, University Hospital and University of Basel, Basel, Switzerland, 3Department of Clinical Research, University of Basel and University Hospital Basel, Basel, Switzerland, 4Division of Cardiology, EOC Ospedale Regionale di Lugano, Lugano, Switzerland, 5Population Health Research Institute, McMaster University, Hamilton Ontario, Canada, 6Medical Image Analysis Center Basel AG and Departement of Biomedical Engineering, University of Basel, Basel, Switzerland, 7Research Department, Reha Rheinfelden, Rheinfelden, Switzerland
On behalf of: Swiss-AF Investigators
Background and aims: Atrial fibrillation (AF) is associated with cognitive decline, with brain atrophy considered one possible explanation. We investigated predictors of brain atrophy in patients with AF.
Methods: Patients with history of AF were enrolled in a prospective, multicenter cohort study and underwent brain magnetic resonance imaging (MRI) at baseline and after 2 years. The primary outcome was the percent change in brain volume after 2 years. We investigated neuronal, glial, and cardiovascular serum biomarkers as well as clinical and MRI characteristics as independent predictors (table 1). A stepwise bi-directional selection procedure based on Akaike’s Information Criterion (AIC) was used to identify the model explaining the most variation in brain atrophy.
Results: Overall, 1070 Swiss-AF patients were included (mean age 71.5 years, 73.5% male). Higher serum levels of osteopontin (coefficient -0.7150, 95% CI [-1-0405; -0.3895], figure 1), history of stroke or TIA (coefficient -0.6357, 95% CI [-1.0405; -0.3895]), and lower mean arterial blood pressure (coefficient +0.0175, 95% CI [0.0076; 0.0275], figure 2) were associated with a greater reduction in brain volume. The best model selected based on all measured biomarkers, clinical and MRI characteristics explained only 8.08% of the observed variance in brain volume change.
Conclusions: In AF patients, the association of higher levels of osteopontin and lower mean blood pressure suggest that inflammatory and hemodynamic mechanisms might contribute to brain atrophy. Despite extensive investigations of clinical, blood-based and neuroimaging predictors, the largest proportion of variance in brain atrophy remained unexplained, highlighting that further mechanisms might play a role.
Disclosures of Interest: No
Abstract N°: 1709
ASSOCIATION BETWEEN STROKE LESION SIZE AND ATRIAL FIBRILLATION DETECTED AFTER STROKE - TRACING NEUROGENIC AFDAS
Markus Klammer*1,2,3, Laura Reimann1,2, Oskar Richter1,2, Simone Lieschke1,2, Helena Stengl2,4, Simon Hellwig1,2,4, Kersten Villringer1,2,4, Matthias Endres1,3,4,5,6,7, Christian Nolte1,2,4,7, Jan Scheitz1,2,4,7
1Center for Stroke Research Berlin (CSB), 2Charité Campus Benjamin Franklin, Berlin, Germany, 3Exzellenzcluster NeuroCure, Berlin, Germany, 4Berlin Institute of Health, Berlin, Germany, 5Charité Campus Mitte, Berlin, Germany, 6Deutsches Zentrum für Herz-Kreislauf-Forschung e.V. (DZHK), Berlin, Germany, 7Deutsches Zentrum für Neurodegenerative Erkrankungen e. V. (DZNE), Berlin, Germany
On behalf of:
Background and aims: Atrial Fibrillation Detected After Stroke (AFDAS) is considered to be influenced by cardiogenic and neurogenic factors.
We hypothesized that patients with AFDAS have larger stroke lesions compared to no atrial fibrillation (no AF) and known AF (KAF). We sought to test the association between stroke lesion volume and AFDAS.
Methods: We retrospectively analyzed ischemic stroke patients consecutively admitted to a university hospital between 10/20 and 01/23 with MRI imaging-confirmed stroke. We categorized patients as no AF, KAF or AFDAS at discharge. Stroke lesion volume was determined on MRI using MRIcron.
Results: In total, we analyzed 1425 patients (median age 78, 47.2% female, median NIHSS 3, median hospital stay 5d, median volume 0.94ml). Of these, 138 had AFDAS (9.7%), 273 had KAF (19.1%) and 1014 had no AF (71.1%).
AFDAS patients displayed a significantly larger stroke lesion volume (median 5.3ml [IQR 1.0-22.0]) compared to no AF and KAF patients (median 0.7 [0.2-4.4] and 1.5 [0.2-8.8] ml, respectively, both p < 0.001).
Lesion volume was independently associated with AFDAS compared to no AF (aOR 1.4, 95%CI 1.2-1.5, per log ml) and KAF (aOR 1.3, 95%CI 1.2-1.4, per log ml).
This association remained stable when excluding 56 patients with AFDAS diagnosed immediately on admission ECG (median 5.3ml) and when excluding 196 KAF patients already on oral anticoagulation (median 1.26ml).
Conclusions: Larger stroke lesions were independently associated with AFDAS diagnosis during index stroke hospitalization highlighting the intricate heart-brain relationship and supporting further exploration of stroke characteristics to comprehensively grasp AFDAS pathogenesis.
Disclosures of Interest: No
Abstract N°: 2157
ATRIAL FIBRILLATION DETECTION ACROSS DURATIONS OF CARDIAC MONITORING AFTER STROKE: A SYSTEMATIC REVIEW AND META-ANALYSIS
Alan Cameron*1, Elizabeth Guilbert1, Georgios Katsas1, Terence J Quinn1, Jesse Dawson1
1University of Glasgow, School of Cardiovascular and Metabolic Health, United Kingdom
On behalf of:
Background and aims: Prolonged cardiac monitoring increases atrial fibrillation (AF) detection after stroke but the optimal monitoring duration is undefined. We explored AF detection rates across durations of cardiac monitoring after stroke.
Methods: We performed a systematic review and meta-analysis. We searched electronic databases for randomised controlled trials (RCTs) and prospective cohort studies of cardiac monitoring after ischaemic stroke or TIA from 2010-2022. The outcome was AF ⩾30 seconds. A network meta-analysis with random effects model compared AF detection across cardiac monitoring durations (⩽7 days versus 7-14 days, 28-30 days or ⩾1 year). Risk of bias was assessed using the Cochrane Risk of Bias Tool (RCTs) or Newcastle-Ottawa Scale (cohort studies).
Results: We identified 5129 studies and nine were included (8 RCTS and 1 cohort study). The studies included 6305 participants and 6.5% (n=409) were found to have AF (95%CI 5.9%-7.1%). The AF detection rates for ⩽ 7 days, 7-14 days, 28-30 days and ⩾1 year of monitoring were 4.20% (145/3456), 6.50% (128/1979), 11.75% (74/630) and 18.96% (106/559) respectively.
Compared to ⩽7 days monitoring, the relative risk of AF detection was 2.50 (95%CI 0.97-6.41) for 7-14 days, 2.96 (1.32-6.63) for 28-30 days and 5.50 (2.64-11.49) for ⩾1 year’s monitoring.
Risk of bias assessment identified some concerns for seven RCTs, high risk of bias for one RCT and good quality for one cohort study.
Conclusions: Our findings demonstrate that more than 7 days cardiac monitoring gives a higher AF detection rate, with incrementally higher AF detection across the duration strata.
Disclosures of Interest: Yes Research grants from Pfizer and honoraria from BMS, Pfizer, AstraZeneca and Boeheringer Ingelheim.
Abstract N°: 2334
CORONARY ANGIOGRAPHY FINDINGS IN ACUTE ISCHAEMIC STROKE PATIENTS WITH MYOCARDIAL INJURY – RESULTS OF THE PRAISE STUDY
Regina von Rennenberg*1,2,3, Simon Litmeier1,2, Ulf Landmesser4,5, Christian Nolte1,2,5,6, Matthias Endres1,2,3,5,6,7
1Charité-Universitätsmedizin Berlin, Department of Neurology with Experimental Neurology, Berlin, Germany, 2Center for Stroke Research Berlin (CSB), Berlin, Germany, 3German Center for Neurodegenerative Diseases (DZNE), Partner Site Berlin, Berlin, Germany, 4Charité-Universitätsmedizin Berlin, Department of Cardiology, Berlin, Germany, 5German Centre for Cardiovascular Research (DZHK), Partner Site Berlin, Berlin, Germany, 6Berlin Institute of Health (BiH), Berlin, Germany, 7Excellence Cluster NeuroCure, Berlin, Germany
On behalf of: the PRAISE investigators
Background and aims: Myocardial injury is common in acute ischaemic stroke patients and may be caused by myocardial infarction (MI). However, the selection of stroke patients for coronary angiography remains challenging.
Methods: The multi-centre, prospective observational PRAISE study included acute ischaemic stroke patients with hs-cTn elevation that met ESC rule-in criteria for suspected MI. Patients underwent standardised coronary angiography and echocardiography. Images were assessed by blinded core laboratories. Patients were diagnosed with type 1, type 2 or no MI by an independent endpoint committee. We performed multivariable logistic regression analyses to identify patient characteristics associated with (1) presence of coronary stenoses (CS), (2) CS severity (percentage of visual diameter reduction), (3) presence of multivessel coronary artery disease (CAD) (affecting >1 vessel).
Results: Of 247 patients included, 131 (53%) had at least one CS. Multivessel CAD was present in 61 (25%) patients. CS were found in 50/50 (100%) patients with type 1 MI and 67/76 (88.2%) with type 2 MI (χ2 p=0.012). Patients with type 1 and type 2 MI did not differ regarding the presence of multivessel CAD or CS severity. Variables independently associated with CS severity were regional wall motion abnormalities (RWMA) on echocardiography (aOR 3.4, 95%CI 1.6-7.3) and higher GRACE scores (aOR 1.1, 95%CI 1.0-1.1). RWMA were independently associated with presence of CS per se (aOR 6.2, 95%CI 2.0-19.1).
Conclusions: CAD and MI are common mechanisms of myocardial injury in ischaemic stroke patients. Echocardiography and the GRACE score may be helpful to select stroke patients for coronary angiography.
Disclosures of Interest: No
Abstract N°: 2395
HISTOLOGY OF PFO-ASSOCIATED STROKE THROMBUS COMPARED TO DEEP VEIN THROMBUS
Maikel Immens*1, Mathijs Stam2, Diederik Dippel2, Geert Lycklama À Nijeholt3, H. Bart van der Worp4, Sjoerd Jenniskens5, Frank-Erik De Leeuw1, Tim Ten Cate6, Heleen M. M. van Beusekom2, Anil Tuladhar1
1Radboud University Medical Center, Neurology, Nijmegen, Netherlands, 2Erasmus MC, Rotterdam, Netherlands, 3HMC Westeinde, Den Haag, Netherlands, 4UMC Utrecht, Utrecht, Netherlands, 5Radboud University Medical Center, Radiology, Nijmegen, Netherlands, 6Radboud University Medical Center, Cardiology, Nijmegen, Netherlands
On behalf of:
Background and aims: A thrombo-embolism travelling through a patent foramen ovale (PFO) is recognized as a potential cause of stroke. It is generally thought that the thrombus originates from the venous circulation. Its histological composition might help to identify its origin. The aim of the study is to characterize the histological composition of thrombi of patients with probable PFO-associated stroke and compare this to venous thrombi from patients with deep venous thrombosis (DVT).
Methods: We included patients with a diagnosis of probable PFO-associated stroke from whom a thrombus was available for histological analyses and patients with symptomatic DVT. Thrombi were fixed, photographed and stored in 4% buffered formaldehyde prior to paraffin embedding. Samples were stained with hematoxylin-eosin as a routine stain and digitized. Digitized images were histologically analyzed using a machine-learning algorithm.
Results: We included three patients with probable PFO-associated stroke (18-55 years), one patient with possible PFO-associated stroke and four patients with DVT. The thrombi of patients with probable PFO-associated stroke contained less red blood cells (RBC) and more fibrine/platelets (F/P) than those with DVT (30.2% vs 91.3% RBC and 67.4% vs 8.5% F/P, p<0.001). The PFO-associated stroke thrombi were similar to thrombi from the MR CLEAN Registry classified as cardioembolic (RBC 25.8% and 67.1% F/B).
Conclusions: The composition of thrombi from patients with probable PFO-associated stroke differs from those with DVT, but is similar to thrombi with a cardioembolic origin. This suggests that the thrombus in patients with PFO-associated stroke might not have originated from the venous circulation in our study population.
Disclosures of Interest: No
Abstract N°: 2586
IMPACT OF GUIDELINE MODIFICATIONS ON PATENT FORAMEN OVALE DIAGNOSIS IN YOUNG PATIENTS WITH ISCHEMIC STROKE IN CATALONIA
EVA GIRALT STEINHAUER*1, Angel Ois1, Elisa Cuadrado-Godia1, Ana Rodriguez-Campello1, Isabel Fernández-Pérez1, Daniel Guisado-Alonso1, Adrià Macias-Gómez1, Antoni Suárez-Pérez1, Jordi Jimenez Conde1, Joan Jiménez-Balado1
1Hospital del Mar, Neurovascular, Barcelona, Spain
On behalf of:
Background and aims: Patent foramen ovale (PFO) is frequently identified in young patients with ischemic stroke (IS), and current ESO guidelines recommend an early detection and closure in patients under 60. Our hypothesis is that revised European guidelines in 2018 has resulted in greater detection of PFO. Besides, we also aim to analyze differences regarding risk of recurrence and mortality among patients with or without PFO diagnosis.
Methods: We conducted a population-based, retrospective cohort study in Catalonia, Spain, using linked health administration databases. We included all IS patients aged 18-60 from 2016 to 2021, registered in the Catalan Service of Epidemiological Surveillance, collecting demographics, comorbidities, stroke recurrence, and mortality.
Results: A total of 13,780 individuals under the age of 60 suffered an IS, representing an average annual rate of 52 cases per 100,000 inhabitants. PFO was detected in 749 (5.4%), and these patients were younger, and had a lower prevalence of male sex and risk factors than patients without PFO (all p-value<0.001, figure-1). When we compared the proportion of strokes with PFO before and after guideline updates, we observed an increase across all age groups (all p-value<0.001, figure-2). Incidence of recurrent stroke after 5 years follow-up was 13% (95%CI: 12.3-13.8%), with no differences between patients with and without PFO. However, all-cause mortality was found to be higher in patients without PFO (p-value<0.001, figure-3).
Conclusions: There is a greater detection of PFO after the update of clinical guidelines. Besides, we found a lower global mortality in young stroke patients with PFO.
Disclosures of Interest: No
Abstract N°: 2598
LEFT ATRIAL APPENDAGE OCCLUSION IN STROKE PREVENTION IN ATRIAL FIBRILLATION
Sandra Elsheikh1,2,3, Muath Alobaida1,2,4, Tommaso Bucci1,5, Benjamin J.R Buckley1,6, Dhiraj Gupta1, Greg Irving3,7, Andrew Hill1,3, Gregory Lip1,2,8, Azmil Abdul-Rahim*1,2,3
1Liverpool Centre for Cardiovascular Science at University of Liverpool, Liverpool John Moores University and Liverpool Heart & Chest Hospital, Liverpool, United Kingdom (UK), 2Cardiovascular and Metabolic Medicine, Institute of Life Course and Medical Sciences, Faculty of Health and Life Sciences, University of Liverpool, Liverpool, UK, 3Mersey and West Lancashire Teaching Hospitals NHS Trust, St Helens, UK, 4Department of Basic Science, Prince Sultan Bin Abdulaziz College for Emergency Medical Services, King Saud University, Riyadh, Saudi Arabia, 5Department of General and Specialised Surgery, Sapienza University of Rome, Italy, 6Cardiovascular Health Sciences, Research Institute for Sport and Exercise Sciences, Liverpool John Moores University, Liverpool, UK, 7Health Research Institute, Edge Hill University, Ormskirk, UK, 8Danish Center for Clinical Health Services Research, Department of Clinical Medicine, Aalborg University, Aalborg, Denmark
On behalf of:
Background and aims: Existing randomised controlled trials assessing the safety and efficacy of left atrial appendage occlusion (LAAO) in atrial fibrillation (AF) were of relatively small sample size, or included patients who could receive oral anticoagulant treatment after device implantation. We compared the outcomes of patients with newly diagnosed AF who received percutaneous LAAO or direct oral anticoagulants (DOAC) treatment, in a large population from a global federated health network (TriNetX).
Methods: Patients with AF treated with percutaneous LAAO were matched with those treated with DOAC between 1st December 2010 and 1st October 2018. Outcomes were all-cause mortality, ischaemic stroke and intracranial haemorrhage (ICH) at 5 years.
Results: We included 200 patients with AF, who received either LAAO or DOAC. The risk of all-cause mortality, ischaemic stroke and ICH at 5 years was not significantly different between the two groups (Risk Ratio [RR] for all-cause mortality: 1.52, 95% confidence interval (CI): 0.97- 2.38, RR for ischaemic stroke: 1.09, 95% CI: 0.51- 2.36, and RR for ICH: 1.0, 95% CI: 0.44- 2.30).
Conclusions: Patients newly diagnosed with AF, eligible for DOAC, showed similar 5-year risk of death, ischaemic stroke, and ICH when comparing those who underwent percutaneous LAAO to those receiving DOAC. Future randomised controlled trials are needed to confirm the findings and advise changes in guidelines.
Disclosures of Interest: Yes Buckley: received research funding from Bristol-Myers Squibb /Pfizer. Gupta: received proctor fees from Abbott for LAAO implants. Lip: Consultant and speaker for BMS/Pfizer, Boehringer Ingelheim, Daiichi-Sankyo, Anthos + co-P.I. of AFFIRMO project.
Abstract N°: 2744
NEUROANATOMIC CORRELATES OF NEWLY DETECTED ATRIAL FIBRILLATION AFTER STROKE
Petr Mikulenka*1, Olivia Murray2,3, Alistair Perry2, James Garrard2,4, George Harston2,5, Michal Mihalovič6, Petr Toušek6, Ivana Štětkářová1, Davide Carone2,4,5
1Department of Neurology, University Hospital Kralovske Vinohrady, Third Faculty of Medicine, Charles University, Prague, Czechia, 2Brainomix, Oxford, UK, 3Division of Informatics, Imaging and Data Science, University of Manchester, Manchester, United Kingdom, 4Radcliffe Department of Medicine, University of Oxford, UK, 5Oxford University Hospitals NHSFT, UK, 6Department of Cardiology, University Hospital Kralovske Vinohrady, Third Faculty of Medicine, Charles University, Prague, Czechia
On behalf of:
Background and aims: Atrial fibrillation is newly detected in up to 20% of patients after stroke. Current evidence suggests AF detected after stroke (AFDAS) might differ from AF that was known before the diagnosis of stroke in both clinical significance and pathophysiology. Previous studies have shown that AFDAS might be precipitated by stroke lesion location within the central autonomic network, but the data are scarce. In this study, we aim to identify neuroanatomical correlates of AFDAS.
Methods: Patients enrolled in a single-centre observational cohort study were screened for AFDAS . Stroke lesions were automatically segmented on follow-up scans (MRI or CT) using Brainomix inhouse-software, and were used to define areas directly injured, and to generate disconnection maps via a DTI template. A voxel-based, multivariate method (Sparse-Canonical-Correlation-Analysis) was used to explore associations between AFDAS and a) areas directly damaged by stroke and b) areas disconnected.
Results: 250 patients were included in the study. 42 had a newly diagnosed AF. No significant association was found between stroke lesion location and AF when only taking in account areas directly damaged. When using disconnection maps, stroke lesion causing disconnection to the hypothalamus, brainstem and cerebellum were significantly associated to AFDAS (p=0.004).
Conclusions: The results from the study suggest an association between lesions causing disconnection to the hypothalamus brainstem and cerebellum, key areas of the central autonomic system, and AFDAS. Incorporating information on disconnection can help better understanding how stroke can affect the autonomic system and might help in differentiating between cardiogenic or neurogenic AF.
Disclosures of Interest: No
Abstract N°: 692
TRIGGERS OF MYOCARDIAL DEMAND ISCHEMIA IN PATIENTS WITH POST-STROKE ACUTE MYOCARDIAL INJURY
Helena Stengl*1,2,3, Sophie Böhme1,2, Markus Klammer1,2,4, Simon Hellwig1,2,3, Oskar Richter1, Regina von Rennenberg1,2,5, Christian Nolte1,2,3,6, Matthias Endres1,2,3,4,5,6, Jan Scheitz1,2,3,6
1Charité Universitätsmedizin Berlin, Department of Neurology, Berlin, Germany, 2Center for Stroke Research Berlin (CSB), Berlin, Germany, 3Berlin Institute of Health (BIH) at Charité – Universitätsmedizin Berlin, Berlin, Germany, 4Excellence Cluster NeuroCure, Charité – Universitätsmedizin Berlin, Berlin, Germany, 5German Center for Neurodegenerative Diseases (DZNE), Partner Site Berlin, Berlin, Germany, 6German Center for Cardiovascular Research (DZHK), Partner Site Berlin, Berlin, Germany
On behalf of:
Background and aims: Acute myocardial injury in the early phase of ischemic stroke is associated with greater disability and higher mortality. Conditions triggering myocardial oxygen demand-supply mismatch, as in type 2 myocardial infarction (MI), may play a relevant role in developing post-stroke acute myocardial injury. However, little is known about triggering factors of myocardial demand ischemia in acute ischemic stroke.
Methods: Acute ischemic stroke patients with acute myocardial injury (defined as elevated high-sensitivity cardiac troponin-T and a rise or fall >20% in serial measurements) were included consecutively from 01.2019 to 12.2020. They were matched by age and sex with stroke patients without acute myocardial injury. Medical records were retrospectively screened for presence of predefined triggers of myocardial demand ischemia.
Results: Of the 508 patients included (mean age 79.4 ± 9.3 years, 52% female), 107 (42%) patients with acute myocardial injury and 61 (24%) of control patients had a predefined trigger of possible myocardial demand ischemia (Figure 1). Patients with a trigger were more likely to be female, had a higher stroke severity on admission (median NIHSS 6 [2-15] vs. 3 [2-8]), more often had insular cortex involvement and large vessel occlusion (all p<0.05). The presence of a trigger was associated with in-hospital mortality (aOR:2.81, 95%CI:1.32-5.98) and unfavorable shift in modified Rankin Scale at discharge (aOR:2.15, 95%CI:1.22-3.78).
Conclusions: Conditions triggering myocardial demand ischemia are common in patients with acute myocardial injury after stroke and are associated with higher stroke severity and worse outcomes. These findings highlight the need for clinical awareness and treatment of respective conditions.
Disclosures of Interest: No
Abstract N°: 1384
QUANTIFYING LEFT ATRIAL APPENDAGE MORPHOLOGICAL CHARACTERISTICS IN ACUTE ISCHEMIC STROKE PATIENTS
Nerea Arrarte Terreros*1,2, Marta Saiz-Vivó3, Daphne Onderwater1,2, Kim Lan Kwa1,2, Shan Sui Nio4, Leon Rinkel4, Jonathan Coutinho4, R. Nils Planken2, Oscar Camara3, Henk Marquering1,2
1Amsterdam UMC, location UvA, Biomedical Engineering and Physics, Amsterdam, Netherlands, 2Amsterdam UMC, location UvA, Radiology and Nuclear Medicine, Amsterdam, Netherlands, 3Universitat Pompeu Fabra, Information and Communication Technologies, Barcelona, Spain, 4Amsterdam UMC, location UvA, Neurology, Amsterdam, Netherlands
On behalf of:
Background and aims: Cardiac thrombi can be detected by the visual assessment of contrast-filling defects in contrast-enhanced computed tomography (CT) images. Such thrombi, commonly found in the left atrial appendage (LAA), can be dislodged and cause an acute ischemic stroke (AIS). Morphological characteristics of the LAA, such as tortuosity or volume, might be markers of thrombus formation risk. We compare LAA morphological characteristics among AIS patients with(out) LAA contrast-filling defects.
Methods: We included AIS patients from the Mind-the-Heart study with available cardiac CTs. LAA contrast-filling defects were visually assessed by experienced cardio-radiologists and, accordingly, classified as normal LAA-flow (no contrast-filling defects), slow LAA-flow (contrast-filling defects above 100HU), or LAA-thrombus (contrast-filling defects below 100HU). Semi-automatic segmentation of the left atrium (LA), including the LAA, was performed using 3D-Slicer (Figure 1). Based on the segmentations, we computed LAA morphological characteristics (including volume, area, tortuosity, and minimum and maximum ostium diameters) and compared them between the contrast-filling defect groups.
Results: We included 69 patients: 30 with normal LAA-flow, 20 with slow LAA-flow, and 19 with LAA-thrombus. There were no significant differences in history of atrial fibrillation (AF) nor anticoagulant usage among the groups, but LAA-thrombus patients more often had AF diagnosed at admission. LAA-thrombus patients had larger LA and LAA volumes, more tortuous LAA, and larger ostium diameters compared to patients with slow and normal flow (Figure 2). LAA-thrombus patients had worse functional outcomes.
Conclusions: Larger ostium, more tortuous LAAs are characteristic of AIS patients with LAA contrast-filling defects. Our study suggests that LAA morphological characteristics influence thrombus formation.
Disclosures of Interest: Yes Cofounder of inSteps, spin-off of the Amsterdam UMC dedicated to in-silico modeling for stroke treatments
Abstract N°: 324
CLINICAL DETERMINANTS AND BIOMARKERS FOR RECURRENT STROKE IN ATRIAL FIBRILLATION: A SYSTEMATIC REVIEW AND META-ANALYSIS
Yuen Cheung*1, Marianne Foley1, Simon Cronin2, Isuru Induruwa3, Mira Katan4, Kayvan Khadjooi3, Margaret O'connor5, Annaelle Zietz4, Peter Kelly6,7, John Mccabe1,6,7
1Mater Misericordiae University Hospital, Stroke Service, Neurology, Dublin, Ireland, 2University College Cork, Department of Neurology, Cork, Ireland, 3University of Cambridge, Department of Clinical Neurosciences, Cambridge, United Kingdom, 4University Hospital Basel, Department of Neurology and Stroke Center, Basel, Switzerland, 5University Hospital Limerick, Stroke Service, Medicine for the Older Person, 6University College Dublin (UCD), School of Medicine, Dublin, Ireland, 7Stroke Clinical Trials Network Ireland, Dublin, Ireland
On behalf of: Dr David Bradley, Dr Tim Cassidy, Prof. Ronan Collins, Dr Eamon Dolan, Dr Sarah Gorey, Dr John Keaney, Prof Martin O’Donnell, Dr Padraig Synott, Prof. David Williams
Background and aims: Anticoagulation reduces recurrent stroke in atrial fibrillation (AF), but a residual risk of 3.5-6.5%/year persists. Therefore, existing secondary prevention strategies are sub-optimal. There is a need for improved risk prediction tools to identify patients at greatest risk and to find new therapeutic targets for secondary-prevention in AF.
Methods: We did a systematic review of studies which investigated clinical factors and echocardiographic, blood, and neuroimaging biomarkers for recurrent stroke in patients with AF-related incident stroke. Studies were included irrespective of anticoagulation use. Risk ratios (RRs) were pooled using random effects.
Results: Of 5427 records searched, 35 reports including 50,470 patients were identified. Age (RR 1.01 [95% CI] [1.00-1.02]), hyperlipidaemia (RR 1.35, [1.08-1.69]), CHA2DS2Vasc (RR 1.22, [1.15-1.30]), qualifying stroke despite anticoagulation (RR 1.56, [1.21-2.02]), CKD (RR 1.86,[1.19-2.92]), malignancy (RR 4.36, [1.85-10.78]), known AF prior to stroke (vs. AF detected after stroke) (RR 1.38, [1.10-1.71]) and NIHSS (RR 0.97,[0.95-0.99]) were associated with stroke recurrence (Figure.1). Neuroimaging markers for recurrence included chronic lacunar infarcts (RR 1.91, [1.29-2.84]), embolic-appearing infarcts (RR 2.76,[1.32-5.77]), and microbleeds (RR 1.29,[1.04-1.59]). Echocardiographic and blood markers included atrial size (RR 1.60,[1.30-1.98]), intra-cardiac thrombus (RR 1.99,[1.38-2.87]), appendage spontaneous echocardiographic contrast (RR 2.91,[1.21-6.17]) or intensity variation (RR 2.81,[1.48-5.32), BNP >300pg/ml (RR 9.2, [1.87-45.01]) and free fatty acids (RR 1.85, [1.15-2.97])(Figure.2).
Conclusions: Several clinical factors were associated with recurrence after AF-related stroke. Biomarkers of atrial cardiopathy, small vessel disease, or prior infarction may also be important prognostic factors. Collaborative efforts are needed to identify and validate new risk factors and biomarkers for recurrent stroke in AF.
Disclosures of Interest: No
Abstract N°: 1442
MULTIVARIATE RELATIONSHIP BETWEEN CIRCULATING CARDIAC BIOMARKERS AND BRAIN FREE-WATER IN A LARGE CROSS-SECTIONAL COHORT STUDY
Felix Nägele*1, Marvin Petersen1, Maximilian Schell1, Bastian Cheng1, Raphael Twerenbold2, Tanja Zeller2, Götz Thomalla1, Märit Jensen1
1University Medical Center Hamburg-Eppendorf, Department of Neurology, Hamburg, Germany, 2University Medical Center Hamburg-Eppendorf, University Center of Cardiovascular Science, University Heart and Vascular Center Hamburg, Hamburg, Germany
On behalf of:
Background and aims: While different studies have demonstrated a relationship between cardiac dysfunction and an increased risk for cognitive decline, the pathophysiology of neurocardial interactions remains elusive. To this end, we studied multivariate associations of circulating cardiac biomarkers, regional brain free-water indicative of microstructural aberrations, and cognitive functioning in 2428 participants from the Hamburg City Health Study.
Methods: We examined data from 2428 community dwelling participants (44% female, mean age: 64 years). Extracellular free-water was derived from diffusion magnetic resonance imaging for 400 cortical, 16 subcortical and 64 white matter regions of interest. After adjusting for cardiovascular risk factors and sociodemographic variables, multivariate relationships between NT-proBNP, MR-proANP, as well as hs-Troponin I, and regional changes in brain free-water were assessed with a partial least squares correlation analysis (PLS). The resulting brain imaging signature was related to different domains of cognitive functioning using linear regression.
Results: The PLS identified one significant latent variable (96.04% explained covariance, Figure 1a) relating higher levels of cardiac biomarkers (Figure 1b) to widespread increases of free-water encompassing fronto-parietal, occipital and temporal regions, subcortical structures and all major white matter tracts (Figure 1d). Imaging scores representing the adherence to this covariance pattern were significantly related to verbal fluency and executive functioning, but not to visuoconstruction or memory (Figure 2).
Conclusions: We identified a single neurocardial dimension explaining most of the covariance between circulating cardiac biomarkers and regional brain free-water. The identified pattern of microstructural changes was associated with performance in different cognitive domains, indicating a potential pathophysiological link between cognitive and cardiac functioning.
Disclosures of Interest: No
Abstract N°: 1623
BRAIN NATRIURETIC PEPTIDE AND ECHOCARDIOGRAPHIC PARAMETERS AS PREDICTORS OF CARDIOEMBOLISM: DATA FROM A LARGE RETROSPECTIVE STUDY
Giovanna De Marco1, Stefano Forlivesi1, Letizia Riva2, Maria Maddalena Viola1, Matteo Paolucci1, Luana Gentile1, Mauro Gentile1, Gianni Casella2, Rita Mancini3, Andrea Zini1
Background and aims: Brain Natriuretic Peptide (BNP) is a widely recognized cardiological biomarker and has recently been investigated in acute ischemic stroke (AIS), emerging as a potential predictor of cardioembolism. We aimed to evaluate the role of BNP and echocardiographic parameters for the prediction of cardioembolic etiology in a large cohort of AIS patients.
Methods: We retrospectively included 2337 consecutive patients admitted for AIS to the Stroke Unit at the Maggiore Hospital (Bologna, Italy) from January 2018 to May 2023. Blood BNP levels were measured within 48 hours from symptom onset. A specific BNP cut-off of 100 pg/ml, commonly employed to exclude congestive cardiac insufficiency, was chosen to classify patients into high and low BNP levels. Clinical and echocardiographic variables were evaluated. Stroke etiology was defined according to the TOAST criteria.
Results: We identified 734 (31.4%) patients with cardioembolic stroke. In the multivariable analysis, high BNP levels (Odds Ratio [OR] 5.10, 95% CI 3.69-7.05, p <0.001), left atrium enlargement (OR 2.37, 95% CI 1.77-3.16, p <0.001), pulmonary arterial hypertension (OR 2.17, 95% CI 1.16-4.04, p = 0.015), left ventricle systolic dysfunction (OR 1.57, 95% CI 1.17-2.12, p=0.002), and higher NIHSS score at admission (OR 1.06, 95% CI 1.04-1.06, p <0.001) were independent predictors of cardioembolic etiology. The BNP cut-off demonstrated a sensitivity and specificity for cardioembolism of 91% and 49% respectively.
Conclusions: BNP levels ⩾100 pg/ml < 48 hours from AIS onset, left atrium enlargement, pulmonary hypertension, and left ventricle systolic dysfunction may be useful biomarkers to predict cardioembolic etiology.
Disclosures of Interest: No
Abstract N°: 2957
POST-TRANSCATHETER AORTIC VALVE IMPLANTATION STROKE: A RETROSPECTIVE ANALYSIS OF RISK FACTORS, CHARACTERISTICS AND CLINICAL OUTCOMES
Eduardo Mariño*1, Guilermo Galeote2, Gerardo Ruiz-Ares1, Carlos Hervás Testal1, Elena de Celis Ruiz1, Raul Moreno2, Santiago Jimenez2, Alfonso Jurado2, Blanca Fuentes1, Ricardo Rigual1
1Department of Neurology and Stroke Center. Hospital La Paz Institute for Health Research-IdiPAZ (La Paz University Hospital-Universidad Autónoma de Madrid), Madrid, Spain, Neurology Department, Madrid, Spain, 2Interventional Cardiology Section, Department of Cardiology. Hospital La Paz Institute for Health Research-IdiPAZ (La Paz University Hospital-Universidad Autónoma de Madrid), Madrid, Spain, Department of cardiology, Madrid, Spain
On behalf of:
Background and aims: Despite advancements in transcatheter aortic valve implantation (TAVI), stroke rates post-procedure has remained consistent. This study aims to explore the incidence, underlying risk factors, acute management stroke received and prognosis of stroke post-TAVI.
Methods: Retrospective, observational study of patients hospitalized with recent stroke post-TAVI between January 2018 and December 2023. We described epidemiologic, clinical, surgical history and outcomes (mortality and modified Rankin scale -mRS-). Additionally, we compared these patients with an historic cohort of 247 patients treated with TAVI not complicated with ischemic stroke (2021-2022).
Results: In the period analyzed, 20 of 660 (3%) patients treated by TAVI suffered a post-procedure ischemic stroke. 12/20 (60%) were woman, median age 80 (IQR 72-88) years. The initial NIHHS median was 7 (IQR 2-19), 15/20 (75%) occurred within the first 4.5 hours after TAVI, large vessel occlusion was described in 7/20 (30%) and 5/20 (25%) were treated by mechanical thrombectomy. At 90-day follow-up 65% presented mRS of 0-2 points and the mortality rate was 21.1%.
Compared to non-stroke TAVI patients, patients with stroke were treated less frequently with balloon valvuloplasty during the procedure (52.6% vs 78.2% p=0.012) and they presented a higher 90-days mortality rate (21.1% vs 1.7%, p=0.001).
Conclusions: In our study, stroke occurred predominantly in the first hours after procedure and 25% of them could be treated with reperfusion therapy. The use of undergoing balloon valvuloplasty may reduce the stroke risk. The high mortality associated with post-TAVI strokes emphasize the need for improved risk stratification and acute management strategies.
Disclosures of Interest: No
Abstract N°: 1288
THE PROGNOSTIC ROLE OF ECHOCARDIOGRAPHIC PARAMETERS IN STORKE PATIENTS WITH ATRIAL FIBRILLATION
Annaelle Zietz*1,2, Alexandros Polymeris1, Beat Kaufmann3, Sabine Schädelin4, Josefin E. Kaufmann1,2, Mira Katan1,5, Urs Fischer1, Philippe Lyrer1, Stefan Engelter1,2, Nils Peters1,2,6
1University Hospital Basel and University of Basel, Department of Neurology and Stroke Center, 2University Department of Geriatric Medicine Felix Platter, University of Basel, Neurology and Neurorehabilitation, 3University Hospital Basel, University of Basel, Department of Cardiology and Cardiovascular Research Institute Basel (CRIB), 4University Hospital Basel, University of Basel, Clinical Trial Unit, Department of Clinical Research, 5University Hospital Zurich, Department for Neurology, 6Klinik Hirslanden, Stroke Center
On behalf of: NOACISP-Investigators
Background and aims: Data on the prognostic importance of functional and structural echocardiographic parameters and their association with cerebral small vessel disease (cSVD) markers in patients with atrial fibrillation (AF) and recent ischemic stroke are scarce.
Methods: We included consecutive AF-associated stroke patients with a recent echocardiogram from the prospective Novel Oral Anticoagulants in Ischemic Stroke Patients (NOACISP) registry. We investigated the association between echocardiographic parameters of the left atrium and ventricle and the composite outcome compromising (i) recurrent ischemic stroke; (ii) intracranial hemorrhage and (iii) all-cause death using unadjusted and adjusted (for age, sex, modified CHA2DS2VASc-Score, hyperlipidemia) Cox proportional hazards regressions. Furthermore, in patients with available MRI we explored the association between echocardiographic parameters and neuroimaging markers of cSVD using logistic regressions
Results: We included 826 AF-associated stroke patients (median age 80, 45.8% female) with a total follow-up of 1295 patient-years. In unadjusted analyses, left ventricular hypertrophy (HR [95 %CI] 1.37 [1.02-1.83], p=0.03) was associated with a higher hazard ratio for the composite outcome, albeit missing statistical significance after adjustment (aHR 1.09 [0.81-1.48], p=0.55). Left atrial dilatation (OR 1.86 [1.26-2.73], p=0.002) and concentric hypertrophy were associated (OR 1.57 [1.01-2.43], p=0.04) with the extent of white matter hyperintensities and left ventricular mass with the presence of cerebral microbleeds (OR 1.01 [1.001-1.01], p=0.03) in unadjusted but not in adjusted analyses.
Conclusions: Structural changes of the left ventricle were associated with future cerebrovascular events or death as well as cSVD marker in AF-associated stroke patients, however not independently of other clinical variables.
Disclosures of Interest: No
Abstract N°: 2707
ASSOCIATIONS BETWEEN HEART AND BRAIN PARAMETERS IN OLDER PATIENTS ON ORAL ANTICOAGULANTS FOR ATRIAL FIBRILLATION: STRAT-AF 2 STUDY
Benedetta Formelli1, Giovanni Minutilli1, Carmen Barbato1, Eleonora Barucci1, Andrea Ginestroni2, Emilia Salvadori3, Enrico Fainardi2, Martina Berteotti4,5, Rossella Marcucci4,5, Anna Poggesi*1,6
1NEUROFARBA Department, University of Florence, Florence, Italy, 2Neuroradiology Unit, Careggi University Hospital, Florence, Italy, 3Department of Biomedical and Clinical Sciences, University of Milan, Milan, Italy, 4Department of Experimental and Clinical Medicine, University of Florence, Florence, Italy, 5Atherothrombotic Diseases Centre, Careggi University Hospital, Florence, Italy, 6Stroke Unit, Careggi University Hospital, Florence, Italy
On behalf of: Strat-AF 2 Study
Background and aims: Neurological complications of Atrial Fibrillation (AF) go beyond cardioembolic stroke. Neuroimaging often shows vascular lesions, such as non-lacunar infarcts and lesions related to cerebral Small Vessel Disease (cSVD), which are possible pathological substrates of neurological manifestations. Mechanisms relating AF with cSVD are still not clear. We aimed at evaluating associations between cardiac parameters and brain markers in a cohort of older AF patients on anticoagulants.
Methods: Strat-AF 2 study (Stratification of cerebral bleeding risk in AF) is an observational single-centre hospital-based study enrolling older AF patients on oral anticoagulants. cSVD and other lesions were visually assessed on brain MRI (56%) or CT (44%). Echocardiography was performed by an expert cardiologist.
Results: Mean age of the 182 enrolled patients was 78.6±6.7years, 58%males. Figure 1a and 1b shows correlation analyses between heart and brain parameters in the two cohorts.
Conclusions: In StratAF2, non-lacunar and SVD total score seem to correlate with higher atrial dimensions. The causal relationship, and clinical/therapeutical implications, needs to be elucidated.
Acknowlegments: Strat-AF 2 study was funded by Tuscany Region (Health Research Program 2018)
Disclosures of Interest: No
Abstract N°: 1460
THE EFFECTIVENESS OF DOAC COMPARED TO WARFARIN ON THE RESOLUTION OF LEFT ATRIAL THROMBUS IN ACUTE STROKE PATIENTS WITH NVAF
1Graduate School of Medicine, Nippon Medical School, Japan, 2Tama-nagayama Hospital, Nippon Medical School, Japan, 3National Cerebral and Cardiovascular Center, Japan, 4National Cerebral and Cardiovascular Center, Japan, 5Jichi Medical University, Japan, 6Brain Attack Center Ota Memorial Hospital, Japan, 7the Jikei University School of Medicine, Japan
On behalf of:
Background and aims: The presence of left atrial thrombus (LAT) in acute stroke patients with NVAF is the major embolic source for recurrent stroke. The aim of this study was to investigate whether DOAC is more effective than warfarin to resolve the LAT detected in acute stroke patients with NVAF.
Methods: Among acute stroke patients admitted to five major comprehensive stroke centers from January 2017 to December 2022, having both NVAF and LAT detected by TEE were selected, and patients with follow-up TEE evaluation were enrolled. All patients were treated with either DOAC or warfarin for LAT. Patients were classified into two groups according to the type of anticoagulation; the DOAC group and the Warfarin group. We compared the clinical characteristics, the resolution of LAT, recurrent stroke and bleeding complications within three months after stroke onset evaluated between the two groups.
Results: Sixty-three patients (male 33 [52%], median age 77) were enrolled. The DOAC group and the Warfarin group had 22 (35%) patients and 41(65%) patients, respectively. Gender, age, NIHSS scores on admission were not different between the two groups. The resolution rate of LAT was significantly high in the DOAC group than the Warfarin group (13 [59%] vs. 14 [34%], P=0.016). Recurrent stroke within three months after stroke was one (5%) in the DOAC group and three (7%) in the Warfarin group (P=1.000). There was no intracerebral hemorrhage up to three month in both group.
Conclusions: In acute stroke patients with NVAF and LAT, DOAC should be more effective than warfarin to resolve LAT.
Disclosures of Interest: No
Abstract N°: 1720
CHARACTERISTICS AND OUTCOMES OF ISCHAEMIC STROKE IN PATIENTS WITH ATRIAL FIBRILLATION KNOWN BEFORE OR FIRST DETECTED AFTER STROKE
Lucio D'ANNA*1, Michele Romoli2, Kirsten Harvey1, Eleni Korompoki1, Roland Veltkamp1
1Imperial College London, Hammersmith Campus, United Kingdom, 2Maurizio Bufalini Hospital, Cesena, Italy
On behalf of:
Background and aims: Atrial fibrillation (AF) can be newly detected after the index stroke (AFDAS) or can be known before (KAF). It remains unclear whether the outcome of ischemic stroke in patients with AFDAS differs from those with KAF. We performed a propensity-matched analysis to investigate the outcome profiles of patients with AFDAS and their counterparts with KAF.
Methods: We analysed a consecutive series of patients enrolled into the EIDASAF study, a single centre, retrospective study of ischemic stroke patients with a diagnosis of AF who had been admitted to the Hyperacute Stroke Unit of Imperial College London between 2010 and 2017.
Results: Overall, our cohort included 959 patients with AF and acute ischemic stroke. After propensity score matching, 541 patients were matched (401 KAF vs 140 AFDAS group).
Patients with KAF were significantly older (p=0.035), had a higher prevalence of heart failure (p=0.006) and were more frequently anticoagulated before the index event (p < 0.001). KAF patients had more often another competing cause of their stroke in addition to AF compared to of AFDAS patients (p < 0.001). The rate of death and of haemorrhagic transformation were significantly higher in KAF patients compared to AFDAS patients. Logistic regression analysis did not reveal a statistically significant effect of subtype of AF on death. However, KAF was associated with an increased probability of haemorrhagic transformation (OR 1.37; CI 1.25-1.52, p=0.015) after the index event.
Conclusions: KAF is associated with an increased risk of haemorrhagic transformation but not of death when compared to AFDAS.
Disclosures of Interest: No
Abstract N°: 2191
RETROSPECTIVE ANALYSIS OF LEFT ATRIAL APPENDAGE CLOSURE IN PATIENTS WITH CEREBRAL AMYLOID ANGIOPATHY
Michael Liu*1, Ryan Coburn1, Jonathan Graff-Radford1, Robert Brown1, Hasan Alarouri2, Agata Sularz2, Eric Yang2, Mohamad Alkhouli2, David Holmes2, Eugene Scharf1
1Mayo Clinic, Neurology, Rochester, United States, 2Mayo Clinic, Cardiology, Rochester, United States
On behalf of: Mayo Clinic Cardiology Research Group
Background and aims: Left atrial appendage (LAA) closure devices are an effective alternative to long term oral anticoagulation for stroke prevention in patients with non-valvular atrial fibrillation. Patients with cerebral amyloid angiopathy (CAA) are at increased risk of intracerebral hemorrhage (ICH) and may have a contraindication to oral anticoagulation. Efficacy and safety of closure device placement in the CAA population has not been well studied.
Methods: We completed a retrospective review of patients who met criteria for possible or probable CAA by Boston Criteria 2.0 and underwent LAA closure at Mayo Clinic sites from 1/1/2015-3/1/2023. Primary outcomes were the development of ischemic stroke (IS) or ICH. Secondary outcomes consisted of procedural safety and mortality. A matched cohort without CAA undergoing closure was utilized to assess for differences between outcomes.
Results: 19 patients were included and underwent successful implantation of LAA closure devices without immediate complication. Peridevice leak was seen in 7 patients with average leak size of 2.9 ± 1.2 mm. One patient had an ICH and 3 patients had an IS over a mean follow-up of 1082 ± 667 days (annualized incidence rate of 1.7% and 5.3% respectively). Four patients died during the study period, none related to study endpoints. The matched cohort had similar rates of IS (3 vs 3 patients, p=1.000), ICH (1 vs 0 patients, p=1.000), and mortality (4 vs 3 patients, p=1.000).
Conclusions: Use of LAA closure devices appear to be a safe and efficacious alternative to anticoagulation in patients with atrial fibrillation and CAA.
Disclosures of Interest: No
Abstract N°: 2233
ASSOCIATION AND DIAGNOSTIC UTILITY OF EPICARDIAL ADIPOSE TISSUE WITH ISCHEMIC STROKE: A META-ANALYSIS
Rukesh Yadav*1
1Institute of Medicine, Maharajgunj Medical Campus, Tribhuvan University, Maharajgunj Kathmandu, Internal Medicine, Kathmandu, Nepal
On behalf of:
Background and aims: The potential use of epicardial adipose tissue (EAT) as an imaging biomarker for cardiovascular disease risk stratification has attracted attention. A potential correlation of EAT with an elevated risk of stroke was demonstrated by recent research. EAT's diagnostic value in cases of ischemic stroke hasn't been thoroughly analyzed, though. A meta-analysis of the literature assessing the correlation between EAT and stroke was conducted.
Methods: Pubmed, Google Scholar and Embase databases were searched from inception till 15 January 2024 for studies that measured EAT thickness of adult patients with ischemic stroke and matched healthy controls. Outcomes included standardarized mean difference (SMD) of EAT thickness between the stroke patients and the healthy controls. Furthermore, the statistical analyses were conducted to obtain adjusted odds ratios (OR) of the association of high EAT thickness with ischemic stroke. The results were combined using a fixed or random effect model as per heterogeneity among the included studies in Revman 5.1 software.
Results: Ten studies comprising 1091 patients were included in this analysis. EAT thickness were significantly higher in ischemic stroke patients as compared to healthy controls [SMD: 2.16, Confidence Interval (CI): 1.66-2.65, I2=86%, P value < 0.00001] (Figure 1). Moreover, the pooled ORs revealed the significant association of high EAT thickness with ischemic stroke [OR:2.97, CI=1.68-5.23, I2=99%, P value < 0.00001] (Figure 2).
Conclusions: The utility of EAT as an imaging biomarker for predicting stroke is promising. EAT represent readily available clinical markers useful in estimating risk of ischemic stroke.
Disclosures of Interest: No
Abstract N°: 2458
REPERFUSION THERAPIES IN PATIENTS WITH ACUTE ISCHAEMIC STROKE AND AF: DATA ON SAFETY AND EFFECTIVENESS FROM A MULTI-CENTRE STUDY
Virginia Cancelloni*1
1Santa Maria della Misericordia Hospital, Stroke Unit and Division of Cardiovascular Medicine, Perugia, Italy
On behalf of: RAF and RAF-NOACs Investigators
Background and aims: Intravenous thrombolysis (IVT) and/or endovascular therapy (EVT) are currently considered best practices in acute stroke patients. Data regarding the efficacy and safety of reperfusion therapies in patients with atrial fibrillation (AF) are conflicting as regards haemorrhagic transformation, mortality, and functional outcome. This study sought to investigate for any differences, in terms of safety and effectiveness, between AF patients with acute ischaemic stroke (AIS) treated and untreated with reperfusion therapies.
Methods: Data from two multicenter cohort studies (RAF and RAF-NOACs) on consecutive patients with AF and AIS were analyzed to compare patients treated and not treated with reperfusion therapies (IVT and/or EVT). Multivariable logistic regression analysis was performed to identify independent predictors for outcome events: 90-day good functional outcome and mortality. A propensity score matching (PSM) analysis compared treated and untreated patients.
Results: Overall, 441 (25.4%) were included in the reperfusion-treated group and 1,295 (74.6%) in the untreated group. The multivariable model suggested that reperfusion therapies were significantly associated with good functional outcome. Rates of mortality and disability were higher in patients not treated, especially in the case of higher NIHSS scores. In the PSM comparison, 173/250 patients (69.2%) who had received reperfusion therapies had good functional outcome at 90 days, compared to 146/250 (58.4%) untreated patients (p=0.009, OR: 1.60, 95% CI:1.11-2.31).
Conclusions: Patients with AF and AIS treated with reperfusion therapies had a significantly higher rate of good functional outcome and lower rates of mortality compared to those patients with AF and AIS who had undergone conservative treatment.
Mortality and disability rates in patients treated and not treated and not treated with IVT and/or EVT, divided by stroke severity. NIHSS National Institute of Health Stroke Scale.
Disclosures of Interest: No
Abstract N°: 3322
MICRORNAS AS BIOMARKERS OF ATRIAL FIBRILLATION IN ISCHAEMIC STROKE PATIENTS
Jansky Petr*1, Tereza Ruzickova1, Anna Olserova1, Václav Maťoška2, Ales Tomek1
1Second Faculty of Medicine, Charles University and University Hospital Motol, Neurology, Praha 5, Czech Republic, 2Na Homolce Hospital, Department of Clinical Biochemistry, Hematology and Immunology, Prague, Czech Republic
On behalf of:
Background and aims: MicroRNAs are non-coding RNA molecules that play a role in posttranscriptional processes and regulate gene expression. Both upregulation and downregulation of different microRNAs were described in patients with atrial fibrillation (AF) and ischaemic stroke. The aim of the study is to evaluate the ability of selected microRNAs as biomarkers of AF in ischaemic stroke patients in comparison with other established biomarkers.
Methods: Case-control study of consecutive ischaemic stroke patients with AF admitted to a comprehensive stroke center. A control group consisted of ischaemic stroke patients with no detection of AF on prolonged (at least 3 weeks) Holter ECG monitoring. As potential biomarkers of AF, we analyzed serum levels of microRNA (mir-21, mir-29b, mir-133b, mir-142-5p, mir-150, mir-499,mir-223-3p) at admission with biochemical (D-dimer, NT-proBNP, high-sensitivity troponin, CRP, eGFR) and echocardiographical biomarkers. The predictive accuracy of biomarkers was assessed by calculating the AUC.
Results: The data of 117 patients were analyzed (62 with AF, 55 with no AF, 46% men, median age 73 years, median NIHSS 6). The diagnostic performance of NT-proBNP for AF had AUC 0.93 (95% CI 0.86–0.98), a cut-off value of > 528ng/mL had a sensitivity of 79% and a specificity of 97%. The diameter of the left atrium had AUC 0.78 (95% CI 0.67-0.90), a cut-off value > 40mm had a sensitivity of 70% and a specificity of 25%. All other biomarkers, including microRNAs levels, were not associated with AF.
Conclusions: Selected microRNAs did not provide useful information over conventional biomarkers in predicting AF diagnosis in our ischaemic stroke cohort.
Disclosures of Interest: No
Abstract N°: 751
IMPLANTABLE LOOP RECORDER FOR DETECTION OF ATRIAL FIBRILLATION AFTER STROKE: GLOBAL/JAPANESE RESULTS FROM THE REVEAL LINQ REGISTRY
1National Cerebral and Cardiovascular Center, Department of Cerebraovascular Medicine, Suita, Osaka, Japan, 2The Jikei University School of Medicine, Department of Neurology, Tokyo, Japan, 3Fujita Health University School of Medicine, Department of Comprehensive Strokology, Toyoake, Japan, 4Hirosaki University Graduate School of Medicine, Department of Cardiology and Nephrology, Hirosaki, Japan, 5Kyorin University School of Medicine, Department of Stroke and Cerebrovascular Medicine, Tokyo, Japan, 6Fukuoka Neurosurgical Hospital, Department of Cerebrovascular Medicine, Fukuoka, Japan, 7Medtronic Inc., Cardiac Rhythm Management, Clinical Department, Minneapolis, 8Medtronic Japan Co., Ltd, Japan Clinical and Medical Affairs, Tokyo, Japan, 9Valley Hospital, Department of Cardiology, Ridgewood, 10Saiseikai Kumamoto Hospital, Division of Cardiology, Kumamoto, Japan
On behalf of: The Reveal LINQ Registry investigators
Background and aims: To quantify the incidence of atrial fibrillation (AF) in cryptogenic stroke patients using an implantable loop recorder (ILR).
Methods: Patients with cryptogenic stroke and implanted with ILR to monitor for covert AF were studied from a large, global, prospective, observational, Reveal LINQ Registry (ClinicalTrials.gov NCT 02746471). AF detection, oral anticoagulation, and stroke recurrence were assessed during up to 36 months of follow-up. A multivariable analysis exploring predictors of AF was performed.
Results: A total of 271 patients (61.6±14.3 years, 170 male, median CHA2DS2-VASc 4, 60 from Japan) were enrolled from Jul/2014 through Jan/2018 from 11 countries. Median time of follow-up was 20 months (IQR 8.0-37.3). AF was detected in 1.5% of patients at 1 month, 18.0% at 18 months, and 28.2% at 36 months. The median time of detection was 7.9 months. The slope of detection rate was relatively steeper in the Japan subgroup for the first 12 months, however, by 36 months the cumulative incidence of AF detection was similar between groups (log-rank P=0.58) (Figure). Only age was independently associated with AF detection (HR 1.05, 95% CI 1.02-1.07, per year). Eleven patients (4.1%) developed recurrent ischemic stroke/TIA; of these, AF was detected in only one. Patients with detected AF were taking oral anticoagulation three times more often than those without AF at the last follow-up.
Conclusions: The overall rate of AF detection was comparable with previous results, with a relatively higher incidence in Japan patients during the first year. This highlights the importance of utilizing ILR for AF management after stroke.
Disclosures of Interest: Yes The Reveal LINQ Registry was sponsored by Medtronic.
Abstract N°: 1066
IS THERE A BENEFIT OF PFO CLOSURE IN OLDER PATIENTS WITH EMBOLIC STROKE OF UNDETERMINED SOURCE; AN OBSERVATIONAL STUDY
Dania Mallick*1,2, Ana Torres1, Mohammad Ahmed2,3, Alan Davis2, Asad Ahrar1, Nadeem Khan1, Muhib Khan4, Malgorzata Miller1, Nabil Wees1, Jiangyong Min1
1Corewell Health Butterworth Hospital, Neurology, Grand Rapids, United States, 2Michigan State University, Grand Rapids, United States, 3Corewell Health Butterworth Hospital, Cardiology, Grand Rapids, United States, 4Mayo Clinic, Neurology, Rochester, United States
On behalf of:
Background and aims: Patent foramen ovale (PFO) closure is recommended for patients below age 60 with embolic stroke of undetermined source (ESUS), but the role of closure in patients older than 60 years is unclear. We aim to investigate the benefit of PFO closure in this age group.
Methods: We included patients older than 60 years with ESUS, who had a PFO closure following presumed PFO-related ischemic stroke. The primary outcome was a composite of recurrent ischemic stroke, transient ischemic attack, or fatal stroke that occurred up to 5 years following PFO closure. The safety outcome was the occurrence of any complications after PFO closure, including new-onset atrial fibrillation (AF).
Results: A total of 64 patients were included (mean age 65.4±5.2), 39 of which were male (61.9%). Mean Risk of Paradoxical Embolism (RoPE) score was 4. Procedure-related complications, including new onset AF were comparable or lower to previous trials (9.4%, 6/64). After a median follow-up of 2.4 years, patients above 60 years demonstrated a high incidence of recurrent ischemic stroke (6.3%, 4/64), recurrent transient ischemic attack (3.1%, 2/64), compared to patients under 60 years from previous clinical trials (1.5% overall recurrent cerebrovascular events). However, no recurrent fatal stroke was seen (0%, 0/64) in this older group.
Conclusions: In patients older than 60 years with cryptogenic stroke, PFO closure demonstrated similar safety profiles but was associated with a relatively high risk of recurrent ischemic stroke compared to their younger counterparts reported in previous trials (CLOSE, CLOSURE-I, DEFENCE-PFO, REDUCE, RESPECT and PC Trial).
Disclosures of Interest: No
Paper Poster - Case Reports
Abstract N°: 786
GLOBAL ORBITAL ISCHEMIA SYNDROME, A RARE, BUT POTENTIALLY DISABLING COMPLICATION OF ENDOVASCULAR THROMBECTOMY
Bridget Schoon*1, Matthijs van der Sluijs2, Pieter Jan van Doormaal2, Diederik Dippel1
1Erasmus MC, University Medical Center, Neurology, Rotterdam, Netherlands, 2Erasmus MC, University Medical Center, Radiology and Nuclear Medicine, Rotterdam, Netherlands
On behalf of:
Background and aims: Global orbital infarction syndrome (GOIS) is a rare, but potentially disabling condition. Its etiology is varied, however, it is often caused by occlusion of the ophthalmic artery. The effects of this (partial) occlusion can be exacerbated by certain anatomical variations of the internal carotid artery and anastomoses of the external carotid artery. Currently, there is no consensus on the optimal treatment of GOIS.
Methods: We present a case of GOIS that occurred shortly after endovascular thrombectomy (EVT) for acute ischemic stroke. The clinical evolution and diagnostic process is discussed.
Results: A 67-year old patient presented at the emergency department with an acute ischemic stroke in the left hemisphere (NIHSS 14). CTA showed a left-sided M1 occlusion and ipsilateral carotid dissection. Directly after undergoing EVT, he complained of severe retro-orbital pain and vision loss. Patient had left-sided proptosis, chemosis and periorbital swelling as well as a visual field defect, with normal eye-movements and no audible bruit. (Figure 1)
There was no evidence for a carotid cavernous fistula on CTA or DSA. However, the procedural DSA showed retrograde flow of in the left ophthalmic artery, attributed to the carotid dissection. There was ischemia of the periorbital structures on MRI (figure 2). After multi-disciplinary review, the diagnosis of GOIS was made. The patient made a spontaneous recovery.
Conclusions: GOIS is a rare periprocedural complication of endovascular thrombectomy. Timely recognition of this disorder is vital to minimize discomfort and reduce the risk of permanent visual disability.
Disclosures of Interest: No
Abstract N°: 2116
EARLY REPEAT THROMBOLYSIS WITH TENECTEPLASE IN RECURRENT ISCHAEMIC STROKE
Hilal Shah1, Georgia Merron1, Mary Donovan1, Chimezie Nzeji1, Barry Moynihan1
1University Hospital Kerry, Tralee, Ireland
On behalf of:
Background and aims: Thrombolysis is usually not recommended within three months of stroke as per the relevant clinical trials. Repeat early thrombolysis with alteplase in early recurrent ischaemic stroke has been described. This case describes repeat thrombolysis with tenecteplase within 10 days of index stroke.
Methods: A 66 year old male presented with right sided weakness with NIHSS 19. Initial CT Angiogram (CTA) showed complete occlusion of left ICA, with M3 occlusion in left MCA territory. He was thrombolysed with 0.25mg/kg tenecteplase and decided not for endovascular thrombectomy on discussion with the thrombectomy centre. Post thrombolysis, a moderate-sized infarct was visible. Repeat NIHSS was 12. Dual antiplatelet therapy was started and neurological deficits improved with rehabilitation. He was mobile with assistance of one person.
10 days later, sudden deterioration occurred with right side weakness, neglect, global aphasia and gaze palsy; NIHSS 20. His CTA showed persistent complete occlusion of left ICA extending to M1 and proximal M2 segments. Due to distance from thrombectomy centre and following discussion with Interventional Neuroradiologist on probability of successful recanalization, he had repeat thrombolysis with 0.25mg/kg tenecteplase.
Results: There was recanalisation post thrombectomy at M1 (complete) and M2 (partial) with unsuccessful left ICA revascularisation. CT brain post thrombolysis showed no haemorrhage. NIHSS 15 post thrombectomy. Ongoing rehabilitation is underway for his residual deficits.
Conclusions: This case report suggests that repeated thrombolysis with tenecteplase in early recurrent ischaemic stroke may be safe, however, further studies are required to establish safety of this approach in the general stroke population.
Disclosures of Interest: No
Abstract N°: 1097
ISCHAEMIC CORONA RADIATA STROKE PRESENTING AS FOIX-CHAVANY-MARIE SYNDROME UNRAVELS CARDIOEMBOLIC CAUSE OF LACUNAR STROKE
Martina Gaia Di Donna*1,2, Maria Rosaria Bagnato1,2, Maria Rita DI Ruzza2, Mario Ferrante2, Emanuele Saggese2, Paola Santalucia2, Maurizio Plocco2
1POLICLINICO TOR VERGATA, NEUROLOGY, ROME, Italy, 2OSPEDALE FABRIZIO SPAZIANI, STROKE UNIT, FROSINONE, Italy
On behalf of:
Background and aims: Foix-Chavany-Marie syndrome (FCMS) is considered the cortical type of pseudobulbar palsy, characterized by dysarthria and bilateral paralysis of the facio-lingual, pharyngeal and masticatory muscles, when bilateral or unilateral lesions of the operculum or adjacent subcortical areas occur.
Methods: FCMS frequently affects individuals who suffered consecutive vascular lesions, in a SVD scenario where deep perforators of MCA are involved.However, stroke in the anterior choroidal artery (AChA) territory can cause clinical presentation of FCSM and previous literature suggested that AchA is rarely related to small vessel occlusion.
Results: Here, we report a case of a 76-year-old male presented with FCMS due to acute left corona radiata stroke in a previously occurred right corona radiata infarct. Although the patient suffered both from hypertension and dyslipidaemia and despite ischaemic leuokoaraiosis emerged from CT scan, a deeper diagnostic examination revealed MRI pattern suggestive of AChA stroke (Fig.1) and an unknown heart failure with concomitant paroxysmal atrial fibrillation.Appropriate preventive therapy with oral anticoagulant drug was set.
Conclusions: Knowledge of neurological semeiotics of rare clinical syndromes is important to evaluate a patient affected by stroke and its possible etiology. FCMS is a condition where cortical-subcortical strategically located insults may mimic an involvement of brainstem.Moreover, it can possibly follow AChA territory infarcts, where a lacunar infarct can be caused not by small vessel disease but by cardioembolism instead, depicting an even more tangled clinical presentation. This evidences suggest that a complete diagnostic workup is mandatory, above all in the clinical atypical presentations.
Background and aims: We report a case of TIA with ipsilateral carotid web associated to atherosclerotic plaque
Methods: Case report
Results: A 23-year-old woman of African descent presented at the emergency department with transient right brachiofacial hypoesthesia. The diagnosis of TIA was made. No other vascular risk factors than the combined oral contraceptive pill were identified. CT angiography of head and neck showed a shelflike protrusion in the posterior wall of the left carotid artery bulb consistent with carotid web (CaW) (Figure 1a). Diffusion weighted imaging revealed no recent ischemic lesion. T1FS imaging of the cervical vessels showed a non-stenotic atherosclerotic plaque with signs of intraplaque haemorrhage associated to the CaW (Figure 1b). Dual antiplatelet therapy was initiated together with a statin and the combined oral contraceptive pill was discontinued. The patient was treated with carotid endarterectomy within a week. Intraoperative findings confirmed the presence of CaW associated to atherosclerotic plaque (Figure 1c). Histological examination revealed intimal hyperplasia with infiltration of spumous macrophages (Figure 1d).
Conclusions: Association of CaW to atherosclerotic plaque is very rare and there are only a few case reports available. With this case report, we aim to raise awareness of CaW possibly being associated to atherosclerotic plaque, even in the young adult presenting symptoms of TIA without recent ischemic lesion on DWI and in the absence of atherosclerotic risk factors. By adding T1FS imaging of the cervical vessels, we were able to identify an intraplaque haemorrhage, which is associated to increased risk of ipsilateral stroke with potential implications on choice of treatment.
Disclosures of Interest: No
Abstract N°: 2877
PREVENTIVE SUPERIOR TEMPORAL ARTERY MIDDLE CEREBRAL ARTERY BYPASS IN A PATIENT WITH BILATERAL OCCLUDED INTERNAL CAROTID ARTERY AND RECURRENT STROKE
Asunción García Maruenda*1, Paula Otero Fernández1, Isabel Martín Sobrino1, M Pilar Nieto Palomares1, Paola Gómez Ramirez1, Maroua El Harmochi Daoud1, Arturo Sánchez Gómez1, José Manuel Flores Barragán1, Luis Moreno Vázquez1
1Hospital General Universitario de Ciudad Real, Neurologia, Ciudad Real, Spain
On behalf of:
Background and aims: Preventive STA-MCA bypass is a neurosurgical procedure usually employed in selected patients affected by cerebrovascular ischemic disease, specially Moya-Moya disease. It is also relied on in cases involving intracranial lesions or aneurysms in the course of which a vessel is required to be sacrificed for complete removal or isolation from the vascular territory respectively.
Methods: We present a clinical case about a 52 year old who experienced a left ACM stroke. Subsequently was repeatedly hospitalized with transient right hemiparesis, amaurosis fugax and speech disturbance because of severe atherothrombotic disease in the form of bilateral occluded internal carotid artery. Ultimately the multidisciplinary team proposed a STA-MCA bypass as secondary prevention treatment. Since the patient wasn’t diabetic he was considered an ideal candidate for the procedure.
Results: A bypass between the parietal branch of the STA and the M4 was performed that went across the trepanation hole of a mini-craniotomy with an ischemia time of 73 minutes. A video of the technique is displayed.
Conclusions: The Japanese EC-IC Bypass Trial demonstrated the efficacy of STA-MCA bypass for occlusive CVD. Patients with chronic retinal ischemia resulting in progressive visual loss, such us our patient, were excluded from COSS and might benefit from EC-IC bypass. After the procedure the patient remains neurologically stable and up until this moment he didn’t suffered a relapse of the symptoms that motivated his treatment.
Disclosures of Interest: No
Abstract N°: 343
A RARE CASE OF UNILATERAL POST-THROMBECTOMY DELAYED HYPOXIC-ISCHEMIC LEUKOENCEPHALOPATHY
Zalan Khan1, Hamidreza Abbasi1, John Hourihane1, Amit Kandel1, Marilou Ching*2,2
1University at Buffalo Jacobs School of Medicine and Biomedical Sciences, Neurology, Buffalo, United States, 2University at Buffalo Jacobs School of Medicine and Biomedical Sciences, Neurology, East Amherst, United States
On behalf of: Zalan Wahid Khan, Hamidreza Abbasi, Jon M Hourihane, Amit Kandel
Background and aims: Delayed hypoxic-ischemic leukoencephalopathy (DHIL) is a rare entity characterized by acute neurologic deterioration and cerebral demyelination occurring days to weeks after clinical recovery from hypoxic-ischemic insult following stroke.
Methods: We report a case of a 66-year-old man with hypertension and hyperlipidemia who presented with complete right internal carotid occlusion.
Results: He underwent emergent thrombectomy with TICI 3 recanalization. NIHSS improved from 19 to 3. Brain MRI post-procedure showed diffusion changes involving the right anterior, medial temporal cortices, and corona radiata without hemorrhagic conversion. He continued to improve until day 10, when there was a steady decline. Follow-up brain MRI on day 13 showed confluent FLAIR/T2 hyperintensities within right hemispheric white matter without apparent restricted diffusion lesions. Workup for metabolic and infective etiologies was unremarkable. On day 35, a lumbar puncture was performed, revealing a CSF protein of 206 with normal glucose, cell count, IgG index, and oligoclonal bands. Bacterial, viral studies and cytology for malignancy were negative. MR spectroscopy showed elevated choline and creatine, decreased N-acetyl aspartate peak, and prominent lactate peak, especially at the right temporal lobe. Right frontal brain biopsy involving all meningeal layers and cerebral parenchyma showed white matter rarefaction and reactive gliosis.
Conclusions: In summary, delayed hypoxic-ischemic leukoencephalopathy does not only occur in the setting of global hypoxia but may occur in patients with large vessel strokes despite successful recanalization. A high index of suspicion and follow-up imaging are crucial in its diagnosis.
Disclosures of Interest: No
Abstract N°: 2601
ALTEPLASE FOR ACUTE CENTRAL RETINAL ARTERY OCCLUSION: CASE REPORT OF FOUR PATIENTS TREATED AT A UNIVERSITY HOSPITAL
Filippo Fratini*1, Francesco Arba2, Maria Lamassa2, Patrizia Nencini2, Mascia Nesi2, Vanessa Palumbo2, Francesca Pescini2, Benedetta Piccardi2, Cristina Sarti1,2, Anna Poggesi1,2
1NEUROFARBA Department, University of Florence, Florence, Italy, 2Stroke Unit, Careggi University Hospital, Florence, Italy
On behalf of:
Background and aims: Central retinal artery occlusion (CRAO) is a medical emergency causing monocular vision loss (MVL). Standard care includes globe compression, anterior chamber paracentesis, without any clear guidelines. Treatment with thrombolysis may be effective and some evidence already exists. We report 4 cases of patients with acute CRAO treated with intravenous (IV) alteplase.
Methods:
Results: A 75 year-old woman with severe cataract in right eye, became acutely blind for MVL in left eye. She came to emergency department (ED) 90 minutes after onset. In the absence of contraindications, neurologist decided IV-alteplase (within 240 minutes after onset, ONT).
A 71 year-old woman experienced acute MVL in right eye. In ED, ophthalmologist diagnosed CRAO. After globe compression and paracentesis no visual improvements were seen. the neurologist started IV-alteplase (ONT 285-min).
A 55 year-old man experienced a sudden MVL in left eye. In ED, ophthalmologist diagnosed CRAO, initially treated with paracentesis. After no improvements, the neurologist started IV-alteplase (ONT 240-min).
A 68 year old man acutely had MVL in right eye. After prolonged global massage by ophthalmologist, without clinical improvement, neurologist started IV-alteplase (ONT 240-min)
No hemorrhagic complications were observed. Visual acuity was gained only for the first patient, while the other 3 did not show any visual improvement.
Conclusions: Early intravenous thrombolysis might be safe in patients with CRAO. There is considerable variability in management of CRAO. Effectiveness should be tested in randomized controlled trial.
Disclosures of Interest: No
Abstract N°: 2869
SUPERNUMERARY PHANTOM LIMB WITHOUT PHANTOM LIMB PAIN IN A PATIENT WITH PONTINE HEMORRHAGE – A CASE REPORT
Yasemin Ronahi Kücük*1, Christina R Kruuse1,2, Charlotte Lützhøft Rath1, Robbert-Jan Roderick van Hooff1
1Department of Brain and Spinal Cord Injury, Copenhagen University Hospital – Rigshospitalet, Glostrup, Denmark, 2Department of Neurology, Neurovascular Research Unit, Copenhagen University Hospital, Herlev Gentofte, Herlev
On behalf of:
Background and aims: In stroke, insight into uncharacteristic symptoms is scarce. Supernumerary phantom limb (SPL) is an awareness of an illusory extra limb in addition to the existing limbs. This illusion can be disturbing to the patient if unrecognized.
Methods: We present a case description of a 44-year-old female patient admitted to the neurorehabilitation unit after a median pontine hemorrhage.
Results: The patient presented upon admission a severe tetraparesis, with a left hemi corporal preponderance, and a sensory impairment to light touch and pain in her left arm and leg.
One month after stroke onset, the patient described the presence of an extra left arm and leg. These extra limbs had been present at onset; however, not identified by staff. She described being able to voluntarily move the extra arm independently from the paretic arm and did not experience any pain. She showed good insight to the presence of the extra limbs and showed no sign of cognitive deficits. The extra limbs disappeared several weeks later as her paretic side improved.
Conclusions: SPL due to cerebral lesions is rare but described in a variety of neurological disorders, though mostly in right hemispheric stroke. SPL is often accompanied by both sensory and motor impairment. This is the first case report of SPL without the presence of concomitant phantom limb in the acute phase after a pontine hemorrhage. A more in-depth examination of a patient’s symptoms is warranted, as SPL may be underreported and overlooked during the acute phase of stroke.
Disclosures of Interest: No
Abstract N°: 966
GELASTIC SEIZURES ARISING FROM A PARIETAL LOBE INTRAPARENCHYMAL HEMORRHAGE SECONDARY TO DURAL VENOUS SINUS THROMBOSIS
Sanghee Lim*1, Eugene Scharf1, Irene Meissner1
1Mayo Clinic, Neurology, Rochester, United States
On behalf of:
Background and aims: Gelastic seizures are characterized by sudden attacks of inappropriate or mirthless laughter occurring in the absence of external stimuli. Hypothalamic hamartomas are most commonly associated with gelastic seizures. Reports of lobar lesions or hemorrhages causing these seizures are exceedingly rare.
Methods: We report a case of a 60 year-old woman who developed gelastic seizures in the setting of a right parietal intraparenchymal hemorrhage secondary to dural venous sinus thrombosis.
Results: The patient presented to the hospital with a 3-day history of progressively worsening severe headaches, nausea, vomiting, and left homonymous hemianopia. CT imaging demonstrated a right parieto-occipital intraparenchymal hemorrhage and dural venous sinus thrombosis involving the right transverse/sigmoid sinuses. Laboratory studies were notable for suppressed TSH, elevated free T4, and elevated thyrotropin receptor antibodies, concerning for Graves’ disease. On hospital day 4, the patient began experiencing recurrent episodes of inappropriate laughter with initial concern for hospital delirium. An EEG was obtained, demonstrating right temporal spike-and-wave discharges with concomitant clinical semiology. Keppra was initiated with resolution of clinical and electrographic seizure activity. Apixaban was started for management of dural venous sinus thrombosis.
Conclusions: We describe, to our knowledge, the first case of gelastic seizures arising from a right parietal hemorrhage. A high index of clinical suspicion was instrumental in making the diagnosis, and response to anti-seizure therapy was robust and sustained.
Head computed tomographic venography image demonstrating right-sided dural venous sinus thrombosis and parieto-occipital intraparenchymal hemorrhage.
Disclosures of Interest: No
Abstract N°: 1023
LIQUEFACTION NECROSIS OF MITRAL ANNULUS ASSOCIATED WITH MULTITERRITORIAL STROKES AND ENDOCARDITIS: A CASE REPORT
Elisa Martínez1, Inhar Esnaola*1, Elena Escriche1, Maria Molina1, Paula Miguel1, Beatriz Zandio1, Maria Carmen Gil Alzueta1
1University Hospital of Navarra, Neurology, Spain
On behalf of:
Background and aims: Liquefaction necrosis of mitral annulus (LNMA) is a rare form of mitral calcification, often underdiagnosed because of its benign and asymptomatic course. Very few cases in the literature relate this condition to embolic stroke, being its treatment complicated and controversial. We present the case of a patient with multiterritorial embolic strokes and LNMA with possible associated endocarditis.
Methods: We present a 73-year-old woman with no vascular risk factors, admitted to the Neurology department for acute confusion. Three months earlier LNMA was diagnosed by an echocardiography performed in our department, after an episode of dysarthria and loss of consciousness.
Neurologic examination revealed bradypsychia, dysarthria and left hemicorporal paresis. In admission, atrial fibrillation was diagnosed.
Results: Emergency Cranial CT was normal. Brain MRI showed multiterritorial ischemic strokes. New echocardiography detected severe mitral insufficiency, likely due to LNMA perforation, possibly associated with infection. Posterior transesophageal echocardiography and PET scan supported endocarditis diagnosis. Empirical antibiotic therapy and anticoagulation were started and valve replacement was performed. Surgical biopsy specimen showed fibrotic tissue with inflammatory cells. No microorganisms were found.
Conclusions: No documented cases of simultaneous presentation of LNMA with endocarditis and multiterritorial strokes have been reported in the current literature. Initial echocardiography performed by the neurologist was key to establish the embolic source. Anticoagulation was initiated due to the high embolic risk, despite of the possibility of endocarditis and the lack of evidence in the literature. Given the exceptional nature of this case, a multidisciplinary approach was considered essential for integral management.
1Northwick Park Hospital, Hyperacute Stroke Unit, Harrow, United Kingdom
On behalf of:
Background and aims: Carotid webs are a rare vascular entity, considered to be a high-risk factor for cryptogenic ischemic strokes due to their alteration of downstream hemodynamics. Currently, no clear evidence or guidelines exist on how to optimally manage patients with carotid webs, symptomatic or asymptomatic.
Methods: A 32-year-old woman with a history of smoking was admitted to our stroke unit after presenting with sudden onset headache, word-finding difficulties and weakness of the right arm and leg. Upon admission her National Institutes of Health Stroke Scale score was 5. Magnetic Resonance Imaging confirmed acute infarcts in the left middle cerebral artery territory. A Young Stroke Screen, including an ECHO, bubble Echo, and Holter monitor, yielded unremarkable results. CT Angiogram of the internal carotid arteries revealed bilateral carotid webs, more marked on the left, accounting for the patient’s left sided infarcts. The left-sided symptomatic carotid web was treated with carotid endarterectomy.
Results: The patient was discharged on dual antiplatelet therapy for 21-days following which she would continue aspirin lifelong. Atorvastatin was initiated for secondary stroke prevention. At four weeks the patient had recovered well from her operation and only reported a mild persistent dysphasia. She was further referred to be seen for the asymptomatic right-sided carotid web, which so far was being medically managed.
Conclusions: Despite representing a very small fraction of stroke aetiology, the management of carotid webs represents a gap in current guidelines and should not be underappreciated. Here we discuss all the medical and surgical options available.
Disclosures of Interest: No
Abstract N°: 1523
EXTRACRANIAL ICA ANEURYSM UNVEILED BY AN ACUTE TANDEM OCCLUSION: A CASE OF REPERFUSION AND SACRIFICE
1251 Hellenic Airforce General Hospital, Interventional Radiology and Neuroradiology Lab., Athens, Greece, 2National and Kapodistrian University of Athens, 1st Radiology Lab.- Areteion Hospital, 3National and Kapodistrian University of Athens, 2nd Radiology Lab.-Attikon Hospital
On behalf of:
Background and aims: Extracranial internal carotid artery (ICA) aneurysms are an exceedingly uncommon etiology of acute tandem occlusions. Only a few cases have been documented in the literature. The main objective during treatment of tandem occlusions is cerebral reperfusion, followed by evaluation of each individual case, weighing risks and benefits, considering the necessity of dual antiplatelet therapy, if a reconstruction precedes or follows reperfusion.
We aim to share our experience treating a rare case in which we chose occlusion rather than reconstruction, following intracranial thrombectomy.
Methods: A 59-year-old-male patient presented to the ER with left-sided hemiplegia-hemianesthesia and dysarthria, scoring 17 on NIHSS, 7 hours after symptoms onset. CT-CTA examination revealed a tandem occlusion with a right M1- middle cerebral artery (MCA) infarction, ASPECTS 7 and retrospectively a dissecting 15mm aneurysm of the cervical RICA. CT-perfusion revealed a mismatch with temporal and basal ganglia core, and we emerged for endovascular recanalization.
Results: Successful recanalization of right MCA, intra and extracranial RICA was achieved after three stent-retriever passes. Control angiographies from the LICA under balloon occluded RICA, revealed satisfactory hemodynamics and patency of the right MCA. Coil embolization of the right subophthalmic ICA was performed ensuring intracerebral patency and preventing new thromboembolic events.
Conclusions: Parent artery occlusion has been a longstanding strategy in Neuroradiology practice for certain aneurysm cases. We implemented this approach for the first time as a final recourse in a complex case of acute ischemic stroke. The patient was transferred ten days later to a rehabilitation center, scoring 8 on NIHSS.]
LATERAL MEDULLARY INFARCT PRESENTING AS FACIAL EPICRANIA FUGAX
Devangi Desai*1, Soaham Desai1
1Shree Krishna Hospital Pramukhswami Medical College Bhaikaka University, Neurology, Anand, India
On behalf of:
Background and aims: Lateral medullary syndrome is characterized by ipsilateral facial and contralateral body sensory loss, with ataxia. Facial epicrania fugax (EF) is characterized by brief paroxysms of lateralized facial pain spreading from a trigger area across the territory of one division of the trigeminal nerve. EF is rare as a presenting symptom of lateral medullary infarction.
Methods: A 63-year-old man presented with acute onset of brief (2-60 seconds) paroxysms of severe right facial pain and hypesthesia rapidly spreading from the infraorbital region to the V2/V3 trigeminal territories, consistent with EF. MRI revealed an acute right lateral medullary infarct.
Results: The patient was treated with aspirin, statin and carbamazepine, and his symptoms resolved over several weeks, except for mild residual right facial sensory loss. We searched PubMed for reports of symptomatic EF associated with brainstem strokes and found 2 cases associated with paramedian pontine infarcts
Conclusions: This unique case expands the clinical spectrum of lateral medullary infarction to include transient symptomatology consistent with EF. It suggests that even with stereotyped lacunar syndromes, localization should be verified with neuroimaging given the variability in vascular supply. EF may result from transient ischemia in trigeminovascular pain pathways within lateral medullary infarcts.
MRI brain showing Right lateral medullary infarct
Disclosures of Interest: No
Abstract N°: 1900
ISCHEMIC STROKE AS THE FIRST PRESENTATION OF POEMS SYNDROME: A CASE REPORT
Nina Žakelj*1, Primož Žužek1
1Neurology Clinic, University Medical Center Ljubljana, Department of Vascular Neurology, Ljubljana, Slovenia
On behalf of:
Background and aims: Polyneuropathy, organomegaly, endocrinopathy, monoclonal plasma cell disorder, and skin changes (POEMS) syndrome is a rare plasma cell dyscrasia associated with an increased risk of ischemic stroke (IS). The underlying mechanisms of IS and its prognosis are unknown and not often debated. We present a 45-year-old patient with a left middle cerebral artery (MCA) stroke as the first manifestation of POEMS syndrome.
Methods: The data was obtained by reviewing the patient’s medical records. We based the discussion on available literature.
Results: We present a case of a 45-year-old patient with arterial hypertension who presented with subacute and progressive motor aphasia and right-sided weakness. Head MRI revealed multiple cortical ischemic lesions in the left MCA territory. His 24h Holter ECG and CTA of the cerebral arteries were unremarkable. Blood analysis showed thrombocytosis. Additional tests revealed concentric left ventricular hypertrophy, monoclonal gammopathy with kappa and lambda light chains, demyelinating polyneuropathy in both upper and lower limbs, and hepatosplenomegaly, thus fulfilling both mandatory and multiple minor criteria for the diagnosis of POEMS syndrome. A lymph node biopsy revealed Castleman syndrome. He was transferred to the Department of Oncology and Haematology for treatment with chemotherapy.
Conclusions: Although rare, POEMS syndrome should be considered in patients with ischemic stroke of unknown aetiology, signs of polyneuropathy, and monoclonal gammopathy.
Disclosures of Interest: No
Abstract N°: 1921
REVERSIBLE CEREBRAL VASOCONSTRICTION SYNDROME IN A PATIENT WITH PROLACTINOMA: IS CABERGOLINE THE FELON?
Faisal S. Alqahtani*1, Jnadi Madkhali2, Nouran Taher2
1King Saud bin Abdulaziz University for Health Sciences (KSAU-HS), College of Medicine, Riyadh, Saudi Arabia, 2Ministry of National Guard - Health Affairs, Division of Neurology, Riyadh, Saudi Arabia
On behalf of:
Background and aims: RCVS is characterized by recurrent thunderclap headaches and segmental constriction of cerebral arteries that resolves spontaneously within 3 months. It is attributed to a transient disturbance in the control of cerebrovascular tone, mainly from exposure to sympathomimetic drugs and the postpartum state. Although it can be associated with major sequelae, there are still unrecognized sporadic classes of drug-induced RCVS. Cabergoline-induced RCVS is extremely rare and reported once only in the literature. Here, we report the second case of RCVS after recent exposure to cabergoline to treat prolactinoma.
Methods: NA
Results: 27 years old single female who is known to have prolactinoma for 7 years under regular follow up. she was seen in gynecology clinic with irregular periods and elevated prolactin level, so she was started on cabergoline 0.5 mg once a week. On the third day of exposure to cabergoline, she presented to the emergence department with thunderclap headache and 1st two episodes of generalized tonic clonic seizure. Her initial neurological examination was non-focal. Brain CT showed left frontal intraparenchymal bleeding which further confirmed by MRI. She underwent digital subtraction angiogram (DSA) which revealed segmental constriction and dilatation of multiple medium and small sized arteries. Cabergoline was stopped and her symptoms were managed conservatively by analgesia and levetiracetam. Six weeks later, DSA was repeated and revealed complete remission of the stenosis, and she recovered completely without any residual symptoms.
Conclusions: Cabergoline should be recognized as a potential trigger of RCVS, and close monitoring is important to avoid the devastating complications of RCVS.
Disclosures of Interest: No
Abstract N°: 2236
UPSIDE DOWN WORDS AS INITIAL CLINICAL PRESENTATION OF AN UNDERLYING ACUTE ISCHEMIC STROKE
Ramuel Spirituel Mattathiah San Juan*1, Neil Ambasing2
1Baguio General Hospital and Medical Center, Neurosciences, Baguio, Philippines, 2Baguio General Hospital and Medical Center, Baguio, Philippines
On behalf of:
Background and aims: We report a diabetic patient who was diagnosed with an acute stroke who presented with a 3-day history of difficulty of reading, described as the words were turned upside down, as if the words were inverted horizontally with associated right homonymous hemianopia and multiple higher cortical function deficits (alexia without agraphia, achromatopsia, prosopagnosia). He has poorly controlled diabetes and hypertension.
Methods: Case Report
Results: Cranial magnetic resonance imaging (MRI) revealed an acute infarct on the left posterior cerebral artery territory. The patient was managed as an acute ischemic stroke and follow up after 6 months revealed improvement of the visual field cut but with persistence of the higher cortical function deficits.
Conclusions: We name this as text reversal metamorphopsia keeping in line with the other metamorphopsias. To the best of our knowledge, we report the first rare occurrence reversal of vision metamorphopsia described as inverted words as the sole initial presentation of an underlying stroke. Our case is extremely rare and it further expands the landscape of metamorphopsias due to its exclusivity to written words and prolonged duration. Knowing these clinical features will help in identifying the lesion locus and may improve subsequent stroke care, especially in time-bound management like intravenous thrombolysis.
Disclosures of Interest: No
Abstract N°: 3033
"WHEN YOU HEAR HOOVES". . .SOMETIMES YOU HAVE TO THINK ZEBRA. A CASE REPORT ABOUT THE RARITY OF GCA INTERLINKED WITH POSTERIOR CIRCULATION STROKE
Georgia Ford*1, Kate Boardman1, Eleanor Skinner1, Helen Harris1
1Torbay Hospital, United Kingdom
On behalf of:
Background and aims: Classically, Giant Cell Arteritis (GCA) presents with symptoms such as unilateral headache, jaw claudication, blurred vision or fever. It’s exceedingly rare for a patient with GCA to present with posterior stroke symptoms. Whilst uncommon, strokes are a severe complication of GCA with high morbidity and mortality rates, making early recognition essential.
Methods: We present our case report of a patient with an atypical presentation of multifocal posterior circulation strokes secondary to GCA.
Results: A 71-year-old female was admitted with 6-week history of headache, visual changes, and ataxia. These symptoms initially responded to steroids. The first MRI scan showed a right cerebellar lesion. Temporal artery ultrasound revealed a normal result, despite rising CRP consistent with active inflammation, and responsiveness to steroids. Rheumatology recommended stopping steroids, the patient later deteriorated with vision loss, dizziness and a further increase in CRP. Steroids were restarted and a repeat MRI revealed new multifocal posterior circulation strokes (right occipital lobe, left thalamic and bilateral cerebellar hemispheres). Subsequent CT angiogram demonstrated thickening and occlusions of both vertebral arteries, in keeping with vasculitis. GCA was later confirmed with a positive temporal artery biopsy. The patient made a marked improvement following reintroduction of steroids.
Conclusions: Through our reflections on this case, we hope to demonstrate the importance of recognising GCA as a cause of stroke and of treating vasculitis in order to reduce risk of subsequent infarcts. We aim to increase awareness of the atypical manifestation of GCA in the context of stroke amongst medical professionals, both in primary and secondary care.
Disclosures of Interest: No
Abstract N°: 3059
INTRAVASCULAR CENTRAL NERVOUS SYSTEM LYMPHOMA PRESENTING WITH UNILATERAL NEURORADIOLOGIC FINDINGS: A CASE REPORT
Sebastiano Giacomozzi*1, Marco Masullo1, Laura Piccolo2, Luigi Cirillo3,4, Matteo Paolucci2, Andrea Zini2
1Department of Biomedical and Neuromotor Sciences (DIBINEM), Alma Mater Studiorum-University of Bologna, Bologna, Italy, 2IRCCS Istituto delle Scienze Neurologiche di Bologna, UOC Neurologia e Rete Stroke Metropolitana, Ospedale Maggiore, Bologna, Italy, 3IRCCS Istituto delle Scienze Neurologiche di Bologna, UOC Neuroradiologia, Ospedale Bellaria, Bologna, Italy, 4Department of Experimental Diagnostic and Specialty Medicine, University of Bologna, Bologna, Italy
On behalf of:
Background and aims: Intravascular lymphoma (IVL) represents a rare subtype of diffuse large B-cell lymphoma distinguished by intraluminal proliferation of lymphomatous cells within small and medium vessels, with a predilection for the central nervous system (CNS) and skin. The diagnosis of IVL is challenging and frequently reached in post-mortem autopsy, because of heterogenous clinical and radiological manifestations and the absence of specific laboratory findings. Here, we report a case of a patient with intravascular CNS lymphoma presenting with unilateral involvement.
Methods: We systematically collected comprehensive data encompassing the patient's medical history, clinical presentation, laboratory results, radiological imaging, and histological findings.
Results: A 42-year-old healthy woman presented with subacute left hemiparesis and hemisensory deficit, followed by progressive cognitive decline. Neurologic examination revealed ideomotor slowing, hypomimia, left hemiparesis and pyramidal signs. Brain MRI showed both acute and chronic ischemic lesions on the right hemisphere (Figure1, A-B), while vessel wall imaging revealed a circumferential contrast enhancement of the right posterior parietal branch (Figure1, C). Cerebral angiography (DSA) showed multiple intracranial distal stenoses of the right MCA (Figure1, D). CSF analysis demonstrated mild lymphocytic pleocytosis and mildly elevated proteins. In the suspicion of primary CNS angiitis, treatment with high-dose glucocorticoids and mofetile micofenolate was started with slight benefit. One month later, after an ischemic stroke recurrence, brain biopsy was performed, revealing a intravascular large B-cell lymphoma. Unfortunately, the patient died few weeks later.
Conclusions: Intravascular CNS lymphoma should be considered in cases with unexplained unilateral recurrent strokes.
Disclosures of Interest: No
Abstract N°: 3155
FUNGAL EMBOLUS AS A RARE CAUSE OF LARGE VESSEL OCCLUSION STROKE – CASE REPORT
Krzysztof Gawrych*1, Artur Dziadkiewicz1, Krzysztof Pawłowski2, Krzysztof Wazny3, Alicja Mączkowiak1
1Pomeranian Hospitals, Department of Neurology and Stroke, Wejherowo, Poland, 2Pomeranian Hospitals, Department of Cardiology and Interventional Angiology, Kashubian Center for Heart and Vascular Disease, Wejherowo, Poland, 3Pomeranian Hospitals, Department of Pathology, Wejherowo, Poland
On behalf of:
Background and aims: The large vessel occlusion stroke is most often caused by artery atherosclerosis or cardioembolic events related to cardiac disease such as atrial fibrillation. Same patients experience rare, potentially treatable causes.
Methods: The 78-year-old patient with an atrial fibrillation and aortic bioprosthetic valve was admitted with symptoms of sudden aphasia and right hemiparesis. The NIHSS score was 24. Additionaly, there were signs of cardiorespiratory failure with elevated white blood cells count. The computed tomography (CT) of the brain was normal (ASPECTS 10), but the computed tomography angiogram (CTA) revealed occlusion of the left middle cerebral artery in the M1 segment (Figure 1). Endovasular thrombectomy (EVT) was performed and the obtained thrombus was sent for histopathological examination. After EVT the patient’s neurological condition improved (The NIHSS score was 14), but the general condition was still serious.
Results: Fungal spores were found in the microscopic image in the thrombus ( Figure 2). Staining for fungi with silver using the Grocott method was positive ( Figure 3 ). Systemic antifungal treatment was initiated. Despite the therapy, the patient’s condition worsened and the patient died after 10 days of hospitalization.
Conclusions: A histopathological examination of the retrieved thrombus is an important element of the etiological diagnosis of stroke. It allows to recognise unusual causes of stroke, such as in this case - fungal sepsis.
Disclosures of Interest: No
Abstract N°: 3216
INTRAVASCULAR LARGE B-CELL LYMPHOMA MISDIAGNOSED AS CEREBRAL AMYLOID ANGIOPATHY: A CHALLENGING CASE PRESENTATION
Navangi Patel*1, Mona Bahouth2
1The Johns Hopkins Hospital, Neurology, Baltimore, United States, 2The Johns Hopkins Hospital, Neurology, Baltimore, United States
On behalf of:
Background and aims: Intravascular large B-cell lymphoma (IVBCL) is a rare variant of extranodal diffuse large B-cell lymphocytes characterized by the presence of lymphoma cells within the lumen of small and medium sized vessels. It poses diagnostic challenges due to its diverse presentation, non-specific laboratory and imaging findings and the necessity for a tissue based diagnosis. Despite its rarity (annual incidence < 0.5 cases per 1,000,000), over 60% of cases manifest neurologic symptoms. This case report highlights the diagnostic complexities associated with IVBCL.
Methods: We report a case of a 70-year-old man presenting with subacute onset of cognitive decline initially treated for possible viral encephalitis and seizures with no improvement. Further work up with MRI brain showed rapidly evolving changes including leptomeningeal enhancement, multifocal cortical and subcortical infarcts and microhemorrhages suggestive of possible cerebral amyloid angiopathy (CAA). But there were no favorable intracranial biopsy sites. Treatment with systemic steroids provided only transient improvement of symptoms. Pancytopenia and increasing LDH prompted a random skin biopsy (left and right abdomen, left thigh).
Results: One out of three biopsy samples (Figure 1) revealed CD20 positive atypical lymphocytes present within vascular spaces of an angioma confirming the diagnosis of IVLBCL.
Conclusions: This patient’s initial misleading presentation as viral encephalitis and CAA emphasizes the importance of considering rare entities. This case illustrates challenge in the diagnosis of IVLBCL. It should be considered as one of the differential diagnoses even with primarily neurological symptoms.
Disclosures of Interest: No
Paper Poster - Cerebrovascular Manifestations of other Infections
Abstract N°: 2030
CEREBROVASCULAR COMPLICATIONS OF INFECTIOUS ENDOCARDITIS OVER THE PAST TWENTY YEARS
Beatriz Martínez García*1, Juan Luis Chico García1, Cristina Moreno López1, Gabriel García Alcántara1, Enrique Navas2, Pilar Martín-Dávila2, Carmen Quereda2, Jaime Masjuan1, Íñigo Corral1
1Ramón y Cajal Hospital, Neurology, 2Ramón y Cajal Hospital, Infectious Diseases
On behalf of:
Background and aims: Symptomatic cerebrovascular complications (SCvC) are the most common neurological involvement of infective endocarditis (IE). Our aim was to analyse the frequency of SCvC, the risk factors for their development and their influence on the clinical outcome and the start of the treatment.
Methods: Retrospective observational study including all the cases of IE who displayed SCvC attended at our institution between 2003 and 2023. Univariate and multivariate models were obtained to assess for risk factors.
Results: Out of 661 patients with IE, 106 (16%) presented SCvC (66% men, median age: 68 years old, IQR: 57-77). Ischaemic stroke (IS) was the most common presentation (77.3%), while remaining patients presented cerebral haemorrhages. In 42 cases (39.6%) the SCvC was the cause of patients’ admission, allowing a definitive diagnosis of IE in 41 patients (38.7%) according to Duke’s criteria. Median time between symptoms onset to antibiotic treatment in the IS group was one day (IQR: 1-2); however, it did not influence the clinical outcome. Left-sided endocarditis was associated with IS (mitral valve [p=0.03] and mitroaortic junction involvement [p=0.01]). Vascular imaging was performed in 48 patients (40.6%), with an increasing preference for using brain computed tomography angiography over digital subtraction angiography over time. Six patients (5.1%) presented unruptured mycotic aneurysms (MA), and one ruptured MA was documented (0.8%). CH presented an OR=4 for death (1.34-11.96, p=0.01) and an OR=4.89 (1.3-18.2, p=0.01) for unfavourable 90-day modified Rankin Scale score.
Conclusions: SCvC remain as the most severe extracardiac complications of IE, particularly CH, which are associated to a poor prognosis.
Disclosures of Interest: No
Abstract N°: 2758
ORAL HEALTH, REGULAR DENTAL CARE, AND INCIDENT ISCHEMIC STROKE
Souvik Sen*1, Stefanie Wood1, Chylee Martin1, James Beck2, Rebecca Gottesman3, Wayne Rosamond2
1University of South Carolina School of Medicine, Neurology, Columbia, United States, 2UNC Gillings School of Global Public Health, Epidemiology, Chapel Hill, United States, 3National Institute of Neurological Disorders and Stroke, Stroke Branch, Bethesda, United States
On behalf of: Atherosclerosis Risk in Communities (ARIC) study group
Background and aims: Periodontal disease (PD) and caries are risk factors for incident ischemic stroke. This study investigated the relationship between PD, caries, stroke, and regular dental care.
Methods: A select group of the Atherosclerosis Risk in Communities dental cohort (n=6271) was followed for stroke incident for 25 years. A full-mouth examination was conducted at visit 4 assessing PD and caries. Adjusted hazards ratio (adj. HR) adjusting for age, sex, race, hypertension, diabetes, smoking, education, BMI and LDL cholesterol were calculated. Regular dental care was assessed.
Results: Of the 6271, 3321 had PD, 1265 had PD + caries and the remaining 1685 had neither, deemed to be in “oral health”. Over the follow-up period, 241/3321 in PD arm, 128/1265 in PD + caries arm and 69/1685 in oral health arm had stroke (Figure 1, Gray’s test p<0.0001). The PD group stroke risk increased after visit 4 and the PD + Caries group risk increased 3 years lag. Both the PD and PD + Caries group had increased risk of stroke, with the PD + Caries group risk being higher [adj. HR 1.50, 95% CI, 1.13–2.01 and adj. HR 2.12, 95% CI, 1.47–3.01] respectively. Regular dental care utilization lowered the chance of PD (odds ratio, 0.27 [95% CI, 0.22–0.34]; P<0.001) and PD + caries (odds ratio, 0.04 [95% CI, 0.03–0.05]; P<0.001).
Conclusions: PD + caries had an independent stronger association with ischemic stroke compared to PD alone. Regular dental care was associated with a lower chance of PD + caries compared to PD.
Disclosures of Interest: No
Abstract N°: 1004
HIGH CONTINUOUS BLOOD PRESSURE VARIABILITY IN HOSPITALIZED COVID-19 PATIENTS IS ASSOCIATED WITH LOWER WHITE MATTER INTEGRITY
Theresa J van Lith*1, Esther Janssen1, Jan-Willem van Dalen1,2, Hao LI1, Menno Huisman3, H. Bart van der Worp4, Anton Meijer5, Anil Tuladhar1, Bas Bredie6, Frank-Erik De Leeuw1
1Radboud University Medical Center, Neurology, Nijmegen, Netherlands, 2Amsterdam UMC, Neurology, Amsterdam, Netherlands, 3Leiden University Medical Center, Department of Thrombosis and Hemostasis, Leiden, Netherlands, 4UMC Utrecht, Neurology, Utrecht, Netherlands, 5Radboud University Medical Center, Medical Imaging, Nijmegen, Netherlands, 6Radboud University Medical Center, Internal Medicine & Health Innovation Labs, Nijmegen, Netherlands
On behalf of: CORONavirus and Ischemic stroke (CORONIS) study group
Background and aims: Increased long-term blood pressure variability (BPV) is associated with cerebrovascular damage and dementia, but it is unknown whether higher short-term BPV is also associated with cerebral white matter (WM) damage. We examined whether short-term BPV, measured in-hospital using continuous monitoring, is associated with WM microstructural integrity in COVID-19 patients.
Methods: We included hospitalized COVID-19 patients from the CORONavirus and Ischemic stroke (CORONIS) study who underwent continuous vital signs monitoring using a wearable device during their stay at the general ward and MRI-DWI imaging shortly after discharge. Systolic BPV was calculated as Average Real Variability (ARV) and Coefficient of Variation (CV) with 1-, 5- and 20-minute intervals. WM integrity was assessed using diffusion tensor imaging (DTI). Associations between BPV and WM integrity were examined using linear regression adjusted for age, hypertension, number of BP measurements and type of respiratory support.
Results: 47 COVID-19 patients (mean age: 59.6 years) were included. BP was measured 6306 ±4343 times per patient (mean admission duration: 11 days). Higher BPV was associated with lower fractional anisotropy (FA) and higher peak width of skeletonized mean diffusivity (PSMD) after adjustment for confounders (ARV: β=-0.42, p=0.008; CV5: β=-0.31, p=0.034; CV20: β=-0.33, p=0.025). Additional adjustment for white matter hyperintensities (WMH) volume confirmed these results. (p<0.02). There was no interaction with WMH volume or hypertension.
Conclusions: High BPV during hospitalization is associated with lower WM integrity in COVID-19 patients, suggesting that BPV may be a target for improving cerebrovascular outcomes. Our findings need validation in hospitalized patients without COVID-19 to examine their generalizability.
Disclosures of Interest: No
Abstract N°: 1466
EXPLORING THE CHAGAS DISEASE-STROKE ‘CONNECTION’: FINDINGS FROM A LARGE MULTICENTER STUDY
Vinicius Montanaro*1, Gisele Sampaio2, Octavio Pontes-Neto3, Jamary Oliveira-Filho4, Gabriel De Freitas5, Fidel Meira6, Eduardo Melo7, Rodrigo Bezerra8, Wilson Oliveira Junior7,7, Luciana Andrade9
Background and aims: Strokes are traditionally attributed to risk factors like aging, hypertension, diabetes, and atherosclerosis. Chagas disease has emerged as an important risk factor for stroke in Latin America. Our study aims at describing the largest cohort of patients with Chagas disease and ischemic stroke and determining variables associated with stroke recurrence and cardioembolic cause.
Methods: This study is the result of a national multicenter cohort study conducted in Brazil. The study spanned from January 2009 to December 2016 and involved a comprehensive retrospective analysis of medical records of patients with both Chagas disease and stroke.
Results: Our findings underscore the significant prevalence of traditional vascular risk factors among Chagas disease patients who had stroke. 81% of patients had hypertension, 56% dyslipidemia and 25% diabetes. We observed a 29.7% recurrence rate. 56% of the patients had embolic stroke of undetermined source (ESUS). Age was a protective factor (OR:0.98, CI 0.970 – 0.997) against cardioembolic etiology. Anticoagulation therapy was associated with reduced risk (OR:0.221 |CI 0.104 – 0.472), highlighting the importance of accurate etiological classification. Female sex(OR:1.83 CI 1.039 – 3.249) emerged as a risk factor for stroke recurrence.
Conclusions: This study significantly advances our epidemiological understanding of the intersection between Chagas disease and stroke. It emphasizes the critical need for extensive epidemiological investigations, a deeper comprehension of stroke recurrence determinants, and accurate etiological classification. Our findings suggests the need of control of vascular risk factors and comorbidities and hold promise for improving patient care and reducing the burden of Chagas disease and stroke worldwide.
Disclosures of Interest: No
Abstract N°: 1006
WHITE MATTER INTEGRITY IN HOSPITALIZED COVID-19 PATIENTS AND ITS ASSOCIATION WITH SHORT- AND LONG-TERM CLINICAL OUTCOMES
Theresa J van Lith*1, Hao LI1, Marte van der Wijk1, Naomi Wijers2, Wouter Sluis3, Marieke Wermer4, Anton Meijer5, Frank-Erik De Leeuw1, Anil Tuladhar1
Background and aims: Many COVID-19 patients experience persistent symptoms including fatigue, cognitive impairment, mood disorders and declined functional outcome, with the underlying mechanisms remaining unclear. This study investigated white matter (WM) integrity in hospitalized COVID-19 patients and its associations with clinical outcomes (including Post COVID-19 condition).
Methods: This study is a part of the CORONavirus and Ischemic Stroke (CORONIS) study. We included COVID-19 patients and controls who underwent MRI-DWI imaging at baseline and 3 months (Table 1) and assessed WM integrity using diffusion tensor imaging and neurite orientation dispersion and density imaging, performing comparisons between groups. Clinical assessment was conducted at 3 and 12 months. Associations between WM integrity and clinical outcomes were evaluated using logistic and linear regression.
Results: 49 patients (mean age 59.5 years) showed higher overall peak width of skeletonized mean diffusivity (PSMD) and lower neurite density index (NDI) in several WM regions compared to 25 controls at baseline (p<0.05), but did not remain significant after adjusting for WM hyperintensities (Figure 1). Orientation dispersion index (ODI) increased in several WM regions within patients after 3 months (p<0.05). Patients exhibited worse clinical outcomes compared to controls, but only decreased NDI at baseline was associated with worse performance on daily function scores after 12 months (p<0.05).
Conclusions: Hospitalized COVID-19 patients had lower WM integrity compared to controls, which is likely explained by the presence of small vessel disease, not due to SARS-CoV-2-infection. WM integrity was not generally associated with clinical outcome measures, suggesting other factors play a role in declined outcomes.
Disclosures of Interest: No
Abstract N°: 3086
CONCEALMENT, BLINDING AND RANDOMIZATION IN A MULTI-CENTER, PRECLINICAL STROKE STUDY—THE SECOND STROKE PRECLINICAL ASSESSMENT NETWORK
Patrick Lyden*1, Jessica Lamb2, Karisma Nagarkatti2, Nabil Alkayed3, Klaus van Leyen4, Yi Zheng4, Robyn Goforth5, Olivia Asfaha6, Theo Hagg7, Evan Unger8
1Zilkha Neurogenetic Institute, Physiology and Neuroscience, 2Unversity of Southern California, Los Angeles, United States, 3Oregon Health Sciences University, 4Massachusetts General Hospital, 5Neurexis Therapeutics, 6Neurexis Therapeutics, Aurora, United States, 7East Tennessee State University, 8NuVox Therapeutics
On behalf of:
Background and aims: The Stroke Preclinical Assessment Network (SPAN) is a randomized, placebo-controlled, blinded, multi-laboratory preclinical study using a Multi-Arm Multi-Stage statistical design to select one or more putative stroke treatments with an implied high likelihood of success in future human clinical stroke trials.
Methods: Through a rigorous NIH-managed peer review process, six independent research laboratories were selected for testing five promising cerebrovascular interventions in SPAN 2.0. The five treatment agents have different solubilities, dose and timing requirements, and physical appearances. Some require delayed initiation. Blinding required iterative cooperation among intervention investigators/drug makers and the SPAN Coordinating Center (CC) to match placebos and coordinate administration schedules.
Results: SPAN successfully implemented treatment blinding, randomization, pre-randomization inclusion and exclusion criteria, and plans blinded assessment of outcomes. Interventions selected are NanO2 (NuvOx) an oxygen delivery emulsion, tatCN19o (Neurexis) a CaM-kinase II inhibitor, GSK2256098 (GlaxoSmithKline/ETSU) a focal adhesion kinase inhibitor, GSK2256294 (GlaxoSmithKline/OHSU) a soluble epoxide hydrolase inhibitor, and BPN-27332 (Loxagen/MGH) a lipoxygenase inhibitor. Intravenous drugs/placebos will be given 5 minutes before MCAo reperfusion over 20 minutes, 90 minutes after reperfusion over 20 minutes, and 180 minutes after reperfusion as a bolus. Intraperitoneal drugs will be given 5 minutes before MCAo reperfusion, and at 6, 24, 48, and 72 hours after reperfusion.
Conclusions: Blinding in a multi-arm, multi-center preclinical trial is complex. Despite dissimilar compounds with differing solubilities and administration schedules, SPAN CC has designed a masked schedule that accommodates very different drugs and dosing schedules into a simplified, 2-tier trial using intravenous and intraperitoneal administration.
Disclosures of Interest: No
Paper Poster - Clinical Practice, Management and Care
Abstract N°: 1431
PERCEPTION AND ACQUAINTANCE OF STROKE PHYSICIANS ON NON-INFERIORITY TRIALS
Aristeidis Katsanos*1, George Howard2, Laetitia Yperzeele3, Kui Kai Lau4, Emily Ramage5, Ivan Koltsov6, Bogdan Ciopleias7, Julia Shapranova8, Philip Bath9
1McMaster University/ Population Health Research Institute, Hamilton, Canada, 2University of Alabama, Birmingham, United States, 3Antwerp University Hospital, Antwerp, Belgium, 4University of Hong Kong, Hong Kong, China, 5University of Melbourne, Melbourne, Australia, 6National Research Medical University (RNRMU), Moscow, Russian Federation, 7County Clinic Hospital Brasov, Brasov, Romania, 8World Stroke Organization, 9University of Nottingham, Nottingham, United Kingdom
On behalf of: World Stroke Organization Future Leaders
Background and aims: The non-inferiority trial design has gained popularity in the evaluation of new interventions for the treatment of patients with stroke. Contrary to a superiority hypothesis, the concept of non-inferiority is more complex and results interpretation becomes more challenging for clinicians.
Methods: We developed a survey to assess the perception and acquaintance of stroke physicians on non-inferiority trials. This survey has been distributed to the members of the World Stroke Organisation (WSO) between November and December 2023.
Results: A total of 120 members responded to our survey (77% neurologists, 5% radiologists, 3% neurosurgeons, 5% internists, 10% other specialists). Eight out of ten responders reported that they practice in an academic hospital. A third of the survey participants reported that they are very familiar with non-inferiority trials, while 6% declared that they are extremely familiar. Of those reporting that they are very or extremely familiar with non-inferiority trials 26% reported that they can name 6-10 non-inferiority trials and 19% can name more than 10. When asked on the impact of non-inferiority trials for advancing the clinical care of stroke patients 42% reported that is high and 45% that is moderate. Eight out of ten responders reported that the findings of non-inferiority trials can affect their clinical practice.
Conclusions: More than 80% of stroke physicians responding to our survey report that non-inferiority trials can have a major impact in their clinical practice and care of stroke patients. However, only 40% report familiarity with the design and interpretation of non-inferiority trials..
Disclosures of Interest: No
Abstract N°: 2633
ASSISTED SUICIDE AFTER RECENT STROKE: EXPERIENCE OF A SWISS ACADEMIC CENTER
1Lausanne University Hospital and University of Lausanne, Stroke Center, Neurology Service, Department of Clinical Neurosciences, Lausanne, 2Lausanne University Hospital and University of Lausanne, Medical Direction, Lausanne, 3Lausanne University Hospital, Legal Affairs Department, Lausanne, 4EXIT, Association for the Right to Die in Dignity, French section of Switzerland, Genève, Switzerland, 5Lausanne University Hospital and University of Lausanne, Psychiatric Liaison Service, Department of Psychiatry, Lausanne, 6Lausanne University Hospital and University of Lausanne, Palliative and Supportive Care Service, Department of Internal Medicine, Lausanne, 7Lausanne University Hospital and University of Lausanne, Clinical Ethics Unit, Institute of Humanities in Medicine, Lausanne
On behalf of:
Background and aims: Assisted suicide (AS) is admitted by Swiss law and deontological rules exist for patients with decision-making capacity and severe diseases or permanent disability and a persistent request for AS. In 2006, our hospital implemented a protocol requiring interdisciplinary evaluation facilitated by an external right-to-die organisation (RTDO) to allow in-hospital AS for patients unable to safely return home. We describe our experience with patients who asked for AS during hospitalisation after a recent stroke and died by AS in-hospital or at home after discharge.
Methods: We extracted data from the hospital’s acute ischemic stroke registry (“ASTRAL") from 2006-2023 of patients who died by AS within 3 months of an IS. We also reviewed their medical records and analysed data anonymously.
Results: Of 6973 consecutively admitted patients, eight (0.1%) died by AS (75% female, median age 89 years (IQR:86-92), admission NIHSS 4.5 (IQR:3-9.3), delay from stroke-to-AS 20 days (IQR:15-33), four of whom in-hospital. Two had non-terminal oncological disease and 7/8 were RTDO-member before stroke. The modified-Rankin-Scale score was 2 (IQR:2-2.3) pre-stroke, and 4 (IQR:3.8-4.3) at the time of AS. All were offered multidisciplinary psychological and spiritual support. All AS occurred without complications after self-administration of pentobarbital prescribed by the RTDO’s physician.
Conclusions: After a recent stroke, very few patients hospitalized in a Swiss academic hospital take the decision to die by AS. An interdisciplinary protocol in collaboration with RTDOs allows in-hospital SA for selected patients unable to return home and gives professionals a clear guidance for their practice.
Disclosures of Interest: No
Abstract N°: 2986
PRE-STROKE CLINICAL FRAILTY SCORE IS A STRONG PREDICTOR OF MORBIDITY AND MORTALITY IN PATIENTS ADMITTED TO A HYPER-ACUTE STROKE UNIT
Benjamin Johnstone*1, Rob Simister2, Arup Sen3, Sadia Saber3
1National Hospital for Neurology and Neurosurgery, Stroke Medicine, London, United Kingdom, 2National Hospital for Neurology and Neurosurgery, Stroke Medicine, Neurology, London, United Kingdom, 3National Hospital for Neurology and Neurosurgery, Stroke Medicine, Geriatric Medicine, London, United Kingdom
On behalf of:
Background and aims: Existing literature demonstrates inconsistent evidence of mRS as a reliable measure of frailty among patients with stroke. This single-centre retrospective cohort study aimed to assess the utility of the Clinical Frailty Score (CFS) in determining functional outcomes in patients admitted to a hyper-acute stroke unit (HASU).
Methods: All patients admitted to a HASU with a diagnosis of ischaemic or haemorrhagic stroke were recruited between September and November 2022. Pre-stroke mRS, pre-treatment NIHSS, and administration of hyper-acute treatment was recorded. CFS was determined from allied health assessment of baseline function. Patients with CFS ⩾ 5 were defined as frail. Outcomes between frail and non-frail patients were compared, including inpatient medical complications, discharge mRS and 30-day mortality.
Results: A total of 292 patients were recruited. 26.6% of frail patients were documented to have a pre-stroke mRS of 0-2. Regression modelling demonstrated that CFS remained a significant predictor of discharge mRS (p=0.024) when adjusted for pre-stroke mRS, age, sex, baseline NIHSS and stroke aetiology. Among patients ⩾65 years of age (n=183), frailty was associated with a significantly higher pre-treatment NIHSS (p=0.022), and significantly increased rates of inpatient medical complications (p=0.040), discharge mRS ⩾3 (p<0.001), and 30-day mortality (p=0.030) compared to non-frail patients.
Conclusions: Frailty was found to be a strong predictor of morbidity and mortality outcomes in patients presenting with hyper-acute ischaemic and haemorrhagic stroke. Pre-stroke mRS was found to underestimate baseline frailty in a significant proportion of patients. CFS may be a useful metric alongside mRS to guide management in this patient population.
Disclosures of Interest: No
Abstract N°: 1146
DESIGN, RATIONALE, AND BASELINE CHARACTERISTICS: REVERXAL STUDY OF PATIENTS HOSPITALISED WITH FXA INHIBITOR–RELATED MAJOR BLEEDS
May Nour*1, Richard Ofori-Asenso2, Masahiro Yasaka3, Hungta Chen4, Vinay Sehgal5, Shoji Yokobori6, Raza Alikhan7, Bruce Koch4, Onivefu Odelade4, Andreas Tiede8
1Department of Neurology, Ronald Reagan University of California, Los Angeles Medical Center, Los Angeles, CA, United States, 2AstraZeneca, Medical and Scientific Affairs, Biopharmaceuticals Medical, London, United Kingdom, 3Department of Cerebrovascular Medicine and Neurology, Cerebrovascular Center, Clinical Research Institute, National Hospital Organization Kyushu Medical Center, Fukuoka Neurosurgical Hospital, Minami-ku, Fukuoka, Japan, 4AstraZeneca, Wilmington, DE, United States, 5University College Hospital London, London, United Kingdom, 6Department of Emergency and Critical Care Medicine, Nippon Medical School, Tokyo, Japan, 7Department of Haematology, University Hospital of Wales, Cardiff, United Kingdom, 8Department of Hematology, Hemostasis, Oncology, and Stem Cell Transplantation, Hannover Medical School, Hannover, Germany
On behalf of: Brooks D. Cash, Marc Maegele, Adam J. Singer
Background and aims: Real-world data on the characteristics, interventions, and associated outcomes of patients who are hospitalised with Factor Xa inhibitor (FXai)-related acute major bleeds are limited. To gain a deeper understanding of patient characteristics and treatment approaches, the REVERXaL study was designed. Here, the design, rationale, and baseline characteristics for REVERXaL, a multinational observational study of patients hospitalised with FXai-related acute major bleeds (intracranial haemorrhage [ICH], gastrointestinal bleeds, and other bleeds; NCT06147830), are described.
Methods: REVERXaL includes two cohorts of patients with FXai-related acute major bleeds of any type from Germany, UK, USA, and Japan. Primary objectives are to describe: 1) patient characteristics, 2) healthcare interventions during hospitalisation, and 3) associations between timing of reversal agent administration and in-hospital outcomes. Secondary/exploratory objectives focus on clinical and patient-reported outcomes at 30 and 90 days. Cohort A is a historical cohort including ~2000 patients hospitalised for FXai-related bleeds, utilising information from medical charts from admission to discharge. Cohort B will prospectively enrol ~2000 patients administered any reversal agent when hospitalised for FXai-related bleeds. Patients are followed up to 90 days, including data collection on clinical and patient-reported outcomes.
Results: First patient data for Cohort A were extracted in December 2023. At ESOC, characteristics of hospitalised patients with FXai-related acute major bleeds, including demographics and clinical presentation of Cohort A, will be presented.
Conclusions: REVERXaL will provide broad, real-world insights on characteristics, treatment approaches, and associated outcomes in hospitalised patients with FXai-related major bleeds of various types (ie, ICH, gastrointestinal bleeds, traumatic bleeds).
Disclosures of Interest: Yes Study participation as subinvestigator
Abstract N°: 26
SCIENTIFIC EVIDENCE SUPPORTING STROKE GUIDELINES
Parth Upadhyaya*1, Ying Xian1
1UT Southwestern Medical Center, Dallas, United States
On behalf of:
Background and aims: Guidelines from the American Heart Association (AHA) and European Stroke Organization (ESO) are important for evidence-based practice. Our objective is to describe changes over time, based on the number, levels of evidence and strength of recommendations.
Methods: AHA recommendations published from 2013 to 2021 and ESO guidelines from 2003 to 2023 were abstracted and described by number of total recommendations, levels of evidence and classes of recommendations.
Results: The total number of recommendations from the AHA, with at least one update, increased from 431 to 617 (+43%) from 2010 to 2021. Recommendations with class A (highest level of evidence) and B level of evidence increased from 14% (60) to 17% (102) and 39% (170) to 52% (319) while class C decreased from 47% (202) to 32% (196). Current AHA guidelines have 17% class A, 51% class B and 32% class C level of evidence. ESO recommendations from 2003 to 2009 increased from 108 to 150 (+39%), with a 58% increase in Level I sources (highest level of evidence). A total of 134 recommendations were added from 2017-2023, of which 6% are Level I sources, 20% Level II, 25% level III and 49% are from Level 4 sources.
Conclusions: The number of recommendations issued by the AHA and ESO have increased over time. Despite increasing number of recommendations with higher level of evidence (Level A in AHA and Level I in ESO), the large majority of AHA and ESO recommendations were developed from lower levels of evidence.
Disclosures of Interest: No
Abstract N°: 2433
ACUTE POST-STROKE HYDRATION CARE – A SYSTEMATIC REVIEW OF INTERNATIONAL CLINICAL PRACTICE GUIDELINE RECOMMENDATIONS
Colette Miller*1, Stephanie Jones1, Elizabeth Boaden1, Alison Mcloughlin1, Caroline Watkins1
1University of Central Lancashire, Stroke Research Team, PRESTON, United Kingdom
On behalf of:
Background and aims: Globally, over 13.7 million people have a stroke each year. Over half of acute stroke patients become dehydrated during their hospital stay. Dehydration is associated with poor outcomes, longer length of stay, and greater costs. Clinical Practice Guidelines (CPGs) summarise the best available evidence to inform, standardise, and improve practice. This review sought to identify, compare, and critically appraise international CPG recommendations regarding acute post-stroke hydration care.
Methods: The review was designed and conducted in accordance with PRISMA guidance. A protocol was prospectively registered on PROSPERO (CRD42020217931). Bibliographic databases (Medline; Embase; HMIC; CINAHL), guideline repositories and websites were searched from 2009-2023. Evidence-based CPGs were included if they made recommendations regarding acute post-stroke hydration care, were endorsed by a national/international organisation, and were available in English. Quality was assessed using the AGREE II Tool. Data were extracted using a bespoke proforma, and mapped to apriori defined categories derived from existing literature.
Results: Searches yielded 5520 results. Of 92 full-texts screened, 73 were excluded (Not CPG N=14; Not stroke-specific N=8; Retired/Superseded N=10; Out of scope N=40; Not English N=1). Nineteen were included, of those 2 provided timescales for the completion of initial assessment. Four CPGs suggested methods of assessment, and 7 discussed management/treatment options, though these varied. No recommendations were made regarding specific diagnostic tools or tests and their reference ranges.
Conclusions: This review highlights the importance of routine hydration care practice after stroke. Clarity is needed to guide practice, standardise care, and improve patient outcomes.
Disclosures of Interest: No
Abstract N°: 3103
IMPROVING EVIDENCE-BASED CARE FOR ISCHEMIC STROKE PATIENTS IN A QUALITY IMPROVEMENT COLLABORATIVE
Charlotte Lens*1,2, Ellen Coeckelberghs1, Deborah Seys1, Kris Vanhaecht1,3, Caroline Weltens4, Robin Lemmens2,5
1Leuven Institute for Healthcare Policy, 2Department of Neurosciences, Experimental Neurology, KU Leuven, 3Department of Quality Management, University Hospitals Leuven, 4Vlaams Ziekenhuis Netwerk, 5Department of Neurology, University Hospitals Leuven
On behalf of: BIC4Stroke working group
Background and aims: Implementation of evidence-based guidelines for stroke care remains challenging despite evidence of, for instance, management of temperature (Fever), Sugar (emergency department and stroke unit) and Swallowing (FeSS) to reduce mortality and disability. We established a collaborative to implement these three interventions and two more recently identified care process activities to improve stroke care, i.e. screening of Activities-of-Daily-Living (ADL) and depression, (FeSS+) with ultimate goal to increase adherence rates.
Methods: This multicentre, intervention study was conducted in 24 hospitals in Belgium. Patient records from the last 30 consecutive patients, diagnosed with ischemic stroke in 2019 (pre-implementation) and 2022 (post-implementation), were retrospectively analysed and results compared. Hospitals were educated about FeSS+-guidelines using a digital learning tool to provide assistance in changing the care pathway.
Results: In total, data was obtained for 1440 patients (720/measurement period). We documented improvements in adherence rates for measuring temperature (pre 18.1%; post 25.2%, p=0.007) and swallowing function screening (pre 36.7%; post 61.6%, p<0.001). Measuring glycaemia at emergency department also increased (pre 92.2%; post 98.6%, p<0,001), but stroke unit glycaemia measurement rates did not (pre 28.3%; post 30.3%, p=0.925). Screening of ADL- (pre 49.6%; post 49.5%, p=0.379) and depression screening (pre 21.8%; post 20.9%, p=0.271) did not differ pre- vs post-implementation.
Conclusions: The digital learning tool increased uptake of guideline recommendations into daily clinical care for most of the FeSS+-interventions. The two additional and more recently identified interventions aimed at screening ADL and depression did not improve with just one intervention
Disclosures of Interest: No
Abstract N°: 3287
BAYESIAN MODELING FRAMEWORK FOR OPTIMIZING INDIVIDUAL PRE-HOSPITAL STROKE TRIAGE DECISIONS
Santiago Ortega-Gutierrez*1, Grant Brown2, Jacob Seedorff2, Anne Zepeski3, Marc Ribo4, Jeffrey Saver5, Natalia Pérez de la Ossa6, Nicholas Mohr7
1University of Iowa Hospitals and Clinics, Neurology, Radiology and Neurosurgery, Iowa City, United States, 2University of Iowa, Biostatistics, Iowa City, United States, 3University of Iowa, College of Medicine, Iowa City, United States, 4Hospital Vall d’Hebron, Neurology, Barcelona, Spain, 5University of Californa Los Angeles, Geffen School of Medicine, Los Angeles, United States, 6Hospital Universitari Germans Trias i Pujol, Neurology, Badalona, Spain, 7University of Iowa Hospitals and Clinics, Emergency Medicine, Iowa City, United States
On behalf of:
Background and aims: The RACECAT trial did not find evidence of improved neurological recovery via early triage of high-risk patients by Emergency medical services (EMS). Its design, however, did not account for time since symptom onset or the distance to either a local “Drip-and-Ship” or EVT-capable “Mothership” center. We developed algorithm to optimize the individual probability of best neurological recovery based on the initial EMS triage strategy, using time decay curves under diagnostic uncertainty from cornerstone EVT and IVT trials, and evaluated RACECAT population in Catalonia.
Methods: We used data from Virtual International Stroke Trials Archive (VISTA), RACECAT, and FAST-MAG. To model prehospital diagnosis, we included patients with any stroke-like illness (ischemic/hemorrhagic stroke, and mimics) at presentation. The primary outcome was 90-day modified Rankin scale (mRS Our model accepts time-from symptoms, location, and capability of all local hospitals as inputs. Bayesian Hierarchical modeling framework to address this decision-making process.
Results: We included 9048 participants with 8600 (95%) ischemic strokes, 1801 (20%) had large vessel occlusion, and 4064 (45%) had a 90-day mRS of 0-2 (good neurologic outcome). The illness specific model coefficients are summarized in Table 1. The estimated median absolute difference in chance of good mRS score between bypass and non-local hospital bypass was 2.3% among 1,320 stroke events in the RACECAT (Figure 2).
Conclusions: Our findings suggest that a uniform EMS destination policy is unlikely to be universally optimal. Personalized approaches, accounting for diagnostic uncertainties, patient characteristics, and geospatial factors, may enhance outcome predictions over simpler strategies.
Destination maps for Catalonia
Disclosures of Interest: No
Abstract N°: 778
THE IMPACT OF TRANSCRANIAL MAGNETIC STIMULATION ON SPEECH RECOVERY IN PATIENTS WITH ISCHEMIC STROKE IN THE ACUTE STAGE
Guzel Gainetdinova1,2, Tatyana Danilova1,2, Dina Khasanova1,2, Saida Ishmanova1,2
1Kazan State Medical University, Department of Neurology, Kazan, Russian Federation, 2Interregional clinical diagnostic center, Department of Neurology, Kazan, Russian Federation
On behalf of:
Background and aims: Speech disorders are a common manifestation of stroke. Repetitive Transcranial Magnetic Stimulation (rTMS) has proven to be an effective method for restoring speech.
Aim: to assess the impact of rTMS on speech recovery in patients in the acute stage of ischemic stroke.
Methods: The thirty-eight patients with severe motor Broca's aphasia included in the study had newly developed ischemic stroke caused by large-artery atherosclerosis or cardioembolism, confirmed by computed tomography and/or magnetic resonance imaging. Aphasiological testing was performed on the first and last day of hospitalization using the validated "screening diagnostics of patients with aphasia". The participants were divided into two groups: the first group (19 patients) received standard rehabilitation, including sessions with a speech therapist, as well as a course of rTMS for therapeutic purposes; the second group (19 patients) underwent rehabilitation measures and speech therapy sessions without rTMS.
Results: After screening diagnostics of aphasia at the end of inpatient treatment, Group 2 (without rTMS) showed no significant improvement in speech function, with an average gain of 1.4 points. In contrast, Group 1 (with rTMS) showed an average gain of 7.4 points. The degree of functional recovery of speech in the patients of the first group was significantly higher compared to the patients of the second group (p < 0.05).
Conclusions: The study results demonstrate a positive impact of rTMS on the degree of speech function recovery in the acute stage of ischemic stroke. Further research with a larger sample size is needed to confirm these findings.
Disclosures of Interest: No
Abstract N°: 1522
THE RAPID-SCORE: RISK ASSESSMENT AND PREDICTION OF DELIRIUM IN ACUTE STROKE PATIENTS BASED ON VERY EARLY CLINICAL PARAMETERS
Johannes Wischmann*1, Pauline Kremer1, Ludwig Hinske2,3, Roland Tomasi2, Andrea Becker-Pennrich2,4, Lars Kellert1
1LMU University Hospital Munich, Department of Neurology, Munich, Germany, 2LMU University Hospital Munich, Department of Anesthesiology, Munich, Germany, 3University Hospital Augsburg, Institute for Digital Medicine, Augsburg, Germany, 4LMU University Hospital Munich, Faculty of Medicine, Pettenkofer School of Public Health, Institute for Medical Information Processing, Biometry and Epidemiology (IBE), Munich, Germany
On behalf of:
Background and aims: Post-stroke delirium (PSD) is a common complication in acute stroke patients, and guidelines recommend routine screening and preventive and treatment measures. However, there is a lack of standardized approaches in diagnostic and therapeutic management of PSD. Here, we aimed to develop a new pragmatic and easily assessable screening tool to predict PSD based on early parameters, which are already integral to acute stroke diagnostics.
Methods: We enrolled acute stroke patients admitted to our stroke unit or intensive care unit and developed the scoring system using retrospective single-center patient data. The Confusion Assessment Method for the Intensive Care Unit was used for prospective score validation. Logistic regression models were employed, analyzing the association of early clinical and paraclinical parameters with PSD development.
Results:N = 525 patients (median age: 76 years; 45.7% female) were enrolled, with 29.7% developing PSD during hospitalization. The resulting score comprises 6 items, including medical history, clinical examination findings, and non-contrast computed tomography results at admission. Scores range from −15 to +15 points, with higher values indicating a higher likelihood of PSD, ranging from 4% to 79%. The accuracy was 0.85, and the area under the curve was 0.89.
Conclusions: The new RAPID (Risk Assessment and PredIction of Delirium in acute stroke patients)-score shows high accuracy in predicting PSD among acute stroke patients and offers precise odds of PSD for each corresponding score value, utilizing routine early clinical and paraclinical parameters. It can identify high-risk populations for clinical study interventions and may be suitable to guide prophylactic PSD measures.
Disclosures of Interest: No
Abstract N°: 2500
NURSE-LED UPGRADED GROIN SURVEILLANCE PROTOCOL AFTERENDOVASCULAR PROCEDURES. ONE-YEAR EXPERIENCE IN A STROKE UNIT
Arantza Lopez de Turiso López*1, Elena González-Holgado1, Macarena Marcos Osuna1, Patricia de la Riva Juez1, Maria Teresa Martínez de Albeniz1, Juan Marta1, José Ángel Larrea1
1Donostia University Hospital, Neurologia, Donostia, Spain
On behalf of:
Background and aims: Femoral artery access site complications are uncommon but likely to become more frequent with the increasing use of endovascular procedures (EP) in stroke patients. Current protocols only assess the physical examination in the first 24h after the EP.
This study aims to describe the feasibility and results obtained one year after implementation of an extended groin surveillance protocol adding basic ultrasonography and auscultation to the physical examination, up to 7 days after the EP and lead by a trained stroke unit nurse team.
Methods: Prospective observational single-center study. The protocol includes systematic physical examination assessing hematoma, lump, local pain and leg arterial pulses, bruise auscultation and basic ultrasonography with longitudinal and axial scans of the artery. Each patient was assessed within 7 days after the EP and if the study was considered non-normal, a regular ultrasonography was performed by a radiologist.
Results: A total of 221 EPs were performed during the year. Of these, 167 patients underwent the protocol and 54 were lost. Eighteen of the protocol studies were considered abnormal and in 10 of them (55.5%) radiology studies confirmed a groin complication: 8 pseudoaneurysms of the femoral artery (PAF) and 2 arteriovenous fistulas. Among the losses, 3 patients had local symptoms and were diagnosed with PAF.
Conclusions: Application of an upgraded groin surveillance protocol including ultrasonography and lead by a trained stroke unit nurse team is feasible and it may help in early detection of potential groin complications after EP in stroke patients.
Disclosures of Interest: No
Abstract N°: 561
TIME INTERVAL OF ESOMEPRAZOLE AND DUAL ANTIPLATELET THERAPY IN PATIENTS WITH CARDIOCEREBROVASCULAR DISEASES
Hyunsoo Kim1, Jong-Hee Choi*1, Man-Seok Park1
1Chonnam National University Hospital, Neurology
On behalf of:
Background and aims: Dual antiplatelet therapy (DAPT) with the combination of clopidogrel and aspirin is recommended for secondary prevention in patients with acute coronary syndrome (ACS) or acute ischemic stroke (AIS). Due to clopidogrel-PPI interactions, separating their administration might be considered. Our study aimed to evaluate clinical outcomes based on administration timing.
Methods: This study included patients with ACS or AIS onset or recurrence of within the last month. Patients who were expected to receive DAPT for at least 6 months and who were currently taking or planning to take esomeprazole were included. Patients were divided into interval administration group (IA group) and concurrent administration group (CA group) according to the interval between esomeprazole and DAPT administration. The time interval was based on 12 hours. The primary outcome was occurrence of MACCEs.
Results: A total of 3600 patients completed this study. The proportions of patients in the two groups were as follows: CA group, 99% (n = 3489) and IA group, 1% (n = 111). The primary outcome occurred in 0.9% of patients in the IA group and 1.8% of patients in the CA group (p = 0.51). There was no significant distinction in the overall bleeding risk of the CA group compared to that of the IA group (2.75% in the CA group and 2.70% in the IA group).Conclusions: There was no significant difference in the occurrence of MACCEs and bleeding issues within 6 months according to the medication administration interval. The majority of patients with DAPT were taking PPIs simultaneously in real-world practice.
Disclosures of Interest: No
Abstract N°: 1116
THE IMPACT OF VISUAL IMPAIRMENT POST-STROKE USING THE BRAIN INJURY ASSOCIATED VISUAL IMPAIRMENT - IMPACT QUESTIONNAIRE (BIVI-IQ)
Lauren Hepworth*1, Jamie Kirkham2, Brin Helliwell3, Elizabeth Perkins1, Fiona Rowe1
1University of Liverpool, United Kingdom, 2University of Manchester, United Kingdom, 3VISable PPI group, United Kingdom
On behalf of:
Background and aims: Post-stroke visual impairment (VI) is common with a prevalence of 73% and can impact on independence, activities of daily living and activities of enjoyment. This has previously been measured using patient reported outcome measures (PROMs) not developed for this population, where VI often co-exists with other stroke sequelae. The aim of this study was to assess the impact of VI post-stroke.
Methods: Stroke survivors with VI were recruited from 18 NHS hospitals and via advertisement. There was no restriction of time post-stroke. Participants completed the Brain Injury-related Visual Impairment Impact Questionnaire (BIVI-IQ). The BIVI-IQ was developed and validated to assess the impact of post-stroke VI: scoring ranges 0-37 - high scores indicating higher degrees of impact. Demographics, social history, stroke details and vision assessment data were collected.
Results: 316 participants completed the BIVI-IQ, of which 93% reported an impact to their vision-related quality of life, with a median score of 13.3 (range 0-33.3). The mean age was 67 years, 64% were male and median time post-stroke was 88 days (range 1-7576). The types of new VI included visual field loss (81%), ocular motility defects (32%), visual inattention (16%), visual perception deficits (16%) and reduced visual acuity (7%): 61% had multiple VI’s. The median scores across the different types of VI ranged from 12.6-17.1.
Conclusions: All types of VI had an impact on quality of life, at acute and chronic stages post-stroke. Further assessment of the wider stroke population with VI is required. This will be supported by the BIVI-IQ easy-read version.
Disclosures of Interest: No
Abstract N°: 2131
ADOPTION OF GUIDANCE ON IMMUNOLOGICAL THERAPIES FOR VITT-ASSOCIATED CEREBRAL VENOUS THROMBOSIS IMPROVED PATIENT OUTCOMES IN THE UK
Wenpeng Zhang*1, Arina Tamborska2, Tom Solomon3, Marie Scully4,5, Alastair Webb6, Christine Roffe7, David Werring1,5, Richard Perry5
1UCL Queen Square Institute of Neurology, United Kingdom, 2The Walton Centre NHS Foundation Trust, Liverpool, United Kingdom, 3Institute of Infection, Veterinary and Ecological Science, University of Liverpool, Liverpool, United Kingdom, 4UCL Institute of Cardiovascular Science, United Kingdom, 5University College London Hospitals Nhs Foundation Trust, United Kingdom, 6Wolfson Centre for Prevention Of Stroke and Dementia, Department of Clinical Neuroscience, University of Oxford, Oxford, United Kingdom, 7University Hospitals of North Midlands NHS Trust, UK
On behalf of: CVT After Immunisation Against COVID-19 (CAIAC) collaborators
Background and aims: Vaccine-induced immune thrombotic thrombocytopenia (VITT) is a rare side-effect of vaccination against COVID-19, and cerebral venous thrombosis (CVT) is its most severe manifestation. New UK guidance on managing VITT-associated CVT (VITT-CVT) was disseminated in March 2021, which recommended immunological therapies (intravenous immunoglobulin, plasma exchange, or both) and avoidance of heparins while managing this condition. However, there is a lack of direct clinical evidence from VITT-CVT research to support the treatments recommended in this guidance.
Methods: We retrospectively analysed data from an observational multicentre cohort of VITT-CVT in the UK. We compared the admission characteristics and functional outcomes of VITT-CVT patients admitted before March 13 (pre-guidance) and after March 18, 2021 (post-guidance).
Results: We received data on 107 patients from 43 hospitals across the UK. 36 CVT patients were excluded because they either had no evidence of VITT or were admitted between March 13 and March 18, 2021, a transition period during which management strategies were very heterogeneous. 71 VITT-CVT patients were included, 14 in the pre-guidance group, and 57 in the post-guidance group. There was no significant difference in admission characteristics between the pre- and post-guidance groups. A favourable outcome (modified Rankin score 0-2) was much more frequent in the post-guidance group (33 of 57 [58%] patients) than in the pre-guidance group (3 of 14 [21%] patients; p=0.015) (Figure).
Conclusions: Adoption of the UK guidance on VITT-specific management appeared to improve the functional outcome of patients with VITT-CVT
Disclosures of Interest: Yes RJP receives grants Randox Labs and The Stroke Association. CR receives grants from NIHR and FirstKind Medical. DJW has received personal fees from Bayer and Alnylam. None of these relate to the work presented here. TS advises the MHRA on vaccines.
Abstract N°: 2163
GENERAL PRACTITIONER AND SPECIALIST CARE IMPROVES SURVIVAL AFTER TIA: A LINKED REGISTRY STUDY
Monique Kilkenny*1,2, Muideen Olaiya1, David Ung3,4, Lachlan Dalli1, Joosup Kim1,2, Dominique A. Cadilhac1,2, Mark Nelson5, Nadine Andrew3,4
1Stroke and Ageing Research, Department of Medicine, School of Clinical Sciences, Monash University, 2Stroke Theme, Florey Institute of Neuroscience and Mental Health, University of Melbourne, 3Peninsula Clinical School, Central Clinical School, Monash University, 4National Centre for Healthy Ageing, 5Menzies Institute for Medical Research, University of Tasmania
On behalf of: PRECISE Investigators
Background and aims: Post-acute care interventions are essential for preventing adverse outcomes after a transient ischemic attack (TIA). Limited information is available on the benefits of medical care by general practitioners (GPs) or specialists post-TIA. We aimed to assess patterns of GP or specialist care within 3-months post-admission following TIA and association with health outcomes.
Methods: Observational study using person-level data from the Australian Stroke Clinical Registry (2012-2016; Queensland and Victoria) linked to government-held administrative datasets. We included patients with TIA (and no prior stroke) who survived >3 months post-discharge. Using medical services data, we categorised medical care received based on 1) regularity of GP visit (continuity of care index ⩾80%); 2) specialist consultation (cardiologist or neurologist). Patients were followed 91-455 days post-discharge. Outcomes were compared based on the type of care using Cox proportional hazards regression, adjusted for age, sex and comorbidities (Charlson Comorbidity Index).
Results: Of 3,894 eligible patients (median age 70 years, 47% female), 180 (4.6%) died within the follow-up period. Overall, 44% regularly saw their GP, 23% saw a cardiologist and 16% a neurologist (32% either specialist). Compared to patients with no medical care within 3 months post-TIA, there was an improvement in survival among patients who saw specialist/s only (HR: 0.57; 95% CI 0.37-0.89) or specialist/s and GP (HR: 0.43; 95% CI 0.26-0.69). There was no significant difference in survival among patients who saw GPs only.
Conclusions: Seeing a specialist in addition to GP visits can improve survival after hospital discharge following a TIA.
Disclosures of Interest: No
Abstract N°: 2445
PRE-HOSPITAL TIMINGS FOR EMERGENCY STROKE PRESENTATIONS IN THE UK: ARE NATIONAL FAST CAMPAIGNS WORKING?
Chris Ashton*1,2, Youssef Hbid1, Kaili Stanley1, Ajay Bhalla1,3, Martin James1,4
1Sentinel Stroke National Audit Programme, King's College, London, United Kingdom, 2Greater Manchester Neurorehabilitation & Integrated Stroke Delivery Network, Salford, United Kingdom, 3Guy’s and St Thomas’ NHS Foundation Trust, London, United Kingdom, 4Royal Devon University Healthcare NHS Foundation Trust, Exeter, United Kingdom
On behalf of:
Background and aims: Although 75% of stroke admissions in the UK arrive by ambulance, stroke presentations via emergency 999 calls represent only 2-3% of overall ambulance activity, and research into these presentations is rare. This comprehensive nationwide study investigated the breakdown of the patient journey from onset to arrival at hospital, including the impact of public education (FAST) campaigns.
Methods: We performed a retrospective observational time series study investigating onset to emergency call, call to incident, time at incident and incident to arrival at hospital. 197,808 Stroke records between April 2019-March 2023 for the 11 ambulance services covering England were extracted and analysed from the Sentinel stroke national audit programme (SSNAP).
Multiple linear regression was used to examine temporal trends in each component of the pre-hospital pathway throughout the study period.
Results: Over 4 years the median onset to arrival time increased from 160 (IQR 91-417) to 185 minutes (IQR 105-475) (p<0.05). All component timings within the pathway increased significantly over this period (p<0.05). Prominently, median time from onset to emergency call increased from 78 (IQR 61-104) to 84 minutes (IQR 64-114), and call to arrival at incident increased from 18 (IQR 11-32) to 26 minutes (IQR 15-47). Median times at incident (27-32 minutes) and incident to hospital (16 minutes), while statistically significant, increased to a lesser extent.
Conclusions: Over the last 4 years, and despite national media campaigns promoting FAST, onset to arrival times for emergency stroke calls in the UK have increased substantially, with potential adverse impacts on reperfusion eligibility and benefit.
Disclosures of Interest: No
Abstract N°: 2575
CONSENT-BIAS – A COMPARISON OF EARLY CLINICAL ENDPOINTS IN STROKE PATIENTS
Annika Söder*1, Susanne Bonekamp1, Markus Möhlenbruch1
Background and aims: Clinical research requires voluntary participation and informed consent. The latter proves to be a major challenge in acute ischemic stroke studies. Often patients are unable to give informed consent either before or immediately after treatment and legal representatives are not routinely appointed. Furthermore, inclusion and exclusion criteria lead to an additional selection of the patient collective. These factors could lead to patients included in a study (group A) differing from patients who were not included in a study (group B) at follow-up.
Methods: The inclusion criteria for this retrospective study were an age of at least 18 years and admission to Heidelberg University Hospital for treatment of an acute ischemic stroke in 2021. There were no exclusion criteria. The data were collected retrospectively from existing study protocols, routine medical records and imaging procedures. Data collected included the National Institutes of Health Stroke Scale (NIHSS) on admission to hospital, after 24 hours and on discharge (from which a shift was calculated).
Results: A significant difference of the NHISS 24 hours after admission (12,5±0,529 vs 6,11±0,477; p<0.001) as well as the change in NIHSS between admission and discharge (3.27±0.631 vs 1.40±0.296; p<0.001) was found.
Conclusions: Group A differed in outcome from group B. This means that the patients who were enrolled into clinical studies were not representative of stroke patients at our centre. These findings underscore the urgency of developing privacy laws and guidelines that allow for the waiver of detailed consent when it comes to minimal risk observations in research.
Disclosures of Interest: No
Abstract N°: 3182
THE DELIVERING OF THROMBOLYSIS AND MECHANICAL THROMBECTOMY IN UKRAINE DURING THE WAR
1Kharkiv National Medical University, Neurology, Kharkiv, Ukraine, 2Feofaniya Clinical Hospital, Neurology, Kyiv, Ukraine, 3Poltava Regional Clinical Hospital named after M.V.Sklifosovskyy, Stroke Center, Poltava, Ukraine, 4Lutsk City Hospital, Stroke Center, Lutsk, Ukraine, 5Dnipro Regional Clinical Hospital named after I.I. Mechnykov, Stroke Center, Dnipro, Uganda, 6Dnipro Regional Clinical Hospital named after I.I. Mechnykov, Stroke Center, Dnipro, Ukraine, 7Vinnytsia National Pirogov Medical University, Neurology, Vinnytsia, Ukraine
On behalf of:
Background and aims: : After the beginning of the war in Ukraine in 2022 stroke care struggled across the whole country despite increasing number of all types of strokes. In the middle of the year healthcare system adopted to the war times and stroke care improved.
Methods: We compared numbers of IV tPA and MT for ischaemic stroke in 2022 and during the first 10 months of 2023 year according to National Health Service of Ukraine data from all Ukrainian stroke units and centres to understand how war can change providing reperfusion therapy in country that suffers the war.
Results: Since the beginning of the war, the percentage of thrombolytic therapy in Ukraine has increased by 37%, and mechanical thrombectomy by 28.6%.
Conclusions: So we can conclude that the war had only short-term negative impact on stroke care. And with correct management of healthcare system all people of Ukraine have a chance for the best stroke service even during the war.
Disclosures of Interest: No
Abstract N°: 854
COPING IN CRISIS: EVALUATING THE IMPACT OF THE COVID-19 PANDEMIC ON STROKE CARE QUALITY FOR DEMENTIA PATIENTS
Tamar Abzhandadze*1,2, Minh Tuan Hoang3, Minjia Mo1, Hong Xu1, Mia Von Euler4, Maria Eriksdotter1, Sara Garcia-Ptacek1
1Division of Clinical Geriatrics, Department of Neurobiology, Care Sciences and Society (NVS), Karolinska Institutet, Stockholm, Sweden, 2Department of Occupational Therapy and Physiotherapy, Sahlgrenska University Hospital, Gothenburg, Sweden, 3Division of Clinical Geriatrics, Department of Neurobiology, Care Sciences and Society (NVS), Karolinska Institutet, Stockholm, Sweden, 4Örebro University, Faculty of Medicine and Health, Department of Neurology and Rehabilitation, Örebro, Sweden
On behalf of:
Background and aims: COVID-19 had profound consequences for healthcare systems worldwide. Many healthcare systems struggled to maintain the same level of quality of care as before the pandemic. We aimed to examine the impact of the COVID-19 pandemic on the quality of stroke care for patients with pre-existing dementia, in comparison to patients with stroke only.
Methods: This was a registry-based study. We included patients with a first stroke between 2019 and 2022, both with and without dementia. The study periods were defined as prepandemic (January 1, 2019, to February 29, 2020), COVID-19 pandemic (March 1, 2020, to February 24, 2022), and post-COVID-19 pandemic period (February 25, 2022, to September 19, 2022). The outcomes examined were stroke admission site, performance of swallowing assessment, reperfusion treatment, assessment for rehabilitation, and early supported discharge.
Results: Out of the 21,795 stroke patients, 1,357 had documented pre-existing dementia, while 20,438 had stroke without a dementia diagnosis. Throughout all study periods, a significantly lower proportion of stroke patients with pre-existing dementia, compared to stroke-only patients, received reperfusion treatment, assessments for rehabilitation, and early supported discharge from stroke units. In the subgroup of stroke patients with pre-existing dementia, no significant associations were found regarding the quality indicators of stroke care between the study periods.
Conclusions: The COVID-19 pandemic revealed disparities in stroke care quality between patients with dementia and those with only stroke, but these differences did not worsen during the pandemic.
Disclosures of Interest: No
Abstract N°: 1234
A SYSTEMATIC-SEARCH-AND-REVIEW OF REGISTERED PHARMACOLOGICAL THERAPIES INVESTIGATED TO IMPROVE NEURO-RECOVERY AFTER A STROKE
Tsong-Hai Lee1, Shinichiro Uchiyama2, Yohanna Kusuma3, Hou Chang Chiu4, Jose Navarro5, Kay Sin Tan6, Jeyaraj Pandian7, Liang Guo8, Yoko Wong8, Narayanaswamy Venketasubramanian*9
1Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan, 2Sanno Medical Center, Tokyo, Japan, 3National Brain Center Hospital, Jakarta, Indonesia, 4Shuang Ho Hospital, Taipei Medical University, Taipei, Taiwan, 5Jose R. Reyes Memorial Medical Center, Manila, Philippines, 6University Malaya Medical Centre, Kuala Lumpur, Malaysia, 7Christian Medical College & Hospital, Ludhiana, India, 8Singapore Clinical Research Institute, Singapore, 9Neuroscience Centre, Raffles Hospital, Singapore
On behalf of: The Asian Stroke Advisory Panel
Background and aims: Stroke burden is largely due to long-term impairments requiring prolonged care with loss of productivity. We aimed to identify and assess studies of different registered pharmacological therapies investigated to improve post-stroke impairments and/or disabilities.
Methods: We performed a systematic-search-and-review (PROSPERO CRD42022376973) of registered or marketed treatments that have been investigated as recovery-enhancing or recovery-promoting therapies in patients with stroke regardless of primary indication. Outcomes reviewed were neurological impairments and functional/disability assessments. “Best available studies” based on study design, size, and/or date of publication were selected and graded for level of evidence (LOE) by consensus.
Results: Our search yielded 7801 citations and we reviewed 665 full-text papers. Fifty-eight publications were selected as “best studies” across 25 pharmacological classes: 31 on ischemic stroke, 21 on ischemic or hemorrhagic stroke, 4 on intracerebral hemorrhage, and 2 on subarachnoid hemorrhage (SAH). Twenty-six were systematic reviews/meta-analyses (SR/MA), 29 randomized clinical trials (RCTs), and three cohort studies.
Only nimodipine for SAH had LOE A of benefit (SR/network MA). Seven interventions had LOE B-R (SR/MA or RCT) of treatment effects. Many studies, some showing treatment effects, were assessed as LOE C-LD mainly due to small sample sizes or poor quality.
Conclusions: Only one commercially available treatment has LOE A for routine use in stroke. Further studies of putative neuroprotective drugs as adjunct to revascularization, and more confirmatory trials on recovery-promoting therapies will enhance the certainty of their benefits. Their use must be guided by the clinical profile, neurological impairments and target outcomes based on the available evidence.
Disclosures of Interest: No
Abstract N°: 226
PATHWAY RESEARCH FOR EYE CARE IN STROKE (PRECIS) STUDY: THE NSW POST-STROKE VISION CARE FRAMEWORK
1University of Technology Sydney, Faculty of Health, Ultimo, Australia, 2University of Liverpool, Liverpool, United Kingdom
On behalf of:
Background and aims: Vision is scarcely addressed in Australian stroke guidelines. The PRECiS study aimed to develop and evaluate a post-stroke vision care framework appropriate for use in Australia.
Methods: The RAND/UCLA Appropriateness Method (RAM) was used to develop and validate the NSW Post-stroke Vision Care Framework. Best practice statements (BPS) were developed by synthesis of evidence from literature and PRECiS: Stage 1 data. BPS were rated on degree of appropriateness by a multidisciplinary expert panel over two rounds, using a modified Delphi process. In a third round, BPS were translated into a diagrammatic care pathway and evaluated via panel meeting. A final consultation process with a sub-sample of stroke survivors was conducted via survey.
Results: 40 BPS were developed across four areas: pre-hospital pathways, screening/ assessment, management/referral, and education. Round one: all 40 BPS were rated as appropriate; 14 BPS had more than two ratings outside the median tertile, indicating some discrepancy between panellists and 31 were revised to for clarity or additional detail. Round two: all BPS were rated as appropriate, with strong agreement (six with 1-2 ratings outside the median tertile) and 12 BPS underwent minor revisions to wording. Round three: three BPS were added, and modifications made to layout and wording of the pathway. Eight of ten stroke survivors felt that use of the framework would have met their post-stroke vision care needs.
Conclusions: Consensus was reached on the NSW Post-stroke Vision Care Framework which is a considerable expansion to current recommendations for vision contained in Australian stroke guidelines.
Disclosures of Interest: No
Abstract N°: 3144
WHAT DO PEOPLE LIVING WITH APHASIA WANT HEALTHCARE PROFESSIONALS TO KNOW WHEN SUPPORTING EMOTIONAL RECOVERY? CODESIGNING A SERIES OF SHORT FILMS
Sarah Northcott1, Amanda Comer1, Abi Roper1, Lydia Davis1, Katerina Hilari*1
1City, University of London, Centre for Language and Communication Science, London, United Kingdom
On behalf of:
Background and aims: Rates of depression for people with post-stroke aphasia are estimated to be between 43-70%; yet healthcare professionals have consistently described lacking confidence in addressing the psychological wellbeing of this client group. This study explored what people living with aphasia and their family members want healthcare professionals to know, prior to co-producing training and awareness-raising films.
Methods: We ran co-design workshops with six experts by experience: four people with aphasia and two family members. The content of the workshops was allowed to evolve in a collaborative manner, with an assumed equality between the facilitators and experts by experience. We then co-produced four films to raise awareness and train healthcare professionals.
Results: The core messages from the workshops fell into two categories: behaviours that harmed emotional wellbeing; and helpful behaviours. Harmful behaviours included: feeling told off; being talked about rather than included; negativity about future recovery; not feeling listened to; not supported to communicate; not feeling treated like a human being. Behaviours perceived to help included: listening to the ups and downs; kindness and patience; noticing family members too; chatting to patients as people; friendly and warm manner; supporting people with aphasia to communicate; keeping hope alive. Link to co-produced films: cityaccess.org/carahub#videos
Conclusions: Workshop members felt strongly that these messages should be heard by all healthcare staff, not just those who elect to go on specialist training courses. Their key message was that psychological care after a stroke is everyone’s responsibility: they urged healthcare professionals to notice the person not just the deficit.
Disclosures of Interest: No
Abstract N°: 138
SAFETY STUDY OF EDARAVONE FOR TREATMENT OF ACUTE ISCHEMIC STROKE AMONG FILIPINO PATIENTS
Laurence Kristoffer Batino*1, Cyrus Escabillas1, Jose Navarro1
1Jose R. Reyes Memorial Medical Center, Stroke and Vascular Neurology, Manila, Philippines
On behalf of:
Background and aims: We aimed to evaluate the safety of intravenous Edaravone for the treatment of Acute Ischemic Stroke among Filipino patients. The study, categorized as Phase IV, spans from December 2022 to November 2023. The primary objective is to document side effects and serious adverse events during the 14-day Edaravone infusion period.
Methods: The protocol gained approval from the Institutional Review Board, and participants provided written consent. Inclusion criteria involved patients aged 18-70 with acute ischemic stroke within 24 hours. Exclusion criteria included extremes of age, pregnancy, severe hepatic impairment, and participation in other clinical trials. Edaravone, administered for 14 days, underwent continuous monitoring, and adverse events were actively recorded.
Results: Out of 64 enrolled patients, 58 completed the treatment, while 4 did not finish, and 2 dropped out. The majority were male (n=35), median age 53.5 years, and 81.03% exhibited moderate stroke severity. Two patients reported headaches, and one reported dizziness. No serious adverse events or other untoward effects were documented. Dropouts, attributed to a low ejection fraction, showed normal laboratory results and no side effects during Edaravone infusion. Thrombolytic therapy were given to 37.93% patients.
Conclusions: Our study contributes insights into Edaravone's safety, revealing a favorable profile with mild side effects, aligning with existing literature. Notably, no serious adverse events occurred, emphasizing Edaravone's tolerability. Headache and dizziness, common side effects, did not lead to treatment discontinuation in most cases. Overall, the findings support the growing evidence of Edaravone's safety in acute ischemic stroke treatment.
Disclosures of Interest: No
Abstract N°: 1726
NUTRITIONAL CARE IN ACUTE CARE AND REHABILITATION OF STROKE PATIENTS: A SYSTEMATIC REVIEW OF CLINICAL PRACTICE GUIDELINES
Karina Siewers*1, Hanne Christensen1
1Bispebjerg Hospital, Department of Neurology, København, Denmark
On behalf of:
Background and aims: The positive impact on outcomes from adequate nutrition during critical medical conditions is increasingly recognized. It is also well-described that malnutrition in stroke patients during hospitalization and rehabilitation is not only prevalent but also overlooked and undertreated, negatively impacting outcomes. Therefore, our aim was to map existing guidelines on nutritional care in stroke patients to obtain an overview of the present state of the art.
Methods: Following registration to PROSPERO (ID 498430), we conducted searches on MEDLINE, EMBASE, NICE database and national medical association websites (Jan 2015-Jan 2024). We sought Clinical Practice Guidelines (CPGs), that included guidance on nutritional care for stroke patients during hospitalization or rehabilitation.
Results: Twelve guidelines were included, from which 73 eligible recommendations were identified. All guidelines covered recommendations on dysphagia. Among them, six CPGs included recommendations on nutritional supplements (without further specification) and malnutrition screening. Recommendations regarding dysphagia were based on a moderate- to a strong level of evidence, whereas recommendations regarding nutritional support and malnutrition were generally based on weak recommendation/moderate- to low- quality, offering limited guidance on specific nutritional interventions.
Conclusions: CPGs on nutritional care for stroke patients primarily emphasize dysphagia management, reflecting a critical aspect of clinical care. However, the paucity of available guidance on nutritional care interventions, specifically addressing the needs of stroke patients, underscores the need for increased focus in both scientific research and clinical practice. A preview of literature on dietary interventions in patients admitted with stroke has been submitted in parallel.
Disclosures of Interest: No
Abstract N°: 2335
DRIP AND SHIFT MODEL IN AN URBAN AREA
Soledad Pérez Sánchez*1, Ana Barragán1, Francisco Moniche Alvarez2, Elena Zapata Arriaza3, Reyes de Torres Chacon1, Asier de Albóniga-Chindurza3, Miguel Angel Gamero Garcia1, Juan Bautista Loscertales Castaños1, Alejandro González3, Joan Montaner1
Background and aims: To analyze efficiency of the two main organizational paradigms developed to manage stroke patients who are potential candidates for endovascular treatment (mothership vs drip-and-shift) in urban settings with short distances to the comprehensive stroke center (CSC).
Methods: A retrospective analysis of a prospective register (ARTISTA) was done to evaluate the two models stablished at each of the two large hospitals from Seville city (1,006,294 habitants). Mothership (patients of the CSC own catchment area) vs drip-and-shift (patients attending the non-CSC hospital with an ESO-certified stroke unit) outcomes were compared.
Results: 1636 thrombectomies were included (from January 2017 to January 2024), of which 629 followed the drip-and-shift model. No significant differences were found between both groups for sex, age, and NIHSS score at admission. Shorter times from symptom onset to puncture (mean 117 vs 180 minutes, p<0.001) and to recanalization (mean 177 vs 230 minutes, p<0.001) existed in the mothership thrombectomy group. However, both groups had similar rates, of successful recanalization (TICI 2b or 3), intracerebral hemorrhage, and 90d mortality. Rates of functional independence at 90 days (mRS 0-2) were also similar (52.95% vs 49.25%, p= 0.154).
Conclusions: Although in urban areas the mothership model may have advantages, both models have similar and acceptable clinical results. Drip-and-shift could be an option in resource-limited areas and low-income regions where stablishing several PSC is not feasible due to high cost or lack of human resources. In any case, frequent audits and short treatment times are necessary to ensure that clinical outcomes remain stable.
Disclosures of Interest: No
Abstract N°: 2476
STATUS OF STROKE CARE, STROKE-METRICS AND OUTCOMES: ANALYSIS OF 2,200 CASES IN PRE-IMPLEMENTATION PHASE OF IMPETUS STROKE STUDY
1All India Institute of Medical Sciences, Department of Neurology, New Delhi, India, 2All India Institute of Medical Sciences, Center for Community Medicine, New Delhi, India
On behalf of: The IMPETUS Stroke Implementation Study Group
Background and aims: In India’s public healthcare system, stroke patients mostly seek care at tertiary-level medical colleges. There are no studies that comprehensively assessed quality of acute stroke care at these facilities. Our aim was to describe the situation in terms of profile of patients, stroke-metrics, care-components, and outcomes.
Methods: IMPETUS stroke is a multicentric, prospective, multiphase, mixed-methods, quasi-experimental implementation study, comprising of three phases, at 22 medical-colleges in India, initiated in October 2021. The present data represents the pre-implementation phase assessment of the existing components of stroke care for prospectively enrolled acute stroke patients.
Results: Of 2,242 participants, mean(SD) age was 59(14) years, 65% were males. 70% had an onset <24 hours; majority were ischemic (59%), followed by ICH (39%); median NIHSS score was 10 (IQR 6, 15); risk-factors included hypertension (66%), diabetes (28%), smoking (31%), alcohol (24%), CAD (10%), RHD (3.6%), AF (5.4%) and previous stroke (21%). Imaging performed was CT (70%), CTA (19%) and MRA (12%). Intravenous thrombolysis was administered in 51% of those eligible, mostly (77%) TPA; most common reason (30%) for not being thrombolysed was in-hospital delay after admission. Median(IQR) time in minutes: onset-to-door was 550(232, 1489), door-to-CT 70(44, 173), onset-to-needle 210(165, 255), CT-to-needle 45(27, 75), and door-to-needle time was 75(54, 110) minutes. In-hospital mortality was 19% and 43% achieved modified Rankin scale score 0–2 at 90-days.
Conclusions: These comprehensive data provide representative baseline of status of acute stroke care in India, which will be useful in comparing implementation assessment and advancements of stroke care.
Disclosures of Interest: No
Abstract N°: 2729
IMPROVING STROKE CARE IN INDIA (IMPROVISE): RESULTS FROM A MULTI-CENTRE FEASIBILITY STUDY
stephanie jones*1, Elizabeth Boaden1, Jane Burnell2, Ranjit Injety3, Catherine Elizabeth Lightbody1, Colette Miller1, Jeyaraj Pandian3, Vasantha Padma4, Pn Sylaja5, Caroline Watkins1
1University of Central Lancashire, School of Nursing and Midwifery, Preston, United Kingdom, 2University of Central Lancashire, Lancashire Clinical Trials Unit, Preston, United Kingdom, 3Christian Medical College and Hospital, Department of Neurology, Ludhiana, India, 4All India Institute of Medical Sciences, Neurology, Department of Neurology, New Delhi, India, 5Sree Chitra Tirunal Institute for Medical Sciences and Technology, Department of Neurology, Thiruvananthapuram, India
On behalf of: on behalf of the NIHR Global Health Research Group on IMPROVIng Stroke CarE in India (IMPROVISE) Collaboration
Background and aims: Stroke is the second leading cause of global disease burden, and the incidence of stroke is increasing in low-middle-income countries (LMICs). Stroke unit care including an organised specialist multidisciplinary team approach and adherence to processes of acute stroke care are associated with reduced mortality. The aim of this study was to explore the feasibility of delivering evidence-based Care Bundles (CB) in an LMIC setting, India.
Methods: A multi-centre, feasibility study using experience-based co-design. We developed three CBs. CB1: a Global Evaluation of Swallowing (GEoS) that uses a range of consistencies, tailored to the local context, and a hydration ‘Osmolarity App’. CB2: a Standardised Neurological OBservation Schedule for Stroke (SNOBSS). CB3: post-discharge patient/carer education in the form of animations. The three CBs were implemented cumulatively at three sites following CB0 (pre-implementation).
Results: 379 participants were recruited, 118 (31%) female, mean age 59 years (12 SD). Swallow assessments increased from 24% (CB0) to 56% (CB1) and assessments maintained in CB2 (61%) and CB3 (55%). Increasing from 0% in CB0, calculated osmolarity was recorded in 63% of participants in CB1 rising to 78% in CB2 and 76% in CB3. In CB2, SNOBSS was recorded in 95% of participants and 93% by CB3. 100% of patients/carers received information about the animations in CB3 and up to 94% of patients/carers accessed the animations post-discharge.
Conclusions: It is feasible to implement context-specific, evidence-based CBs to improve stroke care in an LMIC setting. Further research is needed to measure the impact on patient outcomes.
Disclosures of Interest: No
Abstract N°: 2948
RECANALIZATION THERAPIES FOR ACUTE ISCHEMIC STROKE IN 2 LARGEST HOSPITALS IN ESTONIA: WHY THE DIFFERENCES?
Yousef Quzeih*1,2, Teele Tuularu3, Katrin Sikk3, Riina Vibo1,2, Janika Kõrv1,2
1Tartu University Hospital, Department of Neurology and Neurosurgery, Tartu, Estonia, 2University of Tartu, Department of Neurology and Neurosurgery, Tartu, Estonia, 3North Estonia Medical Center, Department of Neurology, Tallinn, Estonia
On behalf of:
Background and aims: The Estonian Health Insurance Fund's stroke quality indicators reveal variations in recanalization therapy (RT) rates between the two largest hospitals (A and B). Our study aims to analyse factors behind this discrepancy.
Methods: Retrospective chart review for all acute ischaemic (AIS) patients admitted to both hospitals between 01.01.2021 to 30.06.2021 was performed. The mean age, sex, mRS and NIHSS scores upon admission, and contraindications for RT were analysed. Data for RT receivers were analysed based on Safe Implementation of Treatments in Stroke registry.
Results: The rate of RT was significantly higher in hospital A (45%, 151/333) compared to B (30%, 92/302, P<0.001). For RT non-receivers, the mean NIHSS scores on arrival were higher in hospital A versus B (mean 7.3;SD 6.9 and 6.4;SD 7.3, respectively; P=0.041), but no differences were found in other factors. For RT receivers, mild stroke patients (NIHSS=0-5) more often received RT in hospital A than in B (34% versus 16%, respectively, P=0.003). Furthermore, NIHSS scores upon admission were significantly lower in hospital A (median 8; IQR 12) than in B (median 8; IQR 13, P=0.003), while pre-stroke mRS scores were higher in hospital A (median 1; IQR 2) than in B (median 0, IQR 1, P<0.001).
Conclusions: This study showed that AIS patients with mild stroke deficits and lower functional capacity were more frequently treated with RT in hospital A than in B. The contraindications for not receiving RT were similar in both hospitals due to similar stroke protocols.
Disclosures of Interest: No
Abstract N°: 3091
TIME SPENT ON PRESENTING DISCLOSURE SLIDES AT THE ESO CONFERENCE 2023
H. Bart van der Worp*1, Mervyn Vergouwen1
1UMC Utrecht, Neurology and Neurosurgery, Utrecht
On behalf of:
Background and aims: To improve transparency, speakers at the European Stroke Organisation Conference (ESOC) are requested to include a disclosure slide in their presentation. It is unknown whether the audience is given sufficient time for review and consideration. We aimed to count words on disclosure slides and to assess how long these slides were shown in oral presentations at ESOC 2023.
Methods: We used the ESO STroke Education Platform (eSTEP) to assess whether presentations in plenary sessions and those of invited speakers at ESOC 2023 included a disclosure slide and whether a potential conflict of interest was reported. We measured the time this slide was shown and counted the total number of words on this slide, both for slides with disclosures and for those without.
Results: Of 201 presentations available on eSTEP, 21 (10%) did not have a disclosure slide, and two (1%) could not be assessed for technical reasons. The median word count of slides reporting ‘no disclosure’ was 5 (IQR:3-11) and of slides with disclosures 31 (IQR:17-54). The median times the disclosure slides were shown were 3 seconds (IQR:2-5) and 4 seconds (IQR:3-8), respectively (Figure). The median number of words per second of display was 2 (IQR:1-5) for slides reporting ‘no disclosure’ and 7 (IQR:3-14) for slides with disclosures.
Conclusions: At ESOC 2023, slides reporting one or more potential conflicts of interest were shown only slightly longer than those without, and often too briefly for adequate review and contemplation. We propose that speakers limit their disclosures to those really relevant to their presentation.
Disclosures of Interest: No
Paper Poster - Cognition and Vascular Cognitive Impairment
Abstract N°: 1063
THE VALUE OF EARLY-PHASE AMYLOID PET FOR ASSESSING TAU PATHOLOGY IN CEREBRAL AMYLOID ANGIOPATHY
1National Taiwan University Hospital, Nuclear Medicine, Taipei, Taiwan, 2National Taiwan University Hospital, Neurology, Taipei, Taiwan
On behalf of:
Background and aims: Tau, a hallmark of Alzheimer’s disease, is a frequent concomitant pathology in cerebral amyloid angiopathy (CAA). We investigate whether early-phase amyloid PET is a neuroimaging biomarker for the underlying tau pathology.
Methods: Probable CAA patients were recruited from stroke and memory clinics in a single center in Taiwan. All patients received dynamic amyloid and tau PET scans. Early-phase 11C-PiB images were extracted from the dynamic data collected between 1 to 6 minutes. The regional and whole cortex PET data were analyzed using PMOD Software. Diagnostic utility of early-phase amyloid PET for prediction of positive tau PET was assessed using Youden index as cutoff.
Results: 38 probable CAA (24 with ICH and 12 with cognitive impairment) were included. Presence of tau pathology was determined by T807 SUVR > 1.26 in AD-signature meta-temporal ROI. Concomitant tau pathology was found in 20 (52.6%) patients. CAA/Tau(+) showed similar age and sex distributions as CAA/Tau(-), but CAA/Tau(+) were more cognitively impaired (p = 0.010). On early-phase PET, CAA/Tau(+) showed significantly lower SUVR in temporal lobe and precuneus (both P < 0.05) than CAA/Tau(-) (Figure). Early-phase temporal SUVR was associated with tau burden (β = -1.75, 95% CI -3.00 to -0.50, P = 0.007), and the trend remained after adjustment for age and late-phase uptake (P = 0.086). Regarding diagnostic performance, the early-phase SUVR cutoffs afforded sensitivity 55-70% and specific 72-89% in prediction of tau pathology.
Conclusions: Early-phase Amyloid PET potentially serves as an image marker for concomitant Alzheimer’s pathology in CAA.
Disclosures of Interest: No
Abstract N°: 1499
VALIDATION OF DIAGNOSTIC & STATISTICAL MANUAL OF MENTAL DISORDERS (DSM-5) COGNITION SCALE: MINIMAL CLINICALLY IMPORTANT DIFFERENCE
Lisa Woodhouse1, Jason Appleton2, Ellen Backhouse3, Fergus Doubal4, Terence J Quinn5, Joanna Wardlaw4, Philip Bath*1
1University of Nottingham, Stroke Trials Unit, Nottingham, United Kingdom, 2Nottingham University Hospitals NHS Trust, Stroke, Nottingham, United Kingdom, 3University of Edinburgh, Centre for Clinical Brain Sciences (CCBS), Edinburgh, United Kingdom, 4University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom, 5University of Glasgow, School of Cardiovascular and Metabolic Health, Glasgow, United Kingdom
On behalf of: R4VaD and LACI-2 Collaborators
Background and aims: The optimal method for measuring post-stroke cognitive impairment (PSCI) is unclear. DSM-5 (Figure) includes impairments from multiple cognitive domains (so relevant to PSCI) using multiple data sources (so fewer missing data). We assessed the minimal clinically important difference (MCID) for the DSM-5 4- and 7-level ordinal cognition scales.
Methods: We assessed MCID using 3 approaches. A modified Delphi assessment approached members of 3 UK specialist societies using an anonymised Google doc form; DSM-5 was explained and members chose MCID options in the range 0.2-2.0. Anchor analysis used data from the Rates, Risks and Routes to Reduce Vascular Dementia (R4VaD) observational study of PSCI (comparison of participants with severe vs minor stroke using data at 1 year; EurStrokeJ 2021;6:89) and LACunar Intervention Trial-2 (LACI-2, comparison of isosorbide mononitrate vs none with data at 1 year; JAMA 2023;80:682). Distribution analyses were calculated as the common standard deviation (SD) x0.2 (an appropriate multiplier for low cost interventions) using data from LACI-2.
Results: Specialist society members identified MCIDs (N=53): 4-level – median 0.4 (20%), mode 0.5 (24%); 7-level – median/mode 0.5 (26%). MCID from anchor analyses were: DSM-5 4-level – 0.23-0.34; 7-level – 0.41-0.69. The MCID based on distribution analysis was 1.33 (SD) x 0.2 = 0.27.
Conclusions: The DSM-5 4 and 7-level cognitive scales have MCIDs in the range 0.27 to 0.69. Lower values will be relevant for low cost interventions and higher values for more expensive interventions.
Disclosures of Interest: No
Abstract N°: 1711
PREVALENCE OF PURE CEREBRAL SMALL VESSEL DISEASE IN SUBJECTIVE COGNITIVE DECLINE AND MILD COGNITIVE IMPAIRMENT
Chi Kiu Chan*1,2,3,4,5, Siu Ting Fu1,2,3,4,5, Yuan Cai1,2,3,4,5, Chirag Nainani1,2,3,4,5,6, Bonnie Lam1,2,3,4,5, Vincent Ct Mok1,2,3,4,5
1Division of Neurology, Department of Medicine and Therapeutics, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong, 2Li Ka Shing Institute of Health Sciences, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong, 3Margaret K. L. Cheung Research Centre for Management of Parkinsonism, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong, 4Lau Tat-chuen Research Centre of Brain Degenerative Diseases in Chinese, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong, 5Gerald Choa Neuroscience Institute, The Chinese University of Hong Kong, Hong Kong, 6King George V School (KGV), Hong Kong
On behalf of:
Background and aims: Alzheimer's disease (AD) and cerebral small vessel disease [CSVD]) are the two most common causes of cognitive impairment. However, the prevalence of pure CSVD in the absence of AD pathology among stroke-free people with subjective cognitive decline (SCD)/mild cognitive impairment (MCI) remains uncertain. This study aims to investigate the prevalence of pure CSVD among SCD/MCI.
Methods: 97 stroke-free subjects with SCD (n=28) and MCI (n=69) were recruited. All patients underwent structural MRI and 11C-Pittsburgh compound B positron emission tomography to assess the burden of CSVD (V+) and amyloid beta deposition (A+), respectively. We defined presence of CSVD (V+) as showing grade 2 or above on the Fazekas Scale and/or with any lacune on MRI.
Results: Among 97 subjects (mean [SD] age, 67.7 [6.0] years; 44 males [45.4%]), 32 subjects (33%) had CSVD (V+). 21 (21.7%) of these subjects had pure CSVD (V+A-) while the remaining 11 (11.3%) had concurrent AD (V+ A+). On the other hand, 30 subjects (30.9%) were A+ and 19 subjects (19.6%) had pure AD (V-A+).
Conclusions: 1 in 5 elderly subjects with SCD/MCI have pure CSVD and this prevalence is similar to that of pure AD among SCD/MCI.
Disclosures of Interest: No
Abstract N°: 3124
ASSOCIATIONS OF INFLAMMATORY AND ENDOTHELIAL ACTIVATION MARKERS WITH COGNITIVE FUNCTION OVER THREE YEARS AFTER MILD-TO MODERATE ISCHEMIC STROKE
1Carl von Ossietzky-University Oldenburg, Neurology, Oldenburg, Germany, 2Evangelical Hospital Oldenburg, Neurology, Oldenburg, Germany, 3Center for Stroke Research Berlin, Neurology, BERLIN, Germany, 4Charité, Neurology, BERLIN, Germany
On behalf of:
Background and aims: Vascular inflammation is involved in the pathophysiology of post-stroke cognitive impairment. We aimed to assess whether blood-based biomarkers of inflammation and endothelial dysfunction such as interleukin 6 (IL-6), vascular cell adhesion molecule (VCAM-1), and tumor necrosis factor alpha (TNF-α) are associated with cognitive function over time in after first ischemic stroke.
Methods: Data were obtained from the Prospective Cohort with Incident Stroke Berlin (NCT01363856). Cognitive function was assessed with the Telephone Interview for Cognitive Status-modified (TICS-m) at one to three years of follow-up. Associations of baseline levels of IL-6, VCAM-1, and TNF-α with cognitive function over time was estimated using a linear mixed model adjusted for demographics, education, vascular risk factors, stroke severity, ischemic stroke subtype, and white matter lesion severity.
Results: We included 576 ischemic stroke patients with baseline data on biomarker levels. The mean age was 67 (SD ±12), 39% were female, and the median National Institutes of Health Stroke Scale (NIHSS) was 3 (IQR 1–4). Frequency of cognitive impairment defined as TICS⩽ 31 were 22.2 % at year one, 14.7% at year two, and 11.6% at year three. Higher log-transformed levels of IL-6 and VCAM-1 were associated with lower TICS-m scores over time in the adjusted linear mixed model (IL-6: β=-2.4, 95%CI -3.7 to -1.1; VCAM-1: β=-3.9, 95%CI -7.1 to -0.9.)
Conclusions: In patients with mild-to-moderate first-ever ischemic stroke, higher baseline levels of IL-6 and VCAM-1 were associated with lower Telephone Interview for Cognitive Status-modified during three years of follow-up.
Disclosures of Interest: No
Abstract N°: 398
INFLUENCE OF INFARCT MORPHOLOGY AND PATTERNS ON COGNITIVE OUTCOMES AFTER ENDOVASCULAR THROMBECTOMY
Johanna Ospel*1, Leon Rinkel2, Aravind Ganesh1, Andrew Demchuk1, Manish Joshi1, Bijoy Menon1, Michael Tymianski3, Michael Hill1, Mayank Goyal1
1Foothills Medical Centre, Calgary, Canada, 2University of Amsterdam, Amsterdam, Netherlands, 3Nono Inc., Toronto, Canada
On behalf of: the ESCAPE-NA1 Investigators
Background and aims: To assess the association of qualitative and quantitative infarct characteristics and three cognitive outcome tests, namely the Montreal Cognitive Assessment (MOCA) for mild cognitive impairment, the Boston Naming Test (BNT) for visual confrontation naming, and the Sunnybrook Neglect Assessment Procedure (SNAP) for neglect, in large vessel occlusion (LVO) stroke.
Methods: Data are from the randomized controlled ESCAPE-NA1 trial that included stroke patients undergoing endovascular treatment. MOCA, SNAP and 15-item BNT were obtained at 90 days. Total infarct volume, grey matter and white matter infarct volumes were manually measured on 24-hour imaging. Infarcts were also visually classified as either predominantly involving the grey matter or both the grey and white matter and scattered vs. territorial.
Results: Of 1105 patients enrolled in ESCAPE-NA1, 1026 patients with visible infarcts on follow-up imaging were included. Total infarct volume was associated with worse MOCA scores (adjusted common odds ratio[aOR] per 10ml increase: 1.07[95%confidence interval 1.05-1.09]). After adjusting for baseline variables and total infarct volume, grey and white matter involvement (vs. grey matter only (acOR)1.75[95%confidence interval 1.25-2.45]), white matter infarct volume (acOR per 10ml increase 1.34[1.16-1.55]) and territorial (vs. scattered) infarct pattern (acOR 1.49[1.05-2.13]) were associated with worse MOCA scores. Results for SNAP and 15-item BNT were similar, except for territorial infarct pattern, which did not reach statistical significance in multivariable analysis.
Conclusions: Besides total infarct volume, infarcts that predominantly involve the white matter and that show a territorial distribution were associated with worse cognitive outcomes, even after adjusting for total infarct volume.
Disclosures of Interest: No
Abstract N°: 891
DEPRESSIVE SYMPTOMS PROFILES AND COGNITIVE OUTCOMES AFTER STROKE
Giuseppe Scopelliti*1, Emilia Salvadori2, Francesco Mele1, Ilaria Cova1, Pierluigi Bertora2, Simone Pomati1, Leonardo Pantoni2
1Neurology Unit, Luigi Sacco University Hospital, Milan, Italy, 2Stroke and Dementia Lab, Department of Biomedical and Clinical Sciences, University of Milan, Milan, Italy
On behalf of:
Background and aims: Depressive symptoms are a major concern among stroke survivors, often linked with cognitive impairment. This study employs cluster analysis to discern distinct profiles of post-stroke depressive symptoms and their correlation with cognitive profiles.
Methods: We included consecutive patients undergoing neuropsychiatric screening six months after stroke. Cluster analysis incorporated the Center for Epidemiologic Studies Depression Scale score, along with apathy and anxiety item scores from the Neuropsychiatric Inventory questionnaire. Baseline clinical/neuroimaging variables and 6-month cognitive outcomes were compared across identified profiles.
Results: One hundred eighty-nine patients (80% ischemic strokes) underwent 6-month neuropsychiatric screening (mean age 73.7 years, standard deviation 12.0; 62% male). Three distinct profiles emerged: (A) low-depressive symptoms (n=108), (B) high-depressive symptoms plus apathy (n=40); (C) moderate-depressive symptoms plus anxiety (n=41). Compared to patients with low-depressive symptoms, patients with high-depressive symptoms plus apathy exhibited lower Montreal Cognitive Assessment scores at baseline (adjusted odds ratio [adj.OR] 0.91, 95% confidence interval [95%CI] 0.83-0.99). Patients with moderate-depressive symptoms plus anxiety had lower global cortical atrophy scores compared to both low-depressive symptoms (adj.OR 0.92, 95%CI 0.86-0.99) and high-depressive symptoms plus apathy (adj.OR 0.89, 95%CI 0.81-0.97) profiles. High-depressive symptoms plus apathy profile was associated with higher frequency of dementia and attention/executive function impairment compared with the two other groups (both p<0.05); low-depressive symptoms correlated with lower rates of memory impairment compared with the two other groups (both p<0.05).
Conclusions: By integrating apathy and anxiety in our profiling model, depressive symptoms after stroke emerged as heterogeneous neuropsychiatric syndromes, showing different baseline predictors and distinctive cognitive profiles.
Disclosures of Interest: No
Abstract N°: 1696
IMAGING MARKERS IN PATIENTS WITH CAA FROM A MEMORY CLINIC COHORT: EVIDENCE FOR A PATHOPHYSIOLOGICAL TIMELINE
Ana Costa1, Arno Reich1, Omid Nikoubashman2, Jörg B. Schulz1, Kathrin Reetz1, João Pinho*1
1University Hospital, RWTH Aachen University, Department of Neurology, Aachen, Germany, 2University Hospital, RWTH Aachen University, Department of Diagnostic and Interventional Neuroradiology, Aachen, Germany
On behalf of:
Background and aims: The updated Boston criteria v2.0 for the diagnosis of cerebral amyloid angiopathy (CAA) allow the diagnosis of patients with cognitive presentation without hemorrhagic imaging markers. The aim of this study was to compare baseline characteristics of memory clinic patients with CAA according to the type of imaging markers of CAA.
Methods: A retrospective study of patients presenting with suspected cognitive impairment to a memory clinic between 2009-2019. Reasons for exclusion were the unavailability of cerebrospinal fluid (CSF) neurodegeneration markers and/or magnetic resonance imaging, and a set of prespecified causes of cognitive impairment. Patients were selected when fulfilling the updated CAA Boston criteria v2.0. Baseline demographic, clinical, imaging and CSF characteristics were compared between CAA patients with and without hemorrhagic markers.
Results: The final study population consisted of 338 patients fulfilling the CAA Boston criteria v2.0. Patients with hemorrhagic markers were older (76.1 vs. 71.9 years, p<0.001), had longer symptom duration (24 vs. 16 months, p=0.022), lower global cognitive performance (Mini Mental State Examination, 24 vs. 26, p=0.028, Montreal Cognitive Assessment scores, 18 vs. 21, p<0.001) and lower CSF-Aβ1-42 levels (471 vs. 603 pg/mL, p=0.025).
Conclusions: The presence of hemorrhagic markers in CAA patients with cognitive presentation is associated with markers of a more advanced stage of disease, which supports the recently proposed pathophysiological timeline for CAA progression.
Disclosures of Interest: No
Abstract N°: 2597
AGE AND YEARS OF EDUCATION SHOULD BE CONSIDERED IN THE EVALUATION OF ACUTE POST-STROKE COGNITIVE IMPAIRMENT USING THE MOCA
Laura Gallucci*1, Christoph Sperber1, Marcel Arnold1, Roza Umarova1
1University hospital of Bern, Inselspital, Neurology, Switzerland
On behalf of:
Background and aims: The Montreal Cognitive Assessment (MoCA) is a quick and practical screening tool; however, its cutoff of <26 has not been validated. We aimed to establish and validate age- and education-specific MoCA-cutoffs to detect acute post-stroke cognitive impairment (PSCI).
Methods: In a prospective cohort study, non-aphasic patients with acute first-ever ischemic stroke were randomly assigned to the derivation (70% of the sample) and validation cohorts matched by demographic characteristics and stroke severity. PSCI was defined as performance ⩽ -1.5 SD in ⩾ 2 cognitive domains based on a neuropsychological assessment. MoCA-cutoffs were estimated according to the Youden Index.
Results: Of 351 stroke patients (aged 67.4±14.1; 148 female; NIHSS 24h=2.00 [0.00, 3.50]; MoCA=23.7±4.5) 71% had PSCI 2.7±2.0 days post stroke. In the derivation cohort, in patients with >12 years of education, the optimal MoCA-cutoffs indicating PSCI were: <28 in patients aged 22-54 (sensitivity=56.3%, specificity=76.9%), <26 in patients aged 55-70 (sensitivity=63.3%, specificity=85.0%), and <25 in patients >70 years old (sensitivity=64.7%, specificity=88.9%). In patients with ⩽12 years of education, the optimal MoCA-cutoffs were: <26 in patients aged 22-54 and 55-70 (sensitivity=85.7% and 75.0%, specificity=66.7% and 100.0% correspondingly), and <22 in patients >70 years old (sensitivity=60.8%, specificity=92.9%). The cutoffs’ performance in the validation cohort showed similar predictive abilities outperforming those of the original MoCA cut-off <26.
Conclusions: Age and years of education should be considered in the evaluation of acute PSCI using the MoCA. Cutoff performances were suboptimal for young adults and adults with >12 years of education and cautious interpretation of MoCA-score in them is warranted.
Disclosures of Interest: No
Abstract N°: 3040
DOES DEPRESSION WORSEN LONG-TERM OUTCOMES IN PATIENTS WITH POST-STROKE COGNITIVE IMPAIRMENTS?
Katherine Phillips*1, Abdel Douiri1
1King's College London, United Kingdom
On behalf of:
Background and aims: Cognitive impairment and depression are common consequences of stroke and have direct implications on patients’ quality of life and functioning. However, the interaction between cognitive impairment and depression in stroke survivors has not been extensively researched. This study aims to investigate whether depression exacerbates negative long-term outcomes associated with post-stroke cognitive impairment.
Methods: Patient data from the population-based South London Stroke Register between 1995 and 2018 was analysed. A multivariable Poisson regression analysis was conducted to evaluate the relative risks (RR) of the interaction between cognitive impairment and depression on various long-term outcomes including mortality, dependency and activity level after a stroke. Models were adjusted for age, sex, ethnicity, stroke severity and year of occurrence, disability at baseline and pathological stroke subtypes.
Results: A total of 6405 patients with first stroke were registered. Patients with depression in the first three months after post-stroke cognitive impairment had an increased risk of mortality (RR 3.18, 95% CI: 1.87-5.41), physical dependency (RR 1.34: (1.26-1.44)), institutionalisation (RR 1.14: (1.07-1.21)) and inactivity (RR 1.36: (1.29-1.44)). A substantial association between the co-existence of cognitive impairment and depression and increased risk of negative long-term outcomes was observed. Additional long-term outcomes by sex, age, ethnicity, and social economic status were also identified in subsequent analyses.
Conclusions: Depression in patients with post-stroke cognition impairment are at an increased risk of worsened long-term outcomes. Screening stroke patients periodically for depression, might enable the use of novel preventive strategies to reduce the risk of these outcomes.
Disclosures of Interest: No
Abstract N°: 215
CHANGES IN COGNITIVE FUNCTIONS AFTER CAROTID ENDARTERECTOMY AND STENTING: A DECADE-APART COMPARISON
Daniel Václavík*1,2,3, David Pakizer4, Tomáš Hrbáč5,6, Martin Roubec3,4, Václav Procházka7, Tomáš Jonszta7, Roman Herzig2, David Skoloudik3,4
1Hospital Agel Ostrava Vitkovice, Stroke Centre, Department of Neurology, Ostrava, Czech Republic, 2Charles University Faculty of Medicine and Hradec Kralove University Hospital, Comprehensive Stroke Centre, Department of Neurology, Hradec Králové, Czech Republic, 3University Hospital Ostrava, Comprehensive Stroke Centre, Department of Neurology, Ostrava, Czech Republic, 4Faculty of Medicine, University of Ostrava, Centre for Health Research, Ostrava, Czech Republic, 5University Hospital Ostrava, Department of Neurosurgery, Ostrava, Czech Republic, 6Faculty of Medicine, University of Ostrava, Department of Neuroscience, Ostrava, Czech Republic, 7University Hospital Ostrava and Faculty of Medicine, University of Ostrava, Department of Radiodiagnostics, Ostrava, Czech Republic
On behalf of:
Background and aims: Carotid stenosis represents the most common cause of ischemic stroke. Treatment with carotid endarterectomy (CEA) and carotid stenting (CAS) is related with risk of silent cerebral infarctions with possible effect on cognitive function. This study investigated changes in cognitive function in patients with severe carotid stenosis who underwent CEA and CAS over two decades.
Methods: We compared cognitive function within 30 days after the procedure in 267 patients (first 100 each for CEA and CAS in two periods: 2008–2012 and 2018–2022) in a single institution. Assessments used Adenbrooke’s Cognitive Examination–Revised (ACE-R), the Mini-Mental State Examination (MMSE), Speech Fluency Test (SFT), and Clock Drawing Test (CDT), conducted before and 30±2 days after surgery.
Results: 267 patients (181 males, mean age 67.2 years, ⩾70% carotid stenosis) exhibited different cognitive changes over periods. In 2008–2012, significant declines in MMSE (CEA, p=0.049) and CDT (CAS, p=0.015) were observed among asymptomatic patients. On the contrary, in 2018–2022, improvements were observed in ACE-R (p<0.01) and MMSE (p<0.05) for symptomatic and asymptomatic patients undergoing CEA and CAS.
Conclusions: Over a decade, advances in interventional techniques and patient management have reduced risks of cognitive decline in patients with asymptomatic carotid stenosis and also have improved cognitive functions in both symptomatic and asymptomatic individuals.
Disclosures of Interest: No
Abstract N°: 930
PLASMA ANGIOGENESIS-RELATED PROTEINS AS POTENTIAL BIOMARKERS IN POST-STROKE COGNITIVE IMPAIRMENT: A PILOT STUDY
1Shuang-Ho Hospital, Taipei Medical University, Neurology, Taiwan, 2Institute of Population Health Sciences, National Health Research Institutes, Taiwan, 3Graduate Institute of Neural Regenerative Medicine, College of Medical Science and Technology, Taipei Medical University, Taiwan
On behalf of:
Background and aims: Over the past decades, the prevalence of post-stroke cognitive impairment (PSCI) has been on the rise, paralleling the growth in the population affected by stroke. Despite this trend, the identification of precise predictive blood biomarkers remains deficient, hampering early recognition and effective management of PSCI.
Methods: From 2015 to 2022, patients experienced first-ever stroke were enrolled from Shunag-Ho hospital. Baseline characteristics, encompassing age, sex, education, medical history, brain imaging, and mental status examination, were meticulously recorded. Blood samples were obtained within 7 days of the stroke episode. Subsequent to the initial episode, Brain MRI and neuropsychological examinations were conducted at 3-month and 12-month intervals. Plasma angiogenesis-related proteins were measured using commercialized human angiogenesis array kit.
Results: Among the 264 eligible patients for blood analysis, we observed a positive correlation between Endothelin-1 and MoCA scores at the 3-month mark, while Follistatin exhibited a negative correlation. Notably, at the 12-month follow-up, Leptin and Follistatin displayed significance, both showing a negative correlation with MoCA scores (Table 1). Upon employing different cutoff levels, we found that Angiopoietin-2 was associated with development of PSCI at 3-month, defined as MoCA < 23. However, when using a different cutoff level with MoCA < 26, Follistatin and PLGF were linked to the development of PSCI (Table 2).
Conclusions: Among plasma angiogenesis-related proteins, Angiopoietin-2, Follistatin, and PLGF, were identified as being associated with the development of PSCI at the 3-month post-stroke mark. Further research with a larger sample size and longer follow-up is crucial to validate and enhance these findings.
Disclosures of Interest: No
Abstract N°: 1196
EXPLORING NSE AND GFAP AS BIOMARKERS IN COGNITIVE IMPAIRMENT SEVEN YEARS AFTER FIRST-EVER STROKE: A LONGITUDINAL STUDY
1Oslo University Hospital, Department of Neurology, Stroke Unit, Oslo, Norway, 2Bærum Hospital- Vestre Viken Hospital Trust, Department of Medicine, Drammen, Norway, 3Oslo University Hospital, Department of Cardiology, Center for Clinical Heart Research, Oslo, Norway
On behalf of:
Background and aims: The utility of neuron-specific enolase (NSE) and glial fibrillary acidic protein (GFAP) in post-stroke cognitive impairment (PSCI) has not been explored, particularly in longitudinal studies involving cognitive trajectories. This study aimed to assess the association of NSE and GFAP in PSCI seven years post-stroke.
Methods: All patients admitted to Bærum Hospital with a first-ever stroke or TIA during 2007/2008 were consecutively included in the study. The cohort underwent reexamination after one and seven years, involving extensive diagnostic evaluation for cognitive impairment (normal, mild, or dementia) with proposed underlying etiology (vascular, neurodegeneration, or mixed). Circulating levels of NSE and GFAP were measured at the seven years follow-up.
Results: Of the initially recruited 227 patients, 113 completed the seven-year follow-up. At seven years, the mean age was 75.4 (11.1), 46% were women, and 39% had a modified Rankin Scale score ⩾2. Only 41.6% were classified as cognitively normal, while 23.0% fulfilled dementia criteria, with mixed etiology being most prevalent. In logistic regression analysis, no association was observed between NSE or GFAP and cognitive impairment or different trajectories. However, when exploring the association with the proposed underlying etiology, GFAP associated with neurodegenerative and mixed etiology in crude analyses with OR 5.80 (95%CI 1.00,33.68), and OR 6.21 (95%CI 1.11,32.26), respectively. After adjusting for age and sex, the significance was attenuated for neurodegeneration, but remained for mixed etiology with OR 5.99 (95%CI 1.14, 31.25).
Conclusions: The results indicate a subtle tendency of increased GFAP levels in long-term PSCI caused by neurodegeneration.
Disclosures of Interest: No
Abstract N°: 3319
ASSOCIATION BETWEEN AMYLOID-B PET UPTAKE AND COGNITION IN CEREBROVASCULAR DISEASE BEYOND CEREBRAL AMYLOID ANGIOPATHY
Jie Zhang*1,2, Feng Liang2
1University College London, United Kingdom, 2浙江省人民医院, Hang Zhou Shi, China
On behalf of:
Background and aims: The comorbidity of vascular and neurodegenerative pathologies has been gradually observed in patients with cerebrovascular disease (CVD) beyond cerebral amyloid angiopathy (CAA). Therefore, this study aims investigate the association between vascular cognitive impairment (VCI) and amyloid-β deposition measured by positron emission tomography (PET).
Methods: Systematic search was conducted in PubMed, Embase, Web of Science, PsycINFO, and CENTRAL. Observational studies reporting correlation and regression coefficients between cognition and amyloid-PET uptake were respectively merged. Group comparisons of cognitive scores and amyloid load were also extracted for pooling.
Results: 25 eligible studies were included, enrolling a total of 2597 participants. The global cognition performance of non-CAA CVD patients was significantly decreased in the CVD patients with amyloid-β deposition compared to those without AD-like pathology (SMD=-0.41, 95% CI -0.65 to -0.16, p=0.001). The strength of correlations varied across different cognitive domains (executive function: r=-0.41, 95% CI -0.62 to -0.20; memory: r=-0.29, 95% CI -0.42 to -0.17; both p<0.001). The pooled correlation with global cognition were significant in subcortical subtype (r=-0.43, 95% CI -0.56 to -0.30, p<0.001), but milder in post-stroke subtype (r=-0.19, 95% CI -0.53 to 0.15, p>0.05).
Conclusions: The severity of impaired cognition is associated with amyloid-β load in CVD patients beyond CAA. The contribution of amyloid-β deposition to cognitive decline is pronouced in the subcortical vascular disease instead of post-stroke patients. Executive function is the most susceptible domain in VCI when the level of amyloid-β increases.
Disclosures of Interest: No
Paper Poster - Diagnosis/ Investigation of Stroke Etiology
Abstract N°: 2397
RISK OF ISCHEMIC STROKE AFTER TRANSIENT ISCHEMIC ATTACK IN PATIENTS RECEIVING COMPREHENSIVE VS NON-COMPREHENSIVE DIAGNOSTIC WORKUP
Seyyed Sina Hejazian*1, Shima Shahjouei2, Alireza Vafaei Sadr3, Ajith Vemuri1, Vida Abedi3, Ramin Zand1
1The Pennsylvania State University, Neurology, hershey, PA, United States, 2College of Medicine, Pennsylvania State University, Neurology, hershey, PA, United States, 3The Pennsylvania State University, Public Health Sciences, hershey, PA, United States
On behalf of:
Background and aims: Transient ischemic attack (TIA) and minor ischemic stroke (mIS) often indicate an elevated risk of subsequent cerebral ischemic events. We aimed to systematically study if a more comprehensive diagnostic approach to these patients reduces the incidence of post-TIA/mIS ischemic stroke (PT-IS).
Methods: We systematically searched MEDLINE, Web of Science, Scopus, Embase, International Clinical Trials Registry Platform, ClinicalTrials.gov, Trip Medical Database, CINAHL, and all Evidence-Based Medicine review series. Studies providing information on the work-up process of TIA/mIS patients, as well as the incidence of 30-day and 90-day PT-IS, were recorded. Patients’ diagnostic work-up process in each study was evaluated in four distinct aspects, including 1) visit by a stroke professional, 2) performing neuroimaging, 3) vascular imaging, and 4) cardiac assessment. Then, studies were assigned a score based on the number of aspects addressed, ranging from 0 to 4. Finally, the rate of PT-IS was compared between studies with different scores.
Results: A total number of 60 studies were included for metanalysis, which reported 30-day or 90-day PT-IS. The overall estimate of 30-day and 90-day PT-IS rates were 3.3% (CI95%:[1.8%-6.4]), 3.9% (CI95%:[3.3-7.3]). Our analysis showed that studies with a score of 3 or 4 had a significantly lower rate of 30-day PT-IS compared to studies with a score of 1 or 2 (2.2%,CI95%: [1.8-2.6] Versus 4.7%,CI95%:[3.9-5.6]). Similar pattern of results was found for 90-day risk of PT-IS (2.4%,CI95%:[2-2.8] Versus 6.3%,CI95%:[4.8-8]).
Conclusions: We demonstrated that a more comprehensive diagnostic work-up of TIA/mIS patients might improve the outcome of these patients by reducing the likelihood of PT-IS.
Disclosures of Interest: No
Abstract N°: 2446
ACUTE ISCHEMIC STROKE IN PATIENTS ON DIRECT ORAL ANTICOAGULANTS: DISTINGUISHING PSEUDO AND TRUE FAILURES
Francesco Janes1,2,3, Fedra Kuris*2, Simone Lorenzut3, Sara Pez1, Laura Ceccarelli2, Roberto Sperotto2, Roberto Sartor2, Giovanni Merlino1,3, Mariarosaria Valente1,2
1Clinical Neurology Unit, Head-Neck and NeuroScience Department, Udine, Italy, 2Clinical Neurology Unit, Department of Medicine (DAME), Udine, Italy, 3Stroke Unit, Department of Head-Neck and NeuroScience, Udine, Italy
On behalf of:
Background and aims: To investigate acute ischemic stroke (AIS) despite DOACs (Direct Oral Anti-Coagulants) treatment.
Methods: We collected AIS in DOACs treated patients with Atrial Fibrillation, from 1st Jan 2019 to 30th Jun 2023. “DOACs failure” was defined if patients reported optimal adherence and appropriate dosage, otherwise failure was only “apparent”. Other pathogenesis according to TOAST classification, after extensive work-up and 6 months follow-up, were labelled “pseudo failures”; if CE (cardio-embolism) was the only evident mechanism they were considered “true failures”.
Results: We admitted 96 DOACs-related AIS (age= 77,9±9,7 yo; 49,0 % females; NIHSS= 7,8±7,1). 61,4% were “DOAC failure”: among them 54,2% were classified as CE (true failures), 5,1% as LAD, 8,5% as SVD, 3,4% as OTH, and 27,1% were undetermined because at least one cause other than CE coexisted. The mean DOAC plasmatic level (ng/ml) at admission was 102,2±120,3 in the non-CE group (pseudo-failures) vs 71,8±84,4 in the CE group (apparent + true failures), p = 0,17. The levels at trough were 66,8±52,6 vs 33,3±34,8, respectively (p= 0,02). Single daily dose DOACs showed lower levels than double daily dose DOACs: 54,7±57,3 vs 119,6±121,5; (p = 0,02).
Conclusions: AIS related to DOAC’s failure account for up to 10% of AIS, requires a more extensive diagnostic work-up (to reveal intracranial stenosis, acquired thrombophilia, mild unstable epi-aortic atherosclerosis, paradoxical embolism, etc.). Plasmatic dosages may help in discriminating true failures, which present themselves with lower levels, above all at trough. Moreover, single daily dose DOACs seem to be more at risk of “failure”.
Disclosures of Interest: No
Abstract N°: 2488
HIGH THROMBIN EXPRESSION IN ACUTE ISCHEMIC STROKE (AIS) CLOTS MAY BE RELATED TO CARDIOEMBOLIC ETIOLOGY
Nazan Guner Sak*1,2, Cansu Sahin1,2, Alice Giraud3, Pierluca Messina3, Vanessa Chalumeau4, Ivan Vukasinovic5, Marc Ribo6, Nobuyuki Sakai7, Christophe Cognard8, Karen Doyle1,2
1University of Galway, Physiology, Galway, Ireland, 2University of Galway, CÚRAM-SFI Research Centre for Medical Devices, Galway, Ireland, 3Sensome, Massy, France, 4Bicêtre Hospital, Department of Interventional Neuroradiology, Le Kremlin-Bicêtre, France, 5University Clinical Center of Serbia, Center for Radiology and MRI, Clinic for Neurosurgery, Belgrade, Serbia, 6University Hospital Vall d'Hebron, Department of Neurology, Barcelona, Spain, 7Kobe City Medical Center General Hospital, Department of Neurosurgery, Kobe, Japan, 8CHU de Toulouse, Department of Diagnostic and Therapeutic Neuroradiology, Toulouse, France
On behalf of: Vanessa Chalumeau, Ivan Vukašinović, Marc Ribo, Nobuyuki Sakai, Christophe Cognard
Background and aims: High levels of thrombin generation may be associated with increased stroke risk. We investigated the level of expression of thrombin in AIS clots. We assessed etiological differences in expression, the relationship of thrombin expression to other main clot components, and patient characteristics including thrombolysis treatment, age, and sex.
Methods: 86 blood clot samples from Clotbase International Registry (large artery atherosclerosis (LAA) (n=39) and cardioembolic (CE) (n=47) patients) were cut into 3 μm-sections and stained with Martius Scarlett Blue. Immunohistochemistry was performed using anti-thrombin antibody (1:200, ab17199, abcam). Slides were scanned using a slide scanner (VS120, Olympus). The components were quantified via Orbit Image Analysis. Non-parametric statistical tests (Kruskal-Wallis, Spearman’s correlation) were used.
Results: Expression of thrombin was significantly higher in CE than in LAA samples (P=0.008**, U=612.5). Thrombin expression in AIS clots was significantly lower in patients administered thrombolysis than those not given rtPA (P=0.013*, U=605; yes=34, no=52). There was no significant effect of age or sex on thrombin expression. There was a positive correlation between thrombin expression and fibrin (r: 0.28; p: 0.01*) and platelet (r: 0.23; p: 0.04*), and a negative correlation with red blood cells (r: -0.40; p:0.0003***).
Conclusions: Our study showed significantly higher thrombin expression in clots of CE etiology, lower levels following thrombolysis, and a positive association of thrombin with white clot components in AIS clots, suggesting that it may have potential as a useful etiology biomarker candidate. Further study is needed to enhance our understanding of thrombin in AIS clots.
Acknowledgements
SFI (CÚRAM:13/RC/2073_P2), and Sensome
Disclosures of Interest: No
Abstract N°: 2939
DIAGNOSTIC ACUITY OF THE SUBOCCIPITAL APPROACH FOR THE DIAGNOSIS OF RIGHT-LEFT SHUNT BY TRANSCRANIAL DOPPLER
Vanessa Almeida1, Maria Fátima Soares1, Victor Oliveira1, Ana Catarina Fonseca*1
1Hospital de Santa Maria, cerebral hemodynamics lab, lisboa, Portugal
On behalf of:
Background and aims: Patent foramen ovale (PFO) is a cause of stroke, especially in the young. Transcranial Doppler with injection of agitated saline (TCD-c) via a transtemporal window, is frequently used to search for right-to-left shunts (RLS). In about 10% of cases, an inadequate temporal bone window makes it impossible to use TCD-c. Suboccipital insonation may be an alternative to detect RLS. However, there is scarce data regarding the diagnostic accuracy of this strategy.
We aimed to compare the diagnostic agreement between TCD-c performed through a suboccipital approach and with a transtemporal approach to diagnose a RLS.
Methods: A prospective cohort of patients with TIA/stroke that were evaluated at a Neurosonology Laboratory from September 2019 to July 2021 was included. Evaluation of RLS was performed by TCD-c with both a bilateral transtemporal approach (Middle cerebral artery) and a suboccipital approach (Basilar Artery) and with and without a Valsalva Maneuver (VM). Microembolic signals (MES) were quantified as: 0 = negative; 1-25MES = isolated; >25MES= “shower”; countless= "curtain". We compared the category of the number of MES quantified by the two approaches, using Kappa-Cohen statistics.
Results: 184 patients were included, mean age of 51.7 years, ±11.8 (52.4% men). Kappa coefficient without VM was 0.91 with a standard error 0,03. The Kappa coefficient with a VM was 0.93 with a standard error of 0.02.
Conclusions: There was an almost perfect agreement between the two TCD-c approaches. The suboccipital approach should be considered to the search for a RLS, when it is not possible to use a transtemporal approach.
Disclosures of Interest: No
Abstract N°: 852
SPECIFIC FEATURES OF CEREBRAL VENOUS THROMBOSIS ASSOCIATED WITH IRON DEFICIENCY ANAEMIA
Diana Doukhi*1,2, Agnes Aghetti1, Mikael Mazighi1,2,3, Isabelle Crassard1
1Departement of Neurology, Lariboisiere Hospital, FHU NeuroVasc, Paris, France, 2Université Paris Cité, Paris, France, 3INSERM, 1144, F-75006, Paris, France.
On behalf of:
Background and aims: Association between microcytic anemia and cerebral venous thrombosis (CVT) has been reported, but data on characteristics of these types of CVT remain scarce. As iron deficiency is the main cause of microcytic anemia, we aimed to describe the clinical, radiological and follow-up data of patients with CVT and iron deficiency anemia (IDA) and their specific management.
Methods: A retrospective study was performed, including patients with CVT, identified from the Lariboisière cohort (1998-2023), who presented with moderate or severe IDA on admission. Clinical, laboratory and radiological data were collected at admission, 3 and 12 months.
Results: Among 610 patients, 64 (10,5%) had moderate or severe IDA. Sixty-two (97%) were female. The median hemoglobin level was 8.1 g/dL. Anemia was severe in 27 patients (42%). An associated risk factor for thrombosis was present in 42 patients (66%). The cause of IDA was identified in 60 patients (94%), mostly due to gynecological bleeding (45 patients, 70%). Curative anticoagulation was started in all patients. Sixty-one patients (95%) received iron supplementation and 23 patients (36%) received transfusion. When a cause of anaemia was identified, specific treatment was conducted, including gynecological surgery in 16 patients (25%). The outcome was favorable, with excellent outcome (mRS 0-1) in 48 patients/58 (83%) and recanalisation in 37 patients/38 (97%) at 1 year.
Conclusions: Iron deficiency anemia should be systematically sought in cases of CVT. Rapid assessment of the etiology of the anemia is essential for the implementation of targeted therapies in conjunction with anticoagulant treatment, which usually results in a favorable clinical-radiological outcome.
Disclosures of Interest: No
Abstract N°: 1958
COMPARISON OF COMPUTED TOMOGRAPHY ANGIOGRAPHY AND TRANSESOPHAGEAL ECHOCARDIOGRAPHY FOR THE DETECTION OF AORTIC ARCH ATHEROMA
1Service des Urgences Cérébro-Vasculaires, Hôpital Pitié-Salpétrière, AP-HP, Paris, France, 2Sorbonne Université, ACTION Study Group, INSERM UMRS 1166 Institut de Cardiologie, Hôpital Pitié Salpêtrière, AP-HP, Paris, France, 3Service de Neuroradiologie, Hôpital Pitié-Salpétrière, AP-HP, Paris, France, 4Sorbonne Université, Institut du Cerveau et de la Moelle épinière, ICM, INSERM UMRS 1127, CNRS UMR 7225, Paris, France
On behalf of:
Background and aims: Aortic arch atheroma ⩾ 4 mm is a recognised cause of cerebral infarction. The reference method for detecting these high-risk plaques is transesophageal ultrasound (TEE). However, advances in CT angiography in the last decades have made this examination an alternative, fast and less invasive method, which we compared in a cohort of stroke patients.
Methods: Patients hospitalised from 2009 to 2020 at the Pitié-Salpêtrière Hospital for a cerebral ischaemic event underwent TEE and CT angiography within 1 month (n=129). Three segments per patient were studied for a total of 311 segments analysed. The primary aim was to examine the agreement regarding the presence of atheromatous plaques measuring ⩾ 4 mm across all segments of the aortic arch. Secondary objectives included assessing agreement for any plaques and determining the optimal threshold in CT angiography for identifying TEE plaques exceeding 4 mm.
Results: Taking TEE as a reference, CT angiography shows relatively high accuracy (91%) but low sensitivity (44%) and good specificity (94%). The agreement coefficient was relatively low (kappa: 0.33). These performances increased when considering all plaques (kappa: 0.53).
The ROC analysis suggested that a 3 mm CT angiography measurement would better describe a 4 mm TEE measurement.
Conclusions: CT angiography appears to be a reliable method for confirming the presence of aortic atheroma but lacks of sensitivity. In the presence of a non-significant plaque on CT angiography, it seemed legitimate to justify performing a TEE to confirm aortic arch atheroma.
ROC Curve for defining CT angiography threshold.
Disclosures of Interest: No
Abstract N°: 1075
PREVALENCE OF ATRIAL FIBRILLATION AMONG INDIVIDUALS WITH MRI DETECTED SILENT BRAIN INFARCTS IN MIDLIFE: THE ACE 1950 STUDY
1Vestre Viken - Baerum Hospital, Department of Medical Research, Gjettum, Norway, 2University of Oslo Faculty of Medicine, Institute of Clinical Medicine, Oslo, Norway, 3Akershus University Hospital, Division of Medicine, Lørenskog, Norway, 4Oslo University hospital Ullevål, Department of Radiology and Nuclear Medicine, Oslo, Norway, 5Oslo University hospital Ullevål, Stroke Unit, Department of Neurology, Oslo, Norway
On behalf of: The ACE 1950 Study Group
Background and aims: Guidelines recommend cardiovascular risk assessment, including screening for atrial fibrillation (AF), when silent brain infarcts (SBIs) are identified on magnetic resonance imaging (MRI) examinations. Our objective was to investigate the prevalence of subclinical AF, cardiovascular risk and carotid atherosclerosis in subjects with SBI.
Methods: In the prospective Akershus Cardiac Examination 1950 Study, conducted within the general population, cardiovascular risk assessment was conducted at study inclusion from 2012 to 2015. Carotid plaque score quantified the amount of plaque in the carotid arteries, and SCORE2 was calculated to evaluate the overall cardiovascular risk among participants. MRIs were performed in a subgroup of participants between 2017 and 2023. In the event of SBIs, participants were offered 72- hour ambulatory electrocardiography.
Results: MRI was performed in 389 out of 3706 (10.5%) of participants in the ACE 1950 Study. Mean age at the time of MRI examination was 69.9±2.2 years, and 39.8% were women. SBIs were found in 47 (12.1%), of whom one individual (2.1%) had previously known AF and 32 (69.6%) completed prolonged heart monitoring. AF was detected in one individual with SBI (2.1%). There was no difference in the mean carotid plaque score or SCORE2 in participants with SBI compared to those with normal MRI-findings (2.7±2.0 vs. 2.6±2.0, p=0.70, 6.2±1.7 vs. 6.2±2.2, p=0.85, respectively).
Conclusions: In late midlife, the presence of SBI appears not to be associated with elevated cardiovascular risk, as indicated by SCORE2, age-normal carotid plaque burden, and a low prevalence of AF with 72-hour ambulatory electrocardiography.
Disclosures of Interest: No
Abstract N°: 1804
STROKE RISK AFTER EMERGENCY DEPARTMENT VISITS FOR FALL
Jed Kaiser*1, Cenai Zhang1, Hooman Kamel1, Babak Navi1, Ava Liberman1
1Weill Cornell Medicine, Department of Neurology, New York, United States
On behalf of:
Background and aims: Hospitalized patients with stroke misdiagnosis frequently are found to have been admitted from the ED after a fall. We sought to evaluate whether ED visits for falls resulting in discharge to home were associated with increased short-term ischemic stroke risk and thereby suggestive of potential ED misdiagnosis.
Methods: A case-crossover design was used to compare ED visits for fall resulting in discharge to home during case periods (0-15, 16-30, 31-90, and 91-180 days prior to stroke) versus control periods (equivalent time periods 1 year prior to stroke) using Healthcare Cost and Utilization Project data from 10 US states (2016-2020). We used previously validated ICD-10-CM codes to identify fall visits and stroke hospitalizations. Odds ratios (OR) and 95% confidence intervals (CI) were calculated using regression analyses.
Results: We identified 94,059 stroke patients, 9,592 (10.2%) had an ED visit for fall within the 180 days before stroke. Patients with an ED treat-and-release visit for fall were older (mean age 75.3 versus 70.7), more often female (61.9% versus 53.3%), and had higher rates of vascular comorbidities than other stroke patients. ED visits for fall were significantly more common in the 15 days before stroke compared to the 15-day control period 1 year earlier (OR, 2.69; 95% CI, 2.37-3.05; P= 0.006); the association between ED fall visit and stroke decreased in magnitude with increasing temporal distance (Figure 1).
Conclusions: In a large study, ED visits for fall were associated with significantly increased short-term ischemic stroke risk; these visits may be opportunities to improve diagnostic accuracy.
Disclosures of Interest: Yes Conflicts of interest cannot fit in box. Please contact presenting author for conflicts of interest.
Abstract N°: 1829
BNP AND ECHOCARDIOGRAPHIC PARAMETERS AS PREDICTORS OF ATRIAL FIBRILLATION AFTER ESUS: DATA FROM A LARGE RETROSPECTIVE STUDY
Giovanna De Marco1, Stefano Forlivesi1, Letizia Riva2, Maria Maddalena Viola1, Matteo Paolucci1, Luana Gentile1, Mauro Gentile1, Gianni Casella2, Rita Mancini3, Andrea Zini1
Background and aims: Identifying patients at higher risk of atrial fibrillation (AF) in embolic stroke of undetermined source (ESUS) is crucial for determining who may benefit from more intense and prolonged cardiac monitoring. We evaluated the role of brain natriuretic peptide (BNP) and echocardiographic parameters as predictors of AF detection in patients with ESUS from a large cohort of acute ischemic stroke (AIS) patients.
Methods: A total of 2337 consecutive patients admitted for AIS to the Stroke Unit at Maggiore Hospital (Bologna, Italy) from January 2018 to May 2023 were retrospectively enrolled. Blood BNP levels were measured within 48 hours from symptom onset. A BNP cut-off of 100 pg/ml was chosen to classify patients into high and low BNP levels. Clinical and echocardiographic variables were evaluated. Twelve-lead electrocardiography (ECG), continuous ECG monitoring, and loop recorder with external or implantable devices were used to detect new AF in patients with ESUS during 3-month follow-up.
Results: We identified 656 (28%) patients with ESUS and 83 (12% of ESUS) were diagnosed with AF. In the multivariable model, high BNP levels (Odds Ratio [OR] 2.22, 95% Confidence Interval [CI] 1.21-4.07, p=0.009), left atrium enlargement (OR 2.99, 95% CI 1.53-5.83, p=0.001) and arterial hypertension (OR 2.93, 95% CI 1.44-5.95, p=0.003) were independent predictors for the detection of AF in ESUS.
Conclusions: High BNP levels (⩾100 pg/ml), measured within 48 hours from AIS onset, left atrium enlargement and hypertension may be useful biomarkers for predicting new AF in patients with ESUS.
Disclosures of Interest: No
Abstract N°: 2517
CT-PERFUSION VASCULAR TERRITORY MAPS INCREASE INTER-RATER RELIABILITY OF DWI INFARCT ETIOLOGY CLASSIFICATION IN ICAD PATIENTS
Sethu Raman Boopathy1, Søren Christensen1, Kevin Teo*2, Davor Pavlin-Premrl3, Bruce Campbell3, Milad Mohammadzadeh1, Leonard Ll Yeo2, Jing Mingxue2, Yang Cunli4
1See-Mode Technologies, Melbourne, Australia, 2National University Health System, Division of Neurology, Department of Medicine, Singapore, Singapore, 3Melbourne Brain Centre at the Royal Melbourne Hospital, The University of Melbourne, Department of Medicine and Neurology, Parkville, Australia, 4National University Health System, Department of Diagnostic imaging, Singapore, Singapore
On behalf of:
Background and aims: Accurate identification of infarct etiology is crucial for ICAD management as the underlying mechanism determines the optimal treatment. This study compares conventional anatomical classification based on diffusion weighted imaging (DWI) infarcts versus functional, CT perfusion vascular territory maps (VTM) co-registered to DWI imaging.
Methods: Consecutive ICAD patients (N=34) with 50-99% stenosis were retrospectively assessed and the subset (N=27) with CTP & DWI imaging (within 48h) were selected. Using a novel CTP territory mapping technique, vascular territories maps (VTM) of the major cerebral arteries were produced. First, two experienced readers classified the infarcts into 6 categories based on DWI images: hemodynamic borderzone (internal vs external), embolic (borderzone y/n), undetermined type (borderzone y/n). They then repeated the same classification using the (DWI+VTM) maps. Cohen's kappa (k) was used to measure the agreement between readers.
Results: The (DWI+VTM) usage changed the initial (DWI only) decision of the readers in [reader 1: 41% (11/27) and reader 2: 44% (12/27)] of the cases. A fair agreement (k=0.29, p=0.004) was reached between two readers by using DWI with complete agreement in 48% cases. Addition of VTM maps raised the agreement to moderate (k=0.54, p=0.000) with complete agreement in 63% of cases; for embolic & undetermined borderzone types, agreement went from (0/13) to (6/17).
Conclusions: Our study shows promise that CT perfusion vascular territory maps can help provide a more reproducible estimate of infarct etiology between readers. Further prospective studies with larger cohorts are warranted to confirm and extend these results in clinical decision making.
Disclosures of Interest: Yes Employee of See-Mode Technologies
Abstract N°: 2675
CAUSES OF ISCHEMIC STROKE IN PATIENTS WITH SYSTEMIC LUPUS ERYTHEMATOSUS
1Hospital das Clínicas, Brazil, 2University of São Paulo, Brazil
On behalf of:
Background and aims: Systemic lupus erythematosus (SLE) doubles the risk of ischemic stroke (IS) but there is limited information about the subtypes of IS in patients with SLE, particularly in developing countries. We assessed the frequency of stroke etiologies in patients with SLE and IS, in a middle-income country.
Methods: We reviewed data from patients with SLE and history of IS followed from 2010 to 2021 in a Rheumatology tertiary clinic. Medical records were reviewed to apply the Causative Classification System for Ischemic Stroke (CCS). Descriptive analysis was performed.
Results: Fifty-three participants were included; vascular cervical imaging, vascular intracranial imaging, and echocardiogram were performed in 34/53 (64%), 42/53 (79%), and 46/53 (87%) patients, respectively. In six patients (11%), causes were undetermined. The most common category of stroke etiology was "other uncommon causes" (35/53, 71.7%), and the most frequent cause was antiphospholipid syndrome (21/53,39.6%). Large-artery atherosclerosis occurred in 2/53 (3.8%) cases, at a relatively young age (45 and 54 years). Cardio-aortic embolism occurred in 5/53 (9.4% cases, with two cases of Libman-Sacks endocarditis, one case of lupus myocarditis, and one case of atrial fibrillation. One patient (1.9%) presented small-artery occlusion.
Conclusions: The antiphospholipid syndrome and cardio-aortic embolism were the most frequent etiologies but investigation was often incomplete. Efforts should be made to thoroughly investigate stroke etiologies in order to implement effective secondary prevention strategies in patients with SLE.
Disclosures of Interest: No
Abstract N°: 2524
HIGH VALOSIN-CONTAINING PROTEIN (VCP) EXPRESSION IN ACUTE ISCHEMIC STROKE CLOTS OF CARDIOEMBOLIC ETIOLOGY
Cansu Sahin*1,2, Nazan Guner Sak1,2, Alice Giraud3, Pierluca Messina3, Vanessa Chalumeau4, Ivan Vukasinovic5, Marc Ribo6, Nobuyuki Sakai7, Christophe Cognard8, Karen Doyle1,2
1University of Galway, Physiology, Galway, Ireland, 2University of Galway, CÚRAM SFI Research Centre for Medical Devices, Galway, Ireland, 3Sensome, Massy, France, 4Bicêtre Hospital, Interventional Neuroradiology, Le Kremlin-Bicêtre, France, 5University Clinical Center of Serbia, Center for Radiology and MRI, Clinic for Neurosurgery, Belgrade, Serbia, 6University Hospital Vall d'Hebron, Neurology, Barcelona, Spain, 7Kobe City Medical Center General Hospital, Neurosurgery, Kobe, Japan, 8CHU de Toulouse, Diagnostic and Therapeutic Neuroradiology, Toulouse, France
On behalf of: Vanessa Chalumeau, Ivan Vukašinović, Marc Ribo, Nobuyuki Sakai, Christophe Cognard
Background and aims: Acute Ischemic Stroke (AIS) is one of the primary causes of morbidity and mortality worldwide. There is considerable interest in identifying stroke etiological biomarkers. The Ubiquitin (Ub)-Proteasome System (UPS) may play a role in the onset and progression of AIS via multiple pathways. Valosin-Containing Protein (VCP) is important in regulating both UPS and autophagy-mediated protein degradation. This study investigated the expression of Ub and VCP in AIS clots, their relationship with other clot components, patient characteristics and stroke etiology.
Methods: Large-Artery Atherosclerosis (LAA) (n=40) and Cardioembolic (CE) (n=43) clots in the Clotbase International Registry were stained with Martius Scarlett Blue, which differentiates the clot components. Immunohistochemistry was performed using anti-Ubiquitin and anti-VCP antibodies. Components were quantified using Orbit Image Analysis. Non-parametric statistical tests were utilised (Kruskal-Wallis and Spearman's correlation).
Results: VCP expression was significantly higher in CE clots than LAA clots (U=492, p=0.0007). Clots from females (n=32) had higher VCP expression than males (U=519, p=0.007). There was a positive correlation between Ub and VCP expression in AIS clots (r=0.4, p=0.0002). Ub positively correlated with white blood cells (r=0.6). Ub and VCP positively correlated with platelets (r=0.5; 0.4, p<0.0001), and negatively correlated with red blood cells (r=-0.5; -0.4, p<0.0001).
Conclusions: Higher expression of VCP is observed in clots from female AIS patients and may be associated with cardioembolic etiology. Further investigation of the relationship between VCP and AIS clots may lead to advancements in understanding the role of ER stress and abnormal protein processing in AIS.
Acknowledgements
SFI (CÚRAM: 13/RC/2073_P2), Sensome
Disclosures of Interest: No
Abstract N°: 878
ROLE OF TRANSESOPHAGEAL ECHOCARDIOGRAPHY IN ISCHEMIC STROKE DESPITE ADEQUATE ORAL ANTICOAGULANT THERAPY
1IRCCS Istituto delle Scienze Neurologiche di Bologna, UOC Neruologia e Rete Stroke Metropolitana, Ospedale Maggiore, Bologna, Italy, 2AUSL Bologna, UOC Cardiologia, Ospedale Maggiore, Bologna, Italy
On behalf of:
Background and aims: Ischemic strokes in patients on oral anticoagulant therapy (OAT) despite optimal adherence pose a therapeutical challenge. We assessed the utility of transesophageal echocardiography (TEE) in identifying potential competing cardiac causes for stroke that occurred despite adequate OAT.
Methods: This retrospective observational study included patients admitted for acute ischemic stroke between January 2022 and June 2023 who were on OAT for an established long-term indication. Transthoracic and transesophageal echocardiography, along with assessment of OAT adherence (in range INR or adequate DOAC level), were conducted. Demographic data, OAT details, and stroke characteristics were analysed to determine the influence of TEE findings on therapeutic decisions.
Results: We included 26 patients (median age 78.5 [IQR 72-81], 46.2% female; warfarin 27%, DOAC 73%). All patients underwent TEE with a median of 4 days from stroke onset (IQR 3-6). TEE identified potential cardiac competing stroke mechanisms in 88% of cases, with valvular thrombi (31%) and left atrial or appendage thrombus (27%) being predominant (figure 1). Infective endocarditis, often asymptomatic, was unexpectedly prevalent. When performed separately from TEE, Transthoracic echocardiography missed a possible cardioembolic source in 83% of cases, then discovered by a subsequent TEE.
Conclusions: TEE may be crucial for unravelling the mechanisms of ischemic stroke in patients on adequate OAT, guiding precise therapeutic strategies and potentially reducing the risk of recurrent embolic events. Our findings underscore the limitations of standard echocardiography in detecting cardiac embolic sources and emphasise the importance of tailored decision-making in secondary stroke prevention.
Disclosures of Interest: No
Abstract N°: 895
BOLUS TRANSIT-TIME DURING CT ANGIOGRAPHY PREDICTS HEART FAILURE AND CARDIOEMBOLIC AETIOLOGY: AN OBSERVATIONAL STUDY
Simone Bellavia*1, Irene Scala1, Pier Andrea Rizzo1, Jacopo DI Giovanni1, Francesca Colò1, Aurelia Zauli1, Giovanni Frisullo2
Background and aims: Compared to atherothrombotic stroke, cardioembolic stroke can be more challenging in terms of diagnostic workup due to transient cardiac abnormalities and complex and time-consuming diagnostic procedures. The purpose of this study is to evaluate predictive ability for diagnosis of cardioembolic stroke and heart failure of T40HU, a readily available parameter which is the time needed to reach a threshold of 40 HU in the ascending aorta during CT angiography (CTA)
Methods: Patients affected by of ischemic stroke or transient ischemic attack, patients undergoing both CT angiography and echocardiography were included in the study were enrolled. During CTA, T40HU was automatically obtained during arterial phase image acquisition.
Results: Starting from 1058 subjects, we enrolled 382 acute ischemic stroke patients, including 104 affected by cardioembolic stroke. Through the Spearman test, we found an inverse correlation between the ejection fraction (EF) and the T40HU. Moreover, the receiver operating characteristic (ROC) curve demonstrate that T40HU provides good discrimination of heart failure (HF) and cardioembolic stroke diagnosis, with an optimal cut-off of 16.8 seconds (AUC = 0.84 and 0.68, respectively). By multivariate analysis, both the T40HU cut-off and continuous T40HU values were independent predictors of the EF reduction and cardioembolic stroke diagnosis.
Conclusions: The T40HU appear to be a reliable biomarker of HF and cardioembolic stroke and can be useful to tailor the diagnostic workup of the patient, guiding treatment decisions focused on the reduction of the risk of future strokes.
Disclosures of Interest: No
Abstract N°: 2006
DIAGNOSTIC UTILITY OF CARDIAC COMPUTED TOMOGRAPHY IN IDENTIFYING INTRACARDIAC SOURCES OF THROMBUS: A SYSTEMATIC REVIEW AND META-ANALYSIS
Michael Liu*1, Sherief Ghozy2, Hassan Kobeisi2, Deena Nasr1, Alejandro Rabinstein1, David Kallmes2
1Mayo Clinic, Neurology, Rochester, United States, 2Mayo Clinic, Radiology, Rochester, United States
On behalf of:
Background and aims: Cardioembolism is a leading cause of stroke. Investigation traditionally has involved assessment of the heart through transthoracic echocardiography (TTE) or transesophageal echocardiography (TEE). Cardiac computed tomography (CCT) presents as an alternative, non-invasive technique to investigate for intracardiac thrombus. We conducted a meta-analysis to assess the efficacy of CCT compared to TTE and TEE.
Methods: A systematic search of the literature was conducted using the databases PubMed, Scopus, Web of Science, and Embase following PRISMA guidelines. Studies included in our analysis compared CCT to either TTE or TEE. Meta-analyses were performed to assess sensitivity, specificity, and diagnostic odds ratios (DOR) of CCT in detecting intracardiac sources of thrombus as compared to echocardiography. Intracardiac thrombus was defined as thrombus in any chamber of the heart.
Results: 43 articles and 8,540 patients were included in our analysis. When compared to TTE and TEE, sensitivity of CCT in detecting intracardiac sources of thrombus was 98.38% (95%CI 89.20%-99.78%). Specificity was noted to be 96% (95%CI 92.55%-97.88%). DOR was calculated at 98.59 (95%CI 44.05-220.69). Delayed, electrocardiogram gated CCT significantly increased specificity and DOR. Summary receiver operating curve yielded an area under the curve of 0.946. No significant heterogeneity was noted when examining sensitivity (I2=0%, t2=14.514, p=0.767) but was present in specificity (I2=90%, t2=4.075, p<0.001) and DOR (I2=69%, t2=4.126, p<0.001). Regression analysis showed no difference of outcomes with stratified by type of echocardiography.
Conclusions: CCT presents as a sensitive and specific alternative to echocardiography. In particular, electrocardiogram gated and delayed imaging proved to be the most effective imaging modality.
Disclosures of Interest: No
Abstract N°: 2515
COAGULATION FACTOR XIIIA IN ACUTE ISCHEMIC STROKE CLOTS: CORRELATION WITH PATIENT CHARACTERISTICS AND RADIOLOGICAL OBSERVATIONS
Duaa Jabrah*1, Abhay Pandit2,3, Ray Mccarthy4, Katarina Jood5,6, Sarah Power7, Turgut Tatlisumak5,6, Georgios Tsivgoulis8, Istvan Szikora9, Alexandros Rentzos10,11, Karen Doyle1,3
1University of Galway, Physiology, Galway, Ireland, 2University of Galway, CÚRAM–SFI Centre for Research in Medical Devices, Ireland, 3CÚRAM–SFI Centre for Research in Medical Devices, Galway, Ireland, 4Cerenovus, Galway Neuro Technology Centre, Galway, Ireland, 5Sahlgrenska Academy at University of Gothenburg, Department of Clinical Neuroscience, Gothenburg, Sweden, 6Sahlgrenska University Hospital, Department of Neurology, Gothenburg, Sweden, 7Beaumont Hospital, Department of Radiology, Dublin, Ireland, 8National & Kapodistrian University of Athens, Department of Neurology, Athens, Greece, 9National Institute of Neurosciences, Department of Neurointerventions, Budapest, Hungary, 10Sahlgrenska University Hospital, Department of Interventional and Diagnostic Neuroradiology, Gothenburg, Sweden, 11Sahlgrenska Academy at University of Gothenburg, Department of Radiology, Gothenburg, Sweden
On behalf of: Michael Gilvarry, Eric Ceder, Dennis Dunker, Annika Nordanstig, Petra Redfors, Alan O’Hare, Paul Brennan, András Nagy, Ágnes Vadász, Klearchos Psychogios, John Thornton
Background and aims: Coagulation factor XIIIa mediates fibrin cross-linking in contracting clots leading to their stabilisation and retention of clot components. We aimed to investigate FXIIIa composition in acute ischemic stroke (AIS) clots of different etiologies and correlate its expression with clot size, patient characteristics, and radiological observations.
Methods: We analysed AIS clots collected per-pass from 50 cases for each of the three etiologies, cardio-embolism (CE), large artery atherosclerosis (LAA) and cryptogenic in the RESTORE registry. Clot sections were immunohistochemically stained for FXIIIa expression. Martius Scarlet Blue stain identified the histological components. Extracted clot area (mm2) was measured using ImageJ. Quantification of staining was performed on www.orbit.bio. Results were analysed using parametric tests (t-test, 1-way ANOVA, Pearson’s correlation, *p<0.05).
Results:
Conclusions: CE clots contain significantly more FXIIIa than other etiologies. FXIIIa-rich clots are more likely to be small, RBC-poor, platelet-rich clots with low HU on CT and associated with poor recanalisation outcome indicating that it could be a useful marker of etiology for difficult to remove clots.
Acknowledgments
KAU, SFI (13/RC/2073_P2), and Cerenovus.
Disclosures of Interest: No
Abstract N°: 2751
ASSOCIATION OF THROMBUS COMPOSITION WITH CARDIOEMBOLIC ETIOLOGY AMONG STROKES OF UNDETERMINED CAUSE AND COMPARISON WITH ROUTINE BIOMARKERS
Juega Jesús*1, Carlos Palacio1, Laura Melgarejo1, Manuel Requena1, Laura Dorado2, Maria Hernandez Perez2, Alejandro Tomasello1, Marc Ribo1, Carlos A. Molina1, Jorge Pagola1
1Vall d’Hebron Hospital, Stroke Unit, Barcelona, Spain, 2German Trias i Pujol Hospital, Neurology, Badalona, Spain
On behalf of:
Background and aims: Defining a selective biomarker of cardioembolic etiology (CE) among strokes of undetermined cause can help to select patients for advanced diagnostic protocol including early prolonged cardiac monitoring.
Methods: A unicentric observational study among acute strokes of undetermined etiology treated with mechanical thrombectomy. Retrieved intracranial thrombi from each patient were analyzed by Flow cytometry. Thrombi composition, baseline variables, reperfusion treatment features, circulating Troponin, and NT-proBNP were analyzed. All the patients completed a diagnostic work-up with a transthoracic echocardiographic test and at least one month of continuous cardiac monitoring.
Results: Eighty-two patients completed per-protocol analysis. 62 patients ( 75%) were diagnosed of CE: 49 Atrial Fibrillation and 13 structural major cardiac disease. CE stroke thrombi had a higher Monocyte-to-Lymphocyte ratio (MLr) ( 3.47 vs. 1.23; p< 0.01) in comparison with cryptogenic stroke thrombi. CE strokes received higher rates of fibrinolysis ( 61% vs. 35% p= 0.040), had higher levels of NT-proBNP ( 1388 vs.460 ; p < 0.001) and bigger left atrial area ( 22 cm2 vs. 19 cm2; p= 0.026). The area under the curve for MLr, NT-proBNP, and Left Atrial area were 0.812 (0.699-0.897), 0.760 (0.642-0.856) and 0.658 ( 0.533-0.769)respectively.MLr was independently associated with CE strokes ( aOR 1.78, 95% CI 1.12-2.84).
Conclusions: High levels of Monocyte-to-Lymphocyte ratio in flow cytometry analysis of retrieved intracranial thrombi were independently associated with Cardiomebolic etiology among acute strokes of undetermined cause. External validation in a multicentric analysis is warranted.
Disclosures of Interest: No
Abstract N°: 318
IDENTIFYING DIFFERENCES OF MICRORNAS BETWEEN PATIENTS WITH MOYAMOYA DISEASE AND ATHEROSCLEROSIS
Hyuk Sung Kwon*1, Hojin Choi1, Euihyun Sung1, Young Seo Kim1, Hyun Young Kim1, Seong-Ho Koh1, Sung Hyuk Heo2, Dae-Il Chang2
1Hanyang University College of Medicine, Neurology, Seoul, South Korea, 2Kyung Hee University College of Medicine, Neurology, Seoul, South Korea
On behalf of:
Background and aims: Although moyamoya disease (MMD) and intracranial atherosclerotic disease (ICAD) are histopathologically and radiologically different, clinicians often find it difficult to differentiate between two diseases. Accurate and early diagnosis is important in determining treatment and predicting prognosis. In current study, we demonstrated potential micro-ribonucleic acids (miRNAs) in differentiating the MMD and ICAD.
Methods: We analyzed plasma miRNAs in ten patients with MMD or ICAD. The diagnosis of MMD was based on the guidelines of the Research Committee on MMD and RNF213 polymorphisms. We extracted miRNAs and synthesized cDNA that were used for miRNA PCR array analysis. Bioinformatics, including gene ontology (GO) pathway analyses, were also used.
Results: The miRNA array results revealed differential gene expression patterns between the MMD and ICAD groups. A total of 84 miRNAs were inspected and five miRNAs (hsa-miR-100-5p, hsa-miR-10b-5p, hsa-miR-150-5p, hsa-miR-30a-5p, and hsa-miR-7-5p) were significantly downregulated in the MMD group (p<0.05). In addition, three miRNAs (hsa-miR-100-5p, hsa-miR-10b-5p, and hsa-miR-150-5p) showed fold-regulation surpassing ±2.00 values. Bioinformatic analysis revealed that these three miRNAs are related to various genes and pathways involved in biological processes and molecular functions.
Conclusions: We found that these three miRNAs (hsa-miR-10b, hsa-miR-100, and hsa-miR-150) in plasma possess the potential to differentiate between patients with MMD and those with ICAD, which may help pave the way for early diagnosis and prompt treatment. Further prospective studies including follow-up of patients are needed to prove the efficacy of those miRNAs.
Disclosures of Interest: No
Paper Poster - Epidemiology and Risk Factors
Abstract N°: 117
PREVALENCE, DISABILITY BURDEN AND GAPS IN CARE FOR STROKE PATIENTS IN RURAL GUJARAT, INDIA
Soaham Desai*1, Devangi Desai1, Swati Arora1
1Shree Krishna Hospital Pramukhswami Medical College Bhaikaka University, Neurology, Anand, India
On behalf of:
Background and aims: Stroke is a leading cause of disability globally, with a high burden noted in rural parts of low and middle income countries (LMICs). There is limited data on prevalence, disability, risk factors and quality of stroke care from rural areas of India. This study aimed to assess stroke epidemiology and gaps in care in rural Gujarat.
Methods: A cross-sectional, door-to-door survey screened 18,896 adults from 10 villages in Anand District, Gujarat using a validated screening questionnaire. Positive screens underwent confirmation of diagnosis via detailed evaluation by physicians and tele-neurology consultation. Prevalence, risk factors, disability levels and current stroke care practices were assessed.
Results: Among 18896 adults, 100 (0.53%) strokes were diagnosed (88 ischemic, 12 hemorrhagic) - a crude prevalence of 529 per 100,000 population. Mean age was 59 years. Major risk factors were hypertension (76%), diabetes (36%), past stroke/TIA (26%). Significant disability (modified Rankin score 3-5) was present in 46%. Gaps in care included lack of rehabilitation, preventive protocols and non-evidence based medicine use.
Conclusions: A high prevalence of stroke with significant disability burden and gaps in evidence-based care were noted in this rural Gujarat population. Improving availability of protocol-based medicine therapy, secondary prevention and rehabilitation are key to reducing stroke impact.
Disclosures of Interest: No
Abstract N°: 2666
HYPERURICEMIA AND THE RISK OF STROKE INCIDENCE AND MORTALITY: A SYSTEMATIC REVIEW AND META-ANALYSIS
haiyan jiang*1, Jie Yang2
1The First Affiliated Hospital of Chengdu Medical College, neurology, Chengdu, 2Sichuan Provincial People's Hospital, University of Electronic Science and Technology of China, neurology, Chengdu, China
On behalf of:
Background and aims: The relationship between hyperuricemia (HUA) and stroke remains controversial. The aim of this systematic review was to assess the association between hyperuricemia and stroke.
Methods: PubMed, Embase, Web of Science and Cochrane Library were searched from their earliest records to February 3th, 2023, additional papers were identified through a manual search. Prospective studies that provided a multivariate-adjusted estimate of the association between hyperuricemia and risk of stroke incidence and mortality, represented as relative risks (RRs) with 95% confidence intervals (CIs), were eligible.
Results: A total of 22 studies including 770532 adults were eligible and included. Hyperuricemia was associated with a significantly increasing risk of both stroke incidence (combined RR, 1.42; 95%CI, 1.31-1.53) and stroke mortality (combined RR, 1.53; 95%CI, 1.18-1.99) in our meta-analyses. Relative risk of stroke incidence: females (combined RR, 1.67 ; 95%CI, 1.44-1.92) and males (combined RR, 1.13; 95%CI, 1.02-1.25). Relative risk of mortality: female (combined RR, 1.41 ; 95%CI, 1.31-1.52) and males (combined RR, 1.27; 95%CI, 1.20-1.34). The association between hyperuricemia and ischemic stroke (IS) (combined RR, 1.39; 95%CI, 1.31-1.47) was more significant than that of hemorrhagic stroke (HS) (combined RR, 1.13; 95%CI, 1.02-1.26).
Conclusions: Our study found an association between hyperuricemia and stroke, which was more pronounced in females.
Disclosures of Interest: No
Abstract N°: 2983
DIRECT ORAL ANTICOAGULANT TREATMENT FOR THE PREVENTION OF CEREBROVASCULAR EVENTS IN NON-VALVULAR ATRIAL FIBRILLATION PATIENTS; A POPULATION STUDY
Asaf Honig*1, Ruth Smadar1, Anat Horev1, Gal Ifergane1
1Soroka Medical Center, Neurology, Beer Sheva, Israel
On behalf of:
Background and aims: Both efficacy and safety of direct oral anticoagulants (DOAC) treatment for non-valvular AF (NVAF) patients in the prevention of ischemic events and minimizing the risk for spontaneous intracerebral hemorrhage (sICH) respectively remain unclear.
Methods: Within the years 2010-2023, all electronic medical files of health maintenance organization were reviewed for NVAF patients. Compliance was defined as consecutive purchase of DOAC every three months. Imaging was not reviewed to determine stroke type.
Results: A review of 4,602,083 patient charts found that 260,210 were diagnosed with NVAF. 98,839 DOAC treated NVAF patients (age 76.8±10.6, Males 48.7%) met our inclusion criteria and were followed for 256,981 patient years. DOAC treatment included apixaban (60.9%), rivaroxaban (24.9%) and dabigatran (14.2%). Higher dose frequency was 60.2% from the apixiaban treated patients and 40.8% from the Dabigatran treated patients. During follow-up 12% switched DOAC treatment and over 10% switched to apixaban. Ischemic event occurred in 1840 patients (within 2.1±1.9 years of DOAC treatment) and more commonly had preexisting cerebrovascular disease (72.5% vs 37.7%, p<0.001), ischemic heart disease (IHD) (58% vs 45.4%, p<0.001), congestive heart failure (CHF), diabetes mellitus (DM) and chronic renal failure (CRF) and less commonly apixaban treated and strictly compliant. In multivariate analysis, both being non strictly compliant (OR 2.42, 1.4-4.5, p=0.003) and not treated with apixaban (OR 1.7, 1.1- 2.7, p=0.015). sICH occurred in 309 patients (0.3%) within 1.7±1.9 years of DOAC treatment and more commonly with higher DOAC dosages.
Conclusions: Several variables such as type of DOAC and strict compliance are independent predictors of ischemic events.
Disclosures of Interest: No
Abstract N°: 1033
WELL-BEING OF INFORMAL STROKE CAREGIVERS COMPARED TO NON-CAREGIVER FAMILY CONTROLS
Lynda Lisabeth*1, Madeline Kwicklis1, Lewis Morgenstern1
1University of Michigan
On behalf of:
Background and aims: Health consequences of informal stroke caregiving are poorly understood because controlling for having a loved one with stroke is usually not considered.
Methods: We compared outcomes in caregivers and non-caregiver family/friends of stroke survivors (controls) within the Brain Attack Surveillance in Corpus Christi Project, a population-based study in Texas, US. Data were from medical records and interviews. Outcomes included Patient Health Questionnaire-8 (PHQ-8, range 0-24, higher→worse); PROMIS-10 physical (range 16.2-67.7) and mental health (range 21.2-67.6) summary scores (higher→better) at 90 days. Propensity score (PS) methods were used to balance factors by fitting a logistic model with caregiver status as the outcome and predictors including caregiver-control and stroke survivor sociodemographics and measures of stroke severity and outcome. PS were included as splines in regression models of associations between caregiver status and outcomes.
Results: Compared with controls (n=360), caregivers (n=320) had lower socioeconomic status, were more likely female, Mexican American, offspring rather than spouse of care recipient, and to reside with the stroke survivor. Median PHQ-8 scores ranged from mild (median=4, IQR:1-8) to no (median=2, IQR:0-5) depression, and physical (median=47.7, IQR:39.8,54.1; median=50.8, IQR:45.8,56.0) and mental health (median=45.8, IQR:41.1,50.8; median=50.8, IQR:44.9,57.7) scores were good to very good in caregivers and controls, respectively. Caregivers had greater depressive symptoms (β=1.6, 95% CI:0.6-2.5) and worse physical (β=-2.2, 95% CI:-4.0,-0.5) and mental health (β=-3.3, 95% CI:-5.1,-1.5) than controls.
Conclusions: In this study, which controlled for the effect of having a loved one with stroke, caregivers had worse outcomes than controls suggesting caregiver interventions may improve well-being.
Disclosures of Interest: No
Abstract N°: 43
DOES SOCIOECONOMIC POSITION AFFECT KNOWLEDGE OF RISK FACTORS & WARNING SIGNS OF STROKE IN EUROPE?
Katie Stack*1, Wendy Robertson2, Clare Blackburn2
1Queen Elizabeth Hospital Birmingham, United Kingdom, 2University of Warwick, United Kingdom
On behalf of:
Background and aims: Strokes are one of the leading causes of death worldwide. People with a lower socioeconomic position (SEP) are at higher risk of having a stroke. Good knowledge levels about stroke risk factors and warning signs are key to prolonging life and reducing health issues. This systematic review examined differences in knowledge of stroke risk factors and warning signs with regards to SEP in Europe.
Methods: Five databases were systematically searched using appropriate Medical Subject Headings terms and free text, combining search terms with Boolean operators. Two independent reviewers selected studies in two stages, and screened reference lists of included studies.
Results: Screening identified 2118 records. In the final review, 20 articles were included, with 67,309 study participants between them. Out of 17 studies that looked at stroke risk factors, 11 found increasing knowledge to be associated with higher SEP, four found no difference, one showed a mixed pattern and one study found increasing knowledge of risk factors to be associated with lower SEP. Out of 19 studies that looked at stroke warning signs, 15 found there was better knowledge of warning signs with higher SEP, three found no difference, and one study found increasing knowledge of warning signs with lower SEP. Studies that seemed to have a higher quality rating found increasing knowledge of stroke with higher SEP.
Conclusions: In Europe, better knowledge of stroke risk factors and warning signs is associated with a higher SEP. Stroke public health campaigns and educational interventions should be targeted at people with a lower SEP.
Disclosures of Interest: No
Abstract N°: 124
CAUSAL EFFECTS OF SNORING ON STROKE
Qiang He*1, Wenjing Wang2, Chuanyuan Tao1, Lu MA1, Chao You1
1West China Hospital of Sichuan University, Neurosurgery, Chengdu, 2West China Hospital of Sichuan University, Pharmacy, Chengdu
On behalf of:
Background and aims: Multiple risk factors of stroke have been identified in previous studies; however, the causal role of snoring in the onset of stroke is less investigated. To clarify the causal association of snoring on stroke and its subtypes, this study is performed.
Methods: The single nucleotide polymorphisms in relation to snoring were retrieved from the UK biobank cohort with 408,317 participants. The data for stroke and its subtypes of European ancestry (67,162 cases and 453,702 controls) were obtained from the MEGASTROKE consortium. In single-variable Mendelian randomization (SVMR) and multivariable MR (MVMR) analyses, inverse variance weighting was used as the primary estimate, complemented with sensitivity analyses more robust to pleiotropy.
Results: Genetically predicted snoring increased the risk of stroke (odds ratio [OR] = 2.69, 95% confidence interval [CI] = 1.19-6.08, P = 0.016) and ischemic stroke (IS) (OR = 2.82, 95% CI = 1.23-6.44, P = 0.013), but not large artery stroke (LAS) (OR = 3.02, 95% CI = 0.31-29.44, P = 0.339), cardioembolic stroke (CES) (OR = 1.51, 95% CI = 0.58-3.92, P = 0.395). We provide novel genetic evidence that snoring increases the risk of stroke and IS, but not LAS, CES, and SVS.
Conclusions: Our findings provide novel genetic evidence that snoring increases the risk of stroke and IS, but not LAS, CES, and SVS.
Disclosures of Interest: No
Abstract N°: 229
RELATIONSHIP BETWEEN LIFE’S SIMPLE 7 AND CEREBRAL WHITE MATTER HYPERINTENSITIES
Euihyun Sung1, Youngseo Kim*1, Hyuk Sung Kwon1, Hyun Young Kim1
1Hanyang University College of Medicine, Department of Neurology, Seoul, South Korea
On behalf of:
Background and aims: White matter hyperintensities (WMH) have been noticed to be associated with several vascular risk factors and to increase the risk of stroke, dementia, depression, and functional decline in old age. We aimed to investigate the relationship between WMH and Life’s Simple 7 (LS7) score, which is a simple metric developed to define optimal cardiovascular and brain health.
Methods: A total of 2,694 participants were included with available data from the Korean Genome and Epidemiology Study Cardiovascular Disease Association Study. LS7 was analyzed as the total score, behavioral subscore, and biometric subscore, and each was classified as poor, intermediate, or ideal. The total WMH, deep WMH (DWMH), and periventricular WMH (PVWMH) volume and burden were measured quantitatively, while normal or mild WMH was defined as total WMH volume less than 9,600mm3. The relationship between LS7 score and WMH was analyzed.
Results: Ideal LS7 levels and ideal behavioral subscores increased the presence of normal or mild WMH, especially in female participants. All values of WMH, DWMH, and PVWMH appeared to be lower in ideal LS7 and its behavioral subscore, while the biometric subscore only had an association with PVWMH.
Conclusions: LS7 score is negatively associated with WMH. Efforts to achieve optimal cardiovascular health will lessen WMH and can help prevent certain neurologic disorders in turn.
Total WMH, DWMH, and PVWMH volume and burden according to Life’s Simple 7 level.
Disclosures of Interest: No
Abstract N°: 904
VASCULAR RISK FACTORS IN YOUNG STROKE PATIENTS - A TWO YEAR RETROSPECTIVE COHORT STUDY IN A LONDON HYPERACUTE STROKE UNIT
Abigail Rees*1, Zayna Ahmed2, Chaamanti Sivakumar3, Hermaleigh Townsley3, Kate Ellis3, Joseph White3, Arvind Chandratheva3, Graziella Quattrocchi1,3
1North Middlesex University Hospital, London, United Kingdom, 2University College London, London, United Kingdom, 3National Hospital for Neurology and Neurosurgery, Comprehensive Stroke Service, London, United Kingdom
On behalf of:
Background and aims: ‘Young stroke’ signifies a change in risk factor profile from traditional risk factors in older groups to less common aetiologies in younger cohorts. We review the demographics, risk factors and aetiologies of young adult ischaemic stroke patients presenting to a Central London Hyperacute Stroke unit(HASU).
Methods: We retrospectively analysed consecutive records of 261 inpatients aged <55 years attending our HASU with ischaemic stroke between 1 January 2019 and 31 December 2020. Aetiology was classified utilising the TOAST classification system.
Results: Mean age was 46 years(SD=8.2), of which 66%(N=173) were aged 46-55. Mean NIHSS at presentation was 5. 69%(N=180) were male. Most prevalent aetiology was TOAST 5, 37%(N=97), denoting dual or cryptogenic aetiology. 20%(N=52) were cardioembolic(TOAST 2), 15%(N=40) secondary to small vessel disease(TOAST 3) and 15%(N=39) other aetiology (TOAST 4). 12%(N=32) of ischaemic strokes were due to large vessel atherosclerosis(TOAST 1).
Hypertension(48%, N=124) and smoking(41%, N=106) were the most prevalent risk factors. Obesity(BMI >30) was present in 31% of cases, higher than the 2021 Office of National Statistics England prevalence of 26%. Hyperlipidaemia was present in 31%(N=80). 22%(N=56) had pre-existing diagnoses of diabetes mellitus. Risk factors such as valvular heart disease(3%, N=7) and ischaemic heart disease(9%, N=23) were less prevalent.
Conclusions: Traditional vascular risk factors such as smoking and hyperlipidaemia were common. Obesity prevalence was higher than national average in England. This suggests metabolic syndrome and vascular disease should be targeted in ‘young stroke’ cohorts and in primary prevention. Should ‘young stroke’ be redefined instead as stroke with or without conventional risk factors?
Disclosures of Interest: No
Abstract N°: 1106
AGE-SPECIFIC RURAL-URBAN DISPARITIES IN THE INCIDENCE OF ISCHEMIC STROKE IN THE NETHERLANDS
1Radboud University Medical Center, Donders Institute for Brain, Cognition and Behavior, Neurology, Nijmegen, 2Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Department of Epidemiology, Utrecht, Netherlands
On behalf of:
Background and aims: Multiple studies found a higher ischemic stroke incidence in rural areas compared to urbanized areas, but this has rarely been investigated specifically in younger age groups. We aimed to investigate the incidence of ischemic stroke stratified by age (15-49 versus >50 years) in rural and urbanized municipalities within the Netherlands.
Methods: Patients with a first-ever ischemic stroke (15+ years) between 1998-2018 were included in this study through linkage of national administrative registries. Urbanization grade of the municipality was defined by the address density in five subgroups (from most urban; >= 2500 addresses per km2, to rural; <500 addresses per km2). The urbanization grade-specific incidence rate per 100,000 person-years (IR) and incidence rate ratio (IRR) were calculated.
Results: In total, 23,720 patients between 15-49 years (median age=44.7 years [IQR=40.6-48.8], 51.6% women) and 369,107 patients over 50 years (median age=76.7 [IQR=68.8-84.7], 50.8% women) were included. Patients between 15-49 years living in rural areas showed a 25% higher risk of ischemic stroke (IRR=1.25 [IQR=1.18-1.31]) compared to patients in urbanized areas (IR most urban=12.71, IR rural=15.84), whereas for persons over 50 years this risk was decreased (IRR=0.92 [IQR=0.91-0.93); IR most urban=331.10, IR rural=303.97).
Conclusions: The incidence of ischemic stroke is higher among persons between 15-49 years living in rural areas compared to urban areas, while this was reversed among persons over the age of 50. This suggests that different age-specific predictors might play a role in rural-urban disparities in ischemic stroke incidence.
Disclosures of Interest: No
Abstract N°: 1121
THE PRECISION BY THE FACE ARM SPEECH TEST (FAST) IN STROKE CAPTURE, SEX AND AGE DIFFERENCES: A STROKE REGISTRY STUDY
Guri Hagberg*1,2, Håkon Ihle-Hansen3, Tamar Abzhandadze2,4, Malin Reinholdsson2,4, Adam Viktorisson2, Hege Ihle-Hansen1,3, Katharina S. Sunnerhagen2,5
1Oslo University Hospital, Department of Neurology, Stroke Unit, Oslo, Norway, 2Institute of Neuroscience and Physiology, Section for Clinical Neuroscience and Rehabilitation, Gothenburg, Sweden, 3Bærum Hospital- Vestre Viken Hospital Trust, Department of Medicine, Drammen, Norway, 4Sahlgrenska University Hospital, Department of Occupational Therapy and Physiotherapy, Gothenburg, Sweden, 5Sahlgrenska University Hospital, Neurocare, Gothenburg, Sweden
On behalf of:
Background and aims: The shift towards milder strokes and studies suggesting that stroke symptoms vary by age and sex, may challenge the Face-Arm-Speech test (FAST) coverage. We aimed to study the proportion of stroke cases admitted with FAST symptoms, sex and age differences in FAST presentation, and explore any additional advantage of including new item(s) from the NIHSS to the FAST algorithm.
Methods: This registry-based study included patients admitted with acute stroke to Sahlgrenska University Hospital (November 2014 to June 2019) with NIHSS avaliable. FAST symptoms were extracted from the NIHSS at admission. Sex and age differences were explored using descriptive statistics.
Results: Of 5022 patients, 46% were women. Median NIHSS at admission for women was 2(8-0) and for men 2(7-0). In total, 2972 (59%) had at least one FAST symptom, with no sex difference (p=0.22). No sex or age differences were found in FAST coverage when stratifying for stroke severity. 52% suffered mild strokes, whereas 30% had FAST symptoms. The most frequent focal NIHSS items not included in FAST were sensory (29%) and visual field (25%) and adding these or both in modified FAST algorithms led to a slight increase in strokes captured by the algorithms (59 to 67 %). The modified algorithms did not provide enhanced prognostic information to FAST.
Conclusions: 60% had at least one FAST symptom at admission, only 30% in mild strokes. The stroke population of today has symptoms not covered by FAST, and awareness is needed.
Disclosures of Interest: No
Abstract N°: 1364
CONCURRENT COVERT BRAIN INFARCTS AND UNRECOGNISED MYOCARDIAL INFARCTIONS: INCREASED RISK OF ATHEROSCLEROTIC CARDIOVASCULAR DISEASE
Camiel Box*1,2, Julianne van Oortmerssen1, Maryam Kavousi1, Mohammad Kamran Ikram1,3, Frank Wolters1,2
Background and aims: Covert brain infarcts (CBI) are frequent incidental findings, but optimal management is uncertain. We investigated whether the co-occurrence of CBI with unrecognised myocardial infarction (UMI) may identify subgroups of patients at particularly high risk of atherosclerotic cardiovascular disease (ASCVD).
Methods: We included participants with concurrent ECG and brain MRI in a population-based cohort. CBI and UMI were defined as brain infarction on MRI and signs of myocardial infarction on ECG in participants without prior clinical stroke, TIA and myocardial infarction. Co-occurrence was assessed by age/sex-adjusted logistic regression. We determined ASCVD risk (composite of ischemic stroke and myocardial infarction), using Cox proportional hazard models, adjusting for common cardiovascular risk factors.
Results: Among 4,572 participants (mean age: 64 years; 57% women), 334 had CBI (7.3%), 74 UMI (1.6%) and 15 both (0.3%). Individuals with CBI were twice as likely to have UMI as those without CBI (OR [95%CI]: 2.1 [1.2–3.9]). During 45,548 person-years of follow-up, 368 ASCVD events occurred. Among individuals with CBI, those with concurrent UMI were at higher risk of ASCVD (HR: 2.3 [1.0–5.0]), due in particular to ischemic stroke risk. Compared to individuals with neither CBI nor UMI, those with both were at highest risk of ASCVD (HR 3.5 [1.6–7.5], followed by those with only UMI (HR: 1.7 [0.9–3.5]) or CBI (HR: 1.5 [1.1–2.1])
Conclusions: In individuals with CBI, co-occurrence of UMI confers an additional risk of ASCVD. Concurrent UMI may identify a subgroup of patients with CBI that could benefit most from stringent secondary prevention measures.
Disclosures of Interest: No
Abstract N°: 1841
BLOOD PRESSURE LEVELS AND ISCHEMIC STROKE AND MYOCARDIAL INFARCTION IN EARLY TO MIDDLE-AGED ADULTS WITH NEW-ONSET HYPERTENSION
1Korea University Ansan Hospital, Ansan-si, South Korea, 2Seoul National University Hospital, South Korea, 3Soongsil University, South Korea
On behalf of:
Background and aims: The purpose of this study was to determine whether the level of blood pressure control in young, middle-aged, newly onset hypertensive adults was associated with the occurrence of ischemic stroke and myocardial infarction at follow-up.
Methods: This is a retrospective nationwide population-based cohort study using data from the National Health Insurance Corporation. Data were extracted for adult patients with newly diagnosed hypertension from 2009 to 2012. Follow-up was from January 2013 to December 2016. 176,943 patients who were prescribed antihypertensive drugs within 1 year after the diagnosis of hypertension and were reexamined 2 years later were considered for the cohort. Patients with pre-existing cardiovascular disease or over 65 years of age were excluded. Ultimately, 145,697 subjects remained in the baseline cohort group. A multivariate Cox proportional hazards regression model was used to compare the hazard ratios (HR) of stroke or myocardial infarction according to the degree of blood pressure control.
Results: Of 145,697, 43,581 (30%) were unable to control systolic BP (SBP) at ⩽ 140 mmHg and 41,542 (29%) had a diastolic BP (DBP) ⩾ 90 mmHg. A risk of ischemic stroke was increased with a SBP of 150-159 mmHg (HR 1.44; 95% CI, 1.10-1.88), 160-169 (2.10; 1.55-2.84), ⩾ 170 (2.20; 1.51-3.19) and a DBP of 100-109 mmHg (1.70; 1.36-2.12), ⩾ 110 (1.57; 1.05-2.35).
Conclusions: Blood pressure levels are an important risk factor for ischemic stroke, even in young, middle-aged adults with newly onset hypertension. An unhealthy lifestyle can contribute to poor blood pressure control.
Disclosures of Interest: No
Abstract N°: 2716
RAINSTORMS WITH A SPLASH OF BLOOD: MACHINE LEARNING-BASED PREDICTIVE ANALYTICS FOR HEMORRHAGIC STROKE ADMISSION BASED ON WEATHER SYSTEMS
Mate Maros*1, Nandhini Santhanam2, Stefan Muthers3, Andreas Bender4, David Ruegamer4, Franz-Simon Centner5, Wenz Holger6, Michael Neumaier7, Fabian Siegel2
1Medical Faculty Mannheim, Heidelberg University, Departments of Neuroradiology & Biomedical Informatics (DBMI), Mannheim, Germany, 2Medical Faculty Mannheim, Heidelberg University, Department of Biomedical Informatics (DBMI), Mannheim, Germany, 3German Weather Service (DWD), Research Centre Human Biometeorology (ZMMF), Freiburg, Germany, 4Ludwig Maximilian University of Munich, The Statistical Consulting Unit (StaBLab), Department of Statistics, München, Germany, 5Medical Faculty Mannheim, Heidelberg University, Department of Anesthesiology and Surgical Intensive Care Medicine, Mannheim, Germany, 6Medical Faculty Mannheim, Heidelberg University, Department of Neuroradiology, Mannheim, Germany, 7Medical Faculty Mannheim, Heidelberg University, Institute of Clinical Chemistry, Mannheim, Germany
On behalf of: PD Dr. Eva Neumaier Probst, Profs. Dres. Kristina Szabo, Michael Platten, Nima Etminan, Christoph Groden
Background and aims: The climate crisis impacts cardiovascular health and stroke, contributing significantly to the global disease burden. Weather-based disease surveillance for healthcare providers is lacking. Hence, we aimed to forecast the number of daily hemorrhagic stroke admissions based on meteorological parameters by applying machine learning models.
Methods: Hemorrhagic stroke patients diagnosed at the University Medical Center Mannheim, Germany between 01/2015–31/2021 were selected from the local data integration center (DIC). Weather data were obtained from the German Weather Service (DWD). Complex geospatial matching was performed based on clinic-, patients’ home- and closest tower locations at the time of admission. Statistical- (Poisson), support vector- (SVR) and tree-based models (RF, XGB) were evaluated in regression settings within time-stratified nested cross-validation (training-validation: 2015-2020, test set: 2021) for daily, weekly and monthly number of combined bleeding cases.
Results: 2553 hemorrhagic stroke cases (51.8% female) were identified including intracranial- (NICH=1743, 68.3%) and subarachnoid hemorrhages (NSAH=810, 31.7%). Seasonal peaks occurred during February-March and October-November. Among all models, XGB showed the best test performance with the lowest error of 0.8 case/day. Variable importance selected maximum air pressure at sea level and mean lagged two days wind speed as the top predictors. Also, storm-associated increased maximal wind speed within the last 6 days and lower temperatures between 0-8°C were linked to higher number of hemorrhages.
Conclusions: Higher air pressure, wind speed and cold temperature that correspond to weather systems like rainstorms are significantly associated with increased number of hemorrhagic stroke admissions. Hence, these predictive models might be exploited for real-time, optimized resource allocation.
Disclosures of Interest: No
Abstract N°: 2778
ETHNIC DIFFERENCES IN PREVALENCE OF ATRIAL FIBRILLATION AND RELATED RISK FACTORS IN THE UNITED KINGDOM: A META-ANALYSIS
Joseph Kamtchum-Tatuene*1, Peter Rothwell1
1Centre for Prevention of Stroke and Dementia, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
On behalf of:
Background and aims: In US population-based studies, Blacks have lower rates of atrial fibrillation (AF) than Whites despite a higher prevalence of causal risk factors. This “AF paradox” is often attributed to disparities in access to screening. We aimed to determine whether ethnic differences also exist in the UK where publicly funded health services reduce biases.
Methods: We searched PubMed/Ovid-EMBASE for studies of ethnic differences in stroke and related risk factors in the UK, published before July 31, 2023. We compared the prevalence of AF and risk factors by ethnicity using random-effects meta-analysis.
Results: Seventy-six reports (29 studies) were included. In direct comparisons among patients with stroke, Blacks and Asians were less likely than Whites to have AF (pooled OR, 95%CI: 0.25, 0.20-0.32; 0.37, 0.28-0.49), but more likely to have hypertension (1.95, 1.47-2.60; 1.47, 1.02-2.12), diabetes (2.78, 2.40-3.22; 4.15, 3.11-5.53), and obesity (1.52, 1.27-1.83; 1.2, 0.66-2.29). However, other risk factors for AF were less common in Blacks and Asians, including smoking (0.70, 0.50-0.97; 0.57, 0.44-0.74), regular alcohol consumption (0.42, 0.36-0.49; 0.26, 0.13-0.49), and coronary artery disease-CAD (0.48, 0.31-0.76; 1.20, 0.87-1.67). Yet, Blacks were less likely than Asians to have AF (0.67, 0.47-0.95) or CAD (0.30, 0.10-0.80), but more likely to smoke (1.38, 1.02-1.86) and take alcohol regularly (2.09, 1.67-2.62). Most differences were independent of age and were similar in stroke-free populations.
Conclusions: We confirm ethnicity paradoxes for AF and CAD in the UK which are unlikely to solely reflect biases in access to healthcare and suggest different biological susceptibilities.
Disclosures of Interest: No
Abstract N°: 3073
IMPACT OF MULTIPLE VASCULAR CONDITIONS ON STROKE OR MYOCARDIAL INFARCTION PATIENTS? A LIFE COURSE POPULATION BASED STUDY
Youssef Hbid*1, Charles Wolfe1, Abdel Douiri1
1King's College London, Department of Population Health Sciences, London, United Kingdom, United Kingdom
On behalf of:
Background and aims: Cardiovascular diseases, such as myocardial infarction (MI) and stroke, present significant global health challenges. Despite common risk factors linking these conditions, the nuanced relationship between MI and subsequent stroke remains inadequately understood.
Methods: Clinical data from 849,968 patients registered in a large city with diverse population covering the period from 2005 to 2021 were investigated. Two distinct cohorts were analysed: individuals with a history of MI and those with a history of stroke, each compared to non-affected counterparts. Adjustments for age at event onset, sex, and ethnicity were performed using Cox survival models.
Results: Of all registered patients, 9,847 (1.2%) had a record of stroke, mean age 72 years and 47% were female. 5,601 (0.66%) had a record of MI, mean 41, and 28% were female. The median number of morbidities in addition to stroke was 3 (IQR: from 2 to 5). In the MI cohort, Patients with stroke were at 16% risk of mortality adjusted hazard ratio (aHR) 1.16 (95% CI [1.05-1.3]). Conversely, in the stroke cohort, Patients with stroke were 15% risk of mortality aHR 1.15 (95% CI [1.03-1.3]). In both models older age and male gender were associated with mortality but we didn’t observe differences in ethnicity.
Conclusions: Patients with multiple long-term vascular conditions were at significantly greater risk of death, emphasizing the necessity for targeted preventive strategies at first vascular event. This finding showed the importance of tailored secondary preventions strategies for individuals at the first vascular event.
Disclosures of Interest: No
Abstract N°: 1111
INCIDENCE OF POSTOPERATIVE IN-HOSPITAL NEUROLOGIC COMPLICATIONS AMONG OPEN HEART AND MICS PATIENTS IN A TERTIARY HOSPITAL
Jacqueline Costanos*1, Jarungchai Anton Vatanagul1
1Perpetual Succour Hospital of Cebu, Inc., Internal Medicine, Cebu City, Philippines
On behalf of:
Background and aims: Neurological complications have historically been a major concern in cardiac surgery, particularly stroke, negatively impacting survival and quality of life. Despite technological advancements in open, minimally invasive, and endovascular therapies, the recurring issue of neurologic complications persists. This study aims to analyze data from various cardiac procedures, ranging from traditional open-heart surgery to transcatheter valve and aortic therapies, to determine the incidence and predisposing factors of neurologic complications in a Philippine tertiary hospital.
Methods: Retrospective Descriptive Chart Review Study of Adult patients who underwent open heart and minimally invasive cardiovascular surgery.
Results: Total of 211 charts were reviewed. Open-heart group mostly had CABG (63.8%), and minimally invasive group mainly underwent TAVI and EVAR. Predominantly hypertensive, diabetic, with CKD, with mild heart failure symptoms, and preserved ejection fraction. In-hospital neurologic complication rate is 6.2%, primarily observed after open-heart surgery, all developing seizures (100%), mainly within the first 24 hours. Prolonged bypass time duration emerged as a critical factor (p = 0.003), while RHD showed a significant inverse association with post-operative neurologic complications (p = 0.024).
Conclusions: The study revealed that seizures were the most frequent neurologic complication following both open-heart and MICS procedures. Age, hypertension, diabetes, chronic kidney disease, and atrial fibrillation were identified as significant predictors of neurological complications. Notably, patients undergoing MICS exhibited a higher mean age, elevating their risk of perioperative stroke. Prolonged cardiopulmonary bypass times correlated with an increased risk of neurologic complications, while the presence of rheumatic heart disease markedly reduced this risk.
Disclosures of Interest: No
Abstract N°: 1622
RISK OF MACE WITH GLP-1 OR DUAL GIP/GLP-1 RECEPTOR-AGONISTS FOR DIABETES: A SYSTEMATIC REVIEW AND META-ANALYSIS
Georgios Tsivgoulis*1, Maria Ioanna Stefanou1, Aikaterini Theodorou2, Konark Malhotra3, Diana Aguiar De Sousa4, Mira Katan5, Lina Palaiodimou1, Robin Lemmens6, Andrei Alexandrov7, Aristeidis Katsanos8
1“Attikon” University Hospital, School of Medicine, National and Kapodistrian University of Athens, Athens, Greece., Second Department of Neurology, Athens, Greece, 2“Attikon” University Hospital, School of Medicine, National and Kapodistrian University of Athens, Athens, Greece., Second Department of Neurology, Athens, Greece, 3Allegheny Health Network, Pittsburgh, PA., Department of Neurology, Pittsburgh, 4Centro Hospitalar Universitário Lisboa Central and Institute of Anatomy, Faculdade de Medicina, Universidade de Lisboa, Lisbon, Portugal., Stroke Center, Lisboa, Portugal, 5University Hospital Basel and University of Basel, Basel, Switzerland., Department of Neurology, Basel, Switzerland, 6University Hospitals Leuven, KU Leuven - University of Leuven, Leuven, Belgium., Department of Neurology, Leuven, Belgium, 7University of Arizona, Banner University Medical Center, Phoenix, Department of Neurology, Arizona, 8McMaster University/Population Health Research Institute, Hamilton, Ontario, Canada., Division of Neurology, Ontario, Canada
On behalf of:
Background and aims: Glucagon-like peptide-1 receptor-agonists (GLP-1 RAs) have been shown to attenuate cardiovascular risk in type-2 diabetes (T2DM). Tirzepatide is the first-in-class, dual glucose-dependent insulinotropic polypeptide GIP/GLP-1 RA approved for T2DM. We sought to evaluate the cardiovascular efficacy and safety of GLP-1 and GIL/GLP-1 RAs among T2DM-patients.
Methods: We conducted a systematic review and meta-analysis of randomized controlled clinical trials (RCTs) aiming to estimate: (i) the incidence of major adverse cardiovascular events (MACE), all-cause and cardiovascular mortality; and (ii) incidence of all-cause, fatal, and nonfatal stroke in T2DM-patients treated with GLP-1 or GIP/GLP-1 RAs (vs. placebo). Secondary outcomes included stroke subtypes and MACE-recurrence.
Results: Thirteen RCTs comprising 65,878 T2DM patients were included. Compared to placebo, GLP-1RAs or GIP/GLP-1 RAs reduced MACE (OR:0.87; 95% CI:0.81-0.94; p<0.01; I2=37%), all-cause mortality (OR:0.88; 95% CI:0.82-0.96; p<0.01; I2=21%) and cardiovascular mortality (OR:0.88; 95% CI:0.80-0.96; p<0.01; I2=14%), without differences between GLP-1 vs. GIP/GLP-1 RAs detected in subgroup analyses. Concerning stroke, GLP-1 RAs reduced all-cause stroke (OR:0.84; 95% CI:0.76-0.93; p<0.01; I2=0%) and nonfatal stroke (OR:0.85; 95% CI:0.76-0.94; p<0.01; I2=0%). No association between fatal stroke and GLP-1RAs or GIP/GLP-1 RAs was uncovered (OR:0.80; 95% CI:0.61-1.05; p=0.105; I2=0%). In secondary analyses, GLP-1 RAs prevented ischemic stroke and MACE-recurrence, but not hemorrhagic stroke.
Conclusions: GLP-1 and GIP/GLP-1 RAs reduce cardiovascular risk and mortality in T2DM. While there is solid evidence that GLP-1 RAs additionally attenuate the ischemic stroke risk in T2DM, further RCTs are needed to evaluate the efficacy of novel GIP/GLP-1 RAs for primary and secondary stroke prevention.
Disclosures of Interest: No
Abstract N°: 1710
INFLUENCE OF SEX ON PREVALENCE AND MANAGEMENT OF STROKE-ASSOCIATED ATRIAL FIBRILLATION: THE IRISH NATIONAL AUDIT OF STROKE
Meabh Kelly*1,2, Olga Brych3, Joan Mccormack3, Tim Cassidy3, Ronan Collins3, Joseph Harbison4
1Trinity College Dublin, Ireland, 2Tallaght Hospital, Ireland, 3Irish National Audit of Stroke, Dublin, 4St James's Hospital, Ireland
On behalf of:
Background and aims: Recent studies have shown differing care between sexes in managing Atrial Fibrillation (AF), with less anticoagulation used in women. The Irish National Audit of Stroke (INAS) is a national hospital-based stroke registry. We performed an analysis to determine if there was a difference in practice in managing pre-stroke AF between sexes.
Methods: Data collected for INAS between 2017 and 2022 were analysed. All patient data were anonymised and ethics approval obtained.
Results: From 26829 patients (57.1% male), results on 22484 (83.8%) with complete AF data were analysed. Overall 5920 (26.3%) had AF identified. Of these, 3342 had known AF at admission (14.8% of total stroke, 56.5% of total in AF).
Total prevalence of AF was non-significantly higher in women (Men: 25.9% vs. Women: 26.9% (Chi Sq 3.46, p=0.06) but proportion of those with pre-stroke known AF was significantly higher in men (58.1% vs. 54.4% Chi Sq 7.9, p=0.004). The percentage of total strokes who had AF diagnosis after stroke onset was higher in women (10.9% vs. 12.3%. Chi Sq. 10.3 p=0.001).
There was no sex difference in proportion of patients with known AF reported receiving any oral anticoagulation at stroke onset (81.1% vs. 82.7%. Chi Sq 1.4. p=0.23). The proportion of patients receiving DOACs at onset was numerically but non-significantly higher in women (63.7% vs. 64.9%, Chi Sq 0.5, p=0.48).
Conclusions: Women were more likely to present with previously unrecognised AF. Men and women with known AF were equally likely to be anticoagulated pre-stroke.
Disclosures of Interest: No
Abstract N°: 2244
TRENDS IN QUALITY OF ACUTE STROKE AND SECONDARY STROKE PREVENTION CARE IN PATIENTS WITH PRE-STROKE DISABILITY
Vanessa Ha1, Magnus Thorén2, Niaz Ahmed2, Charith Cooray2, Aravind Ganesh*1
1University of Calgary, Clinical Neurosciences, Calgary, Canada, 2Karolinska Institutet, Clinical Neurosciences, Stockholm, Sweden
On behalf of:
Background and aims: Patients with pre-stroke disability (PSD) have worse stroke outcomes. The extent to which the quality of stroke care differs between patients with and without PSD remains uncertain.
Methods: We included patients who were enrolled in the SITS-International Stroke Treatment Registry between 2003-2021 and received IV thrombolysis with or without endovascular therapy. Patients with PSD had a baseline mRS⩾2. We performed regression analyses adjusted for age, sex, year of stroke, stroke severity, and comorbidities. Time-trends were analyzed for each study year.
Results: The mean age of patients with PSD (n=21,414) was 76.88±11.8 and without PSD (n=140,410) was 68.7±13.2. Patients with PSD were less likely to receive thrombectomy (aOR=0.49[95% CI: 0.44, 0.56]), hemicraniectomy (aOR=0.42[95% CIs: 0.19,0.93]), and carotid vascularization (aOR=0.63[95% CIs: 0.47,0.83]) when indicated. Although patients with PSD were more likely admitted to the stroke unit, they were less likely to receive antiplatelet and anticoagulation (aOR=0.61[95%CI: 0.58,0.64]), statin (aOR=0.70[95% CI: 0.67,0.73]), and antihyperglycemic agents (aOR=0.86[95%CI 0.79,0.94]) at discharge. Patients with PSD were more likely to have stroke recurrence at 3 months with no evidence of change in the relationship over time even when adjusted for stroke prevention medications and acute stroke intervention (aOR=1.25[95%CI:1.05,1.49]).
Conclusions: In this observational registry-based study, patients with PSD were not only less likely to receive acute stroke interventions (as might be expected), but were notably less likely to receive secondary stroke prevention therapies. These disparities may explain the higher risk of stroke recurrence in people with PSD, albeit confounding cannot be ruled out.
Disclosures of Interest: No
Abstract N°: 2546
THE EFFECT OF GREEN SPACE AND NOISE EXPOSURE ON THE RISK OF ISCHEMIC STROKE AND ITS SEVERITY; A CASE-CONTROL STUDY
Jad El Masri*1,2,3, Hani Finge3, Tarek Baroud3, Najla Ajaj3, Maya Ghazi3, Diala El Masri3, Mahmoud Younes3, Pascale Salameh3,4, Hassan Hosseini2,5
1American University of Beirut, Beirut, Lebanon, 2Paris 12 Val de Marne University, Créteil, France, 3Lebanese University - Hadat Campus, Beirut, Lebanon, 4Nicosia, Nicosia, Cyprus, 5Henri-Mondor University Hospital, Créteil, France
On behalf of:
Background and aims: Environmental surroundings reduce the rate of several diseases, especially those related to stressful events. Ischemic stroke can be affected by such events, either directly or through its risk factors. Therefore, the present study evaluates the effect of green space and noise exposure on the risk of ischemic stroke.
Methods: A case-control study was carried out, including 200 ischemic stroke cases within the first 48 hours of diagnosis and 200 controls, divided equally into hospitalized and non-hospitalized participants. Controls were matched to cases based on age and gender. Sociodemographic characteristics were assessed, in addition to the exposure to green spaces and noises from home and workplaces. For stroke patients, Modified Rankin Score (mRS) was measured to assess disability.
Results: Living or working in rural areas, living in a house (not building), having a private garden, and taking care of it were associated to a lower risk of stroke (p<0.001 each). Exposure to traffic, industrial and human noises at home and workplaces increased the risk of stroke, while natural sounds decreased it (p<0.001 each). The loudness of home and workplace’s surrounding was also associated to an increase stroke risk (p<0.001). As for disability levels, mRS score was directly correlated to the level of noise in the workplace (p<0.001).
Conclusions: The environmental surroundings were found to affect the risk of ischemic stroke. Higher green space and lower noise exposures have a protective role in stroke and its prognosis, suggesting a possible strategy for preventing stroke through environmental modifications at home and workplaces.
Disclosures of Interest: No
Abstract N°: 3225
THE IMPACT OF PREVIOUSLY DIAGNOSED DEPRESSION ON EARLY AND ONE-YEAR MORTALITY IN PATIENTS WITH ACUTE ISCHEMIC STROKE IN OPOLE PROVINCE, POLAND
Beata Łabuz-Roszak*1, Maja Górniak2, Kacper Wójcicki3, Marek Gierlotka4
1Institute of Medical Sciences, University of Opole, Department of Neurology, Opole, Poland, 2Student Scientific Society at the Department of Neurology, Institute of Medical Sciences, University of Opole, Opole, Poland, 3Student Scientific Society at the Department of Cardiology, Institute of Medical Sciences, University of Opole, Opole, Poland, 4Institute of Medical Sciences, University of Opole, Department of Cardiology, Opole, Poland
On behalf of:
Background and aims: Depression is a known cardiovascular risk factor. However, the impact of preexisting mood disorders on the course of stroke is not clearly defined. Therefore, the purpose of this study was to determine the impact of previously diagnosed depression on mortality in patients with acute ischemic stroke (IS).
Methods: The study was based on the registry created from the administrative database of the only public and obligatory health insurer in Poland (National Health Fund) for the years 2009-2020. The IS cases were selected based on primary diagnosis coded in ICD-10 as I63. Two groups were distinguished; IS-D: patients with IS and a diagnosis of depression within preceding 5 years (n=520), and IS-nD: patients with IS who had never been diagnosed with depression (n=11,505).
Results: The mean age in both groups was similar (72.4±11.6 vs 72.3±12.3 years), while the percentage of women was higher in the IS-D group (71% vs 50%; p<0.001). In-hospital, 30-day and 1-year mortality did not differ significantly between groups (3.8% vs 5.1%, 13.1% vs 12.9%, 27.1% vs 26.8%, respectively). However, when statistical analysis was performed stratified by gender and age, we found a significantly higher 30-day and 1-year mortality in younger men (<65 years old) with IS and prior depression in comparison to those without depression (13.6% vs 3.8%, p<0.001; and 20.3% vs 10.8, p<0.021, respectively).
Conclusions: In patients with IS, special attention should be paid to the presence of depression in medical history, as it can affect prognosis, especially in younger men.
Disclosures of Interest: No
Abstract N°: 82
LONG-TERM INCIDENCE OF STROKE AFTER TIA OR MINOR STROKE: SYSTEMATIC REVIEW AND META-ANALYSIS
Faizan Khan*1, Ale Algra2, Christian Weimar3, Toshiyuki Uehara4, Angel Ois5, Matteo Foschi6, Fredrik Ildstad7, Naja Vinding8, Hong-Kyun Park9, Michael Hill1
1University of Calgary, Cumming School of Medicine, Calgary, Canada, 2UMC Utrecht, Department of Neurology and Neurosurgery, Utrecht, Netherlands, 3Essen University Hospital, Institute for Medical Informatics, Biometry and Epidemiology, Essen, Germany, 4Hyogo Prefectural Harima-Himeji General Medical Center, Department of Neurology, Himeji, Japan, 5Institut Hospital del Mar d'Investigacions Mèdiques (IMIM), Neurovascular Research Group, Barcelona, Spain, 6University of L'Aquila, Department of Biotechnological and Applied Clinical Sciences, L'Aquila, Italy, 7St. Olav's University Hospital, Trondheim, Norway, 8Copenhagen University Hospital, Rigshospitalet, København, Denmark, 9Inje University Ilsan Paik Hospital, Goyang-si, South Korea
On behalf of: PERSIST Collaborators
Background and aims: After a TIA or minor stroke, the long-term risk of stroke is uncertain. We determined the annual and cumulative incidence of subsequent stroke up to 10 years in this patient population.
Methods: Electronic databases were searched (from inception to December 1, 2023) for observational studies reporting subsequent stroke during a minimum follow-up of 1 year in patients with TIA or minor stroke. For the calculation of incidence rates, we requested from the authors of included studies, unpublished aggregate data on the number of subsequent stroke events and the number of exact person-years of follow-up during discrete time intervals (ensuring appropriate censoring of deaths, patients lost to follow-up, and those withdrawn from study). Results across studies were pooled using random-effects meta-analysis.
Results: Fifteen independent cohorts involving 129794 patients were included in the analysis [Table 1]. The pooled incidence rate of subsequent stroke per 100 person-years was 6.4 events in the first year and 2.0 events in the second through tenth years, with cumulative incidences of 14% at 5 years and 21% at 10 years [Table 2]. Based on 10 studies with information available on both fatal stroke and any stroke, the pooled case fatality rate of subsequent stroke was 9.5% (95% CI, 5.9 – 13.8).
Conclusions: The long-term risk of stroke after a TIA or minor stroke is substantial, with one in five patients expected to experience a subsequent stroke within 10 years and every tenth patient expected to die from their subsequent stroke. This information should help inform patient prognosis and improve practice on long-term stroke prevention.
Disclosures of Interest: No
Abstract N°: 121
RISK OF RECURRENT STROKE IN PATIENTS WITHOUT TRADITIONAL RISK FATCTORS AFTER TIA OR MINOR STROKE
Shinichiro Uchiyama*1, Takao Hoshino2, Kazuo Minematsu3, Hugo Charles4, Pierre Amarenco4
1Sanno Medical Center, Center for Brain and Cerebral Vessels, Tokyo, Japan, 2Tokyo Women's Medical University, Department of Neurology, Tokyo, Japan, 3Iseikai International General Hospital, Osaka, Japan, 4Bichat Hospital, Department of Neurology and Stroke Center, Paris, France
On behalf of: TIAregistry.org Investigators
Background and aims: The purpose of this study was to investigate the clinical characteristics and long-term outcome in patients without traditional risk factors (TRFs) after transient ischemic attack or minor ischemic stroke, who were enrolled in the TIAregistry.org, an international, multicenter, prospective cohort.
Methods: TRFs included hypertension, diabetes, hypercholesterolemia, current smoking, and atrial fibrillation. Background characteristics and outcomes at one and five years in patients without TRFs (n=402) were compared to those in patients with TRFs (n=3445). Outcomes analyzed were recurrent stroke and major vascular events. To evaluate the coexistence of causes, we applied the ASCOD (atherosclerosis, small vessel disease, cardiac pathology, other cause, or dissection) grading system.
Results: Age was younger; males, coronary artery disease, and CKD were fewer; physical activity was more common; HDL cholesterol level was higher; triglyceride level and BMI were lower in patients without TRFs. Uses of antiplatelets, anticoagulants and statin were less frequent throughout observation period in patients without TRFs. ABCD2 score in patients without TRFs was comparable despite absence of hypertension and diabetes to that in those with TRFs. Risk of recurrent stroke at one and five years did not differ between patients with and without TRFs. The most significant predictor of major vascular events at one and five years was ipsilateral intracranial or extracranial arterial stenosis (ASCOD A1/A2) in patients without TRFs.
Conclusions: In patients without TRFs, risk of recurrent stroke is underscored and undertreated, and non-TRFs or unknown risk factors for arterial stenosis should be identified and managed appropriately.
Disclosures of Interest: Yes Japan Cardiovascular Research Foundation
Abstract N°: 1439
CARDIOVASCULAR RISK FACTORS CONTROL IN PATIENTS WITH COVERT BRAIN INFARCTS: SILENT STUDY
Alice de Vautibault*1, Valentin Amar1, Marialuisa Zedde2, Rosario Pascarella3, Adnan Mujanovic4, Laurent Roten5, Urs Fischer6, Thomas Meinel6, Marco Pasi1
1CHU de Tours et Université François Rabelais, Neurology Department, Tours, France, 2Azienda Unità Sanitaria Locale-IRCCS di Reggio Emilia, Neurology Unit-Stroke Unit, Reggio Emilia, Italy, 3Azienda Unità Sanitaria Locale-IRCCS di Reggio Emilia, Neuroradiology Unit, Reggio Emilia, Italy, 4Inselspital, Bern University Hospital, University of Bern, Institute of Neuroradiology, Bern, Switzerland, 5Inselspital, Bern University Hospital, University of Bern, Department of Cardiology, Bern, Switzerland, 6Inselspital, Bern University Hospital, University of Bern, Department of Neurology, Bern, Switzerland
On behalf of: for the SILENT group
Background and aims: Covert brain infarctions (CBI) are associated with cardiovascular risk factors (cvRFs) in research cohorts. We aimed to evaluate the presence and yield of assessing modifiable cvRFs in patients with incidentally discovered CBI on routine neuroimaging.
Methods: The SILENT cohort study (NCT05685069) is a prospective, multicenter European cohort recruiting patients without previous manifest stroke after incidental discovery of focal CBI on routinely obtained MRI scans. Presence and control of modifiable cvRFs was assessed using applicable international guidelines for hypertension, dyslipidemia, diabetes, smoking and obesity.
Results: We included 218 patients with a mean age of 65.4 years [Standard deviation: 14.2] and 43% were women. Seventy-five percent of them had at least one, 49% at least two and 12% at least three modifiable cvRFs. Within the group of patients with known risk factors, 163 (91%) patients presented at least one uncontrolled cvRF, 94 (52%) at least two, and 26 (15%) at least three. Most cases of poor control of known cvRFs were dyslipidemia (89/121; 66%), followed by hypertension (71/126; 56%). Active smoking was present in 45/217 (21%) and obesity in 44/214 patients (21%). Work-up identified 39/181 (21%) previously unknown cases of dyslipidemia, 22/213 (10%) of hypertension and 3/188 (2%) of diabetes.
Conclusions: In patients with incidentally discovered CBI in clinical routine, we found a high burden of poorly controlled cvRFs. Our results indicate the importance and yield of a dedicated clinical and laboratory assessment of cvRFs in patients with CBI.
Disclosures of Interest: No
Abstract N°: 1984
TELEPHONE TRAINING TO IMPROVE ECG QUALITY IN REMOTE SCREENING FOR ATRIAL FIBRILLATION
Kethaki Prathivadi Bhayankaram*1, Jonathan Mant1, James Brimicombe1, Andrew Dymond1, Kate Williams1, Peter Charlton1
1Cardiovascular Group, Department of Public Health and Primary Care, Cambridge, United Kingdom
On behalf of: The Screening for Atrial Fibrillation with ECG to Reduce Stroke (SAFER) authorship group
Background and aims: Self-recorded, single-lead ECGs are increasingly used to diagnose arrhythmias. However, they can be of variable quality, which can affect the reliability of interpretation. In this analysis of ECGs collected in atrial fibrillation screening studies, our aims were to: (i) determine the quality of ECGs when recorded unsupervised (at home); and (ii) investigate whether telephone training improved ECG quality.
Methods: Data was obtained from the Screening for Atrial Fibrillation to Reduce stroke (SAFER) programme, where participants recorded single-lead ECGs four times per day for three weeks using a handheld device. ECG quality was assessed using an automated algorithm, and participants who recorded >25% poor quality ECGs from days 4-10 of screening were identified for training. Telephone training to improve ECG recording technique was delivered when research team capacity permitted.
Results: 14,727 participants recorded 1,206,972 ECGs, of which 43,513 (3.6%) were poor quality. Most participants (51.9%) did not record any poor-quality ECGs. 1,105 (7.5%) participants met the threshold for training. Of these, 165 participants received training and 896 did not. Comparing these groups, the mean (95% confidence interval) reduction in the proportion of poor-quality ECGs per participant from before training (days 1-3) to after training (days 11-21) was 21.1 (17.5-23.5) % with training and 15.7 (14.5-16.8) % without training (p<0.05).
Conclusions: Most participants achieved adequate quality ECGs. For those that did not, ECG quality improved over time regardless, and training further improved ECG quality. Therefore, telephone training could be considered in atrial fibrillation screening programmes using single-lead ECG devices.
Disclosures of Interest: No
Abstract N°: 2192
TRENDS IN INTRAVENOUS THROMBOLYSIS FOR EXTENDED TIME WINDOW IN ACUTE ISCHEMIC STROKE IN SOUTH KOREA
1Seoul National University Bundang Hospital, Department of Neurology, Seongnam, South Korea, 2Korea University, Department of Biostatistics, Seoul, South Korea, 3Dong-A University Hospital, Department of Neurology, Busan, South Korea, 4Chonnam National University Hospital, Department of Neurology, Gwangju, South Korea, 5Keimyung University Dongsan hospital, Keimyung University School of Medicine, Department of Neurology, Daegu, South Korea, 6Hallym University Sacred Heart Hospital, Department of Neurology, Anyang, South Korea, 7Seoul National University College of Medicine, Cerebrovascular Disease Center, Seoul National University Bundang Hospital, Department of Neurology, Seongnam, South Korea
On behalf of: CRCS-K investigators
Background and aims: Despite global increases in intravenous thrombolysis (IVT) for acute ischemic stroke (AIS) beyond 4.5 hours from the last normal time (LNT), there's limited data on its real-world application.
Methods: This study analyzed AIS patients presenting within 7 days of symptom onset from January 2015 to December 2022. Data were collected from a prospective, nationwide, multicenter stroke registry (CRCS-K, Clinical Research Collaboration in Korea) in South Korea. The study periods were divided into 3 epochs; 2015-2017, 2018-2020, and 2021-22, considering the publication years of the 2 pivotal trials, WAKE-UP (2018) and EXTEND (2019).
Results: The study included 55,730 patients (mean age 69±13, male 59%). During the period, stroke risk factors such as age, hypertension, and diabetes increased. Additionally, the time from the LNT to the hospital arrival was also delayed. The IVT rate for patients presenting after 4.5 h from LNT decreased from 2.0% to 0.9%, and a similar trend was observed in patient groups that met the eligibility of the two pivotal trials, WAKE-UP(6.3% to 3.2%) and EXTEND(5.6% to 2.5%). The overall IVT rate fell from 14.7% to 10.9%, and the IVT rate for patients arriving within 4.5 h from LNT also declined.
Conclusions: Contrary to the global trend of increasing overall IVT rate, despite the pivotal trials showing the benefits of IVT beyond 4.5 hours from LNT, the IVT rate in South Korea has shown a decreasing trend. Further research will be necessary to enhance IVT treatment in the future.
Disclosures of Interest: No
Abstract N°: 2413
BETTER BRAIN CARE IS GOOD FOR THE HEART AND THE REST OF THE BODY
Jasper Senff*1,2,3,4, Cyprien Rivier5,6, Reinier Tack1,2,3,4, Tamara Kimball1,2,3, Megan Conroy7, Zeina Chemali1,2, Christopher Anderson1,2,8, Jonathan Rosand1,2,3, Guido Falcone5,6, Sanjula D. Singh1,2,3
1Massachusetts General Hospital, McCance Center for Brain Health, Boston, United States, 2Massachusetts General Hospital, Department of Neurology, Boston, United States, 3Broad Institute, Cambridge, United States, 4UMC Utrecht, Department of Neurology, Utrecht, Netherlands, 5Yale School of Medicine, Department of Neurology, New Haven, United States, 6Yale School of Medicine, Yale Center for Brain and Mind Health, New Haven, United States, 7Nuffield Department of Population Health (NDPH), University of Oxford, United Kingdom, 8Brigham and Women's Hospital, Department of Neurology, Boston, United States
On behalf of: Amy Newhouse MD, Valerie Purdie-Greenaway PhD, Gregory Fricchione MD, Rudolph E. Tanzi PhD, Nirupama Yechoor MD
Background and aims:The Brain Care Score (BCS) was developed as a tool to give people agency to make changes in their lifestyle and reduce risk of dementia and stroke (fig. 1). In this study, we investigate the associations between BCS at baseline and incidence of cardiovascular disease (CVD) as well as the three most common cancer types.
Methods: Analyses in the UK Biobank (UKB) were performed in participants with complete BCS data available at baseline. Associations with incident CVD (ischemic heart disease [IHD], stroke, and heart failure) and lung-, colorectal-, and breast cancer were analyzed using Cox proportional hazard regression models.
Results: Among 416,370 UKB participants (mean age:57, female:54%) 33,944 (8.8%) CVD and 16,090 (4.0%) cancer cases were identified (median follow-up: 12.5 years). A five-point higher baseline BCS (indicating better brain care) was associated with lower incidence of CVD (HR:0.57 [95%CI:0.55-0.59]), including IHD (HR: 0.57 [95%CI:0.54-0.59]), and heart failure (HR:0.49 [95%CI:0.44-0.53]). A five-point higher baseline BCS was associated with lower incident overall cancer (HR:0.69 [95%CI:0.66-0.72]), including lung- (HR: 0.34 [95%CI:0.27-0.41]), colorectal- (HR: 0.79 [95%CI: 0.73-0.85]), and breast cancer (HR: 0.84 [95%CI:0.80-0.89]).
Conclusions: The BCS, a simple educational and motivational tool shown to associate with stroke and dementia, may also play an important role in the prevention of coronary heart disease and cancer.
Disclosures of Interest: No
Abstract N°: 2881
UNDERSTANDING EVOLVING SYMPTOM SEVERITY IN THE HYPER-ACUTE PHASE:A MULTIFACTORIAL ANALYSIS OF SERIAL NIHSS ASSESSMENT
Zewen Lu*1,2, Halvor Næss3, Matthew Gittins1,2, Amit Kishore2,4, Craig Smith2,4, Andy Vail1,2
1University of Manchester, Centre for Biostatistics, Manchester, United Kingdom, 2Salford Care Organisation, Northern Care Alliance NHS Foundation Trust, UK, Manchester Centre for Clinical Neurosciences, Geoffrey Jefferson Brain Research Centre, Manchester, United Kingdom, 3Department of Neurology, Haukeland University Hospital, Bergen, Norway, 4University of Manchester, Division of Cardiovascular Sciences, Faculty of Biology, Medicine and Health, Manchester, United Kingdom
On behalf of:
Background and aims: Much research implicitly considers ‘admission NIHSS’ as a fixed marker of stroke severity. However, cross-sectional data suggest higher values with early admission. If symptoms evolve unpredictably, future research could be statistically more efficient if it explicitly recognised this. We therefore sought to explore early changes in serial NIHSS scores and whether routinely recorded baseline characteristics could explain any statistical variation.
Methods: We analysed data from the Bergen NORSTROKE study. Staff routinely recorded serial NIHSS scores for patients at a single stroke unit between 2006 and 2021.
We included patients diagnosed with ischaemic stroke of known onset time who had at least two NIHSS scores recorded within 6 hours of onset and prior to acute intervention. We excluded TIA.
We calculated the average gradient of NIHSS score for each individual and then modelled these gradients on baseline patient characteristics using multifactorial linear regression.
Results: We identified 642 eligible participants: median (IQR) age 75 (63 to 83) y; 46% male; median (IQR) admission NIHSS and time to assessment 2 (1 to 7) and 1.67 (1.00 to 2.58) hrs respectively. Only 221 (34%) had static NIHSS score: 192 (30%) deteriorated; 229 (36%) improved. We did not find any association between NIHSS gradient and factors including age, sex, medical history, and admission time. Our multifactorial model explained <5% of variation.
Conclusions: We need to explore potential statistical gains for epidemiological research from recognising the dynamic nature of symptom severity during the hyper-acute phase.
Disclosures of Interest: No
Abstract N°: 111
LONG-TERM CONTRIBUTION OF STROKE TO OVERALL AND CAUSE-SPECIFIC MORTALITY
Andrea De Alba-Sanchez*1,2, Omar Cárdenas Sáenz1,2, Amado Jimenez-Ruiz1,2, Enrique Gomez Figueroa1,2, Jose Luis Ruiz-Sandoval1,2
1Civil Hospital Fray Antonio Alcalde, Neurology, Guadalajara, Mexico, 2University of Guadalajara, Guadalajara, Mexico
On behalf of:
Background and aims: Stroke mortality is higher in low-income than in high-income countries. In Mexico, information is derived from short-term follow-up of patients, with a high mortality rate related to systemic complications and an early stroke recurrence. Our aim is to describe the long-term contribution of stroke to overall and cause-specific mortality.
Methods: We analysed data from patients with stroke included in the Mexico City Prospective Study (1998-2004), a robust cohort with more than 150,000 baselines ⩾35-year-old subjects with long-term follow-up until December 2022. To evaluate if mortality in stroke patients has different risk factors both the whole cohort and the stroke subset were analyzed. To assess the contribution of stroke to mortality from any cause and cause-specific mortality, Cox regression models were performed adjusted to age, sex, and time (in decades) elapsed from previous stroke to recruitment.
Results: A significant increase in the death risk from any cause was observed in people with stroke (HR: 2.5; CI 1.09-2.68, p<0.001) with an escalation in the HR across the different age subgroups. Examination of cause-specific mortality showed that stroke increases the risk of death of cardiac (HR 3.44, CI 2.92-4.04, p<0.001), renal (HR: 1.99, CI 1.53-2.58; p<0.001) and pulmonary causes (HR 2.23, CI 1.74-2.84, p<0.001).
Conclusions: This cohort confirms the association between a history of stroke and higher mortality from any cause and from cardiac, renal, and pulmonary causes; and showed a higher frequency of cardiovascular comorbidities and deleterious anthropometric and socioeconomic profile in patients who suffered from stroke.
Disclosures of Interest: No
Abstract N°: 2612
AN INTERNATIONAL REGISTRY FOR IATROGENIC CEREBRAL AMYLOID ANGIOPATHY
Gargi Banerjee1, Kanishk Kaushik*2, Floris Schreuder3,4, Robin Lemmens5, Steven Greenberg6, Marieke Wermer2,7, David Werring8
1Institute of Prion Diseases at University College London (UCL), MRC Prion Unit, United Kingdom, 2Leiden University Medical Centre (LUMC), Department of Neurology, Netherlands, 3Radboud University Medical Center (RUMC), Department of Neurology, Nijmegen, Netherlands, 4Donders Institute for Brain, Cognition and Behavior, Radboud University, Nijmegen, Netherlands, 5KU Leuven, Department of Neurology, Leuven, Belgium, 6Massachusetts General Hospital, Department of Neurology, Boston, MA, United States, 7University Medical Center Groningen (UMCG), Department of Neurology, Groningen, Netherlands, 8Stroke Research Centre, UCL Queen Square Institute of Neurology and the National Hospital for Neurology and Neurosurgery, Department of Brain Repair and Rehabilitation, London, United Kingdom
On behalf of: on behalf of all collaborating contributors to the International Registry for Iatrogenic CAA
Background and aims:Iatrogenic cerebral amyloid angiopathy (iCAA) is a recently recognized transmissible subtype of CAA caused by exposure to amyloid-beta protein present during medical procedures. Many cases reported to date have presented with early-onset CAA (typically ⩽55 years). Comprehensive data regarding the disease incidence, phenotype, natural history, and causative exposures for iCAA are scarce. The aim of the International Registry for Iatrogenic CAA is to allow investigators worldwide to perform surveillance and collate data on relevant exposures and natural history.
Methods:Collaborators will be invited to enter completely anonymized data regarding patients with possible or probable iatrogenic CAA via an online data-capture form. Follow up data on cerebrovascular events, cognitive change and mortality will be requested annually. The Registry will provide regular (annual or biennial) reports on the number of cases identified worldwide, and a rolling report on clinical follow-up events. The Registry will also act as a platform to facilitate future sub-studies, for example those relating to fluid-based or neuroimaging biomarkers.
Results:The Registry is now live and collecting data. Ethical approval was granted in September 2023 (Research Ethics Committee Reference: 23/SW/0095). Interim data will be reported at ESOC in May 2024; the first full report is anticipated in Autumn 2024
Conclusions:Establishing this registry is the first step in an important international collaboration to further understand iatrogenic CAA. We warmly encourage clinicians and researchers with experience of iCAA to participate and contribute data to this registry.
Disclosures of Interest: No
Abstract N°: 30
BASILAR ARTERY OCCLUSION STROKES IN THE NEUROLOGICAL CLINIC OF PISA: A 22-YEARS ANALYSIS
Gaia Mignani*1, Nicola Giannini1, Leonardo Ulivi1, Marco Baldini1, Roberto D'agliano1, Giovanni Orlandi1, Mirco Cosottini2, Gabriele Siciliano1, Michelangelo Mancuso1
Background and aims: Basilar artery occlusion (BAO) is a subtype of stroke burdened by high mortality and disability. The aim was to analyze, retrospectively, a cohort of patients with BAO, admitted to the University Hospital of Pisa between January 2001 and December 2022, in order to identify variables related to the outcome at 90 days defined by the modified Rankin Scale (mRS).
Methods: The endpoint was mortality or significant disability at 90 days. We performed a binary logistic regression with the significant variables (p<0.05) at the univariate analysis.
Results: We have analyzed 163 consecutive patients with BAO (median age 73 years). A significant difference between standard medical treatment and an endovascular approach did not emerge, while analyzing the subgroup of patients who underwent endovascular treatment, a trend of significance has been demonstrated in favor of conducting a rescue treatment as opposed to a primary one. Intracerebral haemorrhage (ICH), Glasgow Come Scale (GCS) at admission, tracheostomy care, National Institutes of Health Stroke Scale (NIHSS) score at discharge were associated with worst prognosis at 3 months.
Conclusions: A crucial role in avoiding a negative functional outcome in patients with basilar artery occlusion stroke is played by the prevention of complications during hospitalization in addition to preventing common cardiovascular risk factors, Additionally, it is necessary to consider the Glasgow Coma Scale (GCS) as a prognostic indicator in addition to the NIHSS at onset.
Disclosures of Interest: No
Abstract N°: 1502
THE ASSOCIATION BETWEEN PERIODONTITIS, GINGIVITIS, TOOTH LOSS AND STROKE: AN UMBRELLA STUDY WITH META-ANALYSIS
Jad El Masri1,2,3, Ahmad Malak3, Diala El Masri3, Maya Ghazi*3, Silva Al Boussi3, Yasmina El Masri3, Pascale Salameh3,4, Hassan Hosseini1,5
1Paris Est Creteil, 2American University of Beirut, Beirut, Lebanon, 3Lebanese University - Hadat Campus, Beirut, Lebanon, 4University of Nicosia, Nicosia, Cyprus, 5Henri-Mondor University Hospital, Créteil, France
On behalf of:
Background and aims: Cerebrovascular diseases (CVAs) have several risk factors that are categorized as modifiable and nonmodifiable. Periodontal diseases (PD) have a modifiable role in causing CVA, where several studies suggested a direct or indirect correlations with systemic diseases. This study aims to summarize, evaluate and analyze all the evidence available in literature, to reach a better understanding of the relation between periodontitis, gingivitis, tooth loss and CVA.
Methods: PubMed, Cochrane, Scopus and Web of Science database were searched for all meta-analyses assessing the effect of PD on CVA in accordance with Joanna Briggs Institute guidance for umbrella reviews. Assessment of Multiple Systematic Reviews (AMSTAR) was used for quality assessment. Pooled analysis was performed to assess the effect of periodontitis, gingivitis and tooth loss on CVA, depending on the availability of data using Review Manager Version 5.2.11.
Results: Seven of the identified meta-analyses were of high quality, and they were conducted in different countries. Periodontitis was generally associated with a significant increase of CVA risk (OR= 2.32, 95%CI: 1.70, 3.17, p<0.00001 and RR=1.22, 95%CI: 1.15-1.29, p<0.00001). Similarly, tooth loss was associated with an increase in CVA risk, yet to a lower degree (RR=1.32, 95%CI: 1.12-1.56, p=0.0008). However, gingivitis did not increase the risk of CVA significantly (OR=1.21, 95%CI: 0.32-4.65, p=0.78).
Conclusions: This study highlights the relationship between periodontitis and tooth loss and the risk of CVA, disregarding any significant effect for gingivitis. This relation highlights the importance of monitoring oral health as a preventive measure for CVA.
Disclosures of Interest: No
Abstract N°: 1739
SEASONAL VARIATIONS IN STROKE OCCURRENCE AND ITS SUBTYPES
Vincent Brissette*1, Moira Kapral2,3, Bing Yu3, Jiming Fang3, Tomi Odugbemi3, Michel Shamy1,4, Robert Fahed1,4, Dar Dowlatshahi1,4, Sophia Gocan4,5, Isabelle Martineau4,5
1University of Ottawa, Department of Medicine (Neurology), Department of Medicine and Ottawa Hospital Research Institute, Ottawa, Canada, 2University of Toronto, Department of Medicine and Institute of Health Policy, Management, and Evaluation, Toronto, Canada, 3ICES, Toronto, Canada, 4Ottawa Hospital Research Institute, Neurosciences Program, Ottawa, Canada, 5Champlain Regional Stroke Network, Ottawa, Canada
On behalf of:
Background and aims: Understanding seasonal variations in stroke can help stakeholders identify underlying causes in seasonal trends and tailor resources to times of highest incidence. We evaluated seasonal rates of stroke and its subtypes.
Methods: This retrospective cohort study used administrative data from January 1st, 2003, to December 31st, 2017, in Ontario, Canada. We evaluated seasonal variations of any stroke and its subtypes (ischemic stroke, transient ischemic attack (TIA), intracerebral hemorrhage and subarachnoid hemorrhage) via age/sex standardized rates and adjusted rate ratios using Poisson regressions. We evaluated 30-day case fatality risks by season, adjusted for age, sex, stroke type and comorbid conditions, and used Cox proportional hazard models to estimate the effect of season on fatality.
Results: We observed 394,145 incident stroke or TIA events, with a decrease in monthly hospitalization/emergency department visits per 100,000 people between January 2003 and December 2017 from 24.22 to 17.43. Compared to summer, overall stroke occurrence was similar in spring but slightly lower in fall (adjusted relative risk (RR) 0.97, 95% confidence interval (CI) 0.96 to 0.98) and winter (RR 0.94, 95% CI 0.94 to 0.95). There were minor variations by stroke subtype. (Figure 1) Winter was associated with the highest risk of stroke case fatality compared to summer (12.4% vs. 11.4%, adjusted hazard ratio 1.10, 95% CI 1.07 to 1.13).
Conclusions: We found seasonal variations in stroke occurrence, subtypes, and case fatality, although the absolute differences were small. Further work is needed to understand how environmental or meteorological factors might affect stroke risk.
Disclosures of Interest: No
Abstract N°: 2494
A COMPREHENSIVE EVALUATION OF STROKE MIMICS: A CROSS SECTIONAL STUDY
Bader Mohamed*1,2, Ambreen Fatima2, Fatema Almosawi3, Yee Thu2, Raagaa Vijayabarathy2, Muhammad Shahrukh2, Hnin Thawtar2, Farhad Huwez2, Alexandra Andrews2
1Government Hospitals, Manama, Bahrain, 2Barts Health NHS Trust, United Kingdom, 3Ministry of Health, Sanabis, Bahrain
On behalf of:
Background and aims: The frequency of stroke mimics is variable and depends on where the diagnosis is made.We aimed to do a comprehensive evaluation of stroke mimics.
Methods: All consecutive stroke referrals from ambulance service and ED department, in the period between January to June 2023, were retrospectively analysed using electronic health records, in a large adult tertiary stroke centre in London, UK. We collected demographic data and clinical features for all stroke referrals
Results: After excluding direct MT referrals, 897 total referrals to stroke team. 277 (30.8%) mimics were found. The most common types are shown in table (1). Mean age was 60 years (range 19-90) with equal male and female distribution. 69.5% of patients arrived through ambulance service while 30.5% referred by ED department. During the same period, 142 patients referred through video-triage, 75/142 (52.8%) were stroke mimics.
The median length of stay in ED department was 403 minutes (range 23-1900). 40% admitted to hospital with a median inpatient length of stay of 2 days. Patients with mimics had lower median age (60 in mimics vs 70 in stroke) and fewer cerebrovascular risk factors. 12 patients thrombolysed with no complications. Compared to the data collected from the same centre in 2020, the rate of stroke mimics has improved from 50% to 30.8%.
Conclusions: Stroke Mimics have consequences on the patient and the health system. Protocols should be implemented to accurately diagnose stroke.
Disclosures of Interest: No
Abstract N°: 2645
SEASONAL VARIATION IN STROKE OCCURRENCE BY ISCHEMIC STROKE SUBTYPES: THE KOREAN STROKE REGISTRY
1Seoul National University Hospital, Department of Neurology, Emergency Medical Center, Seoul, South Korea, 2Seoul National University Hospital, Department of Neurology, Seoul, South Korea, 3Seoul National University Hospital, Medical Research Collaborating Center, Seoul, South Korea
On behalf of:
Background and aims: Korea is situated in the mid-latitude zone and exhibits distinct seasonal variations characteristic of a temperate climate. While seasonal variations of cerebrovascular disease have been investigated in various studies, there is limited research on the association with ischemic stroke subtypes. This study aims to explore the occurrence of ischemic stroke subtypes based on seasonal variation.
Methods: We collected data on patients with acute cerebral infarction from 34 hospitals in the nationwide, prospective, multicenter Korean Stroke Registry from 2011 to 2021. We analyzed the total registered patients with ischemic stroke and transient ischemic attack patients classified into each subtype according to the TOAST classification, examining their distribution on a seasonal and monthly basis.
Results: During this period, total 149,017 cases were included. For the overall registered patients, July recorded the highest number, while February had the lowest. Moreover, patients registered during the summer months (July to September) were approximately 9% more prevalent than those in winter (December to February). When examined by TOAST subtype, patients with large artery atherosclerosis exhibited a 1.16-fold higher occurrence during the summer compared to winter; however, other stroke subtypes did not show significant seasonal differences.
Conclusions: We examined patterns of seasonal and monthly variations in ischemic stroke subtypes using nationwide multicenter data. We expect that these findings will contribute to an enhanced understanding of the relationship between stroke and climate.
Disclosures of Interest: No
Abstract N°: 2661
RISK FACTORS FOR ISCHEMIC STROKE IN PATIENTS WITH SYSTEMIC LUPUS ERYTHEMATOSUS
Guilherme Silva1, Carolina Rimkus1, Germana Titoneli1, Emily Yuki1, Raymundo Azevedo Neto2, Gisela Tinone1, Rosa Pereira2, Adriana Conforto*1
1Hospital das Clínicas of the University of São Paulo, Brazil, 2University of São Paulo, Brazil
On behalf of:
Background and aims: Systemic lupus erythematosus (SLE) affects more than three million people worldwide and doubles the risk of ischemic stroke. We compared the frequency of clinical characteristics, results of ancillary tests and use of medications in patients with SLE with and without ischemic stroke (IS).
Methods: We retrospectively assessed data from patients followed at Hospital das Clínicas da Universidade de São Paulo, Brazil, from 2010 to 2021 (n=106). Medical records were reviewed to register history of IS (IS+ or IS-), age, sex, cardiovascular risk factors (hypertension, diabetes, smoking, LDL levels), duration of SLE symptoms, disease activity, profiles of antibodies (anti-DNA ds, anti-Sm, anti-Ro, anti-La, and antiphospholipid antibodies), and treatment (prednisone and hydroxychloroquine). The data were analyzed with Mann-Whitney or Fisher's exact tests.
Results: One hundred and six participants were included; 53 (50%) were IS+. The frequencies of hypertension (IS+, 41/53, 77%; IS-, 23/53, 43%; p < 0.001) and antiphospholipid syndrome (IS+, 22/53, 42%; IS-, 4/53, 8%; p < 0.001) were higher in the group IS+ than in IS-. Conversely, the frequency of hydroxychloroquine use was lower in IS+ than in IS- (IS+, 22/53, 42%; IS-, 37/53, 70%; p = 0.003).
Conclusions: Hypertension, antiphospholipid antibodies were directly associated, and hydroxychloroquine use was inversely associated with IS. Treatment of hypertension, anticoagulation and use of hydroxychloroquine should be tested in randomized clinical trials to prevent IS in patients with SLE.
Disclosures of Interest: No
Abstract N°: 3088
ASSOCIATION BETWEEN INFLAMMATORY BIOMARKERS AND CEREBRAL VENOUS THROMBOSIS
1Neurological Department of Sahloul-Sousse University Hospital- Tunisia, Tunisia, 2Neurological Department of Sahloul-Sousse University Hospital- Tunisia, Sousse, Tunisia, 3Laboratory of hematology Sahloul-Sousse University Hospital- Tunisia, Sousse, Tunisia
On behalf of:
Background and aims: Neuroimaging, in particular magnetic resonance imaging, enables the early detection of cerebral venous thrombosis (CVT) in patients with intracranial hypertension. However, it is not readily available in all facilities and emergency departments. Platelet-to-lymphocyte ratio (PLR) and neutrophil-to-lymphocyte ratio (NLR) are novel thrombo-inflammatory indicators significantly associated with major cerebrovascular events.
We aimed to investigate whether PLR and NLR could be a biomarker for CVT in intracranial hypertension.
Methods: A cross-sectional study was conducted in the stroke unit of the Neurological Department of Sahloul-Sousse University Hospital, Tunisia between 2010 and 2023. Consecutive patients diagnosed with CVT and patients with idiopathic intracranial hypertension defining the control group were retrospectively investigated. Patients underwent demographic data collection and neurological examination. Cell counts were obtained upon hospital admission. PLR and NLR were compared between the two groups.
Results: A total of 143 patients with a mean age± SD of 38.0 ±16.4 years and a female-to-male ratio of 4.1 were included. All patients received an MRI exam. CVT accounted for 37.0% (53) of the total cases. During the acute phase of CVT, PLR and NLR increased compared to the control group with significant statistical differences (p=0.02; p=0.041), while the lymphocyte ratio decreased significantly (p=0.008).
Conclusions: CVT is an important diagnosis to keep in mind when evaluating patients with headaches in the emergency department. Inflammatory biomarkers could ameliorate diagnosis of CVT especially in patients with atypical clinical manifestations.
Disclosures of Interest: No
Abstract N°: 3132
COMPARING SOCIAL/LIFESTYLE DETERMINANTS OF HEALTH BETWEEN STROKE SURVIVORS OF THE US RESIDING INSIDE VS. OUTSIDE OF STROKE BELT
Faezeh Ghanbari Sevari1,2, Seyyed Sina Hejazian*3,4
1Hematology and Oncology Research Center, Tabriz University of Medical Sciences, Tabriz, Iran, 2Tabriz University of Medical Sciences, Public Health, Tabriz, Iran, 3Neurosciences Research Center (NSRC), Tabriz University of Medical Sciences, Tabriz, Iran, 4Immunology Research Center, Faculty of Medicine, Tabriz University of Medical Sciences, Tabriz, Iran
On behalf of:
Background and aims: A collection of southeastern states in the United States (US) is known as the Stroke Belt. It has been shown that the incidence of stroke is much higher in the Stroke Belt compared to the rest of the country. In this study, we aimed to compare the characteristics of stroke survivors residing inside and outside of the Stroke Belt of the US (SBU) during 2022, based on nationally representative data.
Methods: We used the Behavioral Risk Factor Surveillance System dataset of 2022. Participants with a positive history of stroke were first selected and then classified based on whether they resided in the SBU and performed a comparative analysis of their characteristics. The states in the SBU include Alabama, Arkansas, Georgia, Indiana, Kentucky, Louisiana, Mississippi, North and South Carolina, Tennessee, and Virginia.
Results: A total number of 19239 stroke survivors were studied. While stroke survivors made up 3.4% of the population residing outside the SBU, the proportion of stroke survivors inside the SBU was 4.6%. Stroke survivors inside and outside were significantly different in terms of levels of education (p<0.001), annual income (p<0.001), rural residence (p<0.001), health insurance coverage (p<0.001), past medical history of cancer (p<0.001), pulmonary disease (p=0.002), and arthritis (p<0.001), cigarette smoking (p=0.002) and alcohol consumption (p=0.006),and health-related quality of life (p=0.002). No differences in age, sex, and BMI were seen.
Conclusions: Having a better understanding of the difference between stroke survivors residing inside and outside of the SBU improves our knowledge of the increased risk of stroke in the SBU.
Disclosures of Interest: No
Paper Poster - Genetics, 'Omics and Biomarkers
Abstract N°: 2692
MICRORNAS AS POTENTIAL BIOMARKERS OF VULNERABLE PLAQUE: SCREENING STUDY AND SELECTION OF ENDOGENOUS CONTROLS FOR VALIDATION
Laia Carballo-Perich*1, Saima Bashir1,2, Mikel Terceño1,2, Juan Álvarez-Cienfuegos Rodríguez1,2, Víctor Vera-Monge1,2, Alan Murillo1,2, Xavier Xifró3, Yolanda Silva1,2, Joaquin Serena1,2, Carme Gubern-Mérida1
1Institut d’Investigació Biomèdica de Girona (IDIBGI), Cerebrovascular Pathology, Salt, Spain, 2Hospital Universitari Dr. Josep Trueta, Stroke Unit, Girona, Spain, 3Universitat de Girona (UdG), Facultat de Medicina, New Therapeutic Targets Group, Spain
On behalf of:
Background and aims: Carotid stenosis (CS) accounts for approximately 20% of all ischaemic strokes. Vulnerable plaque (VP) identification in patients with asymptomatic CS would be crucial for its optimal treatment and stroke prevention. This study aimed to identify differentially expressed microRNAs in plasma and atherosclerotic plaque (AP) samples from CS patients, to 1) determine the correlation between both sample types and 2) identify circulating microRNAs in asymptomatic CS patients that a) indicate the presence of AP and b) predict its vulnerability. Furthermore, it also seeked to define optimal endogenous microRNAs for normalising and validating the results.
Methods: Histological analysis of AP was performed. 754 microRNAs (TaqMan™OpenArray™) were analysed in 10 APs and 10 plasmas from patients with CS (>70%) symptomatic (Sx), progressive asymptomatic (PASx) and stable asymptomatic (SASx), and 10 plasmas from controls without CS. The best combination of endogenous microRNAs was determined using the summarised stability score.
Results: Plaques from Sx and PASx CS patients exhibited a histological profile of higher vulnerability compared to SASx CS patients. 46 circulating microRNAs were identified as potential diagnostic biomarkers of AP. 9 microRNAs were identified in plasma and 8 in AP as potential prognostic biomarkers of VP, differing between both sample types. The microRNAs selected as endogenous controls were also specific to type of sample.
Conclusions: This study has identified several microRNAs as potential diagnostic and prognostic biomarkers of CS and VP. Our results support the hypothesis of “vulnerable patient” and highlight the importance of the proper selection of endogenous controls.
Disclosures of Interest: No
Abstract N°: 3251
ENHANCED BENEFITS OF THE LIFE’S ESSENTIAL 8 IN APOE EPSILON 4 CARRIERS
Santiago Clocchiatti-Tuozzo*1, Cyprien Rivier1, Daniela Renedo1, Shufan Huo1, Victor Torres-Lopez1, Adam de Havenon1, Kevin Sheth1, Thomas Gill1, Guido Falcone1
1Yale University, Neurology, New Haven, United States
On behalf of:
Background and aims: Adherence to the American Heart Association's Life’s Essential 8 (LE8) reduces the risk of cardiovascular disease. While the APOE-epsilon(ε) 4 variants have been extensively investigated as dementia risk factors, little is known about the APOE-ε4 carriers as a high-risk population. We tested the hypothesis that, compared to non-carriers, APOE-ε4 carriers derive additional neuro-cardiovascular health benefits from LE8 optimization.
Methods: We used longitudinal data from the UK Biobank, a large cohort study. Participants with prior stroke, transient ischemic attack (TIA) or myocardial infarction (MI) were excluded. The exposure was the LE8 score, which captures 8 components (blood pressure, glucose, cholesterol, body mass index, smoking, physical activity, sleep, and diet), divided into categories (poor, intermediate and optimal). The outcome was a composite of stroke, TIA or MI. Multivariable logistic regression models with product terms were used to test for interaction between APOE-ε4 status and LE8 score.
Results: Of the 317,174 participants, 81,877 (26%) were APOE-ε4 carriers (>=1 alleles). Across all participants, optimal LE8 was associated with a 57% reduction in risk when compared to poor LE8 (OR:0.43,95%CI:0.4-0.45,p<0.001). APOE-ε4 status modified the association between the LE8 and the composite outcome (interaction p=0.008): while APOE-ε4 carriers had a 62% reduction in risk (OR:0.38,95%CI:0.34-0.43,p<0.001) when comparing optimal vs. poor LE8, APOE-ε4 non-carriers had a 56% reduction in risk (OR:0.44,95%CI:0.42-0.47,p<0.001).
Conclusions: Compared to non-carriers, middle-aged APOE-ε4 carriers without a history of vascular events derive greater benefit from LE8 optimization. These findings provide information to educate millions of newly genotyped Americans about strategies to improve long-term cerebrovascular outcomes.
Disclosures of Interest: No
Abstract N°: 1315
FREQUENCY AND PHENOTYPE ASSOCIATIONS OF DISEASE-CAUSING TREX1 VARIANTS IN THE UK BIOBANK
Bastien Rioux*1, Sarah Mcglasson1, William Whiteley1, David Hunt1,2
1University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom, 2UK Dementia Research Institute at Edinburgh, Edinburgh, United Kingdom
On behalf of:
Background and aims: Type I interferons are cytokines that may contribute to cerebrovascular disease. Variants in TREX1 can lead to type I interferonopathies, which manifest with increased type I interferon levels, white matter disease, cerebral small and large vessel disease, and autoimmunity. We aimed to determine the frequency and phenotype associations of disease-causing TREX1 variants in a population-based cohort.
Methods: We used whole-exome sequencing and health-related outcomes from 470k UK Biobank participants. We identified carriers of any of 84 disease-causing TREX1 variants, and defined 19 phenotypes (including cerebrovascular, cardiovascular, cognitive, and inflammatory traits, as well as imaging-derived brain volumes) from biologically plausible associations of increased type I interferons. We compared phenotypes in carriers versus non-carriers using logistic and linear regressions (adjusted for age, sex, and the 10 first principal components) and defined statistical significance as p<0.0026 (0.05/19).
Results: We identified 35/84 variants of interest in the UK Biobank (41.7%). The number of alleles per variant ranged from 1 to 619. Carriers, as compared to non-carriers, did not have an increased risk of clinical phenotypes, including ischemic stroke, vascular dementia, and lupus (adjusted OR for any phenotype=0.95; 95% CI: 0.83, 1.08; p=0.450). Imaging-derived traits, including white matter hyperintensity volume, did not differ by carrier status.
Conclusions: In a large population-based cohort with whole-exome sequencing, pathogenic TREX1 variants causing type I interferonopathies were not associated with cerebrovascular disease. We will expand this work through a candidate pathway approach of type I interferon regulators (250 genes) in the risk of stroke.
Disclosures of Interest: No
Abstract N°: 1383
IDENTIFICATION AND CHARACTERIZATION OF EXTRACHROMOSOMAL CIRCULAR DNA IN LARGE-ARTERY ATHEROSCLEROTIC STROKE
Kejie Chen*1, Yanqi Chi1, Hang Cheng2, Min Yang2, Quandan Tan2, Junli Hao3, Yapeng Lin2, Fengkai Mao2, Song He2, Jie Yang4,5
1Chengdu Medical College, School of Public Health, China, 2The First Affiliated Hospital of Chengdu Medical College, China, 3Chengdu Medical College, School of Bioscience and Technology, China, 4Sichuan Provincial People's Hospital, Department of Neurology, China, 5University of Electronic Science and Technology of China, School of Medicine
On behalf of:
Background and aims: Extrachromosomal circular DNA (eccDNA) is a new biomarker and regulator of diseases. However, the role of eccDNAs in large-artery atherosclerotic (LAA) stroke remains unclear.
Methods: Through high-throughput circle-sequencing technique, the length distribution, genomic characteristic, and motifs feature of plasma eccDNA from healthy controls (CON) and patients with LAA stroke were analyzed. Then, we explored the potential functions of the annotated eccDNAs using GO and KEGG pathway analyses.
Results: EccDNAs mapped to the reference genome showed SHN3 and BCL6 were LAA stroke unique transcription factors. The genes of differentially expressed eccDNAs between LAA stroke patients and CON were mainly involved in axon/dendrite/neuron projection development and maintenance of cellular structure via Wnt, Rap1 and MAPK pathways. Moreover, LAA stroke unique eccDNA-targeting genes played a role in regulation of coagulation and fibrinolysis, and there were five LAA stroke unique eccDNAs (Chr2:12724406-12724784, Chr4:1867120-186272046, Chr4:186271494-186271696, Chr7:116560296-116560685 and Chr11:57611780-5761192). Additionally, POLR2C and AURKA carried by ecDNAs (eccDNA size>100kb) of LAA stroke patients were significantly associated with development of LAA stroke.
Conclusions: Our data firstly revealed the characteristics of eccDNA in LAA stroke and discovered the functions of LAA stroke unique eccDNAs and eccDNA-targeting genes, suggesting eccDNA is a novel biomarker and mechanism of LAA stroke.
Disclosures of Interest: No
Abstract N°: 1537
GENETIC UNDERPINNING OF INTRACRANIAL ATHEROSCLEROTIC DISEASE: A META-ANALYSIS AND ENRICHMENT ANALYSIS
Natasha Ong1, Yau Chun En1, Shi Ting Tia2, Benjamin Jun Kiet Chek1, Megan Bi Jia Ng1, Sruthi Ranganathan3, Lai San Poh4, Shaun Loong*1,5, Benjamin Tan6
1Department of Medicine, Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore, 2Department of Biological Sciences, National University of Singapore, Singapore, Singapore, 3School of Clinical Medicine, University of Cambridge, Cambridge, United Kingdom, 4Department of Paediatrics, Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore, 5Cardiovascular-Metabolic Translational Research Program, Yong Loo Lin School of Medicine, National University of Singapore, 6Division of Neurology, Department of Medicine, National University Hospital, Singapore, Singapore
On behalf of:
Background and aims: Intracranial atherosclerotic disease (ICAD) is a major cause of stroke worldwide, especially among East-Asians. RNF213 has been identified to be associated with ICAD. However, the involvement of other genes and the underlying molecular pathways for ICAD pathogenesis require further characterization.
We conducted a meta-analysis and enrichment analysis of genes associated with ICAD to investigate their molecular contributions and shared pathways.
Methods: We searched three databases from inception until 21 November 2022. We included primary studies that reported a significant association of genes with ICAD. We subsequently conducted gene and protein-set enrichment analyses of identified genes.
Results: We identified 39 eligible studies. RNF213 had the most in-depth characterization in ICAD, followed by ApoE, PDE4D, and LPL. 15 case-control studies (8398 patients) investigated the association of three RNF213 variants with ICAD. The rs112735431 and rs371441113 variants are significantly associated with ICAD (Odd ratios 8.97 (4.59, 17.50) and 1.46 (1.00, 2.14) respectively).
Gene-set analysis of 24 implicated genes revealed associations with various cardiometabolic diseases such as coronary artery disease and non-alcoholic fatty liver disease (F1). Pathway analysis also revealed their involvement in the regulation of LDL receptor activity and lipid metabolism. Protein enrichment analysis further revealed no protein-protein interactions between RNF213 with the other genes.
Conclusions: Our enrichment analysis reveals a cardiometabolic underpinning in the pathogenesis of ICAD. Our results further suggest that molecular underpinnings of RNF213-mediated ICAD were distinct from ICAD medicated by the other genes. More work is required for functional analyses to elucidate the underlying mechanistic pathways for ICAD.
Disclosures of Interest: No
Abstract N°: 2346
MONOGENIC CAUSES OF STROKE IN YOUNG PATIENTS
Andreea Ilinca*1,2, Efthymia Kafantari1,3, Joel Wallenius1,3, Andreas Puschmann1,3, Arne G. Lindgren1,3
1Lund, Division of Neurology, Department for Clinical Sciences, Lund University, Lund, Sweden, 2Malmö, Department of Neurology, Skane University Hospital, Malmo, Sweden, Malmö, Sweden, 3Lund, Department of Neurology, Skane University Hospital, Lund, Lund, Sweden
On behalf of:
Background and aims: We aimed to explore the possibilities of increasing the diagnostic yield of monogenic stroke in a stroke population under 56 years of age.
Methods: Fifty probands 55 years old or younger at their first stroke episode were investigated with whole genome sequencing. The patients had one or more of: a) ⩾1Ist or IInd-degree relative with stroke under 60 years or same stroke-causing condition/disease, b) no vascular risk-factors (hypertension, hypercholesterolemia, diabetes, heart disease, smoking), c) an unusual clinical presentation. Rare variants (MAF < 0.01) identified by using a stroke gene panel were further assessed. The stroke-subtypes: “large artery atherosclerotic”, “large artery non-atherosclerotic” (tortuosity, dolichoectasia, aneurysm, non-atherosclerotic dissection or occlusion), “small vessel diseases”, “cardio-embolic” (atrial fibrillation or other arrhythmia, heart defect, cardiomyopathy), “coagulation dysfunctions” (venous thrombosis, arterial thrombosis, bleeding tendency), “intracerebral hemorrhage”, “vascular malformations” (cavernoma, arteriovenous malformations), “metabolism disorders”, and “cryptogenic embolic” were used for genotype-phenotype correlation.
Results: Cryptogenic embolic was the most frequent stroke subtype 18 (36%) followed by cervical dissection 11 (22%), and small vessel disease related stroke 8 (16%). Possible monogenic conditions were detected in 16 (32%) cases: eleven pathogenic/likely pathogenic variants in NOTCH3, APP, MYBC3, F2, ABCC6, MYH7, VWF, TNXB, RNF213 and 5 variants of unclear significance in SHOC2, SOS2, VWF, RAF1, MT-ND4 matching the clinical phenotype. Monogenic conditions were more often detected for cerebral bleeding (100%), cardioembolic (60%) and small vessel disease-related stroke (37,5%).
Conclusions: WGS and a stroke gene panel can detect monogenic causes to early stroke in a considerable proportion of patients.
Disclosures of Interest: No
Abstract N°: 181
IL-6, CRP AND RECURRENCE AFTER STROKE: A TIME-COURSE ANALYSIS OF INDIVIDUAL-PARTICIPANT DATA FROM 9,798 PATIENTS
John McCabe*1,2,3, Sarah Gorey1,2, Pablo Hervella4, Christina Jern5,6, Mira Katan7, Peter Rothwell8, Yuji Ueno9, William Whiteley10,11, Mark Woodward12,13, Peter Kelly1,14
1Stroke Clinical Trials Network Ireland, Dublin, Ireland, 2Mater Misericordiae University Hospital, Stroke Service, Medicine for the Older Person, Dublin, Ireland, 3University College Dublin (UCD), School of Medicine, Dublin, Ireland, 4Neuroimaging and Biotechnology Laboratory (NOBEL), Clinical Neuroscience Research Laboratory, Health Research Institute of Santiago de Compostela, Santiago De Compostela, Spain, 5Institute of Biomedicine, The Sahlgrenska Academy, Gothenburg, Sweden, 6Sahlgrenska University Hospital, Department of Clinical Genetics and Genomics, Gothenburg, Sweden, 7University Hospital Basel and University of Basel, Department of Neurology and Stroke Center, Basel, Switzerland, 8University of Oxford, Wolfson Centre for the Prevention of Stroke and Dementia, Oxford, United Kingdom, 9Juntendo University School of Medicine, Neurology, Tokyo, Japan, 10University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom, 11University of Oxford, Nuffield Department of Population Health, Oxford, United Kingdom, 12George Institute for Global Health, University of New South Wales, Sydney, Australia, 13George Institute for Global Health, Imperial College London, London, United Kingdom, 14Mater Misericordiae University Hospital, Stroke Service, Department of Neurology, Dublin, Ireland
On behalf of: From the Blood Inflammatory markers in Stroke Collaboration (BISC) & Cathal Walsh,Linxin Li, Ramon Iglesias-Rey,Nobukazu Miyamoto,Katie Harris,Catherine Sudlow,Mikel Vicente-Pascual,Francisco Purroy,Joan Montaner,Gian Marco DeMarchis,Markus Arnold
Background and aims: Inflammation promotes atherogenesis and RCTs of anti-inflammatory therapies after stroke are ongoing. IL-6 and high-sensitivity CRP are independently associated with major adverse cardiovascular events (MACE) post-stroke and may guide patient selection in future RCTs. Optimal timing of hsCRP/IL-6 measurement post-stroke is unknown as early blood levels may be confounded by the inflammatory response to brain infarction.
Methods: Using IPD from 9,798 patients (11 studies, 19,891 person-years follow-up), we performed a time-course analysis to investigate the association between hsCRP/IL-6 and recurrent events stratified by timing of blood-sampling. The post-stroke dynamics of IL-6/hsCRP were analysed by plotting their mean concentrations within each tenth of the sampling timeframe. Acute/recovery phases were defined for each biomarker according to the shape of this relationship.
Results: IL-6 was markedly elevated <24hrs post-stroke compared with recovery levels (⩾24hrs) (11.6pg/ml vs. 3.02pg/ml, p<0.001). HsCRP remained elevated for 10days (Fig.1). IL-6 was associated with recurrent MACE if measured in the recovery phase (⩾24hrs, Risk ratio [RR] 1.30, CI 1.19-1.41, per unit logeIL-6), but not in the acute phase (<24hrs,RR 1.10, CI 0.98-1.25, Pinteraction=0.03). After adjustment for risk factors/medication, the association remained for recovery-phase IL-6 when analysed per logeunit (RR 1.16, CI 1.05-1.66) and per quarter increase (RR 1.55, CI 1.19-2.02, Q4 vs Q1), but not if measured acutely. Findings were consistent for recurrent stroke. There was no evidence of time-dependent interaction with hsCRP.
Conclusions: The association between IL-6 and post-stroke recurrence was modified by sample timing, informing future RCT design incorporating biomarker-based selection of patients for anti-inflammatory therapies.
Disclosures of Interest: No
Abstract N°: 1064
IMPACT OF CONTEXTUAL BRAIN AGE ON RECURRENT STROKE ACROSS DIFFERENT TELOMERE LENGTHS
Hongyu Zhou*1, Zixiao LI1, Yongjun Wang1
1Beijing Tiantan Hospital, Capital Medical University, Department of Neurology, Beijing, China
On behalf of:
Background and aims: We aimed to demonstrate the association between brain age based on T2-FLAIR and recurrent stroke in patients with ischaemic cerebrovascular disease stratified by diverse telomere lengths.
Methods: This study included patients from the CNSR-III with imaging and genetic data. For approximating the pre-onset brain state, we proposed a Mask-based Brain Age estimation Network to analyze non-infarcted brain regions, with the derived brain age designated as the Contextual Brain Age (CBA). The disparity between brain and chronological age was the predicted age difference (PAD). The study participants were stratified based on PAD and telomere length.
Results: 6.1% (448/7,325) of patients experienced a new stroke at 3 months, and 9.7% (714/7,325) of patients had a new stroke at 1 year. During the 3-month follow-up, the shorter the telomere length, the weaker the correlation between positive PAD and increased risk of recurrent stroke (T1, adjusted HR 1.82, 95% CI 1.30-2.55; T2, adjusted HR 2.17, 95% CI 1.52-3.10; T3, adjusted HR 2.66, 95% CI 1.83-3.86). Additionally, there was an interaction between telomere length and PAD (P for interaction = 0.04). However, across different telomere length groups, the association between positive PAD and the increased risk of recurrent stroke within 1 year appeared to be similar (T1, adjusted HR 2.08, 95% CI 1.58-2.74; T2, adjusted HR 2.07, 95% CI 1.57-2.73; T3, adjusted HR 2.58, 95% CI 1.92-3.47; P for interaction = 0.09). The results for composite vascular events were consistent.
Conclusions: Telomere length influenced the correlation between CBA and the short-term risk of recurrent stroke.
Disclosures of Interest: No
Abstract N°: 1233
THE EXPRESSION OF SELECTED INFLAMMATORY MIRNAS IN CRYPTOGENIC YOUNG-ONSET STROKE
Riina Vibo*1, Karl Jõgi1, Anu Remm2, Heti Pisarev3, Ana Rebane2, Janika Kõrv1
1University of Tartu, Department of Neurology and Neurosurgey, Tartu, Estonia, 2University of Tartu, Department of Biomedicine, Tartu, Estonia, 3University of Tartu, Faculty of Medicine, Estonia
On behalf of:
Background and aims: About 40% of young onset ischemic strokes are cryptogenic. Our study aims profiling the change of expression of selected inflammatory micro RNAs (miR) in patients with young onset ischemic cryptogenic stroke and to analyse associations with stroke severity and risk factors.
Methods: Clinical data and serum for RNA purification was collected during acute phase and at 1 year follow-up in 48 patients with cryptogenic ischemic stroke from the Estonian Young Stroke Registry. A total RNA was purified and relative miRNA expression of miR-146a, miR-155, miR-21and miR-122 were analysed at both time-points using real-time quantitative PCR. Clinical data and stroke risk factors were analysed using linear regression analysis.
Results: The levels of miRNAs were higher in the active disease phase: most prominent expression of miR-21 (p<0.0001), followed by miR-122 (p=0.0001) and miR-155 (p=0.001). There was significant association between stroke severity and higher expression levels of miR-146a (p=0.0002) and miR-155 (p=0.0036). Significant association was found for preceding infection and miR-146 (p=0.002) and miR-155 (p=0.003) and for dyslipidemia and miR-21 (p=0.02) expressions.
Conclusions: Our results show that selected miRs associated with inflammation and atherosclerosis are upregulated in the acute phase of stroke. Preceding infection, dyslipidemia and stroke severity were associated with higher miR expressions. This indicates that there might be an uniform gene expression fingerprint at miRNA level in patients with cryptogenic stroke.
Disclosures of Interest: No
Abstract N°: 2562
PLASMA EXTRACELLULAR VESICLES AND THEIR PROTEIN CARGO: PROMISING BIOMARKERS FOR ACUTE STROKE DIAGNOSIS
Sandrine Reymond*1, Lyssia Gruaz1, Claire Bridel1, Anna Penalba2, Joan Montaner2,3, Jean-Charles Sanchez1
1University of Geneva, Department of Medicine, Geneva, Switzerland, 2Vall d’Hebron Institute of Research (VHIR), Universitat Autònoma de Barcelona, Barcelona, Spain, 3Institute de Biomedicine of Seville, IBiS/Hospital Universitario Virgen del Rocío/CSIC/University of Seville & Department of Neurology, Hospital Universitario Virgen Macarena, Seville, Spain
On behalf of:
Background and aims: Acute stroke management is challenging and the inclusion of blood biomarkers could improve early diagnosis of stroke. Extracellular vesicles (EVs) enclose a unique molecular cargo reflecting the pathophysiological state of the secreting cell and have the ability to cross the blood-brain barrier. As such, plasma-derived EVs represent a promising source of biomarkers for acute stroke diagnosis and their proteomics analysis could reveal novel biomarker candidates.
Methods: A cohort of age-matched individuals diagnosed with haemorrhagic stroke (n=10), ischemic stroke with large-vessel occlusion (n=10) and small-vessel occlusion (n=10), transient ischemic attack (n=10), stroke mimics (n=10) and healthy controls (n=10) was selected from the StrokeChip and AFRICAT studies. Plasma EVs were isolated by size exclusion chromatography from 150 µL biobanked plasma collected within 6 hours from symptoms onset. Size and particle concentration were determined using nanoparticle tracking analysis (NTA). Quantitative data-independent acquisition mass spectrometry (DIA-MS) was performed on EV samples.
Results: The characterization of EVs confirmed their successful enrichment. No difference in size and particle concentration was observed between the stroke subtypes and controls. Proteomic analysis allowed robust quantification of more than 600 proteins, of which 400 were common to all studied groups. Distinct subsets of differential proteins were observed when comparing stroke subtypes and controls.
Conclusions: Our results demonstrate the feasibility of studying the protein content of plasma-derived EVs from stroke patients, using a minimal sample compatible with clinical applications and research on biobanked samples. Subsequent analysis of differential proteins will provide insights into potential biomarker candidates.
Disclosures of Interest: No
Abstract N°: 1878
ISCHEMIC STROKE INDUCES PERSISTING GUT MICROBIOME DYSBIOSIS AND METABOLOME ALTERATIONS
Philip Melton*1, Rosa Delgado1, Adam Sorbie1, Velma Aho2, Christina Bauer1, Christina Haslinger1, Stefan Roth1, Paul Wilmes2, Corinne Benakis1, Arthur Liesz1
1Institute for Stroke and Dementia Research, LMU University Hospital, LMU Munich, München, Germany, 2LCSB - Luxembourg Centre for Systems Biomedicine, Esch-sur-Alzette, Luxembourg
On behalf of:
Background and aims: Previous studies in experimental models have demonstrated changes to gut-microbiota and (bacteria-derived) metabolomic profiles in AIS. However, the persistence of these microbiome changes is unknown and their clinical validation in stroke patients is still pending. To address this knowledge gap, we used a reciprocal bench-to-bedside approach with longitudinal observation and interventional cohorts in stroke patients and experimental models.
Methods: We performed a prospective, single-center, observational study (n=10) and prospective, single-center, randomized, blinded, placebo-controlled interventional study (n=22) with a probiotic compound being administered for 3-months. In addition to standardized clinical parameters, stool and plasma samples were acquired 7-days and 3-months post-stroke for metagenomic sequencing and mass-spectrometry. Complementary experiments were performed in experimental stroke (MCAo).
Results: Experimental stroke in mice resulted in altered gut-microbiota composition for more than 4-weeks. Chronic gut dysbiosis was associated with stroke-specific alterations in the metabolic profile and intestinal immune cell composition. Correspondingly, the observational patient cohort demonstrated a shift in the metabolic profile, indicative of specific changes to the bacteria-derived metabolites. Specifically, indole and short-chain-fatty-acid concentrations were significantly altered acutely and 3-months post-stroke. Stroke-specific changes to microbiota composition and the abundance of beneficiary bacterial populations were identified 3-months post-stroke. In the interventional cohort, probiotic treatment showed significant effect on gut-microbiota composition and normalized the reduced abundance in beneficial commensal bacteria.
Conclusions: Our research reveals, for the first time, that stroke results in persistent post-stroke dysbiosis, accompanied by alterations in systemic metabolites. We provide evidence that these long-term changes in post-stroke gut microbiota composition can be effectively altered through probiotic supplementation.
Disclosures of Interest: No
Abstract N°: 1003
CCR5Δ32 HETEROZYGOSITY DOES NOT AFFECT EARLY NEUROLOGICAL IMPROVEMENT AFTER RECANALISATION IN ACUTE ISCHAEMIC STROKE
Ádám Annus*1, Zsófia Nagy1, Renáta Fischer2, Rita Maszlag-Török1, Orsolya Horváth1, Katalin Jakab1, Laszlo Sztriha3, Peter Klivenyi4
1University of Szeged, Albert Szent-Györgyi Health Centre, Department of Neurology, Szeged, Hungary, 2Christophsbad GmbH & Co., Fachkrankenhaus KG, Department of Neurology, Göppingen, Germany, 3King's College Hospital, Department of Neurology, London, United Kingdom, 4University of Szeged, Albert Szent-Györgyi Health Centre, Department of Neurology, Szeged
On behalf of:
Background and aims: The expression of the CCR5 chemokine receptor is increased in microglia, astrocytes and neurons after ischaemic stroke, with adverse effects on learning and memory. Stroke patients with CCR5Δ32 loss-of-function polymorphism had better long-term functional and cognitive outcomes, than carriers of wild-type CCR5Δ32. Our study aimed to investigate whether there is a difference in early neurological improvement (ENI) between CCR5Δ32 polymorphism carriers and non-carrier patients after recanalisation.
Methods: Our prospective case-control study included patients with acute ischaemic stroke who had thrombolysis and technically successful thrombectomy (at least TICI 2b). DNA was isolated from venous blood samples. PCR reactions were implemented with fluorescently labeled Taqman probes for allele discrimination. The results were verified by agarose gel electrophoresis. ENI was defined as an improvement in NIHSS score of at least 4 points or becoming asymptomatic from baseline to discharge. The correlation between ENI and the CCR5Δ32 polymorphism was examined by binary logistic regression.
Results: Thirty-nine heterozygous and 187 wild-type CCR5Δ32 carriers were included. We did not find homozygous individuals during the study period. The median age and prevalence of other vascular risk factors were similar in the two groups. ENI was achieved in 35.90% of cases among CCR5Δ32 heterozygous patients and 38.71% among wild-type subjects (p=0.742). CCR5Δ32 heterozygosity was not significantly associated with ENI (OR 0.887, 95%CI 0.433-1.817, p=0.743).
Conclusions: We found no correlation between ENI and CCR5Δ32 heterozygosity after recanalisation in acute ischaemic stroke. Therefore, administration of a CCR5 antagonist in the acute phase of ischaemic stroke would probably not affect early treatment outcomes.
Disclosures of Interest: No
Abstract N°: 2530
PLASMA SYMMETRIC DIMETHYLARGININE AS A METABOLITE BIOMARKER OF SEVERE ACUTE ISCHEMIC STROKE
Saana Pihlasviita*1, Olli Mattila1, Tiina Nukarinen1, Markku Kuisma2, Heini Harve-Rytsälä2, Gerli Sibolt1, Sami Curtze1, Daniel Strbian1, Turgut Tatlisumak3,4, Perttu J. Lindsberg1
1University of Helsinki and Helsinki University Hospital, Neurology and Clinical Neurosciences, Helsinki, Finland, 2University of Helsinki and Helsinki University Hospital, Emergency Medicine and Services, Department of Emergency Care, Helsinki, Finland, 3Institute of Neuroscience and Physiology, Sahlgrenska Academy at University of Gothenburg, Department of Clinical Neuroscience/Neurology, Gothenburg, Sweden, 4Sahlgrenska University Hospital, Department of Neurology, Gothenburg, Sweden
On behalf of:
Background and aims: After severe ischaemic stroke (IS), circulating levels of symmetric dimethylarginine (SDMA) increase. We investigated the performance of SDMA for early differentiation of severe IS and haemorrhagic stroke (HS), to potentially aid with prehospital identification of large vessel occlusion (LVO).
Methods: We performed targeted mass spectrometry (MS) measurements of SDMA in two sequential acute plasma samples (early and secondary) of 50 IS patients with LVO and 49 HS patients. Secondary samples of 227 IS and 84 HS patients with moderate to severe symptoms (NIHSS⩾7) subsequently underwent ELISA validation.
Results: No inter-group differences existed in early samples, but IS patients had significantly higher mean (IQR) SDMA levels in secondary samples in both analyses: 5.8 (5.3 -6.9) vs 5.1 (4.2-5.8) A.U. for HS, p<0.001, with MS; and 0.82 (0.72-1.01) vs 0.71 (0.58-0.85) nmol/mL for HS, p<0.001, with ELISA. Mean (IQR) last-known-well to sampling times for secondary samples were 83 (65-113) and 89 (65-125) minutes for MS and ELISA analyses. For IS patients, higher SDMA levels were associated with cardioembolic stroke: 0.84 (0.73-1.09) vs 0.79 (0.71-0.91) nmol/mL for other aetiologies, p=0.042, and poor outcome: modified Rankin Scale (mRS) 4-6; 0.90 (0.73-1.06) vs 0.80 (0.72-0.97) nmol/mL for mRS 0-3 (p=0.045).
Conclusions: SDMA may prove to have future value in a diagnostic biomarker panel aimed to differentiate LVO from other stroke subtypes, and significant elevation seems already to occur hour and a half after symptom onset.
Disclosures of Interest: No
Abstract N°: 3045
HYPERTENSIVE DISORDERS OF PREGNANCY AND RISK OF STROKE: A MENDELIAN RANDOMIZATION STUDY
Dearbhla Kelly*1, Marios Georgakis2, Stephen Burgess3, Christopher Anderson4,5,6
1University of Oxford, Wolfson Centre for the Prevention of Stroke and Dementia, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom, 2Institute for Stroke and Dementia Research, University Hospital of LMU Munich, Munich, Germany, Munich, Germany, 3University of Cambridge, MRC Biostatistics Unit, Cambridge, United Kingdom, 4Broad Institute of Harvard and the Massachusetts Institute of Technology, Program in Medical and Population Genetics, Cambridge, United States, 5Massachusetts General Hospital, McCance Center for Brain Health, Boston, United States, 6Brigham and Women's Hospital, Department of Neurology, Boston, United States
On behalf of:
Background and aims: Hypertensive disorders of pregnancy (HDPs) are observationally associated with both ischaemic and haemorrhagic stroke risk. Employing a Mendelian randomization approach, we explore the genetic evidence of this association, shedding new light on the complex interplay between maternal health factors and stroke susceptibility.
Methods: We used data from trans-ancestry genome-wide association studies to identify genetic proxies for HDPs (gestational hypertension and preeclampsia) and cerebrovascular disease (ischemic stroke and its subtypes and intracerebral haemorrhage [ICH]). We then used a two-sample Mendelian Randomization (MR) study design to investigate the effect of hypertensive disorders of pregnancy on stroke risk.
Results: Genetically predicted gestational hypertension was associated with a higher risk of multiple stroke subtypes including all stroke [AS] (OR, 1.177; 95% CI, 1.120-1.237; P<0.001), ischaemic stroke [IS] (OR, 1.189, 1.127-1.254; P<0.001), large artery stroke [LAS] (OR, 1.285; 1.084-1.096; P=0.002), and most strongly with small vessel stroke [SVS] (OR, 1.305; 1.154-1.474; P<0.001). Similar associations were evident between genetically predicted preeclampsia and AS (OR, 1.145; 1.022-1.095; P<0.001), IS (OR, 1.158; 1.171-1.218; P<0.001), LAS (OR, 1.185; 1.020-1.377; P=0.026) and SVS (OR, 1.245; 1.108-1.397; P<0.001). No associations were noted between genetically predicted HDPs and cardioembolic stroke or ICH. Findings were similar across a number of sensitivity analyses.
Conclusions: The findings of this study provide genetic evidence supporting an association between HDPs and ischaemic stroke subtypes, particularly small vessel stroke, suggesting a shared susceptibility to microangiopathy. Sex-specific association testing is warranted in future studies.
Disclosures of Interest: No
Abstract N°: 1672
CIRCULAR RNA AS BIOMARKERS FOR ACUTE ISCHEMIC STROKE
Xiao Zhang*1,2, Liqun Jiao3
1Xuanwu Hospital, Capital Medical University, Department of Neurosurgery, Beijing, 2University of Oxford, Sir William Dunn School of Pathology, Oxford, United Kingdom, 3Xuanwu Hospital, Capital Medical University, Department of Neurosurgery, Beijing, China
On behalf of:
Background and aims: Rapid diagnosis of acute ischemic stroke (AIS) patients is still challenging, and reliable biomarkers are needed. Noncoding RNAs are important for many physiological activities, among which circular RNAs (circRNAs) have been proven to be more tissue-specific and conservative. This study aimed to identify circRNAs as potential biomarkers for AIS
Methods: This study has been prospectively registered in PROSPERO (Registration No. 11 CRD42021288033). Published literature comparing circRNA expression profiles between AIS and non-AIS in human and animal models were retrieved from the articles published by January 2023 in major databases. We descriptively summarized the included studies, conducted meta-analysis under a random effects model, and did bioinformatics analysis including Gene Ontology (GO) and Kyoto Encyclopedia of Genes and Genomes (KEGG) enrichment analysis.
Results: Totally 23 studies were included, reporting 18 distinctive upregulated and 20 distinctive downregulated circRNAs. Diagnostic meta-analysis indicated discriminative ability of the circRNAs. Furthermore, circRNA HECTD1, circRNA DLGAP4, circRNA CDC14A, circRNA SCMH1, and circRNA TLK1 were reported with the same regulation trend in more than one study (animal studies included). GO and KEGG enrichment analyses indicated that the target genes of these five circRNAs were enriched in regulating cell proliferation, apoptosis, and oxidative stress.
Conclusions: This study demonstrates that circRNAs (circRNA HECTD1, circRNA DLGAP4, circRNA CDC14A, circRNA SCMH1, and circRNA TLK1) generally are promising as potential biomarkers for AIS. However, due to the limited number of studies, diagnostic value of individual circRNA could not be validated. More in vitro and in vivo functional studies are needed.
Disclosures of Interest: No
Abstract N°: 2560
NEW STRATEGIES FOR THE STUDY OF NEUROVASCULAR DISEASES THROUGH THE IMPLEMENTATION OF COST-EFFECTIVE GENETIC PANELS
Paloma Menéndez-Valladares1, ANA DOMINGUEZ MAYORAL*2, María Pilar Carrasco3, Flora Sánchez1
Background and aims: Genetic neurovascular pathologies can account for up to 5% of all strokes. The most frequent monogenic neurovascular diseases are CADASIL (Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy), familial cerebral cavernous malformations and moyamoya arteriopathy. A multidisciplinary diagnosis approach including a genetic panel is necessary. The aim of the study is to establish the efficacy of setting up a massive sequencing gene panel (NGS) for neurovascular diseases in an autonomic reference unit.
Methods: The follow-up time from the patient’s first visit (with genetic study) to the neurology office until diagnosis has been retrospectively recorded. Until 2021 the study was performed gene by gene, and from 2022 an NGS panel was implemented.
Results: A total of 83 patients with minority neurovascular diseases have been diagnosed, 24.1% (N=20) correspond to familial mutation studies, 10.8% (N=9) to 1-gene studies and 65% (N=54) to NGS panels. Most of the mutations found corresponded to NOTCH3 (55.5%), followed by KRIT1 (16.7%). The mean diagnostic delay in 2021 was 10 months by gene-by-gene analysis, dropping to 3.5 months with the introduction of NGS panels. The use of panels, despite being a more costly technique, has required fewer personnel for reanalysis (extraction, processing and interpretation of the results).
Conclusions: NGS panels will provide greater diagnostic yield given the genetic and clinical heterogeneity of neurovascular diseases, and the large number of genes that may be involved. It has been possible to improve the cost-effectiveness of studies through the creation of a regional reference unit.
Disclosures of Interest: No
Abstract N°: 2818
METABOLIC PROFILING OF YOUNG ISCHEMIC STROKE PATIENTS AT STROKE ONSET, THREE MONTHS AND ONE YEAR AFTER STROKE. A PILOT STUDY
Liisa Kõrv*1,2, Riina Vibo1, Kalle Kilk3, Mihkel Zilmer3, Janika Kõrv1
1University of Tartu, Institute of Clinical Medicine, Department of Neurology and Neurosurgery, 2North Estonia Medical Centre, Department of Neurology, 3University of Tartu, Institute of Biomedicine and Translational Medicine, Department of Biochemistry, Tartu, Estonia
On behalf of:
Background and aims: The aim of the study was to find changes in the serum metabolite levels of young ischemic stroke patients between stroke onset, three months and one year after stroke to better understand the mechanisms of ischemic stroke in this important age-group.
Methods: As a pilot study, metabolic profiling of the serum of the first 62 ischemic stroke patients from the Estonian Young Stroke Registry (strokes in 18-54-year-olds) was performed using mass-spectrometry and the BIOCRATES AbsoluteIDQ® IT180 kit. Statistical analysis was conducted using the one-way repeated measures linear model.
Results: The mean age was 43 (SD 8) years, 44% were female. We identified significant changes in 74 of 188 (39%) metabolites measured between the first two timepoints. There were significant decreases in the levels of 63% acylcarnitines measured at stroke onset when compared to three months. Both the absolute numbers of long-, medium- and short chained acylcarnitines as well as the total esterified carnitine to free carnitine ratio (p<0,0001) were decreased implying a change in beta-oxidation regulation. Significant changes also occurred in 62% of the amino acids measured between the first two timepoints with a trend towards increased levels at onset. There were no significant changes in metabolite levels between three months and one year.
Conclusions: According to our pilot study, there are significant changes in the ischemic stroke metabolic profile between stroke onset and three months with a following basal metabolism level stabilisation. Further studies are planned to investigate changes in metabolite levels by stroke aetiology and outcome more extensively.
Disclosures of Interest: No
Abstract N°: 2841
DIFFERENTIALLY EXPRESSED RNA AND BIOLOGICAL PATHWAYS IN MOYAMOYA: A TRANSCRIPTOMICS SYSTEMATIC REVIEW AND NETWORK META-ANALYSIS
Yunru Chen*1, Eda Liew1, Hao-Xing Lai1, Vijay K Sharma1,2, Leonard Ll Yeo1,2, Shaun Loong1,3, Benjamin Yq Tan1,2
1Yong Loo Lin School of Medicine, National University of Singapore, Department of Medicine, 2National University Hospital, Division of Neurology, Department of Medicine, 3Yong Loo Lin School of Medicine, National University of Singapore, Cardiovascular-Metabolic Translational Research Program
On behalf of: StroCar
Background and aims: Moyamoya Disease (MMD) is a chronic and progressive condition involving a progressive stenosis of bilateral intracranial internal carotid arteries, with an increased prevalence among East Asians. With increasing research into the underpinnings of MMD, there is however a lack of consensus among RNA expression studies. This systematic review and network meta-analysis aims to aggregate transcriptomics studies to identify differentially expressed genes (DEGs) and elucidate biological pathways associated with MMD.
Methods: Databases MEDLINE via PubMed, and EMBASE were searched, and relevant publications up to April 06, 2023 were assessed. Studies were included if they involve RNA transcriptome-wide analysis of human participants diagnosed with MMD. The mRNA functional networks were reconstructed on Enrichr-KG.
Results: The search yielded 7348 studies, of which 1766 were duplicates. 5592 studies were screened and 16 studies were included. Tissues from 605 MMD patients were included. We analysed DEGs from two separate groups of cells – peripheral blood cells and vascular tissue. Functional analysis for peripheral blood cells revealed significant pathways associated with responses to axon injury and reactive oxygen species, alongside a downregulation of intermediate filament bundle assembly and organisation (Table 1). For vascular tissue, there is an overrepresentation of aberrant pathways associated with mitosis and angiogenesis regulation. Meanwhile, complement and coagulation cascades and blood circulation pathways are downregulated (Table 2).
Conclusions: Distinct biological pathways have been found to be enhanced in biologically relevant tissues in MMD patients. With limited treatment options, this analysis seeks to provide potential biomarkers and therapeutic approaches for the risk stratification and treatment avenues for MMD.
Disclosures of Interest: No
Abstract N°: 3037
MICRO-RNA SIGNATURES ASSOCIATED WITH 3-MONTH PROGNOSIS IN YOUNG CRYPTOGENIC STROKE PATIENTS
Guillem Cañellas*1, Aina Medina1, Rosa Diaz Navarro2, Jeronia Llado1, Gabriel Olmos1, Maria Carmen Jimenez Martinez2, Silvia Tur2, Raquel Delgado2, Cristofol Vives-Bauza1
1Universitat de les Illes Balears (UIB), Biology, Palma, Spain, 2Hospital Universitari Son Espases, Neurology, Palma, Spain
On behalf of:
Background and aims: Stroke remains the leading cause of long-term disability worldwide. Around 20%–40% of ischemic strokes (IS) are cryptogenic. The apparent lack of risk factors is a challenge to develop effective therapies to improve functional prognosis. Recovery of the ischemic lesion requires activation of biological processes like angiogenesis, neurogenesis and neuronal plasticity. These processes are tightly regulated by gene expression. MicroRNAs (miRNA) play a pivotal role in this regulation. Aim: To identify miRNAs signatures associated with 3-month prognosis in young patients that suffered a cryptogenic IS.
Methods: Patients ⩽60 years old with cryptogenic IS (n=65) were classified depending on their functional outcome at 3 months after stroke, evaluated with the modified Rankin scale (mRS), and adjusted by initial severity (NIHSS), age and sex. miRNA expression profiles were determined in peripheral blood using the miRNA 3.1 Affymetrix® chip. The five most significantly expressed miRNAs were validated by RT-PCR. To identify their target genes, functional assays, based on gain-and-loss of function experiments, were run in human brain endothelial cells. Cells were transfected with either the MIMIC molecules (analogues of the endogenous miRNAs) or its INHIBITORS (complementary miRNA sequences) and gene expression patterns were determined by microarray expression analyses.
Results: Five miRNAs (miR-1275, miR-3609, miR-941, miR-3201 and miR-625) were significantly downregulated in cryptogenic stroke patients with functional dependence at 3 months. Functional assays and enrichment analysis revealed significant associations with pathways related to inflammation, hematopoiesis, and angiogenesis.
Conclusions: We have identified five miRNAs associated with 3-month outcome in young cryptogenic stroke patients with potential as therapeutical targets.
Disclosures of Interest: No
Abstract N°: 670
ASSOCIATION OF CYP2C19 VARIANTS WITH RECURRENT ISCHEMIC EVENTS IN ACUTE STROKE; NCVC GENOME REGISTRY
1National Cerebral and Cardiovascular Center, Neurology, Suita, Japan, 2National Cerebral and Cardiovascular Center, Cerebrovascular Medicine, Suita, Japan
On behalf of:
Background and aims: We aimed to clarify the association between the CYP2C19 variant and recurrent ischemic events in patients with acute ischemic stroke (AIS) due to large-artery atherosclerotic (LAA) stroke using the National Cerebral and Cardiovascular Center (NCVC) Genome Registry.
Methods: The NCVC Genome Registry is a multicenter, prospective, observational study that enrolled stroke patients within 7 days of stroke onset who consented to CYP2C19 variant testing from 2018 to 2022. Patients with LAA stroke were divided into two groups according to CYP2C19 variants: poor metabolizer (*2/*2, *3/*3, *2/*3) or intermediate metabolizer (*1/*2, *1/*3) group (PM/IM group) and extensive metabolizer (*1/*2, *1/*3) group (EM group). The primary endpoint was recurrent ischemic stroke /transient ischemic attack.
Results: Of 1,612 AIS patients, 367 LAA patients (96 female [26.0%], median age 74 years [IQR, 65-81 years]) were enrolled with a median follow-up period of 3.1 years. Aspirin, clopidogrel, cilostazol, and prasugrel were used at discharge in 72.4%, 56.9%, 8.7%, and 0.8% of patients, respectively. The use of aspirin at discharge was more frequent in the PM/IM group (n=81) compared to the EM group (n=286) (81.5% vs. 69.9%, P=0.05). Multivariate Cox regression analysis showed that PM/IM (hazard ratio 1.63; 95% confidence interval 0.78-3.46, P=0.15) tended to be associated with recurrent ischemic stroke/transient ischemic attack.
Conclusions: In LAA stroke patients, poor or intermediate metabolizers tended to have a higher rate of recurrent ischemic events than extensive metabolizers.
Disclosures of Interest: No
Paper Poster - Hyperacute Management
Abstract N°: 534
INTER-HOSPITAL TRANSFER FOR THROMBECTOMY: TRANSFER TIME IS BRAIN
Pierre Seners*1, Maéva Kyheng2, Julien Labreuche2, Bertrand Lapergue3, Fernando Pico4
1Hôpital Fondation A. de Rothschild, Neurology, Paris, France, 2CHRU Lille, Biostatistics, Lille, France, 3Hôpital Foch, Neurology, Suresnes, France, 4Versailles University Hospital, Neurology, Versailles, France
On behalf of: ETIS investigators
Background and aims: Patients with acute ischemic stroke harboring a large vessel occlusion who present to non-endovascular capable center often require inter-hospital transfer for thrombectomy. Whether inter-hospital transfer time is associated with 3-month functional outcome is currently unknown.
Methods: We retrospectively analyzed acute stroke patients enrolled between January 2015 and December 2022 in the prospective French multicenter ETIS registry. Patients with an anterior circulation large vessel occlusion transferred from a non-endovascular to a comprehensive stroke center for thrombectomy were eligible. Inter-hospital transfer time was defined as the time between imaging in the referring hospital and groin puncture for thrombectomy. The relationship between transfer time and favorable 3-month functional outcome (mRS 0-2) was assessed through mixed logistic regression model adjusting for center, symptom onset-to-referring hospital imaging time, age, diabetes, referring hospital NIHSS score, ASPECTS, occlusion site and intravenous thrombolysis use.
Results: Overall, 3769 patients were included (median inter-hospital transfer time of 161 minutes [IQR, 128-195]; 46% with favorable outcome). Longer transfer time was independently associated with lower rates of favorable outcome (P<0.001). As compared to patients with transfer time below 120 minutes, there was a 15% reduction in the odds of achieving favorable outcome for transfer times between 120-180 minutes (adjusted OR=0.85; 95%CI 0.67-1.07), and a 36% reduction for transfer times beyond 180 minutes (adjusted OR= 0.64; 95%CI 0.50-0.82).
Conclusions: Shorter inter-hospital transfer time is strongly associated with favorable 3-month functional outcome. Fastening inter-hospital transfer is of critical importance to improve outcome.
Disclosures of Interest: No
Abstract N°: 654
INDIVIDUAL- AND COUNTY-LEVEL SOCIAL DETERMINANTS OF HEALTH AND REPERFUSION THERAPIES FOR ISCHEMIC STROKE
1University of Toronto, Division of Neurology, Toronto, Canada, 2University of Toronto, Division of General Internal Medicine, Toronto, Canada, 3Hamilton Health Sciences, Division of Neurology, Hamilton, Canada, 4ICES, Toronto, Canada, 5Michigan State University, East Lansing, United States
On behalf of:
Background and aims: The association between individual- and county-level social determinants of health (SDOH) and reperfusion therapies, thrombolysis, thrombectomy, or both, for ischemic stroke is not well-known.
Methods: We conducted a population-based cohort study of people aged ⩾ 40 years admitted with an ischemic stroke between Jan 1, 2015 and Dec 31, 2019 to a participating Get With The Guidelines-Stroke registry hospital in the United States. We evaluated age, sex, rural residence, and ethnicity/race at the individual level and census derived county-level data on poverty, unemployment, and lack of high-school education based on each patient’s county of residence. Our outcome of interest was receipt of reperfusion therapies. We used log-binomial generalized estimating equations, adjusting for comorbidities, and accounting for clustering at the county-level, to evaluate the association between individual- and county-level SDOH and our outcome of interest, measured by adjusted relative risk (aRR).
Results: We included 1.5 million adults with ischemic stroke, of whom 203,747 (13.4%) received thrombolysis, thrombectomy, or both. Compared to White, Black people (aRR 1.12; 1.10-1.14) and people of Hispanic ethnicity (aRR 1.43; 1.40-1.47) were more likely whereas, those who were older (aRR 0.97; 0.97-0.97) and lived in rural areas (aRR 0.62; 0.61-0.64) were less likely to receive reperfusion therapies. Those residing in counties with lower education were less likely to receive reperfusion therapies (aRR 0.92; 0.91-0.93), and county-level poverty and unemployment were not associated with the outcome.
Conclusions: Knowing the influence of SDOH on receipt of reperfusion therapies can help direct interventions to improve care in all.
Disclosures of Interest: No
Abstract N°: 464
ARTERIAL BLOOD PRESSURE INFLUENCING NEUROLOGICAL SEVERITY IN PATIENTS WITH UNFAVORABLE LEPTOMENINGEAL COLLATERALS GRADE
Joao Andrade*1,2,3,4, Igor Terehoff1, Evelyn Pacheco2, Alexandre Robles4, Rafael Padua Gomes4, Caroline Pergoretti2, Matheus Pellegrino2, Ahmad Majdoub2, Hanna Martins2, Gisele Silva1,3
1Universidade Federal de Sao Paulo, Health Informatics / Neurology, Brazil, 2United Health Group Brazil, 3Hospital Albert Einstein, Brazil, 4Centro Universitário São Camilo
On behalf of:
Background and aims: The association between variables, specifically systolic blood pressure (SBP), and the extent of leptomeningeal collaterals, thereby influencing the clinical-radiological mismatch, remains inadequately elucidated. Our objective is to describe the influence of admission SBP on collateral status among patients afflicted with proximal arterial occlusion, and its consequential effect on neurological severity.
Methods: This is a biprospective study utilizing a national database, encompassing 19 hospitals from 2021 to 2023. Blinded radiologists categorized Alberta Stroke Program Early CT Scores (ASPECTS) and assessed the grade of collaterals according to a standardized protocol. Descriptive analyses, linear regression, and ordinal logistic regression were adopted
Results: The final analysis included 652 patients; 39.6% were male, with a median age of 71[58, 71] years. At admission, median ASPECTS was 8[6, 9], and NIHSS was 11[5, 17]. Large vessel proximal occlusion (LVO) occurred in 41.8% of cases. Collaterals were classified as absent or less than the unaffected side in 53.1% of cases - only in this subgroup, SBP was inversely related to NIHSS upon admission (beta-coefficient -0.20, 95%CI -0.098–0.017, p-value=0.006,R²0.39), adjusted by age, ASPECTS, Time-Last-Known-Well, and left hemisphere. In an ordinal regression, SBP was not associated with collateral grade. The influence of SBP on NIHSS also varied based on ASPECTS and collateral degree, showing an inverted "J-shaped" pattern.
Conclusions: Lower admission SBP values in patients with an unfavorable collateral degree are associated with worse neurological severity. These findings may stimulate randomized studies on blood pressure management and personalization in LVO patients with unfavorable collateral grades, thereby expanding the eligibility for mechanical thrombectomy.
Disclosures of Interest: No
Abstract N°: 1295
PREDICTORS OF STROKE MIMICS IN EMERGENCY DEPARTMENT: AN EASY-TO-USE MIMICS PREDICTION SCORE
Irene Scala*1,2, Mauro Monforte1, Jacopo DI Giovanni2, Pier Andrea Rizzo2, Simone Bellavia2, Aldobrando Broccolini1,2, Paolo Calabresi1,2, Marcello Covino3, Giovanni Frisullo1
1Fondazione Policlinico universitario A. Gemelli IRCCS, Neurology Department, Roma, Italy, 2Catholic University of the Sacred Heart, Neuroscience, Roma, Italy, 3Fondazione Policlinico universitario A. Gemelli IRCCS, Department of Emergency Medicine, Roma, Italy
On behalf of:
Background and aims: Early differential diagnosis between stroke and stroke mimics is a challenge in the management of acute patients in the Emergency Department (ED). The primary aim of this study is to identify diagnostic predictors of stroke mimics based on demographic, clinical parameters and vital signs acquired in the ED during the triage phase of patients with suspected stroke. Secondly, we aimed to develop a diagnostic score predictive of stroke mimics.
Methods: In this retrospective, observational study, we enrolled patients admitted to the ED of a comprehensive stroke center for suspected stroke. Univariate comparisons were performed using Mann-Whitney U-test, Kruskal-Wallis and χ2-test, as appropriate. Logistic regression was used to perform the adjusted analyses. We then computed a predictive score based on each variable’s β coefficient.
Results: 2768 patients with a suspected diagnosis of stroke were included in the study of whom 1189 (43%) with stroke mimics. After multivariate logistic regression we observed that age, systolic blood pressure, speech and motor disorders, previous stroke, hemiplegia and congestive heart failure were independent predictors of stroke, while sensory disorders, headache, seizure, disorientation, syncope, dementia and renal disease were predictors of stroke mimics. Based on machine learning prediction model, we developed an easy-to-use score based exclusively on triage data that can accurately discriminate strokes from stroke mimics.
Conclusions: The identification of independent predictors of stroke mimics and the new mimics score could be useful tools for emergency physicians to stratify patients with suspected stroke and direct them towards a more appropriate diagnostic and therapeutic pathway.
Disclosures of Interest: No
Abstract N°: 1791
IMPACT OF EARLY STATIN ADMINISTRATION ON CLINICAL EVENTS IN PATIENTS WITH ACUTE ISCHEMIC STROKE
Tai Hwan Park1, Kyung Bok Lee2, Byung-Chul Lee3, Joon-Tae Kim4, Jae-Kwan Cha5, Juneyoung Lee6, Ji Sung Lee7, Sung-Il Sohn8, Hee-Joon Bae*9
1Seoul Medical Center, Neurology, Seoul, South Korea, 2Soonchunhyang University Seoul Hospital, Neurology, Seoul, South Korea, 3Hallym University Sacred Heart Hospital, Neurology, Anyang, South Korea, 4Chonnam National University Hospital, Neurology, Gwangju, South Korea, 5Dong-A University Hospital, Neurology, Pusan, South Korea, 6Korea University College of Medicine, Biostatistics, Seoul, South Korea, 7Asan Medical Center, Asan Institute For Life Sciences, Seoul, South Korea, 8Keimyung University Dongsan Hospital, Neurology, Daegu, South Korea, 9Seoul National University Bundang Hospital, Neurology, Seongnam, South Korea
On behalf of: The CRCS-K (Clinical Research Collaboration for Stroke in Korea) investigators
Background and aims: The effectiveness of early statin administration in reducing the risk of clinical events among acute ischemic stroke (AIS) patients remains uncertain, particularly in relation to stroke subtypes. This study aims to address this knowledge gap.
Methods: Data from a multicenter stroke registry (January 2011 - December 2020) included AIS patients admitted within 24 hours of onset. Patients without statin prescriptions during hospitalization or with stroke subtypes other determined or undetermined etiology were excluded. We categorized patients into quintiles based on time from hospital arrival to first statin administration (FSA). Primary and secondary outcomes (recurrent stroke, death, and a composite of myocardial infarction, stroke, and death) were evaluated from 24 hours to 30 days post-stroke. Inverse probability of treatment weighting adjusted for baseline group differences.
Results: The study comprised 22,980 patients (60% male, mean age 68±12 years). Median FSA times ranged from 0 hours in the first quintile (Q1) to 49 hours in the fifth quintile (Q5). Earlier FSA was associated with a lower rate of recurrent stroke across all patients (rates from Q1 to Q5: 8.3%, 8.0%, 9.2%, 8.9%, 10.1%; p for trend <0.01). This association varied among stroke subtypes (p for interaction <0.01), with a notably lower risk in large artery atherosclerosis patients as FSA time decreased (p for trend = 0.03). Similar trends were observed for the composite outcome.
Conclusions: Early administration of statins in AIS patients may reduce the risk of clinical events, with the effect varying according to ischemic stroke subtypes.
Disclosures of Interest: No
Abstract N°: 1812
ASSOCIATION OF GOLDEN HOUR THROMBOLYSIS WITH IMPROVED FUNCTIONAL OUTCOMES
Eliot Smolyansky1, Candice Menezes2,3, Mark Parsons4,5, Andrew Bivard6, Dominic Italiano5, Leonid Churilov2,3,7, Geoffrey Donnan3,5, Stephen Davis3,5, Bruce Campbell3,5, Henry Zhao3,5
1The Royal Melbourne Hospital, Department of General Medicine, Parkville, Australia, 2University of Melbourne Faculty of Medicine, Dentistry and Health Sciences, Carlton, Australia, 3The Royal Melbourne Hospital, Department of Neurology, Parkville, Australia, 4Liverpool Hospital, South Western Sydney Clinical School, University of New South Wales, Department of Neurology, Liverpool, Australia, 5The Royal Melbourne Hospital, Department of Medicine, Parkville, Australia, 6Melbourne Brain Centre at The Royal Melbourne Hospital, Parkville, Australia, 7Austin Hospital, Department of Medicine, Heidelberg, Australia
On behalf of:
Background and aims: Ultra-early thrombolysis within the Golden Hour (GH;⩽60min from onset) is a key benefit of Mobile Stroke Units (MSUs), but it is unknown whether improved outcomes are mediated by such factors as early reperfusion or lower ischaemic core. We therefore aimed to investigate the association of MSU-facilitated GH-treatment with early post-treatment CT-perfusion biomarkers.
Methods: We included MSU patients receiving pre-hospital thrombolysis from 12/2017-12/2022 with post-treatment CT-perfusion on hospital arrival and confirmed infarct. Imaging outcomes were compared between GH and non-GH treatment groups: 1) subthreshold hypoperfusion on hospital CT-perfusion assessed visually as substantial((Tmax>4s-Tmax>6s)/Tmax>4s proportion >80%), partial(20-80%) or minimal(<20%), 2) hypoperfusion(TMax>6s) and core(CBF<30%) volume, and 3) proportion with visually smaller infarct on follow-up(>24h) imaging.
Results: We included n=114 patients, of which 23(20.2%) received GH-treatment. Overall thrombolysis-to-CT-perfusion time was 41min(IQR32-52). GH patients showed no baseline differences but a significant increase in 90-day mRS 0/1/2/return-to-baseline (82.6% vs 57.1%;aOR 4.94[95%CI 1.37-17.84,p=0.015]). On post-treatment CT-perfusion, GH-treatment was not associated with an increase in substantial or partial subthreshold hypoperfusion (30.4% vs 35.2%,p=0.81), nor with lower core volume (8ml[IQR0-23] vs 0ml[IQR0-22],p=0.22). However, there were trends towards higher hypoperfusion volume (64ml[IQR20-153] vs 20ml[IQR0-84],p=0.16) and increased proportion with smaller follow-up infarct (78.3% vs 60.4%,p=0.22).
Conclusions: Pre-hospital GH-thrombolysis dramatically improved outcomes but was not associated with an increase in potential early reperfusion changes or lower ischaemic core. Despite similar baseline severity, GH patients trended towards a larger baseline hypoperfusion volume but higher rates of later reperfusion on follow-up imaging, although further causality analysis is required to determine the contribution of these to treatment effect.
Disclosures of Interest: No
Abstract N°: 2166
CONSENT PRACTICES IN PLATFORM TRIALS
Brian Dewar1, Ubong Udoh1, Zoe Tsai2, Ivy Sebastian3, Michel Shamy*2,4
1Ottawa Hospital Research Institute, Ottawa, Canada, 2University of Ottawa, Ottawa, Canada, 3University of Calgary, Calgary, Canada, 4The Ottawa Hospital Civic Campus, Ottawa, Canada
On behalf of:
Background and aims: Platform and adaptive trials promise new opportunities for research but also present challenges for gaining participant consent. We sought to capture the consent methodologies used in these trials.
Methods: We conducted a systematic review of trials that utilized platform or adaptive methodlogies. Using Covidence software, studies were screened for appropriateness against pre-specified inclusion criteria. Data were extracted utilizing an online extraction form. For all identified trials, the trial protocol was sought to extract further information on consenting practices.
Results: 125 trials were identified. Of these, 85 contained information about consenting practices. A majority of these trials focused on either Covid-19 (n=46) or cancer (n=42), and had central locations in either the United States (n=52) or the UK (n=29). The most common consent methodologies are listed in table 1.
The use of participant information sheets which supplemented or replaced information in the consent form was common (n=14), as was the process of utilizing electronic consenting methodologies (such as digitized forms or informational videos, n=12). Unique to platform trials was a multi-stage consenting process (n=11), in which a participant consents to the trial generally but then provides another consent to whichever domains for which the participant then qualifies.
Conclusions: New trial methodologies have fostered innovation in consenting practices. These innovations should be captured, shared, and incorporated into best practices.
Disclosures of Interest: No
Abstract N°: 2329
SUBARACHNOID HEMORRHAGE AFTER MECHANICAL THROMBECTOMY: PREDICTIVE FACTORS AND INFLUENCE ON PROGNOSIS OF ACUTE ISCHEMIC STROKE
Dolores Fernández Couto*1, Alexia Roel Garcia1, Sabela Cajaraville Martinez1, Maria Jose Feal Painceiras1, Lucía Naya Rios1, Lucia García1, Maria Lopez1, Andrés Da Silva2, Juan Manuel Sánchez3, Mar Castellanos1
1University Hospital of A Coruña, Neurology, A Coruña, Spain, 2A Coruña Biomedical Research Institute, A Coruña, Spain, 3University of Girona, Analytical Chemistry, Girona, Spain
On behalf of:
Background and aims: The efficacy of mechanical thrombectomy (MT) in pacients with acute ischemic stroke has been consistenly reported but the procedure is not free of complications, including the development of subaracnoid hemorrhage (SAH). So far, few studies have analyzed the factors related to this complication. We wanted to determine the variables associated with SAH as well as its influence on the prognosis of patients treated with MT.
Methods: We retrospectively analyzed clinical, neuroimaging and endovascular data as well as previous treaments from patients prospectively treated with MT in our center for a period of 4 years. The presence of SAH was evaluated on CT performed at 24+/-12 h after treatment. Good functional prognosis evaluated at 3 months was considered as a modified Rankin score ⩽ 2.
Results: From a total of 448 patients included, 35 (7.8%) had SAH. Older age, previous treatment with statins, longer groin puncture-reperfusion time, higher number of stent retriever passes and aspirations were associated with SAH. These patients also had more frequency of neurological deterioration and worse functional outcome. Logistic regression showed that number of aspirations (OR 1.567; 95% IC, 1.109-2.213) and previous treatment with statins (OR 2.499; 95% IC, 1.010-6.187) were independently associated to SAH. Moreover, after adjusting for associated variables, SAH was an independent predictor of poor functional outcome (OR 3.249; 95% IC, 1.004-10.516).
Conclusions: SAH after MT is and independent predictor of poor prognosis. Previous treatment with statins and the number of aspirations are associated with this complication.
Disclosures of Interest: No
Abstract N°: 2332
MULTICENTER REGISTRY OF PATIENTS WITH ACUTE CENTRAL RETINAL ARTERY OCCLUSION
ANTONIO CRUZ CULEBRAS*1, Marta Vales2, Beatriz Oyanguren3, Marta Guillan4, Sebastian García Madrona1, Alicia De Felipe1, Consuelo Matute Lozano1, Rocio Vera1, Antonio Gil Núñez2, Jaime Masjuan1
1Ramón y Cajal Hospital, Neurology, Madrid, Spain, 2Gregorio Marañón General University Hospital, Neurology, Madrid, Spain, 3Torrejón University Hospital, Neurology, Torrejón de Ardoz, Spain, 4Hospital Universitario Rey Juan Carlos, Neurology, Móstoles, Spain
On behalf of:
Background and aims: There is limited evidence regarding the proper management of central retinal artery occlusion (CRAO). Early recognition of this condition and the standardization of its management are crucial in healthcare systems, since early treatment with intravenous alteplase can improve visual prognosis, similar to acute ischemic stroke
Methods: Multicenter observational registry of patients with CRAO identified in emergency departments of 4 hospitals with Stroke Units using a specific protocol ('Retina Code') from November 2021 to April 2023. Patients were divided into two groups (treated with intravenous alteplase and managed conservatively)
Results: We registered 46 patients were identified in four hospitals in the Community of Madrid with Stroke Units, of whom 15 (32.6%) received alteplase and 31 (67.3%) were managed conservatively. The baseline visual acuity (VA) in both groups was similar (86.9% of patients had VA in the range of visual disability, with no differences between the groups). In the alteplase group, 5 patients (33.3%) had a VA equal to or greater than 0.7 at 3 months, and 6 patients in the conservative treatment group spontaneously improved (19.3%) without any treatment in the acute phase
Conclusions: Implementing a protocol involving ophthalmology and neurology is crucial in hospitals with Stroke Units to identify patients with CRAO. Thrombolytic therapy is feasible and can be a treatment option to improve visual prognosis in these patients
Disclosures of Interest: No
Abstract N°: 2755
GLUNOMAB: A MONOCLONAL ANTIBODY COUNTERACTING BLOOD-BRAIN BARRIER LEAKAGE CAUSED BY ENDOGENOUS TPA AND THROMBOLYTICS (RTPA/TNK) AFTER ISCHEMIC STROKE
Jonathane Furon1, Potzeha Fanny2,3, Florent Lebrun1,4, Mathys Bellemain-Sagnard1, Pauline Marie1, Nicolas Violle4, Flavie Lesept2,3, Cyrille Orset1,5, Manuel BLANC*2,3, Denis Vivien1,4,5
1PhIND, GIP CYCERON, Caen, France, 2LYS THERAPEUTICS, Lyon, France, 3LYS THERAPEUTICS, GIP CYCERON, Caen, France, 4Etap-Lab, GIP CYCERON, Caen, France, 5ESR3P, GIP CYCERON, Caen, France
On behalf of:
Background and aims: In addition to their profibrinolytic function, both endogenous and exogenous forms of tissue plasminogen activator (tPA/rtPA/TNK) induce toxicity by binding and excessively activating NMDA receptors (NMDAr) on endothelial cells forming the blood-brain barrier (BBB). This action leads to tight junction degradation and subsequent BBB disruption. Our study presents compelling preclinical demonstrations of the therapeutic potential of glunomab, a monoclonal antibody designed to inhibit the interaction between tPA and NMDAr. Glunomab effectively mitigates neuroinflammatory and neuronal cell death pathways associated with the pathogenesis of ischemic stroke by reinstating normal BBB functions.
Methods: We assessed the efficacy of glunomab in diverse animal models of thromboembolic stroke, considering comorbidities and varying therapeutic windows (both early and late). Glunomab was administered either as a standalone treatment or in conjunction with thrombolytics. To investigate glunomab therapeutic effects, we employed a combination of readouts including magnetic resonance imaging, laser speckle flowmetry, behavioral tasks, flow cytometry, and immunohistochemistry.
Results: By restoring BBB function, glunomab decreased neuroinflammation, brain lesion volumes, and the likelihood of hemorrhagic transformations leading to short and long-term neurological improvements. The therapeutic efficacy of glunomab was also demonstrated in conjunction with the standard of care (rtPA or TNK) across diverse therapeutic windows, indicating its potential for clinical translation in stroke patients.
Conclusions: Glunomab markedly attenuates ischemic damages induced by both endogenous and recombinant forms of tPA, including alteplase (rtPA) and its variant tenecteplase (TNK). A humanized form of glunomab has been developed, and a clinical trial in ischemic stroke patients is in preparation.
Disclosures of Interest: No
Abstract N°: 2965
PREHOSPITAL BLOOD PRESSURE IN ACUTE STROKE
Silje Holt Jahr*1,2, Kristin Larsen1,2, Maiken Selseth1,3, Vigdis Hillestad3, Else Charlotte Sandset4,5, Ole Morten Ronning1,2, Espen Saxhaug Kristoffersen2,6
1University of Oslo Faculty of Medicine, Institute of Clinical Medicine, Oslo, Norway, 2Akershus University Hospital, Department of Neurology, Lørenskog, Norway, 3Akershus University Hospital, Department of Diagnostic Imaging, Lørenskog, Norway, 4Oslo University Hospital Ullevål, Department of Neurology, Oslo, Norway, 5The Norwegian Air Ambulance Foundation, Oslo, Norway, 6University of Oslo Faculty of Medicine, Department of General Practice, Oslo, Norway
On behalf of:
Background and aims: Blood pressure (BP) is a potential target for prehospital treatment in patients with suspected stroke. This study investigates the impact of time from symptom onset and pre-stroke hypertension on prehospital systolic BP (SBP) in patients with acute ischemic (AIS) and intracerebral haemorrhage (ICH).
Methods: In a retrospective observational study at a primary stroke center covering 10% of the Norwegian population from January 1st, 2015, to December 31st, 2017, we compared SBP in AIS and ICH patients using electronic medical records, considering time from symptom onset (<6, 7-12, 13-24, 25-48, and > 48 hours) and pre-stroke hypertension.
Results: Of 1663 patients (median age 75, 45% female), 88% had AIS and 12% ICH. 52% arrived within 6 hours of symptom onset, and 64% had known hypertension. Patients with ICH had higher mean SBP (172 ± 35 mmHg) than patients with AIS (160 ± 30; p<0.001), regardless of pre-stroke hypertension. Differences in mean SBP between ICH and AIS were noted only in patients admitted within 6 hours (175 ± 33 mmHg vs. 161 ± 30; p<0.001) and later than 48 hours (170 ± 41 mmHg vs. 157 ± 27; p = 0,049) from symptom onset. Within 6 hours, ICH patients with pre-stroke hypertension (174 ± 33 mmHg) had higher mean SBP than their AIS counterparts (161 ± 31; p <0.005).
Conclusions: Prehospital SBP is higher in ICH than AIS independent of pre-stroke hypertension. Future research should further investigate prehospital BP concerning pre-existing hypertension across different stroke subtypes.
Disclosures of Interest: No
Abstract N°: 470
UMBRELLA REVIEW COMPARING ENDOVASCULAR TO BEST MEDICAL TREATMENT FOR LARGE-VESSEL OCCLUSION ACUTE ISCHEMIC STROKE
1Attikon University Hospital, Neurology, Greece, 2McMaster University and Population Health Research Institute, Neurology, Canada, 3Faculty of Health Sciences, Aristotle University of Thessaloniki, Hygiene, Social-Preventive Medicine & Medical Statistics, Thessaloniki, Greece, 4Clinic for Radiology & Nuclear Medicine, University Hospital Basel, Neuroradiology, Basel, Switzerland, 5GHU Paris Psychiatrie et Neurosciences, Neurology, Paris, France
On behalf of:
Background and aims: The literature on endovascular treatment (EVT) for large-vessel occlusion (LVO) acute ischemic stroke (AIS) has been rapidly increasing after the publication of positive randomized-controlled clinical trials (RCTs) and a plethora of systematic reviews (SRs) showing benefit compared to best medical therapy (BMT) for LVO. An overview of SRs (umbrella review) and meta-analysis of primary RCTs was performed to summarize the literature and present efficacy and safety of EVT.
Methods: MEDLINE via Pubmed, Embase and Epistemonikos databases were searched from January 2015 until October 15, 2023. All SRs of RCTs comparing EVT to BMT were included. The primary outcome was 3-month good functional outcome [modified Rankin scale (mRS) score 0-2].
Results: Three eligible SRs and 4 additional RCTs were included in the overview, comprising a total of 24 RCTs, corresponding to 5,968 AIS patients with LVO. High-quality evidence shows that EVT is associated with an increased likelihood of good functional outcome [RR 1.78 (95%CI:1.54-2.06); 166 more per 1000 patients], independent ambulation [mRS-scores 0-3; RR 1.50 (95%CI:1.37-1.64); 174 more per 1000 patients], excellent functional outcome [mRS-scores 0-1; RR 1.90 (95%CI:1.62-2.22); 118 more per 1000 patients] at 3 months. EVT was associated with reduced 3-month mortality [RR 0.81 (95%CI:0.74-0.88); 61 less per 1000 patients] despite an increase in symptomatic intracranial hemorrhage [sICH; RR 1.65 (95%CI:1.23-2.21); 22 more per 1000 patients].
Conclusions: In patients with AIS due to LVO in the anterior or posterior circulation, within 24 hours from symptom onset, EVT improves functional outcomes and increases the chance of survival despite increased sICH risk.
Disclosures of Interest: No
Abstract N°: 667
THE CLINICAL OUTCOME OF PATIENTS WITH CANCER-RELATED IN-HOSPITAL ONSET STROKE
1Kyorin University, Department of Stroke and Cerebrovascular Medicine, Tokyo, Japan, 2Kyorin University Hospital, Stroke Center, Tokyo, Japan
On behalf of:
Background and aims: Among in-hospital strokes (IHS), cancer-related stroke (CRS) is increasing. The aim was to clarify whether the clinical outcomes of CRS and non-CRS differ among IHS patients.
Methods: We prospectively enrolled IHS patients in our institute. A total of 164 IHS patients (57% male, median age 78 years, median NIHSS score 8) between August 2016 and March 2022 were divided into two groups: CRS group (n=54, 33%) and non-CRS group (n=110, 67%). CRS was defined as acute ischemic stroke during cancer treatment or complicated by cancer of advanced stage.
Results: IHS was recognized frequently by a nurse (63% in CRS group and 71% in non-CRS group). The time from recognition to stroke physician consultation was shorter in CRS group than non-CRS group (40 vs. 91 minutes, p=0.005). The rate of reperfusion therapy was 19% (10/54) in the CRS group and 13% (14/110) in non-CRS group, with no significant difference (p=0.324). The rates of good outcome at discharge (mRS score 0-3, CRS group 31%, non-CRS group 32%) and in-hospital mortality (CRS group 30%, non-CRS group 22%) were similar in both groups. Among 24 patients with reperfusion therapy, the rates of good outcome at discharge were also similar (CRS group 40%, non-CRS group 36%).
Conclusions: One-third of IHS were CRS, and of which one-fifth received reperfusion therapy. The short-term outcome was similar in both groups. Considering that 40% of CRS patients with reperfusion therapy remained functionally independent, reperfusion therapy could enable improved quality of life in CRS patients.
Disclosures of Interest: No
Abstract N°: 771
DETECTION OF LARGE VESSEL OCCLUSION STROKE WITH POINT-OF-CARE ULTRASOUND OF THE COMMON CAROTID ARTERIES: PRELIMINARY RESULTS
João Pinho*1, Pardes Habib2,3, Oliver Matz3, Ramy Abdelnaby3, Omid Nikoubashman4, Martin Wiesmann4, Jörg C. Brokmann5, Jörg B. Schulz3,6, Arno Reich3
1University Hospital, RWTH Aachen University, Department of Neurology, Germany, 2Stanford University School of Medicine, Neurosurgery, 3University Hospital, RWTH Aachen University, Department of Neurology, 4University Hospital, RWTH Aachen University, Department of Diagnostic and Interventional Neuroradiology, 5University Hospital, RWTH Aachen University, Emergency Department, Aachen, Germany, 6JARA Institute of Molecular Neuroscience and Neuroimaging (INM-11), Juelich Research Center GmbH and RWTH Aachen University, Aachen, Germany
On behalf of: POCUS-LVO Study Group
Background and aims: Accurate detection of LVO stroke in the pre-hospital setting allows direct transportation to an endovascular treatment-capable hospital. Our aim was to analyse the diagnostic performance of point-of-care ultrasound of the common carotid arteries (CCA) to detect anterior-circulation LVO (ac-LVO).
Methods: We conducted a prospective single-center study in the emergency department and included patients with suspected stroke. We performed emergent ultrasound of both CCAs in all included patients using a portable point-of-care ultrasound. We measured peak systolic velocities (PSV), end-diastolic velocities (EDV), resistance index (RI) and pulsatility index (PI) of both CCAs. ac-LVO was defined as ICA- or M1-occlusion in CTA/MRA. We analysed the diagnostic performance of CCA spectral waveform parameters.
Results: We included 259 patients with suspected stroke, of whom 133 had ischemic stroke (including 28 with ac-LVO). Among all included patients, CCAs ipsilateral to ac-LVO had lower PSV and EDV, and higher RI and PI (in comparison with CCAs with no ipsilateral ac-LVO). The highest AUC for ac-LVO detection was found for PI-difference between sides (0.91) followed by RI-difference between sides (0.90) and EDV-difference between sides (0.87). Using optimal cut-off values for each parameter, PI-difference between sides and RI-difference between sides had the highest sensitivity (100%), EDV-difference between sides had the highest specificity (88%), and positive likelihood ratio was highest for EDV-difference between sides (6.3).
Conclusions: Spectral waveform parameters of the CCAs have a good diagnostic performance to identify ac-LVO in patients with suspected stroke. These results warrant further studies in a pre-hospital setting.
Disclosures of Interest: No
Abstract N°: 1283
OUTCOMES OF MECHANICAL THROMBECTOMY IN ACUTE BASILAR ARTERY OCCLUSION STROKE WITH MILD TO MODERATE SYMPTOMS
Ettore Nicolini*1,2, Manuela De Michele3, Valentina Saia4, Svetlana Lorenzano1, Antonio Ciacciarelli3, Giovanni Pracucci5, Salvatore Mangiafico6, Niaz Ahmed7, Danilo Toni1, Carlo Cereda8
1Sapienza University of Rome, Human Neuroscience, Roma, Italy, 2Ospedale dei Castelli, Emergency department, Ariccia (Rome), Italy, 3Sapienza University of Rome, Stroke Unit, Emergency department, Roma, Italy, 4Hospital Santa Corona, Pietra Ligure, Italy, 5University of Studies of Florence-Department of Neurofarba, Firenze, Italy, 6IRCCS Neuromed Mediterranean Neurological Institute, Pozzilli, Italy, 7Karolinska Institute, Department of Neurology, Solna, Sweden, 8EOC Ospedale Regionale di Lugano, Stroke Center EOC, Neurocenter of Southern Switzerland, Lugano, Switzerland
On behalf of: On behalf of the IRETAS and the SITS groups
Background and aims: The benefit of mechanical thrombectomy in patients with acute basilar artery occlusion (BAO) and NIHSS<10 is unclear, since this sub-population was mainly excluded from large trials. We aimed to compare the outcomes of patients treated with mechanical thrombectomy (MT) vs intravenous thrombolysis (IVT) in this population.
Methods: We emulated a hypothetical trial including patients with BAO and NIHSS<10, treated with MT (±IVT) from the Italian Registry of Endovascular Stroke Treatments, and with IVT only from the SITS Registry. The primary outcome was a score 0-2 at the 90-day modified Rankin Scale (mRS). We used inverse probability weighting (IPW) adjusted for prespecified covariates to weight each individual’s contribution to the outcome. We used a robust variance estimator to account for potential replications of patients.
Results: After applying IPW, n=710 with MT and n=707 with IVT patients were included. MT was associated with higher odds of 90-day mRS 0-2 (aOR 1.56 [95%CI 1.04-2.03]). MT was also associated with excellent outcome (mRS 0-1) (aOR 2.01 [95%CI 1.37–2.95]), and reduced in-hospital death (aOR 0.448 [95%CI 0.25-0.78]). Among the tested subgroups, MT had a larger effect on independence in patients with NIHSS 6-9 compared to those with NIHSS<6 (p for interaction 0.02).
Conclusions: In a large scale targeted trial emulation, in patients with Stroke from BAO and NIHSS<10 MT was associated with better functional outcomes and lower rates of in-hospital mortality compared to patient treated with IVT alone. Further research is needed for patients with NIHSS<6.
Disclosures of Interest: No
Abstract N°: 711
PREVALENCE OF HEMORRHAGIC TRANSFORMATION AND PREDICTIVE FACTORS AFTER MECHANICAL THROMBECTOMY
Tho Phung*1, Ton Mai Duy1, Phuong Dao1, Linh Pham2
1Bach Mai Hospital, Stroke center, 2Hanoi medical university
On behalf of:
Background and aims: Hemorrhagic transformation (HT) is a serious complication affecting the clinical outcomes and mortality rates in patients with cerebral infarction. This study aimed to identify factors associated with HT following thrombectomy in anterior large vessel occlusion stroke.
Methods: This observational retrospective study enrolled acute ischemia stroke patients with anterior circulation occlusion who underwent mechanical thrombectomy at the Stroke Center of Bach Mai Hospital between October 2022 and July 2023. Logistic regression analysis was employed to determine the significant factors associated with HT.
Results: Of the 166 patients included (mean age: 64 ± 12; male: 51%), 69 individuals (41.6%) developed HT with 23 patients (13.8%) diagnosed with symptomatic HT. The occurrence of HT was associated with ASPECTS < 7 (p = 0.023), mTICI 2b-3 (p = 0.02), systolic blood pressure > 140 mmHg (p = 0.043), cardioembolism (p = 0.036), neutrophil percentage ⩾ 80% (p = 0.002). Following adjustment, mTICI 2b-3 (OR = 2.9, p = 0.037), systolic blood pressure > 140 mmHg(OR = 2.7, p = 0.019), and neutrophil percentage ⩾ 80% (OR = 3.3, p = 0,002) remained significant. Patients with HI exhibited a lower rate of functional independence at 3 months (40.6% vs 49.5%, p = 0.256).
Conclusions: In our study cohort, the rate of HT was 41.6%. Patients who underwent thrombectomy with mTICI 2b-3, systolic blood pressure > 140 mmHg, and neutrophil percentage ⩾ 80% were at an increased risk of developing HT.
Disclosures of Interest: No
Abstract N°: 1685
THE IMPACT OF PROEDURAL TIME OF MECHANICAL THROMEBECTOMY ON ACUTE STROKE OUTCOMES
Eung-Joon Lee*1, Han-Yeong Jeong1, Keun-Hwa Jung1
1Seoul National University Hospital, Neurology, Seoul, South Korea
On behalf of:
Background and aims: Procedural time (PT), groin puncture to recanalization time, affect outcomes of acute ischemic stroke (AIS) patients undergoing mechanical thrombectomy (MT). This study used a nationwide acute stroke registry to investigate the association between PT and clinical outcomes and analyze the significant factors associated with longer PT.
Methods: Patients who underwent MT between January 2015 and December 2021 were included. We investigated the association between PT and successful recanalization (SR) represented as the Thrombolysis in cerebral infarction (TICI) grade 2b and 3 as well as the clinical outcome of the patients identified by modified Rankin scale score (mRS) at discharge. Multivariate models were used to identify factors significantly associated with PT of >60 min.
Results: Using the Korean Stroke Registry, we analyzed 5,432 patients who underwent MT from 54 hospitals. The mean PT was 56.0±37.6 min, and PT was significantly shorter in patients who achieved a mRS score at discharge 0-2 compared to those who did not (50.1±33.3 vs. 59.9±39.8, p<0.001). Also, SR was significantly more likely to be achieved when the PT was less than 60 minutes. After adjusting for confounders, older age (adjusted odds ratio [aOR]=1.01; 95% confidence interval [CI], 1.01–1.02), longer prehospital delay (aOR=1.07; 95%CI, 1.04–1.09) were found to predict PT of >60 min independently. On the contrary, atrial fibrillation (aOR=0.80; 95%CI 0.70-0.91), prior statin use (aOR=0.85, 95% CI 0.74-0.95), and admission at a tertiary referral hospital (aOR=0.68, 95%CI 0.60-0.76) were significantly, negatively associated with PT>60 min.
Conclusions: Shorter PT was significantly associated with SR and favorable clinical outcomes.
Disclosures of Interest: No
Abstract N°: 2851
ENDOVASCULAR TREATMENT IN PATIENTS WITH ACUTE ISCHEMIC STROKE PRESENTING IN THE EXTENDED TIME WINDOW: A COHORT STUDY FROM THE EVA-TRISP COLLABORATION
Nabila Wali*1, Lotte J Stolze1, Mirjam Rachel Heldner2, Susanne Wegener3, Sami Curtze4, Georg Kaegi5, Patrik Michel6, Henrik Gensicke7,8, Stefan Engelter7,8, Paul Nederkoorn1
1Amsterdam UMC, University of Amsterdam, Department of Neurology, Amsterdam, Netherlands, 2Inselspital, Bern University Hospital and University of Bern, Department of Neurology, Bern, Switzerland, 3University Hospital Zurich and University of Zurich, Department of Neurology, Zurich, Switzerland, 4University of Helsinki and Helsinki University Hospital, Department of Neurology, Helsinki, Finland, 5Kantonsspital St. Gallen, St. Gallen, Department of Neurology, St. Gallen, Switzerland, 6Lausanne University Hospital and University of Lausanne, Stroke Center, Neurology Service, Lausanne, Switzerland, 7University Department of Geriatric Medicine FELIX PLATTER, University of Basel, Department of Neurology and Neurorehabilitation, Basel, Switzerland, 8University Hospital Basel and University of Basel, Stroke Center and Department of Neurology, Basel, Switzerland
On behalf of: The EndoVAscular treatment and ThRombolysis for Ischemic Stroke Patients (EVA-TRISP) investigators.
Background and aims: Endovascular thrombectomy (EVT) up to 6 hours after symptom onset or last seen well (LSW) is widely implemented for patients with acute ischemic stroke. After positive findings in recent clinical trials the time window for EVT has been expanded up to 24 hours from symptom onset or LSW. However, real life data are scarce. We aimed to compare EVT patients’ characteristics and outcomes in the early versus extended time window and to compare the outcomes with clinical trial results.
Methods: Data from the EndoVAscular treatment and ThRombolysis for Ischemic Stroke Patients (EVATRISP) cohort study was used. All consecutive EVT patients from 16 European comprehensive stroke centres were included. We compared rates of symptomatic intracranial hemorrhage (sICH), of 90-day favourable outcome (Modified Rankin Scale 0-2), and of mortality between patients treated in the early (<6 hours after onset or LSW) versus extended (6-24 hours after onset or LSW) time windows.
Results: We included 8671 patients, of which 6445 were treated in the early and 2226 in the extended time window. NIHSS score at presentation was lower in patients treated in the extended time window (median 13 [IQR 7-18] vs 15 [IQR 9-19], p<0.001). As expected, favorable outcome rate in the extended window was slightly lower (37.5% vs 42.4%, p<0.001). However, rates of recanalization, sICH, and mortality were similar.
Conclusions: According to this large multicenter cohort study EVT use in the extended time window appears safe and effective.
Disclosures of Interest: No
Abstract N°: 3164
CODE ICH: LOCAL PROTOCOL CHALLENGES FOR BLOOD PRESSURE CONTROL IN INTRACEREBRAL HEMORRHAGE
Anca Negrila*1, Razvan Alexandru Radu1,2, Elena Oana Terecoasa1,2, Raluca Stefania Badea1,2, Bogdan Casaru1, Cristina Tiu1,2
1Emergency University Hospital, Neurology, Bucharest, Romania, 2University of Medicine, and Pharmacy” Carol Davila”, Neurology, Bucharest, Romania
On behalf of:
Background and aims: Early aggressive medical treatment intended to lower the blood pressure (BP) has been proven to improve outcome in patients with intracerebral hemorrhage (ICH).
Methods: We implemented an aggressive blood pressure monitoring protocol for patients diagnosed with ICH in the Neurology Department of our Stroke Centre starting with January 2023. This study focused on assessing compliance with the established protocol and its influence on patient outcomes, through a comparative analysis with a cohort of ICH patients admitted to our centre between 2018 and 2020.
Results: The study included 383 patients with ICH, 113 patients in 2023 group and 270 patients in the 2018-2020 group. There was no difference between cohorts regarding stroke severity, ICH score, GCS at admission and ICH volume. There was no significant difference between the two groups regarding in-hospital mortality (48.51% vs 41.57, p= 0.23) or favourable discharge outcome (30.69% vs 33.33%, p=0.63). However, early control of BP after admission (in less than 2 hours) was achieved for only 42.86% of the ICH patients in 2023. The rate of mortality in the subgroup of patients with efficient early control of BP was significantly lower than in the rest of 2023 group (38.10% vs 58.93%, p=0.04). Patients with efficient early control of BP more frequently had a favourable outcome at discharge. (26.19% vs 12.28%, p=0.07).
Conclusions: Early blood pressure control remains a significant challenge in ICH patients, even with aggressive monitoring protocols in place.
Disclosures of Interest: No
Abstract N°: 815
PATIENT AND CAREGIVER PERSPECTIVES ON THE DESIGN AND EXECUTION OF PLATFORM TRIALS IN ACUTE STROKE
Aravind Ganesh*1, Nora Cristall1, Carol Kenney1, Bijoy Menon1, Michel Shamy2, Nishita Singh3
1University of Calgary Cumming School of Medicine, Clinical Neurosciences, Calgary, Canada, 2University of Ottawa, Ottawa, Canada, 3University of Manitoba Max Rady College of Medicine, Winnipeg, Canada
On behalf of:
Background and aims: Platform trials represent an important paradigm shift in stroke research, allowing multiple questions and treatments to explored simultaneously. We sought to examine how patients and caregivers perceive such trial designs and their potential execution.
Methods: Two focus groups were conducted virtually, attended by a total of 10 patient/caregiver representatives (5 in each) and 7 clinician-researchers/nurses, in which a physician presented a platform trial proposal followed by facilitated discussions. Audio recordings were transcribed and combined with field notes for thematic analysis.
Results: Potential benefits of platform trials perceived by patients/caregivers included opportunities to be randomized to multiple treatments, with accompanying efficiencies and richer data to improve patient care. They emphasized the importance of gatekeeper processes for the addition of candidate treatments to trial platforms with decisions ultimately made by non-conflicted parties, and to ensure examined questions would not interfere with routine care. They appreciated that deferral of consent would be ideal to allow timely randomization/treatment in acute stroke platform trials, as long as patient safety is prioritized in enrolment-related decisions, with family input whenever feasible. They expressed concerns about the risk of unforeseen interactions among multiple treatment arms. They underscored the need for easily accessible trial information in digestible chunks, multiple languages and modalities to facilitate transparency/trust; and endorsed evaluating participant experiences and keeping patients/families updated of trial progress and findings.
Conclusions: Patients and caregivers were supportive of platform trial approaches in acute stroke but expressed important priorities for consideration in the design and execution of such trials.
Disclosures of Interest: No
Abstract N°: 1008
IMPACT OF A CENTRALIZED AI BASED STROKE IMAGING NETWORK ON TRANSPORTATION TIMES FOR THROMBECTOMY VIA DRIP AND SHIP
Istvan Szikora*1, Csaba Ováry2, Ferenc Molnár3, György Pápai3, Gábor Szudi1, Orsolya Szalmás1, Máté Czencz1, Máté Kondor1, Sandor Nardai1, Lorand Eross1
1National Institute of Mental Health Neurology and Neurosurgery, Neurointerventions, Budapest, Hungary, 2Bajcsy Zsilinszky Hospital, Budapest, 3National Ambulance Service, Budapest, Hungary
On behalf of:
Background and aims: A nationwide Artificial Intelligence (AI) based stroke imaging network (Brainomix eStroke) has been installed in 2022 in Hungary. We analyzed its impact on transportation times of drip and ship patients in a large thrombectomy center (TC), serving 15 primary stroke centers (PC).
Methods: Time points, such as first Call of Ambulance (CA), Arrival at PC (APC), Departure from PC (DPC) and Arrival at TC (ATC) were recorded. Data from a 3 month period prior to installation (2021) of the network were compared to those of a 4 months period following installation (2023). Door in- Door Out Time (DiDo) and CA-ATC times were calculated. The 2023 group was divided into those who were further transported by the first ambulance unit (group A) and those, who arrived at the TC by a 2nd ambulance car (group B).
Results: In 2021, complete dataset was available for 50 drip and ship patients within 3 months, the mean DiDo time was 2:33’ and the mean CA-ATC time was 4:18’. In 2023, 114 patient’s data were analyzed. DiDo time was reduced to 1:57’ and CA-ATC time to 3:15’. However, the CA-ATC time was only 1:38’ for 31 (27%) patients in group A, but 3:52’ for 83 (73%) patients in group B.
Conclusions: A centralized AI based stroke imaging network is capable of significantly reducing transportation times for drip and ship patients. The highest reduction can be achieved if the first ambulance unit can complete the transport from the primary to the thrombectomy center.
Disclosures of Interest: Yes Consultant to Brainomix
Abstract N°: 1165
IMPACT OF “SEND AND TELL” FAST TRACK THROMBECTOMY REFERRALS TO A COMPREHENSIVE STROKE CENTRE IN CENTRAL SOUTHERN ENGLAND
Richard Marigold*1, Shivaprasad Siddegowda1, Nic Weir1, Emma Battersby- Wood1, Pamela Crawford1, Sue Evans1, Charis Mavrokordatos2, Ugnius Sukys2
1Wessex Neurological Centre, Stroke Medicine, United Kingdom, 2Queen Alexandra Hospital, Portsmouth, United Kingdom
On behalf of:
Background and aims: Reducing door in door out (DIDO) times is important in speeding up transfer between acute (ASC) and comprehensive stroke (CSC) centres in treating patients with large vessel occlusion (LVO) for mechanical thrombectomy (MT). In a pilot study in which patients who were more “clear cut” cases for MT in the anterior circulation patients were transferred more rapidly using the same ambulance from Portsmouth (ASC) to Southampton (CSC). The CSC was only informed once the patient was en route in a “send and tell” (rapid transfer) pathway.
Methods: Between January 2022 and November 2023, 29 patients were referred using the normal and 39 the “send and tell” pathway. Inclusion criteria for rapid transfer: Mon-Fri 09:00 – 16:00, age <85 years, mRS <3, onset <4 hours, NIHSS >10, ASPECTS>6, LVO in T-ICA, M1 MCA and haemodynamically stable.
Results: 10 patients received tenectplase on normal vs 20 on rapid pathway. Mean DIDO time normal 2hr34min vs rapid 1hr41min, door (ASC) to groin puncture 4hr23min vs 2hr17min, CSC arrival to groin puncture 24min vs 12min. Mean pre-MT NIHSS 16 in both groups and post-MT11 and 8 respectively.
Conclusions: A “send and tell” or rapid transfer approach for clear cut MT candidates resulted in faster DIDO times, door to groin puncture times and better post MT NIHSS scores. Despite being a self selecting group, caution is needed in ensuring patients are fit for transfer when rapid referrals are made, but a more than 2hr reduction in door to groin puncture time resulted in better clinical outcomes.
Disclosures of Interest: No
Abstract N°: 1285
ETHNIC DIFFERENCES IN ACCESS TO CARE AND TREATMENT IN PATIENTS WITH SUSPECTED ACUTE STROKE: A RETROSPECTIVE, COHORT STUDY
Irene Scala*1,2, Jacopo DI Giovanni2, Pier Andrea Rizzo2, Simone Bellavia2, Aldobrando Broccolini1,2, Mauro Monforte1, Paolo Calabresi1,2, Marcello Covino3, Giovanni Frisullo1
1Fondazione Policlinico universitario A. Gemelli IRCCS, Neurology Department, Roma, Italy, 2Catholic University of the Sacred Heart, Neuroscience, Roma, Italy, 3Fondazione Policlinico universitario A. Gemelli IRCCS, Department of Emergency Medicine, Roma, Italy
On behalf of:
Background and aims: Data concerning an unequal healthcare access of the acute stroke patients based on ethnicity or race are inconclusive in Europeans. The primary objective was to evaluate the effect of geographic origin/race on access to acute stroke care and treatments. Secondly, we evaluated the effect of geographic origin/race on stroke risk factors, outcomes, and admission for stroke mimics.
Methods: In this retrospective, cohort study, we enrolled adult patients admitted to the emergency department of a comprehensive stroke center for suspected stroke. Based on geographic origin, patients were divided into two groups: Western Europeans (WE) and non-Western Europeans (nWE). For each nWE subjects we included four sex- and age-propensity score matched patients in the WE group. We then divided patients in three further subgroups (White/Black/Asian) based on race. Univariate comparisons were performed using Mann-Whitney, Kruskal-Wallis and χ2-tests, as appropriate. Logistic regression was used to perform the adjusted analyses.
Results: 618 patients were enrolled in the nWE group and 2444 in the WE group. Belonging to the nWE group is an independent predictor of lower likelihood of receiving intravenous thrombolysis (p=0.005). Considering Black/Asian/White subgroups, ED accesses for stroke mimics were less frequent among racial minority groups (p=0.038). Black and Asian individuals had a higher incidence of brain hemorrhages than Whites (p=0.003). No differences in stroke outcomes were found among groups.
Conclusions: Racial and ethnic disparities in healthcare are a challenging issue even in universal healthcare systems, likely due to differences in socioeconomic status, and it should be addressed promptly through education campaigns of healthcare personnel.
Disclosures of Interest: No
Abstract N°: 285
BENEFIT OF REPERFUSION TREATMENT FOR ISCHEMIC STROKE WITH PREMORBID DISABILITY: RETROSPECTIVE, SINGLE-CENTRE STUDY
Marco Vabanesi*1, Emanuele Dotto1,2, Federico Pedroni1,2, Raffaella Chieffo1, Giacomo Giacalone1, Gianni Cutillo1,2, Mario Orrico1, Marco Bacigaluppi1, Massimo Filippi1,2, Luisa Roveri1
1IRCCS San Raffaele Hospital, Milan, Italy, 2Vita-Salute San Raffaele University, Milano, Italy
On behalf of:
Background and aims: The choice between reperfusion or conservative treatment in patients with acute ischemic stroke (AIS) and premorbid disability can be challenging, because of uncertain benefit of treatment. We aimed to evaluate clinical outcomes in a single-centre cohort with at least moderate premorbid disability (mRS ⩾3).
Methods: From our prospective database we selected consecutive subjects admitted for AIS with large-vessel occlusion between 2012 and 2023, with premorbid mRS ⩾3, presenting within 6 hours from onset. Primary outcome was 90-day mRS distribution (with recovery to premorbid mRS as favourable outcome). Secondary outcomes were NIHSS improvement at hospital discharge and adverse events.
Results: We included 112 AIS patients, with median baseline NIHSS 17 (IQR 12-21), of which 72 received reperfusion treatments (EVT/IVT/combined) and 40 conservatively treated. Ordinal analysis of 90-day mRS showed trend to superior outcome in reperfusion group compared to conservative treatment (generalised OR 1.54 [0.85-2.77], p=0.15; Fig.1) across all stroke severity spectrum (Fig.2), and higher rate of subjects with recovery to premorbid mRS (34.7% vs. 25.0%; OR 1.60 [0.67-3.79]). The reperfusion group showed higher frequency of neurological improvement at discharge, with 51.4% subjects improving ⩾4 NIHSS points from baseline vs. 17.5% in conservative group (OR 4.98 [95% CI: 1.95-12.73], p<0.001). No differences were observed in 90-day mortality (31.9% vs. 40.0%, OR 0.70 [0.32-1.57]) and haemorrhagic transformation rates (OR 0.72 [0.30-1.72]).
Conclusions: Reperfusion treatment was safe and possibly associated with reduced post-stroke disability in this high-premorbid disability cohort. Larger trials evaluating acute treatment outcomes in LVO-AIS patients with prior disability are warranted.
Disclosures of Interest: No
Abstract N°: 1202
INTRAPROCEDURAL HYPOTENSION AND FUNCTIONAL OUTCOMES IN ISCHEMIC STROKE PATIENTS UNDERGOING MECHANICAL THROMBECTOMY
Maria Zuluaga*1, Juan Tascón1, Jaime Ortiz1, Eder Alexander Moreno Vargas2, Natalia Llanos Leyton2, Valentina Mejía Quiñones2, Edgar Folleco2, Pablo Felipe Amaya Gonzalez2
1ICESI University, Cali, Colombia, 2Fundación Valle del Lili Hospital, Cali, Colombia
On behalf of:
Background and aims: Mechanical thrombectomy (MT) stands as an expanding reperfusion strategy for ischemic stroke (IS). Limited data is available on intraprocedural blood pressure targets during MT and subsequent functional outcomes of IS patients
Methods: A cohort study with IS patients undergoing MT between January 2017 and January 2023 at a comprehensive stroke center. Two distinct groups were established: Group A, experiencing hypotension (defined as a decrease in systolic blood pressure exceeding 30 mmHg between triage and anesthesia for MT); and Group B, without hypotension. Primary outcomes included modified Rankin Scale (mRS) at discharge and 90-day, along with mortality. Statistical analysis employed t-student and chi-squared tests, considering significance at p > 0.05, utilizing Stata version 18.
Results: 167 patients (55.7% male, median age 66 years (IQR 53-76 years)) underwent MT. Admission variables, including NIHSS ((A)16; (B)16), ASPECTS (9; 9), and intravenous thrombolysis (45.5%) were comparable between Groups A and B, respectively. The door-to-groin time was 138 vs. 129.5 minutes. A favorable TICI (2b-3) was achieved in 76% vs. 70% (X2=0.92, p=0.33), while unfavorable mRS (>2) at discharge was 70.13% vs. 68.9% (X2=0.03, p=0.86). Discharge mortality was 32.47% vs. 16.67% (X2=8.6, p=0.2), and at 90 days, it was 37.7% vs. 18.9% (X2=15.8, p=0.02).
Conclusions: Despite similar admission variables and thrombectomy outcomes, there was a higher mortality at 3 months in the hypotension group. No statistical difference was observed in functionality.
Disclosures of Interest: No
Abstract N°: 1472
ASSOCIATION OF PROCEDURAL TIME AND FUNCTIONAL OUTCOME IN UNSUCCESSFUL RECANALIZATION AFTER MECHANICAL THROMBECTOMY
Fabrizio Sallustio1, Ettore Nicolini*1,2, Valentina Saia3, Alfredo Paolo Mascolo4, Federico Marrama4, Valerio Da Ros5, Fana Alemseged6, Giovanni Pracucci7, Salvatore Mangiafico8, Danilo Toni2
1Ospedale dei Castelli, Emergency department, Ariccia (Rome), Italy, 2Sapienza University of Rome, Human Neuroscience, Roma, Italy, 3Santa Corona, Pietra Ligure, Italy, 4Hospital Tor Vergata Roma, Department of Systems Medicine, Roma, Italy, 5Hospital Tor Vergata Roma, Department of Biomedicine and Prevention, Roma, Italy, 6The Royal Melbourne Hospital, Department of Medicine and Neurology, Parkville, Australia, 7University of Studies of Florence, Department of Neurofarba, Firenze, Italy, 8IRCCS Neuromed Mediterranean Neurological Institute, Pozzilli, Italy
On behalf of: On behalf of the IRETAS group
Background and aims: The time to stop mechanical thrombectomy (MT) procedures in case of unsuccessful recanalization in acute ischemic stroke (AIS) from large vessels occlusion remains an unanswered question. In our study, we tested the effect of procedural time on outcomes in patients with unsuccessful MT for AIS.
Methods: We selected patients with AIS from M1 and / or M2 segment of middle cerebral artery occlusion and unsuccessful MT (TICI 0-2a) from the Italian Registry of Endovascular Stroke Treatments. Primary outcome was 90-day modified Rankin scale (mRS) 4-6. Secondary outcomes were early neurological deterioration (END), symptomatic intracranial hemorrhage (sICH) according to ECASS II SITS-MOST criteria.
Results: Among 852 selected patients, age (OR:1.039;95%CI:1.022-1.057;p<0.001), previous TIA/stroke (OR:0.294;95%CI:0.118-0.737; p=0.009), M1 occlusion (OR:1.684; 95%CI:1.132-2.506; p=0.010), baseline NIHSS (OR:1.093;95%CI:1.058-1.129;p<0.001) and groin-to-recanalization time (OR:1.007;95% CI:1.002-1.012;p=0.003) were independent predictors of 90-day mRS 4-6. Concerning secondary outcomes, baseline NIHSS (OR:0.958;95%CI:0.929-0.989;p=0.008), general anesthesia (OR:2.589;95%CI:1.522-4.404;p<0.001), groin to recanalization time (OR:1.007;95% CI:1.003-1.011;p=0.002) and intraprocedural vessel perforation or dissection (OR:1.894;95%CI:1.018-3.524;p=0.044) were independent predictors of END. Bridging therapy (OR:2.929;95%CI:1.210-7.089;p=0.017) was associated with sICH per SITS-MOST criteria whereas M1 occlusion (OR:0.354;95%CI:0.182-0.690;p=0.002), bridging therapy (OR:2.025;95%CI:1.073-3.823;p=0.029) and vessel perforation or dissection (OR:5.551;95%CI:2.725-11.311;p<0.001) were associated with sICH per ECASSII criteria. No significant association was found between number of MT attempts and the analyzed outcomes.
Conclusions: Among patients with unsuccessful recanalization procedural time was associated with poor outcome and END, regardless of the number of MT attempts and intraprocedural complications. We suggest a deeper consideration of groin to recanalization time in case of anterior circulation occlusion refractory to MT.
Disclosures of Interest: No
Abstract N°: 1553
BIO-COMPATIBLE CERIA-BASED NANOZYME AS A NOVEL THERAPEUTIC DRUG FOR MASSIVE ISCHEMIC STROKE
Byoungsoo Kim*1,2, Bong Geun Cha1, Joong Pill Park1, Sun Hwa Lee1,2, Seul Ki Ki1,2, Ha Yoon Cho1,2, Ju Hee Han1,2, Jihoon Kim2, Seung-Hoon Lee1,2,3
1Seoul National University Hospital, Department of Neurology, Seoul, South Korea, 2Cenyx Biotech, Seoul, South Korea, 3Seoul National University College of Medicine, Department of Neurology, Seoul, South Korea
On behalf of:
Background and aims: When reperfusion fails, massive (or hemispheric) ischemic stroke (MIS) represents the most severe form affecting the entire territory of the middle cerebral artery (MCA) or internal carotid artery. Reactive oxygen species (ROS)-induced inflammation is the main cause of secondary damage in such strokes. Here, we newly developed a biocompatible ceria-based nanozyme (CX301) as a potent ROS scavenger and investigated its neuroprotective effect in a rodent model of MIS.
Methods: CX301 was developed by combining ceria nanoparticles with polyvinylpyrrolidone polymers, connected by 6-aminohexanoic acids. Its ROS-scavenging capacity was analyzed in vitro. Permanent focal ischemia (PFI) was induced in rats via MCA occlusion to simulate MIS in humans. CX301 (10 mg/kg) was infused intravenously at 1 hour. We analyzed survival rates for 14 days and measured infarct volume, inflammatory cell infiltrations, and neuronal cell death.
Results: We successfully fabricated CX301 (8.84±1.15 nm in size; 0.07±0.11 mV in surface charge). It dramatically reduced ROS levels in cell-free conditions (95.2±3.8% reduction) and cellular conditions (71.8±2.4% reduction). After PFI induction, CX301 infusion resulted in a substantial improvement in survival by 10.5 folds compared to the controls (6.7 vs. 70%). Inflammatory cell infiltrations (41% in microglia/macrophages, 72% in neutrophils), infarct volume (154 vs. 61 mm3; 72% reduction), and neuronal cell death (67 vs. 24%) were substantially decreased by the treatment.
Conclusions: CX301 effectively scavenged ROS, reduced brain inflammation and damage, and improved survival against MIS. These results suggest that CX301 can be used as an emergency rescue drug in MIS.
Disclosures of Interest: No
Abstract N°: 1820
EARLY ANTIHYPERTENSIVE THERAPY AND BLOOD PRESURE MANAGEMENT IN ACUTE ISCHEMIC STROKE: A SYSTEMATIC REVIEW AND META-ANALYSIS
Fengkai Mao*1, Song He1, Jie Yang2
1The First Affiliated Hospital of Chengdu Medical College, Chengdu, China, Department of Neurology, 2Sichuan Provincial People's Hospital, University of Electronic Science and Technology of China, Chengdu, China, Department of Neurology
On behalf of:
Background and aims: Management of elevated blood pressure (BP) for patients with acute ischemic stroke (AIS) remains controversial. Therefore, we conducted a meta-analysis to evaluate the efficacy and safety of early BP reduction for AIS patients.
Methods: English and Chinese databases (PubMed, Embase, et al.) were systematically searched up to 20th October 2023 for randomized controlled trials about BP reduction within seven days of AIS onset. The primary outcomes were disability or death (modified Rankin Scale, mRS⩾3) at 90 days or the end of the trial. Secondary outcomes included all-cause death, the National Institute of Health Stroke Scale, recurrent stroke, and serious adverse events.
Results: Our analysis included 23,358 participants from 26 trials. Pooled results showed that early BP reduction was not associated with significant decrease in disability or death (mRS⩾3) at 90 days or the end of the trial (RR, 1.03; 95% CI, 0.97-1.10; P=0.28), all-cause death at 90 days or the end of the trial (RR, 1.04; 95% CI, 0.94-1.15; P = 0.42), NIHSS at two weeks (MD, 0.58; 95% CI, -1.40 to 2.56; P=0.57), recurrent stroke at one week (RR, 1.42; 95% CI, 0.49-4.11; P=0.52), and SAE within two weeks (RR, 1.40; 95% CI, 0.67-2.96; P=0.37). There was also no significant difference in disability or death (mRS⩾3) at 90 days or the end of the trial in subgroups with thrombolysis/thrombectomy treatment (P=0.37).
Conclusions: Early BP reduction is safe for AIS patients. However, its efficacy should be verified further.
Disclosures of Interest: No
Abstract N°: 1955
EFFECTIVENESS OF ONE-STOP MANAGEMENT WITH ANGIO-CT ROOM FOR TREATMENT OF ACUTE ISCHAEMIC STROKE
1Shinyurigaoka General Hospital, Neurosurgery, Kawasaki, Japan, 2Saitama Medical University International Medical Center, Neurology, Hidaka, Japan
On behalf of:
Background and aims: One-stop management has been proposed to reduce the treatment time for mechanical thrombectomy (MT) for acute ischemic stroke (AIS). Interventional Radiology-Computed Tomography (IVR-CT) system allows for a head to chest CT to diagnosis ischemic stroke using CT perfusion, and pneumonia, and MT, all in one room. It is advantageous to ensure safety of the patient and healthcare workers in COVID-19 pandemic. This study was conducted to determine whether a one-stop management using IVR-CT system can reduce the intrahospital time for MT.
Methods: This is a retrospective study, conducted between April 2020 and June 2023, in a single institute. Patients with anterior circulation occlusion, who underwent MT within 6 hours after symptom onset or with unknown onset time within 24 hours from the last known well, were enrolled. The outcomes between the one-stop management group and the conventional management group were compared.
Results: A total of 62 consecutive AIS patients who underwent MT were enrolled. The one-stop management group demonstrated significantly shorter door-to-puncture (DTP) and door-to-recanalisation (DTR) time compared to conventional management group. The DTP (median, IQR) was 52.5 (46-63) vs. 86.5 (73-128) min. (P<0.01). DTR (median, IQR) was 118 (97-139) vs. 186 (141-215) min. (P<0.01). Favourable outcomes (mRS0-2) were 57.1 vs. 30.1%, (P=0.03) at 90 days. Adequate reperfusion (TICI>2b; 78.5 vs. 78.1 %) was not significantly different between the groups.
Conclusions: One-stop management with IVR-CT system minimises patients pre-examination flow lines which in effect reduces treatment time and ensures patients and healthcare workers safety.
Disclosures of Interest: No
Abstract N°: 2753
TRENDS IN BASILAR ARTERY OCCLUSION TREATMENT. A 13 YEAR RETROSPECTIVE REVIEW
Andres Paipa*1, Helena Quesada1, Blanca Lara Rodriguez1, Ana Núñez-Guillén1, Maria Angels de Miquel1, Lucia Aja1, Oscar Chirife1, Victor Cuba1, Sonia Aixut1, Pere Cardona1
1Hospital Universitari de Bellvitge, Stroke Unit, L'Hospitalet de Llobregat, Spain
On behalf of:
Background and aims: TRENDS IN BASILAR ARTERY OCCLUSION TREATMENT. A 13 YEARS RETROSPECTIVE REVIEW.
Basilar Artery occlusion is an infrequent cause of ischemic stroke. Up until recently, lack of randomized trials in this population made mechanical thrombectomy a compasive use in view of poor natural history. We review our experience and change of practice over the last decade.
Methods: We reviewed a total of 2146 stroke patient with large vessel occlusion treated with thrombectomy,. A total of 190 patients (8.8%) presented with basilar artery occlusion.
Results: No significant differences were found in terms of age, sex, vascular risk factors, presence of atrial fibrillation or anticoagulation prescription. Basilar occlusion patients were less likely to receive tpa (42% vs 27%) due to orotaqueal intubation and unconsciousness at time of arrival and had higher NIHSS scores.
Overall, the percentage of treated basilar artery remained stable overtime, while total thrombectomies increased, reflecting more ample indications for anterior circulation stroke treatment (Figure 1).
A significant improvement on recanalization rates was seen starting 2015, reflecting the more systematic use of stent retriever plus aspiration technique (Figure 2).
Overall, mortality remained higher for basilar artery patients (40% vs 16%).
Conclusions: The increased number of overall stroke interventionism with newer devices has not resulted in an increase of basilar artery occlusion treatments. While better recanalization rate has been achieved, it remains associated with severe morbidity and mortality.
Disclosures of Interest: No
Abstract N°: 3058
IMPROVING STROKE CARE EFFICIENCY: THE IMPACT OF CLINICAL VIDEO ASSESSMENT FOR STROKE (CVAS) IN EMERGENCY DEPARTMENTS
Chak Lam Ip*1, Ian Norris2, Rob Simister1
1National Hospital for Neurology and Neurosurgery, United Kingdom, 2Barking, Havering And Redbridge University Hospitals Nhs Trust, United Kingdom
On behalf of:
Background and aims: In the UK, hyperacute stroke units (HASUs) provide emergency stroke care. Pre-hospital Clinical Video Assessment of possible Stroke (CVAS) improves patient selection and to improve in-hospital stroke treatment times in north London. We aimed to assess the impact of CVAS on Emergency Department flow in one of our participating HASU containing hospitals.
Methods: We reviewed every case referred to the HASU stroke team at Queens Hospital in north London from 1st to 27th March 2023 through three possible referral routes: (1) following prior CVAS contact (CVAS), (2) via non-CVAS emergency ambulance “blue-light” conveyance with ED pre-alert (BLUE-LIGHT) or (3) following non “blue-light” ambulance conveyance or through self-presentation (OTHER).
Results: Between the study dates, 117 patient referrals were accepted through the specified sources: 23 CVAS, 51 BLUE-LIGHT, and 43 OTHER. Median time to first stroke review in each group was 0,0 and 336 minutes and median time to CT scan was 37, 33 and 179 minutes respectively whilst median time to discharge from ED was 330, 161 and 553 minutes. Mimic rate was lowest at 38% following CVAS versus 58% and 53% in the other two groups. Comparison of CVAS versus BLUE-LIGHT revealed no significant differences. CVAS metrics were significantly shorter for time-to-review (p<0.001), time-to-scan (p<0.001) and time-to-disposal (p=0.003).
Conclusions: Pre-hospital CVAS improved ED assessment times for non-emergency presentations and reduces mimic rates. Ambulance conveyed emergency arrivals to the ED and CVAS patients were both seen rapidly on arrival but were more likely to be mimics without CVAS.
Disclosures of Interest: No
Abstract N°: 3106
THROMBECTOMY IN THE ELDERLY : WHICH FACTORS IMPACT THE OUTCOME? RESULTS FROM A 10 YEARS PROSPECTIVE MONO CENTRE REGISTRY
Manar Abomulay*1, François Delvoye1, Carla Ciobanu1, Philippe Desfontaines1
1Clinical Chc Montlégia, Neurology, Comprehensive Stroke Unit, Liège, Belgium
On behalf of:
Background and aims: Little is known about the benefit of thrombectomy and factors impacting outcome in the octogerians (OC) and nonagerians (NO). We compare the outcome with the population under 80 years (YO) and point out the impacting factors.
Methods: We reviewed data from our prospective registry of thrombectomy between 2012 and 2023. We evaluated the association between recanalization (TICI score) and outcome assessed by the modified Rankin scale (mRS) for patients with proximal occlusion. Good outcome (GO) was mRS between 0-3. Demographic predictors including NIH Stroke Scale at admission and procedural predictors was evaluated. Student t test was used for statistical analysis.
Results: Among 642 patients, 38 (5.9%) were nonagerians and 145 (22.5%) were octogerians. Mean NIHSS was similar for all groups (13.5 +/- 1). The rate of good recanalization (TICI >/=2) was significantly lower (p < 0.01) in NO (65%, n=25/38) than in OC (85.7%, n=114/138) and in YO (76.9%, n=310/403). GO was significantly lower (p < 0.0001) in NO (28.9%, n=11/38) and in OC (31.7%, n=46/145) than in YO (59.8%, n=201/336). None of the NO and OC patients with TICI < 2b has a GO. When TICI is >/=2b, the number of GO is higher in OC (34%, n=46/133) than in NO (29%, n=11/37) but not statistically significant (p = 0.08).
Conclusions: In our prospective registry, good recanalization (TICI >/= 2b) seems to be the main impact factor for a good outcome in nonagerians and octogerians. The overall good outcome remains significantly lower than in younger population.
Disclosures of Interest: No
Paper Poster – Imaging
Abstract N°: 838
DEEP LEARNING-BASED CLASSIFICATION OF DIFFUSION-WEIGHTED IMAGING–FLUID-ATTENUATED INVERSION RECOVERY MISMATCH
Joon-seok Jang*1, Seongho Park1
1Inje University Haeundae Paik Hospital, Neurology, Busan, South Korea
On behalf of:
Background and aims: The presence of a diffusion-weighted imaging (DWI)–fluid-attenuated inversion recovery (FLAIR) mismatch can be utilized to identify patients who may benefit from intravenous thrombolytic treatment in situations where the onset time is uncertain. However, the visual assessment of DWI-FLAIR mismatch (DFM) is subject to limitations due to variability among raters, affecting accuracy and consistency. To overcome these challenges, we aimed to develop and validate a deep learning-based classifier to categorize DFM.
Methods: We screened all acute ischemic stroke patients who underwent DWI and FLAIR imaging from a multicenter stroke registry. To establish a reliable ground truth label for DFM, five stroke neurologists performed joint reviews until reaching a consensus, followed by independent reviews. A Convolution Neural Networks-based binary classification algorithm was developed for the secured labels, and its performance was validated using the K-fold cross-validation method.
Results: A total of 2,369 patients were included in the analysis, with 926 showing DWI-FLAIR mismatch and 1,443 matches. The Fleiss Kappa for the agreed-upon labeling among multiple raters was 0.911. The model's performance in classifying DFM in the test set was confirmed with an AUC of 0.87. The calibration slope showed minimal difference between the predicted and observed probability of DFM. The Brier score was 0.02.
Conclusions: Our study showed that the deep learning model reliably classified DFM. This approach offers a more objective tool for clinicians, especially in cases of uncertainty in DFM assessment, and has the potential to aid in selecting patients who would benefit from recanalization therapy.
Ethem Murat Arsava*1, Ezgi Yilmaz1, Ezgi Demirel Ozbek1, Ozlem Aykac2, Zehra Uysal Kocabas2, Baki Dogan3, Murat Polat3, Atilla Ozcan Ozdemir2, Levent Gungor3, Mehmet Akif Topcuoglu1
1Hacettepe University Faculty of Medicine, Neurology, Ankara, Turkey, 2Eskisehir Osmangazi University Faculty of Medicine, Neurology, Eskisehir, Turkey, 3Ondokuz Mayıs University, Faculty of Medicine, Neurology, Samsun, Turkey
On behalf of:
Background and aims: The adequacy of leptomeningeal collateral circulation is variable among stroke patients and is regarded as one of the most critical factors determining tissue and clinical outcome in large vessel occlusions. Herein we assessed how pre-stroke frailty, an aging-related syndrome characterized by loss in the physiologic reserve of numerous body functions, affected the degree of leptomeningeal collateral flow in the setting of acute ischemic stroke.
Methods: A consecutive series of patients with proximal MCA occlusion [n=116; median (IQR) age 78 (71-84) years; 60% female] were enrolled in this prospective, multi-center observational study. Collateral flow was determined by the Regional Leptomeningeal Collateral (rLMC) Score on admission CTA images. Pre-stroke frailty was assessed by the Edmonton Frailty Scale (EFS), based on the information obtained from the relatives of patients. The relationship between collateral flow and frailty was evaluated by bivariate and multivariate analyses taking into consideration the demographic, clinical, and imaging characteristics of patients.
Results: The EFS scores were negatively correlated with rLMC scores on a continuous scale (r=-0.264; p=0.004). A vulnerable or frail (EFS⩾6) status before stroke, imaging studies performed at an earlier phase after contrast injection, and thrombi extending to the proximal half of the M1 portion of MCA were factors significantly related to poor collateral circulation (rLMC score ⩽10). In multivariable analysis, a vulnerable/frail status remained independently associated with poor leptomeningeal collateral flow [OR 2.8 (95%CI 1.2-6.7); p=0.023].
Conclusions: Our findings highlight that the leptomeningeal collateral flow is compromised as part of the diminished physiologic reserve characterizing the frailty status.
Disclosures of Interest: No
Abstract N°: 699
COMPUTED TOMOGRAPHY PERFUSION AS AN EARLY PREDICTOR OF MALIGNANT CEREBRAL INFARCTION
Alejandro Rodríguez Vázquez*1, Carlos Laredo2, Antonio Doncel-Moriano1, Ramón Torné3, Salvatore Rudilosso1, Laura Llull1, Arturo Renú1, Sergio Amaro1, Ángel Chamorro1, Xabier Urra1
1Hospital Clínic de Barcelona, Neurology, Barcelona, Spain, 2Hospital Clínic de Barcelona, Barcelona, Spain, 3Hospital Clínic de Barcelona, Neurosurgery, Barcelona, Spain
On behalf of:
Background and aims: Malignant middle cerebral artery infarction (MCI) necessitates rapid intervention. This study aimed to enhance early MCI diagnosis using computed tomography perfusion (CTP) with varied quantitative benchmarks and segmentation approaches.
Methods: We analyzed 253 patients from a single-center registry presenting with acute, severe proximal large vessel occlusion and available whole-brain CTP imaging. MCI was defined by clinical and imaging criteria, including decreased level of consciousness, anisocoria, death due to cerebral edema, or need for decompressive craniectomy, together with midline shift >5 mm, or infarction of more than 50% of the MCA territory. The predictive accuracy of CTP quantifications for MCI was assessed by receiver operating characteristic (ROC) area under the curve (AUC) and F-score was calculated as an indicator of precision and sensitivity.
Results: Of the cohort, 63 patients (25%) fulfilled MCI criteria. These patients had notably worse clinical and imaging indicators than the non-MCI group. The AUC for MCI prediction was 0.75 using baseline ASPECTS (F-score 0.52), which significantly increased to 0.80 with a cerebral blood flow threshold <35% (F-score 0.64). Grey and white matter-specific thresholds yielded a marginal AUC increase of 0.81. Relative cerebral blood volume obtained better results with an AUC 0.87 (F-score 0.67) for 40% and 45% thresholds.
Conclusions: CTP-based core quantifications provide better MCI prediction than NCCT ASPECTS scores, potentially improving patient monitoring and accelerating the management of life-threatening edema in severe ischemic stroke.
Disclosures of Interest: No
Abstract N°: 740
DEEP LEARNING-BASED PREDICTION OF FINAL INFARCT CORE FROM CT PERFUSION DATA: A COMPARISON TO THE CLINICAL STANDARD
Freda Werdiger*1, Andrew Bivard1, Milanka Visser1, Chushuang Chen2, Christina Lam2, James Kolacz1, Mark Parsons3,4, Longting Lin3, /Christopher Levi/5
1The University of Melbourne, The Royal Melbourne Hospital, Medicine and Neurology, Parkville, Australia, 2The Royal Melbourne Hospital, Neurology, Parkville, Australia, 3Ingham Institute for Applied Medical Research, Southwestern Sydney Clinical School, University of New South Wales, Liverpool, Australia, 4Liverpool Hospital, Neurology, Liverpool, Australia, 5John Hunter Hospital, University of Newcastle, Neurology, Newcastle, Australia
On behalf of: INSPIRE (International Stroke Perfusion Imaging REgistry) Study Group
Background and aims: CT perfusion (CTP) imaging is used in cases of acute ischemic stroke to predict response to treatment. Single value thresholds are applied to CTP-derived maps to estimate tissue response from ischemic core and penumbra. However, this potentially discards valuable data and oversimplifies core and penumbral estimation. Advancing the dichotomous output to a probability model has several advantages such as more sophisticated modelling of pathophysiology and assessing more data to estimate tissue fate. Here we use Deep Learning (DL) to develop such a model and compare it with a threshold-based model, used in a clinical setting.
Methods: Patients from the INSPIRE database were included if they had baseline CTP, a Large Vessel Occlusion which recanalized fully after thrombectomy and follow-up diffusion-weighted imaging. Data was split into training, validation, and testing groups. Training and validation cohorts were used to develop a DL model and performance metrics were derived from the testing set.
Results: Overall, 243 patients were included. The Attention U-Net produced the best prediction of follow-up infarct core on the test set (n=48): mean Dice=0.430±0.213, mean ROC-AUC=0.765±0.095; outperforming the threshold model with a Dice of 0.247±0.167 (paired t-test, p<0.0001) and AUC of 0.604±0.074 (p<0.0001).
Conclusions: The Deep Learning probabilistic CTP model outperformed the current clinical standard, providing a more accurate core estimate than threshold-based measures and demonstrating the potential of DL to improve on current standards.
Individual scores for Deep Learning (DL) probability bands (< 50%, < 70%, < 90% probability of infarct) and single-value thresholding (SVT).
Disclosures of Interest: No
Abstract N°: 1061
EMU ELECTROMAGNETIC BRAIN IMAGING DEVICE IN ACUTE ISCHAEMIC AND HAEMORRHAGIC STROKE
Angela Dos Santos*1,2, Dennis Cordato3, Michael Devlin4, Christian Wight5, Murat Muradoglu5, Zili Xu5, Anna Balabanski1, Andrew Bivard1, Stephen Davis1, Geoffrey A. Donnan1
1Australian Stroke Alliance, Melbourne, Australia, 2University of New South Wales, Randwick, Australia, 3Liverpool Hospital, Liverpool, Australia, 4Princess Alexandra Hospital, Woolloongabba, Australia, 5EMVision Medical Devices Ltd (ASX:EMV), Macquarie Park, Australia
On behalf of:
Background and aims: Mobile CT scanners weigh over 500kg. The Australian Stroke Alliance is collaborating with EMVision to deliver pre-hospital stroke care. EMVision has developed emuTM, a lightweight, portable and affordable electromagnetic imaging device leveraging ultra-high frequency radio signals. It aims to support earlier diagnosis and therefore earlier care of stroke patients. The study aims to acquire brain scans using emuTM and CT/MRI in healthy patients, acute ischaemic and haemorrhagic stroke, and stroke mimics to advance the AI algorithms.
Methods: A 3-stage, multi-centre clinical study was undertaken to acquire matching emu™ and CT/MRI scans. Stage 1 (usability) involved 30 healthy participants. Stage 2 (data collection) involved patients presenting to emergency departments with suspected stroke and includes a minimum 15 haemorrhagic, 15 ischaemic, and various stroke mimics. Stage 3 (verification) continues recruitment of all suspected stroke patients until up to a further 30 haemorrhagic stroke patients are recruited.
All data will be summarized descriptively. Scan data will be used for AI algorithm training and preliminary analysis.
Results: Stage 1 is complete (30 healthy participants aged 63.8 ± 9.29 years). Stage 2 includes 179 patients aged 67.3 ± 15.03 years (93 acute stroke, 18 transient ischaemic attack and 68 mimics). Stage 3 is in progress. No device related adverse events occurred.
Data has been incorporated into AI algorithm advancement. Data from each completed stage will be presented.
Conclusions: The emu™ has further advanced its AI algorithms. A validation study will determine the technology’s potential in a pre-hospital setting to accelerate stroke care.
Disclosures of Interest: No
Abstract N°: 1767
INITIAL CORE VOLUME ASSESSMENT-BASED MACHINE LEARNING ON NON-CONTRAST CT AS A SURROGATE PREDICTOR OF EARLY CLINICAL OUTCOME IN REPERFUSION TREATMENT
Alan Alberto Flores*1, Marta Olive Gadea2, Laia Sero Ballesteros1, Xavier Ustrell Roig1, Ylenia Avivar Saez1, Pere Canals Canals2, Anna Pellisé1, Edgardo Estrada1, Marc Ribo2
1Hospital Universitari de Tarragona Joan XXIII, Stroke Unit, Tarragona, Spain, 2Vall d'Hebron University Hospital, Stroke Unit, Barcelona, Spain
On behalf of:
Background and aims: Among patient candidates for reperfusion treatment, initial core volume (ICV) estimation is helpful for prognostic. We aimed to determine the relation between automated ICV (auto-ICV) assessment-based on machine learning algorithm on non-contrast computed tomography (NCCT) on early clinical outcomes in reperfusion treatment patients.
Methods: Consecutive reperfusion treatment patients were collected from a prospective registry of two stroke-centers (Jan-2022 Dec-2023). ICV on Computed Tomography Perfusion (CTP-ICV) was defined as relative Cerebral Blood Flow<30%. Auto-ICV was predicted on baseline-NCCT by an algorithm (Methinks-AI) trained using UNet architecture with ResNet 34 encoder. Clinical improvement was defined as ⩾8-points drop in NIHSS or 0-1 at 5thday. Final infarct volume was measured on NCCT at 24-36hours.
Results: From 517 treated patients, mean age was 72.7±13.4 SD, median baseline NIHSS 9[IQR:5-17], 259 cases (50%) received thrombectomy. Clinical improvement was observed in 49.1%(n=254). Auto-ICV correlated significantly with ASPECTS (r=-0.624, p<0.001) and CTP-ICV (r=0.292, p<0.001).
Clinical improvement was associated with lower auto-ICV (mean cc; 17.1±29.9 vs. 24.4± 32.9, p=0.02) and CTP-ICV volumes (4.75±12.8 vs 9.27±20.1, p=0.005) but not with ASPECTS (median score:10 vs 10, p=0.158). In a logistic regression adjusted to sex, age, and baseline NIHSS, lower CTP-ICV volume (OR:0.982, CI95%:0.961-0.997, p=0.049) and auto-ICV (OR:0.991, 95%CI:0.983-0.999, p=0.026) emerged as independent predictors of clinical improvement. Final infarct volume was correlated with auto-ICV (r=0.371, p<0.001).
Conclusions: In patients receiving reperfusion treatments, the accuracy in predicting clinical improvement of a machine learning auto-ICV predictor was similar to CTP-ICV thresholds. Further studies exploring the impact of auto-ICV assessment in clinical practice are warranted.
Disclosures of Interest: No
Abstract N°: 1996
DARK DIFFUSION SIGN : A NOVEL MRI PREDICTOR OF HAEMORRHAGIC TRANSFORMATION IN STROKE PATIENTS TREATED WITH ENDOVASCULAR THERAPY?
Victoire Lyon1, Nicolas Raposo2, Fabrice Bonneville2, Rousseau Vanessa2, Chloé Galmiche1, Thomas Tourdias1, Jean-Marc Olivot2, Igor Sibon*1
1Hospital Pellegrin Bordeaux, Neurology, Bordeaux, France, 2Hospital Center University De Toulouse, Neurology, Toulouse, France
On behalf of: FRAME Investigators
Background and aims: Intracerebral haemorrhagic transformation (HT) is associated with poor functional outcome and increased mortality following reperfusion therapies. We identified a novel imaging marker on brain MRI – named Dark Diffusion Sign (DDS) – as potential risk factor of HT following endovascular reperfusion. DDS is characterized by a lenticular infarct with heterogeneous signal on Diffusion Weighted Imaging appearing as hypointense signal surrounded by an hyperintense signal without evidence of bleeding (see figure).
In the prospective observational FRAME cohort study, we evaluated whether the presence of DDS on pre-treatment MRI was an independent predictor of HT following endovascular therapy.
Methods: Participants from the FRAME study with acute ischemic stroke due to large vessel occlusion treated with endovascular therapy within 6h and available pre-treatment MRI were included. DDS and HT were evaluated by two independent readers. Univariable and multivariable analyses were used to assess the association of DDS on pre-treatment MRI with post-treatment HT within the lenticular nucleus at 24h.
Results: 127 patients were included. 57 patients (44.9%) showed DDS on baseline MRI with an inter-rater Kappa of 95.35 [90.85;99.85]. HT in the lenticular nucleus occurred in 55 patients (43%) within 24h following endovascular therapy. DDS was present in 36 patients (65.5%) who experienced post-treatment lenticular nucleus HT compared to 21 (29,2%) in those without HT (p=0.0001). DDS was independently associated with HT in lenticular nucleus at 24h (OR:4.52;IC95%:1.89-11.37;p=0.0009).
Conclusions: In our population, DDS on pretreatment imaging is frequent and associated with the risk of HT. Pathophysiological mechanisms underlying this novel MRI predictor remain to be investigated.
Disclosures of Interest: No
Abstract N°: 2261
THE ROLE OF CT PERFUSION IN THE DIAGNOSIS OF STROKE MIMICS IN THE EARLY TIME WINDOW: A RETROSPECTIVE SINGLE-CENTRE STUDY
Sebastiano Giacomozzi*1, Giacomo Urbinati1, Alice Marucci2, Luana Gentile3, Matteo Paolucci3, Silvia Stagni4, Elisa Sessagesimi4, Stefano Forlivesi3, Luigi Simonetti4, Andrea Zini3
1Department of Biomedical and Neuromotor Sciences (DIBINEM), Alma Mater Studiorum-University of Bologna, Bologna, Italy, 2Department of Medical and Surgical Sciences (DIMEC), Alma Mater Studiorum-University of Bologna, Bologna, Italy, 3IRCCS Istituto delle Scienze Neurologiche di Bologna, UOC Neurologia e Rete Stroke Metropolitana, Ospedale Maggiore, Bologna, Italy, 4IRCCS Istituto delle Scienze Neurologiche di Bologna, UO Neuroradiologia, Ospedale Maggiore, Bologna, Italy
On behalf of:
Background and aims: Stroke mimics are non-ischemic conditions that can clinically mimic a stroke, representing a diagnostic challenge in the hyperacute setting. To avoid unnecessary and potentially dangerous therapy, is essential to promptly recognize these disorders. We investigate the role of the multimodal Computed Tomography (CT) scan, with special attention to CT Perfusion (CTP), in distinguishing between stroke mimics and acute ischemic strokes in the early time window.
Methods: We retrospectively included consecutive patients admitted to our hospital with suspected acute ischemic stroke within a known onset time of 4.5 hours, during the period July 2021-August 2022. All included subjects underwent multimodal CT scan (non contrast CT, multiphase CT Angiography and CTP) in the acute setting and follow-up neuroimaging at 24-48 hours. We conducted an analysis of clinical and neuroradiological characteristics between stroke mimic patients and ischemic stroke patients.
Results: Among 356 subjects, 49 (13.7%) received a final diagnosis of stroke mimic. CTP core expressed as CBF<30% and the final infarct volume (FIV) of the ischemic lesion significantly differed between the two groups. Noteworthy, among stroke mimics patients, only 3 cases showed a perfusion mismatch, easily identifiable as acquisition artifact. The absence of perfusion mismatch in multimodal CT scan has been considered the primary exclusion criterion from intravenous thrombolysis in 26 patients with final diagnosis of stroke mimic (53.1%).
Conclusions: CT perfusion plays a relevant role in identifying stroke mimics in the emergency setting, even in the early time window.
Disclosures of Interest: No
Abstract N°: 2588
LARGE VESSEL OCCLUSION DETECTION IN ACUTE ISCHEMIC STROKE USING NON-CONTRAST CT
ANSAAR RAI*1, Abdulrahman Al Halak2, Thanh N. Nguyen3, Mohamad Abdalkader3, David F. Kallmes4, Waleed Brinjikji4, Alistair Perry5, Zoe Woodhead5, George Harston5,6, Davide Carone5,6,7
1West Virginia University, Rockefeller Neuroscience Institute, Morgantown, United States, 2West Virginia University, Department of Neuroradiology, Morgantown, United States, 3Boston Medical Center, Boston, United States, 4Mayo Clinic Rochester, Rochester, United States, 5Brainomix Limited, Oxford, United Kingdom, 6Oxford University Hospitals NHSFT, Oxford, United Kingdom, 7University of Oxford, Radcliffe Department of Medicine, Oxford, United Kingdom
On behalf of:
Background and aims: This study validated performance of Brainomix 360 Triage Stroke, an FDA-cleared AI-driven software for detection of large vessel occlusions (LVO) on acute stroke non-contrast CT (NCCT).
Methods: Performance was quantified in terms of sensitivity, specificity and positive/negative predictive values modeled on LVO prevalence in two independent datasets from US hospitals. In dataset-A, Triage Stroke’s performance was compared to that of human radiologists. In dataset-B, Triage Stroke was compared to clinical scores and Brainomix 360 Triage LVO, which uses CT angiography to identify suspected LVO.
Results: In dataset-A (112 LVOs, 115 controls), Triage Stroke outperformed radiologists (sensitivity: 69% vs 48%, specificity: 90% vs 89%). In dataset-B (192 LVOs, 193 controls), Triage Stroke performed similarly and outperformed NIHSS. The combination of NIHSS and Triage Stroke increased specificity and PPV for LVO detection. As expected, Triage LVO showed the best performance.
Conclusions: Triage Stroke identified up to 70% of all LVOs whilst retaining high specificity and PPV. Whilst less accurate than using CTA imaging, the device outperformed radiologists and clinical scores and may help centers without access to angiography to identify thrombectomy candidates whilst keeping futile transfers to a minimum.
Disclosures of Interest: Yes AP, ZW, DC and GH are employed by and have share options in Brainomix
Abstract N°: 3198
MAPPING THE HUMAN COLLATEROME IN ACUTE STROKE WITH PERFUSION MRI: OUTCOME-RELEVANT SPATIAL PATTERNS
Alexander Seiler*1, Niklas Helwig2, Marlies Wagner3
1Universitätsklinikum Schleswig-Holstein, Campus Kiel, Neurology, Kiel, Germany, 2Frankfurt University Hospital, Neurology, Frankfurt am Main, Germany, 3Frankfurt University Hospital, Neuroradiology, Frankfurt am Main, Germany
On behalf of:
Background and aims: Despite the fundamental role of pial collaterals in acute ischemic stroke due to large-vessel occlusion (LVO), their direct appearance is underappreciated and outcome-relevant spatial patterns of favorable collateral supply on the cross-sectional level are not well established. We aimed to identify spatial patterns of collateral flow associated with favorable outcome in patients with LVO, using signal variance in magnetic resonance perfusion-weighted imaging (PWI) for automatic segmentation of leptomeningeal collaterals.
Methods: 156 patients (mean age 69.3 ± 15.8 years) with LVO of the anterior circulation were included. T2*-weighted time series from dynamic susceptibility contrast PWI were processed to compute individual maps of leptomeningeal collaterals. Collateral vessel maps of the entire cohort were normalized to standard space and assessed for voxel-wise associations of the collateral vasculature with favorable functional outcome (modified Rankin scale (mRS) score of 0–2) at discharge on the cross-sectional level.
Results: At a significance level of p<0.01 after correction for multiple comparisons, distribution patterns of outcome-relevant collateral flow could be identified, which included pial collateral supply adjacent to the Sylvian fissure, frontal operculum, temporal lobe and the central region of the affected hemisphere. Furthermore, significant associations with favorable early functional outcome were found also on the contralateral unaffected side.
Conclusions: The segmentation of pial collateral vessels based on signal variance in PWI allows for a systematic evaluation of collateral flow patterns associated with early functional outcome on the cross-sectional level. The presented methodology might be useful for future clinical stroke trials and further characterization of pial collateralization as prognostic imaging biomarker.
Disclosures of Interest: No
Abstract N°: 769
ASSOCIATION BETWEEN PERFUSION OF DIFFERENT BRAIN REGIONS AND HEMORRHAGIC TRANSFORMATION AFTER REPERFUSION THERAPY OF ACUTE ISCHEMIC STROKE PATIENTS
Background and aims: To explore the association of cerebral blood flow (CBF) of different brain regions with hemorrhagic transformation (HT) in acute ischemic stroke (AIS) patients with large vessel occlusion.
Methods: AIS patients from the randomized controlled trial with vessel occlusion in the anterior circulation and received reperfusion therapy within 24 hours were included. HT was evaluated using 24-hour repeated CT. CT perfusion source images were post-processed with F-STROKE and co-registered to the Alberta Stroke Program Early CT Score (ASPECTS) template. Absolute CBF was calculated separately and the ratio of CBF on the affected to the contralateral side was defined as the CBF mirror index (CBFmi). Stepwise regression analysis was used to explore the independent variables and receiver operating characteristic (ROC) curve analysis was used to explore the optimal cutoff of regional CBFmi predicting HT.
Results: A total number of 141 patients(age, 67 (57-73)years; 42 [30%] women) were included and 39 patients (27.7%) developed HT. Stepwise logistic regression analysis revealed that a lower CBFmi of the lentiform (L-CBFmi) was associated with an increased risk of any HT(OR= 0.01, 95%CI: 0.001-0.119, P<0.001). L-CBFmi <0.80 was defined as unfavorable according to ROC analysis. An unfavorable perfusion of lentiform was revealed as an independent risk factor for any HT (OR=6.41, 95%CI: 2.48-16.60, P<0.001) and parenchymal hematoma (OR=8.82, 95%CI: 2.61-29.81, P<0.001).
Conclusions: An unfavorable perfusion of lentiform was correlated with increased risk of HT after reperfusion therapy of stroke patients with large vessel occlusion.
Disclosures of Interest: No
Abstract N°: 835
INFARCT GROWTH ON DWI IS A STRONG PREDICTOR FOR FAVORABLE OUTCOME IN ACUTE STROKE PATIENTS RECEIVED ENDOVASCULAR TREATMENT
Background and aims: Diffusion-weighted imaging (DWI) clearly depicts ischemic lesion, and past studies reported various DWI lesion changes following reperfusion therapy. However, the prognostic value of such difference in DWI lesion between initial and follow-up (infarct growth [IG]) for functional outcome in patients who received endovascular treatment (EVT) is not well known. The aims of the present study were to elucidate the relationship between IG and favorable outcome (defined as mRS score 0-2) at 3 months from stroke onset.
Methods: Among consecutive acute stroke patients received EVT from September 2014 through December 2019, pre-morbidly independent (mRS score 0-2) patients were enrolled. DWI was performed on admission and 24 hours after onset. IG was calculated as the difference between infarct volume on DWI 24 hours after onset and that on initial DWI. Factors associated with favorable outcome 3 months after stroke onset were assessed using multivariable analyses.
Results: A total of 251 patients (165 male [66%], median age 75 [IQR 67-81] years, median NIHSS score 15 [7-21]) were enrolled in this study. Patients with favorable outcome (n = 136) had lower IG (2.0 [0.1-7.1] cm3) compared to those with unfavorable outcome (n = 115, 14.3 [2.9-46.3] cm3, p <0.001). Multivariate logistic regression analysis revealed IG was an independent predictor for favorable outcome (OR 0.72, 95% CI 0.60-0.86, p <0.001 for every 10cm3 increment), even adjusting various factors including age, initial NIHSS score, successful reperfusion, and symptomatic intracerebral hemorrhage (Figure).
Conclusions: IG is a strong predictor for favorable outcome in acute stroke patients received EVT.
Disclosures of Interest: No
Abstract N°: 918
QUANTITATIVE ASSESSMENT OF NO-REFLOW ZONES PREDICTS INFARCT GROWTH
Keon Mahmoudi1, Elham Tavakol1, Mersedeh Bahr-Hosseini1, Corey Arnold1, Viktor Szeder1, Geoffrey Colby1, Reza Jahan1, Jeffrey Saver1, David Liebeskind1, Kambiz Nael*2
1UCLA Medical Center, Los Angeles, United States, 2University of California San Francisco Parnassus Campus, Radiology, San Francisco, United States
On behalf of: Mahmoudi K, Kim D, Tavakkol E, Qiao J, Bahr-Hosseini M, Apfel R, Alfonso R, Arnold C, Szeder V, Colby GP, Jahan R, Saver JL, Liebeskind DS, Nael K
Background and aims: Persistent micro-occlusions at the ischemic capillary bed also known as the no-reflow phenomenon has been recently investigated as one of the culprits that can result in infarct growth despite thrombectomy. We aimed to quantify the residual no-reflow perfusion in patients who underwent successful angiographic reperfusion and assess its effect on infarct growth.
Methods: In this retrospective study, patients were included who had anterior circulation LVO, successful reperfusion (TICI ³2b), and pre and posttreatment MRI and MR perfusion. Hypoperfusion volume was calculated on Tmax on both pre and post treatment MRP using Olea Sphere (SP23). Infarct growth was calculated on MR diffusion from pre and post treatment MRIs. The association of baseline demographic, clinical, and imaging variables including hypoperfusion volumes was evaluated to predict infarct growth.
Results: Among 104 patients who met inclusion criteria, 32 (31%) patients had infarct growth ⩾ 10 mL. Residual volumes of posttreatment hypoperfusion (no-reflow) were significant (p<0.05) for prediction of infarct growth with area-under-the curve (AUC) values of 0.669, 0.713, and 0.721 for Tmax volumes of > 2, 4, and 6 sec, respectively. Multivariate logistic regression showed Tmax >6 sec volume as the only independent variable for prediction of infarct growth ⩾ 10 mL (p=0.004). Figure shows sensitivity/specificity for prediction of infarct growth using residual Tmax > 6 sec.
Conclusions: In conclusion, no-reflow zones calculated by residual elevation of Tmax following successful angiographic reperfusion are associated with infarct growth. Residual Tmax volume > 6 sec can be an independent predictor of infarct growth.
Disclosures of Interest: Yes Consultant to Olea Medical and Brainomix, none directly relevant to this study
Abstract N°: 569
AUTOMATIC PROXIMAL AND DISTAL THROMBI SEGMENTATION
Sofía Vargas Ibarra*1,2, Vincent Vigneron1,2, Hichem Maaref1,2, Nicolas Chausson2,3, Didier Smadja3, Yann Lhermitte3, Sonia Garcia4
1Laboratoire de Recherche "IBISC" site Pelvoux, Évry-Courcouronnes, France, 2Paris-Saclay University, Orsay, France, 3Hospital Center Sud Francilien, Corbeil-Essonnes, France, 4Telecom SudParis, Évry-Courcouronnes, France
On behalf of:
Background and aims: In stroke patient treatment, timely decision-making is crucial. Identifying, localizing, and measuring occlusive arterial thrombi during initial imaging is a complex but critical step. And even though some image processing methods [1,2] and deep learning models [3] have been proposed for this purpose, all of them use CT images for acute stroke patients. We present a deep-tech artificial intelligence solution that uses MRI images for hyper-acute proximal and distal thrombi.
Methods: Using a database of 150 patients imaged during the hyper-acute phase of a stroke, with lesions and thrombi manually segmented by experts, we trained a model that computes a cross-modality attention between the diffusion modality (DWI) and the susceptibility-weighted modalities to relate the lesion and the thrombi. A recurrent model is then used to transfer the information in between multiple brain slices. Finally, from the distances between the thrombi and the lesion prediction performed by a classic 3D nnUnet [4], we choose the most probable object among the predicted ones.
Results: We are able to detect all the proximal thrombi and more than 90% for the distal ones on the test set. Incorporating the predicted lesion (having a performance of 77% of surface detection (Dice) with the ground-truth and 95% of detection rate) reduces the false positives to zero and identifies 58% and 52% of the surface (Dice) of distal and proximal thrombi respectively in average.
Conclusions: Our automatic deep learning model swiftly detects and segments thrombi in nearly all patients, providing valuable assistance to clinicians in the initial therapeutic decision.
Disclosures of Interest: No
Abstract N°: 881
CONTINUOUS FLAIR-DWI MISMATCH IS A PREDICTOR OF BLEEDING COMPLICATIONS AND MORTALITY AFTER ENDOVASCULAR THERAPY INDEPENDENT OF THROMBOLYSIS
Silvia Ingala*1,2, Kine Bakke3, Thor Håkon Skattør3,4, Terje Nome5, Brian Enriquez4,6, Mads Nielsen2,7,8, Michael Bachmann Nielsen1,9, Thomas Truelsen9,10, Anne Hege Aamodt5,6, Akshay Pai2
1Copenhagen University Hospital Rigshospitalet, Department of Radiology, København, Denmark, 2Cerebriu A/S, København, Denmark, 3Oslo University hospital, Division of Radiology and Nuclear Medicine, Oslo, Norway, 4Oslo University hospital, Institute of Clinical Medicine, Oslo, Norway, 5Oslo University hospital, Department of Neurology, Oslo, Norway, 6Norwegian University of Science and Technology, Norway, 7Datalogisk Institut, Københavns Universitet (DIKU), København, Denmark, 8Pioneer Centre for AI - KU, København, Denmark, 9Copenhagen University, Department of Clinical Medicine, København, Denmark, 10Copenhagen University Hospital, Rigshospitalet, Department of Neurology, København, Denmark
On behalf of: Marko Bauer, Jacob Johansen, Cecilie Mørck Offersen, Jonathan Frederik Carlsen, Atle Bjørnerud
Background and aims: Hemorrhage is a known post-procedural complication after endovascular therapy (EVT), the gold standard reperfusion treatment for acute ischemic stroke (AIS) due to large-vessel occlusion of the anterior circulation. Existing studies evaluate the role of dichotomous FLAIR-DWI mismatch to define eligibility for and potential complications after thrombolysis. This retrospective study investigates the relationship between continuous FLAIR-DWI mismatch (FDM, %), symptomatic bleeding occurrences within 24hrs (SB) and 1-year survival in AIS patients that underwent EVT.
Methods: We included subjects from a regional register of AIS patients treated with EVT in the period 2017-2021. We retrospectively quantified continuous FDM through Apollo Stroke Insight (Cerebriu A/S).SB occurrences were defined as Heidelberg bleeding classification ⩾ 1c and either NIHSS ⩾ 4 at discharge (compared to arrival) or intubation of the patient within 24hrs of EVT. Two logistic regression analyses were performed to investigate whether FDM is associated a) with SB after correcting for age, sex, the administration of intravenous thrombolysis.and and imaging-to-recanalization time; b) 1-year survival after correcting for age, sex, NIHSS at arrival, administration of intravenous thrombolysis, and SB.
Results: A total of 290 subjects were included in this study. Demographics and clinical characteristics are summarized in Table 1. Lower FDM was associated with higher chances of SB and 1-year mortality (p-value < 0.05, Tables 2 and 3, respectively).
Conclusions: In individuals with AIS, automatic quantification of continuous FLAIR-DWI mismatch could assist prognostic stratification of candidates to reperfusion treatments.
Disclosures of Interest: No
Abstract N°: 922
PERFUSION COLLATERAL INDEX PREDICTS INFARCT GROWTH AFTER SUCCESSFUL REPERFUSION IN ACUTE ISCHEMIC STROKE: A MULTICENTER STUDY
Mark Mcarthur1, Daniel Kim1, Elham Tavakol1, Mersedeh Bahr-Hosseini1, Viktor Szeder1, Geoffrey Colby1, Reza Jahan1, Jeffrey Saver1, David Liebeskind1, Kambiz Nael*2
1UCLA Medical Center, Los Angeles, United States, 2University of California San Francisco Parnassus Campus, San Francisco, United States
On behalf of: McArthur M, Kim D, Tavakkol E, Qiao J, Salehi B, Cai S, Ledbetter L, Cankurtaran CZ, Bahr-Hosseini M, Szeder V, Colby GP, Jahan R, Duckwiler G, Saver JL, Liebeskind DS, Nael K
Background and aims: Perfusion Collateral Index (PCI) and Hypoperfusion Intensity Ratio (HIR) have been shown to correlate with angiographic collaterals. We aimed to assess the ability of PCI and HIR to predict infarct growth in anterior circulation large vessel occlusion (AC LVO) patients who underwent successful reperfusion in a multicenter design.
Methods: In this retrospective study, AC LVO stroke patients from 3 institutions were included if they had pretreatment perfusion (CT or MR), successful reperfusion (mTICI >2b), and follow up MRI within 24 hours from treatment. HIR (defined as volume of Tmax >10 sec/volume of Tmax >6 sec) was calculated by RAPID software (Version 5.0.4). PCI (defined as Volume of Delay2–6 seconds x rCBV) was calculated using Olea Sphere (SP23). Infarct growth was calculated by subtracting baseline ischemic core (ADC < 620 × 10−6 mm2/s on MRI or rCBF<30% on CTP) from posttreatment MRI-DWI volume.
Results: A total of 118 patients were included; time from onset to reperfusion (mean ± SD): 378 ± 240 min, 58 patients (49.1%) had infarct growth 10 mL. ROC analysis for prediction of infarct growth 10 mL revealed AUC/sensitivity/specificity of 0.71/60.6/85.1 for PCI< 60, which was significantly (p<0.01) higher than HIR >0.4 (0.50/50.7/42.6) (Figure). Multivariate logistic regression showed PCI and time-to treatment as only independent variables to predict infarct growth.
Conclusions: In patients with AC LVO stroke, poor baseline collateral perfusion defined by PCI<60 predicts infarction growth > 10 mL despite successful reperfusion. PCI was superior to HIR in the prediction of infarct growth.
Disclosures of Interest: Yes Consultant to Olea, Brainomix, not directly relevant to this study.
Abstract N°: 1637
HAMPERED VENOUS EGRESS AFTER SUCCESSFUL THROMBECTOMY CORRELATES WITH POOR CLINICAL OUTCOME
Francesco Favruzzo*1, Alvise Fattorello Salimbeni1, Matteo Zaccagnino1, Alessandra Pes1, Ludovica De Rosa1, Federica Viaro1, Alessio Pieroni1, Stefano Mozzetta1, Francesco Causin2, Claudio Baracchini1
1Padua University Hospital, Stroke Center, 2Padua University Hospital, Institute of Neuroradiology
On behalf of:
Background and aims: Despite timely and complete recanalization by mechanical thrombectomy, less than half of acute ischemic stroke (AIS) patients are functionally independent at three months. The aim of this study was to investigate whether a hampered venous egress from the ischemic brain is associated with a poor prognosis.
Methods: In this longitudinal study on a cohort of consecutive AIS patients due to proximal middle cerebral artery (MCA) occlusion who underwent mechanical thrombectomy successfully, we analyzed post-interventional digital subtraction angiography (DSA) images. The venous drainage from the MCA territory was divided into superficial (vein of Trolard; superficial middle cerebral vein; vein of Labbé; cortical veins) and deep (deep middle cerebral vein, internal cerebral vein, basal vein of Rosenthal, vein of Galen) venous system. Qualitative scores and quantitative scores were obtained to investigate if venous drainage correlates with ischemic lesion volume, hemorrhagic transformation, and clinical outcome.
Results: Fifty patients [females 29 (58%), mean age 77 years, age range 58-90] met the inclusion criteria. Prolonged venous wash-out times predicted ischemic lesion growth (p < 0.01), hemorrhagic transformation (p = 0.04) and poor 90-day functional outcome (p = 0.03).
Conclusions: In this prospective study of acute stroke patients with MCA occlusion treated successfully with mechanical thrombectomy, hampered venous drainage correlated with ischemic lesion growth and hemorrhagic transformation, and predicted a poor prognosis.
Disclosures of Interest: No
Abstract N°: 1796
FLAIR HYPERINTENSE VESSELS SCORE AS A STRONG PREDICTOR OF PERFUSION MISMATCH IN ACUTE STROKE WITH LARGE VESSEL OCCLUSIONS
1University Medical Center Ho Chi Minh City, Neurology, Ho Chi Minh City
On behalf of:
Background and aims: The National Institute of Health FLAIR Hyperintense Vessels score (NIH-FHV) is a promising surrogate for penumbra estimation. We aimed to determine whether NIH-FHV could be used to accurately identify perfusion mismatch in large vessel occlusions (LVO).
Methods: We performed a retrospective cohort of consecutive patients admitted for terminal ICA or proximal MCA occlusions in extended window or with unknown onset, who were initially assessed with MRI perfusion between December 2019 and December 2023. NIH-FHV was scored by two blinded independent raters. Perfusion parameters were calculated using RAPID software.
Results: A total of 90 patients (median age 62.5, 58.8% men) were included. Median onset-to-imaging time was 482 minutes (IQR 336-704). Median NIH-FHV was 7 (IQR 5-7) and median DWI core volume was 19ml (IQR 11-74.8). Intravenous thrombolysis was used in 16 patients (17.8%) with DWI-FLAIR mismatch. By applying either DAWN or DEFUSE 3 criteria, 57 patients (63.3%) had significant penumbra. In univariate and multivariate analysis, FHV mismatch ratio (NIH-FHV divided by DWI volume) has a strong correlation with significant perfusion mismatch. An optimal cutoff at 0.12 yields a sensitivity of 96.5% and specificity of 81.8%. Area under the curve is 0.921. In patients with core volume greater than 50ml, FHV mismatch ratio was low as FHV disappeared on FLAIR-positive lesion with establised edema.
Conclusions: NIH-FHV in combination with DWI core volume can reliably predict significant perfusion mismatch in LVO. In the setting of unknown onset or extended window, conventional MRI appears to be useful in patient selection for both thrombolysis and thrombectomy.
Disclosures of Interest: No
Abstract N°: 2907
EXTRACRANIAL CAROTID ARTERY DISEASE PERFUSION PROFILES IN ACUTE TANDEM LESION ETIOLOGIES
Darko Quispe-Orozco1, Milagros Galecio-Castillo2, Mahmoud Dibas2, Aaron Rodriguez-Calienes2, Santiago Ortega-Gutierrez*2
1Texas Tech University Health Sciences Center, Neurology, United States, 2University of Iowa Hospitals and Clinics, Neurology, United States
On behalf of:
Background and aims: Perfusion imaging has been used to identify collateral status in patients with acute anterior large-vessel occlusion (LVO). We aimed to study the association between perfusion patterns and extracranial ICA etiology in tandem lesion patients before EVT
Methods: We retrospectively reviewed consecutive EVT stroke patients in our registry from January 2019 to December 2022. Inclusion criteria: (1) patients with acute tandem lesion defined as an extracranial ICA 70-100% stenosis per NASCET criteria with concomitant LVO, (2) patients with CTP before EVT. Patients were divided into those with extracranial ICA atherosclerosis versus non-atherosclerosis disease (dissection, embolism, among others). Perfusion parameters including CBF, CVB, Tmax, and Tmax ratios were post-processed using Rapid software. Multivariable logistic regression identified perfusion parameters independently associated with atherosclerotic extracranial ICA
Results: Among all 624 EVT patients, 70 met inclusion criteria. Of these patients (21 women [41.4%]; median age 68 [60-74] years), 46 (66%) had extracranial ICA atherosclerotic disease. The atherosclerotic group had lower Tmax 10s/6s (median 0.31 versus 0.47, p=0.038) and lower Tmax 10s/4s (median 0.16 versus 0.25, p=0.048). After adjusting for age, gender, smoking, hypertension and admission glucose, patients in the atherosclerotic group had significantly lower Tmax 10s/6s (aOR 0.02; 95%CI: 0-0.56) and lower Tmax 10s/4s (aOR 0.01; 95%CI: 0-0.56) compared with the non-atherosclerotic group.
Conclusions: Tandem patients presenting with extracranial ICA atherosclerotic disease had distinct collateral pattern compared to patients with non-atherosclerotic etiology. Early identification of the underlying etiology may help to individualize the EVT cervical approach.
Disclosures of Interest: No
Abstract N°: 1503
RADIOLOGICAL PROGNOSTIC FACTORS IN CEREBRAL VENOUS THROMBOSIS: A MULTICENTER STUDY
Emma Canada Lahoz*1, Jaime Alonso Maroto1, Carlos Gómez-Escalonilla2, Alicia de Felipe3, Patricia Calleja4, Patricia Simal2, Salvador García-Madrona3, David Seoane4, Carmen Ramos Martín1, Santiago Trillo Senín1
1Hospital Universitario de La Princesa, Neurology, Madrid, Spain, 2Hospital Universitario Clínico San Carlos, Madrid, Spain, 3Hospital Universitario Ramón y Cajal, Madrid, Spain, 4Hospital Universitario 12 de Octubre, Madrid, Spain
On behalf of:
Background and aims: Cerebral venous thrombosis (CVT) is an uncommon pathology with variable evolution. Previous studies suggest that radiological presentation could have a prognostic value, although results are diverse. Our objective is to explore the predictive capacity of radiological presentation in prognosis
Methods: We performed a multicenter retrospective study of patients with CVT treated during the acute/subacute phase in 4 Stroke centers, with cerebral CT as the initial diagnostic technique performed within the first 72 hours. CVT was documented in CT angiography, and the severity of edema and hemorrhage was characterized with scales. The association between findings in CT and CT-angiography with the prognosis at 3 months (mRS-3m) was analyzed
Results: Ninety patients were included (55% women, mean age 49, SD 18.77). 43.3% presented with cerebral edema, 38.9% had hemorrhage on CT. Thrombosis was more common in the transverse/sigmoid sinus (83%) and the sagittal sinus in the posterior region (SSP, 53%). An association was found between SSP thrombosis and mRS-3m>2 (p=0.02). A higher thrombotic burden did not correlate with mRS-3m>2. The presence of unilateral edema in >1 lobe was associated with mRS>2 (p=0.03), as well as the presence of hemorrhage (p=0.016). A significant correlation was found between the degree of hemorrhage and mRS-3m>2 (rho=0.23; p=0.036).
Conclusions: Edema and hemorrhage in the initial CT, along with SSP thrombosis, were associated with worse prognosis, representing a risk group for poor outcome with conventional management. A higher thrombotic burden was not associated with worse prognosis, which shifts the focus of our future studies to other prognostic factors.
Disclosures of Interest: No
Abstract N°: 3231
COMPARISON OF THREE CT PERFUSION PROCESSING SOFTWARE SYSTEMS IN ACUTE STROKE
Viveka Biswas*1, Ammad Mahmood1, Amith Sitaram1, Christopher Pollard2, Keith Muir1
1University of Glasgow, United Kingdom, 2N H S Greater Glasgow & Clyde, United Kingdom
On behalf of:
Background and aims: CT perfusion analysis may modify treatment decisions but few comparisons of different software processing have been undertaken. We investigated CTP analyses by three software systems.
Methods: We analysed CTP in patients recruited to a prospective observational imaging study in which patients were imaged within 24 hours onset of AIS symptoms. EVT was not available at the time of recruitment.
CTP was analysed using RAPID version 4.7 (Ischemaview), Brainomix version 11.001 and MiStar version 3.2 (Apollo). Images were uploaded and analysed separately by two users.
Penumbra was defined as delay time [DT]>3 seconds (MiStar) or Tmax>6 seconds, ischaemic core as DT>3 seconds (MiStar) or Tmax>6 seconds and relative cerebral blood flow [CBF]<30%, and eligibility against DEFUSE3 target mismatch criteria was assessed.
CTA were reviewed by two experienced assessors, confirmed by a third assessor. LVO was defined as ICA or M1 occlusion.
Results: Of 185 patients recruited, 174 had a final diagnosis of AIS or TIA. CTP was undertaken before thrombolysis initiation and analysable on all software in 133 patients.
Figure 1 demonstrates pairwise comparison with a Venn diagram representing DEFUSE 3 eligibilty.
Pairwise comparisons showed small absolute volume biases for core and penumbra but wide LOA - wider for penumbra.
Overall agreement for target mismatch was 94%.
Conclusions: CTP processing software exhibited small mean biases for core, and larger bias for penumbra volume estimates, but wide limits of agreement. While overall agreement on target mismatch criteria was high, variation in hypoperfusion volumes may have consequences for individual treatment decisions.
Disclosures of Interest: No
Abstract N°: 50
ARTIFICIAL INTELLIGENCE ALGORITHMS OUTPUT VARIABILITY BETWEEN RAPID AND VIZ.AI
Mohamad Ezzeldin*1, Saif Bushnaq2, Anita Datta3, Ali Kerro4, Adam Deloraa3, Rime Ezzeldin5, Zuhair Ali6, Tunmi Anwoju6, Layla Nejad7, Ameer Hassan7
1HCA Houston Healthcare Kingwood, Neurointerventional Surgery, Houston, United States, 2Texas Tech University Health Sciences Center, Neurology, Lubbock, United States, 3HCA Houston Healthcare Kingwood, Emergency, Houston, United States, 4HCA Houston Healthcare Conroe, Conroe, United States, 5Jordan University of Science & Technology (JUST), Al-Rumtha, Jordan, 6HCA Houston Healthcare Kingwood, Houston, United States, 7Valley Baptist Medical Center: Harlingen Heliport, Harlingen, United States
On behalf of: Rene Silva MD: Rene.silva01@utrgv.edu Neuroscience and Research Department, VBMC, Harlingen, Texas Yazan Diya Abualnadi MD: yazan-dia@hotmail.com Neuroscience and Research Department, VBMC, Harlingen, Texas Zorain Mustafa Khalil MD: zorainmustafa@hotmail.com Neuroscience and Research Department, VBMC, Harlingen, Texas
Background and aims: Investigate the agreement of decision-making outcomes derived from Rapid and Viz.ai software packages and to identify predictors of inadequate quality CT perfusion (CTP) studies.
Methods: 129 Acute ischemic stroke patients who had CTP processed by the two packages were retrospectively analyzed. Volumetric outputs were compared between packages by performing Spearman’s correlation at early (<6 hours) and extended (>6 hours) time windows. Concordance of selecting patients based on DAWN and DEFUSE3 eligibility criteria were assessed using Mcnemar test.
Results: 108 were found to have adequate quality studies. Spearman correlations were calculated on Tmax >6s volume, Tmax >10s volume, CBF <30% volume, Mismatch Volume, Mismatch Ratio, and Hypoperfusion Index between both software packages with correlation coefficients of 0.82, 0.65, 0.77, 0.78, 0.59, 0.47 respectively. The correlation coefficients remained significant at early and extended time windows. Lower ejection fraction (EF) predicted an inadequate study in RAPID (P = 0.018; 95% CI: 0.01, 0.113) and Viz.ai. (P = 0.024; 95% CI: 0.008, 0.109). In Viz.ai, the presence of metal predicted an inadequate study (P = 0.042; 95% CI: -3.225, -0.057). We applied DAWN and DEFUSE3 criteria using both packages to triage LVO patients and performed a Mcnemar test on the confusion matrix and found no significant difference between triaging classification.
Conclusions: Penumbra and infarct core predictions between both softwares correlated well and resulted in equivalent patient triage based on DAWN and DEFUSE3 eligibility criteria. At larger volumes there was increased variability in predictions between the packages. Lower EF led to inadequate CTP quality study.
1The University of Toledo College of Medicine, Neurology, Toledo, United States
On behalf of:
Background and aims: To assess the prognostic values of hyperdense sign on pretreatment non-contrast head CT scan for successful recanalization (mTICI ⩾2b) and 90-day good functional outcome (mRs 0-2) in patients with acute ischemic stroke (AIS) undergoing mechanical thrombectomy (MT).
Methods: Literature search on PubMed, EMBASE and Cochrane databases from inception up to 01 November 2023 was conducted. Twelve studies which reported hyperdense sign, recanalization and clinical outcomes were included in qualitative synthesis and meta-analysis
Results: Pooled analysis demonstrated a statistically significant association between successful recanalization and hyperdense sign-positive patients who underwent MT (OR = 1.47, 95% CI = 1.03-2.10, p = 0.04). There was a tendency toward cardioembolisim as underlying stroke etiology although did not reach statistical significance (OR: 1.43, 95% CI: 0.98-2.07; P=0.06). No statistically significant association was demonstrated between presence of hyperdense sign and good functional outcome (OR = 1.04, 95% CI = 0.72-1.49, p = 0.86) or symptomatic intracranial hemorrhage sICH (OR = 1.79, 95% CI = 0.72-4.44, p = 0.21)
Conclusions: This meta-analysis demonstrated that pre-intervention hyperdense sign on CT imaging might be useful in prediction of successful recanalization after MT
Disclosures of Interest: No
Abstract N°: 382
ASSOCIATION OF ACUTE CEREBRAL SINUS VENOUS THROMBOSIS WITH CEREBRAL BLOOD FLOW DEMONSTRATED BY [15O]WATER PET
Andreas Harloff*1, Ganna Blazhenets2, Johannes Fostitsch2, Christoph Strecker1, Rick Dersch1, Ernst Mayerhofer1, Philipp Meyer2
Background and aims: Cerebral sinus venous thrombosis (CSVT) is a rare but serious cause of stroke. We assessed the association of acute CSVT and cerebral blood flow (CBF) by [15O]water PET.
Methods: Retrospective analysis of 12 patients with CSVT 10.6±4.6 days after symptom onset and ten healthy volunteers who underwent [15O]water PET (two scans each, 300±14 MBq [15O]water). Static image datasets (15-75 seconds after injection; normalized to cerebellum) reflecting relative CBF (rCBF) were analyzed using voxel- and region-of-interest (ROI)-based analysis (AAL3-atlas). Datasets of patients with left-sided CSVT were mirrored to harmonize the affected hemisphere.
Results: Seven and five patients showed right- and left-sided CSVT, respectively. The superior sagittal sinus (SSS) was involved in 8/12 patients. CSVT patients had extensive rCBF deficits in the voxel-based analysis with accentuation in the right frontal cortex and caudate nucleus compared to controls, which were most pronounced in cortical areas in those with involvement of the SSS (8/12), and in subcortical areas in those without involvement of the SSS (4/12; p<0.05, false discovery rate corrected). ROI-analysis demonstrated significant frontal (p=0.014) and caudate nucleus (p=0.011) rCBF deficits driven by patients with and without SSS occlusion, respectively. Additionally, patients without SSS thrombosis showed an occipital rCBF increase (p<0.001).
Conclusions: Patients with acute CSVT exhibit substantial (up to 30%) rCBF alterations, depending on the site of CSVT, providing novel insight into effects of CSVT. These findings may aid in understanding the pathophysiology and guide future therapy of acute CSVT.
Disclosures of Interest: No
Abstract N°: 1821
MYELIN DAMAGE IN GRAY MATTER IS ASSOCIATED WITH STROKE SEVERITY
Cheol-Woon Kim1, Do Yeon Kim2, Joon Yul Choi*1
1Yonsei University, Department of Biomedical Engineering, 2Seoul National University Bundang Hospital, Department of Neurology and Cerebrovascular Center
On behalf of:
Background and aims: We aimed to investigate the association between the quantity of myelin damage in grey matter and initial stroke severity using myelin-enhanced contrast magnetic resonance imaging (MRI).
Methods: Twelve ischemic patients underwent MRI scans including T1-weighted and T2-weighted images. The acquired T1- and T2-weighted images were utilized to derive whole-brain quantitative myelin-enhanced contrast imaging. The grey matter of the whole brain was segmented and the mean myelin-enhanced value (MEV) of grey matter was measured for each subject. Stroke severity was defined as initial National Institute for Health Stroke cale (NIHSS) of the index stroke. Spearman’s correlation analysis was then conducted to explore the association between MEV and NIHSS score.
Results: Figure 1A illustrates representative T1-weighted, T2-weighted, diffusion-weighted and myelin-enhanced images. The mean MEV of the subjects was 1.073 (± 0.253) and the median initial NIHSS was 3 (interquartile range, 2.75 - 5.25). Visual inspection indicates a lower MEV in regions affected by stroke compared to regions not affected by stroke. The correlation analysis reveals significantly negative rho values (rho = -0.587, p = 0.045), demonstrating that more decreased MEVs correspond to higher NIHSS scores (Figure 1B).
Conclusions: The quantity of myelin damage in grey matter was found to be associated with initial stroke severity. Further investigation into the correlation between the topography of myelin damage and neurologic manifestations or outcomes is warranted.
Acknowledgements
This research was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT)(RS-2023-00251484) and (RS-2023-00249098).
Disclosures of Interest: No
Abstract N°: 2375
QUALITATIVE ASSESSMENT OF THROMBUS PERMEABILITY: PATIENTS’, HISTOPATHOLOGICAL, RADIOLOGICAL CHARACTERISTICS AND OUTCOMES
Megi Meneri*1,2, Luca Caschera3, Gianluca Lopez4,5, Giulia Platania3, Giulia Laura Bianchi4, Sara Bonato2, Gianluca Costamagna1,2
1University of Milan, Dino Ferrari Centre, Department of Pathophysiology and Transplantation (DEPT), Milan, Italy, 2Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, Stroke Unit, Neurology Unit, Milan, Italy, 3Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, Neuroradiology Unit, Milan, Italy, 4Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, Division of Pathology, Milan, Italy, 5University of Milan, Department of Biomedical, Surgical and Dental Sciences, Milan, Italy
On behalf of:
Background and aims: Thrombus apperance on computed tomography angiography (CTA) is affected by occlusion site, thrombus burden and permeability to contrast. We investigated whether residual flow (RF, permeability) on CTA in acute ischemic stroke (AIS) patients is associated with clinical, radiological and histopathological factors, stroke mechanisms, and radiological and clinical outcomes.
Methods: We retrospectively analyzed data between 11/2022-11/2023 from POLISTAR ([Policlinico-Stroke-Thrombi-Analysis-Registry), a consecutive single-center registry of AIS treated with reperfusion therapies in Italy. We compared AIS patients with and without RF (permeability) on CTA images, as defined previously (Menon, JAMA Neurol. 2018), regarding demographic and clinical characteristics, laboratory parameters, stroke mechanisms and outcomes. Other logistic regression and preliminary multiomic analyses on thrombi are ongoing and will be presented at the congress.
Results: Among 67 AIS patients, 56% were women and the median age was 79 years (IQR, 65.5-84.5). Baseline characteristics are presented in Figure 1. In unadjusted analysis, RF is not associated with radiological outcomes (Figure 2). In multivariable analysis, RF is associated with older age (adjusted common OR,1.36 [95%CI,1.10-1.69]), absence of coronaropathy (aOR 0.52 [95%CI, 0.28-0.98)] and lower acute glucose levels (aOR, 0.14 [95%CI, 0.04-0.47]). Longer door-to-imaging intervals and higher clot burden scores were associated with a lower probability of presenting RF (Figure 3).
Conclusions: In a cohort of AIS patients treated with reperfusion therapies, patients with and without RF are similar in most aspects, including thrombus histopathological characteristics, except for age, treatment type, workflow times, thrombus extent and blood glucose levels.
Disclosures of Interest: No
Abstract N°: 2466
COMPARISON OF HYPERACUTE STROKE IMAGING PROTOCOLS FOR TIME EFFICIENT REPERFUSIVE TREATMENT: A TWO-CENTER STUDY
Fabrizio Giammello*1,2, Francesco Grillo2, Ludovica Ferraù2, Valentina Tudisco2, Agostino Tessitore1, Davide Vicari1, Sergio Vinci1, Luigi Simonetti3, Andrea Zini3, Antonio Toscano2
1Policlinico di Messina, Department of Biomedical, Dental Science and Morphological and Functional Images, Messina, Italy, 2Policlinico di Messina, Department of Clinical and Experimental Medicine, Messina, Italy, 3IRCCS Istituto delle Scienze Neurologiche di Bologna, Department of Neurology and Stroke Center, Bologna, Italy
On behalf of:
Background and aims: The three-compartment model of acute ischemic stroke (AIS) includes non-viable tissue (NVT), tissue at risk (TAR), and benign oligoemia. We aimed to assess hyperacute stroke imaging protocols (HSIP) with computed tomography perfusion (CTP) and/or magnetic resonance imaging (MRI) and to better characterize the reliability of the two methods in predicting follow-up infarction.
Methods: We retrospectively reviewed 929 consecutive AIS patients evaluated for the selection for reperfusive treatments at two comprehensive stroke centers, using two different HSIP for proper patient selection. The two CSC employ a FAST MRI based HSIP, including ASL and DWI sequences, and a multimodal CT based HSIP, including mCTA and CTP, respectively.
Results: We enrolled 158 patients undergoing mCT-based HSIP. CTP presented a prognostic accuracy (ACC) of 75.9%. In anterior circulation perfusion deficit, CTP-Tmax >16s overestimated NVT, in patients with favorable clinical-instrumental outcomes. Similarly, CTP-Tmax >9.5s overestimated TAR in patients untreated or with reperfusion treatment failure.
On the other hand, we recruited 349 patients undergoing FAST-MRI based HSIP. MRI with DWI and pcASL presented ACC of 83.9%, when pcASL was positive. In anterior circulation perfusion deficit, DWI was highly reliable for NVT in patients with favorable clinical-instrumental outcomes. Similarly, pcASL tended to overestimate TAR in patients with unfavorable outcome, but the rate of complete overlap with the final infarct was higher.
Conclusions: CTP-Tmax maps for the detection of AIS achieved a sufficiently reliable ACC, but this was not optimal. On the other hand, DWI-pcASL for the detection of AIS achieved a highly reliable ACC.
Disclosures of Interest: No
Abstract N°: 2864
IDENTIFYING AFFECTED VASCULAR TERRITORY IN ANTERIOR CIRCULATION LARGE VESSEL ACUTE ISCHEMIC STROKE BY THE RELATIVE NON-CONTRAST COMPUTED TOMOGRAPHY
Lieselotte Vandewalle*1,2, Praneeta R Konduri3,4, Soren Christensen5, Anke Wouters1, Nicole Yuen5, Maarten Lansberg5, Jelle Demeestere1,2, Robin Lemmens1,2
1Catholic Universities of Leuven, Department of Neurosciences, Division of Experimental Neurology, Leuven, Belgium, 2University Hospitals Leuven, Department of Neurology, Leuven, Belgium, 3Amsterdam UMC - location University of Amsterdam, Department of Biomedical Engineering and Physics, Amsterdam, Netherlands, 4Amsterdam UMC - location University of Amsterdam, Department of Radiology and Nuclear Physics, Amsterdam, Netherlands, 5Stanford Stroke Center, Palo Alto, United States
On behalf of:
Background and aims: Non-contrast computed tomography (NCCT) has limited sensitivity to detect early ischemic changes and is hampered by high interrater variability. The relative NCCT (rNCCT) is a semi-automated NCCT analysis that compares the density of a voxel to the corresponding area in the contralateral hemisphere and generates hypodensity-based ratio maps (doi: 10.1111/jon.12593). We investigated if the rNCCT could identify the approximated affected vascular territory in patients with anterior circulation large vessel occlusion (acLVO) stroke.
Methods: We included 94 patients from the CT Perfusion to Predict Response to Recanalization in Ischemic Stroke Project 2 (CRISP2) study. We created rNCCT images and calculated the volume of tissue above a 1% relative hypodensity threshold, we then compared the volume of the rNCCT lesion within the approximated affected vascular territory to all rNCCT volume in unaffected vascular territories (excluding the cerebellum) in both hemispheres. Correct identification was defined as a larger rNCCT lesion volume in the approximated affected vascular territory compared to unaffected vascular territories.
Results: The mean rNCCT lesion volume in the approximated affected vascular territory was 195 ml (SD 70 ml) and larger than the remaining rNCCT lesion volume (median 124 ml (IQR 98 ml, p < 0.001). The approximated affected vascular territory was correctly selected in 62 of 94 patients (66 %).
Conclusions: rNCCT identified the approximated affected territory in acLVO acute ischemic stroke in 66% of patients. Other rNCCT thresholds may yield higher accuracy and will be studied further.
Disclosures of Interest: Yes P. K.: co-founder and shareholder of inSteps B.V. RL: no personal disclosures, but institutional support for consultancy by iSchemaview.
Abstract N°: 44
MICROENHANCEMENT AS A BIOMARKER FOR CEREBRAL MICROBLEED IN INFLAMMATORY CAA: INSIGHTS FROM HR MRI
Suriya Subramanian1, Peter Sguigna1, Erica Jones1, Brendan. Kelley1, William Moore1, Marco Pinho1, Ty Shang*1
1UT Southwestern Medical Center, Dallas, United States
On behalf of:
Background and aims: Cerebral amyloid angiopathy-related inflammation (CAA-ri) and amyloid-beta-related angiitis (ABRA) are infrequent variants of CAA, characterized by an inflammatory response to amyloid-beta deposits within vessels. Cerebral microbleed (cMB) is a common imaging feature in these conditions. Emerging pathological evidence suggests a focal perivascular inflammatory response acts as a precursor to the evolution of cMBs in CAA. Consequently, there is need for an in vivo imaging biomarker, capable of anticipating the emergence of cMB. We explored the potential of high-resolution MRI (HR-MRI) in offering predictive insights into cMB development in CAA-ri and ABRA patients.
Methods: We conducted a retrospective review of CAA cases recorded in the UT Southwestern Medical Center's HR-MRI registry from 2014-2022, using 3D T1 BrainView Black Blood sequence on Philips MR 3T scanner. Susceptible weighted imaging (SWI) was used to assess cMB.
Results: We identified five cases with pathological confirmation of CAA-ri and ABRA. Observations indicated a consistent pattern where foci of cerebral microenhancement (cME), detectable as punctate and homogeneous contrast enhancement, sometime in clusters, mostly in juxtacortical locations on HR-MRI, preceded the development of cMBs. These cMEs were noted in identical locations where cMBs later emerged. Usually lasted for a few months, but not all cMEs progressed to cMBs; some resolved completely, indicating a potential for reversibility.
Conclusions: In conclusion, cMEs in juxtacortical locations, detectable via HR-MRI, have potential as imaging biomarkers for evaluating cMB risk in CAA-ri and ABRA patients. Upon validation, this tool could extend its utility to a wider CAA and Alzheimer’s disease patients receiving anti-amyloid antibody treatment.
Disclosures of Interest: No
Abstract N°: 367
SUBCORTICAL VOLUMES AND COGNITION IN CADASIL – A PILOT STUDY
1National Taiwan University Hospital, Department of Neurology, Taipei, Taiwan, 2Charité - Universitätsmedizin Berlin, Department of Anesthesiology and Operative Intensive Care Medicine (CCM, CVK), Berlin, Germany, 3National Taiwan University Hospital, Department of Medical Imaging, Taipei, Taiwan
On behalf of:
Background and aims: Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL) represents one of the most common heritable causes of vascular dementia. Subcortical volumes might be proxies of brain reserve capacity and reflective of cognitive function. We explored the impact of subcortical volumes on cognition in CADASIL patients.
Methods: We included 90 patients with pathogenic NOTCH3 variants. They underwent MRI sessions at baseline. The subcortical volumes were calculated by using FreeSurfer and compared them with those of 68 matched controls. Within the CADASIL group, we tested the association of the subcortical volumes, cortical grey matter volume and brain parenchymal fraction (BPF) with scores of Mini-mental state examination (MMSE), cognitive domains, and vascular cognitive impairment (VCI).
Results: Most subcortical volumes differed between CADASIL patients and healthy controls. Within the CADASIL cohort, the thalamus and the putamen were associated with the MMSE [thalamus adjusted beta 21.50 [95%CI 2.15-40.84] p=0.03; R²=0.25; putamen adjusted beta 24.54 [95%CI 10.97-38.10] p=0.0006; R²=0.36] and VCI [thalamus OR per SD-decrement 3.61[95%CI 1.36–9.59] p=0.01; putamen OR per SD-decrement 2.89 [95%CI 1.17 – 7.15] p=0.02]. A larger thalamus volume might also be associated with better executive function and visuospatial perception. The cortical grey matter volume and the BPF showed associations with various cognitive outcomes in all analyses.
Conclusions: Although cortical grey matter volume and the BPF still appear to be robust markers of cognitive performance in CADASIL, the volumes of the thalamus and the putamen might be promising regions of interest for future research.
Disclosures of Interest: No
Abstract N°: 992
IMAGING BIOMARKERS OF CEREBRAL OEDEMA TO PREDICT OUTCOMES AFTER ISCHAEMIC STROKE: A SYSTEMATIC REVIEW
James Garrard1, Davide Carone1, Katie Scandrett2, Yemisi Takwoingi2, James Kennedy*1
1Radcliffe Department of Medicine, University of Oxford, Oxford, United Kingdom, 2Institute of Applied Health Research, University of Birmingham, Birmingham, United Kingdom
On behalf of:
Background and aims: Cerebral oedema is a significant cause of early deterioration after ischaemic stroke. We planned a systematic review and meta-analysis of the prediction of clinical outcomes after stroke using different methods of cerebral oedema quantification.
Methods: Studies indexed in Medline, EMBASE, and Cochrane Stroke databases until July 2023 were included if a method of quantification of cerebral oedema was used to predict: 90-day modified Rankin Scale (mRS), mortality, or a definition of malignant oedema, with the sensitivity and specificity for each study recorded. Study quality was evaluated via QUADAS-2.
Results: Seventeen studies (3687 patients) using six different quantification methods were included. There were five different definitions used for malignant oedema.
All studies were judged high risk of bias, primarily due to post-hoc cut-off value selections. Eleven studies were restricted to large-vessel occlusion stroke patients. Due to a pacity of studies and clinical and methodological differences, meta-analysis was not possible.
Eight studies (1027 patients) used six different quantification methods to predict 90-day mRS (sensitivities: between 0.66 and 1.00; specificities: between 0.47 and 0.91) (see Figure). One study (71 patients) exploring four different methods to predict mortality reported sensitivities between 0.31 and 0.93 and specificities ranging from 0.33 to 1.00. Ten studies (2649 patients) used six different methods to predict malignant oedema (sensitivities: between 0.64 and 0.90; specificities: between 0.71 and 0.97).
Conclusions: Future work should focus on appropriately powered studies of unselected populations of acute stroke patients using agreed definitions to explore the impact of cerebral oedema on prediction of relevant clinical outcomes.
Disclosures of Interest: Yes J Garrard and D Carone are employed part time by Brainomix
Abstract N°: 617
AGREEMENT ACROSS DIFFERENT MEASURES FOR INTERNAL CAROTID ARTERY STENOSIS IN PATIENTS WITH TIA OR STROKE IN THE CONVINCE TRIAL
Louise Maes*1,2, Jo P P Peluso3, Peter Vanacker4,5,6, Geert Vanhooren7, Philippe Desfontaines8, Adinda De Pauw9, Jelle Demeestere1,2, Daniel Bos10,11,12, Peter Kelly13,14,15, Robin Lemmens1,2
1University Hospitals Leuven, Department of Neurology, Leuven, Belgium, 2KU Leuven - University of Leuven, Department of Neurosciences, Experimental Neurology, 3University Hospitals Leuven, Department of Radiology - Division of Neuroradiology, Leuven, Belgium, 4AZ Groeninge, Department of Neurology, Kortrijk, Belgium, 5University Hospitals Antwerp, Department of Neurology, Antwerp, Belgium, 6University of Antwerp, Department of Translational Neuroscience, Antwerp, Belgium, 7AZ Sint-Jan, Department of Neurology, Brugge, Belgium, 8CHC Group Santé, Department of Neurology, Stroke Unit, Liège, Belgium, 9AZ Damiaan, Department of Neurology, Oostende, Belgium, 10Erasmus University Medical Center Rotterdam, Department of Radiology & Nuclear Medicine, Rotterdam, Netherlands, 11Erasmus University Medical Center Rotterdam, Department of Epidemiology, Rotterdam, Netherlands, 12KU Leuven - University of Leuven, Department of Cardiovascular Sciences, Leuven, Belgium, 13Health Research Board (HRB) Stroke Clinical Trials Network Ireland (SCTNI), Dublin, Ireland, 14University College Dublin (UCD), School of Medicine, Dublin, Ireland, 15Mater Misericordiae University Hospital, Department of Neurology - Stroke Service, Dublin, Ireland
On behalf of:
Background and aims: Grade of stenosis in patients with atherosclerosis of the internal carotid artery (ICA) is commonly measured by the NASCET (North American Symptomatic Carotid Endarterectomy Trial) method (% stenosis = [1-(minimum luminal diameter/normal distal diameter)] x 100), initially adapted for 2-D invasive carotid angiography. Semi-automated software techniques for computed tomography angiography (CTA) now offer additional parameters for measurements of stenosis grade. We compared these different stenosis measurements in patients with TIA and stroke.
Methods: We analyzed baseline CTA’s of patients included in the CONVINCE (Colchicine for prevention of vascular inflammation in Non-CardioEmbolic stroke) trial from six Belgian centers. Using semi-automated imaging software, minimal diameter-based stenosis (dia[min]), area-based stenosis (area), and stenosis based on effective diameters calculated from area (dia[area]) and perimeter (dia[perim]) were measured. Within the 30-99% dia[min] subgroup, we assessed agreement between methods using a weighted kappa statistic (κ) and Bland-Altman plots.
Results: We identified 338 atherosclerotic arteries with 0-99% stenosis in 212 patients. Participants had a mean age of 70.4 years (SD 9.6 years) and 163 (77%) were men. Figure 1 illustrates the grade of stenosis by the different methods. Agreement between methods varied: κ=0,73 (dia[min] vs. area), κ=0,55 (dia[min] vs. dia[area]) and κ=0,40 (dia[min] vs. dia[perim]). The Bland-Altman plots showed mean differences of -5,2%, +14,3% and +21,7% between dia[min] and area, dia[area] and dia[perim], respectively.
Conclusions: Different methods for stenosis measurement showed fair to moderate agreement, which affects stenosis gradation. The observed variation underscores the importance of consistently selecting and reporting the method used for patient risk stratification and treatment decisions.
Disclosures of Interest: No
Abstract N°: 1769
DISPARITIES IN ACCESS TO VASCULAR STROKE IMAGING AND CAROTID REVASCULARIZATION: A POPULATION STUDY
Harshil Shah*1,2, Naomi Dyck1,2, Jillian Stang1,3, Christiane Mcintosh1,3, Stephen Wilton1,2, Michael Hill1,2, Aravind Ganesh1,2
1Calgary Stroke Program, Calgary, Canada, 2University of Calgary, Calgary, Canada, 3Alberta Health Services, Calgary, Canada
On behalf of:
Background and aims: CT angiography (CTA), MR angiography (MRA), and ultrasound are non-invasive vascular imaging modalities used in stroke/TIA investigation with variation in use both between and within countries. Vascular imaging decisions may be influenced by various factors ranging from location-based resource considerations to patient characteristics. We used data from an entire Canadian province (population:4.4 million) to investigate disparities in the utilization of vascular imaging modalities and subsequent carotid endarterectomy/stenting.
Methods: We used provincial administrative data encompassing patients presenting to hospital or emergency/urgent-care facilities with a primary diagnosis of either TIA or ischemic stroke from 1-April-2016 to 31-March-2017 and related the vascular imaging received (CTA/MRA/ultrasound/none) to health region, comorbidities, age, and sex using multivariable logistic regressions. The cohort was followed for 5 years with records of any carotid procedures.
Results: Among 7745 patients (median age:71, interquartile-range:22, 48.4% female) with TIA/stroke, females were less likely to receive CTA or any vascular imaging (63.7% males vs 57.7% females, aOR:0.78, 95%CI:0.71-0.86), as were patients older than 71 years (aOR:0.70, 95%CI:0.63-0.78) and those with specific comorbidities (e.g. renal failure). There were also regional differences (phet<0.001). Compared to comprehensive stroke centers, patients at other facilities were less likely to receive CTAs (aOR:0.24, 95%CI:0.22-0.28). Patients receiving only ultrasound or no vascular imaging were less likely to receive carotid revascularization (aOR:0.29, 95%CI:0.20-0.41). After adjustment for other factors, female sex remained associated with lower odds of carotid revascularization (aOR:0.68, 95%CI:0.51-0.90).
Conclusions: Besides regional and comorbidity-related variabilities, age- and sex-related differences were observed in the utilization of vascular imaging and (for sex) subsequent carotid revascularization.
Disclosures of Interest: No
Abstract N°: 2024
COMPARISON OF SMALL VESSEL DISEASE IMAGING MARKERS AT 7-TESLA WITH LOWER FIELD STRENGTHS
Sam Neilson*1, Stephen Makin2, Natasha. E Fullerton3, Keith Muir1
1Queen Elizabeth University Hospital, Stroke Medicine, Glasgow, United Kingdom, 2University of Aberdeen, Centre for Rural Health, Inverness, United Kingdom, 3Institute of Neuroscience, Neuroradiology, Glasgow, United Kingdom
On behalf of:
Background and aims: The higher resolution and better tissue contrast of 7-Tesla MRI may have relevance to small vessel disease (SVD) imaging. Characterisation of SVD visual rating scales SVD at different field strengths is limited. We aim to compare rating scales at 7T with 1.5 or 3T images
Methods: We reviewed imaging from a single-centre prospective study using 7T MRI in recent subcortical infarct. One rater reviewed T1, T2 and SWI sequences and recorded Fazekas score, cerebral microbleed (CMBs) anatomical rating scale (MARS), number of lacunes and enlarged perivascular space (EPVS) scale at routine (1.5 or 3-Tesla) and 7T. Agreement was tested using Intraclass correlation coefficient (ICC) for continuous variables and Cohen’s kappa (ĸ) for ordinal variables.
Results: Twenty people underwent 7-T MRI median 5.5 days after lacunar stroke confirmed on 1.5T (n=15) and 3T MRI (n=5). Comparing routine MRI with 7T there was very good agreement with Fazekas score ĸ=0.932, p<0.001, lacune count ICC 0.958, p<0.001, and CMBs ICC 0.992, p<0.001. Median (IQR) EPVS 4 (3-4) was higher in 7T than lower fields strengths median 3 (2–3), with poor agreement ĸ=0.103, p=0.307. Movement artefact degraded 3 (15%) 7-Tesla images.
Conclusions: Among patients with recent lacunar stroke, there was very good agreement between 7T and lower field strengths for WMH, CMBs and lacune measurement. There was poor agreement for EPVS measurement. Improved image quality might provide additional pathological insight but further characterisation of SVD rating scales at 7T is necessary. Motion artefact degraded a proportion of 7T scans.
Disclosures of Interest: No
Abstract N°: 2080
VESSEL WALL IMAGING DIFFERENTIATORS OF CEREBRAL VASCULITIS AND ATHEROSCLEROSIS
Abbas Kharal*1, Sidonie Ibrikji1, Youssef Farag2, Aaron Shoskes3, Matthew Kiczek1, Shazam Hussain1
1Cleveland Clinic Main Campus, Cleveland, United States, 2Johns Hopkins University, Baltimore, United States, 3University of Utah Hospital, Salt Lake City, United States
On behalf of:
Background and aims: Differentiating atherosclerotic from inflammatory vasculopathy on vessel imaging can be challenging, often leading to misdiagnosis and unnecessary invasive testing in these patients. Vessel wall magnetic resonance imaging (VWMRI) is a useful adjunct tool in differentiating inflammatory from non-inflammatory cerebral vasculopathy, however, significant diagnostic misinterpretation exists due to a lack of quantifiable VWMRI differentiators. We therefore devised three quantifiable VWMRI variables and tested their utility in differentiating intracranial atherosclerosis (IA) from primary CNS vasculitis (PCNSV).
Methods: In this cross-sectional study, we identified patients (⩾18 years old) who presented to our medical center between January 2015 and December 2021 for ischemic stroke due to IA or PCNSV and had 3 tesla VWMRI data available. On VWMRI, for each patient, 20 consistent vessel wall segments were analyzed for percent concentricity, percent irregularity, and concentricity to eccentricity (C/E) ratios. Using logistic regression models, we assessed the diagnostic value of these VWMRI variables in differentiating PCNSV from those with IA.
Results: Thirty-two IA patients (54·2%) and 27 PCNSV patients (45·8%) had VWMRI data available. Twenty-four (75%) IA patients and 6 (22·2%) biopsy-proven PCNSV patients showed large vessel involvement and were included in the analysis. On VWMRI, a C/E ratio >1 (CI, 6·11-2165·95), percent concentricity ⩾50% (95% CI, 4·13-732·71), and percent irregularity <50% (95% CI, 4·13-732·71) indicated a significantly higher odds of PCNSV compared to IA.
Conclusions: Our results suggest that on VWMRI, a higher percent concentricity, lower percent irregularity, and a higher C/E ratio significantly differentiate PCNSV from intracranial atherosclerosis.
Disclosures of Interest: No
Abstract N°: 2333
INTRAVOXEL INCOHERENT MOTION IMAGING IN STROKE: EVALUATING MICROVASCULAR PERFUSION IN CORE AND PENUMBRA FOR LONG-TERM PROGNOSIS
Josua Zimmermann*1,2, Beno Reolon3, Lars Michels3,4,5, Bence Nemeth3, Susanne Wegener1,4,5, Jorn Fierstra5,6, Zsolt Kulcsar3,4, Andreas Luft1,4,5,7, Marco Piccirelli3,4, Tilman Schubert3,4
1University Hospital Zurich, Department of Neurology, Zurich, Switzerland, 2Lake Lucerne Institute, Vitznau, Switzerland, 3University Hospital Zurich, Department of Neuroradiology, Zurich, Switzerland, 4University Hospital Zurich, Clinical Neuroscience Center, Zurich, Switzerland, 5Neuroscience Center Zurich, University of Zurich and ETH Zurich, Zurich, Switzerland, 6University Hospital Zurich, Department of Neurosurgery, Zurich, Switzerland, 7cereneo Center for Neurology and Rehabilitation, Vitznau, Switzerland
On behalf of:
Background and aims: Intravoxel Incoherent Motion (IVIM) imaging has emerged as a contrast agent-free method for assessing microvascular perfusion, demonstrating significant potential in acute stroke imaging. Previous research emphasized diminished microvascular perfusion in the infarct core of acute stroke patients, yet the microperfusion characteristics of the penumbra and its link to clinical outcome remains unclear. Thus, this study aimed to explore microvascular perfusion in the core and penumbra, as well as examining its correlation to long-term clinical outcomes.
Methods: A longitudinal study involving ischemic stroke patients (n analysed=24) was conducted, integrating IVIM and contrast-enhanced perfusion imaging both pre- and post-treatment (24h post-stroke), and at 90 days post-stroke. Delineation of the core and penumbra enabled extraction of imaging parameters specific to these regions. These were used to compare microperfusion characteristics within these regions and their relationship to long-term clinical outcome measured with the NIH Stroke Scale (NIHSS) at 90 days post-stroke.
Results: IVIM parameters were lower in the core but higher in the penumbra compared to adjacent healthy tissue post-treatment. Moreover, employing a machine learning classifier, IVIM parameters demonstrated superior accuracy in separating penumbra from healthy tissue compared to contrast-enhanced perfusion parameters (accuracy 85% vs. 45%). Reduced IVIM measures post-treatment in both core and penumbra were associated with higher NIHSS scores at 90 days post-stroke (r=-0.65 and r=-0.83), which was not seen for contrast-enhanced perfusion measures.
Conclusions: Microvascular perfusion characteristics in the infarct core and penumbra relate to functional recovery in stroke. Moreover, reduced mircoperfusion in core and penumbra were associated with poorer clinical outcome.
Disclosures of Interest: No
Abstract N°: 982
WHOLE BRAIN TOPOGRAPHIC ANALYSIS UTILISING ASPECTS-AAL IN ACUTE ISCHAEMIC STROKE
Jason Vuong*1,2, Tharani Chandran1, Richard Beare3, Marcello Rosa4, Lee-Anne Slater5, Henry MA1,2, Thanh Phan1,2
1Monash University, Department of Medicine, School of Clinical Sciences at Monash Health, Clayton, Australia, 2Monash Health, Department of Neurology, Clayton, Australia, 3Monash University Peninsula Campus, Peninsula Clinical School, Frankston, Australia, 4Monash Biomedicine Discovery Institute, Physiology, Clayton, Australia, 5Monash University, Department of Imaging, School of Clinical Sciences at Monash Health, Clayton, Australia
On behalf of:
Background and aims: The Alberta stroke programme early CT score (ASPECTS) is used to guide reperfusion treatment of acute ischaemic stroke (AIS) and to predict disability after rehabilitation. However, ASPECTS is limited to the central portion of the MCA and does not assess brain parenchyma supplied by the distal MCA, the ACA, or the posterior circulation. We aim to create a digital template covering the entire brain to improve outcome prediction in AIS.
Methods: The 52-point ASPECTS (ASPECTS-AAL) encapsulates the entire (left and right sided) human brain, and is a reduction of the functional automated anatomical atlas (AAL). We used mouse-driven software (FSLeyes) to segment regions of the parcellated AAL. Next, we performed principal component analysis (PCA) and t-distributed stochastic neighbour embedding (t-SNE) to examine if the topographic distribution of the parcellated regions correspond to the vascular territories, and to explore outcomes (R version 4.12).
Results: 26 segmented regions (4-ACA, 13-MCA, 8-PCA and 1 cerebellum) per hemisphere were created, namely the M1–M8, A1–A3, P1–P3, thalamus, temporal, frontal, palladium, hippocampus, parahippocampus, amygdala, caudate, putamen, internal-capsule, insula, and cerebellum (Figure 1a). 109 test subjects (13-ACA, 70-MCA and 26-PCA) were analysed. PCA and t-SNE identified three principal components groups (56% variance) largely correlated to vascular territory (Figure 1b). t-SNE analysis of the MCA cohort identified a cluster of high mRS correlated with involvement of the M8 segment (parietal ASPECTS-ALL).
Conclusions: The 52-point ASPECTS-ALL demonstrates potential to improve patient selection in stroke treatment, and can be made available to researchers in digital format. Further validation is ongoing.
Delin Liu*1, Jichang Luo1, Yifan Yang1, Haozhi Gong1, Long LI1, Tao Wang1, Yan MA1, Liqun Jiao1
1Xuanwu Hospital Capital Medical University, Neurosurgery, Beijing, China
On behalf of:
Background and aims: Reduced cerebral perfusion and insufficient lateral compensation are associated with risk of stroke in intracranial atherosclerotic stenosis (ICAS). Fractional flow reserve (FFR) is a lesion-specific index that determines hemodynamic insufficiency of ICAS. An algorism, based on phase contrast magnetic resonance angiography (pcMRA), called MR-FFR, was developed to non-invasively predict perfusion reversibility. This report presents the correlation and threshold of MR-FFR in functional assessment of ICAS.
Methods: The study recruited patients who underwent angioplasty for symptomatic, anterior circulation ICAS stenosis >50% between April 2020 and August 2022. MR-FFR was calculated from baseline pcMRA, and relative cerebral blood flow (rCBF) was measured by arterial spin labeling before and after operation. The diagnostic value of MR-FFR for patients with reversible cerebral perfusion in the supplying region was analysed.
Results: A total of 33 patients (28 male, 5 female) were included, with 16 having internal carotid artery stenosis and 17 having middle cerebral artery M1 stenosis. The median age was 54.5±11.0 years. Twenty-five (75.8%) patients had redeemable hypoperfusion with preoperative rCBF<0.9 and postoperative rCBV⩾0.9. Cut-off value of MR-FFR was 0.67, with AUC of 0.96, sensitivity of 100%, and specificity of 84% (p<0.001). The reversible hypoperfusion group also had lower baseline levels of white blood cells, international normalized ratio, and hypersensitive C-reactive protein.
Conclusions: Non-invasive MR-FFR demonstrates potential as a reliable factor for assessing the hemodynamic impairment in ICAS and predicting the reversibility of hypoperfusion through neurointervention. Further investigation is needed to determine its clinical efficacy.
Disclosures of Interest: No
Abstract N°: 115
IMAGE-BASED MODEL FOR IDENTIFYING HISTOLOGICAL WALL REMODELING OF UNRUPTURED INTRACRANIAL ANEURYSM
Qingyuan Liu*1, Lei Chen2, Peng Liu1, Mahmud Mossa-Basha3, Michael Levitt4, Jiangan LI5, Shuo Wang1, Chengcheng Zhu3, Hongwei He1
1Beijing Tiantan hospital, Capital Medical University, Department of Neurosurgery, Beijing, China, 2The First Dongguan Affiliated Hospital, Guangdong Medical University, Department of Neurosurgery, Guangdong, China, 3University of Washington, Department of Radiology, Seattle, United States, 4University of Washington, Department of Neurological Surgery, Seattle, United States, 5Jiangnan University Medical Center, Department of Neurosurgery and Emergency Medicine, Wuxi, China
On behalf of:
Background and aims: Intracranial aneurysm wall remodeling (AWR) is associated with high rupture risk. To establish an imaging-based classification model of AWR based on a large-scale pathological cohort of unruptured intracranial aneurysms (UIAs).
Methods: UIA histological samples were prospectively collected, and were grouped as the development cohort (included from January 2017 to October 2021) and validation cohort (included from November 2021 to December 2022). Contrast-enhanced vessel wall-MRI and morphometric analysis were performed before surgery. UIAs were histologically classified as Type A (endothelialized wall with organized cells), Type B&C (thickened and hypocellular wall with disorganized cells) and Type D (extremely thin thrombosis-lined hypocellular wall). The AWR classifier was constructed by a machine-learning algorithm from the development cohort and was then applied to the validation cohort. The accuracy of model in classifying AWR was evaluated using area under the curve (AUC).
Results: This study included 237 UIA samples from 237 patients. Fifty-five (23.2%) UISAs were identified as type A, 105 (44.3%) as type B&C, and 77 (32.4%) as type D. Size ratio, aspect ratio, irregular shape and wall enhancement index were identified as features of AWR. The AWR classifier was established incorporating these features from the development cohort (n=195), and performed well in classifying each type of AWR (AUC=0.92) in the validation cohort (n=42). Sensitivity analysis showed that the model incorporating wall enhancement and morphological features had higher accuracy than morphological features alone (AUC 0.93 vs. 0.73, P<0.001).
Conclusions: Wall enhancement and morphological features can classify AWR of intracranial aneurysms in vivo.
Disclosures of Interest: No
Abstract N°: 294
OVERESTIMATION OF LUMINAL STENOSIS BY MRA OVER CTA AS A PROGNOSTIC MARKER FOR STROKE RECURRENCE IN ICAS
Yuying Liu*1, Shuang LI1, Xuan Tian1, Jill Abrigo2, Bonaventure Ym Ip1, Sze Ho MA1, Sin Ying Fan1, Hing Lung Ip1, Thomas Leung1, Xinyi Leng1
1The Chinese University of Hong Kong, Department of Medicine and Therapeutics, Hong Kong, 2The Chinese University of Hong Kong, Department of Imaging and Interventional Radiology, Hong Kong
On behalf of:
Background and aims: Signals in time-of-flight magnetic resonance angiography (TOF-MRA) are flow-dependent. Hence, it could overestimate the degree of luminal stenosis in intracranial atherosclerotic stenosis (ICAS), particularly in those with significantly reduced flow. We aimed to investigate the clinical relevance of this phenomenon.
Methods: Patients with stroke or transient ischemic attack (TIA) due to 50-99% ICAS confirmed by CT angiography (CTA), who underwent TOF-MRA within one month and received medical treatment, were retrospectively enrolled. The severity of luminal stenosis of each symptomatic ICAS lesion was independently assessed in CTA and MRA, and classified as moderate (50-69%) and severe (70-99%) stenoses. Flow gap with distal vessel filling in MRA was considered severe stenosis. Patients were categorized into Group A with moderate stenosis on both MRA and CTA, Group B with severe stenosis on MRA but moderate stenosis on CTA, and Group C with severe stenosis on both MRA and CTA. The primary outcome was recurrent, same-territory ischemic stroke or TIA within 1 year.
Results: Among 107 patients (mean age 62±10 years; 59.8% males), 34 (31.8%), 33 (30.8%), and 40 (37.4%) were classified into Groups A, B and C respectively. Primary outcome occurred in 18 (16.8%) patients. In multivariate Cox regression, patients in Group B had the highest risk of the primary outcome, followed by Groups C and A (27.3%, 17.5%, 5.9%; adjusted hazard ratio=2.05; p=0.038).
Conclusions: Moderate luminal stenosis on CTA but severe stenosis on TOF-MRA may be a prognostic marker for stroke recurrence in medically treated patients with symptomatic ICAS.
Disclosures of Interest: No
Abstract N°: 442
ARTERIAL FLOATING MURAL THROMBI ARE A CHARACTERISTIC IMAGING PATTERN IN SARS-COV-2-RELATED ISCHEMIC STROKE
1Rabin Medical Center, Neurology, Petah Tikva, Israel, 2Tel Aviv University, Medical School, 3Shamir Medical Center, Neurology
On behalf of:
Background and aims: Acute ischemic stroke (AIS) is a common complication of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. We aimed to explore neurovascular imaging patterns in patients with SARS-CoV-2-related AIS.
Methods: We retrospectively analyzed clinical and radiological data of patients hospitalized between March-2020 and May-2022 with AIS and a SARS-CoV-2 infection prior AIS symptom onset. The control group comprised AIS patients from a pre-COVID-19 pandemic period.
Results: Thirty-five SARS-CoV-2-related stroke patients, and 35 matched controls were included. 20/35 (57%) of patients with SARS-CoV-2-related stroke had either mild or asymptomatic disease. A distinctive imaging pattern of floating arterial mural thrombi was detected in 5 patients (14.3%) in the SARS-CoV-2 group. In four of these patients the floating thrombus was attached to a stenotic atherosclerotic plaque in the proximal internal carotid artery (ICA). In the 5th patient a cardiac CTA showed multiple large mural thrombi in the descending aorta, with only mild underlying atherosclerosis. In the control group, a floating mural thrombus was only detected in one patient (2.9%) with a severe atherosclerotic ICA stenosis (P=0.088). Treatment with dual antiplatelet therapy was associated with thrombus dissolution and good clinical outcome in 3/4 patients with a carotid artery floating thrombus.
Conclusions: Arterial floating mural thrombi attached to atherosclerotic plaques are a common, characteristic neuroimaging pattern in SARS-CoV-2-related AIS. Floating mural thrombi may form on otherwise low-risk plaques in patients with mild or asymptomatic infection and result in ischemic stroke up to 1-2 weeks after SARS-CoV-2 diagnosis.
Disclosures of Interest: No
Abstract N°: 581
PROGNOSTIC VALUE OF EARLY BRAIN MAGNETIC RESONANCE IMAGING IN GLOBAL CARDIOVASCULAR RISK AFTER TRANSIENT ISCHEMIC ATTACK (TIA)
Manuel Pedrero Prieto*1, Diana Tarruella1,2, Lluis Morales Caba1,2, Gerardo Fortea1,2, Jose Ignacio Tembl1,2, Irene Escudero-Martínez1,2
1Hospital Universitari i Politècnic La Fe, Neurology, València, Spain, 2Institut Investigació Sanitària La Fe, Unidad Mixta de Investigación Cerebrovascular (UMIC), València, Spain
On behalf of:
Background and aims: Transient ischemic attack (TIA) is associated with an increased disability rate, independently of the ocurrence of a subsequent ischemic stroke. The aim of this study is to investigate the prognostic value of brain magnetic resonance imaging (MRI) in global cardiovascular risk following a TIA.
Methods: A retrospective observational study with a 5-year longitudinal follow-up was conducted on patients with TIA diagnosis from 2016 to 2018 in a Comprehensive Stroke Center.
Results: 114 patients were included. Major adverse cardiovascular event (MACE) was observed in 17.5% of patients, being recurrent stroke/TIA the most frequent (85%). Regarding MRI findings, 34.2% of patients showed diffusion-weighted imaging (DWI) lesions, 66.7% white matter hyperintensities (WMH), 37.7% chronic lacunar strokes and 14% microbleeds. DWI lesions were associated with motor weakness as clinical presentation (p=0.059) and with vascular atheromatosis (p=0.035). However, they were not associated with subsequent MACE. WMH and microbleeds were associated to MACE (p=0.002 and p=0.01, respectively) and recurrent stroke/TIA (p=0.007 and p=0.02, respectively). Chronic lacunar strokes and microbleeds were also associated with non-cardiovascular mortality (p=0.002 and p=0.034, respectively). Reagrding clinical variables, speech impairment and duration 10-60 minutes were associated with MACE.
Conclusions: In our study, the presence of acute ischemic lesions in MRI after a TIA were not associated with an increased overall cardiovascular risk after a TIA. However, the presence of WMH and microbleeds were associated with an increased risk of MACE. Both findings are related to small vessel disease and large vessel aterosclerosis, which could explain this association.
Disclosures of Interest: No
Abstract N°: 803
USEFULNESS OF SPECTRAL COMPUTED TOMOGRAPHY IN THE MANAGEMENT OF PATIENTS WITH ACUTE ISCHAEMIC STROKE AFTER MECHANICAL THROMBECTOMY
Luis Moreno-Navarro*1,2, Nicolás López-Hernández1,2, Mònica Farrerons-Llopart1,2, Eugenio Ruiz-González3, María-José Ballesteros-Aparicio3, María-Javiera Garfias-Baladrón3, Isabel Beltrán-Blasco1,2, Diego Corona-García1, Raquel Hernández-Lorido1, Luis Concepción-Aramendía3
1Hospital General Universitario Dr. Balmis, Neurology, Alicante, Spain, 2Instituto de Investigación Sanitaria Biomédica de Alicante (ISABIAL), Group 1: Neuroscience Research, Alicante, Spain, 3Hospital General Universitario Dr. Balmis, Radiology, Alicante, Spain
On behalf of:
Background and aims: Mechanical thrombectomy (MT) has improved the prognosis of acute ischaemic stroke (AIS); however, haemorrhagic transformation (HT) is a frequent complication. Spectral computed tomography (CT) distinguishes contrast extravasation (CE) from HT due to the differential behaviour of the materials to dual energy. Our aim is to investigate differences between spectral CT and conventional CT in distinguishing CE from HT on 24-hour control head CT of patients with AIS undergoing MT.
Methods: A retrospective, observational, single-centre study was conducted in a stroke unit in Southeastern Spain that included patients with AIS treated with MT from July 2022 to March 2023. Data collection was carried out using CODICT registry and access to the electronic medical records of our hospital.
Results: This study included 155 patients, with a mean age of 72.5 years, and 50.9% of them were women. In addition, about 40% of the sample had known or newly diagnosed atrial fibrillation. Spectral CT was performed in 63, and conventional CT in 75. In the spectral CT group, 21 hyperdense images were detected, compared to 28 in the conventional CT group. In 42.8% of cases where hyperdensity was detected in the conventional CT group, it was not possible to distinguish between CE and HT, in contrast to the 4.8% in the spectral CT group (p<0.001).
Conclusions: Spectral CT has a sensitivity and specificity for detection of blood close to 100% in patients with AIS undergoing MT. If necessary, this provides high confidence to the neurologist in early resuming anticoagulation therapy.
Disclosures of Interest: No
Abstract N°: 906
INITIAL VALIDATION OF AN AUTOMATED TOOL FOR IDENTIFICATION AND SEGMENTATION OF ACUTE INFARCTS ON MRI IN THE ACT TRIAL
Diana Kim*1, Jianhai Zhang1, Fouzi Bala2, Mao Ding1, Andrew Demchuk1, Mohammed Almekhlafi1, Wu Qiu1, Nishita Singh3, Aravind Ganesh1
1University of Calgary, Department of Clinical Neurosciences, Calgary, Canada, 2Centre Hospitalier Regional Universitaire de Tours, Tours, France, 3University of Manitoba, Winnipeg, Canada
On behalf of:
Background and aims: Machine-learning models for automated infarct detection and segmentation have potential to enhance stroke care delivery and clinical trial data analysis. Manual infarct segmentation is time-consuming and variable, and prior MRI-based segmentation tools have generally relied on a single sequence, typically diffusion-weighted imaging (DWI) leading to misclassification. We developed a novel, automated tool for MRI-based infarct identification and segmentation using DWI and apparent diffusion coefficient (ADC) input sequences.
Methods: A cascade architecture of coarse-to-fine convolutional neural networks was utilized for segmenting acute infarcts. The algorithm was trained using 128 scans with infarcts manually segmented on DWI and ADC, and tested in a clinical trial dataset with post-thrombolysis follow-up MRI. Ground truth for infarct presence was determined by expert readers blinded to algorithm results. Algorithm-generated segmentations were adjudicated to be acceptable or requiring correction based on visual inspection by experts.
Results: Among 534 patients, 437 (81.8%) had infarcts on follow-up MRI. The algorithm achieved the following: sensitivity 96.8% (95%CI 94.7-98.1%) for infarct detection, specificity 86.6% (95%CI 78.4-92.0%), positive predictive value 97.1% (95%CI 95.0-98.3%), negative predictive value 85.7% (95%CI 77.4-91.3%), and accuracy 95.0% (95%CI 92.7-96.5%). Automated segmentation was acceptable by visual inspection in 334/423 (79.0%) true positive cases (Figure 1-2). Examples of corrections are provided (Figure 3). Dice coefficient for 103 manually corrected cases was 0.74 (95%CI 0.67-0.81).
Conclusions: We developed a robust, automated tool for acute infarct segmentation demonstrating high sensitivity, specificity, and accuracy. Future external validation studies will compare the algorithm’s performance to prior tools trained solely using DWI.
Disclosures of Interest: No
Abstract N°: 1247
DIFFERENT RISK FACTORS UNDERLIE VARIABLE DISTRIBUTION OF HAEMORRHAGIC TRANSFORMATION AFTER MECHANICAL THROMBECTOMY
1National Cerebral and Cardiovascular, Department of Neurology, Suita, Japan, 2National Cerebral and Cardiovascular, Department of Cerebrovascular Medicine, Suita, Japan, 3National Cerebral and Cardiovascular, Department of Neurosurgery, Suita, Japan
On behalf of:
Background and aims: Haemorrhagic transformation (HT) is a risk for post-stroke seizure in patients with acute ischaemic stroke, with cortical HT (cHT) being associated with a higher risk than with deep HT (dHT). However, the factors underlying the different distribution of HT remain unknown.
Methods: Our study included patients who underwent EVT for acute stroke of the internal carotid artery or M1 segment of the MCA occlusion between January 2014 and March 2023. HT was classified into cHT and dHT and risk factors were evaluated.
Results: Of the 401 patients who received EVT, 129 had cHT, 78 had dHT, and 41 had both. Patients with cHT had a higher prevalence of diabetes mellitus (aOR 1.68), a higher NIHSS on admission (aOR 1.05), a lower rate of first pass effect (FPE) (aOR 0.53), and a lower rate of expanded Thrombolysis in Cerebral Infarction Scale (eTICI) 2c–3 score (aOR 0.58) compared to patients without cHT. Patients with dHT had a higher NIHSS on admission (aOR 1.04), a lower rate of FPE (aOR 0.55) and a longer time from onset to arrival (aOR 1.01/10 min) than those without dHT. A different interaction between dHT and cHT was observed for diabetes mellitus (p for interaction=0.007) and time from onset to arrival (p for interaction=0.01).
Conclusions: After EVT, the risks for the distribution of HT differ, with cHT being associated with diabetes mellitus, and dHT with time from onset to arrival. These findings may have the potential to help predict future seizures.
Disclosures of Interest: No
Abstract N°: 2549
UTILITY AND YIELD OF EARLY AND INTERVAL MRI IN ACUTE INTRACEREBRAL HAEMORRHAGE - A SINGLE CENTRE CROSS - SECTIONAL STUDY
Bader Mohamed*1,2, Mohammad Aboulwafaali1, Fatema Almosawi3, Sanhita Majumder1, Nadeesha Ahangama1, Sagal Mire1, Farhad Huwez1, Alexandra Andrews1
1Barts Health NHS Trust, United Kingdom, 2Government Hospitals, Manama, Bahrain, 3Ministry of Health, Sanabis, Bahrain
On behalf of:
Background and aims: There is uncertainty regarding which patients are more likely to benefit from a brain MRI following intracerebral haemorrhage (ICH).
We retrospectively assessed the utility of admission and follow-up MRI in detecting secondary causes of ICH.
Methods: All patients with a diagnosis of ICH between January 2022 and December 2022 were retrospectively analysed using electronic health records in a large adult tertiary stroke centre in London, UK.
We collected patients' demographics, clinical and radiological features.
Results: 146 patients were identified (Males: females 87:59), median age was 63 (range 22 to 92). Most patients (80%) had a good baseline function defined by (Modified rankin score of 0 to 3).
ICH's location was at basal ganglia/thalamus (50.5%), lobar (37%), and infratentorial (11.5%).
78 patients (54%) had at least one brain MRI: 25 (17%) at baseline, 70 (47%) on follow-up, and 12 (8%) on both settings.
Median time between ICH onset and admission MRI was 10 days, and 12 weeks for Interval follow-up (range 3-40). Secondary lesions detected in .6/25 (24%) on admission and in 19/70 (27%) on follow up MRI. Detected secondary causes are summarised in Table 1. Patients with positive MRI yield were more likely to be younger, have lobar/infratentorial hematoma, and have an absence of hypertension.
Conclusions: MRI yield in ICH is variable depending on the age, location of the haemorrhage and absence of hypertension.
Disclosures of Interest: No
Abstract N°: 2228
SPINAL CORD STROKES ENHANCE WITH GADOLINIUM
Navangi Patel*1, David Acero-Garces1, Carlos Pardo-Villamizar1
1The Johns Hopkins Hospital, Neurology, Baltimore, United States
On behalf of:
Background and aims: To understand the pattern of gadolinium enhancement in acute spinal cord ischemia.
Methods: We retrospectively analyzed the clinical presentation and MRI of patients diagnosed with spinal cord ischemia in the Myelitis and Myelopathy Center between 2010 and 2023. The MRIs were classified according to the time of acquisition as <48 hours, 2 - 10 days, 11 - 30 days, and >30 days from symptom onset.
Results: We included 165 patients (male 71, female 94). Of the 304 MRIs with T1 weighted + Gadolinium, lesion enhancement was noted in 15.6% within 48 hours, 44.2% between 2-10 days, 53.2% between 11-30 days, and 16% after 30 days of symptom onset.
Conclusions: Most patients with acute spinal cord ischemia had gadolinium enhancement between 11-30 days.
Disclosures of Interest: No
Paper Poster - Intracerebral Haemorrhage
Abstract N°: 422
ENDOSCOPIC VS NON-ENDOSCOPIC INTERVENTION FOR CHRONIC SUBDURAL HEMATOMA: A SYSTEMATIC REVIEW AND META-ANALYSIS OF 1136 PATIENTS
Ibrahim Serag1, Ahmed Aljabali2, Hamed Mustafa3, Mustafa Mohamed Megahed4, Yousef Ahmed Yousef5, Mariam Abdelhady6, Amro Elrosasy*7, Mohamed Abouzid8
1Faculty of Medicine - Mansoura University, Egypt, 2Jordan University of Science & Technology (JUST), , Jordan, 3Faculty of Medicine, Al-Azhar University Damietta, Egypt, 4Faculty of Medicine Al-Azhar University Boy's Branch in Cairo, Egypt, 5Misr University for Science & Technology, Egypt, 6Faculty of Medicine_October 6 University, Egypt, 7Faculty of Medicine, Kasr Alainy, Cairo University, Cairo, Egypt, 8Poznan University of Medical Sciences, Poznań, Poland
On behalf of:
Background and aims: Chronic subdural hematoma (CSDH) is a frequently diagnosed neurosurgical condition that is typically managed using burr hole craniotomy. However, a newer technique known as Endoscopic-assisted evacuation has recently been used for the treatment of CSDH.
Objective: Our primary objective is to compare the safety and effectiveness of Endoscopic-assisted evacuation with non-Endoscopic evacuation for the treatment of CSDH.
Methods: We systematically searched four databases: PubMed, Cochrane Library, Scopus, and Web of Science. Our inclusion criteria for studies were those comparing Endoscopic vs non-Endoscopic intervention for CSDH patients. We used Review Manager Software to conduct statistical analysis and compare the five primary outcomes between the two groups.
Results: We selected nine studies with a total of 1136 patients for inclusion in our meta-analysis. Our statistical analysis showed that there was a significant difference in recurrence rate between the two groups (Odds Ratio (OR)=0.32, 95% Confidence Interval (CI) 0.18 to 0.55, p < 0.0001). In terms of mortality rate, there was no statistically significant difference (OR=0.65, 95% CI 0.26 to 1.26, p=0.35). The morbidity rate for Endoscopic evacuation was superior (OR=0.29, 95% CI 0.16 to 0.51, P=0.0001). Lastly, Endoscopic evacuation patients had a shorter length of hospital stay (days) (Mean Difference (MD)=-1.33, 95% CI -2.31 to -0.34, p=0.008) and length of surgery (minutes) (MD=17.95, 95% CI 12.34 to 19.62, p=0.0003).
Conclusions: Our findings suggest that Endoscopic-assisted evacuation may be a better choice for the treatment of chronic subdural hematoma. However, further research including randomized controlled trials is needed to confirm these findings.
Disclosures of Interest: No
Abstract N°: 418
A COMPARISON OF SUBPERIOSTEAL OR SUBGALEAL DRAINAGE WITH SUBDURAL DRAINAGE ON THE OUTCOME OF CHRONIC SUBDURAL HEMATOMA SURGERY
Ibrahim Serag1, Ahmed Aljabali2, Aboalmagd Hamdallah3, Abdelrahman Ayman Khattab4, Mohammad Al-Jafari5, Mariam Abdelhady6, Amro Elrosasy*7, Mohamed Abouzid8
1Faculty of Medicine - Mansoura University, Egypt, 2Jordan University of Science & Technology (JUST), , Jordan, 3Faculty of Medicine, Al-Azhar University Damietta, Egypt, 4Faculty of Medicine Al-Azhar University Boy's Branch in Cairo, Egypt, 5 , Mouʿtah, Jordan, 6Faculty of Medicine_October 6 University, Egypt, 7Faculty of Medicine, Kasr Alainy, Cairo University, Cairo, Egypt, 8Poznan University of Medical Sciences, Poznań, Poland
On behalf of:
Background and aims: Chronic subdural hematoma (CSDH) is a common neurosurgical condition, especially in the elderly. There are various means to treat CSDH with controversies in operative management. One of the options is whether the placement of subperiosteal /subgaleal position drain (SPGD) or subdural drain (SDD) affects the outcome or not.
we aimed to compare the outcome of SPGD versus SDD in surgically treated patients of CSDH.
Methods: We searched PubMed, Cochrane, Scopus, and Web of Science (WOS) till September 2023. We included observational and controlled trials comparing drain positions following the evacuation of CSDH.
Results: Our analysis included 15 studies involving 4070 patients, 1863 (45.8%) underwent SPGD, and 2207 (54.2%) underwent SDD. The pooled overall recurrence rates demonstrated that the use of an SPGD was associated with a lower recurrence rate compared with the use of an SDD (OR= 0.81; 95% CI [0.66, 1], P-value= 0.05), Pooled results were homogenous (P-value= 0.25, I2= 18%). The pooled overall analysis estimated that the use of an SPGD was associated with a lower brain injury rate compared with the use of an SDD (OR= 0.53; 95% CI [0.30, 0.93], P-value= 0.03), Pooled results were homogenous (P-value= 0.67, I2= 0) No significant differences were identified between the SPD and SDD groups in terms of surgical infection rate (P-value= 0.97), mortality rate (P-value= 0.19), and seizure rate (P-value= 0.85).
Conclusions: Craniotomy with SPGD can be recommended as an effective and safe surgical procedure for CSDH patients. It has a lower recurrence rate and reduced incidence of postoperative brain injuries.
Disclosures of Interest: No
Abstract N°: 951
ASSOCIATION OF PERIHAEMATOMAL OEDEMA & OUTCOME AFTER INTRACEREBRAL HAEMORRHAGE (ICH)-INDIVIDUAL PARTICIPANT DATA META-ANALYSIS
Neshika Samarasekera*1
1Edinburgh, Division of Clinical Neurosciences, Edinburgh, United Kingdom
On behalf of: ICH PHO IPDMA collaboration and VISTA ICH steering committee
Background and aims: Peri-haematomal oedema (PHO) is associated with worse functional outcome after ICH but the association between change in PHO volume and outcome after adjustment for confounders is unclear.
Methods: We aimed to determine if the change in absolute PHO volume between the diagnostic scan and a repeat scan 24 ±12 hours after ICH onset is associated with functional outcome. We did an individual participant data meta-analysis of observational studies, randomised controlled trials and the VISTA ICH collaboration (PROSPERO CRD42021253263). We selected variables a priori based on their known association with ICH outcome and constructed a multivariable logistic regression model of the association between change in PHO volume and poor functional outcome (death or dependency using the modified Rankin scale 90±14 days after ICH onset).
Results: We included 1347 participants (male n= 831 (62%); median age 66 years; IQR 55-75 years) from six cohorts. The median time interval from onset to first scan was 2 (IQR 1-3) hours when median ICH volume was 11 (IQR 6-22) ml, median PHO volume was 4 (IQR 2-11) ml and 425 (32%) had intraventricular extension. After adjustment for sex, age, ICH volume and intraventricular extension, the odds of a poor outcome increased by 4% (95% CI 1-6) per ml increase in PHO volume between the first scan and 24 hours.
Conclusions: Increase in PHO volume between the first scan and a 24 hour scan is associated with worse functional outcome after adjusting for confounders making early change in PHO volume a therapeutic target.
Disclosures of Interest: Yes
Abstract N°: 599
OPTIMAL MAGNITUDE OF BLOOD PRESSURE REDUCTION ON HEMATOMA GROWTH AND FUNCTIONAL OUTCOMES IN INTRACEREBRAL HEMORRHAGE
Qi Li*1, Xinni LV2, Andrea Morotti3, Andrew Warren4, Adnan Qureshi5, Dar Dowlatshahi6, Guido Falcone7, Ashkan Shoamanesh8, Santosh Murthy9, Joshua Goldstein10
1The Second Affiliated Hospital of Anhui Medical University, Neurology, 2The First Affiliated Hospital of Chongqing Medical University, 3Azienda Socio Sanitaria Territoriale Spedali Civili, 4Massachusetts General Hospital, Department of Neurology, 5Zeenat Qureshi Stroke Institute and Department of Neurology, University of Missouri, 6University of Ottawa and Ottawa Hospital Research Institute, Department of Medicine, Division of Neurology, 7Yale School of Medicine, Department of Neurology, 8McMaster University, Population Health Research Institute, Department of Medicine, Division of Neurology, 9Weill Cornell Medicine, Neurology, 10Massachusetts General Hospital, Harvard Medical School, Department of Emergency Medicine
On behalf of:
Background and aims: We sought to ascertain the optimal magnitude of early SBP reduction which would yield the greatest benefit for patients enrolled in Antihypertensive Treatment of Acute Cerebral Hemorrhage 2 trial (ATACH2).
Methods: We performed a post hoc analysis of the ATACH-2 trial of intensive BP reduction. The magnitude of SBP reduction was defined as admission SBP minus minimum SBP at 2h after randomization. Eligible subjects were divided into 5 groups by 15mmHg strata of magnitude of SBP reduction (<40, 55-70, 70-85, 80, ⩾85mmHg). Hematoma expansion was defined as a relative increase >33% from baseline to 24-hour follow-up CT scan as in the main trial. Associations of magnitude of BP reduction on hematoma growth and functional outcomes were assessed using multivariable logistic regression analysis.
Results: A total of 925 (92.5%) patients were included in the analysis. The median magnitude of SBP reduction within 2 hours after ICH were 68 (IQR: 48-88) mm Hg. Of those, 209 (22.6%) experienced hematoma expansion, and 516 (55.8%) had poor outcome. The frequency of hematoma expansion decreased linearly among subjects in five SBP reduction groups (p=0.006). In the adjusted analysis, hematoma growth was less likely to occur in patients with SBP reduction ⩾70mmHg. After adjusting for confounders, a larger magnitude of SBP reduction group (⩾55 mmHg) within 2 hours was associated with lower risks of poor outcome.
Conclusions: A moderate degree of SBP reduction is associated with reduced hematoma growth and improved functional outcome after ICH.
Disclosures of Interest: No
Abstract N°: 716
A SIMPLE CT SCORE PREDICTS EARLY NEUROLOGICAL DISABILITY AND SURVIVAL IN INTRACEREBRAL HEMORRHAGE (IMBES)
Ralf Watzlawick*1, Ahmed Elbaz2, Christian Taschner2, Christian Fung1, Jürgen Beck1
1University of Freiburg, Medical Center, Department of Neurosurgery, Freiburg im Breisgau, Germany, 2University of Freiburg, Medical Center, Department of Neuroradiology, Freiburg im Breisgau, Germany
On behalf of:
Background and aims: Treatment of spontaneous intracerebral hemorrhage (ICH) remains challenging without clear evidence for medical or surgical treatment. Radiological assessment of the initial CT scan after ICH was performed based on three axial slides – resulting in the intracerebral mass and brain edema score (IMBES).
Methods: Primary endpoint was the neurological recovery after acute phase of clinical treatment measured by the modified Rankin Scale (mRS). Two independent reviewers screened each CT scan and IMBES was calculated by visual inspection of three defined CT slides (Figure 1) taking about 30 seconds per patient.
Results: We identified 762 patients treated between 01/2009 and 01/2019. The median age was 75.5 years (IQR: 64.3 – 81.1) and the mean of the ICH volume was 46.1ml (SE: 1.69). After multiple logistic regression patients’ age, documented renal insufficiency, ICH volume and IMBES remained statistically significant. IMBES indicated a clear correlation with clinical outcome and could predict severe impairment (mRS >3) for patients with CT scoring greater than three (Figure 2). Regression for mortality within acute phase confirmed ICH volume, patients’ age and the IMBES as significant. At the control examination (mean: 66.25 days, IQR: 49.0 – 108.0) age and IMBES remained significant for mRS.
Conclusions: Decreased neurological recovery at discharge was observed for high IMBES values. Mortality within the acute phase and neurological outcome at a later control examination confirmed the predictive value. Time efficient scoring can be used to identify patients at high risk for impaired neurological outcome making clinical decisions more transparent.
Disclosures of Interest: No
Abstract N°: 1274
ASSOCIATION OF ANTITHROMBOTIC DRUG USE WITH INCIDENT INTRACEREBRAL HEMORRHAGE LOCATION: A POPULATION-BASED CASE-CONTROL STUDY
Nils Boe*1, Stine Hald1, Alexandra Kristensen1, Sören Möller2,3, Rustam Salman4, Jeseper Hallas5, Luis Rodríguez6, Magdy Selim7, Larry Goldstein8, David Gaist1
1Odense University Hospital, Neurology, Odense, Denmark, 2OPEN, Open Patient data Explorative Network, Odense, Denmark, 3University of Southern Denmark, Clinical research, Odense, Denmark, 4University of Edinburgh, Centre for clinical brain science, Edinburgh, United Kingdom, 5Odense University Hospital, Department of Clinical Pharmacology, Odense, Denmark, 6Calle del Almirante, 28, Centro Español de Investigación Farmacoepidemiológica, Madrid, Spain, 7Beth Israel Deaconess Medical Center, Boston, United States, 8University of Kentucky, Department of Neurology and Kentucky Neuroscience Institute, Lexington, United States
On behalf of:
Background and aims: We aimed to explore the association of various antithrombotic drugs with the risk of ICH by location.
Methods: We verified all cases of incident ICH in people aged ⩾50 years in Southern Denmark from 2009-2018 who we matched by age, sex, and calendar year with general population controls (1:40 ratio). We categorized ICH location as lobar or non-lobar. We used conditional logistic regression to calculate odds ratios adjusted for confounders (aORs) [95% confidence intervals] for the associations between use of clopidogrel, aspirin, vitamin-K-antagonists (VKA), or direct oral anticoagulants (DOACs) and lobar and non-lobar ICH. We used 2-sample Wald test to evaluate differences in strength of location-specific associations for clopidogrel vs aspirin and VKA vs DOAC.
Results: 1,040 lobar (52.1% men, mean age 75.2-years) and 1,263 non-lobar cases (54.2% men, mean age 73.6-years) were matched to 41,651 and 50,574 controls, respectively. Clopidogrel use was more strongly associated with lobar ICH than aspirin use (aOR 3.46 [2.45-4.89] vs. aOR 2.14 [1.74-2.63]; p=0.019), but the associations were similar for non-lobar ICH (aOR 2.44 [1.71-3.49]) vs. aOR 1.77 [1.47-2.15]; p=0.12). VKA use was more strongly associated with lobar ICH than DOAC use (aOR 3.66 [2.78-4.80] vs. aOR 1.66 [1.02-2.70]; p=0.006), but the associations were similar for non-lobar ICH (aOR 4.62 [3.67-5.82] vs. aOR 3.44 [2.33-5.08]; p=0.20).
Conclusions: Use of antithrombotic dugs was associated with an increased risk of ICH with associations that varied by location and drug. This may reflect differences in ICH causes and the mechanisms of drugs’ actions.
Disclosures of Interest: Yes Dr Gaist received speakers’ honoraria from Pfizer and Bristol Myers Squibb outside the submitted work and participated in research outside the submitted work funded by Bayer with funds paid to the institution where he is employed.
Abstract N°: 1276
USE OF ANTITHROMBOTIC DRUGS AND SHORT-TERM SURVIVAL AFTER INTRACEREBRAL HAEMORRHAGE
Christian Jørgensen*1, Nils Boe1, Stine Hald1, Christian Ovesen1,2, Rustam Salman3, Larry Goldstein4, Magdy Selim5, Jesper Hallas6, Luis Rodríguez7, David Gaist1
1Odense University Hospital, Research Unit for Neurology, Odense, Denmark, 2Bispebjerg Hospital, Department of Neurology, Copenhagen, Denmark, 3University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom, 4University of Kentucky, Department of Neurology and Kentucky Neuroscience Institute, Lexington, United States, 5Harvard Medical School, Beth Israel Deaconess Medical Center, Boston, United States, 6University of Southern Denmark, Department of Clinical Pharmacology, Pharmacy and Environmental Medicine, Odense, Denmark, 7Centro Español Investigación Farmacoepidemiológica, Madrid, Spain
On behalf of:
Background and aims: Use of antithrombotic drugs is a risk factor for intracerebral haemorrhage (ICH), but there are few data on the relationship between the type of antithrombotic therapy (i.e., oral anticoagulant (OACs) and platelet antiaggregants (PAs)), and short-term survival in unselected patient cohorts.
Methods: 1,060 patients age ⩾55-years with a first-ever spontaneous ICH in Southern Denmark from 2015-2018 and who had an available index brain CT scan (98% of all eligible patients) were included. Based on filled prescriptions (and for VKA in addition an admission INR>1.5), use of antithrombotic drugs on the date of ICH was classified as OAC use, PA use, or no use of antithrombotic therapy. The primary outcome was 90-day mortality. Relative risk (RR) for death was calculated using binomial regression and potential confounders at ICH onset were adjusted by using standardized mortality ratio weighting.
Results: Compared to patients with no use of antithrombotic therapy (n=440), being prescribed OACs (n=194; 81 direct oral anticoagulant, 113 vitamin K antagonist) was associated with a 56% higher 90-day mortality risk (RR 1.56; 95% CI 1.28-1.90). No evidence was observed for an increased mortality risk among patients prescribed a PA (n=273; RR 1.17; 95% CI 0.99-1.37).
Conclusions: OAC use is associated with a higher risk of 90-day mortality after an ICH. No evidence was observed for an increased mortality risk in patients who were prescribed PAs and had an ICH.
Disclosures of Interest:Yes Dr Gaist received speakers’ honoraria from Pfizer and Bristol Myers Squibb outside the submitted work and participated in research outside the submitted work funded by Bayer with funds paid to the institution where he is employed.
Abstract N°: 1289
TEMPORAL CHARACTERISTICS OF DWI LESIONS IN THE ACUTE AND SUBACUTE PHASE OF SMALL VESSEL DISEASE-RELATED INTRACEREBRAL HAEMORRHAGE
Martina Goeldlin*1, Rosa Kuettner1,2, Bernhard Siepen1, Alexandros Polymeris3, Carlo Cereda4, Susanne Wegener5, Emmanuel Carrera6, Arsany Hakim7, Mira Katan3, David Seiffge1
1Universitätsklinik für Neurologie, Inselspital Bern, Bern, Switzerland, 2, Witten/Herdecke, Germany, 3Universitätsspital Basel, Department of Neurology, Basel, Switzerland, 4EOC Ospedale Regionale di Lugano - Civico, Stroke Center, Department of Neurology, Lugano, Switzerland, 5USZ Neurology Clinic, Zürich, Switzerland, 6Hôpitaux Universitaires de Genève (HUG), Department of Neurology, Genève, Switzerland, 7Universitätsinstitut für Diagnostische und Interventionelle Neuroradiologie, Bern, Switzerland
On behalf of: Swiss Stroke Registry Investigators
Background and aims: Diffusion-weighted imaging (DWI) lesions in patients with intracerebral haemorrhage (ICH) are associated with poor outcomes. Whether they are associated with the underlying small vessel disease (SVD), consequences of acute treatment or secondary brain damage is unknown.
Methods: This study in the Swiss Stroke Registry analyzed patients with SVD-associated ICH who underwent MRI within 14 days after the index ICH. The primary outcome was presence of DWI lesions on the first available MRI. We measured cerebral amyloid angiopathy (CAA) and SVD severity using total MRI marker burden scores. We performed multivariable regression analyses. Timing of MRI was used as continuous variable and dichotomized to hyperacute (=first imaging on admission prior to any treatment) versus subacute (=after admission up to day 14).
Results: We included 645 patients (median age 73 years, IQR 64-79, 46.5% female), 103 (16.0%) had hyperacute and 542 (84.0%) subacute MRI. Overall, 166 patients (25.7%) had DWI lesions. In multivariable analysis, hyperacute (vs subacute) MRI was not associated with presence of DWI lesions, but timing was associated with presence of DWI lesions as continuous variable (aOR 1.06, 95%CI 1.00-1.12 per day, p=0.040). Higher CAA (aOR 1.99, 95%CI 1.40-2.81) and SVD burden scores (aOR 1.64, 95%CI 1.16-2.33) were independently associated with presence of DWI lesions.
Conclusions: DWI lesions in patients with ICH were associated with timing of MRI acquisition and burden of small vessel disease, suggesting that acute treatments, secondary damage and underlying SVD play a role in their pathogenesis.
Disclosures of Interest: No
Abstract N°: 1618
LEAKAGE SIGN FOR PREDICTION OF INTRACEREBRAL HEMATOMA EXPANSION AND NEW STRATEGY FOR OUTCOME IMPROVEMENT
Motohiro Morioka*1,1, Kimihiko Orito1, Jin Kikuchi1, Aya Hashimoto1, Kiyohiko Sakata1, Masaru Hirohata1
1Kurume Univ. School of Medicine
On behalf of:
Background and aims: Hematoma expansion of spontaneous intracerebral hematoma (sICH) is one of the major poor prognosis factors. We established the most reliable predictor of hematoma expansion using contrast enhancement CT; named as “Leakage sign (LS)” which predict hematoma expansion with high specificity and sensitivity of about 90% (Stroke 2016). In this study, we reported the LS characteristics in each sICH location and effectiveness of new therapeutic strategy for prevention of hematoma expansion using LS.
Methods: We performed CTA for over 300 consecutive patients presenting with sICH. Comparing CTA phase and delayed phase (5 minutes after the CTA phase), We defined a positive LS as a >10% increase in Hounsfield units. From 2020, we performed blood pressure active lowering (BPAL) therapy especially only for LS positive patients, in which blood pressure was lowered under 120mmHg only 6 hours just after diagnosis.
Results: Excluding the emergent operated cases, Positive leakage signs were present in about 40 % patients showed hematoma expansion. The highest LS positive rate was found in subcortical hematoma (55.5%) and the lowest rate in cerebellar hematoma (20.2%). The preliminary data (n=27) of BPAL study showed, BPAL therapy significantly decreased hematoma expansion to 10.5 %.
Conclusions: The results indicate that the leakage sign is a useful and sensitive method to predict hematoma expansion and might be useful for surgical indication. Furthermore, BPAL therapy might improve the outcome of LS positive sICH patietnts
Disclosures of Interest: No
Abstract N°: 1947
ASSOCIATION OF CHARLSON COMORBIDITY INDEX AND THE RISK OF HEMORRHAGIC STROKE AMONG PATIENTS WITH ATRIAL FIBRILLATION
Paula Tiili*1,2, Mika Lehto1,2, Olli Halminen3, Jari Haukka2, Miika Linna3,4, Aapo Aro2,5, Pirjo Mustonen6,7, Juha Hartikainen4,8, Juhani Airaksinen6,7, Jukka Putaala2,9
1Helsinki University Hospital, Primary health care unit, Helsinki, Finland, 2University of Helsinki, Helsinki, Finland, 3Aalto University, Department of Industrial Engineering and Management, Espoo, Finland, 4University of Eastern Finland, Kuopio, Finland, 5Helsinki University Hospital, Heart and Lung Center, Helsinki, Finland, 6Turku University Hospital, Turku, Finland, 7University of Turku, Turku, Finland, 8Kuopio University Hospital, Kuopio, Finland, 9Helsinki University Hospital, Department of Neurology, Helsinki, Finland
On behalf of: FinACAF Study Group
Background and aims: The risk of haemorrhagic stroke (HS) rises with oral anticoagulant use. Yet, high-risk patient identification is complicated by the fragility associated with advanced age and comorbidities. Our aim was to assess the predictability of the Charlson Comorbidity Index (CCI) for HS risk among incident atrial fibrillation (AF) patients.
Methods: Analyzing FinACAF study data (2010-2018) with 152,192 incident AF patients without prior intracranial bleeding, we categorized CCI scores as ⩽2 or >2. Additional variables included age, sex, CHA2DS2-VASc, HAS-BLED, and the initial oral anticoagulant purchased (none, warfarin, NOAC) after AF diagnosis. Kaplan-Meier and Cox regression models evaluated HS risk, stratified by CCI score.
Results: The study cohort (50% women, median age 74.3 years) contributed 359,666 person-years and experienced 1,073 first-ever HS events (incidence rate: 2.98 [95% CI 2.80-3.18] per 1000 person-years). [Table 1]
High CCI (>2) patients had significantly higher HS incidence (4.67 vs. 2.74) and distinct Kaplan-Meier curves. [Figure] Adjusting for age, sex, CHA2DS2-VASc, and first OAC after AF diagnosis, CCI >2 correlated with elevated HS risk. Subgroup analyses showed loss of associations in sex, CHA2DS2-VASc, and HAS-BLED scores among high CCI patients, while increasing age had a negative association. NOAC purchase associated with significantly reduced HS risk compared to warfarin or no OAC purchase. [Table 2]
Conclusions: CCI offers valuable insights in identifying AF patients at higher HS risk. Although anticoagulation typically raises bleeding risk, the study found reduced risk among those with a NOAC purchase, suggesting other factors influence both OAC initiation and HS risk.
Disclosures of Interest: No
Abstract N°: 2337
TEMPORAL CLUSTERING OF INTRACEREBRAL HAEMORRHAGE IN CEREBRAL AMYLOID ANGIOPATHY
Simon Fandler-Höfler*1,2, Philip Nash2, Lena Obergottsberger1, Hatice Ozkan2, Larysa Panteleienko2, Rom Mendel2, Kitti Thiankhaw2, Christian Enzinger1, Thomas Gattringer1,3, David J Werring2
1Medical University of Graz, Department of Neurology, Graz, Austria, 2UCL Queen Square Institute of Neurology, Stroke Research Centre, Department of Brain Repair & Rehabilitation, London, United Kingdom, 3Medical University of Graz, Division of Neuroradiology, Vascular and Interventional Radiology, Department of Radiology, Graz, Austria
On behalf of:
Background and aims: While it is known that patients with intracerebral haemorrhage (ICH) are at risk of recurrence, it is unclear whether this risk is linear and whether temporal patterns of recurrence vary according to the underlying small vessel arteriopathy.
Methods: We investigated early recurrent ICH (within 90 days of index ICH) in two large cohorts of consecutive patients with first-ever ICH and available MRI, excluding patients with secondary causes and those without at least six months of follow-up. We classified ICH aetiology based on neuroimaging.
Results: In 682 included patients (median age 68 years, 40.3% female), the median follow-up time was 4.1 years (IQR 1.8-7.7 years). 18 (2.6%) had an early recurrent ICH ⩽90 days after the index ICH. Patients with an early recurrent ICH were older and more frequently had lobar ICH, probable cerebral amyloid angiopathy (CAA), cortical superficial siderosis, lobar microbleeds and enlarged perivascular spaces in the centrum semiovale.
In patients with CAA, the risk of recurrent ICH was increased six-fold within the first three months (10% vs. 1-2% each for months 4-6, 7-9 and 10-12). The temporal recurrence risk appeared linear in ICH not associated with CAA. Among early recurrent ICH, 63% occurred in close proximity to the index ICH. Notably, among survivors of recurrent ICH, the further recurrence risk was low (3.7 per 100 patient-years).
Conclusions: The risk of early recurrent ICH is markedly increased in patients with CAA. Temporal and spatial clustering suggests a transient and localised active bleeding-prone disease process in some patients with CAA.
Disclosures of Interest: No
Abstract N°: 2389
INFLUENCE OF TIME FROM ONSET TO ARRIVAL IN THE OUTCOME OF PATIENTS WITH ACUTE INTRACEREBRAL HAEMORRHAGE: POPULATION-BASED STUDY
Álvaro Lambea-Gil1, Joan Martí-Fàbregas1, Marina Guasch Jiménez*1, Ana Núñez-Guillén2, David Rodriguez-Luna3, Laura Llull4, Yolanda Silva5, Ana Rodríguez-Campello6, Isabel Puig7, Anna Ramos Pachon1
1Hospital de la Santa Creu i Sant Pau, Neurology, Stroke Unit, Barcelona, Spain, 2Hospital Universitari de Bellvitge, Neurology, Stroke Unit, Hospitalet de Llobregat, Spain, 3Hospital Universitari Vall d’Hebron, Neurology, Stroke Unit, Barcelona, Spain, 4Hospital Clínic de Barcelona, Neurology, Stroke Unit, Barcelona, Spain, 5Hospital Dr. Josep Trueta, Neurology, Stroke Unit, Girona, Spain, 6Hospital del Mar, Neurology, Stroke Unit, Barcelona, Spain, 7Hospital Universitari Germans Trias i Pujol, Neurology, Stroke Unit, Badalona, Spain
On behalf of: P Camps-Renom, L Prats-Sánchez, S Abilleira, M Salvat-Planas, N Pérez de la Ossa, S Amaro, O Pancorbo, B Lara, M Gómez-Choco, D Vázquez-Justes, N Guanyabens, D Cocho, L Seró, D Cánovas, E Giralt-Steinhauer, M Puig, J Krupinski
Background and aims: In patients with acute spontaneous intracerebral haemorrhage (ICH), a bundle of care applied within the first hours has been associated with a better prognosis. However, limited data exist on the direct relationship between time from symptoms onset to hospital arrival and functional outcome. Evaluate its impact may be crucial in the organization of stroke care systems, to ensure an appropriate level of care.
Methods: Prospective study using a population-based ICH registry (Catalonia, Spain: March 2020 - March 2022). We analysed adult patients with spontaneous ICH, admitted within the first 24 hours, and a prior modified Rankin scale (mRS) score of 0-3. Demographic, clinical, radiological and therapeutic variables were collected. Certified blinded personnel centrally assessed functional outcomes. The primary outcome was the shift in mRS score at three months. Multivariable ordinal regression analysis (adjusted for age, prior mRS, baseline NIHSS, ICH volume, and intraventricular haemorrhage) examined the association between time from symptoms onset to hospital arrival (OTA) and functional outcome. A sensitivity analysis excluding ICH of unknown onset was performed.
Results: We included 1,842 patients (mean age 70 years, 37.1% women). Median OTA was 167 minutes (IQR 74-540). In multivariable analysis, earlier OTA was not associated with functional outcome. Considering only known-onset ICH, earlier OTA showed direct association with worse functional outcome (cOR 0.97x1h, 95%CI:0.94-0.99). This effect persisted in patients arriving directly at a comprehensive stroke centre.
Conclusions: In Catalonia, for patients with acute known-onset ICH, early hospital arrival was independently linked to worse functional outcome, regardless of the type of centre.
Disclosures of Interest: No
Abstract N°: 2503
INFLUENCE OF FIRST 24H BLOOD PRESSURE CONTROL IN THE OUTCOME OF PATIENTS WITH INTRACEREBRAL HAEMORRHAGE: POPULATION-BASED STUDY
Álvaro Lambea-Gil1, Joan Martí-Fàbregas1, Garbiñe Ezcurra-Díaz*1, Ana Núñez-Guillén2, David Rodriguez-Luna3, Laura Llull4, Yolanda Silva5, Ana Rodríguez-Campello6, Denisse Wenger7, Anna Ramos Pachon1
1Hospital de la Santa Creu i Sant Pau, Neurology, Stroke Unit, Barcelona, Spain, 2Hospital Universitari de Bellvitge, Neurology, Stroke Unit, Hospitalet de Llobregat, Spain, 3Hospital Universitari Vall d’Hebron, Neurology, Stroke Unit, Barcelona, Spain, 4Hospital Clínic de Barcelona, Neurology, Stroke Unit, Barcelona, Spain, 5Hospital Dr. Josep Trueta, Neurology, Stroke Unit, Girona, Spain, 6Hospital del Mar, Neurology, Stroke Unit, Barcelona, Spain, 7Hospital Germans Trias i Pujol, Neurology, Stroke Unit, Badalona, Spain
On behalf of: P Camps-Renom, L Prats-Sánchez, S Abilleira, M Salvat-Planas, N Pérez de la Ossa, S Amaro, O Pancorbo, B Lara, M Gómez-Choco, D Vázquez-Justes, N Guanyabens, D Cocho, L Seró, D Cánovas, E Giralt-Steinhauer, M Puig, J Krupinski
Background and aims: For patients with acute intracerebral haemorrhage (ICH), recent studies suggest potential benefits from a bundle of care during the early phase, including blood pressure (BP) control. We aimed to study the effect of BP control during the first 24 hours in a real-life environment using a population-based registry.
Methods: We performed a retrospective study using a population-based prospective registry of ICH cases (Catalonia, Spain: March 2020 - March 2022). The registry comprised adult patients with a spontaneous ICH, admitted within <24 hours, and a previous modified Rankin scale (mRS) score of 0-3. Demographic, clinical, radiological and therapeutic variables were collected. Certified blinded personnel centrally assessed functional outcomes. The primary outcome was the shift in mRS score at three months follow-up. Multivariable ordinal regression analysis (adjusted for age, prior mRS, baseline NIHSS, ICH volume, and intraventricular haemorrhage) was performed to test the association between achieving BP <140/90mmHg during the first 24h and functional outcome.
Results: We included 1,518 patients (mean age 69.5 years, 37.3% women). A BP goal <140/90mmHg during the first 24h was achieved in 779 (51.32%) patients. In multivariable analysis, BP control was associated with a better functional outcome (cOR 1.49, 95%CI:1.21-1.82). In sensitivity analyses, adjusted by type of centre (primary vs. comprehensive stroke centre) and time from symptoms onset to hospital arrival, the effect remained unchanged.
Conclusions: In our setting, achieving a BP target <140/90mmHg during the first 24 hours in patients with acute ICH, was associated with a better outcome, irrespective of centre type and time from onset to admission.
Disclosures of Interest: No
Abstract N°: 558
TRIPLE ANTIHYPERTENSIVE MEDICATION PREDICTION AFTER INTRACEREBRAL HEMORRHAGE (THE TRICH SCORE)
Charming Yeung1, Koon Ho Chan1, Kui Kai Lau1, Kay Cheong Teo*1
1LKS Faculty of Medicine, University of Hong Kong, Division of Neurology, Department of Medicine, Hong Kong
On behalf of:
Background and aims: Most intracerebral hemorrhage (ICH) survivors have uncontrolled hypertension, leading to elevated long-term cardiac and cerebrovascular risk. As many ICH survivors require ⩾3 antihypertensive medications for blood pressure (BP) control, upfront triple antihypertensives would improve therapeutic inertia and consequent better BP control. However, excessive BP lowering with triple antihypertensives remains a concern, especially in older people. Hence, we aim to develop a score to predict the need for ⩾3 antihypertensives for BP control following ICH.
Methods: We retrospectively analyzed consecutive ICH survivors enrolled in the University of Hong Kong stroke registry from 2011-2020. Outpatient BP and antihypertensive medication prescriptions three months post-ICH were reviewed. Patients with uncontrolled hypertension (systolic BP >130mmHg) while on ⩽2 antihypertensives were considered undertreated and excluded. Predictors of the need for ⩾3 antihypertensives were derived using multivariate logistic regression. A prediction score (TRICH) was created based on the β coefficients.
Results: At three months post-ICH, 43.7% (181/414) of patients were prescribed ⩾3 antihypertensive medications. Age <60, males, estimated glomerular filtrate rate (eGFR) <60mL/min/1.73m2, and higher admission systolic BP were independently associated with the need for ⩾3 antihypertensives three months post-ICH. The 6-point TRICH score (1 point for age <60, 1 for males, 1 for eGFR <60mL/min/1.73m2, 1 for systolic BP 190-220mmHg, and 2 for >220mmHg) has a c-statistic of 0.703. A dichotomized score of ⩾2 predicted the need for ⩾3 antihypertensive with 0.69 sensitivity and 0.66 specificity.
Conclusions: TRICH score has good discrimination ability. Further study and validation of the TRICH score is required for generalizability.
Disclosures of Interest: No
Abstract N°: 1114
THE PROTEOME OF IMMUNE CELLS-DERIVED EXTRACELLULAR VESICLES. APPROACH TO INFECTION-RELATED OUTCOMES IN INTRACEREBRAL HEMORRHAGE
Fernando Laso1, Dolores Piniella2, Laura Casado Fernández1, Rebeca Gallego Ruiz1, Javier Pozo Novoa1, Susana B. Bravo3, Exuperio Díez Tejedor1, Blanca Fuentes1, Maria Alonso de Leciñana1, María Gutiérrez-Fernández*1
1IdiPAZ La Paz University Hospital, Madrid, Spain, 2Universidad Autónoma de Madrid, Madrid, Spain, 3Health Research Institute of Santiago de Compostela, Spain
On behalf of:
Background and aims: Infection is a common complication of patients with intracerebral hemorrhage (ICH) that negatively impact outcome. Identification of biomarkers of the mechanisms involved, would help predict the evolution and identify therapeutic targets
Methods: Patients with acute ICH were prospectively recruited and followed for six months. The occurrence of infections during the acute phase was registered. Extracellular vesicles (EVs) from blood at 7d were grouped according to their cellular origin by immunoprecipitation with anti CD3 (T cells), anti CD14 (monocytes), and anti CD20 (B cells). The proteome was analyzed in the EVs subpopulations according to the occurrence of infections and the good or poor outcome by DIA SWATH MS
Results: Fifty-four patients were included (Fig1). Proteomic study revealed 109 proteins differentially expressed in infected patients. Those with bad outcome showed: 1) In T cells-derived EVs, up expression of PSME1, MTREX, and H2B1C, related with immune response and DNA damage response, and down expression of FBLN1 and DYL2 related with blood coagulation and apoptosis after stroke; 2) In monocyte derived EVs, up-expression of DPP3, related with proteolysis, and down expression of PCSK9, HCD2, and CMC1, related with metabolic processes; 3) In B cell derived EVS, up expression of SDHA, related with the respiratory electron transport chain, and down expression of COHA1, related with cell matrix adhesion.
Conclusions: The proteome in immune system-derived EVs may serve as biomarker of processes possibly involved in the pathogenic mechanisms that may hamper evolution in patients with ICH and infections.
Disclosures of Interest: No
Abstract N°: 1153
PREHOSPITAL IDENTIFICATION OF INTRACEREBRAL HAEMORRHAGE: A SYSTEMATIC REVIEW OF PREDICTION MODELS
Mohammed Almubayyidh*1, Ibrahim Alghamdi1, David Jenkins2, Adrian Parry-Jones1
1The University of Manchester, Division of Cardiovascular Sciences, Manchester, United Kingdom, 2The University of Manchester, Division of Informatics, Imaging and Data Science, Manchester, United Kingdom
On behalf of:
Background and aims: Spontaneous intracerebral haemorrhage (ICH) is a medical emergency necessitating immediate recognition and treatment. Current prehospital stroke assessment tools have limited accuracy in detecting ICH as they were not specifically designed for this purpose. This systematic review aims to evaluate existing prehospital models for distinguishing ICH from other suspected strokes.
Methods: Two independent reviewers systematically searched three databases (MEDLINE, EMBASE, and CENTRAL) via Ovid from their inception to July 2023, using keywords such as "stroke", "intracerebral hemorrhage", "predict", "model", "prehospital", and their associated terms or synonyms. Subsequently, data extraction was conducted, and the methodological quality was assessed using the Prediction Model Risk of Bias Assessment Tool.
Results: A total of nine prediction studies were included. Five aimed to differentiate stroke subtypes, three distinguished between ICH and ischaemic stroke, and one specifically targeted identifying ICH. All studies exhibited a high risk of bias, mainly in the analysis domain. The performance of the models varied, with the area under the receiver operating characteristic curve ranging from 0.73 to 0.91. Common predictors for ICH in these models included impaired consciousness, headache, speech or language disturbance, and high systolic blood pressure.
Conclusions: Studies evaluating prehospital models for discriminating ICH from other causes of suspected stroke are at high risk of bias. Future studies should aim to address these concerns and include a range of unselected suspected stroke cases to develop a reliable model for identifying ICH. Combining prediction models with point-of-care tests might further improve the accuracy of ICH detection.
Disclosures of Interest: No
Abstract N°: 1327
NERVOUS SYSTEM-DERIVED EXTRACELLULAR VESICLES PROMOTE RECOVERY IN A PRECLINICAL MODEL OF INTRACEREBRAL HEMORRHAGE
Rebeca Gallego Ruiz*1, Javier Pozo Novoa1, Iván García Suárez2, Fernando Laso1, Dolores Piniella3, Maripaz López Molina1, Laura Casado Fernández1, Exuperio Díez Tejedor1, Maria Alonso de Leciñana1, María Gutiérrez-Fernández1
1IdiPAZ La Paz University Hospital, Spain, 2San Agustín University Hospital, Spain, 3Universidad Autónoma de Madrid, Spain
On behalf of:
Background and aims: Our group has shown that circulating extracellular vesicles (EVs) participate in endogenous mechanisms of brain repair and functional recovery after intracerebral hemorrhage (ICH). To refine these findings, we performed a study focused on the administration of EVs of neural origin (NEVs) with the hypothesis that they are directly involved in the repair mechanisms triggered in the brain.
Methods: NEVs from serum of patients with ICH and good outcome were obtained by precipitation and immunoisolation using nervous system markers [neurons (L1CAM), astrocytes (GLAST), microglia (CD13)]. Thirty Sprague-Dawley rats were subjected to an ICH in the striatum by stereotactic injection of 0.5U of collagenase-IV and randomly assigned to 3 groups (n=10): healthy; control: ICH+saline; NEVs: ICH+100µg of NEVs administered intravenously 24h after ICH. Hemorrhage was monitored by B mode ultrasound at 24h, 72h and 28d. Motor function was evaluated by Rogers and Ledged Beam Walking tests at baseline, 24h, 72h, 7d,14d and 28d after ICH. NeuN (mature neuron) and VEGF (vascular growth factor) markers were analyzed in the peri-hematoma zone by immunofluorescence at 28d.
Results: NEVs-treated animals showed a significant improvement in the motor function scores (p<0.05) (Fig1). Besides, the treatment significantly increased NeuN and VEGF expression compared to control group (p<0.05) (Fig2).
Conclusions: NEVs are involved in mechanisms of brain protection and repair after ICH. The analysis of the content of these NEVs presents a promising avenue to deepen the knowledge of these mechanisms for potential therapeutic applications.
Disclosures of Interest: No
Abstract N°: 1345
SIGNATURE AND FUNCTION OF PLASMA EXOSOME-DERIVED CIRCULAR RNAS IN PATIENTS WITH HYPERTENSIVE INTRACEREBRAL HEMORRHAGE
Quandan Tan*1,2, Xiaoyuan Cheng3, Kejie Chen4, Jie Yang5
1Chengdu Medical College, Clinical Medicine, Chengdu, China, 2The First Affiliated Hospital of Chengdu Medical College, neurology, Chengdu, 3The First Affiliated Hospital of Chengdu Medical College, Emergency, Chengdu, 4Chengdu Medical College, Public Health, Chengdu, China, 5Sichuan Provincial People's Hospital, School of Medicine, University of Electronic Science and Technology of Chengdu, China, neurology, Chengdu
On behalf of:
Background and aims: Intracerebral hemorrhage (ICH) is one of the major causes of death and disability, and hypertensive ICH (HICH) is the most common type of ICH. Currently, the outcomes of HICH patients remain poor after treatment, and early prognosis prediction of HICH is important. However, there are limited effective clinical treatments and biomarkers for HICH patients. Although circRNA has been widely studied in diseases, the role of plasma exosomal circRNAs in HICH remains unknown.
Methods: The present study was conducted to investigate the characteristics and function of plasma exosomal circRNAs in six HICH patients using circRNA microarray and bioinformatics analysis.
Results: The results showed that there were 499 differentially expressed exosomal circRNAs between the HICH patients and control subjects. According to GO annotation and KEGG pathway analyses, the targets regulated by differentially expressed exosomal circRNAs were tightly related to the development of HICH via nerve/neuronal growth, neuroinflammation and endothelial homeostasis. And the differentially expressed exosomal circRNAs could mainly bind to four RNA-binding proteins (EIF4A3, FMRP, AGO2 and HUR). Moreover, of differentially expressed exosomal circRNAs, hsa_circ_00054843, hsa_circ_0010493 and hsa_circ_00090516 were significantly associated with bleeding volume and Glasgow Coma Scale score of the subjects.
Conclusions: Our findings firstly revealed that the plasma exosomal circRNAs are significantly involved in the progression of HICH, and hsa_circ_00054843, hsa_circ_0010493 and hsa_circ_00090516 would be new biomarkers therapeutic targets of HICH. This provides the basis for further research to pinpoint the best biomarkers and illustrate the mechanism of exosomal circRNAs in HICH.
Disclosures of Interest: No
Abstract N°: 2380
ACCURACY OF PREHOSPITAL STROKE SCALES FOR DETECTION OF LARGE VESSEL OCCLUSION ISCHAEMIC STROKE OR INTRACEREBRAL HAEMORRHAGE
Ruben van de Wijdeven*1, Jasper Daems1,2, Esmee Venema2,3, Martijne Duvekot1,4, Ido van den Wijngaard5,6, Marieke J.H. Wermer7, Nyika Kruyt6, Henk Kerkhoff4, Diederik Dippel1, Bob Roozenbeek1
1Erasmus MC University Medical Center, Department of Neurology, Rotterdam, Netherlands, 2Erasmus MC University Medical Center, Department of Public Health, Rotterdam, Netherlands, 3Erasmus MC University Medical Center, Emergency Department, Rotterdam, Netherlands, 4Albert Schweitzer Hospital, Department of Neurology, Dordrecht, Netherlands, 5Haaglanden Medical Center, Den Haag, Netherlands, 6Leiden University Medical Center, Department of Neurology, Leiden, Netherlands, 7University Medical Center Groningen, Groningen, Netherlands
On behalf of: PRESTO and LPSS investigators
Background and aims: Prehospital stroke scales may be used for detection of anterior-circulation large vessel occlusions (aLVO) in suspected stroke patients, to enable prehospital transportation decision making. Ongoing randomized trials investigating the efficacy of minimally invasive surgery in intracerebral haemorrhage (ICH) may uncover a time-dependent treatment effect, potentially transforming the field of prehospital triage. We studied the diagnostic accuracy of prehospital stroke scales for the detection of a composite outcome of ICH or aLVO.
Methods: We pooled the individual patient data from two prospective cohort studies (PRESTO and LPSS). Paramedics assessed neurological deficits in suspected stroke patients in the ambulance, which enabled reconstruction of eight prehospital stroke scales. We included adult patients with suspected stroke presenting within 6 hours of last seen well. We calculated the area under the curve (AUC) for detection of the composite outcome of aLVO or ICH, and assessed sensitivity for ICH separately.
Results: We included 2358 patients with a suspected stroke. 405 (17%) patients were diagnosed with the composite outcome. Of these, 231 (10%) had an aLVO and 174 (7%) had ICH. Median [IQR] NIHSS was 12 [5-17] for patients with ICH or aLVO and 1 [0-4] for patients without ICH or aLVO. The AUC for the composite outcome ranged from 0.72 (95%CI:0.70-0.75) for FASTPLUS to 0.82 (95%CI:0.79-0.84) for RACE. Sensitivity for ICH ranged from 0.41 (95%CI:0.34-0.49) for CPSS3 to 0.59 (95%CI:0.51-0.66) for LAMS.
Conclusions: Although prehospital stroke scales have acceptable-to-good performance for detection of a composite outcome of ICH or aLVO, better tools are required to improve prehospital ICH detection.
Disclosures of Interest: No
Abstract N°: 2436
ETIOLOGIES OF INTRACEREBRAL HEMORRHAGE IN PATIENTS WITH ATRIAL FIBRILLATION ON OR OFF ORAL ANTICOAGULANTS: THE NEURO-AFIB STUDY
Edip Gurol*1, Alvin Das1, Avia Abramovitz Fouks1, Ofer Rotchild1, Elif Gokcal1, Shadi Yaghi2, Eric Smith3
1Massachusetts General Hospital, Harvard Medical School, Neurology, Boston, United States, 2Brown Neurology, West Warwick, United States, 3University of Calgary, Calgary, Canada
On behalf of: The Neuro-AFib Study Group
Background and aims: Intracerebral hemorrhage (ICH) is the most feared complication of oral anticoagulants (OAC) used to prevent ischemic strokes (IS) in patients with atrial fibrillation (AF). As different ICH etiologic factors correspond to different ICH risks, we aimed to present the causes of ICH in AF patients who were or were not using OAC.
Methods: The Neuro-AFib study is a multicenter effort to elucidate the current causes and consequences of IS and ICH in AF patients. Detailed clinical, laboratory and imaging data were collected from consecutive AF patients admitted to 15 US stroke centers with an IS or ICH between 1/2018-12/2019. ICH etiologies on OAC (OAC-ICH) and off AC (nonAC-ICH) are compared.
Results: A total of 868 AF patients presented with ICH. 571 patients (66%) were on OAC at the time of their ICH [58% on direct OAC (DOAC), 40% on warfarin, 2% on heparin]. OAC-ICH patients were older than nonAC-ICH (76.6+10 vs 74.4+13, p=0.006). CHA2DS2-VASC was higher in OAC-ICH (4.3+1.6 vs 3.9+1.9, p=0.001). Cerebral amyloid angiopathy (CAA) was diagnosed in 42.5% of the ICH patients while hypertensive arteriolosclerosis (HA) in 57.5%. HA was the more common ICH etiology among OAC-ICH (65%) compared to nonAC-ICH (49%). Among OAC-ICHs, DOAC-ICHs tended to have more HA etiology than warfarin-ICH (p=0.09).
Conclusions: Despite the known high ICH risk of CAA, HA was more common among OAC-ICH (especially DOAC-ICH) patients, supporting the view that the presence/absence of HA risk markers such as deep ICH/microbleeds are as important as CAA-markers in determining the optimal stroke prevention method in AF patients.
Disclosures of Interest: Yes Research grants to the Hospital from AVID, Pfizer, Boston Scientific
Abstract N°: 2440
SEX DIFFERENCES IN AETIOLOGY OF ACUTE INTRACEREBRAL HAEMORRHAGE AND ASSOCIATED SMALL VESSEL DISEASE PATTERNS
Linda Fabisch*1, Wenpeng Zhang2, Martina Locatelli2, Yang Du2, Christian Enzinger1, Robert J Simister2, H Rolf Jäger2, Thomas Gattringer1,3, David J Werring2, Simon Fandler-Höfler1,2
1Medical University of Graz, Department of Neurology, Graz, Austria, 2University College London Queen Square Institute of Neurology, Department of Brain Repair and Rehabilitation, London, United Kingdom, 3Medical University of Graz, Department of Radiology, Division of Neuroradiology, Vascular and Interventional Radiology, Graz, Austria
On behalf of: the SIGNAL and Graz ICH collaborators
Background and aims: Underlying pathologies of intracerebral haemorrhage (ICH), in particular small vessel disease (SVD) are subject of current research, and it is unclear whether sex-related factors play a relevant role. Therefore, we aimed to investigate whether there are sex-related differences in aetiology and MRI features of SVD in patients with ICH.
Methods: We included patients from two large observational study cohorts with available MRI at baseline. ICH aetiology was defined based on MRI and clinical findings and grouped as arteriolosclerosis, cerebral amyloid angiopathy, mixed small vessel disease, macrovascular, other secondary causes and cryptogenic. Cryptogenic ICH was defined as both the absence of SVD markers and secondary causes of ICH.
Results: We identified 1043 patients (mean age 66 years, 58% male) with acute ICH. Men had a higher rate of cryptogenic ICH than women (OR 1.64, 95% CI 1.13-2.36, p=0.007), there were no differences in the other aetiological subgroups. After correction for age and hypertension, men had a higher rate of deep lacunes (OR 1.48, 95% CI 1.12-1.96, p=0.006) and severely enlarged perivascular spaces in the basal ganglia (OR 1.45, 95% CI 1.04-2.02, p=0.027), with no differences in cerebral microbleeds or severity of white matter hyperintensities.
Conclusions: While the higher rate of deep lacunes and enlarged perivascular spaces implies a higher severity of arteriolosclerosis in men, the increased rate of cryptogenic ICH in men (possibly caused by transient risk factors or incipient SVD) raises new questions. More research is needed to better understand sex-related differences in ICH.
Disclosures of Interest: No
Abstract N°: 2441
SPECIFIC REVERSAL AGENTS FOR DOACS IN SURGICALLY TREATED INTRACRANIAL HAEMORRHAGE – A REVIEW OF LITERATURE
Laura Zeller*1, Jonas Rohr2, Alexander Kaserer3, Jan-Dirk Studt4, Tilman Schubert5, Christoph Globas6, Giovanna Brandi1, Luca Regli2, Menno Germans2
1University Hospital of Zürich, Neurocritical Care Unit, Zürich, Switzerland, 2University Hospital of Zürich, Department of Neurosurgery, Zürich, Switzerland, 3University Hospital of Zürich, Institute for Anaesthesiology, Zürich, Switzerland, 4University Hospital of Zürich, Department of Medical Oncology and Hematology, Zürich, Switzerland, 5University Hospital of Zürich, Department of Neuroradiology, Zürich, Switzerland, 6University Hospital of Zürich, Department of Neurology, Zürich, Switzerland
On behalf of: This project is part of the COagulation MAnagement in Neurosurgical Diseases Project
Background and aims: Patients with intracranial haemorrhage (ICH) and taking direct oral anticoagulants (DOACs) have increased risk of morbidity and mortality compared to patients without. Emergency neurosurgical management of these patients is sometimes unavoidable. In these cases, pharmacological reversal strategies may play an important role.
The safety and efficacy of the two specific reversal agents idarucizumab and andexanet alfa (AA) in emergency neurosurgery for ICH has not been systematically studied. This study aims to analyze the available literature on this topic.
Methods: We performed a systematic review among various databases from 2015 to 2023. Inclusion criteria were case series of > 5 patients on DOACs diagnosed with ICH and receiving AA or idarucizumab for emergent neurosurgical treatment (<24h after last DOAC intake). Safety was the primary outcome, with thromboembolic events (TE), functional clinical outcome and mortality as secondary outcomes.
Results: For AA, five articles reported on neurosurgically managed cases (range: 8 to 298 subjects). Only two articles performed a subgroup analysis of the neurosurgical group. No neurosurgery-related post-operative bleedings were described and adequate hemostasis was reported in 80-100%. One study investigated TE (8.3%) and in-hospital mortality (50%) in 12 patients. For idarucizumab, two articles reported subgroup analysis of neurosurgical cases (8 and 49 subjects). One study reported on hemostasis efficacy, which was 100 %, while there were no TE. Mortality rates were 12.5% and 4.1%.
Conclusions: The literature on the use of specific reversal agents for DOACs in emergency neurosurgery for ICH is very limited and heterogeneous. Projects to fill this knowledge gap are urgently needed.
Disclosures of Interest: Yes A.K. as received honoraria for lecturing from Bayer AG (Switzerland) and CSLBehring GmbH. All other authors declare no conflict of interest.
Abstract N°: 2619
MINIMALLY INVASIVE INTRACEREBRAL HEMORRHAGE EVACUATION IN ROUTINE HEALTHCARE: IMPACT OF ENRICH CRITERIA TO AN UNSELECTED COHORT
Johan Wasselius*1, Trine Apostolaki-Hansson1, Amir Hillal1, Nathanael Göransson1, Björn Hansen1, Bo G. Norrving1, Birgitta Ramgren1, Teresa Ullberg1
1Lund University, Department of Clinical sciences Lund, Lund, Sweden
On behalf of:
Background and aims: Recently, the Early MiNimally-invasive Removal of IntraCerebral Hemorrhage (ENRICH) trial showed improved outcome for supratentorial intracerebral hemorrhage (ICH) patients treated by minimally invasive surgery (MIS). We aimed to estimate the proportion of ICH patients potentially eligible for MIS in Sweden.
Methods: All patients with spontaneous ICH in the Swedish Stroke Register (RS) during 2016–2020 in Skane county (1.36million) were assessed. Baseline imaging was used for radiological characterization. Clinical data were obtained from RS. Patients eligible for MIS in the total ICH population according to ENRICH criteria were estimated, using different scenarios, and extrapolated to the Swedish population (10.5million).
Results: Of 1618 ICH patients, 6.4% would be eligible for MIS based on ENRICH criteria (ICH volume 30–80ml). By extending the volume limit to 20–80ml, the proportion increased to 8.2%, and by further including patients presenting fully conscious, 11% (ICH volume 30–80ml) and 15.4% (20–80ml) were eligible for MIS. The estimated rate of neurosurgery for ICH could increase from the current 1.46 to 4.39 patients/100 000 population/year (in absolute numbers from 153 to 459 interventions out of 2400 ICHs in Sweden annually).
Conclusions: We show that 6.4% of the Skane ICH population would be eligible for MIS if strict ENRICH criteria are employed in clinical practice. By extending eligibility criteria to include patients presenting alert with a hemorrhage volume of 20–80ml would further increase this proportion to approximately 15% of all ICH patients, corresponding to a tripling of current surgical rates for ICH in Sweden.
Disclosures of Interest: No
Abstract N°: 55
POPULATION-BASED STUDY OF INTRACEREBRAL HEMORRHAGE ON ANTIPLATELETS: AN EVITABLE CATASTROPHE?
Matteo Foschi*1, Raffaele Ornello1, Federico De Santis1, Francesca Gabriele1, Francesco Conversi1, Federica DE Santis2, Berardino Orlandi2, Simona Saaco1
1University of L'Aquila, Department of Biotechnological and Applied Clinical Sciences, L'Aquila, Italy, 2ASL 1 Avezzano-Sulmona-L’Aquila, Department of Neurology and Stroke Unit of Avezzano-Sulmona, L'Aquila, Italy
On behalf of:
Background and aims: To provide updated epidemiological data on first-ever intracerebral hemorrhage occurring on prior antiplatelet therapy (APT-ICH) and to estimate the impact of APT on prognosis.
Methods: Our prospective population-based registry included all cases of first-ever ICH resident in the L’Aquila district, Italy, from January 2011 to December 2020. Indication to APT use was adjudicated according to 2021 ESC recommendations for cardiovascular disease prevention. The number needed to harm (NNH) for ICH 30-day case-fatality related to APT use was calculated from the absolute increase in the risk of death in patients treated with APT compared with those not treated with APT.
Results: We included 606 first-ever ICHs, of whom 251 (41.4%) were APT-related. One-hundred-forty-two APT-ICHs (56.6%) occurred in patients without indication to APT. While the incidence of non-APT-ICH decreased over time, the incidence of APT-ICH was stable. APT-ICH was associated with higher 30-day and 1-year case-fatality rates than non-APT-ICH (44.7% versus 25.6%, 50.6% versus 34.4%; p<0.001). NNH for ICH case-fatality due to APT use was 5. APT intake independently predicted higher 30-day case-fatality (HR 1.48, 95%CI 1.03-2.13; p=0.034).
Conclusions: APT-ICH emerges as a substantial concern exhibiting a sustained incidence over time and considerably elevated mortality. In many patients with ICH, the use of APTs is inappropriate. Urgent initiatives are needed to enhance adherence to established guidelines for APT use to mitigate inappropriate use of APT in primary prevention. This effort has the potential to not only mitigate the risk of ICH but also reduce the associated mortality.
Disclosures of Interest: No
Abstract N°: 799
BRAIN-DERIVED TAU - A NOVEL PLASMA BIOMARKER FOR NEURONAL INJURY IN INTRACEREBRAL HEMORRHAGE
Nicoló Knuth*1, Fernando Gonzalez-Ortiz2,3, Eunice Holbura1, Thomas Liebig4, Marco Duering4,5, Martin Dichgans1,6,7,8, Thomas Karikari2,9, Kaj Blennow2,3, Naomi Vlegels1, Steffen Tiedt1
1Institute for Stroke and Dementia Research (ISD), LMU University Hospital, LMU Munich, Munich, Germany, 2Institute of Neuroscience and Physiology, the Sahlgrenska Academy at the University of Gothenburg, Department of Psychiatry and Neurochemistry, Gothenburg, Sweden, 3Sahlgrenska University Hospital, Clinical Neurochemistry Laboratory, Mölndal, Sweden, 4Institute of Neuroradiology, LMU University Hospital, LMU Munich, Munich, Germany, 5University of Basel, Medical Image Analysis Center (MIAC) and Department of Biomedical Engineering, Basel, Switzerland, 6Munich Cluster for Systems Neurology (SyNergy), Munich, Germany, 7German Center for Neurodegenerative Diseases (DZNE, Munich), Munich, Germany, 8German Centre for Cardiovascular Research (DZHK, Munich), Berlin, Germany, 9University of Pittsburgh, Department of Psychiatry, Pittsburgh, United States
On behalf of:
Background and aims: Treatment options are limited for patients with intracerebral hemorrhage (ICH), partially because of a lack of pathophysiologically meaningful biomarkers. Plasma brain-derived tau (BD-tau) has emerged as a promising biomarker for neuronal injury in patients with ischemic stroke (IS). Here, we examined the value of plasma BD-tau as a biomarker in ICH.
Methods: We conducted the prospective Precision Medicine in Stroke (PROMISE) study (NCT05815836) including 126 patients with spontaneous ICH, 502 patients with IS and 102 healthy controls (HC). BD-tau levels were determined in plasma samples collected upon hospital admission using a single-molecule technology-based assay specifically capturing tau from the brain. We determined whether plasma BD-tau is different between ICH, IS, and HC, its relation to admission hematoma volume, and its value to predict 90-day functional outcome.
Results: ICH patients had a median age of 77 years, hematoma volume of 13.7ml, and time from onset to admission of 2.6h. ICH patients showed higher plasma BD-tau levels compared to HC (P<0.0001) and IS (P<0.0001; Fig.1), but not when matching for hematoma/infarct volume and time-from-onset. In ICH patients, plasma BD-tau correlated with hematoma volume (P=0.0008; Fig.2) and admission NIHSS scores (P=0.03). Plasma BD-tau predicted 24-hour NIHSS scores (P<0.0001) and 90-day functional outcome (odds ratio [95% confidence interval], 4.2 [2.0-10.6], P=0.0007), also when adjusting for hematoma volume (BD-tau P=0.005, hematoma volume P=0.04; Fig.3).
Conclusions: Plasma BD-tau correlates with hematoma volume and independently predicts 90-day functional outcome. As a biomarker of neuronal injury, plasma BD-tau has the potential to inform on ICH pathophysiology and support treatment development.
Disclosures of Interest: No
Abstract N°: 1287
ANTITHROMBOTIC DRUG USE AND CEREBRAL AMYLOID ANGIOPATHY RELATED INTRACEREBRAL HEMORRHAGE: A POPULATION-BASED CASE-CONTROL STUDY
Nils Boe*1, Stine Hald1, Sören Möller2,3, Mark Rodrigues4, Rustam Salman4, Jesper Hallas5, Luis Rodríguez6, Magdy Selim7, Larry Goldstein8, David Gaist1
1Odense University Hospital, Research unit Neurology, Odense, Denmark, 2OPEN, Open Patient data Explorative Network, Odense, Denmark, 3University of Southern Denmark, Department of clinical research, Odense, Denmark, 4University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom, 5Odense University Hospital, Department of Clinical Pharmacology, Odense, Denmark, 6Centro Español de Investigación Farmacoepidemiológica (CEIFE), Madrid, Spain, 7Beth Israel Deaconess Medical Center, Boston, United States, 8University of Kentucky, Department of Neurology and Kentucky Neuroscience Institute, Lexington, United States
On behalf of:
Background and aims: We explored the association of antithrombotic drugs with the risk of incident cerebral amyloid angiopathy-related intracerebral hemorrhage (CAA-ICH).
Methods: Among all persons with incident ICH in Southern Denmark (2015-2018) we selected cases with lobar ICH aged ⩾55-years who we matched by age, sex, and calendar year with general population controls (1:40 ratio). Based on their index brain CT, cases were categorized according to the simplified Edinburgh criteria as high probability CAA (h-CAA-ICH; convexity subarachnoid hemorrhage (cSAH) and finger-like-projections (FLPs)), or intermediate/low probability CAA (l-CAA-ICH; cSAH or FLP, or neither). Using conditional logistic regression, we calculated adjusted odds ratios (aORs) [95% confidence intervals] for the associations between use of aspirin, clopidogrel, vitamin K antagonists (VKAs), or direct oral anticoagulants (DOACs), and h-CAA-ICH or l-CAA-ICH. We used 2-sample Wald test to evaluate differences in strength of h-CAA-ICH vs l-CAA-ICH associations.
Results: 148 h-CAA-ICH (42.6% men, mean age 77.9-years) and 319 l-CAA-ICH cases (52.4% men, mean age 77.3-years) were matched to 5,919 and 12,760 controls, respectively. Aspirin use was more strongly associated with probable h-CAA-ICH (aOR 3.61 [2.11-6.18]), than l-CAA-ICH (aOR 1.44 [0.94-2.20]; p=0.010). All other comparisons were similar for h-CAA-ICH vs l-CAA-ICH (clopidogrel 4.27 [1.97-9.26] vs 3.45 [2.14-5.57], p=0.65; VKA 3.17 [1.44-6.96] vs 4.83 [3.05-7.66], p=0.37; DOAC 2.18 [0.84-5.62] vs 1.95 [1.18-3.22], p=0.78).
Conclusions: All antithrombotic drugs were associated with an estimate compatible with an increased risk of h-CAA-ICH and l-CAA-ICH. The finding of a higher risk of incident h-CAA-ICH than l-CAA-ICH with aspirin use requires further study.
Disclosures of Interest: Yes Dr Gaist received speakers’ honoraria from Pfizer and Bristol Myers Squibb outside the submitted work and participated in research outside the submitted work funded by Bayer with funds paid to the institution where he is employed.
Abstract N°: 1857
RECOMMENCEMENT OF STATINS AFTER ACUTE INTRACEREBRAL HAEMORRHAGE IS ASSOCIATED WITH IMPROVED SURVIVAL
Firas Elfourtia*1, Joshua Au Yeung2, Adrian Parry Jones3, Calvin Heal4
1Salford Royal NHS Foundation Trust, 2CogStack team, Guy's and St Thomas' NHS Foundation Trust, London, UK, 3Geoffrey Jefferson Brain Research Centre, Manchester Academic Health Science Centre, Northern Care Alliance & University of Manchester, Manchester, UK, United Kingdom, 4Division of Population Health, Faculty of Biology, Medicine and Health, University of Manchester, Manchester, UK
On behalf of:
Background and aims: The SPARCL trial of high-dose atorvastatin found a small increased incidence of intracerebral haemorrhage (ICH). Some clinicians thus stop statins in acute ICH but observational studies suggest reduced mortality if statins are continued. Whether this is due to indication bias and the mechanisms behind this association is unclear. We tested whether statin use after acute ICH at our centre is associated with risk of death even after adjusting for bias and investigated potential mediators (inflammation, infection).
Methods: We conducted a secondary analysis of a single centre prospective spontaneous ICH registry including patients admitted between 22/12/2009 to 23/03/2019. We used multifactorial logistic regression to test for an independent association between 30-day case fatality and statin exposure <72 h after onset. A sensitivity analysis, including only those able to take a statin (enteral access, not palliated), was performed. A mediation analysis included white blood cell count, C-reactive protein and common infections (pneumonia or urinary tract infection within 7 days).
Results: 1425 patients were included in our final analysis. Statin exposure post-admission (vs. none) was independently associated with lower case fatality (odds ratio[OR] 0.28; 95% confidence interval[CI] 0.16 to 0.49;p<0.05). Although the association was weaker, this remained significant in our sensitivity analysis (n=1044; OR 0.57; 95%CI 0.33 to 0.98; p<0.05). None of the potential mediators tested were significant.
Conclusions: Exposure to statins (vs. none) after ICH is associated with a higher likelihood of survival at 30 days and remains significant after adjusting for bias. The mechanisms underpinning this association remain unclear.
Disclosures of Interest: No
Abstract N°: 2183
PROBABILITY OF CEREBRAL AMYLOID ANGIOPATHY ACCORDING TO SIMPLIFIED EDINBURGH CT CRITERIA IN A LARGE, UNSELECTED ICH POPULATION
Amir Hillal*1,2, Trine Apostolaki-Hansson2,3, Birgitta Ramgren1,2, Björn Hansen1,2, Bo Norrving2,3, Johan Wassélius1,2, Teresa Ullberg2,3
1Medical Imaging and Physiology, Skåne University Hospital, Lund, Sweden, 2Department of Clinical Sciences, Lund University, Sweden, 3Department of Neurology, Skåne University Hospital, Malmö, Sweden
On behalf of:
Background and aims: Early identification of the underlying cause of intracerebral hemorrhage (ICH) has important treatment and prognostic implications. The aim of this study was to investigate the association of hematoma volume and other clinical parameters on the distribution of CAA probability according to the simplified Edinburgh CT criteria in a large, unselected ICH population.
Methods: Patients with spontaneous ICH residing in Skane county and registered with clinical data in the Swedish Stroke Register 2016–2020 were included. Radiological parameters were evaluated using baseline non-contrast computed tomography for categorization according to the simplified Edinburgh CT criteria into low, intermediate and high probability of CAA by the presence of subarachnoid hemorrhage and fingerlike-projections. Multivariable logistic regression analysis was used to determine factors associated with an increased (intermediate/high) CAA probability.
Results: Of 666 patients with lobar ICH, 190 (29%) had high CAA probability, 92 (14%) intermediate, and 384 (58%) low CAA probability. Patients with increased CAA probability more often presented with decreased level of consciousness, larger hematoma volumes, and had higher 90-day mortality. Female sex, age, and increasing baseline hematoma volume (Odds Ratio up to 30) were associated with increased odds of having an increased CAA probability.
Conclusions: We identified a strong association between baseline hematoma volume and increased CAA probability in lobar ICH patients on NCCT, indicating that large hematoma volumes per se may contribute to the occurrence of FLP and SAH, and act as a confounder for the existing Simplified Edinburgh CT Criteria. Validation against MRI is warranted.
Disclosures of Interest: No
Abstract N°: 2871
STRESS HYPERGLYCEMIA AND EARLY NEUROLOGIC DETERIORATION IN DIABETIC AND NON-DIABETIC PATIENTS WITH INTRACEREBRAL HEMORRHAGE
Carmelo Tiberio Currò*1,2, Federica Ferrari1,2, Giovanni Merlino3, Stefan Moraru1,2, Francesco Bax3, Fedra Kuris3, Lorenzo Nesi3, Mariarosaria Valente3, Federico Mazzacane1,2, Anna Cavallini1
1Mondino Foundation, Stroke Unit, Pavia, 2University of Pavia, Pavia, 3Udine University Hospital, Stroke Unit, Udine, Italy
On behalf of:
Background and aims: Stress hyperglycemia has been proposed as a predictor of unfavorable outcome in intracerebral hemorrhage (ICH). The effect of stress hyperglycemia may be different in diabetic patients with chronic hyperglycemia and non-diabetic patients. The aim of the study was to evaluate the association of stress hyperglycemia indexes, glycemic gap (GGAP) and stress hyperglycemia ratio (SHR) with early neurologic deterioration (END) in diabetic and non-diabetic ICH patients.
Methods: This retrospective study included ICH patients from two stroke centers. Stress hyperglycemia indexes were calculated as follows: SHR as blood glucose divided by 28.7 x HbA1c – 46.7, and GGAP as blood glucose −28.7 × HbA1c + 46.7. END was defined as an increase of ⩾ 2 points on the NIHSS within 48 hours from admission. The association between glycemic measures and END was evaluated in diabetic and non-diabetic subgroups.
Results: We included 206 patients, 49 were diabetics. END was present in 5/49 (10.2%) diabetics and 19/157 (12.1%) non-diabetics patients. GGAP and SHR were significantly associated with END in non-diabetic [GGAP 24.24 vs 19.04, p = 0.024; SHR 1.22 vs 1.02, p = 0.025], but not in diabetic patients [GGAP 44.84 vs 2.13, p = 0.48; SHR 1.25 vs 1.10, p = 0.50].
Conclusions: GGAP and SHR were associated with END in non-diabetic ICH patients but not in diabetic ones. They may serve as simple and low-cost markers to improve prognosis prediction in ICH and can be influenced by previous glycemic status.
Disclosures of Interest: No
Abstract N°: 702
SPONTANEOUS INTRACEREBRAL HEMORRHAGE IN YOUNG ADULTS: DATA FROM A STROKE CENTER IN VIETNAM
Tho Phung*1, Ton Mai Duy1, Phuong Dao1, Dung Nguyentien1
1Bach Mai Hospital, Stroke center
On behalf of:
Background and aims: Intracerebral hemorrhage (ICH) has recently becomes more prevalent in young adults but is still insufficiently studied. This study aimed to investigate the characteristics and outcomes of ICH in young adult patients.
Methods: Between November 2020 and October 2022, we prospectively enrolled a consecutive cohort of ICH patients aged 15-45 years admitted to the Stroke Center of Bach Mai Hospital to investigate risk factors, causes, and 90-day outcomes measured by the modified Rankin Score (mRS).
Results: 207 patients (mean age: 33.8 ± 8.8; males: 70.1%) were enrolled. The most frequent risk factors were hypertension (36.7%), followed by heavy drinking (8.2%), and smoking (3,9%). Notably, 7 (3.4%) patients had a history of coagulopathy or were on anticoagulation therapies. The locations of ICH were basal ganglia/ internal capsule (39,1%), lobar (36.8%) and infratentorial area (9,9%). Specifically, hypertensive ICH (39.6%) and structural vasculopathy (e.g., arteriovenous malformation, cavernoma – 35.3%) were the most common causes, while cryptogenic ICH was considered in 14.5%. At the 90-day follow-up, 126 (59.4%) patients got favorable outcomes (mRS 0-2), and 61 (28.8%) patients died.
Conclusions: ICH in young adults has the most common locations in the basal ganglia/ internal capsule or lobar, and is often caused by hypertension or structural vasculopathy, resulting in a high risk of dependence and 90-day mortality.
Distribution of Causes.
Distribution of mRS at 90 days.
Disclosures of Interest: No
Abstract N°: 3230
NEUROIMAGING AND NEUROPSYCHOLOGICAL BIOMARKERS OF CEREBRAL AMYLOID ANGIOPATHY ASSOCIATED WITH LOBAR INTRACRANIAL HEMORRHAGE: PRELIMINARY STUDY
1Privolzhsky Research Medical University, Department of Neurological Diseases, Russian Federation, 2Saratov State University, Department of Physiology, Russian Federation, 3Lovelace Biomedical Research Institute, United States, 4University of New Mexico Health Science Center, United States
On behalf of:
Background and aims: Cerebral amyloid angiopathy (CAA) is characterized by β–amyloid deposition in the wall of pial or small cerebral vessels. The aim was to study the neuropsychological and neuroimaging biomarkers of CAA associated with lobar intracranial hemorrhage (loICH) vs. hypertensive cerebral microangiopathy (hCMA).
Methods: This retrospective non-randomized single-center study was conducted based on a prospectively maintained database cohort. The patients with loICH (24 women, 32 men, 68±12 years, NIHSS 6±1.7) were stratified into 2 groups matched by sex, NIHSS, and age (32 patients with CAA and 24 patients with hCMA). All patients underwent a battery of neuropsychological assessments (Montreal Cognitive Assessment [MoCA], Frontal Assessment Battery [FAB], and Benson Test) and multimodal CT/MRI examinations. Data are shown as a median [interquartile range]. P<0.05 was considered statistically significant.
Results: In the CAA group, NIHSS, the Benson test, and MoCa test medians were significantly lower than in the hCMA group (4 [3-6], 8 [4-12], P=0,004; 14 [2-16], 17 [16-18], P=0,009, and 13 [10-18], 20 [18-24], P=0,001, respectively). The median FAB score was significantly higher in the CAA group (14.5 [12-16], 9 [5-13], P=0,005). In the hCMA group, perivascular space enlargements in the semioval center and in basal ganglia zones were less frequent than in the CAA group (P< 0.0001)
Conclusions: The CAA patients with loICH had a significantly lower NIHSS score, more pronounced cognitive function impairments, and MRI-derived brain structure disruptions compared with hCMA patients.
Disclosures of Interest: No
Abstract N°: 345
ASSOCIATIONS OF INTRACRANIAL ARTERIAL DOLICHOECTASIA AND CEREBRAL SMALL VESSEL DISEASE IN PATIENTS WITH INTRACEREBRAL HAEMORRHAGE
1Stroke Research Centre, Brain Repair and Rehabilitation, London, United Kingdom, 2Chiang Mai University, Internal Medicine, Chiang Mai, Thailand, 3National Hospital for Neurology and Neurosurgery, University College London Hospitals NHS Foundation Trust, London, United Kingdom, 4National Hospital for Neurology and Neurosurgery, Neuroradiology, London, United Kingdom, 5Faculty of Mathematical & Physical Sciences, University College London, Statistical Science, London, United Kingdom
On behalf of:
Background and aims: Intracranial arterial dolichoectasia (IADE) is associated with cerebral small vessel disease (CSVD) in ischaemic stroke populations. Whether IADE is related to CSVD markers in patients with spontaneous intracerebral haemorrhage (ICH) is unclear but might be relevant for CSVD diagnosis and prognosis. We investigated the prevalence and associations of IADE in patients with ICH.
Methods: In this retrospective, cross-sectional study, consecutive ICH patients who attended a specialist ICH clinic between February 2016 and September 2023 were analysed. IADE was determined using magnetic resonance angiography based on vessel diameter, length, and tortuosity. Neuroimaging markers of CSVD were investigated using magnetic resonance imaging. The associations between IADE and CSVD were assessed using multivariable binary logistic regression.
Results: We included 138 patients with a mean age of 66.7±11.8 years, 58.0% male. IADE was present in 16 patients (11.6%). ICH patients with IADE had significantly higher proportions of deep lacunes (43.8% vs. 18.0%, P = 0.02) and deep cerebral microbleeds (CMBs) (56.3% vs. 27.1%, P = 0.02) compared to individuals without IADE. IADE was independently associated with deep lacunes (adjusted odds ratio (aOR) 3.17, 95% confidence interval (CI) 1.02-9.86, P = 0.04), severe periventricular white matter hyperintensity (aOR 3.40, 95% CI 1.01-11.40, P = 0.04), and deep CMBs (aOR 3.24, 95% CI 1.01-8.31, P = 0.04).
Conclusions: IADE is an arteriopathy that can be found in ICH patients and independently associated with neuroimaging markers of arteriolosclerosis, but not cerebral amyloid angiopathy. The clinical relevance of IADE for diagnosis and prognosis in patients with ICH requires further study.
Disclosures of Interest: No
Abstract N°: 456
INTRACRANIAL INTERNAL CAROTID ARTERY ARTERIOSCLEROSIS AND PROGNOSIS IN INTRACEREBRAL HEMORRHAGE SURVIVORS
1NTUH (National Taiwan University Hospital), Neurology, Taipei, Taiwan, 2NTUH (National Taiwan University Hospital), Medical Imaging, Taipei, Taiwan
On behalf of:
Background and aims: Intracerebral hemorrhage (ICH) survivors are predisposed to long-term vascular events. Intracranial internal carotid artery (ICA) calcification has been linked to stroke risk in general population. We aim to investigate the prevalence and morphological subtypes of ICA calcification and their associations to long-term vascular events in ICH survivors.
Methods: 393 spontaneous patients survived ICH from a single center in Taiwan were included. ICH calcification was assessed on non-contrast CT, and the morphology was evaluated and categorized into intimal, internal elastic lamina (IEL), or mixed subtype (Figure). Patients were followed up for the occurrence of any stroke and vascular death. Associations between follow-up events and calcification subtypes was explored using multivariable Cox regression models.
Results: Of the included subjects, 320 (81.4%) of them had ICA calcifications. 152 patients (38.7%) were categorized as intimal calcification, 150 patients (38.2%) as IEL calcification, 18 patients as mixed type calcification (4.6%) and 73 patients as no calcification (18.6%). Patients with IEL calcification were older than those with intimal or no calcification (both p < 0.001). Age (p < 0.001), diabetes (p = 0.007), and reduced renal function (p = 0.001) were independently associated with IEL calcification. During 2-year follow-up, patients with IEL calcification showed no significant difference for the risk of recurrent ICH (HR=1.6 [0.8-3.3], p=0.149) or incident ischemic stroke (HR=1.3 [0.4-3.9], p=0.651), but had a higher risk of vascular mortality (HR=5.6 [1.5-21.4], p = 0.012).
Conclusions: Intracranial ICA calcification is frequent among ICH survivors while the subtype of IEL calcification serve a potential marker for long-term vascular mortality.
Disclosures of Interest: No
Abstract N°: 533
LEFT ATRIAL APPENDAGE OCCLUSION IN PATIENTS WITH INTRACEREBRAL HAEMORRHAGE ASSOCIATED WITH CEREBRAL AMYLOID ANGIOPATHY
Kitti Thiankhaw*1,2, Jonathan Best1, Sonal Srivastava1, Ishika Prachee3, Smriti Agarwal4, Patrick Calvert5, Ricard Ang3, Oliver Segal3, David Werring1
1Stroke Research Centre, Brain Repair and Rehabilitation, London, United Kingdom, 2Chiang Mai University, Internal Medicine, Chiang Mai, Thailand, 3Barts Heart Centre, St. Bartholomew's Hospital, Cardiac Electrophysiology, London, United Kingdom, 4University of Cambridge, Clinical Neurosciences, Cambridge, United Kingdom, 5University of Cambridge, Cardiovascular Medicine, Cambridge, United Kingdom
On behalf of:
Background and aims: Cerebral amyloid angiopathy (CAA) is a common cause of intracerebral haemorrhage (ICH) with a high recurrence risk. Left atrial appendage occlusion (LAAO) is an alternative method for ischaemic stroke prevention in patients with atrial fibrillation (AF). We aimed to determine the outcomes of AF patients with CAA-associated ICH undergoing LAAO and characterise post-procedure antithrombotic regimens.
Methods: We conducted a multicentre study of patients with CAA-associated ICH and AF treated with LAAO. We pooled findings with data from a systematic review of relevant published studies that reported CAA diagnosis. We collected data on peri- and post-procedure antithrombotic regimens and outcomes of ischaemic stroke and ICH.
Results: We included data from 9 published studies (n=107) and our cohort study (n=37), providing a total of 144 participants (mean age 74.5 ± 8.3 years, 68% male) with CAA-associated ICH and AF treated with LAAO. The median follow-up period was 9.4 months (interquartile range (IQR) 4.2-20.6). The post-procedural antithrombotic regimens varied between single (73.0%) or double antiplatelet therapy (16.2%) or direct oral anticoagulants (10.8%), with a median duration of 42 days (IQR 35–74). Post-procedural complications were uncommon (transient arrhythmias and non-life-threatening tamponade were the common, occurring in 2.1%). The pooled incidence rates of ischaemic stroke and ICH during follow-up were 5.16 (95% confidence interval 1.36-17.48) and 2.73 (0.41-13.94) per 100 patient-years, respectively.
Conclusions: LAAO with short-term antithrombotic therapy may be safe and effective in people with CAA-associated ICH and AF; further randomised controlled trials are needed to determine how LAAO compares to long-term antithrombotic treatment.
Disclosures of Interest: No
Abstract N°: 859
HAEMATOMA AND CORTICOSPINAL TRACT OVERLAP, IDENTIFIED ON CT SCANS, IS CORRELATED TO MOTOR OUTCOME AFTER INTRACEREBRAL HAEMORRHAGE
Ulrike Hammerbeck*1, Olivia Murray2, Sacha Chiuta2, Paul Ryu3, Daniel F. Hanley3, Hiren Patel2, George Harston4, Timothy Cootes2, Adrian Parry-Jones5
1King's College London, Centre for Human and Applied Physiological Sciences, London, United Kingdom, 2University of Manchester, Medical and Human Sciences, Manchester, United Kingdom, 3John Hopkins University, School of Medicine, Baltimore, United States, 4Brainomix Limited, Oxford, United Kingdom, 5University of Manchester, Division of Cardiovascular Sciences, Manchester, United Kingdom
On behalf of:
Background and aims: Corticospinal tract (CST) integrity can predict motor outcome after stroke but requires specialist tests not routinely performed in clinical practice. We investigated whether classification of CST overlap with haematoma on routine clinical CT scans is associated with motor recovery after intracerebral haemorrhage (ICH).
Methods: An expert reader, blinded to outcomes, determined whether haematoma overlapped the CST in the posterior limb of the internal capsule (PLIC) and corona radiata (CR) on baseline CT scans of 100 MISTIE III participants (Fig1). Primary outcome was NIHSS motor scores (ƩQ4,5&6) at Day 180 and secondary outcomes included Stroke Impact Scale (SIS) upper limb impairment and function, NIHSS motor recovery slope, and NIHSS motor recovery extent. We tested for associations between overlap and outcome using multiple linear regression, adjusting for key covariates. For interobserver reliability, three further readers analysed the same scans
Results: Overlap in PLIC only (β-coefficient: 2.49; 95% CI: 0.09 to 4.89; p=0.04) and in both PLIC and CR (β-coefficient: 4.21; 95% CI: 2.55 to 5.87; p=<0.0001) were associated with greater NIHSS motor score at day 180 (Fig2&3). Overlap in PLIC alone or both PLIC and CR was associated with lower SIS scores and less NIHSS recovery. Overlap in both PLIC and CR predicted NIHSS recovery slope. Overlap in CR was associated with lower SIS function scores. Interobserver kappa scores demonstrated a moderate agreement (κ=0.41-0.60).
Conclusions: Haematoma overlap with the CST is strongly associated with motor recovery after ICH and may enhance prognostication. Given moderate interobserver agreement, a more reliable machine-learning classification would be desirable.
Disclosures of Interest: No
Abstract N°: 1080
THE RELATIONSHIP BETWEEN HISTORY OF HYPERTENSION ON ACUTE INTRACEREBRAL HAEMATOMA EXPANSION AND OUTCOMES: DATA FROM TICH-2 TRIAL
Kailash Krishnan*1,2, Zhe Kang Law3, Lisa Woodhouse2, Chaamanti Menon1,2, Robert Dineen4, Philip Bath1,2, Nikola Sprigg1,2
1Queen's Medical Centre, United Kingdom, 2University of Nottingham, Stroke Trials Unit, Nottingham, United Kingdom, 3Malaysia National University Kuala Lumpur Campus, Kuala Lumpur, Malaysia, 4University of Nottingham, United Kingdom
On behalf of:
Background and aims: Hypertension is the most common cause of acute intracerebral haemorrhage (ICH) but the relationship between history of high blood pressure (BP), ICH expansion and prognosis is unclear. We assessed this effect using data from the Tranexamic acid for hyperacute intracerebral haemorrhage (TICH-2) trial.
Methods: Data from 2325 ICH participants recruited within 8 hours of symptom onset were included. Blinded assessors measured ICH volume at baseline and at 24 hours using the semi-automated segmentation method. Logistic regression was used to assess the effects of history of high BP on early death (<7 days), acute neurological deterioration (<7 days), haematoma expansion at 24-hours and death and disability (modified Rankin scale 4-6) at day 90.
Results: 1421 (61.1%) patients had history of hypertension. In adjusted analyses, history of hypertension was associated with risk of death or disability at day 90 (adjusted Odds Ratio, aOR 1.33; 95%CI 1.06-1.66), but not early death (aOR 1.15;0.76-1.74), acute neurological deterioration (aOR 1.01;0.80-1.28) or haematoma expansion at 24 hours (aOR 0.96;0.77-1.18).
Conclusions: A history of hypertension affects death or disability at day 90 after ICH but not early death, neurological deterioration or haematoma expansion.
Disclosures of Interest: No
Abstract N°: 1143
ARE UK STROKE UNITS GETTING BETTER AT DELIVERING ANTICOAGULANT REVERSAL TREATMENT FOR ICH? ANALYSIS OF NATIONAL REGISTRY DATA
Maude Holloway*1, Youssef Hbid1, Martin James1,2, Ajay Bhalla1,3, Kaili Stanley1
1King's College London, 2Royal Devon University Healthcare NHS Foundation Trust, 3Guy's and St Thomas'
On behalf of:
Background and aims: Current clinical guidelines for stroke recommend urgent reversal of anticoagulants in intracerebral haemorrhage (ICH) patients. Using national registry data from SSNAP (the national stroke audit for England, Wales, and Northern Ireland) we examined changes in the practice of anticoagulant reversal in acute ICH.
Methods: SSNAP collected data between 2018-2023 for 158 acute stroke teams using an online proforma. All ICH patients who were on prior anticoagulation were analysed, with comparisons made using Chi-squared and Kruskal-Wallis tests.
Results: Of 45,990 ICH patients admitted over 5 years, 10,002 (21.7%) were on an anticoagulant prior to stroke. No significant difference was seen over time in the proportion treated with a reversal agent. There were no significant differences in the time from arrival to first administration of a reversal agent [Median: 152mins, IQR 81-311] or time from scan to reversal agent [Median: 92mins, IQR 45-178]. There was a significant decrease in the proportion of patients identified as on an anticoagulant prior to ICH (22%-19%, p<0.005).
Conclusions: Despite guidelines recommending urgent anticoagulant reversal in ICH patients, there has been no change in the level or speed of reversal agent administration over the past 5 years in UK stroke units. The decrease in ICH patients on an anticoagulant may reflect the wider use of DOACs in preference to VKAs. As shown in the INTERACT III study, quality improvement should include the faster administration of reversal agents for a greater proportion of patients with anticoagulant-related ICH to reduce variation and improve subsequent outcomes.
Disclosures of Interest: No
Abstract N°: 1167
ANDEXANET ALFA REDUCES SECONDARY HAEMORRHAGE AFTER TRAUMATIC BRAIN INJURY IN MICE
Sarah Gelhard1, Michelle Rosenthal-Rückeis1, Franziska Lieschke1, Christian Grefkes1, Ferdinand Bohmann*1
1Department of Neurology University Hospital Frankfurt, Frankfurt am Main, Germany
On behalf of:
Background and aims: This translational study aims to evaluate the effect of anticoagulation reversal in traumatic brain injury (TBI). For the acute treatment of TBI, especially with no or minimal signs of haemorrhage, the therapeutic dilemma whether and when to use andexanet alfa is challenging. We hypothesize that treatment with andexanet alfa reduces risk of secondary haemorrhage after TBI.
Methods: Forty-eight C57BL/6 mice were pre-treated orally with rivaroxaban 10mg/kg body weight. TBI was induced by control cortical impact (CCI) followed by intravenous application of andexanet alfa or placebo. Haemorrhage volume was quantified by magnet resonance imaging (MRI, Bruker, 7.4 Tesla). Functional outcome was assessed by a blinded investigator (Neurological Severity Score, NSS). Haemostatic efficacy was evaluated by tail vein bleeding time (TVBT).
Results: Andexanet alfa showed a trend to reduce TVBT (without reversal: median 1042s [IQR 836 - 1200] vs. with reversal: 830s [485 - 887], n = 5, p=0.056). Andexanet alfa reduced haemorrhage volume 24h after TBI as compared to control group without reversal of anticoagulation (2.9 ± 1.4µl vs. 5.2 µl ± 3.3 µl, n=14, p=0.022). Regarding functional outcome, andexanet alfa did not improve neurological deficit in comparison to the control cohort 24h after TBI (n=14, p=0.86).
Conclusions: Our experimental data suggest that andexanet alfa reduces the risk of secondary haemorrhage after TBI. However, an effect on neurological deficit could not be shown in this model. Further studies should investigate these aspects in more detail.
Disclosures of Interest: Yes The study was financially supported by Alexion/Astra Zeneca.
Abstract N°: 1183
PREVALENCE AND ASSOCIATIONS OF CEREBRAL SMALL VESSEL DISEASE AND CHRONIC KIDNEY DISEASE IN ACUTE INTRACEREBRAL HAEMORRHAGE
Philip Nash*1,2, Simon Fandler-Höfler3, Gareth Ambler4, Wenpeng Zhang1, Hatice Ozkan1,2, Lena Obergottsberger3, David Wheeler5, Rob Simister1,2, Thomas Gattringer3, David Werring1,2
1UCL Queen Square Institute of Neurology, Stroke Research Centre, London, United Kingdom, 2University College London Hospitals NHS Trust, Comprehensive Stroke Service, London, United Kingdom, 3Medical University of Graz, Department of Neurology, GRAZ, Austria, 4University College London, Department of Statistical Science, London, United Kingdom, 5University College London, Department of Renal Medicine, London, United Kingdom
On behalf of: Martina Locatelli, Yang Du and Hans Rolf Jager at UCL Queen Square Institute of Neurology, London, UK. Gerit Wunsch and Christian Enzinger at the Medical University of Graz, Graz, Austria.
Background and aims: Chronic kidney disease (CKD) may be relevant to the pathogenesis and phenotype of cerebral small vessel disease (SVD), which is the commonest cause of intracerebral haemorrhage (ICH). Therefore, we hypothesised that CKD would be associated with arteriolosclerosis and markers of severe SVD.
Methods: In two cohorts of consecutive MRI-investigated patients with ICH we investigated the frequency and severity of CKD based on established Kidney Disease Improving Global Outcomes criteria, requiring estimated glomerular filtration rate (eGFR) measurements <60 ml/min/1.73² ⩾3 months apart. MRI scans were rated for ICH neuroimaging phenotype (arteriolosclerosis, cerebral amyloid angiopathy, mixed location SVD, or cryptogenic ICH) and SVD markers.
Results: Of 875 patients (mean age 66 years, 58% male), 146 (16.7%) had CKD. After adjusting for age, sex and comorbidities, patients with CKD had higher rates of mixed SVD (relative risk ratio 2.39, 95% CI 1.16-4.94, p=0.019), compared to those with eGFR >60. Severe white matter hyperintensities, deep microbleeds and lacunes were more frequent in patients with CKD in multivariable analysis, as was a higher overall SVD burden score (OR 1.83 per point, 95% CI 1.31-2.56, p<0.001). Patients with eGFR ⩽30 had particularly numerous cerebral microbleeds (median 7 (IQR 1-23) vs. 2 (0-8) for those with eGFR >30, p=0.007).
Conclusions: In patients with ICH, CKD was strongly associated with SVD burden, a mixed SVD phenotype, and markers of arteriolosclerosis. These findings indicate that CKD may independently contribute to the pathogenesis of arteriolosclerosis and mixed SVD, although longitudinal and experimental research is needed to confirm these findings.
Disclosures of Interest: No
Abstract N°: 1194
HEMORRHAGIC STROKE AND ATHEROGENIC MARKERS – IS THERE ANY RELATION?
1Clinical Center University of Sarajevo, Neurology Clinic, Sarajevo, Bosnia-Herzegovina, 2General Hospital "Abdulah Nakas", Department of Cardiology, Sarajevo, Bosnia-Herzegovina, 3Sarajevo Medical School, Sarajevo School of Science and Technology, Department of Pharmacology, Sarajevo, Bosnia-Herzegovina, 4Faculty of Medicine, University of Sarajevo, Sarajevo, Bosnia-Herzegovina, 5University of Gothenburg, Orthopedic Surgery, Sweden
On behalf of:
Background and aims: The triglyceride/high-density lipoprotein (TG/HDL) ratio is a novel indicator of cardiovascular risk. The associaiton between the overall serum lipid status and hemorrhagic stroke (HS) remains unclear, therefore our study aimed to assess the correlation between the novel index and mortality in patients with this subtype of stroke.
Methods: We conducted a study with a retrospective-prospective design, covering the period from January 2020 to August 2023. The study included 104 hospitalized patients diagnosed with HS, whose anamnestic and the values of their lipid profile were analyzed.
Results: Age [OR, 1.078 95% CI, 1.032-1.125; p=0.001], AF [OR, 0.237 95% CI, 0.074- 0.760; p=0.015], glucose [OR, 1.121 95% CI, 1.007-1.247; p=0.037], and TG/HDL [OR, 0.368 95% CI, 0.173-0.863; p=0.020], were found to be independent predictors for in-hospital mortality by both univariable and multivariable logistic regression analysis.
Conclusions: Our findings contribute to the growing body of evidence supporting the TG/HDL index as a valuable component of cardiovascular risk assessment in patients with HS, underscoring the need for a multifactorial approach to risk prediction and management integrating traditional markers with novel indicators.
Disclosures of Interest: No
Abstract N°: 3119
NON-INVASIVE VAGUS NERVE STIMULATION REDUCES HEMATOMA VOLUME AND IMPROVE MOTOR FUNCTION IN A RAT MODEL OF INTRACEREBRAL HEMORRHAGE
Afshin Divani*1, Pascal Salazar2, Denis Bragin3, Michel Torbey1
1University of New Mexico Health Science Center, Neurology, United States, 2Canon Medical Informatics, Inc., United States, 3Lovelace Biomedical Research Institute, United States
On behalf of:
Background and aims: Intracerebral hemorrhage (ICH) carries a high mortality and morbidity among. Here, we assessed the effects of a non-invasive vagus nerve stimulation (nVNS) on reducing the edema, hematoma volume, and motor deficit in a rat model of ICH.
Methods: We used male Wistar rats divided into 2x2 groups: 1) nVNS-treated ICH (treated) and 2) Sham nVNS-treated ICH (control). For each group, ICH was induced using 1.0U or 0.2U of collagenase. We used five 2-min nVNS stimulations, 10 minutes apart, starting 30 minutes post-ICH. At 24 hours post-injury, motor function was assessed using rotarod and beam walking tests. Subsequently, rats were sacrificed, and 2 mm brain slices were photographed for hematoma volume measurements. Spectrophotometric hemoglobin assay method was used for the hematoma volume calculation. For the rats with 0.2U collagenase, the supernatant of homogenized brain samples was used for assessing aquaporin-4 level.
Results: For the 0.1U group, the mean hematoma volume was 8.97mm3 (95%CI:6.48-11.46) for the control (n=7) and 5.51mm3 (95%CI: 3.12-7.89) for the treated (n=7) groups (P=0.030). Rotarod results (P=0.035) and beam-walking results (P=0.013) were significant between the treated (n=10) and control (n=10) groups for the 0.1U dose. For the 0.2 dose groups, the mean hematoma volume was 12.38mm3 for the control (n=14) and 11.19mm3 for the treated (n=13) groups (P=0.38). The aquaporin-4 level difference for the ipsilateral hemispheres was near significant (P=0.053).
Conclusions: For a lower collagenase dose (0.1U), the nVNS treatment was associated with lower volume of hematoma associated with a significant improvement in motor function. Supported by the NIH 1R21NS130423-01
Disclosures of Interest: No
Abstract N°: 3191
DEEP CONVOLUTIONAL NEURAL NETWORK FOR AUTOMATED SEGMENTATION OF HEMORRHAGE, INTRAVENTRICULAR EXTENSION, AND PERIHEMATOMAL EDEMA IN ACUTE ICH
Jawed Nawabi*1, Baumgaertner Georg Lukas2, Schulz-Weddige Sophia2, Dell'orco Andrea1, Helge Kniep3, Federico Mazzacane4, Andrea Morotti5, Uta Meta Paula Hanning3, Jens Fiehler3, Penzkofer Tobias2
1Charité Campus Mitte, Neuroradiology, Berlin, Germany, 2Charité Campus Virchow Clinic, Radiology, Berlin, Germany, 3University Medical Center-Hamburg-Eppendorf, Neuroradiology, Hamburg, Germany, 4Neurological Institute Foundation Casimiro Mondino, Neurology, Pavia, Italy, 5Neurology Clinic, University of Brescia, Department of clinical and experimental sciences, Brescia, Italy
On behalf of: Tobias Orth
Background and aims: To evaluate the performance of a deep learning method based on no-new-U-Net (nnU-Net) for fully automated segmentation of intracerebral hemorrhage (ICH), intraventricular hemorrhage extension of (IVH), and perihematomal edema (PHE) in spontaneous intracerebral hemorrhage on noncontrast Computed Tomography (CT).
Methods: Patients with spontaneous ICH on noncontrast CT admitted at three academic hospitals in Germany and Italy were retrospectively included between 01/2016 and 06/2022. Ground truth segmentation masks were semi-manually generated. Model performance on lesion segmentation and volumetric quantification of ICH, IVH, and PHE was evaluated by calculating the Dice similarity coefficients (DSC) and Pearson correlation coefficient (r).
Results: A total of 1059 patients were included. On the test cohort (n = 189, 10% of the dataset), the nnU-Net achieved a median DSC of 0.9 (interquartile range (IQR), 0.86-0.94), 0.76 (IQR, 0.61-8.85), and 0.71 (IQR, 0.61-0.76), respectively, for ICH, IVH, and PHE segmentation. Correlation of volumetric measurement for ICH (r> 0.97) and of IVH (r> 0.97) were both excellent and good for PHE (r> 0.92), all p-values <0.001. The model took approximately 90 sec to provide automatic volume analysis compared to 15 min in the manual method.
Conclusions: Our model has demonstrated good reliability in automatically segmenting and measuring the volumes of ICH, IVH, and PHE on CT scans in patients with spontaneous ICH. This model has the potential to enhance the diagnostic workflow in clinical settings and assist in future clinical trials.
Disclosures of Interest: No
Paper Poster – Neurointervention
Abstract N°: 780
STENT RETRIEVER VERSUS ASPIRATION BASED THROMBECTOMY: IMPACT ON FIRST-PASS REPERFUSION, PROCEDURAL TIME, AND CLINICAL OUTCOMES
Adrian Karlsson*1, Katarina Jood2, Isabella Björkman-Burtshcer1, Alexandros Rentzos1
1Institute of Clinical Sciences, Sahlgrenska Academy at the University of Gothenburg, Department of Radiology, Gothenburg, Sweden, 2Institute of Neuroscience and Physiology, Sahlgrenska Academy at the University of Gothenburg, Department of Clinical Neuroscience, Gothenburg, Sweden
On behalf of:
Background and aims: First-pass reperfusion (FPR), defined as near-complete reperfusion (eTICI 2c/3) in a single attempt without use of rescue therapy has been proposed as a valid quality metric. However, it remains unclear whether the choice of thrombectomy method influences quality and rate of FPR. We aim to evaluate whether stent retriever and aspiration based thrombectomy differ in FPR rate, technical and clinical outcomes in FPR and multiple-pass reperfusion (MPR).
Methods: This registry study includes consecutive patients treated between 2018 - 2021 in Sweden. Technical outcomes were FPR rate and procedural time. Clinical outcomes were early neurological improvement (improvement of ⩾ 4 points on the National Institutes of Health Stroke Scale [NIHSS] or 0-1 points at 24 hours), favorable functional outcome (modified Rankin Scale [mRS] scores 0-2 or return to pre-stroke mRS at 90 days) and mortality at 90 days.
Results: Of 3,309 included patients, 1,990 underwent stent retriever and 1,319 aspiration based thrombectomy as first-line method. No difference in FPR rate was observed. Patients treated with aspiration based thrombectomy had shorter procedural time in both the FPR (crude p=<0.001, adjusted p=0.004) and MPR (crude p=<0.001, adjusted p=<0.001) groups. Aspiration based thrombectomy was associated with early neurological improvement: cOR 1.21 (95% CI 1.03-1.42), aOR 1.40 (95% CI 1.18-1.67) and favorable functional outcome: cOR 1.00 (95% CI 0.85-1.19), aOR 1.22 (95% CI 1.01-1.47).
Conclusions: Aspiration based thrombectomy is associated with shorter procedural time and better clinical outcome compared to stent retriever. No difference in the FPR rate was found.
Disclosures of Interest: No
Abstract N°: 1629
HYPOPERFUSION INTENSITY RATIO IS CORRELATED WITH THE RISK OF FUTILE REPERFUSION AFTER ENDOVASCULAR TREATMENT
1Beijing Tiantan Hospital Affiliated to Capital Medical University, Neurology, beijing, China
On behalf of:
Background and aims: We aimed to explore the association of hypoperfusion intensity ratio (HIR) and the risk of futile reperfusion (FR) after endovascular treatment (EVT).
Methods: Retrospective data were derived from a multicenter cohort study of patients with large vessel occlusion who underwent EVT between 2017 and 2022 at 7 comprehensive stroke centers in China. HIR was automatically calculated on baseline CT perfusion as the ratio of brain volume with time-to-max (Tmax) delay >10 s over volume with Tmax >6 s. The top quarter of HIR (HIR >0.44) was defined as inadequate baseline perfusion. The primary outcome was FR defined as modified Rankin Scale score of 4-6 at 90 days despite successful recanalizaiton. Safety outcomes were symptomatic intracranial hemorrhage (sICH) within 36 hours and all-cause mortality at 90 days.
Results: In the 897 included patients, we observed FR in 316 (35.2%) patients. More frequent FR at 90 days was seen in patients with inadequate baseline perfusion (51.1% vs. 30.1%; odds ratio [OR], 0.41; 95% confidence interval [CI], 0.30-0.56; P<0.001). The higher HIR was independently associated with higher odds of FR (adjusted OR, 0.54; 95% CI, 0.33–0.88; P=0.01). The rates of sICH were not significant different between 2 groups. HIR>0.44 was numerically correlated with higher rates of 90-day mortality but the difference was not significant after adjusting covariates.
Conclusions: Poorer HIR on admission perfusion imaging was strongly associated with FR occurrence after EVT. This automated and rapidly available perfusion parameter might help to assess prognosis after EVT for ischemic stroke.
Disclosures of Interest: No
Abstract N°: 2123
ACUTE STENTING IN PATIENTS WITH TANDEM LESIONS DUE TO CERVICAL ARTERY DISSECTION: A SECONDARY ANALYSIS OF THE STOP-CAD STUDY
João André Sousa*1, Marc Rodrigo-Gisbert2, Mirjam Rachel Heldner3, Pasquale Mordasini3, Liqi Shu4, Daniel Mandel5,6, João Sargento Freitas1, Shadi Yaghi4,7, Manuel Requena2
1Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal, 2Hospital Universitario Vall d’Hebron, Unidad de Ictus, Servicio de Neurología, Barcelona, Spain, 3Inselspital, Bern, Switzerland, 4Brown University, Providence, United States, 5Department of Neurology, Miami, United States, 6University of Miami Leonard M. Miller School of Medicine, Miami, United States, 7Comprehensive Stroke Center at Rhode Island Hospital, Providence, United States
On behalf of: STOP-CAD investigators
Background and aims: Cervical artery dissection (CAD) accounts for 2% of ischemic strokes but rises to 25% among young adults. There is limited data on the risks and benefits of stenting in patients with tandem occlusions due to dissection and undergoing endovascular treatment (EVT). This study evaluated the risks and benefits of acute stenting in tandem occlusions due to CAD
Methods: A secondary analysis of the STOP-CAD study was conducted including patients with acute ischemic stroke. The primary outcome was 90-day modified Rankin Scale (mRS) 0-2, and the secondary outcome was symptomatic intracranial hemorrhage (sICH). In this analysis, we included patients with tandem occlusions (extracranial ICA and intracranial LVO) who underwent EVT within 2 days from dissection diagnosis. We constructed binary logistic regression models, adjusting for age and NIHSS score to determine associations between stenting and both primary and secondary outcomes.
Results: The study included 328 patients with tandem ICA and intracranial LVO who underwent EVT. Acute stenting was performed in 150 patients (45.7%). In adjusted binary logistic regression models, stenting was associated with similar likelihood of functional independence (aOR 1.23, 95% CI 0.72-2.1, P=0.438), and a similar odds of sICH (aOR 1.03, 95% CI 0.45-2.39, P=0.940).
Conclusions: In patients with CAD, acute stenting in patients with tandem occlusions undergoing EVT was associated with a similar likelihood of functional independence and similar odds of sICH. Studies are needed to validate our findings and investigate subgroups where the benefit of stenting outweighs the risk of sICH.
Disclosures of Interest: No
Abstract N°: 3232
MANAGEMENT FOR FAILED RECANALIZATION OR REOCCLUSION AFTER THROMBECTOMY IN ISCHEMIC STROKE DUE TO ANTERIOR CIRCULATION LARGE VESSEL OCCLUSION
Johannes Gerber*1, Hannes Wahl1, Pawel Krukowski1, Andrij Abramyuk1, Simon Winzer2, Daniel Kaiser1, Dirk Daubner1, Jennifer Linn1, Volker Puetz2
1Medical Faculty and University Hospital Carl Gustav Carus, TUD Dresden University of Technology, Neuroradiology, Dresden, Germany, 2Medical Faculty and University Hospital Carl Gustav Carus, TUD Dresden University of Technology, Neurology, Dresden, Germany
On behalf of:
Background and aims: We sought to evaluate the effect of acute transluminal angioplasty and stenting (PTAS) on 90 day outcome in patients with acute ischemic stroke due to anterior circulation large vessel occlusion (acLVO) and unsuccessful reperfusion or residual stenosis after mechanical thrombectomy (MT).
Methods: We searched our prospective MT database from January 1st 2016 to December 31st 2023 to identify all patients with acLVO and unsuccessful reperfusion (mTICI 0 to 2a) or imminent reocclusion due to residual severe stenosis. Functional outcome at 90 days was compared between patients who had received PTAS as a rescue therapy (group 1), and those who had not (group 2). Favourable outcome was defined as mRS 0-3.
Results: From 2016-01-01 to 2023-12-31 a total of 1647 patients received MT for acLVO. Of these, 131 patients had unsuccessful reperfusion or reocclusion although we could reach the target arterial lesion and complete at least one MT pass. 61 patients (27 women) of them received PTAS (group 1), while 70 patients (45 women) did not (group 2). In group 1, 21 patients had mRS 0-3, compared to only 8 patients in group 2 (p<0.05). Age did not differ between groups (median 73 vs. 77.5), sex did (p<0.05).
Conclusions: In our cohort of acLVO patients with unsuccessful reperfusion or residual severe stenosis after MT, rescue therapy with PTAS was associated with a better clinical outcome.
Disclosures of Interest: No
Abstract N°: 3242
TECHNICAL DETAILS ON THE OCCURRENCE OF VESSEL PERFORATION DURING ENDOVASCULAR THROMBECTOMY FOR ISCHEMIC STROKE
Victor Schulze-Zachau*1, Alex Brehm1, Nikolaos Ntoulias1, Nadja Krug1, Mira Katan2, Urs Fischer2, Marios Psychogios1
1Universitätsspital Basel, Diagnostic and Interventional Neuroradiology Department, Radiology and Nuclear Medicine Clinic, Basel, Switzerland, 2Universitätsspital Basel, Neurology Clinic, Basel, Switzerland
On behalf of: Perforations during endovascular therapy for acute ischemic stroke research collaboration
Background and aims: Due to expanding indications and demographic change, the frequency of thrombectomy in Europe is increasing. Intracranial vessel perforation is a rare, but dangerous complication of thrombectomy which is poorly understood. This study aimed at gathering detailed information on the occurrence of vessel perforation during thrombectomy.
Methods: In this retrospective cohort study, data of patients with vessel perforation during thrombectomy defined as active contrast extravasation during an angiographic run were collected. Data included technical details of the thrombectomy, the occurrence and management of perforation and modified Rankin Scale at 90 days.
Results: 33 centers collected data of 459 consecutive patients with vessel perforation during thrombectomy. All-cause mortality at 90 days was 51.9%. 64.9% of perforations occurred during the first two thrombectomy maneuvers. 6.0% of perforations occurred with interventionalists with < 2 years of experience while 67.7% of perforations occurred with interventionalists with ⩾ 10 years of experience. For patients with at least one thrombectomy maneuver before perforation occurred, the same technique which led to perforation had been used previously without causing a perforation in 81.5%.
Conclusions: This large retrospective cohort challenges the common assumption that most vessel perforations are misadventures of unexperienced interventionalists which occur when a different technique is chosen after several unsuccessful thrombectomy maneuvers. The mortality rate underlines the necessity to investigate on the origin and optimal management of vessel perforations during thrombectomy. This is especially relevant since patients with ischemic stroke and mild neurological deficit are more and more considered for thrombectomy.
Disclosures of Interest: No
Abstract N°: 893
INTERVENTIONALISTS EXPERIENCE DOES NOT DETERMINE THE PREVALENCE OF FIRST-PASS EFFECT IN NEUROTHROMBECTOMY
Jessica Jesser1, Ulf Neuberger1, Jan Purrucker2, Michael Breckwoldt1, Dominik Vollherbst1, Silvia Schönenberger2, Peter Arthur Ringleb2, Markus Moehlenbruch1, Bendszus Martin1, Christian Herweh*1
1Heidelberg University Hospital, Neuroradiology, Heidelberg, Germany, 2Heidelberg University Hospital, Neurology, Heidelberg, Germany
On behalf of:
Background and aims: First-pass effect (FPE), complete recanalization (CR) defined as eTICI grades 2c & 3 at the first thrombectomy attempt, is a known predictor of good clinical outcome in acute ischemic stroke (AIS). The use of a balloon guide catheter (BGC) has been identified as a procedural prerequisite of FPE. Here, we investigated whether the interventionalists experience in years influences the occurrence of FPE.
Methods: AIS patients treated endovascularly for proximal occlusions in the ICA and MCA territory from 2017 to 2022 at a large comprehensive stroke center were analyzed retrospectively regarding FPE.
Results: FPE was achieved in 482 of 1394 patients (34.6%). Baseline characteristics were balanced between patients with and without FPE. Patients with FPE presented earlier (4h15 vs 4h47; p=.03), had more M1 occlusions (54.8 vs 46.2%; p=.02) and BGC use (54.9 vs 45.8%; p=.001), while proximal internal carotid artery occlusion (ICAO) was less frequent (10.4 vs 20.1%; p=<.001). Initial thrombectomy techniques, stent retriever or aspiration, were distributed evenly between groups. Interventionalists experience was inversely correlated with time from puncture to final TICI (r=-.13; p<.001) but was not associated with the number of passes or the occurrence of FPE or any CR. In a multivariate analysis BGC use (aOR 1.4; 1.1-1.8; p=.002), presence of M1 occlusion (aOR 1.4; 1.1-1.8; p=.003), and absence of proximal ICAO (aOR 0.4; 0.2-0.6; p<.001) were significant predictors of FPE.
Conclusions: In this study, BGC use was the only procedural factor that positively predicted FPE, regardless of the interventionalists experience.
Disclosures of Interest: No
Abstract N°: 2240
OUTCOMES OF ANTIPLATELET THERAPY BEFORE ENDOVASCULAR TREATMENT OF ACUTE LARGE VESSEL OCCLUSION: DATA FROM THE ANGEL-ACT REGISTRY
1Beijing Tiantan Hospital, Capital Medical University, 2Beijing Anzhen Hospital, Capital Medical University, 3Boston Medical Center
On behalf of: Xu Tong, MD1; Anxin Wang, PhD; Ning Ma, MD; Feng Gao, MD; Dapeng Mo, MD and ANGEL-ACT group
Background and aims: To investigate whether single or dual antiplatelet therapy (SAPT or DAPT) within 24 hours before endovascular treatment(EVT) could improve the clinical outcomes of patients with large vessel occlusion(LVO).
Methods: Patients from the ANGEL-ACT registry were divided into antiplatelet therapy (APT) and non-APT groups. The APT group was divided into SAPT and DAPT groups. Outcome measurement included 90-day modified Rankin Scale(mRS) distribution, change in the NIHSS at 7 days or discharge, number of passes, first pass recanalization(FPR), successful recanalization, symptomatic intracranial hemorrhage(SICH), and mortality within 90 days. To compare the outcomes, we performed multivariable analyses by adjusting for the propensity score calculated by the logistic regression model.
Results: Of 1611 patients, 1349 were in the non-APT group, while 262(16.3%) were in the APT group (122[46.6%] received SAPT, 140[53.4%] received DAPT). APT, SAPT or DAPT were not associated with a shift to better outcomes (non-APT vs. APT, 3[0-5]vs.3[0-5], common odds ratio[OR], 1.04, 95%confidence interval [CI]:0.82-1.34, P=0.734). DAPT was associated with FPR (OR,2.05,95%CI:1.39-3.01, P<0.001), more NIHSS reduction at 7 days or discharge (β, -2.13, 95%CI: -4.02–0.24,P=0.028), lower number of passes (β,-0.40, 95%CI: -0.68–0.12, P=0.006), and shorter procedure duration (β,-12.4, 95%CI:-23.74--1.05,P=0.032) without increasing odds of successful recanalization, PH within 24 hours and mortality with 90 days.
Conclusions: APT before MT for AIS due to LVO does not affect clinical outcome in 90 days despite a tendency to reduce MT procedure time and number of passes. APT before MT in LVO does not increase SICH or mortality rates
Disclosures of Interest: No
Abstract N°: 2717
PROFILE OF ANTIPLATELET REGIMENS FOR EMERGENT CAROTID STENT INSERTION IN TANDEM OCCLUSION. SYSTEMATIC REVIEW AND META-ANALYSIS
Gianluca De Rubeis*1, Sebastiano Fabiano1, Luca Bertaccini1, Andrea Wlderk1, Gina Moretti2, Enrico Pampana1
Background and aims: To investigate the optimum antiplatelet therapy regimen (APTR) for emergent carotid stent insertion (ECSI) following mechanical thrombectomy (MT) in stroke patients due to tandem occlusion.
Methods: A literature search was performed on Pubmed/OVID/Cochran's CENTRAL database for studies from 2015-2022. Patient characteristics, antiplatelet regimen type, mTICI, mRS, acute in-stent thrombosis (AIST), mortality, intracranial hemorrhage (ICH), and sample size were recorded. Exclusion criteria were non-English literature, no human subjects, sample size < 5 patients, other anticoagulant or antiplatelet therapy, and 100% stent insertion in one study arm. The studies were assessed using MINORS/GRADE systems. Meta-analysis and meta-regression with a random effects model were performed.
Results: Five-hundred-twenty-four studies were retrieved. After applying the exclusion criteria, the final population included 19/534 studies (3.6%) for 880 patients (46.3 per article). I^2 and Q’s Cochrane were 86.4% and 132.5 for mRS, 19.9% and 17.5 for death, 0% and 9.4 for acute in-stent thrombosis and 62.1% and 39.7 for intra-cranial haemorrhages, respectively.
Patients in the aspirin subgroup had a significantly lower rate of functional independence (mRS⩽2) compared with those in the DAPT subgroup (47% [CI95% 42.0%-52.0%] vs. 61.9% [CI95% 50.8 -72.9]; p=0.0007;OR 0.75[CI95% 0.56-1.01], p=0.06). DAPT significantly decreased the death rate compared with aspirin (8.6% [CI95% 5.3% -11.9%] vs. 16.7% [CI95 11.1%-22.2%]; p=0.0012). Anti-GP2b/3a demonstrated a trend of increasing the probability of mortality versus DAPT (OR 1.88[CI95% 0.93 to 3.86], p=0.08.
No other significant differences were observed between AIST and ICH in the treatment groups.
Conclusions: DAPT increases the chances of obtaining mRS⩽2 and reduces mortality.
Disclosures of Interest: No
Abstract N°: 3161
RATES OF DISCONTINUATION AND NON-PUBLICATION OF ENDOVASCULAR STROKE CLINICAL STUDIES: A CROSS-SECTIONAL ANALYSIS
Mariam Abdelhady*1, Ahmed Aljabali2, Ibraheem Alkhawaldeh3, Esraa Zedan4, Marwa Abdelazim5, Dina Essam5, Marwa Kabeel6, Sewar Elejla7, Ahmed Negida8, Rowan H. Elhalag9
1October 6 University, Giza, Egypt, 2Jordan University of Science & Technology (JUST), Irbid, Jordan, 3Mutah University, Al Karak, Jordan, 4Al-Azhar University, Cairo, Egypt, 5Zagazig University, Zagazig, Egypt, 6Kafr El Sheikh University, Kafr El Sheikh, Egypt, 7Al-Quds University - Al-Azhar branch, Gaza, Palestine, 8Virginia Commonwealth University, Virginia, United States, 9Alexandria University, Egypt
On behalf of:
Background and aims: Stroke, a leading cause of morbidity and mortality worldwide, often necessitates endovascular therapy (EVT). Despite its prevalence, EVT clinical trials face high rates of discontinuation and non-publication, potentially impacting evidence-based practices. This study aims to analyze the rates and factors influencing discontinuation and non-publication in EVT stroke trials.
Methods: This retrospective cohort study conducted a systematic review of the ClinicalTrials.gov database, analyzing 88 endovascular stroke clinical trials completed by May 2022. Key parameters such as trial characteristics, participant demographics, funding, and study outcomes were examined. Logistic regression analysis was used to assess the likelihood of study discontinuation and non-publication, considering variables like sample size, number of centers, and funding source.
Results: Of the 88 studies, 25 (28.4%) were discontinued, and 23 (36.5%) of the completed studies remained unpublished. Larger trials (⩾100 participants) were less likely to be discontinued (odds ratio 0.217, p= 0.023) and unpublished (odds ratio 0.0276, p= 0.019). Multicenter trials had a higher discontinuation rate compared to single-center trials. Sample size and multicenter status were significant predictors of trial outcomes.
Conclusions: The study highlights a substantial waste of resources in EVT research, with about 25% of trials discontinued and a significant portion unpublished. It underscores the importance of robust trial designs, particularly in terms of sample size and center type, to mitigate research waste and publication bias. These findings stress the need for strategic planning in clinical trial design and execution, improving transparency, and ensuring public disclosure of all trial outcomes to inform evidence-based practices in EVT stroke treatment.
Disclosures of Interest: No
Abstract N°: 252
ASSOCIATION OF ISCHEMIC CORE HYPODENSITY, ENDOVASCULAR THERAPY TREATMENT EFFECT AND HEMICRANIECTOMY IN LARGE CORE STROKE
Vignan Yogendrakumar*1, Hannah Johns2, Leonid Churilov2, Felix Ng1, Gagan Jyoti Sharma1, Prodipta Guha1, Deep Pujara3, Clark Sitton4, Amrou Sarraj3, Bruce Campbell1
1The Royal Melbourne Hospital, Parkville, Australia, 2The University of Melbourne, Parkville, Australia, 3Case Western Reserve University, Cleveland, United States, 4The University Of Texas Health Science Center, Houston, United States
On behalf of: On behalf of the SELECT-2 Investigators
Background and aims: Core volume is prognostic but does not modify endovascular thrombectomy (EVT) treatment effect. We assessed the association between ischaemic core hypodensity and clinical outcome in the SELECT-2 trial.
Methods: Non-contrast CT-core was manually outlined. The presence of severe hypodensity was defined dichotomously using the lower 99%CI of contralateral thalamic grey matter in Hounsfield units[HU]. A regression model of independent ambulation (mRS0-3) and severe hypodensity volumes was generated and a volume threshold was selected based on intersection of confidence intervals. The treatment effect of EVT on mRS 0-3, 0-2, ordinal mRS, and hemicraniectomy was assessed in subgroups based on the selected volume threshold with adjustment for age, baseline NIHSS, and baseline CT-core volume, in regression models with treatment*volume interactions.
Results: Of 317 patients, median density of non-contrast core was 31HU(IQR:28-33). The severe hypodensity threshold was 26HU, representing 19%(IQR:9-35%) of total core volume. A >26mL threshold was chosen based on modelled confidence intervals for the relationship of severe hypodensity volume and outcome (Figure 1). In patients with ⩾26mL of severe hypodensity, EVT was not associated with mRS0-3 (n=100, aOR=1.02, 95%CI:0.35-3.00) versus patients with <26mL of severe hypodensity (n=217, aOR=7.73, 95%CI:3.55-16.87, p-interaction<0.01), mRS 0-2 (⩾26mL: aOR=0.82, 95%CI:0.19-3.64 versus <26mL: aOR=9.45, 95%CI:3.05-29.27, p-interaction<0.01), or ordinal shift mRS (⩾26mL: acOR=0.83, 95%CI:0.36-1.89 versus <26mL: acOR=0.24, 95%CI:0.13-0.41, p-interaction=0.01), but was associated with hemicraniectomy (⩾26mL: aOR=3.63, 95%CI:1.15-11.41 versus <26mL: aOR=0.75, 95%CI:0.31-1.77, p-interaction=0.03).
Conclusions: Severe hypodensity within a large ischaemic core modifies the treatment effect of EVT and increases the likelihood of hemicraniectomy, independent of total CT-core volume.
Disclosures of Interest: No
Abstract N°: 399
COST-EFFECTIVENESS OF LATE THROMBECTOMY VS. BEST MEDICAL MANAGEMENT IN A CLINICAL TRIAL SETTING AND REAL-WORLD SETTING
Johanna Ospel*1, Charlotte Zerna2, Brian van Adel3, Jai Jai Shankar4, Ryan Mctaggart5, Vitor Pereira6, Donald Frei7, Wolfgang Kunz8, Mayank Goyal1, Michael Hill1
1Foothills Medical Centre, Calgary, Canada, 2Krankenhaus Dresden-Friedrichstadt, Dresden, Germany, 3Hamilton General Hospital, Hamilton, Canada, 4University of Manitoba, Winnipeg, Canada, 5Rhode Island Hospital, Providence, United States, 6St. Michael's Hospital, Toronto, Canada, 7, United States, 8Ludwig Maximilian University of Munich, München, Germany
On behalf of: the ESCAPE-LATE and ESCAPE Investigators
Background and aims: To assess cost-effectiveness of late time-window endovascular treatment (EVT) in a clinical trial setting and a “real-world” setting.
Methods: Data are from the randomized ESCAPE trial and a prospective cohort study (ESCAPE-LATE). Anterior circulation large vessel occlusion patients presenting >6 hours from last-known-well were included, whereby collateral status was an inclusion criterion for ESCAPE but not ESCAPE-LATE. A Markov state transition model was built to estimate lifetime costs and quality-adjusted life-years (QALYs) for EVT in addition to best medical care vs. best medical care only in a clinical trial setting (comparing ESCAPE-EVT to ESCAPE control arm patients) and “real-world” setting (comparing ESCAPE-LATE to ESCAPE control arm patients), Fig 1. Unadjusted analysis used raw 90-day modified Rankin Scale(mRS) as input. Adjusted analysis accounted for differences in baseline factors.
Results: Two-hundred-forty-nine patients were included. Late EVT was cost-effective in the unadjusted analysis both in the clinical trial and real-world setting, with acceptability 96.6%-99.0%. After adjusting for differences in baseline variables between the groups, late EVT was marginally cost-effective in the clinical trial setting(acceptability:49.9%-61.6%), but not the “real-world” setting(acceptability:32.9%-42.6%).
Conclusions: EVT for LVO-patients presenting beyond 6hours was cost-effective in the clinical trial setting and “real-world” setting, although this was largely related to baseline patient differences favoring the “real-world” EVT group. After adjusting for these, EVT benefit was reduced in the trial setting absent in the real-world setting.
Disclosures of Interest: No
Abstract N°: 504
THROMBECTOMY AND THROMBOLYSIS VERSUS THROMBOLYSIS ALONE IN DISTAL MEDIUM VESSEL OCCLUSIONS - RESULTS FROM THE SITS INTERNATIONAL STROKE REGISTER
Boris Keselman*1,2, Michael Mazya1,2, Niaz Ahmed1,2, Daniel Strbian3, Ana Paiva Nunes4, Danilo Toni5, Giovanni Frisullo6, Dalius Jatuzis7,8, Andrea Naldi9, Tiago Holm Moreira1,2
1Karolinska University Hospital, Department of Neurology, Stockholm, Sweden, 2Karolinska Institutet, Department of Clinical Neuroscience, Stockholm, Sweden, 3Helsinki University Hospital, Department of Neurology, Helsinki, Finland, 4Centro Hospitalar Universitario de Lisboa Central, Stroke Center, Lisbon, Portugal, 5University La Sapienza, Emergency Department Stroke Unit, Rome, Italy, 6Policlinico Agostino Gemelli IRCCS, Department of Neuroscience, Rome, Italy, 7Vilnius University, Faculty of Medicine, Vilnius, Lithuania, 8Vilnius University Hospital, Santaros klinikos, Vilnius, Lithuania, 9San Giovanni Bosco Hospital, Neurology, Turin, Italy
On behalf of: Silvia Strumia, MD. Neurology Unit, Pierantoni Hospital, Forli, Italy
Background and aims: Endovascular thrombectomy (EVT) is standard of care for acute ischaemic stroke (AIS) caused by large vessel occlusion. Distal medium vessel occlusions (DMVO) account for 25-40% AIS cases, but recanalization rates with intravenous thrombolysis (IVT) only are often below 50%. Studies have shown better outcomes for EVT in specific DMVO populations. It is unknown whether patients with DMVO benefit from EVT in addition to IVT.
Methods: We included patients in the SITS ISTR 2016–2023, treated with IVT or IVT+EVT for occlusion of the ACA, PCA or distal MCA (M3/more distal), excluding tandem occlusions. Outcomes were distribution of modified Rankin Scale score (mRS), death at three months, and post-treatment haemorrhage. Binomial logistic regression was performed due to baseline imbalances (age, NIHSS and occlusion site).
Results: Of 2198 included patients, 1903 (87%) received IVT, and 295 (13%) had IVT+EVT. IVT+EVT patients were younger (73 vs 75) and had higher median NIHSS: 10 (IQR 6-15) vs 8 (5-12), p<0.001. The most common occlusion site was PCA in the IVT+EVT group, (n=179, 60.7%), and distal MCA (n=1140, 59.9%) in the IVT group. Rates of symptomatic intracerebral haemorrhage were higher in the IVT+EVT group (SICH NINDS: 7.6% vs 3.5%, p=0.003; SICH ECASS-II: 5.4% vs 2.4%, p=0.011). After adjustment, IVT+EVT was associated with worse outcomes at three months (aOR, 95% CI); mRS 0-1: 0.66 (0.50-0.87), mRS 0-2: 0.67 (0.50-0.91) and death: 2.28 (1.48-3.48).
Conclusions: IVT+EVT for DMVO was associated with worse outcomes compared to IVT alone. Results should be interpreted with caution due retrospective observational design, warranting randomized studies.
Disclosures of Interest: No
Abstract N°: 596
RECANALIZATION AND PROCEDURAL COMPLICATIONS IN PATIENTS WITH ISCHEMIC STROKE AND COVID-19 RECEIVING ENDOVASCULAR TREATMENT
João Pedro Marto*1,2, Davide Strambo3, George Ntaios4, Thanh N. Nguyen5, Patrik Michel3
1Hospital de Egas Moniz, Centro Hospitalar Lisboa Ocidental, Lisbon, Portugal, Neurology, Lisbon, Portugal, 2Lisbon Clinical Academic Center, NOVA Medical School, Universidade NOVA de Lisboa, Lisbon, Portugal, Lisbon, Portugal, 3Lausanne University Hospital, Lausanne, Switzerland, Stroke Center, Neurology Service, Department of Neurological Sciences, Lausanne, Switzerland, 4Faculty of Medicine, School of Health Sciences, University of Thessaly, Larissa, Greece, Internal Medicine, Larissa, Greece, 5Boston Medical Center, Boston University Chobanian and Avedisian School of Medicine, Boston, Massachusetts, USA, Radiology and Neurology, Boston, United States
On behalf of: The Global COVID-19 Stroke Registry
Background and aims: COVID-19 is associated with unfavorable outcomes in patients with acute ischemic stroke (AIS) receiving endovascular treatment (EVT). We aimed to evaluate recanalization rates and procedural complications during EVT in patients with AIS and COVID-19, as potential explanations for this finding.
Methods: The Global COVID-19 Stroke Registry is a multicenter retrospective cohort study of consecutive AIS patients receiving revascularization treatment between March-2020 and June-2021 and tested for SARS-CoV-2 infection. For this analysis, patients receiving EVT for intracranial occlusion were included. Recanalization rates were assessed with the modified treatment in cerebral ischemia (mTICI) score using logistic regression analysis. Procedural complications included arterial perforation and reocclusion during the procedure and were assessed with propensity score-matching (PSM). The study protocol was registered in ClinicalTrials.gov (NCT04895462).
Results: 8292 EVT patients were selected for this study, 497 (6.0%) with COVID-19. When compared to controls (COVID-19 negative), patients with COVID-19 had a worse final mTICI score distribution (adjusted odds ratio [aOR] 0.72; 95% confidence interval [CI] 0.59–0.89) and lower rate of successful recanalization (mTICI⩾2b) (aOR 0.59; 95% CI 0.44–0.79). Patients with COVID-19 had higher rates of arterial perforation (PSM-OR 2.14; 95% CI 1.12-4.10) and reocclusion (PSM-OR 2.98; 95% CI 1.75–5.09) during EVT.
Conclusions: Patients with AIS and COVID-19 receiving EVT had lower rates of recanalization and higher rate of arterial perforation and reocclusion during EVT than patients without COVID-19. These findings may partially explain the poorer outcome found in patients with COVID-19 and can be considered for treatment decisions and planning.
Disclosures of Interest: No
Abstract N°: 717
ONSET-TO-DOOR TIME'S IMPACT ON ENDOVASCULAR THERAPY FOR BASILAR ARTERY OCCLUSION
1First Affiliated Hospital of University of Science and Technology of China, Hefei, China, 2the Zeenat Qureshi Stroke Institute and Department of Neurology, 3the UPMC Stroke Institute, 4Department of Neurology and Comprehensive Stroke Center
On behalf of:
Background and aims: Whether onset-to-door time modifies the effect of endovascular treatment (EVT) in patients with acute basilar artery occlusion (BAO) is not determined.
Methods: Retrospective analysis of patients enrolled into the ATTENTION registry (2017-2021) who received EVT or best medical management (BMM) within 24 hours of BAO. The primary outcome was 90-day mRS score. We estimated the EVT effect for time from BAO onset to hospital arrival by using ordinal logistic regression. We entered an interaction term into the model to test for interaction with prespecified BAO onset to hospital arrival subgroups: 0-6h versus >6-12h versus >12-24h.
Results: 2134 patients, 1672 (78.4%) received EVT and BMM and 462 (21.7%) received BMM alone were included in the analysis. Median time from BAO onset to hospital arrival was 333 minutes (IQR, 219 to 584) in the EVT group and was 335 minutes (IQR, 207 to 613) in the BMM group. There was no difference in the effect of EVT among subgroups categorized by the time from BAO onset to hospital arrival, as measured by the 90-day ordinal mRS (acOR at 0-6 hours, 1.60 (95% CI, 1.22 to 2.11); acOR at >6-12h, 1.38 (95%CI, 0.96 to 1.97); acOR at >12-24h,1.63 (95%CI, 0.91 to 2.94); p for interaction=0.92). Likewise, there were no significant differences in the effect of EVT across onset-to-door subgroups in terms of symptomatic intracranial hemorrhage at 24 hours or 90-day mortality.
Conclusions: In patients with BAO presenting within 24 hour window, there was no time dependence in the treatment of patients with EVT compared to BMM.
Disclosures of Interest: No
Abstract N°: 818
SR+CA IS ASSOCIATED WITH REDUCED RISK OF DISTAL EMBOLIZATION THAN CA ONLY IN PATIENTS WITH FIBRIN/PLATELETS-RICH THROMBUS
Li'an Huang*1, Liang Zhang1
1Jinan University First Affiliated Hospital, Neurology, Guangzhou, China
On behalf of:
Background and aims: We examined the relationship between hyperdense artery sign/susceptibility vessel sign (HAS/SVS) and thrombus composition, and evaluated the effect of HAS/SVS status on the association between first-line thrombectomy techniques and outcomes in patients with acute anterior-circulation large vessel occlusion (LVO).
Methods: We retrospectively reviewed consecutive acute anterior-circulation LVO patients who underwent noncontrast computed tomography (NCCT) and/or susceptibility-weighted imaging (SWI) examination before thrombectomy, and in whom the removed clot was available for histological analyses. The presence of HAS and SVS was respectively assessed in NCCT and SWI. Association of first-line thrombectomy techniques [SR combined CA (SR+CA) versus CA] with outcomes was assessed by the HAS/SVS status.
Results: mong 103 included patients, 55 (53.4%) were HAS/SVS(-), and 69 (67.0%) chose first-line SR+CA. Higher relative densities of fibrin/platelets (0.56 vs. 0.51, p<0.001) and lower relative densities of erythrocytes (0.32 vs. 0.42, p<0.001) were observed in HAS/SVS(-) than HAS/SVS(+) patients. First-line SR+CA was associated with reduced odds of distal embolization (aOR, 0.18; 95% CI, 0.04–0.83; p=0.027) and a more favorable 90-day functional outcome (aOR, 5.29; 95% CI, 1.06–26.34; p=0.042) in HAS/SVS(-) patients, and a longer recanalization time (53 min vs. 25 min, p=0.025) and higher risk of subarachnoid hemorrhage (24.2% vs. 0%, p=0.044) in HAS/SVS(+) patients.
Conclusions: Our study suggests that HAS/SVS(-) may indicate a higher density of fibrin/platelets in the thrombus, and first-line SR+CA may have a possible better performance than CA in acute LVO patients without HAS/SVS.
Disclosures of Interest: No
Abstract N°: 940
MONITORED PLATELET FUNCTION AFTER EMERGENT CAROTID ARTERY STENTING
Magnus Peter Kreiberg1, Nicolaj Grønbæk Laugesen*1,2, Andreas Brandt3, Trine Stavngaard3, Joan Hoejgaard1, Klaus Hansen1,2, Thomas Truelsen1,2
1Rigshospitalet, University Hospital Copenhagen, Neurology, Copenhagen, Denmark, 2University of Copenhagen, Faculty of Health Sciences, Copenhagen, Denmark, 3Rigshospitalet, University Hospital Copenhagen, Radiology, Copenhagen, Denmark
On behalf of:
Background and aims: Antiplatelet therapy after emergent carotid stenting (eCAS) represent a challenge balancing risk of intracerebral hemorrhages (ICH) and in-stent thrombosis (IST). Platelet function monitoring can guide antiplatelet therapy and potentially reduce complications.
Methods: Consecutive eCAS patients in 2019-2021 were included in this observational study. Post-procedural platelet inhibition was monitored using Multiplate® (Roche, Mannheim, Germany). Modified Rankin Scale (mRS) at 90 days and safety variables were compared to patients with mechanical thrombectomy of occlusions in the internal carotid artery (ICA) without eCAS. Clinical variables were collected, and multivariate logistic regression for favorable outcome (mRS 0-2) was performed.
Results: One-hundred-and-five patients had eCAS and 28 patients (27%) showed clopidogrel hypo-reactivity and was changed to treatment with ticagrelor. Periprocedural IST occurred in four patients and further two at follow-up. Compared to 196 ICA patients, favorable outcome was more common after eCAS (64% vs. 39%, p<0.001). Symptomatic ICH was similar (6% vs. 7%, p=0.8), however, hemorrhage regardless of clinical worsening was more frequent in eCAS (21% vs. 10%, p=0.01), and affected outcome negatively (OR=0.28, 95% CI 0.08-0.97, p=0.045). Complications were no more frequent in ticagrelor-treated patients. Procedural heparin was associated with post-procedural hemorrhage (27% vs. 6%, p=0.01), while integrillin was not (64% vs. 71%, p=0.60).
Conclusions: One in three eCAS patients had poor clopidogrel response. Hemorrhage without acute symptoms were more common after eCAS and affected functional outcome negatively. In eCAS patients, antiplatelet treatment may be monitored to reduce risk of IST and risk of any type of hemorrhage.
Disclosures of Interest: No
Abstract N°: 1693
TIME TRENDS IN MECHANICAL THROMBECTOMY: DO REAL WORLD-DATA MIRROR PROGRESS IN EVIDENCE FOUND
Christoph Riegler*1,2, Steffen Tiedt3, Felix Bode4, Jörg Berrouschot5, Waltraud Pfeilschifter6,7, Marlena Schnieder8, Kathleen Bernkopf9, Martina Petersen10, Bastian Cheng11, Christian Nolte1,2
1Charité Universitätsmedizin Berlin, Department of Neurology and Experimental Neurology, Campus Benjamin Franklin, Berlin, Germany, 2Center for Stroke Research Berlin, Berlin, Germany, 3University Hospital, Ludwig Maximilians University Munich, Institute for Stroke and Dementia Research, München, Germany, 4University Hospital Bonn, Department of Neurology, Bonn, Germany, 5Klinikum Altenburger Land GmbH, Klinik für Neurologie, Altenburg, Germany, 6Goethe University Frankfurt, Department of Neurology, Frankfurt am Main, Germany, 7Städtisches Klinikum Lüneburg, Department of Neurology and Clinical Neurophysiology, Lüneburg, Germany, 8University Medical Center Göttingen, Department of Neurology, Göttingen, Germany, 9Klinikum rechts der Isar, Technical University of Munich, Department of Neurology, München, Germany, 10Klinikum Osnabrück, Department of Neurology, Osnabrück, Germany, 11University Medical Center Hamburg-Eppendorf, Department of Neurology, Hamburg, Germany
On behalf of:
Background and aims: Following evidence from randomized controlled trials (RCTs), new techniques and indications for mechanical thrombectomy (MT) evolved. We aimed to assess how RCT results affected MT-use in real-world clinical practice.
Methods: The German Stroke Registry, an observational multicentre cohort was analysed. All centres with consecutive data entry from 2017 to 2021 and a 3-month follow-up rate >80% were included. We analysed changes in baseline variables, technical (modified Thrombolysis in Cerebral Infarction scale [mTICI]) and clinical (modified Rankin scale [mRS] at three months) outcomes. Cochran-Armitage and Jonckheere-Terpstra tests were used to assess trends. Adjusted regression analyses were applied to assess association of admission year with outcomes.
Results: Nine centres fulfilled inclusion criteria; 6.931 patients were analysed. The median age(IQR) was 77(66 – 83) years, 52% were female. Between 2017 and 2021, the annual number of patients receiving MT rose from 1.025 to 1.568. We found a relative increase in patients treated > 6h from last-seen-well from 21.5% to 28.5% (p<0.001). The use of perfusion-based imaging grew from 41.1% to 56.3% (p<0.001), while thrombolysis rate decreased from 52.5% to 40.7% (p<0.001). Median time from admission to groin puncture changed from 63(38 – 93) to 70(49 – 95) minutes. Technical outcome improved (mTICI 2b/3 from 84.4% to 86.2%; mTICI 3 from 46.3% to 53.9%), however, clinical outcome worsened (median mRS: from 3 (1–6) to 4 (2–6); aOR (per +1 year): 1.06 (1.02 – 1.11); mortality from 25.9% to 35.5% (aOR 1.11 (1.05 – 1.17)).
Conclusions: Between 2017 and 2021 real-world MT practice changed substantially, possibly affecting technical and clinical outcomes.
Disclosures of Interest: No
Abstract N°: 1910
INTRA-ARTERIAL THROMBOLYSIS SAFELY IMPROVES VISUAL RECOVERY RATES IN NON-ARTERITIC CENTRAL RETINAL ARTERY-OCCLUSION
1Penn State Health Milton S. Hershey Medical Center, Hershey, United States, 2University of California San Diego, La Jolla, United States, 3Mayo Clinic, Scottsdale, United States
On behalf of:
Background and aims: Acute non-arteritic central retinal artery occlusion (naCRAO) is a subtype of ischemic stroke with poor natural visual recovery rate. Limited data exist on the effectiveness and safety of early intraarterial thrombolysis (IAT) administration in patients with naCRAO
Methods: We systematically queried six databases to evaluate visual acuity (VA) improvement in naCRAO patients after intraarterial tissue plasminogen activator (tPA) or urokinase (UK) administration. Logarithm of the Minimum Angle of Resolution (logMAR) was used to quantifying the VA recovery. VA improvement for⩾0.3logMAR, standardized mean change in logMAR, and final VA ⩾20/100 were the study outcomes. We also evaluated the trend of VA recovery within 24h.
Results: Among 565 patients who received IAT within 24h of vision loss (48 studies), 369 patients were included in meta-analyses (42% tPA and 58% urokinase; 12.7% <6h, 50% 6h-12h, 42.3% 12h-24h). VA improvement⩾0.3 logMAR was noted in 57.8% (CI: 49.5%-66.0%) of patients, with 66.4% (CI: 48.8%-84.1%) standardized mean change in logMAR, and final VA⩾20/100 among 25.6% (CI: 16.6%-35.6%) of patients. Although limited by smaller sample size, we observed a decremental trend of VA improvement⩾0.3 logMAR with each 1.5h delay in receiving IAT after the onset of visual loss. Among all reported patients who received IAT, 0.7% patients were complicated with intra-ocular hemorrhage, 0.9% with ischemic stroke, and 1.4% with intracranial hemorrhage.
Conclusions: IAT in naCRAO is safe and may provide improvement of VA compared to natural history. Future large-scale prospective studies are warranted to comparatively study intra-arterial thrombolytic therapy and standard care within the hyperacute phase of visual loss.
Disclosures of Interest: No
Abstract N°: 1934
OUTCOME OF THROMBECTOMY IN ACUTE BASILAR ARTERY OCCLUSION WITH LARGE INFARCTION
Huong Nguyen*1, Thang Nguyen1
1115 People Hospital, Cerebrovascular Disease, Ho Chi Minh
On behalf of:
Background and aims: This study was conducted to investigate outcomes in patients with acute Vertebrobasilar Artery Occlusion (VBAO) characterized by a large core infarction (posterior circulation Alberta Stroke Program Early CT Score, PC-ASPECTS ⩽ 5).
Methods: A prospective study was conducted at People’s Hospital 115 in Ho Chi Minh City, Vietnam from September 2021 to June 2023. There were 210 patients with acute VBAO who underwent recanalization therapy within 24 hours of symptom onset, treated with thrombectomy alone or bridging intravenous thrombolysis and thrombectomy. We analyzed baseline characteristics and outcomes in the patients with PC-ASPECTS scores ⩽ 5. A favorable outcome was defined as a modified Rankin Scale (mRS) score of ⩽ 3 at 90 days, while a good outcome was defined as an mRS score of ⩽ 2.
Results: Of the 210 patients enrolled, 169 (80.5%) had a baseline PC-ASPECTS score of > 5, whereas 41 (19.5%) exhibited PC-ASPECTS scores ⩽ 5. There were 26.8% patients achieved a good outcome, and 17.1% achieved a favorable outcome. The mortality rate among patients with large core infarctions who underwent recanalization therapy was 65.9%. These findings aligned with the results of the studies which investigated the efficacy of thrombectomy in patients with large core infarctions in anterior circulation.
Conclusions: Thrombectomy for acute VABO with a large core infarction is a life-saving strategy. It was associated with improved functional outcomes and reduced mortality compared to the natural history of this condition. Timely intervention remains paramount in achieving optimal outcomes for these patients
Disclosures of Interest: No
Abstract N°: 2348
EARLY VERSUS LATE INITIATION OF ENDOVASCULAR THERAPY IN PATIENTS WITH SEVERE CEREBRAL VENOUS SINUS THROMBOSIS
Philipp Bücke*1, Hans Henkes2, Johannes Kaesmacher3, Mirjam Heldner1, Adrian Scutelnic1, Alexandru Cimpoca2, Thomas Horvath1, Elina Henkes2, Hansjörg Bäzner4, Victoria Hellstern2
1Inselspital, Bern University Hospital, Department of Neurology, Bern, Switzerland, 2Klinikum Stuttgart, Neuroradiologische Klinik, Stuttgart, Germany, 3Inselspital, Bern University Hospital and University of Bern, Institute of Diagnostic and Interventional Neuroradiology, Bern, Switzerland, 4Klinikum Stuttgart, Neurologische Klinik, Stuttgart, Germany
On behalf of:
Background and aims: Endovascular therapy (EVT) for severe cerebral venous sinus thrombosis (CVST) is controversial in terms of indication and clinical benefit. The impact of delay to EVT on functional recovery is unclear. This study aimed to investigate the effect of early versus late initiation of EVT in severe CVST.
Methods: From two EVT and CVST registries, CVST patients were retrospectively identified (January 2010 to October 2022) for this multicenter collaboration. EVT was performed in severe CVST with features prone to a poor prognosis. We compared early (< 24 hours) versus late (> 24 hours) initiation of EVT after the presentation in the emergency department. The main outcome parameter was functional independence (modified Rankin Scale [mRS] 0-2) at 90 days. Secondary outcome parameters included mRS at discharge and mortality at three months.
Results: Out of 363 CVST patients, 45 (12.4%; 31 [early EVT] versus 14 [late EVT]) were included in this study. We found a higher proportion of patients with functional independence at three months among early versus late EVT (66.7% versus 27.3%; odds ratio [OR] 5.3; 95% confidence interval [CI] 1.02-25; p = 0.036). The mortality rate was 16.7% versus 36.4% (mRS 6 at three months; OR 0.34; 95% CI 0.07-1.75; p = 0.217) at 90 days.
Conclusions: We observed a higher frequency of functional independence in early EVT patients. These preliminary findings have to be confirmed and taken into account in subsequent randomized-controlled trials evaluating a time-is-brain paradigm for EVT in CVST.
Disclosures of Interest: No
Abstract N°: 2684
CONTINUOUS SALINE INFUSION LINES REDUCE THE INCIDENCE OF AKI DURING ENDOVASCULAR PROCEDURES FOR STROKE TREATMENT
Gianluca De Rubeis*1, Sebastiano Fabiano1, Luca Bertaccini1, Andrea Wlderk1, Domenica Crupi2, Enrico Pampana1
1San Camillo/Forlanini, Neuroradiology, 2San Camillo/Forlanini, Stroke Unit
On behalf of:
Background and aims: Contrast media, used in mechanical therapies for stroke and myocardial infarction, represents a significant cause of the acute kidney injury (AKI) in acute medical scenarios. While the continuous saline infusion line (CSIL) is a standard procedure to prevent thrombus formation within the catheter during neurovascular interventions of mechanical thrombectomy (MT), it is not utilized in percutaneous coronary interventions (PCI).
Methods: A systematic review of the incidence of AKI after MT for stroke treatment was performed. These data were compared with those reported in literature on the incidence of AKI after PCI during acute myocardial infarction. A random-effect model meta-regression was performed to explore the effects of CSIL on AKI incidence, using clinical details as covariates.
Results: A total of 18 and 33 studies for MT and PCI were included, respectively, with 69,464 patients (30,138[43.4%] for MT and 39,326[56.6%] for PCI). The mean age was 63.6 years±5.8 with male 66.6%±12.8. Chronic kidney disease ranged 2.0%–50.3%. Diabetes prevalence spanned 11.1%-53.0%. Smoking status had a prevalence of 7.5%–72.0%.
The I^2 and Cochrane’s Q were 98.32 and 2984.77, respectively. The incidence of AKI was significantly lower in the MT subgroup than in the PCI subgroup (8.3%[CI95% 4.7–11.9] vs 14.7[CI95% 12.6–16.8]; p<0.05). In multivariate analysis, only the absence of CSIL significantly increased the incidence of AKI (OR 1.08[CI95% 1.001–1.16]; p = 0.03).
Conclusions: The absence of CSIL independently increased the incidence of AKI (OR 1.08[CI95% 1.001–1.16]; P = 0.03) during the endovascular procedure in the acute setting.
Disclosures of Interest: No
Abstract N°: 3314
MECHANICAL THROMBECTOMY ACCESS SCORE: A SYSTEMATIC REVIEW AND MODIFIED DELPHI OF GLOBAL BARRIERS TO ENDOVASCULAR TREATMENT FOR ISCHEMIC STROKE
1University of Texas at Austin, Department of Neurology, Austin, United States, 2University of Iowa Hospitals & Clinics, Department of Neurology, Iowa City, United States, 3University of Illinois Chicago, Department of Neurology, Chicago, United States, 4University of Manitoba, Department of Neurology, Winnipeg, Canada, 5University of Calgary, Calgary, Canada, 6University of California, Los Angeles, Los Angeles, United States, 7New York Medical College, Valhalla, United States, 8University of Miami, Coral Gables, United States
On behalf of:
Background and aims: To create a mechanical thrombectomy access (MTA) score to measure the drivers of access and provide a roadmap to help quantify and accelerate treatment worldwide. We aimed to create a mechanical thrombectomy access (MTA) score to measure the drivers of access and provide a roadmap to help quantify and accelerate treatment worldwide.
Methods: We used systematic review and complement with a modified Delphi method. In the first of three rounds, a systematic literature review using key search terms that drive MT access, following PRISMA guidelines was done. In the second round, a panel of anonymous international experts selected key attributes needed for scoring. I a final meeting, a total of 12 attributes were selected on consensus, each given a score on a 0-3 scale. An ultimate MTA score (range 0-36) was proposed. (Figure 1)
Results: Of 2864 abstracts screened, 121 studies were included in the final systematic review. A total of 34 attributes that potentially drive MT-access were initially identified by the expert. Subsequently a total of 12 attributes were finally selected and weighted as part of the final score. (Table).
Conclusions: The global MTAS represents the first tool to quantify barriers to MT access worldwide. Its implementation aims to objectively measure the magnitude and identify key barriers to guide regional public health interventions to improve MT workflow and access.
Modified Delphi methodology and results.
Final MT Access Score.
Disclosures of Interest: No
Abstract N°: 646
ESTABLISHING A NEW STROKE CENTER IN THE CARIBBEAN: FROM ZERO TO 100
Rodolfo Alcedo Guardia*1,2, Carmen Morales Colon2, Ulises Nobo2, Julio Rodriguez2, Angel Maldonado2, Daniel Reyes2, Juan Ramos Acevedo1, Juan Vicenty Padilla1, Yanitza Lopez Claudio2, Saksham Gupta3
1University of Puerto Rico, Medical Sciences Campus, San Juan, Puerto Rico, 2Hospital Menonita de Caguas, Caguas, Puerto Rico, 3Brigham and Women's Hospital, Boston, United States
On behalf of:
Background and aims: Despite the rapidly rising incidence of ischemic stroke in Puerto Rico, there has been no sustained stroke service. In this study, we describe the development and outcomes of a robust stroke center designed to manage patients in Puerto Rico, overcoming financial and logistical constraints.
Methods: We detail the novel multidisciplinary institutional stroke program with biplane angiography capacity and an institutional case series.
Results: The comprehensive stroke center's development spanned two years and involved multiple stakeholders. In its first 12 months, the center treated 122 patients with mechanical thrombectomy—54 in the first 6 months and 68 in the last 6 months. The median age was 69 (range: 22-95), and 49% were men. The median door-to-needle time was 56 minutes and door-to-groin time was 2.5 hours. Financially, to start the program the investment was 14 millioin USD, the program's annual fixed costs for the first year were 12 million USD, with variable costs per thrombectomy averaging 37,000 USD. Funding came from the hospital and industry partners. Despite financial constraints, the center adheres to U.S. standards due to participation in Medicaid and Medicare programs. The discussion delves into the challenges of starting a new comprehensive stroke center in Puerto Rico, addressing obstacles such as inefficient management by insurance providers, healthcare funding disparities, and the growing need to tackle this pressing health challenge for our patients.
Conclusions: This study provides valuable insights into the challenges faced during the establishment of a comprehensive stroke center in Puerto Rico, offering a comprehensive overview of the process and outcomes.
Disclosures of Interest: No
Abstract N°: 1641
THE ROLE OF STROKE SEVERITY IN THE ASSOCIATION BETWEEN HYPOPERFUSION INTENSITY RATIO AND FUTILE REPERFUSION AFTER THROMBECTOMY
1Beijing Tiantan Hospital Affiliated to Capital Medical University, beijing, China
On behalf of:
Background and aims: The higher National Institutes of Health Stroke Scale (NIHSS) score is an established clinical predictor of futile reperfusion (FR). The hypoperfusion intensity ratio (HIR) was significantly correlated with the NIHSS score in equal direction. We aimed to quantify the direct and indirect effect of HIR on FR.
Methods: We analyzed acute ischemic stroke patients with large vessel occlusion who underwent thrombectomy in a multicenter cohort study between 2017 and 2022 at 7 comprehensive stroke centers in China. HIR was automatically calculated on baseline CT perfusion as the ratio of brain volume with time-to-max (Tmax) delay >10 s over volume with Tmax >6 s. The established threshold HIR >0.44 was regarded as inadequate baseline perfusion. FR was defined as modified Rankin Scale score of 4-6 at 90 days despite successful recanalizaiton. Mediation analysis using the "mediation" package in R 4.2.2 was performed.
Results: Among the 740 analyzed patients, 253 (34.2%) patients had FR at 90 days. Inadequate baseline perfusion was significantly associated with a higher NIHSS score (adjusted common odds ratio [acOR], 2.44 [1.68 – 3.56]) and higher rates of FR (aOR, 0.54 [0.33–0.88]). The baseline NIHSS score was a predictor of FR (aOR, 1.14 [1.09–1.19]). Causal mediation analyses revealed that 39.4% (95% CI, 20.9% – 76.3%) of the relationship between HIR and FR was mediated by the baseline NIHSS score.
Conclusions: The NIHSS score mediates more than 30% of the association between HIR and FR at 90 days. The accurate evaluation of stroke severity at presentation is important for prognosis judgement.
Disclosures of Interest: No
Abstract N°: 1860
A MACHINE LEARNING APPROACH TO PREDICTING FUNCTIONAL OUTCOMES POST-MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE STROKE
Joshua Yeo*1, Benedict Lee1, Kevin Teo1, Benjamin Tan1, Leonard Yeo1
1National University Hospital (NUH) - Singapore, Singapore, Singapore
On behalf of:
Background and aims: Mechanical thrombectomy is the standard of care for select patients who present with acute ischemic stroke. We developed a machine-learning model that would aid the clinician in predicting functional outcome post-mechanical thrombectomy.
Methods: A retrospective cohort of 437 patients with acute ischemic stroke from 2016-2020 was derived. Various relevant clinico-radiological variables were extracted along with their functional outcomes by mRS, including factors such as age, gender, presence of diabetes, National Institute of Health Stroke Scale (NIHSS) score on arrival and door-to-needle time. This data was analyzed with machine-learning algorithms including Random Forests, Support Vector Machines, XGBoost and logistic regression. A test dataset was held out for validation of the models. Simple tuning of hyperparameters also carried out. Good functional outcome was defined as mRS 0-2. Results were assessed using the F1-score and area under Receiver Operating Characteristic(AUROC). Feature importance was also evaluated to identify which variables carried greater weight in making the predictions.
Results: 35.9% (n = 157) of the patients studied achieved a good functional outcome. The best performing model was the Random Forest employing 100 estimators(F1=0.86,AUROC=0.81), while the poorest performing model was the Support Vector Machine(F1= 0.709, AUROC=0.463). Predictive factors which carried the most weight included age, NIHSS on arrival and top-to-bottom distance of the middle cerebral artery as measured on fluoroscopy.
Conclusions: Our model shows good performance in predicting functional outcomes of patients with acute ischemic stroke and may be of help for clinicians who need to make rapid decisions. It incorporates clinically relevant factors and has good explainability.
Disclosures of Interest: No
Abstract N°: 2410
INTENSIVE BLOOD PRESSURE LOWERING AFTER ENDOVASCULAR THERAPY FOR ACUTE ISCHAEMIC STROKE: A SYSTEMATIC REVIEW AND META-ANALYSIS
Elizabet Taylor Weba*1, Rafael Eduardo Streit2, Pedro Henrique Reginato2, Maria Galvão3, Marianna Gerardo Hidalgo Santos Jorge Leite4, Vivian Gagliardi5,6
1State University of the Tocantina Region of Maranhão, Imperatriz, Brazil, 2Federal University of Paraná, Curitiba, Brazil, 3Federal University of Piauí, Teresina, Brazil, 4School of Medicine Santa Marcelina, São Paulo, Brazil, 5Santa Casa de São Paulo, São Paulo, Brazil, 6Albert Einstein Israelite Hospital, São Paulo, Brazil
On behalf of: Elizabet Taylor Pimenta Weba; Rafael Eduardo Streit; Pedro Henrique Reginato; Maria Theresa Leal Galvão; Marianna Gerardo Hidalgo Santos Jorge Leite; Vivian Dias Baptista Gagliardi.
Background and aims: Guideline recommendations to maintain systolic blood pressure (SBP) ⩽180 mmHg for 24 hours after endovascular thrombectomy (EVT) in patients with acute ischaemic stroke (AIS) are based on expert opinion. However, the effect of intensive BP-lowering (<140 mmHg) post-EVT are still uncertain. Therefore, we aimed to perform a meta-analysis to evaluate whether intensive BP-lowering improves clinical outcomes compared with standard BP-lowering.
Methods: We systematically searched PubMed, Embase and Cochrane for studies comparing intensive management with the conventional. The main outcomes were 3-month functional independence and symptomatic intracranial haemorrhage (sICH). Statistical analysis was performed using Review Manager 5.1.7. Heterogeneity was assessed with I2 statistics.
Results: We included 6.569 patients from 11 studies, of which 4 were RCTs. The intensive group included 3.942 (60,01%) patients. Functional independence (OR 1.59; 95% CI 1.00-2.53; p = 0.05) and sICH (OR 0.82; 95% CI 0.56-1.18; p = 0.10) were not significantly different among groups. In sensitivity analysis with just RCTs, the intensive SBP target was associated with a significantly lower functional independence (OR 0.67; 95% CI 0.54-0.82; p = 0.0002) compared with the conventional SBP target.
Conclusions: The findings of this systematic review and meta-analysis suggest that actively BP-lowering to levels <140 mmHg may be associated with a poor functional recovery in patients with AIS post-EVT and a not significantly greater likelihood of sICH.
Disclosures of Interest: No
Abstract N°: 2502
TARA INDUCED CHANGES IN BLOOD PRESSURE DURING ENDOVASCULAR THROMBECTOMY – AN UNDERESTIMATED RISK FACTOR AND THERAPEUTIC TARGET?
Gabriela Siedler*1, Matthias Borutta1, Kosmas Macha1, Svenja Kremer1, Joji B. Kuramatsu1, Tobias Engelhorn2, Iris Mühlen2, Julia Koehn1
Background and aims: Though relevance of periprocedural blood pressure management during endovascular thrombectomy is under intensive investigation, relevance and influence of tachyarrhythmia absoluta (TARA) as a common condition and cause for hypotonia has not been investigated yet. The aims of the study were 1) to generate primary clinical data on prevalence and outcome of TARA in the periinterventional setting and 2) to release real world data of treatment options with amiodarone.
Methods: Data analysis from the prospective STAMINA registry (n=1410, 2015-2019, NCT04357899) including patients with LVO-stroke undergoing endovascular thrombectomy, with functional outcome analysis after 3 months (favorable functional outcome: mRS ⩽3). Perriinterventional TARA was defined as TARA ⩾100bpm for ⩾5min during thrombectomy.
Results: 280 patients had atrial fibrillation, 65 (23%) had periinterventional TARA. Patients with TARA had a higher need for periinterventional catecholamines (59 vs. 74%, p=0.03), a lowe rate of successful reperfusion (TICI ⩾2b: 92 vs. 82%, p= 0.008), and a less favorable functional outcome after three months (37 vs. 19%, p=0.014). Procedural times did not differ. 17/65 patients were treated with Amiodarone (26%). Amiodarone treatment resulted in improved BP (median 30mmHg), whereas no differences in safety parameters occurred (hypertension >185mmHg, kidney failure, thyroid failure, prolongation of QT-time, embolic events). A favorable outcome was seen less often in patients with Amiodarone-treatment(29 vs. 0%, p=0.012).
Conclusions: Periinterventional TARA is common and associated with catecholamine use, less successful reperfusion and less favorable functional outcome. Early treatment with amiodarone appears save. Yet, further research is needed to stratify possible benefits of periinterventional TARA management.
Disclosures of Interest: No
Abstract N°: 2652
EFFICACY AND SAFETY OF MINIMAL-DOSE INTRAVENOUS HEPARIN DURING MECHANICAL THROMBECTOMY
1Inha University Hospital, Neurology, Incheon, South Korea, 2Inha university hospital, Neurosurgery, Incheon, South Korea, 3Soonchunhyang University, Neurology, Seoul, South Korea, 4Dong-Guk Univeristy Hospital, Neurology, Goyang, South Korea
On behalf of:
Background and aims: East Asians are known to have a higher risk of bleeding compared to other races, and they often take low doses of antithrombotics. Previous studies indicated the usual dose heparin(5000 IU bolus followed by 500~1250 IU/h) during mechanical thrombectomy(MT) is associated with an increased risk of hemorrhagic conversion without beneficial effect. However, role of minimal-dose heparin as an adjuvant treatment during MT in East Asians remains unclear.
Methods: We enrolled the patients who underwent MT from the Inha University Hospital Stroke Prospective Registry and compared clinical findings between patients who received heparin during MT and those who did not.
Results: From January 2016 to October 2023, 450 patients (68.8 years, 254 men) were included, and 70(15.6%) subjects received intravenous heparin, dose 500-1000 IU bolus, followed by 500 IU/h. There were no differences in baseline characteristics or procedural parameter including procedural time, device, distal migration and TICI grade between two groups. However, intravenous thrombolysis was performed more frequently in the non-user group than in the heparin group, and the apTT value after the procedure was higher in the heparin group than in the other groups(75.9±12.5 vs 41.6±10.2 sec). The risk of hemorrhagic conversion on image was significantly higher in heparin group than non-user group(31.4% vs 21.8%, p=0.04). However, there was no difference in mRS at 90 days and early neurological deficit between the two groups.
Conclusions: Even minimal dose of intravenous heparin injection during MT was associated with an increased risk of hemorrhagic conversion without significant change in functional outcome or recanalization status.
Disclosures of Interest: No
Abstract N°: 52
EVALUATING THE STRENGTH AND QUALITY OF EVIDENCE IN AMERICAN HEART ASSOCIATION'S GUIDELINES FOR ANEURYSMAL SUBARACHNOID AND INTRACEREBRAL HEMORRHAGE
Syed Gillani*1,2, Mohammed Maan Al-Salihi3, Rehan Ahmed1, Ibrahim Bhatti1, Jonathan Beal4, Christy Cassarly4, Byron Gajewski5, Renee Martin4, Jose Suarez6, Adnan Qureshi1,2
1University of Missouri, Columbia, United States, 2Zeenat Qureshi Stroke Institute, 3University of Wisconsin-Madison, Madison, United States, 4Medical University of South Carolina, Charleston, United States, 5The University of Kansas Cancer Center, Westwood, United States, 6John Hopkins Medical Center | Physical Medicine and Rehabilitation, Baltimore, United States
On behalf of:
Background and aims: Clinical-practice guidelines serve as cornerstones in healthcare decision-making, guiding clinicians through evidence-based practices. We assessed the evidence strength and recommendation quality in American Heart Association/American Stroke (AHA/ASA) Association guidelines for aneurysmal subarachnoid hemorrhage (aSAH) and intracerebral hemorrhage (ICH)
Methods: Our review encompassed current AHA/ASA guidelines for aSAH and ICH with comparisons to previous guidelines. Recommendations were classified based on the Class of recommendation (COR) and Level of evidence (LOE). COR signifies recommendation strength (COR 1: Strong; COR 2a: Moderate; COR 2b: Weak; COR 3: No Benefit/Harm), while LOE denotes evidence quality (LOE A: High-Quality; LOE B-NR: Moderate-Quality, Not Randomized; LOE B-R: Moderate-Quality, Randomized; LOE C-EO: Low-Quality, Expert Opinion; LOE C-LD: Low-Quality, Limited Data).
Results: For aSAH, encompassing 15 guideline categories, 31% were COR I, 30% COR 2a, 17% COR 2b, and 18% were COR 3. A total of 7% were based on LOE A, 10% on LOE B-R, 65% on LOE B-NR, 14% on LOE C-LD. Across 31 ICH guideline categories, 28% were classified COR 1, 32% were COR 2b, and 9% were COR 3. A total of 4% were based on LOE A, 35% on LOE B-NR and 42% on LOE C-LD.
Conclusions: Less than a third of AHA/ASA guidelines on aSAH and ICH are classified as the highest class of recommendation with less than 10% based on highest LOE. There appears to be a decrease in proportion of recommendations based on highest LOE in most recent guidelines. Our analysis suggests areas for enhancing evidence and recommendations in aSAH and ICH guidelines.
Disclosures of Interest: No
Abstract N°: 222
VARIABLES ASSOCIATED TO COLLATERAL CIRCULATION DEGREE IN PATIENTS WITH LARGE-VESSEL OCCLUSION
Joan Martí-Fàbregas*1, Marina Guasch Jiménez1, Garbiñe Ezcurra1, Álvaro Lambea-Gil1, Elena de Celis Ruiz2, Carla Avellaneda3, Maria del Mar Freijo4, Juan F. Arenillas5, Francisco Moniche Alvarez6, Pol Camps Renom1
1Hospital de la Santa Creu i Sant Pau, Neurology, Barcelona, Spain, 2Hospital Universitario La Paz, Neurology, Madrid, Spain, 3Hospital del Mar, Neurology, Barcelona, Spain, 4Hospital Universitario Cruces, Neurology, Baracaldo, Spain, 5Hospital Universitario de Valladolid, Neurology, Valladolid, Spain, 6Hospital Universitario Virgen del Rocío, Neurology, Sevilla, Spain
On behalf of: Ana Aguilera-Simón, Alejandro Martínez-Domeño, Anna Ramos-Pachón, Luis Prats-Sánchez, Rebeca Marín-Bueno, Israel Fernández-Cadenas, José Pablo Martínez-González, Joaquín Ortega-Quintanilla, Isabel Fernández-Pérez, Santiago Trillo-Senin
Background and aims: In patients with acute ischemic stroke (AIS), treated with endovascular therapies (EVT), collateral circulation (CC) degree is associated with outcomes and recanalization success. However, the reasons for the variability in CC degree among patients are uncertain. This study aimed to comprehensively investigate predictors of CC degree before the EVT.
Methods: A multicenter (n=7) and prospective study of patients with AIS and anterior large-vessel occlusion (LVO). We collected demographic data, vascular risk factors, previous treatments, vital signs, baseline laboratory results, time metrics, artery segment occluded, Willis circle (WC) completeness, and presence of an anterior temporal artery (ATA). Automated and validated software (Brainomix Ltd) generated the collateral Score (CS) from the baseline single-phase CT angiography. CS was dichotomized as poor (CC 0-50% compared to the healthy hemisphere) or good (CC 51-100%). We performed bivariate and multivariable logistic regression analyses to predict CS categories.
Results: We included 360 patients (mean age 73.3±13.1, 50.5% were women). CS degree was poor in 86 (24%) and good in 274 (75%) patients. In bivariate analysis CS degree was associated with age, LVO segment, WC completeness, presence of ATA, previous statin therapy and previous ischemic heart disease. Predictors of a good CS were age (OR 0.96, 95% CI 0.94-0.98, p=0.003), presence of ATA (OR 3.1, 95% CI 1.6-5.7, p<0.001), TICA-LVO (OR 0.39, 95% CI 0.2-0.76, p<0.001) and complete WC (OR 3.7, 95% CI 1.35-10.16, p=0.011).
Conclusions: Predictors of CS degree are not modifiable and include age, WC completeness, more proximal LVO and presence of ATA
Disclosures of Interest: No
Abstract N°: 520
PREDICTORS OF FUTILE RECANALIZATION AFTER ENDOVASCULAR THROMBECTOMY IN POSTERIOR CIRCULATION ACUTE ISCHEMIC STROKE
Gaurav Nepal*1, Rajeev Ojha2
1Rani Primary Healthcare Centre, General Medicine, Biratnagar, Nepal, 2Tribhuvan University Teaching Hospital, Neurology, Kathmandu, Nepal
On behalf of:
Background and aims: Acute ischemic stroke (AIS) is a major global cause of disability and death, with posterior circulation AIS accounting for 20-25% of cases. Endovascular treatment (EVT) is the standard care for large vessel occlusion (LVO), but not all patients achieve favorable outcomes due to futile recanalization. This systematic review and meta-analysis aimed to identify predictors of futile recanalization in posterior circulation AIS patients treated with EVT.
Methods: Prospective and retrospective studies in English were included, focusing on AIS patients aged >17 with posterior circulation LVO who underwent EVT. Futile recanalization was defined as poor functional outcome (mRS >2 at 3 months) despite successful recanalization (TICI score 2b or 3).
Results: Five studies met the inclusion criteria. Among the predictors examined, the following were significantly associated with futile recanalization: lower PC-ASPECTS score (MD: -1.14, 95% CI: -1.40 to -0.87, p < 0.05), higher NIHSS score at admission (MD: 9.30, 95% CI: 3.18 to 15.41, p < 0.003), longer groin puncture to recanalization time (MD: 9.69, 95% CI: 3.23 to 16.16, p = 0.0032), elevated blood glucose levels (SMD: 0.19, 95% CI: 0.02 to 0.35, p < 0.026), and higher total leukocyte count (MD: 2.08, 95% CI: -0.12 to 4.29, p = 0.064). Hemorrhagic transformation was also significantly associated with futile recanalization (OR: 2.75, 95% CI: 1.03 to 7.35, p < 0.043).
Conclusions: This meta-analysis identified several predictors of futile recanalization in posterior circulation AIS patients treated with EVT. These predictors can aid clinicians in patient selection and optimizing treatment strategies to improve outcomes.
Disclosures of Interest: No
Abstract N°: 1209
FIRST-PASS ETICI: COMPARISON BETWEEN THE SINGLE AND THE DUAL STENTRIEVER TECHNIQUES
Thomas Fracheboud1, Alexander Salerno*2, Francesco Puccinelli1, Steven David Hajdu1, Bruno Bartolini1, Davide Strambo2, Patrik Michel2, Guillaume Saliou1
1Lausanne University Hospital and University of Lausanne, Department of Diagnostic and Interventional Radiology, Lausanne, Switzerland, 2Lausanne University Hospital and University of Lausanne, Stroke Center, Neurology Service, Department of Clinical Neurosciences, Lausanne, Switzerland
On behalf of: TF and AS contributed equally
Background and aims: Recent developments in mechanical thrombectomy (MT) for acute ischemic stroke (AIS) include the use of a double stentriever (DS) technique, offering promising early results. This study aims to compare the efficacy and safety of the DS technique against the traditional single stentriever (SS) approach.
Methods: We retrospectively analyzed AIS patients undergoing MT for large or medium vessel occlusion in the anterior circulation between 01/2022 and 07/2023, excluding people<18 years old, those treated beyond 24 hours from their last proof of good health, and those not treated with a stentriever as first choice. The primary outcome was first-pass complete recanalization (eTICI 2c-3), and secondary outcomes were safety (procedure-related complications, early neurologic deterioration, symptomatic intracerebral bleeding) and functional outcomes (24-hour NIHSS, 3-month modified Rankin Scale).
Results: Among 187 patients (median age 76 (IQR=65-83), 52% female, median NIHSS 14 (IQR=7-19)), 39/187 (26%) received first-pass DS and 148/183 (74%) first-pass SS, with 16/187 in the SS group later requiring rescue-DS. First-pass complete recanalization was achieved in 29/39 (74%) of DS patients compared to 63/148 (43%) with SS (p<0.01). Procedural complications were lower in the DS group (13%vs26%), with similar rates of early neurologic deterioration (8%vs12%) and symptomatic intracranial bleeding according to ECASSII definition (5%vs5%).
Conclusions: The DS technique appears to be a safe and achieves higher first-pass recanalization rates than SS with fewer procedural complications. Results of secondary functional outcome and multivariable analysis will be presented at the congress. Further research, including prospective randomized trials, is needed to validate these findings.
Disclosures of Interest: No
Abstract N°: 1377
CORTICAL LOW-FREQUENCY OSCILLATIONS (NIRS) - A PROPOSED MARKER OF AUTOREGULATION - DURING ENDOVASCULAR TREATMENT OF ACUTE STROKE
Adam Vittrup Heiberg*1, Troels Lukassen1, Thomas Truelsen1, Henrik Borgwardt2, Götz Bendorff2, Christine Sølling3, Henrik Schytz1, Kirsten Møller3, Klaus Hansen1, Helle Iversen1
1Copenhagen University Hospital - Rigshospitalet, Department of Neurology, Copenhagen, Denmark, 2Copenhagen University Hospital - Rigshospitalet, Department of Diagnostic Radiology, Copenhagen, Denmark, 3Copenhagen University Hospital - Rigshospitalet, Department of Neuroanaesthesiology, Copenhagen, Denmark
On behalf of:
Background and aims: Acute ischemic stroke (AIS) caused by large-vessel occlusion can be treated effectively with endovascular treatment (EVT). Both hypo- and hyperperfusion can cause further tissue damage and worsen clinical outcome.
Near-infrared spectroscopy (NIRS) examines oxygenated haemoglobin (OxyHb) in the cerebral cortex. Low-frequency oscillations (LFO ~ 0.1Hz) in OxyHb have been suggested to reflect cerebral autoregulation (CA).
The study aimed to investigate the CA before and after reperfusion as well as at follow-up after 1 and 90 days.
Methods: We consecutively enrolled AIS patients treated with EVT under general anesthesia. Prefrontal OxyHb recordings (Octamon, Artinis Medical Systems) were obtained immediately before and after reperfusion and at follow-up. CA was evaluated by interhemispheric transfer function analysis of OxyHb LFOs.
Results: 77 of 100 enrolled patients had data segments of sufficient quality for analysis. Patients (39% female, 73 years median age (IQR= [63-80])) had median NIHSS of 16.5 (IQR= [11.0-21.5]) with successful reperfusion in 89.6%. Independent 90-day outcome (mRS 0-2) was 46.8% and 16.9% had died.
Individual LFO gain (amplitude ratio) remained stable over time. Mixed model analysis showed decreasing gain with increasing mRS (-0.04, 95%CI= [-0.07; -0.02], p= 0.002), NIHSS (-1.0%, 95%CI= [-1.8%; -0.1%], p= 0.029) and mortality (-0.21, 95%CI= [-0.35; -0.06], p= 0.005).
Conclusions: CA in AIS patients treated with EVT were increasingly compromised in patients with worse clinical and functional outcome including death. Individual CA values were stable over time. Use of NIRS for monitoring CA could be an important tool for treatment guidance in EVT patients.
Disclosures of Interest: No
Abstract N°: 1584
ENDOVASCULAR TREATMENT OUTCOME FOR ANTERIOR AND POSTERIOR CIRCULATION LARGE VESSEL OCCLUSIONS WITH INTRACRANIAL ATHEROSCLEROSIS
1Hyogo medical university, Neurosurgery, Nishinomiya, Japan, 2University of Tsukuba, Division of Stroke Prevention and Treatment, Faculty of Medicine, Tsukuba, Japan, 3Kobe City Medical Center General Hospital, Neurovascular Research & Neuroendovascular Therapy, Kobe, Japan, 4National Cerebral and Cardiovascular Center, Cerebrovascular Medicine, Suita, Japan, 5University of Tsukuba, Neurosurgery, Faculty of Medicine, Tsukuba, Japan, 6Tohoku university hospital, Development and Discovery of Interventional Therapy, Sendai, Japan
On behalf of: RESCUE AT-LVO investigators
Background and aims: This study aims to investigate the differences in clinical outcomes following endovascular treatment (EVT) between anterior and posterior circulation large vessel occlusions (LVO) associated with intracranial atherosclerotic disease (ICAD).
Methods: Utilizing data from the retrospective multicenter registry on RESCUE AT-LVO, we conducted a post-hoc analysis of 451 patients with LVO caused by ICAD. Patients were categorized as anterior (occlusion of internal carotid artery or M1 or M2 segment of middle cerebral artery) or posterior group (occlusion of basilar artery or intracranial vertebral artery). The primary outcome was a modified Rankin Scale (mRS) score of 0–2 at 90 days.
Results: The posterior group exhibited a higher proportion of male patients, higher NIHSS, and a higher prevalence of diabetes and hypertension The puncture to reperfusion time was significantly longer in the posterior group. The use of stent retrievers was less frequent, and balloon angioplasty was more common in posterior circulation occlusions. Adjusted analyses showed that the posterior group had lower odds ratio of mRS 0-2 at 90 days (adjusted OR 0.58, 95% CI 0.32-1.05, p=0.074) and a higher mortality rate (adjusted HR 2.88, 95% CI 1.67-7.17, p=0.02) compared to the anterior group.
Conclusions: This study, based on real-world data from a large patient registry, highlights the poorer clinical outcomes associated with EVT for ICAD-related LVO in the posterior circulation. The findings emphasize the need for further research to optimize treatment strategies for this specific patient population and improve overall prognosis.
Disclosures of Interest: No
Abstract N°: 1725
OPERATIVE ARTERIAL CLASSIFICATION FOR ENDOVASCULAR TREATMENT USING CT PERFUSION (CAOVA)
Carmen Sánchez-Rodríguez1, Carmen Ramos1, Ainhoa Lorenzo Montilla2, Raquel Berbegal Serralta1, Cristina Sanabria1, Alba Somovilla1, Pablo Iriarte1, Álvaro Ximénez-Carrillo1, Jaime Alonso1, Santiago Trillo*1
1Hospital Universitario de la Princesa, Stroke Center, Department of Neurology, Madrid, 2Hospital Central de la defensa Gómez Ulla, Department of Neurology, Madrid
On behalf of:
Background and aims: The classic classification of arterial occlusion in segments of the MCA can be confusing and hinder the inference of the vascular territory at risk. Our objective is to propose an Operative Arterial Classification according to the Affected Volume (CAOVA), weighing the order of occluded arterial division and the hypoperfused volume, aiming to improve the identification of an occlusion of a dominant artery.
Methods: Retrospective study of patients treated with mechanical thrombectomy for strokes in the MCA/carotid-T territory. A prospective reclassification was performed according to the level of occlusion based on the MCA divisions, from the terminal carotid and M1 segment (undivided trunk) to M4 (artery previously divided three times). The CAOVA considered the order of arterial division along with the number of affected ASPECTS territories in Tmax using conventional software (CAOVA-A) and, alternatively, the hypoperfused volume in Tmax with RAPID (CAOVA-R), reclassifying as more severe occlusions those with affected territories or Tmax above the mean. NIHSS and the difference between baseline mRS and 3 months were used as practical utility measures.
Results: Of 229 analyzed, median NIHSS was 19(IQR:11-23). NIHSS analysis showed rho=-0.27(p<0.001) according to the classic classification, CAOVA-A was superior with rho=-0.30(p<0.001) and using CAOVA-R showed a slight improvement with rho=-0.31(p<0.001). In the correlation with mRSb-3m, no association was identified with the classic classification, but it was present with CAOVA-A and CAOVA-R(p<0.05).
Conclusions: CAOVA classification could be superior to the classic one, allowing to infer the order of occluded arteries and their potential severity more clearly by considering the associated vascular territory.
Disclosures of Interest: No
Abstract N°: 1764
EXTRACRANIAL CAROTID ARTERY STENTING IN ACUTE STROKE - RECONSIDERING THE NEED FOR GLYCOPROTEIN IIB/IIIA INHIBITORS
José Miguel Alves*1, Henrique Coimbra Queirós2, Ana Filipa Fernandes3, Ricardo Veiga2, César Nunes2, João André Sousa1, Gustavo Santo1, Fernando Silva1, Egídio Machado2, João Sargento-Freitas1
1Centro Hospitalar e Universitário de Coimbra, Neurology Department, Coimbra, Portugal, 2Centro Hospitalar e Universitário de Coimbra, Reference Center for Interventional Neuroradiology, Coimbra, Portugal, 3Centro Hospitalar e Universitário de Coimbra, Internal Medicine Department, Coimbra, Portugal
On behalf of:
Background and aims: Acute carotid artery stenting (CAS) is a rescue procedure for extracranial internal carotid artery (ICA) subocclusion or occlusion, requiring antiplatelet agents to prevent intra-stent occlusion. However, hemorrhagic risk in acute stroke requires careful consideration of antiplatelet protocol, with the benefits of glycoprotein IIb/IIIa inhibitors remaining uncertain. The study focused on the impact of a glycoprotein IIb/IIIa inhibitor (eptifibatide) versus other antiplatelet agents in CAS for anterior circulation stroke.
Methods: An historical cohort observational study was conducted at a tertiary hospital to compare the clinical outcomes of patients who underwent acute CAS between 2017 and 2023, with or without eptifibatide administration peri-procedure.
Results: A total of 54 patients underwent acute CAS. Eptifibatide was administered in 35 (64.8%) patients, while 19 (35.25%) received acetilsalicylic acid and P2Y12 inhibitors. Demographics, vascular risk factors, and admission characteristics showed no significant differences between groups. Fibrinolysis before stenting was more frequent without eptifibatide (52% vs. 17.1%, p=0.006). Adjusted ordinal logistic regression for modified Rankin Scale (mRS) at 3 months revealed no significant difference between groups (OR 1.89, 95%CI: 0.65-5.48, p=0.242). Multivariate analysis showed no significant differences in symptomatic intracranial hemorrhages, PH2 intracranial hemorrhages, PH1+PH2 hemorrhages, and intra-stent occlusion.
Conclusions: The administration of eptifibatide during acute CAS did not yield significant impact on functional outcomes, intra-stent occlusion, or hemorrhagic complications. Despite the study's relatively small sample size, it raises pertinent questions about the practicality of eptifibatide administration peri-procedure and emphasizes the necessity for randomized clinical trials to delineate the most appropriate antiplatelet protocol tailored to diverse patient profiles.
Disclosures of Interest: No
Abstract N°: 1771
SAFETY OF ACUTE CAROTID STENTING IN PATIENTS UNDERGOING ENDOVASCULAR THROMBECTOMY: RETROSPECTIVE DATA FROM THE CANADIAN OPTIMISE REGISTRY
George Mendes*1, Gregory Jacquin1, Ariesteidis Katsanos2, Grant Stotts3, Alexandre Y. Poppe1
1Centre Hospitalier de l'Université de Montreal, Neurology, Montreal, 2McMaster University, Neurology, Hamilton, Canada, 3University of Ottawa, Faculty of medicine, Ottawa, Canada
On behalf of:
Background and aims: Optimal management of acute stroke patients with carotid tandem lesions is unknown. Retrospective data suggest improved functional outcomes with acute carotid artery stenting (aCAS) during endovascular thrombectomy (EVT). We sought to assess the relative safety of aCAS in addition to EVT compared to EVT alone in patients undergoing EVT for acute ischemic stroke
Methods: The Optimizing Patient Treatment In Major Ischemic Stroke with EVT (OPTIMISE) registry is a multi-center Canadian prospective database of EVT-treated individuals between January 2018 to December 2021. For this study, we included anterior circulation stroke patients treated with EVT, who had available information regarding the use or non-use of aCAS. We defined the primary outcome as a composite of in-hospital death, long term care facility at discharge, symptomatic intracranial hemorrhage, or any EVT-related procedural complications. Secondary outcomes included each component of the composite outcome individually. Multivariable regression with major confounding factors was performed to compare EVT-aCAS and EVT-only groups.
Results: A total of 4205 patients met inclusion criteria (330 with aCAS-EVT, 3875 with EVT-only) having a mean age of 70.9(±13.9) years. Females comprised 51.3% of the cohort. Baseline median NIHSS was 16 [11-20] and ASPECTS was 8 [7-10]. Adjusted analysis suggested a trend toward a higher proportion of unfavorable safety outcomes with EVT-aCAS (OR=1.35 95%CI[0.97-1.84], p=0.06). Among secondary outcomes, EVT-aCAS was associated with a significantly higher occurrence of procedural complications (10.0% vs 6.1%, p=0.008).
Conclusions: When considering aCAS among patients undergoing EVT for anterior circulation stroke, the possibility of increased procedural complications should inform decision-making.
Disclosures of Interest: No
Abstract N°: 2723
IMPACT ON MORTALITY AT 90 DAYS OF ACUTE KIDNEY INJURIES IN ENDOVASCULARLY TREATED STROKE: A SYSTEMATIC REVIEW, META-ANALYSIS, AND META-REGRESSION
Gianluca De Rubeis*1, Sebastiano Fabiano1, Luca Bertaccini1, Andrea Wlderk1, Elisa Testani2, Enrico Pampana1
1San Camillo/Forlanini, Neuroradiology, 2San Camillo/Forlanini, Stroke Unit
On behalf of:
Background and aims: To investigate the prognostic implication (mortality at 3 months) of acute kidney injury (AKI) in acute ischemic stroke treated with mechanical thrombectomy (MT)
Methods: A literature search was performed using PubMed/OVID/Cochran’s CENTRAL database (time frame: inception to January 2023). Study characteristics, patient status, clinical outcomes, AKI incidence, and sample size were recorded. The exclusion criteria were non-English literature, no human subjects, and <10 patients as the sample size. Studies were assessed using the MINORS/GRADE system. Meta-analysis and meta-regression with a random effects model were performed.
Results: 3314 studies were retrieved. After applying the exclusion criteria, the final population included of 18/3314 studies (0.5%). Among them, only 6/18 (33.3%) studies reported results in two separate groups (AKI vs. non-AKI), allowing for inference statistics for a total population of 3229 (538.2 ± 404.2). The I^2 was 35.8 and Q’s Cochrane was 7.80.
The pooled odds ratio (OR) for mortality at 3 months in patients with AKI was 5.8 (95% confidence interval [95%CI] 95% CI 3.62 to 9.34). Leave-one-out meta-analysis showed no significant sources of heterogeneity. In the meta-regression, diabetes prevalence was associated with a higher mortality rate (OR 1.14, 95% CI 1.03 to 1.28), and lower age and a small amount of contrast media were negatively correlated (0.91 [95% CI 0.83 to 0.99] and OR 0.97 [95% CI 0.94 to 1.00], respectively).
Conclusions: AKI was significantly associated with the mortality rate in MT-treated stroke patients (OR], 5.8 [95% CI 3.62 to 9.34]).
Disclosures of Interest: No
Abstract N°: 2844
ACUTE LARGE VESSEL OCCLUSION STROKE WITH LARGE INFARCT CORE VOLUME- PREVALENCE AND THROMBECTOMY ELIGIBILITY AT A COMPREHENSIVE STROKE CENTER
Paige Banyas*1, Shashvat Desai2, Joshua Catapano3, Lori Graczyk2, Angelina Cooper2, Shyam Kelavkar4, Ruchira Jha3, Andrew Ducruet3, Felipe Albuquerque3, Ashutosh Jadhav1,3
1HonorHealth Scottsdale Osborn Medical Center, Scottsdale, United States, 2Bob Bové Neuroscience Institute at HonorHealth, Scottsdale, United States, 3Barrow Neurological Institute, Phoenix, United States, 4Mid and South Essex NHS Foundation Trust, Southend-on-Sea, United Kingdom
On behalf of:
Background and aims: Recently, multiple randomized trials have demonstrated the safety and efficacy of endovascular thrombectomy (EVT) for large vessel occlusion (LVO) stroke with a large infarct core at presentation. While we await an update to AHA guidelines, we aim to study the prevalence and EVT eligibility per trial criteria at a high-volume comprehensive stroke center (CSC).
Methods: Retrospective chart review of all consecutive strokes at a CSC (January 2021-December 2021). Demographic, clinical, and radiographic data were analyzed to determine EVT eligibility for large core patients per criteria used in large core trials.
Results: 21% (85) of acute ischemic strokes (404) harbor an anterior LVO (ICA/M1/M2). 2.2% (9/404) of acute ischemic strokes and 10.5% (9/85) of anterior circulation LVO strokes met combined trial criteria (ASPECTS 0-5 or infarct volume on NCCT >50 cc within 24 hours) for large core EVT (Figure 1). Eligibility was similar in the early and late time window (0-6 hours vs 6-24 hours). Approximately 12% of additional patients become EVT eligible with expansion of criteria to include large core infarcts.
Conclusions: At a CSC, 2% of acute ischemic strokes and 11% of anterior LVO strokes met large core EVT criteria. This data highlights a large window of opportunity for expansion of EVT services. Extrapolating our results suggests an additional 14,960 US patients and approximately 300,000 patients worldwide are eligible for EVT.
Disclosures of Interest: No
Abstract N°: 3018
FLYING INTERVENTION TEAM FOR ENDOVASCULAR THROMBECTOMY IN RURAL AREAS: IMPACT ON TIME TO TREATMENT AND SAFETY IN LOW-VOLUME HOSPITALS
Isabel Heinrich1, Nikolai Hubert*1, Sophie Herdegen2, Roman Haberl1, Gordian Hubert1
1Munich Clinic, Academic Teaching Hospital of the Ludwig-Maximilians-University, TEMPiS Telestroke Center, Department of Neurology, München, Germany, 2University of Bayreuth, Institute of Medicine Management and Health Science, Bayreuth, Germany
On behalf of: FIT study group
Background and aims: The effectiveness of endovascular thrombectomy (EVT) for acute ischemic stroke is time-dependent, posing challenges in remote areas. Deploying a Flying Intervention Team (FIT) to perform EVT in regional hospitals can significantly reduce time to treatment compared to interhospital patient transfer. Previous studies indicate that the quality of care differs between low- and high-volume hospitals. Aim of this study was to compare FIT and interhospital patient transfer in low-volume hospitals in rural areas.
Methods: This study was a multicenter retrospective observational study with data from 01-2018 to 01-2022. Patients with indication for EVT, admitted to low-volume hospitals (<374 stroke patients/year) were included in the analysis. Primary endpoint was time between EVT decision and groin puncture. Additional endpoints included successful reperfusion, workflow, complications and clinical outcome.
Results: Among 147 patients of 8 low-volume hospitals, 69 were treated by FIT and 78 were transferred to a comprehensive stroke center. Median time from EVT decision to groin puncture was 62 (IQR: 51-73) min in FIT and 148 (120-176) min in interhospital transfer patients (p<0.001). Rate of successful reperfusion was 96% vs. 88%, respectively (p=0.139). Complications and clinical outcome were comparable in both groups.
Conclusions: Deploying a Flying Intervention Team for thrombectomy in low-volume hospitals is safe and significantly faster compared to patient interhospital transfer. Further research is needed to show applicability in other settings.
Disclosures of Interest: Yes N. Hubert, S. Herdegen and G. Hubert received funding from the Bavarian Ministry of Health and the Björn Steiger Foundation.
Abstract N°: 3068
THE EVOLUTION OF MECHANICAL THROMBECTOMY FOR ACUTE ISCHAEMIC STROKE: A DECADE IN DUBLIN
Aisling O'Reilly*1, Muireann Byrne1, Patricia Fearon1, Karl Boyle1, Patrick Nicholson1, Matthew Crockett1, John Thornton1
1Beaumont Hospital, Dublin, Ireland
On behalf of:
Background and aims:
The advent of mechanical thrombectomy(MT) has transformed hyperacute care for stroke patients. We studied changing trends in MT provision over a decade, spanning participation in pivotal randomised controlled trials, evolving neurointerventional techniques, a global pandemic and expanding treatment indications in a comprehensive stroke centre.
Methods: Consecutive patients treated with MT were prospectively recorded between January 2012 and December 2022. We compared baseline clinical and imaging data, treatment times and procedural and clinical outcomes both on an annual basis and across the totality of the epoch.
Results: 2211 MT patients were recorded. Total annual numbers were: 36 (2012), 53 (2013), 46 (2014), 122 (2015), 172 (2016), 248 (2017), 262 (2018), 306 (2019), 301 (2020), 326 (2021) and 338 (2022). Between 2012 and 2022 patients treated with MT became older (mean age: 65.6yrs(SD:13.8) vs 70.0yrs(SD: 14.6); p=0.017), had greater infarct volumes (median baseline ASPECTS: 10(IQR:9-10) vs 9(IQR:8-10): p=0.045) and were treated faster (median door-to-recanalisation: 70mins vs 39 mins; p<0.0001). Patients were less likely to have witnessed stroke onset (100% vs 54%; p<0.0001), receive IV tPA (72% vs 38%; p<0.0001) or have thrombus located in the intracranial ICA or M1-MCA (95% vs 65%: P<0.0001). No significant variations in pre-stroke mRS, baseline NIHSS, onset-to-recanalisation times, rates of successful recanalisation (86% vs 91%: p0.29) or 90-day mRS (0-2: 44% vs 50%; p0.68) were observed.
Conclusions: As our service has evolved, patients presenting for MT have become more complex, are treated faster and continue to achieve excellent clinical and radiological outcomes.
Disclosures of Interest: No
Abstract N°: 637
STENT RETRIEVER ASSISTED LYSIS (SAIL) TECHNIQUE WITH TIROFIBAN: A POTENTIAL BAILOUT ALTERNATIVE TO ANGIOPLASTY AND STENTING
Marc Rodrigo-Gisbert*1, Matúš Hoferica2, Alvaro García-Tornel Garcia-Camba1, Manuel Requena1, Marta Olive Gadea1, Francesco Diana1, Federica Rizzo1, Alejandro Tomasello1, Christophe Cognard2, Marc Ribo1
1Hospital Universitari Vall d’Hebron. Barcelona, Spain, Stroke Unit, Department of Neurology, 2Hôpital Purpan, Centre Hospitalier Universitaire. Toulouse, France, Deparment of Diagnostic Neuroradiology
On behalf of:
Background and aims: Background Angioplasty and stenting (A&S) have been described as bailout technique in individuals with failed thrombectomy. We aim to investigate Stent retriever AssIsted Lysis (SAIL) with tirofiban prior to A&S.
Methods: Patients from 2 comprehensive stroke centers were reviewed (2020-2023). We included patients with failed thrombectomy and/or underlying intracranial stenosis who received SAIL with tirofiban prior to intended A&S bailout.
SAIL consisted in deploying a SR through the occluding lesion to create a by-pass channel and infuse 10ml of tirofiban over 10 minutes either intraarterially (IA) or intravenously (IV). The SR was re-sheathed before retrieval. Primary endpoints were successful reperfusion (eTICI 2b-3) and sICH. Additional endpoints included 90-day mRS 0-2 and mortality.
Results: After a median of 3 (IQR 2-4) passes, 44 patients were considered A&S candidates and received SAIL (43.2% IA-SAIL). Post-SAIL successful reperfusion was obtained in 79.5%. A significant residual stenosis (>50%) after successful SAIL was observed in 45.7%.
No significant differences were detected according to post-SAIL successful reperfusion (IA-SAIL 80.0% vs IV-SAIL 78.9%; p=0.932), post-SAIL significant stenosis (33.3% vs 55.0%; p=0.203), early symptomatic reocclusion (0% vs 8.0%; p=0.207), or sICH (5.3% vs 8.0%; p=0.721). Rescue A&S was finally performed in 15 (34.1%) patients (IA-SAIL 21.0% vs IV-SAIL 44%; p=0.112).
At 90 days, mRS 0-2 (IA-SAIL 50.0% vs IV-SAIL 43.5%;p=0.086) and mortality (26.3% vs 12.0%;p=0.223) were also similar.
Conclusions: In stroke patients in which A&S bailout is considered, SAIL with tirofiban, either intraarterial or intravenous, seems to safely induce sustained recanalization, offering a potential alternative to definitive A&S.
Disclosures of Interest: No
Abstract N°: 708
EFFICACY SAFETY OUTCOMES OF MECHANICAL THROMBECTOMY FOR M2 SEGMENT OF THE MIDDLE CEREBRAL ARTERY
Tho Phung*1, Ton Mai Duy1, Phuong Dao1, Duong Cao2
1Bach Mai Hospital, Stroke center, 2Ha Dong Hospital, ICU
On behalf of:
Background and aims: The evidence supporting the benefits of mechanical thrombectomy (MT) in treating acute ischemic stroke (AIS) patients with occlusion in the M2 segment of the middle cerebral artery (MCA M2) is currently limited. This study aims to assess the efficacy and safety of MT specifically for M2 occlusion in comparison to standard medical treatment among AIS patients.
Methods: Between January 2021 and May 2022, we prospectively enrolled a consecutive cohort of patients admitted to the Stroke Center of Bach Mai Hospital who experienced AIS due to MCA M2 occlusion. We assessed outcomes, including the favorable outcome (defined as a 3-month modified Rankin Scale score of 0-2) and the safety outcome (symptomatic hemorrhage transformation - sHT), among patients receiving MT and those receiving standard medical treatment.
Results: A total of 105 patients were enrolled (mean age: 67 ± 12.6; males: 52.4%). Of these, 53 were treated with MT, while 52 received standard medical treatment. The baseline NIHSS showed no significant difference between two groups ( 12.2 vs. 9.9, p = 0.63). TICI 2b/3 was achieved in 71.7% of patients in the MT group. The MT group exhibited higher rates of favorable outcomes (58.4% vs. 48.1%) and sHT (11.3% vs. 3.8%). However, these differences were not statistically significant (P = 0.28 and 0.15, respectively).
Conclusions: In this study, MT showed a trend toward to higher 3-month functional independence rate without increasing the risk of sHT in patients with AIS due to MCA M2 occlusion.
Disclosures of Interest: No
Abstract N°: 2685
BENEFIT AND SAFETY OF ENDOVASCULAR TREATMENT FROM 6 UP TO 24 HOURS IN PATIENTS WITH A PRE-STROKE MRS 3: A MULTICENTER RETROSPECTIVE STUDY
Ilaria Maestrini*1, Lorenzo Rocchi2, Thanh N. Nguyen3, Alejandro Tomasello4, Giacomo Cester5, Pedicelli Alessandro6, Francesco Garaci7, Marina Diomedi8, Valerio Da Ros9
1University Hospital of Rome “Tor Vergata”, Department of Systems Medicine, Rome, 2University of Cagliari, Department of Medical Sciences and Public Health, Cagliari, Italy, 3Boston Medical Center, Diagnostic and Interventional Neuroradiologist, Boston, United States, 4Interventional Neuroradiology, Vall d'Hebron University Hospital, Barcelona, Spain, 5Department of Neuroradiology, University Hospital of Padova, Padua, Italy, 6IRCCS Catholic University of Rome, UOSA Neuroradiologia Interventistica, Rome, Italy, 7University Hospital of Rome “Tor Vergata”, Department of Biomedicine and Prevention, Rome, Italy, 8University Hospital of Rome “Tor Vergata”, Department of Systems Medicine, Rome, Italy, 9University Hospital of Rome Tor Vergata, Department of Biomedicine and Prevention, Rome, Italy
On behalf of:
Background and aims: Approximately 30% of patients presenting with acute ischemic stroke (AIS) due to large vessel occlusion (LVO) have pre-stroke modified Rankin Scale (mRS) scores ⩾ 2. We aimed to investigate the safety and benefit of endovascular treatment (EVT) in AIS patients with moderate pre-stroke disability (mRS score = 3) in an extended time window (ETW), i.e., 6-24 hours from the last time known well.
Methods: Data were collected from five centers in Europe and United states from January 2018 and January 2023 and included 180 patients who underwent EVT in ETW. Patients were divided into two groups of 90 each (group 1: pre-mRS 0-2; group 2: pre-mRS = 3; 71% women, mean age 80.3±11.9). Primary outcomes were: i) 3-month good clinical outcome, ii) any hemorrhagic transformation (HT), and iii) symptomatic intracranial hemorrhages (sICH). Secondary outcomes were: i) successful and ii) complete recanalization after EVT, and iii) 3-month mortality.
Results: No between-group differences were found in 3-month good clinical outcome (26.6% vs 25.5%, p = 0.974), any HT (26.6% vs 22%, p = 0.733) and sICH (8.9 vs. 4.4%, p = 0.232). By contrast, the improvement in mRS (ΔmRS) was significantly smaller in group 2 compared to group 1 (1.64±1.61 vs 2.97±1.69, p < 0.001). No between-group differences were found in the secondary outcomes.
Conclusions: Albeit equally safe, EVT seems to be less effective in the EWT in AIS patients with pre-stroke mRS 3 compared to those who were functionally independent before AIS (mRS 0-2).
Disclosures of Interest: No
Abstract N°: 438
A SINGLE CENTRE AUDIT OF MECHANICAL THROMBECTOMY RELATED PSEUDOANEURYSM RATES
Weeratunge Malalasekera1,2, Ben Edwards1,2, Jason Macdonald2,2, Richard Marigold*3
1Wessex Neurological Centre, United Kingdom, 2Wessex Neurological Centre, Neuroradiology, United Kingdom, 3Wessex Neurological Centre, Stroke Medicine, United Kingdom
On behalf of:
Background and aims: Femoral artery pseudoaneurysm is a known complication related to endovascular access and in severe cases can lead to life-threatening haemorrhage. As access to mechanical thrombectomy continue to expand, the procedure is now being performed on a more diverse spectrum of the patient population. In presenting our single centre experience we aim to further the understanding of the typical pseudoaneurysm rate in a real-world thrombectomy cohort.
Methods: We performed a retrospective audit of all mechanical thrombectomies performed in a one year period between August 2022 and August 2023 manually collecting relevant clinical data regarding possible risk factors via our institutional RIS and electronic records system.
Results: A total of 183 individual punctures were performed in 182 patients over the audit period. Most were performed without the use of ultrasound (127 without compared to 56 with ultrasound). In total, 13 patients underwent investigations for suspected post-procedural pseudoaneurysms. Of these patients, 6 were diagnosed with pseudoaneurysms (3.28% overall rate). Further subgroup analysis was performed to identify any risk factors for pseudoaneurysm formation but none were found. Four pseudoaneurysms were treated with thrombin injections while two were managed conservatively.
Review of published large scale and seminal randomised control trials found little specific published data on pseudoaneurysm rates though more general reporting of access site complications range from 0.9-7.2%.
Conclusions: Our single centre experience demonstrates a low rate of post-mechanical thrombectomy pseudoaneurysm which to our knowledge is one of the only specifically described descriptions of this complication rate in a real-world cohort.
Disclosures of Interest: No
Abstract N°: 1185
ENDOVASCULAR TREATMENT IN ISCHEMIC STROKE WITH POOR COLLATERAL CIRCULATION IN EXTENDED WINDOW
Carlos Ignacio Gomez-Escalonilla Escobar1, PATRICIA SIMAL HERNÁNDEZ*1, Santiago Rosati2, Manuel Moreu2, Ángela Huete Schmolling2, Carmen Trejo2, José Antonio Egido Herrero1, Alfonso López-Frías López-Jurado2, Carlos Pérez-García2
1Hospital Universitario Clínico San Carlos, Stroke Unit. Neurology Department, Madrid, Spain, 2Hospital Universitario Clínico San Carlos, Interventional Neuroradiology. Radiology Department, Madrid, Spain
On behalf of:
Background and aims: Patients with poor collateral circulation have been excluded from studies of extended-window endovascular treatment (EVT). We analyze the efficacy and safety results of our series in this group of patients
Methods: Retrospective study of a prospective series of patients with ischemic stroke due to large vessel occlusion in the anterior territory undergoing VTE with clinical evolution of more than 6 hours since last seen well and who had low collateral score on CT-angiography in the period from January 2011 to October 2023. The rate of symptomatic intracranial hemorrhage (sICH) and clinical outcome at 3 months were analyzed
Results: 440 patients received EVT, of whom 86 (female 48.8%) met the inclusion criteria. Median age was 72.5 (IQR 57-83), NIHSS 19 (IQR 14-23) and ASPECTS 7 (IQR 6-8). Intravenous thrombolysis was performed in 25.6%. Final TICI score ⩾2b was achieved in 77.9% of patients. Median pass rate was 2 (IQR 1-3). The sICH rate was 9.4%. At 3 months, 29.1% achieved a good functional status (modified Rankin scale ⩽2 or return to baseline) with a mortality of 33.3%.
Conclusions: Despite obtaining worse functional results than patients with good collaterals, 29.1% of patients who received EVT with extended-window and had low collateral score on CT-angiography, achieved a good functional outcome at 3 months. For this reason, this group of patients should not be discouraged for endovascular treatment.
Disclosures of Interest: No
Abstract N°: 1583
EXTERNAL VALIDATION OF A MODEL FOR PERSISTENT PERFUSION DEFICIT IN PATIENTS WITH INCOMPLETE REPERFUSION AFTER THROMBECTOMY
Adnan Mujanovic*1, Felix Ng2, Mattia Branca3, Thomas Meinel4, Leonid Churilov5, Jan Gralla1, Urs Fischer6, Markus Kneihsl7, Bruce Campbell2, Johannes Kaesmacher1
1Inselspital, Department of Diagnostic and Interventional Neuroradiology, Bern, Switzerland, 2Melbourne Brain Centre, Department of Medicine and Neurology, Heidelberg, Australia, 3University of Bern, CTU, Bern, Switzerland, 4Inselspital, Department of Neurology, Bern, Switzerland, 5The Royal Melbourne Hospital, Parkville, Australia, 6Universitätsspital Basel, Department of Neurology, Basel, Switzerland, 7Medical University of Graz, Department of Neurology, Graz, Austria
On behalf of:
Background and aims: We recently developed a model (PROCEED), which predicts the occurrence of a persistent perfusion deficit (PPD) at 24 hours in patients with incomplete reperfusion following thrombectomy. This study aims to externally validate the PROCEED model.
Methods: Individual patient data for external validation were obtained from the EXTEND-IA, EXTEND-IA TNK part 1 and 2 trials and a prospective cohort of the Medical University of Graz. The model’s primary outcome was the occurrence of PPD, defined as the focal, wedge-shaped perfusion delay on 24-hour follow-up perfusion imaging that corresponds to the capillary phase deficit on last angiographic series in patients with <TICI3 reperfusion after thrombectomy. The model’s performance was evaluated with discrimination, calibration accuracy, and clinical decision curves.
Results: We included 371 patients (38% with PPD). The externally validated model had good discrimination (C-statistic 0.81, 95% CI 0.77 – 0.86) and adequate calibration (intercept 0.25, 95% CI 0.21-0.29 and slope 0.98, 95% CI 0.90-1.12). Across a wide range of probability thresholds (i.e. depending on the physicians preferences on how the model should be used), model shows benefit on clinical decision curves, informing physicians on the likelihood of PPD. If a physician’s attitude to false positive and false negative ratings is equal, the model would reduce 4 in 10 unnecessary interventions by correctly predicting complete delayed reperfusion, without missing a patient with PPD.
Conclusions: The externally validated model had adequate predictive accuracy and discrimination. Depending on the acceptable risk threshold, the model accurately predicts persistent incomplete reperfusion and may advise if additional reperfusion attempts should be proceeded.
Disclosures of Interest: No
Abstract N°: 1735
MECHANICAL THROMBECTOMY FOR DISTAL MCA OCCLUSIONS: A SINGLE CENTER STUDY
Carmen Sánchez-Rodríguez1, Carmen Ramos1, Ainhoa Lorenzo Montilla2, Raquel Berbegal1, Cristina Sanabria1, Alba Somovilla1, Pablo Iriarte1, Álvaro Ximénez-Carrillo1, Jaime Alonso1, Santiago Trillo*1
1Hospital Universitario de la Princesa, Stroke Center, Department of Neurology, Madrid, Spain, 2Hospital Central de la defensa Gómez Ulla, Department of Neurology, Madrid, Spain
On behalf of:
Background and aims: Strokes secondary to occlusion of distal segments of the middle cerebral artery(MCA) may produce disabling neurological sequelae despite affecting a less extensive vascular territory. Endovascular treatment(ET) for occlusions in M3 and M4 segments could be considered in selected cases, however, its effectiveness and safety is poorly understood.
Methods: We present a series of patients treated with ET for strokes secondary to occlusion of M3-4 segments. Baseline characteristics and those related to the effectiveness and safety of ET were collected from patients treated during 2021-22.
Results: 17 patients underwent ET for M3-4 occlusion, accounting for 6.5% of the 262 thrombectomies performed during the study period. Among them, 13(76.5%) received ET for M3 segment occlusion, and 4(23.5%) for M4 segment occlusion. Of the documented cases, 8(47%) were female, with a median NIHSS of 11(IQR: 9.5-17.5). Motor deficit was present in 12(70.6%) cases, and 12(70.6%) presented aphasia. 10(58.8%) patients had received intravenous thrombolysis. The stroke laterality was left in 13(76.5%), and in 100% of cases, the involved territory was peri-rolandic. The mean volume of territory with Tmax>6s was 60.8(26.7) ml. Recanalization TICI>2a was achieved in 15(88.2%) cases. Subarachnoid hemorrhage occurred as a complication in 6(35.3%) patients, one of which was moderate to severe. At three months, 13(76.5%) had mRS ⩽2.
Conclusions: Endovascular treatment in distal MCA occlusions is a reality in clinical practice, being treated patients with disabling focality associated with a significant volume of vascular territory affected. Its safety and effectiveness, which were favorable in our study, will be investigated in future multicenter studies.
Disclosures of Interest: No
Abstract N°: 1757
LOCAL, SYSTEMIC AND NEUROLOGIC COMPLICATION OF TRANSFEMORAL CEREBRAL ANGIOGRAPHY, MULTICENTER AND PROSPECTIVE STUDY
1Inje University Busan Paik Hospital, Department Of Neurology, South Korea, 2Inje University Haeundae Paik Hospital, Department Of Neurology, South Korea, 3Kosin University Gospel Hospital, Department Of Neurology, South Korea, 4Ulsan University Hospital, Department Of Neurology, South Korea, 5Gyeongsang National University Changwon Hospital, Department Of Neurology, South Korea, 6Gyeongsang National University Changwon Hospital, Department Of Neurology, South Korea, 7Inje University Busan Paik Hospital, Department of Neurosurgery, South Korea
On behalf of:
Background and aims: We aim to determine the frequency of various local, systemic, and neurological complications that may occur after transfemoral cerebral angiography(TFCA) and interventional treatment, and identify the factors causing their occurrence.
Methods: We included patients who underwent TFCA in adult patients prospectively and excluded spinal angiography or transradial angiography. Outcome variables were investigated during 3 months
Results: A total of six medical institutions began recruiting subjects starting in September 2019 and subjects were finally registered in December 2020. A total of 506 subjects were registered during the study period and 493 subjects were analyzed. Most of the diagnoses for the procedure were ischemic stroke in 36% and unruptured cerebral aneurysm in 44%.
Local complications occurring on the first day after the procedure included pain in 26% and hematoma in 2.4%. Systemic complications included new headache in 10.1%. Neurological complications included hemiplegia, sensory changes, however, many of the neurologic symptoms disappeared within 24 hours in 3.7%, there were persistent cases in 2.4%.
Local complications reported 3 months after the procedure were hematoma in 0.2% and pain in 1.5%.
Conclusions: This study analyzed the frequency and course of various local, systemic, or neurological complications related to cerebral angiography. Compared to previous studies, the study was planned to closely investigate pain-related complications and their prognosis after cerebral angiography. As a result, the frequency of local, systemic, and neurological complications after TFCA and intervention was rare, and it is considered safe in the long term.
Disclosures of Interest: Yes This study was funded by a research grant from Yuhan Corporation, but the independence of the research results was guaranteed.
Abstract N°: 1969
EFFECT OF HAEMOGLOBIN LEVELS ON OUTCOME IN EVT-TREATED STROKE PATIENTS - A COHORT STUDY FROM THE EVA-TRISP COLLABORATION
Valerian Altersberger1, Alessandro Pezzini2, João Pedro Marto3, Christian Nolte4, Susanne Wegener5, Patrik Michel6, Sami Curtze7, Andrea Zini8, Mirjam Rachel Heldner9, Henrik Gensicke*10
1University Hospital Basel, Neurology, Switzerland, 2Parma University Hospital and University of Parma, Stroke Care Program, Department of Emergency, Italy, 3Hospital de Egas Moniz, Centro Hospitalar Lisboa Ocidental, Neurology and Neuroradiology, Portugal, 4Charité – Universitätsmedizin Berlin, Klinik und Hochschulambulanz für Neurologie, Germany, 5University Hospital Zurich and University of Zurich, Neurology, Switzerland, 6Lausanne University Hospital and University of Lausanne, Neurology, Switzerland, 7University of Helsinki and Helsinki University Hospital, Neurology, Finland, 8IRCCS Istituto delle Scienze Neurologiche di Bologna, Maggiore Hospital Bologna, Neurology and Stroke Center, Italy, 9Inselspital, Bern University Hospital and University of Bern, Neurology, Switzerland, 10University Department of Geriatric Medicine FELIX PLATTER and University of Basel, Neurology and Neurorehabilitation, Switzerland
On behalf of: EndoVAscular treatment and Thrombolysis for Ischemic Stroke Patients (EVA-TRISP) collaborators
Background and aims: To study the effect of hemoglobin levels (HL) on functional outcome, mortality and bleeding risk in stroke patients treated with endovascular thrombectomy (EVT).
Methods: In this prospective multicenter study from the EndoVAscular treatment and ThRombolysis for Ischemic Stroke Patients Registry (EVA-TRISP), we compared HL with 3-month poor outcome (mRS 3-6), mortality and symptomatic intracranial hemorrhage (sICH). HL was used as continuous and categorical variable distinguishing anemia (<12g/dl; moderate/severe anemia <10g/dl), normal HL (female:12.0-15.5g/dl, male:12.0-17.0 g/dl) and polyglobulia (female:>15.5g/dl; male:>17g/dl). Unadjusted and adjusted odds ratios with 95% confidence intervals (OR[95%-CI]) from the logistic regression models were calculated.
Results: Among 8425 EVT-treated patients, 6107 (72.5%) had normal HL, 2061 (24.5%) had anemia – of those 514 (6.1%) moderate/severe anemia - and 257 (3.0%) polyglobulia. Decreasing HL (by 1g/dl) independently predicted poor outcome (ORadjusted 1.05[1.02-1.08]) and mortality (ORadjusted 1.12[1.08-1.16]). Anemia was associated with poor outcome (ORadjusted 1.53[1.33-1.76]) and mortality (ORadjusted 1.70[1.46-1.97]). Moderate/severe anemia had the highest odds for poor outcome (ORadjusted 1.82[1.39-2.38]) and mortality (ORadjusted 2.92[2.45-3.81]). Polyglobulia was independently associated with poor outcome (ORadjusted 1.80[1.30-2.49]) and mortality (ORadjusted 1.69[1.20-2.37]). No significant association between HL and occurrence of sICH was found.
Conclusions: Anemia and polyglobulia were independently associated with poor outcome and mortality in EVT-treated stroke patients. The more severe the anemia, the higher the probability of poor outcome and death. Severe anemia might be a target for interventions in the hyperacute setting of stroke to improve outcomes.
Disclosures of Interest: No
Abstract N°: 2256
FUTILE RECANALIZATION AFTER ENDOVASCULAR TREATMENT IN ACUTE ISCHEMIC STROKE WITH LARGE ISCHEMIC CORE
1Chonnam National University Hospital & Medical School, Neurology, Gwangju, South Korea
On behalf of:
Background and aims: Endovascular therapy (EVT) has become the treatment of choice for acute ischemic stroke (AIS) with large vessel occlusion. However, a significant number of patients do not benefit from EVT recanalization, which is called futile recanalization (FR). We aimed to identify the major stroke risk factors and patient characteristics associated with FR in the AIS with large ischemic core.
Methods: 137 patients of AIS with large ischemic core treated by EVT at single comprehensive stroke center were retrospectively included from January 2016 to June 2023. Large ischemic core was defined as DWI ASPECTS < 6. Patient age, sex, mRS, NIHSS, time to treatment, risk factors and radiologic findings were collected, and potential associations with FR were analyzed. FR was successful reperfusion defined as mTICI ⩾ 2b without functional independence at 90 days (mRS ⩾ 3).
Results: Of the 137 initial patients assessed, 120 showed successful recanalization (mTICI ⩾ 2b). 120 patients were divided by those who had FR (n = 80) versus no FR (n = 40). In univariate analysis, older age (p<0.001), atrial fibrillation (p=0.036), hemorrhagic transformation (p=0.001), poor pre-EVT collaterals (p=0.016), higher initial NIHSS (p<0.001), and higher SBP (p=0.035) and lower eGFR (p=0.042) were associated with FR. In multivariate analysis, older age (OR 1.051, 1.002-1.103; p=0.042), higher initial NIHSS (OR 1.161, 1.024-1.317; p=0.020) were independent predictors of FR.
Conclusions: In AIS with large ischemic core, increased age and higher initial NIHSS were independently associated with FR and could predict patients who will not respond well to EVT recanalization therapy.
Disclosures of Interest: No
Abstract N°: 2704
A NOVEL CEREBRAL SMALL VESSEL DISEASE BURDEN SCORE INCLUDING BRAIN ATROPHY PREDICTS COLLATERAL STATUS IN ISCHEMIC STROKE TREATED WITH THROMBECTOMY
Svetlana Lorenzano*1, Andrea Aram2, Sofia Liljeblad2, Manuela De Michele3, Ettore Nicolini4, Marta Iacobucci4, Nicoletta Giuseppa Caracciolo4, Lorenzo Benedetti4, Christine Kremer2, Danilo Toni1
1Sapienza University of Rome, Department of Human Neurosciences, Rome, Italy, 2Lund University, Lund, Sweden, 3Sapienza University of Rome, Policlinico Umberto I hospital, Emergency Department Stroke Unit, Rome, Italy, 4Sapienza University of Rome, Rome, Italy
On behalf of:
Background and aims: Cerebral small vessel disease (cSVD) could impact collateral efficiency. This study had the objective to evaluate whether the total cSVD burden including brain atrophy is associated with the ability to recruit collaterals in acute ischemic stroke (AIS).
Methods: This retrospective study included consecutive adult patients with AIS admitted to the Sapienza University of Rome teaching hospital in 2023 and treated with mechanical thrombectomy (MT) (alone or combined with IV thrombolysis). STRIVE criteria were followed to assess the cSVD signs on MRI. A novel modified cSVD burden score was constructed by adding brain atrophy (measured by the Pasquier’s scale) to the standard score. Collateral status was evaluated by the adapted American Society of Interventional and Therapeutic Radiology/Society of Interventional Radiology (ASITN/SIR) score on pre-treatment CT-Angiography dichotomized into good (3-4) versus poor (0-2).
Results: Overall, 80 patients (51.2% females; mean[SD] age of 73.1[13.8] years) were eligible for analysis; 44(55%) patients had poor collaterals and 41(51.2%) patients had any cSVD sign. Multivariate analysis showed that, conversely to standard cSVD score, a moderate to severe modified total cSVD burden score resulted an independent predictor of poor collateral status (OR adjusted for age 3.733, 95%CI 1.462-9.535, p=0.006; OR adjusted for cSVD risk factors and baseline NIHSS 4.905, 95%CI 1.657-14.515, p=0.004;AUC significantly improved by 20%).
Conclusions: Our study showed that brain atrophy as additional radiological sign of cSVD and index of brain frailty could have a significant role in improving prediction of leptomeningeal collateral recruitment potential in AIS patients treated with MT.
Disclosures of Interest: No
Abstract N°: 2855
RESCUE STENTING VERSUS FAILED MECHANICAL THROMBECTOMY. PROPENSITY SCORE-MATCHED ANALYSIS OF A SINGLE CENTER EXPERIENCE
David Seoane*1,2, Jesús Ramírez Sánchez-Ajofrín3, Fernando Ostos Moliz1,2, Eduardo Barcena4, Maria Gutiérrez Sánchez de la Fuente1,2, David Lora Pablos5, Federico Ballenilla4, Patrica Calleja1,2
1Hospital Universitario 12 de Octubre, Stroke Unit, Madrid, Spain, 2Instituto de Investigación i+12, Neurovascular Sciences, Madrid, Spain, 3Hospital Universitario 12 de Octubre, Neurology, Madrid, Spain, 4Hospital Universitario 12 de Octubre, Interventional Neurorradiology, Madrid, Spain, 5Instituto de Investigación i+12, Biostatistics and Scientific Support, Madrid, Spain
On behalf of:
Background and aims: There is growing evidence favoring rescue intracranial stenting (RS) versus settling for a failed mechanical thrombectomy (FMT), particularly in ICAD, pending trial results. We present the results of RS in a comprehensive stroke center.
Methods: Retrospective case series (2017-2022). Review of records, neuroimaging and outcomes at 3 months. Comparison of RS versus FMT and propensity score matching (PSM) to assess for indication bias.
Results: RS patients were younger and had a higher male proportion than FMT patients. Their main aetiology was ICAD, without other significant baseline differences. TICI 2b-3 recanalization was obtained in 95.8%. 29% received thrombolysis, without association with hemorrhagic transformation. 66.7% reached mRS 0-2 and 8.3% died at 3 months, markedly better outcomes than after FMT, still significant after PSM.
6/24 (25%) of RS patients suffered stent thrombosis, associated with higher recurrence of stroke (50% vs 5.9%, p=0.04) and worse functional outcome (mRS 0-2 33.3% vs 82.4% (p=0.045)). Only 3/6 (50%) had received intraprocedural double antiplatelet therapy, vs 14/17 (82%) (P=0.28).
Conclusions: RS was effective and safe, with good functional outcome in 2/3 cases, improving FMT outcomes, despite high rates of stent thrombosis (1/4) with prognostic impact. Previous thrombolysis was safe and not associated with ICH.
Disclosures of Interest: No
Abstract N°: 3024
FACTORS ASSOCIATED WITH THE FIRST PASS EFFECT IN THE TREATMENT OF ISCHEMIC STROKE BY MECHANICAL THROMBECTOMY
Lorena Lopez Gata*1, María Garcés Pellejero1, Lucia Macarena Olea1, Alberto Barneto1, Juan Carlos Portilla Cuenca1, Ignacio Casado Naranjo1
1Stroke Unit. University Hospital of Caceres, Spain
On behalf of:
Background and aims: In patients with ischemic stroke (IS) and large vessel occlusion (LVO) treated with mechanical thrombectomy (MT), first pass effect (FPE) is associated with a better functional prognosis. Our objective is to know the factors associated with FPE and its influence on the prognosis.
Methods: Retrospective analysis of patients with IS and LVO treated by MT. Define complete recanalization as TICI >2b. Differentiate: group a: FPE and b: no FPE. Early prognosis: NIHSs score at 24 hours and at discharge; the medium-term prognosis: Rankin scale score and mortality at 90d. The main variables included were: demographic characteristics, severity of stroke, location of the occlusion, ASPECT score and endovascular technique.
Results: Included 86 patients; 45 (52.3%) group a. The PEF was achieved more frequently in patients treated by systemic fibrinolysis: 25 (55.6%) vs 15 (36.3%), p 0.05 and the occluded vessel M1: 27 (60%) vs 13 (31.7%), p 0.05. For terminal carotid artery occlusions, combined treatment was associated with a higher frequency of FPE: 42.9% vs 14.3%, p 0.04. The FPE was associated with a better functional prognosis, although without statistical difference: NIHSs 24h: 7 (2.2) vs 16 (8.2), p 0.04 and NIHSs at discharge: 5 (0. 2) vs 12 (5.2), p 0.06; 90-day mRS: 2.8 (0.3) vs 3.6 (0.3), p 0.07 and 90d mortality: 11 (24.2%) vs 14 (34.2%), p 0, 32.
Conclusions: In our center, FPE was common. The location of the occlusion and fibrinolytic treatment were associated with PEF. The FPE was associated with a better functional prognosis of the patients
Disclosures of Interest: No
Abstract N°: 1270
ENDOVASCULAR TREATMENT IN PATIENTS WITH A PRE-STROKE MODERATE DISABILITY
Iker Elosua-Bayés*1, Manuel Requena1,2, Jordi Mayol1, Marta Rubiera1, Marc Rodrigo-Gisbert1, Francesco Diana1, Marta De Dios Lascuevas2, Carlos A. Molina2, Alejandro Tomasello2, Marc Ribó1,2
1Vall d'Hebron University Hospital, Neurology, Barcelona, Spain, 2Vall d'Hebron University Hospital, Interventional Neuroradiology, Barcelona, Spain
On behalf of: Álvaro García-Tornel, Marta Olivé-Gadea, Federica Rizzo, Marian Muchada, Noelia Rodríguez-Villatoro, David Rodríguez-Luna, Jesús Juega, Jorge Pagola, David Hernández
Background and aims: There is a paucity of data about endovascular treatment (EVT) in patients with a pre-stroke moderate disability (modified Rankin scale, mRS 3). This study aims to evaluate the evolution of this profile of patients affected by ischemic stroke undergoing EVT and to identify predictors of good response.
Methods: A retrospective observational study of patients with stroke treated with EVT from January of 2020 to April of 2023 was performed. Patients presented with large vessel occlusion (LVO) stroke were included, describing baseline clinical characteristics, workflow times, and EVT data. Predictors of good response were identified by logistic regression with pre-specified adjustments. A favorable evolution was defined as mRS at 90 days equal to baseline or a one point-increment.
Results: A total of 131 patients were included. At 90 days, 71 patients (54.2%; 95% Confidence Interval-CI: 45.3-62.9%) presented a favorable evolution (40/131, 30.5% with mRS 3 and 31/131, 23,7% with mRS 4). The mortality rate was 38.9% (51/131). Upon adjusting for confounding variables, higher ASPECTS (OR=1.72; 95% CI: 1.12-2.81), lower baseline NIHSS (OR=0.83; 95% CI: 0.74-0.92), final TICI ⩾2b (OR=6.74; 95% CI: 1.64-33.23) and absence of hypertension (OR=0.1; 95% CI: 0.02-0.46) emerged as predictors of a favorable outcome.
Conclusions: A favorable outcome after EVT was observed in over 50% of patients who initially exhibited a moderate level of pre-stroke disability. No previous history of hypertension, higher ASPECTS, lower baseline NIHSS along with a successful reperfusion were predictors of a favorable outcome in this profile of patients.
Disclosures of Interest: No
Paper Poster - Ongoing Trials
Abstract N°: 161
STROKE IN VERY LARGE ISCHAEMIC CORE PATIENTS:ASSESSMENT OF REPERFUSION THERAPY IMPACT ON OUTCOME
Carlos Garcia-Esperon*1, Mark Parsons1, Ferdinand Miteff1, Andrew Bivard2, Leonid Churilov2, Gagan Sharma2, Kenneth Butcher3, Elizabeth Holliday4, Chris Bladin5, Christopher Levi1
1John Hunter Hospital, Neurology Department, New Lambton Heights, Australia, 2University of Melbourne, Parkville, Australia, 3University of NSW, Australia, 4University of Newcastle, Australia, 5The Florey Institute
On behalf of: SICARIO trial group: Spratt NJ, Yan B, Gao L, Cheung A, Easton D, Russell M, Ren S
Background and aims: Endovascular thrombectomy (EVT) is effective for large vessel occlusion (LVO) ischemic stroke patients with small volumes of computed tomography perfusion (CTP)-defined ischaemic core within 24 hours from onset. There is randomized clinical trial data available showing benefit of EVT for patients with large core >70mL, however most of the patients included had an ischemic core between 70 to 100mL. Whether patients with a baseline ischemic core >100mL can benefit from EVT is still an unanswered question. We propose a single arm open-label historical-controlled trial, using volumetric measures of very large core (>100 mL)
Methods:Design: SICARIO is a prospective, international, Bayesian Optimal Phase 2 trial designed to test the promise of effect of EVT on 3-month modified Rankin Scale (mRS), with objective performance criterion derived from the INSPIRE registry. (Sample size: up to 150 patients).
Population: Ischaemic stroke patients with anterior LVO within 24 hours of onset with an ischemic core of >100 mL and a premorbid mRS <3.
Primary Outcome: Proportion of patients with mRS 0-4 (no catastrophic outcome) at 3 months
Results:
Conclusions: SICARIO trial started recruitment in Australia in November 2022, (three active sites at the time of submission) and it will start internationally in early 2024. Five patients have been already enrolled into the trial
Disclosures of Interest: No
Abstract N°: 2457
OUTCOMES OF THROMBECTOMY TECHNIQUES AND FACTORS INFLUENCING FIRST PASS EFFECT FROM INSPIRE-S REGISTRY WITH 804 PATIENTS
Pasquale Mordasini1, Marc Ribo*2, Christophe Cognard3, Nayak Sanjeev4, Markus Moehlenbruch5, Jens Fiehler6
1Kantonsspital St.Gallen, St. Gallen, Switzerland, 2Vall d'Hebron University Hospital, Stroke Unit, Barcelona, Spain, 3Hospital Center University De Toulouse, Toulouse, France, 4UHNM, United Kingdom, 5Heidelberg University, Heidelberg, Germany, 6UMC Hamburg-Eppendorf, Eppdata GmbH, Hamburg, Germany
On behalf of: For the Inspire-S investigators
Background and aims: Three major mechanical thrombectomy (MT) techniques are currently used: stent retriever (SR) only, aspiration (ASP) only, and combination therapy (CT) with a general goal of achieving first-pass recanalization(FPR: TICI⩾2c). Factors influencing FPR are loosely understood and recanalization outcomes achieved persevering with initial vs. switching technique upon unsuccessful FPR (Bailout) remain unknown
Methods: INSPIRE-S is a prospective, imaging core-lab/safety clinical events committee adjudicated, global registry of stroke patients treated with Medtronic Neurovascular devices on the first pass and grouped according to initial MT technique.
Results: From May 2020 to April 2023, 804 patients (30 sites/13 countries) were enrolled: SR:259, ASP:148 and CT:397. MCA-M1/M2 occlusions were present in 75.6%. Mean total number of passes was 1.9±1.3. Among the 3 cohorts, FPR rates were: SR:49.0%, ASP:44.1%, CT:48.6% (p>0.05) and final complete revascularization (eTICI⩾2c) was: 78.7%, 70.3% and 75.6% respectively (p>0.05 in adjusted analyses). Good clinical outcome (mRS⩽2) at 90 days was achieved in 60.9%, 53.1%, and 57.0% respectively (p>0.05 in adjusted analyses). FPR according to occlusion location and bailout analyses to assess outcomes when persevering within the same Vs switching MT technique after an unsuccessful attempt for 2, 3, or >3 passes are ongoing.
Conclusions: Real-world data from a large varied patient population in INSPIRE-S showed comparable outcomes according to first-line MT technique. INSPIRE-S allows unique granular analysis of different bailout strategies in different occlusion locations. The results might guide treatment strategy to further improve procedural and clinical outcomes in the future (will be presented at ESOC).
Disclosures of Interest: Yes I'm a CEC member of Inspire-S (paid by Medtronic)
Abstract N°: 801
OUTCOMES IN PATIENTS WITH HIGH COMORBIDITY BURDEN UNDERGOING ENDOVASCULAR THROMBECTOMY FOR ACUTE ISCHEMIC STROKE
Emma Hall*1, Björn Hansen1, Magnus Esbjörnsson2, Teresa Ullberg2, Johan Wasselius1
1Clinical Science Lund University, Medical Imaging and Physiology Lund University Hospital, Lund, Sweden, 2Clinical Science Lund University
On behalf of:
Background and aims: To maximize the effectiveness of endovascular thrombectomy (EVT) for acute ischemic stroke (AIS), it is crucial to extend treatment beyond the confines of randomized controlled trials. In this nationwide unselected EVT-cohort study, we aimed to analyze potential benefits of EVT for populations with multiple comorbidities, addressing the global increase in comorbidities due to extended life expectancy and modern lifestyles.
Methods: We included all AIS patients treated with EVT in Sweden 2015–2021. Comorbidity burden was assessed using a modified Charlson Comorbidity Index (CCI) and categorized as no (CCI 0), low (CCI 1–2), moderate (CCI 3–5), and high comorbidity burden (CCI ⩾ 6) (Fig 1A). Functional outcome was assessed across the modified Rankin Scale (mRS), and its association with comorbidity burden was explored using X2 test. Patients with unsuccessful recanalization were used as controls. Results were stratified by pre-stroke function.
Results: In 5201 patients, the proportion of favourable outcome (mRS 0-2 after 90 days) ranged between 58.0% (CCI 0) to 15.7% (CCI ⩾ 6) (p=0.001, Fig 1B and 1C). Compared to patients with unsuccessful recanalization, all comorbidity groups appeared to benefit from EVT, but the benefit was only significant within the pre-stroke independent populations (mRS 0-2). Pre-stroke dependency (mRS 3-5, n=524; 10.1%) had a more pronounced impact on outcomes than comorbidity score (Fig 2).
Conclusions: Even though high comorbidity burden is associated with poorer outcomes after EVT, it appears that successful EVT is beneficial for patients with high comorbidity burden as well, and these patients should not be systematically denied treatment.
Disclosures of Interest: No
Abstract N°: 1423
EDOXABAN FOR STROKE PREVENTION IN INTRACRANIAL HEMORRHAGE SURVIVORS WITH ATRIAL FIBRILLATION: ENRICH-AF GLOBAL RANDOMIZED TRIAL
Aristeidis Katsanos*1, Rustam Al-Shahi Salman2, Joan Martí-Fàbregas3, Dar Dowlatshahi4, Robin Lemmens5, Nevine El Nahas6, Jeyaraj Pandian7, Sanjib Sharma8, Matthias Endres9, Georgios Tsivgoulis10
1McMaster University/ Population Health Research Institute, Hamilton, Canada, 2University of Edinburgh, Edinburgh, United Kingdom, 3Hospital de la Santa Creu i Sant Pau, Barcelona, Spain, 4University of Ottawa, Ottawa, Canada, 5University Hospital Leuven, Leuven, Belgium, 6Ain Shams University, Cairo, Egypt, 7Christian Medical College, Ludhiana, India, 8B.P. Koirala Institute of Health Sciences, Dharan, Nepal, 9Charité – Universitätsmedizin Berlin, Berlin, Germany, 10National and Kapodistrian University of Athens,, Athens, Greece
On behalf of: on behalf of the ENRICH-AF Steering Committee
Background and aims: Non-vitamin K oral anticoagulants may provide superior stroke prevention in intracranial hemorrhage (ICrH) survivors with high-risk atrial fibrillation (AF) compared with non-anticoagulant medical therapy.
Methods: ENRICH-AF is an international, prospective, randomized, open-label, blinded endpoint trial comparing edoxaban (60/30 mg once daily) with non-anticoagulant medical therapy. Participants are eligible if they are ⩾45 years with AF (CHA2DS2-VASc⩾2) and previous ICrH (symptomatic and spontaneous intraventricular or non-lobar intraparenchymal hemorrhage, or symptomatic, spontaneous or non-penetrating traumatic subdural hemorrhage; occurring on or off antithrombotic therapy). Patients within 14 days of their ICrH, with secondary causes of ICrH, specific contraindications to edoxaban, absolute indication for non-study assigned antithrombotic treatment, and severe renal impairment are not eligible. The trial is registered in ClinicalTrials.gov:NCT03950076.
Results: An estimated 950 participants will be recruited and followed for a mean of ~2 years until at least 123 primary efficacy outcome events have occurred. The study will have 80% power to detect a 40% relative risk reduction in the primary outcome of stroke with edoxaban. The trial is currently active at 240 sites in 20 countries, and it has enrolled 775 participants as of January 1st, 2024. Due to DSMB concerns regarding excess ICrH risk with edoxaban in patients with lobar and convexity subarachnoid hemorrhages, these patients were excluded from further participation following review of the initial 699 participants.
Conclusions: ENRICH-AF is the largest randomized trial of oral anticoagulation after ICrH in patients with AF and is well positioned to answer unresolved questions surrounding optimal stroke prevention in this patient population.
Disclosures of Interest: No
Abstract N°: 152
MOBILE HEALTH INTERVENTION IN INTRACEREBRAL HAEMORRHAGE SURVIVORS (MOBILE-ICH)
Ching Hei So*1, Roxanna Liu1, Kay Cheong Teo1, Kui Kai Lau1
1Queen Mary Hospital, Hong Kong, Hong Kong
On behalf of:
Background and aims: Intracerebral hemorrhage (ICH) survivors are prone to ICH recurrence, and achieving good blood pressure (BP) control is pivotal to reduce this risk. However, only half of ICH survivors achieved BP targets. Hence, we aim to test the safety and efficacy of a nurse-led, protocol-based, mobile health intervention for the management of hypertension following ICH.
Methods: MOBILE-ICH (Clinical trial.gov: NCT05830305) is an open-label, randomized controlled trial of 140 ICH survivors. Patients were randomized 1:1 to mobile health intervention (mobile) or usual care. Patients will enter their home BP into the WeRise App (Figure 1), Hong Kong’s first mobile stroke platform, and a nurse-led, protocol-based intervention (Figure 2) will be implemented using data from WeRISE. The primary endpoint is the rate of controlled hypertension (systolic BP <130mmHg) 12 weeks after index ICH.
Results: MOBILE-ICH was initiated on the 1st of September 2023. Until the 15th of January 2024, we screened 60 ICH patients, and 12 patients were suitable for recruitment based on inclusion and exclusion criteria. The recruitment rate was 100%, with six subjects in each group. The mean age was 56.3±15.0 years, and 75% were males. Seven patients completed 12 weeks of follow-up. The mean BP change from recruitment to follow-up was -6.5mmHg for the mobile group compared to +6.3mmHg in the usual care group. The rate of controlled hypertension was also higher in the mobile group (100% vs. 66%), with no adverse events reported.
Conclusions: Preliminary analysis of MOBILE-ICH indicated the safety and efficacy of mobile health intervention for hypertension management following ICH.
Disclosures of Interest: No
Abstract N°: 584
A RANDOMIZED TRIAL ON HEMODYNAMIC OPTIMIZATION OF CEREBRAL PERFUSION AFTER ENDOVASCULAR THERAPY IN ACUTE ISCHEMIC STROKE
Joan Martí-Fàbregas*1, Nicolas Lopez2, Herbert Tejada Meza3, Juan Alvarez-Cienfuegos4, Jose Ignacio Tembl5, Ana Rodríguez-Campello6, Maria del Mar Freijo7, Alan Flores8, López Mesonero9, Pol Camps Renom1
1Hospital de la Santa Creu i Sant Pau, Neurology, Barcelona, Spain, 2Hospital de Alicante, Neurology, Alicante, Spain, 3Hospital Universitario Miguel Servet, Neurology, Zaragoza, Spain, 4Hospital Universitari Dr Josep Trueta, Neurology, Girona, Spain, 5Hospital Universitario La Fe, Neurology, Valencia, Spain, 6Hospital del Mar, Neurology, Barcelona, Spain, 7Hospital Universitario Cruces, Neurology, Baracaldo, Spain, 8Hospital Universitari Joan XXIII, Neurology, Tarragona, Spain, 9Hospital Universitario de Salamanca, Neurology, Salamanca, Spain
On behalf of: The HOPE trial
Background and aims: After mechanical thrombectomy (MT) less than half of the patients with large vessel intracranial occlusion (LVO) achieve functional independence. Optimization of blood pressure (BP) after MT could improve clinical outcomes by improving cerebral perfusion and preventing cerebral bleeding and edema.
Methods: ClinicalTrials.gov Identifier: NCT04892511. Standard BP management will be compared with BP targets according to the degree of recanalization, as measured by the TICI (Thrombolysis in Cerebral Infarction) scale after successful MT.
Study design: Multicenter Prospective Randomized Open, Blinded End-point (PROBE) study.
A total of 814 patients with LVO will be allocated to either receive standard treatment (routine local BP management) or hemodynamic optimization, which includes: 1) BP lowering during the 72 hours following MT with different targets according to the TICI score: Intensive (100-140 mmHg systolic BP) after TICI 2c/3; or moderate (140-159mmHg systolic BP) after TICI 2b; 2) Induced hypertension (with isotonic saline serum and intravenous phenylephrine) to reach the desired target if needed .
Primary end-point: Functional outcome assessed by the Rankin scale score at 3 months by a blinded investigator. We will perform a shift analysis to demonstrate differences on the mRS score distribution between both groups. We will compare also the common odds ratio of worsening 1 point on the mRS score between groups using ordinal logistic regression.
Results: We expect to have them in 2025. To date, a total of 255 patients have been enrolled. An interim analysis is scheduled on march 2024.
Conclusions: Protocolised management of BP after MT may improve clinical outcomes.
Disclosures of Interest: No
Abstract N°: 2197
ANTICOAGULATION VERSUS ANTIPLATELETS IN DISSECTION-RELATED ISCHEMIC STROKE: A MULTICENTER STUDY AND META-ANALYSIS OF CASE SERIES
ZHU BINGER*1, Zhang Shufan1, Han Xiang1
1Shanghai, Huashan Hospital Affiliated to Fudan University, Shanghai, China
On behalf of:
Background and aims: The therapy in dissection-related ischemic stroke has not been established.The aim of this study is to figure out the benefits and adverse reactions between antiplatelets and anticoagulants, which could provide more evidences for more suitable selection of clinical treatments.
Methods: Studies from seven databases included two RCTs, sixteen case series and one prospective study by our institution. A meta-analysis of proportions was conducted with a random effects model. Recurrence rate of stroke and transient ischemic attack (TIA) at 90 days was the primary outcome.
Results: A total of 925 patients given antiplatelets and 990 patients given anticoagulants are included. We found there is no significant difference in recurrent stroke and TIA (OR 1.36, 95% CI 0.89-2.08), besides mRS and SICH, between these 2 groups regardless of race or gender subgroups. While the anticoagulant therapy for stroke caused by dissection in posterior circulation has a tendency to reduce the risk of recurrent stroke and TIA (OR 3.96, 95% CI 0.96-14.98).
Conclusions: We found antiplatelets seem to be equally safe and effective to anticoagulation therapy in dissection-related ischemic stroke. While the therapy needs to be individualized based on the location of the vascular lesion.
Disclosures of Interest: No
Abstract N°: 156
RELATIONSHIP LEFT ATRIAL DYSFUNCTION AND CEREBRAL ISCHEMIA IN HIGH-RISK ATRIAL FIBRILLATION PATIENTS (NCT 05772806)
Alba Hernandez-Pinilla*1,1,2, Josep Clua-Espuny2,3, Eva Satue-Gracia1, Francisco Martin-Lujan2,3, Delicia Gentille-Lorente4,5, Ady-Mildred Viveros-Castaño6, Jose-Antonio Izuel-Navarro7, Meritxell Pallejà-Millán3
1Catalonian Health Institute, Primary care, Tarragona, Spain, 2Rovira Virgili University, Primary care, Tarragona, Spain, 3Research Support Unit, Fundació Institut Universitari per a la Recerca a l’Atenció Primària de Salut Jordi Gol i Gurina (IDIAPJGol), Primary care, Reus, Spain, 4Hospital Verge de la Cinta, Cardiology, Tortosa, Spain, 5Institut d'Investigació Sanitària Pere Virgili (IISPV)., Tarragona, Spain, 6Bellvitge University Hospital, Institut Diagnòstic per la Imatge (IDI), L'Hospitalet de Llobregat, Spain, 7Hospital Verge de la Cinta, Institut Diagnòstic per la Imatge (IDI), Tortosa, Spain
On behalf of: PREFATE Research Group
Background and aims: Atrial cardiomyopathy is inherently prothrombotic and silent clinically cerebrovascular ischemic (SI) lesions may be overlooked. Timely identification of patients at risk for AF is crucial for diagnosing and managing such lesions. The study evaluates left atrial dysfunction as an indicator of ischemic risk in high-risk AF patients
Methods: Community-based, prospective cohort study included 150 randomly selected high-risk AF patients according to AFRICAT AF risk calculator. FibricheckR monitoring, Transthoracic echocardiography (TTE), standard electrocardiogram (MVP score), magnetic resonance imaging (Ischemic lesions, cerebral microbleeds, Fazekas score), and Pfeiffer assessment were used. Left atrial dysfunction was defined by criteria such as left atrial biplane volume index (LA-Vi) ⩾34 mL/m2, left atrial ejection fraction (LA-Ef) <50%, and left atrial strain reservoir (LA-r) ⩽26%.
Results: 136 individuals (67% women) underwent MRI, revealing cerebral IS in 14 cases (9.3%), 9 in women In patients diagnosed without IS (n = 6) vs those with SI, significant differences were observed in Fazecas score (0.77±0.7 vs 1.54±0.87; p = 0.001), new diagnosis AF (p = 0.043), and LA-r (29.0±10.9 vs 23.6±8.3; p = 0.067). Lower LA-r, higher the prevalence of cerebral ischemia. No differences were found MVP scores, but markers such as advanced interatrial block and P-wave amplitude in lead I <0.1 mV were correlated with left atrial dysfunction
Conclusions: Left atrial dysfunction criteria serve as potential indicators for the risk of cerebral ischemia in high-risk AF patients. The discriminative power of these criteria for initiating anticoagulant treatment warrants evaluation, even before a diagnosis of AF
Disclosures of Interest: No
Abstract N°: 1982
EECP THERAPY IN PATIENTS WITH SYMPTOMATIC AND SEVERE INTRACRANIAL STENO-OCCLUSIVE DISEASE- A RANDOMIZED CLINICAL TRIAL
Vijay K Sharma*1, Benjamin Tan2, Leonard Yeo2, Bernard Pl Chan3, Lily Yh Wong2, Jin Tao Chen2, Hock Luen Teoh2, Anil Gopinathan2, Arvind Kumar Sinha2
1National University of Singapore, Neurology, Singapore, 2National University Health System, Neurology, Singapore, 3National University Health System, Neurology
On behalf of:
Background and aims: Intracranial atherosclerotic stenosis (ICAS) is a common cause of cerebral ischemia among Asians. While best medical therapy (BMT) carries stroke recurrence rates more than 10% per year, intracranial stenting carries unacceptable peri-procedural ischemic events. Severe ICAS with impaired cerebral vasodilatory reserve (CVR) is associated with higher ischemic events. Enhanced External Counter-Pulsation (EECP) therapy improved myocardial perfusion by facilitating the development of collateral vessels. We evaluated whether EECP therapy is useful in patients with severe stenosis of intracranial internal carotid (ICA) or middle cerebral artery (MCA) with impaired CVR.
Methods: This prospective, randomized, observer-blinded phase-III trial recruited patients with severe ICAS within 3-months of acute cerebral ischemia. All patients demonstrated impaired CVR on transcranial Doppler and Diamox-challenged HMPAO-SPECT of brain. Patients were randomized (1:1) to BMT or BMT plus EECP therapy in a standardised protocol. Cerebral ischemic events, TCD, SPECT and Magnetic Resonance imaging (MRI) of brain were repeated at 4±2months (ClinicalTrials.gov: NCT03921827).
Results: Of 130 participants, 83 (64%) have completed 3-months follow up. Median age (range) was 57 (23-75) years, 53 (64%) men and hypertension (47, 57%) was commonest risk factor. MCA was stenosed in 69 (73%) patients and both groups were well-matched. EECP therapy was well tolerated. Compared to only 2/42 (4.7%) patients in EECP group, 10/41 (24%) patients on BMT developed cerebral ischemic events (p= 0.001). EECP therapy resulted in a median 5.3% (range 3 to 14) net reduction in cerebral metabolic perfusion on SPECT.
Conclusions: EECP therapy combined with BMT, significantly improves cerebral vasodilatory reserve and reduces cerebral ischemic events.
Disclosures of Interest: Yes Received research grant from NMRC Singapore
Abstract N°: 2341
CHINESE HERBAL MEDICINE IN ACUTE INTRACEREBRAL HAEMORRHAGE (CHAIN) RANDOMISED TRIAL: STUDY PROGRESS
1The George Institute for Global Health China, Beijing, China, 2The George Institute for Global Health, University of New South Wales, Sydney, NSW, Australia, 3Neurology Department, The Second Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, China
On behalf of: CHAIN investigators
Background and aims: The Traditional Chinese medicine (TCM) compound FYTF-919 (Zhong Feng Xing Nao Fang) may improve functional recovery in patients with acute intracerebral haemorrhage (ICH) through anti-inflammatory and neuroprotective effects on brain edema, haematoma absorption and the immune system. This study aims to determine the effectiveness and safety of FYTF-919 in acute ICH.
Methods: An ongoing trial of the Chinese Herbal medicine in patients with Acute Intracerabral hemorrhage (CHAIN) is a multicentre, prospective, double-blind, placebo-controlled, randomised trial of FYTF-919 in patients with moderate-severe (NIHSS ⩾8, or GCS 7-14) ICH within 48 hours of onset at 28 hospitals in China. Eligible patients are centrally randomised to receive either FYTF-919 (100 mL per day × 28 d, oral) or matching placebo. A sample size of 1504 patients provides 90% power to detect a 20% difference in average utility-weight scores on the modified Rankin scale (UW-mRS) between groups. Primary outcome is UW-mRS at 90 days. The key safety outcome is any serious adverse events during follow-up.
Results: The first patient was enrolled on November 22, 2021, and final recruitment of 1641 patients have been achieved at the end of 2023. Four Data Safety Monitoring Board meetings were held including 2 interim analyses as planned. The primary outcome assessment will be completed by April 2024.
Conclusions: CHAIN aims to provide reliable assessment of an ancient therapy applied to contemporary clinical practice in China. Trial Registration: ClinicalTrials.gov (NCT05066620).
Disclosures of Interest: No
Abstract N°: 2386
STENOSIS: LONG TERM SINGLE VS DUAL ANTIPLATELET THERAPY IN PATIENTS WITH INTRACRANIAL ATHEROSCLEROTIC DISEASE: A RANDOMISED TRIAL
1All India Institute of Medical Sciences, Department of Neurology, New Delhi, India, 2Christian Medical College, Department of Neurology, Ludhiana, India, 3Postgraduate Institute of Medical Education and Research, Department of Neurology, Chandigarh, India, 4Sree Chitra Tirunal Institute of Medical Science and Technology, Department of Neurology, Thiruvananthapuram, India, 5All India Institute of Medical Sciences, Department of Neuroimaging and Interventional Neuroradiology, New Delhi, India, 6Indian Council of Medical Research, New Delhi, India
On behalf of: The STENOSIS Trial Investigators
Background and aims: Intracranial atherosclerotic disease (ICAD) is a major etiology of ischemic stroke. It is a pathological process that causes progressive stenosis and cerebral hypoperfusion, leading to stroke occurrence and recurrence around the world. In practice, the exact duration of dual antiplatelet therapy (DAPT) for ICAD is unclear in view of long-term risk of bleeding complications. This trial aims to study the safety and efficacy of long-term DAPT in patients with ICAD.
Methods: This is a prospective, randomised, multicentre, double-blind, placebo controlled trial. All ischemic stroke (IS) or transient ischemic attack (TIA) patients, within three months from onset, will be screened for eligibility. Patients with >=50% ICAD in the index territory, and already on DAPT for three months, will be randomized to receive either Clopidogrel 75mg or matching Placebo for the next nine months along with open label Aspirin 75mg. Primary outcomes will be recurrent IS or TIA, any intracranial hemorrhage, or systemic bleeding at the end of 12 months. Secondary outcome is a composite of any stroke, myocardial infarction or death at the end of 12 months.
Results: The estimated sample size is 2200 patients. The trial commenced in September 2022, and is planned for completion by March 2025, corresponding to a total study duration of 30 months. A year into the study, a total of 243 patients have been randomized.
Conclusions: STENOSIS trial will provide level-I evidence on the long term safety and efficacy of DAPT among patients with IS due to ICAD of >=50%.
Disclosures of Interest: No
Abstract N°: 2535
HEAD-OF-BED POSITIONING IN LARGE ARTERY ACUTE ISCHEMIC STROKE- A RANDOMIZED CLINICAL TRIAL
Vijay K Sharma*1, Benjamin Tan2, Leonard Ll Yeo2, Bernard Pl Chan2, Mingxue Jing2, Lily Yh Wong2, Jin Tao Chen2, Hariz Halik2, Arvind Sharma3, Meenakshi Pudugramam Vanchi4
1National University of Singapore, Neurology, Singapore, 2National University Health System, Singapore, 3Zydus Hospital, Neurology, Ahmedabad, India, 4Senthil Multispecialty Hospital, Erode, India
On behalf of:
Background and aims: Flat (0-degree) Head-of-Bed (HOB) positioning may increase blood flow across arterial occlusion in hyperacute large artery ischemic stroke (IS), with some clinical improvement. However, this position may increase the risk of aspiration pneumonia. We evaluate whether 0-degree HOB positioning is associated with neurological stability, without increasing the risk of hospital acquired pneumonia (HAP) in hyperacute large artery IS.
Methods: In this ongoing clinical trial, hyperacute IS patients due to large artery occlusion on CT angiography are randomised to stay in flat HOB or head-elevated (at least 30-degrees) position. Only patients eligible for intravenous thrombolysis and/or mechanical thrombectomy are recruited. Serial NIHSS scoring is performed at 15-minutes interval for 1-hour or until HOB is changed due to medical reasons. Neurological stability is assessed by significant neurological deterioration (NIHSS score increase of 2 or more) during monitoring period. Safety of 0-degree HOB is evaluated by evidence of HAP.
Results: Of the 144 patients recruited so far, 70 (48.6%) were randomized to 0-degree HOB and both groups were well-matched. Median age was 58-years (range 38-76), 66% male with median NIHSS 13-points (range 7-23). Compared to only 4/70 (5.7%) patients in 0-degree HOB, 10/74 (13.5%) patients with elevated HOB developed significant neurological deterioration (p= 0.001). Seventeen (11.8%) patients developed HAP without any difference between the HOB positions (p=0.218). Flat-HOB was an independent predictor of neurological stability (HR 4.106, CI 2.2-10.4; p=0.004).
Conclusions: Flat HOB in hyperacute large artery IS is associated with neurological stability, without any significant increase in aspiration pneumonia.
Disclosures of Interest: Yes Received research grant from NMRC Singapore
Abstract N°: 1481
UNVEILING THE COST OF ACUTE ISCHEMIC STROKE IN LATAM:A COMPREHENSIVE ANALYSIS
Ana Claudia de Souza*1, Ana Paula Etges2, Luiza Dittrich3, Pablo Amaya4, Miguel A. Barboza5, Carisi Polanczyk6, Carlos Abanto7, Andrés Saavedra8, Gustavo Saposnik9, Sheila Cristina Ouriques Martins1
1Hospital Moinhos de Vento, Neurology, Porto Alegre, Brazil, 2Universidade Federal do Rio Grande do Sul, Epidemiology, 3Universidade Federal do Rio Grande do Sul, Engineering, 4Fundación Valle del Lili University Hospital, Neurology, Cali, Colombia, 5Rafael A. Calderón Guardia Hospital, Neurology, Costa Rica, 6Universidade Federal do Rio Grande do Sul, Cardiology, Brazil, 7Instituto Nacional de Ciencias Neurológicas, Neurology, Peru, 8Instituto de Neurología Hospital de Clínicas Facultad de Medicina, Neurology, Uruguay, 9University of Toronto, Department of Medicine |, Canada
On behalf of:
Background and aims: Stroke has an important social and economic impact worldwide. Low and middle-income countries are particularly affected by the high costs of new technologies and treatments related to acute and post-acute stroke and increased indirect costs associated with loss of productivity, caregiver expenses, and institutionalization.
The study aims to assess the real-world costs and outcomes of acute ischemic stroke treatment through accurate costing methods, validate a standard set to drive the cost data collection and outcomes among the acute ischemic stroke care pathway across different countries, and determine the cost-effectiveness of acute ischemic stroke treatment strategies in the same country.
Methods: This is an economic evaluation, and data from stroke patients hospitalized from October 2021 to December 2023 will be collected through accurate costing methods and a standardized data spreadsheet. Approximately 8 high-volume stroke hospitals in Latin America will participate. Cost-effectiveness analysis will be performed to compare different treatment strategies in selected centers in the same country.
Results: We have included 1160 patients in 8 latin american hospitals and intend to present our preliminary findings at the upcoming congress
Conclusions: The results may contribute to better allocating and optimizing resources and implementing treatment strategies to improve patients’ outcomes in the stroke care pathway. We also expect that this study could potentially encourage changes in National Health Policies, reducing the costs and the morbimortality of stroke in Latin America.
Disclosures of Interest: Yes The Research received restricted grant from Boehringer Ingelheim.
Abstract N°: 3213
TENECTEPLASE IN CENTRAL RETINAL OCCLUSION STUDY: TENCRAOS
Stephen James Ryan*1, Øystein Kalnes Jørstad2, Petra Iljas3, Claus Ziegler Simonsen4, Andrej Khanevski5, Robin Lemmens6, Vaidas Matijosaitis7, Michael Mazya8, Louisa Marguerite Christiansen9, Anne Hege Aamodt1
1Oslo University Hospital, Rikshospitalet, Neurology, Oslo, Norway, 2Oslo University Hospital, Ullevål, Ophthalmology, Oslo, Norway, 3Helsinki University Hospital, Neurology, Helsinki, Finland, 4Aarhus University Hospital, Neurology, Aarhus, Denmark, 5Haukeland University Hospital, Neurology, Bergen, Norway, 6UZ Leuven, Neurology, Leuven, Belgium, 7Hospital of Lithuanian University of Health Sciences, Neurology, Kaunas, Lithuania, 8Karolinska University Hospital, Neurology, Stockholm, Sweden, 9Bispebjerg and Frederiksberg Hospital, Neurology, Copenhagen, Denmark
On behalf of: all TenCRAOS collaborators.
Background and aims: Central retinal artery occlusion (CRAO) is an ophthalmologic emergency that, without prompt reperfusion, bears high risk of permanent blindness. No evidence-based treatment is currently available. Whether prompt reperfusion with thrombolytic agents can improve the outcome in CRAO, as proved in ischemic stroke, remains unanswered. The main aim is to assess the effect of systemic tenecteplase within 4.5 hours of onset of central retinal artery occlusion.
Methods: The trial is an ongoing prospective, randomised-controlled, double-dummy, double-blind phase 3 multi-centre trial of TNK 0.25 mg/kg + placebo vs. ASA + placebo (2 arms with 1:1 block randomisation).
Patients are recruited after an ophthalmologist has confirmed CRAO and they can be treated within 4.5hrs. After observation in the stroke unit, patients will be re-examined by an ophthalmologist and a neurologist as an out-patient at 30 and 90-day follow-up.
The primary outcome is the proportion of patients with ⩽ 0.7 logMAR best-corrected visual acuity (BCVA) in the affected eye at 30 days after treatment, representing an improvement in BCVA of at least 0.3 logMAR.
Results: 7 countries are participating with 28 centres already activated. Currently there are 6 countries activated for recruitment. We have recruited 58 patients so far, 25 in Norway, 12 in Denmark, 9 in Finland, 5 in Belgium and 3 in Lithuania. Updated figures will be presented.
Conclusions: Inclusion will continue until 78 patients have been randomized. All patients have been included within the strict parameters of the study.
Disclosures of Interest: No
Abstract N°: 1015
THE DUTCH INTRACEREBRAL HAEMORRHAGE SURGERY TRIAL; MINIMALLY INVASIVE ENDOSCOPY-GUIDED SURGERY IN INTRACEREBRAL HAEMORRHAGE
Axel Wolsink*1,2, Floor N.H. Wilting1,2, Nadia H.C. Colmer3, Floris Schreuder1,2, Ruben Dammers3, Catharina Jm Klijn1,2
1Radboud University Medical Center, Neurology, Nijmegen, Netherlands, 2Donders Centre for Cognitive Neuroimaging, Nijmegen, Netherlands, 3Erasmus MC, Neurosurgery, Rotterdam, Netherlands
On behalf of: The Dutch ICH Surgery Trial Study Group, part of the CONTRAST consortium.
Background and aims: Intracerebral haemorrhage (ICH) accounts for 16-19% of all strokes in Western Europe and contributes profoundly to mortality and disability. Increasing evidence suggests that surgical treatment may be beneficial, in particular with minimally invasive procedures and when performed early. The aim of the Dutch ICH Surgery Trial (DIST) is to assess whether minimally invasive endoscopy-guided surgery within 8 hours of symptom onset in addition to standard medical management improves functional outcome after spontaneous supratentorial ICH when compared to standard medical management alone.
Methods: DIST is a multicentre, prospective, randomised, open clinical trial with blinded outcome assessment. We will include 600 adults (⩾18 years) with a spontaneous supratentorial ICH with a haematoma volume ⩾ 10mL and NIHSS ⩾2. Patients with an underlying aneurysm, arteriovenous malformation or fistula, cerebral venous sinus thrombosis, cavernoma or tumour will be excluded. Patients will be randomised (1:1) to minimally invasive endoscopy-guided surgery performed within 8 hours of symptom onset in addition to standard medical management or to standard medical management alone. The primary outcome is the modified Rankin Scale score at 180 days. The treatment effect estimate will be adjusted for known prognostic variables. Secondary outcomes include technical effectiveness and cost-effectiveness.
Results: DIST has started in November 2022 and will be conducted in 11 neurosurgical centres (currently 5/11) in the Netherlands. Currently, 58/600 participants have been randomized, with a mean age of 59.8 years (SD 12.1 years); 36% female (January 2024).
Conclusions: Results are expected in December 2026.
DIST is registered at ClinicalTrials.gov (NCT05460793).
Disclosures of Interest: Yes Unrestricted funding on behalf of CONTRAST from Penumbra Inc, and Promising Care funding of National Health Care Institute and ZonMw (202138368). Funding sources are not involved in study design, data collection, statistical analyses, or writing.
Abstract N°: 1892
SMART DIAGNOSIS: LEVERAGING IMAGING AND HEALTHCARE DATA FOR ATRIAL FIBRILLATION DETECTION IN ISCHAEMIC STROKE PATIENTS
Meghali Banerjee*1, James Billson2, David Swienton2, Daniel Lawday1, Siyang Song3, Emma Chung1,4,5, Helen Estall6, Lucy Beishon1
1University of Leicester, Cardiovascular Sciences, Leicester, United Kingdom, 2University Hospitals Leicester, NHS Trust, Department of Radiology, United Kingdom, 3University of Leicester, School of Computing and Mathematical Sciences, United Kingdom, 4King's College London, Faculty of Life Sciences and Medicine, United Kingdom, 5University Hospitals Leicester, NHS Trust, Department of Medical Physics, 6University Hospitals Leicester, Imaging Department
On behalf of:
Background and aims: Recent computational advancements enable the development of automated tools to assist clinicians with diagnosis and treatment decisions, employing deep learning models trained with real-world data from electronic health records (EHR). Ischaemic stroke (IS) due to atrial fibrillation (AF) remains challenging to diagnose, often requiring extended periods of cardiac monitoring, but diagnostic yields remain low. This project aims to use deep learning approaches to identify AF from stroke patterns on routinely collected magnetic resonance imaging (MRI) to facilitate earlier diagnosis and therapeutic anticoagulation.
Methods: MRI and EHR were obtained for 962 patients with confirmed IS from the Transient Ischaemic Attack Clinic. Data included demographics, clinical and stroke characteristics, cardiac monitoring and echocardiography reports. An internally validated natural language processing (NLP) algorithm was used to automatically determine AF status from text reports. Diffusion weighted imaging (DWI) will be standardised and deep learning models (transfer learning [resNet] and a custom convolutional neural network) will be applied to determine stroke source based on imaging characteristics.
Results: A preliminary subset of data has been prepared for 180 patients (DWI b=1000: 180, apparent diffusion coefficient: 180), and associated diagnoses of embolic appearance on imaging and AF diagnosis (validated by clinicians in stroke and radiology). Imaging preparation and clinical validation is ongoing for the remainder of patients, with full results expected in October 2024.
Conclusions: A prediction-tool trained with real-world patient data could assist AF diagnosis from routine MRI. This could facilitate earlier diagnosis and therefore anticoagulation, reducing risk of recurrent stroke in occult AF.
Disclosures of Interest: No
Abstract N°: 2467
MR GENTLE - MULTICENTER PHASE 2 RCT OF GHRELIN IN ANTERIOR CIRCULATION ISCHEMIC STROKE TREATED WITH ENDOVASCULAR THROMBECTOMY
Quinty Omes*1, Heleen den Hertog2, Renate Arntz3, Margreet Filius4, Ido van den Wijngaard5, H. Bart van der Worp6, Jeannette Hofmeijer1
Background and aims: About half of the ischemic stroke patients treated with endovascular thrombectomy (EVT) remains dependent or dies in the first 90 days. Ghrelin is a naturally occurring hormone and mildly excitatory neurotransmitter that improved functional, histological, and cytological recovery in ischemia-reperfusion models under experimental in vitro and in vivo conditions. Acyl-ghrelin (i.e., the bioactive form) has demonstrated safety in a range of patient populations. We hypothesize that treatment with acyl-ghrelin improves early recovery and long-term functional outcome in acute ischemic stroke patients treated with EVT.
Methods: MR GENTLE is an investigator-initiated phase two randomized clinical trial in four centers in the Netherlands with open-label treatment and blinded endpoint assessment in eighty patients with acute ischemic stroke in the anterior circulation treated with EVT and a pre-EVT NIHSS score ⩾ 10. Patients are randomized to intravenous acyl-ghrelin, 600µg, twice daily for five days, started within six hours after stroke onset, in addition to standard care or to standard care alone. The primary outcome is the NIHSS score on day seven. Secondary outcomes include infarct size on MRI (day three), adverse events, and functional recovery at 90 days. The primary effect variable will be the adjusted beta for the difference in NIHSS score between the treatment groups, estimated with multi-variable linear regression analysis.
Results: The trial has been ethically approved and registered (ClinicalTrials.gov: NCT05726240) and will start in Q1 2024. Funded by the Dutch Heart Foundation, on behalf of the Collaboration for New Treatments of Acute Stroke 2 (CONTRAST 2).
Conclusions:
Disclosures of Interest: No
Abstract N°: 2576
PHYSICAL ACTIVITY AND LIFESTYLE FACTORS, AND SMALL VESSEL DISEASE BURDEN IN ACUTE ISCHEMIC STROKE
Andreas Gammelgaard Damsbo*1,2, Rolf Ankerlund Blauenfeldt1,2, Rikke Beese Dalby2,3, Grethe Andersen1,2, Janne K Mortensen1,2
1Aarhus University Hospital, Danish Stroke Centre, Neurology, Aarhus, Denmark, 2Aarhus University, Department of Clinical Medicine, Faculty of Health, Aarhus, Denmark, 3South Denmark University Hospital, Radiology, Esbjerg, Denmark
On behalf of: SB Vestergaard, NL Pedersen, KM Orskov, MF Hindsholm, A Bilgin-Freiert, CZ Simonsen
Background and aims: Physical activity (PA) may reduce the development of small vessel disease (SVD). The effect of physical activity and more classical vascular risk factors such as hypertension and diabetes in the development of SVD is debated, however. We aim to investigate the effect modification of physical activity on traditional vascular risk factors and the burden of small vessel disease among acute ischemic stroke patients.
Methods: We have pooled patients from two clinical trials on acute ischemic stroke treatment. The main outcome is an ordinal scale score of quantified MR biomarkers of small vessel disease (SVD) burden based on visually assessed acute stroke scans (T2* or SWI and FLAIR sequences). Biomarkers includes microbleeds, old lacunar infarcts, superficial siderosis, white matter hyperintensities and atrophy. Covariates includes age, sex, pre-stroke physical activity, diabetes, hypertension, atrial fibrillation and previous cardiovascular diseases.
Pre-stroke PA was assessed with a questionnaire on inclusion within a few days after stroke onset. Data will be analyzed using bivariate and multivariate linear regression analysis.
Results: We expect to include a total of around 1000 adult patients admitted to the comprehensive stroke centre at Aarhus University Hospital between 2013-2022. Preliminary results will be presented at ESOC 2024.
Conclusions: Physical activity may be an important factor in modifying the risk of SVD development in stroke patients.
Disclosures of Interest: No
Abstract N°: 2816
OPTIMIZING ACUTE ISCHEMIC STROKE DIAGNOSTICS USING ARTIFICIAL INTELLIGENCE – EXPERIENCE FROM A NATIONAL PROJECT
Linn Heitmann*1, Thor Håkon Skattør2, Jon André Totland3, Brian Enriquez4, Agnethe Eltoft5, Dag Ottar Sætre6, Anette Farmen7, Mayank Goyal8, Atle Bjørnerud9, Anne Hege Aamodt4,10
1Østfold Hospital Trust, Dept. of Neurology, Norway, 2Oslo University Hospital, Dept. of Radiology, Norway, 3University Hospital of North Norway, Tromsø, Dept of Radiology, Norway, 4Oslo University Hospital, Rikshospitalet, Dept. of Neurology, Norway, 5University Hospital of North Norway, Tromsø, Dept. of Neurology, Norway, 6Østfold Hospital Trust, Dept. of Radiology, Norway, 7Innlandet Hospital Trust, Lillehammer, Dept. of Neurology, Norway, 8Hotchkiss Brain Institute, University of Calgary, Dept. of Radiology and Clinical Neurosciences, Canada, 9Computational Radiology and AI (CRAI), Oslo University Hospital, Center for Radiology and Nuclear Medicine, Norway, 10The Norwegian University of Science and Technology, Neuromedicine and Movement Science, Norway
On behalf of: AI-STROKE group
Background and aims: Although the numbers of acute ischemic stroke patients with large vessel occlusions (LVO) being offered endovascular treatment (EVT) are increasing, there is still a need to improve acute diagnostics reducing the time from symptom onset to treatment. The purpose of the project is to streamline the acute stroke pathway by using artificial intelligence to automatically analyze CT images.
Methods: In an ongoing national multicentre study, the use of multiphase CT angiography with software for automatic detection of LVO, calculation of infarct volume and penumbra is compared with standard radiological diagnostics. It is being assessed whether the time to EVT start can be reduced and whether a greater proportion of patients with LVO can be detected using the software compared to standard diagnostics. Time course and proportion of EVTs are compared in hospitals using the software and hospitals with standard diagnostics. 465 patients are planned to be included within a 48-month period.
Results: So far, 131 patients have been included, median age 72 years (IQR 63, 80), 34.4% female patients. Primary stroke centres using using multiphase CT angiography with software for automatic detection of LVO had shorter time from start of CT scan to radiological diagnosis in acute stroke patients compared to hospitals with diagnostics of standard care, 8 minutes (IQR 4, 14) vs 24 minutes (IQR15,52) respectively. More data will be presented at ESOC.
Conclusions: The use of artificial intelligence in acute radiological diagnostics is promising to make the acute stroke pathway more efficient and contribute to equalizing differences in the health service.
Disclosures of Interest: No
Abstract N°: 2969
EFFICACY AND SAFETY OF OTAPLIMASTAT IN PATIENTS WITH ACUTE ISCHEMIC STROKE REQUIRING TPA: A RANDOMISED, DOUBLE-BLIND, PLACEBO-CONTROLLED PHASE 3 STUDY
Jong S. Kim1, Chung Ju*2,3, Byung Su Kim2, Jeiman Ryu2, Won-Ki Kim4
1GangNeung Asan Hospital, Department of Neurology, Gangneung-si, South Korea, 2Research Headquarters, Shin Poong Pharm. Co. Ltd., Anyang-si, South Korea, 3Graduate School of Clinical Pharmacy, CHA University, Pocheon-si, South Korea, 4College of Medicine, Korea University, Department of Neuroscience, Seoul, South Korea
On behalf of: SAFE-TPA Investigators
Background and aims: Otaplimastat (SP-8203) is a neuroprotectant that inhibits the matrix metalloprotease pathway, reducing tPA-induced oedema and intracerebral haemorrhage in animal stroke models. A Phase 1 study demonstrated a favourable safety profile in 72 healthy human volunteers. In Phase 2a and 2b SAFE-TPA studies in acute ischaemic stroke (AIS) receiving tPA (80 and 178 participants, respectively), intravenous otaplimastat adjunctive therapy demonstrated MRI imaging evidence of reduced infarct size and improved functional outcomes compared to placebo, with no symptomatic intracranial haemorrhages (sICHs). This trial is a multicentre, randomised, double-blind, placebo-controlled Phase 3 Study.
Methods: Patients aged 19-80 years with an NIHSS score of 7 or higher will receive six doses of otaplimastat or placebo (1:1 allocation) at 12-hour intervals within 30 minutes after tPA administration, with follow-up for up to 90 days. The primary endpoint is functional outcome at 90 days assessed by the modified Rankin scale (mRS) in the mITT population who require tPA but did not receive endovascular therapy. Secondary outcomes include mRS overall distribution and the NIHSS at 7, 24, 90 days, infarct volume at 5 days, sICH incidence, mortality, and the quality of life at 90 days.
Results: This study is expected to run from 2Q 2024 to 1Q 2025 in Korea. The estimated sample size is ~659 participants. Updates on study design and progression will be presented at the conference.
Conclusions: The study will provide high-quality randomized data supporting the efficacy and safety of otaplimastat in AIS patients requiring tPA as a new therapeutic strategy.
Disclosures of Interest: Yes JSK report grants and non-financial support from Ministry of Health & Welfare, Korea. CJ, BSK, JMR are employees of Shin Poong during the conduct of the study. JSK, WKK reports the grants and personal fees from Shin Poong outside the submitted work.
Abstract N°: 125
TENECTEPLASE VERSUS ALTEPLASE FOR LARGE VESSEL OCCLUSION RECANALIZATION (T-FLAVOR)
1National Cerebral and Cardiovascular Center, Department of Cerebrovascular Medicine, Suita, Japan, 2Kyorin University, Department of Stroke and Cerebrovascular Medicine, Mitaka, Japan, 3National Cerebral and Cardiovascular Center, Department of Data Science, Suita, Japan, 4Kobe City Medical Center General Hospital, Departments of Neurosurgery, Kobe, Japan
On behalf of: T-FLAVOR investigators
Background and aims: The use of tenecteplase has been common in past years and several acute stroke guidelines have recommended its off-label use. In contrast, the drug itself does not exist in Japan and no pharmacy company has or intends to obtain the license to supply tenecteplase. To gain support from the government, we are conducting a physician-initiated clinical trial on the effects of tenecteplase in a certain number of Japanese stroke patients.
Methods: The T-FLAVOR trial (jRCTs051210055, protocol: Kawano H, et al. Eur Stroke J 2022;7:71-75) is an investigator-initiated, phase II, multicenter, prospective, randomized, open-label, masked-endpoint, superiority study. We planned to randomize 220 patients into two groups (1:1), alteplase (0.6mg/kg, n=110) or tenecteplase (0.25mg/kg, n=110). Eligibility criteria include acute ischemic stroke with pre-stroke modified Rankin Scale score ⩽3 and large vessel occlusion (internal carotid artery, middle cerebral artery, or basilar artery) eligible for intravenous thrombolysis ⩽4.5 hours and mechanical thrombectomy ⩽6 hours of stroke onset. The primary efficacy endpoint for the randomized comparative phase is substantial angiographic reperfusion (mTICI grade 2b/2c/3) or absence of retrievable thrombus on the initial angiogram. The primary safety outcome is sICH ⩽24-36 hours and 90-day mortality.
Results: After completing the safety phase involving 4 patients who received non-masked tenecteplase (0.25mg/kg), we started patient enrollment for the randomized phase from August 2022. Until Dec 2023, 126 (57%) patients were enrolled.
Conclusions: The result of this trial may support the use of tenecteplase as a routine clinical strategy before mechanical thrombectomy for Japanese stroke patients.
Disclosures of Interest: No
Abstract N°: 369
ACT-GLOBAL: PROTOCOL FOR AN ADAPTIVE RANDOMIZED CLINICAL TRIAL PLATFORM TO STUDY EFFECTIVE TREATMENTS FOR STROKE
Tolulope Sajobi*1, Leonid Churilov2, Laurent Billot3, Scott Berry4, Xiaoyin Chen3, Mohammed Almeklhafi1, Andrew Demchuk1, Michael Hill1, Craig Anderson3, Bijoy Menon1
1University of Calgary, Calgary, Canada, 2The University of Melbourne, Parkville, Australia, 3The George Institute for Global Health, Barangaroo, Australia, 4Berry Consultants, LLC, Austin, United States
On behalf of: ACT-GLOBAL Investigators
Background and aims: Most advances in stroke management over the last two decades are a result of “traditional” 2-arm parallel randomized clinical trials (RCTs). There is however a pressing need to study better and more effective treatments for improving outcomes in patients with acute ischemic stroke (AIS). Modern statistical designs, such as the adaptive platform design, allow for simultaneous investigation of multiple treatments, flexibility in dropping current treatments when relevant and adding new treatment questions at scale, thus addressing many of the current challenges in conducting RCTs in stroke patients.
Methods: The ACT-GLOBAL trial is an international, multicenter, multi-factorial, multi-arm, adaptive platform trial designed to simultaneously evaluate multiple treatments that may improve outcomes in stroke patients. Key features of trial design include: 1) global foot-print; 2) capacity to address both pragmatic and explanatory research questions across multiple domains and states; 3) Bayesian hierarchical statistical models capable of estimating treatment effects across multiple interventions and patient subgroups; 4) adaptive analyses that allow interventions to be stopped for futility, non-inferiority or superiority based on prespecified decision criteria; 5) integrated single point-of-contact data infrastructure for rapid and easy patient recruitment, data monitoring, linkage and sharing and remote follow ups; and 6) trial management harnessing platform level fiscal and contractual efficiencies.
Results:
Conclusions: The ACT-GLOBAL platform trial will enhance logistical and fiscal efficiencies in the design and conduct of stroke trials at scale globally, thus helping to accelerate the identification of better treatments and novel interventions that improve outcomes for stroke patients.
1Stroke Research Group, Population Health Sciences Institute, Newcastle University, United Kingdom, 2Biostatistics Research Group, Population Health Sciences Institute, Newcastle University
On behalf of: SPEEDY trial investigators
Background and aims: Outcomes from large vessel occlusion (LVO) stroke can be significantly improved by time-critical thrombectomy but treatment is typically only available in comprehensive stroke centres (CSC). Many patients require transfer from a local hospital which delays treatment. Access might be improved if eligible patients were directly admitted to CSCs, but currently no pre-hospital symptom score or diagnostic test has acceptable accuracy for independent use by ambulance clinicians. This on-going trial is evaluating an assessment pathway involving communication between ambulance and CSC clinicians to select pre-hospital patients for direct admission.
Methods: Study design: Multicentre cluster RCT with included health economic and process evaluations (ISRCTN77453332).
Study setting: Ambulance services, local stroke units and CSCs in England.
Cluster randomisation: Ambulance stations or teams.
Intervention: Specialist pre-hospital redirection pathway involving semi-structured telephone communication of information from ambulance to CSC clinicians, who then recommend admission destination according to the likelihood of treatable LVO being present.
Control: Standard care
Study population: All suspected and confirmed stroke in participating regions.
Participant enrolment: Waiver of consent.
Co-primary outcome: Thrombectomy rate and time to treatment
Secondary outcomes: Key aspects of emergency care including time intervals and receipt of other treatments including thrombolysis.
Sample size: Powered on a primary analysis population (ischaemic stroke), 564 thrombectomy procedures will detect at least 30-minutes difference in time to treatment. To observe 564 thrombectomies and address wider service impacts, the overall study population is up to 80,000.
Results: Open in three geographical regions. Results expected in 2026.
Conclusions: N/A
Disclosures of Interest: No
Abstract N°: 761
STUDY DESIGN AND PRELIMINARY RESULTS FROM THE ATRIAL FIBRILLATION SCREENING POST ISCHEMIC CEREBROVASCULAR EVENTS (AF-SPICE) STUDY
Kajsa Strååt*1, Eva Isaksson1, Emma Svennberg2, Per Wester1,3, Johan Engdahl1
1Karolinska Institute Danderyd Hospital, Department of Clinical Sciences, Stockholm, Sweden, 2Karolinska Institute Campus Huddinge, Department of Medicine, Huddinge, Sweden, 3Umeå University, Department of Public Health and Clinical Medicine, Umeå, Sweden
On behalf of: AF-SPICE Study Steering Committee. Johan Engdahl, Per Wester, Kajsa Strååt, Eva Isaksson, Emma Svennberg, Signild Åsberg, Marie Eriksson, Weigang Gu, Kjersti Hellqvist, Bo Norrving, Elisabeth Rooth, Sara Själander, Jakob O Ström, Mia von Euler
Background and aims: Atrial fibrillation (AF) screening with long-term ECG monitoring after ischemic stroke or transient ischemic attack (TIA) is recommended by all major societies in cardiology and cerebrovascular medicine. Data on stroke and mortality reduction post-screening are lacking.
Methods: AF-SPICE is a multicentre, national, investigator-initiated, randomised, parallel-group, register-based trial comparing extended versus standard ECG monitoring in patients submitted for ischemic stroke or TIA, with a composite endpoint of ischemic stroke, all-cause mortality, and intracerebral bleeding. Patients, aged ⩾70 years, without previous AF will be randomised 1:1 to control or intervention by extended ECG monitoring with 14 days ECG patch device twice. The primary outcome will be collected from register data during a 36-month follow-up.
Results: The first patient was included in January 2022. To date (2024-01-10), 24 stroke units have been recruited to the study and 1041 patients (sample size 2948) have been included of which 51% are female. Mean age at inclusion was 79 years. The diagnosis at inclusion was ischemic stroke in 65.4% of the patients and TIA in 34.6%.
In the intervention arm, preliminary results from ECG patch registrations show a diagnostic yield for AF/atrial flutter of 9.8% (48/489) for the first and 3.4% (10/295) for the second ECG patch registration.
In the control group, 8 patients have been diagnosed with AF/atrial flutter, corresponding to a preliminary diagnostic yield of 1.6% (8/489).
Conclusions: The AF-SPICE study is a pragmatic randomised trial investigating the potential benefit of extended AF screening for secondary prevention in elderly patients with ischemic stroke or TIA.
ClinicalTrials.gov-identifier:NCT05134454
Disclosures of Interest: No
Abstract N°: 1100
DIAGNOSTIC AND PREDICTIVE VALUE OF AI SOFTWARE CT EVALUATION FOR FINAL OUTCOME IN PATIENTS WITH ACUTE STROKE – STUDY PROTOCOL
Michal Bar*1,2, Kateřina Dvorníkova1, Veronika Kunešová3, Ondrej Volny1,2, Svatopluk Ostrý4, Robert Mikulík3,5
1University Hospital Ostrava, Department of Neurology, Ostrava, Czech Republic, 2University Ostrava, Faculty of Medicine, Department of Clinical Neurosciences, Ostrava, Czech Republic, 3International Clinical Research Center, Cerebrovascular research program, Brno, Czech Republic, 4Hospital České Budějovice, Department of Neurology, České Budějovice, Czech Republic, 5T. Baťa Regional Hospital Zlín, Neurology Department, Zlín, Czech Republic
On behalf of: CZECHSTROKE Research Network
Background and aims: CT perfusion (CTP) is used for penumbra imaging. It is not clear however, how CTP can add to outcome prediction.
The goal of this study was to find the predictive and diagnostic value of CT parameters (e-ASPECTS, CTP, collateral vessel status, volume and location of final ischemic lesion on 3-month functional outcome defined by the modified Rankin scale(mRS) in patients with stroke after recanalization treatment (IVT and/or MT).
Methods: Multicenter observational study of patients with acute stroke and premorbid mRS ⩽ 4, who are treated with IVT and/or MT in 22 stroke centers involved in Czech Stroke Research Network. Radiological and clinical data will be merged from e-stroke software (Brainomix) and the RES-Q registry. Demographic, clinical and imaging data collection: Age, sex, race, risk factors, time to treatment (OTT, DNT, OGT), TICI, the presence of hemorrhage after IVT or MT (ECAS II), outcome in mRS, etiology of stroke, e-ASPECTS, e-ASPECTS acute ischaemic volume (AIV), thrombus length, CTA collateral score, CTA collateral vessel density, location of large vessel occlusion, ischemic core, hypoperfusion volume, mismatch ratio and volume, final infarct volume, haemorrhage volume and MRI in case of negative follow up NCCT.
Results: We expect to obtain robust clinical and radiological data from 22 centers over a period of 12 months from approximately 6,000 patients. 200 have already been enrolled.
Conclusions: The results can refine diagnostic and prognostic radiological markers in acute stroke patients.
Funding
Supported by STROCZECH within CZECRIN Large Research Infrastructure (No. LM2023049) and by AZV grant NU23-04-00336, ClinicalTrials.gov NCT05864495
Disclosures of Interest: No
Abstract N°: 1263
ENDOVASCULAR THERAPY PLUS BEST MEDICAL TREATMENT (BMT) VERSUS BMT ALONE FOR MEDIUM VESSEL OCCLUSION STROKE (DISTAL)
Marios Psychogios*1, Alex Brehm1, Luzia Balmer1, Urs Fischer2,3
1University Hospital Basel, Department of Neuororadiology, 2University Hospital Basel, Department of Neurology, 3University Hospital Bern, Department of Neurology
On behalf of: the DISTAL Steering Committee
Background and aims: Whether endovascular therapy (EVT) in addition to best medical treatment (BMT) in acute ischemic stroke (AIS) patients with a medium vessel occlusion (MEVO, defined as an occlusion of the co- or non-dominant M2, M3 or M4, A1, A2 or A3, P1, P2 or P3) is beneficial remains a matter of debate. Prior randomized-controlled trials assessing the efficacy of EVT have not included these patients. As they represent a large proportion of AIS patients (approx. 20-40%), randomized-controlled evidence is warranted.
Methods: The trial is conducted at over 50 academic tertiary care centres in Europe to evaluate EVT in patients with AIS. Five hundred twenty-six patients with a MEVO will be randomly assigned in a 1:1 ratio to undergo EVT plus BMT or BMT alone. The primary objective is to determine whether patients experiencing an AIS due to an isolated MEVO have superior functional outcome (measured with the modified Rankin Scale (mRS) at 90 days) when treated with EVT plus BMT compared to patients treated with BMT alone. Secondary objectives are to study causes of mortality, dependency, cognitive function, and quality of life.
Results: DISTAL started recruitment in December 2021 and until now 353 patients have been recruited. We estimate to finish recruitment by December 2024.
Conclusions: DISTAL will provide evidence for the effects of EVT in MeVO stroke patients.
ClinicalTrials.gov Identifier: NCT05029414
Current trial status (Jan 12, 2023): 353 / 526 patients randomised
Disclosures of Interest: No
Abstract N°: 1301
PREHOSPITAL TRIAGE OF PATIENTS WITH A SUSPECTED ACUTE STROKE (PRESTO-2): IMPLEMENTATION AND EVALUATION OF A DECISION SUPPORT TOOL
Ruben van de Wijdeven*1, Esmee Venema2,3, Patrick van der Geest4, Johannes Ijzermans5, Merel Willeboer5, Kirsten Dorresteijn6, Annemarie Wijnhoud7, Henk Kerkhoff8, Diederik Dippel1, Bob Roozenbeek1
1Erasmus MC University Medical Center, Department of Neurology, Rotterdam, Netherlands, 2Erasmus MC University Medical Center, Emergency Department, Rotterdam, Netherlands, 3Erasmus MC University Medical Center, Department of Public Health, Rotterdam, Netherlands, 4Ambulance Rotterdam-Rijnmond, Barendrecht, Netherlands, 5Ambulance Service Zuid-Holland Zuid, Papendrecht, Netherlands, 6Franciscus Gasthuis en Vlietland, Department of Neurology, Rotterdam, Netherlands, 7IJsselland Hospital, Department of Neurology, Capelle aan den IJssel, Netherlands, 8Albert Schweitzer Hospital, Department of Neurology, Dordrecht, Netherlands
On behalf of: PRESTO-2 investigators
Background and aims: Prehospital triage of suspected stroke patients aims to eliminate the need for interhospital transfers for patients with ischaemic stroke caused by a large vessel occlusion (LVO) eligible for endovascular thrombectomy (EVT), reducing onset-to-groin-time and improving long-term functional outcome. This can be facilitated with prehospital stroke scales, but these instruments use crude cut-points and do not account for important characteristics other than stroke severity. We aim to implement and evaluate a novel decision support tool, which provides a personalized triage advice by incorporating the RACE-scale, onset-time, GPS-based driving times, hospital-specific workflow metrics and time-dependent treatment effects.
Methods: We developed the Stroke Triage App, a medical device which will be provided to paramedics. The app will be implemented in two ambulance regions in the Netherlands, encompassing ±1,800,000 inhabitants. The app provides an advice by comparing probability of good functional outcome (mRS0-2) between transportation to the nearest primary stroke center or directly to the thrombectomy-capable center further away. The primary outcome will be difference in onset-to-groin-time in the year before and after implementation, compared to a control region with a difference-in-differences linear regression analysis.
Results: The Stroke Triage App has been developed and CE-certified (class I medical device). We plan to include ±5,000 suspected stroke patients over the course of one year. Patient enrolment started on January 22nd 2024.
Conclusions: We expect that the implementation of the Stroke Triage App will reduce onset-to-groin times in patients with LVO ischaemic stroke, which translates in better functional outcomes.
Disclosures of Interest: No
Paper Poster - Pathophysiology of Stroke/Translational Medicine
Abstract N°: 2930
CEREBROPROTECTIVE EFFECTS OF THE TLR4-BINDING DNA APTAMER APTOLL IN A RAT MODELOF ISCHEMIC STROKE AND THROMBECTOMY RECANALIZATION
Alicia Aliena-Valero*1, Macarena Hernández2,3, Mikahela A. López-Morales1, Eva Tamayo-Torres4, Maria Castelló-Ruiz4, David Piñeiro2, Marc Ribo2,5, Juan Bautista Salom Sanvalero1,4
1Institut d’Investigació Sanitària La Fe de València, València, Spain, 2AptaTargets SL., Madrid, Spain, 3Universidad Complutense de Madrid, Madrid, Spain, 4University of Valencia, València, Spain, 5Vall d'Hebron University Hospital, Barcelona, Spain
On behalf of:
Background and aims: ApTOLL, a TLR4 modulator aptamer, has demonstrated cerebroprotective effects in a permanent ischemic stroke mouse model, as well as safety and efficacy in early phase clinical trials. We carried out reverse translation research according to STAIR recommendations to further characterize the effects and mechanisms of ApTOLL after transient ischemic stroke in rats and better inform the design of pivotal clinical trials.
Methods: Adult male rats subjected to transient middle cerebral artery occlusion were treated either with ApTOLL or vehicle intravenously at different doses and time-points. ApTOLL was compared with TAK-242 (TLR4 inhibitor). Female rats were also studied. After neurofunctional evaluation, brains were removed for infarct/edema volume, hemorrhagic transformation, and histologic determinations. Peripheral leukocyte populations were assessed by flow cytometry.
Results: ApTOLL showed U-shaped dose-dependent cerebroprotective effects. The maximum effective dose (0.45 mg/kg) was cerebroprotective when given both before reperfusion and up to 12 h after reperfusion, and reduced the hemorrhagic risk. Similar effects occurred in female rats. Both, research and clinical ApTOLL batches, induced slightly superior cerebroprotection when compared with TAK- 242. Finally, ApTOLL modulated circulating leukocyte levels, reached the brain ischemic tissue to bind resident and infiltrated cell types, and reduced neutrophil density.
Conclusions: These results show the cerebroprotective effects of ApTOLL in ischemic stroke by reducing infarct/edema volume, neurofunctional impairment, hemorrhagic risk, as well as peripheral and local immune response. They provide information about ApTOLL’s dose-effect, therapeutic window and target population, as well as its mode of action, to be onsidered in the design of pivotal clinical trials.
Disclosures of Interest: No
Abstract N°: 2520
METABOLIC BRAIN CONNECTIVITY IN A RAT MODEL FOR INTRACEREBRAL HAEMORRHAGE
Melissa Lajtos1,2, Silke Proesmans1, Christian Vanhove2, Robrecht Raedt1, Veerle De Herdt*1
14BRAIN Lab, Ghent University, Department of Head and Skin, Ghent, Belgium, 2IBiTech-MEDISIP-Infinity Lab, Ghent University, Department of Electronics and Information Systems, Ghent, Belgium
On behalf of:
Background and aims: Changes in the glucose metabolism of brain tissue could explain some of the pathophysiological consequences of an intracerebral haemorrhage (ICH). As part of a project studying the causes of post-ICH seizures, we investigate changes in metabolic brain connectivity using 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography (PET) imaging in a rat collagenase model.
Methods: Twenty-two male Sprague-Dawley rats were included in this study. In 12 rats, ICH was induced by striatal injection of 0.6U collagenase. 18F-FDG PET scans of the rat brain were acquired at baseline (n=22), and 3 and 7 days post ICH (n=12). Baseline images were used to generate a normal rat brain atlas to which post-ICH PET images were voxel-wise compared using group-level analysis. Metabolic connectivity was compared before and after ICH in an inter-subject manner by calculating Pearson's correlations using 31 brain regions. Permutation tests were performed to statistically compare correlation matrices.
Results: Analysis revealed a region of significantly decreased (p<0.05) glucose metabolism at the site of the ICH lesion 3 days post ICH, but not 7 days post ICH. Significantly decreased connectivity (p<0.05) was observed 3 days post ICH in the following brain regions: metencephalon, basal forebrain, lemniscus, thalamus, hypothalamus and pallidum. 7 days post ICH, reduced connectivity was found in the following regions: tegmentum, hippocampus, metencephalon, thalamus and substantia nigra.
Conclusions: Metabolic brain connectivity using 18F-FDG PET can provide additional information to voxel-based analysis. In this study, 18F-FDG metabolic brain connectivity was reduced post ICH in brain regions remote from the ICH lesion indicating wide-spread effects on brain function.
Disclosures of Interest: No
Abstract N°: 3138
CEREBROVASCULAR DYSFUNCTION IN SMALL VESSEL DISEASE: A MATTER OF IMPAIRED ENDOTHELIAL-PERICYTE CROSSTALK?
1The UK Dementia Research Institute, The University of Edinburgh, Edinburgh, United Kingdom, 2The University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom, 3The University of Edinburgh, High Content Screening Facility, Institute for Regeneration and Repair, Edinburgh, United Kingdom, 4University of Edinburgh, Neuropathology, The Edinburgh Brain and Tissue Bank, Edinburgh, United Kingdom, 5The University of Edinburgh, Simons Initiative for the Developing Brain, Edinburgh, United Kingdom
On behalf of:
Background and aims: Small vessel disease (SVD) is a prevalent disorder of the brain’s microvessels and a common cause of dementia and stroke. Recent evidence suggests a key role involving features of normal ageing in disease progression, including pericyte loss, endothelial dysfunction, and blood-brain barrier breakdown. Here, we aim to examine this relationship through a series of translational investigations.
Methods: Using immunohistochemistry and spinning-disk confocal microscopy, we quantified pericyte coverage and endothelial activation (through VCAM-1 expression) in 8 brain regions in young (n=8, 3-months) and aged (n=8, 12-months) C57Bl/6J wildtype mice. We then similarly quantified pericyte coverage and VCAM-1 expression using multi-spectral imaging and post-mortem tissue from young controls (n=5), mild SVD (n=5) and severe SVD cases (n=5).
Results: Aged mice had a 7.5% reduction in pericyte coverage (β=-7.47,SE=2.15,t=-3.46,p=0.01) and a 99% increase in VCAM-1 expression (β=0.68, SE=0.28, t=2.45, p= 0.03) after adjusting for sex and brain region. Capillary microsegments revealed a 0.75% increase in VCAM-1 coverage for every 10% decrease in pericyte signal (β=-0.08, SE=0.03, t=-0.13, p=0.04). Humans with severe SVD had an 80% decrease in pericyte coverage (β=-1.66, SE=0.35, t=-4.78,p<0.001) and a 47% increase in VCAM-1 expression compared to young controls (β=0.38, SE=0.11,t=3.41, p<0.01), with microvessel segments demonstrating a 64% decrease in VCAM-1 signal corresponding to a 1% increase in pericyte signal (β=-1.03, SE=0.19, t=-5.22, p<0.001).
Conclusions: Our results suggest a significant and progressive reduction in pericyte coverage accompanied by evidence of endothelial activation with a possible interaction in SVD patients compared to controls, and to a lesser extent in normal ageing, as observed in mice and humans.
Disclosures of Interest: No
Abstract N°: 871
REMOTE ISCHEMIC CONDITIONING AFFECTS EXOSOME PROFILING UNDER CONDITIONS OF ISCHEMIC STROKE
Stefan Gerner1, Martin Jünemann1, Hagen Huttner1, Thorsten R. Döppner*1
1University Hospital of Giessen and Marburg, Neurology, Giessen, Germany
On behalf of:
Background and aims: Preclinical studies suggest a beneficial effect of (limb) remote ischemic postconditioning (RIC). Neither the optimal RIC protocol nor the underlying mechanisms, however, have been sufficiently understood. Using a murine stroke model, we therefore analyzed the impact of various RIC protocols with regard to poststroke brain injury, focusing on expression profiles of extracellular vesicles (EV) both in the blood and in the brain.
Methods: Male mice were exposed to cerebral ischemia followed by an observation period of up to eight weeks. Thereafter, mice were subject to various protocols of hindlimb RIC. Brain injury, EV profiles including non-coding RNA contents, and neurological recovery were analyzed thereafter.
Results: Seven cycles of RIC performed on a daily basis during the first two weeks poststroke yielded profound neuroprotection and neurological recovery for as long as eight weeks. EV derived from plasma samples displayed increased levels of distinct miRNA and non-coding RNA as was the case with EV obtained from CSF samples, albeit the latter differed in detailed expression patterns. Interestingly, direct cerebral postconditioning did not affect EV profiles in stroke mice, neither in the CSF nor in the blood. EV harvested from CSF of stroke mice undergone RIC modulated neuronal cell injury in cultivated neurons exposed to hypoxia by inhibiting the ubiquitin-proteasome-system. On the contrary, plasma-derived EV did not affect the ubiquitin-proteasome-system, suggesting a different mode of action for these EV.
Conclusions: RIC attenuates poststroke brain injury by modulating EV profiles both in the blood and even more so in the CSF.
Disclosures of Interest: No
Abstract N°: 875
A NOVEL ANIMAL MODEL AND NEW MECHANISM OF CEREBRAL VENOUS SINUS THROMBOSIS
Baoshan Qiu*1,2, Nan Wang1,2, Yilong Wang1,2
1Beijing Tiantan Hospital, Capital Medical University, Neurology, Beijing, 2Chinese Institute for Brain Research, Beijing, China
On behalf of:
Background and aims: Cerebral venous and sinus thrombosis (CVST) accounts for approximately 1.0% of all strokes and is more common in younger populations. Despite being clinically rare, CVST is often misdiagnosed or overlooked, carrying a high disability and mortality rate. Additionally, the pathophysiological mechanisms remain unclear, and there is a lack of suitable animal models and specific treatment methods. This study aims to establish a novel animal model of venous sinus thrombosis and explore its pathophysiological mechanisms.
Methods: The success and stability of the model were assessed through laser speckle blood flow imaging, behavioral evaluation, and immunofluorescence staining. Further insights into the novel mechanisms of brain damage caused by CVST were revealed through transcriptome sequencing, single-cell sequencing, immunofluorescence, and drug interventions.
Results: The study successfully established a simple, high success rate, and reproducible mouse model of cerebral venous sinus thrombosis. RNA-sequence of brain tissues revealed a significant upregulation of pathways related to neutrophil migration and chemotaxis, suggesting a more pronounced myeloid immune response in venous sinus thrombosis compared to arterial ischemic stroke. Moreover, 24 hours after venous sinus thrombosis formation, a large number of immune cells, predominantly neutrophils, gathered in the dura mater. Depleting neutrophils significantly reduced the size of venous sinus thrombosis and the damaged area, improving mouse motor abilities.
Conclusions: Local photoactivation of rose bengal in the venous sinus is a simple and efficient method for creating a mouse model of venous sinus thrombosis. The myeloid immune response, represented by neutrophils, plays a crucial role in the brain damage following venous sinus thrombosis.
Disclosures of Interest: No
Abstract N°: 914
ELIMINATION OF SENESCENT ENDOTHELIAL CELLS PROTECTS BLOOD-BRAIN BARRIER FROM AGE-RELATED DYSFUNCTION
Ulvi Bayraktutan*1, Jingyuan Ya1
1University of Nottingham, Clinical Neuroscience
On behalf of:
Background and aims: Accumulation of senescent endothelial cells (ECs) plays an important role in age-related blood–brain barrier (BBB) dysfunction. Selective clearance of senescent cells by senotherapeutics has been determined to delay the development of senescence of the neighbouring cells. This study investigated whether a cocktail of senotherapeutics mitigate EC senescence and associated BBB dysfunction.
Methods: Replicative senescence was induced through repetitive culture of human brain microvascular ECs (HBMECs). An in vitro model of BBB, composed of HBMECs, astrocytes and pericytes, was used to explore how HBMEC senescence may affect BBB integrity and function, assessed by measurements of transendothelial electrical resistance (TEER) and paracellular flux. HBMECs were treated with a cocktail of dasatinib and qurecetin (D+Q) from passage 16 to passage 20. Senescence-associated β-galactosidase activity, γ-H2AX staining, telomere length and p16 expression were studied as markers of HBMEC senescence. Expression of tight junction proteins and the activation of matrix metallopeptidases (MMPs) were measured to explore the mechanism involved in BBB dysfunction.
Results: At passage 20, over 70% of HBMECs stained positive for SA-β-galactosidase and γ-H2AX and displayed shortened telomere length, increased expression of p16 and MMP-2 and decreased expression of tight junction proteins. BBB established with senescent HBMECs displayed significantly decreased TEER value and increased paracellular flux. Treatment with the D+Q delayed EC senescence and protected the BBB function.
Conclusions: Prevention of senescent EC accumulation in cerebrovasculature may help preserve BBB function during chronological ageing.
Disclosures of Interest: No
Abstract N°: 916
INHIBITION OF P38MAPK DELAYS ENDOTHELIAL CELL SENESCENCE AND PROTECTS BLOOD-BRAIN BARRIER FROM AGE-RELATED DYSFUNCTION
Ulvi Bayraktutan*1, Jingyuan Ya1
1University of Nottingham
On behalf of:
Background and aims: Endothelial cell (EC) senescence plays a key role in age-related blood-brain barrier (BBB) disruption. Considering the prominent role of p38 mitogen-activated protein kinase (p38MAPK) in cellular senescence, this study investigated whether targeting this signalling pathway may prevent EC senescence and protect BBB function in an in vitro setting of chronological ageing.
Methods: Replicative senescence was induced through repetitive culture of human brain microvascular ECs (HBMECs). HBMECs were treated with BIRB796, a p38MAPK inhibitor, from passage 16 to 20. Senescence-associated β-galactosidase activity, γ-H2AX staining, telomere length and p16 expression were probed as senescent markers. An in vitro model of BBB, composed of HBMECs, astrocytes and pericytes was used to explore how HBMEC senescence may affect BBB integrity and function, assessed by measurements of transendothelial electrical resistance (TEER) and paracellular flux. Expression of tight junction proteins and the activation of matrix metallopeptidases (MMPs) were measured to explore the mechanisms that may contribute to BBB dysfunction.
Results: Replicative senescence was deemed present at passage ⩾19 where over 70% of HBMECs stained positive for SA-β-galactosidase and γ-H2AX and displayed shortened telomere length and increased p16 expression. BBB established with senescent HBMECs displayed significantly impaired integrity and function. Inhibition of p38MAPK rendered HBMECs more resistant to replicative stress and preserved BBB function by increasing expression of tight junction proteins while inhibiting MMP-2 activity.
Conclusions: Inhibition of p38MAPK pathway delays EC senescence and help prevent age-related BBB dysfunction.
Disclosures of Interest: No
Abstract N°: 1155
INCOMPLETE MICROVASCULAR REPERFUSION IN A SWINE MODEL OF RECANALIZED ACUTE ISCHEMIC STROKE
Meiqi Wang*1, Aladdin Taha1,2, Jadey Raben1, Romy Noort1, Mathijs Stam1, Dirk Duncker1, Diederik Dippel2, Joaquim Bobi1, Heleen M. M. van Beusekom1
1Erasmus MC University Medical Center, Department of Cardiology, Rotterdam, Netherlands, 2Erasmus MC University Medical Center, Department of Neurology, Rotterdam, Netherlands
On behalf of:
Background and aims: Incomplete microvascular reperfusion (IMR) might impair regained functionality in stroke patients despite early recanalization. Gyrencephalic large-animal models of acute ischemic stroke (AIS) are gaining attention in translating preclinical to clinical stroke research, as brain anatomy and hemostasis are more similar to humans. We aimed to study occurrence and relevance of IMR in swine AIS-models with recanalization.
Methods: Anesthetized female Yorkshire-Landrace swine (n=23) underwent craniotomy and right-sided middle cerebral arteries occlusion using aneurysm clips. Clips were released 1 (n=5), 2 (n=5), or 4 (n=5) hours after occlusion followed by 4 hours recanalization. As controls, clips were left in place (8 hours, non-recanalized AIS, n=5) or not placed at all (sham, n=3). 3D angiography confirmed occlusion and recanalization. After sacrifice, brain slices were stained with TTC and processed for histology. Infarct size by TTC was expressed as %-infarcted hemisphere. Histologic sections (upper quadrants, both hemispheres) were immuno-stained (α-CD61) to visualize microvascular platelet aggregates. Intravascular aggregates (Fig.2A) were quantified using automated software analysis (Orbit) (CD61+ aggregates/mm2).
Results: Infarct size increased significantly with duration of occlusion (Fig.1, p=0.006) and showed significantly increased microvascular platelet-aggregates in the infarcted hemisphere (Fig.2, p=0.014). Groupwise comparison showed only a trend (p=0.075) for more aggregates after 4 hours occlusion. Linear regression could not identify whether infarct size and duration of occlusion were independent predictors of the number of platelet aggregates in the infarcted hemisphere (p=0.191).
Conclusions: IMR occurs in this swine model of AIS showing microvascular platelet aggregates. Further analysis is needed to elucidate which predictors can explain intravascular platelet aggregation.
Disclosures of Interest: No
Abstract N°: 1839
REVASCULARIZATION FEATURES BY MULTIPLE BURRHOLES AND ERYTHROPOIETIN IN ACUTE STROKE PATIENTS WITH PERFUSION IMPAIRMENT
Seong-Joon Lee1, So Young Park1, Geun Hwa Park1, Ji Soo Lee1, Yong Cheol Lim2, Ji Man Hong*1
1Ajou University Medical Center, Neurology, Suwon-si, South Korea, 2Ajou University Medical Center, Neurosurgery, Suwon, South Korea
On behalf of:
Background and aims: Transdural collaterals, primarily originating from the extracalvarial superficial temporal artery (STA) and intracalvarial middle meningeal artery (MMA) via the external carotid artery (ECA), have been identified following revascularization surgery. However, the precise source of these collaterals in stroke patients with perfusion insufficiency remains unclear. This study aimed to investigate revascularization patterns and characteristics based on the origin of these collaterals.
Methods: We employed erythropoietin pretreatment and performed multiple burr holes under local anesthesia to achieve transdural revascularization in acute stroke patients with perfusion insufficiency. After a 6-month period, transfemoral cerebral angiography was performed to assess revascularization patterns. Collaterals were categorized into three groups: intracalvarial ECA-dominant (MMA-dominant), extracalvarial ECA-dominant (STA-dominant), and balanced groups. Various imaging parameters were compared among these groups.
Results: Overall, 87 patients with 103 treated hemispheres participated in the study. Among them, 57.3% were classified as intracalvarial ECA-dominant, 20.4% as extracalvarial ECA-dominant, and 22.3% as balanced. Most hemispheres with intracalvarial or extracalvarial collaterals (vs. balanced collaterals) exhibited successful revascularization (78/80 [97.5%] vs. 12/23 [52.1%]), p<0.001). In ultrasonographic hemodynamic changes related to revascularization patterns, only intracalvarial ECA-dominant revascularization was significantly associated with specific alterations in ECA blood flow, resulting in the conversion to a low-resistance ECA Doppler sonography waveform.
Conclusions: Our findings highlight the pivotal role of intracalvarial ECA-dominant revascularization in the development of transdural collaterals following combination therapy. Furthermore, these distinct changes in ECA hemodynamics can be non-invasively identified through bedside ultrasound studies. This research contributes to a better understanding of collateral formation mechanisms in acute stroke patients with perfusion impairment.
Disclosures of Interest: No
Abstract N°: 2142
VON WILLEBRAND FACTOR ANTIGEN, VWF PROPEPTIDE AND ADAMTS13 ACTIVITY IN TIA/ISCHAEMIC STROKE PATIENTS CHANGING ANTIPLATELET THERAPY
Deirdre Smith*1, Soon Tjin Lim2, Stephen Murphy3, Fionnuala Hickey4, Sinead Murphy3, Rónán Collins5, Bridget Egan6, James O' Donnell7, Jamie O' Sullivan8, Dominick J. H. Mccabe1
1Vascular Neurology Research Foundation, Dept of Neurology and Stroke Service, Tallaght University Hospital / AMNCH; Academic Unit of Neurology, School of Medicine, Trinity College Dublin, Dublin, Ireland, 2Dept of Neurology and Stroke Service, Tallaght University Hospital/ AMNCH; Dept of Clinical and Movement Neurosciences, Royal Free Campus, UCL Queen Square Institute of Neurology, London, U.K, 3Dept of Neurology, Tallaght University Hospital / AMNCH; Academic Unit of Neurology, School of Medicine, Trinity College Dublin, Dublin, Ireland, 4Dept. of Clinical Medicine, School of Medicine, Trinity College Dublin, Dublin, Ireland, 5Age-Related Health Care Department and Stroke Service, Tallaght University Hospital / AMNCH; Academic Unit of Neurology, School of Medicine, Trinity College Dublin, Dublin, Ireland, 6Dept of Vascular Surgery, Tallaght University Hospital / AMNCH, Dublin, Ireland, 7National Coagulation Centre, St James’s Hospital, Dublin, Ireland; Irish Centre for Vascular Biology, Royal College of Surgeons in Ireland, Dublin, Ireland, 8Irish Centre for Vascular Biology, Royal College of Surgeons in Ireland, Dublin, Ireland
On behalf of: Optimal Antiplatelet Therapy in TIA and Ischaemic Stroke (OATS) study group: The OATS study research group also includes Offiah C MRCPI, O’Neill D FRCPI and Coughlan T FRCPI
Background and aims: Data are limited on the impact of commencing antiplatelet therapy on von Willebrand Factor Antigen (VWF:Ag) or von Willebrand Factor propeptide (VWFpp) levels and ADAMTS13 activity, and their relationship with platelet reactivity following TIA/ischaemic stroke.
Methods: In this pilot, observational study, VWF:Ag and VWFpp levels and ADAMTS13 activity were quantified in 48 patients ⩽4 weeks after TIA/ischaemic stroke (baseline), and 14days (14d) and 90days (90d) after commencing aspirin, clopidogrel or aspirin+dipyridamole. Platelet reactivity was assessed at moderately-high shear stress (PFA-100®Collagen-Epinephrine/Collagen-ADP/INNOVANCE P2Y assays), and low shear stress (VerifyNow®Aspirin/P2Y12, and Multiplate®Aspirin/ADP assays).
Results: VWF:Ag levels decreased and VWFpp/VWF:Ag ratio increased between baseline and 14d and 90d in the overall population (P⩽0.03). In the clopidogrel subgroup, VWF:Ag levels decreased and VWFpp/VWF:Ag ratio increased between baseline and 14d and 90d (P⩽0.01), with an increase in ADAMTS13 activity between baseline vs. 90d (P⩽0.03). There was an inverse relationship between VWF:Ag and VWFpp levels with PFA-100 C-ADP closure times at baseline (R2⩾0.25; P⩽0.04) and 14d (R2⩾0.28; P⩽0.03), and an inverse relationship between VWF:Ag and PFA-100 INNOVANCE P2Y closure times at 14d (P=0.001) in the aspirin+dipyridamole subgroup. There was a positive relationship between ADAMTS13 activity and PFA-100 C-ADP closure times at baseline in the aspirin+dipyridamole subgroup (R2=0.25; P=0.04).
Conclusions: Commencing/altering antiplatelet therapy, mainly attributed to commencing clopidogrel monotherapy, was associated with reduced endothelial activation status over time following TIA/ischaemic stroke. Endothelial biomarkers, especially VWF:Ag and VWFpp levels, influence ex-vivo platelet reactivity at high shear stress after TIA/ischaemic stroke.
Disclosures of Interest: No
Abstract N°: 3177
DRAG-REDUCING POLYMER EFFICACY DEPENDENCE FROM THE TIME OF APPLICATION IN A RAT MODEL OF PERMANENT MIDDLE CEREBRAL ARTERY OCCLUSION
Denis Bragin1, Jun Wu2, Zefeng Peng3, Olga Bragina1, Edwin Nemoto4, Alexey Trofimov5, Afshin Divani*6
1Lovelace Biomedical Research Institute, United States, 2Central South University, China, 3Central South University, Department of Neurosurgery, China, 4University of New Mexico Health Science Center, United States, 5Privolzhsky Research Medical University, Department of Neurological Diseases, 6University of New Mexico Health Science Center, Neurology, United States
On behalf of:
Background and aims: Current treatments for ischemic stroke are not focused on microvascular cerebral blood flow (mvCBF). Previously, we demonstrated that drag-reducing polymers (DRPs), administered just after permanent middle cerebral artery occlusion (pMCAO) in rats, effectively restored mvCBF. This study aimed to assess the efficiency of DRPs administered at various time points post-ischemia in a rat model of pMCAO.
Methods: DRPs (2 μg/ml) or saline was injected intravenously 0.5, 3, or 6 hours after pMCAO (n=10/group). In-vivo 2-photon laser scanning microscopy assessed mvCBF, hypoxia (NADH), and blood-brain barrier (BBB). MRI and behavioral testing evaluated cerebral infarction, CBF, and neurological outcomes 24 hours, 1, and 3 weeks post-pMCAO. Two-way ANOVA for multiple comparisons was used to test intergroup differences.
Results: pMCAO progressively decreased cortical mvCBF, causing tissue hypoxia and BBB disruption (p<0.032). DRPs increased capillary perfusion and tissue oxygenation while protecting BBB compared to saline (p<0.026). MRI studies demonstrated reduced infarct expansion and mitigated CBF disturbances in all DRPs-treated groups (p<0.027). Neurological function was more preserved in all DRP groups than in the saline group (p<0.042). DRP efficacy reduced with the time of application from 0.5 h to 6 hours after pMCAO but remained significant (p<0.034).
Conclusions: DRPs (administered 0.5, 3, and 6 hours post-occlusion) effectively restored mvCBF after pMCAO, reducing tissue hypoxia and BBB damage, leading to reduced infarct size and improved neurological outcome in a time-dependent manner. DRPs can be used as an adjunct therapy for ischemic stroke even without reperfusion and after delayed administration following the stroke onset.
Disclosures of Interest: No
Abstract N°: 1303
A DIRECT INTRA-ARTERIAL ANTI-INFLAMMATORY STRATEGY TO TREAT CEREBRAL ISCHEMIA
Paula García-Rodríguez*1, Daisy Guamán1, Anna Penalba1, Marcel Lamana-Vallverdú1, Alejandro González2, Anna Rosell1, Joan Montaner1,2
1Vall d'Hebron Institut de Recerca (VHIR), Universitat Autònoma de Barcelona, Neurovascular Research Laboratory, Barcelona, Spain, 2Institute of Biomedicine of Seville, IBiS/Hospital Universitario Virgen del Rocío-Macarena/CSIC, University of Seville, Stroke Research Program, Sevilla, Spain
On behalf of:
Background and aims: Despite the effectiveness of the current treatment for ischemic stroke - intravenous thrombolysis and mechanical thrombectomy - these therapies may not effectively address the inflammatory response after the event. Our project aims to develop a novel reprofiling approach for treating ischemic stroke by using intra-arterial administration of an anti-inflammatory agent to enhance the survival of recently reperfused brain tissue.
Methods: Focal cerebral ischemia was performed in C57BL/6 mice by the filament occlusion model of the middle cerebral artery removed after 60 minutes, resembling a thrombectomy procedure. The anti-inflammatory agent was administered at reperfusion intra-arterially or intravenously by the retro-orbital route (four groups of n=9 animals per group were tested: intra-arterial/retro-orbital study drug vs. intra-arterial/retro-orbital vehicle). Intra-arterial administration was performed in the ischemic stroke model by cannulation of the external carotid artery with a micro-catheter directed to the internal carotid artery and connected to an infusion pump. Functional tests to assess the outcome were performed 24 hours after the event.
Results: The intra-arterial administration of the anti-inflammatory agent was safe and effective in reducing by 32.81% the total infarct volume compared to the control group [12.22(10.88-26.89) vs. 45.03(27.38-48.60) respectively, p=0.024]. No differences were seen in the retro-orbital treated group compared to the control group.
Conclusions: The targeted delivery throughout the intra-arterial administration of our therapeutic anti-inflammatory agent reduces brain infarct volume and could be considered a promising adjuvant strategy in the context of mechanical thrombectomy to treat ischemic stroke.
Disclosures of Interest: No
Abstract N°: 1605
INTERACTION BETWEEN THE ENDOPLASMIC RETICULUM STRESS AND ONE-CARBON METABOLISM REGULATES NEURONAL SURVIVAL AFTER STROKE
Yikui Liu*1, Liuguan Bian1, Yuhao Sun1
1ruijin hospital, shanghai jiaotong university, department of neurosurgery, Shanghai, China
On behalf of:
Background and aims: Emerging evidence has revealed the association of oxidative stress to neuronal damage and disruptions in mitochondrial and endoplasmic reticulum (ER) function following intracerebral hemorrhage (ICH). However, there is limited evidence elucidating their coordinated role in maintaining neuronal homeostasis.
Methods: We established ICH models in vivo and hemin-induced primary neuronal damage models in vitro. Metabolomics, RNA-seq, CUT&Tag-seq, western blotting and RT-qPCR were used to investigate the underlying mechanism of interaction between the PERK/ATF4 branch of endoplasmic reticulum stress (ERS) and mitochondrial one-carbon (1C) metabolism in the neuronal resistance to oxidative stress. In addition, the association between mitochondrial 1C metabolism and the PERK/ATF4 branch of the ERS after ICH was investigated using transcription factor motif analysis, immunofluorescence, and co-immunoprecipitation (co-IP).
Results: The findings revealed interactions between the GRP78/PERK/ATF4 branch of the ERS and mitochondrial 1C metabolism, which played an important role in preserving neuronal homeostasis after ICH. Mechanistically, ATF4 was identified as an upstream transcription factor directly regulating key genes involved in mitochondrial morphology, function, NADPH production and neuronal survival, including SHMT2, MTHFD2 and ALDH1L2. Additionally, the GRP78/PERK/ATF4 branch of the ERS formed a negative regulatory loop with MTHFD2 due to the interaction between GRP78 and MTHFD2.
Conclusions: This study presents the first evidence of disrupted 1C metabolism and the occurrence of ERS in neurons post-ICH and that supplementing exogenous NADPH or interfering with the PERK/ATF4 branch of the ERS could reduce symptoms related to neuronal injuries, suggesting new prospects for improving the outcomes of ICH patients.
Disclosures of Interest: No
Abstract N°: 1920
G6PD DEFICIENCY DISRUPTS PERICYTE RECRUITMENT AND BLOOD–BRAIN BARRIER REPAIR IN MICE AFTER ISCHEMIC STROKE
Yuangui Cai*1, Jiating Wei1, Jinsheng Zeng1
1The First Affiliated Hospital, Sun yat-sen University, Department of Neurology, Guangzhou, China
On behalf of:
Background and aims: Ischemic stroke causes blood-brain barrier (BBB) disruption due to the damage to the integrity of BBB and pericytes play an essential role in the modulation of BBB function. Recent studies have shown that glucose-6-phosphate dehydrogenease(G6PD), the key rate-limiting enzyme in pentose phosphate pathway, is required for establishing vascular mural cells coverage of the dorsal aorta in zebrafish. Considering G6PD deficiency is the most common enzyme disorder worldwide and G6PD-deficient patients have poorer outcomes after ischemic stroke, we investigated the effect of G6PD on the regulation of pericyte recruitment and BBB dysfunction in mice after stroke.
Methods: We performed a transient middle cerebral artery occlusion in both wild-type and CRISPR-mediated G6PD-deficient mice and compared neurobehavioral outcomes, infarct volume, BBB permeability and other histological changes between the two groups.
Results: In the ischemic cortex, G6PD was increased at the onset of reperfusion, reached the peak level 3 hour after reperfusion and returned to baseline levels within a week. We found larger infarct volumes, more BBB leakage and poorer neurobehavioral outcomes in G6PD-deficient mice than in control mice after stroke. Control mice showed increased numbers of pericytes in the ischemic lesion, while G6PD-deficient mice did not.
Conclusions: G6PD appears to regulate pericyte recruitment to support BBB maintenance and repair after ischemic stroke. Further studies are needed to confirm the underlying mechanism.
Disclosures of Interest: No
Abstract N°: 2781
PRECLINICAL SYSTEMATIC REVIEW AND META-ANALYSIS OF THE IMPACT OF AGE AND COMORBIDITIES ON ISCHAEMIC STROKE OUTCOME AND TREATMENT EFFICACY
1Berlin Institute of Health at Charité Universitätsmedizin Berlin, QUEST Center for Responsible Research, Berlin, Germany, 2University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom, 3University of Manchester, Division of Neuroscience & Experimental Psychology, Manchester, United Kingdom
On behalf of:
Background and aims: Insufficient consideration of relevant patient characteristics such as age and comorbidities when modelling stroke in preclinical studies may contribute to difficulties in translating their findings to human health. Here, we present the results of three systematic reviews on the effect of modelling advanced age; hypertension; and diabetes, obesity, and metabolic syndrome, on outcome and treatment effects in animal models of ischaemic stroke.
Methods: For each review we published a study protocol, searched three databases, and performed screening, data extraction and risk of bias (RoB) assessment in duplicate. We identified reports of the impact of stroke modelling and the effect of treatment in aged or comorbid animals and assessed infarct volume, neurofunctional deficits, and mortality outcomes using random-effects multilevel modelling. We assessed study design and quality variables as potential sources of heterogeneity using meta-regression.
Results: We included more than 500 studies. Advanced age and comorbidities resulted in worse outcome, with substantial heterogeneity in the datasets relating to factors including age, sex, and animal species. Meta-regression analyses suggest distinct age-related and comorbidity-specific patterns in response to therapeutic interventions. Poor reporting quality resulted in an unclear RoB assessment for several domains.
Conclusions: These results offer insights into the determinants of ischaemic stroke modelling in animal models and the complex interrelationships between age, comorbidities, and treatment efficacy. We identify factors that may contribute to poor translation, helping to facilitate improved design of future animal studies.
Disclosures of Interest: No
Abstract N°: 1330
BAZEDOXIFENE PROMOTES THE MICROGLIA M2 PHENOTYPE AND PROTECTS THE BLOOD BRAIN BARRIER IN RATS AFTER ISCHEMIC STROKE
Maria Castelló-Ruiz*1, Alicia Aliena-Valero2, Mikahela A. López-Morales2, Julia Baixauli-Martín2, Maria C. Burguete3, Germán Torregrosa2, Juan Bautista Salom Sanvalero2
1Universitat de València, Biología Celular, Biología Funcional y Antropología Física, Valencia, Spain, 2Instituto de Investigación Sanitaria La Fe, Unidad Mixta de Investigación Cerebrovascular, Valencia, Spain, 3Universitat de València, Fisiología, Valencia, Spain
On behalf of:
Background and aims: Inducing microglial polarization from the M1 (pro-inflammatory) to the M2 (anti-inflammatory) phenotype is emerging as a potential strategy for stroke treatment. Bazedoxifene (BZA), a selective estrogen receptor modulator, reduces brain damage in a rat model of transient middle cerebral occlusion (tMCAO) under normoglycemic and diabetic conditions. We hypothesized that the cerebroprotective effects of BZA could be due by its ability to induce microglial polarization towards an M2 phenotype, thus, contributing to the maintenance of the blood-brain barrier (BBB) integrity.
Methods: Male Wistar normoglycemic and streptozotocin-induced diabetic rats were subjected to tMCAO and treated with BZA (1mg/kg, s.c. + 3mg/kg/day, i.p.) or vehicle (DMSO). Neurofunctional tests were performed after 24 h of reperfusion and brain tissue collected to determine cerebral infarct and edema volumes, and expression of mRNA markers of M1/M2 phenoypes and BBB integrity by RT-qPCR.
Results: Treatment with BZA induced significant reduction of brain damage, increases in the expression of the M2 markers (Arg1, Cd206, Il10, and Tgfb1), and decreases of the M1 markers (Cd16, Nos2, Il1b and Tnfa) in the ischemic hemisphere. On the other hand, BZA induced a significant increase of Anxa1, and a significant decrease of Mmp9. Similar results were obtained under diabetic conditions.
Conclusions: BZA induces microglial polarization towards an M2 phenotype. This anti-inflammatory effect contributes to maintain the BBB integrity, may partly explain its cerebroprotective effects, and points to BZA as an effective and safe adjuvant treatment for normoglycemic and diabetic stroke patients subjected to mechanical thrombectomy.
Supported by grant RD21/0006/0014 from ISCIII and FEDER.
Disclosures of Interest: No
Abstract N°: 1337
CIRCULATING NITRIC OXIDE AND COLLATERAL CIRCULATION IN PATIENTS WITH ACUTE ISCHEMIC STROKE TREATED WITH MECHANICAL THROMBECTOMY
Ana Aguilera-Simón*1, Pol Camps Renom2, Marina Guasch Jiménez2, Francisco Moniche Alvarez3, Isabel Fernández-Pérez4, Elena de Celis Ruiz5, Maria del Mar Freijo6, Juan F. Arenillas7, Santiago Trillo Senin8, Joan Martí-Fàbregas2
1Institut de Recerca Sant Pau (IR SANT PAU), Barcelona, Spain, 2Hospital de la Santa Creu i Sant Pau, Neurology, Barcelona, Spain, 3Hospital Universitario Virgen del Rocio, Neurology, Sevilla, Spain, 4Hospital del Mar, Neurology, Barcelona, Spain, 5Hospital Universitario La Paz, Neurology, Madrid, Spain, 6Hospital Universitario Cruces, Neurology, Baracaldo, Spain, 7Hospital Universitario de Valladolid, Valladolid, Spain, 8Hospital Universitario de La Princesa, Neurology, Madrid, Spain
On behalf of: Álvaro Lambea-Gil; Rebeca Marín; Cristina Gallego-Fabrega; Luis Prats-Sánchez; Anna Ramos-Pachón; Jose Pablo Martínez-González; Alejandro Martínez-Domeño; Garbiñe Ezcurra-Díaz
Background and aims: Nitric oxide (NO) is a signalling molecule involved in processes such as vasodilation and neuroprotection. We aimed to study whether the circulating NO levels are associated with collateral circulation (CC) in patients with acute ischaemic stroke (AIS) and large-vessel occlusion (LVO) treated with mechanical thrombectomy (MT).
Methods: Prospective multicentre study of patients with anterior circulation AIS due to LVO (M1, tandem or TICA) treated with MT. Blood samples were obtained at admission. Plasma NO levels were quantified by Nitrate/Nitrite Colorimetric Assay. We collected demographic data, vascular risk factors, previous treatments, vital signs, baseline laboratory results, time metrics, artery segment occluded, Willis circle (WC) completeness, and presence of an anterior temporal artery (ATA). The primary outcome was CC at admission classified by Collateral Score (CS). The CS was assessed by automated software (Brainomix®) from baseline CT angiography and was classified as: poor (filling of ⩽10% of the ischemic area compared to the healthy hemisphere); moderate (11-50%); good (51-90%); excellent (>90%). Bivariate and ordinal logistic regression analyses were performed to predict CS.
Results: We included 238 patients (mean age 73.5±13.4 years, 50.4% women). Median baseline NO was 18.4µM (IQR 14.1-24.4). We observed an inverse association between levels of circulating NO and a higher CS (cORx1 increase NO quartiles=0.74, 95%CI 0.58-0.94; p=0.013). However, this association was no longer significant after adjusting for age, time from stroke onset to admission, WC completeness and presence/absence of ATA.
Conclusions: Circulating NO levels are not an accurate plasmatic biomarker for predicting collateral status in patients with AIS due to LVO.
Disclosures of Interest: No
Abstract N°: 1530
WHITE MATTER PRECONDITIONING AGAINST ISCHEMIC INJURY
Hung Nguyen1, Sarah Zerimech1, Isabela Harmon1, Selva Baltan*1
1Oregon Health & Science University, Department of Anesthesiology and Perioperative Medicine, Portland, United States
On behalf of:
Background and aims: Ischemic preconditioning (IPC) is mainly studied in gray matter, despite white matter injury (WMI) and axon dysfunction contributing to clinical deficits in patients. The need for clinically applicable approaches preconditioning the brain against ischemia is unmet. Casein Kinase 2 (CK2) mediates WMI via Cdk5 and Akt signaling pathways in a spatiotemporal manner. During ischemia Cdk5 inhibition protects WM while Akt/GSK3β inhibition confers post-ischemic protection. CX-4945 exerts WM protection during and after ischemia by inhibiting CK2. We investigated CK2 inhibition preconditioning WM against ischemic injury via signaling pathways as a function of age and sex.
Methods: Isolated optic nerves (MONs) from Thy1 CFP+ mice (male and female, 2–4 and 12–14-month-old) were perfused with artificial cerebrospinal fluid (ACSF) at 37 °C, saturated with oxygen and had extracellular compound action potentials (CAPs) evoked every 30 seconds to record baseline axonal responses for one hour. Ischemia was induced by glucose-free nitrogen saturated ASCF (1 hour with five recovery hours) and 30 minutes before ischemia CX-4945 (5μM) treatment was applied. Selective Cdk5 or phosphorylated Akt (p-Akt) inhibitors deciphered preconditioning signaling pathways; for downstream histological assessment MONs were fixed with 4% paraformaldehyde (PFA).
Results: Young and aging MONs of both sexes withCK2 inhibition using CX-4945 preconditioned axon function and Cdk5 inhibition with Roscovitine preconditioned MONs, but p-Akt inhibition with ARQ092 did not. Oxygen glucose deprivation translocated Cdk5 cytoplasm to the nucleus while Roscovitine prevented Cdk5 translocation.
Conclusions: CK2 inhibition differentially preconditioned WM by regulating the Cdk5 signaling pathways as a function of age and sex.
Disclosures of Interest: No
Abstract N°: 1558
PRECLINICAL REPLICATION STUDY OF PSD-95 INHIBITOR NA-1
Ha Kim1, Seungbum Choi1, Dong-Eog Kim*1
1Dongguk University Ilsan Hospital, Neurology, Goyang, South Korea
On behalf of:
Background and aims: Nerinate (NA-1), a postsynaptic density protein-95 inhibitor, is a clinical-stage stroke neuroprotectant. In a phase-III clinical trial (ESCAPE-NA1), a single intravenous dose of NA-1 did not improve the proportion of patients achieving favorable 3-month functional outcomes after endovascular thrombectomy compared with patients receiving placebo. Thus, we conducted a preclinical replication study to test therapeutic efficacy of NA-1 under the same experimental settings as the dose-translation study that showed significant reduction of infarct volume by ~25% in a mouse model of transient middle cerebral artery occlusion (tMCAO) for either 30 or 60 minutes.
Methods: Male 12-week-old C57BL/6 mice (n=74) underwent tMCAO for 30 or 60 minutes. Mice were randomly assigned to a group treated intravenously with either vehicle control (n=10 and 21, respectively) or 10 nM/g NA-1 (n=10 and 21, respectively). At 1-day poststroke, brain was harvested and sliced in 2-mm thickness for 2,3,5-triphenyl-tetrazolium chloride (TTC) staining after neurological scoring.
Results: The vehicle group and the NA-1 group showed similar infarct volumes at 1 day after either 30 minutes (32.5±6.4 mm3 and 44.7±8.7 mm3; t-test P=0.27) or 60 minutes of tMCAO (113.4±7.6 mm3 and 108.2±7.6 mm3; P=0.63). Neurological scores did not show significant inter-group differences, either (all P>0.05).
Conclusions: We were unable to reproduce the positive results of a prior study, i.e., neuroprotective effects of NA-1 to reduce infarct volume at 1 day after tMCAO for 30 or 60 minutes. Implementation of multicenter animal studies is warranted to enhance the reproducibility and generalizability of preclinical observations.
Disclosures of Interest: No
Abstract N°: 3142
EXPLORING THE ANTI-INFLAMMATORY POTENTIAL OF INHALED NITRIC OXIDE IN EXPERIMENTAL ISCHEMIC STROKE
1Institute for Stroke and Dementia Research (ISD), Experimental Stroke Research, Munich, Germany
On behalf of:
Background and aims: Inhaled nitric oxide (iNO) is known to selectively increase collateral blood flow after ischemic stroke. Since iNO exhibits also anti-adhesive properties on adhering leukocytes we hypothesized that iNO, in addition to its cerebral blood flow modulation, may protect the brain by inhibiting post-ischemic inflammation.
Methods: Male C57BL/6 mice underwent 60 minutes of middle cerebral artery occlusion, followed by inhalation of 50 ppm NO upon reperfusion. Visualization of leukocyte-endothelial interactions (LEI) was conducted in vivo using deep brain 2-photon microscopy. Five hours post-reperfusion, plasma and tissue samples were collected for the analysis of cytokines, adhesion molecules, leukocyte numbers, nitric oxide synthases, and NO metabolites through qPCR, Western blot, ELISA, or chemiluminescence.
Results: iNO application significantly increased NO-related metabolites, nitrite and nitrate, in plasma four-fold (p < 0.001). Furthermore, iNO reduced leukocyte rolling and adhesion by 75% (p < 0.05) and 98% (p < 0.001), respectively. Additionally, iNO downregulated cytokine and ICAM-1 expression by 60% (p < 0.05) and 75% (p < 0.01), respectively.
Conclusions: In the context of focal cerebral ischemia, iNO demonstrated a reduction in inflammatory signaling within cerebral vessels. This suggests the potential for iNO as a novel therapeutic approach for ischemic stroke, emphasizing the need for clinical evaluation to further validate its efficacy in reducing vascular inflammation.
Disclosures of Interest: No
Paper Poster - Pre-Hospital Service Organisation
Abstract N°: 2059
MOBILE STROKE UNIT IN STROKE CARE: IMPACT ON LENGTH OF STAY, DISCHARGE AND COST EFFECTIVENESS
Ayush Arora*1, Kareem El Naamani2, James Glessner3, Roha Herial4, Maureen Deprince5, Stavropoula Tjoumakaris2, Michael Reid Gooch2, Pascal Jabbour2, Robert Rosenwasser2, Nabeel Herial2
1Sidney Kimmel Medical College, Philadelphia, United States, 2Thomas Jefferson University, Philadelphia, United States, 3Jefferson Torresdale Hospital, Philadelphia, United States, 4Jefferson Abington Hospital, Abington, United States, 5Thomas Jefferson University Hospital, Philadelphia, United States
On behalf of:
Background and aims: Mobile Stroke Units (MSUs) allow for expedited delivery of care and proven to improve clinical outcomes in ischemic stroke. Benefits of MSUs in management of hemorrhagic stroke, particularly cost-effectiveness in stroke care remains to be established. We evaluate clinical utility and cost-effectiveness of MSUs
Methods: Retrospective review of stroke inpatient registry at a Thrombectomy-Capable Stroke center of a large health system was conducted. Data reviewed from Aug 2019 – Feb 2023 as part of an ongoing study included patient characteristics, treatment time and response, length of stay (LoS), discharge and estimated cost of hospitalization. Analysis was restricted to ischemic or hemorrhagic stroke and TIA. Cost-effectiveness was evaluated using billing records, LoS, insurance reimbursements compared to conventional evaluation
Results: A total of 482 patients were evaluated by MSU, 145 (30%) were diagnosed with ischemic, 31 (6.4%) with hemorrhagic stroke and 96 (20%) with TIA. Mean age was 74 yrs (37-99), majority were women (55%) and most patients arrived from home (91%). Mean time from arrival to thrombolysis decision was 20 min (SD 7.9). Rate of thrombolysis and thrombectomy were 12.6% and 5.2%. Prehospital RACE score of ⩾5 was reported in 43 (9%). Average LoS was 7 days and common discharge destination was home (30%) and acute rehab (29%) of patients
Conclusions: MSU evaluation was associated with faster treatment times and favorable clinical outcomes with discharge to home or acute rehab. Comparison with conventional transport and triage and cost effectiveness of MSU utilization in a health system will be detailed
Disclosures of Interest: No
Abstract N°: 487
PREHOSPITAL NEUROLOGIC ASSESSMENT USING MOBILE PHONES: COMPARISON BETWEEN NEUROLOGISTS AND EMERGENCY MEDICINE PHYSICIANS
1National Taiwan University Hospital, Department of Emergency Medicine, Taiwan, 2National Taiwan University Cancer Center, Department of Medicine, Taiwan, 3National Taiwan University Hospital, Department of Neurology, Taiwan, 4National Taiwan University Hospital Yun-Lin Branch, Department of Emergency Medicine, Taiwan
On behalf of:
Background and aims: Ambulance-based telestroke may be a promising solution to improving stroke care. We assessed technical feasibility and reliability of prehospital evaluations using commercial mobile phones with fifth-generation wireless communication technology.
Methods: Six standardized patients portrayed scripted stroke scenarios during ambulance transport in an urban city and were remotely evaluated by independent raters using tablets (three neurologists and three emergency physicians) in a hospital, assisted by paramedics (trained in NIHSS assessment) in the ambulance; commercial cellular networks were utilized for videoconferencing transmission. The primary outcomes were mean difference (MD) and correlation of NIHSS scores between the face-to-face and remote assessments. We also examined the Bland-Altman plot for itemized NIHSS components, and Kaplan–Meier curves were used to compare the differences in the duration of the two evaluations between neurologists and emergency physicians.
Results: We conducted 32 ambulance runs and successfully completed all NIHSS examinations. No significant difference was found between the face-to-face and remote evaluations (MD, 0.782; 95% confidence interval [CI], -0.520-0.395). The correlation of NIHSS scores between the two assessment methods was 0.994 (95% CI, 0.945-1.026), and three items (facial palsy, sensation, and extinction and inattention) exhibited score differences between the two methods. There were no significant differences between neurologists and emergency physicians in the mean evaluation duration and NIHSS scores for the two methods.
Conclusions: Prehospital evaluation using commercial mobile phones with fifth-generation wireless communication technology is feasible and reliable during ambulance transport in urban areas. Emergency physicians and neurologists performed similarly in stroke evaluations.
Disclosures of Interest: No
Abstract N°: 492
A DECISION-ANALYTIC MODEL TO EVALUATE COST-EFFECTIVENESS OF REGIONAL IMPLEMENTATION OF A MOBILE STROKE UNIT
Peter van Hulst*1,2, Ruben van de Wijdeven1, Esmee Venema3,4, Florentina Pinckaers5,6,7, Myriam Hunink2,8,9, Aad van der Lugt2, Diederik Dippel1, Hester Lingsma4, Daniel Bos2,8, Bob Roozenbeek1
1Erasmus MC University Medical Center, Department of Neurology, Rotterdam, Netherlands, 2Erasmus MC University Medical Center, Department of Radiology and Nuclear Medicine, Rotterdam, Netherlands, 3Erasmus MC University Medical Center, Emergency Department, Rotterdam, Netherlands, 4Erasmus MC University Medical Center, Department of Public Health, Rotterdam, Netherlands, 5Maastricht University Medical Center, Department of Radiology and Nuclear Medicine, Maastricht, Netherlands, 6Maastricht University Medical Center, School for Cardiovascular Diseases, Maastricht, Netherlands, 7Maastricht University Medical Center, Care and Public Health Research Institute, Maastricht, Netherlands, 8Erasmus MC University Medical Center, Department of Epidemiology, Rotterdam, Netherlands, 9Harvard T.H. Chan school of Public Health, Center for Health Decision Sciences, Boston, United States
On behalf of:
Background and aims: Mobile stroke units (MSU) have the potential to improve outcome of ischemic stroke patients, through shortening onset-to-treatment times. Previous studies have a limited generalizability to non-metropolitan settings and did not evaluate long-term cost-effectiveness. We aimed to develop a regionally adaptable decision model, to evaluate cost-effectiveness of the implementation of an MSU.
Methods: We developed a microsimulation model comparing addition of MSU to dispatch of emergency medical services (EMS), responding to stroke calls with onset-to-alarm time <6 hours, to dispatch of EMS alone. Health states were based on quality-adjusted life years (QALY), translated from the modified Rankin Scale. Discount rates were 1.5% for QALY and 4.0% for cost. We used the South-West of the Netherlands (1,770,000 inhabitants, 7 primary stroke centers, 2 comprehensive stroke centers) as an example. Region-specific inputs for the model, such as population density, age distribution, and driving times, were obtained at the level of postal codes. We assessed the long-term (lifetime horizon) cost-effectiveness from a health care perspective of one-year MSU implementation.
Results: We estimated that, in one year, the MSU was dispatched to 2080 patients with a suspected stroke, resulting in a lifetime gain of 361 additional QALYs and €6,500,000 cost savings. The evaluated MSU+EMS strategy dominated the EMS alone strategy.
Conclusions: Our model suggests that adding an MSU to the dispatch strategy for patients with suspected stroke is cost-effective in our study region. The model facilitates future evaluation of the cost-effectiveness of different scenarios of MSU implementation in other regions with varying characteristics.
Disclosures of Interest: No
Abstract N°: 2122
EARLY DISTINCTION BETWEEN STROKE AND STROKE MIMIC AMONG SUSPECTED STROKE PATIENTS TRANSPORTED BY AMBULANCE
Walid Moudrous*1,2, Luuk Dekker3, Jasper Daems2,4, Esmee Venema4, Henk Kerkhoff5, Ido van den Wijngaard6, Diederik Dippel2, Marieke Wermer7, Nyika Kruyt3, Bob Roozenbeek2
1Maasstad Hospital, Neurology, Rotterdam, Netherlands, 2Erasmus MC, Neurology, Rotterdam, Netherlands, 3Leiden University Medical Center (LUMC), Neurology, Leiden, Netherlands, 4Erasmus MC, Public Health, Rotterdam, Netherlands, 5Albert Schweitzer Hospital, Neurology, Dordrecht, Netherlands, 6HMC Westeinde, Neurology, Den Haag, Netherlands, 7University Medical Center Groningen, Neurology, Groningen, Netherlands
On behalf of: on behalf of the PRESTO and Leiden Prehospital Stroke Study investigators
Background and aims: Early distinction between stroke and stroke mimics is crucial to guide acute treatment. The aim of this study was to compare pre-hospital and in-hospital characteristics of patients with strokes versus mimics and to assess the performance of the paramedic-assessed RACE scale and physician-assessed NIHSS scale in distinguishing both.
Methods: We pooled individual patient data from two prospective observational cohort studies with stroke-code patients transported by ambulance: PRESTO (n=1313) and LPSS (n=2007). Paramedics assessed vital signs and neurological deficits measured with the FAST and RACE scales. Trained stroke physicians performed in-hospital assessments, including the NIHSS. Outcome was the final diagnosis at discharge or 3-month follow-up. Performance of the scales was expressed as the area under the receiver operating characteristic curve (AUC). We used regression modeling to assess associations of patient characteristics and RACE and NIHSS subitems with having a stroke.
Results: Of 3320 included stroke code patients, 2241 (67.5%) had a stroke. Older age, male sex, atrial fibrillation and hypertension were associated with stroke. The AUC of RACE was 0.62 (95%CI: 0.60-0.65) and NIHSS 0.69 (95%CI: 0.67-0.71). The following subitems of RACE had the strongest association with stroke: arm (OR 2.39; 95%CI: 2.0-2.86) and leg (OR 2.32; 95%CI: 1.92-2.8). For NIHSS, these were extinction (OR 6.61; 95%CI: 4.4-9.94), visual deficits (OR 5.70 (95%CI: 3.98-8.17), and gaze deviation (OR 4.84; 95%CI: 3.54-6.63).
Conclusions: The RACE scale is insufficient for early distinction between strokes and stroke mimics. However, in-hospital NIHSS assessment of visual deficits, gaze deviation, and extinction symptoms are the best discriminating.
Disclosures of Interest: No
Abstract N°: 2294
EXAMINING PATTERNS OF PREHOSPITAL STROKE CARE USING AN AMBULANCE DATABASE
BENJAMIN CLISSOLD*1,2, Albert Phan2, Richard Beare3, Velandai Srikanth3, Henry MA2, Thanh Phan2, Ziad Nehme4, Peter Cameron5, John Mcneil2
1Monash Medical Centre, Clayton, Australia, 2Monash University, Faculty of Medicine, Nursing and Health Sciences, Clayton, Australia, 3Monash University Peninsula Campus, Frankston, Australia, 4Ambulance Victoria Research and Evaluation, Melbourne, Australia, 5The Alfred, Melbourne, Australia
On behalf of:
Background and aims: Organised pre-hospital care is critical to ensuring appropriate treatment for all patients with acute ischaemic and haemorrhagic stroke. Ambulance Clinical Practice Guidelines support transfer of patients to dedicated stroke centres for reperfusion therapies and early access to stroke units. The aim of this study is to examine the raw data on ambulance demand in each suburb to identify ambulance resource requirements.
Methods: Retrospective analysis of Victorian Ambulance Clinical Information System (VACIS) prehospital dataset for all patients with a paramedic final primary assessment (diagnosis) of stroke and TIA from January 2017 to December 2021, for the state of Victoria, Australia and dispatch category 1 (time critical/lights and sirens) and 2 (urgent).
Results: The daily number of paramedic diagnosis of stroke and TIA increased from 24 cases in 2017 to 34 cases in 2020 with time series forecasting (Autoregressive integrated moving average) prediction of 39 cases in 2025. Case numbers (>100) were observed to be higher in a zone approximately 10 kilometres from the city centre. Figure 1 shows this zone as yellow and orange coloured suburbs. There was a statistically significant linear relationship between high number of ambulance call-out for stroke and suburbs with high number of populations aged >60-year-old (R2 =0.91, p<0.01).
Conclusions: Understanding sociodemographic data at a suburban level will improve time critical ambulance response to stroke. This analysis may guide future allocation of ambulance services and deployment of ambulances at the suburban level.
Acknowledgements
Ambulance Victoria Centre for Research and Evaluation
Disclosures of Interest: No
Abstract N°: 2604
A HIGHLY SPECIFIC BLOOD BIOMARKERS PANEL TO IDENTIFY ICH AT THE AMBULANCE MIGHT HELP TO START THE INTERACT-3 BUNDLE ON THE ROAD
Ana Barragán*1, Leire Azurmendi2, Rosa Delgado1, Sandrine Reymond2, Antonia Romero Hidalgo3, Ismael Muñoz Martínez4, Antonio Gómez Rodríguez4, Rafael Canto Neguillo5, Jean Charles Sanchez6, Joan Montaner1
1Hospital Universitario Virgen Macarena, Sevilla, Spain, 2Hôpitaux Universitaires de Genève (HUG), Genève, Switzerland, 3Centro de Emergencias Sanitarias 061, Sevilla, Spain, 4Dispositivos de Cuidados Críticos de Urgencias (DCCU), Sevilla, Spain, 5Hospital Sierra Norte High Resolution, Constantina, Spain, 6ABCDx, Barcelona, Spain
On behalf of: BIOFAST study collaborators
Background and aims: Several tools are being investigated to identify stroke patients subtypes out of the hospital to start treatments or shift them directly to the most appropriate stroke center. The aim is to validate a panel of blood biomarkers to differentiate intracerebral hemorrhage (ICH) from ischemic stroke (IS) and mimics in the hyperacute phase.
Methods: Patients with suspected stroke (<6h) were enrolled in BIO-FAST study in an ambulance network (Biomarkers for Initiating Onsite and Faster Ambulance Stroke Therapies, ClinicalTrials.gov:NCT04612218). Blood sample was collected at the ambulance or ED. Glial fibrillary acid protein (GFAP) and N-terminal proB-type natriuretic peptide (NT-proBNP) were measured by immunoassays and integrated with clinical data into panels. Cutoff points were obtained for 100% specificity for ICH using the Panelomix software.
Results: 305 patients were recruited (17% ICH, 66% IS and 17% mimics). ICHs had significantly higher GFAP and IS higher NT-proBNP. Clinical parameters such as neurological scales, blood pressure, heart rate and time to blood sampling enriched panels accuracy. Three different panels containing clinic-biological info were able to identify 47.4%, 45.7% and 51.4% of the ICH patients (sensitivity) with 100% specificity. A less restrictive cutoff yielded a sensitivity of 65.8%, 57.1% and 60% for a specificity of 95.8%, 95.8% and 97.2% respectively.
Conclusions: GFAP and NT-proBNP in combination with simple clinical data reaches 100% specificity for ICH diagnosis in the hyperacute phase. This opens the possibility of applying the INTERACT-3 bundle at the prehospital evaluation in at least half of ICH patients using a point-of-care algorithm.
Disclosures of Interest: No
Abstract N°: 3105
PREHOSPITAL STROKE SCALES FOR MINOR STROKE, A PARANASPP SUBGROUP STUDY
1Norwegian Air Ambulance Foundation, Oslo, Norway, 2University of Oslo Faculty of Medicine, Oslo, Norway, 3Oslo University hospital Ullevål, Department of Neurology, Oslo, Norway, 4OsloMet, Oslo, Norway
On behalf of:
Background and aims: Identification of minor stroke in the prehospital system is challenging, yet 1/3 of Norwegian stroke patients have NIHSS of 0-2 at admission. Studies evaluating prehospital stroke scales have an overall higher median NIHSS at admission and more knowledge on how prehospital stroke scales perform on minor stroke identification is needed.
Methods: Data from the stepped-wedge, cluster-randomised controlled ParaNASPP trial was used to reconstruct 9 prehospital stroke scales (NIHSS, FAST/CPSS, BE-FAST, LAPSS, MASS, MedPacs, OPSS, PreHAST and sNIHSS-EMS), based on presenting symptoms of patients with suspected acute stroke. We assessed whether the presenting symptom in stroke patients with NIHSS 0-2 at admission would be captured and examined by the scales.
Results: 431 patients in the ParaNASPP trial had NIHSS 0-2 at admission. 153(35%) of these had a stroke. The paramedics reported that symptom remission had occurred in 48(18.5%) of the patients. 60(39%) of the patients had TIA. All the scales captured symptoms in a higher proportion of patients with stroke compared with mimics. NIHSS captured symptoms in the highest proportion of stroke patients 141(93%) and mimics 221(79%), while LAPSS captured the least strokes 68(45%) and mimics 57(20%). NIHSS missed 11(7%) of the strokes, whereas LAPSS missed 84(55%).
Conclusions: For patients with suspected acute stroke and NIHSS 0-2 at admission both strokes and mimics have symptoms captured by prehospital stroke scales. Increasing the number of strokes identified comes with the price of more mimics to evaluate, illustrating the difficulty of prehospital identification of minor stroke.
Disclosures of Interest: No
Abstract N°: 495
COMPARISON OF PREHOSPITAL SCALES FOR DETECTING ANTERIOR LARGE-VESSEL OCCLUSION ISCHAEMIC STROKE BY AMBULANCE PARAMEDICS
Luuk Dekker1, Jasper Daems*2,3, Mariam Ali1, Martijne Duvekot4, Ido van den Wijngaard1,5,6, Henk Kerkhoff4, Diederik Dippel2, Marieke Wermer1,7, Bob Roozenbeek2, Nyika Kruyt1,6
1Leiden University Medical Center, Department of Neurology, Leiden, Netherlands, 2Erasmus MC University Medical Center, Department of Neurology, Rotterdam, Netherlands, 3Erasmus MC University Medical Center, Department of Public Health, Rotterdam, Netherlands, 4Albert Schweitzer Hospital, Department of Neurology, Dordrecht, Netherlands, 5Haaglanden Medical Center, Department of Neurology, The Hague, Netherlands, 6University NeuroVascular Center (UNVC) Leiden-the Hague, Netherlands, 7University Medical Center Groningen, Department of Neurology, Groningen, Netherlands
On behalf of: LPSS and PRESTO investigators
Background and aims: Many prehospital scales have been developed for detecting anterior-circulation large-vessel occlusion (aLVO) ischaemic stroke in the ambulance. We aimed to compare the diagnostic performance of existing scales with individual patient data from two large prehospital cohorts.
Methods: We performed a systematic literature search to identify all aLVO scales published until January 2023. We used individual patient data from two large prospective multicentre cohort studies: PRESTO and LPSS. In both studies, stroke code patients who presented <6 hours after onset were assessed by ambulance paramedics and a standard set of neurological deficits was documented before hospital arrival. Scales that could be reconstructed from the prehospital assessments were compared for their ability to detect symptomatic aLVO ischaemic stroke, as diagnosed by stroke physicians in the hospital and based on neuroimaging. Diagnostic performance was assessed with the scales’ area under the receiver operating characteristic curve (AUROC), and sensitivity and specificity at the scales’ prespecified cut points.
Results: The systematic search yielded 63 aLVO scales of which 15 could be reconstructed from the available prehospital assessments. Of 2358 stroke code patients, 231 (10%) had an aLVO ischaemic stroke. The AUROCs ranged from 0.65 (CPSS+gaze, 95%CI:0.61-0.68) to 0.81 (RACE, 95%CI:0.78-0.84). Sensitivity ranged from 0.35 (CPSS+gaze, 95%CI:0.29-0.41) to 0.85 (EMSA and LVOS, 95%CI:0.80-0.90), whilst specificity ranged from 0.58 (EMSA and LVOS, 95%CI:0.56-0.61) to 0.94 (CPSS+gaze, 95%CI:0.93-0.95).
Conclusions: Prehospital aLVO scales have acceptable-to-good diagnostic performance for detecting symptomatic aLVO ischaemic stroke. Performance variation was very large. RACE discriminated best between patients with and without aLVO.
Disclosures of Interest: No
Abstract N°: 2507
PREHOSPITAL SCALE TO DIFFERENTIATE INTRACEREBRAL HEMORRHAGE FROM LARGE-VESSEL OCCLUSION PATIENTS
Albert Freixa Cruz*1, Gerard Mauri Capdevila1, Yhovany Gallego1, Miriam Paul Arias1, Emilio Ruiz Fernández1, Sara Salvany2, Agustín Sancho Saldaña1, Eduardo San Pedro Murillo1, Daniel Vázquez-Justes1, Francisco Purroy1
1Hospital Universitari Arnau de Vilanova, Neurology, Lleida, Spain, 2INSTITUT DE RECERCA BIOMÈDICA DE LLEIDA, Lleida, Spain
On behalf of:
Background and aims: Scales to detect large vessel occlusion (LVO) permit early referrals to a thrombectomy-capable center in the prehospital stroke code setting. Nevertheless, they entail a significant number of false positives corresponding to intracranial hemorrhages (ICH), which delay in medical attention could be potentially harmful. Our study aims to identify easily collectible variables for the development of a scale to differentiate ICH from LVO patients in a prehospital context.
Methods: We conducted a prospective cohort study of stroke code patients between May/2021 and January/2023. Patients were evaluated with CT/CT-Angiography at arrival. We compared clinical variables and vascular risk factors between ICH and LVO patients to design a prehospital ICH screening scale (PreICH).
Results: Out of 989 stroke code patients, we included 190 (66.7%) LVO and 95 (33.3) ICH cases. In the multivariate analysis, headache (odds ratio [OR] 3.56; 1.50-8.43), GCS<8 (OR 8.19; 3.17-21.13), SBP>160mmHg (OR 6.43; 3.37-12.26) and male sex (OR 2.07; 1.13- 3.80) were associated with ICH, while previous hypercholesterolemia (HCL) (OR 0.35; 0.19-0.65) with LVO. The scale was designed assigning a score to each significant variable based on its specific weight: +2 points for SBP>160, +1 for headache, +1 for male sex, +2 for GCS<8, and -1 for HCL. The area under the curve (AUC) was 0.82 (0.77-0.87). A score ⩾4 exhibited a sensitivity of 0.10, specificity of 0.99, and negative predictive value of 0.98.
Conclusions: We present the development of a prehospital scale to discriminate between ICH and LVO patients based on easily detectable variables in the prehospital setting.
Disclosures of Interest: No
Abstract N°: 1810
PREHOSPITAL NOTIFICATION ON A TELESTROKE NETWORK ASSOCIATED TO LOWER DOOR-TO-NEEDLE TIMES FOR ACUTE ISCHEMIC STROKES
1Unidad de TeleACV, Departamento de Salud Digital, Ministerio de Salud de Chile, Santiago, Chile, 2Clinica Alemana, Unidad de Neurología Vascular, Servicio de Neurología, Departamento de Neurología y Psiquiatría, Facultad de Medicina Clínica Alemana Universidad del Desarrollo, Santiago, Chile, 3Universidad del Desarrollo, Centro de Estudios Clínicos, Instituto de Ciencias e Innovación en Medicina, Facultad de Medicina Universidad del Desarrollo Clínica Alemana, Santiago, Chile, 4Universidad del Desarrollo, Escuela de Medicina, Facultad de Medicina Clínica Alemana Universidad del Desarrollo, Santiago, Chile
On behalf of: RUTA Registry: Mirya Arevalo, Fiorella Celsi, Andres Gallardo, Felipe Jurado, Lorena Lara, Diego Rocha, Diego Rojas
Background and aims: Door-to-needle time (DNT) is an important process measure in acute ischemic stroke (AIS) patients receiving intravenous thrombolysis. The purpose of this study was to examine the impact of prenotification by the emergency medical service (EMS) on DNT in a telestroke network of 10 spokes.
Methods: from January 2019 to June 2023 consecutive AIS patients evaluated by the telestroke unit were included. Prenotified AIS patients were compared with those not-prenotified by the EMS to the on-call neurologist.
Results: 2096 AIS patients were evaluated, 48% women. The mean age was 65 years (SD 15.1). 518 (24.7%) were prenotified. 1061 patients were thrombolysed with a median DNT of 52 minutes (IQR 41-66). Prenotification was not associated with a higher rate of thrombolysis (33% vs 36%, p=0.1). Among those thrombolysed patients the DNT was significantly lower in prenotified patients compared to those not-prenotified (46 min IQR 38-57 vs 55 min IQR 43-69, p=0.001). Door-to-CT was also lower in prenotified patients (6 min IQR 4-12 vs 15 min IQR 8-27, p=0.001).
Conclusions: prehospital notification was associated to lower DNT in AIS thrombolysed patients assisted by telestroke. These results highlight the importance of training EMS teams on prenotification of AIS patients, which probably may also impact in functional recovery.
Disclosures of Interest: Yes E.Mazzon reports an educational grant from Boehringer Ingelheim
Abstract N°: 3126
AWARENESS OF SOCIAL INEQUALITY TO INCREASE CAMPAIGN EFFECTIVENESS IN A DANISH STROKE CAMPAIGN
1Copenhagen University Hospital – Herlev and Gentofte, Department of Neurology, Neurovascular Research Unit, Herlev, Denmark, 2University of Copenhagen, Department of Public Health, Copenhagen, Denmark, 3University of Copenhagen, Department of Clinical Medicine, Neuroscience, Copenhagen, Denmark, 4Copenhagen University Hospital Rigshospitalet, Department of Brain and Spinal Cord Injury, Glostrup, Denmark, 5Danish Resuscitation Council, Herlev, Denmark
On behalf of:
Background and aims: Public stroke campaigns appear to have lower effects on recognition of stroke among individuals with shorter education. Research into campaign impacts across educational levels is limited. We aimed to identify effect of a national stroke campaign on knowledge and symptom recognition, examining potential educational disparities.
Methods: In a cross-sectional study spanning 2019-2022, YouGov conducted six post-campaign surveys using a national responder panel. Logistic regression was performed to test associations between campaign recall, knowledge of stroke, symptom recognition, and knowledge of correct call-to-action. Data were stratified by educational level.
Results: Of 7001 individuals (56.7 % women) 44.8% in total recalled the campaign during the period, with increased recall over time. Recall was associated with increased knowledge of stroke (OR: 1.57, 95% CI: 1.42; 1.74) and symptom recognition (OR: 2.11, 95% CI: 1.89; 2.36). The stratified analyses showed that people with shorter education with campaign recall were associated with lower OR for symptom recognition. This difference is for example seen in those who recalled the campaign, individuals with graduate degrees or more had higher OR for symptom recognition (OR: 2,59 95% Cl: 1,95; 3,44) compared to individuals with vocational education (OR 1,93, 95% Cl: 1,59; 2,35).
Conclusions: Campaign recall was associated with improved knowledge of stroke and symptom recognition. In individuals with shorter education the association between campaign recall and symptom recognition was smaller. Such variable impacts of a stroke campaign related to educational levels should be considered when designing and evaluating effect of future stroke campaigns.
Disclosures of Interest: No
Abstract N°: 3139
FACTORS INFLUENCING INTER-HOSPITAL TRANSFER TIME FOR THROMBECTOMY IN FRANCE
1Service SAMU-Urgences, Centre Hospitalier Universitaire Édouard Herriot, Hospices Civils de Lyon, Lyon, France, 2Department of Biostatistics, Hospices Civils de Lyon, Lyon, France, 3INSERM U1290 (RESHAPE), Université Claude Bernard Lyon 1, Lyon, France, 4Réseau Urg'ARA, Lyon, France, 5Unité de Soins Intensifs Neurovasculaires, Department of Neurology, Hôpital Neurologique, University of Lyon, Lyon, France, 6CarMeN Laboratory, INSERM U1060, University Lyon 1, Lyon, France
On behalf of:
Background and aims: Up to 70% of acute ischaemic stroke (AIS) patients with LVO are first evaluated at a hospital without endovascular therapy (EVT) capabilities and need to be tranferred to a center that performs thrombectomy. Reducing inter-hospital transfer time (IHTT) is an important issue as prolonged times to accessing EVT may reduce benefits for eligible patients. We aimed to describe the factors influencing IHTT for EVT.
Methods: This is a retrospective analysis of IHTT of AIS patients for EVT from 34 hospitals to the Lyon University stroke center, covering a population of 3.4 million people in the Auvergne Rhone Alpes region (from January 2018 to December 2020). Univariate linear regression models were constructed in order to identify factors influencing IHTT. All models were adjusted for distance.
Results: 683 patients were transferred to the Lyon University stroke center for EVT. Median transfer time was 81 minutes [IQR 59 ;101]. Median distance was 51 kilometers [IQR 14 ;111]. Linear regression models show that patients transported by Emergency Medical Services (EMS) ambulances (with a nurse on board) and EMS helicopters have a significantly reduced IHTT as compared to patients transported by private ambulances (reduction of 13 minutes and 22 minutes respectively) and a significantly reduced stroke onset to arterial puncture time. Age, gender, clinical severity, occlusion site, intravenous thrombolysis use, admission during off-hours, and admission in an emergency department had no significant influence. The mode of transport was the only factor influencing IHTT.
Conclusions: Our findings emphasize readily modifiable factors that are likely to reduce IHTT for thrombectomy.
Disclosures of Interest: No
Abstract N°: 36
A2L2 SCORE IN ACUTE ISCHEMIC STROKE PATIENT TRIAGE: A LOCAL SITS REGISTRY ANALYSIS
Pasquale Scoppettuolo*1, Jean-Marc Raymackers2, Matthieu Pierre Rutgers3, Jean-François Poma4, Pierre Goffette5, Frank Hammer5, André Peeters1
Background and aims: Two or more National Institutes of Health Stroke Scale (NIHSS) points on each motor items (A2L2 score) have shown good accuracy in predicting large vessel occlusion (LVO) in the prehospital setting. We aimed to study this score for LVO prediction in our stroke network and the impact on clinical outcome of direct admission to comprehensive stroke center (CSC) versus referred from primary stroke centers (PSC) for mechanical thrombectomy (MT).
Methods: From the Safe Implementation of Thrombolysis in Stroke (SITS) registry of patients receiving reperfusion therapy, we retrospectively computed the A2L2 score from the admission NIHSS to test the diagnostic accuracy for LVO prediction. Outcome from patients with LVO directly coming to the CSC or referred from PSC were subsequently compared.
Results: From the 853 patients with acute ischemic stroke (67% LVO), A2L2 was positive in 52%. A2L2 score (Odds-ratio 4.6; p=0.001), smoking (Odds-ratio 2.1; p=0.017), atrial fibrillation (Odds-ratio 1.6; p=0.015) and younger age (Odds-ratio 0.98; p=0.008) were independent predictors of LVO. A2L2 score showed 82%/49% positive/negative predictive values with 68% accuracy (64%/72% sensitivity/specificity) for LVO prediction. The 3-month modified-Rankin scale did not differ in CSC vs referred from PSCs patients with LVO. A2L2 score (Odds-ratio 2.2; p=0.004), atrial fibrillation (Odds-ratio 4.1; p=0.001), longer onset-to-groin time (Odds-ratio 1.003; p=0.007) and MT procedure (Odds-ratio 1.01; p=0.001) were independent predictors of poor outcome.
Conclusions: A2L2 score is an independent predictor of LVO and poor outcome after reperfusion therapy. Patient profile and procedure-related factors influence clinical outcome more than CSC admission.
Disclosures of Interest: No
Abstract N°: 172
AMBULANCE DURATION AT HOSPITAL FOR STROKE CALLS BEFORE AND DURING THE COVID-19 PANDEMIC IN IRELAND
Emma Mccarthy1, Edel Burton*1, Rory Quinn2, Kieran Crosbie-Staunton3, Patricia Kearney1, Vera Mccarthy4, Claire Buckley1, David Willis5, Siobhán Masterson2, Cathal O'donnell2
1University College Cork, School of Public Health, Cork, Ireland, 2National Ambulance Service, Clinical Directorate, Dooradoyle, Ireland, 3National Ambulance Service, National Emergency Operations Centre, Tallaght, Ireland, 4University College Cork, School of Nursing and Midwifery, Cork, Ireland, 5National Ambulance Service, Portfolio Management Office, Tralee, Ireland
On behalf of: Prehospital Care of Stroke (PHoCoS) Consortium
Background and aims: Prehospital management of stroke/transient ischemic attacks (TIA) aims to shorten time to diagnosis and treatment. The aim of this study was to investigate the impact of the COVID-19 pandemic on “duration at hospital time” for suspected stroke/TIA in Ireland.
Methods: A quasi-experimental study of patients ⩾ 18 years with suspected stroke/TIA from 2018-2021, based on data from a national ambulance service, was conducted. The COVID-19 period was defined as 01/03/2020-31/12/2021 and pre-COVID-19 as 01/01/2018-29/02/2020. The Health Protection Surveillance Centre defines 5 waves of COVID-19. Partial data for wave 5 is included. Duration at hospital time is the time the resource (vehicle) reaches the hospital until time clear/stood down. A t-test was used to compare duration at hospital time between pre-COVID-19 and COVID-19. An ANOVA and post-hoc Tukey test was used to compare this time interval between pre-COVID-19, and waves 1-5 of COVID-19.
Results: Of 40,004 cases, 19,826 and 20,178 were during the pre-COVID-19 and COVID-19 period respectively. Mean duration at hospital time increased from 41.5 minutes (± 24.4) pre-COVID-19 to 47.4 minutes (±27.2) during COVID-19 (p<0.001). An ANOVA test showed differences in duration at hospital time between the time periods (f=321, p<0.001). The post-hoc test showed a statistically significant difference in duration at hospital time for all comparisons, except for pre-COVID-19 and wave 1; pre-COVID-19 and wave 2; wave 4 and wave 5.
Conclusions: Our findings indicate that mean duration at hospital increased during the COVID-19 period, with the most significant increase occurring from wave 4 onwards.
Disclosures of Interest: No
Abstract N°: 896
EFFECT OF INTER-HOSPITAL TRANSFER IN PATIENTS WITH LARGE VESSEL OCCLUSION STROKE AND MILD SYMPTOMS
Eva Groenendijk*1,2, Nabila Wali2, Jeffrey Stolp2, Maritta van Stigt1,2, Henk Marquering3,4, Paul Nederkoorn2, Jonathan Coutinho2
1Amsterdam UMC, location AMC, Department of Clinical Neurophysiology, Amsterdam, Netherlands, 2Amsterdam UMC, location AMC, Department of Neurology, Amsterdam, Netherlands, 3Amsterdam UMC, location AMC, Department of Radiology and Nuclear Medicine, Amsterdam, Netherlands, 4Amsterdam UMC, location AMC, Department of Biomedical Engineering and Physics, Amsterdam, Netherlands
On behalf of:
Background and aims: Prehospital stroke triage methods typically focus on identifying large vessel occlusion (LVO) strokes and diagnostic accuracy is assessed across all LVO stroke patients, irrespective of stroke severity. The effect of inter-hospital transfer for endovascular thrombectomy (EVT) has, however, primarily been studied in moderately to severely affected patients. We aimed to determine the effect of inter-hospital transfer on LVO stroke patients with mild symptoms.
Methods: We included LVO stroke patients with mild symptoms (baseline NIHSS score <6) from a single comprehensive stroke centre. The primary outcome of the study was functional independence (90-day modified Rankin Scale [mRS] score of 0-2). Secondary outcomes included time from first presentation to intravenous thrombolysis (DNT) and to groin puncture (DGT).
Results: Out of 83 included patients, 64 (77%) LVO stroke patients with mild symptoms were transferred. Intravenous thrombolytics were administered in 39/64 (61%) vs 7/19 (37%) patients, and EVT was performed in 38/64 (59%) vs 14/19 (74%) patients. Transferred patients had similar DNTs (median: 28 [IQR=20-49] vs 30 [IQR=25-120] minutes; P=0.40), but longer DGTs (median: 156 [IQR=113-258] vs 64 [IQR=49-82] minutes; P<0.001). In spite of this treatment delay, there was no statistically significant difference in the rate of functional independence (42/64 (66% [95% CI 54%-77%]) vs 15/19 (79% [95% CI 61%-97%]); P=0.40; Figure 1).
Conclusions: Among patients with LVO stroke and mild symptoms, inter-hospital transfer was associated with longer treatment times. However, there was no statistically significant difference in functional independence.
90-day outcome of transferred and directly presented patients.
Disclosures of Interest: No
Abstract N°: 3092
PREHOSPITAL DELAY AND RATE THROMOBOLYSIS IN ACUTE POSTERIOR CIRCULATION CEREBRAL STROKES: A LATIN-AMERICAN MULTICENTRY STROKE REGISTRY (LA COFRADIA)
Andrés Alberto Mercado Pompa*1, Idarmis Reyes-Cortes1, Charles Huamani2, David Vidal-Gonzalez3, Vanessa Cano Nigenda1, Victor Oré-Montalvo4, Hebert Puente-Vila5, Melissa Pérez6, Iván Baracaldo-Santamaría7, Antonio Arauz Gongora1
1Instituto Nacional de Neurología y Neurocirugía Manuel Velasco Suárez, Stroke Clinic, Mexico, City, Mexico, 2Universidad Andina del Cusco, Cusco, Peru, 3Hospital de Especialidades Centro Médico Nacional de Occidente, IMSS, Guadalajara, Mexico, 4Hospital Nacional Adolfo Guevara Velasco, Cusco, Peru, 5Hospital Nacional Guillermo Almenara Irigoyen, Lima, Peru, 6Hospital Nacional Carlos Seguín, Arequipa, Peru, 7Clínica Nueva, Bogotá, Colombia
On behalf of: Enriquez-Peregrino K, Garcia-Rivera J, Moreno-Arias J, Camacho-Gamez I, Romero-Vucovich R, Pereda-Castillo A, López-Pizano A, Aguilar-Parra L, López-Gonzalez A, García-Quintero R
Background and aims: Intravenous thrombolysis(IVT) has a very narrow therapeutic window. Posterior circulation stroke(PCS) presents with symptoms that are difficult to associate with an emergency, which can contribute to delays in arrival to stroke centers. Our aim was to evaluate the arrival time in patients with PCS and the probability of receiving IVT when compared to Anterior Circulation Stroke(ACS).
Methods: Multicenter study in Peru, Colombia and Mexico in adults with acute stroke, treated between 2019 to 2023. Demographic characteristics: initial NIHSS, times from onset of symptoms to admission(O-D), door-image(D-I) and door-needle(D-N) were evaluated. The probability(OR) of receiving thrombolysis was calculated according to compromised circulation.
Results: We included 1,192 patients, 657(55.1%) were male, median age was 70yo[IQR 59-79], 420(35.2%) had PCS. We found differences in median O-D time (PCS 16 hours,IQR 6- 48 vs ACS 9 hours, IQR 4-22, p<0.001 and the rate of thrombolysis (PCS 6.1% vs QCS 15.7%, p<0.001). Arriving in therapeutic window(<4.5h) was the most strongly associated variable with receiving thrombolysis(aOR 71, 95% CI 30-166), while the compromised circulation (PCS vs ACS) only showed significant association in the crude analysis but not after the adjust model
Conclusions: We found a greater delay in arrival time in patients with PCS, in addition to a lower rate of thrombolysis. Not arriving <4.5 hrs was strongly associated with no thrombolysis regardless of compromised circulation. These resultsprobably reflect that PCS symptoms are poorly identified by patients, therefore tools to improve their recognition could reduce arrival time and increase therate of thrombolysis.
Disclosures of Interest: No
Abstract N°: 3120
PREHOSPITAL STROKE DIAGNOSTICS USING THREE DIFFERENT SIMULATION MODULES - A PRAGMATIC PILOT STUDY
Emma Christensen1, Helge Fagerheim Bugge1,2,3, Jostein Hagmo2, Karianne Larsen2,3, Astrid Karina Harring4, Jørgen Ibsen5, Mona Guterud1,2, Else Charlotte Sandset2,3, Maren Ranhoff Hov*2,3,4
1University of Oslo Faculty of Medicine, Oslo, Norway, 2Norwegian Air Ambulance Foundation, Oslo, Norway, 3Oslo University hospital Ullevål, Oslo, Norway, 4OsloMet, Oslo, Norway, 5Ringerike Hospital, Norway
On behalf of:
Background and aims: The optimal pathway for ultra-early diagnostics and treatment in patients with acute stroke remains uncertain. The aim of this study was to investigate the use of 3 modalities of prehospital CT for acute stroke patients in rural areas on time to prehospital treatment decision.
Methods: In this pragmatic, simulation, pilot study three modalities of prehospital CT were investigated: a regular ambulance with transport to a paramedic run rural stationary CT machine, a Mobile Stroke Unit (MSU), and a helicopter with a simulated CT machine. Each modality completed 20 real life dispatches combined with predetermined animated patient cases with acute stroke symptoms and CT images. The primary endpoint of the study was time from alarm to prehospital treatment decision.
Results: Median time spent from alarm to the treatment decision differed significantly between the three groups (p=0.0005), with 38 minutes for regular ambulance with rural CT, 33 minutes for the MSU and 30 minutes for the helicopter. There was no difference in time when comparing regular ambulance with MSU, nor when comparing the MSU with the helicopter. There was a difference in time to treatment decision between the regular ambulance and the helicopter (p<0.0001).
Conclusions: Prehospital CT can be organized in several ways depending on geography, resources and need. Further research on rural MSU, stationary paramedic run CT and helicopter CT is needed to find the optimal strategy.
Disclosures of Interest: No
Abstract N°: 3123
PREVALENCE AND PATTERNS OF PRE-HOSPITAL DELAY IN ACUTE STROKE - A MIXED-METHODS OBSERVATIONAL COHORT STUDY IN AN IRISH COMPEHENSIVE STROKE CENTRE
Deirdre McCartan*1, Anne Hickey1, David Williams1
1Royal College of Surgeons in Ireland, Dublin, Ireland
On behalf of:
Background and aims: Pre-hospital delay in acute ischaemic stroke (AIS) remains a barrier to increased intervention rates. The decision to attend hospital for assessment is complex involving emotional, cognitive and behavioural responses, and is influenced not only by stroke symptom type and severity, but also the context in which they are experienced. We aimed to gain a deeper understanding of factors that may lead to delayed presentations in an Irish stroke population.
Methods: Consecutive patients admitted to the stroke service in an Irish comprehensive stroke centre between June and December 2023 were assessed against inclusion criteria. A survey interview was completed with participants, with integration of survey results and interview findings. Questions posed related to knowledge and awareness of stroke, stroke interventions and best first response to symptoms. Patient-reported behavioural responses to their symptoms and factors influencing decision to attend hospital and transportation mode were recorded.
Results: 396 patients were assessed for inclusion. 293 had a confirmed diagnosis of AIS of which 91 were recruited. 31% of those recruited presented outside of thrombolysis or thrombectomy windows. Onset time was known in just 37%. Patient factors associated with delayed presentations included hesitation and denial, moral rationalisation regarding personal health care utilisation and knowledge of available acute interventions.
Conclusions: A disparity exists between patient awareness of symptoms of stroke and their knowledge of improvements in acute stroke pathways and time-dependent treatments. Local health system challenges can impact willingness to act quickly in response to symptoms. Bridging this gap may improve the proportion of patients presenting within treatment windows.
Disclosures of Interest: No
Paper Poster – Prevention
Abstract N°: 2994
THE PREVENTION OF STROKE IN HIGH-RISK HYPERTENSIVE PATIENTS
1Tashkent medical academy, Neurology, Tashkent, Uzbekistan
On behalf of:
Background and aims: Blood-pressure-lowering drug therapy is a major strategy of preventing stroke among hypertensive patients. However, the optimal preventive drug therapy is still uncertain. We compared the stroke prevention efficacy with the combination of amlodipine with diuretics or angiotensin II receptor blocker.
Methods: In a prospective, randomized, open-label, blinded-endpoint trial, 13542 hypertensive patients at high risk for cardiovascular events were assigned to receive treatment with either amlodipine plus amiloride/hydrochlorothiazide (n = 6776) or telmisartan (n = 6766). Patients were recruited from 180 clinical centers across China and followed up for the incidence of stroke and prespecified cardiovascular outcomes.
Results: The median follow-up was 41 months. Compared with the baseline, mean blood pressure declined similarly, by 26.4/14.8 mm Hg in amlodipine-diuretics group and 26.3/14.9 mm Hg in amlodipine-telmisartan group. The primary cardiovascular outcome was reduced significantly in the amlodipine-diuretics group (hazard ratio [HR], 0.78, p = 0.011). Of note, there were 290 stroke events over the course of the trial: 127 (1.9%) in the diuretics-based group and 163 (2.4%) in the telmisartan-based group, resulting in a 21.3% risk reduction (HR, 0.79, p = 0.044). There were similar trends toward reduction in ischemic stroke (HR, 0.80; p = 0.073) and hemorrhagic stroke (HR, 0.72; p = 0.321) between the two treatment groups.
Conclusions: The diuretics-based combination treatment was more efficacious in preventing stroke than telmisartan-based therapy in hypertensive patients with high cardiovascular risk, independent of blood pressure reduction.
Disclosures of Interest: No
Abstract N°: 190
CLOPIDOGREL PREVENTIVE EFFECT BASED ON CYTOCHROME P450 2C19 GENOTYPE IN ISCHAEMIC STROKE
Yo Han Jung1, Sang Won Han2, Tae-Jin Song3, Jinkwon Kim4, Young Dae Kim5, Jong Yun Lee6, Seong Hwan Ahn7, Hye Sun Lee8, Kyung-Yul Lee*1
1Gangnam Severance Hospital, Yonsei University College of Medicine, Neurology, Seoul, South Korea, 2Sanggye Paik Hospital, Inje University College of Medicine, Neurology, Seoul, South Korea, 3Seoul Hospital, College of Medicine, Ewha Womans University, Neurology, Seoul, South Korea, 4Yongin Severance Hospital, Yonsei University College of Medicine, Neurology, Seoul, South Korea, 5Severance Hospital, Yonsei University College of Medicine, Neurology, Seoul, South Korea, 6National Medical Center, Neurology, Seoul, South Korea, 7Chosun University Hospital, Chosun University School of Medicine, Neurology, Gwangju, South Korea, 8Biostatistics Collaboration Unit, Yonsei University College of Medicine, Research Affairs, Seoul, South Korea
On behalf of:
Background and aims: Cytochrome P450 2C19 (CYP2C19) genotypes (extensive metabolizer (EM), intermediate metabolizer (IM), and poor metabolizer (PM)) are related to the metabolism of clopidogrel for the prevention of cardiovascular disease and cerebral infarction. This study aimed to investigate differences in the efficacy and safety outcome in patients with acute ischaemic stroke according to CYP2C19 genotypes.
Methods: Multicentre, prospective, observational, clinical trial conducted from September 2019 to January 2023. We included patients who had an acute ischaemic stroke and received clopidogrel within 72 hours after onset. CYP2C19 genotyping was performed to classify patients based on their metabolizer status (PM, IM, and EM). The primary efficacy outcome was the composite of stroke, myocardial infarction, or cardiovascular death within 6 months. The safety outcome was all-cause mortality and fatal bleeding.
Results: A total of 2,927 patients were enrolled in the PLATELET trial from 37 clinical sites. The mean age was 65.3 years, and 66.3% were men. Among these patients, 15 were excluded. Of the remaining 2,912 patients, 61.3% were PM or IM, and 38.7% were EM. The primary outcome occurred more frequently in the PM/IM group compared to the EM group (2.8% [49 of 1,785] vs 1.6% [18 of 1,125], log-rank p-value = 0.048). Safety outcomes did not show any significant differences in major bleeding and cause of death (p=0.559, 0.525, respectively).
Conclusions: This study showed that patients with CPY2C19 genotype of PM/IM metabolizer had more likelihood in composite cardiovascular events, especially recurrent stroke after ischaemic stroke. (Trial registration number NCT04072705).
Disclosures of Interest: No
Abstract N°: 319
OVERWEIGHT AND OBESITY IN A MULTICENTER ASYMPOTMATIC CAROTID ATHEROSCLEROSIS TRIAL
James Meschia1, Tanya Turan*2, Jenifer Voeks2, Carlos Mena-Hurtado3, Michael Jones4, Wayne Clark5, Navdeep Sangha6, Lloyd Edwards7, George Howard7, Thomas Brott1
1Mayo Clinic, Neurology, Jacksonville, United States, 2Medical University of South Carolina, Neurology, CHARLESTON, United States, 3Yale School of Medicine, Vascular Surgery, New Haven, United States, 4Baptist Heart and Vascular Institute, Cardiology, Lexington, United States, 5Oregon Health & Science University, Neurology, Portland, United States, 6Southern California Permanente Group/Kaiser Permanente, Neurology, Los Angeles, United States, 7University of Alabama at Birmingham, Biostatistics, Birmingham, United States
On behalf of:
Background and aims: CREST-2 is a pair of parallel randomized trials of intensive medical management (IMM) with or without endarterectomy and IMM with or without stenting in patients with asymptomatic high-grade carotid atherostenosis. Primary risk factor targets are a systolic BP < 130/90 mmHg and LDL <70 mg/dL. Overweight and obesity are secondary risk factors, for which centralized diet and exercise counseling are given. Semaglutide was recently shown to lower the risk of a composite endpoint of stroke and death in patients with preexisting cardiovascular disease and overweight or obesity. Our aim was to estimate how many CREST-2 patients would be potential candidates for obesity pharmacotherapy.
Methods: Patients are periodically assessed by central review of site-provided data on height, weight, blood pressure, and lipid levels. Site study staff are instructed when to consider further action for patients who are out of target on primary risk factors. Patients also receive lifestyle coaching via telephone. Trial data were reviewed as of 12/13/23.
Results: 2376 patients were included in this analysis. At baseline 42.4% were overweight and 37.2% obese in the endarterectomy trial. At baseline, 40.2% were overweight and 38.2% were obese in the stenting trial. For both trials at last follow-up 40.1% were overweight (BMI 25 - 29.9 kg/m²) and 30.7% were obese (BMI≥30 kg/m²). Of the 1821 patients with BMI 25 at baseline, 55.7% were not diabetic.
Conclusions: There are several opportunities to improve on control of overweight and obesity in the CREST-2 trial and new pharmacotherapies should be considered.
Disclosures of Interest: No
Abstract N°: 1396
EFFECT OF FACTOR XIA INHIBITION BY MILVEXIAN ON COAGULATION BIOMARKERS IN PATIENTS WITH ACUTE IS OR TIA IN THE AXIOMATIC-SSP TRIAL
Zhaoqing Wang*1, Aiqing He1, Warren Anderson1, Anja Kahl1, Grigor Abelian1, Matthias Endres2, Mark Donovan1, Danshi LI1, Dave Gailani3, Mike Sharma4
1Bristol Myers Squibb, 2Dept Neurology and Center for Stroke Research Berlin, Charité- Universitätsmedizin Berlin, 3Vanderbilt University Medical Center, 4Population Health Research Institute
On behalf of:
Background and aims: In the AXIOMATIC-SSP phase 2b trial (ClinicalTrials.gov:NCT03766581), oral milvexian was associated with fewer symptomatic ischaemic strokes (IS) compared to placebo without increased fatal or intracranial bleeding. Coagulation and thrombosis biomarkers were measured to evaluate pharmacodynamics and mechanisms of anticoagulation effect of milvexian in this study.
Methods: Participants were randomized to one of 5 doses of milvexian or placebo and treated for 90 days on top of antiplatelet therapy. Plasma samples were obtained at Baseline (Day1 Pre-dose), Day1, Day21 and Day90 and analysed for activated partial thromboplastin time (aPTT), prothrombin time (PT) and D-dimer at the central laboratory.
Results: Milvexian prolonged aPTT at all time points and doses; at Day90, mean percentage increases from baseline were 38.7% (25mg QD), 58.3% (25mg BID), 97.3% (50mg BID), 140.8% (100mg BID), and 193.6% (200mg BID) (Figure 1). D-dimer decreased in all groups from baseline. Milvexian treatment at 25mg BID and above resulted in greater decrease of D-dimer compared to placebo (Figure 2), the mean percentage decreases from baseline were -17.8% (placebo), -22.4% (25mg QD), -28.4% (25mg BID), -24.7% (50mg BID), -29.9% (100mg BID), and -36.4% (200mg BID) at Day90. There were minimal changes in PT in all groups.
Conclusions: Milvexian prolonged aPTT in a dose-dependent manner with minimal effects on PT, demonstrating pharmacodynamic effects consistent with milvexian’s mechanism of action as a highly selective inhibitor of FXIa. Additionally, milvexian decreased D-dimer levels compared to placebo, suggesting milvexian reduced hypercoagulability in patients with stroke and transient ischaemic attack (TIA).
Disclosures of Interest: Yes ZW is an employee of Bristol Myers Squibb and may hold stock in Bristol Myers Squibb.
Abstract N°: 2283
DUAL VERSUS SINGLE ANTIPLATELET THERAPY IN PATIENTS WITH ACUTE ISCHEMIC NON-CARDIOEMBOLIC STROKE AND AVAILABLE MRI - PLACEHOLDER
Gian Marco De Marchis*1,2, Anna Toebak1,2, Tolga Dittrich1,2, Angela Wang3, Ashkan Shoamanesh3, Eric Smith4, Hardi Mundl5, Pablo Colorado6, Stuart Connolly7, Robert Hart3
1Cantonal Hospital St. Gallen, Department of Neurology and Stroke Center, St. Gallen, Switzerland, 2University of Basel, Department of Clinical Research, Basel, Switzerland, 3McMaster University, Population Health Research Institute, Division of Neurology, Hamilton, Canada, 4Hotchkiss Brain Institute, Cumming School of Medicine, University of Calgary, Department of Clinical Neuroscience, Calgary, Canada, 5Bayer AG, TA Thrombosis and Vascular Medicine, Wuppertal, Germany, 6Bayer US Pharmaceuticals, Hanover, United States, 7McMaster University, Population Health Research Institute, Department of Medicine, Hamilton, Canada
On behalf of:
Background and aims: Dual antiplatelet therapy (DAPT) is recommended over single antiplatelet therapy (SAPT) to prevent early recurrence after an acute, non-cardioembolic stroke and NIHSS⩽3. In clinical practice, DAPT is prescribed also to patients with NIHSS>3 or with large infarcts. We aimed to compare DAPT versus SAPT in a broad population of patients with stroke.
Methods: Post-hoc analysis within the PACIFIC-STROKE Trial, which enrolled patients with non-cardioembolic stroke and NIHSS⩽15. Participants were prescribed DAPT or SAPT at the discretion of the treating physician and were randomized to placebo or asundexian, a factor XIa inhibitor. The efficacy endpoint was the rate of recurrent symptomatic ischemic stroke during follow-up or covert brain infarcts on MRI at 26 weeks. The safety endpoint was the rate of major or clinically relevant non-major bleeding over total study follow-up.
Results: Among 1590 patients (32% with NIHSS over 3 points), 634 (40%) received DAPT. Median follow-up was 11.5 months. The rates of the efficacy endpoint did not differ between the DAPT and SAPT arm (16.9% versus 16.7%, respectively, punivariate=0.36, pmultivariable=0.24). A trend for significant effect modification by index stroke size on MRI was present: the odds ratio (OR) for the efficacy endpoint between the DAPT and SAPT arm was 0.67 (95%CI 0.43-1.03) in patients with qualifying infarcts <15mm vs. 1.15 (95%CI 0.80-1.66) in patients with infarcts ⩾15mm (pinteraction=0.06). The rate of the safety endpoint was 2.7% versus 4.6% in the SAPT versus DAPT arm (p=0.047). Additional analysis including safety endpoints will be presented at ESOC24.
Conclusions: Pending: PLACEHOLDER ABSTRACT.
Disclosures of Interest: Yes Authors were part of the steering committee of PACIFIC Stroke
Abstract N°: 114
EARLY-START ANTIPLATELET THERAPY AFTER SURGERY IN PATIENTS WITH SPONTANEOUS INTRACEREBRAL HEMORRHAGE
Qingyuan Liu1, Jun Wu1, Shaohua Mo1, Kaiwen Wang*1, Michael Levitt2, David Hasan3, Chengcheng Zhu4, Yong Cao1, Shuo Wang1, Jizong Zhao1
1Beijing Tiantan Hospital, Capital Medical University, Department of Neurosurgery, Beijing, China, 2University of Washington, Department of Neurological Surgery, Seattle, United States, 3Duke University, Department of Neurosurgery, Durham, United States, 4University of Washingto, Department of Radiology, Seattle, United States
On behalf of:
Background and aims: The effect and safety of early staring antiplatelet therapy postoperatively for patients with spontaneous intracerebral hemorrhage has not been extensively studied.
Methods: We conducted a multicenter, prospective, open-label, randomized trial involving patients with spontaneous intracerebral hemorrhage and at a high risk of ischemic events postoperatively (with previous cadio-/cerebrovascular ischemic diseases or Atherosclerotic Cardiovascular Disease Risk Estimator 10-year risk >10%). Patients were randomly assigned in a 1:1 ratio on the 72 hours after surgery to undergo early starting antiplatelet therapy (aspirin, 100 mg once daily, starting on 72 hours after surgery) or normal starting antiplatelet (aspirin, 100 mg once daily, starting on 30 days after surgery). The primary efficacy outcome was new major cardiovascular, cerebrovascular, peripheral vascular events (MACCPE), and the primary safety outcome was any intracranial bleeding events, both within 90 days after surgery.
Results: A total of 269 patients were enrolled; 134 were assigned to the early-starting group and 135 to the normal-starting group. MACCPE occurred within 90 days after surgery in 27 patients (20.1%) in the early-start group and in 42 patients (31.1%) in the normal-start group (treatment effect, 0.56; 95% confidence interval, 0.32 to 0.98; P=0.041). Any intracranial bleeding occurred in 1 patient (0.7%) in the early-start group and in 4 patients (3.0%) in the normal-start group.
Conclusions: In a trial conducted in China, patients with spontaneous intracerebral hemorrhage had a lower risk of MACCPE postoperatively with early starting antiplatelet therapy than with normal starting antiplatelet therapy, with no increasing risk of bleeding events.
Disclosures of Interest: No
Abstract N°: 278
EXPLORING ASSOCIATION BETWEEN DAYTIME HEART RATE VARIABILITY AND INTRACRANIAL ATHEROSCLEROSIS BY HIGH RESOLUTION MRI
1The Hong Kong Polytechnic University, Department of Health Technology and Informatics, HONG KONG, Hong Kong, 2Shanghai General Hospital, Department of Neurology, Shang Hai, China, 3The Second Affiliated Hospital of Guangzhou University of Chinese Medicine, Department of Brain Function, Guang Zhou, China
On behalf of:
Background and aims: Low heart rate variability (HRV), a surrogate of cardiac autonomic dysfunction, has been associated with increased cardiovascular mortality and incident stroke. In Asian, intracranial atherosclerosis (ICAS) is a major cause of ischemic stroke which carries a higher risk of stroke recurrence. In this community-based study in Hong Kong, we aimed to investigate the relationship between daytime HRV measured by 3-minute ECG monitoring and ICAS identified by high-resolution magnetic resonance imaging (HR-MRI).
Methods: Consecutive 227 adults (mean age, 64.0±6.5; male, n= 98) were recruited from November 2022 to October 2023. Based on 3-minute ECG monitoring, HRV was assessed as the standard deviation of normal-to-normal intervals (SDNN), which was categorized into quartile for data analysis. On HR-MRI vessel wall scanning, the prevalence and severity of ICAS were assessed in middle cerebral artery (MCA), vertebral artery (VA) and basilar artery (BA), together with plaque characteristics (eccentricity, thickening patterns, remodelling index, and surface morphology).
Results: A total of 181 arterial lesions caused by ICAS were detected in 55% subjects, including MCAs (71/454,), VAs (75/436), and BAs (35/227). Eighty-one subjects with significant HRV deviation had a higher degree of intracranial arterial stenosis (p= 0.010) and more eccentric plaques (p = 0.041). In multivariate analyses, lower SDNN was independently associated with the presence of ICAS (OR 1.68, 95% CI 1.15 – 2.46, p=0.007).
Conclusions: Our study suggested that lower HRV was correlated with an increased risk of ICAS. Further prospective evidence is needed to validate the causal relationship between HRV and ICAS.
Disclosures of Interest: No
Abstract N°: 1394
ASSOCIATION BETWEEN ALDH4A1 BLOOD LEVELS AND MANIFEST ATHEROSCLEROTIC DISEASE: RESULTS FROM THE BIOSIGNAL STUDY
Tolga Dittrich*1,2, Annaelle Zietz2,3, Felix Gross4, Lilian Kriemler5, Markus Arnold4, Gawinecka Joanna6, Arnold von Eckardstein7, Mira Katan2,3,4, Gian Marco De Marchis1,2
1Cantonal Hospital St. Gallen, Department of Neurology and Stroke Center, St. Gallen, Switzerland, 2University of Basel, Department of Clinical Research, Basel, Switzerland, 3University Hospital Basel, Neurology and Stroke Center, Basel, Switzerland, 4University Hospital and University of Zurich, Department of Neurology, Zürich, Switzerland, 5Catonal Hospital of Schaffhausen, Clinic of Internal Medicine, Schaffhausen, Switzerland, 6University Hospital of Zurich, Switzerland, Institute of Clinical Chemistry, 7University Hospital of Zurich, Institute of Clinical Chemistry, Switzerland
On behalf of: BIOSIGNAL Study Team
Background and aims: The role of Aldehyde Dehydrogenase 4 Family Member A1 (ALDH4A1) in patients with atherosclerotic diseases remains unclear. We explored the association of circulating ALDH4A1 with atherosclerotic disease outcomes in stroke patients.
Methods: Multicenter study using data from the prospective BIOSIGNAL cohort, including patients with acute ischemic stroke between 2014 and 2017. ALDH4A1 plasma levels were measured in stored samples collected within 24 hours after stroke onset. Primary outcome was large artery atherosclerotic stroke (LAAS) origin. Secondary outcomes were atherosclerotic disease outcomes such as the maximum intima-media-thickness (IMT), the degree of stenosis on ultrasound, and a composite for atherosclerotic disease burden (large artery atherosclerotic index stroke, history of myocardial infarction, coronary artery disease, or peripheral artery disease). Logistic regression analyses were performed to examine the association between ALDH4A1 plasma levels (absolute and log-transformed) and the primary and secondary outcomes.
Results: Of 1,759 stroke patients, 84.5% had available ALDH4A1 measurements. We found no consistent association between circulating ALDH4A1 levels and LAAS (logALDH4A1 aOR 0.97, 95%CI 0.79-1.21, p=0.81) nor the secondary outcome measures including the maximum IMT, stenosis degree or the composite for atherosclerotic disease burden. Sensitivity analysis using inverse probability of treatment weighting were in line with the main findings.
Conclusions: In acute stroke patients, no association was found between clinically relevant atherosclerotic disease outcomes and circulating ALDH4A1 levels. In addition, the maximum IMT – as a subclinical marker of atherosclerosis – was also not associated with elevated ALDH4H1 levels.
Disclosures of Interest: No
Abstract N°: 2581
EFFICACY OF ADD ON THERAPY WITH ASPIRIN OR CLOPIDOGREL TO STANDARD MEDICAL THERAPY ALONE IN TUBERCULAR MENINGITIS: ACT-TBM TRIAL
1All India Institute of Medical Sciences, Department of Neurology, New Delhi, India, 2Postgraduate Institute of Medical Education and Research, Department of Neurology, Chandigarh, India, 3All India Institute of Medical Sciences, Department of Neuroradiology, New Delhi, India, 4All India Institute of Medical Sciences, Center for Community Medicine, New Delhi, India, 5All India Institute of Medical Sciences, Department of Medicine, New Delhi, India, 6Postgraduate Institute of Medical Education and Research, Department of Emergency Medicine, Chandigarh, India
On behalf of: The ACT-TBM group: Achal Srivastava, Vishnu V.Y, Ashutosh Biswas, Sanjeev Sinha, Naval K Vikram, V. Sreenivas, Navneet Sharma, Paramjeet Singh, Kusum Sharma, Bikash Medhi, Chirag Ahuja
Background and aims: Vascular complication in Tubercular meningitis (TBM) is an important cause of mortality and morbidity. Intervention with antiplatelets may help reduce the complication. We hypothesised that add-on therapy with aspirin or clopidogrel and antitubercular-therapy (ATT) will be safe and effective in reducing cerebral infarction and/or clinical stroke in TBM compared with ATT alone.
Methods: This was a randomized, open-label, superiority trial with blinded outcome assessment. Patients with suspected TBM were randomised to receive either add-on oral aspirin-75mg, clopidogrel-75mg along with ATT or only ATT. MRI-brain and MR-Angiogram at baseline, 1- and 3-months from randomisation were performed. Primary outcome was reduction in occurrence of either imaging-based cerebral infarction or clinical stroke at 1- and 3-months. Safety outcome: occurrence of minor/major bleeding. Secondary outcome: mortality at 1- and 3-months.
Results: 237 TBM patients were randomised – group-1 Aspirin (77,32.48%), group-2 Clopidogrel (77,32.48%) and group-3 Standard (88,37.13%). Occurrence of imaging-based infarction at 1-month was 6(9.8%) in group-1, 8(12%) in group-2 and 7(11%) in group-3 (p>0.9); at 3-month was 2(3.5%), 3(5.0%) and 2(3.6%) respectively (p>0.9). Occurrence of stroke at 1-month was 1(1.4%) in group-1, none(0.0%) in group-2 and 3(4.3%) in group-3 (p=0.12); at 3-month was 2(3.3%), 1(1.6%) and 2(3.4%) respectively (p=0.7). Composite outcome (imaging-based infarction/clinical stroke) was 9(12%) in group-1, 10(13%) in group-2 and 11(13%) in group-3 (p>0.9). There was no difference in minor/major bleeding and mortality between the groups.
Conclusions: No difference was observed by an add-on therapy of antiplatelets to standard care compared to standard care alone on imaging-based cerebral infarction, clinical stroke or mortality.
Disclosures of Interest: No
Abstract N°: 1924
INSULIN RESISTANCE AND WHITE MATTER MICROSTRUCTURAL ABNORMALITIES IN NONDIABETIC ADULT: A POPULATION-BASED STUDY
Mengyuan Zhou*1, Yilong Wang2
1Beijing Tiantan Hospital Affiliated to Capital Medical University, Neurology, Beijing, China, 2Beijing Tiantan Hospital, Department of Neurology, Beijing, China
On behalf of:
Background and aims: Insulin resistance is of growing concern yet its association with white matter integrity remains controversial. We aimed to investigate the association between insulin resistance and white matter integrity in nondiabetic adults.
Methods: This cross-sectional analysis was conducted based on the PolyvasculaR Evaluation for Cognitive Impairment and vaScular Events (PRECISE) study. A total of 1709 Nondiabetic community-dwelling adults with available brain magnetic resonance imaging and diffusion tensor imaging data and completed oral glucose tolerance test were included. Insulin resistance was measured non-invasively by insulin sensitivity indices (ISI), including ISIcomposite and ISI0,120, as well as homeostasis model assessment of insulin resistance (HOMA-IR). White matter microstructure abnormalities were identified by diffusion tensor imaging along with tract-based spatial statistics analysis to compare diffusion metrics between groups. The multivariable linear regression models were applied to measure the association between white matter microstructure abnormalities and insulin resistance.
Results: We found that insulin resistance was associated with a significant increase in mean diffusivity, axial diffusivity, and radial diffusivity extensively in cerebral white matter in regions such as the anterior corona radiata, superior corona radiata, anterior limb of internal capsule, external capsule, and body of corpus callosum (Fig. 1). The pattern of association was more marked for ISIcomposite and ISI0,120.
Conclusions: Our findings indicate a significant association between insulin resistance and white matter microstructural abnormalities in nondiabetic middle-aged community residents. It was suggested that prophylactic strategies of maintaining a low insulin resistance status may ameliorate disturbances in white matter integrity.
Disclosures of Interest: No
Abstract N°: 2315
THE 6-MONTHS FOLLOW-UP OF THE TREAT-CAD TRIAL: ASPIRIN VERSUS ANTICOAGULATION FOR STROKE PREVENTION IN CERVICAL ARTERY DISSECTION
Stefan Engelter1,2,3, Lukas Enz*2,3, Flavia Ravanelli2,3, Josefin Kaufmann1,2,3, Sandro Fischer1,2,3, Christian Nolte4,5, Hanne Christensen6,7, Susanne Wegener8,9, Philippe Lyrer2,3, Christopher Tränka1,2,3
1Universitäre Altersmedizin FELIX PLATTER, Basel, Switzerland, 2Universität Basel, Basel, Switzerland, 3Universitätsspital Basel, Department of Neurology and Stroke Center, Basel, Switzerland, 4Berlin Institute of Health, Berlin, Germany, 5Charité – Universitätsmedizin Berlin, Department of Neurology with Experimental Neurology, Berlin, Germany, 6Copenhagen University, Department of Neurology, København, Denmark, 7Bispebjerg Hospital, Department of Neurology, København, Denmark, 8University of Zurich, Division of Vascular Neurology and Neurorehabilitation, Zürich, Switzerland, 9University Hospital of Zürich, Division of Vascular Neurology and Neurorehabilitation, Zürich, Switzerland
On behalf of: TREAT-CAD-Investigators
Background and aims: Cervical artery dissection (CeAD) is a major cause of stroke in the young and the optimal choice and duration of antithrombotic treatment for stroke prevention are debated. The aim of this analysis was to compare occurrence of ischaemic and haemorrhagic events in the 3-6 months period after CeAD in participants on aspirin versus anticoagulation.
Methods: We used data from the extended follow-up of the randomised controlled TREAT-CAD trial (TREATment of Cervical Artery Dissection). Exposure was Aspirin (100-300mg/d) or anticoagulation (Vitamin-K-antagonists, target-INR 2-3). We report ischaemic and haemorrhagic outcomes occurring 3-6 months after randomisation, stratified (i) to the treatment taken from 3-6 months (as-treated-analysis) and (ii) to the treatment randomised to and taken from 0-3 months (per-protocol-analysis). Main outcomes were new clinical (ischaemic stroke, intracranial/major extracranial bleeding, death) and new MR-imaging outcomes (ischaemic or haemorrhagic brain lesion).
Results: Among the 122 participants of the as-treated-analysis, 3/92 (3.3%) aspirin-treated participants had new clinical (n=1, a gastrointestinal-bleed) or MR-imaging outcomes (n=2; haemorrhagic brain lesions) at 6 months, while 1/29 (3.4%) anticoagulated participant had a MR-imaging outcome (n=1, haemorrhagic brain lesion), yielding an absolute difference between groups of 0.2% (95%-CI -8.0% to 7.5%). These results were virtually identical to those of the per-protocol-analysis (0.15% (95%-CI -6.1% to 6.4%).
Conclusions: For the period 3-6 months after CeAD - no advantage of either aspirin or anticoagulation was observed. All outcome events between 3-6 months were haemorrhagic outcomes, while ischaemic outcomes in the trial had only occurred within 0-3 months (mostly within 7-14 days.
Disclosures of Interest: No
Abstract N°: 202
EVALUATING THE IMPACT OF OMEGA-3 FATTY ACID ON LIPID PROFILES IN ADULTS WITH PPARG POLYMORPHISMS
Evgeny Pokushalov*1,1,2, Andrey Ponomarenko1, Sevda Bayramova1, Claire Garcia2, Inessa Pak1, Evgenya Shrainer1, Elena Voronina3, Ekaterina Sokolova3, Michael Johnson2, Richard Miller2
1Center for New Medical Technologies, Research & Development, NOVOSIBIRSK, 2Triangel Scientific, Scientific research laboratory, San Francisco, United States, 3Institute of Chemical Biology and Fundamental Medicine, Siberian Branch of the Russian Academy of Sciences, Genetic, Novosibirsk, Russian Federation
On behalf of:
Background and aims: Emerging evidence suggests that PPARG gene polymorphisms may influence lipid metabolism and cardiovascular risk, with omega-3 fatty acids proposed to modulate these effects. This study aims to assess the effects of fish oil supplementation on cardiovascular markers among adults with PPARG gene polymorphisms in a randomized, double-blind, placebo-controlled trial.
Methods: A cohort of 102 patients, aged 40-75 with LDL-C 70-190 mg/dL, was randomized to receive either 2000 mg of omega-3 fatty acids or a placebo daily for 90 days. Lipid and metabolic panels were evaluated at baseline and study conclusion.
Results: Ninety-nine participants completed the trial. In the omega-3 group with PPARG polymorphisms, LDL-C was reduced by 15.4% (95% CI: -19.8% to -11.0%), compared with a 2.6% decrease in the placebo group (95% CI: -4.1% to -1.1%; p<0.01). In the omega-3 group without PPARG polymorphisms, LDL-C was reduced by 3.7% (95% CI: -6.9% to -0.6%), not significantly different from the placebo group's reduction of 2.9% (95% CI: -5.1% to -0.8%; p=0.28). The reduction in LDL-C was notably 11.7% greater in those with PPARG polymorphisms than in those without (95% CI: -19.3% to -4.0%; p<0.01). Triglycerides decreased by 21.3% in omega-3 recipients with PPARG polymorphisms (95% CI: -26.5% to -16.2%; p<0.01), with no significant changes in HDL-C, total cholesterol, or hsCRP levels in any groups. Minor allele frequencies and baseline characteristics were comparable, ensuring a balanced genetic representation.
Conclusions: Omega-3 fatty acids significantly reduce LDL-C and triglycerides in carriers of PPARG polymorphisms, underlining the potential for genetic-driven personalization of cardiovascular interventions.
Disclosures of Interest: No
Abstract N°: 1305
IMAGING FEATURES OF ATRIAL FIBRILLATION-ASSOCIATED ISCHEMIA IN CRYPTOGENIC STROKE PATIENTS, THE NOR-FIB STUDY
Anna Tancin Lambert1,2, Dag Ottar Sætre3, Barbara Ratajczak-Tretel1,2, Jostein Gleditsch2,3, Gudrun Anette Hoeie4, Riadh Al-Ani4, Maiju Pesonen5, Dan Atar2,6, Anne Hege Aamodt*7
1Østfold Hospital Trust, Department of Neurology, Grålum, Norway, 2University of Oslo, Institute of Clinical Medicine, Oslo, Norway, 3Østfold Hospital Trust, Department of Radiology, Grålum, Norway, 4Østfold Hospital Trust, Department of Cardiology, Grålum, Norway, 5Oslo University Hospital, Center for Biostatistics and Epidemiology, Oslo, Norway, 6Oslo University hospital Ullevål, Department of Cardiology, Oslo, Norway, 7Oslo University Hospital, Rikshospitalet, Department of Neurology, Oslo, Norway
On behalf of: The NOR-FIB study group
Background and aims: Specific imaging features might identify cryptogenic stroke (CS) patients with high risk of underlying atrial fibrillation (AF) in need of prolonged monitoring with insertable cardiac monitors (ICMs). The purpose of this study was to evaluate brain imaging features in CS patients and their utility as AF predictors.
Methods: Single-center analysis of the AF incidence in a CS population rhythm-monitored by ICMs for 12 months. Brain computed tomography or magnetic resonance imaging were assessed for chronic and acute infarctions and white matter hyperintensities (WMH) and included in a score for AF prediction. Receiver operating characteristics (ROC) curve was used to evaluate the discriminative ability of the score and for its dichotomization for predictive model.
Results: Age, periventricular WMH (PVWMH), acute lesion size, and medium vessel occlusion were significantly associated with underlying AF. Chronic cortical and cerebellar stroke, and acute cortical stroke were numerically more frequent in the AF than non-AF group. A score consisting of six features (range of 0-6 points) was proposed (Table 1). Area under ROC curve was 0.735 and a score of ⩾ 3 points was a predictor of AF, odds ratio 12.90 [95% confidence interval (CI) 2.86−58.15] (Figure 1).
Conclusions: Suggested combination of imaging and clinical features was shown to identify CS patients with an increased risk of underlying AF.
Disclosures of Interest: Yes Devices used in the study were partially financed by Medtronic
Abstract N°: 2732
WARFARIN BUT NOT NOAC IN ADDITION ON ANTIPLATELET THERAPY SHOULD BE ASSOCIATED WITH INCREASE OF MORTALITY IN PATIENTS WITH INTRACEREBRAL HEMORRHAGE
Koichi Nomura*1, Satoshi Suda2, Kazumi Kimura3
1Shioda Hospital, Neurology, Katsuura, Japan, 2Saitama Medical School, Neurology, Hidaka, Japan, 3Nippon Medical School, Neurology, Tokyo, Japan
On behalf of:
Background and aims: Prior concomitant use of vitamin K antagonists (VKAs) and antiplatelet (AP) therapy increase the hematoma volume and mortality compared with VKA monotherapy in patients with intracranial hemorrhage (ICH). However, the prior concomitant use of non-vitamin K oral antagonists (NOACs) and AP has not been clarified.
Methods: We conducted a PASTA registry study, which was an observational, multicenter, registry of 1043 patients with stroke receiving oral anticoagulants (OACs) in Japan. In the present study, ICH from the PASTA registry was used to analyze the clinical characteristics including mortality among the four groups (NOAC, VKA, NOAC and AP, and VKA and AP).
Results: Among the 216 patients with ICH, 118 (54.6%), 27 (12.5%), 55 (25.5%), 16 (7.4%) were taking NOAC monotherapy, NOAC and AP, VKA, and VKA and AP, respectively. In-hospital mortality rates were the highest in VKA and AP (31.3%) than in NOACs (11.9%), NOACs and AP (7.4%), and VKA (7.3%). Multivariate logistic regression analysis demonstrated that the concomitant use of VKA and AP (odds ratio [OR], 20.57; 95% confidence interval [CI], 1.75–241.75, p €i0= 0.0162), initial National Institutes of Health Stroke Scale score (OR, 1.21; 95%CI, 1.10–1.37, p €i0< €i00.0001), hematoma volume (OR, 1.41; 95%CI, 1.10–1.90, p €i0= 0.066), and systolic blood pressure (OR, 1.31; 95%CI, 1.00–1.75, p €i0= 0.0422) were independently associated with in-hospital mortality.
Conclusions: Although VKA in addition to AP therapy could increase the in-hospital mortality, NOAC and AP did not increase the hematoma volume, stroke severity, or mortality compared to NOAC monotherapy.
Disclosures of Interest: No
Abstract N°: 635
AVERTTO DETECTS LARGE VESSEL OCCLUSION VIA CAROTID MONITORING
Hilla Ben-Pazi*1, Shady Jahshan2, Sam Zibman1, Samuel Goldstein1, Shirley Ackerman1, Ornit Yanai1, Sagi Har Nof3, Marc Ribo Jacobi4
1Avertto Medical, Aderet, Israel, 2Galilee Medical Center, Nahariyya, Israel, 3Rabin Medical Center, Petah Tikva, Israel, 4La Vall d'Hebron, Barcelona, Spain
On behalf of:
Background and aims: To detect acute large vessel occlusions (LVOs) via continuous, noninvasive monitoring of carotid pulse waves.
Methods: In an open, prospective multi-center study in Rabin and Galilee Medical Centers, Israel, and Val d’Hebron, Spain, skin displacement over the carotid arteries was recorded using a custom-built, first-generation noninvasive bi-lateral bimorph piezoelectric sensor-based system (Avertto101) during endovascular procedures, such as balloon inflation creating temporary LVOs. To maximize signal quality, we applied signal analysis, comparing patients’ pulse waves to prototypical waveforms. We then used a Deep Learning to learn each patient’s baseline activity. Occlusions were detected as sustained deviations from the personalized baseline. We optimized the alert threshold to minimize false negatives.
Results: Most (38/59) participants underwent prolonged balloon occlusion (>30 seconds), mainly during carotid artery stenting (CAS), which provided sufficient length to train the model. Of those, we recorded high-quality bilateral pulse waveforms in 27 patients (age 70±8 years; M: F, 25:2). The model learned personalized baseline hemodynamic activity during a calibration period in each participant. Following this period, the model continuously outputs an LVO probability measure, which can trigger an alarm when it passes a threshold. When using the deviation from the personal baseline, we detected LVOs with 83% accuracy (median of 100%), applying a threshold of 50% occlusion probability. Accuracy was affected by false positives in five participants and failure to detect the occlusion in another eight. The threshold did not vary according to gender, age, and BMI.
Conclusions: Carotid pulse wave changes can be detected during acute LVO using a noninvasive device.
Disclosures of Interest: Yes H Ben Pazi, MD, is the founder and CEO of Avertto.
Abstract N°: 501
TRANSCRANIAL DOPPLER BUBBLE STUDY TECHNIQUE IN A CLINICAL TRIAL: VALSALVA AND BODY POSITION MATTER, IV LOCATION DOES NOT
Mark Rubin*1, Ruchir Shah2, Teddy Youn3, John Volpi4, Aaron Stayman5, Theodore Lowenkopf6, Georgios Tsivgoulis7, Andrei Alexandrov8
1Edward Hines, Jr. VA Hospital, Neurology, Hines, United States, 2CHI Memorial Hospital - Chattanooga, Chattanooga, United States, 3Barrow Neurological Institute, Phoenix, United States, 4Houston Methodist Hospital, Houston, United States, 5Swedish Hospital - First Hill Campus, Seattle, United States, 6Providence Portland Medical Center, Portland, United States, 7National and Kapodistrian University of Athens, Athens, Greece, 8Banner - University Medicine Neurosciences Clinic, Phoenix, United States
On behalf of:
Background and aims: This is a secondary analysis of BUBL (NCT04604015) to ascertain the effects of transcranial Doppler (TCD) bubble study technique on right to left shunt (RLS) presence and size. Valsalva maneuver, body positioning and IV placement have been reported to affect results in observational studies but not in the setting of a clinical trial.
Methods: We conducted a prospective, single-arm device clinical trial of robot-assisted TCD (raTCD) versus TTE for RLS diagnosis at 6 clinical sites in patients who presented with an event suspicious for embolic cerebrovascular ischemia. Robot-assisted TCD was performed with standard TCD bubble study technique, including runs with and without Valsalva, supine and at 45o incline. IV location was tracked, acknowledging recommendations for right antecubital placement as technically ideal.
Results: A total of 154 patients were enrolled, 129 evaluable (intent to scan) and 121 subjects had complete data per protocol. In the intent to scan cohort, mean age was 60±15 years, 47% were women, and all qualifying events were diagnosed as ischemic stroke or transient ischemic attack. Valsalva maneuver and bed positioning increased RLS grade in 28% and 19%, respectively, including patients from RLS absence to presence and “small” to “large” grades. Antecubital IV placement had a RLS positivity rate of 63.6% and “other location” had a RLS positivity rate of 63.2%.
Conclusions: Technical aspects of TCD bubble study performance matter, including Valsalva maneuver and upright positioning, increasing not only sensitivity but the size grade of the RLS. IV location does not affect rate of RLS detection.
Disclosures of Interest: Yes Consultant, NovaSignal (study sponsor)
Abstract N°: 1840
INTEGRATED CARE IMPROVES LONG TERM-FOLLOW-UP AFTER TRANSIENT ISCHEMIC ATTACK OR MINOR STROKE PATIENTS
Francisco Purroy*1,2,3, Maria Oro4, Meritxell Juanos4, Ines Cruz4, Gisela Galindo4, Antoni Plana4, Yhovany Gallego Sánchez1,3, Gerard Mauri Capdevila1,3
1Hospital Universitari Arnau de Vilanova de Lleida, Neurology, Lleida, Spain, 2Universitat de Lleida, Lleida, Spain, 3IRBLLEIDA, Lleida, Spain, 4Institut Català de la Salut, Lleida, Spain
On behalf of: Lleida TIA Intervention Study
Background and aims: The Lleida TIA Intervention Study (LLETIS) was a clinical trial aimed at evaluating the effects on vascular risk factors control (VRF), stroke recurrence (SR) and other vascular events (composite endpoint [CE]) of an intervention program designed to enhance the implementation of recommended stroke prevention strategies in primary care (ClinicalTrial.gov number: NCT04524078).
Methods: TIA and minor stroke (NIHSS<=3) subjects were recruited and randomly allocated into two groups: The usual care group (CG] (n=50) and the intervention group (IG)(n=50). Patients in the IG were attended to by primary care physicians and nurses, both previously trained in secondary stroke prevention. The primary endpoint was the improvement in the control of VRF at 12 months, while the secondary endpoint included the reduction of SR and CE, assessed at 12 months, 5 years, and 10 years.
Results: The baseline demographic, clinical, and imaging characteristics were comparable between the two trial groups, however there were a higher proportion of atheromatous etiology episodes in the CG (22% vs. 8%). At 12-months, a higher proportion of IG patients achieved blood pressure objectives (52.2% vs. 36.4%; P= 0.263) compared to CG. There were no differences in the control of other VRF. After a median follow-up of 10.0 (6.4-10.1) years, SR tended to be lower (HR 0.47; 0.20-1.09 and the risk of CE adjusted by etiology was significantly lower (HR 0.36; 0.15-0.87) in the IG.
Conclusions: The LLETIS model tended to demonstrate superiority over usual care for the early control of some VRF, and reduced the risk of CE in the long-term follow-up.
Disclosures of Interest: No
Paper Poster - Prognosis and Outcome after Stroke
Abstract N°: 3171
UTILIZING THE MODIFIED RANKIN SCALE AS A PROGNOSTIC TOOL FOR COMMUNITY PARTICIPATION IN STROKE SURVIVORS AFTER HOSPITAL DISCHARGE
Te-Hsun Hung*1, Shih-Pin Hsu1, Feng-Hang Chang1,2
1Graduate Institute of Injury Prevention and Control, College of Public Health, Taipei Medical University, New Taipei City, Taiwan, 2Department of Physical Medicine and Rehabilitation, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan
On behalf of:
Background and aims: Inpatient services often provide limited insight into the post-discharge evolution of community life. Establishing prognostic evidence for long-term participation outcomes is essential and warranted. This study aims to delineate group participation trends among individuals with different functional statuses and make comparisons between each subgroup.
Methods: This study presents a secondary analysis of a cohort derived from two prospective observational studies. Six hundred and forty-four first-ever stroke survivors, assessed at discharge, 3-month, and 1-year follow-ups, were included. Participants were stratified by the modified Rankin Scale score at discharge for dichotomous and trichotomous comparisons of participation courses, measured by the Participation Measure–3 Domains, 4 Dimensions (PM-3D4D). Mixed-effect regression models were employed to establish predictive models and identify differences in trends.
Results: Individuals achieving independence in activities of daily living (ADL) at discharge demonstrate greater progress and overall participation compared to those requiring assistance. Similarly, individuals who can walk independently but still need assistance with ADL show a comparable pattern in social participation to those who are independent in ADL. However, they demonstrate a less favorable trend in community participation. Conversely, individuals needing constant care exhibit less favorable trends, engaging in fewer social activities and facing heightened challenges post-discharge.
Conclusions: Dichotomous and trichotomous analyses of modified Rankin Scale scores are found to provide informative prognosis information regarding the long-term recovery course. The study underscores the imperative need for services and interventions for individuals requiring constant care at discharge to facilitate their return to the community setting.
Disclosures of Interest: No
Abstract N°: 2820
POST-STROKE DEPRESSION IN THE CONTEXT OF THE COVID-19 PANDEMIC
Isabella Stuckart1, Jessica Barlinn1, Simon Winzer*1, Uwe Helbig1, Nastasja Pfaff1, Lisa Frost1, Sandy Klewin2, Bernhard Rosengarten2, Timo Siepmann1, Kristian Barlinn1
1Faculty of Medicine and University Hospital Carl Gustav Carus, Technische Universität Dresden, Germany, Department of Neurology, Dresden, Germany, 2Klinikum Chemnitz gGmbH, Department of Neurology, Chemnitz, Germany
On behalf of:
Background and aims: Post-stroke depression (PSD) affects about one-third of stroke survivors within the first year. The COVID-19 pandemic imposed containment measures like social distancing that might have impacted PSD risk. Considering the pandemic as a model for investigating effects of critical life events on mental health, we aimed to investigate its impact on PSD risk among stroke survivors.
Methods: We analyzed prospective data from our post-stroke care program (SOS-Care) including patients with TIA, ischemic stroke and intracerebral hemorrhage. According to social distancing measures mandated by authorities in the study region, the COVID-19 pandemic was categorized into pre-pandemic (11/11-03/20), pandemic (04/20-02/22) and post-pandemic (03/22-to date). PSD was assessed using the Patient Health Questionnaire-9 (PHQ-9) at 6 and 12 months, with scores ⩾10 indicating depression.
Results: Of 1580 patients enrolled between 11/11 and 12/22, 1016 patients with PHQ-9 data were analyzed (mean age 70±12.7, 46% female, median baseline NIHSS score 2 [IQR 4]). There were no differences in 6- and 12-month PSD rates across pre-pandemic (32.4% and 22.1%), pandemic (34.5% and 21.3%) and post-pandemic (33.1% and 25.9%) periods (p=ns). Similarly, no differences were observed between pandemic (34.5% and 21.3%) and any non-pandemic (37.7% and 23.3%) periods (p=ns). Time series analysis adjusted for sex and baseline NIHSS scores, showed no association between the pandemic and changes in PHQ-9 scores (p=ns).
Conclusions: The pandemic did not appear to significantly affect the frequency of PSD in our cohort of stroke survivors. Further analysis will explore its impact on health-related quality of life and anxiety after stroke.
Disclosures of Interest: No
Abstract N°: 1572
STATINS FOR PREVENTING THE RISK OF RECURRENT STROKE IN PATIENTS WITH FIRST EVER STROKE - A NETWORK META-ANALYSIS
1All India Institute of Medical Sciences, Clinical Research Unit, New Delhi, India, 2All India Institute of Medical Sciences, Neurology, New Delhi, India
On behalf of:
Background and aims: Statins, renowned for their lipid-lowering and potential pleiotropic effects, have emerged as promising candidates for preventing recurrent strokes. This study aims to conduct a comprehensive Network Meta-Analysis to evaluate the efficacy of statins in preventing the risk of recurrent stroke in patients having first-ever stroke.
Methods: An extensive literature search utilizing PubMed, EMBASE, Web of Science, clinicaltrials.gov, and Google Scholar for randomized controlled Trials (RCTs) published upto 31st Dec 2023 was performed. Outcomes including risk of recurrent stroke, all-cause mortality and functional recovery associated with Statin use vs. Placebo were examined.
Results: A total of 18 RCTs involving 6409 stroke patients in Statin use and 6432 stroke patients in placebo group were included. Upon comparing various statins, administration of atorvastatin 80 mg/daily [Risk Ratio (RR)= 0.69; 95% CI, 0.42 to 0.78] followed by simvastatin 40 mg/day (RR)= 0.71; 95% CI, 0.35 to 0.83) were associated with the significant reduction of recurrent stroke in Stain vs. placebo was noted. However, Statin use did not significantly alter for all-cause mortality and good functional recovery.
Conclusions: Our Network Meta-Analysis reveals promising prospects for statins as effective agents in preventing the risk of recurrent strokes among patients with a history of first-ever stroke. Our evidence suggests that further guidelines can be developed, recommending the use of statins as a means to provide protection against the recurrent stroke.
Disclosures of Interest: No
Abstract N°: 1381
AUTOMATICALLY QUANTIFIED FOLLOW-UP IMAGING BIOMARKERS AS PREDICTORS OF CLINICAL OUTCOMES AFTER ACUTE ISCHAEMIC STROKE– A RWE STUDY
George Harston*1,2, Davide Carone1,2, Stephen Gerry3, Zoe Woodhead2, Orell Mielke4, Mark Heise5, Agnieszka Swierczak6, Greg Bass6, Sonya Abraham5
1Oxford University Hospitals NHSFT, Oxford, United Kingdom, 2Brainomix Limited, Oxford, United Kingdom, 3Centre for Statistics in Medicine, Nuffield Department of Orthopaedics, Rheumatology & Musculoskeletal Sciences, University of Oxford, Oxford, United Kingdom, 4CSL Behring, Marburg, Germany, 5CSL Behring, King of Prussia, United States, 6CSL Innovation, Melbourne, Australia
On behalf of:
Background and aims: Follow-up infarct volume (FIV) is a proposed surrogate endpoint for proof-of-concept clinical studies in acute ischaemic stroke (AIS). This study aimed to validate an automated multimodal FIV algorithm and describe the association between FIV and clinical outcome to support use of this endpoint.
Methods: Data were gathered for adult AIS patients undergoing mechanical thrombectomy with follow-up imaging 12–96h from initial assessment. Image processing used the AI-powered software Brainomix 360 Stroke (Brainomix Ltd, Oxford, UK) and Brainomix core lab research software. Measures included total FIV and composites: ischaemic injury, haemorrhagic transformation and oedema. Primary endpoint was modified Rankin Scale (mRS) at 3 months. Secondary endpoint was NIHSS at 24 hours.
Results: Imaging was available for 979 patients (median age 71 years), representative of the thrombectomy stroke population. Median premorbid mRS was 0 and baseline NIHSS was 16 (IQR: 12–21). Median 24h NIHSS was 11 (5–17); 35% of patients had mRS 0–2 at 3 months. Median FIV was 28.1mL (11–112mL).
FIV was significantly associated with 3-month mRS (concordance 0.73, p<0.001) and NIHSS at 24h (adj R2 0.21, p<0.001). Oedema, infarct growth, penumbral salvage and haemorrhagic transformation were significantly associated with clinical outcomes. In multivariate analysis, FIV remained strongly associated with 3-month mRS. Association was greatest for follow-up imaging >36h from baseline. FIV showed a bimodal distribution consistent with success/failure of recanalisation during thrombectomy.
Conclusions: This study validates the prognostic significance of automated FIV and its composites as mechanistic endpoints for early-stage trials in AIS.
Disclosures of Interest: Yes GC, DC & ZW are employed by and have share options in Brainomix. SG has no conflicts of interest to declare. OM, MH, AS, GB & SA are employed by and own stock in CSL.
Abstract N°: 1471
TOWARD AN EFFICIENT, ROBUST, AND RELEVANT ASSESSMENT OF INDEPENDENCE IN ACTIVITIES OF DAILY LIVING
1University of Glasgow, Glasgow, United Kingdom, 2Cardiff University, Cardiff, United Kingdom
On behalf of:
Background and aims: Assessment of independence in extended Activities of Daily Living (ADLs) is integral to stroke research and practice. Patient Reported Outcome Measures (PROMs) including the Nottingham Extended Activities of Daily Living (NEADL) have previously been criticized for the number of items and their lack of contemporary relevance.
Methods: To address this issue, we designed a program of work with three strands: Work Package (WP) 1 utilized data from 722 stroke survivors at 6 months post stroke to derive a short form NEADL (SF-NEADL) and evaluate its psychometric properties. An online survey of 2244 participants for WP2 captured the frequency with which older adults perform tasks included in common ADL scales and identify common omitted tasks. The ongoing survey for WP3 aims to further validate the SF-NEADL and additional contemporary tasks with common ADL and Quality of Life scales.
Results: WP1 data led to the derivation of a 5-item SF-NEADL capturing mobility and kitchen items with good internal constancy (α .863), a very strong relationship with the NEADL (.944), strong convergent validity with both the Barthel Index (.787), and the Modified Rankin Scale (-.656). WP2 identified multiple redundant ADL scale tasks and common omitted tasks, including online banking and shopping.
Conclusions: WP1 introduces a robust tool for efficient and valid assessment of stroke survivors’ perceived independence in extended ADLs. WP2 emphasizes redundant tasks included in ADL scales and emerging tasks of daily living. Feedback from participants highlights the need for robust ADL tools containing items of contemporary relevance.
Disclosures of Interest: No
Abstract N°: 1927
OUTCOMES OF DEPRESSION UP TO 15 YEARS AFTER STROKE: A POPULATION-BASED STUDY
Lu Liu*1, Iain Marshall1, Ajay Bhalla1, Ruonan Pei1, Charles Wolfe1, Matthew DL O’connell1, Yanzhong Wang1
1King's College London, Population Health Sciences, London, United Kingdom
On behalf of:
Background and aims: Data on the long-term outcomes of post-stroke depression (PSD) are limited. We aim to estimate various outcomes of PSD up to 15-years after stroke and assess the differences by age
Methods: Data were from the South London Stroke Register (1997-2022). Depression was assessed using the Hospital Anxiety and Depression Scale at 3-months post-stroke. Outcomes included mortality, recurrent stroke and yearly follow-up functional outcomes (physical ability, activity of daily living, cognitive function and quality of life). Cox proportional hazards models were used to estimate the association between depression and mortality and stroke recurrence. The associations with functional outcomes over 15-years post-troke were estimated using Generalized estimating equation (binary outcomes) and linear regression models (continuous outcomes), adjusting for age, sex, ethnicity, stroke severity, anti-depression medications and comorbidities
Results: 2574 stroke survivors were assessed at 3-months and 913 (35.5%) had depression. Survivors with depression had higher risk of mortality (aHR 1.16, 95% CI 1.05–1.27), but similar risk of stroke recurrence (0.93 [0.70-1.23]) compared to those without depression to 15-years post-stroke. Patients with depression also had poorer physical abilities (aRR 1.79, [1.48-2.17]), higher risks of inactive activity of daily living (2.57, [2.06-3.18]) and cognitive impairment (1.33,[1.05-1.69]) and poorer physical (β=−2.75, -3.50 to-2.00) and mental quality of life (β=−6.29,-7.22 to-5.35). These associations were more pronounced in patients< 65 years
Conclusions: PSD is associated with higher mortality, poorer functional outcomes and reduced quality of life up to 15-years after stroke and this association was more evident in younger patients. PSD doesn’t affect stroke recurrence.
Disclosures of Interest: No
Abstract N°: 2033
FACTORS AFFECTING STROKE READMISSIONS WITHIN THE US VETERANS AFFAIRS SYSTEM
Seemant Chaturvedi*1, Jason Sico2, Anthony Perkins3, Laura Myers4, Joanne Daggy3, Stanley Taylor4, Brian Koo2, Laura Burrone5, Ali Sexson4, Dawn Bravata4
1University of Maryland School of Medicine, Neurology, Baltimore, United States, 2Yale University School of Medicine, Neurology, 3Indiana University School of Medicine, 4Indianapolis VA Hospital, 5West Haven VA Hospital
On behalf of:
Background and aims: Ischemic stroke patients are at risk for readmission following the index event. We sought to explore factors associated with readmission within a national healthcare system
Methods: This retrospective cohort study included patients with ischemic stroke/TIA who were admitted to 36 Veterans Affairs (VA) hospitals between 2019-2021. Clinical variables were obtained from electronic health record data, along with health measures reflecting cumulative vascular burden (CHADS-VASC) or medical comorbidities. We examined all-cause readmission within 90 days using logistic regression models.
Results: Among 5392 patients, the mean age was 70.2 years and 95.6% were men. The rates of hypertension, diabetes, and drug use were 84.5%, 48.8%, and 13.4%, respectively. The index event was stroke in 77%, TIA in 23%. The median Charlson comorbidity index was 2.0 and median CHADS-VASC was 4.9. The 90-day readmission rate was 25.8%. Factors significantly associated (all P<0.05) with readmission are presented in the Table (area under ROC 0.654).
Conclusions: Patients admitted to the intensive care unit (ICU), along with those with COPD, drug abuse, motor weakness, and an elevated CHADS-VASC and APACHE scores are at increased risk for hospital readmission. Targeted interventions to ensure that high-risk patients receive needed care and services early after discharge might reduce the burden of hospital readmissions.
Disclosures of Interest: No
Abstract N°: 2176
PREVALENCE, NATURAL HISTORY, AND PREDICTORS OF NON-MOTOR OUTCOMES AFTER STROKE: A SYSTEMATIC REVIEW AND META-ANALYSIS
Hatice Ozkan*1,2, Gareth Ambler3, Taniya Esmail2, Gargi Banerjee2,4, Rob Simister1,2, David Werring1,2
1UCL Queen Square Institute of Neurology, London, UK, 2National Hospital for Neurology and Neurosurgery, University College London Hospitals NHS Foundation, Queen Square, London, 3Department of Statistical Science, University College London, Gower Street, London, UK, 4MRC Prion Unit at UCL, Institute of Prion Diseases, London, UK
On behalf of:
Background and aims: Adverse patient-reported non-motor outcomes after stroke have substantial impact on health-related quality of life, but knowledge of their prevalence, natural history and predictors remains limited. We aim to synthesise existing data and identify knowledge gaps through a thorough systematic review and meta-analysis of cohort studies.
Methods: We searched the PubMed, Embase, Medline, and PsycINFO databases for English articles published between 1st January 1999 and 30th June 2023. We included cohort studies reporting at least one of the following non-motor outcomes in adults after stroke: anxiety; depression; fatigue; sleep disturbance; social participation; pain; bladder dysfunction; bowel dysfunction (constipation, faecal incontinence); and sexual dysfunction. Meta-analysis, and meta-regression models were used to report the findings.
Results: We included 279 studies (n=117440 median age 64.9 years, 75% male) with a median follow-up duration of 6.4 years. The most prevalent adverse non-motor outcomes were: sleep disturbance (in 59.9% of patients); sexual dysfunction (59.8%); constipation (58.2%); reduced social participation (56.5%); bladder dysfunction (45.9%); and fatigue (45.2%); all showed significant heterogeneity (I2 52.3% to 98.7%, p<0.05). There was little improvement with time for 8 of 10 adverse non-motor outcomes; only pain and sexual dysfunction showed reducing prevalence. Female sex, stroke due to intracerebral haemorrhage, and older age were associated with adverse non-motor outcomes in multiple domains.
Conclusions: Adverse non-motor outcomes are common after stroke, have impact across multiple health domains, and largely persist over time; our findings emphasise the need for future research and clinical strategies to characterise, detect, prevent, and manage them.
Disclosures of Interest: No
Abstract N°: 310
LONG-TERM POST-COVID CONDITIONS AMONG STROKE SURVIVORS OF THE UNITED STATES, 2022 BEHAVIORAL RISK FACTOR SURVEILLANCE SYSTEM
Seyyed Sina Hejazian*1, Alireza Vafaei Sadr2, Shima Shahjouei3, Ajith Vemuri1, Vida Abedi2, Ramin Zand1
1The Pennsylvania State University, Neurology, State College, United States, 2Pennsylvania State University, Public Health Sciences, hershey, PA, United States, 3Penn State Health Milton S. Hershey Medical Center, Neurology, hershey, PA, United States
On behalf of:
Background and aims: Persistent post-COVID conditions (PCCs) have become unavoidable challenges for individuals who have survived COVID. The National Research Plan on Long COVID-19 underscores the priority of addressing post-COVID conditions (PCCs) within specific subgroups of the United States (US) population. This study aimed to investigate the prevalence and factors associated with PCCs among stroke survivors in the US.
Methods: We utilized the Behavioral Risk Factor Surveillance System (BRFSS) 2022 dataset. First, we identified respondents with a positive history of both COVID-19 and stroke. Subsequently, we categorized these respondents based on whether they experienced PCCs and conducted a comparative analysis of their characteristics. Additionally, our study included a comparison of our findings with those among individuals who have survived myocardial infarction (MI) and cancer, which are the two conditions associated with the highest mortality rates in the US.
Results: A total of 3999 stroke, 5406 MI, and 10551 cancer survivors were included. The estimated prevalence of PCCs among stroke survivors was 30.6%, compared to 22.4%, 29.2%, and 24.6% among non-stroke (p<0.001), MI, and cancer survivors, respectively. Fatigue, dyspnea, and taste/smell loss were the most common primary symptoms. Among stroke survivors, Tennessee (47.3%) and Pennsylvania (14.8%) had the highest and lowest PCCs prevalence. In multivariate regression analysis, women (aOR:1.61, CI95%:[1.4-1.6]), stroke-belt residence (aOR:1.54, CI95%:[1.04-2.27]), pulmonary disease (aOR:1.99,CI95%:[1.44-2.74]), depression (aOR:1.47, CI95%:[1.03-2.09]), arthritis (aOR:1.44, CI95%: [1.03-2.02]) were independent PCCs risk factor among stroke survivors. Additionally, age>64 years was a protective factor (aOR:0.61, CI95%: [0.42-0.88]).
Conclusions: Our study highlights a considerable prevalence of PCCs among stroke survivors, particularly among younger women and individuals with other chronic conditions.
1West China Hospital, Sichuan University, Department of Neurology and Center of Cerebrovascular Diseases, Chengdu, China, 2The Chinese University of Hong Kong, Department of Medicine and Therapeutics
On behalf of:
Background and aims: Animal studies suggest that higher heme oxygenase-1 (HO-1) levels are linked to reduced infarct size and milder neurologic deficits in ischemic stroke. However, the relationship between HO-1 and human ischemic stroke outcome remains unclear, which was investigated in this study.
Methods: Acute ischemic stroke patients admitted within 24 hours were enrolled. Serum HO-1 levels at baseline were measured via ELISA. Poor 3-month functional outcome was defined as modified Rankin Scale (mRS) score 3-6. Multivariable-adjusted binary logistic regression and restricted cubic spline models were employed to examine association between serum HO-1 and functional outcome. HO-1's additive prognostic utility, on top of conventional clinical factors including thrombolysis and/or endovascular therapy, was assessed by net reclassification index (NRI) and integrated discrimination improvement (IDI).
Results: Of 194 eligible patients (median age 66; 63.9% males), 79 (40.7%) developed poor functional outcomes at the 3-month follow-up. The highest quartile of serum HO-1 was independently associated with a lower risk of poor functional outcome (adjusted OR 0.13, 95% CI 0.04-0.45; P=0.001) compared with the lowest HO-1 category. The relationship between higher HO-1 levels and reduced risk of poor functional outcome was linear and dose-responsive (P=0.002 for linearity). Incorporating HO-1 into the analysis with conventional factors significantly improved reclassification for poor functional outcome (NRI=41.2%, P=0.004; IDI=5.0%, P=0.004).
Conclusions: Elevated serum HO-1 levels at baseline were independently associated with improved 3-month functional outcomes post-ischemic stroke. Serum HO-1 measurement may enhance outcome prediction beyond conventional clinical factors.
Disclosures of Interest: No
Abstract N°: 2568
PROXIES OF COGNITIVE RESERVE ARE ASSOCIATED WITH NON-COGNITIVE STROKE OUTCOME: A SYSTEMATIC REVIEW AND META-ANALYSIS
Laura Gallucci1, Mirjam Rachel Heldner1, Christoph Sperber1, Marcel Arnold1, Roza Umarova*1
1University hospital of Bern, Inselspital, Neurology, Switzerland
On behalf of:
Background and aims: The inter-individual variability in stroke outcome remains less understood. In neurodegenerative diseases, this variability has been explained by the construct of cognitive reserve (CR). We conducted a systematic review and meta-analysis to investigate the association of multiple CR-proxies with stroke outcome to implement the understanding of its inter-individual variability and improve its prediction.
Methods: We systematically searched PubMed, Cochrane, EMBASE, and Web of Science for studies reporting the association between CR-proxies (e.g. level or years of education, occupational attainment, crystallized intelligence) and non-cognitive stroke outcome (NIHSS, modified Rankin Scale etc.). Estimates were pooled using a random-effects model.
Results: Of 4129 articles screened, nine studies involving 19’287 patients were included. Low CR increased the risk of poor stroke outcome (standardized mean difference [SMD] 0.12, 95% CI 0.03-0.21). Subgroup analysis showed that CR operationalized as occupational attainment (SMD 0.34, 95% CI 0.10-0.57) or level of education (SMD 0.24, 95% CI 0.11-0.37) has higher predictive value than years of education (SMD 0.03, 95% CI -0.02-0.08). The effect of CR was stronger at ⩽ 3 months post-stroke (SMD 0.19, 95% CI 0.09-0.29) than in the chronic phase (SMD 0.03 95% CI -0.03-0.08).
Conclusions: Low CR increases the risk of higher stroke severity, functional disability, and dependency. This systematic review and meta-analysis demonstrates that CR might explain inter-individual variability after stroke and its proxies should be considered to improve outcome prediction.
Disclosures of Interest: No
Abstract N°: 2609
ESTIMATING INDIVIDUAL TREATEMENT EFFECTS FOR LVO STROKE PATIENTS BASED ON NON-CONTRAST CT AND CLINICAL DATA
Lisa Herzog*1,2, Nelly Blindenbacher2, Arnolt-Jan Hoving3, Charles Majoie3, Wim Van Zwam4, Aad van der Lugt5, Beate Sick6, Susanne Wegener1,2
1University of Zurich, Zürich, Switzerland, 2University Hospital of Zürich, Neurology, Zürich, Switzerland, 3University of Amsterdam, Department of Radiology and Nuclear Medicine, Amsterdam, Netherlands, 4Maastricht UMC+, Maastricht, Netherlands, 5Erasmus University Medical Center, Rotterdam, Netherlands, 6University of Zurich, Epidemiology, Biostatistics & Prevention Institute, Zürich, Switzerland
On behalf of:
Background and aims: Treatment decisions in large vessel occlusion (LVO) stroke patients are challenging, as clinical recovery of those patients treated with mechanical thrombectomy (MT) is variable. Clinical decision support tools are therefore highly desired. We aimed at developing an outcome prediction model to derive individual treatment effects in LVO stroke patients using clinical and imaging data.
Methods: We included 499 LVO stroke patients of the MRCLEAN trial to develop a deep learning based logistic regression model predicting favorable vs. unfavorable outcome in terms of the modified Rankin Scale of 0-2 vs. 3-6 at 3 months after stroke. The deep learning approach using raw non-contrast CT (NCCT) and clinical data was compared to standard logistic regression including the same clinical data and the ASPECTS score. All models were evaluated in a five-fold cross validation.
Results: Only 32.6% of the 233 patients treated with MT had a favorable outcome. Additionally including imaging information in terms of raw NCCT (AUC of 0.681 [0.628, 0.733]) or the ASPECTS (AUC of 0.718 [0.665, 0.771]) into models yielded similar prediction results as clinical data only (AUC of 0.704 [0.649, 0.759]). The estimated average treatment benefit (13.9%, 95%-CI [8.8%, 18.9%]) was in agreement with the estimated average across individual treatment effects (12.6%). However, individual treatment effects varied between 8.2% and 18.1% in 75% of the patients.
Conclusions: Adding CT imaging to clinical data has not much value in predicting treatment benefit. We will now include other raw imaging modalities like angiography to improve individual outcome prediction.
Disclosures of Interest: No
Abstract N°: 2786
CHARACTERISTICS OF PATIENTS WITH CEREBRAL SINUS VENOUS THROMBOSIS AND ANTIPHOSPHOLIPID SYNDROME: A MULTI-CENTER STUDY
Naaem Simaan1, Hen Hallevi2, Asaf Honig3, Rani Barnea4, Shorooq Aladdin5, Rom Mendel6, Ronen R Leker7, Jeremy Molad*2
1Ziv Medical Center, Department of Neurology, Safed, Israel, 2Tel-Aviv Sourasky Medical Center, Department of Neurology & Stroke, Tel-Aviv, Israel, 3Soroka Medical Center, Department of Neurology, Beer-Sheva, Israel, 4Rabin Medical Center, Department of Neurology, Petach-Tikva, Israel, 5Sheba Medical Center, Departments of Neurology, Ramat-Gan, Israel, 6Assuta Medical Center, Department of Neurology, Ashdod, Israel, 7Hadassah-Hebrew University Medical Center, Departments of Neurology, Jerusalem, Israel
On behalf of:
Background and aims: Antiphospholipid syndrome (APS) is an important cause for venous thrombotic events. Current data regarding the characteristics and prognosis of cerebral sinus vein thrombosis (CSVT) among APS patients is limited. We aimed to describe the clinical features and prognostic implications of APS patients presented with CSVT.
Methods: Data from a prospectively enrolled database of CSVT patients from six academic medical centers was retrospectively analyzed. APS diagnosis was based on the Sydney criteria. Demographics, clinical presentations, risk factors, radiological and outcome parameters were compared between patients with and without APS.
Results: 556 CSVT patients (mean age 42.0 ±18.5, 66% females) were included in the current study, among them 64 patients (11.5%) were diagnosed with APS. Patients with and without APS had similar rates of favorable outcome (82.8% versus 79.6%, p=0.554), however APS patients had lower rates of venous infarct, near significant lower mortality rates, and higher rates of complete recanalization (10.9% versus 14.4%, p=0.017, 0% versus 5.6%, p=0.052, 60.0% versus 44.0%, p=0.043 respectively). Triple positive APS patients had higher rates of previous thrombotic event, recurrent CSVT and complete recanalization compared with non-APS patients (27.8% versus 8.4%, p=0.005, 2.7% versus 11.1%, p=0.043, 44.1% versus 66.7%, p=0.06, respectively).
Conclusions: The results of the current study suggests that CSVT related APS patients have similar neurological prognosis and better complete recanalization rates compared with patients without APS. Triple positive APS only was associated with higher rates of recurrent thrombotic events, which may lead to worse long term outcomes among these patients.
Disclosures of Interest: No
Abstract N°: 2911
EARLY BILINGUALISM AS A POSSIBLE NEUROPROTECTIVE FACTOR FOR ACUTE STROKE APHASIA
Federica Palacino*1, Marcello Naccarato1, Giovanni Furlanis1, Paola Caruso1, Laura Mancinelli1, Gabriele Prandin1, Emanuele Vincis1, Paolo Manganotti1
1Province of Trieste, Clinical Unit of Neurology, University of Trieste, Cattinara University Hospital (ASUGI), Trieste, Italy., Trieste, Italy
On behalf of:
Background and aims: Aphasia affects functional outcomes and quality of life. Recent studies suggest that bilingualism could be associated with a better linguistic improvement in chronic stroke patients compared to monolingualism. The aim of this study is to verify if bilingualism is a protective factor for acute stroke aphasia investigating language recovery, functional outcome and discharge characteristics.
Methods: A suggestive early-bilingual (Italian-Slovenian or Italian/Croatian) stroke aphasic sample (n=71) was recruited and compared to monolingual ones (n=207) from January 2020 to December 2023. The two groups were statistically compared for demographic characteristics; cardiovascular risk factors; stroke characteristics; acute treatment, National Institutes of health Stroke Scale (NIHSS), modified Rankin Scale (mRS) at admission and discharge; speech therapy; aphasia’s outcome; and discharge destination. Univariate and multivariate analysis were performed using SPSS 13.0.
Results: The two cohorts were similar in relation to demographical data, cardiovascular risk factors, type of stroke (ischemic or hemorrhagic), acute intervention (thrombolysis, thrombectomy, surgical intervention), neurological disability at admission/discharge, and radiological features. Notheworthy, our data showed that early bilinguals had a statistically significant admission-discharge improvement in language-NIHSS-items (i.e. at least 2 points) at 7 days (p<0,001) in both univariate and multivariate analysis.
Conclusions: Early bilingualism is a protective factor for linguistic improvement in the acute post-stroke period.
Disclosures of Interest: No
Abstract N°: 24
LONG-TERM COMORBIDITIES ARE OF HIGH IMPORTANCE WHEN PREDICTING 30-DAY AND 1-YEAR READMISSION AFTER STROKE
Raed Hailat*1, Gustavo de Los Campos1, Michael Thompson2, Adrienne Nickles3, John Adam Oostema4, Mathew Reeves1
1Michigan State University, Epidemiology and Biostatistics, East Lansing, United States, 2University of Michigan, Cardiac Surgery, Ann Arbor, United States, 3Michigan Department of Health and Human Services, Lansing, United States, 4Michigan State University, Emergency Medicine, Grand Rapids, United States
On behalf of:
Background and aims: Although several US-based stroke readmission prediction models exist, the relative importance of individual predictor variables remains uncertain. We used LASSO logistic regression to identify the most important predictors in 30-day and 1-year readmission risk models.
Methods: We probabilistically linked data from acute stroke discharges (ICD-10 I61-I63) recorded by 31 hospitals in the Michigan Acute Stroke registry between 2016-2020 to statewide multipayer claims data. Registry data included demographics, stroke clinical features, comorbidities, procedures, and in-hospital outcomes. Claims data was used to identify all-cause readmissions within 30-day and 1-year. We used multivariable LASSO logistic regression to predict readmission. We applied a hospital-split internal validation method to generate 31 hospital-specific models and reported the overall pooled AUC. The relative importance of individual predictors were identified according to the rank order that they were selected by the 31 models.
Results: Of 19,382 linked stroke discharges, 2,724 (14.1%) and 8,169 (42.1%) were readmitted within 30-days and 1-year, respectively. The pooled 30-day and 1-year readmission AUCs were 0.68 (95% CI: 0.65-0.70) and 0.67 (95% CI: 0.65-0.69), respectively. In both models, variables that were selected early and thus had the highest importance included discharge disposition, length of stay, chronic renal disease, and heart failure (Figure). In contrast, clinical features of stroke (e.g., NIHSS, stroke etiology) were less important in terms of rank in the 30-day model and were almost absent in the 1-year model.
Conclusions: Clinical features of stroke are less important than the burden of long-term comorbidities in predicting post-stroke readmission, especially over longer periods of time.
Disclosures of Interest: No
Abstract N°: 126
LONGITUDINAL RETINAL STRUCTURE CHANGES DIFFERED BETWEEN THALAMIC AND EXTRA-THALAMIC SSI PATIENTS
Ruosu Pan*1, Chen Ye1, William Kwapong1, Bo Wu1
1West China Hospital, Sichuan University, Department of Neurology, Chengdu, Sichuan Province, China
On behalf of:
Background and aims: Cerebrovascular lesions in the visual pathway have been associated with retinal neurodegeneration via the retrograde degeneration (RD). We aimed to use optical coherence tomography (OCT) to assess the effects of the strategic single subcortical infarction (SSI) location on retinal neurodegeneration and its longitudinal impacts.
Methods: Patients with SSI were enrolled and stratified by lesion location into the thalamic infarction group and extra-thalamic infarction group. Healthy controls (HC) were also recruited. Retinal nerve fiber layer (RNFL) and ganglion cell-inner plexiform layer (GCIPL) were quantified using OCT. Generalized estimating equation (GEE) models were used for cross-sectional analyses and linear mixed models for longitudinal analyses.
Results: We included 283 eyes from 149 SSI patients. Of these, 115 eyes with follow-up were included in the longitudinal analyses. Cross-sectionally, thalamic group had reduced retinal thickness compared with extra thalamic group (p = 0.026 for RNFL, and p = 0.026 for GCIPL). Longitudinally, SSI patients showed greater retinal thinning compared with HC (p = 0.040 for RNFL, and p < 0.001 for GCIPL), and thalamic group exhibited faster rates of GCIPL thinning compared with extra-thalamic group (p < 0.001).
Conclusions: Our study demonstrates a distinct effect of subcortical infarction lesion site on the retina both at the early stage of disease and at the 1-year follow-up time. These results present evidence of associations between strategic infarction locations and retinal neurodegeneration. It may provide insights for research on RD in stroke patients and facilitate individualized recovery therapeutic strategy.
Disclosures of Interest: No
Abstract N°: 341
ACUTE MYOCARDIAL INJURY IN SPONTANEOUS INTRACEREBRAL HEMORRHAGE: A SECONDARY OBSERVATIONAL ANALYSIS OF THE FAST TRIAL
Michela Rosso1, Helena Stengl2, Jan Scheitz2, Jennifer Lewey1, Stephan A Mayer3, Shadi Yaghi4, Scott Kasner1, Jens Witsch*1
1University of Pennsylvania, Philadelphia, United States, 2Charité – Universitätsmedizin Berlin, Berlin, Germany, 3New York Medical College, White Plains, United States, 4Brown University, Providence, United States
On behalf of:
Background and aims: As acute myocardial injury is associated with poor outcomes and mortality in ischemic stroke patients, we investigated whether acute myocardial injury and the direction of the cardiac troponin I (cTnI) change (rising vs. falling) affect outcomes also in intracerebral hemorrhage (ICH) patients.
Methods: We conducted a secondary analysis of the Factor Seven for Acute Hemorrhagic Stroke (FAST) trial. Acute myocardial injury was defined as at least one cTnI value above the upper reference limit with a rise/fall of>20%. Binary and ordinal logistic regression analyses were performed for associations of acute myocardial injury and rising/falling cTnI patterns with poor outcomes (modified Rankin Scale 4-6) and mortality.
Results: Among the 841 FAST participants, 785 patients were included (Fig.1). Acute myocardial injury was detected in 29% (n=227); 170 had rising cTnI. At 15 and 90 days, respectively, those with acute myocardial injury had higher odds of poor outcomes (adjusted odds ratios (aOR)=2.3 [1.3-3.9] and aOR 2.5 [1.6-3.9]; shift analysis in Fig.2), and mortality (aOR=2.4 [1.4-4.3] and aOR=2.2 [1.3-3.6]). Rising cTn was associated with the highest risk of poor outcomes and mortality, while the risk for patients with falling pattern was similar to those without acute myocardial injury (Tab.1).
Conclusions: In this post-hoc analysis of the FAST trial, acute myocardial injury was common and associated with poor outcomes and mortality. The direction of the cTn change might provide additional risk stratification in ICH patients. Further characterization of types of cardiac events associated with different cTn patterns might be relevant for future targeted diagnostic and therapeutic approaches.
Disclosures of Interest: No
Abstract N°: 626
DATA DRIVEN ANALYSIS REVEALS CORTICAL INFARCTION PATTERNS CORRELATED WITH INFLAMMATION AND PROGNOSIS
Wenjie Wang*1, Lingling Ding1, Zixiao LI1
1Beijing Tiantan Hospital, department of neurology, Beijing, China
On behalf of:
Background and aims: We aim to identify the distinct lesion patterns and regions associated with functional outcome and inflammation in acute ischemic stroke (AIS) patients, and investigate whether the association between lesion patterns and functional outcome was mediated by inflammation.
Methods: We performed non-negative matrix factorization to derived low-dimensional lesion patterns (atoms) and Bayesian linear regression models were applied to explore the associations of lesion patterns with inflammatory factors including high sensitivity C reactive protein (hs-CRP) and interleukin-6 (IL-6), as well as functional outcome (defined as modified Rankin Scale score at 3-month). The difference distribution mean and 95% highest probability density interval (HPDI) were calculated. Mediation analysis was used to examine the mediating effects of inflammation on the relationships between lesion patterns and functional outcome.
Results: Seven lesion patterns were derived from 5,914 AIS patients. Lesion patterns distributed in the cortical regions and inflammatory response, including atom 1 (IL-6: mean =0.113, 95% HPDI =0.073–0.162; hs-CRP: mean=0.082, 95% HPDI=0.038–0.123) and atom 4 (IL-6: mean=0.113, 95% HPDI=0.071–0.167; hs-CRP: mean=0.108, 95% HPDI=0.058–0.165). These lesion patterns were also significantly associated with functional outcome (atom 1, mean =1.958, 95% HPDI=1.538–2.383; atom 4: mean=2.245, 95% HPDI=1.773–2.741). Mediation analysis suggested that IL-6 explained 15.34% and 7.47% in the association of atom 1 and atom 4 with functional outcome, respectively.
Conclusions: Certain lesion patterns that associated with both inflammation and functional outcome of AIS, especially cortical infarction may play a role in functional outcome through modulating inflammatory reactions.
Disclosures of Interest: No
Abstract N°: 766
PREDICTORS OF EARLY NEUROLOGICAL DETERIORATION IN ACUTE ISCHEMIC STROKE OF POSTERIOR
Sung-Il Sohn*1, Hyesoo Kwon1
1Keimyung University Dongsan Hospital, Department of Neurology, Daegu, South Korea
On behalf of:
Background and aims: We aimed to evaluate the predictive factors of neurological deterioration (ND) and explore the outcome in patients with acute ischemic stroke (AIS) involving posterior circulation. Methods: Based on single center stroke registry for 5 years, 900 (25.7%) patients with acute ischemic stroke of posterior circulation confirmed with computed tomography (CT) or diffusion-weighted MRI were included. ND was defined as any new neurologic symptoms or signs or neurologic worsening that satisfies a change of ⩾ 1 point in the motor or level of consciousness sub-items of the NIHSS score or ⩾ 2 points in other NIHSS sub-items during hospitalization in neurology department within 3 weeks of symptom onset. Results: Of the included 900 patients (mean age 67 years, 41% female) of AIS of posterior circulation, 133 (14.8%) had ND. The most common etiology of ND was stroke progression (81%), followed by medical condition (8%), symptomatic hemorrhagic transformation (6%), and stroke recurrence (5%). In multivariable logistic regression analysis, independent predictors of ND were onset to arrival time (OR 0.999, CI 0.9997-0.9999, P = 0.017), ischemic damage reflected in pc-ASPECTS (OR 0.415, CI 0.167-0.996, P = 0.015), initial systolic blood pressure (OR 1.009, CI 1.001-1.017, P = 0.027), and the presence of any stenosis (OR 1.920, CI 1.024-3.472, P = 0.035) or occlusion (OR 4.803, CI 1.726-13.781, P = 0.003) of the basilar artery (BA). Conclusions: The predictors of ND in AIS of posterior circulation are early arrival, poor neuroimaging findings, any stenosis or occlusion in the BA and high initial blood pressure.
Disclosures of Interest: No
Abstract N°: 947
EFFECT OF SMALL VESSEL DISEASE ON BLOOD PRESSURE LOWERING IN THROMBOLYZED PATIENTS WITH ISCHEMIC STROKE: THE ENCHANTED TRIAL
1Department of Neurology, West China Hospital, Sichuan University, China, 2The George Institute for Global Health, Faculty of Medicine, University of New South Wales, Australia
On behalf of:
Background and aims: It remains unknown whether the effects of intensive blood pressure (BP) lowering interact with cerebral small vessel disease (SVD) in thrombolyzed patients with acute ischemic stroke (AIS). We aimed to quantify the interaction of SVD features and the effect of BP lowering (intensive vs. guideline) on functional outcome and intracranial haemorrhage (ICH) in the international ENCHANTED trial.
Methods: Patients with available baseline brain computerized tomography (CT) were included. We assessed SVD features including old lacunar infarcts, white matter changes, and brain atrophy blinded to clinical data. Outcome measures were poor functional outcome (defined as modified Rankin scale 3-6) at 90 days and any ICH on central CT adjudication.
Results: Of 2115 AIS patients included, 496 (34.8%, 496/1424) had old lacunar infarcts, 596 (42.5%, 596/1404) had white matter changes, and 891 (63.2%, 891/1409) had brain atrophy. 699 (33.2%, 699/2106) patients had poor functional outcome and 337 (15.9%, 337/2115) had any ICH. There was no significant interaction between intensive BP lowering and old lacunar infarcts on poor functional outcome (with old lacunar infarcts, OR 1.09, 95% CI 0.81-1.49 and without old lacunar infarcts, OR 1.06, 95% CI 0.71-1.61; p for interaction=0.80), and any ICH (with old lacunar infarcts, OR 0.84, 95% CI 0.57-1.23 and without old lacunar infarcts OR 0.70, 95% CI 0.41-1.18; p for interaction=0.55). Similar non-significant results applied for white matter changes and brain atrophy.
Conclusions: SVD does not modify the effect of BP-lowering therapy on functional outcome or ICH in thrombolyzed AIS patients.
Disclosures of Interest: No
Abstract N°: 1378
ASSOCIATION OF SYSTOLIC DYSFUNCTION AND REHOSPITALISATION/MORTALITY 2-YEARS AFTER ISCHEMIC STROKE: ANALYSES OF THE SICFAIL STUDY
Kathrin Ungethüm*1,2, Felipe A. Montellano1,3, Viktoria Rücker1, Caroline Morbach4,5, Stefan Frantz5, Stefan Störk4,5, Christoph Kleinschnitz6, Karl Georg Häusler3, Peter Heuschmann1,2,4,7
1University Würzburg, Institute of Clinical Epidemiology and Biometry, Würzburg, Germany, 2University Hospital Würzburg, Institute for Medical Data Sciences, Würzburg, Germany, 3University Hospital Würzburg, Department of Neurology, Würzburg, Germany, 4University and University Hospital Würzburg, Comprehensive Heart Failure Center, Würzburg, Germany, 5University Hospital Würzburg, Deparment of Internal Medicine I, Würzburg, Germany, 6University Hospital Essen, Department of Neurology, Essen, 7University Hospital Würzburg, Clinical Trial Unit, Würzburg, Germany
On behalf of: SICFAIL study group
Background and aims: About 10% of patients with acute ischemic stroke (AIS) exhibit systolic dysfunction (SD). We hypothesized that SD in AIS affects the risk of rehospitalisation and mortality within two years after the index event.
Methods: Data were collected within the prospective hospital-based single-centre SICFAIL study. At the time of the index stroke, patients were comprehensively phenotyped including medical history anamnesis, standardized echocardiography by expert sonographer, and blood sampling. SD was defined as left ventricular ejection fraction <52% (men) or <54% (women). Information on rehospitalisation and vital status were collected yearly using postal/phone interviews, or information from next of kin or residents’ registration offices. Cox proportional hazard regression models were calculated to analyse the association of SD with the combined endpoint (all-cause death or rehospitalisation) using adjustment for baseline characteristics (age, NIHSS score, pre-stroke dependency) and comorbidities (history in stroke/TIA, coronary heart disease, atrial fibrillation, diabetes, treated/untreated hypertension). Study patients without echocardiographic (n=52) or outcome information were excluded (n=166).
Results: Overall, 478 (median 71.0 years(quartiles 60.0-78.0), 64% men) AIS patients were included in the present analysis, including 41(9%) with SD at baseline. Within the 2-year follow-up period, 269(56%) patients were rehospitalised (n=206) and/or died (n=63). After adjustment for baseline variables and comorbidities, the combined endpoint was independently associated with SD (HR=1.68 95%CI(1.03-2.72)), NIHSS score (HR=1.04 per point 95%CI (1.01-1.08)) and history of stroke/TIA (HR=1.66 95%CI(1.19-2.31)) before enrolment.
Conclusions: SD appears to influence clinical outcome after AIS. Ongoing analyses of the SICFAIL 5-year follow-up will investigate the role of SD in the course after AIS.
Disclosures of Interest: No
Abstract N°: 1380
CLINICAL OUTCOMES BY STROKE SEVERITY USING NATIONAL INSTITUTE OF HEALTH STROKE SCALE (NIHSS) SCORE AMONG PATIENTS WITH IS OR TIA
Priyanka Gaitonde1, Jenny Jiang1, Meg Crighton2, Merena Henderson*1
1Bristol Myers Squibb, 2Janssen Research & Development, LLC
On behalf of:
Background and aims: Despite current therapies, stroke remains a leading cause of disability, and ~25% patients experience a secondary stroke within 5 years . Stroke prevalence has increased in younger patients, contributing to economic and healthcare burdens. We assessed clinical outcomes by NIHSS scores in hospitalised patients with non-cardioembolic ischaemic stroke (IS) and transient ischaemic attack (TIA).
Methods: Optum® US de-identified Clinformatics® Data Mart claims (01Oct2015-31Mar2023) were analysed retrospectively. Patients with IS/TIA were included if they had no atrial fibrillation-related stroke or oral anticoagulant use. Outcomes were analysed across index NIHSS score categories (0-7, 8-15 and 16-42).
Results: Among 54,381 patients, 75.0%(n=40,805), 14.3%(n=7,788) and 10.6%(n=5,788) had NIHSS scores of 0-7, 8-15 and 16-42. During follow-up, median length of stay (LOS) was 4, 6 and 7 days in patients with scores 0-7, 8-15 and 16-42. Rates per 100 person-years were 6.7, 11.7 and 14.3 for recurrent stroke; 2.9, 4.2 and 4.3 for major bleeding; and 9.6, 20.0 and 28.7 for death in the 0-7, 8-15 and 16-42 categories. For readmissions due to overall recurrent stroke and major bleeding, 73.1% and 77.0% were from the 0-7 category, and 67.0% of deaths were attributed to the 0-7 category.
Conclusions: Although the 0-7 category represents a less severe stroke, quantitatively this category represents the largest number of patients, with significant clinical outcomes of recurrent stroke, major bleeding and death. This category also contributed significantly to healthcare resource use via extended LOS and readmissions. This demonstrates the need for more clinically-effective therapies, beyond current guideline-recommended antiplatelet therapies such as DAPT and SAPT.
Disclosures of Interest: Yes PG, JJ, and MH are employees of Bristol Myers Squibb and may hold stock in Bristol Myers Squibb. MC is an employee of Janssen Research & Development, LLC and may hold stock in Johnson & Johnson.
Abstract N°: 1511
PROGNOSIS AND DISTRIBUTION OF ISCHEMIC STROKE WITH NEGATIVE DIFFUSION-WEIGHTED IMAGING: A SYSTEMATIC REVIEW AND META-ANALYSIS
Ahmed Alkhiri*1, Fahad Alturki2, Nayef M. Alansari1, Ahmed A. Almaghrabi1, Basil A. Alghamdi1, Aser F. Alamri2, Saeed Alghamdi3, Seraj Makkawi1,4
1King Saud Bin Abdulaziz University for Health Sciences, College of Medicine, Jeddah, Saudi Arabia, 2King Saud Bin Abdulaziz University for Health Sciences, College of Medicine, Riyadh, Saudi Arabia, 3King Faisal Specialist Hospital and Research Centre, Neuroscience department, Jeddah, Saudi Arabia, 4Ministry of the National Guard-Health Affairs, Department of Neuroscience, Jeddah, Saudi Arabia
On behalf of:
Background and aims: Magnetic resonance diffusion-weighted imaging (DWI) is the most sensitive modality for ischemic stroke (IS) diagnosis. However, DWI may fail to detect ischemic lesions in a notable proportion of patients. In this review, we aimed to assess the distribution and the prognostic value of DWI-negative IS
Methods: A systematic search of three electronic databases (Medline, Embase, and Web of Science) was conducted through October 13, 2023. The inclusion was confined to English literature with sufficient reporting. Proportions of DWI-negative IS were pooled. For binary variables, odds ratios (ORs) were computed using the random-effects model.
Results: Fourteen studies (16,268 patients) were included. DWI-negative IS was reported in 16% (95% CI: 10-24%; after sensitivity analysis: 11% [95% CI: 8-15%]) of included patients. The rates were higher among minor stroke patients (24% [95% CI 12-42%]). Predictors of DWI-negative scans included posterior circulation stroke, history of ischemic heart disease, prior stroke, and prior transient ischemic attack. Atrial fibrillation increased the likelihood of positive DWI findings. Patients with DWI-negative IS had higher odds of good functional outcomes (mRS of 0-1) (OR, 2.26; 95% CI: 1.03-4.92), lower odds of stroke recurrence (OR, 0.68; 95 % CI: 0.48-0.96), and lower odds of severe disability or mortality (mRS of 3-6) (OR, 0.44; 95 % CI: 0.34-0.57) compared to patients with positive DWI. Rates of symptomatic intracerebral haemorrhage after intravenous thrombolysis were comparable.
Conclusions: DWI-negative findings were present in a notable proportion of IS patients and may be utilised as a marker for a favourable prognosis.
Disclosures of Interest: No
Abstract N°: 1515
AORTIC-BRACHIAL PULSE WAVE VELOCITY DIFFERENCE IS INDEPENDENTLY ASSOCIATED WITH EARLY AND LATE OUTCOME AFTER ISCHAEMIC STROKE
Kamil Kowalczyk*1, Mariusz Kwarciany1, Krzysztof Narkiewicz2, Bartosz Karaszewski1, Dariusz Gasecki1
1Medical University of Gdańsk, Department of Adult Neurology, Gdansk, Poland, 2Medical University of Gdańsk, Department of Hypertension and Diabetology, Gdansk, Poland
On behalf of:
Background and aims: Increased aortic pulse wave velocity (PWV) is considered an unfavourable prognostic factor following ischaemic stroke (IS). An increase in the physiological stiffness difference between the aortic and muscular artery stiffness may lead to damage in the microcirculation. Whether arterial stiffness difference is related to outcome after ischemic stroke has never been demonstrated.
Methods: Aortic-brachial PWV difference (PWVdiff) was defined as carotid-femoral (cf-PWV)−carotid-radial PWV and was measured in IS patients on day 6 after stroke onset. Early (EFO) and late favourable outcomes (LFO) were defined as modified Rankin scale score=0–1 at discharge and on day 90, respectively.
Results: Among 185 patients, aged 63 (56–70) years, 67% males, National Institutes of Health Stroke Scale (NIHSS) score of 5 (3–8), 91 (49%) had EFO. 13 (7%) patients were lost to follow-up, and 89 (52%) patients had LFO. Patients with EFO compared to those without EFO had lower cf-PWV [9.2 (8.0–11.1)m/s vs. 10.8 (8.2–12.8)m/s, p=0.014) and PWVdiff (0.92±2.54m/s vs. 2.36±3.14m/s, p=0.001). In multivariate analysis including confounding factors (age, sex, previous stroke, intravenous thrombolysis, initial NIHSS score, mean blood pressure, heart rate), lower PWVdiff, but not cf-PWV, was associated with EFO (OR, 1.15; 95%CI, 1.00–1.32; p=0.048 and OR, 1.13; 95%CI, 0.96–1.32, p=0.139; respectively). Lower PWVdiff was associated with LFO in univariate [0.90 (−0.4–2.7)m/s vs. 1.8 (0.0–4.6)m/s, p=0.009) and multivariate analysis [OR, 1.207; 95%CI, 1.02–1,43, p=0,026].
Conclusions: Lower aortic-brachial pulse wave velocity difference is independently associated with better early and late outcome after ischaemic stroke.
Disclosures of Interest: No
Abstract N°: 1654
CLINICAL OUTCOMES OF RADIATION-INDUCED CAROTID STENOSIS
Xiao Zhang*1,2, Liqun Jiao1
1Xuanwu Hospital, Capital Medical University, Department of Neurosurgery, Beijing, 2University of Oxford, Sir William Dunn School of Pathology, Oxford
On behalf of:
Background and aims: Clinical outcomes of radiation-induced carotid stenosis are still unclear. Therefore, this study is aimed to evaluate the short-term and long-term outcomes after surgery for radiation-induced carotid stenosis.
Methods: PubMed, EMBASE, the Cochrane Library and Web of Science were searched for relevant RCTs and observational studies which reported short- and long- term outcomes after carotid endarterectomy (CEA) and carotid angioplasty and stenting (CAS) for carotid stenosis induced by radiation. Risk of bias were assessed through different scales according to study design. I2 statistic were used to evaluate the heterogeneity, and meta-regression and sub-group analysis were performed to investigate the source of heterogeneity.
Results: A total of 26 studies with 1002 patients were included. CEA was performed in 364 patients and CAS in 638 patients. The estimated rate of short-term stroke was 0.19% (95% CI=0-0.90%), and the rate of long-term stroke was 2.68 % (95% CI=1.19-4.57%). The rate of CNI in CEA group was significantly higher than that in CAS group [risk ratio (RR)=6.03, 95% CI=1.63-22.22, P=0.007)], however, there was a tendence of decreasing year after year. The univariate meta-regression analysis showed that the risk of stroke in CAS group were significantly higher than CEA group in both short-and long term [incidence rate ratio (IRR) =3.62, 95% CI=1.21-10.85, P=0.22; IRR=2.95, 95% CI=1.02-8.59, P=0.046), respectively].
Conclusions: This study provided the worldwide profile of outcome of treatment for radiation-induced carotid stenosis, and also found that CEA can yield better results for these patients than CAS.
Disclosures of Interest: No
Abstract N°: 1664
SHORT-TERM RECURRENCE, MORTALITY, AND FUNCTIONAL OUTCOME IN PATIENTS WITH STROKE IN PERFORATING ARTERY TERRITORIES
1Jichi Medical University, Division of Neurology, Department of Medicine, Japan
On behalf of:
Background and aims: The present study aimed to explore the underlying clinical factors and those effect to prognosis in acute ischemic stroke patients in only the perforating artery territories.
Methods: We assessed acute ischemic stroke patients with lesions in only the perforating artery territories. Background clinical factors including atrial fibrillation (AF) and carotid and intracranial large artery atherosclerotic occlusion or stenosis of 50% or more (LAA) were investigated in all patients. We observed stroke recurrence or all-cause mortality within 3 months of the onset, as well as a 3-month functional outcome measured by the modified Rankin scale (mRS).
Results: Out of the 779 patients diagnosed with acute ischemic stroke in only the perforating artery territories, 106 (13.6%) had AF and 199 (25.5%) had LAA. Thirty patients (3.9%) had both AF and LAA. In the multivariate analysis including AF/LAA subgroups (AF+LAA+, AF+LAA-, AF-LAA+, and AF-LAA- group), the AF+LAA+ group demonstrated the highest risk for stroke recurrence or all-cause mortality in contrast to the AF-LAA- group (Odds Ratio [OR] 3.14, 95% Confidence Interval [CI] 1.14-8.68, p=0.0273). The AF-LAA+ group also showed higher risk for stroke recurrence or all-cause mortality than the AF-LAA- group. In the AF+LAA+ group, the risk of 3-month functional poor outcome (mRS score of 3 to 6) was relatively higher than the AF-LAA+ group.
Conclusions: In patients with acute ischemic lesions in only the perforating artery territories, AF and LAA were not rare and were associated with short-term stroke recurrence or all-cause mortality and poor functional outcome.
Disclosures of Interest: No
Abstract N°: 1795
DETERMINING OPTIMAL AGE FOR EXTRACRANIAL-INTRACRANIAL BYPASS SURGERY: A POST-HOC ANALYSIS OF THE CMOSS STUDY
Xin LI1, Xinjuan Xu2, Xuesong Bai3, Yan MA3, Tao Wang*3, Tong Chen1, Liqun Jiao3
1North China University of Science and Technology Affiliated Hospital, Department of Neurosurgery, Tangshan City, China, 2The Affiliated Cardiovascular Hospital of Shanxi Medical University and Shanxi Cardiovascular Hospital, Department of Neurosurgery, Shanxi, China, 3Xuanwu Hospital Capital Medical University, Beijing, China, Department of Neurosurgery, Beijing, China
On behalf of: for the CMOSS Investigators
Background and aims: Due to the rising incidence of cerebrovascular hemodynamic insufficiency in elderly patients, although there's a lack of thorough studies examining the optimal age for Extracranial-Intracranial (EC-IC) bypass surgery in this demographic.
Methods: A post hoc analysis of data from the Carotid or Middle Cerebral Artery Occlusion Surgery Study (CMOSS) to explore the association between age and EC-IC bypass surgery. Primary outcome was stroke or death within 30-day or ischemic stroke in the qualifying artery territory beyond 30-day through 2-year. Baseline characteristics of participants in different ages were compared. Receiver operating characteristic (ROC) curve and Kaplan-Meier survival function were used to evaluate performance. The risk of outcomes in different groups was tested using cox regression.
Results: Primary outcome occurred in surgical group(13/161 [8.1%]) and medical group(19/163 [11.7%]) patients. In the surgical group, the cutoff value of age predicting primary outcome was 55.5 (odds ratio [OR], 5.972 [95% CI, 1.468-24.295]; p= .013) and no significant differences in medical group. Surgical group had a lower risk of primary outcome in participants aging ⩽55.5-year-old (p= .024), but >55.5-year-old group had no significant differences(p= .441). Compared with medical group, the risk of primary outcome(2.9%[3/102] vs 16.9%[10/59]; hazard ratio[HR], 0.255 [95% CI, 0.071-0.916]; p= .036) yielded surgical group had a lower risk in ⩽55.5-year-old participants, but >55.5-year-old participants had no significant differences (16.9%[10/59] vs 12.7%[8/63]; HR 1.438[95% CI, 0.567-3.643]; p= .444).
Conclusions: Patients ⩽55.5-year-old with carotid or middle cerebral artery occlusion may benefit more from EI-CI bypass surgery than medical therapy alone.
Disclosures of Interest: No
Abstract N°: 1866
SERIAL CHANGES IN BLOOD BRAIN BARRIER PERMEABILITY (BBBP) AFTER THROMBECTOMY AND THEIR ASSOCIATION WITH FUNCTIONAL OUTCOME
Nadja Korajkic*1, Christopher Steward2,3, Vijay Venkatraman2,3, Peter Mitchell2,3, Mark Parsons4,5, Vincent Thijs1, Bruce Campbell6,7, Patricia Desmond2,3, Richard Leigh8, Felix Ng1,6,7
1Austin Health, Department of Neurology, Heidelberg, VIC, Australia, 2The University of Melbourne, Department of Radiology, Parkville, VIC, Australia, 3The Royal Melbourne Hospital, Department of Medical Imaging, Parkville, VIC, Australia, 4Hunter Medical Research Institute, Newcastle, NSW, Australia, 5University of New South Wales Southwestern Sydney Clinical School, Ingham Institute for Applied Medical Research, Liverpool Hospital, Department of Neurology, Sydney, NSW, Australia, 6The Royal Melbourne Hospital, University of Melbourne, Department of Medicine, Parkville, VIC, Australia, 7The Royal Melbourne Hospital, Department of Neurology, Parkville, VIC, Australia, 8Johns Hopkins University, Department of Neurology, Baltimore, MD, United States
On behalf of:
Background and aims: Increased BBBP after ischemic stroke may be a therapeutic target to prevent secondary injury. In experimental models of stroke, it fluctuates with time. We sought to measure serial changes in BBBP during the first 72 hours following thrombectomy and assess association with modified Rankin score (mRS) at 3-months.
Methods: In a prospective, longitudinal study at two comprehensive stroke centres, patients with successful angiographic reperfusion (TICI2b-3) for anterior circulation large vessel occlusion underwent 3T-MRI immediately (timepoint 1 [TP1]) and at 48±24 hours (timepoint 2 [TP2]) post-thrombectomy. BBBP index derived from dynamic susceptibility contrast-enhanced perfusion-weighted imaging and expressed as the average of voxels with pathologically increased permeability, was calculated using published methods within the infarct lesion at both timepoints.
Results: Our population included 55 patients (median age 73 [IQR 58-80]), with a median NIHSS 15 (IQR 10-20). TP1-MRI occurred at median 185 minutes (IQR 124-282 minutes) from reperfusion and TP2-MRI at median of 48 hours (IQR 27.7 – 71.8-hours). BBBP of the infarct lesion was similar between TP1 and TP2 (p=0.415). BBBP at both timepoints was associated with 3-month mRS on univariable analysis (TP1 p<0.005; TP2 p<0.002) and on multivariable analysis after adjusting for age, NIHSS, pre-morbid mRS and core volume on CT-perfusion (TP1 p=0.004; TP2 p=0.014).
Conclusions: In humans, infarct lesion BBBP is static within the first 72-hours in the setting of successful reperfusion and is consistently associated with long-term outcome. Future clinical studies measuring BBBP beyond 72-hours after treatment will further characterise natural history of BBB disruption.
Disclosures of Interest: No
Abstract N°: 1893
STRESS HYPERGLYCEMIA AND FUTILE RECANALIZATION: RESULTS OF A MULTICENTER STUDY
Laura Ceccarelli*1, Michele Romoli2, Matteo Foschi3, Raffaele Ornello3, Lucio D'anna4, Francesco Cordici2, Banerjee Soma4, Simona Sacco3, Mariarosaria Valente1, Giovanni Merlino1
1Stroke Unit and Clinical Neurology, Udine University Hospital, Udine, Italy, 2Stroke Unit, Bufalini Hospital, AUSL Romagna, Cesena, Italy, 3Stroke Unit, Avezzano Hospital, L'Aquila, Italy, 4Stroke Unit, Charing Cross Hospital, Imperial College Healthcare NHS Trust, London, United Kingdom
On behalf of:
Background and aims: Mechanical thrombectomy (MT) is the standard treatment for acute ischemic stroke (AIS) due to large vessel occlusion (LVO). Despite successful recanalization, many of these stroke patients remain disabled after three months. Mechanisms that can cause futile recanalization (FR) are still largely unknown. We decided to perform a multicentric study to investigate if stress hyperglycemia (SH) might be a significant predictor of FR in patients who underwent MT for anterior LVO.
Methods: From January 2021 to December 2022, consecutive patients with successful recanalization, defined as a mTICI score >2b, were included in this multicenter retrospective study. Included patients were treated in four thrombectomy capable centers: Udine University Hospital, Udine (Italy); Bufalini Hospital, AUSL Romagna, Cesena, (Italy); Charing Cross Hospital, Imperial College Healthcare NHS Trust, London (UK); Avezzano Hospital, L’Aquila (Italy). SH was estimated by the GAR index (glucose-to-glycated hemoglobin ratio).
Results: A total of 691 subjects were included. After multivariate analysis, independent predictors of FR were the following: age (OR: 1.04, CI 95%: 1.02-1.06, p <0.001), GAR index (OR: 1.08, CI 95%: 1.03-1.14, p =0.003), NIHSS at admission (OR: 1.16, CI 95%: 1.11-1.22; p <0.001), and procedure length (OR: 1.01, CI 95%: 1.00-1.02; p =0.009). We observed that the model combining age, GAR index, NIHSS at admission, and procedure length has good predictive accuracy (AUC 0.78, 95% CI 0.74–0.81, p <0.001).
Conclusions: SH, in addition to age, NIHSS at admission, and procedure length, represents an independent predictor of FR in AIS patients with anterior LVO undergoing MT.
Disclosures of Interest: No
Abstract N°: 2091
STROKE IN VERY OLD PATIENTS
Karl Matz*1, Yvonne Teuschl1
1Danube University Krems, Clinical Neurosciences and Preventive Medicine, Krems an der Donau, Austria
On behalf of: Austrian Stroke Unit Registry Investigators
Background and aims: Demographic changes in our societies confer a continuously increasing burden of stroke patients in advanced age. The study aimed to elucidate which factors influence stroke outcome in very old stroke patients and how do they differ from younger age groups
Methods: Data of 155 814 patients treated between 2001 and 2023 extracted from the Austrian Stroke Unit Registry were used. The target group of analysis were patients aged > 85 years, various younger age groups were used as comparison groups. In univariate analysis groups were compared regarding demographic variables, risk factors and outcome variables. Possible associations with different outcomes were investigated by age groups above and below 85 years in logistic regression models.
Results: 25795 patients > 85a with ischemic stroke and 3206 patients >85a with intracerebral hemorrhage were compared to 111746 and 15067 patients <85a, respectively. Very old patients with cerebral hemorrhage have a very high mortality rate after three months (73%). Multivariate analysis of outcomes showed no significant differences. In ischemic strokes of patients >85a a high proportion of women, a higher stroke severity and a higher proportion of strokes due to atrial fibrillation were found. Infections and cardiac disorders were particularly frequent complications in very old patients. Three-month mortality is significantly increased with 41.3% vs. 12.7%. In multivariate analysis of outcomes thrombolysis and thrombectomy were significantly associated with favorable outcomes comparable to younger patients
Conclusions: Stroke in very old stroke patients is characterized by a significantly higher severity and mortality. The effect of guideline-oriented therapy is comparable to younger patients.
Disclosures of Interest: No
Abstract N°: 2224
RISK OF RECURRENCE IN AF PATIENTS WITH ACUTE ISCHEMIC STROKE: THE IMPACT OF CONCOMITANT MAJOR CEREBRAL ARTERY STENO-OCCLUSIONS
Hyung Seok Guk*1, Do Yeon Kim1, Beom Joon Kim2, Joon-Tae Kim3, Byung-Chul Lee4, Jun Lee5, Keon-Joo Lee6, Ji Sung Lee7, Juneyoung Lee8, Hee-Joon Bae2
1Seoul National University Bundang Hospital, Department of Neurology and Cerebrovascular Center, Seongnam-si, South Korea, 2Cerebrovascular Center, Seoul National University Bundang Hospital, Department of Neurology, Seoul National University College of Medicine, Seongnam-si, South Korea, 3Chonnam National University Hospital, Department of Neurology, Gwangju, South Korea, 4Hallym University Sacred Heart Hospital, Department of Neurology, Anyang-si, South Korea, 5Yeungnam University Hospital, Department of Neurology, Daegu, South Korea, 6Korea University Guro Hospital, Department of Neurology, Seoul, South Korea, 7Asan Medical Center, University of Ulsan College of Medicine, Clinical Research Center, Asan Institute for Life Sciences, Seoul, South Korea, 8Korea University College of Medicine, Department of Biostatistics, Seoul, South Korea
On behalf of: EAST-AF and CRCS-K Investigators
Background and aims: Atrial fibrillation (AF) patients presenting with acute ischemic stroke (AIS) often exhibit cerebral atherosclerosis, a notable prognostic factor for stroke. However, its prognostic significance in such patients remains unclear.
Methods: Utilizing the EAST-AF (East Asian ischemic STroke with Atrial Fibrillation) Part II study, a prospective multicenter cohort, data were collected from patients who underwent MR Angiography during admission. Concomitant large artery steno-occlusion (cLASO) was evaluated across 26 segments of major cerebral arteries. Ischemic stroke recurrence (ISR) risk was analyzed based on cLASO presence, severity (mild 1-49%; moderate-to-severe 50-99%; occlusion), and relevance (potential to cause infarction or residual stenosis post-thrombectomy) using cause-specific hazard models, considering death as a competing risk.
Results: Of 2035 patients (mean age 74.9; 55% male), 67% had cLASO. Among these, 33% had mild, 27% moderate-to-severe, and 40% occlusion; 43% had relevant steno-occlusion. Discharge treatments included 85% on anticoagulants and 22% on antiplatelets (13% on both). Over a median follow-up of 756 days, incidences of ISR varied significantly with cLASO presence, severity, and relevance (P’s<0.01; Figure). Approximately half of the 3-year ISRs occurred within 3 months. Adjusted hazard ratios for cLASO presence, moderate-to-severe stenosis, and relevance were 1.79 (95% confidence intervals; 1.47-2.18), 2.26 (1.38-3.70), and 3.47 (2.66-4.53), respectively.
Conclusions: cLASO, particularly of higher degree or relevance, markedly raises recurrent stroke risk in AF patients with AIS, notably in the first 3 months. Prompt risk stratification and management are crucial.
Disclosures of Interest: Yes This study was supported in part by Bristol–Myers Squibb Korea and the Korea Centers for Disease Control and Prevention (no. 2020ER620200f)
Abstract N°: 2304
CONTEXTUAL BRAIN AGE, TELOMERE LENGTH AND POOR FUNCTIONAL OUTCOME IN PATIENTS WITH ISCHEMIC CEREBROVASCULAR DISEASE
Hongyu Zhou*1, Zixiao LI1, Yongjun Wang1
1Beijing Tiantan Hospital, Capital Medical University, Department of Neurology, Beijing, China
On behalf of:
Background and aims: We aimed to investigate the relationship between brain age based on T2-FLAIR and poor functional outcome in patients with acute ischemic stroke or transient ischemic attack (TIA) with different telomere lengths.
Methods: A total of 7325 patients with imaging and genetic data from the CNSR-III were included. To analyse the non-infarcted brain regions and approximate the pre-onset brain state, we proposed a Mask-based Brain Age estimation Network to predict brain age, called contextual brain age (CBA). The disparity between brain and chronological age is called the predicted age difference (PAD). The study participants were stratified based on PAD and telomere lengths. Poor functional outcome was defined as the mRS score of 3 to 6.
Results: Through the 3-month follow-up, positive PAD increased the risk of poor functional outcome in the T1 group (T1, adjusted OR 1.45, 95% CI 1.13-1.86). However, in the T2 and T3 groups, there was no significant association between positive PAD and poor functional outcome (T2, adjusted OR 1.21, 95% CI 0.94-1.56; T3, adjusted OR 1.27, 95% CI 0.99-1.64). During the 1-year follow-up, positive PAD was correlated with an increased risk of poor functional outcome across different telomere length groups (T1, adjusted OR 1.49, 95% CI 1.16-1.92; T2, adjusted OR 1.48, 95% CI 1.13-1.92; T3, adjusted OR 1.44, 95% CI 1.10-1.87). There was no significant interaction between telomere length and PAD at 3 months and 1 year.
Conclusions: Telomere length has a complex relationship with CBA in the risk of poor functional outcome, especially in the short term.
Disclosures of Interest: No
Abstract N°: 2331
TRIMETHYLAMINE N-OXIDE (TMAO) DOES NOT IMPROVE RISK STRATIFICATION AFTER ACUTE ISCHEMIC STROKE – RESULTS FROM THE BIOSIGNAL STUDY
benjamin jeker*1, Frenger Johannes1, Markus Arnold2, Gian Marco De Marchis3, Carlo Cereda4, Timo Kahles5, Joan Montaner6, George Ntaios7, Müller Daniel1, Mira Katan1,2
1Universitätsspital Basel, Basel, Switzerland, 2University Hospital of Zürich, Zürich, Switzerland, 3Kantonsspital St.Gallen, St. Gallen, Switzerland, 4EOC Ospedale Regionale di Lugano - Civico, Lugano, Switzerland, 5KSA Kantonsspital Aarau, Aarau, Switzerland, 6Hospital Universitario Virgen Macarena, Department of Neurology, Sevilla, Spain, 7Larissa General University Hospital, Greece
On behalf of: the BIOSIGNAL consortium
Background and aims: Recent studies in patients with myocardial infarction and atrial fibrillation have underscored the significance of trimethylamine N-oxide (TMAO) as a valuable blood biomarker for predicting major adverse cardiovascular events (MACE). However, its role after ischemic stroke remains underexplored. This study aims to elucidate the association between TMAO levels and MACE as well as functional outcome after stroke.
Methods: We measured plasma TMAO levels in 1726 acute ischemic stroke patients (within 24 hours from symptom onset) from the multicenter BIOSIGNAL cohort. Measurements were blinded to all outcomes. We investigated the association of TMAO with MACE within 365 days and functional outcome at 90 days using cox respectively logistic regression models adjusting for demographic and vascular risk factors.
Results: In a univariate analysis patients with higher TMAO levels did not have a significant higher risk of MACE (n=320) within 365 days after stroke (unadj HR per unit increase of log(TMAO) 1.07 and 95% CI 0.91-1.26). Moreover, we also did not find an independent association with unfavorable outcomes (adj. OR per unit increase of log(TMAO) 1.07 95% CI 0.89-1.28) in a multivariate logistic regression model. The results did not change when looking at pre-defined interactions (i.e. stroke etiology, stroke severity and the presence versus absence of comorbidities).
Conclusions: In the BIOSIGNAL cohort, TMAO does not appear to be independently associated with an increased risk for MACE, or adverse functional outcomes following stroke thus TMAO does not represent a clinically useful prognostic marker in the stroke population.
Disclosures of Interest: No
Abstract N°: 2401
EFFECT OF FIBRINOGEN ON EFFICACY OF ALTEPLASE PPST STROKE
1Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China, China National Clinical Research Center for Neurological Diseases, Beijing Tiantan Hospital, Capital Medical University, Beijing, China
On behalf of:
Background and aims: The effect of IV thrombolysis might depend on hemostasis factors affecting clot structure, notably the fibrinogen. The dynamic changes in fibrinogen levels are associated with intracranial hemorrhage in patients treated with intravenous rt-PA. However, the data for poor outcomes (mRS 0-6) after 3 months are limited. Our study aims to determine the effect of fibrinogen level on poor functional outcomes in stroke patients treated with alteplase.
Methods: TRACE II is a multicenter, prospective, open-label, blinded-endpoint, randomized controlled, non-inferiority trial, including adults with an acute ischemic stroke within 4·5 h, received intravenous alteplase (0.9mg/kg). The fibrinogen plasma level was measured before and 24 hours after thrombolysis. The efficacy outcome was the proportion of participants who had an mRS score of 2-6 at 90 days. All statistical analyses were performed with SAS software, version 9.4.
Results: 704 patients received rt-PA intravenous thrombolysis. Among them, 266 (37.6%) had poor outcomes at 3 months with a mean age of 68 (60-75) and male dominance (67%). In multivariable regression analysis, plasma fibrinogen level was independently associated with poor outcomes adjusted for cardiovascular risk factors. On admission, fibrinogen level was significantly associated with risk of mRS (2-6) (OR: 1.3; CI 95% (1.08-1.57); p=0,005), after 24 h of rt-PA thrombolysis the fibrinogen increasing 1.52-fold the risk of poor outcome (OR: 1.52; CI 95% (1.24-1.86); p<0.001).
Conclusions: The fibrinogen level could be a predictor biomarker of poor outcomes after 30 months in patients receiving rt-PA intravenous thrombolysis.
Disclosures of Interest: No
Abstract N°: 2648
PERIVASCULAR SPACES AND THE RISK OF HEMORRHAGE AFTER INTRAVENOUS THROMBOLYSIS
Iris Deppe*1, Domenique Ahrens2, Tim Bastian Brämswig3, Jochen B. Fiebach1, Christian Nolte3, Jan Scheitz3, Kersten Villringer1
1Center for Stroke Research Berlin, Charité-Universitätsmedizin Berlin, Berlin, Germany, 2Department of Radiology, Charité-Universitätsmedizin Berlin, Berlin, Germany, 3Department of Neurology with experimental Neurology, Center for Stroke Research Berlin, Charité-Universitätsmedizin Berlin, Berlin, Germany
On behalf of:
Background and aims: Perivascular spaces (PVS) have been identified as a marker of small vessel disease(SVD) and have been associated with increased risk of stroke1. However, data on a possible association between PVS count and the risk of symptomatic hemorrhage(sICH) after intravenous thrombolysis (iv-TPA) is lacking.
Methods: We analyzed radiological, clinical data as well as outcomes of stroke patients who received iv-TPA using 3-T-MRI as primary diagnostic imaging between 2008 and 2017. The number of PVS was evaluated by two raters (ID=senior radiologist, DA=radiological technologist) using the Potter visual rating scale2 on B0 images in the basal ganglia(BG) and the centrum semiovale(CSO). The association between PVS count and both hemorrhagic transformation(HT) and sICH was evaluated cross-sectionally using binary logistic regression. Outcome was assessed using modified Rankin Scale day 90(mRS-d90).
Results: Interrater Agreement was good (Kappa=0.86 BG, Kappa=0.78 CSO). Out of 664 patients (mean age 74 +/-12, 64% female) 149 patients had HT. Fifty-five were classified as sICH (ECASS II)3. There was no association of increased PVS with either sICH (BG: OR 1.003(0.596-1.687), CSO: OR 0.960 (0.572-1.612)) or HT (BG: OR 0.918(0.644-1.309) CSO: OR 1.001 (0.719-1.421)). There was no association between PVS count and mRS-d90 either (BG: OR 0.849(0.614-1.174) CSO: OR 0.874(0.642-1.191)). An association was found between hypertension and increased PVS count in the BG (OR 1.075(1.018-1.135), as well as with increased SVD-Score4 and unfavourable outcome (>2 mRS-d90)(OR 0.785(0.662-0.93)).
Conclusions: There was no increased risk of sICH after ivTPA in acute stroke patients with increased PVS count.
Disclosures of Interest: No
Abstract N°: 2784
THE INFLAMMATION AND RECURRENCE RISK IN ISCHAEMIC STROKE (IRIS) SCORE: DERIVATION AND VALIDATION
Sarah Gorey*1, Cathal Walsh2, Gian Marco De Marchis3,4, Mira Katan5, Annie Pedersen6, Francisco Purroy7, Peter Rothwell8, Cathie Sudlow9, John Mccabe10, Peter Kelly10
1UCD School of Medicine, Dublin, Ireland, 2Trinity College Dublin, Ireland, 3Universitätsspital Basel, Basel, Switzerland, 4Kantonsspital St.Gallen, Klinik für Neurologie & Stroke Center, St. Gallen, Switzerland, 5Universität Basel, Basel, Switzerland, 6University of Gothenburg, Sweden, 7Institut de Recerca Biomèdica de Lleida Fundació Dr. Pifarré, Lleida, Spain, 8Department of Clinical Neurosciences (DCN), Medical Sciences Division, United Kingdom, 9The University of Edinburgh, United Kingdom, 10The Mater Misericordiae University Hospital, Ireland
On behalf of: On behalf of the BISC Biomarkers in Stroke Collaboration; Markus Arnold, Sarah Coveney, Joan Marti-Fabregas, Pablo Hervella, Ramon Iglesias-Rey, Christina Jern, Linxin Li, Joan Montaner, Mikel Vicente-Pascual, Yuji Ueno, William Whiteley.
Background and aims: High sensitivity C-reactive protein (hsCRP) is not routinely-measured for risk-stratification of recurrent vascular events after stroke. We aimed to develop a risk prediction score including hsCRP and investigate its clinical utility.
Methods: BISC includes individual-patient-data of 10,520 participants from 12 prospective cohort studies. Outcomes were (1) major adverse cardiovascular event (MACE) (2) fatal/nonfatal stroke (3) fatal/nonfatal major cardiac event. The cohort was divided into derivation (n=7290) and validation (n=3230) sets. We derived and externally-validated a risk-prediction model using multivariate stepwise Cox regression. We then created a points-based risk score for clinical use.
Results: Derivation-set median follow-up was 96 days (IQR 90-366). Recurrence rates were: MACE 12%, stroke 10.5%, major cardiac events 1.2%. The final model included 7 independent variables, including highest hsCRP quarter (⩾8mg/L) (p<0.05). A 10-point clinical-risk score (IRIS) was derived (Table). Derivation-set C-statistics were: MACE 0.58 (CI 0.55-0.60); stroke 0.53 (CI 0.51-0.55); major cardiac event 0.70 (CI 0.66-0.74). In the validation-set, C-statistics were: MACE 0.56 (CI 0.53-0.59); stroke 0.53 (CI 0.49-0.57); major cardiac event 0.65 (CI 0.59-0.71). Validation-set observed and predicted risks were consistent indicating good calibration. Net reclassification improvement was 14.5. Recurrence risk increased across ordinal IRIS categories (ptrend<0.001).
Conclusions: A risk prediction score incorporating hsCRP was externally-valid and performed best for improving identification of patients with fatal/non-fatal coronary events after stroke.
Disclosures of Interest: No
Abstract N°: 2840
PREVALENCE AND FACTORS ASSOCIATED WITH SEXUAL FUNCTION AFTER STROKE: A MULTI-CENTRE OBSERVATIONAL STUDY
Hatice Ozkan*1,2, Lisa Woodhouse3, Rosalind Brown4, Ellen Backhouse4, Richard Mcmanus5, Philip Bath3, Adrian Parry-Jones6, Nikola Sprigg3, Joanna Wardlaw4, David Werring1,2
1UCL Queen Square Institute of Neurology, London, UK, 2National Hospital for Neurology and Neurosurgery, University College London Hospitals NHS Foundation, Queen Square, London, 3Stroke Trials Unit, Mental Health & Clinical Neurosciences, School of Medicine, University of Nottingham, 4Centre for Clinical Brain Sciences, University of Edinburgh, Edinburgh, UK, 5Department of General Practice, University of Oxford, UK, 6Division of Cardiovascular Sciences, School of Medicine, Faculty of Biology, Medicine & Health, Manchester Academic Health Science Centre, The University of Manchester, Manchester, UK
On behalf of:
Background and aims: Stroke frequently causes sexual dysfunction and patients commonly perceive this as emotionally challenging. Nevertheless, knowledge about post-stroke sexual function remains limited.
Methods: We included data from R4VaD (Rates, Risks, and Routes to Reduce vascular dementia), a UK-wide multicentre prospective observational cohort study. We investigated 6-week prevalence and baseline factors associated with sexual dysfunction (problems with sexual response, desire, orgasm or pain) after cerebral ischaemic stroke, transient ischaemic attack (TIA), and intracerebral haemorrhage (ICH).
Results: We included 338 stroke patients, with an 83% follow-up rate. Median age was 64.7 years (range: 18–83), and 31% were female. At 6 weeks post-stroke, the prevalence of sexual dysfunction was 43%. Patients with ICH were significantly more likely to report sexual dysfunction (50%) compared to patients with ischemic stroke (41%) or TIA (48%), p=0.049. Factors associated with sexual dysfunction included:modified Rankin Scale (mRS) score >2 (OR 3.80, 95% Cl 1.67 – 5.63, p= 0.018); male sex (OR 2.17, 95% Cl 1.29 – 3.09, p= 0.042); pre-stroke cognitive impairment (OR 2.03, 95% Cl 1.73 – 2.41, p= 0.033); and pre-stroke depression (OR 1.87, 95% Cl 1.29 – 2.18, p= 0.007).
Conclusions: Sexual dysfunction affects over 40% of individuals six weeks post-stroke yet remains overlooked in clinical practice. Male sex, functional disability, pre-stroke cognitive impairment and depression could identify people at highest risk so aiding Improved recognition and management strategies.
Full list of authors: Hatice Ozkan1,2, Lisa J Woodhouse3, Rosalind Brown4, Ellen Backhouse4, Richard McManus, Hugh Markus, Philip M Bath3, Adrian Parry-Jones7, Yee-Haur Mah8, Nikola Sprigg3, Joanna Wardlaw4, David J Werring1,2, R4VaD investigators
Disclosures of Interest: No
Abstract N°: 2878
INFLUENCE OF ASYMPTOMATIC HAEMORRHAGIC TRANSFORMATION FOLLOWING ENDOVASCULAR TREATMENT ON FUNCTIONAL OUTCOME IN PATIENTS WITH ACUTE ISCHEMIC STROKE
Marina Guasch Jiménez*1, Pere Cardona2, Noelia Rodriguez-Villatoro3, Alejandro Rodríguez Vázquez4, Meritxell Gomis5, Tomàs Xuclà Ferrarons6, Ana Rodríguez-Campello7, David Cánovas8, Mercè Salvat-Plana9,10, Pol Camps Renom1
1Stroke Unit, Department of Neurology, Biomedical Research Institute Sant Pau (IIB-Sant Pau), Hospital de la Santa Creu i Sant Pau, Universitat Autònoma de Barcelona (Department of Medicine) Barcelona, Spain., Spain, 2Bellvitge University Hospital, Neurology, L'Hospitalet de Llobregat, Spain, 3Vall d'Hebron University Hospital, Neurology, Barcelona, Spain, 4Hospital Clínic de Barcelona, Neurology, Barcelona, Spain, 5Hospital Germans Trias i Pujol, Neurology, Badalona, Spain, 6Hospital Universitari de Girona Doctor Josep Trueta, Neurology, Girona, Spain, 7Hospital del Mar, Neurology, Barcelona, Spain, 8Park Taulí University Hospital, Neurology, Sabadell, Spain, 9Agència de Qualitat i Avaluació Sanitàries de Catalunya, Barcelona, Spain, 10CIBER Epidemiology and Public Health, Barcelona, Spain., Barcelona, Spain
On behalf of: Laia Seró-Ballesteros10, Francisco Purroy11 and the CICAT registry. 10Stroke Unit, Neurology, Hospital Universitari Joan XXIII, Tarragona, Spain. 11Stroke Unit, Neurology, Hospital Universitari Arnau de Vilanova, Lleida, Spain.
Background and aims: In patients with acute ischemic stroke (AIS), the association between symptomatic intracerebral haemorrhage (sICH) after endovascular treatment (EVT) and unfavourable outcomes has been established. However, the influence of asymptomatic haemorrhagic transformation (HT) following EVT on functional outcome remains unclear.
Methods: We performed a retrospective study using an official and mandatory population-based prospective stroke code registry in Catalonia (CICAT). All patients with an anterior circulation AIS (January2017-March2023) who underwent EVT were included. We excluded patients without data on the presence of HT or functional outcome. HT was categorised according to the ECASS-2 classification. Functional outcome was centrally assessed using the modified Rankin Scale (mRS) by certified blinded personnel. The primary outcome was the shift on the mRS score at three months of follow-up. After excluding sICH, multivariable ordinal regression analyses (adjusted by age, prior mRS, baseline NIHSS, ASPECTS and mTICI⩾2b) were performed to test an association between asymptomatic TH and the primary outcome.
Results: We included 3067 patients [72.0 years, 50.7% women]. sICH was present in 179 (5.8%) and asymptomatic HT in 612 (21.2%). In multivariable analysis, any asymptomatic TH was associated with a worse functional outcome (cOR 2.24, 95CI: 1.89-2.66) and higher mortality (OR 1.50, 95%CI: 1.17-1.91) at three months. In sensitivity analyses by HT subtypes, the association with functional outcome remained significant for any subtype, with asymptomatic PH2 showing higher odds of a worse outcome (cOR 3.15, 95%CI: 1.46-6.83).
Conclusions: In patients with AIS treated with EVT, we found that any asymptomatic HT was associated with a worse functional outcome.
Disclosures of Interest: No
Abstract N°: 3236
HIGHER HDL CHOLESTEROL IS ASSOCIATED WITH IMPROVED FUNCTIONAL OUTCOME AND REDUCED BLEEDING RISK AFTER THROMBECTOMY FOR ANTERIOR CIRCULATION STROKE
Annahita Sedghi1, Sonja Schreckenbauer1, Daniel Kaiser2, Ani Cuberi2, Martin Arndt1, Jessica Barlinn1, Kristian Barlinn1, Volker Puetz1, Timo Siepmann*1
1University Hospital Carl Gustav Carus, Department of Neurology, Dresden, Germany, 2University Hospital Carl Gustav Carus, Department of Neuroradiology, Dresden, Germany
On behalf of:
Background and aims: The role of high-density lipoprotein cholesterol (HDL-C) in the pathophysiology of acute ischemic stroke (AIS) and in the response to acute recanalization therapy is controversial. We studied the impact of serum HDL-C on outcome after thrombectomy for AIS and scrutinized its dependence on preceding thrombolysis.
Methods: We analyzed data from consecutive anterior circulation large vessel occlusion (acLVO) patients from our prospective thrombectomy registry treated from 01/2017 to 09/2022 at a German tertiary stroke center. We evaluated the association of HDL-C levels and 90-day functional outcome quantified via modified Rankin scale (mRS) applying multivariate lasso regression with interaction terms with subsequent sensitivity analyses using propensity score matching.
Results: In our study population of 942 acLVO patients who received thrombectomy (486 females, median age 77 [67-84, IQR]) higher HDL-C emerged as predictor of better functional outcome [ß=-0.4; 95% CI [-0.7-0.1]; p=0.02) and lower risk of intracranial hemorrhage [OR=0.6; 95% CI [0.3-0.9]; p=0.03] independent of thrombolysis with adjustment for demographic and cardiovascular risk profiles, clinical and imaging stroke characteristics, grade of reperfusion, distal thrombus migration and onset-to-recanalization time. We could reproduce the beneficial association of high HDL-C levels and improved functional outcome on propensity score analysis, where an increase of 1 mg/dl in HDL-C led to a 0.32 decrease in 90-day mRS [p= 0.03].
Conclusions: Higher levels of HDL-C are independently associated with improved functional outcome in patients with acLVO, likely mediated by a decreased risk of ICH but not explainable by modulation of the pharmacodynamic effect of rtPA alone.
Disclosures of Interest: Yes Prof. Siepmann received speaker fees from Astrazeneca
Abstract N°: 283
HEMORRHAGIC TRANSFORMATION IS ASSOCIATED WITH POOR FUNCTIONAL OUTCOME AFTER SUCCESSFUL ENDOVASCULAR TREATMENT OF STROKE
Faustin Cloet*1, Stefanos Finitsis2, Alain Viguier1, Christophe Cognard3, Jean-François Albucher1, Lionel Calviere1, Nicolas Raposo1, Bertrand Lapergue4, Benjamin Gory5, Jean-Marc Olivot1
1Department of Neurology Acute Stroke Unit-CIC 1436-UMR 1214, CHU Toulouse, Toulouse, France, 2Department of Neuroradiology, Aristotle University of Thessaloniki, Ahepa Hospital, Thessaloniki, Greece, 3Department of Interventional and Diagnostic Neuroradiolology, CHU Toulouse, Toulouse, France, 4Department of Neurology, Foch Hospital, Versailles Saint-Quentin en Yvelines University, Suresnes, France, 5Diagnostic and Therapeutic Neuroradiology, Université de Lorraine, IADI, INSERM U1254, Nancy, France
On behalf of: The ETIS Registry Investigators
Background and aims: Despite a 90% recanalization rate, more than 50% of patients experiencing a large-vessel occlusion related acute ischemic stroke (LVO-AIS) successfully treated by endovascular treatment (EVT) have a poor functional outcome. We aimed in this study 1- to evaluate the relationship between post-endovascular reperfusion hemorrhagic transformation (HT) and poor functional outcome and 2- to identify factors associated with HT.
Methods: We reviewed data from consecutive patients enrolled in the “Endovascular Treatment for Ischemic Stroke” registry with LVO-AIS in the anterior or posterior circulation successfully (TICI2b-3) treated by EVT. The occurrence of HT was assessed according to European Collaborative Acute Stroke Study classification. Poor functional outcome was defined by a modified Rankin Scale > 2 at 3 months.
Results: 3759 patients with anterior circulation stroke and 352 patients with posterior circulation stroke were included. HT occurred among 1597 (42.5%) in the anterior and 76 (21.6%) in the posterior circulation patients. Any HT occurrence and its severity were associated with poor outcome. After multivariate analysis, post-treatment parenchymal hemorrhage (i.e PH1 and PH2) in the anterior circulation was associated with higher systolic blood pressure and blood sugar level at admission, initial stroke severity (i.e higher NIHSS and lower ASPECT scores), drip-and-ship management and CT imaging selection. For the posterior circulation, a lower pre-treatment PC-ASPECT score was associated with any HT.
Conclusions: HT after the successful endovascular treatment of anterior and posterior LVO-AIS is frequent and associated with poor outcome. Expedited transfer and adjunctive therapy treatment mitigating HT may improve clinical response to endovascular reperfusion.
Disclosures of Interest: No
Abstract N°: 394
QUANTIFICATION OF THE IMPACT OF LEPTOMENINGEAL COLLATERALS DURING STROKE – A COMPUTATIONAL FRAMEWORK INCORPORATING IN VIVO DATA
Robert Epp1, Chryso Lambride2, Chaim Glück3, Nadine Binder4, Mohamad El Amki4, Bruno Weber3, Susanne Wegener4, Patrick Jenny1, Franca Schmid2
1Institute of Fluid Dynamics, ETH Zurich, Zurich, Switzerland, 2ARTORG Center for Biomedical Engineering Research, University of Bern, Bern, Switzerland, 3Institute of Pharmacology and Toxicology, University of Zurich, Zurich, Switzerland, 4Dept. of Neurology, University Hospital Zurich and University of Zurich, Zurich, Switzerland
On behalf of:
Background and aims: Leptomeningeal collaterals (LMCs), i.e., anastomoses at pial level, are known to be beneficial for stroke outcome. However, quantifying the precise impact of the extent of collaterals in maintaining perfusion during stroke remains challenging.
Methods: We performed blood flow simulations in four semi-realistic microvascular networks derived from two LMC-rich (C57BL/6) and two LMC-poor (BALB/C) mice. By artificially modifying the number of LMCs, their impact on perfusion could be studied in an isolated manner and across all vessel types, including arteries, veins, and the capillary bed.
Results: We showed that after middle cerebral artery (MCA) occlusion LMCs caused a redistribution of flow from the anterior cerebral artery (ACA) territory towards the MCA territory. Flow redistribution was enhanced by dilation of LMCs, arterial dilation, and the extent of collateralization. For example, within 250 µm from the LMCs, the summed flow rate through all descending arterioles (DAs) was 714% larger for 100% LMCs and 431% larger for 50% LMCs if compared with no LMCs. Importantly, the beneficial effect of LMCs was also apparent at the capillary level but generally came at the cost of slightly reduced flow rates in ACA-sided DAs and capillaries.
Conclusions: Our results highlight the relevance of LMCs in maintaining perfusion after MCA occlusion. This likely contributes to preserving vascular functionality, which seems crucial for successful treatment. Moreover, as our simulation framework is directly aligned with in vivo experiments, it is ideally suited for follow-up studies on the impact of vascular alterations during stroke and interventions.
Disclosures of Interest: No
Abstract N°: 481
CLINICAL COURSE, CAUSES OF WORSENING, AND OUTCOMES FROM SEVERE ACUTE ISCHAEMIC STROKE: A PROSPECTIVE MULTICENTRE COHORT STUDY
Simiao Wu*1, Yanan Wang1, Cairong Zhu2, Craig Anderson3, Ming Liu1
1West China Hospital, Sichuan University, Department of Neurology, Chengdu, China, 2West China School of Public Health and West China Fourth Hospital, Sichuan University, Department of Epidemiology and Health Statistics, Chengdu, China, 3The George Institute, Global Brain Health, Sydney, Australia
On behalf of:
Background and aims: To investigate clinical course, causes of worsening, and outcomes of severe ischaemic stroke.
Methods: This prospective, multicentre cohort study enrolled adult patients <30 days after acute ischaemic stroke. Severe stroke was defined as National Institutes of Health Stroke Scale (NIHSS) score ⩾15. Neurological worsening was defined as an increase of 2 in NIHSS from baseline. Outcomes were unfavourable outcome (modified Rankin scale, mRS ⩾3) at 3 months and 1 year.
Results: Of 4201 patients enrolled, 854 patients (20.3%) had severe stroke on admission and 607 patients (14.4%) had neurological worsening. Brain oedema (n=244, time from onset to worsening, median 45h) was the leading cause of worsening, followed by progressive stroke (n=142, median 49h) and haemorrhagic transformation (HT, n=137, median 45h). Of 141 patients (3.4%) with late-developed severe stroke, HT (n=40) was the leading cause. Intravenous thrombolysis was associated with increased risk of neurological worsening (adjusted OR 1.96, 95% CI 1.40-2.75), and reduced risk of 3-month (adjusted OR 0.72, 95% CI 0.53-0.97) and 1-year (adjusted OR 0.58, 95% CI 0.42-0.81) unfavourable outcomes; recanalization reduced the risk of worsening (adjusted OR 0.47, 95% CI 0.25-0.87), and unfavourable outcomes at 3 months (adjusted OR 0.36, 95% CI 0.17-0.79) and 1 year (adjusted OR 0.35, 95% CI 0.16-0.75), after adjusting for the effect of age, NIHSS, diabetes, and large infarct.
Conclusions: Neurological worsening mainly occurred in the first 3 days after stroke, with brain oedema as the leading cause. HT was the main cause for late-developed severe stroke. Recanalization reduced the risk of worsening and improved outcomes.
Disclosures of Interest: No
Abstract N°: 508
DETERMINING AEROMEDICAL RISK IN PILOTS WHO HAVE HAD A STROKE – WOULD YOU FLY WITH THESE PILOTS?
Timothy Ingall*1
1Mayo Clinic, Neurology, Scottsdale, United States
On behalf of:
Background and aims: For pilots requesting certification following a stroke, the risks of stroke recurrence and post-stroke seizures, and recurrent stroke risk mitigation management, should be assessed. It is unclear how the European, UK, and USA aviation authorities determine aeromedical risk when assessing pilots with cerebrovascular disease.
Methods: Published regulations from the European Union Aviation Safety Agency (EASA), the UK Civil Aviation Authority (CAA), and the US Federal Aviation Administration (FAA) regarding the evaluation of pilots with cerebrovascular conditions were reviewed to determine if an aeromedical risk assessment based on the risks of recurrent stroke and post-stroke seizures, and recurrent stroke risk mitigation management, is required.
Results: EASA and FAA regulations do not specifically mention an assessment of the risks of recurrent stroke or post-stroke seizures, or stroke risk mitigation management when assessing a pilot with a stroke for certification. The UK CAA performs no individual aeromedical risk assessment for Class 1 pilots with a history of stroke based on a determination that their risk of stroke recurrence always exceeds 1%/year.
Conclusions: Aviation authority regulations in the USA and Europe regarding the aeromedical assessment of pilots with cerebrovascular disorders are vague and opaque, while in the UK, no Class 1 pilot with a history of stroke can be certified. Professional Stroke associations should work with aviation authorities to ensure that the evaluation of pilots with cerebrovascular disorders include an assessment of the risks of recurrent stroke and post-stroke seizures, and recurrent stroke mitigation management, to determine if they can be certified as medically safe to fly.
Disclosures of Interest: No
Abstract N°: 862
IMPACT OF PRE-STROKE FRAILTY ON OUTCOME IN ACUTE STROKE: A THREE-YEAR FOLLOW-UP STUDY FROM NOR-COAST
Ragnhild Munthe-Kaas1,2, Stian Lydersen3, Terence J Quinn4, Stina Aam5, Sarah T Pendlebury6,7, Hege Ihle-Hansen*8,9
1Kongsberg Hospital,Vestre Viken Hospital Trust, Norway, Department of Medicine, 2Bærum Hospital, Vestre Viken Hospital Trust, Norway, Department of Medicine, 3Regional Centre for Child and Youth Mental Health, Faculty of Medicine and Health Science, NTNU-Norwegian University of Science and Technology, Trondheim, Norway, Department of Mental Health, 4University of Glasgow, Institute of Cardiovascular and Medical Sciences, Glasgow, United Kingdom, 5Faculty of Medicine and Health Science, NTNU-Norwegian University of Science and Technology, Trondheim, Norway, Department of Neuromedicine and Movement Science, 6Oxford University Hospitals NHS Foundation Trust, Oxford, UK, Departments of Acute Internal Medicine and Geratology, 7Wolfson Centre for Prevention of Stroke and Dementia, Nuffield Department of Clinical Neurosciences, University Of Oxford, and the NIHR Biomedical Research Centre Oxford University Hospitals NHS Foundation Trust, Oxford, UK, 8Institute of Clinical Medicine, University of Oslo, Oslo, Norway, 9Oslo University Hospital, Ullevaal, Oslo, Norway, Stroke Unit, Department of Neurology
On behalf of:
Background and aims: Frailty is a state of vulnerability with an increased risk of adverse health outcomes. We aimed to explore the predictive value of pre-stroke frailty index (FI) on functional dependency and mortality three years after stroke.
Methods: Based on the Rockwood’ 36-item FI score, we generated pre-stroke FI from medical conditions recorded at baseline in the multicentre prospective Norwegian Cognitive Impairment after Stroke (Nor-COAST) 2015-2017. Participants with a FI score and a modified Rankin scale (mRS) 0-6 at three years were included in the study. We used logistic regression with mRS 0-2 versus over 2 and logistic regression with dead at three years as outcome, unadjusted and adjusted for the following variables one at a time: Age, sex, years of education, NIHSS at admission and stroke progression. We report OR per 0.10 increase in FI.
Results: At baseline, the 609 included patients had mean age 72.8 (SD 11.8), 261 (43%) were females, and had a FI mean score of 0.16 (SD 0.12), range 0 to 0.69. During three years, 138 (23%) had died.
FI was a strong predictor (OR=4.1, 95% CI 3.2 to 5.2) for bad function post stroke (mRS>2). Only adjusting for age (OR=2.8) affected the result. FI was a strong predictor for death before 3 years (OR=2.2, CI 2.2 to 3.6), adjusted for age and sex. Adjusting for any of the other listed variables gave approximately the same results.
Conclusions: As a strong predictor of poor outcome, FI can be included in prognostication after stroke.
Disclosures of Interest: No
Abstract N°: 938
TO WEIGHT OR NOT TO WEIGHT: CONSIDERATIONS FOR ANALYZING MODIFIED RANKIN SCALE IN ACUTE STROKE TRIALS
Ayoola Ademola1, Michael Hill1, Bijoy Menon1, Tolulope Sajobi*1
1University of Calgary, Calgary, Canada
On behalf of:
Background and aims: The utility-weighted-modified Rankin Scale (UW-mRS) is a patient-centered, approximately continuous scale that is increasingly used as an outcome measure in stroke trials. This study examines the performance of regression approaches on the mRS and the UW-mRS
Methods: Computer simulations were used to evaluate the performance of ordered probit regression, UW-mRS-based linear regression, unweighted-mRS linear regression, and logistic regression for analyzing mRS data. Simulation data were generated based on ordinal regression model with patient distribution across the mRS scale obtained from Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Times (ESCAPE) trial and Intravenous Tenecteplase compared with Alteplase for acute Ischaemic stroke in Canada (AcT) trials. Type I error and statistical power were used to evaluate comparative performance of these models.
Results: While all the models demonstrated reasonable control over the Type 1 error rate (i.e., < 5%), they differed with respect to the statistical power under a variety of data characteristics. The UW-mRS-based linear regression showed greater power than logistic regression, but it has less power than the unweighted-mRS linear regression and ordered probit regression models.
Conclusions: The selection of an appropriate analytical method should by be guided by considerations for statistical power, interpretability of associated effect size, and the type of research question being addressed.
Disclosures of Interest: No
Abstract N°: 948
THE DEEP LEARNING-BASED PREDICTION MODEL FOR MORTALITY AFTER ISCHEMIC STROKE
Mi-Young Oh*1, Changi Kim2, Jun Myoung Kwon3, Sang Won Park4, Chulho Kim5
1Bucheon Sejong Hospital, Department of Neurology, 2Seoul national university, Department of bioengineering, 3Medical AI Inc, Medical Research team, 4Kangwon National University, Department of Medical Informatics, 5Hallym University College of Medicine, Department of Neurology
On behalf of:
Background and aims: Most prognostic indexes for ischemic stroke mortality lack radiologic information. We aimed to create and validate a deep learning-based mortality prediction model using brain diffusion weighted imaging (DWI), apparent diffusion coefficient (ADC), and clinical factors.
Methods: Data from patients with ischemic stroke who admitted to two tertiary hospitals during acute periods from 2013–2019 were collected and split into training (n = 1,109), validation (n = 437), and internal test (n = 654). Data from patients from secondary cardiovascular center was used for external test set (n = 507). The algorithm for predicting mortality, based on DWI and ADC (DLP_DWI), was initially trained. Subsequently, important clinical factors were integrated into this model to create the integrated model (DLP_INTG). The performance of DLP_DWI and DLP_INTG was evaluated by using time-dependent area under the receiver operating characteristic curves (TD AUCs) and Harrell concordance index (C-index) at one-year mortality.
Results: The TD AUC of DLP_DWI was 0.643 in internal test set, and 0.785 in the external dataset. DLP_INTG had a higher performance at predicting one-year mortality than premise score in internal dataset (TD- AUC: 0.859 vs. 0.746; p =0 .046), in external dataset (TD- AUC: 0.876 vs. 0.808; p =0 .007). DLP_DWI and DLP_INTG exhibited strong discrimination for the high-risk group for one-year mortality.
Conclusions: A deep learning model using brain DWI, ADC and the clinical factors was capable of predicting mortality in patients with ischemic stroke.
Disclosures of Interest: No
Abstract N°: 1079
THE RELATIONSHIP BETWEEN REPERFUSION THERAPY AND EARLY NEUROLOGICAL DETERIORATION
Tony Yu*1,2, Cameron Lee1, Mohammed Mallah1,3, Yassine Noui1,4, Maria Lucia Uribe Mz Recaman1, Beatrix Sari1, Samantha Roberto1, Carol Belo1, Yee Mah1,5
1King's College Hospital, United Kingdom, 2Auckland District Health Board, Auckland, New Zealand, 3St George's Hospital, United Kingdom, 4Uppsala University, Uppsala, Sweden, 5King's College London, School of Biomedical Engineering and Imaging Sciences, United Kingdom
On behalf of:
Background and aims: Reperfusion therapy (Intravenous Thrombolysis [IVT] or Mechanical Thrombectomy [MT]) is frequently used to treat ischaemic strokes, but its influence with developing Early Neurological Deterioration (END) is not entirely clear. This project aims to further examine the relationship between reperfusion therapy and END
Methods: All stroke admissions between 1 Jan- 30 Jun 2022 (inclusive) to the Hyper Acute Stroke Unit at King's College Hospital, London were manually reviewed for END occurring within the first 14 days from stroke onset
Results: There were 477 stroke admissions within this time period (41 episodes excluded - medical notes not available for review). 384 patients presented with an acute ischaemic stroke. Of these, 93 received IVT and 59 received MT, with an overlap of 28 patients who received both. Compared against no reperfusion therapy, only MT (alone or in combination with IVT) was associated with a greater risk of END. Arrival NIHSS scores in those who received MT were significantly higher than those without reperfusion therapy. However, within the MT cohort, there was no significant difference in arrival NIHSS scores between those who did and did not exhibit END
Conclusions: (1) The risk of END is higher in those receiving MT compared with no reperfusion treatment. (2) Within the MT cohort, the increased risk of END appears related to arrival NIHSS score. (3) Reperfusion treatment shifted the probability density function for END risk towards higher arrival NIHSS scores and suggests at these higher scores, intervention may increase the risk compared with no treatment.
Disclosures of Interest: No
Abstract N°: 1154
DOPPLER TRANSCRANEAL COMO HERRAMIENTA PRONÓSTICA FUNCIONAL EN VASCULITIS DEL SISTEMA NERVIOSO CENTRAL
José de Jesús García Rivera1, Kevin Giuseppe Enriquez Peregrino1, Idarmis Brisseida Reyes Cortés1, Jacqueline Moreno Arias1, Vanessa Cano Nigenda*1, Antonio Arauz Gongora1, Andrés Alberto Mercado Pompa1, Adrian Pereda-Castillo1, Andony Isabel Camacho Gámez1, Ricardo Romero Vucovich1
1Instituto Nacional de Neurología y Neurocirugía, Mexico
On behalf of: Liliana Escobar Pérez, Luis Esteban Ramírez González, Paul Jhovanny Rodríguez Flores, Thalia Esmeralda Morfín Morales, Jefferson Ramirez, Enrique Isaac Tetlalmatzi Azuara
Background and aims: Transcranial Doppler(TCD) is a low-cost, noninvasive test that can provide accurate information on intracranial blood flow velocities. Information on its use as a diagnostic tool in Central Nervous System(CNS) vasculitisis is scarce.
Methods: retrospective cohort since 2016-2023 in patients with diagnosis of CNS vasculitis. Vessels evaluated in TCD: Anterior Cerebral Artery(ACA), Middle Cerebral Artery(MCA) and Posterior Cerebral Artery(PCA). Their association with an unfavorable functional outcome (mRS 3-6) at 3 months was evaluated. Descriptive and inferential statistics were performed.
Results: Total 187 participants of which 148 with complete records were included, 85(57.4%) men, mean age 39.9(±13.6), 45(30.4%) were infectious vasculitis and 103(69.6%) of undetermined etiology. The most frequent infectious etiologies were 23(46%) for cryptococcosis, 12(24%) tuberculosis and 8(16%) neurocysticercosis, 43(30.9%) patients had immunodeficiency, the most frequent: HIV 28(59.6%), diabetes 13(27.7%), immunosuppressant use 2(4.3%). MRI studies showed infarction in 29(28.2%), hemorrhage in 4(5.3%), pachymeningitis in 21(20.4%) and 33(32%) were normal. Parameters of the first TCD, Mean Velocity
(MV) and Pulsatility Index(PI) were: ACA MV 59.8 cm/s(±24.93) and PI 1.03(±0.30); MCA MV 92.3cm/s(±80.1) and PI 1.01(±0.34); PCA MV 45.6 cm/s(±13.4) and PI 0.97(±0.31). MV elevation in MCA at initial TCD was associated with an increased likelihood of having an unfavorable functional outcome at 3-month follow-up (OR 4.06;95% CI 1.55-10.63; p=0.003).
Conclusions: TCD is a valid adjunctive tool to assess the functional prognosis of patients with CNS vasculitis. Increased MV in the MCA in the initial TCD study is associated with an unfavorable functional outcome at 3 months in CNS vasculitis.
Disclosures of Interest: No
Abstract N°: 1332
EARLY RECURRENCE OF ISCHEMIC STROKE IN YOUNG ADULTS: A MULTICENTRE COHORT STUDY
Charlene Kok*1, Gabriel Yi Ren Kwok2, Hock-Luen Teoh3, Sarah ML Tan3, Nur Hafizah Mohd Amin4, Maznah Marmin4, Fadhlina Hassan4, Leonard Ll Yeo3,5, Aftab Ahmad4, Benjamin Yq Tan3,5
1Imperial College London, United Kingdom, 2Barts and The London School of Medicine and Dentistry, United Kingdom, 3National University Hospital (NUH) - Singapore, Singapore, Singapore, 4Ng Teng Fong General Hospital, Singapore, Singapore, 5Yong Loo Lin School of Medicine, Singapore, Singapore
On behalf of:
Background and aims: Ischaemic stroke (IS) recurrence, especially in early phase, remains a significant prognostic challenge despite secondary prevention strategies. This is especially devastating for young adult patients, who are in their most productive years, but factors influencing stroke recurrence remains under-studied in this growing and clinically distinct subgroup of patients.
Methods: We performed a retrospective cohort study of all consecutive acute IS patients aged 18-50 years admitted to 2 Singapore tertiary hospitals from 2020-2022, encompassing the country’s entire western region (n=566). Patients were followed up for a duration of 90 days. We compared demographic characteristics, TOAST aetiologies, cerebrovascular risk factors and 90-day modified Rankin Scale (mRS) score between patients with and without recurrent IS and/or transient ischemic attack (TIA) using chi-squared and Mann-Whitney U tests, as well as univariate and multivariate logistic regression.
Results: Overall, 2.83% (16/566) of patients experienced a recurrent stroke or TIA. There was significantly higher prevalence of diabetes mellitus (62.5% vs. 20%, p<0.001) and prior stroke/TIA (62.5% vs. 7.5%, p<0.001) in this group of patients. In univariate logistic regression analysis, diabetes mellitus (OR 6.65, 95% CI 2.42-19.92, p<0.001) and prior stroke/TIA (OR 20.65, 95% CI 7.30-63.41, p<0.001) were significantly associated with stroke recurrence (Table 2). Both associations with diabetes mellitus (aOR 5.63, 95% CI 1.79-19.34, p=0.04) and prior stroke/TIA (aOR 20.78, 95% CI 6.54-74.23, p<0.001) remained significant in multivariate analysis (Table 3).
Conclusions: Patients with diabetes mellitus and prior stroke or TIA are more likely to have a recurrent event. Large observational studies are needed to confirm these findings.
Disclosures of Interest: No
Abstract N°: 2223
SRAGE AND ITS ISOFORMS AS PROTECTIVE BIOMARKERS FOR FUNCTIONAL DEPENDENCE AFTER ACUTE ISCHEMIC STROKE
1Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China, China
On behalf of:
Background and aims: The present study aimed to investigate the relationship between sRAGE and its isoforms [cleaved RAGE (cRAGE) and endogenous secretory RAGE (esRAGE)] with clinical outcomes following acute ischemic stroke.
Methods: A total of 3189 acute ischemic strokes were included. The concentration of cRAGE was calculated by subtracting esRAGE from sRAGE. The primary outcome was functional dependence, defined as a modified Rankin Scale (mRS) score of 3-6. The association between sRAGE and its isoforms (cRAGE and esRAGE) with stroke outcomes was analyzed using a Cox proportional hazards model, and hazard ratios (HRs) with 95% confidence intervals (95% CIs) were calculated.
Results: The plasma cRAGE and esRAGE were positively correlated with sRAGE (R=0.942 and 0.781, respectively). There were 426 (13.5%) and 409 (13.1%) patients with functional dependence within 90 days and 1 year, respectively. Compared with the bottom quartile levels of sRAGE, cRAGE, and esRAGE, the adjusted HRs (95% CI) of functional dependence in the top quartiles were 0.65 (0.47–0.91), 0.71 (0.51-0.99) and 0.51 (0.36–0.72) within 90 days and 0.66 (0.48–0.91), 0.69 (0.50-0.95), and 0.54 (0.39-0.76) at 1 year, respectively. Similar results were not observed in stroke recurrence, ischemic stroke recurrence, or combined vascular events within 90 days and 1 year after stroke.
Conclusions: Plasm cRAGE and esRAGE showed a positive correlation with sRAGE level within 7 days, and sRAGE and its isoforms all acted as protective biomarkers for short- and long-term functional dependence in patients with acute ischemic stroke.
Disclosures of Interest: No
Abstract N°: 2249
DRIVING AFTER STROKE, TRAFFIC ACCIDENTS AND INJURY SEVERITY - A SWEDISH NATIONWIDE REGISTRY-BASED STUDY
Hanna C Persson*1,2, Katharina Stibrant Sunnerhagen1, Helena Selander1,3
1Institute of Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg, Department of Clinical Neuroscience, Gothenburg, Sweden, 2Sahlgrenska University Hospital, Department of Occupational Therapy and Physical Therapy, Gothenburg, Sweden, 3Swedish National Transport Research Institute, Gothenburg, Sweden
On behalf of:
Background and aims:To resume driving after a stroke can be challenging, and little is known regarding the prevalence and type of road traffic accidents after stroke. The aim of the present study was to examine what types of road traffic accidents that were associated with drivers with stroke, compared to a group of individuals with ulcerative colitis or Crohn’s disease (the comparison group).
Methods: This retrospective national wide, registry-based study included all drivers involved in road traffic accident (driving car, bus/truck, moped/motorcycle) in Sweden from 2010-2019, based on the Swedish Traffic Accident Data Acquisition database. Data on pre-existing diagnoses were retrieved retrospectively from the National Patient Registry. Data analyses included group comparisons and binary logistic regression.
Results: In total, 4670 drivers were registered to have been involved in a road traffic accident, where of 2727 with stroke, and 1943 in the comparison group. Within 3 months post stroke, few (<5) registered accidents occurred. Mean time since diagnose in months at the time of the accident were, 87 (58.2) after stroke, and 118 (64.3) in the comparison group (p <0.001). People with stroke were more often involved in accidents with vulnerable road users i.e. pedestrian/bicycle/moped (p<0.001). People with stroke were more severity injured when driving a moped/motorcycle (p<0.001), however, the number of severe/fatal injuries were overall low.
Conclusions: Drivers with stroke were more often involved in accidents with vulnerable road users, and drivers of risk may therefore be individually assessed to reduce the burden of traffic accidents. This may be important also several years after the stroke.
Disclosures of Interest: No
Abstract N°: 2578
PLASMA BRAIN-DERIVED TAU AS A BIOMARKER OF POST-STROKE COGNITION
Lukas Holmegaard*1,2, Fernando Gonzalez-Ortiz3,4, Tara Stanne5,6, Henrik Zetterberg3,4, Hans Samuelsson1,2, Katarina Jood1,2, Kaj Blennow3,4, Christina Jern5,6
1Institute of Neuroscience and Physiology, Department of Clinical Neuroscience, Gothenburg, Sweden, 2Sahlgrenska University Hospital, Region Västra Götaland, Department of Neurology, Gothenburg, Sweden, 3Institute of Neuroscience and Physiology, Department of Psychiatry and Neurochemistry, Gothenburg, Sweden, 4Sahlgrenska University Hospital, Region Västra Götaland, Clinical Neurochemistry Laboratory, Mölndal, Sweden, 5Institute of Biomedicine, Department of Laboratory Medicine, Gothenburg, Sweden, 6Sahlgrenska University Hospital, Region Västra Götaland, Department of Clinical Genetics and Genomics, Gothenburg, Sweden
On behalf of:
Background and aims: Cognitive impairment is common and contributes to work disability in ischemic stroke survivors. There is a large variation in post-stroke cognitive outcomes, and there is no predictive blood-based biomarker. The novel biomarker brain-derived tau (BD-tau) selectively reflects tau of central nervous system origin. Here, we investigate BD-tau for associations to long-term post-stroke cognitive outcome in working aged individuals.
Methods: Plasma levels of BD-tau were measured in 182 adult patients with acute ischemic stroke before 70 years of age. Index brain infarcts were manually delineated from Magnetic Resonance Imaging (MRI) scans, volumes calculated, and adjusted for intracranial volumes by one neurologist (LH). Cognitive outcome was assessed by the Barrow Neurological Institute Screen (BNIS) for Higher Cerebral Functions 7 years post-stroke. Association between BD-tau or infarct volumes and cognitive outcome were investigated in linear regression models adjusted for Model 1: age, sex, day of blood draw, and level of education; and Model 2: also stroke severity (NIHSS).
Results: Median age at inclusion was 55 (48-62) years, 65% were males, and median BNIS score was 40 (IQR 37-44). BD-tau and infarct volumes were strongly correlated (r=0.75, p=1x10-31). Higher BD-tau and infarct volumes were both associated with lower BNIS scores (standardized β per standard deviation increase Model 1: -0.262, p<0.001 and -0.278, p<0.001; Model 2: -0.174, p=0.02 and -0.196, p<0.01, respectively).
Conclusions: Plasma BD-tau is a promising non-invasive and accessible biomarker for cognitive outcome that may provide similar predictive information as advanced neuroimaging, and future studies in larger cohorts are warranted.
Disclosures of Interest: No
Abstract N°: 2637
PATIENTS HAVE HIGHER QUALITY OF LIFE COMPARED TO THEIR INFORMAL CAREGIVERS IN THE IMMEDIATE AFTERMATH OF ACUTE STROKE
Anton Schmick*1, Pascal Sommerhalder1, Roland von Känel2, Jonathan Amstutz1, Clara Meny1, Robert Weber1, Tina Maria Binz3, Ulrike Held4, Susanne Wegener1
1University Hospital of Zurich, Department of Neurology, Zürich, Switzerland, 2University Hospital of Zurich, Department of Consultation-Liaison Psychiatry and Psychosomatic Medicine, Zürich, Switzerland, 3Center for Forensic Hair Analysis, Zurich Institute of Forensic Medicine, University of Zurich, Zürich, Switzerland, 4Epidemiology Biostatistics and Prevention Institute, University of Zurich, Zürich, Switzerland
On behalf of:
Background and aims: Stroke, the third leading global cause of death and a major contributor to disability, affects both, survivors and their informal caregivers. Stroke induces caregiver burden, depression, and reduced quality of life (QoL) for both parties. This study aims to evaluate stress, QoL, depression, and anxiety in the psychosocial aftermath of acute stroke.
Methods: Conducted longitudinally, our study involves 150 stroke-survivor caregiver pairs, with 20 control-pairs for normative data. Assessments occur post-stroke, at 3 and 12 months. Perceived Stress Scale 10 (PSS-10), Distress-Thermometer and biological parameters linked to chronic stress (hair cortisol, CRP etc.) are used to quantify stress. QoL is evaluated using SF-36, Stroke Impact Scale (SIS-3.0), and EuroQol-5. Anxiety, depression, sexual behavior, and caregiver burden are assessed with standardized measures. Statistical analysis involves descriptive statistics and multiple linear regression models.
Results: Preliminary findings from 13 pairs indicate that during the acute phase following a stroke patients exhibit lower stress levels in patients comparison to their caregivers (Distress-Thermometer 4.3 vs. 5.6; PSS-10 21 vs. 24p). Patients show higher emotional well-being (SF-36-EWB 86 vs. 68), social functioning (SF-36-SF 85 vs. 69), and self-perceived health (SF-36-GH 55 vs. 50) than caregivers. Additional time points' will be assessed, respective data will be presented at the conference.
Conclusions: The acute stroke burden appears to affect caregivers' QoL and stress levels more than those of stroke-survivors'. Acute denial may contribute and further data is needed to eliminate confounding factors. The project continues to assess the psychosocial burden in patients and informal caregivers post-stroke.
Disclosures of Interest: No
Abstract N°: 2811
USE OF STACKED PROPORTIONAL BAR GRAPHS TO VISUALISE FUNCTIONAL OUTCOME DISTRIBUTIONS IN OBSERVATIONAL STUDIES: A META-RESEARCH STUDY
Meghan R. Forrest*1,2,3, Tracey Weissgerber4, Emma S. Lieske3,4, Lydia Jones1,5, Marco Piccininni1,3, Jessica L Rohmann1,3
1Charité - Universitätsmedizin Berlin, Institute of Public Health, Berlin, Germany, 2Charité – Universitätsmedizin Berlin, Berlin School of Public Health, Berlin, Germany, 3Charité - Universitätsmedizin Berlin, Center for Stroke Research Berlin, Berlin, Germany, 4QUEST Center for Responsible Research, Berlin Institute of Health at Charité – Universitätsmedizin Berlin, Berlin, Germany, 5Federal Joint Committee, Berlin, Germany
On behalf of:
Background and aims: Stacked proportional bar graphs (nicknamed “Grotta bars”) are commonly used to visualise functional outcome scales in stroke research. When these visualisations are not generated reflecting the adjustment strategy employed within an observational study, they visualise confounded associations and can be misleading. In a sample of recent observational neurology studies with confounding-adjusted effect estimates, we aimed to determine the frequency with which Grotta bars were used to visualise functional outcomes, how often unadjusted Grotta bars were presented without an accompanying adjusted version. We also assessed the methods used to generate adjusted Grotta bars.
Methods: Our sample included all observational studies published in top Clinical Neurology journals between 2020-2021 with an ordinal functional outcome and confounding-adjusted effect estimates. We determined whether a Grotta bar was present, whether these visualisations were adjusted, and which adjustment strategies were applied.
Results: 250 neurology studies met all inclusion criteria. Of these, 93 (37.2%) used a Grotta bar to depict functional outcome scale distributions, with 73 (81.7%) depicting exclusively unadjusted visualisations (n=76; 81.7%). In the 17 studies that presented adjusted Grotta bars, the adjustment strategies included propensity score matching (n=10; 58.8%), regression (n=6; 35.3%), and inverse probability weighting (n=1; 5.9%). Most studies that included a Grotta bar (n=87;87.9%) were stroke studies.
Conclusions: In observational neurology research, especially stroke, papers that present adjusted associations for functional outcome results commonly show only unadjusted Grotta bars, which may be misleading. Our recommendations help authors generate Grotta bars that align with their effect estimates and readers to interpret them.
Disclosures of Interest: Yes M.P. reports having received partial funding from Novartis Pharma and being awarded a research grant from the Center for Stroke Research Berlin (private donations).
Abstract N°: 2908
THE WORSE DISABILITY IN PATIENTS WITH COVID-19 AT THE ONSET OF A STROKE IS NOT SEEN AT 2 YEARS IN THE UK MULTICENTRE STUDY SETICOS
Riham El Sayed*1, Craig Smith2, Rob Simister1, Christine Roffe3, David Werring4, Richard Perry1
1University College London Hospitals Nhs Foundation Trust, London, United Kingdom, 2The University of Manchester, United Kingdom, 3Keele University, Keele, United Kingdom, 4UCL Queen Square Institute of Neurology, United Kingdom
On behalf of:
Background and aims: We previously reported that COVID-19 at the onset of a stroke is associated with greater disability at discharge. Here, we examine whether a worse outcome persists at two years.
Methods: Two years (± 2 months) from stroke onset, patients from 18 UK hospitals were sent a patient questionnaire followed by a telephone call during which their disability was assessed using the modified Rankin scale. We present results in patients who had COVID-19 at stroke onset (CSO) and in patients who acquired COVID-19 during their admission (CDA), compared with patients who did not have evidence of COVID-19 (NC).
Results: At discharge, functional independence appeared to be less common in groups CSO (47%, 16/34, p=0.06) and CDA (31%, 4/13, p=0.04) than in group NC (64%, 172/270). At two years, however, the proportion of patients achieving independence was similar between groups CSO (67%, 22/33) and NC (64%, 164/257), but was much lower in group CDA than group NC (8%, 1/13, p<0.001). The sum of median scores on the Stroke Impact Scale (SIS) was also similar between groups CSO and NC (690 vs 700), whereas group CDA scored worse than group NC (370, p<0.001). Additionally, PROMIS-10 mental health score was much lower in group CDA than group NC (9, 12, p=0.004).
Conclusions: At two years, the adverse effect on stroke outcome of having had COVID-19 at onset was no longer apparent, whereas contracting COVID-19 during admission was still associated with increased disability.
Acknowledgements
Supported by The Stroke Association
Disclosures of Interest: No
Abstract N°: 61
ENDOVASCULAR THERAPY IN ACUTE ISCHEMIC STROKE WITH AND WITHOUT TANDEM OCCLUSION: PREDICTION FOR COMPLETE RECANALIZATION
1Beijing Tiantan Hospital, Capital Medical University, Department of neurology
On behalf of:
Background and aims: Acute ischemic stroke (AIS) with tandem lesions (TLs) harbors worse prognosis. Although RCTs have proven the benefits of mechanical thrombectomy (MT) in such patients, there is debate on the optimal acute endovascular therapy, such as intravenous thrombosis, stenting and balloon dilatation. This study aims to compare the effects of different endovascular procedures on acute reperfusion for AIS with and without TLs.
Methods: This was a multicenter, cross-sectional study that recruited AIS receiving MT from Jan 2017 to June 2022 in China. Demographics, previous histories, endovascular procures conducted, and the modified Thrombolysis in Cerebral Infarction (mTICI) score etc. were collected. Patients were divided into non-TLs group and TLs group. The primary outcome was complete recanalization defined as mTICI 3. Multivariate logistics were conducted for independent predictors for complete recanalization for AIS with and without TLs respectively.
Results: Totally 799 AIS patients were included (119 with and 680 without TLs). Multivariate logistics revealed that: for non-TLs, conduction of stenting (adjusted OR=2.88; 95% CI 1.27 -6.51; P=0.011) and absence of AF (adjusted OR=1.77; 95% CI 1.23-2.54; P=0.002) were independently associated with higher rate of complete recanalization; for TLs, conduction of balloon angioplasty (adjusted OR=3.68; 95% CI 1.26-10.74; P=0.017), and absence of history of hyperlipidemia (adjusted OR=4.71; 95% CI 1.49-14.93; P=0.008) were independently associated with higher rate of complete recanalization.
Conclusions: AIS with TLs requires different optimal endovascular therapy from AIS without TLs, and balloon dilatation may increase the rate of complete recanalization.
Disclosures of Interest: No
Abstract N°: 69
ANTIPLATELET THERAPY AS RISK FACTOR FOR SYMPTOMATIC INTRACRANIAL HAEMORRHAGE IN PATIENTS WITH ACUTE ISCHEMIC STROKE
Lukas Nussbaum1,2, Mira Katan1,2, Gian Marco De Marchis2,3, Philippe Lyrer*1,2
1Universitätsspital Basel, Department of Neurology and Stroke Centre, Basel, Switzerland, 2Universität Basel, Medizinische Fakultät, Basel, Switzerland, 3Kantonsspital St.Gallen, Department of Neurology and Stroke Centre, St. Gallen, Switzerland
On behalf of: Swiss Stroke Registry Investigators
Background and aims: Are patients with acute ischemic stroke while on antiplatelet therapy at higher risk of symptomatic intracranial haemorrhage (sICH) compared to patients without antiplatelets?
Methods: Retrospective analysis of the Swiss Stroke Registry, group analysis: single antiplatelet therapy (SAPT) vs no antiplatelet therapy (nAPT), dual antiplatelet therapy (DAPT) vs SAPT. Primary outcome: frequency of sICH, secondary: recurrent ischemic stroke, all cause mortality, functional outcome from hospital admission to 90-days follow-up, corrected for covariates and acute revascularization treatment (intravenous thrombolysis (IVT) or intraarterial treatment (IAT)).
Results: At 90-days patients with SAPT compared to nAPT had significantly increased risk of sICH (OR 1.330 (1.100 to 1.610), p<0.01), no differences in all cause mortality, recurrent IS or functional outcome. Patients with DAPT compared to SAPT did not have increased risk of sICH or mortality but had more often recurrent IS (OR 1.474 (1.166 to 1.863), p<0.01) and a worse functional outcome (OR 1.158 (1.037 to 1.293), p<0.01). IVT and IAT did not seem to increase the risk of sICH. Patients with SAPT compared to nAPT received the same rate of IVT and IAT. Patients with DAPT compared to SAPT receive less IVT (OR 0.601 (0.511 to 0.707), p <0.01) and the same amount of IAT.
Conclusions: Stroke patients with SAPT compared to nAPT have an increased risk of sICH. Patients with DAPT compared to SAPT have an increased risk of recurrent stroke but the acute treatment did not further increase the risk of sICH. There seems to be no reason to withdraw IVT or IAT based on prior DAPT.
Disclosures of Interest: No
Abstract N°: 174
THE ASSOCIATION BETWEEN NEIGHBORHOOD SOCIO-ECONOMIC STATUS AND FUNCTIONAL OUTCOME THREE MONTHS AFTER ENDOVASCULAR THROMBECTOMY
Bridget Schoon*1,2, Daniël Hansen1,3, Bob Roozenbeek1, Wouter van der Steen1, Manon Kappelhof4, Yvo Roos5, Aad van der Lugt2, Charles Majoie6, Frank van Lenthe3, Diederik Dippel1
1Erasmus MC, University Medical Center, Neurology, Rotterdam, Netherlands, 2Erasmus MC, University Medical Center, Radiology and Nuclear Medicine, Rotterdam, Netherlands, 3Erasmus MC, University Medical Center, Public Health, Rotterdam, Netherlands, 4Amsterdam University Medical Center, location AMC, Radiology and Nuclear Medicine, Amsterdam, Netherlands, 5Amsterdam University Medical Center, location AMC, Neurology, Amsterdam, Netherlands, 6Amsterdam University Medical Center, location AMC, Radiology and Nuclear Medicine, Amsterdam, Netherlands
On behalf of: MR CLEAN NO-IV and MR CLEAN MED investigators
Background and aims: Neighborhood socio-economic status (nSES) is associated with stroke incidence and functional outcome. However, few studies have investigated its effect on patients treated with endovascular thrombectomy (EVT). We aim to examine the association of nSES on both degree of neurological deficit at 24 hours as functional outcome three months after EVT.
Methods: Analyses were performed using data from the MR CLEAN-MED and MR CLEAN NO-IV trials, collected between 2018 and 2021. As a proxy for nSES, a per postcode composite score of education, employment and household income (SES-WOA score, as created by ‘Statistics Netherlands’) was used. The association of nSES with degree of neurological deficit (NIHSS) at 24 hours and functional outcome (mRS) at 90 days was analyzed using linear regression and ordinal logistic regression respectively. Analyses were adjusted for relevant patient characteristics, including baseline NIHSS, sex and age.
Results: A total of 948 patients (45.3% female, mean age 70.3, median baseline NIHSS 15) were included. The association of nSES with NIHSS at 24 hours was not statistically significant (β -1.68 (95%CI -3.78, 0.42)). However, patients with a lower SES-WOA score had significantly less favorable mRS at 90 days (OR 0.52(CI95% 0.33, 0.80)).
Conclusions: Our results suggest that, although the degree of neurological deficit at 24 hours was not associated with nSES, patients with lower nSES had a less favorable functional outcome at 90 days. This suggests disparities in post-stroke care depending on nSES, and highlights the importance of the continuing to work towards health equity for stroke patients.
Disclosures of Interest: No
Abstract N°: 402
IMPACT OF PLEURAL EFFUSION ON CLINICAL OUTCOMES IN PATIENTS WITH ISCHEMIC STROKE
Joong-Goo Kim*1, Gil Myeong Seong2
1Jeju National University College of Medicine, Neurology, Jeju, 2Jeju National University College of Medicine, Internal medicine, Jeju
On behalf of:
Background and aims: Pleural effusions can be observed in initial computed tomography in patients with acute ischemic stroke; however, the impact on clinical outcomes is not well characterized. This study aims to demonstrate the clinical outcomes of acute ischemic stroke patients with pleural effusion.
Methods: All patients who underwent acute ischemic stroke between 2018 and 2022 at a tertiary care university hospital were included in this observational, cross-sectional analysis.
Results: Of 1,137 patients who underwent acute ischemic stroke during the study period, 961 (84.5%) patients had no pleural effusion and 178 (15.6%) patients had pleural effusion. After propensity matching, the mortality of patients with pleural effusion was 7.3% higher than those with no pleural effusion (p < 0.001). Neurointensive care unit (NICU) stay was longer for those with pleural effusions (8 [IQR 6–11] days, 3 [IQR 2–7] days for those without pleural effusion, p < 0.001). Patients with pleural effusions had a higher incidence of early neurological deterioration (END, 21 [11.8%] with pleural effusions, 66 [6.8%] without pleural effusions). Patients with pleural effusion were more likely to be associated with congestive heart failure and atrial fibrillation (22.1% vs. 5.7% and 34.6% vs. 17.5%)
Conclusions: Pleural effusions are highly associated with worse outcomes, including increased mortality, longer length of NICU stay, and higher END rates. These insights may be of stroke neurologists alike to foster research into innovative methods for preventing and treating pleural effusions to improve outcomes for patients with acute ischemic stroke.
Disclosures of Interest: No
Abstract N°: 484
HUMAN URINARY KALLIDINOGENASE IN TREATMENT OF ACUTE ISCHEMIC STROKE: ANALYSIS OF A MULTICENTER, CLINICAL TRIAL (CASTOR) IN CHINA
Diandian Huang1, Haiqiang Jin*1
1Peking University First Hospital, Department of Neurology, Beijing, China
On behalf of:
Background and aims: To measure whether human UrinaryKallindinogenase (HUK) has benefits for patients with acute ischemic stroke (AIS) after discharge and the 3-months after time of onset of this disease.
Methods: In this prospective, multiple centers, real world study involving 80 hospitals in China registered with ClinicalTrials.gov (NCT02470624), patients with AIS were treated following the Chinese stroke guideline and local practice. Real-world data on treatment regimens and clinical outcomes are collected at baseline and subsequent visits. Patients were analyzed whether or not receiving preconditioned Human Urinary Kallindinogenase (HUK group) or standard treatment alone (control group). The primary outcome was the alteration of the score on the modified Rankin Scale (mRS) between the discharge and the 3 months re-investigation. Secondary measurements included alteration in NIHSS at discharge after admission and the classification of the shift of mRS(including the age and gender)
Results: A total of 10002 cases were recruited. After the criteria filter and propensity score matching (PSM), 2319 cases were ultimately analyzed in the study with 1:1 ratio of HUK or non-HUK group, seperatively. Baseline characteristics were not different between groups. There was significant difference between the groups in the shift of mRS score (p< 0.001) and the HUK group performed the improvement with larger numbers with statistical significance.
Conclusions: HUK treatment was associated with improvements in the shift from discharge to 3-month mRS score. However, large scale Randomized clinical trials(RCT), especially the underlying cerebral hemodynamics mechanism still need further study.
Disclosures of Interest: No
Abstract N°: 673
CHALLENGES OF RECANALIZATION THERAPY IN ACUTE STROKE PATIENTS TAKING DOACS
Jessica Seetge*1, László Szapáry1
1University of Pécs, Department of Neurology, Pécs, Hungary
On behalf of:
Background and aims: Direct oral anticoagulants (DOACs) and vitamin K antagonists (VKAs) are the recommended primary therapy for preventing acute ischemic stroke (AIS) in patients with atrial fibrillation. Nonetheless, an annual AIS risk of 1-2% endures despite their effectiveness. Intravenous thrombolysis (IVT) and mechanical thrombectomy (MT) are interventions capable of reducing AIS-related morbidity. Herein, we assess the safety and efficacy of recanalization therapy in anticoagulated patients.
Methods: Within the prospective TINL-STROKE-registry, AIS patients admitted to the Department of Neurology, between February 2023 and March 2024 were investigated. The study’s objective was to assess the association between oral anticoagulant (OAC), choice of reperfusion therapy, proportion of functionally independent patients at 90 days (modified Rankin Scale [mRS] ⩽ 2), and clinical improvement (National Institute of Health Stroke Scale [NIHSS] ⩽1 or change from baseline [∆ NIHSS] ⩾4) after 72 hours. Outcomes were compared with (ordinal) logistic regression analyses adjusted for confounding factors.
Results: 627 eligible patients (DOAC, n=72 and VKA, n=40 vs. non-anticoagulated, n=515) was included. 307 patients underwent reperfusion therapy (133 IVT, 131 MT, 43 IVT+MT), the remaining 320 received standard care (SC). Anticoagulated patients (n=112) showed less favorable outcomes than non-anticoagulated patients (n=515): 29,2% vs. 49,4% 90-day mRS ⩽2, 29,5% vs. 36,3% NIHSS ⩽1, 23,2% vs. 26,2% ∆ NIHSS ⩾4 and 90-day mortality: 26,8% vs. 13,8%. However, this difference was no longer apparent after adjustment for baseline prognostic factors.
Conclusions: Our study adds evidence to the safety and efficacy of recanalization therapy in patients with prior therapeutic anticoagulation.
Disclosures of Interest: No
Abstract N°: 1126
CLINICAL OUTCOMES AFTER ACUTE ISCHEMIC STROKE IN PATIENTS WITH COMORBID CANCER
1Kyushu University, Department of Health Care Administration and Management, Graduate School of Medical Sciences, Fukuoka, Japan, 2Kyushu University, Department of Medicine and Clinical Science, Graduate School of Medical Sciences, Fukuoka, Japan
On behalf of: the Fukuoka Stroke Registry
Background and aims: Comorbid cancer was not uncommon in patients with stroke. This study aimed to determine whether comorbid cancer is associated with functional outcomes after acute ischemic stroke.
Methods: We investigated data on patients with acute ischemic stroke who were hospitalized in 7 stroke centers in Fukuoka, Japan, between June 2007 and September 2019. Comorbid cancer was categorized into non-active and active cancer based on its status at stroke onset. Clinical outcomes included poor functional outcome (modified Rankin Scale [mRS] score of 3-6), all-cause death, and functional dependency (mRS score of 3–5) at 3 months. Logistic regression analysis was performed to adjust for multiple confounding factors.
Results: Of 13,047 patients (aged 71.1±12.3 years, 62.8% men) without pre-stroke disability, 1,384 (10.8%) patients had non-active cancer, and 622 (4.8%) had active cancer at stroke onset. Active cancer was associated with poor functional outcome (multivariable-adjusted odds ratio [95% confidence interval], 2.26 [1.85-2.76]), death (5.99 [4.42-8.14]), and functional dependency (1.62 [1.30-2.02]) even after adjusting for covariates, whereas no association was found between non-active cancer and the clinical outcomes. These associations were maintained when clinical outcomes were assessed at discharge. The associations of active cancer with 3-month unfavorable functional outcomes were still found even after excluding patients with previous stroke, or patients who had recurrent stroke within 3 months after onset.
Conclusions: Active cancer but not non-active cancer was associated with an increased risk of unfavorable functional outcomes as well as death at 3 months after acute ischemic stroke.
Disclosures of Interest: No
Abstract N°: 1386
STROKE OUTCOMES USING UTILITY-WEIGHTED MODIFIED RANKIN SCALE SCORES: RESULTS FROM A LARGE COMMUNITY-BASED STUDY IN CHILE
Carlos Delfino*1, Paula Muñoz Venturelli1,2,3, Gabriel Cavada4, Lorena Hoffmeister1, Pablo Lavados2,4
1Instituto de Ciencias e Innovación en Medicina, Facultad de Medicina Clínica Alemana Universidad del Desarrollo, Santiago, Chile, las condes, Chile, 2Clinica Alemana, Servicio de Neurología, Departamento de Neurología y Psiquiatría, Clínica Alemana de Santiago, Facultad de Medicina, Vitacura, Chile, 3The George Institute for Global Health, Faculty of Medicine, University of New South Wales, Barangaroo, Australia, 4Unidad de Investigación y Ensayos Clínicos, Clínica Alemana de Santiago, Facultad de Medicina Clínica Alemana Universidad del Desarrollo, Santiago, Chile
On behalf of:
Background and aims: A promising approach to Patient-Reported Outcome Measures in stroke is the transformation of mRS (modified Rankin Scale) scores according to respective utilities of health-related quality of life questionnaires. We aimed at mapping mRS functional status and the EQ5D-3L to derive utility-weighted (UW) stroke outcomes from a representative national cohort.
Methods: The UW-mRS was obtained by analysing the EQ5D-3L and mRS scores at 180 days after any stroke in the ÑANDU study, a large prospective community-based study in Chile. The mRS prediction was estimated using a linear regression adjusted by the EQ5D-3L tariff. A misclassification matrix was used to classify each patient into a new ‘‘matched’’ mRS category. Formal agreement between the ''current'' and ''matched'' mRS was estimated by correspondence analysis. STATA v18.0 was used.
Results: In this analysis, 958 patients with a stroke in 2015-2016 were considered: 48% were women, had a mean age of 71 (SD 13.8) years, and 85% had an ischemic stroke. UW-mRS values for mRS categories 0–6 at 180 days were 0.88, 0.69, 0.47, 0.36, 0.15, 0.03, and 0. When comparing the mRS weighted by EQ5D-3L (matched) with the current mRS, between 32-72% of patients in all mRS scores were considered in a worse mRS, with a higher discrepancy in patients with mRS 4. (figure 1)
Conclusions: Our findings, derived from a nationally representative cohort, underscore the need to develop novel outcome assessment methods for stroke patients describing their health status more comprehensively.
Disclosures of Interest: No
Abstract N°: 1443
THE STRUCTURAL CONNECTOME IS ASSOCIATED WITH COGNITIVE PERFORMANCE OVER TIME IN YOUNG STROKE SURVIVORS
Esther Boot*1, Mijntje Schellekens1, Jamie Verhoeven1, Merel Ekker1, Hao LI1, Roy Kessels2, Anton Meijer3, Frank-Erik De Leeuw1, Anil Tuladhar1
1Radboud University Medical Centre; Donders Institute for Brain, Cognition and Behaviour, Neurology, Nijmegen, Netherlands, 2Radboud University Medical Centre; Donders Institute for Brain, Cognition and Behaviour, Medical Psychology, Nijmegen, Netherlands, 3Radboud University Medical Centre; Donders Institute for Brain, Cognition and Behaviour, Radiology, Nijmegen, Netherlands
On behalf of:
Background and aims: Post-stroke cognitive impairment is common among young stroke survivors, but its mechanisms remain unclear. We aimed to study the relationship between brain network measures and cognitive performance in this population, focusing on hub regions.
Methods: A cohort of young stroke survivors (ages 18-49) with confirmed cerebral ischemia from the ODYSSEY study underwent MRI and neuropsychological assessments at baseline (n=60) and follow-up (n=46). We used Diffusion Tensor Imaging (DTI) based connectivity matrices for graph analysis. Lesion impact scores (combining affected voxel percentage and mean betweenness centrality) and rich club scores (quantifying affected voxels in rich club areas) were calculated using a normative brain atlas derived from DTI data from 23 stroke-free controls. Participants were categorized as no/mild or major vascular cognitive disorder (VCD) and group differences were examined.
Results: Among 60 participants (median age: 39.2 (IQR 27.9-46.2) and 52% female), 20 had major VCD. The major VCD group exhibited larger lesions (p=0.02), lower global efficiency (p=0.03), local efficiency (p=0.047) and density (p=0.03) compared to the no/mild VCD group, persisting at follow-up. At follow-up, the major VCD group showed significantly higher lesion impact scores and rich club scores, however validation analysis in a larger cohort (n=287) could not replicate these findings.
Conclusions: Our findings indicate a significant association between brain network measures and cognitive function in young stroke survivors, indicating a role of network disruption in post-stroke cognitive impairment. However, specific associations with hub region were only evident in a limited subgroup and not replicable in a larger cohort.
Disclosures of Interest: No
Abstract N°: 2302
THE HEALTH-RELATED QUALITY OF LIFE AMONG STROKE SURVIVORS WITH POST-COVID CONDITIONS LIVING IN THE UNITED STATES
Seyyed Sina Hejazian*1, Alireza Vafaei Sadr2, Shima Shahjouei3, Ajith Vemuri1, Vida Abedi2, Ramin Zand1
1The Pennsylvania State University, neurology, hershey, PA, United States, 2The Pennsylvania State University, Public Health Sciences, hershey, PA, United States, 3Penn State Health Milton S. Hershey Medical Center, Neurology, hershey, PA, United States
On behalf of:
Background and aims: It is well-known that a considerable number of COVID-19 survivors suffer from post-COVID conditions (PCCs) following the acute infection. As stroke survivors are at an elevated risk of PCCs compared to the general population, we aimed to evaluate the effect of PCCs on the health-related quality of life (HRQL) among stroke survivors of the US.
Methods: We used the Behavioral Risk Factor Surveillance System data 2022. Respondents with a positive history of COVID-19 infection and stroke were first selected and then classified based on whether they experienced PCCs. Finally, the HRQL-related items, including self-reported general health (SRGH), were compared between the two groups. We also compared our findings with those among the whole population of COVID-19 survivors. P-value<0.05 was significant.
Results: Overall, 108273 respondents with a positive history of COVID-19 (COVID-survivors) and 3988 respondents with a positive history of COVID-19 and stroke (STRCOV-survivors) were enrolled. Individuals with PCCs had significantly worse HRQL than those without PCCs among COVID and STRCOV-survivors. While unfavorable SRGH was more prevalent among STRCOV-survivors aged>64 years, same-age COVID-survivors had better SRGH. Consistent in all study groups, males aged>64 years and females aged<64 years had worse SRGH compared to same-age males. Among PCC-positive COVID-survivors, unfavorable SRGH was more prevalent in southern and western states. Based on multivariate regression analysis, PCCs independently increase the odds of unfavorable SRGH among COVID-survivors (aOR=1.41, CI95%: [1.29-1.54],p<0.001) but not among STRCOV-survivors (aOR=1.1, CI95%:[1.29-1.54], p=0.580).
Conclusions: The compromised HRQL among COVID and STRCOV survivors with PCCs underscores the importance of these conditions and necessitates developing novel strategies for patient-oriented treatments.
Disclosures of Interest: No
Abstract N°: 2374
ISOLATED CEREBELLAR STROKE: CLINICAL CHARACTERISTICS AND OUTCOME PREDICTORS
Petra Redfors*1,2, Malin Reinholdsson3,4, Adam Viktorisson3, Katarina Jood1,2, Katharina Stibrant Sunnerhagen3,5
1Institute of Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg, Department of Clinical Neuroscience, Gothenburg, Sweden, 2Department of Neurology, Sahlgrenska University Hospital, Gothenburg, Sweden, 3Institute of Neuroscience and Physiology, The Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden, 4Department of Occupational Therapy and Physiotherapy, Sahlgrenska University Hospital, Gothenburg, Sweden, 5Rehabilitation Medicine, Neurocare, Sahlgrenska University Hospital
On behalf of:
Background and aims: Isolated cerebellar strokes (ICS) represent 2-3% of all strokes, with up to 50% resulting in poor outcomes, especially in hemorrhagic cases. However, large, detailed studies on ICS are scarce. This study aims to elucidate the acute presentation, treatment, and factors influencing outcome.
Methods: We identified ICS cases from the Väststroke register (November 2014-December 2019). Data on clinical characteristics and infarct volumes were extracted from the Swedish stroke register Riksstroke, medical records, and neuroimaging. Comorbidities were assessed using the Charlson Comorbidity Index. Multivariable logistic regression determined predictors of poor outcome (modified Rankin Scale (mRS) 3-6) at 3 months.
Results: Among 245 patients, common symptoms were vertigo (87%), nausea (77%), inability to walk (61%), and ataxia (43%). Cerebellar hemorrhage occurred in 26.5%, with these patients presenting higher NIH Stroke Scale scores (median 2 vs. 0, p<0.01), older age (mean 74 vs. 65 years, p<0.001), and higher pre-admission independence (83% vs. 93%). Stroke volumes measured by CT (58%) and MRI (42%), were similar across subtypes. Among the cerebellar infarction subtype, 4.4% underwent mechanical thrombectomy and 6.7% received intravenous thrombolysis. Decompressive surgery was performed in 3.2% of all cases. Of those independent pre-stroke (n=222), 74% maintained low disability (mRS 0-2) at follow-up. Hemorrhage subtype and higher NIHSS scores correlated with worse outcomes, irrespective of age, sex, comorbidities, and stroke volume.
Conclusions: Neurological outcome in this ICS cohort was generally more favorable than previously reported. Hemorrhagic subtype and increased stroke severity predicted poor outcome. Recognizing presentation symptoms might enhance the low reperfusion treatment rate.
Disclosures of Interest: No
Abstract N°: 3281
IMPACT OF SOCIOECONOMIC STATUS ON STROKE RISK FACTORS AND OUTCOMES
Federica Rizzo*1, Marta Olive-Gadea2, Rodrigo Marc1, Francisco Purroy3, Xavier Ustrell4, Joaquin Serena5, Natalia Perez de la Ossa6, David Cano7, Carlos Molina1, Marta Rubiera2
1Vall d'Hebron University Hospital, Neurology, Barcelona, Spain, 2Vall d'Hebron University Hospital, Barcelona, Spain, 3Hospital Universitari Arnau de Vilanova, Lleida, Spain, 4Hospital Universitari de Tarragona Joan XXIII, Tarragona, Spain, 5Hospital Doctor Trueta, Girona, Spain, 6Hospital Germans Trias i Pujol, Badalona, Spain, 7NORA bio, Sant Cugat del Vallès, Spain
On behalf of: On Behalf of the HARMONICS consortium
Background and aims: Socioeconomic status (SES) represents an important and underestimate predictor of outcomes in stroke patients. Patient-reported outcomes (PROMs) are key in value-based healthcare, revealing disparities. We aim to describe the impact of SES on acute stroke baseline characteristics and outcomes.
Methods: Consecutive acute stroke patients admitted to 5 Catalan University Hospitals participating in HARMONICS (an EU-funded High-value Stroke care project), were offered a digital follow-up by a PROMs-through-App-program (NORA). PROMs included: HADs(anxiety/depression), PROMIS-10(global physical and mental health), global health quality (GHQ) and Fatigue Assessment Scale (FAS). mRS was also determined at 3 months. SES was evaluated by the TIRS scale (social risk indicators test; score 0-7, ⩾1 presence of social risk and >3 high socioeconomic risk (HSER))
Results: 1283 patients were included, 38.3% female, median age 69y. Only 0,9% patients had not social risk, and X% showed HSER. HSER patients were older (72 vs 65), had worse pre-stroke mRS (1vs0) and higher prevalence of vascular risk factors (Hypertension 73,1%vs59,5%, Dyslipidemia 52,9%vs43,5%, Diabetes 33,7%vs22,5%, Atrial Fibrillation 14,5%vs10,4%, low Physical activity 20,0%vs32,3%, p<0.05 for all).HSER patients showed worse clinician- (mRS at 90 day (2vs1 p<0.001)) and patient- reported outcomes in all timepoint except for HAD-anxiety (Figure1-2).
In a logistic regression adjusted by age, sex and baseline mRS, SES emerged as an independent predictor of functional outcome at 90 days (OR 0.62, p<0.001)
Conclusions: A poor SES is related to higher vascular risk factors and worse outcomes after acute stroke. Social evaluation and interventions should be mandatory to improve stroke management.
Disclosures of Interest: No
Abstract N°: 302
MECHANICAL THROMBECTOMY OUTCOMES IN PATIENTS WITH FRAILTY & UTILITY OF THE CLINICAL FRAILTY SCALE TO GUIDE REFERRAL DECISIONS
1Royal Hampshire County Hospital, Stroke, Winchester, United Kingdom
On behalf of:
Background and aims: Pre-stroke frailty has been independently associated with poor outcomes. There is limited data on the best ways of assessing frailty to guide patient selection for mechanical thrombectomy (MT). We reviewed all thrombectomy referrals at a district general hospital in Hampshire, and assigned a clinical frailty scale (CFS) score to all cases, and evaluated outcomes post-MT.
Methods: Data was collated on all referrals over an 18-month period. Pre-morbid and discharge mRS scores were recorded. Pre-morbid and discharge CFS scores were retrospectively identified. A sub-analysis of patients with frailty characterised by a pre-mRS >= 3 and/or pre-CFS >=4 was undertaken to evaluate functional outcomes.
Results: 55 patients were referred for MT. 9.1% had a pre-morbid mRS of >=3 and 35% had a pre-morbid CFS>=4. Over a third (37%) of patients with a CFS>=4 underwent MT. All cases achieved a TICI score of >2 suggesting good recanalisation. All patients had worse CFS score post MT compared to the pre-admission score.
Conclusions: The CFS identified a greater number of patients with frailty compared to the mRS suggesting this is a better predictive tool. Those with frailty had worse outcomes post-MT despite good recanalization, versus those with lower frailty scores. The CFS appears to be a useful tool in identifying pre-stroke frailty and could be easily incorporated into pre-MT assessments to facilitate referral decisions. We plan to integrate the CFS into our electronic stroke admissions form.
Disclosures of Interest: No
Abstract N°: 451
SICKNESS ABSENCE AND DISABILITY PENSION BEFORE AND AFTER ISCHEMIC STROKE:A SWEDISH LONGITUDINAL COHORT STUDY W/ MATCHED REFERENCES
Mihae Roland*1, Ann-Sofie Rudberg2, Kristina Alexanderson1, Christina Sjöstrand1
1Karolinska Institutet, Department of Clinical Neuroscience, Sweden, 2Danderyd Hospital, Department of Clinical Sciences, Sweden
On behalf of:
Background and aims: To determine ischemic stroke patients’ sickness absence (SA) and disability pension (DP) before and after stroke, and compare these to that of matched references.
Methods: A nationwide longitudinal cohort study of working-aged individuals (aged 18-61) in Sweden with incident ischemic stroke in 2000, 2005, 2010, or 2015, respectively. Each cohort was followed one year prior to the stroke and three years after. Five matched references per stroke patient were randomly selected from the population. Rates and mean days of diagnoses-specific SA and DP among stroke patients and references were calculated. Trajectory modelling was used to compute trajectories of mean annual SA and DP days over time. Multinomial regression analyses were used to identify predictors of high SA and DP.
Results: Among patients with incident ischemic stroke in 2000 (N=2728), 2005 (N=2738), 2010 (N=2767), and 2015 (N=2531), mean age (53 years) for stroke remained unchanged over the study years as did rate of men (64%). About 30% of stroke patients had SA in the year prior their stroke, corresponding proportions for references were 10-15%. Mean annual SA and DP days were significantly higher among stroke patients than references. Factors associated with patient’s future high mean number of SA and DP days, compared to low, were elementary educational level; adjusted OR (95%CI) 3.47(2.38-5.05), being single; 1.67(1.29-2.16), diabetes; 1.86(1.18-2.92), and aged >50; 2.25(1.69-2.98) in most cohorts.
Conclusions: Ischemic stroke patients have higher rates of sickness absence and disability pension both before and after stroke compared to matched references.
Disclosures of Interest: No
Abstract N°: 1954
CORTICAL AND DEEP VENOUS OPACIFICATION AFTER THROMBECTOMY - A MARKER OF GOOD PROGNOSIS
Keshet Pardo1,2, Liron Snapir2, Rani Barnea1, Ahmad Atmna1, Alain Perlow1, Ran Brauner1, Guy Raphaeli1, Eitan Auriel1, Michael Findler1
1Rabin medical center, Neurology, Petach Tikva, Israel, 2Tel Aviv University, Israel
On behalf of:
Background and aims: Imaging in acute ischemic stroke prior thrombectomy helps predict the clinical outcomes of patients. In recent years the role of venous outflow in stroke prognosis has become apparent. We aimed to explore the correlation between opacification profile of anastomotic cortical and deep veins, and clinical outcome.
Methods: A retrospective study of patients who undergone thrombectomy for large vessel occlusion of the anterior circulation. Digital subtraction angiography (DSA) images were reviewed to determine the venous opacification profile (VOP) based on contrast filling of vein of Labbe, vein of Trolard, Superficial Middle Cerebral vein, and Deep vein complex. Prognostic evaluation based on the VOP was analyzed with respect to 90 days modified Rankin Scale, mortality rates, and intracranial haemorrhage (ICH) rates.
Results: A total of 84 patients were included, 61 had a favorable VOP and 23 unfavorable VOP. There was no difference between groups regarding baseline and stroke characteristics. There were higher percentages of asymptomatic ICH with the unfavorable VOP group (39.1% and 14.8%, respectively, P=0.034). The favorable VOP group had lower rates of mortality (11.5% and 34.8%, respectively, P=0.023) and higher percentages of good clinical outcomes (49.2% and 21.7%, respectively, P=0.027). There was a significant correlation between favorable VOP and good clinical outcome and lower mortality rates.
Conclusions: A favorable venous opacification profile based on DSA images is a good prognostic factor for functional independence at day 90 and lower mortality rates in patients post-M1 thrombectomy. This study underlines the importance of venous outflow for brain tissue integrity.
Disclosures of Interest: No
Abstract N°: 3145
NEUTROPHIL/LYMPHOCYTE RATIO IS ASSOCIATED WITH THE SEVERITYOF ISCHEMIC STROKE IN THE FIRST 72 HOURS
1Faculdade de Ciências Médicas da Santa Casa de São Paulo, São Paulo, Brazil, 2Irmandade da Santa Casa de Misericórdia de São Paulo - Hospital Central, Brazil
On behalf of:
Background and aims: Ischemia resulting from a stroke triggers an inflammatory response in the central nervous system. The neutrophil/lymphocyte ratio (NLR) in peripheral blood can serve as a reliable marker of systemic inflammation in various diseases. The present study aims to quantify the NLR in patients diagnosed with ischemic stroke in the first 72 hours and investigate the correlation between NLR values, risk factors and its severity - according to the National Institutes of Health Stroke Scale (NIHSS).
Methods: It is a retrospective study based on medical records of patients aged over 18 years, who had ischemic stroke between 2017 and 2022. The clinical data includes the type of ischemic stroke and the presence of risk factors. NLR values was performed by analyzing blood count data from the patients' medical records.
Results: Of the 194 stroke patients, 80 % had NLR values exceeding 2, a value considered non-physiological. Patients with a more severe condition, according to the NIHSS scale, had a higher NLR in the first 72 hours. No statistically significant correlation was found between NLR, types of strokes and the presence of risk factors.
Conclusions: Stroke patients exhibit a higher neutrophil-lymphocyte ratio, which is associated with the severity of the condition.
Percentage of individuals in NLR ranges less than 2, between 2 and 4 and greater than 4, in individuals with stroke (n = 194) and healthy patients (n = 24).
Percentage of patients with NLR ≤ 2, between 2 and 4 and ≥ 4, according to NIHSS. P = 0.002.
Disclosures of Interest: No
Abstract N°: 191
RISK FACTORS AND THE OUTCOMES OF HEMORRHAGIC TRANSFORMATION IN AF-RELATED ACUTE ISCHEMIC STROKE
Po-Lin Chen*1,2, Chi Sheng Wang1, Jin-AN Huang1
1Taichung Veterans General Hospital, Cerebral Vascular Disease, Taichung, Taiwan, 2College of Medicine, National Chung Hsing University, Department of Post-Baccalaureate Medicine, Taichung, Taiwan
On behalf of:
Background and aims: This study aimed to investigate the risk factors for hemorrhagic transformation (HT) and its outcomes in patients with AF-related acute ischemic stroke.
Methods: Patients admitted within 48 hours after onset were retrospectively screened and classified into the HT or non-HT group according to the brain MRI beyond 48 hours after onset. The risk factors for HT and the outcomes were analyzed.
Results: One hundred and two and 362 patients were in the HT and non-HT groups, respectively. The HT group had higher NIHSS scores (15 [7–22] vs 6 [2–15], p<0.001), fewer patients with oral anticoagulant use (OAC) before stroke (58.8% vs 70.2%, p=0.031) and oral antiplatelet (OAP) within 48 hours after stroke (77.5% vs 85.9%, p=0.039), and more patients with endovascular thrombectomy (EVT, 29.4% vs 13.3%, p<0.001). Multivariate regression showed that a higher NIHSS score and EVT were significantly associated with a higher risk of HT, while OAC before stroke and OAP within 48 hours after stroke onset were significantly associated with a lower risk of HT. All-cause mortality within 90 days was similar (Figure 1). Analyses of the mRS adjusted for age and NIHSS score showed that HT was less likely to have favorable outcomes (mRS⩽1) at 90 days (Figure 2, 16.7% vs 39.0%; OR, 0.46; 95% CI, 0.24–0.86, p=0.016).
Conclusions: Higher NIHSS scores, no OAC before stroke, no OAP within 48 hours after stroke onset, and EVT are risk factors for HT. HT was associated with an unfavorable function outcome at 90 days.
Disclosures of Interest: No
Abstract N°: 439
MECHANICAL THROMBECTOMY IN THE FRAIL ELDERLY – SOUTHAMPTON EXPERIENCE AND PREDICTORS OF OUTCOME
Richard Marigold*1, Nic Weir1, Shivaprasad Siddegowda1, Sue Evans1, Emily Tjerkstra1, Pamela Crawford1, Emma Battersby Wood1
1Wessex Neurological Centre, Stroke Medicine, United Kingdom
On behalf of:
Background and aims: Mechanical thrombectomy (MT) is used to treat 10-15% of patients with large vessel occlusion (LVO) and indications for treatment have recently expanded. One challenging area is clinical frailty, and deciding which patients benefit most from intervention. University Hospital Southampton is a medium sized comprehensive stroke centre (CSC) in southern England admitting 1200 stroke patients and treating 200 patients with MT in 2023. In this retrospective audit, we reviewed our outcomes in patients treated with MT over 80 years of age.
Methods: 48/179 patients were over the age of 80 treated with MT in 2023. Data were analyzed to assess the pre-MT clinical frailty score (CFS), modified 5-item frailty (MFI-5) index, and post MT 90 day modified Rankin score (mRS).
Results: The mean mRS at 90 days was 4.2. 17/48 patients had an mRS 0-3. 11/48 patients died (mRS 6). The MFI-5 score did not correlate well with 90-day mRS, but a CFS of 5 or 6 was highly correlated with an mRS at 90 days of 5 or 6. 16/48 patients had pre-MT CFS 5-6- and 90-day mRS 5-6.
Conclusions: Our data supports the use of the clinical frailty score (CFS) as a potential screening tool in predicting poor outcomes after thrombectomy. Current trials use different assessment scales with considerable heterogeneity in the results, but further analysis of the CFS as a screening tool may aid clinicians in making better informed decisions when treating frail patients with multiple comorbidities.
Disclosures of Interest: No
Abstract N°: 675
THE PROGNOSTIC ROLE OF IRON DEFICIENCY IN ACUTE ISCHEMIC STROKE PATIENTS. A PROSPECTIVE MULTICENTRIC COHORT STUDY
Antonio Ciacciarelli*1, Anne Falcou1, Aldobrando Broccolini2, Giovanni Frisullo2, Serena Abbruzzese2, Irene Scala2, Sabrina Anticoli3, Ennio Montinaro4, Elisa Testani3, Danilo Toni1
1Sapienza University of Rome, Emergency Department, Rome, Italy, 2Università Cattolica del Sacro Cuore, Department of Neurosciences, Rome, Italy, 3AO S. Camillo, Stroke Unit, Rome, Italy, 4Azienda Ospedaliera Santa Maria Terni, Neurology Division, Terni, Italy
On behalf of:
Background and aims: Iron deficiency (ID) holds prognostic significance in heart failure and acute coronary syndrome. However, its role in cerebrovascular diseases is controversial. This study aims to determine the impact of ID on the outcome of acute ischemic stroke (AIS) patients.
Methods: This is an ongoing observational prospective multicentric cohort study. From January to September 2023, we enrolled AIS patients admitted to the stroke units of two University Hospitals. Venous blood samples were collected at admission to determine the iron status (serum iron, ferritin, transferrin). ID was defined as a serum ferritin concentration <100 ng/mL or 100–299 ng/mL with transferrin saturation (TSAT) <20%. The primary endpoint was the functional outcome at 90 days measured by the modified Rankin Scale (mRS).
Results: The analysis included 153 patients (mean age 74±12, 48.4% female, mean NIHSS 10±7, 69.2% treated with IVT±EVT). ID prevalence was 56.9%. Binary logistic regression for mRS 0-2 at 90 days revealed that ID, along with admission NIHSS and CRP, was independently associated with poorer functional outcome regardless of age, anemia, or large vessel occlusion (table 1). Patients with ID were older, more frequently female, diabetics, and displayed lower serum cholesterol levels. Hemoglobin levels, CRP, and Neutrophil to Lymphocytes ratio predicted TSAT levels in linear regression analysis.
Conclusions: Preliminary analysis indicated an ID prevalence of 56.9% among ischemic stroke patients, independently linked to worse functional outcome at 90 days. Expanding the sample size is needed to validate these findings.
Disclosures of Interest: No
Abstract N°: 1772
LIMITED BENEFIT OF SWALLOWING REHABILITATION IN SEVERE DYSPHAGIA DURING ACUTE ISCHAEMIC STROKE HOSPITALISATION
Background and aims: Swallowing rehabilitation is important in acute ischemic stroke. Oral intake impairment at admission has been reported to be associated with dysphagia recovery impairment. However, whether the degree of swallowing function affects dysphagia recovery has been fully investigated. In this study, we examined the effect of swallowing function at admission on dysphagia recovery.
Methods: We examined consecutive patients with acute ischemic stroke from our single-center stroke registry between 2018 and 2020 (1034 patients were enrolled). Swallowing function was assessed by the food oral intake scale (FOIS) at two points: at admission and 14 days after hospitalization. In this study, patients with severe dysphagia, defined as FOIS 1-3 which requires alternative nutrition, were enrolled. The outcome was poor dysphagia recovery, defined as FOIS 1-3 on day 14. We evaluated the effect of each FOIS score at admission for dysphagia recovery.
Results: Among 237 patients, 88 (37%) experienced dysphagia recovery. The prevalence of dysphagia recovery was extremely lower only in FOIS 1 (couldn’t be taken orally at all) compared with FOIS 2 and 3, with 1%, 63%, and 59%, respectively. The logistic regression analysis also showed FOIS 1 was independently associated with poor dysphagia recovery (adjusted OR 95.1; 95%CI:12.3-735.0).
Conclusions: In acute ischemic stroke, FOIS 1 at admission had an extremely lower dysphagia recovery rate and was independently associated with poor dysphagia recovery. In patients with FOIS 1 at admission, early initiation of alternative nutrition should be considered.
Disclosures of Interest: No
Abstract N°: 1880
CIRCOGDH AS A NEW BIOMARKER FOR THE DIAGNOSIS AND OUTCOME PREDICTION IN ACUTE ISCHEMIC STROKE
Min Peng*1,2,3, Man Ke1,2,3, Dan Lu1,2,3, Anding Xu1,2,3
1The First Affiliated Hospital of Jinan University, Department of Neurology and Stroke Center, Guangzhou, China, 2The First Affiliated Hospital of Jinan University, Clinical Neuroscience Institute, Guangzhou, China, 3The First Affiliated Hospital of Jinan University, Key Lab of Guangzhou Basic and Translational Research of Pan-vascular Diseases, Guangzhou, China
On behalf of:
Background and aims: Circular RNAs are a class of non-coding RNAs that show promise as stroke biomarkers. This study aims to investigate the diagnostic and prognostic significance of CircOGDH for acute ischemic stroke (AIS).
Methods: Patients with AIS were enrolled from a multicenter hospital-based stroke registry in China. Blood plasma samples were collected for CircOGDH assessment on days 1 (admission), 3, and 7. The modified Rankin Scale (mRS) was used to assess neurological function at 90 days post-stroke. Ischemic penumbra volume was assessed by CT perfusion (CTP).
Results: A total of 444 patients were included for further analysis. There was an increase in CircOGDH in AIS when compared to healthy controls (444 vs. 83). CircOGDH have a good predictive value for the diagnosis of both AIS and the penumbra (AUC=0.843 and 0.819, respectively). Compared to patients with poor outcome (mRS 3−6), patients with favorable outcomes (mRS 0−2) had elevated CircOGDH levels on Day (D) 1 and the differences in values between D1 and D7 (P=0.028 and 0.023, respectively). Multiple logistic regressions showed that the differences in log-transformed values between Day 1 and Day 3, denoted as log (D1/D3) (OR=2.959, 95%CI:1.548−1.815) and log (D1/D7) (OR=2.314, 95%CI:1.141−4.967) were independent predictors for favorable outcomes of AIS after adjusted for confounders. In the subgroup of large vessel anterior circulation occlusion, elevated log (D1/D7) remains a strong predictor for AIS.
Conclusions: CircOGDH is a marker of the ischemic penumbra and AIS diagnosis. The dynamic change in CircOGDH levels could serve as a potential biomarker for AIS outcome prediction [ChiCTR23 00072569].
Disclosures of Interest: No
Abstract N°: 2136
RISK OF BIAS ASSESSMENT OF MACHINE LEARNING PREDICTIVE MODELS OF POST-STROKE MORTALITY
Mariam Desouki1, lan Soh*2, Abdelrahman M. Saad1, Nicole Maria Radley3, Milindu Wickramarachchi4, Amelia Dawson5, Jeremy Ng Chieng Hin6, Abhrajit Giri7, Asad Ali8
1Alexandria university, Faculty of Medicine,Egypt., 2St George's, University of London, 3Imperial College London, 4school of clinical medicine, university of Cambridge, 5Kavanagh, Chesterfield Royal Hospital foundation trust, 6Wirral University Teaching Hospital NHS foundation trust, 7Nottingham University Hospitals NHS Trust, 8Lancaster University
On behalf of:
Background and aims: Stroke is a debilitating neurological condition with short and long-term medical consequences. It can at times be both challenging to diagnose and unpredictable.
This encouraged the development of advanced technology like machine learning to better predict its prognosis. The aim of this systematic review is to provide reliable evidence from previously published scientific literature whether machine learning is beneficial for the prediction of post-stroke mortality or not.
Methods: We searched PubMed, Scopus, Cochrane and Web of Science databases for original publications on machine learning applications in stroke mortality prediction, published between January 2011, and January 2024. Risk of bias was evaluated using the tailored PROBAST tool.
Results: Of the 9,775 studies retrieved, 10 retrospective studies were included. The ML models demonstrated a favorable range of AUC for mortality prediction (0.81-0.95). In the included articles, the models were applied for both short-term and long-term post stroke mortality. The number of explanatory features used in the models to predict mortality ranged from 6 to 47, with substantial overlap in the variables included. Age, high NHISS score, hyperlipidemia and creatinine, were identified as important predictors for mortality. Almost all studies had a high risk of bias in at least one category. However, there is a variation in the degree of bias displayed in the included retrospective cohorts.
Conclusions: The application of machine learning in the prediction of both long-term and post-stroke mortality demonstrated promising beneficial effects. Nonetheless, more prediction models needs to be developed to be more transparent and clear in terms of the methodology used.
Disclosures of Interest: No
Abstract N°: 2501
IMPACT OF COLLATERAL STATUS ON OUTCOMES OF MECHANICAL THROMBECTOMY – IN-VITRO STUDY
Magda Jablonska*1,2, Jiahui LI1,2, Riccardo Tiberi1,2, Alejandro Tomasello2,3, Marc Ribo1,2
1Vall d´Hebron Hospital, Stroke Unit, Barcelona, Spain, 2Vall d’Hebron Research Institute, Stroke Research, Barcelona, Spain, 3Vall d’Hebron University Hospital, Neurointerventional Radiology Department, Barcelona, Spain
On behalf of:
Background and aims: The presence or lack of an extensive cerebral collateral net is becoming more widely considered as an independent prognostic factor in stroke patients. We aimed to assess whether the extent of collaterals had modifying effects on first pass recanalization (FPR) and distal emboli measures in mechanical thrombectomy (MT).
Methods: Two in-vitro neurovascular models were created: good collaterals model (GCM) and poor-collaterals model (PCM). The two models were identical up to the M2 segment of middle cerebral artery (MCA). The GCM included anastomoses of the M2-MCA branches with anterior cerebral arteries and vertebrobasilar circulation. In the PCM these anastomoses were missing. Synthetic uniform clots (stiffness = 95.77±5.80 kPa) were embolized to the M1-MCA. In all cases MT was performed using Solumbra technique (Solitaire 4x40mm + React 71). The primary outcome measure was FPR. The secondary outcomes assessed distal embolization parameters.
Results: A total of 60 MTs were performed (30 experiments per study arm). Overall rate of FPR was 30%. FPR was higher in GCM (52%) than in PCM (8%; p<0.01). Maximum distal embolus size (1.51±1.31mm vs. 0.58±0.46mm; p<0.05), mean size of the embolus (0.95±1.1 vs. 0.35±0.28; p<0.05), total area of emboli (2.49±3.45 vs. 0.42±0.64; p<0.05) and total count of particles >1mm (0.97±1.03 vs. 0.27±0.69; p<0.01) were also lower in GCM than in PCM.
Conclusions: The degree of collateral circulation may modify mechanical thrombectomy outcomes. Good collaterals might facilitate the achievement of FPR and prevent distal embolization.
Disclosures of Interest: No
Abstract N°: 2812
VERY LONG-TERM RECURRENCE IN HEMORRHAGIC STROKE: A COMPARATIVE ANALYSIS WITH ISCHEMIC STROKE
Antoni Suárez-Pérez*1, Angel Ois1,2, Adrià Macias-Gómez1,2, Marta Vallverdú-Prats1, Elisa Cuadrado-Godia1,2, Eva Giralt-Steinhauer1,2, Isabel Fernández-Pérez1,2, Ana Rodríguez-Campello1,2, Jordi Jiménez-Conde1,2, Joan Jiménez-Balado1
1Hospital del Mar Research Institute, Neurovascular Research Group, Barcelona, Spain, 2Hospital del Mar, Neurology, Barcelona, Spain
On behalf of:
Background and aims: While extensive research has focused on ischemic stroke recurrence, recurrence following a hemorrhagic stroke remain less explored. Our study aims to analyze risk factors associated with long-term ischemic or hemorrhagic recurrence (SR) in patients who have experienced a first hemorrhagic stroke, comparing these with a similar ischemic stroke cohort.
Methods: The study analyzed 83 hemorrhagic and 604 ischemic stroke survivors from a prospective registry spanning 2005-2017, with follow-up until January 2023. Demographic factors (sex, age dichotomized at 55 years) and vascular risk factors (hypertension, diabetes, dyslipidemia, atrial fibrillation, heart failure, and smoking) were analyzed. Kaplan-Meier and Cox proportional hazards regression models were used to identify significant SR predictors.
Results: The median follow-up period was 6.39 years (IQR 2–10 years). SR was registered in 130 cases (18.9%): 119 (19.7%) and 11 (13.3) in ischemic and hemorrhagic stroke survivors respectively. In the hemorrhagic stroke group, Cox regression analysis revealed that only atrial fibrillation (HR [95%CI]: 3.99 [1.17-13.68]) was significantly associated with SR. In contrast, among ischemic stroke survivors, significant associations with SR were observed for diabetes (HR [95%CI]: 1.64 [1.14-2.35]), heart failure (HR [95%CI]: 1.68 [1.02-2.77]), and female gender (HR [95%CI]: 1.64 [1.14-2.35]).
Conclusions: Our study underscores distinct risk factor for SR in hemorrhagic versus ischemic strokes. Atrial fibrillation significantly predicts SR in hemorrhagic, but not in ischemic strokes. Diabetes, heart failure, and female gender are linked to higher SR in ischemic strokes. We hypothesize this difference might be due to anticoagulant drug removal following a hemorrhagic stroke.
Disclosures of Interest: No
Abstract N°: 2834
CALORIC INTAKE DURING HOSPITAL STAY AND IMPACT ON THE SURVIVAL AMONG PATIENTS WITH INTRACEREBRAL HEMORRHAGE
Natasha Gupta*1, Padmini Sekar2, Marlene Deguzman2, Anay Dalal2, Lee Gilkerson2, Matthew Flaherty2, Shea Wright2, Stacie Demel2, Daniel Woo2
1University of Cincinnati College of Medicine, Cincinnati, United States, 2University of Cincinnati, Cincinnati, United States
On behalf of:
Background and aims: Overweight patients have better survival after intracerebral hemorrhage (ICH). We hypothesized that a higher caloric intake during hospitalization would improve survival for ICH patients.
Methods: Between 2008-2021, the Genetic and Environmental Risk Factors for Hemorrhagic Stroke and the Ethnic/Racial Variations of Intracerebral Hemorrhage studies prospectively recruited spontaneous ICH cases. To evaluate strict caloric intake, we utilized patients who exclusively received tube feeds and had a follow-up examination at 3 months. Patient weights were collected at admission, during admission, at discharge. Patient malnutrition status was estimated using admission serum albumin levels. Caloric consumption and IV fluid intake were collected. The outcome metric, patient survival, was defined as mortality or discharge to hospice care. All variables with p<0.05 in univariate analysis were included and then backward eliminated to best fit utilizing multivariate logistic regression.
Results: After exclusions, 86 patients were included. By 3-month follow-up, 18 patients died (mean±SD age 73.3±9.7; 50% female) and 68 patients survived (mean±SD age 65.5±14.4; 37% female). Multivariate analysis to discharge outcome is presented (Table 1).
Conclusions: Routine variation in caloric replacement was not associated with improved survival suggesting that either greater calories are needed or other explanations for the obesity paradox in ICH should be explored.
Disclosures of Interest: No
Abstract N°: 2896
LONG-TERM FUNCTIONAL OUTCOME AND QUALITY OF LIFE 2.5 YEARS AFTER THROMBOLYSIS IN ACUTE ISCHEMIC STROKE
Marie Schäbitz1,2, Leona Möller1, Anja Friedrich3, Nele Klein2, Alkisti Kitsiou2, Isabell Greeve2, Anja Gerstner1, Wolf-Rüdiger Schäbitz*2, Lars Timmermann1, Andreas Rogalewski2,4
1Philipps University Marburg, Department of Neurology, Marburg, Germany, 2Evangelisches Klinikum Bethel, University Hospital OWL of the University Bielefeld, Campus Bielefeld-Bethel, Department of Neurology, Bielefeld, Germany, 3Bielefeld University, Department of Psychology, Bielefeld, Germany, 4Sankt Elisabeth Hospital Gütersloh, Catholic Hospital Association of East Westfalia (KHO), Department of Neurology, Gütersloh, Germany
On behalf of:
Background and aims: Evaluation of outcome after stroke is largely based on assessment of gross function 3 months after stroke onset using scales such as mRS. Cognitive or social functions, level of symptom burden or emotional health are not usually assessed, nor are data available on long-term functional outcomes years after stroke.
Methods: Analysis of 1141 patients with AIS treated with IVT from two major German hospitals between 2017 and 2020. Patient characteristics and short-term outcome were analysed from patient records. Long-term outcome of 228 patients with prior written informed consent was assessed via telephone survey using mRS and PROMs (EQ-5D-5L, EQ-VAS) 2.5 years after stroke.
Results: Predictors of excellent to good long-term outcome were younger age, event to door time ⩽ 2 h, NIHSS ⩽ 6 on admission and NIHSS ⩽ 6 after IVT. Stroke recurrence was a negative predictor. Predictors of excellent quality of life at 2.5 years included age < 73 years, lower NIHSS after IVT, absence of hypertension. Quality of life was rated in all dimensions with a medium score of 1 and a medium EQ-VAS of 70, representing the good general health status of this stroke population.
Conclusions: Main predictors of an excellent to good long-term outcome and excellent QoL 2.5 years after stroke are younger age, lower NIHSS, and event to door time ⩽ 2 h. Research on long-term outcome and treatment is important, as it has the ability to reveal the true functional outcome and quality of life and to provide information on the status of independence and self-esteem.
Disclosures of Interest: Yes WRS received honoraria for lectures/consulting from Argenx/AstraZeneca/Bayer HealthCare/Biogen/Bristol-Myers Squibb Daiichi Sankyo. LT received honoraria for lectures/consulting by BostonScientific/AbbVIE/Novartis/Neuraxpharm/Teva/MovementDisordersSociety/DIAPLAN
Abstract N°: 3005
EFFICACY OF INTERMITTENT THETA-BURST TRANSCRANIAL MAGNETIC STIMULATION IN PATIENTS WITH DYSPHAGIA AFTER STROKE
1Faculty of Medicine, Al-Azhar University, Cairo, Egypt
On behalf of:
Background and aims: The intermittent Theta-burst Transcranial Magnetic Stimulation (iTBS) is an emerging protocol of Repetitive Transcranial Magnetic Stimulation (rTMS). However, its efficacy in patients with dysphagia after stroke hasn't been proven. We aim to investigate the efficacy of iTBS in post stroke dysphagia patients.
Methods: PubMed, Scopus, Cochrane CENTRAL, Embase and Web of Science were searched. We included studies that tested iTBS in post stroke dysphagia patients. We conducted a single arm meta-analysis to prove the efficacy of iTBS in different brain locations and then we compare it with sham TBS in the studies comparing them. With the Review Manager software for statistical analysis, we used the mean difference (SMD) and its 95% confidence interval to compare continuous outcomes applying the random effect model.
Results: Three randomized controlled trials (RCT) were yielded with four different groups to compare. iTBS showed a significant improvement in Standardized swallowing assessment (SSA), Rosenbek Penetration-Aspiration Scale (PAS), YPRS (severity of pyriform fossa residue), Murray Secretion Scale (MSS) and Oral Motor Function Scale (OMFS) with the following values respectively (MD=-6.72, 95% CI [-7.74,-5.70], p<0.0001), (MD=-2.55, 95% CI [-3.06,-2.05], p<0.0001), (MD=-1.39, 95% CI [-2.36,-0.41], p=0.005), (MD=-0.69, 95% CI [-1.08,-0.31], p=0.0004) and (MD=16.25, 95% CI [3.36,29.15], p=0.01). SSA, PAS And YPRS were also statistically significant in favor of iTBS compared to sham (MD=3.44, 95% CI [1.79,5.09], p<0.0001), (MD=1.22, 95% CI [0.66,1.79], p<0.0001) and (MD=0.83, 95% CI [0.42,1.24], p<0.0001).
Conclusions: iTBS showed a promising result as a treatment for post stroke dysphagia patients
Disclosures of Interest: No
Paper Poster - Rare Causes Incl. Dissection
Abstract N°: 1518
BIOPSY-PROVEN PACNS: RESULTS FROM THE LARGE, MULTICENTER COHORT OF CEREBRAL VASCULITIS PATIENTS
Milani Deb-Chatterji*1, Parnia Aghel2, Hans Pinnschmidt3, Christina Krueger4, Juliane Herm5, Julia Nordsiek6, Hebun Erdur7, Felix Bode6, Christian Nolte5, Tim Magnus4
1University Hospital Schleswig-Holstein Campus Kiel, Department of Neurology, Kiel, Germany, 2University Medical Center Hamburg Eppendorf, Department of Neurology, Hamburg, Germany, 3University Medical Center Hamburg Eppendorf, Institute of Medical Biometry and Epidemiology, Hamburg, Germany, 4University Medical Center Hamburg Eppendorf, Department of Neurology, Ham, Germany, 5Charite Universitätsmedizin Berlin, Department of Neurology, Berlin, Germany, 6University Hospital Bonn, Department of Neurology, Bonn, Germany, 7Asklepios Fachklinikum Teupitz, Department of Neurology, Teupitz, Germany
On behalf of:
Background and aims: Reports of Primary angiitis of the CNS (PACNS) are mainly restricted to clinically highly suspected cases but biopsy-proven ones are rare. Here, we present results from the largest multicenter cohort of patients with biopsy-proven PACNS (BP-PACNS).
Methods: BP-PACNS patients treated in three university hospitals between 1999–2021 were analyzed. The outcome was assessed by modified Rankin Scale (mRS). Between-group comparisons were perfor-med by Kruskal-Wallis-, Chi2- or Fisher’s Exact tests.
Results: In total, 57 patients were analyzed (52% male). Of these, n=37 (65%) had a lymphocytic (L-PACNS), n=9 (16%) an ABRA, n=8 (14%) a granulomatous (G-PACNS) and n=3 (5%) a necrotizing (N-PACNS) pattern. Median follow-up was 41.5 months (IQR 7.5-73.5). At time of diagnosis, age differed significantly between groups (median age [years] L-PACNS 47, ABRA 64.5, G-PACNS 37, N-PACNS 65; p=0.008). L-PACNS and ABRA mostly had a monophasic course (65% and 63%), while 75% G-PACNS patients showed a relapsing-remitting type. Worst outcome (mRS 4 at last follow-up) and numerically highest mortality (25%) were seen in G-PACNS. Good induction treatment response (combined steroid and cyclophosphamide therapy) was achieved in 77% BP-PACNS patients and was numerically lowest in G-PACNS (43%).
Conclusions: In this large, multicenter series of BP-PACNS patients G-PACNS had a worse functional outcome, a predominant relapsing-remitting disease and a less treatment response to the induction therapy. Another first-line treatment for G-PACNS patients, i.e. with infliximab, should be discussed and further examined in larger studies.
Disclosures of Interest: No
Abstract N°: 3021
REFINING THE PHENOTYPE OF INTRAVASCULAR LYMPHOMA WITH CENTRAL NERVOUS SYSTEM INVOLVEMENT: LESSONS FROM A FRENCH COHORT OF 17 PATIENTS
1Lariboisière Hospital, Assistance Publique-Hôpitaux de Paris, Neurology Departement, Paris, France, 2Pitié-Salpêtrière Hospital, Assistance Publique-Hôpitaux de Paris, Neuro-oncology departement, Paris, France, 3Saint-Louis Hospital, Assistance Publique-Hôpitaux de Paris, Neuro-oncology departement, Paris, France, 4Lariboisière Hospital, Assistance Publique-Hôpitaux de Paris, Neuro-radiology Departement, Paris, France
On behalf of:
Background and aims: Intravascular lymphoma (IVLBCL) is a rare large B-cell lymphoma characterized by clonal lymphocytic proliferation confined to small and medium-sized vessel lumen. Involvement of central nervous system (CNS) is reported over 50% of patients in Western countries, where IVLBCL represents a rare cause of stroke. The diagnosis is often delayed as symptoms lack of specificity. We aimed to refine the phenotype of IVLBCL with CNS involvement (CNS-IVLBCL), through the analysis of 17 French patients, intending to facilitate its early diagnosis.
Methods: We retrospectively analysed clinical, biological and radiological data of 17 biopsy-proven CNS-IVLBCL patients recruited through collaboration with the French Expert Network for Oculo-Cerebral Lymphomas.
Results: Fifteen patients had ⩾ 1 focal neurological deficit (FND), with an acute-onset in 68% of FND, suggesting a vascular origin. Most showed recurrent FND during the course of the disease, averaging 2 FND/patient. Clinical fluctuations were frequently reported, especially during the first FND episode (64%). Rapid cognitive deterioration occurred in 88% patients, and pre-existed before FND in half of cases. Brain MRI showed DWI-positive lesions in 81% of patients, which accumulated over time. All patients exhibited unusual ischemic pattern such as progressive growth (23%), persistent DWI-hypersignal >1 month (69%), or a location within or at the edge of a larger FLAIR hypersignal (100%). Early-onset inflammatory syndrome, and increased LDH levels were observed in > 90% of cases.
Conclusions: Clinical fluctuations, unusual ischemic MRI pattern, elevated CRP and LDH levels are «red flags» that should prompt consideration of CNS-IVLBCL diagnosis in stroke patients.
Disclosures of Interest: No
Abstract N°: 695
ISCHEMIC STROKE DUE TO CAROTID ARTERY DISSECTION ASSOCIATED WITH ELONGATED STYLOID PROCESS
1The Second Affiliated Hospital of Soochow University, Suzhou, China
On behalf of:
Background and aims: Internal carotid artery dissection (ICAD) represents a major cause of ischemic stroke in young adults. To investigate the clinical and neuroradiological features of patients with carotid artery dissection associated with elongated styloid process.
Methods: Retrospective data was collected from registration system in our stroke center over 10 years. All patients with ischemic stroke due to ICAD were identified from individuals who underwent computer topography angiography of the neck. Available data on comorbidity, laboratory parameters, treatment administered, clinical evolution, bilateral styloid process length and angulation in the axial and rostral-caudal planes, and proximity to the carotid artery were measured.
Results: 395 ischemic stroke patients with ICAD were identified. 108 (27.3%) patients had Eagle syndrome, of which 10 (0.9%) had bilateral dissection, accounting for 18.5% (20 of 108) of ischemic strokes in young patients (⩽45 years). Bilateral ICAD accounts for 30% (6 of 20) of young stroke patients with elongated styloid process. In patients with Eagle syndrome, 87% (94 of 108) patients had elongated styloid process, and the left and right sides accounted for 43.5% and 43.5%, respectively. And average styloid process length was 3.46 cm for left side and 3.52 cm for right side. 10 patients had direction abnormality accounting for 9.3%, and styloid process-internal carotid distance was 5.2 mm.
Conclusions: when dealing with ischemic stroke and ICAD, especially in young stroke adults, elongated styloid process must be taken into account by neurologists.
Disclosures of Interest: No
Abstract N°: 2125
INCIDENCE, MANAGEMENT AND OUTCOME IN PATIENTS WITH TRAUMATIC CEREBROVASCULAR INJURY
Tracey Fan*1, Meredith Yang2, Shyam Prabhakaran1
1University of Chicago, Department of Neurology, Biological Science Division, Chicago, United States, 2The University of Chicago Pritzker School of Medicine, Chicago, United States
On behalf of:
Background and aims: Traumatic cerebrovascular injury (TCI) has important immediate and long-term implications. We aim to report its incidence, management, and impact on outcomes.
Methods: Medical charts of patients⩾18 years who presented from 11/1/2021 to 10/1/2023 with isolated TBI or polytrauma and completed CT angiogram (CTA) of head and neck were reviewed, and relevant information were extracted.
Results: Among 307 patients (median age 45 [IQR 31-64], 27% female, 61% African American, 25% with penetrating brain injuries), 28% (n=87) had TCI on initial CTA (66 arterial, 25 venous, and 7 both). Among those with arterial injuries, 82% (n=54) had vascular injury Biffl scale grade<3; 86% (n=57) had subsequent CTA (median 3 days [IQR 2-6]) and 25% (n=14) showed improvement or resolution of TCI; Thirty-five percent (n=23) were started on single antiplatelet agents (87% aspirin, median 3 days from admission [IQR 3-9], 13% (n=8) were started on therapeutic anticoagulation (median 11 days from admission [IQR 2-14]), 15% (n=10) had endovascular procedures, and 23% (n=15) had ischemic stroke at median 4 days from admission (IQR 2-6). Among patients with venous injuries, 76% (n=19) involved the superior sagittal sinus, 92% (n=23) had no propagation on subsequent imaging, and only 3 patients were anticoagulated. Patients with TCI had higher mRS (5 vs. 3, p=0.004) at discharge than patients without TCI and were less likely to be discharged home (22% vs. 45%, p<0.001).
Conclusions: TCI is common after isolated TBI or polytrauma and associated with high stroke risk. Larger prospective studies are needed to better understand the optimal management.
Disclosures of Interest: No
Abstract N°: 3087
DOES THROMBOTIC MICROANGIOPATHY DRIVE THE OCCURRENCE AND PATTERN OF CEREBROVASCULAR INJURY IN MALIGNANT HYPERTENSION ?
Peter Chen1, Yannis Lombardi2, Cédric Rafat2, Cedi Koumako3, Alice Doreille2, Cyril Mousseaux2, Michel Paques4, Stephen Delorme1, Sonia Alamowitch*1
1Hôpitaux Universitaires Pitié-Salpétrière, AP-HP, Urgences Cérébro-Vasculaires, Paris, France, 2Hôpital Tenon, AP-HP, Soins Intensifs et Rein Aigu, Paris, France, 3Hôpital Saint-Antoine, AP-HP, Service de Radiologie, Paris, France, 4Centre Hospitalier National d'Ophtalmologie des Quinze-Vingts, Paris, France
On behalf of:
Background and aims: Malignant hypertension (MHT) is characterized by diffuse microvascular damage caused by severe hypertension. Cerebrovascular injury stands as a hallmark of the disease, identified in up to half of patients. Thrombotic microangiopathy (TMA) also emerges as a frequent complication of MHT, but its role in cerebrovascular disease (CVD) remains unexplored. The objectives of this study were to explore the role of TMA in acute ischemic stroke (AIS) and to provide a comprehensive description of MHT-associated CVD.
Methods: We retrospectively assessed brain MRIs of patients admitted to the kidney intensive care unit at Tenon hospital for MHT during the 2017-2023 period. Brain MRIs were systematically performed and independently reviewed by two blinded operators. Acute CVD, defined as AIS, intracerebral hematoma (ICH) or posterior reversible encephalopathy syndrome (PRES), was assessed. Underlying cerebral small vessel disease (CSVD) was evaluated using a validated score.
Results: A total of 60 patients were admitted for malignant hypertension, with a mean age of 42.9 years. Chronic CVSD was present in 33 patients (55.0%). Acute injury occurred in 27 patients (45.0%). AIS was the most frequent (33.3%), followed by PRES (21.7%) and ICH (1.7%). Among patient with AIS, 14 (70.0%) presented with multiple simultaneous lesions. TMA was present at admission in 34 patients (56.7%). In an exploratory analysis, AIS was associated with the presence of CVSD (p=0.013), but not with TMA (p=0.79).
Conclusions: Our study confirmed the high incidence of acute CVD during MHT. Underlying chronic CVSD increased the incidence of ischemic brain injury, but not TMA.
Disclosures of Interest: No
Abstract N°: 3235
PERSISTENT TRIGEMINAL ARTERY AS A RARE CAUSE OF VERTEBROBASILAR INSUFFICIENCY SYMPTOMS: A CASE SERIES STUDY
Alberto Velayos Galán*1, Elena Resa Serrano1, Laura Velayos Galán1, Pablo del Saz Saucedo1, Rafael Huertas Arroyo1
1Hospital General La Mancha Centro, Neurology, Alcázar de San Juan, Spain
On behalf of:
Background and aims: Persistent trigeminal artery (PTA) is the fetal carotid-basilar anastomosis that most frequently persists in adults. Most cases are diagnosed incidentally, without associated symptoms. Occasionally, PTA could cause vertebrobasilar (VB) insufficiency sypmtoms.
Methods: Two cases of PTA with VB symptoms are presented. A 80-year-old woman evaluated in neurology clinics because of attacks and a 50-year-old man hospitalized in neurology due to transient repeated episodes of facial asymmetry and dysarthria.
Results: Doppler ultrasound of the supraortic and transcranial trunks was performed, revealing, in the first patient, both V4 and the proximal basilar inversion and in the second, right vertebral inversion from its origin and throughout its trajectory, without repercussions. In addition, brain MRI and MRI angiography were performed, finding hypoplasia of both AV and BA and the presence of Salzman type I PTA in the first patient and severe stenosis of the right prevertebral subclavian artery, hypoplasia of proximal basilar and presence of Salzman type II PTA in the second.
Conclusions: Some cases of PTA are associated with vertebrobasilar insufficiency, especially if it is associated with proximal basilar hypoplasia. The association of PTA with a subclavian steal syndrome may favor a hemodynamic deficit on the basilar. The diagnosis of PTA is made through the vascular study of the WP by CT angiography or MRI angiography, which should be performed in patients with symptoms of VB insufficiency.
Disclosures of Interest: No
Abstract N°: 1382
BRAZILIAN CAROTID WEB REGISTRY – AN ONGOING COHORT
Alessandra Braga Cruz Guedes de Morais*1,2, Ana Silvia Sobreira Lima Verde1, George Mendes1,3, Lara Oliveira1, Adson Freitas de Lucena1, Francisco Mont'alverne1, Joao Andrade2,4, Fernanda Martins Maia Carvalho1,5, Gisele Sampaio2,4, Fabrício Oliveira Lima1
1Fortaleza General Hospital, Fortaleza, Brazil, 2Federal University of São Paulo, São Paulo, Brazil, 3CHUM - Centre hospitalier de l'Université de Montréal, Montréal, Canada, 4Hospital Albert Einstein, Brazil, 5UNIFOR University of Fortaleza, Brazil
On behalf of:
Background and aims: Carotid web (Web-Ca) is considered an underrecognized cause of stroke. The lack of prospective studies results in a poor understanding of its clinical characteristics, recurrence rate, treatment strategies, and stroke prevention. We present a prospective ongoing Brazilian cohort to describe the epidemiology, treatment outcomes, and long-term prognosis of patients diagnosed with Web-Ca.
Methods: Patients admitted to our stroke unit or attended in our stroke clinic were systematically evaluated. This involved an in-depth review of neuroimaging data (CT Angiography and/or MR Angiography) at our center, from 2017 to 2023. Two experienced stroke neurologists confirmed the diagnosis. Data on demographics, risk factors, treatment, and patient outcomes were gathered using a standardized questionnaire.
Results: A total of 42 cases were identified (57.1% female) with a median age of 50.5 (IQR 42.25-58). Most of the patients were identified after an ischemic stroke, and the initial NIHSS median was 11 (IQR 4-15.5). Twenty-two patients (52.4%) were treated with either endarterectomy or angioplasty, and 32 (78%) were considered symptomatic. There were three cases of colorectal neoplasm associated (7.7%). In addition, Web-Ca was identified in two cases of Intracranial hemorrhage, one case of subdural hematoma, and five cases of subarachnoid hemorrhage.
Conclusions: The ongoing Brazilian cohort study provides valuable insights into epidemiology, treatment outcomes, and long-term prognosis of patients with Web-ca. This study underscores the importance of recognizing Web-Ca in the differential diagnosis of ischemic stroke etiology and also in non-ischemic stroke patients. Suggesting the necessity for further research on its management and prevention.
Disclosures of Interest: No
Abstract N°: 1566
THE ASSOCIATION OF CARDIAC ABNORMALITIES AND STROKE IN FABRY DISEASE
Adi Shemesh*1, Elad Shemesh2, Patrick Deegan3
1Carmel Medical Centre, Neurology, Haifa, Israel, 2Tel Aviv Sourasky Medical Center - Ichilov, Endocrinology & Metabolism, Tel Aviv-Yafo, Israel, 3Addenbrooke's Hospital, United Kingdom
On behalf of:
Background and aims: Fabry disease (FD), an X-linked lysosomal storage disorder, is a well-established risk factor for stroke. The pathogenesis of stroke in FD is multifaceted, involving small and large vessel disease, as well as cardioembolism. However, the specific contribution of each factor remains partially understood. This study aims to elucidate the cerebrovascular consequences of cardiac involvement in FD
Methods: A retrospective analysis was conducted on 98 FD patients at Cambridge University Hospitals from 2003-2019. Diagnostic tools included ECG, cardiac biomarkers, and cardiac imaging. Cerebrovascular events (CE) were defined as a composite of CVA and/or TIA
Results: 98 participants (525 visit years, 60 with classic mutations) were included. 15 patients experienced CE - 80% having classic mutations, 46% females. Mutation types in CE patients was similar to the general FD cohort. Mean age at first visit for CE patients was 49±13. Hypertension & dyslipidemia rates were similar. At first cardiac assessment, 85% of FD patients who subsequently developed CE exhibited left ventricular hypertrophy on echocardiography (compared to 56% in the general FD cohort), and 35% had elevated troponin/nt-proBNP. One-third had atrial fibrillation.
Conclusions: In FD, traditional stroke risk factors such as hypertension, diabetes, dyslipidemia appear not to contribute significantly to the elevated stroke risk. Cardiac hypertrophy might be an early marker for increased stroke risk, highlighting the potential role for cardioembolic pathogenesis. While mutation type and sex are established predictors for the severity of cardiovascular complications in FD, their impact on cerebrovascular events remains unclear.
Disclosures of Interest: No
Abstract N°: 160
LONG-TERM STROKE RISK IN MOYAMOYA DISEASE
Peter Birkeland1, Victoria Hansen*2, Vinosha Tharmabalan1, Jens Lauritsen3, Troels Nielsen4, Thomas Truelsen5, Sverre Rosenbaum6, Paul von Weitzel-Mudersbach7
1Copenhagen University Hospital, Department of Neurosurgery, København, Denmark, 2Aalborg University Hospital, NEurology Department, Stroke Unit, Aalborg, Denmark, 3Odense University Hospital, Department of Orthopaedic Surgery, Odense, Denmark, 4Odense University Hospital, Department of Neurosurgery, Odense, Denmark, 5Copenhagen University Hospital, Department of Neurology, Copenhagen, Denmark, 6Department of Neurology, Bispebjerg Hospital, Copenhagen, Denmark, 7Aarhus University Hospital, Department of Neurology, Aarhus, Denmark
On behalf of:
Background and aims: Moyamoya disease is considered a progressive disease with an ongoing risk of recurrent stroke. However, there is a lack of long-term observational data to quantify the extent of the stroke risk
Methods: This study aimed to provide insight into the long-term stroke risk in MMD and explore possible risk factors for stroke. Records from all patients diagnosed with MMD in 13 clinical departments from six different Danish hospitals between 1994 and 2017 were retrospectively reviewed until 2021.
Results: The cohort comprised 50 patients (33 females and 17 males). Patients were followed up for a median of 9.4 years, with more than 10 years of follow-up for 24 patients. Ten patients had 11 new stroke events - 6 ischemic strokes and 5 brain hemorrhages. Events occurred at a median of 7 years and up to 25 years after diagnosis. The overall Kaplan-Meier 5-year stroke risk was 10%. Patients with bypass performed had significantly fewer events than conservatively treated patients (HR 0.25, 95% CI 0.07 - 0.91, p<0.05). All but one event occurred in females, a difference that reached statistical significance.
Conclusions: The study provides data on the extent of the risk of recurrent stroke in MMD. Bypass surgery patients had fewer stroke events than those treated conservatively. There was a trend toward a higher stroke risk in females.
Disclosures of Interest: No
Abstract N°: 2740
CLINICAL PROFILE AND OUTCOME OF CEREBRAL VENOUS THROMBOSIS WITHOUT SIGNS OF PARENCHYMAL INJURY
Emma Roustaei*1, Erik Lindgren1, Patrıcia Canhao2, Diana Aguiar De Sousa3, Mirjam Rachel Heldner4, Ronen R Leker5, Jukka Putaala6, Jonathan Coutinho7, Turgut Tatlisumak1,6, Katarina Jood1
1Sahlgrenska University Hospital, Institute of Neuroscience and Physiology, Gothenburg, Sweden, 2Hospital de Santa Maria, Department of Neurosciences and Mental Health (Neurology), Lisboa, Portugal, 3Centro Hospitalar Universitário Lisboa Central, Stroke Centre, Lisboa, Portugal, 4University of Bern, Department of Neurology, Bern, Switzerland, 5Hadassah Ein Kerem Hospital, Department of Neurology, Jerusalem, Israel, 6University of Helsinki, Department of Neurology, Helsinki, Finland, 7University of Amsterdam, Department of Neurology, Amsterdam, Netherlands
On behalf of: The international CVT consortium: Sweden;A.K. Switzerland; A.S,M.A. Netherlands; K.K,M.S,S.S,S.Z. Finland; S.H. Iran; M.M,M.G. Turkey; E.E,M.S,N.Y. Portugal; M.R,E.S. Australia; C.G. Italy; A.V,P.A. Israel; N.S,J.M. Spain; D.G. Costa Rica; M.B. Mexico; A.A
Background and aims: Not all patients with cerebral venous thrombosis (CVT) develop clinical or neuroimaging signs of parenchymal injury (PI). We aimed to describe characteristics and risk factors for CVT without PI and factors associated with poor functional outcome in this subgroup.
Methods: We included consecutive adult patients with neuroimaging confirmed CVT from the International CVT Consortium between 1995-2021. Based on admission data, patients were categorized into CVT with PI (focal deficit and/or hemorrhagic or non-hemorrhagic parenchymal lesion) or CVT without PI (no focal deficit and no parenchymal lesion). Poor functional outcome was defined as modified Rankin Scale score 2-6 at follow-up.
Results: Among 1478 patients (median age: 41[IQR 29-53]; 70% female), 448 (30%) had no signs of PI at admission. In univariate analysis, headache (92% vs. 83%), subacute or chronic onset (82% vs. 68%) and systemic inflammatory disease (13% vs. 7%), were more frequent, while coma (<1% vs. 8%) and deep cerebral venous thrombosis (3% vs. 14%) were less frequent among patients without PI compared to patients with PI(p<0.01 throughout). New focal deficits or decreased consciousness during hospital stay occurred among 5% of patients without PI. At follow-up (median 6 months[IQR 6-12]), 16% without PI experienced poor functional outcome, compared to 37% among the patients with PI(p<0.001). In multivariate analysis, higher age was associated with poor functional outcome in the group without PI(p=0.035).
Conclusions: One-third of patients with CVT presents without PI. Despite a more favorable presentation, every sixth patient without PI experienced poor functional outcome at follow-up, associated with higher age.
Disclosures of Interest: No
Abstract N°: 3223
PREDICTORS OF ACUTE SYMPTOMATIC SEIZURES IN CEREBRAL VENOUS THROMBOSIS PATIENTS – A MULTICENTER COHORT STUDY
Naaem Simaan1, Jeremy Molad2, Hen Halevi2, Rani Barnea3, Shorooq Aladdin4, Rom Mendel3, Ronen R Leker5, Asaf Honig*6
1Ziv Medical Center, Neurology, Israel, 2Ichilov Medical Center, Neurology, Israel, 3Rabin Medical Center, Neurology, Israel, 4Sheba Medical Center, Neurology, Israel, 5Hadassah-Hebrew University Medical Center, Neurology, Jerusalem, Israel, 6Soroka Medical Center, Neurology, Beer Sheva, Israel
On behalf of:
Background and aims: We aimed to identify predictors of acute symptomatic seizures (ASYS) in CVT patients.
Methods: Prospective CVT databases from four academic centers were retrospectively analyzed. Patients with and without ASYS within seven days from presentation were compared.
Results: From 529 included patients (mean age 42.4±18.6 years, 64.3% females), 106 (20%) had ASYS. ASYS patients had higher rates of chronic hypertension (19.8% vs. 12.3%, p = 0.045), diabetes (14.1 vs. 7.3, p=0.026) and presented more often with focal neurological deficits (50% vs. 22%, p < 0.001) but less often with papilledema (13.2% vs. 29.3%, p < 0.001) and headache (63% vs. 80%, p < 0.001). Radiological variables associated with ASYS included presence of intracerebral hemorrhage (ICH) (42.5% vs. 11.1%, p < 0.001), venous infarction (36.8% vs. 9.4%, p < 0.001), superior sagittal sinus (SSS) thrombosis (59.4% vs. 32.4%, p < 0.001), isolated cortical vein thrombosis (28.3% vs. 8.7%). ASYS patients had lower rates of favorable outcomes, as measured by 90-day-mRS 0-1 (51.9% vs. 83.9%, p < 0.001). status epilepticus was more common in previous Diabetes, hypertension, and active malignancy associated with worse prognosis (88.9% vs 11.1%, p=0.042) and mortality (50.0% vs 6.1%, p=0.002).
On multivariate analysis, ICH (OR 3, 95%CI 1.5-6, p = 0.002), SSS involvement (OR 2.48, 95%CI 1.3-4.8, p = 0.006) and isolated cortical thrombosis (OR 4.2, 95%CI 1.9-9.2, p < 0.001), were independent predictors of ASYS. Conversely, presentation with papilledema (OR 0.39, 95%CI 0.17-0.9, p=0.03) negatively predicted ASYS.
Conclusions: ASYS has unique predictors in CVT patients suggesting a different course of disease.
Disclosures of Interest: No
Abstract N°: 704
PREDICTING EARLY IN-HOSPITAL MORTALITY IN CEREBRAL VENOUS THROMBOSIS USING VOXEL BASED – LESION SYMPTOM MAPPING
1Christian Medical College, Neurology, Vellore, India
On behalf of:
Background and aims: Cerebral venous thrombosis (CVT) is an important cause for stroke in the young. The mortality rates ranging from 6% to 15%. Majority of deaths occur within 30 days. The leading cause of death is hemorrhagic conversion of large venous infarcts causing herniation. In our study we aim to study whether lesion location is a predictor of early in-hospital mortality.
Methods: This was a hospital-based retrospective study conducted . 36 patients had a diagnosis of CVT and had died within one week of hospitalization and were recruited as cases. Patients who were age matched with the cases, with a diagnosis of CVT, had parenchymal lesions and had survived were taken as controls. MRI brain images of all patients were viewed, and individual lesions were mapped onto the Montreal Neurological Institute (MNI) space manually using MRIcron. Nonparametric mapping toolbox software was used for voxel-based lesions symptom analysis. The Liebermeister test was used for statistical analysis, and the resultant statistical map was displayed on the MNI template using MRIcron.
Results: Results of Multivariate Analysis showed GCS < 12 0R 1.38(CI 1.1-1.8), Left Parietal hemorrhagic lesion OR 3.9 (CI 1.9 – 8.3), Associated Subarachnoid hemorrhage OR 4.7 ( CI 2.7-9.7) and straight sinus involvement OR 4.2 (CI 3.3-5.6 ) associated with early in-hospital deaths.(See figure for lesion mapping )
Conclusions: Apart from known predictors of mortality, like low GCS, straight sinus involvement and subarachnoid hemorrhage, left parietal hemorrhagic lesions increases the risk for early in hospital mortality in patients with CVT.
Disclosures of Interest: No
Abstract N°: 1429
VERTEBRAL BODY AND SPINAL CORD INFARCTION IN A PILE-DRIVER OPERATOR WITH FIBRO-CARTILAGINOUS DISC EMBOLISM
Stephen Murphy1, Dominick J. H. McCabe*2, Rory O'donohoe3, Allan Mccarthy2
1Chelsea and Westminster Hospital, United Kingdom, 2Tallaght Hospital, Ireland, 3St. Vincent's University Hospital, Ireland
On behalf of:
Background and aims: Fibrocartilaginous disc embolism (FCDE) is a rare stroke syndrome proposed to arise from embolism of contents of the fibrocartilaginous nucleus pulposus of an intervertebral disc into the spinal vasculature. Heavy machinery operators exposed to continuous vibration may be at increased risk of fibrocartilaginous embolic events.
Methods: We describe the case of a male heavy-machinery operator who presented from work with a rapidly evolving spinal cord syndrome.
Results: Examination revealed normal cranial nerves, a mild spastic paraparesis, a T10 spinal sensory level to soft touch, pin-prick and temperature, but intact proprioception and vibration sensation. Serial spinal magnetic resonance imaging (MRI) over 6 days revealed evolving low thoracic spinal cord and vertebral body infarction, with increasing mild thoracic intervertebral disc prolapse, attributed to FCDE with early discordance between clinical findings of anterior spinal artery territory infarction and mainly posterior spinal cord signal changes on spinal MRI (Figure 1).
Conclusions: Fibrocartilaginous disc embolism should be considered as one of the aetiological mechanisms of acute spinal cord infarction in pile-driver/heavy machinery operators, especially in association with adjacent vertebral body infarction and intervertebral disc prolapse. Magnetic resonance imaging (MRI) changes may evolve, warranting early follow-up MRI in appropriate cases.
Schmorl’s node and hyperintense endplate changes at T11 (thin arrow); hyper-intense endplate changes also at T11-12 (thick arrow); Figure 1b: Evolving hyper-intense posterior T11 vertebral body infarction (thick arrow); evolving mild T11-12 disc prolapse (dashed arrow). Figures 1c & 1d: Evolving hyper-intense ‘posterior’ spinal cord infarction from T8/9-T11 (dashed arrows).
Disclosures of Interest: No
Abstract N°: 1133
CLINICAL CHARACTERISTICS AND NEUROIMAGING OF CERVICOCEPHALIC ARTERY DISSECTION IN A VIETNAM COHORT
1The People’s Hospital 115, Department of Cerebrovascular Disease, Viet Nam, 2University Medical Center HCMC, Department of Neurology, Viet Nam, 3University Medical Center HCMC, Department of Diagnostic Imaging, Viet Nam, 4University of Medicine & Pharmacy HCMC, Viet Nam, 5Pham Ngoc Thach University of Medicine, Viet Nam
On behalf of:
Background and aims: Cervicocephalic arterial dissection (CAD) is rare disease and a major cause of stroke in young adults. However, clinical data on CAD are limited in East Asia countries. We aimed to describe CAD's clinical characteristics and neuroimaging in Vietnamese patients.
Methods: We retrospectively included all CAD patients admitted to the University Medical Center in Ho Chi Minh City, Vietnam, from January 2016 to November 2022. All patients met the vascular imaging diagnostic criteria of the European Stroke Organization for CAD.
Results: Of the 6053 patients who were screened, 93 patients had CAD (1,5%). CAD occurred in the following locations: intracranial artery dissection-posterior circulation (IAD-PC) (37,6%), extracranial artery dissection–anterior circulation (EAD-AC) (35,5%), EAD-PC (19,4%), IAD-AC (7,5%). Mean age: 50,9±15,9 years, 67 patients (72%) were males. The history of head/neck trauma was 13%. Median admission NIHSS was 4 (1-4, IQR). A good clinical outcome (mRS ⩽ 2) was observed in 60 patients (64,5%). Detection of major CAD by MR angiography (MRA) (67,7%), and high-resolution MR imaging (HR-MRI) additionally identified 22,6% (IAD (8,6%), EAD (14%)) not previously seen on MRA. Typical neuroimaging in dissection: intramural hematoma (44,1%), double lumen (37,6%), long tapering stenosis (8,6%), intimal flap (5,4%), pseudoaneurysm (1,1%).
Conclusions: In our study, CAD resulted in almost mild strokes with good neurological outcomes. IAD-PC was the most common site of dissection. MRA proved to be a valuable imaging method for diagnosing CAD, with HR-MRI enhancing detection, especially in cases of IAD.
Disclosures of Interest: No
Abstract N°: 2018
CANCER AND EMBOLIC STROKE OF UNDETERMINED SOURCE: ANALYSIS FROM THE COMPREHENSIVE STROKE CENTER
Stanislav Chazov*1, Aleksey Kulesh1, Sergey Mekhryakov1, Lyudmila Syromyatnikova1
1Perm State Medical University, Perm
On behalf of:
Background and aims: According to the CHALLENGE ESUS/CS registry in cryptogenic stroke active cancer was detected in 6,1% of cases and 7,5% of patients had a history of inactive cancer. In 2–10% of patients with ESUS, cancer is detected within a year after stroke. The aim was to assess the incidence of cancer and its characteristics in patients with ESUS.
Methods: This study retrospectively enrolled 129 patients with MRI-verified ESUS (January 2017 to December 2022). The presence of cancer was established on the basis of anamnesis and routine examination without conducting a targeted oncological search. Active cancer was defined as cancer diagnosed or under treatment within 6 months before index stroke onset or detected on imaging examination and newly diagnosed during hospitalization. Inactive cancer was defined as cancer treated within >6 months before stroke onset, and remission or complete recovery was confirmed at the time of admission without any evidence of active cancer on imaging investigation during the hospital stay
Results: Of the total 129 patients (age, 65.1±13.5 years; 70 men), 5 (3,9%) had active cancer (skin, intestines, larynx, prostate, lymphoma), 6 (4,7%) had a history of inactive cancer. In 4 out of 5 patients, stroke can be considered cancer-associated. During an average follow-up period of 29 (17-45) months, cancer was diagnosed in another 4 patients - 3,1% (prostate gland, lungs, pancreas, leukemia). The cumulative prevalence of cancer was 11,6%.
Conclusions: Cumulative prevalence of cancer in ESUS was 11,6% during 2,5 years of follow-up period. Possible cancer-associated stroke was observed in 3,1% of patients.
Disclosures of Interest: No
Abstract N°: 2471
ACUTE ISCHEMIC STROKE IN ACTIVE CANCER PATIENTS RESTARTING VS NON-RESTARTING CANCER TREATMENT AFTER STROKE
Gianluca Costamagna*1, Andreas Hottinger2, Françoise Livio3, Alexander Salerno1, Davide Strambo1, Babak Navi4, Patrik Michel1
1Lausanne University Hospital and University of Lausanne, Department of Clinical Neurosciences, 2Lausanne University Hospital and University of Lausanne, Lundin & Family Brain Tumor Research Center, Services of Neurology and Oncology, 3Lausanne University Hospital and University of Lausanne, Switzerland, Service of Clinical Pharmacology, Lausanne, Switzerland, 4Weill Cornell Medicine, New York, NY, Feil Family Brain and Mind Research Institute and Department of Neurology, New York, United States
On behalf of:
Background and aims: whether to initiate or restart cancer treatment (IRCT) in patients with active cancer (AC) after an acute ischemic stroke (AIS) remains uncertain. We aimed to estimate the rate of IRCT after AIS in AC patients and to compare these patients’ characteristics, stroke mechanisms, and outcome with non-IRCT patients.
Methods: we retrospectively analyzed a consecutive large academic single-center stroke registry between 1/2003-12/2021. We defined AC following standard definitions. We compared IRCT-patients within 3 months after AIS with non-IRCT patients regarding patients’ characteristics, stroke mechanisms, medium-term disability, and medium- and long-term mortality, and cerebrovascular recurrences. Univariable analysis is provided; other logistic and Cox regression analyses are ongoing and will be presented at the congress.
Results: among 6686 AIS patients, 260 (3.9%) had AC. Of these, 39% were women and the median age was 73.2 years (IQR 16.5). One hundred seventeen (45%) patients initiated or restarted cancer treatment after AIS. IRCT patients were younger, had fewer urogenital tumors, and more often had recently received chemotherapy. Unadjusted analysis demonstrated less 3-month disability (ordinal) and mortality for IRCT patients and no difference in long-term mortality and recurrences. At 12 months, mortality was high in both groups (IRCT, 38%; non-IRCT, 48%), and the cerebrovascular recurrence rate was 20% in IRCT and 17% in non-IRCT patients
Conclusions: within 3 months after AIS, 45% of patients with AC had initiated or restarted cancer treatment. These patients were generally younger and had fewer urogenital cancers. IRCT may be associated with less 3-month disability and mortality.
Disclosures of Interest: No
Abstract N°: 2922
VESSEL DIAMETER IN PRIMARY ANGIITIS OF THE CENTRAL NERVOUS SYSTEM (PACNS): ETIOLOGICAL AND PROGNOSTIC IMPLICATIONS
Franziska Frank*1, Salomé Jacques1, Alexander Seiler2
1Frankfurt University Hospital, Frankfurt am Main, Germany, 2University of Kiel, Kiel, Germany
On behalf of:
Background and aims: Cerebral vasculitis, characterized by segmental inflammation and necrosis of cerebral blood vessels, presents a clinically diverse spectrum ranging from mild to severe, with varied symptoms like headaches, cognitive issues, seizures, and neurological deficits. This study focuses on primary angiitis of the central nervous system (PACNS) to characterize individual disease courses by vessel size involvement and assess clinical outcomes, relapses, and demographic data.
Methods: This single-center retrospective study, conducted from January 2010 to April 2022 included 105 patients diagnosed with cerebral vasculitis. PACNS patients (n=49) were the primary focus of this study. They were classified into four groups based on radiological manifestations of vessel involvement: Group 1 (large vessels), Group 2 (large and medium-sized vessels), Group 3 (small, peripheral vessels), and Group 4 (mixed vessel involvement). Data analyzed included demographics, laboratory findings, vascular risk factors, clinical outcomes and imaging results.
Results: There is a preference for anterior cerebral circulation involvement seen in our PACNS cohort accompanied by a high number of experienced cerebral infarctions (95.9%). Significant differences in BMI were observed across the four mentioned groups, particularly higher in patients with mixed vessel involvement. Variations in the usage of estrogen-containing medication and cyclophosphamide were noted among groups, favoring a higher usage in the small vessel comprising group. However, a notably lower risk of intracranial bleeding was observed in patients with exclusive large vessel involvement.
Conclusions: This study underscores the importance of vessel size in understanding the heterogeneity of PACNS. It reveals associations between vessel involvement and demographic factors, treatment choices, and clinical outcomes.
Disclosures of Interest: No
Abstract N°: 3054
ARE THERE DIFFERENCES BETWEEN TRAUMATIC AND SPONTANEOUS CERVICAL ARTERY DISSECTIONS?
Issa Metanis*1, Naaem Simaan1, Yoel Schwartzmann1, Tamer Jubeh1, Hamza Jubran1, Asaf Honig1, Jad Magadle1, Jose Cohen1, Ronen R Leker1
1hadassah medical center, Jerusalem, Neurology, Jerusalem, Israel
On behalf of:
Background and aims: Cervical arterial dissections (CeAD) are a common cause of stroke, which can be spontanious (sCeAD) or traumatic (tCeAD). Weather these types differ in outcome remain largely unexplored
Methods: Patients with CeAD were retrospectively identified and divided between sCeAD and tCeAD. Demographics, risk factors and clinical features were compared between the groups. favorable outcome determined as a modified Rankin score (mRS)<2 at 90days post presentation were determined on multivariate logistic regression analyses.
Results: Overall, 154 patients were included (106 sCeAD, 48 tCeAD). Patients with sCeAD were significantly older (mean±SD 46±12 vs. 35±14, p<0.001) and more likely to have hyperlipidemia (19% vs. 4%, p=0.016) but other risk factors did not differ between the groups. Patients with tCeAD less often had signs of early infarction on the admission CT (21% vs. 49%, p=0.001) and lower stroke severity on admission (NIHSS, median, interquartile range [IQR] 0 (0-9) vs. 2 (0-4), p=0.012) but more often had symptomatic intracranial hemorrhages (12.5% vs. 2%, p=0.006). recurrent stroke and recurrent dissections did not differ between the groups but patients with tCeAD less often had favorable outcomes at 90 days (78% vs. 97%, p<0.001). On regression analysis the only variables that were associated with favorable outcome were age (Odds ratio [OR] 1.13 95% confidence intervals [CI] 1.03-1.24], initial stroke severity (OR 0.84 95% CI 0.73-0.97), degree of vessel stenosis (OR 0.35 95% CI 0.14-0.83) and involvement of multiple vessels on presentation (OR 0.04 95% CI 0.02-0.70).
Conclusions: Dissection subtype isn’t an independent modifier of the chances of attaining functional independence at 90 days.
Disclosures of Interest: No
Paper Poster - Rehabilitation and Recovery
Abstract N°: 2019
RELATIONSHIP OF POSTURAL CONTROL WITH SENSORIMOTOR FUNCTION, BALANCE AND SPATIAL NEGLECT IN PATIENTS WITH ACUTE STROKE
Ceren Bayrak*1,2, Ela Tarakci3, Hatice Yelda Yildiz2, Yakup Krespi2
1Istanbul University- Cerrahpasa, Physiotherapy and Rehabilitation Department, İstanbul, 2Istinye University Hospital, Brain Angiography and Stroke Center, İstanbul, 3Istanbul University- Cerrahpasa, Physiotherapy and Rehabilitation Department, İstanbul
On behalf of:
Background and aims: The importance of early evaluation of sensory and cognitive problems as well as motor deficits associated with postural control in patients with ischemic stroke in the acute phase.
Methods: Between January and August 2023, 65 individuals with acute ischemic stroke were included in the study. Postural control impairment was assessed with the Posture Assessment Scale for Patients with Stroke (PASS T), upper and lower extremity motor function with the Stroke Rehabilitation Assessment of Movement (STREAM), neglect phenomenon with the Extinction and Inattention subscale of the NIHSS (National Institutes of Health Stroke Scale) and the Broken Hearts subtest of the Oxford Cognitive Screen (OCS). Within sensory functions, superficial sensation, position sensation and vibration sensation with diapozon were examined.
Results: As a result of the evaluations, a significant correlation was found between postural control and upper and lower extremity motor function, vibration sensation, balance and unilateral spatial neglect in individuals with acute ischemic stroke (p<0,001). When the severity of postural control was divided into two groups as severe and mild postural control disorder with a cut-off value of 12,5 points of PASS T, upper extremity motor function, vibration, superficial and position sense, balance and unilateral spatial neglect were significantly different in patients with severe postural control disorder (p<0,05). According to logistic regression analysis, upper extremity motor function and vibration sensation had a significant effect on postural control impairment severity (p<0,05).
Conclusions: This study underscores the importance of integrating sensory and cognitive treatment approaches with motor rehabilitation in acute stroke rehabilitation.
Disclosures of Interest: No
Abstract N°: 1615
CHANGES IN MICROARCHITECTURE OF WHITE MATTER TRACTS AFTER INTRA-ARTERIAL CELL THERAPY IN AIS. THE DTI-STUDY OF THE IBIS TRIAL
JUAN ANTONIO CABEZAS RODRIGUEZ*1,2, Carles Biarnes3, Marc Comas-Cufí3, Marian Martí-Navas3, Manuel Medina-Rodriguez1,2, Pilar Piñero4, Joaquin Ortega-Quintanilla4, Alejandro González2,5, Josep Puig Alcantara3, Francisco Moniche Alvarez1,2
1Virgen del Rocio University Hospital, Stroke Unit, Seville, Spain, 2Seville Biomedical Research Institute, Neurovascular Research Program, Seville, Spain, 3Girona Biomedical Research Institute (IDIBGI), Hospital Universitari de Girona Dr Josep Trueta, Radiology, Girona, Spain, 4Virgen del Rocio University Hospital, Radiology, Seville, Spain, 5Virgen del Rocio University Hospital, Interventional Neuroradiology, Seville, Spain
On behalf of:
Background and aims: Bone marrow mononuclear cell (BM-MNC) intra-arterial transplantation has emerged as a potential therapy for the treatment of stroke. We aimed to determine whether BM-MNC therapy induces significant changes in diffusion tensor imaging (DTI) metrics of the major white matter tracts (WMT).
Methods: IBIS trial was a multicentre phase 2, randomised, controlled, investigator-initiated, assessor-blinded, clinical trial, in four centres in Spain. We included patients (aged 18-80 years) with a non-lacunar, middle cerebral artery ischaemic stroke within 1-7 days from stroke onset and with a NIHSS score of 6-20. 20 treated with BM-MNCs and 17 controls underwent MRI at study entry and 6 months later. DTI-metrics (fractional anisotropy [FA] and mean diffusivity [MD]) for superior longitudinal fasciculi, corpus callosum and corticospinal tracts from ICBM DTI-81 atlas were obtained. We determined the average changes in DTI-metric values over the course of the follow-up.
Results: The mean age was 62 years (SD 13.4), 19 (50%) were men, and 31 (81.6%) received thrombectomy. The median NIHSS score before randomisation was 12 (IQR 8.5-15), with intra-arterial BM-MNC injection done a median of 6 days (5-7) after stroke onset. Comparable DTI-metric values were observed between groups at baseline. The FA values of patients treated with BM-MNC decreased less in six of seven tracts analyzed. Similarly, the mean variations of MD values were reduced in patients who had been treated.
Conclusions: Intra-arterial BM-MNC transplantation modified the microstructure of WMT, suggesting that this therapy may mitigate acute stroke damage.
Variations in fractional anisotrophy values from baseline to 6 months of follow-up.
Disclosures of Interest: No
Abstract N°: 1449
PHOSPHODIESTERASE4 INHIBITOR ROFLUMILAST TO IMPROVE COGNITION AFTER STROKE AN OPEN-LABEL EXTENSION STUDY
Jill Kerckhoffs*1, Ieke Winkens1, Arjan Blokland1
1Maastricht University Psychology Neurosciences Department (FPN), Neuropsychology & Psychopharmacology, Maastricht, Netherlands
On behalf of:
Background and aims: Currently, there are no pharmacological treatments for post-stroke cognitive impairment (PSCI). PDE4 inhibitors, e.g. roflumilast, have been found to enhance neuronal plasticity. Accordingly, positive effects of roflumilast were found on memory performance in healthy students and elderly, without side effects. The current study extends a double-blind placebo-controlled RCT on the use of 100 µg q.d. roflumilast in chronic stroke patients for 3 months. After this study, the patients who received placebo could participate in a 3-month open-label study to measure the effects of roflumilast and adverse side effects.
Methods: The current study was an open-label extension study that followed a placebo-controlled double-blind RCT. 42 participants completed the study, they were 41-70 years old; > 1-year post-stroke; and screened for memory complaints (< normative score on Verbal Word Learning Test: VLT). Participants were treated with roflumilast (100 µg q.d.) for three months. The primary outcome was the delayed recall of the VLT. Secondary outcomes focused on other cognitive functions and subjective effects in daily life.
Results: The GLM analysis revealed a significant improvement in memory on immediate (p<0.001) and delayed recall of the VLT (p=0.050), and the immediate (p=0.007) and delayed recall (p=0.016) of the Rivermead Behavioural Memory Test, and the Everyday Memory Questionnaire (p=0.014). Improvements were also observed for secondary outcomes assessing cognitive functions and daily life.
Conclusions: The current open-label study demonstrates significant improvements while taking 100 µg Q.d. roflumilast for 3 months on objective and subjective measures of memory and other cognitive functions. These results encourage further stronger powered, multi-center studies.
Disclosures of Interest: Yes Arjan Blokland has a proprietary interest in the PDE 4 inhibitor roflumilast.
Abstract N°: 3002
VERY EARLY MOBILISATION OF ACUTE ISCHEMIC STROKE IS SAFE AND FEASIBLE: A CLINICAL TRIAL
1Hamad General Hospital, Physiotherapy, Doha, Qatar, 2Hamad General Hospital, Head of Stroke Service, Senior Consultant Neurologist, Doha, Qatar
On behalf of:
Background and aims: Early mobilisation (EM) after 24hrs of stroke onset is recommended. The safety and feasibility of very early mobilisation (VEM) within 24 hrs. is conflicting. The pathophysiology and management of ischemic and hemorrhagic stroke differs. EM may have different effect on subtypes and should have different protocol. VEM studies including AVERT have both subtypes with same protocol. VEM of ischemic stroke (Tong Yet al, 2019) with 3hrs mobilisation per day resulted in unfavorable outcome.
Aim: To find safety and feasibility of VEM in acute ischemic stroke with a low intensity and frequency of mobilisation.
Methods: Subjects with base line similairty were grouped into VEM and EM and both received same mobilisation for seven days. The stroke severity is measured using Canadian Neurological Scale (CNS) and Mobility Scale for Acute Stroke Patients (MSAS) for mobility on day one and seven. Blinded outcome assessment done on day seven. Clinical deterioration and adverse effects were noted.
Results: VEM group had 138 subjects and 162 in the EM. There is a significant difference within the group analysis in CNS and MSAS (P=0.001). Non-significant difference exists in CNS (p=0.653) and MSAS (p=0.604) between the groups at discharge. No clinical deterioration noted in both the groups.
Conclusions: Both the group improved in mobility and stroke severity reduced by seventh day. VEM protocol is successful among acute ischemic stroke patients without any complications. This is a pragmatic trial conducted in a clinical setting. The mobilisation dosage is practical and can be successfully implemented elsewhere compared to AVERT trial.
Disclosures of Interest: No
Abstract N°: 499
MOTOR SKILL LEARNING DURING ACUTE STROKE: GOOD LEARNERS, POOR LEARNERS
Yves Vandermeeren*1,2,3, Regnier Maxime4, Dricot Laurence5, Herman Benoit2,6, Van Ravestyn Coralie1,2,3, De Coene Beatrjis7, Mulquin Nicolas7, Bihin Benoît4, Lejeune Thierry8, Gerardin Eloïse1,2,3
1CHU UCL Namur - Godinne, Neurology, Stroke Unit / Motor Learning Lab, Yvoir, Belgium, 2UClouvain, Louvain Bionics, Louvain-la-Neuve, Belgium, 3UCLouvain, Institute of NeuroScience (IoNS), NEUR division, Brussels, Belgium, 4CHU UCL Namur (Godinne), Scientific Support Unit (USS), Yvoir, Belgium, 5UCLouvain, Institute of NeuroScience (IoNS), COSY division, Brussels, Belgium, 6UCLouvain, Institute of Mechanics, Materials and Civil Engineering, Louvain-la-Neuve, Belgium, 7CHU UCL Namur (Godinne), Radiology, Yvoir, Belgium, 8Cliniques universitaires Saint-Luc, Physical Medicine and Rehabilitation, Brussels, Belgium
On behalf of:
Background and aims: Whereas recovery is fast early after stroke, knowing whether patients can learn new motor skills with the contralesional/affected upper limb (UL) would determine how to individualise neurorehabilitation. We explored whether (sub)acute stroke patients achieved motor skill learning (MSkL) and compared them to healthy individuals (HI) and chronic patients.
Methods: 43 HI, 20 chronic and 116 acute patients were randomized to train during three days on a robot with either the serious game CIRCUIT (involving MSkL with a speed/accuracy trade-off (SAT)) or BRICKBUSTER (repetitive movements with limited MSkL). Patients used their contralesional/affected UL, HI their non-dominant UL. The primary outcomes were the SAT on CIRCUIT and Distance on BRICKBUSTER.
Results: In the HI (n=21), chronic (n=11) and acute (n=88) groups training with CIRCUIT, the SAT progressions were similar (all p⩾0.9) and larger than in the groups training with BRICKBUSTER (all p<0.001). The proportion of good learners (SAT progression ⩾76%) was larger in the HI (86%) and chronic (73%) groups than in the acute group (58%) training with CIRCUIT. Whereas there were no poor learners (SAT progression ⩽25%) in the HI and chronic groups training with CIRCUIT, 14% in the acute group were poor learners.
Conclusions: Acute patients achieved MSkL at the group level but the proportion of good learners was larger in the HI/chronic groups than in the acute group. Furthermore, poor learners were found exclusively in the acute group, suggesting that MSkL was impaired during the (sub)acute stroke phase, highlighting the need for individualised neurorehabilitation.
Disclosures of Interest: No
Abstract N°: 2187
TREATMENT OF UPPER LIMB PARESIS WITH REPETITIVE PERIPHERAL SENSORY STIMULATION: POST-TREATMENT FOLLOW-UP
1University of São Paulo, Brazil, 2Hospital das Clínicas, Brazil, 3Hospital Albert Einstein, Brazil
On behalf of:
Background and aims: In a previous randomized, placebo-controlled, proof-of-principle clinical trial, active or sham repetitive peripheral sensory stimulation (RPSS) were delivered as add-on interventions to task-specific training (TST) and functional electrical stimulation (FES) to 38 subjects with moderate to severe upper limb motor impairment in the chronic phase after stroke, three times per week, for six weeks. Increases in grasp and pinch force were significantly greater in the active than in the sham group, after treatment. We investigated, in a subgroup of patients who complied with at least 80% of the interventions, if gains in pinch and grasp strength remained, one month after the end of treatment.
Methods: The outcomes were assessed in 19 patients. Ten subjects were included in the active and nine, in the sham group. Within-group changes in performance (post-treatment versus 1 month later) were compared with the Wilcoxon test.
Results: Baseline characteristics were similar between the two groups. There were no significant within-group differences between performance after treatment and one month later: pinch, active group, p=0.105; pinch, sham group, p=0.570; grasp, active group, p=0.557; grasp, sham group, p=0.859
Conclusions: Gains in hand strength observed after treatment were sustained, one month after the end of treatment, in the active and sham groups. These results suggest that RPSS may have long-lasting benefits in patients with moderate to severe upper limb motor impairments.
Disclosures of Interest: No
Abstract N°: 2424
GERIATRIC NUTRITION RISK INDEX PREDICT DYSPHAGIA RECOVERY IN ACUTE ISCHEMIC STROKE
1Sendai City Hospital, Division of Neurology, Sendai, Japan
On behalf of:
Background and aims: Malnutrition inhibits dysphagia recovery in the chronic stage of stroke rehabilitation. The effects of nutritional state at admission on dysphagia recovery have not yet been investigated in the acute stage.
Methods: We retrospectively analyzed acute ischemic stroke patients with dysphagia in our institute from January 2018 to December 2020 (1034 patients were enrolled). Swallowing function was assessed using the Food Oral Intake Scale (FOIS) and patients with initial FOIS levels 1–3, which represent tube dependent nutrition were enrolled. Dysphagia recovery was defined as FOIS levels 4-7 on day 14 after admission, which represent non-tube dependent nutrition. Nutritional status was assessed using the Geriatric Nutritional Risk Index (GNRI) at admission. GNRI >98 suggests no risk, 92-98 as mild nutrition risk, 82-92 as moderate nutrition risk, and <82 as severe nutrition risk. The association between GNRI and dysphagia recovery was assessed.
Results: Of 196 patients (median age, 85 years; male, 39%), dysphagia recovered in 70 patients (36%). The dysphagia recovery group had higher GNRI and lower NIHSS score. In multivariate logistic regression analysis, higher GNRI was independently associated with dysphagia recovery (continuous value; adjusted odds ratio [OR] 1.03, 95% confidence interval [CI] 1.00–1.06). As categorical value, no nutritional risk was independently associated with dysphagia recovery (adjusted OR 2.70, 95% CI 1.12–6.67, compared with moderate and severe risk).
Conclusions: In acute ischemic stroke patients, high GNRI at admission was independently associated with dysphagia recovery.
Disclosures of Interest: No
Abstract N°: 2886
DEVELOPING AN EFFICIENT ADAPTIVE PLATFORM TRIAL FOR MULTIPLE POST-STROKE INTERVENTIONS ALIGNED WITH NATIONAL RESEARCH PRIORITIES: THE LEAP PLATFORM
Amanda Farrin*1, Audrey Bowen2, Florence Day1, Lauren Moreau1, Geraldine Murden1, Holly Schofield1, Alexandra Wright-Hughes1, Anne Forster1
1University of Leeds, United Kingdom, 2The University of Manchester, United Kingdom
On behalf of: The LEAP Collaboration
Background and aims: Long-term problems, including emotional difficulties, impaired communication, and/or reduced mobility, persist for many stroke survivors. Randomised controlled trials testing single interventions are inefficient, expensive and poorly aligned to stroke survivors’ complex, varying needs. To address this, we are developing an innovative platform trial to test multiple ways of improving life after stroke in a single efficient study.
Methods: Active collaboration between stroke survivors, researchers and clinicians underpinned trial development. Objective criteria to prioritise platform interventions were agreed, with candidate interventions identified through comprehensive review of Life After Stroke evidence and stroke survivor engagement. All stakeholders agreed the platform focus on post-stroke emotional difficulties. We selected candidate non-pharmacological interventions with strongest evidence of efficacy, feasibility and acceptability. Outcomes were determined by appraising psychometric properties and relevance. Detailed statistical simulation informed optimal platform design features.
Results: We will present our proposed adaptive platform protocol testing five predetermined non-pharmacological interventions for post-stroke emotional difficulties, with futility stopping rules and robust procedures for including new interventions. We will report agreed criteria for prioritising interventions, candidate interventions for the platform trial, proposed outcome assessments, core data sets and trial design choices.
Conclusions: A platform trial to address longer-term outcomes after stroke is a step-change in trial design, reducing research waste and accelerating evidence generation to inform improved service provision and enhance long-term outcomes for people and their families after stroke. We seek to promote platform trial methodology and share resources for researchers and clinicians, to maximise research efficiency, take-up and impact.
Disclosures of Interest: No
Abstract N°: 2585
THE EFFECT OF A NURSE-LED PROGRAM ON PSYCHOSOCIAL PROBLEMS AND QUALITY OF LIFE IN STROKE PATIENTS
1Çanakkale Onsekiz Mart University, Faculty of Health Sciences, CANAKKALE, Turkey, 2Istanbul University-Cerrahpasa, Institute of Graduate Studies, ISTANBUL, Turkey, 3Istanbul University-Cerrahpasa, Florence Nightingale Faculty of Nursing, ISTANBUL, Turkey, 4Istinye University Liv Hospital Bahcesehir, Stroke Center, ISTANBUL, Turkey, 5Istinye University, Medical Faculty, ISTANBUL, Turkey
On behalf of:
Background and aims: Psychosocial problems such as depression, anxiety, cognitive impairment and fatigue are common in stroke patients. This study investigated the effect of a nurse-led follow-up program on psychosocial problems and quality of life in stroke patients.
Methods: A total of 104 patients (55 in the intervention and 49 in the control group) participated in this pretest-posttest randomized controlled study. Stroke severity, functional status, cognitive function, anxiety, depression, sleep quality, fatigue, reintegration to normal life, and quality of life were assessed. A nurse follow-up program was applied to the patients and they were followed up for three months. The control group was discharged with the routine protocol of the clinic. At the third month, two groups were evaluated by independent evaluators.
Results: Patients in the experimental group were younger (p=0.013) and reported a good income level (p=0.071) more than the control group. They also had better cognitive test scores (p=0.50). Minor stroke and independent patients were predominant in both groups. When the primary outcome measures of the patients at the third month after the program were evaluated, there was no difference between the two groups in terms of improvement achieved at the third month compared to baseline (discharge). Within-group comparison showed that sleep quality increased in the experimental group (p=0.001); an improvement tendency was found in anxiety (p=0.084), reintegration to normal life (p=0.076) and quality of life (p=0.059) scores.
Conclusions: The nurse-led follow-up program may be beneficial in improving the psychosocial outcomes and quality of life of the patients.
Disclosures of Interest: No
Abstract N°: 934
EXERCISE INTERVENTIONS FOR PELVIC FLOOR DYSFUNCTIONS IN WOMEN WITH STROKE - A SCOPING REVIEW
Sanya Anklesaria*1, Rukmini Padiyar1, John Solomon1,2, Kari Bø3,4, Preetha Ramachandra1
1Manipal Academy of Higher Education, Manipal College of Health Professions, Department of Physiotherapy, Manipal, India, 2Centre for Comprehensive Stroke Rehabilitation and Research, Manipal Academy of Higher Education, India, 3Norwegian School of Sport Sciences, Department of Sports Medicine, Oslo, Norway, 4Akershus University Hospital, Department of Obstetrics and Gynecology, Lørenskog, Norway
On behalf of:
Background and aims: Pelvic floor dysfunctions (PFD) are common following stroke yet, are rarely addressed. In this review, we aimed to identify existing exercise interventions and their effectiveness in managing PFD in women with stroke.
Methods: We searched The Cochrane Library, Medline, Scopus, CINAHL, Embase, Web of Science, ProQuest, and Google Scholar from inception to date using appropriate keywords and search strings. We included RCTs and quasi-experimental studies comparing exercise to control interventions/alternate treatments. Two reviewers independently screened the title and abstract, to determine included studies. A third author resolved disputes.
Results: We identified 12 studies of which 9 focused on the management of urinary incontinence (UI), one on fecal incontinence (FI), and two on the management of sexual dysfunctions (SD). Pelvic floor muscle training (PFMT) was predominantly used to manage UI independently or combined with other forms of treatment such as timed voiding, intermittent catheterization, acupuncture, and drug therapy. FI was managed using anal sphincter strengthening exercises, PFMT, and bowel training. Management of SD included comfortable and safe sexual position training, stretching, and strengthening of pelvic floor muscles. Studies found significant improvement in terms of symptoms of bladder and bowel incontinence, number of incontinence episodes, pelvic floor muscle strength and function, Functional independence measure score, International consensus on incontinence questionnaire score, 24-hour pad test, Electromyography readings, sexual knowledge, sexual satisfaction, sexual activity frequency and quality of life.
Conclusions: Exercise interventions help persons with PFD following stroke. Effective management of PFD can improve long-term outcomes in women with stroke.
Disclosures of Interest: No
Abstract N°: 2268
PERSPECTIVES OF HEALTHCARE PROFESSIONALS AND STROKE SURVIVORS ON SEXUAL HEALTH AND INTIMACY IN A SINGAPORE TERTIARY HOSPITAL
Siti Rohaida Rahmat*1, Kaavya Narasimhalu1, Szu Chyi Ng2, Fung Peng Woon2, Wai May Ng1, Dian Handayani2, Shamala Thilarajah2, Kinjal Doshi3, Il Fan Tan1, Deidre Anne De Silva1
1National Neuroscience Institute, Singapore, Singapore, 2Singapore General Hospital, Singapore, Singapore, 3National University Singapore, Singapore, Singapore
On behalf of:
Background and aims: Sexual health is fundamental to the overall well-being of individuals. Stroke can profoundly impact sexual health and intimacy. This study explored the perspectives of sexual health after stroke among healthcare professionals as well as stroke survivors and their partners.
Methods: This is a descriptive cross-sectional study via an anonymised online survey developed with the help of psychologists, a physiotherapist, and a sexual health therapist. It was administered to healthcare professionals and stroke survivors and their partners in a tertiary stroke centre from April to December 2023.
Results: Of the 75 healthcare professionals who responded, 77.3% was not highly confident to discuss sexual health with their patients and have cited this aspect to not be of clinical priority. 34.7% of healthcare professionals thought stroke survivors should abstain from sex.
Among the 36 survivor and partner responses, 61.1% stated there was a role change in relation to sexual behaviour after stroke. 66.5% stroke survivors valued sexual health to be at least somewhat important after stroke. More than 50% has expressed interest to further discuss sexual and intimacy health with healthcare professionals after their stroke.
Conclusions: Preliminary findings of this study demonstrates mismatched perceptions of sexual health and intimacy need between healthcare professionals and stroke survivors. This highlights the need for knowledge building across healthcare professionals and design an intervention program to integrate and optimize sexual health recovery as part of standard routine stroke care.
Disclosures of Interest: No
Abstract N°: 2628
“I FELT A BOX HAD JUST BEEN TICKED” – STROKE SURVIVOR’S PERSPECTIVE ON REHABILITATION PROVISION AND HOW IT NEEDS TO BE IMPROVED
Hannah Jarvis*1, Philip Nagy1, Daniel Allen1, Ewan Dean1, James Smith1, Annabel Riding1
1Lancaster University, Lancaster Medical School, Lancaster, United Kingdom
On behalf of:
Background and aims: The ability to walk after a stroke is critical to mobilising independently and a key aim of stroke survivors. Understanding what rehabilitation is provided, where, by whom and how it can be improved as part of routine healthcare to aid the ability to walk after stroke is not well documented. The aim was to determine stroke survivor perspectives on rehabilitation provision, effectiveness and what could be improved in helping them walk.
Methods: Twenty-two participants aged 45-80years and experienced a stroke within the last 5-years were provided with a questionnaire on what aspects of their rehabilitation did they feel helped them walk better, where it took place and what would they change. Inductive thematic analysis was used to extract key themes.
Results: Most participants stated that rehabilitation was provided at home via the health service or self-learnt at least three days per week. One participant used a treadmill and another an ankle-foot orthosis. Acceptance, “returning to normal”, being able to walk with family, pets, and negotiate stairs were critical. Participants described needing more rehabilitation and better support from community services.
Conclusions: Practicing walking over ground indoors and outdoors after their stroke with health care professionals, family or friends was key to improving their ability to walk, but despite being recommended by clinical guidelines, few used a treadmill or orthoses. Whilst home-based rehabilitation is core for stroke survivors to return home there is a risk of isolation. Increasing duration of rehabilitation and community led group-based sessions are vital.
Disclosures of Interest: No
Abstract N°: 1357
CONTEXTUALIZED CLINICAL PRACTICE GUIDELINES FOR STROKE REHABILITATION: AN UNMET NEED IN LOW AND MIDDLE-INCOME COUNTRIES
1Christian Medical College & Hospital, Department of Neurology; College of Physiotherapy, Ludhiana, India, 2Northumbria University, Department of Social Work, Education, and Community Wellbeing, Newcastle Upon Tyne, United Kingdom, 3College of Medicine and Health Sciences, University of Rwanda, Department of Physiotherapy, School of Health Sciences, Kigali, Rwanda, 4St Stephen`s Hospital, Department of Neurology, Delhi, India, 5SARAH Network of Rehabilitation Hospitals, Brasilia, Brazil, 6Christian Medical College & Hospital, Department of Neurology, Ludhiana, India, 7St John`s Medical College Hospital, Department of Physiotherapy, Bangalore, India, 8Research Organization for Health Education and Rehabilitation-Cameroon (ROHER-CAM), Bamenda, Cameroon, 9Manchester Metropolitan University, Department of Health Professions, Manchester, United Kingdom, 10University of Leicester, Institute of Precision Health, Ulverscroft Eye Unit, Leicester, United Kingdom
On behalf of: GCSR Collaborators
Background and aims: Stroke is the third-leading cause of death and disability combined; reducing it is an immense challenge among low and middle-income countries (LMICs). The limited scope and quality of clinical practice guidelines (CPGs) for stroke rehabilitation in these nations, could hinder effective translation to clinical practice. This systematic review aims to evaluate the availability, scope, and quality of these CPGs in LMICs.
Methods: Four major electronic databases (Medline, EMBASE, CINAHL and PEDro) were searched using keywords related to the objective of the review, including grey literature and hand search. The availability of the CPGs and their content were narratively summarised. The quality of the included guidelines, developed de novo, was analyzed using AGREE REX and AGREE II.
Results: 11 CPGs from 9 countries for stroke rehabilitation were identified and included in this review. Guidelines from Pakistan, Sri Lanka, and India were developed de novo; whereas those from Kenya, Philippines, South Africa, Cameroon, Mongolia & Ukraine were contextualised guidelines from high-income countries. Most contextualizations lacked stakeholder involvement or local healthsystems or patient pathway analysis. Nine countries included recommendations for physiotherapy, seven for communication and swallowing, and five for occupational therapy services post-stroke. Quality assessment using AGREE REX and AGREE II showed low rigor in the development and applicability of the CPGs.
Conclusions: Contextualised CPGs for stroke rehabilitation in LMICs are limited and indaequate. There is a need to develop context-specific, culturally relevant CPGs for better clinical implementation to improve the quality of stroke rehabilitation and service delivery in LMICs.
Disclosures of Interest: No
Abstract N°: 3300
ASSESSING COMPETENCE TO DELIVER EARLY STROKE SPECIFIC VOCATIONAL REHABILITATION (ESSVR) IN THE RETURN-TO-WORK AFTER STROKE TRIAL: A FEASIBILITY STUDY
Kathryn Radford*1,1, Katie Powers1, Julie Philips1, Jain Holmes1, David Clarke2, Ruth Tyerman1, Kristelle Craven1, On Behalf of the Retake Research Group1,2
1University of Nottingham, Centre for Rehabilitation and Ageing Research, Nottingham, United Kingdom, 2University of Leeds, Academic Unit for Ageing and Stroke Research, Leeds, United Kingdom
On behalf of: RETAKE Research Group
Background and aims: Therapist incompetence could compromise trial outcomes. We developed methods to assess occupational therapists’ (OTs) competence to deliver ESSVR and assessed its feasibility in the RETAKE trial.
Methods: OTs attended ESSVR training, 6m refresher-training plus monthly-mentoring during intervention delivery. Competency assessed using case vignettes 1) immediately following initial (T1) and refresher-training (T2) and by reviewing randomly-selected intervention records (one/OT), 9-12m after commencing delivery (T3). Competency criteria included intervention process knowledge (40%), clinical reasoning (50%) and communication skills (10%). Scores mapped to a rubric identified OTs as highly-competent (⩾70%), competent (50-69%) or needing support (⩽49%). Feasibility determined by time/effort in competency assessment and data completeness. Acceptability assessed using interviews. Factors influencing competency were explored using logistic regression.
Results: 60 OTs assessed at T1; 38 at T2 and T3. At T1, 45(75%) were competent and 15(25%) required support. At T2, 33(69%) competent, 4(8%) highly-competent; 1(2%) needed support. At T3, 28(58%) were competent, 10(21%) highly-competent and 2(4%) required support. Both methods were feasible/acceptable, taking 45-90 minutes to mark. Data completeness was impacted by OT dropout at T2/T3, and incomplete/missing records at T3. OTs with prior-VR-experience more likely to be competent at T1 (OR=1.3, CI 95% = [1.01, 1.67]).
Conclusions: Competency assessment identified OTs needing support to implement ESSVR. Repeat-testing assured us OTs remained competent during RETAKE. Intervention records offered insights into competency not-evident from vignettes. Competency increased with ESSVR experience. Some OTs required support throughout. Research should identify optimum methods of competency assessment and relationships between competence, fidelity, and outcomes.
Disclosures of Interest: No
Abstract N°: 1469
STROKE-SPECIFIC VIRTUAL ASSISTANT AS A COMPANION IN RECOVERY
1University of Glasgow, Glasgow, United Kingdom, 2Aalborg University, Aalborg, Denmark
On behalf of: RES-Q+ consortium
Background and aims: RES-Q+ project partners have been developing a virtual assistant (VA) for stroke survivors, their families, and caregivers. The primary purpose of the VA is to provide users with quality assured information in response to common questions regarding stroke. The VA also aims to allow users to check in on their mental wellbeing, functional recovery and rehabilitation progress.
Methods: Interviews and focus groups were conducted with stroke survivors and their families and caregivers in Scotland, Northern Ireland, Denmark, and the Czech Republic. Overall, 30 stroke survivors across 15 interviews interacted with the VA and answered Patient Recorded Outcome Measures on the VA interface and in a human interview. The corpus of 35 sessions with 40 participants was transcribed verbatim by the partner teams. Thematic analysis identified key overarching themes of barriers to using the VA, its relative advantages compared to human check-ins, and perceptions of the VA as a human-like companion.
Results: Barriers to use included lack of familiarity and comfort with technology, and scepticism toward information found online. The VA’s relative advantages included increased ease of access and comfort around sensitive topics compared to conversations with humans. Perceptions of the VA as a human-like companion emerged as participants used human terms to describe its role as an additional, trustworthy and personable source of information and support, rather than a replacement to resource-intensive human check-ins.
Conclusions: Our findings highlight the need of stroke survivors for an additional, readily available, and trustworthy source of support post discharge.
Disclosures of Interest: No
Abstract N°: 72
LESION LOCATION INFLUENCES MOTOR SKILL RETENTION IN SUBACUTE STROKE
Bernat de las Heras*1, Jacopo Cristini1, Lynden Rodrigues1, Janice Eng2, Alexander Thiel3, Ada Tang4, Joyce Fung1, Marc Roig1
1McGill University, School of Physical and Occupational Therapy, Montréal, Canada, 2University of British Columbia, Vancouver, Canada, 3McGill University, Department of Neurology and Neurosurgery, Montréal, Canada, 4McMaster University, School of Rehabilitation Sciences, Hamilton, Canada
On behalf of:
Background and aims: Motor learning is essential for upper-limb motor recovery after stroke. Lesion location influences motor impairment and functional recovery, but whether it affects different stages of motor learning is unknown. We investigated the impact of lesion location on motor skill acquisition and retention in individuals with cortical (CO) and subcortical (SC) stroke.
Methods: Fifty-seven CO (n=22) and SC (n=35) patients (63.9±23.4 days post-stroke) performed four blocks of a visuomotor task requiring handgrip force modulation with the hand contralateral to the lesioned hemisphere at baseline and after four weeks. Acquisition was calculated as the mean score difference between the first and best block of practice at baseline, and retention as the difference between the best block at baseline and the first block at four weeks. Upper-limb impairment was assessed with the Fugl-Meyer Assessment. Linear mixed models were controlled for age and impairment.
Results: The mean Fugl-Meyer was lower in the SC group but this difference was not significant (55.11±11.46 vs. 60±5.29, p=0.079). Both groups exhibited comparable improvements in skill acquisition (F(3, 82)=1.70, p=0.17). In contrast, compared to the SC group, the CO group showed greater deficits in skill retention (F(1, 52)=5.27, p=0.02).
Conclusions: Stroke location has no effect on the acquisition of motor skills in a visuomotor task. Nevertheless, individuals with cortical lesions exhibit deficits in retaining acquired skills. These findings underscore the significant role of cortical networks in storing sensorimotor information and offer insights with potential clinical implications for tailoring upper-limb rehabilitation strategies for individuals recovering from stroke.
Disclosures of Interest: No
Abstract N°: 2640
EEG DELTA NETWORK PROPERTIES AT ADMISSION PREDICT NIHSS AT DISCHARGE AFTER ISCHEMIC STROKE
Giuseppe Reale*1, Chiara Iacovelli2, Aurelia Zauli1, Marco Moci1, Paolo Calabresi1, Pietro Caliandro1
1Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Department of Neuroscience, Sensory organs and Chest, Rome, Italy, 2Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Emergency, Anaesthesiology and Intensive Care Medicine, Rome, Italy
On behalf of: COMMAS Research Group
Background and aims: Following a stroke, brain network overall balance between local specialization (Cw) and global integration (Lw), known as "Small-worldness" (Sw), experiences complex changes. In particular, stroke causes a reduction of delta network Sw and an increase of alpha network Sw. In this multicentric study, we explored whether specific networks characteristics at admission and at discharge are associated with different clinical evolution patterns.
Methods: We recruited patients with acute anterior circulation stroke; we recorded an EEG within 24 hours and another EEG within 5 days. Connectivity analysis was performed with eLORETA for each EEG frequency band (figure). We performed a regression analysis using NIHSS as dependent variable and network parameters as independent variables.
Results: We enrolled 80 consecutive patients (57% female, median age 75). Median NIHSS at admission was 11 (IQR:6-15), 5.5 (IQR:2-12) at discharge.
The regression model found an indirect association between alpha 1 Sw at first acquisition and NIHSS at admission (p=0.043) and a direct association between delta Sw at second acquisition and NIHSS at discharge (p<0.0001). Finally, the regression model found a direct association between delta Sw at first acquisition and NIHSS at discharge (p=0.024) and delta Cw at first acquisition and NIHSS at discharge (p=0.029).
Conclusions: While brain connectivity dynamically changes in stroke acute phase, delta network rearrangements have a potential prognostic role. In fact, a higher delta Sw at admission predicts greater stroke severity at discharge. Such rearrangement seems to depend more strongly on modifications of local specialization (Cw) induced by the lesion itself.
Disclosures of Interest: No
Abstract N°: 35
PROTECTIVE EFFECTS OF ARTIFICIAL HYPOTHERMIA AND OLANZAPINE INDUCED HYPOTHERMIA
Seong MI Heo1, Jae Seong Noh1, Da Som Han1, Joong Bum Moon1, Myoung Cheol Shin1, Taek Geun Ohk1, Tae-Kyeong Lee2, Ji Hyeon Ahn3, Jun Hwi Cho*1
1Kangwon National University, Emergency Medicine, Chuncheon, South Korea, 2Hallym University, Food Science and Nutrition, Chuncheon, South Korea, 3Youngsan University, Physical Therapy, Yangsan, South Korea
On behalf of:
Background and aims: The blood–brain barrier (BBB) is a crucial physiological barrier which separates the central nervous system (CNS; brain and spinal cord) from the CNS circulation that contains inflammatory mediators. The BBB controls molecular and cellular exchange for normal functions between the CNS blood vessels and parenchyma. It has been reported that neuroinflammation can destroy the BBB, resulting in various CNS diseases.
Methods: In this study, 15-minute transient cerebral ischemia (ischemia-reperfusion, IR) was developed in gerbils. The striatum, which is an important brain structure in extrapyramidal motor system, was used to compare the protective effects of artificial hypothermia and drug-induced hypothermia against BBB disruption on day 5 after IR, when striatal neuronal death occurred in the ischemic striatum.
Immediately after IR, artificial hypothermia was induced by body surface cooling using ice and drug-induced hypothermia was developed using olanzapine, an antipsychotic medication able to treat several mental health conditions (i.e., schizophrenia and bipolar disorder), that has been discovered to have some beneficial effects beyond its original effectiveness.
Results: The effects of artificial hypothermia against IR-mediated neuronal loss, AFE damage (loss), caveolin-1 increase, and IgG and albumin leakage were tenuous; however, olanzapine-induced hypothermia significantly protected IR-induced damages.
Conclusions: Collectively, our findings revealed that olanzapine administration after IR apparently protected RI-induced BBB disruption, which might be closely related with IR-mediated neuroinflammation, in ischemic gerbil striatum. Thus, olanzapine can be a therapeutic agent for brain IR injury by protecting BBB disruption following cerebral ischemic insults.
Disclosures of Interest: No
Abstract N°: 724
AUTONOMIC CHALLENGE MANEUVERS REVEAL RECOVERY OF CARDIOVASCULAR AUTONOMIC DYSFUNCTION THREE AND SIX MONTHS AFTER STROKE-ONSET
Ruihao Wang*1,2, Julia Koehn1, Bernd Kallmünzer1, Martin Köhrmann3, Christian Blinzler1, Max Hilz1,4
1University of Erlangen-Nuremberg, Department of Neurology, Erlangen, 2Academic Teaching Hospital Bamberg, University of Erlangen-Nuremberg, Department of Psychiatry, Bamberg, 3University Hospital Essen, Department of Neurology, Essen, 4Icahn School of Medicine at Mount Sinai, Department of Neurology, New York
On behalf of:
Background and aims: Stroke may cause cardiovascular autonomic dysfunction (CAD). We previously showed that CAD at rest may recover within days. It is unclear whether autonomic challenge-maneuvers uncover post-stroke CAD after several months. Therefore, we assessed cardiovascular autonomic modulation in stroke patients during autonomic challenges within one week, three and six months after stroke-onset.
Methods: In 65 patients with ischemic stroke [26 women, mean age 64.2±8.6 years, median NIHSS 1], we recorded RR-intervals (RRI), systolic, diastolic blood-pressure (BPsys, BPdia), and respiration during metronomic-deep-breathing (MDB), Valsalva-maneuver, and standing-up within one week, three and six months after stroke-onset. We calculated E/I-ratios, Valsalva-ratios, and 30/15-ratios. Values lower than the age-dependent reference values of our laboratory were considered abnormal.
Results: Within one week, three and six months after stroke-onset, E/I-ratios were abnormal in 9/65, 3/65, and 3/65 patients respectively; Valsalva-ratios were abnormal in 4/65, 0/65, and 0/65 patients respectively, 30/15-ratios were abnormal in 2/65, 1/65, and 1/65 patients respectively. Three months after stroke, E/I-ratios, Valsalva-ratios, and 30/15-ratios were significantly higher than the respective values assessed within the first week after stroke. Six months after stroke, Valsalva-ratios and 30/15-ratios also were higher than the respective values of the first week assessment.
Conclusions: The autonomic challenge-maneuvers unveiled CAD only in rather few patients, probably due to the low stroke-severity. MDB was most sensitive and demonstrated post-stroke CAD in 13.8% of patients during the first week, in 6.2 % three and six months after stroke. Valsalva-ratios and 30/15-ratios upon standing-up were less sensitive but also showed CAD-recovery after three and six months.
Disclosures of Interest: No
Abstract N°: 942
EXPLORING THE IMPACT OF POST-STROKE SHOULDER PAIN ON UPPER EXTREMITY FUNCTIONS, KINESIOPHOBIA, ANXIETY, AND QUALITY OF LIFE
Sevtap Gunay Ucurum1, Onur Kortelli2, Yusuf EMUK*3
1Izmir Katip Çelebi University, Physiotherapy and Rehabilitation, Izmir, Turkey, 2Beykent University, Physiotherapy and Rehabilitation, Istanbul, Turkey, 3Izmir Katip Çelebi University, Faculty of Health Sciences Department of Physiotherapy and Rehabilitation, Izmir, Turkey
On behalf of:
Background and aims: This study aims to examine the impact of post-stroke shoulder pain on upper extremity motor functions, kinesiophobia, anxiety, and quality of life.
Methods: The study included 53 patients (35 males, 18 females) in the chronic phase of stroke, with a mean age of 61.28±10.07 years. The pain severity of patients was assessed using the Resting Numerical Pain Rating Scale, Activity Numerical Pain Rating Scale, and Shoulder Pain and Disability Index. The evaluation of upper extremity motor functions utilized the Arm Motor Test, kinesiophobia was assessed with the TAMPA Kinesiophobia Scale, anxiety with the Beck Anxiety Scale, and the Stroke Specific Quality of Life Scale was employed for assessing the quality of life.
Results: A positive correlation emerged between post-stroke shoulder pain and anxiety level (p<0.01). Conversely, a negative correlation was identified between shoulder pain and both upper extremity motor functions and quality of life (p<0.01). No statistically significant relationship was found between shoulder pain and kinesiophobia. Additionally, a negative correlation was observed between the time elapsed after stroke and shoulder pain. Furthermore, it was noted that the severity of shoulder pain is higher in women compared to men.
Conclusions: This study highlights the detrimental impact of post-stroke shoulder pain on the psychological state, quality of life, and motor functions of individuals. The holistic evaluation of shoulder pain, a prevalent complication following stroke, is crucial. Understanding its comprehensive effects on individuals' lives is essential for raising awareness and comprehending the consequences of post-stroke shoulder pain.
Disclosures of Interest: No
Abstract N°: 1044
PHYSICAL ACTIVITY EVALUATION OF PERSONS WITH ACUTE STROKE AT A SPECIALISED UNIT IN SOUTH AFRICA: A FEASIBILITY STUDY
1Stellenbosch University, Health and Rehabilitation Sciences, South Africa, 2Karolinska Institutet, Neurobiology, Care Sciences, and Society, Sweden
On behalf of:
Background and aims: Physical activity (PA) is often impacted negatively after stroke. PA engagement is not only paramount for functional recovery but may contribute to lowering recurrent stroke risk. Early PA evaluations, as in the acute setting, may be crucial for secondary prevention. The aim of this study was to evaluate the feasibility of sensor-derived PA measures during specialised acute care in a low resourced healthcare setting.
Methods: A cross-sectional design was used to evaluate process and scientific feasibility. Participants needed to be admitted to the specialised acute unit, have a confirmed stroke diagnosis, and be able to ambulate independently upon screening. Process feasibility included recruitment rates, ease and acceptability of assessments, and valid days of PA assessment, while scientific feasibility related to PA outcomes.
Results: Of the eighty-two consecutive participants screened, 26 (32%), with a mean age of 46 years (SD:12), met the inclusion criteria. All assessments were perceived to be acceptable and completed with relative ease besides the assessment of the global impression scale which required a psychiatrist. Twenty participants (77%) had valid PA data. Participants spent 904 ± 183 minutes in sedentary, 103 ± 38 minutes in light PA, and 9 ± 8 minutes in moderate-to-vigorous PA states.
Conclusions: Although it may be feasible to objectively assess PA in an acute setting, participation (reach) rates appear low which may be contextual, whereby those with more severe strokes are admitted to the specialised unit. Further research is required to establish the additional value of a sensor-derived PA marker during acute care.
Disclosures of Interest: No
Abstract N°: 2721
NUTRITIONAL INTERVENTIONS DURING ACUTE CARE AND REHABILITATION OF STROKE PATIENTS: A SCOPING REVIEW
Karina Siewers*1, Hanne Christensen1
1Bispebjerg Hospital, Department of Neurology, København
On behalf of:
Background and aims: Malnutrition is reported in up to half of patients during hospitalization and rehabilitation after stroke and negatively impacts mortality, infection rate, and functional prognosis. Guidelines provide advice on dysphagia but not on specific nutritional interventions in stroke. This scoping review aimed to explore the field of nutritional care interventions in stroke patients undergoing acute care and rehabilitation.
Methods: A systematic search of MEDLINE and Embase was conducted for relevant articles published from 2015 to 2024, with some older articles included. Eligible studies were randomized controlled designs investigating the effects of nutritional care interventions compared to control interventions including usual care in stroke patients during in-patient rehabilitation.
Results: The search identified 17 experimental studies involving a total of 5,532 patients; median number of participants were 73. Nutritional care interventions were heterogeneous, with a predominant focus on the investigation of oral protein supplements. The interventions with number of trial participants are presented in Table 1; interventions with reported statistically positive results have been marked with *.
Conclusions: At least 15 different nutritional interventions have been tested in patients with stroke during rehabilitation. Most studies were underpowered, interventions lacked consistent pathophysiological support and study designs were heterogeneous measuring different outcomes. The findings underscore the imperative for future methodologically robust research to address this gap and provide evidence-based recommendations for nutritional interventions in stroke patients.
Disclosures of Interest: No
Abstract N°: 2793
RESILIENCE OF BRAIN NETWORKS AFTER STROKE: IMPACT OF NEW EVENTS ON SPECIALIZATION AND INTEGRATION
Elisabeth Dirren*1, Julian Klug1, Cecilia Jarne1,2,3,4, Emmanuel Carrera1
1Hôpitaux Universitaires de Genève (HUG), Genève, Switzerland, 2National University of Quilmes, Bernal, Argentina, 3CONICET, Buenos Aires, Argentina, 4Aarhus University, Aarhus, Denmark
On behalf of:
Background and aims: Brain networks reorganization has been investigated in association with recovery of function after stroke. Here, based on a novel approach using virtual lesions, we tested the hypothesis that specific changes in brain networks organization after stroke reflect an increase in resilience to potential recurrent events.
Methods: We used a dataset of 75 first-time patients with resting-state connectivity assessed at three time-points after stroke: 2 weeks (TP1), three months (TP2), one year (TP3). Functional connectivity matrices were computed for each subject and TP. Resilience of network integration R(integration) was defined as the difference between network global efficiency before and after virtual lesions and resilience of network specialization R(specialization) was defined as the difference of modularity. Virtual lesions were simulated by removing nodes corresponding to 122 strokes masks.
Results: Compared to controls, R(integration) to virtual lesions was higher in patients at TP1 (0.133, p=0.04) and TP2 (0.135, p=0.04) but not at TP3 (0.023, p=0.854). R(specialization) was higher in patients at TP1 (0.661, p<0.001), TP2 (0.316, p=0.073) and TP3 (0.456, p=0.007), albeit not significantly at TP2. Lesion side, site, patient age, acute NIHSS, gender and handedness modulated resilience, but not lesion size.
Conclusions: Network reorganization after stroke strengthens resilience of network integration and specialization to recurrent lesions. These results demonstrate that reorganization of brain network architecture after stroke is not only associated with clinical improvement but also with reinforcement of resilience to future lesions.
Disclosures of Interest: No
Abstract N°: 247
THE EFFECTS OF EXERCISE-BASED REHABILITATION ON BALANCE AND GAIT IN STROKE PATIENTS AT THE TERAMO STROKE UNI
SIMONE SERRONI*1
1Asl Teramo, MEDICINA, TERAMO
On behalf of:
Background and aims: Post-stroke depression (PSD) is common in 18 to 33% of cases, and is associated with higher mortality, more difficult recovery, more pronounced cognitive deficits, and lower quality of life than stroke without depression.
Methods: Patients admitted to the Stroke Unit of the Neurology Unit of the Teramo Hospital suffering from collaborative strokes were subjected to the self-assessment test: Beck Depression Inventory (BDI) in order to evaluate the presence and degree of the depressive state.
Results: All patients underwent a rehabilitation program, which took place with double daily sessions lasting approximately 60 minutes each (only one session except Saturday) for six days a week for both neuromotor re-education and language re-education. The depressed patients were all treated with SSRIs and SNRIs.
Conclusions: PSD plays an unfavorable role on prognosis, rehabilitation treatment, functional recovery, length ofhospital stay, quality of life and patient survival. The more serious the depressive state, the worse the evolution of the pathology.
Disclosures of Interest: No
Abstract N°: 872
WHAT ARE PHYSIOTHERAPY STAFF’S PERCEPTIONS OF PHYSIOTHERAPY DELIVERED IN ACUTE STROKE REHABILITATION IN A 3:2 FLOAT REHAB MODEL
Sophie Badcock*1, Jimmy James1
1St Thomas' Hospital, London, United Kingdom
On behalf of:
Background and aims: An alternate model of physiotherapy provision is being implemented on an acute stroke unit whereby two patients are concurrently treated by 3 physiotherapy staff whereby one physiotherapist “floats”. Preliminary data has shown this model to deliver similar amounts of patient physical activity with fewer resources. The aim of this project is to understand physiotherapy staff’s perception of the 3:2 float rehab model.
Methods: Focus group discussion with staff allocated to attend one of two focus groups. Inclusion eligbility: physiotherapy staff who had worked on the unit in the last 6 months. 11 physiotherapy staff (bands 3-7) participated. Each group was facilitated by either author, with audio-recordings transcribed before being thematically analysed. Both authors coded the data independently before developing possible themes. Collaborative development of themes was completed using a series of mind-maps, tables and colour coding to develop the final four themes.
Results: 4 main themes were identified:Two themes encompassed the perceived benefits & considerations for physiotherapists completing the model;The other two themes were related to those experiencing the model, both patient and staff perspective.
Conclusions: This research suggests that float sessions are perceived as a positive, efficient and effective rehab model by the physiotherapy team, with benefits to both staff and patients. With increased practice and familiarity, it becomes more efficient. However there may be some considerations needed around using it with all patients. Further research is needed to look at functional outcomes for those patients receiving rehab in a 3:2 rehab model.
Disclosures of Interest: No
Abstract N°: 1691
POST-STROKE QUALITY OF LIFE LEVEL AND ITS ASSOCIATED FACTORS: A CROSS-SECTIONAL STUDY
Khader Almhdawi*1, Alza Alazrai1, Hanan Jaber1
1Jordan University of Science & Technology (JUST), Rehabilitation Sciences, Irbid, Jordan
On behalf of:
Background and aims: Individuals post-stroke might demonstrate significant declines in their mental health and quality of life which might hinder their functional independence and well-being. This study aimed to investigate quality of life level among individuals with stroke in Jordan and to identify this level associated factors.
Methods: A cross-sectional design was conducted using the 12-item Short-Form Health Survey (SF-12) to assess quality of life level. Possible associated factor included fatigue, mental health status, cognition, upper limb functional abilities, gait, and life-style variables. Multiple variable linear regression analysis was used to identify quality of life significant associated factors.
Results: the study recruited 153 participants with stroke with a mean age of 55.8 (±10.8) years. Participants’ overall total SF-12 total score was 55.6 (±14.4). The study regression model significantly explained 69.6% of the variance in participants’ quality of life level (r2=0.696, F=36.1, P < 0.001). Participants’ quality of life level was significantly and negatively associated with fatigue, worse sleep self-evaluation, worse health self-evaluation, depression, and worse diet self-evaluation. On the other hand, quality of life level was significantly and positively associated with better ten-meter walk speed.
Conclusions: Participants showed a relatively a low level of quality-of-life post-stroke. Possible predictors of post-stroke quality of life level included fatigue, sleep, health status, sleep, diet, and walking speed. Quality of life level and its significantly associated factors should be carefully considered by healthcare and rehabilitation practitioners working with individuals’ post-stroke.
Disclosures of Interest: No
Abstract N°: 2316
OCCUPATIONAL THERAPY INTERVENTION IN STROKE PATIENTS (AS INPATIENT AND OUTPATIENT) IN SOCIAL INTEGRATION - REINTEGRATION
Stavroula Bakatsi*1, Eleni Michailidou2, Sofia Sivetidou2, Ioannis Alexandros Tzanos2, Elisavet Tzani2, Nefeli Anna Papageorgiou2, Maria Nianiarou2, Aikaterini Kotroni2
1KAT GENERAL HOSPITAL, PRM, Kifisia, Greece, 2KAT GENERAL HOSPITAL, Kifisia, Greece
On behalf of:
Background and aims: Stroke is the leading cause of disability in adults, with a significant impact on the family. Early occupational therapy intervention (in-hospital and post-discharge) has a positive effect on patient’s independence during reintegration.
Methods: Stroke patients (N=56) hospitalized in rehabilitation clinic from 2018 to 2023. At the start of the program they were assessed with the Barthel index (BI), the Mini Mental State Examination (MMSE) and participated in a training program with basic activities of daily living and cognitive deficits training, with 5 sessions per week for 4 months. After discharge, they continued the occupational therapy sessions as outpatients. The evaluation was done at the beginning and end of the program with: BI, MMSE, Time Up and Go (TUG), Balance Berg Scale (BBS) and Community Integration Questionnaire (CIQ) for participation in household tasks, social participation and return to work. The program included the solving of the daily problems at home, the commuting to the community and the returning to work to increase their independence, with 3 sessions per week for 3 months.
Results: After completion of the rehabilitation program, reassessment with the CIQ showed an increase in independent participation in the community activities
Conclusions: It seems that occupational therapy combined with the ability of stroke patients to express the real problems they confront in the process of their reintegration into previous tasks, is a very important practice for their substantial and more independent reintegration.
Disclosures of Interest: No
Abstract N°: 2924
DEVELOPING A TELEHEALTH ASSESSMENT TOOLKIT FOR SPEECH AND LANGUAGE THERAPISTS USING THE COM-B AND TDF MODELS FOR BEHAVIOUR CHANGE
Amanda Comer1, Nicholas Behn1, Sarah Northcott1, Roper Abi1, Niamh Devane1, Katerina Hilari*1
1City, University of London, Language and Communication Science, London, United Kingdom
On behalf of: FATE-A Group - Dr S. Vitoratou (King's College London); Dr H. Gimeno (Barts Health); Dr A. Hill (The University of Queensland); V. Bedford (East London Foundation Trust); A. Posada (St George's NHS Trust); Dr S. Kramer (Whittington Health NHS Trust)
Background and aims: A survey of UK speech and language therapists (SLTs) suggests increased telehealth use due to the COVID-19 pandemic (Hilari et al., 2023), however few outcome measures have been tested for telehealth administration and little is known about how best to facilitate this process. Data gathered from UK SLTs and people with aphasia (PWA) explored their experiences and views on telehealth assessment, including ethnographic observations of telehealth assessment administration. The COM-B and Theoretical Domains Framework (TDF) provide a structured approach to identifying barriers and facilitators to behaviour (Cane et al., 2012; Atkins et al., 2017). This study aimed to investigate what the barriers and facilitators are to SLTs delivering telehealth assessment; and explore which intervention functions are salient in the design of a telehealth assessment toolkit.
Methods: Qualitative data exploring the views and experiences of PWA and SLTs in the UK were synthesised using a meta-ethnography approach. Iterative themes identified were barriers, facilitators and desires of telehealth assessment. Themes were deductively mapped to the TDF, and intervention functions identified, in order to develop a telehealth assessment toolkit.
Results: Environmental factors and beliefs in consequences were highlighted as both barriers and facilitators to telehealth assessment. Intervention functions directly influenced the design of the prototype toolkit, drawing on existing resources for SLT telehealth delivery and creating new content.
Conclusions: Using the TDF COM-B models of behaviour change is suggested as a systematic and feasible method for designing a stakeholder informed telehealth assessment toolkit.
Disclosures of Interest: No
Abstract N°: 610
ASSOCIATION BETWEEN THE EXECUTIVE DYSFUNCTION AND DYNAMIC BALANCE FUNCTION IN PATIENTS WITH STROKE
1Tokyo Metropolitan University, Faculty of Health sciences, Tokyo, Japan, 2Reiwa Rehabilitation Hospital, Department of rehabilitation, Chiba, Japan, 3Moriyama Neurological Center Hospital, Department of Rehabilitation, Tokyo, Japan, 4Keio University School of Medicine, Department of Rehabilitation of Medicine, Tokyo, Japan, 5Sendai Seiyo Gakuin University, Department of Rehabilitation, Sendai, Japan
On behalf of:
Background and aims: Previous study has shown an association between executive dysfunction and dynamic balance in patients with stroke. However, it is unclear which factors mediate the association between executive dysfunction and dynamic balance. Therefore, the aim of this study was to investigate the association between executive dysfunction and dynamic balance and to identify mediating factors using mediation analysis.
Methods: This study was a cross-sectional design. The study included 107 patients with stroke (age: 67.0 ± 11.8, time since stroke; 73.5 ± 55.7 days). Executive function was assessed using the Trail Making Test (TMT) part B. Dynamic balance was assessed using the Timed Up and Go Test (TUGT). Other variables assessed were Brunnstrom Recovery Stage (BRS) lower limb, sensory, cognitive functions. Statistical analysis was performed using partial correlation analysis with age as a control factor. Subsequently, a model was created with TUGT as the dependent variable, TMT part B as the independent variable and BRS lower limb as the mediating variable, and mediation analysis was conducted.
Results: TMT part B value was 156.5 ± 103.8 s. TUGT was 14.25 ± 9.29 s. BRS lower limb was median 6 (min: 1, max:6). TMT part B correlated with TUGT (r=0.41) and BRS lower limb (r=-0.22). Mediation analysis showed a significant indirect effect as a result of mediation of the BRS lower limb between TMT part B and TUGT (P < 0.05).
Conclusions: Executive dysfunction and dynamic balance were associated, and the degree of paralysis associated with them in patients with stroke.
Disclosures of Interest: No
Abstract N°: 1336
(THE TRUTH ABOUT) GAIT RECOVERY IN PATIENTS WITH CHRONIC STROKE: A SYSTEMATIC REVIEW
Jose Lopez1, Dolores Villalobos2, Jorge Alegre Ayala1, Paula Fragoso*1, Benjamin Peralta Wieland1, Adrian Plaza Garcia1, Pietro Lais1, Daniel Jimenez Masa1, Elena Marabotto1
1Centro de Neurorehabilitación CEN, Neurorehabilitation, Madrid, Spain, 2UCM Faculty of Psychology, Pozuelo de Alarcón, Spain
On behalf of:
Background and aims: The idea regarding the impossibility of significant recovery in chronic stroke patients is strongly established. Nowadays, it is considered that the most significant improvements occur in the first few weeks or months after the stroke, with posterior less significant recovery. After 6 months, in chronic stroke phase, spontaneous and induced recovery is usually considered at its limit. This systematic review aims to explore the literature performed in this field and analyze if gait recovery is possible in patients with a chronic stroke
Methods: The systematic search of literature was conducted until October 2023, in the electronic databases: Scopus, Medline, Cochrane Library and Web of Science.
Results: 48 articles were finally included (from 2000 to 2023). Were included 1600 chronic stroke patients. We described the baseline gait profile, the measures tool and the different interventions found in the literature. Finally, we analyzed the intervention results, focus on the significant improvements described in terms of gait resistance, gait speed and balance (and also in other aspects such as fear of falling, functional mobility or deficit). In general, despite the heterogeneous interventions, outcome measures showed improvements after the intervention in a high number of studies.
Conclusions: The belief of the six months as a maximum time to achieve recovery, has a negative impact in the attitudes of patients towards their rehabilitation and on therapists making optimal training plans. Nevertheless, the literature shows that besides the different rehabilitation techniques, improvements of some stroke-induced deficits can even be achieved in the chronic phase.
Disclosures of Interest: No
Abstract N°: 1433
DEVELOPING A MULTI-DISCIPLINARY TEAM LED EDUCATION PROGRAMME FOR CAREGIVERS ON A SPECIALIST STROKE INPATIENT REHABILITATION UNIT
Sushmita Mohapatra*1, Rebecca Sleath1
1Betsi Cadwaladr University Health Board, United Kingdom
On behalf of:
Background and aims: Stroke has a huge impact on stroke survivors’ (SS) support system, predominately consisting of family members who take the main responsibility for supporting someone after a stroke. Caregivers have a range of unmet needs, amongst which, information needs to support caring for the SS and caring for themselves (National Guidelines for Stroke UK). Although the Stroke Association Wales (SAW) provides a wealth of online resources, the need for focused, specific discussion was identified by family members.
This study describes the development process of the pilot programme.
Methods: A participatory open co-design method was used to co-create a pilot multi-disciplinary education programme, by involving family caregivers of SS, who were ‘experts by experience’ in designing solution. The pilot was completed in collaboration with SAW, committed to supporting the particular challenge.
Results: Six caregivers and 12 staff contributed to the development of the programme, deciding the content, format, length and delivery. Six sessions of educational content were developed to be delivered face to face, over six consecutive weeks, for SS family receiving rehabilitation in the stroke unit. Preliminary analysis of data highlighted the programme was appropriate, useful and added to the caregivers’ confidence on understanding the stroke survivor’s post-stroke needs.
Conclusions: The co-designed education programme can be an effective way to meet caregivers’ need for information immediately after stroke, preparing them for the caregiving role. This could address the emotional need of caregivers to be heard and build peer support. The impact on their understanding, resource allocation and cost effectiveness needs further evaluation.
Disclosures of Interest: No
Abstract N°: 1560
SHINING A LIGHT INTO THE BLACK BOX: QUALITATIVE RESULTS FROM THE TAKING CHARGE AFTER STROKE (TACAS) TRIAL
Vivian Fu1, Kathryn Fernando2, Felicity Bright3, Judith Riley2, Harry Mcnaughton*2
1University of Calgary, Department of Clinical Neurosciences, Calgary, Canada, 2Medical Research Institute of New Zealand, Wellington, New Zealand, 3Auckland University of Technology, Auckland, New Zealand
On behalf of: the Taking Charge After Stroke (TaCAS) trial investigators
Background and aims: Take Charge (TC), an intervention designed to enhance intrinsic motivation and self-determination, significantly improves quality of life, social functioning, and independence up to a year after acute stroke. We sought to understand how TC supports the subacute phase of recovery after stroke.
Methods: We conducted a qualitative study nested within the TaCAS trial. We identified potential participants at the 12-month outcome assessment using a purposive, intensity sampling approach, and we determined that all participants had received either one or two TC sessions. We conducted semi-structured interviews and analysed data using interpretive description.
Results: We interviewed six participants. A core feature that participants valued in TC was the value of being listened to. TC also enabled its stroke survivors to focus on personal goals that were important to them. Over time, this led to a sense of coming to their own wisdom, that they knew best how and what to prioritise in their recovery. Participants also described two major external factors that impacted recovery: being well-supported was a positive factor, while the paternalism of healthcare was a detrimental barrier.
Conclusions: Take Charge is an effective, subacute intervention that supports stroke survivors through self-determination and intrinsic motivation. Stroke survivors who received TC felt heard and viewed TC as a tool which helped to focus on prioritising their personal goals. They were then able to develop a sense of confidence in themselves and their expertise.
Disclosures of Interest: No
Abstract N°: 1901
FROM NEWCOMER TO EXPERT: THE MEANING OF PARTICIPATING IN A FACEBOOK GROUP FOR STROKE SURVIVORS
Malin Tistad1,2, Lill Hultman1, Annica Wohlin Wottrich1, Lena Von Koch*1,3
1Karolinska Institutet Campus Huddinge, Neurobiology, Care Sciences and Society, Sweden, 2Dalarna University, Sweden, 3Karolinska University Hospital, Sweden
On behalf of:
Background and aims: Facebook groups are digital arenas available for sharing experience-based knowledge of a diagnosis or specific symptoms. The aim of this study was to increase the knowledge about the lived experience of taking part in a Facebook group as described by stroke survivors or people with fatigue after acquired brain injury.
Methods: Members of two Facebook groups were invited to participate in the study. Semi-structured interviews were conducted in which the participants (stroke n=14, fatigue n=8) were encouraged to describe their experiences of participating in the Facebook group in a narrative manner. The interviews were audio-recorded, transcribed verbatim and analyzed using the empirical phenomenological psychological method.
Results: The lived experience of being a member in a Facebook group for people with a diagnosis or a specific symptom presented a common meaning structure with three main characteristics: learning through others’ experiences, confirming a new self, and finding a new role in supporting others. Together the categories reflected a process whereby members moved from being newcomers with more pronounced needs to learn from others' experiences and have their own experiences validated, to taking on a role as adviser and supporting others. The participants valued that the information from peers was accessible 24/7 and unique i.e., not available elsewhere, built on true understanding and different from information supplied by health care professionals.
Conclusions: A Facebook group has the potential to provide relevant and accessible peer-support. Thus, training in the use of social media could be part of stroke rehabilitation when relevant.
Disclosures of Interest: No
Abstract N°: 2743
WHAT IS BEING SHARED IN A FACEBOOK GROUP FOR STROKE SURVIVORS?
Malin Tistad*1,2, Lill Hultman1, Ulla-Karin Schön3, Elisabet Åkesson1, Jeanette Nelson1, Fredrik Sandman1, Mikael Åkerlund1, Lena von Koch1
1Karolinska Institutet, 2Dalarna University, 3Stockholm University
On behalf of:
Background and aims: Facebook groups are arenas where stroke survivors and relatives share their experiences of life after stroke. With the view of Facebook groups as peer-support groups in which stroke survivors set the agenda, the aim of this study was to increase the knowledge about what is being shared in posts and comments in a Facebook-group for stroke survivors.
Methods: People with own experience of stroke were co-researchers in all phases of the research project. We collected data on posts and comments in a Facebook group for stroke survivors during a 3-month period and analysed the posts (n=397) using the principles of qualitative content analysis.
Results: The six categories of posts; Consequences of stroke and their challenges in everyday life, Living in proximity to health care services and bodily symptoms, The path to or from the labor market, Setbacks and frustration, Enjoying everyday life and making progress, and Everyday life goes on described experiences of everyday life, stories of everyday events and requests to take part of other members’ experiences. In the comments generated by the posts, members confirmed experiences described in the posts and provided additional perspectives based on their experience. In addition, new discussions on related topics and occasionally also conflicts arose in the comment threads.
Conclusions: Sharing experiences of living with the consequences of stroke, learning from others’ experiences and getting recognition of what you are going through seemed valuable. Rehabilitation services could inform stroke survivors about Facebook-groups for stroke survivors when relevant.
Disclosures of Interest: No
Abstract N°: 3202
RECOVERY OF LANGUAGE AND DOMAIN-GENERAL ABILITIES DURING THE FIRST THREE MONTHS AFTER ANTERIOR CIRCULATION ISCHEMIC STROKE
Jon Martin Prieto*1, Karen Arellano Garcia2, Nerea Gorostiola Oyarzabal2, Alejandra Gomez1, Alain Luna1,3, Tomas Perez-Concha1,3, Aida Laguela1, Ventura Anciones1, Simona Mancini2, Maria del Mar Freijo Guerrero1,3
1Hospital Universitario Cruces, Neurology, 2Basque Center on Cognition, Brain and Language, 3Biocruces-Bizkaia Health Research Institute.
On behalf of:
Background and aims: The extent to which language disorders concur in left hemispheric strokes with impairments in non-linguistic general domain skills (GDs), such as attention, memory and reasoning, is still under debate. The aim of this study is to observe for 3 months the recovery of these domains in patients admitted to our centre for anterior circulation ischemic stroke.
Methods: 25 patients divided according to the affected hemisphere (left, LH, n=14; right, RH, n=11) completed the study. Exclusion criteria were: a) previous stroke, b) previous cognitive impairment and c) any other condition that could interfere with the performance of the tasks. Different linguistic (LNG) levels -phonology, grammar, semantics-, and GD abilities -attention (A), reasoning (R), memory (M)- were evaluated at three different time points: first week (TP1), one month (TP2) and three months (TP3) post-stroke.
Results: Clinical data and test scores are summarised in Table 1 and 2.
Conclusions: Left-sided stroke patients showed deficits not only in LNG but also in GD abilities. The recruitment of more patients for follow-up with moderate to severe language impairments may allow confirmation of these findings and the importance of exhaustive linguistic and non-linguistic assessment in stroke patients.
Disclosures of Interest: No
Abstract N°: 3298
MULTI-MUSCLE TMS MAPPING FOR THE ASSESSMENT OF MOTOR-CORTEX REORGANIZATION DURING HAND MOTOR-SKILL ACQUISITION
Anastasia Sukmanova1, Anastasia Asmolova2, Milana Makarova1, Pavel Novikov1, Vadim Nikulin3, Maria Nazarova*4
1National Research University Higher School of Economics, 2Max Planck School of Cognition, Germany, 3Max Planck Institute for Human Cognitive and Brain Sciences, 4Aalto University, The Department of Neuroscience and Biomedical Engineering, Espoo, Finland
On behalf of:
Background and aims: Here we investigated MCR changes using multi-muscle navigated transcranial magnetic stimulation (nTMS) motor mapping after finger individuation training in healthy subjects to translate the approach to stroke patients.
Methods: 31 right-handed male volunteers (18-36y.o.) underwent two nTMS mapping sessions separated by ten sessions of biofeedback training. Participants learned to abduct their thumb keeping the little finger still and vice versa. Apart from probing the ability to perform abductor pollicis brevis (APB) and abductor digiti minimi (ADM) independent contraction, we tested muscle strength and hand dexterity using a 9-hole peg test (9HPT).
Results: Muscle independence increased for both muscles (p<0.001), while muscle strength did not change significantly. 9HPT performance improved for right/left hands (p=0.001/0.01). There was a tendency for APB resting motor threshold (RMT) decrease (p=0.05). No group-level change was observed for MCR areas or APB-ADM MCR overlap. In comparison with SDC the TMS output substantial changes observed individually were non consistent, e.g., APB-ADM MCR overlap decreased and increased in 2 participants.
Conclusions: The finger independence training for the right hand increased hand dexterity in both hands, but no hand strength changes were observed, which is consistent with the studies in stroke showing that hand strength and dexterity do not recover in parallel (Xu et al., 2015; Barry et al., 2020). While previous studies with muscle peripheral constraint showed a decrease in the overlap between MCRs (Raffin & Siebner, 2019), using active muscle relaxation we saw non unidirectional changes, suggesting that muscle relaxation as an active process may increase the MCR area.
Disclosures of Interest: No
Abstract N°: 2447
DYNAMIC RESPONSES OF THE PREFRONTAL CORTEX DURING CELLO PERFORMANCE: INSIGHTS FROM FNIRS MONITORING IN PROFESSIONAL CELLISTS
Jong Wook Shin*1, Dae-Hyun Kim2
1Chungnam National University Sejong Hospital, Neurology, Sejong, South Korea, 2Dong-A University Hospital, Neurology, Busan, South Korea
On behalf of:
Background and aims: The impact of music on cerebral cortical activity is well-established, yet the specific influence of music-related tasks on prefrontal cortex activation remains an area of exploration. Utilizing functional near-infrared spectroscopy (fNIRS), we investigate the dynamic responses of the prefrontal cortex during music-related tasks, particularly in professional cellists.
Methods: Fifteen professional cellists (average age: 30.5 years) participated in the study, performing Johann Sebastian Bach's 'Suites for Cello Solos No. 1 in G Major, BWV 1007: I. Prelude.' Using a streaming video for consistent playing time, each session comprised resting, observing a scrolling sheet without sound, observing with listening sound, and playing the cello. Channels were categorized based on anatomical locations in the prefrontal area.
Results: Significant prefrontal activation was observed in the left upper medial frontal lobe during experimental tasks (p = 0.025), notably pronounced during cello playing. Even after motion correction (p = 0.008), sustained activation persisted. Hemispheric asymmetry surrounding the dorsolateral prefrontal lobe was exclusively detected during cello playing (p = 0.034). Epoch analysis revealed hyperactivation, especially in the first and second quarters of the music, across all channel groups.
Conclusions: Our study unveils the prefrontal cortex's involvement in music-related tasks, with playing the cello inducing substantial activation, particularly within the dorsolateral prefrontal cortex. Despite confinement to the prefrontal lobe, our findings provide nuanced insights into the effects of music-related tasks, emphasizing the significant role of the dorsolateral prefrontal cortex during cello performance.
Disclosures of Interest: No
Paper Poster - SAH, Aneurysms and Vascular Malformations
Abstract N°: 2641
ASSOCIATION BETWEEN FEMALE-SPECIFIC RISK FACTORS AND THE INCIDENCE OF ANEURYSMAL SUBARACHNOID HEMORRHAGE IN THE UK BIOBANK
Maaike J.A. van Eldik*1, Jos P. Kanning1, Ynte Ruigrok1
1UMC Utrecht, Neurology and Neurosurgery, Utrecht, Netherlands
On behalf of:
Background and aims: Aneurysmal subarachnoid hemorrhage (ASAH) occurs more often in women than in men, suggesting that female-specific risk factors may play an important role in this disease. Previous research has explored the association of such factors with ASAH, but with conflicting results, while some factors remain unexplored. Therefore, we aimed to assess the association between female-specific risk factors and the incidence of ASAH in a large population-based cohort.
Methods: Using data from the prospective UK Biobank study, the association between gestational hypertension, preterm delivery, oral contraceptive (OC) use, hormonal replacement therapy (HRT) use, parity and age at menarche and incident ASAH was assessed using Cox regression analysis. Participants with a previous history of ASAH at baseline or missing data were excluded. We adjusted for the known risk factors for ASAH age, family history of stroke, hypertension, smoking status, alcohol consumption, and educational level.
Results: Of the 242 644 included female participants, ASAH occurred in 475 (0.20%) during a median follow-up time of 6 years (IQR 4-9). HRT use was associated with an increased risk of ASAH (HR 1.26 [95%CI 1.03–1.54]). In addition, OC use (HR 1.24 [95%CI 0.98-1.56]) and parity (HR 1.10 [95%CI 0.98-1.19]) were associated with ASAH, although these findings were not statistically significant. Other risk factors showed no association with ASAH.
Conclusions: HRT use, and possibly OC use and parity, are female-specific risk factors for ASAH. Further research is needed to identify additional female-specific risk factors contributing to the female predominance in ASAH.
Disclosures of Interest: No
Abstract N°: 870
ASSOCIATION OF EXTERNAL VENTRICULAR DRAIN DURATION AND CEREBRAL INFARCT IN ANEURYSMAL SUBARACHNOID HEMORRHAGE
Ali Mahta*1,2, Ariyaporn Haripottawekul2, Wendy Gonzalez2, Elijah M. Persad-Paisley1, Sarah Uriarte1, Karen Furie1
1Warren Alpert Medical School of Brown University, Neurology, Providence, United States, 2Brown University, Providence, United States
On behalf of:
Background and aims: The optimal duration of external ventricular drain (EVD) in patients with aneurysmal subarachnoid hemorrhage (aSAH) is debatable. We sought to determine the association of EVD duration with outcomes, including cerebral infarct.
Methods: We performed a retrospective study of a prospectively collected cohort of consecutive patients with aSAH who were admitted to an academic center from 2016 to 2023. Multivariate logistic regression was used to determine the association of EVD duration with outcomes, including cerebral infarct prior to discharge (excluding immediate post aneurysm securement infarcts) and a shift in 3-month modified Rankin Scale (mRS). Hospital mortalities were excluded in functional outcome ordinal shift analysis.
Results: We reviewed 429 cases of aSAH and included 306 patients who received EVD with mean age 57.9 years (SD 13.9), 67% female and 69% white. EVD duration was longer in patients with cerebral infarcts compared to those without infarcts (mean 15.8 days [SD 13.7] vs 13 [11.8]; p=0.016). Longer EVD duration was associated with higher odds of cerebral infarct (OR 1.04 for each day increase, 95% CI 1.01-1.07; p=0.003) independent of age, sex, Hunt and Hess grade, modified Fisher score and aneurysm securement mode. However, EVD duration was not associated with worse functional outcome (OR 1.02, 95% CI 0.98-1.06; p=0.23) when adjusted for other predictors.
Conclusions: Longer EVD duration may not improve functional outcome and can be associated with more cerebral infarcts in patients with aSAH. Unnecessary prolongation of EVD duration should be discouraged. Larger prospective studies are needed to confirm these findings.
Disclosures of Interest: No
Abstract N°: 1190
EFFICACY AND SAFETY OF INTRAARTERIAL RESCUE THERAPIES FOR THE MANAGEMENT OF REFRACTORY DELAYED CEREBRAL ISCHEMIA
Amr Abdulazim*1, Neele Riemann1, Hannah Roth1, Marina Heilig1, Fabian Wenz1, Katharina Hackenberg1, Christoph Groden2, Mervyn Vergouwen3, Gabriel Rinkel1,3, Nima Etminan1
1University Medical Center Mannheim, University of Heidelberg, Department of Neurosurgery, Mannheim, Germany, 2University Medical Center Mannheim, University of Heidelberg, Department of Neuroradiology, Mannheim, Germany, 3UMC Utrecht Brain Center, University Medical Center Utrecht, Utrecht University, Department of Neurology and Neurosurgery, Utrecht, Netherlands
On behalf of:
Background and aims: We analysed the risk-benefit-ratio of intraarterial rescue therapies for intractable delayed cerebral ischemia (DCI) after aneurysmal subarachnoid haemorrhage (SAH).
Methods: A prospective cohort of 379 SAH patients between January 2016 and December 2022 was treated using a standardized, escalating treatment protocol in case of refractory DCI: 1) induced hypertension, 2) twice solitary intraarterial nimodipine bolus, 3) intraarterial catheter for continuous nimodipine administration over 48 hours with CT Perfusion imaging in between each escalating step. Efficacy was evaluated by means of clinical (recovery of a neurological deficit) and/or radiological (resolution of a CT perfusion deficit) improvement. Safety was evaluated by means of treatment associated complications.
Results: Among the 379 SAH patients, 126 received at least one intraarterial nimodipine bolus application. Clinical improvement occurred in 33 (26.2%) and radiological improvement in 42 (33.3%) patients. A second intraarterial nimodipine bolus was performed in 64 (51%) patients. Of those, 15 (23%) had clinical and 30 (47%) radiological improvement. An intraarterial catheter was used in 16 (25%) among those patients. Overall, a total of 43 patients received an intraarterial catheter. Clinical and/or radiological improvement was notable in 25 (58%) patients; however, the unfavourable outcome rate was 65.1%. The overall catheter-associated complication rate was 27.9%, comprising catheter dysfunction (33.3%), catheter-associated haemorrhages (16.7%), catheter-associated infarctions (16.7%).
Conclusions: Intraarterial rescue therapy for intractable DCI is associated with clinical or radiological improvement in one out of 2 to 4 patients. This beneficial effect may be offset by treatment associated complications. Matched-pair analyses are warranted to further elucidate the impact on unfavourable outcome.
Disclosures of Interest: No
Abstract N°: 1432
PREVALENCE OF VITAMIN D DEFICIENCY AMONG HOSPITALIZED PATIENTS WITH ANEURYSMAL SUBARACHNOID HAEMORRHAGE AND TRAUMATIC BRAIN INJURY
Andia Mirbagheri*1, Nima Etminan1, Gabriel Rinkel1
1Mannheim University Hospital, Neurosurgery, Mannheim, Germany
On behalf of:
Background and aims: Inflammatory processes lead to the development and rupture of intracranial aneurysms. Vitamin D has shown to attenuate neuroinflammation. The aim of this study was to assess the prevalence of vitamin D deficiency in hospitalized patients with aneurysmal subarachnoid haemorrhage (aSAH) vs. a control group consisting of patients with traumatic brain injury (TBI).
Methods: We included patients diagnosed with aSAH (ICD-10 I60) and TBI (ICD-10 S06). Data about vitamin D deficiency (ICD-10 E55) for both diagnoses were collected. In a subgroup analysis, we distinguished between children/adolescents (<20 years), adults and elderly (>65 years). Data were obtained from the German Federal Statistical Office (DeStatis) and covered hospitalized and discharged patients with the respective diagnoses in Germany during the time period between January 1st and December 31st, 2022.
Results: 16,835 aSAH patients and 309,598 TBI patients were admitted in the one-year study period. The prevalence of Vitamin D deficiency was 2.07 % in aSAH vs. 1.23 % in TBI patients (OR=1.70, 95% confidence intervals (CI)=1.52-1.90). The prevalence of Vitamin D deficiency in children was 0% in aSAH vs. 0.04 % in TBI (OR infinite with zero cases/Haldane-corrected OR≈11.97, CI≈0.73-197.03), in adults 1.3 % in aSAH vs. 0.29% in TBI (OR=4.47, CI=3.43-5.81) and in elderly 2.4% in aSAH vs. 2.19% in TBI (OR=1.10, CI=0.97-1.25).
Conclusions: The prevalence of Vitamin D deficiency was distinctly higher in aSAH than TBI patients. Future studies with adjusted analysis for vascular risk factors are necessary to further assess potential benefits of nutritional supplementation for hospitalized patients.
Disclosures of Interest: No
Abstract N°: 1581
ASSOCIATION OF EPIGENETIC AGE ACCELERATION AND THE PRESENCE OF MULTIPLE ANEURYSM IN ANEURYSMAL SUBARACHNOID HEMORRHAGE
Elisa Cuadrado-Godia*1, Adria Macias1, Antoni Suárez-Pérez1, Marta Vallverdu-Prats1, Isabel Fernández-Pérez1, Ana Rodríguez-Campello1, Eva Giralt-Steinhauer1, Angel Ois1, Jordi Jiménez-Conde1, Joan Jimenez-Balado1
1Hospital del Mar Research Institute, Neurology, Barcelona
On behalf of:
Background and aims: The contribution of epigenetics on the development of cerebral aneurysms is poorly understood. We studied the link between epigenetic age acceleration (AgeAcc) and the occurrence of multiple aneurysms (MA) in patients with aneurysmal subarachnoid hemorrhage (aSAH).).
Methods: Prospective study including patients with aSAH and available DNA methylation data obtained from peripheral blood within the first 24 hours via the Illumina-EPIC chip. Biological age (B-age) was determined using various epigenetic clocks (Hannum, Horvath, Levine, Zhang-EN, and Zhang-BLUP). AgeAcc was calculated as the residual from regressing chronological age (C-age) against the difference between C-age and B-age. Differences in AgeAcc based on the presence of single or MA were assessed through an ANCOVA model adjusted for potential confounders: sex, hypertension, diabetes, smoking status and time since onset of symptoms
Results: We recruited 277 patients and average C-age was 55.0 years, with a predominance of females (66.8%). A total of 88 (31.7%) had MA. We found a significant association between higher AgeAcc, as indicated by Levine’s clock, and MA (Average AgeAcc: 0.96 years [95%CI: -0.17 to 2.08] vs -0.46 years [95%CI: -1.22 to 0.30]; p-value = 0.040). No significant differences were observed for other epigenetic clocks. (Figure-1)
Conclusions: aSAH patients with MA showed a higher AgeAcc in Levine’s clock, implicating Epigenetic Biological Age in cerebral aneurysm pathogenesis. Levine's clock, incorporating biomarkers and factors like hypertension and smoking, both associated with aSAH pathophysiology, provides enhanced understanding of age-associated changes contributing to cerebral aneurysm formation. Further replication of these findings is warranted.
Disclosures of Interest: No
Abstract N°: 1824
VASODILATATION AFTER INTRA-ARTERIAL NICARDIPINE OR DANTROLENE INFUSION IN ANIMAL MODEL OF CEREBRAL VASOSPASM
Young Dae Cho*1
1Seoul National University, South Korea
On behalf of:
Background and aims: Intra-arterial (IA) infusions of calcium channel blockers (CCBs) have been widely applied in treating medically refractory vasospasm. However, surprisingly little is known regarding their vasodilatory duration. This study was undertaken to compare attributes of nicardipine and dantrolene, focusing on efficacy and capacity for sustained vasodilation.
Methods: In New Zealand white rabbits (N=22), vasospasm was individually provoked through experimentally induced subarachnoid hemorrhage and confirmed via conventional angiography, grouping animals by IA-infused drug (nicardipine vs dantrolene). Controls received normal saline. After chemoangioplasty, follow-up angiography was performed at intervals of 1-3 hours for 6 hours to compare vasospastic and dilated (ie, treated) arterial diameters. Drug efficacy, duration of action, and changes in mean arterial pressure (relative to baseline) were analyzed by group.
Results: Compared with controls, effective vasodilation was evident in both nicardipine and dantrolene test groups after IA infusion. Vasodilatory effects of nicardipine peaked at 1 hour, returning to former vasospastic states at 3 hours. In dantrolene recipients, vasodilation endured longer, lasting >6 hours. Only the nicardipine group showed a significant 3-hour period of lowered blood pressure.
Conclusions: Unlike the vasodilatory action of a CCB, sustained for <3 hours after IA infusion, the effect of dantrolene endured for >6 hours. This outcome suggests that IA dantrolene infused alone or together with a conventional CCB infusion may be a new means of prolonging vasodilatory effect. Further research is needed to assess durations of IA-infused vasodilatory drug based on perfusion status.
Disclosures of Interest: No
Abstract N°: 2407
PATIENT-SPECIFIC BLOOD CLEARANCE AFTER ANEURYSMAL SUBARACHNOID HEMORRHAGE. A 5-YEAR PROSPECTIVE OBSERVATION OF DCI PREVENTION
Roland Roelz*1, Peter Reinacher1, Juergen Beck1
1Medical Center - University of Freiburrg, Neurosurgery, Freiburg im Breisgau, Germany
On behalf of:
Background and aims: Delayed cerebral infarction (DCI) is a severe complication after aneurysmal subarachnoid hemorrhage (aSAH). Clearance of intracranial blood targets the root cause of vasospasm and may reduce the DCI-risk. We have introduced four methods for blood clearance into the management of aSAH patients. Here, we report the results of their patient-tailored application in a prospective aSAH population.
Methods: 220 aSAH admitted 01/2019-12/2023 were included in a prospective registry. Exclusions: Patients not at risk for DCI (30 with early mortality/withdrawal of care <4 days) and 2 with admission delay, 7 patients who enrolled in a clinical trial precluding blood clearance.
78 of 181 patients (43%) were considered at risk for DCI and selected for intracranial blood clearance. Patient-specifically, intracranial blood clearance was enabled by either of these Methods: 1) n=35 (19%): stereotactic or endoscopic catheter ventriculocisternostomy (STX-VCS/eVCS), 2) n=20 (11%) intraoperative placement of a cisterno-ventricular catheter via the fenestrated lamina terminalis (oVCS), 3) n=19 (10%) ventriculo-lumbar (VLI), 4) n=4 (2%) lumbo-lumbar irrigation (LLI). Irrigation therapy was performed using the fibrinolytic urokinase and, upon detection of vasospasm, nimodipine. The primary endpoint was delayed infarction.
Results: We observed signs of overdrainage in 3 patients with lumbar catheters. Otherwise, no procedure-related complications occurred. Delayed infarcts occurred in 13 of 181 patients (7.2%). DCI was minor in 5 (3%) and moderate or severe in 8 (4%) patients.
Conclusions: We developed and implemented four interventions for intracranial blood clearance to prevent delayed infarction after aSAH. This patient-specific paradigm leads to a low rate of DCI.
Disclosures of Interest: No
Abstract N°: 2852
CLINICAL AND PATIENT-REPORTED OUTCOMES OF PATIENTS WITH SPINAL CAVERNOUS MALFORMATIONS
Abel Sandmann*1, Rens Kempeneers2, Rene van den Berg3, Dagmar Verbaan2, William Peter Vandertop2, Jonathan Coutinho1
Background and aims: We report clinical and patient-reported outcomes of patients with a spinal cavernous malformation (SCM), a rare neurovascular disorder.
Methods: We included consecutive patients with a SCM, diagnosed in 1995-2023. Patients were selected from our prospective neurovascular registry. We extracted data from medical records, and conducted follow-up by telephone and questionnaires, which included EQ-5D-5L and PROMIS-29. Domain sum scores were transformed to T scores, and compared with Dutch reference populations.
Results: Of 2548 patients in the registry, 27 (1%) patients had a SCM (median age 45 years [IQR 35-61]; 67% male). Six (22%) patients presented with symptomatic hemorrhage (SH), 12 (44%) with focal neurological deficits (FNDs) without hemorrhage, and 9 (33%) were asymptomatic. Localizations were cervical (n=7), thoracic (n=19), and lumbar (n=1). The median SCM size was 7 mm (IQR 4-11). Twenty-six (96%) patients were initially managed conservatively, while one patient underwent surgery after diagnosis due to the patient’s preference following a SH with urinary retention. During 66 months (IQR 45-120) median follow-up, 10 (37%) patients experienced a clinical event (SH [n=4]; FNDs [n=6]), and 5 (19%) underwent surgery. No patients died. The median EQ health score was 70/100 (IQR 54-80). Most PROMIS-29 T scores were similar to Dutch reference populations, but SCM patients reported more Anxiety/Fear (57.5 versus 50.3, p=0.002), Sleep Disturbance (55.9 versus 49.9, p=0.035), and problems in Social Roles/Activities (54.7 versus 49.2, p=0.029).
Conclusions: One-third of the SCM patients suffered a clinical event during follow-up. Patient-reported outcomes were comparable with Dutch reference populations, but worse regarding anxiety, sleep, and social participation.
Disclosures of Interest: No
Abstract N°: 3250
RISK FACTORS AND IMPACT ON OUTCOME OF DELAYED CEREBRAL ISCHEMIA AFTER ANEURYSMAL SUBARACHNOID HAEMORRHAGE: A MULTICENTER OBSERVATIONAL STUDY
Ingrid Marques*1, Carla Rynkowski2, Carolina Rouanet3, Natalia Vasconcellos3, Vanessa Colares3, Erica Adissy3, Cássia Shinotsuka4, Fernando Bozza1, Gisele Sampaio3, Pedro Kurtz4
1IDOR - Instituto D'Or de Pesquisa e Ensino, Neurology, Rio de Janeiro, Brazil, 2Hospital Cristo Redentor, Neurointensive Care Unit, Porto Alegre, Brazil, 3São Paulo Hospital, Vascular neurology, São Paulo, Brazil, 4Instituto Estadual do Cérebro Paulo Niemeyer, Neurointensive Care Unit, Rio de Janeiro, Brazil
On behalf of:
Background and aims: Predicting delayed cerebral ischemia (DCI) after aneurysmal subarachnoid haemorrhage (SAH) remains challenging, especially in middle-income countries, where resources are limited, and data is scarce. We aimed to identify risk factors for cerebral infarction associated with DCI and evaluate the impact of DCI on outcomes.
Methods: Data were collected prospectively between 2016 and 2022 in three centres with high volume of SAH hospitalisations. Demographic, clinical, and radiological data were collected, as well as functional outcomes at hospital discharge. Mixed logistic regression models were used to investigate the association between risk factors and the development of cerebral infarction.
Results: 1,280 patients were analyzed. The median age was 55 (46, 63) years, 73% were female, and 28% had poor clinical grade on admission (World Federation Neurological Surgeons – WFNS – 4 or 5). 297 (23%) patients developed cerebral infarction due to DCI. Hospital mortality was 25%, and 50% had poor functional outcomes at hospital discharge (modified Rankin 4 to 6). In multivariable mixed regression, premorbid arterial hypertension (Odds ratio [OR] 1.4, 95%CI 1.04-1.9), poor clinical grade (OR 1.72, 95%CI 1.24-2.4), and modified Fisher (mFisher) 3 or 4 (OR 1.65, 95%CI 1.2-2.29) were associated with DCI, after adjusting for covariates. Moreover, patients with DCI were 3 times more likely to have an unfavorable outcome at hospital discharge.
Conclusions: Hypertension and measures of clinical and radiological severity were the main risk factors for cerebral infarction after SAH in this large cohort from a middle-income country.
Disclosures of Interest: No
Abstract N°: 235
ADDITIONAL RELEVANT INTRACRANIAL FINDINGS IN PERSONS SCREENED WITH MR FOR INTRACRANIAL ANEURYSMS
Philippine B. van Wijngaarden*1, Gabriël J.E. Rinkel1, Irene C. van der Schaaf2, Liselore A. Mensing1, Ynte M. Ruigrok1, Mervyn D.I. Vergouwen1
1University Medical Centre Utrecht, Department of Neurology and Neurosurgery, 2University Medical Centre Utrecht, Department of Radiology
On behalf of:
Background and aims: Radiological screening for intracranial aneurysms (IAs) may identify other relevant intracranial findings. We investigated their prevalence on MR in persons screened for IAs.
Methods: We included all persons who were screened for the presence of IAs with brain MRI/MRA between 1996-2022 because of a family history of aneurysmal subarachnoid haemorrhage (aSAH) or autosomal dominant polycystic kidney disease (ADPKD). We reviewed radiology reports of initial and repeated brain MR to identify additional intracranial findings that needed follow-up or treatment, or carried a risk of becoming symptomatic.
Results: We included 766 persons (positive family history of aSAH: n=681; ADPKD: n=85) who had 1446 MRI/MRAs. At initial screening, 49 additional relevant intracranial findings were reported in 47 persons (6.1%;95%CI:4.7-8.1%). Of all included persons, 338 (44%) underwent one (n=154) or more (n=184) follow-up screenings (total MRI/MRAs at follow-up: n=680). In 15/338 persons (4.4%;95%CI:2.7-7.2%), 16 new additional relevant findings were reported at a median follow-up duration of 10 years (IQR 5-12).
Conclusions: Persons who are counselled for screening for IAs should be informed that there is a six percent chance of identifying an additional finding that requires follow-up or treatment, or may become symptomatic. Additionally, after 10-year follow-up screening there is a four percent chance of identifying a new additional relevant finding. The impact of such findings on quality of life needs further study.
Disclosures of Interest: No
Abstract N°: 1519
SEX DISPARITIES IN INTRACRANIAL ANEURYSM TRIAL PARTICIPATION
Helena Janssen*1, Paut Greebe2, Melanie Anderson3, Gabriel Rinkel2, Joanna Schaafsma1
1Toronto Western Hospital, Department of Neurology, Toronto, Canada, 2UMC Utrecht, Department of Neurology, Utrecht, Netherlands, 3Toronto Western Hospital, University Health Network - Library and Information Services, Toronto, Canada
On behalf of:
Background and aims: Underrepresentation of women in controlled clinical trials (CCT) could affect results, reduce the generalizability and therefore validity of evidence guiding treatment. Around 65% of patients with aneurysmal subarachnoid haemorrhage (aSAH) and unruptured intracranial aneurysms (UIAs) are women (1,2), therefore female underrepresentation in clinical trials may distort evidence in particular in these diseases. We performed a systematic review and analysis to assess female participation in clinical trials on aSAH and UIAs and to determine associated factors with their participation.
Methods: Ovid Medline, Embase, Cochrane Central, Clinicaltrials.gov, and International Clinical Trials Registry (ICTRP) were searched for all human CCTs on aSAH and UIAs, published from inception to June 2023, with a minimal sample size of 100 patients and that required informed consent for participation. Two independent authors performed screening and data extraction. The primary outcome was the proportion of women enrolled.
Results: The search identified 6727 records. After deduplication, we screened title and abstract from 3667 records, assessed full-text from 225 records, and included 160 CCTs. Of 42,631 included patients (mean age 55) 27,522 were women, resulting in a proportion of 64.6% (95% CI: 64.1-65.0).
Conclusions: Preliminary analyses showed that overall women are not underrepresented in clinical trials on intracranial aneurysms and aneurysmal subarachnoid haemorrhage. Further analyses will explore time trends and geographical variance and will assess for sex disparities according to intervention type, recruitment and consent procedure, sex of principal investigator/author and burden of trial participation.
Disclosures of Interest: No
Abstract N°: 1942
PROGNOSTIC RELEVANCE OF BRAIN MYELIN VOLUME AFTER SAH: A LONGITUDINAL QUANTITATIVE SYNTHETIC MRI STUDY
Daniel Santana*1, Laura Llull2, Carlos Laredo3, Eloy Martínez-Heras3, Luigi Zattera4, Gabriel Pujol4, Antonio Lã³pez-Rueda5, Sara Llufriu2, Ramon Torné6, Sergio Amaro2
1Hospital Germans Trias i Pujol, Neurology, Badalona, Spain, 2Hospital Clínic de Barcelona, Neurology, Barcelona, Spain, 3Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Magnetic Resonance Core Facility, Barcelona, Spain, 4Hospital Clínic de Barcelona, Anaesthesiology, Barcelona, Spain, 5Hospital Clínic de Barcelona, Neurorradiology, Barcelona, Spain, 6Hospital Clínic de Barcelona, Neurosurgery, Barcelona, Spain
On behalf of:
Background and aims: Spontaneous subarachnoid haemorrhage (SAH) induces an early and diffuse white matter and myelin injury. We aimed to evaluate the prognostic relevance of myelin volume loss after SAH
Methods: We included 73 SAH sufferers (mean age=53, WFNS=I-III 61%, Fisher 4=56%) evaluated longitudinally with quantitative Synthetic-MRI at 5+/-2 days (T0) and 90 days (T90) after bleeding. Synthetic-MRI allowed the automatic extraction of intracranial volumes, including the myelin fraction volume (MyFV). Poor clinical outcome was defined as a modified Rankin Scale score >2 at 90 days. Adjusted logistic regression analyses were used to assess the association of MyFV with clinical outcome.
Results: Overall, lower MyFV at T0 and T90 were significantly associated with older age and with higher initial clinical and radiological bleeding severity. MyFV at T90 was also associated with the incidence of delayed cerebral ischemia. Patients with poor clinical outcome had lower MyFV both at T0 (poor versus good clinical outcome, mean [SD] 10.3[1.4]% versus 11.9[1.8]%, p=0.004) and at T90 (10.5[2.1]% versus 12.5[1.6]%, p<0.001). In multivariate regression models adjusted by confounders, lower MyFV remained associated with poor clinical outcome both at T0 (aOR=0.63, 95%CI=0.41-0.98, p=0.040) and at T90 (aOR=0.50, 95%CI=0.30-0.82), p=0.007). MyFV increased significantly from T0 to T90 in patients with good clinical outcome (+0.6%, p<0.001) but not in those with poor outcome (+0.2%, p=0.621).
Conclusions: These findings suggest that in SAH survivors, persistently low MyFV is associated with poor clinical recovery. Myelin protection and/or repair could represent a potential therapeutic goal for improving clinical recovery after SAH.
Disclosures of Interest: No
Abstract N°: 2043
IMPACT OF ACUTE HYDROCEPHALUS AFTER ANEURYSMAL SAH ON LONGITUDINAL NEUROPSYCHOLOGICAL OUTCOME
Vincens Kälin1, Menno Germans2, Philippe Bijlenga3, Roy Thomas Daniel4, Thomas Robert5, Johannes Goldberg6, David Bervini6, Luca Regli2, Martin Stienen1, Isabel Charlotte Hostettler*1
On behalf of: On behalf of the MOCA-DCI study group
Background and aims: Hydrocephalus occurs about 67% of patients with aneurysmal subarachnoid hemorrhage (aSAH). It is associated with increased morbidity and mortality. While a deletrious effect of acute hydrocephalus on short-term cognitive functions is known, its longitudinal effect, is poorly understood. The aim of this study was to evaluate its effect on longer-term cognitive outcome.
Methods: Prospective, observational multicenter study (8 Swiss centers) including patients from all cultural and linguistic Swiss areas. Alert patients (Glasgow Coma Scale ⩾13 points 48h-72h after aSAH) underwent serial neuropsychological assessments (Montreal Cognitive Assessment [MoCA]) by a trained, independent neuropsychologist getting baseline (first assessment < 72 hours after aSAH), short- (14-28 days [discharge]) and longterm assessment (3 months).
Results: We included 112 patients (87.5%). Mean age was 53.9 years (13.9 SD), 66.1% were female. Forty patients (35.7%) developed acute hydrocephalus, ten (25%) needed a permanent ventriculo-peritoneal shunt. MoCA z-score was significantly lower in the hydrocephalus group both at baseline (-2.84 vs -1.12, p<0.001) and at discharge (0.53 vs -3.35, p<0.001). Patients with hydrocephalus were more likely to experience a decline of ⩾2 points at discharge (OR 2.76, 95% CI 1.16–6.53; p=0.02). However, this effect was not evident at the 3 month follow-up (OR 1.22, 95% CI 0.32-4.62; p=0.77).
Conclusions: Lower-grade aSAH patients with hydrocephalus have worse short-term but noth 3 months cognitive function compared to those without. This likely indicates the beneficial effect of restored cerebro-spinal fluid flow or its permanent diversion. Hydrocephalus is an independent risk factor for a temporary, but clinically meaningful decline in neurocognitive function.
Disclosures of Interest: No
Abstract N°: 2909
INTRACRANIAL ANEURYSMS RISK STRATIFICATION USING RADIOMICS
Elena Sagues Sese*1, Arshaq Saleem2, Sricharan Veeturi3, Diego Ojeda1, Carlos Dier Melo1, Edgar Samaniego1
1University of Iowa Hospitals & Clinics, Neurology, Iowa City, United States, 2Roy J. and Lucille A. Carver College of Medicine, Iowa City, United States, 3University at Buffalo (South Campus), Buffalo, United States
On behalf of:
Background and aims: Radiomics is a novel image analysis tool that offers a voxel by voxel quantification of medical images signal, shape and texture characteristics. Our aim is to determine if radiomics analysis of intracranial aneurysms (IAs) can help predict their symptomatic presentation.
Methods: Patients with saccular, >2mm IAs were scanned using a high-resolution vessel wall imaging 3T MRI at the University of Iowa. After corregistration of the T1 and T1+Gd sequences, Slicer 3D was utilized to segment the aneurysms shell and radiomic features using PyRadiomics extension (Figure 1). Machine learning was used to analyze the data in conjunction with the morphology and clinical variables to create nomograms (Figure 2).
Results: Ninety patients with 104 IAs were included. Twenty-nine were symptomatic, defined as cranial nerve palsy or sentinel headache. We selected 87 radiomic features that were significantly different between symptomatic and asymptomatic IAs. The clinical nomogram combining clinical, morphological and radiomic features achieved an AUC=0.83, 89% sensitivity and 73% specificity in predicting IAs symptomatic presentation.
Conclusions: Radiomics may improve the prediction of IAs symptomatic presentation and may aid in the stratification of their risk of rupture. This information is essential to guide therapeutical management of unruptured IAs.
3T HR-MRI image acquisition and segmentation in 3D Slicer.
Nomogram for symptomatic presentation prediction.
Disclosures of Interest: No
Abstract N°: 2923
NEUTROPHIL EXTRACELLULAR TRAPS IN SUBARACHNOID HEMORRHAGE (NET-SAH): A PROSPECTIVE OBSERVATIONAL STUDY
1University Hospital Augsburg, Neurology, Augsburg, Germany, 2Center for Molecular and Vascular Biology, KU Leuven, Cardiovascular Sciences, Leuven, Belgium, 3University of Pennsylvania, Neurology, Philadelphia, United States
On behalf of:
Background and aims: Delayed cerebral ischemia (DCI) is a dreaded complication in patients with subarachnoid hemorrhage (SAH). Biomarkers of DCI might help to define an early therapeutic time window during which DCI could be preventable. NETs are the product of neutrophil hyperactivation and have been shown to be involved in inflammatory and thrombotic processes. The overall goal of NET-SAH is to measure NETs biomarkers in the plasma of SAH patients with and without DCI.
Methods: NET-SAH is a prospective single-center study at the University Hospital Augsburg, Germany (DRKS, #DRKS00025118). SAH patients were enrolled within 48 hours of symptom onset. Biomarker assays were performed on plasma samples collected on days 2, 7, and 10 after onset (NET components cell-free DNA; myeloperoxidase (MPO)-DNA complexes; citrullinated histone H3-DNA complexes; along with DNase activity and peptidylarginine deiminase 4 (PAD4)).
Results: From November 2021 to January 2023, 40 SAH patients were enrolled. All NET biomarkers were elevated throughout the follow-up period, with increase from day 2 to 7. DNase levels ranged from 41.3-318.9% of a reference value on day 2 and rose up to 786.4% on day 10. We will report on further results of plasma analyses of NET components comparing SAH patient with and those without DCI and will present further analyses using clinical, imaging and NET plasma data.
Conclusions: The results of our single-center study will identify a potential role of neutrophil extracellular traps as predictive biomarkers of DCI in patients with subarachnoid hemorrhage.
Disclosures of Interest: No
Abstract N°: 1448
VITAMIN D DEFICIENCY ASSOCIATED WITH HIGHER INCIDENCE OF ANEURYSMAL SUBARACHNOID HAEMORRHAGE
Andia Mirbagheri*1, Svetlana Hetjens2, Jos Kanning3, Kristiina Rannikmae4, Nima Etminan1, Ynte Ruigrok3, Gabriel Rinkel1,3
1Mannheim University Hospital, Neurosurgery, Mannheim, Germany, 2Mannheim University Hospital, Medical Statistics and Biomathematics, Mannheim, Germany, 3UMC Utrecht, Neurology, Utrecht, Netherlands, 4University of Edinburgh, Centre for Medical Informatics, Usher Institute of Population Health Sciences and Informatics, United Kingdom
On behalf of:
Background and aims: Aneurysmal subarachnoid haemorrhage (aSAH) has been described as an inflammatory disease. Vitamin D has systemic anti-inflammatory properties. and may therefore reduce the risk of aSAH. We studied the association between vitamin D deficiency and the occurrence of aSAH in the UK Biobank (UKBB).
Methods: We analysed data from UKBB, a prospective population-based cohort study with 502,411 participants. We performed multivariate logistic regression analysis, adjusting for demographic characteristics and vascular risk factors, to compare serum 25-hydroxyvitamin D [25(OH)D] levels at baseline between participants who developed SAH and those who did not. 25(OH)D levels were categorized as sufficient (> 50nmol/L), deficient (<50nmol/L) and severely deficient (<30nmol/L).
Results: 1,447 aSAH occurred during the follow up period (April 2006 - May 2022). Compared to the general population, aSAH patients had a female preponderance (60.23% vs. 51.71%, p<0.0001) with a higher prevalence of smoking (67.09% vs 60.40%, p<0.0001) and higher systolic blood pressure (142.7 mmHg vs. 140mmHg, p<0.0001). Compared to participants with sufficient 25(OH)D levels, the odds ratio for those with vitamin D deficiency was 1.45 (95% Confidence intervals (CI) 1.04 – 2.20) and for those with severe vitamin D deficiency 2.05 (95%CI 1.28 – 3.29).
Conclusions: The incidence of aSAH was increased in patients with vitamin D deficiency and severe vitamin D deficiency in the large cohort study of the UK Biobank. Mendelian randomization will be used in a subsequent analysis to contextualise our results with regards to gene variant modulation.
Disclosures of Interest: No
Abstract N°: 282
HIGH RATES OF STROKE OR DEATH WITH ENDOVASCULAR OR NEUROSURGICAL TREATMENT OF RUPTURED BRAIN ARTERIOVENOUS MALFORMATIONS
Burak Konya*1, H. Bart van der Worp1, Joost Schouten2, Jeroen Boogaarts3, Pieter Jan Van Doormaal4, Albert van der Zwan1, Bart Emmer5, Ynte Ruigrok1, Irene van der Schaaf6
1UMC Utrecht, Neurology and Neurosurgery, Utrecht, Netherlands, 2Erasmus MC, Neurosurgery, Rotterdam, Netherlands, 3Radboud University Medical Center, Nijmegen, Netherlands, 4Erasmus MC, Radiology & Nuclear Medicine, Rotterdam, Netherlands, 5Amsterdam UMC, Radiology and Nuclear Medicine, Amsterdam, Netherlands, 6UMC Utrecht, Radiology, Utrecht, Netherlands
On behalf of:
Background and aims: Guidelines recommend interventional treatment for most patients with a brain arteriovenous malformation (bAVM) who present with intracranial haemorrhage. We assessed the risk of stroke or death in patients with a ruptured bAVM undergoing endovascular or neurosurgical treatment.
Methods: We performed a multicentre, retrospective cohort study in three university hospitals in the Netherlands of adult patients with a ruptured bAVM who underwent endovascular or neurosurgical treatment between 2012 and 2021. Treatment groups were based on the modality of the first treatment. The primary outcome was stroke or death at three months (±45 days) after the final treatment. A secondary outcome was dependency or death (mRS>2) at this timepoint.
Results: We included 202 patients, of whom 118 had an endovascular intervention and 84 neurosurgery. The primary outcome stroke or death occurred in 34 (28.8%) patients in the endovascular group and in 12 (14.3%) in the neurosurgical group. Stroke occurred in 33 (28.0%) and 12 (14.3%) patients, respectively, and death in 8 (6.8%) and 5 (6.0%). Most strokes were haemorrhagic. Before treatment, 36 (30.5%) patients in the endovascular and 30 (35.7%) in the neurosurgical group were functionally dependent. At final follow-up, 37 (31.4%) and 27 (32.1%) patients, respectively, were dependent or dead.
Conclusions: In this cohort of patients with ruptured bAVM, both endovascular and neurosurgical treatment were associated with a considerable risk of stroke or death, without an increase in long-term dependency. Data on the risk of treatment complications and on functional outcomes from other multicentre studies are needed.
Disclosures of Interest: No
Abstract N°: 848
A SURVEY FOR PATIENTS WITH INCIDENTAL CEREBRAL ANEURYSM IN EXPECTANT MANAGEMENT: THE SPICE STUDY
Jorge Rodriguez-Pardo*1, Jesús García-Castro1, Carlos Ignacio Gomez-Escalonilla Escobar2, Araceli García Torres3, Andrés García-Pastor4, Jose Vivancos5, Jose Fernandez-Ferro6, Antonio Cruz Culebras7, Joaquin Carneado-Ruiz8
1La Paz University Hospital, IdiPAZ, Neurology, Madrid, Spain, 2Hospital Clinico Universitario San Carlos, Neurology, Madrid, Spain, 3Hospital Universitario Fundación Jiménez Díaz, Neurology, Madrid, Spain, 4Gregorio Marañón General University Hospital, Neurology, Madrid, Spain, 5Hospital de La Princesa, Neurology, Madrid, Spain, 6Hospital Universitario Rey Juan Carlos, Neurology, Móstoles, Spain, 7Ramón y Cajal University Hospital, Neurology, Madrid, Spain, 8Puerta de Hierro Majadahonda University Hospital, Neurology, Majadahonda, Spain
On behalf of: on behalf of the Madrid Stroke Network
Background and aims: The increasing availability of neuroimaging has led to a rise in the identification of incidental cerebral aneurysms (CA). While surgical or endovascular treatment is recommended in specific cases, managing unruptured small aneurysms lacks substantial evidence. Typically, imaging follow-up is advised, but the optimal duration and frequency remain uncertain.
Methods: We conducted a multicenter cross-sectional study involving patients undergoing clinical-radiological follow-up for CA. Patients with history of stroke, polycystic kidney disease, symptomatic CA or neurosurgery were excluded. Patients received a 40-question survey via QR code, assessing the frequency and impact of clinical-radiological follow-up on their daily activities and quality of life. Responses were collected anonymously.
Results: Of 183 surveyed patients from 8 hospitals, we obtained 68 complete responses. 50 (74%) were women, median age (IQR) 62 (55-70). 53 (78%) underwent imaging at least once a year, and only 6 (9%) found them excessive. 39 (67%) patients found control imaging relieving, and 12 (18%) expressed concerns about the results. 19 patients (28%) reported a healthier lifestyle after diagnosis and 13 (19%) reported a negative impact (unchanged for 53%). 7 (10%) believed they would fare better without knowledge of their condition. 47 (69%) patients acknowledged to avoid or condition at least one activity/situation from a list. Overall, 81% reported their quality of life as good or better.
Conclusions: The diagnosis of incidental CA appears to significantly influence the activities of most patients. Encouragingly, expectant management does not appear to adversely affect the quality of life in most patients, who are comfortable with periodic imaging follow-ups.
Disclosures of Interest: No
Abstract N°: 1952
ENLARGED PERIVASCULAR SPACES AFTER SAH: DYNAMICS AND ASSOCIATION WITH EARLY BRAIN INJURY BIOMARKERS
M Angels Calderón1, Daniel Santana2, Carlos Laredo3, Luigi Zattera4, Gabriel Pujol4, Antonio Lã³pez-Rueda5, Ramon Torné6, Laura Llull7, Salvatore Rudilosso7, Sergio Amaro*7
1Universitat de Barcelona, School of Medicine, Barcelona, Spain, 2Hospital Germans Trias i Pujol, Neurology, Badalona, Spain, 3Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Magnetic Resonance Core Facility, Barcelona, Spain, 4Hospital Clínic de Barcelona, Anaesthesiology, Barcelona, Spain, 5Hospital Clínic de Barcelona, Neurorradiology, Barcelona, Spain, 6Hospital Clínic de Barcelona, Neurosurgery, Barcelona, Spain, 7Hospital Clínic de Barcelona, Neurology, Barcelona, Spain
On behalf of:
Background and aims: In preclinical models, subarachnoid haemorrhage (SAH) induces an acute dysfunction of the glymphatic system (GS). Enlarged perivascular spaces (EPVS) are essential components of the GS, but their association with early brain injury (EBI) biomarkers after SAH has not been described
Methods: In this longitudinal study we evaluated qualitatively the load of EPVS in centrum semiovale in 114 SAH sufferers who had MRI acquisitions within one week (T1) and at 3 months (T2) after bleeding and in 19 age and sex-matched controls (subjects with unruptured incidental aneurysms). EPVS were qualified with a validated scale (0:no EPVS; 1:<10; 2:11–20; 3:21–40; 4:>40). The change of EPVS from T1 to T2 was calculated after score subtraction. The association of EPVS with EBI biomarkers was evaluated with contingency tables.
Results: SAH sufferers had a significantly higher EPVS score both at T1 and T2 (median (IQR) 2 [2-3]) than controls (median (IQR) 1 [1-1]), p<0.001. From T1 to T2, EPVS burden increased in 17 (15%), remained stable in 85 (75%) and decreased in 12 (11%) patients. EPVS burden was higher in T1 than in T2 in patients with worse WFNS grade at hospital admission (p=0.032) and those with with global cerebral oedema (p=0.016) at initial neuroimaging
Conclusions: These findings suggest that SAH induces an increase in the burden of EPVS from the acute phase of bleeding that seems to be associated with a more severe disease, thus suggesting that the GS could be dysregulated after SAH.
Disclosures of Interest: No
Abstract N°: 313
PATIENT-REPORTED OUTCOMES OF PATIENTS WITH CONSERVATIVELY MANAGED CEREBRAL CAVERNOUS MALFORMATIONS
Abel Sandmann*1, Rens Kempeneers2, Rene van den Berg3, Dagmar Verbaan2, William Peter Vandertop2, Jonathan Coutinho1
Background and aims: There is uncertainty whether patients with a cerebral cavernous malformation (CCM) should be treated surgically or conservatively, resulting in practice variation among hospitals. Our aim was to collect patient-reported outcomes (PROs) from patients with conservatively managed CCMs.
Methods: We included consecutive adult patients with a CCM, diagnosed in 2000-2023, who were primarily managed conservatively. Patients were followed-up with telephone consultations and questionnaires, which included EQ-5D-5L and PROMIS-29. Domain sum scores were transformed to T scores, and compared with Dutch reference populations.
Results: We invited 246 patients to participate (median age 46 years [IQR 35-57]; 44% male), of whom 205 (83%) completed the questionnaire, median 62 months (IQR 38-95) after diagnosis. The median EQ health score was 75/100 (IQR 60-86). Most PROMIS-29 T scores were comparable to Dutch reference populations (Figure), but CCM patients reported more Anxiety/Fear (T score 54.1 versus 50.3, p<0.001) and Depression/Sadness (T score 52.4 versus 50.3, p=0.005). Interestingly, CCM patients experienced less pain than the Dutch reference population (T score 41.6 versus 55.6, p<0.001). Patients who presented with symptomatic hemorrhage (SH) more often reported anxiety and depression symptoms (45/96 [47%], versus 35/109 [32%], p=0.033), and overall reported worse quality of life (utility weighted EQ index scores 0.82 versus 0.85, p=0.037), than patients who presented with other or no symptoms.
Conclusions: In patients with conservatively managed CCMs, PROs were generally comparable to Dutch reference populations, except for mental domains. Presentation with SH was associated with worse PROs. These data imply that a primary conservative approach should be considered in CCM patients.
Disclosures of Interest: No
Abstract N°: 409
THE IMPACT OF ENTERAL NIMODIPINE ON ENDOTHELIAL CELL APOPTOSIS IN AN ANIMAL SUBARACHNOID HEMORRHAGE MODEL
Jeongwook Lim*1, Young Dae Cho2, Kwang Hyon Park1, Taeeun Yun1, Young Il Won1
1Chungnam University Sejon Hospital, Neurosurgery, Sejong, South Korea, 2Seoul National University Hospital, Radiology, Seoul, South Korea
On behalf of:
Background and aims: Enteral nimodipine is the most evidence-based and widely used drug for the treatment of delayed cerebral ischemia and is known to have various neuroprotective functions. However, the neuroprotective mechanism of nimodipine still remains unclear and the effects of nimodipine remain ambiguous. Herein, we studied the effect of enteral nimodipine on endothelial apoptosis after subarachnoid hemorrhage (SAH).
Methods: SAH was experimentally introduced in white rabbits (n=42) that were grouped: enteral nimodipine (group N, n=14); a control that received normal saline (group S, n=13); and a control without hemorrhage (group C, n=15). On the third day after SAH induction, the brain stem, including the vertebrobasilar vascular system, was extracted. The effects of enteral nimodipine were analyzed by group using histopathologic analysis, including immunohistochemical staining of apoptosis-related proteins (Bcl2 and Bax).
Results: Cytoplasmic vacuolation of smooth muscle cells was observed in groups S and N, and was more prominent in group S. Endothelial desquamation was observed only in group S. For the basilar artery, expression of Bcl2 and Bax in group N was lower than in group S, but significant differences were not observed. In penetrated arterioles, the expression of Bax in group N was significantly lower than that of group S (p < 0.001). The thickness of the tunica media in the basilar artery was thinner in group N than in group S (p < 0.001).
Conclusions: This study suggests that enteral nimodipine may have a neuroprotective function by inhibiting endothelial apoptosis in small arterioles and preventing smooth muscle cell proliferation in large arteries.
Disclosures of Interest: No
Abstract N°: 1193
THE EFFECT OF AN EXTENSIVE VERSUS A RESTRAINED MANAGEMENT FOR DELAYED CEREBRAL ISCHEMIA ON RADIOLOGICAL AND FUNCTIONAL OUTCOME
Amr Abdulazim*1, Hannah Roth1, Neele Riemann1, Marina Heilig1, Fabian Wenz1, Katharina Hackenberg1, Christoph Groden2, Mervyn Vergouwen3, Gabriel Rinkel1,3, Nima Etminan1
1University Medical Center Mannheim, University of Heidelberg, Department of Neurosurgery, Mannheim, Germany, 2University Medical Center Mannheim, University of Heidelberg, Department of Neuroradiology, Mannheim, Germany, 3UMC Utrecht Brain Center, University Medical Center Utrecht, Utrecht University, Department of Neurology and Neurosurgery, Utrecht, Netherlands
On behalf of:
Background and aims: The appropriate management of delayed cerebral ischemia (DCI) after aneurysmal subarachnoid haemorrhage (SAH) remains controversial. We compared outcomes between two high-volume SAH centres with considerably different approaches to DCI monitoring and treatment.
Methods: A prospective cohort of 379 SAH patients at centre E(xtensive) (January 2016 to December 2022) underwent regular CT-perfusion monitoring and escalating treatment for persistent DCI, including induced hypertension and intra-arterial rescue therapies. This group was compared to 591 SAH patients at centre R(estrained), managed through mere clinical monitoring and treatment targeting physiological medical conditions, without induced hypertension or rescue therapy. We compared DCI-related infarction and unfavourable outcome (modified Rankin scale 3-6) at 3 months. Odds ratios (OR) were calculated with 95% confidence intervals, adjusting for age, WFNS grade, modified Fisher score (mFS), aneurysm treatment modality (aOR*) and, additionally, external ventricular drain (EVD) treatment (aOR**).
Results: Centre E had a higher proportion of poor WFNS grade IV/V (40.1% vs. 31.1%), lower mFS (76.5% vs. 83.1%), and more surgical aneurysm repair (56.2% vs. 40.4%;) and EVD application (75.7% vs. 33.8%;). Incidence of clinical DCI was significantly higher in centre E (42.0% vs. 25.7%). DCI-related infarction rates were 18.2% (E) vs. 18.8% (R) (OR: 0.96 [0.69-1.34]). Adjusted ORs were aOR*: 0.85 [0.60-1.22] and aOR**: 0.68 [0.46-1.00]. Unfavourable outcome rates were 47.1% (E) vs. 40.3% (R) (OR: 1.32 [1.02-1.71]). Adjusted ORs were aOR*: 1.01 [0.74-1.39] and aOR**: 0.71 [0.50-1.02].
Conclusions:
Disclosures of Interest: No
Abstract N°: 2100
CLINICAL OUTCOME AND COMPLICATIONS AFTER ENDOVASCULAR SPASMOLYSIS IN PATIENTS WITH ANEURYSMAL SUBARACHNOID HEMORRHAGE
Julian Schwarting*1,2, Carolin Albrecht3, Dominik Trost1, Isabel Hostettler3,4, Martin Renz1, Bernhard Meyer3, Claus Zimmer1, Jannis Bodden1, Maria Wostrack3, Tobias Boeckh-Behrens1
1Technical University of Munich, Germany, School of Medicine, Klinikum rechts der Isar, Department of Diagnostic and Interventional Neuroradiology, Munich, Germany, 2Institute for Stroke and Dementia Research, München, Germany, 3Technical University of Munich, Germany, School of Medicine, Klinikum rechts der Isar, Department of Neurosurgery, Munich, Germany, 4Cantonal Hospital St. Gallen, Department of Neurosurgery, Switzerland
On behalf of:
Background and aims: Despite targeted standard therapy, aneurysmal subarachnoid hemorrhage (aSAH) frequently leads to cerebral vasospasms (CVS) of large cerebral arteries, reduced oxygen supply of the brain tissue, known as delayed cerebral ischemia (DCI), subsequent development of manifest cerebral infarction and poor neurological outcome. The objective of this study was to examine the potential benefits of endovascular therapy in the treatment of CVS following aSAH.
Methods: In our retrospective, monocentric cohort study, we included 310 aSAH patients developing CVS during the hospital stay and evaluated their clinical and radiographic outcomes. Severe vasospasm was defined by a mean velocity of >200 cm/sec in transcranial Doppler ultrasound and/or occurrence of new neurological deficits, and/or decrease of at least 2 points on the Glasgow Coma Scale (GCS), respectively.
Results: 92 patients (29.7%) underwent endovascular spasmolysis (eSL) due to persistent symptoms despite conservative therapy. Among endovascularly treated patients, 86% (n=79) improved in terms of angiographic results, 71% (n = 44) of 62 patients who underwent eSL due to symptomatic deterioration improved clinically. Clinical worsening due to progressive CVS occurred in 18% of cases (n=11). Periprocedural complications were observed in 4% (n=4).
Conclusions: eSL emerges as a safe and effective therapy for individuals experiencing delayed ischemic neurologic deficits triggered by large-artery vasospasm following aSAH. The implementation of a standardized, multi-step process for detection and medical management, coupled with well-defined criteria for endovascular interventions, proves to be an efficient preventative approach to enhance neurological outcomes after aSAH.
Disclosures of Interest: No
Abstract N°: 1440
RISK PREDICTION MODEL FOR OUTCOME IN ANEURYSMAL SUBARACHNOID HAEMORRHAGE(ASAH) BASED ON A DIRECTED ACYCLIC GRAPH (DAG)
Carlo Berzuini1, Louise Dulhanty2, James Galea3, Hiren Patel*2
1University of Manchester, Biostatistics, Manchester, United Kingdom, 2Geoffrey Jefferson Brain Research Centre, Manchester, United Kingdom, 3University hospital Wales, Cardiff, United Kingdom
On behalf of: British Neurovascular Group
Background and aims: Available aSAH prediction models lack generalisability and interpretability because they ignore causal relationships and overlook the relationship between variables which may influence prognosis. Our study aims to enhance predictive accuracy and usefulness of aSAH models by making the process of selection and confounding explicit, and fitting a model directed by the assumptions of a DAG.
Methods: Uk&Ireland data were analysed. Model development was performed using data from English centres (n=8963). Data from non-English centres were used for external validation (n=2226). We fitted several fixed effects models using accumulating information at key landmark times (At admission (Adm), External Ventricular Drain insertion (EVD) and aneurysm treatment (Rx)) to predict unfavourable (Glasgow Outcome score 1-3) outcome at 3 months. Discrimination and calibration characteristics were used to assess model performance.
Results: In the validation cohort, Adm, EVD and Rx models all had good discrimination with AUC statistics of (.841) (.864) and (.871) and good calibration characteristics. In the Adm model ( Age, hypertension, WFNS (injury severity), Fisher (blood load), centre, centre* WFNS, centre* Fisher) presence of interactions* suggest potential inter-centre differences in selection for admission. For the EVD model (Age, hypertension, WFNS, Fisher, centre, centre* WFNS, centre* Fisher, rebleed, EVD, EVD * WFNS), significant interaction between EVD and injury severity suggested heterogeneity of the effect of an EVD on outcome.
Conclusions: Reliable model fitting on a causal pathway in aSAH is possible using DAGs. Interpretation of the observed interactions in conjunction with the DAG may improve understanding of the cause of poor outcome in aSAH patients.
Disclosures of Interest: No
Paper Poster - Secondary Prevention
Abstract N°: 1081
THE LONGITUDINAL COURSE OF PHYSICAL ACTIVITY VARIES AMONG DISTINCT SUBPOPULATIONS POST-STROKE
1Norwegian University of Science and Technology, Department of Neuromedicine and Movement Science (INB), Trondheim, Norway, 2Yale University, School of Medicine, New Haven, United States
On behalf of:
Background and aims: Mean estimates of post-stroke physical activity (PA) may mask the heterogeneity during recovery. We aimed to objectively describe the longitudinal course of PA post-stroke and to uncover heterogeneity in activity patterns
Methods: We included stroke survivors who had at least 2 follow-up periods with a thigh-worn accelerometer for at least 3 days at 3-, 18-, and 36-months post-stroke. Linear mixed-effect modeling (LMM) estimated the overall course of PA measured as upright time (standing/walking), considering pre-stroke PA (HUNT1-questionnaire Index) as primary exposure variable. A multi-trajectory model, adjusted for sex, age, education, BMI, and single living identified groups of individuals exhibiting similar patterns in minutes of daily light PA, moderate PA, and the number of sit-to-stand transitions over 36-months.
Results: Altogether, 277 individuals (age: 70.1 (SD=10.9), 116 (41.9%) female) with mild to moderate strokes were included. The LMM showed that each additional unit of pre-stroke PA was associated with 20 min (95% CI 7 to 32) increase of upright time post-stroke. Four distinct PA trajectories were identified: 1) “Infrequent and Low” (25.6%); 2) “Infrequent and Intermediate” (32.4%); 3) “Frequent and Intermediate” (20.8%), and 4) “Frequent and High” (21.2%) (Figure 1).
Conclusions: The strong association of pre-stroke PA engagement with post-stroke upright time, emphasizes the habitual component of PA behavior. Individuals exhibit unique PA patterns that can be categorized into 4 distinct trajectory groups. The link between PA trajectory groups and recovery is yet to be established.
Disclosures of Interest: No
Abstract N°: 1213
EARLY STATIN USE FOR SECONDARY PREVENTION IN PATIENTS WITH ATRIAL FIBRILLATION AND RECENT ISCHAEMIC STROKE
Sylvia Choi1,2, Tommaso Bucci1,2,3, Jiayi Huang4, Kelvin K. H. Yiu4, Christopher Tsang4, Gary Lau4, Gregory Y. H. Lip1,2,5, Azmil Abdul-Rahim*1,2,6
1Liverpool Centre for Cardiovascular Science at University of Liverpool, Liverpool John Moores University and Liverpool Heart & Chest Hospital, Liverpool, United Kingdom, 2Department of Cardiovascular and Metabolic Medicine, Institute of Life Course and Medical Sciences, University of Liverpool, Liverpool, United Kingdom, 3Sapienza University of Rome, Department of General Surgery and Surgical Specialties “Paride Stefanini”, Italy, 4The University of Hong Kong, Cardiology Division, Department of Medicine, Hong Kong, China, 5Danish Center for Health Services Research, Aalborg University, Department of Clinical Medicine, Aalborg, Denmark, 6Whiston Hospital, Mersey and West Lancashire Teaching Hospitals NHS Trust, Stroke Division, Department of Medicine for Older People, Rainhill, United Kingdom
On behalf of:
Background and aims: We investigated the benefits of early statin use for secondary prevention of ischaemic stroke (IS) in patients with AF.
Methods: We conducted a propensity score matched analysis using data within TriNetX, a global federated healthcare database, comparing patients with AF and recent IS, who received statins within 28 days of their index stroke with those who did not. Primary outcomes included the 2-year risk of recurrent IS and major adverse cardiovascular events (MACE). Secondary outcomes included the 2-year risk of transient ischaemic attack (TIA), and intracranial haemorrhage (ICH).
Results: We identified 20,902 patients with AF and recent IS, of whom 7,500 (35.9%) received statins within 28 days of their stroke and 13,402 (64.1%) did not. We included 11,182 well-matched patients (mean age 73.7±11.5; 5,277 (47.2%) female). Patients who received early statins had significantly lower risk of the primary and secondary outcomes, including recurrent IS (Hazard Ratio [HR]: 0.45, 95% Confidence Interval [CI]: 0.41–0.48, p<0.001), MACE (HR: 0.48, 95%CI: 0.45-0.52, p<0.001), TIA (HR: 0.37, 95%CI: 0.30-0.44, p<0.001), and ICH (HR: 0.59, 95%CI: 0.47-0.72, p<0.001) (Figure.1). Subgroup analyses (Figure.2) using: (1) patients with optimal LDL-cholesterol; (2) low, moderate and high intensities of statins; and (3) lipophilic vs hydrophilic statins demonstrated a lower risk of recurrent IS. A significant reduction in ICH was only observed in the lipophilic subgroup (vs. hydrophilic subgroup).
Conclusions: Early statin use may have an important role in secondary prevention of recurrent stroke and MACE (including ICH) in patients with AF and recent ischaemic stroke.
Subgroup analyses.
Disclosures of Interest: No
Abstract N°: 1682
NET BENEFIT OF LIFELONG ANTIPLATELET THERAPY AFTER CRYPTOGENIC STROKE AT YOUNG AGE
Nina Hilkens*1, Wietske Kievit2, Edo Richard1, Frank-Erik De Leeuw1
1Radboud University Medical Center, Neurology, Nijmegen, Netherlands, 2Radboud University Medical Center, Health Evidence, Nijmegen, Netherlands
On behalf of:
Background and aims: Young patients with cryptogenic stroke are prescribed lifelong antiplatelet therapy, based on extrapolation from guidelines for older patients. It is unknown whether benefits of antiplatelet therapy outweigh harms in young patients without atherosclerosis, who are at low risk of ischemic events. We assessed net benefit of long-term antiplatelet therapy after cryptogenic stroke at young age.
Methods: We developed a state-transition model based on published literature to assess consequences of stopping or continuing antiplatelet therapy three years after cryptogenic stroke at young age, over a time-horizon of 30 years. Outcomes were number of ischemic events (ischemic stroke, myocardial infarction), major bleeds and quality adjusted life years (QALYs). Because the effect of long-term antiplatelet therapy on ischemic events is unknown in patients with cryptogenic stroke, we modelled three scenarios: no effect, 12.5% and 25% relative risk reduction (similar to the effect of antiplatelet therapy in older patients).
Results: The number of major bleeds prevented (54-57/1000 patients) outweighs the number of ischemic events caused (2-39/1000 patients) by antiplatelet discontinuation for all scenarios. Antiplatelet discontinuation results in QALY gain in the first and second scenario (QALY gain 50 and 9 years respectively), but not in the third scenario (QALY loss 40 years).
Conclusions: Based on a state-transition model, antiplatelet discontinuation after cryptogenic young stroke could be beneficial, as it prevents more major bleeds than it causes ischemic events. Whether antiplatelet discontinuation results is QALY gain depends on the effect of antiplatelet therapy on ischemic events, which should ultimately be assessed in a RCT.
Disclosures of Interest: No
Abstract N°: 1587
TIMING OF ANTICOAGULANTS INITIATION FOR ATRIAL FIBRILLATION AFTER ACUTE ISCHEMIC STROKE: A SYSTEMATIC REVIEW AND META-ANALYSIS
Lina Palaiodimou*1, Maria Ioanna Stefanou1, Aristeidis Katsanos2, Gian Marco De Marchis3,4, Diana Aguiar De Sousa5, Jesse Dawson6, Mira Katan7,8, Konstantinos Toutouzas9, David Seiffge10, Georgios Tsivgoulis1
1National and Kapodistrian University of Athens, Second Department of Neurology, “Attikon” University Hospital, Athens, Greece, 2McMaster University/Population Health Research Institute, Department of Medicine (Neurology), Hamilton, Canada, 3University of Basel, Department of Clinical Research, Basel, Switzerland, 4Kantonsspital St. Gallen, Department of Neurology and Stroke Center, St. Gallen, Switzerland, 5University of Lisbon, Department of Neurosciences (Neurology), Hospital de Santa Maria, Lisbon, Portugal, 6University of Glasgow, Institute of Cardiovascular and Medical Sciences, Glasgow, United Kingdom, 7University of Zurich, Department of Neurology, University Hospital of Zurich, Neuroscience Center Zurich, Zurich, Switzerland, 8University Hospital and University of Basel, Department of Neurology, Basel, Switzerland, 9National and Kapodistrian University of Athens, First Department of Cardiology, Athens, Greece, 10University of Bern, Department of Neurology, Inselspital, Bern University Hospital, Bern, Switzerland
On behalf of:
Background and aims: There is a longstanding clinical uncertainty regarding the optimal timing of initiating oral anticoagulants (OAC) for atrial fibrillation (AF) following acute ischemic stroke (AIS). Current international recommendations are based on expert opinions, while significant diversity among clinicians is noted in everyday practice.
Methods: We conducted an updated systematic review and meta-analysis including all available randomized-controlled clinical trials (RCTs) and observational cohort studies that investigated early versus later OAC-initiation for AF after AIS. The primary outcome was defined as the composite of ischemic and haemorrhagic events and mortality at follow-up. Secondary outcomes included the components of the composite outcome (ischemic stroke recurrence, intracranial haemorrhage, major bleeding and all-cause mortality). Pooled estimates were calculated with random-effects model.
Results: Nine studies (two RCTs and seven observational) were included comprising a total of 4,946 patients with early OAC-initiation vs 4,573 patients with later OAC-initiation. Early OAC-initiation was associated with reduced risk of the composite outcome (RR=0.74; 95%CI:0.56-0.98; I2=46%) and ischemic stroke recurrence (RR=0.64; 95%CI:0.43-0.95; I2=60%) compared to late OAC-initiation. Regarding safety outcomes, similar rates of intracranial haemorrhage (RR=0.98; 95%CI:0.57-1.69; I2=21%), major bleeding (RR=0.78; 95%CI:0.40-1.51; I2=0%) and mortality (RR=0.94;95%CI:0.61-1.45; I2=0%) were observed. There were no subgroup differences, when RCTs and observational studies were separately evaluated. Early OAC-initiation was associated with reduced risk of the composite outcome (RR=0.72; 95%CI:0.53-0.98; I2=0%) and recurrent ischemic stroke (RR=0.63; 95%CI:0.41-0.98; I2=0%) in the RCT-subgroup.
Conclusions: Early OAC-initiation in AIS patients with AF appears to have a better efficacy and similar safety profile compared to later OAC-initiation.
Disclosures of Interest: No
Abstract N°: 811
STENTING VS. OPTIMAL MEDICAL THERAPY FOR SYMPTOMATIC EXTRACRANIAL VERTEBRAL ARTERY STENOSIS: A SYSTEMATIC REVIEW AND META-ANALYSIS
Pedro Henrique Reginato1, Rafael Eduardo Streit*1, Marianna Gerardo Hidalgo Santos Jorge Leite2, Elizabet Taylor Weba3, Maria Galvão4, Vivian Gagliardi5,6
1Federal University of Parana, Curitiba, Brazil, 2School of Medicine Santa Marcelina, Sao Paulo, Brazil, 3State University of the Tocantina Region of Maranhão, Imperatriz, Brazil, 4Federal University of Piauí, Teresina, Brazil, 5Santa Casa de São Paulo, Sao Paulo, Brazil, 6Albert Einstein Israelite Hospital, Sao Paulo, Brazil
On behalf of: Pedro Henrique Reginato; Rafael Eduardo Streit; Marianna Gerardo Hidalgo Santos Jorge Leite; Elizabet Taylor Pimenta Weba; Maria Theresa Leal Galvão; Vivian Dias Baptista Gagliardi
Background and aims: For individuals with recent ischemic stroke or transient ischemic attack and extracranial vertebral artery (VA) stenosis who continue to exhibit symptoms despite receiving optimal medical therapy (OMT), the effectiveness of stenting remains uncertain. We aimed to perform the first systematic review with meta-analysis comparing stenting plus OMT with OMT alone.
Methods: We systematically searched PubMed, Cochrane and EMBASE, from inception to 2nd December 2023, for studies comparing stenting plus OMT against OMT alone. Assessed outcomes were stroke during the entire follow-up period, stroke or TIA during the entire follow-up period and all-cause mortality during follow-up. Statistical analysis was performed using RevMan 5.4.1. Heterogeneity was assessed with I² statistics.
Results: We included 342 patients from 3 studies, of which 2 were RCT. Stenting plus OMT was used to treat 165 (42%) patients. Follow-up ranged from 3 to 41 months. All-cause mortality during the entire follow-up period (RR 0.68; 95% CI 0.26 - 1.79; p = 0.44; I² = 0%) and stroke during the entire follow-up period (RR 0.58; 95% CI 0.27 - 1.22; p = 0.15; I² = 0%) were not significantly different among groups.
Conclusions: This meta-analysis suggests evidence regarding the safety of stenting therapy concerning all-cause mortality. Also, the low heterogeneity and potential signals of efficacy in reducing stroke in any arterial territory highlights the need for more RCTs to provide more robust data regarding the effect of stenting therapy plus OMT in symptomatic patients with extracranial VA stenosis.
Disclosures of Interest: No
Abstract N°: 1095
ACCURACY OF ROUTINELY COLLECTED DATA FOR IDENTIFYING CARDIOVASCULAR OUTCOMES IN A RANDOMISED TRIAL OF SECONDARY PREVENTION
Alice Hosking*1, Jacqueline Stephen2, William Whiteley1,3, Cathie Sudlow2,3, Rustam Al-Shahi Salman1
1University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom, 2University of Edinburgh, Usher Institute, Edinburgh, United Kingdom, 3Health Data Research UK, British Heart Foundation Data Science Centre, United Kingdom
On behalf of: On behalf of the RESTART collaboration.
Background and aims: Routinely collected healthcare data (RCHD) could substantially reduce clinical trial costs. RESTART (ISRCTN71907627, n=537) was a randomized clinical trial in the UK, of adults taking antithrombotic therapy when they developed intracerebral haemorrhage. Participants were then randomly allocated to start or avoid antiplatelet therapy. Our aim was to assess the accuracy of RCHD as the sole method of follow-up for RESTART.
Methods: RESTART participants participants were followed-up through annual participant and GP questionnaires, with central blinded outcome adjudication. The primary outcome was recurrence of intracerebral haemorrhage. The secondary outcome was a composite of major haemorrhagic and thrombotic events. We obtained data on outcomes through RCHD for all participants in England and Scotland (n=496). We compared RCHD alone to best-available outcomes ascertained from adjudicated follow-up combined with RCHD; and compared the difference between the treatment effect found in RCHD with the original trial result.
Results: For the primary outcome, RCHD had sensitivity of 84% (95% CI 66% to 95%), and positive predictive value of 68% (51% to 82%). For the secondary outcome, RCHD had sensitivity of 84% (76% to 91%) and positive predictive value of 78% (69% to 85%). For the primary outcome, survival analysis demonstrated an identical hazard ratio using RCHD alone (HR=0.51, 95% CI 0.27-0.98), compared with the original trial data (HR=0.51, 0.23-1.03).
Conclusions: RCHD is moderately accurate for follow-up of cardiovascular outcomes in a trial of stroke secondary prevention, and showed very similar treatment effect to traditional adjudicated follow-up. RCHD could be an efficient alternative to adjudicated follow-up.
Disclosures of Interest: No
Abstract N°: 1152
STATIN EFFECT ON QUALITY OF LIFE AND FUNCTIONAL OUTCOME OF OLDER ISCHEMIC STROKE PATIENTS: A SYSTEMATIC REVIEW AND META-ANALYSIS
Susanna R. Prins*1, Sarah Vermeer2, Birgit A. Damoiseaux-Volman3,4, Simone Priester-Vink5, Nathalie van der Velde4,6, Renske M. Van den Berg-Vos7,8
1Amsterdam UMC location University of Amsterdam, Neurology, Amsterdam, Netherlands, 2Rijnstate Hospital, Neurology, Arnhem, Netherlands, 3Amsterdam UMC location University of Amsterdam, Medical Informatics, Amsterdam, Netherlands, 4Amsterdam UMC location University of Amsterdam,, Amsterdam Public Health Research Institute, Amsterdam, Netherlands, 5OLVG, Research and Epidemiology, Amsterdam, Netherlands, 6Amsterdam UMC location University of Amsterdam, Geriatrics, Amsterdam, Netherlands, 7Amsterdam UMC location University of Amsterdam,, Neurology, Amsterdam, Netherlands, 8OLVG, Neurology, Amsterdam, Netherlands
On behalf of:
Background and aims: Existing reviews on the efficacy of statin therapy in older ischemic stroke or transient ischemic attack (TIA) patients often overlook patient-related outcome measures (PROMs) like quality of life (QoL).
Methods: We conducted a systematic review and meta-analysis, identifying relevant studies in Medline, Embase, Cochrane Central Register of Controlled Trials and Web of Science. We included studies comprising older patients (mean age >65) with a recent ischemic stroke or TIA, that compared statin use versus no statin use on QoL or functional outcomes. We assessed study quality using two Cochrane Collaboration tools for bias evaluation, and used R software with a significance level of p<0.05.
Results: We included 22 studies totalling 66,627 patients, comprising 6 randomized controlled trials (RCTs) and 16 observational studies. No study focused solely on older individuals, and 10 studies excluded patients with premorbid poor functioning or severe comorbidities. The RCTs within our study provided inconclusive evidence regarding the effect of statins on both functional outcomes and QoL. The meta-analysis of observational studies revealed a small statistically significant positive effect of statin therapy on functional outcomes (effect size: 0.35, CI 0.21-0.50) after three months. Notably, we observed high to critical bias in all observational studies, as well as a potential presence of publication bias.
Conclusions: This study, including predominantly non-frail individuals, did not demonstrate a clear effect of statin use on QoL or functional outcomes in older individuals after an ischemic stroke or TIA.
Disclosures of Interest: No
Abstract N°: 1822
POPULATION EFFECT OF CHRONIC DISEASE MANAGEMENT POLICIES ON TRAJECTORIES OF MEDICATION ADHERENCE AFTER STROKE
Lachlan Dalli*1, Monique Kilkenny1,2, Muideen Olaiya1, David Ung3,4, Joosup Kim1,2, Leonid Churilov5, Dominique A. Cadilhac1,2, Vijaya Sundararajan6, Mark Nelson7, Nadine Andrew3,4
1Stroke and Ageing Research, Department of Medicine, School of Clinical Sciences at Monash Health, Monash University, Clayton, Australia, 2Stroke Division, Florey Institute of Neuroscience and Mental Health, Heidelberg, Australia, 3National Centre for Healthy Ageing, Peninsula Clinical School, Central Clinical School, Frankston, Australia, 4Department of Medicine, Peninsula Clinical School, Central Clinical School, Monash University, Frankston, Australia, 5Melbourne Medical School, The University of Melbourne, Parkville, Australia, 6Department of Medicine, St Vincent’s Hospital, The University of Melbourne, Fitzroy, Australia, 7Menzies Institute for Medical Research, University of Tasmania, Hobart, Australia
On behalf of: PRECISE Investigators
Background and aims: It is unclear whether primary care incentives for chronic disease management (CDM) improve trajectories of medication adherence after stroke. We aimed to evaluate differences in trajectories of medication adherence after stroke, based on evidence of a CDM claim.
Methods: A target trial was emulated using population-wide linked data obtained for the PRECISE project. Community-dwelling survivors of stroke or transient ischemic attack (TIA) were identified from the Australian Stroke Clinical Registry (42 hospitals; Victoria and Queensland; 2012–2015). These registrants had their data linked with government-held datasets, including pharmaceutical dispensing and primary care data. Only adults alive at 18 months with regular primary care visits were included. The 7–18 month post-stroke/TIA exposure was a primary care CDM claim (vs no claim). The 19–30 month post-stroke/TIA outcome was group-based trajectories of monthly medication adherence. We used multi-level logistic regression, with inverse probability treatment weights, to compare trajectories by CDM exposure.
Results: Among 11,580 participants (median age: 70 years, 42% female), 45% had a CDM claim. Four distinct trajectories of medication adherence were identified: non-use, declining adherence, high adherence, and near-perfect adherence. After adjustment, having a CDM claim (vs no claim) promoted a high adherence trajectory for antihypertensive (adjusted odds ratio [aOR]: 1.33 [95%CI 1.24–1.44]) or lipid-lowering (aOR: 1.26 [95%CI 1.16–1.37]) medications. For antithrombotic medications, having a CDM claim (vs no claim) promoted a near-perfect adherence trajectory (aOR: 1.16 [95%CI 1.08–1.25]).
Conclusions: Receipt of government-funded CDM policies promoted favourable trajectories of medication adherence after stroke/TIA.
Disclosures of Interest: No
Abstract N°: 3248
RISK STRATIFICATION FOR SECONDARY PREVENTION OF AF-RELATED AIS: DEPLOYING MACHINE LEARNING FOR ROBUST VALIDATION AND UPDATING OF CHA2DS2-VASC
Jenny Simon*1,2, Lukasz Krainski3, Karlinski Michal Adam4, Maciej Niewada1
1Medical University of Warsaw, Department of Experimental and Clinical Pharmacology, Warszawa, Poland, 2The Open University, School of Mathematics and Statistics, Kents Hill, United Kingdom, 3Warsaw School of Economics, Warszawa, Poland, 4Institute of Psychiatry and Neurology, Warszawa, Poland
On behalf of:
Background and aims:This two-paper study consists of an original article and accompanying statistical analysis plan (SAP).
Guidelines recommend oral anticoagulation for primary and secondary prevention of atrial
fibrillation-related acute ischaemic stroke on the basis of CHA2DS2-VASc. However, adherence is poor for secondary prevention. This is partly because patients with and without previous stroke were not routinely differentiated in CHA2DS2-VASc validation studies. We aimed to develop a risk stratification scheme bespoke to secondary prevention.
Quality of reporting has been found to be poor across the literature as researchers tended to develop more stroke clinical prediction rules (CPRs), in lieu of validating existing ones.
Methods: 11,138 AF-AIS patients were extracted from the VISTA repository. To validate the existing scheme, association between CHA2DS2-VASc score and 90-day recurrence was assessed using logistic regression and naive Bayes models. To update the scheme, deep learning and decision tree ensemble models were constructed and Shapley value-based feature importance employed to inform each predictor's coefficient. Schemes were compared on grounds of discrimination, calibration, and consistency.
Results: Discrimination of the existing scheme was unsatisfactory-to-modest (C-statistic=0.55-0.68), while the updated scheme achieved good discrimination (C-statistic=0.74-0.88). The updated scheme was better calibrated to recurrence risk (Kendall’s rank correlation coefficient = 0.77 versus 0.45) and more consistent across same-scoring patients (CV=0.16 versus 1.10).
Conclusions: In harnessing machine learning, the literature may become more validation-oriented and systematic as researchers forgo continual development of new stroke CPRs. The time is opportune to make SAPs a reporting standard as ML-based methodologies present novel challenges.
Disclosures of Interest: No
Abstract N°: 2182
ADHERENCE AND THE LONG-TERM BENEFIT OF EARLY POSITIVE AIRWAY PRESSURE (PAP) THERAPY AFTER ACUTE ISCHEMIC STROKE
1Hallym University Dongtan Sacred Heart Hospital, Neurology, Hwaseong-si, South Korea
On behalf of:
Background and aims: Sleep disordered breathing (SDB), is under-recognized risk factor for stroke and the gold standard of managmeent of SDB is positive airway pressure (PAP) therapy.There are no clear guidelines when to start the PAP therapy after acute ischemic stroke. This study aims to examine the adherence and long-term benefit of early PAP after acute cerebrovascular events.
Methods: Acute stroke patients within 5 days of symptom onset and with a STOP-Bang score of 3 or higher on the sleep questionnaire were screened. After getting informed consent, the patients underwent type 1 polysomnography (PSG). Patients whose Apnea-Hypopnea Index (AHI) was 5 or higher started PAP therapy within 7 days of stroke onset during hospitalization.
Results: From Dec. 2021 to October 2023, 191 patients agreed to participate in the study. From the type I PSG, 169 patients were diagnosed with OSA. Among them, 95 initiated PAP therapy during the hospitalization. Three months later, 45 patients (47.4%) performed good adherence to PAP and 36 individuals (37.9%) continued the good adherence to PAP therapy over 12 months. The patients who had good adherence to PAP therapy had lower glucose level (115.7 mg/dL vs. 117.6 mg/dL) and lower systolic blood pressure (128.1 mmHg vs. 130.8 mmHg).
Conclusions: The adherences of early PAP therapy at the 3 months and 12 months are tolerable. The 1 year follow-up data showed well-controlled vascualr risk factors in the good adherence group to PAP therapy.
Disclosures of Interest: No
Abstract N°: 458
PATTERNS AND PREDICTORS OF STATIN THERAPY AFTER ISCHEMIC STROKE AND TIA: INSIGHTS FROM THE LIPYDS MULTICENTER STUDY
Angelo Cascio Rizzo*1, Ghil Schwarz1, Anna Cavallini2, Paolo Candelaresi3, Simona Marcheselli4, Marina Diomedi5, Maria Luisa Zedde6, Danilo Toni7, Andrea Zini8, Elio Clemente Agostoni1
1ASST Grande Ospedale Metropolitano Niguarda, Neurology and Stroke Unit, Milan, Italy, 2IRCCS Fondazione Mondino, U.C. Malattie Cerebrovascolari e Stroke Unit, Pavia, Italy, 3A.O.R.N. Cardarelli, Neurology and Stroke Unit, Naples, Italy, 4IRCCS Humanitas Research Hospital, Neurologia d'Urgenza e Stroke Unit, Rozzano-Milan, Italy, 5University of Rome Tor Vergata, Stroke center, Department of Systems Medicine, Rome, Italy, 6Azienda Unità Sanitaria Locale-IRCCS di Reggio Emilia, Neurology and Stroke Unit, Reggio Emilia, Italy, 7Sapienza University of Rome, Department of Human Neurosciences, Rome, Italy, 8IRCCS Istituto delle Scienze Neurologiche di Bologna, Neurologia e Rete Stroke Metropolitana, Ospedale Maggiore, Department of Neurology and Stroke center, Bologna, Italy
On behalf of: LIPYDS study group
Background and aims: Patients with ischemic stroke (IS) or TIA face an elevated cardiovascular risk, warranting intensive lipid-lowering therapy. Despite recommendations, adherence to guidelines is suboptimal, leading to frequent undertreatment. This study aims to evaluate the patterns and predictors of statin use after IS and TIA.
Methods: LIPYDS (Lipid-lowering therapy and LDL-C after IS/TIA in Italy) is a multicenter, observational, retrospective study including >18-year-old patients discharged after IS/TIA from 19 Italian centers in 2021. Multivariable logistic regression analysis was used to determine (1) the association at discharge between statin prescription (Any-Statin versus No-Statin), type (High-Intensity Statin versus Other-Statin) with stroke etiology (TOAST), (2) clinical variables independently associated with statin prescription in the entire cohort and within TOAST categories.
Results: We included 3,740 patients (median age 75 [IQR 64-82]; median LDL-C 173 [IQR 145-204]). At discharge, 1,971 (52.7%) received a High-Intensity Statin, 969 (25.9%) no statin therapy. Among patients not previously on statins (N=2686[71.8%]), 50.1% initiated High-Intensity Statin (78.2% Large-Artery-Atherosclerosis [LAA], 60.8% Small-Vessel-Disease [SVD], 34.7% Cardioembolic [CE], 47.4% Undetermined etiology); in 33% the choice to not initiate statin therapy persisted (14.5% LAA, 21.8% SVD, 48% CE, 29.3% Undetermined). LAA showed the strongest association with Any-Statin (aOR 3.07 [95%CI 2.39-3.95], p<0.001) and High-Intensity Statin (aOR 4.51 [95%CI 3.39-6.00], p<0.001), while CE showed an inverse association (respectively, aOR 0.36 [95%CI 0.31-0.43], p<0.001 and aOR 0.52 [95%CI 0.44-0.62], p<0.001). Stepwise regression highlighted LDL-C and previous statin therapy as consistent predictors of statin prescription at discharge.
Conclusions: A considerable under-prescription of statins, especially at high-intensity, is observed following IS/TIA, especially among cardioembolic and non-atherosclerotic strokes.
Disclosures of Interest: No
Abstract N°: 1597
DUAL ANTIPLATELET THERAPY FOR ISCHEMIC STROKE WITH INTRACRANIAL ARTERIAL STENOSIS: A SYSTEMATIC REVIEW
1Department of Neurology, Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, Chengdu, China, 2Department of Neurology, The First Affiliated Hospital of Chengdu Medical College, Chengdu, China, 3The George Institute for Global Health, University of New South Wales, Sydney, NSW, Australia, 4Department of Medicine & Therapeutics, The Chinese University of Hong Kong, Hong Kong, China, 5The George Institute for Global Health, Faculty of Medicine, University of New South Wales, Sydney, Australia
On behalf of:
Background and aims: The effectiveness and safety of dual antiplatelet therapy (DAPT) in ischemic stroke patients with intracranial artery stenosis (ICAS) are debated.This study aims to evaluate the efficacy and safety of DAPT in this patient group.
Methods: We searched PubMed, Embase, Cochrane Library, ClinicalTrials.gov, CNKI, WanFang, VIP, and SinoMed from inception through June 20, 2023, for randomized controlled trials that compared efficacy and safety of DAPT versus single antiplatelet therapy (SAPT) in ischemic stroke patients with ICAS. The primary outcome was composite endpoint events (ischemic and bleeding events). Secondary outcomes were stroke (cerebral infarction and cerebral hemorrhage), ischemic events, and cerebral infarction separately. Safety outcomes were bleeding events, cerebral hemorrhage, and death seperately.. Pooling risk ratios (RRs) with 95% confidence intervals (CIs) were calculated using Review Manager 5.4.
Results: Our analysis included 21 randomized controlled trials of 3591 patients. Compared to SAPT, DAPT significantly reduced the rate of composite endpoint events (RR=0.53; 95% CI: 0.46-0.60, P<0.001) and stroke (RR=0.37; 95% CI: 0.30-0.45, P<0.001). The increase in the risk of bleeding events (RR=1.34; 95% CI: 0.97-1.85, P=0.07) and cerebral hemorrhage (RR=0.47; 95% CI: 0.17-1.31, P=0.15) was not significant.
Conclusions: DAPT is both effective and safe for ischemic stroke patients with ICAS, offering a significant reduction in stroke and composite endpoint events without a substantial increase in bleeding risks.
Disclosures of Interest: No
Abstract N°: 1819
PRIOR ANTIPLATELET IS ASSOCIATED WITH BETTER OUTCOME FOR ACUTE ISCHEMIC STROKE PATIENTS TREATED WITH ENDOVASCULAR TREATMENT
Yapeng Lin*1, Jie Yang2
1The First Affiliated Hospital of Chengdu Medical College, neurology, Chengdu, China, 2Sichuan Provincial People's Hospital, University of Electronic Science and Technology of China, neurology, Chengdu, China
On behalf of:
Background and aims: There has been limited evidence and inconsistent results on the safety and effectiveness of prior antiplatelet (PA) for acute ischemic stroke (AIS) patients treated with endovascular treatment (EVT).
Methods: We prospectively enrolled consecutive patients from two comprehensive stroke centers from June 2015 to June 2019. The efficacy outcomes were vascular recanalization rate, early neurological function improvement (24-hour NIHSS decreased ⩾4), poor prognosis at 90-day (mRS 3-6), and death at 90-day. The safety outcomes were intracranial hemorrhage (ICH) and symptomatic intracranial hemorrhage (sICH). Post hoc univariate and multivariate logistic regression was performed with SPSS 22.0.
Results: A total of 298 AIS patients were included. Of them, 54 (18.1%) patients were taking antiplatelet agent before stroke. PA (OR=0.40, 95% CI 0.16-0.98, p=0.046) significantly reduced the three-month death, and this difference persisted after adjusting for clinical confounders (adjusted OR =0.29, 95% CI 0.10-0.83, p=0.021). PA (adjusted OR=0.52, 95% CI 0.26-1.06, p=0.075) was not a significant indicator for three-month death or disability. There were no significant difference in successful recanalization, early neurological improvement, ICH and sICH between groups.
Conclusions: For AIS patients with EVT, prior antiplatelet is safe, and might reduce the odds of three-month death.
Disclosures of Interest: No
Abstract N°: 841
REAL WORLD EVIDENCE IN MANAGEMENT OF DYSLIPIDEMIA IN STROKE PATIENTS: A HARMONICS COHORT DESCRIPTIVE ANALYSIS
Ylenia Avivar Saez*1,2, Anna Bordas Sanchez2,3, Jose Maria Gonzalez de Echevarri1,2, Alan Alberto Flores1,2, Laia Seró1,2, Noelia Canela2, Xavier Ustrell Roig1,2
1Institut d'Investigació Sanitària Pere Virgili, 2Hospital Universitari Joan XXIII, 3Secretaria Territorial ICS Camp de Tarragona
On behalf of: on behalf of the HARMONICS (an EU-funded project) investigators
Background and aims: The imperative for secondary prevention in cases of ischemic stroke (IS) and transient ischemic attack (TIA)) is crucial to forestall recurrence. Dyslipidemia management recommendations from the American Stroke Association/American Heart Association (ASA/AHA) differ notably from the European Society of Cardiology/European Atherosclerosis Organization (ESC/EAS) guidelines in target LDL levels post-stroke. This study aims to provide real-world insights in secondary prevention for dyslipemia based on a Tarragona cohort.
Methods: We conducted a descriptive analysis of the HARMONICS database (an EU-funded High-value Stroke care project in Catalonia) community in Tarragona from April 2022 to July 2023. The primary analysis compared lipid profiles at hospitalization and twelve weeks post-discharge to determine the rate of patients within required ranges according to the different guidelines.
Results: Out of 710 patients, 56 were excluded as they didn’t belong to our sanitary region. Of the remaining 654 patients, 546 had experienced IS or TIA. Only 24.73% exhibited proper lipid profiles three months post-event, regardless of etiology. Analysis exposed significant deficiencies in control measures, with only 46.3% of patients within the threshold of 70 mg/dL proposed by the ASA/AHA and only 22.4% within the threshold of the ESC/EAS guidelines.
Conclusions: In conclusion, the HARMONICS community analysis underscores significant risks for patients who have experienced cerebrovascular events as less than a quarter of patients had an adequate follow-up for dyslipidemia. Addressing these care gaps is crucial to enhance patient outcomes and minimize the risk of further incidents.
Disclosures of Interest: No
Abstract N°: 604
DIFFERENT EFFECTS OF GASTROINTESTINAL SURGERY ON THE EFFICACY OF WARFARIN VERSUS DOACS IN PATIENTS WITH ATRIAL FIBRILLATION
1Seoul National University Hospital, Neurology, Seoul, South Korea, 2Seoul National University Hospital, Medical Research Collaborating Center, Seoul, South Korea
On behalf of:
Background and aims: Potential malabsorption of direct oral anticoagulants (DOACs) after gastrointestinal (GI) surgery and exclusion of patients with altered GI tracts in DOAC trials raise concern for the efficacy of DOAC post-GI surgery. Conversely, warfarin is noted for reduced dose requirements post-GI surgery. Yet, there is still a lack of evidence for optimal anticoagulant prescription after GI surgery. We aimed to investigate the efficacy of warfarin and DOACs with GI surgery in patients with nonvalvular atrial fibrillation (NVAF).
Methods: We performed a retrospective cohort study on patients with NVAF taking oral anticoagulants, using claim-based national data from Korean Health Insurance Review and Assessment Service database from 2013 to 2020. We estimated the hazard ratios (HR) for stroke occurrence after GI surgery in warfarin and DOACs, using the Cox proportional hazard models with time-varying covariates. Inverse probability of treatment weighting was used to adjust the confounders.
Results: Of 308,041 included patients with NVAF (age; 71.85±11.17yrs, male; 56.8%), 4,959 underwent GI surgery. Warfarin and DOACs were prescribed in 10.2% and 89.9%, respectively. GI surgery was associated with a higher risk for ischemic stroke in patients taking warfarin (HR 2.52, 95% confidence interval [CI] 1.207-5.267), in contrast to those taking DOACs (HR 1.005, 95% CI 0.733, 1.379).
Conclusions: GI surgery demonstrated an increased risk of ischemic stroke in patients with NVAF and taking warfarin, compared to DOACs. Additional research is necessary to guide the optimal prescription of OACs in patients after GI surgery based on comprehensive clinical data and rational pharmacological interpretation.
Disclosures of Interest: No
Abstract N°: 739
FACTORS ASSOCIATED WITH RECURRENT ISCHEMIC STROKE WITHIN 2 YEARS AFTER THROMBOLYSIS IN ALGARVE, SOUTHERN PORTUGAL
Teresa Abegão1,2, Teresa Tomásia1, Sofia Andraz1, Catarina Maria Frias Rodrigues1, Tiago Branco2, Ana Marreiros2, Ana Paula Fidalgo1, Hipolito Nzwalo*1,2
1University Hospital Center of Algarve, Faro, Stroke Unit, Faro, Portugal, 2FMCB - Faculdade de Medicina e Ciências Biomédicas da UAlg - Edif. 2, Aging and Cerebrovascular Research Group, Faro, Portugal
On behalf of:
Background and aims: Recurrent ischemic stroke (RIS) is associated with disability, higher case fatality, and increased health costs. Identifying preventable factors for RIS is therefore crucial. Our objective was to evaluate sociodemographic, clinical, and process of care risk factors for RIS in a consecutive case series of stroke survivors treated with thrombolysis.
Methods: We conducted a case-control study, including stroke patients and their time-matched controls (1:2 ratio) from a consecutive case series of ischemic stroke (IS) patients treated with fibrinolysis (n=556, 2006-2018). Sociodemographic factors (age, sex, poverty, municipality), clinical factors (discharge modified Rankin/mRS, cerebrovascular risk factors, comorbidities), and process of care (post-stroke consultations, family doctor) were analyzed. The outcome was defined as RIS within 2 years, and predictors were evaluated using multivariate logistic regression analysis.
Results: The 2-year cumulative recurrence rate was 14.8% (84 cases). The mean age in RIS cases was 71.1 years and 69.2 in the controls (n=168). Not having recommended follow-up stroke consultations (odds ratio [OR]: 3.230; 1.588-6.573, p = 0.001) and untreated dyslipidemia (OR: 4.484; 2.226-9.031; p=0.000) emerged as predictors of RIS. Having regular family doctor consultations (OR: 0.532; 0.339-0.836; p=0.006) and an mRS ⩽ 2 at discharge (OR: 0.280; 0.138-0.568) reduced the likelihood of RIS.
Conclusions: Ensuring an adequate post-stroke process of care, specifically stroke follow-up consultations and primary health care to identify and manage cerebrovascular risk factors, is central to reducing the risk of RIS. Our study reinforces the need for regular access to post-stroke follow-up to decrease the likelihood of stroke recurrence.
Disclosures of Interest: No
Abstract N°: 919
PILOT FEASIBILITY STUDY OF A NOVEL MULTICOMPONENT DIGITAL PROGRAM FOR SECONDARY PREVENTION OF STROKE
Liam Allan*1,2, David Silvera-Tawil2, Jan Cameron1, Jane LI2, Marlien Varnfield2, Vanessa Smallbon2, Julia Bomke2, Muideen Olaiya1, Natasha Lannin3, Dominique Cadilhac1
1Monash University, Stroke and Ageing Research, School of Clinical Sciences at Monash Health, Victorian Heart Institute, Clayton, Australia, 2Commonwealth Scientific and Industrial Research Organisation, Australian e-Health Research Centre, Herston, Australia, 3Monash University, Brain Recovery and Rehabilitation Group, Central Clinical School, Melbourne, Australia
On behalf of:
Background and aims: The Care Assistant and support Program for people after Stroke or TIA (CAPS) was co-designed with consumers to support secondary prevention of stroke. The program combines clinician-led goal setting with risk-factor monitoring, enabled by a mobile application, wearable devices, SMS messages, and a clinician portal. Aims: To determine the acceptability and feasibility of the CAPS program.
Methods: Open label, single group pilot study of the program delivered over 12 weeks. Participants were recruited through the Australian Clinical Stroke Registry. Eligibility: diagnosed with stroke/TIA in preceding 6 months - 3 years, ⩾18 years old, smartphone ownership, and live in the community. Participants set 1-2 secondary prevention goals, were provided a wearable device and training in technology use. Feasibility outcomes included recruitment, usability, and acceptability. Health outcomes were collected assessed at baseline, 6 and 12 weeks. Change from baseline was analysed using Cohen’s d.
Results: Following 600 invitations, 58 responded, 36 were eligible, 34 commenced the program and 1 withdrew (73% male, median age 70 years). The usability of the CAPS app was rated as ‘Good’ to ‘Excellent’, and 70% of participants believed the program beneficial for secondary prevention. Significant improvements at 12 weeks from baseline (p<0.05) were reported for cardiovascular health (d = 0.71), one domain of mental health (d = 0.63), and self-efficacy (d = 0.40).
Conclusions: The CAPS program was feasible to deliver and acceptable to participants, with promising signals in improved aspects of health and self-efficacy. Findings have informed the design of an effectiveness trial.
Disclosures of Interest: No
Abstract N°: 1578
TEMPORAL TRENDS IN CARDIOVASCULAR HEALTH (CVH) IN AUSTRALIAN POPULATION WITH PREVIOUS STROKE AND HEART DISEASE
Sabah Rehman*1, Seana Gall1
1Menzies Institute for Medical Research, University of Tasmania, Hobart, Australia
On behalf of:
Background and aims: Changes in CVH in people with previous stroke/heart disease may reflect the success of secondary prevention strategies. This remains unexplored among adult Australians over time.
Methods: We included people from Australian National Health Surveys in 2011-12 (n=9522), 2014-15 (n=11,071) and 2017-18 (n=12,253). Five items aligned with American Heart Association’s guidelines (smoking, blood pressure, body mass index, diet and physical activity) and were used to create a CVH score (range: 0 [worst] to 10 [best]) grouped as poor (0-4), intermediate (5-6) or ideal (7-10). We compared the proportions achieving ‘ideal’ and ‘intermediate’ to ‘poor’ CVH scores at each time point over time for people with and without stroke/heart disease. Multinomial logistic regression analyses estimated the relative risk ratio (RRR 95% CI) for ‘intermediate’ and ‘ideal’ scores in 2014-15 and 2017-18 compared with the reference of ‘poor’ score in 2011-12 adjusting for sex, age, and demographic factors.
Results: The proportion of people with stroke and heart disease was 6% in each survey (stroke [1%]/heart disease [5%]). People with previous stroke/heart disease more often had poor CVH than those without a history (Figure 1). In those with previous stroke/heart disease there was evidence of a non-significant reduction in CVH scores while (Figure 2, top) no change was noted in those without stroke/heart disease (Figure 2, bottom).
Conclusions: CVH has not changed over time in people with previous stroke and heart disease requiring better strategies to address poor risk factors in high-risk groups.
Acknowledgement
Australian Bureau of Statistics
Disclosures of Interest: No
Abstract N°: 1798
ASSOCIATION BETWEEN PLATELET AGGREGATION FUNCTION AND PROGNOSIS WITHIN 24H OF REPERFUSION THERAPY FOR ACUTE ISCHEMIC STROKE
Hongwei Deng*1, Yifang Tang Tang1, Jie Yang2
1The First Affiliated Hospital of Chengdu Medical College, Chengdu, China, Department of Neurology, 2Sichuan Provincial People's Hospital, University of Electronic Science and Technology of China, Chengdu, China, Department of Neurology
On behalf of:
Background and aims: The maximal platelet aggregation rate (MPA) can be used to visually depict platelet aggregation function after reperfusion therapy for acute ischemic stroke(AIS). We performed a study assessing the association between changes in MPA and prognosis among AIS patients within 24 hours post-reperfusion therapy.
Methods: This prospective, observational study was conducted at a single center and enrolled 67 patients with AIS(37 receiving intravenous thrombolysis, 14 receiving mechanical thrombolysis, and 16 receiving bridging therapy) from November 2018 to December 2020. The MPA was assessed using LTA(light transimission aggregometry) at baseline (0h) and at 6h, 12h, 18h, and 24h post-treatment. Primary outcomes were good recovery of nerve function (NIHSS score) within 7 days and good prognosis (mRS 0-2) at 90d after treatment. Additionally, the association between baseline data, MPA and progrosis was evaluated.
Results: Hypertension, diabetes, smoking, platelet count, D-dimer level, Triglyceride level, puncture to arterial opening time (PTR), and TOAST classification were identified as influential factors for MPA, with variations observed among treatment groups. There was no significant difference in MPA among AIS patients prior to treatment with different reperfusion methods (60.00±22.13 vs. 64.53±19.68 vs. 56.69±30.53, P=0.671). However, significant differences in MPA were observed at five different time points within 24 hours post-treatment (P < 0.001). Ultimately, MPA at five time point within 24 hours was not associated with prognosis (P > 0.05).
Conclusions: A dynamic change in MPA was observed within 24 hours after reperfusion therapy in patients with AIS. However, it was not associated with the prognosis.
Disclosures of Interest: No
Abstract N°: 2060
ON-TREATMENT PLATELET REACTIVITY AND PLATELET ACTIVATION STATUS ON ASPIRIN OR CLOPIDOGREL IN PATIENTS WITH TIA OR ISCHAEMIC STROKE
Soon Tjin Lim1,2,3, Stephen Murphy1,2, Deirdre Smith1,2,4, Rónán Collins2,5, Sinead Murphy1,6, Allan Mccarthy1,2,6, Bridget Egan7, Su-Yin Lim8, Dermot Cox9, Dominick J. H. McCabe*1,2,3,4,6
1Dept Of Neurology, Tallaght University Hospital / AMNCH, Dublin, Ireland, 2Stroke Services, Tallaght University Hospital / AMNCH, Dublin, Ireland, 3Dept of Clinical and Movement Neurosciences, Royal Free Campus, UCL Queen Square Institute of Neurology, London, United Kingdom, 4Vascular Neurology Research Foundation, Tallaght University Hospital / AMNCH, Dublin, Ireland, 5Age Related Healthcare, Tallaght University Hospital / AMNCH, Dublin, Ireland, 6Academic Unit of Neurology, School of Medicine, Trinity College Dublin, Dublin, Ireland, 7Dept of Vascular Surgery, Tallaght University Hospital / AMNCH, Dublin, Ireland, 8Faculty of Health and Medical Sciences, Taylor’s University, Malaysia, 9School of Pharmacy and Biomolecular Sciences, Royal College of Surgeons, Dublin, Ireland
On behalf of: Optimal Antiplatelet Therapy in TIA and Ischaemic Stroke (OATS) study group: The OATS study research group also includes O’Neill D FRCPI and Coughlan T FRCPI
Background and aims: Simultaneously-collected data regarding platelet reactivity and activation status in ischaemic cerebrovascular disease (CVD) patients commencing commonly-prescribed antiplatelet agents are limited.
Aims: To assess platelet reactivity and activation in whole blood in CVD patients commencing aspirin or clopidogrel.
Methods: This prospective pilot study assessed TIA/ischaemic stroke patients before (baseline; N=73), and 14 +/-7 days (14d) and ⩾90 days (90d) after commencing aspirin or clopidogrel monotherapy. Platelet reactivity at low shear-stress (Multiplate® Aspirin/ADP assays) and platelet activation status (% expression of CD62P, CD63 and leucocyte-platelet complexes on whole blood flow cytometry) were quantified. Prevalence of high on-treatment platelet reactivity (HTPR) was determined on the Multiplate analyser with ‘case-control’ definitions (Aspirin-HTPR: >40U on Aspirin assay; Clopidogrel-HTPR: >46 U on ADP assay)
Results: Prevalence of Aspirin-HTPR was 23.8% (5/21) at 14d, and 30.8% (4/13) at 90d. Prevalence of Clopidogrel-HTPR was 60.5% (23/38) at 14d, and 52% (13/25) at 90d. Commencing aspirin or clopidogrel did not significantly affect platelet activation status on flow cytometry (P⩾0.05). However, median % lymphocyte-platelet complexes significantly decreased between baseline and 14d (2.35% vs. 1.24%, P=0.019), and median % monocyte-platelet complexes decreased between baseline and 90d (6.5% vs. 5.1%, P=0.017) only in the patient subgroup without Clopidogrel-HTPR. Increasing percentages of lymphocyte-platelet complexes were associated with a greater likelihood of having Clopidogrel-HTPR at 14d (Exp(B)=13.81, P=0.013). Two of four patients with recurrent vascular events had Clopidogrel-HTPR.
Conclusions: An important proportion of CVD patients have Antiplatelet-HTPR at low shear-stress. % leucocyte-platelet complexes influence Clopidogrel-HTPR status, and these data could inform personalised-antiplatelet regimen approaches.
Disclosures of Interest: No
Abstract N°: 2078
TREATMENT OF HYPERLIPIDEMIA IN ARMENIA IN PATIENTS AT RISK FOR STROKE
Arianna Mesrobian1, Arevik Bichakhchyan2,3, Marine Balasanyan*3, Lilit Minasyan3, Mariam Grigoryan3, Ani Shiroyan3, Mikael Muratoglu4, Viken Babikian5, Nune Yeghiazaryan2,3
1Temple University, St. Luke’s School of Medicine, Philadelphia, United States, 2National Institute of Health, Neurology and Neurosurgery, Yerevan, Armenia, 3Erebuni Medical Center, Department of Neurology & Comprehensive Stroke Center, Yerevan, Armenia, 4University of Alberta, Department of Medicine, Edmonton, Canada, 5Boston Medical Center, Department of Neurology, Boston, United States
On behalf of:
Background and aims: Early treatment of hyperlipidemia is key for primary and secondary stroke prevention. Real world data regarding treatment in Caucasian countries are limited. We studied the prevalence and treatment of hyperlipidemia in acute stroke patients presenting to medical attention in Yerevan, Armenia.
Methods: We prospectively enrolled consecutive patients with symptoms of acute cerebral ischemia admitted over a 30-day period in 2023 to the Erebouni Stroke Center. Data obtained as part of routine evaluations were tabulated. Based on the 2019 European Society of Cardiology Guidelines, we used LDL-cholesterol thresholds for moderate and high-risk patients.
Results: 129 patients were enrolled; 83 (64.3%) were men. Mean-age was 67.8 years. A pre-admission diagnosis of stroke had been made in 16 (12.4%) patients, myocardial infarction in 33 (25.6%), hypertension in 98 (76.0%), diabetes in 40 (31.0%), and hyperlipidemia in 25 (19.4%).
At admission, 18 (14.0%) patients were on a statin. Average LDLs in patients on or off a statin were respectively 2.74 mmol/L (n=17) and 3.54 mmol/L (n=93, p=0.011). LDL was screened in 110 (85.3%) patients; in 99 (90.0%) it was >1.8 mmol/L, and in 75 (68.2%) >2.6 mmol/L
At discharge, 109 (84.5%) were on a statin; 77 (72.0%) on high, and 22 (20.6%) on moderate, intensity doses; 20 (15.5%) patients remained untreated, including 3 with an LDL >2.6mmol/L.
Conclusions: Hyperlipidemia was highly prevalent and poorly treated in patients with increased stroke risk at admission, and treatment improved after hospitalization. Education of the public and of primary care and stroke physicians is in order.
Disclosures of Interest: No
Abstract N°: 2713
THE EFFECT OF HYPERTENSION MANAGEMENT ON STROKE: REAL-WORLD EVIDENCE FROM A MEGA-CITY IN CHINA 2017-2021
Yuqian Chen*1,2, Xiaohui Hou2, Yuhan Liu2, Kun Fang3, Fen LI2
1Shanghai University of Political Science and Law, School of Economics and Management, Shanghai, China, 2Shanghai Health Development Research Center, Department of Health Policy Study, Shanghai, China, 3Huashan Hospital, Department of Neurology, Shanghai, China
On behalf of:
Background and aims: Hypertension is a vital independent risk factor for stroke. This study aims to investigate the effect of hypertension management (HM) on stroke attacks and the post-stroke long-term lifetime in hypertension patients.
Methods: Hypertension patients included were collected from a database of a district Residences Community Health Records from January 2017 to December 2021. Their outpatient and inpatient records were extracted from the China Statistical Survey of Health Resources and Services Program database. Hypertension management was represented by hypertension follow-up and periods visits,. The multi-variable Logistic regression models were used to evaluate the effect of HM on stroke attacks. The Kaplan-Meier survival curves with log-rank tests and multiple Cox regression models were used to assess the effect of HM on the long-term life of hypertension patients after the stroke attack.
Results: 278,167 patients with hypertension were collected, and 16758 (6.02%) patients died from all-cause mortality by December 2021. The Logistic models indicated that HM in the latest year was significantly associated with lower morbidity in the next year: hypertension patients with followed up, periodic visits, and both of them in the latest year had lower hazard ratio The Cox regression models showed the stroke patients with hypertension follow-up, periodic visits and both in the latest year had lower hazard ratios of 0.89, 0.88, 0.79 in the next year on all-cause mortality after a stroke attack.
Conclusions: The management of hypertension could effectively reduce the risk of stroke in patients in terms of stroke onset and post-stroke long-term lifetime.
Disclosures of Interest: No
Abstract N°: 3200
OFF-LABEL DUAL ANTIPLATELET THERAPY FOR NON-MINOR ISCHEMIC STROKE: A SYSTEMATIC REVIEW AND META-ANALYSIS
Ahmed Alkhiri*1, Ahmed A. Almaghrabi1, Aser F. Alamri2, Basil A. Alghamdi1, Shatha Alqurashi1, Razan Alabdulqader3
1King Saud Bin Abdulaziz University for Health Sciences, College of Medicine, Jeddah, Saudi Arabia, 2King Saud Bin Abdulaziz University for Health Sciences, College of Medicine, Riyadh, 3King Faisal University, College of Medicine, Alahsa, Saudi Arabia
On behalf of:
Background and aims: The role of dual antiplatelet therapy is well-established in the secondary prevention of high-risk transient ischemic attack (TIA) and minor stroke. However, limited evidence exists regarding the optimal antiplatelet regimen for non-minor stroke patients (NIHSS >3).
Methods: A systematic search of Medline, Embase, and Web of Science databases was conducted in November 2023. Studies reporting outcomes of non-minor stroke patients treated with either dual (DAPT) or single antiplatelet therapy (SAPT) were included. Risk ratios (RRs) with their respective 95% confidence intervals (CIs) were calculated for binary variables. Prescription patterns and patient outcomes were analyzed for those treated with DAPT versus SAPT.
Results: Seven studies (49,111 patients) deemed eligible for qualitative synthesis. Of those, four studies (8308 patients) provided data for quantitative analysis. Out of the total 49,111 patients included, 48.5% (23,837 patients) received DAPT. DAPT was more commonly prescribed for patients with a history of stroke or TIA, hypertension, and diabetes. No significant differences were observed between DAPT and SAPT in terms of stroke recurrence (RR, 0.92 [95% CI, 0.82–1.04]), composite outcomes of stroke recurrence, ischemic heart disease, and/or death (RR, 0.97 [95% CI, 0.76–1.24]), and major bleeding rates (RR, 0.99 [95% CI, 0.23–4.20]).
Conclusions: In this meta-analysis of non-minor stroke patients, nearly half of the patients received DAPT for secondary stroke prevention. The outcomes associated with DAPT were similar to those with SAPT. Nevertheless, the restricted number and quality of included studies emphasize the necessity for additional evidence.
Disclosures of Interest: No
Paper Poster - Service Organisation and Quality Improvement
Abstract N°: 809
THE INFLUENCE OF DRIVING DISTANCE FROM COMPREHENSIVE STROKE CENTRES ON ACUTE STROKE TREATMENT ACCESSIBILITY IN ONTARIO, CANADA
Foad Taghdiri*1, Manav Vyas1, Moira Kapral1,2, Lauren Lapointe-Shaw1, Peter Austin2, Peter Gozdyra2, Yue Chen2, Jiming Fang2, Amy Yu1,2
1University of Toronto, Medicine, Toronto, Canada, 2ICES, Toronto, Canada
On behalf of:
Background and aims: Endovascular thrombectomy (EVT) and intravenous thrombolysis improve outcomes after ischemic stroke, but ensuring rapid access to treatment is challenging in regions with vast geography. We assessed the associations between distance to EVT-capable stroke centers and revascularization treatments in Ontario, Canada.
Methods: We used administrative data to identify community-dwelling adults hospitalized with ischemic stroke from 2017-2022. Ontario is home to 15 million residents in an area larger than France and Spain combined. Utilizing the Ontario Road Network File and patient postal codes, we estimated the driving times to EVT centers. We used multivariable logistic regression, adjusted for baseline differences, to estimate the association between driving time (modeled as a continuous variable using restricted cubic splines) and receipt of thrombolysis or EVT as two separate outcomes.
Results: Among 57,706 patients (median age 74 years; 45.8% female), we found no significant association between driving time and thrombolysis. However, the odds of EVT decreased with increasing driving time (Figure). For instance, compared to patients within 20 minutes of an EVT center, those 180 minutes away were less likely to undergo EVT (adjusted adds ratio and 95% confidence intervals 0.78 [0.62, 0.97]) and those 240 minutes away were even less likely to have this treatment (0.60 [0.46, 0.79]).
Conclusions: While thrombolysis is equitably accessible across Ontario, use of EVT decreases with increasing distance from EVT centers, likely because current systems of care were designed for thrombolysis. New policies and systems must be developed to ensure equitable access to EVT.
Disclosures of Interest: No
Abstract N°: 1489
THE SPANISH NATIONAL STROKE STRATEGY EVALUATION SHOWS A SIGNIFICANT DECREASE IN STROKE MORTALITY RATES SINCE ITS ADOPTION
1Hospital Universitario Clínico San Carlos, Neurology Department, Madrid, Spain, 2Spanish Ministry of Health, General Subdirectorate of Quality Healthcare, General Directorate of Public Health and Health Equity, Madrid, Spain, 3Spanish Ministry of Health, General Subdirectorate of Health Information Systems, Madrid, Spain
On behalf of:
Background and aims: The Spanish National Stroke Strategy, approved in 2008 for the Interterritorial Council of the National Health System, was a major breakthrough in improving stroke care in Spain. We present the main results of the evaluation carried out to assess the achievement of the objectives set out in the Strategy.
Methods: The Strategy was structured in 5 priority lines, each of them establishing different objectives and recommendations: health promotion and primary and secondary stroke prevention (7 objectives); acute stroke care (8); rehabilitation (5) and restoration of life (3); education (1); research (2). Quantitative variables were measured through quality indicators. The objectives for which quantitative information was not available were evaluated by means of surveys of the different health managers in the Autonomous Communities of Spain. The achievement of the objectives was established in 5 levels: not started, started, partially achieved, practically achieved, achieved.
Results: 12/20 (60%) of the objectives were practically achieved or achieved, especially those in acute stroke care and prevention. Notably, there was a decline in adjusted mortality rates (from 20,3-52,4/100.000 inhabitants in 2008 to 14,9-31,6/100.000 inhabitants in 2018), a decline in premature mortality due to stroke, in addition to a decline in inter-territorial stroke mortality variability over time.
Conclusions: The implementation of the National Stroke Strategy in Spain has led to a significant improvement in stroke prevention and care, resulting in a decline in stroke mortality.
Disclosures of Interest: No
Abstract N°: 1718
IMPACT OF A STROKE THROMBOLYSIS RUCKSACK IN THE REDUCTION OF DOOR TO NEEDLE TIMES: WITHIN AN ENGLISH HOSPITAL
Suzanne Lucas*1, Louise Vincent1
1Royal United Hospitals NHS Foundation Trust, Acute Stroke, Bath, United Kingdom
On behalf of:
Background and aims: Rapid use of intravenous thrombolysis to treat hyper-acute ischaemic strokes lead to better outcomes with early reperfusion. Delayed access to equipment and medication contributes to longer door to needle times (DTNt) and increased morbidity.
To evaluate the DTNt following the introduction of a stroke thrombolysis rucksack containing equipment and medication for use by the Stroke Medical Nurse Practitioners (SMNPs), who facilitate the rapid assessment and treatment of hyper-acute stroke patients within the emergency department.
Methods: Analysis of the DTNt held in the Sentinel Stroke National Audit Programme (SSNAP) for the centre, over a 9-month period pre and post the introduction of the rucksack. This study measured the rucksack use by the SMNPs and when it was not, or when administered by emergency department (ED) staff outside of SMNPs service hours. The mean averages were then calculated and compared. A qualitative survey evaluated SMNPs’ attitudes to use of the rucksack.
Results: The DTN time was found to be significantly reduced when the rucksack was used by SMNPs. SMNPs reported improvement in their experience of delivering thrombolysis. Data showed an increase in the number of patients thrombolysed.
Conclusions: SMNPs experience and DTNt improved with the introduction of stroke thrombolysis rucksack. Greater awareness of the stroke team and importance of the service was achieved across the hospital by the visibility of the rucksack. Further study needs to be completed to examine all factors involved.
Disclosures of Interest: No
Abstract N°: 1698
THROMBOLYSIS RATES ACCORDING TO AGE AND SEX: AN ANALYSIS USING DATA FROM THE IRISH NATIONAL AUDIT OF STROKE
Meabh Kelly*1, Olga Brych2, Joan Mccormack2, Tim Cassidy2, Ronan Collins2, Joseph Harbison3
1Trinity College Dublin, Ireland, 2Irish National Audit of Stroke, 3St James's Hospital, Ireland
On behalf of:
Background and aims: When considering differences in stroke care and management between sexes, studies have previously demonstrated lower thrombolysis rates in women. Few data is available describing thrombolysis rates in respect of age and sex in Ireland. The Irish National Audit of Stroke (INAS) is a national hospital-based registry of stroke patients in Ireland. We performed an analysis to investigate Irish stroke thrombolysis rates between sexes.
Methods: A retrospective analysis of data collected for INAS between 2017 and 2022 was done. All patient data were anonymised and ethics approval obtained. Pre specified data were extracted including: Sex, age group, stroke subtype (ischaemic versus haemorrhagic), and rates of ischaemic stroke thrombolysis. Data on Subarachnoid Haemorrhage were not included. Statistical analysis of data was done using the Chi squared test.
Results: Data on 26,829 patients were analysed, 15,322 male (57%).Women had a lower proportion of ischaemic stroke versus ICH, (men: 13,336/1986, [87% ischaemic], women: 9715/1792 [84.8% ischaemic] chi sq 36.8 p<0.0001).
Overall, 10.2% (1366/15,322) of men with ischaemic stroke were treated with thrombolysis, versus 10.7% of female ischaemic strokes (1041/11,507) (p=0.31). Thrombolysis rates were 10.6% in men <80 years, compared with 8.9% in men >80 years (p=0.01). In women, thrombolysis rates were 11.3% <80 years versus 9.7% >80 years (p=0.14).
Conclusions: Women were more likely to have suffered haemorrhagic stroke. We found no statistically significant differences in Irish stroke thrombolysis rates between sexes at any age but both men and women younger than 80 years were more likely to get thrombolysis.
Disclosures of Interest: No
Abstract N°: 2439
ACCESS TO STROKE TREATMENT IN A MOUNTAINOUS REGION: IMPLEMENTATION ANALYSIS
ENRICA FRANCHINI*1, Leonardo Carbonera2, Mateus Boiani3, Leonardo Dorneles3, Ana Claudia de Souza2, Marcio Dorn3, Sheila Cristina Ouriques Martins2, Gordian Hubert4
1Bolzano Central Hospital, Department of Neurology, Bolzano-Bozen, Italy, 2Hospital Moinhos de Vento, Department of Neurology, Porto Alegre, Brazil, 3Universidade Federal do Rio Grande do Sul, Institute of Informatics, Porto Alegre, Brazil, 4TEMPiS telestroke center, Department of Neurology, München Klinik gGmbH, Munich, Germany
On behalf of:
Background and aims: To provide access to acute stroke treatments within 45 minutes to 90% of the population is a defined goal. In mountainous areas, acute stroke treatments are difficult to provide due to limited access. We aim to evaluate the current availability of acute stroke care in our region and analyze the effect of implementing stroke care in more hospitals.
Results: The three existing ASCs cover 69.37% of the population within a 45-minute drive range. The coverage would increase to above 90% if in five PASCs stroke care was implemented, and to the maximum of 93.67% if all PASCs were converted. By additionally including one AP in the northwest area, 95% would be achieved (Figure 1).
Conclusions: The MAPSTROKE tool can be used to plan acute stroke care in underserved areas.
The map shows population coverage of stroke centers within a 45-minute drive radius from each hospital: existing (dark blue), potential (light blue), and artificial (red). The total coverage of the three colors is 95%.
Disclosures of Interest: Yes This project has received limited grants from the World Stroke Organization and the Angels Initiative (contract number 782566).
Abstract N°: 3112
GEOGRAPHICAL DIFFERENCES IN THE STROKE CARE AVAILABILITY IN THE CZECH REPUBLIC
Martin Sramek*1,2, Ales Tomek3, Robert Mikulík4, Ondrej Skoda5, Marian Rybar6, Ladislav Wagner7
1Second Faculty of Medicine, Charles University in Prague and Motol University Hospital, Department of Neurology, Czech Republic, Prague, Czech Republic, 2Military University Hospital Prague, Department of Neurology, Prague, Czech Republic, 3Second Faculty of Medicine, Charles University in Prague and Motol University Hospital, Department of Neurology, Czech Republic, Prague, 4Tomas Bata Regional Hospital, Department of Neurology, Zlin, Czech Republic, 5Hospital Jihlava, Department of Neurology, Jihlava, Czech Republic, 6Czech Technical University in Prague, Faculty of Biomedical Engineering, Prague, Czech Republic, 7Health Insurance Bureau, Prague, Czech Republic
On behalf of:
Background and aims: Although the performance of stroke service at the national level in the Czech Republic is satisfactory (10 mil population, 46 stroke centers, 31% of ischemic stroke thrombolysed and 9% undergoing thrombectomy), there is concern that access to stroke care differs by the district. Our study therefore aimed to identify regional disparities in stroke care across the country's 76 districts.
Methods: Health insurance company data covering the whole stroke population were analyzed. Cases were identified by ICD code I6 as discharge diagnoses. The general practitioner's residency address was used as a proxy for the patient's residential address.
Results: The percentage of stroke patients treated in a stroke center varied from 99.7% to 22% across different districts. The administration of thrombolysis of ischemic stroke ranged from 37% to 10%. Thrombectomy for ischemic stroke was performed in a range from 0.29% to 12.94%. Mortality rates varied from 9% to 23% across different districts.
Conclusions: In certain districts, patients have several-fold less access to stroke unit treatment, thrombolysis, and thrombectomy. Our work showed large district differences in the care provided for stroke patients. It underscored the need to analyze access to stroke services at the hospital or national level and at the district level. Our results serve as a basis for planning to improve the organization of stroke services.
Percentage of patients with stroke treated in stroke centers in districts of Czech Republic
Disclosures of Interest: No
Abstract N°: 3211
RECRUITMENT IN STROKE STUDIES: HYPERACUTE STROKE RESEARCH CENTRES (HSRC) VERSUS NON-HSRC CENTRES IN THE UK
Peter Wilding*1,2, Yin-Leng Tan3, Paul Bentley1,2
1Imperial College Healthcare NHS Trust, Stroke, London, United Kingdom, 2Imperial College London, Brain Sciences, London, United Kingdom, 3University of Reading, Henley Business School, Reading, United Kingdom
On behalf of:
Background and aims: In the UK, accredited Hyperacute Stroke Units (HASUs) provide hyperacute diagnosis and treatment for stroke. HASUs that meet demanding research criteria (including imaging-infrastructure, out-of-hours research coverage and annual review of performance) can also be accredited as Hyperacute Stroke Research Centres (HSRCs). There are 13 HSRCs and over 100 non-HSRCs. In contrast to HASUs, empirical data examining the value of HSRCs is limited, we therefore examined this using national recruitment data.
Methods: We analysed data on large multi-centre interventional stroke RCTs in the UK at both HSRC-sites (1-12 depending on study) and non-HSRC-sites (1-101 depending on study) from 2009-2023. The primary measure was whether sites met their agreed local recruitment target or not for each study. We then compared the aggregated results of each study at HSRC-sites versus non-HSRC-sites.
Results: Our findings showed that, overall, HSRCs met their recruitment target at a higher rate than non-HSRCs for hyperacute, commercially sponsored, and acute/secondary prevention RCTs. Hyperacute RCTs (n=12) at HSRCs met agreed recruitment targets on average 71% of the time versus non-HSRCs at 44%. For acute/secondary prevention studies (n=14), HSRCs were 73% versus non-HSRCs at 51%. Commercial studies (n=6) at HSRCs were 55% versus non-HSRCs at 11%. See figures 1–3 for details.
Conclusions: HSRCs consistently demonstrated value in terms of meeting agreed recruitment targets. Further research is warranted. This should explore the concept of HSRCs, as well exploring factors that influence performance between HSRCs in terms of infrastructure and leadership, to better enable and expand inclusive, diverse, high-quality recruitment to stroke studies.
Disclosures of Interest: No
Abstract N°: 3243
A SYSTEMATIC REVIEW AND META-ANALYSIS OF THE EFFECT OF STROKE UNIT AND STROKE CENTER CERTIFICATION ON WORKFLOW AND OUTCOME
Diederik DIPPEL*1, Aleksandras Vilionskis2, Apostolos Safouris3, Bjorn Thorarinsson4, Ana Catarina Fonseca5, Cristina Hobeanu6, Marta Nowakowska-Kotas7, Thomas Gattringer8, Vlad Tiu9, Tobias Neumann-Haefelin10
1Erasmus University Medical Center, Neurology, Rotterdam, Netherlands, 2Vilnius university, Clinic of Neurology and Neurosurgery, Vilnius, Lithuania, 3"Attikon" University Hospital,, Second Department of Neurology, Athens, Greece, 4Landspitali University Hospital, Reykjavík, Iceland, 5Lisbon School of Medicine, Lisboa, Portugal, 6Bichat-Claude Bernard Hospital, Dept of Neurology and Strokecenter, Paris, France, 7Klinika Neurologii, Wrocław, Poland, 8Medical University of Graz, Neurology, Graz, Austria, 9Spitalul Universitar de Urgență Elias, București, Romania, 10Klinikum Fulda, Neurology, Fulda, Germany
On behalf of: ESO SU Certificaton committee, including Francesca Romana Pezzella,Stroke Unit AO S Camillo Forlnini, Roma fpezzella@scamilloforlanini.rm.it
Background and aims: Programs of stroke-unit and stroke-centre certification are meant to raise the standard of care and make high quality centres recognisable. We aimed to quantify the association of certification with acute stroke treatment, workflow, complications and outcome.
Methods: We performed a systematic search of Pubmed with the following key words: “(certification OR accreditation) AND stroke [ti]”. We included controlled and before-after studies that described a program of certification by an official organization on a national or international level and used controls to estimate effects. We considered workflow and outcome measures including door-to-CT (DtCT) and door-to-needle time (DtNT), dysphagia screen, DVT-prophylaxis, number of IV-thrombolytics and thrombectomy, and occurrence of pneumonia and death within 30 days.
Results: Our search led to 568 hits. Finally, 19 studies were included. Sixteen contrasted with not-certified control centres, and 3 studies were before-after studies. Patients admitted to centres with certification were more likely to have a DtCT of less than 25 minutes (OR:1.18;1.15-1.21), DtNT less than 60 minutes (OR:1.52;1.45-1.60), IV thrombolytics (OR:1.43;1.42-1.45); thrombectomy (OR:1.53;146-1.61), dysphagia screen (OR:5.27;4.23-5.56) and DVT prophylaxis (OR:3.56;3.31-3.81). Both pneumonia (OR 0.89;0.86-0.92) and death within 30 days occurred less often (OR 0.93;0.92-0.94). Few of the studies adjusted for centre level, but all effects in each study were in the same direction and statistically significant There was considerable heterogeneity of effect (I-squared >90%).
Conclusions: Stroke unit and stroke centre certification is associated with increased quality of stroke care. Therefore, centres should enrol in a national certification program, or apply for ESO certification.
Disclosures of Interest: Yes all authors are members of the ESO Stroke Unit Certification Committee.
Abstract N°: 3328
IMPLEMENTATION OF CLOPIDOGREL-BASED PHARMACOGENOMIC PRECISION MEDICINE IN STROKE
Benjamin Jaa Ming New*1, Shayan Aziz1, Alexandre Matos1, David Baty1, Alexander Doney2, Wai Meng Yu1
1Ninewells Hospital, United Kingdom, 2School of Medicine - University of Dundee, United Kingdom
On behalf of:
Background and aims: Clopidogrel is an antiplatelet prodrug used in secondary prevention of non-cardioembolic ischaemic cerebrovascular events (NCIE). About 30% of white Europeans carry a genetic variant of the CYP2C19 gene resulting in impaired clopidogrel metabolism (ICM). Such individuals remain at greater risk of harm from recurrent ischaemic events when prescribed clopidogrel and can be identified by a simple pharmacogenetic test. We describe a clinical pathway developed in our acute stroke unit in NHS Scotland to reduce harm from ICM.
Methods: A one year pilot commenced in April 2022. A Taqman-based assay for relevant CYP2C19 variants (*2 *3 and *17) was developed to NHS genetics laboratory standards. A clinical pathway, led by a specialist pharmacist, was implemented for test requesting at diagnosis of NCIE, as well as follow-up reporting and communication with primary care. Results were reported to the stroke team within one week. Aspirin, dipyridamole, ticagrelor or their combinations were prescribed for individuals identified as ICM.
Results: During the pilot, 723 tests were reported with 204 (28.2%) identified as ICM and alternative antiplatelets prescribed to 168 (23.2%) individuals. Based on an estimated number needed to treat of 10, we considered 16.8 recurrent ischaemic events were prevented. The pilot pathway has been adopted long term and to-date 1887 genetic tests have been done with 570 (30.2%) ICM identified.
Conclusions: We have demonstrated the feasibility of integrating a clinical pharmacogenetic pathway for clopidogrel in an acute stroke unit to reduce harm. This initiative is being considered for rollout to other hospitals in Scotland.
Disclosures of Interest: No
Abstract N°: 730
RES-Q REGISTRY FOR MONITORING THE QUALITY OF STROKE CARE 2017-2023 IN N.MACEDONIA
Anita Arsovska*1
1University Clinic of Neurology, University “Ss. Cyril and Methodius”-Faculty of Medicine, Urgent Neurology, Skopje, Macedonia
On behalf of:
Background and aims: The Registry of Stroke Care Quality (RES-Q) was launched by ESO-EAST (Enhancing and Accelerating Stroke Treatment) in 2016, and N. Macedonia has participated since 2017. This registry is an important tool for achieving and implementing the overarching targets of the Stroke Action Plan for Europe (SAP-E). The aim was to analyze the results from the RES-Q registry for N. Macedonia for the 2017-2023 period.
Methods: Consecutive patients with acute stroke were prospectively registered in RES-Q registry. Data on demographics, risk factors, neuroimaging, treatment and outcome at discharge were evaluated and compared for each year in the period 2017-2023. Statistical analyses were done in SPSS, with p for significance <0.05.
Results: Total number of enrolled patients was 2101. Their mean age was 69 years; 75.8% had ischemic stroke. Our results showed improvement in recanalization rates (IVT from 4.4% to 16%, with maxiumum of 20.99% in 2022), and use of mechanical thrombectomy (from 0 to 2%), with variable door-to needle time, depending on internal organizational factors. COVID-19 pandemic dramatically reduced the number of hospitalized patients with stroke due to the fact that our hospital became a COVID center. We saw improvement in NIHSS performance, dysphagia screening as well as use of statins and direct oral anticoagulants in secondary stroke prevention (p<0.05).
Conclusions: We should encourage more hospitals to take part in the stroke registry in order to harmonize and improve stroke care in N. Macedonia.
Disclosures of Interest: No
Abstract N°: 1333
BEYOND FACE ARM AND SPEECH TEST (BEYOND FAST), A PREDICTED PROBABILITY-BASED STROKE IDENTIFICATION SCALE
1The University of Chester, Chester Medical School, Chester, United Kingdom, 2Countess of Chester Hospital Accident and Emergency Department, Chester, United Kingdom, 3Mersey and West Lancashire Teaching Hospitals NHS Trust, Rainhill, United Kingdom
On behalf of:
Background and aims: Despite its widespread usage in stroke identification, the FAST test exhibits modest accuracy. This study assesses the effectiveness of integrating additional clinical parameters to distinguish strokes and stroke mimics.
Methods: A retrospective analysis of 39 clinical parameters was undertaken, involving patients suspected of having a stroke and brought to two hyperacute stroke units in the UK via '999' calls from 2021 to 2023. Clinical notes were reviewed, and final diagnoses of stroke/TIA or mimic were independently coded by stroke consultants. Data from Whiston Hospital was used for model development, with Countess of Chester Hospital data reserved for validation. Logistic regression was utilised to determine model-predicted probabilities.
Results: The study encompassed 273 patients from Whiston Hospital. Six parameters – increased age, new onset of speech loss, unilateral arm weakness, absence of loss of consciousness, absence of seizures, and presence of neurological signs – were statistically significant in the multivariate model (p<0.05). The validation dataset from the Countess of Chester Hospital included 398 patients. The probability-based model exhibited high sensitivity at the lower cutoff, where patients may not need to travel to comprehensive stroke centres, and high specificity at the higher cutoff level, where calls from the paramedics can be taken directly by the stroke nurses, as illustrated in Table 1, Figures 1 and 2.
Conclusions: Employing a predictive probability scale rather than a binary threshold scale could more effectively guide patients to suitable stroke services. This approach has the potentials to reduce pre-hospital delays and improve stroke identification accuracy.
Disclosures of Interest: No
Abstract N°: 1420
DISSEMINATION AND POLICY CHANGES AS A RESULT OF THE IMPROVING STROKE CARE IN INDIA (IMPROVISE) STUDY
Ranjit Injety*1,2, Stephanie Jones3, Elizabeth Boaden3, Catherine Elizabeth Lightbody3, Jeyaraj Pandian1, Vasantha Padma4, Pn Sylaja5, Caroline Watkins3
1Christian Medical College & Hospital, Department of Neurology, Ludhiana, India, 2University of Leicester, Institute of Precision Health, Ulverscroft Eye Unit, Leicester, United Kingdom, 3University of Central Lancashire, Stroke Research Team, School of Nursing, Preston, United Kingdom, 4All India Institute of Medical Sciences, Department of Neurology, New Delhi, India, 5Sree Chitra Tirunal Institute for Medical Sciences and Technology, Neurology, Department of Neurology, TIruvananthapuram, India
On behalf of: NIHR Global Health Research Group on IMPROVIng Stroke CarE in India (IMPROVISE) Collaboration
Background and aims: The incidence of stroke is increasing in low-middle-income countries. IMPROVISE was a multi-centre, feasibility study using experience-based co-design to develop and implement three Care Bundles (CBs). CB1: a Global Evaluation of Swallowing tool and hydration ‘Osmolarity App’. CB2: a Standardised Neurological Observation Schedule for Stroke. CB3: post-discharge patient/carer education in the form of animations. We aimed to disseminate the findings and associated training from IMPROVISE to hospitals across India to build stroke capacity and influence national policy.
Methods: Endorsed by the regional ministries for Health and Family Welfare, capacity building was delivered through two training programs. Health Care Professionals from the states of Punjab and Assam with an interest in stroke were eligible to attend. Training covered: stroke and its prevention, IMPROVISE CBs1-3, the implementation of stroke unit care. In addition, a stakeholder/policy maker meeting was conducted in New Delhi with representation from the Indian Council of Medical Research, Angels Initiative, National Accreditation Board for Hospitals (NABH), World Health Organization, Ministry of Health and Family Welfare, and the National Health Authority.
Results: 598 Health Care Professionals representing 96 hospitals attended the training. Inclusion of the three CBs within stroke unit care forms fundamental criteria to determine if accreditation from NABH is awarded. These criteria and accreditation will apply to all stroke unit across India.
Conclusions: Engagement of stakeholders at every level of stroke patient care including policy makers can improve dissemination, training and policy impact with the potential to improve delivery of stroke care and patient outcomes.
Disclosures of Interest: No
Abstract N°: 2338
BARRIERS AND FACILITATORS TO DATA COLLECTION FOR THE IRISH NATIONAL AUDIT OF STROKE (INAS)
Agnes Jonsson*1, Isabelle Jeffares1, Catherine Moran1, Joan Mccormack2, Lisa Mellon1, David Williams1,3, Anne Hickey1
1Royal College of Surgeons in Ireland, Ireland, 2National Institute of Clinical Audit, Ireland, 3Beaumont Hospital, Dublin, Ireland
On behalf of:
Background and aims: The audit of stroke care facilitates service evaluation and quality improvement initiatives and is becoming increasingly important as acute stroke treatment is rapidly changing. In Ireland, the National Office of Clinical Audit has managed the Irish National Audit of stroke (INAS) since 2019.
This study is part of a wider project titled “Maximising the Quality of Stroke Care in Ireland – Development of a National Stroke Audit” which aims to further develop the INAS.
Methods: As part of the overarching project, semi-structured interviews were conducted with health professionals involved in stroke audit data collection, including nurses, health and social care professionals and administrators. Qualitative data relating to data collection for INAS were extracted and analysed for recurring themes using NVIVO.
Results: The most frequent barriers to data collection were: 1. Lack of time and resources; 2. Infrastructural challenges (access to computers, desk space and IT systems); 3. Perceived uselessness of the audit.
Facilitators were: 1. Systems of organisation that allow shared responsibility of data input; 2. Leadership from managers that perceive the data collection as important and beneficial for local service.
Professionals who valued the audit as an important clinical tool were more likely to have a positive view of the work required to input data for INAS.
Conclusions: INAS is a crucial instrument for understanding the demographic characteristics and care received by stroke patients in Ireland. Streamlining data collection procedures is an important part in developing INAS. There are resource and time limitations that need to be considered for future audit development.
Disclosures of Interest: No
Abstract N°: 2571
WHAT MAKES AN EFFECTIVE PRINCIPAL INVESTIGATOR (PI)? INVESTIGATING LEADERSHIP QUALITIES IN STROKE RESEARCH
Peter Wilding*1,2, Yin-Leng Tan3
1Imperial College Healthcare NHS Trust, Stroke, London, United Kingdom, 2Imperial College London, Brain Sciences, London, United Kingdom, 3University of Reading, Henley Business School, Reading, United Kingdom
On behalf of:
Background and aims: The exciting prospect of effective stroke treatments that prevent or reduce disability and death, or enhance recovery, drive the research agenda. At the site-level the Principal Investigator is responsible for the delivery of research in accordance with ethical and legal requirements, and is empowered to delegate other investigators and research staff to support delivery, commensurate with their qualifications and suitability. There is, however, an absence of studies exploring the effectiveness of PIs in terms of characteristics and leadership qualities in stroke research.
Methods: Using a qualitative method, we conducted eight semi-structured interviews with Hyperacute Stroke Research Centre (HSRC) team-members and related stakeholders. Thematic analysis was used to determine perceptions of effectiveness and leadership qualities of PIs in stroke research, grounded by service science theory and practice.
Results: Our findings revealed that ineffective PIs were characterised by an I-shaped skillset, i.e., stroke-specialism without recognised leadership skills. Effective PIs, in contrast, had a T-shaped skillset, i.e., not only the stroke-specialism but also additional (hence T-shaped) leadership skills. Three themes emerged for the T-shaped PI: (1) establishing psychological safety among the research team; (2) clarity of purpose and strategy; and co-creating aims and solutions with (3) collaboration and action.
Conclusions: Effective PIs can be characterised using the service science T-shaped leadership profile. This is the first time, to our knowledge, it has been applied to stroke research. We recommend that stroke services assess for, develop, and hire, research-active consultants and others based on their proven record of T-shaped leadership-qualities.
Disclosures of Interest: No
Abstract N°: 3166
GUIDELINES IN STROKE AND VASCULAR NEUROLOGY – AN ANALYSIS FROM 2012 TO 2023
Hanna Martins1, João Brainer de Andrade*1, Gisele Silva1, Renato Lopes2, Marcella Santos1, Eva Rocha1
1Universidade Federal de São Paulo, neurology and neurosciences, São Paulo, Brazil, 2Duke Clinical Research Institute, Cardiology, Durham, United States
On behalf of: Carlos Felipe Romera Lopes; Gustavo Rodrigues Ferreira Gomes; Jorge Luiz de Brito de Souza; Nathalia Souza de Oliveira; Paula Sanchez Nascimento; Raissa Kaori Ikeda; Rebeca Bessa Maurício; Vitória Maia Torres Peixoto
Background and aims: Clinical guidelines have become an essential tool for updating medical professionals. Their use lessens the possibility of medical harm and promotes proper medical practices.
Methods: Review of the European, American and Brazilian Academies of Neurology guidelines on stroke and vascular neurology, published between 2012 and 2023, evaluating the number and proportion of recommendations made.
Results: Sixty-one articles were analyzed. The GRADE classification was used in 31 guidelines, 22 used level/class of evidence and 8 used only level of evidence to classify the recommendations made. Overall, 2547 recommendations were published. There were 98 strong recommendations (17.88%), of which 17 had high-quality evidence (3.10%) and 24 with very low quality evidence (4.37%). There were 171 recommendations of weak strength (31.20%), 2 of which had high quality evidence (0.36%) and 62 with very low quality evidence (11.31%). Among the articles that did not use the GRADE classification system, there were 430 level A recommendations (16.88%) and 785 level C (30.82%). Regarding the class of evidence, there were 698 class I recommendations (27.40%). Only 242 recommendations received an IA classification (9.50%). There have been 27 guidelines published in the last 4 years (2020-2023), which were responsible for 709 recommendations (27.83%). The average number of recommendations per guideline in this period was lower when compared to previous years – 26.25 recommendations per guideline versus 54.05.
Conclusions: New approaches to conducting clinical research are needed to enable the generation of high-quality evidence in a more pragmatic and efficient way.
Disclosures of Interest: No
Abstract N°: 3199
FRAGILITY FRACTURE RISK IN STROKE PATIENTS: A QUALITY IMPROVEMENT PROJECT
Oriane Grant*1, Lucy Sykes2
1Royal Hampshire County Hospital, United Kingdom, 2Royal Hampshire County Hospital, Winchester, United Kingdom
On behalf of:
Background and aims: Fragility fractures cost the NHS £4.4 billion p.a. and result in high morbidity and mortality for patients1. Strokes are associated with an elderly population and falls are the most common complication post-stroke2,3, giving stroke patients a significant risk of fragility fracture4.
Aim: To assess and improve identification of fracture risk and prescription of appropriate bone protection in a stroke unit.
Methods: Clinical notes of 90 patients were retrospectively reviewed to establish baseline practice. A QFracture score was estimated for each patient to establish their risk of fragility fracture5,6. An investigation table was then integrated into clinical noting and included a prompt to check vitamin D and QFracture. A teaching session was also conducted. A preliminary re-audit of 30 patients was completed 2 months later, with a full re-audit taking place in January-February.
Results: No patients were started on bone protection during admission and only 1 had their vitamin D checked. 1 patient was re-admitted after discharge with a wrist fracture. 78% qualified for bone protection based on QFracture score. Preliminary re-audit results showed that 80% of patients either had their vitamin D checked during admission or were already established on protection. 78% of patients who had their vitamin D checked were deficient and 100% of these were started on replacement.
Conclusions: The surveyed stroke unit had no current bone health prescribing practice, despite 78% of patients being risk of fragility fracture. Initial results suggest a significant improvement in vitamin D monitoring and replacement. Full results are expected by March.
Disclosures of Interest: No
Abstract N°: 5
META-ANALYSIS OF AUDITS MEASURING ANTITHROMBOTICS WITHIN 48 HOURS FOR ISCHEMIC STROKE
Andy Lim*1, Grace Phillips2, Henry MA1, Thanh Phan1
1Monash University, Stroke and Aging Research Group, Department of Medicine, Monash University, Melbourne, Australia., Clayton, Australia, 2Monash University, Faculty of Medicine, Nursing and Health Sciences, Clayton, Australia
On behalf of:
Background and aims: Meta-analysis of clinical trials supports the use of early antithrombotic medication in ischemic stroke and transient ischemic attack. It is not known whether this therapy is delivered within the 85% threshold that is acceptable in North America’s Get With The Guidelines (GWTG) stroke program. Our aim is to investigate the pooled proportion of patients receiving antiplatelet therapy within 48 hours of ischemic stroke.
Methods: PubMed to November 2022 was searched for studies reporting “stroke”, “audit”, “antithrombotic”, “national” and “registry” (Figure 1). Multilevel random effects meta-analysis was used to cluster studies by country.
Results: There were 45 studies describing 1,178,595 patients. Pooled proportion of patients receiving antithrombotic therapy within 48 hours was 81.1%, (95% CI 74.5, 87.8, p<0.0001, I2=99.99%) (Figure 2). The high heterogeneity was due to within-country (I2Level 3=55.4%) and between-country heterogeneity (I2Level 2=44.6%). There was no statistical significance (p=0.35) between low- to middle- income countries (LMIC) – 81.8%, (95% CI 76.1, 87.4, p<0.01, I2=100%) and high-income countries (HIC) – 86.8%, (95% CI 81.2, 92.3, p<0.01, I2=99.7%) nor any difference between contemporary studies (⩾2008) – 86.5%, (95% CI 82.3, 90.8, p<0.01, I2=100%) – and studies published before 2008 – 69.9%, (95% CI 57.4, 82.4, p<0.01, I2=99.7%). Sensitivity analysis showed no difference when excluding single-centre studies, observations with n<500, or both. Meta-regression showed proportion of antiplatelet administration to increase significantly with subsequent year of publication (β=0.01, 95% CI 0.00, 0.02, p<0.05).
Conclusions: This study is a wake-up call as the majority of countries do not yet provide early antiplatelet therapy at a level acceptable by GWTG hospitals.
Disclosures of Interest: No
Abstract N°: 10
IN-PATIENT CODE STROKE: A MULTI-CENTRE RETROSPECTIVE COHORT STUDY IN EASTERN SPAIN
Luis Moreno-Navarro*1,2, Diego Corona-García1, Mònica Farrerons-Llopart1,2, Diana Tarruella-Hernández3, Helena Benetó-Andrés4, Isabel Beltrán-Blasco1,2, Raquel Hernández-Lorido1, José Tembl-Ferrairó3, Cristina Soriano-Soriano4, Nicolás López-Hernández1,2
1Hospital General Universitario Dr. Balmis, Neurology, Alicante, Spain, 2Instituto de Investigación Sanitaria Biomédica de Alicante (ISABIAL), Group 1: Neuroscience Research, Alicante, Spain, 3Hospital Universitari i Politècnic La Fe, Neurology, Valencia, Spain, 4Hospital General de Castelló, Neurology, Castellón de la Plana, Spain
On behalf of:
Background and aims: In-Hospital Stroke (IHS) refers to a stroke that occurs in a patient already admitted for another disease. It accounts for 4-17% of acute stroke events. However, there is little scientific literature on this topic. Our aim is to investigate differences in baseline characteristics and acute management between IHS and Community-Onset Stroke (COS) patients.
Methods: A multi-centre retrospective cohort study was conducted through the collaborative participation of 3 Stroke Units in Eastern Spain. The study included Code Stroke activations from July 2020 to December 2022. Data collection was carried out using CODICT registry.
Results: A total of 1874 patients with stroke were enrolled, of whom 106 had IHS (5.7%). The mean age of IHS cases was 70.8 years and 57.5% were male. IHS patients were most frequently observed in the Cardiology department (30.8%) and exhibited longer response times compared to COS patients (median door-to-imaging time (minutes): IHS 32.5, COS 20, p<0.001; median door-to-needle time (minutes): IHS 80, COS 39, p<0.001; median door-to-groin time (minutes): IHS 118.5, COS 79, p<0.001). Furthermore, IHS cases showed a notably lower use of intravenous fibrinolysis (IHS 5.6%, COS 42.6%, p<0.001) and mechanical thrombectomy (IHS 21.1%, COS 41.2%, p<0.001). Most common contraindication reasons for intravenous fibrinolysis among IHS cases were active use of anticoagulants (35.3%) and recent major surgery (32.4%).
Conclusions: Acute management of IHS cases experiences significant delays in response times compared to COS patients, along with a reduced application of revascularization therapies. This highlights the need to develop specific algorithms for IHS.
Disclosures of Interest: No
Abstract N°: 879
DEVELOPMENT OF THE IRISH NATIONAL AUDIT OF STROKE (INAS): MONITORING THE QUALITY OF ACUTE STROKE CARE IN IRELAND
Catherine Moran*1, On Behalf of the Hrb-Apa Stroke Audit Development Research Steering Group Rcsi1
1RCSI University of Medicine & Health Sciences, Dublin, Ireland
On behalf of: Steering Group & Co-Authors: I. Jeffares, N.A. Merriman, J. McCormack, J. Harbison, E. Sexton, D. Williams, P.J. Kelly, F. Horgan, R. Collins, M. Ní Bhreacáin, E. Byrne, J. Thornton, C. Tully, A. Hickey
Background and aims: This project aims to develop internationally-benchmarked, core minimum datasets for acute and non-acute stroke care for integration into the newly-developed Irish National Audit of Stroke (INAS).
Methods: In the acute phase, a scoping review of international practice identified 21 stroke registries/audits with national coverage and continuous data collection. Audit documentation was retrieved and acute stroke care data items were extracted, translated, and charted. Data charting was performed to compare Irish and international items to identify commonalities and/or gaps in coverage.
Results: A synthesised inventory of acute care data items, including existing Irish items (n=103), the most frequently-collected international items (n=97) and additional expert-suggested items (n=22), were reviewed by key stakeholders in a three-stage Delphi process to obtain their expert perspectives as to the worthiness and appropriateness of items for integration (or retention) in INAS. Consensus agreement was obtained and a core minimum dataset of 86 acute stroke care and 35 thrombectomy items was finalised. Examples of items considered for addition to INAS include items that examine risk factors for stroke and associated secondary prevention.
Conclusions: The minimum datasets, as guided by best practice international standards, local priorities, and iterative cycles of stakeholder engagement, will act as the “gold standard” for monitoring stroke care in Ireland with the ultimate aims of enhancing patient recovery and supporting local and national quality improvement. This work represents the “ideal” core outcomes dataset for acute stroke care in Ireland but additional resourcing would be required if these recommended items were to be added to INAS.
Disclosures of Interest: No
Abstract N°: 1867
5-YEAR EXPERIENCE ON RES-Q REGISTRY FOR MONITORING THE QUALITY OF STROKE CARE IN CROATIA (FROM 2019 TO 2023 YEAR)
Hrvoje BUDINCEVIC*1, Ivan Peric2, Zdravka Poljakovic2, David Bonifacic3, Marina Roje Bedeković4, Arijana Lovrenčić Huzjan4, Klementina Korda5, Robert Marčec6, Karla Sabolek Lovrec6, Igor Cindrić7
1Clinical Hospital "Sveti Duh", Zagreb, Croatia, 2University Hospital Centre Zagreb, Zagreb, Croatia, 3Clinical Hospital Center Rijeka, Rijeka, Croatia, 4Sisters of Charity Hospital, Zagreb, Croatia, 5General Hospital Vinkovci, Vinkovci, Croatia, 6County Hospital Čakovec, Čakovec, Croatia, 7General Hospital Virovitica, Virovitica, Croatia
On behalf of: Croatian RES-Q Stroke Study Group: Andrija Meštrović, Doroteja Lehpamer, Maida Seferović, Danijela Erak, Antonija Švinger-Muić, Ervin Jančić, Irena Pintarić, Borislav Vuković, Mateja Bošković, Sanja Svalina, Siniša Majski, Miljenko Crnjaković, Stela Rutović, Ruža Kostanjevec, Emina Pavlekovic, Simona Milić, Marinko Dikanović, Frederic-Ivan Silconi, Tihana Gržinčić, Marina Šimunović, Juraj Mark Poje, Maro Vodopić, Andrijana Bogoje Raspopović, Ivan Miletić, Ana Gorupić, Zurap Raifi
Background and aims: Stroke registry might be used as a tool for improving stroke care. The Registry of Stroke Care Quality (RES-Q) was launched by ESO-EAST (Enhancing and Accelerating Stroke Treatment) in 2016, and Croatia is participating since 2017. The aim was to compare results captured from the RES-Q registry in Croatia for the first quarters of the last five years (2019 to 2023).
Methods: Data on demographics, stroke care pathway, specific acute treatment issues, and stroke prevention issues in all acute stroke admissions in Croatia during the first years’ quarters from 2019 to 2023. were analysed.
Results: Acute hospitals which provide stroke treatment recruited 3582 patients. Figure 1. shows the map of Croatia with all centers (green – > three periods, yellow – two periods, red – one period, black–no data). Table 1. shows the number of patients recruited by site and time period. Table 2. shows patients' main baseline characteristics and outcome measures.
Conclusions: Our results showed improvement in percentage of stroke patients across Croatia treated with recanalization therapy (IVT from 10% to 20.6% in 2022, and MT from 4.0 to 7.8%), with reaching a median DTN time of 39 minutes in 2021 and DTG time of 57.5 minutes in 2021. Secondary stroke prevention might be improved by increasing the usage of statins with performing smoking cessation programs. There is a substantial need for involvement of all stroke centers in a stroke registry to achieve more accurate data and improve stroke care in Croatia.
Disclosures of Interest: No
Abstract N°: 2041
REPORTING OF DATA COLLECTION METHODS AND RESOURCING OF NATIONAL STROKE REGISTRIES: A SYSTEMATIC REVIEW
Agnes Jonsson*1, Nicole Cosgrave1, Anna Healy2, David Williams2, Anne Hickey1
1Royal College of Surgeons in Ireland, Ireland, 2Beaumont Hospital, Dublin, Ireland
On behalf of:
Background and aims: National disease registries are powerful tools for improving stroke care and advancing research. With the evolution of newer treatments for stroke, registries have become instrumental in measuring changes and pinpointing areas for improvement in care. We aim to describe the methodology and resourcing of existing national stroke registries.
Methods: We conducted a systematic search of the published, peer-reviewed literature and grey literature looking for descriptions of the data collection methods and resourcing of national stroke registries or audits. The systematic review was registered in PROSPERO.
Results: 97 references relating to 21 audits in 19 countries were identified. They universally employed web-based platforms for data collection. The principal profession of data collectors was nursing. The scope of variables collected varied. All included the acute phase of care, 24% (6) also registered the pre-hospital (ambulance) phase and 23% (5) included rehabilitation. 71% (15) collected outcome data. The audits varied in their approach to outcome data collection; in 9 registries it was collected by hospitals themselves, in 3 it was collected directly by the audit/registry, and 7 had access to national administrative databases allowing follow-up of a limited number of end points. Creating a comparative table to evaluate resourcing of the audits was challenging due to the diverse nature of management structures and variables.
Conclusions: We highlight the role of clinical stroke audits as instruments for quality improvement in healthcare, as well as providing data that can be used for research. Future work could involve creating a central repository of stroke registries to facilitate international comparisons.
Disclosures of Interest: No
Abstract N°: 2434
QUALIFICATION NEEDS AND CAREER PERSPECTIVES IN NEURO NURSING IN GERMANY – A QUALITATIVE INTERVIEW STUDY
1University of Applied Sciences Saarland, Social Science, Saarbrücken, Germany, 2University of Cologne, Köln, Germany, 3University of Applied Sciences Saarland, School of Social Science, Saarbrücken, Germany, 4University of Lübeck, Institute of Social Medicine and Epidemiology, Lübeck, Germany
On behalf of:
Background and aims: The prevalence and complexity of neurological diseases stress the need for nursing expertise. In Germany, there is a lack of high-quality education programs for neuro nurses, and nurses face challenges like high workloads and low retention rates. The study aims to identify qualification needs and expand the scope of action required to develop neurology as an attractive nursing practice field.
Methods: We conduct a mixed-methods study applying a Delphi process. Semi-structured, guideline-based expert interviews were conducted with experienced nurses and physicians working in neurological settings. The interviews were analyzed according to Mayring’s qualitative content analysis method. Two subsequent quantitative waves with standardized online surveys are planned.
Results: 22 interviews were conducted with 12 nurses and 10 neurologists. The experts were generally receptive to qualification and expanded fields of nursing action. However, they reported a number of challenges in Germany that make it difficult to implement expanded results. Based on the interviews, we identified:
Qualification needs: strategic alignment and content of qualification programs for neuro nurses.
Possible autonomous fields of nursing action: e.g. screening & assessment, basic invasive procedures, medication management, follow-up examinations, patient education, knowledge transfer and research.
Barriers and enablers: Structural, traditional, financial, legal and personal conditions for implementing high-quality education programs and greater autonomy in nursing action.
Conclusions: Experts considered the academization of neuro nurses and various non-academic career paths to be necessary. The quantitative waves will investigate qualification requirements and possible autonomous fields of action in a larger sample of neuro specialists.
Disclosures of Interest: No
Abstract N°: 3009
DISCRETE EVENT SIMULATION MODEL OF AN ACUTE STROKE TREATMENT PROCESS AT A COMPREHENSIVE STROKE CENTER
Background and aims: Ischemic stroke is treatable with thrombolysis and/or endovascular thrombectomy (EVT). However, faster treatment increases the probability of good outcomes. This study develops a discrete event simulation model of the acute stroke treatment process at the Comprehensive Stroke Center in Nova Scotia, Canada. Several improvement strategies were trialed to determine reduction of treatment.
Methods: The sub-tasks in the treatment process were modelled using a discrete-event simulation in Python. Nine scenarios were proposed based on different phases in the process, and the impact of each scenario was investigated. Scenarios were tested individually and in combinations. The results were compared using the Mann-Whitney U Test. The primary outcomes of the model were DTCT (door-to-CT time), DNT (door-to-needle time), and DGPT (door-to-groin-puncture-time).
Results: The simulation model was run 30 times to simulate 185 patients. Collecting patient history on the way to the CT scanner (rather than in ED) showed the highest impact on reduction for DTCT (14.3 vs 12.5 minutes, p<0.001) and DNT times (40.1 vs 37.2 minutes, p<0.001). Reduction of treatment decision time by 50% resulted in lower DNT (40.1 vs 35.8 minutes, p<0.001) and DGPT times (67.0 vs 63.1 minutes, p<0.001). The combinations of each phase scenarios with all the patients were treated by stroke neurologists resulted in the lowest DTCT (14.3 vs 10.9 minutes, p<0.001), DNT (40.1 vs 30.0 minutes, p<0.001), and DGPT (67.0 vs 47.8 minutes, p<0.001).
Conclusions: The proposed simulation model provides improvement strategies that will result in significant treatment time reduction.
Disclosures of Interest: No
Abstract N°: 3264
REDUCING DOOR-TO-NEEDLE AND DOOR-TO-PUNCTION TIMES IN ACUTE ISCHEMIC STROKE: A QUALITY IMPROVEMENT STUDY
Murilo Souza*1, Alexandre Drayton1, Gabriel Xavier1, Humberto Castro-Lima1,2, Mateus Do Rosário1, Daniel Abreu1, Guilherme Almeida1, Lidianne Neri1, Barbara Costa1, Caio Souza2
1Hospital Cárdio Pulmonar, Neurology, Salvador, Brazil, 2BAHIANA - School of Medicine and Public Health, Salvador, Brazil
On behalf of:
Background and aims: In-hospital delay from symptom onset to reperfusion therapy decrease treatment efficacy of ischemic stroke. Therefore, institutional protocols designed to reduce door-to-needle time (DTN) and door-to-puncture (DTP) are crucial for best care of acute stroke. This single-center observational study aimed to describe the impact of the our stroke protocol in reducing delays in treatment.
Methods: This retrospective observational study included all patients eligible for Alteplase or Thrombectomy from 2011 to 2023. The Impacts of the protocol were evaluated by calculating frequencies and the annual median DNT and DTP. The protocol mandated: 1) Early recognition of stroke and direct referral to CT during triage; 3) Protocol and mock stroke training; 4) Real-time feedback to the emergency room staff.
Results: 966 patients were admitted under the stroke protocol between january 2011 and december 2023, with a median age of 73 years and a NIHSS score of 8. Reperfusion Therapy was offered to 170 patients. We observed a significant increase in thrombolysis rate from 7.9% to 15% (P<0.001), and thrombectomy rate from 1.1% to 7.6%. (P<0.001) when comparing 2012-2014 to 2015-2023. Differences in DTN among years are statistically significant (P=0.007). The DNT decreased from a median of 89 minutes (84-116) in 2012 to 31 minutes (18-51) in 2015, and to 28 minutes (17-43) in 2019. Notwithstanding the COVID outbreak, the DNT did not surpass the 45-minute mark, reaching 31 minutes (20-46) in 2023.
Conclusions: The implementation of validated strategies effectively reduced treatment delays and improved reperfusion therapy rates.
Disclosures of Interest: No
Abstract N°: 518
OPTIMALISATION OF THE DOOR-IN DOOR-OUT TIME WITHIN THE STROKE CARE NETWORK TROMBVZ
Sofie Vanneste*1, Sofie De Blauwe1, Annelies Depreitere2, Marie-Christine Hasenbroekx3, Penka Kirilova4, John Lebbink5, Leen Sinnaeve6, Annelies Terwecoren4, Marie-Damienne Verhalle4, Geert Vanhooren1
Background and aims: In XXX, thrombectomy is performed at S2 centers. "XXX" in XXX is serving as hub (S2 center) for 8 spokes (S1 center) in the XXX stroke care network. The Door-In Door-Out (DIDO) is the epoch between entering and leaving an S1 center. It is considered as process quality indicator recommended to be below 60 minutes.
The aim is to optimize the DIDO time within XXX.
Methods: Time indicators of the DIDO process and local process details were collected by a quantitative pre-measurement (2014-2021) and semi-structured interviews. Individual quality improvements advice was given to each S1 center based on interim analysis findings. Also, two more possibly interesting data points (First-Contact time and Decision time) were identified and implemented in further analysis. A quantitative post-measurement was conducted from July 2022 – 2023.
Results: The dataset included data on 556 patients (378 pre-intervention, 178 post-intervention). Median DIDO pre-intervention was 78 minutes, not significantly different from the post-intervention 80 minutes. Imaging is considered as a local decision point for thrombolysis/thrombectomy. The Door-In-to-Imaging was only 15 minutes (19% of DIDO), while the Imaging-to-Door-Out was 65 minutes. Introducing the new time points showed an Imaging-to-First-Contact time of 36 minutes, constituting 45% of the total DIDO process. The Decision-to-Door-Out time was 22 minutes.
Conclusions: Continued investment in enhancing the DIDO process could yield a median time below 60 minutes. The new time indicators emphasize potential time savings during the Imaging-to-First-Contact process and also the Decision-to-Door-Out epoch. A new round of individualized advice is planned.
Disclosures of Interest: No
Abstract N°: 663
FACTORS ASSOCIATED WITH DECREASING RATE OF INTRAVENOUS THROMBOLYSIS IN KOREA
1Soonchunhyang University Seoul Hospital, Neurology, Seoul, South Korea, 2ASAN Medical Center, Clinical Research Center, Seoul, South Korea, 3Seoul National University Bundang Hospital, Neurology and Cerebrovascular Center, Seongnam, South Korea, 4Seoul National University Hospital, Neurology, Seoul, South Korea, 5Inha University Hospital, Neurology, Incheon, South Korea, 6Seoul Medical Center, Neurology, Seoul, South Korea, 7Uijeongbu Eulji Medical Center, Neurology, Euijeongbu, South Korea, 8Dong-A University Hospital, Neurology, Busan, South Korea
On behalf of:
Background and aims: Recently, the rate of intravenous thrombolysis (IVT) for hyperacute ischemic stroke has been declining in Korea. This study aimed to investigate the factors affecting the IVT implementation rate.
Methods: This study analyzed the data of 28,800 patients admitted in 248 hospitals which participated in the 8th nationwide assessment of acute stroke treatment quality by National Health Insurance Review and Assessment Service. Among them, 124 hospitals with 3 or more IVTs performed for 6 months were included. The IVT rates of individual hospitals were divided into quartiles (⩾12.2%, 8.8-12.1%, 6.5-8.7%, <6.4%), and the characteristics of each group were compared. Number of specialists, 24-hour IVT availability, endovascular thrombectomy case volume, stroke unit beds, and accreditation of center were additionally obtained.
Results: The mean of IVT rates was 9.75±4.71%. The median door-to-imaging time was 13.1 minutes, 13.3 minutes, 16.5 minutes, and 15.3 minutes for each quartile. Door-to-needle time was not statistically different: 54.4 minutes, 46.4 minutes, 51.6 minutes, and 50.2 minutes. The higher the IVT implementation rate, the higher the endovascular thrombectomy rate: 11.9%, 8.0%, 7.5%, and 6.8%. The ambulance use rate was significantly lower in the hospitals with lower IVT implementation rate: 64.2%, 61.3%, 57.4%, and 56.1%. The onset-to-visit time was also delayed in those hospitals: 3.2 hours, 4.0 hours, 5.1 hours, and 5.4 hours.
Conclusions: Hospitals with low IVT rates had a lower rate of ambulance use and a longer hospital visit time from stroke onset. Unimproved patients’ recognition and the ambulance system may be important causes of recent declining IVT rate in Korea.
Disclosures of Interest: No
Abstract N°: 1120
ADDITIONAL ENDOVASCULAR THROMBECTOMY-CAPABLE STROKE CENTERS IN THE NORTHERN NETHERLANDS: A COST-EFFECTIVENESS MODELING STUDY
Chi Nguyen*1,2,3, Maarten Lahr2,4, Willemijn Maas2, Ido van den Wijngaard5,6, Wim Van Zwam7,8, Diederik Dippel9, Yvo Roos10, Erik Buskens1,2, Durk-Jouke van der Zee1,2, Maarten Uyttenboogaart11,12
1Faculty of Economics and Business, University of Groningen, Operations, Netherlands, 2University Medical Center Groningen, Epidemiology, Netherlands, 3Hanoi University of Pharmacy, Pharmaceutical Management and Economic, Viet Nam, 4University of Groningen, Aletta Jacobs School of Public Health, Netherlands, 5Haaglanden Medical Center, Neurology, Netherlands, 6Leiden University Medical Center, Neurology, Netherlands, 7Maastricht University Medical Center, Radiology and Nuclear Medicine, Netherlands, 8Maastricht University, School for Cardiovascular Diseases (CARIM), Netherlands, 9Erasmus University Medical Center, Neurology, Netherlands, 10Amsterdam University Medical Center, Neurology, Netherlands, 11University Medical Center Groningen, Neurology, Netherlands, 12University Medical Center Groningen, Radiology, Medical Imaging Center, Netherlands
On behalf of: CONTRAST consortium
Background and aims: To improve the accessibility for endovascular thrombectomy (EVT) upgrading primary stroke centers (PSCs) to EVT-capable stroke centers appears to be a logical solution. We assessed the cost-effectiveness of one extra EVT-capable stroke center, and two extra EVT-capable stroke centers versus current practice. Currently, patients with large vessel occlusion (LVO) are transferred from seven PSCs to a single EVT-capable stroke center in the Northern Netherlands.
Methods: We developed a simulation model combined with a decision tree and Markov model to estimate total costs, total quality-adjusted life years, and net monetary benefit (NMB) assuming a willingness-to-pay threshold of €50,000 over a 15-year time horizon. Data were derived from the MR CLEAN Registry. Costs were obtained from a healthcare-payer perspective. Probabilistic sensitivity analysis and scenario analysis were performed to assess robustness of results.
Results: Two extra EVT-capable centers yielded the highest NMB (€120,502), followed by one extra center (€119,803), and current practice (€116,278). The probability of two additional centers being cost-effective was 64%, 34% for one extra center, and 2% for current practice. However, when taking into account the volume of EVT per year on quality of care (i.e., a center with ⩾100 EVT cases vs. < 100 EVT cases), extra EVT-capable stroke centers resulted in a lower NMB (€115,575 for one extra center, €115,600 for two extra centers) compared to current practice (€116,278).
Conclusions: Introduction of additional EVT-capable stroke centers in the Northern Netherlands only appeared to be cost-effective if all the EVT-capable centers would achieve substantial EVT volumes.
Disclosures of Interest: No
Abstract N°: 1434
IMPROVING STROKE PREVENTION IN DEVICE-DETECTED ATRIAL FIBRILLATION THROUGH AN MDT PATHWAY BETWEEN CARDIOLOGY AND STROKE SERVICES
Nick Mills*1, Sarah Finlay1, Viki Carpenter1, Elizabeth Warburton1, Isuru Induruwa1, Kayvan Khadjooi1
1CB2 0QQ, United Kingdom
On behalf of:
Background and aims: The Stroke Prevention in AF (SOS-AF) service at Cambridge University Hospital screens medical admissions for AF, advises secondary and primary care and holds outpatient clinics. Historically, if AF was detected on a pacemaker or implantable loop recorder by Cardiac Rhythm Management (CRM) team, a generic letter would be sent to the GP, however, anticoagulation rates and time to prescription were very poor.
Methods: A multidisciplinary pathway was developed to initiate collaboration between CRM team and SOS-AF service. On receipt of an electronic referral, SOS-AF team holistically considers each case. Patients are contacted via a remote consultation, fully consulted and educated on AF to make an informed decision on anticoagulation. Same day letters are emailed to GPs, covering comprehensive management plans.
Results: In the first 12 months, 100 referrals received: median age 80 (72-86), CHA2DS2-VASc 4 (3-5).
● 100% triaged within 24 hours;
● Median time between referral to first-input: 3 days (1-12.5);
● 99%: a final documented plan for stroke prevention within a few days of referral;
● 53 letters recommending GP to start anticoagulation sent (52: started anticoagulation);
● 29: advised anticoagulation not indicated or contraindicated;
● 18: already on anticoagulation, dose correction advised in 4.
Conclusions: This innovative pathway has led to considerable improvement in patient safety and satisfaction through rapid triage, timely contact with patients and GPs, delivering education, advice and a practical management plan. This has led to a 98% anticoagulation rate in device-detected AF who are eligible for anticoagulation, while decreasing workload and saving time for primary care at no additional costs.
Disclosures of Interest: No
Abstract N°: 2132
ESTABLISHMENT OF THE NEUROVASCULAR UNIT IN ORAN (2014-2024): 10 YEARS OF EXPERIENCE
Douniazed Badsi*1,2
1Etablissemnt hospitalo-universitaire -Oran EHU, Medecine,neurology, oran, 2faculté d emedecine Oran, Medecine,neurology, oran
On behalf of:
Background and aims: Stroke is one of the leading causes of death and disability worldwide.
The stroke unit has proven its effectiveness in all studies on mortality and functional disability of a stroke patient.The aim of our presentation is to share our experience of stroke management in our region by presenting our results of 10 years, from the creation of the UNV to the certification project.
Methods: This is a descriptive, single-center study. It took place from February 2015 to 02 January 2024. The Neurovascular Unit was set up on February 2, 2015, open 24 hours a day.
Results: During the study period, we hospitalized 3000 patients with acute neurovascular pathologies including 1900 patients (80%) with ischemic stroke, 640 with hemorrhagic stroke (15%), 200 with cerebral venous thrombosis and 80 with subarachnoid hemorrhage.
240 (10%) of strokes were thrombolyzed.The initial NIHSS was between 8-15 in 70% of patients.The Door To Needle Time to less than 60.The average time of arrival at the hospital since the onset of symptoms was 02 hours, the majority of patients lived in ORAN.
Our UNV is a pilot training center for emergency physicians in neurovascular pathology, a telemedicine activity has been set up with teams from the south of the country. we have been honored with 07 Angels awards.Our center is a candidate for certification
Conclusions: The establishment of a stroke unit, the training of nursing staff, the organization of the stroke sector improves the care of patients with neurovascular pathology in our region.
Disclosures of Interest: No
Abstract N°: 2190
CAROTID INTERVENTION IN ACUTE NON-DISABLING STROKE OR TIA PATIENT WITH SIGNIFICANT SYMPTOMATIC EXTRACRANIAL CAROTID STENOSIS
Marwa Hamdan*1, Joumana Janbieh2, Asmaa Al-Noori3
1Royal Hallamshire Hospital, Stroke department, Sheffield, United Kingdom, 2Royal Hallamshire Hospital, Neuroscience department, United Kingdom, 3Royal Hallamshire Hospital, United Kingdom
On behalf of:
Background and aims: Extracranial carotid artery stenosis is considered a potentially treatable cause of ischemic strokes. Carotid revascularization has been established as an effective treatment in reducing the risk of stroke. The intervention is recommended to be done within 14 days of the symptoms onset. We aimed to evaluate the adherance to NICE guidelines at Sheffield Teaching Hospitals and to ensure that all eligible candidates are being referred and assessed within the recommended timeframe.
Methods: We have reviewed 1789 patients who had carotid doppler ultrasound done between 1st March 2022 until 31st January 2023. All cases with significant carotid stenosis meeting NASCET criteria for vascular referral have been retrieved. We reported three phases to assess the median time and IQR from symptoms to carotid endarterectomy.
Results: A total of 68 patients had carotid stenosis meeting the NASCET criteria in 11 months period. A total of 32 (48.5%) patients have had surgical intervention done. 14 (43.7%) patients had the intrevention done within 14 days. The median time from symptom onset to surgical intervention was 16 days. The median times for the three phases were as follow; Onset of symptoms to vascular referral; 2 days (IQR 1-10). From referral to vascular team to being assessed; 3 days (IQR 2-7). From being assessed by vascular to the intervention; 12 days (IQR 4-15). 2.9% have developed major complcaitions, this is in keeping with rate reported by national vascular registry.
Conclusions: 48.5% of eligible patients who presented with acute stroke/TIA and significant symptomatic carotid stenosis had their intervention within 14 days.
Disclosures of Interest: No
Abstract N°: 2377
UNDERSTANDING PERFORMANCE IMPROVEMENT FOR PARTICIPANTS IN CODE STROKE SIMULATION TRAINING
Lauren Sanders*1,2, Jayne Lysk3, Stuart Marshall4,5
1St Vincent's Hospital, Melbourne, Department of Neurosciences, Australia, 2The University of Melbourne, Department of Medicine, Australia, 3The University of Melbourne, Department of Medical Education, Australia, 4Peninsula Health, Department of Anaesthesia, Australia, 5The University of Melbourne, Department of Critical Care, Australia
On behalf of:
Background and aims: Code stroke simulation is associated with improvements in clinician knowledge, performance metrics and clinical outcomes. Although increasingly incorporated into neurology curriculums and stroke team training, little is known about why stroke simulation is effective or how to enhance learning outcomes. We sought to understand how learning occurs during code stroke simulation in order to optimise training delivery and facilitation.
Methods: Debriefs of six multi-level learner code stroke simulations were recorded and transcribed. Sessions were conducted in the hospital simulation centre with a simulated participant. Participants were the on-call stroke and radiology teams with a simulation trained neurologist facilitating. Data were evaluated using reflexive thematic analysis with interpretation through a Situated Learning Theory lens.
Results: Although several topics (“Communication”, “Knowledge”, “Processes Efficiency”, “Team Factors”) demonstrated expected overlap with principles of crisis resource management, the most frequently identified topics were “Self-Reflection” and “Feedback”. The central theme was “Development of identity as a stroke team member” which identified participants’ efforts not just to retain and make meaning of learnings but to situate learnings in the context of their role, expectations and performance as stroke team member. This included subthemes of how learners define and view themselves as clinicians, how performance expectations influence communication with senior clinicians and drivers of both positive and negative interdisciplinary interactions.
Conclusions: Self-reflection and development of clinician identity are significant components of the learning that occurs during simulation debriefs. Attention to these factors, in addition to usual knowledge and process consolidation, may assist facilitators in optimising translation of learnings to clinical care.
Disclosures of Interest: No
Abstract N°: 2739
INTEGRATED STROKE CARE IN THE NETHERLANDS: RESULTS OF SELF-ASSESSMENT STUDY AMONG REGIONAL STROKE SERVICE NETWORKS
Bert Vrijhoef*1, Tamar Kwakkel1, Lucas Koester1, Monique Bergsma1
On behalf of: Aligned Integrated Stroke Care Networks in the Netherlands
Background and aims: To support the enhancement of integrated stroke care delivery, regional stroke service networks in the Netherlands participated in a self-assessment study. The previous (2012, 2015, 2019) and new (2023) insights aim to enable networks in their quality improvement initiatives.
Methods: Coordinators of networks filled out an online self-assessment survey in 2023. The validated survey is based on the Development Model for Integrated Care and consist of 97 items, representing 9 themes. Cluster scores indicate proportions of activities implemented to achieve integrated stroke service delivery. Data were analysed descriptively (mean±SD) and compared with data from previous years.
Results: Data were obtained from 17 networks initiated between 1995 and 2022. The smallest network counts 5 organisations, the largest 21. Overall, networks implemented 68.6(±12.5) % of items in 2023. On cluster level, 3 clusters score below average and 6 above. Networks are least active in ‘Performance Management’ (59.5±24.6) and ‘Delivery system’ (61.8±16.5), and most active in ‘Interprofessional Teamwork’ (92.2±14.6) and ‘Roles & Tasks (87.5±12.5). On item level, most challenging activities are sharing patient record and using incentives for continuous quality improvement (both 0%). The results for 2023 are to a high degree comparable to 2019 and better than results from 2012 and 2015.
Conclusions: Dutch regional stroke service networks remain highly active in the provision of integrated care. To further improve the quality of care, the Dutch Stroke Knowledge Network will use the study results to support the coordinators of regional networks in overcoming barriers and sharing improvement strategies.
Disclosures of Interest: No
Abstract N°: 2800
IMPACT OF ASSISTENTIAL QUALITY IN PATIENT REPORTED OUTCOMES POST-STROKE
Sara Bernardo-Castro*1, Ana Margarida Ferreira2, David Cano3,4, Giorgio Colangelo3,4, Francisco Purroy5, Xavier Ustrell Roig6, Yolanda Silva7, Alejandro Bustamante8, João Sargento Freitas1, Carlos A. Molina4,9
1Centro Hospitalar e Universitário de Coimbra, Neurology department, Coimbra, Portugal, 2Centro Hospitalar e Universitário de Coimbra, Physical and Rehabilitation Medicine Department, Coimbra, Portugal, 3Nora Health, Barcelona, Spain, 4VHIR - Vall d’Hebron Institute of Research, Barcelona, Spain, 5Hospital Univesitari Arnau de Vilanova, Stroke Unit, Neurology department, Lleida, Spain, 6Hospital Universitari Joan XXIII, Stroke Unit, Neurology department, Tarragona, Spain, 7Hospital Universitari Dr. Jose Trueta, Stroke Unit, Neurology department, Girona, Spain, 8Hospital Universitari Germans Trias i Pujol, Stroke Unit, Neurology department, Badalona, Spain, 9Hospital Universitari Vall d’Hebron, Stroke Unit, Neurology Department, Barcelona, Spain
On behalf of:
Background and aims: Patient-Reported Experience Measures (PREMs) assess hospital-stay satisfaction and follow-up. Despite their relevance in a system aiming at high-value healthcare, it is still not established whether better PREMs improve functional outcomes and Patient-Reported Outcome Measures (PROMs). We aimed to examine the impact of PREMs on clinical outcomes and PROMs post-stroke.
Methods: Consecutive stroke patients admitted to 6 hospitals of two southern Europe countries, were followed using a PREMs/PROMs electronic application, in the frame of an EU-funded high-value stroke care project. PREMs included quality of hospital care (7 days) and follow-up (90 days). PROMs (90 days) included HADs (anxiety/depression), PROMIS-10 (physical and mental health), global health quality (GHQ 0-100), and functional outcomes using the modified Rankin Scale (mRS).
Results: From 2022, 1372 patients were included (60.8% men, mean age 68years). A better perception of hospital care was associated with lower incidence of depression (OR 0.860 CI 0.764-0.968), mental and physical impairments (OR 0.883 CI 0.795-0.982; OR 0.900 CI 0.813-0.997). Follow-up quality was also associated with reduced anxiety, depression (OR 0.876 CI 0.797-0.964; OR 0.824 CI 0.746-0.910), and physical or mental changes (OR 0.804 CI 0.768-0.919; OR 0.825 CI 0.755-0.903). Quality of care and follow-up (B 1.002 CI 0.19-2.026; B 2.125 CI 1.326-2.924) increased GHQ and decreased mRS values (OR 0.880 CI 0.81-0.960 and OR 0.840 CI 0.78-0.90); p<0.05 for all.
Conclusions: The perceived quality of hospital and post-hospitalisation care improves functional outcomes and well-being. These findings highlight a new target for organizational improvement with potential to change current practices.
Disclosures of Interest: No
Abstract N°: 3169
IMPLEMENTATION OF THE ROADMAP FOR THE DEVELOPMENT OF CARE SYSTEM FOR HEART ATTACK AND STROKE IN KYRGYZSTAN: SUCCESSES AT THE MIDTERM REVIEW
Francesca R. Pezzella*1, Alexey Yakovlev2, Asel Kerimkulova3, Nurlan Omorov3, Sverdlova Irina3, Alexander Timukhin3, Aliina Altymysheva4, Jill L. Farrington5
1San Camillo Forlanini Hospital, Neuroscience, Rome, Italy, 2Almazov Center, Cardiology, St Petersburg, Russian Federation, 3National Hospital of Neurology, Stroke Unit, Bishkek, Kyrgyzstan, 4World Health Organization Country Office for Kyrgyzstan, NCD, Bishkek, Kyrgyzstan, 5WHO Regional Office for Europe, København,, Denmark
On behalf of:
Background and aims: Cardiovascular disease (CVD) are main cause of premature mortality and disability in Kyrgyzstan, hence, combating CVD has been a priority of the health national programs. The CVD Road Map (RM) was developed in 2018-19 under the coordination of the WHO Regional Office for Europe and the WHO Country Office, to create and transform existing networks and CVD system of care: update and implement clinical guidelines, use resources more effectively, improve infrastructure and performance management. The RM outlines core acute care interventions in acute myocardial infraction and stroke with key design of services and proposes strategic directions to accelerate gains in CVD management
Methods: The following coordinated tools/activities were used to implement RM: ministerial orders, dissemination of written materials, national and international KOL, off and online workshops. Results were monitored through snapshot audits conducted in main regional public hospitals and private services (7 regions + Capital city Bishkek) measuring infrastructure and process indicators
Results: Since 2019 Fast test campaigns and use raise from 0 to 66,2% (capital city and 5 out of 7 regions); availability of neuroimaging in public service raise form 0 to to 66,2% (capital city and 5 out of 7 regions); prescription of low-dose acetylsalicylic acid for ischaemic stroke (public and/or private ) is maintained (100% in 2019 and 2023); dysphagia test and management raised from 11% to 100 % (capital city and all regions)
Conclusions: the RM drove improvement in CVD care and it could be considered as an effective model for other low-middle income countries
Disclosures of Interest: No
Paper Poster - Sex, Gender and Stroke
Abstract N°: 3340
SEX DIFFERENCES IN STROKE SEQUELAE AMONG SURVIVORS IN THE UNITED STATES
Eduard Valdes*1, Imama Naqvi1
1Columbia University Irving Medical Center, Division of Stroke and Cerebrovascular Disease, New York, United States
On behalf of:
Background and aims: Post-stroke disability often varies by sex, with women consistently exhibiting poorer outcomes than men. Despite advancements in stroke care, the predictors of these sex-related differences, particularly concerning age, remain unclear.
Methods: We conducted a comprehensive cross-sectional study using National Health Interview Survey data spanning 2008 to 2018. Examining 73,604,258 weighted stroke survivors, we assessed seven crucial disability domains: perceived health, pain, activities of daily living (ADLs), functional limitations, mood disturbances, healthcare delays, and financial stress. Temporal trends were analyzed using Wald tests, and weighted multivariable logistic regression models identified predictors for each disability domain.
Results: Among stroke survivors (47.6% men, 52.4% women, mean age 65.6 and 65.7 years, respectively), 93-96% of men and 96-98% of women reported at least one disabling condition. Notably, 83.4% reported functional limitations, 73% reported impaired ADLs, 64.5% reported mood disturbances, 55% reported chronic pain, 48.2% reported poor perceived health status, 25.5% reported healthcare delays, and 17.8% reported financial stress. Women faced increased risks for chronic pain (adjusted odds ratio [aOR] 1.8, p<0.001), functional limitations (aOR 1.8, p<0.001), mood disturbances (aOR 1.7, p<0.001), healthcare delays (aOR 1.3, p<0.001), and financial stress (aOR 1.4, p<0.001).
Conclusions: This study highlights persistent sex-related disparities in post-stroke outcomes, emphasizing the need for targeted interventions to enhance the well-being and quality of life for female stroke survivors. Understanding the factors contributing to these disparities is crucial for developing personalized rehabilitation and support approaches.
Disclosures of Interest: No
Abstract N°: 2674
SEX DIFFERENCES IN NEUROIMAGING UTILIZATION FOR ACUTE ISCHEMIC STROKE AT A COMPREHENSIVE STROKE CENTER IN ATLANTIC CANADA
Mukesh Kumar*1, Sherry Hu2, Steven Beyea3, Noreen Kamal1
1Dalhousie University, Department of Industrial Engineering, Halifax, Canada, 2Dalhousie University, Department of Medicine (Neurology), Halifax, Canada, 3Dalhousie University, Department of Diagnostic Radiology, Halifax, Canada
On behalf of:
Background and aims: Limited knowledge exists about sex differences in neuroimaging use for acute ischemic stroke(AIS) in Canada. We examined these differences in Atlantic Canada, marked by an aging population and potential healthcare delivery gaps.
Methods: This linked-registry study examined AIS patients admitted to one of three comprehensive stroke centers in Atlantic Canada, from 2015 to 2019. Presentation characteristics were age, wake-up stroke, ambulance arrival, ASP activation, symptom recognition to arrival, and stroke severity. Potential sex differences in neuroimaging utilization were investigated using stepwise logistic regression models: 1) unadjusted, 2) age-adjusted, and 3) age, stroke severity, and ambulance arrival- adjusted.
Results: Among 1,956 patients, 931 (47.6%) were females. Presentation characteristics were comparable, except for older age (median age 75 vs. 70, P<0.001), higher ambulance arrival (66.6% vs. 59.4%, P<0.001), and higher stroke severities (26.6% vs. 19.0%, P<0.001) in females. Utilizations of non-contrast computed tomography (NCCT), CT angiography (CTA), and CT perfusion (CTP) were comparable, while magnetic resonance imaging (MRI) utilization was significantly lower among females (Table).
Conclusions: Sex differences in CTP utilization increased non-significantly with stepwise covariates introduction, whereas differences in MRI utilization lowered. MRI usage retained significance across all three models, indicating a notable disparity. However, the confounding in outcomes is limited by the unavailability of comorbidities, gender-specific, and socioeconomic variables.
Disclosures of Interest: No
Abstract N°: 3308
SEX DIFFERENCES IN PROGNOSTIC MARKERS: EXPLORING OUTCOME VARIABILITY AFTER MECHANICAL THROMBECTOMY IN LARGE VESSEL OCCLUSION STROKE
Hannes Schacht1, Maria Marburg1, Linda Rudolf1, Christine Matthis1, Alexander Neumann1, Constantin Schareck2, Peter Schramm1, Georg Royl1, Philipp J Koch*1
Background and aims: Sex-related disparities in long-term outcomes after large vessel occlusion (LVO) following mechanical thrombectomy (MT) have been repeatedly shown. Notably, women exhibit a lower likelihood of achieving functional independence 90 days post-stroke. So far, it remains unclear whether there is sex difference in the prognostic values of established clinical and neuroradiological parameters. Therefore, our investigation aimed to discern the divergent prognostic values of multiple clinical markers between sexes.
Methods: In a retrospective analysis, we examined 195 stroke patients with LVO. All patients were admitted to the University Medical Center Lübeck within the early time window and received MT. Utilizing multivariate logistic regression models, we explored the interaction between sex and various parameters including ASPECTS, Lesion core volume, penumbra volume, collateral status and time to reperfusion, in relation to favorable outcomes 90 days post-stroke. Models were adjusted for the influence of sex, age, initial symptom severity, and recanalization status.
Results: The lesion core volume, ASPECTS and the collateral status exhibited sex-dependent associations with favorable outcome 90 days after stroke. Subgroup analyses revealed that these biomarkers were exclusively meaningful for men.
Conclusions: Our findings suggest that the prognostic value of the lesion core as well as the collateral status is sex-specific, emphasizing their relevance primarily in men. Further investigations are warranted to comprehensively understand sex-specific differences in functional outcome after stroke and to identify most promising prognostic markers for the functional outcome following MT in women. Unraveling sex-specific prognostic biomarkers of recovery holds potential to further develop precision medicine and individualized clinical management in stroke.
Disclosures of Interest: No
Abstract N°: 546
ISCHEMIC STROKE IN YOUNG ADULTS: A COMPARISON OF OUTCOMES, STROKE RISK FACTORS AND ETIOLOGIES BETWEEN MALES AND FEMALES
Pamela Correia*1,2,3, Alexandre Y. Poppe1,2,4, Laura Gioia1,2,4, George Mendes1,2, Hanan Alhazmi5, Yan Deschaintre1,2,4, Gregory Jacquin1,2,4, Céline Odier1,2,4, Christian Stapf1,2,4, Olena Bereznyakova1,2,4
1Université de Montréal, Department of Neurosciences, Montréal, Canada, 2Centre Hospitalier de l'Université de Montréal, Department of Medicine (Neurology), Montréal, Canada, 3Biel Hospital Center, Stroke Unit, Department of Neurology, Biel, Switzerland, 4Centre de Recherche du Centre Hospitalier de l'Université de Montréal (CRCHUM), Neurovascular Group, Neurosciences Axis, Montréal, Canada, 5Université de Montréal, Department of Interventional Neuroradiology, Montréal, Canada
On behalf of:
Background and aims: Few studies have explored sex differences in functional outcomes after ischemic stroke in young adults. The primary aim was to determine if functional outcomes among young adults with stroke differed based on sex. The secondary aim was to identify differences in stroke risk factors and etiologies between females and males.
Methods: We conducted a retrospective analysis of consecutive acute ischemic stroke patients aged 18 to 55 years from a single centre stroke registry between 2018 to 2022. Using multivariable logistic regression, we analysed if modified Rankin Scale at 3-6 months (mRS, dichotomized 0-2 versus 3-6) was associated with sex.
Results: We included 315 patients (127 female) with a median age of 48 years (IQR 42-52), median NIHSS 10 (IQR 4-19) and median mRS (3-6 months) 2 (IQR 1-3). Following adjustment for vascular risk factors, clinical stroke characteristics, baseline mRS, thrombolysis, stroke time metrics and unknown onset of symptoms, there was no significant difference in mRS (3-6 months) based on sex (p=0.40). Female patients were more likely to have an unknown time of stroke onset (p=0.03), while known atrial fibrillation (p=0.03), drug use (p=0.003) and large-artery atherosclerosis as a stroke etiology (p=0.01) were more frequent in males.
Conclusions: Patient-oriented outcomes maybe of interest in future studies as functional outcomes based on mRS do not differ between young male and female stroke patients. Males had a higher prevalence of large-artery atherosclerosis and risk factors including drug use and atrial fibrillation. These findings could help develop targeted stroke prevention strategies.
Disclosures of Interest: No
Abstract N°: 1913
SEX DIFFERENCES IN THE UTILISATION OF INTRAVENOUS THROMBOLYSIS AND OUTCOMES: POPULATION-BASED COHORT STUDY BETWEEN 2004 AND 2020
Min Xu*1, Iain Marshall1,2, Charles Wolfe1,2, Matthew DL O‘connell1,2, Abdel Douiri1,2
1King's College London, London, School of Life Course & Population Health Sciences, United Kingdom, 2NIHR Applied Research Collaboration (ARC) South London, London, United Kingdom
On behalf of:
Background and aims: Evidence on sex disparities in thrombolysis use in stroke patients and their response to this treatment remains controversial. We examined sex differences in the utilisation of intravenous thrombolysis (IVT) therapy and compared outcomes between men and women.
Methods: Data from the population-based cohort study of first-ever strokes between 2004 and 2020. Logistic regression was used to model sex differences in thrombolysis use. Cox proportional hazards model and logistic regression were used to analyse mortality and activity of daily living (ADL) disability after thrombolysis, respectively. Models were adjusted for age, pre-morbid status, stroke severity and risk factors.
Results: There were 47% women (mean age 71 years, SD 16.4) and 53% men (66 [14.8]) in 4041 participants. More women presented with severe strokes (12.1% vs 9.7%, p<0.001) and atrial fibrillation (18.9% vs 15.3%, p=0.003). 398 patients received thrombolysis therapy after stroke, with 49.5% being women. Adjusted analysis showed no significant difference in thrombolysis utilisation between men and women (Adjusted Odds Ratio 1.06; 95% Confidence Interval 0.84-1.34). Despite the absence of statistical significance, compared to men, there was a trend toward better survival for women (AHR at 1 year: 0.63 [0.38, 1.05]; 5 years: 0.77 [0.54,1.10]) but poorer ADL (AOR: 1.60 [0.63, 4.02]; 1.67 [0.43,6.58]) after thrombolysis.
Conclusions: We did not observe sex-related differences in the use of thrombolysis. However, women tended to have better survival but poorer ADL after thrombolysis.
Disclosures of Interest: No
Abstract N°: 2128
ARE THERE SEX DIFFERENCES POST-CAROTID ENDARTERECTOMY FOR SYMPTOMATIC CAROTID STENOSIS? A SYSTEMATIC REVIEW AND IPD META-ANALYSIS
Ya Yuan Rachel Leung*1, Sothida Nantakool2, Kittipan Rerkasem2, Alan Dardik3, Jean-Louis Mas4, Gioele Simonte5, Luca Mezzetto6, Mario D'oria7, Elena Giacomelli8, Dominic Pj Howard1
1Centre for Prevention of Stroke and Dementia, Department of Clinical Neurosciences, University of Oxford, Oxford, United Kingdom, 2Chiang Mai University, Chiang Mai, Thailand, 3Yale Department of Surgery Departments of Surgery and Cellular and Molecular Physiology, United States, 4Université Paris Descartes and Sainte-Anne Hospital, Department of Neurology, France, 5Università degli Studi di Perugia, Surgical and biomedical sciences department, Italy, 6zienda Ospedaliera Universitaria Integrata Verona, Verona, Italy, 7University of Padova, Department of Cardiac, Thoracic and Vascular Sciences, Padova, Italy, 8University of Florence, Italy
On behalf of:
Background and aims: Results on post-carotid endarterectomy (CEA) stroke/death risk in females varied between observational studies and trials. Controversies remain on whether trials recruited fewer female participants may affect generalizability. Few meta-analysis included all study types and differentiated outcome by symptomatology, of which none included individual patient data (IPD). Our IPD meta-analysis aim to investigate any sex differences in safety and efficacy of CEA for symptomatic carotid stenosis.
Methods: We performed a systematic review and meta-analysis (PROSPERO CRD:42023425278) on all published studies reporting stroke and mortality by sex and symptom status post-operation (30-day) and up to 5-year. IPD from 10 prospective studies enabled multivariate and survival analysis.
Results: In 44 studies, including 7 RCTs, 10 registries, and 27 cohorts (female n= 97,176, male n= 190,384), there was no sex differences in postoperative stroke across study types, but overall effect showed higher risks in female (OR 1.1 [95%CI 1.01-1.19]). Postoperative mortality was higher in female overall (1.22 [1.12-1.32]) and in registries, but not in trials and cohort studies. IPD multivariate analysis (n= 45,048) showed female sex was not associated with postoperative stroke (1.33 [0.97-1.82]) and death (1.25 [0.88-1.77]), while stroke as presenting symptom was independently associated with postoperative stroke (3.94 [1.98-7.8]) and death (6.62 [1.83-24.1]) (Table1). Survival and stroke risk up to 5-years were similar between sex in octogenarians and nonoctogenarian respectively (Figure 2).
Conclusions: There were no sex differences in postoperative adverse outcomes and long-term survival and stroke risk post-CEA for symptomatic stenosis. We confirm the safety and efficacy of CEA for female with symptomatic stenosis.
Disclosures of Interest: No
Abstract N°: 2660
WOMEN WITH MINOR STROKES MAY BE LESS LIKELY TO RECEIVE OPTIMAL CARE
Lina Grosset*1,2, Peggy Reiner1, Antoine Guillonnet3, Ruben Tamazyan4, Joseph Benzakoun5, Hugues Chabriat1,2, Catherine Oppenheim5, Mathieu Zuber2,4, David Calvet6, Eric Jouvent1,2
1Lariboisière Hospital AP-HP, Neurology, Paris, France, 2Université Paris Cité, Paris, France, 3Lariboisière Hospital AP-HP, Neuroradiology, Paris, France, 4Hospital Paris Saint-Joseph, Neurology, Paris, France, 5Hospital Sainte-Anne, Neuroradiology, Paris, France, 6Hospital Sainte-Anne, Neurology, Paris, France
On behalf of:
Background and aims: Minor strokes may be under-diagnosed in women as they are less likely to seek medical attention and their symptoms may be less recognised. We sought to test this hypothesis by evaluating a cohort of minor stroke patients admitted to a stroke unit, expecting to find a smaller proportion of women with, on average, more severe symptoms than men, due to non-admission of women with the least severe symptoms.
Methods: We evaluated patients admitted to the stroke unit at Lariboisière Hospital in Paris and included in an ongoing prospective cohort of MRI-proven minor subcortical ischemic strokes (NCT03552926). Inclusion began in 2018 with a planned follow-up of 5 years. Comparisons between groups were made using appropriate statistical tests, with p-values < 0.05 considered significant.
Results: At the time of writing, 174 patients had been included, of whom only 47 (27%) were women, which is lower than the sex ratio of ischemic stroke patients in our stroke unit (43% [183/430 in 2023], p<0.001). The inclusion rate of eligible patients did not significantly differ between men and women (33% and 38% respectively, p>0.05). Although not significantly older (66±12 vs 63±12, p>0.05), women had more severe NIHSS scores (median: 1.5, interquartile range: [0.0-3.0] vs 1.0 [0.0-2.0], p=0.03).
Conclusions: In a cohort of minor strokes, women are under-represented, and their strokes are less “minor” than those of their male counterparts. Our results support the hypothesis that women with very mild strokes may be under-diagnosed and/or less often admitted to stroke units.
Disclosures of Interest: No
Abstract N°: 2738
HIGHER RISK OF STROKE IN FEMALE POST-CAROTID ENDARTERECTOMY FOR ASYMPTOMATIC CAROTID STENOSIS: A SYSTEMATIC REVIEW AND IPD META-ANALYSIS
Ya Yuan Rachel Leung*1, Sothida Nantakool2, Kittipan Rerkasem2, Alan Dardik3, Gioele Simonte4, Jean-Louis Mas5, Mario D'oria6, Elena Giacomelli7, Luca Mezzetto8, Dominic Pj Howard1
1Centre for Prevention of Stroke and Dementia, Department of Clinical Neurosciences, University of Oxford, Oxford, United Kingdom, 2Chiang Mai University, Chiang Mai, Thailand, 3Yale Department of Surgery Departments of Surgery and Cellular and Molecular Physiology, United States, 4Università degli Studi di Perugia, Perugia, Italy, 5Paris-Cité University, Department of Neurology, Paris, France, 6University of Padova, Padova, Italy, 7University of Florence, Florence, Italy, 8Azienda Ospedaliera Universitaria Integrata Verona, Verona, Italy
On behalf of:
Background and aims: Results from observational studies and trials on sex-related stroke and death risks post-carotid endarterectomy (CEA) for asymptomatic stenosis were inconclusive. Moreover, sex differences in long-term stroke risk post-CEA from observational data are scarce. Our IPD meta-analysis aim to investigate any sex differences in the safety and efficacy of CEA for asymptomatic carotid stenosis in all study types.
Methods: We performed a systematic review and meta-analysis (PROSPERO CRD:42023425278) on all published studies reporting stroke, myocardial infarction (MI), and mortality by sex and symptom status post-operation (30-day) and up to 5-year. IPD from 10 prospective studies enabled multivariate and survival analysis.
Results: In 41 studies, including 6 RCTs, 11 registries, and 23 cohorts (female n= 211,486, male n= 329,229), postoperative stroke was higher in female overall (OR 1.20 [95%CI 1.09-1.32]) and in observational studies, but not in trials (1.21 [0.85-1.71]). There were no sex differences in postoperative MI (1.04 [0.96-1.14]) and mortality (0.9 [0.72-1.14]) (Figure 1). Subgroup by patching, shunting, and degree of stenosis showed similar findings. In IPD multivariate analysis (n=45,048), female sex was independently associated with postoperative stroke (1.82 [1.22-2.72]), and stroke/death (1.39 [1-1.93]). Diabetes was associated with postoperative mortality and stroke/death (Table 1). 5-year survival and 4-years stroke risk were similar between male and female overall, and in octogenarians and nonoctogenarian respectively (Figure 2).
Conclusions: We confirmed higher risk of postoperative adverse events in female post-CEA for asymptomatic stenosis. Caution should be exercised when selecting and operating on females for asymptomatic stenosis, particularly in diabetic patients.
Disclosures of Interest: No
Abstract N°: 3299
GENDER-RELATED DIFFERENCES IN PATIENTS WITH INTRACEREBRAL HEMORRHAGE ADMITTED TO A TERTIARY CARE CENTER HOSPITAL FROM CAMPANIA REGION, ITALY
Emanuele Spina*1, Antonio De Mase1, Stefano Barbato1, Nicola Capasso2, Giovanna Servillo1, Giuseppe Leone1, Massimo Muto1, Paolo Candelaresi1, Mario Muto1, Vincenzo Andreone1
Background and aims: Intracerebral hemorrhage (ICH) accounts for 20% of total stroke. Controversial data have been published over gender differences in baseline features and long-term outcome for ICH patients regarding gender differences. The aim of this study is to investigate possible gender-differences in admission and long-term outcome in ICH patients.
Methods: we analyzed consecutive patients admitted to our hospital (Naples, Campania, Southern Italy) suffering from non-traumatic ICH, collecting demographic, radiological and biochemical features at baseline. We set as primary outcome disability shift (measured by modified Rankin Scale) at baseline and at 3-months evaluation; as secondary outcome in-hospital mortality and discharge nihss.
Results: we enrolled 199 patients in our analysis, with a female ratio of 43.2% (86/199). Significant gender differences at baseline were mean diastolic arterial pressure (86 mmHg vs 91 mmHg, p < 0.05), platelet count (239 vs 212 x 10’3 /ul) and disability at baseline (p=0.01); no differences were found in presence of hypertension, diabetes, dyslipidemia, typical versus atypical ICH. Analysis of variance for repeated measures (baseline and 3-months evaluation) showed a better outcome for the interaction between gender and time (p=0.00) on disability as measured with mRS score; no gender-differences were found in rate of in-hospital mortality and nihss at discharge.
Conclusions: despite a worse grade of disability at admission, female patients suffering from non-traumatic ICH showed a better long-term clinical evolution.
Disclosures of Interest: No
Abstract N°: 3062
SEX DISPARITIES IN CLINICAL OUTCOMES: INTRACEREBRAL HAEMORRHAGE DUE TO CEREBRAL AMYLOID ANGIOPATHY – TICH-2 TRIAL DATA
Chaamanti Menon*1, Iris Isheanesu Mhlanga1, Kailash Krishnan2, Zhe Kang Law3, Robert Dineen4, Michael Desborough5, Philip Bath1, Nikola Sprigg1
1University of Nottingham, Stroke Trials Unit, Mental Health and Clinical Neurosciences, Nottingham, United Kingdom, 2Queen's Medical Centre, Stroke Medicine, Nottingham, United Kingdom, 3Malaysia National University Kuala Lumpur Campus, Department of Medicine, Kuala Lumpur, Malaysia, 4University of Nottingham, Radiological Sciences, Nottingham, United Kingdom, 5Oxford University Hospital Trust, Departmental of Haematology, Nottingham, United Kingdom
On behalf of:
Background and aims: Cerebral amyloid angiopathy (CAA) is a significant risk factor for lobar intracerebral haemorrhage (ICH). We explored the sex disparities in functional outcome after ICH in those with CAA.
Methods: We used data from the Tranexamic Acid for Hyperacute Primary Intracerebral Haemorrhage 2 trial (TICH-2), a double-blind, placebo-controlled study examining the effects of tranexamic acid in patients presenting with acute, spontaneous ICH. We assessed CT images using the Boston Criteria (version 1) to classify scans as probable, possible, or no CAA. Logistic regression analyses, adjusted for prognostic factors, was conducted to investigate sex disparities in functional outcome (modified Rankin scale, mRS) at 90 days among participants with bleeds secondary to CAA.
Results: Women were more likely to have CAA compared to men (57% vs 43%). Table 1 summarises the baseline differences between sexes with possible and probable CAA. At 90 days there was no significant functional outcome differences in men or women with probable or possible CAA (aOR 1.23 95% confidence interval(CI) [0.88;1.72]). There was no difference in death at day 7 or day 90 between sexes (aOR, 95% CI; 0.862 [0.45-1.66], 1.03 [0.61-0.73 respectively].
Conclusions: Our analysis shows that although women are older, have worse stroke symptoms and higher blood pressure, mRS or death at 90 days does not differ between sexes after adjustment
Disclosures of Interest: No
Abstract N°: 1131
STROKE CHAMELEONS AND SEX/GENDER ASPECTS: A SINGLE-CENTER NESTED CASE-CONTROL STUDY
1Unisanté, Health and Gender Unit, Lausanne, Switzerland, 2CHUV, Stroke Center, Neurology Service, Department of Clinical Neurosciences, Lausanne, Switzerland
On behalf of:
Background and aims: To analyze if the gendered socioeconomic position (SEP) of patients is associated with acute ischemic stroke chameleons (AIS-Cs).
Methods: We performed a nested case-control study, using data collected from March 2003 to December 2020 from a single stroke center registry. AIS-Cs were compared with a randomly selected control sample in a 1:1 ratio. We extracted 6 gender-related socioeconomic variables (civil status, living situation, education level, professional categories, being professionally active, having children). Associations between AIS-Cs and sex/gender as well as the gender-related socioeconomic variables were investigated using logistic regression. A gendered SEP score was constructed reflecting the level of conformity with feminine characteristics. The association between the score and an AIS-C was investigated using logistic regression.
Results: AIS-Cs represented 182 (3%) of all admitted AIS, 80 (44%) of which were women. No association between sex/gender and AIS-Cs was found (OR 1.25, 95% CI 0.78-2.00). Women in the middle professional category had higher odds of an AIS-C compared to women in the lower professional category (OR 3.93, 95% CI 1.19-13-03). Men with higher education had lower odds of an AIS-C compared to men with lower education (OR 0.31, 95% CI 0.10-0.92). For women, increase in the gendered SEP score (high conformity) was associated with lower odds of an AIS-C (OR 0.66, 95% CI 0.46-0.94).
Conclusions: There is no difference in the risk of AIS-C between men and women. However, interacting sex/gender with SEP identified diverging trends for men and women. Conformity to expected gendered norms may have a protective effect against AIS misdiagnosis.
Disclosures of Interest: No
Abstract N°: 1884
SEX DIFFERENCES IN PATIENTS WITH SYMPTOMATIC INTRACRANIAL STENOSIS IN THE ANTERIOR CIRCULATION
Kateryna Antonenko*1, Adrian Scutelnic1, Marina Krasteva1,2, Philipp Bücke1, Nedelina Slavova1, Marcel Arnold1, Arsany Hakim3, Piotr Radojewski3,4, Pasquale Mordasini3,5, Mirjam Rachel Heldner1
1Inselspital, University Hospital and University of Bern, Department of Neurology, Bern, Switzerland, 2University Hospital Queen Giovanna, Department of Neurology, Sofia, Bulgaria, 3Inselspital, University Hospital and University of Bern, Institute of Diagnostic and Interventional Neuroradiology, Bern, Switzerland, 4Translational Imaging Center, Sitem-Insel, Bern, Switzerland, 5Kantonsspital St. Gallen, Netzwerk Radiologie, St.Gallen, Switzerland
On behalf of:
Background and aims: The aim of this study was to investigate sex differences in patients with symptomatic intracranial stenosis in the middle cerebral or carotid artery.
Methods: Patients, which got admitted to our Bernese Stroke Centre from 05/2012 till 06/2023 were consecutively included in this observational cohort study. We compared baseline characterstics and outcome between women and men.
Results: 119 patients (43.7% women, median age 72.2 years) were analyzed. Women were older in comparison to men (77.3 versus 66.9 years, p=0.004) and median time delay from symptom onset to admission was shorter (2.69 versus 6 hours, p=0.032). Strokes (86.6% versus 59.6%) compared to TIA were more frequent in men than in women (p=0.003). Men had more often known coronary hearth disease compared to women (22.4% versus 7.7%, p=0.042), women had higher LDL levels on admission (2.98 versus 2.75 mmol/l, p=0.05). Stroke and stenosis severity, intracranial stenosis location as well as the treatment approaches did not differ between groups. We did not find any differences for outcome (in women versus men: in-hospital sICH: 0% versus 4.5%, unadjusted-p=0.256, adjusted-p=0.995, favourable outcome at 3 months in women versus men: 77.3% versus 77.0%, unadjusted-p=0.979, adjusted-p=0.760, median mRS at 3 months: 2 versus 2, unadjusted-p=0.600, adjusted-p=0.618).
Conclusions: Although women with symptomatic intracranial stenosis in the anterior circulation were older, had higher admission LDL levels, but a shorter median time delay from symptom onset, less known coronary heart disease and more often presented with TIA than stroke, the study found similar outcomes between women and men.
Disclosures of Interest: No
Paper Poster - Small Vessel Disease
Abstract N°: 2594
MONITORING BLOOD BRAIN BARRIER LEAKAGE CHANGES IN YOUNG HYPERTENSIVE PATIENTS
Esther Janssen*1, Joost de Jong2, Esmée Verburgt1, Marnix Maas3, Anton Meijer3, Jaap Deinum4, Niels Riksen4, Anil Tuladhar1, Walter Backes2, Frank-Erik De Leeuw1
1Radboud University Medical Center, Department of Neurology, Nijmegen, Netherlands, 2Maastricht UMC+, Department of Radiology and Nuclear Medicine, Maastricht, Netherlands, 3Radboud University Medical Center, Department of Medical Imaging, Nijmegen, Netherlands, 4Radboud University Medical Center, Department of Internal Medicine, Nijmegen, Netherlands
On behalf of:
Background and aims: Hypertension presumably leads to disruption of the Blood Brain Barrier (BBB). BBB disruption is thought to be involved in the etiology of cerebral small vessel disease (SVD), but this has only been demonstrated in patients with long-lasting SVD. It remains unknown if BBB disruption already occurs prior to the development of SVD. We aim to determine if Dynamic Contrast Enhanced (DCE) MRI can detect BBB leakage in young patients with hypertension at risk for SVD and examine changes in BBB leakage over time.
Methods: This is a preliminary analysis of the Hyperintense study, an ongoing observational study in hypertensive adults (18-55 years). In a subset of participants, MRI was repeated at different time-points following antihypertensive medication start and withdrawal for diagnostic purposes to assess effects of changes in blood pressure (BP) on BBB leakage. 3Tesla DCE-MRI was used to measure BBB leakage. Linear regression adjusted for age was used to determine relation between BP at baseline and BBB leakage.
Results: BBB leakage was assessed at baseline (n=23, median age: 37 [18-55] years) and at follow-up (n=4). BBB leakage at baseline was detected in the white and grey matter and was higher in participants with higher BP (Table 2). Longitudinal leakage maps are shown in figure 1.
Conclusions: BBB leakage already occurs in young hypertensive patients and is more prominent with higher BP, emphasizing the importance of early BP treatment. Changes in BBB leakage can be detected before and during drug withdrawal. Follow-up of our participants will disclose if BBB leakage precedes SVD development.
Disclosures of Interest: No
Abstract N°: 787
QUANTITATIVE VESSEL SIZE IMAGING REVEALS ALTERED CEREBRAL MICROVASCULAR DENSITY IN PATIENTS WITH CEREBRAL SMALL VESSEL DISEASE
Maud van Dinther1, Paulien H.M. Voorter2, Gerhard S. Drenthen2, Elles P. Elschot2, Julie Staals1, Robert J. van Oostenbrugge1, Walter H. Backes2, Jacobus F.A. Jansen2
1Maastricht University Medical Center, Neurology, Maastricht, Netherlands, 2Maastricht University Medical Center, Radiology & Nuclear Medicine, Netherlands
On behalf of:
Background and aims: Microvascular rarefaction, the reduction in perfused microvessels and microvascular density, is an understudied, but potentially important pathophysiological mechanism in cerebral small vessel disease (cSVD). We investigated quantitative microvascular alterations in patients with cSVD.
Methods: 40 patients with clinically overt cSVD (age 70±9 years, 32% women) and 21 controls (age 67±7 years, 29% women) underwent 3T brain MRI with vessel size imaging, which provides voxel-based quantitative estimates of vessel density (Q) and size (VSI). Differences between white matter hyperintensities (WMH) and normal appearing white matter (NAWM) were assessed using paired-samples T-test. Patient/control group differences in Q and VSI for NAWM and gray matter (GM) were assessed using linear regression accounting for age, sex and cardiovascular risk factors.
Results: Q was lower (0.28s-1/3 vs 0.38s-1/3, p <0.001), and VSI higher (33.1 µm vs 18.7 µm, p<0.001) in WMH compared to NAWM. Q was lower (β -0.020 [95% CI -0.035 - -0.006], p=0.007), and VSI higher (β 2.266 [95% CI 0.920-3.612], p=0.001), in GM in patients with cSVD compared to controls. No significant group differences were found in NAWM. Higher age and male sex were significantly associated with lower Q and higher VSI in NAWM and GM.
Conclusions: We found lower vessel density and larger vessel size in WMH compared to NAWM, and in the GM of patients with cSVD compared to controls. Our findings support a role of microvascular rarefaction (possibly leaving the larger, or more dilated vessels) in the pathophysiology of cSVD. Ageing and sex affect these microvascular alterations.
Disclosures of Interest: No
Abstract N°: 867
HAEMOSIDERIN DEPOSITS SIGN ON SUSCEPTIBILITY-WEIGHTED IMAGING IN RECENT SMALL SUBCORTICAL INFARCTS
Yu-Yuan Xu*1, Francesca Chappell1, Carmen Arteaga Reyes1, Una Clancy1, Stewart Wiseman1, Michael Stringer1, Michael Thrippleton1, Maria Valdes-Hernandez1, Fergus Doubal1, Joanna Wardlaw1
1University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
On behalf of:
Background and aims: The long-term evolution of recent small subcortical infarcts (SSIs) remains insufficiently characterized. Haemosiderin deposits (HDs) have been noted in SSIs at subacute and chronic stages and might be confused with haemorrhage. We aimed to determine the frequency and morphology of HDs in SSIs and associated factors.
Methods: We evaluated 108 index infarcts of SSI patients prospectively who underwent serial imaging at 6 and 12 months. Using susceptibility-weighted imaging (SWI), HDs in SSIs were categorized into four types: spots, smudge, rim, and cluster. We assessed SWI at all available timepoints and the associations between HDs and the SSIs overall appearance, demographic and stroke-related factors.
Results: Amongst 108 enrolled SSIs patients (63.76±11.45 years, 74 men [68.5%]), there were 141 SSIs. HDs were observed in 43 SSIs (55.0%) at baseline and 83 (100%) at 12-month follow-up. The predominant initial type was ‘smudge’. A ‘rim’ pattern occurred in >25% SSIs at all follow-up timepoints, mainly in the lentiform/internal capsule region (50.0%) or thalamus (36.4%). Infarct volume (OR=1.003, 95% CI 1.001-1.006; P=0.004) and SVD score at baseline (OR=2.50, 95% CI 1.28-4.86, P=0.007) independently predicted HDs occurrence at 12-months. Although HDs did not associate with anterior or posterior circulation SSI location, the rate of HDs in the subtentorium was lower than that in the supratentorial area.
Conclusions: The presence of HDs in SSIs detected through SWI may be associated with RSSIs volume and SVD score. ‘Rim’ is common in SSIs so caution is needed to avoid mistaking for primary haemorrhage in the subacute and chronic stages.
Disclosures of Interest: No
Abstract N°: 987
PREVALENCE, CHARACTERISTICS AND RISK FACTORS OF INCIDENTAL DWI-POSITIVE LESIONS IN CAA AND CADASIL
Annemieke Ter Telgte*1,2, Anna de Kort3, Anna Dewenter4, Anna Kopczak4, Benno Gesierich5, Catharina Jm Klijn3, Marco Duering5, Marcel Verbeek3,6, Floris Schreuder3
1VASCage GmbH, – Centre on Clinical Stroke Research, Innsbruck, Austria, 2Medical University of Innsbruck, Department of Neurology, Innsbruck, Austria, 3Department of Neurology, Donders Institute for Brain, Cognition and Behaviour, Radboud University Medical Center, Department of Neurology, Nijmegen, Netherlands, 4Institute for Stroke and Dementia Research (ISD), LMU University Hospital, LMU Munich, Munich, Germany, 5Medical Image Analysis Center and Department of Biomedical Engineering, University of Basel, Basel, Switzerland, 6Department of Human Genetics, Radboud University Medical Center, Nijmegen, Netherlands
On behalf of:
Background and aims: Small acute brain infarcts detected as incidental diffusion-weighted imaging (DWI)-positive lesions are increasingly seen on MRI in ageing. They are considered an emerging feature of cerebral small vessel disease (SVD), but more research into their causes and pathology is required to conclude these lesions as established markers of SVD. Hence, we investigated the prevalence and risk factors of incidental DWI-positive lesions on high-resolution MRI in two well-phenotyped SVD populations, including CAA and CADASIL.
Methods: 43 patients with probable CAA (mean age 71 years [SD±6], all >3 months post-ICH) and 77 patients with CADASIL (mean age 53 [SD±10], all >3 months post-stroke, without atrial fibrillation) underwent advanced 3T DWI-MRI at baseline (all), and month 18 and 36 (CADASIL). All DWI scans were manually screened by 1 rater, followed by a consensus meeting with 1 other rater. Risk factors included cardiovascular risk factors and SVD MRI markers.
Results: At baseline, the prevalence of incidental DWI-positive lesions in CAA was 56% (95% CI 40-68%) and in CADASIL 22% (95% CI 14-33%). In CAA, 43/67 (64%) DWI-positive lesions were in cortical location whereas in CADASIL almost all lesions, i.e. 58/61 (95%), were located subcortically. In CADASIL, DWI-positive lesions were significantly associated with hypertension, and MRI markers of SVD (lacunes and white matter hyperintensities). No significant associations were seen in CAA.
Conclusions: Incidental DWI-positive lesions are highly prevalent in CAA and CADASIL. Their location in the brain largely reflects their putative underlying microangiopathy suggesting that these lesions are a feature of SVD.
Disclosures of Interest: No
Abstract N°: 1137
ASSOCIATION OF GLYCEMIC VARIABILITY ON CONTINUOUS GLUCOSE MONITORING WITH CEREBRAL SMALL VESSEL DISEASES IN TYPE 2 DIABETES
1National Cerebral and Cardiovascular Center, Department of Neurology, Suita, Osaka, Japan, 2National Cerebral and Cardiovascular Center, Department of Cerebrovascular Medicine, Suita, Osaka, Japan, 3National Cerebral and Cardiovascular Center, Department of Diabetes and Lipid Metabolism, Suita, Osaka, Japan
On behalf of:
Background and aims: Diabetes mellitus is a significant cardiovascular risk factor, but the impact of glycemic variability on the brain remains unclear. We explored the association between high and low blood glucose variability and cerebral small vessel disease (SVD) in patients with type 2 diabetes mellitus.
Methods: Patients aged 65-85 with type 2 diabetes, who visited our hospital from June 2018 to March 2020 and exhibited mild cognitive impairment (MoCA 17-25), were included. We conducted continuous blood glucose monitoring using the FreeStyle Libre Pro system (Abbott) for 7-14 days. Brain MRI assessed asymptomatic lacunar infarcts, cerebral microbleeds, white matter lesions (WML), and perivascular spaces as markers of SVD. The blood glucose variability was measured using the Mean Amplitude of Glycemic Excursions (MAGE).
Results: Out of 109 patients enrolled, 101 (median age: 77 years, 68 males) with available MRI images were analyzed. Based on median MAGE (92.9 mg/dL), we categorized into high and low MAGE groups. No significant differences in age, sex, or HbA1c were observed. However, the high MAGE group exhibited significantly higher Fazekas scores for WML (periventricular area) compared to the low MAGE group (median 1.00 vs. 2.00, p = 0.028). Multivariable analysis confirmed high MAGE as an independent predictor for increased WML (periventricular area) (Adjusted Odds ratio 1.75, 95% CI 1.04-3.06, p=0.041).
Conclusions: Elevated glycemic variability in patients with type 2 diabetes mellitus is independently associated with worsening cerebral white matter lesions, especially in periventricular area.
Disclosures of Interest: No
Abstract N°: 1861
VASCULAR NOTCH3 DEPOSITION LOAD IN ASSOCIATION WITH NOTCH3 GENOTYPE AND CADASIL PHENOTYPE
1National Taiwan University Hospital, Department of Neurology, Taipei, Taiwan, 2National Taiwan University Hospital, Department of Medical Imaging, Taipei, Taiwan, 3National Taiwan University, Department of Anatomy and Cell Biology, College of Medicine, Taipei, Taiwan
On behalf of:
Background and aims: Vascular NOTCH3 deposition is the pathological hallmark of CADASIL. We aimed to explore the relationship between NOTCH3 deposition load, NOTCH3 variant genotype, and cerebral small vessel disease phenotype.
Methods: 54 subjects, including 39 index CADASIL patients and 15 asymptomatic NOTCH3 pathogenic variant carriers, were enrolled and underwent skin biopsy for the quantification of dermal vascular NOTCH3 deposition load using immunohistochemistry staining. The NOTCH3 deposition load was compared among carriers of NOTCH3 p.R544C heterozygotes (n=46), p.R544C homozygotes (n=3), and pathogenic variants located in EGFr 1-8 (n=5). In subjects with heterozygous NOTCH3 p.R544C, we further investigated the association between NOTCH3 deposition load and various clinical and imaging phenotypes of cerebral small vessel disease using regression models adjusted for age, sex, and vascular risk factors.
Results: The NOTCH3 deposition load was higher in subjects with NOTCH3 variants located in EGFr 1-8 (93.21 vs. 16.37%, p=0.0002) and in p.R544C homozygotes (56.63 vs. 16.37%, p=0.0179) compared to p.R544C heterozygotes. In subjects with heterozygous NOTCH3 p.R544C, no statistically significant associations were found between NOTCH3 load and stroke (p=0.393), Mini-Mental State Examination (MMSE) (p=0.330), or the modified Rankin Scale (mRS) (p=0.931 for mRS >=2 vs. mRS 0-1). With Regard to MRI features, the cerebral microbleed count was associated with a higher NOTCH3 load (B=0.073, 95% CI=0.014-0.133, p=0.017) after adjustment for age, sex, and hypertension.
Conclusions: The NOTCH3 variant genotype is the primary determinant of vascular NOTCH3 deposition load. In subjects with heterozygous NOTCH3 p.R544C, the cerebral microbleed count is associated with NOTCH3 deposition load.
Disclosures of Interest: No
Abstract N°: 2622
RECURRENT CEREBROVASCULAR EVENTS AFTER RECENT SMALL SUBCORTICAL INFARCTION
Melanie Haidegger*1, Nina Klock1, Simon Fandler-Höfler1, Markus Kneihsl1,2, Sebastian Eppinger1,2, Stephan Seiler1, Christian Enzinger1, Thomas Gattringer1,2
1Medical University of Graz, Department of Neurology, Austria, 2Medical University of Graz, Division of Neuroradiology, Vascular and Interventional Radiology, Department of Radiology, Austria
On behalf of:
Background and aims: Recent small subcortical infarcts (RSSI) are the neuroimaging hallmark feature of small vessel disease (SVD)-related acute lacunar stroke. Data on recurrent cerebrovascular events including their aetiology after RSSI are scarce.
Methods: This retrospective study included all consecutive ischaemic stroke patients with an MRI-confirmed RSSI (in the supply area of a small single brain artery) at University Hospital Graz between 2008 and 2013. We investigated associations between clinical and SVD features on MRI (STRIVE criteria) and recurrent cerebrovascular events, using multivariable Cox regression adjusted for age, sex, vascular risk factors and MRI parameters.
Results: We analysed 332 consecutive patients (mean age 68 years, 36% women; median follow-up time 5.4 years, IQR=9 years). Recurrent ischaemic cerebrovascular events occurred in 70 patients (21.1%; 54 ischaemic strokes, 22 TIA) and were mainly attributed to SVD (68%); 26 patients (7.8%) developed intracranial haemorrhage.
Diabetes (HR 2.36, 95% CI 1.44-3.88), WMH severity (HR 1.87, 95% CI 1.06-3.29), presence of lacunes (HR 1.63; 95% CI 1.01-2.65) and cerebral microbleeds (HR 2.13, 95% CI 1.25-3.66) on baseline MRI were related to recurrent ischaemic stroke/TIA, while only presence of cerebral microbleeds increased the risk for intracranial haemorrhage (HR 2.87, 95% CI 1.22-6.75). A widely-used CSVD summary score indicated high risks of recurrent ischaemic (HR 1.27, 95% CI 1.04-1.55) and haemorrhagic cerebrovascular events (HR 1.48, 95% CI 1.05-2.05).
Conclusions: RSSI patients have a substantial risk for recurrent cerebrovascular events – particularly those with coexisting chronic CSVD features. Recurrent events are mainly related to SVD.
Disclosures of Interest: No
Abstract N°: 2719
SKIN SINGLE CELL RNA-SEQUENCING AND BLOOD PROTEOMICS IDENTIFY POTENTIAL CADASIL BIOMARKERS AND THERAPEUTIC TARGETS
Paula Villatoro-González*1,2, Isabel Sala3, Olga Maisterra-Santos4, Alba Marcos-Sierra5, Victoria Ros5, Luis Puig6, Narcís Cardoner7, Israel Fernández-Cadenas1, Elena Muiño1,5
1Institut de Recerca Sant Pau (IR Sant Pau), Stroke Pharmacogenomics and Genetics group, Barcelona, Spain, 2Universitat Autònoma de Barcelona, Department of Medicine, Bellaterra, Spain, 3Hospital de la Santa Creu i Sant Pau, Memory Unit (Neurology Service), Barcelona, Spain, 4Vall d'Hebron University Hospital, Barcelona, Spain, 5Hospital de la Santa Creu i Sant Pau, Epilepsy Unit, Barcelona, Spain, 6Hospital de la Santa Creu i Sant Pau, Dermatology service, Barcelona, Spain, 7Hospital de la Santa Creu i Sant Pau, Barcelona, Spain
On behalf of:
Background and aims: CADASIL, a rare disease without treatment, is due to mutations of NOTCH3, which is mainly expressed in vascular smooth muscle cells (VSMC) in adults. Higher brain atrophy, small subcortical infarcts, male sex, and mutations affecting Notch3 EGFr 1-6 carry a worse prognosis. Nevertheless, no marker monitors disease progression or assesses the efficacy of future treatments. We aimed to identify potential biomarkers and/or therapeutic targets by performing single-cell RNA sequencing (scRNA-seq) and proteomic analysis in human CADASIL samples.
Methods: Eight CADASIL patients balanced by sex and mutation location were chosen for skin biopsies for scRNA-seq. The eight CADASIL patients and 39 healthy controls were studied with the OLINK discovery panel, analysing 3.072 proteins in plasma. Differential expression analysis was performed according to cognitive impairment, which was determined by DSM-V criteria. A principal component (PC) analysis was performed in the plasma proteome, as well as a study to find proteins associated with CADASIL regardless of age, sex, and first four PC.
Results: 833 VSMC were obtained from the skin biopsies and 132 transcripts were significantly associated with cognitive impairment after Bonferroni correction. PC1 in the blood proteome study completely differentiates cases from controls and 510 proteins were significantly associated with CADASIL. Gene set enrichment analysis (GSE) showed that the significant molecules are involved in intracellular and protein transport, cell adhesion and extracellular matrix, among others.
Conclusions: We found 132 transcripts and 510 proteins that are potential biomarkers and/or therapeutic targets for CADASIL. These molecules are involved in alterations already known in CADASIL.
Disclosures of Interest: No
Abstract N°: 2833
THE RELATIONSHIP BETWEEN PLASMA SOLUBLE LOW-DENSITY LIPOPROTEIN RECEPTOR-RELATED PROTEIN-1 AND WHITE MATTER LESIONS
Xiang Lu1, Beilei Chen*1
1Northern Jiangsu People’s Hospital, Clinical Medical College, Yangzhou University, Department of Neurology, China
On behalf of: Tiantian Han,Haina Zhao,Jingwen Wang,Chao Jiang
Background and aims: The soluble Low-Density Lipoprotein Receptor-Related Protein-1 (sLRP-1) is a soluble extracellular protein involved in various biological processes including neurotransmitter regulation, cell apoptosis, and inflammatory response.This study aims to investigate the levels of sLRP-1 in the plasma of patients with white matter lesions (WMLs) and its relationship with cognitive function.
Methods: A total of 181 patients with WMLs and 46 healthy subjects were included in the study. The severity of WMLs was categorized as mild (n=91), moderate (n=63), and severe (n=27) using the Fazekas scale. The levels of sLRP-1 in the plasma were assessed using an enzyme-linked immunosorbent assay.
Results: Compared with healthy subjects, patients with WMLs demonstrated significantly lower levels of sLRP-1 in their plasma (p<0.001).Binary logistic regression analysis revealed that age [OR=1.084,95%CI (1.039-1.132)],glycated hemoglobin [OR=1.593, 95%CI (1.079-2.353)], and alanine aminotransferase [OR=1.079, 95% CI (1.018-1.143)] were independent risk factors for WMLs, whereas sLRP-1 [OR=0.977, 95%CI (0.966-0.988)] was identified as a protective factor. The ANOVA analysis revealed significant differences in sLRP-1 levels between the mild and moderate WMLs groups, as well as between the mild group and the severe group (p<0.05).Furthermore, the binary logistic regression analysis indicated that homocysteine [OR=1.235, 95%CI (1.1-1.386)] was an independent risk factor, while sLRP-1 [OR=0.975, 95%CI (0.961-0.990)] was found to be a protective factor for cognitive impairment in WMLs patients. Additionally, the Pearson correlation analysis demonstrated a positive correlation between plasma sLRP-1 levels and delayed-recall scores (r=0.401, p<0.001) in WMLs patients.
Conclusions: These findings suggest that reduced plasma sLRP-1 levels may contribute to the development of WMLs and cognitive impairment.
Disclosures of Interest: No
Abstract N°: 3282
PREVALENCE AND RECURRENCE RATE OF CEREBRAL AMYLOID ANGIOPATHY-RELATED INFLAMMATION: A SINGLE-CENTER COHORT
Reinier van der Zwet*1, Sabine Voigt1,2, Emma Koemans1, Ingeborg Rasing1, Kanishk Kaushik1, Matthias van Osch2, Gisela Terwindt1, Marianne van Walderveen2, Marieke Wermer1,3, Ellis van Etten1
1Leiden University Medical Center (LUMC), Neurology, Leiden, Netherlands, 2Leiden University Medical Center (LUMC), Radiology, Leiden, Netherlands, 3University Medical Center Groningen, Neurology, Groningen, Netherlands
On behalf of:
Background and aims: Cerebral amyloid angiopathy-related inflammation (CAA-ri) is a rare variant of CAA, which often presents with headache or rapid neurological impairment. Our study aims to determine the prevalence and recurrence of CAA-ri in sporadic CAA patients.
Methods: In this retrospective cohort study, we included patients with probable CAA according to the Boston Criteria V2 who presented to the vascular neurology outpatient clinic of Leiden University Medical Center between January 2012 and December 2020. Patients were diagnosed with CAA-ri based on clinicoradiological criteria. We calculated the prevalence and used survival analysis for the recurrence rate and 5-year mortality.
Results: We included 109 patients with sCAA; 18 (16.5%) showed at least 1 episode of CAA-ri (range 1-3 episodes). Cognitive impairment was the most common presenting symptom (12/18; 67%), followed by focal neurological symptoms (8/18; 44%), and epilepsy and headache (both 5/18; 28%). The median follow-up time for patients with CAA was 1.1 years (range 0.1–5.3 years). Nine recurrent CAA-ri episodes occurred during follow-up, giving a recurrence rate of 26.9 per 100 person-years. All first recurrences occurred within one year after the first episode. Twelve out of 18 (67%) CAA-ri patients received immunosuppressive therapy; Six patients were not treated since they were retrospectively diagnosed with CAA-ri. These patients had no recurrences. The 5-year mortality rate was 28.6% in CAA-ri patients and 19.3% in other patients with CAA.
Conclusions: In a selected cohort at an expert center, CAA-ri occurs frequently, has a high recurrence rate and a higher mortality rate compared with other patients with CAA.
Disclosures of Interest: No
Abstract N°: 2625
SUBCLINICAL CEREBRAL LESIONS IN MIGRAINE AND PLATELET AGGREGATION
Ilaria Maestrini*1, Mariaignazia Curreli2, Giada Giuliani3, Costanza Giannì3, Marta Altieri4, Patrizia Pantano4, Fabio Pulcinelli2, Vittorio DI Piero4
1University Hospital of Rome “Tor Vergata”, Department of Systems Medicine, Rome, 2Sapienza University of Rome, Department of Experimental Medicine, Rome, 3Sapienza University of Rome, Department of Human Neurosciences, Rome, Italy, 4Sapienza University of Rome, Department of Human Neurosciences, Rome
On behalf of:
Background and aims: Cerebral white matter lesions (WMLs) are more frequently found in migraine patients (Mig) than in general population. Their nature, albeit not known, is hypothesized to be micro-ischemic. Although platelet aggregation (PA) has long been investigated in Mig, there are no data according to brain injuries. Our aim was to evaluate PA in Mig presenting WMLs to correlate lesions with an ischemic pathophysiology.
Methods: We enrolled all consecutive Mig diagnosed at our Headache center with episodic and chronic migraine, with and without aura (ICHD3 criteria). Exclusion criteria were concomitant antiplatelet therapy, hereditary platelet defects or thrombophilia. All patients underwent brain MRI (3D T1 weighted, DP T2 and 3D T2 FLAIR). A neuroradiologist, blinded to diagnosis and clinical data, quantified WMLs total volume (TV) in mm3. PA was evaluated in response to different agonists in Mig compared to a group of Healthy Volunteers (HV) matched for age and gender.
Results: 42 Mig were enrolled including 26 with and 16 without WMLs. We found that PA in response to Adrenaline was lower in Mig compared to HV. Among Mig, patients who had a TV ⩾150 mm3 (median value), presented a higher aggregation induced by Adrenaline than those with a TV <150 mm3 or no lesions (p<0,001).
Conclusions: In our study migraine was associated with a reduced platelets responsivity to aggregation stimuli compared to HV. When we divided Mig according to lesion load, Mig in whom the TV is considerable, presented an increased PA compared to those with a less load.
Disclosures of Interest: No
Abstract N°: 2572
NON-CONTRAST CT MARKERS AS A PREDICTOR FOR UNDERLYING CEREBRAL AMYLOID ANGIOPATHY
Sanne Schriemer*1, Ole de Bruin1, Marieke Wermer2, Ellis van Etten1
1Leiden University Medical Center (LUMC), Neurology, Leiden, Netherlands, 2University Medical Centre Groningen, Neurology, Groningen, Netherlands
On behalf of:
Background and aims: Non-contrast CT (NCCT) markers of intracerebral haemorrhage (ICH) are associated with haematoma expansion and poor clinical outcome. However, their prevalence in different ICH aetiologies, such as sporadic cerebral amyloid angiopathy (sCAA), Dutch-type hereditary CAA (D-CAA), and deep perforator arteriopathy (DPA), remains unclear. We assessed the prevalence of NCCT markers in ICH-patients and established if they can predict CAA as underlying aetiology.
Methods: We assessed CT scans of initial and recurrent ICHs of consecutive patients with sCAA, D-CAA, and DPA, for the presence of 9 NCCT markers: black hole sign, blend sign, island sign, satellite sign, swirl sign, irregular shape, fluid level, hypodensity, and heterogeneous density. We compared their prevalence between the three aetiologies and used binomial regression models to identify NCCT markers predictive for underlying CAA (sCAA and D-CAA) compared to DPA.
Results: We assessed 316 NCCT scans from 231 ICH-patients (mean age 69, 52% female): 64 with sCAA, 67 with D-CAA, and 100 with DPA. In 40% of NCCTs no markers were present. The blend, island, and satellite sign were seen more often in both sCAA and D-CAA patients, while hypodensity was found more often in patients with DPA (all p<0.01). In regression analyses, the island (OR=7.0,95%CI:1.4-34.4), blend (OR=4.8,95%CI:1.4-16.7), and satellite signs (OR=4.0,95%CI:1.8-8.9) were associated with underlying CAA, while CAA was less often present in case of hypodensity (OR=0.4, 95%CI:0.2-0.7).
Conclusions: The blend, island, and satellite sign are associated with underlying CAA, while hypodensity is associated with DPA. These markers may help identify the underlying cause of ICH.
Disclosures of Interest: No
Abstract N°: 3237
ASSOCIATION OF BLOOD BIOMARKERS OF ENDOTHELIAL AND PERICYTE DYSFUNCTION WITH COGNITIVE IMPAIRMENT AND MRI MARKERS OF SPORADIC SMALL VESSEL DISEASE
Daniela Jaime Garcia*1,2, Una Clancy1, Carmen Arteaga1, Maria Valdés-Hernandez1, Francesca Chappell1, Michael Thrippleton1,3, Michael Stringer1,3, Axel Montagne1,2, Fergus Doubal1, Joanna Wardlaw1,2
1The University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom, 2UK Dementia Research Institute, The University of Edinburgh, Edinburgh, United Kingdom, 3The University of Edinburgh, Edinburgh Imaging Facility (Royal Infirmary of Edinburgh), Edinburgh, United Kingdom
On behalf of: on behalf of the Mild Stroke Study 3 (MSS3) research group
Background and aims: Despite evidence supporting the role of endothelial and pericyte dysfunction in small vessel disease (SVD), the relationship between circulating biomarkers and disease burden remains unclear. We investigated associations between biomarkers of pericyte and endothelial dysfunction and SVD MRI markers and cognitive impairment in a mild-stroke cohort.
Methods: In patients with a non-disabling ischaemic stroke, we related serum concentrations of PDGFRB, PDGF-BB, VCAM-1, ICAM-1, E-selectin and P-selectin to MRI SVD markers, including: white matter hyperintensity (WMH) severity (Fazekas scale), lacunes, and compounded SVD score (based on the presence/severity of WMH, microbleeds, lacunes, and enlarged perivascular spaces) as well as mild cognitive impairment (MCI) (score <26 on the Montreal Cognitive Assessment). Ordinal and logistic regression models were adjusted for age, sex, vascular risk-factors, premorbid intelligence and stroke subtype.
Results: Biomarker data were available for 181 participants (69%male,mean age:65(SD:11)). Participants in the highest 3 quartiles of PDGF-BB and E-selectin levels had an increased risk for worse WMH burden (OR:1.26,95%CI:0.66,2.39 and OR:1.34,95%CI:0.72,2.53, respectively). Participants in the highest 3 quartiles of ICAM-1 concentrations had a two-fold increased risk for the presence of lacunes (OR:2.23,CI:1.06,4.78). ICAM-1, E-selectin and PDGF-BB were associated with increased SVD score (Q2-4 vs Q1: OR:1.62,95%CI:0.87,3.06 and OR:1.21,95%CI:0.65,2.26; and OR:1.10,95%CI:0.59,2.03, respectively). Higher VCAM-1 and PDGFRB concentrations were associated with an increased risk of MCI (OR:1.88,95%CI:0.83,4.26; OR:1.13,95%CI:0.51,2.43).
Conclusions: Our results support a role for pericyte and endothelial dysfunction in distinct SVD manifestations. Longitudinal outcomes and assessing the predictive value of these and other biomarkers remain the focus of our ongoing analyses.
Disclosures of Interest: No
Abstract N°: 338
RETINAL SUB-LAYER THICKNESSES, PRESENCE OF LACUNES, AND THEIR INTERACTION WITH COGNITIVE PERFORMANCE IN RSSI
William Robert Kwapong1, Jingyu Cui*1, Yu-Ying Yan1, Le Cao1, Chen Ye1, Shuai Jiang1, Bo Wu1
1West China Hospital, Sichuan University, Department of Neurology, Cheng Du Shi, China
On behalf of:
Background and aims: Recent single subcortical infarction (RSSI) leads to cognitive decline and dementia, and previous studies have shown that retinopathy is associated with RSSI severity. We explored the association between optical coherence tomography (OCT) metrics and the presence of lacunes on cognitive performance in RSSI.
Methods: 132 RSSI underwent magnetic resonance imaging (MRI) and small vessel disease markers were assessed. Retinal nerve fiber layer (RNFL) and ganglion cell-inner plexiform (GCIPL) thicknesses were measured with OCT. Montreal Cognitive Assessment (MoCA) was done and patients were stratified as non-cognitively impaired (NCI) (⩾22) and cognitively impaired (CI) (⩽ 21).
Results: We showed RNFL (ß = 0.366, p = 0.042), GCIPL (ß = 0.093, p = 0.034) thicknesses and presence of lacunes (ß = -1.478, p = 0.029) significantly correlated with MoCA scores in RSSI patients. A significant interaction was seen between RNFL (ß = 0.712, p = 0.036) and GCIPL thicknesses (ß = 0.209, p = 0.013) and the presence of lacunes on MoCA scores in RSSI patients respectively. We showed that changes in retinal sub-layer thicknesses and the presence of lacunes jointly influence cognitive performances in RSSI patients.
Conclusions: Our study suggests that OCT metrics with the presence of lacunes may hold promise as a screening tool for monitoring the trajectory of cognitive decline following RSSI.
Disclosures of Interest: No
Abstract N°: 1149
PLASMA PHOSPHORYLATED TAU 217 AS A DISCRIMINATIVE BIOMARKER FOR CEREBRAL AMYLOID ANGIOPATHY
1NTUH (National Taiwan University Hospital), Neurology, Taipei, Taiwan, 2NTUH (National Taiwan University Hospital), Department of Nuclear Medicine, Taiwan, 3NTUH (National Taiwan University Hospital), Medical Imaging, Taiwan
On behalf of:
Background and aims: Blood-based biomarker offers a non-invasive approach for diagnosing cerebral amyloid angiopathy (CAA), especially in the early stage. Our study evaluates the utility of plasma phosphorylated tau-217 (p-tau217) in differentiating CAA from Alzheimer’s disease (AD) and hypertensive small vessel disease (HTN-SVD).
Methods: Patients of AD (N = 24, age 74.1±7.2 years), probabe CAA (N=36, 73.9±7.2 years), and HTN-SVD (N=19, 61.8±9.1 years) were enrolled from memory and stroke clinics in a medical center in Taiwan. All participants received amyloid and tau PETs, and measurements of plasma biomarkers via SIMOA immunoassay platform (Quanterix). Diagnostic utility of p-tau 217 was assessed using ROC analyses and Yunden cutoff. The association between plasma p-tau 217 and neuroimaging variables were explored in CAA.
Results: Patients of CAA (T-) had lower plasma p-tau 217 (0.67±0.93 vs. 1.16±0.92 pg/mL, p < 0.001) compared to AD (A+T+), but had higher levels than HTN-SVD (A-) (0.67±0.93 vs. 0.46±0.85 pg/mL, p < 0.01). Plasma Aβ40, Aβ42, Aβ40/Aβ42 and total tau showed no differences among groups. Plasma p-tau 217 offers moderate diagnostic utility in differentaiting CAA from AD (sensitivity 0.83, specificity 0.64, AUC 0.771) and from HTN-SVD (sensitivity 0.58, specificity 0.90, AUC 0.751). In CAA, p-tau 217 significantly correlates to lobar microbleed count (p < 0.001).
Conclusions: Plasma p-tau217 potentially serve as a biomarker in differenting CAA from AD and HTN-SVD.
CAA vs. HTN-SVD: comparison of plasma biomarkers.
AD vs. CAA: comparison of plasma biomarkers.
Disclosures of Interest: No
Abstract N°: 1293
GYRAL SWELLING AND SULCAL HYPERINTENSITIES ARE COMMON IN CEREBRAL AMYLOID ANGIOPATHY-RELATED INFLAMMATION
Larysa Panteleienko*1,2, Gargi Banerjee3,4, Dermot Mallon5,6, Michael Zandi4,7, Rolf Jäger6,8, Frederik Barkhof9,10, David Werring1,4
1UCL Queen Square Institute of Neurology, Stroke Research Centre, Department of Brain Repair and Rehabilitation, London, United Kingdom, 2Bogomolets National Medical University, Department of neurology, Kyiv, Ukraine, 3UCL Institute of Prion Diseases, MRC Prion Unit, London, United Kingdom, 4National Hospital for Neurology and Neurosurgery, Queen Square, University College London Hospitals NHS Foundation Trust, London, United Kingdom, 5UCL Queen Square Institute of Neurology, London, UK, Neuroradiological Academic Unit, London, United Kingdom, 6National Hospital for Neurology and Neurosurgery, Lysholm Department of Neuroradiology, London, United Kingdom, 7UCL Queen Square Institute of Neurology, Department of Neuroinflammation, London, United Kingdom, 8UCL Queen Square Institute of Neurology, Neuroradiological Academic Unit, London, United Kingdom, 9Centre for Medical Image Computing (CMIC), University College London, London, United Kingdom, 10UCL Queen Square Institute of Neurology, Department of Brain Repair and Rehabilitation, London, United Kingdom
On behalf of:
Background and aims: Cerebral amyloid angiopathy-related inflammation (CAA-ri) is a rare form of CAA, and our understanding of the condition is likely affected by reporting bias. The current diagnostic criteria can be of limited application in a “real-life” setting, particularly when considering mimics. Quantitative phenotyping might further refine these criteria.
Methods: We retrospectively reviewed patients with CAA-ri assessed at our quaternary referral centre, and applied a standardised MRI-rating scale developed for ARIA (Amyloid-Related Imaging Abnormalities; an inflammatory response to anti-amyloid-beta immunotherapies in Alzheimer’s disease), which quantifies parenchymal (white matter) hyperintensities, gyral swelling and sulcal hyperintensities.
Results: We included 27 patients (52% men, mean age 71.8 years); comorbidities, including autoimmune diseases (48%), malignancy (33%), and other conditions associated with longstanding inflammation (33%), were common (Table 1). In our cohort, acute presentations (within 24 hours), were as common as the subacute (up to 4 weeks) presentations classically associated with CAA-ri. On review of the imaging (Table 2), nearly all patients had white matter hyperintensities (96%; usually confluent, asymmetric and involving ⩾2 lobes) and gyral swelling (92%; mainly colocalized with white matter hyperintensity). Sulcal hyperintensities were observed in 64%; these were mostly localized and in 2 patients with neuropathologically proven CAA-ri, this was the only observed MRI abnormality.
Conclusions: In our cohort of patients with CAA-ri, comorbid conditions associated with systemic inflammation were common, which might be of pathophysiological relevance. Patients with CAA-ri have MRI features associated with another inflammatory beta-amyloidosis (ARIA); the inclusion of gyral swelling and sulcal hyperintensities might improve the diagnostic accuracy of current criteria.
Disclosures of Interest: No
Abstract N°: 1509
CEREBROSPINAL FLUID AND PLASMA BIOMARKERS IN CEREBRAL AMYLOID ANGIOPATHY: A SYSTEMATIC REVIEW AND META-ANALYSIS
Aikaterini Theodorou*1, Maria Ioanna Stefanou1, Simona Saaco2, Aristeidis Katsanos3, Ashkan Shoamanesh4, David Werring5, Charlotte Cordonnier6, Lina Palaiodimou7, Thorsten Steiner8, Georgios Tsivgoulis1
1“Attikon” University Hospital, School of Medicine, National and Kapodistrian University of Athens, Athens, Greece., Second Department of Neurology, Athens, Greece, 2University of L’Aquila, via Vetoio, Italy, Department of Biotechnological and Applied Clinical Sciences, L’Aquila, via Vetoio, Italy, 3McMaster University/Population Health Research Institute, Hamilton, Canada, Division of Neurology, Ontario, Canada, 4McMaster University/Population Health Research Institute, Hamilton, Canada, Division of Neurology, Ontario, Canada, 5UCL Queen Square Institute of Neurology, London, United Kingdom, Stroke Research Centre, London, United Kingdom, 6University Lille, Inserm, CHU Lille, U1172, LilNCog, Lille Neuroscience and Cognition, France, University Lille, Lille, France, 7“Attikon” University Hospital, School of Medicine, National and Kapodistrian University of Athens, Athens, Greece., Second Department of Neurology, Athens, Greece, 8Klinikum Frankfurt Höchst, Frankfurt and Heidelberg University Hospital, Heidelberg, Germany., Departments of Neurology, Frankfurt, Germany
On behalf of:
Background and aims: Limited data exist regarding cerebrospinal fluid (CSF) and plasma biomarkers among patients with Cerebral Amyloid Angiopathy (CAA). We sought to investigate the levels of four biomarkers [β-amyloids (Aβ42 and Aβ40), total (tau) and phosphorylated tau (p-tau)] in CAA patients compared to healthy controls (HC) and Alzheimer disease (AD) patients.
Methods: We conducted a systematic review and meta-analysis including all available studies with data on CSF and plasma biomarkers and our single center experience, in sporadic CAA versus HC and AD patients. Biomarkers’ comparisons were investigated using random-effects models based on the ratio of mean (RoM) biomarker concentrations. RoM<1 and RoM>1 indicate lower and higher biomarker concentration in CAA compared to either HC or AD patients.
Results: We identified 10 cohorts, comprising 352 CAA patients with available data on CSF biomarkers. CSF Aβ42 [RoM:0.47; 95%CI:0.37–0.60; p-value<0.0001] and Aβ40 levels [RoM:0.72; 95%CI:0.64–0.82; p-value=0.0001] differentiated CAA from HC. CSF Aβ40 levels [RoM:0.73; 95%CI:0.65–0.82; p-value<0.0001] differentiated CAA from AD. CSF tau and p-tau levels differentiated CAA from HC [RoM:1.69; 95%CI:1.41–2.01; p-value<0.0001 and RoM:1.43; 95%CI:1.21–1.68; p-value=0.0006, respectively] and from AD [RoM:0.61; 95%CI:0.54–0.69; p-value<0.0001 and RoM:0.58; 95%CI:0.49–0.69; p-value<0.0001. respectively]. Plasma Aβ42 [RoM:1.14; 95%CI:0.89–1.45; p-value=0.2079] and Aβ40 [RoM:1.07; 95%CI:0.91–1.25; p-value=0.3306] levels were comparable between CAA and HC.
Conclusions: CAA is characterized by a distinct CSF biomarker pattern with lower Aβ40 levels compared to HC and AD patients. Tau and p-tau levels are higher in CAA compared to HC, but lower in comparison to AD patients.
Disclosures of Interest: No
Abstract N°: 2894
RELATIONSHIP BETWEEN PERIVENTRICULAR WHITE MATTER HYPERINTENSITY BURDEN AND POOR COLLATERALS IN ISCHEMIC STROKE TREATED WITH MECHANICAL THROMBECTOMY
Andrea Aram*1, Sofia Liljeblad1, Svetlana Lorenzano2, Manuela De Michele3, Marta Iacobucci4, Ettore Nicolini4, Nicoletta Giuseppa Caracciolo4, Martina Lombardi4, Christine Kremer1, Danilo Toni2
1Lund University, Lund, Sweden, 2Sapienza University of Rome, Department of Human Neurosciences, Rome, Italy, 3Sapienza University of Rome, Policlinico Umberto I hospital, Emergency Department Stroke Unit, Rome, Italy, 4Sapienza University of Rome, Rome, Italy
On behalf of:
Background and aims: White matter hyperintensity (WMH) might influence leptomeningeal collateral recruitment. The objective of this study was to investigate whether cSVD and, in particular, WMH burden are associated with poor collateral circulation in acute ischemic stroke (AIS).
Methods: This retrospective study included consecutive adult patients with AIS admitted to the Sapienza University of Rome teaching hospital in 2023 and treated with mechanical thrombectomy (MT). STRIVE criteria were followed to assess cSVD signs on MRI; Fazekas scale was used to grade WMH (periventricular, deep, total). Collateral status was evaluated by the adapted American Society of Interventional and Therapeutic Radiology/Society of Interventional Radiology (ASITN/SIR) score on pre-treatment CT-Angiography dichotomized into good (3-4) versus poor (0-2).
Results: Overall, 80 patients (51.2% females; mean[SD] age of 73.1[13.8] years) were eligible for analysis; 44 (55%) patients had poor collaterals, and 41 (51.2%) patients had any cSVD sign. Multivariate analysis did not show significant association between standard total cSVD burden score and collateral status. However, when the single components of the score were analysed, total moderate/severe WMH (OR 5.897, 95%CI 1.949-17.840, p=0.002) and, particularly, any degree of periventricular WMH (OR 2.834, 95%CI 1.281-6.273, p=0.010) resulted independent predictors of collateral status after adjustment for the well-known risk factors for cSVD and baseline NIHSS.
Conclusions: Our study showed that the burden of WMH and, especially, of periventricular WMH, more than other signs of cSVD, could have a significant role in predicting cerebral collateral recruitment potential in AIS patients treated with MT.
Disclosures of Interest: No
Abstract N°: 3090
CLINICAL, IMAGIOLOGICAL AND GENETIC PROFILES OF PATIENTS WITH CADASIL: THE REALITY OF A PORTUGUESE COHORT
Diogo Damas*1, José Miguel Alves1, Henrique Queirós2, Carolina Fernandes1, Maria Rosário Almeida3, Gustavo Santo1
1Coimbra University Hospital, Neurology Department, 2Coimbra University Hospital, Neuroradiology Department, 3University of Coimbra, Center for Neuroscience and Cell Biology
On behalf of:
Background and aims: Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is a rare genetic form of cerebral small vessel disease that is caused by mutations in the NOTCH3 gene. Despite being the most common vascular inherited disease, there is still need to elucidate the clinical and genetic features of CADASIL in the portuguese population.
Methods: We conducted an observational retrospective study in a tertiary medical center in Portugal and reported the clinical, imagiological and genetic data from medical records of patients with genetic confirmation of CADASIL.
Results: We identified 56 patients (57% females) with causative mutations in NOTCH3 gene and the mean age of diagnosis was 52±11.08 years. Ischemic stroke was the first manifestation of the disease in only 10 patients (18%), but a positive family history was present in 26 patients (46%). The most prevalent vascular risk factors were dyslipidaemia and arterial hypertension with 36% and 34%, respectively. Approximately a third of patients had recurrent migraines, and 31% (7 patients) with aura. Regarding imaging features, the median Fazekas score was 2, and the majority had white matter hyperintensities in the external capsule and temporal lobes. The genetic testing showed 80% of subjects with cysteine-altering variants, seven cysteine-sparing variants and four nonsense mutations, located mainly in the exons 11 and 8.
Conclusions: This study presents the most extensive series of portuguese CADASIL patients to date. In spite of the high variability of CADASIL, most of our clinical and epidemiological patterns have significant similarities with european cohorts.
Disclosures of Interest: No
Abstract N°: 3245
FREQUENCY, EVOLUTION AND LOCATION OF WHITE MATTER HYPERINTENSITIES IN A MULTI-SPOT PATTERN IN SPORADIC AND DUTCH-TYPE CEREBRAL AMYLOID ANGIOPATHY
Reinier van der Zwet*1, Isabel Kohlmann1, Manon Schipper2, Rosemarie van Dort1, Erik van Zwet3, Ellis van Etten1, Gisela Terwindt1, Matthias van Osch2, Marianne van Walderveen2, Marieke Wermer1,4
1Leiden University Medical Center (LUMC), Neurology, Leiden, Netherlands, 2Leiden University Medical Center (LUMC), Radiology, Leiden, Netherlands, 3Leiden University Medical Center (LUMC), Medical Statistics, Leiden, Netherlands, 4University Medical Center Groningen, Neurology, Groningen, Netherlands
On behalf of:
Background and aims: White Matter Hyperintensities (WMH) in a multi-spot pattern is a new MRI biomarker for Cerebral Amyloid Angiopathy (CAA) and part of the revised Boston Criteria-v2. We explored the frequency, localization, and progression of WMH spots to evaluate their potential as a biomarker for future trials.
Methods: We analyzed baseline and 1-year 3T-FLAIR scans of patients with sporadic (sCAA) and pre- and symptomatic Dutch-type hereditary CAA (D-CAA). We assessed the number of WMH spots, the frequency of a multi-spot pattern (>10 spots), and the distribution within the cerebral lobes with a Chi-squared Goodness-of-Fit-test, adjusted for lobar volume.
Results: We included 46 patients with sCAA and 57 patients with D-CAA (31 presymptomatic). Forty of 46 (87%) patients with sCAA and 41/57 D-CAA mutation carriers (72% overall, 48% presymptomatic) had WMH in a multi-spot pattern. The median spot count was 46 (range 2-227; IQR 15-71) in sCAA, 67 (range 0-218; IQR 5-113) in D-CAA overall, and 5 (range 0-71) in presymptomatic mutation carriers. The spots were most often (61.4%) present in the frontal lobe (24.3% parietal, 11.1% temporal, 3.1% occipital). The mean one-year increase of spots was 4 (SD:11) in sCAA and 8 (SD:9) in D-CAA (6; SD:5 in presymptomatic, 9; SD:10 in symptomatic). Sixty-two% of patients with sCAA and 89% of mutation-carriers with D-CAA (91% of presymptomatic) showed progression of spots after one year.
Conclusions: WMH in a multi-spot pattern is a common and progressive biomarker in early and advanced stages of CAA, with potential to be used in future trials.
Disclosures of Interest: No
Abstract N°: 2287
PROXIMAL AND DISTAL MIDDLE CEREBRAL ARTERY DIAMETER RATIO AND LENTICULOSTRIATE ARTERY INFARCTION
Jun Sang Yoo1, BumJoon Kim*1
1Asan Medical Center
On behalf of:
Background and aims: Subcortical infarctions in the lenticulostriate territory (LSA) can be attributed to two distinct pathophysiological mechanisms: lipohyalinotic degeneration (LD) and branch atheromatous disease (BAD). This study aims to identify the association between the diameter ratio between proximal and distal middle cerebral artery and the two different pathomechanisms of LSA infarction.
Methods: Acute LSA infarctions due to small vessel occlusive disease were included. Demographic and clinical data, along with MCA geometrical variables were collected. LD and BAD were differentiated based on length of infarction diameter and number of axial slices (LD: less than 00 mm in diameter and 00 axial slices). The geometrics of MCA were compared between LD and BAD. Independent factors associated with LD was investigated.
Results: A total of 117 patients were included, with 64 (54.7%) classified as BAD and 53 (45.3%) as LD. LD was associated with hypertension, lesion located at more distal, and better clinical outcomes compared to BAD. MCA geometric variables revealed that LD had a higher M1 diameter ratio, indicating a potential distinguishing factor. Multivariate analysis confirmed the independent association between LD and M1 diameter ratio. The M1 diameter ratio also showed positive correlation with the number of ipsileional lacunes.
Conclusions: Despite both LD and BAD occurring in the same vascular territory, they exhibit distinct pathophysiological differences. The study suggests that MCA geometry, particularly the M1 proximal/distal ratio, may serve as an independent factor for identifying lipohyalinotic degeneration.
Disclosures of Interest: No
Abstract N°: 2290
THE GLOBAL BURDEN OF CEREBRAL SMALL VESSEL DISEASE – A SYSTEMATIC REVIEW AND META-ANALYSIS
Bonnie Lam*1, Yuan Cai1, Ami LI1, Huijing Zheng1, Vincent Ct Mok1
1The Chinese University of Hong Kong, Division of Neurology, Department of Medicine and Therapeutics, Hong Kong, Hong Kong
On behalf of: The International Society for Vascular Behavioural and Cognitive Disorders (VasCog) Working Group
Background and aims: The prevalence of radiologically defined cerebral small vessel disease (cSVD) is variable across geographical regions. Previous studies on cSVD prevalence are mostly based on single geographically-defined cohorts. This study aimed to systematically review the prevalence of cSVD globally.
Methods: Articles were searched from the Ovid MEDLINE and EMBASE databases from 1st Jan 2000 to 31st March 2022, without language restrictions. Title/abstract screening, full-text review, and data extraction were performed. The prevalence of cSVD was extracted by world region and health status. The Risk of Bias for Non-randomized Studies tool was used. The protocol was registered on PROSPERO (CRD42022311133). A random-effects meta-analysis was performed to assess factors contributing to the prevalence of cSVD, adjusted for age and sex.
Results: Of 11,753 studies identified, 145 studies spanning 30 global regions were included in the systematic review (Figure 1). The pooled prevalence of cSVD in the community was 27% for moderate-to-severe white matter hyperintensities (WMH); 13% for lacunes; and 12% for cerebral microbleeds (CMB) (Figure 2). The prevalence of cSVD was higher in Latin America (WMH: 57%) and South Asia (lacunes: 50%). Meta-regression showed that having stroke or dementia predicted the prevalence of CMB (β = 1.61, p= 0.018, 95% CI= 0.28-2.95). Men participants were overrepresented in the included studies.
Conclusions: This is the first systematic review and meta-analysis of the global prevalence of cSVD. A higher prevalence of cSVD was found in LMICs and may be due to lifestyle, diet, socio-economic factors, risk factor control, genetic contributions, etc.
Disclosures of Interest: No
Abstract N°: 347
ASYMPTOMATIC DIFFUSION-WEIGHTED IMAGING POSITIVE LESIONS IN PATIENTS WITH CADASIL
1National Taiwan University Hospital, Department of Neurology, Taipei, Taiwan, 2National Taiwan University Hospital, Department of Medical Imaging, Taipei, Taiwan
On behalf of:
Background and aims: Asymptomatic diffusion-weighted imaging positive (aDWI+) lesions on brain MRI are occasionally detected in patients with small vessel disease (SVD). We aimed to investigate the prevalence and features of aDWI+ lesions in patients with CADASIL.
Methods: We enrolled patients from the Taiwan CADASIL Registry who received at least one brain MRI study between January 2019 and September 2023. aDWI+ were defined as incidentally detected DWI lesions without corresponding neurological deficits. Clinical characteristics, radiological markers of SVD, and the temporal evolution of the aDWI+ lesions were analyzed.
Results: Among the 155 enrolled patients (62±10 years, 52% male), 16 (10%) ever had aDWI+ lesions detected. Demographics and vascular risk factors were comparable between patients with and without aDWI+ lesions. Patients with aDWI+ lesions had more lacune (median 8 vs 2), microbleeds (20 vs 5), and anterior temporal white matter hyperintensity (WMH; 44% vs 14%) compared to those without. In the multivariate analysis, anterior temporal WMH was independently associated with aDWI+ lesions (OR 5.34, 95% CI 1.29-22.12). Compared to 18 patients with symptomatic DWI+ lesions, the aDWI+ lesions were more likely to be microinfarct (<1 cm; 81% vs 33%) and less likely to have corticospinal tract involvement (12.5% vs 94%). Among the 9 aDWI+ lesions with available follow-up MRI, 1 evolved into a lacune, 1 merged into WMH, and 7 disappeared (Fig 1.)
Conclusions: The presence of aDWI+ lesions in patients with CADASIL is not uncommon and closely associated with a greater burden of SVD markers. Its clinical implications in the long-term outcomes warrant further investigation.
Disclosures of Interest: No
Abstract N°: 1031
WHITE MATTER LESION BURDEN, BLOOD-BRAIN BARRIER DISRUPTION, AND WORSE COGNITIVE PERFORMANCE IN PATIENTS WITH CADASIL
Richard Leigh*1, Kyle Kern2, Joseph Snow3, Govind Nair4, Sherrell Apugo5, Alessandra Brofferio5, Manfred Boehm5, Elisa Ferrante5
1Johns Hopkins University, Neurology, Baltimore, United States, 2University of California, Los Angeles, Los Angeles, United States, 3National Institute Of Mental Health, Bethesda, United States, 4National Institute of Neurologic Disorders and Stroke, Bethesda, 5National Heart Lung & Blood Institute, Bethesda, United States
On behalf of:
Background and aims: In cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL), T2 white matter hyperintensity (WMH) accumulate on MRI, particularly in the anterior temporal lobes, distinguishing it from sporadic cerebral small vessel disease (SCSVD). Blood-brain barrier disruption (BBBD) has been implicated in SCSVD pathogenesis, although its role in CADASIL remains disputed. We investigated the relationship between WMH, BBB disruption, and cognitive performance in patients with genetically confirmed CADASIL.
Methods: Patients with CADASIL enrolled in a natural history study were included if they had cognitive assessment and dynamic susceptibility contrast (DSC) MRI. FLAIR and T1 were used to segment brain white matter and WMH. WMH burden was expressed as the fraction of white matter with WMH. DSC was used to calculate mean BBBD across white matter and expressed as percent leakage. Neuropsychological testing scores were used to quantify cognitive performance globally and 7 distinct cognitive domains: visuospatial, attention, verbal memory, visual memory, language, processing speed, and executive function. Comparisons used univariate linear regression.
Results: All sixteen patients included demonstrated BBBD (figure 1). Mean WMH fraction was 0.13 and mean BBBD was 1.5%. Greater WMH fraction was associated with greater BBBD (p=0.016) and worse cognitive performance in all domains except visuospatial. The strongest association was with global cognition (R2=0.653, p<0.001) (figure 2). Greater BBBD was associated with worse performance in language (p=0.048) and executive function (p=0.043) (figure 3).
Conclusions: In this small CADASIL cohort, BBBD was common, worse with greater WMH burden and associated with worse cognitive performance in multiple domains.
Disclosures of Interest: No
Abstract N°: 1684
IMAGING PATTERNS AND PROGNOSIS OF SMALL SUBCORTICAL INFARCTS
Stefano Mombelli*1, Chiara Rinaldi1, Vanessa Palumbo2, Anna Poggesi2, Patrizia Nencini2, Gabriele Vandelli3, Giorgio Busto4, Rosario Pascarella5, Marialuisa Zedde3, Francesco Arba2
1Careggi University Hospital, NEUROFARBA Department, University of Florence, Firenze, Italy, 2Careggi University Hospital, Stroke Unit, Firenze, Italy, 3Arcispedale Santa Maria Nuova, Neurology Unit, Stroke Unit, Azienda Unità Sanitaria Locale-IRCCS di Reggio Emilia, Reggio Emilia, Italy, Reggio Emilia, Italy, 4Careggi University Hospital, Neuroradiology Unit, Department of Experimental and Clinical Biomedical Sciences, University of Florence, Florence, Italy, Firenze, Italy, 5Arcispedale Santa Maria Nuova, Neuroradiology Unit, Azienda Unità Sanitaria Locale-IRCCS di Reggio Emilia, Reggio Emilia, Italy, Reggio Emilia, Italy
On behalf of:
Background and aims: Small subcortical infarcts (SSI) are one of the hallmarks of cerebral small vessel disease. We investigated radiological differences and prognosis of proximal and distal SSI (p-SSI and d-SSI, respectively).
Methods: We retrospectively reviewed records of consecutive patients admitted at two Stroke Units. We assessed location, shape and axial diameter of p-SSI and d-SSI with computed tomography (CT) and/or magnetic resonance (MR) imaging blinded to clinical data. Outcomes were: progression (worsening of at least two points at NIHSS compared with baseline), length of hospital stay, modified Rankin Scale (mRS) three months after the index stroke. We assessed independent associations between type of subcortical stroke and outcomes with logistic regression adjusting for age, sex, baseline NIHSS, i.v. thrombolysis.
Results: We included 292 patients, mean (±SD) age 67.42 (±12.41) years, 205 (70%) males, median (IQR) NIHSS=4 (2-5); 67 (23%) received i.v. thrombolysis, 169 (58%) had an ischemic lesion visible only with MR. P-SSI was detected in 85 (29%) patients. Progression occurred in 57 (20%) patients overall. Compared with d-SSI, p-SSI was associated with non-rounded shape (82%vs 65%,p=0.005), lesion diameter>15 mm (34% vs 10%,p<0.001), absence of white matter changes (22% vs 12%,p=0.035). Progression occurred more frequently in p-SSI (44% vs 10%,p<0.001; OR=7.23;95%CI=3.73-14.03). In p-SSI length of stay was more frequently longer than six days (58% vs 40%,p=0.005; OR=1.78;95%CI=1.04-3.07) and a shift towards worse mRS (cOR=2.47;95%CI=1.46-4.18) was observed.
Conclusions: Small subcortical infarcts have two distinct imaging lesion patterns with different prognostic implications, with p-SSI associated with both worse outcomes and functional status.
Disclosures of Interest: No
Abstract N°: 1704
GENERATION OF HUMAN IPSCS WITH EXONIC VARIANTS FROM CADASIL PATIENTS AND PROTEOMIC COMPARATIVE ANALYSIS
ANA BUGALLO-CASAL*1, Elena Muiño-Acuña2, Israel Fernández-Cárdenas2, María Rosa Martorell-Riera3, Cristòfol Vives-Bauzá4, Rita Quintas-Rey5, Enrique Vara-León5, Antonio Dopico-López1, Francisco Campos-Pérez1
1Health Research Institute of Santiago de Compostela (IDIS), Translational Stroke Laboratory Group (TREAT), Clinical Neurosciences Research Laboratory, Santiago de Compostela, Spain, 2Institut de Recerca de l'Hospital de la Santa Creu i Sant Pau, Stroke Pharmacogenomics and Genetics Group, Barcelona, Spain, 3Hospital Universitari Son Espases, Secció Genètica, Palma, Spain, 4Hospital Universitari Son Espases, Neurobiology Laboratory, Research Unit, Palma, Spain, 5Galician Public Foundation of Genomic Medicine, Molecular Medicine Group, Santiago de Compostela, Spain
On behalf of:
Background and aims: CADASIL (Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy) is a rare genetic condition caused by mutations in the NOTCH3 gene, inherited in an autosomal dominant manner. Previous studies suggest that the mutation's location may influence diagnosis and symptom severity. Our study aims to assess whether the mutation's position affects the generation of induced pluripotent stem cells (iPSCs) and observe whether the accumulation of Notch3 could already be visible in the early stages of cellular development. Additionally, we aim to conduct a proteome analysis to understand altered protein pathways and identify potential disease causes.
Methods: Six stable iPSC lines, derived from four CADASIL patients and two control subjects, underwent comprehensive characterization through genetic and molecular tests. Immunofluorescence was employed to examine intracellular and extracellular Notch3 accumulation. A quantitative proteomic study was employed to compare patients with mild and severe disease forms. A subsequent qualitative proteomic study identified protein profiles in severe versus mild disease forms.
Results: The iPSCs have been shown to maintain their chromosomal stability and pluripotency. Notch3 accumulation was already observed in iPSCs-derived CADASIL patients. A comparative proteomic profile revealed significant differences in the cell lines generated.
Conclusions: The mutation's position does not hinder the formation of iPSCs. Notch3 accumulation is evident in the early stage of pluripotency before cell differentiation into the pathologically affected vascular smooth muscle cells. Proteomic analysis revealed disruptions in key proteins related to cellular organization and function, particularly in pathways related to cellular structure.
Disclosures of Interest: No
Abstract N°: 1802
RADIOMICS-BASED FUNCTIONAL OUTCOME PREDICTION IN ACUTE SINGLE SUBCORTICAL INFARCTION
Tang Yang*1, Shuai Jiang1, Yuying Yan1, Yajun Cheng1, Bo Wu1
1West China Hospital, Sichuan University, neurology, China
On behalf of:
Background and aims: Diffusion-weighted imaging (DWI) and perfusion-weighted imaging (PWI) radiomics could be used as prognostic biomarkers in acute ischemic stroke. We aimed to build a model incorporating radiomic features and clinical factors to predict functional outcomes of patients with acute single subcortical infarction.
Methods: A total of 148 patients with acute single subcortical infarction were randomly divided into training (n=118) and test (n=30) cohorts. According to the modified Rankin Scale (mRS) score at 3 months after symptom onset, prognosis was dichotomized into excellent (mRS⩽1) and unfavorable (mRS>1). We extracted and selected the radiomic features on DWI and PWI to develop a radiomic model. Multivariable logistic regression was performed to construct a clinical model. Finally, a combined model was built using both the clinical and radiomics features. Receiver operating characteristic curves were used to evaluate these models.
Results: Early neurological deterioration, hypertension, baseline National Institutes of Health Stroke Scale score, and infarct volume were independently associated with functional outcomes and were included in the clinical model, which had an area under the curve (AUC) of 0.891 vs. 0.769 in the training and test cohorts. The radiomics and the combined model showed an improved AUC: 0.774 vs. 0.907 for the training cohort and 0.824 vs. 0.846 for the test cohort.
Conclusions: The clinical-radiomics model allows the accurate prediction of unfavorable outcome in patients with acute single subcortical infarction, which may add more value to the current clinical decision-making process.
Disclosures of Interest: No
Abstract N°: 1933
GLYMPHATIC SYSTEM MEDIATED THE ASSOCIATIONS BETWEEN PERIVASCULAR SPACES IN BASAL GANGLIA AND OTHER MARKERS OF SMALL VESSEL DISEASE
Yu Tian*1, Yuesong Pan1, Yilong Wang1
1beijing tiantan hospital, China
On behalf of:
Background and aims: MRI visible perivascular spaces(PVSs) are thought to be associated with small vessel disease (SVD) and to be important for interstitial fluid drainage. However, it is not clear whether the relationship between the PVSs and other neuroimaging markers of CSVD was mediated by glymphatic system.
Methods: We included 2219 participants from a community-based population in China. We estimated glymphatic pathway using the diffusivity along perivascular spaces based on diffusion tensor imaging(DTI-ALPS index). We rated white matter hyperintensity(WMH) and lacunes according to STRIVE2 guideline. We performed mediation effect analyses to to explore the associations between BG-PVSs, DTI-ALPS index and other CSVD markers by using linear and logistic regression models.
Results: The mean age was 61.3 (SD 6.6) years, and 1019 (45.9%) participants were men. The average DTI-ALPS index was 1.67±0.14. After adjusting for potential confounders, the DTI-ALPS index played a partial mediation role in the relationship of PVSs in basal ganglia with total WMH (11.70%, 95% CI 3.74-19.66, P=0.004), deep WMH(9.13%, 95% CI 2.36-15.90, P=0.02) and periventricular WMH (9.04%, 95%CI 1.87-16.22, P=0.01). Moreover, DTI-ALPS index played a partial mediating role of 17.01 (5.24-28.78, P=0.005) % in the association between PVSs in basal ganglia and lacunes.
Conclusions: Glymphatic system mediated less than 20% of the association between PVSs in basal ganglia and WMH and lacunes among community-dwelling participates, and PVSs in basal ganglia were partly associated with WMH and lacunes via impaired glymphatic system.
Disclosures of Interest: No
Abstract N°: 2343
MRI PATTERNS OF IATROGENIC CEREBRAL AMYLOID ANGIOPATHY
Simon Fandler-Höfler*1,2,3, Kanishk Kaushik3, Benedetta Storti4, Slaven Pikija5, Jacopo C. Difrancesco6, Thomas Gattringer1,7, Anna Bersano4, Marieke J.H. Wermer3,8, Gargi Banerjee2,9, David J Werring2
1Medical University of Graz, Department of Neurology, Graz, Austria, 2UCL Queen Square Institute of Neurology, Stroke Research Centre, Department of Brain Repair & Rehabilitation, London, United Kingdom, 3Leiden University Medical Center, Department of Neurology, Leiden, Netherlands, 4Fondazione IRCCS Istituto Neurologico Carlo Besta, Cerebrovascular Unit, Milan, Italy, 5Christian-Doppler-Clinic, Paracelsus Medical University, Department of Neurology, Salzburg, Austria, 6Fondazione IRCCS San Gerardo dei Tintori, Department of Neurology, Monza, Italy, 7Medical University of Graz, Division of Neuroradiology, Vascular and Interventional Radiology, Department of Radiology, Graz, Austria, 8University Medical Center Groningen, University of Groningen, Department of Neurology, Groningen, Netherlands, 9MRC Prion Unit at UCL, Institute of Prion Diseases, London, United Kingdom
On behalf of:
Background and aims: Iatrogenic cerebral amyloid angiopathy (iCAA) is presumed to be caused by the transmission of pathological amyloid-ß through neurosurgical procedures, particularly those involving cadaveric dura. Whether iCAA has distinct neuroimaging characteristics is yet unknown.
Methods: We collected patient-level longitudinal clinical and radiological data from the three largest published iCAA case series. Patients meeting criteria for probable or possible iCAA were included. MRIs were centrally analysed for inflammatory features, haemorrhagic and non-haemorrhagic markers of CAA using validated rating scales.
Results: We included 51 patients (68.6% male, median age at presentation 48 years, at exposure 9 years), 54.9% with probable and 45.1% with possible iCAA. We evaluated 219 MRIs (median 4 per patient) over a median follow-up time of 4 years (IQR 2-7). 23 patients (45.1%) presented with intracerebral haemorrhage, and 43 symptomatic haemorrhages occurred during the follow-up period in 33 individual patients (16.7/100 patient-years), and one patient died.
Patients with previous supratentorial brain surgery showed a regional spread of haemorrhagic markers (microbleeds, cortical superficial siderosis and intracerebral haemorrhages) into adjacent areas. 14/51 (27.5%) patients demonstrated transient cortical oedema suggestive of inflammation. 48/51 (94.1%) had severely enlarged perivascular spaces in the centrum semiovale. During follow-up, there was extensive progression of haemorrhagic markers (microbleeds, cortical superficial siderosis, small intragyral haemorrhages).
Conclusions: Patients with iCAA appear to have distinctive MRI characteristics, and typically develop new haemorrhagic markers close to the site of suspected beta-amyloid inoculation. These features might help to differentiate iCAA from other CAA-types, and provide new insights into underlying mechanisms of haemorrhage.
Disclosures of Interest: No
Abstract N°: 2360
CLINICAL RELEVANCE AND POSSIBLE PREDICTORS OF EVOLUTION OF RECENT SINGLE SUBCORTICAL INFARCT AND SURROUNDING WHITE MATTER
Yuying Yan*1, Anqi Zhang2, Shuai Jiang1, Lan Hong2, Congjun LI1, Simiao Wu1, Ming Liu1, Xin Cheng2, Bo Wu1
1West China Hospital, Sichuan University, Neurology, Chengdu, China, 2Huashan Hospital, Fudan University, Neurology, Shanghai, China
On behalf of:
Background and aims: Morphologic evolution of recent single subcortical infarcts (RSSIs) and secondary changes of perilesional white matter are not well understood. We aimed to investigate long-term changes of RSSI, its relevance for stroke outcome and possible predictors.
Methods: RSSI Patients within 72 hours after stroke onset in the stroke registry database who conducted baseline magnetic resonance imaging (MRI) and computed tomography perfusion (CTP) and at least one follow-up MRI (⩾90 days) were retrospectively enrolled. CTP metrics, MRI features, modified Rankin Scale (mRS) scores at 90 days and 1 year and imaging evolution were evaluated.
Results: On follow-up MRIs of 52 RSSI patients, 44 (84.6%) index infarcts had complete or partial cavitation, 6 (11.5%) stayed non-cavitated white matter lesions, and 2 (3.8%) almost vanished with a median follow-up period of 14.05 months. New white matter hyperintensity (WMH) adjacent to the infarct was observed in 26 (50.0%) patients. Patients without new WMH showed better functional outcome at 3 months (P <0.001) and 1 year (P <0.001), while no significant difference was found between varied lesion evolution types. After adjusting for baseline lesion volume, cerebral blood flow (CBF) in the region contralaterally mirrored to the infarct (OR=0.870, P=0.015), lesion located within corticospinal tract (OR=32.336, P=0.004) and follow-up duration (OR=1.214, P=0.008) were independently associated with new WMH.
Conclusions: The presence of new WMH surrounding the index infarct indicated worsening functional outcome in RSSI. CBF of mirrored region and lesion location might be predictive of white matter injury.
Disclosures of Interest: No
Abstract N°: 2437
COMPARISON OF PARANASAL SINUS OPACIFICATION BETWEEN PATIENTS 3 MONTHS POST STROKE AND HEALTHY, AGED COMMUNITY DWELLING INDIVIDUALS
Grant Kirkwood*1, Maria Valdes-Hernandez1, Michael Stringer1, Javier Escudero Rodriguez2, Una Clancy1, Fergus Doubal1, Michael Thrippleton1,3, Susana Munoz Maniega1, Joanna Wardlaw1,3
1Centre for Clinical Brain Sciences and UK Dementia Research Institute, Edinburgh, United Kingdom, 2Institute for Digital Communications, Edinburgh, United Kingdom, 3Edinburgh Imaging (University of Edinburgh), Edinburgh, United Kingdom
On behalf of: The 1936 Lothian Birth Cohort Collaboration Group and the Mild Stroke Study 3 Collaboration Group
Background and aims: Paranasal sinuses are vascularised structures situated adjacent to neurovascular bundles and meningeal lymphatics draining to cervical lymph nodes. Given known inflammatory response post-ischaemic stroke, we compare paranasal sinus opacification in mild stroke patients and healthy-aged cerebrovascular-matched individuals.
Methods: We acquired 3T T2-weighted MRI brain scans within 3-months of mild ischaemic stroke (Mild Stroke Study 3, MSS3) and 1.5T/3T T2-weighted MRI brain scans at five 3-years intervals between ages 72-85 of the community-dwelling, aged 1936 Lothian Birth Cohort (LBC). Paranasal sinus opacification was assessed using established scoring methods (Lund-MacKay (LM) and Zinreich, Figure 1). We selected age, sex, Fazekas scores, and vascular risk factors (diabetes, hypercholesterolaemia and hypertension)-matched cohorts and compared presence (LM) and severity (Zinreich) of opacification using Wilcoxon signed-rank test.
Results: We found opacification generally increased with age in older community-dwelling adults (e.g. 72 vs 85 years, z= -5.836,p<0.001, n=672, 180). In the matched sample (N=91, 76.6(4.4) years, 39(42.9%) female, 2[1 3] Fazekas PV, 2[1 2] Fazekas Deep, 25(27.5%) diabetics, 69(75.8%) with hypercholesterolaemia and 71(78%) hypertensive, in each), patients with stroke had higher LM scores than community-dwelling elderly (z=-4.394,p=<0.001). In the frontal, anterior and posterior ethmoid, opacification presence (all z<-2.982,p<0.003) and severity (all z<-2.220,p<0.026) were higher in patients with stroke, maxillary sinus opacification presence was also higher (z<-2.183,p<0.029).
Conclusions: We found patients 3-months post-stroke had higher levels of paranasal sinus opacification compared to a community-dwelling, aged and cerebrovascular-matched community cohort. Thence suggests a relationship between stroke and sinus opacification, with further exploration into underlying pathophysiology required.
Disclosures of Interest: No
Paper Poster – Stroke Complications
Abstract N°: 2649
SPASTICITY AFTER STROKE: AN UNDERRECOGNIZED NEED IN POST-STROKE CARE – PRELIMINARY RESULTS FROM A PROSPECTIVE COHORT STUDY
Isabella Stuckart1, Kristian Barlinn1, Nastasja Pfaff1, Lisa Frost1, Uwe Helbig1, Henry Lemkau1, Simon Winzer*1, Timo Siepmann1, Jessica Barlinn1
1Faculty of Medicine and University Hospital Carl Gustav Carus, Technische Universität Dresden, Germany, Department of Neurology, Dresden, Germany
On behalf of:
Background and aims: Spasticity is frequently underrecognized in stroke survivors. We implemented a screening algorithm to identify patients at risk of developing spasticity in our organized post-stroke care program (SOS-Care).
Methods: This prospective cohort study enrolled acute stroke patients with motor deficits (⩾1 point in NIHSS motor items) at hospital admission who participated in SOS-Care. We assessed strength and spasticity using the modified Ashworth Scale (MAS) in 12 muscle groups at hospital discharge, 3 and 12 months post-stroke. Patients with persistent motor deficits underwent further follow-up assessments. Non-pharmacological and pharmacological antispasticity therapies provided in routine ambulatory care were recorded.
Results: Between 07/22 and 01/24, 95 patients (ischemic stroke, n=83; intracerebral hemorrhage, n=12) were included: median age was 70 (IQR, 18) years, 41% were women and NIHSS score was 7 (IQR, 11) points. Among the patients who completed their respective follow-up assessments to date, 57.9% (55/95) had persistent motor deficits and 7.4% exhibited spasticity (median MAS: 0 [IQR, 0]) at discharge. At 3 months, 49.8% (47/95) still had persistent motor deficits and 20% showed spasticity (median MAS: 8.5, [IQR, 8.5]). Of the nine patients who completed 12-months follow-up, eight showed spasticity (median MAS: 6 [IQR, 10]). Overall, 13 patients received occupational therapy, two were prescribed oral antispasticity medication and one patient was treated with botulinum neurotoxin type A.
Conclusions: Our preliminary observations from standardized spacticity screening in a prospective cohort of stroke survivors undergoing organized post-stroke care highlight the need for improved recognition and management of spasticity in post-stroke survivors.
Disclosures of Interest: No
Abstract N°: 2677
CHANGES IN SEXUAL ACTIVITY POST-STROKE
Marti Boix Coll*1, Isaac Nuño1, Laura Pérez1, David Collado1, Monica Millan1, Marina Martínez-Sánchez1, Alejandro Bustamante1, Lucia Muñoz Narbona1, Rosa López1, Natalia Pérez de la Ossa1
1Hospital Germans Trias i Pujol, Neurology, Badalona, Spain
On behalf of:
Background and aims: Sexual dysfunction is a poorly studied post-stroke consequence. We aim to evaluate the changes produced in the sexual activity of patients who have suffered a stroke, determining their degree of affectation and their needs
Methods: Observational study of patients between 18 and 85 years old admitted for ischemic or hemorrhagic stroke from June to November 2019. Information about sexual activity was recorded through an ad hoc survey, evaluated by telephone between 6-12 months after suffering a stroke. Demographic and clinical variables were obtained from our prospective stroke database.
Results: Of 212 patients with inclusion criteria, 27% were not located, 35% refused to participate and 81 were included (average age 63 years, 67% men, 75% mRS 0-1 at discharge). Sexual desire after stroke was reduced in 14% of participants, sexual activity decreased in 20%, physical abilities were affected in 17% (erection 15%, lubrication 3%) and level of sexual arousal decreased by 37%. Dissatisfaction with their sexual activity increased by 16% (from 20% to 36%). Only 11% received specific information, although 52% considered it necessary.
Conclusions: Sexual activity and dysfunction are a common problem after a stroke. It affects up to 20% of patients, causing concern and changes in the patient's interest in their sexual activity. Our results suggest devoting greater attention to this common problem in stroke survivors.
Disclosures of Interest: No
Abstract N°: 1627
MEDICAL COMPLICATIONS DURING INTERHOSPITAL TRANSFER IN PATIENTS WITH ACUTE ISCHEMIC STROKE AND LARGE VESSEL OCCLUSIONS
Damjan Mirkov*1, Ekkehart Jenetzky2, Andrea Thieme1, Christoph Gumbinger1, Wolfgang Wick1, Peter A. Ringleb1, Timolaos Rizos1
1Heidelberg University Hospital, Department for Neurology, Heidelberg, Germany, 2Faculty of Health/School of Medicine, Witten/Herdecke University, Witten, Germany
On behalf of:
Background and aims: Studies exploring complications during transfer between primary stroke centers (PSC) to comprehensive stroke centers (CSC) in ischemic stroke (AIS) patients with large vessel occlusions (LVO) are rare. It remains unknown how often medical interventions by emergency physicians (EP) are needed during these transfers.
Methods: In this retrospective observational study, all AIS patients transferred between 01/2015 and 10/2021 from PSCs to our CSC to undergo thrombectomy were included. Complications were classified being major (MACO) or minor (MICO), based on a predefined list and according to the necessity of an EP.
Results: We included 985 patients into analysis. MACO occurred in 16 (1.6%), MICO in 144 (14.6%). Patients with MACO were more severely affected by stroke (p=0.026); transport duration was longer (p=0.05) but geographical distances between PSC and CSC did not differ (p=0.892 and p=0.757). Patients with MICO were more often treated with thrombolysis (p<0.001) and antihypertensives prior to thrombolysis (p<0.001) and more often transported with an emergency physician (p=0.004). Overall, thrombolysed patients had more often any complication compared to patients without thrombolysis (11.9 % vs 4.4%; p<0.001); however, this was driven by patients with MICO (p<0.001): MACO were not associated to thrombolysis (p=0.389). Neither in thrombolysed nor in non-thrombolysed patients, significant associations between stroke severity and complications were observed.
Conclusions: No patient-specific factor increasing the risk of complications was identified and our results do not indicate that thrombolysis increases major complications. Our data suggest that interhospital transfer without additional emergency physicians is reasonable in most patients.
Disclosures of Interest: No
Abstract N°: 822
IMPACT OF CORTICAL SUPERFICIAL SIDEROSIS ON SEIZURE CONTROL OF POST-STROKE EPILEPSY
1National Cerebral and Cardiovascular, Neurology, Suita, Japan, 2National Cerebral and Cardiovascular, Cerebrovascular Medicine, Suita, Japan
On behalf of:
Background and aims: Post-stroke epilepsy (PSE) is generally well-controlled. However, 20-30% of cases are refractory to antiseizure medications (ASM), presenting with recurrent seizures. Identifying specific features in refractory PSE cases can be valuable in guiding treatment strategy.
Methods: A retrospective study of cases with PSE from 2014 to 2019 analyzed differences between well-controlled and refractory groups. PSE was defined as a seizure occurring more than seven days after stroke. Cases without head MRI or prescription of ASM were excluded. Cases in which seizure control was achieved with a single ASM were defined as well-controlled group, while cases requiring > 1 and > 2 ASMs were defined as refractory and super-refractory groups, respectively.
Results: Among 208 cases with PSE (median age: 74 years; 37.0% female), 130 received newer-generation ASM, 44 older-generation ASM, and 34 both. Single ASM control (453 days seizure-free) was achieved in 68.3%, with 31.7% refractory. The refractory group tended to be male (72.7% vs. 58.5%), hemorrhagic stroke (60.6% vs. 43.0%), and had a higher craniotomy frequency (27.2% vs. 11.3%) than the well-controlled group. Cortical superficial siderosis (cSS) was significantly more prevalent in the refractory group (65.2% vs. 45.1%). Multivariable analysis adjusting for age, sex, stroke type, stroke size, and other factors confirmed the association of cSS with the refractory group (odds ratio: 1.96, 95% CI: 1.01-3.82). Super-refractory group had a much higher prevalence of cSS (74.2%).
Conclusions: The presence of cSS is associated with ASM resistance in PSE, offering a crucial insight for future interventions in refractory cases.
Disclosures of Interest: No
Abstract N°: 2286
EARLY NEUROLOGICAL IMPROVEMENT AFTER ENDOVASCULAR THROMBECTOMY AS A PROTECTIVE FACTOR AGAINST STROKE ASSOCIATED PNEUMONIA. A RACECAT SUBANALYSIS
Bárbara Yugueros-Baena*1, Marina Martínez-Sánchez1, Anna Ramos2, Monica Millan1, Daniel Santana1, Sònia Abilleira3, Marc Ribo4, Natalia Pérez de la Ossa1, Xabier Urra5, Alejandro Bustamante1
1Hospital Germans Trias i Pujol, Neurology, Badalona, Spain, 2Hospital de la Santa Creu i Sant Pau, Neurology, Barcelona, Spain, 3Institut Català de la Salut, Salut,, Barcelona, Spain, 4Vall d'Hebron University Hospital, Neurology, Barcelona, Spain, 5Hospital Clínic de Barcelona, Neurology, Barcelona, Spain
On behalf of:
Background and aims: Stroke-associated pneumonia (SAP) contributes to a greater morbimortality in stroke. The effects of successful recanalization on the risk of developing SAP have not been fully investigated. We aim to assess whether the absence of early neurological improvement (ENI) after endovascular thrombectomy (EVT) represents a risk factor for SAP.
Methods: Retrospective analysis of the prospective, randomized RACECAT trial. We selected patients with ischemic stroke who underwent EVT. Demographic data, clinical information and ENI (defined as improvement of 8+ points in the National Institutes of Health Stroke Scale (NIHSS) or NIHSS <2 in the first 24h) were compared regarding the development of SAP (defined as suspected respiratory infection requiring antibiotics). Independent risk factors for SAP were assessed by logistic regression analysis and its importance was assessed by random forest.
Results: Among 417 patients treated with EVT, 89 (21%) developed SAP. Patients without ENI had a higher risk of pneumonia (84% Vs 49%, p<0.0001), being an independent risk factor for SAP (OR 9.4, 95% CI 2.0-43.4), together with age, male sex, history of diabetes mellitus, higher diastolic blood pressure, posterior circulation occlusion, use of general anesthesia and higher baseline NIHSS. Transfer protocol or complications during transfer were not associated with higher risk of SAP. Absence of ENI was the variable with the highest importance in random forest.
Conclusions: ENI represents the main protective factor against SAP in patients treated with EVT, on top of pre-treatment factors. Studies looking for enriched populations with higher rates of SAP may benefit from focusing on patients without ENI after EVT.
Disclosures of Interest: No
Abstract N°: 2787
QUANTITATIVE EEG CHARACTERISTICS OF POST-STROKE DELIRIUM
Fenne Vandervorst*1,2, Edwin van Dellen3, Amber Maselis4, Arjen Slooter1,2,3, Sebastiaan Engelborghs1,2, Sylvie De Raedt1,2
Background and aims: Delirium after ischemic stroke (IS) is associated with worse outcome. Studying EEG characteristics among patients with post-stroke delirium (PSD) may improve our insight in underlying pathophysiological processes. Our aim was to study multiple EEG characteristics among homogeneous groups of patients with and without PSD.
Methods: In a previously published dataset of 514 patients with IS, 39% patients developed a PSD. 213 of 514 patients underwent a usable EEG, including 50 patients with an EEG during PSD and 163 patients without PSD. Subsequently, case control matching analysis was performed, using SPSS, for the patients with versus without delirium. We matched on following variables: stroke location, NIHSS score on admission and age (tolerance variables respectively 0, 5 and 10). For each patient, the first 8 artifact-free epochs of 8 seconds were selected and EEG characteristics were calculated and averaged over all channels and epochs. Parameters were compared using a Mann-Whitney-U-test.
Results: We included 82 patients (74 patients with middle cerebral artery (MCA) infarction, 8 with vertebrobasilar stroke). Median age was 76 in both groups, median NIHSS was 12 in the delirium group and 9 in the non-delirium group. Relative delta power (RDP) is significantly increased (0,542 versus 0,454, p-value 0,011) in patients who develop PSD. In patients with MCA infarction with PSD, RDP was increased in both the affected and the unaffected hemisphere compared to those without PSD.
Conclusions: The RDP is increased in patients with PSD compared to patients with similar stroke characteristics without PSD.
Disclosures of Interest: No
Abstract N°: 2879
CLINICAL FRAILTY IS ASSOCIATED WITH POST-STROKE DELIRIUM
Eduard Druyts1, Marijke Desmet1,2, Isaline Demarcin1,2, Robin Gens1,2, Fenne Vandervorst1,2, Sylvie De Raedt*1,2
1UZ Brussel, Neurology, Jette, Belgium, 2Vrije Universiteit Brussel, Center for Neurosciences (C4N), Ixelles, Belgium
On behalf of:
Background and aims: Post-stroke delirium is a common complication after ischemic stroke (IS), linked to poor outcome, however the underlying mechanisms are still unclear. Clinical frailty is also linked to poor stroke outcome. The aim of our study is to investigate the role of pre-stroke clinical frailty in the development of post-stroke delirium (PSD).
Methods: In a previously published dataset of 514 patients with IS, 39% (201) patients were diagnosed with PSD using a chart review, based on the DSM-5 criteria. A 35 item Frailty Index (FI) list was created. The total number of conditions present was divided by the total number of items defined on the index list to generate frailty scores for each patient (range 0-1). Four frailty categories were identified: non-frail = FI <0.1, pre-frail = 0.1 < FI ⩽ 0.21, frail = FI > 0.21 and most frail = FI ⩾0 .45. We used a logistic regression analysis to determine factors associated to post-stroke delirium.
Results: In our dataset, median age was 75 (IQR 20), NIHSS on admission 7 (IQR 12) and FI 0.11 (IQR 0.14). FI ranged from 0 to 0.46. 212 (41%) patients were non-frail, 200 (39%) were pre-frail, 98 (19%) were frail, and 4 (0.8%) most frail. In logistic regression analysis, clinical frailty (FI > 0.1) was associated to post-stroke delirium (OR 1.77, 95% CI 1.08-2.88, p = 0.023), independent of age and NIHSS.
Conclusions: Pre-stroke clinical frailty is associated with the development of post-stroke delirium.
Disclosures of Interest: No
Abstract N°: 154
IMAGING BIOMARKERS INDICATING RISK FOR DELIRIUM AFTER THROMBECTOMY OF LARGE VESSEL OCCLUSION STROKE
Marianne Hahn*1, Lavinia Brockstedt2, Sonja Gröschel1, Ahmed Othman2, Klaus Gröschel1, Timo Uphaus1
1University Medical Center of the Johannes Gutenberg University Mainz, Department of Neurology, Mainz, Germany, 2University Medical Center of the Johannes Gutenberg University Mainz, Department of Neuroradiology, Mainz
On behalf of:
Background and aims: Post-stroke-delirium has been linked to worse outcome in patients with acute cerebrovascular disease; identification of individuals at risk may prevent delirium and thereby improve outcome. We investigate prognosis and factors associated with post-stroke-delirium in patients with large vessel occlusion (LVO) ischemic stroke treated by mechanical thrombectomy (MT).
Methods: All 747 patients (53.4% female) prospectively enrolled in the Gutenberg-Stroke-Study (May 2018-November 2022) were analyzed with regard to diagnosis of delirium during hospital stay; patient-, stroke- and treatment characteristics as well as native computed tomography (CT)-imaging based parameters of cerebral atrophy (global cortical atrophy [GCA] score, posterior atrophy score [Koedam], medial temporal lobe atrophy [MTA] score) and white matter lesions (Fazekas score) were compared on univariate level. Multiple logistic regression analyses were conducted to identify independent predictors of delirium and to investigate the association of delirium with functional outcome at 90-day follow-up.
Results: We report 8.2% of patients (61/747) developing delirium following MT of LVO. Independent predictors of delirium were older age (aOR[95%CI]:1.034[1.005-1.065], p=0.023), male sex (aOR[95%CI]: 2.173[1.182-3.994], p=0.012), general anesthesia during MT (aOR[95%CI]:2.455[1.385-4.352], p=0.002), infectious complications (aOR[95%CI]:1.845[1.031-3.305], p=0.039), “other determined” stroke etiology (aOR[95%CI]:2.424[1.100-5.345], p=0.028), and a MTA score exceeding age-specific cut-offs (aOR[95%CI]:2.126[1.065-4.244], p=0.033). Delirium was independently associated with worse functional outcome (aOR[95%CI]:2.902[1.005-8.383], p=0.049) at 90-day follow-up.
Conclusions: Delirium is independently associated with worse functional outcome after LVO, stressing the importance of preventive measures. Besides conventional risk factors, pathological MTA scores and use of general anesthesia during MT may be easy-to-apply criteria to identify individuals at risk of developing delirium following MT of LVO.
Disclosures of Interest: No
Abstract N°: 468
PREDICTING PNEUMONIA RISK AFTER STROKE DISCHARGE USING MACHINE LEARNING-BASED SURVIVAL ANALYSIS
1Ditmanson Medical Foundation Chia-Yi Christian Hospital, Division of Neurology, Department of Internal Medicine, Chia-Yi, Taiwan, 2Ditmanson Medical Foundation Chia-Yi Christian Hospital, Pulmonary medicine, Chia-Yi, Taiwan, 3Ditmanson Medical Foundation Chia-Yi Christian Hospital, Clinical Medicine Research Center, Department of Medical Research, Chia-Yi, Taiwan, 4National Taiwan University Hospital, Yunlin Branch, Department of Neurology, Douliu, Taiwan, 5National Cheng Kung University, Department of Biomedical engineering, Tainan, Taiwan
On behalf of:
Background and aims: Post-stroke pneumonia (PSP) is common in stroke patients. PSP occurring after hospital discharge still predisposes stroke survivors to poor functional outcomes and death. Currently, no prediction model is designed to predict PSP beyond the acute stage of stroke. This study examined machine learning (ML) methods for predicting the risk of PSP after hospital discharge.
Methods: This study analyzed data from 5754 hospitalized stroke patients. The dataset was randomly split into a training set and a holdout test set in a 4:1 ratio. Various clinical and laboratory variables were used as predictors, and different ML algorithms were used to model time-to-event data. A model-agnostic method based on Shapley additive explanations was used to interpret the ML model.
Results: The study found that 5.7% of the study patients experienced pneumonia within one year after discharge. The random survival forest (RSF) model had the highest C-index than other ML algorithms and traditional Cox regression analysis based on repeated 5-fold cross-validation on the training set. The final RSF model achieved a C-index of 0.787 with a 95% confidence interval of 0.737–0.840 on the holdout test set. The top three important predictors were the Glasgow Coma Scale score, age, and length of hospital stay.
Conclusions: The RSF model showed superior discriminative ability compared to other ML algorithms and traditional Cox regression analysis, suggesting a non-linear relationship between predictors and outcomes. The ML model generated can be integrated into the hospital information system to offer personalized risk assessments.
Disclosures of Interest: No
Abstract N°: 886
AETIOLOGY OF ACUTE RESPIRATORY FAILURE IN PATIENTS WITH ISCHAEMIC STROKE STUDIED BY CHEST CT SCAN
1University Hospital Bonn, Division of Vascular Neurology, Department of Neurology, Bonn, Germany, 2University Hospital Bonn, Department of Diagnostic and Interventional Neuroradiology, Bonn, Germany
On behalf of:
Background and aims: Acute respiratory failure (ARF) is a serious complication of acute ischaemic stroke. This study aimed to investigate the aetiologies of ARF in stroke patients. By systematically analysing chest CT images, we aimed to identify the specific respiratory conditions that most frequently lead to ARF as well as their impact on functional outcome and mortality.
Methods: We included acute ischaemic stroke patients admitted to our University Hospital from 2017 to 2022, who underwent chest CT scans for ARF. All chest CT scans were re-evaluated by a radiologist. We established a database encompassing demographic, clinical, radiological and laboratory data. This dataset was then analysed using descriptive statistics and regression analyses.
Results: 236 stroke patients with a mean age of 71.3 years and a median NIHSS on admission of 7 were included. Re-evaluation of chest CT scans revealed acute respiratory complications including bronchitis (66.1%), pleural effusion (60.6%), pneumonia (53%), pulmonary oedema (37.3%) and pulmonary artery embolism (27.5%). Patients had varying numbers of pulmonary diagnoses, with 2.1% having five different conditions, while the majority (53%) had at least three diagnoses. In adjusted regression analyses, bronchitis was the only respiratory complication that independently predicted in-hospital mortality. Regarding functional outcome, the subtype of respiratory complication did not adversely affect the modified Rankin Scale score on discharge.
Conclusions: The study revealed diverse aetiologies of ARF in ischaemic stroke patients. Intriguingly, the specific pulmonary condition itself did not significantly affect functional outcome, while bronchitis was associated with an increased mortality risk.
Disclosures of Interest: No
Abstract N°: 1728
RELATION OF POST-STROKE HEADACHE TO CEREBROVASCULAR PATHOLOGY AND HEMODYNAMICS
Elsayed Abed*1
1Al-Azhar University, Neurology, Cairo, Egypt
On behalf of:
Background and aims: Despite the high prevalence of cerebrovascular stroke, headache attributed to ischemic strokes is often undertreated and overlooked. The aim is to detect the relation of a post-stroke headache to cerebrovascular pathology and changes in hemodynamics through a high-resolution duplex ultrasound examination.
Methods: The study was conducted on 239 patients who were presented with an acute ischemic stroke. Patients were subdivided into two groups; Group I included patients with headache attributed to ischemic stroke (cases) and Group II included headache-free stroke patients (controls). Clinical and radiological examination were preformed to detect the type of stroke. Ultrasound duplex examination of the extracranial and intracranial cerebrovascular system was carried out for both groups.
Results: Group I included 112 patients (mean age 57.66 ±6.59 years), Group II included 127 patients (mean age 57.73±7.89 years). Post-stroke headache was more frequent in patients with posterior circulation infarction (58%). Post-stroke headache was reported within 7 days post-stroke in (61.6%) of patients. Pre-stroke headache was an independent predictor for post-stroke headache occurrence (OR=28.187, 95%CI; 6.612-120.158, P<0.001). Collateral opening and various degrees of intracranial vascular stenosis were strong predictors of headache occurrence (OR=25.071, 95% CI; 6.498-96.722, P<0.001).
Conclusions: Post-stroke-headache is a common phenomenon especially in patients with pre-stroke headache, history of old stroke, posterior circulation infarction, and large artery disease. This headache was of moderate-intensity with clinical characteristics of tension-type. The intracranial cerebrovascular pathological changes including opening of the collateral channels and variable degrees of stenosis of cerebrovascular systems were implicated in the production of that headache.
Disclosures of Interest: No
Abstract N°: 1779
PRACTICE VARIATIONS IN GJ/PEG INSERTION FOR DYSPHAGIA AFTER ISCHEMIC STROKE IN THE US
Lily Zhou*1, Thalia Field1, Kim Mcgrail1, Jason Sutherland1, Robert Holloway2
1The University of British Columbia, Vancouver, Canada, 2University of Rochester, Rochester, United States
On behalf of:
Background and aims: Among patients with post stroke dysphagia (PSD), the optimal timing for insertion of surgical percutaneous gastric-jejunal (GJ) tubes, most common percutaneous endoscopic gastrostomy (PEG) tubes, is unclear. The AHA recommends GJ/PEG if PSD persists for >2-3 weeks based on low-level evidence.
Methods: Using the 2019 and 2020 National Readmissions Database (NRD), we identified adults discharged with AIS (ICD-10-CM I63*) as the principal diagnosis who received a GJ/PEG for PSD. We compared patient demographics, discharge disposition and readmission by timing of GJ/PEG insertion. We examined rates of GJ/PEG insertion and median time to insertion by hospital.
Results: 21,941/560,707 (3.91%) patients with AIS received a GJ/PEG before discharge. The median time to insertion was 8 days after admission (IQR 4-12, 81.9% prior to 2 weeks). Receiving a GJ/PEG in the earliest quartile(Q) (Q1=<5 days; Q2=5-8d; Q3=9-12d; Q4>12d) was associated with higher inpatient mortality (15.2% vs. 7.4% vs. 6.6% vs. 6.6%, p<0.001) and fewer readmitted days for the remainder of the year (11.7d vs. 12.0d vs. 13.7d vs. 15.5d, p<0.001); both effects remained significant after controlling for age, sex, and stroke severity. In hospitals where >5 GJ/PEG tubes were inserted for PSD annually (2019=569; 2020=557), the median time to insertion by hospital ranged from 0-21 days.
Conclusions: There is significant practice variation with regards to GJ/PEG insertion and the majority are inserted earlier than guidelines recommend. More research is needed to explain the higher mortality seen in patients receiving GJ/PEGs <5 days from admission and if delaying the procedure would improve patient outcomes.
Disclosures of Interest: No
Abstract N°: 1962
PREDICTORS OF APPENDICULAR SKELETAL MUSCLE LOSS AFTER ACUTE STROKE
Naomi Whitehead*1, Laura Johnson1, Sheharyar Baig1, Jessica Redgrave2, Arshad Majid1, Elizabeth Williams1, Ali Ali1
1The University of Sheffield, United Kingdom, 2Sheffield Teaching Hospitals NHS Foundation Trust, United Kingdom
On behalf of:
Background and aims: Stroke related sarcopaenia may be related to factors such as immobility, nutritional deficiency and inflammation, all of which are prevalent after acute stroke. We aimed to identify which of these factors were most predictive of skeletal muscle loss after acute stroke.
Methods: 30 patients admitted within 1 week of stroke were recruited into this longitudinal observational study. Weekly measures of bioelectrical impedance analysis (BIA), hight and weight were used to estimate appendicular skeletal muscle mass (ASM) from validated formulae (European Working Group on Sarcopaenia in Older People). Stroke severity (NIHSS) ambulation status and self-care status were recorded, weekly assessment of protein (g/Kg body weight) and calorie (Kcal/Kg body weight) intake was estimated from food charts, Functional Oral Intake Scale (FOIS) detailed swallow status, and the Modified Glasgow Prognostic Score (mGPS) was used as a valid surrogate of inflammation. NIHSS, self-care status, protein and calorie intake, FOIS and mGPS were entered into stepwise multiple regression alongside age and comorbidities to understand their influence on change in ASM.
Results: Patients experienced a significant decline in ASM of 3.7% during the inpatient stay (p= 0.028). Univariate regression revealed significant correlations between change in ASM and stroke severity (NIHSS, p= 0.017), mGPS (p= 0.035), ability to self-care (p= 0.023) and FOIS (p= 0.041). However only stroke severity remained an independent predictor of loss of ASM on multivariate analysis (p= 0.015).
Conclusions: Stroke severity independently predicts muscle loss, while the role nutrition and inflammation play are still uncertain and require further exploration in larger studies.
Disclosures of Interest: No
Abstract N°: 2130
EFFICACY OF NON-INVASIVE CEREBELLAR STIMULATION IN PATIENTS WITH POST-STROKE DYSPHAGIA: A SYSTEMATIC REVIEW AND META-ANALYSIS
1Kasr Alainy Medical School, Cairo University, Faculty of Medicine, Cairo, Egypt, 2Al-Azhar university, Faculty of Medicine, Cairo, Egypt, 3Zagazig University, Faculty of Medicine, El-sharkia, Egypt, 4Alexandria University, Faculty of Medicine, Alexandria, Egypt, 5Tanta University, Faculty of Medicine, Tanta, Egypt, 6Helwan University, Faculty of Medicine, Helwan, Egypt
On behalf of:
Background and aims: Post-stroke dysphagia (PSD) is one of the most common stroke complications. The optimal protocol and target area for PSD using repetitive transcranial magnetic stimulation (rTMS) or theta-burst stimulation (TBS) remain uncertain. Existing studies often focus on the hemispheric cortex, neglecting the cerebellum. Limited studies explore cerebellar rTMS and TBS in PSD, so we aim to assess their efficacy.
Methods: Following the PRISMA guidelines. We searched databases to identify the relevant RCTs. Using RevMan 5.4 software, the analyzed primary outcome was Fiberoptic Endoscopic Dysphagia Severity Scale (FEDSS) with subgroups based on the follow-up duration, side of stimulation (bilateral or unilateral) and stimulation modality (rTMS or TBS). Pooled standardized mean differences (SMD) and their 95% confidence intervals (CI) were analyzed using inverse variance.
Results: We included seven RCTs with a total of 358 patients. Compared to the sham group (control), Patients who received cerebellar rTMS had significantly greater improvement in FEDSS, with the four-week subgroup showing slightly better improvement than the two-week subgroup (SMD=-0.71; 95%CI [-0.98, -0.43]) and (SMD=-0.50; 95%CI [-0.93, -0.06]) respectively. Patients who received rTMS or bilateral stimulation (SMD=-0.88; 95%CI [-1.16, -0.61]) and (SMD= -1.12; 95%CI [-1.63, -0.61]), respectively, showed slightly better improvement than those who received TBS or unilateral stimulation (SMD=-0.52; 95%CI [-1.02, -0.02]) and (SMD= -0.85; 95%CI [-1.43, -0.26]), respectively, with all subgroups showing significant improvement compared to control.
Conclusions: Cerebellar stimulation using rTMS or TBS is significantly efficacious in improving PSD, with TBS being more cost and time convenient. Further RCTs on more diverse populations still need to be conducted.
Disclosures of Interest: No
Abstract N°: 2672
EFFECT OF THE PHARMACOLOGICAL INHIBITION/ABSENCE OF TLR4 IN BACTERIAL TRANSLOCATION AFTER EXPERIMENTAL STROKE AND IT'S INFLAMMATORY CONSEQUENCES
CRISTINA GRANADOS-MARTINEZ*1, Nuria Alfageme1, Maria Encarnación Fernández-Valle1, David Castejón1, David Sevillano2, Luis Alou2, Macarena Hernandez-Jimenez1, Maria Angeles Moro3, Ignacio Lizasoain4, Jesus Miguel Pradillo2
1Complutense University of Madrid, Pharmacology and Toxicology, Madrid, Spain, 2Complutense University of Madrid, Microbiology, Madrid, Spain, 3National Center for Cardiovascular Research Carlos III (CNIC), 412 de Octubre Hospital, Madrid, Spain
On behalf of:
Background and aims: Post-stroke infections is one of the main complications in this disease. It has been demonstrated that bacterial translocation(BT) might be a possible reason to cause this type of complications. It has bee also demonstrated an altered inflammatory response due to BT. Since our group demonstrated the significant role of TLR4-receptor in this disease, a potential antagonist of these receptor (ApTOLL) has proved to be beneficial experimentally and clinically. Then, our objective here is to determine the role of the absence/pharmacological inhibition of TLR4 in the scenario of stroke and BT.
Methods: Wistar-male rats with MCAO administered with vehicle/ApTOLL and male C57BL/6 and TLR4-KO mice were used. In naïve and at 72h in stroke groups BT was analyzed by microbiological cultures of peritoneal cavity organs, infarct volume in T2W-MRI-images, peripheral inflammation by flow cytometry and central inflammation by immunofluorescence.
Results: At 72h after stroke, the TLR4 inhibition with ApTOLL significantly reduced the infarct volume, BT, improved the peripheral inflammation and decreased the number of infiltrated T-lymphocytes inside the ischemic brain compared with untreated animals. In mice, the absence of TLR4 also reduced the infarct volume, the BT, decreased the infiltrated T-cells levels inside the lesion and improved peripheral immune cell levels.
Conclusions: Our results show that the inhibition/absence of TLR4 not only reduces the infarct volume, but also the BT process and its inflammatory consequences.
Disclosures of Interest: No
Abstract N°: 823
REDUCED RISK OF POST-ISCHEMIC STROKE EPILEPSY: THE ASSOCIATION WITH ACE INHIBITOR AND ANGIOTENSIN RECEPTOR BLOCKER THERAPY
Kuo-Cheng Chang*1, Ching-Heng Lin2, Jin-AN Huang1
1Taichung Veterans General Hospital, Division of Neurology, Neurological Institute, Taichung City, Taiwan, 2Taichung Veterans General Hospital, Department of Medical Research, Taichung City, Taiwan
On behalf of:
Background and aims: Post-stroke epilepsy (PSE) is a common complication after ischemic stroke, especially in patients with hypertension. This study investigates the association between the use of angiotensin-converting enzyme inhibitors (ACEI) or angiotensin receptor blockers (ARB) for hypertension treatment and the risk of PSE in patients with ischemic stroke.
Methods: A population-based retrospective cohort study was conducted using the Taiwan National Health Insurance Research Database between 2000 and 2015. Hypertensive patients with a history of ischemic stroke were categorized according to their use of ACEI/ARB. Prevalent ACEI/ARB users were further classified into continuing or discontinued users, based on their post-stroke medication adherence. We employed multivariate Cox regression models, adjusted for demographics and comorbidities, to assess the risk of PSE among different ACEI/ARB usage groups.
Results: Our study included 182,983 ACEI/ARB users and 38,365 non-users. Non-users exhibited a higher risk of PSE (adjusted hazard ratio [aHR], 1.72; 95% confidence interval [CI], 1.63-1.82). Both prevalent and non-users had higher risks compared to new ACEI/ARB users, with respective aHRs of 1.30 (95% CI, 1.22-1.37) and 1.95 (95% CI, 1.82-2.08). Discontinued ACEI/ARB users showed the highest risk of PSE (aHR, 2.27; 95% CI, 2.09-2.47), suggesting the importance of continuing use of ACEI/ARB after stroke. A significant interaction was observed between age and ACEI/ARB treatment regarding the risk of PSE, indicating that this protective effect was more pronounced in younger patients.
Conclusions: The use of ACEI/ARB after ischemic stroke in hypertensive patients is associated with a reduced risk of PSE, especially among younger patients.
Disclosures of Interest: No
Abstract N°: 2366
DECOMPRESSIVE CRANIECTOMY FOR MALIGNANT ISCHEMIC STROKE BEYOND CLINICAL PRACTICE GUIDELINES: RESULTS FROM A TERTIARY CENTER
Carlota Villar Rodriguez*1, Antonio Cristobal Luque-Ambrosiani1, Diego Villagran Sancho1, Manuel Medina-Rodriguez1, Juan Antonio Cabezas Rodriguez1, Leire Ainz1, Pablo Baena Palomino1, Blanca Pardo-Galiana1, Francisco Moniche Alvarez1
1University Hospital Virgen del Rocio, Neurology, Sevilla
On behalf of:
Background and aims: Decompressive craniectomy has shown to reduce mortality in patients with malignant ischemic stroke, although there is controversy about its impact on functional status.
Aims: To compare functional outcome and mortality in patients undergoing decompressive craniectomy after malignant ischemic stroke who did not meet clear indication criteria according to clinical practice guidelines (CPG) and those who did.
Methods: A retrospective analysis of prospective regional registry (2016-2022) was made. We analyzed baseline characteristics, time to procedure and complications, comparing the functional status according to the modified Rankin Scale (mRS) of those patients with no clear indication by CPG.
Results: We included 25 patients (68% men), age 50±12 years. The median time to craniectomy was 30.5h. At discharge 40% presented a favorable functional status (mRs⩽4); with 56% at 3 months, 66.7% at 6 months and 69.6% at 12 months.
A total of 48% of treated patients did not meet clear craniectomy criteria according to CPG (12% >60 years, 28% >48h to surgery and 28% signs of incipient herniation). Of them, 83% of patients presented an unfavorable functional status at discharge, while only 38.5% in the group that met criteria (p=0.04). However, there were not significant differences in mortality or functional status at 3, 6 and 12 months.
Conclusions: Craniectomy is effective reducing mortality associated with malignant infarction, even in patients who do not strictly fit CPG criteria. Although these patients showed worse functional outcome at discharge, this difference did not persist in time, suggesting that the intervention could be safely performed in selected cases.
Disclosures of Interest: No
Abstract N°: 113
IS INFECTION PRECEDING STROKE ASSOCIATED WITH WORSE OUTCOMES WITH STROKE-ASSOCIATED PNEUMONIA?
Crystal Sing Chiek Teoh*1, Calvin Heal2, Craig Smith1,3, Amit Kishore1,3
1Greater Manchester Comprehensive Stroke Centre, Geoffrey Jefferson Brain Research Centre, Manchester Academic Health Science Centre, Northern Care Alliance, Salford Royal Foundation Trust, Stroke Neurology, Greater Manchester, United Kingdom, 2Centre for Biostatistics, University of Manchester, Manchester Academic Health Science Centre, Greater Manchester, United Kingdom, 3Division of Cardiovascular Sciences, Faculty of Biology, Medicine and Health, University of Manchester, Manchester, Greater Manchester, United Kingdom
On behalf of:
Background and aims: Infections commonly precede, and complicate stroke. Stroke-associated pneumonia (SAP) is associated with a higher risk of poor outcome, but it is not known how infection preceding stroke affects this relationship. We therefore investigated the association between infection treated with antibiotics in the month prior to stroke onset and mortality from SAP.
Methods: We conducted a retrospective analysis of in patients with SAP who were admitted to Manchester Centre for Clinical Neurosciences between 2013-2021. Kaplan-Meier survival curves were generated to assess parameters associated with survival at 1 year and 5 years. Association between prior infection and time-to-mortality were tested using multivariable Cox regression models.
Results: 471 patients with SAP were included in the analysis. Of these the median age was 80y (IQR 71y-87y), with 241 (51%) being male; Median baseline NIHSS was 8 (IQR 2-17). 85 (18%) had used antibiotics in the 4 weeks prior. The most commonly identified preceding treated infections were chest (71%) and urinary tract (17%). Mortality within 1 year and 5 years were 50/85 (59%) and 65/85 (76%) respectively for those with prior infection compared to 202/386 (52%) and 254/386 (66%) for those with no prior infection. In the multivariable analyses, time-to-mortality in SAP was not associated with prior infection (Hazard ratio 1.10, 95% CI 0.84 to 1.45, p =0.49).
Conclusions: Although the study was limited by the small population size and retrospective nature, in patients with SAP, there was no significant increase in risk of death for those with antibiotic treated infection preceding stroke.
Disclosures of Interest: No
Abstract N°: 243
INTRACRANIAL HEMORRHAGE PREDICTION IN ACUTE MCA INFARCTION THROUGH EARLY ISCHEMIC CT CHANGES PRECEDING INTRAVENOUS THROMBOLYSIS
1Faculty of Medicine, Chiang Mai University, Internal Medicine, Chiang Mai, Thailand
On behalf of:
Background and aims: The association between the Alberta Stroke Programme Early CT Score (ASPECTS) and intracranial hemorrhage (ICH) in acute ischemic stroke (AIS) remains unclear. The study aimed to determine the association between ASPECTS and thrombolysis-associated outcomes, particularly symptomatic (sICH) and asymptomatic (aICH) ICH.
Methods: AIS patients with middle cerebral artery (MCA) territory treated with intravenous thrombolysis were enrolled. Eligible patients were categorized into favorable (8-10) and unfavorable (7 or less) ASPECTS. The primary outcome was sICH and aICH. Secondary outcomes included ICH management, modified Rankin Scale (mRS), and mortality.
Results: We included 622 patients with mean age of 66.1 ±13.5 years, 50.5% male; 95 (15.3%) had unfavorable ASPECTS. Those with unfavorable ASPECTS exhibited higher sICH but not aICH (21.1% vs. 4.9%, P <0.001 and 16.9% vs. 17.3%, P = 1.00, respectively). The unfavorable ASPECTS was associated with sICH (adjusted odds ratio 5.1; 95% confidence interval 2.7–9.7, P <0.001). From multivariate analysis, factors associated with lower ASPECTS were age ⩾65 years, body weight <60 kg, atrial fibrillation, onset to needle time ⩾120 minutes, and anemia. Patients with lower ASPECTS showed significantly higher mortality and unfavorable mRS (>2) at discharge, 14- and 90-day (74.7% vs. 50.1%, P <0.001 for 90-day mRS >2).
Conclusions: The ASPECTS is a simple tool to predict rt-PA-associated sICH; however, no predictive potential was observed in aICH patients. Patients with an ASPECTS lower than eight should be cautioned about the risk of complications and poor functional outcomes. Alternative treatments, such as mechanical thrombectomy, might be advisable in these patients.
Disclosures of Interest: No
Abstract N°: 383
PREVALENCE OF MEDICAL COMPLICATIONS IN ACUTE ISCHEMIC STROKE
1Medical University "Prof. Paraskev Stoyanov", Neurology and Neuroscience, Varna, Bulgaria, 2University Hospital "St. Marina", Second Clinic of Neurology with ICU and Stroke Center, Varna, Bulgaria, 3Medical University "Prof. Paraskev Stoyanov", Optometry and Occupational Diseases, Varna, Bulgaria
On behalf of:
Background and aims: Medical complications are frequent in acute ischemic stroke (AIS), as they can increase the risk of death or interfere with the best possible outcome. The aim of the study is to examine the prevalence of predefined somatic and neurological complications in AIS.
Methods: The current retrospective study included 898 unselected AIS patients at a mean age of 70.6±11.6 who were admitted to a comprehensive stroke center between October 2020 and March 2021. Throughout their hospital stay, they had evaluations for sixteen prespecified medical complications.
Results: Of the 898 patients, 452(50.3%) experienced at least one complication (Figure 1). Inflammatory conditions were the most commonly occurring in 334(37.8%) patients: urinary tract infection in 158(17.6%), pulmonary infection in 124(13.8%), and undefined infection in 79(8.8%) cases. A worsening of the neurological deficit, which was indicative of a stroke progression, was noted in 218(24.3%), delirium in 90(10%), and epileptic seizures in 29(3.2%) of the participants. Thromboembolic complications were rare in 14 patients (1.6%) with peripheral artery embolism, and myocardial infarction and pulmonary embolism were each present in 5(0.6%) of the patients. Additional complications such as renal failure were recorded in 84 patients (9.4%), non-serious falls in 31(3.5%), pressure sores in 51(5.7%), and bleeding in 10(1.1%) (Figure 2). The single most significant risk factor for complications was the severity of the stroke at admission (p<0.001).
Conclusions: Thromboembolic complications are relatively uncommon, while inflammatory conditions are the most common complications, followed by the stroke progression. Improving the outcome of AIS requires prompt recognition and treatment of any medical complications.
Disclosures of Interest: No
Abstract N°: 2076
ACTIVITY OF DAILY LIVING, SOCIAL SUPPORT, AND SELF-EFFICACY AMONG POST-STROKE PATIENTS ON SAUDI ARABIA: A CROSS-SECTIONAL STUDY
ALI ALSALEH*1, Ahmad Nahari2
1National Neuroscience Institute, Nursing administration, Riyadh, Saudi Arabia, 2College of Nursing, Riyadh, Saudi Arabia
On behalf of:
Background and aims: Stroke remains to be a leading cause of morbidity and mortality worldwide. It is a stunning global cost resulting from increased stroke incidence and prevalence. More than 12 million new cases globally and one in four people are affected by stroke in their lifetime. Post-stroke patients experience a number of physical and psychosocial changes, which can impact their quality of life. Little is known about the physical and psychosocial changes among post-stroke patients in Saudi Arabia. This study aims to explore activity of daily living (ADL), social support, and self-efficacy among post-stroke patients in Saudi Arabia.
Methods: This study utilized a descriptive, cross-sectional design. The study took place in stroke clinics from six healthcare facilities in three regions in Saudi Arabia. Convenience sampling approach was used. The study included 158 patients, through an online survey. Data were analyzed using descriptive statistics, correlation coefficients, and linear regression.
Results: The study showed that the participants had higher levels of ADL, social support, and self-efficacy. Also, the results revealed that self-efficacy, stroke frequency, income, and stroke onset played significant roles in ADL among post-stroke patients. Although ADL and social support significantly predicted self-efficacy, mediation analysis showed that self-efficacy did not mediate the relationship between social support and ADL.
Conclusions: The study highlighted the importance of promoting self-efficacy as a mean to improve ADL. optimizing ADL, and providing overall support held promising opportunities for improving self-efficacy and facilitating the experience of post-stroke patients.
Disclosures of Interest: No
Abstract N°: 2323
MUSCLE MEASURES OF ACUTE DECONDITIONING AFTER STROKE
Naomi Whitehead*1, Laura Johnson1, Nik Kudiersky2, Sheharyar Baig1, Arshad Majid1, Elizabeth Williams1, Ali Ali1
1The University of Sheffield, United Kingdom, 2Sheffield Hallam University - City Campus, United Kingdom
On behalf of:
Background and aims: Stroke-related sarcopaenia is a recognised complication of stroke that contributes to poor prognosis. Estimates suggest over a third of stroke survivors are sarcopaenic at 6 months, however, little existing data inform us how quickly such changes to muscle occur.
Methods: This single-centre, longitudinal observational study recruited individuals admitted within the first week of stroke (Sheffield, UK). Socio-demographic and clinical details were recorded, alongside weekly assessment of mid-femoral circumference (MFC), mid-humeral circumference (MHC), and bioelectrical impedance analysis (BIA). Appendicular skeletal muscle mass (ASM) was estimated from validated formulae (European Working Group on Sarcopaenia in Older People) and muscle strength using unaffected handgrip strength (HGS, Kg). Weekly assessments continued until discharge from hospital. Wilcoxon Signed Rank tests and one-way ANOVA were then used to investigate timings and significance of these changes accordingly.
Results: 30 participants were enrolled, mean (SD) age 72.7 (11.5) years, 59% female, mean (SD) NIHSS 9.5 (6.0), average length of inpatient stay 28.2 days. Statistically significant reductions in affected and non-affected limb MFC (-1.03 cm,p=0.039; -1.14cm,p=0.003 respectively), affected limb MHC (-0.81cm,p=0.021) and ASM (-0.7kg,p=0.028) were observed, while non-affected MHC and HGS were unaffected. Within the first 2 weeks non-affected MFC reduced by 2.1% (p= 0.012) and ASM 6.0% (p= 0.277).
Conclusions: Significant changes to muscle mass can be detected within the first 2 weeks of stroke, suggesting physiological muscle changes occur before this time. Potential interventions mitigating muscle loss may need to be initiated in the hyper-acute period after stroke in order to be effective.
Disclosures of Interest: No
Abstract N°: 2767
POST-STROKE FATIGUE IN PATIENTS WITH SPONTANEOUS SUBARACHNOID HEMORRHAGE WITH NO RESIDUAL FOCAL DEFICITS. OBSERVATIONAL RESTROSPECTIVE STUDY
Gemma Reig Roselló*1, Paula Paños Basterra1, Laura Estallo Guijarro1, Celia Romero DEL Rincon1, Pablo Iriarte1, Carmen Sánchez-Rodríguez1, Alba Somovilla1, Cristina Sanabria Gago1, Florentino Nombela1
1Hospital de La Princesa / IIS IP, Neurology, Madrid, Spain
On behalf of:
Background and aims: To assess frequency of post-stroke fatigue and its potential risk factors in patients with spontaneous subarachnoid hemorrhage (SAH) without residual focal deficits in our population.
Methods: Descriptive cross-sectional observational study was conducted in a cohort of patients admitted to our tertiary hospital between 2020 and 2022. Telephone evaluations were performed using validated scales: FSS, MFIS, PHQ-9, and EuroQoL-5D. Data on demographic, clinical, and lifestyle variables were collected.
Results: 38 patients met inclusion criteria, N=28 agreed to participate. Mean age 58.82 years (SD=14.31), 60.7% female. The median time since the event was 14 months. Fatigue was found in 42.9% (n=12) according to FSS (cut-off point ⩾ 4) and MFIS (cut-off point ⩾ 38). Patients with decreased physical activity after SAH (p<0.05), intellectual job (p<0.05), and pre-SAH sedentary lifestyle (p<0.05) exhibited higher levels of fatigue. Older age (>65 years, p=0.03), absence of vasospasm (p=0.04), and non-aneurismatic etiology (p=0.06) were associated with lower levels of fatigue. Depression (PHQ-9 ⩾ 5) was significantly associated with fatigue (OR=2 for FSS and OR=2.8 for MFIS). Patients with higher levels of fatigue were unable to return to work. There was an inverse correlation between quality of life (EQ-5D) and fatigue FSS (-0.37,p=0.05) and MFIS (-0.49,p<0.05).
Conclusions: Over 40% of patients with non-focal residual SAH may experience post-stroke fatigue during follow-up, predominantly affecting those of working age and impacting their quality of life. Physical activity and weight management could be potential areas for preventive or therapeutic intervention, to be explored in future studies.
Disclosures of Interest: No
Abstract N°: 3143
CLINICAL, RADIOLOGICAL AND PROCEDURAL INDICATORS OF REPERFUSION INJURY IN MCA STROKE PATIENTS: A CLINICAL STUDY
1University of Rome "Tor Vergata", Stroke Unit, Italy, 2Ospedale Fabrizio Spaziani, Stroke Unit, Frosinone, Italy, 3Hospital Tor Vergata Roma, Stroke Unit, Roma, Italy
On behalf of:
Background and aims: Reperfusion injury is a complication of ischaemic stroke, worsening its prognosis. Identifying markers may improve outcome. Our study examined possible predictors of haemorrhagic infarction (ICH).
Methods: Patients aged ⩾18 years with MCA stroke were selected from our prospective register. Clinical, radiological, and procedural data were collected.
The primary outcome was the presence of ICH at 24-hour CT-scan in all patients and in subgroups of patients treated with MT< 6 or >6 hours after symptom onset. The secondary outcome was the occurrence of symptomatic ICH (sICH).
Results: 398 patients were selected (38,2% men, mean age 74,5), 32,6% developed ICH, 4,2% had sICH.
Higher blood glucose levels, neutrophils percentage and NRL, lower lymphocyte count and ⩾3 passages in MT, resulted associated with ICH (p< 0,05). IVT treatment resulted protective against ICH (p=0,05) and poor collaterals related to sICH (p=0,05).
Patients presenting ICH showed higher 24-hours-NIHSS and mRS at 3 months (p<0,001), highlighting its impact on prognosis.
ICH frequency was similiar in the two subgroups in relation to treatment time (>6 hours 37.5%; <6 hours 32.3%). Higher onset-NIHSS and longer duration of procedure, related to the risk of ICH, p<0,05, in >6hours.
Conclusions: MTs with multiple passages and prolonged duration may increase risk of reperfusion injury. Interventional radiologist's expertise and proper device selection could be crucial as well as thrombolysis administration before procedure. The grade of collateral is confirmed to be useful for patient-tailored treatment. Moreover, both inflammation and blood glucose take part in reperfusion injury, and thus could be targeted to prevent it.
Disclosures of Interest: No
Paper Poster - Stroke in the Young and Pediatric Stroke
Abstract N°: 2003
ASSOCIATION OF FAMILY HISTORY OF STROKE WITH EARLY-ONSET CRYPTOGENIC ISCHEMIC STROKE
Liisa Tomppo1, Maximilian Sihvo1, Radim Licenik2, Giovanni Malferrari3, Jaana Autere4, Katarina Jood5, Ulla Junttola6, Christine Holbe7, Steven Kittner8, Jukka Putaala*1
1Department of Neurology, Helsinki University Hospital and University of Helsinki, Helsinki, Finland, 2Stroke, Peterborough City Hospital, Peterborough, United Kingdom, 3Azienda Unità Sanitaria Locale - IRCCS, Reggio Emilia, Italy, 4Department of Neurology, Kuopio University Hospital, Kuopio, Finland, 5Department of Clinical Neuroscience, Institute of Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg and Department of Neurology, Region Västra Götaland, Sahlgrenska University Hospital, Gothenburg, Sweden, 6Department of Neurology, Oulu University Hospital, Oulu, Finland, 7Department of Neurology, University Medicine Greifswald, Greifswald, Germany, 8Department of Neurology, University of Maryland School of Medicine, Baltimore, United States
On behalf of:
Background and aims: Familial aggregation of stroke is pronounced in younger patients, and may provide clues on potential mechanisms, especially in cryptogenic ischemic stroke (CIS). We analyzed the prevalence and strength of the association of a positive family history of stroke (FHS) in young patients with CIS.
Methods: We included 508 patients with CIS (median age 41 years; 46.5% women) and 520 matched controls from a multicenter case-control study. We asked FHS in parents, grandparents, siblings, and offspring with a structured questionnaire. We used logistic regression adjusting for demographics and 12 well-documented stroke risk factors to determine independent associations.
Results: Compared to controls, patients reported more frequently FHS among any family member (52.9 vs. 41.9 %, P=0.009), parents (17.8 vs. 12.9%, P=0.032), grandparents (47.0 vs. 38.6%, P=0.011), and both parents and grandparents (51.7 vs. 44.4%, P=0.021), whereas no difference emerged among, siblings or offspring (Figure 1). In the adjusted logistic regression, FHS among any family member (odds ratio 1.54, 95% CI 1.17-2.03), parents (1.51, 1.01-2.24), grandparents (1.44, 1.07-1.93) and both parents and grandparents (1.48, 1.12-1.96) were associated with CIS. The associations were stronger with the male sex.
Conclusions: FHS is an independent risk factor for early-onset CIS, even after adjustment for cardiovascular and lifestyle risk factors. This is suggestive of genetic risk and highlights the need for further studies focusing on the genetic background of CIS.
Disclosures of Interest: No
Abstract N°: 2757
LOW THROMBIN INACTIVATION CAPACITY IS ASSOCIATED WITH AN INCREASED RISK OF RECURRENT CARDIOVASCULAR EVENTS IN YOUNG PATIENTS WITH ISCHEMIC STROKE
Janneke Spiegelenberg*1,2, Mark Roest2, Bas Laat, de2, Romy De Laat-Kremers2, Marleen Gelder, van3, Saskia Middeldorp1, Anil Tuladhar4, Frank-Erik De Leeuw4, Jenneke Leentjens1
1Radboud university medical center, Internal medicine, Nijmegen, Netherlands, 2Synapse Research Institute, Maastricht, Netherlands, 3Radboud university medical center, Health Evidence, Nijmegen, Netherlands, 4Radboud university medical center, Donders Institute for Brain, Cognition and Behaviour, Neurology, Center for Neuroscience, Nijmegen, Netherlands
On behalf of:
Background and aims: Patients with ischemic stroke at young age (18-50 years) have a long-term increased risk of recurrent ischemic events. Hypercoagulability may be of greater etiologic significance in young patients. We aimed to explore associations between in/ex vivo coagulation parameters and the risk of recurrent ischemic events after a first ischemic stroke or TIA in young patients.
Methods: We included patients with first-ever TIA or ischemic stroke between 1980 and 2010 from the prospective FUTURE cohort. Blood was collected in 2010 and patients were followed for recurrent ischemic events between 2010 and 2023. Pro- and anticoagulation biomarkers and thrombin generation (TG) were measured. Prothrombin conversion and thrombin inactivation were calculated. We applied Fine and Gray regression analysis to estimate hazard ratios per one standard deviation increase.
Results: During a mean follow-up of 6.5 years, 70 of 332 included patients experienced recurrence. We found a higher risk for recurrent ischemic events in patients with lower antithrombin activity (adjusted HR=0.76 [95% CI 0.58-0.99]) and in patients with higher fibrinogen levels (adjusted HR=1.31 [1.00-1.72]; table 1). Plasma thrombin generation was not associated with recurrence. The pro- and anticoagulant processes underlying thrombin generation were studied separately through computational analysis (table.2). This revealed negative associations between recurrence and the capacity to form thrombin-antithrombin complexes and the overall capacity to inhibit thrombin (HR=0.77 [0.60-0.99] and 0.69 [0.53-0.90]).
Conclusions: Low thrombin inactivation capacity, attributable to low antithrombin levels and high fibrinogen levels, is associated with higher risk of recurrent ischemic events after an acute ischemic stroke or TIA at young age.
1Midlands Partnership NHS Foundation Trust, United Kingdom, 2Royal Stoke University Hospital, United Kingdom
On behalf of:
Background and aims: 25% of strokes occur under age 65. Young stroke survivors have unique rehabilitation needs leading to health inequalities relating to their age. These were identified to develop a bespoke service known as YOUNGER.
Methods: Unmet needs were identified using mixed methods. Qualitatively this involved two focus groups (patients and stakeholders from national organisations). Quantitative methods included a bespoke young patient questionnaire and prospective identification and documentation of unmet needs in 373 patients over 12 months in a regular physician led young stroke clinic.
Results: Thematic analysis of the focus groups identified three main themes: unmet needs, lack of a young stroke network and lack of personalised care. Within ‘unmet needs’ key subthemes included: lack of vocational rehabilitation, peer support and misconceptions around younger stroke prevalence and emergency care. The patient survey identified commonly unmet needs including fatigue (27%), physical (26%), cognitive (15%), employment (18%), relationships (7%). Prospective data analysis demonstrated the 3 most commonly unserved needs documented by specialists as: fatigue management, lifestyle advice and physiotherapy.
Conclusions: Significant needs in the care of young people with stroke in our region were identified by patients, specialists, and stakeholders. Given the heterogeneity of these needs, a one size fits all approach is inappropriate.
YOUNGER is a new innovative pathway encompassing a multi-disciplinary approach including a specialist young stroke clinic (providing physician, physiotherapy, occupational therapy, nursing and psychological assessment), peer support group, personalised rehabilitation pathway and app-based education – that aims to meet the needs of the young stroke population.
Disclosures of Interest: No
Abstract N°: 990
RISK FACTORS, MECHANISMS AND 6-MONTH OUTCOME AFTER STROKE IN YOUNG ADULTS: PROSPECTIVE OBSERVATIONAL COHORT STUDY
Raafiah Mussa*1, Gareth Ambler2, Kitti Thiankhaw3, Hatice Ozkan1,4, Rob Simister1,4, Arvind Chandratheva1,4, David Werring1,4
1UCL Queen Square Institute of Neurology, Department of Brain Repair and Rehabilitation, London, United Kingdom, 2University College London, Department of Statistical Science, London, United Kingdom, 3Chiang Mai University, Department of Internal Medicine, Chiang Mai, Thailand, 4National Hospital for Neurology and Neurosurgery, Comprehensive Stroke Service, London, United Kingdom
On behalf of: ULYSSES and SIGNAL
Background and aims: The incidence of stroke in younger adults is increasing worldwide. We aimed to identify the spectrum of risk factors, mechanisms, and functional outcome post-stroke in a young cohort to improve our understanding of stroke in this age group.
Methods: We included consecutive young adults (<55 years) with ischaemic stroke or intracerebral haemorrhage (ICH) presenting to a specialist stroke centre serving a multi-ethnic population of 1.6 million people between 2017-2020. Ischaemic stroke was classified using the TOAST criteria. ICH was classified as probable cerebral small vessel disease (cSVD); macrovascular; other secondary cause; or undetermined aetiology. Multivariable logistic regression was performed to identify predictors of poor functional outcome (modified Rankin Scale (mRS) >1) 6 months post-stroke.
Results: 554 patients were included (median age 47 (IQR 41-51); 33.6% female). Common risk factors included dyslipidaemia (57.3%), hypertension (39.5%), and cigarette smoking (33.6%). The most frequently identified cause of ischaemic stroke was cardioembolism (22.3%); 33.7% remained undetermined. Probable cSVD was the most common ICH aetiology (53%). Poor functional outcome was prevalent in 254/507 (50.1%) patients at 6 months and was significantly associated with female sex (OR 1.61, 95%CI 1.02–2.54, p=0.039), ICH (OR 2.03, 95%CI 1.14–3.59, p=0.016), stroke severity (OR 1.11, 95%CI 1.07–1.16, p<0.001) and pre-morbid mRS 2-5 (OR 3.16; 95%CI 1.11–9.04, p=0.031).
Conclusions: This study provides detailed data regarding baseline characteristics and their associations with poor functional outcome post-stroke in younger adults. These findings could help to improve strategies for stroke prevention, treatment, and rehabilitation in this age group.
Disclosures of Interest: No
Abstract N°: 1189
RETROSPECTIVE ANALYSIS OF CLINICAL AND LABORATORY ANTIPHOSPHOLIPID ANTIBODY PHENOTYPE IN YOUNG ADULT ISCHAEMIC STROKE
Abigail Rees*1, Hannah Cohen2, Prabal Mittal2, Zayna Ahmed3, Chaamanti Sivakumar4, Hermaleigh Townsley4, Kate Ellis4, Joseph White4, Graziella Quattrocchi1,4, Arvind Chandratheva4
1North Middlesex University Hospital, London, United Kingdom, 2University College Hospital London, Department of Haematology, London, United Kingdom, 3University College London, 4National Hospital for Neurology and Neurosurgery, Comprehensive Stroke Service, London, United Kingdom
On behalf of:
Background and aims: Antiphospholipid syndrome (APS) is a cause of young ischaemic stroke. We aim to phenotype a cohort of young adult ischaemic stroke with APS.
Methods: Retrospective analysis was performed on all ischaemic stroke admissions aged 17-55years to a London Hyperacute Stroke Unit from 1 January 2019-31 December 2020. Clinical characteristics, antibodies and aGAPSS (Adjusted Global Anti-Phospholipid Syndrome Score), assessing risk of thrombosis in APS, were recorded.
Results: Of 261, 205(79%) were tested for antiphospholipid antibodies (aPL). 34(17%) were aPL-positive. Of those, 48%(n=21) had lupus anticoagulant, 43%(n=19) anticardiolipin antibodies a(aCL), and 9%(n=4) anti-beta-2glycoprotein 1 antibodies (aß2GP1). 2(6%) were triple aPL-positive.
Of these 34 patients, 27%(n=9) were reviewed, the remainder discharged to respective local stroke units. 7/9 were persistently aPL positive at ⩾12 weeks and anticoagulated with warfarin, high-intensity (target INR 3.0-4.0) unless contraindicated. 29%(n=2) were triple aPL-positive. 60%(n=3) of females had previous recurrent miscarriages.
The mean age of the APS cohort was 41 vs 46years for the overall cohort; mean NIHSS for both cohorts was 5.The proportion of females within the APS cohort was 71%(n=5) versus 31%(m=81) in the total cohort. Mean aGAPSS was 9/17(SD=4) suggestive of medium thrombotic risk; 86%(n=6) had medium-to-high thrombotic risk. Obesity(BMI >30) and hyperlipidaemia were seen in 57%(n=4) of the APS patients, versus 31% (n=80) of the total cohort. Hypertension was seen in 29%(n=2) of APS vs 48%(n=124) of the total cohort.
Conclusions: Antiphospholipid antibodies were present in 17% of young adult strokes investigated. We found female predominance, and vascular risk factors, particularly obesity and hyperlipidaemia, were common.
Disclosures of Interest: No
Abstract N°: 2905
ASSESMENT OF ATRIAL CARDIOPATHY BY CARDIAC MAGNETIC RESONANCE IN YOUNG PATIENTS WITH AN UNDETERMINED STROKE ETIOLOGY
Ana Catarina Fonseca*1, João Pedro Marto2, Nuno Inacio3, Pedro Nascimento Alves1, Mariana Dias1, Miguel Baptista2, Teresa Pinho e Melo1, Ana G. Almeida1
1Hospital de Santa Maria, Neurology, Lisboa, Portugal, 2Hospital Egas Moniz, Centro Hospitalar Lisboa Ocidental, Neurology, Lisboa, Portugal, 3Hospital Beatriz Angelo, Neurology, Loures, Portugal
On behalf of:
Background and aims: Evidence of atrial cardiomyopathy has been found in ischemic stroke patients older than 50 years old with an undetermined stroke etiology. There is lack of data regarding the presence of atrial cardiomyopathy in young ischemic stroke patients. We compared the characteristics of the left atrium (LA) and left atrial appendage (LAA) of young stroke patients with an undetermined stroke etiology and stroke due to cervical artery dissection (CAD).
Methods: Consecutive sample of patients with ischemic stroke (< 50 years-old) admitted to two university hospitals from January 2019 to June 2022. We included patients with an undetermined stroke etiology after a complete investigations and patients with non-traumatic CAD. Stroke etiology was classified according to TOAST.
A 3 Tesla cardiac magnetic resonance was performed within the first month after stroke onset. We compared the indexed LA volume, LA ejection fraction, LA strain, LAA and LA fibrosis between patients with an undetermined etiology and CAD.
Results: Sixty-one patients were included with a median age of 44.0 years (IQR 7). Sixty-five per cent were men.Nineteen patients had CAD (31.1%). There was no difference between patients with undetermined cause versus CAD regarding indexed LA volume (p=0.80), LA ejection fraction (p=0.88), LA strain (p=0.73), LAA and LA fibrosis (p=0.83 and 0.33 respectively)
Conclusions: In our cohort, markers of atrial cardiomyopathy were similar in patients with an undetermined stroke etiology and in CAD. Atrial cardiomyopathy does not seem to be a significant mechanism of stroke in young ischemic stroke patients with an undetermined etiology.
Disclosures of Interest: No
Abstract N°: 3060
WILL ROUTINE HEALTH SCREENING PREVENT YOUNG STROKE? POPULATION-BASED STUDY
Cathy Scott*1, Linxin LI1, Peter Rothwell1
1Wolfson Centre for Prevention Of Stroke and Dementia, Oxford, United Kingdom
On behalf of:
Background and aims: Stroke incidence at younger ages is increasing. One solution might be to extend routine health screening to younger people, as is proposed in England, where the 5-yearly NHS Health Check will include all individuals aged 30-39, using predicted 10-year CV-risk (QRISK3®CV score) to target prevention. We aimed to assess whether this approach could improve prevention.
Methods: In a population-based study (OXVASC/2002-2023) of all acute vascular events, we calculated premorbid 10-year QRISK3®CV score and QRISK®-Relative Risk(RR) scores for participants with a first event at age 30-45 from face-to-face examination and primary care records.
Results: Among 173 individuals aged 30-45 years with a vascular event (figure-1), 49/28% were already in a health check program. Of the remaining 122 individuals who would have been eligible for the new health check, the median 10-year QRISK®3 score was 2.8% (IQR=1.1-4.9%). Although 91% were higher than optimal risk (QRISK®-RR scores >1), in terms of treatment thresholds, 116/95% were nevertheless categorised as not requiring treatment (low risk), including all women, 6 (5%) were eligible for lifestyle advice and reassessment of risk at 3 months (moderate risk), and none were high risk (figure-2).
Conclusions: Using the QRISK3®-score the vast majority of men and all women with vascular events aged 30-45 who were not already eligible for screening were categorised as having a pre-morbid 10-year risk score insufficient to merit intervention, although 91% had at least one vascular risk factor. Without improved risk models, or lower treatment thresholds, additional screening will prevent few events and risks harm due to false reassurance.
Disclosures of Interest: No
Abstract N°: 1601
AGE- AND SEX-SPECIFIC CONTRIBUTION OF WELL-DOCUMENTED RISK FACTORS ON EARLY-ONSET CRYPTOGENIC ISCHEMIC STROKE
Jukka Putaala*1, Nicolas Martinez-Majander1, Tomi Sarkanen2, Maria Luisa Zedde3, Pekka Jäkälä4, Petra Redfors5, Juha Huhtakangas6, Bettina von Sarnowski7, Pauli Ylikotila8, Nilufer Yesilot9
1Helsinki University Hospital, Neurology, 2Tampere University Hospital, Neurology, 3Arcispedale Santa Maria Nuova IRCCS, Neurology, 4Kuopio University Hospital, Neurology, 5Sahlgrenska University Hospital, Neurology, 6Oulu University Hospital, Neurology, 7Greifswald University Hospital, Neurology, 8Turku University Hospital, Neurology, 9Istanbul Faculty of Medicine, Istanbul University, Neurology
On behalf of: SECRETO Collaborators
Background and aims: Risk factors for cryptogenic ischemic stroke (CIS) remain sparsely studied. In a multicenter study, we explored the contribution of well-documented stroke risk factor (WDSRF) burden on early-onset CIS
Methods: Of the 598 prospectively enrolled patients aged 18-49 years (mean age 39.4 years; 45.3% women) with a recent CIS and 551 sex- and age-matched stroke-free controls, 576 cases and 521 controls with complete data were included. We determined WDSRF burden by counting preexisting cardiovascular disease, hypertension, diabetes, hypercholesterolemia, abdominal obesity, physical inactivity, current smoking, unhealthy diet, heavy drinking, psychosocial stress, and depression. We used logistic regression adjusting for demographics to determine associations.
Results: Compared to controls, patients had a higher WDSRF count (overall mean 3.1±1.7 vs. 2.1±1.4) across both sexes and age groups (Figure 1). In patients, mean WDSRF increased from 2.8±1.4 in the youngest to 3.5±1.7 in the oldest age group and was higher in men (3.3±1.6 vs. 2.8±1.6). Each incremental WDSRF was associated with a 50% higher risk for CIS (odds ratio 1.51, 95% CI 1.38-1.65) and the association was significant across all age groups for both sexes (Figure 2), with exposure-response patterns according to categorical count of WDSRF (Figure 3). Adjusting for the presence of high-risk PFO did not change the overall association; however, in subgroup analysis, WDSRFs showed a stronger association for those without high-risk PFO (P=0.004 for interaction).
Conclusions: WDSRFs contribute robustly to the risk of early-onset CIS regardless of sex and age. The presence of high-risk PFO modulates this association.
Disclosures of Interest: No
Abstract N°: 2169
PREDICTION OF RECURRENCE AND FUNCTIONAL STATUS IN YOUNG ISCHEMIC STROKE PATIENTS
Vinicius Montanaro*1, Mina Jacob2, Rui LI3, Kay Sin Tan4, Eleonora Oliveira5, Thiago Hora5, Gabriel De Freitas6, Frank-Erik De Leeuw7
1SARAH network of rehabilitation hospitals, Brasilia, 2Radboud University Medical Center, Netherlands, 3Cambridge University, United Kingdom, 4University of Malaya Medical Center, Malaysia, 5SARAH network of rehabilitation hospitals, 6Universidade Federal Fluminense, 7Radboud University Medical Center
On behalf of: GOAL(Global Outcome Assessmeny Life-long After Stroke) consortium
Background and aims: Ischemic stroke in young adults poses a significant socio-economic challenge. Each year, approximately two million individuals aged 18-50 worldwide experience a stroke. Rapid identification of risk factors linked to recurrent events and stroke outcomes is vital for optimizing personalized treatment and secondary prevention. New machine learning techniques may potentially predict recurrence and post-stroke functional status more effectively than traditional methods. We investigated these outcomes in young stroke patients using machine learning and compared with traditional statistical methods.
Methods: This study is part of the Global Outcome Assessment Lifelong After Stroke in Young Adults (GOAL) initiative, collecting individual patient data from hospital-based young ischemic stroke cohorts (18-50 years) worldwide. We employed machine learning and traditional regression techniques to determine the best model for predicting stroke recurrence and functional outcome, as measured by the modified Rankin scale, at three months.
Results: Data from 7937 patients for functional outcome and 9366 for stroke recurrence were available, spanning 29 countries across all continents. Machine learning models performed comparably to logistic regression: Sensitivity 0.64x0.62, accuracy 0.85x0.83 and AUC 0.95x0.89 for functional outcome (as measured by the modified Rankin scale, in three months post-event.)and sensitivity 0.64x0.64, accuracy 0.62x0.61 and AUC 0.64x0.64 for stroke recurrence.
Conclusions: Our work underscores the potential application of artificial intelligence in predicting stroke outcomes, which could be integrated into clinical practice. However, in this specific cohort, for predicting stroke functional status and recurrence, it did not enhance the traditional statistical models. Therefore, its use is not deemed superior to traditional regression models in our sample.
Disclosures of Interest: Yes
Abstract N°: 2534
ASSOCIATION BETWEEN EARLY-ONSET CRYPTOGENIC ISCHEMIC STROKE AND INVASIVE DENTAL PROCEDURES IS MODERATED BY PATENT FORAMEN OVALE
Jaakko Leskelä*1, Jukka Putaala1, Nicolas Martinez-Majander1, Lauri Tulkki1, Muhammed Manzoor1, Juha Sinisalo1, Pirkko Pussinen1, Susanna Paju1
1University of Helsinki and Helsinki University Hospital
On behalf of:
Background and aims: Periodontitis is a disease affecting tooth supporting tissue, mediated by chronic oral infection and inflammation, and an independent risk factor for cardiovascular diseases, but the evidence is incomplete for early-onset cryptogenic ischemic stroke (CIS). Invasive dental procedures cause transient bacteremia, potentially triggering systemic inflammatory responses, and more importantly, they are signs of ongoing dental ailment. We investigated the relationship between CIS, periodontitis, and recent dental procedures and whether the associations are moderated by the patent foramen ovale (PFO) status.
Methods: 18–49-year-old Finnish CIS patients (n=146) and their sex- and age-matched (±5 years) controls were examined by a periodontologist approximately three months after the CIS incidence. Recent invasive dental procedures within three months before the incidence (or recruitment for controls) were asked with a structured questionnaire. Statistical analysis used conditional logistic regression adjusted for age, waist-to-hip ratio, smoking, PFO status, regular dentist visits, and hypertension. Interaction analysis used logistic regression models adjusted for age and sex.
Results: CIS was associated with periodontitis (at least stage III and grade B; odds ratio 4.11; confidence interval 1.15–14.6) and with recent invasive dental procedures (2.54; 1.01–6.39). In interaction analysis, association with recent invasive dental procedures was strong for those with PFO (6.26; 1.72–40.3), but not for those without PFO. The presence of PFO did not interact with periodontitis status.
Conclusions: Periodontitis and recent invasive dental procedures are associated with CIS. Interestingly, PFO status moderates the association with recent invasive dental procedures, but not with periodontitis.
Disclosures of Interest: No
Abstract N°: 2695
STROKE IN YOUNG ADULTS: IMPACT OF THE COVID-19 PANDEMIC
Cai Hua Sim1, Tian Xu2, Nadia Novichkova1, Rita Ghatala1, Ana Margarida Castanheira1, Kate Kennedy1, Boglarka Toth-Zilahi1, Sarah Fanning1, Liqun Zhang*1
1St George's University Hospitals NHS Foundation Trust, Stroke Research/Neurology, London, United Kingdom, 2Affiliated Hospital of Nantong University, Neurology, Nantong, China
On behalf of:
Background and aims: Increasing evidence suggests that COVID-19 is associated with ischaemic stroke, although the risk factors and mechanisms are not fully understood. Nationally enforced restrictions considerably affected everyday life, especially in young adults. This pilot study aims to explore the pandemic’s impact on young stroke patients.
Methods: Data was extracted from Sentinel Stroke National Audit Programme (SSNAP) at a comprehensive stroke centre in three periods: before (2018-2019), during (2020-2021), and after (2022-2023) the pandemic. Demographics, stroke type, and stroke risk factors for all young stroke admissions (⩽ 50 years old) were analysed.
Results: A total of 649 patients were reviewed. Differences in young stroke admission rates were not statistically significant among the studied periods (10.0%, 10.8%, and 9.3% respectively). However, there was a significantly higher number of ischaemic strokes (79.9%, 84.6%, and 73% respectively, p=0.017) compared to haemorrhagic stroke. Based on TOAST classification, cardioembolic ischaemic strokes were significantly high (22.7%, 23.6%, and 11.2%, p=0.01) while cryptogenic ischaemic strokes were low (12.3%, 9.7%, and 18.9%, p=0.05). Stroke risk factors significantly increased: hypertension (27.2%, 29.1%, and 39.3% respectively, p=0.016), hyperlipidaemia (17.3%, 22.5%, and 29.1% respectively, p=0.001) and drug abuse (9.8%, 13.8%, and 18.9%, p=0.04).
Conclusions: Consistent with previous findings, there was an increase in ischaemic strokes compared to haemorrhagic strokes in young patients during the pandemic. However, we observed a variation in the causes of stroke throughout the study period. This study also showed an increase in modifiable risk factors, with important public health implications. Further studies are needed to confirm these findings.
Disclosures of Interest: No
Abstract N°: 3173
DETERMINED VS. UNDETERMINED ETIOLOGIES OF STROKE IN YOUNG ADULTS: A NATIONWIDE SWISS STUDY
Tolga Dittrich1, Thomas Schneider*2, Mira Katan3, Marcel Arnold4, Emmanuel Carrera5, Carlo Cereda6, Leo Bonati7, Alexander Tarnutzer8, Gian Marco De Marchis2
1Kantonsspital St.Gallen, St. Gallen, Switzerland, 2Kantonsspital St.Gallen, Klinik für Neurologie, St. Gallen, Switzerland, 3Universitätsspital Basel, Klinik für Neurologie, Basel, Switzerland, 4Inselspital, Klinik für Neurologie, Bern, Switzerland, 5Hôpitaux Universitaires de Genève (HUG), Department of Neurology, Genève, Switzerland, 6EOC Ente Ospedaliero Cantonale, Department of Neurology, Bellinzona, Switzerland, 7Reha Rheinfelden, Klinik für Neurologie, Rheinfelden, Switzerland, 8Kantonsspital Baden AG, Klinik für Neurologie, Baden, Switzerland
On behalf of: Swiss Stroke Registry Investigators
Background and aims: The rising prevalence of stroke in young adults, particularly with undetermined etiology, is a growing health concern. This study aims to bridge the knowledge gap regarding their risk factors, treatment options, and outcomes.
Methods: This retrospective Swiss study analyzed young adults aged 18-55 with acute ischemic stroke (AIS) from January 2014 to September 2022. Stroke etiology was determined using the modified TOAST classification. The study focused on the prevalence of vascular risk factors, acute treatments (recanalization therapies, antiplatelets, anticoagulation), 90-day functional outcomes, and AIS recurrence. Statistical analyses included logistic regression, Fine-Gray proportional hazards models, and etiology comparisons.
Results: Patients with undetermined etiology showed – compared to those with determined etiology – higher rates of overweight (62% vs. 56%, p=0.003), dyslipidemia (59% vs. 54%, p=0.007) and smoking (43% vs. 37%, p=0.001), but less diabetes, than. Intravenous thrombolysis administration was performed more frequently in the undetermined group (31% vs. 27%, p=0.046), with comparable endovascular treatment rates. Approximately two-thirds of patients attained favorable 90-day functional outcomes, more commonly in the undetermined etiology group (70% vs. 66%, p=0.053), but with a higher 90-day stroke recurrence risk (HR = 1.72, CI =[1.01, 2.94], p=0.047). Comparisons between the undetermined stroke etiology group and other specific etiology groups reveal that the undetermined group falls intermediate across all examined aspects, complicating its characterization.
Conclusions: Young adults with AIS of undetermined etiology show distinct risk factor- and treatment patterns from those with determined etiologies. They have better short-term outcomes despite a higher recurrence risk, underscoring the need for targeted prevention and further research.
Disclosures of Interest: No
Abstract N°: 970
EPIDEMIOLOGICAL AND FUNCTIONAL OUTCOMES OF PERINATAL STROKE INJURY IN CATALONIA: LESSONS FROM OUR COHORT
Gloria Arque*1, Ares Regué2, Raul Hileno3, Nuria Visa4, Fernando Paredes4, Francisco Purroy5
1IRBLleida - Universitat de Lleida, Clinical Neuroscience research group, Lleida, Spain, 2IRBLleida, Clinical Neuroscience Research group, Lleida, Spain, 3Institut Nacional d'Educació Física de Catalunya (INEFC Lleida), Lleida, Spain, 4Hospital universitari Arnau de Vilanova, Lleida, Spain, 5Hospital universitari Arnau de Vilanova, IRBLleida - Clinical Neuroscience research group, Lleida, Spain
On behalf of:
Background and aims: Perinatal acute ischemic stroke (PAIS) outcomes are often poor, and most survivors have lifelong disabilities (cerebral palsy, cognitive consequences, behavioral problems and epilepsy). Despite this situation, little high-quality evidence exists regarding incidence, pathophysiology and predictors of outcomes. Our aim was to conduct a systematic review and meta-analysis in all series that include patients with perinatal ischemic stroke or presumably perinatal ischemic stroke who have had subsequent clinical follow-up; to describe epidemiological profile on Catalonia of PAIS patients to bring specific information on risk factors and real incidence; and to assess the impact of perinatal ischemic stroke on the longitudinal neuropsychological performance of the patients.
Methods: For that, we have established the incidence of PAIS in Catalonia, and we have characterized retrospectively a cohort of PAIS patients to validate a diagnostic criterion and treat children ideally before permanent brain damage occurs.
Results: Forty-one studies were included in the meta-analysis with a total number of 1808 patients included. Patients with an affection of the internal capsule showed higher risk of epilepsy than those without. The retrospective study showed no significant differences compared to the normative population on neuropsychological performance. The clinical variables of injury location and laterality showed no differences on the cognitive development of children.
Conclusions: These results could contribute to a better understanding of the effects of perinatal ischemic stroke on children's neuropsychological performance and help develop more effective and individualized neurotherapeutic interventions aimed at improving the neurodevelopment and quality of life of these patients.
Disclosures of Interest: No
Abstract N°: 1206
ESTABLISHING A NEW HEALTH SERVICE MODEL TO SUPPORT LIFE AFTER YOUNG ADULT STROKE
Karen Borschmann1, Emma Power2, Dana Wong3, Natasha Lannin4, Brooke Parsons1, Daniel Capurro5, Dominique A. Cadilhac4, Maria Crotty6, Julie Bernhardt1, Vincent Thijs*1
1The Florey Institute of Neuroscience and Mental Health, Stroke Theme, Heidelberg, Australia, 2University of Technology Sydney, Ultimo, Australia, 3La Trobe University, Bundoora, Australia, 4Monash University, Melbourne, Australia, 5The University of Melbourne, Parkville, Australia, 6Flinders Medical Centre, Bedford Park, Australia
On behalf of: Young Stroke Service project team
Background and aims: Despite increasing incidence of young stroke, most health services are designed for older stroke survivors, leaving young adults under-diagnosed and under-served.
Here we overview a co-designed, inclusive, digitally-supported outpatient health service being developed for young Australians (18-45 years) with stroke.
Key aims: 1) establish a digital platform to engage with service users, 2) establish a suite of screening and assessment tools, 3) validate new clinical pathways, 4) establish a curated patient dataset to inform future research.
Methods: A new collaboration of >70 clinicians, researchers, lived experience contributors, IT specialists, politicians, and stroke advocates are building and testing the service model across two state-lines.
Workplans are underpinned by principles of co-design, communication accessibility, evaluation, and sustainability. Patients’ unmet needs inform clinical pathway development, particularly for neuropsychological assessment and intervention, and return to work and driving.
Results: 171 patients (mean (IQR) age 44 (38, 51), 57% female) have engaged with the service to date. Commonly reported unmet needs are fatigue, memory/ thinking, and return to work or study.
Best practice policies have been established:
- Establishment and engagement with Lived Experience Contributor Group
- Communication accessibility to improve equity of access to services.
- Patient feedback content and style
- Evaluation of digital platform usability, communication accessibility, user acceptance, health economics, and service provision audits
Conclusions: Two years since project inception, Young Stroke Service is filling a critical healthcare gap for many young people. Our next phase of targeted patient recruitment and evaluation will inform ongoing developments and sustainability beyond the five-year funding period.
Disclosures of Interest: No
Abstract N°: 2522
RETROSPECTIVE SINGLE-CENTRE STUDY OF CLINICAL MANIFESTATIONS AND IMAGING FINDINGS IN MOYAMOYA DISEASE
Background and aims: Moyamoya disease is a progressive vaso-occlusive disease of large intracranial arteries with characteristic collaterals formation. We report a case series of 50 patients with Moyamoya disease.
Methods: This is a retrospective study of Moyamoya disease from a single centre in south India. The clinical manifestations and imaging findings were assessed retrospectively.
Results: There were 24 males and 26 females. The mean age at presentation was 18.6±13.7 years. The median time from the onset of symptoms to diagnosis was 13 months. Stroke (n=45, 90%) was the most common presentation followed by migranious headache(n=17, 34%); recurrent TIA(N=16, 32 %); and seizure(n=13, 26%). Two patients presented with choreiform movement disorders. MRI brain showed the most common type of stroke was watershed infarct in 25(50%) patients followed by MCA territory in 6, ACA territory in 4 and PCA territory in 3 patients. Interventricular haemorrhage appeared in 4(8%) patients and one had a putaminal bleed. All patients had bilateral stenosis of supraclinoid ICA. Magnetic Resonance Angiography showed involvement of anterior circulation in all patients and involvement of posterior circulation in 16(32%) patients. Collateral in the form of lenticulostriate, thalamoperforators and pial were found in 40(80%), 39(78%), and 33(66%) patients respectively. Eleven(22%) patients underwent surgery while the remaining patients were managed medically.
Conclusions: We should consider Moyamoya disease as a differential in paediatric and young adult stroke presented with the above mentioned characteristics clinical features and imaging findings.
Disclosures of Interest: No
Abstract N°: 3104
MENTAL HEALTH, SMOKING AND EXERCISE LEVELS AMONG YOUNG STROKE PATIENTS PRE- AND POST-STROKE
Minni Timberg*1, Riina Vibo1, Janika Kõrv1
1University of Tartu, Department of Neurology and Neurosurgery, Tartu, Estonia
On behalf of:
Background and aims: The aim of our study was to evaluate the associations between mental health and behavioural risk factors in young ischemic stroke patients.
Methods: Patients from the Estonian Young Stroke Registry, who were hospitalized in 01.01.2013–31.12.2022 and had filled in both the initial and one year follow-up questionnaires, were included. Depressive symptoms and stress levels in the past 30 days were assessed with a single screening question, each. Smoking was defined as either occasional or daily smoking; physical activity as exercising (a minimum of 30 minutes) on < 2 days a week. The degree of disability at follow-up was evaluated with modified Rankin Scale (mRS).
Results: A total of 233 patients (56% males, mean age at stroke onset 43.8 years (SD±8.5)) were included. At one year post-stroke, 70.8% of patients had a mRS score of 0–1, and the remaining had a score of 2–3. The prevalence of behavioural risk factors reduced significantly between admission and follow up, being 44.2% vs. 33.5% for smoking (p=0.02) and 68.8% vs. 56.6% for low exercise levels (p=0.01). Patients who reported being stressed were more likely to have low exercise levels upon admission (75.3% vs. 63.5%, p=0.07), but the difference was not significant at follow-up.
Conclusions: While mental health complaints are common among young stroke patients, they were not directly associated with behavioural risk factors. However, patients who reported high stress levels were less physically active before stroke onset.
Disclosures of Interest: No
Abstract N°: 3310
ISCHAEMIC STROKE IN YOUNG ADULTS - A RETROSPECTIVE COHORT ANALYSIS
Hongying Chen*1, Ahmed Gabr2, Caitlin Gibson2, Razan Habiballa2, Claire Collins2, Marwa Mustafa2, Nora Cunningham2, Ida Carroll2, Abdirahman Mohamed2, Margaret O'connor2
1University Hospital Limerick, Department of Neurology, Limerick, Ireland, 2University Hospital Limerick, Department of Aging and Therapeutics, Limerick, Ireland
On behalf of: On behalf of Department of Neurology, University Hospital Limerick, Ireland
Background and aims: Stroke is the second most common cause of death and disability worldwide. The rising prevalence of young strokes warrant public health attention given the personal and economic cost of disability. This study aimed to explore the aetiology, clinical characteristics, and outcomes of stroke presentations to a tertiary hospital in Ireland in patients under 50 years over a one-year period.
Methods: Acute ischaemic strokes in patients aged 18-50 years old were identified from a retrospectively maintained Hospital In-Patient Enquiry (HIPE) database using International Classification of Diseases (ICD-10) coding. Intracerebral haemorrhage, transient ischaemic attacks, and intracranial malignancies were excluded. Data were collected on patient demographics, clinical presentation, risk factors, acute stroke care, investigations and clinical outcomes.
Results: 28 patients were included with a mean age of 42.8 years (range 28 to 50 years) and a higher male preponderance of 64.3%. Alcohol consumption and smoking remain the most common risk factors. Large artery atherosclerosis (8/28) and cardioembolic source (7/28) represented the most common aetiologies followed by arterial dissection (6/28). Patent foramen ovale (PFO) was identified in 25%, all of whom underwent successful closure without complications. The stroke unit admission rate was 71.4%. The overall median length of stay was 10 days with a discharge Modified Rankin Scale of 1.7.
Conclusions: Traditional lifestyle-related risk factors remain critical in the secondary prevention of young strokes. This study highlights the need for a streamlined stroke pathway with targeted management and diagnostic evaluation of acute ischaemic stroke in young adults.
Disclosures of Interest: No
Paper Poster – Technology Innovations
Abstract N°: 309
IMPACT OF REPEATED TRANSCRANIAL MAGNETIC STIMULATION ON ENHANCING BLOOD CIRCULATION IN THE BRAIN
Sang-Hun Lee*1, Kisoo Pahk2
1Korea University Ansan Hospital, Korea University College of Medicine, Neurology, Ansan, South Korea, 2Korea University Anam Hospital, Korea University College of Medicine, Nuclear Medicine, seoul, South Korea
On behalf of:
Background and aims: Repetitive transcranial magnetic stimulation (rTMS) is recognized for its capacity to promote neurogenesis and angiogenesis. This study investigates the influence of rTMS on perfusion in individuals with middle cerebral artery stenosis or occlusion, exploring the potential benefits of heightened neural activity on blood flow.
Methods: In this prospective, randomized, open-label, blinded end-point pilot study conducted from June 2020 to May 2022, 16 patients were randomly assigned to either the rTMS intervention or non-intervention (control) group. Both groups received antiplatelet drugs for vascular steno-occlusion treatment. The intervention group received targeted rTMS at the stenotic and obstructed region, while perfusion rates were assessed using single-photon emission computed tomography/computed tomography (SPECT/CT)
Results: Analysis of 15 patients (8 in the rTMS group, 7 in the control group) revealed a significant increase in the standardized uptake value ratio (SUVr) in the rTMS group compared to the control group. Specifically, four rTMS patients exhibited a ⩾20% increase in SUVr compared to none in the control group. Changes in SUVr were significantly different between initial and follow-up SPECT/CT in the rTMS group (p = 0.033), while no significant difference was observed in the control group (p = 0.481).
Conclusions: Our study suggests a notable enhancement in perfusion in stroke patients with middle cerebral artery steno-occlusion following rTMS stimulation. These findings, derived from a 6 to 12-month post-stimulation perfusion test, highlight the potential of rTMS as a therapeutic intervention in vascular-related neurological disorders.
Disclosures of Interest: No
Abstract N°: 632
LIFEGLOV FOR STROKE REHABILITATION. PATIENT CO-DESIGN: AN NHS - BIOLIBERTY COLLABORATION
Wendy Juner1, Charlie Chung1, Yvonne Chun1,2, Rowan Armstrong3, Conan Bradley3
1NHS Lothian, 2NHS Borders, 3Bioliberty Limited
On behalf of:
Background and aims: Stroke is the second-leading cause of death in the UK and third leading cause of death and disability worldwide. Evidence-based stroke clinical guidelines now recommend a minimum of 3 hours of multidisciplinary therapy a day which is challenging to provide with current resources.
Lifeglov is an innovative soft robotic glove with accompanying software to support goal orientated rehabilitation and with the potential to increase therapy intensity within existing staffing levels, and at home.
Laboratory data and patient co-design activities are integral in developing the Lifeglov system to optimize its potential clinical application. The current study represents an ongoing user co-design activity which will inform the next version (Beta prototype) of Lifeglov.
Methods: 20 stroke survivors from NHS Lothian and NHS Borders, Scotland, UK with varying degrees of upper limb impairement will undergo semi-structured interviews to provide user feedback on the latest Lifeglov prototype (alpha).
This will involve Demonstration and user experience on the donning and doffing aspect of Lifeglov Alpha Demonstration of the robotic-powered hand movements, the use of the control box and accompanying software.
Quantitative and qualitative data will be obtained using a semi-structured interview and a questionnaire.
Results: Quantitative and qualitative data obtained from this co-design activity will be presented.
Conclusions: The Lifeglov system could potentially play a vital part in increasing rehabilitation intensity for stroke patients. The latest patient co-design findings inform the next version (Beta) of Lifeglov, which will undergo clinical evaluation in rehabilitation settings.
Disclosures of Interest: No
Abstract N°: 186
ARTIFICIAL INTELLIGENCE SOFTWARE TO EXPEDITE ELECTRONIC HEALTH RECORD REVIEW IN ACUTE STROKE
Cameron Brown*1,2, Sean Denham3, Alistair Meikle3, Shadia Mikhael3, Hannah Watson3, Murray Cutforth3, Keith Goatman3, Alison O'neil3, Alexander Weir3, Keith Muir1,2
1University of Glasgow, School of Psychology & Neuroscience, Glasgow, United Kingdom, 2NHS Greater Glasgow and Clyde, Queen Elizabeth University Hospital, Glasgow, United Kingdom, 3Canon Medical Research Europe, Edinburgh
On behalf of:
Background and aims: We have developed software that utilises Natural Language Processing (NLP) to identify information relevant to acute stroke reperfusion therapy decisions from free text within Electronic Health Records (EHR). We compared EHR review interval when using either Artificial Intelligence (AI) enhanced or routine EHR software.
Methods: 24 evaluators individually reviewed 6 EHR from patients previously attending our University Hospital Emergency Department with possible acute stroke.
We randomised evaluators to groups with differing case order and software access. EHR contained documents from 01/01/2011 until admission date (mean=61 (95%CI:47-76) documents/case).
Evaluators recorded information influencing reperfusion therapy suitability electronically and were asked to complete this rapidly. Reviews >10mins were considered incomplete. Review time was captured automatically upon electronic form submission.
We compared review time using time-to-event analysis, determining significance with log-rank test. We undertook binary logistic regression comparing review completion per software access, adjusting for evaluator stroke experience, case and case order.
Results: Median review time was 6.1mins (4.7-8.4) and 126 (87.5%) reviews were complete.
Review time was significantly shorter with AI-enhanced software (AI=5.7mins (4.7-6.6) vs Routine EHR=6.4mins (5.4-7.3), p=0.032)(fig.1). Less experienced evaluators (n=12) had a larger difference in review time per software access (AI=7.1mins (5.9-8.2) vs Routine EHR=9.1mins (8.0-10.2), p=0.001)(fig.2).
EHR review completion was significantly more likely with AI-enhanced software (OR:4.7 (1.4-15.8), p=0.012) and previous stroke experience (OR:10.2 (2.2-47.4), p=0.03).
Conclusions: AI-enhanced software significantly expedited EHR review and increased completion <10mins. Less experienced evaluators had greater benefit from AI assistance. There is potential for AI-enhanced software using NLP to assist EHR review in acute stroke cases.
Disclosures of Interest: No
Abstract N°: 354
DEEP LEARNING MODELS USING PERFUSION IMAGES ARE USEFUL FOR PREDICTING THE PROGNOSIS OF PATIENTS WITH LARGE VESSEL OCCLUSION
1Kurashiki Central Hospital, Neurosurgery, Kurashiki, Japan, 2The University of Tokyo, Division of Radiology and Biomedical Engineering, Bunkyo Tokyo, Japan
On behalf of:
Background and aims: Machine learning models utilising multiple preoperative variables and diffusion-weighted images have been shown to be useful in predicting outcomes for patients with large vessel occlusions. However, there are few reports on the feasibility of models using perfusion images.
Methods: We identified a total of 124 patients with large vessel occlusion in the internal carotid artery and the middle cerebral artery (M1) undergoing mechanical thrombectomy with successful recanalisation. Patients were randomly allocated into the training group (75 patients), the validation group (25 patients), or the test group (24 patients). We employed 3D-DenseNet to build predictive models, which were trained with extensive data augmentation to compensate for the small size of the training dataset. DICOM data of perfusion images were used for the input, and three-dimensional resizing was performed. The modified Rankin Scale score at discharge was set as the targeted label. The study task was designated as three-dimensional image classification, and the performance of each predictive model was evaluated based on the receiver operating characteristic area under the curve (AUC).
Results: Utilising the best of the three predictive models, the highest performance observed in the validation group was AUC ± SE 0.7430 (±0.0995) and in the test group AUC ± SE 0.7812 (±0.0950). The mean AUC ± SEM for the test group across the three different models was 0.7604 (±0.0113).
Conclusions: Deep learning models, constructed by extracting features from preoperative perfusion images, are useful for predicting the prognosis of patients with large vessel occlusion.
Disclosures of Interest: No
Abstract N°: 557
AUTOMATED DIAGNOSIS OF LACUNAR STROKE BY CT PERFUSION AND MACHINE LEARNING
James Thomas*1, Milanka Visser2, Carlos Garcia-Esperon3, Neil Spratt3, Cecilia Cappelen-Smith4, Dennis Cordato4, Andrew Bivard2, Longting Lin1, Mark Parsons1
1University of New South Wales, South Western Sydney Clinical School, Liverpool, Australia, 2University of Melbourne, Melbourne Brain Centre, Melbourne, Australia, 3John Hunter Hospital, Department of Neurology, Newcastle, Australia, 4Liverpool Hospital, Department of Neurophysiology, Liverpool, Australia
On behalf of:
Background and aims: Lacunar strokes, accounting for about 25% of ischemic strokes, present diagnostic challenges due to the limitations of traditional imaging techniques like non-contrast CT, CT angiography, and CT perfusion (CTP). Acute DWI is the gold standard for detection, but its accessibility is limited in many stroke centers. This study explores the use of an AI machine learning model to detect lacunar strokes on CTP maps, with accuracy compared against expert assessment.
Methods: The study involved patients with confirmed lacunar strokes and stroke mimics from two comprehensive stroke centers in New South Wales, Australia. CTP images were processed into cerebral blood volume (CBV), flow (CBF), mean transit time (MTT), and delay time (DT) maps. A stroke neurologist selected cases with clear CTP abnormalities for AI training. The AI model, trained on 100 cases with individual and combined CTP maps, was refined with 13 additional cases and evaluated on another 13.
Results: Results showed that the AI model, using MTT maps, matched expert sensitivity and specificity, indicating a high accuracy in identifying lacunar strokes in this patient subset. The model with DT maps was slightly less accurate, and those using CBV or CBF maps could not effectively differentiate between strokes and mimics.
Conclusions: In conclusion, the AI model shows potential in detecting lacunar strokes on raw MTT maps, performing on par with expert assessment. These promising results support further development of AI in diagnosing lacunar strokes, although further validation in a larger, more heterogeneous dataset is necessary.
Disclosures of Interest: No
Abstract N°: 1320
MULTIMODAL DEEP LEARNING FOR FUNCTIONAL OUTCOME PREDICTION IN ENDOVASCULAR THERAPY
Frank te Nijenhuis*1, Ruisheng Su1, Pieter Jan Van Doormaal1, Jeannette Hofmeijer2,3, Jasper M Martens4, Wim Van Zwam5, Aad van der Lugt1, Xucong Zhang6, Theo van Walsum1
Background and aims: The efficacy of EVT in LVO of the anterior circulation depends on adequate patient selection. Patients can be selected based on their predicted functional outcome after EVT.
Methods: Using a dataset composed of 1929 patients, we compare the functional outcome prediction performance of clinical models, including the clinically validated **** decision tool, with a CTA image based pipeline and a multimodal approach integrating CTA and clinical data. Clinical data is split into radiologically- and non-radiologically derived features, where radiological features require a radiologist to assess the images. For image analysis we employ Med3D as a deep learning backbone. The predicted outcome measure is dichotomized mRS, 90 days after EVT. Classifier performance is quantified using the AUC. AUCs are compared using DeLong’s test.
Results: On the dataset containing images only, the Med3D based pipeline performs best. On the dataset containing images as well as clinical features, Logistic Regression (LR) performs best. None of the comparisons are statistically significant. See Table 1.
Conclusions: Combining clinical features with imaging information extracted through deep learning does not significantly improve the performance of functional outcome prediction methods compared to a baseline model based on clinical data. The proposed multimodal approach can however replace radiologically derived biomarkers, potentially alleviating radiologist workload in the acute stroke setting.
Test set performance of the models, expressed as AUC values. MLP: Multilayer Perceptron.
Disclosures of Interest: No
Abstract N°: 1498
GENERATING HIGH RESOLUTION TOF-MRA DATA FOR DEEP LEARNING APPLICATIONS IN STROKE USING STYLEGAN
Orhun U. Aydin*1, Adam Hilbert1, Alexander Koch1, Felix Lohrke1, Dietmar Frey1
1Charité Campus Mitte, CLAIM - Charite Lab for Artificial Intelligence in Medicine, Berlin, Germany
On behalf of:
Background and aims: Deep learning image analysis applications in stroke require large datasets that can be time-consuming and resource-intensive to gather. We apply a generative AI model to synthesise vessel neuroimaging data to overcome privacy concerns and data scarcity.
Methods: Time-of-flight Magnetic Resonance Angiography (TOF-MRA) data from a total of 1,783 healthy patients from 6 open-source datasets were included. Images were registered to a custom TOF-MRA template. 32 axial slices covering the Circle of Willis and the adjacent anatomy were extracted from each 3D scan, resulting in 57,056 axial slices for the training dataset. StyleGANv2 architecture was utilized for the generative modelling with a target resolution of 256x256 voxels. The quality of the generated images was quantitatively evaluated using the Fréchet-Inception-Distance (FID), by applying a vessel segmentation model trained on vasculatures of real stroke patients and visually inspecting the segmentation outputs.
Results: The generated images showed realistic anatomical structures with diverse representations of the Circle of Willis variations achieving an FID score of 15.72 compared to an FID score of 1.15 between real axial slices (Figure_1). The vessel segmentation model trained on real data from stroke patients produced high-quality segmentations when applied to the synthesised data (Figure_2).
Conclusions: The generation of anatomically realistic high-quality vessel data can improve heterogeneity of datasets and the generalisation of deep learning models. Generated data can be used for data augmentation in deep learning applications, for clinical use in stroke such as large vessel occlusion detection, automated collateral score assessment and vessel segmentation.
Disclosures of Interest: No
Abstract N°: 2177
WHY CARE SHOULD BE EXERCISED WHEN USING ORDINAL NON-INFERIORIRTY ANALYSES IN STROKE
Hannah Johns*1, Bruce Campbell2, Fabiano Cavalcante3, Pooja Khatri4, Leonid Churilov1
1The University of Melbourne, Department of Medicine, Parkville, Australia, 2The Royal Melbourne Hospital, Department of Neurology, Parkville, Australia, 3University of Amsterdam, Department of Radiology and Nuclear Medicine, Amsterdam, Netherlands, 4University of Cincinnati, Department of Neurology, Cincinnati, United States
On behalf of:
Background and aims: Ordinal logistic regression has been used to analyse mRS outcomes in noninferiority studies by establishing a common odds ratio (cOR) noninferiority margin derived from the relevant margin for absolute risk difference (ARD) at a reference mRS cut point (e.g. IRIS collaboration meta-analysis). We aim to investigate the consequences of violating the proportional odds assumption for various underlying mRS distributions and to provide recommendations on ordinal noninferiority analyses for stroke researchers.
Methods: We performed in-silico experiments examining the behaviour of the methodology for performing ordinal non-inferiority analysis as used by IRIS, using its control-arm mRS distributions and small effects where proportional odds was either true or violated. For each combination of factors, we identified when noninferiority was not achieved for ARD where it should have been based on the postulated cOR margin.
Results: The cOR noninferiority margin derived from a particular dichotomised mRS ARD margin will vary widely based on the underlying control-arm reference mRS proportion and is at its maximum when it is 50%. The relationship between cOR and ARD margins is consistent when the proportional odds assumption holds, but under even minor deviations from this assumption an intervention substantially inferior on the ordinal ARD margin may be declared noninferior based on the cOR margin.
Conclusions: When using ordinal noninferiority analysis based on the cOR, noninferiority margins derived from an ARD to a reference proportion depend on the rate of outcomes in the control arm. Violations of proportional odds assumption can lead to non-inferiority claims despite substantially inferior outcomes.
Disclosures of Interest: No
Abstract N°: 2542
CAN ARTIFICIAL INTELLIGENCE DIAGNOSE STROKES? PERFORMANCE OF A RADIOLOGICAL AI-TOOL WITH CLINICAL NEUROLOGY AS A REFERENCE
Malini Sagar*1,2, Christian Krag2,3,4, Karen Lind Gandrup3, Mads Nielsen5, Henriette Raaschou3,4, Jonas Asgaard Bojsen6,7, Ole Graumann8,9, Mikael Boesen2,4,10, Helle Christensen2,11, Christina R Kruuse1,2,12
1Copenhagen University Hospital, Herlev and Gentofte, Department of Neurology, Herlev, 2University of Copenhagen, Department of Clinical Medicine, Copenhagen, Denmark, 3Copenhagen University Hospital, Herlev and Gentofte, Department of Radiology, Herlev, 4Copenhagen University Hospital - Herlev and Gentofte & Bispebjerg and Frederiksberg, Radiological AI Test Center, Copenhagen, Denmark, 5University of Copenhagen, Department of Computer Science, Copenhagen, Denmark, 6University of Southern Denmark, Research and Innovation Unit of Radiology, Odense, Denmark, 7Odense University Hospital, Department of Radiology, Odense, Denmark, 8Aarhus University Hospital, Department of Radiology, Aarhus, Denmark, 9Aarhus University, Department of Clinical Research, Aarhus, Denmark, 10Copenhagen University Hospital - Bispebjerg and Frederiksberg, Department of Radiology, Copenhagen, Denmark, 11University of Copenhagen, Zealand Emergency Services, Sorø, Denmark, 12Copenhagen University Hospital - Rigshospitalet, Department of Brain and Spinal Cord Injury, Glostrup, Denmark
On behalf of:
Background and aims: Non-comprehensive stroke treatment is time sensitive, where brain imaging is a therapeutically consequential aspect, distinguishing ischemic and hemorrhagic etiologies. A commercially available artificial intelligence (AI) algorithm (Apollo version 2.1.1 by Cerebriu), with a sensitivity of 89% and specificity of 90% for brain ischemia on magnetic resonance imaging (MRI), may facilitate swift workups. We aimed to test this radiological AI-tool in comparison to clinical diagnoses.
Methods: We retrospectively included patients with suspected strokes, admitted consecutively in 2020 to our non-comprehensive stroke unit, with brain MRI included in their inpatient workups. Clinical diagnoses upon discharge were determined based on ICD-10 codes and review of medical records and subclassified as “acute ischemic stroke” (AIS), “transitory ischemic attack” (TIA), “intracerebral hematoma” or “other”. The AI-algorithm interpreted the MRI scans and provided dichotomous outputs of “suspected ischemia” and/or “suspected hemorrhage”. If both were present simultaneously, the AI-read was classified as “hemorrhage”.
Results: Of 627 included patients, 353 (56%) were female, and the average age was 67 years, 137 had AIS, 98 had TIA and 6 had hemorrhages. The sensitivity for ischemic etiologies (AIS/TIA) was 46% [39; 52%] and specificity was 90% [88; 93%]. For hemorrhagic etiologies, sensitivity was 67% [22; 96%] and specificity was 90% [88; 93%]. If TIA-patients were excluded, with 529 patients remaining, sensitivity and specificity for ischemia were 66% [58; 74%] and 91% [88; 93%] respectively.
Conclusions: For suspected stroke, MRI-based AI-tools may supplement clinical factors, provide decision support, and especially help identify scans without ischemia or hemorrhage present.
Disclosures of Interest: Yes MVS: none, CHK: consulting fees from Cerebriu, KLG: none, MN: employed at Cerebriu, HR: none, JAB: none, OG: none, MPB: none, HCC: none, CK: none.
Abstract N°: 3185
LVOCHECK: A RAPID POINT-OF-CARE BLOOD TEST FOR THE MANAGEMENT OF CEREBROVASCULAR DISORDER PATIENTS IN THE AMBULANCES
Leire AZURMENDI*1, Lisa Kjonigsen2, Yolanda Fernandez2, Sandrine Reymond1, Rosa Delgado3, Carmen de Jesús-Gil3, Joan Montaner3, Jean-Charles Sanchez1
1University of Geneva, Human Protein Sciences, Geneva, 2ABCDx SL, BHH, Barcelona, 3Hospital Universitario Virgen Marcarena, Sevilla
On behalf of:
Background and aims: While D-dimer, NT-proBNP, and H-FABP individually indicate conditions like pulmonary embolism, heart failure, and myocardial infarction, their combined analysis with clinical parameters is crucial for identifying Large Vessel Occlusion (LVO). The LVOCheck system, designed for rapid point-of-care testing (POCT) in suspected acute stroke patients using whole blood samples, integrates data with a mobile app.
Methods: The POCT device incorporates a single strip with assays for D-Dimer, H-FABP, and NT-proBNP. Using sandwich enzyme immunoassay techniques, 30 µL of whole blood flows through the nitrocellulose membrane, forming antibody-antigen complexes that generate visible pink bands in three reaction zones. A dedicated smartphone app reads and analyzes the triplex POCT results for precise diagnostics.
Results: Excellent linearity was observed across a wide range for NT-proBNP (125-6000 pg/mL), H-FABP (3-40 ng/mL), and D-Dimer (156 ng/mL to 10 ug/mL). The lower limit of quantification was set at 125 pg/mL for NT-proBNP, 2.5 ng/mL for H-FABP, and 156 ng/mL for D-Dimer in whole blood samples. Strong Spearman correlation coefficients (ρ>0.8, p<0.001) between classical ELISA and LVOCheck concentrations indicated robust concordance.
Conclusions: The LVOCheck system, with its triplex POCT and smartphone app integration, is a valuable tool for acute stroke diagnosis. Demonstrating impressive linearity, sensitivity, and strong correlation with established methods, this innovation holds promise for revolutionizing early diagnosis and management in suspected acute stroke cases. The potential for more precise and timely interventions could significantly improve patient outcomes and streamline healthcare processes.
Disclosures of Interest: No
Abstract N°: 2189
FEDERATING EUROPEAN REGISTRIES FOR STROKE (FERES): AN ESO-EAN-HBP ENDORSED PROJECT
Alexander Salerno*1, Mira Katan2, Stefan Kiechl3, Joseph Harbison4, Leonardo Renieri5, Valeria Caso6, Danilo Toni7, Georgios Tsivgoulis8, Patrik Michel1, Philippe Ryvlin9
1Lausanne University Hospital and University of Lausanne, Stroke Center, Neurology Service, Department of Clinical Neurosciences, Lausanne, Switzerland, 2University Hospital and University of Basel, Department of Neurology, Basel, Switzerland, 3Medical University of Innsbruck, Department of Neurology, Innsbruck, Austria, 4Dublin, Stroke Service, Dublin, Ireland, 5University Hospital Careggi, Interventional Neuroradiology Unit, Florence, Italy, 6Santa Maria Della Misericordia Hospital, University of Perugia, Stroke Unit, Perugia, Italy, 7Policlinico Umberto I Hospital, Sapienza University of Rome, Emergency Department Stroke Unit, Department of Human Neurosciences, Rome, Italy, 8"Attikon" University Hospital, School of Medicine, National and Kapodistrian University of Athens, Second Department of Neurology, Athens, Greece, 9Lausanne University Hospital and University of Lausanne, LTE2C, Department of Clinical Neurosciences, Lausanne, Switzerland
On behalf of: FERES collaborators; Georges Melissargos; Viktoria Schmid Bastic; Wilfried Lang; Soeren Paaske Johnsen; Charlotte Cordonnier; Laurent Puy; Lina Palaiodimou; Peter Kelly
Background and aims: Understanding current stroke management in real-world settings is crucial for shaping stroke care policies. Multicenter registry data are an essential source of information for this purpose, yet face challenges due to technical constraints and General Data Protection Regulation (GDPR) regulations. A federated framework overcomes these by structuring information and keeping source data at its original location (node), sharing only necessary, anonymized data with the central node (Medical Information Platform, MIP) in an iterative way only during statistical federated-analysis. This way data is readily available to be analyzed and is not stocked in the central node. Our aim is to develop a robust stroke framework to impulse the re-use of health data collected in European National Stroke Registries and Electronic Health Records (EHR) in a fully General Data Protection Regulation (GPDR)-compliant way.
Methods: FERES is a European Stroke Organization (ESO), European Academy of Neurology (EAN) and Human Brain Project (HBP) endorsed initiative. It comprises three concurrent phases: A) Harmonizing and mapping metadata across stroke registries to create a Common Data Element (CDE); B) Establishing technical infrastructure in each country and connecting to the central framework; C) Handling specific national regulatory and legal aspects.
Results: Our framework successfully integrates aggregate data from multiple European stroke registries (Figure 1). Currently, three registries have completed metadata, technical, and administrative tasks, shortly becoming operational for initial analyses. More centers are progressing in technical implementation.
Conclusions: This project showcases a powerful tool for retrospective stroke care research across Europe.
Disclosures of Interest: No
Abstract N°: 2311
VALIDATE APP: A TRUSTWORTHY-AI POWERED MOBILE APPLICATION FOR CLINICAL DECISION SUPPORT IN ACUTE ISCHEMIC STROKE TREATMENT
Adam Hilbert*1, Ingo Werren2, Marta Rubiera3, Ronen Leker4, Martin Bendszus5, John Kelleher6, Giorgio Colangelo7, Arlene Wilkie8, Vince Madai9, Dietmar Frey1
1Charité Universitätsmedizin Berlin, Charite Lab for AI in Medicine (CLAIM), Berlin, Germany, 2IBM iX GmbH Berlin, Digital Health, Berlin, Germany, 3University Hospital Vall d'Hebron, Neurology Department, Barcelona, Spain, 4Hadassah-Hebrew University Medical Center, Department of Neurology, Jerusalem, Israel, 5Heidelberg University Hospital, Department of Neuroradiology, Heidelberg, Germany, 6Trinity College Dublin, Dublin, Ireland, 7Nora Health, Research and Development, Barcelona, Spain, 8Stroke Alliance for Europe, SAFE, London, United Kingdom, 9Berlin Institute of Health (BIH), Charité UniversitätsmedizinBerlin, QUEST Centre for Responsible Research, Berlin, Germany
On behalf of: On behalf of the VALIDATE consortium - EU HorizonEurope No. 101057263
Background and aims: In acute ischemic stroke, reperfusion treatments showed significant benefits across different stroke subtypes. However, several features and their combination may influence outcomes and are not usually considered in routine clinical practice.
To this end, we developed a tool that enhances the available patient information by predicting the functional outcome according to different treatment options. Our aim is to provide a clinical decision support system to guide the decision-making process of clinicians regarding treatment selection based on individual patient data.
Methods: Careful stakeholder requirement research and co-creation by a multidisciplinary team of clinicians, ethicists, designers and developers was employed. A specifically developed ethical framework guided the fulfilment of trustworthy-AI criteria during development. To derive predictions of patient outcomes, a Neural Network model was trained on multi-center retrospective data of more than 5000 patients. Outcome was determined by the full modified Rankin Scale (mRS) at 3 months.
Results: An iOS-based application was created with high usability allowing feature capture in the hyperacute setting. The user obtains the predicted full and dichotomized mRS distributions according to different treatment options before the treatment decision. The app additionally displays input feature importance and model confidence. The tool is being validated in a prospective, observational study in three clinical centers.
Conclusions: Our unique solution arms clinicians with individualized information about likely outcomes while our development process provides a case study for trustworthy-AI development, testing and validation in healthcare.
Depicts selected screens with artificial data, real-time use can be demonstrated in case of acceptance.
Disclosures of Interest: No
Abstract N°: 2698
A FAST AND SIMPLE BLOOD TEST USING A SMARTPHONE READER PREDICTS OUTCOME AMONG THROMBECTOMY TREATED STROKE PATIENTS
Joan Montaner*1, Ana Barragán1, Marcel Lamana Vallverdu2, Ana Asensio1, Rosa Delgado1, Carmen de Jesús-Gil1, Aynara Zamora1, Diego Villagran Sancho3, Antonio Cristobal Luque-Ambrosiani3, Alejandro González3
1Hospital Universitario Virgen Macarena, Sevilla, Spain, 2Vall d'Hebron Institut de Recerca, Barcelona, Spain, 3Hospital Universitario Virgen del Rocio, Sevilla, Spain
On behalf of:
Background and aims: Fatty Acid Binding Protein (FABP) and NT-proBNP are brain damage blood biomarkers with prognostic value among stroke patients. A smartphone APP reading a rapid blood test measuring those biomarkers has been developed to be used at the angio-suite to predict outcome among large vessel occlusion (LVO) patients that receive thrombectomy.
Methods: Consecutive patients (n=300) with confirmed LVO and receiving thrombectomy included in the ARTISTA prospective registry were recruited. Blood samples were obtained at thrombectomy, samples were centrifuged, and plasma was biobanked. A rapid POC test measuring both markers at the same time and scanned with a smartphone APP that offered quantitative values of each biomarker was performed. Functional outcome at 3 months was the main endpoint.
Results: Following thrombectomy 139 patients (46.5%) remained independent (mRS 0-2) and 54 died (18%) at 90 days. Clinical factors significantly associated with poor outcome in multivariate models were age, baseline NIHSS, previous mRS, diabetes and time from symptoms onset to blood sampling. FABP was highly elevated among dependent and deceased patients (p<0.001). Using Panelomix software we identified optimal cutoffs in two panels of biomarkers+clinical parameters to predict outcome with excellent specificity; for mRS>2: specificity= 98.3% and sensitivity= 50.6% (panel=NIHSS/FABP/NT-proBNP/age/previous mRS/sampling time) and for mortality: specificity = 0.99 and sensitivity = 0.40 (panel= NIHSS/FABP/NT-proBNP/sampling time).
Conclusions: A friendly smartphone device might predict outcome among those patients that get endovascular therapies. This might aid in future decisions about limiting endovascular therapies efforts or adding neuroprotectants in those with predicted poor outcome despite successful reperfusion.
Disclosures of Interest: No
Abstract N°: 86
INTEGRATING HEMODYNAMICS, MORPHOLOGY, AND MEDICAL HISTORY: DYNAMIC AI ANALYSIS OF CEREBRAL ANEURYSMS
1NYU Tandon School of Engineering, Mechanical and Aerospace Engineering, Brooklyn, United States, 2NYU School of Medicine, Department of Neurology, New York, United States, 3CARA Systems Inc., Brooklyn, United States
On behalf of:
Background and aims: Cerebral arteries are at high risk of aneurysm development. Due to their high prevalence and the morbidity and mortality of their rupture, cerebral aneurysms are of particular clinical importance and there is a need for predictive tools that can effectively risk-stratify individuals. Our model uses patient medical history and Navier-Stokes equations to dynamically simulate cerebral aneurysms over time, identifying key risk factors and predicting rupture risk.
Methods: We conducted a retrospective study of 30 patients, 15 with ruptured and 15 with unruptured aneurysms, and collected potential risk factors from their medical history. This data, along with the morphological parameters of the aneurysm and the dynamic modeling data such as arterial flow velocity, pressure distribution, and Wall Shear Stress (and the related indices Time Average Wall Shear Stress, Oscillatory Shear Index, and Relative Residence Time) will be analyzed using Artificial Intelligence (AI) and Machine Learning (ML) techniques to gain valuable insights into the risk of rupture (RoR) and progression of the presented aneurysms.
Results: We expect the generated data to match the actual data, identifying key risk factors that correlate with RoR and demonstrating that our model accurately predicts the RoR for the study sample.
Conclusions: Our model uses Navier-Stokes equations with AI/ML techniques to identify key risk factors and offers clinical insight into the RoR of aneurysms within the Circle of Willis in an efficient and non-invasive manner using CT/MRI, emphasizing ease-of-use and reducing repetitive imaging costs
Disclosures of Interest: No
Abstract N°: 690
WHEN BLOOD GOES TO YOUR HEAD: MICROGRAVITY CHANGES DETECTED BY CAROTID HEMODYNAMIC MONITORING IN ASTRONAUTS
Itamar Machol1, Hilla Ben-Pazi*2, Sam Zibman2, Samuel Goldstein2, Meron Ben Pazi2, Ori Shriki2, Shady Jahshan3, Marc Ribo Jacobi4, Sagi Har Nof1, Harel Baris5
1Rabin Medical Center, Petah Tikva, Israel, 2Avertto Medical, Aderet, Israel, 3Galilee Medical Center, Nahariyya, Israel, 4La Vall d'Hebron, Barcelona, Spain, 5Sheba, Ramat Gan, Israel
On behalf of:
Background and aims: to test if microgravity-related changes in the can be detected carotid arteries.
Methods: Pulse wave data was recorded using piezoelectric sensors placed on the carotid arteries and external jugular veins of 4 male astronauts before and after an 11-day space mission. Advanced signal processing and machine learning were employed to calculate hemodynamic changes.
Results: Significant hemodynamic changes were observed in the carotid artery; a decrease in mean PWV was noted following the space mission. Also the deep learning algorithm effectively identified waveform changes. Pulsewaves were clustered into 3 variants. The predominant variant during baseline accounted for >50% (58±2%) during baseline dropping to under 50% (46±13.3%) upon returning to earth and partially recovering to account for 50% (50±11%) within 24 hours later. Upon landing there was an increase in the other 2 variantes (from 16±12% and 26±8% before take off to 25±8% and 28±9% after landing, respectively). Here too there was a partial recovery within 24 hours as these variants decreased towards baseline (25±11% and 2±8% respectively). A 2x3 repeated measures ANOVA of time (Before takeoff vs After landing) by variant type revealed a trend of p=0.086, supporting the observation that extended exposure to microgravity causes an increase in variability of pulsewave types.
Conclusions: Neck sensors detected microgravity-induced changes in the carotid arteries. Further investigation is needed to evaluate the potential of continuous carotid artery monitoring for space missions.
Disclosures of Interest: Yes H Ben Pazi, MD, is the founder and CEO of Avertto.
Abstract N°: 1032
AI-ECG FOR PREDICTION OF SUBCLINICAL ATRIAL FIBRILLATION IN PATIENTS WITH STROKE WHO UNDERGO PROLONGED CARDIAC MONITORING
Carmen Holmes*1, Ahmed Mohamed Ahmed2, Kathryn Mangold1, Peter Noseworthy1, Francisco Lopez-Jimenez1, Jonathan Graff-Radford1, Alejandro Rabinstein1, Stephen English1
1Mayo Clinic, Rochester, United States, 2Mayo Clinic, Jacksonville, United States
On behalf of:
Background and aims: Evaluate the performance of an AI-ECG algorithm to predict atrial fibrillation(AF) detection on prolonged cardiac monitoring(PCM) after index stroke.
Methods: Retrospective study of patients with ischemic stroke evaluated at Mayo Clinic with baseline electrocardiogram(ECG) and PCM between 2018-2020. Demographics, clinical features, stroke mechanism, PCM duration, and PCM outcome(AF vs no-AF) recorded. ECGs were analyzed using the AI-ECG algorithm to determine likelihood of AF capture with PCM. Stroke etiology was adjudicated using TOAST classifications. The ability of the AI-ECG algorithm to predict AF detected by PCT was assessed via receiver operating characteristics(ROC) analysis, calculating the area under curve(AUC). Sensitivity and specificity analyses were performed for each tool using optimal cutoffs.
Results: 863 patients were included; median age was 69 years, 496(57.5%) were male, and 561(65%) patients were categorized as embolic stroke of undetermined source(ESUS). PCT detected AF in 85(9.8%) patients. Median duration of PCM was 30(IQR 25-30) days. AI-ECG identified a significant difference in probability of AF on PCM. For its optimal cutoff of 0.24, AI-ECG had a NPV of 94.2%(95% CI 92.2-95.9) and a specificity of 81.8%(95% CI 78.9-84.4) for excluding AF on PCM. However, the ROC analysis revealed suboptimal AUC(0.69). There was no significant difference in AUC when comparing the ESUS vs non-ESUS subgroups(p=0.417).
Conclusions: AI-ECG may identify patients who are unlikely to have AF on PCM. Future studies should evaluate the relationship between AI-ECG AF probability and AF detection on PCM of longer duration and compare the performance of both methods in predicting of stroke recurrence.
Disclosures of Interest: No
Abstract N°: 1464
‘MY STROKE COMPANION’: A FEASIBILITY STUDY EVALUATING A PERSONALISED DIGITAL SUPPORT PACKAGE CO-DESIGNED WITH STROKE SURVIVORS AND THEIR FAMILIES
Louis Stokes1, Daisy Allington1, Alice Wood1, Rob Simister2, Arvind Chandratheva2
1Cognitant Group Ltd., Oxford, United Kingdom, 2UCL Queen Square Institute of Neurology, United Kingdom
On behalf of:
Background and aims: Stroke survivors are seldom discharged from hospital with specific and accessible information about stroke, making navigating the post-stroke pathway challenging - contributing to worse outcomes and non-compliance. ‘My Stroke Companion’ is an accessible digital support package (DSP) providing personalised, reliable, and localised information about type of stroke, post-stroke care plans (including prescribed medicines and rehabilitation) and local support. Life after stroke is emphasised including driving, work, and sex and relationships. Following an initial pilot and iterative development, this feasibility study presents acceptability and usability data collected from stroke survivors and their families.
Methods: Five UK NHS hospitals “prescribed” the DSP to stroke survivors at discharge over an 8-month period by selecting content using the clinician web-interface, and then sharing a personalised weblink with each patient. Platform engagement and anonymous feedback surveys were analysed.
Results: Clinicians generated 504 “prescriptions”, and subsequently 400 users accessed the DSP 555 times, with an average session duration of 6-minutes. Of 42 users, 31% self-reported a ‘good’ or ‘excellent’ understanding of stroke before accessing the DSP, compared to 88% after accesing the platform. Additionally, 91% felt information was easy to understand, 81% felt it was personalised, and 91% were satisfied overall. Feedback also indicates increased knowledge in all domains - including medicines, rehabilitation, accessing support, and preventing further stroke.
Conclusions: ‘My Stroke Companion’ is an innovative way to share information with stroke survivors, empowering them to better navigate life after stroke. Our data suggests the benefits of providing multi-format, digital content and user feedback indicates high acceptability.
Disclosures of Interest: No
Abstract N°: 1512
HOW MUCH BRAIN COULD BE SAVED BY REMOTE ROBOTIC THROMBECTOMY?
1Besançon University Hospital, Interventional Neuroradiology, Besançon, France, 2Besançon University Hospital, Neurology, Besançon, France, 3Foch Hospital, Interventional Neuroradiology, Paris, France, 4St Michalel's Hospital, RADIS Lab, Toronto, Canada
On behalf of:
Background and aims: Feasibility of robotic endovascular therapy has recently been demonstrated. This technology could lead to remote endovascular treatment (EVT) of acute ischemic stroke (AIS). Therefore current regional telestroke network should prepare to implement this technology and select the best sites for remote robotics. The aim of this study was to propose a method to select the best remote robotic sites for AIS EVT.
Methods: We retrospectively analyzed a regional telestroke network with one hub providing EVT and 7 remote hospitals (called A to G) addressing AIS patients. We tried to assess the number of minutes lost each year for every site by multiplying the annual number of EVT by real-life inter-hospital transfer times. We also did projections of expected EVTs, using the Hub EVT/AIS ratio on each site.
Results: Site C had the larger minutes lost per year at 3024 followed by sites G and D with respectively 1938 and 2047. Hub had an EVT/AIS ratio of 8.8%. Projecting this figure on remote sites, the larger expected minutes gain were seen on the same sites C, G and D with 4869, 2799 and 2867 mn respectively. Regarding only site C, suppression of inter-hospital transfer time by remote robotics could potentially save 56 years of disability and 39 billions neurons.
Conclusions: Analysis of current telestroke networks are needed to target the best sites for future remote robotics. We propose a simple method to quantify and classify potential candidates.
Disclosures of Interest: No
Abstract N°: 2098
USABILITY TESTING OF A NOVEL REMOTE ISCHEMIC CONDITIONING SYSTEM FOR PRE-HOSPITAL STROKE CARE
1University of Calgary, Clinical Neurosciences, Calgary, Canada, 2University of Calgary, Graduate Science Education, Calgary, Canada, 3Northern Alberta Institute of Technology, Centre for Advanced Medical Simulation, Edmonton, Canada
On behalf of:
Background and aims: For acute ischemic stroke, often-prolonged hospital transport times present an opportunity for early interventions to salvage at-risk brain tissue. Remote ischemic conditioning (RIC), where brief cycles of ischemia-reperfusion in a limb are induced to protect the brain from injury, is a promising treatment for this setting. We assessed the usability of a novel miniaturized RIC system in a simulated emergency response scenario.
Methods: Following a brief introduction to operating the RIC device (Image 1) for upper-limb application, participating paramedics were asked to use it in a simulated scenario, involving emergency care and ambulance transport for a stroke patient (manikin). Feedback on device use was collected through questionnaires, including the System Usability Scale (SUS; max. score: 100), and a semi-structured interview. Questionnaire responses were summarized using descriptive statistics; interview transcripts were analyzed thematically.
Results: Eight paramedics completed the simulation – five female; mean age 34.8±11.8-years (SD); mean 9.75±11-years of professional experience. As reiterated during interviews, questionnaire responses indicated high device usability (mean SUS score 86.9±12.9). Seven paramedics stated they would use the device in daily practice. Expressed concerns related to: interference with standard procedures, cable management, device durability, and patient discomfort. Suggested improvements included enabling attachment of the activation unit to the cuff.
Conclusions: Our RIC system was found to be highly usable. Feedback on the importance of seamless integration of novel procedures with those already established, robustness of equipment, and effective paramedic-patient communication will be used to refine our prototype, and may help inform the design of other, future pre-hospital stroke interventions.
Disclosures of Interest: Yes Dr. Ganesh has a patent filed (U.S. 17/317,771) for the device being studied in this project, which is being assigned to his start-up SnapDx Inc.
Abstract N°: 2179
DEEP LEARNING-BASED PREDICTION OF INFARCT GROWTH IN ACUTE ISCHEMIC STROKE PATIENTS
Heylen Ewout*1, Anke Wouters2, Maarten Lansberg3, Soren Christensen3, Nicole Yuen3, Michael Mlynash3, Praneeta R Konduri4,5, Lieselotte Vandewalle2,6, Frederik Maes1, Robin Lemmens2,6
1KU Leuven, Department of Electrical Engineering (ESAT), Leuven, Belgium, 2KU Leuven, Department of Neurosciences Division of Experimental Neurology, Leuven, Belgium, 3Stanford Stroke Center, Palo Alto, United States, 4Amsterdam UMC Location University of Amsterdam, Department of Biomedical Engineering and Physics, Amsterdam, Netherlands, 5Amsterdam UMC Location University of Amsterdam, Department of Radiology and Nuclear Medicine, Amsterdam, Netherlands, 6University Hospitals Leuven, Department of Neurology, Leuven, Belgium
On behalf of:
Background and aims: In acute ischemic stroke, perfusion imaging based on deconvolution can assess the size of the core and penumbra. Recently, we have developed a deep learning model to predict infarct core growth based on native CT Perfusion (CTP) images and clinical metadata. Here, we aimed to validate the growth model by evaluating the CTP-based prediction versus Diffusion Weighted Imaging (DWI) at a follow-up timepoint before reperfusion was achieved.
Methods: We included data from patients with an anterior circulation large vessel occlusion admitted at a primary stroke center (PSC) at which CTP was acquired, before transfer to a thrombectomy capable comprehensive stroke center (CSC) at which DWI was obtained. Based on the predicted growth rate by the deep learning model and transfer time between the two imaging studies, we could compare the predicted infarct core versus the actual lesion on DWI before initiation of endovascular treatment.
Results: We report results of 33 patients with a median transfer time of 160 minutes (IQR 68 minutes) and a median DWI lesion volume of 15.0 ml (IQR 29.0 ml) in the CSC. When comparing the estimation of the DL model to the DWI lesion, the mean absolute volume difference was 17.0 ml (SD 22.1 ml) which corresponded to a mean dice score of 0.34.
Conclusions: Deep learning models can predict infarct growth rates in acute stroke patients which may be of benefit for future neuroprotection trials. We will further evaluate the accuracy of this model in a larger dataset to obtain more robust data.
Disclosures of Interest: No
Abstract N°: 2270
UTILIZING RAPID AI FOR AUTOMATED DETECTION AND VOLUME ESTIMATION OF INTRACRANIAL HEMORRHAGE TO ENHANCE STROKE TREATMENT
Vishal Jani*1,2, Jenny Hammond1, Craig Rabb1, Douglas Hardesty1, Alexander Yang1, Omar Akbik1, Ruchika Jani1, Zachary Depew1, Douglas Moore1, Steven Leitch1
1CHI Health Creighton University Medical Center - Bergan Mercy, Omaha, United States, 2Creighton University School of Medicine, Department of Neurology, Omaha, United States
On behalf of: Klaus Thaler MD, Adam Highley MD, Venketraman Sahasranaman MD, Nikhil Jagan MBBS, Jason E. Lambrecht MD, Barb Leonard, Kathy Jesus RN, Kathleen Wolter, Korrine Bowers, Douglas Page, Lindsey Amato APRN, Candy Garner APRN, Drew Wallenstein
Background and aims: Intracranial hemorrhage (ICH) accounts for 10-20% of strokes with high morbidity and mortality. Rapid identification on CT is critical for treatment decisions. However, small bleeds are often missed, delaying diagnosis. Rapid ICH uses a convolutional neural network (CNN) to automatically detect ICHs with volumes of 0.4 ml or larger with high sensitivity and specificity. The Rapid Hyperdensity module provides accurate ICH volumes.
Methods: Rapid software and was integrated into imaging workflow at our comprehensive stroke center in June 2023. The software processes CT scans in <1 minute and alerts physicians via apps, email and EMR regarding suspected ICH, including location/volume. The impact on clinical documentation, door-to-needle times, and 30-day mortality was assessed for 6 months post-integration.
Results: RapidICH detected ICH with 98.1% sensitivity and 99.7% specificity (excluding hemorrhagic transformations) in validation studies based on >1,000 patients. At our center, appropriate documentation of hemorrhage severity scores rose from 30% pre-integration to 95% following integration (P<0.05).
Conclusions: Rapid ICH integration led to substantial gains in speed and accuracy of hemorrhage identification. Ensuing process improvements demonstrate significant benefits across the care cycle, including facilitated clinical decision-making and reduced delays in treatment and mortality rates. Further studies are warranted to evaluate the impact of Rapid ICH on individualized clinical decision-making and patient outcomes. Leveraging automated quantification of brain hemorrhage through innovations like Rapid ICH shows immense potential to optimize and personalize hemorrhagic stroke management.
Disclosures of Interest: Yes I have served in an advisory role for RAPID AI to provide scientific consultation.
Abstract N°: 1238
GEMINI: DIGITAL TWINS OF ISCHEMIC AND HEMORRHAGIC STROKE PATIENTS
Henk Marquering*1, Charles Majoie1, Alfons Hoekstra2
1Amsterdam UMC, Radiology and Nuclear Medicine, 2University of Amsterdam, Informatics Institute
On behalf of: Gemini collaborators
Background and aims: The introduction of Digital Twins in Healthcare for stroke opens up unmet opportunities to improve treatment, management, and trial design involving stroke patients. Digital Twins in Healthcare represent patients by integrating all information for this specific patient. This allows the simulation of (new) treatments giving valuable insight into patient-specific treatment selection illustrating potential complications such as thrombus fragmentation during mechanical thrombectomy.
Methods: Gemini brings together a consortium of 19 organizations from 12 countries including computer science institutions, hospitals, large industry, and small and medium enterprises. Gemini will address a large scale of aspects of stroke from fundamental physiological cascade initiated with the onset of stroke up to the patient-specific functional deterioration after a treated stroke.
Results: Gemini will bring mechanistic models of cerebral blood flow, brain perfusion and metabolism, and thrombosis along the heart-brain axis utilizing these to population-based ischemic and hemorrhagic stroke digital twins, which will subsequently be utilized to enable patient-specific digital twin generation. The value of the availability of a digital twin in clinical practice will be evaluated in a clinical trial in which outcomes of patients will be evaluated for situations with and without the presentation of digital twin results.
Conclusions: With Gemini a consortium has been established that will establish and make available Digital Twins of stroke patients, which can be used to improve fundamental understanding of the complex physiological processes involved in stroke, treatment selection of specific patients, up to the development of novel treatments and design of clinical trials.
Disclosures of Interest: Yes HM is co-founder of Nicolab, TrianecT, and inSteps
Abstract N°: 1150
STROKE AI-BASED DETECTION IN EMERGENCIES: DEVELOPING A VIRTUAL ASSISTANT BASED ON AI TOOLS FOR ACUTE STROKE (SAID-E)
Alessandro Bufi*1, Valeria Caso1, Virginia Cancelloni1
1Hospital Santa Maria della Misericordia in Perugia, Perugia, Italy
On behalf of:
Background and aims: In medical AI, stroke diagnosis and management are increasingly important. Quick and accurate diagnosis is key to effective treatment. Stroke care demands a coordinated, protocol-driven process from a skilled multidisciplinary team. Patient care is routed through HUB and SPOKE centers within a structured network, determined by case complexity and treatment needs. The emergency physician is crucial in initial stroke management, working with neurologists to follow established diagnostic and treatment pathways. This study aims to create a Virtual Assistant (VA) with software capable of recognizing ischemic stroke patients. The VA will undergo a learning process based on data collection and analysis to improve its accuracy in stroke patients in the emergency setting.
Methods: A prospective, longitudinal, interventional, non-profit, single-center study will be conducted. The study will last from 01/02/24 to 28/02/2025 and consists of five phases, from creating VA to validating SPOKE centers. Patient recruitment will span 12 months, beginning 01/03/2024, and will include consecutive patients presenting to the Emergency Department of the Perugia Hospital with suspected ischemic stroke. The VA utilizes advanced deep learning techniques through Tensorflow to analyze stroke-related symptoms specifically. It employs convolutional neural networks for detecting changes in facial symmetry and vocal patterns indicative of stroke events, enhancing classification accuracy with metadata.
Results: The preliminary results will be announced at ESOC 2024.
Conclusions: The VA may be a new tool to support emergency physicians in recognizing and treating stroke more swiftly, improving patient outcomes.
Disclosures of Interest: No
Abstract N°: 1668
COMPUTERIZED DECISION SUPPORT SYSTEMS IN ACUTE STROKE CARE: A SCOPING REVIEW
1Amsterdam University Medical Centers, University of Amsterdam, Amsterdam Neuroscience, Department of Radiology and Nuclear Medicine, Amsterdam, Netherlands, 2Haaglanden Medical Center, Department of Radiology, The Hague, Netherlands, 3Amsterdam University Medical Centers, University of Amsterdam, Amsterdam Neuroscience, Department of Neurology, Amsterdam, Netherlands, 4Amsterdam University Medical Centers, University of Amsterdam, Amsterdam Neuroscience, Biomedical Engineering & Physics, Amsterdam, Netherlands, 5Amsterdam University Medical Centers, University of Amsterdam, Department of medical informatics, Amsterdam, Netherlands
On behalf of:
Background and aims: Decision making in acute stroke care is becoming increasingly complex and dependent on multiple information sources. Computerised decision support systems (CDSS) can assist stroke specialists in gathering and interpreting information and improving treatment time metrics. However, real-world experience with these tools is often unsatisfactory. We investigated the involvement of users in the development of CDSS for acute stroke care.
Methods: We performed a scoping review of publications reporting the development of CDSS for acute stroke care. We extracted information on target users’ definitions and involvement in the development and implementation of CDSS for acute stroke care. Additionally, the authors’ affiliations were used to identify the participation of clinical and technical experts. A secondary analysis focused on CDSS for automated neuroimaging analyses.
Results: We identified 93 publications reporting 85 unique CDSS. Target users were mentioned in 60% of the publications, with only 15% reporting their involvement in the development of the CDSS. Overall, 38% of the studies had both at least one author affiliated with a technical department and one author affiliated with a clinical department. Publications with both clinical and technical authors more frequently defined target users and described involvement of users in the development of the CDSS in their publications.
Conclusions: Publications reporting the development of the CDSS for acute stroke care frequently lack details regarding the target user and how the user requirements were considered.
Disclosures of Interest: No
Abstract N°: 1967
ALTERNATIVE CHOICE OF NIHSS TRAINING: VIRTUAL REALITY PROVIDE EQUAL TRAINING OUTCOMES AND ENHANCE LEARNING MOTIVATION
Yu-Ming Chang*1, Chun Min Wang1, Wei-Jung LI2, Yu-Lien Shen2, Chien-Hsu Chen2, Pi-Shan Sung1
1National Cheng Kung University Hospital, Department of Neurology, 2National Cheng Kung University, Department of Industrial Design
On behalf of:
Background and aims: NIHSS remains a vital stroke severity assessment in evaluating acute ischemic stroke patients. Virtual reality (VR) had shown its strength in immerse reality that it could help simulation training in medical fields. We developed a new NIHSS training program in National Cheng-Kung University Hospital via VR system. This study aimed to investigate the training outcomes and learning motivation between VR training model and traditional training protocol.
Methods: We prospectively enrolled medical students from Sep 2022 to May 2023. They would be randomly divided into video training (VT) group or virtual reality training (VR) group. Once they completed the program, objective structured clinical examination (OSCE) was held for direct assessment of their NIHSS clinical ability. Situational Motivation Scale (SIMS) was used to evaluate the scale motivation. The testing results from pre-lecture tests, post-lecture tests, between-test difference, OSCE and SIMS were compared between two groups.
Results: We had enrolled 61 students. There were no differences in the outcomes of pre- lecture test, post-lecture test, between-test difference and OSCE performance. In motivation questionnaire SIMS, VT group showed a lower score in intrinsic motivation (17.84 vs. 21.38, p=0.001) but higher score in external regulation (18.84 vs. 16.00, p=0.007) and amotivation (12.25 vs. 9.83, p=0.031) in comparison with VR group. Thus, in self-determination index, VT group was lower than VR group (12.47 vs. 27.07, p<0.001).
Conclusions: NIHSS training via virtual reality system had proven similar training effect in comparison with traditional video training, but enhanced much more motivation in learning for the trainees.
Disclosures of Interest: No
Abstract N°: 2768
IN-SILICO SIMULATION FOR DEVELOPMENT OF NOVEL THROMBECTOMY DEVICES
Shashvat Desai*1, Praneeta R Konduri2, Sara Bridio3, Nerea Arrarte Terreros2, Giulia Luraghi3, Francesca Berti3, Ashutosh Jadhav4, Charles Majoie2, Henk Marquering2, Francesco Migliavacca3
1HonorHealth Research and Innovation Institute, Phoenix, United States, 2Amsterdam University Medical Center, Netherlands, 3Politecnico di Milano, Italy, 4Barrow Neurological Institute
On behalf of:
Background and aims: While in-vitro analysis is the gold standard for pre-clinical device development, in-silico evaluation (virtual stroke model) has the potential to accelerate and optimize development of next-generation thrombectomy devices. We aim to demonstrate the utility of in-silico simulation for the development of a novel stent-retriever..
Methods: A prototype of Gravity Medical Technology’s SuperNova Stent-retriever was the device under investigation. Anatomy of the virtual model was built based on digital subtraction angiography of an in-vitro model (Sim Agility, Mentice, Inc). In-silico analysis was performed using a virtual thrombectomy model (fine-grained finite-element model), to estimate the probability of successful recanalization and emboli. In-vitro experiments of two thrombectomy scenarios based on thrombus occlusion pattern were performed and replicated with in-silico models. Rates of recanalization and emboli formation were compared between in-vitro and in-silico models along with qualitative assessment.
Results: Rate of successful recanalization and rate of emboli formation with stent-retriever prototype was comparable for different thrombectomy simulations in similar in-vitro and in-silico models (Table1). A schematic representation comparing in-vitro and in-silico thrombectomy simulation for a Y-shaped clot in the M1-M2 bifurcation, mechanism of clot engagement, withdrawal, and potential complications such as clot fragmentation is provided in Figure 1.
Conclusions: In-silico models can replicate in-vitro thrombectomy experiments. In-silico models can evaluate the performance of novel devices in different thrombectomy scenarios and have the potential to accelerate and optimize development of novel thrombectomy technology.
Disclosures of Interest: No
Paper Poster – Thrombolysis
Abstract N°: 2479
VARIATION IN THROMBOLYSIS USE AND THE POTENTIAL EFFECT ON OUTCOMES IN ENGLAND AND WALES: AN OBSERVATIONAL MACHINE LEARNING STUDY
Kerry Pearn1, Michael Allen1, Anna Laws1, Martin James*2
1University of Exeter, Medical Scool, Exeter, United Kingdom, 2Royal Devon University Healthcare NHS Foundation Trust
On behalf of:
Background and aims: We have previously identified that the most significant source of the five-fold between-hospital variation in thrombolysis use in the UK is differences in hospitals' willingness to use thrombolysis. Where hospitals differ in their approach to treatment, the question arises 'which results in better outcomes?'. We used machine learning to compare thrombolysis selection and outcomes based on the comprehensive national stroke registry SSNAP.
Methods: We built three machine learning models based on 172,001 patients across 119 hospitals between 2016 and 2021. All patients had modified Rankin Scale (mRS) estimated prior to stroke, and on hospital discharge. XGBoost was used to predict the likelihood of receiving thrombolysis, the outcome (mRS), and the benefit (mRS shift) from thrombolysis. SHAP explainability models investigated the relationship between patient characteristics and model predictions.
Results: Key factors associated with thrombolysis choice were: arrival-to-scan time, stroke type, stroke severity, whether stroke onset was known precisely (rather than estimated), pre-stroke disability, hospital, use of anticoagulants, and onset-to-arrival time. Key factors associated with outcome were pre-stroke disability, stroke severity, hospital, age, and use/time of thrombolysis. Key factors associated with the predicted benefit from thrombolysis were age, time to thrombolysis, and stroke severity. Though pre-stroke disability and whether stroke onset was known precisely affected choice to use thrombolysis, they had little association with the predicted benefit from thrombolysis.
Conclusions: Machine learning combined with large national clinical registry data allows detailed analysis of clinical variation in use of thrombolysis, and the subsequent effect on outcomes.
Disclosures of Interest: No
Abstract N°: 2978
EARLY RECANALIZATION FOLLOWING INTRAVENOUS THROMBOLYSIS FOR ANTERIOR CIRCULATION STROKE WITH A THROMBUS LENGTH OF 8 MM OR MORE
Omar Khashaba*1,2, Michael Mazya3,4, Mariam Willny5, Ibrahim Libida1,2, Mohamed Abo-Warda1,2, Ahmed El-Sammak1,2, Michael Söderman4,5, Åsa Kuntze Söderqvist4,5
1Zagazig University Hospitals, Department of Diagnostic and Interventional Radiology, Zagazig, Egypt, 2Faculty of Medicine, Zagazig University, Department of Diagnostic and Interventional Radiology, Egypt, 3Karolinska University Hospital, Department of Neurology, Sweden, 4Karolinska Institutet, Department of Clinical Neuroscience, Sweden, 5Karolinska University Hospital, Department of Neuroradiology, Sweden
On behalf of:
Background and aims: It has previously been reported that intravenous thrombolysis (IVT) has nearly no potential to recanalize cerebral arterial thrombi with a length of more than 8 mm within the anterior circulation. Based on clinical observations, we aimed to test the hypothesis that early recanalization of long thrombi in IVT patients is more common than previously reported.
Methods: We used data from the National Stroke Registry on patients with a large vessel occlusion (LVO) anterior circulation stroke and a thrombus length of ⩾ 8 mm, transferred from a Primary Stroke Center (PSC) to a Comprehensive Stroke Center (CSC) for thrombectomy during 2019–20. LVO was defined as any thrombus occupying the intracranial ICA, M1, M2, A1 or A2. Patients were divided according to IVT administration into IVT group and No IVT group. Time between the first radiological image at PSC and repeated imaging upon arrival to CSC had to be one hour or more. We analyzed early recanalization (ER) by comparing imaging from the CSC versus the PSC and comparing ER rates in the IVT versus the No IVT groups.
Results: Early recanalization occurred in 27/215 (12.5%) patients in the IVT and 2/162 (1.2%) in the No IVT groups respectively. The median thrombus length among the 27 ER patients in the IVT group was 15 mm.
Conclusions: IVT administration prior to a long transfer is associated with recanalization of large artery occlusions in patients with anterior circulation stroke and thrombus length of 8 mm or more.
Disclosures of Interest: No
Abstract N°: 316
MECHANICAL THROMBECTOMY WITH AND WITHOUT BRIDGING THROMBOLYSIS IN POSTERIOR CIRCULATION LVOS – INSIGHTS FROM STAR
Ev-Christin Heide1, Sami Al Kasab2, Ali Alawieh3, Adam Arthur4, Waleed Brinjikji5, Shakeel Chowdhry6, Roberto Crosa7, Hugo Cuellar8, Alejandro Spiotta2, Ilko Maier*1
1University Medicine Göttingen, Neurology, Göttingen, Germany, 2Medical University of South Carolina - Main Campus, 3Emory University, 4University of Tennessee Health Science Center/Semmes Murphey Foundation, 5Mayo Clinic in Minnesota, 6NorthShore University HealthSystem, 7Médica Uruguaya, 8LSU Health Shreveport
On behalf of: De Leacy R, Dumont T, Ernst M, Ezzeldin M, Fragata I, Howard B, Jabbour P, Kan P, Kim JT, Levitt MR, Mascitelli J, Matouk C, Moss M, Navia P, Osbun J, Park MS, Polifka A, Psychogios MN, Rai A, Starke R, Wolfe SQ, on behalf of STAR Investigators
Background and aims: Multiple randomized trials did not demonstrate non-inferiority of mechanical thrombectomy (MT) alone compared with prior bridging thrombolysis (BT) in anterior circulation large vessel occlusion (LVO) stroke. The role of BT in posterior circulation LVO remains controversial.
Methods: In this multicenter, retrospective study, stroke patients with LVO in the posterior circulation who received mechanical thrombectomy (MT) alone or with BT were selected from the stroke thrombectomy and aneurysm registry (STAR) between 2013 to 2021. Effects of BT on favorable functional outcome (defined as modified Rankin scale ⩽ 3 at 90 days) and change in National Institutes of Health Stroke Scale (NIHSS) from presentation to discharge were investigated using multivariable logistic and linear regression models.
Results: Of the 588 included patients, 67% (n=394) were treated with MT alone and 29% (n=170) with BT and in 4% (n=24) this variable was imputed. Controlling for multiple confounding factors, BT was not associated with a higher likelihood of favorable functional outcome at 90 days (OR 1.04, 95%CI 0.52-2.09, p=0.901). There was a trend towards a higher improvement in NIHSS in the BT-group (linear regression coefficient -3.31, 95%CI -6.71-0.09, p=0.056) with an effect size of 3 points. MT alone did not show any safety advantages compared with those receiving BT.
Conclusions: Similar functional outcomes and complication rates were seen in patients with posterior circulation LVO treated with MT alone vs BT. Further non-inferiority studies are required to determine the utility of BT in posterior circulation stroke, especially in patients being directly admitted to thrombectomy centers.
Disclosures of Interest: No
Abstract N°: 850
THROMBECTOMY WITH OR WITHOUT INTRAVENOUS THROMBOLYTICS IN BASILAR ARTERY OCCLUSION
Stefanos Foinitsis*1, Benjamin Maïer2, Mikael Mazighi3, Bertrand Lapergue4, Gaultier Marnat5, Igor Sibon5, Sébastien Richard6, Christophe Cognard7, Jean Marc Olivot7, Benjamin Gory6
1School of Visual & Applied Arts A.U.TH, Greece, 2Hôpital Saint-Joseph, Paris, France, 3Université Paris Cité, Paris, France, 4Hôpital Foch Suresnes, Service de Neurologie, Suresnes, France, 5Hopital Universitaire, Bordeaux, Bordeaux, France, 6University De Lorraine, Nancy, France, 7Hospital Center University De Toulouse, Toulouse, France
On behalf of: ETIS Registry Investigators
Background and aims: Two randomized trials demonstrated the benefit of endovascular therapy (EVT) in patients suffering from stroke due to a basilar artery occlusion (BAO). However, intravenous thrombolytic (IVT) use before EVT was low in these trials, questioning the added value of this treatment in this setting. We sought to investigate the efficacy and safety of EVT alone compared to IVT + EVT in stroke patients with a BAO.
Methods: We analyzed data from the ETIS registry, a prospective, observational study, encompassing 21 comprehensive stroke centers in France (January 2015 to 31 December 2021). Patient with BAO and/or intracranial vertebral artery occlusion were divided in a EVT vs and a IVT + EVT group. Efficacy outcomes were modified Rankin Scale [mRS] 0-3 and functional independence mRS 0–2 at 90 days. Safety outcomes were symptomatic intracranial hemorrhages and all-cause mortality at 90 days.
Results: Among 385 patients, 243 (134 EVT alone and 109 IVT + EVT) were included after PS matching. There was no difference regarding good functional outcome ([aOR] labeling = 1.27, 95%CI, 0.68–2.37, p = 0.45) and functional independence (aOR = 1.50, 95% CI, 0.79–2.85, p = 0.21). Symptomatic intracranial hemorrhage and mortality were also similar (aOR = 0.42, 95% CI, 0.10–1.79, p = 0.24 and aOR = 0.56, 95% CI, 0.29–1.10, p = 0.09, respectively).
Conclusions: In this analysis, EVT alone seemed to lead to similar neurological recovery than IVT + EVT, with comparable safety profile. However, further studies are needed to confirm these findings.
Disclosures of Interest: No
Abstract N°: 1830
IV THROMBOLYSIS BEFORE COMPLETE ANGIOGRAPHIC REPERFUSION: BEYOND ANGIOGRAPHIC ASSESSMENT TO TARGET MICROVASCULAR OBSTRUCTION?
Stefanos Foinitsis*1, Benjamin Gory2, Jean Marc Olivot3, Sébastien Richard4, Gaultier Marnat5, Igor Sibon6, Christophe Cognard7, Mikael Mazighi8, Bertrand Lapergue9, Benjamin Maïer10
1Aristotle University of Thessaloniki, Thessaloniki, Greece, 2University De Lorraine, Nancy, France, 3Hospital Center University De Toulouse, Toulouse, France, 4Hospital Center Regional And University De Nancy Hospital Central, Nancy, France, 5University Hospital of Bordeaux, Bordeaux, France, 6, Bordeaux, France, 7University of Toulouse, Toulouse, France, 8Hospital Foundation Adolphe De Rothschild, Paris, France, 9Hospital Foch, Suresnes, France, 10Hospital Paris Saint-Joseph, Paris, France
On behalf of: ETIS Registry Investigators
Background and aims: Ineffective tissue reperfusion despite successful angiographic reperfusion may be partly responsible for unfavorable outcomes after endovascular therapy (EVT) and might be modulated by intravenous thrombolysis (IVT) before EVT. To decipher the effect of IVT before EVT, we compared outcomes of patients with complete reperfusion at the end of EVT according to IVT use.
Methods: The ETIS registry encompasses 21 centers that perform EVT in France. We included patients with ICA or MCA occlusion and complete reperfusion with EVT within 6 hours (January 2015 to December 2021) and divided them into two propensity score matched groups according to IVT use before EVT. Primary outcome was the mRS shift in at 90 days. Secondary outcomes included mRS 0–2 at 90 days. Safety outcomes included symptomatic intracranial hemorrhage and 90-day mortality.
Results: 1,093 were included, of whom 651 patients with complete recanalization treated with IVT before EVT. After PSM, 488 patients with IVT before EVT were compared to 337 patients without IVT. The IVT+EVT group had a favorable shift in the overall mRS distribution ( [aOR] = 1.41, 95%CI= 1.04–1.91, p = 0.023) and higher rates of favorable outcome (61.1% vs 48.7%, aOR = 1.49, 95% CI = 1.02–2.20, p = 0.041) at 90 days compared with the EVT alone group. Rates of symptomatic intracerebral hemorrhage were comparable (6.0% vs 4.3%, aOR = 1.16, 95% CI = 0.53–2.54, p = 0.709).
Conclusions: Even after complete angiographic reperfusion by EVT, prior IVT use improves clinical outcomes of patients without increasing bleeding risk.
Disclosures of Interest: No
Abstract N°: 454
PREDICTORS OF EARLY VERSUS DELAYED NEUROLOGICAL DETERIORATION AFTER THROMBOLYSIS FOR ACUTE ISCHEMIC STROKE: THE ENCHANTED STUDY
1Suzhou TCM Hospital Affiliated to Nanjing University of Chinese Medicine, Suzhou, China, 2The Second Affiliated Hospital of Soochow University, Neurology, Suzhou, China, 3Fukuoka University, Fukuoka, Japan, 4West China Hospital, Sichuan University, Neurology, Chengdu, China, 5The George Institute for Global Health, Faculty of Medicine, University of New South Wales, Sydney, Australia
On behalf of: the ENCHANTED Investigators
Background and aims: We aimed to determine predictors of early (END) and delayed neurological deterioration (DND) and their association with functional outcome in patients with acute ischemic stroke (AIS) in the international Enhanced Control of Hypertension and Thrombolysis Stroke Study (ENCHANTED) (NCT01422616).
Methods: END and DND were defined as ⩾2 point increase on the National Institutes of Health Stroke Scale (NIHSS) or ⩾1 point decrease on Glasgow coma scale (or death), from baseline to 24 hrs and 24-72 hrs, respectively. Multivariable logistic regression models were used to determine independent predictors of END and DND and their associations with 90-day outcomes (dichotomous scores on the modified Rankin scale of 2-6 vs 0-1 and 3-6 vs 0-2, and death).
Results: Of 4496 patients, 871 (19.4%) and 302 (8.4%) patients experienced END and DND, respectively. Higher baseline NIHSS score, older age, large artery atheroma occlusion, cardioembolic stroke, and any ICH within 24 hrs, were independent predictors for both END (all P ⩽0.01) and DND (all P ⩽0.03). Moreover, higher baseline systolic blood pressure (BP), higher diastolic BP variability within 24 hrs, and patients from Asia, were the only independent predictors for END (all P ⩽0.03). Asian ethnicity was negatively associated with DND (P=0.004). END and DND were all associated with a poor functional outcome at 90 days (all P<0.001).
Conclusions: There are overlapping demographic and clinical predictors of END and DND post-thrombolysis for acute ischemic stroke. Both END and DND predict unfavorable outcomes at 90 days.
Disclosures of Interest: No
Abstract N°: 660
COMPARISON OF THE EFFECTIVENESS AND SAFETY OF BRIDGING REPERFUSION THERAPY BETWEEN POSTERIOR AND ANTERIOR CIRCULATION STROKE
1Soonchunhyang University Seoul Hospital, Neurology, Seoul, South Korea, 2Uijeongbu Eulji Medical Center, Neurology, Euijeongbu, South Korea, 3Seoul Medical Center, Neurology, Seoul, South Korea, 4Inje University Ilsan Paik Hospital, Goyang, South Korea, 5Nowon Eulji Medical Center, Neurology, Seoul, South Korea, 6Dong-A University Hospital, Neurology, Busan, South Korea, 7Daejeon Eulji University Medical Center, Neurology, Daejeon, South Korea, 8Korea University College of Medicine, Seoul, Biostatistics, Seoul, South Korea, 9Seoul National University Bundang Hospital, Neurology and Cerebrovascular Center, Seongnam, South Korea
On behalf of: Clinical Research Collaboration for Stroke in Korea (CRCS-K) Investigators
Background and aims: Combination of intravenous thrombolysis and endovascular thrombectomy (bridging therapy, BT) is recommended in hyperacute ischemic stroke. However, there are still concerns about bleeding risk for posterior circulation stroke (PCS). This study aims to compare the effectiveness and safety of BT between anterior circulation stroke (ACS) and PCS.
Methods: A total of 3,067 patients treated with BT between January 2011 to November 2021 in multicenter stroke registry database were enrolled. Clinical characteristics, time to treatment and stroke severity were compared between ACS and PCS. Early neurological deterioration (END), functional outcome and mortality were prospectively captured from hospitalization to 1 year.
Results: The patients received BT included 2,817 ACS (85.3%) and 419 PCS (13.7%). The median of National Institute of Stroke Scale was 15 in PCS and 14 in ACS (P=0.014). Door-to-needle time (38 min VS 33 min, P=0.01) and door-to-puncture time (104 min VS 100 min, P=0.02) were delayed in PCS. Stroke progression was more in PCS (16.9% VS 12.0%, P<0.001) while symptomatic intracranial hemorrhage was less in PSC (2.2% VS 5.0%, P=0.004). In-hospital mortality was higher in PCS (9.8% VS 6.0%, P=0.001) which may be mediated by increased C-reactive protein. Poststroke functional independence was not different in ACS and PCS at discharge, 3 months, and 1 year.
Conclusions: Although BT in PCS was provided in patients with severe stroke and later time compared to ACS, it was associated with more stroke progression but lesser symptomatic intracranial hemorrhage. These results suggest that intravenous thrombolysis should be actively considered before endovascular thrombectomy in PCS.
Disclosures of Interest: No
Abstract N°: 1055
THE HEALTH EQUITY IMPACT OF ALTEPLASE FOR ACUTE ISCHEMIC STROKE IN THE UNITED STATES: A DISTRIBUTIONAL COST-EFFECTIVENESS ANALYSIS
Thomas Majda1, Elizabeth Mearns*1, Barbara Purdon1, Stacey Kowal1
1Genentech, South San Francisco, United States
On behalf of:
Background and aims: We performed a distributional cost-effectiveness analysis (DCEA) to evaluate how the use of alteplase for acute ischemic stroke (AIS) impacts health equity in the US.
Methods: Using a published CEA, a DCEA was built from a US payer perspective. The US population was divided into 25 equity-relevant subgroups based on race/ethnicity and county-level social vulnerability index. Inputs for AIS outcomes, AIS incidence, and receipt of alteplase were varied across subgroups based on published estimates.
Results: Alteplase treatment results in larger relative health gains in more vulnerable subgroups due to the increased AIS incidence and lower receipt of alteplase. Alteplase utilization improves social welfare by improving both population health (45,606 QALYs gained) and reducing existing overall US inequities annually. Health benefits are driven by cost savings from reduced disability post hospital discharge. Additionally, equity benefits are driven by the higher risk of AIS in more vulnerable patients who experience larger relative health gains given their lower baseline length and quality of life. Conclusions were robust across all sensitivity analyses. Further, health system scenarios that reduced care gaps (e.g. reduced time to treatment) led to additional gains in population health and reductions in existing inequalities.
Conclusions: Under current treatment patterns, this DCEA demonstrated that use of alteplase for AIS increases population health while also improving health equity. Given the disproportionate burden of AIS in more vulnerable population subgroups, it is critical to address care gaps to lead to more equitable thrombolytic access across race, ethnicity, and geography.
Disclosures of Interest: Yes All authors disclose employment at GNE and stock with Roche
Abstract N°: 1204
GOLDEN HOUR THROMBOLYSIS FOR ACUTE ISCHEMIC STROKE: A SYSTEMATIC REVIEW AND META-ANALYSIS
Fahad S. Alajlan1, Ahmed Alkhiri2, Aser F. Alamri3, Basil A. Alghamdi2, Ahmed A. Almaghrabi2, Abdullah R. Alharbi4, Nayef Alansari2, Ahmed Z. Almelibary2, Jeffrey L. Saver5, Adel Alhazzani1
1King Faisal Specialist Hospital and Research Centre, Neuroscience Center, Riyadh, Saudi Arabia, 2King Saud Bin Abdulaziz University for Health Sciences, College of Medicine, Jeddah, Saudi Arabia, 3King Saud Bin Abdulaziz University for Health Sciences, College of Medicine, Riyadh, Saudi Arabia, 4King Abdullah Medical City, Department of Neurology, Makkah, Saudi Arabia, 5David Geffen School of Medicine, UCLA, Department of Neurology, Los Angeles, United States
On behalf of:
Background and aims: The benefits of intravenous thrombolysis are time-dependent, with maximum efficacy when administered within the first “golden” hour after onset. Nevertheless, the impact of golden hour thrombolysis has not been well quantified.
Methods: Medline, Embase, and Web of Science databases were systematically searched from inception to August 27, 2023. We included studies reported on the safety and efficacy outcomes of golden hour thrombolysis vs later treatment window in patients with acute ischemic stroke. The primary outcome was an excellent functional outcome, defined as a modified Rankin scale (mRS) of 0-1 at 90 days. Secondary efficacy outcomes were a good functional outcome (defined as mRS of 0-2) and complete recanalization. The main safety outcome was symptomatic intracerebral haemorrhage (sICH).
Results: Seven studies involving 78,826 patients met the selection criteria. Golden hour thrombolysis was associated with higher odds of 90-days excellent functional outcomes (OR, 1.40 [95% CI, 1.16-1.67]), 90-days good functional outcomes (OR, 1.42 [95% CI, 1.24-1.62]) and complete recanalization (OR, 3.05 [95% CI, 1.48-6.31]) compared to thrombolysis outside the golden hour. The number needed to treat to benefit for golden hour thrombolysis to reduce disability by at least one level on the mRS per patient was 2.6. Rates of sICH and mortality were similar between groups.
Conclusions: Golden hour thrombolysis significantly improved acute ischemic stroke outcomes. The findings provide a rationale for intensive efforts aimed at expediting thrombolytic therapy within the golden hour window following the onset of acute ischemic stroke.
Disclosures of Interest: No
Abstract N°: 2412
IN VITRO COMPARATIVE ANALYSIS OF RT-PA VS TIROFIBAN EFFECTS ON HUMAN BLOOD CLOTS
Judith Cendrero*1,2, Miguel Serôdio3, Riccardo Tiberi2, Jia Hui LI2, Olga Miñarro1, Mariona Sangenis1, Angel Guillermo Arevalo1, Jorge Pagola1, Juega Jesús1, Marc Ribo1
1Vall d'Hebron University Hospital, Stroke Unit, Barcelona, Spain, 2VHIR - Vall d'Hebron Institut de Recerca, Barcelona, Spain, 3Centro Hospitalar Lisboa Ocidental, Department of Neurology, Lisbon, Portugal
On behalf of:
Background and aims: Complete recanalization after endovascular treatment (EVT) in stroke is linked to better clinical outcomes. Intraarterial thrombolytic such as Alteplase (rt-PA) or antiplatelet such as Tirofiban during EVT might enhance recanalization rates. We aimed to compare the in vitro effect of these drugs on clots retrieved during EVT.
Methods: For each patient, the retrieved clot was divided into two fragments and blood samples were obtained: plasma was separated and mixed with 5 mL of drug (Tirofiban or rt-PA) and 5 mL of physiological saline. Each clot fragment was embolized in a 3D printed arterial model connected to a flow pump creating a closed circuit where the study solution was circulated for 5 minutes. Clots where weighted before and after experiments.
Results: From May to December 2023, 41 thrombus (82 experiments) were tested. In the overall analysis, the median weight reduction was: rt-PA 18.10% vs. Tirofiban 21.71% (p=0.086). According to stroke etiology, the median weight reduction was, cardioembolic: rt-PA 19.72% vs. Tirofiban 21.30% (p=0.454), non-cardioembolic: rt-PA 16.67% vs. Tirofiban 22.98% (p=0.10). According to initial stroke occlusion, the median weight reduction was, TICA: rt-PA 20.84% VS Tirofiban 29.71% (p=0.06), M1-MCA: 15.38% VS Tirofiban 20.00% (p=0.053).
Conclusions: In our experimental setting, we observed a trend towards higher lytic effect of Tirofiban as compared to rt-PA on retrieved clots from patients undergoing EVT. Experiments are ongoing and additional results, including the effect of the Tirofiban/tPA combination, will be presented at ESOC24.
Disclosures of Interest: No
Abstract N°: 453
24-HOUR NIHSS POST-THROMBOLYSIS AS A STRONGER PREDICTOR OF FUNCTIONAL RECOVERY IN ACUTE ISCHEMIC STROKE: THE ENCHANTED STUDY
1The Second Affiliated Hospital of Soochow University, Neurology, Suzhou, China, 2West China Hospital, Sichuan University, Neurology, chengdu, China, 3The George Institute for Global Health, Faculty of Medicine, University of New South Wales, Sydney, Australia, 4Fukuoka University, Preventive Medicine and Public Health, Fukuoka, Japan, 5Suzhou TCM Hospital Affiliated to Nanjing University of Chinese Medicine, Neurology, Suzhou, China
On behalf of: ENCHANTED Investigators
Background and aims: To compare predictive ability of National Institutes of Health Stroke Scale (NHISS) measurements at baseline, 24 hours, and changes from baseline to 24 hours, on functional recovery from acute ischemic stroke in the ENCHANTED (Enhanced Control of Hypertension and Thrombolysis Stroke Study) dataset (NCT01422616).
Methods: Absolute (baseline minus 24 hours) and percentage (absolute change/baseline x 100) changes in NIHSS scores were calculated. Receiver operating characteristics curve analyses assessed performance of different NIHSS measurements on 90-day favorable functional recovery (modified Rankin Scale [mRS] 0-2) and excellent recovery (mRS 0-1). Youden index used to identify optimal predictor cut-off points.
Results: There were 4410 patients in ENCHANTED. 24-hour NIHSS had the highest discriminative ability for predicting favorable 90-days functional recovery (mRS 0-2) (AUC 0.846 vs 0.739, 0.680, 0.753; P <0.001) than baseline, absolute and percentage change of NIHSS, respectively. The optimal cut-off point of 24 hour NIHSS for predicting favorable functional recovery was ⩽4 (sensitivity 66.45%, specificity 87.13%, adjusted odds ratio 9.44; 95% confidence interval 7.77-11.48). 24-hour NIHSS (⩽3) was the best predictor of 90-day excellent functional recovery (mRS 0-1). Findings were consistent across subgroups, including sex, race and age.
Conclusions: In thrombolysis-eligible acute ischemic stroke patients, 24-hour NIHSS score (optimal cut-point of 4) is the strongest predictor on 90-day functional recovery over baseline and early change of NIHSS.
Disclosures of Interest: No
Abstract N°: 1896
CT-PERFUSION IS BENEFICIAL FOR THE PREDICTION OF HEMORRHAGIC TRANSFORMATION AFTER THROMBOLYSIS
Aviva Alpernas*1, Hen Hallevi1, Udi Sadeh2, Tali Jonas Kimchi2, Einor Ben Assayag1, Issa Metanis3, Ronen R Leker3, Jeremy Molad1
1Tel Aviv Sourasky Medical Center - Ichilov, Neurology - Stroke, Tel Aviv-Yafo, Israel, 2Tel Aviv Sourasky Medical Center - Ichilov, Invasive Neuroradiology, Tel Aviv-Yafo, Israel, 3Hadassah Ein Kerem Hospital, Neurology, Jerusalem, Israel
On behalf of:
Background and aims: CT-perfusion is the most widely used method for the prediction of salvageable tissue and treatment selection in acute ischemic stroke. Most studies have discussed CTP role in the setting of endovascular thrombectomy. However, CTP ability to predict hemorrhagic transformation (HT) after thrombolysis was not assess to date. We aim to examine the inter-relation between CTP parameters, HT and outcome among patients treated with thrombolysis solely.
Methods: The study included ischemic stroke patients treated with thrombolysis only from two comprehensive stroke centers. All patients underwent CTP on admission, and follow-up CT 24-hours post-thrombolysis. CTP parameters including core and penumbra volumes were analyzed. We examined CTP parameters association to HT and prognosis.
Results: 482 patients were included, of whom 427 (88.6%) had adequate CTP acquisition (core volume 6.3±15.1. penumbra volume 29.5±41.0). Poor CTP acquisition was associated with worse premorbid mRS, atrial fibrillation, lower rates of favorable outcome and higher rates of mortality. CTP core presence and volume, but not penumbra volume was associated with the presence and the degree of HT (p<0.001, p=0.008). CTP core and penumbra presence and volumes were associated with the rates of worse outcome (p<0.001, P=0.001). After multivariate analysis, CTP core presence remained significantly associated with HT, worse outcome and mortality (p=0.02, p= 0.025, p=0.008, respectively).
Conclusions: CTP core presence, but not penumbra, is associated with the rates of HT, worse outcome and mortality among acute stroke patients treated with thrombolysis solely. Further larger studies are needed to examine CTP parameters role in patient selection for thrombolysis.
Disclosures of Interest: No
Abstract N°: 2057
THE RED BLOOD CELL: A DETERMINANT OF THROMBUS FIBRIN CONTENT AND FIBRINOLYTIC ACTIVITY – A PROTEOMIC STUDY OF CEREBRAL THROMBI
1AP-HM, La Timone, Stroke Unit, Marseille, France, 2C2VN, Marseille, 3TIRO-MATOS, Nice, 4AP-HM, La Timone, Radiology Department, Marseille, France
On behalf of:
Background and aims: Cerebral thrombus composition determines fibrinolytic activity. Because histological techniques only partially analyze thrombi leading to contradictory data, we carried out proteomic analyses of whole thrombi in order to establish the determinants of fibrin content and fibrinolytic activity.
Methods: In Retro-MATISSE Study, the proteome of 104 thrombi extracted by mechanical thrombectomy (±rt-PA: 47/104) was established by mass spectrometry coupled to liquid chromatography. Proteins detected in 90% of samples and specific to a thrombus component were selected. Thrombus fibrinolytic activity was estimated outside (FA-out: D-Dimers level in thrombus rinsing fluid) and inside (FA-in: fibrinogen α degradation ratio). The clinico-biological determinants of fibrin content and fibrinolytic activity were determined by linear regression adjusted for the use of IV rt-PA.
Results: Fibrin level in thrombi was significantly negatively correlated with erythrocyte-specific proteins, admission blood hematocrit and hemoglobin. FA-out (p<0.0001) and FA-in (p=0.0147) were conditioned by rt-PA administration, admission glycemia and thrombus composition. Indeed, fibrin-rich thrombi showed greater FA-out than erythrocytes-rich thrombi, explained by more (r)t-PA substrates. Thus, cardioembolic thrombi (72/104), richer in fibrin, showed greater FA-out (p=0.030). Inside the thrombus, opposite results were found, reflecting a penetrability of (r)t-PA hampered by the density of the fibrinous cap. In a sub-group of comparable patients (n=82), only FA-out was significantly associated with reduction of thrombus weight, higher recanalization rate and better clinical outcome.
Conclusions: Although less studied than other components, erythrocytes seem to condition the density of the thrombus fibrinous cap and consequently fibrinolytic activity and clinical response. The search for new fibrinolytic strategies must consider this neglected actor.
Disclosures of Interest: No
Abstract N°: 2099
IMPACT OF PRIOR ANTIPLATELET THERAPY ON POST-THROMBOLYTIC OUTCOMES IN AIS PATIENTS: A SYSTEMATIC REVIEW AND META-ANALYSIS OF 120,427 PATIENTS
Ahmed Naeem*1, Hesham Kelani2, Abdelrhman M. Abdelwahab3, Omar Abdelnasser A. Mohamed4, Mostafa Mahmoud Naguib5, Salem Elshenawy3, Rowan H. Elhalag3, Hazem Mohamed Salamah6, Abdelrahman Mahmoud7, Omar Elsayed Rageh8
1Al-Azhar University, Faculty of Medicine, Asyut, Egypt, 2SUNY Downstate at OBH, Neurology Department, 3Alexandria University, Faculty of Medicine, 4Ain Shams University, Faculty of Medicine, 5Al-Azhar University, 6Zagazig Faculty of Medicine, 7Minia University, 8Tanta University
On behalf of:
Background and aims: Due to conflicting data on the impact of antiplatelet pretreatment (AP) on the safety and effectiveness of intravenous thrombolysis (IVT) for acute ischemic stroke (AIS), we conducted a comprehensive systematic review and meta-analysis to explore the relationship between AP and outcomes in AIS patients treated with intravenous alteplase.
Methods: We performed a systematic query in PubMed, Scopus, WOS, and the Cochrane Library from inception to November 14, 2023. Data were extracted from 31 articles for comparison and synthesis using the R language.
Results: We included 31 studies involving 120,427 patients in our meta-analysis. Prior AP therapy was associated with increased odds of symptomatic intracranial hemorrhage (OR, 1.42; 95%CI [1.35, 1.50]; p<0.01), intracranial hemorrhage (OR, 1.54; 95%CI [1.18, 2.01]; p<0.01), and mortality (OR, 1.34; 95%CI [1.17, 1.53]; p<0.01).
However, we found no statistically significant differences regarding successful recanalization (OR, 0.84; 95%CI [0.37, 1.91]; p=0.68), excellent functional outcome [modified Rankin Scale 0-1] (OR, 0.97; 95%CI [0.80, 1.17]; p=0.75), good functional outcome [modified Rankin Scale 0-2] (OR, 0.91; 95%CI [0.67, 1.25]; p=0.57), and poor functional outcome [modified Rankin Scale 3-6] (OR, 1.42; 95%CI [0.53, 3.76]; p=0.48).
Conclusions: Our findings suggest that while antiplatelet pretreatment may be associated with certain adverse events, its influence on the overall functional outcomes of patients with AIS receiving intravenous alteplase remains inconclusive. Therefore, further studies are warranted.
Disclosures of Interest: No
Abstract N°: 2777
RATES OF THROMBOLYSIS IN ATRIAL FIBRILLATION ASSOCIATED STROKE DISEASE
Thomas Cloney*1, Joan Mccormack2, Olga Brych2, Ronan Collins2,3, Tim Cassidy2,4, Joseph Harbison1,2,5
1St James' Hospital, Neurovascular Department, Dublin, Ireland, 2National Office of Clinical Audit, Irish National Audit of Stroke, Dublin, Ireland, 3Tallaght University Hospital, Medicine for Older Persons & Neurovascular Department, Dublin, Ireland, 4St Vincent's Hospital, Stroke, Dublin, Ireland, 5Trinity College Dublin, Associate Professor Medical Gerontology, Dublin, Ireland
On behalf of:
Background and aims: The rate of anticoagulation for Atrial Fibrillation (AF) in Ireland has doubled since the introduction of the Direct Oral Anticoagulants (DOACs. Breakthrough strokes occur on DOACs, but thrombolysis is currently contraindicated. We examined rates of thrombolysis in AF associated strokes in relation to different anticoagulation statuses.
Methods: Data on subjects from the Irish National Audit of Stroke admitted 2017-2022 with Ischaemic stroke (ICD10: i63) and AF detected during admission were analysed. Data for patients with previously undetected AF (undetected) was compared with that of patients with previously detected and anticoagulated AF (treated) and detected but not anticoagulated AF (untreated).
Results: Results on 5920 patients analysed are tabulated below. Patients with previously undetected AF were younger (Treated: Chi sq 106.9, p=0.0001) (Untreated: Chi SQ 12.9, p=0.0003). There were proportionally more males in the treated group (Chi Sq 9.3, p=0.002). There was a higher proportion thrombolysed in the undetected group than in the untreated group (16.6% vs. 13.0%. Chi Sq 4.4, p=0.03) and a dramatically lower rate in the treated group (3.2% Chi Sq 268.6 p<0.0001). The thrombolysis rate was significantly lower in those taking DOACs than Warfarin (2.4% vs. 7.1%. Chi Sq 26.9 p<0.0001).
Conclusions: Existing DOAC therapy in AF associated stroke patients is associated with a significantly lower rate of thrombolysis even than for patients receiving Warfarin.
Disclosures of Interest: No
Abstract N°: 517
INFLUENCE OF CEREBRAL MICROBLEEDS ON HEMORRHAGIC TRANSFORMATION AFTER SUCCESSFUL THROMBECTOMY WITH ACUTE ISCHEMIC STROKE FROM LAO
Seung Young Chung*1, Jae Guk Kim2, Soo Joo Lee2
1Daejeon Eulji Medical Center, Eulji University School of Medicine, Department of Neurosuregery, Daejeon, South Korea, 2Daejeon Eulji Medical Center, Eulji University School of Medicine, Department of Neurology, Daejeon, South Korea
On behalf of:
Background and aims: This prospective cohort study aimed to investigate the relationship between the presence and burden of CMBs and the occurrence of hemorrhagic transformation (HT) following successful thrombectomy with acute ischemic stroke from LVO.
Methods: A total of 132 patients with acute ischemic stroke with successful recanalization by thrombectomy for emergent LVO, were enrolled in this study. CMBs and HT assessed using T2-MRI with a validated scale. The primary outcome measure was the occurrence of HT following thrombectomy. We examined the association between the presence and burden of CMBs and HT. The secondary outcome was defined as a poor functional outcome, with mRS ranging from 3 to 6, assessed at 3 months after stroke onset.
Results: Among 132 patients (mean age 66.9±14.0 years, 68.9% male), 24 (18.2%) exhibited CMBs, and 59 (44.7%) developed HT. A total of 47 (49.2%) experienced a poor functional outcome, and the mortality rate was 11.3%. Statistical analysis revealed a significant association between the presence of CMBs and the occurrence of HT after successful thrombectomy (77.8% vs. 38.9%; P=0.002). Moreover, the presence of CMBs was significantly correlated with a higher likelihood of a poor functional outcome (77.8% vs. 42.9%; P=0.007) after adjustment of initial stroke severity and diffusion lesion volume. However, there was no observed association between the presence of CMBs and mortality (16.7% vs. 8.25%; P=0.426).
Conclusions: The presence of CMBs is significantly associated with the occurrence of HT and a poor functional outcome following successful thrombectomy. However, it does not appear to impact mortality rates in these patients.
Disclosures of Interest: No
Abstract N°: 1256
COMPARISON OF OUTCOMES IN THE EXTENDED VERSUS EARLY TIME WINDOW AFTER INTRAVENOUS THROMBOLYSIS AND MECHANICAL THROMBECTOMY
Laura Mannismäki*1, Nicolas Martinez-Majander1, Olli Suomalainen1, Gerli Sibolt1, Maria Girfanova1, Miranda Nybondas1, Hanna Nissinen1, Sami Curtze1
1Helsinki University Hospital and Clinical Neurosciences, University of Helsinki, Neurology, Helsinki, Finland
On behalf of:
Background and aims: Recent trials have not proven non-inferiority of mechanical thrombectomy (MT) compared to intravenous thrombolysis (IVT) plus MT, in eligible patients, in the early time window (TW), 0 to 4.5 hours from last seen well (LSW). Whether this also concerns the extended TW, 4.5 to 9 hours from LSW, is yet unclear. We compared the functional and safety outcomes with matched controls in the extended versus early TW in real-life retrospective data.
Methods: All patients (n=134) treated with IVT, MT, or IVT plus MT in the extended TW between 1/2021 and 12/2022 were matched with controls, treated in the early TW, between 1/2016 and 12/2020, at Helsinki University Hospital. Logistic regression was applied on functional outcome at three months, evaluated on Modified Rankin Scale (mRS) and if possible, on the incidence of symptomatic intracerebral hemorrhage (sICH) by European Cooperative Acute Stroke Study -II criteria.
Results: Functional outcomes did not significantly differ between the extended versus early TW in patients with IVT, MT, or IVT plus MT; in patients with IVT plus MT, the adjusted odds ratio (aOR) for a favorable outcome shift was 1.15 (95% CI 0.54-2.4, p=0.71), respectively. In the extended versus early TW, aOR for sICH was 1.04, 95% CI 0.15-7.4, p=0.97.
Conclusions: No significant difference was detected in the functional or safety outcomes in patients treated with IVT plus MT in the extended versus early TW. This might support our current clinical treatment guidelines not to omit IVT in the extended TW for eligible patients.
Disclosures of Interest: No
Abstract N°: 1399
INTRAVENOUS THROMBOLYSIS IN ACUTE ISCHEMIC MINOR STROKE: A DANISH NATION-WIDE COHORT STUDY
Daniel Harsfort*1,2, Jakob Nebeling Hedegaard2, Søren Paaske Johnsen2, Boris Modrau1,2
1Aalborg University Hospital, Department of Neurology, Aalborg, Denmark, 2Aalborg University, Department of Clinical Medicine, Aalborg, Denmark
On behalf of:
Background and aims: In patients with minor stroke, intravenous (i.v.) thrombolysis is recommended only for those with disabling symptoms. However, there is no standardised definition, and the decision to treat relies on the subjective judgement of each investigator. This study aims to assess the effect of thrombolysis in minor stroke using real world data.
Methods: Danish nation-wide register-based cohort study on minor stroke patients defined as Scandinavian Stroke Scale (SSS) ⩾45 from 2011-2021. Vascular risk factors, demographic data, and clinical characteristics were adjusted for using inverse probability of treatment weighting. Patients were categorised as having mild strokes (SSS 45-49) and very mild strokes (SSS 50-58) in order to pragmatically distinguish between disabling and non-disabling symptoms. Return-to-work, use of homecare, typical stroke complications, recurrent stroke, and mortality were compared in patients treated with and without thrombolysis.
Results: A total of 31,007 patients were included. Of these, 1,910 patients with mild strokes and 4,052 patients with very mild strokes received thrombolysis. In patients with mild strokes, thrombolysis was associated with higher chance of return-to-work (adjusted hazard ratio 1.33 (1.07-1.64)), lower risk of pneumonia (adjusted relative risk (aRR) 0.40 (0.25-0.62)), and lower mortality (aRRs 0.58 (0.34-0.97), 0.50 (0.35-0.72), and 0.50 (0.40-0.64) at 30, 90, and 365 days, respectively). In patients with very mild strokes, thrombolysis was not associated with improved outcomes, except lower mortality at 365 days (aRR 0.78 (0.65-0.94)).
Conclusions: I.v. thrombolysis was more often associated with better outcomes in patients with mild strokes than in patients with very mild strokes.
Disclosures of Interest: No
Abstract N°: 1833
ESTIMATED RECANALIZATION TIME PREDICTED THE BENEFIT OF INTRAVENOUS THROMBOLYSIS WITH TENECTEPLASE
Lan Hong*1, Chushuang Chen2, Andrew Bivard3, /Christopher Levi/4, Yifeng Ling1, Lumeng Yang1, Mark Parsons5, Qiang Dong1, Xin Cheng1, Longting Lin1
1Huashan Hospital, Fudan University, Department of Neurology, Shanghai, China, 2Faculty of Health, University of Newcastle, Newcastle, Australia, 3Melbourne Brain Centre, Royal Melbourne Hospital, University of Melbourne, Melbourne, Australia, 4John Hunter Hospital, Newcastle, Australia, 5South Western Sydney Clinical School, University of New South Wales, Sydney, Australia
On behalf of: INSPIRE study group
Background and aims: The aim of this study was to describe the recanalization process after tenecteplase treatment, and to explore an appropriate time-point of recanalization assessment.
Methods: Eligible patients from an international registry study were included. Patients were grouped according to time of recanalization from thrombolysis estimated by core growth rate (early: within 1 hour; delayed: 1-6 hours; late: 6-24 hours). The association between recanalization time, accumulative recanalization, futile recanalization and 3-month good clinical outcome (modified Rankin Scale 0-2) was explored using logistic regression models. The area under the receiver operating characteristic curve (ROC-AUC) analysis was performed to explore an appropriate time-point of recanalization assessment to predict clinical outcome.
Results: A number of 87 tenecteplase-treated patients were included. The odds of accumulative recanalization and the risk of futile recanalization increased with recanalization time (Accumulative recanalization: OR=1.03, P=0.02, per hour; Futile recanalization: Delayed vs. early: OR=25.2, P=0.01; Late vs. early: OR=70.0, P=0.001). Recanalization within 6 hours after treatment was associated with a better 3-month clinical outcome compared with non-recanalization (Early: OR=24.5, P<0.001; delayed: OR=14.2, P=0.046), while late recanalization was associated with an increased risk of bleeding (OR=16.6, P=0.02). Recanalization estimated within 6 hours after treatment demonstrated the highest AUC to predict clinical outcome (ROC-AUC=0.73).
Conclusions: The odds of accumulative recanalization as well as the risk of futile recanalization increased with time from tenecteplase treatment. Six hours after treatment could be an appropriate time-point to assess recanalization to predict clinical outcomes, therefore, serving as an ideal substitute endpoint for relevant clinical trials.
Disclosures of Interest: No
Abstract N°: 2493
MODELLING DISABILITY-LEVEL AND UTILITY OUTCOMES DEPENDING ON TIME TO THROMBOLYSIS AND MECHANICAL THROMBECTOMY
Anna Laws1, Michael Allen1, Kerry Pearn1, Martin James*2
1University of Exeter, 2Royal Devon University Healthcare NHS Foundation Trust
On behalf of:
Background and aims: Hyper-acute stroke care requires the national coverage of thrombolysis (IVT) and thrombectomy (MT). In the UK, IVT is provided in all emergency stroke units, but MT is provided in fewer regional centres often requiring secondary transfer. Patients may gain more rapid access to IVT by using local IVT-only units, but at the expense of delayed access to MT. Optimal configuration of stroke services, comparison between 'drip-and-ship' and 'mothership' configurations and the population benefit from bypass models of pre-hospital care could be guided by a model that predicts outcomes based on times to IVT and MT.
Methods: We have synthesized clinical trial and five-year national stroke registry data to develop a disability-level outcome model and extended it to include utilities of resulting health states, that may be applied to analysis of organization of stroke services, and applied it to England and Wales.
Results: We have produced a mathematical model of stroke outcome (available at https://samuel-book.github.io/stroke_outcome/), and have made this available to other healthcare systems as a Python package (see https://pypi.org/project/stroke-outcome/). Illustrative output of the disability and utility benefits from differing access to IVT and MT are in figure 1.
Conclusions: A disability-level model of stroke outcome, with resultant utility values, based on times to IVT and/or MT has been developed, and made freely available. This has potential to guide the configuration of hyper-acute stroke care, particularly in systems like the UK with limited access to centres offering MT for which most patients require secondary transfer.
Disclosures of Interest: No
Abstract N°: 2916
REAL-WORLD DATA OF TIME EFFICIENCY OF TNK VS. ALT IN PATIENTS UNDERGOING THROMBOLYSIS OR COMBINED STROKE THERAPY IN THE NORTH REGION OF PORTUGAL
Daniel Oliveira Ferreira*1,2, Sofia Marques3, Luís Fontão4, José Roriz4, Carla Ferreira3, Pedro Castro1,2
1Unidade Local Saúde São João, Porto, Portugal, Serviço de Neurologia, 2Faculdade de Medicina da Universidade do Porto, Porto, Portugal, Departamento de Neurociências Clínicas e Saúde Mental, 3Unidade Local Saúde de Braga, Braga, Portugal, Serviço de Neurologia, 4Unidade Local Saúde de Entre o Douro e Vouga, Santa Maria da Feira, Portugal, Serviço de Neurologia
On behalf of:
Background and aims: Shorter times between stroke onset and reperfusion are associated with improved functional outcome. Tenecteplase (TNK) has a higher fibrin specificity and longer half-life than alteplase (ALT), permitting the convenience of single-bolus administration. We aimed to evaluate the real-world data of time efficiency in stroke protocol procedures between patients undergoing thrombolysis (IVT) or combined stroke therapy, in the same or different hospital centers.
Methods: Retrospective analysis of a multicenter cohort study from 3 centers in the north region of Portugal of patients who received IVT from 01/01/2020 to 31/08/2021. Primary outcomes were the time intervals between stroke protocol interventions and adjustment for distances between hospital centers was calculated.
Results: 520 patients (TNK: 146; ALT: 374) were included, with 247 presenting primary indication for endovascular treatment (EVT; TNK: 65; ALT: 182). The Door-to-Needle (DTN) time was inferior in the TNK group (ALT: 46 ± 36 vs. TNK: 38 ± 24 minutes; p=0.001). This result was also observed in the group with primary indication for EVT (DTN: ALT 45 ± 36 vs. TNK 37 ± 24 minutes; p=0.011), where a significant difference was present in the needle-to-groin time only in patients undergoing EVT at the same hospital (ALT: 70 ± 134 vs. 48 ± 54 minutes, p=0.016; unadjusted beta -0,127 [95% CI: -0,495 to -0,004], p=0.047).
Conclusions: Our study provides real-world data supporting that TNK is associated with faster timelines in stroke. These advantages might extend to patients undergoing combined therapy, particularly, in those without the need of interhospital transport.
Disclosures of Interest: No
Abstract N°: 3222
REAL-WORLD DATA OF SAFETY AND EFFECTIVENESS OF TENECTEPLASE VERSUS ALTEPLASE IN STROKE PATIENTS TREATED IN THE NORTH OF PORTUGAL
Sofia Marques*1, Luís Rufo Costa2, Daniel Oliveira Ferreira3, Luís Fontão4, José Mario Coutinho Roriz4, Jose Nuno Alves1, Pedro Castro3, Carla Ferreira1
1Braga Public Hospital, Serviço de Neurologia, Braga, Portugal, 2ULSAM - Hospital de Santa Luzia, Viana do Castelo, Viana do Castelo, Portugal, 3Hospital de São João, Viana do Castelo, Porto, Portugal, 4Centro Hospitalar de Entre Douro e Vouga (CHEDV), Viana do Castelo, Santa Maria da Feira, Portugal
On behalf of:
Background and aims: A number of randomized controlled trials have demonstrated its safety and when comparing the effectiveness of both thrombolytics, TNK has invariably been considered non-inferior to ALT. The aim of this study is to assess the outcome of TNK compared with ALT in a real-world setting in a region of the north of Portugal.
Methods: We conducted a multicenter observational retrospective study on patients with acute ischemic stroke (AIS) who received intravenous thrombolysis (IVT) between August 1st 2019 and August 31st 2021. Primary outcomes were the occurrence of symptomatic intracranial hemorrhage (sICH), defined as any ICH causing an increase in NIHSS⩾4, and functional outcome at 3 months, assessed using the mRS score.
Results: Were included in the study 520 patients, 374 (71.9%) treated with alteplase and the remaining 146 (28.1%) with tenecteplase; 247 (47.5%) patients were also candidates to mechanical thrombectomy (ALT: 182, TNK: 65). In respect of sICH, no significant difference was noted between groups (ALT: 16, TNK: 10, p=0.218). Median ASPECTS 24 hours after treatment was lower in the alteplase group [ALT: 8 (4), TNK: 9 (3), p=0.017]. Notwithstanding, no differences were noted in mRS⩽2 at 90 days (ALT: 172, TNK: 72, p=0.190).
Conclusions: Our study provides real-world evidence of comparable safety and efficacy between the two thrombolytics. These data, allied with the convenience of a single bolus injection, favor the use of tenecteplase in the management of ischemic stroke patients.
Disclosures of Interest: No
Abstract N°: 2208
SAFETY AND EFFICACY OF INTRAVENOUS THROMBOLYSIS BY INFARCT TYPE IN PATIENTS WITH NO VISIBLE OCCLUSION: ANALYSIS OF THE ACT TRIAL
Zohaib Siddiqi*1, Katrina Ignacio2, Chitapa Kaveeta2, Fouzi Bala3, Mohammed Almekhlafi2,4,5, Richard Swartz6, Bijoy K. Menon2,4,5, Nishita Singh1
1University of Manitoba, Division of Neurology, Rady Faculty of Medicine, Winnipeg, Canada, 2Cumming School of Medicine, University of Calgary, Department of Clinical Neurosciences, Calgary, 3Tours University Hospital, Department of Radiology, Tours, France, 4University of Calgary, Department of Community Health Sciences and O'Brien Institute for Public Health, Calgary, Canada, 5University of Calgary, Department of Radiology, Calgary, Canada, 6Hurvitz Brain Sciences Program, Sunnybrook Health Sciences Centre, Department of Medicine (Division of Neurology), Toronto, Canada
On behalf of:
Background and aims: Stroke patients with no visible occlusion(NVO) might be denied intravenous thrombolysis(IVT) for safety concerns. In this study we assessed safety and efficacy of IVT in patients with NVO by infarct type.
Methods: This is a post-hoc analysis of the AcT trial to assess the safety of IVT in subgroups of patients with NVO. NVO were divided based on 24h imaging (MRI/CT) into lacunar (single infarct, ⩽15mm, in subcortical region or pons), non-lacunar infarct, and no infarct groups. Outcomes included symptomatic intracerebral hemorrhage (SICH), any intracerebral hemorrhage on imaging at 24h, and modified Rankin Scale (mRS). Mixed-effects regression models adjusted for age, sex, stroke severity, thrombolytic type, and onset-to-needle time were used.
Results: 456 of 1577 patients (29.9%) had NVO and follow-up imaging (MRI: 41.2%). 93 (20.4%) had lacunar infarcts, 171 (37.5%) non-lacunar, and 192 (42.1%)(MRI:7.3%) no visible infarcts. Baseline characteristics were similar across groups. 66% of lacunar patients received tenecteplase vs 50% of non-lacunar and 45.7% of no visible infarct. SICH occurred in 4 patients (2.3%) in the non-lacunar infarct group but none in the lacunar infarct and no visible infarct groups. Any intracerebral hemorrhage was seen in 21 (12.4%) in the non-lacunar infarct group (MRI: 81.4%), compared to 4 (4.3%) in the lacunar (MRI:100%), and 2 (1.0%) in the no visible infarct (MRI: 0%) groups. Functional outcomes (Figure) including adjusted analyses were similar across groups. There was no significant interaction between thrombolytic type and outcomes.
Conclusions: In the AcT trial, IVT was safe across all infarct types in patients with NVO.
Disclosures of Interest: No
Abstract N°: 192
SAFETY AND FEASIBILITY OF INTRAVENOUS THROMBOLYSIS IN PATIENTS WITH CADASIL – A MULTICENTER STUDY
1NTUH (National Taiwan University Hospital), Neurology, Taiwan, 2National Cerebral and Cardiovascular Center, Division of Neurology, Suita, Japan, 3Taipei Veterans General Hospital, Taiwan
On behalf of:
Background and aims: Existing guidelines did not recommend the use of intravenous thrombolysis (IVT) in patients with CADASIL, due to unknown safety and efficacy profile. We described the results of IVT use in patients with CADASIL from a multicenter study in East Asia.
Methods: We included patients who had received IVT for acute ischemic stroke from three ongoing CADASIL registries in Taiwan and Japan. Clinical manifestations, imaging markers of cerebral small vessel diseases, and post-thrombolysis outcome were documented.
Results: From a total of 396 CADASIL patients, eight patients (2%) had ever received IVT. Six of them carried NOTCH3 R544C, one with R141C, and one with C1250R mutation. Genetic diagnosis preceded IVT in one case. For the stroke episodes, the median National Institutes of Health Stroke Scale was 6 (IQR 4-7), and onset-to-thrombolysis time was 160 min (95-170). On follow-up imaging, six had small subcortical infarcts, two had no visible new lesion (Figure 1). Most cases had moderate to severe white matter hyperintensity (Figure 2); the median number of lacunes was 2 (1-4) and cerebral microbleeds was 5 (4-7; maximum 23). No hemorrhagic transformation occurred post-IVT. The majority (88%) achieved an excellent outcome (modified Rankin Scale 0 or 1) at 3 months.
Conclusions: We demonstrated the safety of IVT use in patients with CADASIL, even in the presence of a high burden of cerebral small vessel disease. Given the rising discovery of NOTCH3 variants in stroke and general populations, our study provided vital insights in the field.
Disclosures of Interest: No
Abstract N°: 193
EFFICACY AND SAFETY OF NON-IMMUNOGENIC STAPHYLOKINASE FOR ISCHEMIC STROKE IN REAL-WORLD PRACTICE
Andrey Alasheev*1, Elena Lantsova2, Dmitriy Tretyakov3
1Sverdlovsk Regional Clinical Hospital #1, Stroke unit, 2Sciencefiles, 3Sverdlovsk Health Insurance Fund
On behalf of:
Background and aims: To compare the efficacy and safety of non-immunogenic staphylokinase and alteplase in patients with ischemic stroke in real-world practice.
Methods: The real-world data between 01 Jan 2021 and 31 Dec 2022 from the register of the Health Insurance Fund was analyzed. The proportion of patients with a favorable outcome, the degree of disability at baseline and discharge, the duration of hospitalization, the hospital mortality in the groups of non-immunogenic staphylokinase and alteplase were evaluated.
Results: The data of 1238 patients from 26 stroke units of Sverdlovsk region (Russia) were included. There were no statistically significant differences in the proportion of a favorable outcome between the groups of non-immunogenic staphylokinase and alteplase (26% and 25% respectively, p = 0,845). Mediana of duration of hospitalization in the non-immunogenic staphylokinase group was one day less, which is statistically significant compared to the alteplase group (9 [7;12] and 10 [7;13] respectively, p <0,001). There were no differences in the frequency of mortality (11% and 13% respectively, p = 0,331). The hospital, the year and month of hospitalization, the level of disability at the baseline have a statistically significant effect on the outcome of hospitalization. The choice of a thrombolytic drug did not have a statistically significant effect on the frequency of favorable outcome.
Conclusions: The comparable efficacy and safety of non-immunogenic staphylokinase and alteplase in ischemic stroke has been proven previously in clinical trial and confirmed now by real-world evidence.
Disclosures of Interest: No
Abstract N°: 2023
THROMBUS MIGRATION IN PATIENTS TREATED WITH TENECTEPLASE VERSUS ALTEPLASE PRIOR TO MECHANICAL THROMBECTOMY
Gabriel García-Alcántara1, Juan Luis Chico García1, Patricia Garay1, Beatriz Martínez García1, Consuelo Matute Lozano1, Sebastian García Madrona1, Alicia De Felipe1, Rocio Vera1, Jaime Masjuan1, ANTONIO CRUZ CULEBRAS*1
1Ramón y Cajal Hospital, Neurology, Madrid, Spain
On behalf of:
Background and aims: The aim of the study was to describe the rate of thrombus migration/recanalization from large vessel to distal segments in patients with acute ischemic stroke (AIS) who received intravenous thrombolysis (IVT) with tenecteplase (TNK) versus alteplase prior to mechanical thrombectomy (MT), as well as to determine if there is a relationship between thrombus migration and the patient's functional prognosis
Methods: We conducted a retrospective analysis of a series of consecutive patients treated at Ramón y Cajal University Hospital who presented with acute ischemic stroke with large vessel thrombus from November 2017 to April 2023 and were treated with IVT (TNK or alteplase divided into two different groups) and mechanical thrombectomy
Results: A total of 197 patients were included (96 received TNK and 101 received alteplase). Thrombus migration/recanalization was observed in baseline arteriography in 25 patients (26%) in the TNK group and in 13 patients (13%) in the alteplase group, with significant differences in the thrombus migration rate (OR=2.63, 95% confidence interval: 1.01; 6.82). Migration to a highly distal unrecoverable segment occurred in 4 patients (4%) with TNK and in 2 patients (2%) with alteplase, without significant differences (p>0.05). Thrombus migration was not significantly associated with a different functional prognosis (measured by the Rankin scale at 3 months).
Conclusions: The rate of thrombus migration after fibrinolysis was significantly higher with tenecteplase than with alteplase. We observed that the migration of thrombi to more distal segments, theoretically less accessible with MT, did not differ between both groups and was not significantly associated with a worse functional prognosis.
Disclosures of Interest: No
Abstract N°: 3228
CATHETER- BASED INTRACORPOREAL SHOCK WAVE THROMBOLYTIC THERAPY ACCOMPANIED BY INTRAVENOUS PLGA- BASED ENCAPSULATED TPA NANOPARTICLES ADMINISTRATION
Hossein Mehrad*1,2,3, Solmaz Tasdighi Matanagh2
1Islamic Azad University, Department of Physics, Tabriz, Iran, 2Mehrad Research Lab, Division of Translational Medicine Development of Noninvasive Treatments, Tabriz, Iran, 3Islamic Azad University, Laboratory of Novel Technologies in Non- Invasive Treatments, Tabriz, Iran
On behalf of:
Background and aims: A plaque may rupture with high risk of subsequent thrombus mediated acute clinical events such as myocardial infarction and stroke. The middle cerebral artery (MCA) is the most common artery involved in acute stroke.The aim of this study was to generate a rabbit model of thromboembolic occlusion and the subsequent investigating the feasibility of intracorporeal shock wave- mediated inertial cavitation thrombolytic therapy in combination with simultaneous, intravenous PLGA- based encapsulated tPA nanoparticles administration in this model
Methods: Briefly, New Zealand White rabbits were submitted to thromboembolic occlusion by injecting autologous blood clots through MCA artery. Then treatment group underwent catheter- based shock wave (15 Kv, F= 2 Hz, Impulses= 120)- mediated inertial cavitation thrombolytic therapy accompanied by simultaneous intravenous PLGA - based encapsulated tPA nanoparticles (0.8 mg/kg) administration, wherein diagnostic B- mode ultrasound is combined with therapy system, with a goal of increased safety
Results: Results from ultrasound imaging concurrent with catheter- based shock wave-mediated thrombolytic therapy, showed the generation of inertial cavitation in the MCA artery and its thrombous content reduction. Also, histopathology results, showed a significant reduction in the mean value for thrombus content at the embolic region in the treatment group compared with the other groups (P < 0.05)
Conclusions: Enhanced thrombolytic effect of shock wave, induced by inertial cavitation effect of collapsed capsules, can cause to enhance the anti- thrombotic effect of tPA and significantly reduce the thrombus content and dilate the luminal cross-sectional area at the embolic region and lower treatment time and reduce total costs of treatment.
Disclosures of Interest: No
E-Poster - Acute and Hyperacute Management
Abstract N°: 166
RECOMBINANT HUMAN ERYTHROPOIETIN PRODUCES FAVORABLE FUNCTIONAL OUTCOME IN ACUTE ISCHEMIC STROKE
Jun-beom Lee*1
1Hongik Hospital, Neurology, Seoul, South Korea
On behalf of:
Background and aims: Until now, there is no prior study focused on the effects of erythropoietin (EPO) administration within 12 hours of onset in acute ischemic stroke patients ineligible for tPA or mechanical thrombectomy.
This study evaluate the impact of EPO treatment on functional outcomes in acute ischemic stroke patients presenting within 12 hours.
Methods: The intervention group received a subcutaneous injection of recombinant human erythropoietin 8000 units on day 1, followed by subsequent administrations every 48 hours (on days 3, 5, and 7). They also received the same conventional drug therapy as the control group, which included dual antiplatelet therapy (aspirin and clopidogrel), a statin, cerebrolysin, and argatroban.
Outcome measurements included NIHSS scores at discharge, as well as modified Rankin Scale (mRS) assessments at discharge and 3 months post-treatment.
Results: There were no other significant differences between the two groups (table 1).
At 3 months post-treatment, the EPO group showed a statistically significant lower mRS score compared to the control group (EPO group 1.9 ± 0.1, Control group 2.9 ± 0.6, p=0.012) (table 2).
There was no significant difference in the occurrence of side effects between the two groups. (table 2)
Table 1. Patient demographics.
Table 2. Comparison of functional outcome and side effects.
Conclusions: The administration of EPO in acute ischemic stroke patients within 12 hours of onset resulted in significantly improved functional outcomes.
Patient demographics.
Comparison of functional outcome and side effects.
Disclosures of Interest: No
Abstract N°: 754
DUAL ANTIPLATELET THERAPY IN DIFFERENT SUBTYPE OF WATERSHED INFARCTION
Chenhui Liu1, Ying Gao1, Zhangxinyi Liu1, Wei Qi Chen1, S. Claiborne Johnston2, Pierre Amarenco3, Philip Bath4, Yuesong Pan1, Yongjun Wang1, Yilong Wang*1
1Beijing Tiantan Hospital, the Department of Neurology, Beijing, China,2University of California, Department of Neurology, San Francisco, China,3Assistance Publique-Hôpitaux de Paris (APHP), Bichat Hospital, Department of Neurology and Stroke Center, Paris, France,4University of Nottingham, Stroke Trials Unit, Mental Health & Clinical Neuroscience, Nottingham, United Kingdom
On behalf of:
Background and aims: The pathogenesis of watershed infarction is complex, which has a high recurrence risk. It is unclear whether patients with different watershed infarction types benefit differently from dual antiplatelet therapy.
Methods: In this imaging subgroup of Intensive Statin and Antiplatelet Therapy for High-risk Intracranial or Extracranial Arterial Stenosis (INSPIRES), patients with infarctions were divided into cortical watershed infarction (CWI), internal watershed infarction (IWI), CWI+IWI, and no-watershed infarction. The primary efficacy and safety outcomes were new stroke and moderate-to-severe bleeding at 90 days, respectively.
Results: A total of 5299 patients were included. Patients with CWI+IWI had a higher risk of new stroke than those with CWI at 90 days (8.47% versus 14.15%, Adjusted HR, 1.71; 95%CI, 1.14-2.57; P<0.001). New stroke occurred in 20 patients (8.20%) in CWI group receiving clopidogrel-aspirin and 21 patients (8.75%) receiving aspirin (Adjusted HR, 0.88; 95%CI, 0.47-1.64), in 18 patients (9.47%) and 35 patients (16.67%) in IWI group (Adjusted HR, 0.54; 95% CI, 0.30-0.97), in 23 patients (11.27%) and 35 patients (16.99%) in CWI+IWI group (Adjusted HR, 0.51; 95%CI, 0.29-0.87), and in 147(7.3%) and 175(8.79%) in no-watershed infarction group (Adjusted HR, 0.82; 95%CI, 0.66-1.03), respectively (Pinteraction=0.36). The risks of moderate-to-severe bleeding in clopidogrel-aspirin versus aspirin were similar among 4 groups.
Conclusions: Among patients with mild ischemic stroke of atherosclerotic origin, we found no antiplatelet treatment by watershed infarction subgroup interaction, but identified a greater absolute risk reduction of new stroke at 90 days after treatment with clopidogrel plus aspirin versus aspirin alone in patients with IWl or CWl+lWl than those without.
Disclosures of Interest: No
Abstract N°: 953
EFFICACY AND SAFETY OF INTRAVENOUS THROMBOLYSIS BY T-PA IN THE ACUTE PHASE OF MINOR ISCHEMIC STROKE OVER A 7-YEARS PERIOD
VERONIQUE QUENARDELLE*1, Takuefou Brigitte1, Lauer Valerie1, Pierre Paul Irene1, Gheoca Roxana1, Goetsch Thibaut1, Valérie Wolff1
1Hôpitaux universitaires de Strasbourg, unité neurovasculaire, STRASBOURG, France
On behalf of:
Background and aims: Intravenous thrombolysis (IVT) by tPA is the gold standard treatment in acute ischemic stroke (IS). However, patients with minor stroke (MS), representing more than half of the IS, were excluded from pivotal IVT studies. An unfavorable functional prognosis in 1/3 of MS leads many teams to propose «off label» IVT. We evaluated the efficacy and safety of IVT in MS hospitalized in our department.
Methods: From January 2015 to December 2021, in Strasbourg University Hospital Stroke unit, we prospectively collected individual patient data with IS treated by a recanalization therapy. From this database, we retrospectively selected patients with initial NIHSS⩽5 having IVT alone, and we studied the characteristics of this subgroup and their evolution at discharge and 3-6 months.
Results: During this 7-year period, 477 MS received tPA treatment. Median age of patients was 69.5±15 years [17-96]. Median NIHSS score before IVT was 1±1.6 and 81% of patients (n=388) had NIHSS⩽3. Median time between symptoms and admission and door to needle were respectively 101±94 min [0-960], and 75±46 min [7-402]. 86% of them (n=387) were independent at 3-6 months (Rankin score ⩽1). There were 5 symptomatic intracerebral hemorrhages (1%), including 3 fatal.
Conclusions: This study confirms in real-life the effectiveness of IVT in the initial management of minor IS but with a significant hemorrhagic risk. The risk-benefit balance must be assess on robust clinical and radiological data before each IVT decision, especially in minor IS. Large-scale studies are needed to define the optimal management of these patients.
Disclosures of Interest: No
Abstract N°: 979
IMPACT OF MULTIPLE PASS EFFECT ON INTENSIVE BLOOD PRESSURE CONTROL AFTER ENDOVASCULAR THROMBECTOMY
Jae Wook Jung1, Kwang Hyun Kim1, Jaeseob Yun1, Young Dae Kim1, Ji Hoe Heo1, Hyo Suk Nam*1
1Yonsei University College of Medicine
On behalf of: the OPTIMAL-BP trial investigators
Background and aims: Multiple attempts of thrombectomy have been linked to a higher risk of intracerebral hemorrhage and worsened functional outcomes, potentially influenced by blood pressure (BP) management strategies. Nonetheless, the impact of intensive BP management following multiple attempts recanalization remains uncertain.
Methods: This was a secondary analysis of the OPTIMAL-BP trial, a comparison of intensive and conventional BP management during the 24 hours after successful reperfusion. Patients were divided into the first-pass effect (FPE) group and the multiple-pass effect (MPE) group. Effects of BP managements were compared within groups. The primary outcome was functional independence at 3 months (modified Rankin Scale score ⩽2). Safety outcomes were symptomatic intracerebral hemorrhage within 36 hours and mortality within 3 months.
Results: Of the 305 patients (median 75 [66-82] years; 182 [59.7%] men), 203 (66.6%) were the FPE group and 102 (33.4%) were the MPE group. In the FPE group, the proportion of patients with functional independence at 3 months was not significantly different between the intensive and conventional managements. However, the intensive management was significantly associated with a lower rate of functional independence in the MPE group (intensive, 32.7% vs conventional, 54.9%; adjusted OR, 0.33 [95% CI, 0.12-0.90]; P=0.03). Rates of symptomatic intracerebral hemorrhage and mortality were not significantly different according to BP managements in both FPE and MPE strata.
Conclusions: Among stroke patients with MPE, intensive BP management for 24 hours resulted in a reduced chance of functional independence at 3 months and did not reduce symptomatic intracerebral hemorrhage following successful reperfusion by endovascular thrombectomy.
Disclosures of Interest: No
Abstract N°: 1024
CHANGES IN THE TIMING OF REPERFUSION TREATMENT AND EFFECT ON THE CIRCADIAN VARIATION IN STROKE
Estefanía García Molina*1, Maria Esther Llorente Iniesta1, Francisco Martinez García1, Ainara Sanz Monllor1, Laura Albert Lacal1, Ángel Valero López1, Carmen Sánchez García1, María Rodriguez Martin2, Ana María Morales Ortiz1
1Virgen of Arrixaca University Clinical Hospital, El Palmar, Spain,2School of Medicine, Murcia, Spain
On behalf of:
Background and aims: The stroke has a circadian rhythm, but there are not too many studies about the response to the acute treatment depending on the day time.
Methods: Patients with a diagnosis of ischemic stroke in whom acute reperfusion with thrombolysis (IVT) is performed. Those are divided according to time slot depending on the IVT time, in day time between 6am-6pm, and night time between 6pm-6am. We compare the functional outcome, mortality, and complications between groups.
Results: 458 patients with ischemic stroke treated with IVT between 2018-2022, man 52%, median age 73. IVT alone 54,1% and IVT plus mechanical thrombectomy 45,9%. There are no differences in basal characteristics between groups, in complications or modificated rankin scale (mRS) at 90 days. There are significative differences in: hospital mortality (12,2% at night time vs 5,2% at day time) and 90 days mortality (20,9% at night time vs 11,5% at day time). Finally, if we divide the 24h time in tertials and in 6-hour slots, we continue to see differences, with higher mortality at the end of the day, from 5-6 pm to midnight.
Conclusions: The patients treated with IVT during night hours, especially those from 6pm to midnight, have a higher risk of death in hospital and 90 days mortality.
Disclosures of Interest: No
Abstract N°: 1051
MECHANICAL THROMBECTOMY FOR VERTEBROBASILAR ARTERY THROMBOSIS
Aung Phyoe*1, Chit Hmu1
1Norfolk and Norwich University Hospital, Stroke Medicine, Norwich, United Kingdom
On behalf of:
Background and aims: Basilar artery occlusion is a life-threatening condition which is salvageable if timely treated.
This discussion aims to emphasize the benefits of mechanical thrombectomy for basilar artery occlusion.
Methods: Case Studies
Results: All the patients below did not receive thrombolysis.
A 42-year-old man with a history of abusing cocaine and anabolic steroids woke up with right neck pain and upper limb paraesthesia. CT-angiogram showed basilar artery occlusion. NIHSS 2. He underwent the thrombectomy in 15 hours. He had right posterior-inferior cerebellar infarct. The discharge mRS was 1.
A 45-year-old man with left sided symptoms and drowsiness had basilar occlusion with NIHSS 16. Despite the delayed triage, he received the mechanical thrombectomy at 29 hours from the onset. He suffered subacute pontine infarct with mild subarachnoid haemorrhage but survived. The discharge mRS was 4 with a long stay.
A 62-year-old man with 1-day-long headache, vomiting, vacant episodes, right hemiplegia, and facial weakness suffered the distal right vertebral and basilar artery occlusion. NIHSS 5. PC-ASPECTS score 10. He received mechanical thrombectomy in 12 hours of admission. His discharge mRS was 1 in 7 days.
Conclusions: The Stroke-Guideline-UK recommends the mechanical thrombectomy for vertebrobasilar occlusion with the following criteria – confirmed vertebra-basilar occlusion, NIHSS>=10, favourable PC-ASPECTS/Pons-Midbrain-Index.
BAOCHE and ATTENTION trials supported it with a higher percentage of good functional outcome at 90 days. From our small sample of case studies, we also witnessed the functional benefits.
However, more studies are needed for different ethnic populations to further prove the benefits from Basilar Artery Thrombectomy.
Disclosures of Interest: No
Abstract N°: 1339
MECHANICAL THROMBECTOMY IN PATIENTS WITH TANDEM OCCLUSIONS AT UNIVERSITY HOSPITAL SOUTHAMPTON: A CASE SERIES
Deborah Inyang1, Lorraine Lemke1, Richard Marigold*1, Donald Adjorlolo1, Shivaprasad Siddegowda1
1University Hospital Southampton NHS Foundation Trust, Stroke Medicine, Southampton, United Kingdom
On behalf of:
Background and aims: Acute ischaemic strokes due to tandem occlusions (TO) account for 15-30% of all large-vessel occlusion strokes. Mechanical Thrombectomy (MT) has been associated with positive functional outcomes in TO. We present this case series, detailing the procedural and clinical outcomes of patients with ischaemic strokes secondary to TO who underwent MTs at University Hospital Southampton, UK.
Methods: This is a retrospective review of single-center data from 47 patients with TO who underwent an MT from May 2021 to April 2023. Data regarding clinical presentation, angiographic results, medical treatment, MT procedure, MT outcome, and clinical outcomes were recorded and analysed.
Results: After 6 months 12/47 patients (25.5%) died (mRS 6). Remaining 23/35 patients (68.6%) were successfully followed up: 11 patients had no mRS data recorded, and 1 patient refused MT follow-up. The median mRS at 6 months was 3 (range 0 to 5). Overall, 11/35 (31.4%) patients had a good functional outcome (mRS 0-2), whilst 24/35 (68.6%) patients had poor functional outcomes (mRS 3-5). 14/47 patients (29.8%) experienced post-procedural complications but did not affect the outcome. There was trend towards better functional outcome among patients did not have carotid stent and this group also showed an increased mortality trend compared to those who did not have carotid intervention.
Conclusions: MT resulted in successful reperfusion in 66% of patients with acute stroke secondary to TO, with 48% patients having a good functional outcome at 6 months.
Disclosures of Interest: No
Abstract N°: 1363
ANGIOPLASTY AND / OR STENTING FOLLOWING SUCCESSFUL MT FOR ICAS-LVOS (ASSET) : PROTOCOL OF A MULTICENTRE RCT
1the First Affiliated Hospital of Jinan University, Department of Neurology, Guangzhou, China,2Guangdong Provincial People’s Hospital, Guangzhou, China,3Nanfang Hospital, Southern Medical University, Department of Neurology, Guangzhou, China,4Guangdong Medical University, Zhanjiang, China
On behalf of:
Background and aims: Mechanical thrombectomy (MT) is the preferred treatment recommended by the guidelines for the patient with intracranial atherosclerotic stenosis-related emerge large vessel occlusive stroke (ICAS-LVOs). However, the management of residual stenosis after thrombectomy is still unknown.
Methods: This is a prospective,multicentre, radomization,blinded endpoint study. After successful MT in patients with acute anterior circulation ICAS-LVOs, the responsible vessel can maintain at flow grade extended Thrombolysis in Cerebral Infarction(eTICI) 2b50~3 for 20 minutes.About 360 patients are divided into a observation group and a control group according to 1:1 ratio randomisation, the observation group undergo emergency balloon angioplasty and/or stenting in combination with standard medication and the control group undergo standard medical treatment.
Results: The primary outcome is the incidence of ischemic stroke in responsible vessel, which will be assessed at 90 (±7) days following randomisation. is the ncidence of ischemic stroke in responsible vessel, which will be assessed at 90 (±7) days following randomisation. Secondary endpoint indicators:1.Rate of reocclusion of the responsible vessel within 7(±1) days of randomization.2.The modified Rankin Scale(mRS) 0-2 score at 90(±7) days after randomization. Additionally, the safety outcomes will be evaluated, including symptomatic intracranial haemorrhage within 24(±3) hours, severe procedure-related complications and mortality within 90 (±7) days.
Conclusions: The aim of this study is to generate substantial evidence regarding the efficacy and safety of remedial intracranial angioplasty as a treatment for residual stenosis after successful MT in patients with LVO.
Disclosures of Interest: No
Abstract N°: 1536
A NOVEL NOMOGRAM INTEGRATING RETINAL MICROVASCULATURE AND CLINICAL INDICATORS FOR INDIVIDUALIZED PREDICTION OF END IN RSSI
Chen Ye*1,2, William Robert Kwapong1, Le Cao1, Hui Xu3, Ruosu Pan1, Ruilin Wang4, Junfeng Liu1, Wendan Tao1, Bo Wu1
1West China Hospital, Sichuan University, Neurology, Chengdu, China,2West China Hospital, Sichuan University, Center of Cerebrovascular Diseases, Chengdu, China,3West China Hospital, Sichuan University, Radiology, Chengdu, China,4West China Hospital, Sichuan University, Ophthalmology, Chengdu, China
On behalf of:
Background and aims: Early neurological deterioration (END) is a relatively common occurrence among patients with single subcortical infarction (SSI). Accurate and early prediction of END in SSI is challenging and could contribute to enhancing prognosis.
Methods: This prospective observational study enrolled SSI patients who arrived within 24 hours from symptom onset at a single center between December 2020 and March 2023. The least absolute shrinkage and selection operator (LASSO) regression model was applied to optimize feature selection for the predictive model. A nomogram was generated based on multivariate logistic regression analysis, to identify potential predictors associated with risk of END. The performance and clinical utility of the nomogram were generated using Harrell’s concordance index, calibration curve, and decision curve analysis (DCA).
Results: Of 166 acute SSI patients, 45 patients (27.1%) developed END after admission. The appearance of END is associated with 4 routine clinical factors (NIHSS score, serum neuron-specific enolase, uric acid, periventricular white matter hyperintensity) and 2 retinal microvascular indicators (ipsilateral superficial and deep vascular complexes). Incorporating these factors, the nomogram model achieved a concordance index of 0.922 (95% CI 0.879 – 0.964) and had a well-fitted calibration curve and good clinical application value by DCA. A cutoff value of 203 was determined to predict END via this nomogram.
Conclusions: This novel nomogram exhibits high accuracy in predicting END in SSI patients. It could guide clinicians to identify SSI patients with a high risk of END at an early stage and initiate necessary medical interventions, ultimately leading to a better prognosis.
Disclosures of Interest: No
Abstract N°: 1746
CLINICAL FEATURES TO DISTINGUISH VESSEL OCCLUSION IN THE HYPERACUTE MANAGEMENT 4.5-24H OF SYMTOM ONSET
Melker Artborg1, Elisabeth Rooth*2
1Danderyds hospital, Department of Neurology, danderyd,2Karolinska Institute, Danderyd Hospital
On behalf of:
Background and aims: Several prehospital stroke scales aiming at identifying EVT-eligible patients have been developed, but none apply to the unselected group of patients admitted to a non-thrombectomy hospital. Aim of this study was to determine the associations between preselected NIHSS-items and the presence of vessel occlusion (VO) in patients within the EVT treatment time window.
Methods: Patient records were retrospectively studied in patients diagnosed with ischemic stroke May 1 - October 31 2022 with 4.5-24h of symptom onset. Patients were divided into two groups if CT-angio showed occlusion or not. We calculated OR with 95% confidence intervals (CI) for the associations of eight NIHSS items, as well as a composite score combining these items, and vessel occlusion. In a subgroup analysis, OR with 95% CI for the association of the composite score and VO was calculated.
Results: Patients with VO (n=25) had higher admission NIHSS (6 vs 4), more likely to have unknown symptom onset (44% versus 8.7%) but less likely a wake-up stroke (32% versus 65%). NIHSS items found to be significantly associated with vessel occlusion were complete hemianopia (OR 10.4, 95% CI 1.18-91.0), pronounced limb paresis (OR 6.2, 95% CI 1.45-26.1) and an NIHSS total score ⩾6 (OR 6.4, 95% CI 1.77-23.1). The composite score was significantly associated with vessel occlusion, sensitivity of 92% and a specificity of 35%.
Conclusions: A composite score of eight NIHSS items had high sensitivity in detecting patients with vessel occlusion, making it a tool to be used in our emergency departments to screen for EVT-eligible patients.
Disclosures of Interest: No
Abstract N°: 1864
LOCAL ANAESTHESIA VERSUS GENERAL ANAESTHESIA DURING MECHANICAL THROMBECTOMY FOR ANTERIOR CIRCULATION STROKE
1Beijing Tiantan Hospital, Capital Medical University, Beijing, China,2China National Clinical Research Centre for Neurological Diseases, Beijing, China,3Chinese Institute for Brain Research, Beijing, China
On behalf of:
Background and aims: The optimal anaesthetic approaches during endovascular treatment is still an active subject of debate. We aimed to compare the effectiveness and safety of local anaesthesia (LA) and general anaesthesia (GA), with real-world data for anterior circulation stroke (ACS) patients who underwent mechanical thrombectomy (MT).
Methods: Retrospective data were derived from a multi-centre registry cohort study of patients with large vessel occlusion who underwent MT at 7 comprehensive stroke centres in China. Our analysis included consecutive ACS patients who achieved successful recanalization and finished Computed Tomography angiography (CTA)+CT perfusion (CTP) imaging before MT between 2017 and 2021. The primary outcome was favourable functional outcome defined as 90-day modified Rankin Scale (mRS) scores of 0-2. Safety outcomes comprised symptomatic intracranial haemorrhage (sICH) within 24 hours and mortality at 90 days. We used multiple imputation to address missing data at admission, and multivariable regression analysis to adjust for confounding factors.
Results: Of 277 included patients, 153 (55.2%) received LA and 124 (44.8%) received GA. 77 (50.3%) in the LA group and 87 (70.2%) in the GA group had mRS scores of 0-2 at 90 days (adjusted odds ratio [aOR], 0.6; 95% confidence interval [CI], 0.3 to 1.2; adjusted P=0.145). Additionally, MRI-confirmed infarct volume at 24 hours was similar between groups (adjusted P=0.911). There were no significant differences observed in rates of mortality (adjusted P=0.979) and sICH (adjusted P= 0.243).
Conclusions: LA demonstrated similar effectiveness and safety profile with GA for ACS patients undergoing MT.
Disclosures of Interest: No
Abstract N°: 1889
INTENSIVE BP LOWERING AND RENAL SAFETY IN ACUTE ISCHAEMIC STROKE AFTER THROMBECTOMY: SECONDARY ANALYSIS OF ENCHANTED2/MT
1Shanghai East Hospital, School of Medicine, Tongji University, Neurology Department, Shanghai, China,2The George Institute for Global Health China, Beijing, China,3The George Institute for Global Health, Faculty of Medicine, University of New South Wales, Sydney, Australia
On behalf of: For the investigators of ENCHANTED2/MT
Background and aims: Acute ischaemic stroke (AIS) patients with large vessel occlusion and elevated blood pressure (BP) have relatively vulnerable renal function due to the use of contrast agents and the renal arteriosclerosis. This study aimed to evaluate the renal safety in the Enhanced Control of Hypertension and Thrombectomy Stroke Study (ENCHANTED2/MT).
Methods: It was a secondary analysis of ENCHANTED2/MT, a multi-center randomised controlled trial comparing more intensive BP lowering (systolic BP, SBP target <120 mmHg) with less intensive BP lowering (SBP target 140-180 mmHg) after successful thrombectomy. Estimated glomerular filtration rate(eGFR) calculated by the Chronic Kidney Disease–epidemiology Collaboration equation (CKD-EPI) using serum creatinine collected at hospital admission and day 1. Renal safety outcomes were short-term change of eGFR (∆eGFR = 24 h – baseline eGFR) and acute kidney injury (AKI) (serum creatinine increased ⩾26.5 µmol/L within 24 hours), analyzed using linear and logistic regression with adjustment for clinical variables.
Results: Of 729 participants (mean age 67.3 years; 38.1% female) included with available baseline eGFR, there were significant differences in mean SBP 119.0±9.1 vs 139.6±12.9 [D20.6 mmHg] (P<0.0001) within 24 hours. There was no significant difference in ∆eGFR (adjusted mean difference -2.40, 95% confidence interval [CI] -5.34 to 0.54; P=0.110) and AKI (adjusted odds ratio 1.03, 95% CI 0.42 to 2.57; P=0.945) between randomised groups.
Conclusions: More intensive BP lowering with SBP targeted less than 120 mmHg didn’t show harm to renal function within 24 hours after successfully thrombectomy.
Disclosures of Interest: No
Abstract N°: 1911
DIFFRENT IMPACT OF AGE ON THE INFARCTION PROGRESSION IN GOOD COLLATERAL STATUS IN CTA AFTER ENDOVASCULAR THROMBECTOMY
Hyungjong Park*1
1Daegu, Department of Neurology, Keimyung University School of Medicine, Dalseogu, South Korea
On behalf of:
Background and aims: Age is associated with decreasing in number, diameter and increasing in tortuosity of leptomeningeal collateral vessel. As an age increases, the likelihood of becoming a fast progressor can be high, even with good collateral. We investigated the impact of age on infarction progression in patients with good collateral after EVT
Methods: A consecutive 208 patients who were older than 75 years with good collateral with successful recanalization after EVT was included. Patients dichotomized into two groups: Group 1 (Age 75-84 years) and Group 2 (Age ⩾85 years). Good functional outcome was defined as mRS ⩾2. Propensity score (PS) matching for age, ASPECTS and pre mRS by 1:1 ratio. We tested whether the likelihood of good outcome by onset to reperfusion time was differentbetween two groups.
Results: Mean age of the patient was 83.2 ± 12.9. Median NIHSS was 10 [8-19]. Mean ASPECTS was 7 [6-9]. Pre mRS was 1 [0-2]. After PS matching, 104 patients were selected as 1 to 1 ratio. In spline curve for the likelihood for good functional outcome by onset to reperfusion time, Group B (⩾85 years) showed significantly a rapid ascent followed by a swift descent compared to group A (Age 75-84yrs), which is indicative of fast progressor in more elderly group.
Conclusions: Despite good collateral and ASPECTS, Age (⩾85 years) may be fast progressor compared to age between 75 to 84. As age increases, the faster and organized systemic pre-hospital process for reducing onset to reperfusion time seems to be needed.
Disclosures of Interest: No
Abstract N°: 2089
ENDOVASCULAR TREATMENT FOR ACUTE ISCHEMIC STROKE DUE TO TANDEM LESION IN ANTERIOR CIRCULATION
Jarmila Neradova1, David Cernik*1, Štěpánka Brušáková1, Veronika Hliněná1, Filip Cihlar1, David Cihlar2
1Masaryk Hosp, Krajska Zdravotni as, Usti Nad Labem, Czech Republic, Neurology Department,2Jan Evangelista Purkyně Univ in Ústí nad Labem, Ústí nad Labem, Czech Republic, Department of Physical Education and Sports
On behalf of:
Background and aims: Acute insertion of a carotid stent in the absence of antiaggregation premedication often leads to acute stent occlusion with clinical impact. Conversely, early anticoagulation or anticoagulant therapy after intravenous thrombolysis can lead to hemorrhagic complications. Early reocclusion may also occur if the carotid artery is left with residual stenosis for elective treatment. Our aim was to analyze the clinical outcome of patients with tandem lesions (TL).
Methods: Patients who underwent mechanical thrombectomy (MT) between 2008 and 2022 were included in the retrospective study. Most underwent intravenous thrombolysis (IVT) at the same time. Neurological deficit was assessed using the National Institutes of Health Stroke Scale (NIHSS) and clinical outcome using the modified Rankin Scale (mRS).
Results: 1350 patients were included in the study. 225 patients underwent MT for a tandem lesion. (age 72.9 ± 12.5 years, 52.4 % men). Successful recanalization (TICI ⩾ 2b) was achieved in 83.1 % (79.9 % at non TL group, p=0,269). A good clinical outcome(mRS ⩽ 2) was achieved by 54.7 % of patients (43.4 % at non TL group, p=0,002). A relatively good clinical result (mRS ⩽ 3) was achieved by 61.8 % of patients (50 % at non TL group, p=0,001) Mortality (90 days) was 25.3 % (34.6 % at non TL group, p=0,007).
Conclusions: A tandem lesion in the anterior circulation is a frequently feared finding in acute cerebrovascular accident. However, endovascular treatment can have a significantly good clinical result here as well. In our cohort, this is the subgroup with the best prognosis.
Disclosures of Interest: No
Abstract N°: 2106
RESULTS OF MECHANICAL THROMBECTOMY IN THE VERTEBROBASILAR AREA IN REAL CLINICAL PRACTICE:
Jarmila Neradova1, David Cernik*1, Štěpánka Brušáková1, Veronika Hliněná1, Filip Cihlar1, David Cihlar2
1Masaryk Hosp, Krajska Zdravotni as, Usti Nad Labem, Czech Republic, Neurology Department,2Jan Evangelista Purkyně Univ in Ústí nad Labem, Ústí nad Labem, Czech Republic, Department of Physical Education and Sports
On behalf of:
Background and aims: There are significantly fewer data from large randomized trials for MT in the posterior circulation (MT from a basilaris, a.vertebralis, a.cerebri posterior) than in the anterior circulation. We present the results of a monocentric retrospective study from the real practice of treatment in the posterior circulation.
Methods: Patients who underwent MT between 2008 and 2022 were included in the retrospective study. Most underwent intravenous thrombolysis (IVT) at the same time. Neurological deficit was assessed using the National Institutes of Health Stroke Scale (NIHSS) and clinical outcome using the modified Rankin Scale (mRS). Symptomatic bleeding was assessed according to the SITS-MOST criteria. The achieved recanalization was evaluated using the Thrombolysis in Cerebral Infarction scale (TICI).
Results: 1350 patients were included in the study. 161 MT were performed in the posterior area (age 68.9 ± 12.9 years, 62.7 % men). Successful recanalization (TICI ⩾ 2b) was achieved in 78.9 % (80.7 % in anterior circulation, p=0,594). A good clinical result (mRS ⩽ 2) was achieved by 34.8 % of patients (46.7 % in anterior circulation, p=0,004). Mortality (90 days) was 50.3 % (30.7 % in anterior circulation, p=0,000001).
Conclusions: Stroke in the posterior circulation generally have a worse prognosis, even in our group when a similar rate of recanalization using MT is achieved. Nevertheless, one third of patients with AIS in the vertebrobasilar area achieve self sufficiency within three months of the incident.
Disclosures of Interest: No
Abstract N°: 2295
INFLUENCE OF RENAL FUNCTION ON MORTALITY AFTER EVT: POST HOC ANALYSIS OF THE ENCHANTED2/MT TRIAL
Xinwen Ren*1,2, Yang Zhao1,2, Craig Anderson1,2,3, Lili Song1,3
1The George Institute for Global Health, Beijing, China,2The George Institute for Global Health, University of New South Wales, Sydney, Australia,3Royal Prince Alfred Hospital, Neurology, Sydney, Australia
On behalf of:
Background and aims: The relation of renal impairment to outcome after endovascular thrombectomy (EVT) is unclear. We determined associations of renal impairment and clinical outcomes, and any modification by intensity of BP control, in the second Enhanced Control of Hypertension and Thrombolysis Stroke Study (ENCHANTED2/MT).
Methods: Post hoc analysis involving 816 ENCHANTED2/MT post-EVT patients who were randomly allocated to more-intensive (SBP target <120 mmHg) versus less-intensive (SBP target 140-180 mmHg) BP-lowering. Logistic regression models were used to define associations between eGFR and 90-day mortality and any heterogeneity in the treatment effect.
Results: Of 729 patients with available baseline eGFR (mean age 67 years; 38% female), 366 (50.2%), 258 (35.4%), and 105 (14.4%) had normal (eGFR ⩾90 mL/min/1.73 m2), mild impaired (60-89) and moderate-to-severe impaired (<60) renal function, respectively. Compared with normal group, the odds of mortality was higher in those with moderate-to-severe renal impairment (aOR 2.0, 95%CI 1.10-3.61; p=0.04 for trend). There was no heterogeneity in the treatment effect by grades of renal function (p for interaction 0.42).
Conclusions: Moderate-to-severe renal impairment is associated with increased mortality in patients with acute ischemic stroke who receiver EVT. Renal function does not modify the effect of more intensive BP-lowering on mortality in this patient group.
Disclosures of Interest: No
Abstract N°: 2423
IMPACT OF TIME TO TREATMENT WITH NICARDIPINE ON CLINICAL OUTCOMES OF PATIENTS WITH HYPERACUTE INTRACEREBRAL HEMORRHAGE
John Christopher Ruiz*1, Marian Irene Escasura1
1East Avenue Medical Center, Neurosciences, Quezon City, Philippines
On behalf of:
Background and aims: Recent evidences suggest that timing of treatment with anti-hypertensive medication in hyperacute intracerebral hemorrhage leads to limited hematoma expansion and improved clinical outcomes. This study aims to determine if time to treatment, with blood pressure lowering agent, leads to decreased mortality and improved functional outcomes in patients with hyperacute intracerebral hemorrhage.
Methods: We retrospectively assessed 125 patients who were categorized based on the time that the first dose of intravenous nicardipine was started. Sixty percent (n=75) received treatment within sixty minutes of arrival at the Emergency Room while forty percent (n=50) was given treatment beyond sixty minutes. Stroke mechanisms and clinical outcomes were then identified and determined for each group.
Results: Improved functional outcomes (Modified Rankin Score 0-2) was seen in patients who received intravenous nicardipine greater than sixty minutes (n = 20, 39.2% vs. n = 15, 20.3%). In addition, lower mortality (n=18, 35.3%), decreased need of intensive care unit (ICU) admission (n=16, 31.4%) and adverse events (n=17, 33.3%) were also seen in these patients. However, there is no significance in the rate of rebleeding between two groups.
Conclusions: Time to treatment with intravenous nicardipine greater than 60 minutes is associated with good functional outcome, lower mortality rate, decrease ICU admission and incidence of adverse events. However, rebleeding rates between two groups were similar.
Disclosures of Interest: No
Abstract N°: 2610
ISCHEMIC STROKE DUE TO THE OCCLUSION OF THE CERVICAL INTERNAL CAROTID ARTERY: SAFETY AND EFFICACY OF EMERGENT CEA AND IVT
Roman Herzig*1, Svatopluk Ostrý2, Veronika Kunešová3, Adéla Kondé4, Martin Kovář5, René Jura6, Jan Fiksa7, Petr Geier8, Ondřej Škoda9, Peter Vaško10
1Charles University Faculty of Medicine and University Hospital Hradec Kralove, Department of Neurology, Hradec Kralove, Czech Republic,2Ceske Budejovice Hospital, Department of Neurology, Ceske Budejovice, Czech Republic,3International Clinical Research Center, Cerebrovascular Research Program, Brno, Czech Republic,4Technical University of Ostrava, Faculty of Electrical Engineering and Computer Science, Ostrava, Czech Republic,5Na Homolce Hospital, Department of Neurology, Prague, Czech Republic,6University Hospital Brno, Department of Neurology, Brno, Czech Republic,7First Faculty of Medicine, Charles University and General University Hospital in Prague, Department of Neurology, Prague, Czech Republic,8Pardubice Hospital – Hospital Pardubice Region, Inc., Department of Neurology, Pardubice, Czech Republic,9Hospital Jihlava, Department of Neurology, Jihlava, Czech Republic,10Third Faculty of Medicine, Charles University and Faculty Hospital Kralovske Vinohrady, Department of Neurology, Prague, Czech Republic
On behalf of: Emergent CEA in Acute Ischemic Stroke Study Group
Background and aims: Acute ischemic stroke (AIS) caused by cervical internal carotid artery occlusion (ICAo) is often associated with a severe and persistent neurological deficit and a high mortality rate. IVT is the only standard treatment method. An emergent CEA represents an experimental alternative. The aim was to assess the safety and efficacy of IVT and CEA in AIS patients with cervical ICAo.
Methods: In a retrospective, multicentre study, the CEA group consisted of 39 patients (21 males; median age 71 [66–78] years), and the IVT group of 32 patients (23 males; median age 65 [60–78] years). Neurological deficit was assessed using NIHSS score on admission and after 24 h and 3-month mRS (with favorable outcome defined as mRS 0–3).
Results: In the CEA vs. IVT groups, the median (IQR) NIHSS value was 7 (4–12) vs. 6 (4–9) on admission, and 4 (2–9) vs. 3 (1–5) after 24 h; the median decrease of 2 (0–4) in both groups was significant (p<0.001) and did not differ between both groups (p>0.05). The recanalization rate was significantly higher (91.4% vs. 21.7%; p<0.001) and 3-month mortality was significantly lower (5.1% vs. 25.0%; p=0.035) in CEA vs. IVT patients. A favorable 3-month clinical outcome was present in 86.1% of CEA vs. 65.2% of IVT patients (p>0.05).
Conclusions: In this multicentre retrospective comparison, emergent CEA in patients with AIS with cervical ICAo was associated with a higher recanalization rate and lower mortality when compared to standard IVT.
AcknowledgementsSupported by STROCZECH (No. LM2023049).
Disclosures of Interest: No
Abstract N°: 2796
POTENTIAL OF THE NEUROLOGICA OMNITOM ELITE MOBILE PHOTON-COUNTING DETECTOR IN THE DIFFERENTIATION BETWEEN BLOOD AND IODINE
Iris Grunwald1,2, Leah White1, Grant Milne2, Chloe Voutsas1, Pamela Barr1, Michelle Cooper1, Anna Podlasek1, Helen Donald-Simpson1, Stephanie Clark1
1Tayside Innovation MedTech Ecosystem, University of Dundee, Dundee, United Kingdom,2NHS Tayside, Dundee, United Kingdom
On behalf of:
Background and aims: Differentiating between blood and contrast extravasation due to a disrupted blood-brain barrier is often impossible due to similar Hounsfield units. We aimed to evaluate the potential of the NeuroLogica OmniTom Elite mobile photon-counting detector (PCD) computed tomography (CT) scanner in differentiating between blood and iodine.
Methods: Human blood and a concentration of iodine were scanned in the NeuroLogica OmniTom Elite mobile PCD scanner. Images were obtained in vitro in scintillator tubes positioned in a Gammex phantom, and ex vivo in the brain of a cadaveric model. Regions of interest were analysed within the scintillator tubes to obtain Hounsfield units of the samples. Virtual non-contrast images and iodine density maps were generated, and material decomposition was performed.
Results: Region of interest analysis showed similar Hounsfield units for the tubes containing blood and iodine. Iodine density maps enabled detection of iodine in vitro, and ex vivo in the brain of a human cadaveric model.
Conclusions: PCD iodine maps allow material decomposition and differentiation between blood and iodine, both in vitro and ex vivo.
Disclosures of Interest: No
Abstract N°: 2884
CHARACTERISTICS OF MECHANICAL THROMBECTOMY IN ACUTE ISCHEMIC STROKE AMONG PATIENTS IN SAUDI ARABIA A DESCRIPTIVE ANALYSIS: A SINGLE CENTER EXPERIENCE
Background and aims: Mechanical thrombectomy (MT) for acute ischemic stroke (AIS) in large vessel occlusion (LVO) results in excellent outcome. There is limited data on the outcome from the Middle East.We present our experience from Riyadh, Saudi Arabia.
Methods: Data from the Riyadh thrombectomy registry between January 2021 to December 2023 from King Faisal Specialist Hospital and Research Centre, Riyadh, Saudi Arabia was analyzed.
Results: There were 356 participants (median age of 58 years [IQR: 47-70]), including 36.8% females with a median BMI of 27.8 (IQR: 24.7-31.6). The median time from onset to groin puncture was 140 minutes. The most common sites of occlusion were in the M1 (50.8%) followed by M2 (22.7%). Tissue plasminogen activator (IV tPA) and intra-arterial (IA tPA) were administered to 33.6% and 40.1%, respectively. The pre-treatment NIH Stroke Scale (NIHSS) score was 15 (IQR: 10-19). Post-EVT modified treatment in cerebral ischemia (mTICI) score of 3 was achieved in 41.2%. Immediate post-EVT NIHSS score was 11 (IQR: 5-16).NIHSS scores at 24 and 48 hours were 9 (IQR: 3-15) and 5 (IQR: 1-13), respectively. Functional outcomes measured by 90-days modified Rankin Scale (mRS) of 0-2 was evident in 52.5% of patients.
Conclusions: Our experience from Riyadh is similar to the results of large clinical trials. Whereas a mTICI score of 3 was achieved in 41.2% of patients, a good to excellent outcome was seen in 52.5% of patients.These preliminary results are encouraging. Further studies are necessary to understand the underlying mechanisms and prognosis of LVO in Saudi Arabia.
Disclosures of Interest: No
Abstract N°: 3031
TANDEM OCCLUSION STROKE MANAGEMENT: A SINGLE-CENTER CASE SERIES
David Seoane*1,2, Jesús Ramírez Sánchez-Ajofrín3, Fernando Ostos Moliz1,2, Eduardo Barcena4, Maria Gutiérrez Sánchez de la Fuente1,2, Federico Ballenilla4, Patrica Calleja1,2
1Hospital Universitario 12 de Octubre, Stroke Unit,2Instituto de Investigación i+12, Neurovascular Sciences,3Hospital Universitario 12 de Octubre, Neurology,4Hospital Universitario 12 de Octubre, Interventional Neurorradiology
On behalf of:
Background and aims: Endovascular management for tandem occlusion strokes (TS), which account for 10-15% of LVO-strokes, remains controversial pending trial results. Emergent carotid artery stenting and retrograde approach (intracranial recanalization first) are generally advocated.
Methods: Retrospective single-center series of TS (cervical occlusion or >90% stenosis) between 2016-2022. Review of records, neuroimaging and outcomes at 3 months.
Results: 133 TS patients. Intracranial occlusion predominantly M1 (48%) and terminal ICA (32%). TICI 2b-3 achieved in 92.3%. Compared to the general population of LVO: younger age (median): 68 vs 76 years; higher male proportion (63,9% vs 46%); predominant large-artery atherosclerosis aetiology (62%), followed by dissection (9%); mRS 0-2 44.4% vs 52.0% with equivalent mortality (23,3% vs 20,6%) and sICH (5,3% vs 3,1%). Higher rate of complications (7.5% vs 3.9%) and any ICH (28.6% vs 22.2%), without impact of prior thrombolysis, which therefore seems safe.
Standard practice was periprocedural single antiplatelet therapy (Inyesprin), early (6-12 hours) control CT and subsequent start of double antiplatelet therapy if deemed safe, maintained 3-6 months. Stent permeability was assessed by Doppler-ultrasound (64%) or angioCT (20%). Stent thrombosis occurred in 18 patients (13.5%), associated with futile recanalization but not with recurrent stroke. No outcome differences found between closed-cell and open-cell stents.
Functional outcome in patients treated with emergent cervical stenting seemed better than with angioplasty alone (mRS 0-2 48.2% vs 36.9%, without reaching statistical signification).
Conclusions: TS benefit from emergent stenting plus conventional thrombectomy, also in patients with prior thrombolysis despite the general concern, and regardless of the underlying lesion aethiology.
Disclosures of Interest: No
E-Poster - Cardioembolism and Heart-Brain Interactions
Abstract N°: 297
DISCONTINUATION OF ORAL ANTICOAGULANTS AND RISK OF RECURRENT ISCHEMIC STROKE IN PATIENTS WITH ATRIAL FIBRILLATION
Mette Hindsholm*1,2, Edip Gurol3, Luis Alberto García Rodríguez4, Jesper Hallas5, Birgit Høyer6, Sören Möller7, Axel Brandes8, Claus Ziegler Simonsen1,2, David Gaist9
1Aarhus University Hospital, Department of Neurology, Aarhus, Denmark,2Aarhus University, Department of Clinical Medicine, Aarhus, Denmark,3Massachusetts General Hospital, Department of Neurology, Boston, United States,4Centro Español Investigación Farmacoepidemiológica, CEIFE, Madrid, Spain,5University of Southern Denmark, Department of Clinical Pharmacology, Odense, Denmark,6Odense University Hospital, Odense Patient Data Explorative Network (OPEN), Odense, Denmark,7University of Southern Denmark, Department of Clinical Research, Odense, Denmark,8University of Southern Denmark, Department of Regional Health Research, Odense, Denmark,9Odense University Hospital, University of Southern Denmark, Research Unit for Neurology, Odense, Denmark
On behalf of:
Background and aims: Studies exploring the relationship between OAC-discontinuation and risk of recurrent ischemic stroke (recurrent-IS) in patients with atrial fibrillation (AF) are limited. We sought to estimate the risk of recurrent-IS associated with OAC discontinuation in unselected patients with AF.
Methods: This register-based nested case-control study included all patients in Denmark aged ⩾50 years with AF and hospitalized with IS January 2014-December 2021, who initiated or restarted OAC within 30 days after their stroke. Follow-up continued until first recurrent-IS, or censoring (intracranial bleed, emigration, death, or end-of-study (June 2022)). Within the cohort, incident cases of recurrent-IS were matched to controls on time since entry-stroke and calendar year of recurrent-IS. We disregarded all information on medication use occurring after selection as case or control.
Results: 663 cases with recurrent-IS (274 [41.3%] women; mean [SD] age, 80.1 [9.2] years; median CHA2DS2-VASc score 4.0 [IQR 3.0-5.0]) were matched with 2652 controls (1148 [43.3%] women; mean [SD] age, 78.6 [9.4] years; median CHA2DS2-VASc score 4.0 [IQR 2.0-5.0]). OAC discontinuation was associated with a higher risk of recurrent-IS (cases 13.4%, controls 6.8%, aOR 2.13; 95% CI [1.57-2.89]) than non-discontinuation. Patients who had a recurrent-IS and discontinued OAC more often had a more severe stroke (aOR 2.10; 95% CI [1.31-3.36]) and higher 30-days mortality (28.1% vs. 10.9%) than patients who continued OAC at the time of their recurrent-IS.
Conclusions: Patients with AF and IS who discontinue OAC treatment have twice the risk of recurrent-IS, have more severe strokes, and have higher mortality than patients who continue OAC treatment.
Disclosures of Interest: No
Abstract N°: 298
RECURRENT ISCHEMIC STROKE RISK IN PATIENTS WITH ATRIAL FIBRILLATION ON ORAL ANTICOAGULANTS
Mette Hindsholm*1,2, Edip Gurol3, Luis Alberto García Rodríguez4, Jesper Hallas5, Birgit Høyer6, Sören Möller7, Axel Brandes8, Claus Ziegler Simonsen1,2, David Gaist9
1Aarhus University Hospital, Department of Neurology, Aarhus N, Denmark,2Aarhus University, Department of Clinical Medicine, Aarhus, Denmark,3Massachusetts General Hospital, Department of Neurology, Boston, United States,4Centro Español Investigación Farmacoepidemiológica, CEIFE, Madrid, Spain,5University of Southern Denmark, Department of Clinical Pharmacology, Odense, Denmark,6Odense University Hospital, Odense Patient Data Explorative Network (OPEN), Odense, Denmark,7University of Southern Denmark, Department of Clinical Research, Odense, Denmark,8University of Southern Denmark, Department of Regional Health Research, Odense, Denmark,9Odense University Hospital, University of Southern Denmark, Research Unit for Neurology, Odense, Denmark
On behalf of:
Background and aims: Prior ischemic stroke (IS) is one of the strongest prognostic factors for recurrent-IS in patients with atrial fibrillation (AF). Data from randomized trials indicate that patients with AF and IS while on oral anticoagulants (OACs) are at increased risk of recurrent-IS and death. Data from an unselected patient-population are lacking. We sought to estimate the cumulative incidence of recurrent-IS and mortality in patients with AF who initiated/restarted OAC after an IS.
Methods: This nationwide register-based cohort study included all patients in Denmark aged ⩾50 years with AF hospitalized with an IS January 2014 and December 2021 who initiated or restarted OAC within 30 days after their stroke. Follow-up continued until first recurrent-IS, or censoring (intracranial bleed, emigration, death, or end-of-study (June 2022)).
Results: We included 8.119 patients (4.392 [54.1%] men; mean [SD] age, 78.4 [9.6] years; median CHA2DS2-VASc score 4.0 [IQR 3.0-5.0]). The crude cumulative incidence of recurrent-IS at 1 year was 4.28% (95% CI, 5.92-7.10) and all-cause mortality at 1 year was 15.44% (95% CI, 14.67-16.25). A history of IS prior to start of follow-up was associated with higher cumulative incidence of recurrent-IS (6.47% [95% CI, 5.06-8.26] vs 3.96% [95% CI, 3.51-4.46]) and all-cause mortality (19.12% [95% CI, 16.84-21.66] vs 14.91% [95% CI, 14.09-15.76]). Adjusted analyses showed similar results. Based on redeemed prescriptions, 80.4% of patients were still on OACs at the time of their recurrent-IS.
Conclusions: Patients with IS and AF have a high risk of recurrent-IS and death despite OAC use.
Disclosures of Interest: No
Abstract N°: 477
THE ROLE OF ATRIAL CARDIOPATHY AS POTENTIAL CAUSE OF EMBOLIC STROKE OF UNDETERMINED SOURCE
Angelo Cascio Rizzo*1, Ghil Schwarz1, Andrea Bonelli2, Andrea DI Pietro3, Martina DI Pietro4, Francesco Aruta1, Cristina Motto1, Benedetta Carla De Chiara2, Antonella Moreo2, Elio Clemente Agostoni1
1ASST Grande Ospedale Metropolitano Niguarda, Neurology and Stroke Unit, Milan, Italy,2ASST Grande Ospedale Metropolitano Niguarda, Cardiology, De Gasperis Cardio Center, Milan, Italy,3AORN Sant’Anna e San Sebastiano, Neurology, Caserta, Italy,4“F.Renzetti” Hospital, Neurology and Stroke Unit, Lanciano, Italy
On behalf of:
Background and aims: Atrial cardiopathy (AC) is considered a potential mechanism of embolic stroke of undetermined source (ESUS). Etiological misclassification may have limited our understanding of the link between AC and ESUS due to the heterogeneous ESUS construct. After application of a recently proposed ESUS update, we investigated the role of AC in ESUS.
Methods: A retrospective single-center study on consecutive ESUS patients from 2018-to-2022 was conducted. According to the proposed ESUS criteria we excluded patients with high-risk PFO, high-risk supracardiac non-stenosing atherosclerosis, cancer-related hypercoagulability. AC was defined as left atrial enlargement measured by left atrial volume index (LAVI) >34mL/m2. We assessed clinical and radiological features of AC(+)/ESUS and the association (univariate and multivariate logistic regression analyses) between AC and stroke severity, 90-day functional outcome, stroke recurrence and atrial fibrillation detection after stroke (AFDAS).
Results: Among 414 eligible ESUS, 298 patients (72%) were included. AC prevalence was higher in ESUS classified according to the revised criteria compared to traditional criteria (42% vs. 36%). AC(+)/ESUS were older, had more frequently hypertension, coronary-artery-disease, supracardiac atherosclerosis, cortico-subcortical lesions compared to AC(-)/ESUS. Recurrent ischemic stroke occurred in 17 patients (5.9%) and AFDAS in 28 (9.7%). No significant association was found between AC and stroke severity (aOR 1.17 [95%CI 0.78-1.75],p=0.442), 90-day outcome (aOR 2.48 [95%CI 0.97-6.31],p=0.056), stroke recurrence (aOR 1.56 [95%CI 0.53-4.64],p=0.420). AFDAS was independently associated with AC (aOR 4.63 [95%CI 1.77-12.10],p=0.002).
Conclusions: AC is associated with AFDAS, but not with stroke severity, stroke recurrence, or 90-day functional outcome in ESUS classified according to the proposed construct update.
Disclosures of Interest: No
Abstract N°: 1104
CAN BETA-BLOCKERS BE USEFUL TO ANTAGONIZE STROKE HEART SYNDROME?
Gabriele Prandin*1, Giovanni Furlanis1, Laura Mancinelli1, Federica Palacino1, Emanuele Vincis1, Paola Caruso1, Marcello Naccarato1, Paolo Manganotti1
1University of Trieste, Clinical Department of Medicine, Surgery and Health Sciences, Trieste, Italy
On behalf of:
Background and aims: the Stroke Heart Syndrome (SHS) is a frequent complication of acute stroke and consists in the cardiac injury following the cerebrovascular event. The main pathogenetic hypothesisis the cytokines storm involving the sympathetic system. A biomarker of ongoing SHS is the “rise and fall” over 30%. troponin pattern within 72h since the event. There are no studies which explore the possible role of cardio-selective beta-blockers (BB) taken chronically before the acute event in preventing SHS.
Methods: we collected retrospectively data of 890 patients admitted to the Stroke Unit of Trieste from 2018 to 2021. We excluded hemorrhagic strokes, stroke mimics, TIAs and patients with incomplete data. We compared clinical characteristics, stroke location and troponin ”rise and fall” pattern in 142 patients divided into 2 groups: troponin elevation above 30% (SHS) and no troponin variation (no SHS).
Results: SHS and no-SHS have similar cardiovascular risk factors, except for age. Higher NIHSS on baseline, non-lacunar etiology and insular involvement were significantly more frequently in SHS group, as well as NT-proBNP, maximum troponin level and cardioembolic etiology. The BB use was similar in the two groups. In the multivariate analysis (logistic regression) only age is significantly associated with our endpoint (OR 1.092 CI95%, 1.026-1.161)
Conclusions: Chronically BB-treated patients may not be protected by SHS. More studies are needed to better understand the therapeutic role of BB in eventually antagonizing the sympathetic storm after ischemic strokes.
Disclosures of Interest: No
Abstract N°: 1457
THE UTILITY OF CARDIAC RHYTHM MONITORING IN YOUNG ADULTS WITH STROKE
Zayna Ahmed*1, Abigail Rees2, Chaamanti Sivakumar3, Hermaleigh Townsley3, Kate Ellis1, Joseph White1, Robert Bell4, Graziella Quattrocchi2,3, Arvind Chandratheva3
1University College London Medical School, London, United Kingdom,2North Middlesex University Hospital, London, United Kingdom,3Comprehensive Stroke Service, National Hospital for Neurology and Neurosurgery, London, United Kingdom,4University College London Hospitals Nhs Foundation Trust, United Kingdom
On behalf of:
Background and aims: We aimed to evaluate the utility of cardiac rhythm monitoring in young patients with Stroke.
Methods: Consecutive stroke patients ⩽55 years old admitted to a London Hyperacute Stroke Unit from 1st January 2019-31st December 2020 were retrospectively reviewed. Demographics, vascular risk factors, aetiology (TOAST criteria), 24-to-72 hours-ECG-Holter were recorded.
Results: Of 350 patients, 260(74%) had ischemic stroke, 69% of which were male, mean age 46 (SD-8.2). Stroke location was anterior in 158(61%), posterior in 81(31%), multi-territory in 19(7%) and retinal in one (0.4%), 2(0.8%) unknown location. Most prevalent aetiology was TOAST 5, 37%, denoting dual or cryptogenic aetiology, 13% large vessel atherosclerosis (TOAST 1), 20% cardioembolic(TOAST 2), 15% small vessel disease(TOAST 3) and 15% other aetiology(TOAST 4).
Of 148 acute ECG, 68% showed normal sinus rhythm and 13% atrial fibrillation(AF). 87 underwent Holter Monitoring(HM) of which 11(13%) were found to have AF on HM, of which 4(5%) known. 19(11%) showed signs of LVH, 3(2%) showed LAD. 8(9%) had supraventricular tachycardia of which 5 were <1%.
All seven patients with new diagnoses of AF were identified on acute ECG. All had at least two vascular risk factors, most commonly smoking and BMI>30. Median CHADSVASC was 2 (range:1-3). Six(7%) had ventricular tachycardia of which 67% had mild valvular dysfunction, most commonly mitral regurgitation(MR).
Conclusions: Prolonged cardiac monitoring was of low yield with new AF found in only 2%, of which all cases were identified by their acute ECG. All had at least two vascular risk factors or valvular dysfunction. Alternative non-AF arrhythmias were rare.
Disclosures of Interest: No
Abstract N°: 1496
GAIN AND LOSS OF CARDIAC FUNCTION IN CEREBROVASCULAR DISEASE
Background and aims: Cardiovascular reactivity (CR) was defined by beat indices, ratio (R) or difference (D) between higher maximal or minimal heart rate on higher maximal or minimal pulse rate. A value <1 or >1 were considered as negative (NCR) or positive (PCR), respectively [Fiori P. et al, 2020].
The aim of the present study was to examine the correlation between CR and lesional load at MRI.
Methods: Lesional load was calculated according to Fazekas’ criteria. Moreover, we considered juxtacortical ischaemic lesions and microbleeds, evaluated as rare (1:1-3), sporadic (2:3-6), multiple (3:>6) at FLAIR-T2 and SWI-Weighted-MRI sequences.
Results: The following correlations (r) were found:
Conclusions: Pulse rate may be considered a reflex of heart rate. Low cardiovascular reactivity stands for a low cardiac output syndrome, reduced capillary flow because of arteriosclerosis, increased transit time, lacunar encephalopathy, higher risk of disability and worst prognosis in case of acute events.
Although high heart rate correlates with greater total lesion volume and higher number of micro- and macro-structure WML [Fuhrmann D. et al, 2019], low CR may help in predicting both irreversible ischaemic sufferance and high haemorrhagic risk.
Disclosures of Interest: No
Abstract N°: 1872
ATRIAL IMAGING AND CARDIAC RHYTHM IN CRYPTOGENIC EMBOLIC STROKE: THE ARIES STUDY
Ricardo Rigual1, Sergio Castrejón-Castrejón2, Lucía Fernández-Gassó3, Jorge Rodriguez-Pardo*1, Maria Alonso de Leciñana1, Exuperio Díez Tejedor1, Esther Pérez-David3, Gerardo Ruiz-Ares1, Jose Luis Merino2, Blanca Fuentes1
1Department of Neurology and Stroke Centre. Hospital La Paz Institute for Health Research-IdiPAZ (La Paz University Hospital-Universidad Autónoma de Madrid), Madrid (Spain)., Madrid, Spain,2Robotic and Cardiac Electrophysiology Unit, Department of Cardiology. Hospital La Paz Institute for Health Research-IdiPAZ (La Paz University Hospital-Universidad Autónoma de Madrid), Madrid, Spain,3Cardiac Image Unit, Department of Cardiology. Hospital La Paz Institute for Health Research-IdiPAZ (La Paz University Hospital-Universidad Autónoma de Madrid), Madrid, Spain
On behalf of:
Background and aims: In cryptogenic stroke (CS), long-term EKG monitoring is used to search atrial fibrillation (AF) but usually finds high burden of ectopic atrial activity (HBEA) with uncertain significance. We aim to analyze the risk of developing AF or HBEAs in patients with CS and compare their atrial function using advanced echocardiography and their clinical outcome.
Methods: Observational, prospective study including patients with CS admitted to a comprehensive Stroke Centre. We analyzed the frequency of AF and HBEAs in two consecutive 30-day ECG records and compared echocardiographic signs of left atrial (LA) dysfunction according to rhythm classification: AF, HBEAs and normal sinus rhythm (NSR). We also evaluated stroke recurrence and mortality at 12-months follow-up.
Results: We included 109 patients. AF was found in 35 (32.1%) patients, HBEAs in 27 (24.8%) and NSR in 47 (43.1%). In multivariate analysis, patients with AF compared with NSR patients presented significative higher values in LA volume, LA index volume, 3D LA index volume, 3D-telediastolic LA volume, 3D-telesistolic LA volume, lower rates of LA ejection fraction, LA strain in reservoir and contraction. After adjusting for confounders HBEAs patients showed no significant differences compared to NSR. There were no significant differences in clinical outcomes between the three groups.
Conclusions: Patients with CS who developed AF exhibited significant changes in LA volume, LA function and reservoir and contraction strain, while those with HBEAS showed fewer structural changes in echocardiography. These results suggest that advanced LA echocardiography could be a useful tool for better patient selection for long-term EKG monitoring.
Disclosures of Interest: No
Abstract N°: 1882
ANTICOAGULATION STRATEGIES IN ACUTE ISCHEMIC STROKE PATIENTS WITH NON-VALVULAR ATRIAL FIBRILLATION REAL-WORLD REGISTRY STUDY
1The Second Affiliated Hospital of Soochow University, Department of Neurology, Suzhou Clinical Research Center of Neurological Disease, Suzhou, China
On behalf of:
Background and aims: This study aims to investigate the risk of thromboembolism, intracranial hemorrhage, extracranial hemorrhage and all-cause mortality in acute ischemic stroke (AIS) patients with non-valvular atrial fibrillation (NVAF) who received anticoagulant therapy.
Methods: We consecutively included AIS patients with NVAF in 2 centers from January 2019 to December 2021. Baseline data, laboratory and imaging biomarkers and anticoagulation therapy were recorded. Each patient had follow-up at least once.
Results: 623 patients were included, average age 75.48 ± 8.84 years, 45.1% female. The median follow-up time was 18 months. Patients who used non oral anticoagulants significantly increased hemorrhagic risks within 3 months (adjusted OR=4.73, 95% CI: 2.34-9.56) and 1 year (adjusted OR=4.08, 95% CI: 2.17-7.65). Patients who initiated anticoagulation therapy within 2-14 days had a lower risk of composite outcomes (adjusted OR=0.50, 95%CI:0.30-0.85), hemorrhagic events (adjusted OR=0.42, 95%CI:0.23-0.76) within 3 months and hemorrhagic events within 1 year (adjusted OR=0.51, 95%CI:0.29-0.92). No statistical difference was found in functional outcome between two groups (adjusted OR=0.76, 95% CI:0.45-1.29). Patients using rivaroxaban ⩽ 10mg QD(versus ⩾10mg QD) had similar rate of composite outcomes (adjusted OR=0.53, 95% CI:0.23-1.19) and functional outcome (adjusted OR=0.59, 95% CI:0.29-1.17)
Conclusions: Use of non-oral anticoagulants didn’t reduce thromboembolism risk but the risk of hemorrhagic increased. Initiated anticoagulants within 2-14 days (versus other time intervals) had no statistical differences in function prognosis but combined with lower risks of composite outcomes and hemorrhagic events within 3 months. Prospective studies are demanded to confirm the safety and effectiveness of low-dose rivaroxaban in Chinese patients.
Disclosures of Interest: No
Abstract N°: 2005
CARDIO-CEREBRAL INFARCTION PATIENTS' OUTCOMES: A SINGLE CENTRE RETROSPECTIVE STUDY
Tamanna Agarwal1, Aravinth Sivagnanaratnam*1, Julia Jenkins1, Mariana Nalmpanti1
1Northwick Park Hospital, Harrow, United Kingdom
On behalf of:
Background and aims: Cardio-cerebral infarction (CCI) belongs to an area of growing interest within cerebrovascular medicine as it refers to the concurrence of acute ischaemic stroke (AIS) and acute myocardial infarction (AMI) usually within 72 hours. A scenario where both the heart and brain sustain a catastrophic ischemic insult can be devastating.
Methods: A retrospective analysis of AIS patients admitted to a Hyperacute Stroke Unit between Jan 2020- Dec 2021, was performed to investigate occurrence of concurrent AIS and AMI. Patients were initially included, if they had elevated troponins upon admission to the stroke unit, following which they were excluded or included based on the diagnosis and treatment of MI within 72 hours of AIS or vice versa. We describe the clinical characteristics on admission, clinical progression, management, and outcome of patients suffering from CCIs.
Results: The number of AIS patients analysed was 1921. Of these 302(16%) patients had elevated troponin and 35 (1.8%) patients were treated as acute coronary syndrome. 17(0.9%) patients had CCI.Further analysis of CCI patients showed in-hospital death occurred in 7(41%) patients. The median length of stay was 6 days (range 1-44 days). Angioplasty was used to treat MI in 5(29%) patients and the rest were medically managed or died.
Conclusions: Although rare, CCI has exceedingly high mortality and therefore recognising and choosing the appropriate therapy is vital when attempting to re-perfuse both vital organs. Collaboration between stroke physicians, neuro interventionalists and the cardiologists with a clear CCI pathway will enable better management and outcome to these patients.
Disclosures of Interest: No
Abstract N°: 2108
PERCUTANEOUS CLOSURE OF THE PATENT FORAMENT OVALE IN PATIENTS WITH ISCHEMIC STROKE: EXPERIENCE FROM A UNIVERSITY HOSPITAL
Albert Freixa Cruz*1, Gerard Mauri Capdevila1, Daniel Vázquez-Justes1, Miriam Paul Arias1, Yhovany Gallego1, Anna Garcia Díaz1, Cristina Nieva Sánchez1, Juan Manuel Casanova Sandoval2, Marcos García Guimaraes2, Francisco Purroy1
1Hospital Universitari Arnau de Vilanova, Neurology, Lleida, Spain,2Hospital Universitari Arnau de Vilanova, Cardiology, Lleida, Spain
On behalf of:
Background and aims: Patent foramen ovale (PFO) is a highly prevalent condition and even higher in patients <55 years of age who suffered a cryptogenic stroke. After ruling out other potential etiologies, the concept of stroke associated with PFO has been coined. Several clinical trials and meta-analyses changed the treatment paradigm in selected patients.
The objective is to establish the profile of patients with ischemic stroke followed in our hospital by percutaneous closure of PFO.
Methods: Ischemic stroke patients who have undergone percutaneous closure of PFO between 2021 and 2023 have been reviewed retrospectively. Demographic data, medical history, characteristics of the cerebral ischemic event, percutaneus closure procedure, and complications have been considered.
Results: 13 patients with ischemic stroke underwent percutaneous closure of PFO. 76.9% were men. The mean age was 46.6 years, of whom 76.9% did not have vascular risk factors and 15.4% had migraine. Majority (61.5%) had RoPE score ⩾7. According to Oxfordshire classification, the most frequent strokes were POCI (61.5%) and initial etiology was ESUS/Cryptogenic. Three cases coincided with Valsalva maneuvers. 92.3% had an mRS ⩽2 at discharge. All PFO were massive and in 46.1% were associated with atrial septal aneurysm. The mean time until closure was 2.21 years. As complications, 1 patient (7.7%) presented transient atrial fibrillation. Effective closure was verified in all. No recurrences have been recorded.
Conclusions: Percutaneous PFO closure is feasible in selected stroke patients. In our sample, transient AF was identified in 7.7%. it is necessary to optimize the time between the event and percutaneous closure.
Disclosures of Interest: No
Abstract N°: 2444
ANTICOAGULATION THERAPY AND ISCHEMIC STROKE IN ATRIAL FIBRILLATION PATIENTS: A PROSPECTIVE STUDY
1Medical University - Pleven, Neurology and neurosurgery, Плевен, Bulgaria,2Dr. Georgi Stranski University Hospital, Neurology clinic, Pleven, Bulgaria
On behalf of:
Background and aims: Anticoagulation therapy, including both Vitamin K antagonists (VKA) and non-vitamin K oral anticoagulants (NOACs), is considered effective for stroke prevention in patients with non-valvular AF. This study aims to investigate the relationship between ischemic stroke(IS) severity and lesion localization in patients with AF.
Methods: Of all the 1175 IS patients, admitted to the Neurology Clinic, UMHAT Pleven, Bulgaria, from January 2022 to December 2023, 221 (108 women, median age 77 years) had AF. The patients with AF and IS were divided into four groups:control group of 117 patients without previous anticoagulation; 57 patients on NOACs; 15 patients taking VKA, with INR>=2, and 32 patients taking VKA, but with INR<=2. IS severity on admission was assessed using the National Institutes of Health Stroke Scale (NIHSS).
Results: In the control group, anterior circulation infarction (ACI) experienced 75% of patients (n=103) with 65% of them had moderate to severe neurological deficits on admission (NIHSS>=10). In the NOAC group, 84% (n=48) had ACI, and 37.5% (n=18) of them had NIHSS>=10. In the well-controlled VKA group, 60% presented with ACI (n=9), and only one had a moderate stroke. In the subtherapeutic VKA group, 81% (n=26) had ACI, with 32% of them presenting with moderate to severe IS.
Conclusions: IS in patients with AF is more common in the anterior circulation. Patients on VKA treatment and INR in therapeutic range experience a lower incidence of ACI and less severe stroke. Such findings implement that individualized anticoagulation for patients with AF is the best therapeutic option for stroke prevention.
Disclosures of Interest: No
Abstract N°: 2565
CENTRAL AUTONOMIC SYSTEM DISCONNECTION IS ASSOCIATED WITH ACUTE MYOCARDIAL INJURY FOLLOWING ACUTE STROKE
Petr Mikulenka*1, Olivia Murray2,3, Alistair Perry2, James Garrard2,4, George Harston2,5, Michal Mihalovič6, Petr Toušek6, Ivana Štětkářová1, Davide Carone2,4,5
1Department of Neurology, University Hospital Kralovske Vinohrady, Third Faculty of Medicine, Charles University, Prague, Czechia,2Brainomix, Oxford, UK,3Division of Informatics, Imaging and Data Science, University of Manchester, Manchester, United Kingdom,4Radcliffe Department of Medicine, University of Oxford, UK,5Oxford University Hospitals NHSFT, UK,6Department of Cardiology, University Hospital Kralovske Vinohrady, Third Faculty of Medicine, Charles University, Prague, Czechia
On behalf of:
Background and aims: Myocardial injury (MI) can be frequently observed in patients with acute stroke. It has been hypothesised that stroke lesion location within the central autonomic network might precipitate MI. However neuroimaging studies offer conflicting results and the neuroanatomical basis of stroke-related MI is not yet fully understood. In this study, we explored how lesion location, and its impact on brain connectivity is associated with MI in acute stroke patients.
Methods: Stroke patients enrolled in a single-centre observational cohort study were screened for acute MI by serial troponin sampling. Stroke lesions were automatically segmented on follow-up scans (MRI or CT) using Brainomix inhouse-software, and were used in conjunction with a DTI template to generate disconnection spatial maps. A voxel-based, multivariate method (Sparse-Canonical-Correlation-Analysis was used to explore associations between new MI and a) areas directly damaged by stroke and b) areas disconnected.
Results: 250 patients were included in the study. 37 had a newly diagnosed MI. Stroke lesions causing disconnection to a number of regions comprising the central autonomous network such as the brainstem, the insula and the hypothalamus were found to be significantly associated with new MI (p<0.001).
Conclusions: The results presented suggests that MI in acute stroke is associated with disconnection to a wide number of cerebral areas comprising the central autonomic system. A network connectivity approach might be better suited in identifying patients at risk of MI in acute stroke.
Disclosures of Interest: No
Abstract N°: 3130
HEART INJURY MARKERS ACROSS CEREBRAL HAEMORRHAGES AND UNTREATED ISCHEMIC STROKES: IS THE HEMISPHERE INVOLVED RELEVANT?
Laura Mancinelli*1, Gabriele Prandin1, Federica Palacino1, Emanuele Vincis1, Giovanni Furlanis1, Paola Caruso1, Marcello Naccarato1, Paolo Manganotti1
1University of Trieste, Department of Medical Surgical and Health sciences, Trieste, Italy
On behalf of:
Background and aims: Stroke-heart syndrome (SHS) consists in cardiac injury following an acute stroke, ranging from ECG changes to sudden cardiac death. This applies to cerebral haemorrhage, especially when extensive. The aim of this study is to compare the relevance of the side affected in the SHS between cerebral haemorrhages (HS) and untreated ischemic strokes (IS).
Methods: We included 205 patients (2018-2022) in our Stroke Unit, divided between HS and IS, 98 have right hemisphere involved, 107 the left. We compared the event (HS vs IS), demographic-clinical features (sex, age, comorbidities, insula cortex’s involvement) and markers of cardiac injury (maximum TnI level reached, NT-proBNP, Tn pattern elevation over 30% baseline). Statistical analysis was performed with SPSS using X² test/Fisher-Yates test/Mann-Whitney U-test.
Results: No statistical differences between the clinical features were observed in the two cohorts (right vs left), specifically the type of event (50%/54% in HS right/left; 49%/46% in IS right/left), p=0.547, the only item bordering on significance is the insula cortex’s involvement (29%/18% in right/left, p=0.071); the cardiac marker of injury were not statistically significant between the two groups, in particular NT-proBNP (624; IQR 187-1863 in right and 539; IQR 205-1847 in left; p=0.528), maximum TnI level reached in right (16; IQR 8-43) and left (14; IQR 8-45), p=0.278. The troponin elevation pattern up to 30% was 21%/25%, respectively right/left (p=0.611).
Conclusions: This study suggests there are no significant differences considering the event and the side involved in the acute phase. The raise and fall pattern is superimposable.
Disclosures of Interest: No
E-Poster – Case Reports
Abstract N°: 336
A RARE CASE OF BILATERAL MEDIAL MEDULLARY INFARCT: HEART-SHAPED BRAINSTEM STROKE
1University at Buffalo Jacobs School of Medicine and Biomedical Sciences, Neurology, Buffalo, United States,2University at Buffalo Jacobs School of Medicine and Biomedical Sciences, Neurology, East Amherst, United States
On behalf of: Huasheng Wang, Minahil Shahid, Zalan Wahid Khan, Hamidreza Abbasi
Background and aims: Bilateral medial medullary infarcts (BMMI) is a rare stroke subtype and often leads to paralysis, sensory disturbance, ataxia, dysphagia, and death. It is usually caused by occlusion of the anterior spinal artery or vertebrobasilar arteries. Stenosis, ipsilateral vertebral artery dissection, and cardioembolism are other possible etiologies.
Methods: We report a case of a 77-year-old Caucasian female with hypertension, hyperlipidemia, chronic alcohol use of 30 years, and newly diagnosed atrial fibrillation.
Results: She initially presented to the emergency department for left-sided numbness and was discharged after CTA of the head and neck and MRI of the brain were reported as unremarkable. She returned a week later due to persistent numbness that now involved her fingers and lower extremities bilaterally. This time, she complained that her "knees gave out." Examination revealed facial diplegia, right ptosis, normal tongue movement, and 5/5 motor strength throughout. She had diminished sensation to pinprick in both feet. Follow-up MRI of the brain demonstrated the pathognomonic rostral medulla Y-shaped "heart sign." A review of her prior brain MRI showed similar, less prominent bilateral medullary diffusion changes with ADC correlate not mentioned on the radiology report. Apixaban was started. She had an NIHSS of 1 for sensory changes and a Modified Rankin score of 2 at discharge.
Conclusions: In summary, our patient had the classic MRI findings of bilateral medial medullary infarct but astonishingly few clinical deficits. This case demonstrates significant differences in patient presentation and outcomes, as well as highlights the fascinating variability in brainstem stroke syndromes.
Disclosures of Interest: No
Abstract N°: 344
UNILATERAL NUMBNESS OF THE ORAL CAVITY: A UNIQUE PRESENTATION IN A PATIENT WITH THALAMIC INFARCT
Zalan Khan1, Hamidreza Abbasi1, Marilou Ching*2
1University at Buffalo Jacobs School of Medicine and Biomedical Sciences, Neurology, Buffalo, United States,2University at Buffalo Jacobs School of Medicine and Biomedical Sciences, Neurology, East Amherst, United States
On behalf of: Zalan Wahid Khan, Hamidreza Abbasi
Background and aims: Pure sensory stroke is a well-defined entity in which hemisensory symptoms predominate in the absence of other concomitant neurological signs. It is an infrequent lacunar syndrome accounting for approximately 5.4% of acute ischemic strokes and 17.4% of lacunar syndromes.
Methods: We report a case of a 60-year-old man with hypertension, diabetes, hyperlipidemia, and obstructive sleep apnea who presented with an acute onset of numbness involving the left half of the tongue and upper and lower gums while at dinner.
Results: He best described his symptoms as akin to an injection of local anesthetic before a dental procedure. His general physical and neurological examinations were within normal limits. His vital signs were unremarkable except for elevated blood pressure of 184/116 mmHg. Pertinent laboratory includes HBA1c of 6.5% and LDL of 150 mg/dL. CTA of the head and neck were negative for intracranial or extracranial stenosis or aneurysms. MRI of the brain revealed diffusion changes in the right anterior thalamus. Given the patient's vascular risk factors, the etiology of his stroke was felt to be secondary to small vessel disease. His treatment consisted of dual antiplatelet agents, high-intensity statin, and risk factor modification.
Conclusions: In summary, acute thalamic stroke can present with a variety of sensory and motor deficits based on the topographic area of infarction. We highlighted a unique case of pure sensory thalamic syndrome, specifically involving the parvicellular portion of the ventropostero-medial nucleus of the thalamus, which plays a fundamental role in relaying gustatory information to the cortex.
Disclosures of Interest: No
Abstract N°: 359
PAROXYSMAL POSTERIOR ALIEN LIMB SYNDROME SECONDARY TO ACUTE ISCHEMIC LEFT PARIETAL INFERIOR MCA TERRITORY INFARCTION
AHMED ALI*1, Ganesh Subramanian1
1Queen's Medical Centre, Stroke, Nottingham, United Kingdom
On behalf of:
Background and aims: Alien Limb Syndrome is a rare ill-defined neurological phenomenon characterized by an individual's perception of disownership and estrangement from one's own limb, often coupled with the limb's seemingly autonomous, purposeful actions. AHS, generally regarded as persistent, but rarely maybe observed as paroxysmal.
Methods: A 72-year-old man presented with atypical behaviour involving his right arm, perceiving it as unfamiliar. He encountered paroxysmal episodes of attempting self-strangulation using his other hand, coupled with difficulties in finding words. With a medical history including atrial fibrillation, past tuberculosis, he ceased oral anticoagulants under the impression that it would aid the healing of a leg ulcer. Following a routine CT head, high-dose aspirin was initiated, and he was referred to the TIA clinic. Subsequent MRI findings disclosed an infarction in the left parietal inferior middle cerebral artery territory, confirming a diagnosis of stroke, likely attributed to cardiac embolism. Aspirin was discontinued, and Apixaban resumed in the management plan.
Results: While most Alien Hand Syndromes (AHS) are linked to anterior pathway insults, this case highlights a paroxysmal manifestation associated with a posterior lesion, specifically from an acute ischemic infarction.The precise pathophysiology is unknown regarding how parietal lobe disruption can lead to AHS, although it is believed to be from error in neuronal connections
Conclusions: This case sheds light on the unique presentation of Posterior Alien Limb Syndrome, introducing a paroxysmal aspect of it. Clinicians should be vigilant in distinguishing AHS from other conditions, such as extrapyramidal movement disorders and epileptic seizures, during the differential diagnosis process.
Disclosures of Interest: No
Abstract N°: 379
RECURRENT BRAIN ISCHEMIA IN A 27-YEAR OLD MAN
Daniel Richter*1, Jeyanthan Charles James2, Özkan Neriman3, Ulrich Sure3, Ralf Gold4, Carsten Lukas4, Christos Krogias1
Background and aims: The causes of an ischemic stroke in young adults include functional compression syndromes such as “Bow hunter`s syndrome” (rotational vertebral artery compression), which is a diagnostic challenge.
Methods: We present a case of a 27-year-old man with recurrent cerebral ischemia in the vertebrobasilar vascular area with the diagnosis of rotational vertebral artery compression that was suggested by dynamic Doppler and duplex sonography (DDS) and confirmed by digital subtraction angiography (DSA).
Results: A 28-year-old patient was repeatedly admitted to different hospitals due to recurrent cerebral ischemia in the vertebrobasilar vascular area that were treated with systemic thrombolysis in several times. Extended etiological examinations were unremarkable. DDS suggested a compression of the V3 segment of the right vertebral artery during head rotation that was confirmed by DSA. Reevaluation of CTA images using 3D reconstructions finally revealed a shark fin-like osseous condyle at the right sided skull base in close relationship to the horizontal part of the V3 segment. Extirpation of this bone spur resulted in the absence of further ischemic events.
Conclusions: Unexplained recurrent ischemic insults in the vertebrobasilar territory, especially in young adults, should lead to the differential diagnostic consideration of rotational vertebral artery compression, where dynamic Doppler and duplex sonography can be helpful in the diagnostic work-up. Dynamic DSA in neutral and rotated positions remains the gold standard to make a definite diagnosis. Careful re-evaluation of CT and MRI as well as additional 3D reconstruction of CT scans may help to precisely identify the underlying etiologies.
Disclosures of Interest: No
Abstract N°: 397
REVERSIBLE CEREBRAL VASOCONSTRICTION SYNDROME ASSOCIATED WITH ANTIPHOSPHOLIPID SYNDROME IN A POSTPARTUM PATIENT WITH PREECLAMPSIA
1University College London Medical School, London, United Kingdom,2University College London Hospitals NHS Foundation Trust, Department of Haematology, LONDON, United Kingdom,3National Hospital for Neurology and Neurosurgery, Comprehensive Stroke Service, London, United Kingdom
On behalf of:
Background and aims: A 42-year-old woman had sudden onset occipital pain and word-finding difficulties three days post-twin delivery by emergency caesarean-section. Symptoms resolved after two hours. She developed transient binocular horizontal diplopia a few days later. Her third-trimester had been complicated by hypertension, proteinuria, mild thrombocytopenia (nadir platelet count 100x109/L) and liver function test abnormalities, managed as preeclampsia. Medical history included three first-trimester miscarriages (2/3 attributed to chromosomal abnormalites).
Methods:
Results: MRI brain showed an acute left frontal lobe infarct. CT-angiography revealed focal stenosis and irregularity in the left middle cerebral artery. Reversible cerebral vasoscontriction syndrome (RCVS) was suspected, and supported by resolution of angiographic abnormalities after four months. Antiphospholipid antibody (aPL) testing identified moderate positive IgG anti-beta-2 glycoprotein antibodies, persistent beyond 12 weeks, and combined with the history of preeclampsia, suggested obstetric antiphospholipid syndrome (OAPS). She made a full recovery. Despite persistent aPL, antithrombotic therapy was not considered neccessary as the neurological event was non-thrombotic. However, given the association of both preeclampsia and OAPS with future cardiovascular/thrombotic disease, optimisation of modifiable risk factors was recommended.
Conclusions: RCVS may be idiopathic or precipitated by various factors, including pregnancy-related conditions. There are few case reports of RCVS in association with aPL. This, to our knowledge, is the first report of RCVS occuring with preeclampsia and probable OAPS. The question arises whether aPL may have a direct pathophysiological role in RCVS, particuarly considering the association of aPL with other conditions of vascular spasm, notably Raynaud's phenomenon and livedo reticularis, and known role of endothelial cell dysfunction in aPL-pathogenicity.
Disclosures of Interest: No
Abstract N°: 412
PROGRESSIVE MULTIFOCAL LEUKOENCEPHALOPATHY MASQUERADING AS ACUTE ISCHEMIC STROKE IN A HIV PATIENT WITH I.R.I.S
Muhammad Ishaq Khan*1, Ahmed Ali1, Sumbal Saleem2, Muhammed Nawaz2, Abdul Aziz3
1Queen's Medical Centre, Nottingham, United Kingdom,2Sandwell General Hospital, Birmingham, United Kingdom,3Royal Derby Hospital, Stroke Medicine, United Kingdom
On behalf of:
Background and aims: Progressive multifocal leukoencephalopathy is a demyelinating infectious disorder of the CNS typically observed in immunocompromised individuals with a history of AIDS, hematologic malignancies, or immunosuppressive drug therapy. This case highlights the challenging diagnostic scenario of an undiagnosed HIV patient presenting with subacute left-sided weakness, initially resembling an acute stroke.
Methods: A 56-year-old previously healthy woman reported a two-week history of left-sided numbness, progressing rapidly to severe left-sided weakness within three days. On admission, the recorded NIHSS score was 8. Imaging revealed enhancement along the right parietal gyrus on MRI. Widespread lymphadenopathy detected by whole-body CT raised suspicions of haematological malignancy. Neuro-oncology recommendation of tumour markers was inconclusive. Positive HIV serology prompted investigation for PML, confirmed by the presence of JC Virus in her CSF. Unfortunately, initiation of HAART led to the development of IRIS, complicating the clinical course. Despite interventions, the patient's condition rapidly deteriorated and lead to become the cause of her death.
Results: PML's subacute presentation can mimic a stroke, emphasizing the importance of understanding its background and potential complications, particularly in patients with HIV/AIDS or other immunocompromised conditions. Delayed diagnosis due to the absence of known immunocompromised status underscores the need for heightened awareness and early initiation of antiretroviral therapy.
Conclusions: PML, often misdiagnosed as a stroke mimic, demands careful consideration in patients who are young, requiring clinicians to be adept at distinguishing between these entities. Adding HIV and syphilis serology to any patient coming as a young stroke patient can reduce the delays in diagnosis.
Disclosures of Interest: No
Abstract N°: 421
IRON-DEFICIENCY ANEMIA AS A PRECURSOR TO CEREBRAL VENOUS SINUS THROMBOSIS: A CASE REPORT
Elena Simeonovska Joveva*1,2, Lichkova Elena2, Marija Trajkova Petkovska2, Stefan Petrovski1, Marija Karakolevska Ilova1
1"Goce Delchev" University, Faculty of Medical Sciences, Stip, Republic North Macedonia, Штип, Macedonia,2Clinical Hospital Shtip, Shtip, Macedonia
On behalf of:
Background and aims: Cerebral venous sinus thrombosis (CVST) poses a rare yet severe neurological challenge, with multifactorial etiology encompassing prothrombotic conditions, infections, trauma, medical procedures, hormonal factors, inflammatory disorders, dehydration, malignancies, and rare inherited disorders. This case report explores the association between iron deficiency anemia and the development of CVST, shedding light on the non-specific symptoms.
Methods: A 41-year-old female presented with: headache, dizziness, nausea, and vomiting. Examination revealed impaired consciousness, left-sided hemiplegia, and brisk reflexes. Diagnosis of CVST was made with computed tomography (CT) and computed tomography angiography (CTA). A comprehensive assessment, including blood count and iron studies, was conducted to evaluate the patient's iron-deficiency anemia. The case was initially managed with anticoagulation therapy and two units of packed red blood cells.
Results: Imaging studies displayed bilateral subarachnoid hemorrhage, intracerebral hematomas, and a filling defect in the superior sagittal sinus. Laboratory results indicated iron-deficiency anemia and thrombocytosis. Subsequent CT scans revealed hyperdense hemorrhagic changes, persistent SAH, and intracerebral hematomas. Physiologically, iron deficiency induces a prothrombotic state through increased platelet aggregation, alterations in clotting factor function, and impaired fibrinolysis. Additional links include endothelial dysfunction, elevated homocysteine levels, and reduced nitric oxide bioavailability.
Conclusions: This case underscores the significance of recognizing iron deficiency as a significant contributor to a hypercoagulable state in the context of CVST. The interplay of iron in physiological processes, coupled with its deficiency, heightens the susceptibility to thrombotic events. Recognition and management of iron deficiency anemia are crucial in mitigating the risk of complications associated with CVST.
Bilateral cerebral oedema.
Disclosures of Interest: Yes
Abstract N°: 462
ANTON’S SYNDROME: A RARE AND UNUSUAL FORM OF BILATERAL OCCIPITAL INFARCT
Tariq Soliman1, Tahir Ismail1, Abul Azim*1, Juliana Delos Reyes1
1West Suffolk Hospital, Bury St Edmunds, United Kingdom
On behalf of:
Background and aims: Anton's syndrome is a condition in which patients are in denial of loss of vision (i.e., visual anosognosia) associated with confabulation in presence of obvious visual loss and cortical blindness. It is a syndrome that results from injury to the visual association cortex while the anterior visual pathways remain intact. It is a very rare condition; only 28 cases have been recorded between 1965 and 2016. It is most commonly reported after cerebrovascular accident but has been reported in other causes such as encephalopathy, head trauma, MS, MELAS, adrenoleukodystrophy and HIV.
Methods: An 89-year-old patient, known to have stroke and hypertension, presented to the stroke services at West Suffolk hospital in September 2023 with bilateral occipital infarcts. Despite his obvious blindness, he expressed denial of visual loss and demonstrated confabulation in his accounts of his surroundings consistent with a diagnosis of Anton's syndrome.
Results: CT head scans confirmed large left PCA territory infarct and small right PCA territory infarct involving occipital lobes.
Conclusions: A suspicion of Anton's syndrome should be considered in patients with a denial of visual loss with evidence of occipital lobe injury. As in our patient, cerebrovascular disease is the most common cause of Anton's syndrome. However, any condition that may cause cortical blindness can lead to Anton's syndrome. The recovery of visual function depends on the underlying etiology, in our case due to the bilateral occipital lobe infarction being less likely to result in complete recovery. Management was focused on secondary prevention and rehabilitation.
Disclosures of Interest: No
Abstract N°: 466
EFFECTS OF COMBINING A STANDING UNSTABLE BOARD AND ELECTRICAL STIMULATION TO THE NECK MUSCLE ON SITTING BALANCE: TWO CASES STUDY
1Sonodakai Medical Corporation, Hanahata Rehabilitation Hospital, Department of Rehabilitation, Adachi-ku, Tokyo, Japan,2Tokyo Metropolitan University, Graduate School of Human Health Sciences, Department of Physical Therapy, Arakawa-ku, Tokyo, Japan,3Sendai Seiyo Gakuin College, Department of Rehabilitation, Japan,4International University of Health and Welfare Graduate School, Department of Health and Medical Sciences, Occupational Therapy, Japan
On behalf of:
Background and aims: Previous studies reported that unstable board and neck muscle stimulation (NMS) improves balance of stroke patients. Combining them would acquire more effects. This case series aimed to clarify the combined effect of the unstable board and NMS in standing.
Methods: Two patients with chronic stroke participated, case 1, a 74-year-old woman with right hemiplegia, and case 2, a 75-year-old woman with left hemiplegia. The intervention was conducted in a 1-week AB design. During period A, an unstable board was applied on the non-paralyzed leg with usual physiotherapy. During period B, transcutaneous electrical nerve stimulation (TENS, 100 Hz, 200 µs, 20 min) to the sternocleidomastoid muscle on the paralyzed side was added to the period A intervention. Evaluations were performed on the trunk impairment scale (TIS) and the center of pressure (COP) movement distance during the righting reaction (RR) from a tilted sitting at the beginning and end of each period.
Results: After period A, the TIS scores were almost unchanged. For the RR to the non-paralyzed side, the COP movement distance increased to 2.86 mm in case 1 and 6.17 mm in case 2. After period B, the TIS score was unchanged in case 1 and improved by 8 points in case 2. Under the same condition, the COP movement distance increased by 4.4 mm in case 1 and 9.4 mm in case 2.
Conclusions: It was suggested that combining an unstable board and TENS was more effective. We believed that NMS activated the vestibular function.
Disclosures of Interest: No
Abstract N°: 503
A CASE REPORT OF MOYAMOYA SYNDROME PRESENTING AS MIGRAINES IN A 31-YEAR-OLD HONG KONG CHINESE WOMAN
Charlie Saunders*1, Sudhakar Unnam1, Sandip Ghosh1
1University Hospital Crosshouse, Crosshouse, United Kingdom
On behalf of:
Background and aims: Moyamoya Disease (MMD) is an occlusive cerebrovascular condition with progressive stenosis of the internal carotid arteries (ICA) and their branches, resulting in a formation of collateral vessels. In Moyamoya Syndrome (MMS), individuals have an underlying disease resulting with a vasculopathy similar to MMD. We present a case where an individual presented with complex migraines was found to have MMS
Methods: Describe an individual with underlying MMS that presented with migraines.
Results: A 31-year-old female was referred to neurovascular clinic in May 2023 with ischaemic lesion on MRI. She reported 2 years of transient right hemiparesis, expressive dysphasia and scotoma associated with twice-weekly hour-long headache. Her background consisted of Grave’s Disease.
Her first event of right arm sensory disturbance in 2021 triggered hospitalisation. She fully recovered, CT imaging was normal and was diagnosed with migraine. MRI in September 2022 showed frontal T2 hyper-intensities with repeat MRI confirming the lesions being ischaemic initiating her referral. In May 2023, the neurological events were less frequent and she had no focal neurology. CTA in June showed bilateral narrowing of the terminal ICAs and M1 segments with bilateral abnormal collateral circulation. MRA in October showed no interval change. Diagnosis of MMS was made, adequate thyroid control recommended, with further imaging assess for progression.
Conclusions: The case highlights that MMS can present with recurrent migraine-like episodes. When investigating young adults with recurrent headaches and neurological deficits, vascular events and MMS should be considered. Particularly if there is concurrent underlying disease including hyperthyroidism
Disclosures of Interest: No
Abstract N°: 685
BEGINNING ANTICOAGULANTS FOR ACUTE LIMB ISCHEMIA IN A POST-HEMICRANIECTOMY PATIENT WITH A LARGEHEMISPHERIC INFARCT, A CASE REPORT
Enrique Lorenzo Panganiban*1, Cymbeline Perez-Santiago2
1St. Luke's Medical Center - Global City, Institute for Neurosciences, Taguig, Philippines,2St. Luke's Medical Center - Global City, Taguig, Philippines
On behalf of:
Background and aims: Timing the initiation of anticoagulants after large hemispheric infarct cases from cardioembolic events has always been a balance between preventing further strokes, and a hemorrhagic transformation. However, bedridden patients may also be afflicted with the formation of other thrombi in other vascular beds. The authors present a stroke case, who underwent decompressive hemicraniectomy, but required acute medical management with alteplase for an acute limb ischemia within four days of ictus and two days of surgery.
Methods: A 62-year-old male, poorly compliant to his medications for his permanent atrial fibrillation, presented with drowsiness, left sided weakness, and anarthria. Able to follow commands, he suffered from an acute large hemispheric infarct involving the right proximal-M1, mid-A4, and distal-P3 segments and had to undergo decompressive hemicraniectomy on the second day post-ictus. Over two consecutive days, the patient developed an acute limb ischemia of the right arm from the right proximal subclavian artery to the proximal brachial artery, and the right leg below the popliteal artery (Rutherford Classification 2b and 2a, respectively).
Results: He underwent balloon angioplasty for both limbs, suctioning of the systemic cardio-emboli, catheter directed thrombolysis, and intra-arterial alteplase drip. After shifting this to Dabigatran, the patient continue to improve clinically and radiological monitoring only showed minimal hemorrhagic conversion. Eventually the patient was discharged.
Conclusions: Cardio-embolism is always a threat to multiple vascular beds. In this case, the importance of a multi-disciplinary approach in deciding to prevent limb loss with an anticoagulant prevailed over the risk for hemorrhagic transformation of a large hemispheric infarct post-operatively.
Disclosures of Interest: No
Abstract N°: 1089
CATASTROPHIC MULTIPLE RECURRENT CEREBRAL ISCHEMIA IN A PATIENT WITH NEWLY DIAGNOSED HYPEREOSINOPHILIA: A CASE REPORT
Maria Rosaria Bagnato*1,2, Martina Gaia DI Donna1,2, Maria Rita DI Ruzza2, Emanuele Saggese2, Mario Ferrante2, Temistocle Lo Giudice2, Paola Santalucia2, Maurizio Plocco2
1University Tor Vergata, Rome, Neurology, Rome, Italy,2Hospital Fabrizio Spaziani, Stroke Unit, Frosinone, Italy
On behalf of:
Background and aims: Ischemic strokes from rare causes are insidious conditions sometimes underling systemic diseases like hyperosinophilia, as in this case.
Methods: An 82-year-old man, no home therapy, arrived in E.R. for dysarthria and right hemiataxia. Brain CT and angio-CT were normal. He underwent intravenous thrombolysis, with recovery. On blood tests, hypereosinophilia(24.000/mm3) of neodiagnosis, was found. Infectious, autoimmune and other secondary aetiologies were ruled out. EKG was sinusal. Brain MRI showed multiple recent ischemic strokes in border zones (Fig.1a,b). Total-body CT-scan was performed showing splenomegaly. In the suspicion of chronic myeloproliferative disease, molecular investigation of BCR/ABL and FIP1L1/PDGFRa were performed, resulting negative. Corticosteroid therapy was started. 2 weeks after, the patient presented with left motor deficit. The eosinophils were 19,000/mm3. Brain MRI showed new ischemic lesions in border zones. Oncocarbide was started. The Bone Marrow Aspiration and Biopsy report confirmed a chronic myeloproliferative disease. After two weeks, eosinophil count remained elevated and Imatinib was started. Despite treatment, the patient presented new ischaemic episodes, and died 4 weeks later, following a brainstem stroke.
Results: Ischaemic stroke in hypereosinophilic syndromes (autoimmune, infectious, idiopathic or secondary disorders) is common. The ischemic lesions may involve large vessels for cardioembolism or border zones, possibly related to the stagnation of eosinophils and release of substances damaging endothelium, from granules.
Conclusions: Myeloproliferative forms may increase in frequency with the ageing of population, thus, it would be useful identifying prognostic factors to guide haematological treatment for stroke recurrence prevention.
SECONDARY STROKE PREVENTION IN INTRACRANIAL ATHEROSCLEROSIS GUIDED BY SEQUENTIAL VESSEL WALL IMAGING: A CASE SERIES
Beatrice Del Bello*1,2, Federico Mazzacane1,2, Elisa Rognone3, Federica Ferrari1,2, Anna Pichiecchio1,3, Anna Cavallini2
1University of Pavia, Department of Brain and Behavioural Sciences, Pavia,2IRCCS Mondino Foundation, Department of Cerebrovascular Disease/Stroke Unit, Pavia, Italy,3IRCCS Mondino Foundation, Department of Neuroradiology, Pavia, Italy
On behalf of:
Background and aims: Secondary stroke prevention in ischemic stroke due to intracranial atherosclerotic disease (ICAD) relies on dual antiplatelet therapy (DAPT). A neuroimaging approach with vessel wall MRI (VWMRI) may help guiding decisions about treatment duration, ensuring a better balance between ischemic recurrence and hemorrhagic risk.
Methods: We retrospectively selected patients admitted to our stroke unit for ischemic stroke due to ICAD who underwent sequential VWMRI from 01/11/2021 to 01/09/2022. Clinical and radiological characteristics, stroke recurrence and hemorrhagic events were retrieved from follow-up visits at 3, 6 and 12 months. Plaque enhancement and degree of stenosis were assessed.
Results: Three patients were included. The time points for VW imaging were <1 month (T0), 4±1 months (T1) and 11±1 months (T2). One patient had an atherosclerotic plaque resulting in >50% stenosis, the other two had non-stenotic lesions. Baseline VWMRI revealed atherosclerotic lesions with vivid contrast enhancement in all patients. They were treated with DAPT and high-dose statins. At T1, lesions presented persistent enhancement and stable degree of stenosis. An asymptomatic recurrence in the same vascular territory was recorded in one patient. Patients were kept on DAPT. At T2, lesions presented minimal/absent enhancement. A reduction of the stenosis degree was appreciated in the stenotic lesion. Patients were started on SAPT. No symptomatic recurrence or hemorrhagic events occurred during follow-up.
Conclusions: Plaque risk features can be sequentially assessed non-invasively by VWMRI. The integration of radiological and clinical data may help to provide a tailored secondary prevention approach. Further studied are needed to assess the potential benefits of this approach.
Disclosures of Interest: No
Abstract N°: 1294
USING ORBITAL ULTRASOUND TO ASSIST IN EARLY DIAGNOSIS AND MANAGEMENT OF CENTRAL RETINAL ARTERY OCCLUSIONS
CHU PENG HOI*1, Wa Hou Tai2, Mat Mat Lam1
1Hospital Centre S. Januario, Neurology, Macao, China,2Hospital Centre S. Januario, Neurosurgery, Macao, China
On behalf of: Wai I Leong, Paulo Lo, Iek Hou Chu, Si Si Ieong
Background and aims: Central retinal artery occlusion (CRAO) is an ophthalmologic emergency with high morbidity and potential for long-term vision loss. CRAO is a form of acute ischemic stroke that was suggested to be treated with intravenous or intra-arterial thrombolysis as quickly as possible. The gold standard for diagnosis is to perform a dilated fundoscopic exam which reveals a pale retina with a “cherry-red spot” on the fovea. However, a dilated fundoscopic exam is often time-consuming and technically challenging in an emergency department (ED) setting. Alternatively, orbital ultrasound is a fast and non-invasive tool that is already widely used in the ED and can assist in diagnosis. The aim of this paper is to demonstrate the effectiveness of orbital ultrasound in the early diagnosis and management of CRAO.
Methods: A case of CRAO was described and a literature review was conducted.
Results: We report the case of a 44-year-old previously healthy woman who presented to the ED with sudden onset of painless vision loss of her right eye. An orbital ultrasound revealed a retrobulbar “spot sign” and she was subsequently diagnosed with CRAO (Figure 1). Her right eye visual function was improved after treatment with intravenous alteplase 3 hours after symptom onset.
Conclusions: Orbital ultrasound is a reliable and effective alternative tool to help diagnosis CRAO early and shorten the time for reperfusion therapy.
Disclosures of Interest: No
Abstract N°: 1441
ACUTE STROKE GOES VIRAL: CASES OF YOUNG AND OLD STROKE SECONDARY TO PRIMARY VARICELLA ZOSTER INFECTION
Kalpesh Kondalkar*1, Sam Craik1, Busayo Osineye1, Meena Srinivasan1
1Princess Royal Hospital, Stroke Medicine, Telford, United Kingdom
On behalf of:
Background and aims: Varicella zoster is a documented risk factor for development of ischemic stroke for up to 1 year following infection. Multiple cases of stroke following zoster reactivation have been reported previously. Here we outline two admissions to our ward in 2023 in which a stroke developed following primary zoster infection.
Methods: An 18 year old woman was admitted with right hand numbness, speech disturbance and headache. A CT angiogram revealed occlusion of the left middle cerebral artery. She was treated with dual antiplatelets. A lumbar puncture was performed and cerebrospinal fluid was positive for Varicella zoster. On further history the patient revealed she had chicken pox 3 months prior. She was treated with intravenous aciclovir and discharged with her neurological symptoms largely resolved.
Results: A 75 year old male with a background of Non-Hodgkin lymphoma was admitted with acute confusion and right sided weakness and high fever. Examination also revealed a rash to the torso and head. CT revealed an area of low attenuation in the right basal ganglia, MRI revealed multiple bilateral infarctions. Lumbar puncture was performed due to suspected encephalitis and PCR was positive for Varicella zoster. The patient was treated with intravenous aciclovir however suffered a drop in consiousness. A repeat CT revealed catastrophic intracerebral bleed extending into the ventricles. The patient received palliative care and died one day later.
Conclusions: Varicella zoster infection is an important risk factor for stroke in both younger and older adults and should be considered in unusual presentations.
Disclosures of Interest: No
Abstract N°: 1462
CEREBRAL SINUS VENOUS THROMBOSIS IN THE SETTING OF ULCERATIVE COLITIS
Lichkova Elena*1, Elena Simeonovska Joveva2, Marija Trajkova Petkovska1, Natasha Vasileska Pirganoska3, Keti Mihailovska1, Blagica Djidrova1, Maja Bozinovska4
Background and aims: Cerebral venous sinus thrombosis (CVST) is a rare and severe complication of inflammatory bowel disease (IBD), including ulcerative colitis (UC) and Crohn's disease (CD). UC, a subtype of IBD, exhibits diverse neurological manifestations, with increased thrombotic complications. A 56-year-old male with concomitant UC was diagnosed with cerebral venous thrombosis (CVT) after presenting to the emergency department with epileptic seizures and right-sided extremity weakness.
Methods: Neuroimaging assessments, MRI, and MRV, were conducted to confirm the diagnosis.
Results: MRI revealed thrombotic masses in the transverse sinus, extending into the right sigmoid sinus. A small hypersignal change in the right temporo-occipital region lacked pathological contrast accumulation, indicating hemorrhage. Ischemic alterations in the left cerebellum were attributed to sagittal sinus thrombosis. MRI venography: findings include hypointense filling defects within the lumens of the superior sagittal sinus, inferior sagittal sinus, as well as the right sigmoid and right transverse sinuses.
Conclusions: UC is linked to an increased risk of deep venous thrombosis and pulmonary thromboembolism. CVT, though rare, occurs in both UC and CD cases. Proposed mechanisms for UC-related thrombosis include hyper-coagulation, hypo-fibrinolysis, platelet abnormalities, endothelial dysfunction, and immunological issues. Considering IBD as a potential cause of CVT is crucial for early diagnosis and management, improving the typically poor prognosis. Prophylactic anti-coagulation should be considered, especially during severe IBD flares.
Disclosures of Interest: No
Diffuse brain sinus thrombosis.
Abstract N°: 1483
BRAIN ABSCESS CAUSED BY ESCHERICHIA COLI AFTER EMBOLIZATION OF A GIANT ARTERIOVENOUS MALFORMATION. CLINICAL CASE
Andrii Netliukh*1, Andrian Sukhanov1, Oleh Kobyletskyi1
1MNE "First Territorial Medical Association of Lviv", Lviv, Ukraine, neurosurgery, Lviv, Ukraine
On behalf of:
Background and aims: Reports of infectious complications after endovascular procedures are rare, as are reports of brain abscesses caused by Escherichia coli. Review of this clinical case shows how to choose the most effective treatment option and improve the patient's quality of life managing the harmful complications.
Methods: A 37-year-old patient admitted with complaints of convulsive attacks, fever, speech impairment, and right-sided hemiparesis, who developed a brain abscess 1 month after the third stage of embolization of a giant brain arteriovenous malformation (AVM). Cultures of the abscess showed a positive result for Escherichia coli.
Results: This case presents a unique clinical phenomena of spontaneous brain abscess caused by E. coli in the background of a giant AVM in an adult male without the known route of infection spread and without immunosuppression. During the long course of treatment, several recurrences of the abscess were observed, in each of which complex approaches were used in a combination of neurosurgical resection of an abscess with antibiotic therapy, AVM partial bipolar cauterization.
Conclusions: Although abscess formation after embolization is extremely rare, it is a serious condition that requires immediate treatment. The probability of unexpected infectious complications should be taken into account during endovascular treatment of brain AVMs. Long and repeated procedures, incomplete embolization of the AVM, the use of a large amount of embolization material can significantly increase the risk of infection during endovascular intervention.
Disclosures of Interest: No
Abstract N°: 1729
SAFETY AND EFFECTIVENESS OF EMERGENT CEA COMBINED WITH IVT AND EVT IN TANDEM ACUTE ISCHEMIC STROKE - A CASE SERIES
Renato Simonetti*1, Federica Pes2, Andrea Saletti3, Cristiano Azzini2, Marina Padroni2, Luca Traina4, David Rodriguez-Luna5, Alessandro De Vito2
1Vall d'Hebron Institut de Recerca, Stroke Unit, Barcelona, Spain,2Ospedale Sant'Anna, Stroke Unit, Ferrara, Italy,3Ospedale Sant'Anna, Dpt of Neuroradiology, Ferrara, Italy,4Ospedale Sant'Anna, Dpt. of Vascular Surgery, Ferrara, Italy,5Hospital Vall d'Hebron, Stroke Unit, Barcelona, Spain
On behalf of:
Background and aims: Acute ischemic strokes resulting from Large Vessel Occlusion (LVO) with tandem lesions account for 15-30% of all LVO strokes. These strokes typically have poorer outcomes and are less responsive to IVT. (Hebert D et al, 2022). This case series aims to highlight the role of emergent Carotid Endarterectomy (CEA) as an alternative to carotid stenting.
Methods: The prospective database of carotid surgery of the Azienda Ospedaliero-Universitaria of Ferrara, Italy was reviewed (2013-2023) Series involve 9 patients presented with stroke-in-evolution, with CTA determination of tandem occlusion (ICA+MCA/ACA) treated with emergency CEA combined with IVT/EVT.
Results: Patients had a mean age of 74 and were predominantly male (77.8%). 33.3% had hypertension and 11.1% had diabetes. Only 22.2% of patients was on antiplatelet therapy, and none was on anticoagulants. The median NIHSS score at admission was 16, reduced to 3 at discharge. The median ASPECTS score at admission was 9. Treatment involved Endovascular Treatment (EVT) with CEA in 44.4% of cases or Intravenous Thrombolysis (IVT) combined with EVT and CEA in 55.6%. 33.3% had unfavorable outcomes (mRS > 2) at 90 days, with minimal post-surgical complications. None of the patients experienced recurrences in the subsequent 90 days.
Conclusions: Emergent CEA, combined with EVT or IVT+EVT, is a promising option for acute ischemic stroke resulting from tandem occlusion. This series encourages further research to validate the effectiveness and safety of emergent CEA, considering its significant impact on NIHSS score, patient independence, and the low rate of complications.
Disclosures of Interest: No
Abstract N°: 1836
HYPERACUTE HYPOFIBRINOGENEMIA AS A COMPLICATION OF THE RT-PA THERAPY IN STROKE PATIENT
Lusine Martirosyan*1, Khachik Petrosyan1
1Saint Gregory the Illuminator Medical Center, Department of general and vascular neurology, Yerevan, Armenia
On behalf of:
Background and aims: IVT is an evidence-based therapy for acute ischemic stroke. Severe hypofibrinogenemia after intravenous thrombolysis (IVT) with rt-PA is rare, potentially misdiagnosed complication, which occurs with using rt-PA in nearly 5% of AIS cases, with huge increase of the risk of major bleedings. There are no clear data on when the peak decrease in fibrinogen develops and when hypofibrinogenemia is regulated.
Methods: We have observed a case of hyperacute rt-PA-related hypofibrinogenemia and subsequent sustained low fibrinogen levels for about 76 hours.
Results: A 74-year-old woman was admitted with acute-onset vague speech, prosoparesis and left limb weakness for 1 hour. An MRI was performed, FLAIR negative ischemic stroke was detected, with occlusion of the right M1 distal segment. Pre-stroke mRs-0, NIHSS-11, DTI- 6min, DTN-19min, DTP-48min. During the infusion bleeding from the nose and gums was observed, followed by bruises spreading to the upper and lower limbs. Pre-infusion fibrinogen level: 318 mg/dL, immediate post-infusion level: 39 mg/dL. After cessation of epistaxis and gingival bleeding and exclusion of intracranial hemorrhage, mechanical thrombectomy was performed considering the stability of other parameters. Fibrinogen replacement therapy was not realized, due to documented patient' intolerance to plasma. In dynamics, no major bleeding complications developed, fibrinogen level was 212mg/dL after 76 hours.
Conclusions: Severe hypofibrinogenemia may occur after rt-PA, which increase the risk of major bleedings and mortality. Acute diagnosis of hypofibrinogenemia is crucial for preventing complications. We recommend routine check-up the fibrinogen level after i/v rt-PA and fibrinogen replacement therapy should be rapidly available to stroke centers.
Disclosures of Interest: No
Abstract N°: 1842
ACCOUNTING ISSUES OF DWI/FLAIR MISMATCH USE IN WAKE-UP STROKE: A CASE REPORT
Martina Gaia Di Donna*1,2, Maria Rosaria Bagnato1,2, Mario Ferrante2, Maria Rita DI Ruzza2, Temistocle Lo Giudice2, Emanuele Saggese2, Maurizio Plocco2
1Hospital Tor Vergata Roma, NEUROLOGY, Roma, Italy,2Ospedale Fabrizio Spaziani, STROKE UNIT, Frosinone, Italy
On behalf of:
Background and aims: In patients with acute wake-up stroke, rTPA is guided by a mismatch between DWI and FLAIR in the region of ischaemia.
Methods: We describe the case of a 33 years-old man, found in the early morning by his father on the floor, coming to E.R. with drowsiness, dysarthria, multidirectional nystagmus.Brain angio-CT showed left VA occlusion, no radiological signs of acute ischemia were revealed at basal CT. Based on WAKE-UP trials results,emergency-performed brain-MRI showed multiple ischemic lesions in posterior circle,among them a wide cerebellar lesion both DWI+ and FLAIR+,while a left emipontine lesion only DWI+ but no FLAIR+ was revealed.Because of FLAIR+ of the cerebellar lesion,considering the risk of haemorrhagic transformation, rTPA treatment was excluded (Fig.1).In the following hours drowsiness and dysarthria worsened and the patient developed right hemiplegia.
Results: 25% of patients with ischemic stroke become aware of their symptoms upon awakening from sleep.However,comparing MRI characteristics of patients with wake-up ischemic stroke and with ischemic stroke with known onset time,several studied found that DWI-FLAIR mismatch decreased gradually as the time from symptom onset to MRI increased,but there was no significant difference between the two groups within 2 h from the first noted symptoms to MRI examination.
Conclusions: Differences in degree and location of DWI/FLAIR mismatch should be considered as additive parameters to rTPA.A major clarification of the role of DWI/FLAIR mismatch in wake-up stroke in estimating the time of symptoms onset seems to be mandatory to guide clinical practice.
Disclosures of Interest: No
DWI/FLAIR mismatch of the emipontine lesion(left)compared to DWI/FLAIR overlap of the cerebellar lesion(right).
Abstract N°: 2026
INTRAVENOUS THROMBOYSIS FOR ACUTE ISCHAEMIC STROKE IN A PATIENT WITH A PITUITARY MACROADENOMA
Andrew Evans1, Jahanzeb Rehan*1
1King's Mill Hospital, Stroke Medicine, Sutton-In-Ashfield, United Kingdom
On behalf of:
Background and aims: According to many current guidelines, an intra-cranial tumour is a contra-indication to stroke thrombolysis, because of the assumed increased risk of intra-cranial haemorrhage. We present a case where the decision to proceed with thrombolysis was complicated by an incidental finding of an intra-cranial tumour.
Methods: A 64-year-old man with no significant past medical history presented with acute onset right sided limb weakness, facial droop and dysarthria. A diagnosis of acute stroke was made; NIHSS was 10. Thrombolysis was planned, pending exclusion of intra-cranial haemorrhage.
Results: A CT Brain revealed no haemorrhage or infarct but incidentally revealed a large Sellar mass. The decision was made to proceed with thrombolysis. The patient had excellent functional recovery in the hours after administration, NIHSS improving to 4. They did not suffer any intra-cranial haemorrhage. A subsequent MRI revealed acute symptomatic infarction and confirmed a Pituitary Macroadenoma. At discharge they had minimal symptoms, and the MRS was 1. At clinic review 3 months later, their MRS was 0.
Conclusions: Although some, though not all, guidance would exclude patients with intra-cranial neoplasms from thrombolysis, the evidence is limited. Original randomised controlled trials of stroke thrombolysis excluded this patient group and there have been none since. Published case reports and series are heterogenous in their conclusions. In this case the decision was made to proceed with thrombolysis, despite detection of a Sellar mass, and the outcome was positive but it is clear that further studies are needed to allow guidelines to be clarified.
Disclosures of Interest: No
Abstract N°: 2055
ATYPICAL POSTERIOR FOSSA POSTERIOR REVERSIBLE ENCEPHALOPATHY SYNDROME IN MULTIPLE SCLEROSIS UNDER INTERFERON-BETA, A CASE REPORT
Nikolaos S. Avramiotis*1, Matthias Mehling1, Matthias Mutke2, Ramona-Alexandra Todea2, Marios Psychogios2, Urs Fischer1, Joachim Christian Fladt1
1University Hospital Basel and University of Basel, Department of Neurology and Stroke Center, Basel, Switzerland,2University Hospital Basel and University of Basel, Department of Neuroradiology, Clinic of Radiology and Nuclear Medicine, Basel, Switzerland
On behalf of:
Background and aims: Posterior reversible encephalopathy syndrome (PRES) manifests with acute or subacute onset of neurological symptoms along with typical occipital signal alterations on cerebral MRI, likely to resolve with timely antihypertensive treatment. We present a case of atypical PRES of a patient with multiple sclerosis treated with Interferon-beta (IFN-b).
Methods: A 36-year-old man with relapsing multiple sclerosis (RMS) under IFN-b presented with blurry vision of one week and known, yet intensified tension type headaches. The neurological examination was normal, while the blood pressure was markedly elevated. Fundoscopy showed bilateral hypertensive retinopathy, without signs of optic neuritis.
Routine MRI one month prior had revealed new FLAIR/T2-hyperintense cerebellar lesions without contrast enhancement, suggesting active RMS. Admission MRI showed extensive confluent bilateral cerebellar FLAIR/T2 hyperintensities with multiple contrast enhancing cerebellar lesions, consistent with RMS progression. Antihypertensive treatment was promptly initiated and broad blood- as well as CSF-workup was performed to rule out potential infectious or other immune related etiologies (including PML), as steroid treatment was withheld. Follow-up MRI showed complete regression of the new lesions supporting the diagnosis of PRES.
Results: -
Conclusions: This case reflects the diagnostic challenge of recognizing an atypical PRES manifestation over RMS activity, a serious treatment complication such as PML, or other possible diagnoses, in a patient population with commonly few cerebrovascular comorbidities. Increased tissue susceptibility attributable to underlying RMS activity, as well as interference of endothelial cell function through IFN-b may play a role in this atypical disease localization.
Disclosures of Interest: No
Abstract N°: 2109
CT PERFUSION: SIMILAR APPEARANCES, DIFFERENT DIAGNOSES
1Whiston Hospital, Stroke Medicine, Liverpool, United Kingdom
On behalf of:
Background and aims: CT brain perfusion (CTP) scans are frequently used by stroke centres to assess stroke patients. In increasing availability of CTP we have found that their diagnostic value is high in both assessing mismatch volumes in ischaemic areas, and offering alternative diagnoses. Our aim is to illustrate the importance of correlation between CTP, clinical presentation and the findings of unenhanced CT/MRI brain and CT/MR angiogram.
Methods: We have reviewed two cases of patients presenting with stroke-like symptoms with similar looking CTP scans on admission. We have examined their initial clinical presentations and imaging, including unenhanced CT head, CT angiogram and MRI brain.
Results: Both CTP scans showed hyperperfusion indicative of seizure activity. In the first case, the patient’s clinical presentation was more in keeping with seizure activity and subsequent MRI brain excluded stroke as the cause of his symptoms. In the second case, the patient’s clinical presentation was more in keeping with stroke and despite CTP not identifying a mismatch he was appropriately treated with intravenous thrombolysis with subsequent MRI brain confirming pontine infarcts.
Conclusions: In depth analysis of these two cases illustrates the importance of correlating CTP imaging with clinical presentation and other forms of imaging including unenhanced CT head, MRI brain and CT/MR angiogram to diagnose and differentiate hyperacute stroke from mimics and treat patients appropriately.
Disclosures of Interest: No
Abstract N°: 2168
STATUS EPILEPTICUS AND ULCERATIVE COLITIS AS MANIFESTATION OF CEREBRAL VENOUS THROMBOSIS WITH INTRACEREBRAL HEMORRHAGE. A CASE REPORT
Beatriz Rodríguez García*1, Antonio Manuel González García1,Miriam Ravelo Leon1, Diana Stefania Gomez de la Torre Morales1, Juan Alberto Aguilera Aguilera1, Juan Sebastián Rodríguez Carrillo1, José Miguel Velázquez Pérez1, Francisco Javier González Terriza1, López Mesonero1, María Esther Ramos Araque,1
1Hospital Universitario de Salamanca, Neurology, Salamanca, Spain
On behalf of:
Background and aims: The cerebral venous thrombosis (CVT) is an infrequent and multifactorial entity, with variable clinical presentation including seizures. In up to 40% of the cases is found an intracerebral hemorrhage. We report a case of CVT presented as status epilepticus in a young patient caused by sepsis and the debut of an unknown Inflammatory Bowel Disease (IBD).
Methods: A 19-year-old man with episodic migraine history who developed acute decreassed consciusness and tonic-clonic convulsive status epilepticus. Previous weeks he had presented tonsillitis treated with antibiotics and bloody diarrheal stools.
Results: An urgent multimodal head computed tomography (CT) showed right temporo-occipital hyperdensity surrounded by hypodense area with permeability of the venous system (Fig. 1). A cerebral angiography revealed thrombosis of right posterior parietal cortical veins (Fig. 2) and therapeutic dose low-molecular-weight heparin was administered.
The etiological study of CVT revealed a right basal pneumonia and IBD type Ulcerative Colitis (UC) previously unknown, that caused a respiratory and digestive sepsis, and was treated with corticosteroids and empirical antibiotic therapy.
After three weeks of hospitalization the patient was discharged neurologically asymptomatic, and acenocoumarol, levetiracetam and prednisolone were continuous.
After 6 months of follow-up, a brain magnetic resonance imaging (MRI) showed a right parieto-occipital malacic area and resolution of the cortical veins’ thrombosis (Fig. 3), and the patient was asymptomatic, hence anticoagulant and antiseizure treatments were withdrawn.
Conclusions: It’s important to suspect CVT in intracerebral hemorrhages and delve into the underlying cause to begin treatment early.
There’s still controversy over how long antiepileptic and anticoagulant treatment should be maintained.
Disclosures of Interest: No
Abstract N°: 2171
MECHANICAL THROMBECTOMY IN THE CONTEXT OF MALIGNANCY: CASES SERIES OF REAL WORLD EXPERIENCES
Adam Young*1, Kinza Ali1, Jessica Gill1, George Thomas1
1The James Cook University Hospital, United Kingdom
On behalf of:
Background and aims: Advances in the last decade have established Mechanical Thrombectomy (MT) as a vital treatment in acute ischaemic stroke (AIS) with large vessel occlusion (LVO). The patient selection criterion for MT is explicit but does not give consideration to co-morbidity. This leaves uncertainty over whether to offer MT to patients with cancer, which is common in the UK, because concomitant cancer may considerably affect the patient’s outcome but is not an exclusion. We present our experience in a case series of LVO patients who had MT with concurrent cancer.
Methods: Review of routinely collected notes and imaging.
Results: Between 2021 and 2023, 3 patients (2 men, 1 woman) with cancer underwent MT. The average age was 72 years. The cancer diagnosis was varied; metastatic Bladder cancer, Lung cancer, and metastatic Vulval cancer. Baseline mRS was 0 for two patients and 2 for one patient. The average baseline NIHSS was 22. Average ASPECTS score was 8. Average collateral score was 2. 2 patients were thrombolysed prior. Post procedure TICI scores were 2a in one patient and 2b in two patients. The average 24-hour NIHSS was 14. At 90 days, 2 had a mRS of 3 and 1 a mRS of 6.
Conclusions: This small case series demonstrates these cancer patients had severe AIS syndromes despite favourable ASPECTS and collateral scores. Though they had successful recanalisation, their post-procedure outcomes were poor. It is likely there are other unrecognised factors influencing outcomes in these patients. Further research could help us understand this better.
Disclosures of Interest: No
Abstract N°: 2225
ANTICOAGULATION DECISION IN SETTING OF INOPERABLE INTRACRANIAL ANEURYSM AND ATRIAL FIBRILLATION TO PREVENT STROKE
Background and aims: The standard treatment for subarachnoid hemorrhage in the setting of aneurysm rupture is to secure the aneurysm. The standard treatment to prevent stroke in setting of atrial fibrillation and embolic strokes is anticoagulation. Here, we report a case of a patient who had an unsecured aneurysm not amenable to surgery or intervention and new onset atrial fibrillation with cardioembolic strokes.
Methods: This was a 51-year-old male with history of drug use, hypertension and hyperlipidemia who presented with syncope and severe headache, found to have extensive subarachnoid hemorrhage with extension into the ventricles. He had a diagnostic cerebral angiogram demonstrating a 2.5mm fusiform dilatation in the distal left posterior communicating artery (PComm) connected to the left posterior cerebral artery (PCA). Later, the patient went into new onset atrial fibrillation and was noted to have small infarcts involving right anteromedial frontal subcortical region adjacent to the genu of corpus callosum, left paramedian frontal cortical region and left posterior cerebellum.
Results: The fusiform dilation in the distal left PComm was not operable without sacrificing the left PCA. Given unsecured aneurysm and history of drug use, patient was not felt to be a candidate for anticoagulation for strokes in setting of atrial fibrillation. Watchman device was placed for occlusion of the left atrial appendage. The patient was discharged on dual antiplatelet therapy with minimal neurological deficits.
Conclusions: Left atrial appendage occlusion is an alternative to consider when a patient presents with intracranial hemorrhage, inoperable vascular abnormalities and concurrent atrial fibrillation with strokes.
Disclosures of Interest: No
Abstract N°: 2312
SIMULTANEOUS SPINAL CORD AND VERTEBROBASILAR STROKE
Alexandre Montalvo*1,2, Sarah Oliveira3, José Duro4, Ângelo Dias5, Pedro Mota6, Luísa Biscoito5, Nuno Gaibino2,6, Mariana Carvalho Dias1,2
1Unidade de Acidentes Vasculares Cerebrais, Serviço de Neurologia, Departamento de Neurociências e Saúde Mental, Hospital de Santa Maria, Centro Hospitalar Universitário Lisboa-Norte, Lisboa, Portugal,2Faculdade de Medicina, Universidade de Lisboa, Lisboa, Portugal,3Serviço de Anestesiologia, Hospital de Santa Maria, Centro Hospitalar Universitário Lisboa-Norte, Lisboa, Portugal,4Serviço de Medicina Interna, Hospital de Santa Maria, Centro Hospitalar Universitário Lisboa-Norte, Lisboa, Portugal,5Serviço de Imagiologia Neurológica, Departamento de Imagiologia, Hospital de Santa Maria, Centro Hospitalar Universitário Lisboa-Norte, Lisboa, Portugal,6Serviço de Medicina Intensiva, Hospital de Santa Maria, Centro Hospitalar Universitário Lisboa-Norte, Lisboa, Portugal
On behalf of:
Background and aims: Spinal cord stroke represents 1% of all strokes. In rare cases it is associated with brain stroke. We present a case report of simultaneous medullary and brain ischemia.
Methods:
Results: A 25-year-old male presents with weakness and paraesthesia of the four limbs and urinary retention. He reports a brief episode of bright flashes in his left visual field. He denied headache or cervical pain. No trauma was reported. No relevant background history, besides having started surfing lessons two days before.
Neurological examination disclosed asymmetric tetraparesis (predominantly in lower limbs and left hemibody), thermo-algic anaesthesia with C8-D1 level and neurogenic shock with hypotension and bradycardia. Spinal cord MRI showed anterior ischemic stroke at C5 level and brain MRI showed multiple ischemic lesions in the vertebrobasilar territory. Cervical and intracranial angioCT were normal.
He was admitted to ICU with vasopressor support and lumbar drainage catheter was placed for 72 hours, with slight tetraparesis improvement. Antiaggregation was started. Etiologic studies, including fat-suppression-MRI, embolic source investigation, blood and CSF analysis were negative. He was discharged to rehabilitation clinic on wheelchair (mRankin 4). Three months later he was independent for daily activities with slight tetraparesis (mRankin 2).
Conclusions: No etiology was identified, but we propose a spontaneous vertebral artery dissection (possibly associated with surfing practice) with embolization to the anterior spinal and basilar arteries as the most likely hypothesis. Treatment is individualized - IV-thrombolysis, antiaggregation and systemic/medullary hypotension prevention may be considered. Although prognosis is frequently incapacitating, this case represents excellent recovery at 3 months.
Disclosures of Interest: No
Abstract N°: 2354
THROMBOLYSIS FOR ISCHAEMIC STROKE IN HEREDITARY HAEMORRHAGIC TELANGIECTASIA
Benjamin Jaa Ming New*1, Danisha Bhuckory1
1Ninewells Hospital, United Kingdom
On behalf of:
Background and aims: There is limited data around the efficacy and safety of intravenous thrombolysis (IVT) in patients with hereditary haemorrhagic telangiectasia (HHT) and acute ischaemic stroke (AIS). HHT often manifest with epistaxis, gastrointestinal bleeding, as well as AIS. We report on an elderly gentleman who presented with 1 hour onset of left-sided ataxic hemiparesis. His NIHSS was 9 and premorbid mRS was 1. He is known to have HHT and untreated atrial fibrillation (AF).
Methods: HHT is associated with arteriovenous malformations (AVM), mainly in the cerebral, pulmonary, and gastrointestinal vessels. AVMs are relative contraindications to IVT due to the risk of haemorrhage. An urgent CT Brain and angiography was performed, which ruled out both intracerebral AVM and large vessel occlusion. He had no recent epistaxis or haemorrhagic episodes, and no pain in his chest or abdomen. Systemic examination revealed stable vitals with no bleeding or bruising. After discussion with the patient, we proceeded with IVT using Alteplase.
Results: Our patient remained well with no signs of haemorrhage over the next 24-hours, with early improvements in his neurological symptoms. A post thrombolysis CT brain at 24-hours showed only a subtle right lacunar ischaemic infarct. Apixaban was commenced on the 4th day following his AIS. He was safely discharged home after 1 month of rehabilitation, NIHSS 2 and mRS of 2.
Conclusions: Although HHT is commonly associated with AVMs, it should not preclude the use of IVT if clinically indicated. Haemorrhagic cerebral AVM is an important association to exclude when deciding IVT in patients with HHT.
Disclosures of Interest: No
Abstract N°: 2356
CHIARI NETWORK: UNVEILING A “PATENT” RISK FACTOR FOR RECURRENT STROKE?
Miguel Serôdio*1, Marta Magriço1, Danna Krupka1, Bárbara Rodrigues1, Rita Ventura1, João Pedro Marto1,2
1Centro Hospitalar Lisboa Ocidental, Department of Neurology, Lisbon, Portugal,2Faculdade de Ciências Médicas, NOVA Medical School, Universidade NOVA de Lisboa, Chronic Diseases Research Centre (CEDOC), Lisbon, Portugal
On behalf of:
Background and aims: High-risk characteristics associated with patent foramen ovale (PFO) heighten the likelihood of stroke, which may justify its closure. Chiari network (CN), an embryonic remnant often linked to PFO, has been suggested as a potential embolic source and may impede PFO visualization during transoesophageal echocardiography (TEE). This case-report aims to highlight CN’s role as an underrecognized high-risk feature of PFO and its implications in stroke management.
Methods: Case-report.
Results: A 22-year-old female, active smoker, and illicit drug user, with metabolic syndrome and intellectual development disorder, presented with a left MCA stroke. After endovascular treatment, the patient had a favourable clinical outcome. On etiological evaluation, a high-volume intracardiac mass was documented on TEE. After excision, histological evaluation confirmed the presence of an intracardiac thrombus. Patient was lost to follow-up and failed to adhere to secondary prevention measures. 3 years after, the patient was admitted again with a right MCA stroke. No reperfusion treatment was offered due to an established right hemispheric ischemic lesion. Evaluation identified a PFO with right-left shunt and the presence of CN on TEE. Notably, no alternative aetiology was found. Apixaban was started and PFO closure was planned.
Conclusions: CN remains underrecognized as a high-risk feature in PFO patients, leading to a lack of established strategies for its management. Heightened awareness of CN's significance may aid in preventing recurrent strokes, particularly in individuals presumed to have "low-risk" PFO profiles.
Disclosures of Interest: No
Abstract N°: 2510
STEROID NON-RESPONSIVE DELAYED BRAIN EDEMA OF GIANT BASILAR ANEURYSM AFTER ENDOVASCULAR TREATMENT CAUSED BY WATER-HAMMER EFFECT
PETRA MIKLAVCIC*1,1, Anita Resman1, Tanja Lavric1, Vid Zgonc1, Dimitrij Lovric2
1University Medical Centre Ljubljana, Department of Vascular Neurology, Ljubljana, Slovenia,2University Medical Center Ljubljana, Department of Radiology, Ljubljana, Slovenia
On behalf of:
Background and aims: Despite advances in endovascular treatment, the management of giant brain aneurysms remains challenging. We describe a case of delayed extensive brain edema after endovascular treatment of unruptured giant basilar aneurysm.
Methods: 52-year-old female presented with 6 months history of right-sided facial numbness. CT of the brain and CT-angiography revealed 25 mm large proximal basilar artery aneurysm with mass effect. She was treated with placement of flow-diverter (FD) and coils on dual antiplatelet therapy. Because of the mass effect she was treated with dexamethasone and discharged home a week later without new neurological deficit on oral methylprednisolone for 10 days.
Results: Five weeks later, she was admitted due to symptom worsening. Dysarthria, central nystagmus, abducens palsy, right-sided facial palsy, and right-sided limb ataxia were found. MRI revealed extensive edema in mesencephalon, pons and right cerebellum with compression of 4th ventricle and hemorrhage into aneurysmal wall. She was treated with high dosages of dexamethasone for 36 days, with no improvement. Control MRIs showed no regression of edema. DSA revealed water-hammer effect in incompletely occluded aneurysm necessitating additional FD placement. She even had two half a day lasting episodes of coma with dilated pupil and skew deviation. She regained consciousness after mannitol treatment. Brainstem edema gradually improved and she remained stable.
Conclusions: Steroid therapy is the first-line treatment for perianeurysmal edema. When not efficient, persistent water-hammer effect against residual lumen of aneurysm should be suspected, warranting further endovascular treatment.
Disclosures of Interest: No
Abstract N°: 2737
A MULTI MIMIC SURGICAL ‘STROKE’
Orla Kemple1, Mikar Singh1, Ronán Collins1
1Tallaght University Hospital, Stroke / Age-Related Healthcare, Dublin, Ireland
On behalf of:
Background and aims: Stroke mimics account for 50% of acute emergency department (ED) presentations of suspected stroke (1). However, surgical pathologies are rarely considered in the differential diagnoses
Methods: N/A
Results: A 75-year-old lady presented to ED with right upper and lower limb weakness and expressive dysphasia. Past medical history included a prior anterior cerebral artery (ACA) territory infarct and PE in 2017, hypertension, hypercholesterolemia, and active smoking. Computed tomography (CT) imaging noted an old established ACA infarct only without large vessel occlusion.
Further examination revealed pallor, reduced sensation and temperature and absent peripheral pulses in right lower limb. Patient had focal right shoulder tenderness on examination with limited range of movement. Urgent angiographic imaging of the lower limbs revealed a proximal right external iliac filling defect with a right tibial occlusion. X- ray imaging of the right shoulder revealed an acute humeral fracture.
In view of the patient’s dysphasia and previous stroke, she was admitted to acute stroke unit where subsequent magnetic resonance imaging (MRI) confirmed no acute infarct. Her speech deficit resolved. She required complex multidisciplinary management with control of pain, immobilisation of shoulder and IV unfractionated heparin, with eventual surgical repair of her shoulder and rehabilitation.
Conclusions: This case highlights the unpredictable nature of stroke mimics. Although unusual, it is likely her right lower limb weakness due to acute limb ischaemia caused a fall at ictus with subsequent unilateral shoulder injury. Expressive dysphasia was likely caused by post stroke ‘recrudescence’. A FAST response does not obviate the need for careful history and examination.
Disclosures of Interest: No
Abstract N°: 2745
A WINDOW OF UNCERTAINTY: THROMBOLYSIS IN METHOTREXATE-INDUCED STROKE-LIKE SYNDROME - A CLINICAL DILEMMA
Background and aims: Methotrexate-induced stroke-like syndrome (SLS) or leukoencephalopathy is a rare neurological complication associated with intrathecal or high-dose Methotrexate (MTX) administration. The mechanisms involve unclear neurotoxic pathways, including the alteration of folate homeostasis in the CNS and/or direct neuronal toxicity. Incidence rates range from 0.8-3.8%, manifesting within 14-21 days of MTX exposure.
Methods: Case report
Results: An 18-year-old with B cell lymphoblastic lymphoma undergoing MTX and 6 Mercaptopurine chemotherapy presented with sudden-onset weakness in the right upper and lower limbs with a weak hand grip, right hemianopia, and an extensor plantar response on the right side. NIHSS score was 4. Emergency CT Brain during the thrombolytic window showed no abnormalities (ASPECTS 10). However, MRI revealed hyperacute infarcts, prompting IV Tenecteplase thrombolysis. Re-examination after 24 hours showed complete symptom resolution. A repeat MRI brain taken 10 days later showed complete resolution of findings, confirming that the previous observations were indeed indicative of cytotoxic edema.
Conclusions: This case underscores diagnostic challenges in Methotrexate-induced SLS, emphasizing consideration of rare complications in chemotherapy. Transient symptoms complicate decision-making, especially in distinguishing SLS from life-threatening conditions. Variable neurologic outcomes highlight the need for clinical suspicion and a thorough differential diagnosis. Treatment options, from observation to thrombolysis, pose a dilemma when symptoms mimic an evolving stroke within the thrombolytic window. This presentation contributes insights into managing Methotrexate-induced SLS, urging vigilance in recognizing this uncommon yet serious neurological complication in cancer chemotherapy.
Disclosures of Interest: No
Abstract N°: 2780
CONGENITAL SUBCLAVIAN STEAL SYNDROME IN A CASE OF RIGHT SIDED AORTIC ARCH WITH COMPLETE ISOLATED LEFT INNOMINATE ARTERY
Ya-Ju Lin*1, Helen Po1, Kun-Shou Huang1
1MacKay Memorial Hospital, Neurology, Taipei, Taiwan
On behalf of:
Background and aims: Right aortic arch (RAA) anomalies is rare in the general population (~0.1%). Most of the patients are asymptomatic, and it is discovered incidentally. It causes symptoms when associated with other vascular anomalies (vascular ring) with local compression or because of reversal of flow through the vertebral-basilar vasculature resulting in symptoms of cerebral/limbs ischemia. That is, the type III RAA with isolation of left subclavian artery (1.5%) lead to congenital subclavian steal syndrome (SSS) and vertebrobasilar insufficiency (VBI). We presented a case of RAA with complete isolation of left innominate artery with complete left SSS.
Methods: case report
Results: This 58-year-old female patient with history of hypertension and hyperlipidemia under regular treatment complained of intermittent dizziness, blurred vision and left arm soreness after exercise and found different BP in both arms. Left subclavian steal syndrome was impressed and confirmed by duplex sonography, which also showed hypoplasia of left CCA and ICA with some reversed flow from left ECA. Dynamic CTA showed atresia of left innominate artery, complete left subclavian steal phenomenon with partial filling to left CCA, and cervical trunk branches to left CCA with good intracranial collateral. Antiplatelet and statin were used for secondary stroke prevention. Her symptoms were relieved partially if avoidance of strenuous exercise.
Conclusions: RAA with isolated left subclavian artery will lead to congenital subclavian steal syndrome. This single-steal type have the best prognosis and present latest with symptoms of VBI or left arm claudication. Well control of vascular risk factors is mandatory.
Disclosures of Interest: No
Abstract N°: 2874
INTRAARTERIAL TREATMENT OF SEVERE SYMPTOMATIC VASOSPASM AFTER GLIOMA RESECTION
Frans Van den Bergh*1, Martijn Verdam1, Yacine Boudiba1, Koenraad Nieboer1, Fenne Vandervorst2, Johny Duerinck3, Michael Bruneau3, Sylvie De Raedt2
Background and aims: Cerebral vasospasm-induced delayed cerebral ischemia is a well-recognized complication following subarachnoid hemorrhage. Conversely, cerebral hypoperfusion resulting from vasospasm after brain tumor resection is frequently overlooked and can be a debilitating complication.
Methods: A 39-year-old man underwent a partial resection of an insular frontotemporal glioma. On the first postoperative day, an MRI revealed typical postoperative findings and a patent left middle cerebral artery (MCA). However, a CT scan on the sixth day displayed a hematoma in the resection cavity. Postoperatively, he received medication for headaches but reduced the dosage independently due to drowsiness. Corticoids were tapered on postoperative day 10. Then, two days later, the patient experienced progressive speech problems, severe headaches persisted. An EEG showed no ictal changes. MRI demonstrated a left MCA stenosis and a hypoperfusion zone within the left MCA territory. A tentative diagnosis of vasospasm induced by blood components was established.
Results: In the angio-suite, a severe vasospasm was identified in the M1 segment of the left MCA. A total of 3 mg of nimodipine and 4 milligrams of milrinone were administered intra-arterially. The vasospasm had nearly disappeared on the final angiogram. Speech problems were fully resolved. On a follow-up CT angiogram, no more vasospasm was shown in the left MCA.
Conclusions: Any new neurological deficit after brain tumor resection that cannot be explained by hemorrhage, seizures or infection should be investigated by MR or CT angiography. Early endovascular therapy can reverse the vasospasm.
Disclosures of Interest: No
Abstract N°: 2954
ENDOVASCULAR TREATMENT OF THROMBOSIS OF CEREBRAL VENOUS SINUS - CASE REPORT
David Cernik*1, Vojtech Smolka2
1Krajská zdravotní as, Masaryk hospital, Comprehensice stroke center, Neurology, Ústí nad Labem, Czech Republic,2J.E. Purkinje University and KZ a.s, Masaryk Hospital, Dept. of Radiology, Ústí nad Labem, Czech Republic
On behalf of:
Background and aims: Thrombosis of cerebral vessels with a complication can be a life-threatening condition. Anticoagulation treatment has its limits and endovascular treatment is the last option. We present a case of a combined approach to the management of extensive intracranial thrombosis.
Methods: A patient (female, 45 years old) with a history of schizophrenia was admitted after an epileptic seizure. There was deterioration into aphasia and right lateralization. According to the CT, massive bleeding was found (subarachnoid hemorrhage, and small intracerebral hematomas and small hemocephalus). Ct venography showed occlusion of the sigmoid sinus, right transversus sinus, superior sagittal sinus. Despite the bleeding, anticoagulation therapy with low-molecular-weight heparin was used as the only therapeutic option. The patient was transferred to a comprehensive stroke center. Here, she was treated with continuous heparinization and partial embolectomy of all vessels was performer.A microcatheter was inserted for local application of Actilyse 20mg/20h. At an interval of 20 hours, a second endovascular intervention was performed, and in another 10 hours, a third one with complete recanalization of all sinus. Continuous heparinization was carried out at the same time. On follow-up CT, a small right temporal ischemia developed, without a hemorrhagic complication.
Results: The clinical condition has completely returned to normal. The patient was discharged home on anticoagulation therapy. The etiology of the thrombosis has not yet been established.
Conclusions: Thrombosis of cerebral venous sinus with complications is an emergency condition that must be addressed. Endovascular treatment can be more effective when divided into several procedures in combination with prolonged local action of thrombolytics.
Disclosures of Interest: No
Abstract N°: 3014
A GOOD HISTORY - NOT TO BE SNEEZED AT?
Bradly Woolfenden1, Patrick Doyle*1, Helena Dolphin1, Rónán Collins1
1Tallaght University Hospital, Stroke Service, Dublin, Ireland
On behalf of:
Background and aims: Patent Foramen Ovale (PFO) the most common congenital heart defect, present in up to 25% of the adult population. It is a potential source of paradoxical embolism. A temporal association between Valsalva-inducing manoeuvres and stroke symptoms should prompt investigations to out-rule PFO.
Methods: Case report
Results: A 54-year-old left hand dominant man presented to our Emergency Department with a 30-minute episode of left arm and leg weakness and associated sensory disturbance at presentation. Sudden onset of these symptoms was heralded by a sneeze which occurred while bending over. Past history included hypertension and allergic rhinitis. Social history was notable for recreational scuba diving. The National Institute of Health Stroke Scale(NIHSS) on arrival was 2. Initial CT brain and intracranial angiogram were normal. MRI Brain demonstrated a small region of acute ischaemia in the right frontal cortex, and two old lacunar infarcts within the left corona radiata. A Transoesophageal Echocardiogram was performed with bubble study, which demonstrated the right to left shunt of a PFO on Valsalva manoeuvre. The patient was commenced on aspirin and was referred for consideration of PFO closure. He was advised against scuba diving and prescribed topical treatment for allergic rhinitis.
Conclusions: Sneezing precipitating a paradoxical embolism via PFO is rarely described in the literature. This case highlights the importance of clarity in history-taking to guide aetiological investigation and treatment considerations.
Acute infarct right frontal cortex on MRI diffusion weighted imaging.
Acute infarct right frontal cortex on MRI diffusion weighted imaging.
Disclosures of Interest: No
Abstract N°: 3159
SYMPTOMATIC CEREBELLAR THROMBOSED DEVELOPMENTAL VENOUS ANOMALY: A CASE REPORT
Owen Feely*1, Muireann Byrne1, Patrick Nicholson1, Patricia Fearon1
1Beaumont Hospital, Dublin, Ireland
On behalf of:
Background and aims: With the rising prevalence of advanced neuroradiological imaging, detection of incidental developmental venous anomalies (DVAs) is more commonplace. DVAs are rarely symptomatic (<2%). Typically, symptoms arise due to flow-related complications or mechanical effects. Of particular concern is venous thrombosis, a frequent flow-related complication, which can cause venous ischemia or haemorrhage. Thus, early recognition and intervention is important.
Methods: We describe a case of a 54-year-old male, with background of hypertension, presenting three days after sudden onset headache, ataxia, and diplopia. Initial clinical examination revealed bidirectional horizontal gaze-evoked nystagmus, skew deviation, and decreased temperature sensation of the left face. Ophthalmological examination identified left inferior rectus limitation.
Results: Initial non-contrast CT brain identified hypoattenuation in the right pons, suggestive of sub-acute infarction. Secondary prevention was initiated. Subsequent MRI revealed hyperattenuation on T2 and FLAIR in the pons, right middle cerebellar peduncle, and right cerebellar hemisphere without restricted diffusion. SWI sequences identified an abnormal venous structure in the right cerebellum, with increased signal within it, suggestive of thrombus. The patient was diagnosed with a thrombosed DVA with associated venous oedema. Symptoms had resolved on dual antiplatelet therapy without anticoagulation.
Conclusions: This case highlights the potential for DVAs, generally considered a benign entity, to become symptomatic with associated parenchymal damage and a rare, but important, stroke mimic.
a - CTB, 1b, FLAIR, 1c, DWI.
SWI.
Disclosures of Interest: No
Abstract N°: 3210
AN UNEXPECTED TWIST OF A PTOSIS
Meryem El Azhari*1, Zineb Yacoubi1, Yasmine Mimouni1, Sara Lhassani1, Asmaa Hazim1, Jehanne Aasfara1, Hamid Ouhabi1
1Cheikh Khalifa International Hospital, Neurology, Casablanca, Morocco
On behalf of:
Background and aims: Cerebral venous thromboses impact a substantial global population, stemming from various causes like infections and autoimmune disorders. Symptoms often include headaches, vomiting, reduced visual acuity, and oculomotor issues. An essential aspect is determining the cause for comprehensive management. Common causes in women involve contraceptives, autoimmune diseases, and neoplastic conditions.
Methods: We present the case of a 46-year-old female with likely immunological thrombocytopenia, who underwent splenectomy and was admitted for pyelonephritis treatment. During hospitalization, she developed diplopia and an incomplete right third nerve palsy, including a subtle ptosis of the right eye. Neurological examination showed no additional signs. Imaging revealed bilateral cavernous sinus thrombosis, predominantly on the right side. Elevated protein levels and lymphocytic pleocytosis were noted in a lumbar puncture. Immunological assessment showed doubtful anti-sm and anti-RNP/sm antibodies. The clinical course suggested lupus with renal, pulmonary, and neurological involvement. Therapeutic-dose low-molecular-weight-heparin improved neurological symptoms, resolving ptosis and trigeminal nerve deficits. Unfortunately, the patient succumbed to renal and pulmonary complications.
Results: Cerebral venous sinus thrombosis can coincide with systemic lupus erythematosus (SLE). In our case, the patient met three SLE criteria: hemolytic anemia, thrombocytopenia, and renal involvement. The pathogenesis involves vasculitis and a hypercoagulable state; however, antiphospholipid antibodies were absent. Standard treatment for SLE-related cerebral venous sinus thrombosis includes anticoagulants, steroids, and immunosuppressants. Managing thrombocytopenia poses a challenge, leading to the deferral of anticoagulant therapy due to bleeding risks.
Conclusions: Fast diagnosis and treatment of cerebral venous sinus thrombosis are crucial for a positive prognosis, especially with thrombocytopenia in SLE
Disclosures of Interest: No
E-Poster - Clinical Practice, Management and Care
Abstract N°: 20
ASSESSMENT OF DONOR-VESSEL AFTER STA-MCA BYPASS FOR MOYAMOYA DISEASE USING HANDHELD DOPPLER
Satoshi Takahashi*1, Masahiro Toda1
1Keio University, Neurosurgery, Tokyo, Japan
On behalf of:
Background and aims: To clarify the blood flow changes in donor vessels from immediately after direct revascularization for moyamoya disease using a handheld Doppler.
Methods: The study included 12 hemispheres of 9 patients with moyamoya disease who underwent direct-indirect revascularization. The parameters (PSV, MV, RI, FV) of the STA on the operated side were measured using a handheld Doppler before and after surgery.
Results: Patency of the STA-MCA bypass was confirmed by MRA performed on all 12 sides of 9 patients within the first 2 postoperative days. There was a statistically significant increase in the PSV (p=0.0201) and the MV (p=0.0110) and a decrease in the RI (p=0.0177) in the STA after surgery when compared with those measured before surgery. None of the changes from the immediate postoperative period to POD1 were statistically significant. Postoperative TNEs occurred in 3 patients (25%) in the first 2 weeks after 12 surgeries. The FV of the three sides associated with perioperative TNEs was significantly higher than that of the nine sides that were not associated with perioperative TNEs (p=0.0273).
Conclusions: From the early stage after moyamoya disease bypass surgery, it was clarified that the parameter of the STA changed in which the PSV and the MV increased and the RI decreased. It was clarified that the increase in the FV, which is the blood flow rate that flows through the STA in the immediate postoperative period, may be a predictor of the development of TNEs during the perioperative course.
Disclosures of Interest: No
Abstract N°: 329
THE EFFECTS OF ALPHA-LIPOIC ACID SUPPLEMENTATION ON POST-STROKE PATIENTS
Hamid Abbasi*1,2, Neda Jourabchi1, Ranasadat Abedi1, Kiarash Tajernarenj1, Mehdi Farhoudi2
1Tabriz, Student Research Committee, Tabriz University of Medical Sciences, Tabriz, Iran., Tabriz, Iran,2Tabriz, Neurosciences Research Center (NSRC), Tabriz University of Medical Sciences, Tabriz, Iran., Tabriz, Iran
On behalf of:
Background and aims: Alpha lipoic acid (ALA), fat- and water-soluble, coenzyme with sulfuret content, has received considerable attention for its potential therapeutic role in diabetes, cardiovascular diseases, cancers, and central nervous disease. This investigation aims to evaluate the probable protective effects of ALA in stroke patients.
Methods: Based on Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines, This meta-analysis was performed. The PICO criteria for this meta- analysis were as follows: Population/Patients (P: stroke patients); Intervention (I: ALA); Comparison (C: control); Outcome (O: blood glucose, lipid profile, oxidative stress,inflammatory factors).In addition, Studies that were excluded from the analysis consisted of in vitro, in vivo, and ex vivo studies, case reports, quasi-experimental studies. Scopus, PubMed, Web of Science, EMBASE databases were searched until August 2023.
Results: Of 496 records that were screened in the title/abstract stage, 9 studies were included in this meta-analysis. The sample sizes in the included studies vary between 28 and 90. The result of risk of bias was performed via risk of bias (RoB) in randomized-controlled trials (RCTs) based on the second version of the Cochrane RoB assessment tool. 8 studies had a definitely high risk of bias.
Conclusions: In conclusion, we found ALA supplementation might be effective on blood glucose, Superoxide dismutase, and high-density lipoprotein levels. Nonetheless, to comprehensively assess the beneficial effects of ALA consumption on oxidative stress and inflammatory indices, there is a need for additional trials encompassing larger populations, extended durations, elevated ALA dosage, and more specific participant criteria.
Disclosures of Interest: No
Abstract N°: 613
STROKE SURVIVORS, CAREGIVERS AND HEALTHCARE PROFESSIONALS’ PERSPECTIVES OF ACUTE STROKE CARE DURING COVID-19 IN IRELAND
1University College Cork, School of Public Health, Cork, Ireland,2University College Cork, School of Nursing and Midwifery, Cork, Ireland,3National Ambulance Service, Clinical Directorate, Limerick, Ireland,4University College Cork, College of Medicine and Health, Cork, Ireland,5University of Galway, Discipline of General Practice, Galway, Ireland,6Cork University Hospital, Department of Neurology, Cork, Ireland,7University College Cork, School of Medicine, Cork, Ireland,8University College Cork, School of Pharmacy, Cork, Ireland
On behalf of:
Background and aims: The management of time-sensitive conditions like acute stroke and transient ischaemic attack (TIA) serves as a key gauge for assessing the COVID-19 pandemic's impact on healthcare access and delivery. Thus our aim was to investigate stroke survivors, caregivers and healthcare professionals' perspectives on the emergency/pre-treatment phase of acute stroke care in Ireland during the COVID-19 pandemic.
Methods: In this qualitative study from April to August 2023, we conducted semi-structured interviews with stroke survivors, caregivers and healthcare professionals engaged in both prehospital and hospital-based stroke care. Included stroke survivors had a stroke/TIA during the COVID-19 pandemic in Ireland ( March 2020 - February 2022). Participants were purposively sampled from four hospitals in one region. Data were analysed using reflexive thematic analysis and patient journey mapping.
Results: We included thirty participants in this study; fifteen healthcare professionals (seven prehospital practitioners, four nurses and four doctors), eight stroke survivors and seven caregivers. Six main themes were constructed from the data: Acute stroke care pathway during COVID-19; Barriers and facilitators to timely hospital presentation; Stroke/TIA presentations during COVID-19; COVID-19 public health measures; Lessons learned from COVID-19, and Stroke workforce during COVID-19. The same themes emerged from both the healthcare professional and stroke survivor/caregiver interviews.
Conclusions: Preliminary results from this study highlight factors which can influence healthcare seeking behaviour in the context of time-dependent conditions during healthcare crises. Furthermore, the effects of initiatives and circumstances introduced during COVID-19 on survivors and caregivers can provide learnings for future acute stroke care.
Disclosures of Interest: No
Abstract N°: 1444
PHYSICIANS SURVEY ON ACCEPTED NON-INFERIORITY MARGINS IN STROKE TRIALS
Aristeidis Katsanos*1, Philip Bath2, Vasileios-Arsenios Lioutas3, Teresa Ullberg4, Linxin LI5, Maria Khan6, George Howard7
1McMaster University/ Population Health Research Institute, Hamilton, Canada,2University of Nottingham, Nottingham, United Kingdom,3Beth Israel Deaconess Medical Center - Harvard Medical School, Boston, United States,4Lund University, Lund, Sweden,5University of Oxford, Oxford, United Kingdom,6Rashid Hospital, Dubai, United Arab Emirates,7University of Alabama, Birmingham, United States
On behalf of: World Stroke Organization Future Leaders
Background and aims: Non-inferiority trials test whether a new intervention is not unacceptably worse than the standard treatment by more than a predefined margin. The selection of this margin is one of the most challenging steps in the design of non-inferiority trials.
Methods: We designed a survey to assess the perception of stroke physicians on non-inferiority margins in stroke trials evaluating new interventions. This survey was distributed to World Stroke Organisation (WSO) members between November and December 2023.
Results: A total of 120 members responded to our survey. When asked on who should define the non-inferiority margin in a trial they ranked investigators first, followed by expert consortia, patient-caregiver groups, regulatory agencies, sponsors and hospital administration. Ease of administration, relative effect of the standard treatment, clinical implication of inappropriately introducing the new treatment, availability, price and ease of storage and shipping of the new treatment were ordered as factors that should influence the selection of the margin. Non-inferiority margins considered acceptable by responders were highly variable. Less familiarity on non-inferiority was associated with larger acceptable margins. Median values of non-inferiority margins considered acceptable by responders declaring to be very knowledgeable on this topic was 5% in the setting of acute ischemic stroke treatment and 2% in secondary stroke prevention.
Conclusions: Perception of stroke physicians on factors that should influence non-inferiority margins may differ from other stakeholders. There is high variability on margins that are considered acceptable by physicians. The width of an acceptable margin seems to correlate with the acquaintance of an individual with non-inferiority trials.
Disclosures of Interest: No
Abstract N°: 1705
FEASIBILITY STUDY OF ADVANCE CONSENT IN ACUTE STROKE TRIALS: PRELIMINARY RESULTS
Rena Patricia Seeger*1, Emma Cummings2, Brian Dewar3, Ubong Udoh2, Dar Dowlatshahi4, Michel Shamy5
1University of Ottawa, Stroke Program,2Ottawa Hospital Research Institute, Stroke Program,3Ottawa Hospital Research Institute, Neurology,4University of Ottawa, Neurology,5University of Ottawa, Neurology
On behalf of:
Background and aims: Obtaining consent for participation in acute stroke trials is widely recognized as a significant challenge. Advance consent, in which patients at risk of stroke consent to participate in trials before they experience a stroke, could address these challenges. We seek to assess the feasibility of advance consent in this context.
Methods: In this feasibility study, we approach patients deemed at risk of stroke in stroke prevention clinic, and invite them to complete a questionnaire about advance consent. Patients who respond positively are offered the opportunity to consent in advance to participate in active enrolling acute stroke trials. If a patient decides to provide advance consent, this decision will be recorded in their electronic medical record, remaining valid for a year. We aim to screen 2000 consecutive patients, of whom we expect 800 to be eligible, and 400 to participate in this study.
Results: Since July 2023, we have screened 671 patients (34%), of whom 187 (28%) were eligible to participate. Of the patients who were eligible, 45 (24%) completed the initial questionnaire, and 6 (13%) have provided advance consent to one of the two ongoing clinical trials. Of the patients who completed the questionnaire, 95% would be open to the idea of providing advance consent.
Conclusions: Recruitment is progressing slower than anticipated, though preliminary results support the acceptability of advance consent in patients at risk of stroke for participation in acute stroke trials.
Disclosures of Interest: No
Abstract N°: 1717
AGE AND SEX AS DETERMINANTS OF STROKE UNIT ADMISSION RATES: THE IRISH NATIONAL AUDIT OF STROKE
Meabh Kelly*1,2, Olga Brych3, Joan Mccormack3, Tim Cassidy3, Ronan Collins3, Joseph Harbison1,4
1Trinity College Dublin, Ireland,2Tallaght Hospital, Ireland,3Irish National Audit of Stroke,4St James's Hospital, Ireland
On behalf of:
Background and aims: Stroke Unit (SU) care is associated with improved outcome and is a central recommendation of the Stroke Action Plan for Europe. Ireland has a target of 90% admission of patients to SU but this has never been met. We examined what factors influenced admission in the Irish National Audit of Stroke.
Methods: Anonymised INAS data between 2017-2022 were analysed after ethics approval. Data on Sex, age group, Length of Stay (LoS) and Post stroke Modified Rankin Score (mRS) were collected. Chi square analyses were used.
Results: Data on 26808 patients were analysed, 15310 male (57.1%). 70.7% of both men and women were admitted to a SU. Subjects >70 years were slightly more likely to be admitted (71.1% vs. 68.9% Chi Sq 9.2 p=0.002).
LoS was longer for all SU admitted subgroups. There was no significant difference in discharge mRS.
Conclusions: Patients admitted to SU were older and had a longer LoS, possibly due to less impaired patients being discharged before SU admission.
Disclosures of Interest: No
Abstract N°: 1888
HOW DO HEALTHCARE PROFESSIONALS MANAGE POST-STROKE FACIAL PALSY IN THE UK? – AN INTERDISCIPLINARY SURVEY
Havva Eroglu*1,2, Audrey Bowen2,3, Matthew Checketts4, Claire Mitchell1,2
1The University of Manchester, Division of Psychology, Communication and Human Neuroscience, Faculty of Biology, Medicine and Health, Manchester, United Kingdom,2Northern Care Alliance & University of Manchester, Geoffrey Jefferson Brain Research Centre, The Manchester Academic Health Science Centre, Manchester, United Kingdom,3The University of Manchester, Division of Psychology and Mental Health, Faculty of Biology, Medicine and Health, United Kingdom,4University of Glasgow, School of Psychology & Neuroscience, United Kingdom
On behalf of:
Background and aims: Post-stroke facial palsy, affecting 50% of stroke survivors, significantly impairs speech, eating, and quality of life. Management remains unclear and we lack clinical guidelines and research on this topic. We aimed to describe the assessment and treatment currently used in UK clinical practice for post-stroke facial palsy.
Methods: A Qualtrics online survey was distributed among UK healthcare professionals working in stroke care via professional networks, conferences, and social media platforms (July 4 and December 31, 2023).
Results: 96/138 respondents completed the survey. 41 physiotherapists, 38 speech and language therapists, 9 nurses, 5 stroke doctors 2 occupational therapists and 1 orthoptist. Healthcare professionals use a range of assessment tools and treatments. The most used assessments were NIHSS (40%) for screening, clinical observation methods (85%) for diagnosis and, Sunnybrook Facial Grading System (SFGS) (40%) for measuring outcomes. The most commonly used treatment approaches were orofacial exercises (61%) and facial massage (52%).
Conclusions: As anticipated physiotherapists and speech and language therapists were the professions most interested in reporting their approaches to post-stroke facial palsy. Having determined the most commonly used assessment (clinical observation) and treatment (orofacial exercises) it would be useful to explore their effectiveness. This could remedy the absence of national guidance on post-stroke facial palsy.
Disclosures of Interest: No
Abstract N°: 1936
EFFECTS OF BRAINWAVE MUSIC ON POST-STROKE FATIGUE IN PATIENTS WITH ACUTE ISCHEMIC STROKE
YUN WANG*1
1Sichuan Academy Medical Sciences & Sichuan Provincial People's Hospital, Neurology Department, Cheng Du, China
On behalf of:
Background and aims: There is scare evidence on the topic that Brainwave music may alleviate post-stroke fatigue (PSF) in acute patients with ischemic stroke (AIS). So, it is critical to investigate risk factors associated with the occurrence of PSF and explore the effects of brainwave music on PSF, neurological function and anxiety in AIS patients.
Methods: 64 patients with AIS were divided into control and intervention groups randomly. The control group were exposed to regular nursing methods. Whereas the intervention group, in addition to regular nursing, also underwent a brainwave music intervention which brainwave music of healthy adults in a resting state was delivered to patients for 30 minutes once a day for 7 days. The FSS, NIHSS, BI and SAS were used to assess the severity of fatigue, degree of neurological deficits, autonomous self-care ability and to measure the anxiety level between the two groups both before and after the intervention.
Results: PSF is at high risk in patients with AIS. The risk factors for PSF are the degree of impaired neurological function and anxiety level.Brainwave music can significantly reduce the fatigue and anxiety levels for patients with AIS (P<0.05).
Conclusions: Brainwave music can alleviate the occurrence of PSF and reduce anxiety levels for patients with AIS, thus improving the patient’s quality of life and confidence in recovery. Brainwave music serves as an important potential intervention for stroke patients with fatigue, and these results provide a clinical evidence warranting further trial.
Disclosures of Interest: No
Abstract N°: 2160
DEVELOPING A MODEL OF ADVANCE CONSENT FOR PARTICIPATION IN ACUTE STROKE TRIALS
Rena Seeger*1, Ubong Udoh2, Brian Dewar2, Stuart Nicholls2, Mark Fedyk3, Sophia Gocan4, Victoria Shepherd5, Dar Dowlatshahi4, Michel Shamy4
1University of Ottawa, Ottawa, Canada,2Ottawa Hospital Research Institute, Ottawa, Canada,3University of California, Davis, Davis, United States,4The Ottawa Hospital Civic Campus, Ottawa, Canada,5Cardiff University, United Kingdom
On behalf of:
Background and aims: Advance consent, in which participants at risk for stroke may consent to trial participation in advance of meeting eligibility criteria, could address many of the limitations traditional consenting methods pose to participation in acute stroke trials. We sought to develop a model of advance consent to be tested in a real-world feasibility study.
Methods: We integrated data from a series of preliminary studies with institutional policy and feedback from our institutional review board to justify a model of advance consent to be tested in a real-world feasibility study.
Results: Individuals found to be at risk of stroke after assessment in the stroke prevention clinic are invited to consent to participate in active enrolling acute stroke trials, with the intention that they be enrolled in those studies without delay should they experience a stroke and be eligible in the future. A decision to accept or decline participation will be communicated to the patient's substitute decision-maker and will be documented in the medical record. Consent given in advance will only be used to enroll a participant into a clinical trial if the participant meets eligibility criteria for a trial within one year and is unable to provide informed consent for herself or himself at that time.
Conclusions: Individuals identified as being at risk of stroke will be invited to review informed consent forms for active enrolling acute stroke trials, and to consent or decline to participate in advance. This practice could serve as a model for research in other emergency conditions.
Disclosures of Interest: No
Abstract N°: 2178
ADDRESSING HEALTH INEQUALITIES BY DELIVERING A PILOT STROKE AWRENESS EDUCATION PROJECT IN SCHOOLS IN DEPRIVED AREAS
Kirsty Harkness*1,2, Jaimie Shepherd1, Gavin Church1, Gemma Hayden1, Zara Kabir1, Jane Douthwaite1, Michelle Campbell1, Matt Crowder1, Nazeen Iqbal1
1South Yorkshire Integrated Stroke Delivery Network, Oak House, Rotherham, United Kingdom,2Sheffield Teaching Hospitals NHS Trust, Neurology, Sheffield, United Kingdom
On behalf of:
Background and aims: The National Stroke Service Model: Integrated Stroke Delivery Networks (NSSM) published in 2021, has prevention and health inequalities as a key ambition and is a key priority for the South Yorkshire Integrated stroke delivery network (SYISDN).
Analysis of hospital admissions shows a social gradient, with the most deprived areas have significantly higher admission rates than the South Yorkshire (SY) average. SYISDN planned an education pilot to proactively target schools in areas of deprivation. To educate on stroke prevention, including the FAST message and how to reduce the modifiable risk factors of a Stroke.
Methods: A virtual interactive learning package, over 3 sessions including participation of stroke survivors and MDT professionals was delivered in partnership with the Sheffield University Technology college, students (aged 15-16).
This was followed by project work by the students to create a social media package to raise awareness of Stroke in the community.
Feedback was obtained via an electronic questionnaire.
Results: Education package was delivered over 3 sessions to 29 students. 76% female, 24% male. 41% ethnic minority, 59% white British. Prior to the sessions 72% reported little awareness of stroke and only 1% after the package. 28% reported a lot of knowledge about stroke before and 99% after.
Conclusions: The pilot was successfully delivered by SYISDN and has now been implemented as a training package delivered by Sheffield schools.
Disclosures of Interest: No
Abstract N°: 2382
ACUTE STROKE TRAINING – KEEPING PACE WITH MODERN ADVANCEMENTS IN EDUCATION
Caitlin Gibson1, Hongying Chen*2, Ahmed Gabr1,3, Natasha Slattery4,5, Anne Belcher6, Ida Carroll1,3,7, Abdirahman Mohamed1,3, Mélanie Suppan8, Laurent Suppan8, Margaret O’connor1,3,9
1University Hospital Limerick, Department of Ageing and Therapeutics, Ireland,2University Hospital Limerick, Department of Neurology,3University of Limerick, Ageing Research Centre, Castletroy, Ireland,4University Hospital Limerick, Ireland,5University of Limerick, Castletroy, Ireland,6Johns Hopkins University, Baltimore, United States,7University Hospital Limerick, Nursing and Midwifery, Ireland,8Hôpitaux Universitaires de Genève (HUG), Genève, Switzerland,9HRB Stroke Clinical Trials Network Ireland, Dublin, Ireland
On behalf of: The Ageing Research Centre: Rose Galvin, Katie Robinson, Nora Cunningham, Marwa Mustafa; The Stroke Clinical Trials Network Ireland (SCTNI): Peter Kelly, John McCabe, Joe Harbison; The National Stroke Program: Sinead Coleman, Ronan Collins
Background and aims: Stroke is a leading cause of death and disability. Stroke reperfusion therapies are rapidly evolving with time-critical management associated with improved patient outcomes. Educational interventions have proven benefit for both learners and patients. Our aim was to conduct a comprehensive and systematic needs assessment to inform the development of an acute stroke course curriculum, aligned with Kern’s six-step approach and formulated through the lens of educational theory.
Methods: An exploratory, qualitative research design was applied in accordance with COnsolidated criteria for REporting Qualitative research (COREQ) guidelines. Participants perspectives were gathered through semi-structured focus groups followed by expert interviews. Reflexive thematic analysis of transcripts was conducted using NVivo software and adhered to Braun and Clark’s six-step approach.
Results: Two focus groups (n=13) and eight interviews were conducted (January 2022-December 2023). The major themes identified were curricular design, pedagogical considerations, and quality of care and patient safety. A blended learning format incorporating the following principles was recommended: 1) interactive pre-course learning as a foundation, 2) in-person training centred around simulation/case-based discussion, 3) competence-based approach, 4) innovative strategies for learner engagement, 5) interprofessional education and 6) promoting quality of care and patient safety.
Conclusions: This study informs a needs assessment for curriculum development of an acute stroke course, based on expert and clinician perspectives, grounded in clinical practice and linked to the needs of learners and patients. Future research will focus on gaining expert consensus via Delphi methodology on curricular design and content for an acute stroke course.
Disclosures of Interest: No
Abstract N°: 2448
DEVELOPMENT AND IMPLEMENTATION OF A POST-STROKE HYDRATION SCREENING TOOL; RESULTS FROM A MULTI-CENTRE FEASIBILITY STUDY IN INDIA
Colette Miller*1, Stephanie Jones1, Elizabeth Boaden1, Jane Burnell2, Catherine Elizabeth Lightbody1, Jeyaraj Pandian3, Gordon Prescott2, Vasantha Padma4, Pn Sylaja5, Caroline Watkins1
1University of Central Lancashire, Stroke Research Team, PRESTON, United Kingdom,2University of Central Lancashire, Lancashire Clinical Trials Unit, PRESTON, United Kingdom,3Christian Medical College & Hospital, Department of Neurology, Ludhiana, India,4All India Institute Of Medical Sciences, Department of Neurology, New Delhi, India,5Sree Chitra Tirunal Institute for Medical Sciences & Technology, Department of Neurology, Thiruvananthapuram, India
On behalf of: the NIHR Global Health Research Group on IMPROVIng Stroke CarE in India (IMPROVISE) Collaboration.
Background and aims: In India, stroke is the fourth leading cause of death and the fifth leading cause of disability. Of those surviving, around half will experience dysphagia and decreased oral intake, increasing their risk of dehydration. Dehydration is associated with poor outcomes, and reported prevalence in the acute stroke population ranges from 29-70% but there are currently no data representing the Indian population. Calculated Osmolarity (cOsm) has been shown to be a reliable and cost-effective predictor of hydration status. This study aimed to co-design, develop, and implement a context-specific hydration screening tool (HST).
Methods: A multi-centre, feasibility study using the principles of experience-based co-design. Informed by existing literature, stroke guidelines, and expert knowledge, the HST included common methods of hydration assessment, a user guide, and an “Osmolarity App”. Using the Khajuria and Krahn formula, the App calculated expected serum osmolarity from routinely collected data (sodium, potassium, urea and glucose). Pre- and post-implementation data were collected on demographics (age, sex, stroke type, stroke severity) and the number of completed hydration assessments. Participants included consecutively admitted stroke patients aged ⩾18 years.
Results: Fifty-three nurses completed HST training. Participants were recruited to the pre-implementation group (n=92), and the implementation group (n=91). cOsm informed hydration assessment was not routine practice pre-implementation. Following implementation, cOsm was assessed in 66 (73%) participants. Of those, 15 (23%) participants were dehydrated.
Conclusions: This study demonstrates that cOsm informed hydration assessment is a feasible approach to the identification of post-stroke dehydration in India, and has the potential to improve stroke practice in LMICs.
Disclosures of Interest: No
Abstract N°: 2769
CO-DESIGN, DEVELOPMENT AND IMPLEMENTATION OF A GLOBAL EVALUATION OF SWALLOWING (GEOS) FOR ACUTE STROKE PATIENTS IN INDIA: A FEASIBILITY STUDY
Elizabeth Boaden*1, Stephanie Jones1, Jane Burnell2, Elizabeth Lightbody1, Colette Miller1, Jeyaraj Pandian3, Gordon Prescott2, Padma Srivastava4, P.N. Sylaja5, Caroline Watkins1
1University of Central Lancashire, Stroke Research Team, Preston, United Kingdom,2University of Central Lancashire, Lancashire Clinical Trials Unit, Preston, United Kingdom,3Christian Medical College and Hospital, 3Department of Neurology, Ludhiana, India,4All India Institute of Medical Sciences, Department of Neurology, New Delhi, India,5Sree Chitra Tirunal Institute for Medical Sciences and Technology, 5Department of Neurology, Thiruvananthapuram, India
On behalf of: the NIHR Global Health Research Group on IMPROVIng Stroke CarE in India (IMPROVISE) Collaboration.
Background and aims: India’s stroke burden is increasing, with over a million new strokes each year. Staff (regardless of profession) need the knowledge and skills to provide timely and effective patient care.
With our partners in India, patients, carers, and stakeholders, we aimed to co-design, develop and implement a context-specific swallowing assessment, to reduce the proportion of patients screened (water only) and increase the number of patients fully assessed (different consistencies).
Methods: A multi-centre, feasibility study using experience-based co-design was used to develop and implement a context-specific GEoS, in three hospitals in India. We provided training, competence assessment and supportive implementation. Participants included consecutively admitted patients aged ⩾18 years, with a clinical diagnosis of acute stroke.
Pre and post-implementation data was collected on demographics (age, sex, stroke type, severity), and the number of swallow screens and/or assessments undertaken in the first 3 days. Demographic characteristics were summarised by descriptive analysis: mean and standard deviation or median and interquartile ranges, frequencies and percentages.
Results: Fifty-three nurses completed training and competence assessments. Participants were recruited to the pre-implementation group (n=92), and the implementation group (n=91). The number of screens undertaken decreased in the implementation period from 30 (33%) to 14 (15%) and the number of patients receiving an assessment increased from 22 (24%) to 51 (56%).
Conclusions: To our knowledge this is the first study to co-design a context-specific swallowing assessment for the extended healthcare team in India, resulting in increased staff competence to assess and manage swallowing difficulties post-stroke.
Disclosures of Interest: No
Abstract N°: 2902
DOAC ADHERENCE IN ATRIAL FIBRILLATION
Aaizza Naqvi*1, Anuvita K Sharma1, Sana Mushtaq1
1Royal Hallamshire Hospital, Hyper Acute Stroke Unit, United Kingdom
On behalf of:
Background and aims: Atrial fibrillation (AF) increases stroke risk by five times as compared to usual population. This risk can be reduced by about 70% with anticoagulation. Direct oral anticoagulants (DOACs) have widely replaced warfarin due to their efficacy, less interactions and lack of need for monitoring. However, they need to be taken meticulously as advised for effective anticoagulation due to the nature of their individual pharmacokinetics. This audit was primarily undertaken to see if AF patients were taking their specific DOAC correctly and if they received advice on initiation.
Methods: Data was collected on 50 randomly selected patients admitted to our stroke unit between 2022 and 2023.We conducted structured interview regarding taking their specific DOAC meticulously and whether they were given appropriate instructions on initial prescription.
Results: We found only 34% of the total patients were taking their medication correctly. 20% were on Rivaroxaban, 54% on Apixaban and 26% on Edoxaban and only 8%, 20% and 4% of them respectively were taking DOAC as per recommendations. It was further noted that 72% of the total patients did not receive appropriate instructions when first initiated on the DOAC.
Conclusions: Our project highlighted poor adherence to DOACs which was concerning. We took simple but specific measures to improve adherence like clear instructions on each DOAC box when dispensed and handing out pictorial information leaflets regarding their anticoagulant on discharge from the ward to raise awareness. We will reassess our service post implementation of these actions soon.
Disclosures of Interest: No
Abstract N°: 2912
ACUTE STROKE TREATMENT PROCESS ACROSS CANADA: A QUALITATIVE STUDY OF SIMILARITIES AND VARIATIONS
Background and aims: Stroke is one of the leading causes of death and disability across Canada. There is an apparent divide in proportion of patients that receive treatment and timeliness of treatment between urban and rural hospitals. This qualitative study explores the similarities and variations in available resources, process workflow, adapted practices, and information collected across hospitals in Canada, through examining perspectives on stroke treatment by clinicians in primary and comprehensive stroke centers.
Methods: Semi-structured interviews were conducted with healthcare practitioners involved in stroke treatment. Expert participants were selected using non-probability purposive sampling. The interviews focused on treatment process practices, challenges faced, and information collected. Interview results were examined using a thematic analysis to understand similarities and variations in acute stroke treatment across various sites.
Results: 14 participants were interviewed across 7 different hospitals in 5 provinces. Analysis showed there were concerns about resource variation, as small hospitals lacked enough clinical staff and hospital beds for clinicians to go with the patient to the CT scanner. When asked about adoption of practices, participants in small centers found documenting treatment metrics was often delayed or unfinished. For process challenges, gathering accurate information early and communicating it throughout the process was a common challenge discussed. Considering data collection, most hospitals had a combination of paper and electronic data collection, resulting in re-entering data into their electronic system.
Conclusions: There are noticeable variations in available resources and standardization of best practices in stroke treatment, primarily affecting rural centers.
Disclosures of Interest: No
Abstract N°: 2966
RESTLESS LEGS SYNDROME IN STROKE SURVIVORS: PREVALENCE, SEVERITY AND IMPACT ON QUALITY OF LIFE
Soaham Desai1, Devangi Desai*1, Jay Darji1
1Shree Krishna Hospital Pramukhswami Medical College Bhaikaka University, Neurology, Anand, India
On behalf of:
Background and aims: Restless Legs Syndrome (RLS) is characterized by an irresistible urge to move the legs. The prevalence in the general population ranges from 5-15%. Secondary RLS can occur due to underlying conditions like stroke. This study aimed to determine RLS prevalence and features among stroke patients at a rural Indian hospital. Additionally, RLS impact on quality of life and daytime sleepiness was evaluated using the Patient Health Questionnaire-9 (PHQ-9) and Epworth Sleepiness Scale (ESS).
Methods: This cross-sectional study enrolled consecutive consenting 106 stroke patients over a two year period. RLS diagnosis was based on International RLS Study Group criteria. Severity was graded via the International RLS Rating Scale. Demographic and stroke data were gathered. PHQ-9 and ESS evaluated quality of life and sleepiness.
Results: RLS prevalence among stroke patients was 15.1%, higher in older, female patients with unilateral, hemorrhagic strokes. Patients with RLS showed significantly higher PHQ-9 and ESS scores escalating with RLS severity. A correlation was observed between greater RLS severity and poorer quality of life and increased daytime sleepiness.
Conclusions: A significant RLS prevalence of 15% exists among stroke patients, detrimentally impacting their quality of life and daytime wakefulness. Systematic RLS screening among stroke patients is recommended. Healthcare professionals must recognize RLS in stroke patients to minimize associated disability and impairment. Addressing secondary RLS should constitute comprehensive post-stroke care.
Disclosures of Interest: No
Abstract N°: 2979
LIPID OPTIMISATION FOR ACUTE STROKE PATIENTS: BENCHMARKING AGAINST UK NATIONAL GUIDELINE
Charlotte Perry*1, Alexandra Cann1, Puneet Singh1, Soma Banerjee2, Jaimini Cegla2, Joseph Kwan2
1Imperial College Healthcare NHS Trust, London, United Kingdom,2Imperial College London, London, United Kingdom
On behalf of:
Background and aims: Lipid optimisation is vital for patients admitted to the Hyperacute Stroke Unit (HASU). In the UK, AHSN published the National Guideline “Lipid Optimisation Pathway Following an Acute Cardiovascular Event” in March 2023. We benchmarked our current lipid optimisation practices against the gold standard of the AHSN Guideline (version 2, 2022).
Methods: We conducted an audit within the HASU of a major London Comprehensive Stroke Centre. Routine clinical data including lipid lowering treatments (LLT) were retrospectively collected from electronic patient records of 100 admissions (mean age 70 years, 43% female) into HASU between 1/1/23-7/2/23. Deceased patients were excluded.
Results: Of 100 patients, 85% had lipid profile checked (mean total cholesterol 4.98, LDL 3.04, triglyceride 1.54); of these, 86% had LDL>1.8. Pre-admission, 38% were taking statin and 3% taking ezetimibe only. Compliance to LLT was documented in only 10%, and 9% had documented intolerance to statin and/or ezetimibe. Of the 25 patients who had previous strokes/TIA, only 52% were on a statin and 35% had LDL<1.8. On discharge, 61% of patients had high-intensity statin (1 also on ezetimibe), 22% had lower-dose statin, 2% had lower-dose statin plus ezetimibe, and 1% had ezetimibe only. Overall, only 39% of LLT prescriptions adhered to AHSN Guideline. After discharge, 21% of local patients had lipid profiles re-checked.
Conclusions: There are significant gaps in lipid optimisation management along the entire hyperacute stroke pathway, with enormous long-term clinical outcome implications. Targeted education and training of the stroke professionals on the lipid optimisation pathway is urgently needed.
Disclosures of Interest: No
Abstract N°: 3019
ENHANCING STROKE PROFESSIONAL TRAINING: A COMPREHENSIVE ASSESSMENT OF LEVEL 1 PSYCHOLOGICAL CARE PROFICIENCY
Carleen Scott1, Kausik Chatterjee*2, Steven Green3, Suzanne Ragab4
1Essex Partnership University NHS Foundation Trust, Runwell, United Kingdom,2Countess of Chester NHS Foundation Trust, Stroke and Care of the Elderly, Chester, United Kingdom,3The Queen Elizabeth Hospital King's Lynn NHS Foundation Trust, United Kingdom,4University Hospitals Dorset NHS Foundation Trust, United Kingdom
On behalf of:
Background and aims: For healthcare professionals treating stroke patients, addressing psychological challenges like intense emotions and cognitive issues is vital. However, the lack of consistent coverage in standard training results in varied levels of knowledge, often based on personal experience. This inconsistency makes it challenging to develop a bespoke training programme that meets the diverse training needs of all professionals involved in stroke care.
Methods: Between October and December 2023, a survey was carried out throughout the UK, aiming to identify the training requirements of professionals in stroke care, with a particular focus on improving Level 1 psychological care. The survey was developed with contributions from a range of stakeholders, including patient groups, included 24 questions, some utilising a Likert scale from 1 to 10, to assess the professionals' skills and confidence in various aspects of Level 1 psychological care.
Results: Data from 304 healthcare professionals across various roles highlighted the influence of experience and access to clinical psychologists on confidence and skills in Level 1 psychological care (Figure 1), while a random forest model in Figure 2 confirmed the strong link between self-reported confidence & skills and their proficiency in managing psychological issues. Thematic analysis highlighted specific training requirements for two distinct groups based on confidence levels. The favoured training methodologies encompass face-to-face, interactive online, hybrid, and video-assisted options, ranked in order of preference.
Conclusions: The variability in skill and confidence among healthcare professionals underscores the need for tailored training programmes, accounting for their experience in psychological care.
Disclosures of Interest: No
E-Poster - Cognition and Vascular Cognitive Impairment
Abstract N°: 846
EVALUATING SHORT SWEDISH MOCA (S-MOCA-SWE) AS AN EARLY PREDICTOR FOR 6-MONTH COGNITIVE OUTCOMES AFTER STROKE
Tamar Abzhandadze*1,2, Olga Berg3, Elias Lindvall3, Erik Lundström3
1Institute of Neuroscience and Physiology, the Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden,2Department of Occupational Therapy and Physiotherapy, Sahlgrenska University Hospital, Gothenburg, Sweden,3Department of Medical Sciences, Neurology, Uppsala University, Akademiska Sjukhuset, Uppsala, Sweden
On behalf of:
Background and aims: Cognitive dysfunction is prevalent among stroke survivors; therefore, international guidelines recommend routine cognitive screening. The short Swedish version of the Montreal Cognitive Assessment (s-MoCA-SWE) has been developed for efficient application in acute stroke settings. Our objective was to determine whether early post-stroke cognitive screening with s-MoCA-SWE could predict intact cognition at 6 months. Additionally, we aimed to compare the discriminative ability and psychometric properties of s-MoCA-SWE with those of the full MoCA version.
Methods: A cohort of stroke patients from 35 Swedish stroke and rehabilitation centers was had cognitive screening with the full version of the Montreal Cognitive Assessment (MoCA) at 2-15 days post-stroke and again at 6 months. Scores from the full MoCA were converted to the s-MoCA-SWE equivalents for statistical analysis, with early s-MoCA-SWE scores serving as the primary predictor and the 6-month full MoCA scores as the outcome variable.
Results: 1141 patients were included (38% female, mean age 71). With each increasing s-MoCA-SWE point, the odds of having a normal cognitive function at 6 months rose by 43% (95% CI [1.36, 1.51], p<0.001). At the 6-month assessment, the s-MoCA-SWE yielded results in cognitive function discrimination that were equivalent to those obtained by the full MoCA. However, early s-MoCA-SWE had higher sensitivity (92.3%) than the early full version MoCA (89.7%) in detecting impaired cognitive function at 6 months.
Conclusions: Early s-MoCA-SWE can predict cognitive function at 6 months after stroke, suggesting a potential value of s-MoCA-SWE as a brief cognitive screening tool.
Disclosures of Interest: No
Abstract N°: 981
MANAGEMENT OF POST-SUBARACHNOID HEMORRHAGE COGNITIVE IMPAIRMENT A SYSTEMATIC REVIEW AND META-ANALYSIS
Background and aims: Subarachnoid hemorrhage ( SAH) is a cataclysmic disease causing high mortality and morbidity rates. Around 50 % of SAH survivors are cognitively affected despite neurological recovery affecting quality of life. Thus we aimed to conduct a meta-analysis and systematic review about the studied interventions for post-SAH cognitive impairment
Methods: Search was conducted using the keywords: SAH, cognition, management, and intervention among PubMed, Scopus, Web of Science, Embase and Cochraine library databases.
Results: After screening, 40 studies were included (N:3835) ; 32 studies examined SAH rat models ( N:3148, 82.09%) and 8 studies examined patients with SAH ( N: 687, 17.91%). Intervention methods were highly variable (Figure.1) however the most studied mechanism of intervention among all the studies was Neuro-inflammation ( 27.87%) followed by apoptosis ( 25.92%).
The mean time of intervention and cognitive evaluation among SAH rat models was 4.5 +/- 8.46 hours, 10.317+/- 8.37 days compared to 92.43 +/- 144.38, 165.83 +/- 121.26 days for SAH patients. Regarding the efficacy of interventions to improve SAH related cognitive impairment, that was reported in (100%) of SAH rat models and only ( 40.32 %) of SAH patients ( P-Value < 0.001)
Conclusions: Our systematic review showed the efficacy of the studied potential methods of intervention for post SAH cognitive impairment. Better results among the SAH rat models can be explained by the shorter time to intervention, early cognitive evaluation and lack of the early brain injury (EBI) event created by the sudden intracranial pressure rise in SAH.
Disclosures of Interest: No
Abstract N°: 1789
INFLUENCE OF HBA1C AND WHITE MATTER DISEASE ON CORRELATION BETWEEN COGNITION AND CEREBROVASCULAR RESERVE INCVD
1Nerima Hikarigaoka Hospital, Neurosurgery, Tokyo, Japan,2Saitama Medical Center, Jichi Medical University, Neurosurgery, Saitama, Japan,3Edogawa Hospital, Neurosurgery, Tokyo, Japan,4International University of Helth and Welfare Hospital, Tochigi, Japan
On behalf of:
Background and aims: Cognitive impairment has been reported in patients with steno-occlusive disease of a main cerebral artery and without causative lesions on magnetic resonance imaging. We investigated the correlation between cognitive function and factors, cerebral blood flow (CBF), cerebrovascular reserve (CVR), white matter disease (as an indicator of chronic cerebral ischemia) and HbA1c (as an indicator of hyperglicemia) in the patients.
Methods: Total cognitive scores, CBF, CVR, periventricular hyperintensity (PVH) grade, and HbA1c were examined by stepwise multiple regression analysis in 43 patients with steno-occlusive disease of a main cerebral artery. Total COGNISTAT scores and the factors were also analyzed in low and high HbA1c groups, and low and high PVH grade groups.
Results: Patients with lower COGNISTAT score had significantly lower CVR [standardized partial regression coefficient (SPRC) = 0.229, p < 0.0001] and lower CBF (SPRC = 0.156, p = 0.0462), judging from multiple regression analysis. The statistical significant correlation between COGNISTAT scores and CVRs was demonstrated in the each group. The SPRCs (0.176 and 0.196) of the correlation between COGNISTAT scores and CVRs were lower in the higher HbA1c PVH grade groups, compared to SPRCs (0.221 and 0.245) of the lower HbA1c and PVH grade groups, respectively.
Conclusions: The significant correlation between COGNISTAT scores and CVRs were demonstrated in patients with steno-occlusive disease of a main cerebral artery. This correlation may be low in patients with high HbA1c (hyperglicemia) or a high PVH grade (chronic cerebral hypoperfusion).
Disclosures of Interest: No
Abstract N°: 2288
SCREENING FOR COGNITIVE IMPAIRMENT WITH THE MOCA IN YOUNG MINOR STROKE PATIENTS: FINDINGS FROM A PROSPECTIVE OBSERVATIONAL STUDY
Jakob Leyrer*1,2,3, Alexander Tinchon1,2,3, Elisabeth Freydl1,2,3, Melanie Huber1,2, Stefan Oberndorfer1,2,3
1Karl Landsteiner University of Health Sciences, Krems, Austria,2University Hospital St. Pölten, Neurology, St. Pölten, Austria,3Karl Landsteiner Society, Institute for Clinical neurology and neuropsychology, St. Pölten, Austria
On behalf of:
Background and aims: About half of all stroke patients under the age of 50 have cognitive deficits. If these are subtle, they may escape routine neurological examination. The aim of this study was to investigate whether the Montreal Cognitive Assessment (MoCA), an internationally recommended screening tool for cognitive assessment in stroke patients, is suitable for detecting cognitive deficits in younger stroke patients with a minor stroke.
Methods: Patients aged 18 to 55 years with a minor (NIHSS ⩽5) ischemic stroke were eligible for inclusion in this prospective observational study. The primary endpoint was to assess the sensitivity of the MoCA. Secondary endpoints were specificity, positive and negative predictive value. A comprehensive neuropsychological assessment (CNA) and the MoCA were completed at least 3 days after stroke. The CNA assessed memory, attention, language, visuospatial and executive functions with multiple tasks for each domain.
Results: Of 121 patients who met the inclusion criteria between April 2021 and December 2023, 34 were enrolled. Median age was 48 years (41; 52) and 35% were female. The median interval between stroke and screening was 5 days (4; 7). Half of the patients scored 1.5 standard deviations below the population norm in at least one cognitive domain. The MoCA detected this impairment in only four cases (cut-off <26), giving a sensitivity of 24%. The specificity, positive predictive value and negative predictive value were 88%, 66% and 54% respectively.
Conclusions: Our data suggest that the MoCA is not sensitive to cognitive impairment in young minor stroke patients.
Disclosures of Interest: No
Abstract N°: 2398
VALIDATION OF DIAGNOSTIC & STATISTICAL MANUAL OF MENTAL DISORDERS (DSM-5) 4-& 7-LEVEL ORDINAL SCALES OF COGNITION: THE R4VAD STUDY
Ellen Backhouse1, Lisa Woodhouse2, Martin Taylor-Rowan3, Philip Bath2, Fergus Doubal1, Terence J Quinn4, Joanna Wardlaw*1
1University of Edinburgh, Centre for Clinical Brain Sciences, United Kingdom,2University of Nottingham, Stroke Trials Unit, Mental Health & Clinical Neurosciences, School of Medicine, United Kingdom,3University of Glasgow, School of Health and Wellbeing, United Kingdom,4University of Glasgow, School of Cardiovascular and Metabolic Health, United Kingdom
On behalf of: R4VaD collaborators
Background and aims: Consensus on how best to measure post-stroke cognitive impairment (PSCI) is limited. DSM-5 counts impairments similarly in any cognitive domain (not just memory, so more relevant to PSCI), using multiple data sources (so few missing data). We validated the DSM-5 4 and 7-level ordinal cognition scales using expert dementia adjudication in the R4VaD prospective multicentre study of PSCI.
Methods: We categorised cognition at ⩾1-year post-stroke into DSM-5 7-and 4-level ordinal scales in R4VaD, n=2442. In a subsample (n=250, 10%), we tested 3 models: basic model (Figure 1), model 2 (basic model+ details of cognition in casenotes and verbal fluency score), model 3 (model 2+ subjective memory complaints, Stroke Impact Scale cognitive questions). Trained researchers completed dementia adjudication using clinical casenotes, (e.g. formal dementia diagnosis, cognitive concerns, relevant prescribing, imaging data) and cognitive study data, interpreted accounting for confounding factors (e.g. low mood, speech problems). We conducted intraclass coefficient analysis (ICC) to determine agreement between the 3 cognitive algorithms and the expert dementia adjudication.
Results: We found excellent agreement between expert dementia adjudication and cognitive algorithms in all models (basic model: Cog-4 ICC= 0.97, Cog-7 ICC=0.99; model 2: Cog-4 ICC=0.96, Cog-7 ICC=0.98; model 3: Cog-4 ICC=0.96, Cog-7 ICC=0.96). Model 2 included 9 and model 3 17 more than basic model.
Conclusions: The DSM-5 4 and 7 level cognitive scales are valid measures of post-stroke cognitive status, are robust to missing data, and may provide a standardised method of cognitive categorisation for use in future clinical trials on PSCI.
Disclosures of Interest: No
Abstract N°: 2498
NEUROVASCULAR COUPLING ASSESSMENT BY TRANSCRANIAL DOPPLER IN ACUTE STROKE COULD BE INFORMATIVE OF LONG-TERM COGNITIVE STATUS
Juliana Ferreira*1, Frederica Alves1, Tiago Pedro2, Ana Luísa Aires1,3, Luísa Fonseca4, Guilherme Gama4, Goreti Moreira4, Elsa Azevedo1,3, Pedro Castro1,3
1Faculty of Medicine of the University of Porto, Porto, Portugal, Department of Clinical Neurosciences and Mental Health, Porto, Portugal,2Centro Hospitalar Universitário São João, Porto, Portugal, Deparment of Neuroradiology, Porto, Portugal,3Centro Hospitalar Universitário São João, Porto, Portugal, Deparment of Neurology, Porto, Portugal,4Centro Hospitalar Universitário São João, Porto, Portugal, Deparment of Internal Medicine, Porto, Portugal
On behalf of:
Background and aims: Neurovascular Coupling (NVC) is compromised in cerebrovascular pathologies. Recent studies suggest a relationship between microcirculatory damage and cognitive impairment. We aimed to study if NVC in acute stroke is related to long-term cognitive impairment.
Methods: This is a prospective study of consecutive patients with ischemic stroke, without prior cognitive deficit and eligible for Transcranial Doppler monitoring within 7 days after a stroke, recruited from the stroke unit (CHUSJ, Portugal) between September 2021 and August 2022. 40 controls with similar age, gender and vascular risk factors were recruited. NVC was determined by the peak relative increase in CBv, recorded in the P2 segments of PCA, during a visual stimulus paradigm of each of 5 cycles of increasing length. The main outcome was the cognitive status at 12 moths of follow-up which was based in 7-scale cognitive score was operationalized from Montreal Cognitive Assessment.
Results: The final analysis involved 141 patients and 41% (n=58) presented cognitive impairment. Globally, NVC exhibited a non-linear relationship with cognitive outcome with extreme quintiles having no significant effect on cognitive impairment but intermediate values showing increasing NVC being associated with reduced odds worse cognitive status (aOR= 0.50, CI95% 0.28 –0.97, p= 0.048) (Figure 1). Same results were independent of stroke severity, age, and educational class in a multivariate model.
Conclusions: NVC assessment with TCD in acute stroke could provide information on long-term cognitive status. Modulating CBv responses might be the focus of future trials to enhance post-stroke cognitive impairment.
Cognitive Score Classes Distribution by Quintiles of NVC.
Disclosures of Interest: No
Abstract N°: 2920
AMBULATORY BLOOD PRESSURE MONITORING IN VASCULAR COGNITIVE IMPAIRMENT: TOLERABILITY AND CHARACTERISTICS
1Faculty of Medicine, Transilvania University, Neurology, Brașov, Romania,2County Clinical Emergency Hospital of Brașov, Neurology, Brașov, Romania
On behalf of:
Background and aims: Abnormal blood pressure is an important factor in the pathogenesis of vascular cognitive impairment (VCI). There are few studies available on ambulatory blood pressure monitoring (ABPM) in VCI and its tolerability in vascular dementia.
The aim of this study is to assess the tolerability of ABPM in a group of patients with different forms of vascular cognitive impairment.
Methods: we evaluated 65 patients with VCI, 67.78 ± 11.23 years and 58.46% males. We used an extensive battery of tests, which included MMSE, MoCA, Neuropsychiatry Inventory (NPI) and MRI. A patient was considered tolerant if he/she kept the device for 24 hours. The percentage of 70% was considered the minimum limit of correct measurements from the total expected.
Results: there were 48 VCI no dementia (VCIND) and 17 with different degrees of vascular dementia. The number of patients who did not tolerate the ABPM were 4/48 (8.33%) in VCIND group and 9/17 (52.17%) in vascular dementia group. From the patients who tolerated the ABPM there were 5/44 (11.36%) in VCIND and 3/8 (37.5%) in vascular dementia group who did not reach the minimum number of required measurements. Patients with vascular dementia had lower levels of daytime and nighttime diastolic blood pressure comparing with VCIND.
Conclusions: ABPM is quite well tolerated in VCI with no dementia but it is challenging in more advanced vascular dementia.
Disclosures of Interest: No
Abstract N°: 3011
HIGH-RESOLUTION DIFFUSION-WEIGHTED IMAGING IDENTIFIES ISCHEMIC LESIONS IN PATIENTS WITH COGNITIVE IMPAIRMENT AFTER TRANSIENT ISCHEMIC ATTACKS
María Rocío Córdova Infantes*1, Sandra Bartolomé Alberca2, Noelia Valverde Mata3, Andrea Parejo3, Marina Mesa Rubio3, Jose M Ramirez-Moreno3,4
1University Virgen de Valme Hospital, Neurology Department, Seville, Spain,2University Hospital of Badajoz, Neurology Service, Badajoz, Spain,3University Hospital of Badajoz, Stroke Center. Neurology Service, Badajoz, Spain,4Extremadura University, Department of Biomedical Science, Badajoz, Spain
On behalf of:
Background and aims: Temporary and permanent cognitive changes after a transient ischemic attack or minor stroke (TIA/MS) have been described previously. It is unknown whether persistent cognitive deficits in these patients correlate with acute infarction identified by magnetic resonance imaging. We tested the hypothesis that cognitive impairment is associated after TIA/MS with lesions on diffusion-weighted imaging.
Methods: Patients with acute TIA/MS (NIH Stroke Scale score ⩽3) within 24 h of onset were prospectively enrolled. Patients underwent a Montreal cognitive assessment and MRI, including diffusion-weighted imaging and fluid-attenuated reverse recovery sequences, at baseline in the acute phase. Cognitive testing was repeated on day 90. Diffusion-weighted imaging injury and fluid-attenuated reverse recovery. Chronic white matter and basal ganglia hyperintensity volumes were measured using the ARWMC scale. Cognitive impairment was defined a priori as a Montreal Cognitive Assessment score <26.
Results: Ninety patients were imaged. Acute ischemic lesions occurred in 66 (73.3%) patients. Rates of cognitive impairment were significantly higher in patients with (49/60, 74.2%) and without diffusion-weighted imaging lesions (11/24, 45.8%; p=0.011). We found no relationship between the ARWMC scale either at the level of changes in the white matter (p=0.525) or in the basal ganglia (p=0.927) and the Montreal Cognitive Assessment scores on day 90.
Conclusions: Most patients with TIA/MS suffer acute cognitive impairment after the event. Deficits after 90 days of onset correlate with ischemic brain injury on high-resolution DWI sequences and provide evidence that these lesions would impair the ability to compensate for the cognitive effects of acute ischemic strokes.
Disclosures of Interest: No
E-Poster - Diagnosis/Investigation of Stroke Etiology
Abstract N°: 234
ARTERY-TO-ARTERY EMBOLISM IN INTRACRANIAL ATHEROSCLEROTIC STENOSIS: HIGH WALL SHEAR STRESS AND DIABETICS
Shuang Li*1, Yuying Liu1, Xuan Tian1, Bonaventure Ym Ip1, Hing Lung Ip1, Jill Abrigo2, Sin Ying Fan1, Sze Ho MA1, Xinyi Leng1, Thomas Leung1
1The Chinese University of Hong Kong, Medicine and therapeutics,2The Chinese University of Hong Kong, Imaging and Interventional Radiology
On behalf of:
Background and aims: Diabetics mellitus (DM) was more likely to cause artery-to-artery embolism (AAE) in intracranial atherosclerotic stenosis (ICAS), however, the underlying mechanisms has not been well studied. We aimed to explore whether DM can alter the relationship between wall shear stress (WSS) and AAE.
Methods: Patients with 50-99% atherosclerotic stenosis of M1 middle cerebral artery on CT angiography (CTA) were included in this cross-sectional study. Probable stroke mechanism was assessed based on the infarct topology in diffusion-weighted MR imaging. Those with small cortical infarcts, or territorial infarcts outside borderzone regions were classified as AAE group, otherwise, non-AAE group. WSS ratio (WSSR) was quantified on CTA-based computational fluid dynamics models, calculated as WSS measured at the stenotic throat divided by WSS at proximally normal vessel. WSSR was divided as moderate or high WSSR, by the 4th quartile. Logistic regression analyses were conducted to explore the WSSR-baseline DM interactions on the presence of AAE.
Results: Among 102 eligible patients (median age 62, 73 [71.6%] males), 40 (39.2%) had AAE. Logistic regression analyses revealed significant high WSSR-baseline DM interactions on the presence of AAE (p=0.034): high WSSR was positively associated with AAE in baseline DM patients (odds ratio [OR]=4.18, 95% confidential interval [CI]=1.32-13.23, p=0.015), however, the association was not significant among non-DM patients, (OR=4.09, 95%CI=0.69-24.24, p=0.121).
Conclusions: In DM patients, moderate WSS across an ICAS lesion could also cause AAE, possibly by the activating inflammation response.
Disclosures of Interest: No
Abstract N°: 817
VARIATION IN BLOOD VISCOSITY BASED ON THE POTENTIAL CAUSE OF TRANSIENT ISCHEMIC ATTACK
Sang Won Han*1, Jae Hyeon Park1, Kyung-Yul Lee2
1Sanggye Paik Hospital, Inje University College of Medicine, Neurology, Seoul, South Korea,2Gangnam Severance Hospital, Yonsei University College of Medicine, Neurology, Seoul, South Korea
On behalf of:
Background and aims: Transient ischemic attack (TIA) is defined as brief episodes of neurological dysfunction resulting from focal cerebral ischemia and without evidence of acute infarction. TIA is etiologically heterogeneous disorders. An accurate and precise etiologic classification of TIA may impact its evaluation and treatment. Our previous study suggested that blood viscosity (BV) levels differed depending on the potential cause of the stroke in the stroke of undetermined etiology, negative evaluation (SUDn) group. SUDn with potential atherothrombosis (SUDn-AT) patients had a higher BV levels than those with possible embolism (SUDn-E) group. This study investigated differences in BV levels based on the potential cause of TIA.
Methods: Patients were categorized into two groups: TIA-AT and TIA-E. In TIA-AT group, patients should have evidences of systemic atherosclerosis, including: 1) atherosclerosis in one or more major brain arteries, 2) coronary artery disease, and/or 3) peripheral artery disease.
Results: A total of 86 TIA patients were included for analysis. Of these, 56 (65%) were classified as TIA-AT and 35% as TIA-E. No significant differences were observed in the baseline characteristics and laboratory findings between the groups except BV levels. TIA-AT patients had a higher systolic BV (SBV) (p=0.033) and diastolic BV (DBV) (p=0.031) levels than TIA-E group. Hct-adjusted partial correlation analysis showed that TIA-AT subtype was significantly associated with increased SBV (r=0.279, p=0.010) and DBV (r=0.258, p=0.017) levels.
Conclusions: While the role of BV in the mechanism of TIA requires further elucidation, two distinct TIA entities according to the potential etiology might be distinguishable.
Disclosures of Interest: No
Abstract N°: 1714
DEVELOPING A CLINICAL FINDING SCALE FOR LARGE VESSEL ISCHEMIC STROKE FOR RESOURCE LIMITED EMERGENCY SETTING
Apratim Chatterjee*1
1ILS, NEUROINTERVENTION, KOLKATA, India
On behalf of:
Background and aims: Large vessel ischemic strokes are notorious to cause huge mortality and morbidity and are crucial to be treated acutely. Hence a clinical charting of key symptoms may help pick up Large Vessel Occlusion ( LVO) in emergency setting by emergency physicians and even by paramedics in resource limited settings.
The Key symptoms listed were Aphasia, Dense Hemiplegia, Neglect, Conjugate Eye Deviation(CED), Seizure at onset. One or more of the above symptoms or findings with a NCCT brain with no bleed is proposed to be suggestive of LVO.
Methods: This was a prospective study done over one year with analysis of symptoms identified in the emergency to activate “code brain” for a suspected stroke. We analysed the emergency “code brain “calls for 240 patients at a comprehensive stroke centre. NCCT scans without bleeds were taken for study and symptoms analysed to form a clinical analyser in emergency resource poor setting.
Results: Aphasia was the most common finding which was identified with LVO 96 (40%) calls. Other common symptoms were dense hemiplegia(n = 72, 30%) and CED(n = 62, 26%). Loss of consciousness was often missed as stroke symptoms. Neglect was most frequently missed finding among LVO. Seizure at onset although identified as a prospective symptom of LVO during code brain was often missed.
Conclusions: Developing a clinical finding checklist with no bleed in CT brain is a very effective tool in early identification of LVO in resource poor setting where only CT machine is available.
Disclosures of Interest: No
Abstract N°: 1738
INFLAMMATION IN EMBOLIC STROKE OF UNDETERMINED SOURCE (ESUS)
Maurizio Acampa*1, Pietro Enea Lazzerini1, Riccardo Accioli1, Carlo Domenichelli2, Viola Salvini1, Francesca Guideri1, Rossana Tassi2
1University of Siena; Italy, Department of Medical Sciences, Surgery and Neurosciences, University of Siena;,2Azienda Ospedaliera Universitaria Senese
On behalf of:
Background and aims: Evidence strongly suggests that inflammation plays a crucial role in various pathogenic subtypes of ischemic strokes (large artery atherosclerosis, cardioembolic, lacunar, and stroke of undetermined causes). Among these, embolic strokes of undetermined source (ESUS) account for one third of ischemic strokes and include heterogeneous and distinct clinical phenotypes. The aim of our study was to investigate if inflammatory markers can be associated with specific ESUS phenotypes.
Methods: 226 patients with ESUS (105M, 121F) were stratified into two groups based on their high-sensitivity C-reactive protein (CRP) levels: normal-CRP ESUS (<0.5 mg/dl) and high-CRP ESUS group (>0.5 mg/dl). The inclusion criteria were determined according to the ESUS definition proposed by the Cryptogenic Stroke/ESUS International Working Group.
Results: High-CRP ESUS patients were older than normal-CRP patients (75±13 vs. 67±12; p<0.0001). Additionally, they presented with a more pronounced neurological deficit, as evidenced by a higher NIHSS score at admission (12±8 vs. 6±6; p<0.0001). Despite similar cardiovascular risk factors in both groups, those with high CRP levels showed a higher prevalence of minor-risk potential embolic sources, specifically mitral valve calcifications and some markers of atrial cardiopathy such as increased left atrium size (20±6 vs. 18±5 cm2, p=0.04) and elevated P wave dispersion levels (54±14 vs. 44±13, p<0.0001). Interestingly, there was no significant difference in the presence of carotid artery non-stenotic plaques between the two patient groups.
Conclusions: In ESUS patients, inflammatory markers are particularly associated with a more severe neurological deficit and with the presence of the phenotype related to atrial cardiopathy.
Disclosures of Interest: No
Abstract N°: 1886
CEREBRAL THROMBI ANALYSIS FOR IDENTIFYING INFECTIVE ENDOCARDITIS-RELATED STROKES
Beatrice Dell'Acqua*1,2, Aurora Semerano2, Ghil Schwarz3, Francesca Sanvito4, Pietro Panni5, Patrik Michel6, Massimo Filippi1, Gianvito Martino2, Davide Strambo6, Marco Bacigaluppi1,2
1San Raffaele Hospital, Milan, Italy, Department of Neurology, Stroke Unit, Milan, Italy,2San Raffaele Scientific Institute, Milan, Italy, Neuroimmunology Unit, Division of neuroscience, Institute of Experimental Neurology,3Niguarda Ca’ Granda Hospital, Milan, Italy, Department of Neurology,4San Raffaele Hospital, Department of Pathology,5San Raffaele Hospital, Milan, Italy, Department of Neuroradiology,6Lausanne University Hospital, Switzerland., Department of Clinical Neurosciences, Stroke Centre, Neurology Service
On behalf of:
Background and aims: Infective endocarditis (IE) is a life-threatening condition that can cause stroke, and its diagnosis can be challenging. Our objective is to evaluate whether the microbiological and histological analysis of cerebral thrombi obtained through endovascular thrombectomy from stroke patients with IE could contribute to a definitive diagnosis of this condition.
Methods: We compared cerebral thrombi from three groups of ischemic stroke patients with large vessel occlusion stroke: definite IE (n=10), cardioembolic stroke plus other concomitant infections (n=10 CE-I+), and cardioembolic stroke without infections (n=30 CE-I-). Our multiparameter analysis encompassed histological examinations, molecular biology and microbiological tests to detect microorganisms within the thrombi and to comprehensively assess their structural composition and immune signatures.
Results: We directly detected invading pathogens through either histology, PCR or thrombus culture in all cerebral thrombi from IE patients, whereas none of the control thrombi showed such pathogens. Thrombi from IE patients exhibited significantly lower content of red blood cells and CD14+ monocytes, increased von Willebrand Factor density, and a cell-dominant pattern of Neutrophil Extracellular Traps (NETs) deposition. These four thrombus components displayed good discriminative ability between IE and controls, with AUC values ranging between 0.84 and 0.89.
Conclusions: Multimodal analysis of cerebral thrombi in stroke patients with suspected infective endocarditis supports early and definitive diagnosis by detecting pathogens and reflecting immunothrombotic changes.
Disclosures of Interest: No
Abstract N°: 1983
NON-STENOTIC CAROTID PLAQUES IN EMBOLIC STROKE OF UNDETERMINED SOURCE
Manuraj N*1, Adarsh Anil Kumar2, Santhosh Kumar K2, Sapna Erat Sreedharan1, Arya Devi K S1, P N Sylaja1
1Sree Chitra Tirunal Institute for Medical Sciences & Technology, Comprehensive stroke care Program,Department of Neurology, Thiruvananthapuram, India,2Sree Chitra Tirunal Institute for Medical Sciences & Technology, Department of imaging sciences and Interventional Radiology, Thiruvananthapuram, India
On behalf of:
Background and aims: Identifying the possible underlying mechanism of stroke in Embolic Stroke of undetermined Source (ESUS) will help in better planning of secondary prevention strategies. The aim is to determine the prevalence of ipsilateral non-stenotic carotid plaques in patients with ESUS and identify the high-risk plaque characteristics and analyse the infarct pattern in them.
Methods: This is a hospital based retrospective cohort study of patients with ESUS between 2012 to 2022.The CT angiogram were reviewed for presence of non-stenotic carotid plaques and plaque characteristics. The infarct pattern were also analysed and compared with ESUS without non-stenotic carotid plaques.
Results: Two hundred and forty patients with ESUS were included (Mean age - 57.96 ± 12.59 years; Males: 65.83%). The prevalence of non-stenotic carotid plaques ipsilateral to stroke was 10.7% [27/240] and contralateral to stroke was 6.2% [15/240] (p = 0.056). Of the plaque characteristics on imaging, except plaque irregularity (14.6% vs 8.6%, p= 0.045), none of the features like plaque thickness, ulceration, and hypodensity were significantly associated with ipsilateral stroke. Among the infarct pattern, compared to the patients without non-stenotic carotid plaques, watershed infarcts (18.5 vs 3.8 %, p = 0.002) and embolic pattern (22.2 %vs 5.2 %, p= 0.001) were more frequent in the ESUS with non-stenotic plaques which was significant.
Conclusions: In patients with ESUS, non-stenotic carotid plaques with irregular surface were more common on the side of the ischemic stroke, suggesting it to be a stroke mechanism in them. Identifying the infarct pattern in this subgroup reinforces this as a possible stroke etiology.
Disclosures of Interest: No
Abstract N°: 2113
ENDOTHELIN-1 IN EMBOLIC STROKE OF UNDETERMINED SOURCE PATIENTS WITH COMPLICATED NON-STENOSING INTRACRANIAL ATHEROSCLEROTIC PLAQUES
Federico Mazzacane*1, Beatrice Del Bello1, Federica Ferrari1, Elisa Rognone2, Anna Pichiecchio1, Anna Cavallini3
1University of Pavia, Department of Brain and Behavioral Sciences, Pavia, Italy,2IRCCS Mondino Foundation, Department of Neuroradiology, Pavia, Italy,3IRCCS Mondino Foundation, Department of Emergency Neurology and Stroke Unit, Pavia, Italy
On behalf of:
Background and aims: Artery to artery embolization from non-stenosing intracranial complicated atherosclerotic plaques has been suggest as one of the main etiologies of embolic stroke of undetermined source (ESUS). These lesions are often missed by conventional imaging. Vessel wall MRI (VWMRI) can identify high-risk intracranial atherosclerotic plaques but is not widely available. Endothelin-1 (ET-1) has been proposed as a marker of complicated atherosclerotic disease and could be a promising marker to identify ESUS patients with atherosclerotic etiology, to guide the subsequent diagnostic workup.
Methods: We included in the study all consecutive ESUS patients with single territory strokes, after a standard diagnostic workup consisting in CT angiography of intracranial and epiaortic vessels, transthoracic echocardiogram, and 72h ECG monitoring. Included patients underwent VWMRI with gadolinium contrast agent administration within 1 month and blood sampling to measure plasma ET-1 concentration at 3 ± 1 days from onset.
Results: The first 18 patients have been enrolled in the study. Median (IQR) age was 63 (9.5) and 6 patients (33%) were female. VWMRI revealed complicated intracranial non-stenosing atherosclerotic plaques in the involved vascular territory in 6 patients (33.3%). ET-1 plasma concentration was higher in patients with culprit intracranial atherosclerotic lesions detected by VWMRI [2.476 (0.883) vs 4.242 (1.159), p = 0.002].
Conclusions: Serum ET-1 concentration in the acute phase after ischemic stroke are higher in ESUS patients with a culprit intracranial complicated atherosclerotic lesion detected by VWMRI. Our preliminary data suggest that plasma biomarkers may assist in patients’ selection for advanced vascular imaging in cryptogenic stroke.
Disclosures of Interest: No
Abstract N°: 2532
C-REACTIVE PROTEIN EXPRESSION IN ACUTE ISCHEMIC STROKE (AIS) BLOOD CLOTS
Wenyi Liu*1, Cansu Sahin1,2, Alice Giraud3, Pierluca Messina3, Vanessa Chalumeau4, Ivan Vukasinovic5, Marc Ribo6, Nobuyuki Sakai7, Christophe Cognard8, Karen Doyle1,2
1University of Galway, Physiology, Galway, Ireland,2University of Galway, CÚRAM SFI Research Centre for Medical Devices, Galway, Ireland,3Sensome, Massy, France,4Bicêtre Hospital, Interventional Neuroradiology, Le Kremlin-Bicêtre, France,5University Clinical Center of Serbia, Center for Radiology and MRI, Clinic for Neurosurgery, Belgrade, Serbia,6University Hospital Vall d'Hebron, Neurology, Barcelona, Spain,7Kobe City Medical Center General Hospital, Neurosurgery, Kobe, Japan,8CHU de Toulouse, Diagnostic and Therapeutic Neuroradiology, Toulouse, France
On behalf of: Vanessa Chalumeau, Ivan Vukašinović, Marc Ribo, Nobuyuki Sakai, Christophe Cognard
Background and aims: C-reactive protein (CRP) is a prototypic marker of inflammation. Elevated plasma CRP concentration is associated with an increased risk of cerebrovascular events. To determine whether CRP could be a useful biomarker of stroke etiology, we investigated CRP expression in AIS clots from cardioembolic (CE), large artery atherosclerosis (LAA) and cryptogenic subtypes.
Methods: We collected clot samples from AIS patients of different etiologies: CE (n=50), LAA (n=39) and cryptogenic (n=29). Assessment of clot composition was carried out using Martius Scarlet Blue stain. Immunohistochemistry was used to investigate CRP expression and immunofluorescence was used to detect colocalisation between CRP and clot components including platelets and fibrin. Statistical analysis used Mann-Whitney and Chi-square tests.
Results: Overall, 30% (38% of CE, 21% of LAA, 28% of Cryptogenic) of clot samples expressed CRP. The proportion of CRP expression in CE was higher than LAA samples (X2(1,89)=3.170). Significantly higher expression of CRP was observed in clots from female patients compared to males (X2(1,114)=5.094,P=0.02). Clots expressing CRP had significantly higher fibrin content than clots with no CRP expression (U=1508; P=0.03). Confocal microscopy showed colocalization of CRP with fibrin but not platelets.
Conclusions: Significantly more AIS clots of CE origin expressed CRP compared to LAA clots, suggesting CE strokes may be more strongly linked to inflammation. Significantly more clots from female patients expressed CRP suggesting a sex difference. Further study of the relationship between fibrin and CRP in clots may improve our understanding of the processes of thromboinflammation.
AcknowledgementsChinese Scholarship Council; SFI (CURAM:13/RC/2073_P2), and Sensome
Disclosures of Interest: No
Abstract N°: 2608
RETROSPECTIVE ANALYSIS OF ATHEROSCLEROTIC INTRACRANIAL ARTERIAL STENOSIS: A CROSS - SECTIONAL STUDY
Bader Mohamed*1,2, Fatema Almosawi3, Sanhita Majumder1, Nadeesha Ahangama1, Lampros Nikolopoulos1, Alexandra Andrews1, Ambreen Ali Sheikh1
1Barts Health NHS Trust, United Kingdom,2Government Hospitals, Manama, Bahrain,3Ministry of Health, Sanabis, Bahrain
On behalf of:
Background and aims: Intracranial atherosclerotic disease (ICAD) is a major risk factor for stroke and cognitive decline. We aimed to determine the clinical features and outcome of ICAD-related stroke.
Methods: All patients with a diagnosis of ICAD related stroke, in the period between July to December 2022 were retrospectively analysed using electronic health records in a large adult tertiary stroke centre in London, UK.
We collected patients' demographics and clinical features.
Results: 140 cases identified. Mean age was 70 (26- 96 years). 6/140 (4.2%) were younger than 50 years of age. Male represented 60% of the subjects. 52% (n = 66) were from ethnic minorities including Asian and Black. Most patients (70%) had (Modified Rankin score of 0-2). 66.5% (n=93) had a mild or moderate stroke as stratified by NIHS score. 77% of subjects had anterior circulation strokes, while 14% (n=20) had posterior circulation and (8.5%, n=12) had TIA.
Arteriopathy in other major vessels was found to be common in such cases with 20% of subjects had carotid disease, 16% had ischemic heart disease, and 3% had Peripheral artery disease. 26% (n = 36) had recurrent strokes at presentation, 5% of these cases had recurrent strokes or TIA despite being on best medical treatment and 9% died within 6 months.
Only 50% were discharged on Dual anti-platelet (DAPT) and the duration of DAPT was not stated in 30% of cases.
Conclusions: Aggressive, individualised risk stratification, patient education, communication with primary carers at discharge and self-management are key areas to be considered to improve patient outcomes.
Disclosures of Interest: No
Abstract N°: 2891
DISCORDANCE RATES AND CLINICAL USEFULNESS OF MULTIMODALITY IMAGING IN THE ASSESSMENT OF PATIENTS WITH SYMPTOMATIC CAROTID STENOSIS
Jessica Redgrave1, Sara Lomzynska*2, Stephen Goode3
1Sheffield Teaching Hospitals, Sheffield, United Kingdom,2University of Sheffield,3Sheffield Teaching Hospitals
On behalf of:
Background and aims: Narrowing of the carotid artery (carotid stenosis) is a common cause of ischemic stroke. Patients with > 50% stenosis on the symptomatic side may be recommended for carotid endarterectomy (CEA). Ultrasound (US) is commonly used to screen for carotid stenosis in the UK; however, if a stenosis >50% is found, a second imaging modality e.g. magnetic resonance angiography (MRA) is usually performed to confirm. If a discrepancy is found between the first and second scan, a third modality is recommended; usually a computed tomography (CTA). We assessed how much time was taken to perform additional imaging, and how often the 2nd imaging modality altered patient management.
Methods: A list of patients who underwent an MRA for “? carotid stenosis” at the Sheffield NHS Trusts between 03.10.2021 and 05.05.2022 (n= 46). Stenosis levels were categorised into 8 groups (0-29%, 30-49%, 50-59%, 60-69%, 70-79%, 80-89%, 90-99%, 100%), with discordance being classed as modalities reporting different categories of stenosis.
Results: 13 (25%) patients had discordant results on imaging. In 10 (4.6%) cases, one modality found <50% stenosis whilst the other found >50%. In 2 cases, one modality found complete occlusion of the artery (100%) while the other found some flow. The mean days between the first and second imaging modality was 2 (SD: 6.550). Management was changed for 12 patients based on the results of the second imaging modality.
Conclusions: Multi-modality imaging provided useful clinical information in a significant proportion of patients carotid stenosis but in some cases increased delay to CEA.
Disclosures of Interest: No
Abstract N°: 3140
ISCHEMIC STROKE SECONDARY TO RECURRENT THROMBOTIC THROMBOCYTOPENIC PURPURA (TTP): A CASE SERIES
Earl Biag1, Monika Manchanda*1
1University of New Mexico, Neurology
On behalf of:
Background and aims: Stroke develops in <10% of patients admitted with Thrombotic Thrombocytopenic Purpura (TTP). The rate of “recurrent TTP” and ischemic strokes, is even more rare and not well documented.
Methods: Patients diagnosed with recurrent TTP with confirmation of ADAMTS13 activity and inhibitor levels, who developed clinical and neuroimaging evidence of acute ischemic stroke, were reviewed retrospectively, and included in the study.
Results: Two patients were identified. A 36-year-old male patient presented with speech difficulties and was found to have ischemic strokes involving bilateral cerebellum and left occipital lobe. His platelet count was 10,000/uL and ADAMTS13 activity was low at <2.2%. He received glucocorticoids and underwent five sessions of plasmapheresis. One year later, he presented with left homonymous hemianopia, with MRI brain showing acute left frontal lobe and right occipital lobe infarcts. His ADAMTS13 level was <5% with the inhibitor level of 2.9 (reference normal <0.4). He was diagnosed with recurrent TTP and ischemic stroke, and treated with plasmapheresis and glucocorticoids again, with recovery in platelets. He further received Caplacizumab and rituximab thereafter. Similarly, a 59-year-old female patient was also diagnosed with ischemic stroke due to recurrent TTP and was placed on rivaroxaban and clopidogrel after the initial flare. The outcome was favorable in both cases; with Modified Rankin score of 0 for both at one year.
Conclusions: We report two cases of ischemic stroke due to recurrent TTP here in hopes to pull this rare phenomenon into established knowledge for both neurologists and hematologists.
Disclosures of Interest: No
Abstract N°: 3214
YIELD OF PROLONGED ECG MONITORING IN AN ISCHEMIC STROKE/TIA COHORT: COULD WE HAVE BETTER TARGETED THE PATIENTS ELIGIBLE FOR THE TEST?
Elena Escriche*1, Inhar Esnaola1, Karmele Gil Alzueta1, Idoia Rubio1, Julian Librero2, Maria Herrera Isasi1
Background and aims: Selection of patients with a higher pretest probability of PAF-related stroke would allow physicians to use cardiac monitoring devices (CMDs) more effectively and ultimately reduce the secondary stroke burden. Our aim was to analyze the yield of outpatient CMDs and the identification of factors of high negative predictive value (NPV) for better patient selection.
Methods: We analyzed a retrospective cohort of 277 consecutive patients who underwent 28-day mobile cardiac outpatient telemetry from sept22 to sept23 after stroke or TIA. Bivariate and multivariable analyses (stepwise logistic and regression trees) were performed to identify predictive factors associated with presence or absence of PAF in first CMD or further on.
Results: PAF detection percentage was 9,7% in patients with stroke/TIA (27/277), 11,1% (27/244) in patients with undetermined TOAST stroke/TIA, and 18.75% (27/144) when patients met non PFO-ESUS criteria. 24.1% of 29 initially negative monitoring showed PAF when repeated. Age, valvular cardiopathy, hyperthyroidism, large vessel occlusion, total supraventricular streak number, supraventricular streak length, CHA2DS2-VASc scale and HAVOC scale were significantly associated with PAF presence. After multivariate analysis, younger age (OR 0.89; CI 95%: 0.84-0.94) and absence of large vessel occlusion (OR 0.23; CI 95%: 0.08-0.68) were independently associated with PAF absence.
Conclusions: The CMD yield after stroke/TIA in our hospital aligned with findings from previous studies. Besides, in order to enhance patient selection for the test, a more meticulous classification based on the TOAST scale and a comprehensive investigation of non-cardioembolic causes in younger patients and/or in the absence of large vessel occlusion would be of interest.
Disclosures of Interest: No
Abstract N°: 3258
CAROTID IMAGING – THE WEAK LINK IN ACUTE STROKE CARE IN ROMANIA. DATA FROM THE RES-Q REGISTRY
Cristina Tiu*1,2, Bogdan Casaru1, Anca Negrila1, Razvan Alexandru Radu1,2, Vlad Tiu2,3, Cristina Panea2,3, Elena Oana Terecoasa1,2
1Emergency University Hospital Bucharest, Neurology, București, Romania,2Carol Davila University of Medicine and Pharmacy, București, Romania,3Spitalul Universitar de Urgență Elias, Neurology, București, Romania
On behalf of:
Background and aims: Vascular imaging plays a crucial role in the management of patients with ischemic stroke or TIA, especially in selecting those cases which would benefit most from a revascularization procedure. The RES-Q Registry helps us to establish the level at which this diagnostic procedure is performed throughout the country and to set new goals for the future.
Methods: RES-Q Registry data from all the 38 participating centers in Romania since 2017 until 2023 was analyzed.
Results: A total of 12.528 patients were included in the RES-Q Registry nationwide between 2017 and 2023 on a one month per year basis. For this analysis we included only ischemic strokes and TIA, in a total number of 10.892 cases. The percentage of patients for which carotid imaging was done during the hospital admission has varied from a minimum of 45.44% in 2021 to a maximum of 66.5% in 2023. A symptomatic carotid stenosis > 50% was identified in as low as 4.21% of the patients screened in 2022 and in a maximum of 16.17% of the total cases in 2023. Regarding the procedures of revascularization for symptomatic carotid stenosis, the numbers draw a grim picture, with a minimum of 17.14% benefiting from this intervention in 2020 and a maximum of 31.62% in 2019.
Conclusions: According to our data, there is still a vast proportion of cases which remain undiagnosed in Romania. The gap between the number of identified symptomatic carotid stenosis and revascularization procedures is still wide, so there is an urgent need to address this issue.
Disclosures of Interest: No
E-Poster - Epidemiology and Risk Factors
Abstract N°: 49
SEASONAL VARIATIONS IN MORBIDITY AND MORTALITY OF STROKE IN BISHKEK, KYRGYZ REPUBLIC
Mirgul Yrysova*1
1I.K.Akhunbaev Kyrgyz State Medical Academy, General and Clinical Epidemiology, Bishkek, Kyrgyzstan
On behalf of:
Background and aims: There is no evidence of long-term studies of seasonal variations in stroke in the Kyrgyz Republic. The purpose of this study was to investigate seasonal variation in stroke morbidity and mortality using data from stroke registry of general population in Bishkek
Methods: A retrospective analysis of data from all patients with stroke admitted to city hospitals by ambulance from January 2016 to December 2019 was carried out. To study the seasonal variation of stroke, patients were divided according to the time of stroke occurrence by month and season of the year, also a seasonality index was calculated. The corresponding monthly meteorological data to the study period were obtained.
Results: From 2016 to 2019 we identified a total of 4059 stroke cases, of which 3353 cases had ischemic stroke, and 706 had intracerebral hemorrhage. The mortality rate was 1206 cases. Strokes are recorded throughout the year, but the largest number of strokes occurred in the spring (29.2%). Analysis of seasonality by stroke subtypes revealed that ischemic strokes and hemorrhagic strokes also predominated in the spring (28.7% and 31.4%, respectively). Mortality rates from stroke were 28.7% in winter and 33.3% in spring. Indices of seasonal fluctuations in stroke demonstrated the spring seasonality
Conclusions: The identified season of peak rhythm of stroke morbidity and mortality (with an increase in winter and early spring) can be used for adequate planning of treatment and preventive care for the population
Disclosures of Interest: No
Abstract N°: 93
COVID-19 AND STROKE IN THE PHILIPPINES
Gabriel Alejandro Baroque*1, Jose Navarro1, Alejandro II Baroque1, Johnny Lokin1, Ericka Samantha Teleg2, Annabelle Lao-Reyes3, Priscille Ogena4, Maritoni Abbariao5, Joseree Ann Catindig1, Suni Grace Castillo6
1University of Santo Tomas Hospital, Neuroscience and Behavioral Medicine, Manila, Philippines,2Grand River Hospital, Department of Internal Medicine, Ontario, Canada,3Southern Philippines Medical Center, Department of Neurology, Davao, Philippines,4Jose R. Reyes Memorial Medical Cennter, Department of Neurology, Manila, Philippines,5Dr. Jose N. Rodriguez Memorial Hospital, Department of Neurology, Caloocan, Philippines,6Veterans Memorial Medical Center, Department of Neurology, Quezon City, Philippines
On behalf of: Maningo, Jason Rey T., MD (Department of Neurology Southern Philippines Medical Center, J.P. Laurel Avenue, Bajada, Davao City, 8000 Davao del Sur, Philippines) and Zamora, Maria Rheena Flor C., MD (Department of Neurology Southern Philippines Medical Center, J.P. Laurel Avenue, Bajada, Davao City, 8000 Davao del Sur, Philippines)
Background and aims: COVID-19 has slowly emerged as a multi-organ system disease which predominantly is a pulmonary disease; however, involvement of the cerebrovascular system have been observed. Our aim is to have a better demographic data of the stroke patients with COVID-19 to be able to better allocate and prioritize resources for these patients. With the review of pathogenesis of the disease and its involvement with cerebrovascular diseases, we wanted to confirm if there is a correlation with the COVID-19 disease and stroke.
Methods: This is a cross-sectional, multi-center collaborative study with representative institutions in the country utilizing chart and electronic databases from patients who were admitted for stroke from March 2020 to March 2021.
Results: Out of a total of 10,298 patients diagnosed with COVID-19 and admitted in the centers included in the study, 216 patients were diagnosed with stroke (2.1%). Vascular risk factors such as diabetes mellitus, cardiac diseases and alcohol use were seen to be significantly increased in patients with COVID-19. Large artery atherosclerosis and small vessel diseases were seen more in patients with COVID-19. Inflammatory markers were significantly elevated in stroke patients with COVID-19.
Conclusions: The incidence of stroke in COVID-19 patients are comparable with other incidence studies with the same population of interest. Looking at the different characteristics of patients, it was noted that inflammatory processes from COVID-19 may have led to a hypercoagulable state. Furthermore, stroke must be considered as a possible complication in patients with COVID-19 with associated vascular risk factors.
Disclosures of Interest: No
Abstract N°: 269
CAN WE CREATE AN EFFECTIVE VIRTUAL NATIONAL STROKE REGISTER? A NATIONAL DATA LINKAGE AND VALIDATION STUDY
Marine Corbin1, Hayley Denison1, Mina Whyte2, Jeroen Douwes1, Anna Ranta*2,3
1Massey University, Research Centre for Hauora and Health, Wellington, New Zealand,2University of Otago, Wellington, Medicine, Wellington, New Zealand,3Wellington Hospital, Neurology, Wellington, New Zealand
On behalf of: REGIONS Care Study Group
Background and aims: To assess the validity of administrative data to identify stroke patients, risk factors, and outcomes in New Zealand (NZ), we compared data from Statistics NZ Integrated Data Infrastructure (IDI) with nationwide prospectively collected data from the REGIONS Care study.
Methods: We matched prospective stroke study patients admitted between 1/5/2018-31/10/2018 to administrative IDI discharges for the same period and compared case ascertainment, stroke diagnosis, risk factors, and outcomes using novel composite administrative variables.
Results: Of 1719 REGIONS Care patients, 1422 (82.7%) had a primary stroke hospitalisation in the IDI. Of the remaining patients, 102 (5.9%) had a secondary IDI stroke diagnosis, 111 (6.5%) were admitted within one week of the study period, and 57 (3.3%) had no hospitalisation record. Sensitivity and specificity for IDI favourable outcome vs. mRS 0-3 were 0.87 and 0.82 and the kappa coefficient was 0.67. Kappa coefficients for stroke risk factors ranged from good for atrial fibrillation (0.75) and diabetes (0.78), to moderate for smoking (0.71), prior stroke (0.69), hypertension (0.54), and TIA (0.53), to fair for dyslipidaemia (0.33). IDI and REGIONS Care patients had similar age (77.6 (19.5) vs 77 (19) years), stroke type (13% vs 12% haemorrhagic), and length of stay (4 (5) vs 4.9 (5.6) days) respectively.
Conclusions: NZ administrative data is an imperfect, but reasonably accurate tool to identify stroke patients, type and outcomes and several key risk factors. Development of an administrative virtual stroke register to track stroke patients for health service planning appears feasible using the developed variables.
Disclosures of Interest: No
Abstract N°: 529
CHARACTERISTICS OF ACUTE ISCHEMIC STROKE PATIENTS WITH INTRACRANIAL ATHEROSCLEROTIC STENOSIS IN VIETNAM
Trung Vuong Xuan*1, Ton Mai Duy1, Phuong Dao1, Tho Pham-Quang1, Trung Vuong-Xuan1
1Bach Mai Hospital, Stroke Center, Ha Noi, Viet Nam
On behalf of:
Background and aims: Intracranial atherosclerotic stenosis (ICAS) is an important cause of ischemic stroke, especially in Asia populations. There is a limited number of studies on this disease in Vietnamese people. This study aimed to evaluate the clinical and imaging features of Vietnamese acute ischemic stroke patients due to ICAS.
Methods: A cross-sectional descriptive study was conducted at the Stroke Center - Bach Mai Hospital from April 2022 to April 2023. We recruited all AIS patients diagnosed with intracranial atherosclerotic stenosis and admitted within 24 hours from onset.
Results: 135 patients (mean age 64.9 ± 12.6, male 65.9%) were recruited for this study. Among these AIS patients due to ICAS, hypertension is the leading risk factor (62.2%), followed by smoking and diabetes mellitus (35.6% and 23%, respectively). At admission, median NIHSS score was 5 (2-9). The stenosis site was mainly in the anterior cerebral circulation (85.9%), including internal carotid artery and middle cerebral artery. The common mechanisms of stroke were artery-to-artery embolism and thrombotic occlusion (65.2%). Patients with moderate (50-69%) versus severe (70-99%) intracranial artery stenosis accounted for 27.4% and 72.6%, respectively. After three months, there was no difference in recurrence rate and neurological function outcomes between these two groups.
Conclusions: This study gave a glance at Vietnamese acute ischemic stroke patients due to intracranial atherosclerotic stenosis. Despite some limitations, it is the basis for further study in Vietnam.
Disclosures of Interest: No
Abstract N°: 697
ACUTE ISCHEMIC STROKE IN THE PATIENTS WITH INFLAMMATORY ARTHRITIS: AN ANALYSIS OF DATA FROM NATIONAL HEALTH INSURANCE SERVICE
Jun Hong Lee*1
1National Health Insurance Service Ilsan Hospital, Neurology, Goyang-si, South Korea
On behalf of:
Background and aims: Inflammation is an important mechanism of stroke and inflammatory arthritis. We evaluated the risk of stroke and compared the medical expenses between the patients of inflammatory arthritis and matched population, using data from National Health Insurance Service
Methods: We defined the patients of ankylosing spondylitis, seropositive rheumatoid arthritis, and psoriatic arthritis and enteropathic spondyloarthropathy. Control group was defined by 1:5 propensity score matching. Newly developed stroke was defined as the patients with the main diagnosis and 1) brain imaging, or 2) prescription of stroke medication or related intervention.
Results: Seropositive rheumatoid arthritis was associated with more frequent stroke occurrence in patient group of seropositive rheumatoid arthritis (Hazard ratio 1.11, 95% CI 1.02-1.20, p value=0.012). In-patient medical expense related to stroke in seropositive rheumatoid arthritis patients with stroke, showed the tendency to be larger than the control group.
Conclusions: Seropositive rheumatoid arthritis was a predictor of the more frequent stroke occurrence. To decrease the comorbid stroke and following burden of social cost, the careful concern is needed for the early diagnosis and active management of inflammatory arthritis, especially seropositive rheumatoid arthritis. Further studies involving the long-term follow-ups of clinical outcomes are warranted to elucidate the underlying correlation between the inflammatory arthritis and the stroke.
Disclosures of Interest: No
Abstract N°: 701
VASCULAR RISK FACTORS AND MEDICATION COMPLIANCE IN STROKE PATIENTS IN ARMENIA
1Erebuni Medical Center, Department of Neurology & Comprehensive Stroke Center, Yerevan, Armenia,2National Institute of Health, Department of Neurology and Neurosurgery, Yerevan, Armenia,3Temple University, St. Luke’s School of Medicine, Philadelphia, United States,4University of Alberta, Department of Medicine, Edmonton, Canada,5Boston Medical Center, Department of Neurology, Boston, United States
On behalf of:
Background and aims: The early treatment of vascular risk factors treatment is pivotal for primary and secondary stroke prevention. Data regarding patient compliance in taking prescribed medications for these conditions are limited in the Caucasus. In this study, we assessed the prevalence and treatment of risk factors in patients with acute stroke seeking medical attention in Yerevan, Armenia.
Methods: We prospectively enrolled consecutive patients admitted over a 30-day period, in 2023, to the Erebouni Comprehensive Stroke Center with a diagnosis of acute stroke. Based on a questionnaire prepared a priori, their histories and laboratory test results, obtained as part of their routine evaluations, were extracted, and tabulated.
Results: 129 patients were included. Mean age was 67.4 years. 37.2% were women. Ischemic stroke was diagnosed in 83,72%, hemorrhagic in 12.4% and TIA in 3,87%. In-patient case fatality rate was 8.3% for ischemic, and 25.0% for hemorrhagic, stroke. Admission prevalence of vascular risk factors and patient compliance in taking medications prescribed to treat stroke risk factors are presented in the table.
Conclusions: Vascular risk factors were highly prevalent in this population. Patient compliance in taking prescribed medications was suboptimal and was a factor affecting treatment outcome. Further investigation regarding the causes of the non-compliance, effective prevention strategies, and patient education are indicated.
Disclosures of Interest: No
Abstract N°: 712
IMPACT OF THE OCCUPATIONAL STRESS ON THE ASYMPTOMATIC CEREBROVASCULAR DISEASE
Vladina Dimitrova-Kirilova1,2, Alexandra Yankova1,2, Dimitrinka Dimitrova1,2, Mihael Tsalta-Mladenov*2,3, Veselinka Nestorova1
1Medical University "Prof. Paraskev Stoyanov", Optometry and Occupational Diseases, Varna, Bulgaria,2University Hospital "St. Marina", Second Clinic of Neurology with ICU and Stroke Center, Varna, Bulgaria,3Medical University "Prof. Paraskev Stoyanov", Neurology and Neuroscience, Varna, Bulgaria
On behalf of:
Background and aims: Asymptomatic cerebrovascular disease (ACVD) is acknowledged as a socially significant condition and has been correlated with an increased risk of dementia and stroke. Occupational stress affects a large percentage of the working population and has been associated scientifically with a higher risk of cerebrovascular disease. The purpose of our research is to determine the impact of occupational stress on ACVD.
Methods: Our study included 151 working-age individuals with at least one vascular risk factor who had never experienced a stroke or transient ischemic attack. ACVD was described as brain atrophy, lacunar strokes, cerebral microhaemorrhages, and hyperintense white matter lesions of vascular origin found in magnetic resonance imaging (MRI). The participants were divided according to the presence (N=41) or absence (N=110) of MRI changes. A specific self-reporting questionnaire, the Workplace Stress Scale (WSS), was utilized to measure the levels of work-related stress.
Results: The mean WSS points in patients with MRI alterations were found to be higher - 21.34±5.47 - than in the control group (19.08±4.29)(p=0.009). Those with MRI changes are most likely to fall into the "severe stress level" category (31.7%), while those without MRI changes are more likely to fall into the "fairly low stress level" category (44.5%)(p<0.001). Elevated occupation stress levels were associated with a higher chance of MRI abnormalities (OR:2.61,95%CI,1.478–4.611) and correlated with them (rho=213, p=0.009).
Conclusions: Excessive work-related stress raises the risk of asymptomatic MRI lesions and is related to ACVD. Reducing work stress levels could contribute to the prevention of cerebrovascular diseases.
Disclosures of Interest: No
Abstract N°: 1136
COMPARISON OF ACUTE STROKE CARE AND OUTCOMES IN KOREA BETWEEN 2013/2014 AND 2018
Jun Yup Kim*1, Jihoon Kang1, Beom Joon Kim1, Moon-Ku Han1, Seong-Eun Kim1, Juneyoung Lee2, Yong Uk Kwon3, In Ok Bae3, Gui Ok Kim3, Hee-Joon Bae1
1Seoul National University Bundang Hospital, Department of Neurology, Seongnam-si, South Korea,2Korea University College of Medicine, Department of Biostatistics, Seoul, South Korea,3Health Insurance Review and Assessment Service, Wonju, South Korea
On behalf of:
Background and aims: Quality of acute stroke care can be improved through nationwide compulsory quality assessment. Acute stroke quality assessment (ASQA) covers most acute stroke patients in Korea. We evaluated the changes of acute stroke management and outcomes between 2013/2014 and 2018
Methods: Patients with ischemic stroke (IS), subarachnoid hemorrhage (SAH), and intracerebral hemorrhage (ICH), who were admitted via emergency rooms within 7 days at hospitals treating 10 or more cases during the each 3-month (2013, 2014) and 6-month (2018) survey period were selected. We grouped 2013 and 2014 into one group and compared them with 2018.
Results: In 2013/2014, 19,599 acute stroke cases were enrolled at 216 nationwide hospitals, while in 2018, 28,286 cases were enrolled at 248 hospitals. Patient age increased slightly, and the severe stroke cases decreased. More hospitals had stroke units. IV thrombolysis (IVT) decreased to 6.3% (8.7% in 2013/2014), and endovascular treatment (EVT) increased to 9.8% in 2018 (5.3% in 2013/2014). IVT in patients aged over 80 dropped from 1.3% to 0.2%, while EVT increased from 0.7% to 2.4%. Decompressive surgery in ICH patients fell from 28.0% to 25.2%. SAH clipping rates dropped from 34.7% to 24.3%, and coiling rates increased from 39.8% to 53.0%. One-year mortality declined from 22.0% to 18.2% across all stroke patients, also at 1 and 3 months, and for IS, ICH, and SAH patients.
Conclusions: This study showed that while stroke patients had improved outcomes from 2013/2104 to 2018 in Korea, there is still room for improvement, particularly in IVT rates.
Disclosures of Interest: No
Abstract N°: 1188
PREDICTORS OF STROKE OUTCOME IN SUBPOPULATION ADHERENT TO DIRECT ORAL ANTICOAGULANTS
Hamidreza Abbasi1, Thomas Covey1, Zalan Khan1, Marilou Ching*2
1University at Buffalo Jacobs School of Medicine and Biomedical Sciences, Neurology, Buffalo, United States,2University at Buffalo Jacobs School of Medicine and Biomedical Sciences, Neurology, East Amherst, United States
On behalf of: Hamidreza Abbasi, Thomas Covey, Zalan Wahid Khan
Background and aims: Direct oral anticoagulants (DOAC) are the mainstay for stroke prevention in non-valvular atrial fibrillation (NVAF). Nevertheless, patients may have embolic strokes (ES) despite compliance. We sought to determine whether certain variables are more predictive of recurrent ES in this population.
Methods: A case control study was conducted between November 2011 to January 2021. Only patients admitted with ES while adherent with DOAC were included. Age, gender and race matched controls comprised of NVAF patients on DOAC without stroke. Past medical history, laboratory and demographics were obtained. Logistic regression model was used to analyze whether certain variables were predictive of stroke. Variables entered in the model included family history, sleep apnea, heart valve replacement (HVR), atrial fibrillation, diabetes, LDL, fasting glucose, creatinine, BMI, triglycerides, and HBA1c.
Results: A total of 114 patients (62 controls, 52 patients) were included. Age (mean ± SD) was 74.77 ± 12.08. There were 63 (55.3%) females, 95 (83.3%) Caucasians, 17 (14.9%) African Americans. Stroke recurrence was predicted by the variables in the model (χ2 = 26.76, p = .005), with a Nagelkerke R2= .280. Stroke outcome was significantly predicted by history of HVR (1.6 % vs. 11.5%, p=0.04) and creatinine (1.01 ± 0.35 vs. 1.1± 0.34, p=0.048). There was a trend for BMI (p=0.098) however it was not statistically significant.
Conclusions: In summary, HVR and creatinine are factors found to be independent predictors of embolic stroke in patients adherent with DOAC in our study population.
Disclosures of Interest: No
Abstract N°: 1387
RISK OF RECURRENT STROKE IN SURVIVORS OF A FIRST ISCHEMIC STROKE: RESULTS FROM THE NORTHERN FRANCE STROKE REGISTRY
Roberto Gonzalez Sanchez1, Marie-Pierre Dumont1, Isabelle Jakobek1, Nadine Marécaux1, Luc Dauchet1, Aghiles Hamroun1, Philippe Amouyel1, Jean Dallongeville1, Aline Meirhaeghe1, Victoria Gauthier*1
1Univ. Lille, INSERM, CHU Lille, Institut Pasteur de Lille, U1167 - RID-AGE - Facteurs de risque et déterminants moléculaires des maladies liées au vieillissement, LILLE, France
On behalf of:
Background and aims: Ischemic stroke recurrence rates differ in the literature depending on geographic area and methodological differences. The objective of this study was to characterize the risk of recurrence among survivors of an incident ischemic stroke in a French population-based registry.
Methods: From the morbi-mortality registry in northern France, all cases of incident ischemic stroke have been recorded since 2008. Each patient was followed for 5 years or until the occurrence of a new episode or the patient's death. Factors associated with the occurrence of a recurrence were analyzed using the Cox model adjusted for age and sex.
Results: A total of 2188 incident ischemic strokes were recorded. The cumulative probability [95%CI] of recurrent stroke was 5.0%[4.1-6.0] the first year and 11.8%[10.1-13.7] over five years, with variability across ischemic type: 15.7%[12.1-19.6] for cardioembolic, 12.0%[7.3-18.0] for small-vessel occlusion, 11.3%[7.4-16.2] for atherosclerotic, 10.7%[4.3-20.5] for other determined etiology and 9.1%[6.8-12.0] for undetermined etiology.
The risk of recurrence was higher in cardioembolic stroke than in other ischemic strokes (HR=1.5[1.1-2.1]), in patients over 75 years old (HR=1.4[1.0-2.0]) and in those with known atrial fibrillation (HR=2.0[1.4-2.9]).
In contrast, NIHSS (HR=1.0[1.0-1.1]), a history of ischemic heart disease (HR=1.3[0.7-2.3]), TIA (HR=1.1[0.6-2.2]), hypertension (HR=1.2[0.9-1.8]), diabetes (HR=1.3[0.9-1.9]), or dyslipidemia (HR=1.0[0.7-1.4]) were not significantly associated with stroke recurrence risk at 5 years.
Conclusions: In this recent stroke registry data, the rate of recurrence after an incident ischemic stroke occurs mainly in the first year and depends on the etiology of the ischemic stroke. Older age and atrial fibrillation were stronger predictors of the risk of recurrence.
Disclosures of Interest: No
Abstract N°: 1598
CLINICAL OUTCOMES OF ACUTE ISCHEMIC STROKE PATIENTS WITH INTRACRANIAL ATHEROSCLEROTIC STENOSIS IN VIETNAM
Trung Vuong Xuan*1, Ton Mai Duy1, Phuong Dao1, Tho Pham-Quang1
1Bach Mai Hospital, Stroke Center, Ha Noi, Viet Nam
On behalf of:
Background and aims: Intracranial atherosclerotic stenosis (ICAS) is an important cause of ischemic stroke, especially in Asia populations. There is a limited number of studies on this disease in Vietnamese people. This study aimed to evaluate the clinical outcomes of Vietnamese acute ischemic stroke (AIS) patients due to ICAS.
Methods: A cross-sectional descriptive study was conducted at the Stroke Center - Bach Mai Hospital from April 2022 to April 2023. We recruited all AIS patients diagnosed with intracranial atherosclerotic stenosis and admitted within 24 hours from onset. Multivariable regression analysis was used to find out predictors of 3-month clinical outcomes.
Results: 135 patients (mean age 64.9 ± 12.6, male 65.9%) were recruited for this study. The number of patients admitted within 4 hours and 4.5-6 hours from onset were 40% and 9.6% respectively. At admission, the median NIHSS score was 5 (2-9). There were 26 (19.3%) patients receiving thrombolysis and 12 (8.9%) patients treated with mechanical thrombectomy. Acute stenting procedure was carried out for 2 patients. After 3 months, 86 (63.7%) patients had favorable outcomes (mRS 0-2) and 8 (5.9%) patients died. AIS recurrence was seen in 18 patients. Multivariable regression analysis pointed out some predictors of unfavorable outcomes (mRS 3-6), including admission NIHSS score (OR 1.26, 95% CI: 1.13-1.39) and dual-antiplatelet therapy (OR 0.30, 95%CI: 0.14-0.67).
Conclusions: This study gave a glance at Vietnamese acute ischemic stroke patients due to intracranial atherosclerotic stenosis. Despite some limitations, it is the basis for further study among this group of patients in Vietnam.
Disclosures of Interest: No
Abstract N°: 1883
FRANK’S SIGN: A CLINICAL PREDICTOR OF ISCHAEMIC STROKES?
Annie Renju*1, Aravinth Sivagnanaratnam1
1Northwick Park Hospital, United Kingdom
On behalf of:
Background and aims: Frank’s sign is a diagonal crease in the earlobe extending from the tragus to the edge of the auricle. Past studies have associated Frank’s sign with coronary artery disease.
This observational study aims to determine whether there is an association between Frank’s sign and ischaemic strokes.
Methods: Consecutive patients admitted to a stroke and Care of Elderly ward over 3 months were inspected for Frank’s sign. Patient’s electronic medical records were used for data such as age, sex and medical history.
Patients with ischaemic stroke were identified and examined for Frank’s sign. We also identified whether they had any history of cardiovascular disease which could be contributing to a positive Frank’s sign.
Results: We identified 137 patients, of which 72 were admitted with or had a history of ischaemic stroke. There was a statistically significant association between ischaemic stroke and a positive Frank’s sign.
We then excluded patients with a history of cardiovascular disease from the dataset to identify if there was a true link between Frank’s sign and ischaemic strokes. There still remained a statistically significant association.
Conclusions: Frank’s sign can be a clinical predictor for ischaemic stroke. Identifying Frank’s sign could be beneficial in primary care to trigger assessing and managing stroke risk factors. Further research should be done to identify other factors causing a positive Frank’s sign in order to determine the strength of association to ischemic strokes.
Disclosures of Interest: No
Abstract N°: 1940
TOP OF THE BASILAR ARTERY SYNDROME: CLINICAL AND IMAGING HALLMARKS IN A STROKE CENTER SAMPLE OF 96 PATIENTS
Franziska Lieschke*1, Maximilian Rauch2, Bastian Roller1, Jan Hendrik Schaefer1, Martin Alexander Schaller-Paule1
1Department of Neurology University Hospital Frankfurt, Frankfurt am Main, Germany,2Department of Neuroradiology University Hospital Frankfurt, Frankfurt, Germany
On behalf of:
Background and aims: Clinical symptoms and neuroradiological findings in patients with top of the basilar artery syndrome (TOBS) are known to vary. The aim of this retrospective, monocentric cohort study was to determine clinical and imaging factors associated with clinical outcome at discharge in patients with TOBS.
Methods: Consecutive patients with radiological confirmed TOBS presenting to our comprehensive stroke center were analyzed. Clinical and imaging parameters such as National Institutes of Health Stroke Scale (NIHSS), Glasgow Coma Scale (GCS), mode of recanalization, posterior circulation Alberta Stroke Program Early CT score (pcASPECTS) and infarct localization were assessed. Functional outcome parameters included modified Rankin Scale (mRS) and Barthel Index (BI).
Results: We identified 96 patients with a mean age of 70.32 years, 41.67% of whom were female. Factors significantly associated with functional dependence at discharge as measured by mRS and BI included NIHSS (r= 0.52, p <0.0001; r= -0.5567, p <0.0001 respectively), GCS (r= -0.46, p <0.0001; r= -0.3396, p= 0.0007 respectively), presence of ataxia (r= 0.48, p <0.0001; r= -0.4917, p <0.0001 respectively) at admission, and success of recanalization assessed by TICI (r= -0.49, p <0.0001; r= 0.4219, p <0.0001 respectively).
Conclusions: To our knowledge this is the largest cohort study of patients with TOBS identifying primarily the initial stroke severity measured by NIHSS and GCS as well as the success of recanalization assessed by TICI for clinical and neuroradiological outcome predictors, supporting the use of mechanic thrombectomy for posterior circulation strokes.
Disclosures of Interest: No
Abstract N°: 2004
EPIDEMIOLOGY OF TRAUMATIC CERVICAL ARTERY DISSECTIONS
Zafer Keser*1, Kim Griffin1, Helena Xeros1, William Harmsen1, Giuseppe Lanzino1, Robert Brown1
1Mayo Clinic, Rochester, United States
On behalf of:
Background and aims: Unlike spontaneous cervical artery dissection (CeAD), the incidence of CeAD after a major trauma is not well characterized. In this population-based cohort study, we reported trends of traumatic CeAD incidence.
Methods: We utilized the resources of the Rochester Epidemiology Project, Rochester, MN which allows essentially complete case ascertainment. We only included patients with CeAD attributable to major trauma. We estimated age- and sex-adjusted incidence rates using the US decennial census, with rates expressed as per 100,000 person-years. We also divided the data into two 10-year intervals to assess longitudinal trends. Poisson regression analysis was used to investigate the sex, age, and year period trends.
Results: Between 2002 and 2020, we identified 21 patients with traumatic CeAD (7 women, 14 men, median age of 57.5 [range 20.1-87.6]). Dissections involved the internal carotid in 42.9% and the vertebral artery in 57.1% of the cases. CTA was the most commonly used initial diagnostic test (81%). The majority of the cases did not have symptoms related to the traumatic CeAD and transient ischemic attack/ischemic stroke at presentation was uncommon. The incidence of traumatic CeAD was 0.85 per 100,000 person-years in 2002-2020, with a significant increase in the 2012-2020 period compared to 2002-2011 (1.29 vs. 0.37, p=0.005).
Conclusions: The diagnosis of traumatic CeAD, although still less common than spontaneous CeAD, is on the rise, potentially due to more routine usage of arterial imaging in emergency settings. Unlike spontaneous CeAD, most cases of traumatic CeAD were incidentally diagnosed.
Disclosures of Interest: No
Abstract N°: 2104
THE ASSOCIATION BETWEEN GREEN SPACES AND ATHEROSCLEROSIS BURDEN: A RETROSPECTIVE COHORT STUDY
1Schulich School of Medicine & Dentistry, London, Canada,2Western University, London, Canada,3Schulich School of Medicine & Dentistry, Epidemiology and Biostatistics, London, Canada,4Stroke Prevention & Atherosclerosis Research Centre, London, Canada,5Schulich School of Medicine & Dentistry, Pathology and Laboratory Medicine, London, Canada,6Western University, Clinical Neurological Sciences, London, Canada
On behalf of:
Background and aims: Individual-based risk factors for stroke such as hypertension and blood glucose levels, and their association with atherosclerotic plaque burden have been heavily investigated. However, such traditional risk factors only account for 57% of atherosclerotic carotid plaque. There is a need for understanding the association between environmental variables and cardiovascular disease; this study aims to explore whether there is any association between green spaces, and atherosclerotic burden. Our primary objective is to investigate whether a relationship between the greenness of spaces and the burden of atherosclerotic plaque of people near those spaces exists. Our secondary objective was to determine whether higher amounts of greenness in regions are associated with plaque progression or regression.
Methods: Data on the greenness of spaces was collected from the Canadian Urban Environmental Health Research Consortium in the form of the annual Normalized Difference Vegetation Index (NDVI) for different postal codes, from 1984-2019. Data on the atherosclerotic plaque burden for 556 patients was collected and measured as the total plaque area (TPA), and patients were followed from 1 to 26 ultrasound examinations.
Results: Data analysis for the collected information is still ongoing, however a preliminary analysis calculated the unadjusted correlation coefficient to be -0.13, however this crude estimate has yet to be adjusted for confounders like age, sex, and comorbidities.
Conclusions: These early results suggest that as the NDVI for a postal code region increases, the mean TPA for patients from that region likely decreases.
Disclosures of Interest: No
Abstract N°: 2119
HIGH PREVALENCE OF CAROTID ARTERY AND TANDEM OCCLUSIONS IN STROKE PATIENTS TREATED WITH MECHANICAL THROMBECTOMY IN NORTH KASHUBIAN REGION
Artur Dziadkiewicz*1, Krzysztof Pawlowski2, Krzysztof Gawrych1, Marek Szołkiewicz2, Alicja Maczkowiak1
1Pomeranian Hospitals, Florian Ceynowa Hospital, Neurology an Stroke, Wejherowo, Poland,2Pomeranian Hospitals, Kashubian Center for Heart and Vascular Diseases, Cardiology and Inteventional Angiology, Wejherowo, Poland
On behalf of:
Background and aims: Carotid artery proximal occlusion and tandem occlusion (ICA-o) are related to higher risk of peri- and post-procedural complications and worse final clinical outcome. The prevalence presented in studies is 12-21%. Study presents the group of patients with LVO in anterior circulation, treated in Thrombectomy-capable centre in Wejherowo, North Kashubia.
Methods: The group of 118 AIS patients treated in 8/2020-10/2023. Two subgroups were compared: ICA-o group (34patients, 28.81%) and anterior circulation of other location (84patients). Analysis was done with Chi-square and U-Mann-Whitney tests.
Results: ICA group: Age 68.6±9.6, M/F 23/11
Anterior group: Age 68.5±12.6, M/F 46/38.
Tables presented below.
Conclusions: Higher prevalence of ICA-o in presented group: 28.81%. No significant difference in two subgroups in: haemorrhage transformation, mRS at 3months, death rate, comorbidities, except atrial fibrillation. Less and slower improvement in clinical outcome (NIHSS), longer time from onset and groin puncture to first pass and recanalisation in ICA and tandem group. Further studies are conducted.
Disclosures of Interest: No
Abstract N°: 2350
ANTI-NMDA-RECEPTOR GLUN1 ANTIBODY SEROSTATUS IS ROBUST IN ACUTE SEVERE STROKE
Pia Sophie Sperber*1,2,3,4, Benjamin Hotter1, Matthias Endres1,2,4,5, Harald Prüß1,5, Andreas Meisel1,2,4
1Charité – Universitätsmedizin Berlin, Neurology with Experimental Neurology,2Charité – Universitätsmedizin Berlin, Center for Stroke Research Berlin (CSB),3Max Delbrueck Center for Molecular Medicine & Charité – Universitätsmedizin Berlin, Experimental and Clinical Research Center (ECRC),4Charité – Universitätsmedizin Berlin, Neuroscience Clinical Research Center (NCRC),5German Center for Neurodegenerative Diseases (DZNE)
On behalf of:
Background and aims: Anti-N-Methyl-D-Aspartate GluN1 IgM and IgA antibodies (NMDAR1-abs) are associated with unfavorable stroke outcomes and may be risk factors thereof. However, to utilizing NMDAR1-abs serostatus for risk assessment in acute stroke, it is crucial to understand the robustness of serostatus during this phase. Therefore, here we investigated the robustness of NMDAR1-abs serostatus and titer levels up to seven days after stroke.
Methods: In this exploratory analysis of the multicenter STRAWINSKI trial (identifier:NCT01264549), patients with a severe ischemia (NIHSS>=9) in the middle cerebral artery territory were included. The first blood drawing was conducted within 36h, and following daily, from day two to seven, post-stroke. We firstly measured NMDAR1-abs in the total cohort on day 1 after stroke. Subsequently, in samples from initially seropositive participants and a seronegative control group we measured NMDAR1-abs at each of the following days. NMDAR1-abs were measured from sera with cell-based assays. Titer dilutions started from 1:10 up to 1:1000. Seropositivity was defined as any titer>0.
Results: Out of 171 patients (mean age=76[SD=11], median NIHSS=15[IQR=12-18]), 16(9%) were NMDAR1-abs seropositive. Seropositive patients on day 1 after stroke remained seropositive and matched seronegative participants remained seronegative over sequential measurements. Although titer levels remained largely unchanged, a few patients showed fluctuating titers.
Conclusions: The status of NMDAR1-abs seropositivity is stable during the acute stroke phase, with little or no variation in titer levels.
Disclosures of Interest: Yes Private donation of family Gohla to CSB. M.E.: DFG–EXC-2049 – 390688087, ReTune TRR 295- 424778381, BMBF, DZNE, DZHK, EU, Corona Foundation. ME & AM: DFG–KFO 5023 BeCAUSE-Y, project 2 EN343/16-1, Fondation Leducq.
Abstract N°: 2556
EMERGING AGE TRENDS IN ACUTE ISCHEMIC STROKE INCIDENCE: A 13-YEAR RETROSPECTIVE SINGLE-CENTER ANALYSIS
Paul Ciucur*1, Elena Oana Terecoasa1,2, Raluca Stefania Badea1,2, Ileana Voda1, Anca Negrila1, Ruxandra Iatan1, Ionut Somoiag1, Daiana Dafinescum1, Cristina Tiu1,2
1Emergency University Hospital Bucharest, Neurology, București, Romania,2Carol Davila University of Medicine and Pharmacy, Neurology, București, Romania
On behalf of:
Background and aims: Acute ischemic stroke (AIS) is traditionally associated with the elderly; however, its rising incidence in younger cohorts signals a shifting epidemiological pattern. This retrospective analysis aims to delineate the incidence trends of AIS in patients under 50 years admitted in our department over a thirteen-year span.
Methods: Hospital records from 2010 to 2023 were scrutinized to ascertain the proportion of AIS patients aged 18- 35 and 35-50. We assessed year-on-year percentual changes and divided the data by sex within each age bracket, providing insight into demographic shifts and potential etiological factors.
Results: An upsurge was observed in the under-50 category, rising from 6.17% in 2010 to 8.13% in 2023, with male proportions increasing from 3.45% to 5.49%, and female rates exhibiting a peak in 2020 at 2.84%. The 35-50 age bracket had an overall incidence elevation from 5.21% in 2010 to 7.00% in 2023. Notably, the male subgroup within this bracket demonstrated a more pronounced increase compared with the female counterpart (3.17 % in 2010 – 5.04% in 2023 versus 2,04% – 1,96%). The over-50 demographic still constituted the bulk of AIS cases.
Conclusions: Results from this single-center retrospective study suggests a growing AIS burden in under-50 populations, with a distinct gender disparity accentuating male susceptibility, especially among the 35–50-year-olds. This necessitates a re-evaluation of stroke prevention paradigms, especially in younger demographics, to thwart the advancing tide of AIS in these younger cohorts.
Disclosures of Interest: No
Abstract N°: 2643
CIRCULATING OMEGA-3 POLYUNSATURATED FATTY ACIDS AND PROGNOSIS IN INTRACEREBRAL HAEMORRHAGE
Tomàs Xuclà Ferrarons*1, Iolanda Lázaro López2, Carme Gubern-Mérida3, Joan Martínez Sancho3, Antonia Escanelles Forteza2, Mikel Terceño1, Maria Lucas-Parra3, Joaquin Serena1, Aleix Sala Vila2, Yolanda Silva1
1Hospital Universitari de Girona Doctor Josep Trueta, Girona, Spain,2Institut Hospital del Mar d'Investigacions Mèdiques (IMIM), Barcelona, Spain,3Institut d'Investigació Biomèdica de Girona Dr. Josep Trueta (IDIBGI), Salt, Spain
On behalf of:
Background and aims: The intake of omega-3 fatty acids (EPA and DHA) has been associated with protection against ischemic events due to their anti-aggregant properties. However, it has been suggested that they may amplify damage in hemorrhagic events. We have investigated whether blood omega-3 levels are associated with a worse prognosis in patients with intracerebral haemorrhage (ICH).
Methods: Retrospective and observational study of 177 consecutive patients prospectively admitted to our hospital. The percentage of EPA and DHA in serum phospholipids was determined by gas chromatography. Clinical and neuroimaging data (hematoma growth >33% and/or 6 ml at 24-72 hours; in-hospital mortality and 90-day mortality) were collected. Logistic regression models were created.
Results: In this cohort (mean age, 71.5±12.5 years; 62.1% men), in-hospital mortality was 15.3%, and 24.3% at 90 days. 50 patients (29.1%) suffered hematoma growth. The percentage of EPA at admission was associated with a lower in-hospital mortality (OR 0.121; 95% CI 0.015-0.66; p = 0.028) in multivariable logistic regresion models, after adjusting for age, volume and localization of ICH and NIHSS. No significant differences were found for 90-day mortality, neurologic deterioration, hematoma growth nor recurrence. In secondary analysis for lobar haemorrhages alone, higher levels of marine omega-3 fatty acids were associated with a lower in-hospital mortality (OR 0.449; 95%CI 0.189-0.828; p = 0.030) and a lower probability of neurologic deterioration (OR 0.49; 95% CI 0.229-0.853; p = 0.032).
Conclusions: Higher levels of marine omega-3 fatty acids could be associated with a better prognosis in intracerebral haemorrhages.
Disclosures of Interest: No
Abstract N°: 2646
DOES INTRACRANIAL ARTERIOSCLEROSIS EXPLAIN THE ASSOCIATION BETWEEN HYPERTENSION AND STRUCTURAL BRAIN CHANGES IN STROKE PATIENTS?
Xi Li*1, Brian Berghout2, Mohammad Kamran Ikram2, Bob Roozenbeek3, Daniel Bos2
Background and aims: Hypertension is a major risk factor of cerebral small vessel disease (CSVD) and brain atrophy. To better understand the underlying mechanism, we investigated whether intracranial carotid artery calcification (ICAC), as a proxy for intracranial arteriosclerosis, explains the association between hypertension and structural brain changes in stroke patients.
Methods: 864 patients (mean age 62.3 years) with TIA or ischemic stroke, who underwent non-contrast CT (NCCT) and CT-angiography (CTA) were included in this study. Presence and subtypes of ICAC were assessed on NCCT, where ICAC was categorized into intimal and internal elastic lamina (IEL) type calcification. ICAC volume (mm3) was calculated on CTA. The degree of brain atrophy, periventricular and deep white matter lesions (WML), and lacunes were assessed on NCCT. Causal mediation analysis was performed using ICAC, ICAC volume, and ICAC subtypes as the mediator.
Results: The presence of ICAC explained 8% of the effect of hypertension on periventricular WML and 23% of the effect on lacunes. Hypertension was associated with more severe brain atrophy through the mediation of ICAC (OR: 1.03, 95% CI: 1.00-1.05). In subgroup analyses, IEL calcification partly explained the effect of hypertension on periventricular WML (13%), deep WML (10%), and brain atrophy (OR: 1.15, 95% CI: 1.02-1.33). We observed no evidence of mediation through intimal calcification.
Conclusions: ICAC partially explained the association between hypertension and periventricular WML, lacunes, and brain atrophy. Although a higher prevalence of intimal calcification was found in stroke patients, IEL calcification takes the leading role of explaining the association between hypertension and structural brain changes.
Disclosures of Interest: No
Abstract N°: 2686
THE INFLUENCE OF OBSTRUCTIVE SLEEP APNOEA IN THE EFFICACY/SAFETY RESPONSE TO ORAL ANTICOAGULANTS IN PATIENTS WITH CARDIOEMBOLIC STROKE
Natalia Cullell*1,2, Cristina Gallego-Fabrega1, Gemma Sansa3, Júlia Ferrer3, Jara Cárcel-Márquez1, Elena Muiño Acuña1, Anna Ramos Pachon4, Laia Llucia Carol1, Israel Fernandez Cadenas1, Jerzy Krupinski2
1Stroke Pharmacogenomics and Genetics Group, Institut d'Investigació Biomèdica Sant Pau (IIB SANT PAU), Barcelona, Spain.,2Fundació per a Docencia I Recerca, Mútua Terrassa, Terrassa (Barcelona), Spain.,3AdSalutem Instituto del Sueño, Barcelona, Spain,4Stroke Unit, Department of Neurology, Biomedical Research Institute Sant Pau, Hospital de la Santa Creu i Sant Pau, Universitat Autònoma de Barcelona (Department of Medicine), Barcelona, Spain.
On behalf of:
Background and aims: Obstructive sleep apnoea (OSA) is a risk factor for incident and recurrent stroke and it influences the pharmacokinetics of some drugs, including oral anticoagulants (OA) (the main secondary prevention in cardioembolic stroke (CS)). This study is to evaluate whether OSA is a risk factor for stroke recurrence and other vascular events in stroke patients treated with OA
Methods: Interventional study including 23 CS patients treated with OA, from which 16 underwent a post-stroke eight-hours sleep polysomnography (PSG) and were followed-up 2 years. The association between the PSG apnoea/hypopnea index (AHI) and the risk of stroke recurrence, major cardiovascular events (MACE) and composite of both was studied with Krustal-Wallis test. The association between OSA severity (mild (AHI<5)/moderate (AHI⩾5-<30)/severe (AHI⩾30)) with the risk of events was assessed with ANOVA test. We evaluated the causal association between OSA and stroke risk with mendelian randomization (MR) using the most recently Genome-Wide Association Studies for OSA and ischemic stroke (n=362,638 and n=1,296,908, respectively)
Results: All but one patient were diagnosed with OSA (4 mild, 7 moderate and 4 severe). The 41.2%, 29.4% and 17.6% of the patients presented any event, MACE and stroke recurrence, respectively. The AHI index was significantly associated with an increased risk of stroke recurrence (p-value = 0.037). The risk of composite events was significantly increased (p-value=0.023) in patients with more OSA severity The MR showed that OSA was causally associated with IS risk (inverse variance weighted p-value=0.037)
Conclusions: This study suggests that OSA could be a modulator of the efficacy response to OA
Disclosures of Interest: Yes This study (ID: BMS-ACE-2019-02) was funded by Bristol Myers Squibb (BMS) and Pfizer alliance
Abstract N°: 2750
MEDIATION EFFECT OF ECONOMIC BURDEN ON THE INTEGRATED STROKE PREVENTION AND TREATMENT SYSTEM AND MORTALITY
1Shanghai Health Development Research Center, Health Policy Research, Shanghai, China,2Shanghai University of Political Science and Law, shanghai, China,3Shanghai Municipal Health Commission Financial Management Affairs Center, shanghai, China
On behalf of:
Background and aims: Stroke is the main cause of cardiovascular diseases, disability and death all over the world. Due to the implementation of the integrated stroke prevention and treatment system in China, the incidence and mortality of stroke have been reduced. However, the casual pathway is poorly investigated. This study is aimed to research whether the effect of system on mortality was mediated by economic burden.
Methods: 66,775 patients with hypertension stroke comorbidities from 2017-2020 were included in the study. Part of people attended the integrated stroke prevention and treatment system. The economic burden was obtained by outpatient and inpatient records from the diagnosis and treatment database. The death information was collected from centers for disease and control. Causal mediation analyses were used to separate the whole effects of participating in the system on death into direct effects and indirect effects.
Results: 4,905 death events occurred finally. The mortality of patients participanting in the system was 4.39%. The analysis showed that attending the system was associated with the risk of death (hazard rate: 0.41;95% confidence interval [CI], 0.32-0.50). Mediation analysis reveals 4.89% of the association between attending system and death was mediated by economic burden (P<0.05).
Conclusions: Mediation effect of economic burden on the integrated stroke prevention and treatment system and mortality is existed. Reasonable control in the cost of treatment can not only reduce the mortality, but also save medical resources and help patients reduce the economic burden.
Disclosures of Interest: No
Abstract N°: 2774
STROKE PROFILE OF PATIENTS WITH HIGH RISK OF OBSTRUCTIVE SLEEP APNEA: A TRANSVERSAL STUDY
Juliana Cerqueira Gomes1, Aurea Maria Lago Novais*1, Beatriz Santos Rogério2, Marina Soledad Benitez Bitencourt1, Thaise Braga De Oliveira1, Renan Carvalho Castello Branco1
1Bahiana School of Medicine and Public Health,2Federal University of Bahia
On behalf of: Research Group of Vascular Neurology (GEPNeV)
Background and aims: Obstructive sleep apnea (OSA) is a disease of upper airways,diagnosed with polysomnography,that is well associated with stroke through diverse mechanisms.Despite that,it still lacks studies about stroke profile in patients with high risk of OSA.This study aims to describe the differences between stroke profile in patients with different risks of OSA.
Methods: We performed a transversal study,part of a cohort of stroke patients.Patients were evaluated of risk of OSA with STOP-BANG and SOS;also, data of stroke characteristics and death during internment were collected.Comparison between both groups was done using Mann-Whitney,T test or chi-square(considering p<0.05).
Results: We obtained 323 patients.Data of stroke characteristics are in tables 1 and 2.68% were classified as high risk with STOP-Bang and 82% had ischemic stroke(28% were cardioembolic,27% atherothrombotic and 27% indeterminate;p=0.474); 6% evolved to death(84% of high risk;OR=2.5;CI 95% 0.7-9;p=0.127). 50% were classified as high risk with SOS and 81% had ischemic stroke(28% were cardioembolic,27% atherothrombotic and 27% indeterminate; p=0.474);6% evolved to death(84% high risk;OR=1.76;CI 95% 1.4-2.2;p=0.002). Comparing both groups,we obtained stroke type(p=0.033) and type of hemorrhagic transformation (p=0.02).
Conclusions: Stroke profile of patients with high risk of OSA is similar to the same verified in literature.Although patients with high risk arrive with better NIHSS, evolve more to hemorrhagic transformation and death,suggesting a “lucid interval” of OSA,underlying mediated mechanism for these outcomes not evolving the characteristics of stroke itself.Finally,a higher–and significant–rate of ischemic stroke and indetermined etiology of it lead us to hypothesize whether OSA is the true cause of stroke.
Disclosures of Interest: No
Abstract N°: 2802
DO RESEARCHERS CONSIDER THE INTER-RELATIONSHIP BETWEEN TIME TO ASSESSMENT AND ADMISSION SEVERITY IN ACUTE STROKE?
Zewen Lu*1,2, Matthew Gittins1,2, Amit Kishore2,3, Craig Smith2,3, Andy Vail1,2
1University of Manchester, Centre for Biostatistics, Manchester, United Kingdom,2Salford Care Organisation, Northern Care Alliance NHS Foundation Trust, UK, Manchester Centre for Clinical Neurosciences, Geoffrey Jefferson Brain Research Centre, Manchester, United Kingdom,3University of Manchester, Division of Cardiovascular Sciences, Faculty of Biology, Medicine and Health, Manchester, United Kingdom
On behalf of:
Background and aims: Stroke severity evolves but is recorded typically as NIHSS on admission. Time to admission may depend on symptom severity. Failure to recognise this dynamic inter-relationship may lead to sub-optimal statistical analysis. We sought to assess whether and, if so, how stroke researchers account for this data structure. We sought to compare this with approaches used by perinatal researchers considering a similar statistical relationship between gestational age and birthweight.
Methods: Two reviewers systematically reviewed papers in leading specialty journals published in 2019 using NIHSS at admission and birthweight respectively as an explanatory factor in the statistical analysis. We targeted a minimum of 50 articles from each field to ensure 90% to identify approaches used in 5% or more of studies.
Results: 110 (stroke group:57; perinatal group:54) studies were reviewed. Perinatal researchers considered the temporal variable gestational age more often than time to assessment in stroke studies (89% vs. 7%, chi-squared p<0.001). It was consequently included more often (56% vs. 5%, chi-squared p<0.001). Four methods including stratification, distribution, regression and combined approaches were found. Time to assessment was only included as a continuous (n=2) or categorical (n=1) factor alongside admission NIHSS in three studies. Methods for covariate selection, essential for interpretation of statistical models, were rarely specified.
Conclusions: Few researchers explore the inter-relationship between baseline stroke severity and time to assessment, in sharp contrast to consideration of timing in perinatal prognosis. Future research will investigate whether time to assessment or repeated measurement of NIHSS in the hyper-acute phase could benefit clinical practice and epidemiological research.
Disclosures of Interest: No
Abstract N°: 2832
IS BLOOD PRESSURE SELF-MONITORING FOR THE MANAGEMENT OF PRE-HYPERTENSION FEASIBLE AND ACCEPTABLE; THE REVERSE STUDY?
Emma Bray*1, Lucy Hives2, Valerio Benedetto3, Nefyn Williams4, Andrew Clegg3, Paul Rutter5, Calvin Heal6, Julie Cook7, Clare Thetford1, Caroline Watkins1
1University of Central Lancashire, Stroke research team, Preston, United Kingdom,2University of Central Lancashire, School of Community Health and Midwifery, Preston, United Kingdom,3University of Central Lancashire, Synthesis, Economic Evaluation and Decision Science Group, Preston, United Kingdom,4University of Liverpoo;l, Department of Primary Care and Mental Health, Liverpool, United Kingdom,5University of Portsmouth, School of Biomedical Sciences, Portsmouth, United Kingdom,6University of Manchester, Division of Population Health, Health Services Research & Primary Care, Manchester, United Kingdom,7University of Central Lancashire, Research Facilitation and Delivery Unit, Preston, United Kingdom
On behalf of: The REVERSE study team
Background and aims: Prehypertension (PHT) affects 40% of UK adults and is associated with increased risk of cardiovascular disease, stroke, and progression to hypertension. Self-monitoring of blood pressure (BP) is highly effective in managing hypertension, but it’s role in PHT is unknown.
This study explored the feasibility and acceptability of self-monitoring BP for management of PHT.
Methods: A prospective, non-randomised, mixed-methods, feasibility study. Individuals with BP between 120-139/80-89mmHg identified from GP registers or pharmacy health checks were invited to participate. Participants home-monitored their BP for 6-months following a protocol. Outcome data were collected at baseline, 6- and 12-months. Semi-structured interviews were conducted with individuals and healthcare professionals (HCPs), and an evaluation survey sent to participants.
Results: 1501 people were invited to participate, 156 (10%) expressed an interest, 80 (80/156; 51%) were enrolled, and 75 (75/80; 94%) started self-monitoring. 66 (66/80; 83%) completed the 6-month follow-up. Although the overall recruitment target was not met, the GP target was exceeded. Despite high levels of interest from pharmacies, their recruitment was poor.
The sample lacked ethnic diversity (99% White) and most were well educated (56.4% >=degree-level) and from a high SES group (41%).
Interview and survey data showed that HCPs and participants thought self-monitoring for PHT was feasible and acceptable. Minor concerns regarded future implementation. Valuable suggestions for future development were provided.
Conclusions: REVERSE is feasible and acceptable in GP, but unlikely in pharmacy. Improvements to the diversity and inclusivity are vital. Useful information to inform a future effectiveness trial of self-monitoring of PHT was collected.
Disclosures of Interest: No
Abstract N°: 2872
STROKE AWARENESS IN THE CITY OF SÃO PAULO, BRAZIL IN 2023: A CROSS-SECTIONAL STUDY
Júlia Giordano*1, Rubens Gagliardi1, Vivian Gagliardi2, Larissa Oliveira1, Gabriella Chinaglia Zanin1, Maria Eduarda Amaral3, Ana Carolina Straub Bullentini3
1Faculdade de Ciências Médicas da Santa Casa de São Paulo, Neurologia, São Paulo, Brazil,2Santa Casa de São Paulo and Albert Einstein Israelita Hospital, Neurology, São Paulo, Brazil,3Faculdade de Ciências Médicas da Santa Casa de São Paulo, Neurology, São Paulo, Brazil
On behalf of:
Background and aims: Lack of knowledge about stroke can impact its treatment and its outcomes. This study aimed to evaluate the current knowledge of the Brazilian population about stroke symptoms and its treatment.
Methods: A cross-sectional study was done in Sao Paulo, Brazil, in October 2023. A RedCap questionnaire about stroke awareness was applied in 7 different subway stations across the city. The questionnaire had questions about the basic knowledge of stroke symptoms and what the participants thought were its treatment options.
Results: This study included 372 participants; an average of 54.9 years old, 57.1% female, 28.3% graduated secondary school. 28% did not know what a stroke is. In contrast, 31,8% knew what a stroke is, but 89.7% didn't know that they should be aware of the initial time of the event. 6,6% of the participants did not know they should go to an emergency room when suspected of a stroke.
Conclusions: Although stroke is a very prevalent disease, most people in a developing country still don't know how to recognize it or how to deal with a patient who seems to be having a stroke, which impacts their outcome.
Disclosures of Interest: No
Abstract N°: 3049
RATES OF COVID INFECTION AND CHANGES IN STROKE DEMOGRAPHICS AND OUTCOME: A REVIEW OF NATIONAL AUDIT DATA
Ruth Comber*1, Joan Mccormack2, Olga Brych2, Rónán Collins3, Tim Cassidy4, Joseph Harbison2
1St James's Hospital, Dublin, Ireland,2National Office of Clinical Audit, Irish National Audit of Stroke, Dublin, Ireland,3Tallaght Hospital, Stroke Service, Dublin, Ireland,4St. Vincent's University Hospital, Dublin, Ireland
On behalf of: Irish National Audit of Stroke Contributors and Governance Committee
Background and aims: Recent US data revealed an increase in the rate of stroke deaths since the beginning of the Covid epidemic in 2020. Ireland imposed prolonged lockdowns and had a high vaccination rate and OECD has recently reported had no Covid related excess mortality 2020-2022. We evaluated data for Covid and stroke in Ireland looking for changes in demographics and outcome over this period.
Methods: Data from 2018-2022 for the Irish National Audit of Stroke and Hospital Inpatient Enquiry were evaluated. Comparisons were made using Chi Square Statistics.
Results: There was no significant change in average annual increase in stroke admissions between 2013-2017 (2.11%) and 2018-2022 (2.03). Proportion of patients with a co-diagnosis of stroke and Covid increased (2020: 1.2%, 2021: 3.1%, 2022: 9.8%). No change was identified in any outcome measure across the period. There was an increase in the proportion of strokes in younger people starting 2018 (23.4%-27.8%. Chi sq 21.8, p<0.0001) and in the proportion of ischaemic strokes in 2022 (83.1%-85.4%. Chi Sq 8.79 p=0.003).
Conclusions: Although there were demographic changes over the period no change in these or outcome measure were contemporaneous with the Covid pandemic.
Disclosures of Interest: No
Abstract N°: 3078
CIRCULATING MAGNESIUM LEVEL AND RISK OF STROKE: A SYSTEMATIC REVIEW AND META-ANALYSIS
Amit Kumar*1, Charan Mahendran2, Pradeep Kumar3, Dhiraj Khurana1
1Postgraduate Institute of Medical Education and Research, Department of Neurology, Chandigarh, India,2Postgraduate Institute of Medical Education and Research, Department of Psychiatry, Chandigarh, India,3All India Institute of Medical Sciences, Clinical Research Unit, New Delhi, India
On behalf of:
Background and aims: Stroke remains a prevalent global health concern, contributing significantly to morbidity and mortality. Identifying modifiable risk factors is imperative for effective prevention strategies. Magnesium (Mg), an essential mineral known for its cardiovascular effects, has been implicated in modulating stroke risk. This study aimed to explore the association between circulating Mg levels and the risk of stroke.
Methods: A comprehensive literature search was conducted in databases including PubMed, EMbase, Web of Science, Cochrane Library and Google Scholar up to 31st December 2023 to identify relevant studies. Observational studies reporting on the association between circulating Mg levels and stroke risk were included. Methodological quality was assessed by New castle Ottawa Scale. A Pooled Standard mean deviation (SMD) and 95% confidence interval [CI] was employed to estimate pooled effect sizes.
Results: A total of nine case-control studies with a total sample size of 1,464 were included. A significant increased risk of stroke was found to be associated with lower circulating Mg levels (SMD= -2.89,95% CI; -3.74 to -2.03). Further subgroup analyses based on ethnicity, type of stroke and source of sample demonstrated consistent findings.
Conclusions: Our observed inverse association underscores the potential of Mg in reducing the risk of stroke. However, further research is warranted to elucidate underlying mechanisms and establish optimal mg levels for effective stroke risk reduction.
Disclosures of Interest: No
Abstract N°: 3110
INTERMEDIATE STAGE ATHEROSCLEROTIC PLAQUE REGRESSION, USING FOCUSED ULTRASOUND ACCOMPANIED BY HIGH- DOSE ATORVASTATIN ADMINISTRATION
Hossein Mehrad*1,2,3, Solmaz Tasdighi Matanagh2
1Islamic Azad University, Department of Physics, Tabriz, Iran,2Mehrad Research Lab, Division of Translational Medicine Development of Noninvasive Treatments, Tabriz, Iran,3Islamic Azad University, Laboratory of Novel Technologies in Non- Invasive Treatments, Tabriz, Iran
On behalf of:
Background and aims: Intermediate stage atherosclerosis is highlighted by infiltration of oxidized low-density lipoprotein and foam cell formation, resulting in the thickening of arterial walls and decreased arterial lumen space. In this study, we aimed to investigate the effect of histotripsy therapy on atherosclerosis regression, wherein diagnostic ultrasound is combined with the therapy system, with a goal of increased safety.
Methods: Briefly, Golden Syrian hamsters underwent endothelial denaturation using ballooning at the carotid artery, before being fed a 1.5% cholesterol-rich diet. After four weeks, the histopathology results showed foam cells-rich plaque formation, resulting in vessel wall thickening and intermediate stage atherosclerosis formation in all of the hamsters' arteries. Then treatment group underwent pulsed, high- intensity focused ultrasound (F=750KHz, I=150W/cm2, PD=200ms) histotripsy therapy accompanied by simultaneous, intravenous high-dose atorvastatin (5 mg/Kg/day)-loaded PESDA (Perfluorocarbon- Exposed Sonicated Dextrose Albumin) microbubbles (100ml/kg, 2-5×105 bubbles/ml) administration
Results: Results from ultrasonography and histology at the stenotic region showed a significant reduction in the mean value for foam cells, smooth muscle cells, collagen, and immune cells density and blood mean velocity, wall mean thickness and the percentage of luminal cross-sectional area of stenosis and a significant increase in the mean value for blood volume flow in the treatment group compared with the other groups (P<0.05).
Conclusions: Enhanced sonoporation effect of ultrasound, induced by inertial cavitation effect of collapsed microbubbles, accompanied by anti- atherogenic effect of atorvastatin and plaque destructive effect of focused ultrasound- based histotriosy, can cause to Intermediate stage atherosclerotic plaque regression and significantly dilate the luminal cross-sectional area of stenosis.
Disclosures of Interest: No
Abstract N°: 3133
CHEMO-SONODYNAMIC COMBINATION THERAPY OF EARLY STAGE ATHEROSCLEROSIS USING HEMATOPORPHYRIN NANOPARTICLES AND DOCETAXEL (DTX)
Hossein Mehrad*1,2,3, Solmaz Tasdighi Matanagh2
1Islamic Azad University, Department of Physics, Tabriz, Iran,2Mehrad Research Lab, Division of Translational Medicine Development of Noninvasive Treatments, Tabriz, Iran,3Islamic Azad University, Laboratory of Novel Technologies in Non- Invasive Treatments, Tabriz, Iran
On behalf of:
Background and aims: In atherosclerosis, local inflammation and associated macrophage activity can lead to foam cell- rich plaque formation, which results to plaque rupture and thrombosis, making inflammation an important therapeutic target in stroke and cardiovascular disease. Foam cells are generated by uncontrolled uptake of modified LDL, especially oxidized LDL. In this study, we developed an experimental chemo-sonodynamic anti- inflammation therapy protocol, and investigated its effectiveness on macrophage foam cells density reduction, wherein diagnostic ultrasound is combined with sonodynamic therapy, with a goal of increased safety.
Methods: Briefly, Golden Syrian hamsters underwent primary balloon dilatation injury at the carotid artery followed by a 1.5% cholesterol-rich diet injury for three weeks. Histopathology results showed early stage atherosclerosis formation in all of the hamsters' arteries. Then animals’ arteries in the treatment group at the lesion region, treated using intravenous lipid- based encapsulated hematoporphyrin nanoparticles (10mg/kg) and docetaxel (20mg/kg) administration accompanied by extracorporeal low level focused- electrohydraulic shock wave (V=15 Kv, F=2Hz, Impulses=50) sonodynamic therapy. Foam cells density were evaluated in the treatment group compared with the control group using B-mode ultrasonography and histology.
Results: Results from ultrasonography and histopathology showed a significant reduction in the mean value for foam cells and immune cells density within the injured region, in the treatment group compared with the control group (p< 0.05).
Conclusions: Enhanced anti- proliferative effect of hematoporphyrin, induced by electrohydraulic shock wave sonodynamic therapy effect and inertial cavitation- mediated sonoporation effect of collapsed capsules, accompanied by anti- proliferative effect of docetaxel, can cause to reduce the early stage atherosclerosis.
Disclosures of Interest: No
Abstract N°: 3154
EFFECT OF COMBINED HDL THERAPY AND ULTRAVIOLET LASER PHOTOTHERAPY ON BIOMECHANICAL PARAMETERS OF CAROTID ARTERY WITH FIBROATHEROMATIC PLAQUE
Hossein Mehrad*1,2,3, Solmaz Tasdighi Matanagh2
1Islamic Azad University, Department of Physics, Tabriz, Iran,2Mehrad Research Lab, Division of Translational Medicine Development of Noninvasive Treatments, Tabriz, Iran,3Islamic Azad University, Laboratory of Novel Technologies in Non- Invasive Treatments, Tabriz, Iran
On behalf of:
Background and aims: The thickening of the artery wall, altered arterial elasticity, smooth muscle contraction, increased sensitivity to pharmacological stimulation, and increased arterial viscoelasticity, i.e., arteriosclerosis, are examples of mechanical alterations. The goal of the current study was to determine how combined high-density lipoprotein (HDL) treatment and ultraviolet (UV) phototherapy, affected the mechanical characteristics of the carotid artery with fibroatheromatic plaque.
Methods: Primary intravascular radiofrequency thermal balloon angioplasty and a 12-week 1% cholesterol rich- diet were used to damage the carotid artery arteries of Golden Syrian hamsters. According to histology findings, the arteries of the hamsters developed fibroatheromatic plaque. The lesion area underwent combined PESDA (Perfluorocarbon- Exposed Sonicated Dextrose Albumin) microbubbles (100 ml/kg, 2-5 × 105 bubbles/ml) loaded with HDL (80 mg/kg)- mediated pulsed low- level focused ultrasound (F=750 KHz, P=13 W, PD=250 ms) sonoporation therapy and catheter- based low-level ultraviolet laser (λ= 280 nm, E/A=150 J/cm2) phototherapy. A new ultrasound image- based automatic image processing software, were used to assess the groups' arterial biomechanical characteristics.
Results: The treatment group's mean values for shear elastic modulus, and resistance index and intraplaque fibrotic content were significantly lower than those of the other groups, whereas the mean values for radial strain, compliance, and distensibility were significantly higher (P<0.05).
Conclusions: Improved arterial biomechanical parameters and a significant reduction in fibroatheromatic plaque content, can result from the enhanced sonoporation therapy impact of ultrasound, which is caused by the inertial cavitation effect of collapsed microbubbles in conjunction with the anti- proliferative effect of UV phototherapy and anti-atherogenic effect of HDL therapy.
Disclosures of Interest: No
Abstract N°: 3167
THE INCIDENCE AND MORTALITY OF SPONTANEOUS INTRACEREBELLAR HEMORRHAGE IN A NORWEGIAN POPULATION
1Akershus University Hospital, Department of Neurology, Lørenskog, Norway,2Akershus University Hospital, Department of Diagnostic Imaging, Lørenskog, Norway,3University of Oslo, Institute of Clinical Medicine, Lørenskog, Norway,4Oslo University Hospital, Department of Neurosurgery, Oslo, Norway,5Oslo University Hospital, Department of Neurology, Oslo, Norway,6University of Oslo, Department of General Practice, Oslo, Norway
On behalf of:
Background and aims: The majority of data on cerebellar hemorrhage (cICH) are from tertiary referral centres not reflecting an unselected cICH population. The purpose of this study was to explore the incidence, risk factors, clinical presentation, and mortality of cICH in an unselected population.
Methods: A retrospective observational study conducted at a University Hospital, serving as the primary hospital for 10% of Norway. Patients were identified through electronic chart reviews based on manually screening for the relevant ICD-10 codes for all ICH-cases from January 1st, 2009, to December 31st, 2023. Only patients with spontaneous cICH were included.
Results: 123 patients aged 26-102 years were included, median age 75 years (IQR 68-83) and 46% were females. The overall incidence of cICH was 2.03 (95%CI 1.65–2.42) per 100 000/year. 31 % were associated with on-going anticoagulant therapy. The median hematoma volume was 8.0 ml (IQR 3.4-17.5). Median NIHSS was 3 (IQR 1-7). Reduced level of consciousness was seen in 52%. Acute IV anti-hypertensive medication was given to 44%. A Do Not Resuscitate order was issued for 44%. Neurosurgeons were consulted for 71% of the cases, and 14% underwent surgery. In-hospital mortality was 29%, overall 3 months and 1 year mortality was 33% and 40%. 29% had a modified Rankin Scale score of 0-2 three months after the event while 56% were dependent or dead.
Conclusions: The incidence of cICH in this unselected population was 2.03/100 000/year. Few patients underwent surgery. The mortality rates were similar to those of supratentorial ICH.
Disclosures of Interest: No
Abstract N°: 3197
THE IMPACT OF 2 YEARS OF THE COVID-19 PANDEMIC ON STROKE AND MYOCARDIAL INFARCTION HOSPITALIZATION AND MORTALITY; SEX AND AGE DIFFERENCES
Julia Anna Kent*1, Petra Sedova1,2,3,4,5, Jiri Jarkovsky6,7, Ingrid Kovacova8, Marek Lichter6, Robert D. Brown, Jr.2, Robert Mikulik1,3,5
1Masaryk University, Faculty of Medicine, Brno, Czech Republic,2Mayo Clinic, Department of Neurology, Rochester, United States,3St. Anne's University Hospital Brno, International Clinical Research Center, Brno, Czech Republic,4University Hospital Brno, Department of Internal Medicine and Cardiology, Brno, Czech Republic,5St. Anne's University Hospital Brno, Department of Neurology, Brno, Czech Republic,6Institute of Health Information and Statistics of the Czech Republic, Prague, Czech Republic,7Masaryk University, Faculty of Medicine, Institute of Biostatistics and Analyses, Brno, Czech Republic,8Masaryk University, Brno, Czech Republic
On behalf of:
Background and aims: Since the beginning of the COVID-19 pandemic many countries have reported a decline in admission rates for stroke and MI without clear explanation. This nationwide study spanning two COVID-19 years aims to analyze whether this reduction is linked to pandemic intensity, lockdown measures, and evaluate sex and age differences.
Methods: Comparing the first (March 1, 2020, to February 28, 2021) and second (March 1, 2021, to February 28, 2022) pandemic years with the preceding year (March 1, 2019, to February 28, 2020), we utilized data from the National Register of Reimbursed Health Services for MI volumes and patient characteristics. Mortality data were extracted from the Czech National Mortality Registry
Results: During the first and second pandemic year, MI admissions declined by 10.6% (p<0.001) and 8.9% (p<0.001) respectively. The observed decline was greater in women than in men in both years of the pandemic (-11.8% vs -10.0% and -10.8% vs -7.9%, p<0.001 respectively).
For stroke, admission rates dropped by 7.4% (p<0.001) in the first year of the pandemic and 7.2%, (p<0.001) in the second year. Women were more affected than men during both years of the pandemic (-9.0% vs -5.9%; -9.7% vs -4.8%, p<0.001 respectively).
Conclusions: The decline in both stroke and MI admissions during the COVID-19 pandemic was unrelated to COVID-19 incidence. Notably, during both years of the pandemic, this decrease primarily affected older women. The 30-days mortality rate of stroke and MI patients was increased during both years of the pandemic.
Disclosures of Interest: No
Abstract N°: 3207
ISCHAEMIC STROKE IN PATIENTS WITH ATRIAL FIBRILLATION AFTER CORONAVIRUS DISEASE
1National Scientific Center "Institute of Cardiology, Clinical and Regenerative Medicine named after Academician M.D.Strazhesko of the National Academy of Sciences of Ukraine", Clinical Arrhythmology and Electrophysiology, Kyiv
On behalf of:
Background and aims: In patients with atrial fibrillation (AF), a factor in the genesis of cerebral ischemia is a thromboembolic mechanism, but other factors may also be involved, including acquired coronavirus disease (COVID-19). To determine the features of the course of AF in patients with cerebral ischemia after the COVID-19.
Methods: The study included 116 patients aged 63,8 ± 0,6 years (48,3% men, 51,7% women). The first group (G1) - 36 patients who developed AF for the first time after COVID-19. The second group (G2) - 25 patients in whom the transformation of the paroxysmal form of AF into persistent, or persistent AF into its permanent form occurred. The third group (G3) - 55 patients in whom the form of AF did not change. This group is divided into subgroup 3A - 35 patients, which included patients whose frequency and duration of paroxysms increased and subgroup 3B - 20 patients in whom the frequency and duration of paroxysms did not change.
Results: Acute cerebrovascular accident was registered in 4 people out of 116, which was 3.4% of patients in the main group. Three out of four patients belonged to subgroup 3A, i.e. patients in whom the form of AF remained after the coronavirus infection, but its course worsened, compared to patients in subgroup 3B, in whom the course of this arrhythmia remained unchanged (8.6% vs 0.0 %, p<0.0001).
Conclusions: Patients with atrial fibrillation who suffered from the coronavirus disease (COVID-19) and had a history of ischemic stroke had a more unfavorable course of this arrhythmia.
Disclosures of Interest: No
Abstract N°: 3209
ANTI-INFLAMMATORY EFFECT OF MESENCHYMAL STEM CELLS AMELIORATES ENDOTHELIAL DYSFUNCTION IN THE RAT CAROTID ARTERY INJURY MODEL
Hossein Mehrad*1,2,3, Solmaz Tasdighi Matanagh2
1i, Department of Physics, Tabriz, Iran,2Mehrad Research Lab, Division of Translational Medicine Development of Noninvasive Treatments, Tabriz, Iran,3Islamic Azad University, Laboratory of Novel Technologies in Non- Invasive Treatments, Tabriz, Iran
On behalf of:
Background and aims: The preservation of vascular homeostasis involving antioxidant, anti-inflammatory, pro-fibrinolytic, anti-adhesive, or anticoagulant effects depends on healthy endothelial cells. The primary indicator of endothelial dysfunction is a problem in controlling vascular tone. It is common knowledge that the majority of cases of atherosclerosis begin with vascular injury, inflammation, and endothelial dysfunction. Mesenchymal stem cells (MSCs) are cells that can renew themselves and differentiate into different cell types in a variety of human tissues. They also have anti-inflammatory and immunomodulatory effects. In this study, we looked into the anti-inflammatory impact of mesenchymal stem cells on endothelial function in a rat carotid artery damage model.
Methods: Briefly, rats were injured by balloon dilatation at the right common carotid artery. Following two days, MSCs administration was used to treat the treatment group's common carotid arteries in the lesion region. In order to evaluate endothelial-dependent relaxation, acetylcholine-mediated dilation (AMD) was measured during the infusion of acetylcholine at a rate of 0.5 µg/kg/min and endothelial independent relaxation was evaluated by measuring nitroglycerin mediated dilation (NMD) during the infusion of nitroglycerin at a rate of 5 µg/kg/min.
Results: Results from B-mode ultrasound images showed significant differences in AMD between the treated and the non- treated rats (p<0.05), whereas there were no significant differences in NMD between the treatment and normal groups (p>0.05). No microscopic intimal lesions were seen in the normal and treated rats, but intimal thickening was observed in the histological studies in the non-treated rats.
Conclusions: Administration of mesenchymal stem cells improves endothelial dysfunction by lowering vascular inflammation.
Disclosures of Interest: No
Abstract N°: 3217
FRAGILITY AS A PREDICTIVE FACTOR FOR STROKE IN ELDERLY PATIENTS WITH ATRIAL FIBRILLATION
Natalie Burgos Bencosme1, Jorge Eduardo Herrera Parra2, Lucia Antuña Montes2, Lucia Ovies Menéndez2, Elena Valle Calongue2, Aurea Álvarez Abellaa1, Sara Fueyo Álvarez2, Julieth Caballero Velásquez2, José Gutiérrez Rodríguez2, Montserrat Gonzalez Delgado*3
1Hospital Monte Naranco, Geriatric, Oviedo, Spain,2Hospital Monte Naranco, Geriatrics, Oviedo, Spain,3Hospital Universitario Central de Asturias, Neurology, Oviedo, Spain
On behalf of:
Background and aims: In the context of an ageing population, it is crucial to understand how the characteristics of elderly individuals with atrial fibrillation (AF) influence the incidence of stroke.
To assess the relationship between clinical and demographic characteristics of elderly individuals with AF and the incidence of stroke.
Methods: A prospective observational study was conducted with 200 patients with AF between 2019 and 2021. Demographic data, comorbidities, frailty and cognitive function, as well as the type and adequacy of anticoagulation, were collected. Statistical tests such as the Mann-Whitney U and Chi-square, in addition to logistic regression analysis, were used.
Results: 65% were women, with an average age of 89.23±0.63 years. The Barthel index was 65.23±2.4, and 39% showed cognitive impairment. The most common comorbidities were valvular heart disease (36%), anemia (31%), and previous stroke (31.5%). The thromboembolic risk (CHA2DS2-VASc) was 5.74±0.17, and the hemorrhagic risk (HAS-BLED) 2.94±0.6. 75.32% were anticoagulated (47.62% with antivitamin K, 27.7% with direct anticoagulants). Frailty measured by the Short Physical Performance Battery showed 43.5% disabled, 47% frail, 7.5% pre-frail, and 2% robust.
When assessing the relationship between these variables and the incidence of stroke, frailty demonstrated a statistically significant association (p= 0.033) with an ischaemic stroke rate at 6 months (23.4% frail, 6.7% pre-frail, 6.9% disabled, and 0% robust).
Conclusions: This study highlights frailty as a determining factor in the predisposition to stroke in elderly patients with AF, which could guide more effective prevention and treatment strategies in the future.
Disclosures of Interest: No
Abstract N°: 3240
PHOTOFRIN NANOPARTICLES - MEDIATED B- MODE ULTRASOUND- GUIDED SONODYNAMIC THERAPY AFTER LASER ANGIOPLASTY OF CAROTID ARTERY WITH FIBROTIC PLAQUE
Hossein Mehrad*1,2,3, Solmaz Tasdighi Matanagh2
1Islamic Azad University, Department of Physics, Tabriz, Iran,2Mehrad Research Lab, Division of Translational Medicine Development of Noninvasive Treatments, Tabriz, Iran,3Islamic Azad University, Laboratory of Novel Technologies in Non- Invasive Treatments, Tabriz, Iran
On behalf of:
Background and aims: The risk of associated disorders is decreased by treating carotid advanced atherosclerotic stenosis. The present laser atherectomy techniques lead to irritation and a subsequent restenosis. This study's objective was to assess how sonodynamic therapy affected the decrease of intimal hyperplasia and inflammation following laser angioplasty. A diagnostic ultrasound was combined with therapy system with a goal of increased safety
Methods: Briefly, primary intravascular radiofrequency (F= 23.7 MHz, P= 10 W) thermal balloon angioplasty- mediated endothelial injury at the carotid artery was used to cause advanced atherosclerosis with severe stenosis in New Zealand White rabbits. This was followed by a 0.5% cholesterol-rich diet injury for 12 weeks. The findings of the histopathology revealed the development of progressive atherosclerosis with fibrotic plaque that led to significant stenosis ( > 70%) in every artery of the rabbits. The treatment group next had angioplasty using an ArF excimer laser (193 nm), followed by extracorporeal electrohydraulic low- level focused shock wave-mediated sonodynamic therapy and simultaneous intravenous injection of lipid-based encapsulated photofrin (porfimer sodium) nanoparticles (10 mg/Kg)
Results: According to histopathology and ultrasonography findings, the treatment group's mean value for immune cells density, smooth muscle hyperplasia cells density was significantly lower than other groups (p <0.05)
Conclusions: Reduced fibrotic content (including collagen, foam cell, extracellular matrix, smooth muscle cell) of atherosclerotic plaque can be brought about by shock waves' enhanced photofrin's toxicity and anti-proliferative activity. Also, photofrin- mediated sonodynamic therapy, can be enhanced by enhanced sonoporation effect of shock waves, induced by inertial cavitation effect of collapsed capsules
Disclosures of Interest: No
Abstract N°: 3270
NEOATHEROSCLEROSIS REGRESSION WITH COMBINED PROTOPORPHYRIN-IX- MEDIATED SONODYNAMIC THERAPY AND ATORVASTATIN- MEDIATED ANTI- ATHEROGENIC THERAPY
Hossein Mehrad*1,2,3, Solmaz Tasdighi Matanagh2
1Islamic Azad University, Department of Physics, Tabriz, Iran,2Mehrad Research Lab, Division of Translational Medicine Development of Noninvasive Treatments, Tabriz, Iran,3Islamic Azad University, Laboratory of Novel Technologies in Non- Invasive Treatments, Tabriz, Iran
On behalf of:
Background and aims: Neoatherosclerosis is a significant clinical entity in vascular surgery, because it reduces the long-term effectiveness of surgical and endovascular interventions. We developed an experimental sonodynamic therapy protocol in this study and tested its efficacy in reducing neoatherosclerosis. In order to increase safety, diagnostic ultrasonography is paired with focused ultrasound in this protocol.
Methods: Using ballooning at the carotid artery, Golden Syrian hamsters underwent primary endothelial denaturation damage. They then consumed a 0.5% cholesterol-rich diet for eight weeks. After eight weeks, the balloon angioplasty procedure was repeated on the treatment group, who then endured a 1.5% cholesterol-rich diet for four weeks. All of the hamster's arteries had developed neoatherosclerosis, according to histopathology findings. Then, the treatment group received high-dose atorvastatin (5 mg/kg/day) and pulsed, low-level focused ultrasound (F= 750 KHz, P= 25 W, PD= 150 ms) together with protoporphyrin-IX-loaded PESDA (Perfluorocarbon Exposed Sonicated Dextrose Albumin) microbubbles (100 ml/kg,2-5 × 105 bubbles/ml).
Results: The treatment group's mean values for lumen wall mean thickness, percentage of luminal cross-sectional area of stenosis, intraplaque smooth muscle cells, immune cells, foam cells density, and lipid content were significantly lower than other groups, according to histopathology and sonogrphy results (p <0.05).
Conclusions: Neoatherosclrotic plaque content can be reduced and the luminal cross-sectional area of stenosis can be significantly enlarged as a result of the enhanced cytotoxicity and anti- proliferative effect of protoporphyrin-IX, induced by pulsed, low level focused ultrasound, and inertial cavitation effect of collapsed microbubbles, and as well as anti- atherogenic and anti- inflammatory effects of high- dose atorvastatin.
Disclosures of Interest: No
E-Poster - Genetics, 'Omics and Biomarkers
Abstract N°: 844
EXPLORING THE PATHOPHYSIOLOGICAL MECHANISMS OF CEREBRAL VENOUS SINUS STENOSIS BASED ON MULTI-SAMPLES AND MULTI-OMICS
Nan Wang*1, Baoshan Qiu1, Dapeng Mo2, Yilong Wang1
1Beijing Tiantan Hospital Affiliated to Capital Medical University, Department of Neurology,2Beijing Tiantan Hospital Affiliated to Capital Medical University, Neurointerventional Department
On behalf of:
Background and aims: Cerebral venous sinus stenosis is the main cause of idiopathic intracranial hypertension. In recent years, it has been found that the incidence of idiopathic intracranial hypertension is increasing year by year. Female gender and obesity are important risk factors for idiopathic intracranial hypertension. The latest view is that idiopathic intracranial hypertension should be treated as a systemic metabolic disease. However, there is currently a lack of systematic research to support this idea.
Methods: This study included patients with not stent treatment group (NSTG) and stent treatment follow-up group (STFG). Metagenomic and untargeted metabolomic measurements of feces. Untargeted metabolomic measurements were performed on cerebrospinal fluid, femoral vein blood samples, and blood samples from cerebral venous sinus stenoses. Demographic and clinical data were combined to explore the underlying pathophysiological mechanisms of cerebral venous sinus stenosis based on a metabolic perspective.
Results: A total of 86 patients were included, 94.2% were women, there was no difference in BMI between the two groups (26.89 vs 27.82, p=0.378), and intracranial pressure was significantly reduced in STFG patients (183.00 vs 285.08, p<0.001). Importantly, there were significant differences in the structure and function of the gut microbiota between the two groups of patients. In addition, there are also many differences in metabolites in feces, cerebrospinal fluid, and blood samples from different parts between the two groups.
Conclusions: Stent treatment of cerebral venous sinus stenosis can change the structure and function of intestinal flora, and the metabolites in feces, cerebrospinal fluid, and blood samples from different parts will also change significantly.
Disclosures of Interest: No
Abstract N°: 971
CIRCULATING MIRNAS AS POTENTIAL BIOMARKERS OF HAEMATOMA GROWTH IN INTRACEREBRAL HAEMORRHAGE: A PILOT STUDY
Maria Lucas-Parra1, Carme Gubern-Mérida*1, Carla Herminia Vera Caceres2, Laia Carballo-Perich1, Mikel Terceño1,2, Saima Bashir1,2, Tomàs Xuclà-Ferrarons1,2, Juan Álvarez-Cienfuegos Rodríguez1,2, Joaquin Serena1,2, Yolanda Silva1,2
1Institut d’Investigació Biomèdica de Girona (IDIBGI), Cerebrovascular Pathology, Salt, Spain,2Hospital Universitari Dr. Josep Trueta, Stroke Unit, Girona, Spain
On behalf of:
Background and aims: Haematoma growth (HG) is the main cause of early neurological impairment and poor clinical outcome in spontaneous non-traumatic intracerebral haemorrhage (ICH) patients. Predicting HG from a blood sample obtained upon hospital admission would be highly valuable in clinical practice. Our aim was to evaluate circulating miRNAs as HG predictive biomarkers.
Methods: Circulating RNA was extracted from citrated-plasma samples at admission of 20 ICH patients (13 without HG and 7 with HG after ICH onset). 754 miRNAs were assessed by Open Arrays and relative quantification value for each miRNA was obtained by global normalisation method and the mean value of the most stable endogenous miRNAs based on the summarised stability score. Candidate miRNA biomarkers were selected according to their fold change (±1.5) and p-value (p<0.1).
Results: Our study cohort, matched for age, sex, baseline NIHSS, intraventricular extension and arterial hypertension, presented higher basal haematoma volume in HG patients (p=0.046). We identified miR-425-5p and miR-484 as the most stable miRNAs and they were used as endogenous miRNAs for data normalisation. A specific profile of deregulated circulating miRNAs differentiated ICH patients with and without HG. Twelve miRNAs were found to be upregulated and three miRNAs were found to be downregulated in patients who suffered HG.
Conclusions: Although further validation is needed, this study has identified 2 suitable endogenous miRNAs and 15 miRNAs as promising predictive biomarkers of HG in ICH patients.
Disclosures of Interest: No
Abstract N°: 1279
NEXT GENERATION SEQUENCING AND WHOLE-EXOME SEQUENCING OF PATIENTS WITH SPONTANEOUS CERVICAL ARTERY DISSECTIONS
Irene Scala*1,2, Valentina Trevisan3, Pier Andrea Rizzo2, Simone Bellavia2, Jacopo DI Giovanni2, Paola Concolino4, Angelo Minucci4, Aldobrando Broccolini1,2, Chiara Leoni3, Giovanni Frisullo1
1Fondazione Policlinico universitario A. Gemelli IRCCS, Neurology Department, Roma, Italy,2Catholic University of the Sacred Heart, Neuroscience, Roma, Italy,3Fondazione Policlinico universitario A. Gemelli IRCCS, Center for Rare Diseases and Birth Defect, Roma, Italy,4Fondazione Policlinico universitario A. Gemelli IRCCS, Departmental Unit of Molecular and Genomic Diagnostics, Roma, Italy
Background and aims: Several evidence support genetic predisposition in the pathogenesis of spontaneous Dissection of the Cervical Arteries (sCeAD)1,2. This study aims to find pathogenic variants (PV) prevalence in sCeAD patients.
Methods: We enrolled consecutive adult patients with sCeAD who met at least one of the following: 1)multiple vascular wall abnormalities; 2)family history of arterial dissections/cerebrovascular disease; 3)clinical/radiological/dysmorphic findings suggestive of genetic diseases. Exclusion criteria were: 1)recent trauma; 2)connective tissue diseases. All patients underwent total-body CT and dysmorphological examination. Next Generation Sequencing (NGS) of the clinical exome was performed, analyzing a panel of 38 genes associated with vascular fragility conditions. In patients whose NGS was inconclusive, but who met ⩾2/3 inclusion criteria, Whole Exome Sequencing (WES) was performed.
Results: NGS was performed in 11 patients: a woman showed a heterozygous c.4565T>C variant of uncertain significance of MYLK gene; another woman showed a heterozygous likely PV c.3469G>A of COL1A1 gene, and a man a heterozygous PV c.1862G>A of COL3A1 gene. WES was performed in five subjects and found a heterozygous PV c.2371C>T of COL4A3 gene in a woman. The prevalence of genetic mutations was 36.4%. Among patients with genetic variants, a positive family history was the most represented risk factor (75%), while multiple vessel alterations and suggestive clinical/radiological/dysmorphic findings were present in 50% of patients.
Conclusions: We found a genetic variant in 36.4% of our selected patients suggesting that family history and whole-body vascular anatomy should always be investigated. Genetic analyses should be performed when ⩾1 suggestive criterion is satisfied.
Disclosures of Interest: No
Abstract N°: 1633
AGE-RELATED CHANGES IN COAGULATION AND FIBRINOLYSIS IN HEALTHY DONORS, CEREBRAL SMALL VESSEL DISEASE, AND ISCHEMIC STROKE
Ivan Koltsov*1,2, Mikhail Martynov1,2, Albina Yasamanova2, Oleg Brusow3, Natalia Karpova3, Yuri Shilov3, Ivan Shchukin1,2, Mihkail Fidler2
1Federal Center of Brain Research and Neurotechnologies, Moscow, Russian Federation,2Pirogov Russian National Research Medical University, Moscow, Russian Federation,3Mental Health Research Center, Moscow, Russian Federation
On behalf of:
Background and aims: Ischemic stroke (IS) patients show a hemostatic shift towards hypercoagulation/hypofibrinolysis that may influence stroke outcomes, including post-stroke cognitive impairment severity (Koltsov et al., 2021, 2022, 2023). The goal of this post-hoc study was to analyze the age-dependent global changes in coagulation and fibrinolysis in healthy donors, cerebral small vessel disease (CSVD), and IS.
Methods: Data for 49 IS patients, 17 CSVD patients, and 45 healthy donors were used for a post-hoc analysis. In IS patients, blood plasma samples were obtained at admission, on the 7th and 14th day. In CSVD patients and healthy donors, blood samples were obtained once. Dynamic thrombophotometry assay was used in conjunction with the Karmin software to calculate Coagulation Brightness (CB), Fibrinolysis Brightness (FB), and Hemostatic Brightness (HB). The local ethical committee approved the study.
Results: Across all groups, there was a significant age-dependent shift hypercoagulation (r=0.506, p<0.001) and hypofibrinolysis (r=-0.612, p<0.001). Moreover, HB was significantly lower in more aged patients (r=-0.672, p<0.001), indicative of the loss of physiological balance between coagulation and fibrinolysis systems. Changes were similar in all stroke subtypes.
Conclusions: It is well known there is a prothrombotic tendency in the elderly, especially in IS patients. This study shows that this prothrombotic shift is due not only to the coagulation activation but also due to the loss of coagulation/fibrinolysis balance. More population studies are needed to assess the role of different vascular risk factors across various age groups to understand the age-associated changes in coagulation/fibrinolysis balance. The study was funded by presidential grant SP-2404.2022.4.
Disclosures of Interest: No
Abstract N°: 2263
LAMININ-AUGMENTED PORCINE BRAIN-DECELLULARIZED ECM: A STRATEGY FOR HUMANIZED NEURAL MODELING
Hyungseok Kim1, Jongtae Park*1, Sujin Lee2
1Chonnam National University Medical School, Department of Forensic Medicine,2Chonnam National University Hospital, Biomedical Researsh Instisute
On behalf of:
Background and aims: The quest for humanized physiological neural models is often impeded by the limited brain-specificity and safety concerns of non-neural extracellular matrix (ECM) applications. Brain-derived ECM, while richer in neural components, suffers from loss of critical elements during decellularization, necessitating augmentation.
Methods: This study introduces a laminin-augmented porcine brain-decellularized ECM (P-BdECM), which is depleted of xenogeneic factors and supports the regulation of human neurons, astrocytes, and microglia. Comparative analysis confirms that P-BdECM's composition closely mirrors human brain-derived ECM in terms of brain-specificity, as assessed through matrisome and gene ontology-biological process analysis.
Results: The incorporation of laminin 111 supplements in P-BdECM synergistically enhances neural functions, complementing laminin 521. Key components, Annexin A1 (ANXA1) and Peroxiredoxin (PRDX), in P-BdECM, stabilize microglial and astrocytic activities under standard conditions while facilitating active neuroinflammation in response to neuropathological stimuli. Additionally, supplementing brain-specific molecules in non-neural matrices similarly mitigates glial cell inflammation, as observed with P-BdECM.
Conclusions: Our findings demonstrate that the P-BdECM augmentation strategy effectively recreates pathophysiological cerebral environments, offering a promising avenue for neurological studies. This approach paves the way for more accurate humanized models in neurological research, potentially enhancing our understanding and treatment of cerebral pathologies.
Disclosures of Interest: No
Abstract N°: 2555
PREDICTIVE VALUE OF GFAP, NFL AND TDP-43 LEVELS IN ISCHEMIC STROKE
Ventura Anciones*1, Alain Luna1,2, Leire Campos2, Leire Iglesias2,3, Raffaela Cipriani3, Estibaliz Capetillo-Zarate3, Covadonga Fernández-Maiztegi1,2, Aida Lagüela1, Abraham Martín3,4, María del Mar Freijo1,2
1Cruces University Hospital, Neurology Department, Barakaldo, Vizcaya, Spain,2Instituto investigación Sanitaria Biocruces-Bizkaia, Barakaldo, Vizcaya, Spain,3Achucarro Basque Center of Neuroscience, Leioa, Vizcaya, Spain,4Ikerbasque Basque Foundation of Science, Bilbao, Vizcaya, Spain
On behalf of:
Background and aims: Glial fibrillary acidic protein (GFAP), neurofilament (NFL) and transactive response DNA binding protein 43 kDa (TDP-43) are biomarkers of brain damage which have been associated with different subtypes of neurodegenerative diseases. Despite this, the predictive value of all three biomarkers at the acute phase of ischemic stroke has been scarcely evaluated so far. Thus, the main objective of this study is to analyze the levels of these biomarkers and their predictive value in patients with ischemic stroke.
Methods: We included patients with ischemic stroke treated with reperfusion therapies. We analyzed levels of GFAP, NFL and TDP-43 in plasma in the first hours using SIMOA. We recorded: age, sex, vascular RF, previous stroke, NIHSS (arrival and 24 hours), type of treatment, delay from symptoms and extraction, and functional status before, at discharge, and 3 months(mRankin). Finally, we compared and analized these variables between patients and controls.
Results: We analyzed 78 patients and 30 sex-matched controls. Women: 35(44.9%); average age: 75(68-82); thrombectomy:71(91%); NIHSS arrival:10(6-18), at 24 hours:2(1-6); previous stroke:10(12.8%); mRankin at discharge:1(0-2), at 3 months:1(0-2).
GFAP and NFL showed higher values in stroke compared to controls(p<0.05). Increased GFAP levels were associated with:age, severity, functional limitation and delay from symptoms to extraction(p<0.05). NFL levels were only associated with functional limitation at 3 months(p<0.05).
Finally, plasmatic TDP-43 levels are currently being evaluated for the first time to date.
Conclusions: GFAP and NFL showed elevated plasmatic values in the first hours. These biomarkers could be predictive of diagnosis and poor functional prognosis.
Disclosures of Interest: No
Abstract N°: 2616
ACUTE-PHASE SERUM BIOMARKERS AND ISCHEMIC STROKE SEVERITY
Federica Ferrari*1, Federico Mazzacane1, Beatrice Del Bello1, Silvia Scaranzin2, Chiara Morandi2, Matteo Gastaldi2, Alessandra Persico3, Anna Cavallini3
1University of Pavia, Department of Brain and Behavioral Sciences, Pavia, Italy,2IRCCS Fondazione Mondino, Neuroimmunology Unit, Pavia, Italy,3IRCCS Fondazione Mondino, U.C. Malattie Cerebrovascolari e Stroke Unit, Pavia, Italy
On behalf of:
Background and aims: One of the most challenging research fields in cerebrovascular disease is to identify reliable etiologic and prognostic biomarkers. The aim of this prospective observational study is to evaluate which biomarkers are most suitable to be included in an acute-phase prognostic panel.
Methods: We included patients with acute stroke at neuroimaging, >18y, onset<24h, NIHSS>1, pre-stroke mRS=0-1. Exclusion criteria were age>80y, previous stroke/TBI/other neurological disease, pre-stroke immunosuppression, eGFR<30mL/min. Patients were treated as standard of care. Stroke severity (NIHSS) was evaluated every 24hrs until discharge. Serum concentrations of inflammatory cytokine Interleukin-6 (IL6), vasoconstrictor endothelin-1 (ET1) and neurofilament-light-chain (NfL) were determined with ELLATM on samples collected within 24h (T0) and after 7±2 days from onset (T1).
Results: We included 55 patients (36 males, mean age 62.73±13.84). At onset, 49.1% had NIHSS1-4, 41.8% NIHSS5-15, 9.1% NIHSS>16. Biomarker median values were T0: IL6=4.9pg/mL [IQR=5.93], ET1=3.73pg/mL[IQR=2.47], NfL=34.4pg/mL [IQR=50.4]; T1: IL6=5.97pg/mL[IQR=12.12], ET1=2.98pg/mL [IQR=1.72], NfL=119pg/mL[IQR=194.6]. ET1 was higher at T0vsT1 (p=0.014), IL6 was not different, while NfL was higher at T1vsT0 (p<0.001). NfL at both time-points correlated with ET1-T0 and IL6-T2. At discharge, NIHSS positively correlated with ET1 and NfL at T0, and with IL6 and NfL at T1.
Conclusions: IL6 and ET1 are released with different kinetics after stroke, being their serum peak concentrations correlated with the extension of brain damage assessed by NfL. ET1 correlates with stroke severity and it is known to be higher in complicated atherosclerotic disease: it could predict both the prognosis and the etiopathogenetic mechanism and so be a good candidate for an acute-phase biomarker panel.
Disclosures of Interest: No
Abstract N°: 2620
INVESTIGATING ISOPROSTANE EXPRESSION TO DIFFERENTIATE BETWEEN TRANSIENT ISCHAEMIC ATTACKS (TIAS), MINOR STROKES, AND TIA MIMICS
Deeksha Sharma*1, Erik Noschka1, Emilie Mas2, Suzanne Edwards1, Austin Milton3, Joshua Mahadevan3, Craig Kurunawai3, Timothy Kleinig3, Jim Jannes3, Anne Hamilton-Bruce3
1The University of Adelaide, Adelaide, Australia,2SA Pathology, Adelaide, Australia,3Central Adelaide Local Health Network, Adelaide, Australia
On behalf of: Dr Tomas Rozek, Enzo Ranieri, Dr Thierry Durand, Dr Camille Oger, Dr Jean-Marie Galano, Prof Simon Koblar
Background and aims: TIAs are an important predictor for ischaemic stroke and an opportunity for risk mitigation if managed urgently. However, misdiagnoses are common due to overlaps with other neurological conditions. Oxidative stress is a key component of the ischaemic cascade and isoprostanes in plasma have been investigated as a stable and specific marker for this. The aim is to investigate isoprostanes to improve identification of TIAs.
Methods: Patients presenting to the Royal Adelaide Hospital with TIA-like symptoms £48 hours of onset were enrolled (n=104). Plasma samples were collected (£10mL) and all patients were clinically classified retrospectively by a panel of vascular neurologists as TIA/TIA Mimic/Minor Stroke. A modified methodology for quantitative isoprostane profiling was utilised for plasma investigation using UPLC–MS/MS. Data output was collected using MultiQuant prior to statistical analysis using SAS and visualisation with MetaboAnalyst. A p value £0.002 was considered statistically significant following a Bonferroni correction.
Results: The first phase of analysis was conducted with 50 patient plasma samples (29 Females, 21 Males) aged 39-94 (Median: 72y) at time of sample collection. All patients were classified based on clinical data, with 56% established as a TIA mimic. Univariate linear regressions were performed on the logarithmic transformation of 25 isoprostanes. Although no statistically significant associations were found, data visualisation identified minor dysregulation across 6 isoprostanes.
Conclusions: This pilot investigation has helped establish methodology and elucidate minor dysregulation between the clinical groups. The primary limitation has been the sample size, with further analysis in a larger cohort (n=104) underway.
Disclosures of Interest: No
Abstract N°: 2925
SECRETOME FROM SYMPTOMATIC CAROTID PLAQUES PRESENT HIGHER CONTENT OF INFLAMMATORY AND ANTIOXIDANT MOLECULES COMPARED TO ASYMPTOMATIC PLAQUES
Núria Puig1, Pol Camps Renom*2, Belén Pérez3, Ana Aguilera-Simón4, Arnau Solé1, Mercedes Camacho5, Francesc Jiménez-Altayó3, Sònia Benítez1
1Institut de Recerca - Hospital Santa Creu i Sant Pau, Cardiovascular Biochemistry, Barcelona, Spain,2Hospital de la Santa Creu i Sant Pau, Stroke Unit - Departmen of Neurology, Barcelona, Spain,3Universitat Autònoma de Barcelona, Department of Pharmacology, Therapeutics and Toxicology, School of Medicine, Bellaterra, Spain,4Institut de Recerca - Hospital Santa Creu i Sant Pau, Stroke Unit, Barcelona, Spain,5Institut de Recerca - Hospital Santa Creu i Sant Pau, Barcelona, Spain
On behalf of:
Background and aims: Atherosclerotic internal carotid plaques (CP) secrete multiple molecules related to inflammation and oxidative stress. We aimed to identify the different profile of molecules secreted by asymptomatic and symptomatic CP (aCP and sCP, respectively) from patients undergoing carotid endarterectomy.
Methods: Prospective study of patients with carotid stenosis ⩾50% who underwent carotid endarterectomy (aCP=19, sCP=19). Carotid plaque explants (100 mg) were cultured in 5%CO2 with DMEM medium, and after 20h the medium with secreted molecules (secretome) was collected. Proteomic analysis was performed by mass spectrometry. The results were corroborated by ELISA for inflammatory molecules and by biochemical kits for oxidation/cell viability. Other plaque explants were kept frozen in RNA later until real-time PCR (RT-PCT) analysis in order to assess changes in gene expression.
Results: In the proteomic analysis, 131 proteins, mainly related to inflammation, lipids, and oxidation, differed between aCP and sCP. In secretome from sCP a 30% increase in the antioxidant capacity (74.91±7.66 μM vs 49.28±7.18 μM Trolox equivalents, p=0.026) was found compared to aCP. Secretome from both CPs showed high concentration of inflammatory molecules, being some of them significantly higher in sCP, such as IL6 (7.29±0.62 vs 4.76±0.84 ng/mL, p=0.026) and IL8 (15.02±2.93 vs 8.18±1.82 ng/mL, p=0.03). A trend to higher gene expression of inflammatory genes was observed in sCP compared to aCP. A strong trend to higher cell mortality was also found in secretome from sCP.
Conclusions: sCP release higher content of inflammatory molecules than aCP, and show a greater antioxidant microenvironment, likely as a response to exacerbated oxidative stress.
Disclosures of Interest: No
Abstract N°: 2998
DECIPHERING THE DIAGNOSTIC AND PROGNOSTIC ROLE OF MICRORNAS IN STROKE: A SYSTEMATIC REVIEW AND META-ANALYSIS
1All India Institute Of Medical Sciences, Neurology, New Delhi, India,2Yale University, Neurology, New Haven, United States,3All India Institute Of Medical Sciences, Clinical Research Unit, New Delhi, India
On behalf of:
Background and aims: MicroRNAs (miRNAs) are a class of small, non-coding RNA molecules that play a crucial role in gene regulation. Studies have shown that miRNAs can be involved in the pathogenesis of many diseases, including stroke. Stroke is a major public health problem and a leading cause of death and disability worldwide. In this systematic review and meta-analysis, we aimed to investigate the role of miRNAs in stroke.
Methods: We conducted a comprehensive search of several databases, including PubMed, Embase, and Cochrane Library, from inception to November 2023. We included studies that reported miRNA expression in stroke patients compared to healthy controls or in stroke patients with different stroke subtypes. We performed a meta-analysis using a random-effects model to estimate the pooled effect size.
Results: A total of 34 studies were included in this systematic review and meta-analysis. The meta-analysis showed that the expression of miR-21 was significantly upregulated in stroke patients compared to healthy controls (standardized mean difference [SMD]=1.35, 95% confidence interval [CI]: 0.99-1.71, p<0.001). In addition, the expression of miR-145 was significantly downregulated in stroke patients compared to healthy controls (SMD=-1.09, 95% CI: -1.47 to -0.71, p<0.001). Furthermore, the expression of miR-221 was significantly upregulated in ischemic stroke patients compared to hemorrhagic stroke patients (SMD=1.13, 95% CI: 0.57-1.68, p<0.001.
Conclusions: Our systematic review and meta-analysis provide evidence that miRNAs play a role in the pathogenesis of stroke. The upregulation of miR-21 and downregulation of miR-145 in stroke patients suggest their potential as diagnostic and therapeutic targets for stroke.
Disclosures of Interest: No
E-Poster - ICH and SAH
Abstract N°: 189
ASSOCIATION OF INTENSIVE BLOOD PRESSURE LOWERING WITH EARLY NEUROLOGICAL DETERIORATION AFTER ICH
Daniel Vázquez-Justes*1, Gerard Mauri Capdevila1, Yhovany Gallego Sánchez1, Miriam Paul Arias1, Albert Freixa Cruz1, Francisco Purroy1
Background and aims: The benefit of intensive lowering of Blood pressure (BP) has been demonstrated in patients with intracerebral Hemorrhage (ICH). However, the underlying mechanisms for this benefit are not well understood. Early Neurological Deterioration (END) is the clinical worsening during the first 24 hours after ICH onset, and is a contributor to poor outcomes after ICH
We aimed to analyze if BP intensive lowering were related to fewer rates of END in a cohort of patients with ICH
Methods: We retrospectively analyzed data of consecutive patients with ICH who were admitted to our hospital. Variables related to END in bivariate analysis with p value of <0,05 were included in a multivariate logistic regression analysis. Optimal BP control was considered when the target of both less than 140mmHg of SBP and less than 105mmHg of DBP were achieved and maintained during the first 24 hours in patients hemodynamically stable. Hematoma expansion (HE) was defined as an increase of 6ml or 33% or more in the neuroimaging at 24 hours
Results: 148 patients were analyzed. Laboratory parameters (cholesterol, LDL, hemoglobin, glycaemia, interleukin 6) were not related to END. Age, anticoagulants use, baseline NIHSS scale, volume, HE and optimal BP control were related to END. In the multivariate analysis, only HE (OR, 14,4; 95% CI, 3,69-55,6; P<0.01) and BP control (OR, 0,28; 95% CI, 0,079-1,00; P=0.05) remained statistically significant.
Conclusions: Intensive BP lowering could lead to lower rates of END, and this could independently explain the better outcomes after BP lowering.
Disclosures of Interest: No
Abstract N°: 364
INFLUENCE OF HOSPITAL TYPE ON OUTCOMES OF PATIENTS WITH ACUTE SPONTANEOUS INTRACEREBRAL HEMORRHAGE. A POPULATION-BASED STUDY
Joan Martí-Fàbregas*1, Anna Ramos Pachon1, Luis Prats-Sánchez1, Ana Núñez-Guillén2, David Rodriguez-Luna3, Sergio Amaro4, Ana Rodríguez-Campello5, Yolanda Silva6, Natalia Pérez de la Ossa7, Pol Camps Renom1
1Hospital de la Santa Creu i Sant Pau, Neurology, Barcelona, Spain,2Hospital Universitari de Bellvitge, Neurology, Hospitalet de Llobregat, Spain,3Hospital Universitari Vall d'Hebron, Neurology, Barcelona, Spain,4Hospital Clínic, Neurology, Barcelona, Spain,5Hospital del Mar, Neurology, Barcelona, Spain,6Hospital Universitari Dr Trueta, Neurology, Girona, Spain,7Hospital Universitari Germans Trias i Pujol, Neurology, Badalona, Spain
On behalf of: Sònia Abilleira, Mercè Salvat-Planas Isabel Puig, Laura Llull, Olalla Pancorbo, Blanca Lara, Manuel Gómez-Choco, Daniel Vázquez-Justes, Nicolau Guanyabens, Dolores Cocho, Laia Seró, David Cánovas, Eva Giralt-Steinhauer, Marc Puig, J. Krupinski
Background and aims: Outcomes depending on the type of hospital where patients with spontaneous intracerebral hemorrhage (ICH) are admitted is uncertain. We aimed to determine the influence on functional outcomes of hospital type at admission: telestroke centre (TSC)/primary stroke centre (PSC) or comprehensive stroke centre (CSC).
Methods: A multicentre, population-based, prospective observational study of a cohort of consecutively recruited patients with ICH (March 2020-March 2022) in Catalonia (Spain). We excluded patients with a previous modified Rankin Scale (mRS) score>3 and those admitted >24h post-onset. Primary endpoint: 3 month mRS obtained by blinded investigators. mRS was tested using adjusted ordinal logistic regression to estimate the shift in mRS scores. A propensity score matching (PSM) analysis was performed for the subgroup of transferred patients (n=331) from a TSC/PSC to a CSC
Results: We included 1961 patients [mean age 70 (14.1) years, 713 (38%) women]; 641 were admitted to a TSC/PSC and 1320 to a CSC. After adjusting for confounders (age, National Institute of Health and Stroke Scale score, intraventricular haemorrhage, hematoma volume and previous mRS), type of hospital of initial admission (CSC vs TSC/PSC) was not associated with outcomes (adjusted common OR 1.13, 95% CI: 0.93-1.38). A PSM analysis indicated that transfer to a CSC was not associated with more favourable outcomes (OR 0.77, 95% CI: 0.55-1.10; p=0.16).
Conclusions: Hospital types were not associated with functional outcomes. Additionally, for patients who were transferred from a TSC/PSC to a CSC, outcomes were similar to non-transferred patients. Our findings suggest that patient characteristics are more important than hospital characteristics.
Disclosures of Interest: No
Abstract N°: 416
LOCAL ANESTHESIA WITH SEDATION AND GENERAL ANESTHESIA FOR THE TREATMENT OF CSDH: A SYSTEMATIC REVIEW AND META-ANALYSIS
Mariam Ahmed Abdelhady1, Ibrahim Serag2, Ahmed Aljabali3, Mohammad Al-Jafari4, Amr Elrosasy*5, Ahmed Atia5, Aya Ehab6, Shrouk F Mohammed7, Ibraheem M Alkhawaldeh4, Mohamed Abouzid8
1Faculty of Medicine_October 6 University, Egypt,2Faculty of Medicine - Mansoura University, Egypt,3Jordan University of Science & Technology (JUST), الرمثا, Jordan,4جامعة مؤتة, Mouʿtah, Jordan,5Faculty Of Medicine Kasr Al-Ainy, Cairo University, Egypt,6Faculty of Medicine - Aswan University, Egypt,7Alexandria Faculty of Medicine, Egypt,8Poznan University of Medical Sciences, Poznań, Poland
On behalf of:
Background and aims: Surgery is the primary treatment for chronic subdural hematoma, and anesthesia significantly impacts the surgery's outcomes. A previous systematic review compared general anesthesia to local anesthesia in 319 patients. Our study builds upon this research, analyzing 4,367 cases to provide updated and rigorous evidence
Methods: We systematically searched five electronic databases, PubMed, Cochrane Library, Scopus, Ovid Medline, and Web of Science, to identify eligible comparative studies. All studies published until September 2023 were included in our analysis. We compared six primary outcomes between the two groups using Review Manager Software.
Results: Eighteen studies involving a total of 4,367 participants were included in the meta-analysis. The analysis revealed no significant difference between the two techniques in terms of 'recurrence rate' (OR= 0.95, 95% CI [0.78 to 1.15], P=0.59), 'mortality rate' (OR= 1.02, 95% CI [0.55 to 1.88], P=0.96), and 'reoperation rate' (OR=0.95, 95% CI [0.5 to 1.79], P=0.87). Local anesthesia demonstrated superiority with a lower 'complications rate' than general anesthesia, as the latter had almost 2.4 times higher odds of experiencing complications (OR=2.4, 95% CI [1.81 to 3.17], P<0.00001). Additionally, local anesthesia was associated with a shorter 'length of hospital stay' (SMD =1.19, 95% CI [1.06 to 1.32], P<0.00001) and a reduced 'duration of surgery' (SMD=0.94, 95% CI [0.67 to 1.2], P<0.00001).
Conclusions: Surgery for chronic subdural hematoma under local anesthesia results in fewer complications, a shorter length of hospital stay, and a shorter duration of the operation.
Disclosures of Interest: No
Abstract N°: 419
CLOPIDOGREL VS TICAGRELOR IN DUAL ANTI-PLATELET THERAPY FOR INTRACRANIAL ANEURYSM PATIENTS UNDERGOING NEUROENDOVASCULAR TREATMENT
Mostafa Hossam El Din Moawad1, Ibrahim Serag2, Ibraheem Alkhawaldeh3, Abdulrahman Sharaf4, Sumaya Alsalah5, Mohamed Smail Aissani6, Mona Mahmoud Elsakka7, Amro Elrosasy*8, Osama Bisht9
1Alexandria University, Egypt,2Faculty of Medicine - Mansoura University, Egypt,3faculty of medicine Mutah university, Jordan,4Salmaniya Medical Complex, Manama, Bahrain,5inistry of Health, Primary Care, governmental health centers, Egypt,6Blida, Blida, Algeria,7Damanhour University, Egypt,8Faculty of Medicine, Kasr Alainy, Cairo University, Cairo, Egypt,9Ketschendorfer Str. 33, Coburg, Germany
On behalf of:
Background and aims: Patients with cerebral aneurysms often undergo neurointerventional treatments involving stent implantation or flow diversion. These treatment options are associated with high risk of thromboembolic complications. However, there is some conflicting data regarding the use of more potent P2Y12-Inhibitors (e.g., Ticagrelor) when compared to standard combination therapy with clopidogrel.
Objective: We aimed to investigate the safety and effectiveness of clopidogrel versus ticagrelor in addition to aspirin as a part of DAPT regimen after successful endovascular treatment of cerebral aneurysms
Methods: We searched PubMed, Web of Science, and Scopus for comparative studies that fit the eligibility criteria including observational studies and randomized controlled trials up to November 2023. The analysis was performed using a fixed effect model since no or minimal heterogeneity was present.
Results: we selected 13 eligible articles. There was no difference between clopidogrel and ticagrelor in thromboembolic complications, hemorrhagic complications, stroke, ischemic stroke, stent thrombosis, modified Rankin scale (mRs) 0-2 and all-cause mortality (OR= 0.92, 95% CI [0.73, 1.16], p=0.46), (OR= 1.06 .95% CI : 0.82–1.36), (OR= 1.06, 95% CI [0.72, 1.57], p=0.76), (OR= 1.06, 95% CI [0.67, 1.69], p=0.79), (OR= 0.88, 95% CI [0.46, 1.71], p=0.71), (OR=0.86, 95% CI 0.51 to 1.45; P=0.56), and (OR= 1.01 with 95% CI [0.59, 1.73], p=0.97), respectively. The overall odds ratio between the clopidogrel and ticagrelor in mRs worsening favored ticagrelor (OR= 0.52, 95% CI [0.32, 0.83], p=0.007).
Conclusions: clopidogrel could be used as first-line according to the recommended guidelines, with the use of ticagrelor as an alternative for patients with inadequate response to.
Disclosures of Interest: No
Abstract N°: 490
ANY IMPROVEMENT FROM 24-HOURS TO 7-DAYS PREDICTS FAVORABLE FUNCTIONAL RECOVERY AFTER INTRACEREBRAL HEMORRHAGE: INTERACT2 STUDY
1The Second Affiliated Hospital of Soochow University, Neurology, Suzhou, China,2The George Institute for Global Health,Faculty of Medicine, University of New South Wales, Newtown, Sydney, Australia,3Suzhou TCM Hospital Affiliated to Nanjing University of Chinese Medicine, Suzhou, China
On behalf of: the INTERACT Investigators
Background and aims: The significance of late neurological improvement (LNI) after acute intracerebral hemorrhage (ICH) is unknown. We investigated the frequency and prognostic effect of LNI on 90-days functional outcome after ICH in the INTERACT2 (second Intensive Blood Pressure Reduction in Acute Intracerebral Hemorrhage Trial; NCT00716079).
Methods: LNI included any, moderate and significant, neurological improvement defined as ⩾1, ⩾2 and ⩾3 point decrease on the National Institutes of Health Stroke Scale (NIHSS) from 24-hour to 7-day post-ICH, respectively. Logistic regression models were used to assess associations of LNI and death or major disability (mRS 3-6), major disability (mRS 3-5), and death alone.
Results: Of 2602 patients included in analyses, 1506 (57.9%), 1069 (41.1%) and 738 (28.4%) experienced any, moderate and significant, LNI from 24-hours to 7-days post-ICH. After adjustment for key confounders, any LNI were associated with 49%, 25% and 65% reduced risks of death or major disability (OR 0.51, 95% CI 0.42-0.63), major disability (OR 0.75, 95% CI 0.63-0.90), and death (OR 0.35, 95% CI 0.24-0.50), respectively. Moderate and significant LNI were also significantly associated with decreased odds of poor 90-day functional outcome. Any LNI for reduced poor functional outcome was consistent across most subgroups including age, baseline hematoma volume and early hematoma expansion.
Conclusions: Half of mild-moderate ICH patients experience LNI from 24-hour to 7-days, with any neurological improvement being significantly associated with favorable functional outcome.
Disclosures of Interest: No
Abstract N°: 591
PREDICTIVE FACTORS OF DEVELOPING EPILEPSY IN PATIENTS WITH ARTERIO-VENOUS MALFORMATION
1County Emergency Hospital Cluj-Napoca, Neurology, Cluj-Napoca, Romania,2Lariboisiere Hospital, FHU NeuroVasc, APHP Nord, Neurology, Paris, France,3Univ. Lille, CHU Lille, ULR 2694 - METRICS : évaluation des technologies de santé et des pratiques médicales, F-59000, Lille, France,4CHU Lille, Département de Biostatistiques, F-59000 Lille, France, Lille, France,5INSERM UMR 1144, Université Paris Cité, Paris, France
On behalf of:
Background and aims: Data focusing on time-to-onset for epilepsy in patients with arterio-venous malformations (AVM) are lacking. We aimed to characterize the predictive factors and timing of developing epilepsy in AVM patients.
Methods: We conducted a retrospective analysis on 200 AVM patients treated between 2000-2023. We used univariate and multivariate analyses to assess the association between baseline characteristics and seizures. The risk of developing seizures during follow-up was estimated using nonparametric survival analysis for interval-censored data.
Results: In the present cohort, 90/200 patients (45%) had epilepsy at baseline. Epileptic patients were predominantly men (71.1%), alcohol users (18.8%), and presented with AVM located more often in the frontal lobe (55.6%) as compared to non-epileptic patients (40%, 7.4%, 23.6% respectively). Male gender (OR, 3.81, 95%CI, 1.77 to 8.24) was associated with higher prevalence of seizures at inclusion, while headaches (OR, 0.19, 95%CI, 0.09 to 0.41), focal deficit (OR, 0.22, 95%CI, 0.09 to 0.49) and AVM occipital localization (OR, 0.16, 95%CI, 0.05 to 0.47), remained associated with lower prevalence of epilepsy at inclusion. Among patients without epilepsy at baseline, 79.4% remained non-epileptic after 5 years. Ruptured AVM (HR, 3.77, 95%CI 1.50 to 9.44) and surgery (HR, 7.75, 95% CI 2.04 to 29.45) were predictors of seizure occurrence.
Conclusions: Male patients and frontal AVM topography were associated with higher risk of epilepsy as initial symptoms. Among non-epileptic patients, ruptured AVM and surgery were predictors of epilepsy at 5 years.
Disclosures of Interest: No
Abstract N°: 853
PREDICTORS OF FUNCTIONAL RECOVERY PATTERN IN PATIENTS WITH ACUTE INTRACEREBRAL HEMORRHAGE AFTER MINIMALLY INVASIVE SURGERY
1The George Institute for Global Health, Global Brain Health,2Linyi People’s hospital
On behalf of:
Background and aims: The efficacy of minimally invasive surgery for functional recovery in acute spontaneous intracerebral hemorrhage (ICH) remains unclear. Our study focuses on identifying prognostic factors for functional recovery in ICH patients to refine criteria for future randomized controlled trials.
Methods: A single-center register study was conducted on acute ICH patients with basal ganglia hemorrhage, treated with enhanced frameless minimally invasive stereotactic soft channel brain haemorrhage evacuation and thrombolysis therapy (MIS) from January 2020 to October 2023. We used to binary logistic regression identify predictors of unfavorable outcomes (modified Rankin scale scores 4-6) and death within 3-6 months.
Results: Of the 792 registered ICH cases (35% female, average age 58±13 years), the median time from onset to MIS was 23 hours(IQR 11-32), and the median Glasgow Coma Scale score was 9 (IQR 7-11). Within 3-6 months, 30% of patients died, and 50% experienced unfavorable outcomes. Multivariate analysis indicated that older age, more severe ICH, longer time to surgery, greater baseline hematoma volume, and higher admission glucose levels were significant predictors of death or unfavorable outcomes.
Conclusions: This study provides real-world evidence on the use of MIS for hematoma evacuation in acute ICH. The findings will inform clinical guidelines and assist in selecting and managing patients for future trials targeting hematoma evacuation.
Disclosures of Interest: No
Abstract N°: 929
NEW TREATMENT STRATEGY FOR SEVERE SUBARACHNOID HEMORRHAGE WITH INTRACEREBRAL HEMATOMA
JIN KIKUCHI*1, Sosho Kajiwara1, Kimihiko Orito1, Masaru Hirohata1, Motohiro Morioka1
1Kurume University School of Medicine, Neurosurgery, kurume, Japan
On behalf of:
Background and aims: The outcome of severe subarachnoid hemorrhage (SAH) is poor. Although one of important pathology is increased intracranial pressure (ICP), there is still no effective treatment. Barbiturate therapy is known to decrease the ICP, but barbiturate has some serious side effect. Recently we developed a novel safe barbiturate therapy, named “step down barbiturate therapy (SDB) for severe brain traumatic injury, which decreased ICP well and has no serious side effect. In this study, we examined the efficacy of this SDB for severe SAH patients; prospective SDB treated group vs historical control group.
Methods: Of 342 SAH patients treated by surgery at our hospital from January 2010 to May 2022, 17 patients with ruptured middle cerebral artery aneurysm with intracerebral hematoma(ICH) graded as WFNS Grade IV or V, to whom hematoma removal, aneurysmal clipping or coiling and external decompression were included. These patients were historically divided into two groups; group A treated with SDB and Group B treated without SDB. Thiamylal sodium was started immediately after surgery at 4 mg/kg/h and tapered to 3, 2, 1.5, and 1 every 24 hours after the start of administration with normothermia.
Results: There were 7 cases in group A and 10 cases in group B. The patient number of good outcome (mRS 0~2) of group A was 4 (57.4%), and that of group B was 1(10.0%). There was no death in Group A and no serious side effects associated with barbiturate.
Conclusions: For severe SAH with ICH, SDB reduced ICP well without serious side effect and improved outcome.
Disclosures of Interest: No
Abstract N°: 976
ENDOVASCULAR TREATMENT OF SAH RELATED VASOSPASM-SINGLE CENTRE EXPERIENCE. WHEN TO START AND WHEN TO STOP?
Mislav Budisic*1, Vladimir Kalousek2, Marijana Bosnar-Puretić1, Lidija Dežmalj-Grbelja1, Lara Pilepić1, Sara Drnasin1, Josip Sekovanic2, Branimir Čulo2, Marko Gavrančić1, Marina Roje Bedeković1
1University hospital "Sestre Milosrdnice", Neurology, ICU, Zagreb, Croatia,2University hospital "Sestre Milosrdnice", Radiology, Zagreb, Croatia
On behalf of:
Background and aims: Cerebral vasospasm (CVS) is present in 30-70% of patients after aneurysmal subarachnoid haemorrhage (aSAH) and is a main contributor to delayed cerebral ischemia (DCI). DCI occurs in 20-40% of patients and is a major predictor of poor outcome after aSAH. After the failure of baseline management of CVS, endovascular treatment (EVT) is reasonable option for refractory vasospasm. However, the effect and safety of repeated EVT has not yet been clearly investigated. The aim of this study is to show the benefit and evaluate safety of repeated EVT in combination with medical vasodilatation in cases of recurrent or refractory CVS.
Methods: We report 24 patients with CVS after aSAH who received EVT (98 vessel segments, 44 procedures). In 12 patients (50%) we performed EVT once and in 12 (50%), two or more EVT were done due to refractory or recurrent vasospasm. All EVT were combined with intra-arterial application of nimodipine.
Results: In our research 59% of patients who had two or more EVT had significantly better functional outcome (mRS 0–2) after 3 months (p=0.047) as opposed to 42 % of patients who had one EVT, reflecting the trend towards lower rates of DCI (58% vs. 67%) in patients with repeated EVT despite refractory or recurrent vasospasm. We found no EVT related complications.
Conclusions: Our results are suggesting that repeated EVT in combination with medical vasodilatation is safe and efficient as rescue therapy of CVS. Repeated vasodilatation is worthwhile strategy in recurrent or persistent vasospasm and prevention of DCI.
Disclosures of Interest: No
Abstract N°: 1078
PERIPHERAL BLOOD CELL RATIOS AS PREDICTIVE INDICATORS FOR DELAYED CEREBRAL INFARCTION IN PATIENTS WITH INTRACRANIAL ANEURYSM
Hyun Kyung Kim1, Kee Ook Lee1, Seung-Hun Oh1, Kyung-Yul Lee2, Ok Joon Kim1, YEON SOO HA*3
1CHA Bundang Medical Center, School of Medicine, CHA University, Department of Neurology, Seongnam-si, South Korea,2Yonsei University College of Medicine, Department of Neurology, Seoul, South Korea,3Presbyterian (Jesus) Medical Center, Department of Neurology, jeonju, South Korea
On behalf of:
Background and aims: Although DCIN is now understood to be a multistep process that progresses over time, its pathophysiology is still unclear. The aim of this study was to analyze the inflammatory and platelet related thrombotic markers for rupture risk of IA and verify the predictive value of the markers for DCIN in subarachnoid hemorrhage (SAH) caused by ruptured IA.
Methods: A total of 1536 patients, including 1231 with unruptured IA and 305 with ruptured IA, were enrolled in this study. Logistic regression was used to analyze the risk factors for DCIN. Receiver operating characteristic (ROC) curve analysis was performed to test the combined ability of the inflammatory and platelet related thrombotic markers to predict DCIN.
Results: Compared with the unruptured IA group, the ruptured IA group had lower platelet-to-neutrophil count (PNR), platelet-to-white blood cell count (PWR), and higher neutrophil-to-lymphocyte count (NLR), platelet-to-lymphocyte count (PLR). In multivariate analysis, the risk of DCIN was negatively correlated with PWR (p = 0.001) and positively correlated with system inflammation response index (SIRI) and mean platelet volume (MPV) (p = 0.020, p = 0.006, respectively).
Conclusions: Our findings suggest a correlation between the peripheral blood markers and DCIN risk of ruptured IA patients. The use of the PWR combined with SIRI and MPV shows a good diagnostic performance for DCIN prediction in patients with SAH of ruptured IA. However, additional long-term, large-scale prospective studies are needed to explore potential mechanisms underlying this association.
Disclosures of Interest: No
Abstract N°: 1302
SHORT-TERM MORTALITY AFTER INTRACEREBRAL HAEMORRHAGE BY TYPE OF ANTICOAGULANT AND ANTIPLATELET DRUG
Christian Jørgensen*1, Nils Boe1, Stine Hald1, Christian Ovesen1,2, Rustam Salman3, Larry Goldstein4, Magdy Selim5, Luis Rodríguez6, Jesper Hallas7, David Gaist1
1Odense University Hospital, Research Unit for Neurology, Odense, Denmark,2Bispebjerg Hospital, Department of Neurology, Copenhagen, Denmark,3University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom,4University of Kentucky, Department of Neurology and Kentucky Neuroscience Institute, Lexington, United States,5Harvard Medical School, Beth Israel Deaconess Medical Center, Boston, United States,6Centro Español Investigación Farmacoepidemiológica, Madrid, Spain,7University of Southern Denmark, Department of Clinical Pharmacology, Pharmacy and Environmental Medicine, Odense, Denmark
On behalf of:
Background and aims: Studies of mortality after intracerebral haemorrhage (ICH) in patients with prior use of direct oral anticoagulants (DOACs) compared to vitamin K antagonists (VKAs) report conflicting results. Data reflecting the relationship of prior use of clopidogrel vs aspirin and short-term mortality are limited. We aimed to assess the associations between DOAC vs VKA and clopidogrel vs aspirin use before ICH and post-ICH survival in an unselected patient cohort.
Methods: All patients age ⩾55-years with a first-ever spontaneous ICH in Southern Denmark between 2015-2018 were identified. From this population, patients who had a dispensed prescription for antithrombotic drugs at ICH onset (and for VKA in addition an admission INR>1.5) were identified and classified into two groups: DOAC vs VKA (reference group) and clopidogrel vs aspirin (reference group). Adjusted relative risks (aRRs) and corresponding 95% confidence intervals (CIs) for 90-day mortality were calculated. We adjusted for potential confounders by using inverse probability of treatment weighting.
Results: Among 1,060 patients in the ICH cohort, 89 were prescribed a DOAC, 122 a VKA, 111 clopidogrel and 177 aspirin. Adjusted for potential confounders, no evidence was observed for a difference in short-term mortality between patients prescribed a DOAC versus VKA (aRR=0.83; 95% CI 0.68-1.02) or between those prescribed clopidogrel versus aspirin (aRR 1.09; 95% CI 0.91-1.30).
Conclusions: No evidence was observed for a difference in short-term survival after ICH between those prescribed a DOAC versus a VKA or between those prescribed clopidogrel versus aspirin.
Disclosures of Interest: Yes Dr Gaist received speakers’ honoraria from Pfizer and Bristol Myers Squibb outside the submitted work and participated in research outside the submitted work funded by Bayer with funds paid to the institution where he is employed.
Abstract N°: 1398
CHARACTERISTICS OF PATIENTS WITH A DIAGNOSIS OF BRAIN DEATH AND ORGAN DONATION AFTER SPONTANEOUS INTRACEREBRAL HEMORRHAGE
Miriam Paul Arias*1, Daniel Vázquez-Justes1, Albert Freixa Cruz1, Yhovany Gallego Sánchez1, Gerard Mauri Capdevila1, Francisco Purroy1
1Arnau de Vilanova University Hospital, Neurology Service, Lleida, Spain
On behalf of:
Background and aims: Spontaneous intracerebral hemorrhage (ICH) is a subtype of stroke with high morbidity and mortality, and is currently the main cause of brain death (BD) and organ donation (OD).
Our objective was to compare patients with ICH who were diagnosed with BD from those who died due to cardiorespiratory death and from those who ultimately became OD.
Methods: We reviewed those patients who died in hospital after ICH between 2016-2022. Patients diagnosed with BD were compared with those who died due to cardiorespiratory death and those who were OD with those who were not OD.
Results: Of 325 patients with ICH, 109 (33.5%) died during admission and, of these, 23 (21.1%) were diagnosed with BD and 20 became OD. 8 were OD by controlled asystole. Patients diagnosed with BD were younger (66 vs 76 years), had lower GCS [4 (IQR 3-6) vs 7 (IQR 6-10)] and shorter survival time (all of them p<0.05).
Patients with ICH who were OD compared to non-OD were younger (67 vs 77 years), with a lower initial GCS [4 (IQR 3-7) vs 7 (IQR 6-11)], higher NIHSS [30 (IQR 25-31) vs 20 (IQR 15-24)], with a higher ICH volume [75 (IQR 40-120) vs 50 (IQR 20-80)] and had more intraventricular extension.
Conclusions: In our center, ICH is the leading cause of BD and OD. In both cases the patients are younger, with a lower initial GSC and shorter survival time. The OD had larger volumes and extension to the ventricular system.
Disclosures of Interest: No
Abstract N°: 1456
CAUSAL DIRECTED ACYCLIC GRAPH (DAG) TO TEST THE EFFECT OF TREATMENT(S) IN ANEURYSMAL SUBARACHNOID HAEMORRHAGE (ASAH)
Carlo Berzuini1, Ian Anderson2, Diederik Bulters3, Ahmed Toma4, Daniel Walsh5, Louise Dulhanty6, James Galea7, Hiren Patel*6
1University of Manchester, Centre for Biostatistics, United Kingdom,2Leeds General Infirmary, Neurosurgery, Leeds, United Kingdom,3Wessex Neurological institute, Neurosurgery, Southampton, United Kingdom,4National Hospital for Neurology and Neurosurgery, London, United Kingdom,5King's College Hospital, London, United Kingdom,6Geoffrey Jefferson Brain research centre, Neurosurgery, Manchester, United Kingdom,7University Hospital of Wales, Neurosurgery, Cardiff, United Kingdom
On behalf of:
Background and aims: Randomized Controlled Trials are considered the most reliable method to assess the effect of medical interventions. Observational studies (OS) are considered less dependable becasue of selection and confounding. DAGs are useful in visualizing confounders and causal links between variables and can facilitate adjustments to estimate causal effects. Our study aimed to record and describe a DAG designed to assess the causal effects of treatment(s) in aSAH using OS.
Methods: Our DAG was collaboratively created by causal inference and aSAH experts. DAG describing how variables (presenting characteristics, interventions, patient responses) affect outcome for a typical aSAH patient was created. Each node of the DAG representing a one or more variables in the problem was associated with relevant definitions, and an explanation of reasons for inclusion and exclusion. The DAG was inspected for causality sequence and the biological plausibility of each variable.
Results: Figure 1. DAG representing assumptions about how variables causally relate to Outcome acknowledging that each node is informed by everything known to that time. Unobserved variables and selection are acknowledged though (U-0) and (D-Admit). HTN- hypertension, WFNS- World Federation of Neurological Sciences, mRS- modified Rankin Score, CVS- cardiovascular, GCS- Glasgow Coma Scale, Admit- Admission, H’cephalus- Hydrocephalus, ICP-intracranial pressure, DCI-delayed cerebral ischaemia, Rx-treatment, D-decision.
Conclusions: The described DAG is designed to help guide data collection and analysis to evaluate the effect of treatments using observational data
Disclosures of Interest: No
Abstract N°: 1461
IMPLEMENTATION OF INTERACT3 BUNDLE OF CARE FOR INTRACEREBRAL HAEMORRHAGE PATIENTS IN LATIN AMERICA: A DELPHI STUDY
Maria Ignacia Allende Echanez1, Paula Muñoz Venturelli*1,2,3, Francisca Mccawley1,4, Francisca Bascur Gutiérrez1, Craig Anderson2, Menglu Ouyang2, Baltica Cabieses Valdes5, Alexandra Obach5, Vanessa Cano Nigenda6, Antonio Arauz Gongora7
1Centro de Estudios Clínicos, Facultad de Medicina Universidad del Desarrollo, Las Condes, Chile,2The George Institute, University of New South Wales, Barangaroo, Australia,3Departamento de Neurología y Psiquiatría, Facultad de Medicina Clínica Alemana Universidad del Desarrollo, Vitacura, Chile,4Facultad de Ciencias de la Salud Blanquerna, Universitat Ramón Llull, Barcelona, Spain,5Centre for Global Intercultural Health (CeSGI), Universidad del Desarrollo, Las Condes, Chile,6Instituto nacional de Neurología y Neurocirugía, Departamento de Neurología, Ciudad de México, Mexico,7Instituto nacional de Neurología y Neurocirugía, General director of the institute, Ciudad de México, Mexico
On behalf of:
Background and aims: Recently, the INTERACT3 care bundle results showed improved clinical outcomes for patients with intracerebral haemorrhage (ICH), however its implementation in Latin American countries (LAC) faces unique challenges. We aimed to establish recommendations for the integration of the INTERACT3 care bundle across LAC.
Methods: A Three-phase Delphi study was performed among 32 healthcare workers from 14 LAC. A comprehensive review of the INTERACT3 process evaluation generated the first statements across 7 domains: training, resources and infrastructure, education to patients, blood pressure, temperature, glycemic control, and reversal of anticoagulation. Panelists rated statements in each round, with the final round allowing for ranking. Consensus threshold was predefined at 75%.
Results: All 43 statements reached consensus by the conclusion of the third round, and an additional 12 new statements emerged throughout the rounds. The highest-ranked statements in each domain emphasized critical aspects, placing particular emphasis on ensuring minimal resources for successful implementation. Key priorities included continuous training for all healthcare workers involved in managing ICH patients, the establishment of protocols aligned with available resources, and fostering a collaborative approach through the creation of communication channels between professionals and healthcare institutions support networks. Notably, statements related to anticoagulation reversal were the highest ranked among all statements highlighting the limited availability of treatments and the overall lack of knowledge regarding anticoagulation reversal in the region.
Conclusions: The findings of the study provide key aspects to address integration of the INTERACT3 care bundle in LAC, in effort to mitigate the disparities in ICH outcomes.
Disclosures of Interest: Yes PMV receives research grants from ANID Fondecyt Regular 1221837, Pfizer and Boehringer Ingelheim.
Abstract N°: 1538
PRIMARY VENTRICULAR HEMORRHAGE: CLINICAL CHARACTERISTICS AND OUTCOMES
1National Cerebral and Cardiovascular Center, Department of Cerebrovascular Medicine, Suita, Osaka, Japan,2National Cerebral and Cardiovascular Center, Department of Neurology, Suita, Osaka, Japan,3National Cerebral and Cardiovascular Center, Department of Neurosurgery, Suita, Osaka, Japan
On behalf of: Ryo Usui
Background and aims: Primary intraventricular hemorrhage (PIVH), defined as intracerebral hemorrhage (ICH) confined to intraventricular system (IVH) of unknown cause, is rare and poorly understood.
Methods: We performed a retrospective study in the prospectively collected single-center stroke registry between 2010 and 2022. Patients with ICH were classified as non-IVH, PIVH, and secondary-IVH defined as IVH with known causes. The unfavorable outcome was defined as mRS 4–6 at discharge. Hematoma volume was assessed by visual-ratings as IVH score on initial CT. The demographic and clinical profile of PIVH were compared to those with non-IVH, using logistic regression analysis. Factors associated with unfavorable outcome were evaluated, using univariate analysis.
Results: Among 2,310 patients with ICH, 2,285 patients (98.9%) were classified as non-IVH (female 43.2%, age 71±13), 23(1.0%) as PIVH (43.5%, 73±11), and 2(0.1%) as secondary-IVH. Compared to non-IVH, PIVH had a higher frequency of diabetes (PIVH 34.8% vs non-IVH 16.2%), atrial fibrillation (34.8% vs 12.5%), prior antithrombotic agents (65.2% vs 27.4%), and lower diastolic blood pressure (median 91[interquartile range 75-103] vs 99[84-112]) and initial NIHSS (4[0-11] vs 13[5-23]) (all p<0.05). Prior antithrombotic agents were independently associated with PIVH (adjusted OR 3.44[1.21-9.80]) after adjusting for variables showing significant differences in univariate analysis. There was no difference in the frequency of unfavorable outcome (43% vs 62%, p=0.09). Initial NIHSS and IVH score were each associated with unfavorable outcome in PIVH (all p<0.05).
Conclusions: PIVH accounted for 1.0% of ICH and was associated with prior antithrombotic agents compared to non-IVH.
Disclosures of Interest: No
Abstract N°: 1574
CEREBRAL AMYLOID ANGIOPATHY-RELATED INFLAMMATION PRESENTED WITH REPEATED RECURRENT LOBAR INTRACEREBRAL HEMORRHAGE: A NEW ENTITY?
CHU PENG HOI*1, Wa Hou Tai2, Iek Hou Chu1
1Hospital Centre S. Januario, Neurology, Macao, China,2Hospital Centre S. Januario, Neurosurgery, Macao, China
On behalf of: Xian Lun Zhu, Ka Ming Chan, In Chao Ho, Han Tian Huang, Wai I Leong, Paulo Lo, Mat Mat Lam, Si Si Ieong, Kay Cheong Teo
Background and aims: Cerebral amyloid angiopathy (CAA) is a major cause of lobar intracerebral hemorrhage (ICH) in older adults. CAA-related inflammation (CCA-ri) is an aggressive CAA variant characterized by diffused T2-weighted white matter hyperintensity on magnetic resonance imaging with pathological evidence of vascular or perivascular inflammation. Treatment with steroids can improve the prognosis of CAA-ri. However, the diagnostic criteria of CAA-ri does not include ICH. We report two patients with CAA-ri who presented with repeated recurrent lobar ICH, with one histologically confirmed, that improved significantly after steroid treatment. The aim of this paper is to explore the possbility that repeated recurrent lobar ICH may represent a new clinical entity for CAA-ri.
Methods: Two cases were reported and review of literature were conducted.
Results: The first case is a 70-year-old man who developed four recurrent lobar ICHs in 12 months (Figure 1). Brain biopsy and histopathological study revealed characteristic findings of CAA-ri (Figure 2). Prednisolone therapy was initiated, and there was no recurrent ICH for three years. Unfortunately, the ICH recurred again two months after the reduction of prednisolone from 10mg to 7.5mg daily. In the second case, a 73-year-old man had four recurrent lobar ICHs in the previous six years. Recurrent ICH was prevented again with prednisolone therapy.
Conclusions: Repeated recurrent lobar ICH may be a new clinical entity for CAA-ri. There might be a benefit of steroid or other immunosuppressive therapy in patients with recurrent lobar hemorrhage related to CAA.
Disclosures of Interest: No
Abstract N°: 1671
THE EFFICACY OF STEREOTACTIC EVACUATION AT THE SUBACUTE PERIOD FOR PUTAMINAL HEMORRHAGE
Background and aims: We have performed stereotactic evacuation of hematoma in the subacute period for patients, who don’t require emergent surgical treatment. We evaluated the efficacy of stereotactic evacuation for putaminal hemorrhage.
Methods: 203 patients with putaminal hemorrhage retrospectively, who were admitted to our institute between 2012 and 2022, were included. Except for the patients who received emergent surgical treatment, we performed stereotactic evacuation at the subacute period for the patients whose consciousness disturbance was prolonged and/or whose neurological findings didn’t improve within 7-14 days of admission. We evaluated the efficacy of our treatment in independence 3 months after admission between the surgical and conservative groups using the FIM (Functional Independence Measure) score.
Results: Among all 203 putaminal hemorrhage patients, 65 patients were surgically treated. 36 of 65 patients underwent stereotactic evacuation 7-14 days after admission. Focusing on the patients who suffered putaminal hemorrhage of CT classification IVa (hematoma extended to anterior and posterior internal capsule without intraventricular hematoma; n=28), there were some advantages of stereotactic evacuation; the average change of cognitive FIM score was 8.9±1.7 in the surgical group (n=14). While the conservative treatment group (n=14) showed an average change of cognitive FIM score of 3.3±1.6 (p=0.14).
Conclusions: Compared to conservative treatment, stereotactic evacuation for putaminal ICH in the subacute period suggested the potential to improve FIM, especially cognitive FIM.
Disclosures of Interest: No
Abstract N°: 1855
EXPLORING THE PATHOPHYSIOLOGY OF INTRACEREBRAL HEMORRHAGE THROUGH PROTEOMIC ANALYSIS OF CIRCULATING EXTRACELLULAR VESICLES
Laura Casado Fernández*1, Fernando Laso1, Susana B. Bravo2, Blanca Fuentes1, Elisa Alonso-López1, Jorge Rodriguez-Pardo1, Gerardo Ruiz-Ares1, Exuperio Díez Tejedor1, María Gutiérrez-Fernández1, Maria Alonso de Leciñana1
1La Paz University Hospital, Neurological Sciences and Cerebrovascular Research Laboratory, Department of Neurology and Stroke Centre, Neurology and Cerebrovascular Disease Group, Neuroscience Area, Madrid, Spain,2Foundation Health Research Institute of Santiago de Compostela (IDIS), Proteomic Unit, Santiago de Compostela, Spain
On behalf of:
Background and aims: The protein cargo of extracellular vesicles (EVs) may reflect the mechanisms underlying damage and repair following intracerebral hemorrhage (ICH). To ascertain whether circulating EVs could serve as biomarkers for these processes, we aimed to explore the protein content of EVs derived from individuals experiencing acute ICH in comparison to healthy subjects.
Methods: Patients with acute non-traumatic supratentorial ICH, without previous disability or severe comorbidities were included. Demographic and clinical data were recorded. EVs were obtained from blood samples within 24-48 hours from symptom onset. Healthy subjects who gave their informed consent were recruited as control group. EVs were isolated from serum by precipitation and immunoisolation. Protein content was analysed with quantitative mass spectrometry (DIA-SWATH) and compared between groups (differential expression defined as Fold-change>2 or <0.5 and p<0.05).
Results: Fourty-eight ICH patients and ten controls were included. There were 212 proteins identified in EVs from the global cohort. Seventeen were exclusive to the ICH group, mainly immunoglobulins and complement activation-related proteins. In the differential expression analysis of the proteins present in both groups, there were 35 up-expressed and 53 down-expressed proteins in the ICH group compared to controls. In the ICH group there was a higher expression of proteins associated to coagulation, complement activation and the innate immune system, and lower expression of proteins related to lipid metabolism, transport and cell-cell signalling.
Conclusions: During the acute phase of ICH, circulating EVs show differential proteomic signature. These findings may support the role of circulating EVs as biomarkers of the pathophysiological processes underlying ICH.
Disclosures of Interest: No
Abstract N°: 1887
OPTIC NERVE SHEATH DIAMETER DOES NOT CORRELATE WITH INTRACRANIAL PRESSURE IN PATIENTS WITH INTRACEREBRAL HEMORRHAGE
Mario Trappe1, Ibrahim Allam1, Lars-Olav Harnisch2, Onnen Mörer2, Tammam Abboud3, Silvia Hernandez3, Ilko Maier*1
1University Medical Center Göttingen, Neurology, Göttingen, Germany,2University Medical Center Göttingen, Anesthesiology, Göttingen, Germany,3University Medical Center Göttingen, Neurosurgery, Göttingen, Germany
On behalf of:
Background and aims: Multiple studies showed an association between transorbital ultrasound (toUS) measurements of the optic nerve sheath diameter (ONSD) and increased intracranial pressure (ICP). However, published measurement techniques and cut-off values vary widely casting doubt on the utility of the technique. Aim of the study was to investigate longitudinal changes of ONSD in patients with intracranial hemorrhage (ICH).
Methods: Monocenter, prospective, longitudinal study with serial toUS in patients with ICH on two neurointensive care units receiving invasive ICP-monitoring. We measured diameter of the optic nerve (ON), the ONSD from the inner- (irONSD) and outer reflex of the dura mater (orONSD) 3 mm behind the optic disc after insertion of invasive ICP-monitoring once daily for at least 4 consecutive days (see Fig. 1). We fitted linear mixed-effects models for all diameters.
Results: Fifty-five patients with a median of 6 (IQR, 4-7) consecutive toUS-examinations resulting into 660 ON and ONSD measurements, respectively, were included. With a median ICP of 9.50 (IQR, 2-93) mmHg, the mean diameter of the ON was 3.13±0.36, of the irONSD 5.53±0.49 and orONSD 6.68±0.57 mm. Among the whole cohort, there was no difference of the ON/ONSD diameters in ICH patients with ICP <15, 15-20, 20-25 and >25 mmHg.There was only a weak association between orONSD diameters and ICP (β 0.008, CI95% 0.001-0.015, p=0.027). Change in ON/ONSD was not associated with change in ICP nor predicted significant ICP-peaks (p=n.s.).
Conclusions: Our data indicates that ON/ONSD measurements are not a reliable marker to determine or to predict increased ICP in ICH-patients.
Disclosures of Interest: No
Abstract N°: 1918
GLYCAEMIC STATUS PROFILING THROUGH CONTINUOUS GLUCOSE MONITORING IN SPONTANEOUS SAH AND ASSOCIATION WITH FUNCTIONAL OUTCOME
Daniel Santana*1, Laura Llull2, Alejandra Mosteiro3, Carlos Laredo4, Leire Pedrosa5, Ricard Mellado6, Gabriel Pujol6, Antonio Lã³pez-Rueda7, Ramon Torné3, Sergio Amaro2
1Hospital Germans Trias i Pujol, Neurology, Badalona, Spain,2Hospital Clínic de Barcelona, Neurology, Barcelona, Spain,3Hospital Clínic de Barcelona, Neurosurgery, Barcelona, Spain,4August Pi i Sunyer Biomedical Research Institute (IDIBAPS), Magnetic Resonance Core Facility, Barcelona, Spain,5August Pi i Sunyer Biomedical Research Institute (IDIBAPS), Barcelona, Spain,6Hospital Clínic de Barcelona, Anaesthesiology, Barcelona, Spain,7Hospital Clínic de Barcelona, Neurorradiology, Barcelona, Spain
On behalf of:
Background and aims: Glycaemic dysregulations in the acute phase of spontaneous SAH are related to worse prognosis, although studies are based on finger-prick testing with low temporal resolution. Continuous Glucose Monitoring devices (CGM) allow frequent and automated measurements, and assessment of novel glycaemic indicators. We assessed the feasibility and prognostic relevance of CGM-derived metrics obtained during the Early Brain Injury (EBI) phase of SAH.
Methods: Single-center, prospective cohort of 66 spontaneous SAH patients (50% female, mean age 55 years). CGM was placed upon admission and kept for at least 72h. Demographics, SAH severity indicators and CGM indicators were prospectively collected. The association of CGM indicators with unfavourable outcome (Rankin>2) at 3 months was assessed with logistic regression models adjusted by age, baseline WFNS and modified Fisher scores and premorbid Rankin score.
Results: In adjusted analysis, several CGM-derived indicators were associated with unfavourable outcome including higher mean glucose [adjusted-OR (95% CI)=1.06 (1.01-1.11)], time spent above 140mg/dL [1.08 (1.01-1.14)], high blood glucose index [9.19 (1.63-59.85)], glucose management indicator [10.86 (1.33-88.96)] and J index [1.24 (1.04-1.48)]. From these indicators, high blood glucose index -a measure of hyperglycaemia load and glucose variability- had the highest prognostic accuracy. CGM-derived indicators outperformed standard finger-prick measures and no device-related safety concerns were detected.
Conclusions: CGM seems a feasible and safe tool in acute phase of SAH and outperforms traditional finger-prick testing in assessing glycaemic status. This could eventually lead towards a more personalized management of SAH sufferers during the EBI period and to improve glucose management protocols.
Disclosures of Interest: No
Abstract N°: 1941
HIGH MIP-1A/CCL3 AND EOTAXIN/CCL11 CONCENTRATIONS ARE ASSOCIATED WITH SURVIVAL IN ACUTE INTRACEREBRAL HEMORRHAGE
Mikhail Fidler1, Mikhail Martynov1,2, Ivan Shchukin1,2, Vladimir Chubykin1, Ivan Koltsov*1,2
1Pirogov Russian National Research Medical University, Moscow, Russian Federation,2Federal Center of Brain Research and Neurotechnologies, Moscow, Russian Federation
On behalf of:
Background and aims: Chemokines play a significant role in brain injury and recovery in acute intracerebral hemorrhage (ICH). Proinflammatory chemokines MIP-1α/CCL3 and eotaxin/CCL11 are potent attractants of immune cells. Previously, it was shown that MIP-1α concentration is associated with poor perihematomal perfusion (Shchukin et al., 2021). This study aimed to evaluate the complex interactions between MIP-1α and eotaxin in ICH.
Methods: A post-hoc analysis of 24 patients with acute hypertensive ICH was performed. MIP-1α and eotaxin blood concentrations at admission were measured using a multiplex immunoassay. ICH outcome data were obtained from medical records. The study was approved by the Local Ethics Committee.
Results: Complex multidirectional relationships between different levels of systemic concentrations of these chemokines were identified. An optimal chemokine profile in ICH at admission was computed. A combination of MIP-1α concentration of >15 pg/ml and concentration of >200 pg/ml was associated with better outcomes. A logistic regression model confirmed the prognostic significance of the estimated threshold values. The combination of high levels of MIP-1α and eotaxin at admission was associated with a significant increase in the likelihood of 28-day survival in ICH (OR 45.000, 95% CI 2.160 – 937.321, p=0.014).
Conclusions: Blood chemokine concentrations may be promising predictors of ICH functional outcomes. The combination of high MIP-1α concentration and high eotaxin concentration may be helpful in predicting survival in acute ICH.
Disclosures of Interest: No
Abstract N°: 2010
THE HEMORRHAGE-HEART SYNDROME: PREDICTORS OF CARDIAC TROPONIN-ELEVATION IN PATIENTS WITH ACUTE INTRACEREBRAL HEMORRHAGE
Felix Hess*1, Enayatullah Baki1, Julian Mcginnis1, Tun Wiltgen1, Christian Maegerlein2, Jan Kirschke2, Claus Zimmer2, Bernhard Hemmer1, Silke Wunderlich1, Mark Mühlau1
1Klinikum rechts der Isar der Technischen Universität München, Neurology, München, Germany,2Klinikum rechts der Isar der Technischen Universität München, Neuroradiology, München, Germany
On behalf of:
Background and aims: Myocardial damage, indicated by an elevation of high-sensitive Troponin (hs-cTnT), is a frequent stroke-related complication and the most common phenotype of stroke-heart syndrome. Most studies investigated patients with ischemic stroke, but only little is known about its occurrence in patients with intracerebral hemorrhage (ICH). This study aimed to evaluate the frequency of myocardial injury and associated lesion patterns in ICH patients.
Methods: Our retrospective analysis included 322 ICH patients. Datasets were categorized according to peak hs-cTnT level (⩽0.0014ng/ml vs. >0.0014ng/ml). Changing pattern as a biomarker of acute myocardial injury was defined as a 50% rise or fall of hs-cTnT. We used nnU-Net, a deep-learning-based framework, for automatic lesion segmentation.
Results: The prevalence of hs-cTnT elevation was 63% (20% changing pattern). It was associated with age, stroke severity, pre-existing cardiac disease and midline shift (p <0.05). Patients with Troponin elevation had a worse outcome and higher mortality (p <0.05). Elevation of hs-cTnT was associated with abnormal electrocardiographic findings and a higher frequency of adverse cardiac events (p <0.01). Compared to stable troponin elevation, hs-cTnT-changing pattern correlated with higher scores on the NIHSS, worse outcomes, larger lesion volumes, and midline shift (p <0.05), but not with pre-existing cardiac diseases.
Conclusions: Myocardial injury is a frequent complication of ICH. Especially acute myocardial injury, indicated by a changing pattern of hs-cTnT, which is associated with poor functional outcomes and higher mortality, primarily occurs in patients with severe, space-occupying ICH and is less dependent on premorbid cardiac status.
Disclosures of Interest: No
Abstract N°: 2032
CEST-MRI CHARACTERIZES PH CHANGES IN A PATIENT WITH STROKE DUE TO INTRACEREBRAL HAEMORRHAGE – CASE REPORT FROM A PILOT STUDY
Alicia Cronin1, Robert Bartha1, Sebastian Fridman2, Alexander Khaw*2
1Western University, Medical Biophysics, Robarts Research Institute, Schulich School of Medicine & Dentistry, London, Canada,2Western University, Clinical Neurosciences, Schulich School of Medicine & Dentistry and Lawson Research Institute, London, Canada
On behalf of:
Background and aims: Determinants of the extent and course of perifocal oedema, a predictor of functional outcome after acute intracerebral haemorrhage (ICH) and a potentially modifiable biomarker, are poorly understood. We sought to test feasibility of chemical exchange saturation transfer (CEST) MRI for characterizing pH alterations in patients with acute stroke from ICH.
Methods: Adult patients with first-ever ICH underwent 7T-MRI at 48-96 hours after stroke onset and a second scan at 10 days or before discharge. CEST images were acquired at 50 frequency offsets (1.2-6.6 ppm), with an isotropic resolution of 3.3 mm3. pH-weighted CEST contrast can be generated using a ratiometric contrast, amine/amide concentration independent detection (AACID). The AACID difference map was calculated by subtracting the AACID map from timepoint 1 from timepoint 2. We present a first single case of ‘pH imaging’ in a patient with right temporal ICH.
Results: The figure illustrates the ICH with hypointense susceptibility artifacts (haematoma deoxyhaemoglobin) and hyperintense perifocal oedema on FLAIR which extends from the right lateral ventricle to the cortex (A). In the AACID difference map (C) calculated from the CEST-imaging single slices (B) at the same level as the FLAIR slice, positive AACID difference indicates lower pH corresponding with the haematoma area, whereas FLAIR-hyperintense parenchyma suggestive of perifocal oedema did not differ from the ICH-remote ipsilateral or the unaffected contralateral parenchyma.
Conclusions: CEST imaging on a 7T magnet is feasible in stroke patients with ICH and may visualize shifts in brain parenchyma acidity within and around the haematoma.
Disclosures of Interest: No
Abstract N°: 2148
FACTORS ASSOCIATED WITH HEMATOMA EXPANSION IN DEEP VERSUS LOBAR INTRACEREBRAL HEMORRHAGE
Francesco Arba*1, Jawed Nawabi2, Qi LI3, Federico Mazzacane4, Giacomo Urbinati5, Ilaria Casetta6, Enrico Fainardi7, Alessandro Padovani8, Andrea Zini9, Andrea Morotti8
1Careggi University Hospital, Firenze, Italy,2Charité – Universitätsmedizin Berlin, Berlin, Germany,3Anhui University, Hefei, China,4Neurological Institute Foundation Casimiro Mondino, Italy,5Dibinem Unibo, Bologna, Italy,6Ospedale Sant'Anna, Ferrara, Italy,7University of Florence, Firenze, Italy,8University of Brescia, Brescia, Italy,9Major Carlo Alberto Pizzardi Hospital, Bologna, Italy
On behalf of:
Background and aims: Identification of factors associated with hematoma expansion (HE) in patients with primary intracerebral hemorrhage (ICH) is crucial for optimization of their management and therapeutic strategies. We investigated whether such factors differed in supratentorial ICH location, comparing deep versus lobar ICH.
Methods: Retrospective analysis of patients with primary ICH admitted at six Hospitals. HE was defined as growth >=6 mL and/or >=33% from baseline to follow-up imaging. We evaluated independent associations using multivariable logistic regression models adjusted for age, sex, baseline hematoma volume, anticoagulants and antiplatelets use and other relevant confounders identified in univariate analyses.
Results: A total of 1644 patients were included (mean age 70 years, 57% males) of whom 948 (58%) had deep and 696 (42%) had lobar ICH. Age and baseline hematoma volume were shared predictors of HE in lobar and deep ICH. Conversely, anticoagulant use (OR=1.65;95%CI=1.07-2.56) and lower Glasgow Come Scale (OR=0.91;95%CI=0.86-0.96) were associated with HE only in lobar ICH, whereas the associations between systolic blood pressure >140 mmHg (OR=1.62;95%CI=1.08-2.42), history of diabetes (OR=1.83;95%CI=1.29-2.61) and HE were observed only in patients with deep ICH.
Conclusions: We found some shared factors associated with HE between deep and lobar ICH, whereas other factors appear to be location-specific. Our findings may reflect different physiopathology underlying different location of ICH and might improve stratification of HE risk in clinical practice or randomized trials.
Disclosures of Interest: No
Abstract N°: 2230
SENTINEL HEADACHE BEFORE RUPTURE OF SACCULAR INTRACRANIAL ANEURYSMS
Elena Lebedeva*1, Alexandr Shamov2, Vladimir Kolotvinov2, Denis Gilev3, Jes Olesen4
1the Ural State Medical University, Yekaterinburg, Russia, International Medical Centre “Europe-Asia”, Yekaterinburg, Russia, Yekaterinburg,2City Clinical Hospital №40, Neurosurgery, Yekaterinburg,3Ural Federal University, Economics, Yekaterinburg, Russian Federation,4Copenhagen University, København, Denmark
On behalf of:
Background and aims: Sentinel headache is a warning symptom and represents a new type of headache or a previous type of headache with altered characteristics (severe intensity and frequency) which arises before stroke or subarachnoid haemorrhage (SAH). The exact type and distinctive features of this headache were, however, not studied before the first-ever aneurysmal SAH.
Methods: This cross-sectional study included 181 patients (93 females and 88 males, mean age: 43.4) with first-ever ruptured saccular intracranial aneurysms (SIA). All patients were professionally interviewed soon after admission to the hospital about unusual headaches before rupture of SIA and these headaches were compared with past usual headaches during one year before rupture. Patients with speech and memory problems were excluded. Diagnoses were made according to the International Classification of Headache Disorders 3rd edition criteria. Aneurysms were diagnosed by conventional cerebral angiography.
Results: Sentinel headache was found in 43 out of 181 patients (23.7%) with ruptured SIA, 65% females, mean age: 43.8 years. Sentinel headache was of a migraine-like type in most cases (76.7%). Sentinel headache developed during the month before rupture of SIA (76.7%), usually 2-4 weeks before rupture (39.5%) and in the remaining patients during 2-3 months before rupture. Sentinel headache had localization in frontotemporal (48.8%) or occipital (23.3%) regions, was unusually severe (69.8%), constant (27.9%) or attack-wise (72.1%) with high frequency and no effect of painkillers (45.5%).
Conclusions: The sudden onset of unusually severe migraine-like headaches in patients after 40 years of age should require the exclusion of sentinel headache and intracranial aneurysm by additional examinations.
Disclosures of Interest: No
Abstract N°: 2325
COLLAGEN BREAKDOWN PRODUCTS AS BIOMARKERS FOR EFFICACY OF ACETYLSALICYLIC ACID TREATMENT IN PATIENTS WITH INTRACRANIAL ANEURYSMS
Katharina Hackenberg*1, Judith Dremel1, Oluwadamilola Akanji1, Amr Abdulazim1, Gabriel Rinkel1, Nima Etminan1
Background and aims: Biomarkers for the structural stability of unruptured intracranial aneurysms (UIA) are needed. The main molecular constituent of IA is type I collagen, which undergoes permanent turnover. Our previous study indicated that collagen breakdown products were elevated in patients with unstable compared to stable IA. Acetylsalicylic acid (ASA) had a protective effect on IA stability in previous studies. We studied if collagen breakdown products could serve as biomarkers for the efficacy of ASA treatment and IA stability.
Methods: This ongoing prospective, longitudinal study includes patients with UIA. We determined C-telopeptide (CTx) and c-terminal-telopeptide (ICTP) as breakdown products of collagen in venous blood at baseline, at 3, 6, 12, 24 months.
Results: Since 04/2022, we included 53 patients with UIA. Mean age was 57.2±11.3 years, 37(70%) were female. Mean UIA size was 3.6±1.4mm. Twenty-seven (51%) patients were under ASA treatment at baseline. Regarding CTx/ICTP 44/53(83/100%) samples were analyzed at baseline, 35/48(66/91%) at 3, 34/46(64/87%) at 6 months.
In Figure 1 CTx and ICTP levels according to ASA treatment are shown. In female patients with ASA intake CTx levels were lower compared to no intake at any time point (Figure 2).
Conclusions: Our preliminary data provide molecular evidence that risk factor modification might result in stabilization of UIA and that CTx may serve as a biomarker for efficacy of risk factor treatment in female patients. Larger sample sizes and longer follow-up are needed to validate our findings.
Disclosures of Interest: No
CTx(a), ICTP(b) levels according to ASS treatment.
CTx levels in female(a), male(b) patients according to ASS treatment.
Abstract N°: 2854
POPULATION CHARACTERISTICS OF PRIMARY INTRACEREBRAL HAEMORRHAGE IN RELATION TO ANTICOAGULATION STATUS
Thomas Cloney*1, Joan Mccormack2, Olga Brych2, Ronan Collins2,3, Tim Cassidy2,4, Joseph Harbison1,2,5
1St James' Hospital, Neurovascular Department, Dublin, Ireland,2National Office of Clinical Audit, Irish National Audit of Stroke, Dublin, Ireland,3Tallaght University Hospital, Medicine for Older Persons & Neurovascular Department, Dublin, Ireland,4St Vincents University Hospital, Stroke, Dublin, Ireland,5Trinity College Dublin, Associate Professor Medical Gerontology, Dublin, Ireland
On behalf of:
Background and aims: Anticoagulation is recognised to be associated with increased risk of haemorrhagic stroke but how do the characteristics of people with haemorrhagic stroke on Anticoagulant therapy differ from those not receiving anticoagulation?
Methods: National data on patients from 2017-2022, admitted with Primary Intracerebral Haemorrhage (ICD 10 classification i61) (PICH) were extracted from the Irish National Audit of Stroke (INAS) database for analysis following ethical approval. Data, including modified Rankin Scale (mRS) at discharge, were identified, for patients on no anti thrombotic therapy (ATT), Direct Oral Anticoagulants (DOAC) and Warfarin.
Results: Data on 3477 patients with full medication data were identified. Forty were excluded for being on dual antiplatelet/anticoagulant therapy and 36 for being on antiplatelet therapy. Results are in Table 1 below.
Compared to untreated patients, those on anticoagulants were significantly older. (DOAC: Chi Sq 91.2 p<0.0001. Warfarin: Chi Sq 13.3, p=0.0002). Patients on Warfarin were more likely to be male (Chi Sq 7.8, p=.005) and had a higher median discharge mRS. Patients on anticoagulants were more likely to die (mRS =6) (DOAC: Chi Sq 6.9, p=0.009. Warfarin Chi Sq 9.1, p=0003).
Conclusions: Patients suffering PICH on Anticoagulants are older than untreated patients and typically suffer worse outcomes.
Disclosures of Interest: No
Abstract N°: 2870
THE ROLE OF GUT MICROBIOTA METABOLITES IN INTRACRANIAL ANEURYSMS; A SYSTEMATIC REVIEW
Jad El Masri*1,2,3, Rahaf Al Sabsabi3, Maya Ghazi1,3, Abdo Jurjus1
1American University of Beirut, Beirut, Lebanon,2Paris 12 Val de Marne University, Créteil, France,3Lebanese University - Hadat Campus, Beirut, Lebanon
On behalf of:
Background and aims: Several studies investigated the implication of the gut microbiota (GM) in the formation and progression of intracranial aneurysms (IA), suggesting a key role for GM metabolites in aneurysmal pathogenesis and prognosis. This systematic review aims to collect key findings concerning the role of GM-related metabolites in IA development and rupture.
Methods: A PubMed, Medline, Embase, and Web of Science database search was conducted in accordance with PRISMA guidelines for systematic reviews, targeting all studies assessing the role GM in IA till 2023.
Results: Of 292 papers, data from 7 articles were included. According to established sources, unruptured intracranial aneurysms (UIA) development was accompanied by gut dysbiosis, a decrease in the intestinal bacteria’s biosynthesis of many amino acids (threonine, lysine. . .), and the depletion of several gut-derived circulating amino acids (taurine, L-histidine. . .) and fatty acids (linoleic acid). The metabolism of propionate was also reduced while peptidoglycan synthesis was enriched in symptomatic UIAs. Moreover, the administration of Hungatella hathewayi or taurine decreased the rate of aneurysmal rupture and IA’s incidence by reducing VSMCs apoptosis, ameliorating MMP activation, and alleviating the strong inflammatory response in UIA. This response was usually induced by the elevated TNF-α and IL-6 levels and the accumulation of macrophages and neutrophils in perivascular spaces. Furthermore, the downregulation of CAV1 and MYH11 genes associated with IA formation was reversed after gut probiotics supplementation.
Conclusions: The alteration of the gut microbial composition and the consequent changes in metabolic pathways and inflammatory responses play a potentially important role in IA development, prognosis, and rupture.
Disclosures of Interest: No
Abstract N°: 3022
EXPERIMENTAL SAH IN RATS. CHANGES IN THE CELLULAR RESPONSE OF THE HIPPOCAMPUS DEPENDING ON DRUG THERAPY
Oleksii Polkovnikov*1, Sergiy Tertyshnyi1
1Zaporizhzhia State Medical and Pharmaceutical University, Ukraine, Neurosurgery, Zaporizhzhia, Ukraine
On behalf of:
Background and aims: Immunohistochemical study of rat hippocampal neurons and astocytes at different time-points of experimental SAH treated with acelysin and nimotop.
Methods: SAH was modeled according to R.V. Dudhani. Using 35 Wistar rats which were divided into 7 groups. The 1 and 2, for 4 and 7 days respectively received acelysin at a dose of 15 mg/kg once a day; 3 and 4 received nimodipine at a dose of 0.3 mg/kg every 8 hours. In 5, 6 (control), SAH was modeled without treatment, 7 intact animals. Hippocampal CA1 fields were studied immunohistochemically evaluating the expression of CASP3, NeuN, GFAP by the relative area of immunostaining in ImageJ.
Results: CASP3 expression in hippocampal neurons increases by 2.3 and 5.7 times on day 4 and by 1.8 and 3.9 times on day 7 compared to intact group. GFAP expression increases in all observation groups compared to intact animals with the maximum values in the 5 gr.– by 8.14 times. The dynamics of NeuN expression in hippocampal neurons when using acelisin and nimotop corresponds to the inverse dynamics of CASP3 expression. The NeuN expression increases maximally on the 7 day of acelisin use and is equal to 91.76% of the intact group values.
Conclusions: The use of acelisin and nimotop leads to a decrease in the expression of CASP3 in the hippocampus, which reflects the positive effect of the therapy on preventing death of hippocampal neurons. The results of experimental study provide a theoretical justification of the feasibility of including used drugs in the basic therapy of SAH.
Disclosures of Interest: No
Abstract N°: 3276
THE RELATIONSHIP BETWEEN GUT MICROBIOTA COMPOSITION AND INTRACRANIAL ANEURYSMS: A SYSTEMATIC REVIEW
Jad El Masri*1,2,3, Rahaf Al Sabsabi3, Maya Ghazi1,3, Abdo Jurjus1
1American University of Beirut, Beirut, Lebanon,2Paris 12 Val de Marne University, Créteil, France,3Lebanese University - Hadat Campus, Beirut, Lebanon
On behalf of:
Background and aims: Several studies investigated the role of gut microbiota (GM) in the formation and progression of aneurysms, suggesting a key role for dysbiosis in its pathogenesis and prognosis. This systematic review aims to collect key findings concerning the role of GM in intracranial aneurysm (IA) development and its rupture.
Methods: A PubMed, Medline, Embase, and Web of Science database search was conducted in accordance with PRISMA guidelines for systematic reviews, targeting all studies assessing the GM’s role in IA till 2023.
Results: Data from 6 out of 292 non-duplicated studies were included. Based on the published literature, Odoribacter splanchnicus was increased in unruptured intracranial aneurysms (UIAs), Lawsonibacter was positively correlated with aneurysmal diameter, and ruptured IAs were concomitant with Campylobacter ureolyticus abundance. On the other hand, Ruminiclostridium and Burkholderia were negatively correlated with aneurysmal diameter. Oscillospira and Paraprevotella genera were associated with a reduced UIA risk. Furthermore, the administration of Hungatella hathewayi probiotic prevented IA development and rupture by several mechanisms: ameliorating MMP-9 activity in cerebral arteries, reducing TUNEL-positive VSMCs apoptosis, enhancing extracellular matrix remodeling, and alleviating the strong inflammatory response induced by the amplified TNF-α and IL-6 levels in case of a UIA. Moreover, subarachnoid hemorrhage (SAH) risk in IAs was increased with Streptococcaceae family abundance and decreased with the Porphyromonadaceae family and Bilophila genus abundance.
Conclusions: IA is accompanied by an increase and a decrease in specific intestinal bacteria, affecting the aneurysm’s prognosis and rupture. Therefore, the alteration of the gut microbial composition paves the way for promising preventive and therapeutic approaches in IA cases.
Disclosures of Interest: No
Abstract N°: 3324
OUTCOMES OF INTRACEREBRAL HEMORRHAGE TREATMENT REQUIRING MECHANICAL VENTILATION: SINGLE CENTRE EXPERIENCE OF EARLY SURGICAL ICH EVACUATION
nika zorko garbajs*1, Nataša Milivojević1
1Neurology Clinic, vascular neurology, Ljubljana, Slovenia
On behalf of:
Background and aims: Efficacy of early ICH surgery is controversial, with conflicting results of clinical trials. The aim of this retrospective study was to assess relevant critical care outcomes in patients presenting with symptomatic spontaneous intracerebral hemorrhage depending on neurosurgical treatment.
Methods: We retrospectively included adult spontaneous supratentorial ICH patients requiring mechanical ventilation admitted to our tertiary center from January 1, 2014, through December 31, 2019. Patients with catastrophic, surgically unattainable ICH, or surgery > 24 hours post ictus were excluded. We abstracted patient demographic data, surgical treatment, and outcome data.
Results: A total of 1228 patients with ICH were admitted to our institution in the study period. 177 met eligibility criteria. The mean age at admission was 64 years, 75 (42%) patients were female. 117 (66.1%) patients had a history of arterial hypertension, 53 (29.9%) had used anticoagulant or antiplatelet drugs. 81 (45.8%) had EVD placement. 48 (27.7%) patients died, 25 patients (14.5%) had good outcome (mRS 0-3) at discharge. The mean ICU LOS was 13.8 ± 10.6 days, and the mean hospital LOS was 31.8 ± 29.2 days. 104 (58.8%) had surgical ICH evacuation, the rest had best medical treatment with or without EVD placement. There was significantly shorter ICU (p=0.011, 95% CI 2.39-18.64) and lower mortality (p<0.001, 95% CI 0.190-0.465).
Conclusions: There is a role of surgical ICH evacuation in selected patient, as it can reduce ICU LOS and lower mortality.
Disclosures of Interest: No
Abstract N°: 3339
IDENTIFICATION OF INTRACRANIAL HEMORRHAGE PATIENTS AT RISK OF BRAIN DEATH IN TELESTROKE
Daniela Schoene*1, Martin Arndt1, Konrad Pleul2, Eyad Altarscha1, Timo Siepmann1, Kristian Barlinn1
1Faculty of Medicine and University Hospital Carl Gustav Carus, TU Dresden, Department of Neurology, Dresden, Germany,2Deutsche Stiftung Organtransplantation (DSO), Frankfurt am Main, Germany
On behalf of:
Background and aims: Given the global shortage of available organs, proper identification of patients at risk of brain death is essential. We aimed to investigate how frequently patients at risk of brain death were identified among patients with intracranial hemorrhages (ICH) within a telestroke network.
Methods: We analyzed data from our telestroke network (SOS-TeleNet), which comprises 13 spoke hospitals without on-site neurology services. We identified patients who died from non-traumatic ICH, were mechanically ventilated and had no recorded contraindications for organ donation. Patients not initially evaluated for brain death were retrospectively reassessed by expert intensivists to determine the potential for impending brain death during hospitalization, based on available clinical and neuroimaging data.
Results: Between 01/2019 and 12/2022, 170 patients died from non-traumatic ICH in the spoke hospitals of our telestroke network (mean age 82.1±8.9 years, 60% women). Majority of patients had ICH (85%), followed by subdural hematoma (8%) and subarachnoid hemorrhage (7%). Among these, 27 patients (15.9%) were mechanically ventilated. None of the patients were diagnosed with brain death, nor did any undergo deceased organ donation. Upon retrospective reassessment, impending brain death was deemed possible in 7/170 patients (4.1%, 95%CI 1.9-8.4%). No justifications for omitting brain death evaluations in these cases were documented.
Conclusions: There might be an under-recognition of patients progressing to brain death within spoke hospitals of a telestroke network, despite a low number of cases identified.
Disclosures of Interest: Yes DS received funding from the German organ procurement organization (DSO). KP served as a paid employee for the DSO. KB served as a paid consultant for the DSO. The other authors declare that they have no competing interests.
E-Poster – Imaging
Abstract N°: 183
COMPARISON OF OUTCOMES IN PATIENTS WHO UNDERWENT EVT USING DIFFERENT PERFUSION MODALITIES
Jiali Gao*1, Li'an Huang1
1The First Affiliated Hospital of Jinan University, Neurology, Guangzhou, China
On behalf of:
Background and aims: Advanced perfusion modalities are increasingly popular for various diseases. However, few studies have focused on contrasting perfusion patterns. Compare the time efficiency and clinical outcomes of patients with acute ischemic stroke (AIS) who underwent endovascular treatment (EVT) before one-stop arterial spin labeling (ASL) and computed tomography perfusion (CTP) protocols.
Methods: This study retrospectively included 362 patients with AIS who have accepted EVT within 24 hours of onset from four comprehensive stroke centers between October 2017 and September 2022. After 1:1 matching of the propensity scores, 202 patients were separated into two groups: the ASL group (n=101) and the CTP group (n=101).
Results: Functional independence at 90 days (modified Rankin Scale [mRS] 0-2; p=0.574), onset-to puncture time (p=0.231), door-to-puncture time (p=0.136), and door-to-perfusion time (p=0.646) were not significantly different between the two groups. There were significant differences in EVT complications (31.7% in the ASL group vs. 14.9% in the CTP group, p=0.005) and symptomatic intracranial hemorrhage at 24 h (23.8% in the ASL group vs. 9.9% in the CTP group, p=0.008). The ischemic core volume was a common predictor of favorable outcome in both the ASL (p<0.001) and CTP (p<0.001) groups.
Conclusions: No significant differences in time efficiency and efficacy outcomes between the two groups of patients receiving one-stop ASL and CTP. The proportion of symptomatic intracranial hemorrhage at 24 hours and EVT complications of patients in CTP group were lower than ASL group. The ischemic core volume was an independent predictor for favorable outcome.
Disclosures of Interest: No
Abstract N°: 198
TRANSCRANIAL DOPPLER ULTRASOUND TO FIND PATENT FORAMEN OVALE BEFORE LEFT VENTRICULAR ASSIST DEVICE
Kelly Matmati*1,2, Ryan Tudino3,4, Sanjay Anandaram2, Patricia Oates2, Nabil Matmati1, Scott Feitell2
1St. Vincent's Medical Center, Neurology, Bridgeport, United States,2Rochester General Hospital, Neurology, Rochester, United States,3Brown University, Internal Medicine, Providence, United States,4Qunnipiac University, Frank H. Netter School of Medicine, North Haven, United States
On behalf of:
Background and aims: Detection of patent foramen ovale (PFO) has become important with the increasing use of left ventricular assist devices (LVAD) for advanced heart failure. After LVAD implantation there may be increased right to left shunting through a PFO causing hypoxemia. Pre-operative screening can identify PFO so that closure can be planned. Transcranial Doppler Ultrasound (TCD) with agitated saline has previously been shown to have high sensitivity for detection of left to right shunt compared to transthoracic echocardiography (TTE) and is less invasive than transesophageal echocardiography (TEE). This study calculates sensitivity and specificity of TCD for PFO compared to the gold standard of intraoperative identification in patients receiving LVAD implantation.
Methods: Charts of 103 patients who received an LVAD were reviewed. Rates of detection of PFO were identified with TCD with agitated saline, and TTE with agitated saline. The sensitivity and specificity of these techniques compared to the gold standard of intraoperative identification with TEE or direct visualization were calculated.
Results: TTE was found to have sensitivity of 26.7% and specificity 96.2%. TCD had sensitivity of 23.1%, and specificity 92.6%. Using TTE and TCD in combination resulted in sensitivity of 33.3%, specificity 94.0%.
Conclusions: Sensitivity of TCD and TTE in this population was lower than published rates. This could be due to the high reliability of the gold standard, intraoperative detection. Adding TCD to TTE improved sensitivity from 26.7% to 33.3%. TCD can be used to find additional PFOs that are not detected by TTE in this patient population.
Disclosures of Interest: Yes Dr. Feitell has worked as a consultant for Abbott
Abstract N°: 250
THE SPEEDY STUDY: MIDDLE CEREBRAL ARTERY STENOSIS MORPHOLOGY BY ULTRASOUND
Giorgia Arnone1, Matteo Paolucci*1, Giovanni Malferrari1, Ludovica Migliaccio1, Mauro Gentile1, Stefano Forlivesi1, Simone Galluzzo2, Luigi Simonetti2, Andrea Zini1
1IRCCS Istituto delle Scienze Neurologiche di Bologna, UOC Neurologia e Rete Stroke metropolitana, Bologna, Italy,2IRCCS Istituto delle Scienze Neurologiche di Bologna, UO Neuroradiologia, Bologna, Italy
On behalf of:
Background and aims: Intracranial arterial stenosis is a common cause of stroke worldwide. The burden is therefore high for healthcare systems, making their correct identification crucial. The morphological characterization of intracranial stenosis can have prognostic value for cerebrovascular risk and, to date, is a privilege of neuroradiology.
This is an observational, multicenter study on Transcranial Color-Coded Doppler to better classify intracranial stenosis of the middle cerebral artery (MCA) by adding a new technique “Advanced Harmonic Ultrasonic Enhancement (AHUSE)”.
Methods: The study includes intracranial stenoses of the MCA identified through neurosonological or neuroradiological examinations performed within ⩽7 days of each other, in patients referred to the neurosonology clinics of the centers.
Velocity, Color, Power, and AHUSE were performed, stratifying the stenoses. This set of data were compared with radiological data obtained by CT angiography.
The morphological criteria included the length and single or multiple points of stenosis.
Results: On 19 stenosis AHUSE showed good sensitivity (84.62%), and moderate specificity (66.67%) in assessing the stenosis length (> 5 mm).
In the focality assessment, AHUSE showed low sensitivity (44.44%).
Measuring stenosis by NASCET on AHUSE was sensitive as well as doing the same diagnosis by Doppler velocity criteria in stenosis > 50%.
Measuring > 50% stenosis by AHUSE (NASCET) compared with CTA has good sensitivity at 89% and low specificity.
Conclusions: The good performance of AHUSE in detecting long stenosis is useful in adding an extra prognostic element to the standard velocity-based evaluation.
Disclosures of Interest: No
Abstract N°: 270
GOOD VENOUS OUTFLOW IS ASSOCIATED WITH FAVORABLE FUNCTIONAL OUTCOMES OF MECHANICAL THROMBECTOMY
guangshuo li*1, Yunyun Xiong1, Xingquan Zhao1
1Beijing Tiantan Hospital, Neurology, Beijing, China
On behalf of:
Background and aims: A new collateral cascade was proposed including arterial, tissue and venous levels of collateralization. We aimed to investigate whether arterial, tissue or venous levels of collateral blood flow was correlated with functional outcome of mechanical thrombectomy (MT)
Methods: We conducted a single-center, retrospective study to include patients with ischemic stroke due to large vessel occlusion of anterior circulation treated with MT. The arterial level of collateral blood flow was assessed by a 4-point scale based on CTA. The tissue level of collateral blood flow was assessed with hypoperfusion intensity ratio (volume ratio: T-max > 10s / T-max > 6s). The venous level of collateral blood flow, also known as venous outflow (VO) was assessed with opacification of the vein of Labbé, sphenoparietal sinus, and superficial middle cerebral vein based on CTA. The study outcome was defined as mRS 0-2 at discharge in our study.
Results: One hundred and sixty-five patients were included in our analysis according to inclusion criteria. Seventy-five (45.45%) patients achieved favorable functional outcome (mRS 0-2). Compared with arterial and tissue levels of collateralization, VO was independently correlated with favorable functional outcome (adjusted OR 1.378, 95% CI 1.083-1.754, P=0.009). Shift analyses showed that the COVES 4-6 group had a more favorable mRS distribution (P=0.012), compared with the COVES 0-3 group.
Conclusions: Our study showed that, compared with pial collateralization and HIR, VO might be a superior imaging marker associated with functional outcomes of MT.
Disclosures of Interest: No
Abstract N°: 636
EARLY ISCHEMIC CHANGE AT LATE ISCHEMIC STROKE PRESENTATION IS UNCOMMON: A POPULATION-BASED STUDY
Yasmin Aziz*1, Achala Vagal2, Heidi Sucharew3, Brady Williamson2, Vivek Khandwala2, Lily Wang2, Thomas Maloney2, David Robinson1, Robert Stanton1, Pooja Khatri1
1University of Cincinnati, Department of Neurology and Rehabilitation Medicine, Cincinnati, United States,2University of Cincinnati, Department of Radiology, Cincinnati, United States,3University of Cincinnati, Department of Emergency Medicine, Cincinnati, United States
On behalf of: The Assessing Population-Based Radiological Brain Health in Stroke Epidemiology (APRISE) Investigators
Background and aims: Acute ischemic stroke (AIS) treatment and prognosis depend on injury sustained at time of presentation. Anterior circulation stroke is characterized using the semiquantitative Alberta Stroke Program Early CT Score (ASPECTS). We sought to determine the distribution of baseline ASPECTS at a population level.
Methods: Clinical imaging was collected from hospitalized stroke/TIA patients ascertained in a population of 1.3 million in the Greater Cincinnati/Northern Kentucky Stroke Study. Trained central neuroradiologists blinded to clinical presentation characterized ASPECTS on initial CTs. For this analysis, patients presenting to an ED in 2015 within 24 hours of anterior circulation AIS were included. Large vessel occlusion (LVO) status was inconsistently available.
Results: Among 1,518 patients presenting with physician diagnosis of AIS to the ED within 24 hours, 984 (65%) were anterior circulation, including 969 (98%) with baseline ASPECTS. Among these 969 (mean age 71[SD 14] years, median ED arrival time 5.1 [IQR1.3-13.1] hours, median NIHSS 4 (IQR [1-9]), 940 (97%) had ASPECTS ⩾6. Among 175 patients with NIHSS ⩾6 and presenting beyond 4.5 hours, 153 (87%) had ASPECTS ⩾6 (Figure 1).
Conclusions: In our population, most (87%) had ASPECTS ⩾6 even when limiting to presentation beyond 4.5 hours from onset with NIHSS ⩾6. Assuming 1/3 would harbor LVOs and all cases with ASPECTS<6 were among those with LVOs, only a minority (14%) of patients with LVO would have ASPECTS 0-2. These results can inform resource utilization and clinical trial design.
Disclosures of Interest: No
Presenting ASPECTS by Time of Onset in Patients with NIHSS⩾6.
Abstract N°: 902
CEREBRAL VASOMOTOR REACTIVITY IN THE ACUTE PHASE AND AFTER 6 MONTHS IN NON-DISABLING STROKE/TIA: A PROSPECTIVE COHORT STUDY
Nicoletta Brunelli*1, Claudia Altamura1, Marilena Marcosano1, Sergio Soeren Rossi1, Carmelina Maria Costa2, Adriana Fallacara3, Marcel Bach-Pages4, Mauro Silvestrini5, Carlo Augusto Mallio6, Fabrizio Vernieri1
1Fondazione Policlinico Universitario Campus Bio-Medico, Department of Medicine and Surgery, Unit of Headache and Neurosonology, Unit of Neurology, Università Campus Bio-Medico di Roma, Rome, Italy,2Sondrio Hospital, Neurology Unit, Sondrio, Italy,3Policlinico of Bari “Aldo Moro”, Neurology Unit, Bari, Italy,4University of Oxford, Department of Biology, Oxford, United Kingdom,5Marche Polytechnic University, Neurological Clinic, Ancona, Italy,6Fondazione Policlinico Universitario Campus Bio-Medico, Unit of Radiology, Università Campus Bio-Medico di Roma, Rome, Italy
On behalf of:
Background and aims: Cerebral Vasomotor Reactivity (VMR), is a fundamental property of cerebral hemodynamics that protects from cerebrovascular disease. We aimed to explore the longitudinal changes in VMR in patients with acute non-disabling stroke/Transient Ischemic Attack (TIA) to better understand its implication in the etiopathogenesis of stroke.
Methods: VMR by Transcranial Doppler Breath Holding test was performed at 48-72 h from stroke onset (T1) and after 6 months (T2) on MCA of the non-affected hemisphere and PCA of the affected hemisphere
Results: We consecutively enrolled 124 patients (71% men) with a median age of 66.0 (IQR 54.75-74.25) years with acute non-disabling stroke/TIA (median NIHSS 2, IQR 1-3). Since 15 patients dropped out after baseline evaluation, VMR evaluations at 6 months are available for 109 patients. Both MCA of the non-affected hemisphere (1.38 %/s SD 0.58) and PCA of the affected hemisphere (1.35 %/s SD 0.75) BHI at T1 did not differ among different stroke subtypes (p=0.067 and p=0.350; N=124). MCA and PCA BHI decreased from T1 to T2 (respectively 1.39 %/s SD 0.56 vs 1.18%/s SD 0.44 and 1.30 %/s SD 0.69 vs 1.20 %/s SD 0.51; N=109) regardless of the stroke subtype (respectively p<0.0001 and p=0.111). Neither vascular risk factors nor sex influenced the decrease in BHI at T2.
Conclusions: The VMR is higher in acute phase than at 6 months in patients with non-disabling stroke/TIA, regardless of etiopathogenesis. The higher VMR in acute phase could be sustained by an increased Cerebral Blood Flow due to collateral circulation activation supporting the ischemic zone.
Disclosures of Interest: No
Abstract N°: 925
VALUE OF MR IMAGING OF LEPTOMENINGEAL COLLATERAL FLOW IN ACUTE ISCHEMIC STROKE PATIENTS WITH OCCLUSION OF MIDDLE CEREBRAL ARTERY
Dong Woo Park*1, Sohi Bae1
1Hanyang University Guri Hospital, Radiology, Guri-si, South Korea
On behalf of:
Background and aims: Poor leptomeningeal collateral flow is related to worse clinical outcome in acute ischemic stroke. This study aims to evaluate the value of MR imaging (MRI) of leptomeningeal collateral flow in acute stroke patients with an occlusion of middle cerebral artery (OMCA).
Methods: 328 acute stroke patients who underwent MRI study due to OMCA were included. In acute stroke patients with OMCA, MRI findings of leptomeningeal collateral flow were retrospectively analyzed as follows; negative MRI with no leptomeningeal collateral flow (-MRI), positive MRI with delayed enhancing vessel on contrast enhanced T1WI (CET1WI) and/or FLAIR hyperintense vessel. The relationship of MRI findings of leptomeningeal collateral flow was statistically analyzed comparing with clinical outcome as modified Rankin Scale.
Results: In acute stroke patients with OMCA, MRI findings of leptomeningeal collateral flow were classified and ranked in order of clinical outcome from poor to good as follows; -MRI (125, 38%), delayed-enhancing vessel (62, 19%), FLAIR hyperintense vessel (77, 23%), and both delayed enhancing vessel and FLAIR hyperintense vessel (64, 20%), which were each statistically significant (p < 0.05).
Conclusions: MR imaging of leptomeningeal collateral flow in acute stroke patients with OMCA correlates with clinical outcome. Therefore, it can be applied as a prognostic MRI marker in acute stroke patients.
Disclosures of Interest: No
Abstract N°: 937
DUAL DEEP LEARNING MODEL TO DETECT CEREBRAL INFARCTS ON DIFFUSION-WEIGHTED IMAGING USING APPARENT DIFFUSION COEFFICIENTS
Ho Kyu Kim*1, Moses Lee1, Wi-Sun Ryu2, Chi-Kyung Kim1
1Korea University Guro Hospital, Neurology, Seoul, South Korea,2JLK Inc, Artificial Intelligence Research Center, Seoul, South Korea
On behalf of:
Background and aims: In this study, we aimed to address a common challenge in deep learning algorithms for identifying acute ischemic lesions in diffusion-weighted imaging (DWI): the tradeoff between sensitivity and specificity.
Methods: Our primary model, based on the U-net algorithm, was trained on a substantial dataset of 8,359 DWI b1000 images from nine hospitals in Korea, achieving exceptionally high sensitivity. To enhance specificity, we introduced an apparent diffusion coefficient (ADC) threshold of ⩽500 × 10–6 mm²/s on the segmented mask of the b1000 image, creating a secondary model. We evaluated the performance of our dual deep learning model using an external dataset of 581 DWIs from a single stroke center. Two neurologists categorized these images as normal, ischemic stroke, or other abnormalities.
Results: Without ADC thresholding, the primary model displayed perfect sensitivity (1.0) but limited specificity (0.42). However, after applying the ADC threshold, sensitivity remained high (0.88), while specificity improved significantly (0.77; p < 0.001). The ADC thresholding effectively corrected issues like the T2 shine-through effect, non-stroke high signal on b1000, and artifacts. Furthermore, after excluding non-stroke brain abnormalities, the secondary model demonstrated a sensitivity of 0.88 and a specificity of 0.92.
Conclusions: Our study demonstrates that implementing ADC thresholding can substantially boost the specificity of deep learning models in detecting ischemic lesions on DWI. This approach offers a promising solution to the sensitivity-specificity tradeoff, potentially enhancing the clinical utility of deep learning algorithms for identifying acute ischemic lesions with both high sensitivity and high specificity.
Disclosures of Interest: No
Abstract N°: 1268
CT PERFUSION IN ACUTE STROKE-RELATED APHASIA: CORRELATION BETWEEN HYPOPERFUSED BRAIN VOLUME AND APSAA PERFORMANCE
Emanuele Vincis*1, Giovanni Furlanis1, Gabriele Prandin1, Laura Manicinelli1, Federica Palacino1, Alina Menichelli2, Paola Caruso1, Miloš Ajčević3, Marcello Naccarato1, Paolo Manganotti1
1Trieste University Hospital - ASUGI, Clinical Unit of Neurology, Trieste, Italy,2Trieste University Hospital - ASUGI, Neuropsychology Service, Rehabilitation Unit, Trieste, Italy,3University of Trieste, Department of Engineering and Architecture, Trieste, Italy
On behalf of:
Background and aims: Aphasia is a common presenting symptom of ischemic stroke. To characterize patients’ linguistic deficits, clinicians can administer screening tests, such as the Aphasia Post-Stroke Acute Assessment (ApsAA). The correlation between CT perfusion (CTP) imaging and the performance of aphasic patients in these tests has been poorly investigated so far. We aimed to determine whether the hypoperfused brain volume calculated on CTP maps correlates with ApsAA performance in patients with stroke-related aphasia.
Methods: Demographic, clinical, and imaging data along with ApsAA assessment of patients with acute stroke-related aphasia were retrospectively analyzed. CTP was aquired immediatly before Stroke Unit admission. Total hypoperfused volume calculated on MTT map and core volume calculated on CBV map, assessed by manual segmentation, were then correlated with ApsAA assessment (0-65 points, where lower scores indicate more severe aphasia) administered at Stroke Unit admission.
Results: 30 aphasic patients were considered. Median age was 80 years (IQR 72-84) and median baseline NIHSS was 8 (IQR 5-16). Median volume of prolonged MTT was 84.08 cm3 (IQR 31.65-126.62) and median volume of decreased CBV was 3.22 cm3 (IQR 3.22-16.34). Median ApsAA score was 0 points (IQR 0-27). We found an inverse correlation between both prolonged MTT volume and decreased CBV volume and ApsAA performance (respectively p 0.001, ρ -0.57 and p 0.002, ρ -0.53).
Conclusions: In the acute phase, both CTP total hypoperfused volume and core volume correlate with stroke-related aphasia severity as measured by the ApsAA test.
Disclosures of Interest: No
Abstract N°: 1359
ASSOCIATION OF BASELINE BLOOD PRESSURE AND HEMISPHERIC CEREBRAL BLOOD FLOW IN ACUTE SMALL SUBCORTICAL INFARCTS
1Huashan Hospital, Department of Neurology, National Center for Neurological Disorders, National Clinical Research Centre for Aging and Medicine, Shanghai, China
On behalf of:
Background and aims: Increased baseline blood pressure (BP) is common in acute ischemic stroke. However, the association between baseline BP and the state of hemispheric perfusion in patients with acute small subcortical infarcts (SSIs) has not been studied in detail. The aim of this study was to investigate the relationship between baseline BP and hemispheric cerebral blood flow (CBF) in acute SSIs.
Methods: This retrospective study included 101 patients with acute SSIs. Baseline BP was measured in the emergency room (ER). Baseline hemispheric CBF was assessed through coregistration of baseline CT perfusion imaging and follow-up diffusion-weighted imaging (DWI). The association between baseline BP, CBF, and different cerebral small vessel disease (CSVD) biomarkers were assessed.
Results: Baseline systolic BP (SBP) and diastolic BP (DBP) were negatively associated with contralateral hemispheric CBF after multivariate-adjusted linear analysis (SBP: β=-0.001, 95%CI: -0.002-0.000, P=0.030; DBP: β=-0.002, 95%CI: -0.003~0.001; P=0.006). Among other CSVD biomarkers, the presence of any cerebral microbleeds (CMBs) showed a significant association with lower CBF in the contralateral hemisphere of the infarct lesion (r=-0.270, P=0.035).
Conclusions: In patients with acute SSIs, increased baseline BP was associated with reduced CBF in the contralateral hemisphere of the infarct lesion, which probably could be interpreted by the exacerbation of the CSVD burden.
Disclosures of Interest: No
Abstract N°: 1525
UTILITY OF HYPOPERFUSION INTENSITY RATIO IN MILD ANTERIOR CIRCULATION LARGE VESSEL OCCLUSION STROKES
Anusha Nallaparaju*1, Jia-Yi Wang2, Marc Fisher3, Vasileios-Arsenios Lioutas4, Magdy Selim3
1Beth Israel Deaconess Medical Center, Stroke Division,2Beth Israel Deaconess Medical Center,3Beth Israel Deaconess Medical Center, Stroke Division, Boston, United States,4Beth Israel Deaconess Medical Center, Boston, United States
On behalf of:
Background and aims: The progression of clinical deficits in anterior large vessel occlusion (A-LVO) strokes may be attributed to the degree of collateral flow. We investigated the association between hypoperfusion intensity ratio (HIR), a perfusion marker associated with collateral status, and clinical outcomes in mild A-LVO strokes (mLVOs).
Methods: We conducted a retrospective cohort study of consecutive patients from 2019-2023 with mLVOs (NIHSS⩽5), who presented within 24 hours and underwent CT perfusion. We dichotomized the sample based on median HIR and analyzed patients without initial mechanical thrombectomy (iMT). The primary outcome was early neurologic deterioration (END), ⩾4-point worsening on NIHSS within 3 days, attributed to the A-LVO without ICH. Secondary outcomes included symptomatic ICH, 3-month mRS and mortality. Results were analyzed using Fisher’s exact test and univariate logistic regression.
Results: We identified 37 patients. Median HIR was 0.2. Excluding ten patients who underwent iMT, we had 17 in HIR⩽0.2 and 10 in HIR>0.2 groups. Baseline NIHSS was higher in the HIR>0.2 group (4 vs 2; p=0.04). Remaining baseline characteristics, tPA use, and A-LVO location were similar between groups. There was no between-group difference in END (OR 1.16, p=0.879); mRS 0-1, adjusting for NIHSS (aOR 0.15, p=0.146); symptomatic ICH or mortality (p=0.178).
Conclusions: In our exploratory analysis, median HIR was lower in mLVOs (0.2) compared to previously reported HIR in moderate-to-large A-LVO strokes (0.4). We found no association between HIR and END or functional outcome. Larger prospective studies evaluating the role of HIR in outcome prediction and decision-making of mLVOs are needed.
Disclosures of Interest: No
Abstract N°: 1582
PRE-TRANSFER CTP MISMATCH MORE ACCURATELY PREDICTS MECHANICAL THROMBECTOMY FOLLOWING TRANSFER OF LVO STROKE PATIENTS THAN ASPECTS
Malgorzata Miller1, Esam Abobaker*1, Brian Wideman1, Stephanie Mueller2, Lindsey Ouellette3, Nadeem Khan1, Muhib Khan4, Mathew Reeves5, John Adam Oostema6
1Corewell Health - West / Michigan State University Neurology,2Research Operations, Corewell Health,3Michigan State University,4Department of Neurology, Mayo Clinic, Rochester, MN,5Department of Epidemiology and Biostatistics, MSU,6Department of Emergency Medicine, MSU CHM
On behalf of:
Background and aims: The optimal imaging strategy (NCCT, CTA, CTP) to be performed at the regional facilities and after the transfer to the comprehensive stroke center (CSC) in acute LVO ischemic stroke is unclear. The aim of this study was to compare rural CTP and NCCT profiles in predicting treatment with mechanical thrombectomy (MT) following transfer to the CSC.
Methods: We included 44 patients who were evaluated for LVO stroke at a regional facility and transferred to a CSC for possible MT between 11/2021 and 04/2023. All patients received NCCT, CTA and CTP at the regional and CSC hospitals. A favorable CTP imaging profile was defined as perfusion mismatch/core infarct volume ratio >1.8. NCCT favorable profile was defined as ASPECTs ⩾6
Results: The median age was 69 (IQR 60-79), 57% were female, median NIHSS was 15 (IQR 3-21) at regional facility and 11 (IQR 4-18) at CSC. Twenty patients (45%) received thrombolytic therapy at the regional facility and 18 patients (40%) underwent MT. Regional CTP imaging profile agreed with the CSC imaging in 86.4% of cases (K= 0.66, 95% CI 0.42-0.90) and in 81.8% based on NCCT criteria (K= 0.41, 95% CI 0.09-0.37). Favorable regional CTP profile predicted MT in 59.1% of cases (p=0.024) as compared to 47.4% of cases when ASPECTs criteria were used (p=0.312).
Conclusions: The agreement of regional and CSC CTP imaging profiles was higher than regional and CSC ASPECT score-based profiles. Regional CTP profile was also associated with MT attempt while regional ASPECTs profile was not
Disclosures of Interest: No
Abstract N°: 1908
NEURORADIOLOGICAL EXPERIENCES WITH ARTIFICIAL INTELLIGENCE (AI) BASED DECISION SUPPORTING SYSTEM IN ACUTE STROKE MANAGEMENT
Orsolya Szalmás*1, Gábor Szudi1, Eszter Gerencsér1, Eszter Vraukó1, Anita Andrássy1, Kinga Pozsár1, Péter Várallyay1, Istvan Szikora1
1National Institute of Mental Health, Neurology and Neurosurgery, Neuroradiology, Budapest
On behalf of:
Background and aims: The AI-powered decision support CT-analytic system for stroke assessment by Braionomix is available for all Hungarian stroke centers from 03-10-2022. The aim of the study was to check the diagnostic accuracy of the software on a large volume center.
Methods: In the National Institute of Mental Health, Neurology and Neurosurgery (Budapest, Hungary) we reviewed 735 CT and CTA studies of stroke patients during 1 year, including 355 cases of MCA M1 and distal ICA occlusions. AI based and human readings were compared retrospectively.
Results: Regarding ASPECTS, AI results matched the neuroradiologists’ reading in 79%. In case postcontrast scans were submitted for AI evaluation, contrast enhancement confused the ASPECTS results in 23%. For large-vessel occlusion, average sensitivity and specificity were 0,9, but the phase of CTA scanning made a difference. Sensitivity was 0,95 in peak arterial CTA-phase, but was only 0,9 in early arterial and 0,85 in equilibrium phase.
Conclusions: The AI-based CT analytic system is safe because the incidence of the relevant errors is low. The phase of CTA affects the sensitivity of the software which is the highest in peak arterial phase. Evaluation of postcontrast brain CT series should be avoided, since it can result in false ASPECT scores.
Disclosures of Interest: Yes Consultant to Brainomix
Abstract N°: 1993
NONINVASIVE IMAGING OF CAROTID PLAQUE CALCIFICATION: A SYSTEMATIC REVIEW AND DIAGNOSTIC ACCURACY META-ANALYSIS
David Pakizer*1, Jiří Kozel1, Patrick Taffé2, Jolanda Elmers3, Janusz Feber1,4, Patrik Michel5, David Skoloudik1, Gaia Sirimarco5,6
1Center for Health Research, Faculty of Medicine, University of Ostrava, Ostrava, Czech Republic,2Center for Primary Care and Public Health, Division of Biostatistics, University of Lausanne, Lausanne, Switzerland,3Medical Library, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland,4Division of Nephrology, Department of Pediatrics, Children’s Hospital of Eastern Ontario, University of Ottawa, Ottawa, Canada,5Stroke Center, Service of Neurology, Department of Clinical Neurosciences, Lausanne University Hospital, Lausanne, Switzerland,6Neurology Unit, Department of Internal Medicine, Riviera Chablais Hospital, Rennaz, Switzerland
On behalf of:
Background and aims: Carotid plaque calcification seems to have a negative association with ipsilateral ischemic events but an increased risk of post-stroke cognitive impairment and a significant risk for stroke/death in patients undergoing carotid stenting. The study aimed to estimate the diagnostic accuracy of non-invasive plaque imaging modalities (ultrasound [US], computed tomography [CT], magnetic resonance imaging [MRI]) to detect carotid plaque calcification when compared to histology in patients with symptomatic and asymptomatic carotid plaques.
Methods: Medline Ovid, Embase.com, Cochrane Library, and Web of Science Core were searched without any search limitation. We performed quality assessment of included studies by QUADAS-2 and univariate and bivariate random-effect meta-analysis to analyze the results.
Results: 21 studies investigating carotid plaque calcification using three different imaging methods (5 CT, 10 MRI, and 6 US studies) were included. In univariate meta-analyses, CT showed the highest accuracy (sensitivity 88% [95% CI: 72-95], specificity 93% [95% CI: 52-99], accuracy 90% [95% CI: 58-98]) closely followed by MRI (sensitivity 84% [95% CI: 80-88], specificity 93% [95% CI: 90-95], accuracy 89% [95% CI: 87-91]) and US (sensitivity 72% [95% CI: 57-84], specificity 89% [95% CI: 71-97], accuracy 85% [95% CI: 67-94]) in detecting plaque calcifications. Bivariate analysis showed no significant difference between the diagnostic accuracy of CT, MRI and US (p>0.05).
Conclusions: The noninvasive imaging modalities investigated (CT, MRI, and US) showed similar and very high diagnostic accuracy to detect carotid plaque calcification, allowing to better assess the patient’s risk profile.
Disclosures of Interest: No
Comparison of detection of calcification by CT/MRI/US, based on HSROC curves (solid lines).
Abstract N°: 2203
CT PERFUSION VS NON-CONTRAST CT IN PREDICTING OUTCOMES IN ACUTE STROKE PATIENTS WITH LARGE ISCHAEMIC CORE
Chushuang Chen*1, Longting Lin2, Bernard Yan3, Henry MA4, Thanh Phan5, Peter Mitchell6, Mark Parsons2
1The University of Newcastle, School of Medicine and Public Health, Callaghan,2The University of New South Wales, South Western Clinical School, Faculty of Medicine, Sydney, Australia,3The University of Melbourne, Medicine, Parkville, Australia,4Monash University, School of Clinical Sciences, Department of Medicine, Australia,5Monash University, Neuroscience Research, Monash Health & Stroke & Aging Research Group, Clayton, Australia,6The Royal Melbourne Hospital, Radiology, Parkville, Australia
On behalf of: the INSPIRE and the MOSES study group
Background and aims: Recent trials confirm treatment-benefit of endovascular therapy (EVT) in large ischaemic cores. However, there is variation in definitions for large-core with various neuroimaging modalities. Our study aimed to compare the precision in clinical outcome correlation between NCCT Alberta Stroke Program Early CT Score (NCCT-ASPECTS) and CT perfusion (CTP) core in large ischaemic-core patients.
Methods: We included patients enrolled in the INternational Stroke Perfusion Registry (INSPIRE) and Monitoring of Stroke Endovascular Services (MOSES) Registry. Patients with baseline CTP-core ⩾70mL or NCCT-ASPECTS(3-5) were included. The association of EVT vs.non-EVT with good (modified Rankin Score (mRS) 0-2) and poor (mRS 5-6) outcomes in patients with CTP-core ⩾70mL or NCCT-ASPECTS (3-5) were assessed.
Results: In patients (n=186) who met the ASPECTS (3-5) criteria, EVT was not associated with higher proportion of good outcome (37.1% EVT vs.30.1% non-EVT, aOR 1.5 95% CI 0.5-7.1, p=0·56), nor a lower rate of poor outcome (43.6% vs.58.5%, p=0.067). With CTP-core ⩾70ml, EVT was strongly associated with less poor outcomes. There was a lower rate of sICH in CTP-core ⩾70ml patients (5.2% EVT vs.20.0% non-EVT, aOR 0.11, 95% CI 0.01-0.8, p=0·028), lower mortality rate (32.5% EVT vs.56.6% non-EVT, aOR 0.5, 95% CI 0.3-0.8, p=0·021), and lower proportion of poor mRS outcome (48.7% EVT vs.76.6% non-EVT, aOR 0.5 95% CI 0.3-0.8, p=0·011).
Conclusions: The CTP-defined large core of 70mL strongly predicts less poor outcomes with EVT. ASPECTS(3-5) defined large core does not.
Disclosures of Interest: No
Abstract N°: 2284
WOW - WITH OR WITHOUT: MEASURING IMPACT OF E-ASPECTS SOFTWARE ON CONVENTIONAL CT REPORTING IN ACUTE ISCHEMIC STROKE
Julija Vlahovic1, Iris Grunwald2, Anna Podlasek*2,3
1Anglia Ruskin University, Chelmsford, United Kingdom,2University of Dundee, Tayside Innovation MedTech Ecosystem, Dundee, United Kingdom,3University of Nottingham, Radiological Sciences, Nottingham, United Kingdom
On behalf of:
Background and aims: Rapid and accurate diagnosis of acute ischemic stroke (AIS) is crucial for improved outcomes. This research aimed to compare the impact of an automated AI tool (Brainomix, e-ASPECTS) on scoring CT scans of patients with AIS.
Methods: This prospective, multicenter, randomized study involved 39,780 ASPECTS regions in 39 patients with AIS. A total of 51 scorers from six medical backgrounds were recruited, including junior (7) and consultant (10) stroke doctors, junior (10) and consultant (7) radiologists, neuroradiologists (7), and cardiologists (10). Each scorer scored the ASPECTS regions twice, with (Fig. 1.) and without assistance from the e-ASPECTS software. Agreement with the ground truth and scoring time were evaluated between clinicians and clinician groups.
Results: Compared to unassisted scoring, agreement of ASPECTS score with the ground truth was improved with e-ASPECTS. Cohen's kappa improved from 0.29 to 0.58 (p<0.05). The Junior Stroke Doctors showed the most improvement (from 0.09 to 0.54) and consultant neuroradiologists the least (from 0.27 to 0.46). We observed overall time saving of -8 sec (95% CI -11, -4), and in each group of participants.
Conclusions: The e-ASPECTS software is a valuable tool for clinicians in the rapid and accurate diagnosis of acute ischemic stroke. The use of AI in stroke diagnosis has the potential to enable the identification of AIS patients in centres without neuroradiology expertise, improving access to life-saving treatment.
Disclosures of Interest: Yes IQG is a co-founder of Brainomix
User interface.
Abstract N°: 2468
COLLATERAL STATUS AND OUTCOMES AFTER ENDOVASCULAR TREATMENT IN ACUTE ATHEROSCLEROTIC AND CARDIOEMBOLIC LARGE VESSEL OCCLUSION
Xinyi Leng*1, Ximing Nie2,3, Lina Zheng2,3, Hongyi Yan2,3, Yuesong Pan2,3, Weibin Gu4, Zhongrong Miao2,3, Thomas W Leung1, Liping Liu2,3
1The Chinese University of Hong Kong, Department of Medicine and Therapeutics,2Beijing Tiantan Hospital, Capital Medical University, Department of Neurology,3China National Clinical Research Center for Neurological Diseases,4Beijing Tiantan Hospital, Capital Medical University, Department of Radiology
On behalf of:
Background and aims: We aimed to investigate the prognostic values of pretreatment collateral status for outcomes after endovascular treatment in patients with acute large vessel occlusion (LVO) due to large artery atherosclerosis (LAA) and cardioembolism (CE).
Methods: In a prospective, nationwide registry, we enrolled patients with acute intracranial anterior-circulation LVO due to LAA or CE, who underwent endovascular treatment within 24 hours. Pre-treatment leptomeningeal collaterals was assessed in digital subtraction angiography by ASITN/SIR Collateral Flow Grading System, and classified as good and poor collaterals. Primary outcome was good functional outcome at 3 months (modified Rankin Scale [mRS] 0-2). Secondary outcomes included 3-month mRS distribution, successful recanalization, early neurological deterioration, symptomatic intracranial hemorrhage (sICH) within 7 days, and 3-month mortality.
Results: Among 805 eligible patients (median age 66 years, 60.3% males), 355 had LVO due to CE and 450 due to LAA. In CE patients, good collaterals was associated with a higher chance of good functional outcome (adjusted odds ratio [OR]=1.78; 95% CI 1.13-2.80) and lower mRS at 3 months (adjusted generalized OR=0.57; 95% CI 0.39-0.83). In LAA patients, good collaterals was associated with fewer sICH (adjusted OR=0.34; 95% CI 0.15-0.80) and deaths within 3 month (adjusted OR=0.51; 95% CI 0.27-0.94). There was no significant association between collateral status and other outcomes in either CE or LAA patients, or significant CE/LAA and collateral status interaction on any outcome.
Conclusions: Pretreatment collateral status may have different protective effects for outcomes after endovascular treatment, in patients with LVO due to LAA and CE. The mechanisms warrant further investigations.
Disclosures of Interest: No
Abstract N°: 2593
CONTRAST-ENHANCED ULTRASOUND IN POST-STENTING EVALUATION OF CAROTID ARTERIES
Dae-Hyun Kim*1, Jong-Wook Shin2
1Dong-A University Hospital, Department of Neurology, Busan, South Korea,2Chungnam National University Sejong Hospital, South Korea, Department of Neurology, Sejong CIty, South Korea
On behalf of:
Background and aims: Carotid artery stenting (CAS) has become a standard intervention for treating carotid artery stenosis. Conventionally, post-stenting evaluation involves the use of angiography and Doppler ultrasound. This research investigates the viability of contrast-enhanced ultrasound (CEUS) in assessing patients following carotid artery stenting. The objective is to enhance diagnostic accuracy and gain further insights into neointima and atherosclerotic plaques linked to restenosis.
Methods: This study included patients experiencing restenosis after CAS, who have received antiplatelet agents and statins. Among these individuals, a total of five post-carotid stenting patients with restenosis underwent CEUS examinations, utilizing the contrast agent Sonovue®. We assessed the visualization of the stented segment, extending from the proximal neointima to the restenosis region, while also examining the presence of neovascularization
Results: Carotid artery stenting was performed on three patients for symptomatic and two patients for asymptomatic stenosis. The average follow-up period was 4.4 years post-procedure. In all patients with carotid artery restenosis, intense neovascularization was observed in at least one region within the neointima or plaque in the restenosis area. Three patients exhibited neovascularization in both areas, while two patients depicted neovascularization in one of the areas. Compared with pre-enhancement, a reclassification of stenosis degree was observed in two patients, transitioning from mild to moderate.
Conclusions: The enhanced visualization capabilities provided by CEUS enable a dynamic assessment of vascular integrity, particularly in cases of carotid artery restenosis. The notable presence of intense neovascularization within neointima or restenosis areas highlights the potential role of CEUS in elucidating the pathophysiological aspects associated with post-stenting complications.
Disclosures of Interest: No
Abstract N°: 2733
HYPODENSITY ON NON-CONTRAST COMPUTED TOMOGRAPHY BEYOND THE ISCHEMIC CORE
Lieselotte Vandewalle*1,2, Praneeta R Konduri3,4, Soren Christensen5, Anke Wouters2, Nicole Yuen5, Maarten Lansberg5, Jelle Demeestere1,2, Robin Lemmens1,2
1University Hospitals Leuven, Department of Neurology, Leuven, Belgium,2Catholic Universities of Leuven, Department of Neurosciences, Division of Experimental Neurology, Leuven, Belgium,3Amsterdam UMC - location University of Amsterdam, Department of Biomedical Engineering and Physics, Amsterdam, Netherlands,4Amsterdam UMC - location University of Amsterdam, Department of Radiology and Nuclear Physics, Amsterdam, Netherlands,5Stanford Stroke Center, Palo Alto, United States
On behalf of:
Background and aims: Hypodensity on non-contrast computed tomography (NCCT) in ischemic stroke is assumed to result predominantly from vasogenic oedema. We aimed to determine tissue changes in areas adjacent to the ischemic core by assessing subtle hypodensity, detected using relative NCCT, a semi-automated NCCT analysis that compares the density of a voxel to the corresponding area in the contralateral hemisphere and generates hypodensity-based ratio maps (doi: 10.1111/jon.12593).
Methods: We included 94 patients with anterior circulation large vessel occlusion (acLVO) from the CT Perfusion to Predict Response to Recanalization in Ischemic Stroke Project 2 (CRISP2) with baseline NCCT at the referring hospital and DWI (diffusion weighted imaging) prior to endovascular treatment at the comprehensive stroke centre. We compared rNCCT lesion volume with 1% relative hypodensity threshold within the approximated affected vascular territory, but outside the co-registered DWI lesion, e.g. ‘non-infarcted rNCCT lesion’, to the ‘rest’ of the rNCCT lesion (excluding the cerebellum) in all non-affected vascular territories.
Results: The median DWI volume was 16 ml [IQR 73 ml]. The non-infarcted rNCCT lesion volume was larger than the rest rNCCT volume (mean 165 ml [SD 69 ml] vs median 125 ml [IQR 102], p = 0.048). Figure 1 shows cases with large rNCCT volumes in the affected vascular territory outside the DWI lesion.
Conclusions: In patients with acLVO, we report subtle relative hypodensity on baseline NCCT within the approximated affected vascular territory but outside the DWI lesion. Further research will focus on assessing the presence of these findings in perfusion imaging confirmed penumbral tissue.
Disclosures of Interest: Yes P. K.: co-founder and shareholder of inSteps B.V. RL: no personal disclosures, but institutional support for consultancy by iSchemaview.
Abstract N°: 3052
POTENTIAL OF TCCS- AND NIRS-BASED ACUTE STROKE IMAGING FOR DECISION-MAKING ON INTRAVENOUS THROMBOLYSIS TREATMENT
Erik Freitag*1, Heinrich Audebert1, Hebun Erdur2, Ahmed Khalil1, Peter Harmel3, Maximilian Kaffes1, Christoph Schmitz4, Joachim Weber3
1Charité Universitätsmedizin Berlin, Neurology, Berlin,2Asklepios Fachklinikum Teupitz, Department of Neurology,3Charité Universitätsmedizin Berlin, Berlin Institute of Health at Charité, Berlin,4Hochschule für Technik und Wirtschaft (HTW), Berlin
On behalf of:
Background and aims: Mobile Stroke Units (MSU) shorten time to intravenous thrombolysis (IVT) and improve functional outcome, but they rely on computed tomography (CT) making them highly specialized and costly. Alternative technologies can potentially identify imaging-based IVT contraindications like intracranial haemorrhage (ICH) or malignancies, e.g. by transcranial color-coded sonography (TCCS) and near-infrared spectroscopy (NIRS).
Methods: Using a simulation approach, we analysed magnetic resonance imaging (MRI) scans of patients with suspected stroke and within 4.5 hours of symptom onset to determine whether TCCS and NIRS could identify imaging-based IVT contraindications. The conservative scenario defined TCCS to detect acute deep-brain haemorrhages or tumours >20mm from scalp surface or >10ml in volume or causing >4mm midline-shift, while NIRS was defined to detect them <20mm from scalp surface with a volume >3.5ml. The optimistic scenario defined TCCS to detect intracranial or subarachnoid acute/subacute hematoma or tumours >20mm from scalp surface or >5ml in volume or causing >2mm midline-shift, while NIRS was defined to detect them <35mm from the scalp surface with volume >3.5ml.
Results: We assessed 1089 consecutive patients undergoing acute MRI, with 69 having imaging-based IVT contraindications. Among the 29 patients without non-imaging-based contraindications, TCCS/NIRS would detect 15 of 25 haemorrhages and 3 of 4 malignant tumours in the conservative scenario. In the optimistic scenario 18 of 25 haemorrhages and all malignant tumours would be detected.
Conclusions: While TCCS and NIRS technologies exhibit potential for identifying IVT contraindications in pre-hospital settings, comprehensive evaluation in real-world scenarios is imperative to ascertain their operational constraints.
Disclosures of Interest: Yes C.H.S. reports receiving personal fees from NIRx. H.J.A. reported receiving personal fees from Astra Zeneca, Boehringer Ingelheim, Novo Nordisk, and Roche. The other authors have nothing to report.
Abstract N°: 3266
DIFFERENTIAL IMPACT OF PIAL COLLATERAL SUPPLY ON TISSUE OXYGEN METABOLISM IN ACUTE STROKE
Alexander Seiler*1, Franziska Frank2, Marlies Wagner3
1Universitätsklinikum Schleswig-Holstein, Campus Kiel, Neurology, Kiel, Germany,2Frankfurt University Hospital, Neurology, Frankfurt am Main, Germany,3Frankfurt University Hospital, Neuroradiology, Frankfurt am Main, Germany
On behalf of:
Background and aims: In acute ischemic stroke (AIS) of the anterior circulation, collaterals are the key element for limiting the progression of the ischemic tissue damage and the main determinant of stroke severity. However, the pathophysiology underlying leptomeningeal collateral flow with regard to preservation of a relatively stable hemodynamic and metabolic situation in the hypoperfused peri-infarct tissue for maintaining its structural integrity is currently not well understood. We aimed to characterize the association between leptomeningeal collateralization and parameters of tissue oxygen metabolism in AIS using combined perfusion and oxygenation-sensitive magnetic resonance imaging (MRI).
Methods: Data from patients with AIS due to middle cerebral artery (MCA) and/or internal carotid artery (ICA) occlusion were analyzed. All patients received intravenous thrombolysis after exclusion of contraindications and underwent endovascular thrombectomy (EVT). The MR imaging protocol comprised diffusion- and perfusion-weighted imaging (DWI and PWI) as well as multiparametric quantitative BOLD (mq-BOLD) imaging. Pial collateral supply was calculated based on signal variance in T2*-weighted PWI time series, while mq-BOLD was used to compute maps of the relative tissue oxygen extraction fraction (rOEF) and cerebral metabolic rate of oxygen (rCMRO2).
Results: In patients with poor collateral supply, the collateral vessel abundance showed a significant negative correlation with the ischemic core volume as well as with rOEF in hypoperfused peri-infarct tissue (p<0.05 and p=0.006), while a significant positive association between collateral supply and rCMRO2 was observed (p=0.02).
Conclusions: In AIS, elevated oxygen extraction under poor collateral flow is ineffective for limiting ischemic tissue damage and is associated with metabolic compromise and infarct growth.
Disclosures of Interest: No
Abstract N°: 3317
ANALYSIS OF CLOT CHARACTERISTICS IN ACUTE ISCHEMIC STROKE PATIENTS USING MULTIPHASE CT ANGIOGRAPHY AND SUSCEPTIBILITY WEIGHTED IMAGING
Jeonghoon Bae*1
1Chung-Ang University Gwangmyeong Hospital, neurology
On behalf of:
Background and aims: Rapid assessment of the occlusion site and clot characteristics in acute ischemic stroke is crucial. Among various imaging techniques such as CT angiography, FLAIR, and SWI, the optimal choice remains uncertain. This study aims to compare the utility of multiphase CT angiography (mCTA) and SWI in analyzing occlusion sites and clots in acute ischemic stroke.
Methods: This retrospective study, conducted at a single center, included acute ischemic stroke patients admitted to Chung-Ang University Gwangmyeong Hospital from April 1, 2022, to November 30, 2023. Patients with confirmed occlusion sites through TFCA underwent analysis of images obtained from both mCTA and SWI at the initial assessment. The clot location and size were compared.
Results: Out of 353 cases, 27 were included, with one case excluded due to self-recanalization confirmed during TFCA. Clot size analysis was feasible in 13 cases for both mCTA and SWI, showing no significant difference in clot size estimation (average size, mCTA 16.0mm vs. SWI 17.2mm, p=0.62). Clot location was consistent between mCTA and TFCA in all cases, but SWI failed to confirm clot location in 6 cases. SWI did not allow clot size and localization analysis in all ICA occlusions, while mCTA provided partial information. Among cases where mCTA failed to analyze clot size, 8 of 9 cases (89%) were M2 occlusions, excluding ICA occlusions.
Conclusions: In clot size estimation, mCTA and SWI yielded similar results. However, SWI demonstrated higher applicability in clot size estimation, while mCTA showed greater applicability in clot localization.
Disclosures of Interest: No
E-Poster - Ongoing Trials
Abstract N°: 150
EVALUATING THE SAFETY AND EFFICACY OF LT3001 IN ACUTE ISCHEMIC STROKE PATIENTS UNDERGOING EVT
Sheng-Wen Yeh*1
1Lumosa Therapeutics, Taipei City, Taiwan
On behalf of:
Background and aims: LT3001 is an innovative small molecule, specifically crafted to enhance endogenous thrombolysis while also reducing inflammation and free radicals. Its proven safety and efficacy, based on various animal stroke models, indicate its potential benefits. Preliminary results from a phase 2a study suggest that administering a single dose of LT3001 within 24 hours of an AIS onset was safe and could lead to improved neurological and functional outcomes.
Objective: The aim of the phase 2 study is to assess the safety and efficacy of LT3001 for AIS patients, especially those are planned for IA EVT within the first 24 hours post-stroke symptoms onset (NCT05198323)
Methods/Design: The study is a two-part, multicenter, randomized, placebo-controlled clinical trial.
Intervention: Enrolled participants are randomized (2:1 ratio) to either receive IV doses of LT3001 or placebo, administered prior, during or after completion of EVT.
Population: The study aims to recruit 66 participants aged 18-90 years who have had an AIS (with the LKN < 24 hours before drug administration). Those thrombectomy candidates with a NIHSS score greater including 6, and not scheduled for IV thrombolysis are eligible.
Outcome: Primary focus revolves around safety measures. Secondary outcomes encompass various metrics including neurological, functional and imaging outcome observed at 24 hour and up to 90 days.
Results: Recruitment has commenced in the United States and Taiwan.
Conclusions: The result would provide valuable insights into the safety and potential benefit of LT3001 for AIS patients, particularly those undergoing IA EVT.
Disclosures of Interest: Yes Lumosa employee
Abstract N°: 268
SEARCH (A RANDOMISED CONTROLLED TRIAL OF SCANNING EYE TRAINING AS A REHABILITATION CHOICE FOR HEMIANOPIA AFTER STROKE)
Fiona Rowe*1
1University of Liverpool, Institute of Population Health, Liverpool, United Kingdom
On behalf of: Michaela Brown, Kausik Chatterjee, Avril Drummond, Christine Hazelton, Brin Helliwell, Lauren Hepworth, Claire Howard, Stevie Johnson, Carmel Noonan, Catherine Sackley, Laura Wright
Background and aims: Visual scanning/search training is potentially beneficial to treat hemianopia. This randomised controlled phase III trial aims to determine the clinical effectiveness of visual scanning training to treat homonymous hemianopia in stroke survivors.
Methods: Recruitment was undertaken in 34 hospitals. Inclusion criteria: clinically diagnosed stroke, 18+ years, stable hemianopia, >4 weeks and <26 weeks post-stroke onset, able to engage in training, informed/proxy consent. Exclusion criteria: inability to undertake treatment (severe cognition problems), unwilling to participate, <4 weeks and >26 weeks post-stroke onset, presence of severe visual inattention, other serious concomitant medical condition. The intervention was a visual scanning strategy compared to sham training. Minimum duration of treatment was for 6 weeks with follow-up for 26 weeks. The primary outcome measurement was the National Eye Institute Visual Function Questionnaire 25. Secondary outcome measurements included the Nottingham Extended Activities of Daily Living, EQ-5D-5L, BIVI-IQ, visual field measurement, visual scanning performance and adverse events.
Results: The first patient was randomised on 04/05/2021. The last patient was randomised on 31/07/2023. 161 were randomised. For 158 participants, baseline characteristics were available: mean age 65.22 years (SD 13.95), 114 male (72.2%), 44 female (27.8%), mean time from onset to randomisation, 98.97 days (SD 43.03), stroke type (ischemic 145 (91.8%), haemorrhagic 13 (8.2%)), mean Barthel index 8.96 (SD 2.48). Partial homonymous hemianopia was documented for 126 (79.7%) and complete for 32 (20.3%).
Conclusions: The sample size target for the SEARCH trial was met. Next steps are to complete follow-up to 26 weeks for remaining participants.
Disclosures of Interest: Yes Funding for research: NIHR, Stroke Association, Fight for Sight.
Abstract N°: 295
FINDING THE RIGHT DOSE: A SCOPING REVIEW EXAMINING FACILITATION AS AN IMPLEMENTATION STRATEGY FOR EVIDENCE-BASED STROKE CARE
Oyebola Fasugba1,2, Heilok Cheng1,2, Simeon Dale1,2, Kelly Coughlan1,2, Elizabeth Mcinnes1,2, Dominique A. Cadilhac3, Kelvin Hill4, Anna Ranta5, /Christopher Levi/6,7, Sandy Middleton*1,2
1Australian Catholic University, St Vincent’s Health Network Sydney & St Vincent’s Hospital Melbourne, Australia,2Australian Catholic University, School of Nursing, Midwifery and Paramedicine, Australia,3Monash University, Stroke and Ageing Research, Department of Medicine, School of Clinical Sciences, Australia,4Stroke Foundation, Melbourne, Australia,5University of Auckland, School of Nursing, Faculty of Medical and Health Sciences, New Zealand,6University of Newcastle, Department of Medicine, Callaghan, Australia,7John Hunter Hospital, John Hunter Health & Innovation Precinct, New Lambton Heights, Australia
On behalf of: QASC Australasia Trialist
Background and aims: Facilitation supports implementation of evidence into clinical practice. However, facilitation ‘dose’ or intensity required for optimal uptake of interventions and/or how ‘dose’ is measured in trials evaluating facilitation is unknown. A scoping review was undertaken as part of the Quality in Acute Stroke Care Australasia Trial, which is testing two different facilitation intensities to support delivery of the Fever Sugar Swallow Protocols for stroke patients. The review aimed to determine if, and how, facilitation dose is reported and measured, and what facilitation strategies have been used to implement interventions in stroke trials.
Methods: Cochrane, CINAHL and MEDLINE databases were searched (January 2017 to July 2023) to identify randomised trials and quasi-experimental studies of stroke/TIA interventions. Narrative synthesis of the data was undertaken.
Results: Ten studies (23 papers) were included. Only one study reported facilitation ‘dose’, measured as external facilitator interaction with hospital site member. Facilitation strategies ranged from remote contact via online resources, to face-to-face workshops from an external facilitator and ongoing telephone/email support, to continuous engagement using on-site internal facilitators. Facilitator roles were broad: site-specific briefing, action planning and/or goal setting; identifying enablers and barriers to change; coaching, training, education or feedback; and network support. Only two studies reported using recommended guidelines to support intervention replication.
Conclusions: There was a paucity of information on facilitation ‘dose’ and reporting on specific details of intervention delivery in stroke. Given the complexity of implementing healthcare interventions and the implications for resourcing of higher facilitation ‘doses’, precise reporting of facilitation ‘dose’ is warranted.
Disclosures of Interest: No
Abstract N°: 420
ASUNDEXIAN FOR STROKE PREVENTION IN PATIENTS WITH ACUTE NON-CARDIOEMBOLIC ISCHEMIC STROKE OR HIGH-RISK TIA: DESIGN OF THE OCEANIC-STROKE TRIAL
Ashkan Shoamanesh1, Stuart Connolly2, Qiang Dong*3, Evija Miglane4, Jaime Masjuan5, Hee-Joon Bae6, Andrew Demchuk7, Pablo Colorado8, Eva Muehlhofer9, Mike Sharma1
1McMaster University / Population Health Research Institute, Medicine (Neurology), Hamilton, Canada,2McMaster University / Population Health Research Institute, Medicine (Cardiology), Hamilton, Canada,3Huashan Hospital, Fudan University, Neurology, Shanghai, China,4Pauls Stradins Clinical University Hospital, Riga Stradins University, Riga, Latvia,5Hospital Universitario Ramón y Cajal, Universidad de Alcalá, Neurology, Madrid, Spain,6Seoul National University Bundang Hospital, Neurology, Seongnam, South Korea,7Hotchkiss Brain Institute, Cumming School of Medicine, University of Calgary, Calgary Stroke Program, Departments of Clinical Neurosciences and Radiology, Calgary, Canada,8Bayer LLC, Clinical Development, Whippany, United States,9Bayer AG, Thrombosis, Wuppertal, Germany
On behalf of: OCEANIC-STROKE Steering Committee
Background and aims: Patients with non-cardioembolic ischemic stroke and high-risk transient ischemic attack (TIA) remain at a high risk of stroke recurrence despite current best practice. In the PACIFIC-STROKE phase II randomized trial, factor XIa inhibition with asundexian was suggested to reduce recurrent symptomatic ischemic stroke and TIA in patients with acute non-cardioembolic ischemic stroke without significantly increasing bleeding when compared with placebo on top of background standard antiplatelet treatment.
Methods: OCEANIC-STROKE is an international, double-blind, event-driven, phase III randomized trial comparing oral asundexian 50 mg once daily with placebo, on top of standard antiplatelet treatment, in patients with acute non-cardioembolic ischemic stroke or high-risk TIA. Participants aged ⩾18 years with non-cardioembolic ischemic stroke or high-risk TIA within 72 hours of symptom onset, presence of systemic/cerebrovascular atherosclerosis or qualifying non-lacunar stroke are eligible.
Results: The primary efficacy outcome is time to first ischemic stroke and the primary safety outcome is time to first ISTH major bleeding. The planned sample size of 9300 participants will be recruited from over 700 sites in 36 countries.
Conclusions: OCEANIC-STROKE is likely to be a landmark clinical trial with significant implications for the clinical management of large numbers of patients with non-cardioembolic ischemic stroke or high-risk TIA (Clinicaltrials.gov. NCT05686070).
Disclosures of Interest: Yes The trial is sponsored by Bayer AG
1Royal Stoke University Hospital, United Kingdom,2Firstkind Ltd, United Kingdom,3Bournemouth University, United Kingdom,4University of California, Irvine, Irvine, United States,5Keele University, Keele, United Kingdom,6Independent Stroke Research Advisor, Birmingham
On behalf of:
Background and aims: Venous thromboembolism (VTE) is a potentially fatal complication of stroke. Intermittent Pneumatic compression (IPC) is recommended for prevention. However, 30% of patients have contraindications to or cannot tolerate IPC. Surface neuromuscular electrostimulation of the peroneal nerve using the geko™ device leads to rhythmic dorsiflexion of the foot improving venous flow. It is easier to use and better tolerated than IPC. The aim of this study is to assess whether using the geko™ device is more effective than IPC at preventing VTE.
Methods: This is a prospective, multicentre, randomized controlled trial to compare neuromuscular electrostimulation using the geko™ device with IPC for 30 days or until independently mobile. Adults admitted with acute stroke, unable to mobilize independently and within 36 hours of symptom onset will be included. Exclusion criteria include: DVT at screening, allergy to hydrogel, contraindications to IPC, palliative care. DVT will be assessed by leg Dopplers at day 7 and 14. Clinical suspicion of VTEs will also be recorded. The primary outcome is any VTE at 30 days. Secondary outcomes include device tolerance, neurological recovery, disability, quality of life, and home time at 90 days.
Results: First study site opened June 2023 and to date 15/1200 patients have been recruited.
Conclusions: We are still reviewing centres. Please contact Christine.roffe@uhnm.nhs.uk for details.
This study is funded by the NIHR i4i Challenge (NIHR203425). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Disclosures of Interest: Yes Christine Roffe's Department has received funds from Firstkind Ltd for an audit of VTE prevention, and Prof Roffe has also received a travel grant. Wing To and Kieron Day are employees of the Study Sponsor.
Abstract N°: 900
RAPID ASSAY DIAGNOSTIC FOR ACUTE STROKE RECOGNITION (RADAR):PORTABLE BLOOD TEST TO DETECT LARGE VESSEL OCCLUSION (ONGOING TRIAL)
Lisa Shaw*1, David Burgess2, Anand Dixit3, Edoardo Gaude4, Clare Lendrem5, Graham Mcclelland6, Phil White1, Cameron Williams5, Gewei (Becky) Zhu1, Chris Price1
1Newcastle University,2Service user (contact via Newcastle University),3Newcastle upon Tyne Hospitals NHS Foundation Trust,4UpFront Diagnostics,5NIHR Newcastle MedTech and In-vitro diagnostics Co-operative (MIC),6Northumbria University
On behalf of:
Background and aims: Large vessel occlusion (LVO) stroke is effectively treated by time-critical thrombectomy but the procedure is typically only available in Comprehensive Stroke Centres (CSC). Many patients require transfer for treatment following initial assessment at a local hospital, resulting in delays. This diagnostic accuracy study is evaluating the hospital performance of a new rapid test for LVO stroke. If accurate, the test could be used in the future by ambulance practitioners to help select patients for direct CSC admission.
Methods: Study design: Prospective observational cohort study (ISRCTN 12414986).
Setting: Emergency departments and stroke units.
Study population: Adults with new face weakness and/or arm weakness and/or speech disturbance who are known to be <6 hours of symptom onset, or are last known well between 6-24 hours.
Index test: Two portable lateral flow assays which use fingerprick capillary blood to detect D-Dimer and Glial Fibrillary Acidic Protein (GFAP) concentrations associated with the presence of LVO.
Reference standard: Independently adjudicated standard CT brain +/- CT/MR angiography plus expert clinician opinion will establish the following diagnoses: ischaemic stroke +/- LVO; intracerebral haemorrhage; transient ischaemic attack; stroke mimic.
Main analyses: Sensitivity, specificity, negative and positive predictive values for LVO stroke identification.
Sample size: A primary analysis population of 276 participants (FAST ⩾ 2, symptom onset known <6 hours) can demonstrate a test specificity of 92%. The total study population of 552 participants allows evaluation for milder symptoms and/or unknown onset times.
Results: Recruiting participants at 4 NHS organisations. Results expected in 2025.
Conclusions: N/A
Disclosures of Interest: Yes This work is done in collaboration with a commercial company (UpFront Diagnostics)
Abstract N°: 959
MUSIC AND ART THERAPY IN PATIENTS UNDERGOING REHABILITATION
Rathi Ratha Krishnan*1
1Tan Tock Seng Hospital, Rehabilitation Medicine, Singapore, Singapore
On behalf of:
Background and aims: Music therapy is effective in improving both socioemotional and functional aspects of care. Music can address the emotional issues that arise due to hospitalisation, independence loss and adjustment. Dealing with emotions in a rehabilitation setting is important as these may impact patient’s ability or willingness to participate. The literature regarding art therapy in rehabilitation is sparse. Studies done are mainly in geriatric or palliative populations. The aim of this study is to evaluate the impact of music therapy and art therapy on inpatients in an inpatient tertiary Rehabilitation Centre
Methods: This is a pilot feasibility study. We will use a randomised case control study design. The interventions group will receive music therapy alone or art therapy alone in addition to standard therapy prescribed by their primary team. Patients in the control group will not receive music or art therapy. Patients will be recruited over a 1-year period. These inpatients may be admitted following stroke, TBI, SCI or orthopaedic related diseases.
Results: We plan to recruit 54 patients for the music or art therapy intervention and 27 patients as controls (2:1). The study outcome measures include FIM, HADS, Fugl Meyer scores and pain score. Subjective assessments in the form of a simple questionnaire will also be administered. The study is expected to be commenced by March 2024.
Conclusions: Our hypotheses are that there will be little or nil impact on quantitative outcome measures and there will be a positive impact recorded in subjective reporting (in terms of improved mood or pain relief).
Disclosures of Interest: No
Abstract N°: 977
EUROPEAN BLOOD PRESSURE INTENSIVE CONTROL AFTER STROKE – PILOT TRIAL (EPICS-PILOT)
Pádraig Synnott*1,2, David J Williams1,3, Rónán Collins1,4, Kirstyn James1,5, Tim Cassidy1,2,6, David Bradley1,7, Michael Marnane1,2,8, John J Mccabe1,2,8, Sarah Coveney1,4, Peter J Kelly1,8
1Health Research Board (HRB), Stroke Clinical Trials Network Ireland (SCTNI), Dublin, Ireland,2University College Dublin, School of Medicine, Dublin, Ireland,3Royal College of Surgeons in Ireland (RCSI), University of Medicine and Health Sciences, Department of Geriatric and Stroke Medicine, Dublin, Ireland,4Tallaght University Hospital, Geriatric and Stroke Medicine, Dublin, Ireland,5Cork University Hospital, Department of Geriatric Medicine, Cork, Ireland,6St Vincent’s University Hospital, Department of Geriatric Medicine, Dublin, Ireland,7St James' Hospital, Department of Neurology, Dublin, Ireland,8Mater Misericordiae University Hospital, Stroke Service, Dublin, Ireland
On behalf of:
Background and aims: ESO guidelines recommend office-measured blood pressure (BP) reduction for secondary prevention, with a target systolic BP (SBP) <130mmHg. However, high rates of failure to achieve guideline BP targets are reported in clinical practice. Uncertainty also remains regarding the safety of BP reduction in important groups (eg. older patients) and the benefit of SBP reduction to even lower levels. Home blood pressure measurement with telemonitoring (HBPM-TM) is a promising strategy to improve compliance with current guidelines, and evaluate safety and tolerability of very low SBP targets. However, few data exist on HBPM-TM after ischaemic stroke or TIA.
Methods: EPICS-Pilot (trial registration NCT04647292) is a prospective, open-label, blinded endpoint assessed (PROBE) randomised, parallel group pilot/feasibility clinical trial, comparing the efficacy of HBPM-TM plus protocol-guided titration of antihypertensive medication versus usual care (scheduled office-based BP measurement) to achieve guideline-based SBP targets and assess safety/tolerability of intensive SBP reduction. Included patients have non-cardioembolic ischaemic stroke or high-risk TIA and SBP⩾140mmHg at baseline. The primary outcome will be the difference in mean SBP office measurement between the intervention and control arms at 12 months. Safety data will be reported. Target recruitment is 142 patients (71 per arm).
Results: Patient recruitment has begun as of January 2024 with results expected in 2025.
Conclusions: EPICS-Pilot will provide important evidence for the efficacy and safety of HBPM-TM to achieve guideline-based SBP targets compared with standard care post-stroke.
Disclosures of Interest: No
Abstract N°: 1214
CO-DESIGN OF LOVE YOUR BRAIN: A DIGITAL PLATFORM FOR STROKE PREVENTION
Monique Kilkenny*1,2, Rosanne Freak-Poli1,3, Catherine Burns1, Christine Farmer4, Tara Purvis1, Seamus Barker4, Dominique A. Cadilhac1,2, Jan Cameron1, Andrea Sanders5, Seana Gall4
1Stroke and Ageing Research, Department of Medicine, School of Clinical Sciences, Monash University,2Stroke Theme, Florey Institute of Neuroscience and Mental Health, University of Melbourne,3School of Public Health and Preventive Medicine, Monash University,4Menzies Institute for Medical Research, University of Tasmania,5Stroke Foundation
On behalf of: Love Your Brain Investigators
Background and aims: Love Your Brain is a three-armed randomised controlled trial, evaluating the effectiveness of a Massive Open Online Course, individualised text messages, and minimal control on health knowledge of Australians in stroke prevention. We aimed to develop the Love Your Brain digital platform through co-design.
Methods: Using snowballing methods, 20 community members and 16 stroke knowledge experts (e.g. health professionals, researchers) from across Australia expressed interest and were invited to participate. Of which, 12 community members and 10 experts participated in at least one of the seven online focus groups (as separate cohorts). The focus groups were designed to provide input into the structure of, and content for the digital platform (e.g. stroke signs, risk factors and management). The facilitated group discussions, live chats & interactive polls were analysed using an inductive thematic approach.
Results: Findings from focus groups include:
Use simple, easy to understand language and layout.
Use a variety of statistics, personal stories and expert information (“tell a story”).
Videos are preferred over text (make transcripts available).
Use impact to engage (“Stroke impacts everything”).
Personalise content (age, sex, location and risk factors).
Provide options for simplified/advanced information (provide trusted links)
Emphasise the importance of going to the doctor for stroke prevention.
Assist with materials to enact change (“it is difficult”).
Conclusions: The co-design informed the development of the Love Your Brain digital health platform. The platform is currently being piloted in a feasibility trial prior to a larger randomised controlled trial.
Disclosures of Interest: No
Abstract N°: 1228
MLC1501 STUDY ASSESSING EFFICACY IN POST STROKE SUBJECTS WITH MOTOR DEFICITS (THE MAESTOSO STUDY)
Christopher Chen*1, Narayanaswamy Venketasubramanian2, Romulo Esagunde3
1National University of Singapore, Singapore,2Raffles Hospital, Singapore,3Jose R. Reyes Memorial Medical Center, Manila, Philippines
On behalf of: The MAESTOSO Investigators
Background and aims: MLC601/MLC901, containing extracts from 9 herbs, has neuroprotective, anti-inflammatory and neurorestorative properties in pre-clinical models of cerebral ischemia. Clinical trials showed benefits in improving long-term recovery in patients with ischemic stroke (IS). MLC1501, with only 4 herbal components, showed similar properties in pre-clinical models of cerebral ischemia.
Our primary objective is to determine, in a multicentre clinical trial, the efficacy of MLC1501 on motor recovery measured as improvement on Fugl-Meyer motor Assessment (FMA) at 24 weeks after IS. Secondary objectives are to assess the safety of MLC1501, and to determine its efficacy on improving FMA upper or lower extremity scores at 12 and 24 weeks, modified Rankin Scale (mRS) score, Patient Reported Outcome Measurement Information System – Global Health (PROMIS-10), and NIHSS score at 4, 12 or 24 weeks.
Methods: 300 eligible patients will be randomized to receive MLC1501 high-dose, MLC1501 low-dose, or matching placebo orally for 24 weeks in a multi-centre double-blind study. Key inclusion criteria are age ⩾18 years, ischemic stroke with compatible brain imaging in the prior 2 to 10 days, NIHSS score of 8 to 18 with a combined score of ⩾3 on motor items 5A, 5B, 6A and/or 6B, and candidacy for active rehabilitation. Efficacy assessments are FMA, mRS, PROMIS-10 and NIHSS.
Results: From 21 July 2023 to 10 January 2024, 69 patients were randomized: mean age 57.1±14.4 years, Women n=29 (42%), mean baseline NIHSS 11.0±2.8, mean baseline FMA 29.3±23.8.
Conclusions: Awaiting completion.
Disclosures of Interest: No
Abstract N°: 1229
GENOTYPE GUIDED ANTIPLATELET THERAPY IN ISCHEMIC STROKE: A RANDOMIZED CONTROLLED TRIAL
1National Neuroscience Institute, Neurology (SGH Campus), Singapore, Singapore
On behalf of:
Background and aims: Clopidogrel is one of the mainstays of secondary prevention in patients with ischemic stroke. CYP2C19 loss of function (LOF) mutations impair the effectiveness of clopidogrel. The prevalence of LOF mutations is approximately 60% in Asia, rendering the effectiveness of empiric clopidogrel treatment doubtful. Therefore, we aimed to determine the feasibility and clinical impact of genetic testing guided antiplatelet therapy in ischemic stroke patients on the prevention of major adverse cardiovascular or cerebrovascular events (MACCE).
Methods: We designed a prospective randomized open blinded end point study (NCT05763862) where clopidogrel naïve ischemic stroke or TIA patients aged 21 and above will be randomized to genetic testing guided antiplatelet therapy or standard medical therapy within 1 week of their index stroke. Patients who test positive for an LOF mutation will be offered alternative antiplatelet therapy in the form of aspirin or ticagrelor (for those with monotherapy) or aspirin plus ticagrelor (for those who need dual antiplatelet therapy). Patients who test negative for LOF mutation will continue on clopidogrel.
Results: The primary clinical outcome is the composite MACCE over 12 months from recruitment following the index stroke. Secondary outcomes include clinically significant bleeding as per GUSTO criteria (Global Use of Strategies to Open Occluded Arteries) of severe/life threatening bleeding event, ischemic events (ischemic stroke or TIA, myocardial ischemic events, or death from vascular causes). Cox regression analyses will be used to analyse the primary and secondary outcomes.
Conclusions: The study is still ongoing with active recruitment.
Disclosures of Interest: No
Abstract N°: 1255
A MULTIMODAL INDIVIDUALIZED LONG-TERM INTERVENTION TO PREVENT FUNCTIONAL DECLINE AFTER STROKE. THE LAST-LONG TRIAL
Torunn Askim*1, Anne Hokstad1, Elin Bergh1,2, Øystein Døhl1,3, Hanne Ellekjær1,4, Håkon Ihle-Hansen5, Bent Indredavik1,4, Sara Langlo1, Anne Silja Mäkitalo Leer1,3, Bente Thommessen2
1Norwegian University of Science and Technology, Department of Neuromedicine and Movement Science, Trondheim, Norway,2Akershus University Hospital, Department of Neurology, Lørenskog, Norway,3Trondheim Municipality, Health and welfare, Trondheim, Norway,4St. Olav's University Hospital, Department of Stroke, Trondheim, Norway,5Bærum Hospital, Department of Stroke, Bærum, Norway
On behalf of: LAST-long study group: Stian Lydersen, Jon Magnussen, Ingvild Saltvedt and Yngve M. Seljeseth
Background and aims: Physical and cognitive impairments present substantial barriers to maintaining functionality following a stroke. The main objective of the LAST-long trial is to investigate the benefits of regular follow-up conducted by a stroke-coordinator. This coordinator will develop a tailored treatment plan S. to address the specific needs of individuals, with the intention of preventing long-term functional decline post-stroke.
Methods: A pragmatic randomised controlled trial, with repeated measures at 6, 12, and 18 months after inclusion, is applied. Patients admitted to four Norwegian hospitals; age ⩾18, modified Rankin Scale <5, able to understand Norwegian and willing to sign informed consent, were screened for inclusion 3-months after stroke. Patients with short life expectancy or diagnosed with severe illnesses were excluded.
The intervention comprises regular meetings with a community-based stroke-coordinator. Using a comprehensive checklist, the coordinator will assess the patients’ risk-profile encompassing physical health, lifestyle, mobility, ADL function, cognitive function, and social function. Following this assessment, the coordinator will establish an action-plan aligned with national guidelines, with the overarching goal of achieving the guidelines’ specified treatment goals.
Mixed models will be used to evaluate differences between the groups for the primary (disability) and secondary endpoints (cognition, motor function, extended ADL, self-perceived health, quality-of-life, frailty, vascular events, caregivers’ burden, health costs, etc.) across the 4 time points.
Results: Recruitment was concluded by March 2023, at St. Olavs Hospital (n=136), Akershus University Hospital (n=91), Bærum Hospital (n=67) and Ålesund Hospital (n=7).
Conclusions: The intervention and follow-up assessments will be concluded by august 2024.
Disclosures of Interest: No
Abstract N°: 1427
COLCHICINE FOR THE PREVENTION OF VASCULAR EVENTS AFTER AN ACUTE INTRACEREBRAL HEMORRHAGE (COVASC-ICH)
1McMaster University/ Population Health Research Institute, Hamilton, Canada,2University of British Columbia, Vancouver, Canada,3University of Calgary, Calgary, Canada,4Queen's University, Kingston, Canada,5Western University, London, Canada,6University of Toronto, Toronto, Canada,7University of Alberta, Edmonton, Canada,8Centre hospitalier de l'Université de Montréal, Montreal, Canada
On behalf of: on behalf of the CoVasc-ICH investigators
Background and aims: Intracerebral hemorrhage (ICH) survivors are at high risk of ischemic vascular events. Colchicine is a promising treatment for ICH survivors as its anti-inflammatory effects may attenuate secondary (inflammatory) brain injury following an acute ICH, and reduce ischemic major adverse cardiovascular events (MACE) without increasing the risk of bleeding
Methods: CoVasc-ICH is a randomised, double-blind, placebo-controlled trial. The vanguard phase aims to determine the feasibility of conducting a main phase trial. Consenting adults within 48 hours of spontaneous ICH onset and who have vascular risk factors or established atherosclerosis are randomly assigned (1:1) to either oral colchicine 0.5mg once daily or matching placebo. The primary efficacy outcome collected in anticipation of continuation to a main phase trial is MACE over a median of 12 months. Safety outcomes include symptomatic ICH expansion and recurrent ICH. An MRI sub-study is investigating whether colchicine attenuates perihematomal edema volume and number of DWI hyperintense lesions on 10-day MRI. This trial is registered (NCT05159219) and is open to recruitment.
Results: Up to January 1, 2024 a total of 69 participants have been enrolled at 11 high volume Canadian stroke centres and recruitment into the vanguard phase will continue to reach a target of 100 patients.
Conclusions: Colchicine is a low-cost widely available treatment that has the potential to change clinical practice and improve outcomes after ICH. The vanguard phase will provide information related to safety, efficacy outcomes and feasibility to help refine the design of the subsequent main phase trial.
Disclosures of Interest: No
Abstract N°: 1797
SAFETY AND TOLERABILITY OF ADJUNCTIVE TBO-309 IN REPERFUSION FOR STROKE (STARS), TRIAL UPDATE
Candice Delcourt*1,2, Simone Schoenwaelder3, Christopher Levi4, Mark Parsons5,6, Shaun Jackson3
1The George Institute for Global Health, The University of New South Wales, Sydney, Australia,2Macquarie University, Department of clinical medicine, Faculty of Medicine, Health and Human sciences, Sydney, Australia,3Heart Research Institute, Charles Perkins Centre, University of Sydney, Sydney, Australia,4John Hunter Hospital, University of Newcastle, Hunter Medical Research Institute, Newcastle, Australia,5Department of Neurology, Liverpool Hospital, Liverpool, Australia,6The University of New South Wales, Sydney, Australia
On behalf of:
Background and aims: Adding an antiplatelet agent to acute stroke therapies holds the promise to overcome the limitations of acute stroke therapy in terms of eligibility and efficacy. TBO-309 is an enzyme PI 3-kinase (PI3K) inhibitor Type Ia p110β isoform which is a safe and effective way to inhibit pathological thrombus formation without causing bleeding based on robust animal and healthy volunteers’ trials. This is related to its ability to modulate, rather than completely block Glycoproteins IIb/IIIa and to specifically target platelet function under conditions of shear stress which occurs in pathological clotting (thrombosis). The STARS trial is a phase IIa, dose escalation study to evaluate the safety and tolerability of adjunctive TBO-309 in adult patients with acute ischaemic stroke.
Methods: We will include ~80 patients with acute ischaemic stroke receiving thrombolysis with or without thrombectomy. TBO-309 is given as a bolus and 3-hour infusion in addition and concomitantly to acute stroke management. Patients are included according to the continual reassessment method. The primary outcome is intracerebral haemorrhage associated with clinical deterioration. Secondary outcomes include imaging and clinical outcomes.
Results: Recruitment of the first cohort of the STARS trial is ongoing at the dose of 30 mg.
Conclusions: If the trial shows safety of the AZD6482, further trials will be conducted to assess its efficacy. Trial registration: NCT05363397.
Disclosures of Interest: No
Abstract N°: 1975
THE MIND-PRO TRIAL - PROTOCOL OF A RANDOMIZED CONTROLLED HYBRID EFFECTIVENESS-IMPLEMENTATION TRIAL
Anne Roos van der Endt*1, Marieke P. Hoevenaar-Blom2, Eric P. Moll van Charante2, Martien J.H. Kas3, Esther van der Berg4, Ron Handels5, Edo Richard1
1Radboud University Medical Center, Department of Neurology, Nijmegen, Netherlands,2Amsterdam UMC, locatie AMC, Department of Public and Occupational Health, Amsterdam, Netherlands,3University of Groningen, Groningen Institute for Evolutionary Life Sciences, Groningen, Netherlands,4Erasmus MC, Department of Neurology and Alzheimer Center Erasmus MC, Rotterdam, Netherlands,5Maastricht University, Department of Psychiatry and Neuropsychology, Maastricht, Netherlands
On behalf of: NDPI Consortium
Background and aims: Dementia and stroke share many risk factors. Specifically among lower socioeconomic status (SES) and migrant populations, risk factors are more common and less well controlled. This highlights the importance of prevention strategies for these groups. The aim of the mHealth Intervention for Dementia Prevention through lifestyle Optimisation (MIND-PRO) study, is to evaluate the effectiveness and implementation of a culture-sensitive smartphone app that supports lifestyle modification to lower dementia risk factors through self-management and remote coaching.
Methods: This prospective randomized open-label blinded endpoint (PROBE) trial will follow a type 2 hybrid effectiveness-implementation design with a 12-months intervention. Entry criteria include age 50-75 years, low SES and/or migration background, one or more dementia risk factors (hypertension, dyslipidaemia, diabetes mellitus, physical inactivity, smoking, and overweight) or manifest cardiovascular disease, and owning a smartphone. Participants are randomized to a coach-supported, interactive app facilitating self-management of dementia risk factors or a control app with static health information.
Results: The MIND-PRO study aims to enrol 692 participants in the Netherlands. The primary effectiveness outcome is a composite score of systolic blood pressure, total cholesterol, and BMI. Implementation outcomes include coverage, adoption, acceptability, appropriateness, feasibility, fidelity, and sustainability of the intervention. Main secondary outcomes are change in CAIDE dementia risk score, change in individual risk factors, daily distance moved measured by BeHapp (remote behavioural monitoring app), and cost-effectiveness.
Conclusions: The results of this proof-of-concept study are expected in 2026 and may inform future large-scale RCTs with tailored, culture-sensitive, dementia risk reduction strategies, which may also reduce the risk of stroke.
Disclosures of Interest: No
Abstract N°: 2015
RE-OPEN: RANDOMISED TRIAL OF BIOSIMILAR TNK VERSUS TPA DURING ENDOVASCULAR THERAPY FOR ACUTE ISCHEMIC STROKE DUE TO LVO
Rohit Bhatia*1, Angel T Miraclin2, Srijithesh Pr3, Biman Kanti Ray4, Dhiraj Khurana5, Vijaya Pamidimukkala6, Jeyaraj Pandian7, Pn Sylaja8, Vivek Nambiar9, Roy Jayanta10
1All India Institute of Medical Sciences, Department of Neurology, New Delhi, India,2Christian Medical College, Department of Neurology, Vellore, India,3National Institute of Mental Health and Neurosciences, Department of Neurology, Bangalore, India,4Bangur Institute of Neurosciences and IPGMER, Department of Neurology, Kolkata, India,5Postgraduate Institute of Medical Education and Research, Department of Neurology, Chandigarh, India,6Lalitha Superspeciality Hospital, Department of Neurology, Guntur, India,7Christian Medical College, Department of Neurology, Ludhiana, India,8Sree Chitra Tirunal Institute of Medical Science and Technology, Department of Neurology, Thiruvananthapuram, India,9Amrita Institute of Medical Sciences, Department of Neurology, Kochi, India,10Institute of Neurosciences, Department of Neurology, Kolkata, India
On behalf of: The RE-OPEN Trial Investigators
Background and aims: The choice of thrombolytic agent during bridging therapy in acute ischemic stroke (AIS) due to large vessel occlusion (LVO) remains uncertain. The current study aims to observe if Intravenous Tenecteplase (TNK) is superior to intravenous Alteplase (rTPA) during bridging therapy as well as provide evidence for the efficacy of a biosimilar Tenecteplase within 4.5 hours.
Methods: The RE-OPEN study is an ongoing prospective, randomized, multicentre, open label trial with blinded outcome analysis (PROBE) design. All consecutive AIS patients with LVO presenting within 4.5 hours and meeting eligibility criteria will undergo web-based randomization to either Intravenous rTPA or Intravenous TNK, prior to the endovascular treatment (EVT) procedure. Primary outcomes are the proportion of patients with mRS <=2 at three months and grade 2b/3 recanalization on mTICI score at first angiography run and end of the EVT procedure. Secondary outcomes include proportion of patients with early neurological improvement defined as improvement of NIHSS by 4 points at 24 hours, rate of symptomatic ICH, rate of any ICH, rate of any systemic major or minor bleeding, and duration of hospital stay. Safety outcome includes any intracranial bleeding or symptomatic ICH.
Results: The estimated sample size is 372 patients. The trial started in September 2022, and is planned for completion by March 2025. One year and three months into the study, a total of 109 patients have been randomized.
Conclusions: Results from the RE-OPEN trial will provide class-I evidence about the choice of thrombolytic agent during bridging therapy, and effectiveness of intravenous biosimilar Tenecteplase.
Disclosures of Interest: No
Abstract N°: 2201
SYMPTOMATIC CAROTID OUTCOMES REGISTRY WITH MULTI-CENTER EVALUATION (SCORE)
Seemant Chaturvedi*1, Helmi Lutsep2,3, Magdy Selim4, Brian Silver5, Bijoy Menon3, Thanh N. Nguyen6, Luciano Sposato7,7
1University of Maryland School of Medicine,2University of Oregon Health Sciences Center,3Calgary Health Sciences Center,4Harvard Medical School,5Univ. of Massachusetts Medical Center,6Boston University School of Medicine,7London Health Sciences Center
On behalf of:
Background and aims: Current treatment of symptomatic carotid stenosis relies on data that are more than 30 years old. There is no reliable information on the stroke rate with modern, intensive medical therapy. The aim of this pragmatic registry is to provide an estimate of the ipsilateral stroke rate for patients with 50-99% symptomatic carotid stenosis who have at least one feature suggesting reduced stroke risk.
Methods: Intensive medical therapy (IMT) will be provided to all participants. IMT consists of dual antiplatelet therapy (short-term), high potency statins, blood pressure control, and lifestyle modification with risk factor education. Criteria for enrollment include any of three clinical or radiologic markers. Clinical 1) Women 2) Retinal ischemic event only 3) Last symptomatic event >2 weeks ago. Radiologic: 1) TCD negative for emboli 2) MRI negative for intraplaque hemorrhage 3) High risk TIA with negative DWI. Follow-up is one year.
14 centers in the US, Canada, and Denmark are approved for enrollment.
Primary endpoint: Ipsilateral ischemic stroke within 12 months of enrollment.
Results: Study began enrollment in late 2022.
Sample size 114 patients
Enrollment as of Jan 2023: 14
Conclusions: SCORE Registry will provide valuable information on the stroke rate in patients with symptomatic carotid stenosis treated with intensive medical therapy. These data will allow clinicians to refine carotid stenosis decision making in symptomatic patients with >50% stenosis and potentially justify a future phase III RCT.
Disclosures of Interest: No
Abstract N°: 2227
DETERMINING OPTIMAL EARLY REHABILITATION AFTER STROKE (AVERT DOSE) ONGOING TRIAL UPDATE 2024
Julie Bernhardt1, Vincent Thijs*1, Leonid Churilov2, Jeyaraj Pandian3, Peter Langhorne4, Bent Indredavik5, Richard Lindley6, Katijjahbe MD Ali7, Geoffrey A. Donnan2, Avert Dose Trialist Collaboration1
1The Florey Institute of Neuroscience and Mental Health, Heidelberg, Australia,2University of Melbourne, Parkville, Australia,3Christian Medical College and Hospital, Ludhiana, India,4University of Glasgow, Glasgow, United Kingdom,5Norwegian University of Science and Technology, Trondheim, Norway,6University of Sydney, Sydney, Australia,7Universiti Kebangsaan Malaysia, Kuala Lumpur, Malaysia
On behalf of: On behalf of the AVERT DOSE Collaboration
Background and aims: Mobility training started within 48 hours of stroke should be safe and effective given the right dose. AVERT DOSE is using an adaptive trial design to define the optimal mobility training for mild and moderate ischemic stroke patients in the acute phase.
Methods: This is an ongoing global Multi-Arm, Multi-Stage, Covariate-Adjusted, Response-Adaptive randomised trial. Patients in mild (NIHSS 0-7) and moderate (NIHSS 8-16) stroke severity strata are randomised to one of four mobility training regimens (including a pre-specified reference group), starting within 48 hrs of stroke and up to 14 days. Inclusion criteria: Ischaemic stroke within 48 hours, ⩾18 years. Exclusion criteria: Severe stroke (NIHSS>16), medically unwell, no evident mobility problems. Primary Outcome: Blinded Assessment of proportion of participants achieving a favourable outcome (mRS score 0-2) at 3 months post stroke. With a goal to recruit ~2,500 patients, adaptive sample size re-estimation provides 80% power to detect a 10% absolute treatment effect or larger compared to the pre-specified reference group, with a significance threshold of p=0.025 per stratum. Analyses will be intention-to-treat.
Results: All regions (Australia, Singapore, Malaysia, India, UK, Ireland and Brazil) are actively recruiting with 594 participants. Trial recruitment is slower than expected. Main reasons for non-inclusion: presentation to hospital >48 hours (26.3%), no mobility issues (25.5%), discharge within 3 days (9.4%).
Conclusions: Participants are presenting to hospital later and discharged earlier than expected requiring new strategies to increase recruitment. Results will provide reliable guidance about the dose of early rehabilitation after ischaemic stroke and will be globally generalisable.
Disclosures of Interest: No
Abstract N°: 2279
FEVER, HYPERGLYCEMIA, SWALLOWING, AND HYPERTENSION MANAGEMENT IN ACUTE STROKE - PHASE II
1All India Institute of Medical Sciences, Department of Neurology, New delhi, India,2Rajendra Institute of Medical Sciences, Department of Neurology, Ranchi, India,3Fortis Vasant Kunj, Department of Neurology, New Delhi, India,4All India Institute of Medical Sciences, Department of Neurology, Rishikesh, India,5Institute of Human Behaviour and Allied Sciences, Department of Neurology, New Delhi, India,6Dr Ram Manohar Lohia Hospital, Department of Neurology, New Delhi, India
On behalf of:
Background and aims: Stroke is the second-leading cause of death. In India, it is estimated that there are 16 lakh new cases of stroke every year, out of these two-third suffer from either mortality or morbidity after stroke. A cluster randomized study conducted in Australia showed the wide applicability of FeSS (management of fever, sugar, swallowing) in comparison to other interventions and 15.7% improvement in patient’s survival.
Methods: The Pilot study of this intervention involving 12 hospitals (six medicals and six district hospitals) has been completed which indicated the feasibility of the intervention. The design of current ongoing study is “stepped wedge cluster randomized trial with cross-sectional data collection” with 20 centers. Each sub center enters into intervention phase at a time period, and eventually all centers get intervention by the end of randomization process. The intervention targets to prompt nursing assessment of fever, sugar, swallowing, hypertension, along with standard of care in line of clinical treatment protocols and stroke care pathways developed by clinicians.
Results: AIIMS, New Delhi, one of the centre is under control arm and not been randomized in the intervention arm yet. Baseline data of cases and control patients enrolled in the study is maintained in the RedCap.Telephonic follow up of each enrolled case is done after three months from enrollment and their mRS and barthel index is scored.
Conclusions: It is an ongoing trial, till date (15-01-24) 314 patients have been screened out of which 93 cases and 27 healthy controls have been enrolled at our centre.
Disclosures of Interest: No
Abstract N°: 2416
EXPLORING VASCULAR CONTRIBUTIONS TO COGNITIVE IMPAIRMENT AND DEMENTIA (ENIGMA): PROTOCOL FOR A PROSPECTIVE OBSERVATIONAL STUDY
Andreas Gammelgaard Damsbo*1,2, Sigrid Breinholt Vestergaard1,2, Niels Lech Pedersen2,3, Katrine Zachariassen1, Kim Ryun Drasbek4, Leif Østergaard4, Grethe Andersen1,2, Rikke Beese Dalby2,5, Janne K Mortensen1,2
1Aarhus University Hospital, Danish Stroke Centre, Neurology, Aarhus, Denmark,2Aarhus University, Department of Clinical Medicine, Faculty of Health, Aarhus, Denmark,3Aarhus University Hospital, Department of Radiology, Aarhus, Denmark,4Aarhus University, Center of Functionally Integrative Neuroscience, Aarhus, Denmark,5South Denmark University Hospital, Department of Radiology, Esbjerg, Denmark
On behalf of:
Background and aims: Post-stroke cognitive decline is common. However, no treatment of post-stroke cognitive decline exists, and the underlying pathophysiology remains largely unknown. Finding markers that can predict, which patients may experience post-stroke cognitive decline, could be a first step towards better screening and management.
Capillary dysfunction may accompany cerebral small vessel disease and predict cognitive decline. Extracellular vesicles (EVs) carry molecules between cells and may therefore act as disease biomarkers.
We aim to investigate capillary dysfunction and EV profiles as predictors of cognitive function one year after acute ischemic stroke (AIS) and transient ischemic attack (TIA).
Methods: The ENIGMA study is a single-centre prospective clinical observational study conducted at Aarhus University Hospital, Denmark. Consecutive patients with magnetic resonance imaging (MRI)-verified AIS and TIA are included and followed for one year with follow-up visits at three and 12 months. An MRI is performed at 24 hours and 12 months after admission. EV profiles will be characterised from blood samples drawn at 24 hours and three months after admission. Cognitive function is assessed three and 12 months after AIS and TIA using the Repeatable Battery for the Assessment of Neuropsychological Status.
Results: No results to present yet.
Conclusions: Using novel imaging and molecular biological techniques the ENIGMA study will provide new knowledge about the vascular contributions to cognitive decline and dementia.
Disclosures of Interest: No
Abstract N°: 2478
DOES PHARYNGEAL ELECTRICAL STIMULATION IMPROVE SWALLOWING IN ACUTE STROKE DYSPHAGIA? THE PHEAST TRIAL
Lisa Woodhouse1, Tim England1, Lisa Everton2, Shaheen Hamdy3, Tiffany Hamilton1, Marilyn James4, Alan Montgomery4, Cameron Skinner11, Craig Smith5, Philip Bath*1
1University of Nottingham, Stroke Trials Unit, Mental Health & Clinical Neurosciences, Nottingham, United Kingdom,2Nottingham University Hospitals NHS - QMC, Speech and Language Therapy, Nottingham, United Kingdom,3University of Manchester, Division of Diabetes, Endocrinology & Gastroenterology, Manchester, United Kingdom,4University of Nottingham, Nottingham Clinical Trials Unit, Nottingham, United Kingdom,5University of Manchester, Division of Cardiovascular Sciences, Manchester, United Kingdom
On behalf of: the PhEAST Trial Investigators
Background and aims: Dysphagia (swallowing difficulties) is common post stroke and an independent predictor of poor outcome, but there are no standardised treatment guidelines. Pharyngeal electrical stimulation (PES) is licensed for use in the UK and Europe but lacks a definitive evidence-base and so is not widely used. We aim to assess whether PES is safe and effective at improving post-stroke dysphagia.
Methods: PhEAST is an international prospective, randomised, open-label, blinded-endpoint (PROBE) trial. 800 adults with recent (4-21 days) ischaemic or haemorrhagic anterior or posterior circulation stroke, and clinical dysphagia with a reliance on non-oral nutrition will be recruited.
Patients will be randomised (1:1), with stratification on country and minimisation on age, sex, dysphagia severity rating scale (DSRS), impairment, stroke type, circulation and time to randomisation, to receive either PES or No PES. The PES group will receive six, once daily (10 minute) treatments of PES. Both groups will receive standard dysphagia rehabilitation.
The primary outcome is dysphagia status, assessed using the Dysphagia Severity Rating Scale (DSRS) at day 14. Secondary outcomes include PES threshold and tolerability at day 7, dysphagia status, dependency, disability, quality of life, cognition, mood and disposition at 90 and all-cause mortality at day 365.
Results: As of 15th January 2024, 157 participants have been recruited to the PhEAST trial.
Conclusions: PhEAST will provide definitive evidence for the use of PES in acute stroke. The results may directly inform clinical decision making and support decisions on guidelines for standardised practice in dysphagia treatment.
Disclosures of Interest: No
Abstract N°: 2497
SALICORNIA RAMOSISSIMA EXTRACT ADMINISTERED TO TIA PATIENTS: A RANDOMIZED, PLACEBO-CONTROLLED, PILOT TRIAL
Soledad Pérez Sánchez*1,2, Ana María Najar Moyano1,2, Carmen del Rio Mercado2, Cristina López Ázcarate1, Carmen Domínguez Ruiz1, Reyes de Torres Chacon1,2, Ana Barragán1,2, Ana Dominguez Mayoral1,2, Rosa Acevedo Aguilera1, Joan Montaner1,2
1Hospital Universitario Virgen Macarena, Neurology, Sevilla, Spain,2Instituto de Biomedicina de Sevilla, Neurovascular, Sevilla, Spain
On behalf of:
Background and aims: A substantial proportion of strokes are attributed to unhealthy lifestyle habits and could be prevented by applying a multifactorial approach including dietary interventions. Regular intake of dietary polyphenols has been shown to reduce the incidence of cardiovascular events. Preclinical studies on animal models of ischemia showed the neuroprotective effect of supplementation with polyphenol-rich extracts of the halophyte plant Salicornia.
We aimed to explore the safety of administering a Salicornia extract in patients who had suffered a recent (in last 24 months) transient ischemic attack (TIA).
Methods: We performed a randomized, parallel-group and doble-blind pilot study to assess the safety of administering 1 gram of Salicornia extracts versus placebo for 11 months to TIA patients (NTC06076122). The total polyphenol content of each Salicornia extract capsule was 8.6±1.2 mg GAE/g. We report the interim analysis for safety purpose at 6 months (visit 2) after the onset of treatment.
Results: 80 participants were enrolled, with a mean age of 67.92 years. No differences in the risk factors profile existed between groups. The rate of adverse events related to the treatment was similar in the two arms (10% vs 7.5%, p=0.813). There were no differences between groups in the analytical data analyzed (lipid and renal profile).
Conclusions: Our study shows that supplementation with polyphenols-rich Salicornia extracts in patients with TIA is safe and the study continues to the end. This encourages to explore the efficacy of Salicornia extracts in primary and secondary stroke prevention.
Disclosures of Interest: No
Abstract N°: 2561
CAROTID ARTERY STENTING DURING ENDOVASCULAR TREATMENT OF ACUTE ISCHEMIC STROKE (CASES) – A MULTICENTER RANDOMIZED CLINICAL TRIAL
Louise Maes*1,2, Theodora Van Elk3, Anne van der Meij4,5, Paul Nederkoorn4, Robin Lemmens1,2, Maarten Uyttenboogaart3,6
1University Hospitals Leuven, Department of Neurology, Leuven, Belgium,2KU Leuven - University of Leuven, Department of Neurosciences, Experimental Neurology, Leuven, Belgium,3University Medical Center Groningen, Department of Neurology, Groningen, Netherlands,4University Medical Center Amsterdam, Department of Neurology, Amsterdam, Netherlands,5Leiden University Medical Center, Department of Neurology, Leiden, Netherlands,6University Medical Center Groningen, Department of Radiology - Medical Imaging Center, Groningen, Netherlands
On behalf of: CASES Executive Committee
Background and aims: The optimal management of tandem lesions in acute ischemic stroke patients is unclear. Our aim is to assess the efficacy and safety of immediate carotid artery stenting (CAS) in patients undergoing endovascular treatment (EVT) for intracranial large vessel occlusions (LVOs) and concomitant carotid artery stenosis.
Methods: CASES is a phase 3 multicenter randomized clinical trial with open-label treatment and blinded outcome assessment (PROBE design) and a non-inferiority design. We aim to include 600 patients with a CT-angiography proven intracranial LVO in the anterior circulation and a severe ipsilateral proximal carotid artery stenosis (>50%) or occlusion of presumed atherosclerotic origin. Patients will be randomized to either immediate CAS during EVT or to EVT and a deferred strategy with carotid endarterectomy (CEA), CAS or medical management alone according to the national guidelines. The primary endpoint is functional outcome at 90 days, assessed with the modified Rankin Scale (mRS). Secondary outcomes include the mRS overall distribution at 90 days, stroke severity measured with the NIHSS at 24 hours and 5-7 days and recurrence of ischemic events, carotid re-occlusion, symptomatic intracranial haemorrhage, mortality and the quality of life at 90 days.
Results: CASES will be conducted in 29 EVT centers in Belgium and the Netherlands. The first patient was included on July 5th 2023. Currently, 71/600 patients have been randomized in 16 different centers.
Conclusions: This study will provide high-quality randomized data on the efficacy and safety of immediate CAS in patients undergoing endovascular treatment for acute ischemic stroke due to a carotid tandem lesion.
Disclosures of Interest: No
Abstract N°: 2567
EFFICACY OF NITRIC OXIDE IN STROKE-2(ENOS-2): RATIONALE DESIGN OF A PHASE-IIB SINGLE-BLIND RANDOMISED CONTROLLED SINGLE-CENTRE
Philip Bath*1, Amanda Buck2, Tiffany Hamilton1, Lisa Woodhouse1, Amanda Hedstrom2, Kailash Krishnan2, Kennedy Cadman1, Sharon Ellender1, Iris Isheanesu Mhlanga1, Nikola Sprigg1
1Stroke Trials Unit, Division of Mental Health & Clinical Neurosciences, Nottingham, United Kingdom,2Stroke Research Team, Division of Mental Health and Clinical Neurosciences, Nottingham, United Kingdom
On behalf of: Nottingham Hospital’s Charity Research fund.
Background and aims: High blood pressure (BP) common in stroke, is associated independently with increased recurrence, dependency, or late death. Nitric oxide (NO) donors including glyceryl trinitrate (GTN) are candidate treatments for acute stroke. Whether GTN improves outcome through reducing expansion and recurrence or worsens it through reducing cerebral blood flow remains unclear.
We aim to assess the feasibility of recruitment and safety of GTN to inform the design of a definitive trial.
Methods: 120 adult patients [100 ischaemic stroke(IS) and 20 intracerebral haemorrhages(ICH)], characterised by systolic BP >120mmHg, will be recruited within 3-5 hours of onset. Exclusion criteria include; seizure, mRS⩾4, glucose <3mmol/l, GCS<8, known stroke mimic, life expectancy <6months, known sensitivity to Duoderm and contraindications to GTN.
Patients will be randomised (1:1) to receive 5mg GTN or matching comparator Duoderm patch placed on back or shoulders applied for 2 days. Patients, researchers, and outcome assessors will be masked to treatment allocation.
Feasibility outcomes include recruitment of 100 IS and 20 ICH patients, rate of recruitment, proportion of patients approached being randomised, adherence to treatment and follow up. Secondary outcomes include BP and heart rate over the first 2 days, discharge destination, serious adverse events up to day 2, fatal SAEs up to day 90, mortality, disability, cognition, mood, and quality of life at day 90.
Results: As of 15th Jan 2024, 36 participants have been recruited to the ENOS-2 trial.
Conclusions: ENOS-2 will provide definitive evidence for the use of GTN in acute stroke.
Disclosures of Interest: No
Abstract N°: 2582
MANNITOL FOR CEREBRAL OEDEMA AFTER INTRACEREBRAL HAEMORRHAGE (MACE-ICH): A FEASIBILITY TRIAL
Kailash Krishnan*1, Jesse Dawson2, Robert Dineen3, Tim England4, David Hewson5, Mary Joan Macleod6, Christine Roffe7, Nikola Sprigg4, Lisa Woodhouse4, Philip Bath4
1Nottingham University Hospitals NHS Trust, Stroke, Nottingham, United Kingdom,2University of Glasgow, Cardiovascular & Metabolic Health, Glasgow, United Kingdom,3University of Nottingham, Radiological Sciences, Mental Health & Clinical Neurosciences, Nottingham, United Kingdom,4University of Nottingham, Stroke Trials Unit, Mental Health & Clinical Neurosciences, Nottingham, United Kingdom,5Nottingham University Hospitals NHS Trust, Department of Anaesthesia & Critical Care, Nottingham, United Kingdom,6University of Aberdeen, Department of Medicine and Therapeutics, Aberdeen, United Kingdom,7Keele University, School of Medicine, Keele, United Kingdom
On behalf of: the MACE-ICH Investigators
Background and aims: After spontaneous intracerebral haemorrhage (ICH), a key question is the management of significant cerebral oedema, estimated to affect ~1,500 patients in the UK each year. Mannitol, an osmotic diuretic, is readily available and licensed to treat cerebral oedema. MACE-ICH will determine the feasibility of screening, assessing eligibility, approaching potential participants, randomisation, administering mannitol and completing follow-up for acute ICH patients with cerebral oedema, or at risk of cerebral oedema, to inform a definitive trial.
Methods: MACE-ICH is a multicentre, prospective, randomised, open-label, blinded-endpoint trial and will recruit adults with spontaneous ICH with estimated largest diameter >2cm, presenting within 72 hours of onset with, or at risk of cerebral oedema with or without mass effect (limited GCS score <9 (eye opening and motor only) and NIHSS>8). Participants will be randomised (1:1:1) to receive either: (a) 1g/kg 10% single-dose mannitol infusion at 10ml/min with standard care; (b) 1g/kg 10% mannitol at 10 ml/min, followed by a second dose at 24 hours (if serum osmolality <320mOsm/Kg and sodium <160mEq/L after the first dose) with standard care; or (c) standard care alone.
Results: 45 participants will be recruited from ten UK, NHS hospitals providing acute stroke services.
Conclusions: MACE-ICH will inform the design and conduct of an adequately powered, pragmatic, prospective multicentre randomised controlled trial testing mannitol as a treatment for cerebral oedema in spontaneous ICH.
Disclosures of Interest: No
Abstract N°: 2605
ENHANCEMENT OF STROKE REHABILITATION WITH LEVODOPA (ESTREL) - PROGRESS OF THE MULTICENTRE PLACEBO-CONTROLLED RANDOMISED TRIAL
Stefan Engelter1,2, Josefin E. Kaufmann*1,2, Annaelle Zietz1,2, Karin Wiesner1, Sandro Fischer1,2, Eveline Brunner1,2, Jeremia Held3,4, Gary Ford5, Andreas Luft6, Christopher Kenan Traenka1,2
1FELIX PLATTER, University of Basel, Switzerland, Neurology and Neurorehabilitation, University Department of Geriatric Medicine, Basel, Switzerland,2University Hospital Basel and University of Basel, Department of Neurology and Stroke Center, Basel, Switzerland,3University Hospital Zurich, Vascular Neurology and Neurorehabilitation, Stroke Center, Zurich, Switzerland,4Valens Clinics, Rehabilitation Triemli Zurich, Zurich, Switzerland,5University of Oxford, Oxford University Hospitals NHS Foundation Trust, Oxford, United Kingdom,6Center for Neurology and Rehabilitation, Vitznau, Cereneo, Vitznau, Switzerland
On behalf of: ESTREL investigators
Background and aims: The ESTREL trial investigates whether Levodopa given in addition to usual rehabilitative therapies results in a patient-relevant enhancement of motor recovery after acute stroke.
Methods: ESTREL (Enhancement of Stroke REhabilitation with Levodopa) is a multicentre, placebo-controlled, double-blind randomised superiority trial. Patients with an acute ischaemic or haemorrhagic stroke and disabling hemiparesis requiring in-hospital rehabilitation are enrolled in 12 acute care centres within 7 days of onset and later transferred to neurorehabilitation centres. Participants receive Levodopa 100mg/Carbidopa 25mg three times daily or a matching placebo for 5 weeks in addition to standardised rehabilitation therapy. The primary outcome is the in-between-difference of the Fugl-Meyer Motor Assessment score 3 months after randomisation. We present the characteristics of the first 500 of 610 patients to be enrolled.
Results: 422 patients (84.4%) had an ischaemic stroke. Participants had a median age of 73 [IQR 63-82] years and 40.2% were female. At baseline, the median NIH-Stroke scale score was 7 [5-10]. Three-month visits were performed in 464 patients (92.8%); 22 (4.4%) died before the 90-day visit, 9 (1.8%) withdrew from the study and 5 (1.0%) patients missed the clinical visit.
Conclusions: The ESTREL study progresses successfully, and few patients are withdrawing. The last patient-in is expected in summer 2024. This large trial in the field of neurorehabilitation will provide evidence of whether Levodopa is safe and improves functional outcome in stroke rehabilitation.
Nikola Sprigg*1, Tiffany Hamilton1, Chaamanti Menon1, Brittany Hare1, Joseph Dib1, Solomon Adegbola1, Christopher Cheung1, Lisa Woodhouse1, Iris Isheanesu Mhlanga1, Philip Bath1
1Stroke Trials Unit, Mental Health and Clinical Neurosciences, Nottingham, United Kingdom
On behalf of: the National Institute of Health and Care Research (NIHR); Programme Hospitalier de Recherche Clinique (PHRC), France and Sweden, project (HTANIHR129917).
Background and aims: ICH a medical emergency causes more than 1.7 million strokes worldwide/year with over 40% mortality. Tranexamic acid(TXA) when given early, reduces mortality and haematoma expansion in spontaneous ICH. The haemostatic effect of TXA was demonstrated in prior pilot studies. We aim to assess the clinical effectiveness of TXA after ICH and determine whether TXA should be used in clinical practice.
Methods: TICH-3 is a pragmatic phase III prospective double-blinded randomised placebo-controlled trial. 5500 patients(⩾18years) with spontaneous ICH (including direct oral anticoagulants(DOACs) associated ICH) will be recruited within 4.5hrs of onset across UK and International sites. Exclusion criteria include known indication for TXA, contraindications for TXA, known to be on anticoagulation (except DOACs), massive ICH(>60ml), severe coma(GCS<5) and palliative care.
Rapid emergency consent will take place and patients will be randomised(1:1) by simple randomisation to receive intravenous TXA 2g; 1g bolus loading dose given as 100ml infused over 10-minutes, followed by another 1g in 250ml infused over 8hrs or matching comparator. Patients, relatives, researchers, and outcome assessors will be masked to treatment allocation.
The primary outcome is mortality by day 7. Secondary outcomes include dependency(using mRS), Quality of Life at day 180, SAE’s up to 7-days, and fatal SAEs up to day 180.
Results: By 15th of January 2024, 621(11.3%) participants have been recruited by 61 UK and 7 International countries (Malaysia, Georgia, Finland, Denmark, Ireland, France and Italy) into TICH-3 trial.
Conclusions: TICH-3 results will provide definitive evidence for the effectiveness of TXA clinical usage which could change clinical practice globally.
Disclosures of Interest: No
Abstract N°: 2696
METOCLOPRAMIDE FOR AVOIDING PNEUMONIA AFTER STROKE(MAPS-2): SINGLE-BLIND RANDOMIZED CONTROLLED TRIAL OF MCL FOR PREVENTION OF PNEUMONIA AFTER STROKE
Christine Roffe*1, Anushka Warusevitane1, Craig Smith2, Anand Dixit3, Nikola Sprigg4, Julius Sim5, Sue Jowett6, Reuben Ogollah7, Lisa Woodhouse4, Philip Bath4
1Royal Stoke University Hospital, Stoke-on-Trent, United Kingdom,2Division of Cardiovascular Sciences, University of Manchester, Manchester, United Kingdom,3Freeman Hospital, Newcastle upon Tyne, United Kingdom,4Stroke Trials Unit, Division of Mental Health and Clinical Neurosciences, Nottingham, United Kingdom,5School of Medicine, Health and Social Sciences, Staffordshire, United Kingdom,6Health Economics Unit, Institute of Applied Health Research, Birmingham, United Kingdom,7Nottingham Clinical Trials Unit, Nottingham, United Kingdom
On behalf of: NIHR HTA
Background and aims: Pneumonia causes more deaths than neurological damage after stroke. Stroke-associated pneumonia is caused by aspiration of vomited/regurgitated gastric content.
MAPS-2 assesses whether the antiemetic metoclopramide reduces mortality in patients with dysphagia after stroke, and prevents pneumonia and improves neurological recovery when given for 2 weeks after stroke.
Methods: 2100 adults with a clinical diagnosis of acute stroke, within 24-hours of stroke-onset with moderate to severe neurological impairment(NIHSS⩾10) or dysphagia and NIHSS⩾6, without contraindications to metoclopramide, pneumonia at screening, pregnancy, or life-limiting comorbidities will be recruited from ⩾60 UK-hospitals.
Patients are randomised(1:1) by minimisation on age, mRS, NIHSS, type of centre and time from onset, to 10mg of metoclopramide solution or placebo three times a day via slow IV injection or nasogastric tube for 14 days. Follow-up is at day 14 in person and at 6-months by telephone.
The primary outcome is all-cause mortality by 6-months. Secondary outcomes include pneumonia, antibiotic treatment, quality of life(QOL), dysphagia, and neurological recovery at day 14 and mRS, frailty, quality of life, dysphagia, and home time at 6-months.
Results: By 9th of January 2024, 575(27.4%) participants were recruited. Baseline characteristics are: mean(SD) age 77.6(11.9) years, median[IQR] pre-stroke mRS 1.0 [0.0, 2.0], NIHSS 17.0[13.0, 21.0], and Glasgow-Coma-Scale 14.0[12.0, 15.0]. By 14 days 168(37.7%) patients had at least 1 episode of pneumonia. Mortality by day180 is 133(23.1%).
Conclusions: MAPS-2 is recruiting the target population of severe strokes at high risk of pneumonia and will show whether metoclopramide given for 2 weeks reduces pneumonia and mortality.
Disclosures of Interest: No
Abstract N°: 2890
RANDOMIZATION TO EXTEND STROKE INTRAVENOUS THROMBOLYSIS IN EVOLVING NON-LARGE VESSEL OCCLUSION WITH TNK (RESILIENT- EXTEND-IV)
1Hospital Albert Einstein, Neurology, São Paulo, Brazil,2Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto, Neurology, Brazil,3Moinhos de Vento Hospital, Neurology and Neurosurgery, Porto Alegre, Brazil,4São Paulo Hospital, Neurology, São Paulo, Brazil,5Fortaleza General Hospital, Neurology, Fortaleza, Brazil,6Faculdade de Medicina da Bahia da Universidade Federal da Bahia, Neurology, Salvador, Brazil,7Hospital de Base do Distrito Federal, Neurology, Brasilia, Brazil,8University of Pittsburgh Medical Center, Neurology, Pittsburgh, United States
On behalf of: RESILIENT EXTEND-IV Investigators
Background and aims: Patients with AIS caused by large vessel occlusion (LVO) treated in the extended time window obtained better outcomes with tenecteplase (TNK) versus tPA regarding arterial reperfusion and clinical outcomes. None of these trials compared TNK in non-LVO AIS in the extended time window using clinical-radiological mismatch or CTP.
Methods: Prospective, multicenter, randomized, controlled, double-blinded trial. The randomization employs a 1:1 ratio of intravenous thrombolysis with TNK versus placebo in patients who suffer a non-LVO AIS between 4.5 and 12 hours from the TLSW and have evidence of salvageable brain with a clinical-radiological mismatch. The primary outcome is the rate of good clinical outcome using sliding dichotomy (mRS 0-1 for baseline mRS 0; mRS ⩽ 2 for baseline mRS 1) as evaluated by two separate assessors at the central core lab, with local reading as a backup.
Results: The study recruitment is ongoing, with the final analysis planned for 2026, including 360 patients with completed 90-day follow-ups. Enrollment is ongoing at 17 sites. Until now, 39 patients have been enrolled.
Conclusions: The RESILIENT EXTEND-IV trial may provide inputs on the efficacy and safety of TNK use in non-LVO AIS in the extended time window.
Disclosures: This study is supported by Boehringer Ingelheim (BI) for providing the drug/placebo. BI has no role in the results' design, analysis, or interpretation. BI was allowed to review the manuscript for medical and scientific accuracy and intellectual property considerations. This research is funded through PROADI-SUS, Hospital Moinhos de Vento. ClinicalTrials.gov registry: NCT05199662.
Disclosures of Interest: No
Abstract N°: 2949
RANDOMIZATION TO ENDOVASCULAR TREATMENT ALONE OR PRECEDED BY SYSTEMIC THROMBOLYSIS WITH TNK IN AIS DUE TO LVO - RESILIENT DIRECT-TNK
Octavio Pontes1, Gisele Sampaio2, Leonardo Carbonera*3, Ana Claudia de Souza3, Daniel Bezerra4, Fabrício Oliveira Lima5, Francisco Mont'alverne5, Mário Bernardes Wagner6, Raul Nogueira7, Sheila Cristina Ouriques Martins3
1Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto, Neurology, Ribeirão Preto, Brazil,2Hospital Albert Einstein, Neurology, São Paulo, Brazil,3Moinhos de Vento Hospital, Neurology and Neurosurgery, Porto Alegre, Brazil,4Hospital Pró-Cardíaco, Neurology, Rio de Janeiro, Brazil,5Fortaleza General Hospital, Neurology, Fortaleza, Brazil,6Universidade Federal do Rio Grande do Sul, Statistics, Porto Alegre, Brazil,7University of Pittsburgh Medical Center, Neurology, Pittsburgh, United States
On behalf of: RESILIENT DIRECT-TNK Investigators
Background and aims: Recent studies have questioned the benefit of IV thrombolysis with alteplase before mechanical thrombectomy (MT) in acute ischemic stroke (AIS) patients with large vessel occlusion (LVO). Other studies suggested that tenecteplase (TNK) before MT might provide higher recanalization rates than alteplase.
Methods: Randomized, prospective, multicenter, placebo-controlled clinical trial in patients with AIS due to LVO of the anterior circulation (ICA, MCA-M1, or MCA-M2) below 4.5 hours from symptoms onset. Randomization is 1:1 according to reperfusion treatment modalities: (A) direct mechanical thrombectomy (placebo-controlled) vs. (B) Intravenous thrombolysis with TNK (0.25 mg/kg) plus mechanical thrombectomy. The primary outcome is be the ordinal distribution from the modified Rankin scale (mRS) at 90 days.
Results: The study recruitment is ongoing, with the final analysis planned for late 2026, including 390 patients with completed 90-day follow-ups. Enrollment is ongoing at 13 sites. Until now, 104 patients have been enrolled.
Conclusions: The RESILIENT DIRECT TNK trial will evaluate the hypothesis that in AIS patients with anterior LVO < 4.5 hours of symptoms, MT preceded by TNK is superior to MT alone to achieve more favorable outcomes measured by mRS scores at 90 days.
Disclosures: This study was supported by Boehringer Ingelheim (BI) and Medtronic for providing the drug/placebo and devices, respectively. BI and Medtronic have no role in the results' design, analysis, or interpretation. BI was allowed to review the manuscript for medical and scientific accuracy and intellectual property considerations. This research is funded through PROADI-SUS, Hospital Moinhos de Vento. ClinicalTrials.gov registry: NCT05199194.
Disclosures of Interest: No
Abstract N°: 3201
STENTING OF SYMPTOMATIC LOW GRADE STENOSES OF THE PROXIMAL INTERNAL CAROTID ARTERY WITH A NOVEL BRAIDED HIGH COVERAGE CAROTID STENT
Naomi Larsen*1, Hannes Nordmeyer2, David Schild3, Franziska Dorn4, Simgen Andreas5, Olav Jansen1, Fritz Wodarg1
1University Hospital Schleswig-Holstein Campus Kiel, Department of Radiology and Neuroradiology, Kiel, Germany,2Städtisches Klinikum Solingen, Department of Neuroradiology, Solingen, Germany,3Acandis GmbH, Pforzheim,4University of Bonn, Department of Neuroradiology, Bonn,5Westpfalz-Klinikum Kaiserslautern, Department of Neuroradiology, Kaiserslautern, Germany
On behalf of:
Background and aims: Stenting or carotid endarterectomy for proximal carotid artery stenosis is generally recommended in patients with 50-99% symptomatic stenosis. In patients with recurrent stroke without a competing source of emboli and mild (<50%) stenosis, invasive treatment can be considered when imaging features of the carotid plaque indicate a high risk of future cerebrovascular events. Plaque coverage with a low porosity stent offers a novel treatment option. We report our first experience with the new CARESTO®heal stent.
Methods: In this multicentre case series patients with symptomatic mild carotid stenosis treated with the CARESTO® heal stent are included. Patient selection comprises plaque characterization by MRI and CTA. Technical outcome measures include wall apposition and surface remodelling. Safety outcome measures are periprocedural ischemic events, stroke, mortality at six weeks and six months follow-up.
Results: So far fifteen patients have been included. Technical success rate was 100%. There were no major peri-procedural complications. Post-interventional MRI revealed asymptomatic DWI lesions in 1 patient. 3 months follow-up has been performed in 6 patients so far, showing no recurrence of stenosis or neurological events.
Conclusions: Vulnerable carotid plaques are suspected to be the source of embolism in a substantial number of patients with embolic stroke of undetermined source, and there is evidence suggesting a potential benefit of invasive treatment in selected patients. A dedicated device has not been available before. A stent with a high mesh density designed for the treatment of low grade stenoses and optimal plaque coverage could be a feasible treatment option.
Disclosures of Interest: Yes Consultant for Acandis GmbH
Abstract N°: 3274
THE OSLO STUDY OF VISUAL IMPAIRMENT AFTER STROKE: STROKEVIS
Stephen James Ryan*1, Øystein Kalnes Jørstad2, Anna-Kathrina L. Jørstad2, Moten C. Moe2, Fiona Rowe3, Anne Hege Aamodt1
1Oslo Universtiy Hospital, Rikshospitalet, Neurology, Oslo, Norway,2Oslo University Hospital, Ullevål, Ophthalmology, Oslo, Norway,3University of Liverpool, Primary Care and Mental Health, Liverpool, United Kingdom
On behalf of: all StrokeVIS collaborators
Background and aims: Studies have shown that up to 60% of patients have some form of new visual impairment after stroke (Rowe et al., 2019).
In the annual report of the Norwegian Stroke Register from 2021, only 16% of stroke patients were registered with visual impairment. Notably, this figure is significantly lower than expected from the literature and indicates a significant under-reporting and/or under-diagnosis.
Methods: Studies have shown that up to 60% of patients have some form of new visual impairment after stroke (Rowe et al., 2019).
In the annual report of the Norwegian Stroke Register from 2021, only 16% of stroke patients were registered with visual impairment. Notably, this figure is significantly lower than expected from the literature and indicates a significant under-reporting and/or under-diagnosis.
The Oslo study of visual impairment (StrokeVIS) intends to measure the prevalence of visual impairment after stroke, validate a Norwegian version of the VISA screening tool (Rowe et al., 2020) and evaluate vision outcomes of acute stroke patients.
Results: So far, 121 patients have been included. Recruitment is still ongoing at Oslo University hospital, with a completion date of March 30th 2024.
Conclusions: Preliminary findings indicate feasibility for the use of VISA as a screening tool in Norway in the subacute setting and highlight the difficulty of assessing visual impairment in the acute stroke patient.
Disclosures of Interest: No
E-Poster - Pathophysiology of Stroke / Translational Medicine
1National Neuroscience Institute, Research, Singapore, Singapore
On behalf of:
Background and aims: Reperfusion injuries such as oedema and haemorrhagic transformation are common following reperfusion therapy, limiting the use of this potent therapy with a narrow time window. Recently, transient receptor potential melastatin 4 (TRPM4) channels has emerged as a potential target for vascular protection and neuroprotection in stroke management. We aim to develop a novel TRPM4 blocker for stroke therapy
Methods: We have developed a novel TRPM4-specific antibody M4P which binds to a region close to the channel pore. Biochemical, eletrophysiological, and animal studies were performed to characterize this therapeutic antibody.
Results: M4P could inhibit TRPM4 current and downregulate TRPM4 surface expression, therefore preventing hypoxia-induced cell swelling in both neurons and vascular endothelial cells. In a rat model of 3-h stroke reperfusion, application of M4P at 2 h after occlusion ameliorated reperfusion injury by improving blood–brain barrier integrity and enhanced functional recovery. In a delayed 7-h stroke reperfusion model, M4P treatment could improve vascular morphology and attenuate vascular leakage, leading to a reduction of infarct volume and animal mortality rate.
Conclusions: TRPM4 blocking antibody could attenuate reperfusion injury in both early and delayed stroke recanalization. When applied together with reperfusion treatments, TRPM4 blocking antibody has the potential to extend the therapeutic time window for acute ischemic stroke. We are currently developing a humanized version of TRPM4 blocking antibody for stroke and other neurological diseases.
Disclosures of Interest: No
Abstract N°: 34
ISCHEMIA AND REPERFUSION UNDER HYPERTHERMIA AGGRAVATES NEURONAL DEATH
Seong MI Heo1, Jae Seong Noh1, Da Som Han1, Myoung Cheol Shin1, Taek Geun Ohk1, Joong Bum Moon1, Tae-Kyeong Lee2, Ji Hyeon Ahn3, Jun Hwi Cho*1
1Kangwon National University, Emergency Medicine, Chuncheon, South Korea,2Hallym University, Food Science and Nutrition, Chuncheon, South Korea,3Youngsan University, Physical Therapy, Yangsan, South Korea
On behalf of:
Background and aims: Impaired oxidant/antioxidant balance and excitotoxicity due to glutamate transporter dysfunction are well known as the major causes of selective neuronal death (loss) in the hippocampus after ischemia-reperfusion injury (IRI). Hyperthermia (HT) deteriorates ischemic neuronal damage in the hippocampus, but the underlying mechanisms remain unclear. This experiment was conducted to investigate the mechanisms of worse neuronal damage due to IRI under hyperthermia in gerbil hippocampal CA1 region following IRI.
Methods: Normothermia (NT; 37.5±0.2°C) or HT (39.5±0.2°C) was controlled for 30 min before and during IRI. The gerbils received IRI and were sacrificed 0 h, 3 h, 6 h, 12 h, 1 day, 2 days, and 5 days after IRI. Neuronal loss using NeuN immunohistochemistry and Fluoro-Jade B histofluorescence was examined. Oxidative stress, excitotoxicity, and reactive astrogliosis were evaluated using immunohistochemistry for 8-hydroxy-2'-deoxyguanosine (8OHdG; an oxidative DNA damage marker) and superoxide dismutase 2 (SOD2; an endogenous antioxidant enzyme), glutamate transporter 1 (GLT1), and glial fibrillary acidic protein GFAP.
Results: Neuronal loss of pyramidal neurons was earlier detected in HT-IRI group than NT-IRI group. 8OHdG and SOD2 immunoreactivity in the HT-IRI group was significantly higher than NT-IRI group. Reactive astrogliosis was informal in both groups util 1 day post-IRI, showing that, at 2 and 5 days post-IRI, GFAP immunoreactivity was significantly stronger in the HT-IRI group.
Conclusions: This experiment indicated that severer oxidative stress and greater reduction in GLT1 in the HT-IRI group mighty contribute to earlier and severer neuronal death under hyperthermia in the hippocampal CA1 region.
Disclosures of Interest: No
Abstract N°: 461
CORRELATION OF THROMBOELASTOGRAPHIC PARAMETERS WITH INFARCT SIZE AND SEVERITY IN ACUTE ISCHEMIC STROKE
Background and aims: Acute ischemic stroke (AIS) is a complex neurological emergency, and understanding the role of hypercoagulability in its pathophysiology is crucial for improved patient outcomes. The primary aim was to discern whether hypercoagulability, identified through Thromboelastographic parameters correlated with larger infarct sizes.
Methods: This is a prospective observational study conducted at the Department of Neurology, Aster Ramesh Hospitals, Guntur over 18 months. It included 100 AIS patients diagnosed within 24 hours of onset, with TEG assessments and MRI scans. Reaction time (R), clot kinetics (K), angle (alpha), Maximum Amplitude (MA), and Lysis at 30 min (LY30) were the thromboelastographic parameter analyzed alongwith infarct volumes measured through MRI and NIHSS score to assess stroke severity.
Results: A moderate positive correlation (r = 0.434, p < 0.001) was found between MA and the size of the infarct. Additionally, there was significant difference in MA between patients with and without large vessel occlusion (p < 0.001). The study further investigated the correlation between the size of the infarct and clinical outcomes. A moderate positive correlation was observed between the size of the infarct and the National Institutes of Health Stroke Scale (NIHSS) score (r = 0.485, p < 0.001). This correlation was also explored in relation to thromboelastography, indicating a moderate positive correlation between MA and NIHSS score (r = 0.391, p < 0.001).
Conclusions: The correlation between TEG parameters and infarct size, along with the association with NIHSS scores, emphasizes the clinical relevance of coagulation dynamics in the pathophysiology of acute cerebral infarction.
Disclosures of Interest: No
Abstract N°: 774
NEUROPROTECTION AFFORDED BY AN ENRICHED MEDITERRANEAN-LIKE DIET IS MODIFIED BY EXERCISE IN A RAT MODEL OF CEREBRAL ISCHEMIA
Daniel Romaus-Sanjurjo*1,2, Maria Castañon3,4,5, Esteban Lopez-Arias1, Antía Custodia1,2, Cristina Martin-Martín6, Alberto Ouro1,2, Elena Lopez-Cancio3,4,5, Tomás Sobrino1,2
1Health Research Institute of Santiago de Compostela (IDIS), Santiago de Compostela,2Centro de Investigación Biomédica en Red en Enfermedades Neurodegenerativas (CIBERNED), Madrid, Spain,3Hospital Universitario Central de Asturias (HUCA), Departament of Neurology, Oviedo, Spain,4Instituto de Investigación Sanitaria del Principado de Asturias (ISPA), Oviedo, Spain,5Universidad de Oviedo, Oviedo, Spain,6Translational Inmmunology, Instituto de Investigación Sanitaria del Principado de Asturias (ISPA), Oviedo, Spain
On behalf of:
Background and aims: Currently, there are no treatments allowing a remarkable better outcome in patients after ischemic stroke, and so, it is mandatory to seek new approaches preventing stroke. Multiple preclinical and clinical studies highlighted the potential beneficial roles of exercise and a Mediterranean diet following stroke. Here, we examined whether a Mediterranean-like diet supplemented with hydroxytyrosol with/without physical exercise improves the outcome of animals submitted to cerebral ischemia.
Methods: SD male rats were randomly divided in sham group, control group (Western-like [W] diet), diet group (Mediterranean-like rich in polyphenols[M] diet), PA group (W diet) diet/PA group (M diet). PA and diet/PA groups performed physical activity sessions during the 4 weeks prior to transient middle cerebral artery occlusion and for 3 weeks after surgery. Same timeline applied to the food strategy. MRI imaging, several functional tests and flow cytometry were used. Milliplex and ELISA assays, and immunohistochemistry studies were carried out.
Results: We found that an enriched Mediterranean-like diet decreased infarct and edema volumes, delayed acute immune response (modulates cytokines/chemokines levels), reduced oxidative stress, and increased acute functional recovery after ischemic injury. Strikingly, although physical exercise did improve cellular and some functional outcomes compared to control animals, it did not synergize with the Mediterranean-like diet but even impaired the positive short-term outcomes.
Conclusions: Overall, these data provide the first preclinical evidence that a preemptive enriched Mediterranean diet modulates cytokines/chemokines levels downwards that eventually has an important role during the acute phase following ischemic damage, likely mediating neuroprotection.
Disclosures of Interest: No
Abstract N°: 923
EFFECTS OF LOW-PRESSURE VALSALVA MANEUVER ON CEREBROVASCULAR CHANGES
1Gil Medical Center, Gachon University College of Medicine, Neurology, Incheon, South Korea,2Neuroscience Research Institute, Gachon University, Research Center of Cerebrovascular Disease, Incheon, South Korea,3Gachon Advanced Institute for Health Sciences & Technology, Health Sciences and Technology, Incheon, South Korea,4Gachon University Graduate School, Health Science, Incheon, South Korea,5Gil Medical Center, Gachon University College of Medicine, Rehabilitation, Incheon, South Korea,6Gil Medical Center, Gachon University College of Medicine, Neurosurgery, Incheon, South Korea,7College of Health Science, Gachon University, Radiological Science, Incheon, South Korea
On behalf of:
Background and aims: The effect of different exhalation force pressures for Valsalva maneuver (VM) on cerebrovascular response is not clearly understood. Therefore, this study aimed to investigate the effect of low-pressure VM on cerebrovascular physiology and hemodynamic function.
Methods: 27 healthy participants performed VM at two different levels of pressures (30 and 40 mmHg). Cerebrovascular physiology was measured using near-infrared spectroscopy (NIRS), including regional oxygen saturation, oxygenated and deoxygenated hemoglobin. Hemodynamic function was measured using diagnostic ultrasound, including peak systolic velocity (PSV), resistance index (RI), pulsatile index (PI), pulse wave velocity (PWV) and heart rate (HR) in right common carotid artery.
Results: Both 30 and 40 mmHg VM had significant effects on PSV and PWV after VM. PSV increased by 5.44 cm/s (30 mmHg, p = 0.031) and 4.48 cm/s (40 mmHg, p = 0.04). In addition, PWV decreased by 0.69 mm/s (30 mmHg, p < 0.001) and 0.34 mm/s (40 mmHg, p = 0.022). On the other hand, RI increased significantly by 0.04 (p = 0.035) and HR decreased by 1.53 bpm (p = 0.003) after VM only at 40 mmHg VM.
Conclusions: Both 30 and 40 mmHg VM induced significant changes in cerebrovascular physiology and hemodynamic function. The increased PSV and decreased vascular stiffness can attribute to facilitate cerebrovascular oxygen exchange even at 30 mmHg VM. However, 40 mmHg VM showed the significant increased RI due to the high arterial pressure, influencing a decrease in the efficiency of cerebral oxygen exchange. Therefore, 30 mmHg VM appears to be more effective in promoting cerebrovascular change.
Disclosures of Interest: No
Abstract N°: 1314
TOWARDS NOVEL INTRACEREBRAL HAEMORRHAGE STROKE MODELS BY ENDOVASCULAR APPROACH IN SWINE
Alexia García-Serran*1, Carlos Castaño2, Marc Melià-Sorolla1, Núria De Gregorio-Rocasolano1, Octavi Martí-Sistac3, Teresa Gasull1
1Germans Trias i Pujol Research Institute, Cellular and Molecular Neurobiology Research Group, Badalona, Spain,2Germans Trias i Pujol Hospital, Neurointerventional Radiology Unit, Badalona, Spain,3Universitat Autònoma de Barcelona, Department of Cellular Biology, Physiology and Immunology, Bellaterra (Cerdanyola del Vallès), Spain
On behalf of:
Background and aims: Intracerebral haemorrhage (ICH) stands as a major cause of disability and death. Most experimental therapies tested in rodents failed in stroke patients. Rodent ICH models via craniotomy alter intracranial blood pressure and do not mimic the human pathology. We intended to establish an endovascular approach to generate new ICH models in swine, a mammal with gyrencephalic brain and akin white-to-grey matter ratio to humans.
Methods: Brain venous drainage was studied in vivo with angiography. To create an ICH model in pigs, catheterisation of the venous brain vasculature was performed in order to reach the thalamostriatal vein. Then, the vein was perforated and 1.5mL of arterial blood were injected along 2.5min. MRI sequences were obtained in vivo at different timepoints, and brains were obtained at the end of the procedure.
Results: Specific brain regions of interest (striatal areas or occipital cortex) were reached through the pig’s brain veins. After perforation and blood injection, we observed ICH in all the pigs as assessed 1-hour post-ICH in the CT. The area of the haemorrhage was quantified using both, in vivo longitudinal MRI multimodal imaging at 90min, 24h, and 1week, and ex vivo assessment in brain slices. The haemorrhage did not progress beyond 90min. The pigs showed neurological impairment in the form of evident aberrant circling behaviour.
Conclusions: We have successfully developed novel ICH models in pig using a craniotomy-free endovascular approach.
AcknowledgementsWe are deeply grateful to the Comparative Medicine and Bioimage Centre of Catalonia staff and Canon Medical Systems.
Disclosures of Interest: No
Abstract N°: 1521
EXPLORING CELL-TYPE-SPECIFIC VULNERABILITY TO ISCHEMIA USING MIDDLE CEREBRAL ARTERY RAT MODEL
Allison Brookshier*1, Lillie Eckstein1, Heather Chang1, Sophie Liska1, Will Alton1, Patrick Lyden1
1University of Southern California, Dept. of Physiology and Neuroscience, Los Angeles, United States
On behalf of:
Background and aims: There has been limited success in the development of effective stroke treatments. Treatments that are effective in pre-clinical models fail to show the same level of success in human clinical trials. The evaluation of these treatments often assesses the survival of neurons but fails to consider the health of the other components of the neurovascular unit. We demonstrated cell-type-specific vulnerability to oxygen-glucose deprivation using in vitro cultures (Rajput, 2018). Here we sought to find evidence supporting cell-type-specific vulnerability to ischemia in vivo.
Methods: We used equal numbers of male and female Sprague Dawley rats in a middle cerebral artery occlusion (MCAo) model, randomly assigning them to 2, 4, 6, or 12 hours of MCAo followed by 30 minutes reperfusion. After fixation, 25µm mid-parietal cortex sections were stained with Sytox, anti-GFAP, anti-NeuN, and anti-Tie2. Three z-stacks were imaged in the stroke, ipsilateral cingulate, and contralateral cortex homotopic to the stroke region. Cell death was expressed as the ratio of Sytox-positive to total cell-type marker-positive cells.
Results: We found no significant differences in cell death numbers among cell types in the contralateral cortex. We found a significant difference among cell types in the ipsilateral cingulate (p<0.0001) and the stroke region (p<0.05). Neuronal cell death peaked at 4 hours, while astrocytes’ peaked at 12 hours; endothelial cells’ remained minimal at all durations.
Conclusions: These findings suggest an inherent biological difference among the cell types concerning their response to ischemic injury, which should be considered during the evaluation of stroke treatments.
Disclosures of Interest: No
Abstract N°: 2047
ENDOTHELIN 1-INDUCED ISCHEMIA-REPERFUSION MODEL IN THE PIG BRAIN
Jose Fernandez-Ferro*1, Javier Sanchez Gonzalez1, Carlos Galan Arriola1, Agustin Clemente Moragon1, Borja Ibáñez Cabeza1
1CNIC - Centro Nacional de Investigaciones Cardiovasculares, Neurology, Madrid, Spain
On behalf of:
Background and aims: Endothelin 1 (ET1) has been previously used to achieve effective ischemia in the pig brain as an alternative to the classical endovascular model. We describe our experience while trying to achieve an experimental model of ischemia-reperfusion using ET1.
Methods: Three different methods were tested to achieve effective brain infarcts using ET1 through a burr hole in the cranium: an intraparenchymal injection, a blinded subarachnoid releasing; and artery-targeted subarachnoid releasing. All the experiments were performed at the Centro Nacional de Investigaciones Cardiovasculares in Madrid-Spain and all ethical aspects in animal manipulation and care where carefully considered and monitored.
Results: A stereotaxic system attached to an engine-powered pump was developed to deliver a fixed dose of ET1 into the brain parenchyma. We describe two methods for releasing of ET1 into the subarachnoid space: one blinded, and a second using a TOF-MRA to achieve a targeted delivering on a specific superficial brain artery. Effectiveness, infarct volumes, artifacts and other problems related with each technique are revised.
Conclusions: Difficulties with the classical endovascular approach forced us to look for new approaches. An artery-targeted subarachnoid releasing of the strong vasopressor ET1 seems the most promising way to achieve effective ischemia-reperfusion brain lesions.
Disclosures of Interest: No
Abstract N°: 2776
AN ADJUNCT THERAPY TO MECHANICAL THROMBECTOMY – LOCALLY ADMINISTERED ACIDIFIED MALONATE PROTECTS AGAINST STROKE ISCHAEMIA/REPERFUSION INJURY
Jordan Lee*1, Hiran Prag1, Karthik Chary2, Jiro Abe1, Shinpei Uno3, Annabel Sorby-Adams4, Joshua Kaggie2, Ferdia Gallagher2, Michael Murphy3, Thomas Krieg1
1University of Cambridge, Department of Medicine, Cambridge, United Kingdom,2University of Cambridge, Department of Radiology, Cambridge, United Kingdom,3University of Cambridge, MRC Mitochondrial Biology Unit, Cambridge, United Kingdom,4Massachusetts General Hospital and Harvard Medical School, Department of Neurology and the Center for Genomic Medicine, Boston, United States
On behalf of: Chak Shun Yu, Olga Sauchanka, Amin Mottahedin
Background and aims: Mechanical thrombectomy provides the opportunity for targeted drug delivery into ischaemic tissue upon reperfusion; however, equivalent pre-clinical animal models are lacking. Malonate, a competitive inhibitor of succinate dehydrogenase, preferentially enters ischaemic tissue on reperfusion via monocarboxylate transporter 1 (MCT), and potentially MCT2 and MCT4 due to the low tissue pH and ameliorates ischaemia/reperfusion injury (IRI). We aimed to develop a method for the local administration of acidified malonate and determine its efficacy as an adjunct therapy in a pre-clinical model of stroke.
Methods: C57BL/6J mice were treated with saline or malonate at physiological or low pH (6.0) either intravenously or intra-arterially via the thrombectomy catheter. Metabolites were measured by liquid chromatography-tandem mass spectrometry. For transient middle cerebral artery occlusion (tMCAO), mice were subjected to 30 mins ischaemia followed by either 2 or 24 hours reperfusion. Brain infarct size was assessed by TTC-staining or MRI. mtDNA amplification, complex I activity, and lipid peroxidation (MDA) assays were used as oxidative damage markers.
Results: Intravenous malonate treatment significantly reduced infarct size at both 2 and 24 hours post-stroke compared to saline controls. Administration of acidified malonate locally to drive its uptake via MCT1 significantly enhanced brain uptake, consequently leading to reduced infarct size at lower administered doses. In addition, local acidified malonate administration significantly reduced the extent of oxidative damage, mean apparent diffusion coefficient and neurological score were also improved.
Conclusions: Malonate is neuroprotective against stroke IRI, and is an attractive candidate as an adjunct therapy for mechanical thrombectomy.
Disclosures of Interest: Yes JJL, HAP, MPM and TK have pending patents on targeting succinate metabolism in ischaemia/reperfusion injury. MPM and TK are directors of Camoxis Therapeutics Ltd.
Abstract N°: 2887
HISTOLOGICAL AND RADIOLOGICAL ASSESSMENT OF THROMBI RETRIEVED VIA ENDOVASCULAR THROMBECTOMY IN CEREBRAL VENOUS THROMBOSIS
Ghil Schwarz*1, Angelo Cascio Rizzo1, Martina DI Como2, Antonio Macera3, Maria Costanza Aquilano2, Marco Bacigaluppi4, Francesco Ruggieri5, Mariangela Piano3, Maria Sessa1, Elio Clemente Agostoni1
1Niguarda, Stroke Unit - Neurology, Milan, Italy,2Niguarda, Hematology, Oncology and Molecular Medicine, Milan, Italy,3Niguarda, Neuroradiology, Milan, Italy,4San Raffaele Hospital, Neuroimmunology Unit, Italy,5Niguarda, Neurointensive Care Unit, Milan, Italy
On behalf of:
Background and aims: Endovascular thrombectomy (EVT) allows histological analysis of thrombi, potentially improving pathophysiology understanding and treatment approaches. We aimed to analyze EVT-retrieved thrombi in cerebral venous thrombosis (CVT), compare them with acute ischemic stroke (AIS) thrombi, and correlate their composition with computed-tomography (CT) density.
Methods: Retrospective study (2020-2023; at two comprehensive Italian Stroke Centers) including 5 CVT patients and 10 (randomly-selected) AIS cases treated with EVT (5 large-artery atherosclerosis and 5 cardioembolic). Thrombi were histologically examined (Hematoxylin and Eosin, Picro Mallory, Prussian Blue; anti-CD61, anti-MPO, anti-CD3, anti-CD20, anti-CD34, anti-CD68, anti-citH3) and quantified using image analysis algorithms (Orbit). Relative CT density (rHU) was also assessed. Two more CVT cases (and 4 AIS-controls) are under analysis.
Results: CVT thrombi had a high red blood cell (RBC) content and were larger (median size: 185.6 mm2 [IQR 83.0-237.9]) compared to AIS thrombi (median size: 21.8 mm2 [IQR 8.8-77.8];p=0.028). Fibrin content was lower in CVT (median 16.6% [IQR 13.9-31.5]) than in AIS thrombi (median 46.5% [IQR 25.1-49.5];p=0.036). There was a significant negative correlation between fibrin content and rHU (R -0.9;p=0.047), and a positive correlation between RBC-to-fibrin ratio and rHU (R 0.9;p=0.047).
Conclusions: Our findings indicate that CVT thrombi are larger than AIS thrombi, characterized by a high RBC content and lower fibrin levels, corresponding to their CT density. This study, for the first time, deepens our understanding of CVT pathophysiology and may inform potential improvements in treatment. Ongoing analysis of two additional CVT cases may further validate our results.
Disclosures of Interest: No
Abstract N°: 3137
IMPROVED CSF SAMPLING ALLOWS VALIDATION OF QUANTITATIVE PROTEOMICS IN MICE
Athanasios Lourbopoulos*1,2, Stephan Müller3,4, Georg Jocher3,4, Manfred Wick5, Nikolaus Plesnila1,6, Stefan Lichtenthaler3,4,6
1Institute for Stroke and Dementia Research (ISD), LMU University Hospital, LMU Munich, Laboratory of Experimental Stroke Research, Munich, Germany,2Schön Klinik Bad Aibling, Neurointensive Care Unit, Bad Aibling, Germany,3German Center for Neurodegenerative Diseases (DZNE), Munich, Germany,4Neuroproteomics, School of Medicine, Klinikum Rechts der Isar, Technical University of Munich, Munich, Germany,5Institute of Laboratory Medicine, LMU University Hospital, LMU Munich, Munich, Germany,6Munich Cluster for Systems Neurology (SyNergy), Munich, Germany
On behalf of:
Background and aims: Low CSF volume and frequent blood contaminations of mouse cerebrospinal fluid (CSF) block multiple mass-spectrometry (MS) and molecular analysis from single animals. We aimed to improve this.
Methods: We single-sampled mouse CSF from the cisterna magna of anesthetized animals (19 C57bl6; 3, 6 and 12 months-old) or re-sampled 3 months afterwards (n=6, initially 3 months-old), and controlled CSF for absent blood/tissue contamination (Hemoglobin-ELISA, Neubauer). We analyzed single CSF samples with MS, plus ⩾3 immunoassays (ELISA, WB or Simoa). We validated our methodology in transgenic 5xFAD and their littermates (n=10, 7 months-old). We used an absolutely quantified external standard (AQES) via MS to estimate for the first time concentrations for all detected mouse CSF proteins.
Results: We routinely collected 19-30 µl (median 26) of pure CSF from individual mice. All samples were devoid of free hemoglobin (below ELISA detection limit) or blood cells (Neubauer); we now provide a Quality Control workflow for contamination-free, MS-suitable, murine CSF sampling. Aging of wild type mice induced mild inflammatory, lysosomal and secreted-proteins CSF changes mainly between 3 and 6 months, while repeated sampling triggered a sustained inflammatory and fibrotic CSF response after 3 months. Amyloid pathology in the 5xFAD mouse model of Alzheimer’s disease massively changed CSF proteome: neurofilament light chain and TREM2 were strongly upregulated and validated in single CSF samples using immunoassays. AQES-MS proteomics provided single concentrations in fmol/ml for selected mouse samples.
Conclusions: Our refined murine CSF collection method overcomes all previous limitations in mouse CSF sampling and analysis
Disclosures of Interest: No
E-Poster - Prevention and Secondary Prevention
Abstract N°: 676
OUTCOME AND SECONDARY PREVENTION AFTR ISCHAEMIC STROKE IN THREE DIFFEERENT SOCIOECONOMIC ENVIRONMENTS IN EUROPE
Charlotte Berger*1, Helly Hammer1, Costa Marino1, Adrian Scutelnic1, Kateryna Antonenko1, Claudio Bassetti1, Andriy Yagensky2, Chwojnicki Kamil3, Marcel Arnold1, Mirjam Rachel Heldner1
1University Hospital and University of Bern, Department of Neurology, Inselspital, Bern, Switzerland,2Lutsk, Regional Center for Cardiovascular Disease, Lutsk, Ukraine,3Gdańsk, Department of Neurology, Gdańsk, Poland
On behalf of: SEPAIS collaboration
Background and aims: There is limited knowledge regarding the impact of socioeconomic environment on long-term outcomes and secondary prevention after ischaemic stroke in Europe.
Methods: In this observational multicenter cohort study, we analyzed patient baseline characteristics, reperfusion treatment, outcome, and secondary prevention in patients with acute ischaemic stroke admitted to three teaching hospitals in diverse socioeconomic environments: Bern/CH/n=293, Gdansk/PL/n=140 and Lutsk/UA/n=188.
Results: We analyzed 621 patients (43.2% women, median age=71.4y), admitted between 07-12/2019. Significant differences were observed in median BMI (CH=26/PL=27.7/UA=27.89), stroke severity [(median NIHSS CH=4(0-40)/PL=11(0-33)/UA=7(1-30)], initial neuroimaging (CT:UA=71.3%/PL=50.7%/CH=21.6%) and conservative treatment (CH=34.1%/PL=38.6%/UA95.2%), (each p<0.001), in arterial hypertension (CH=63.8%/PL=72.6%/UA=87.2%), atrial fibrillation (CH=28.3%/PL=41.4%/UA=39.4%), hyperlipidaemia (CH=84.9%/PL=76.4%/UA=17%) (each p<0.001) and active smoking (CH=32.2%/PL=27.3%/UA=10.2%) (p<0.007). Discharge destination was most often home in PL=52.1%/UA=84.1% and to another acute care facility in CH=43.5% (un-/adjusted-p<0.001).
3-months favourable (mRS=0-2) outcome was seen in CH=63.1%/PL=50%/UA=59% (unadjusted-p=0.01, adjusted-p CH-PL/CH-UA= 0.601/0.981), excellent (mRS=0-1) outcome in CH=48.5%PL=32.1%/UA=27% (unadjusted-p<0.001, adjusted-p CH-PL/CH-UA=0.201/0.08 and adjusted-OR CH-UA=2.094). 3-months mortality was similar between groups (CH=17.2%/PL=15.7%/UA=4.8%) (unadjusted-p=0.71, adjusted-p CH-PL/CH-UA=0.087/0.24). 3-months recurrent stroke/TIA occurred in CH=3.1%/PL=10.7%/UA=3.1%/adjusted-p/OR CH-PL= 0.038/0.318).
3-months follow-up medication adherence rates were the same for antihypertensives. Statin/OAC use was lowest in UA=67.1%/25.5% (CH= 87.3%/39.2%/PL=87.3%/41.5%/unadjusted-p<0.001/0.006/adjusted-p CH-PL/CH-UA=0.795/0.02;0.892/0.012/adjusted-OR CH-UA=2.326/ 2.18). Oral antidiabetics’ use was lowest in CH=10.8% (PL=15.7%/UA=16.1%/unadjusted-p=0.245/adjusted-p CH-PL/CH-UA=0.061/0.002/adjusted-OR CH-UA=0.249). Smoking rates in comparison to baseline decreased in all groups.
Conclusions: This study provides a comparative analysis of stroke patients, their baseline characteristics and outcome in different socioeconomic environments, highlighting the complex interplay of socioeconomic, cultural, and healthcare factors shaping stroke outcomes and the need for targeted interventions and addressing disparities in treatment and secondary prevention strategies.
Disclosures of Interest: No
Abstract N°: 874
SAFETY, BIOAVAILABILITY AND PHARMACOKINETICS OF ASUNDEXIAN: GUIDANCE ON DRUG ADMINISTRATION IN PATIENTS WITH DYSPHAGIA
Friederike Kanefendt1, Sven Stein2, Christine Brase3, Katharina Sommer4
Background and aims: Asundexian is a reversible and selective inhibitor of activated factor XI currently under investigation in the Phase III OCEANIC-STROKE study (NCT05686070) for stroke prevention in at-risk patients. Asundexian is highly permeable, with low solubility, and can be administrated independently of food. Many patients suffer from dysphagia after having a stroke, which also hampers swallowing an intact tablet. This abstract provides supporting evidence for the administration of asundexian in patients with dysphagia to ensure continuous treatment.
Methods: A Phase I, open-label, single-centre, randomised two-fold cross-over study investigated the effects of administration of asundexian 50 mg as an intact or crushed tablet in 14 healthy participants (fasted state) (EudraCT 2022-003284-26). In addition, in vitro investigations were performed to provide supporting evidence for administration of asundexian via an enteral feeding tube.
Results: Asundexian was generally well tolerated (Table 1). Crushing and resuspending the asundexian 50 mg tablet in apple sauce had no clinically relevant effect on the bioavailability of asundexian in healthy participants (Figures 1 and 2). Furthermore, in vitro data will be reported supporting the administration of asundexian via enteral tube, e.g., recovery, compatibility with tube material and stability.
Conclusions: Administration of oral tablets can be challenging for patients who have experienced a stroke event, as they may have difficulty swallowing due to stroke. Asundexian can be administered as a crushed tablet mixed with liquids or soft food to facilitate drug intake.
Disclosures of Interest: Yes FK, SS and CB: employees of Bayer AG and own shares or share options in the company. KS: Employee of ClinStat GmbH and reports consulting or advisory roles of her contract research organisation with Bayer AG.
Abstract N°: 884
EFFECTS OF AGE, SEX, KIDNEY FUNCTION AND HEPATIC IMPAIRMENT ON THE PHARMACOKINETICS, PHARMACODYNAMICS AND SAFETY OF ASUNDEXIAN
Friederike Kanefendt*1, Christine Brase1, Sebastian Schmitz2, Katharina Sommer3
Background and aims: Asundexian is a reversible and selective inhibitor of activated factor XI (FXIa). It is currently under investigation for the prevention of thrombotic events in at-risk patients; these patients are often characterised by advanced age, impaired organ function and comorbidities.
Methods: Three Phase I studies were included in this analysis, which investigated the effects of intrinsic factors on the pharmacokinetics, pharmacodynamics and safety of asundexian. Study 1 investigated the effect of age and sex, study 2 of chronic kidney disease (CKD) (stages 2–4; EudraCT 2020-000626-25) and study 3 of hepatic impairment (Child–Pugh A and B; EudraCT 2022-000196-38).
Results: Overall, asundexian pharmacokinetics were not meaningfully affected by intrinsic factors (age, sex, CKD stage and liver disease; Figure 1). Differences in pharmacodynamic-time profiles were driven by differences in the pharmacokinetics of asundexian, as expected per its mode of action. The pharmacodynamics for both activated partial thromboplastin time and FXIa activity (as ratios to baseline) were not relevantly affected by intrinsic factors (Figure 2). In addition, asundexian was well tolerated across all three studies (Table 1).
Conclusions: Results of these studies indicate that dose adjustments based on age, sex, kidney disease and hepatic impairment are unlikely to be needed.
Disclosures of Interest: Yes FK, CB and SS: employees of Bayer AG and own shares or share options in the company. KS: Employee of ClinStat GmbH and reports consulting or advisory roles of her Contract Research Organisation with Bayer AG.
Abstract N°: 908
LYMPHOCYTES SUBPOPULATIONS VALUES IN PATIENTS WITH ATRIAL FIBRILLATION AND FLUTTER
1NSC M.D. Strazhesko Institute of Cardiology, Clinical and Regenerative Medicine NAMS of Ukraine, Clinical arrhythmology and electrophysiology, Kyiv, Ukraine,2NSC M.D. Strazhesko Institute of Cardiology, Clinical and Regenerative Medicine NAMS of Ukraine, Clinical Immunology, Kyiv, Ukraine
On behalf of: Professor Oleg Sychov, Professor Tetiana Talaieva, Dr Taisia Getman
Background and aims: The aim is to compare immune status in patients (pts) with atrial fibrillation (AF) and atrial flutter (AFl) associated with hypertension and pts without rhythm disturbances and almost healthy people.
Methods: The study involved 103 patients with hypertension and arrhythmias who were divided into three groups: 1 (n = 35) - with paroxysmal atrial fibrillation (AF), 2 (n = 38) - with persistent form of AF, 3 (n = 30) - with persistent form of atrial flutter (AFl). Control groups were formed: 4 (n = 23) - patients with hypertension, but without arrhythmias and 5 (n = 21) - almost healthy people. The immune status was assessed by the level of monocytes (Mc), lymphocytes subpopulations and T-regulatory cells (T-reg) in the peripheral blood using flow cytometry.
Results: The number of classical CD14++CD16- and intermediate CD14++CD16+ Mc was significantly higher in pts with persistent AF and AFl comparing with patients without arrhythmias and healthy people (p<0.005). Amount of non-classical CD14+CD16++ Mc was lower in the 2 group (p<0.005). The count of T cells with natural killer (TNK) activity was higher in all groups comparing to normal value, so significance was observed only compared to the 5 group. The highest quantity of T-reg cells was found in healthy people comparing to other groups.
Conclusions: An increased activity of proinflammatory subpopulation of monocytes, higher amount of T-cells with natural killer activity and reduced T-regulatory cells was determined, whose main function is to control the immune response.
Disclosures of Interest: No
Abstract N°: 924
HETEROGENEITY OF POST-ISCHEMIC STROKE CARDIAC MONITORING: A UK PERSPECTIVE FOR THE DIVERT STUDY
Amit Kishore*1,2, Crystal Sing Chiek Teoh1, Kunal Sareen1, Mirko de Melis3, Karah Neisen4, Michael Chandler4, Roberto Carta4, David Z Rose5
1Greater Manchester Comprehensive Stroke Centre, Geoffrey Jefferson Brain Research Centre, Manchester Academic Health Science Centre, Northern Care Alliance, Salford Royal Foundation Trust, United Kingdom,2Division of Cardiovascular Sciences, Faculty of Biology, Medicine and Health, University of Manchester, Manchester, United Kingdom,3Medtronic, Inc., Cardiac Rhythm Management, Clinical, Maastricht, Netherlands,4Medtronic, Inc., Cardiac Rhythm Management, Clinical, Mounds View, United States,5University South Florida College of Morsani Medicine, Vascular Neurology, Tampa, United States
On behalf of:
Background and aims: To characterize etiological work-up post-ischemic stroke in the DiVERT (SeconDary Stroke PreVention ThRough Pathway ManagemenT) study. A retrospective analysis of patients admitted to the Manchester Centre for Clinical Neurosciences was conducted between 2019 and 2020 using Stroke National Audit database and electronic records.
Methods: Demographic, etiological investigations, mortality data were collected, and a summary statistical analysis was performed.
Results: In total, 189 patients were included; 51.9% were male, 23.8% were diabetic and 48.1% had hypertension. Etiology of ischemic strokes were classed as large vessel disease (16.9%), small vessel disease (32.3%) and cryptogenic stroke (50.8%). Non-invasive ambulatory ECG monitoring with an R-test event monitor for up to 7 days was performed in 68.8%. Implantable loop recorder (ILR) was inserted in 5.8% and hospital readmission rate was 15.3% within 180 days.
Conclusions: Wide variations in post-stroke cardiac monitoring and high readmission rates were observed. This warrants a standardized diagnostic pathway to streamline the etiology reclassification, provide faster access to cardiac monitoring improving the detection of atrial fibrillation and potentially reduce recurrent stroke.
Disclosures of Interest: No
Abstract N°: 926
CLINICIAN PERCEPTIONS OF A NOVEL MULTICOMPONENT DIGITAL PROGRAM FOR THE SECONDARY PREVENTION OF STROKE
Liam Allan*1,2, Jan Cameron1, David Silvera-Tawil2, Jane LI2, Marlien Varnfield2, Vanessa Smallbon2, Julia Bomke2, Muideen Olaiya1, Natasha Lannin3, Dominique Cadilhac1
1Monash University, Stroke and Ageing Research, School of Clinical Sciences at Monash Health, Victorian Heart Institute, Clayton, Australia,2Commonwealth Scientific and Industrial Research Organisation, Australian e-Health Research Centre, Herston, Australia,3Monash University, Brain Recovery and Rehabilitation Group, Central Clinical School, Melbourne, Australia
On behalf of:
Background and aims: The novel digital Care Assistant and support Program for people after Stroke or TIA (CAPS) was co-designed with end-users to improve secondary prevention. CAPS was evaluated for feasibility among 33 people living with stroke/TIA. Aims: To capture clinician perceptions of the program to refine it for future evaluation.
Methods: Clinicians experienced in stroke care were invited to participate in semi-structured interviews. The program components were demonstrated to participants including the clinician portal, goal-setting procedure with aligned SMS messages, risk factor monitoring supported by a smartphone application (app) and a wearable device. We sought feedback regarding the program components, potential modifications, perceived benefits, and future implementation. Interviews were transcribed and thematically analysed.
Results: Ten clinicians participated, including three nurses, two neurologists, one stroke consultant, one general practitioner (GP), and three allied health professionals. Eight participants had positive perceptions of the program, with six mentioning it was user-friendly. Five participants saw the value of CAPS for improving patient self-management and secondary prevention, indicating that health measures collected through the app were appropriate and captured “vital information”. Three recommended adding tracking for atrial fibrillation. Seven participants believed that the program would be most appropriate if delivered within three months post-discharge, when patients are the “most motivated”. Six believed that GP-led multidisciplinary care is the most appropriate model to deliver CAPS.
Conclusions: Feedback from clinicians supports usefulness of the CAPS program as a novel, digitally-enabled secondary prevention program for people living with stroke/TIA. Feedback to improve the design is being incorporated.
Disclosures of Interest: No
Abstract N°: 1208
DIFFERENCES IN RACE, ETHNICITY, SEX, AND STROKE SUBTYPE COMPREHENSIVE VS NON-COMPREHENSIVE STROKE CENTERS: DIVERT PHASE I
David Z Rose*1, Dhanunjaya Lakkireddy2,3, Ruchir Shah4, Josh Snavely5, Stephen Adams6, Marla Hairston7, Noreli Carolina Franco8, Karah Neisen8, Roberto Carta8, Thomas Devlin4,9
1University South Florida Morsani College of Medicine, Vascular Neurology, Tampa, United States,2HCA Regional Medical Center, Overland Park, United States,3HCA Regional Medical Center, Kansas City Heart Rhythm Institute, Overland Park, United States,4CHI Memorial, Vascular Neurology, Cha, United States,5Virginia Mason Franciscan Health, Franciscan Neurology Associates, Tacoma, United States,6CHI Memorial, Chattanooga, United States,7University South Florida Morsani College of Medicine, Clinical Research, Tampa, United States,8Medtronic, Inc., Cardiac Rhythm Management, Clinical, Mounds View, United States,9CHI Memorial Neuroscience Institute, Vascular Neurology, Chattanooga, United States
On behalf of: On behalf of the DiVERT Phase I Investigators
Background and aims: Racial-ethnic and sex disparities in stroke care can lead to inequality in outcomes and performance metrics. Differences in these disparities among comprehensive stroke centers (CSC) and non-comprehensive stroke centers (NCSC) have not been studied.
Methods: DiVERT Phase I was a retrospective clinical study evaluating care pathways for patients hospitalized at CSC and NCSC with cryptogenic, large vessel disease, or small vessel disease ischemic stroke. Data was obtained through clinician interviews across cardiology and neurology and electronic health records from 2017-2019. Baseline demographics and cardiac monitoring at 6 months post-discharge were evaluated.
Results: Overall, stroke patients (N= 6347) in DiVERT were aged 67.5 ± 13.9 years and 49.8% were female. Within CSC (n=4 CSC hospitals), greater diversity was seen for sex (p=0.009), race (p<0.001), ethnicity (p<0.001) and ischemic stroke subtype classification (p<0.001) compared to NCSC (n=9 NCSC hospitals) (Table). Also, patients evaluated at CSC were more likely to receive any post-stroke cardiac monitoring than those at NCSC.
Conclusions: Significant differences in demographic diversity (race, ethnicity, sex, and stroke subtype) were seen among hospitals designated as either CSC or NCSC. Plausible explanations are insurance status, socioeconomic status and payor mix. Whether this discrepancy results in disparity in care, particularly for post-stroke cardiac monitoring, needs further study.
Disclosures of Interest: Yes DZR has received honoraria/grant funding from Atricure, Boston Scientific, Chiesi, CSL-Behring, Medtronic and Viz.
Abstract N°: 1372
REDUCING RISK BEHAVIOURS AFTER STROKE: AN OVERVIEW OF REVIEWS INTERROGATING PRIMARY STUDY DATA USING THE TDF
1University College Dublin, School of Public Health, Physiotherapy and Sports Science, Dublin, Ireland,2Glasgow Caledonian University, Department of Nursing and Community Health, Glasgow, United Kingdom,3University College Dublin, School of Nursing, Midwifery and Health Systems, Dublin, Ireland
On behalf of:
Background and aims: Lifestyle changes, in addition to preventive medications, optimise stroke secondary prevention. Whilst evidence from systematic reviews(SR) support behaviour-change interventions, understanding of the theory-driven mediators that affect behaviour-change post-stroke is lacking.
Methods: Electronic databases were searched to March 2023 for SRs addressing behaviour-change post-stroke. Primary studies from identified SRs were interrogated for evidence supporting theoretically-grounded interventions. Data were synthesized in new meta-analyses examining behaviour-change domains of the Theoretical Domains Framework(TDF) and secondary prevention outcomes.
Results: From 71 identified SRs, 246 primary studies were screened. Only 19 trials (N=2530 participants) were identified that employed theoretically-grounded interventions and measured associated mediators for behaviour-change. Identified mediators mapped to 5 of 14 possible TDF domains. No studies addressed primary outcomes of recurrent stroke or cardiovascular mortality and/or morbidity. Lifestyle interventions targeting mediators mapped to the TDF Knowledge domain may improve the likelihood of medication adherence; physical activity participation and smoking cessation post-stroke, supported by low certainty evidence; Lifestyle interventions targeting mediators mapping to both TDF domains of Knowledge and Beliefs about Consequences may improve medication adherence post-stroke (very low certainty evidence); Lifestyle interventions targeting mediators mapped to Beliefs about Capabilities and Emotions domains may modulate low mood post-stroke (low certainty evidence).
Conclusions: Limited theory-based research and use of behaviour-change mediators exists within stroke secondary prevention trials. Knowledge, Beliefs about Consequences, and Emotions are the domains which positively influence risk-reducing behaviours post-stroke. Behaviour-change interventions should include these evidence-based constructs known to be effective. Future trials should address cardiovascular outcomes and ensure adequate follow-up time.
Disclosures of Interest: No
Abstract N°: 1409
THROMBOELASTOGRAPHY-GUIDED ANTIPLATELET THERAPY FOR CEREBROCARDIOVASCULAR DISEASE PATIENTS: A SYSTEMATIC REVIEW AND META-ANALYSIS
Song He*1, Quandan Tan1, Haifeng Shao2, Fengkai Mao1, Xinyi Leng3, Xia Wang4, Xiaoling Chen2, Hongwei Deng1, Yapeng Lin1, Jie Yang2
1The First Affiliated Hospital of Chengdu Medical College, Chengdu, China, Department of Neurology,2Sichuan Provincial People's Hospital, University of Electronic Science and Technology of China, Chengdu, China, Department of Neurology,3The Chinese University of Hong Kong, Department of Medicine & Therapeutics,4The George Institute for Global Health, Faculty of Medicine, University of New South Wales, Sydney, Australia
On behalf of:
Background and aims: Thromboelastography (TEG) is a reliable, economical, and user-friendly method for assessing platelet aggregation function. The effectiveness of thromboelastography (TEG)-guided antiplatelet therapy in patients with cerebrocardiovascular diseases is not well-established. This systematic review evaluates the efficacy and safety of TEG-guided antiplatelet therapy compared to standard treatment in patients with cerebrocardiovascular diseases, including ischemic stroke and coronary artery disease.
Methods: A comprehensive search was conducted in databases like PubMed, Embase, China National Knowledge Infrastructure, and Wanfang Data up to August 31, 2023. The search aimed to find randomized controlled trials and observational studies comparing TEG-guided antiplatelet therapy with standard therapy in patients suffering from ischemic stroke (IS) or coronary artery disease (CAD). The primary efficacy measure was a composite of ischemic and hemorrhagic events as defined by the trials. Secondary efficacy measures included any ischemic events, while safety was assessed by the occurrence of bleeding events.
Results: Ten studies involving 1,678 patients were included. Compared to standard antiplatelet therapy, TEG-guided therapy significantly reduced the risk of composite events (Odds Ratio [OR] 0.26, 95% Confidence Interval [CI] 0.19 to 0.37; P<0.00001), ischemic events (OR 0.28, 95% CI 0.19 to 0.41; P<0.00001), and bleeding events (OR 0.31, 95% CI 0.16 to 0.62; P=0.0009) in patients with IS or CAD.
Conclusions: TEG-guided antiplatelet therapy appears to be both effective and safe for patients with ischemic stroke or coronary artery disease. These findings support the use of TEG testing to tailor antiplatelet therapy in individuals with cerebrocardiovascular diseases.
Disclosures of Interest: No
Abstract N°: 1946
HEALTH ECONOMIC BURDEN OF MEDICAL STROKE PREVENTION IN ISCHEMIC STROKES - ANALYSIS OF ANNUAL DRUG COSTS IN A REAL-WORLD ATTEMPT
Konstantin Kohlhase*1, Ferdinand Bohmann1, Christian Grefkes-Hermann1, Laurent Willems1
1Goethe University Frankfurt, Department of Neurology, Frankfurt, Germany
On behalf of:
Background and aims: Medical secondary prevention represents a cornerstone to reduce the risk of ischemic stroke recurrency. During the last decade various drugs and therapy regimen have been developed with relevant differences in their respective costs. The aim was to evaluate the cost distribution of medical stroke prevention in a real-world attempt.
Methods: Annual treatment costs were calculated using the costs per defined daily dosage (DDD) for acetylsalicylic acid (ASA), ADP-inhibitors, direct oral anticoagulants (DOACs), vitamin K antagonists, lipid-lowering drugs (LLD), antihypertensives (AHT) and oral antidiabetics (OD) based on the discharge medication of a representative stroke cohort treated in 2020 at a tertial referral hospital in Germany. Kruskal-Wallis test was used to calculate intergroup differences.
Results: 422 patients were included – subdivided into 25.6% cardioembolism, 29.9% large-artery atherosclerosis, 17.8% small-vessel occlusion and 26.8% undetermined etiology. Total drug expenditure per year was € 241,808.40 of which 51.5% accounted for DOACs (p<0.01), followed by 20.0% for AHTs, 15.7% for ODs and 8.7% for LLDs. Drug costs for permanent ASA or transient DAPT accounted for 1.6% and 2.5%, respectively. Cardioembolism due to atrial fibrillation resulted in the highest annual treatment costs per patient that were 7.0-7.5 times higher compared to other etiologies (p<0.001). There were no significant differences between costs for ODs or LLDs across etiologies with higher expenses for AHTs in cardioembolic strokes (p<0.026).
Conclusions: DOACs after cardioembolic strokes represented the largest cost factor in medical secondary stroke prevention outranging the costs for permanent ASA, transient DAPT or drugs for cardiovascular risk factors.
Disclosures of Interest: No
Abstract N°: 2025
EFFECTIVENESS OF SELF-MONITORING OF BLOOD PRESSURE IN HYPERTENSION DETECTION IN PRIMARY-CARE: THE EASE-BP RANDOMISED TRIAL
1All India Institute of Medical Sciences, Department of Neurology, New Delhi, India,2All India Institute of Medical Sciences, Center for Community Medicine, New Delhi, India,3All India Institute of Medical Sciences, Department of Cardiology, New Delhi, India
On behalf of:
Background and aims: Hypertension diagnosis remains a major gap in the care continuum, especially in low-middle-income countries. Studies have reported self-monitoring of blood pressure (SMBP) enhanced hypertension detection, however, evidence is limited from India. We aimed to assess whether an intervention targeting SMBP better detects hypertension in a primary care set-up in India.
Methods: EASE-BP was an open-label randomized trial that recruited self-reported non-hypertensives (⩾30 years) in 2023 between April-November. Participants randomised to intervention group (N=212) received a validated BP device for SMBP and control group (N=212) were advised to monitor BP at their nearest health center. Both groups received education on hypertension and atherosclerotic disease. Frequency of BP measurements was advised for at least twice or more and recorded in a logbook provided at enrolment. The outcome was a logbook detected SBP ⩾140 and/or DBP ⩾90 for three months from randomisation. https://ctri.nic.in/Clinicaltrials NO CTRI/2023/02/049949.
Results: 212 (100%) individuals in intervention group and 206 (97.2%) in control group completed the trial. At 3-month follow-up, hypertension incidence was higher in intervention group compared with control group [intervention: 46 (21.7%) vs control: 17 (8.0); P<0.001]. The likelihood of hypertension detection increased with intervention [adjusted OR 4.6 (95% CI: 2.3-9.1); P<0.001)]. Incidence rate was 7.2 per 100 person-month in intervention group and 2.7 per 100 person-month in control group.
Conclusions: SMBP intervention in a non-hypertensive population led to better hypertension detection compared to BP monitoring at health centers. Our study sets an opportunity to implement this strategy at national level for timely management of hypertension.
Disclosures of Interest: No
Abstract N°: 2247
EFFECTIVENESS OF SELF-MONITORING OF BLOOD PRESSURE IN MEDICATION ADHERENCE IN A RURAL COMMUNITY: THE EASE-BP RANDOMISED TRIAL
1All India Institute of Medical Sciences, Center for Community Medicine, New Delhi, India,2All India Institute of Medical Sciences, Department of Neurology, New Delhi, India,3All India Institute of Medical Sciences, Department of Cardiology, New Delhi, India
On behalf of:
Background and aims: Sub-optimal adherence to antihypertensive medication is a substantial challenge among hypertensive individuals in India. It increases the risk of stroke, ischemic heart disease, and mortality. We aimed to assess whether self-monitoring of blood pressure (SMBP) enhances anti-hypertensive medication adherence in a rural community set-up in India.
Methods: In an open-label randomized trial we recruited participants aged 18 years and above, with known/treated hypertension in April-2023. Participants in intervention group received validated BP devices for SMBP, while those in control group received advice to monitor BP at the nearest health center. Both groups received education on hypertension prevention and risk-factor modification. Medication adherence was estimated using the pill counting method (proportion of days participants consumed medicine as prescribed) and a five-item Medication Adherence Reporting Scale (MARS-5). Outcome was the rate of medication adherence at 3-month follow-up. https://ctri.nic.in/Clinicaltrials NO CTRI/2023/02/049949.
Results: A total of 175 individuals were recruited in each arm. At 3-month follow-up, medication adherence was higher in intervention group compared with control group in both pill counting method [(intervention: 54% vs control: 39%); P<0.001] and MARS-5 [(intervention: mean(SD) 18.1(8.5) vs control: mean(SD) 15.5(8.8)); P<0.001]. Intervention was associated with both pill counting [β=0.11; P<0.001] and MARS-5 [β=1.90; P=0.02], adjusted for age, sex, marital-status, education, waist-circumference, hip-circumference, smoking, family-history IHD, baseline-BP.
Conclusions: SMBP at a rural community set-up in India led to better medication adherence at 3-months. Its integration into national programs may provide an innovative solution to address medication adherence among hypertensive individuals, and thus help meet the NCD goals in India.
Disclosures of Interest: No
Abstract N°: 2782
SECONDARY PREVENTION AND OUTCOMES AFTER ISCHEMIC STROKE, WITH FOCUS ON DYSLIPIDEMIA: A PROSPECTIVE STUDY
Costa Marino1, Charlotte Berger1, Kateryna Antonenko1, Marieta Peycheva*2, Marina Krasteva1,3, Adrian Scutelnic1, Helly Hammer1, Roza Umarova1, Pasquale Mordasini4,5, Mirjam Rachel Heldner1
1Inselspital, University Hospital and University of Bern, Department of Neurology, Bern, Switzerland,2Medical University Plovdiv, Department of Neurology and Research Institute, Plovdiv, Bulgaria,3University Hospital Queen Giovanna, Department of Neurology, Sofia, Bulgaria,4Inselspital, University Hospital and University of Bern, Institute of Diagnostic and Interventional Neuroradiology, Bern, Switzerland,5Kantonsspital St. Gallen, Netzwerk Radiologie, St. Gallen, Switzerland
On behalf of:
Background and aims: The aim of this study was to compare stroke patients with serum LDL>1.8 mmol/L versus ⩽1.8 mmol/L.
Methods: Patients with a first ischemic stroke aged >18years admitted to our Bernese Stroke Centre between 06/2021-03/2022 were consecutively included in this prospective cohort study. Follow-up assessments were obtained at 3 months.
Results: 381 patients (LDL>1.8 mmol/L [n=305], LDL⩽1.8 mmol/L [n=76]) were analyzed. Patients with LDL>1.8 mmol/L versus ⩽1.8 mmol/L were younger (median age 73 vs. 78, p=0.001), less frequent female (13.1% versus 24.9%, p=0.005), most often had stroke of undetermined aetiology (45.6% versus 30.3%, p=0.036), less frequent had previous vascular events (4.6% versus 11.8%, p=0.018), previous myocardial infarction (5.9% versus 23.7%, p<0.001), atrial fibrillation (20.7% versus 43.3%, p<0.001), diabetes mellitus (15.4% versus 36.8%, p<0.001) and endovascular treatment (12.1% versus 21.1%, p=0.044). 3 months outcome was as follows: median NIHSS: 0 versus 0, p=0.294; median mRS: 2 versus 1, p=0.166; recurrent cerebrovascular events: 4.8% versus 19%, p<0.001; at home with family: 59.7% versus 63.2%, p<0.001; no memory difficulties: 67.4% versus 53.9%, p=0.013; smoking: 16.5% versus 5.3%, p=0.002; regular exercise: 73.6% versus 63.2%, p=0.030; dietary counseling received: 12% versus 21.1%, p<0.001; no lipid lowering therapy: 8.6% versus 13.2%, p=0.006).
Conclusions: This study compared stroke patients with LDL>1.8 mmol/L to those with LDL⩽1.8 mmol/L. Of 381 patients, those with higher LDL were younger, had different risk factors, and showed different outcomes at 3 months, including recurrent cerebrovascular events, living situation, memory difficulties, lifestyle factors and treatment adherence.
Disclosures of Interest: No
Abstract N°: 2857
INEFFECTIVE CITY-HOSPITAL INTERACTIONS FOR OPTIMAL BLOOD PRESSURE CONTROL IN PATIENTS WITH MINOR STROKE WISHING TO PARTICIPATE IN COHORTS
Lina Grosset*1,2, Agnes Aghetti1, Ana Dimitrovic1,2, Antoine Guillonnet3, Antoine Dusonchet4, Hugues Chabriat1,2, Catherine Oppenheim5, Mathieu Zuber6, David Calvet4, Eric Jouvent1,2
1Lariboisière Hospital AP-HP, Neurology, Paris, France,2Université Paris Cité, Paris, France,3Lariboisière Hospital AP-HP, Neuroradiology, Paris, France,4Hospital Sainte-Anne, Neurology, Paris, France,5Hospital Sainte-Anne, Neuroradiology, Paris, France,6Hospital Paris Saint-Joseph, Neurology, Paris, France
On behalf of:
Background and aims: Secondary prevention after ischaemic stroke is effective, but targets are rarely achieved. In patients discharged early from hospital, achieving blood pressure targets probably requires even more effective city-hospital collaboration. We sought to assess blood pressure at 6 months in a cohort of patients with minor stroke.
Methods: We evaluated patients admitted to stroke units at Lariboisière, Sainte-Anne or Saint-Joseph hospitals in Paris and included in an ongoing prospective cohort of patients with MRI-proven minor subcortical ischaemic stroke (NCT03552926). In this cohort, after early discharge from hospital, care is provided in the community. Patients are then systematically reassessed in the recruiting hospital after 6 months. After 30 minutes' rest, 3 blood pressure measurements are taken at 5-minute intervals and the average of the last 2 calculated.
Results: At the time of writing, 166 patients (median inclusion NIHSS 1, interquartile range [0-2]) had been reassessed at 6 months. A further 39 patients reached the end of the follow-up but were not reassessed (6 died, 2 became too disabled, 16 were lost to follow-up, 15 missed the assessment). Of the patients reassessed (63±12 years old, 72% men), only 95 (61%) reached <140/90 and 50 (32%) <130/80.
Conclusions: Despite the selection bias due to their willingness to participate in a cohort study, minor stroke patients showed a less than optimal level of achievement of blood pressure targets at 6 months. New approaches are urgently needed to strengthen and facilitate interactions between hospital and post-hospital care to ensure effective prevention.
Disclosures of Interest: No
Abstract N°: 2972
CODESIGNING A BEHAVIOURAL INTERVENTION TO SUPPORT HEALTHY LIFESTYLE PARTICIPATION AFTER STROKE
Patricia Hall*1,2, Eric Asaba3,4, Paula Peniche5, Deirdre Mccartan2, Geraldine O Callaghan2, Olive Lennon1
1University College Dublin, School of Public Health, Physiotherapy and Sports Science, Dublin, Ireland,2RCSI University of Medicine and Health Sciences, iPASTAR (improving pathways for acute stroke and rehabilitation) Collaborative Doctoral Award, Division of Population Health Sciences, Dublin, Ireland,3Karolinska Institutet, Department of Neurobiology, Care Sciences and Society (NVS), Division of Occupational Therapy, Stockholm, Sweden,4Stockholms Sjukhem Foundation, Unit for Research, Development, and Education, Stockholm, Sweden,5Universidade Federal de Minas Gerais (UFMG), Departamento de Fisioterapia (Department of Physical Therapy), Brazil
On behalf of:
Background and aims: Lifestyle measures in addition to pharmacotherapy are recommended to optimise stroke secondary prevention. This study used codesign to develop a novel theory and evidence-based secondary prevention intervention that supports healthy lifestyle participation post-stroke. The aim was to capitalise on the evidence from previous related studies (overview of reviews and qualitative research) and an expert stakeholder group.
Methods: Guided by the principles of design thinking (human-centred and creative mindset), multistakeholder representation was sought to participate in a series of facilitated workshops to generate ideas, plan, refine and execute development of an iterative codesigned intervention prototype. Participants included experienced stroke secondary prevention academic researchers and clinicians, key advocacy and service provider stakeholders, and representatives of an established patient and public involvement (PPI) panel. Three facilitated online workshops and one in-person workshop were hosted October/November 2024. A variety of multimedia data gathering modes were utilised including observation, open-ended questions, screenshots, online white-boards, post-its, flip-charts, iterations/artefacts.
Results: Core components of a multimodal healthy lifestyle intervention through an iterative and dynamic process were developed and agreed. These included: clinical/risk factor baseline assessment; stroke secondary prevention and lifestyle education; activity-based goal setting; real-life examples with peer-learning and support; practice opportunities; emotional self-regulation and self-management. A number of recommendations on frequency, intensity and time/timing were proposed and refined.
Conclusions: A theory and experience-driven codesign approach in the development of components in a stroke secondary prevention intervention are explored. Next steps include testing and refining the iterative prototype in line with the evidence base and theoretical framework.
Disclosures of Interest: No
Abstract N°: 3043
EMERGING ROLE OF A STROKE CLINICAL NURSE SPECIALIST (CNS) IN EARLY SUPPORTED DISCHARGE:CNS AND ADVANCED NURSE PRACTITIONER SURVEY RESULTS
Sarah-Jane Byrne*1,2, David Williams1,3, Declan Patton4, Frances Horgan5
1Beaumont Hospital, Department of Geriatric and Stroke Medicine, Dublin, Ireland,2RCSI University of Medicine and Health Sciences, School of Postgraduate Studies, Dublin, Ireland,3RCSI University of Medicine and Health Sciences, Department of Geriatric and Stroke Medicine, Dublin, Ireland,4RCSI University of Medicine and Health Sciences, School of Nursing and Midwifery, Dublin, Ireland,5RCSI University of Medicine and Health Sciences, School of Physiotherapy, Dublin, Ireland
On behalf of:
Background and aims: Early Supported Discharge (ESD) improves patient recovery after stroke and reduces recurrent admission. The role of the clinical nurse specialist (CNS) in ESD helps to reduce post-discharge challenges for patients, can support treatment compliance and secondary prevention; however, it is not well described in the literature. The aim of this study is to describe the current role of CNS and ANP in Ireland in ESD.
Methods: A survey was circulated to stroke CNSs and stroke advanced nurse practitioners (ANP) to establish what elements of their role are transferable and could be implemented in a pathway for the Stroke CNS in ESD. The survey included open-ended questions to explore three areas, (i) secondary prevention at first patient contact in hospital, (ii) secondary prevention on discharge from hospital, and (iii) secondary prevention in ESD. The study received ethics approval from RCSI.
Results: There was a 50% response rate of 17 CNSs and 3 ANPs. 100% of respondents were female. 95% reported first patient contact in hospital. 37% had a stroke CNS as part of their ESD Team. 70% reported that a phone-call or house visit by the ESD CNS on discharge would benefit all stroke patients. Information was provided on the current service they deliver regarding education on secondary prevention and medication compliance.
Conclusions: The information gained from this survey will inform the development of an education pathway for the stroke CNS in Early Supported Discharge as part of a larger study on the role of the stroke CNS in ESD in Ireland.
Disclosures of Interest: No
Abstract N°: 1177
INVESTIGATION OF THE POTENTIAL OF LEVONORGESTREL FOR STROKE PROTECTION
Tom Skyhøj Olsen*1, Gasper Letnar2, Klaus Kaae Andersen2
1Bispebjerg University Hospital, Neurology, Copenhagen, Denmark, 2Omicron ApS, Copenhagen, Denmark
On behalf of:
Background and aims: The progestin, levonorgestrel influence hemostasis towards less coagulation. Used in combined oral contraceptives it modifies thrombogenic effects of ethinylestradiol thereby reducing stroke risk. However, the impact of levonorgestrel alone on risk of ischemic stroke (IS) has not been studied. Currently use of levonorgestrel alone is administered through levonorgestrel-releasing intra-uterine devices (IUDs) for contraceptive purposes. We investigated risk of IS and intracerebral hemorrhage (IH) in women receiving levonorgestrel via IUDs in comparison with women not using hormonal contraceptives.
Methods: In this Danish cohort study (2003-2021) we followed non-pregnant women (18-49 years) registering incident IS and IH during use of IUDs/non-use of hormonal contraceptives using Danish high-quality registries with nation-wide coverage. Poisson regression models adjusting for age, ethnicity, education, calendar-year, and stroke risk factors were utilized.
Results: A total of 1,735,306 non-pregnant women contributed 16,933,276 person-years (py) of observation. Mean age was 29.1 years; 3403/432 had IS/IH. IUD users contributed 1,720,931 py to the study while non-users of hormonal contraceptives contributed 10,297,380 py. Incidence rate of IS/IH among IUD users was 19.2/3.0 and among non-users 25.2/3.1 per 100,000 py. After adjustment relative risk for IS was 0.77 (CI: 0.68; 0.86), and for IH 0.93 (CI: 0.68; 1.26).
Conclusions: Use of IUDs was associated with a 23% lower risk of IS without raising risk of IH thus pointing to IUDs as a good choice of contraception for women in high-risk populations. It is still too early to claim a stroke[1]protective effect of levonorgestrel, but our results justify and calls for further investigation of this potential possibility.
Disclosures of Interest: No
E-Poster - Prognosis and Outcome after Stroke
Abstract N°: 25
PREDICTORS FOR INTRACEREBRAL HEMORRHAGE AFTER INTRAVENOUS OR INTRAARTERIAL RECANALIZATION IN ACUTE MAJOR CEREBRAL ARTERY OCCLUSION IN KOREAN PATIENTS
Byung-Rae Cho*1, Dong-Sub Kim1, Dong-Kyu Jang1
1Incheon St. Mary's Hospital, Colloge of Medicine, The Catholic University of Korea, Neurosurgery, Incheon, South Korea
On behalf of:
Background and aims: To evaluate predictors for intracerebral hemorrhage and 1-month mortality after intravenou or intraarterial recanalization therapy for major cerebral artery occlusion in Korean patients.
Methods: From 2011 to 2015, we prospectively gathered data from consecutive patients treated with IV/IA recanalization within 8 h of symptoms in a single center. The effects of demographic, clinical, laboratory, and radiological factors on ICH within 2 weeks were assessed, as well as 1-month mortality.
Results: From a total of 183 patients, symptomatic intracerebral hemorrhage occurred in 32 patients (17.5%), and asymptomatic ICH occurred in 37 patients (20.2%). The mortality rate at 1 month in ICH patients was 37.7%. The international normalized ratio (INR) (p = 0.046), glucose (p = 0.023), medium-volume infarct (15–69.9 mL) (p = 0.03), large-volume infarct (⩾70 mL) (p = 0.001), and angioplasty or stenting (p = 0.006) were predictors of any ICH. Hyperlipidemia or statin medication (OR, 4.17; 95% CI, 1.38–12.59; p = 0.011), INR (OR, 7.13; 95% CI, 0.94–54.22 p = 0.058), and large-volume infarct (⩾70 mL) (OR, 7.96; 95% CI, 2.31–27.39; p = 0.001) were predictors of SICH. Hypertension (OR, 5.77; 95% CI, 1.43-23.3; p = 0.014), initial NIHSS score (OR, 1.09; 95% CI, 1.01–1.18; p = 0.27), and SICH (OR, 15.7; 95% CI, 4.04–61.08; p < 0.001) were predictors of 1-month mortality.
Conclusions: INR and glucose may be strong modifiable predictors of critical ICH leading to death after IV/IA recanalization therapy in acute cerebral artery occlusion.
Disclosures of Interest: No
Abstract N°: 96
RETINAL THICKNESS CHANGES AS A MEDIATOR OF VISUAL LOSS IN OCCIPITAL LOBE INFARCTION
Le Cao*1, Hang Wang1, William Robert Kwapong1, Bo Wu1
1West China Hospital, Sichuan University, Neurology, China
On behalf of:
Background and aims: Visual loss has been reported in occipital lobe infarction (OI) but the pathophysiological changes of clinical outcomes including vision is underexplored.We explored the relationship between optical coherence tomography angiography (OCT)/ OCT angiography (OCTA) metrics and clinical outcomes in occipital lobe infarction (OI).
Methods: Twenty-six OI patients and 28 controls underwent macular OCT/OCTA scans; retinal nerve fiber layer (RNFL), ganglion cell-inner plexiform layer (GCIPL), and superficial vascular complex (SVC) were measured by the OCT/OCTA tool. All participants underwent visual acuity examination. Disease duration, neurological deficit, and infarct diameter were recorded in patients.
Results: OI patients presented thinner GCIPL thickness (p = 0.018) and SVC density (p = 0.002) compared to the controls. GCIPL thickness significantly correlated with infarct diameter (p = 0.024) and visual acuity (p = 0.007) while SVC density also significantly correlated with infarct diameter (p = 0.028). Infarct diameter had a total (p = 0.004) and direct effect (p = 0.036) on reduced visual acuity in OI patients. We also showed infarct diameter had a significant indirect effect (p = 0.048) on reduced visual acuity in OI patients via GCIPL thinning.
Conclusions: GCIPL thinning may account for the effect of infarct diameter in OI patients on visual acuity. Future prospective studies are needed to assess OCT/OCTA as a potential surrogate marker of visual loss in OI.
Disclosures of Interest: No
Abstract N°: 119
THYROID AXIS HORMONE LEVELS ASSOCIATIONS WITH HEALTH-RELATED QUALITY OF LIFE AFTER ISCHAEMIC STROKE
Saulius Taroza*1, Julius Burkauskas1, Aurelija Podlipskyte1, Nijolė Kažukauskienė1, Narseta Mickuvienė1
1Laboratory of Behavioral Medicine, Neuroscience Institute, Lithuanian University of Health Sciences, Palanga, Lithuania
On behalf of:
Background and aims: A history of stroke diminishes individual’s health-related quality of life (HRQoL). Enhancing the ability to predict the risk of deteriorating future HRQoL may serve as a foundation for timely targeted interventions. We aimed to evaluate associations between thyroid axis hormones serum levels and HRQoL in individuals following acute ischaemic stroke (aIS).
Methods: Individuals on admission due to aIS underwent assessment using National Institutes of Health Stroke Scale, considering pre-stroke disability and prior stroke history. HRQoL was measured using EQ-5D five-level (EQ-5D-5L) instrument at the end of the first week. Individuals answers were categorized into two groups: EQ-5D-5L estimated £ 3 in every dimension as positive outcome and all others as negative outcome. Blood samples were taken to evaluate thyroid stimulating hormone (TSH), free triiodothyronine (fT3), free tetraiodothyronine (fT4) and reverse triiodothyronine (rT3). Analysis was performed applying logistic regression.
Results: In sum, 168 individuals (mean age 66 ± 10 years, 95 [59.7%] men and 73 [40.3%] women) participated in the study. Comparative analysis revealed significantly higher mean levels of TSH (1.77 vs. 1.38 UI; p = 0.047 ), fT3 (0.29 vs. 0.27 ng/dl; p = 0.017), rT3 (35.96 vs. 29.69 ng/dl; p = 0.003) in positive HRQoL outcome group compared to negative. Multivariable logistic regression analysis showed that only higher fT3 (OR = 2.11, 95% CI 1.16 – 3.83; p = 0.014) remained associated with positive HRQoL outcome.
Conclusions: Higher fT3 serum levels on admission after experiencing aIS were associated with increased probability of better HRQoL at the end of the first week.
Disclosures of Interest: No
Abstract N°: 168
STROKE MECHANISM IN SYMPTOMATIC INTRACRANIAL ATHEROSCLEROTIC DISEASE: A MODIFIED CLASSIFICATION
Shuang Li*1, Xuan Tian1, Yuying Liu1, Bonaventure Ym Ip1, Hing Lung Ip1, Jill Abrigo2, Sin Ying Fan1, Sze Ho MA1, Thomas Leung1, Xinyi Leng1
1The Chinese University of Hong Kong, Medicine and therapeutics, China,2The Chinese University of Hong Kong, Department of Imaging and Interventional Radiology, Hong Kong
On behalf of:
Background and aims: In patients with symptomatic intracranial atherosclerotic stenosis (sICAS), hypoperfusion was widely considered as a stroke mechanism in internal and cortical borderzone (IBZ/CBZ) infarcts. Yet, recent evidence has suggested an association between artery-to-artery embolism (AAE) and CBZ infarcts.
Methods: We recruited patients with 50-99% sICAS in the anterior circulation. Stroke mechanisms were categorized as parent artery atherosclerosis occluding penetrating artery, AAE, hypoperfusion, and mixed mechanisms, using two systems. In Classification I, the probable stroke mechanisms of IBZ and CBZ infarcts were both considered as hypoperfusion, which were respectively considered as hypoperfusion and AAE in Classification II. Other classification criteria were the same in the two systems. We investigated and compared the predictive values of the two systems in predicting recurrent same-territory ischemic stroke (SIT) within 90 days and 1 year.
Results: Among 134 patients (median age, 62 [interquartile range, 52-70] years), 92 (68.7%) were males. The number of patients with parent artery atherosclerosis occluding penetrating artery, AAE, hypoperfusion and mixed mechanisms in classification I was 20 (14.9%), 16 (11.9%), 52 (38.8%), 46 (34.3%) and in classification II was 20 (14.9%), 42 (31.3%), 29 (21.6%), 43 (32.1%). Overall, 10 (7.5%) and 18 (13.4%) patients respectively had 90-day or 1-year recurrent SIT. Compared with Classification I, Classification II could better predict the risk of 90-day recurrent SIT (0.693 vs 0.773, Z=2.19, p=0.029).
Conclusions: In stroke mechanism classification in sICAS patients, reclassifying CBZ infarcts from the hypoperfusion category to the AAE category may be associated with improved risk stratification of affected patients.
Disclosures of Interest: No
Abstract N°: 196
DEEP LEARNING DISCONNECTOMES TO ACCELERATE & IMPROVE PREDICTIONS FOR POST-STROKE SYMPTOMS
Anna Matsulevits*1,2,3, Pierrick Coupe4, Huy-Dung Nguyen5, Lia Talozzi6, Chris Foulon7, Parashkev Nachev8, Maurizio Corbetta9, Thomas Tourdias10, Michel Thiebaut DE Schotten11
1Bordeaux University - Campus Carreire, Bordeaux, France,2Groupe d’Imagerie Neurofonctionnelle, Institut des Maladies Neurodégénératives- UMR 5293, CNRS, CEA, Bordeaux, France,3Brain Connectivity and Behaviour Laboratory, Sorbonne Universities, Paris, France.,4University Bordeaux, Bordeaux, Gironde,5Bordeaux University - Campus Carreire,6Stanford Medical School, Stanford, CA,7Groupe d'Imagerie Neurofonctionnelle (GIN), Institut des Maladies Neurodegeneratives-UMR 5293, CNRS, Bordeaux, FRANCE,8UCL Queen Square Institute of Neurology, London, London,9Clinica Neurologica, Department of Neuroscience, University of Padova, Padova, Italy,10University Bordeaux, Bordeaux, Gironde,11University Bordeaux, Institut des Maladies Neurodégénératives CNRS UMR 5293 Université de Bordeaux, Bordeaux, Gironde
On behalf of:
Background and aims: Anticipating the risk of developing impairments following stroke could help refer the patients to dedicated training to improve their outcomes.
Methods: We implemented a 3D-U-Net network for predicting individual deep-disconnectomes from binary masks of infarcts that was trained on N=1333 synthetic lesions and their corresponding disconnectomes, and tested on N=1333 real stroke lesions. To predict clinical scores, we embedded the deep-disconnectomes of the 1333 patients within a 2D-morphospace using UMAP. With the achieved association between location within the morphospace and neuropsychological scores, we were able to predict scores for an out-of-sample population.
Results: The trained model was able to capture most information obtained in conventional disconnectomes, but output a deep-disconnectome 720 times faster. Through the morphospace, the deep-disconnectomes predicted neuropsychological outcome at 1-year with an average accuracy of 85.2% (R2=0.208) which was significantly better (p=0.009) than prediction from the conventional disconnectome approach. Assessing the structure of the morphospace suggests a greater differentiation for deep-disconnectomes derived from similar stroke lesions. This may have improved the segregation between similar profiles of white-matter damage and, accordingly, led to better modeling of fine differences within the same neuropsychological assessment.
Conclusions: The deep-learning model accurately resembles the ground truth, producing a deep-disconnectome from a binary lesion mask. For long-term stroke outcome predictions, the deep-disconnectome's predictive power outperformed the conventional disconnectomes. This demonstrates the potential of practical application of AI-driven models for clinical settings, which might enhance efficiency within healthcare systems, and ultimately contribute to an improved quality of life for stroke survivors.
Disclosures of Interest: No
Abstract N°: 798
MODIFIED RANKIN SCORE (MRS) 6 – THE IMPORTANCE OF PALLIATIVE CARE ON THE HYPERACUTE STROKE UNIT (HASU)
Agampodi Umanda De Thabrew*1,2, Lady-Namera Alexander1,2, Maria Francisca Rocha1,2, Benjamin Sacks1,2, Jai Mathur1,2, David Turner1,2
1National Hospital for Neurology and Neurosurgery, United Kingdom,2University College Hospital, United Kingdom
On behalf of:
Background and aims: Five million annual stroke deaths occur globally, 50% of which occur in hospital. End of life (EOL) decisions are a challenging aspect of inpatient stroke care (1,2). Our study characterises the journey of dying stroke inpatients with a view to enhancing EOL care.
Methods: A retrospective cohort analysis conducted over an 8 month period (March-October 2023). Patients who died <24 hours after admission or under neurosurgical or intensive care were excluded.
Results: A total of 30 patients were included. Mean age of death was 83 years (SD +/- 13.9 years). Major presenting complaints were sudden onset weakness (66%), reduced GCS (17%) and fall (17%). Mean length of stay (LOS) was 15 days (SD: +/-15.69/IQR: 20.5). Total LOS across all patients was 465 days. Commonest diagnoses were middle cerebral artery (MCA) ischaemic stroke (44%) and intracranial haemorrhage (ICH) (31%). Causes of death (COD) were ischaemic stroke (40%), primary or secondary ICH (37%) and aspiration pneumonia (20%). 73% of patients had EOL pathway documentation completed. Mean time on EOL pathway was 3.13 days (SD: +/-3.67). 75% of patients had a nasogastric tube (NGT) during admission, 67% had a syringe driver. Mean NGT duration was 7.13 days (SD: +/-10.6). Syringe driver duration was 2.63 days (SD: +/-3.54).
Conclusions: EOL patients had long admissions, and mean NGT duration was >1 week. Comparatively, EOL pathway and syringe driver durations were short. Palliative care is needed everyday on HASU, and should be a key part of resource planning and education for Stroke services.
Disclosures of Interest: No
Abstract N°: 888
ROLE OF TCCD WITH COGIF SCORE IN PREDICTING CLINICAL IMPROVEMENT AFTER SUCCESSFUL EVT IN ISCHEMIC STROKE PATIENTS
Matteo Paolucci*1, Sabrina Rossi2, Giorgia Arnone1, Ludovica Migliaccio1, Mauro Gentile1, Guido Bigliardi3, Michele Romoli4, Georgios Tsivgoulis5, Andrea Zini1, Giovanni Malferrari1
1IRCCS Istituto delle Scienze Neurologiche di Bologna, UOC Neurologia e Rete Stroke Metropolitana, Italy,2Azienda Ospedaliera Arcispedale Sant'Anna, Stroke Unit - UO Neurologia, Cona, Ferrara, Italy,3Azienda Ospedaliero-Universitaria di Modena, SC Neurologia-Stroke Unit Clinica Neurologica, Modena, Italy,4AUSL Romagna, UOC Neurologia, Ospedale "M. Bufalini", Cesena, Italy,5National and Kapodistrian University of Athens, School of Medicine, Athens, Greece., Second Department of Neurology, "Attikon" Hospital, Greece
On behalf of: on behalf of HYS Study Group: Cristiano Azzini, Donatella Mastria, Giuseppe Pulito, Vittoria Sarra, Marco Longoni, Daniela Monaco, Vincenzo Inchingolo, Monia Russo, Lorenzo Coppo
Background and aims: This study aimed to assess the utility of the COGIF score, a systematic consensus for standardizing Transcranial Color-Coded Doppler (TCCD) in multicenter studies, to predict clinical outcomes in patients undergoing successful endovascular treatment (EVT) for ischemic stroke.
Methods: We conducted a multicentric prospective study with consecutive patients with ICA or MCA M1-M2 segments occlusion treated with successful EVT (TICI 2b-3), evaluating TCCD within 48 hours post-EVT. TCCD flow was graded by COGIF score (1: no flow; 2-3: low flow; 4a: normal; 4b: residual stenosis; 4c: hyperperfusion). Clinical improvement was defined as a decrease of 8 points/30% on NIHSS at day 7 compared to baseline.
Results: 186 ischemic stroke patients were included (female: 48%; mean age 72.2 yo, SD 14.3; TICI 2b-c 23%). Median NIHSS was 16 (IQR 10-19) at admission and 2.5 (IQR 1-8) at day 7/discharge. 26 patients did not show clinical improvement (69% had TICI 3). COGIF was 4a in 78.6% of TICI 2b-c and 83.9% of TICI 3. TICI 2b-c and 3 had similar percentage of COGIF 3 (2.4% vs 2.2%, respectively) but differred for COGIF 4b and 4c (19% vs 3.6% and 0% vs 10.2%, respectively). Absence of clinical improvement was significantly more frequent in COGIF 3 and 4b compared to COGIF 4a and 4c (p<.001; figure).
Conclusions: COGIF score grading by TCCD in the first 24-48h after EVT may help identifying patients with lack of clinical improvement at day 7. Specifically, the spectrum structure may indicate inadequate perfusion or potential leptomeningeal activation.
Disclosures of Interest: No
Abstract N°: 949
THE RELATIONSHIP BETWEEN SERUM INFLAMMATORY BIOMARKERS AND HEMORRHAGIC TRANSFORMATION AFTER ACUTE ISCHEMIC STROKE
1Department of Neurology, West China Hospital, Sichuan University, China
On behalf of:
Background and aims: Inflammation plays a crucial role in the process of hemorrhagic transformation (HT). We aimed to investigate the relationship between serum inflammatory biomarkers (including CTSB, NLRP3, ferritin, HMGB1 and MMP9) and HT in patients with acute ischemic stroke.
Methods: Consecutive patients with ischemic stroke within 24 h of onset evaluated from January 2016 to December 2019 were included. HT was defined as the presence of hemorrhage within the infarct territory or parenchymal hemorrhage outside the infarct zone, which was not visible on the initial CT or MRI but was detected on follow up CT or MRI. Multivariable regression analyses were performed to explore the association between each serum biomarker and HT. Area under curve (AUC) was calculated for biomarkers to predict HT.
Results: Of the 1119 included patients, 170 (15.2%) developed HT. In multivariable analyses, a panel of serum biomarkers (CTSB ⩾ 3.69 ng/ml + HMGB1 ⩾ 196.35 ng/ml + NLRP3 ⩽ 820.59 pg/ml + ferritin ⩾ 205.9 ng/ml) was found to have the largest AUC of 0.709 (95%CI 0.649-0.764; P<0.001) for predicting HT (sensitivity: 62.86%; specificity: 68.33%). When incorporated with conventional risk factors, this panel significantly improved predictive values for HT (net reclassification improvement: 71.65%, 95%CI 36%-107.30%, P<0.001; integrated discrimination index: 6%, 95%CI 2.51%-9.49%, P=0.001).
Conclusions: We found a clear relationship between serum inflammatory biomarkers and risk of HT. Incorporation of a combination of multiple biomarkers observed substantially improved the risk stratification for HT.
Disclosures of Interest: No
Abstract N°: 1039
POST-STROKE FATIGUE IN PATIENTS IN WORKING AGE AT THREE MONTHS AFTER ISCHEMIC STROKE: PILOT ANALYSIS FROM THE FRAILTY STUDY
Daniel Sanak*1, Elena Gurkova2, Lenka Sturekova2, Sarka Sanakova2, Jana Zapletalova3, David Franc4, Daniela Bartonickova5
1University Hospital Olomouc, Comprehensive Stroke Center, Dept. of Neurology, Olomouc, Czech Republic,2Palacký University, Faculty of Health Sciences, Department of Nursing, Olomouc, Czech Republic,3Department of Biophysics and Statistics, Palacký University Medical School, Olomouc, Czech Republic,4University Hospital Olomouc, Department of Neurology, Olomouc, Czech Republic,5Palacký University, Faculty of Health Sciences, Department of Nursing, Olomouc, Czech Republic
On behalf of:
Background and aims: Post-stroke fatigue (PSF) is known sequel after ischemic stroke (IS), however its incidence and contributing factors remains controversial or not well established, especially in younger population. Our aim was to assess PSF in the patients in working age (18-65 years) three months after IS and evaluate possible association to post-stroke depression (PSD), anxiety (PSA), and other factors.
Methods: Consecutive IS patients in working age enrolled in the prospective FRAILTY (Factors Affecting the Quality of Life After Ischemic Stroke in Young Adults; ClinicalTrials.gov: NCT04839887) were analysed. PSF was assessed using Fatigue Severity Scale (FSS) and Neuro_QoL_Fatigue scale (NQFs), PDS and PSA using Hospital Anxiety and Depression Scale (HADS) at three months after IS. Subgroup comparison according to FSS scores was performed to identify possible predictors of PSF.
Results: In total, 94 (56.4% males, mean age 53.7 ± 12.8 years) IS patients were analyzed and 81 (86.2%) of them had mRS 0-1 after three months. Mean FSS score was 4.37 ± 2.14 (borderline fatigue) and 41 (43.2%) patients had FSS score ³ 5 (severe fatigue). Mean NQFs score was 2.58 ± 0.91 and 62 (66%) patients had NQFs score > 2.0 (fatigue). No association was found between PSF scores and age, sex, mRS, NIHSS and HADS scores.
Conclusions: 66% of patients had PSF and 43.2% severe form of PSF after three months after IS. No associations between PSF and age, sex, NIHSS, mRS, PSD and PSA were found.AcknowledgmentSupported by the grant of Ministry of Health CR, n. NU22-09-00021.
Disclosures of Interest: No
Abstract N°: 1159
INFLAMMATION SERUM MARKERS, CLINICAL AND NEURORADIOLOGICAL PARAMETERS IN ACUTE ISCHEMIC STROKE: A NEW COMPOSITE PROGNOSTIC SCORE
Pier Andrea Rizzo*1, Simone Bellavia1, Irene Scala1, Jacopo DI Giovanni1, Giovanni Frisullo1,2
1Università Cattolica del Sacro Cuore, Neurology, Roma, Italy,2Agostino Gemelli University Policlinic, Neurology, Roma
On behalf of:
Background and aims: Inflammation plays a significant role in the pathophysiology of ischemic and the identification of specific inflammatory markers is still an open challenge. The aim of this study is to identify the predictors of outcome among serum markers of inflammation and clinical and neuroimaging parameters and, consequently, to develop a prognostic score.
Methods: We included all consecutive ischemic stroke patents which performed, in emergency department within the first 24 hours from stroke onset, inflammatory serum markers such as CRP, leukocyte formula, fibrinogen and ESR, clinical and neuroradiological evaluation.
Results: Starting from 824 subjects, we enrolled in the final analysis 341 acute ischemic stroke patients. CRP, ESR, SIRI (systemic inflammation response index), age, pre-admission mRS, admission NIHSS and ASPECT score were predictor of both good vs poor outcome and death. Moreover, through ROC curve analysis, we identified a CRP cut-off of 21,9 mg/L as a good predictor of both 3 months outcome (AUC=0.642) and mortality (AUC=0.850). After multivariate analysis, CRP, pre-admission mRS, and ASPECT score were independent predictor of worse prognosis. On the basis of the multivariate analysis, we elaborated a score and an app in order to predict the long-term outcome in acute stroke patients.
Conclusions: Elevated CRP appears to be a reliable predictor of poor outcome and mortality in ischemic stroke. The CRP cut-off and composite prognostic score could be a useful tool in the risk stratification of acute stroke patients in the emergency department.
Disclosures of Interest: No
Abstract N°: 1335
THE UTILITY OF NIHSS IN THE PREDICTION AND IDENTIFICATION OF EARLY NEUROLOGICAL DETERIORATION
Cameron Lee*1, Tony Yu1,2, Maria Lucia Uribe Mz Recaman1, Beatrix Sari1, Samantha Bayhonan1, Carol Belo1, Mohammed Mallah1,3, Yassine Noui1,4, Yee Mah1,5
1King's College Hospital, United Kingdom,2Auckland District Health Board, Auckland, New Zealand,3St George's Hospital, United Kingdom,4Uppsala University, Uppsala, Sweden,5King's College London, Biomedical Engineering and Imaging Sciences, United Kingdom
On behalf of:
Background and aims: Between 5-40% of Acute Ischaemic Stroke (AIS) presentations are complicated by Early Neurological Deterioration (END). There is an array of underlying aetiologies and this heterogeneity makes it challenging to precisely define clinical criteria for the identification of END. Worsening NIHSS has been proposed as a defining feature; here we evaluated the relationship between NIHSS and the risk of END to establish its utility in identifying END.
Methods: All stroke admissions to the Hyper Acute Stroke Unit at King’s College Hospital, London, from Jan-Jun 2022 were manually reviewed for END occurring within the first 14 days from stroke onset. END was identified using clinical documentation, GCS and radiological evidence and did not include changes in NIHSS.
Results: Of the 477 stroke admissions between 1 Jan-30 Jun 2022, 50 AIS patients developed END. Overall, a higher arrival NIHSS was associated with a greater risk of END.
In those receiving reperfusion therapy, logistic regression analysis showed patients with no change or an improvement in NIHSS still had up to a 20% risk of END. Greater worsening of NIHSS was associated with increased END risk.
Conclusions: Arrival NIHSS is a predictor of END risk in AIS. However, by excluding NIHSS in the identification of END during our review process, we have shown the arrival NIHSS and change in NIHSS is far less useful at identifying this cohort. We therefore recommend that future studies investigating END should consider alternative methods to define their END cohort due to the high false negative rate.
Disclosures of Interest: No
Abstract N°: 1373
PREDICTION OF IN-HOSPITAL MORTALITY OF ACUTE ISCHEMIC STROKE PATIENTS TREATED WITH INTRAVENOUS THROMBOLYSIS: SCORE-BASED APPROACH
Raissa Cariello*1, Raissa Soares2, Ana Carolina Do Couto Andrade3, Natasha Matsunaga3, Helena Rezende1, Rodrigo Castro1, Eduardo Damasceno1, Clara Monteiro Antunes Barreira1, Marco Tulio Araujo Pedatella1
1Hospital Estadual de Urgências de Goiás Dr. Valdemiro Cruz, NEUROLOGY, GOIANIA, Brazil,2Santa Casa de Misericórdia de Goiânia, NEUROLOGY, GOIANIA, Brazil,3Universidade Federal De Goiás, GOIANIA, Brazil
On behalf of:
Background and aims: Global burden and mortality from stroke are higher in lower-income and lower-middle-income countries. National studies on predictors of in-hospital mortality in acute stroke remain scarce. Our aim was to develop an applicable tool for mortality risk stratification of patients with acute stroke treated with intravenous thrombolysis in an emergency unit in Brazil.
Methods: In this retrospective study, we collected data on demographic and clinical variables of each patient profile. After exploratory data analysis, multivariate logistic and stepwise regression were used to identify statistically significant predictors of in-hospital mortality to compose a risk stratification score (FAST GAIN) validated through crossed validation. ROC curve was used to test the accuracy of the final model.
Results: A sample of 238 patients (50.8% women) were included between March, 2022 and November, 2023. Mortality rate was 22.3%. In 31 variables analyzed, the ones significantly associated with unfavorable outcome were: age ⩾75 years, NIHSS of admission ⩾12, kidney dysfunction in the first 72h from admission, hemorrhagic transformation (more importantly hematoma than petechial), ASPECTS ⩽7, and use of nasoenteral tube. Furthermore, the presence of atrial fibrillation or flutter and admission capillary glucose ⩾140 mg/dL were also relevant in the analysis of confidence interval and odds ratio. In the ROC curve analysis, the optimal point was 0.2310.
Conclusions: The variables mentioned above constitute the acronym FAST GAIN. This prognostic score had an accuracy rate of 85,92% and can be a helpful tool for directing strategies of multidisciplinary clinical care.
Disclosures of Interest: No
Abstract N°: 1474
INTRACRANIAL ARTERIOSCLEROSIS AND PROGNOSIS AFTER ENDOVASCULAR TREATMENT FOR ACUTE ISCHEMIC STROKE
Alicia Sierra Gómez*1, Maria Esther Ramos-Araque2,3, Sven Luijten4, Mercedes de Lera Alfonso1, Ana Isabel Calleja Sanz1, Beatriz Gomez Vicente1, Francisco Javier Reyes Muñoz1, Mario Martínez Galdámez5, Daniel Bos4,6, Juan F. Arenillas1,7
1University Clinical Hospital of Valladolid, Department of Neurology, Valladolid, Spain,2Hospital Clínico Universitario de Valladolid, Department of Neurology, Spain,3Salamanca University Hospital, Department of Neurology, Salamanca, Spain,4Erasmus MC, Department of Radiology & Nuclear Medicine, Rotterdam, Netherlands,5University Clinical Hospital of Valladolid, Department of Radiology, Valladolid, Spain,6Erasmus MC, Department of Epidemiology, Rotterdam, Netherlands,7University of Valladolid, Clinical Neurosciences Research Group. Department of Medicine, Spain
On behalf of: Stroke program HCU Valladolid
Background and aims: Intracranial arteriosclerosis (ICAR) is a major stroke cause worldwide, but its role in acute ischemic stroke (AIS) prognosis remains unclear. We investigated the ICAR effect on the prognosis of large vessel occlusion (LVO) AIS in patients undergoing endovascular treatment (EVT), with specific focus on ICAR subtypes.
Methods: Longitudinal prospective cohort study in consecutive AIS patients with anterior circulation LVO treated with EVT. We assessed intracranial carotid artery calcification (ICAC), as ICAR hallmark, using baseline non-contrast-CT, quantifying ICAC volume and establishing the predominant subtype (intimal, internal elastic lamina (IEL) calcification, mixed). We recorded procedural (first pass effect (FPE)), short-term (24h-infarct volume) and long-term outcomes (poor functional outcome (mRs>2), disability (mRs 0-6)). Multivariate-adjusted linear and logistic regression models were used.
Results: From January 2021 to February 2022, 181 patients met inclusion criteria. ICAC was present in 172 (95%) patients. IEL calcification was predominant in 103 (57%) patients, intimal in 52 (29%), and mixed in 17 (9%). Larger ICAC volumes were associated with greater FPE probability (aOR, 1.45 [95% CI: 1.01-2.11]), and lower mortality (aOR, 0.47 [95% CI: 0.26-0.85]). Intimal ICAC was associated with lower FPE likelihood (aOR, 0.42 [95% CI:0.21-0.84]), higher infarct volume (ab, 22.19 [95% CI: 0.71-43.67]), poorer functional outcome (aOR, 2.18 [95% CI: 1.13-4.21]) and higher mortality (aOR, 2.84 [95% CI: 1.14-7.08]).
Conclusions: In LVO AIS patients undergoing EVT, a predominant intimal subtype, linked with underlying atherosclerosis, is associated with larger infarct volume, worse 90-day functional outcome, and higher mortality. Intracranial atherosclerosis appears as a relevant factor hampering the clinical benefit after EVT.
Disclosures of Interest: No
Abstract N°: 1688
COMPARING DUAL-TASK COSTS BETWEEN STROKE PATIENTS AND HEALTHY CONTROLS: A PILOT STUDY
Yusuf EMUK*1, Nurcan Akbulut2, Zeynep Tanriverdİ3
1Izmir Katip Çelebi University, Faculty of Health Sciences Department of Physiotherapy and Rehabilitation, Izmir, Turkey,2Izmir Katip Çelebi University, Neurology, Izmir, Turkey,3Izmir Katip Çelebi University, Faculty of Medicine Department of Neurology, Izmir, Turkey
On behalf of:
Background and aims: Cognitive-motor and motor dual tasks are significant factors in everyday activities. The objective of this study was to assess and compare the dual-task costs across various activities in both stroke survivors and healthy individuals.
Methods: The study comprised 19 individuals diagnosed with stroke (62 years old (25-75th percentiles: 52–64) and 11 healthy participants (49 years old (25-75th percentiles: 42–59) and. The lower extremity performance was assessed using the 10-Meter Walk Test (10MWT), while the upper extremity was evaluated through the Box and Block Test. Participants underwent the tests under conditions of a single task, an additional motor task, and a cognitive task.
Results: The study results demonstrated that, with regards to upper extremity performance, individuals with stroke incurred a higher dual-task cost compared to healthy individuals in all parameters, except for the dominant hand motor-motor dual task. During the motor-cognitive dual task in the lower extremity, no significant difference was observed between the groups. However, motor-motor dual-task cost was higher in individuals with stroke. Furthermore, in individuals with stroke, the dominant hand motor-cognitive dual-task cost was significantly higher than the motor-motor dual-task cost.
Conclusions: Our findings indicate an increase in dual-task costs across various performances involving both lower extremity and upper extremity in individuals with stroke. We believe that integrating dual-task training into treatment programs may be beneficial for enhancing the improvements in stroke rehabilitation.
Disclosures of Interest: No
Abstract N°: 1752
PREDICTORS OF ACUTE HEADACHE AT STROKE ONSET: A PROSPECTIVE STUDY; CLINICAL AND RADIOLOGICAL EVALUATION
Elsayed Abed*1
1Al-Azhar University, Neurology, Cairo, Egypt
On behalf of:
Background and aims: The clinical and radiological predictors for the occurrence of acute headache at stroke onset do not meet great attention in various studies.We aimed to assess and identify the possibly associated clinical and radiological predictors for the post-stroke headache to provide better prophylactic management.
Methods: This study is an observational case-control study in which 112 patients fulfilling the criteria of the ICHD-3 for post-stroke headache were evaluated by a control group including 127 matched patients who didn’t report headache. The present study focuses on possibly associated clinical and radiological predictors for the occurrence of a post-stroke headache
Results: The case group included 112 patients and the control group included 127 matched patients. There was a statistically significant difference between the two groups as regards the history of lack of sleep, increased body mass index above 25, presence of pre-stroke headache, old stroke, and posterior circulation infarction (P< 0.001). The most prevalent site of infarction demonstrated with brain imaging was in the territory of the posterior circulation (34%) with statistically significant differences between the two groups as regards the cerebellar site (P< 0.001). Moreover, only infarcts >15 mm were associated with headache production (P< 0.001).
Conclusions: We can predict the development of post-stroke headache through several clinical and radiological factors. on the concept of post-stroke headache was developed within 7 days after stroke onset in most of the case group, our study could help further studies with a new scope to provide better prophylactic management for a post-stroke headache once we predict it.
Disclosures of Interest: No
Abstract N°: 1845
COMPARING ISCHEMIC STROKES TREATED IN EXTENDED AND CONVENTIONAL TIMES IN PISA OVER A YEAR; POPULATION OUTCOMES ANALYSIS
Gaia Mignani*1, Roberto D'agliano1, Marco Baldini1, Nicola Giannini1, Giovanni Orlandi1, Mirco Cosottini2, Riccardo Morganti3, Gabriele Siciliano4, Michelangelo Mancuso4
1University of Pisa, Neuroscience, Pisa, Italy,2University of Pisa, Department of Translational Research and New Technologies in Medicine and Surgery, Pisa, Italy,3University of Pisa, Section of Statistics, Pisa, Italy,4University of Pisa, Neurological Sciences, Pisa, Italy
On behalf of:
Background and aims: The study aimed to analyze the clinical outcomes of ischemic stroke patients eligible for reperfusion therapies. It compared patients treated within < 4.5 hours for IVT and/or < 6 hours for EVT to those treated in the extended time window (EXTEND, DAWN, DEFUSE-3 criteria). Furthermore, the study identified clinical and anamnestic variables associated with worse outcomes in disability (efficacy outcome) and safety (major hemorrhagic complications) within the entire population.
Methods: Data were collected from Stroke Unit patients in Pisa from July 2022 to July 2023. Two subgroups, treated within conventional and extended time windows, were compared by analyzing mRs change using the Mann-Whitney U test. Univariate analyses used the Mann-Whitney U test for mRS at 3 months and the chi-square test for hemorrhagic complications. Subsequent multivariate analysis employed significant variables from univariate analyses, using shift analysis and binary logistic regression.
Results: No inferiority was observed in treating within the extended time window compared to traditional timings regarding mRs at 3 months (p=0.102). Worse efficacy outcomes in the overall population were associated with nosocomial infections, dysphagia, and NIHSS onset. Worse safety outcomes correlated with current neoplasm, dysphagia, and NIHSS at onset.
Conclusions: Non-inferiority of treatment within the extended time window compared to traditional timings was demonstrated, aligning with current guidelines. Effective in-hospital management is crucial to prevent infections and dysphagia. The presence of an ongoing neoplasm may influence the development of hemorrhagic complications.
Disclosures of Interest: No
Abstract N°: 1953
PREDICTORS OF GOOD FUNCTIONAL RECOVERY IN PATIENTS WITH ACUTE ISCHEMIC STROKE AT THREE MONTHS OF THE EVENT
1All India Institute of Medical Sciences, Neurology, New Delhi, India
On behalf of:
Background and aims: Stroke is the fourth leading cause of death and fifth leading cause of disability in India. Our aim was to assess predictors of good functional outcome(mRS 0-2) at three months & ENI(Early Neurological Improvement= NIHSS 0/1) at 24 hours in acute ischemic stroke patients.
Methods: A single-centre prospective-cohort study recruiting 311 adult acute ischemic stroke patients with pre-stroke mRS⩽1, within 72 hours of ictus, fulfilling the inclusion and exclusion criteria, was conducted from February 2022- November 2023.
Results: 66% were males, having mean age of 56 years(±16.18). Mean Systolic Blood pressure, Diastolic Blood pressure, GCS, NIHSS at presentation, CT-ASPECTS, Collateral score, time to hospital arrival, time to thrombolysis & time to thrombectomy were 147 mm Hg(±28.8), 86 mm Hg(±16.4), 6(±1), 12(±8), 6(±3), 4(±1), 11 hours(±4), 4 hours(±2) & 6 hours(±2) hours respectively. 52% had LVO. 36% achieved ENI. Younger age at presentation (OR 1.04 with 95% CI 1.00-1.09, p=0.04), Low NIHSS at presentation(OR 1.35 with 95% CI 1.09-1.66), IVT(OR 5.24 with 95% CI 0.86-32.01), Higher albumin(OR 8.08 with 95% CI 1.05-62.34) & ENI (OR 6.53 with 95% CI 1.36-31.28) were associated with good functional outcome, whereas poor collateral score(OR 0.33 with 95% CI 0.15-0.74) was associated with bad functional outcome at three months. Lower NIHSS at 24 hours (OR 4.49 with 95% CI 2.26-8.95) & higher GCS at presentation (OR 22.188 with 95% CI 3.94-125.02) were associated with ENI at 24 hours.
Conclusions: Improving our knowledge about predictive factors might enhance rehabilitative procedures in acute ischemic stroke patients.
Disclosures of Interest: No
Abstract N°: 1957
PERSONAL EXPERIENCES OF LASTING CHALLENGES FOUR MONTHS AFTER TRANSIENT ISCHEMIC ATTACK
Birgitte Hede Ebbesen1, Boris Modrau*2, Michael Rathleff3, Søren Johnsen4, Jane Andreasen5
1Aalborg University Hospital, Department of Physiotherapy and Occupational Therapy,2Aalborg University Hospital, Department of Neurology,3Aalborg University, Department of Health Science and Technology,4Aalborg University, Department of Clinical Medicine,5Aalborg Municipality
On behalf of:
Background and aims: Paradoxically, 1/3 of patients with transient ischemic attack (TIA) experience lasting challenges as fatigue, depression, anxiety, and cognitive difficulties. The aim is to explore how TIA impacts patients’ lives during four months after discharge. Furthermore, to identify what patients believed facilitated return to everyday life.
Methods: Qualitative semi-structured interviews.
Results: 15 patients were included. Four themes were identified; 1) “They say it is transient – no, not for me” where all describe lasting challenges emphasizing invalidating fatigue and impaired social participation, 2) “I am a changed person, how does this impact my future?” which reflects altered identify and elevated alertness for symptoms, 3) “Time has been my ally and new perspectives have evolved” where most communicate improvement over time and a few considered TIA as a needed wake-up call to change lifestyle. Lastly 4) “What would have helped me recover?” which unfolds that close, trustful relations influence coping abilities positively. On the contrary the system failed to support. Participants described pressure to return to work and lack of trust and negative experiences when involving their general practitioner.
Conclusions: During the four months since diagnosis participants experienced limitations impacting physical, psychological and/or social domains. They felt uninformed that lasting challenges could affect them. Different coping strategies were used, and participants with close, supportive relations managed better. A pressure to return to work and lack of trust in the general practitioner affected negatively. Overall, the return to everyday life after TIA can be stressful and appropriate support was not provided.
Disclosures of Interest: No
Abstract N°: 2007
SIGNIFICANT ASSOCIATION OF NIGHTTIME SYSTOLIC BLOOD PRESSURE WITH CLINICAL OUTCOMES FOR ACUTE ISCHEMIC STROKE
1Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Department of Neurosurgery, Beijing,2Peking University Shenzhen Hospital, Department of Neurosurgery,3Hainan General Hospital, Hainan Affiliated Hospital of Hainan Medical University, Hainan Province Clinical, Medical Center and Hainan Academician Innovation Platform, Department of Neurology,
On behalf of:
Background and aims: Blood pressure (BP) is a crucial factor for clinical outcomes of patients with acute ischemic stroke (AIS) receiving endovascular thrombectomy (EVT). However, the current study is unclear as to which BP parameter is most associated with clinical outcomes in AIS.
Methods: This retrospective observational study was conducted at three hospitals in China from 2016 to 2022. A total of 370 consecutive patients with AIS who underwent EVT and thereafter continuous 24-hour BP monitoring were included in the analysis. The 3-month mRS score and symptomatic intracranial hemorrhage were considered the clinical outcomes in the study. The association between different BP parameters and these outcomes was assessed using logistics models.
Results: 166 (44.9%) of 370 patients were functionally dependent, and 51 (13.8%) experienced sICH. Restricted cubic spline (RCS) analysis revealed a linear relationship between BP indexes and the mRS, as well as sICH. Higher value of systolic BP (SBP) and diastolic BP (DBP) were associated with greater risk of functional dependence, but only nighttime SBP was associated with sICH (OR: 1.329, 95% CI: 1.062-1.673 per 10 mmHg). After adjusting for other BP indexes, 24-hour SBP and daytime SBP lost their association with functional outcome, but nighttime SBP remained strongly correlated with outcome, both in the unadjusted and adjusted analyses.
Conclusions: In patients with AIS after EVT, nighttime SBP remained significantly associated with outcomes even after adjusting for other BP indexes. Therefore, nighttime SBP should be considered the optimal measurement for assessing outcomes in AIS patients.
Disclosures of Interest: No
Abstract N°: 2012
BASELINE CHARACTERISTICS OF POSTERIOR CIRCULATION STROKE - IS THERE A CORRELATION TO THE OUTCOME AT DISCHARGE?
1National Institute of Neurology and Neurovascular Diseases, Neurology, Bucharest, Romania,2Carol Davila University of Medicine and Pharmacy, Bucharest, Romania,3Emergency University Hospital Bucharest, Internal Medicine, Bucharest, Romania
On behalf of:
Background and aims: The National Institutes of Health Stroke Scale (NIHSS) is widely used for stroke patients; however, it seems to underestimate the clinical severity in posterior circulation stroke (PCS). Our aim is to evaluate the correlation between baseline presentation of PCS and the outcome at discharge.
Methods: All patients admitted to our clinic in 2022 with PCS were retrospectively evaluated based on demographic features, the baseline NIHSS and the accompanying PCS related phenomena. Patients who underwent revascularization were excluded. The outcome was defined based on the modified Rankin Scale (mRS) at discharge.
Results: 239 patients with PCS were included in the analysis (mean age 68.74 years (± 12.36), 41% female). A positive correlation between NIHSS and mRS was found (r=0.53). Univariate analysis demonstrated that age is statistically significantly associated with the outcome (p < 0.0001). Headache (p = 0.0009), vertigo (p = 0.005), diplopia (p = 0.001) and dysphagia (p < 0.0001) are statistically significantly associated with mRS at discharge, but only dysphagia is associated with a poor outcome. Multivariate analysis revealed age (p < 0.0001) and dysphagia (p < 0.0001) as independently associated with the outcome. For patients with NIHSS ⩽ 4 (144 patients) only age (p < 0.0001) was an independent determinant of mRS.
Conclusions: NIHSS and dysphagia in the acute stage of PCS were associated with mRS at discharge. In patients with low NIHSS, age was the only predictor of the outcome. Future studies are needed to examine these findings and their importance in clinical practice.
Disclosures of Interest: No
Abstract N°: 2051
GAIT DISTURBANCES AMONG LACUNAR STROKE PATIENTS
Reyes de Torres Chacon*1, Ana Maria Najar Moyano2, Cristina López Ázcarate2, Miriam Camino2, Carmen del Rio Mercado2, Carmen Domínguez Ruiz2, Emilio Montero Ramírez1, Enrique Rodriguez Rua1, Soledad Pérez Sánchez1, Joan Montaner1
1Hospital Virgen Macarena, Neurology, Spain,2Instituto de Biomedicina de Sevilla, Neurology, Spain
On behalf of:
Background and aims: Lacunar stroke is associated with motor, sensory and cognitive deficits that can limit patient's independence. Moreover, gait and balance deficits, especially in elderly patients, can limit their daily activities. This study aims to describe the gait pattern of patients with a lacunar stroke using advanced gait analysis technologies
Methods: Gait parameters are assessed in a cohort of patients who suffered a lacunar stroke in the last 24 months with mRS⩽3. Protocols and devices used for gait assessment are the Six Minutes Walking Test, the Berg test, and the automatic measurement of gait patterns using a GAITRite Electronic System®.
Results: 78 patients (70.5% male) with a median age of 67 years were included. According to their Functional Ambulatory Profile, most patients had a functional gait (median 93.5 out of 100 points). The main items used for the assessment of gait showed the following values: the Berg test (median 55 out of 56 points), the area of the base of the supporting surface =median left side 10.4cm and right side 10.7cm) and the step length =median left step 56 cm and right step 56.4 cm.
Conclusions: Lacunar stroke patients in our cohort have a functional gait pattern but linked to the acquisition of compensations in stride length, stride velocity, and base of support amplitude. These results suggest that, despite apparent functionality, there is a deficit in the patient's balance, strength, and proprioception. This type of analysis can help to detect non-obvious gait defects that can be treated to improve independence.
Disclosures of Interest: No
Abstract N°: 2105
IMPACT ON HEALTH-RELATED QUALITY OF LIFE IN RELATION TO DEPRESSION AND ANXIETY AFTER TRANSIENT ISCHEMIC ATTACK AND MINOR STROKE
María Rocío Córdova Infantes*1, Noelia Valverde Mata2, Andrea Parejo2, Marina Mesa Rubio2, Jose M Ramirez-Moreno2,3
1University Virgen de Valme Hospital, Neurology Department, Seville, Spain,2University Hospital of Badajoz, Stroke Center. Neurology Service, Badajoz, Spain,3Extremadura University, Department of Biomedical Science, Faculty of Medicine and Health Sciences, Badajoz, Spain
On behalf of:
Background and aims: Some patients may present depression or anxiety after a transient ischemic attack (TIA) or minor stroke. However, health-related quality of life (HRQOL) in these patients is little known. We aimed to explore the presence of depression and anxiety and consequences in HRQOL after TIA or minor stroke.
Methods: We consecutively enrolled 90 patients with first-ever TIA/minor stroke (18-70 years) from the Stroke Unit and were assessed 3 months later using Hamilton Depression Rating Scale (HDRS), Hamilton Anxiety Rating Scale (HARS) and European Quality of Life index (EQ-5D-5L).
Results: 27,8% had depression and 75,6% anxiety. Depressive patients had lower EQ-5D-5L than without depression (p=0.007). Patients with anxiety perceived worse QOL than without anxiety patients (p=0.002). Higher scores of depression and anxiety scores were associated with lower EQ-5D-5L index: correlation between depression and EQ-5D-5L index r=-0,613 (p<0,001) and between anxiety and EQ-5D-5L index r=-0,629 (p<0,001).
Conclusions: Depression and anxiety after TIA/minor stroke showed a significative impact on the health-related quality of life, although TIA or minor stroke are considered no disabling entities.
Disclosures of Interest: No
Abstract N°: 2210
ASSOCIATION BETWEEN CHANGES IN CALF CIRCUMFERENCE DURING HOSPITALIZATION AND FUNCTIONAL OUTCOMES IN PATIENTS WITH STROKE
1Kansai Medical University,2Niigata University of Health and Welfare,3Hyogo University of Health Sciences, Kobe, Japan,4Konan Medical Center, Kobe, Japan
On behalf of:
Background and aims: Calf circumference (CC) is a straightforward tool for assessing muscle mass and may predict functional outcomes in patients with stroke. However, the impact of CC reduction during hospitalization on these outcomes is not well established. This study investigates the association between CC at admission, its reduction during hospitalization, and functional outcomes in patients with stroke.
Methods: In this retrospective cohort study, CC was measured in hospitalized stroke patients at admission and discharge, with the change in CC (ΔCC; discharge CC minus admission CC) calculated. The primary outcome, measured by the modified Rankin Scale (mRS) at 3 months after stroke, was defined as a poor outcome, indicated by mRS > 2 in patients who had a premorbid mRS ⩽ 2, or any increase in mRS score for patients with premorbid mRS ⩾ 3. Multiple logistic regression analysis assessed the relationship between admission CC, ΔCC, and poor outcomes.
Results: Among 351 stroke patients (median age 78 years), 223 (63%) presented with low calf circumference (CC) at admission, and 157 (45%) experienced a reduction in CC (ΔCC ⩽ -0.5) during their hospital stay. Patients with reduced CC were more likely to have poor outcomes (p<0.001) (Fig.1).After adjusting for confounding factors, both low CC at admission (aOR: 2.04, 95%CI: 1.04-3.97, p=0.037) and CC reduction during hospitalization (aOR: 2.59, 95%CI: 1.49-4.50, p=0.007) were independently associated with poor outcomes (Fig.2).
Conclusions: Low CC at admission and CC reduction during hospitalization are associated with poor outcomes in patients with stroke, underscoring the importance of monitoring CC changes during hospitalization.
Disclosures of Interest: No
Abstract N°: 2255
MACHINE LEARNING–BASED CLINICAL PREDICTION MODELS FOR ACUTE ISCHEMIC STROKE BASED ON SERUM XANTHINE OXIDASE LEVELS
1Clinical Medical College of Yangzhou University, Department of Neuro Intensive Care Unit, Yangzhou City, China,2Northern Jiangsu People’s Hospital, Department of Neurology, Yangzhou City, China,3Medical College of Yangzhou University, School of Nursing, Yangzhou City, China,4Northern Jiangsu People’s Hospital, Department of Echocardiography, Yangzhou City, China,5Medical College of Yangzhou University, School of Public Health, Yangzhou City, China,6Northern Jiangsu People’s Hospital, Department of Cardiac Intensive Care Unit, Yangzhou City, China,7Northern Jiangsu People’s Hospital, Institute of Neurosurgery, Yangzhou City, China
On behalf of:
Background and aims: Early prediction of the onset, progression and prognosis of acute ischemic stroke (AIS) is helpful for treatment decision-making and proactive management. Xanthine oxidase (XO) is a form of xanthine oxidoreductase (XOR), which plays an important role in redox reactions and ischemia‒reperfusion injury. The purpose of this study was to utilize serum XO levels and clinical data to establish machine learning models for predicting the onset, progression and prognosis of AIS.
Methods: We enrolled 328 consecutive patients with AIS and 107 healthy controls from October 2020 to September 2021. Serum XO levels and stroke-related clinical data were collected. We established five machine learning models—the logistic regression (LR), support vector machine (SVM), decision tree, random forest, and K-nearest neighbor (KNN) models—to predict the onset, progression and prognosis of AIS. The area under the receiver operating characteristic curve (AUROC), accuracy, sensitivity, specificity, negative predictive value and positive predictive value were used to evaluate the predictive performance of each model.
Results: Among the five machine learning models predicting AIS onset, the LR model showed the best AUROC value (AUROC=0.9586, 95% CI 0.927-0.991). The LR model still showed the highest AUROC value for the progression of AIS (AUROC=0.6543, 95% CI 0.453-0.856). We compared the value of five machine learning models in predicting the prognosis of AIS, and the LR model showed the best predictive value (AUROC=0.8124, 95% CI 0.715-0.910).
Conclusions: Among the five machine learning models, we found that the LR model showed the best predictive performance.
Disclosures of Interest: No
Abstract N°: 2281
PREMORBID FRAILTY, STRESS HYPERGLYCEMIA RATIO AND FUNCTIONAL OUTCOME INPATIENTS WITH ACUTE ISCHEMIC STROKE
Piergiorgio Lochner*1,2, Marialuisa Zedde3, Andrea Pilotto4, Andrea Morotti4, Stoegbauer Jakob2, Janitscke Daniel2, Rosario Pascarella4, Merzou Fatma2
1Saarbrücken, Neurology, Saarbrücken, Germany,2Neurology, Saarland University Center, Homburg Saae, Germany,3AUSL-IRCCS di Reggio Emilia, Neurology Unit, Stroke Unit, Reggio Emilia, Italy,4University of Brescia, Department of Clinical and Experimental Sciences, Brescia, Italy
On behalf of:
Background and aims: Frailty, defined as multidimensional prognostic index (MPI), is a strong
predictor of disability and mortality in the elderly with acute ischemic stroke (AIS) treated
with IV-rtPA. The stress hyperglycemia ratio (SHR) is a recently introduced stroke biomarker
significantly associated with poor outcome, and 3-months mortality.
This study aimed to investigate in what extent frailty, measured by MPI, affects
the 3-months outcome of patients > 65 years-old with AIS.
Methods: Consecutive patients with AIS > 65 years-old who underwent intravenous thrombolysis (IVT) from 2015 to 2019 were enrolled in a German Stroke Unit. Baseline fasting plasma glucose and glycated hemoglobin (HbA1c) levels were collected to measure stress hyperglycemia. The SHR was calculated by dividing the fasting plasma glucose at admission with HbA1c. Demographics data, stroke-related variables, including baseline and post-treatment NIHSS score were evaluated in order to determine the correlation to stroke outcome. The 3-months functional outcome was evaluated by using modified Rankin scale (mRS); good outcome was defined as mRS 0-2.
Results: 155 AIS patients were enrolled in the study. Median MPI was 0.19 [0.13-0.31]; 118 (76.1%) patients were classified as “robust” and 37 (23.9%) as “frail”. In regression analysis, age, NIHSS and MPI demonstrated as the most significant predictor of 3-months good outcome in the whole cohort. In robust patients, SHR values were significantly associated with the outcome.
Conclusions: MPI is a comprehensive and strong predictor of 3-months good outcome. SHR seems to be a reliable predictor of 3-months poor outcomes in “robust” patients but not in frial patients.
Disclosures of Interest: No
Abstract N°: 2293
THE CLINICAL VALUE OF INDOLE-3-PROPIONIC ACID LEVEL IN PATIENTS WITH ACUTE CEREBRAL INFARCTION
1Northern Jiangsu People’s Hospital, Department of Neurology, Yangzhou City, China,2Northern Jiangsu People’s Hospital, Department of Neuro Intensive Care Unit, Yangzhou City, China,3Northern Jiangsu People’s Hospital, Department of Neurosurgery, Yangzhou City, China
On behalf of:
Background and aims: This study aimed to explore the correlation between the serum level of indole-3-propionic acid (IPA) and the progression and prognosis of acute cerebral infarction (ACI).
Methods: This study enrolled 197 patients with ACI, and 53 examinees from a community stroke screening program from the same period were included as the control group. The patients with ACI were divided into quartiles of serum IPA. A logistic regression model was used to compare them. The receiver operating characteristic (ROC) curve was drawn to evaluate IPA’s predictive value.
Results: Compared with the healthy control group, the ACI group had lower serum IPA (P < 0.05). Serum IPA was an independent factor for acute ischemic stroke (OR=0.992, 95% CI: 0.984-0.999, P=0.035). Serum IPA was lower in patients with progressive stroke or poor prognosis than in patients with stable stroke or good prognosis (P < 0.05). Patients with ACI with low serum IPA were prone to progression and poor prognosis. The best cutoff value for predicting progression was 193.62 pg/mL (sensitivity, 67.5%; specificity 83.7%), and that for poor prognosis was 193.77 pg/mL (sensitivity, 71.1%; specificity, 72.5%).
Conclusions: The serum level of IPA was an independent predictive factor for ACI and had certain clinical predictive value for stroke progression and prognosis in patients with ACI.
Disclosures of Interest: No
Abstract N°: 2298
EARLY NEUROLOGICAL DETERIORATION IS ASSOCIATED WITH HIGH IMMATURE PLATELET IN ACUTE ISCHEMIC STROKE
Sungwook Yu*1, Bang-Hoon Cho1, Kyung-Hee Cho1
1Korea University Anam Hospital, Department of Neurology, Seoul, South Korea
On behalf of:
Background and aims: Early neurological deterioration (END) in acute ischemic stroke is relatively common event. The underlying pathomechanisms are not well known. Immature platelet is the useful marker of increased platelet production and turnover which could occur in patients with increased platelet activation. We aimed to investigate the association between the level of immature platelet and the END in acute ischemic stroke patients.
Methods: A total 1655 of acute ischemic stroke patients in single tertiary academic center was enrolled from January 2013 to October 2020 via stroke registry. IPF levels were quantified by whole blood flow cytometry with automated assays. High immature platelet was defined as the level was more than 5%. Early neurological deterioration was defined as an increment change of at least one point in motor power or total National Institute of Health Stroke Scale (NIHSS) score deterioration ⩾2 points within the first week after admission.
Results: A total of 72 patients (4.4%) experienced END. END was more prevalent in the patients with high IPF [13 (11.7%) vs 59 (3.8%), p<0.0001]. Multivariate logistic regression analysis showed high IPF was an independent predictor of the prevalence of END (adjust odds ratio = 1.32; 95% confidence interval = 1.03–1.70).
Conclusions: END was associated with high immature platelet in acute ischemic stroke patients.
Disclosures of Interest: No
Abstract N°: 2396
RELIABILITY AND VALIDITY ACROSS EXISTING VERSIONS OF THE MODIFIED RANKIN SCALE FOR STROKE: SYSTEMATIC REVIEW AND META-ANALYSIS
1University of Glasgow, School of Cardiovascular & Metabolic Health, Glasgow, United Kingdom
On behalf of:
Background and aims: The Modified Rankin Scale (mRS) measures functional outcome after stroke. Aside the standard unstructured mRS, multiple structured versions of the scale exist. We aimed to summarize and compare inter-rater reliability (IRR) and validity of all available versions of mRS for stroke.
Methods: Multidisciplinary databases were searched from December 2008 to June 2023, following prespecified inclusion criteria: adult human stroke participants, original data, psychometric properties of mRS evaluated. Two researchers independently reviewed abstracts, extracted data and conducted risk of bias analysis, using the COSMIN and GRRAS tools. Primary outcome variables for a random effects meta-analysis were IRR measured by kappa and weighted kappa (kw). Validity and inter-modality reliability measures (Spearman’s rho, kw) were summarized.
Results: From the initial 897 titles, 281 abstracts were reviewed, and 32 studies met all inclusion criteria, resulting in 7309 stroke participants (57% males), age = 67.2(SD=3.77). There was a high risk of bias in five reliability and seven validity studies. Overall, the IRR was excellent (kw=0.84, 95%CI: 0.78 – 0.91). Across versions of the mRS, the IRR was highest for the Rankin Focused Assessment (RFA) (kw=0.99, 95%CI: 0.98 – 1), and lowest for the mRS decision tool (kw=0.68, 95%CI: 0.56 – 0.79). Validity ranged from poor to excellent, with an excellent overall concurrent validity of structured scales with the standard mRS (kw=0.86, 95%CI: 0.75 – 0.97).
Conclusions: The mRS has an excellent IRR overall. However, validity and reliability vary across different versions of the scale with more recent structured scales being more reliable than the standard mRS.
Disclosures of Interest: Yes One of the authors, Prof. Quinn, has contributed to the creation of mRS training materials that are used commercially; he has advised on mRS administration for Shiongi and MedTronic; he developed a mRS platform that has been used by commercial trials.
Abstract N°: 2422
THE SIGNIFICANCE OF SOME LABORATORY BIOMARKERS AS SHORT-TERM OUTCOME INDICATORS IN PATIENTS WITH ACUTE ISCHEMIC STROKE
1University Hospital St. Anna - Sofia, Department of Clinical Laboratory, Sofia, Bulgaria,2University Hospital St. Anna - Sofia, Neurology, Sofia, Bulgaria,3“St. Anna” University Hospital, Neurology, Sofia, Bulgaria,4South-West University “Neofit Rilski” (SWU), Medical and social sciences, Blagoevgrad, Bulgaria,5Medical University of Sofia, Department of Clinical Laboratory, Sofia, Bulgaria,6South-West University “Neofit Rilski” (SWU), Logopedics, Blagoevgrad, Bulgaria,7University Hospital, Alexandrovska, Central Clinical Laboratory, Sofia, Bulgaria
On behalf of:
Background and aims: The diagnosis of stroke is made based on a good clinical assessment, laboratory and radiological studies. In this work, we focus on the dynamic changes of the biomarker panel (CRP, Fibrinogen, D- dimer) in acute ischemic stroke and the functional outcome of the treatment during the hospital stay.
Methods: The present prospective study included 118 patients with acute ischemic stroke, aged 63-83 years, admitted to the Stroke Center of the University Hospital St. Anna, Sofia. The severity of the stroke was assessed with the National Institutes of Health Stroke Scale, and for poor outcome (PO) we accepted a severe functional deficit at the end of the hospital stay, assessed with NIHSS ⩾15 points, and for good outcome (GO) – NIHSS ⩽ 14 points. In all patients, we monitored the dynamics /at admission, 6th, 24th and 72nd hours/ of the indicators CRP, Fibrinogen, D-dimer and evaluated their predictive value regarding the good and bad outcome of the disease.
Results: The best positive predictive value at admission was D-dimer (OR=5.886, 89% CI 1.683-20.590; p<0.001). At 24 hours from admission, only CRP could be used to predict poor treatment outcome (OR=8.437, 92% CI 2.938-24.234; p<0.001) as well as at 72 hours of admission (CRP: OR=5.614, 86% CI 2.127-14.821; p<0.001).
Conclusions: Routine biomarkers of atherothrombosis, coagulation and fibrinolysis (CRP, Fibrinogen, D-dimer) alone or in combination could be simple, reliable and economical laboratory parameters in decision making, monitoring the healing process, assessing the risk of early neurological deterioration or death during hospital treatment.
Disclosures of Interest: No
Abstract N°: 2451
ACUTE-TO-CHRONIC GLYCAEMIC RATIO AS AN OUTCOME PREDICTOR IN ISCHEMIC STROKE
Ana Rodriguez Campello*1, Elisenda Climent2, Joan Jiménez-Balado3, Angel Ois1, Eva Giralt-Steinhauer1, Jordi Jiménez-Conde1, Elisa Cuadrado-Godia1, Gemma Llauradó2, Juana Flores1, Juan José Chillarón2
1Hospital del Mar, Neurology, Barcelona, Spain,2Hospital del Mar, Barcelona, Spain,3Municipal Institute of Medical Research, Barcelona, Spain
On behalf of: Isabel Fernández Pérez, Adriá Macias, Antoni Suárez, Lidia Bojtos, Julia Peris, Sergio Vidal Notari
Background and aims: Acute hyperglycemia is recognized as an independent determinant of adverse outcomes in acute ischemic stroke (AIS). While the impact of the acute-to-chronic glycemic ratio (ACR) has been studied in COVID-19 and heart failure, its influence on AIS prognosis remains partially understood. The aim of this study was to determine whether the ACR was associated with outcome at 3-months follow-up in AIS patients.
Methods: Prospective descriptive design with retrospective analysis of patients admitted for AIS. The database includes demographic data, sex, age, acute treatment, severity, vascular risk factors, and outcome (mRS 0-2 vs. 3-6). Chronic glucose levels (CGL) were estimated using the formula eCGL=[28.7xHbA1c (%)]-46.7, and ACR (glycemia at admission/eCGL) was calculated for all subjects.
Results: The study involved 2774 AIS patients admitted between 2005 and 2021. Baseline characteristics were stratified based on ACR tertiles. Multivariate analysis revealed that age (OR 1.04; 95% CI: 1.03-1.05; p<0.001), presence of diabetes (OR 1.55; 95% CI: 1.20-1.90; p<0.001), baseline NIHSS (OR 1.19; 95% CI: 1.16-1.21; p<0.001), and ACR (OR 1.07; 95% CI: 1.04-1.11; p<0.001) were independently associated with poor prognosis (OR 1.62; 95% CI: 1.28-2.06; p<0.001) and mortality (OR 1.88; 95% CI: 1.26-2.83; p = 0.002). However, in ROC curves, adding the ACR variable to the classical clinical model did not enhance the prediction of AIS prognosis (0.786 vs. 0.781).
Conclusions: Higher ACR correlated positively with poor outcomes at 3 months in AIS patients. These findings suggest that ACR may serve as a prognostic biomarker in ischemic stroke patients, warranting further investigation as a potential therapeutic target.
Disclosures of Interest: No
Abstract N°: 2460
HIGH RATE OF EEG ABNORMALITIES IN ACUTE LARGE VESSEL OCCLUSION
1National Cerebral and Cardiovascular Center, Department of Neurology, Osaka, Japan,2Gifu University Graduate School of Medicine, Department of Emergency and Disaster Medicine, Gifu, Japan,3National Cerebral and Cardiovascular Center, Department of Cerebrovascular Medicine, Osaka, Japan
On behalf of:
Background and aims: Patients with acute large vessel occlusion (LVO) often present with convulsive or nonconvulsive seizures. EEG monitoring has been utilized to detect electrographic seizures in critical care patients with altered consciousness but is not commonly performed in patients with LVO in the acute phase.
Methods: atients transferred to our institute for acute LVO between June and September 2023 were included. A long-term EEG (at least 3 hours) was performed within 72 hours of admission and assessed for interictal epileptiform discharges (IEDs), spike/sharp and wave (SW), periodic discharges (PDs), and rhythmic delta activity (RDA).
Results: Six (23.1%) of the 26 study participants had occlusions in the internal carotid artery, 17 (65.4%) in the middle cerebral artery, and 3 (11.4%) in the vertebral or basilar artery. Endovascular therapy was performed in 21 (81.8%), and 3 (11.5%) had clinical seizures. On EEG, 13 (50.0%) had abnormal findings, including IEDs in 7 (28.0%), SW in 2 (8.0%), PDs in 4 (16.7%), and RDA in 12 (48.0%). The patients with abnormal EEG findings had a higher NIHSS score (20 [11–28] vs. 4 [2–17]), and a worse mRS score at discharge (5 [3–5] vs. 4 [2–5]).
Conclusions: Abnormal EEG findings were found in half of the patients with LVO, who had a more severe cerebral infarction and a worse functional prognosis. EEG performed in the acute setting of LVO may help predict the prognosis.
Disclosures of Interest: No
Abstract N°: 2627
EARLY RENAL DAMAGE BIOMARKER AS AN INDEPENDENT PREDICTOR OF POOR OUTCOME AFTER ISCHEMIC STROKE
1Medical Univeristy of Gdańsk, Department of Adult Neurology, Gdańsk,2Medical Univeristy of Gdańsk, Department of Clinical Nutrition, Gdańsk, Poland,3Medical Univeristy of Gdańsk, Department of Nephrology, Transplantology and Internal Diseases, Gdańsk, Poland
On behalf of:
Background and aims: The neutrophil gelatinase–associated lipocalin (NGAL) has been shown a reliable early detector of acute kidney injury, and a marker of high risk in subjects with cardiovascular disease. Aortic stiffness, as reflected by the carotid-femoral pulse wave velocity (PWV), has been found to be independently related with functional outcome in patients with acute ischemic stroke (AIS). The aim of the study was to assess the relationship between NGAL and stroke severity and to evaluate its potential role as a predictor of functional outcome in patients with AIS.
Methods: We enrolled 78 AIS patients (52 males, age 64.5 ± 11.6 years, median NIHSS score 5(3-7.5) points). Urinary NGAL excretion to creatinine excretion (NGAL/cr ratio) was measured at admission. Carotid-femoral PWV were measured (SphygmoCor®) within several (6±2) days after stroke onset. Functional outcome was evaluated 90 days after stroke using the modified Rankin Scale (mRS) with an mRS score of 0 to 1 (no significant disability) considered as a favourable outcome.
Results: The NGAL/cr ratio was significantly lower in patients with favorable compared to those with poor functional outcome (32.7±24.2 vs 73.2±83.9; p = 0.01). In a multivariate analysis, the NGAL/cr ratio was significantly associated with functional outcome after controlling for age, sex, stroke severity, previous stroke, diabetes, PWV and use of rtPA (adjusted OR = 1.03; 95% CI, 1.00-1.05; p=0.04).
Conclusions: NGAL might be a useful predictor of functional outcome in patients with acute ischemic stroke, independent of traditional and new vascular factors, including arterial stiffness.
Disclosures of Interest: No
Abstract N°: 2919
FRAILTY PREVALENCE IN STROKE PATIENTS AT A GERMAN STROKE UNIT: INSIGHTS FROM CLINICAL, PHYSICAL, AND NUTRITIONAL ASSESSMENTS
Stefan Gerner*1, Hagen Huttner1, Angelina Radüchel1, Marc Schneider1, Martin Jünemann1, Thorsten R. Döppner1
1University Hospital Giessen, Department of Neurology, Giessen, Germany
On behalf of:
Background and aims: Frailty, a complex syndrome marked by reduced physiological capacity and increased vulnerability to stressors, is notably impactful on stroke outcomes. This study's objective is to examine the prevalence and assessment diversity of frailty in stroke patients, integrating clinical scales, muscle strength, sarcopenia, and nutritional status evaluations in a German stroke unit.
Methods: In this cross-sectional analysis, stroke patients admitted to a German stroke unit from August to December 2023 were studied. The evaluation of pre-stroke frailty included the Clinical Frailty Scale (CFS), Groningen Frailty Indicator (GFI), grip strength measurements, and sonographic sarcopenia analysis in both upper and lower limbs. Mobility, nutritional status, and laboratory markers (FI-LAB) were also assessed. Patient outcomes were determined using the Modified Rankin Scale (mRS) at discharge, with subsequent follow-ups planned at 3 and 12 months.
Results: The study comprised 220 stroke patients, averaging 67.2 (±15.4) years. Frailty prevalence in this cohort varied significantly, with rates of 20.3% (CFS⩾5), 26.9% (GFI⩾4), 24.5% (FI-LAB), and 27.8% (sonographic sarcopenia). The range of unfavorable outcomes (mRS ⩾3) at discharge according to CFS scores spanned from 10.2% (CFS=1 or 2) to 100% (CFS=7 or 8), regardless of age.
Conclusions: This study revealed a varied prevalence of frailty in stroke patients, as determined by different assessment methods, underscoring frailty's intricate nature and its significance in tailoring stroke rehabilitation. The importance of early, comprehensive frailty assessment is emphasized by the observed disparities in Modified Rankin Scale scores, highlighting its role in enhancing patient outcomes.
Disclosures of Interest: No
Abstract N°: 3030
CAROTID REVASCULARIZATION’S IMPACT ON LONG-TERM LANGUAGE ABILITY IN STROKE INDUCED APHASIA: FIRST EVIDENCE
Mariacristina Musso*1, Marina Bucher1, Isabelle Caseley1, Ema Vaidelyte1, Cornelius Weiller1
1Faculty of Medicine, University of Freiburg, Germany, Department of Neurology and Neurophysiology, Medical Center—University of Freiburg, 79106
On behalf of:
Background and aims: Are reperfusion stroke therapies relevant for determining the severity of long-term stroke-aphasia? Is there a clinical score that would predict in the acute phase the presence of chronic aphasia?
Methods: 91 patients with confirmed aphasia in the Aachen Aphasia Test (AAT) at a median of 5 days after a first-ever left hemispheric stroke received a clinical follow-up after a median of 6 months (T1). Demographic scores, stroke-related data, cardiovascular risicofactors, intercurrent diseases, T1 testing time, economic status, familial impact, rehabilitation and language therapies were first included in a backward regression, and the significant factors were analyzed using hierarchical regression. Receiver operating characteristic (ROC) was used to determine the clinical cut-off. For analyses IBM SPSS Statistics, version 28 was used.
Results: The strongest hierarchical models determining chronic aphasia severity assessed by AAT stanine in T1 reached an adjusted R2 of 0.652. Age, lesion volume, NIHSS, poorly controlled arterial hypertension, and the occurrence of intercurrent diseases were markers of poorer outcomes. The carotid recalculation therapy and the use of antidepressants showed significant positive effects. The ROC curve analysis for the optimal age-specific cut-off for NIHSS at 72h showed an AUC of 0.80 (95% CI 0.71 - 0.89).
Conclusions: This study provides first evidence that carotid intervention has an impact on long-term language ability in patients with stroke-induced aphasia. In addition, the combination of two data points that are routinely collected in the stroke unit should allow accurate prediction of the presence of chronic aphasia already in the acute setting.
Disclosures of Interest: No
Abstract N°: 3129
LIPOPROTEIN(A) AT THREE MONTHS AFTER ISCHEMIC STROKE
Nina Sørensen*1, Lotta Larsson1, Ulriche-Sophie Pedersen1, Pia Kamstrup2, Børge Nordestgaard2, Christina Kruuse1
1Herlev and Gentofte Hospital, Department of Neurology, Herlev, Denmark,2Herlev and Gentofte Hospital, Department of Clinical Biochemistry, Herlev, Denmark
On behalf of:
Background and aims: Increased Lipoprotein(a) (Lp(a)) is associated with ischemic stroke, mainly large artery atherosclerosis (LAA) by the Trial of Org 10172 in Acute Stroke Treatment (TOAST)-classification. However, longitudinal data of Lp(a) alterations post-stroke are few. The aims of this study were to explore 1) overall change in Lp(a) levels from admission until three months follow-up and 2) subgroup differences by baseline TOAST classification and Lp(a) levels.
Methods: Patients with ischemic stroke were prospectively included when admitted to Herlev-Gentofte Hospital from 2013 to 2014 and followed up after 3 months. Lp(a) was measured at baseline and follow-up. TOAST-classification was performed retrospectively. Baseline and follow-up Lp(a) were assessed by one-way ANOVA. Temporal alterations, and subgroup analyses were assessed by mixed-effects models.
Results: A total of 382 patients with ischemic stroke was included, hereof 175 patients were followed up. There was no difference in Lp(a) levels between TOAST-groups at baseline (p=0.914), or at follow-up (p=0.957). There was no significant temporal change in Lp(a) overall, or by TOAST group. When excluding patients with Lp(a) ⩾50.0 (n=39), however, the level of Lp(a) decreased from baseline until follow-up (p<0.001), whereas all patients with Lp(a) ⩾50.0 at baseline remained at levels >50.0. Levels of total cholesterol, low-density lipoprotein, and triglycerides were significantly higher at baseline in patients with LAA and lacunar infarctions as compared to patients with cardio embolic stroke (all p<0.01).
Conclusions: Long-term focus should be on patients with Lp(a) levels ⩾50.0, as their levels do not decrease post-stroke.
Disclosures of Interest: No
Abstract N°: 3188
MACHINE LEARNING IN UNBALANCED DATASET BUILDING PREDICTION MODELS FOR NEW-ONSET ATRIAL FIBRILLATION IN ICU POST-STROKE PATIENTS
Yang Chen*1, Yang Liu1, Ying Gue1, Garry Mcdowell1
1University of Liverpool, Liverpool, United Kingdom
On behalf of:
Background and aims: Atrial fibrillation is the most common arrhythmia encountered in the Intensive Care Unit (ICU), leading to high mortality. Stroke and AF have a close relationship, especially new-onset AF after stroke, which may lead to a high risk of death and risk of stroke recurrence. This study aimed to analysis the association between new-onset atrial fibrillation (NOAF) and ICU mortality, and predict the NOAF by machine learning (ML).
Methods: Patients were collected from Medical Information Mart for Intensive Care database. Logistic regression was employed to analyze the association between NOAF and ICU death. Inverse probability treatment weighting and propensity score matching were also used. Various ML algorithms were employed, including K nearest neighbors, support vector machine, random forest, and LightGBM, then compared their performance.
Results: Of 2225 stroke patients, mean age and SD were 65.88 (12.65) years, 52.9% was male, 114 (5.1%) were identified as NOAF. The ICU mortality of NOAF patients was 28.1%. NOAF were significantly associated with high risk of ICU mortality (OR: 3.52, 95%CI: 2.04, 5.98) after adjusting covariables. Similar results were found after inverse probability treatment weighting (OR: 3.86, 95%CI: 3.14-4.73) and propensity score matching (OR: 2.58, 95%CI: 1.28-5.20). Prediction models were constructed by selected clinical features. Among all ML algorithms, random forest showed the best C-index (0.874) in test cohort.
Conclusions: NOAF in post-stroke patients in the intensive care unit increases the risk of ICU mortality. Machine learning models, particularly random forest models, provide valuable insights for early identification and intervention in the ICU setting.
Disclosures of Interest: No
Abstract N°: 3295
IMPACT OF COGNITIVE IMPAIRMENT ON STROKE REHABILITATION OUTCOMES – SHOULD WE BE CALLING FOR MORE TIMELY CEILINGS OF REHABILITATION?
Mathilde Pauls1, William Tai*1
1Addenbrooke's Hospital, United Kingdom
On behalf of:
Background and aims: Population ageing presents challenges beyond increasing stroke incidence. Stroke patients are often older with multi-morbidities, frailty, and cognitive impairment. We have anecdotally observed in our rehabilitation unit that such patients lean towards poorer engagement and outcomes, and lengthier admissions. There is general reluctance to make early decisions to switch focus from rehabilitation to discharge planning. Our aim was to more objectively evaluate outcomes between stroke patients with-and-without cognitive impairment on our rehab unit.
Methods: 103 older patients discharged between 2021-2 were retrospectively evaluated. Data were collected on demographics, pre-and-post stroke mRS, death, cognitive impairment at any stage, dysphasia, and engagement. Cognitive impairment and engagement were determined by close review of documented entries.
Results: More than half of our sample (n=59 / 103) had cognitive impairment (pre- and/or post). 37.3% of these were deceased at 12 months compared to 6.8% without impairment. In the sub-cohort of moderate/severe cognitive impairment (n=30 / 59), median length of stay was around 10 days longer than those without to mild. Any degree of cognitive impairment with poor engagement (n=39) had a similarly long length of stay, saw the most discharge mRS 5, and had the highest 12-month mortality at 55.9%. 97% of this cohort were discharged with mRS 4 or more.
Conclusions: Cognitive impairment lead to higher discharge mRS and 12-month mortality numbers. Patients with any cognitive impairment and poor rehabilitation engagement saw the highest length of stay, discharge mRS, no functional independence, and highest mortality at 12 months.
Disclosures of Interest: No
E-Poster - Stroke Complications
Abstract N°: 1161
THE PROFILE OF EARLY NEUROLOGICAL DETERIORATION AT KING’S COLLEGE HOSPITAL
Mohammed Mallah1,2, Samantha Roberto*1, Beatrix Sari1, Maria Lucia Uribe Mz Recaman1, Caroline Domingos Belo1, Tony Yu1,3, Cameron Lee1, Yassine Noui1,4, Yee Mah1,5
1King's College Hospital, United Kingdom,2St George's Hospital, United Kingdom,3Auckland District Health Board, Auckland, New Zealand,4Uppsala University, Uppsala, Sweden,5King's College London, School of Biomedical Engineering and Imaging Sciences, United Kingdom
On behalf of:
Background and aims: Early Neurological Deterioration (END) is a serious complication following an acute stroke. Patients who exhibit END are associated with a poorer prognosis and worse long-term outcomes. Despite this data related to END is not widely reported in the UK or other countries. The aim of this poster is to provide an overview of the distribution and characteristics of END at a major London Stroke Unit.
Methods: The medical records of all stroke admissions to the Hyper Acute Stroke Unit (HASU) at King’s College Hospital, between 1 Jan 2022 and 30 Jun 2022 were manually reviewed for deteriorations within the first 14 days of stroke onset.
Results: 477 admission episodes were reviewed. Complete records for 41 episodes were not accessible. 50 admissions of the remaining 436 were associated with END (11.5%).
96% of END associated admissions occurred within the first 3 days of stroke onset, reaching 100% after 7 days. Cerebral oedema, haemorrhagic transformation and seizures were the 3 most common cause of END.
Age, sex, pre-admission independence level congestive cardiac failure, hypertension, atrial fibrillation, and diabetes are not associated with a higher incidence of END.
Conclusions: (1) The incidence of END at a Hyper Acute Stroke Unit performing thrombolysis and mechanical thrombectomy is 11.5. (2) END occurs primarily within the first 3 days from stroke onset. (3) Cerebral oedema, haemorrhagic transformation and seizures were the 3 most common cause of END. (4) The incidence of END was not significantly influenced by demographics, level of pre-admission independence and common co-morbidities.
Disclosures of Interest: No
Abstract N°: 2103
DURATION OF HOSPITAL STAY IN PATIENTS WITH ACUTE CEREBRAL STROKE AS A RISK FACTOR FOR POST-STROKE DEPRESSION
1Petro Mohyla Black Sea National University, Therapeutic Disciplines, Myckolayv, Ukraine,2MC "Expert Health", Odesa, Ukraine
On behalf of:
Background and aims: The purpose of the study was to assess the effect of the duration of hospital stay in patients with acute cerebral stroke on the incidence of post-stroke depression.
Methods: The study was carried out on the basis of the Expert-Health MC in 2020-2023. The medical records of 83 patients who developed depression within a year after a stroke were retrospectively reviewed. The diagnosis of depression was made according to the DSM-5 criteria. Depression severity was assessed using Beck Depression Inventory (BDI). The severity of depression was compared with the duration of inpatient treatment. As a control, data from the medical records of 50 stroke patients without post-stroke depression were analyzed. In terms of stroke severity, patients in both groups were comparable (NIHSS scores in the range of 5-15 points). Variance and correlation analysis was performed using Statistica 14.0 software (TIBCO, USA).
Results: The average BDI score in patients with post-stroke depression was 19.8±0.3 points, in patients in the control group – 8.4±0.2 points (p<0.05). The duration of hospital stay was 14.7±0.4 days in patients with post-stroke depression, and 10.1±0.5 days in the control group (p<0.05) and correlated with BDI scores (r=0.62 p<0.05). It should be noted that in 21 of 83 (25.3%) manifestations of depression arose while in hospital, which could affect the overall length of inpatient stay.
Conclusions: Long-term hospital stay increases the risk of post-stroke depression in the first year after a stroke.
Disclosures of Interest: No
Abstract N°: 2836
RISK FACTORS AND SCALES PREDICTIVE OF HEMORRHAGIC TRANSFORMATION IN MECHANICAL THROMBECTOMY OF MCA
Pablo Iriarte*1, Jaime Alonso1, Alba Somovilla1, Carmen Sánchez1, Raquel Berbegal1, Ainhoa Lorenzo2, Gemma Reig2, Juan Vega3, Carmen Ramos2, Santiago Trillo Senin2
1Hospital de La Princesa, Neurology, Madrid, Spain,2Hospital Central de La Defensa Gómez Ulla, Neurology, Madrid, Spain,3Hospital de La Princesa, Radiology, Madrid, Spain
On behalf of:
Background and aims: Hemorrhagic transformation(HT) in patients treated with mechanical thrombectomy(MT) is a frequent complication, with uncertain prediction and prognostic significance. This study aims to investigate predictors of the different subtypes of HT, especially in symptomatic HT(SHT).
Methods: We performed a retrospective study with prospective data collection. We included patients with middle cerebral artery(Carotid-T/M1-MCA) treated at our center in 2021-22 with TM. We analyzed risk factors associated with petechial HT(HT-IH), parenchymal HT(HT-P) and subarachnoid HT(HT-SAH) as well as SHT. The usefulness of predictive scales of HT(HAT, SEDAN) was also studied.
Results: 173 patients were included. Higher mortality was associated with HT-P(p<0.01) and SHT(p<0.01). In the univariate analysis, hypertension (OR2.14;p=0.05), diabetes mellitus (OR2.62;p=0.01), ASPECTS (OR0.8;p=0.02), and mismatch (OR1.01;p=0.01) were associated with HT-IH. For HT-P, significant factors included ASPECTS (OR3.53;p=0.01), blood glucose (OR4.83;p=0.01), collateral flow (OR3.79;p=0.02), and witnessed onset(OR0.36;p=0.05). TH-SAH was identified with MT time (OR2.25;p=0.02), TICI>2b (OR0.2;p=0.02), and onset-to-CT time (OR1.01;p=0.03). SHT was associated with blood glucose (OR4.82;p=0.01), ASPECTS (OR0.76;p=0.02), pre-stroke mRS (OR1.31;p=0.02), MT time>60 minutes (OR4.39;p=0.02), documented onset (OR0.32;p=0.03), and number of passes (OR1.31;p=0.02). HAT score>5(OR 8.06;p<0.01) and SEDAN score>6 (OR 8.80; p<0.01) predicted THS. Multivariate analysis related mismatch (OR1.01;p=0.01) and ASPECTS(OR0.83;p=0.05) with HT-IH. For TH-P, glucose (OR4.4;p=0.04) was associated. TH-HAS was related to onset-to-CT time (OR1.01;p=0.01), number of passes (OR1.33;p=0.02), and pre-stroke mRS (OR1,55;p=0.03). THS was associated with glucose (OR4.4;p=0.04), MT duration (OR1.01;p=0.01), and pre-stroke mRS(OR1.66;p<0.01).
Conclusions: There are factors associated with different subtypes of hemorrhagic transformation (HT), with the most relevant ones, due to their association with prognosis, being the predictors of HT-PH and SHT. Future studies could enable the development of predictive tools for HT with a prognostic capacity superior to those analyzed in our work.
Disclosures of Interest: No
E-Poster - Rare Causes incl. Stroke in the Young
Abstract N°: 236
THE IMPORTANCE OF A COMPLETE WORKOUT FOR PATIENTS WITH POSTERIOR REVERSIBLE ENCEPHALOPATHY SYNDROME
Bianca Oana Pîrlog*1,2, Agnes Aghetti2, Mikael Mazighi2,3, Peggy Reiner2
1County Emergency Hospital Cluj-Napoca, Neurology, Cluj-Napoca, Romania,2Lariboisière Hospital AP-HP, Neurology, Paris, France,3INSERM UMR 1144, Université Paris Cité, Paris, France
On behalf of:
Background and aims: Cervical artery dissection (CAD), reversible cerebral vasoconstriction syndrome (RCVS), and posterior reversible encephalopathy syndrome (PRES) share common risk factors such as post-partum status. Associations between RCVS and CAD or RCVS and PRES have already been described and similar pathophysiology is suspected. However, having 3 pathologies simultaneously are extremely rare.
Methods: We report five cases diagnosed with concomitant PRES, RCVS, and CAD admitted in our stroke unit.
Results: Five women, including 4 during post-partum, between day 0 and day 10 were on average 33 years old. Two patients had eclampsia criteria and one had pre-eclampsia. All patients had headaches as the first symptom, 3 had encephalic signs. Only two patients had recurrent thunderclap headaches and 2 had cervicalgia. PRES was diagnosed, between days 1 and 8; one patient of those had right vertebral CAD. RCVS was detected after a mean of 6 days from the initial CT scan for 4 patients, while for one patient this diagnosis was retained retrospectively. CAD was detected between days 0 and 13 by CTA/Doppler Ultrasound or MRI. None of the patients had cerebrovascular ischemic complications. Three out of 5 patients had subarachnoid hemorrhage. At follow-up, at 5 months, all morphological abnormalities regressed, and patients had no disabling symptoms.
Conclusions: These unique 5 cases stress the importance for a complete and repeated evaluation of brain arteries including cervical segments. Particular attention should be paid to patients during post-partum status, especially if pre-eclampsia. It also reinforces the hypothesis of a shared pathophysiology between those disorders.
Disclosures of Interest: No
Abstract N°: 705
RISK FACTORS IN YOUNG ISCHEMIC STROKE AND OUTCOMES OF REPERFUSION THERAPIES
Tho Phung*1, Ton Mai Duy1, Phuong Dao1, Dung Pham1
1Bach Mai Hospital, Stroke center
On behalf of:
Background and aims: The incidence of ischemic stroke among younger adults is on the rise; however, comprehensive data regarding risk factors in young acute ischemic stroke (AIS) and the outcomes of reperfusion therapies remain limited. Our objective was to investigate prevalent risk factors and the outcomes associated with reperfusion therapies among young individuals with AIS.
Methods: Between January 2021 and May 2022, we prospectively enrolled a consecutive cohort of AIS patients aged 18-45 years admitted to the Stroke Center of Bach Mai Hospital. Our investigation focused on identifying risk factors and assessing 90-day outcomes, measured using the modified Rankin Scale.
Results: A total of 171 patients were enrolled (mean age: 38 ± 5.9; males: 68.4%). The most prevalent risk factors were dyslipidemia (84.2%), smoking (24.6%), and hypertension (23.4%). Among these patients, 57 received reperfusion therapy. At the 90-day follow-up, 82.4% of patients showed favorable outcomes (mRS 0-2), while 5.3% had died, and 14% experienced hemorrhage transformation.
Conclusions: Dyslipidemia emerged as the predominant risk factor in young AIS cases. Favorable functional outcomes at the 90-day mark were observed among patients who underwent reperfusion therapies.
Disclosures of Interest: No
Abstract N°: 1090
ISCHEMIC STROKE FROM FOCAL INTRACRANIAL CAROTID ARTERY VASCULITIS: CLINICAL AND RADIOLOGICAL FEATURES, AND OUTCOME
1UNIL - Université de Lausanne, Lausanne, Switzerland,2CHUV Radiologie et radiodiagnostic, Lausanne, Switzerland,3Lausanne University Hospital, Immunology, Lausanne, Switzerland,4Hospital Du Valais, Neurology, Sion, Switzerland,5Lausanne University Hospital, Neurology, Lausanne, Switzerland
On behalf of:
Background and aims: In exceptional cases, vasculitis involving the central nervous system is limited to a single arterial segment, such as the termination of the internal carotid artery (ICA). Only a few cases of such occurrences have been documented, therefore this condition remains largely unexplored. This study aims to present a clinico-radiological description of patients with focal ICA vasculitis.
Methods: From 2017 to 2023, we collected a single-center prospective case series of patients with ischemic stroke (IS) in the carotid territory and vasculitis involving the intracranial ICA with or without extension to its primary division branches.
Results: We included 10 patients with median age of 35 years, 50% were women. One patient had a known history of Crohn's disease, one was diagnosed with Horton giant cell arteritis, and the remaining had no systemic autoimmune or vasculitis diseases. Six patients underwent vessel wall imaging MRI, and eight had cerebral angiography. Lumbar puncture was performed in nine patients, revealing increased leukocytes in the cerebrospinal fluid in one, increased proteins in two, and oligoclonal bands in one. All patients received antithrombotic treatment following IS, and 6 immunosuppressive therapies. At follow-up, ICA pathology improved in two patients, worsened in four, and remained stable in the remaining. The one-year stroke recurrence rate was 40%, and median 3-month mRS was 2.
Conclusions: Focal ICA vasculitis predominantly affects young patients and can occur either in isolation or, less frequently, in conjunction with systemic autoimmune or vasculitis disorders. This condition is characterized by a high rate of stroke recurrence and medium-term disability.
Disclosures of Interest: No
Abstract N°: 1180
CADASIL PATIENT SERIES – A SINGLE DEPARTMENT REPORT
Ivana Karla Franić*1, Snježana Juren Meaški1, Vladimir Miletić1, Branko Malojcic1,2
1University Hospital Centre Zagreb, Department of Neurology, Zagreb, Croatia,2University of Zagreb, School of Medicine, Zagreb, Croatia
On behalf of:
Background and aims: Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is an autosomal dominantly inherited small vessel disease. Mutations of the NOTCH 3 gene on chromosome 19 cause an angiopathy of the small cerebral vessels which manifests mostly as recurrent transitory ischemic attacks (TIA)/strokes and white matter lesions in young and middle-aged individuals. Other common symptoms include migraines, dementia, and psychiatric changes. Our aim is to report first Croatian series of patients with genetically confirmed CADASIL who were treated in our department from 2017 until today and compare genotype and phenotype characteristics of our cohort with similar case series found in literature.
Methods: We analysed genetic, clinical, and radiological features of genetically confirmed CADASIL patients in our cohort. The spectrum of NOTCH3 variants found in our patients and the clinical features associated with those variants were compared with other European and Asian CADASIL patient series.
Results: Our cohort currently has six genetically confirmed CADASIL patients in the follow up, with mean age of 57.8 years. Three patients had mutations on exon 4 of NOTCH3 gene and for others, exons were not specified. All six mutations were various, no predominance of certain mutation was found. Five patients presented with TIA/stroke and migraines, one had exclusively cognitive disturbances. Five patients have positive family history for cerebrovascular disease. All patients are stable during the follow-up.
Conclusions: Literature review showed that phenotype and genotype characteristics of Croatian CADASIL patients in this single-department cohort are consistent with other European CADASIL patient series.
Disclosures of Interest: No
Abstract N°: 1894
STROKE IN A YOUNG FEMALE WITH ULLRICH CONGENITAL MUSCULAR DYSTROPHY (UCMD)
Jessie Gew*1, Sissi Ispoglou2
1Queen Elizabeth Hospital Birmingham, Neurology,2Queen Elizabeth Hospital Birmingham, Stroke
On behalf of:
Background and aims: Ullrich Congenital Muscular Dystrophy (UCMD) is a severe neuromuscular disorder caused by mutations in genes encoding collagen-VI (COLVI). It is characterised by muscle weakness, joint laxity and respiratory failure. Vascular complications are not common. Only one case of non-ischaemic carotid artery dissection in a UCMD patient has been described. The objective of the study is to report a case of stroke due to chronic bilateral carotid artery dissection (CAD) in UCMD.
Methods: Case report
Results: A 27-year-old female with UCMD (de novo mutation of gene encoding COLVI and history of pneumothoraces) self-presented to a small district general hospital, reporting transient right hemiparesis and dysphasia, preceded by headache for a week. Initial CT head was normal. Her symptoms recurred whilst at the emergency department, but baseline disability contributed to delayed stroke recognition. Repeat imaging showed an evolving acute infarct. A CT angiogram demonstrated bilateral chronic internal carotid artery dissections with near occlusion of left M2. NIHSS was 17. By the time of transfer to our unit, she was well outside the lysis window, whilst mechanical thrombectomy was considered to outweigh the benefit. She had a long inpatient rehabilitation course and was discharged home with ongoing speech and language therapy for her dysphagia.
Conclusions: Stroke needs to be considered in patients with UCMD presenting with acute neurological deficit and there should be low threshold for vascular imaging in these patients.
Disclosures of Interest: No
Abstract N°: 1979
"USE OF INTRAVASCULAR ULTRASOUND (IVUS) IN CAROTID WEB"
Mouna Ennazeh el Khaili1, Alvaro Jamilena Lopez1, José Clemente Segundo Rodriguez1, Paula Lobato Casado*1, Mar Morín1
1Stroke Unit, Complejo Hospitalario Universitario de Toledo, Neurology, Toledo
On behalf of:
Background and aims: Carotid web have been associated with ischemic stroke in the young, attributed to embolization from flow stasis/thrombosis within the carotid web pocket. Carotid web is a shelf-like linear filling defect in the posterior aspect of the internal carotid bulb, representing an intimal variant of fibromuscular dysplasia. The diagnosis of carotid web is traditionally restricted to digital subtraction angiography, CT/MR angiography and duplex ultrasonography.
Methods: A 46-year-old woman with a history of hypertension presented with repeated right-eye amaurosis fugax. CT-scan and MRI showed no abnormalities, the transthoracic-echocardiogram and the 24 hour-Holter monitoring were normal. Carotid duplex ultrasound showed an isoechoic membrane at the level of the right ICA bulb.A CT-angiography showed a shelf-like, smooth filling defects, located along the posterior wall of the internal right carotid artery.
Results: At that moment a focal arterial dissection with partial thrombosis cannot be ruled out, so the patient underwent vascular surgery. A digital subtraction arteriography displayed a shelf-shaped filling defect in the wall of the right carotid bulb. An intravascular ultrasound (IVUS) was performed to assess the nature of the lesion. The 018 IVUS probe under roadmap guidance into the mid-cervical ICA. The images demonstrated a thin isoechoic ridge/lesion at the posterior aspect of the carotid bulb without evidence of trombus or plaque. The patient underwent stent placement and follow-up showed satisfactory integration of the stent into the vessel wall
Conclusions: Intravascular ultrasound may have relevance at the approach of carotid web.
Disclosures of Interest: No
Carotid duplex ultrasound and CT-angiography.
Intravascular ultrasound (IVUS).
Abstract N°: 1997
PREDICTION OF CEREBRAL ARTERY DISSECTION USING POLYGENIC RISK SCORES IN CHINESE POPULATION
Shufan Zhang*1, Xiang Han1
1Huashan Hospital, Fudan University, Department of Neurology, China
On behalf of:
Background and aims: We performed genome-wide association study (GWAS) and computed polygenic risk score (PRS) to explore the genetic susceptibility factors and prediction model of CeAD based on Huashan hospital cases.
Methods: A total of 210 CeAD patients and 280 controls were enrolled from June 2017 to September 2022 in Department of Neurology, Huashan Hospital. We performed GWAS in 140 CeAD patients and 210 control individuals according to a case and control 1:1.5 design rule in the training dataset, while the other 70 cases and 70 controls were used as validation. Then, we constructed a PRS by capturing all independent GWAS SNPs in the analysis and explored the predictivity of PRS, age, and sex for CeAD.
Results: Through GWAS analysis of the 140 cases and 210 controls in the training dataset, we identified 10 SNPs were annotated in or near (in the upstream and downstream regions of ±500Kb) 10 functional genes. We computed PRS including 32 independent SNPs and constructed predictive model for CeAD by using age, sex and PRS as predictors both in training and validation test. The area under curve (AUC) of PRS predictive model for CeAD reached 99% and 95% in the training test and validation test respectively, which were significantly stronger than the age and sex model of 83% and 86%.
Conclusions: The present study showed that ten risk loci were associated with CeAD susceptibility. The PRS derived from risk variants was associated with CeAD incidence after adjusting for age and sex both in training test and extra validation.
Disclosures of Interest: No
Abstract N°: 2156
POSTPARTUM BILATERAL VERTEBRAL ARTERY DISSECTION IN A PATIENT OF LATE ECLAMPSIA WITH POSTERIOR REVERSIBLE ENCEPHALOPATHY SYNDROME
Chen-En Tsai1, Ya-Ju Lin*1, Pai Ching Tsui1, Helen Po1
1MacKay Memorial Hospital, Neurology, Taipei, Taiwan
On behalf of:
Background and aims: Postpartum cervical arterial dissection (CAD) is uncommon, though those with a history of a hypertensive disorder of pregnancy and postpartum state are at high risk. Vertebral artery dissection (VAD) is quite rare. Posterior reversible encephalopathy syndrome (PRES) may be an important cause of postpartum headache and seizures (late eclampsia). Concomitant postpartum VAD and PRES after childbirth is rare. Here we presented a case of postpartum eclampsia with PRES in a 33-year-old woman who began experiencing severe headache and neck pain with high blood pressure 2 days after delivery. VAD was diagnosed via extracranial duplex ultrasound and confirmed by MRA.
Methods: case report
Results: This 33-year-old G1P0 female patient received cesarean section due to 41-week of gestation. Generalized tonic-clonic seizure happened about 1 hour after delivery. High blood pressure and severe headache developed about 2 days later. The pain was over bi-occipital and nuchal area which got worse in supine but relieved when upright without any focal neurologic deficits. MRI of brain was compatible with PRES and MRA showed diffuse vasoconstriction and irregular segmental stenosis in bilateral VA. Extracranial duplex sonography showed extensive dissecting membrane from V1 to V2 segment. Antiplatelet and antiseizure agents were prescribed to prevent stroke and seizure. Her symptoms resolved near fully about 10 days after.
Conclusions: Postpartum vertebral arterial dissections associated with late eclampsia and PRES are rare but should be highly suspected if patient with severe orthostatic headache. Prognosis is usually favorable in patients with early diagnosis and prompt treatment.
Disclosures of Interest: No
Abstract N°: 2222
CURRENT PRACTICE IN INVESTIGATIONS AND MANAGEMENT OF ISCHAEMIC STROKE IN YOUNG (⩽55 YEARS) PATIENTS AT A UK TERTIARY STROKE CENTRE
Amna Mohsin1,2, Zong Lee3, Aina Chang4, Emma Bennion-Pedley5, Elizabeth Bearblock6, Eoin O'brien1, Smriti Agarwal*1
1Addenbrooke's Hospital ( Cambridge University NHS Foundation Trust ), Stroke Medicine, Cambridge, United Kingdom,2Lister Hospital ( East and North Hertfordshire NHS Trust), Acute Internal Medicine and Stroke Medicine, Stevenage, United Kingdom,3West Suffolk NHS Trust, Internal medicine,4King's College Hospital NHS Foundation Trust, Internal medicine, London, United Kingdom,5Calderdale and Huddersfield NHS Foundation Trust, Internal medicine, Huddersfield, United Kingdom,6Nottingham University Hospital NHS Trust, Internal medicine, Nottingham, United Kingdom
On behalf of:
Background and aims: 10% of hospitalised ischaemic stroke patients are ⩽55 years. 50% of the cases remain cryptogenic.
We reviewed current practice for investigations and management of a cohort of young stroke patients at a tertiary stroke centre.
Methods: Retrospective analysis of electronic records for patients ⩽55 years-old, discharged with a diagnosis of ischaemic stroke at UK tertiary stroke centre, between January 2021-December 2022.
Results: n=123 patients were included, with a median follow-up of 21.2 months. The mean age was 45 (n=66 male; n=57 female).
Partial anterior circulation strokes were commonest (31.7%), followed by posterior circulation strokes (28.5%), lacunar events (25.2%) and total anterior circulation strokes (10.6%). In line with published data, cardioembolic aetiology was predominant (33.3%), followed by small vessel disease (23.6%), cryptogenic (19.5%), and other determined causes (16.3%).
21% of the cohort had newly diagnosed PFO (patent foramen ovale); 4.9% had new AF and treated accordingly. The most common risk factors were hypercholesterolaemia (42%) and hypertension (38%).
50% had infection screening including HIV, syphilis, hepatitis etc.16.2% of all patients had genetic testing for aortopathy/cardiomyopathy and small vessel disease. 40% had thrombophilia screening.54% had testing for antiphospholipid syndrome; only n=1 patient was diagnosed with true APS and received treatment.
Conclusions: Despite extensive investigations, a significant proportion of young strokes remain cryptogenic. Addressing vascular risk factors is important, while investigating for cardioembolic aetiology. Wider use of genetic testing for rarer causes of small vessel disease or inherited vasculopathy may be needed.
Disclosures of Interest: No
Abstract N°: 2455
A CASE OF RUPTURED ANTERIOR INFERIOR CEREBELLAR ARTERY DISSECTION
1International university of health and welfare hospital, Tochigi, Japan,2Saiseikai Yokohamashi Tobu Hospital, Neurosurgery, Yokohama, Japan,3International University of Health and Welfare Mita Hospital, Neurosurgery, Minato City, Japan,4Edogawa Hospital, Edogawa City, Japan,5Saitama Medical Center, Jichi Medical University, Neurosurgery, Saitama, Japan,6Nerima Hikarigaoka Hospital, Neurosurgery, Nerima City, Japan
On behalf of:
Background and aims: A subarachnoid hemorrhage (SAH) caused by a dissecting aneurysm of anterior inferior cerebellar artery (AICA) is a rare condition. Occlusion of the AICA for effective treatment may result in cerebellar and brainstem infarction. The causes of AICA dissection are not known.
Methods: A 65-year-old woman arrived at the emergency room, reporting a headache and vomiting for the past 5 days. She had contracted COVID-19 10 days prior to the onset of these symptoms. After being referred to Neurosurgical department, a CT scan revealed that she had SAH and intraventricular hemorrhage in the fourth ventricle. In the MR and CT angiographies, a dissecting aneurysm was observed in the a2-a3 segment, along with vasospasm of the right AICA in the SAH. The angiography conducted before coiling indicated an intramural pooling sign in the AICA. The rupture of the dissecting aneurysm of the AICA was identified as the cause of her SAH.
Results: The patient underwent endovascular surgery 18 days after the initial SAH. The parent artery was successfully occluded using coiling, with no issues of hearing disturbance, cranial nerve palsy, or infarction. 7 weeks after SAH, she underwent ventriculoperitoneal shunt surgery to address hydrocephalus. 2 weeks after the procedure, she was discharged from the hospital with no neurological deficit, achieving a modified Rankin Scale score of 0.
Conclusions: We reported a rare case of dissecting aneurysm of AICA. The parent artery occlusion by coiling was performed without neurological deficit and infarction. The mechanism of dissection is unknown, but COVID-19 may increase susceptibility to AICA dissection.
Disclosures of Interest: No
Abstract N°: 2537
SIMULTANEOUS STROKE AND MYOCARDIAL INFARCTION SECONDARY TO LARGE-VESSEL VASCULITIS
Itziar Abad-Inchaurrondo*1, Georgina Figueras- Aguirre1, Victor Silva1, Joan Maria Mercade2, Carlos Feijoo2, Nicolás Augusto Romero Flórez3, David Cánovas1
1Park Taulí University Hospital, Neurology, Sabadell, Spain,2Park Taulí University Hospital, Internal Medicine, Sabadell, Spain,3Park Taulí University Hospital, Radiology, Sabadell, Spain
On behalf of:
Background and aims: Stroke and myocardial infarction are unusual presentation of large vessel vasculitis. The two best known are Takayasu's arteritis and giant cell arteritis (GCA).
Methods: We present a case of concurrent cardio-cerebral infarction secondary to large-vessel vasculitis.
Results: A 62-year-old woman with no cardiovascular risk factors, was admitted to our center with right hemispheric syndrome (NIHSS 18) with stablished ischemia in the CT brain. EKG showed ST-elevation suggestive of inferolateral myocardial infarction. Treatment was declined as considered subacute heart attack and patient was admitted to the Intensive Care Unit.
During hospitalization, echocardiography confimed inferolateral akinesia without thrombus and MRI excluded cardiac viability. Chest CT angiography was performed, excluding acute aortic syndrome and showing signs of aortitis. Blood analysis manifested a persistently elevated inflammatory markers with negative serological and autoimmunity tests.
Study was completed with a PET/TC revealing cranial and extracranial large-vessel vasculitis and signs of polymyalgia rheumatic. Diagnosis of GCA was established due to age presentation, and clinical and radiologic features. Immunosuppressant treatment was initiated.
Conclusions: Ischemic complications may be a presenting symptom of large-vessel vasculitis. We highlight the importance of consider it as an etiology in the absence of cardiovascular risk factors in conjunction with the presence of elevated inflammatory markers. Early diagnosis is essential to start treatment and reduce morbidity and mortality.
Disclosures of Interest: No
Abstract N°: 2671
ETHICAL CONSIDERATIONS ON DISCLOSURE OF PRESUMED IATROGENESIS IN CEREBRAL AMYLOID ANGIOPATHY
Kanishk Kaushik*1, Marleen Eijkholt2, Nienke de Graeff2, Gargi Banerjee3, David Werring4, Gisela Terwindt1, Martine De Vries2, Ellis van Etten1, Marieke Wermer1,5
1Leiden University Medical Centre, Department of Neurology, Leiden, Netherlands,2Leiden University Medical Centre, Department of Medical Ethics and Health Law, Leiden, Netherlands,3Institute of Prion Diseases at University College London (UCL), MRC Prion Unit, London, United Kingdom,4Stroke Research Centre, UCL Queen Square Institute of Neurology and the National Hospital for Neurology and Neurosurgery, Department of Brain Repair and Rehabilitation, London, United Kingdom,5University Medical Center Groningen (UMCG), Department of Neurology, Groningen, Netherlands
On behalf of:
Background and aims: Cerebral amyloid angiopathy (CAA) causes stroke and cognitive decline. The recently identified iatrogenic CAA-subtype (iCAA) is thought to be transmitted through medical procedures that took place decades earlier. The recognition of iCAA raises ethical questions concerning disclosure.
Methods: We consider ethical arguments concerning three disclosure-related questions. Should clinicians disclose their suspicion of iCAA to patients presenting with CAA and a history of relevant exposure? Should clinicians recommend the additional tests needed for iCAA-diagnosis? Should clinicians proactively identify and notify asymptomatic at-risk individuals who are unaware of their risk?
Results: Our ethical analysis offers the following answers to these questions: (1) Physicians should fulfill their professional responsibility to inform patients of the presumed iatrogenesis and related uncertainties, regardless of whether iCAA is the most likely diagnosis (e.g., confirmed exposure to cadaveric material) or if diagnostic uncertainties persist (e.g., missing clinical documentation). Though the expected clinical benefit is limited, disclosure facilitates autonomous (non-medical) decision-making of patients. The benefits of disclosure likely outweigh the possible psychological harms for most patients. (2) While a definite iCAA diagnosis is unattainable, additional diagnostics can provide diagnostic support and exclude other causes. (3) Notification of confirmed at-risk (but asymptomatic) individuals might be reasonable as it facilitates patient autonomy, potentially provides clinical benefits, and maintains trust in the medical profession. However, proactive identification of this group is challenging and might have psychosocial consequences.
Conclusions: Understanding iCAA has major scientific and public health implications; our arguments should be critically re-evaluated as knowledge advances.
Disclosures of Interest: No
Abstract N°: 2849
STROKE IN YOUNG PATIENTS WITH INTRACRANIAL ATHEROSCLEROSIS (SYINCAT)
Joshua Yeo1, Benjamin Tan1, Megan Ng1, Jia Wen Tan*1
1National University Hospital (NUH) - Singapore, Singapore, Singapore
On behalf of:
Background and aims: The incidence of ischemic stroke in young adults has accelerated in Asia. The impact to healthcare systems in caring for young stroke patients lends urgency to studying this population. SYINCAT (Stroke in Young patients with INtraCranial ATherosclerosis) is a prospective cohort study that evaluates young adults with ischemic stroke (IS) or transient ischemic attack (TIA) due to intracranial artery stenosis (ICAS).
Methods: Young adults(<60 years) presenting with IS or TIA secondary to ICAS were recruited from 2023-2024. Inclusion criteria included an ICAS culprit lesion of at least moderate severity involving the intracranial internal or middle cerebral artery with 50–99% stenosis. Montreal Cognitive Assessment(MoCA) was performed. Cognitive impairment was defined as a MoCA score <26.
Results: The mean age of the cohort was 47.4(S.D8.5). 51.5% were male. The median NIHSS was 2. In this cohort, 36.9% had diabetes mellitus, 52.0% had dyslipidemia, 71.5% had hypertension and 30% were chronic smokers.
Amongst the 58 patients recruited, 13(22.4%) exhibited cognitive impairment. These patients had higher NIHSS(P-value=0.037).
Conclusions: The initial results from SYINCAT suggest that young stroke patients with ICAS are at risk of cognitive impairment.
Disclosures of Interest: No
Abstract N°: 3111
FREQUENCY AND CHARACTERISTICS OF BOTHERSOME HEADACHE AFTER CEREBRAL VENOUS THROMBOSIS
Alva Kjellberg*1, Erik Lindgren1, Sini Hiltunen2, Emma Roustaei1, Mattias Linde1, Turgut Tatlisumak2, Jukka Putaala2, Katarina Jood1
1Sahlgrenska University Hospital, Institute of Neuroscience and Physiology, Gothenburg, Sweden,2Helsinki University Hospital, HUS Neurocentrum
On behalf of:
Background and aims: Headache is frequently reported at follow-up after cerebral venous thrombosis (CVT). We aimed to describe the occurrence, characteristics and factors associated with bothersome headache post-CVT.
Methods: We included adult patients with consecutively diagnosed, radiologically confirmed, CVT from two local hospital-based registries in Sweden (1996-2020) and Finland (1987-2022). We defined bothersome headache as; headache ⩾1day/month and either intensity over 1.7 (⩾17mm) on a visual analogue scale (VAS), associated nausea/vomiting and/or ⩾15headache-days/month. Data on demographics, risk-factors, clinical presentation, and neuroimaging was extracted from the registries. Headache characteristics were assessed at long-term follow-up using patient-reported questionnaires. Potential risk-factors for bothersome headache were evaluated with multivariate logistic regression.
Results: Of 380 survivors, 304 patients (median age 43 [IQR 30-55], 65% female, median follow-up 26 months [IQR 11-58, range 0.5-293months, 1172 patient-years]) with complete follow-up questionnaires were included. Headache persisting ⩾3 months post-CVT diagnosis was present among 41% and 90 patients (30%) fulfilled criteria for bothersome headache.
Reported headache frequency was 8 (IQR 4-20) days/month, described as attacks (74%) or continuous in 44% of patients, with reported median intensity VAS-7 (IQR 4.5-9). Associated features included light- and/or sound-sensitivity (55% and 49%, respectively), nausea/vomiting (31%) and sleep-interruption (43%). Patients reported worsening headache with mental (53%) and physical exertion (46%. Most patients (88%), used analgesics, experiencing at least moderate alleviation (97%). In multivariate analysis, no significant risk-factors for bothersome headache were identified.
Conclusions: Bothersome headache occurs frequently post-CVT and is not associated with any known factor. Although bothersome, most patients experience some headache-alleviation with medication.
Disclosures of Interest: No
E-Poster - Rehabilitation and Recovery
Abstract N°: 33
WHOLE-BODY ISCHEMIA AND REPERFUSION-INDUCED NEURONAL LOSS
Seong MI Heo1, Jae Seong Noh1, Da Som Han1, Myoung Cheol Shin1, Taek Geun Ohk1, Joong Bum Moon1, Tae-Kyeong Lee2, Ji Hyeon Ahn3, Jun Hwi Cho*1
1Kangwon National University, Emergency Medicine, Chuncheon, South Korea,2Hallym University, Food Science and Nutrition, Chuncheon, South Korea,3Youngsan University, Physical Therapy, Yangsan, South Korea
On behalf of:
Background and aims: Until now, CA/CPR-induced spinal cord injury has been investigated in the anterior motor nucleus at the lumbar spinal cord levels, but few studies on neuronal damage, and blood-spinal cord barrier (BSCB) disruption and leakage have been reported in all subregions (dorsal horn, intermediate zone and ventral horn) of the lumbar gray matter after CA/CPR.
Methods: This experiment investigated survival rate, physiological variables, neuronal damage/death, and BSCB disruption and leakage according to all subregions after CA (for 5 min)/CPR in rats. Sham group was given sham asphyxial CA/CPR operation, and CA/CPR group received asphyxial CA/CPR operation until the return of spontaneous circulation (ROSC) was obtained.
Results: Neuronal loss was examined using Fluoro-Jade B histofluorescence: the neuronal loss was detected in all subregions at 12 h and thereafter gradually enhanced. BSCB disruption was investigated using immunohistochemistry for caveolin-1and glial fibrillary acidic protein (GFAP; a marker for astrocyte): strong caveolin-1 immunoreactivity was shown in endothelial cells at 48 h after CA/CPR and GFAP-immunoreactive astrocyte endfeet disappeared apparently at 48 h after CA/CPR. BSCB leakage was observed using immunohistochemistry for immunoglobulin G (IgG): weak and strong Ig immunoreactivity was detected in the parenchyma of all subregions at 24 h and 48 h, respectively, after CA/CPR.
Conclusions: In brief, neuronal loss, and BBB disruption and leakage occurred similarly in all subregions of the lumbar spinal gray matter within 48 h after CA/CPR. This finding indicated that IRI after CA/CPR occurred earlier when compared with IRI in the brain.
Disclosures of Interest: No
Abstract N°: 390
ANALYSIS OF OPTIMAL ACCELERATION/DECELERATION DISTANCE IN GAIT SPEED TESTS WITH OPTITRACK MOTION SYSTEM IN POST-STROKE
Rosa Cabanas-Valdés*1, Aida Cadellans-Arroniz1, Silvia Ortega-Cebrián1, Carlos-Antonio Zárate-Tejero2, Victor Zárate-Lozano2, David Blanco-de-Tena Davila2
1Universitat Internacional de Catalunya, Physiotherapy, Barcelona, Spain,2Universitat Internacional de Catalunya, Physiotherapy, Barcelona, Spain
On behalf of:
Background and aims: Gait impairment is one of the prevalent physical limitations contributing to stroke-related disability and impacting the performance of activities of daily living. Gait speed is an important measure for stroke survivors. However, different protocols exist. The aim of this study is to analyse what is the optimal accelerate/decelerate distance for the 4-meter walk test (4mWT) and the 6-meter walk test (6mWT) at comfortable and fast speeds in chronic stroke survivors.
Methods: A cross-sectional study was performed at laboratory of the Universitat Internacional de Catalunya. The primary outcome was to analyse in Visual3D with OptiTrack system (Fig.1-2) the optimal distance to accelerate/decelerate for 4mWT and 6mWT at comfortable and fast speeds. The optimal distance is the mean of the repetitions for each condition (90% individuals). ClinicalTrials.gov (NCT05679011).
Results: Twenty individuals were recruited (Table 1). They performed randomly 12 conditions (3 at comfortable speed for 4mWT and 6mWT and 3 at fast speed for 4mWTand 6mWT) with 8 reflective markers (Fig.3). The optimal distances for 90% of individuals are described in Table 2. The mean speed for 4mWT was 0,76 (0,31) m/s and 0,99 (0,44) m/s at comfortable and fast speed respectively and for 6mWT was 0,83 (0,33) m/s and 1,08 (0,45) m/s at comfortable and fast speed respectively.
Conclusions: According to our results, it takes more distance to decelerate than to accelerate. For the 4mWT timed a corridor of 7 meters would be necessary and for the 6mWT timed a corridor of 10 meters for chronic stroke survivors.
Disclosures of Interest: No
Abstract N°: 548
THE FEASIBILITY OF INCREASING PHYSICAL ACTIVITY THROUGH AN ACTIVITY GROUP ON AN ACUTE STROKE UNIT
Naomi Felthouse*1
1Guy’s and St Thomas’ NHS Foundation Trust
On behalf of:
Background and aims: People after stroke frequently become deconditioned with reduced levels of cardiovascular fitness and muscle strength (Saunders et al 2020). As a result, recent UK national stroke guidelines recommend people remain active for up to six hours a day, and engage in activities promoting cardiovascular fitness. One possible delivery method to target this is through a physical activity group, but the feasibility providing this on an acute stroke unit is unknown
Methods: A 30 minute physical activity group was implemented on an acute stroke unit five days a week. Feasibility was determined by: group attendance, minutes of physical activity completed during attendance, the impact of attending the group on participating in scheduled physiotherapy sessions, and frequency of group occurrence over a four-month period. Physical activity minutes were recorded through direct observation. Data were analysed with descriptive statistics.
Results: 36 patients attended the group over a four-month period. Attendance ranged from 2 to 6, median attendance was 3. Mean physical activity time was 33.6 minutes, and included activity associated with traveling to the group. Attendees participated in 59% more physical activity than in standard therapy sessions alone. Attendees participated in 5.6 (mean) of their 6 weekly physiotherapy sessions scheduled. 79.6% of planned group sessions successfully occurred.
Conclusions: It appears feasible to implement a weekday physical activity group on an acute stroke unit. The group increased attendee’s physical activity with little impact on physiotherapy session attendance. Further work should explore patient’s experience in attending the group and understand exercise behaviours upon discharge from hospital.
Disclosures of Interest: No
Abstract N°: 887
A QUALITATIVE STUDY ON THE EDUCATIONAL NEEDS OF MIGRANT DOMESTIC WORKERS CARING FOR STROKE SURVIVORS
Wai Ping Alfred Seng*1, Ri-Ann Tan2, Shuen-Loong Tham1
1TTSH-Integrated Care Hub (ICH), Rehabilitation Medicine, Singapore, Singapore,2Lee Kong Chian School of Medicine, Singapore, Singapore
On behalf of:
Background and aims: Migrant domestic workers (MDWs) caring for stroke survivors play a key role in supporting them through rehabilitation and recovery. Caregiver training (CGT) provided by healthcare professionals (HCPs) in rehabilitation wards aims to equip MDWs with the ability to care for stroke patients after discharge. However, there is limited understanding of the educational needs of MDWs. This qualitative study aims to identify gaps in current CGT frameworks for MDWs caring for stroke survivors.
Methods: HCPs were recruited from an inpatient stroke rehab unit in Singapore. Qualitative in-depth interviews were conducted with 10 HCPs to obtain their experiences and perceptions on providing CGT for MDWs. Interviews were transcribed and analysed using thematic analysis.
Results: HCPs included physiotherapists, occupational therapists, speech therapists and rehab nurses. Three main themes were derived, each with two subthemes. The main themes were: having individualised education, facilitating communication, and transitioning to care in the community. These findings identify the deficiencies in CGT and education to MDWs, and present as areas for HCPs to improve their training methodology.
Conclusions: MDWs face significant challenges in caring for stroke survivors in a foreign country. Providing individualised education, facilitating communication between MDWs and family members, as well as supporting MDWs in the transition from hospital to home could lead to better outcomes for stroke survivors and safeguard the well-being of MDWs.
Disclosures of Interest: No
Abstract N°: 909
PROVISION OF COMMUNITY REHABILITATION SERVICES FOR LIFE AFTER STROKE IN THAILAND
Noppanan Chaiyapoom*1,2, Arina Nurfianti1 3, Lisa Kidd4, David Hunter5, Anne Rowat1
1Nursing & Health Care School, University of Glasgow, Glasgow, United Kingdom,2Faculty of Nursing, Khon Kaen University, Thailand,3School of Nursing, Faculty of Medicine, Universitas Tanjungpura, Indonesia,4School of Health and Life Sciences, Glasgow Caledonian University, United Kingdom,5School of Health and Life Sciences, University of the West of Scotland, United Kingdom
On behalf of:
Background and aims: Long-term needs after stroke are being increasingly recognised and the organisation of community services in supporting life after stroke remains a top James Lind Alliance research priority. Although, there is emerging evidence to support the provision of community stroke care, the implications of this evidence for longer-term community support in Thailand is not yet known. This study aims to examine the provision and implementation of community care for people with stroke in rural Thailand.
Methods: This study included the following phases: 1) a literature review of international stroke guidelines (2011-2021) to determine the recommendations for the community provision and long-term support for stroke survivors; and 2) qualitative interviews with key stakeholders, including clinical leads and managers of community-based teams working in rural Thailand. Guideline recommendations were synthesised using Content Analysis and the qualitative interviews were analyzed using Thematic Analysis.
Results: From 15 eligible guidelines, recommendations of long-term community stroke services focused on rehabilitation, life after stroke, secondary prevention and carer support, by coordinated multidisciplinary and peer support. The interviews revealed that community stroke service focused mainly on rehabilitation and secondary prevention rather than broader life after stroke support. Psychosocial and carer support is not delivered routinely in Thailand. Multidisciplinary teams deliver services with reliance on carer, volunteers and local organizations. Challenges included service discontinuation, multidisciplinary incoordination, and lack of stroke specialists.
Conclusions: There needs to be further research to understand stroke survivors’ and families’ needs for life after stroke support in rural Thailand to inform the provision and implementation of services.
Disclosures of Interest: No
Abstract N°: 1140
STROKE-SPECIFIC EMOTIONAL AND PSYCHOLOGICAL SUPPORT - NORTHERN IRELAND
Sarah Belson*1
1Stroke Association
On behalf of: Róisín O’Connor
Background and aims: In the Stroke Association’s “Struggling to Recover” Report, 90% of stroke survivors in Northern Ireland said their emotional and cognitive needs were not met after discharg from hospital. Stroke-Specific Emotional and Psychological Support (STEPS) was developed to meet that need. Building on our counselling pilot programme started in 2019, and The National Lottery-funded 6-month project “First Steps” in response to COVID 19, in 2021 a successful bid was made to the National Lottery Community Fund for a 3 year project.
Methods: The service delivers counselling remotely to anyone impacted by stroke.
Results: In the 2 years to date we have had 272 referrals and delivered 837 counselling sessions. Clinical impact is measured using the CORE Outcome Measure. Year 2 CORE data from clients shows that 83% achieved clinical and reliable change.
Conclusions: Life After Stroke care must recognise the huge emotional impact of stroke. A remote counselling service staffed by counsellors with specialised stroke training allows survivors and families space to process the trauma of stroke diagnosis and deal with issues such as grief, relationship issues, depressions and anxiety. We recognise the cognitive and communication issues that people might be dealing with, allowing for greater insight than generic counselling services. Remote delivery removes barriers caused by mobility issues, fatigue, and time restraints faced by carers. This model is easily adaptable to other locations working with the stroke population. STEPS is a vital part of people’s recovery, and allows for increased mental wellness and capacity for thriving after stroke.
Disclosures of Interest: No
Abstract N°: 1232
EFFECTS OF TRAINING WITH AN END-EFFECTOR REHABILITATION ROBOT ON UPPER LIMB FUNCTION IN PATIENTS WITH CHRONIC STROKE
Dong Hyun Ye*1, Min Ho Chun1, Jung Il Chung1, An Na Lee2, Hyo Jin Jeon2
1Asan Medical Center, Department of Rehabilitation Medicine, Seoul, South Korea,2Asan Medical Center, Asan Institute for Life Sciences, Seoul, South Korea
On behalf of:
Background and aims: This study aimed to examine the effects of training with Rebless PlanarÒ on upper limb function in patients with stroke.
Methods: The study included patients with hemiparetic stroke and assigned them randomly to either the robotic treatment group (Rebless PlanarÒ) or the control group (conventional rehabilitation program using MOTOmedÒ).
Results: Overall, 20 patients were enrolled, of which 10 were in the Rebless PlanarÒ group and 10 in the control group. The baseline characteristics of the two groups were not significantly different. The Rebless PlanarÒ group showed significant improvements (p < 0.05) in the Fugl–Meyer assessment of the upper extremity (FMA-UE) and Korean version of the modified Barthel index (K-MBI) after 10 sessions of robot-assisted exercise, and the improvement of FMA-UE and K-MBI scores were better than those in the control group. No significant improvement in spasticity was found in both groups. The duration of point-to-point reaching exercise measured by Rebless PlanarÒ showed significant improvement in the Rebless PlanarÒ group, and the improvement was better than that in the control group.
Conclusions: Rebless PlanarÒ can help in improving the upper extremity function and activities of daily living of patients with chronic hemiparetic stroke. More studies with a larger sample size or population with earlier onset may help further identify the efficacy and effectiveness of the rehabilitation device.
Disclosures of Interest: No
Abstract N°: 1252
EFFECTS OF TRAINING WITH A REHABILITATION DEVICE (REBLESS®) ON UPPER LIMB FUNCTION IN PATIENTS WITH CHRONIC STROKE
Dong Hyun Ye*1, Jong Yoon Chang1, Min Ho Chun1
1Asan medical center, Department of Rehabilitation Medicine, Seoul, South Korea
On behalf of:
Background and aims: This study aimed to explore the clinical effectiveness of upper limb training using a rehabilitation robotic device (Rebless®) for patients with stroke.
Methods: In this prospective, unblinded, randomized controlled trial, patients were randomly assigned to receive robotic training (experimental group; n = 15) or conventional therapy (control group; n = 15). Both groups received upper limb training lasting for 30 min per session with a total of 10 training sessions within 4 weeks. Motor function, functional evaluation, and spasticity were clinically assessed before and after training. Cortical activation was measured using functional near-infrared spectroscopy at the 1st and 10th training sessions.
Results: The experimental group demonstrated a significant improvement in the Fugl–Meyer assessment-upper extremity (FMA-UE) score and modified Ashworth scale grade in elbow flexors. The cortical activity of the unaffected hemisphere significantly decreased after 10 training sessions in the experimental group compared with the control group.
Conclusions: Training with Rebless® may help patients with chronic stroke in restoring upper limb function and recovering the contralateral predominance of activation in motor function.
Disclosures of Interest: No
Abstract N°: 1325
BRINGING A STROKE RECOVERY SERVICE AND POST STROKE REVIEWS TO OXFORDSHIRE, UK
Sarah Belson*1
1Stroke Association
On behalf of: Tara Lakin
Background and aims: There is no community stroke or neuro team in Oxfordshire. From acute hospital discharge patients go to the in-bed stroke rehab unit, or get 12 weeks of ESD rehab. Otherwise there is a void of longer term community provision and no data on needs at 6 months to evidence gaps and unmet needs.
Methods: We set up a Stroke Association service in January 2023 to address the inequity in Oxfordshire. The objectives were:
Establish a stroke recovery service in Oxfordshire.
Supporting levelling up access to 6 month reviews.
Ensure equity to a stroke recovery service for all newly diagnosed stroke survivors and for those whose needs have not previously been addressed.
Provide a person-centred service that empowers individuals to self-manage their condition(s).
Identify unmet needs of stroke survivors to inform future service planning/ evaluation.
Results: Through a data protection impact assessment and information governance procedure we were able to integrate the service with local services. This has allowed streamlined access to data and does not take up clinician time unnecessarily. It allows co-working with ESD.
Conclusions: Data will consider the cohorts of patients that benefit from this model, and which cohorts require qualified clinical intervention at a later stage. We are measuring confidence at entry to service and discharge, outcome and experience at discharge, mRS and EQ5D at 6 months.
Disclosures of Interest: No
Abstract N°: 1392
CHANGES IN HEART RATE VARIABILITY AT REST AND DURING EXERCISE IN PATIENTS AFTER STROKE: A PRELIMINARY STUDY
Jittima Saengsuwan*1,2, Lars Brockmann2, Corina Schuster-Amft2,3,4, Kenneth Hunt2
1Khon Kaen University, Department of rehabilitation medicine, Faculty of medicine, Khon Kaen, Thailand,2Bern University of Applied Sciences, The Laboratory for Rehabilitation Engineering, Institute for Human Centred Engineering, Biel, Switzerland,3Reha Rheinfelden, Research Department, Rheinfelden, Switzerland,4University of Basel, Department of Sport, Exercise and Health, Basel, Switzerland
On behalf of:
Background and aims: The aim of this preliminary study was to investigate time- and intensity-dependent changes in heart rate variability (HRV) at rest and during exercise in patients after a stroke using a biofeedback-enhanced robotics-assisted tilt table (RATT).
Methods: Twelve patients completed two separate measurement sessions. The first session involved familiarization and system identification, which in turn allowed determination of the parameters of a feedback system for automatic control of heart rate (HR). The second session consisted of 14 min of rest and 20 min of active exercise, during which HR was stabilised using feedback control. Heart rate data were collected using a chest-belt HR sensor, and raw RR intervals were employed for HRV analysis.
Results: Twelve patients, including 7 women and 5 men, aged 55.3 ± 15.6 years (mean ± SD), were enrolled. All HRV metrics exhibited substantially lower values during the exercise phase compared to the rest phase, consistent with a substantially higher HR intensity during exercise. All HRV values during the 0-7 min interval of rest were lower than during the 7-14 interval, consistent with a slight decrease in HR over the whole rest period. During the exercise period, all HRV values during the 5-12.5 min interval were higher than those observed during the 12.5-20 min interval, pointing to a purely time-dependent decrease in HRV.
Conclusions: All HRV metrics exhibited intensity-dependent changes—lower HRV at higher intensity, i.e. exercise vs. rest—and time-dependent changes—decreasing HRV over time when cardiovascular drift is eliminated.
Disclosures of Interest: No
Abstract N°: 1591
AN ADAPTED CARDIAC REHABILITATION (CR) IMPROVES FITNESS AND FATIGUE AFTER STROKE
Sabah Rehman*1, Michele Callisaya1, Martin Schultz1, Gregory Peterson1, Helen Castley2, Sue Sanderson2, Seana Gall1
1Menzies Institute for Medical Research, University of Tasmania, Hobart, Australia,2Royal Hobart Hospital, Hobart, Australia
On behalf of:
Background and aims: We adapted a cardiac rehabilitation (CR) to improve secondary prevention for stroke survivors. We aimed to examine if the program changed short-term outcomes.
Methods: The Cardiac REhabilitation for the Secondary prevention of Stroke (CARESS) intervention comprised a 7-week co-designed program with 1-hour group exercise and 1-hour group discussion. Outcomes included fitness (6-minute walk test), fatigue, and depression (Patient Health Questionnaire), before and 6 weeks after the program available in CARESS participants and a historical control group (n=31) from a study about physical activity after stroke. Propensity score matching (age and sex-matched) and ‘teffects’ was used to measure the average treatment effect (ATE). Difference in difference (DiD) estimates the average effect of CR between treated and control groups.
Results: There were n=7 treated (mean age 68±7 years) matched to n=14 controls (mean age 70±13 years). The ATEs were statistically significant for 6 min walk test in those receiving CR (139.03 meters, 95% CI 44.34, 233.72, p=0.004) and fatigue (-4.7, 95% CI -8.9, -0.45, p=0.03) with a non-significant decrease in depression (-0.79, 95% CI -1.77, 0.18). The DiD showed that CR was associated with an average 61 meters increase in 6-min walk, a 4 unit decrease in fatigue and a 0.85 unit decrease in depression compared to the control group.
Conclusions: Our CR program co-designed with people with stroke and health professionals showed improvement in some outcomes in stroke survivors showing its potential benefits.
Disclosures of Interest: No
Abstract N°: 1898
THE EFFECT OF GALVANIC VESTIBULAR STIMULATION ON THE BRAIN ACTIVITY DURING RIGHTING REACTION IN THE HEALTHY ADULT
1Tokyo Metropolitan University, Graduate School of Human Health Sciences, Department of Physical Therapy,2Saiseikai Higashi Kanagawa Rehabilitation Hospital,3Sendai Seiyo Gakuin University
On behalf of:
Background and aims: A previous study reported that galvanic vestibular stimulation (GVS) affects postural control in stroke patients. However, there are few reports on the effects of GVS on sitting balance, and no studies on brain activity during righting reaction with GVS. Therefore, the purpose of this study was to investigate brain activity during righting reaction with GVS in healthy participants using functional near-infrared spectroscopy (fNIRS).
Methods: Participants were 28 healthy young right-handed adults. Participants performed the righting reaction in the sitting position with a sham GVS and then performed the righting reaction while receiving either a left cathode GVS or a right cathode GVS, which were randomly assigned. For the righting reaction task, the participant’s seat was tilted 10 degrees to the left side. Brain activity was measured with fNIRS. Regions of interest were the bilateral motor association and temporal area, and the oxygenated hemoglobin concentration (Oxy-Hb) was compared between the sham GVS and with GVS during the righting reaction task.
Results: Under LC-GVS conditions, Oxy-Hb values during righting reaction were significantly increased compared to sham during left tilt in primary somatosensory cortex (S1), pre-motor. (PMC) and supplementary motor cortex (SMC), S1, and subcentral area (p=0.043). Oxy-Hb values during righting reaction with RC-GVS conditions were significantly increased in the pars triangularis Broca’s area, supramarginal gyrus part, supramarginal gyrus part, supramarginal gyrus part of Wernicke’s area, PMC and SMC were significantly decreased compared to sham.
Conclusions: GVS may affect cerebral blood flow during righting reaction.
Disclosures of Interest: No
Abstract N°: 2093
THE USE OF CIMT IN UPPER LIMB REHABILITATION IN THE SUBACUTE STAGE OF ISCHEMIC STROKE
1Petro Mohyla Black Sea National University, Therapeutic Disciplines, Myckolayv, Ukraine
On behalf of:
Background and aims: Constraint-induced movement therapy (CIMT) has been found to be effective for rehabilitation of upper limb function in chronic and subacute stroke in adults.
The purpose of the study was to evaluate the effectiveness of CIMT in restoring upper limb function in patients in the subacute stage of ischemic stroke.
Methods: The study was carried out in the MC „Expert Health“ MC in 2019-2023. 56 patients in the subacute stage of ischemic stroke with impaired function of the upper limb were examined. All patients underwent rehabilitation with the involvement of a multidisciplinary team (neurologist, physical therapist, occupational therapist). 30 patients were randomly selected to undergo CIMT (main group), the remaining patients (n=26) formed the control group. Upper limb function was assessed using the modified ARAT+ test in three and six months after stroke. Statistical processing was performed by analysis of variance using Statistica 14.0 software (TIBCO, USA)
Results: The average age of the patients was 64.6±0.7 years. Patients of both groups were comparable in stroke severity (NIHSS score in the acute period 9.1±0.2 and 9.5±0.3 points) and the severity of upper limb dysfunction after three months (ARAT+ results were 47.7±0, 4 points in the main group and 47.4±0.5 points in the control group). After six months, upper limb function improved in all patients, and the increase in ARAT+ was higher in the main group (56.8±0.6 vs 54.9±0.3 points, p<0.05).
Conclusions: The use of CIMT improves upper limb function in the subacute stage of ischemic stroke
Disclosures of Interest: No
Abstract N°: 2096
REVOLUTIONIZING STROKE REHABILITATION: A SOFT ROBOTICS-BASED APPROACH FOR UPPER LIMB RECOVERY
Muhammad Umair Ahmad Khan*1, Rabbia Muneer1, Arsalan Ali1, Muhammad Faisal1
1University of Engineering and Technology (Narowal Sub-Campus), Narowal, Pakistan
On behalf of:
Background and aims: Stroke annually affects more than 12.2 million individuals globally, resulting in over 5 million survivors struggling with motor dysfunction and limb paralysis. While traditional physiotherapy shows promise in early rehabilitation, limited access due to a scarcity of trained professionals, inadequate facilities, and financial barriers poses significant challenges. This study introduces an innovative approach to surmount these obstacles in upper limb rehabilitation.
Methods: A novel, portable, cost-effective, soft robotics-based wearable device is developed, specifically tailored for upper limb rehabilitation. This device incorporates soft robotics based artificial muscles constructed from elastomeric bladders and threaded mesh as outer coverings, eschewing traditional motor-based systems. It operates in two modes: a continuous mode for regular rehabilitation exercises and an "Interactive Neuromuscular Facilitation (INF)" mode. In the INF mode, the device detects the patient’s movement intention through surface electromyography, subsequently assisting in the execution of the movement.
Results: Preliminary testing indicates that the device significantly aids in the rehabilitation of upper limbs in stroke patients. This is evidenced by a marked reduction in muscle activity, which is a key indicator of improved neuromuscular control and reduced spasticity. Reduced muscle activity indicates more efficient movement and improved functional rehabilitation results, especially beneficial for stroke patients with muscle weakness or partial paralysis.
Conclusions: The development of this soft robotic rehabilitation device, particularly with its INF mode, marks a substantial advancement in stroke rehabilitation for upper limbs. It provides a practical and accessible solution for patients, potentially revolutionizing stroke recovery and rehabilitation practices.
Disclosures of Interest: No
Abstract N°: 2303
THE USAGE OF THE JACOBSON’S RELAXATION TECHNIQUE IN PATIENTS WITH ACUTE VASCULAR PATHOLOGY
Nataliya Nekrasova*1, Ivan Darii1, Iuliia Panasenko2
1Kharkiv National Medical University, Neurology, Kharkiv, Ukraine,2Kharkiv Regional Hospital, Neurology, Kharkiv, Ukraine
On behalf of:
Background and aims: The restoration of impaired functions in case of brain injury occurs mostly due to the compensation of intact functional systems. This process is carried out thanks to the plasticity of nerve centers. Neurorehabilitation measures can significantly increase the plastic functions of the brain, which is clinically reflected in the form of a decrease in motor, sensory, cognitive disorders. The psychological state of a patient who has suffered a stroke is decisive for neurorehabilitation. Assuming, that patients feel that relaxing the muscles could relax the mind as well, use of Jacobson’s relaxation technique (JRT) can be useful in the rehabilitation of this group of patients.
Methods: We examined 77 patients, aged 64±7.1 years, who were treated in the neurological department of the Kharkiv regional clinical hospital with a verified diagnosis of ischemic stroke. Stroke survivors completed the Hospital Anxiety and Depression Scale-Anxiety Subscale (HADS-A) during the initial screening and on the 14th day of hospitalization. In order to help patients deal with anxiety, patients performed JRT. In control group the strokes survivals were not performed JRT.
Results: According the results of conducting HADS-A assessment 2 groups of patients were formed. In 1gr. (67% of patients) HADS-A revealed clinically expressed level of anxiety/depression. In 2 gr. (33%), HADS-A indicated on subclinically expressed level of anxiety/depression. After 14 days of treatment the indexes of HADS-A both groups were significantly decreased (p 0.⩽05).
Conclusions: The results indicate the need to implement JRT as a inexpensive intervention for post-stroke anxiety into the treatment of these patients.
Disclosures of Interest: No
Abstract N°: 2411
THE THERAPEUTIC CONNECTION BETWEEN ART AND STROKE RECOVERY
1North Middlesex University Hospital, Medical Photography, London, United Kingdom,2North Middlesex University Hospital, Acute Stroke Unit, London, United Kingdom
On behalf of:
Background and aims: Drawing attention to stroke recovery through the provision of art is important in our community. Stroke patients experience emotional, physical and social difficulties during their rehabilitation that can negatively affect their quality of life. Art can provide the practical and emotional support needed for a quicker recovery as well as making rehabilitation more pleasant.
Methods: Through our Patient Arts Programme we run weekly art sessions for patients on the acute stroke unit. During these sessions patients are encouraged to visualise and verbalise their creative abilities and to practise their fine motor and cognitive skills in a relaxed, safe environment. These opportunities for social interaction and self-expression often lead to enjoyable and rewarding experiences for patients, particularly for those with aphasia and cognitive communication impairments. Our facilitators provide art materials, tips and tuition to help patients create pieces of art with deep personal importance.
Results: The art sessions are beneficial for the recovery and emotional and physical rehabilitation of our stroke patients. Patients say they enjoy and look forward to the art activities and benefit from socialising with other patients during the sessions. The artwork created by patients is publicly displayed in the hospital and has been positively received.
Conclusions: The Patient Arts Programme makes a vital contribution to the healing environment, improving the experience of recovery and rehabilitation for stroke patients in hospital.
Disclosures of Interest: No
Abstract N°: 2464
CADASIL PATIENT RECOVERY ANALYSIS USING MICROPHILLAR ELECTRODE ARRAY CHIP
Chi Kyung Kim*1, Ho Kyu Kim1, Hyun Myung Doo1
1Korea University Guro Hospital, Neurology, Seoul, South Korea
On behalf of:
Background and aims: This study leverages a novel microphillar electrode array chip to investigate synapse formation in CADASIL patients, addressing the limitations of traditional neuroglial cell analysis methods for neurological diseases.
Methods: Employing the microphillar electrode array chip, we conducted real-time and quantitative analysis of synapse formation in cultured neuroglial cells, comparing it with conventional imaging techniques.
Results: The microphillar electrode array chip demonstrated a distinct, delayed yet robust pattern of synapse formation in CADASIL patients. It provided quantitative data superior to traditional imaging, revealing significant differences in synaptic recovery patterns. This method proved effective in real-time monitoring, contrasting with the time-consuming nature of image analysis. It also enabled precise measurement of synapse formation at various stages of cell culturing, offering insights into the recovery trajectory post-stroke.
Conclusions: This study highlights the microphillar electrode array chip as a breakthrough in neuroglial cell analysis, offering real-time, quantitative insights into the recovery process in CADASIL patients.
Disclosures of Interest: No
Abstract N°: 2518
PROSPECTS FOR THE DEVELOPMENT OF NEUROREHABILITATION IN UKRAINE (ACURE PROJECT)
1Karazin Medical University, Neurology, Kharkiv, Ukraine,2State Institution “Institute of Neurology, Psychiatry and Narcology of the National Academy of Medical Sciences of Ukraine”, Neurology, Kharkiv, Ukraine,3NGO “Ukrainian Society of Physical and Rehabilitation Medicine", Rehabilitation Medicine, Kyiv,4Shupyk National Univercity of Healthcare in Ukraine, Rehabilitation Medicine, Kyiv,5Transcarpathian Regional Centre of Neurosurgery and Neurology, Neurology, Uzhorod, Ukraine
On behalf of:
Background and aims: ACURE (Austrian Cooperation Ukraine Rehabilitation) is a programme of cooperation between Austrian rehabilitation centres and the All-Ukrainian Society of Neurorehabilitation, the Association of Neurologists, Psychiatrists and Narcologists of Ukraine, the Ukrainian Society of Physical and Rehabilitation Medicine, and Shupyk National Healthcare University of Ukraine.
Objective: To create intensive trainings on the basic principles of organising and conducting post-stroke rehabilitation for multidisciplinary rehabilitation teams in different regions of Ukraine.
Methods: The ACURE project aims to education and continuous professional development of doctors; providing rehabilitation care after stroke in the acute and subacute rehabilitation periods; clinical practice in neurorehabilitation.
Results: The ACURE project began in 2019, when Austrian colleagues and Ukrainian rehabilitation specialists visited Ukrainian rehabilitation units with different levels of professional development. Three Ukrainian doctors completed internships at Austrian rehabilitation hospitals and began implementing trainings for neurologists, PRMs, occupational therapists, and physical therapists who provide a neurorehabilitation for patients after stroke and TBI. Since February 2020 about 1 000 medical workers were trained at 40 trainings, they received relevant certificates. In August 2023 two speech and language therapists from Ukraine participated in 2nd course on dysphagia in Lyon, since then trainings on dysphagia have become a mandatory part of ACURE. These activities contributed to the introduction of modern standardised neurorehabilitation approaches into practice and the improvement of stroke and TBI rehabilitation.
Conclusions: The main goal of the project remains its implementation and deepening of cooperation between Ukraine and Austria in the field of rehabilitation of patients after stroke and TBI.
Disclosures of Interest: No
Abstract N°: 2928
EVOLVREHAB – MOVEWELL TELEREHABILITATION FOR UPPER LIMB REHABILITATION EARLY AFTER STROKE: FEASIBILITY AND PROOF OF CONCEPT
Philip McBride*1, Jemma Perks1,2, Mae Mansoubi1, Philip Clatworthy3, Claire Hulme1, Gordon Taylor1, Martin Warner4, Helen Dawes1,2
1University of Exeter, Medical School, Exeter, United Kingdom,2University of Oxford, Department of Paediatrics, Oxford, United Kingdom,3North Bristol NHS Trust, Bristol, United Kingdom,4University of Southampton, Southampton, United Kingdom
On behalf of:
Background and aims: Unilateral upper-limb impairments, including “compensatory” movements, are common in people who have had a stroke. “EvolvRehab–MoveWell” is a telerehabilitation system which uses game-based activities to assess and correct compensatory movements. This study aimed to assess the initial feasibility of a telerehabilitation programme, using EvolvRehab–MoveWell, in people who have recently had a stroke; before progressing into a larger trial.
Methods: This initial feasibility work recruited five participants who had recently had a stroke and were referred by treating clinicians as requiring upper-limb rehabilitation. Participants were given an EvolvRehab–MoveWell Kit to use in their homes for one week, with access to a personalised rehabilitation programme. To assess the feasibility of a larger trial, quality of life, physical activity, and physical function were measured at baseline and after one week of use. Interviews with users were conducted after the intervention, as well as a log of issues and adverse events.
Results: The five participants (aged 46 ± 13 years) were primarily left side affected (80%) and were 121 ± 93 days post-stroke. Participants saw a range of beneficial changes across the outcomes of interest, including handgrip strength (mean change 1.7kg [-2.39, 5.79]), EQ-VAS (7.25 [-1.79, 16.29]), EQ-Index (0.17 [-0.42, 0.76]), and SAFE score (0.6 [-0.51, 1.71]). Feedback on the intervention was largely positive. Limited technical issues were reported. There were no study-related adverse events.
Conclusions: With some updates to the software, a larger, longer duration trial of EvolvRehav–MoveWell appears to be feasible in a stroke population.
Disclosures of Interest: No
Abstract N°: 2999
ALAMEDA, AN OPORTUNITY FOR AT-HOME NEUROLOGIC REHABILITATION-INTERIM NEUROCOGNITIVE REHABILITATION RESULTS
Mara Moldovan*1, Athena Cristina Ribigan1,2, Raluca Stefania Badea1,2, Patricia Anda Ioan1, Alexandra Niculae1, Alexandru Sorici3, Lidia Bajenaru3, Adina Magda Florea3, Florina Antochi1
1Emergency University Hospital Bucharest, București, Romania,2Carol Davila University of Medicine and Pharmacy, București, Romania,3POLITEHNICA București National University for Science and Technology, București, Romania
On behalf of:
Background and aims: The second most prevalent reason for mortality and a primary contributor to adult disability within the European Union is stroke. Although stroke center designation has advanced, survivors often struggle with persistent impairments.
The Alameda research project aims to develop technologies for monitoring the rehabilitation process, encompassing three pilot studies in Greece (Parkinson’s disease), Italy (MS) and Romania (Stroke) with 15 international partners.
Methods: The stroke pilot study enrolled 15 patients undergoing a 12-month rehabilitation program, employing diverse measurement devices: belt (troncular ataxia), insoles (walking), smartwatch (physical activity), smartmattress (sleeping), smartbracelet (muscle strength), smartphone and a tablet used for questionnaires/games (emotional/cognitive status). The Montreal Cognitive Assessment (MOCA) scale was used to monitor cognitive domains across four visits. Results await correlation with the cognitive game scores, specifically the virtual supermarket and the line tracking test.
Results: MOCA revealed no variability of the Memory Domain with scores starting at 0.53 (SD = 1.13). MOCA-Attention Domain exhibited a gradual increase from 4.6 (SD = 1.35) to 5.5 (SD = 0.76), and MOCA-Language Domain scores slightly fluctuated around 2.0. MOCA-Abstraction showed a minor decrease from 2.0 to 1.88, while MOCA-Word Recall scores fluctuated around 3.07 (SD = 1.79). MOCA-Orientation scores remained around 5.7. MOCA-Total Score displayed a slight increase from 23.4 (SD = 3.14) to 25.13 (SD = 3.64).
Conclusions: In conclusion, the MOCA domain scores provide insights into the cognitive functions of the participants. These findings offer valuable perspectives on the cognitive impact of the exercises, highlighting the need for tailored rehabilitation strategies in stroke care.
Disclosures of Interest: Yes This project has received funding from the European Union`s Horizon 2020 research and innovation programme.
Abstract N°: 3048
EVALUATION OF THE USABILITY AND USER EXPERIENCE OF FIVE DIFFERENT NON-IMMERSIVE GAMIFIED HOME-BASED EXERCISES FOR STROKE SURVIVORS
Hatem Lazem*1,2, Abi Hall2, Maedeh Mansoubi2, David Harris3, Sallie Lamb2, Carlos Monteiro4, Helen Dawes2
1Faculty of physical therapy, Cairo university, Basic science department, Cairo, Egypt,2The university of Exeter, Medical School, Faculty of Health and Life Sciences, Exeter, United Kingdom,3The university of Exeter, School of Public Health and Sport Sciences, Exeter, United Kingdom,4university of São Paulo, School of arts, science and humanities, São Paulo, Brazil
On behalf of:
Background and aims: Gamified exercises can be a promising motivating tool in stroke telerehabilitation. This study aimed to explore the potential of repurposing and adapting established non-immersive virtual reality gaming systems, by evaluating the usability and user experience of five gamified exercise platforms with stroke survivors.
Methods: Chronic stroke survivors were invited to a session to try five different games with various levels of difficulty and settings with a focus on training the upper limb and challenging balance in sitting or standing positions. Participant demographics, and the usability and user experience of the system were evaluated using the System Usability Scale (SUS), the User Experience Questionnaire(UEQ) with open-ended questions asking about their satisfaction, and house of quality analysis.
Results: Eleven chronic stroke survivors (subtypes: 63% hemorrhagic, 37% ischemic;45.5% female) (Fugl-Meyer Assessment of Upper Extremity mean(SD)=41(19.4)), (time from stroke median(IQR)= 44(78) months) with mild to moderate spasticity ( Modified Ashworth Scale mean(SD)=1.4(0.5)) perceived the usability of the five games as very good to excellent for four games, median SUS=85% and poor for one game SUS=52.5%. All UEQ scales (Attractiveness, Pragmatic Quality, Hedonic Quality) showed good to excellent acceptance among most of the games with the best mean values for one Game being 1.85, 1.51, and 1.98 respectively.
Conclusions: All games were perceived positively by the participants, which may increase their motivation to increase their exercise dose and adhere to their exercise routine, thus improving their quality of life. Clinical trials should be conducted to investigate the efficacy of these non-immersive gamified exercises as a telerehabilitation tool.
Disclosures of Interest: No
E-Poster - Service Organisation
Abstract N°: 70
IMPLEMENTATION OF NOSIP IN IMPROVING REPERFUSION TREATMENT IN A CSC IN SOUTHERN ENGLAND
Richard Marigold*1, Lawrence Lee1, Elvina Cerejo1, Ahmed Elserafy1
1University Hospital Southampton NHS Foundation Trust, Department of Stroke Medicine, Southampton, United Kingdom
On behalf of:
Background and aims: National Clinical Guidelines for Stroke in the UK have strongly recommended the implementation of the National Optimal Imaging Pathway (NOSIP) to improve detection of patients eligible for thrombolysis and mechanical thrombectomy
Methods: We compared the use of CT,CTA and CTP between 2022 and 2023 in our unit following an education campaign across the hospital and in the department to raise awareness about the importance of advance imaging in detecting large vessel occlusion (LVO) and identifying patients for thrombolysis and thrombectomy We also assessed the number of non strokes being admitted.
Results: In 2022, CTA was performed in 25/54 (46%) patients. 15/54(27%) showed an LVO. 6/52(11%) had CTP. 6/54 (11%) received thrombolysis 3/54 (5%) mechanical thrombectomy and 1/54 both. In 2023 CTA was performed in 61/99 (61%). 37/99 (37%) showed an LVO. 32/99 (32%) received reperfusion therapy including 6/99 (6%) thrombolysis, 16/99 (16%) mechanical thrombectomy and 10/99 (9%) both.
Conclusions: A hospital based education programme and raising awareness about NOSIP significantly increased the proportion of patients receiving CTA by 15%, leading to a 10% rise in LVO detection and doubling the rates of thrombolysis and mechanical thrombectomy. The proportion of patients admitted with a stroke diagnosis to HASU increased from 45% to 70% between 2022 and 2023.
Disclosures of Interest: No
Abstract N°: 541
CHANGES IN THE TREATMENT OF ACUTE ISCHEMIC STROKE IN SUZHOU: A COMPARATIVE STUDY OF KEY QUALITY CONTROL INDICATORS OVER 5 YEARS
1The Second Affiliated Hospital of Soochow University, Department of Neurology, Suzhou Clinical Research Center of Neurological Disease, Suzhou, China,2Affiliated Hospital of Jiangnan University, Department of Geriatrics
On behalf of:
Background and aims: This study aims to compare the trends in the acute phase of patients with AIS in Suzhou from 2014 to 2019, focusing on key quality control indicators for patients treated with IVT and providing clinical data for the improvement of regional stroke center construction.
Methods: Baseline data 5 years ago were obtained from the SUMMITS study phase I and the Suzhou branch database of ENCHANTED clinical study from December 2013 to May 2014. Data in 2019 was obtained from the SUMMITS Study Phase II. Data about basic information, reperfusion therapy, complications and prognosis were compared.
Results: 5316 patients were included. Thrombolysis rate was higher in 2019 (P<0.001). DNT, OTT and prehospital delay ware all reduced from 2014 to 2019 (P<0.05). 66.1% of patients achieving a DNT ⩽60 in 2019. In-hospital delays improved more significantly than pre-hospital delays. Patients were older in 2019 (P=0.002), with lower median baseline NIHSS score (P=0.007), higher proportion of mild strokes with an NIHSS score ⩽5 (P<0.001), and higher prevalence of diabetes (P=0.048). Patients in 2019 had a lower incidence of pulmonary infections, electrolyte disturbances, and asymptomatic hemorrhagic transformation, a heel segment of hospital days, a lower proportion of in-hospital deaths, and a lower discharge NIHSS score (all P<0.05).
Conclusions: The key quality control indicators for patients treated with IVT were significantly improved in Suzhou over a five-year period. Patients treated with IVT had a significant decrease in in-hospital mortality and better improvement in neurological function at discharge.
Disclosures of Interest: No
Abstract N°: 678
FIRST EXPERIENCE OF STROKE SECONDARY PREVENTION SERVICE (POST-STROKE FOLLOW-UP) IMPLEMENTATION IN UKRAINE
1Chernivtsi central city clinical hospital, City stroke center, Chernivtsi, Ukraine,2Kharkiv National Medical University, Neurology, Kharkiv, Ukraine
On behalf of:
Background and aims: Stroke patients after discharge are accompanied by family physicians in Ukraine. In May 2023 secondary stroke prevention (follow-up) service started to work as a part of stroke unit.
Methods: A telephone-based follow-up service was implemented in a stroke unit in Ukraine, contacting patients 30 and 90 days post-stroke. The service focused on mRS assessment, complication detection, treatment adjustments, referrals, and risk factor management. Data from the first 8 months of the service were analyzed.
Results: Total number of patients who were examined after stroke is 213(33,8% of all discharged patients), 60(9,5%) – repeatedly on 90 (±7) day. Treatment correction was performed in 123(57,7%) of all examined patients: 82(38,4%) – antihypertensive drugs, 23 (17,8%) – statins, 32(15%) – antiplatelet/anticoagulants. In 15(7%) patients any other medications were prescribed. In 29(13,6%) cases post-stroke complications were detected and treated: depression – 12(9,7%), pain – 12(9,7%), incontinence – 5(2,3%), seizures – 8(3,7%). 41(19,2%) patients undergone rehabilitation course. Physical activity and diet issues were solved in 198(92,9%) cases. On 90 day we observed better compliance of medication intake and lifestyle modification.
Conclusions: Post-stroke follow up service will help to gain better compliance in patients, reach better risk factors control, track mRS in patients after stroke, detect and treat post-stroke complications in patients. We cannot estimate reduction of recurrent stroke because of short term observation, but probably we can assume it in longer perspective (e.g. 5 or more years).
Disclosures of Interest: No
Abstract N°: 783
REHABILITATION IN PRIMARY CARE NETWORKS FOR PEOPLE WITH ACQUIRED BRAIN INJURY IN THE NETHERLANDS: INSIGHTS FROM A NATIONWIDE SURVEY
On behalf of: Learning Network Implementation of Guidance for Rehabilitation in Primary Healthcare
Background and aims: The way services for people with Acquired Brain Injury (ABI) are organised is fundamental to the quality of care. To strengthen primary care networks providing interdisciplinary rehabilitation for people with ABI, a national guidance was developed. The guidance holds recommendations for healthcare professionals and networks. This study aimed to investigate the baseline of networks to support the implementation of the guidance.
Methods: A self-developed, online survey was distributed among primary care networks in the Netherlands. Multiple items were used to collect data regarding organisation of care in a network, criteria for knowledge and skills of allied health professionals and visibility and findability of healthcare providers and networks for patients and providers. Data were analysed descriptively.
Results: Out of the 38 identified networks, 23 completed the questionnaire (RR 61%). The networks range in number of healthcare providers from <25 (36%), 25-100 (45%) to >100 (18%). The most frequent professions are physiotherapist (100%), occupational therapist (74%) and speech therapist (74%), whereas in 78% the general practitioner is not actively involved. Of networks, 86% has a set of quality standards, 66% has a minimum caseload for its participants, and 30% has appointed a coordinator. Visibility and findability are most often guaranteed by a website (83%). Most networks (95%) offer training to participants.
Conclusions: Rehabilitation in primary care networks for people with ABI varies in the Netherlands. To support the nationwide implementation of the guidance, baseline data indicate the need for an implementation strategy that is responsive to regional variation.
Disclosures of Interest: No
Abstract N°: 915
FACTORS IMPACTING ACUTE STROKE REPERFUSION RATES IN A TERTIARY STROKE CENTRE IN NEW ZEALAND
Dong Hyun Kim1, Lillian Choy1
1Waikato Hospital, Neurology, Hamilton, New Zealand
On behalf of:
Background and aims: Reperfusion treatment is one of the four stroke indicators reported to the New Zealand Ministry of Health, with a target of 12% of acute ischaemic stroke patients treated with thrombolysis or clot retrieval. Monthly stroke indicator reports have consistently shown rates of less than 10% in this hospital. We wanted to determine potential reasons for this.
Methods: A list of patients discharged with acute stroke between May to July 2023 was retrieved. Information including patient demographics, modified Rankin score (mRS), stroke aetiology, National Institutes of Health Stroke Score (NIHSS), type of imaging, and treatment were collected.
Results: There were 107 patients discharged with acute ischaemic stroke; 15 patients (14%) received acute reperfusion therapy. When compared to the monthly report, the number of patients receiving acute reperfusion therapy was the same, however there was a big difference in the reported number of acute ischaemic stroke patients (107 versus 184). The main reasons why patients did not have treatment were: being out of window (47%), low NIHSS (15%) and having contraindications (8%). This audit did not identify any patients who missed out on acute reperfusion therapy.
Conclusions: This audit showed that the apparent low rates of acute reperfusion treatment reported each month may be due to differences in the clinical coding of acute ischaemic stroke. The results provided reassurance that no patients meeting criteria for reperfusion therapy missed out on treatment. The audit also highlighted that public awareness of stroke symptoms needs to be improved.
Disclosures of Interest: No
Abstract N°: 974
CHALLENGES IN PERFORMING A STRUCTURED STROKE FOLLOW-UP IN NURSING HOME RESIDENTS: A PILOT FEASABLITY STUDY
Ingrid Lindgren*1,2, Åsa Rejnö3, Hélène Pessah-Rasmussen2
1Lund University, Department of Health Sciences, Lund, Sweden,2Skåne University Hospital, Department of Neurology, Rehabilitation Medicine, Memory Disorders and Geriatrics, Lund, Sweden,3University West, Department of Health Sciences, Trollhättan, Sweden
On behalf of:
Background and aims: Multidisciplinary team-based follow-up is recommended for all stroke patients in Sweden including those discharged to nursing homes. The nursing homes are organized by the municipalities and staffed daily by assistant nurses with access to registered nurses. The aims were to explore the feasibility of a structured follow-up with the Post Stroke Checklist, PSC, in nursing home residents and to map stroke related problems and planned interventions.
Methods: Due to a complex recruitment process and low recruitment rate, the study protocol was adapted to an explorative design. Nine health professionals and five nursing home residents participated. Data included health professionals’ views on usefulness of the PSC (questionnaire and interviews), results from the PSC and description of ongoing or planned interventions.
Results: The health professionals were generally satisfied with the PSC, but adjustments were suggested. Lack of coordination between different stakeholders, fear for increased paperwork and lack of referral options for some of the suggested interventions were identified as obstacles for the implementation of routine structured stroke follow.
All nursing home residents reported problems with ADL, mobility, spasticity, incontinence, mental fatigue and performing former activities. Several inexpensive ongoing or planned interventions were considered.
Conclusions: A structured post-stroke follow up was difficult to perform in nursing homes in a Swedish context. However, the need for identifying stroke related problems in this vulnerable population was highlighted. The professionals perceived PSC feasible with smaller adjustments. The need to build a suitable organization able to act for identified problems was acknowledged.
Disclosures of Interest: No
Abstract N°: 1091
EVOLUTION OF STROKE CARE IN UKRAINE FROM 2017 TO 2022
1Kharkiv National Medical University, Neurology, Kharkiv, Ukraine,2Feofaniya Clinical Hospital, Stroke Center, Kyiv, Ukraine,3Lutsk City Hospital, Stroke Center, Lutsk, Ukraine,4Poltava Regional Clinical Hospital named after M.V.Sklifosovskyy, Stroke Center, Poltava, Ukraine,5Dnipro Regional Clinical Hospital named after I.I. Mechnykov, Stroke Center, Dnipro, Ukraine,6Vinnytsia National Pirogov Medical University, Neurology, Vinnytsia, Ukraine
On behalf of:
Background and aims: According to World Bank data, Ukraine is grappling with a population decrease while stroke instances escalate. The study assesses the progression of stroke treatment in Ukraine from 2017 to 2022, developed from the post-Soviet healthcare framework.
Methods: Analysis involved data from all Ukrainian stroke units and centers per the National Health Service of Ukraine.
Results: The Angels Initiative since 2016 has propelled medical education for professionals and citizens, leading to a simulation center in Poltava in 2019 and localizing the BEFAST acronym to MOZOK CHAS for awareness.
Conclusions: Ukraine’s acute stroke care has significantly evolved in 6 years, with thrombolysis rates surging from 0.36% in 2017 to 6.4% in 2022. Despite hurdles, IVtPA and MT rates have consistently climbed, marking stroke care as a pivotal healthcare focus by the Ministry of Health and the National Health Service.
Disclosures of Interest: No
Abstract N°: 1147
CREW RESSOURCE MANAGEMENT (CRM) BASED SIMULATION TRAINING FOR TELEMEDICALLY SUPPORTED STROKE CARE
Christina Laitenberger*1, Ferdinand Bohmann2, Gabriele Rossner1, Jennifer Abels1, Bernadette Wehrle1, Gordian Hubert1, Yvonne Schombacher1
1München Klinik gGmbH, TEMPiS telestroke center, Department of Neurology, München, Germany,2Frankfurt University Hospital, Department of Neurology, Frankfurt am Main, Germany
On behalf of:
Background and aims: CRM-based simulation training is established in many disciplines of medicine but not regularly in acute telemedically supported stroke care. We integrated the teleconsultation process into the trained process flow of a simulation training. Aims were to analyze staff confidence when dealing with acute stroke patients and acceptance of this training format.
Methods: Based on the Stroke-Team-Training by Frankfurt University Hospital, the training concept was adapted to the specific circumstances of our telemedical setting and conducted simulation trainings in 5 spoke hospitals of the telemedical stroke network in Southeast Bavaria (TEMPiS). It consisted of briefing including basics of acute stroke care and the CRM concept, implementation of the actual simulation training and subsequent CRM-based debriefing. It took place in real settings of the emergency department with an interdisciplinary team. Training period covered the entire door-to-needle-process, including the teleconsultation process. We conducted a survey before and after the training. Outcome parameters were self rated confidence, and acceptance.
Results: Of 78 participants, 59 participated in the survey. Before training, 50% of participants said they felt confident in dealing with acute stroke patients, compared to 89% afterwards. In the after-training-survey, 92% rated it as realistic, 97% welcomed that it took place at the actual workspace and 80% saw relevance to their everyday work. Overall, 98% rated the training format as positive and regular repetition was requested by 100%.
Conclusions: Training format was well received and led to greater confidence when dealing with acute stroke patients.
Disclosures of Interest: No
Abstract N°: 1251
EMS STROKE ASSESMENT – SUITABILITY OF CURRENT TRIAGE TOOLS FOR YOUNG ADULTS?
Nedim Leto*1,2, Elisabeth Farbu1,3, Paul Barach4, Thomas Lindner2
1University of Bergen, Department of Clinical Science, Bergen, Norway,2Stavanger University Hospital, The Regional Centre for Emergency Medical Research, Stavanger, Norway,3Stavanger University Hospital, Department of Neurology, Stavanger,4Thomas Jefferson University, Philadelphia
On behalf of:
Background and aims: The incidence of stroke is increasing among younger adults. Unawareness and misinterpretation of symptoms among the public and health care providers may lead to treatment delays. We aimed to investigate EMS stroke identification rates, symptom presentation and time delays in young adults with acute ischaemic stroke (AIS).
Methods: We included patients with confirmed AIS who were transported by the EMS in Western Norway with initial contact made with the Emergency Medical Dispatch Centre (EMDC) in 2021. We collected the EMDC suspicion of stroke, stroke symptoms, NIHSS at admission, prehospital and in-hospital time metrics, including reperfusion treatments. Patients were dichotomized based on age under (young adults) or over 60 years of age.
Results: In total, 91/771 (12 %) of the included patients were young adults. The patients tended to have higher rates of EMDC stroke suspicion (62 (68 %) vs 419 (62 %) (OR 1.33 (95% CI 0.83,2.12; p=0.23). Young adults also had lower NIHSS scores (2 vs 4; p=0.038) and presented more often with symptoms such as dizziness, ataxia, diplopia, and unconsciousness (33 (37 %) vs 155 (23); (OR 1.94 (95% CI 1.22,3.08; p=0.005). The ambulance on-scene times (11 vs 13 minutes); (p=0.019) were also shorter for these patients. Door-to-needle (22 vs 23 minutes; p=0.24) and door-to-groin times (84 vs 68 minutes; p=0.38) were similar in both groups.
Conclusions: EMS showed comparable stroke identification and response times in young adults and those over 60 with AIS, but young adults had lower NIHSS scores at admission.
Disclosures of Interest: No
Abstract N°: 1297
THE DEVELOPMENT OF A NEW STROKE UNIT WEBSITE: IMPROVING ACCESS TO INFORMATION ABOUT ACUTE STROKES AND INPATIENT CARE
Background and aims: Stroke survivors and relatives would like more information during the post-stroke period. A website was developed for the local acute stroke unit, detailing stroke resources and ward information. However, service users’ awareness and perceptions of the website were unknown. This project aims to evaluate the readability and usefulness of the existing stroke unit website, and subsequently improve it as a resource and raise website awareness.
Methods: A Google survey of patients and relatives assessed website usefulness, reliability, and readability, and collected free-text suggestions. Interventions were designed using Plan-Do-Study-Act (PDSA) cycle methodology.
2nd PDSA cycle: ward leaflet promoting the website distributed; website views counted before and afterwards.
Results: Pre-intervention survey: 17 responses. 7.0/10 for usefulness, 7.7/10 for readability and 5.9/10 for reliability. 23.5% rated it up-to-date. Recommendations: improve accuracy, more information on stroke and support.
Post-intervention survey: 18 responses. 9.3/10 for usefulness, 9.4/10 for readability and 9.5/10 for reliability. 94.4% rated it up-to-date. Free-text suggestions: promotional leaflets, update content.
Website awareness was 28.6%. The month before leaflet distribution the website had 0 visits. Months 1 and 2 post-distribution it had 6 and 39 visits respectively.
Conclusions: An updated website including information about staff roles objectively improved readability, usefulness, and accuracy. Lack of website awareness prompted a second PDSA cycle and promotional leaflet. Improving access to information can address common post-stroke questions and support individuals’ understanding of rehabilitation. A website with a supporting leaflet is effective in disseminating such information. Future goals include improving accessibility for communication difficulties.
Disclosures of Interest: No
Abstract N°: 1425
PEOPLE WITH STROKE AND CAREGIVERS’ PREFERENCES AND EXPERIENCES REGARDING SUPPORTS PROVIDED AT TRANSITION FROM HOSPITAL TO HOME
Geraldine O’Callaghan*1, Martin Fahy2, Sigrid O’meara2, Sebastian Lindblom3, Lena Von Koch3, Peter Langhorne4, Rose Galvin5, Frances Horgan2
1RCSI, RCSI School of Population Health, Dublin 2, Ireland,2RCSI, RCSI School of Physiotherapy, Dublin 2, Ireland,3Karolinska Institutet, Department of Neurobiology, Care Sciences and Society, Stockholm, Sweden,4University of Glasgow, School of Cardiovascular and Metabolic Health, Glasgow, United Kingdom,5University of Limerick, School of Allied Health, Faculty of Education and Health Sciences, Limerick, Ireland
On behalf of:
Background and aims: For people with stroke (PWS) and their caregivers (CGs), the transition from structured setting to home presents many challenges, as they navigate through complex uncertainties. This qualitative study seeks to bridge gaps in our understanding of appropriate support interventions for managing the transition home by exploring the perspectives of PWS and their CGs regarding their support experiences and preferences during this period.
Methods: Audio-recorded, semi-structured interviews were conducted with PWS and their CGs within six months of hospital discharge. All interviews were transcribed, imported into NVivo software, and analysed using reflexive thematic analysis.
Results: Sixteen interviews were conducted with PWS (n = 9) and CG (n = 7). Three themes relevant to their experiences and preferences were identified (i) quest for understanding and connection, (ii) left in limbo, (iii) inequity of access.
Conclusions: This study highlights the difficulties PWS and families face during the transition phase, irrespective of the discharge route and even with formal support systems in place. Furthermore, it highlights many inequitable aspects and disparities in care experiences in the transition phase. A partnership approach to this critical transition period is required; which includes improved communication and goal-setting amongst healthcare providers, support organisations, PWS and their families.
Disclosures of Interest: No
Abstract N°: 2001
PREDICTIVE VALUE OF THE GAZE-FACE-ARM-SPEECH-TIME SCALE FOR LARGE VESSEL OCCLUSION IN ACUTE STROKE PATIENTS
HANG TRAN*1,2, Loc Phan2, Trung Nguyen2, Anh Truong1,2, Thang Nguyen1,2
1Pham Ngoc Thach University of Medicine, Neurology, Ho Chi Minh City, Viet Nam,2People’s Hospital 115, Cerebrovascular Diseases, Ho Chi Minh City, Viet Nam
On behalf of:
Background and aims: Prehospital stroke scales have been developed to identify large vessel occlusion (LVO) in acute ischemic stroke (AIS) patients for direct transport to thrombectomy-capable hospitals; however, its perfomance in Vietnamese population remains unknown. We aims to evaluate the predictive value of the gaze-face-arm-speech-time (G-FAST) scale for LVO detection in Vietnam.
Methods: A prospective study of consecutive AIS patients who admitted at our hospital between November 2022 and August 2023. All patients was assessed the G-FAST scale with four items: gaze deviation (0–1), facial palsy (0–1), arm weakness (0–1), and speech disturbance (0–1). LVO was confirmed by CTA, or MRA. Receiver operating curve, sensitivity, specificity, and accuracy of G-FAST were analyzed to evaluate its predictive value for LVO.
Results: 312 patients were included, 36.9% (115/312) had LVO. The G-FAST score was strongly associated with LVO (P<0.001). Receiver operating curves showed capacity to predict LVO of G-FAST scale with area under the curve (AUC) of 0.767. Optimal cutoff was ⩾3.5 with sensitivity=0.54, specificity=0.92, PPV=0.81, NPV=0.77, and overall accuracy=0.78. High-sensitivity threshold was observed for G-FAST⩾3 (OR=5.7 [95% CI, 2.6–12.5] for LVO, sensitivity=0.93, specificity=0.30, PPV=0.44, and NPV=0.88). G-FAST⩾3 had higher sensitivity for detecting LVO in AIS patients in the 6-24-hour window than within 6 hours (AUC=0.75 vs.0.79, sensitivity=0.95 vs.0.89, specificity=0.25 vs.0.37).
Conclusions: The G-FAST scale is a simple screening tool that can accurately identify AIS patients with LVO. This tool may be useful to early detection of LVO patients and should be validated at prehospital setting in Vietnam.
Disclosures of Interest: No
Abstract N°: 2088
DEVELOPMENT OF A NATIONWIDE STROKE SIMULATION PROGRAMME – THE UK AND REPUBLIC OF IRELAND ACUTE STROKE SIMULATION COURSE (ASSC)
Ella Sherman1, Zehra Mehdi*2, Louise Shaw3
1Musgrove Park Hospital, Stroke and Geriatric Medicine Department, Taunton, United Kingdom,2Royal Hampshire County Hospital, Stroke Department, Winchester, United Kingdom,3Royal United Hospital, Stroke Department, Bath, United Kingdom
On behalf of: UK and Republic of Ireland Acute Stroke Simulation Working Group
Background and aims: Stroke simulation-based education (SBE) has proven to improve door-to-needle times1, clinical pathways1, outcomes1 and endovascular proficiency2. Across our five nations, access to stroke simulation training is inequitable. We describe the development of the first national Acute Stroke Simulation Course (ASSC).
Methods: In 2021, a working party comprising individuals from the United Kingdom (UK) and Republic of Ireland (ROI) interested in stroke simulation was convened. An initial mapping exercise revealed significant geographical variations. Consequently, the ASSC was developed. A bespoke course website was created with the British and Irish Association of Stroke Physicians (BIASP). Multiple pilots preceded the official launch.
Results: Pilot feedback was collated. Candidates responded to pre- and post-course questionnaires regarding their confidence in managing reperfusion. Data was analysed using Wilcoxon Signed-Rank testing. Table 1 demonstrates a significant improvement in confidence levels.
Thematic analysis revealed three key themes: scenarios were realistic and relevant; trainers were friendly and knowledgeable and the debriefing sessions outlined techniques to improve team communication. Several candidates suggested that the course should be made a mandatory requirement for stroke practitioners.
Conclusions: Resulting from collaborative working across five nations, the ASSC should facilitate a standardised approach to hyper-acute stroke simulation based education, addressing an unmet training need. There are plans to embed the course into medical and advanced practice training curricula, aligned to the Stroke Specific Education Framework3
Disclosures of Interest: Yes This course has received financial support from Medtronic.
Abstract N°: 2146
CHARACTERISTICS OF HIGH-PERFORMANCE HOSPITALS IN LOW STROKE VOLUME CENTERS
1Seoul National University Hospital, Department of Neurology, Emergency Medical Center, Seoul,2Seoul National University Bundang Hospital, Department of Neurology and Cerebrovascular Center, Seongnam,3Soonchunhyang University Hospital, Department of Neurology, Seoul
On behalf of:
Background and aims: Generally, it is known that in stroke centers, a larger patient volume is associated with better outcomes. However, especially in regions with low population density, time-sensitive stroke patients may need to visit low-volume centers. This study aims to investigate the performance of low-volume centers and identify characteristics of hospitals that demonstrate favorable performance despite of low stroke volume.
Methods: Using the combined data of 8th audit of Acute Stroke Quality Assessment Program (ASQAP) in 2018, claims data for reimbursement, the total of nationwide 248 hospitals were included. Hospitals that treat fewer than 100 stroke patients per year were classified as low-volume centers, and those with a defect-free care rate of more than 75% were defined as high-performance centers. The primary outcome measure was the mortality rate at 1 year.
Results: The 1-year mortality rate for acute stroke patients was higher in low-volume centers compared to high-volume centers (24.8% vs. 17.6%, adjusted p < 0.01). In the low-volume center group, the 1-year mortality rate was lower in high-performance centers compared to low-performance centers (21.1% vs. 26.9%, adjusted p = 0.036). There was no difference in the number of hospital beds or the annual volume of stroke admissions between the high- and low-performance centers. There was a significant difference in the number of physicians, especially neurologists (p = 0.01).
Conclusions: This study identified and characterized the performance of low-volume centers, which is unavoidable in stroke care. We found that improving human resources is important for improving patient outcomes in the low-volume centers.
Disclosures of Interest: No
Abstract N°: 2213
OPTIMIZING ACUTE STROKE TREATMENT IN ATLANTIC CANADA: A CFIR-BASED ANALYSIS OF A QUALITY IMPROVEMENT COLLABORATIVE IMPLEMENTATION
Shadi Aljendi*1,2, Kelly Mrklas3, Adam Forward1, Noreen Kamal1,4,5
1Dalhousie University, H-COAL, Department of Industrial Engineering, Halifax, Canada,2UNB Faculty of Computer Science, Fredericton, Canada,3Alberta Health Services, Strategic Clinical Networks, Provincial Clinical Excellence, Calgary, Canada,4Dalhousie University, Department of Community Health and Epidemiology, Faculty of Medicine, Halifax, Canada,5Dalhousie University, Department of Medicine (Neurology), Halifax, Canada
On behalf of:
Background and aims: Efficient approaches in acute stroke treatment are essential to reduce treatment time and increase the proportion of patients treated. This study investigates the facilitators and barriers encountered in the implementation of a Modified Quality Improvement Collaborative (mQIC) across four Atlantic provinces in Canada, aiming to improve stroke treatment practices. The mQIC was 6 months long and consisted of 2 full-day workshops with action planning, and participants were also supported with virtual site visits and webinars.
Methods: Utilizing a qualitative approach, semi-structured interviews were conducted with healthcare professionals that particiated in the mQIC, including stroke coordinators, physicians, nurses, imaging technicians, emergency medical services and admistrators. The Consolidated Framework for Implementation Research (CFIR) was the framework used in the evaluation.
Results: A total 33 healthcare professionals participated in the interviews. There were 1141 intances of facilitators and 236 instances of barriers. The study identified work infrastructure and culture as pivotal, serving dual roles as barriers and facilitators. Key barriers included resource availability, innovation complexity, and compatibility issues. Conversely, facilitators were notably leadership engagement, effective communication and partnerships as well as external pressure. The modified design and flexibility of the mQIC played a critical role in leveraging facilitators, with most barriers being external to the mQIC’s control.
Conclusions: The mQIC was positively received, indicating its potential for broader implementation. The predominance of facilitators over barriers suggests its adaptability to varied settings, offering valuable insights for future healthcare innovations.
Disclosures of Interest: No
Abstract N°: 2481
MEASURING AND IMPROVING THE QUALITY OF INTEGRATED CARE SERVICES FOR ISCHAEMIC STROKE: A QUALITATIVE ANALYSIS
Daniël Hansen*1,2, Henk Kerkhoff3, Diederik Dippel1, Hester Lingsma2, Bob Roozenbeek1
1Erasmus Medical Centre, Neurology, Rotterdam, Netherlands,2Erasmus Medical Centre, Public Health, Rotterdam, Netherlands,3Albert Schweitzer Hospital, Neurology, Dordrecht, Netherlands
On behalf of:
Background and aims: Care for ischaemic stroke is organized in integrated services, consisting of regional networks of providers collaborating during the acute, rehabilitation and chronic phase of stroke care. We previously developed a dashboard with quality indicators to measure and improve quality of integrated stroke care. We aimed to gain insight in how stakeholders value this dashboard.
Methods: We performed a qualitative study with stakeholders of integrated stroke care: vascular neurologists, rehabilitation professionals, and patient representatives. The focus groups reviewed the dashboard – consisting of patient characteristics and indicators of structure, process, and outcome – prior to the meeting. Data was collected in three one-hour meetings. The meetings were recorded and the transcript was coded to identify thematic findings.
Results: Healthcare providers agreed that the dashboard could provide novel insight in integrated care services, e.g. patient flow and outcomes. However, neurologists found the goal of the dashboard currently unclear, specifically since they also used other dashboards. Rehabilitation professionals found the indicators too hospital-centred and suggested to include rehabilitation relevant outcomes. Patient representatives indicated they found the dashboard useful to improve quality of care, specifically at transitions between providers, but not for themselves. All participants emphasized the need for high-quality data but to limit the burden of data collection.
Conclusions: Stakeholders consider the use of quality indicators of integrated stroke care services an important means to improve regional collaboration and quality of care. However, the current dashboard needs to be improved by clearly defining its goal, using high-quality data and including relevant indicators for the full care cycle.
Disclosures of Interest: No
Abstract N°: 2659
CO-CREATING A PUBLIC INVOLVEMENT GROUP (PPI) FOR A HYPERACUTE STROKE UNIT (HASU) AND HYPERACUTE STROKE RESEARCH CENTRE (HSRC)
Peter Wilding*1,2, Jennifer Crow1,2, Vaishali Dave1, Salwa Elmamoun1,3, Marney Williams4
1Imperial College Healthcare NHS Trust, Stroke, London, United Kingdom,2Imperial College London, Brain Sciences, London, United Kingdom,3Chelsea and Westminster Hospital NHS Foundation Trust, Stroke, London, United Kingdom,4NIHR Stroke National Specialty Group, United Kingdom
On behalf of:
Background and aims: Patient, Carer, and Public Involvement are key components of both Hyperacute Stroke Unit (HASU) and Hyperacute Stroke Research Centre (HSRC) re-accreditation for UK centres specialising in hyperacute stroke treatment and research. It is also required by major funders of stroke research. Despite the importance of PPI there is a scarcity of such groups in the UK. We wanted to share our approach to successfully co-creating a PPI Group.
Methods: We used an Agile/Scrum project management modality. Our Steering Group consists of 4-members, including a PPI-specialist and stroke survivor; selected for high-levels of motivation, diversity of experience and viewpoint, clinical and research expertise. Our meetings were non-hierarchical and collaborative: We prioritised individuals/interactions and responding to change by having 9 x 90-minute weekly-meetings. Each meeting had a clear goal, achieving the smallest amount necessary to deliver. Decisions were made and executed swiftly. We also visited a neighbouring stroke support group for inspiration and to invite participants, as well as using our networks to invite patients.
Results: We successfully established and launched a Stroke PPI Group within two months, with ambitious plans for both service and research development. The Agile/Scrum mind-set enabled us to co-create incrementally and effectively select a highly-motivated multi-disciplinary Steering Group that recruited 9 members affected by stroke from diverse backgrounds for our first-ever local Stroke PPI Group.
Conclusions: An Agile/Scrum modality can be used to establish a successful Stroke PPI Group in approximately 2 months, and establish co-ordinates for the future of the Group.
Disclosures of Interest: No
Abstract N°: 2976
STROKE UNIT ADMISSIONS AT A REGIONAL HOSPITAL: A RETROSPECTIVE AUDIT
Dawn Ryan*1, Margaret O’connor2, Ahmad Gabr3, Jethen Maharaj4, Marwa Mustaffa4, Javad Ghassemi Rad3, John Peacock3, Nora Cunningham3
Background and aims: The world stroke organisation estimates that there are 12.2M strokes each year. Stroke unit care is associated with improved clinical outcomes. The national clinical guideline for stroke recommends admission to a stroke unit as soon as possible. The national stroke strategy 2022-2027 outlines a key performance indicator that at least of 90% of patients should be admitted to a stroke bed for at least 90% of their admission.
This audit aims to examine the following data during 2020-2022:
1. The proportion of stroke patients admitted to a stroke unit.
2. The proportion of stroke patients who spent 90% or more of their admission on a stroke unit.
Methods: Patient data was collected each year and input into Microsoft Excel. Data was analysed to determine the number of patients admitted to a stroke unit, and the % of admission spent on the unit.
Results: 444, 447 and 512 stroke patients were admitted in 2020, 2021 and 2022. 78.8%, 74.8% and 65% of patients were admitted to a stroke unit. In 2020, 2021 and 2022, 53%, 51% and 45% of total stroke patients spent 90% or more of their admission in the stroke unit. The top reasons for non-admission included ‘bed not available’, ‘infection control risk’ and ‘other’.
Conclusions: Compliance with the identified KPI declined each year of the audit, as did the proportion of patients admitted to a stroke unit. The biggest issue affecting stroke unit admission is the availability of beds. Patients requiring infection control precautions are disadvantaged.
Disclosures of Interest: No
Abstract N°: 3025
END OF LIFE CARE PATHWAY IN STROKE: PATTERN, IMPLEMENTATION AND OUTCOME
Pramol Ale*1, Olubunmi Omojowolo1, Martin Kawabata1, Mary Harawa1, Doom Joy Chen-Unongo1, Wasif Hoque1, Chinedu Okafor1, Rami Abdallah1, Imran Zafar1, Rami Mohammed1
1Kent And Canterbury Hospital, Stroke Medicine, Canterbury, United Kingdom
On behalf of: George Thomas, Saidu Abubakar, Hardeep Baht, Gunaratnam Gunathilagan, Ibrahim Balogun, Thomas Webb, Yogish Pai, Abinas Gurung, David Hargroves
Background and aims: The issue of end-of-life care in patients who are terminally ill is very sensitive and involves a lot of ethical considerations.
This study is aimed at reviewing the pattern, utilization and implementation of EOL pathway in stroke patients.
Methods: This was a retrospective study of patients admitted into the stroke unit who either died or fast - tracked from January 2021 to August 2023 (Total no. of patients 288).
Results: There were 189 patients (66%) with ischemic stroke while 87 patients (30 %) those with haemorrhagic stroke. Unspecified categories were 12(4.0%). Non stroke patients were excluded.
Admission modified rankin scale score was significantly higher compared to premorbid score.
The most common co-morbidities were hypertension and diabetes.
Clinicians initiated EOL discussion with the family in 255(88.5%) as death was anticipated. Proper documentation was done for 244(84.7%) patients.
Unfortunately, 44 patients (15.3%) died suddenly and their death was not anticipated hence no EOL paperwork documentation or clear discussion with family was documented.
5 patients (1.74%) had the EOL reversed due to sustained clinical improvement while 7(2.4 %) were fast track discharged.
The mean time to death was 1 week/8days from the moment the patients were put of EOLC
DNACPR form were available for 275(98.0%) of the patient as at the time of death.
Conclusions: This study showed that the uptake in incorporating palliative and end of life care in acute stoke setting is improving gene. However, there is a need for the development of a stroke-specific guidelines.
Disclosures of Interest: No
Abstract N°: 3032
COST-EFFECTIVENESS OF METOCLOPRAMIDE, PARACETAMOL AND CEFTRIAXONE IN THE TREATMENT OF ELDERLY PATIENTS WITH ACUTE STROKE
Mathyn Vervaart1, Anne Hege Aamodt*2,3, Jeroen de Jonge4, Wouter Sluis4, H. Bart van der Worp4
1Oslo University Hospital, Clinical Trial Unit, Oslo, Norway,2Oslo University Hospital, Neurology, Oslo, Norway,3The Norwegian University of Science and Technology, Neuroscience and Movement Sciences, Norway,4Brain Center, University Medical Center Utrecht, Department of Neurology and Neurosurgery, Utrecht
On behalf of: the PRECIOUS investigators
Background and aims: Infections and fever after stroke are associated with poor outcomes. Evidence on the health and economic consequences of pharmacological treatments to improve stroke outcomes is however scarce.
Our study aimed to evaluate the cost-effectiveness of metoclopramide, paracetamol and ceftriaxone, either as monotherapies or in combination, compared to standard of care in the treatment of elderly patients with acute stroke.
Methods: We conducted a model-based analysis to estimate lifetime costs, quality-adjusted life years (QALYs), and net monetary benefit (NMB), given a willingness-to-pay threshold of 50,000 euros per QALY gained. The model synthesized data from long-term observational studies and short-term outcomes from an international randomised, controlled trial in elderly acute stroke patients. We evaluated the impact of parameter uncertainty on the model’s results through probabilistic and value of information analyses.
Results: Combination therapy with metoclopramide, ceftriaxone and paracetamol yielded the highest NMB and was the optimal choice in terms of cost-effectiveness. When compared to standard care, this treatment option decreased costs by 5,958 euros and increased QALYs by 0.10. The probabilistic analysis indicated a 30% probability of combination therapy with metoclopramide, paracetamol, and ceftriaxone being the optimal choice. Value of information analysis showed that uncertainty about the optimal treatment option was largely driven by uncertainty about the initial modified ranking scale probabilities.
Conclusions: Combination therapy with metoclopramide, paracetamol and ceftriaxone is expected to be the optimal choice in terms of cost-effectiveness for treating elderly patients with stroke.
The trial was funded by the European Union’s Horizon, 2020 research and innovation programme.
Decision tree structure (a) and state-transition model structure (b). mRS, modified Rankin Scale.
Cost-effectiveness acceptability frontier. Cef, Ceftriaxone; Met, Metoclopramide; Par, Paracetamol; SoC, Standard of Care..
Per person Expected Value of Partial Perfect Information (NMB) for groups of input parameters given a willingness-to-pay threshold of 50,000 euros per QALY gained. Cef, Ceftriaxone; Met, Metoclopramide; mRS, modified Rankin Scale; Par, Paracetamol; SoC, Standard of Care.
Disclosures of Interest: No
Abstract N°: 3291
VIDEO-BASED PREHOSPITAL TELETRIAGE FOR ACUTE STROKE : RESULTS FROM A REGIONAL PILOT-STUDY
Gregory Jacquin1,2, Christian Stapf2, Olena Bereznyakova*2, Nicole Daneault2, Yan Deschaintre2, Céline Odier2, Alexandre Y. Poppe2, Laura Gioia2
Background and aims: Only limited data exist on the potential benefit of prehospital video-based teletriage for patients with acute stroke.
Methods: During a 6-month period (March-September 2023), all prospective patients from a defined geographical catchment area with a 911 call for acute stroke were screened by the paramedic team on site. Those with known symptom onset of <6h underwent video-based teletriage for transfer to either the closest tertiary (for suspected LVO occlusion) or to the closest secondary stroke centers (for unlikely LVO occlusion). Patients referred for thrombectomy by same the secondary stroke centers without teletriage during the same period served as control.
Results: Overall, 33 patients were teletriaged: ten (30%) were directed to the closest secondary stroke center, while 23 (70%) were bypassed to the tertiary center. Of the latter, 13 (mean age 76y, 8 (62%) women, median NIHSS 19) underwent thrombectomy (+/- iv thrombolysis). During the same period, 22 patients (mean age 76y, 13 (59%) women; median NIHSS 17) were referred for thrombectomy without teletriage. The median time from 911 to thrombectomy was 129 [IQR 51] min after teletriage, as compared to 196 [74] min in controls (p=0.015). The median NIHSS at 24h after thrombectomy was 6 in the teletriage group versus 14.5 in controls (p=0.07). None of the patients triaged to a secondary stroke center had an acute LVO stroke (NPV 100%).
Conclusions: Video-based prehospital teletriage for acute stroke is feasible, reliably identifies patients without LVO stroke and significantly improves the delay between stroke alert and thrombectomy in eligible LVO stroke patients.
Disclosures of Interest: No
Abstract N°: 3341
ARE WE DOING JUSTICE TO ALL STROKE PATIENTS?
Ramya Satyadi1, Phyo MA MA Thu Khine1, Aaizza Naqvi*1
1Royal Hallamshire Hospital, Sheffield Teaching Hospitals NHS Foundation Trust, Sheffield, United Kingdom
On behalf of:
Background and aims: Prompt thrombolysis and thrombectomy have been a game changer in stroke management. However not many patients are eligible for hyperacute interventions (HAI). Whilst all efforts are directed towards prompt HAI, often there is underemphasis on promptly giving aspirin to patients who are not eligible for HAI despite having evidence of benefit. Our project aims to evaluate our current practice with regards to timings of aspirin given to such patients to take measures to improve our practice and patient outcomes.
Methods: Retrospective data was collected of all stroke admissions to our stroke unit in October 2023. Excluding those eligible for HAI, we analysed paper and electronic data to establish key timelines since symptom onset to aspirin administration and their relationship with patient demographics.
Results: Our analysis revealed that 0% of patients received aspirin within an hour of arrival. 20.7%, 28.3%, 15%, 3.7%, 3.7%, 3.7%, 1.8% and 5.6% of patients were given aspirin within 3 hours, 3-5 hours, 5-7 hours, 7-9 hours, 9-12 hours, 12-15 hours, 15-18 hours, and after 24 hours respectively. For 17% of patients, the time of arrival was not recorded. 15%, 18.8%,7.54%,9.43%, 3.7%, were given aspirin within 6 hrs, 6-12hrs,12-18hrs,18-24hrs,24-36hrs and after 36hrs of symptom onset respectively. For 35.8% of patients, the time of symptom onset was unknown.
Conclusions: Our findings reflect that aspirin is not given as promptly in patients not eligible for HAI. There is a need for emphasis of prompt delivery of aspirin for such patients.
Disclosures of Interest: No
E-Poster - Sex, Gender and Stroke
Abstract N°: 1132
STROKE RISK FACTORS IN POST-MENOPAUSAL WOMEN
Anita Arsovska*1
1University Clinic of Neurology, University "Ss. Cyril and Methodius"-Faculty of Medicine, Urgent Neurology, Skopje, Macedonia
On behalf of:
Background and aims: In the period of menopause, many women develop vascular risk factors and increase the risk of stroke. This risk is doubled during the first decade after menopause. The aim of this study is to identify the frequency ofstroke risk factors (hypertension, atrial fibrillation, diabetes mellitus, previous stroke, dyslipidemia, obesity, smoking and carotid atherosclerosis)in postmenopausal women (aged > 51 years) compared to men at the same age.
Methods: A retrospective analysis of 78 postmenopausal women (mean age 70.5 years) and 94 men (mean age 68 years) hospitalized with stroke during a 1 year period was performed. Statistical analyses were done in SPSS, with p for significance <0.05.
Results: There was no statistically significant difference in the presence of hypertension, atrial fibrillation, diabetes mellitus and recurrent stroke (p>0.05). Dyslipidemia and obesity were more prevalent in postmenopausal females (p<0.05), while smoking and carotid atherosclerosis was dominant in men (p<0.05). There was no difference in the frequency of risk factors for first and recurrent stroke in the post-menopausal women (p<0.05).
Conclusions: Proper management of stroke risk factors (especially dyslipidemia and obesity) is important in order to reduce the burden of stroke in postmenopausal women.
Disclosures of Interest: No
Abstract N°: 2993
SEX DISPARITIES IN FUNCTIONAL OUTCOMES BY HAEMATOMA LOCATION: TICH-2 TRIAL DATA
Chaamanti Menon*1, Iris Isheanesu Mhlanga1, Kailash Krishnan2, Zhe Kang Law3, Michael Desborough4, Robert Dineen5, Philip Bath1, Nikola Sprigg1
1University of Nottingham, Stroke Trials Unit, Mental Health and Clinical Neurosciences, NOTTINGHAM, United Kingdom,2Queen’s Medical Centre, Stroke Medicine, Nottingham, United Kingdom,3Malaysia National University Kuala Lumpur Campus, Department of Medicine, Kuala Lumpur, Malaysia,4Oxford University Hospital Trust, Department of Haematology, Oxford, United Kingdom,5University of Nottingham, Radiological Sciences, Nottingham, United Kingdom
On behalf of:
Background and aims: The tranexamic acid for intracerebral haemorrhage trial (TICH 2) data has shown previously that female patients with intracerebral haemorrhage (ICH) were more likely to have lobar bleeds compared to men. We further explored the sex disparities in functional outcomes within the subgroups of deep and lobar haemorrhages.
Methods: Using the TICH-2 trial data, a double-blind study exploring tranexamic acid effects in acute ICH, we grouped frontal, parietal, temporal, occipital and cerebellar bleeds as lobar, and basal ganglia, thalamic and brainstem bleeds as deep, bleeds. Using adjusted ordinal logistic regression analysis, we analysed the primary outcome (modified Rankin Score, mRS) at 90 days post stroke in the deep vs lobar ICH subgroups.
Results: Lobar ICH were more common in women (56.2% vs 43.8%) and deep ICH were more common in men (61.7% vs 38.1%). Table 1 summarises the baseline characteristic differences between sexes with deep or lobar ICH. mRS at 90 days did not differ between sexes in lobar or deep ICH (aOR [95% confidence interval]; 1.14 [0.87;1.50], 1.05[0.86;1.28]).
Conclusions: Despite woman having a worse prognosis being older with worse strokes, at 90 days functional outcome between sexes in lobar or deep bleeds showed no significant disparities after correction for prognostic factors.
Disclosures of Interest: No
Abstract N°: 3192
THE IMPACT OF SEX DIFFERENCE ON FUNCTIONAL OUTCOME AFTER STROKE
Jeong-Min Kim*1, Patrik Michel2
1Seoul, Neurology, Seoul, South Korea,2Lausanne, Lausanne, Switzerland
On behalf of:
Background and aims: Several studies have suggested female sex is associated with worse outcome after acute ischemic stroke (AIS). We investigated the relationship between gender and functional outcome after stroke by analyzing two different ethnic groups.
Methods: The two hospital based AIS registries between 2015 and 2022, Seoul National University Hospital Korean Stroke Registry (SNUH_KSR) and the Acute Stroke Registry and Analysis of Lausanne (ASTRAL) in Switzerland were analyzed. We first compared the demographic and clinical variables between male and female stroke patients, followed by acute revascularization rates and functional 3-month outcome. Multivariable logistic regression model was constructed to identify whether female sex was independently associated with neurological outcome of modified Rankins ⩽ 2 three months after stroke.
Results: Female stroke patients were older and associated with more severe neurological deficit at initial presentation and at discharge than male patients from the two stroke registries, which included 3548 patients from SNUH_KSR and 3449 patients from ASTRAL. Cardioembolic stroke subtypes and atrial fibrillation were more prevalent among the female patients, whereas atherosclerotic stroke and diabetes mellitus were more prevalent among male patients. The rate of receiving recanalization treatment was not different between two sexes. Multivariable logistic regression analysis including clincal variables and interaction between recanalization treatment and sex revealed that female sex was an independent factor of neurological outcome (SNUH_KSR: odds ratio=0.80, 95% confidence interval=0.64 – 0.99, ASTRAL: odds ratio=0.70, 95% confidence interval=0.58 – 0.86).
Conclusions: Female stroke patients were associated with poor functional outcome, probably due to prevalent cardioembolic stroke etiology.
Disclosures of Interest: No
E-Poster - Small Vessel Disease
Abstract N°: 497
VASCULAR PARKINSONISM IN CADASIL: PREVALENCE AND CLINICAL FEATURES
1NTUH (National Taiwan University Hospital), Department of Neurology, Taipei City, Taiwan,2NTUH (National Taiwan University Hospital), Department of Medical Imaging, Taipei City, Taiwan
On behalf of:
Background and aims: To investigate the prevalence and clinical features of vascular parkinsonism (VaP) among patients with CADASIL.
Methods: Patients in the prospective Taiwan CADASIL Registry underwent evaluation using the United Parkinson’s Disease Rating Scale. VaP was diagnosed if they had gait impairment or bradykinesia not explained by stroke-related paresis. MRI features and plasma alpha-synuclein were analyzed. Furthermore, comparisons were made with patients having idiopathic Parkinson’s disease (IPD) of similar age and sex.
Results: In 75 patients with CADASIL (age 64 [57-72], male 52%), 55 (73%) exhibited parkinsonism feature, while 45(60%) had stroke (Figure 1). Patients with VaP were older, had thinner cortical thickness, and larger white matter hyperintensity (WMH). WMH volume was associated with the presence of VaP (OR 1.03, 95% CI 1.00 – 1.07), while thinner cortical thickness was associated with motor severity in patients with VaP. Compared with patients with IPD (n=158, age 70 [62-76] male 51%), patients with VaP had comparable Hoehn-and-Yahr stage (2 [1-3] vs 2 [1-3]), but lower UPDRS-III scores (median 12 [7-26] vs 18 [12-25]), lower plasma alpha-synuclein (0.08 [0.07-0.13] vs 0.95 [0.24-1.99] pg/mL), thinner cortical thickness (2.35 [2.23-2.39] vs 2.44 [2.36-2.53] mm), higher Fazekas score (6 [5-6] vs 2 [1-3]), number of lacunes (7 [3-12] vs 0 [0-0]) and CMB (21 [4-61] vs 0 [0-0]). Plasma alpha-synuclein was associated with UPDRS-III only in patients with IPD, not in patients with CADASIL (Figure 2).
Conclusions: VaP is not uncommon among patients with CADASIL. The burden of small-vessel disease, but not alpha-synuclein, may contribute to its development.
Disclosures of Interest: No
Abstract N°: 583
DO AGE, SEX, OR BASELINE WHITE MATTER HYPERINTENSITY VOLUME INFLUENCE WHITE MATTER HYPERINTENSITY REGRESSION VS PROGRESSION?
Angela Jochems*1, Susana Munoz Maniega1, Una Clancy1, Carmen Arteaga Reyes1, Daniela Jaime Garcia1, Maria Valdes-Hernandez1, Francesca Chappell1, Michael Stringer1, Fergus Doubal1, Joanna Wardlaw1
1University of Edinburgh, Centre for Clinical Brain Sciences and UK Dementia Research Institute, Edinburgh, United Kingdom
On behalf of: MSS-3 Study Group
Background and aims: Well-known risk factors for white matter hyperintensity (WMH) progression are older age and larger baseline WMH volumes. Despite accumulating evidence for WMH regression, including potential clinical benefits, factors related to regression are unknown. We assessed whether WMH regression is related to age, sex or baseline WMH.
Methods: We recruited patients with minor, non-disabling, ischaemic stroke who underwent MRI within 3 months post-stroke and one year later. We calculated WMH volumes (% intracranial volume [ICV]), excluding stroke lesions. Regression is defined as overall WMH volume decrease between baseline and one year and progression as overall increase. We used one logistic regression to obtain odds ratios (OR), and included baseline age, sex and WMH volume predicting WMH regression and progression.
Results: 198 participants (32.8% female, baseline mean age=65.5 years[SD=11.1]) had useable WMH volumes. Mean WMH regression (N=77) was -0.068 (%ICV, SD=0.089; range: -0.563, -0.000) and mean WMH progression (N=121) 0.142 (SD=0.170; range: 0.000, 0.809). A one-year increase in age decreased the odds of WMH regression by 1.03 (OR=1.03[95%CI 1.00, 1.06]). The odds for women to have WMH regression were lower than for men (OR=0.44; 95%CI [0.22,0.86]). A one %ICV larger baseline WMH volume might decrease the odds of WMH regression (OR=1.36; 95%CI [0.99, 2.00]).
Conclusions: Younger age, male sex, and, possibly, lower baseline WMH volume seem to favour WMH regression. WMH in older age might be more established. While men appeared more likely to have WMH regression, in this sample women were on average older; hence sex differences in WMH change require confirmation.
Disclosures of Interest: No
Abstract N°: 633
CRITICAL CLOSING PRESSURE MEDIATES THE ASSOCIATION BETWEEN INTRACRANIAL ARTERY CALCIFICATION AND WHITE MATTER HYPERINTENSITIES
Xuelong Li*1, Xiang-Yan Chen1
1The Hong Kong Polytechnic University
On behalf of:
Background and aims: This study sought to investigate the severity of intracranial artery calcification (IAC) in relation to white matter hyperintensities (WMH), and whether the association was mediated by cerebral autoregulation as determined by critical closing pressure (CCP).
Methods: A total of 144 patients with cerebral small vessel disease were included in this study. The severity of IAC was evaluated on non-contrast head computed tomography (CT) images. IAC was classified as intimal or medial calcification. CCP, determined by analyzing pressure-flow velocity relationships in the middle cerebral artery. The severity of WMH was assessed using Fazekas scores in FLAIR images. Mediation analyses were conducted to examine the direct association between IAC and WMH, as well as the mediated effect of CCP on this association.
Results: A significant relationship was observed between IAC scores and higher CCP values (β, 0.329; 95% confidence interval [CI], 0.129–0.528; P = 0.001). IAC scores were also found to be associated with WMH scores (β 0.364; 95% CI, 0.133-0.409; P <0.001). Mediation analyses revealed that CCP partially mediated 10.3% of the association between higher IAC scores and increased WMH severity. The proportions of mediations were higher in participants with predominantly medial calcification (13.9%) than intimal calcification and non-calcification IAC (−8.5%).
Conclusions: Higher IAC scores may contribute to the severity of WMH in patients with cerebral small vessel disease, and this association is partially mediated by cerebral autoregulation as indicated by CCP, especially for the patients with predominantly medial calcification.
Disclosures of Interest: No
Mediation Analyses (all participants).
Abstract N°: 1311
CLINICAL RELEVANCE OF DIFFERENT LOADS OF PERIVASCULAR SPACES ACCORDING TO THEIR LOCALIZATION IN PATIENTS WITH A LACUNAR STROKE
Caterina Sozzi1, Carla Brenlla2, Andres Girona2, Emma Muñoz-Moreno2, Carlos Laredo2, Angels Calvet2, Alejandro Rodríguez Vázquez2, Xabier Urra2, Salvatore Rudilosso*2, Angel Chamorro2
1University of Milan Bicocca, Resident in Neurology, Milano, Italy,2Hospital Clínic de Barcelona, Neuro, Barcelona, Spain
On behalf of: The study was supported by a grant of the Catalan Society of Neurology Foundation
Background and aims: Cerebral perivascular spaces (PVS) are typically enlarged in small vessel disease (SVD). However, PVS patterns according to different brain regions have still an uncertain clinical significance. We aimed to describe the PVS distribution in patients with a lacunar stroke and analyse their correlations with clinical and imaging factors.
Methods: In a cohort of 50 consecutive lacunar stroke patients with complete clinical data, including the Pittsburgh Sleep Quality Index (PSQI), and investigational 3T-MRI, we segmented and quantified the PVS percentage in white matter (WM-PVS), basal ganglia (BG-PVS), brainstem (BS-PVS), and the WM/BG and WM/BS PVS ratios. We applied a log transformation to these variables to achieve a normal distribution. We analysed the Pearson correlation coefficient between PVS regional loads, and the association with clinical and MRI-SVD features (WMH, number of lacunes and microbleeds) in univariable and multivariable linear regressions adjusted for age and history of hypertension.
Results: In our cohort (mean age 70 years; 36% female) the correlations (r) between WM-PVS/BG-PVS, WM-PVS/BS-PVS, and BG-PVS/BS-PVS were 0.67, 0.61, and 0.59 (all p<0.001). Higher PVS loads were globally associated with age, hypertension and most SVD markers in univariable analyses. In adjusted models, BG-PVS was associated with lacunes (p=0.005) and WMH (p=0.001); WM-PVS was associated with lacunes (p=0.003) and microbleeds (p=0.021); WM/BG-PVS ratio was associated with PSQI.
Conclusions: PVS burdens in different regions are highly correlated to each other in patients with a lacunar stroke but with different SVD lesion patterns. Sleep-quality impairment might affect waste removal mechanisms differently in WM and BG regions.
Disclosures of Interest: No
Abstract N°: 1360
IMAGING EVIDENCE OF NEURODEGENERATION IN IATROGENIC CEREBRAL AMYLOID ANGIOPATHY
1UCL Queen Square Institute of Neurology, London, UK, Stroke Research Centre, Department of Brain Repair and Rehabilitation, London, United Kingdom,2Bogomolets National Medical University, Department of neurology, Kyiv, Ukraine,3UCL Institute of Prion Diseases, MRC Prion Unit, London, United Kingdom,4National Hospital for Neurology and Neurosurgery, Queen Square, University College London Hospitals NHS Foundation Trust, London, United Kingdom,5UCL Queen Square Institute of Neurology, Neuroradiological Academic Unit, London, United Kingdom,6National Hospital for Neurology and Neurosurgery, Queen Square, University College London Hospitals NHS Foundation Trust, Lysholm Department of Neuroradiology, London, United Kingdom
On behalf of:
Background and aims: Iatrogenic cerebral amyloid angiopathy(iCAA) describes amyloid-β(Aβ) deposition in small cortical and leptomeningeal arterioles resulting from transmission of Aβ during medical procedures, with disease onset occurring decades later. Parenchymal Aβ deposits are also found in Alzheimer’s disease (AD). In both sporadic (non-iatrogenic) CAA and AD, parenchymal and vascular Aβ frequently co-exist. It is not known whether this is also the case for iCAA.
Methods: We retrospectively assessed 10 patients with probable iCAA. We measured medial temporal lobe atrophy score (MTA; a neuroimaging biomarker of AD) and global cortical atrophy (GCA) score.
Results: Six patients were male, and mean age was 42 years; all had exposure to cadaveric dura mater at a mean age of 6 years with a mean latency to clinical onset of 36 years. Most patients presented with intracerebral haemorrhage (n=6); none had cognitive symptoms or neuroimaging evidence of atrophy at presentation. Two years later, four patients had developed MTA (score range 2 to 3; Figure 1); of these, three also had GCA (all scoring 2). Histopathological data at follow-up for two of these four patients showed Alzheimer-type pathology (parenchymal Aβ and tau deposition).
Conclusions: We found that 40% of patients with iCAA develop neuroimaging evidence of neurodegeneration within 2 years of presentation, which might reflect co-existing AD pathology. It is unclear whether this neurodegeneration occurs because of iCAA or develops independently due to additional transmission of AD-associated Aβ (or tau) at the time of exposure. We suggest monitoring for cognitive symptoms in iCAA to allow early identification and appropriate management.
Disclosures of Interest: No
Abstract N°: 1592
AGE-RELATED RISK FACTORS AND PRIMARY HEMOSTASIS: A PILOT STUDY OF SMOKING IN ELDERLY AND YOUNG MALE INDIVIDUALS
Minh Duc Tran1, Albina Yasamanova1, Ivan Koltsov*1,2, Ivan Shchukin1,2, Mikhail Fidler1, Vladimir Chubykin1, Georgy Avakyan1,2
1Pirogov Russian National Research Medical University, Moscow, Russian Federation,2Federal Center of Brain Research and Neurotechnologies, Moscow, Russian Federation
On behalf of:
Background and aims: In patients with chronic cerebrovascular disease (CCVD), the persistent risk factors continue to contribute to symptom progression, worsening the prognosis. Smoking can cause degenerative changes in arteries and arterioles, leading to accelerated atherosclerosis and stenosis. This pilot study aims to investigate the impact of smoking on vessel walls in young individuals without nervous system disorders and in CCVD patients.
Methods: Adenosine-diphosphate-induced platelet aggregation (ADP-IPA), ristocetin-induced platelet aggregation (RIPA), and von Willebrand factor activity (vWF) were assessed using a Biola aggregometer. The study included 20 elderly patients with CCVD (10 non-smokers and 10 smokers) and 12 young healthy individuals (6 smokers and 6 non-smokers). Blood samples of smokers were assessed before and 30 minutes after smoking; non-smokers’ samples were assessed once.
Results: In CCVD participants, the ADP-IPA was 64.0% [55.5-65.3] pre-smoking and 68.5% [61.5-71.5] post-smoking (p=0.046). Their pre- and post-smoking RIPA was 64.5% [61.8-68.3] and 73.5% [66.8-76.5], respectively (p=0.083). There was a nonsignificant trend towards higher RIPA post-smoking in both smokers and non-smokers. The pre- and post-smoking vWF in CCVD patients was 94.0% [84.3-98.5] and 93.0% [89.0-101.5], respectively (p=0.646). Both pre- and post-smoking ADP-IPA, the post-smoking RIPA in CCVD individuals were significantly higher than those in young individuals (p=0.012, p=0.006, p=0.044, respectively). There were no statistically significant differences in ADP-IPA, RIPA, and vWF between young smokers and non-smokers.
Conclusions: Smoking contributes to considerably increased RIPA and ADP-IPA in the elderly with CCVD. Further studies are needed to improve understanding of the age-dependent effect of smoking on primary hemostasis.
Disclosures of Interest: No
Abstract N°: 1749
CEREBRAL SMALL VESSEL DISEASE AS A MEDIATOR BETWEEN HEART FAILURE WITH PRESERVED EJECTION FRACTION AND COGNITIVE DECLINE
Patrick Müller*1, Katja Neumann2, Horndasch Laslo1, Hendrik Mattern3, Thomas Groscheck1, Sven Meuth4, Alexander Schmeißer1, Daniel Behme5, Stefanie Schreiber2, Rüdiger Braun-Dullaeus1
1University Hospital Magdeburg; Division of Cardiology and Angiology, Magdeburg, Germany,2University Hospital Magdeburg; Division of Neurology, Magdeburg, Germany,3Biomedical Magnetic Resonance, Faculty of Natural Sciences, Otto-von-Guericke University, Magdeburg, Germany,4Department of Neurology, Medical Faculty, Heinrich Heine University of Düsseldorf, Düsseldorf, Germany,5University Hospital Magdeburg, Department of Neuroradiology, Magdeburg, Germany
On behalf of: HIM-Study
Background and aims: Patients with heart failure with preserved ejection fraction (HFpEF) show a high prevalence of cerebral small vessel disease (CSVD) and cognitive dysfunction, whereas the causal relation is still topic of ongoing research. Our aim was to investigate the impact of CSVD on the interrelation of HFpEF and cognitive decline.
Methods: Twenty-five participants (14 HFpEF patients, 11 healthy controls, age 68.5 ± 9.9) were prospectively included and underwent the CERAD-Plus neuropsychology test battery. HFpEF severity was assessed using the H2FpEF-score (including clinical characteristics such as hypertension and echocardiographic parameters such as diastolic dysfunction). Three-Tesla brain MRI was used to quantify CSVD severity (summary SVD scores) according to the STRIVE criteria.
Results: Compared to controls, patients were characterized be a high H2FpEF-score [H(1) = 16.58, p ⩽.001]. Additionally, the demonstrated pronounced CSVD severity [H(1) = 14.69, p ⩽.001] and worse cognitive performance [H(1) = 15.27, p ⩽.001]. The H2FpEF-score correlated with cognition (r = -.75, p ⩽.001) and CSVD severity (r = .65, p ⩽.001). CSVD partially mediated the relation between HFpEF and cognition (Figure 1).
Conclusions: Microvascular brain tissue damage (CSVD) partially mediates cognitive decline in HFpEF patients. Our data demonstrate the urgent need for interdisciplinary heart-brain research investigating interrelated pathophysiological mechanisms of HFpEF and CSVD.
Disclosures of Interest: No
Mediation Analysis. Summary SVD scores partially mediated the relation between heart failure with preserved ejection fraction (H2FpEF score) and cognitive decline. Age was included as covariate. Significant paths are marked with */**/*** for p < .05/.01/.001.
Abstract N°: 2042
MICROSTRUCTURAL INTEGRITY ON DIFFUSION TENSOR IMAGING PREDICTS ’CAP’ AND ’TRACK’ FORMATION ADJACENT TO LACUNAR INFARCT
Yajun Cheng*1,2, Carmen Arteaga Reyes1, Una Clancy1, Daniela Jaime Garcia1, Maria Valdes-Hernandez1, Michael Thrippleton1,1, Angela Jochems1, Susana Munoz Maniega1, Fergus Doubal1, Joanna Wardlaw1
1University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom,2Sichuan University, Department of Neurology, West China Hospital, Chengdu, China
On behalf of: Edinburgh SVD Group
Background and aims: Half of symptomatic lacunar infarcts develop secondary hyperintense changes in the adjacent superior or inferior white matter (‘cap’ or ‘track’ respectively) and are associated with long-term dependency. However, ’cap/track’ pathophysiology remains unknown. We aimed to assess the relationship between baseline microstructural integrity of normal-appearing white matter (NAWM) and ‘cap/track’ formation at 1-year after lacunar stroke.
Methods: We prospectively enrolled patients with a recent symptomatic lacunar infarct who underwent MRI at baseline and 1-year post-stroke. We measured baseline NAWM microstructural integrity as diffusion tensor imaging fractional anisotropy (FA) and mean diffusivity (MD). We identified ‘cap/track’ present at 1-year on FLAIR, classified as none; ’cap’ alone; ‘track’ alone; both ‘cap’ and ‘track’. We performed multinominal logistic regression to assess the association between baseline NAWM FA/MD and 1-year ‘cap/track’ presence, adjusted for demographics, vascular risk factors, and infarct size.
Results: We included 172 patients (mean age 64, SD 11). Eighty-five (49%) patients developed any ‘cap/track’ (17 ‘cap’ alone, 31 ‘track’ alone, 37 both). Baseline NAWM-MD (but not FA) differed by ‘cap/track’ category (median 0.76 [0.74-0.78] for none, 0.77 [0.76-0.79] for ‘cap’ or ‘track’ alone, 0.78 [0.76-0.80] for both, p=0.023). Higher NAWM-MD was associated with the formation of both ‘cap’ and ‘track’ (OR=1.90, 95%CI 1.18-3.05, p=0.008).
Conclusions: Elevated baseline NAWM-MD increases the risk of ‘cap/track’ formation adjacent to index lacunar infarcts at one year. Poor NAWM microstructural integrity may predispose to secondary white matter damage and hence worse clinical outcome after lacunar stroke.
Disclosures of Interest: No
Abstract N°: 2762
CEREBRAL SMALL VESSEL DISEASE IN PATIENTS WITH SYSTEMIC LUPUS ERYTHEMATOSUS
Guilherme Silva1, Carolina Rimkus1, Germana Titoneli1, Emily Yuki1, Raymundo de Azevedo Neto2, Gisela Tinone1, Rosa Pereira2, Adriana Conforto*1
1Hospital das Clínicas, Brazil,2University of São Paulo, Brazil
On behalf of:
Background and aims: Cerebral small vessel disease (cSVD) is a candidate biomarker of increased stroke risk in patients with systemic lupus erythematosus (SLE). We assessed the presence and subtypes of cSVD in patients with SLE with and without ischemic stroke.
Methods: Retrospective, case-control study of patients in a tertiary SLE clinic, who performed brain MRI as part of the clinical routine, with and without a history of ischemic stroke (IS+ and IS-) from 2010 to 2021. Two neuroradiologists independently assessed cSVD. A cSVD score ranging from 0 to 4 was calculated. The data were analyzed with Mann-Whitney or Fisher’s exact tests.
Results: One hundred and six participants were included: 53 IS+ and 53 IS-. The median age was 41 years and 98/106 (92%) were women. IS+ patients had a higher median score of the cSVD score (1 (0,1) versus 0 (0,0), p < 0.001). Higher scores were associated with a progressively greater likelihood of being in the IS+ group (0: 36%, 1: 65%, 2: 90%, 3: 100%, and 4: 100%). Microbleeds (IS+, 34%; IS-, 11%), lacunes of presumed vascular origin (IS+, 28%; IS-, 4%) and white matter hyperintensities of presumed vascular origin (IS+, 79%; IS-, 32%) were more common in IS+ patients (p < 0.05).
Conclusions: cSVD was more frequent in patients with SLE, IS+ than in those IS-. Prospective studies to validate prediction of stroke risk in patients with SLE should consider including cSVD in their models.
Disclosures of Interest: No
Abstract N°: 2825
SEX-SPECIFIC ASSOCIATIONS IN GUT MICROBIOTA DYSBIOSIS AND CEREBRAL SMALL VESSEL DISEASE IN MIDDLE-AGED CHINESE: A METAGENOMIC SEQUENCING ANALYSIS
Mandy Yuen-Man Chan*1, Chelsea C.W. Lo1, Gordon Qian2, Yick Hin Chow1, Yiu Hei Tse1, Crystal P.I. Lee1, Tin Wai Hung1, Marco Choi1, Preeti Dinesh Virwani1, Kui-Kai Lau1
1Department of Medicine, School of Clinical Medicine, LKS Faculty of Medicine, The University of Hong Kong, Pokfulam, Hong Kong,2School of Biomedical Sciences, LKS Faculty of Medicine, The University of Hong Kong, Pokfulam, Hong Kong
On behalf of: Hani EL-NEZAMI, Kay Cheong TEO, Joshua Wing Kei HO, HKU Stroke Team
Background and aims: Gut microbiota (GM) dysbiosis has been implicated in the pathogenesis of cerebral small vessel disease (CSVD). However, previous studies were limited by use of 16S rRNA gene sequencing, did not stratify by sex, nor adjusted for 24-hour blood pressure (BP). We applied whole-genome shotgun metagenomics to investigate sex-specific associations between GM dysbiosis (at species level) and white matter hyperintensity (WMH) burden.
Methods: In 188 (51% males, mean age 54±6years, 38% with hypertension) Chinese without symptomatic cerebrovascular/neurodegenerative diseases, we sequenced their stool samples with shotgun metagenomics and performed brain MRI to evaluate their WMH volume. Sex-stratified associations of GM species abundances with WMH volume were studied in linear regression models adjusted for age, smoking, education, body-mass index, and 24-hour BP.
Results: Although Firmicutes/Bacteroidetes ratio was positively associated with WMH volume in females only, the species abundance of Alistipes shahii, Ruminococcus lactaris, Firmicutes bacterium, Bacteroides salyersiae, Bacteroides coprophilus and Bacteroides cellusilyticus were significantly associated with an increased WMH volume in males (all p<0.01) but not females. Apart from a negative association between Bacteroides coprophilus abundance with WMH volume, no bacterial species were associated with WMH volume in females. Stool proprionic acid was strongly associated with WMH volume in males but not females.
Conclusions: Independent of age and 24-hour BP, GM dysregulation appears to be more strongly associated with WMH burden in males, which may be mediated through short-chain fatty acids. Gut microbiota dysbiosis may be a novel risk factor which may account for the observed sex differences in CSVD.
Disclosures of Interest: No
Abstract N°: 3065
SPATIAL PREDILECTION OF CEREBRAL SMALL VESSEL DISEASE WITHIN BORDER ZONES REGIONS OF THE BRAIN
Davy Vanderweyen*1, Samantha Coté2, Julia Huck1,3, Karim Fathy4, Sarah Remahi5, François Rheault3, Ann-Marie Beaudoin6, Kevin Whittingstall1
1Centre Hospitalier Universitaire de Sherbrooke, Département de Radiologie Diagnostique, Sherbrooke, Canada,2Centre Hospitalier Universitaire de Sherbrooke, Département de Pédiatrie, Sherbrooke, Canada,3Université de Sherbrooke, Département d’informatique, Sherbrooke, Canada,4Université de Sherbrooke, Département de médecine nucléaire et radiobiologie, Sherbrooke, Canada,5Université de Sherbrooke, Faculté des sciences, Sherbrooke, Canada,6Centre Hospitalier Universitaire de Sherbrooke, Département de Neurologie, Sherbrooke, Canada
On behalf of:
Background and aims: Border zone regions (BZRs) in the brain are parenchymal areas located at the farthest point between vascular territories, where the brain is more susceptible to ischemia. Cerebral small vessel disease, often secondary to chronic ischemic insults, frequently occurs in regions in proximity to BRZs. However, the topological link between them has not been quantitatively assessed.
Methods: The arterial tree was segmented into groups from the anterior (ACA), middle (MCA), and posterior cerebral arteries (PCA) using a semi-automatic approach on time-of-flight magnetic resonance angiography performed on 340 stroke-free participants from 2 different centers. Distances between each voxel on T2-FLAIR sequences and its nearest arterial group branch were computed. Vascular territories were defined as voxels closest to a particular artery, and BZRs as zones equidistant from two arteries but closer than to the third artery. The intersection between white matter hyperintensities (WMH) and BZRs was computed and compared to WMH outside border zones.
Results: Vascular territories conformed to known atlases but showed intersubject variability. On average, MCA territory accounted for 46% of brain parenchyma, ACA 31%. and PCA 23%. 80% of WMH accumulated within BZRs, compared to randomly generated brain masks of the same volume.
Conclusions: Vascular territories and BZRs were highly spatially reproductible, albeit with some variation among participants. WMH showed a predilection for occurrence in BZRs. This mapping of cerebral small vessel disease within BZRs provides valuable insights into the disease’s localization and may guide future research on its mechanisms and therapeutic interventions.
Disclosures of Interest: No
Abstract N°: 3272
IDEALIZED AND PATIENT-SPECIFIC COMPUTATIONAL ANALYSIS OF BIOFLUID MECHANICS OF CEREBROVASCULAR DISEASE AND STROKE
AMAR SHRIVASTAVA*1, Ashish Suri2, Sitikantha Roy1
1Indian Institute Of Technology Delhi (IIT Delhi), Applied Mechanics, New Delhi, India,2All India Institute Of Medical Sciences, Neurosurgery, New Delhi, India
On behalf of:
Background and aims: Cerebrovascular diseases affect the blood vessels in the brain leading to a decrease in oxygen and nutrient supply. These diseases include ischemic strokes, hemorrhagic strokes, and transient ischemic attacks (TIAs). Stroke is the primary cause of long-term disability and the third most common underlying cause of death in the United States. Moyamoya is a type of cerebrovascular disease, a Japanese word meaning something hazy, like a puff of cigarette smoke floating in the air. It describes an unusual angiographic image that reveals blood vessels located at the base of the brain, collaterals formation and blockage of the internal carotid artery. The goal of this study broadly is to perform steady-state and pulsatile bio-fluid dynamic simulations of Magnetic angiography based Moyamoya patient-specific geometries to predict stroke and TIAs.
Methods: Governing equations for cerebrovascular disease and stroke’s computational modelling are the Continuity and Navier-Stokes equations. Blood is modelled as a Non-Newtonian fluid using the Carreau-Yasuda model.
Results:In silico biomechanical CFD simulation showed that Superficial Temporal Artery-Middle Cerebral Artery bypass surgery has improved the wall shear stress (WSS) of the artery, MCA distal branches have lower total pressure, the bypass shows higher total pressure, making it easier for blood to enter these veins. Low WSS zones are more prone to developing atherosclerosis, causing ischemic stroke and transient ischemic attack (TIA).
Conclusions: Patient-specific 3D bio-fluid simulations of Moyamoya (cerebrovascular disease) can be helpful for diagnosis and prognosis of disease, pre-surgical planning, clinical decision-making, and efficient stroke management.
Disclosures of Interest: No
Abstract N°: 3294
CEREBRAL ATROPHY OVER 5 YEARS IN TRANSIENT ISCHEMIC ATTACK COMPARED TO CONTROLS AND RELATIONSHIPS TO BASELINE CEREBRAL SMALL VESSEL DISEASE
Ryan Muir1, Britney Denroche*1, George S. Tadros1, Dhanae Mogan1, Aravind Ganesh1, Philip Barber1
1University of Calgary, Calgary, Canada
On behalf of:
Background and aims: In this study we evaluated potential differences in cerebral atrophy measures over 5 years of follow up and relationships to baseline cerebral small vessel disease (CSVD).
Methods: TIA patients (n=57) and controls (n=50) underwent serial MRI at baseline and 5-years. CSVD burden was measured using validated rating scales for microbleeds (CMBs), lacunes, enlarged perivascular spaces (PVS), and white matter hyperintensities (WMHs). Percent brain volume change (PBVC) and percent ventricular volume change (PVVC) over 5 years were computed using FSL. Multiple linear regression models evaluated PBVC and PVVC as outcome measures and TIA status and CSVD as the main predictors while adjusting for age, sex, and vascular risk factors.
Results: TIA patients were older (65.86 (sd:9.16)) than controls (61.26 (8.26)). Those with TIA had a mean PBVC of -4.25% (1.88) vs -3.21% (1.87) in controls (not significant after adjustment for age). Increasing age (β=-0.07, p<0.0001) and the presence of hypertension (β=-0.88, p=0.021), but neither TIA status, sex, dyslipidemia nor CSVD predicted PBVC. Additionally, PVVC was higher in TIA (28.04% (13.07)) vs controls (24.35% (17.74)) (not significant). This difference was not related to TIA status, hypertension, dyslipidemia or CSVD, but was related to male sex (β=-6.98, p=0.01) and age (β=0.61, p<0.0001. WMHs, lacunes, CMBs and PVSs did not predict PBVC or PVVC in either TIA or controls.
Conclusions: Neither CSVD nor TIA status predicted differences in PBVC or PVVC. Brain atrophy may be more related to aging and vascular risk factors, while TIA and CSVD may exert effects on brain health independent of atrophy.
Disclosures of Interest: No
E-Poster - Technology Innovations
Abstract N°: 56
USE OF ARTIFICIAL INTELLIGENCE IN CARDIAC SOURCE IDENTIFICATION AMONG ESUS PATIENTS: META-ANALYSIS
Background and aims: Stroke is the second most common cause of mortality worldwide with about 41.1 per 100,000 related annual deaths (1).
ESUS is a subtype of ischemic stroke represent 17% of all strokes with 4.5% recurrence rate. ESUS harbors a heterogeneous group of etiologies with cardio-embolic sources being the most important to detect due to higher risk or recurrence (2).
AI (Artificial intelligence) is a computer based science that has recently developed. AI has been studied for etiological determination of stroke patients (3).
In our paper, we did a meta-analysis and review about the potential use of AI to detect cardio-embolic sources in ESUS patients.
Methods: Performing search using the keywords including ESUS, cryptogenic, AI, machine learning, among databases including Pubmed, Scopus, Web of science, Embase and Cochrane library.
Results: After screening, 10 articles were included, total number of included patients was 2542, 52% males (N=1094) and 48% females, mean age 65.4+/- 14.7; input data included Echo, clinical risk factors and labs as most common data type (62%, N=1576).
Machine learning classification mode was the most common AI method used (59.36%), followed by deep learning (17.23%) and neuronal network (13.1%).
Most studies used AI for occult cardiac etiology including AF (58.18%, N=1479) with compared efficacy to Holter ECG (51.37 %) and less commonly to ambulatory ECG (20.02%) with a mean C- index of 0.87 and mean odds ratio of 2.903+/-0.495
Conclusions: Our systematic review documents the accuracy and feasibility of using AI and machine learning in detection of cardio-embolic subgroup of ESUS patients
Disclosures of Interest: No
Abstract N°: 1470
INITIAL EXPERIENCES IN DESIGNING A STROKE-SPECIFIC VIRTUAL ASSISTANT
1University of Glasgow, Glasgow, United Kingdom,2Aalborg University, Aalborg, Denmark
On behalf of: RES-Q+ consortium
Background and aims: RES-Q+ project partners have been developing a Virtual Assistant (VA) for stroke survivors, their families, and caregivers. The VA will provide users with quality assured information in response to common questions regarding stroke. The VA also aims to allow users to check in on their mental wellbeing, functional recovery and rehabilitation progress.
Methods: Interviews and focus groups were conducted with stroke survivors and their families and caregivers in Scotland, Northern Ireland, Denmark, and the Czech Republic. Participants interacted with the VA and answered Patient Recorded Outcome Measures (PROMs) on the VA interface and in a human interview. The corpus of 35 sessions with 40 participants was transcribed verbatim by the partner teams. Thematic analysis was performed to identify barriers to using the VA and expectations for its functions.
Results: Our quantitative results from 30 stroke survivors in 15 interviews explore the impact of PROM question delivery on response and preference for the checking-in feature of the VA. Barriers to use included lack of familiarity and comfort with technology, and scepticism toward information online. Perceptions of the VA as a companion emerged as participants used human terms to describe its role as an additional, trustworthy and personable companion.
Conclusions: Our empirical evidence highlights the importance of additional prompts to help stroke survivors understand questions in PROMs. This would facilitate checking in with a conversational VA that meets users’ expectations without sacrificing accuracy. Our findings highlight the need for an additional, readily available, and trustworthy source of support post discharge.
Disclosures of Interest: No
Abstract N°: 1585
COLLABORATIVE DESIGN OF A PATIENT PORTAL WITH STROKE SURVIVORS AND CARERS
Mahnoor Mustafa*1, Sophie Rowland-Coomber2, Iain Marshall2,3, David Wyatt2
1GKT School of Medical Education, King’s College London,2King’s College London, Department of Population Health Sciences,3NIHR Applied Research Collaboration (ARC) South London at King’s College Hospital NHS Foundation Trust
On behalf of:
Background and aims: Electronic health portals have emerged as a pivotal tool enabling patients to actively participate in their healthcare and help manage their chronic conditions. By collaborating with stroke survivors and their carers we have developed a patient portal specifically catering for this group dealing with long-term post-stroke effects.
The objective of this study was to investigate stroke survivors’ perspectives to fine-tune the design of our patient portal to better cater to their healthcare needs.
Methods: A literature review identified barriers hindering the regular use of patient portals, such as language proficiency, race, advanced age, and socioeconomic status. Recruitment efforts involved reaching out to stroke charities to ensure a diverse and representative participant cohort. Semi-structured interviews were conducted with participants who were presented with a preliminary patient portal design. Thematic analysis of interview transcripts was completed using NVivo software. Analysis is ongoing at the time of this report, based on a set of seven interviews.
Results: Positive responses included satisfaction with healthcare teams’ access to information and user-friendly features like simple language and visual aids. Negative feedback focused on limited interest in certain portal aspects, such as recording health data or medication reminders. Suggested improvements revolved around staying updated on stroke research and enhancing mental well-being tracking features.
Conclusions: The study’s preliminary findings emphasize the specific support needs of stroke survivors, highlighting the importance of user-friendly portal design, comprehensive health information, and stroke-related education. The feedback obtained will be used to refine and customize the patient portal.
Disclosures of Interest: No
Abstract N°: 1938
A WEARABLE PNEUMATIC-PIEZOELECTRIC SYSTEM FOR QUANTITATIVE ASSESSMENT OF MUSCLE SPASTICITY IN STROKE
KENG KONG*1, Dace Gao2, Lei Tay1, Matthew Tan3, See Lee3, Jian Chen3
1Tan Tock Seng Hospital,2Nanyang Technological University, School of Materials Science and Engineering,3Nanyang Technological Institute
On behalf of:
Background and aims: There is currently no good objective tool to measure spasticity. Here we present a wearable pneumatic-piezoelectric system (WPPS) to quantify spasticity in stroke patients.
Methods: The WPPS comprises of 2 components: a) a wearable cuff that incorporates an elastomer-based pneumatic actuator and a flexible piezoelectric sensor to enable in vivo and rapid measurement of muscular elasticity in muscles, and b) a pneumatic pump which pumps air to inflate the actuator. During testing, the actuator compresses the muscle beneath which deforms the piezoelectric sensor to register a voltage spike whose peak value is correlated to the muscle’s elastic modulus. The device was tested in the biceps muscle of 8 healthy subjects and 15 stroke survivors with varying degrees of elbow flexor spasticity.
Results: During the test, the wearable cuff was wrapped around the biceps muscle. For healthy subjects, WPPS tests were performed with their arms posed naturally at ~90° flexion and ~180° extension, respectively. WPPS waveforms recorded from flexed and extended joint positions exhibit minimal discrepancy. In the 15 stroke patients, static testing with the elbow fully extended showed reduced waveform voltage compared to healthy subjects. In dynamic testing where the biceps was quickly stretched from flexion to extension, a voltage dip and prolonged coupling time was seen and this correlated positively with the severity of spasticity.
Conclusions: In summary, WPSS system offers a novel wearable solution that measures spasticity, and is potentially applicable to other quantitative assessments of muscular biomechanics with ease and reliability.
Disclosures of Interest: No
Abstract N°: 2107
PREDICTING BRAIN AGE IN CADASIL PATIENTS USING AI
Katerina Benesova*1, Ales Tomek1, David Kala2, Jakub Otahal2, Anna Olserova1, Silvia Kmetonyova1, Jaroslava Paulasova Schwabova1, Petr Jansky1, Tereza Sramkova1, Hana Magerova1
1Motol University Hospital and Second Faculty of Medicine, Department of Neurology, Prague, Czech Republic,2Department of Pathophysiology, Second Faculty of Medicine, Charles University, Czech Republic
On behalf of:
Background and aims: CADASIL (Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy) is the most common progressive hereditary cerebral microangiopathy. Brain age reflects the estimated age based on quantitative brain MRI analysis with deep learning and AI techniques. The aim of the project was to use brainageR software to predict brain age in CADASIL patients.
Methods: Patients with genetically confirmed CADASIL were examined using 3 Tesla MRI (Siemens Vida Magnetom). The T1-weighted scans were analysed in a brainageR 2.1. Age gap was calculated (difference between predicted and actual chronological age). Pearson’s correlation was used to determine the strength and direction of a linear relationship between predicted and chronological age. Simple linear regression was used to determine how much of the variation in the expected age is explained by the chronological age.
Results: 24 CADASIL patients (14 women, mean age 48.9, SD 13.5) were included. Mean age gap in CADASIL was 3.1 years. A strong positive correlation between predicted and chronological age in CADASIL patients was established, r=0.71. The correlation was stronger in patients under 50 (r=0.64, n=13) than in older ones (r=0.48, n=11). The AI model made a statistically significant prediction of the chronological age and it accounted for 50.2% of its explained variability.
Conclusions: The software performance was significantly worse in CADASIL patients (r=0.71) than in healthy individuals (r=0.97). A positive brain age gap suggests accelerated aging. With targeted training of the model, there is a potential application in the automated assessment of sequential MRI.
Funding Project was supported by grants: nr.NU21-02-00289, nr.LX22NPO5107
Disclosures of Interest: No
Abstract N°: 2336
IMPACT ON THE QUALITY-OF-LIFE PERCEPTION OF USING 3D PRINTING IN THE INFORMATION OF PATIENTS WITH INCIDENTAL CEREBRAL ANEURYSMS
Laura González Martín1, David Fernández Escudero1, Elisa Alonso López1, Laura Casado Fernández1, Carlos Hervás1, Gerardo Ruiz Ares1, Ricardo Jaime Rigual1, José Tadeo Borjas Gómez1, Pedro Navia1, Blanca Fuentes1
1La Paz University Hospital, Madrid, Spain
On behalf of:
Background and aims: The higher demand and accessibility of MRI studies has led to an increase in the diagnosis of incidental cerebral aneurysms in healthy people, which might cause stress and anxiety with a negative impact on the patient’s quality of life. We aim to analyse the results of global health tests in patients diagnosed of cerebral aneurysm with the support of 3D printed models and neuroimaging and to assess the degree of understanding.
Methods: prospective cohort study including patients with incidental intracranial aneurysms. We analyse the differences in patient satisfaction through a Likert scale and the PROMIS-10 questionnaire depending on the type of information received.
Results: we included 51 patients (70.8% women,). The diagnostic tests used for the aneurysm diagnosis were CT scan 17.8% and MRI 46.7%, mostly requested because of stroke (26.7%) headache (20%) and vision impairment (13.3%). To explain the diagnosis, there were used neuroimaging (24.4%), drawings (33.3%), verbal explanation (24.4%), or 3D printed model (8.9%). Up to 66.7% reported information was adequate, rated their health as good and were satisfied with the information method received. We found a greater level of satisfaction in those patients informed with neuroimaging or 3D models (3.2/4 and 3.0/4) compared with those informed verbally (2.0/4 and 2.43/4) with fewer doubts and anxiety regarding the diagnosis (1.2-1.33/4 vs 1.42-1.5/4).
Conclusions: Patients who were informed of an incidental cerebral aneurysm with neuroimaging and 3D printed models were more satisfied with the information received, reporting fewer doubts and anxiety.
Disclosures of Interest: No
Abstract N°: 2665
ASSESSING SAFETY OF THROMBECTOMY DEVICE AND TECHNIQUE USING A NOVEL IN-VITRO DEFLECTION MODEL
1HonorHealth Research and Innovation Institute,2Barrow Neurological Institute, Phoenix, United States
On behalf of:
Background and aims: Endovascular thrombectomy (EVT) devices and techniques are evolving rapidly to improve safety-efficacy of EVT-mediated recanalization of large vessel occlusion strokes, and to access medium and distal vessel occlusions. We aim to assess the safety of thrombectomy using an aspiration catheter only versus a combined technique (aspiration catheter stent-retriever) in an in-vitro stroke model.
Methods: We utilized Q™ Aspiration Catheter (MIVI-Neuroscience)and Solitaire™ StentRetriever (Medtronic) in an in-vitro stroke model (Mentice). The thrombectomy devices were deployed in M2-segment of middle cerebral artery using an 0.014-inch guide wire and 0.021-inch microcatheter. After unsheathing in the M2-segment, in the presence of blood clot, the microcatheter was withdrawn back into the petrous internal carotid artery, and the system was withdrawn as a rate of 5mm/second. Maximum deflection of the M1-M2 and MCA-ACA junctions (from resting position to largest displacement) was measured in 3-axes using a specialized camera set-up.
Results: Maximum 3-dimensional deflection was lower with Q5 catheter alone compared to Q5 catheter and Solitaire stent-retriever mediated thrombectomy at the M1-M2 (1mm vs 5.1mm) and MCA-ACA (1.4mm vs 5.4mm) junctions during retrieval of the devices. It was comparable during delivery of the devices (1mm M1-M2 and 1.4mm MCA-ACA)(Table1). Figure1 demonstrates the degree of deflection from resting position at the M1-M2 junction during retrieval of the devices.
Conclusions: Delivery of thrombectomy devices does not lead to a large vessel deflection. Combined technique leads to a five-fold increase in vessel deflection during retrieval of thrombectomy devices when compared to only aspiration catheter mediated thrombectomy simulation.
Disclosures of Interest: No
Abstract N°: 2827
VIRTUAL REALITY TO ACCELERATE THE ACTIVATION OF THE ICTUS CODE. VIRTUAL IMMERSION AS AN EDUCATIONAL TOOL IN THE IDENTIFICATION OF SIGNS OF A STROKE
Aida Lagüela*1, Jon Martín1, Ventura Anciones1, Leire Campos2, Jon Eneko Idoyaga2, Alejandra Gómez1,2, Idoia Revilla3, Iratxe Ugarriza1,2, Alain Luna1,2, María del Mar Freijo1,2
1Cruces, Neurology, Baracaldo, Vizcaya, Spain,2Cruces, Biocruces Bizkaia Health Research Institute, Baracaldo, Spain,3Osakidetza Emergency Unit, Baracaldo, Spain
On behalf of:
Background and aims: The time elapsed between the onset of stroke symptoms and their treatment is a determining factor in functional prognosis, making it essential for the general population to be able to identify the initial symptoms. We seek to evaluate the usefulness of a virtual reality (VR) system in recognising the symptoms of a stroke and knowing how to act.
Methods: The testing product is a video played on VR goggles. Patients over 50 years of age who have suffered an ischemic stroke and a control group are included and clinical and demographic data are collected. They are administered an Objective Structured Clinical Examination (OSCE) and a stroke knowledge test (SIT) before and after viewing the video.
Results: 52 subjects were included: 32 patients (21 males) and 22 controls (8 males). Patients: mean age (SD): 64 (9). 40% active smokers, 54.17% hypertensive, 25% diabetic, 50% dyslipidaemic and 4.17% had atrial fibrillation. Both case and control groups improved test scores (p <0,05). No episodes of cerebral ischemia were observed in any of the subjects.
Conclusions: The product was well-tolerated and all patients learned the information presented; this suggests that it could be used as an educational tool in people in this age group. Extending the population, following it up with a subsequent reassessment to confirm long-term learning. Also comparing it with traditional techniques in the population with vascular risk factors could corroborate its usefulness.
Disclosures of Interest: No
E-Poster - Thrombolysis and Neurointervention
Abstract N°: 60
CAROTID ARTERY STENTING OUTCOMES BY NEUROINTERVENTIONAL SURGEONS (CASONI)
Mohamad Ezzeldin*1, Ameer Hassan2, Ali Kerro3, Osman Mir4, Zuhair Ali1, Tunmi Anwoju1, Rime Ezzeldin5, Osama Zaidat6, Farhan Siddiq7
1HCA Houston Healthcare Kingwood, Houston, United States,2Valley Baptist Medical Center: Brownsville, Brownsville, United States,3HCA Houston Healthcare Conroe, Conroe, United States,4Texas Stroke Institute - Plano, Plano, United States,5Jordan University of Science & Technology (JUST), الرمثا, Jordan,6Mercy St. Vincent Medical Center, Toledo, United States,7University Hospital, Columbia, United States
On behalf of: 1. Dr. Maria Martucci: martucm2@ccf.org Cleveland Clinic, Cleveland, Ohio 2. Dr. M. Shazam Hussain hussais4@ccf.org Cleveland Clinic, Cleveland, Ohio 3. Dr. Bains Navpreet bainsn@umsystem.edu University Hospital Missouri, Columbia, Missouri 4. Dr. Faheem Sheriff fsheriff@ttuhsc.edu Texas Tech University Health Sciences Center, El Paso, Texas 5. Dr. Varun Chabal vrnchbl@gmail.com St. Vincent Medical Center, Toledo, Ohio 6. Dr. Peter Kan ptkan@utmb.edu University of Texas Medical Branch (UTMB), Galveston, Texas 7. Dr. Chizoba Ezepue Chizoba.Ezepue@ssmhealth.com SSM Health Saint Louis University Hospital, St. Louis, Missouri 8. Dr. Nazli Janjua nazli.janjua@apcsi.org Asia Pacific Comprehensive Stroke Network; Pomona Valley Hospital Medical Center 9. Dr. Nazli Janjua nazli.janjua@apcsi.org Asia Pacific Comprehensive Stroke Network; Pomona Valley Hospital Medical Center 10. Dr. Kaiz S. Asif kaiz.asif@gmail.com Ascension Health and University of Illinois, Chicago, Illinois 11. Dr. Ramesh Grandhi ramesh.grandhi@hsc.utah.edu University of Utah, Salt lake city, Utah 12. Dr. Ali Alaraj alaraj@uic.edu University of Illinois Chicago (UIC), Chicago, Illinois 13. Dr. Muhammad Niazi mniazi@wellspan.org WellSpan Health, York, Pennsylvania. 14. Dr. Osama Mansour yassinossama@yahoo.com Alexandria University, Alexandria, Egypt 15. Dr. Michael Chen michael_chen@rush.edu Rush University Medical Center, Chicago, Illinois 16. Dr. Saif Bushnaq bushnaq10@gmail.com Texas Tech University, Lubbock, Texas 17. Dr. Omar Tanweer omar.tanweer@bcm.edu Baylor St. Lukes Medical Center, Houston, Texas 18. Dr. Mohammad Ammar Abdulrazzak abdulrm@ccf.org Cleveland Clinic, Cleveland, Ohio 19. Dr. Hamzah Saei hamzah.saei@hcahealthcare.com Valley Baptist Medical Center, Brownsville, Texas 20. Dr. Gustavo Rodriguez gustavo.j.rodriguez@ttuhsc.edu Texas Tech University Health Sciences Center, El Paso, Texas 21. Dr. Mohammand AlMajali malmajali@mercy.com St. Vincent Medical Center, Toledo, Ohio 22. Dr. Gautam Edhayan gaedhaya@utmb.edu University of Texas Medical Branch (UTMB), Galveston, Texas 23. Dr. Amer Alshekhlee amer.alshekhlee@ssmhealth.com SSM Health, DePaul Hospital 24. Dr. Christopher Hadjialiakbari christopher.hadjialiakbari@hcahealthcare.com HCA Houston Healthcare Kingwood 25. Dr. Musaab Froukh Musaab.Froukh@vituity.com Ascension Health, Chicago, Illinois 26. Dr. Walid Salah walid.salah@hsc.utah.edu University of Utah, Salt lake city, Utah 27. Dr. Adrusht Madapoosi amadap2@uic.edu University of Illinois Chicago (UIC), Chicago, Illinois 28. Dr. Yazan Radiaideh yazangrad@gmail.com Rush University Medical Center, Chicago, Illinois 29. Dr. Darko Quispe darko.quispe@ttuhsc.edu Texas Tech University, Lubbock, Texas 30. Dr. Oz Haim oz.haim@bcm.edu Baylor St. Lukes Medical Center, Houston, Texas 31. Dr. Noel Garza noelgarza@live.com Valley Baptist Medical Center, Brownsville, Texas 32. Dr. Alberto Maud alberto.maud@ttuhsc.edu Texas Tech University Health Sciences Center, El Paso, Texas 33. Dr. Morgan Rolon-Newton rolonnew@med.umich.edu Texas Tech University Health Sciences Center, El Paso, Texas 34. Dr. Benan Barakat BBarakat@mercy.com St. Vincent Medical Center, Toledo, Ohio 35. Dr. Tejas Gowda Tgowda@mercy.com St. Vincent Medical Center, Toledo, Ohio 36. Dr. Muhammad Monk muhammad.monk@hcahealthcare.com HCA Houston Healthcare Kingwood, Kingwood, Texas
Background and aims: Report the complication rate in Carotid Artery stenting (CAS) performed exclusively by fellowship-trained neurointerventionalists (NIR).
Methods: Retrospective data was collected regarding symptomatic and asymptomatic carotid stenosis eligible for CAS at multiple comprehensive stroke systems (CSCs) across the USA and one international center. We excluded CAS for acute tandem occlusions and conditions other than atherosclerosis. The primary endpoints included a composite of complications including procedure-related mortality, myocardial infarction (MI) and symptomatic stroke. We also looked at rates of secondary complications. Chi-squared tests were performed for categorical variables and Welch’s T-Test was used for continuous variables on complications and whether or not patients were symptomatic prior to the procedure. Cutoffs in continuous variables were estimated using a grid search optimization.
Results: 1445 CAS performed by 38 NIR physicians were included. 71.8% were performed by neurologists, 19.3% by neurosurgeons and 8.9% by neuroradiologists. Median age of patients was 69 years. Majority were symptomatic (93.0%), white (70.4%), men (65.8%). CAS technical success was 99.52%, and transfemoral access was the most common method (73.96%). Primary complication rate was only 1.8%. Symptomatic ischemic stroke, symptomatic intracranial hemorrhage, procedure-related mortality and MI occurred in 8 (0.55%), 4 (0.28%), 5 (0.35%) and 1 patient (0.07%) respectively. There was a statistically significant increase of complications in women (p=0.012), in patients older than 73 years (p=0.002) and in patients with aortic arch type 3 (p=0.0133).
Conclusions: CAS performed by NIR fellowship trained physicians in CSC’s demonstrate low complication rate which might be explained by physician training and effectuation of CAS in a CSC.
Disclosures of Interest: Yes Dr. Mohamad Ezzeldin: Speaker for Viz AI. Stocks at Galaxy therapeutics Dr. Ameer Hassan: 1.Consultant/Speaker: Medtronic, Microvention, Stryker, Penumbra, Cerenovus, Genentech, GE Healthcare, Scientia, Balt, Viz.ai, Insera therapeutics, Proximie, NeuroVasc, NovaSignal, Vesalio, Rapid Medical, Imperative Care, Galaxy Therapeutics, Route 92 and Perfuze. 2.Principal Investigator: COMPLETE study – Penumbra, LVO SYNCHRONISE – Viz.ai, Millipede Stroke Trial - Perfuze, RESCUE - ICAD - Medtronic. 3.Steering Committee/Publication committee member: SELECT, DAWN, SELECT 2, EXPEDITE II, EMBOLISE, CLEAR, ENVI, DELPHI, DISTALS 4.DSMB - COMAND trial Dr. Peter Kan: Stryker Consultant Dr. Ali Alaraj: Consultant for Cerenovus Dr. Omar Tanweer: Consulting Agreements: Viz.AI, Inc., Penumbra, Inc, Balt, Inc, Stryker Inc, Imperative Inc., Q’Apel Inc. Proctor: Microvention Inc, Medtronic Inc. Dr. Farhan Siddiq: Consultant Microvention, Grants from NIH, CNS, SNIS, non related to this project.
Abstract N°: 110
IMPACT OF DIRECT ORAL ANTICOAGULANT LEVELS ON OUTCOMES AFTER ENDOVASCULAR THROMBECTOMY
1National Taiwan University Hospital, Pharmacy, Taipei,2National Taiwan University, School of Pharmacy,3National Taiwan University Hospital, Neurology, Taipei,4National Taiwan University Hospital, Medical Imaging, Taipei,5National Taiwan University, School of Pharmacy, Taipei
On behalf of:
Background and aims: To access the association between emergent direct oral anticoagulant (DOAC) levels and functional independence after endovascular thrombectomy (EVT).
Methods: Participants with atrial fibrillation, pre-morbid modified Rankin Scale (mRS) ⩽ 3, and received EVT for acute stroke were enrolled. In pre-stroke DOAC users, drug level upon hospital arrival was measured. The primary outcome was the functional independence at 3 months (mRS score 0 to 2 or return to pre-morbid status for patients with pre-morbid mRS of 3).
Results: A total of 250 patients, included 42.0% of antithrombotic agent non-users (AT non-users), 34.0% oral anticoagulant therapy users (OAC), and 24.0% antiplatelet therapy users were enrolled. Primary outcomes did not differ between three groups. Among OAC users, 78.8% were using DOAC. Out of the 59 DOAC users with measured drug levels, 62.7% had low levels (defined as <50 ng/mL). Low-level patients were less likely to achieve functional independence compared to high-level patients: 29.7% versus 63.6%, respectively (adjusted OR [aOR] 0.26 [0.08, 0.87]). Compared to AT non-users, OAC users with therapeutic anticoagulation were more likely to achieve functional independence (aOR 2.83 [1.18, 6.78]), while those with inadequate anticoagulation were not (aOR 0.97 [0.43, 2.17]). Symptomatic ICH occurred in 3 DOAC users with low level group (8.1%), 1 DOAC user with high level group (4.5%) and 4 AT non-users (3.8%).
Conclusions: Among AF patients under DOAC therapy, those with low DOAC levels were less likely to achieve functional independence. Furthermore, OAC users with therapeutic anticoagulation displayed better functional outcome than AT non-users.
Disclosures of Interest: No
Abstract N°: 530
ENDOVASCULAR TREATMENT OF SYMPTOMATIC BASILAR ARTERY STENOSIS
Taemin Kim*1, Sang Hyun Suh1
1Gangnam Severance Hospital, Yonsei university, neurology, Seoul
On behalf of:
Background and aims: While symptomatic basilar artery (BA) stenosis is associated with a higher risk of recurrent stroke or death, there is no consensus on the management of these patients who are refractory to antiplatelet therapy. This study retrospectively assesses the outcomes of endovascular treatment (EVT) for symptomatic BA stenosis.
Methods: We conducted a retrospective review of patients with symptomatic BA stenosis who underwent EVT, including angioplasty or stenting, from 2006 to 2018. A total of 15 patients, who experienced transient ischemic attacks or strokes despite dual antiplatelet therapy, were included. EVT was performed under local anesthesia after pretreatment with antiplatelet medications. Angiographic follow-up was performed at 12 and 24 months post-EVT. Clinical outcomes were evaluated using the modified Rankin Scale (mRS).
Results: EVT was successfully completed in all patients. Peri/post-procedural complications occurred in 33% of cases, including in-stent thrombosis, intracranial hemorrhage, and pontine infarction. At long-term follow-up (mean 98.5±80.5 months), 73.3% of patients achieved a favorable functional outcome (mRS⩽2) without disability or mortality. Patients with unfavorable outcomes had previous infarcts, with 2 experiencing new pontine infarctions after stenting.
Conclusions: This study suggests that EVT, including angioplasty and stenting, may offer promise as a treatment option for symptomatic BA stenosis refractory to medical therapy. However, the procedure carries a notable risk of complications, especially in patients with severe stenosis and previous infarcts. Careful patient selection, based on clinical and radiological criteria, is crucial.
Disclosures of Interest: No
Abstract N°: 553
RADIOMIC SIGNATURES ON NON-CONTRAST CT SCANS OF HYPERDENSE ARTERY SIGNS
Elena Sagues Sese*1, Ariel Vargas Sanchez1, Samantha Saenz Hinojosa1, Diego Ojeda1, Carlos Dier Melo1, Alex Hanson1, Malik Ghannam1, Edgar Samaniego1
1University of Iowa Hospitals & Clinics, Neurology, Iowa City, United States
On behalf of:
Background and aims: The presence of the hyperdense artery sign (HAS) on non-contrast CT (NCCT) in acute ischemic strokes has been correlated with improved endovascular therapy (EVT) outcomes. However, its determination traditionally relies on subjective visual evaluation. This study explores the application of radiomics as an objective quantitative method for assessing the HAS.
Methods: We analyzed patients with acute ischemic stroke that underwent EVT at our institution during 2022-23. CT angiography (CTA) served as a guide to locate the occlusion and estimate the clot location in NCCTs. To objectively define a HAS, we calculated a Hounsfield Units ratio between the affected side and the contralateral vessel, aiming for >1.15. 3D Slicer was then employed to segment and extract radiomic features (RFs) of the clot and the contralateral vessel. (Figure 1).
Results: We included 50 patients in our analysis. We observed differences between signal intensity and textural RFs of the clot and the contralateral vessel (Table 1). Furthermore, five of those texture RFs predicted first pass effect with high accuracy: Joint Average, Sum Average, High Gray Level Emphasis, High Gray Level Run Emphasis and Long Run High Gray Level Emphasis (AUC=0.680, 0.680, 0.675, 0.672 and 0.639 respectively).
Conclusions: Radiomics on NCCT may help identify HAS and predict reperfusion outcomes.
Disclosures of Interest: No
Pipeline to extract RFs from the NCCT.
Abstract N°: 655
CHARACTERISTICS, TEMPORAL TRENDS, AND OUTCOMES OF INTRAVENOUS THROMBOLYSIS IN STROKE PATIENTS AGED > 80 YEARS IN CHINA
1Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, China,2China National Clinical Research Center for Neurological Diseases, Beijing Tiantan Hospital, Capital Medical University,3China National Clinical Research Center for Neurological Diseases, Beijing Tiantan Hospital, Capital Medical University, China
On behalf of:
Background and aims: To evaluate temporal trends in alteplase use, clinical characteristics, and outcomes in acute ischemic stroke (AIS) patients over 80 years of age in China.
Methods: Data were collected from The China Stroke Center Alliance program, which is a nationwide, multicenter, prospective registry at 1751 hospitals in 31 provinces, between January 1, 2018, and December 14, 2022.The primary outcome was a modified Rankin scale score (mRS) of 0-2 at discharge, and the secondary study outcomes were an mRS score 0-1 and independent ambulation at discharge. The safety outcomes included in-hospital mortality and symptomatic intracranial hemorrhage(sICH).
Results: 30,902 patients eligible for thrombolysis were aged > 80 years; among them, 8,673 patients (median [IQR] age, 84 [82-87] years) were treated with alteplase, 52.7% of whom were female (n=4570). Patients treated with alteplase had better short-term functional outcomes, including mRS scores 0-2 (adjusted OR [aOR] 1.13, 95% CI 1.08-1.19, p<0.001), mRS scores 0-1 (aOR 1.14, 95% CI 1.09-1.20, p<0.001), and independent ambulation at discharge (aOR 1.27, 95% CI 1.19-1.39, p<0.001). Furthermore, there was no increased risk of in-hospital mortality (aOR 0.92, 95% CI 0.79-1.08, p=0.31). However, alteplase was associated with a higher risk of sICH (aOR 2.85, 95% CI 2.48-3.27, p<0.001).
Conclusions: Elderly patients receiving IVT with alteplase had better short-term functional outcomes without an increased risk of in-hospital mortality; however, elderly patients are at higher risk of developing symptomatic intracranial hemorrhage.
Disclosures of Interest: No
Abstract N°: 721
CEREBRAL COMPLIANCE IN PSEUDOTUMOR CEREBRI AND TRANSVERSE SINUS STENOSIS UNDERGOING VENOPLASTY OR CSF PUNCTURE
Lorena Souza Viana*1,2, Fabiano Moulin de Moraes2, Sandro Luiz De Andrade Matas2, Gisele Sampaio2
1Albert Einstein Israelite Hospital, Brazil,2Federal University of São Paulo, Brazil
On behalf of:
Background and aims: Pseudotumor cerebri (PTC) has a high prevalence among women, and 30% to 93% of patients have transverse sinus stenosis (TSS). In addition, venoplasty improves symptoms in up to 87% of patients. Intracranial complacency (IC) can be a surrogate marker for intracranial hypertension. The FDA approved a non-invasive Brazilian method for monitoring intracranial pressure waves, Brain4care (B4C), in 2021. We aimed to compare the IC in patients with PTC and TSS only with lumbar punctures (LP) versus venoplasty.
Methods: This is an observational and single-centered study from 2020 to 2022. Inclusion criteria: ⩾18 years with PTC; with presence of TSS. Data were reported as mean (± SD) or median (± IQR). Categorical variables were reported as percentage and compared using the X2 test or Fisher’s test. P-values were considered significant when <0.05, using SPSS.
Results: We enrolled 158 patients, among whom nine were excluded due to age: 12 without PTC, 13 without stenosis, 22 with CVT and 35 with missing data. In tables 1- 2: In the LP group (50), we found 100% female, mean age 37.6 (SD: 11.6), B4C mean TTP 0.24 (SD: 0.07) in lay-position and 0.23 (SD: 0.06) in sit-position. In the venoplasty group (17), we noticed 88.2% females, with a mean age of 45.6. (SD: 12.6), B4C mean TTP 0.24 (SD: 0.07), and 0.23 (SD: 0.06) in positions. There were no differences in IC between the two groups.
Conclusions: We demonstrated no significant difference in IC between patients with PTC associated with TSS submitted only to LP vs venoplasty.
Disclosures of Interest: No
Abstract N°: 727
RETROSPECTIVE STUDY OF THROMBECTOMY FOR ACUTE ISCHEMIC STROKE AFTER CARDIAC SURGERY OR INTERVENTION
Rosa M. Eckert*1, Christoph Leithner1, Christoph J. Ploner1, Wolf U. H. Schmidt1, Sarah Zweynert1, Jörg Brandes2
1Charité – Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt- Universität zu Berlin, Department of Neurology and Experimental Neurology, Berlin, Germany,2Deutsches Herzzentrum der Charité - Campus Virchow-Klinikum, Department of Cardiothoracic and Vascular Surgery, Berlin, Germany
On behalf of:
Background and aims: Acute ischemic stroke caused by large vessel occlusion is a potentially devastating complication of cardiac surgeries or interventions. However, intravenous thrombolysis is mostly not feasible in these patients. Rapid mechanical thrombectomy may provide a treatment option, but only few studies have evaluated treatment of acute ischemic stroke in this setting so far.
Methods: We retrospectively analysed consecutive patients with mechanical thrombectomy for acute ischemic stroke and large vessel occlusion after cardiac surgery or intervention in a German heart centre. Demographics, acute imaging reports, thrombectomy characteristics and functional neurologic outcome (modified Rankin Scale {mRS}) were assessed.
Results: From January 2018 to January 2022, 39 patients were identified (median age, 66 years {58-76, IQR}; female sex, 13 {33.3 %}). Among those, 6 (15.4%) had left ventricular assist device (LVAD) surgeries, 5 (12.8%) had coronary bypass grafting, 5 (12.8%) coronary angiography or heart catheterization, 3 (7.7%) trans-catheter aortic valve implantation (TAVI) and 13 (33.3%) had combined surgeries/interventions prior to stroke. Fourteen patients (35.9%) experienced an occlusion of the first segment of the middle cerebral artery (M1). Recanalization was technically successful (TICI 2b/3) in 31 patients (83.8%). Seven of 33 patients (20.6%) had good functional outcome (mRS 0-2), whereas 12 (35.3%) had died at 90 days.
Conclusions: In a large heart centre, a relevant number of patients experience acute stroke with large vessel occlusion following cardiac surgeries/interventions. Good functional outcome is possible after thrombectomy. Our data argue for interdisciplinary standardised diagnostic and treatment algorithms adapted to this specific setting.
Disclosures of Interest: No
Abstract N°: 840
ANGIOPLASTY VERSUS ANGIOPLASTY PLUS STENTING FOR UNDERLYING ATHEROSCLEROTIC STENOSIS IN ACUTE LARGE VESSEL OCCLUSION
Byung Hyun Baek*1, Woong Yoon2, Seul Kee Kim1, You Sub Kim2
1Chonnam National University Hospital, Radiology, Gwangju, South Korea,2Chonnam National University Hospital, Neurosurgery, Gwangju, South Korea
On behalf of:
Background and aims: The optimal treatment strategy for patients with acute large vessel occlusion (LVO) due to underlying intracranial atherosclerotic stenosis (ICAS) is unclear. The aim was to investigate the safety and efficacy of angioplasty and angioplasty plus stenting for underlying ICAS in such patients.
reocclusion, and positive remodeling
Methods: A total of 138 patients underwent angioplasty without and with stenting for the rescue therapy of underlying atherosclerotic stenosis during endovascular treatment for acute LVO. Procedural complications and clinical outcomes were compared between 2 groups. A patency of treated artery was assessed with follow up CT angiography for the assessment of recoil of the treated artery, early reocclusion, and positive remodeling
Results: Fifty patients received angioplasty and 88 patients were treated with angioplasty plus stenting. Instant reocclusion occurred in 16 patients (11.6%) during procedure. Extravasation occurred in 2 patients of stenting group. Subarachnoid hemorrhage was found in 26 patient (18.8%) on immediate brain CT. The rates of procedural complications are not different between 2 groups. Recoil was more frequently observed in the angioplasty group than the angioplasty plus stenting group (28.0% vs 1.1%, p<0.005), whereas positive remodeling was more common in the angioplasty plus stenting group than the angioplasty group (22.7% vs 4.0 %, p=0.004). There were no significant differences in the rates of early reocclusion, symptomatic hemorrhage, and favorable outcome.
Conclusions: Both angioplasty and angioplasty plus stenting are both safe and effective for underlying ICAS in acute LVO paients. Additional stenting might be helpful for preserving arterial patency after angioplasty in such patients.
Disclosures of Interest: No
Abstract N°: 1362
ENDOVASCULAR TREATMENT IN ISCHEMIC STROKE WITH POOR COLLATERAL CIRCULATION
Carlos Ignacio Gomez-Escalonilla Escobar1, PATRICIA SIMAL HERNÁNDEZ*1, Alfonso López-Frías López-Jurado2, Carlos Pérez-García2, Ángela Huete Schmolling2, Carmen Trejo2, José Antonio Egido Herrero1, Santiago Rosati2, Manuel Moreu2
1HOSPITAL UNIVERSITARIO CLÍNICO SAN CARLOS, STROKE UNIT. NEUROLOGY DEPARTMENT, MADRID, Spain,2HOSPITAL UNIVERSITARIO CLÍNICO SAN CARLOS, INTERVENTIONAL NEURORADIOLOGY. RADIOLOGY DEPARTMENT, MADRID, Spain
On behalf of:
Background and aims: Patients with acute ischemic stroke (AIS) with poor collateral circulation have a worse functional prognosis after endovascular treatment (EVT). We analyze the results of efficacy and safety in this group of patients and the factors associated with a good clinical outcome (modified Rankin scale ⩽ 2 or return to previous status).
Methods: Retrospective study of a prospective series of patients with AIS due to large vessel occlusion in the anterior territory, undergoing EVT up to 24 hours since last seen well, who had low collateral score on CT-angiography, from April 2009 to October 2023. Rate of symptomatic intracranial hemorrhage (sICH) and clinical outcome at 3 months were analyzed.
Results: 1150 patients received EVT, of whom 313 (women 52.4%) met the inclusion criteria. Median age was 74 (IQR 64-83), NIHSS 20 (IQR 16-23) and ASPECTS 7 (IQR 6-9). Intravenous thrombolysis (IVT) was performed in 41.5%. TICI ⩾2b was achieved in 74.1%, median number of passes of 2(IQR 1-3). sICH rate was 6.1%. At 3 months 30.7% achieved good clinical outcome. Mortality rate was 29.5%. Factors associated with a good functional outcome in the multivariate analysis were: lower age, lower baseline glycemia, lower number of passes, lower NIHSS, shorter procedure times, higher ASPECTS, higher rates of TICI⩾2b recanalization, adjunctive IVT and non-general anesthesia.
Conclusions: In our series, patients with AIS with poor collateralization undergoing EVT achieved good functional outcome almost in one third of the patients. Factors associated with a good prognosis include IVT and non-general anesthesia in the procedure.
Disclosures of Interest: No
Abstract N°: 1459
A NON-INFERIORITY META-ANALYSIS OF THE SAFETY AND EFFICACY OF TENECTEPLASE VERSUS ALTEPLASE IN LARGE VESSEL OCCLUSION STROKE
Hassan Salamatullah*1,2, Bader Bashrahil1,2, Abdulaziz Alghamdi1,2, Faisal Alsharm1,2, Osama Alkulli1,2, Ziyad Alzahrani1,2, Ahmed Alkhiri1,2, Saeed Al Ghamdi3, Seraj Makkawi1,3,4
1King Saud Bin Abdulaziz University for Health Sciences, College of Medicine, Jeddah, Saudi Arabia,2King Abdullah International Medical Research Center, Jeddah, Saudi Arabia,3King Faisal Specialist Hospital and Research Center, Neuroscience Department, Jeddah, Saudi Arabia,4Ministry of the National Guard-Health Affairs, Department of Neuroscience, Jeddah, Saudi Arabia
On behalf of:
Background and aims: Alteplase is the established medical intervention for acute ischemic stroke (AIS) within a 4.5-hour window. Tenecteplase, a modified tissue plasminogen activator, has distinct pharmacological properties. Multiple randomised controlled trials (RCTs) have examined the efficacy and safety of both in AIS patients with large vessel occlusion (LVO). This study conducts a non-inferiority meta-analysis to compare safety and efficacy outcomes between the interventions.
Methods: This systematic review adhered to PRISMA guidelines, utilizing three databases to identify relevant RCTs comparing the efficacy and safety of tenecteplase against alteplase for AIS patients with LVO. Exclusions comprised review articles, observational studies, case reports, and series. Data synthesis employed risk ratios (RRs) and 95% confidence intervals (CIs).
Results: Four RCTs and a secondary analysis of two RCTs were conducted to investigate endpoints in patients with LVO subjected to the distinct interventions. Both therapeutic modalities exhibited comparable rates of modified Rankin Scale (mRS) 0-1 (Risk Ratio = 1.18, 95% CI [1.00-1.40], P = 0.05) and mRS 0-2 (RR = 1.18, 95% CI [0.90-1.54], P = 0.23). Similarly, mortality rates (RR = 0.98, 95% CI [0.57-1.69], P = 0.94) and symptomatic intracranial haemorrhage (sICH) rates (RR = 1.13, 95% CI [0.60-2.13], P = 0.70) demonstrated no significant differences between the two interventions.
Conclusions: Our research findings affirm that tenecteplase exhibits non-inferiority to alteplase and demonstrates promising efficacy in patients with LVO. The ease of administration further advocates for the consideration of tenecteplase as a viable alternative to alteplase.
Disclosures of Interest: No
Abstract N°: 1480
EXPANDING STROKE THROMBOLYSIS ELIGIBILITY USING ADVANCED NEUROIMAGING TECHNIQUES: A SYSTEMATIC REVIEW AND META-ANALYSIS OF RCTS
Adel Alhazzani1, Ahmed Alkhiri*2, Ahmed Almaghrabi2, Aser Alamri3, Basil Alghamdi2, Hassan Salamatullah2, Mohammed Aldriweesh4, Bruce Campbell5, Gregory Albers6, Fahad Al-Ajlan1
1King Faisal Specialist Hospital and Research Centre, Neuroscience Center, Riyadh, Saudi Arabia,2King Saud Bin Abdulaziz University for Health Sciences, College of Medicine, Jeddah, Saudi Arabia,3King Saud Bin Abdulaziz University for Health Sciences, College of Medicine, Riyadh, Saudi Arabia,4King Abdulaziz Medical City, National Guard Health Affairs, Department of Neurology, Riyadh, Saudi Arabia,5Melbourne Brain Centre at the Royal Melbourne Hospital, University of Melbourne, Department of Medicine and Neurology, Parkville, VIC, Australia,6Stanford Hospital, Department of Neurology, CA, United States
On behalf of:
Background and aims: Time restrictions prevent a substantial proportion of acute ischemic stroke (AIS) patients from receiving intravenous thrombolysis (IVT), and advanced neuroimaging has a promising value in extending IVT eligibility.
Methods: We conducted a prospectively registered systematic review and meta-analysis of randomised clinical trials (RCTs) reported on IVT treatment in the extended window or with unknown onset. Patient selection for inclusion in the analysis relied on the implementation of advanced imaging. Proportions and risk ratios (RRs) with the corresponding 95% confidence intervals (CIs) were computed using the random-effects model.
Results: Six RCTs (1070 patients) were included. IVT was administered to 584 patients, whereas 486 patients were in the control group. Rates of excellent functional outcomes (mRS 0-1) and functional independence (mRS 0-2) at 90-days following IVT were 43% (95% CI, 36–50%) and 59% (95% CI, 50–68%), respectively. Compared to control, IVT increased the chances of excellent functional outcomes (RR, 1.21 [95% CI, 1.04–1.40]) and functional independence (RR, 1.13 [95% CI, 1.03–1.25]). Symptomatic intracerebral haemorrhage (sICH) occurred in 2% (95% CI, 1–5%) of the IVT group. sICH occurred more frequently in the IVT arm (RR, 4.70 [95% CI, 1.36–16.29). Mortality rates at 90-days were similar between groups. Rates of patients alive with significant disability (mRS 4-5) preferred IVT over control.
Conclusions: For AIS patients not meeting the 4.5 h eligibility criteria, IVT resulted in better functional outcomes when advanced neuroimaging protocols were employed. Although sICH rates were higher with IVT, mortality rates were comparable.
Disclosures of Interest: No
Abstract N°: 1643
MECHANICAL THROMBECTOMY AFTER ISCHEMIC STROKE IN PATIENTS AGED ⩾ 85 YEARS: SURVIVAL AND FUNCTIONAL OUTCOMES
Cristina Moreno López*1, Rodrigo López Rebolledo1, Gabriel García Alcántara1, Antonio Cruz Culebras1, Alicia De Felipe1, Consuelo Matute Lozano1, Sebastian García Madrona1, Jaime Masjuan1, Rocio Vera1
1Ramón y Cajal Universitary Hospital, Department of Neurology, Madrid, Spain
On behalf of:
Background and aims: Age is no longer an exclusion criterion for endovascular treatment of ischemic stroke. However, the progressive aging of the population raises questions about the efficacy and safety of mechanical thrombectomy (MT) in the older population.
Methods: Retrospective study of a prospective database of patients treated with MT at our center between 2017- 2023. We compared our experience using MT in patients aged ⩾ 85 years to those aged < 85 years.
Results: Among the 647 patients treated with MT, 94 (14.5%) were ⩾ 85 years old (median age, 87.4± 2.4). Both groups had similar stroke severity evaluated by the NIHSS scale (16.5 in ⩾ 85 years old vs 16 in the younger group, p= 0,116) and had a similar proportion of fibrinolysis treatment (50% vs 53.7%, p= 0.526). We found no significant differences in the complete recanalization rate (87.7% vs 87.7%, p= 0.903) or symptomatic hemorrhagic transformation (4.3% vs 4.9%, p= 0.792) between both groups. However, there were significant differences in the functional outcome at 3 months with a smaller proportion of independence (38% vs 53.9%, p= 0.014) and higher mortality (21% vs 13.3%, p= 0.029) in older patients. In this group, we also found higher hospital mortality differences close to significant (17% vs 10.7%, p= 0.07).
Conclusions: In our experience, treatment with MT in the older population with ischemic stroke has a high rate of recanalization with no increment in the risk of hemorrhagic transformation but with higher mortality and worse functional outcome at 3 months comparing it with the younger population.
Disclosures of Interest: No
Abstract N°: 1731
PHYSICAL THROMBUS CHARACTERISTICS: IMPACT ON ENDOVASCULAR OUTCOMES IN ACUTE ISCHEMIC STROKE WITH MIDDLE CEREBRAL ARTERY OCCLUSION
Pablo Iriarte*1, Carlos Molina2, Raquel Berbegal1, Ainhoa Lorenzo3, Carmen Ramos1, Alba Somovilla1, Jaime Alonso1, Juan Vega2, Jose Vivancos1, Santiago Trillo Senin1
1Hospital de la Princesa, Neurology,2Hospital de la Princesa, Radiology,3Hospital Gómez Ulla, Neurology
On behalf of:
Background and aims: The physical characteristics of the thrombus, such as its length (LT) and contrast perviousness (PT), could be associated with the outcome of endovascular treatment (ET) in stroke due to middle cerebral artery (MCA) occlusion. We have studied the association of both variables with ET characteristics, as well as their possible association with the degree of collateral blood flow(CBF).
Methods: We performed a retrospective study with prospective data collection. Patients with MCA occlusion (carotid T/M1-MCA) treated by ET in our center during 2019-2022 were included. LT was estimated in late phase of perfusion CT. PT was calculated with a dynamic technique, subtracting the average Hounsfield Units (HU) of MCA hyperdensity between baseline CT and late phase perfusion CT. CC was estimated using RAPID software (HIR parameter). The variable penetrable thrombus(T-PEN) was defined as low LT(<5mm) and high PT(>13HU).
Results: A total of 174 patients were included. Median LT was 10mm[IQR 7-13], median PT was 13HU[IQR 5-24]. Significant correlation was identified between LT and PT (rho=-0.21;p0.01). High contrast perviousness (>13HU) was associated with lower pre-treatment NIHSS(p=0.02), shorter ET duration(p<0.01), lower number of passes(p<0.01), lower infarct core (CBF<30s;p=0.03) and better CBF (p=0.03). LT >10mm was associated with greater infarct core (CBF<30s);=p0.04) and worse CBF (p<0.01). T-PEN was associated with a higher probability of recanalization, TICI>2a(p=0.006).
Conclusions: In our study, physical characteristics of the thrombus, such as PT and LT, could predict the technical difficulty of ET in MCA stroke. The association of these factors with CC suggests that retrograde collateral flow could affect patency and length.
Disclosures of Interest: No
Abstract N°: 1748
INTRAVENOUS THROMBOLYSIS WITH RT-PA IN PATIENTS WITH ACUTE ISCHEMIC STROKE: CLINICAL EXPERIENCE FROM TWO EGYPTIAN CENTERS
Elsayed Abed*1
1Al-Azhar University, Neurology, Cairo, Egypt
On behalf of:
Background and aims: We aimed to identify the barriers which prevent utilization of rt-PA in a proper time in the clinical context of persons suspected of acute stroke for reducing delays for revascularization therapies, and in the meantime limit secondary brain damage.
Methods: This retrospective study was conducted on patients who presented with acute ischemic stroke and were treated with Intravenous rt-PA within 4.5 hours of the onset of symptoms according to the inclusion and exclusion criteria of the ECASS III study. Early deterioration was defined as 2-point NIHSS deterioration within 24 hours post-rt-PA infusion, new headache,the hemorrhagic transformation was occurred or death.
Results: A total of 167 patients (mean age of 62.55 ± 9.94 years) and included 94 males (56.2%) were included. Based on arrival time to the emergency department, door-to-needle time of ⩽60 minutes was achieved by only 32.8% (42/128) of patients who arrived within 0-2 hours of their symptom onset compared to 48.7% (19/39) of those who arrived at the emergency department within 2-3.5 hours of their symptom onset.There was no mortality due to rt-PA treatment complications; however, pneumonia due to COVID-19 infection was the cause of death in 15 patients (8.9%) who received thrombolytic therapy during the era of the COVID-19 pandemic.
Conclusions: The extremely low number of stroke patients receiving rt-PA in the developing countries was attributed to several barriers which included lack of public awareness about revascularization therapy, and Inaccessibility to emergency medical services especially restrictions and logistic rules of many hospitals during the era of the COVID-19 pandemic.
Disclosures of Interest: No
Abstract N°: 1843
COMPARING POST-CAROTID INTERVENTION DWI LESIONS: CAS VS. CEA
JUN LEE*1, Doo Hyuk Kwon1
1Yeungnam University Medical Center, Neurology, Daegu, South Korea
On behalf of:
Background and aims: Carotid endarterectomy (CEA) and carotid stenting (CAS) are established procedures for stroke prevention in patients with carotid artery stenosis. Diffusion-weighted imaging (DWI) detects new brain lesions, enabling outcome comparisons. This study investigates associations between new DWI lesions and procedural variables.
Methods: We retrospectively analyzed data from 159 patients undergoing CEA or CAS over six years. Stenosis severity was assessed via transfemoral cerebral angiography (TFCA), and new ischemic lesions were identified on post-intervention DWI within three days of the procedure. Data on cardiovascular risk factors, surgical details, and intraoperative transcranial Doppler (TCD) monitoring were collected.
Results: Among 164 patients, seven with post-operative neurological deficits underwent post-procedural DWI. Within a subgroup of 116 patients (72 CEA, 44 CAS) with both pre- and post-intervention DWI, 53 exhibited new ischemic lesions. CAS correlated significantly with more post-intervention DWI lesions than CEA (70.5% vs. 30.6%, p < 0.001). No significant associations were found between new DWI lesions and stenosis severity or symptomatic stenosis. After adjusting for age and gender, CAS had an odds ratio of 6.0 (95% CI; 2.6 to 14, p < 0.001) for detecting new DWI lesions. Intraoperative TCD showed a trend between higher microembolic signals (MES) quartiles and new DWI lesions (p = 0.053). Shunt use during CEA predicted new DWI lesions (OR 6.9, 95% CI 1.6 to 29.9, p = 0.008).
Conclusions: This study highlights more post-CAS DWI lesions than CEA. Selective shunting during CEA reduces new lesions. TCD aids shunt use, preventing unpredictable ischemic lesions. These findings impact carotid intervention outcomes.
Disclosures of Interest: No
Abstract N°: 2040
MEMBRANECTOMY FOR THE TREATMENT OF CHRONIC SUBDURAL HEMATOMA: AN UPDATED META-ANALYSIS
Mariam Abdelhady*1, Ahmed Aljabali2, Ibraheem Alkhawaldeh3, Ibrahim Serag4, Hadeer Aboelfarh5, Rowan Elhalag6, Muhammad Husain7, Abdulhameed Alhadeethi8, Ahmed Negida9, Mohamed Abouzid10
1October 6 University, Faculty of Medicine, Giza, Egypt,2Jordan University of Science and Technology, Faculty of Medicine, Irbid, Jordan,3Mutah University, Faculty of Medicine, AL Karak, Jordan,4Mansoura University, Faculty of Medicine, Mansoura, Egypt,5Mansoura University Hospital, Department of Neurology, Mansoura, Egypt,6Alexandria University, Faculty of Medicine, Alexandria, Egypt,7Al-Azhar University, Faculty of Medicine, Cairo, Egypt,8Al-Salam Teaching Hospital, Faculty of Medicine, Ninevah, Iraq,9Virginia Commonwealth University, Department of Neurology, Virginia, United States,10Poznan University of Medical Sciences, Department of Physical Pharmacy and Pharmacokinetics, Poznan, Poland
On behalf of:
Background and aims: Chronic Subdural Hematoma (CSDH) is a significant neurosurgical challenge, especially prevalent in the elderly. This meta-analysis evaluates the effectiveness of membranectomy in conjunction with other neurosurgical interventions in CSDH treatment.
Methods: A comprehensive literature review was performed across Ovid, PubMed, and Cochrane Library databases, covering studies up to September 2023. The inclusion criteria were based on the PICO framework, targeting CSDH patients undergoing membranectomy. The primary outcomes assessed included mortality, morbidity, recurrence, reoperation rates, and length of hospital stay, analyzed using Open Meta-Analyst.
Results: From 1,486 screened articles, 16 studies (15 retrospective cohorts and one RCT) were included, involving 1,490 CSDH patients treated with membranectomy. The meta-analysis revealed a recurrence rate of 15.3% (95% CI: 10.2-20.3% p<0.001), reoperation rate of 13.1% (95% CI: 7.7-18.5% p<0.001), and a mortality rate of 5.8% (95% CI: 2.9-8.7% p<0.001). The complication incidence was 15.7% (95% CI: 10.8-20.6% p<0.001), with an average hospital stay of 25 days (95% CI: 16.6-33.4, P<0.001). These outcomes suggest a higher rate of complications and recurrence compared to previous studies and alternative minimally invasive techniques.
Conclusions: The study indicates that membranectomy, combined with other neurosurgical procedures, may lead to better patient outcomes in CSDH management. However, the rates of Complications, Recurrence, and Reoperation were considered higher than the previous literature and minimally invasive interventions and call for a cautious approach. Further research with comparable studies is highly indicated for a definitive conclusion.
rates.
Disclosures of Interest: No
Abstract N°: 2045
THE IMPACT OF SERUM D-DIMER LEVELS AFTER INTRAVENOUS THROMBOLYSIS ON SHORT-TERM OUTCOMES IN PATIENTS WITH ACUTE ISCHEMIC STROKE
Jovana Ivanovic*1, Maksim Sarcevic1, Vanja Radisic1, Katarina Djurdjevic1, Mladen Jankovic1, Tamara Svabic1, Visnja Padjen1, Ivana Berisavac1, Dejana Jovanovic1, Stanarcevic Predrag1
1Neurology Clinic, Univertisty Clinical Center of Serbia, Blegrade, Serbia
On behalf of:
Background and aims: D-dimer is a fibrin-degradation product. The aim of our study was to evaluate the association between serum d-dimer values after intravenous thrombolysis (IVT) and short-term outcomes in patients with acute ischemic stroke (AIS).
Methods: We included 100 consecutive patients, 66% males, with AIS treated with IVT, during 2022 in our Stroke Unit. Mean age at the disease onset was 66.5 (± 12.7) years. Serum d-dimer levels were measured at baseline and 24h after IVT. Patients were devided in four groups by post-IVT plasma d-dimer levels: Quartile 1 (0.15-28.575 mg/L), Quartile 2 (28.567-57.001 mg/L), Quartile 3 (57.002-85.427 mg/L) and Quartile 4 (⩾ 85.428 mg/L).
Results: The mean onset to needle time was 211.6 (± 157.8) minutes. The median baseline d-dimer level was 0.69 mg/L (± 1.93) and post-IVT was 2.72 mg/L (± 13.89). In our cochort, higher post-IVT d-dimer levels were in statistically significant correlation with the occurence of haemorragic transformation (HT); p=0.008, k=0.27. Higher d-dimer levels was also associated with worse neurological post-stroke recovery, quantified with The Modified Rankin Score (mRS ⩾3); p=0.00004, k=0.404. Cut off value for d-dimer and higher risk of HT occurence was 3.270 mg/L (area under the curve 0.685, CI 95%, CI 0.57-0.8, sensitivity 73%, specificity 65%) and poor mRS was 1.910 mg/L (area under the curve 0.7336, CI 95%, CI 0.633-0.834, sensitivity 78%, specificity 66%).
Conclusions: Higher post-IVT d-dimer levels were in statistically strong correlation with HT occurence and poor discharge mRS (⩾3) in our patients with AIS treated with IVT.
Disclosures of Interest: No
Abstract N°: 2064
ENDOVASCULAR THROMBECTOMY IN LARGE ISCHEMIC STROKE: EXPERIENCE AT A TERTIARY HOSPITAL
Marina Lara González1, Blanca Hidalgo Valverde1, Manuel García Ruiz1, Alfonso López-Frías López-Jurado2, PATRICIA SIMAL HERNÁNDEZ*1, Carlos Pérez-García2, Santiago Rosati2, José Antonio Egido Herrero1, Manuel Moreu2, Carlos Ignacio Gomez-Escalonilla Escobar1
1Hospital Clínico San Carlos, Stroke Unit. Neurology Department, Madrid, Spain,2Hospital Clínico San Carlos, Neuroradiology Unit. Radiology Department, Madrid, Spain
On behalf of:
Background and aims: The benefit of endovascular thrombectomy (ET) in patients with large ischemic stroke due to large-vessel occlusion within 24 hours after onset has not been clearly defined.
Methods: Descriptive and retrospective study enrolled patients with large ischemic stroke (ASPECTS⩽5) due to large vessel occlusion in anterior territory who underwent ET within 24 hours after onset in our hospital, between July 2009 and March 2023. Efficacy outcome was favorable functional outcome at 90 days, defined as modified Rankin Scale score (mRS) of 0 to 3. Safety outcomes were symptomatic intracranial hemorrhage (sICH) and mortality at 90 days.
Results: Ninety-two patients (44,6% females) were included. The median age was 68 years (IQR 56-77). The median NIHSS was 21 (IQR 18-23) and median ASPECTS was 5 (IQR 3-5). Intravenous fibrinolysis was performed in 42.4%. Median time from last baseline to arterial puncture was 306 minutes (IQR 210-450.5). The rate of TICI⩾2b (successful recanalization) was 68.5% and of sICH was 11%. At 90 days, a favorable functional outcome was achieved in 39.1% and mortality rate was 29.3%. In patients with successful recanalization, a higher percentage of favorable functional outcome (49.2% vs 17.2%) and lower mortality (22.2% vs 44.8%) was achieved at 90 days.
Conclusions: In our study, approximately 40% of patients with large ischemic stroke who underwent ET within 24 hours after onset achieved a favorable functional outcome. The best results were observed in those with successful recanalization.
Disclosures of Interest: No
Abstract N°: 2149
STROKE UNIT IN AN ALGERIAN OUTLYING HOSPITAL: NECESSITY AND CHALLENGES
1EHS El Maham, Department of Neurology, Cherchell, Algeria,2EHS El Maham, Cherchell, Algeria
On behalf of:
Background and aims: The aim of this study is to evaluate the outcomes of stroke patients in an outlying Algerian hospital, identify potential gaps, and suggest solutions.
Methods: We conducted a prospective observational study in patients who presented at the emergency with an acute stroke, during the period from March 2022 to January 2024.
These patients underwent a neurological examination, an evaluation of the NIHSS score, and the ASPECT score. We also noted the method and times of arrival, as well as the times and results of intravenous thrombolysis.
Results: Out of 7722 the patients seen in the emergency room, 1222 presented with acute stroke symptoms. Of these, 232 (18.98%) arrived at the hospital within 4.5 hours of which 18.10% received intravenous thrombolysis within an average of 30 minutes. The rest were excluded due to contraindications. Among those who underwent thrombolysis, 35.7% fully recovered, 35.7% partially, and 12% had a similar NIHSS score. Unfortunately, 16.6% passed away due to a massive ischemic stroke.
Conclusions: The proportion of patients arriving within 4.5 hours and receiving thrombolysis remains low (3.43%), mainly due to poor stroke awareness among the public and doctors. This encourages us to conduct awareness campaigns. Monitoring is needed for those with a transient ischemic attack or low NIHSS to prevent extensive strokes.
IV thrombolysis remains the most common acute stroke treatment but many patients don’t benefit from it. Better organisation of our neurovascular unit and raising awareness among all its stakeholders should enhance the effectiveness of this therapy.
Disclosures of Interest: No
Abstract N°: 2321
EFFECTS OF A BIASED ANGIOTENSIN II TYPE 1 RECEPTOR AGONIST IN AN EXPERIMENTAL STROKE MODEL
Melissa Colin*1,2, Laura Ponsaerts3, Peter Leenders4, Mathilde Achard5, Samir Acherar5, Caroline Perrin-Sarrado1, W Matthijs Blankesteijn4, Annelies Bronckaers3, François Dupuis1, Sébastien Foulquier2,4
1Université de Lorraine, CITHEFOR, Vandoeuvre-Lès-Nancy, France,2Maastricht University, Department of Pharmacology and Toxicology, MHeNS - School for Mental Health and Neuroscience, Maastricht,3Hasselt University, Biomedical Research Institute, Hasselt, Belgium,4Maastricht University, Department of Pharmacology & Toxicology, CARIM - Cardiovascular Research Institute Maastricht, Maastricht,5Université de Lorraine, LCPM, Nancy, France
On behalf of:
Background and aims: During ischemic stroke, AngII-mediated vasoconstriction and neuroinflammation via AT1 receptor (AT1R) is deleterious as it reduces cerebral blood flow (CBF) and increases lesion size. The use of AT1R antagonists (ARBs) counteracts the harmful effects of AT1R mediated by G protein signaling. However, AT1R activation can also be protective in the acute phase after stroke via activation of b-arrestin signaling. To study this, we aimed to investigate the effects of TRV120027, an AT1R biased agonist (receptor-specific ligands able to selectively activate a single signaling pathway) on CBF and neuroinflammation in an ischemic stroke mouse model.
Methods: 9- to 10-week-old C57BL6/JOlaHsd male mice underwent a distal middle cerebral artery occlusion (dMCAO) or a Sham surgery. Mice were distributed in three groups: sham + saline (n=11), dMCAO + saline (n=11) and dMCAO + TRV120027 (5nmol/kg) (n=12). CBF was measured transcranially using Laser Speckle Contrast Imaging. CBF was recorded before and 24h after the surgery. Treatment (TRV120027 or saline) was administered 15 min after the occlusion. Lesion size was assessed by a TTC staining.
Results: CBF was reduced in both dMCAO groups vs Sham (dMCAO+saline -55±7%, one-way anova, p=0.0001; dMCAO+TRV120027 -43±21%, p=0.0001). TRV120027 treatment did not improve CBF vs Sham (p=0.52) but decreased the lesion size (4.11±2.84%, vs dMCAO+saline 6.62±2.71% p=0.030).
Conclusions: TRV120027 treatment reduced the size of the ischemic lesion without a direct improvement of the CBF in the dMCAO mouse model. The impact of TRV1200027 treatment on neuroinflammation is being assessed.
Disclosures of Interest: No
Abstract N°: 2324
MECHANICAL THROMBECTOMY IN INTERNAL CAROTID ARTERY DISSECTION WITH ACUTE ISCHEMIC STROKE
Rikke Puggaard1, Nicolaj Grønbæk Laugesen*1,2, Andreas Brandt3, Trine Stavngaard3, Thomas Truelsen2,3
1Copenhagen University Hospital, Rigshospitalet, Neurology, København, Denmark,2Copenhagen University, Faculty of Health Sciences, København, Denmark,3Copenhagen University Hospital, Rigshospitalet, Radiology, København, Denmark
On behalf of:
Background and aims: Mechanical thrombectomy (MT) has not been independently investigated in internal carotid artery dissection (ICAD), while MT has shown efficacy in occlusion of the internal carotid artery (ICA). We compared patients undergoing MT due to either ICAD or other pathology of the ICA.
Methods: In 2017-2021, patients with MT for ICAD or for other pathology of the ICA were enrolled in this observational study. The primary outcome was modified Rankin Scale (mRS) of 0-2 at 90 days (favorable outcome). Multivariate regression was used to test for factors associated with outcome with the significance level at p<0.05.
Results: A total of 454 patients undergoing MT were included, of which 67 patients had ICAD (15%). While ICAD patients more often achieved favorable outcome compared to patients with other ICA pathology (77% vs. 42%, <0.001), ICAD was not significantly associated with outcome in multivariate analysis. Patients with ICAD were significantly younger (median 53 years [IQR 47-61] vs. 72 years [IQR 64-79]) and had significantly better pre-stroke mRS (mRS 0 in 93% vs. 64%), which in turn was associated with favorable outcome with aOR 0.95 (95% CI: 0.93-0.98) and 0.58 (95% CI: 0.40-0.82), respectively. Procedural complications were no different and post-procedural symptomatic intracranial hemorrhage no more frequent (8% vs. 9%).
Conclusions: Despite marked differences in patient and procedural characteristics both outcome and safety after MT was comparable in ICAD and other ICA pathologies.
Disclosures of Interest: No
Abstract N°: 2369
THE PREDICTIVE FACTOR OF SYMPTOMATIC INTRACRANIAL HEMORRHAGE POST INTRAVENOUS THROMBOLYSIS WITH TENECTEPLASE
1Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China, China National Clinical Research Center for Neurological Diseases, Beijing Tiantan Hospital, Capital Medical University, Beijing, China
On behalf of:
Background and aims: Intravenous thrombolysis is the most commonly applied pharmacological intervention for managing acute ischemic stroke (AIS). However, the risk of symptomatic intracranial hemorrhage (sICH) persists. Our study aimed to identify the predictors of intracranial hemorrhage in stroke patients treated with Tenecteplase.
Methods: Tenecteplase versus alteplase in an Acute ischemic Cerebrovascular Events-2 (TRACE-II) is a multicenter, prospective, randomized, controlled trial, including patients aged at least 18 years who had received intravenous thrombolysis with tenecteplase within 4.5 hours of the AIS. All stroke patients’ clinical, radiological, and laboratory data were collected and analyzed. The safety outcomes were the presence of sICH within 36h. Statistical analysis was performed using SAS software, version 9.4.
Results: We enrolled 704 patients who received intravenous thrombolysis with Tenecteplase, between June 12, 2021, and May 29, 2022. The median age was 65 years, with a male predominance (68%). After 36 hours, 15 patients, or 2% had a sICH, with a mean age of 71 (66-78) years, and a sex ratio equal to 1.1. Univariate analysis showed that the risk of sICH was associated with age (p: 0.02), gender (p: 0.01), and history of diabetes mellitus (p: 0.03). after further adjustments of several factors, the association between sICH occurrence and history of diabetes mellitus was still significant with an increase of 4.8-fold this risk (ORAdjusted: 4.80; IC 95% [1.63-13.95]; p<0.00).
Conclusions: The history of diabetes mellitus in AIS patients treated with Tenecteplase intravenous thrombolysis increases the risk of the risk of sICH.
Disclosures of Interest: No
Abstract N°: 2392
COMPARATIVE ANALYSIS OF INTRAVENOUS THROMBOLYSIS EFFICACY IN STROKE BEYOND MEDIAN LIFE EXPECTANCY IN REPUBLIC OF MOLDOVA
Cristian Bour*1,2, Natalia Ciobanu2, Stanislav Groppa1,2
1Nicolae Testemitanu State University of Medicine and Pharmacy of the Republic of Moldova, Department of Neurology nr. 2, Chișinău, Moldova,2Institute of Emergency Medicine, Neurology Department, Chișinău, Moldova
On behalf of:
Background and aims: Our research investigates the effectiveness of intravenous rt-PA (recombinant tissue-type plasminogen activator) for ischemic stroke within the demographic setting of the Republic of Moldova, where the average life expectancy is 69 years for men and 75 years for women.
Methods: The study encompassed 103 acute ischemic stroke patients treated with rt-Pa in Institute of Emergency Medicine in Republic of Moldova from 1 July 2022 to 1 December 2023 and logged in the RES-Q (Registry of Stroke Care Quality) database.
Results: For males aged 60-69 (23 patients), the in-hospital mortality rate was 21.74%, with 4.35% showing unchanged NIHSS (National Institutes of Health Stroke Scale), improvements by 1-3 points in 8.70%, and by 4+ points in 56.52%. In the female 66-75 cohort (32 patients), the in-hospital mortality rate stood at 25%, with 18.75% improving by 1-3 points, and 56.25% by 4+ points. Among the 70+ male group (28 patients), in-hospital mortality reached 32.14%, with 10.71% showing unchanged NIHSS, 10.71% improving by 1-3 points, improved by 4+ points in 39.29% and deteriorated in 7.14%. In the 76+ female group (20 patients), the in-hospital mortality rate was 25%, with NIHSS improvements of 1-3 points in 10% and 4+ points in 65%.
Conclusions: The study indicates an increased mortality rate in men post-average life expectancy, potentially linked to lifestyle and health management practices, women exhibited a consistent mortality rate across age groups. Comorbidities and lifestyle choices may be a more powerful independent predictor play than age in determining the outcomes of thrombolysis in ischemic stroke.
Disclosures of Interest: No
Abstract N°: 2525
RESIDUAL STENOSIS AFTER INTRACRANIAL ACUTE STENTING: IS GOOD ENOUGH GREAT?
Fábio Gomes*1, Henrique Queirós2, Carolina Maia2, César Nunes2, Ricardo Veiga2, Gustavo Santo1, Fernando Silva1, João Sargento-Freitas1, Egídio Machado2, João André Sousa1
1Centro Hospitalar e Universitário de Coimbra, Neurology, Coimbra, Portugal,2Centro Hospitalar e Universitário de Coimbra, Medical Imaging, Neuroradiology Unit, Coimbra, Portugal
On behalf of:
Background and aims: Intracranial atherosclerosis (ICAD) is associated with the highest recurrence among stroke etiologies. We aimed to evaluate the impact of residual stenosis in patients with ICAD submitted to acute stenting.
Methods: Retrospective single-center study including patients who underwent acute intracranial stenting, comparing patients with (RS) and without (no-RS) post-procedural residual stenosis.
Results: We included 31 patients with ICAD submitted to acute phase intracranial stenting. A total of 14 (42.4%) patients had residual ⩾50% stenosis (RS), while 17 (51.5%) had no or <50% residual stenosis (no-RS). Successful recanalization (TICI 2c/3) was similar in both groups (RS= 55.6% vs. no-RS= 44.4%, p=0.275). No differences were found in the rate of symptomatic ICH (RS= 7.1% vs. no-RS=11.8%, p=1.0). In 8/14 (57.2%) RS vs. 10/17 (58.8%) no-RS patients there was infarct expansion from baseline to control CT (p=1.0). Median volume of infarct expansion was 6.7 (0.8-39.6) in RS vs 1.9 (0.6-2.3) in no-RS groups (p=0.29). Median NIHSS point reduction from baseline to discharge was 6.5 (2.5-10.0) in RS patients vs 2 (1.0-9.5) no-RS patients (p=0.6). In RS group 4/14 (28.5%) patients achieved 90-day functional independence (mRS 0-2) vs. 7/17 (41.2%) in no-RS group (p=0.7).
Conclusions: Residual stenosis after acute stenting was not associated with worse clinical or imaging outcomes. We can argue that a more aggressive approach aiming for a perfect recanalization of ICAD does not provide additional benefits. Larger studies are needed.
Disclosures of Interest: No
Abstract N°: 2566
MULTIDISCIPLINARY MANAGEMENT OF ACUTE ISCHEMIC STROKE IN PREGNANCY: SUCCESSFUL RECANALIZATION WITH THROMBOLYSIS AND THROMBECTOMY
Dae-Hyun Kim*1, Jong-Wook Shin2
1Dong-A University Hospital, Department of Neurology, Busan, South Korea,2Chungnam National University Sejong Hospital, Department of Neurology, Sejong, South Korea
On behalf of:
Background and aims: Acute ischemic stroke in pregnant patients is a rare occurrence, and the exclusion of this population from clinical trials has resulted in a lack of established guidelines for their management. Managing acute ischemic stroke in pregnant patients poses a unique challenge, necessitating careful consideration by stroke physicians regarding the use of thrombolysis or thrombectomy.
Methods: We present the successful application of both thrombolysis and thrombectomy in a 32-year-old woman at 33 weeks and 2 days of pregnancy. The patient presented with left-sided weakness and dysarthria, and a diagnosis of acute cerebral infarction with right MCA M1 occlusion was established. A comprehensive treatment plan, involving the administration of a regular dose of intravenous tissue plasminogen activator and subsequent endovascular intervention, was implemented. The collaborative efforts of a multidisciplinary team, including the obstetric department, played a crucial role in assessing the fetal status both before and after thrombolysis.
Results: During thrombectomy, a lead protector was strategically placed over the estimated fetal position to minimize radiation exposure. The obstetric department ensured the safety of both the mother and the fetus post-thrombectomy. With a multidisciplinary approach, we successfully performed recanalization treatment, allowing the patient to have a normal delivery on the scheduled day.
Conclusions: This case underscores the feasibility and safety of acute thrombolysis and thrombectomy in pregnant patients, highlighting the pivotal role of a multidisciplinary approach in achieving successful outcomes. Furthermore, we advocate for the establishment of a proper protocol for pregnant ischemic stroke patients in similar situations.
Disclosures of Interest: No
Abstract N°: 2697
BENEFITS AND SAFETY OF PCSK9 INHIBITOR INJECTION IN PATHIENTS IMMEDIATELY BEFORE MECHANICAL THROMBECTOMY
1Inha university hospital, Neurology, Incheon, South Korea,2International ST. Mary`s Hospital, Neurology, Incheon, South Korea,3Soonchunhyang University Seoul Hospital, Soonchunhyang University School of Medicine, Neurology, Seoul, South Korea
On behalf of:
Background and aims: Evolucumab is a PCSK9 inhibitor(PCSK9i) and a fast-acting lipid lowering agent with beneficial effects during chronic stroke period. However, the clinical effect of PCSK9 inhibitor injection around mechanical thrombectomy(MT) is still unclear. Here we showed the efficacy and safety of PCSK9i injection immediate before MT.
Methods: All subjects underwent MT at Inha University Hospital from April 2019 to March 2023. Clinical profiles between the evolucumab group and the non-user group were analyzed.
Results: Of the 263 patients enrolled,112 (42.6%) were male and the mean age was 69.1 years. Of these, 42 patients received a single dose of a PCSK9i immediately prior to MT. There were no significant differences between the two groups in age, gender ratio, major risk factors, stroke etiology, or prior statin treatment. Evolucumab group had a higher stent recovery rate than the non-user group (70.7 vs 53.4%, p = 0.04). However, there were no significant difference in TICI grade, or symptomatic hemorrhage. Compared with non-user group, Evolucumab group had the lower NIHSS score on discharge (12.41 vs 8.83, p=0.03) and seemed to have the lower in-hopital mortality(12.2 vs 2.4% p=0.06). Cardiovascular and other adverse events within 3 months were similar in both groups.
Conclusions: Evolocumab added to statin therapy was well tolerated and appeared to be associated with lower in-hospital mortality and lower NIHSS scores at discharge without additional side effects. Further large randomized clinical trials might be needed to investigate the beneficial effects of PCSK9i during hyperacute stroke period.
Disclosures of Interest: No
Abstract N°: 2783
ASSOCIATION OF CAROTID INTIMA MEDIA THICKNESS WITH REPERFUSION RATE AND OUTCOME IN STROKE PATIENTS UNDERGOING ENDOVASCULAR THERAPY
Simon Winzer*1, Katharina Laske1, Daniel Kaiser2, Timo Siepmann1, Kristian Barlinn1, Johannes Gerber2, Witold Polanski3, Volker Puetz1, Lars-Peder Pallesen1
1Department of Neurology, Dresden, Germany,2Institut und Poliklinik für Diagnostische und Interventionelle Neuroradiologie, Dresden, Germany,3Department of Neurosurgery, Dresden, Germany
On behalf of:
Background and aims: Atherosclerotic large arteries are potentially associated with more complicated procedures and worse reperfusion rates in stroke patients with anterior circulation large vessel occlusion (acLVO) undergoing endovascular therapy (EVT). We sought to determine the impact of carotid intima media thickness (cIMT) measured by duplex sonography on reperfusion success and functional outcome.
Methods: We analysed consecutive patients with acute ischemic stroke due to acLVO from our prospective EVT database. We determined cIMT on routinely performed duplex-ultrasound examinations and categorized cIMT into normal or increased according to age-dependent thresholds. We measured functional outcomes with mRS at 90 days and defined favourable outcome as mRS 0-2. Successful reperfusion was defined as modified treatment in cerebral infarction (mTICI) score of 2b or 3. We performed multivariable analysis to test for an association of cIMT with favorable outcome.
Results: Among 298 patients (median age 75 years [IQR 17], 142 [48%] male, baseline NIHSS 16 [IQR 8], 62% IV-thrombolysis), 174 patients (58.4%) had increased cIMT. Compared to those with altered cIMT patients with normal cIMT showed higher successful reperfusion rates (114/121 [94%) vs. 151/174 [87%], OR 2.481, 95%CI 1.003 - 6.13) and were more likely to have a favourable outcome (median mRS 3 [IQR 3] vs. 4 [IQR 3], p<0.001). Multivariate logistic regression adjusted for NIHSS, age, IVT and peri-procedural complications also indicated that normal cIMT was associated with functional outcome (aOR 2.69, 95%CI 1.51 – 4.80).
Conclusions: Normal cIMT was associated with higher reperfusion rate and improved functional outcomes in patients with acLVO undergoing EVT.
Disclosures of Interest: No
Abstract N°: 2831
CAROTID ARTERY STENTING: INFLUENCE OF TAILORED ANTIPLATELET THERAPY
Pavol Vigláš1, Filip Cihlář1, Vojtech Smolka1, Jan Raupach2, Alex Hejčl1, David Černík1
1Masaryk Hospital, Czech Republic,2Fakultní nemocnice Hradec Králové, Czech Republic
On behalf of:
Background and aims: The objective of this study was to determine if routine antiplatelet responsiveness testing for patients undergoing carotid artery stenting (CAS) was associated with lesser incidence of tromboembolic complications and death.
Methods: All consecutive patients treated with CAS in a single institution were enrolled in a retrospective study. Antiplatelet therapy function test was performed and efficient antiplatelet therapy was set before the procedure. Incidence of procedure-related stroke or death within periprocedural period (0-30 days) have been evaluated and compared with results of large randomized control trials (RCT).
Results: A total of 241 patients were treated for atherosclerotic carotid stenosis, seven patients undergo CAS on both sides over time. There was 138 symptomatic (55,6%) and 110 asymptomatic stenoses (44,4%) Five tromboembolic complications (2,01%) occoured, four of them (1,61%) was procedure-related. Two patients died because of procedure-related stroke (0,82%). Incidence of procedure-related stroke or death was significant lesser compared to the results of CREST study (2,01 % vs. 4,81 %, p=0,0243) in the entire cohorts, and to the results of ICSS study in the symptomatic cohorts (2,86 % vs. 7,37 %, p=0,0243), respectively.
Conclusions: Tailored antiplatelet therapy in carotid stenting is safe and seems to be related with lesser incidence of procedure-related stroke/death rate.
Disclosures of Interest: No
Abstract N°: 2910
ENDOVASCULAR TREATMENT OF CEREBRAL VENOUS THROMBOSIS. A MULTICENTRIC STUDY
Jaime Alonso*1, Emma Canada Lahoz1, Carmen Ramos1, Carlos Ignacio Gomez-Escalonilla Escobar2, Alicia De Felipe Mimbrera3, Patricia Calleja4, Patricia de la Riva5, Carlos Tejero6, Laura Llull Estrany7, Santiago Trillo Senin1
1Hospital Universitario de La Princesa,2Hospital Clínico San Carlos,3Hospital Universitario Ramón y Cajal,4Hospital Universitario 12 de Octubre,5Hospital Universitario Donostia,6Hospital Clínico Universitario Lozano Blesa,7Hospital Clinic
On behalf of:
Background and aims: Cerebral venous thrombosis (CVT) stands as a potential clinical challenge whose treatment is based on anticoagulation. However, endovascular treatment (EVT) is occasionally necessary as rescue therapy. Our objective is to define the clinical and radiological profile of CVT undergoing EVT, as well as its evolution and prognosis.
Methods: Retrospective observational study with prospective data collection of patients with CVT treated with EVT between 2008 and 2022 in 7 national stroke centers. Their clinicoradiological profile, therapeutic management, technique, complications, evolution and prognosis were recorded.
Results: N=17 CVT undergoing EVT, 25% due to critical situation at baseline and 75% upon clinical or radiological worsening despite anticoagulation. Age 43 years(SD18), 70,5% women, baseline mRS 0(0-1). Upon decision of EVT: GCS 12(9-15), NIHSS 9(3-17), encephalopathy 53%, status epilepticus 11%, brain edema 77,7%, hemorrhagic infarction 66,6%. Technique: aspiration 80%, disruption and extraction 20%, venous stenting 10%, local thrombolysis 33,3%. Complications during EVT: 1 basilar artery thrombosis successfully recanalized, 1 obstructed venous sinus rupture (5,8%); after EVT: herniation necessitating craniectomy 16,7%, in-hospital mortality 17.6%, mRS3m>3 42,9% of survivors
Conclusions: In our study we observed how EVT was performed for patients who were critically ill at baseline or as rescue therapy for those worsening despite medical therapy. A larger multicentric study is needed to analyze the ideal candidate for these therapies in order to understand its potential.
Disclosures of Interest: No
Abstract N°: 2944
IMPACT OF RISK OF OBSTRUCTIVE SLEEP APNEA IN POST THROMBOLYSIS CONTEXT OF STROKE PATIENTS: A TRANSVERSAL STUDY
Thaise Braga De Oliveira1, Aurea Maria Lago Novais*1, Beatriz Santos Rogério2, Juliana Cerqueira Gomes1, Marina Soledad Benitez Bitencourt1, Renan Carvalho Castello Branco1
1Bahiana School of Medicine and Public Health,2Federal University of Bahia
On behalf of: Research Group of Vascular Neurology (GEPNeV)
Background and aims: Obstructive sleep apnea(OSA)is a disease of upper airways well associated with stroke through diverse mechanisms.Despite that,it still lacks studies about its role in outcomes after thrombolysis in stroke patients.This study aims to elucidate the difference of post thrombolysis outcomes in stroke patients with different risks of obstructive sleep apnea(OSA).
Methods: We performed a cohort.Patients were evaluated of risk of OSA with STOP-Bang and SOS scores; also, data of previouscomorbidities were collected. Outcomes evaluated were CTI time, internment time, delirium,infection,and death during internment.Patients were accompanied with Barthel and Rankin during 3,6 and 12 months.We compared groups with T test, Mann-Whitney, or chi-square(considering p<0.05).
Results: We obtained 323 patients,of which 36 were submitted to thrombolysis. 69% (64% male, mean age) high risk with STOP-Bang,and 47%(71% female)with SOS. Most relevant fidings in comparison between groups are summarized in tables 1,2 and 3.There were no differences between outcomes.
Conclusions: The risk oh the OSA changes the patient’s admission profile (patients with higher risk have better Rankin, admissional NIHSS and previous use of medications), however, it does not affect post-thrombolysis outcomes. Thrombolysis has the same safety profile, regardless of the risk of obstructive sleep apnea, but with a higher absolute number of hemorrhagic transformations in the high-risk group. The extended needle holder time on the context social vulnerability had Implication on outcomes.This study shows that, although OSA is a known risk factor of stroke and appears to be determinant in recovery, it does not impact differently in the context of post thrombolysis.
Disclosures of Interest: No
Abstract N°: 3008
SAFETY OF STENTING IN SYMPTOMATIC EXTRACRANIAL VERTEBRAL ARTERY STENOSIS: A SINGLE-ARM META-ANALYSIS AND SYSTEMATIC REVIEW
Rafael Eduardo Streit*1, Pedro Henrique Reginato1, Marianna Gerardo Hidalgo Santos Jorge Leite2, Elizabet Taylor Weba3, Maria Galvão4, Vivian Gagliardi5,6
1Federal University of Parana, Curitiba, Brazil,2School of Medicine Santa Marcelina, São Paulo, Brazil,3State University of the Tocantina Region of Maranhão, Imperatriz, Brazil,4Federal University of Piauí, Teresina, Brazil,5Santa Casa de São Paulo, São Paulo, Brazil,6Albert Einstein Israelite Hospital, São Paulo, Brazil
On behalf of: Rafael Eduardo Streit; Pedro Henrique Reginato; Marianna Gerardo Hidalgo Santos Jorge Leite; Elizabet Taylor Pimenta Weba; Maria Theresa Leal Galvão; Vivian Dias Baptista Gagliardi
Background and aims: Stenting is an important surgical treatment for symptomatic extracranial vertebral artery stenosis. However, the rates of clinical complications related to this procedure are uncertain. Therefore, we aimed to conduct a systematic review and single-arm meta-analysis in order to assess this procedure’s risks.
Methods: We systematically searched PubMed, Cochrane and EMBASE, from inception to 2nd December 2023, for studies analyzing the occurrence, during the entire follow-up period, of stroke, in-stent restenosis and all-cause mortality in patients who underwent surgery for stent placement in the extracranial portion of a symptomatic vertebral artery. Statistical analysis was performed using OpenMeta[Analyst]™ version 12.11.14. Heterogeneity was assessed with I² statistics.
Results: A total of 1641 patients from 25 studies were included. Follow-up ranged from 3 to 59 months. During the entire follow-up period, all-cause mortality occurred in 80 of 1252 patients (proportion of 0.04; 95% CI 0.019 – 0.061; p < 0.001), stroke in 29 of 1281 patients (proportion of 0.018; 95% CI 0.011 – 0.025; p = 0.870) and in-stent restenosis in 221 of 1417 patients (proportion of 0.137; 95% CI 0.094 – 0.180; p < 0.001).
Conclusions: The findings from this single-arm meta-analysis suggest that employing stents in the surgical management of symptomatic extracranial vertebral artery stenosis is deemed safe and has a low correlation to all-cause mortality and the incidence of stroke.
Disclosures of Interest: No
Abstract N°: 3015
EFFECT OF HOLMIUM: YAG LASER IRRADIATION CONCURRENT WITH PLGA- BASED ENCAPSULATED TPA NANOPARTICLES ADMINISTRATION ON ATHEROTHROMBOTIC STENOSIS
Hossein Mehrad*1,1,2,3, Solmaz Tasdighi Matanagh2
1Islamic Azad University, Department of Physics, Tabriz, Iran,2Mehrad Research Lab, Division of Translational Medicine Development of Noninvasive Treatments, Tabriz, Iran,3Islamic Azad University, Laboratory of Novel Technologies in Non- Invasive Treatments, Tabriz, Iran
On behalf of:
Background and aims: Thrombus formation on a disrupted atherosclerotic plaque is a key event that leads to atherothrombosis. The aim of this study was to generate a hamster abdominal aorta model of atherothrombotic stenosis with morphological similarities to the human disease and the subsequent assessment of the reliability of B- mode ultrasound- guided Holmium: YAG laser therapy accompanied by PLGA- based encapsulated tPA nanoparticles administration in this model
Methods: Briefly, Golden Syrian hamsters were submitted to abdominal aorta atherothrombotic stenosis by primary balloon injury followed 1.5% cholesterol- rich diet injury for 12 weeks and finally perivascular severe cold injury. Then treatment group underwent catheter- based Holmium: YAG laser-induced liquid jet knife-mediated thrombolysis, concurrent with PLGA- based encapsulated tPA nanoparticles (0.8 mg/kg) administration, wherein diagnostic B- mode ultrasound is combined with the therapy system, with a goal of increased safety
Results: Results from color Doppler and B-mode ultrasonography and histopathology, showed a significant reduction in the mean value for thrombus content, blood mean velocity and the percentage of luminal cross-sectional area of stenosis and a significant increase in the mean value for blood volume flow at the stenotic region in the treatment group compared with the other groups (p <0.05)
Conclusions: Enhanced photoporation effect of Holmium: YAG laser, induced by inertial cavitation effect of collapsed capsules, can cause to enhancement of tPA nanoparticles penetration within the thrombus. Furthermore, catheter- based Holmium: YAG laser-induced liquid jet knife-mediated thrombolysis effect, can cause to enhance anti-thrombotic effect of tPA nanoparticles and significantly dilate the luminal cross- sectional area of stenosis
Disclosures of Interest: No
Abstract N°: 3149
THROMBOLYTIC VS DUAL ANTIPLATELET TREATMENT IN SELECTED PATIENTS WITH PRESUMED NON-EMBOLIC STROKE
Marta Olive Gadea*1, Federica Rizzo1, Marc Rodrigo-Gisbert1, Maria Angeles Muchada Lopez1, Marta Rubiera1, Alvaro García-Tornel Garcia-Camba1, Jordi Mayol1, Renato Simonetti1, Noelia Rodriguez-Villatoro1, Marc Ribo1
1Vall d’Hebron University Hospital, Stroke Unit, Neurology, Barcelona, Spain
On behalf of:
Background and aims: Dual antiplatelet therapy (DAPT) has shown non-inferiority to intravenous thrombolysis (IVT) in non-disabling minor strokes. After IVT, antiplatelet treatment delay and tighter blood pressure controls could be associated to early neurological deterioration due to residual thrombus progression or hemodynamic impairment. We aim to compare the impact of IVT vs DAPT therapy in selected patients with presumed non-embolic stroke.
Methods: We performed a single-center retrospective (January 2020 to December 2023) analysis of consecutive patients with mild to moderate ischemic stroke (NIHSS 1-9) presenting within 6 hours of onset, and received either acute DAPT or IVT. Patients with confirmed arterial occlusion, CTP maps suggestive of distal emboli or cortical symptoms were excluded. We evaluated the association between treatment and clinical improvement at discharge, 90-day mRS and neurological complications.
Results: Of the 136 patients included the analysis, 51 (38%) received IVT. Patients in the IVT group had higher baseline NIHSS (4[2-5] vs 3[1-4], p<0.001). There were no differences in baseline variables including mRS or onset-to-door times. After adjusting by baseline NIHSS, acute treatment was not associated with neurological improvement at discharge (aOR 0.97[0.49-1.92; p= 0.918]) or with 90-day mRS (aOR 2.03[0.81-4.02], p=0.132). No sICH occurred in either group, but one death related to a systemic hemorrhage occurred in the IVT group. Rates of early stroke recurrence and neurological deterioration (+4 NIHSS points) were IVT: 4(7.8%) vs DAPT: 2(2.4%) (p=0.131).
Conclusions: No treatment effect was observed between IVT and DAPT groups for neurological outcomes in a cohort of selected patients with initially presumed non-embolic stroke.
Disclosures of Interest: No
Abstract N°: 3195
IMPACT OF NEUROINTERVENTION - BASED PHOTOBIOMODULATION THERAPY USING POLARIZED YELLOW LIGHT EMITTING DIODES, ON ARTERIAL STRUCTURAL CHARACTERISTICS
Hossein Mehrad*1,2,3, Solmaz Tasdighi Matanagh2
1Islamic Azad University, Department of Physics, Tabriz, Iran,2m, Division of Translational Medicine Development of Noninvasive Treatments, Tabriz, Iran,3Islamic Azad University, Laboratory of Novel Technologies in Non- Invasive Treatments, Tabriz, Iran
On behalf of:
Background and aims: A blood vessel aneurysm is a bulge that develops due to a weakening in the vessel wall, typically where it branches. The blood pressure causes a small area to expand outwards when the blood flows through the blood vessel that has become weak. This study’s objective was to assess the impact of photobiomodulation therapy on carotid artery aneurysm
Methods: Briefly, carotid artery aneurysm was induced in New Zealand white rabbits by placing sterile cotton gauze directly on the artery for 40 minutes while it was saturated with 1.2 mol/L calcium chloride. The media layer was thinned, the collagen dispersion was significantly increased, and the elastin fibers were fragmented, according to histopathology findings. The animals were administered catheter- based polarized yellow light LEDs photobiomodulation therapy (570 ±15 nm, 120 J/cm2). A computerized analytic technique was employed to analyze ultrasound images in the rabbits’ artery’s wall.
Results: Histology and ultrasound results showed a significant increase in the mean value for the smooth muscle cells and collagen density, arterial thickness, radial strain, longitudinal strain, compliance and distensibility index and significant reduction in the mean value for the elastic modulus, resistive and pulsatility index in the treatment group compared with the other groups (p<0.05)
Conclusions: Yellow light phototherapy modifies matrix metalloproteinase expression and activity, as well as collagen formation, extracellular matrix protein expression, smooth muscle cell proliferation, and the pro-inflammatory cytokine interleukin(IL)-1β gene expression from arterial cells. The aneurysm- artery structural characteristics and biomechanical parameters can be improved by yellow light photobiomodulation therapy.
Disclosures of Interest: No
Abstract N°: 3224
A NEW SIMPLE SCORE TO PREDICT DISTAL BALLOON GUIDE CATHETER PLACEMENT
Givi Lengvenis*1, Alicija Krasavceva2, Marius Kurminas1, Andrius Berukstis1, Rokas Gircius1, Andrej Afanasjev3, Algirdas Edvardas Tamosiunas1
1Vilnius University Faculty of Medicine, Institute of Biomedical Sciences, Department of Radiology, Nuclear Medicine and Medical Physics, Vilnius, Lithuania,2Vilnius University Faculty of Medicine, Vilnius, Lithuania,3Republican Vilnius University Hospital
On behalf of:
Background and aims: The Balloon Guide Catheter (BGC) is employed in mechanical thrombectomy (MTE) for flow reversal. Positioning the BGC distally in the cervical internal carotid artery (ICA) is important for achieving the best results; however, this is not always possible due to cervical ICA tortuosity. We have developed a score for predicting distal BGC positioning from preprocedural computed tomography angiography (CTA) images.
Methods: We prospectively enrolled 90 patients with M1 and M2 occlusions. Patients with cervical ICA tortuosity and kinks ipsilateral to the intracranial occlusion were included. Two radiologists measured angles in the proximal, middle, and distal thirds of the cervical ICA on the preprocedural CTA and assigned points according to the proposed score (Table).
Results: Median age was 75 (IQR 66–82), and 54.4% were women. The median NIHSS was 12 (IQR 8–16), with final TICI 2C-3 recanalization achieved in 70% of cases. Straightening of the cervical ICA and distal placement of the BGC were achieved in 63.3%. The area under the ROC for the proposed score was 0.949 (95% CI 0.897–1.000; p<0.001). The optimal cut-off value was 8, with 93% sensitivity and 97% specificity.
Conclusions: Our novel score shows promising results for predicting BGC distal placement. This tool could help plan MTE procedures and save time. Further validation in a larger cohort is planned.
Disclosures of Interest: No
Abstract N°: 3256
MECHANICAL THROMBECTOMY IN ACUTE ISCHEMIC STROKE IN THE OLDER ADULTS
Dominika Jakubowicz-Lachowska*1, Anna Mironczuk1, Anna Milewska2, Alina Kulakowska1, Jan Kochanowicz1
1Medical University of Bialystok, Poland, Department of Neurology, Bialystok, Poland,2Medical University of Bialystok, Department of Biostatistics and Medical Informatics, Poland
On behalf of:
Background and aims: The mechanical thrombectomy (MT) has been established as a standard treatment for acute large artery occlusion. Despite the lack of an upper age limit, this procedure in people over 80 years of age carries a greater risk of failure. The aim of our study was to investigate the safety, functional laboratory outcomes of elderly patients treated with MT.
Methods: We retrospectively reviewed the records of ischemic stroke patients treated with MT, referred to our neurology department during the period (12/2017–12/2023). 254 patients (119 women and 135 men) were included in the study. We divided patients into older (<80 years) and younger (<80 years) groups. Variables included baseline NIHSS score, blood glucose (BG), lipids, presence of hypertension (H), atrial fibrillation (AF), age, gender, BMI, IV tPA, TICI score. Outcome measures were hemorrhagic transformation (HT) on 24-hour postoperative head CT and modified Rankin Scale (mRS) after hospital discharge.
Results: Among 254 patients (68,7±12), 93 (36,6%) experienced HT after thrombectomy. Compared with the older group, the younger group had higher CHOL levels (p=0,0002), also had more higher LDL CHOL levels (p=0,0002) and TG levels (p=0,04). Younger patients had statistically significantly more often mRS score £2 upon discharge (p=0,042). A statistical relationship was also demonstrated between age and: gender (p=0,0006), H (p=0,01), AF (p=0,01), IVtPA (p=0,0004), LDL (p=0,002) and TG (p=0,01). No difference was detected of HT between two groups.
Conclusions: Increasing age is associated with a low rate of favorable functional outcomes and high mortality rates.
Disclosures of Interest: No
Abstract N°: 3296
REAL WORLD ANALYSIS OF FIRST PASS EFFECT AND SECOND PASS EFFECT AT A COMPREHENSIVE STROKE CENTER
Randy Bravo1, Shashvat Desai1, Paige Banyas1, Angelina Cooper1, Lori Graczyk1, Felipe Albuquerque2, Andrew Ducruet2, Ashutosh Jadhav2
1HonorHealth Research Institute, Neuroscience, Scottsdale, United States,2Barrow Neurological Institute, Neurosurgery, Phoenix, United States
On behalf of:
Background and aims: Mechanical thrombectomy (MT) is an effective treatment option for reperfusion of large vessel occlusions (LVOs). Achieving fast and complete reperfusion on the first pass, known as the first pass effect (FPE), is optimal. Achieving a second pass effect (SPE) is also ideal if a FPE is not attained. We aim to compare the occlusion locations and technique patterns seen in FPE, non-FPE, and SPE patients at our comprehensive stroke center (CSC).
Methods: A retrospective analysis was performed on a MT database between August 2019 – November 2021. The clinical and procedural information were analyzed amongst FPE and non-FPE patients with LVO strokes in the internal carotid artery (ICA), middle cerebral arteries (MCA-M1/M2), and basilar artery.
Results: 110 patients underwent EVT between August 2019 and November 2021. Mean age was 70 and 49% were females. FPE was observed in 18% (20) of patients. Patients with FPE had lower proportion of ICA occlusions (10% vs 33%, p=0.02) and higher utilization of manual aspiration thrombectomy (MAT) (65% vs 42%, p=0.06) compared to non-FPE patients. Amongst non-FPE patients, SPE was observed in 25.5% (23). Similarly, patients with SPE had lower proportion of ICA occlusions (9% vs 52%, p<0.01) and higher utilization of manual aspiration thrombectomy (MAT) (52% vs 21%, p=0.01) compared to non-SPE patients.
Conclusions: Rates of first pass effect and second pass effect at a CSC were 18% and 26%, respectively. Absence of internal carotid artery occlusions and utilization of manual aspiration thrombectomy were associated with first and second pass effect.
Disclosures of Interest: No
Abstract N°: 3311
DIRECT ORAL ANTICOAGULATION AS A REASON OF NON-THROMBOLYSIS IN PATIENTS WITH ACUTE ISCHEMIC STROKE
Espen Saxhaug Kristoffersen*1, David Seiffge2, Silje Holt Jahr1, Ole Morten Ronning1, Thomas Meinel2
1Akershus University Hospital, Department of Neurology, Lørenskog, Norway,2Inselspital Bern University Hospital and University of Bern, Department of Neurology, Bern, Switzerland
On behalf of:
Background and aims: International guidelines advise against intravenous thrombolysis (IVT) in patients with acute ischemic stroke (AIS) and recent ingestion of direct oral anticoagulants (DOAC). We aimed to determine the proportion of AIS in patients with recent DOAC intake (<48h) otherwise qualifying for IVT.
Methods: A retrospective study conducted at a University Hospital, serving as the primary hospital for 10% of the population in Norway. Consecutive patients with AIS between January 1st, 2015, and December 31st, 2023 were included. Time from symptom onset to admission, stroke severity, indications for IVT, DOAC (type, dosage, indication, last known ingestion), and imaging findings including large vessel occlusion were recorded.
Results: Almost 6000 patients were included. Overall, 10% of all patients with AIS had preceding DOAC use (median age 80 (IQR 74-86), 40% female). 12% of those arriving at the hospital within 4.5 hours had a recent intake of DOAC with increasing rates over the study period. Among those excluded from IVT due to DOAC use, 46% had National Institute of Health Stroke Scale score >3 and 30% had large vessel occlusion. Detailed information on the % that fulfill the criteria of a hypothetical randomized controlled trial and in-depth analysis including time trends will be presented at ESOC.
Conclusions: A substantial and increasing proportion of patients with AIS are disqualified from IVT due to recent DOAC ingestion. RCTs are feasible and urgently warranted to assess safety and efficacy of IVT in these patients. Our data helps to inform upcoming RCTs on this burning topic.
Disclosures of Interest: No
Abstract N°: 3336
OUTCOMES FOLLOWING MECHANICAL THROMBECTOMY FOR PATIENTS WITH LARGE INFARCT CORE IN A REAL-WORLD OBSERVATIONAL REGISTRY
Muireann Byrne*1, Aisling O’reilly1, Karl Boyle1, Patrick Nicholson2, Patricia Fearon1
1Beaumont Hospital, Department of Stroke Medicine, Dublin, Ireland,2Beaumont Hospital, Department of Interventional Neuroradiology, Dublin, Ireland
On behalf of:
Background and aims: The recent publication of several randomised controlled trials reporting net clinical benefit of mechanical thrombectomy(MT) for patients presenting with large infarct core volumes has been a hot topic amongst stroke clinicians tasked with re-organising referral pathways. Our centre has previously treated occasional patients with larger infarct core volumes. We aimed to describe outcomes for large core thrombectomy patients in a real-world observational registry.
Methods: Consecutive patients treated with MT were prospectively recorded between January 2012 and December 2022. Large infarct core was defined as a baseline ASPECTS score of ⩽ 5. Primary outcome was 90-day mRS.
Results: A total of 2211 patients treated with MT were recorded. We excluded 45 patients with missing baseline ASPECTS (2%) and a further 111 patients with posterior circulation vessel occlusion. Of the remaining 2055 patients, 59 had a baseline ASPECTS of ⩽5. Mean age was 63.9years (SD:17.8), median baseline NIHSS was 19 (IQR: 15,20) and all but 3 patients had pre-stroke mRS of zero. Successful recanalization was achieved in 52/59 patients (90%). Median onset to recanalization time was 399 mins (IQR:305, 675). Good functional outcome (mRS 0-2) was achieved in 30%, ambulant outcome (mRS 0-3) in 46%, bedbound outcome (mRS 5) in 11% and death (mRS 6) in 16%. Of the 6 patients aged ⩾80 years, all had mRS 5/6 at 90-day follow up.
Conclusions: Outcomes for patients with large infarct core treated with mechanical thrombectomy in a real world observational registry have achieved clinical outcomes that closely reflect recent RCT results.
Disclosures of Interest: No
Abstract N°: 794
Category: 4.27 BRAIN REORGANISATION AND RECOVERY
THE EFFECT OF A HIGH- VERSUS LOW-SALT DIET COMPARED TO A STANDARD DIET ON STROKE RECOVERY
Frederike Anne Straeten*1, Jan-Kolja Strecker1, Louisa Müller-Miny1, Mailin Hannah Marie Koecke1, Lucia Härtel1, Maike Hoppen1, Birgit Schmeddes1, Antje Schmidt-Pogoda1
1Münster University Hospital, Department of Neurology with Institute of Translational Neurology, Münster, Germany
On behalf of:
Background and aims: The global incidence of stroke in the younger population compared to older generations is alarmingly increasing. This represents an unmet need of exploring lifestyle interventions to attenuate stroke-associated disability and prevent secondary non-motor consequences of stroke. These are not only caused by the lesion itself, but also by a deranged and sustained proinflammatory immune reaction after stroke. Non-pharmacological interventions to skew the immune response into a rather regulatory one are of special interest. High sodium intake induces pathogenic T helper cells associated with tissue inflammation and pronounced secretion of pro-inflammatory cytokines. The phagocytic capacity of macrophages – essential for clearing debris and thereby supporting tissue regeneration – is attenuated upon a high-salt diet. We have previously shown that regulatory T cells are essential for stroke recovery. Our aim here is to investigate the immunological effect of a high- vs. low-salt diet compared to standard diet in the subacute recovery phase after stroke and its functional implications.
Methods: 27 mice were subjected to photothrombotic stroke (n = 9 each; high-salt diet containing 4% sodium chloride, low-salt diet containing <0.03% sodium chloride and standard diet). Over 7 weeks we performed weekly functional testing (foot fault and adhesive tape test). After the experiment we performed histological and molecular analyses regarding infarct volume, connectivity, and inflammatory gene expression.
Results: Preliminary results indicate a worse functional outcome upon a high-salt diet. Further results shall be presented at the ESOC 2024.
Conclusions: The conclusion shall be presented at the ESOC 2024.
Disclosures of Interest: No
Abstract N°: 2082
Category: 4.10 PROGNOSIS AND OUTCOME AFTER STROKE
DIFFERENTIAL CLINICAL-RADIOLOGICAL CHARACTERISTICS OF CEREBRAL VENOUS THROMBOSIS ASSOCIATED WITH HORMONAL CONTRACEPTIVES
CELIA ROMERO DEL RINCON*1, Carmen Ramos1, Jaime Alonso1, Carmen Sánchez-Rodríguez1, Alba Lopez Bravo2, Herbert Tejada Meza3, Alicia De Felipe Mimbrera4, Santiago Trillo Senin1
1Hospital de La Princesa, Madrid, Spain,2Hospital Reina Sofía, Tudela, Spain,3Miguel Servet University Hospital, Zaragoza, Spain,4Ramón y Cajal Hospital, Madrid, Spain
On behalf of:
Background and aims: The use of Hormonal Contraceptives(HC) in patients suffering from cerebral venous thrombosis(CVT) is prevalent. We investigated whether the clinical and radiological characteristics of CVT in women taking HC differ from those in patients who do not.
Methods: A multicenter observational retrospective study was conducted. Patients with CVT treated at 11 centers in Spain from 2008 to 2021 were included. Clinical, radiological, and prognostic variables were recorded and compared between the non-HC-associated group(CVT-noHC) and the HC-associated group(CVT-HC).
Results: N=256. Males 127(49.6%), females 129(50.4%), of which 48(37.2%) were taking HC. The mean age differed between CVT-HC 32.02(SD=9.31) and CVT-noHC 53.99 (SD=17.92)(p<0.001). No differences were found in clinical presentation. Regarding radiological characteristics, the non-HC group showed a significantly higher percentage of normal baseline CT (40.1% vs. 20.8%)(p=0.02), lower sinus or vein hyperdensity (21.3% vs. 37.5%)(p=0.03), a tendency towards less edema or infarction (8.5% vs. 15.2%)(p=0.18), and a lower combination of signs(16.4% vs. 22.9%)(p=0.39), although hemorrhage was more frequent in CVT-noHC (15% vs. 4.2%)(p=0.07). The initial admission location differed between CVT-noHC and CVT-HC patients with(7.7% vs. 12.5%) in the ICU,(33.7% vs. 52%) in the Stroke Unit, and(58.7% vs. 35.4%) in conventional hospitalization(p=0.014). No differences were found in prognosis.
Conclusions: Our study suggests that patients with CVT associated with HC are younger, with a higher percentage admitted to the ICU or Stroke Unit, without differences in clinical severity but with a higher percentage of abnormalities in the initial baseline CT compared to patients not taking HC. No differences were observed in prognosis.
Disclosures of Interest: No
Abstract N°: 2271
Category: 4.17 INTRACEREBRAL HAEMORRHAGE
DECOMPRESSIVE HEMICRANIECTOMY WITHOUT EVACUATION OF HEMATOMA IN INTRACEREBRAL HEMORRHAGE IN THE PHILIPPINES
Rodelia Pascua*1, John Harold Hiyadan2
1Baguio General Hospital and Medical Center, Neurology, Baguio, Philippines,2Baguio General Hospital and Medical Center, Baguio, Philippines
On behalf of:
Background and aims: Decompressive hemicraniectomy (DC) is well-established in ischemic stroke. It is important in the management of increased intracranial pressure thus improving clinical outcomes. DC and its application to intracerebral hemorrhage (ICH) without the evacuation of hematoma remains to be unclear.
Methods: This is a tertiary hospital-based, observational, review of records that enrolled 65 patients who were admitted in the Neuroscience department from January 2017- August 2022. We analyzed the clinical, radiological characteristics and the surgical inclusion time to DC.
Results: Of all the 59 patients with ICH score < 3, 28 had mRS < 3, none died. All of them had mild to moderate stroke based on NIHSS. Among 6 patients with ICH score 3 and NIHSS > 18, all patients died. All patients with ICH score 4 and 5 and NIHSS > 25 also died. The increase in ICH score and NIHSS was associated with poor clinical outcome in the present study despite undergoing decompressive hemicraniectomy. Mortality rate was found to be high when the size exceeded 50 cm3 and those who underwent secondary phase of edema. Overall mortality was 9%, and morbidity (mRS 3/4/5) was 28% among patients who underwent decompressive hemicraniectomy without evacuation of hematoma within 48 hours. Three underwent decompressive hemicraniectomy during the secondary phase of edema (> 48 hours) with 66% morbidity rate and 33% mortality rate.
Conclusions: Decompresive hemicraniectomy without hematoma evacuation might be a safe and effective in patients based on the clinical manifestations, hematoma volume and time of surgical intervention.
Disclosures of Interest: No
Abstract N°: 2613
Category: 4.06 EPIDEMIOLOGY & RISK FACTORS
REAL-WORLD DIAGNOSIS OF ATRIAL FIBRILLATION IN THE SUBGROUP OF PATIENTS WITH ENDOVASCULAR TREATMENT AND UNKNOWN ETIOLOGY
Pere Cardona P.*1, Blanca Lara Rodriguez1, Andres Paipa1, Anna Nuñez1, Elena Quesada1, Anna Escrig Avellaneda2, Ester Catena3, Sergio Campoy4, Maria Angeles De Miquel5, Manuel Gomez Choco6
1Hospital Universitari Bellvitge, Department of Neurology, L’Hospitalet de Llobregat,2Parc Sanitari Sant Joan de Deu Sant Boi., Department of Neurology, Sant Boi,3Consorci Sanitari Garraf -Penedès., Department of Neurology, Vilafranca Penedès.,4Hospital Viladecans, Department of Neurology, Viladecans,5Hospital Universitari Bellvitge, Department of Neuroradiology, L’Hospitalet de Llobregat,6Hospital Moises Broggi, Department of Neurology, Sant Joan Despí
On behalf of:
Background and aims: Atrial fibrillation (AF) could be the main cause of large vessel occlusion strokes of unknown sources. New devices for prolonged recording of heart rhythm and algorithms are used since 2019 for the diagnosis of AF after hospital discharge with 5.2% AF detection in our population in the first month. However, its impact on actual and routine healthcare is challenging.
Methods: We review and follow-up patients treated with endovascular treatment (EVT) of unknown cause from 2010 to 2019. We analyzed the percentage of new diagnosis of atrial fibrillation and stroke recurrence in our National Electronic Healthcare Database during follow-up. We analyze several epidemiologic variables, functional recovery and other relevant pathologies.
Results: A total of 201 patients of unknown etiology were analyzed during mean 6.2 years of follow-up time, 9.5% of patients were diagnosed of AF in this period after stroke. Variables associated with statistically significance to AF finding were >6 supraventricular extrasystoles or tachycardia in 24Holter test and severe auricular dilatation (>41 mm) evaluated during hospitalization.
However, only two cases (1.9%) were associated to recurrence of minor stroke and none with mortality.
Other diagnoses were malignant neoplasm (5%) and delayed seizures (4.2 %).
Conclusions: The incidental diagnosis of atrial fibrillation at long-term follow-up of patients requiring EVT and unknown etiology is discrete (9,5%), but stroke recurrence is rare (<2%). It could be a good Key Performance Indicator of our stroke diagnostic strategy. We must select efficiently patients for detection of atrial fibrillation by long-term heart rhythm recording based on signs of atrial impairment.
Disclosures of Interest: No
Abstract N°: 2624
Category: 4.19 COGNITION AND VASCULAR COGNITIVE IMPAIRMENT
COGNOSPEAK: A FEASIBILITY PILOT STUDY OF AUTOMATED SPEECH ANALYSIS TO AID COGNITIVE ASSESSEMENT POST STROKE
Simon Bell*1, Bahman Mirheidari2, Kirsty Harkness3, Mary Sikaonga4, Jonathan Gardner4, Madalina Roman4, Jo Howe4, Emma Richards4, Heidi Christensen2, Daniel Blackburn1
1Sheffield Institute for Translational Neuroscience, Neuroscience, Sheffield, United Kingdom,2The University of Sheffield, Computer Science, Sheffield, United Kingdom,3Sheffield Teaching Hospitals NHS Foundation Trust, Neurology, Sheffield, United Kingdom,4Sheffield Teaching Hospitals NHS Foundation Trust, Stroke Medicine, Sheffield, United Kingdom
On behalf of:
Background and aims: Stroke survivors (SSs) often experience cognitive decline following initial stroke, necessitating repeat cognitive assessments. Current methods of assessment, such as Montreal Cognitive Assessment (MoCA), are time-consuming and rely on health-care professionals. Addressing these challenges, our paper introduces the first system of its kind using an automated system to assess cognition in SS.
Methods: CognoSpeak is an automated cognitive assessment system that is used initially on the ward post-stroke and subsequently at home. CognoSpeak assesses cognitive decline via a user interface of a virtual agent. SS answer questions and complete cognitive tests. CognoSpeak then uses Artificial intelligence methods to extract and process speech, language, and interactional cues for cognitive decline.
Results: In a cohort of 55 SS, CognoSpeak successfully predicted MoCA scores and identified cognitive decline predicated on a MoCA-based threshold (score < 26). Excellent performance on both predicted methods was seen when compared to recorded MOCA scores. Best regression result (Normalized Root Mean Squared Error (N-RMSE)) of 0.092. Direct classification of the MoCA score cutoff of < 26 yields a Specificity of 0.73, Sensitivity of 0.75. Demonstrating the first evidence of the system’s robustness in SS.
Conclusions: CognoSpeak can be used successfully in the acute stroke setting to predict cognitive scores of SS highlighting its use in streamlining and improving post-stroke cognitive assessment. Challenges of automated assessment on the stroke pathway include patient computer access, anxiety in using information technology resources and post-stroke apathy.
Disclosures of Interest: No
Abstract N°: 3128
Category: 4.29 CASE REPORTS
CAROTID WEB – THE OVERLOOKED CONTENDER
Samantha Wakerlin*1, Ahmed Gabr1, Sanam Lasi1, Nora Cunningham1, Maged Henin1, Averil Kenny2, Liga Akmenkalne2, Eamon Kavanagh2, Michael O’reilly3, Jude Ryan1
Background and aims: Carotid web (CW) is a rare, often underdiagnosed cause of cryptogenic stroke and is considered an atypical form of fibromuscular dysplasia. Despite optimal medical management, the stroke recurrence rate remains high, with a reported 17% risk over two years. Surgical intervention, either carotid endarterectomy (CEA) or stenting, is the treatment of choice, particularly in those with recurrent ischemic events. We present a case of cryptogenic stroke secondary to CW, retrospectively diagnosed following neuroradiology-stroke multidisciplinary discussion (MDM).
Methods: A 64-year-old male without significant cardiovascular risk factors presented outside of the thrombolysis window with symptoms of right MCA stroke. CT brain and angiogram (CTA) showed no evidence of acute infarction or large vessel occlusion. Laboratory investigations, Holter and blood pressure monitoring, and transoesophageal echocardiography were unremarkable.
Results: MRI brain demonstrated embolic right MCA territory infarction (Figure 1). Carotid ultrasonography revealed bilateral atheroma without significant stenosis. The patient was discharged home on optimal medical management with planned discussion at MDM. Neuroradiology highlighted CW as a possible aetiology, however a thrombus adherent to a ruptured carotid plaque could not be excluded, thus interval imaging was recommended. Repeat CTA showed persistence of a 3mm shelf-like projection from the posterior right carotid bulb (Figure 2), consistent with a CW. CEA was performed and a smooth structure that uniformly traversed the vessel wall, without appreciable atherosclerotic calcification, was identified (Figure 3). Neointimal hyperplasia was confirmed with histopathology.
Conclusions: CW should always be suspected in cryptogenic strokes. This case highlights the importance of MDM approach, particularly when the aetiology remains uncertain.
Disclosures of Interest: No
Abstract N°: 443
Category: 4.10 PROGNOSIS AND OUTCOME AFTER STROKE
COMORBITIES INFLUENCE ON SURVIVANCE AND FUNCTIONAL PROGNOSIS IN ELDERLY ISCHEMIC STROKE PATIENTS UNDERGOING SUCCESSFUL MECHANICAL THROMBECTOMY
Mario Bautista Lacambra*1,2, Herbert Tejada Meza1,2,3,4, Beatriz Pardinas Baron1,2, Diego Rodríguez-Gascón1,2, Esther Garcés-Antón5, Marta Serrano1,2,4, Marta Palacín-Larroy1,2,4, Cristina Moreno Loscertales2,6, Christian Josué Hernández-Rodríguez3, Javier Marta-Moreno1,2,4
1Miguel Servet University Hospital, Department of Neurology, Zaragoza, Spain,2IIS Aragon. Unidad de Investigación Clínica HUMS, Grupo de Investigación en Neurociencias, Zaragoza, Spain,3Miguel Servet University Hospital, Interventional Neuroradiology Unit, Department of Radiology, Zaragoza, Spain,4Miguel Servet University Hospital, Stroke Unit. Department of Neurology, Zaragoza, Spain,5Hospital Clinico Universitario Lozano Blesa, Department of Neurology, Zaragoza, Spain,6Hospital Ernest Lluch Martin, Department of Neurology, Calatayud, Spain
On behalf of:
Background and aims: we aim to investigate which comorbidities play a significant role in the functional prognosis of elderly patients who suffer an ischemic stroke and undergo mechanical thrombectomy, achieving successful reperfusion.
Methods: This retrospective hospital-based study focused on elder patients (>80 years) who experienced a stroke and underwent mechanical thrombectomy (N=250). We exclusively selected those patients who experienced a successful reperfusion and presented a favourable previous functional outcome (mRS⩽2) (n=204). We studied clinical information related to stroke assistance, comorbidities and functional outcome at three months.
Results: Women represented 57.8% of patients. Mean age was 86 (80-90) years. The most prevalent comorbidity was hypertension (83.3%), followed by atrial fibrillation (61.3%). When assessing the functional prognosis at three months, 31.4% of patients demonstrated a favourable functional outcome (mRS⩽2), while 24.2% had died. The most common aetiology of stroke was a cardioembolic source (65.2%). Multivariate analysis of mortality at three months revealed statistical differences in smoking, coronary artery disease, rheumatoid arthritis, heart failure, NIHSS, and time from symptom onset to reperfusion. Our model adjusts mortality better than Charlson (AUCmodel=0,825 vs AUCCh=0,662). Multivariate analysis of a favourable functional outcome at three months showed statistical differences in NIHSS and previous mRS, with no differences in comorbidities.
Conclusions: The decision-making process in the treatment of ischemic stroke in elderly is complex. Previous comorbidities could help to determine the risk of decease and could guide clinical decisions and management. However, more studies and models are needed as percentage of older patients rises in our clinical setting.

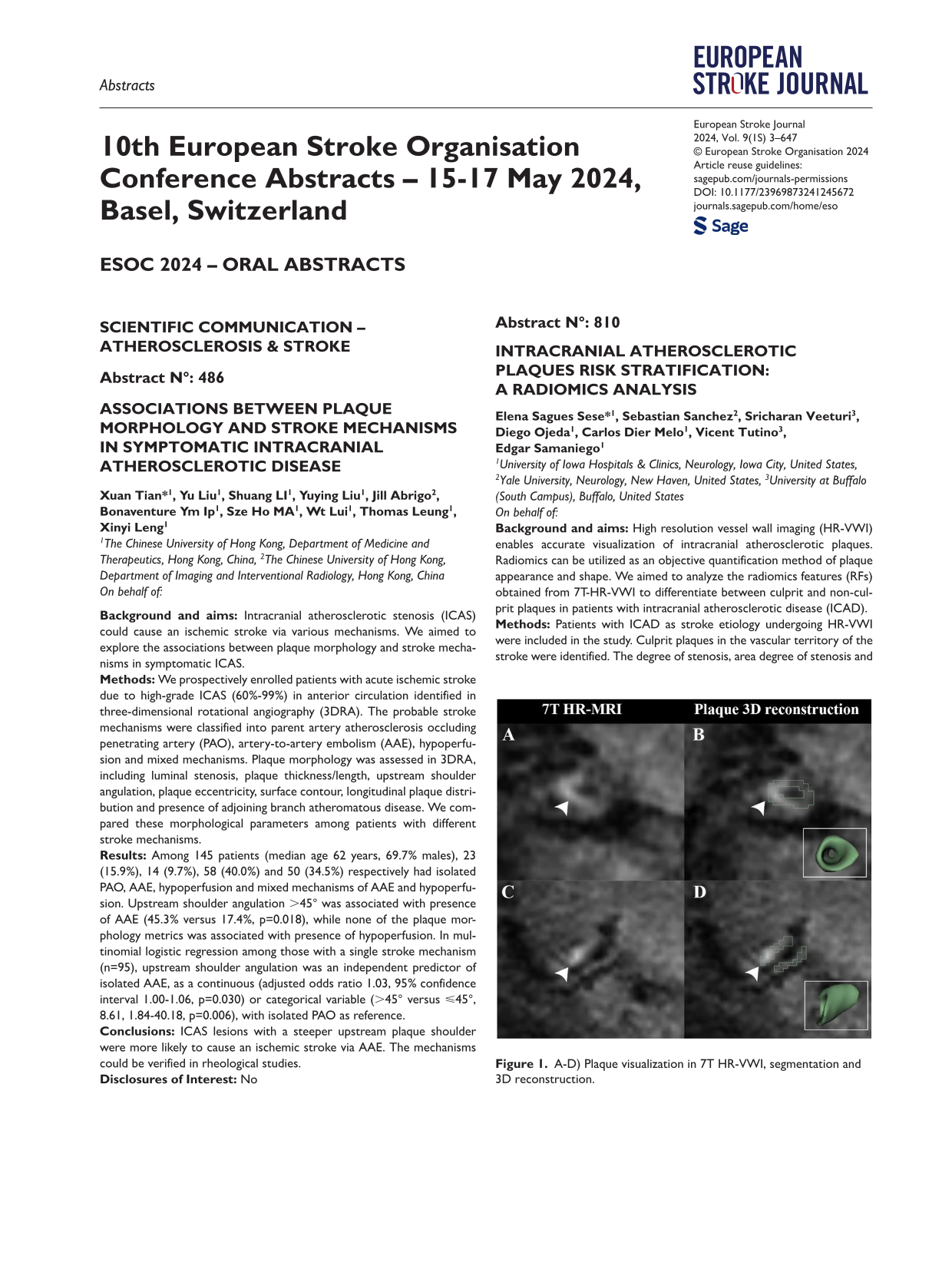
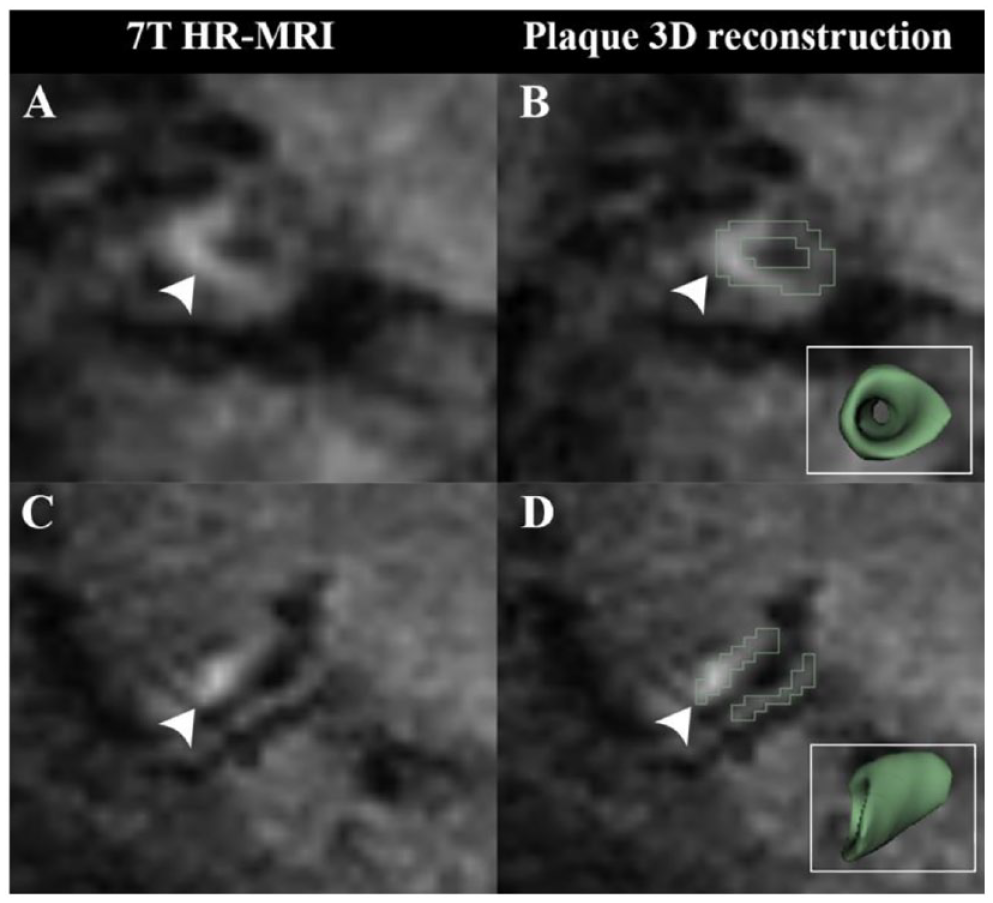
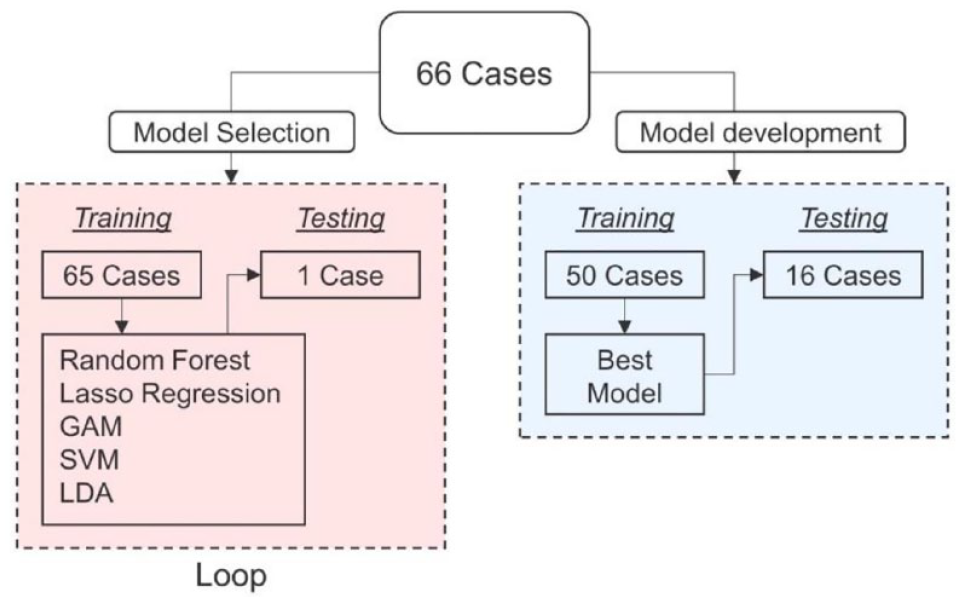
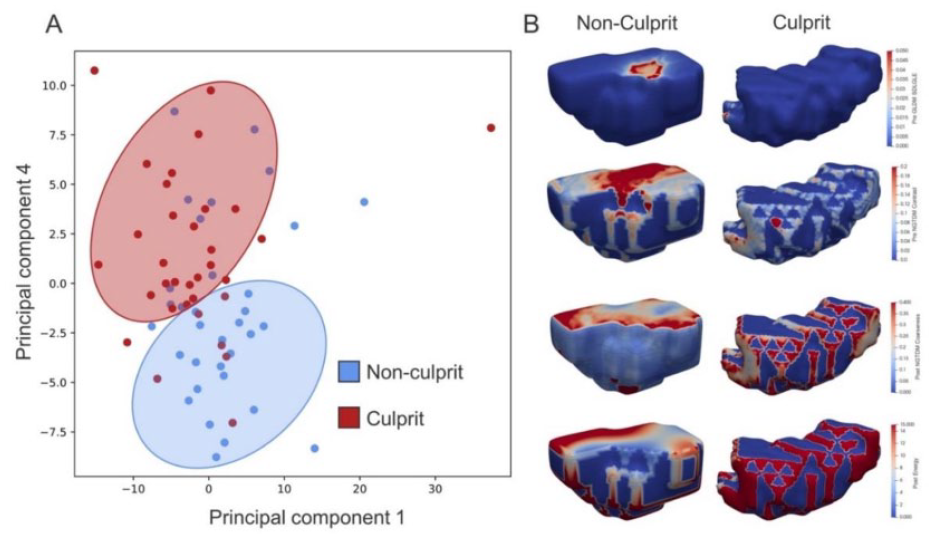
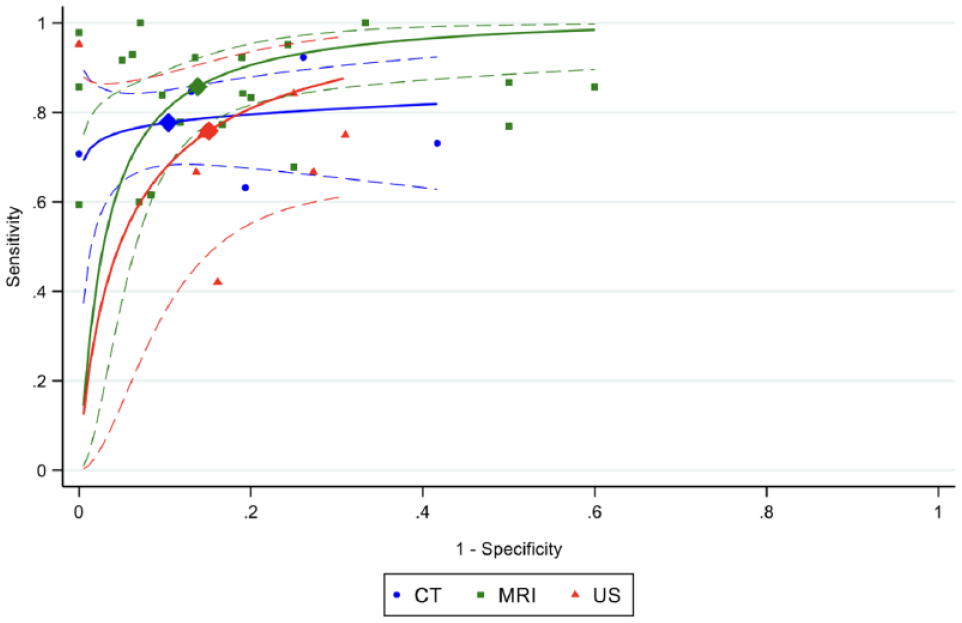
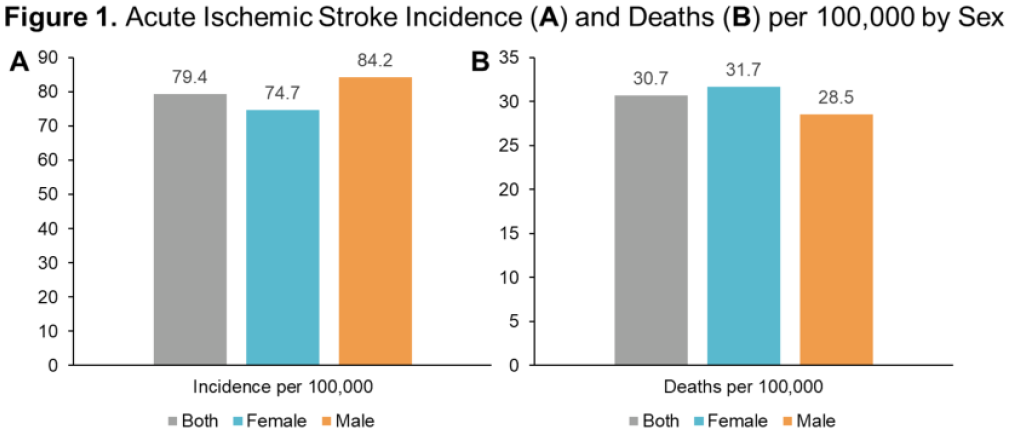
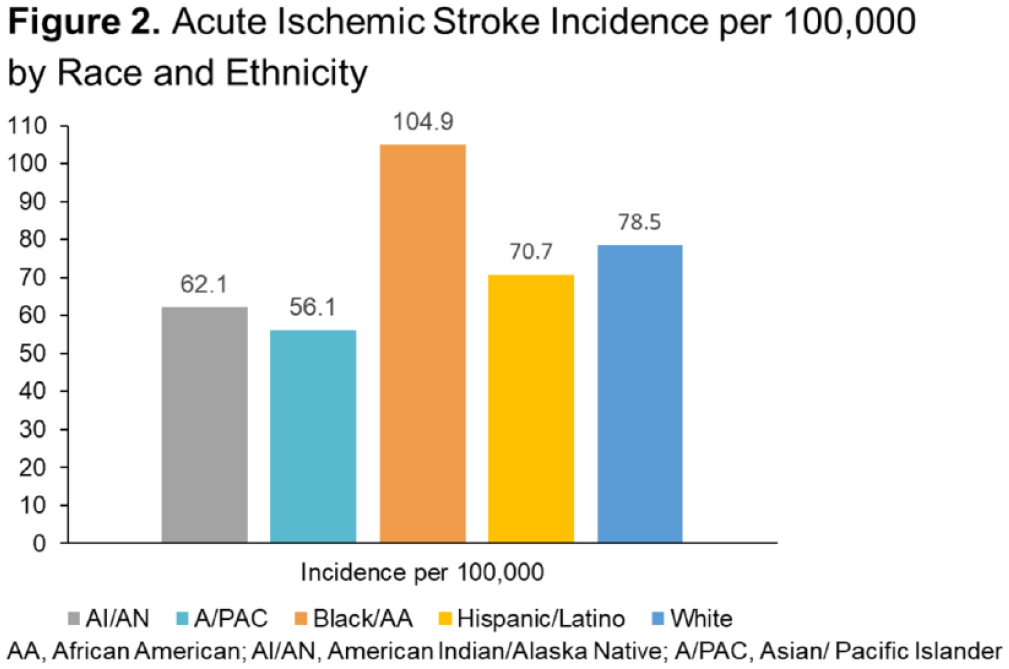
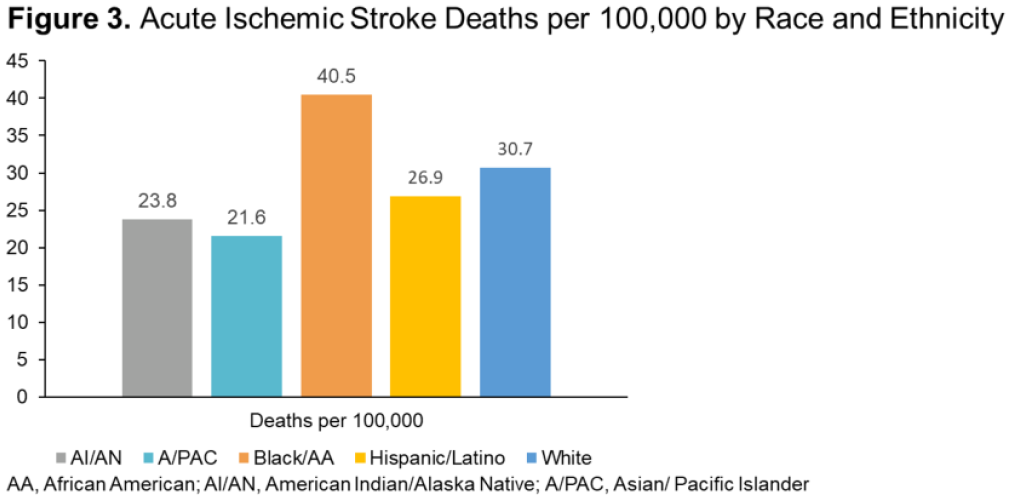
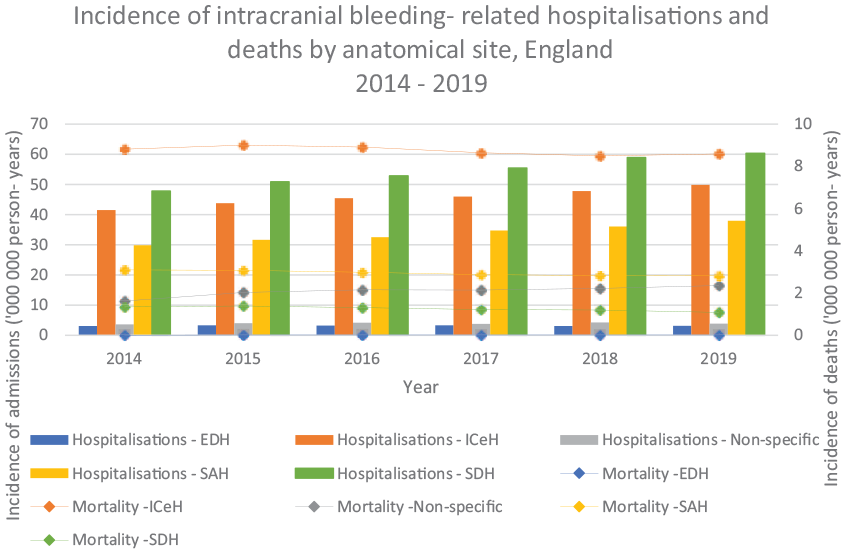
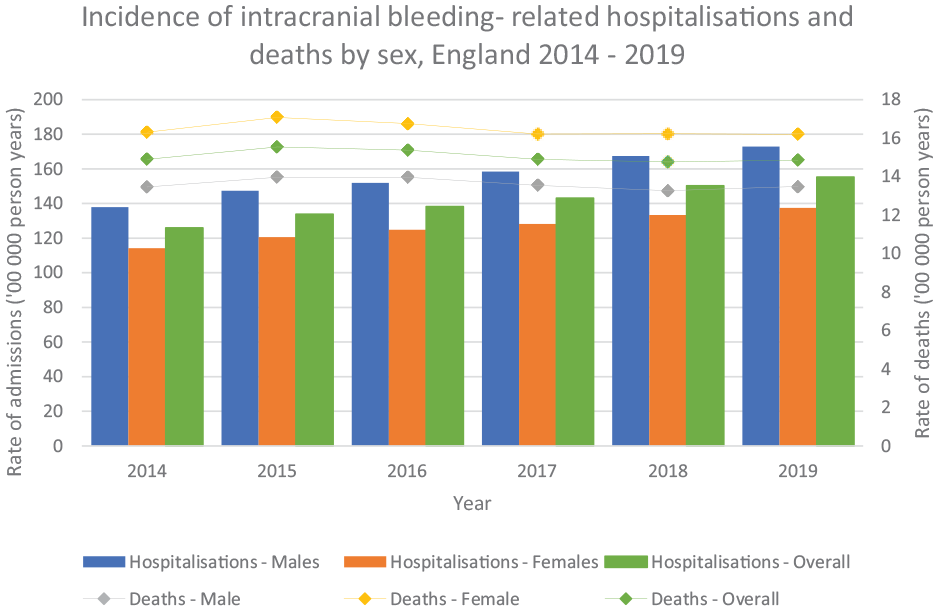
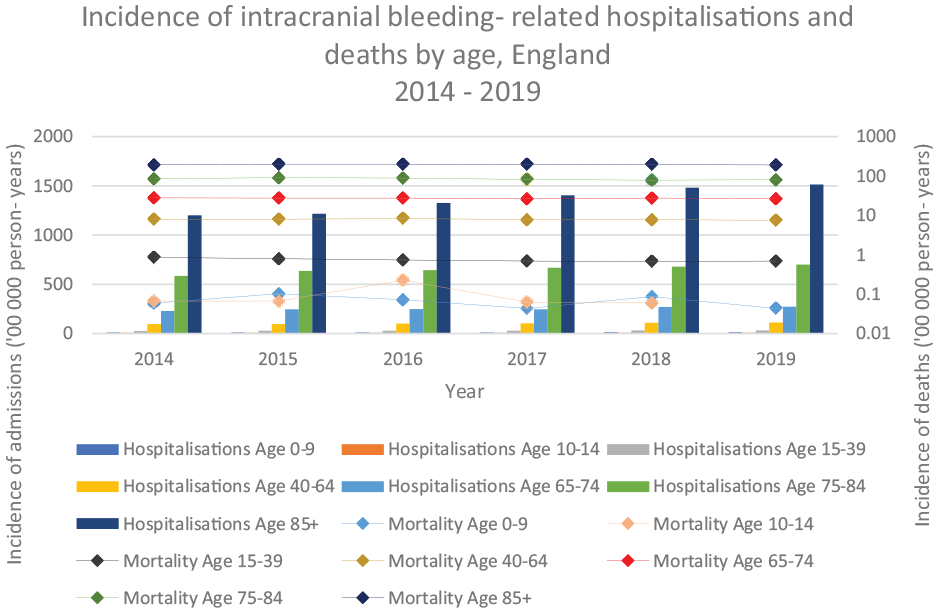
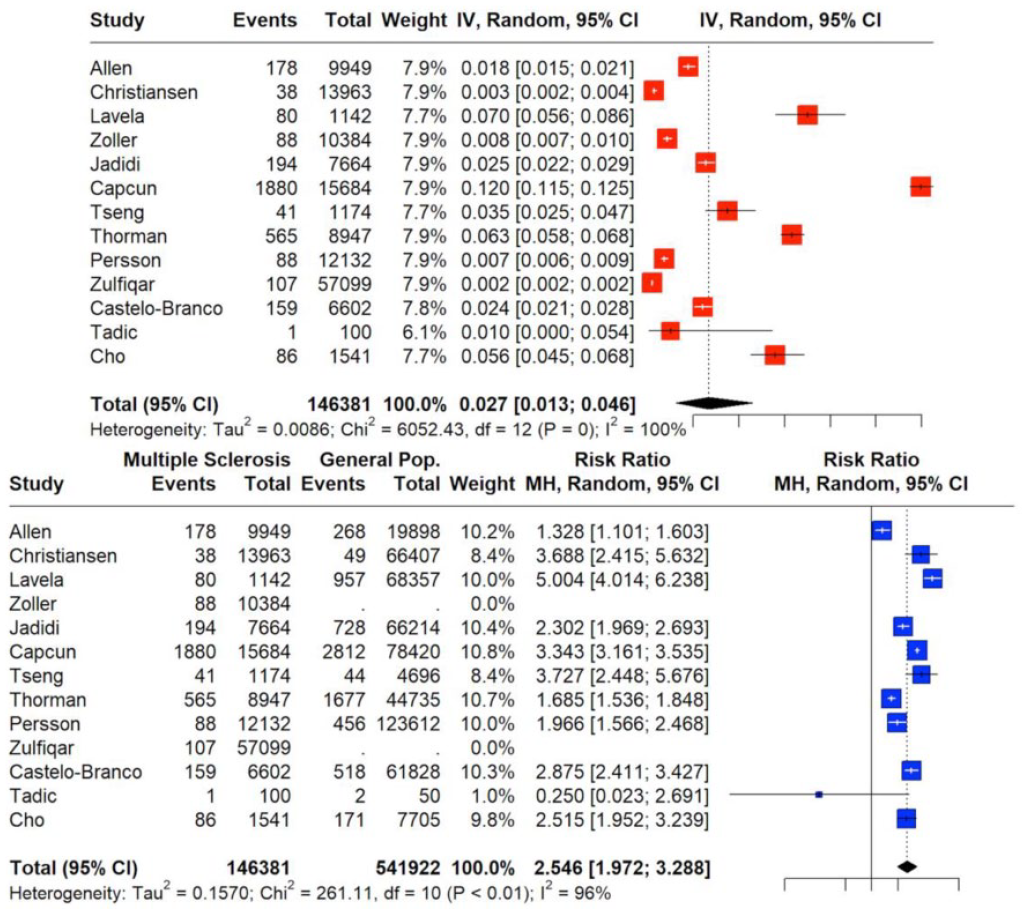
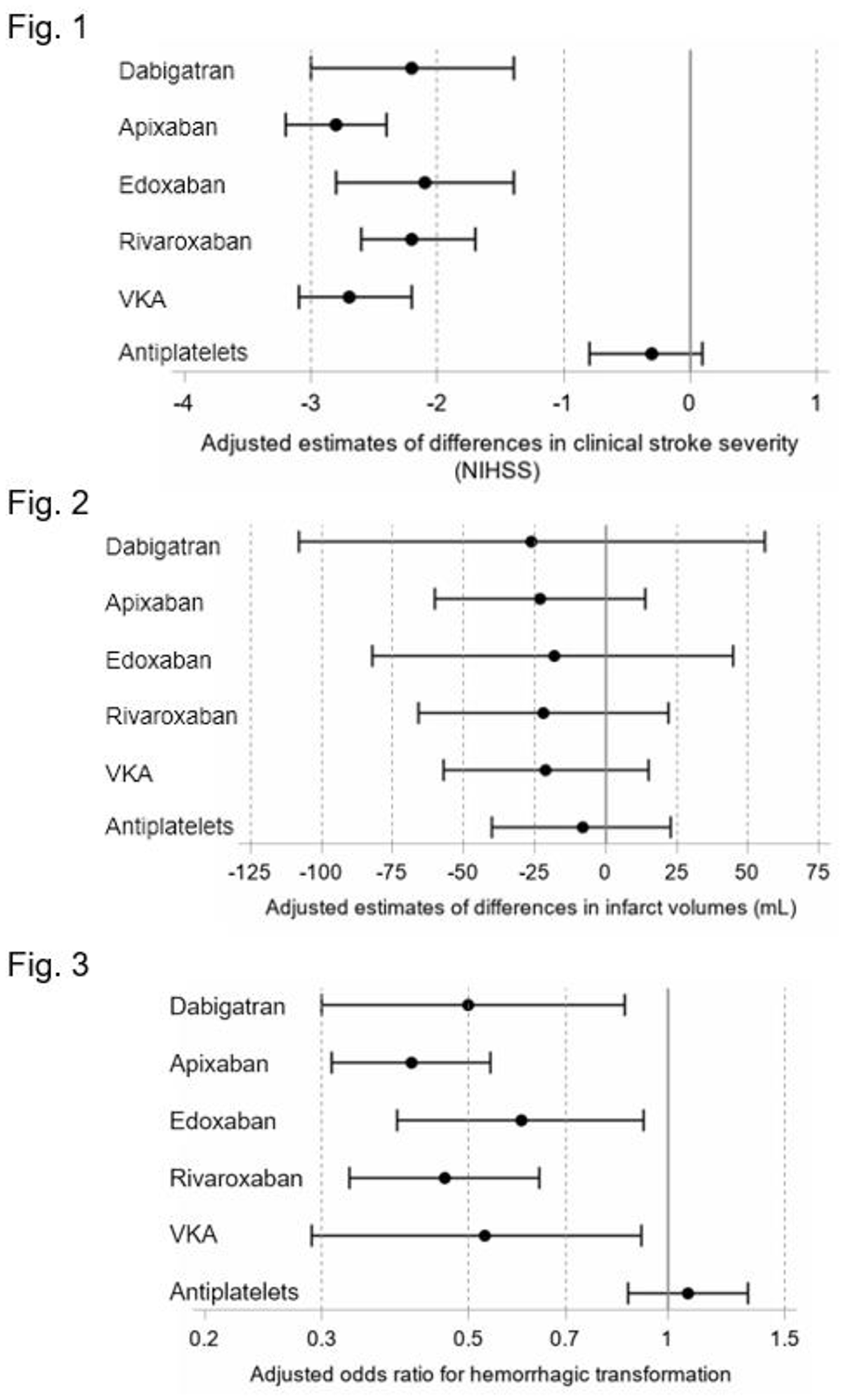
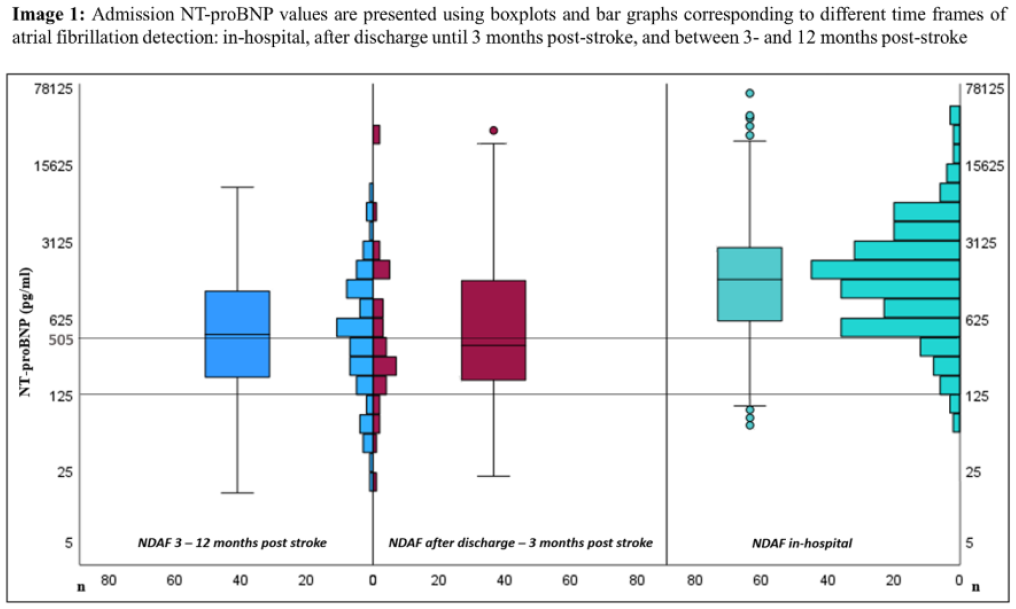
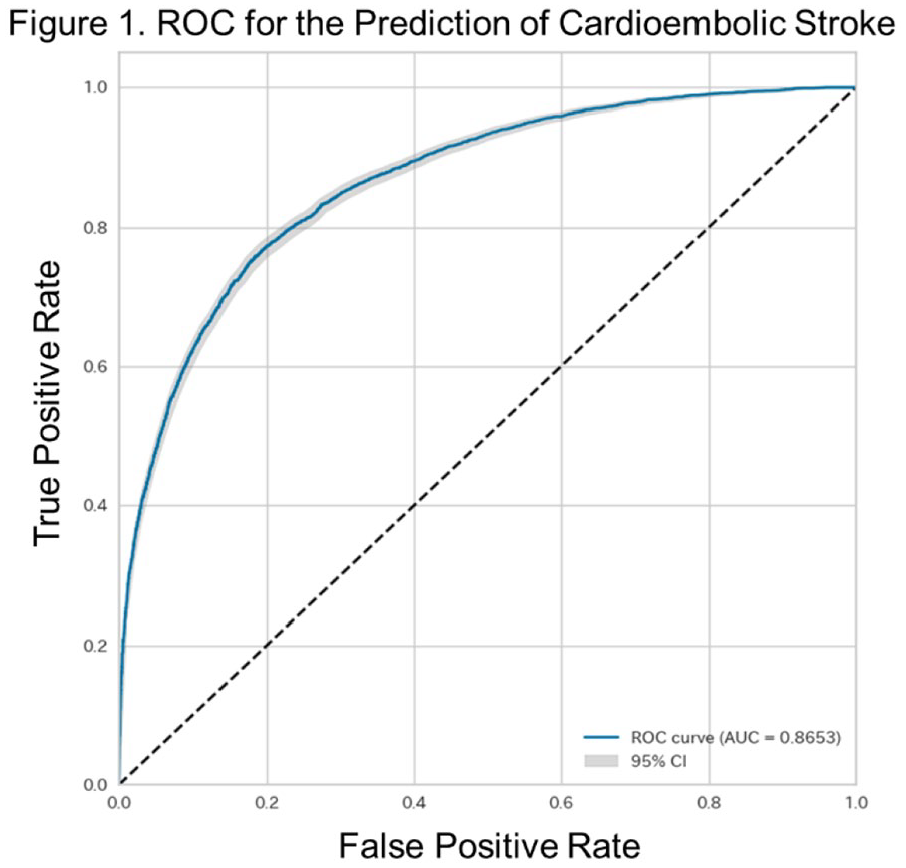
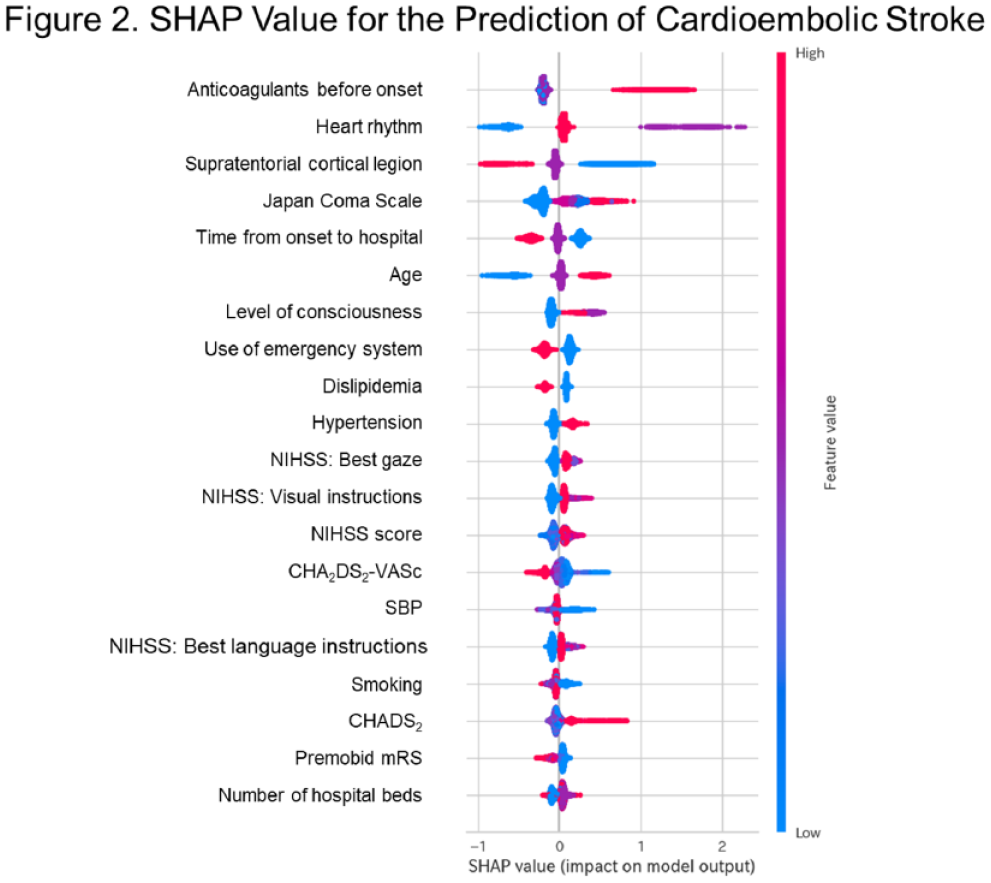
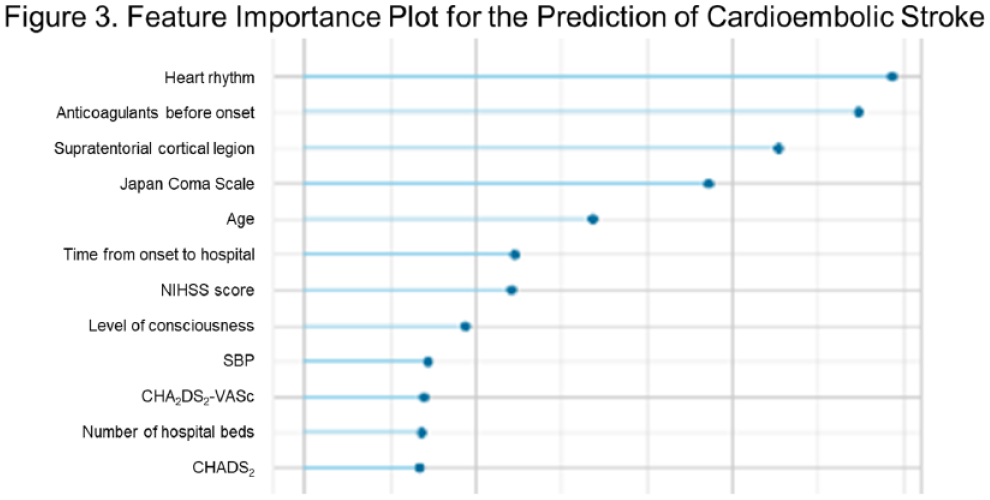
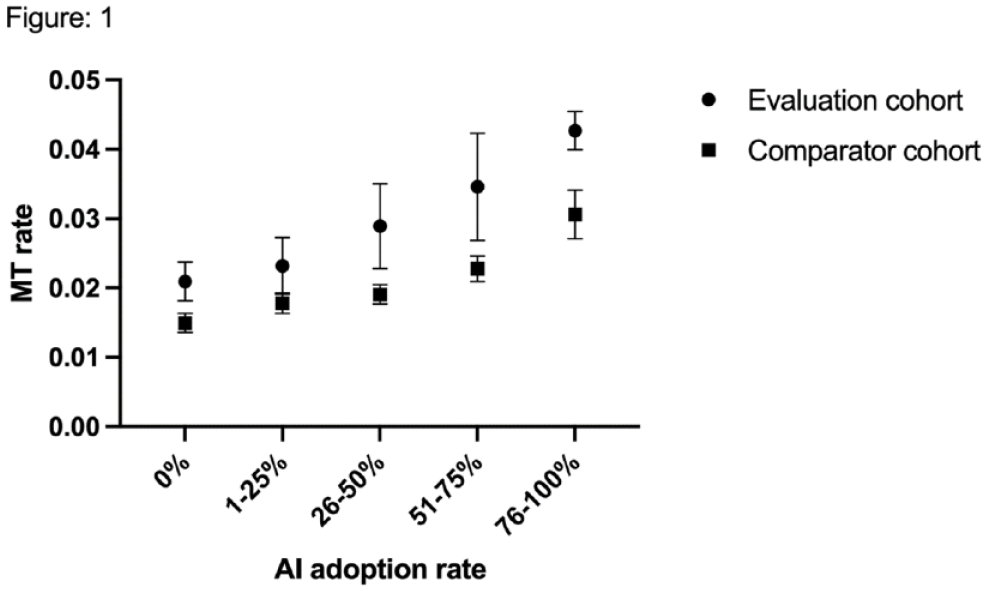
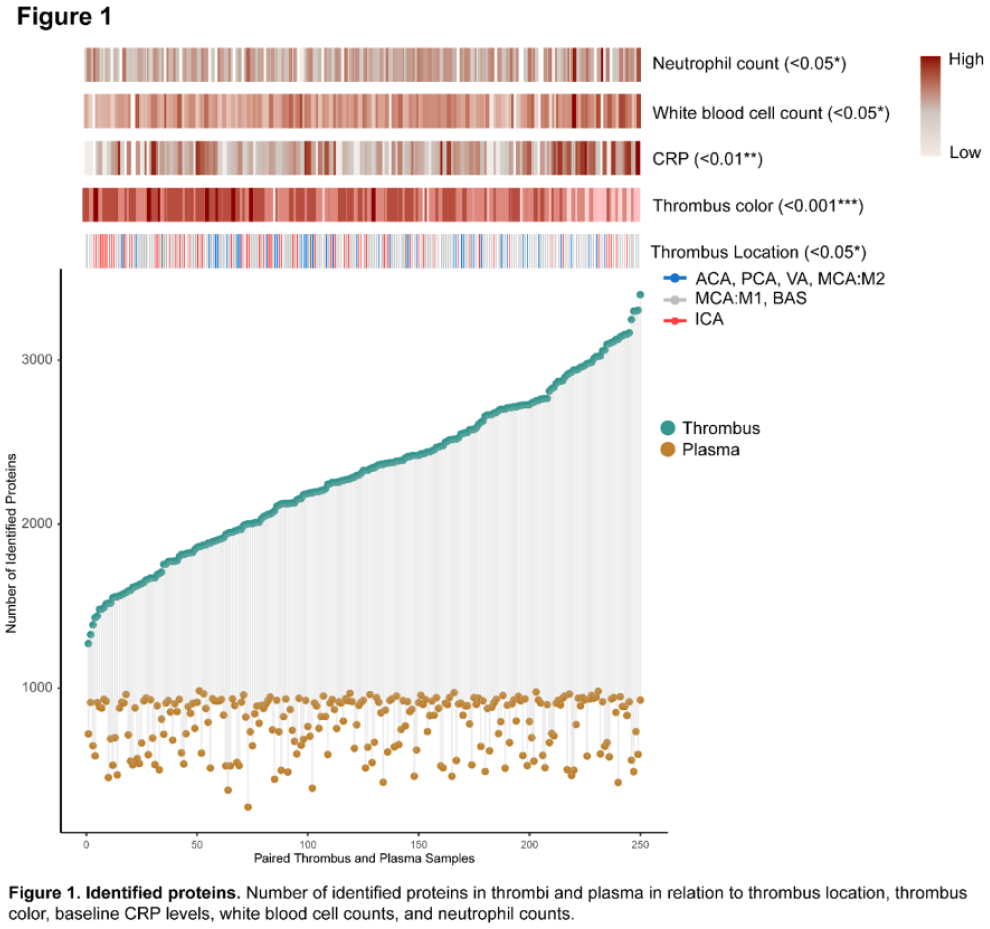
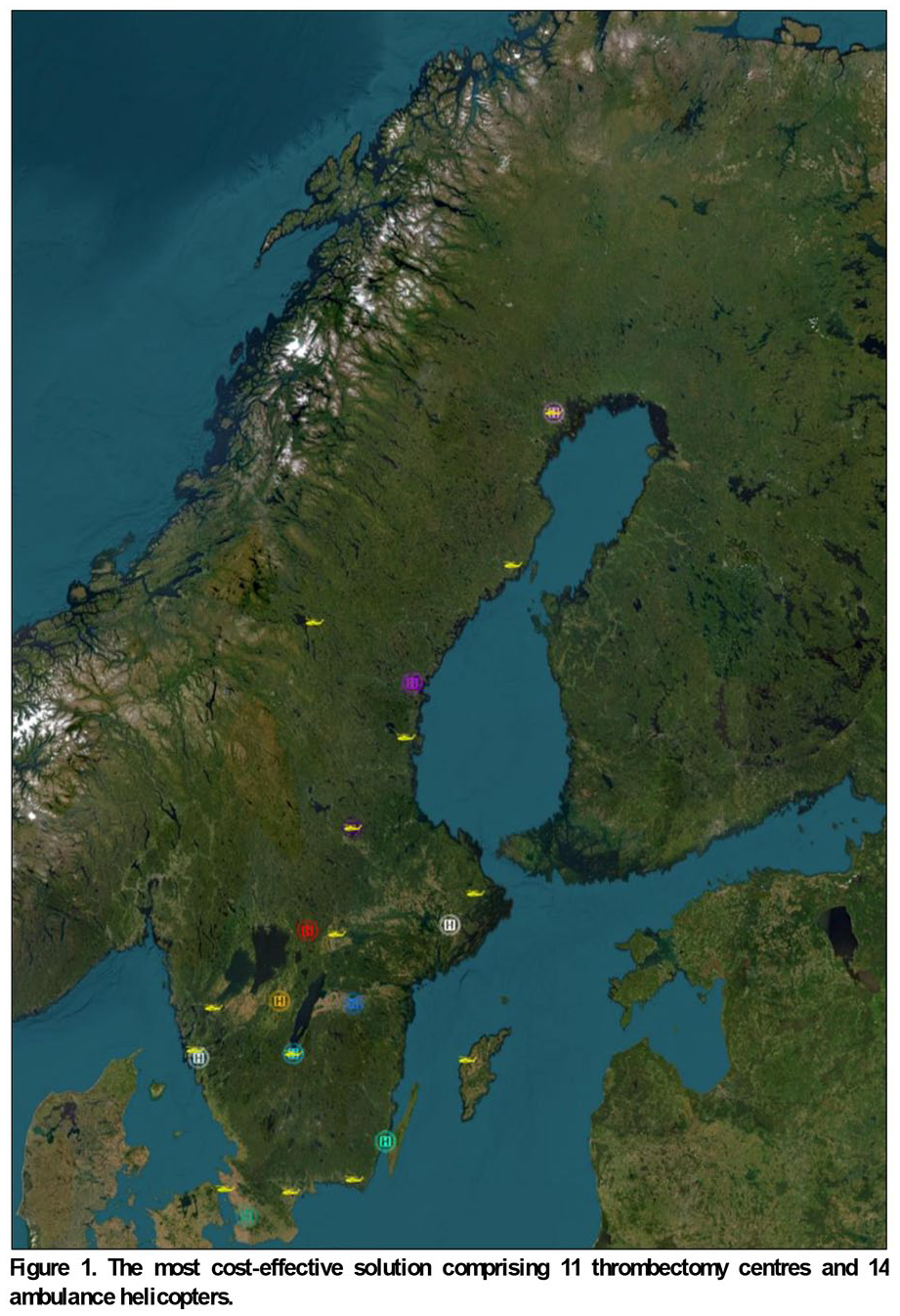
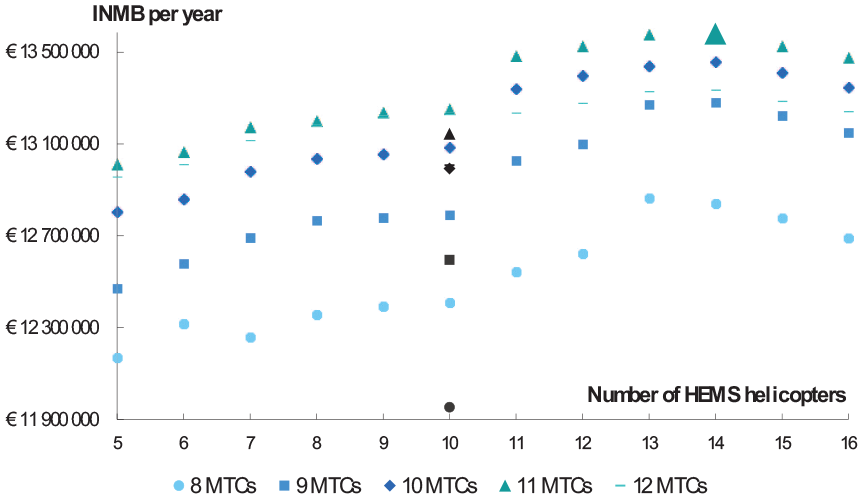
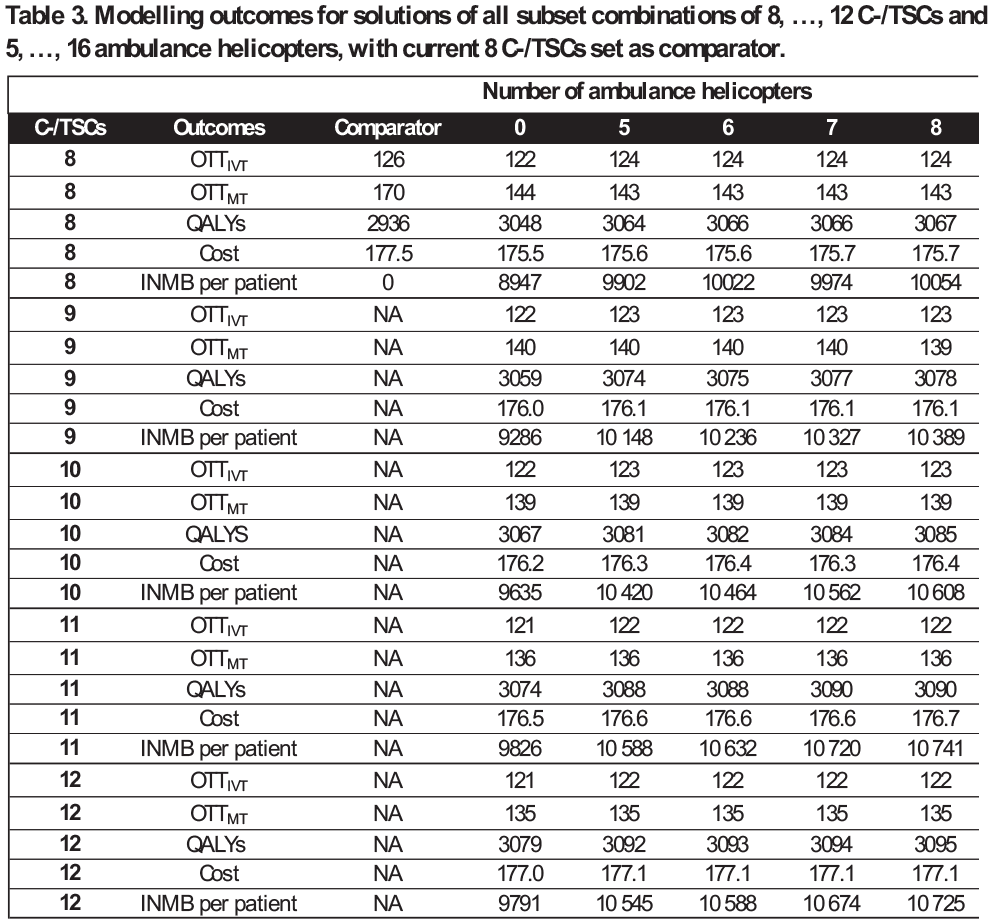
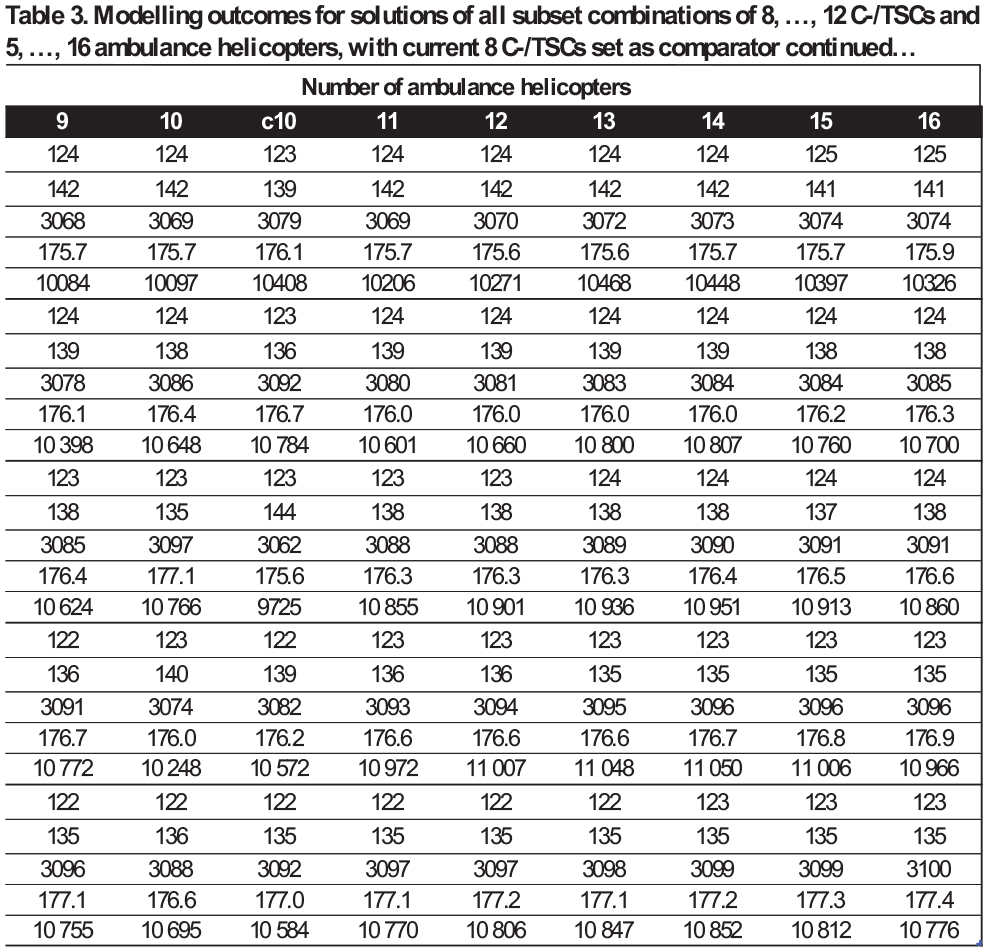
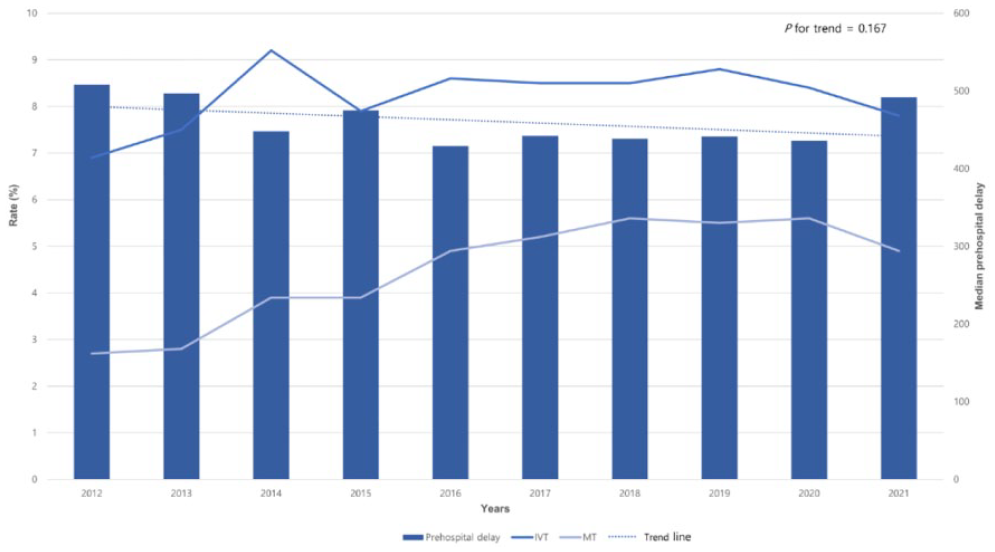
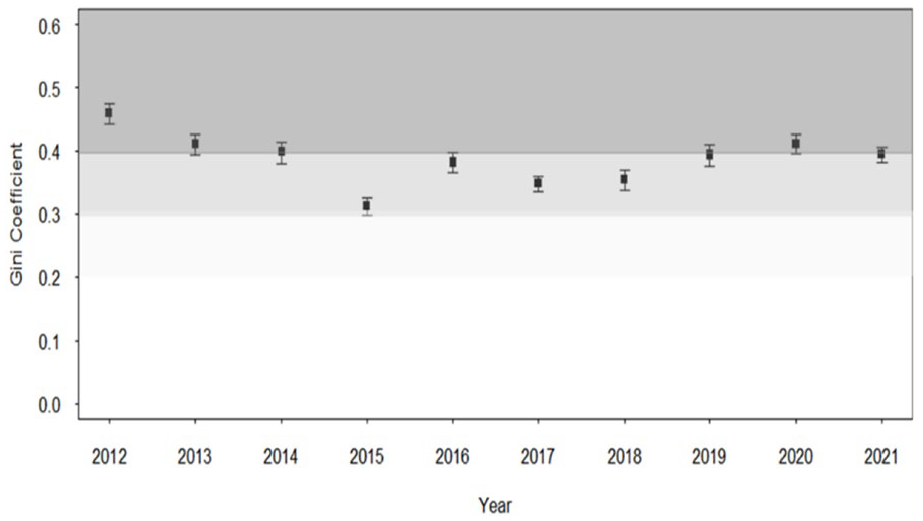
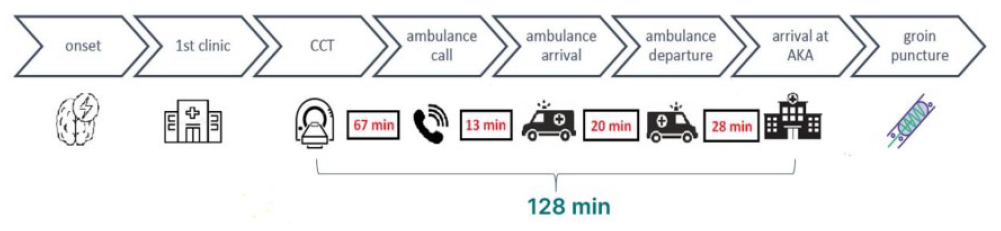
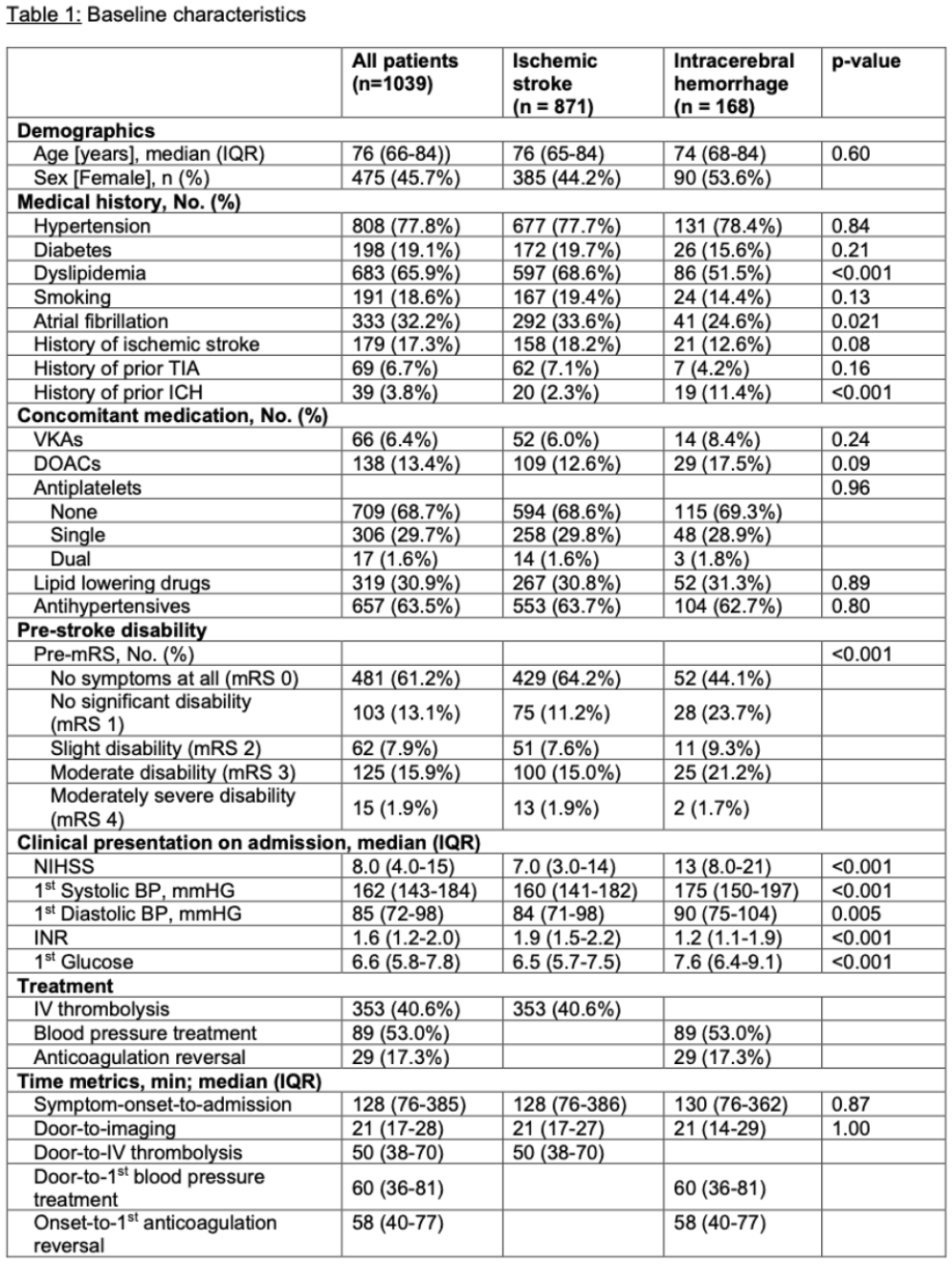
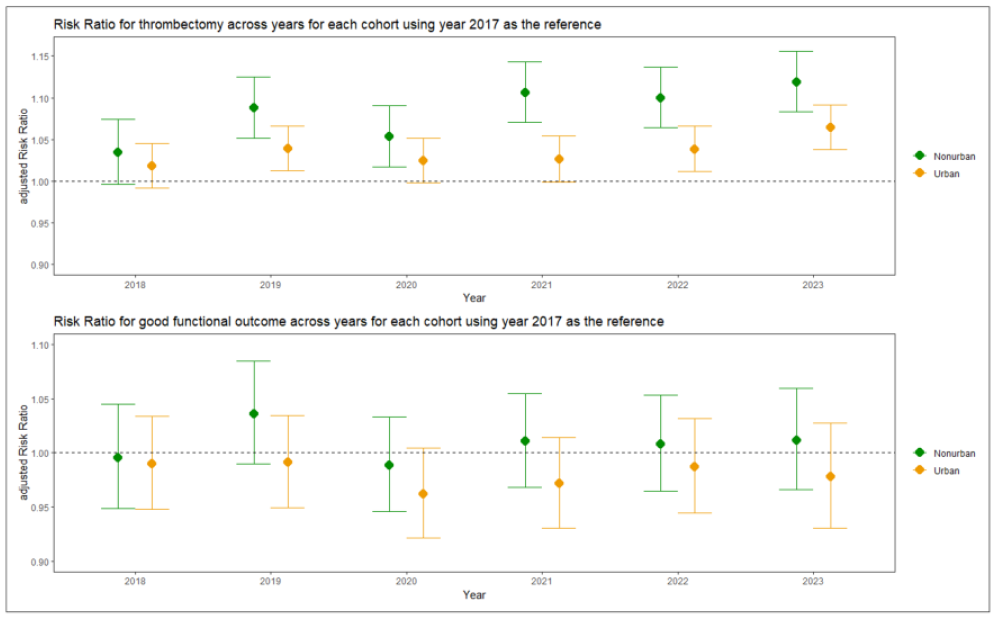
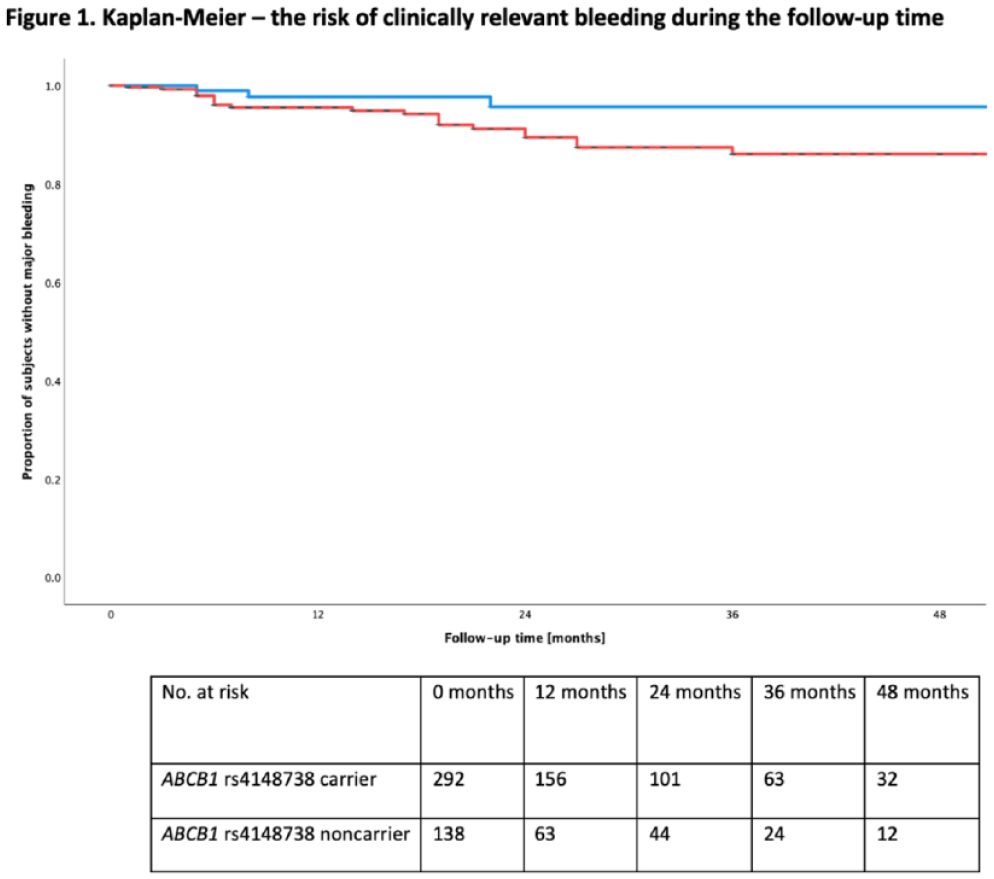
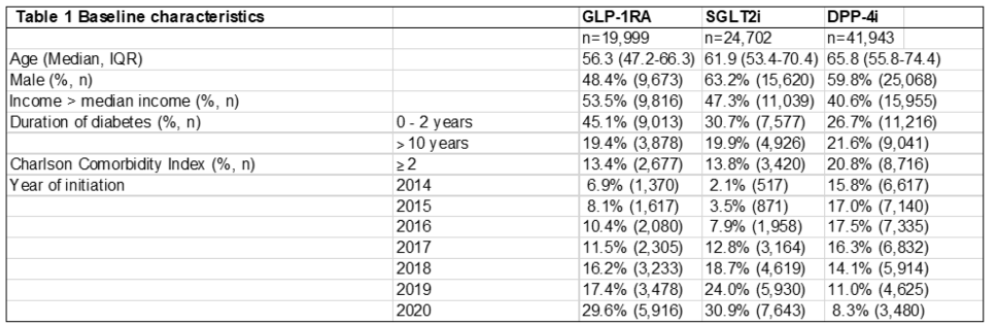
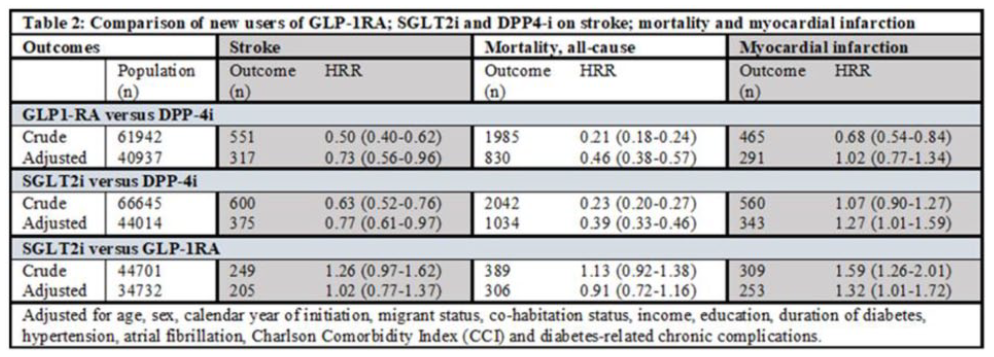
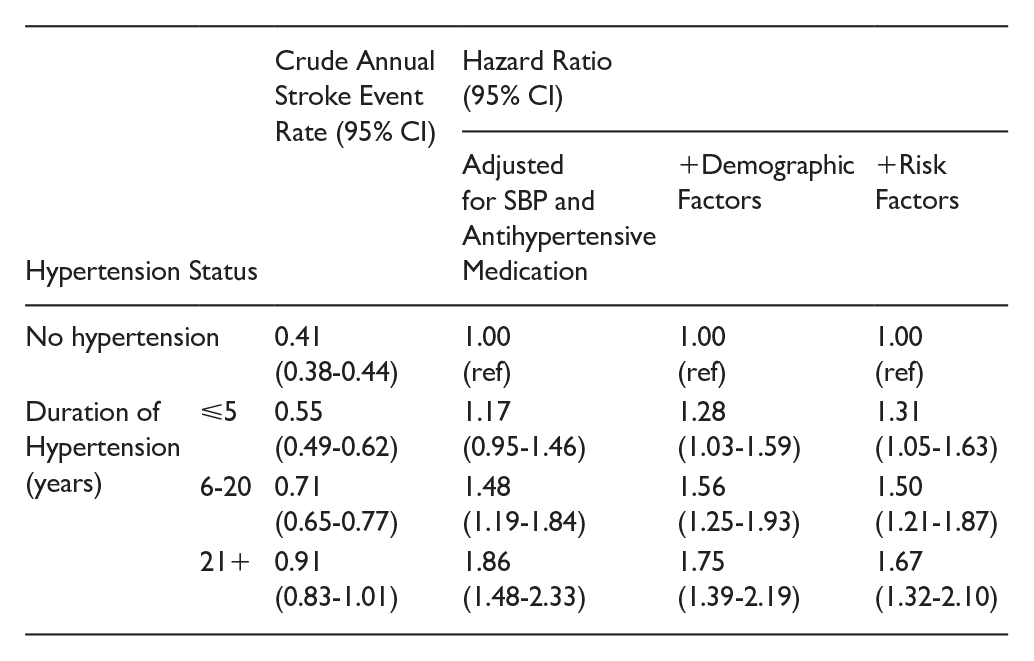
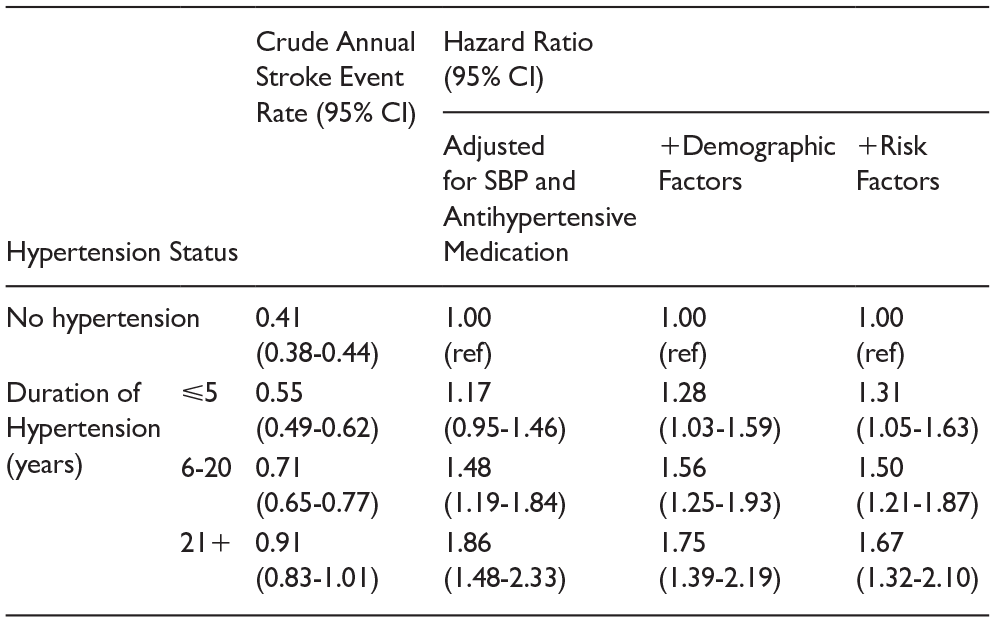
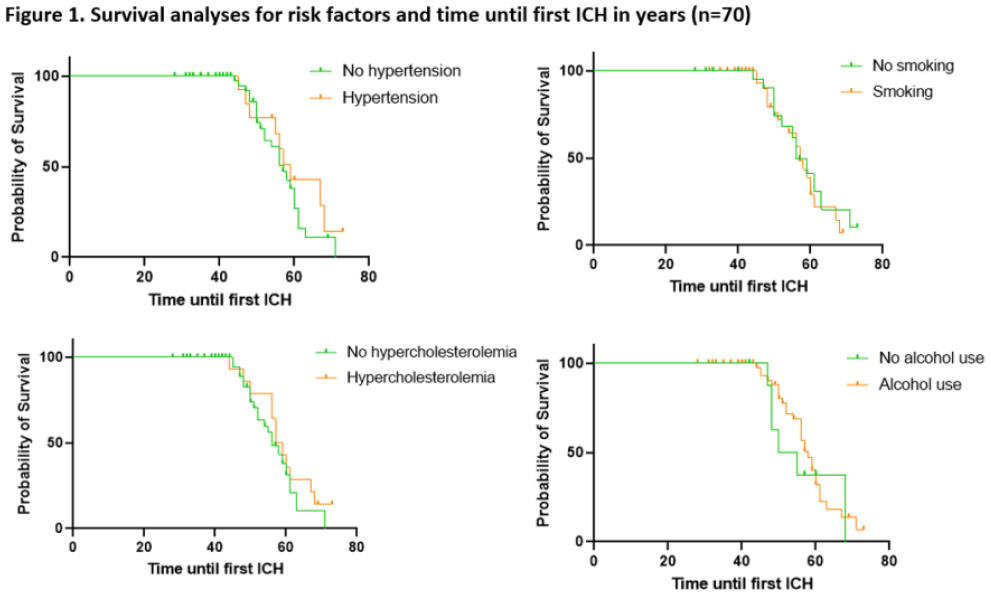
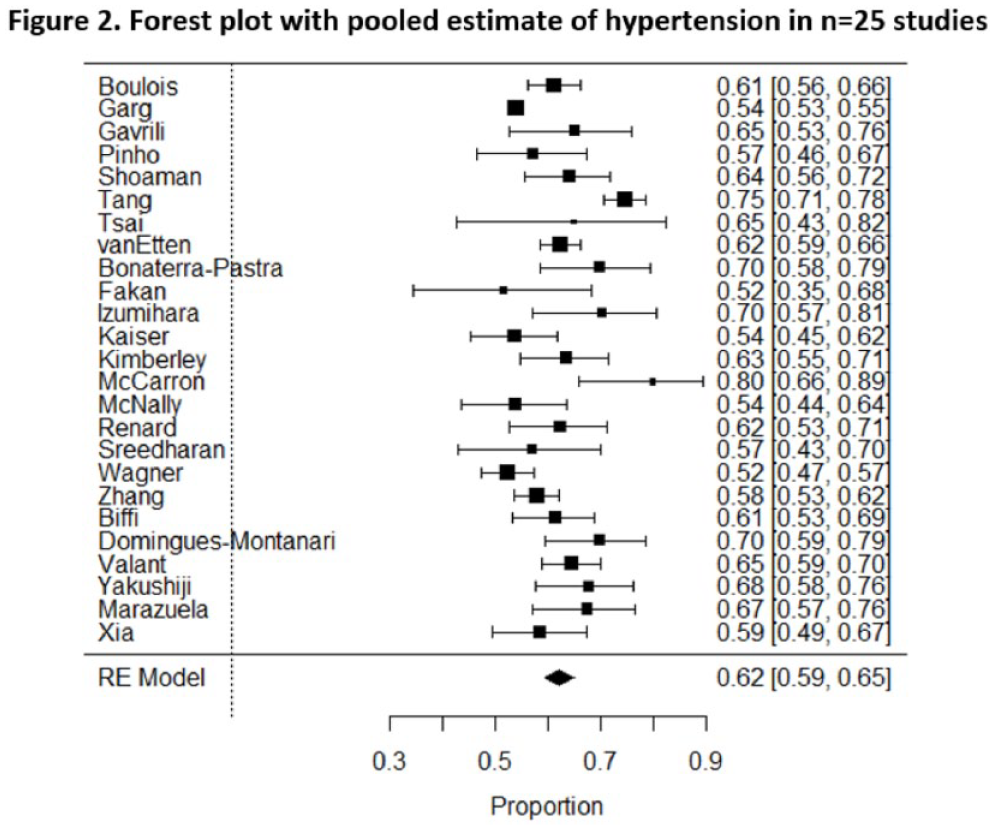
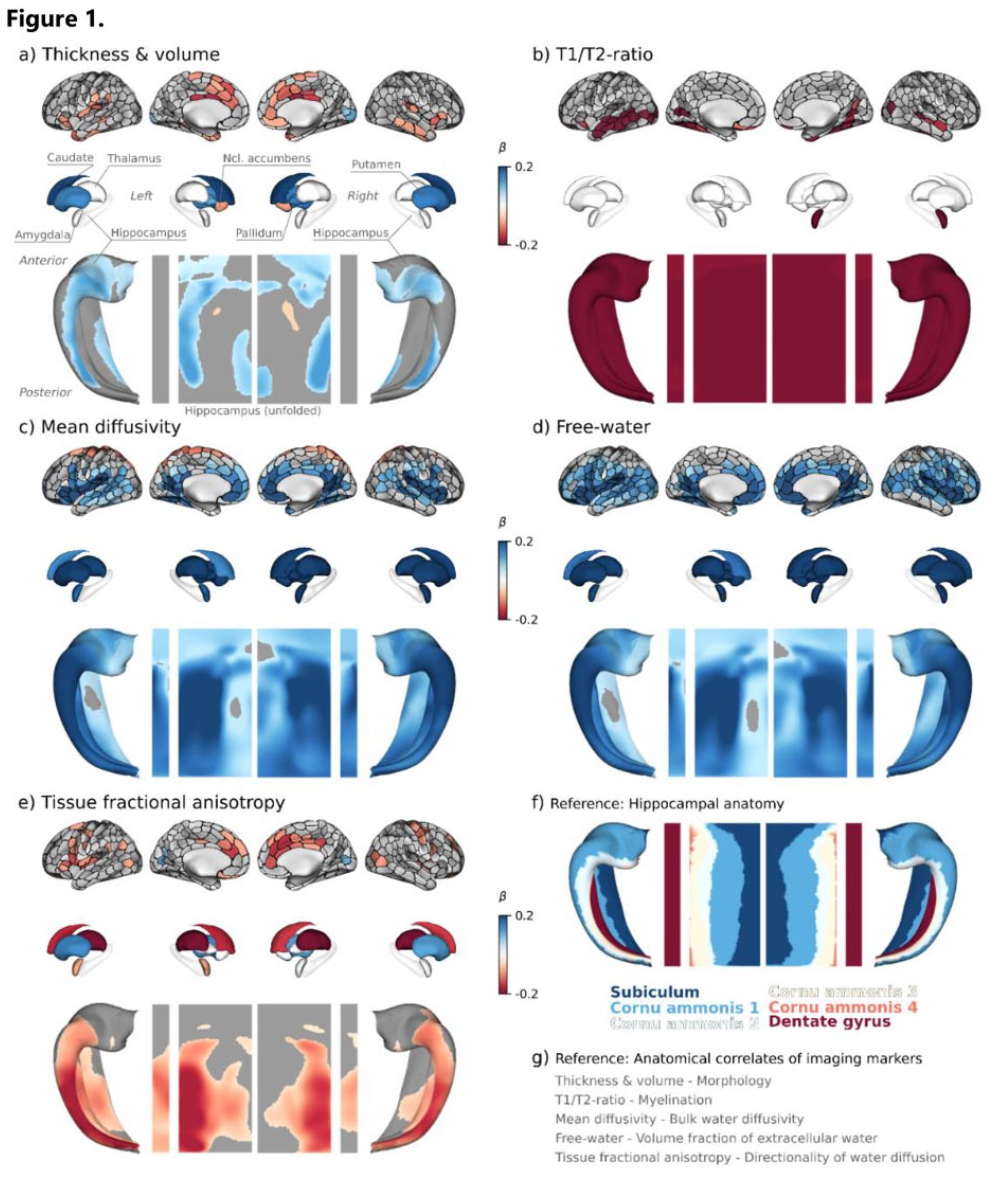
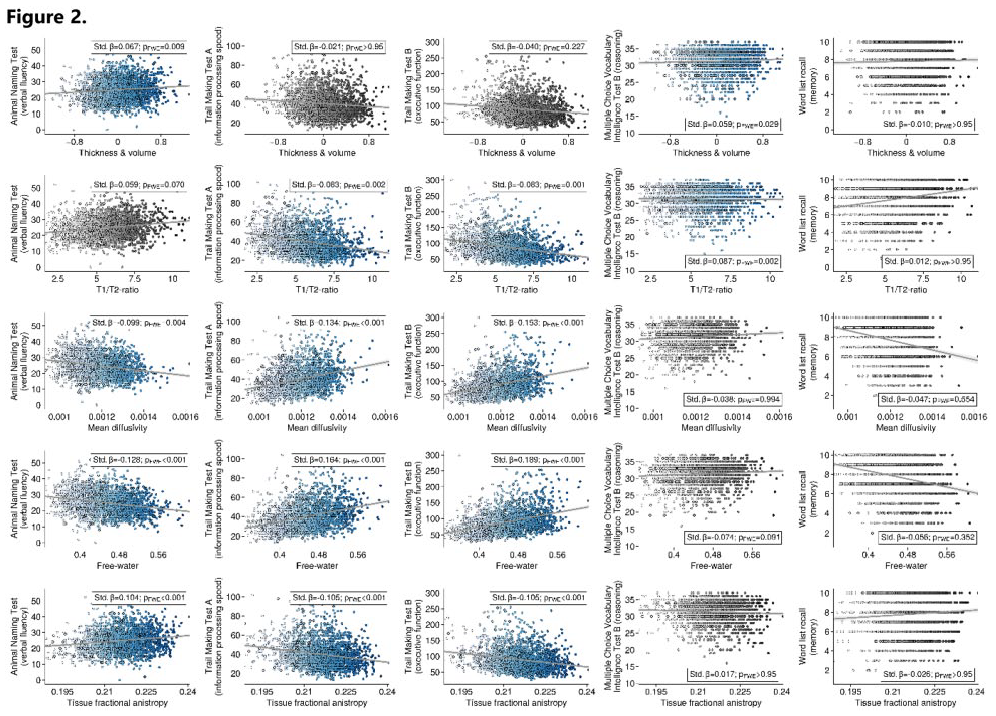
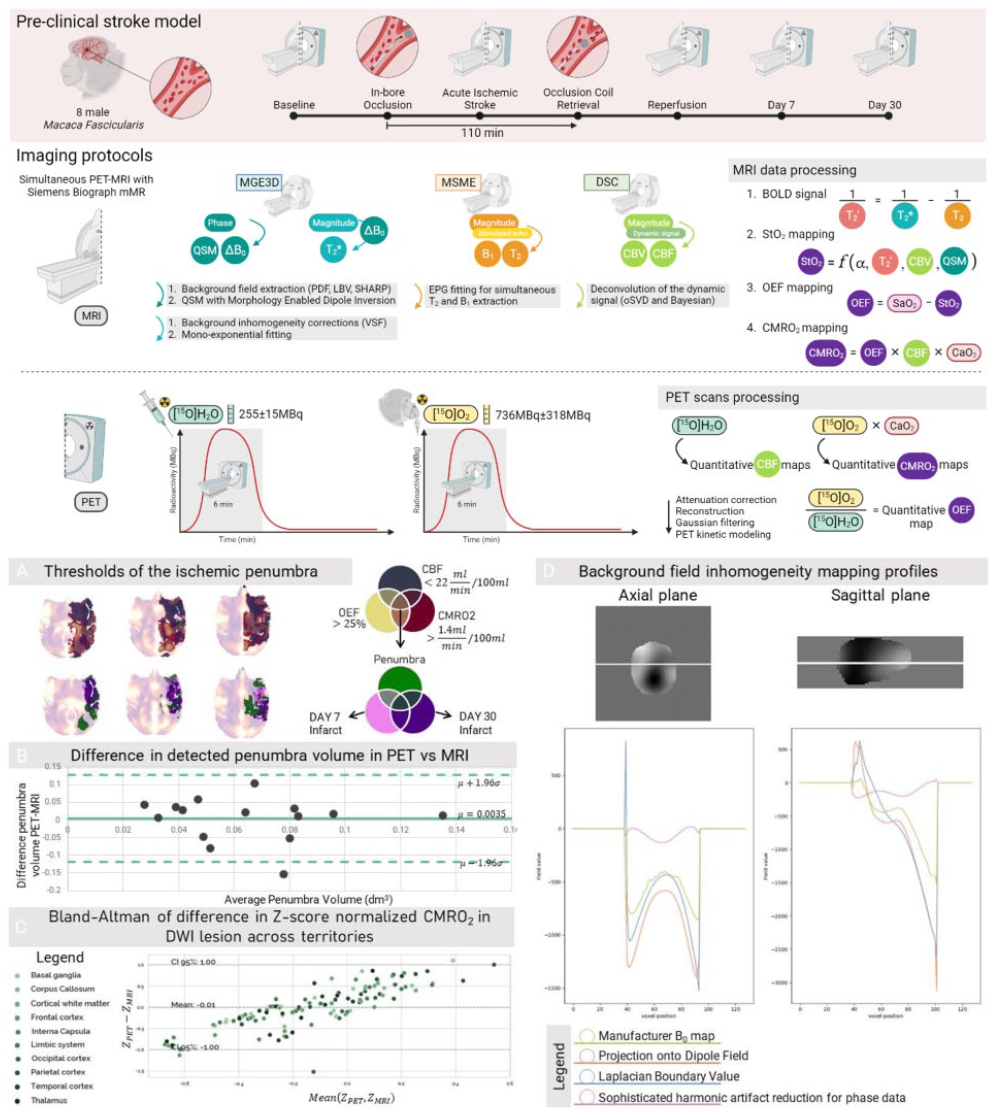
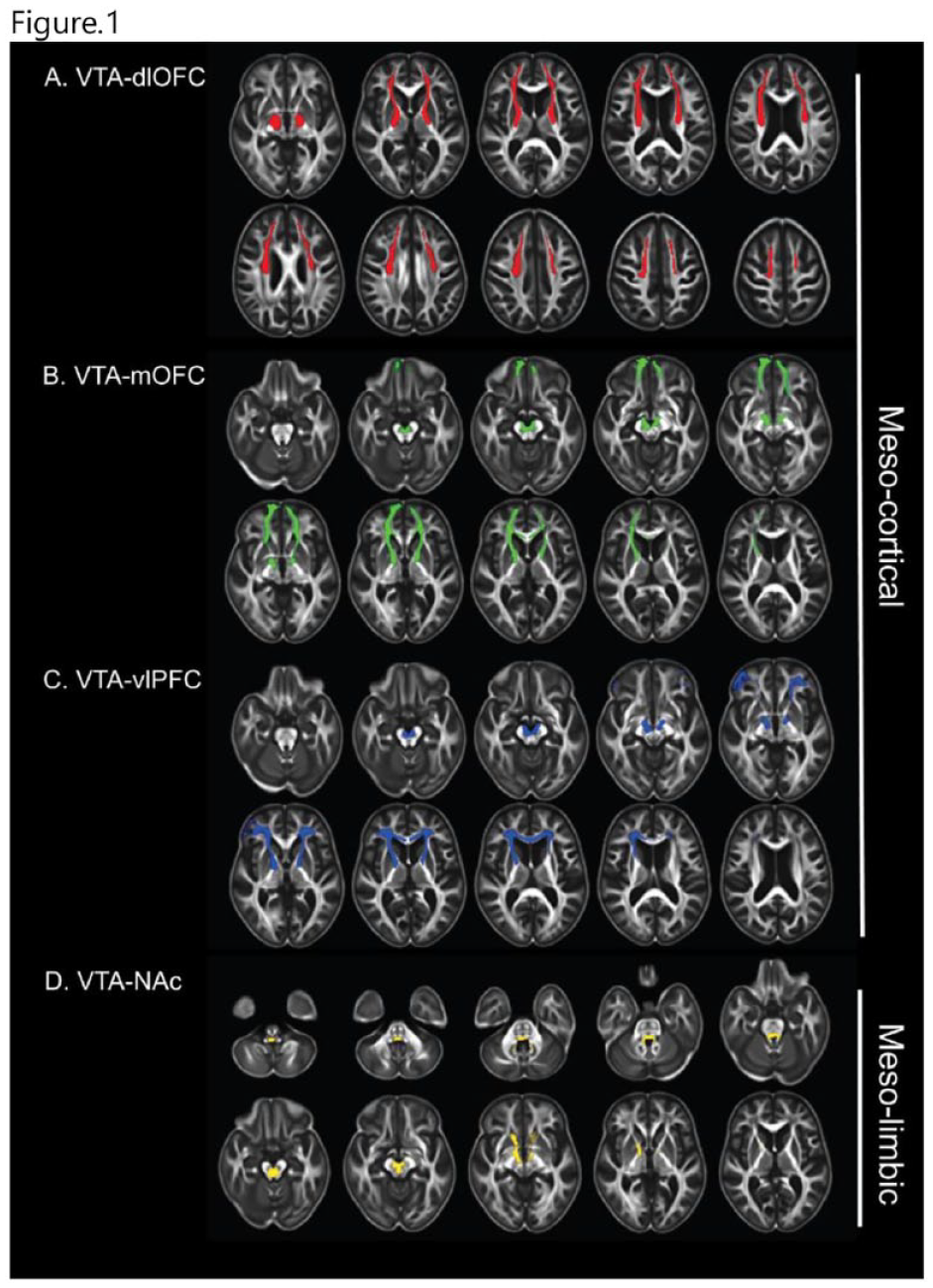
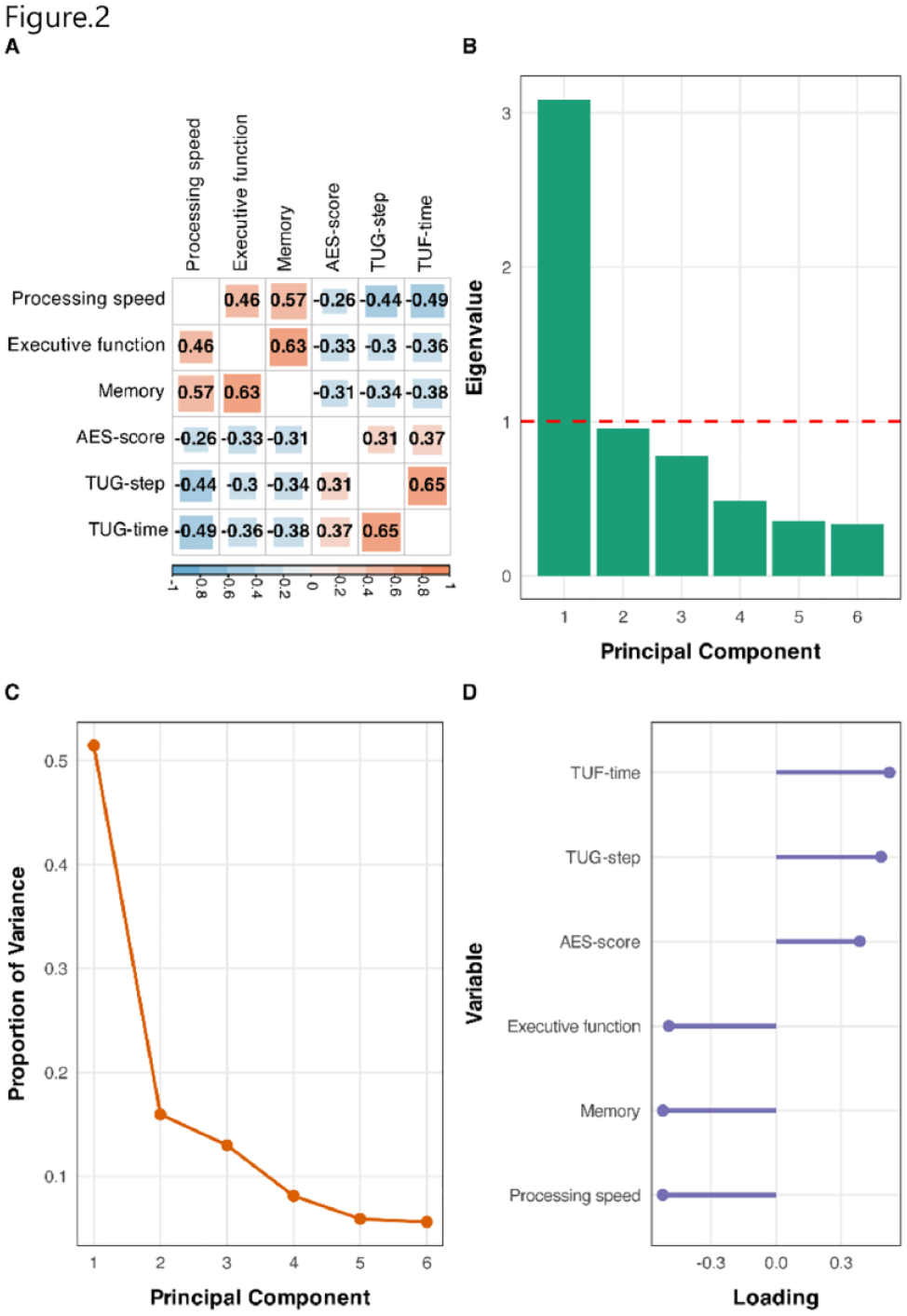
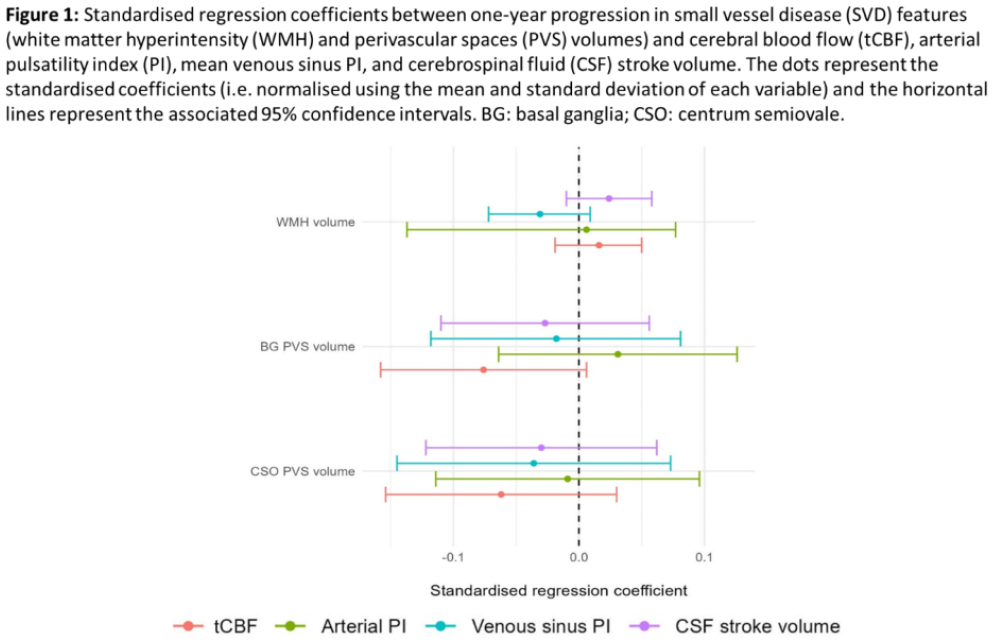
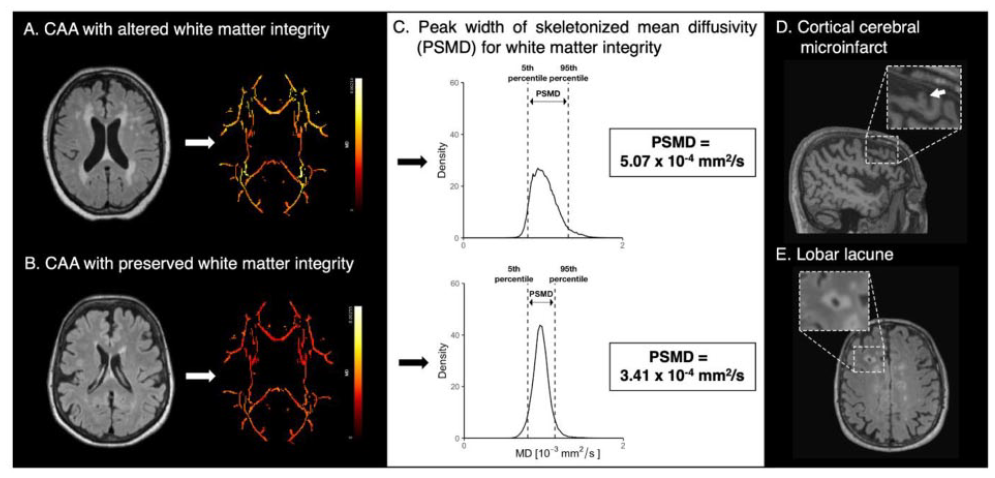
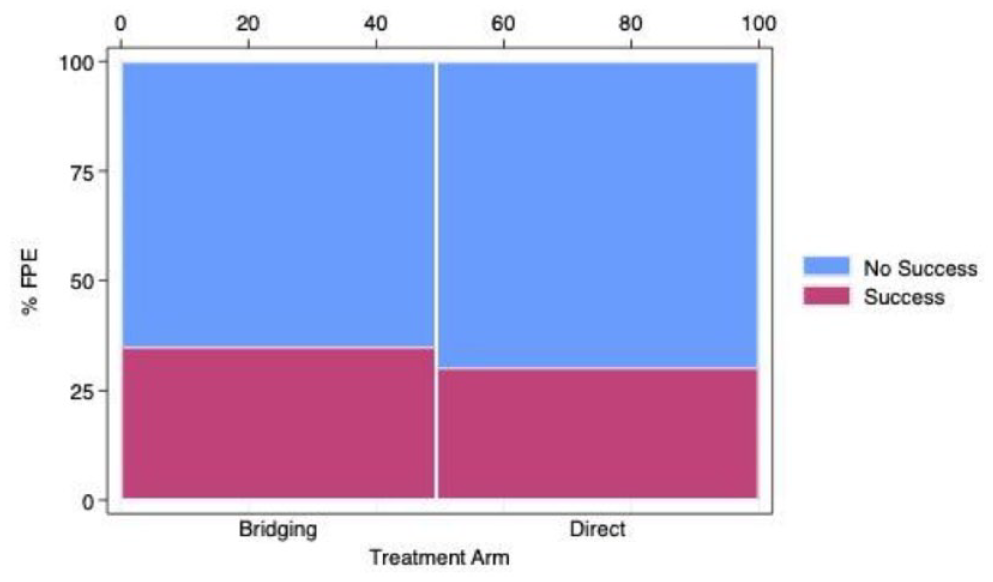
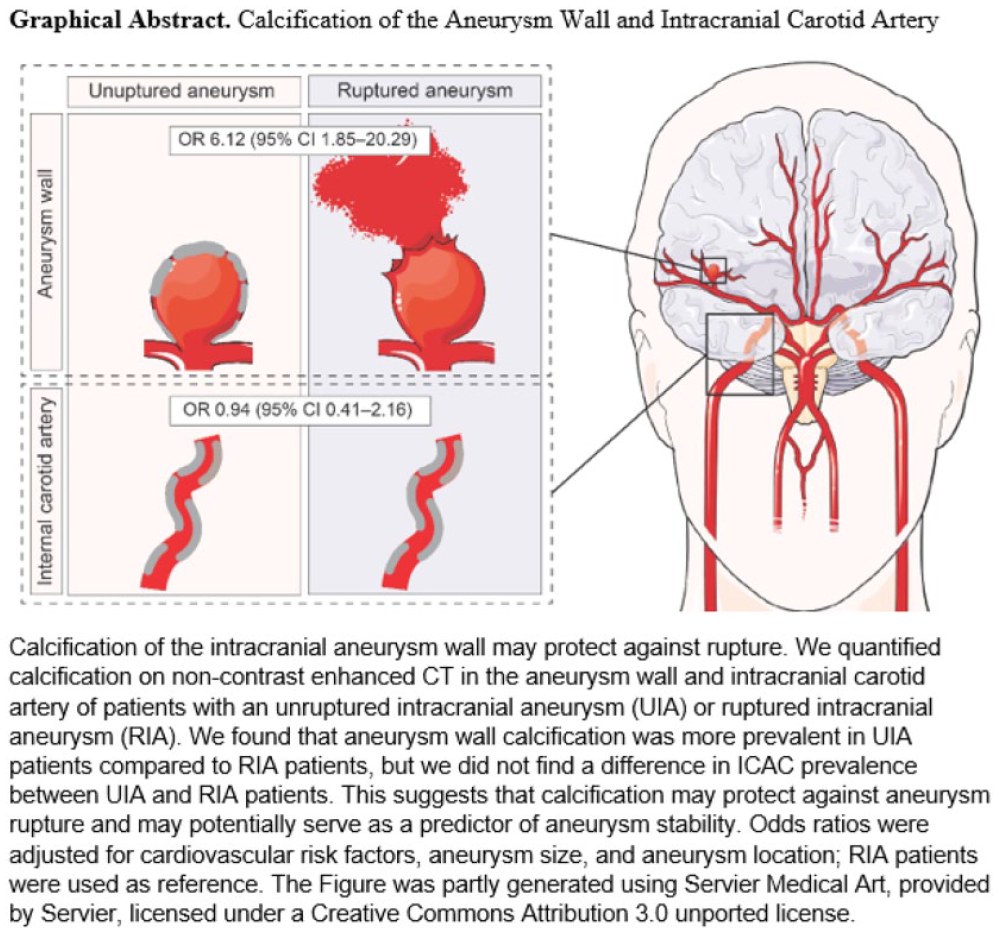
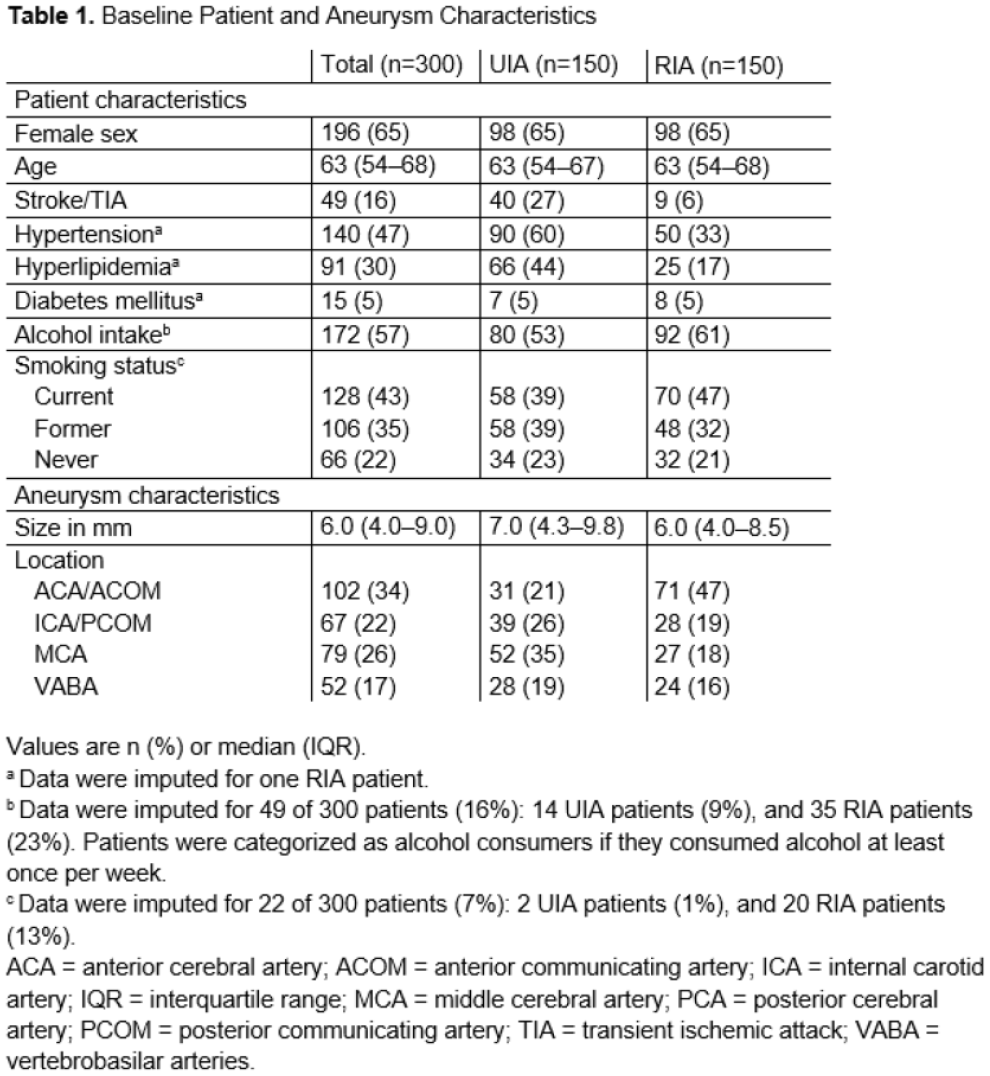
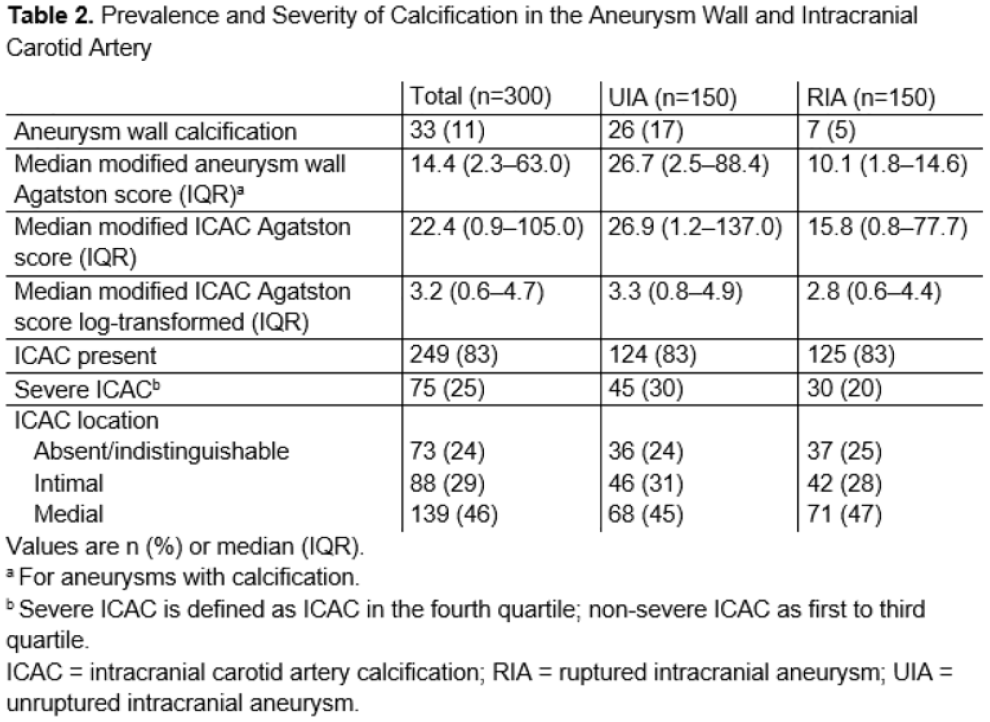
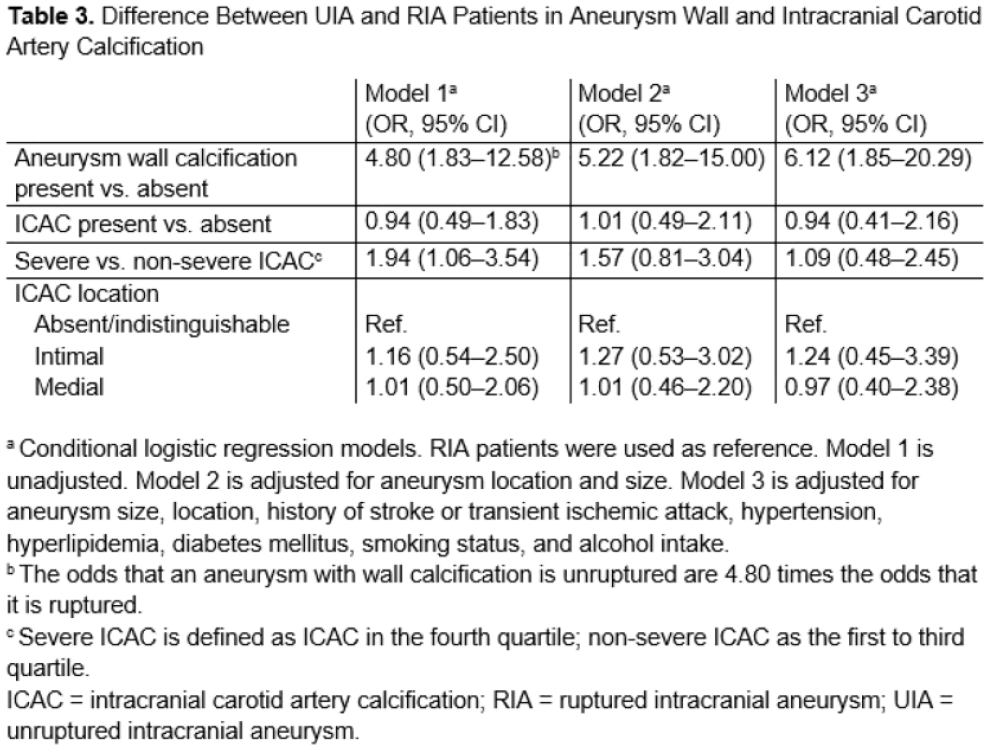
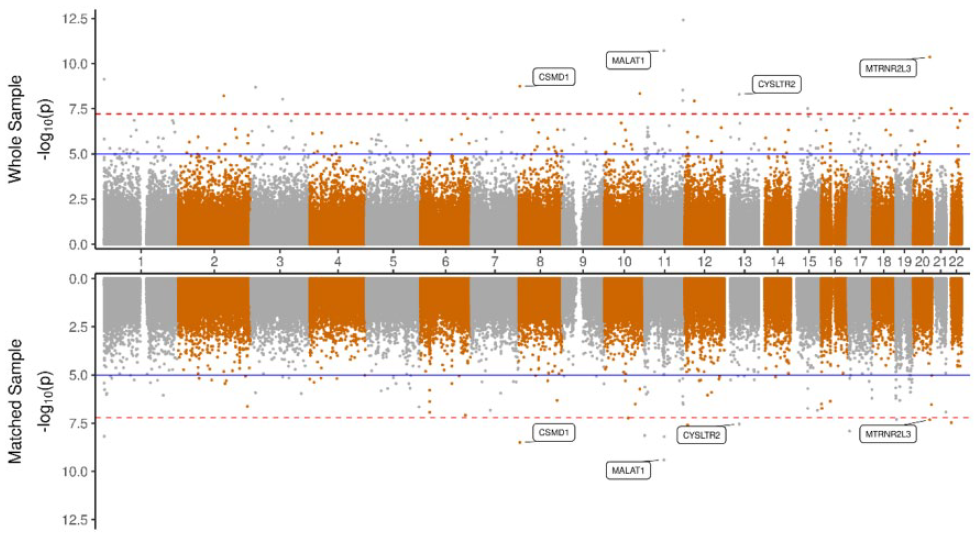
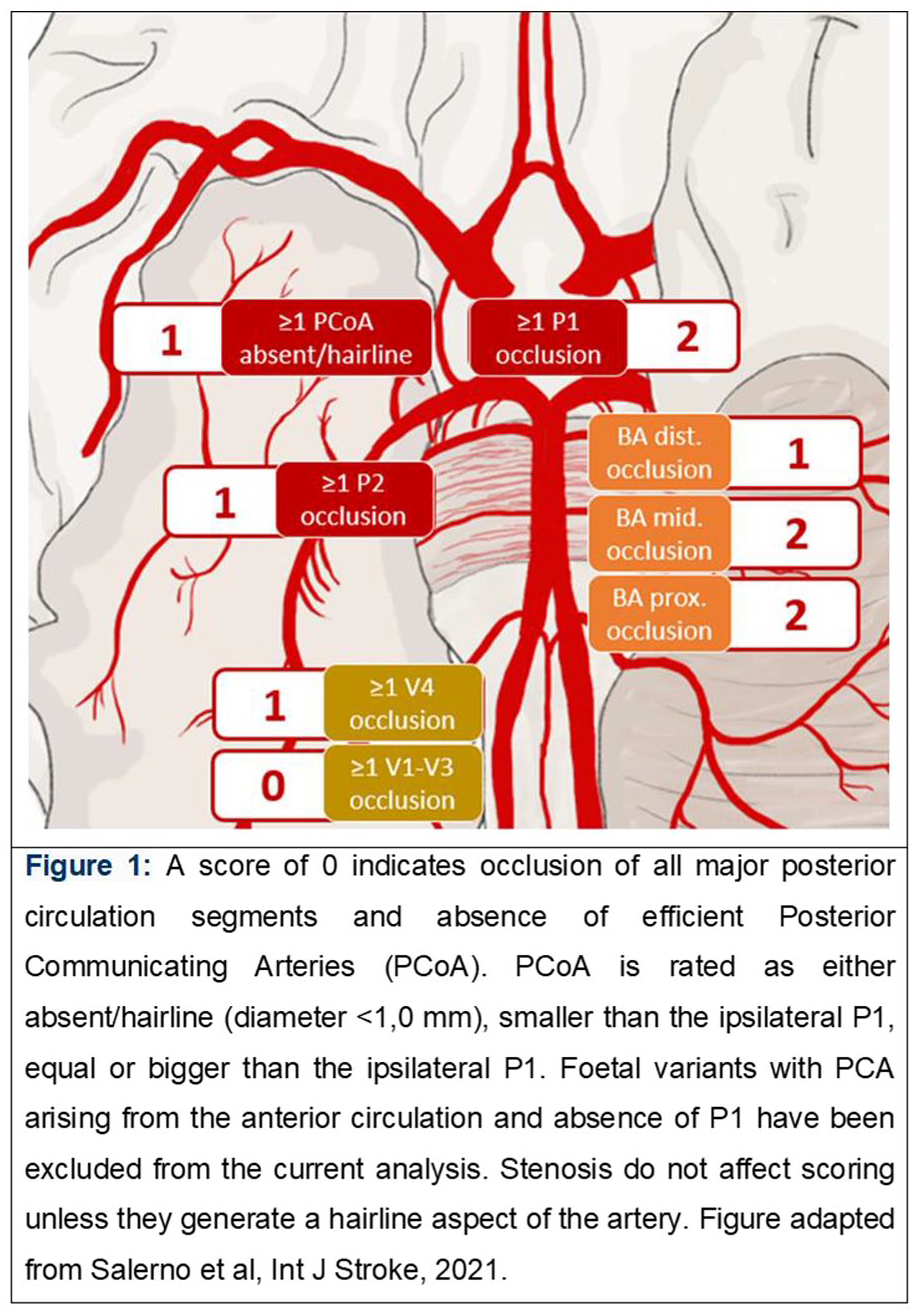
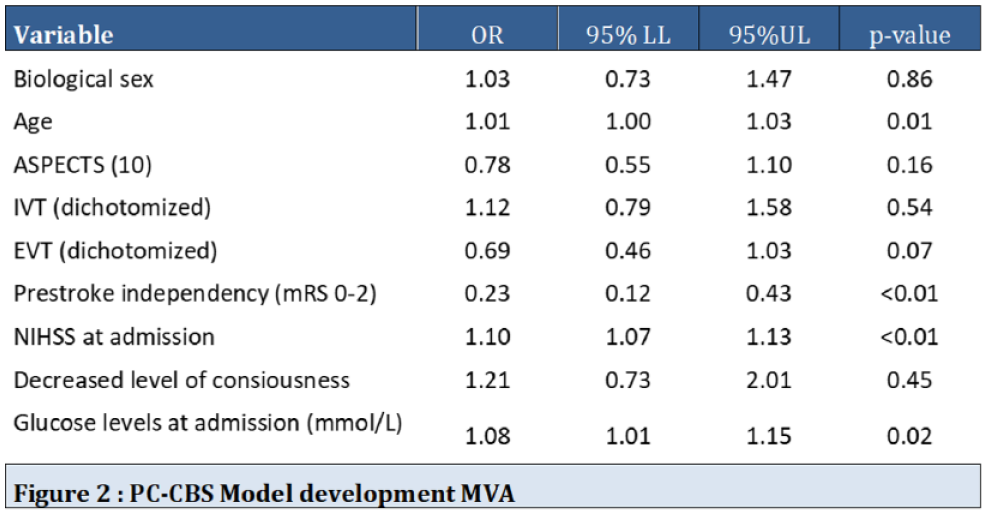
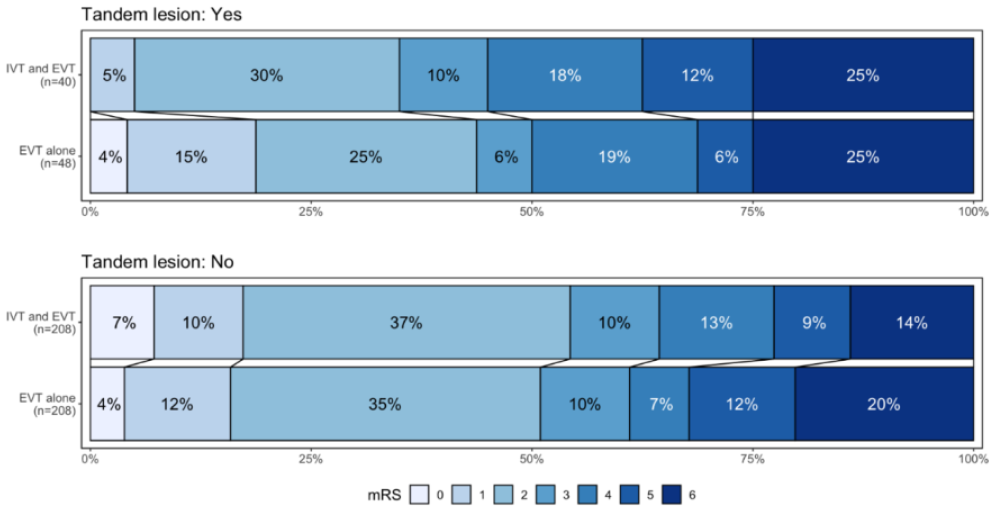
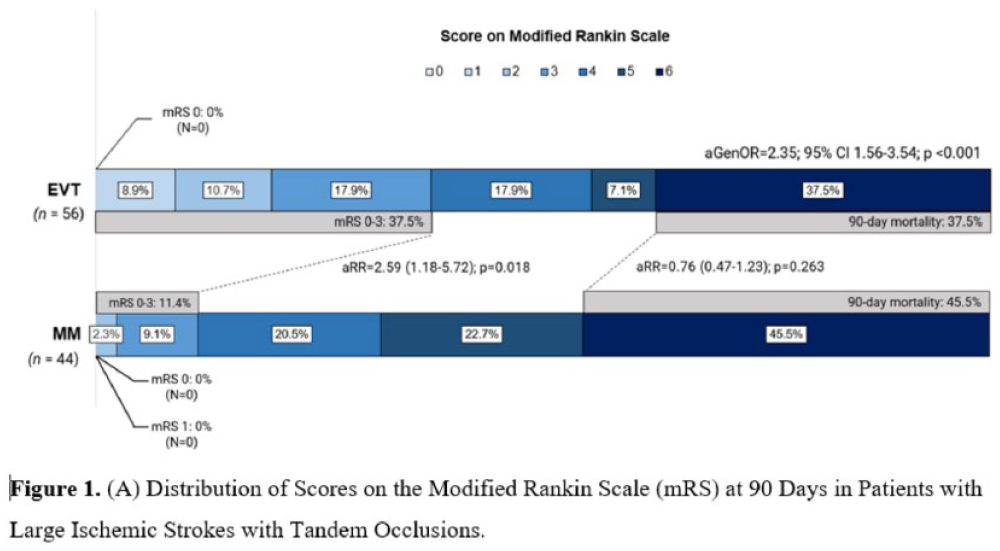
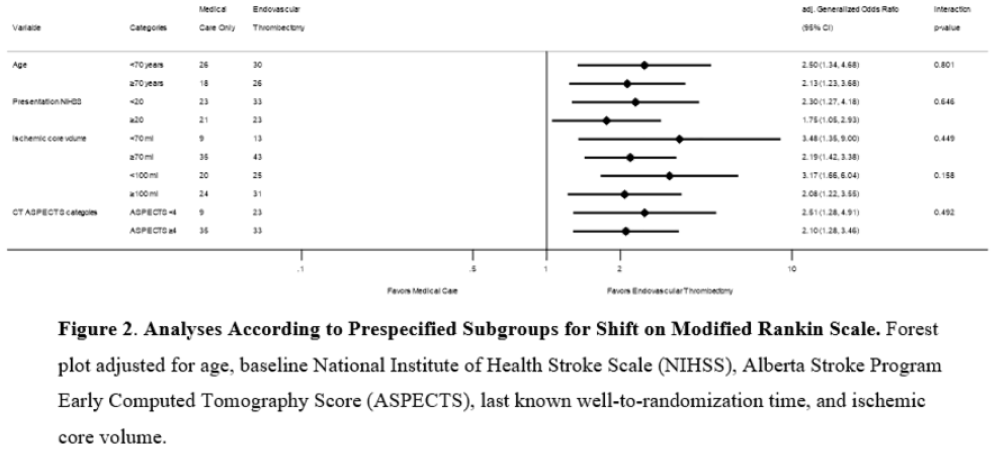
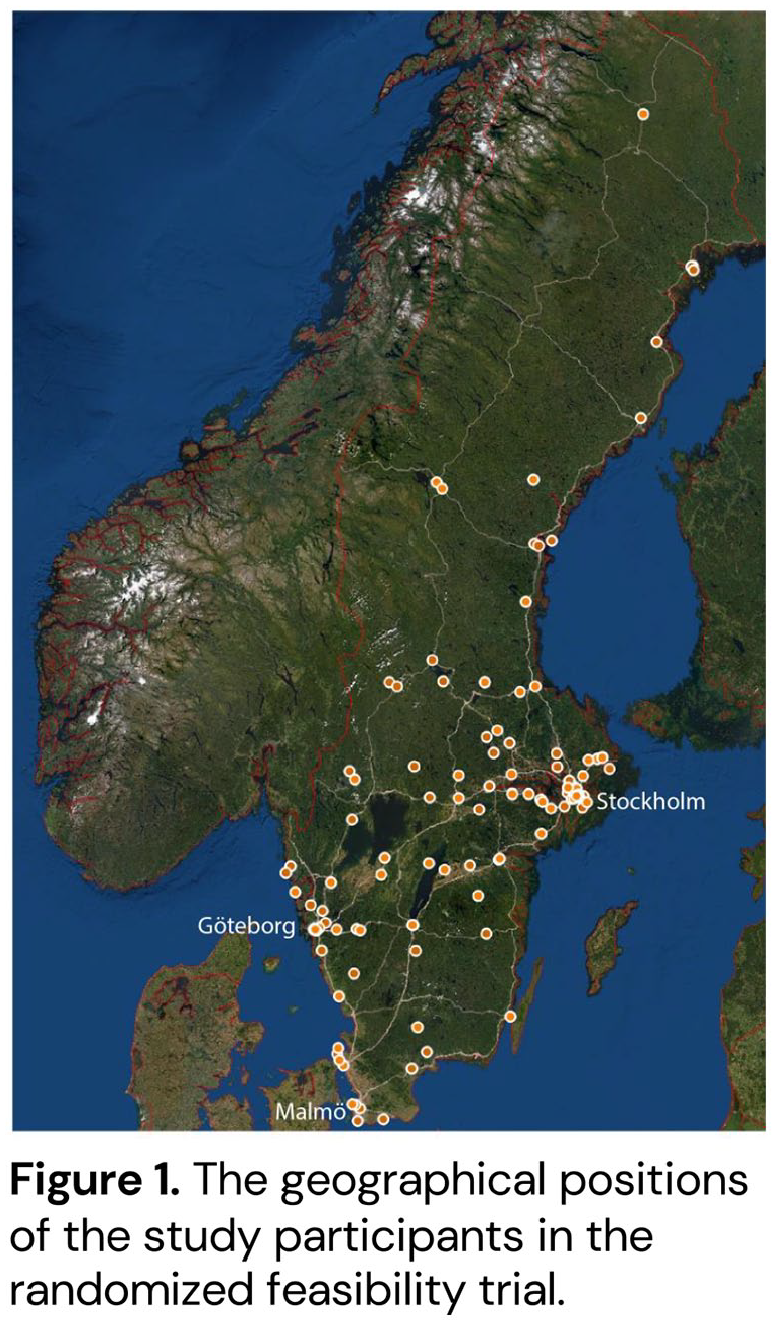
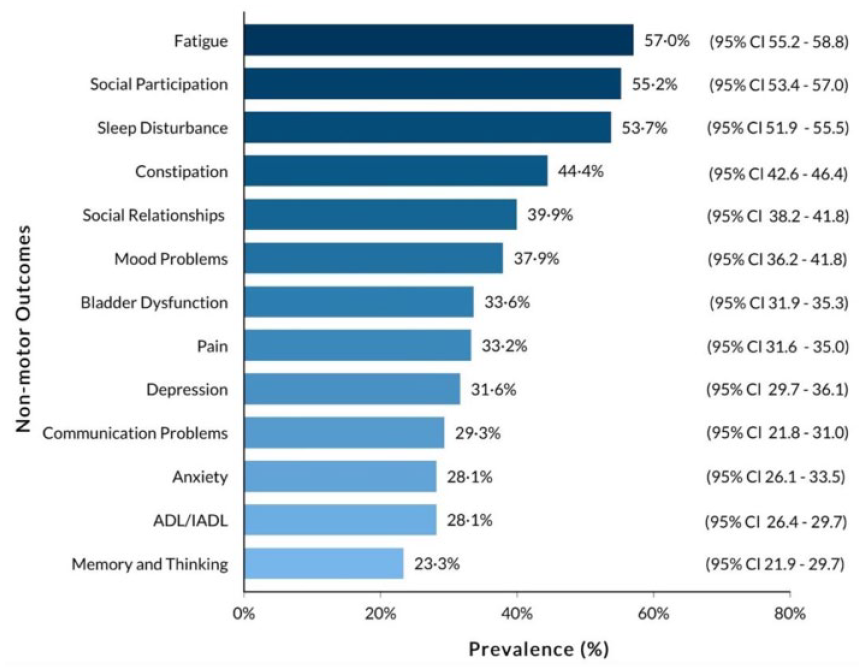
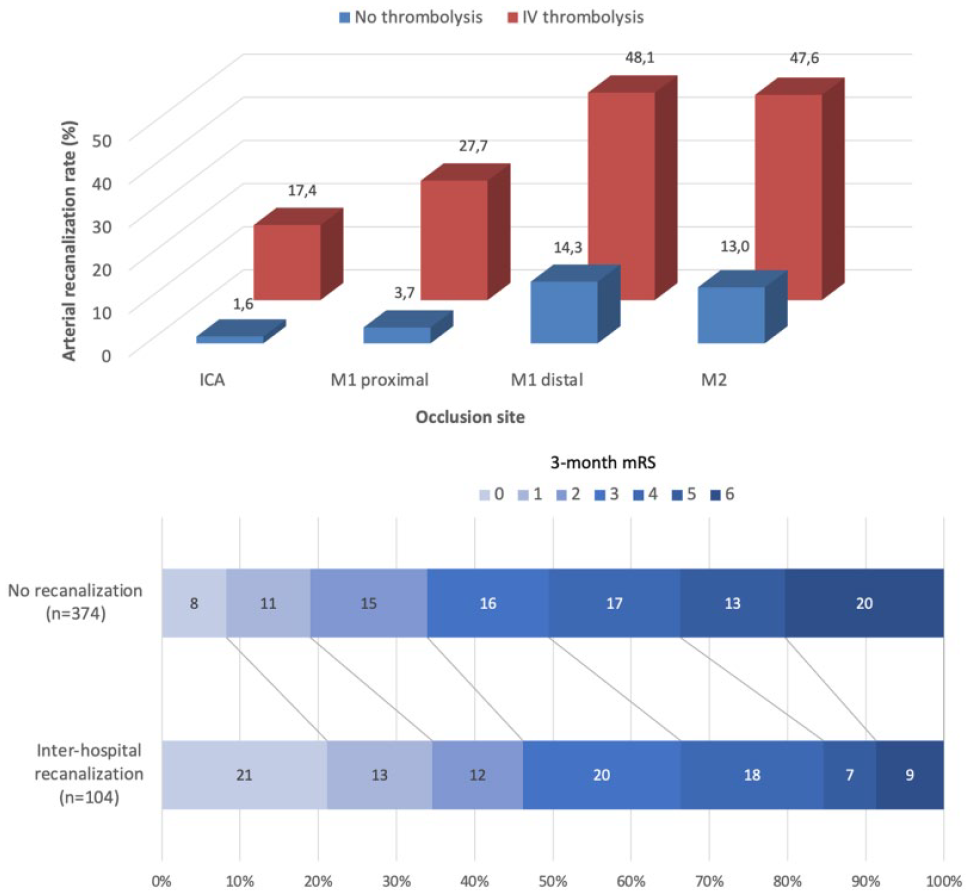
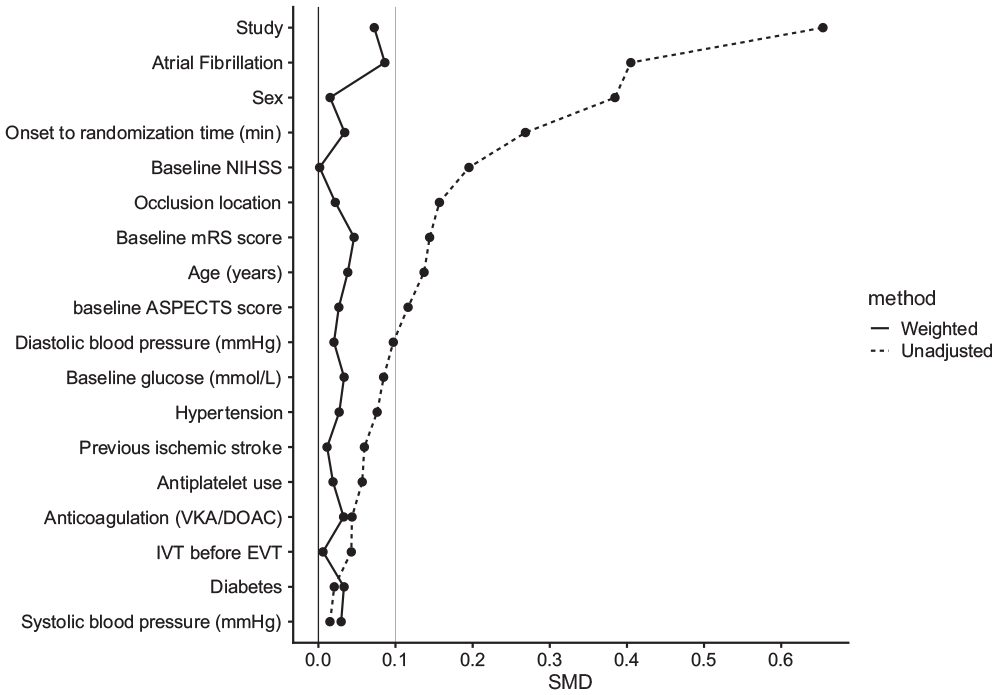
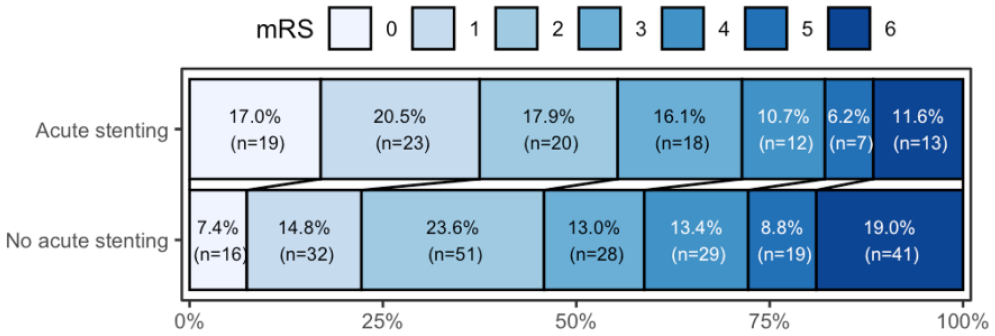
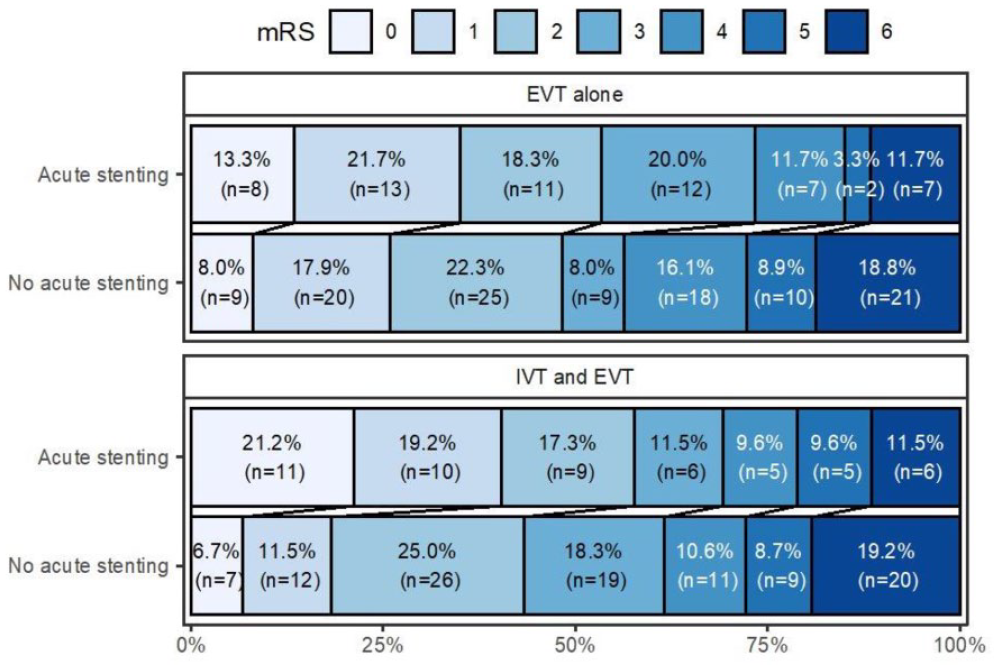
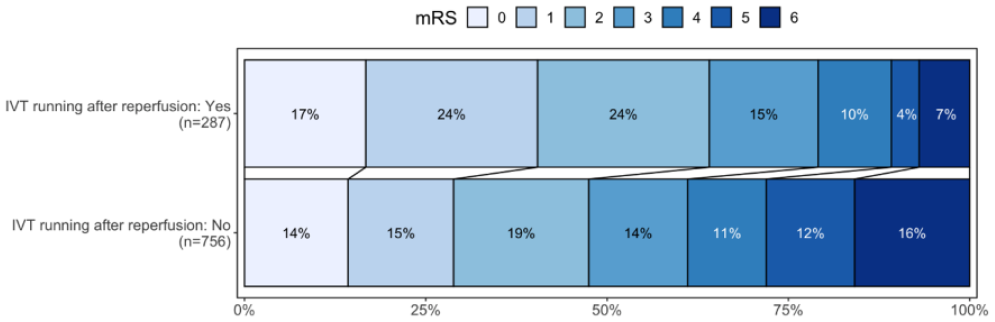
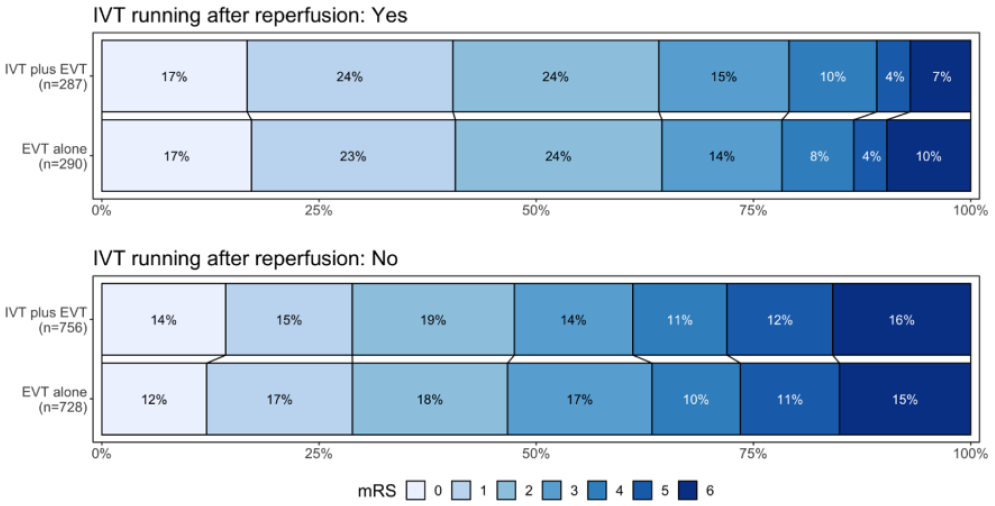
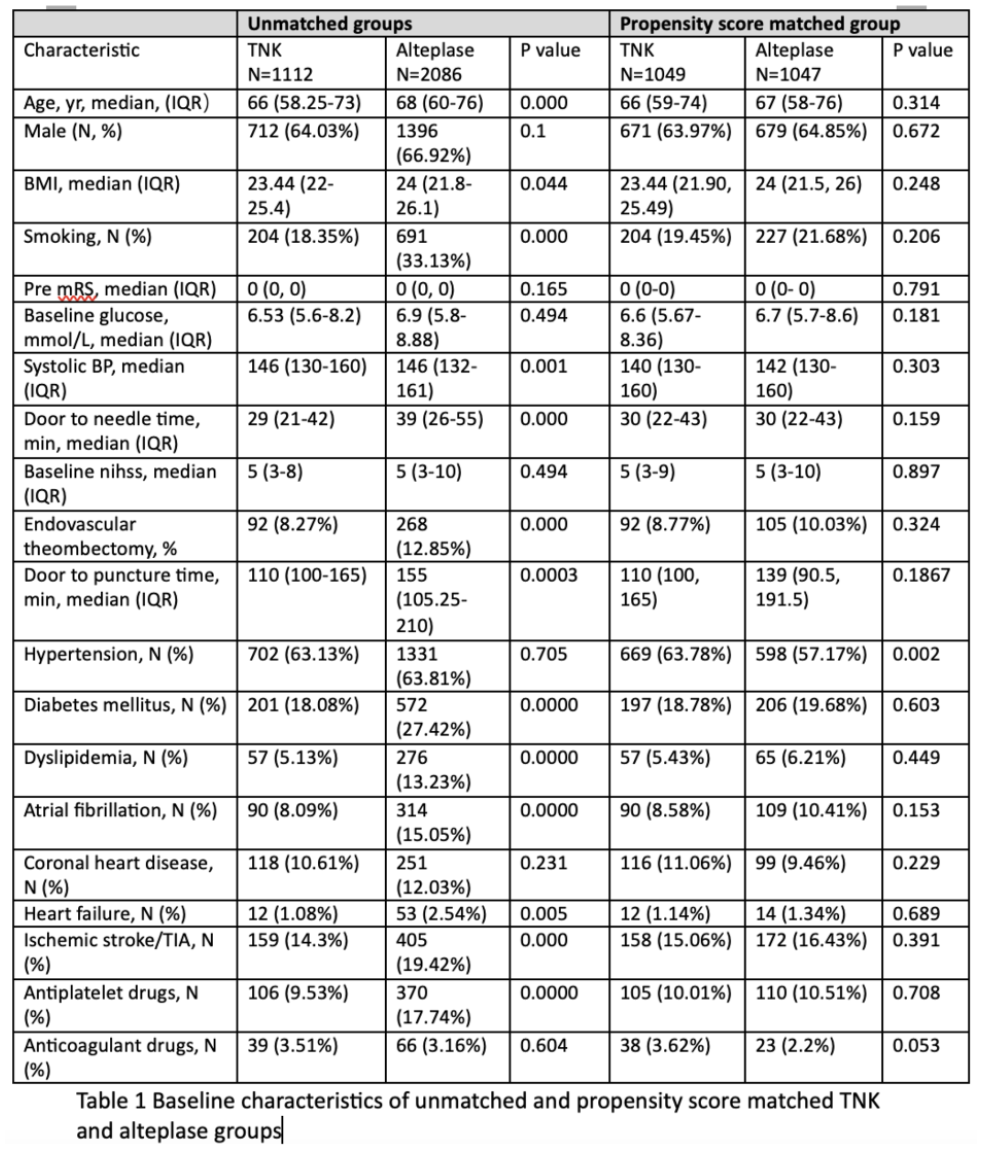
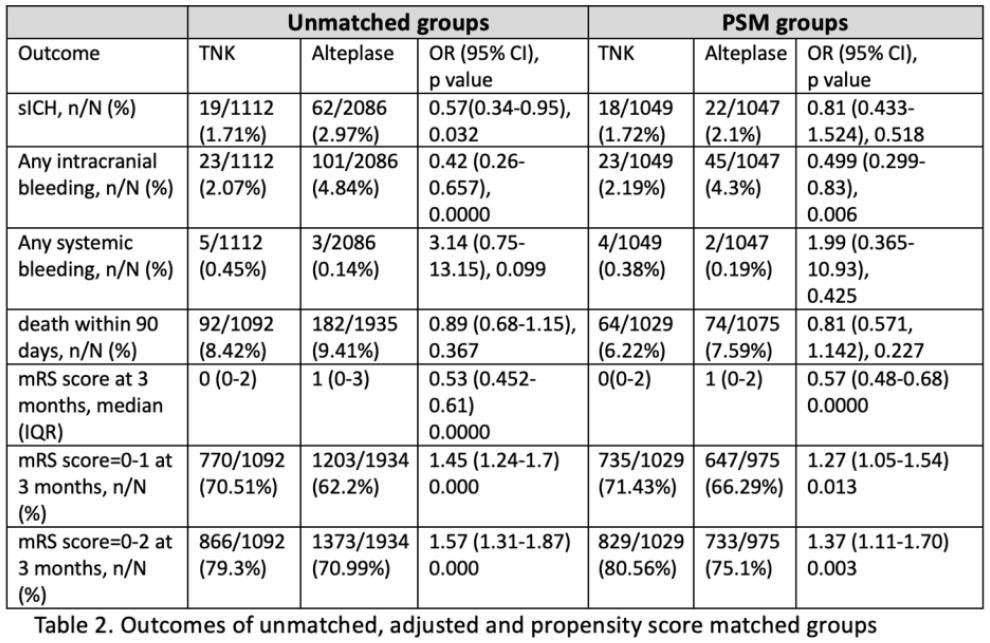
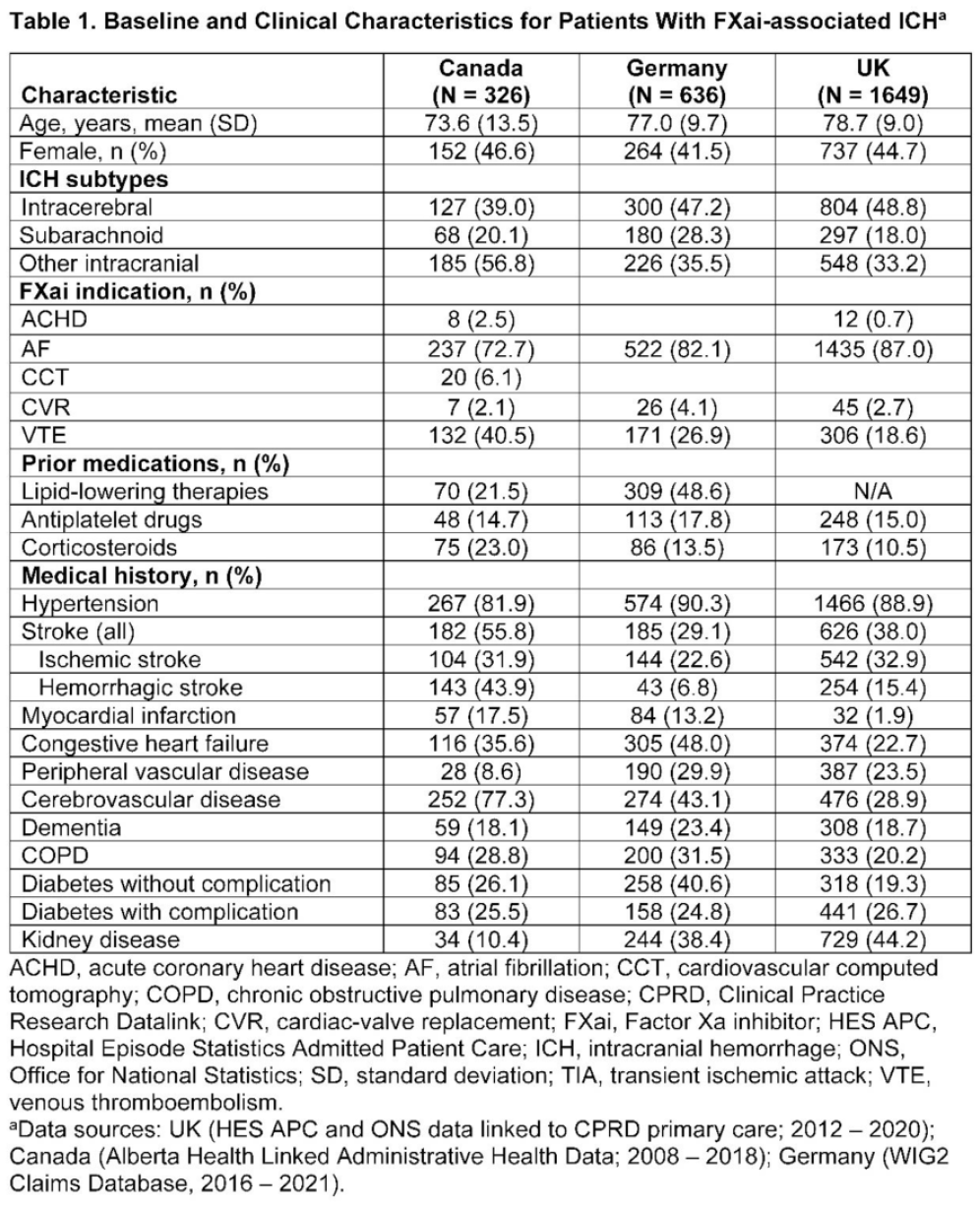
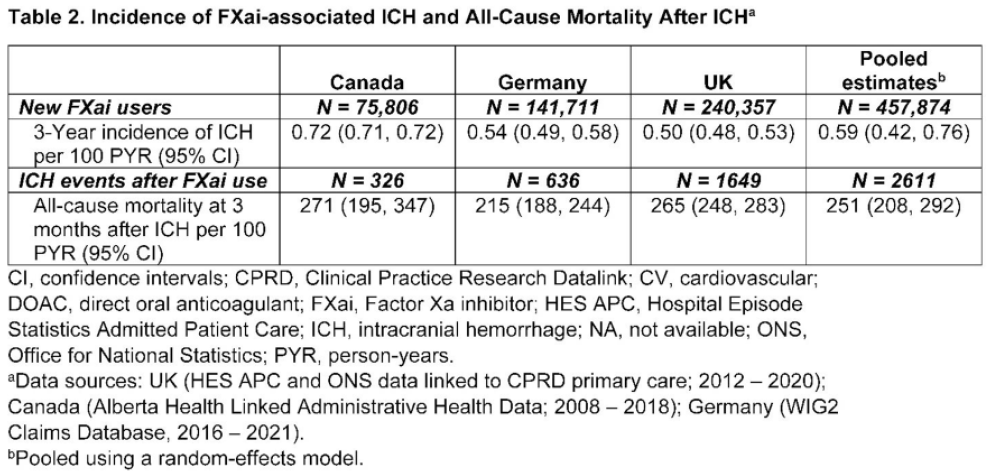
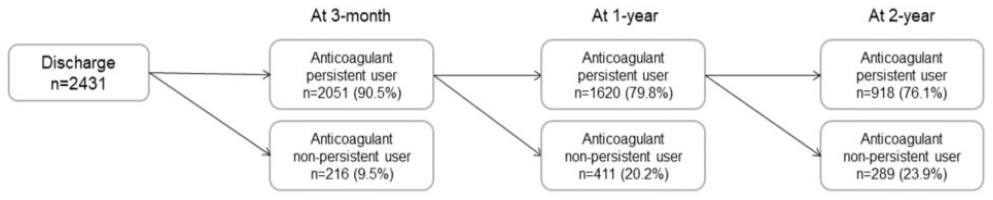
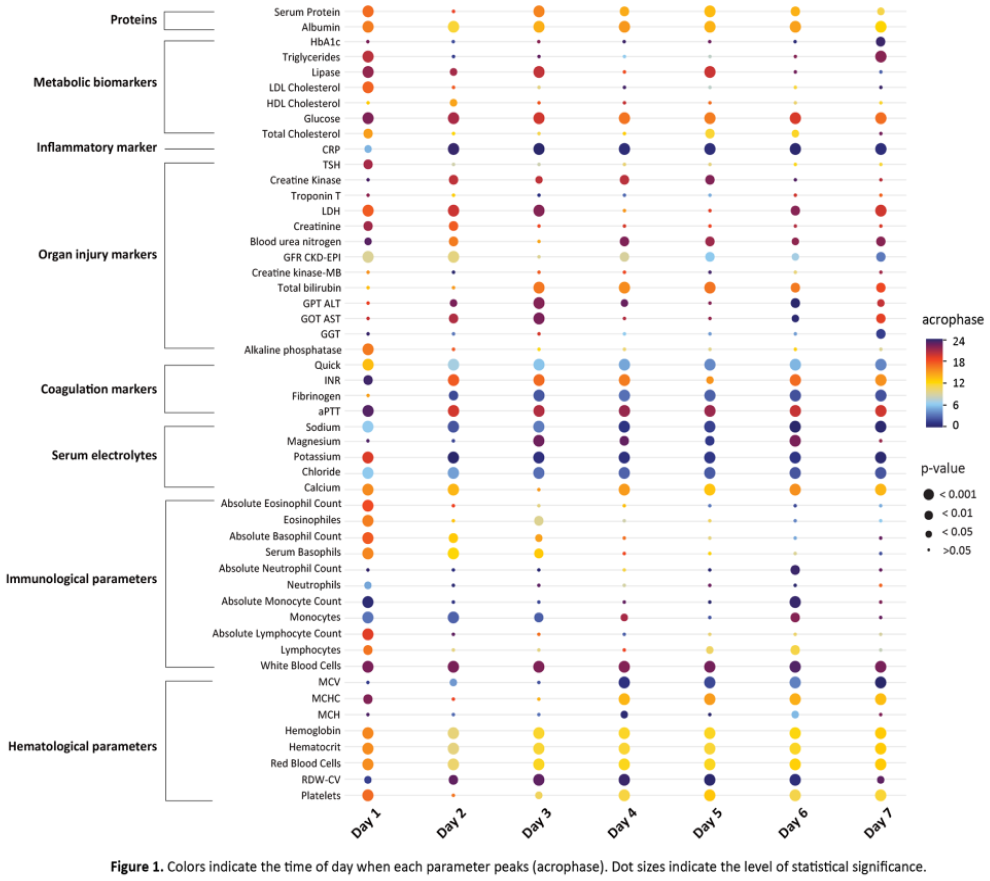
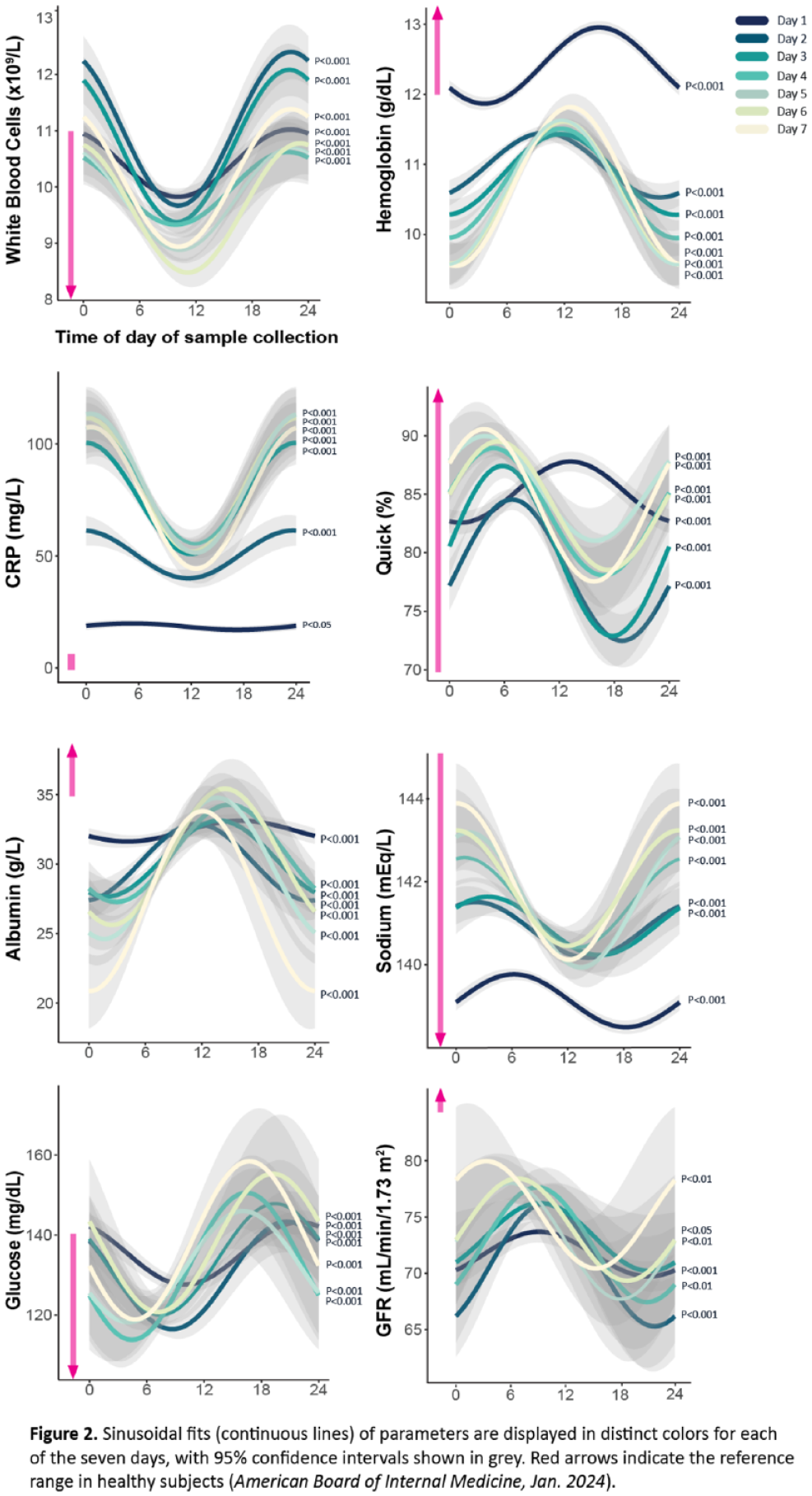
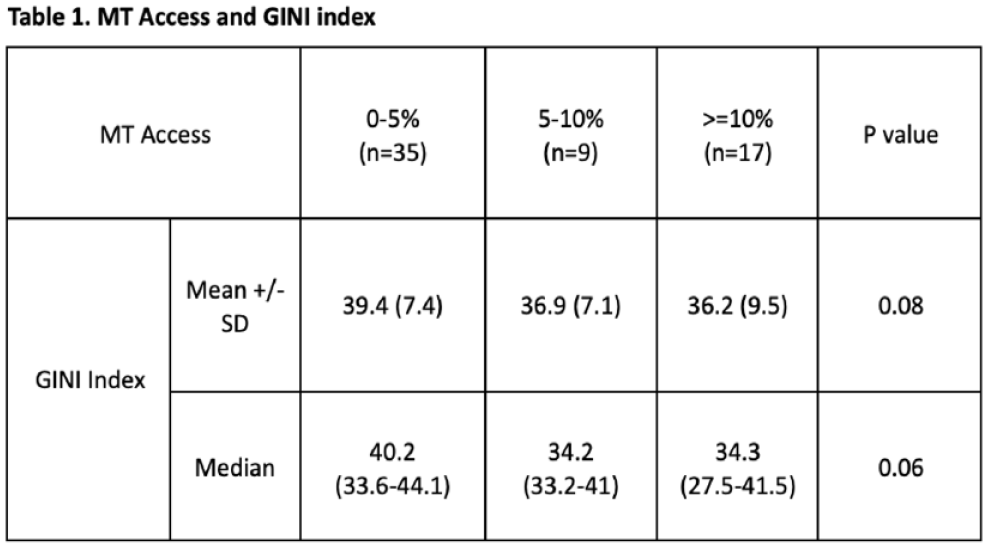
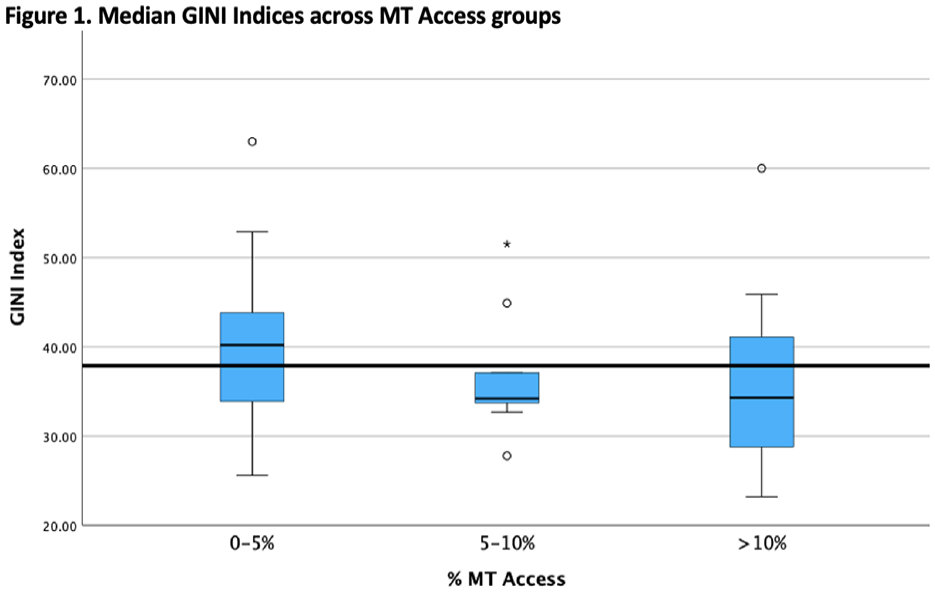
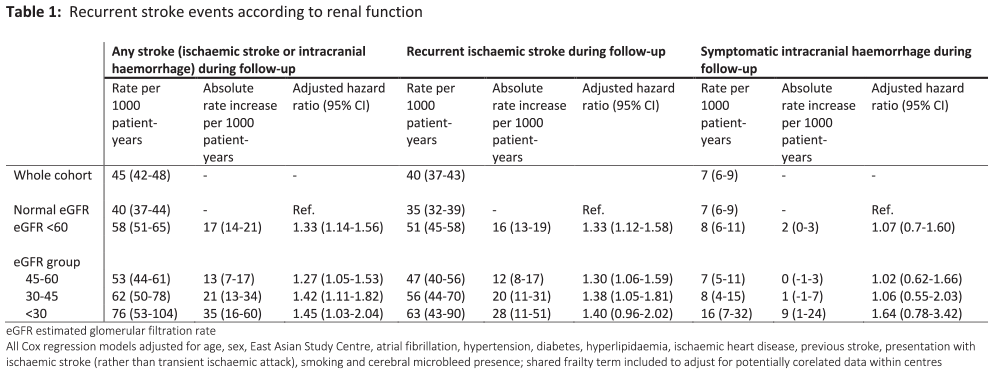
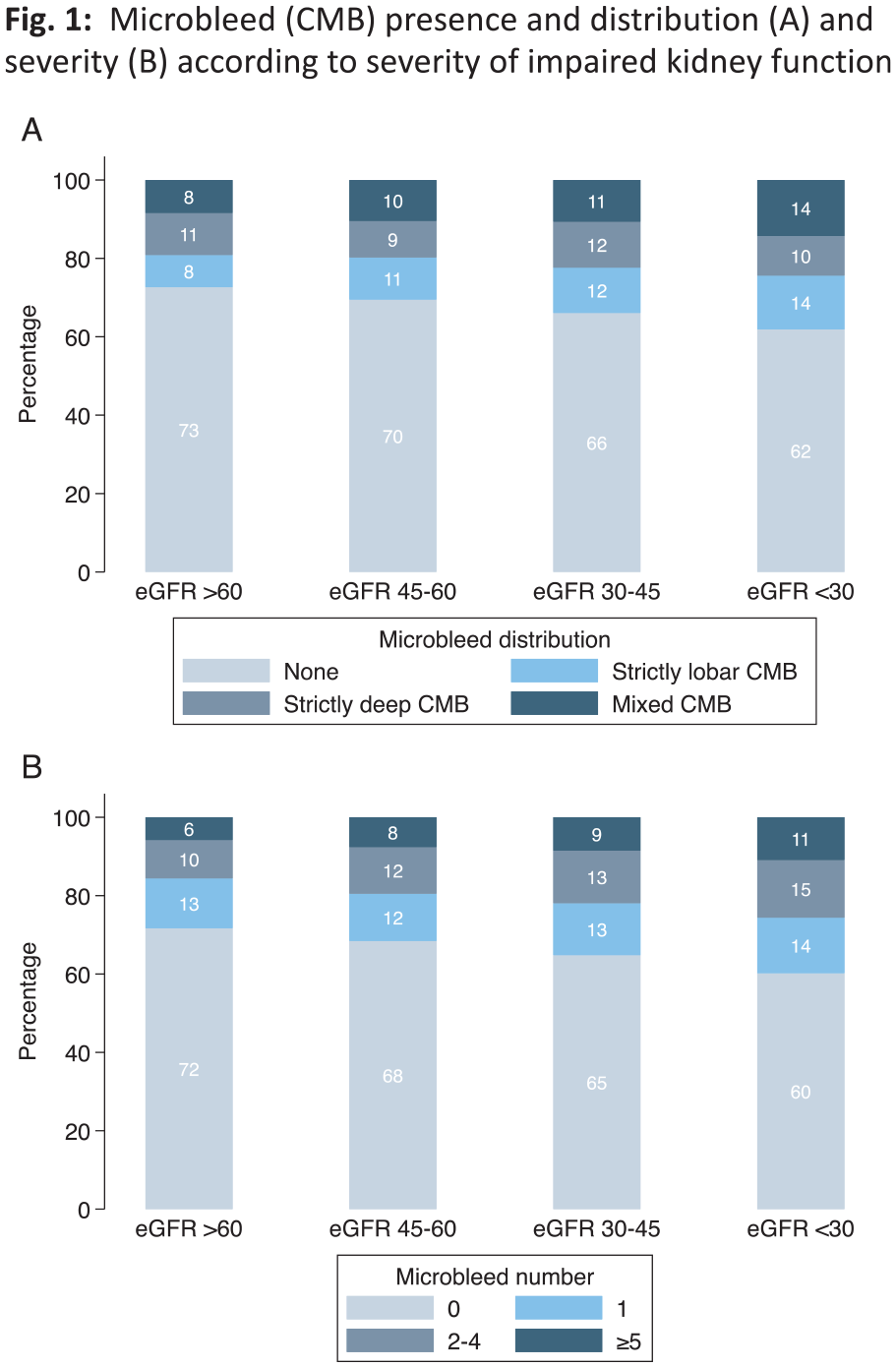
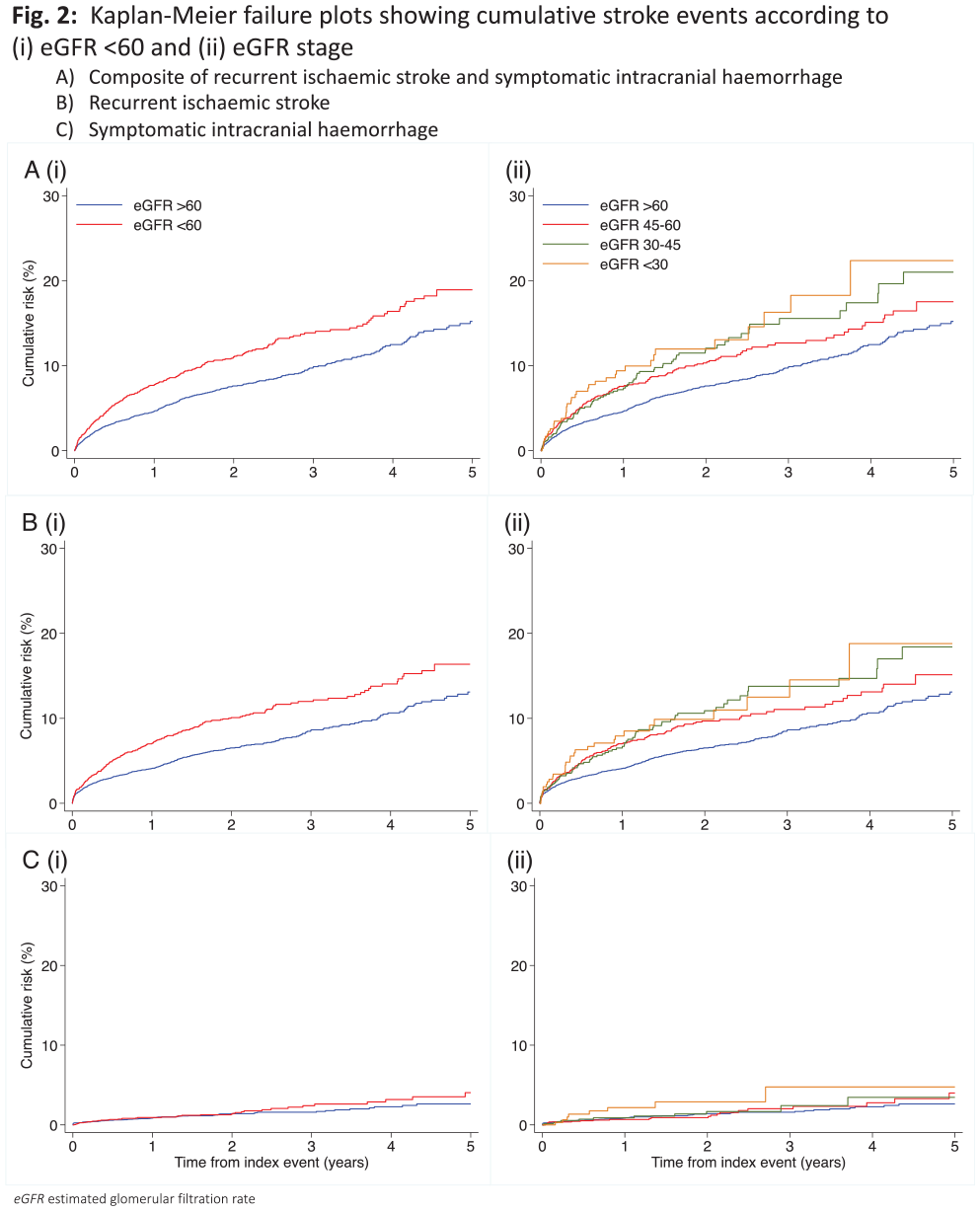
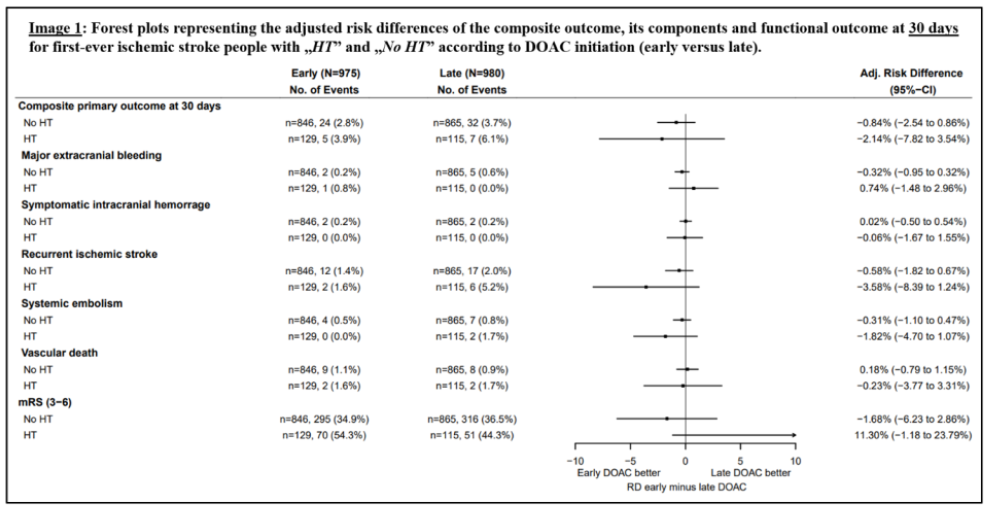
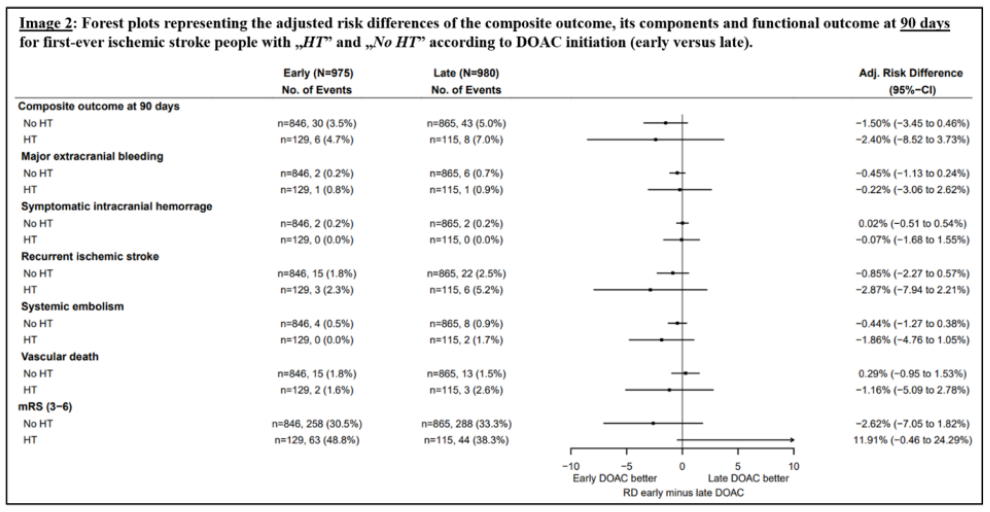
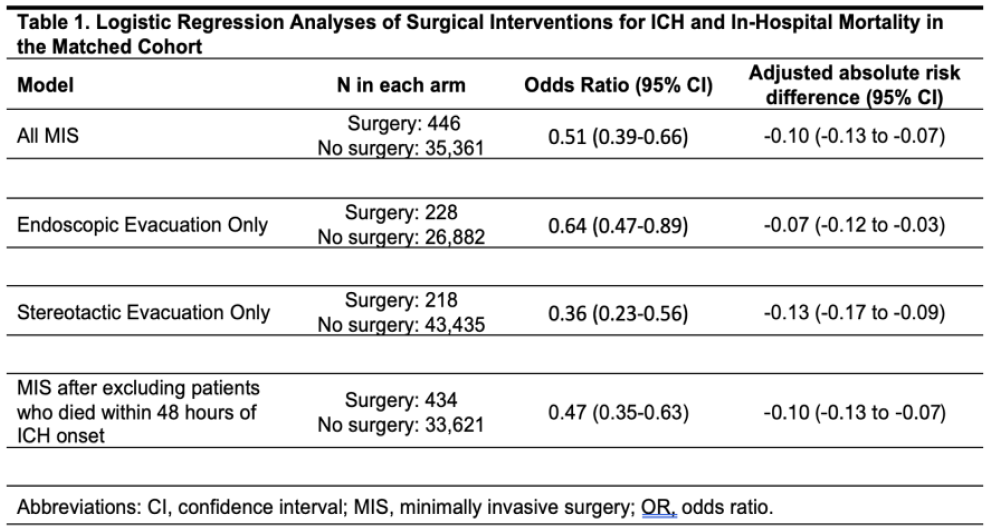
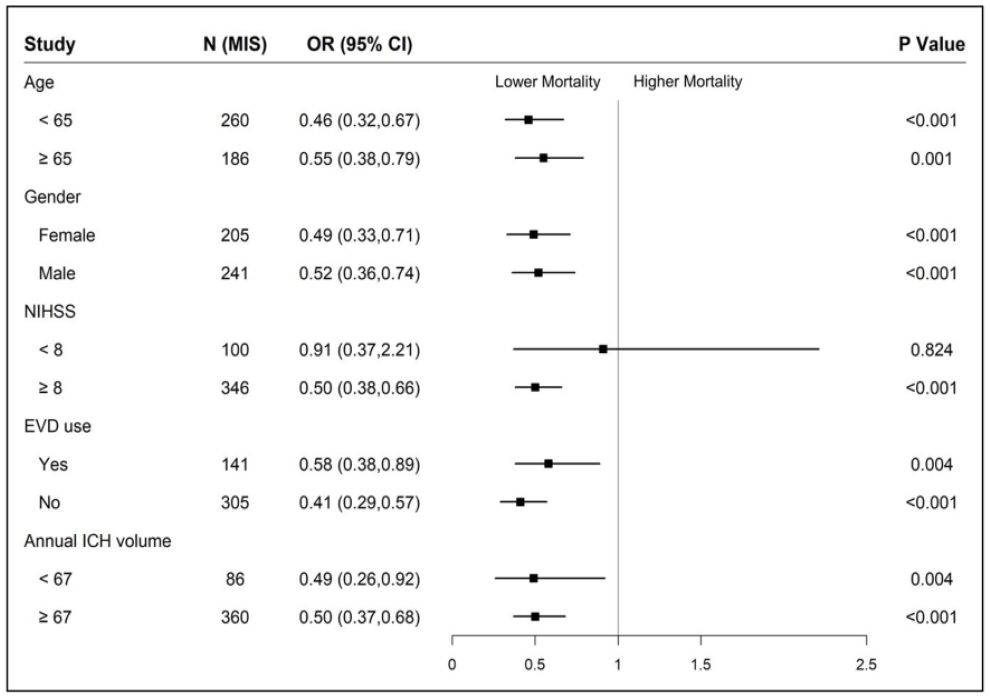
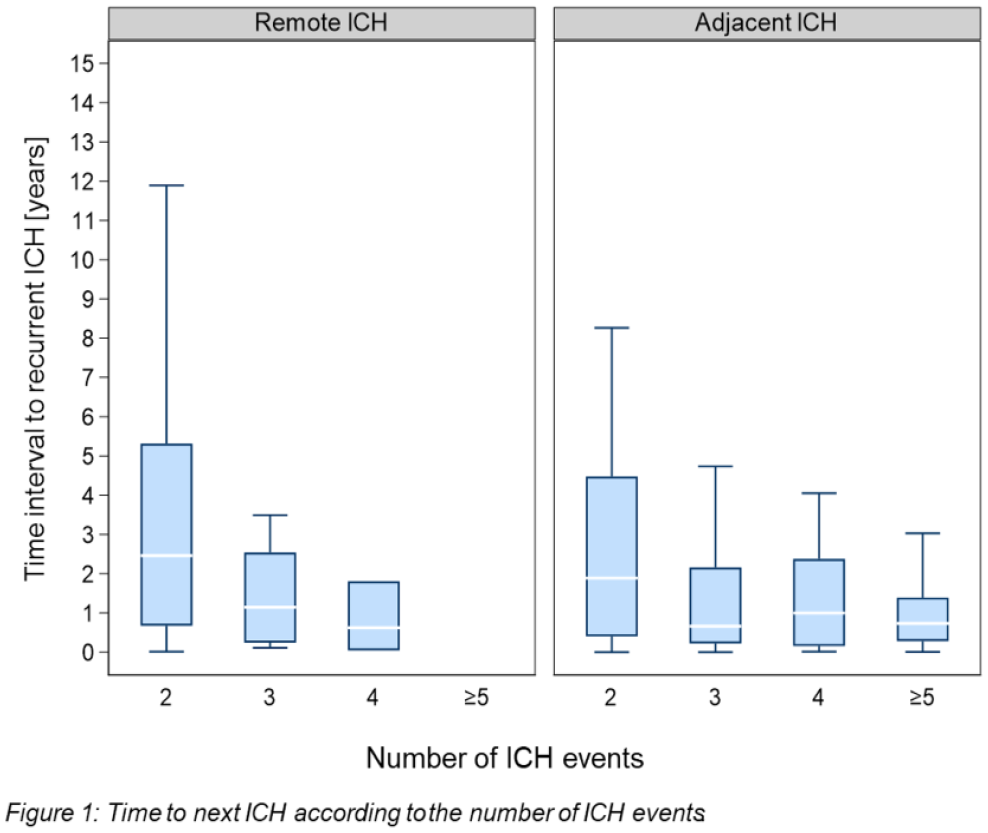
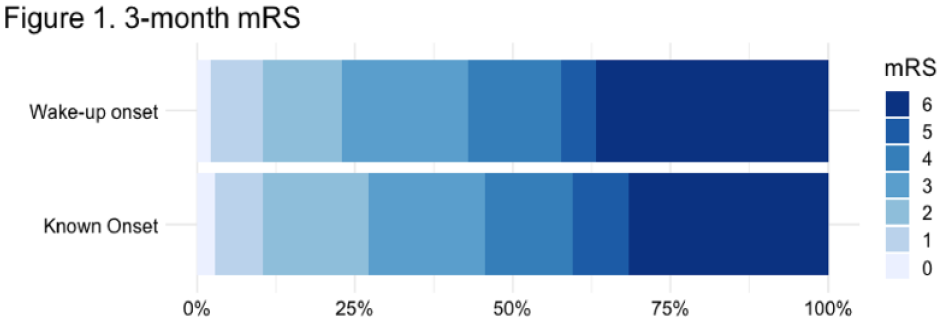
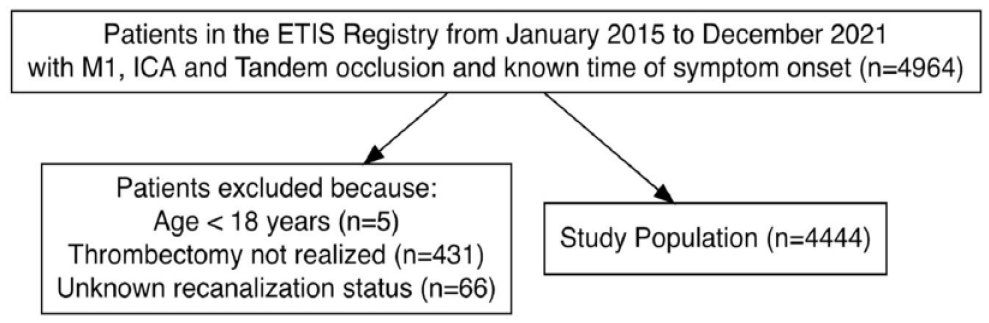
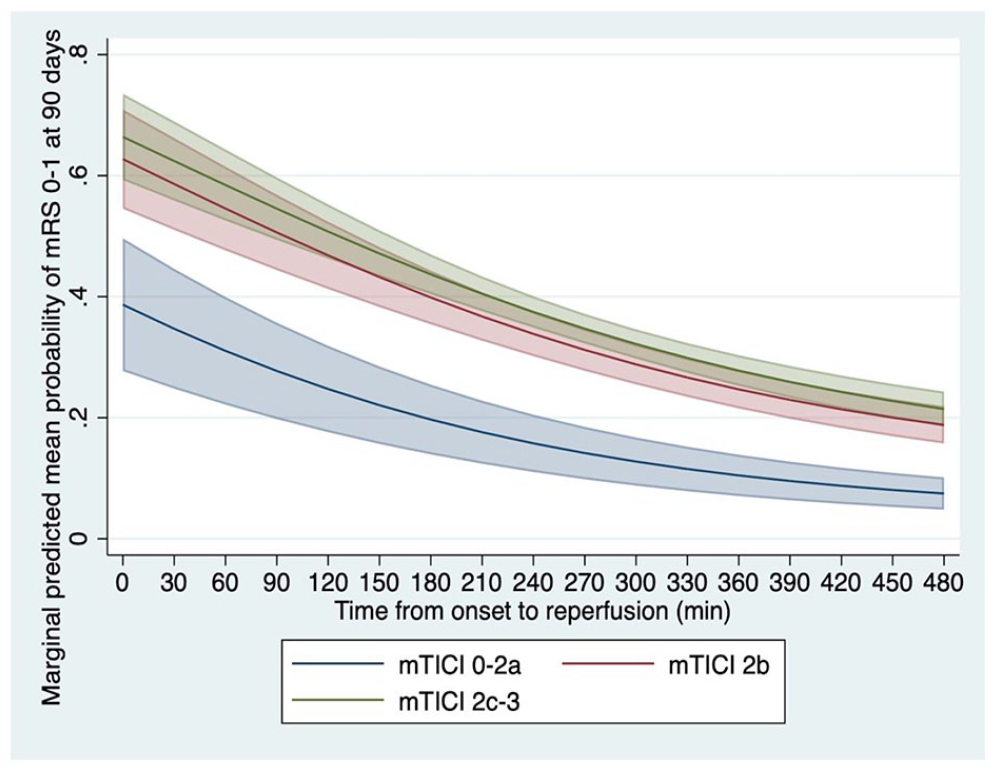
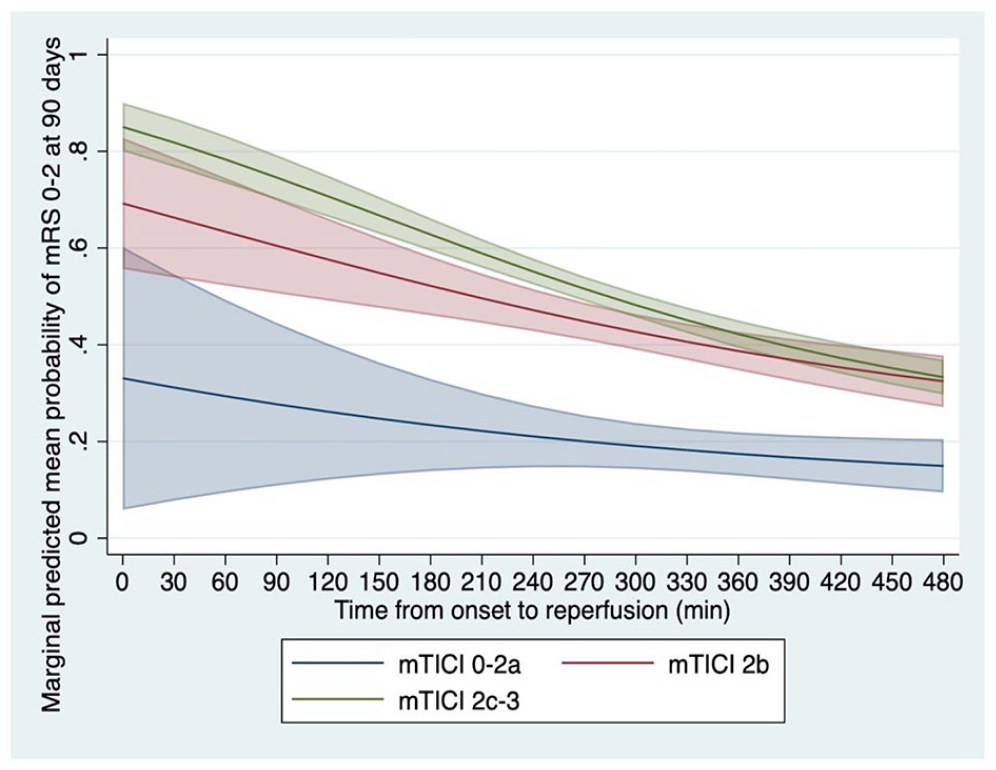
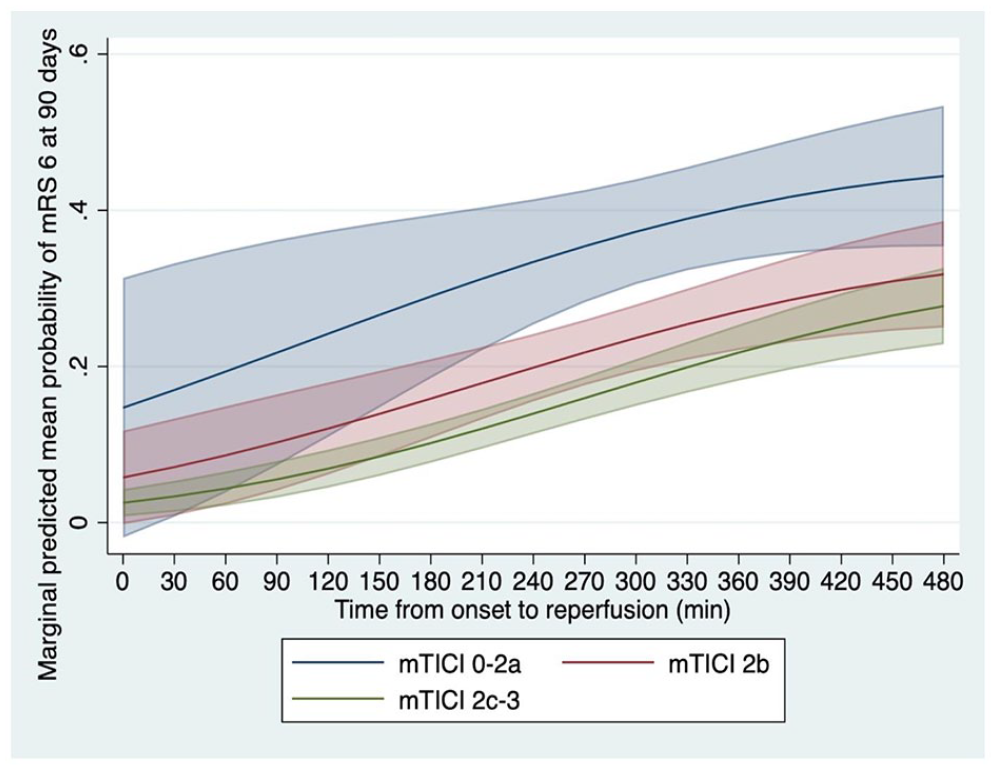
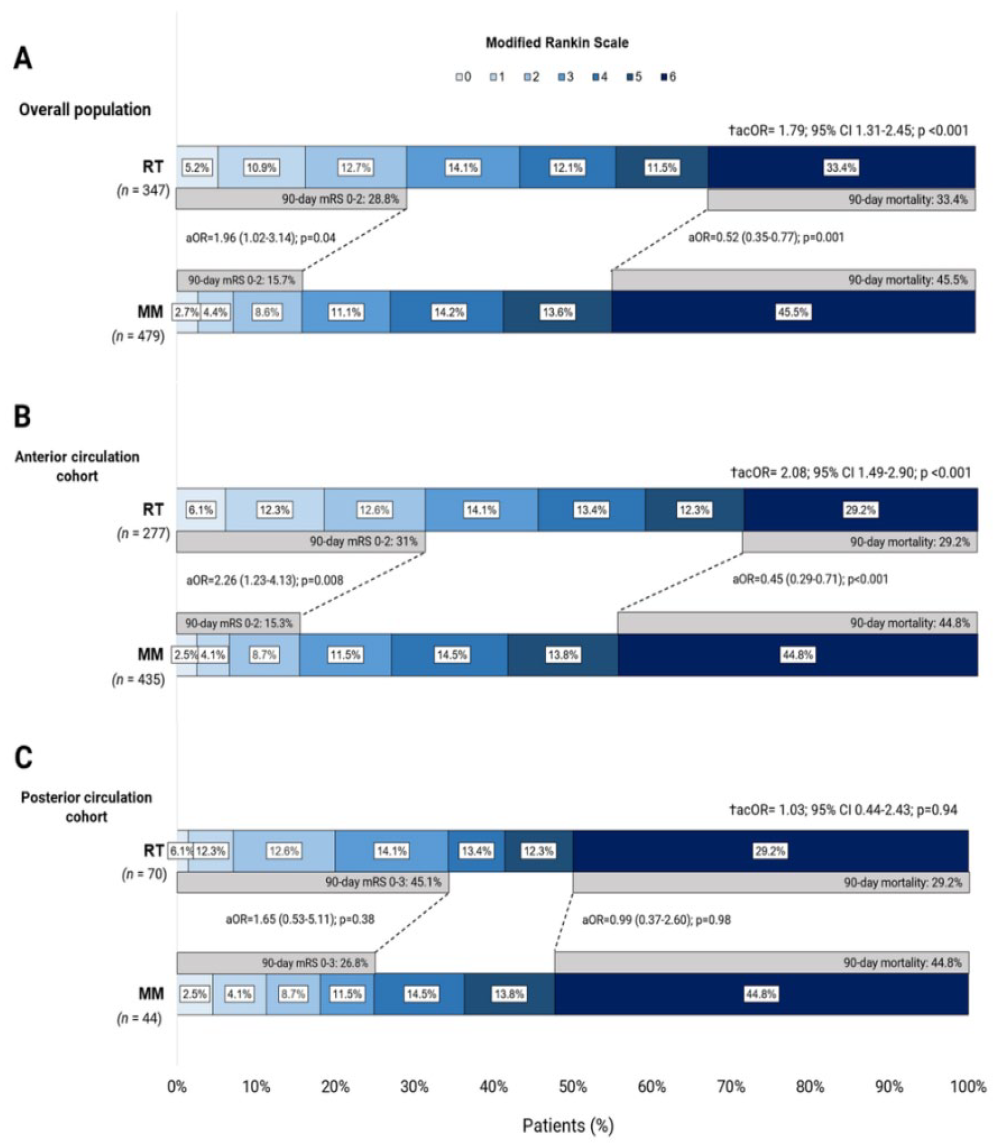
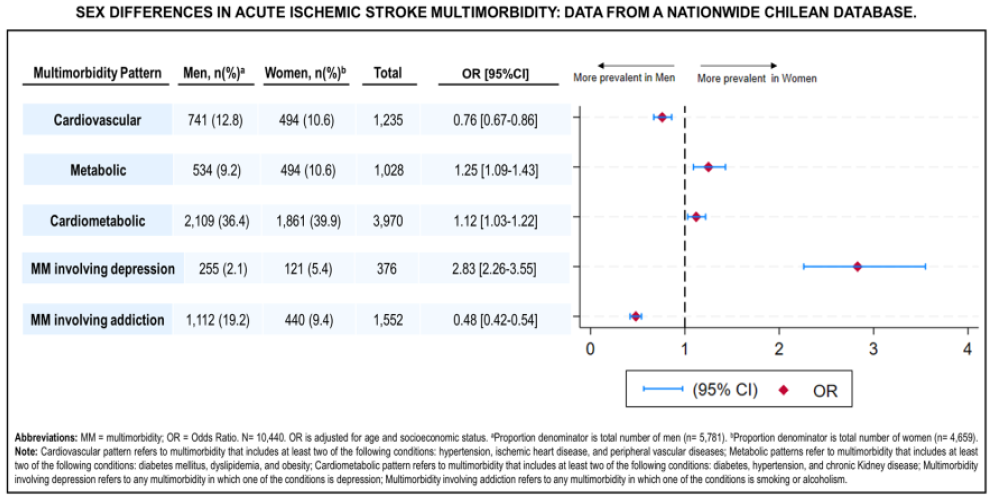
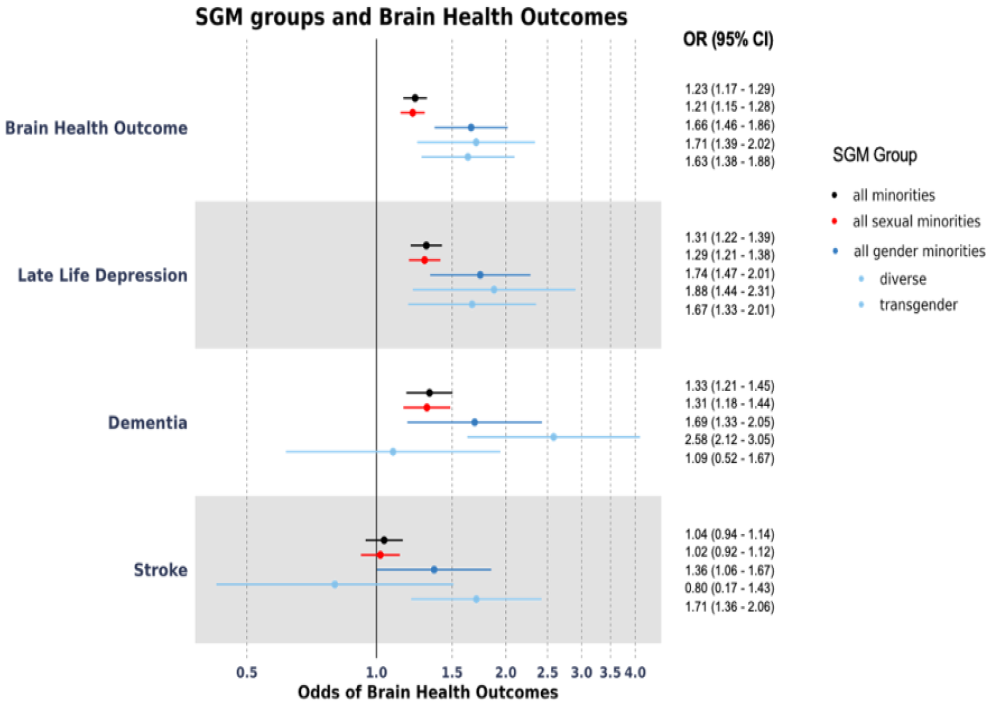
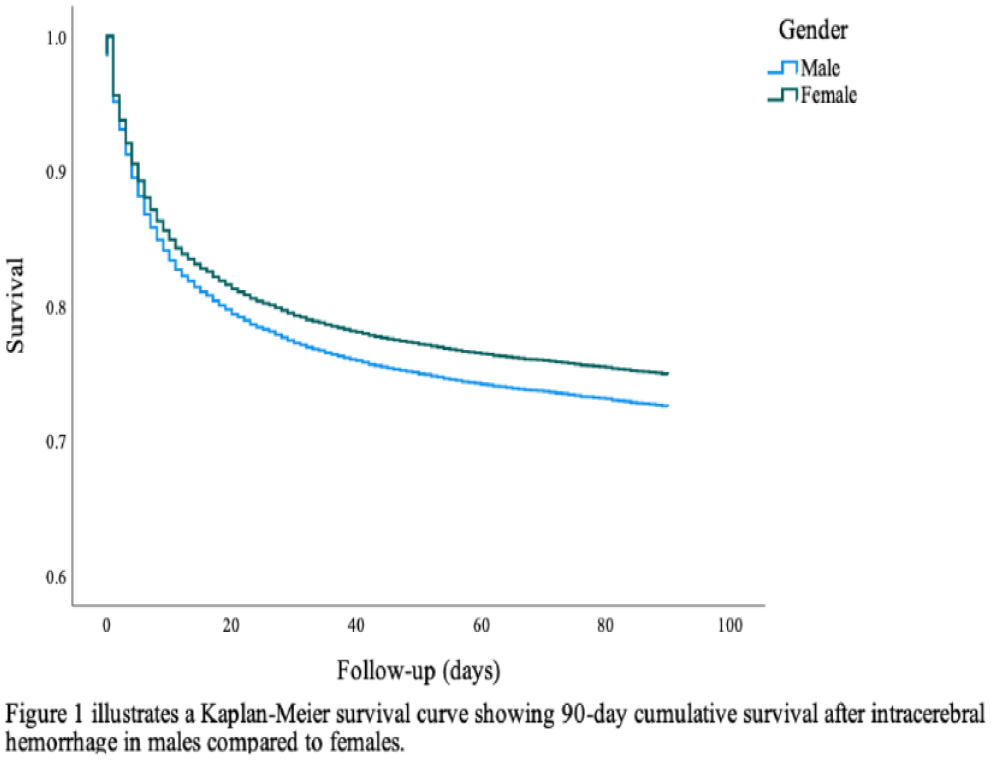
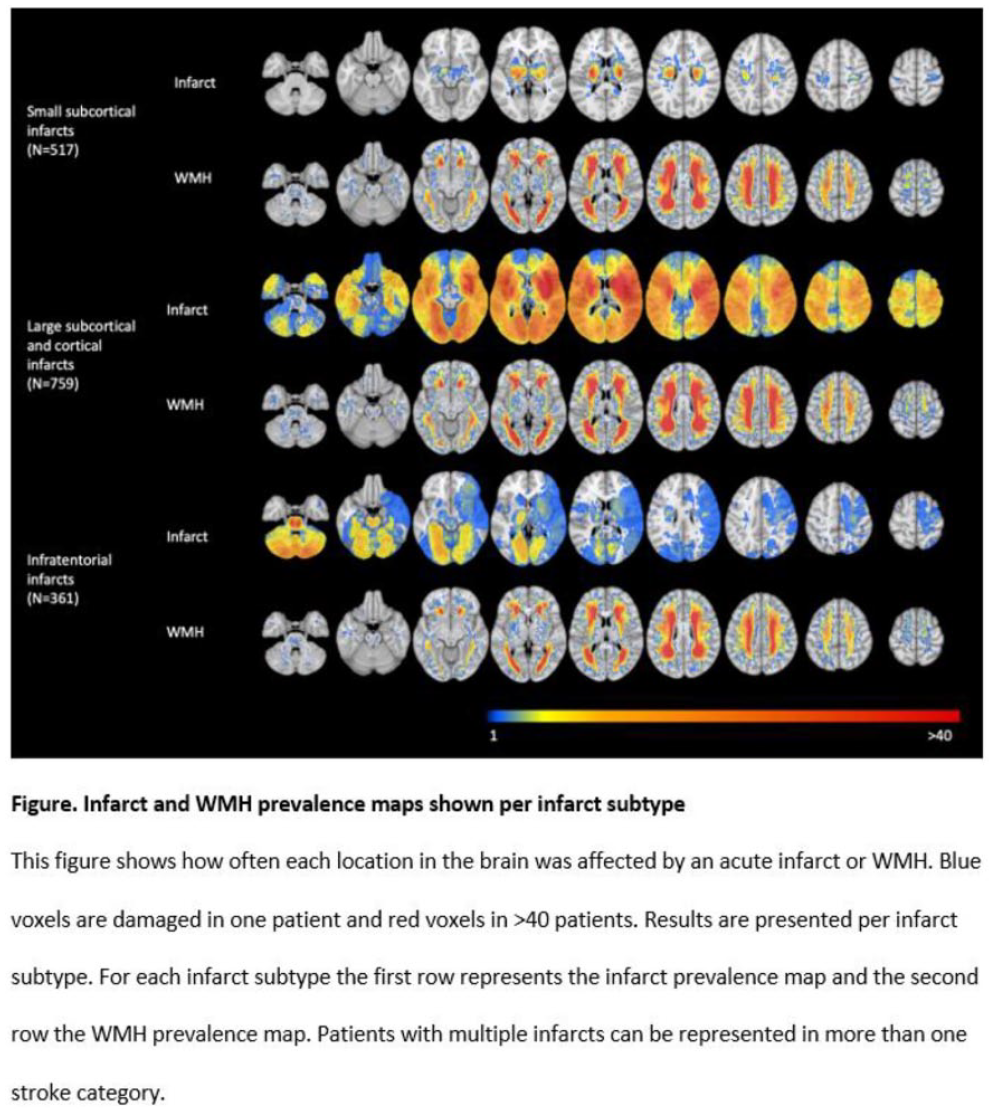
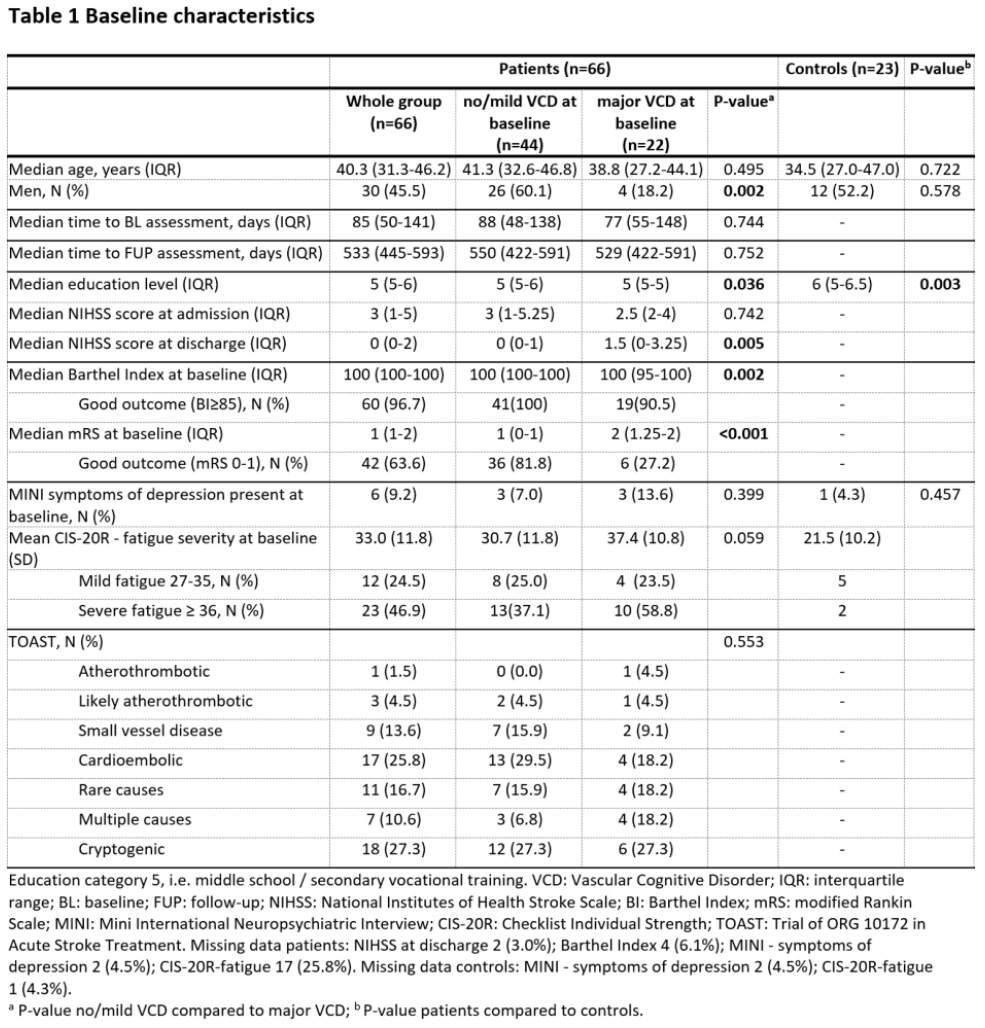
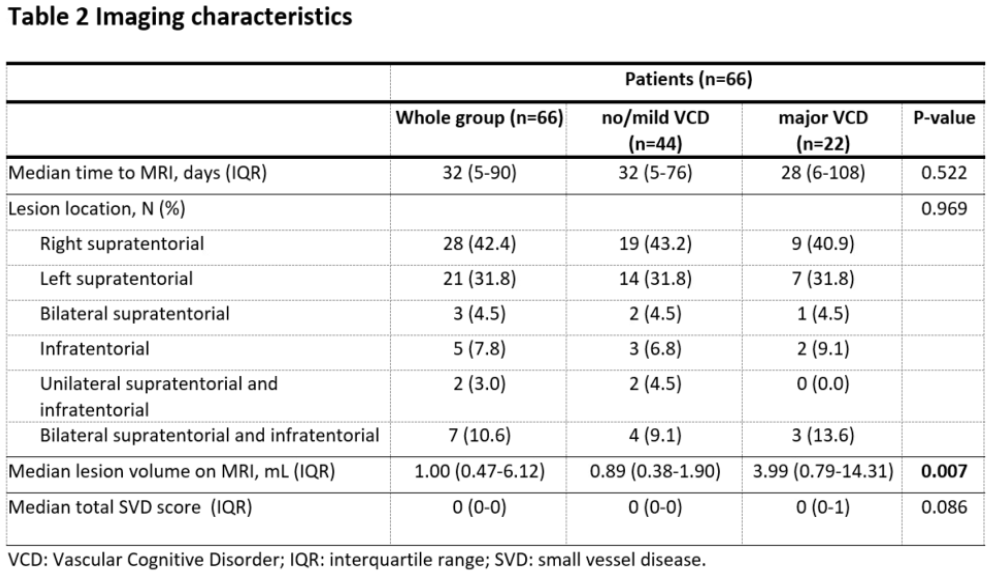
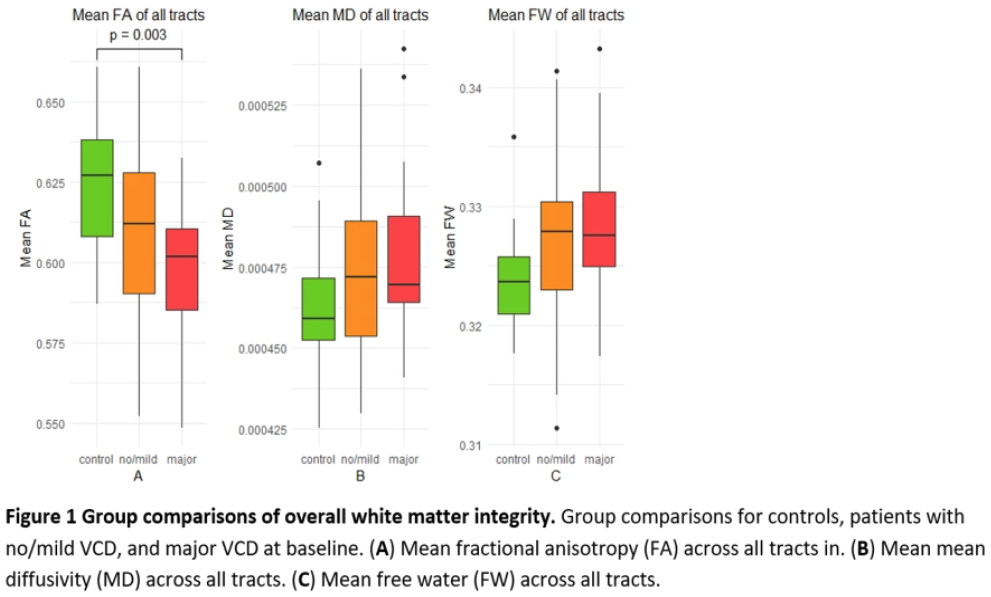
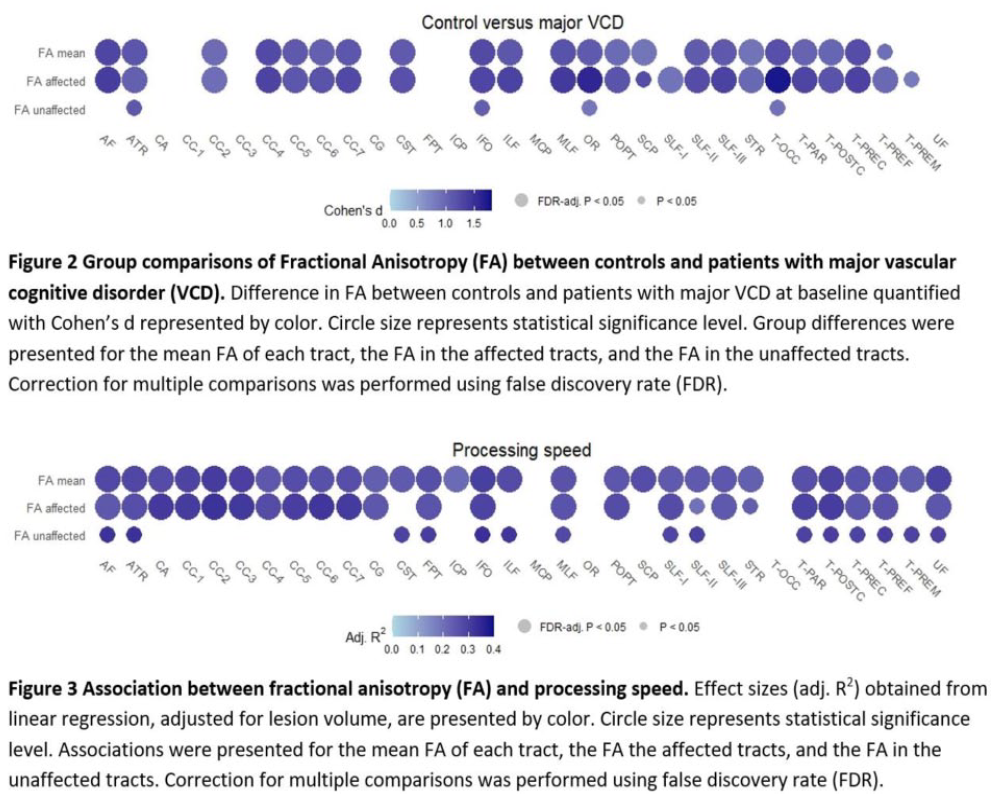
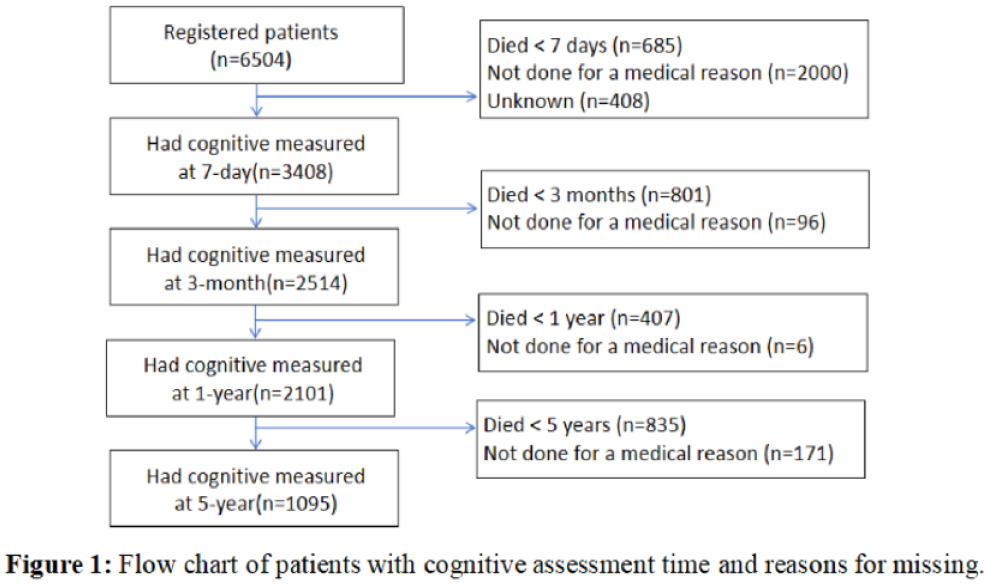
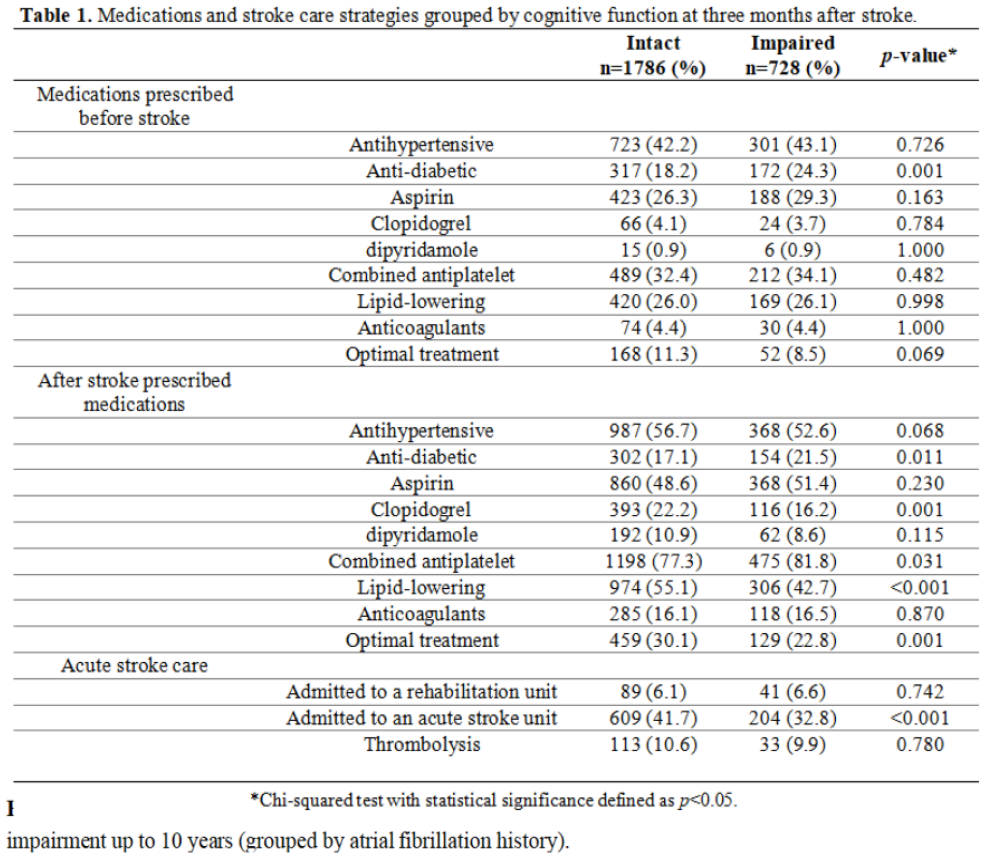
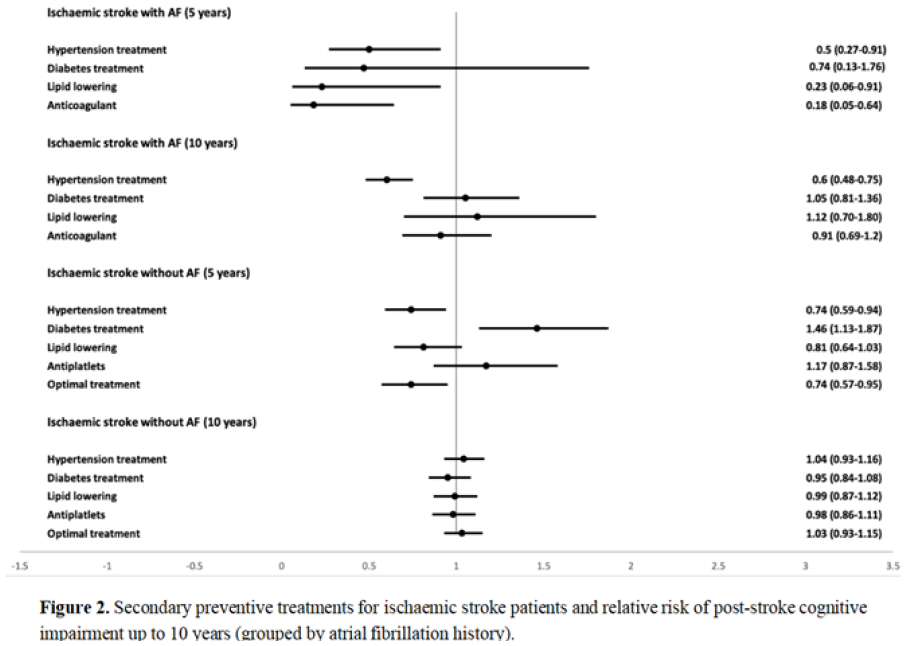
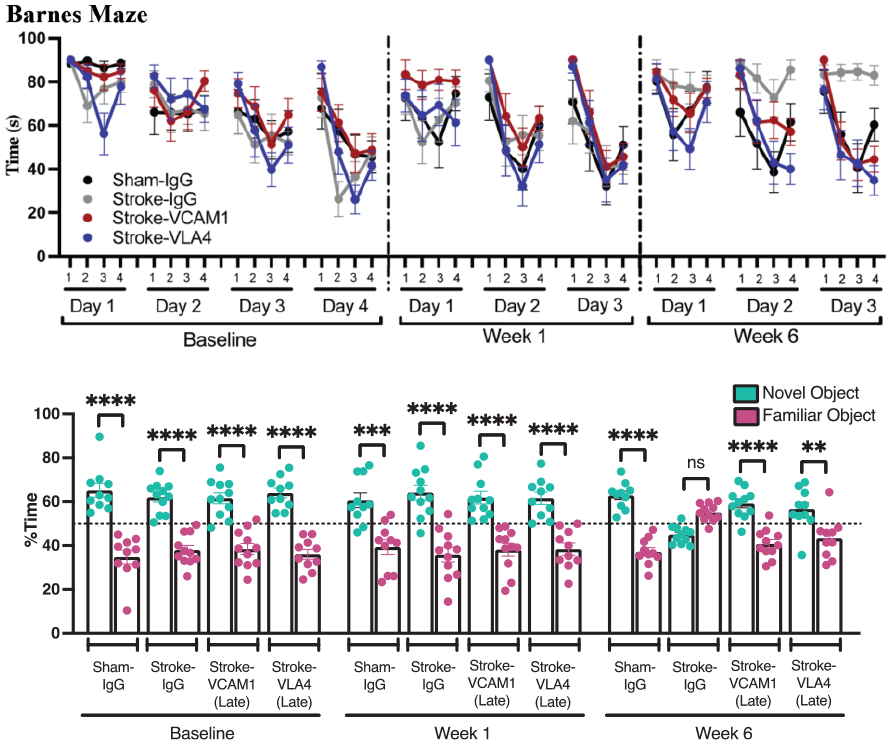
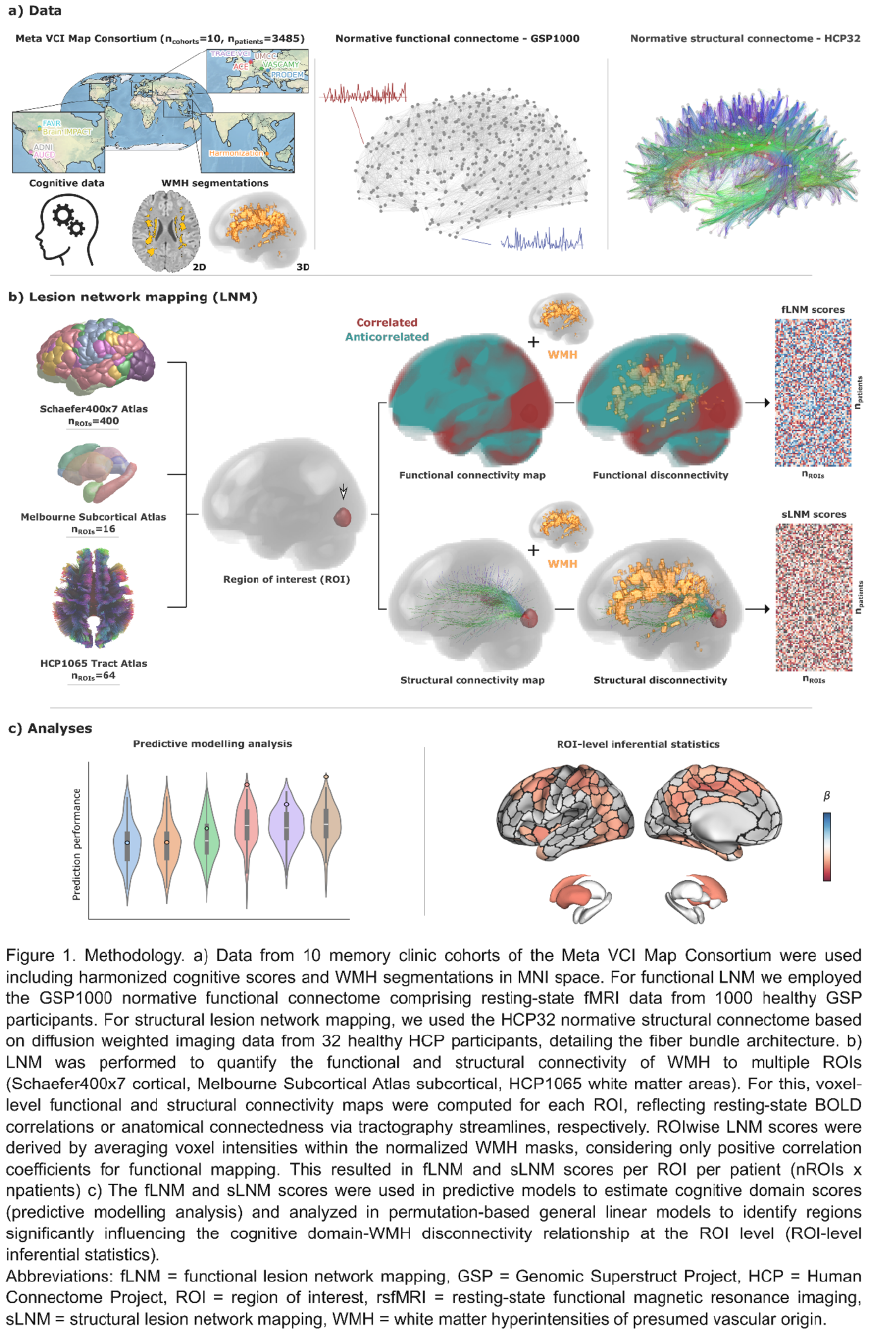
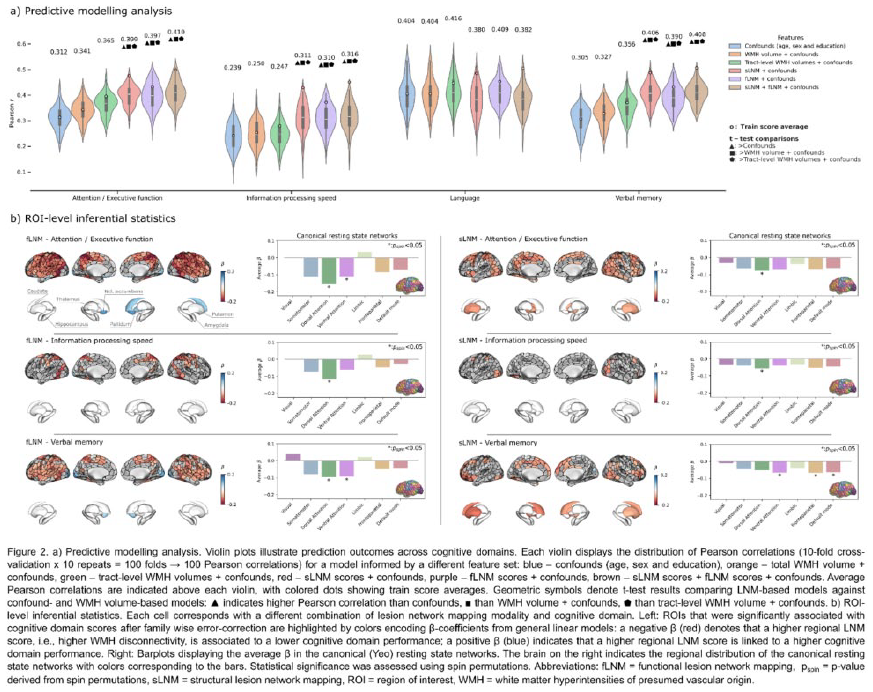
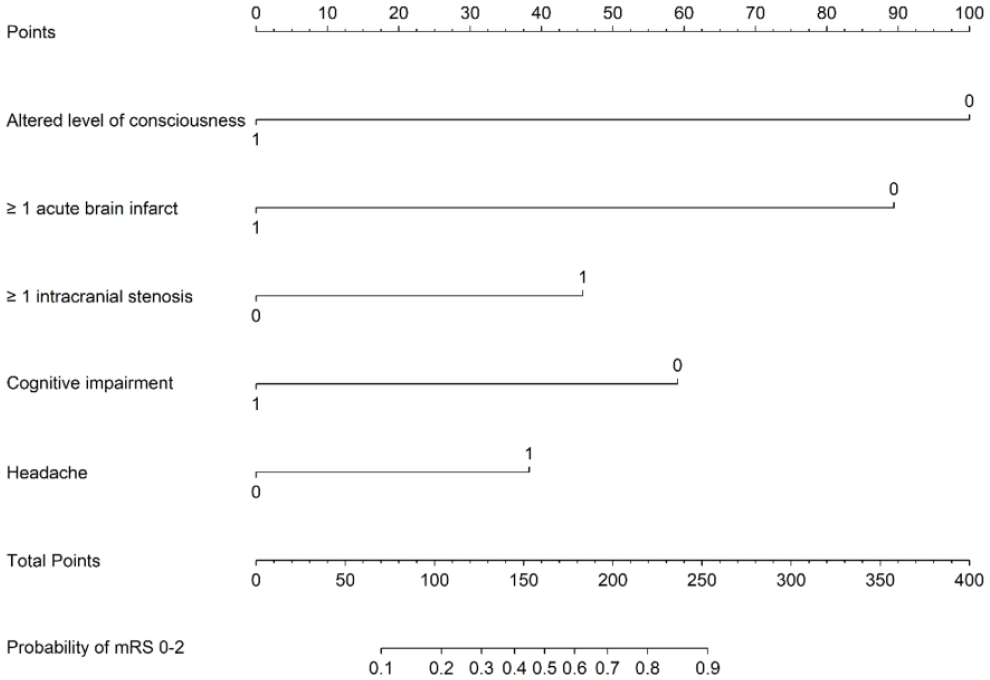
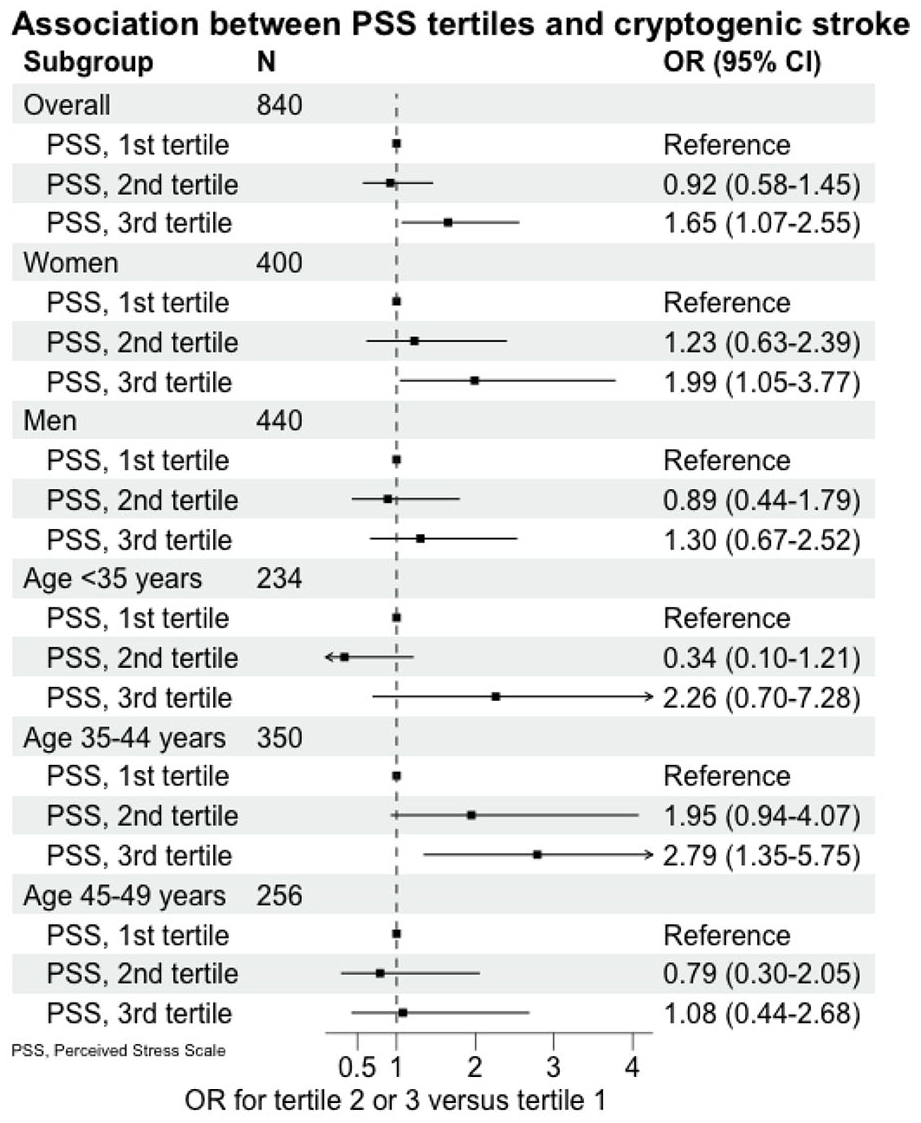
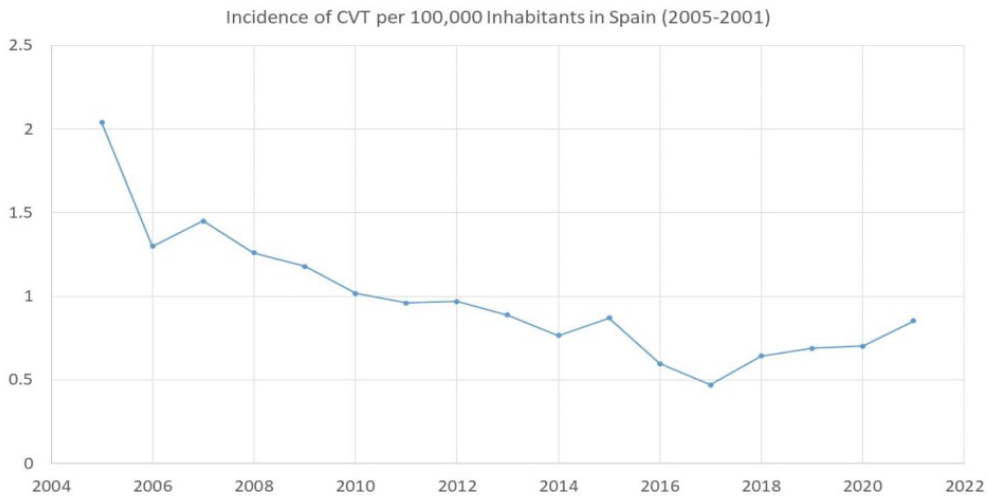
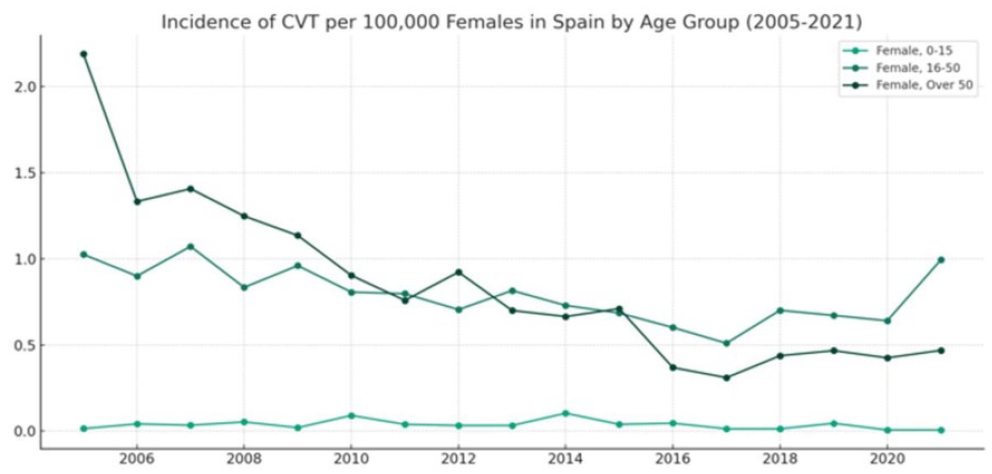
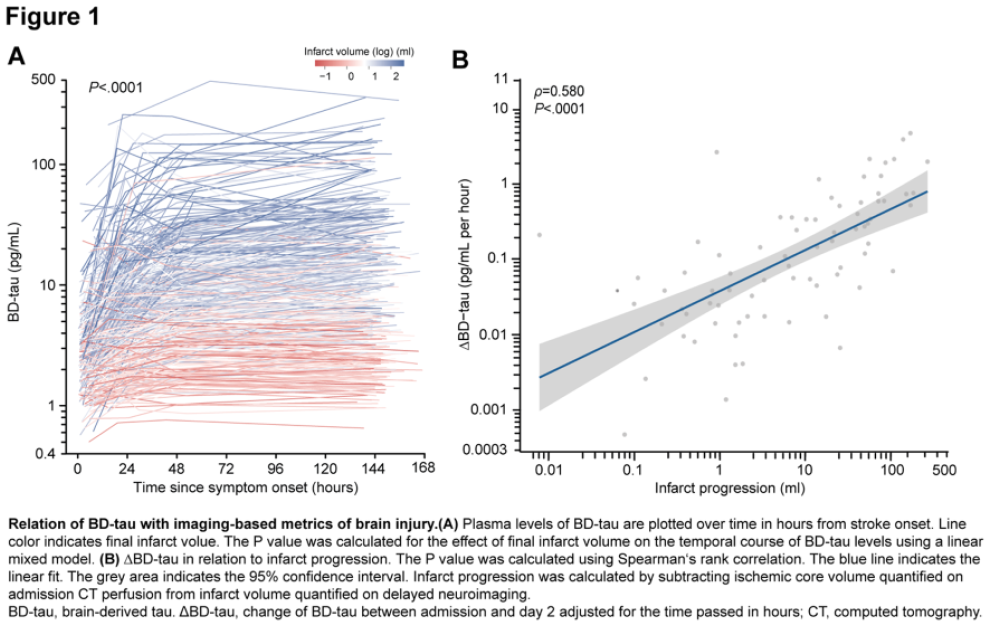
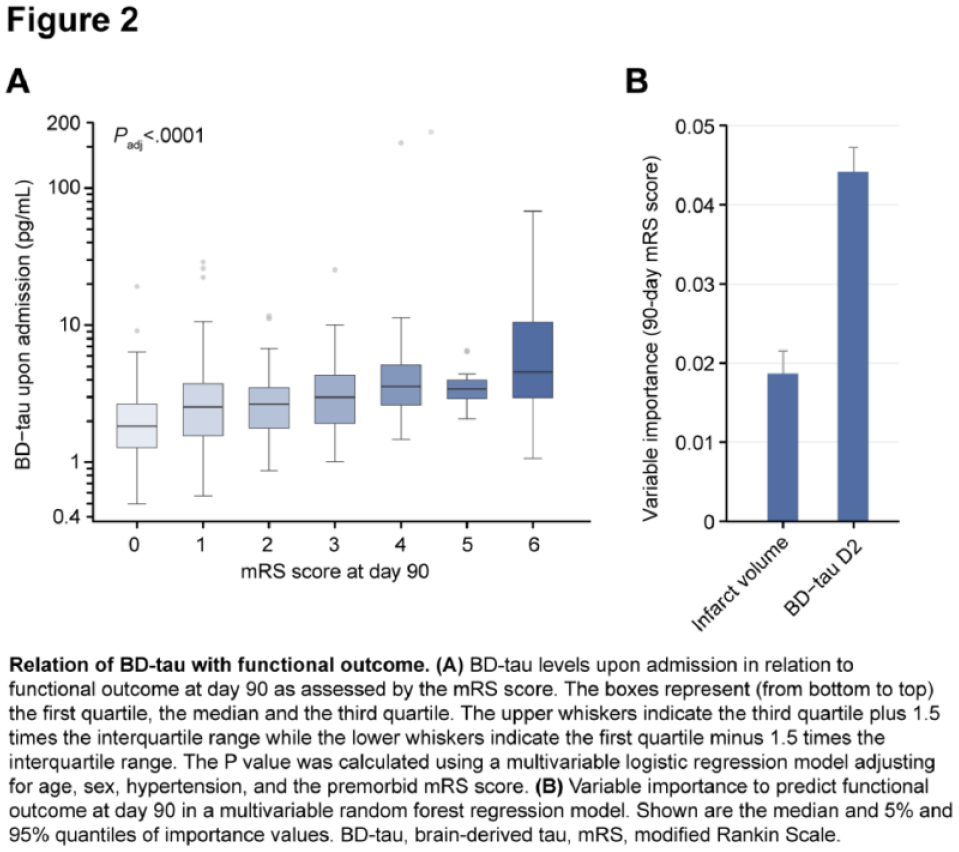
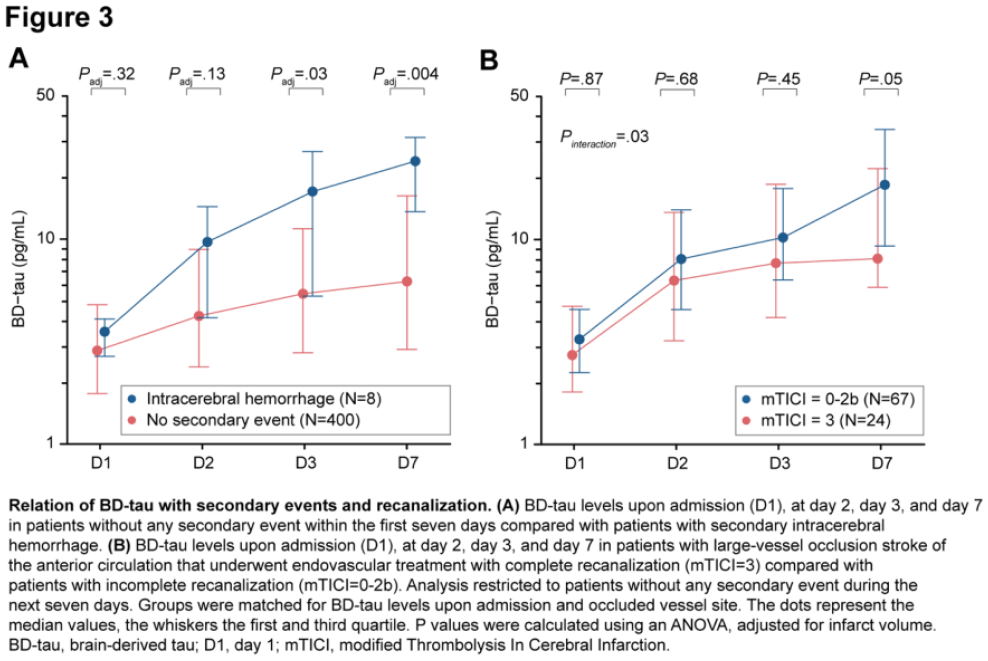
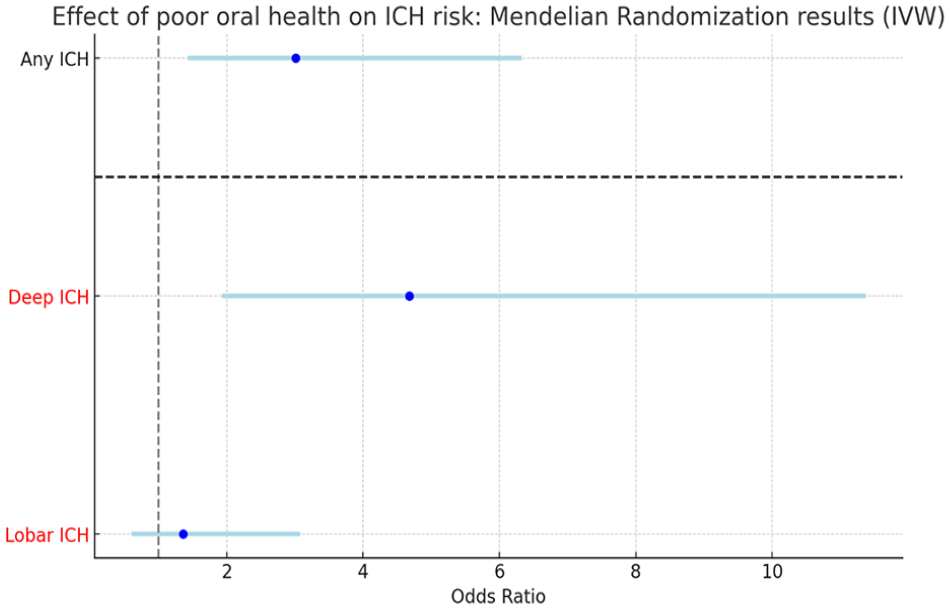
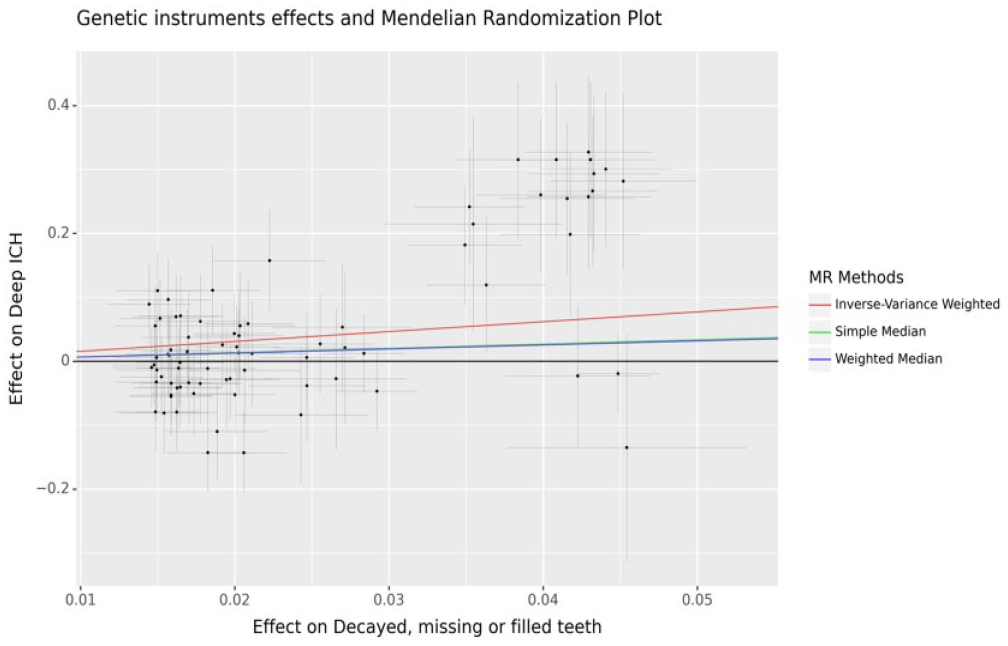
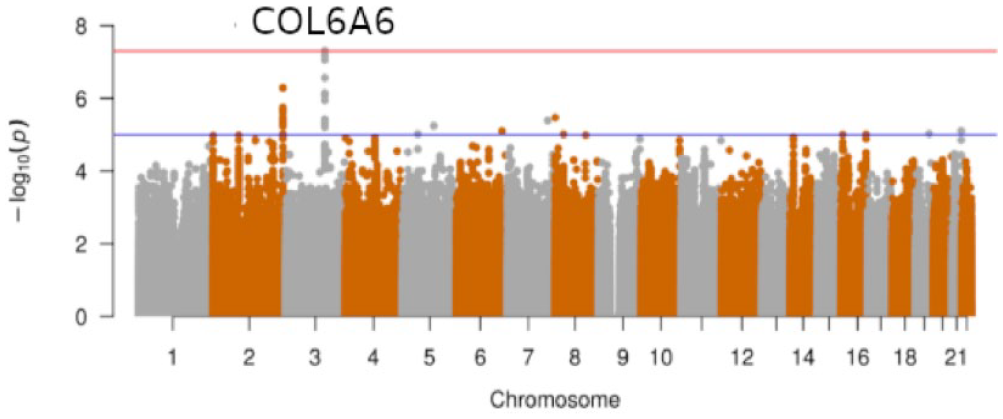
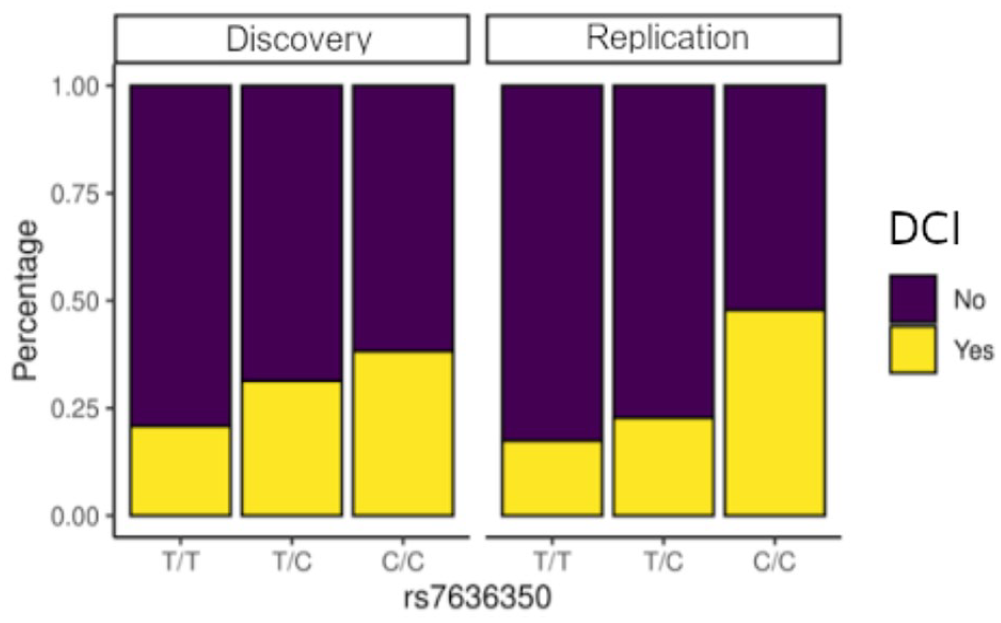
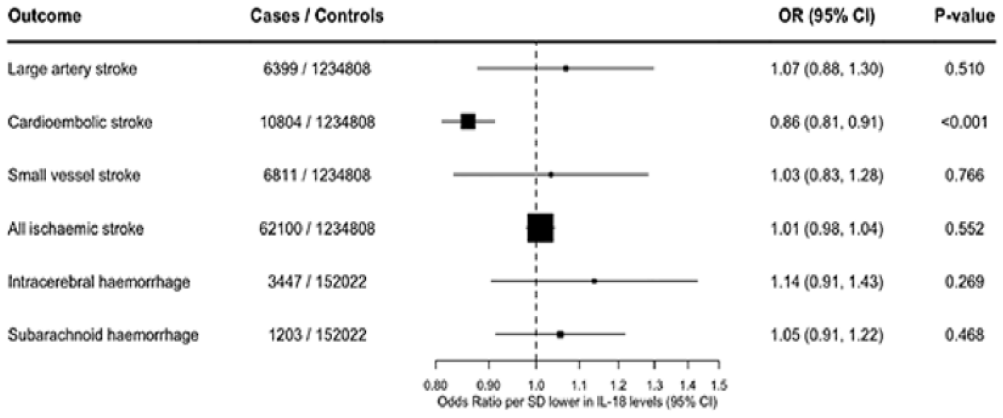
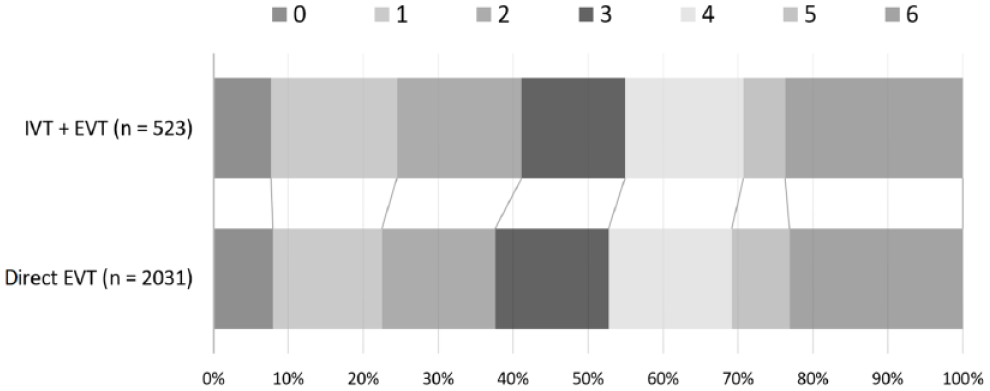
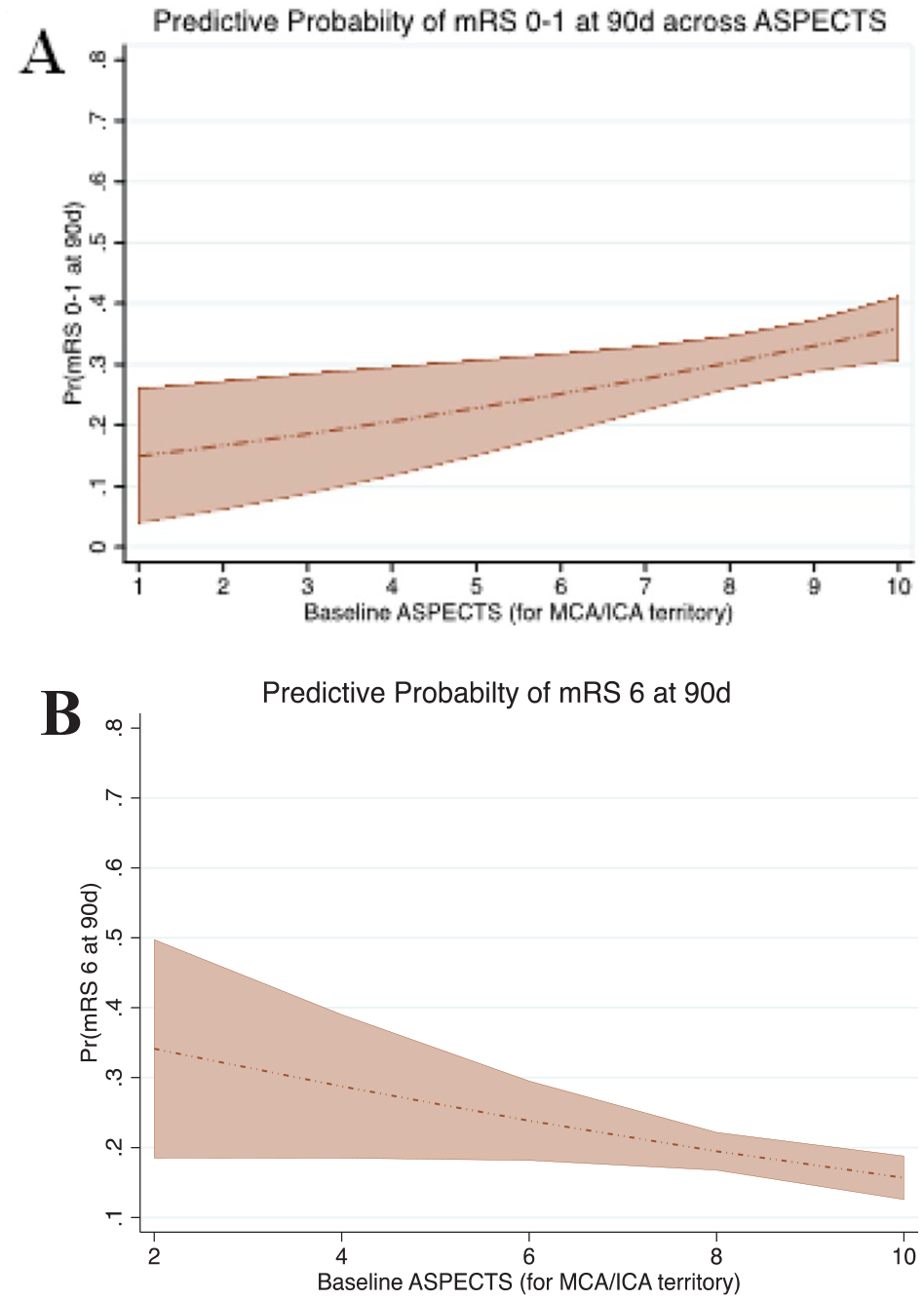
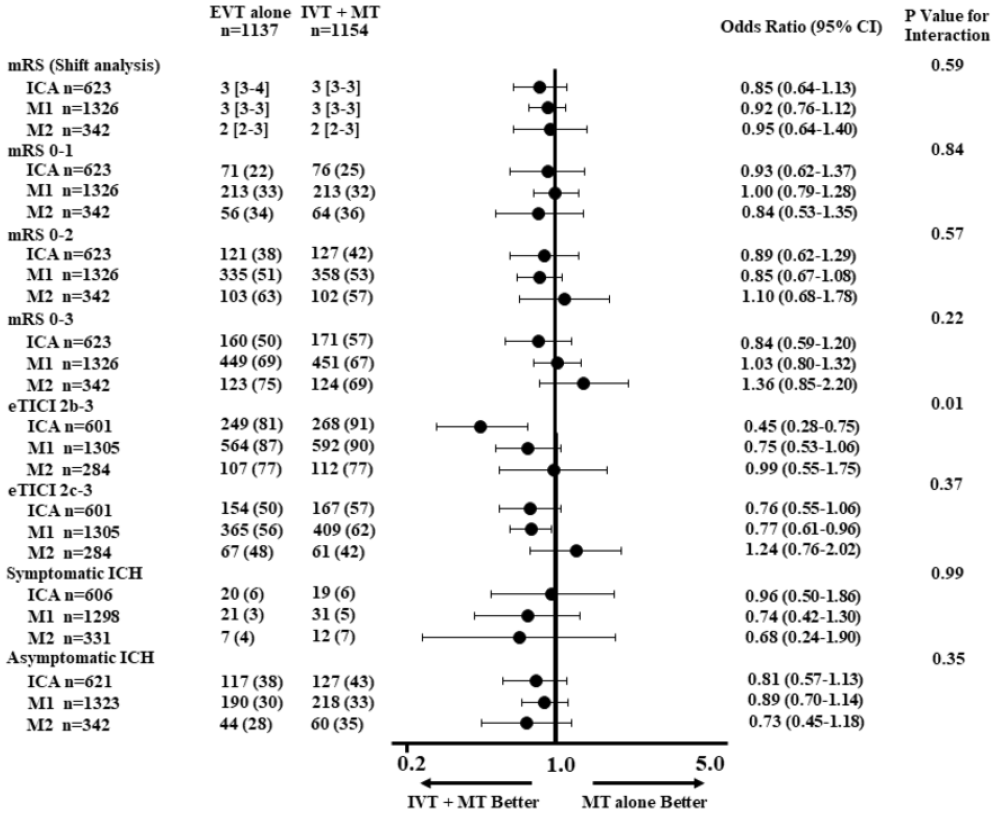
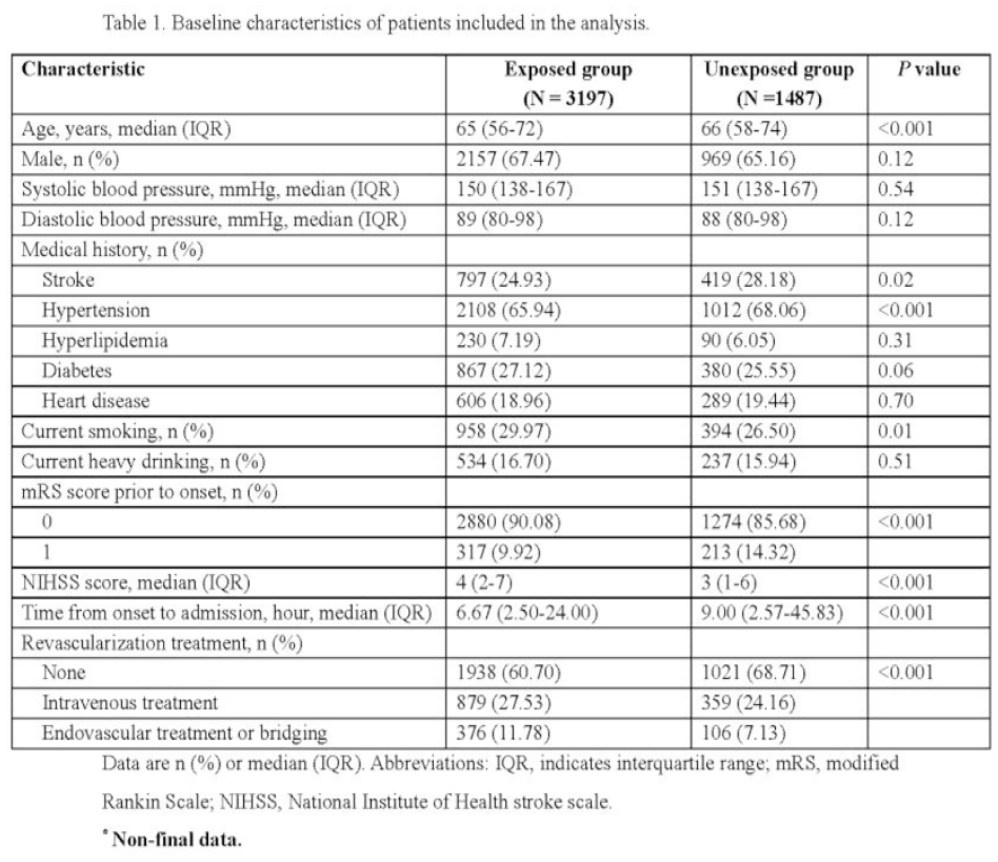

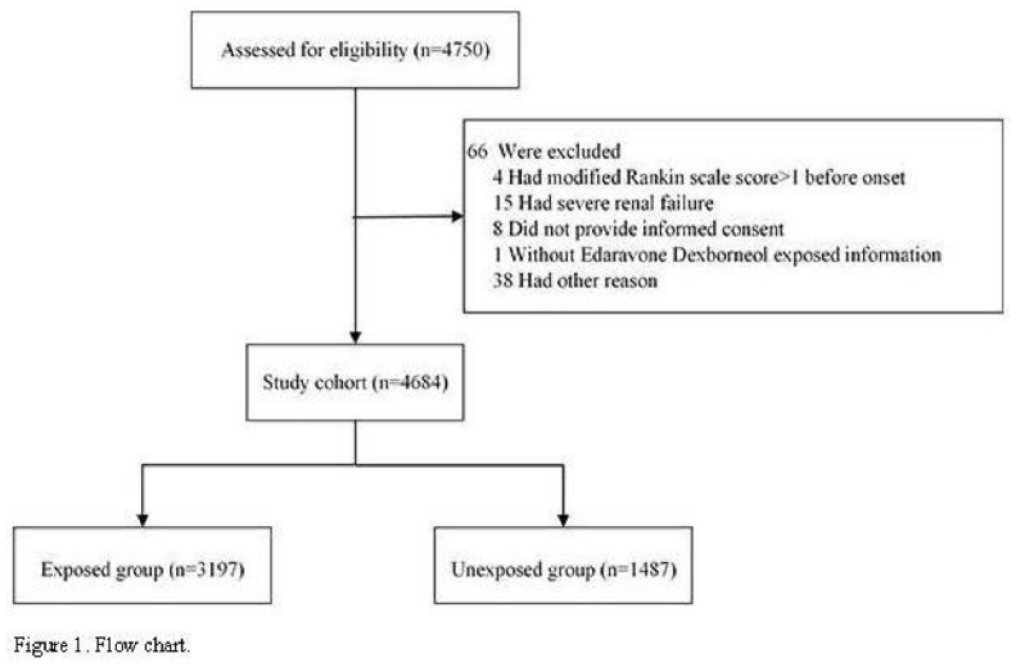
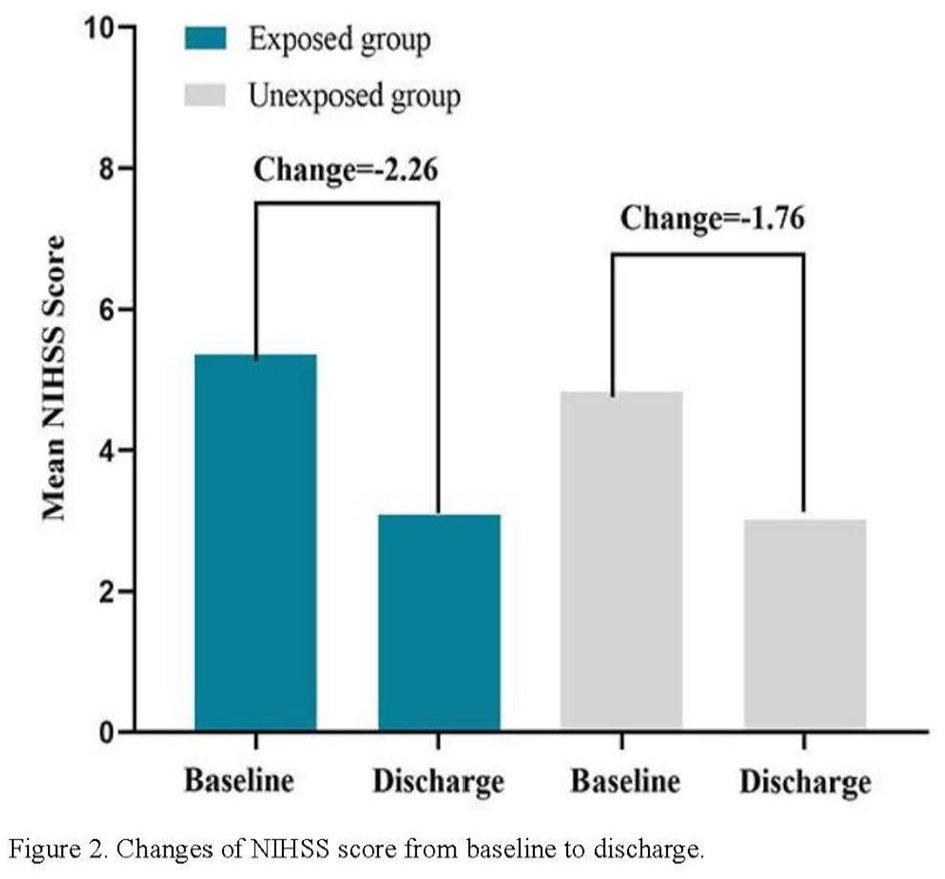
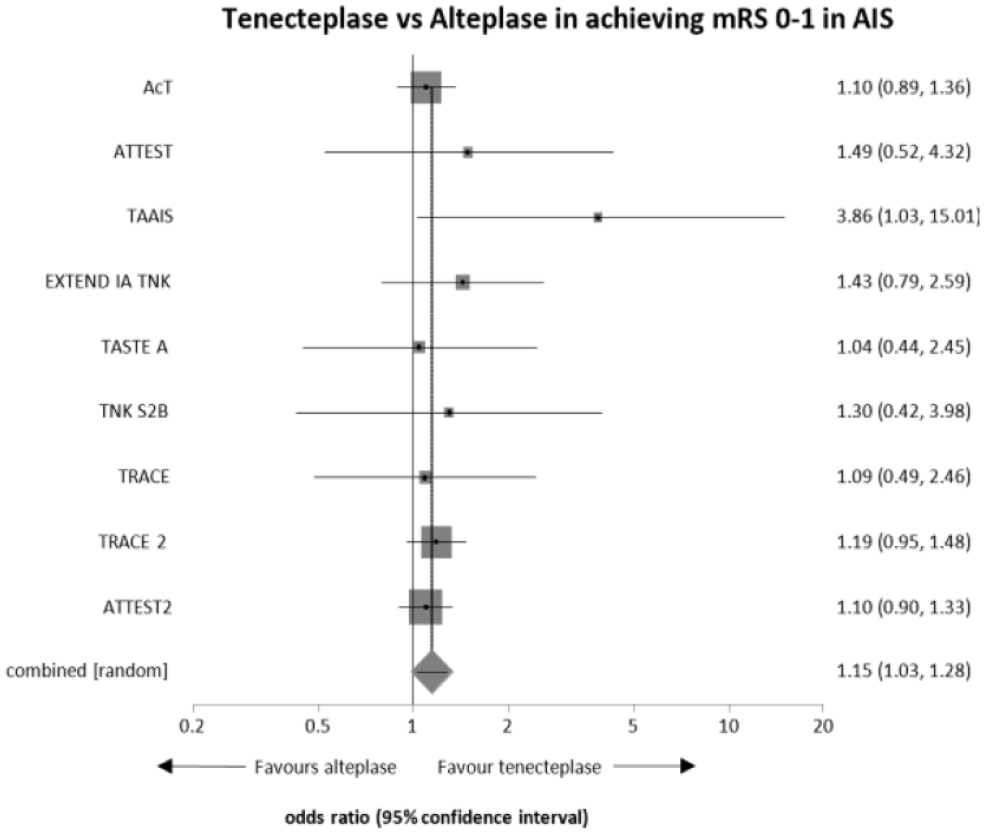
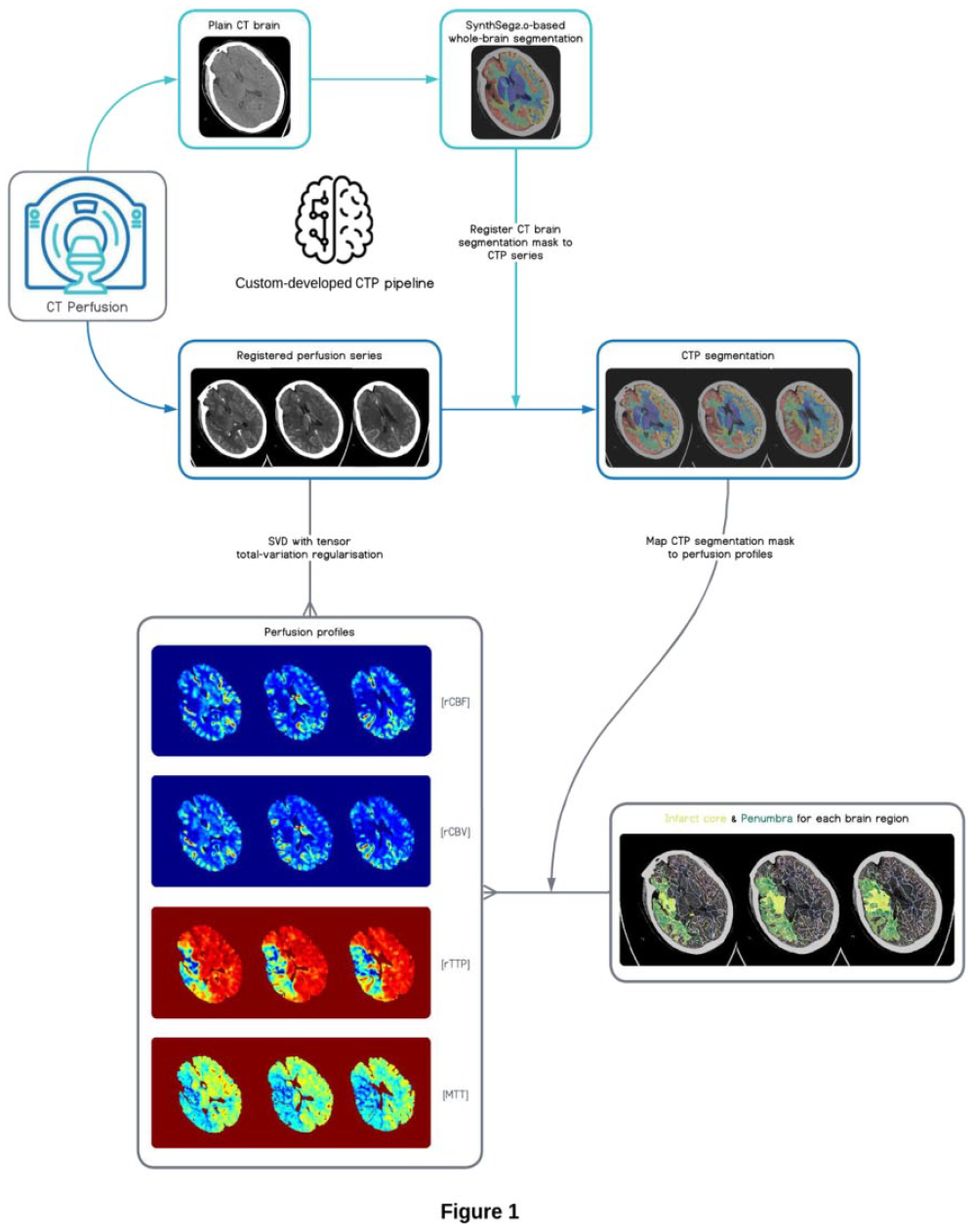
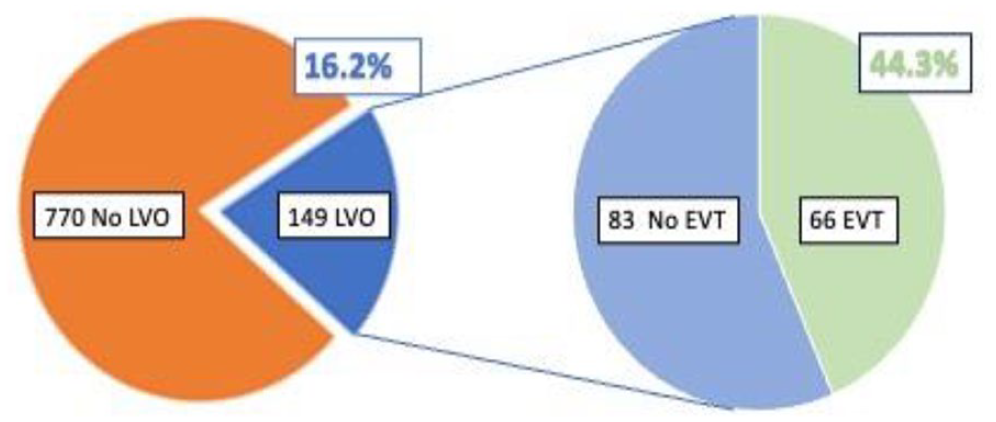
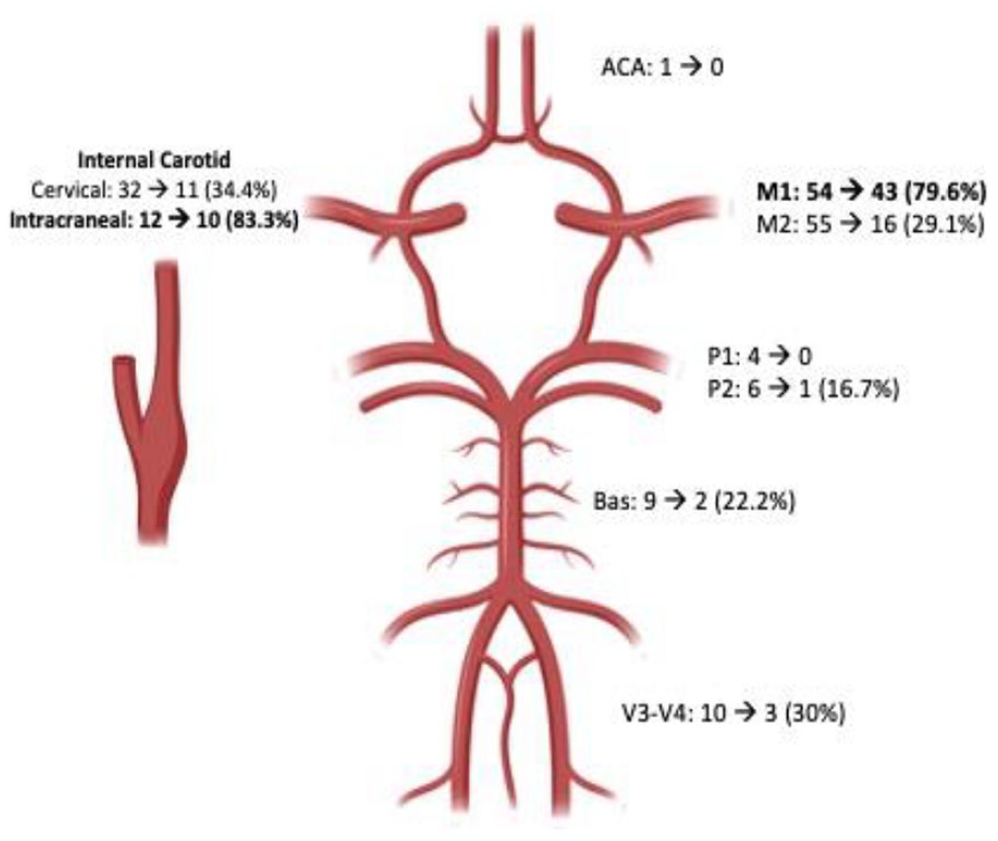
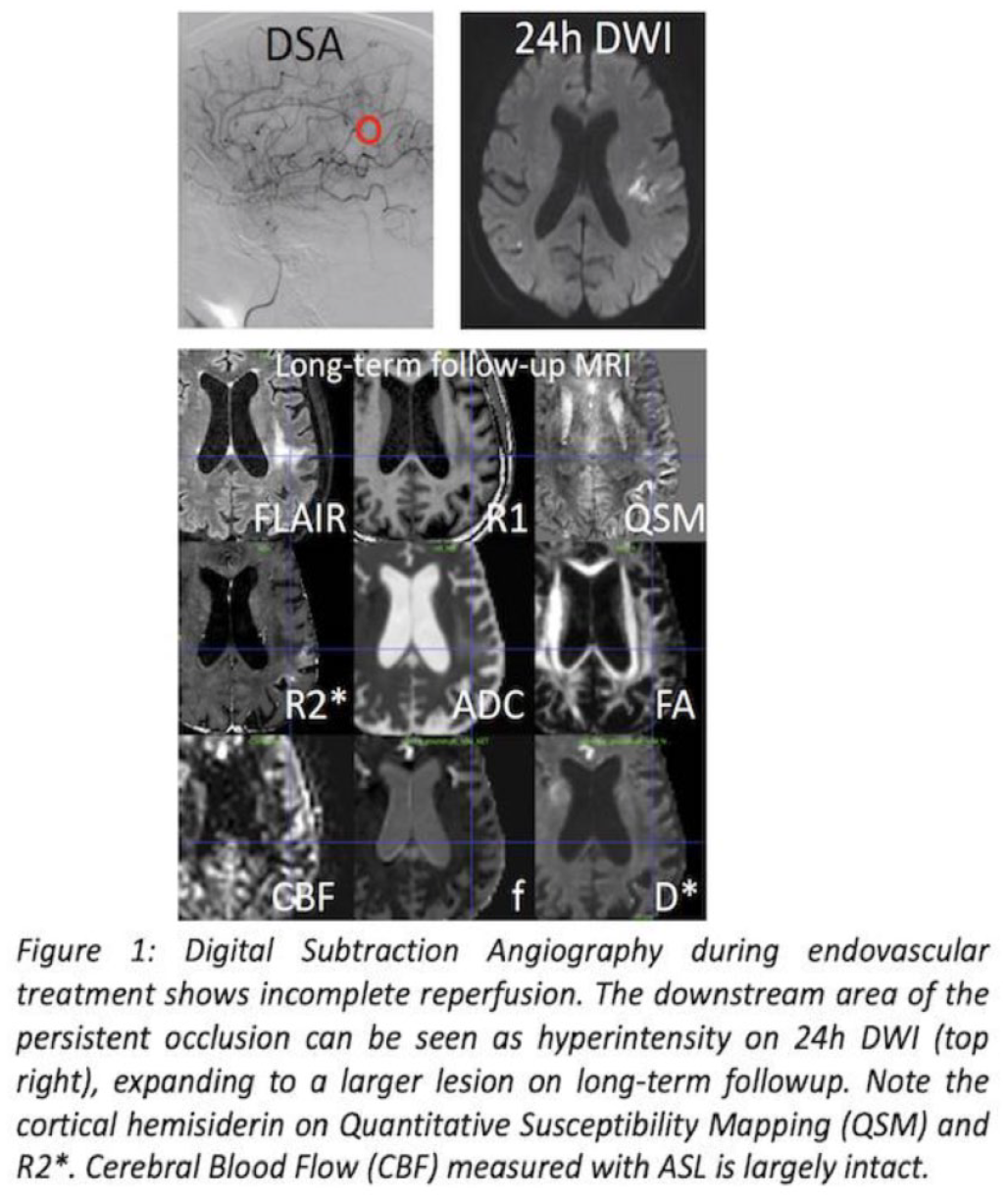
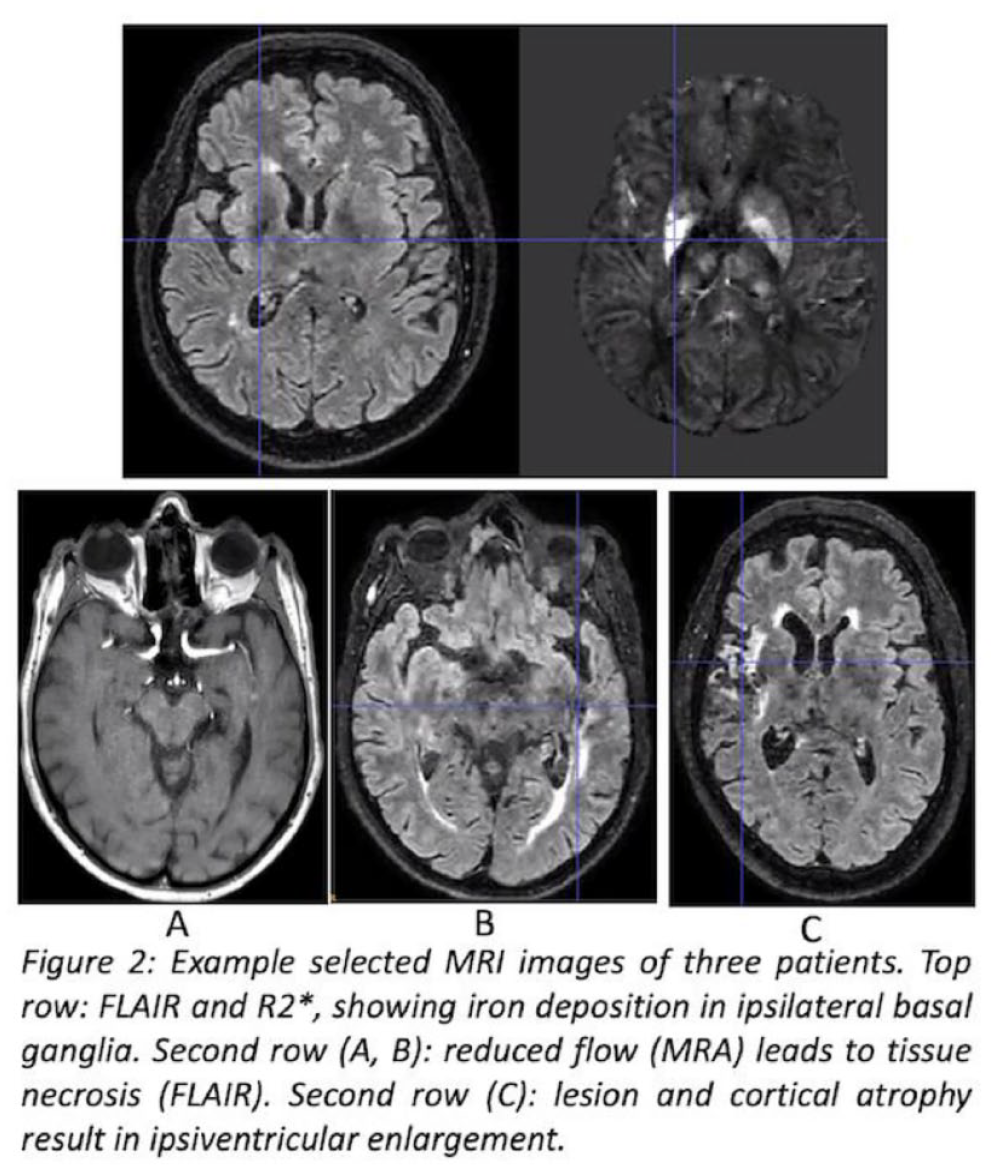
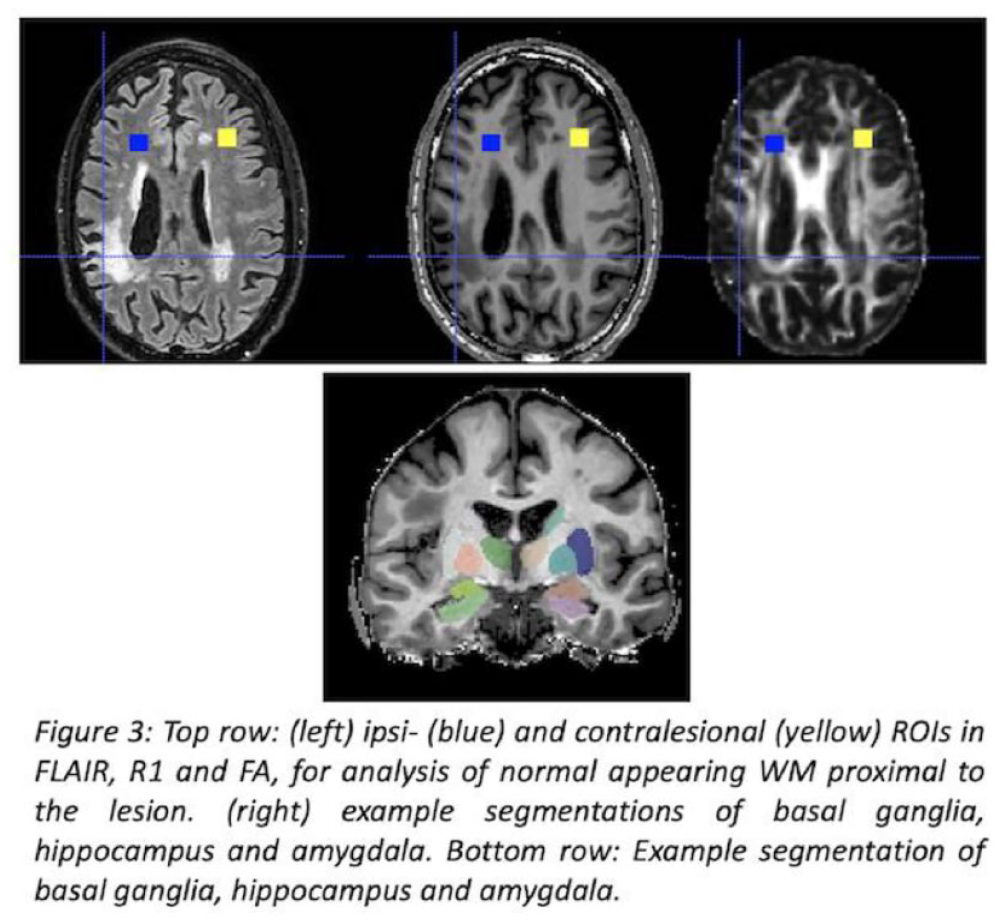
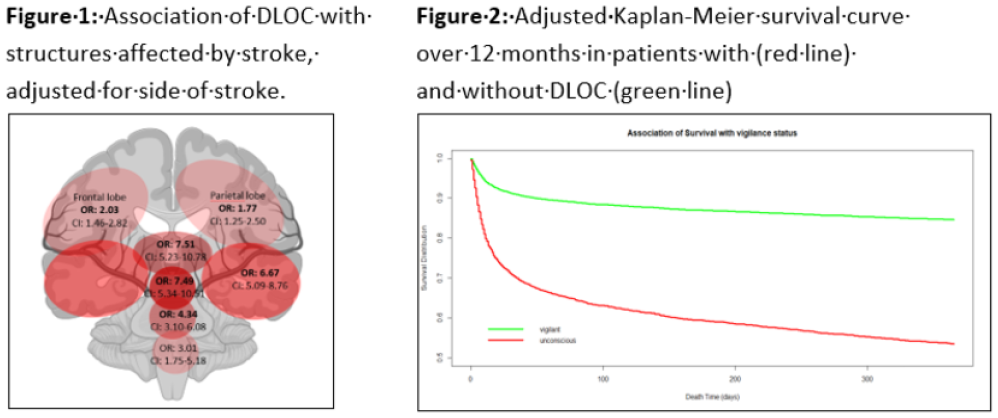
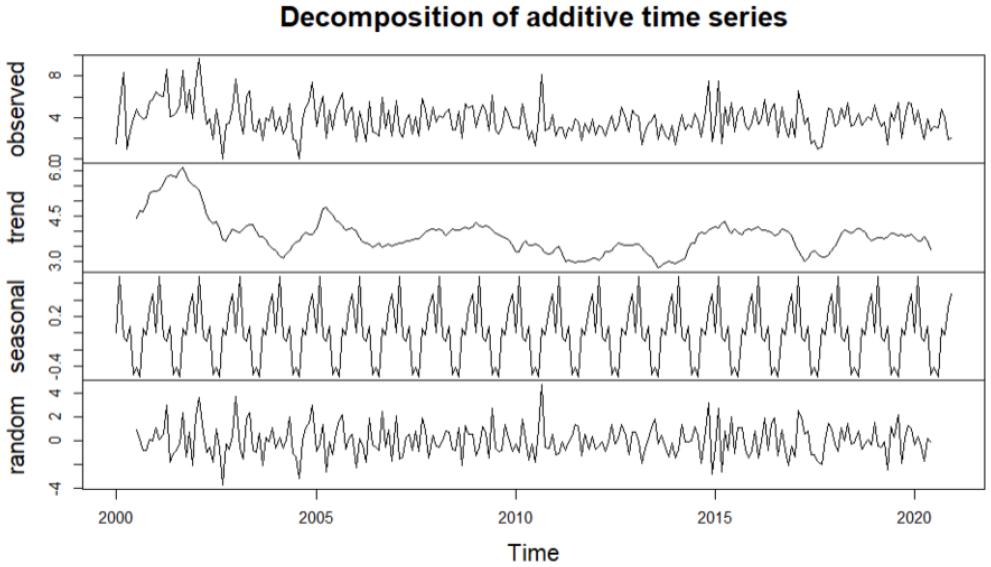
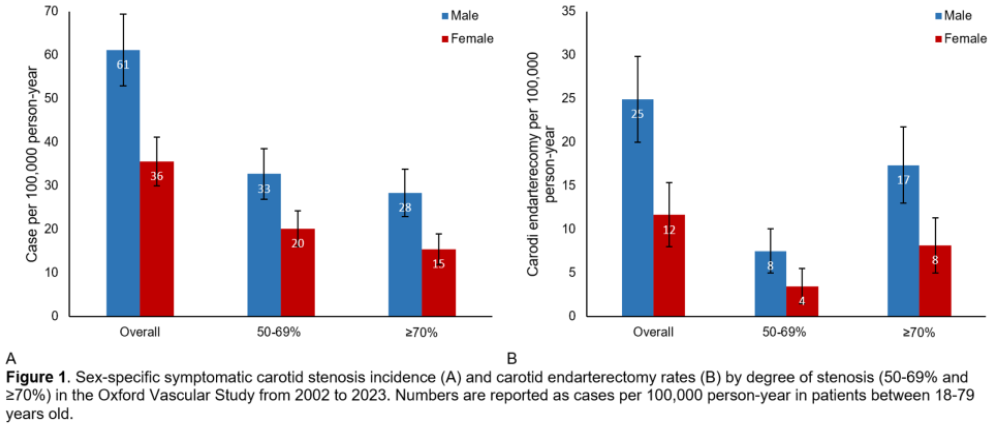
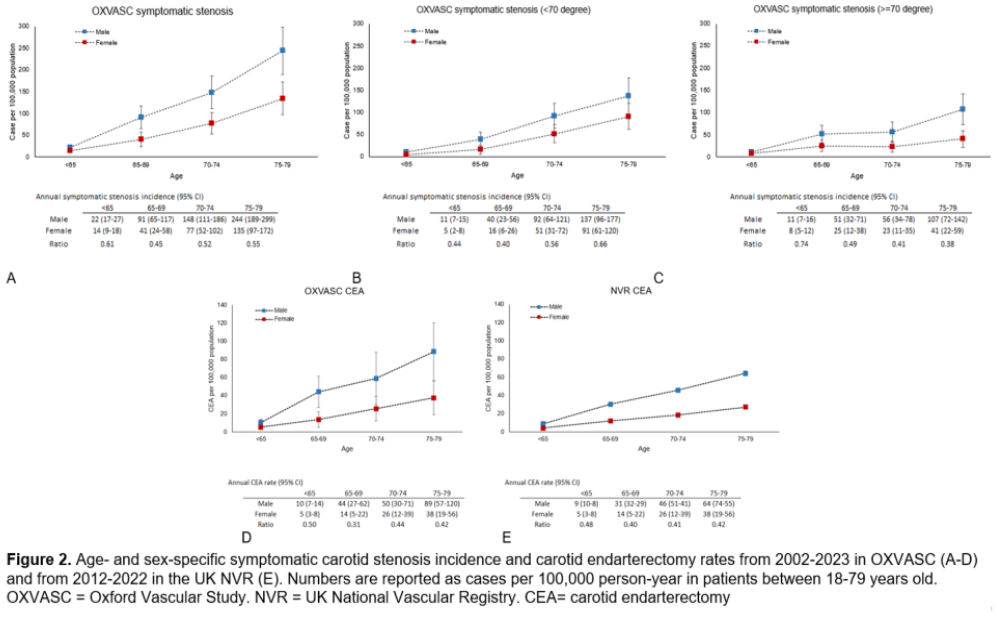
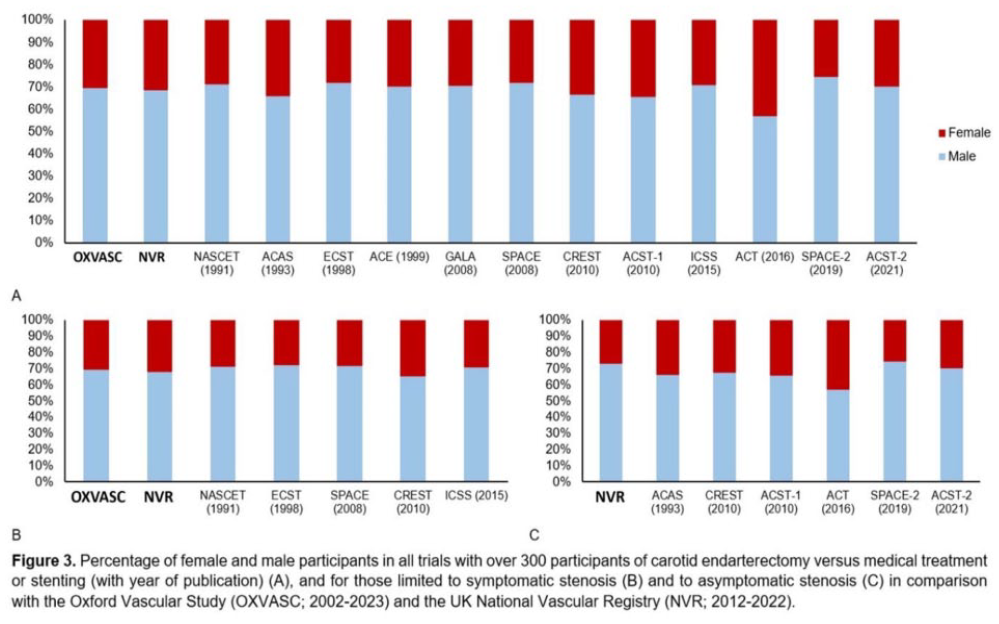
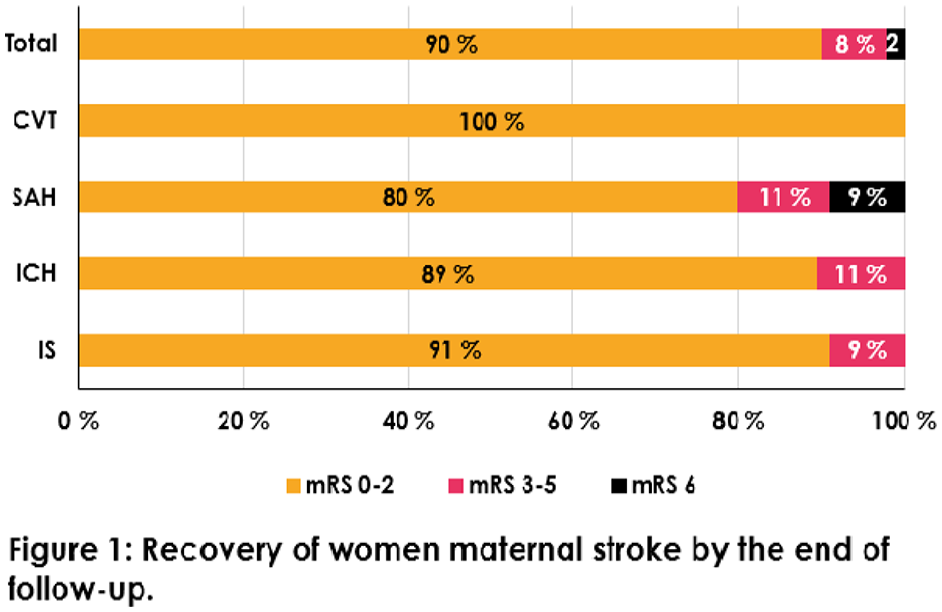
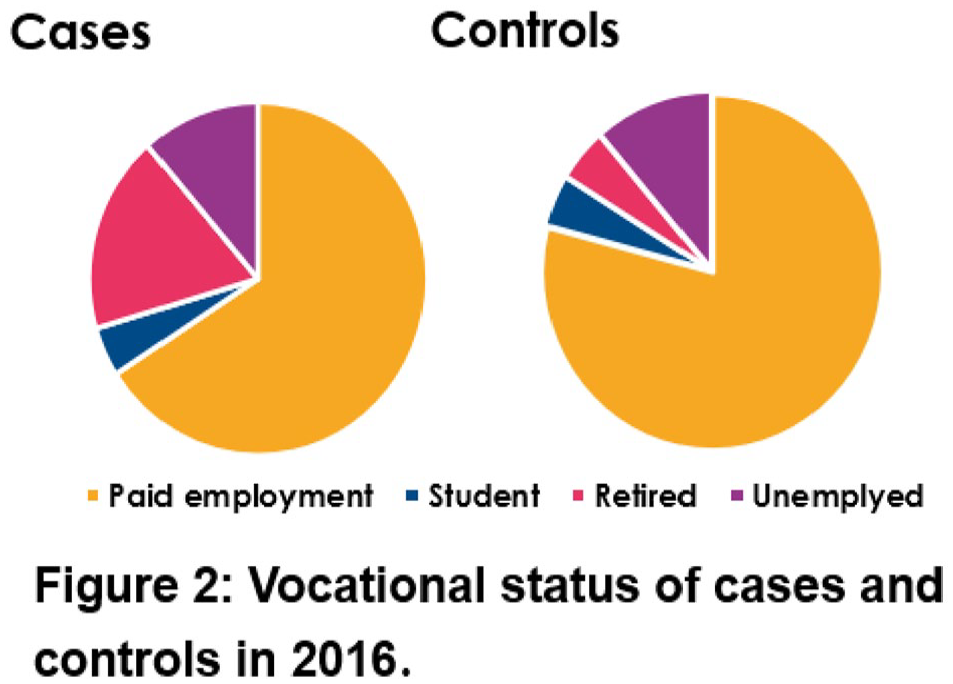
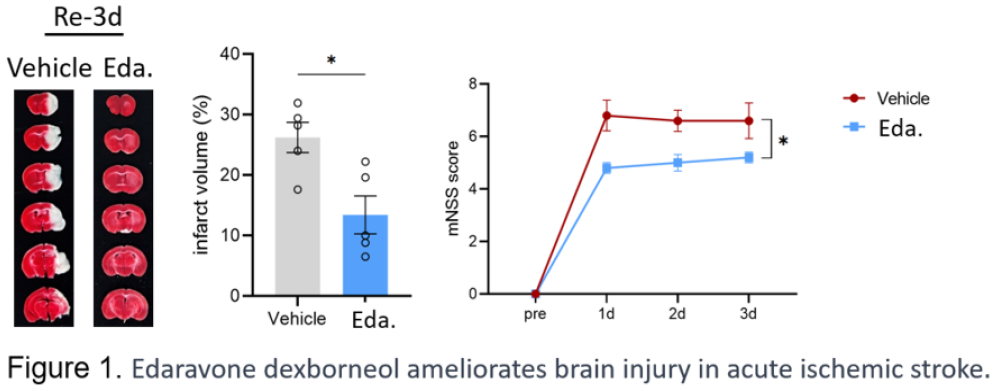
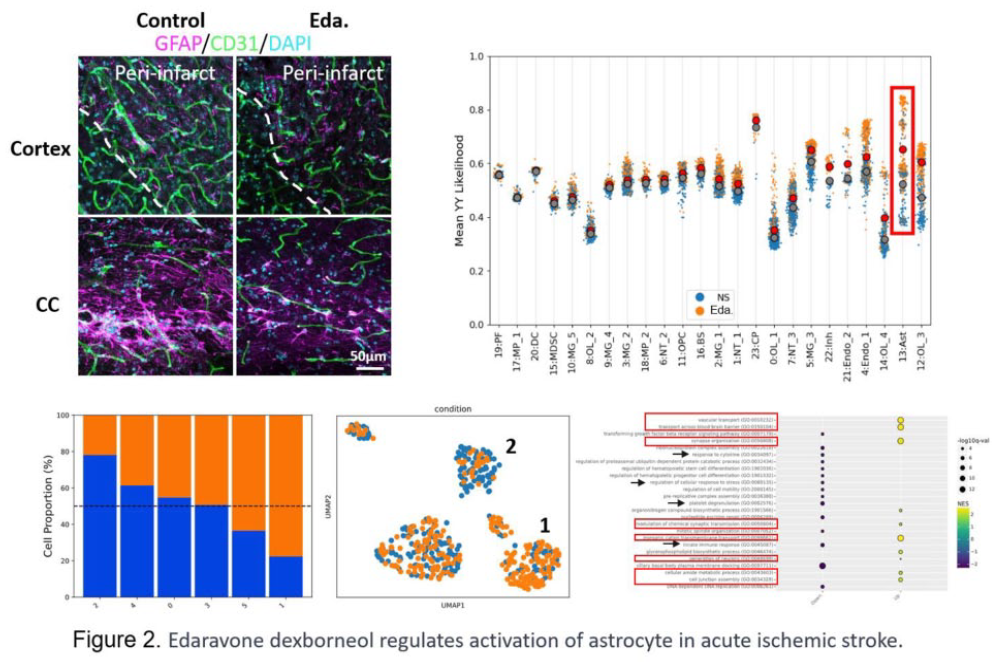
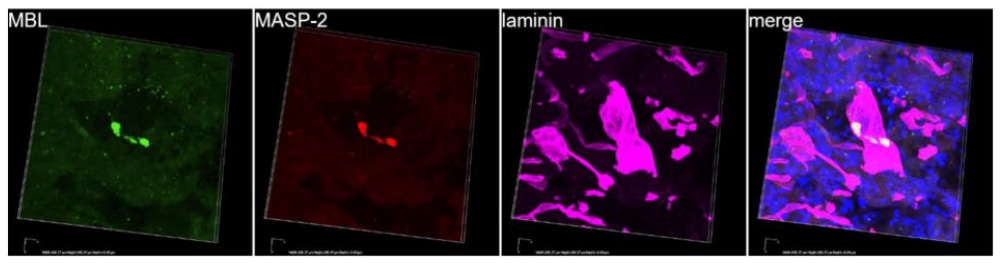
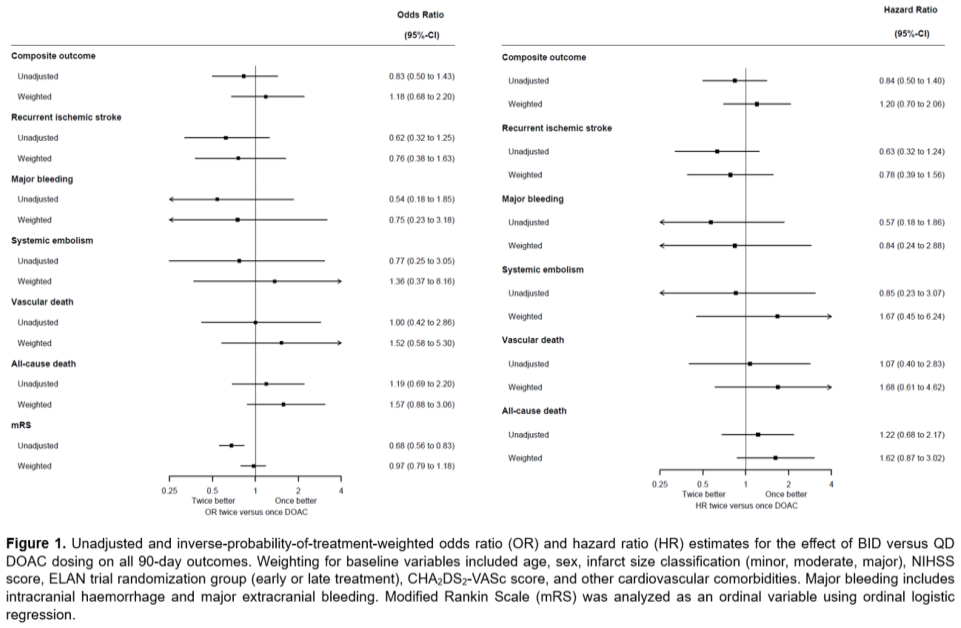
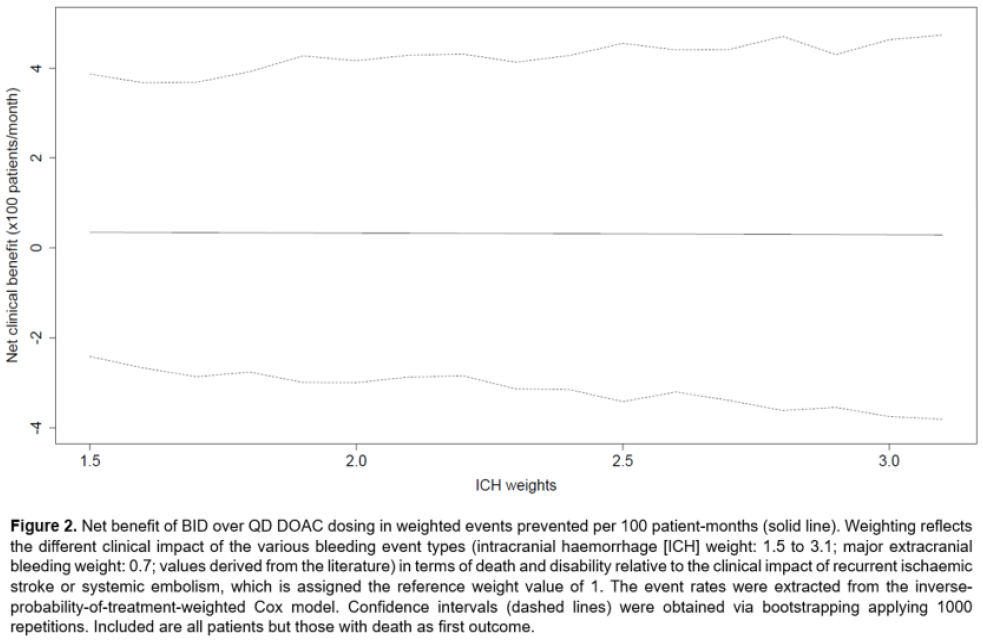
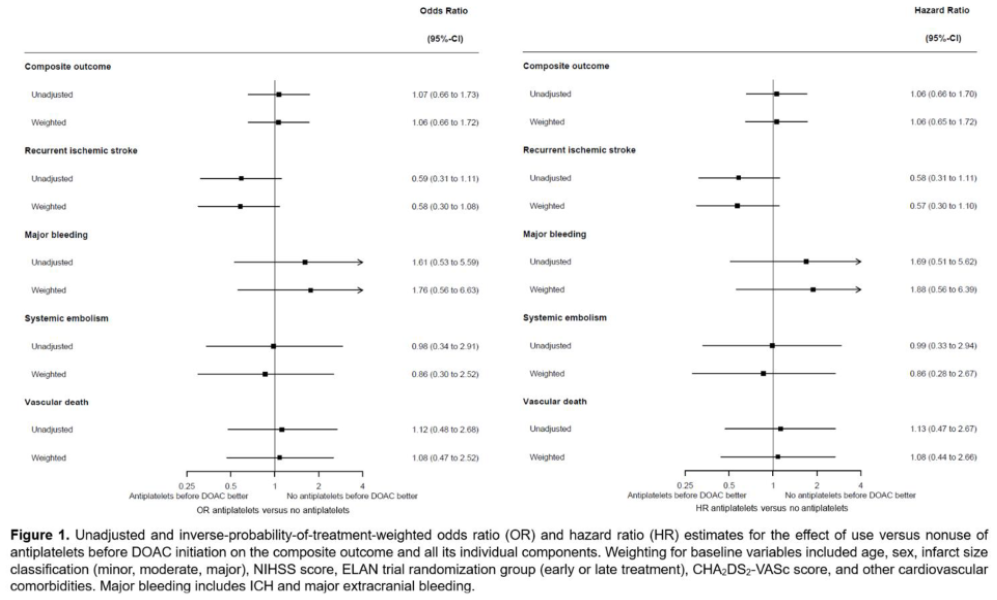
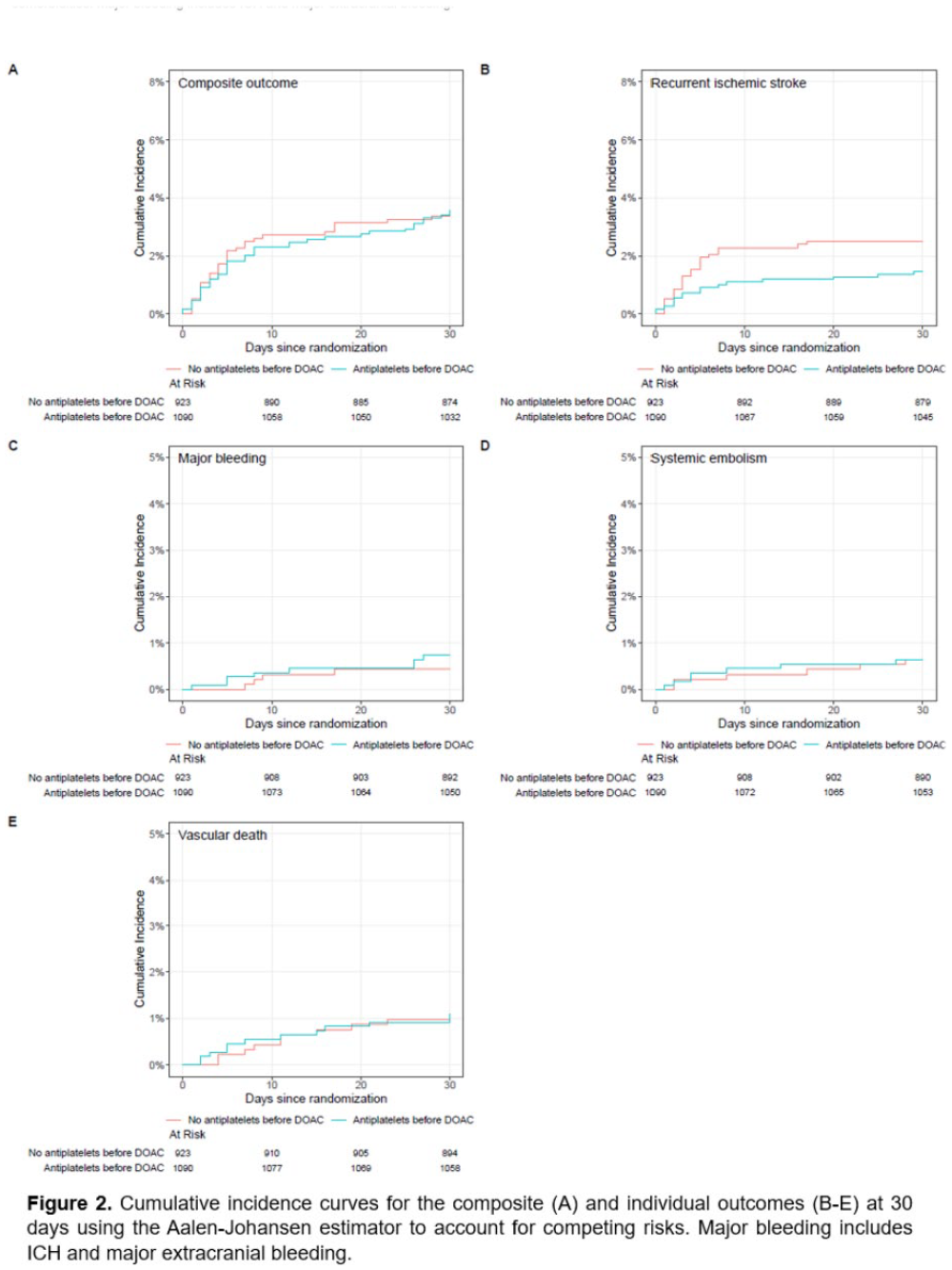
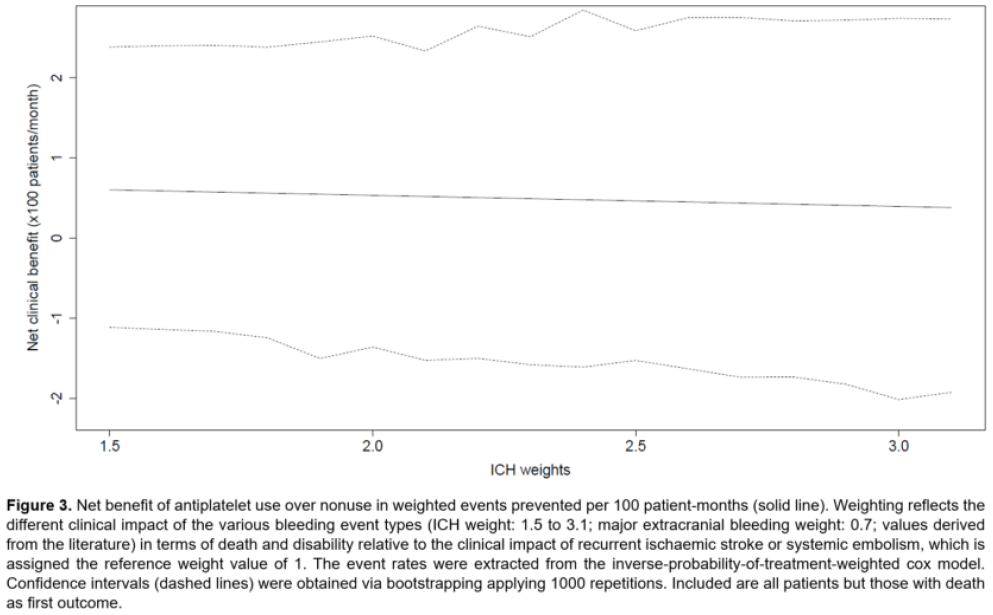
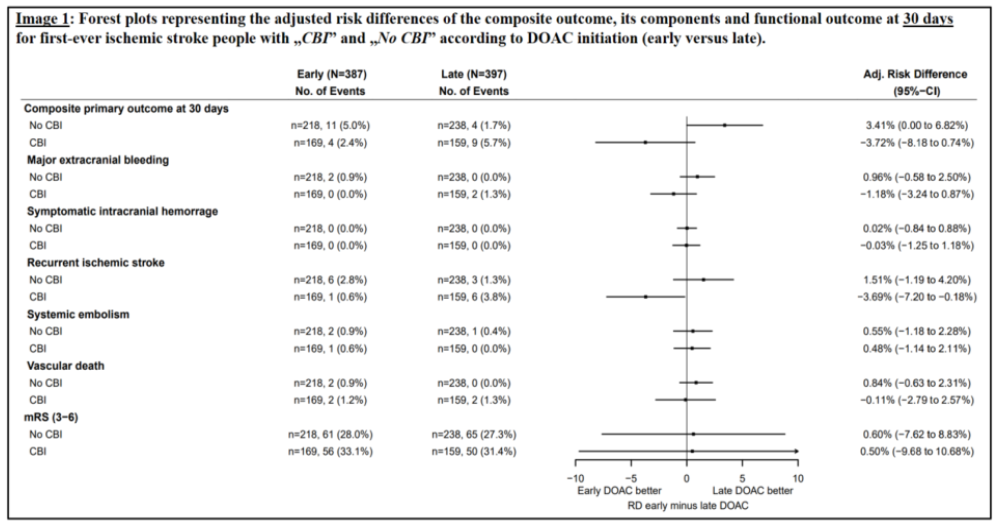
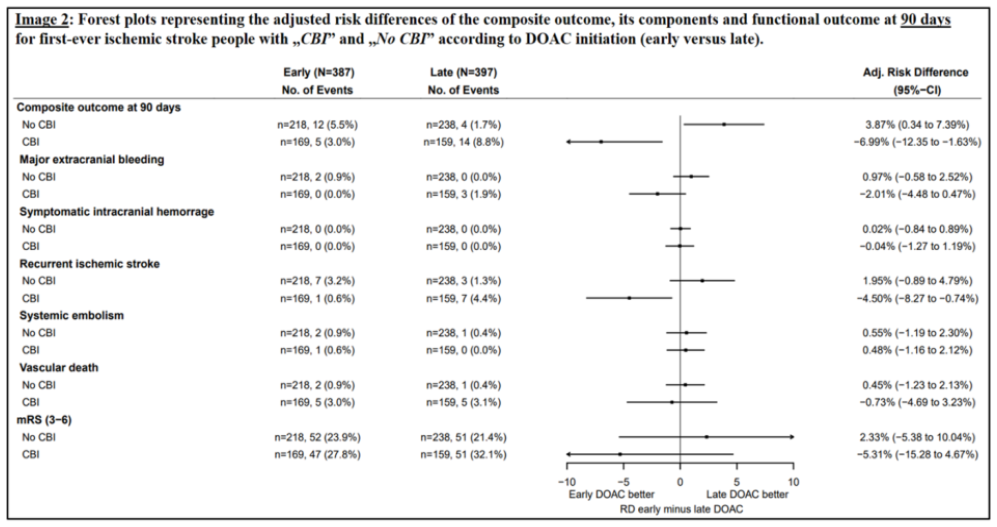
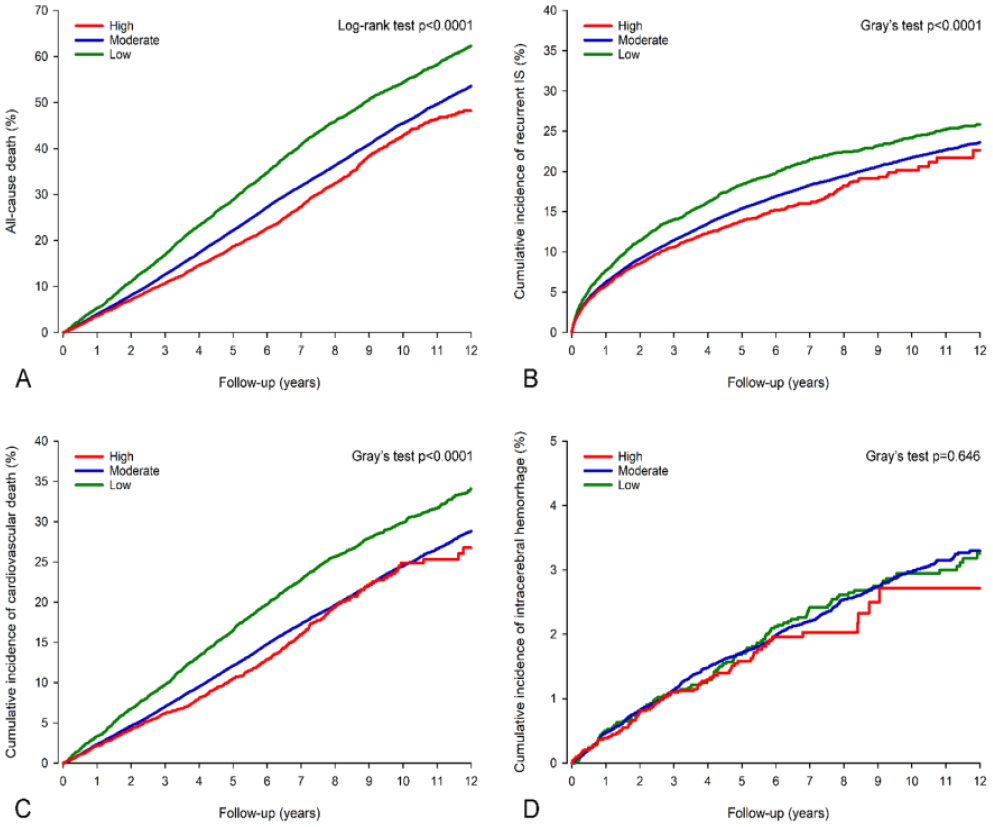
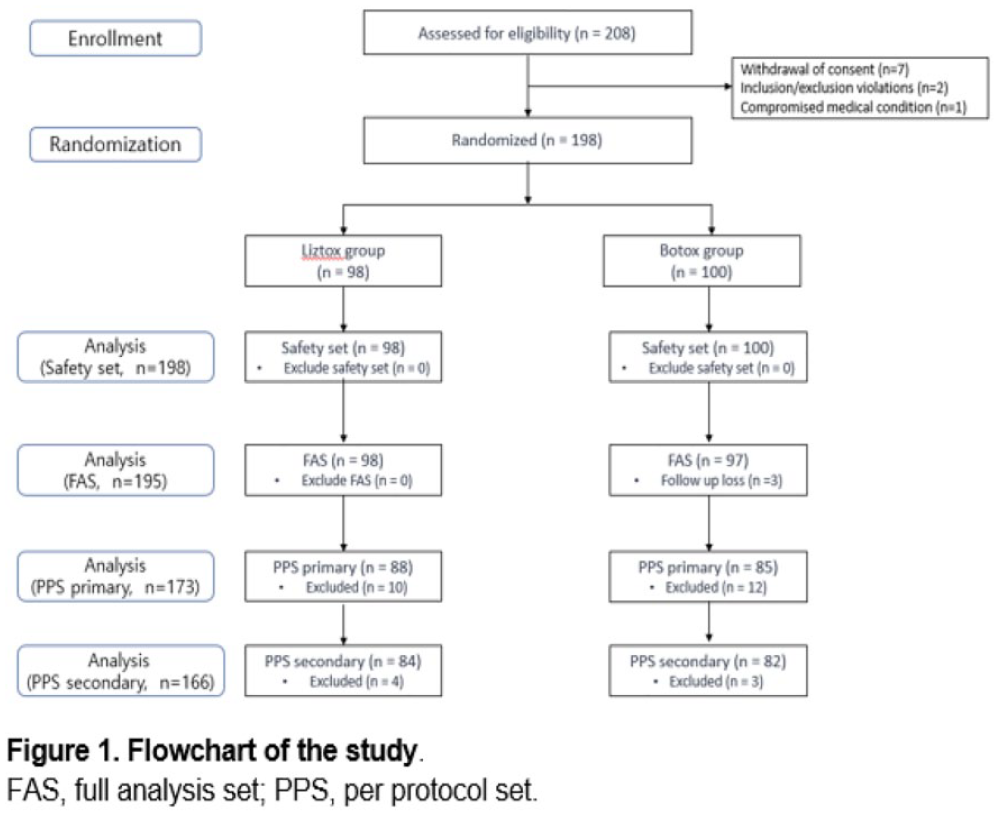
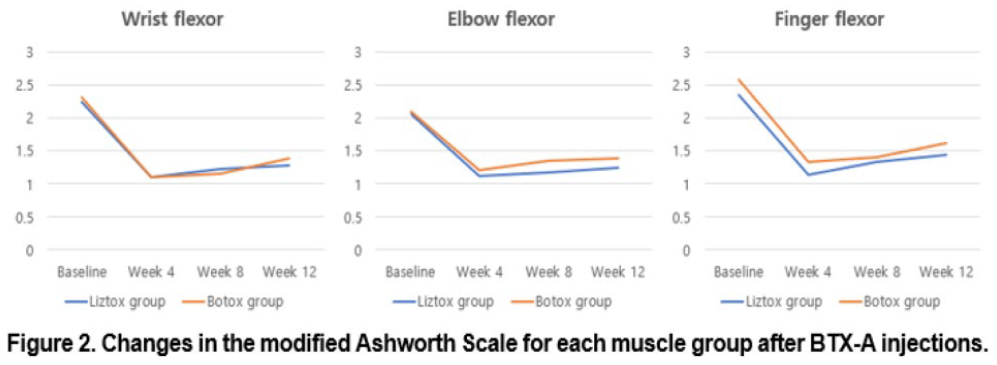
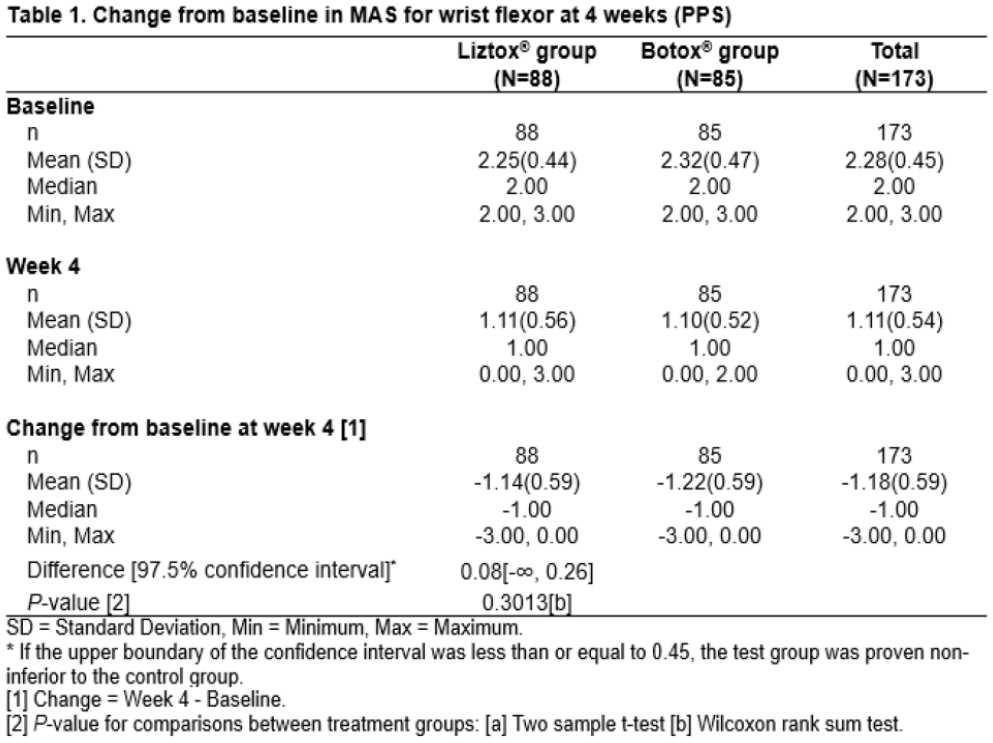
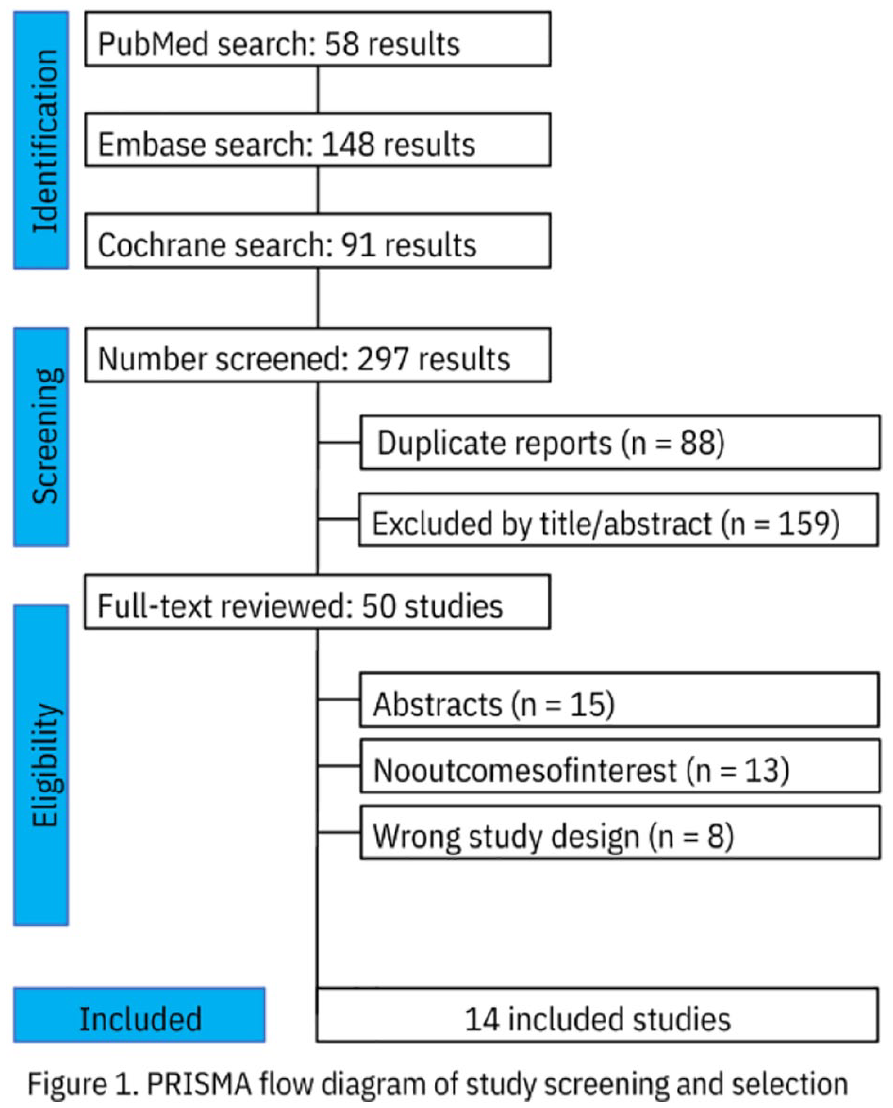
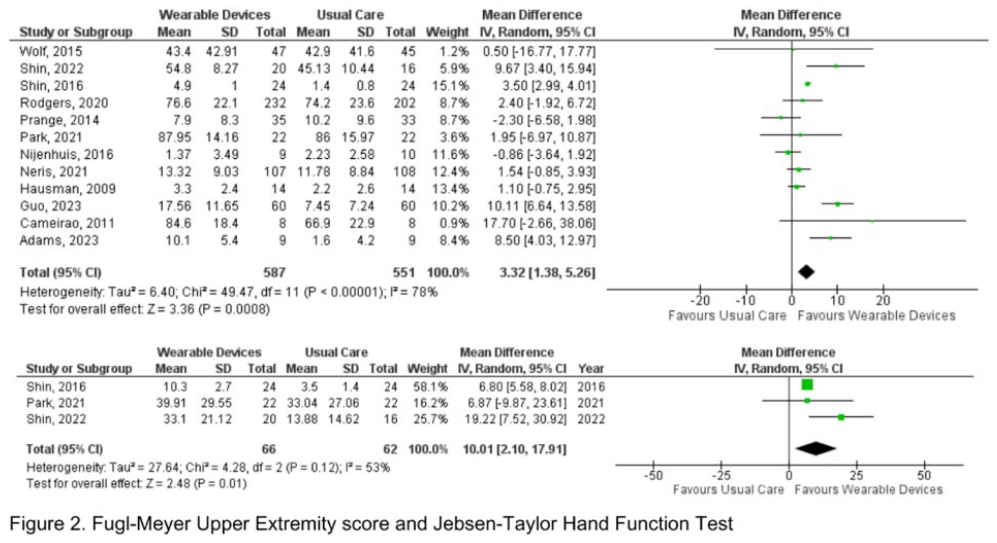
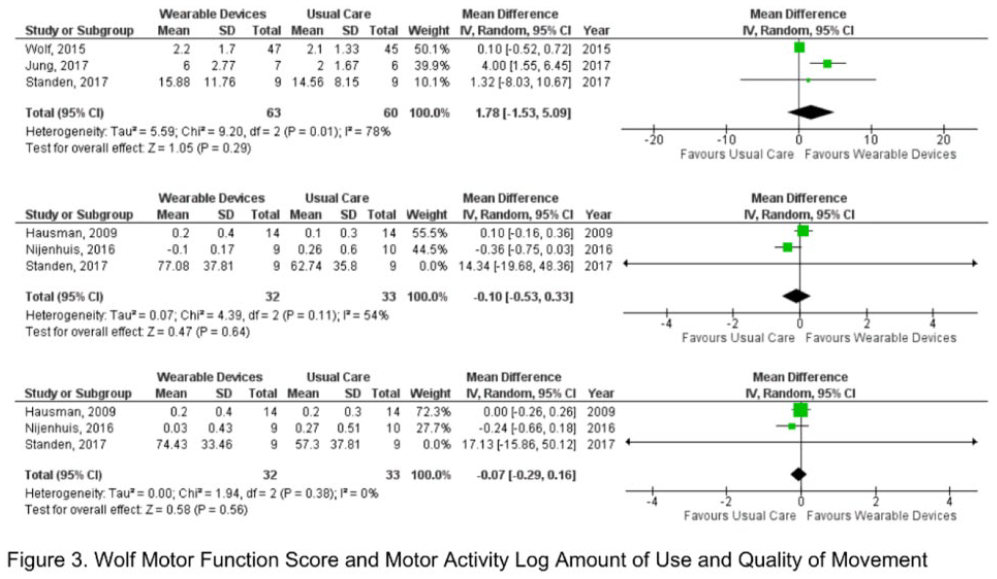
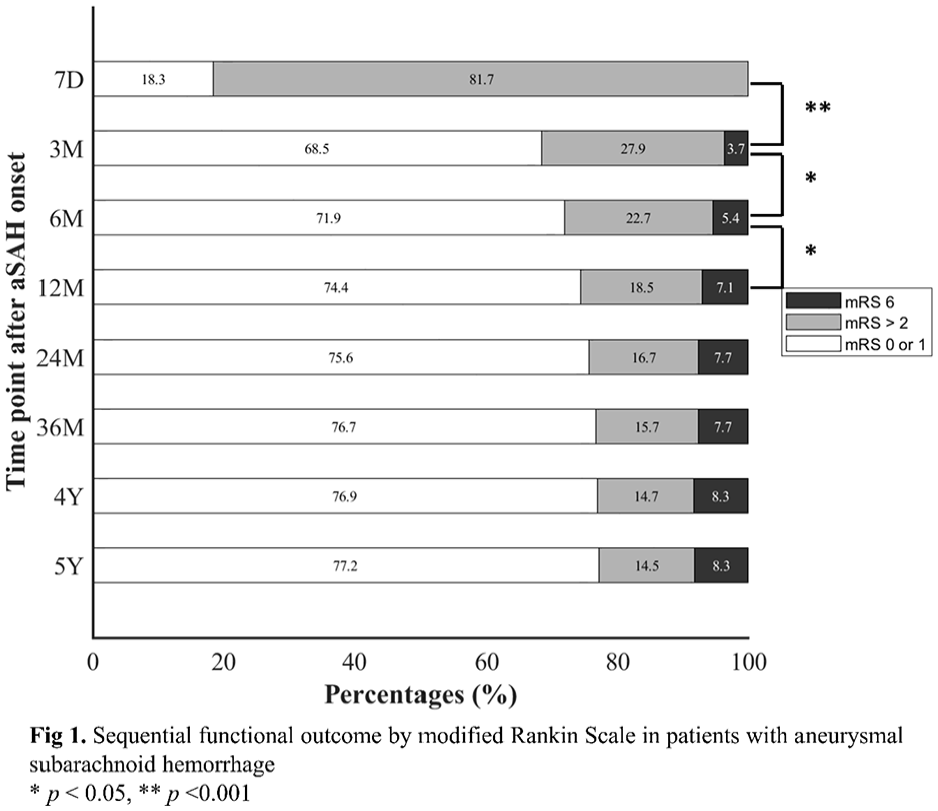
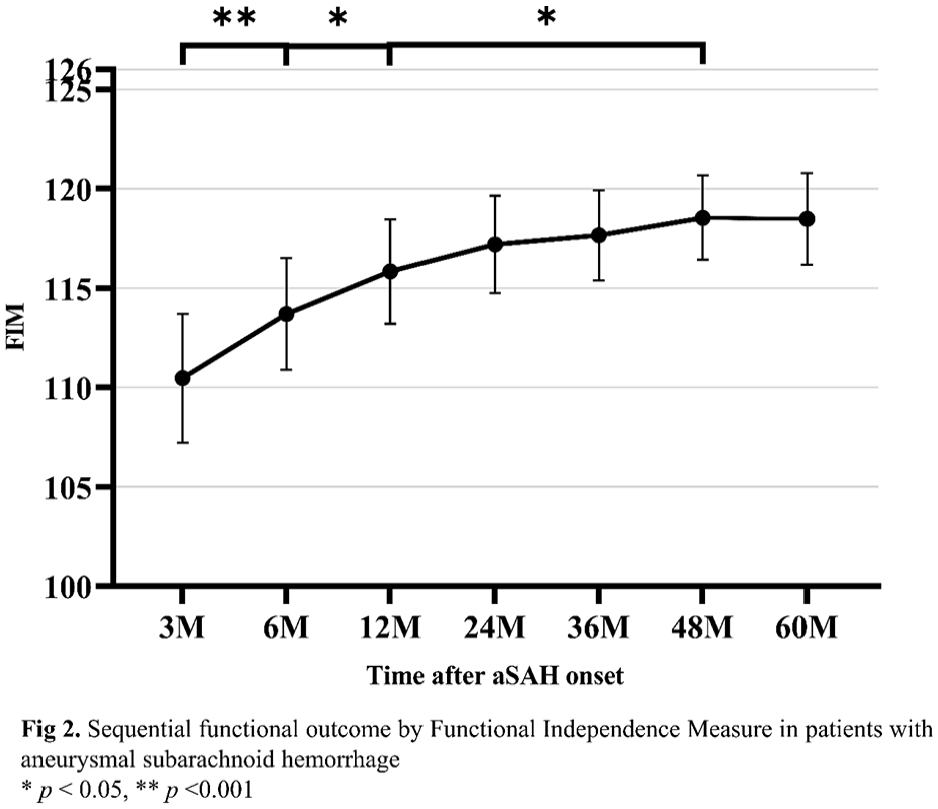
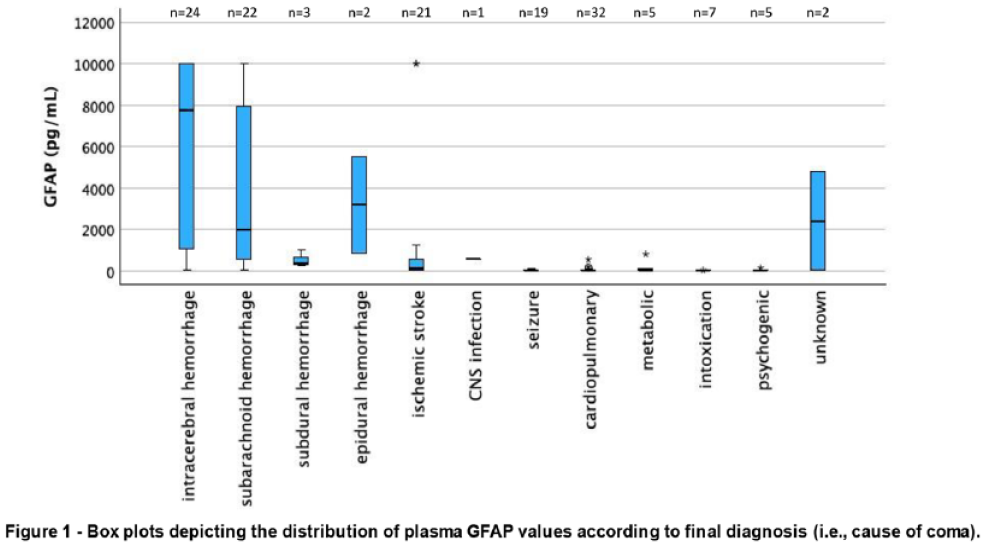
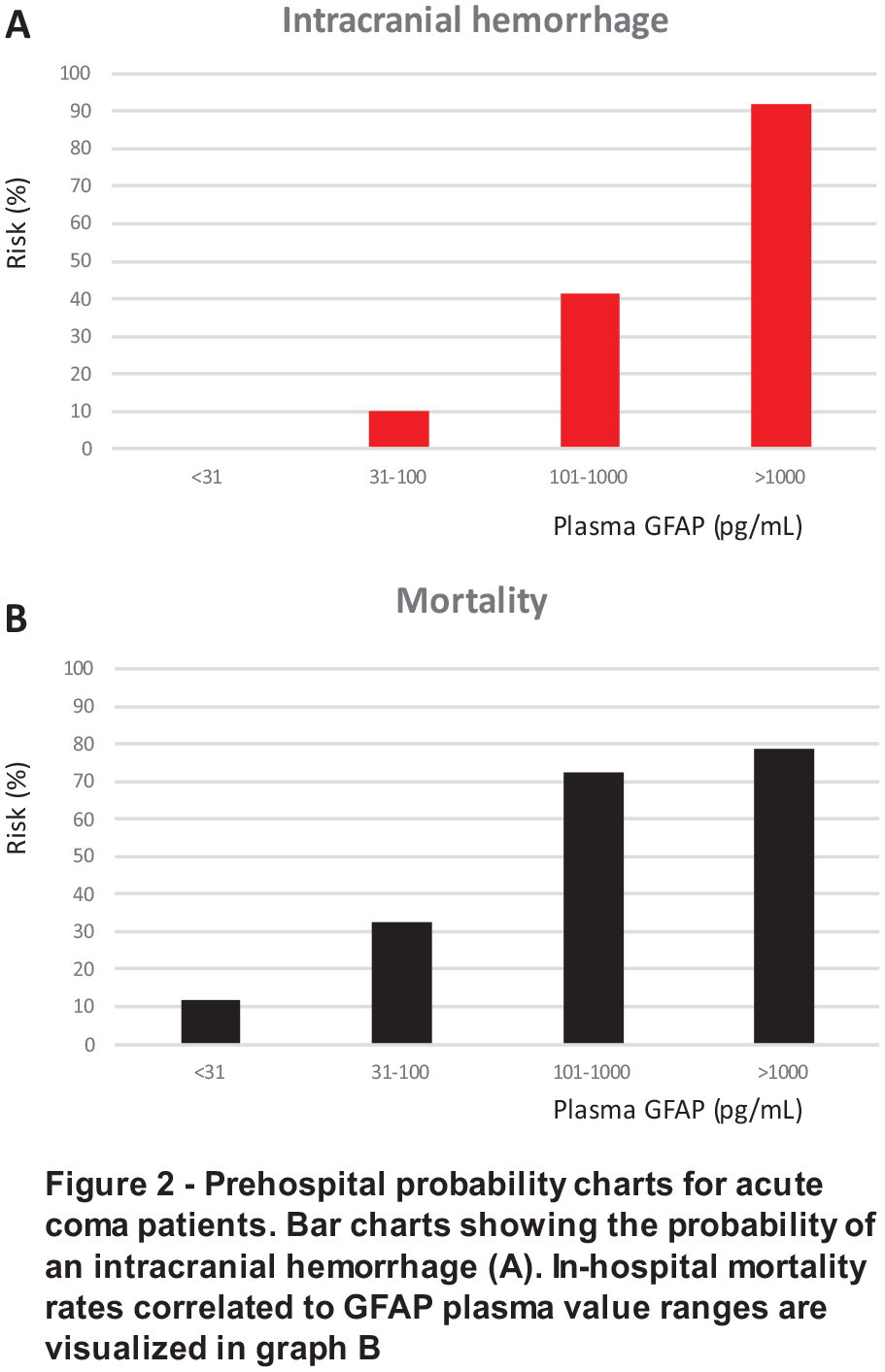
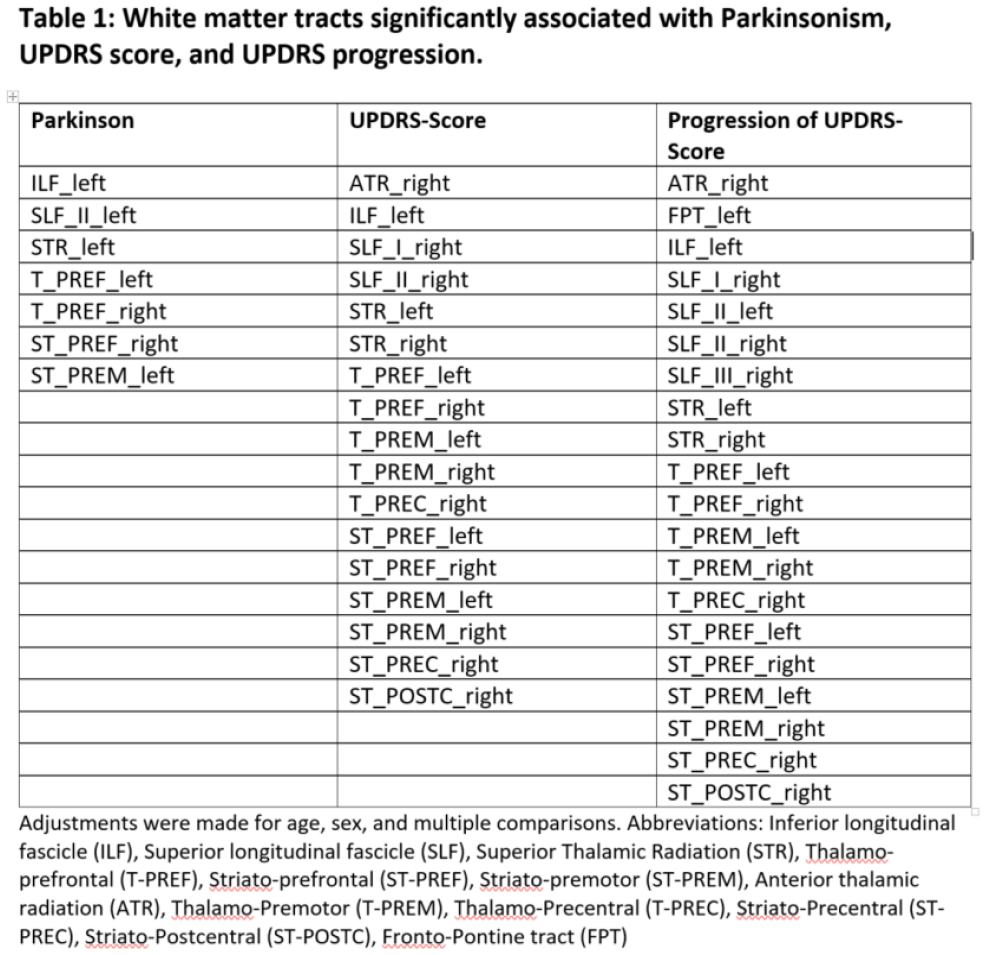
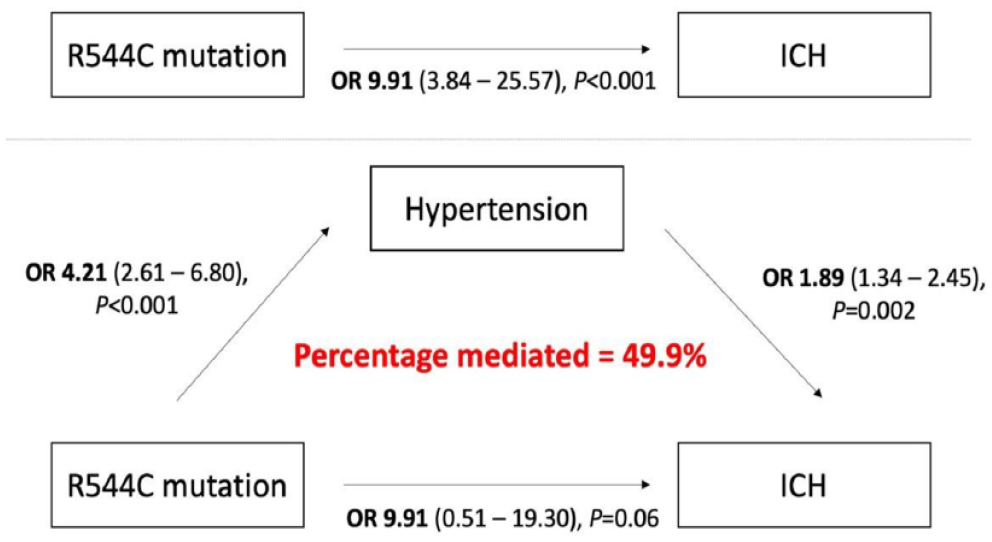
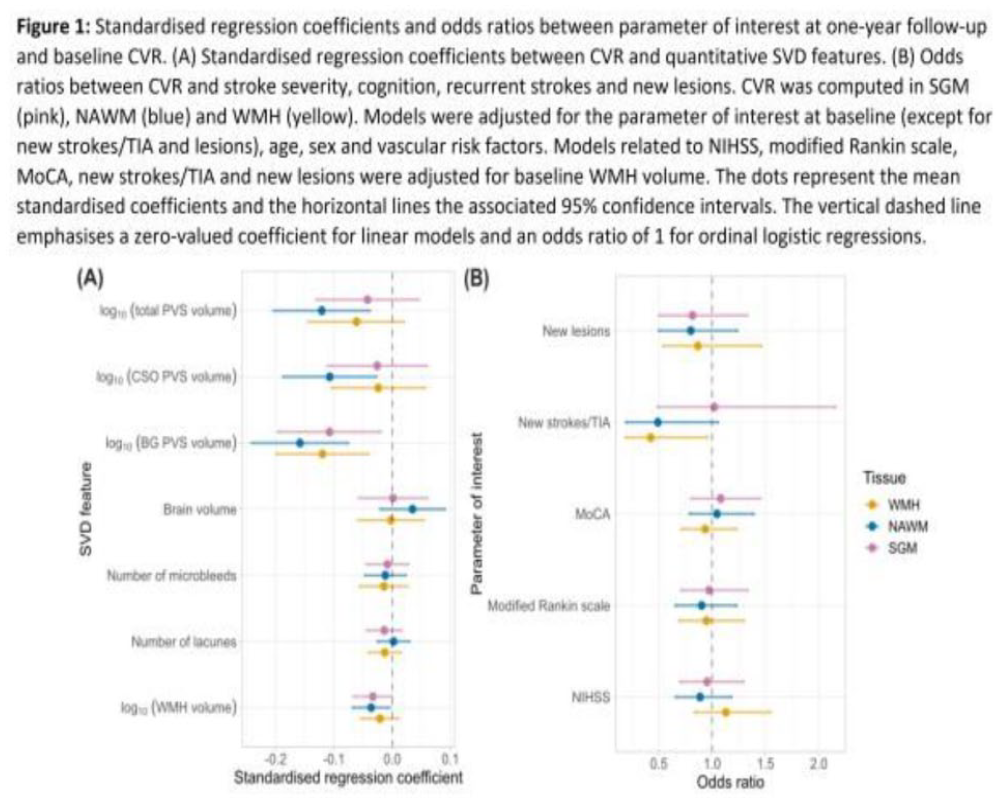
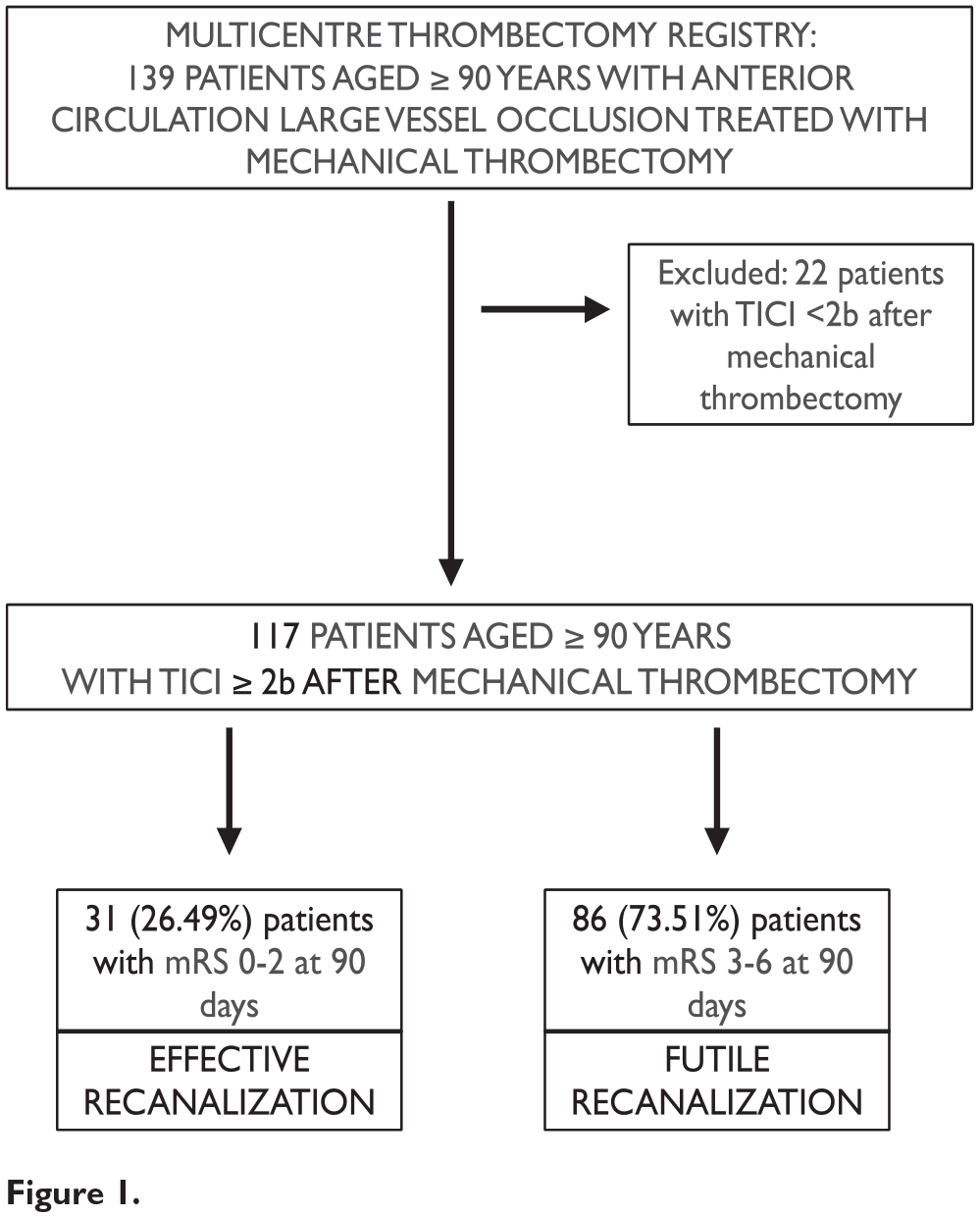
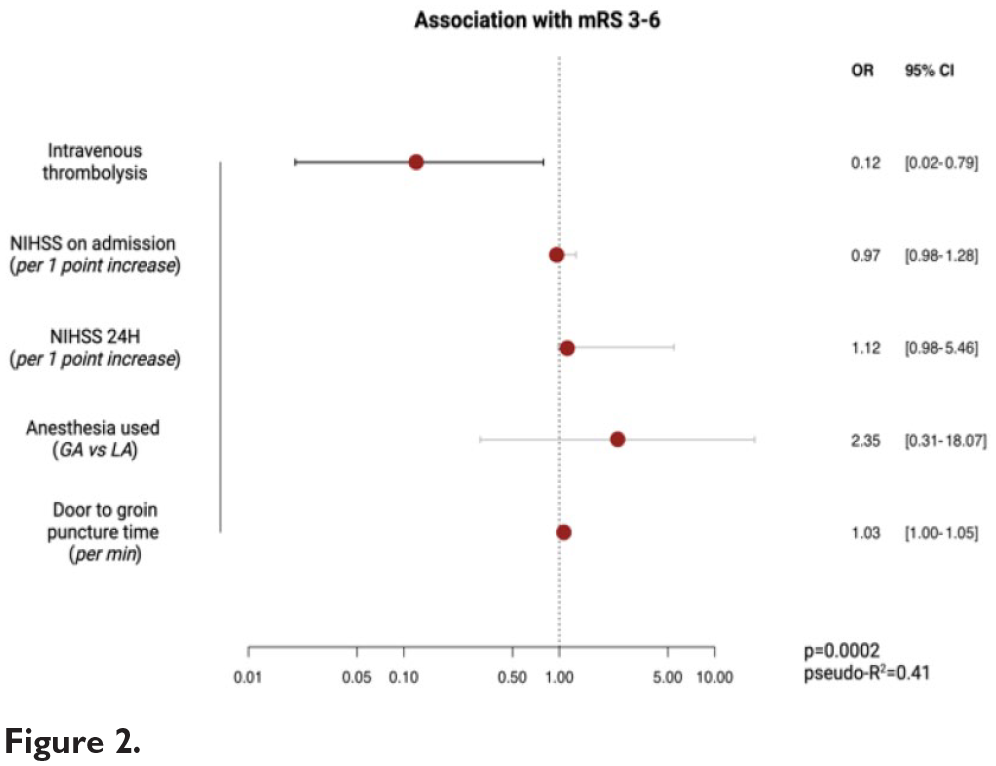
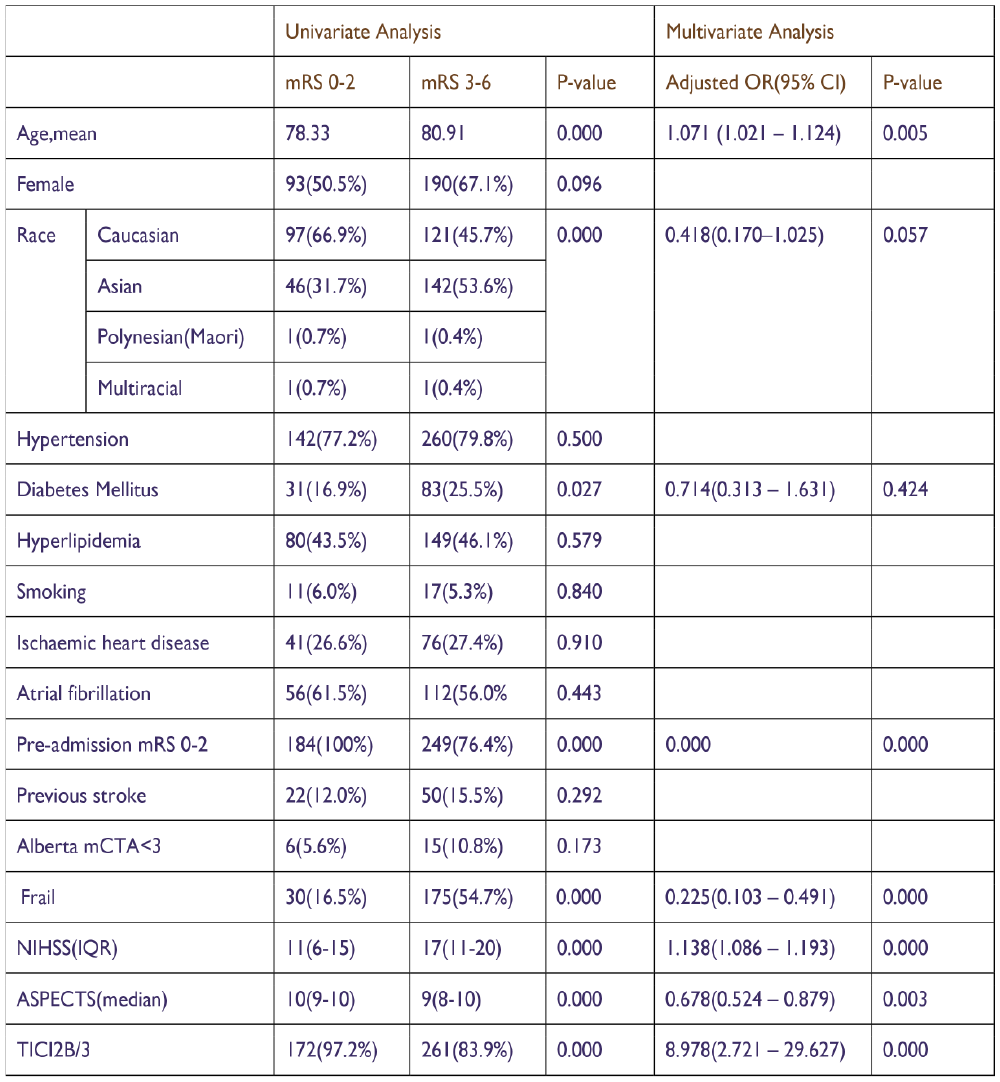
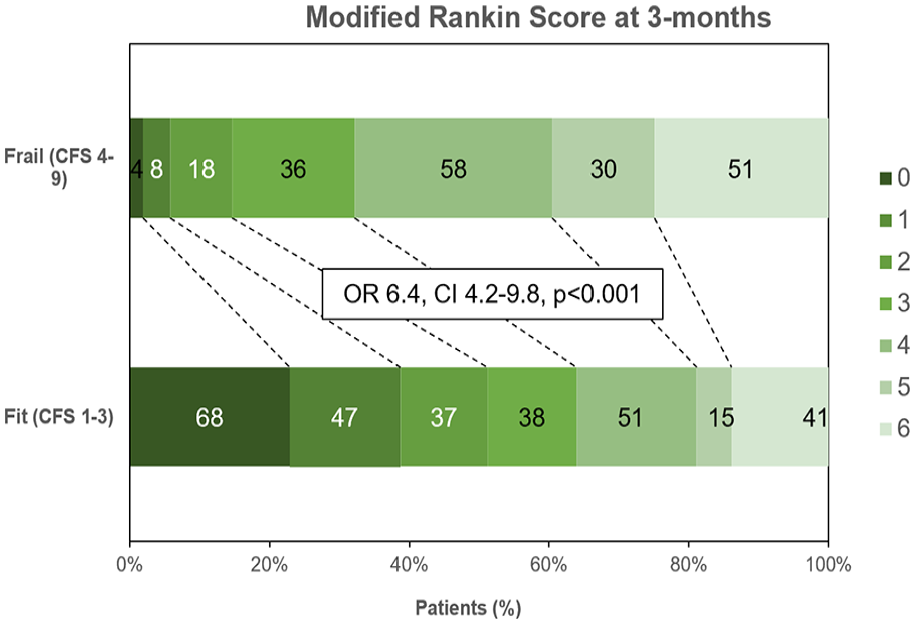
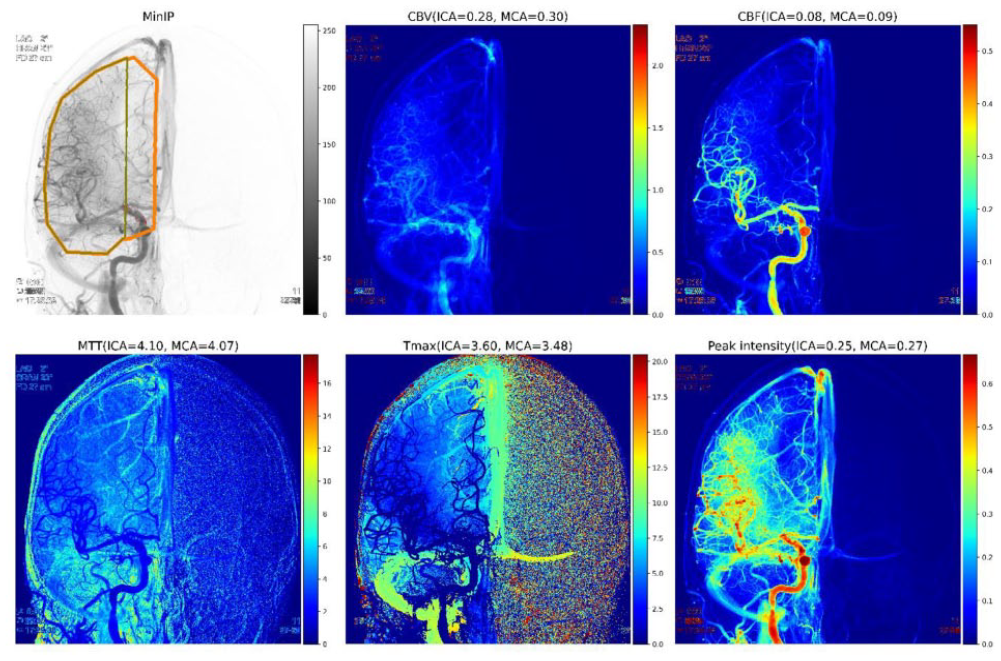
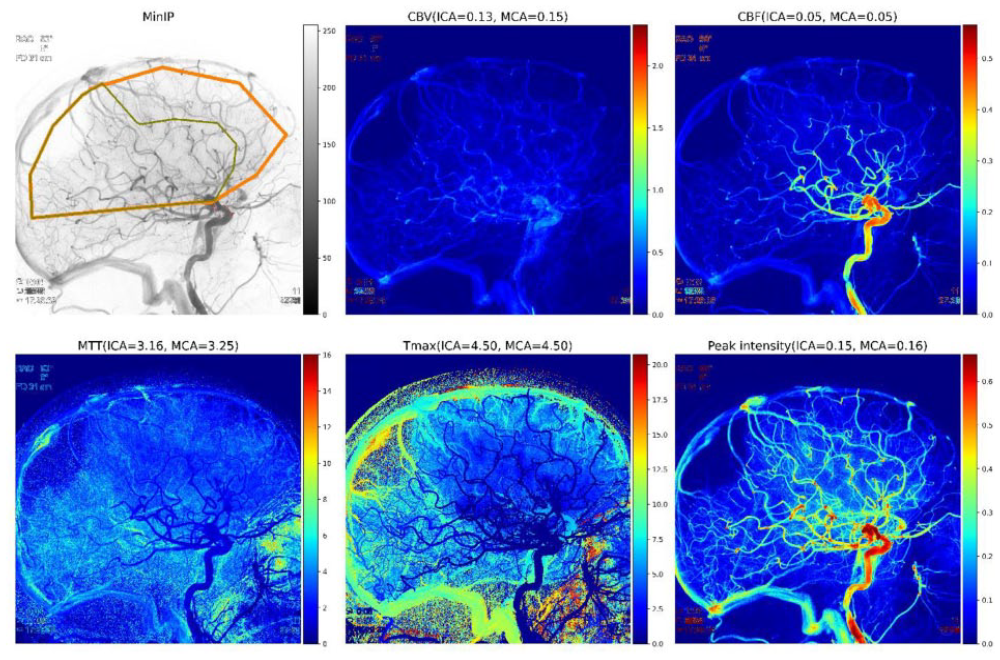
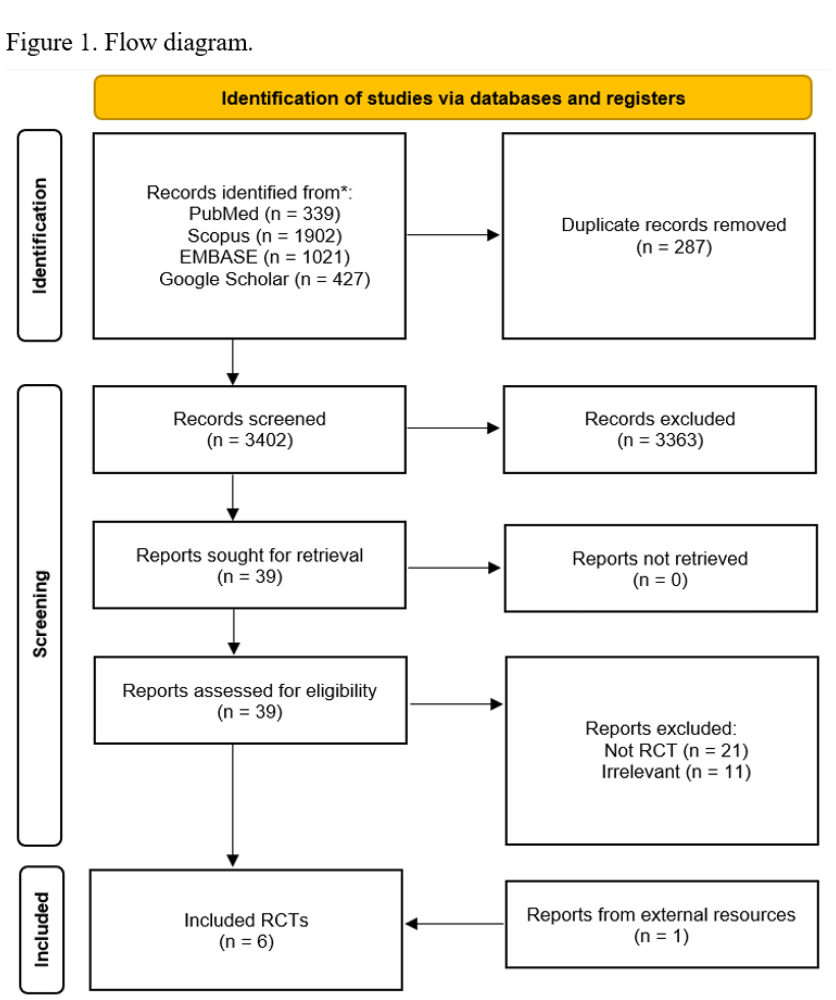
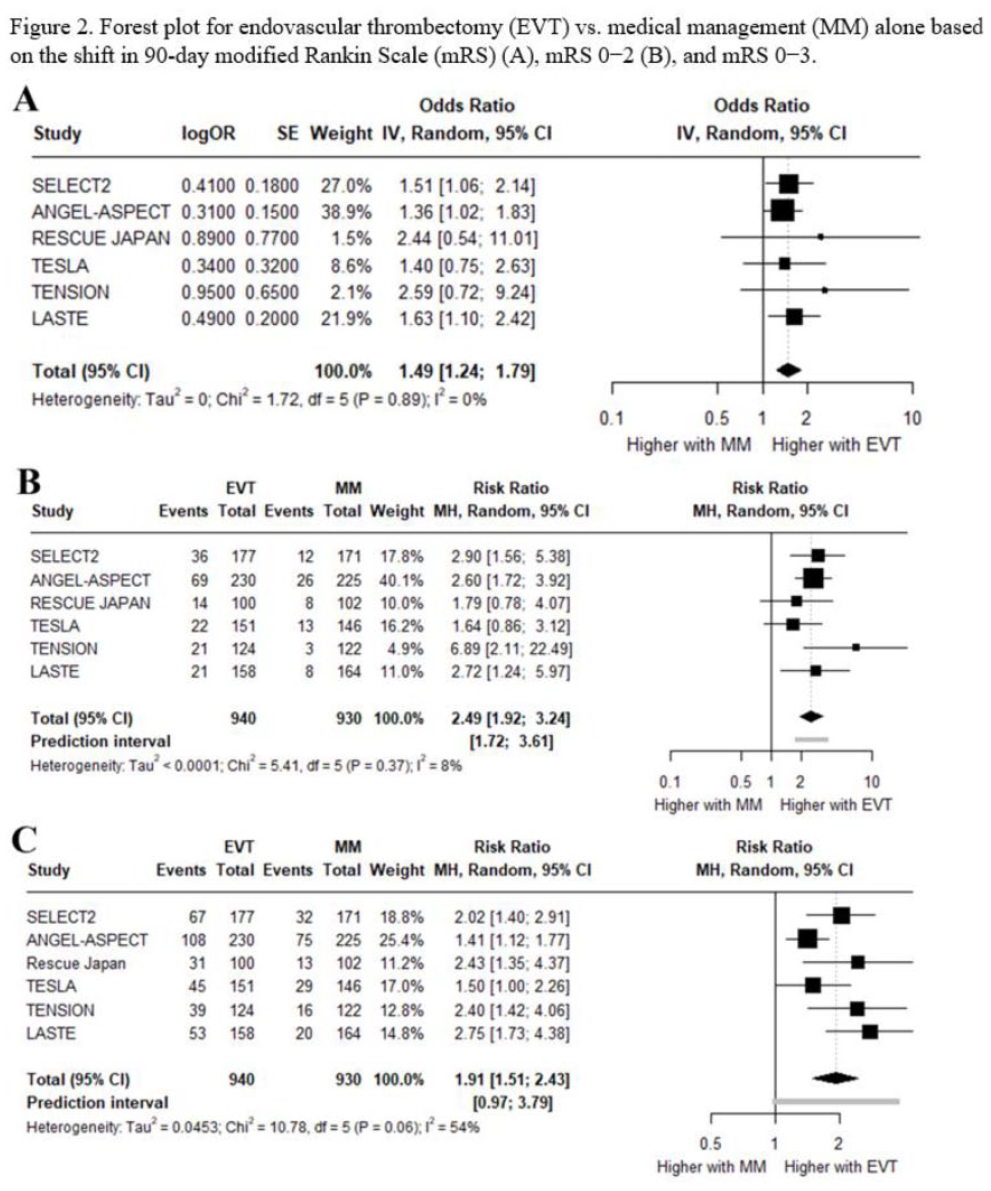
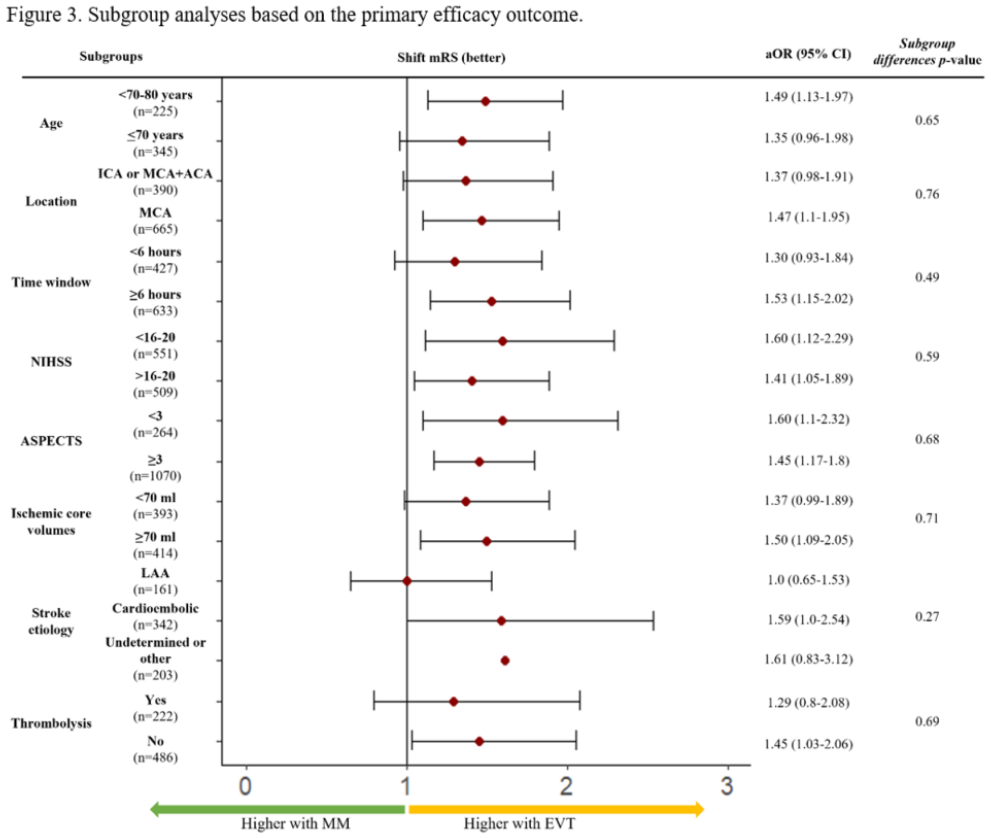
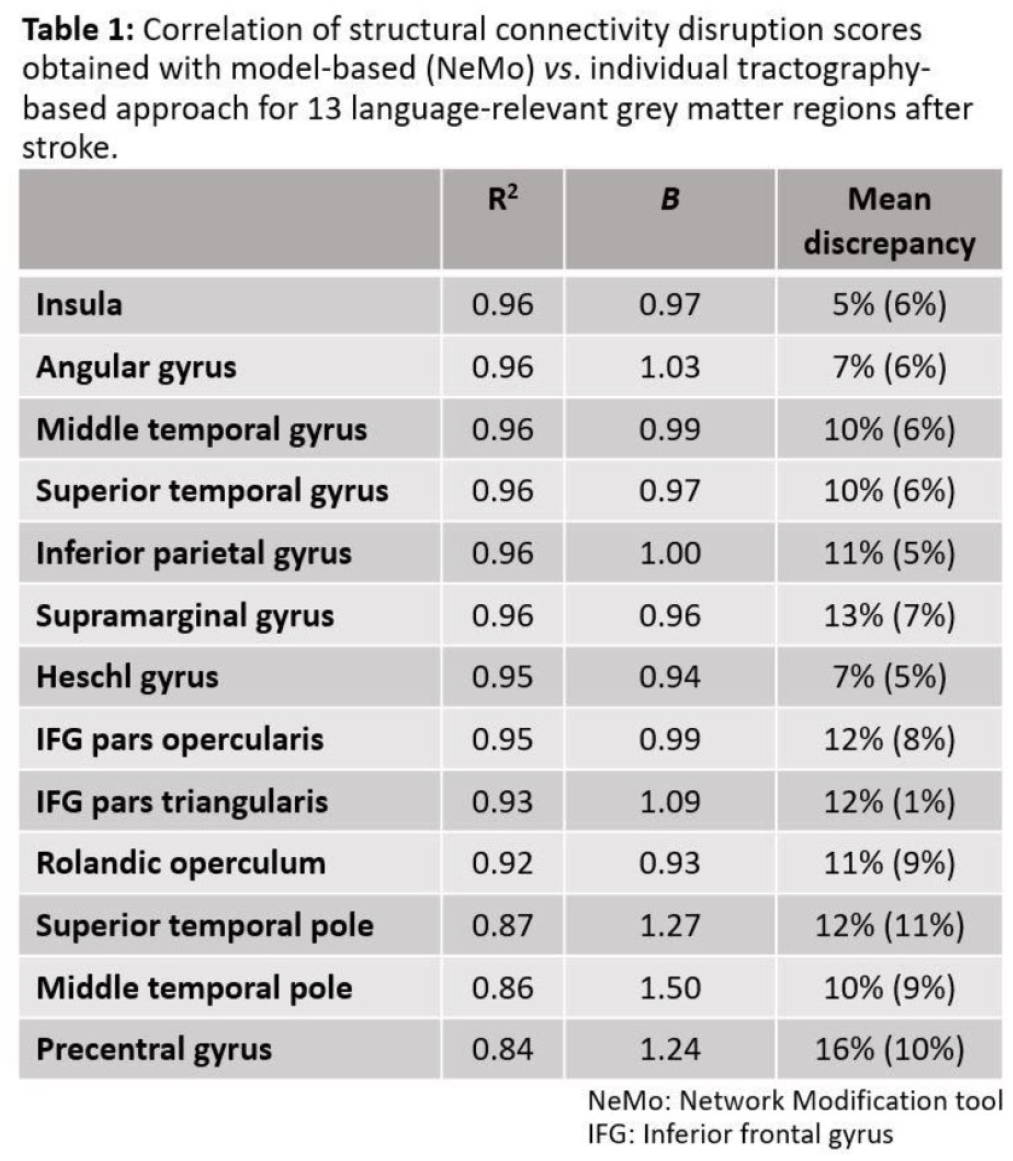
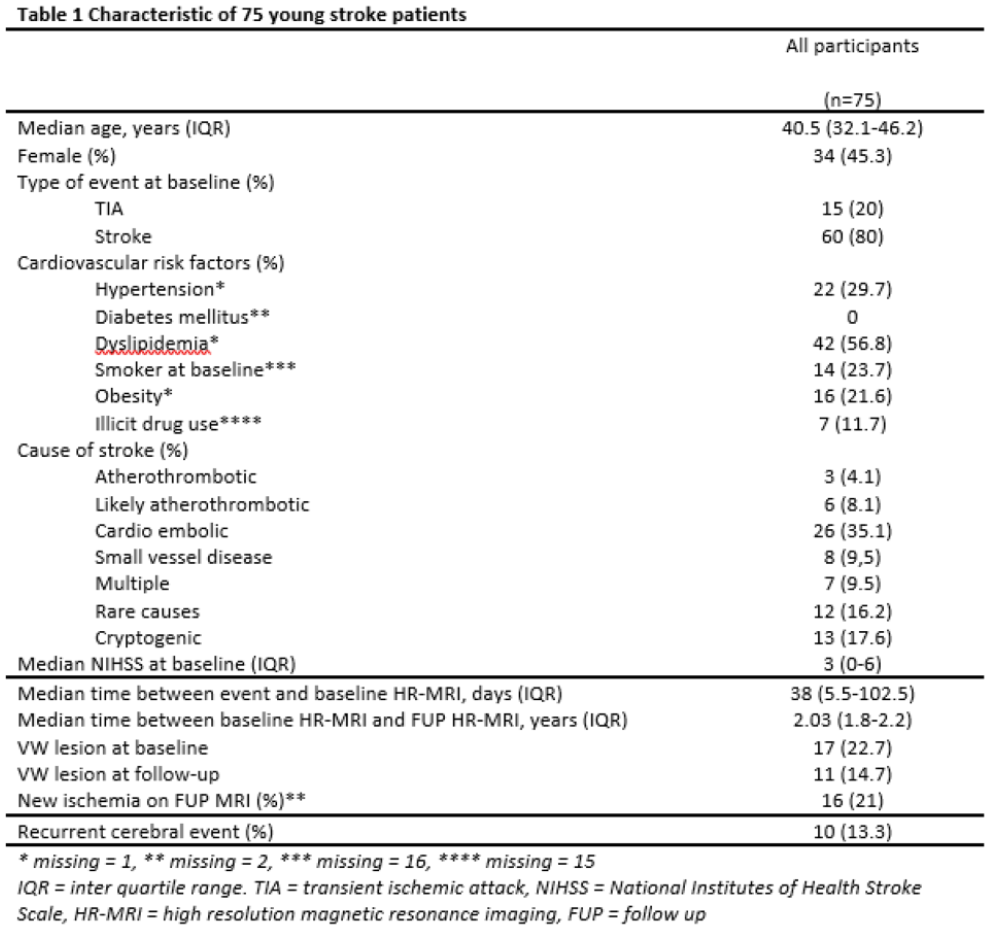
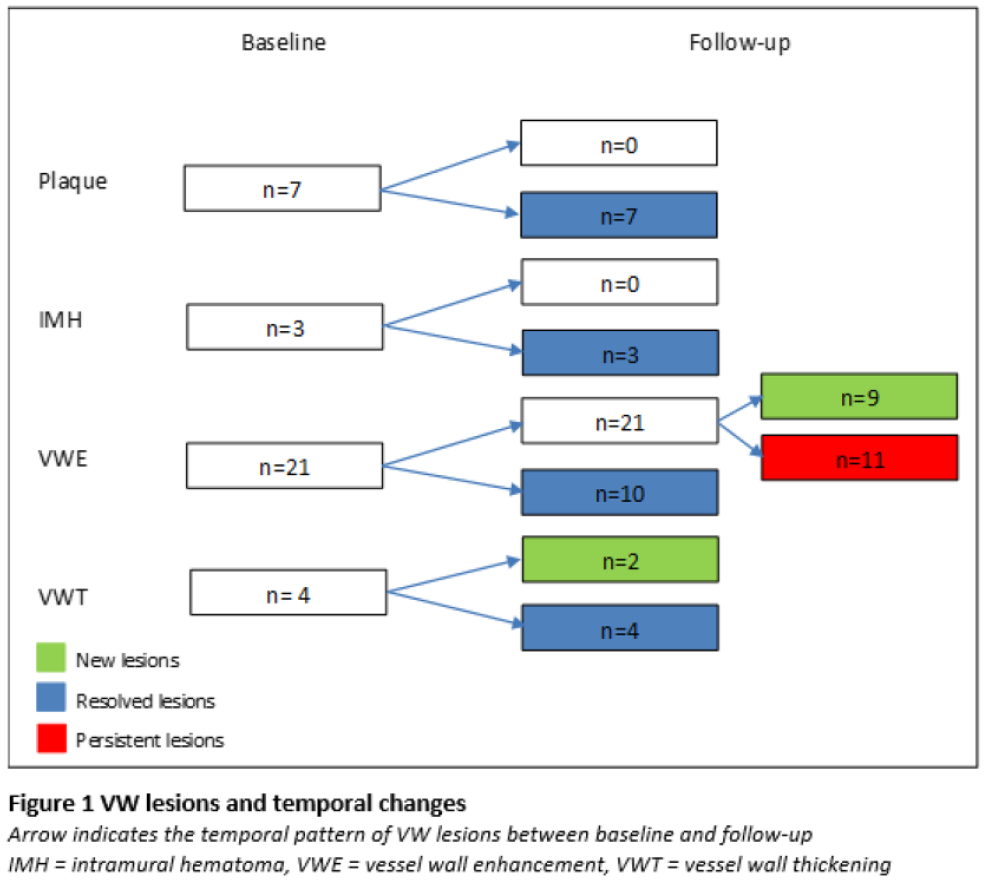
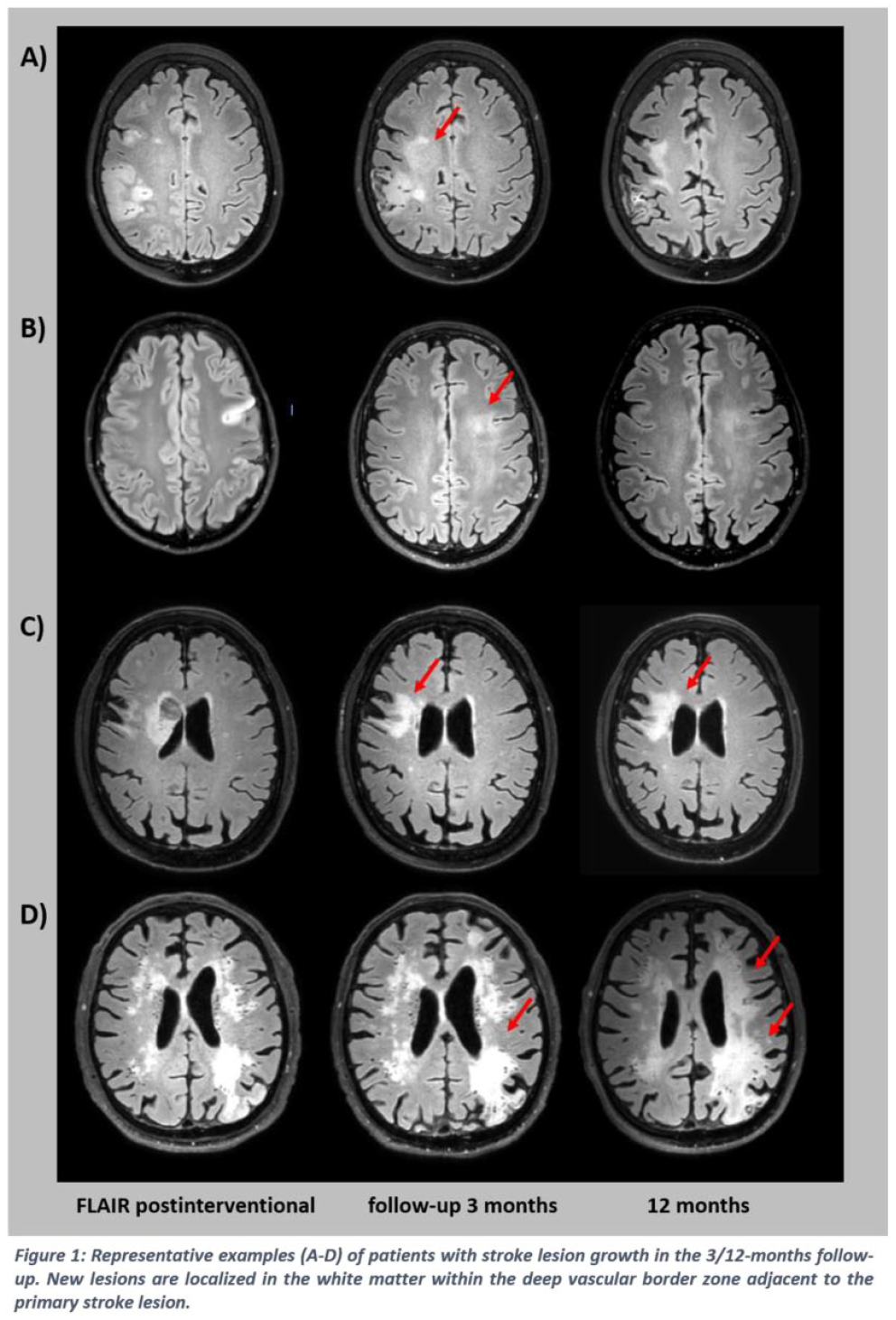
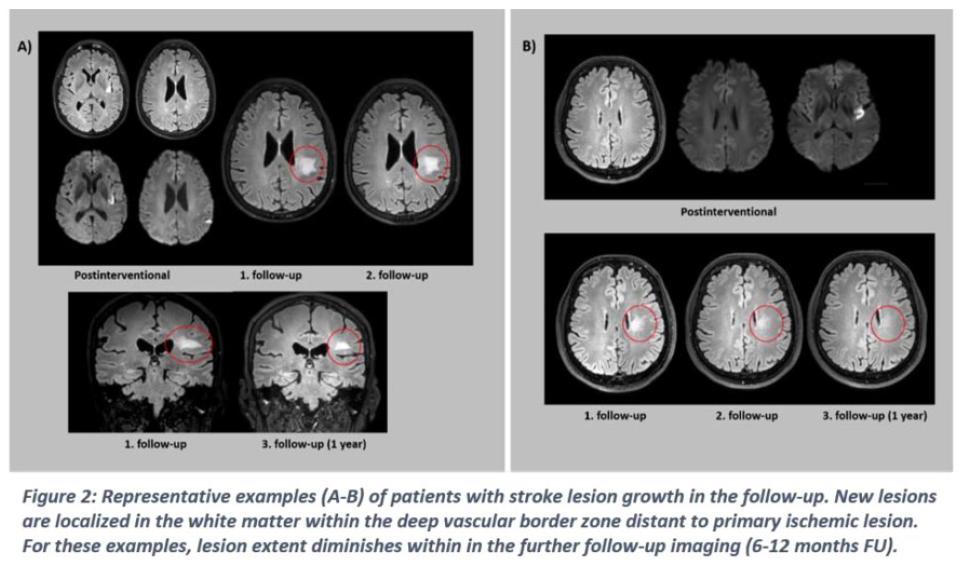
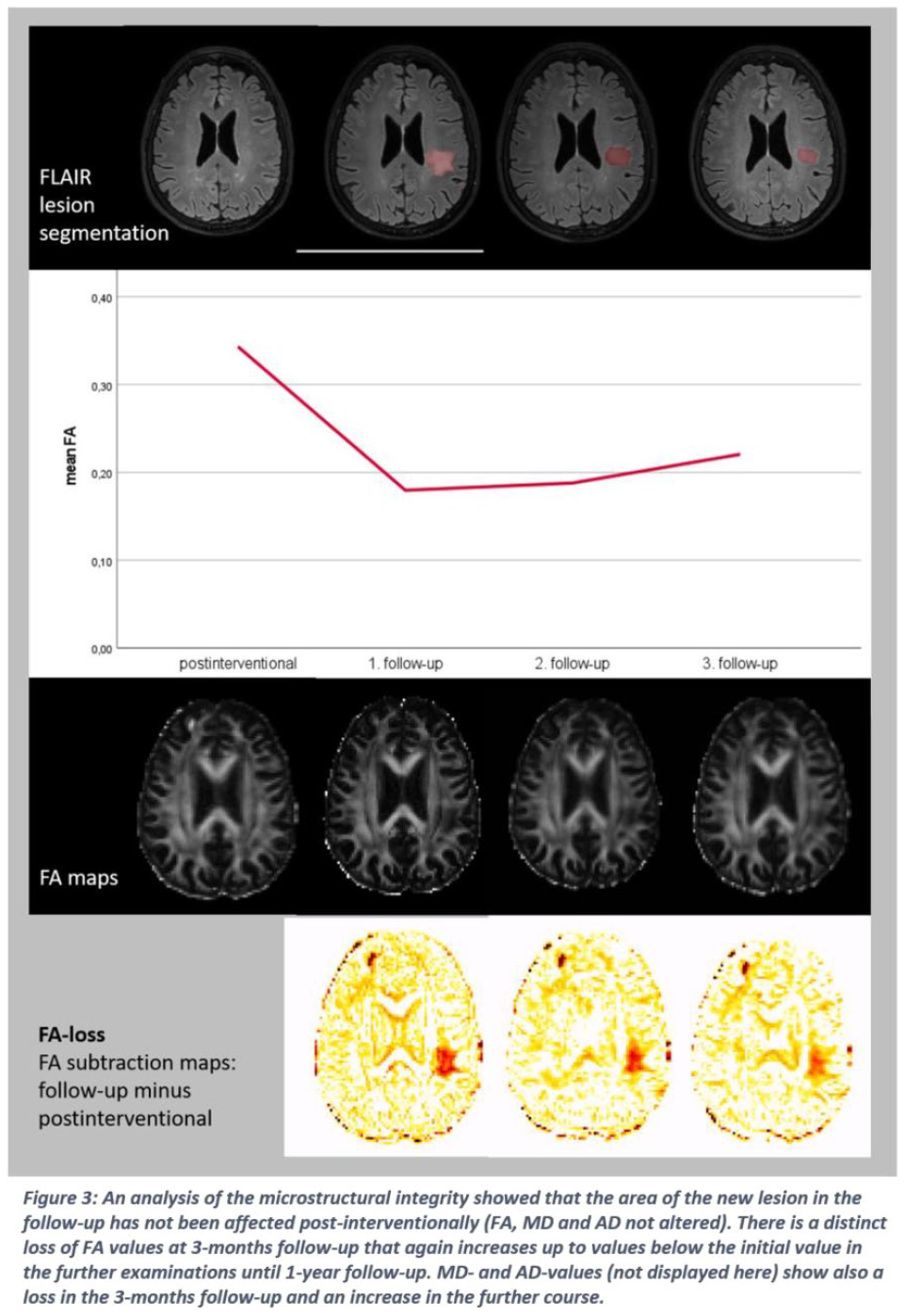
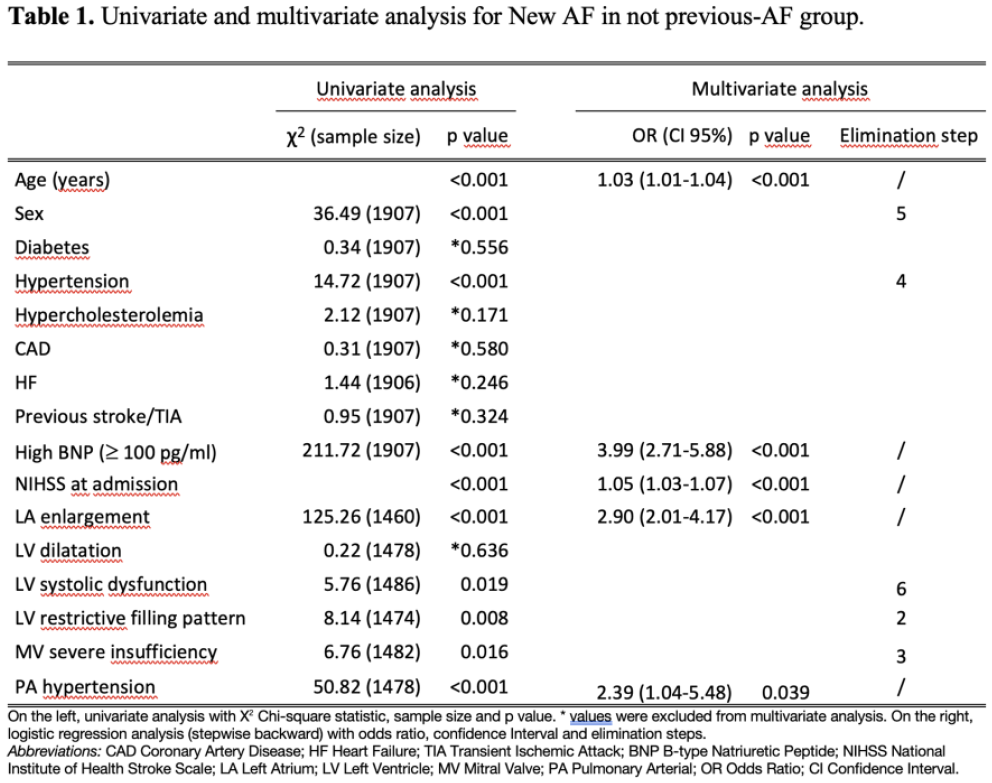
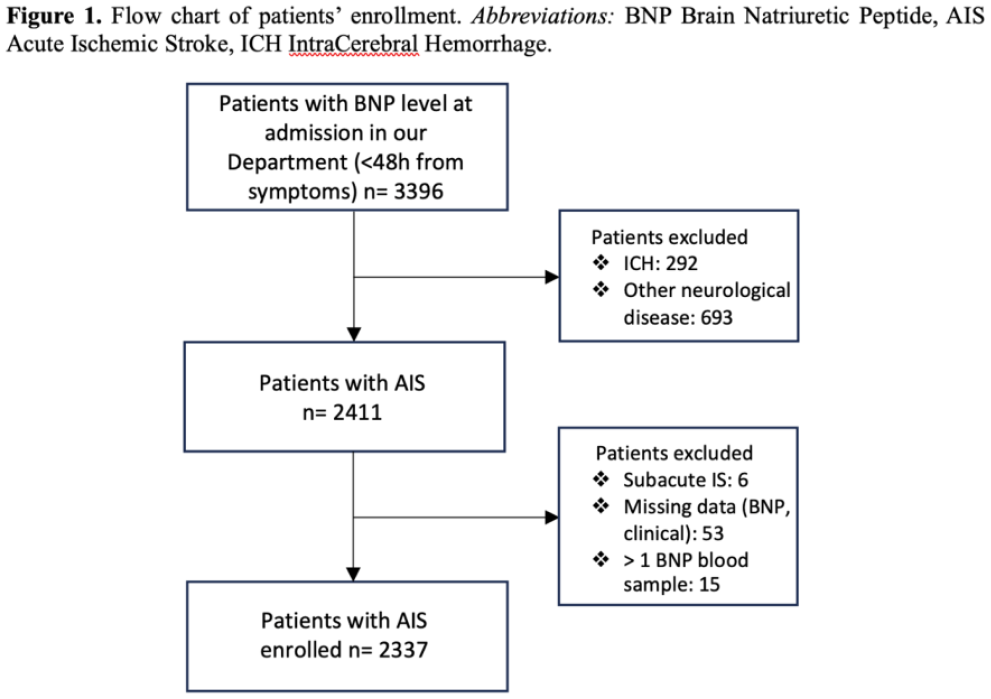
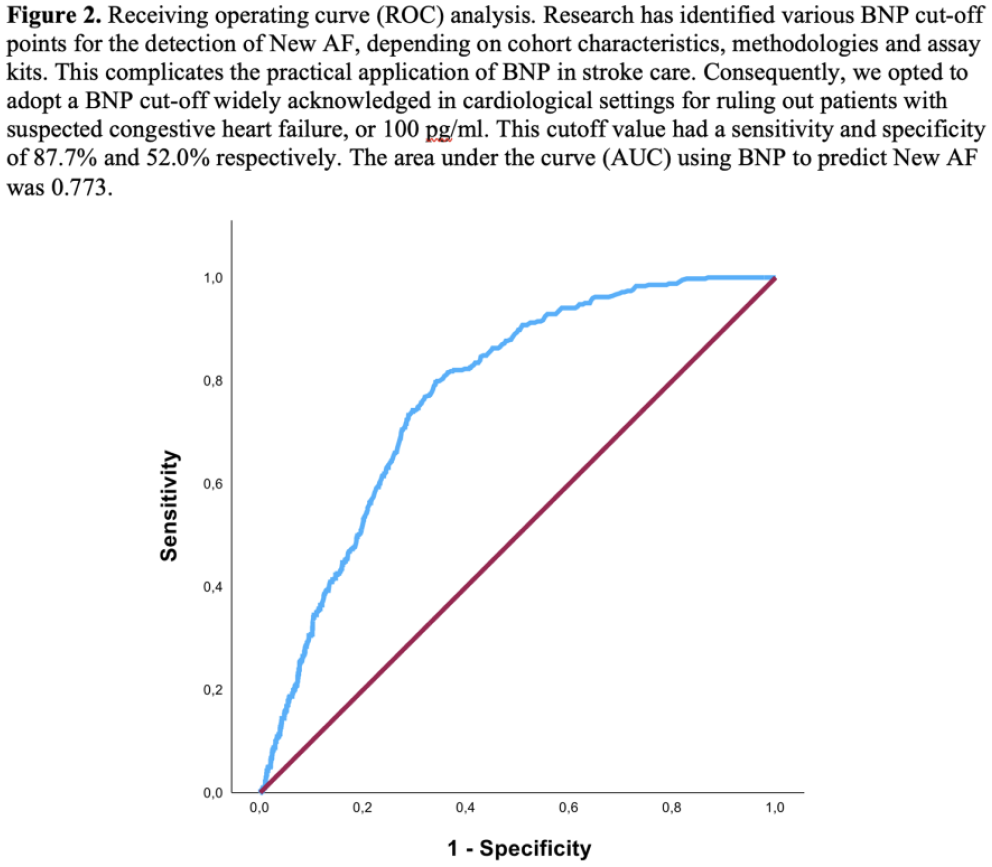
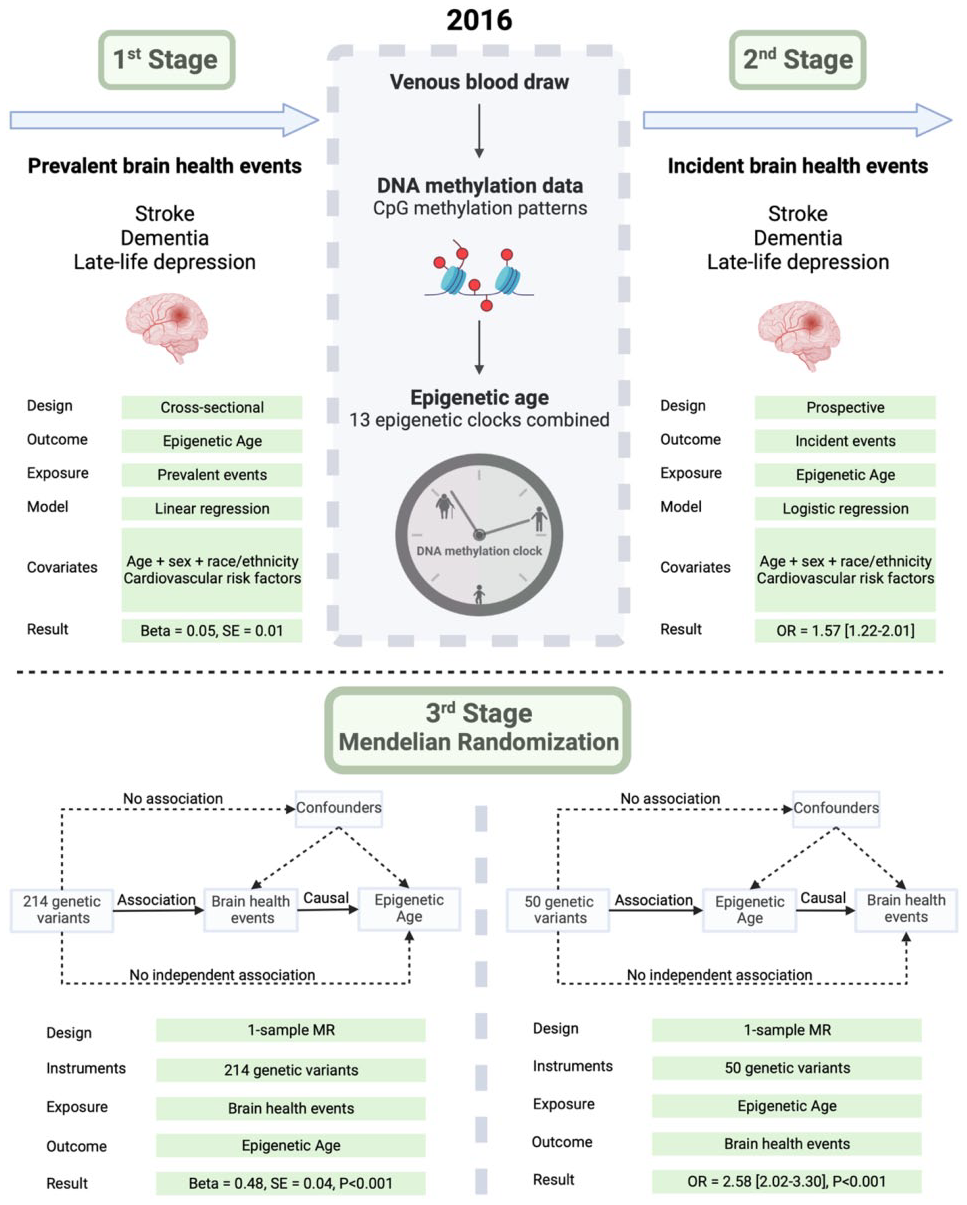
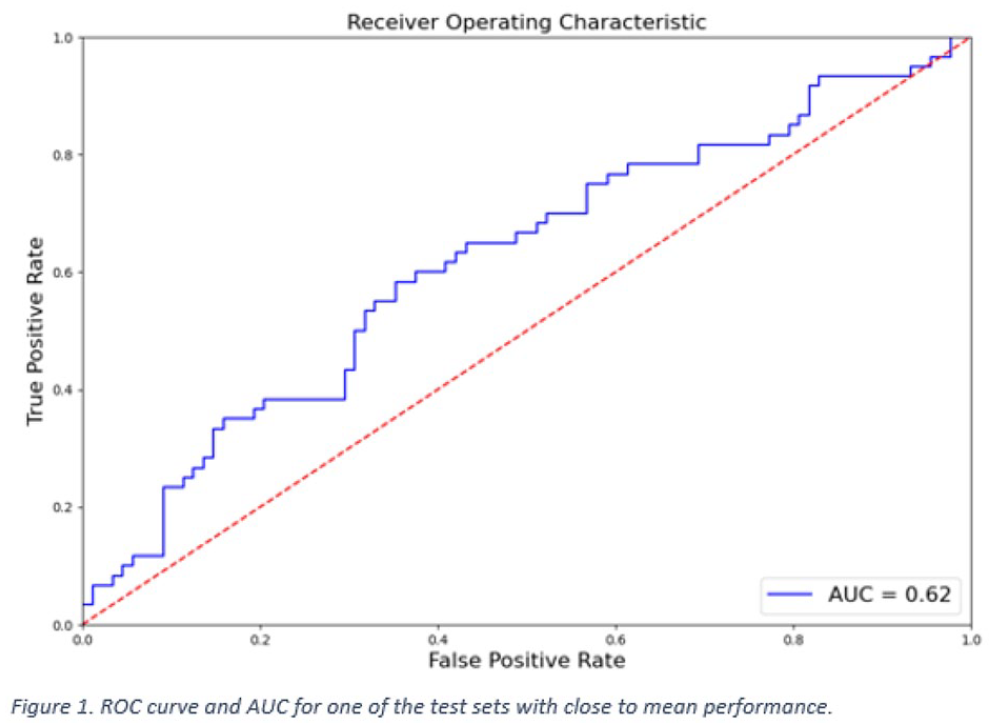
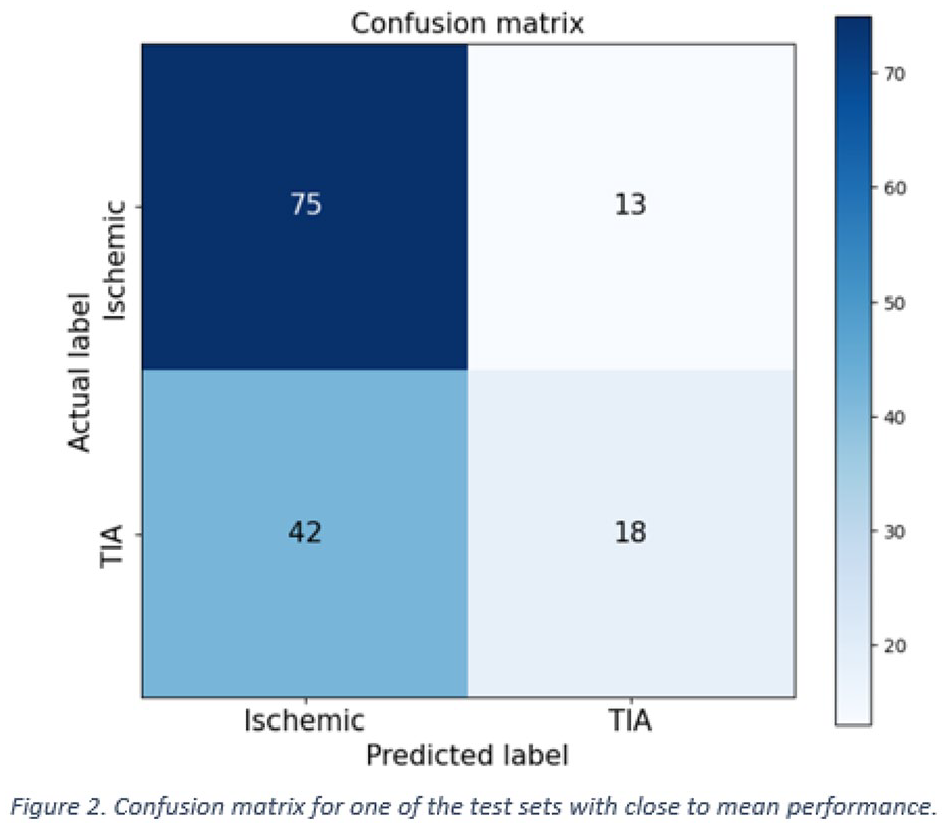
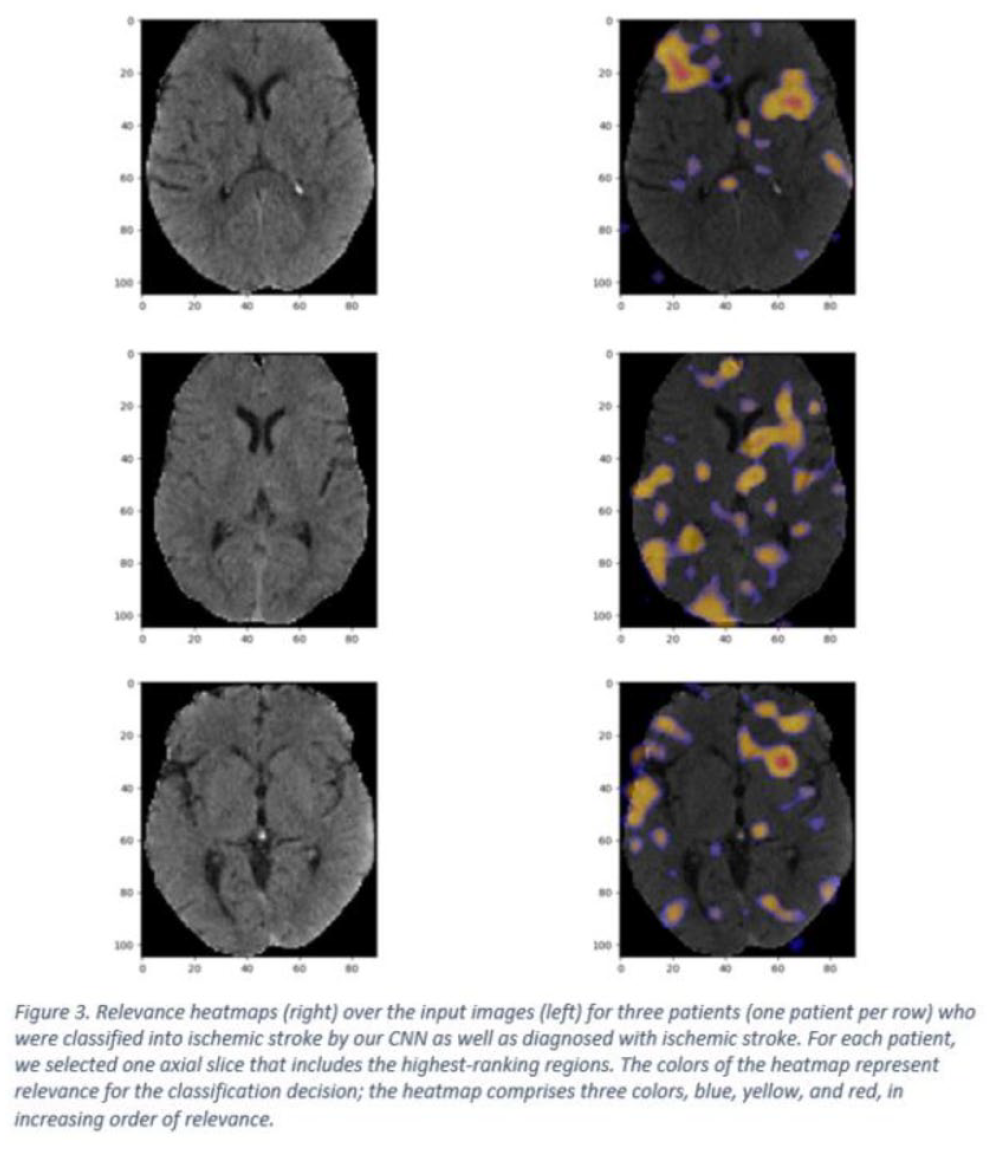
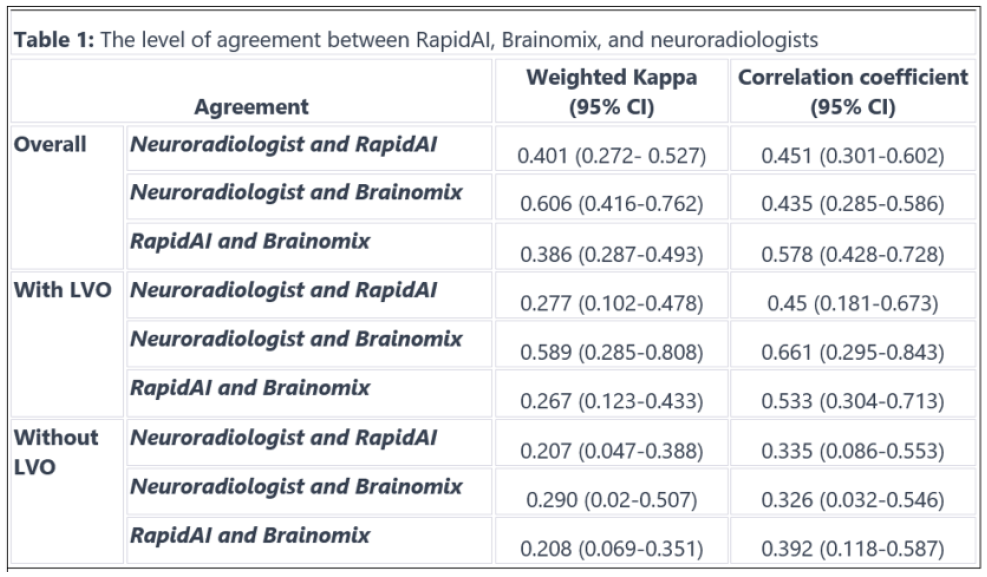
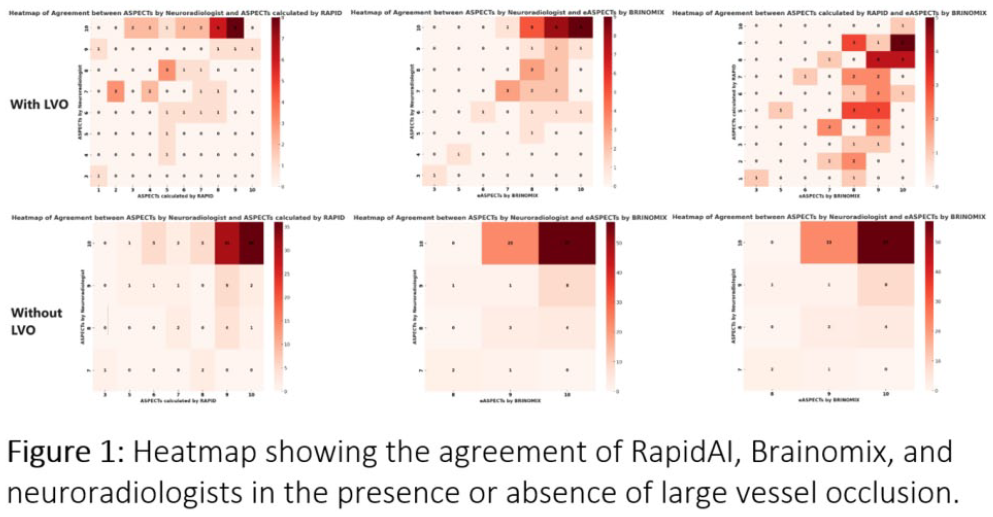
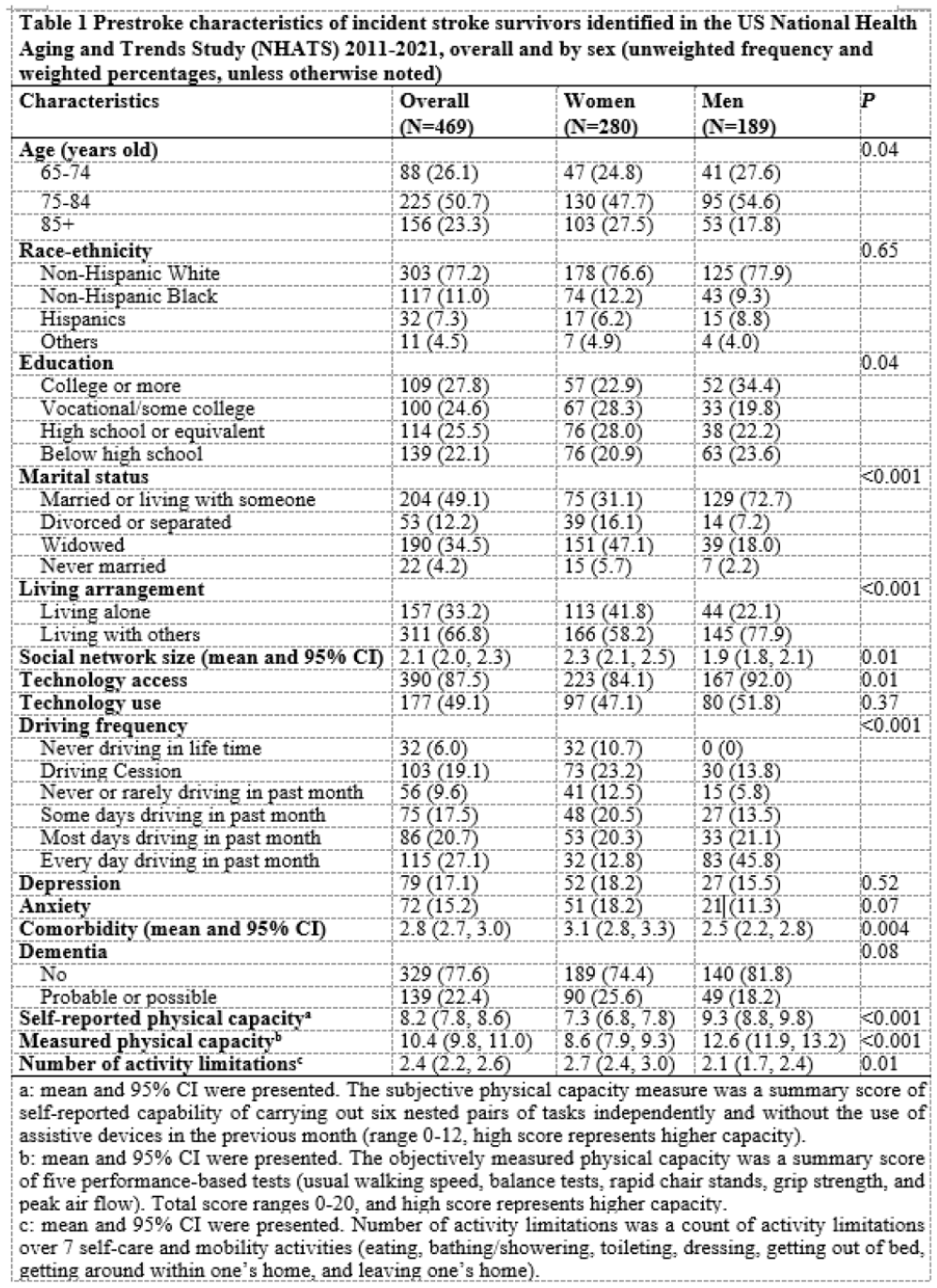
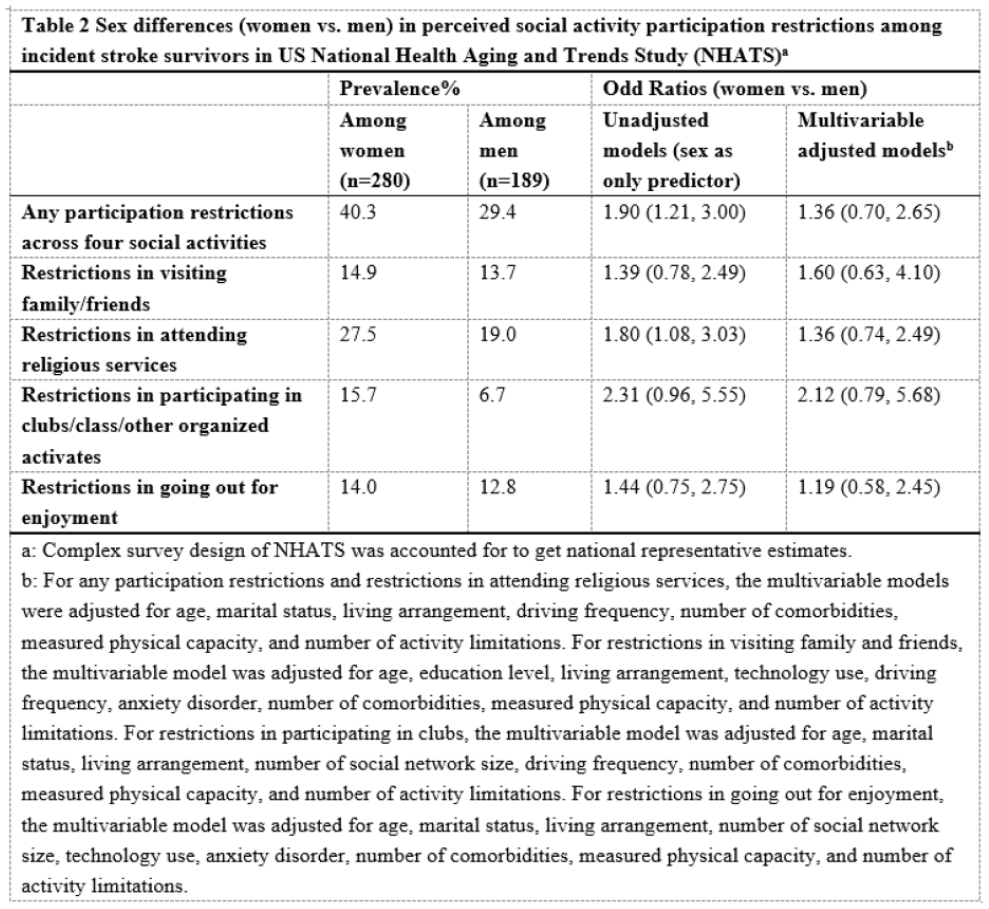
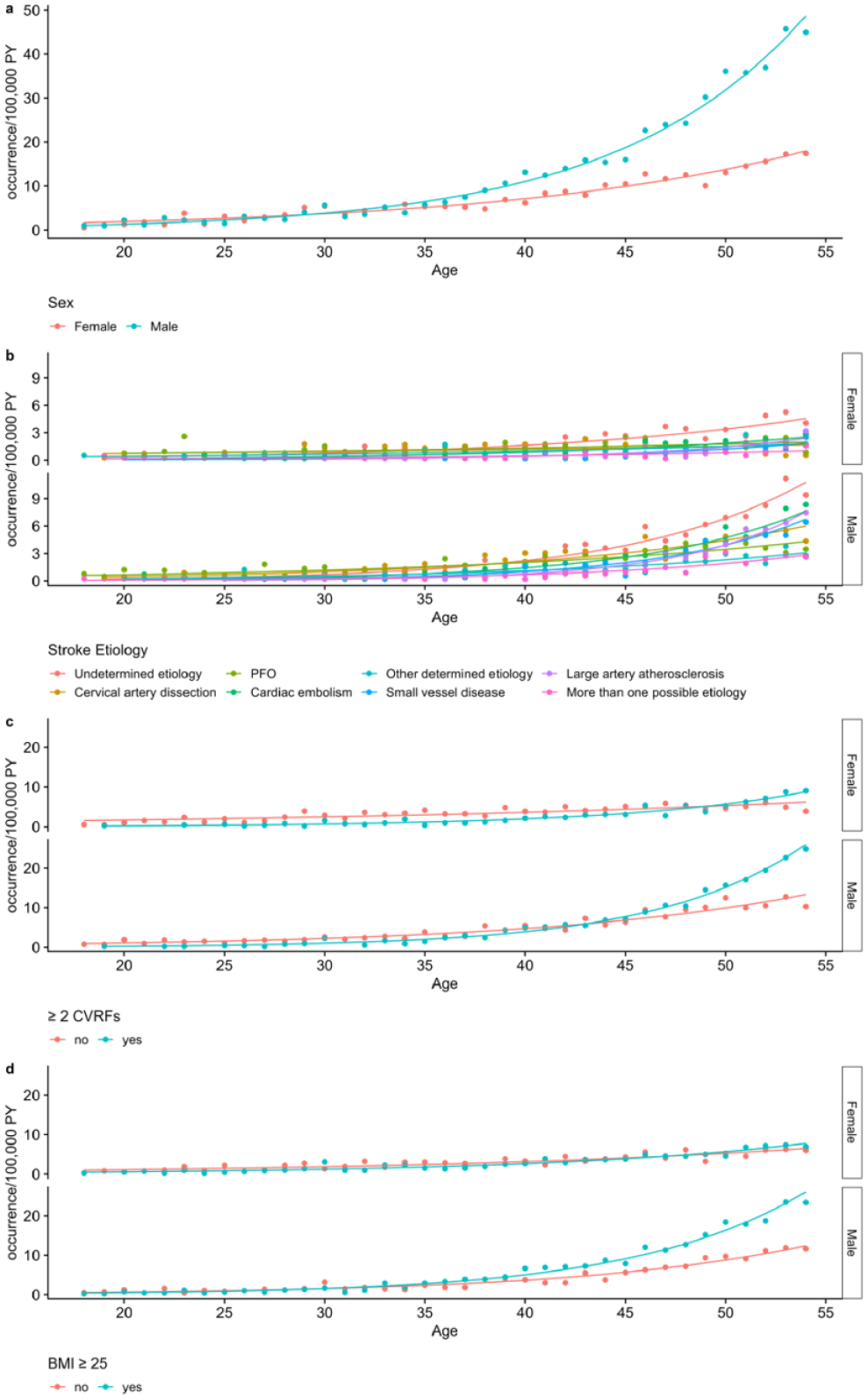
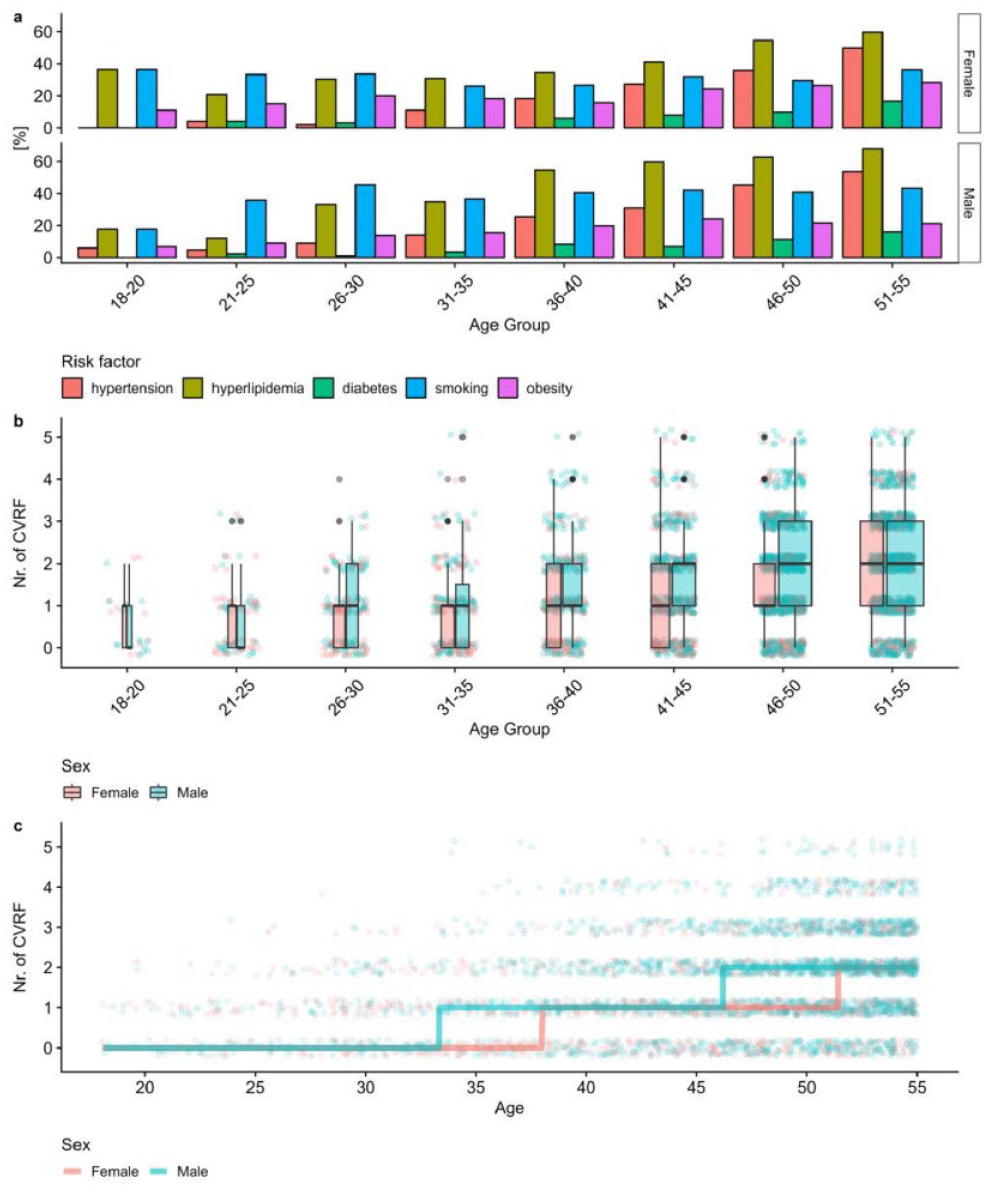
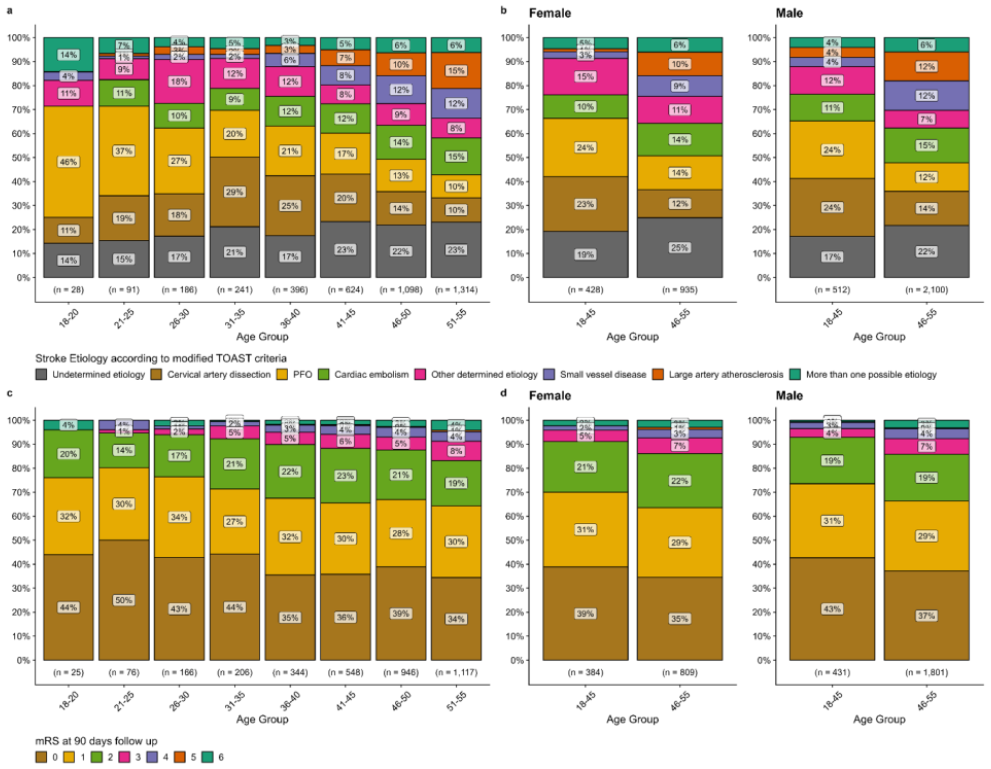
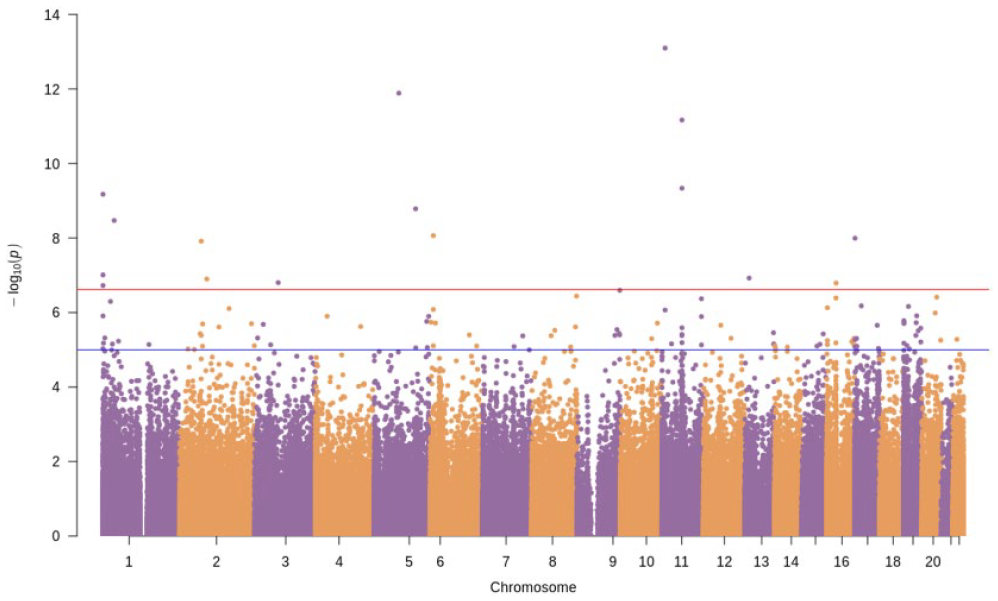
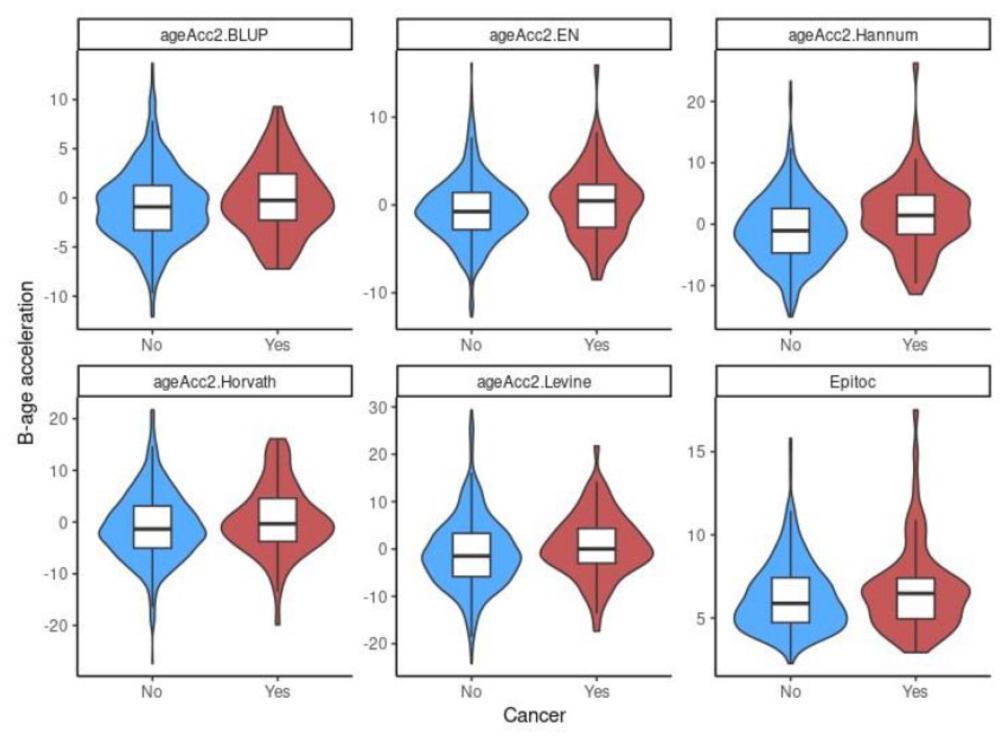
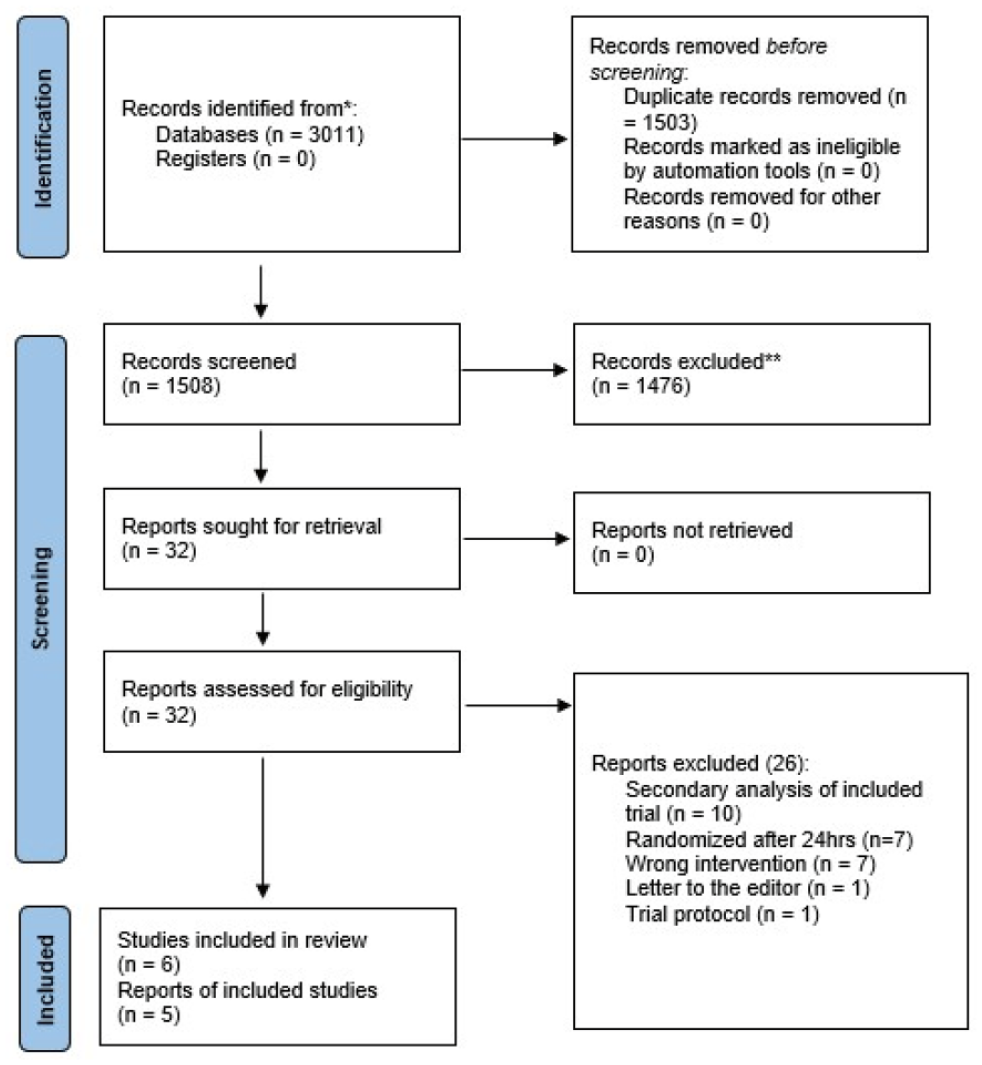
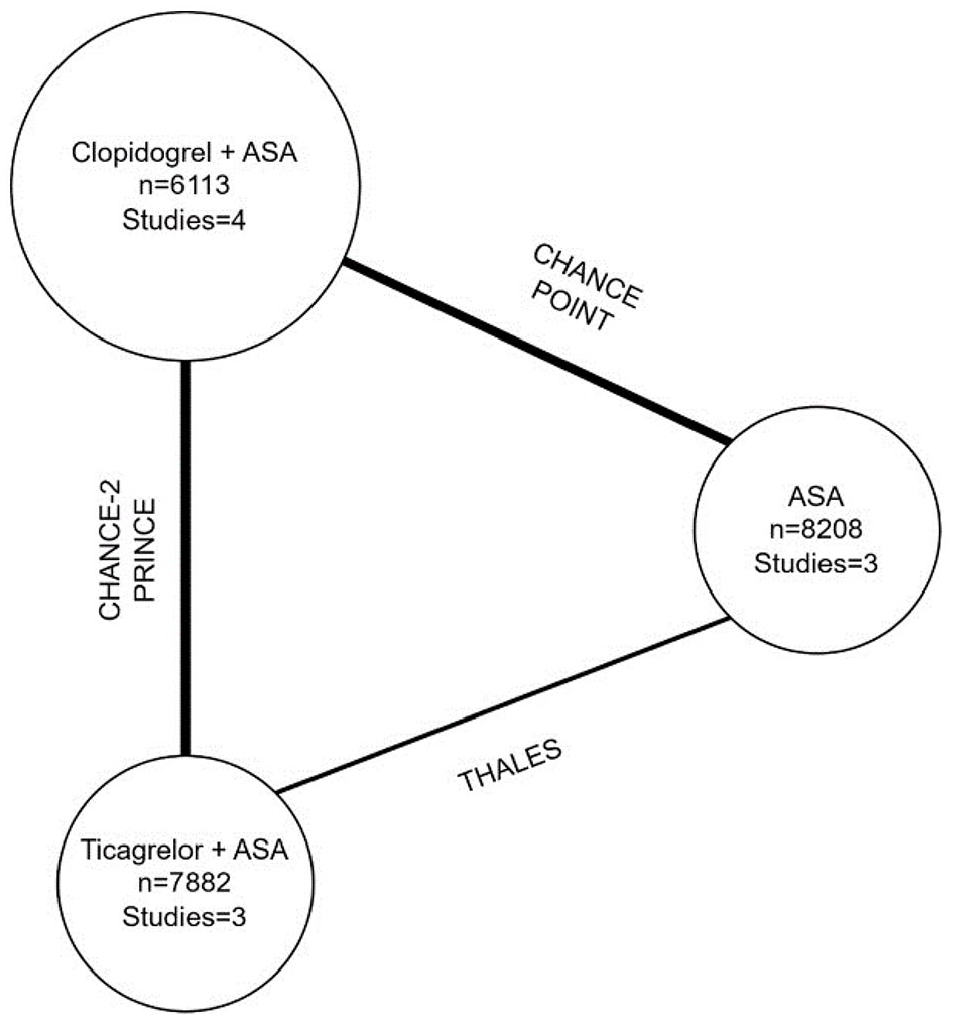
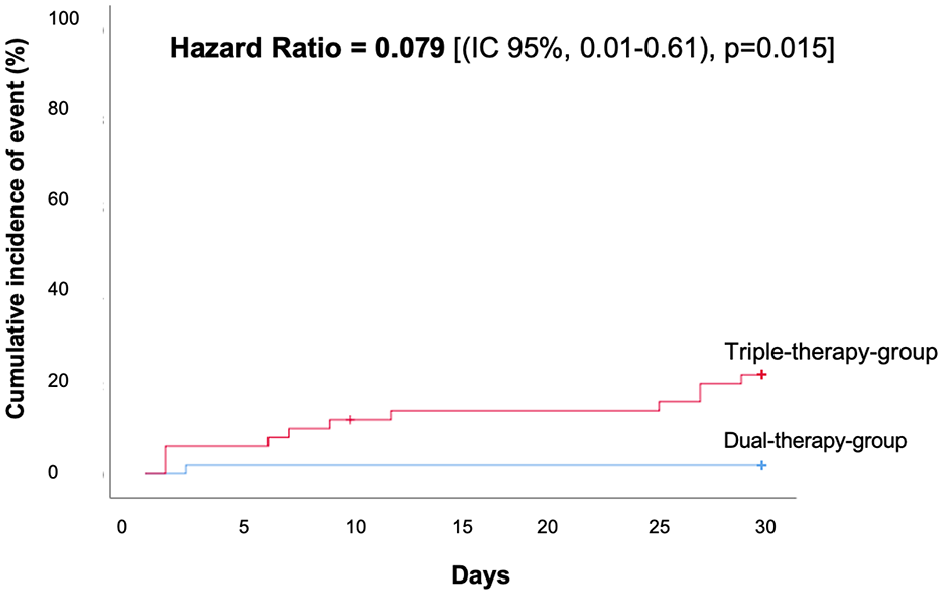
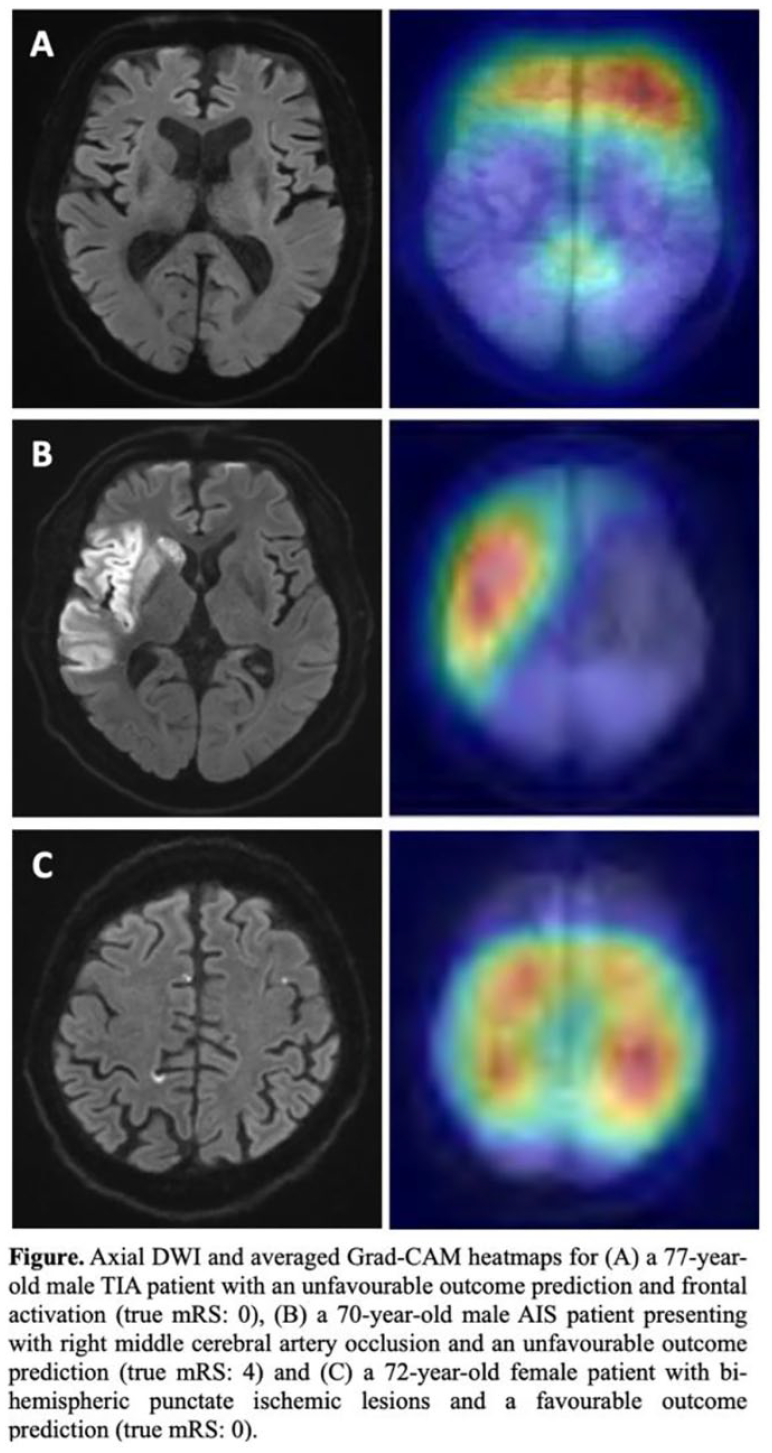
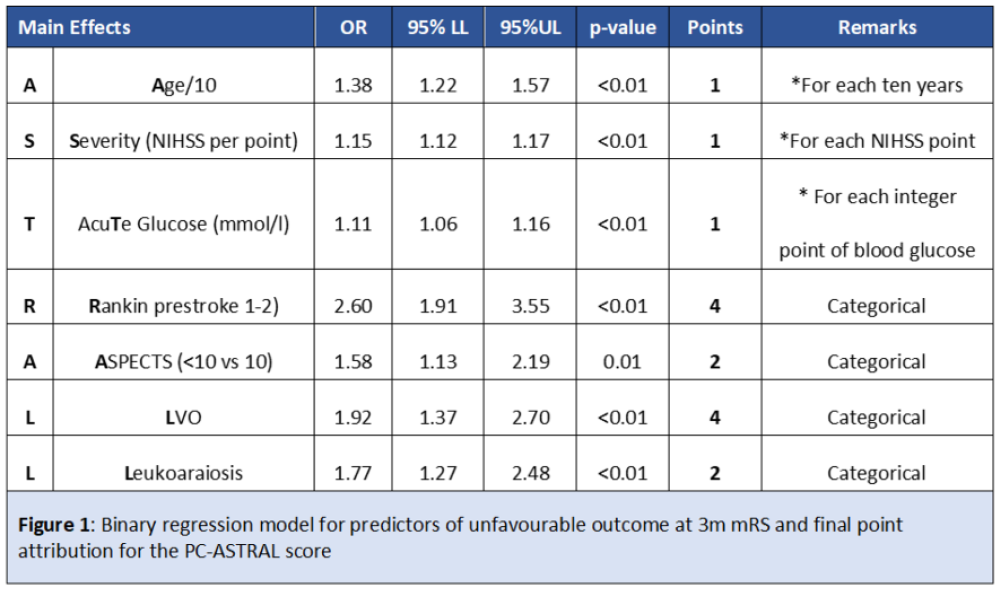
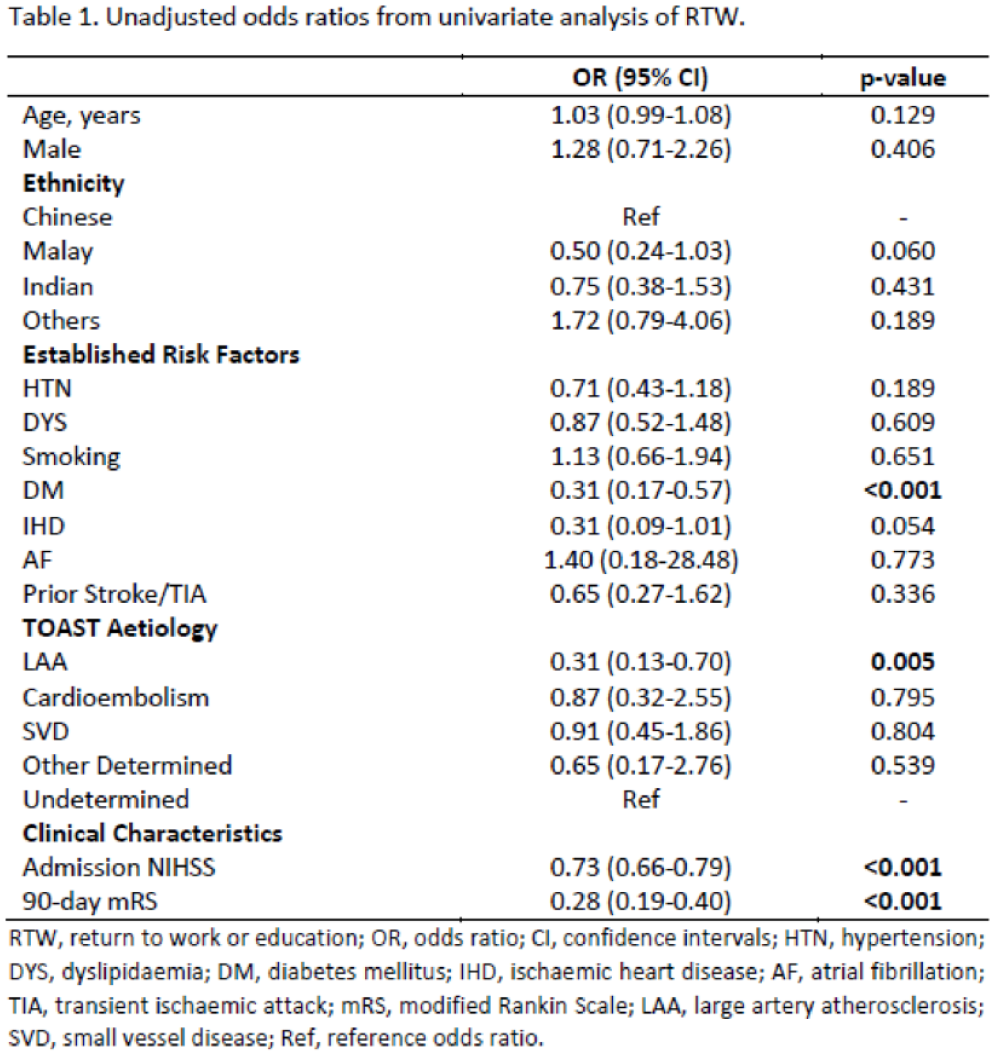
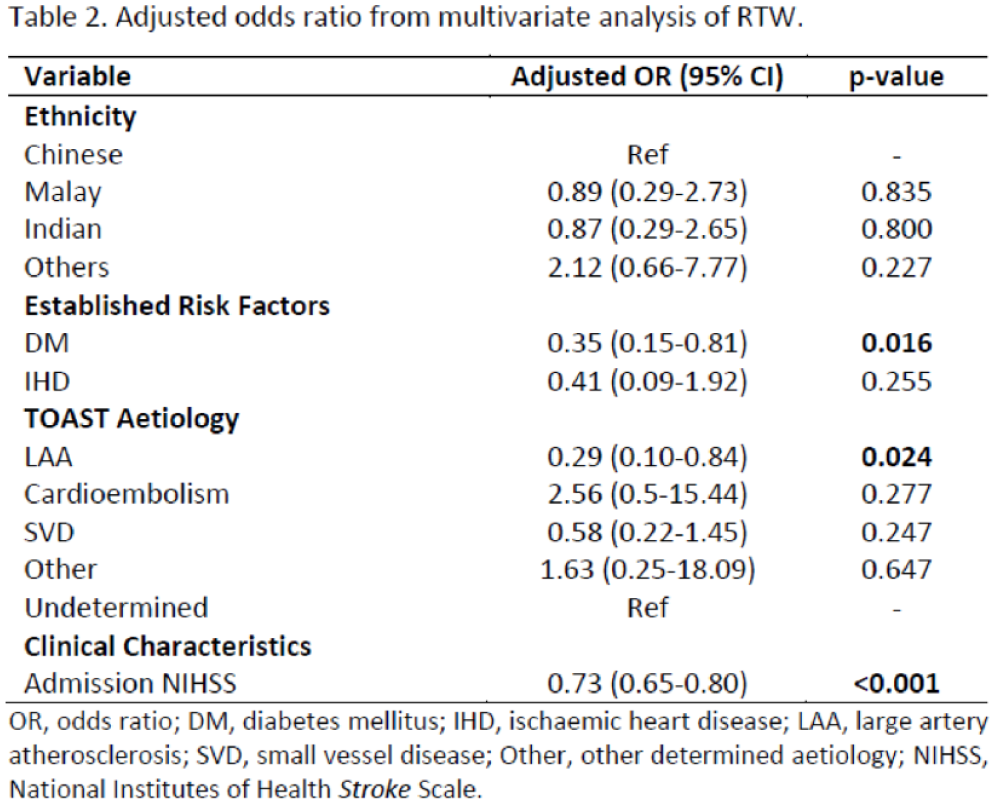
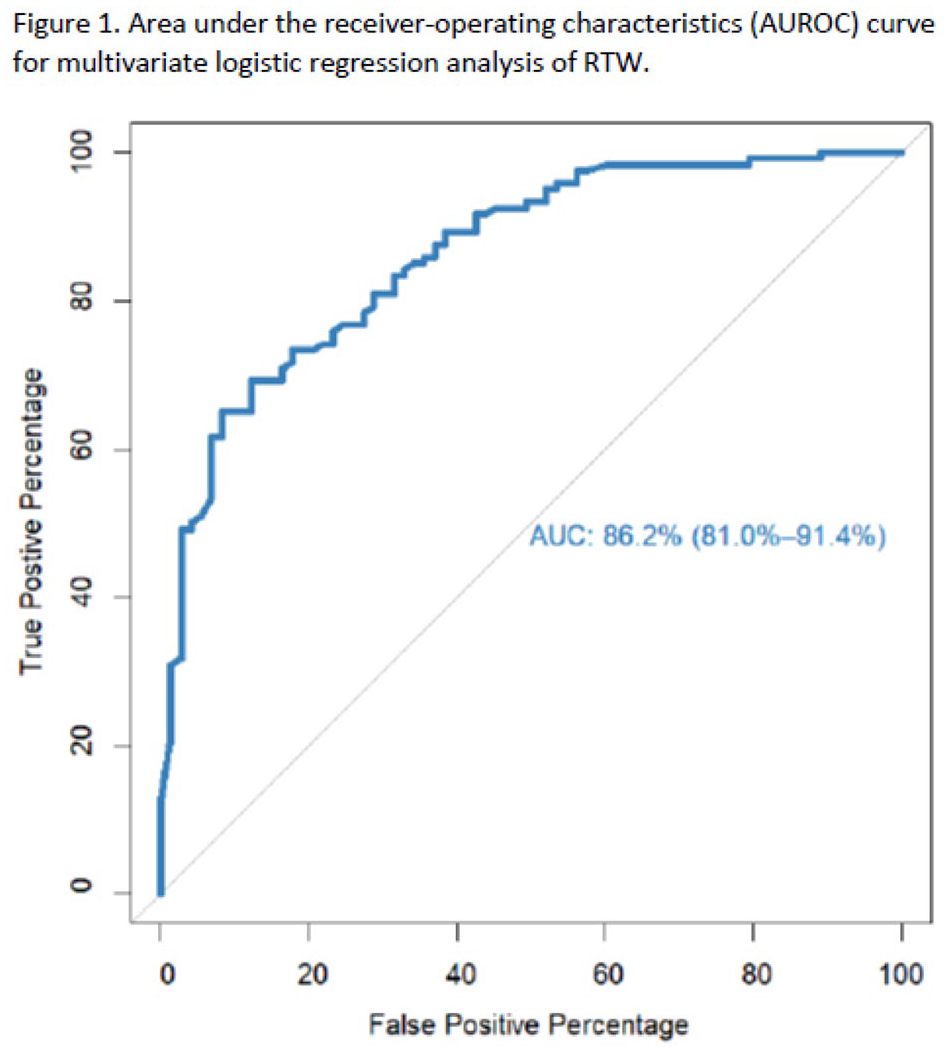
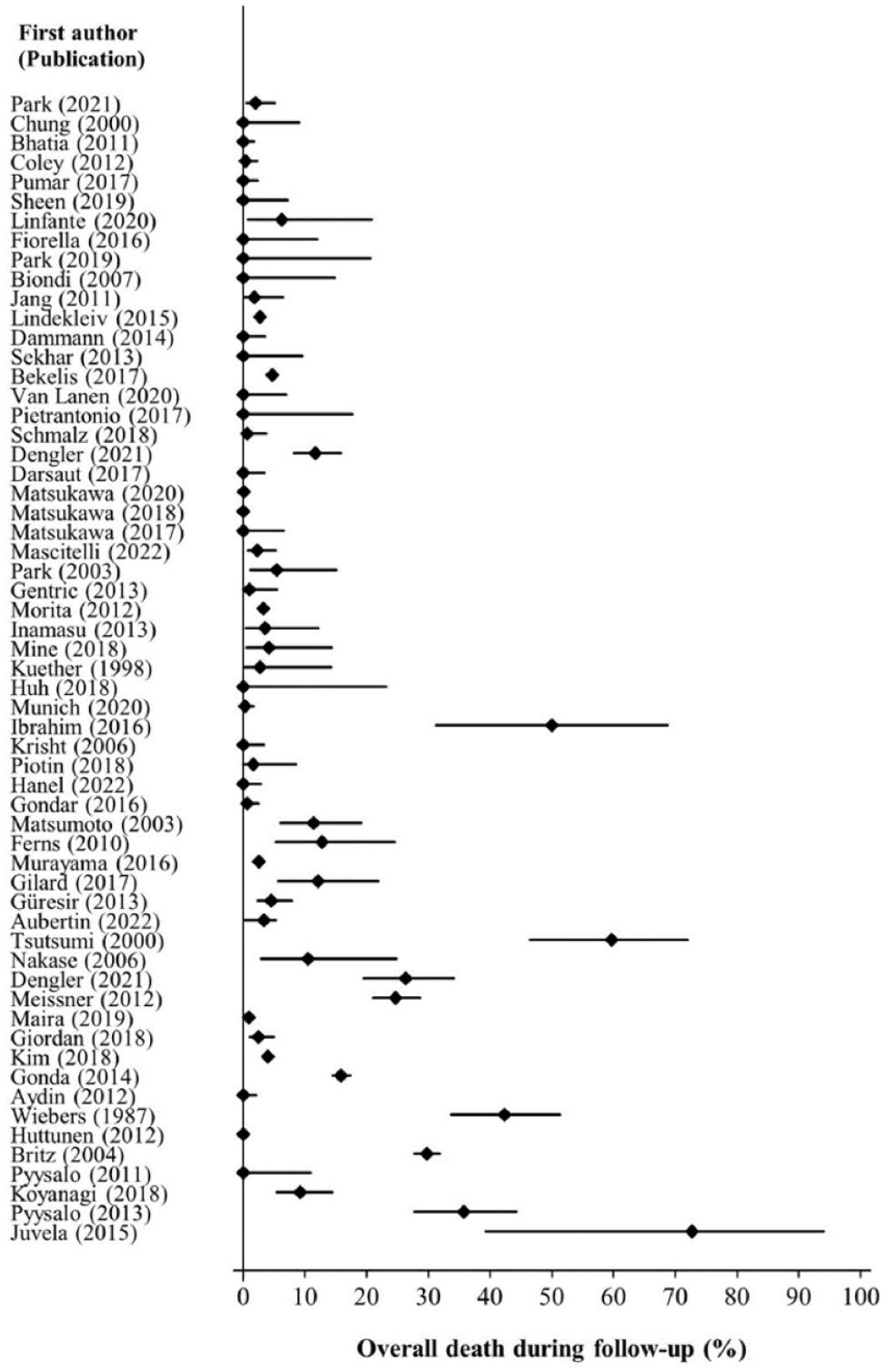
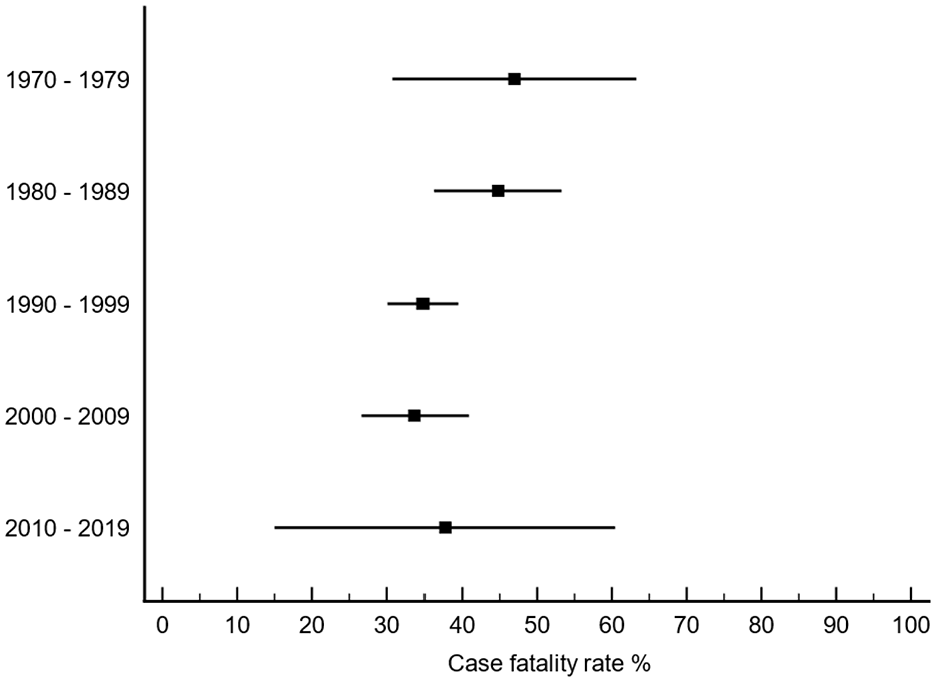
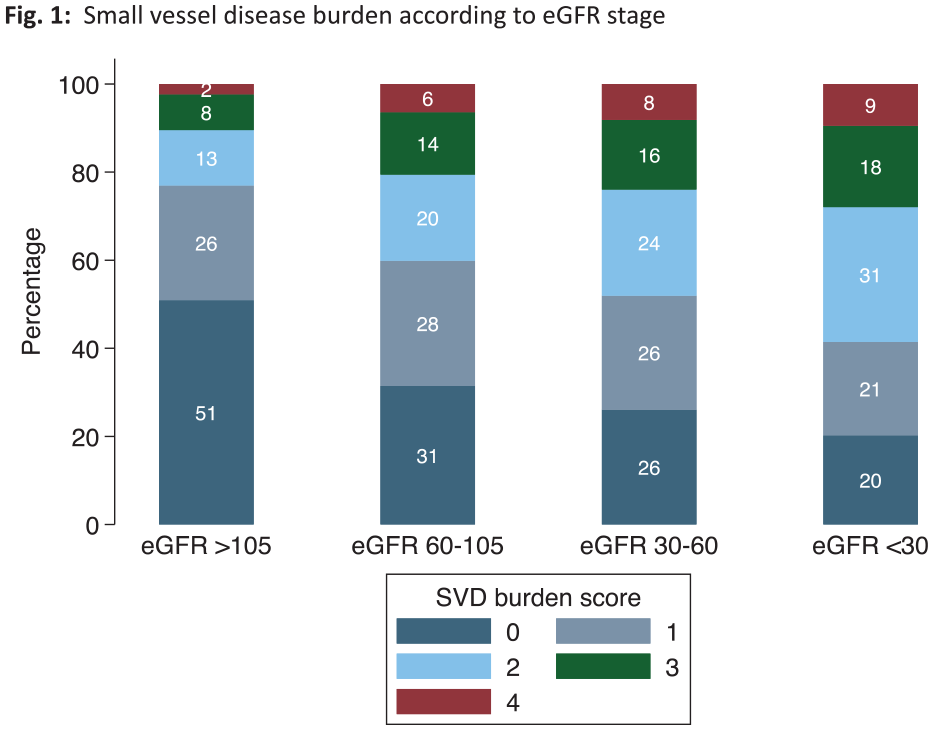
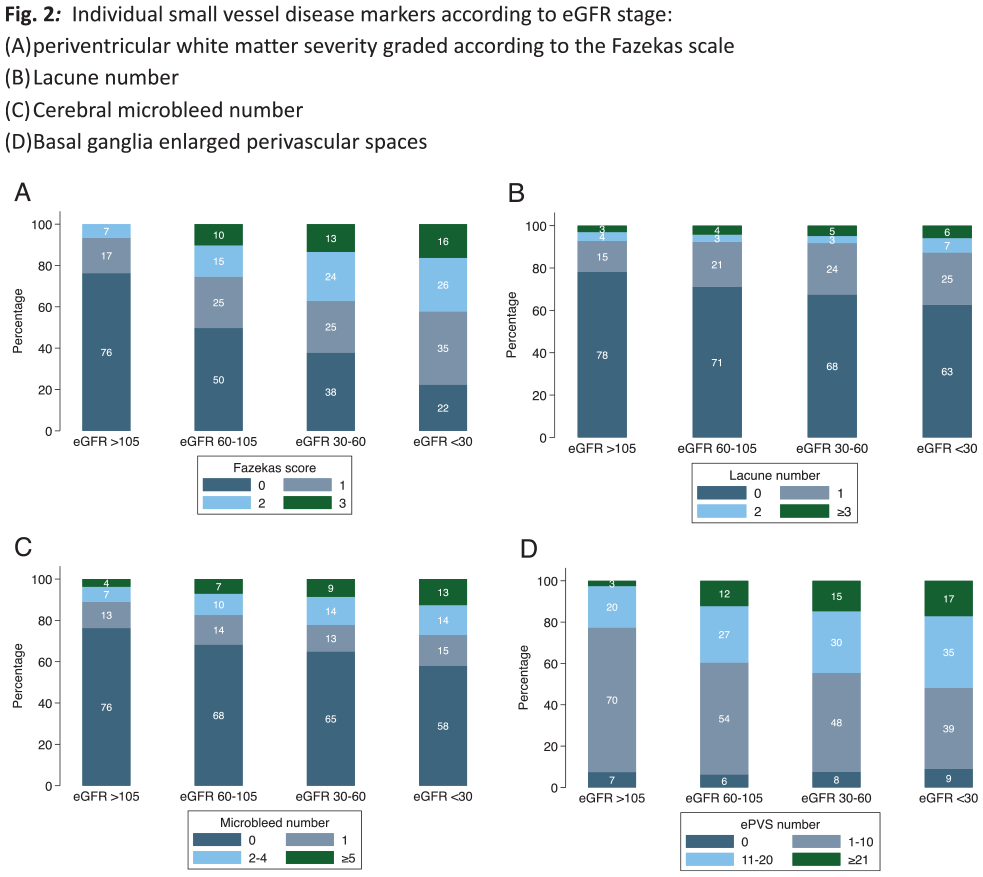
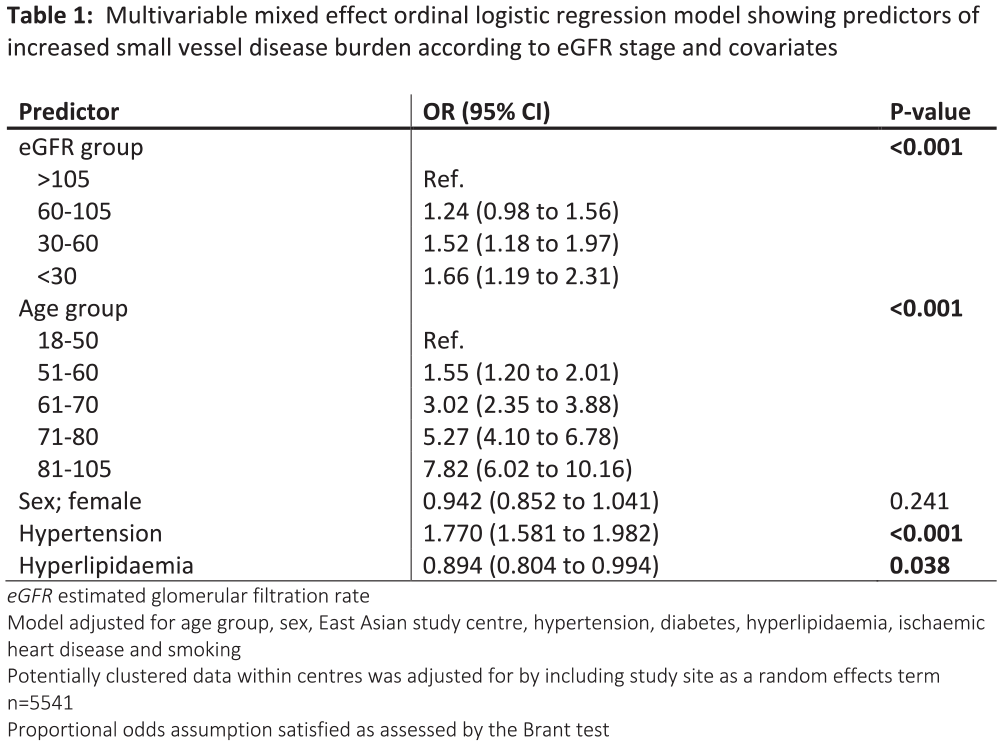
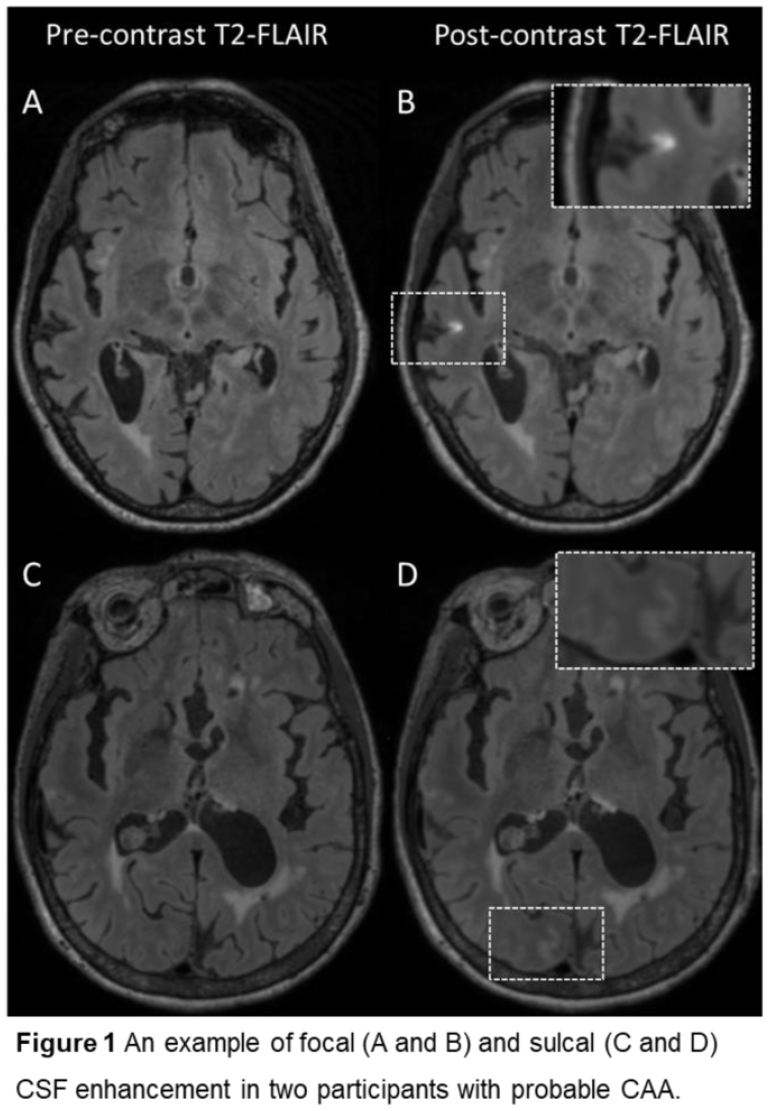
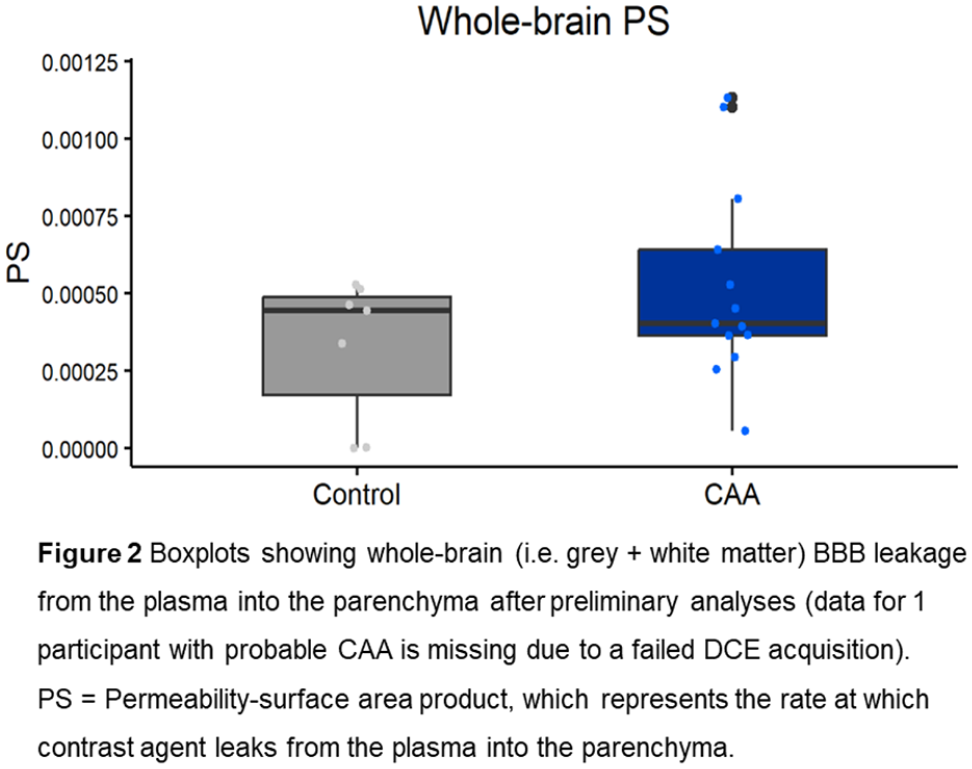
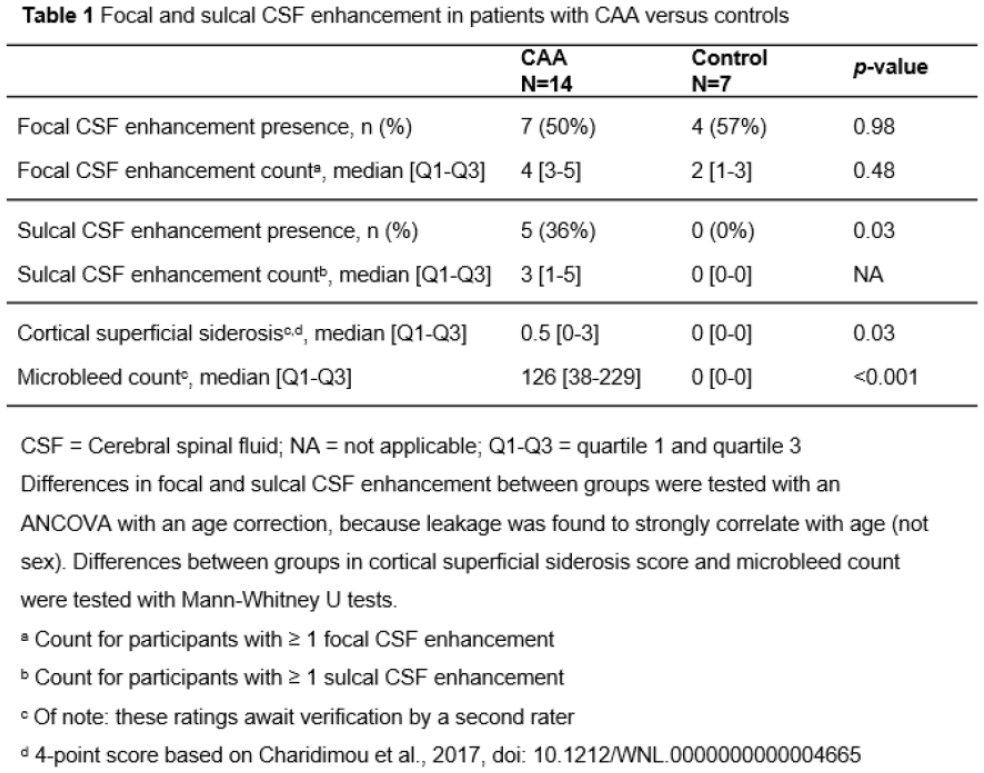
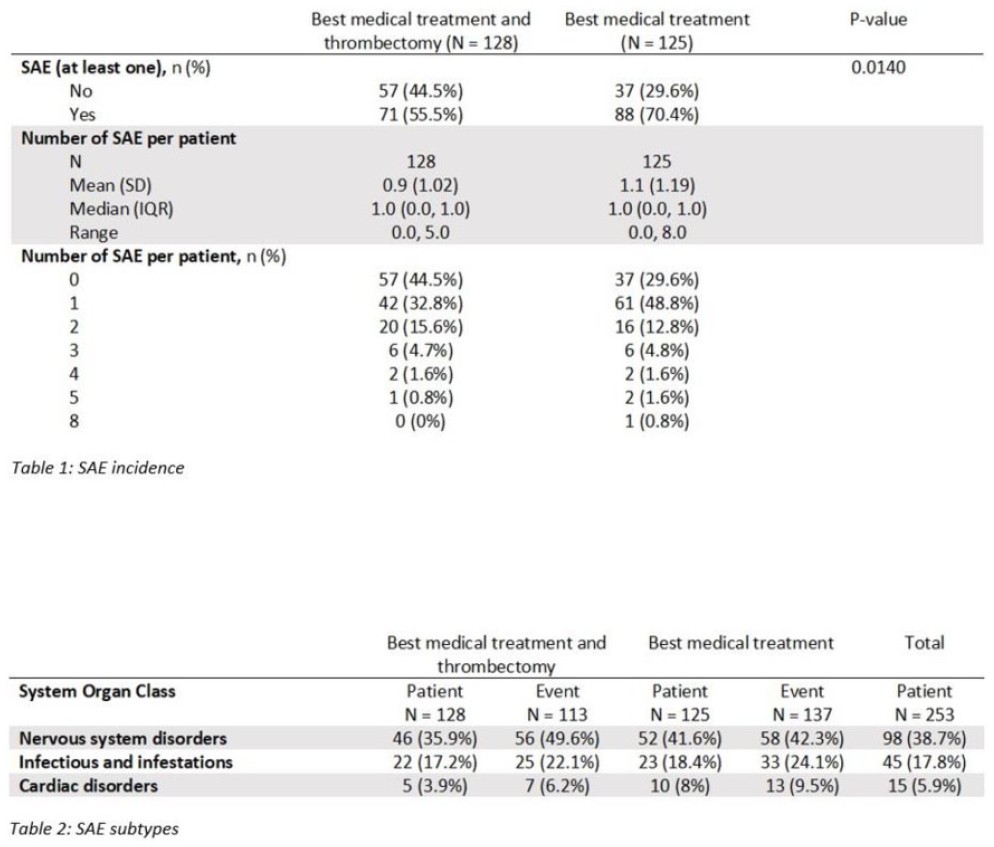
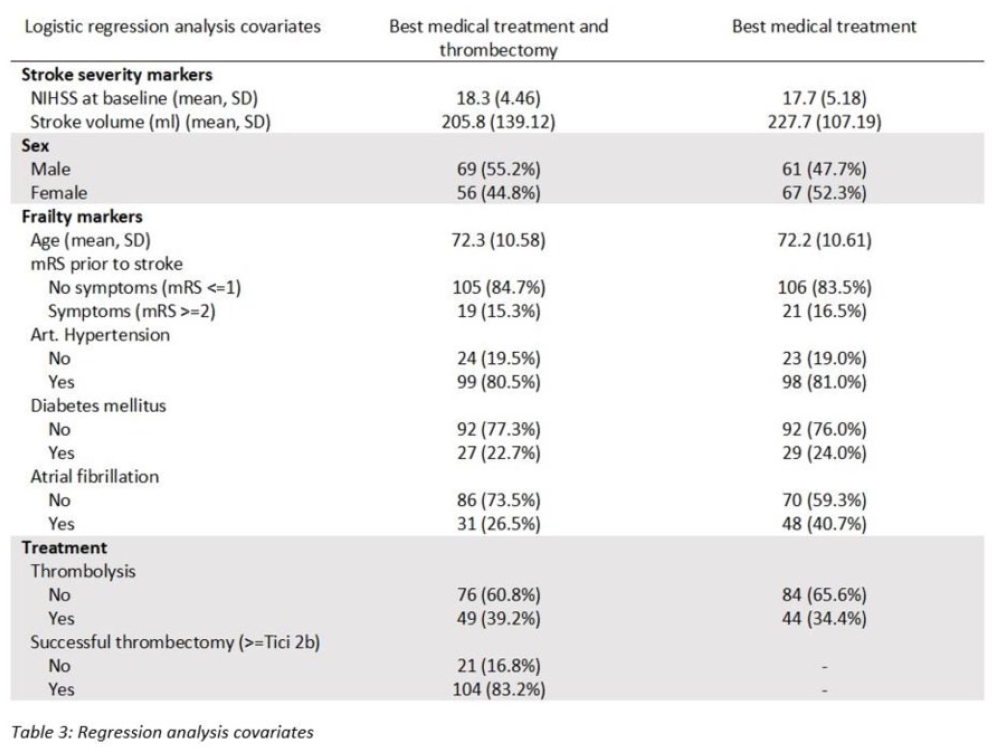
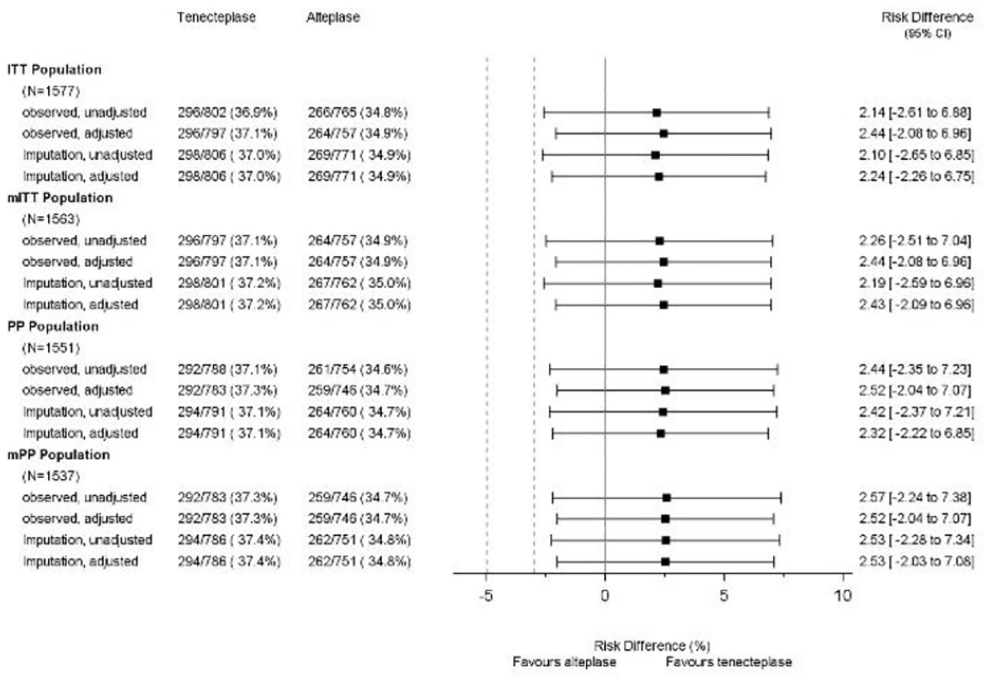
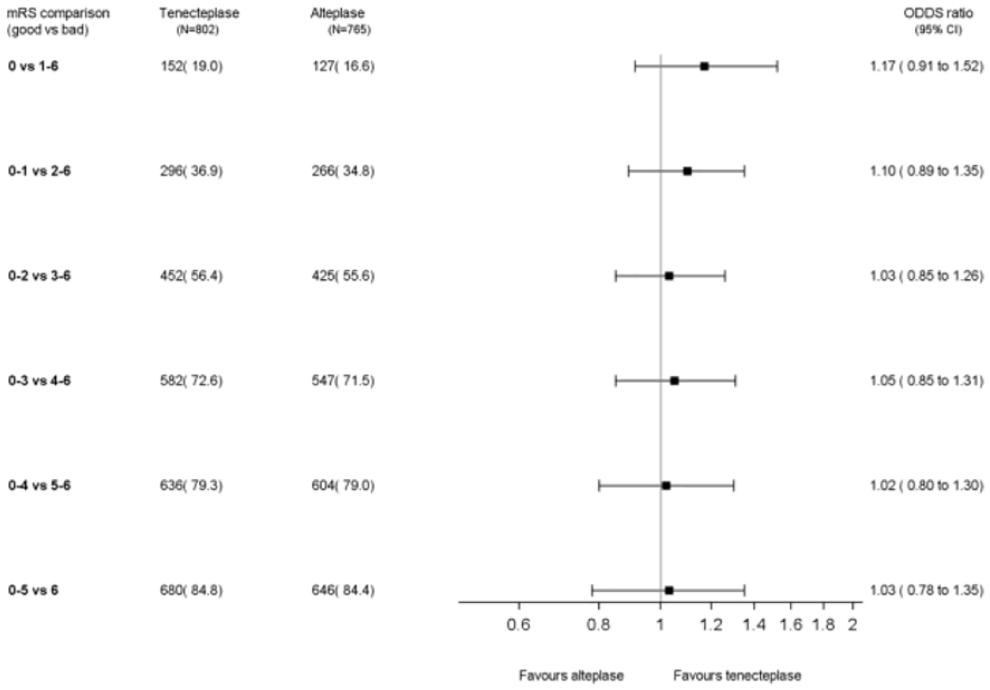
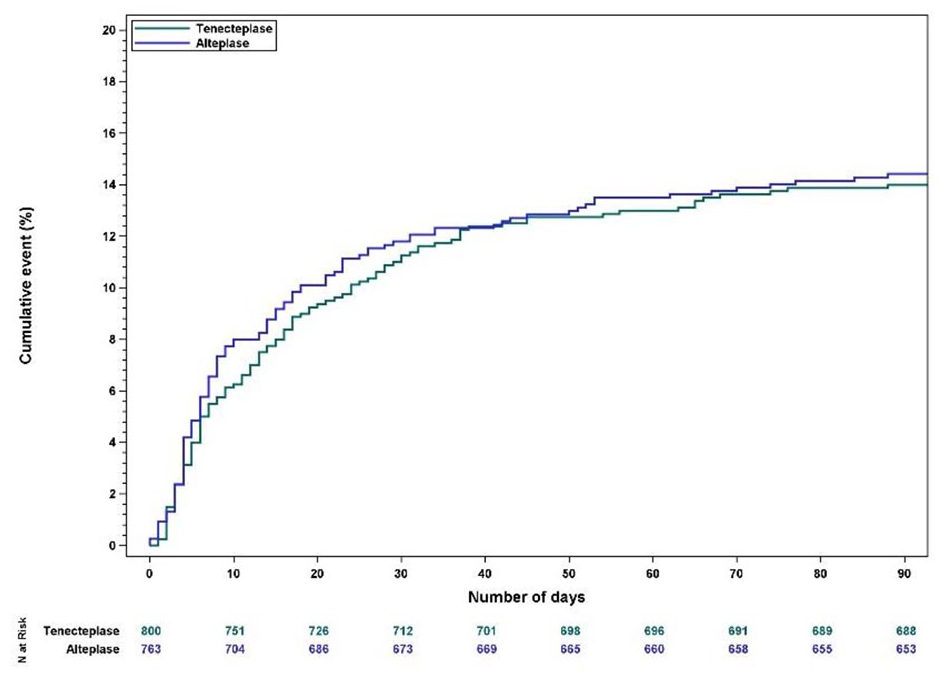
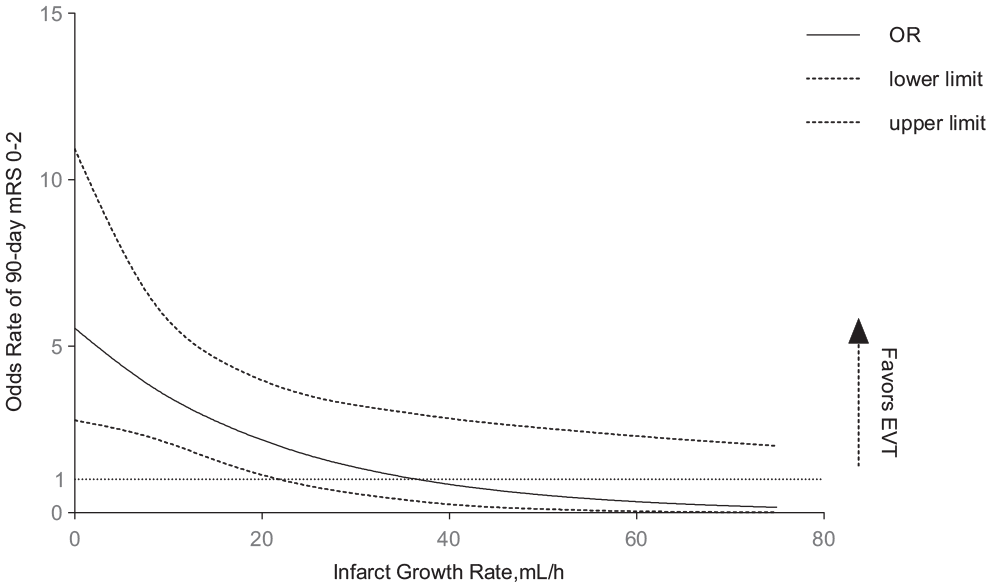
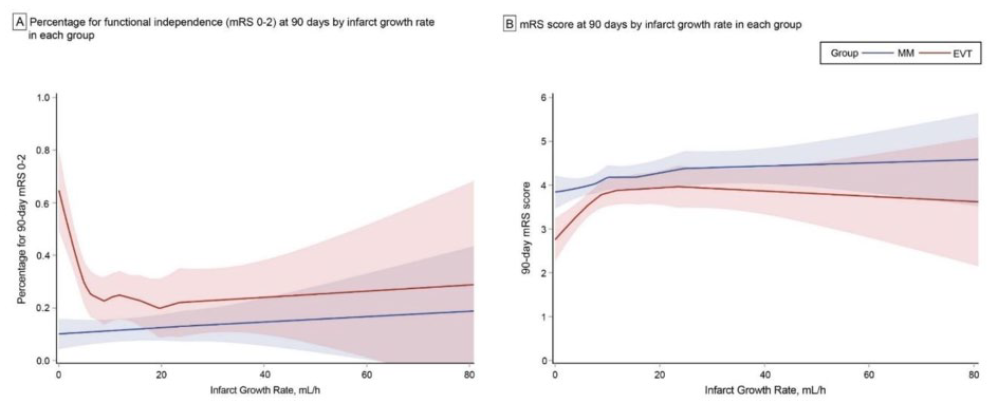
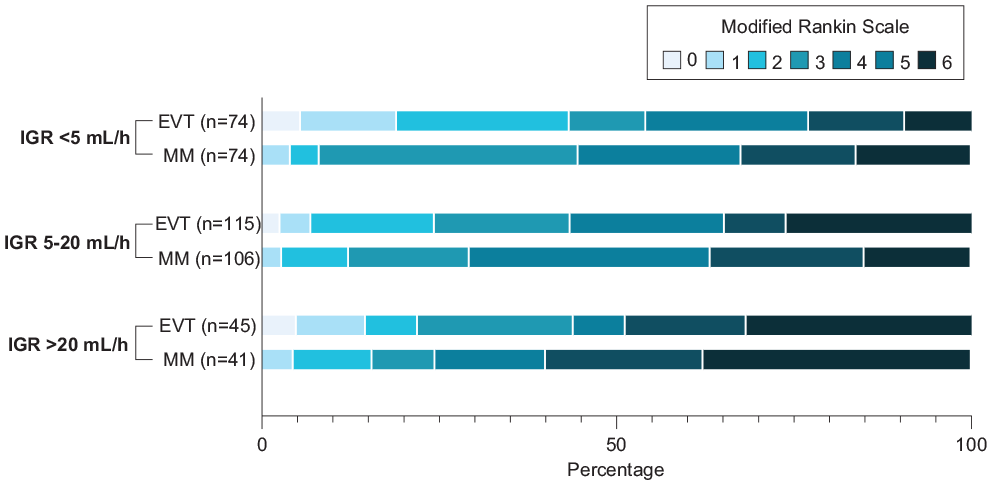
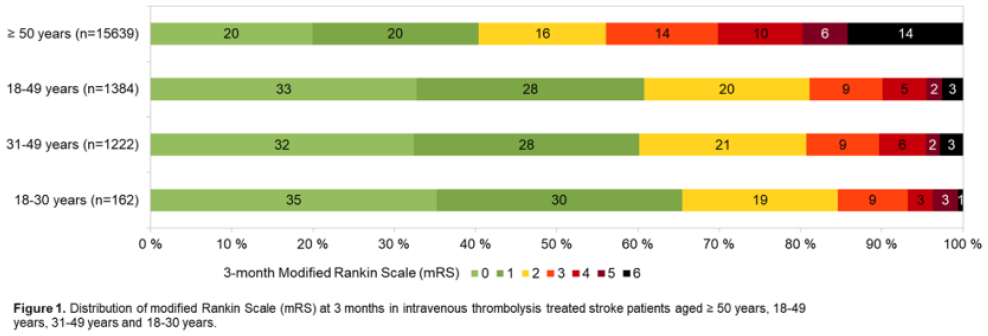
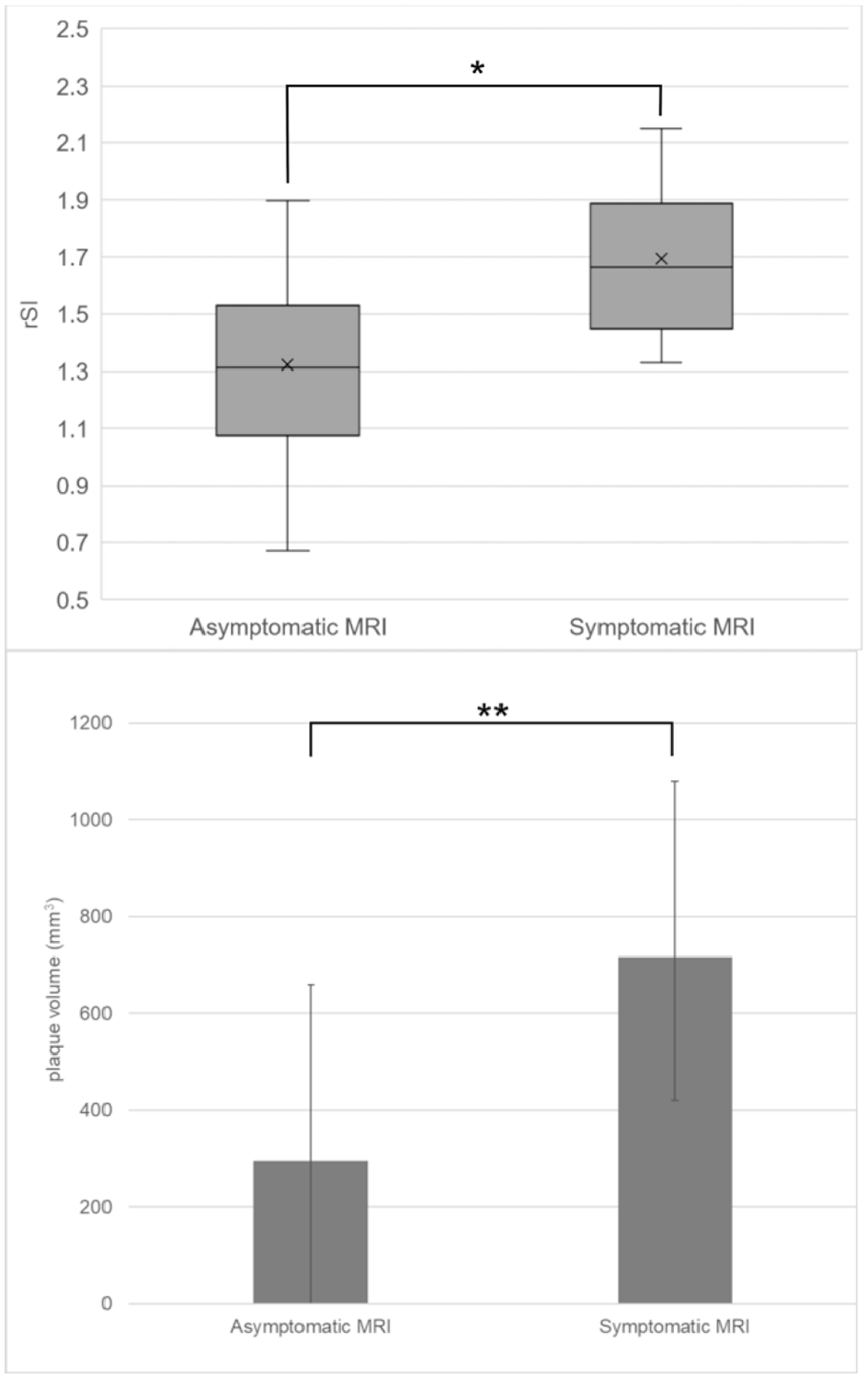
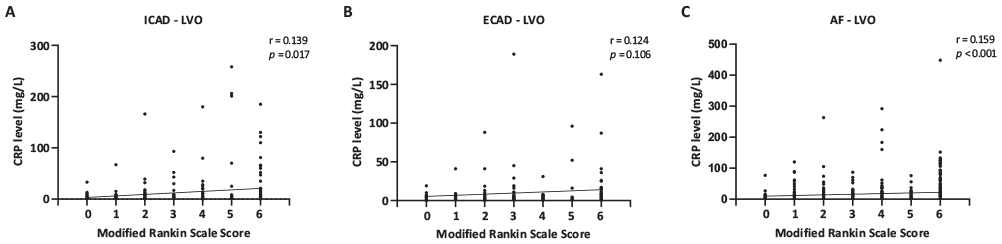
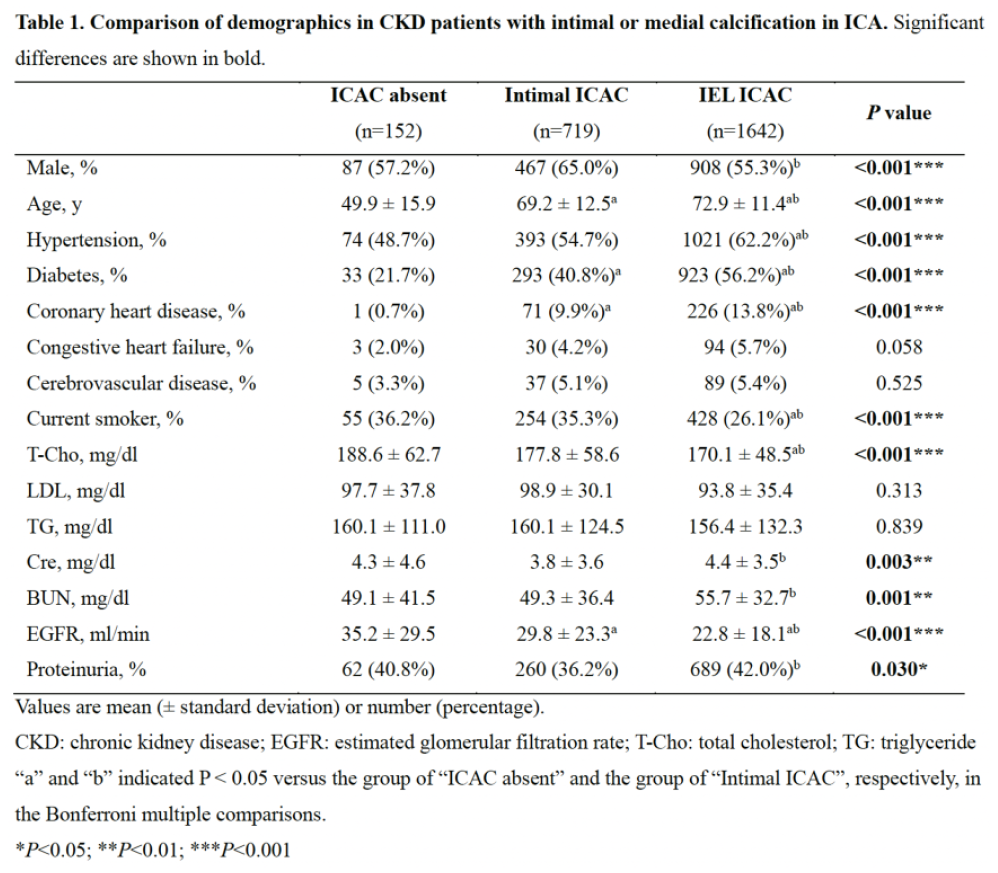
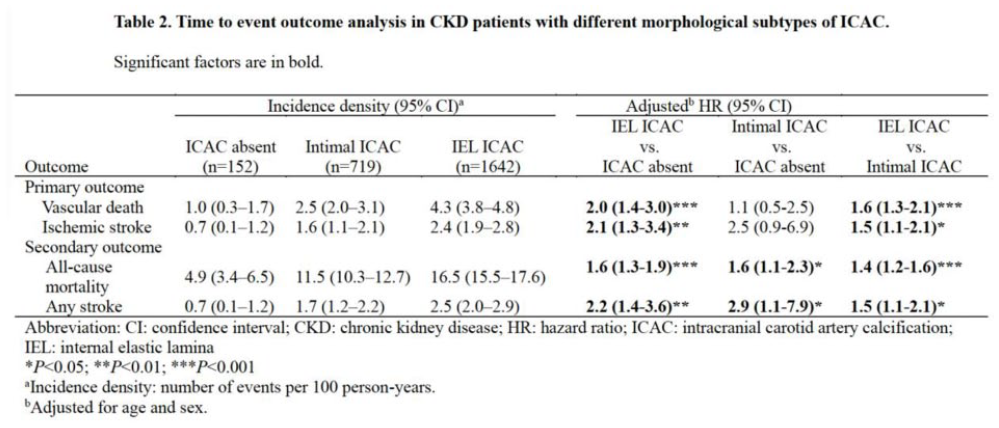
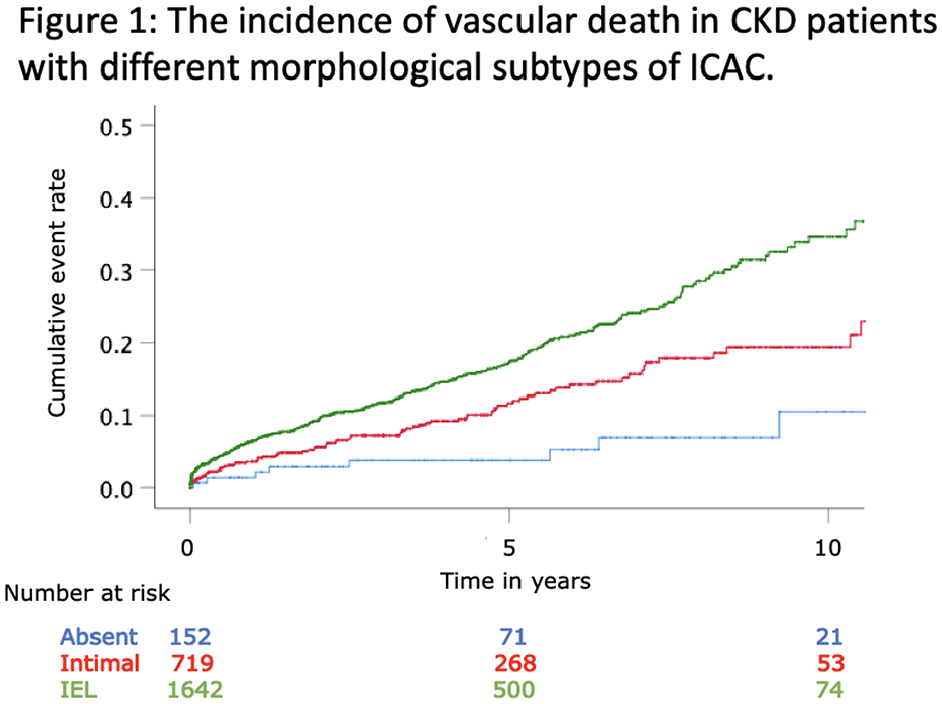
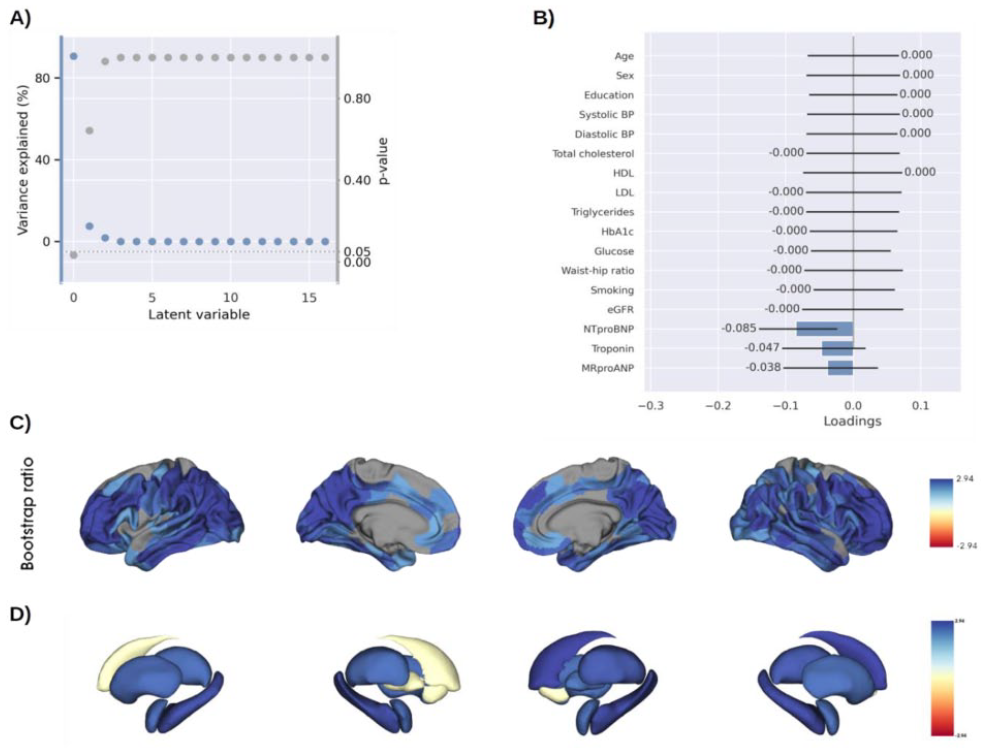
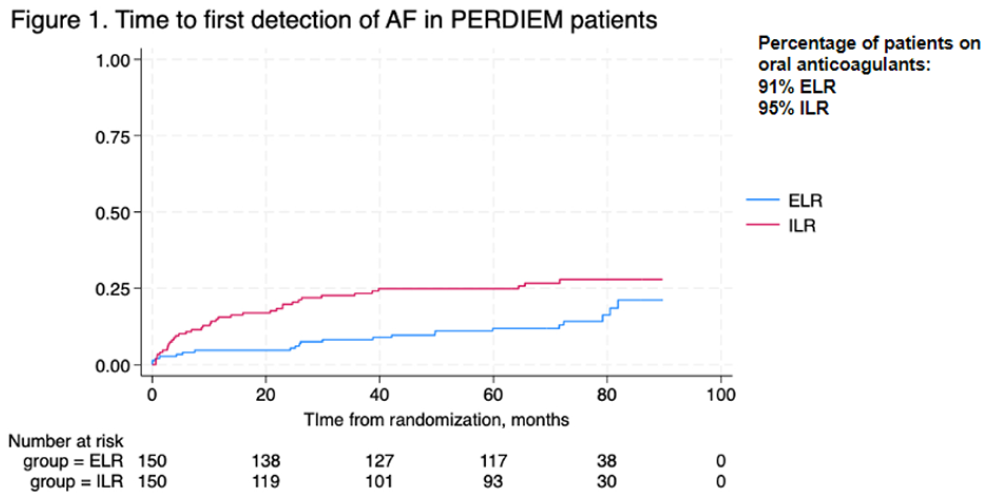
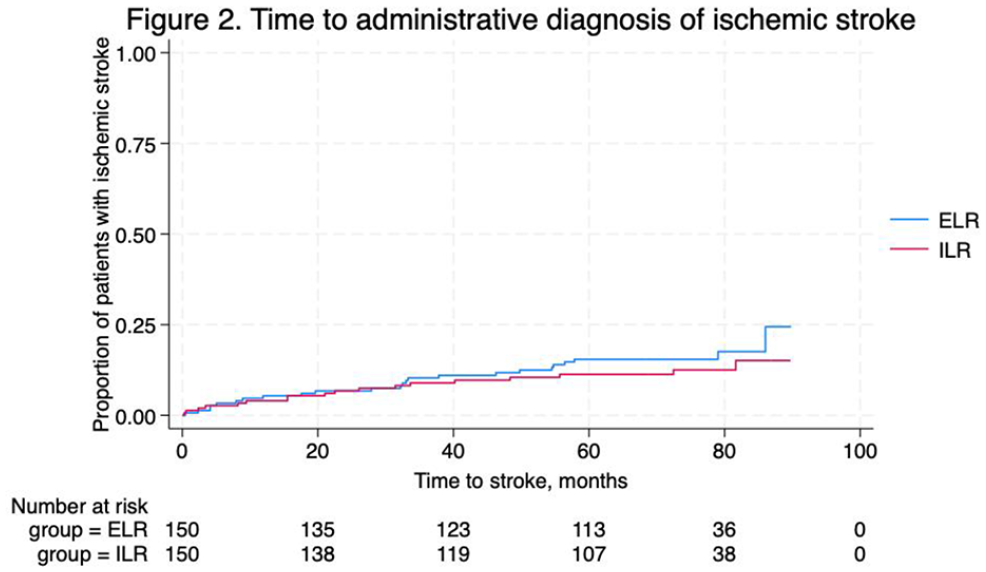
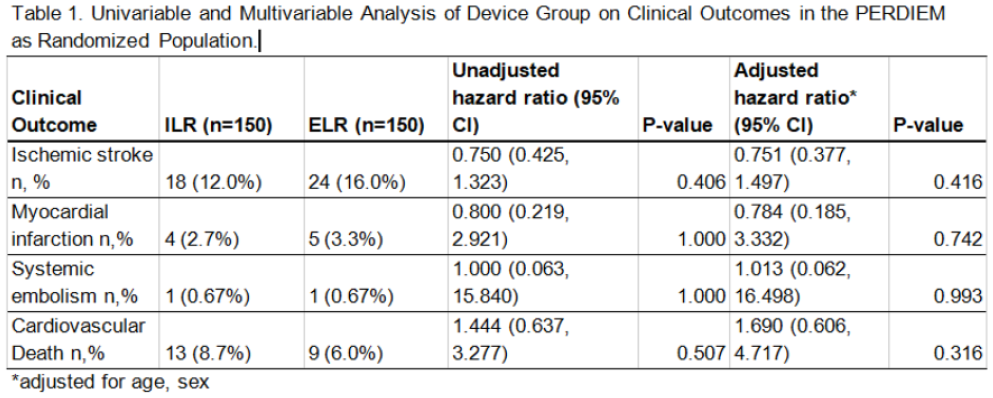
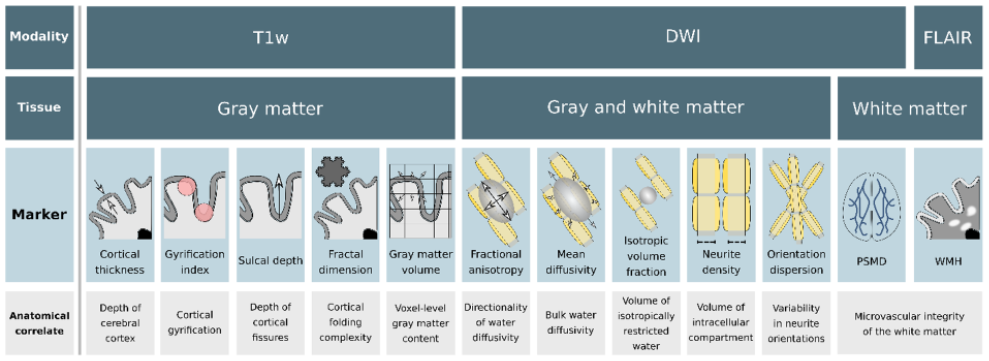
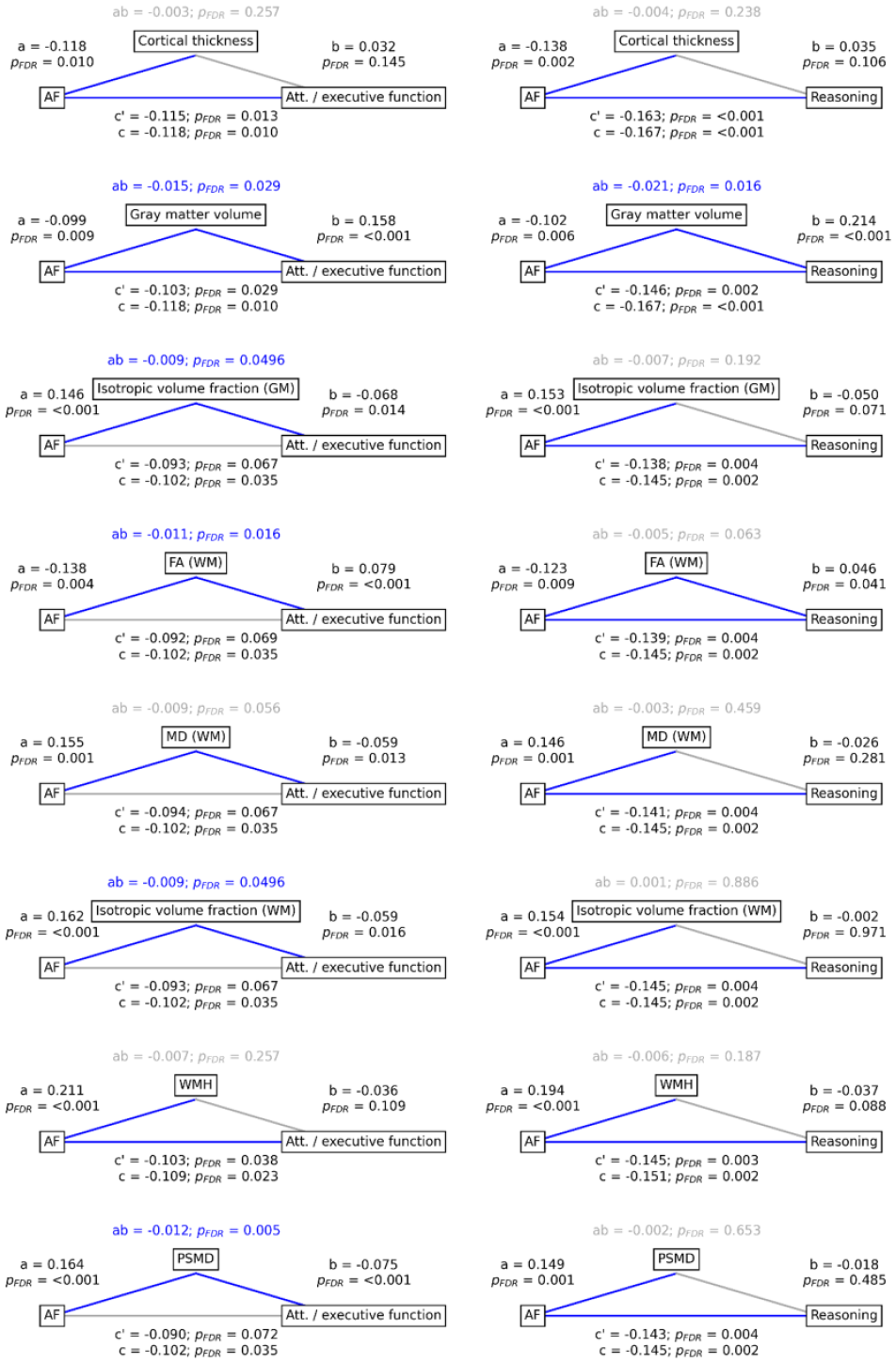
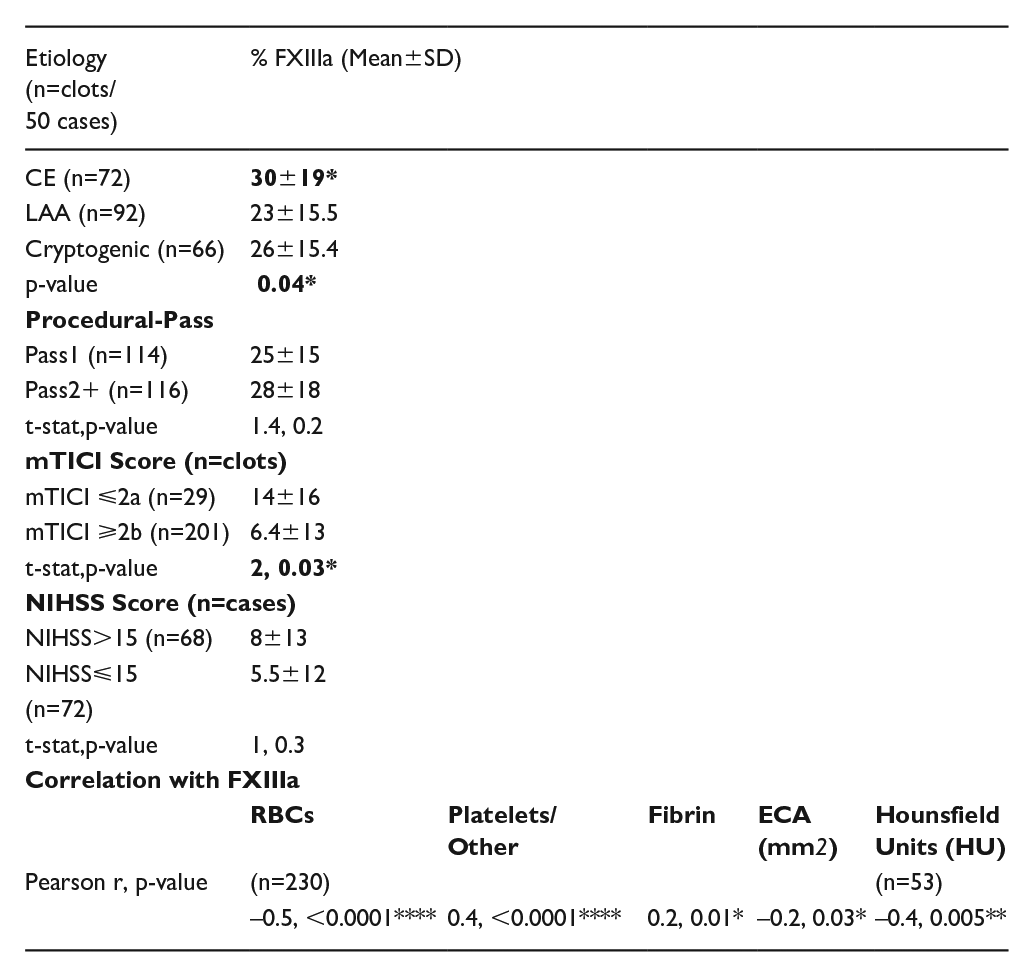
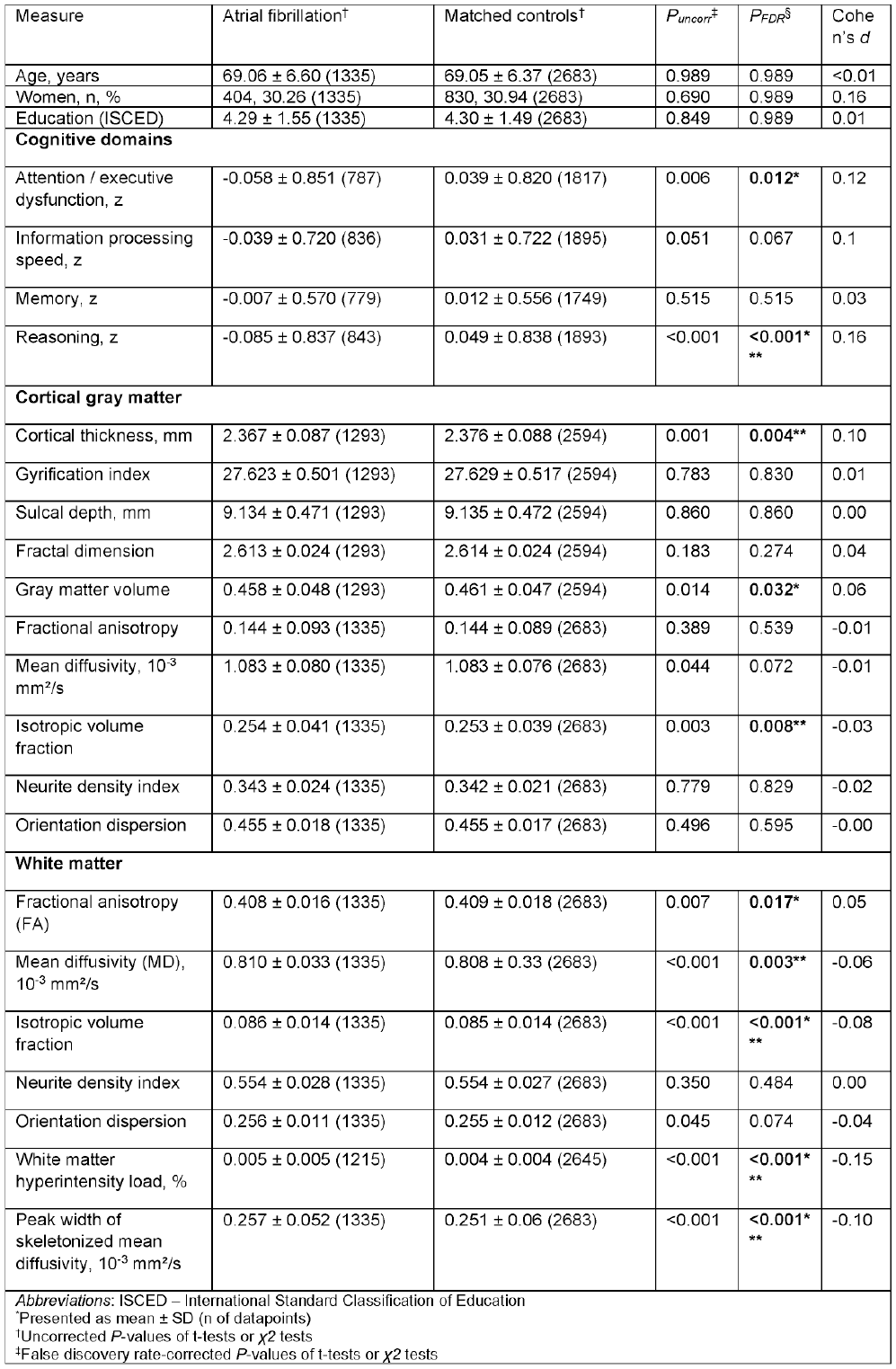
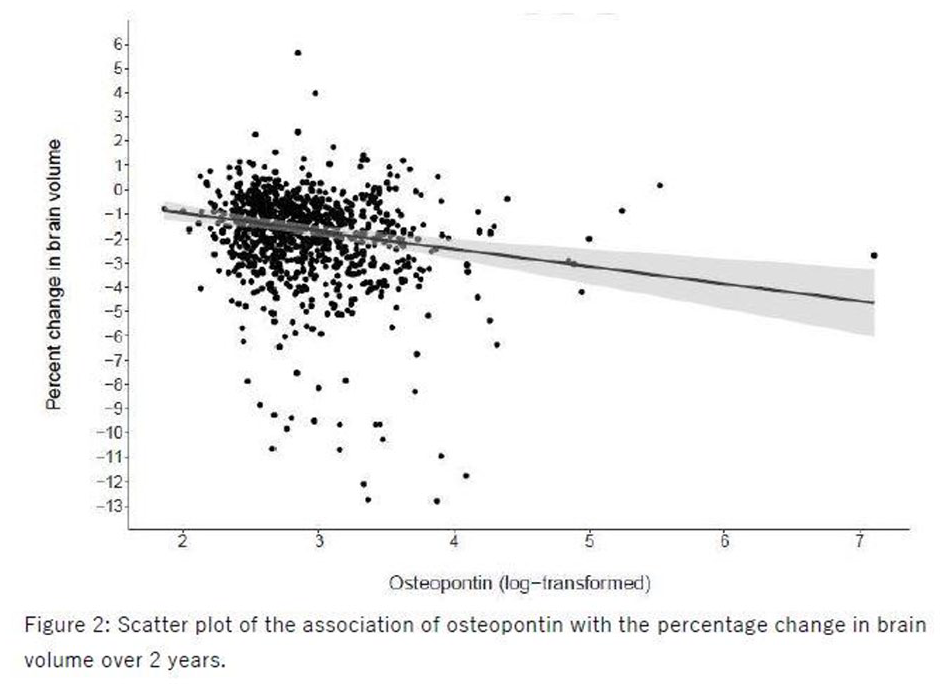
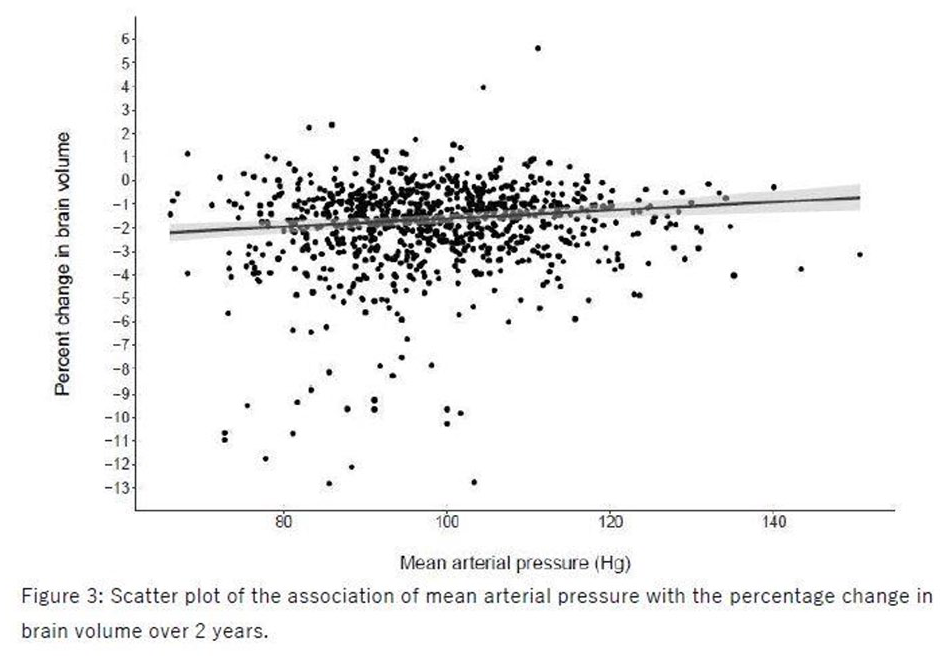
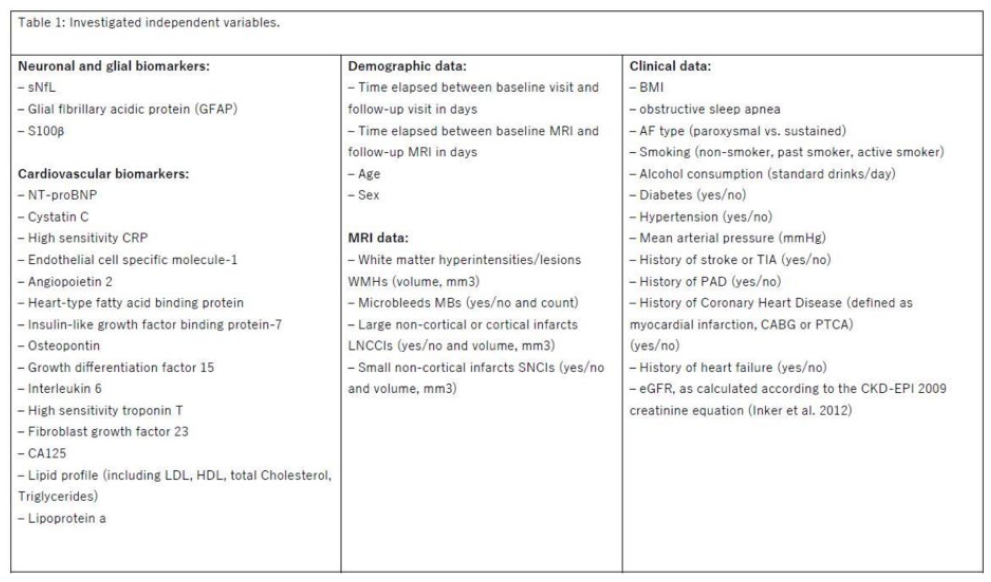
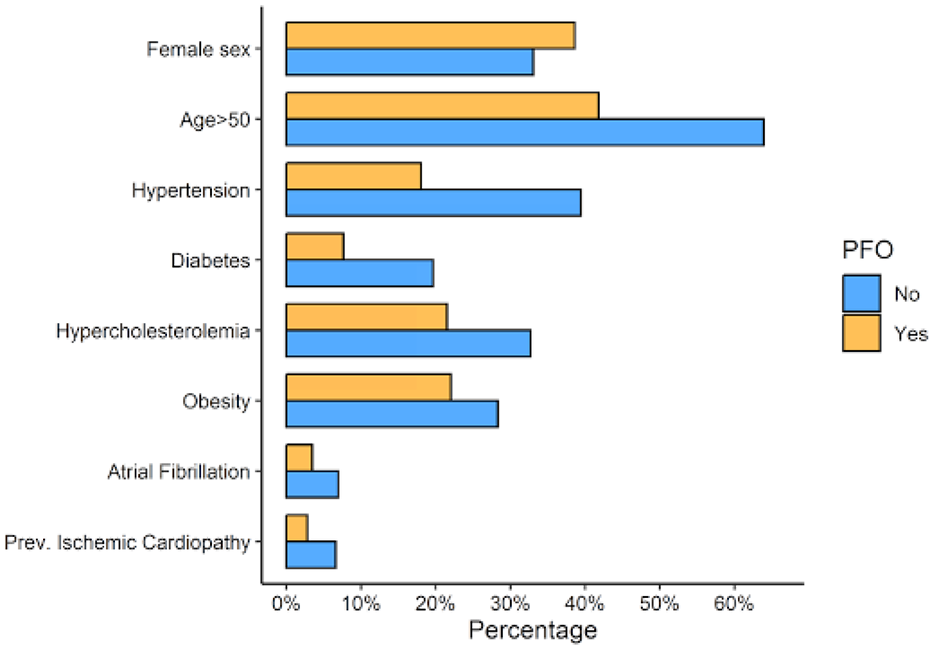
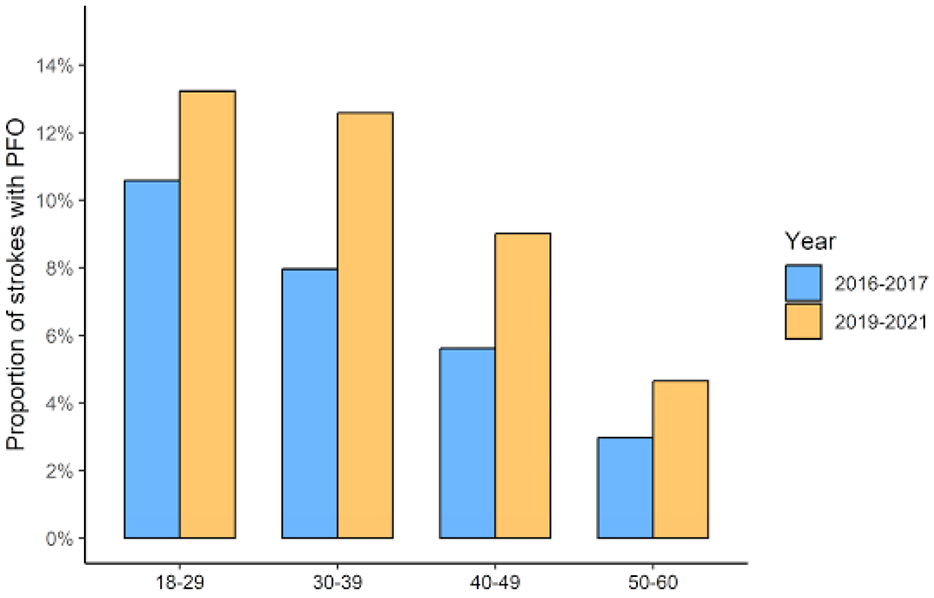
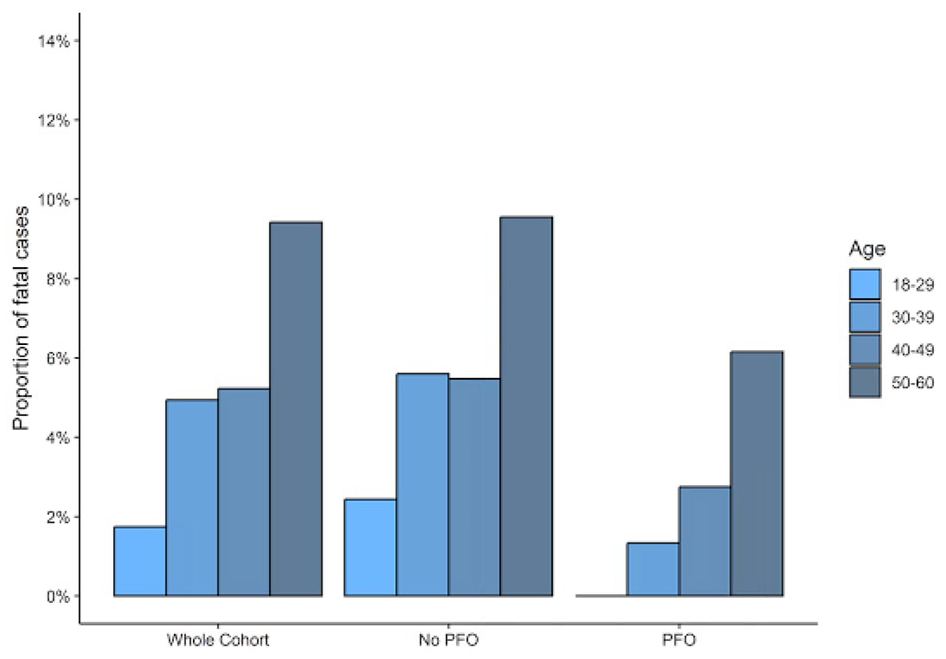
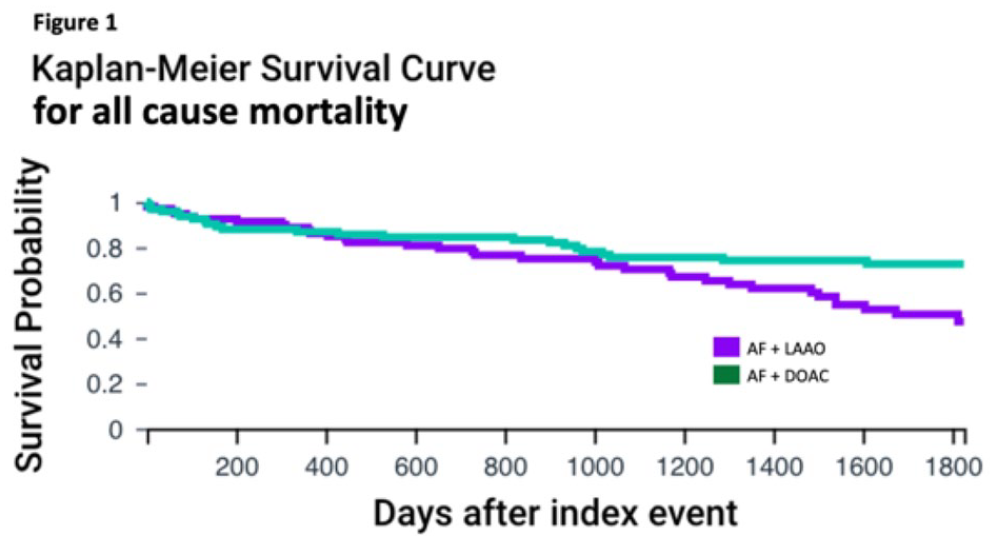
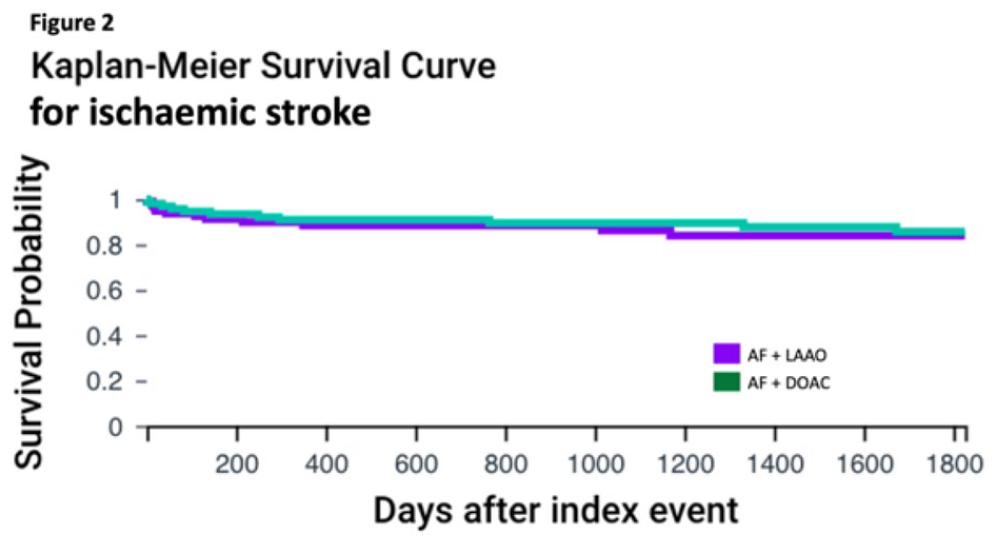
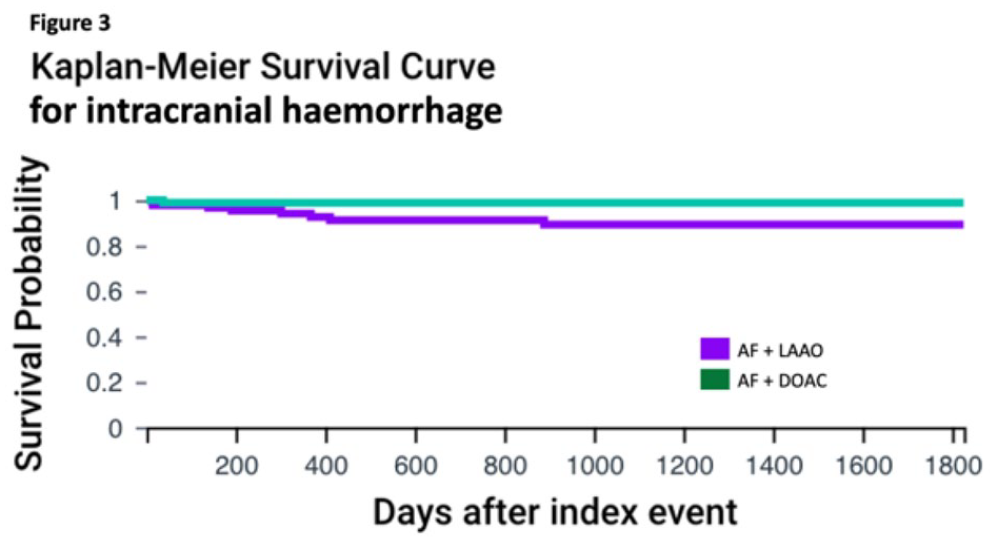
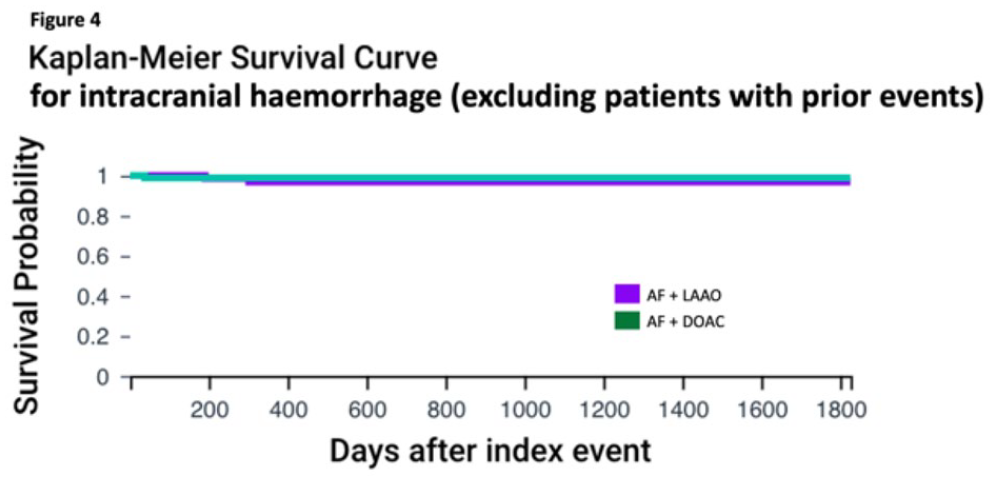
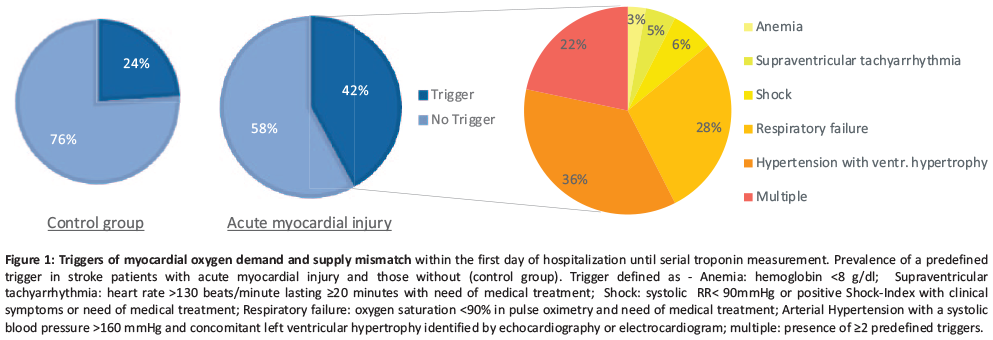
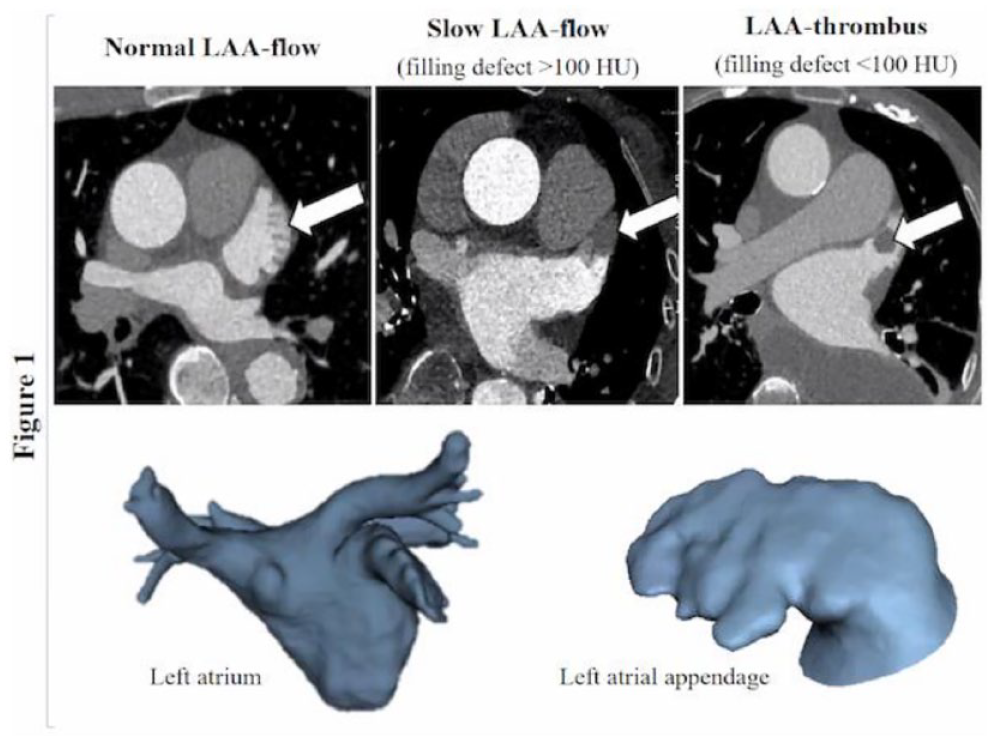
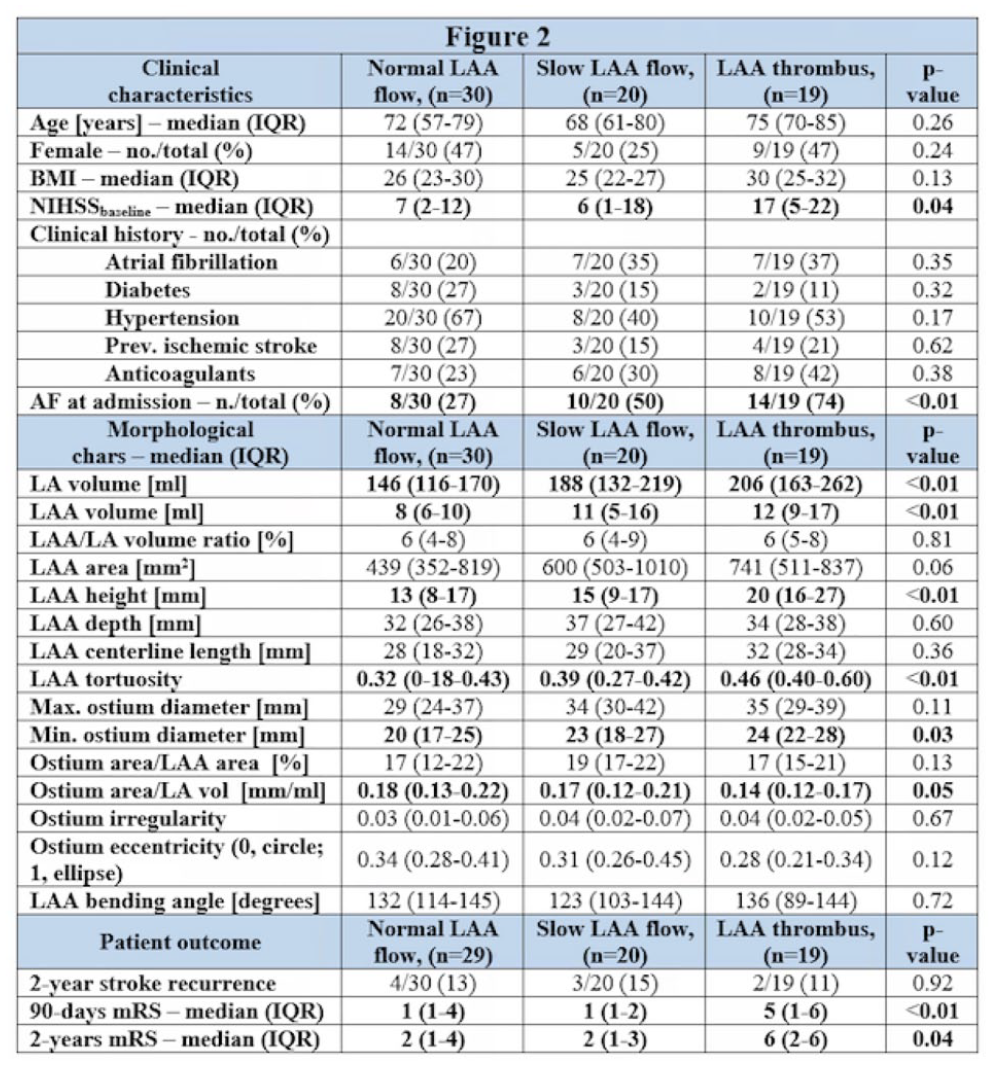
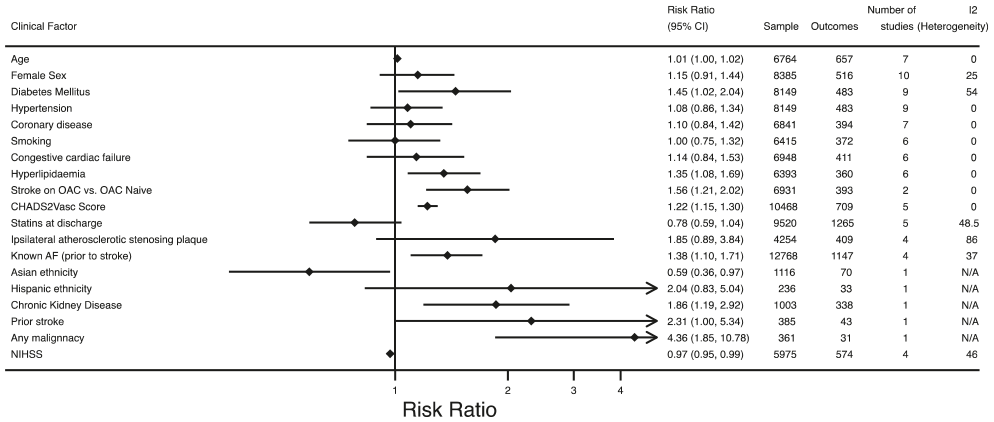
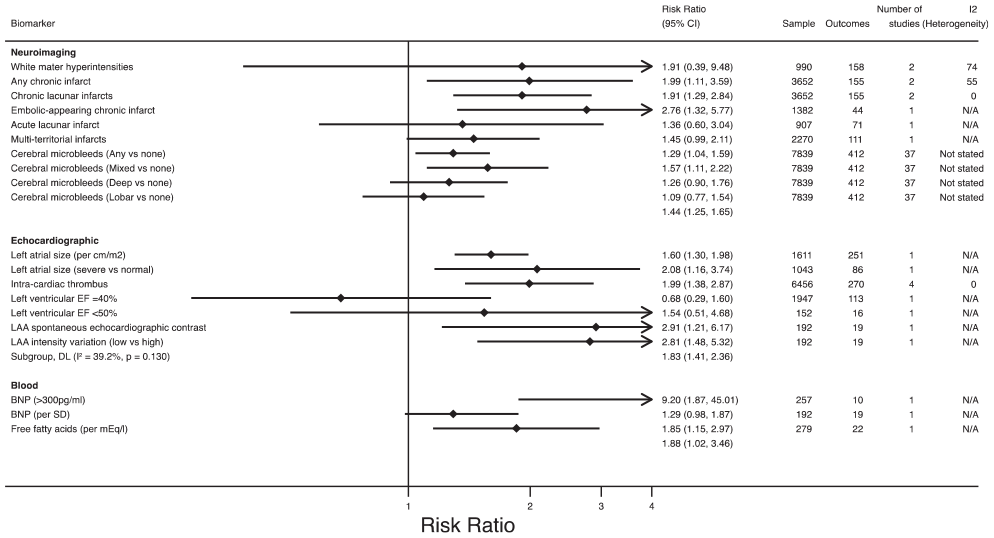
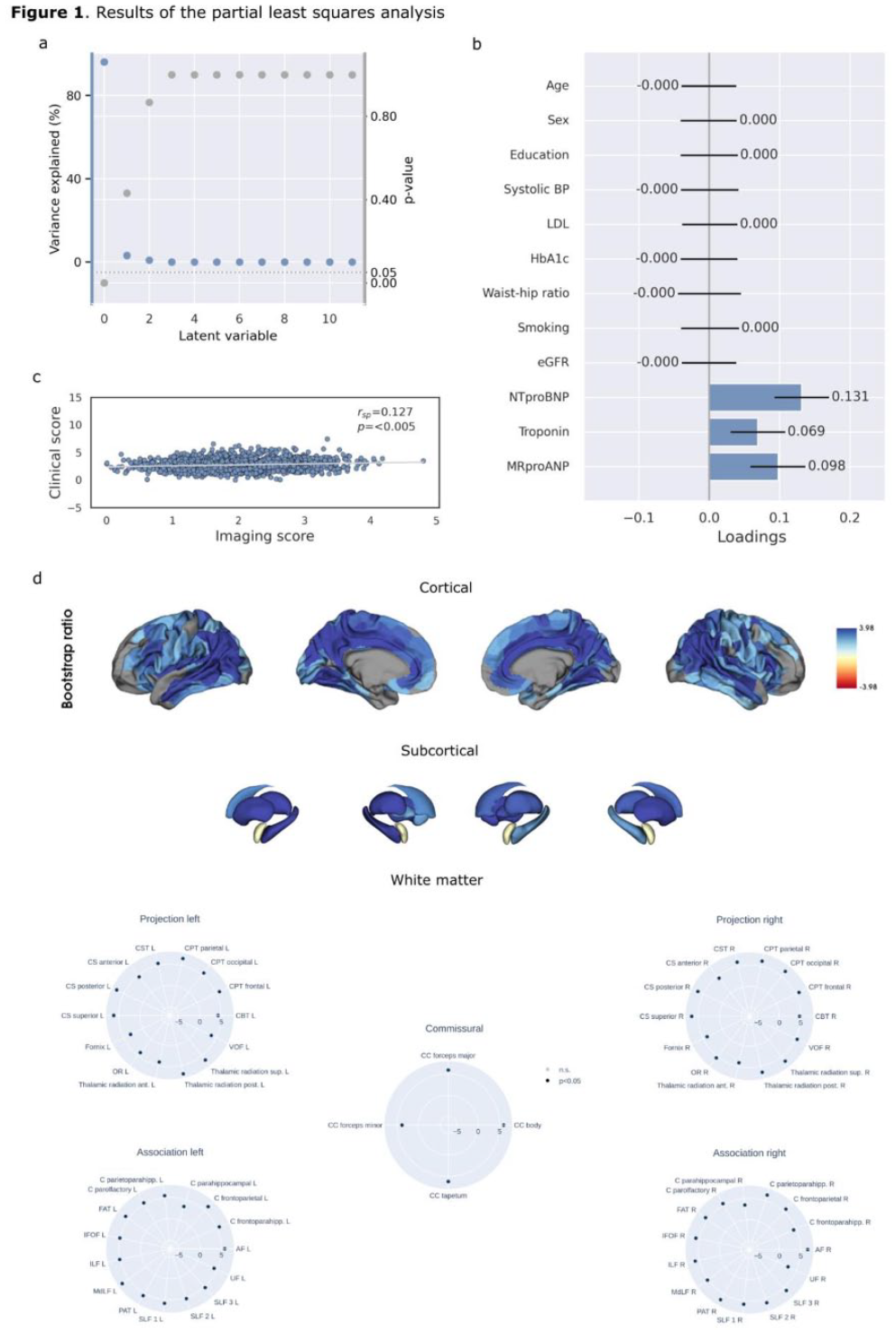
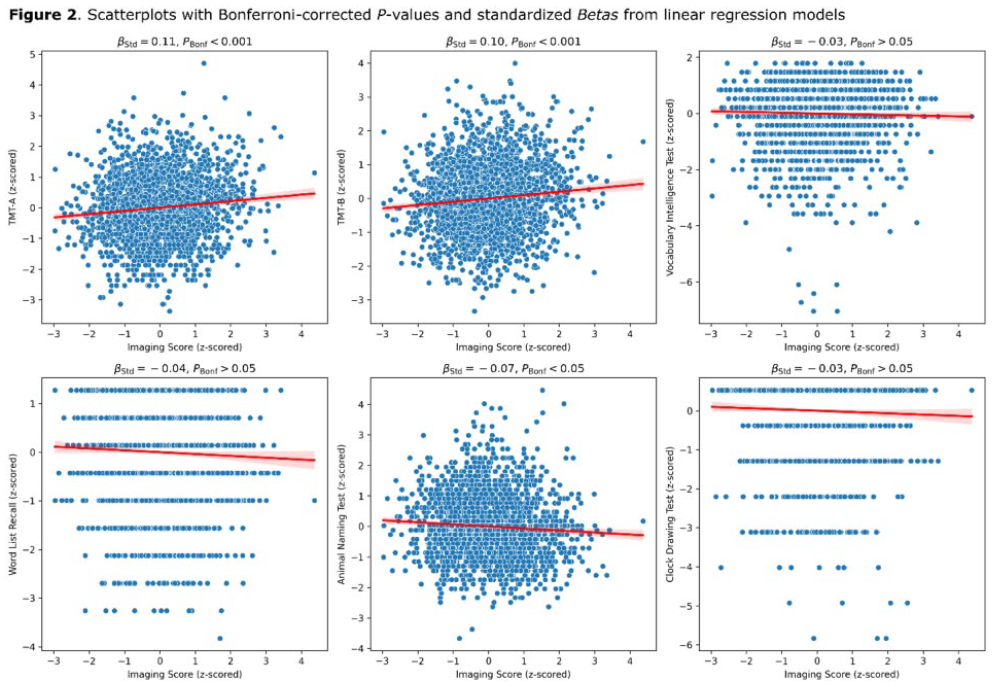
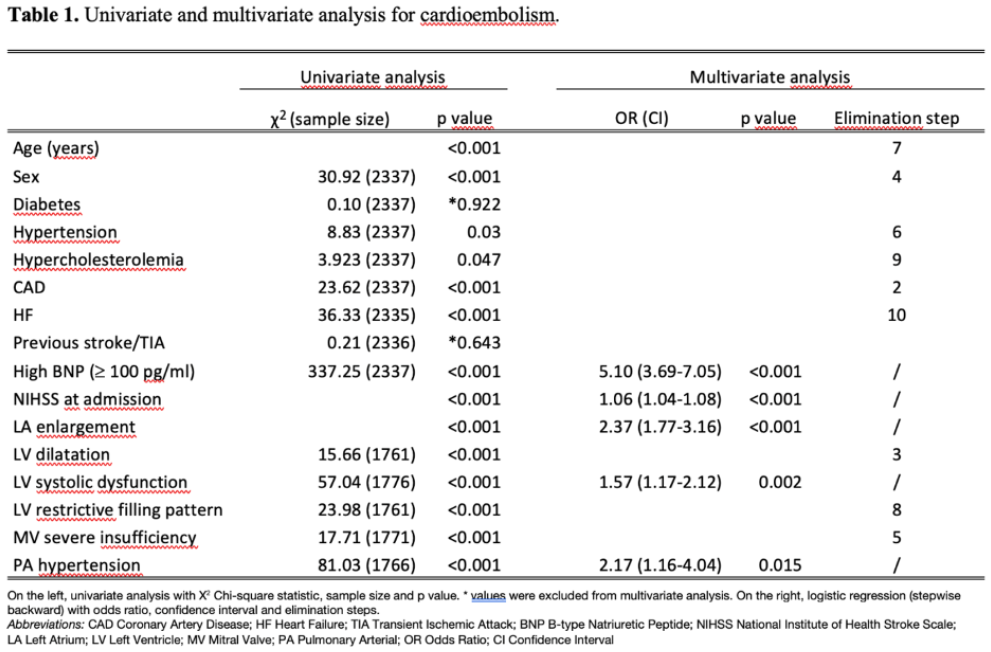
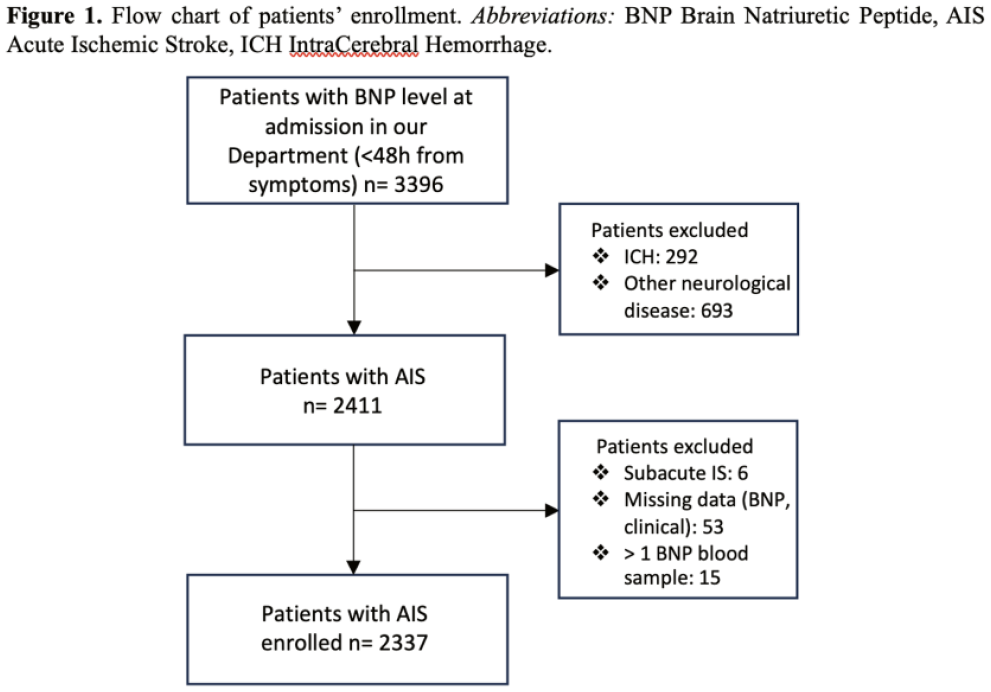
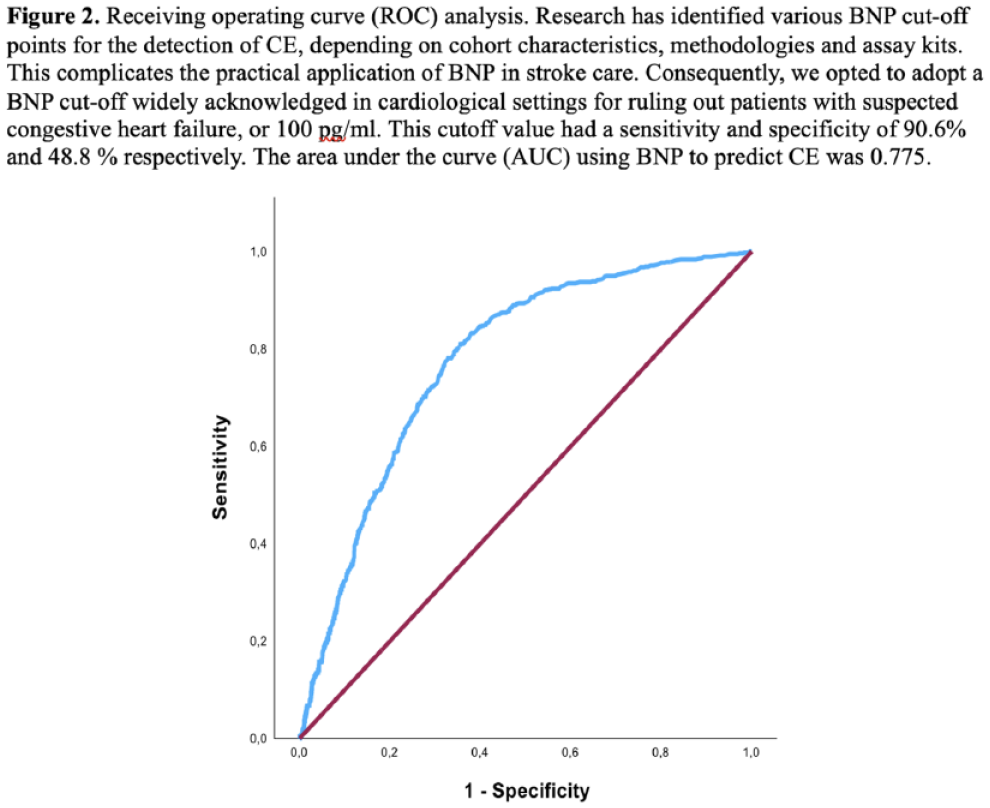
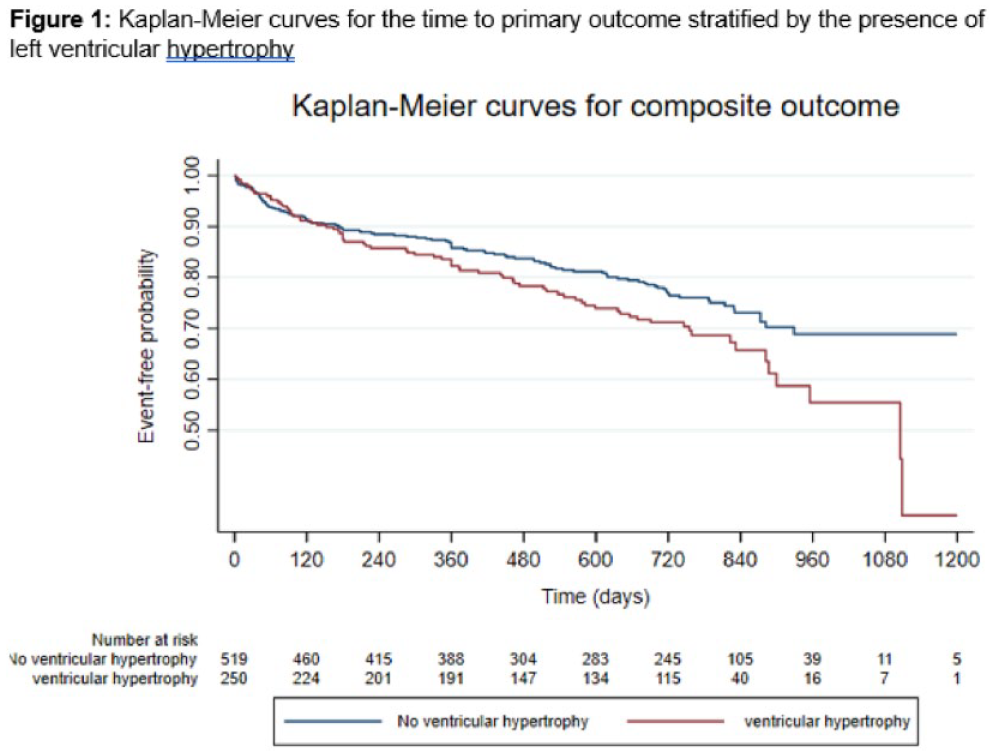
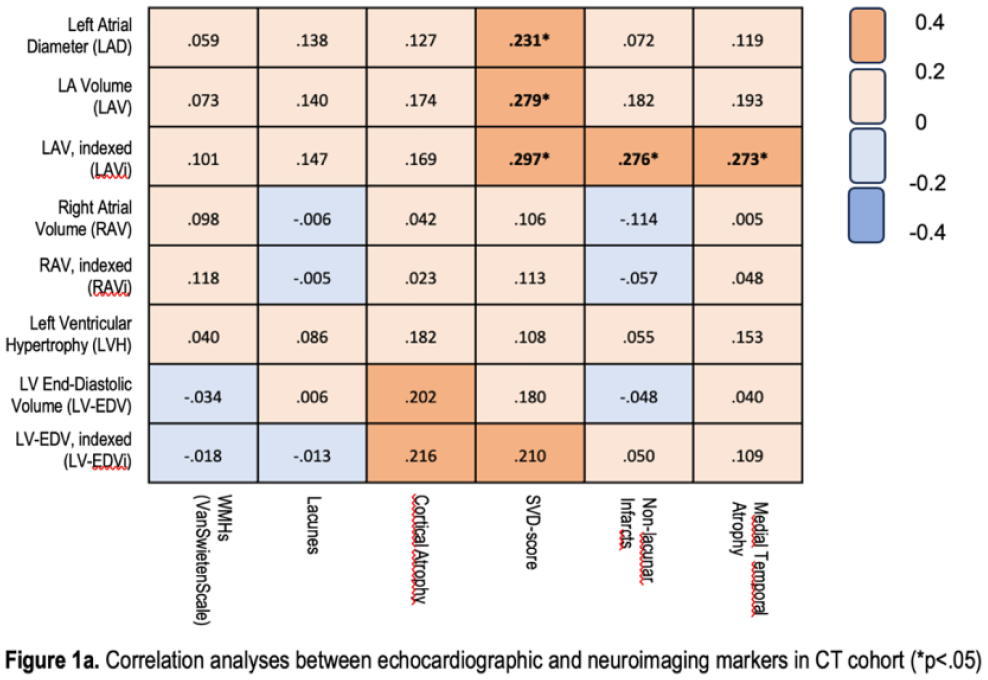
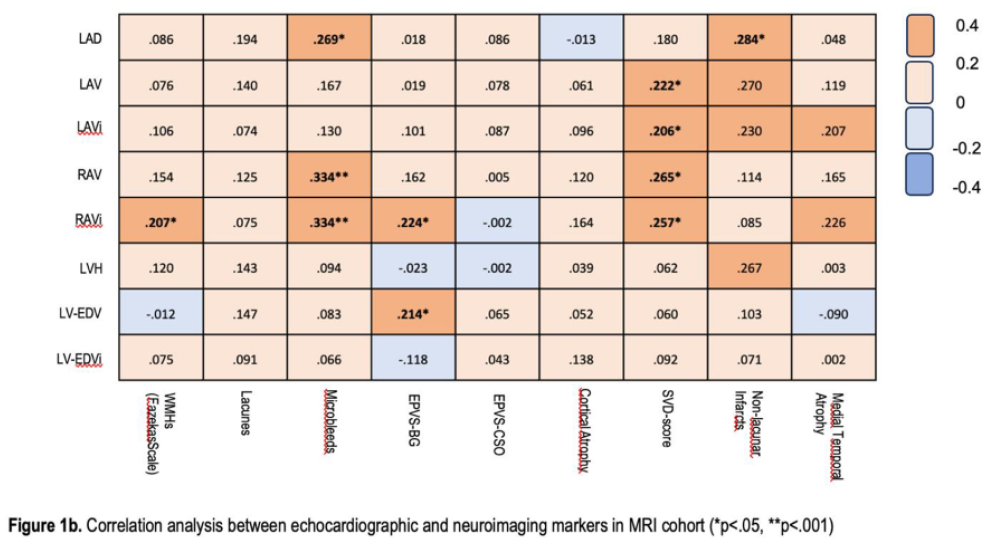
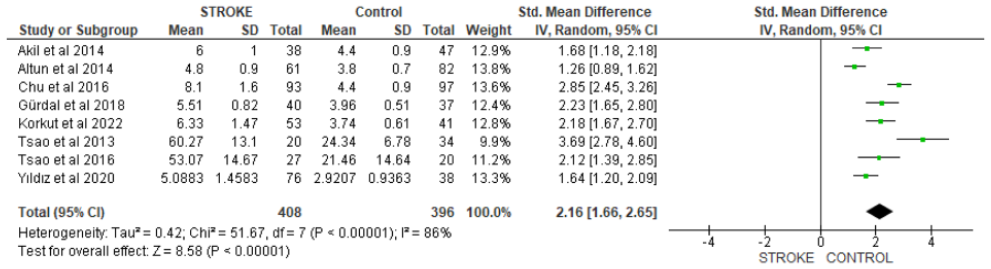
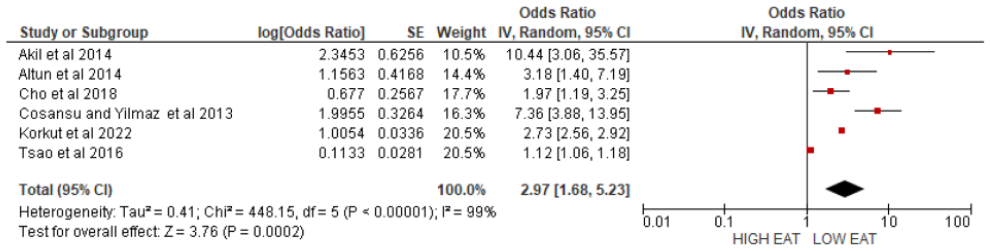
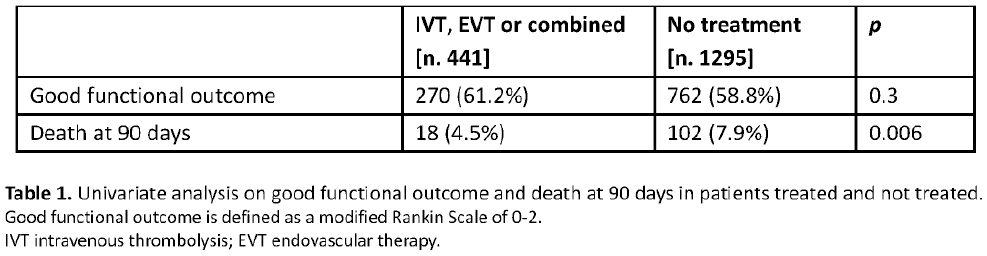
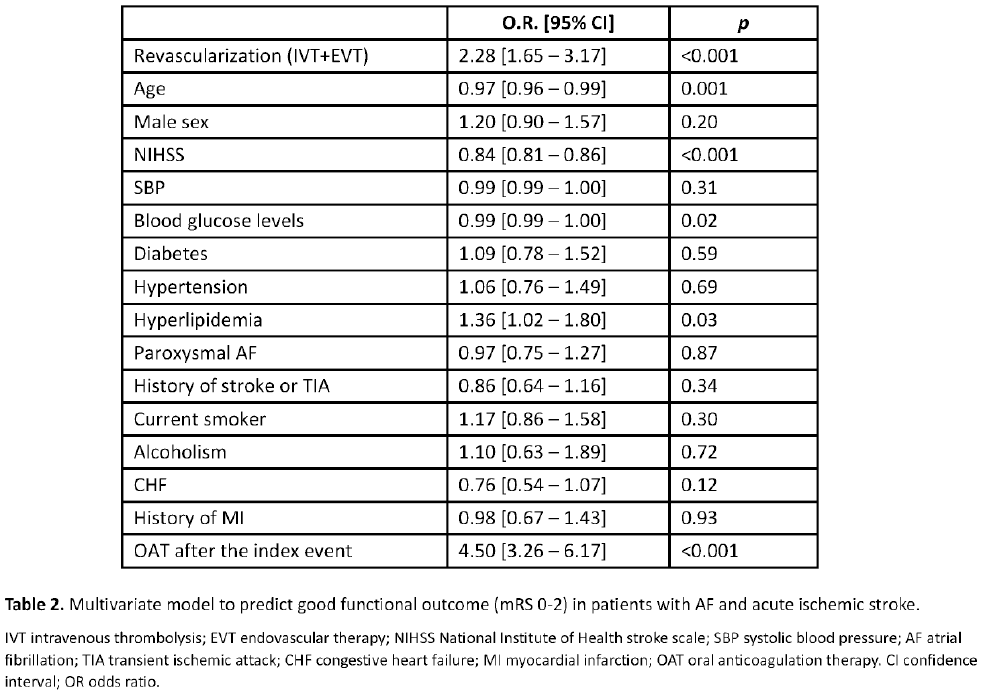
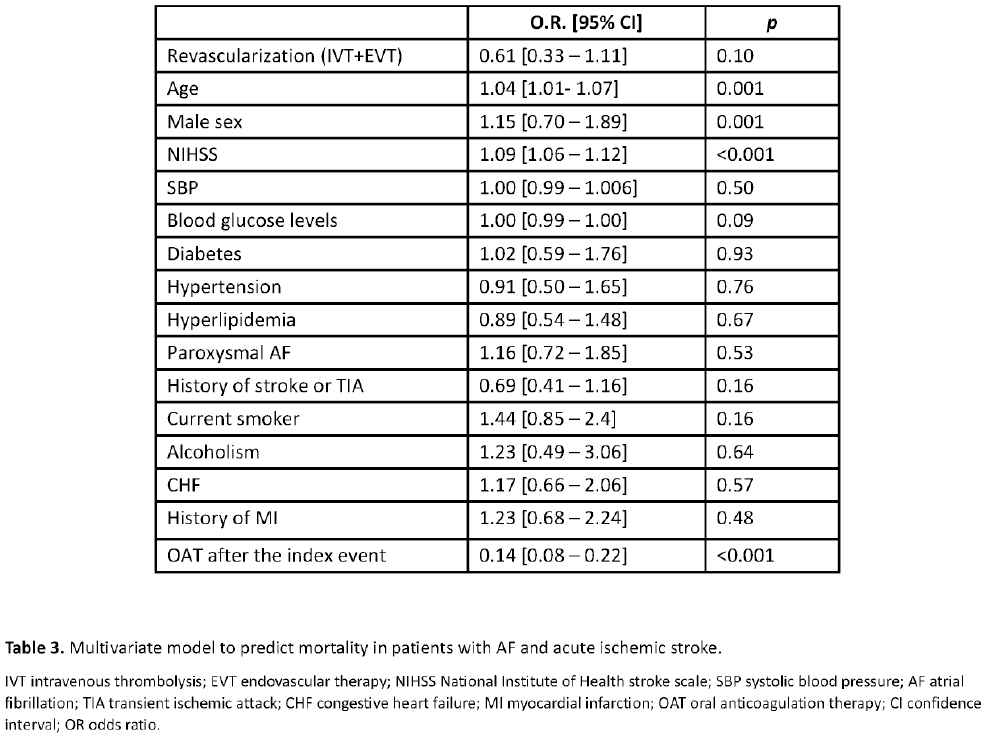
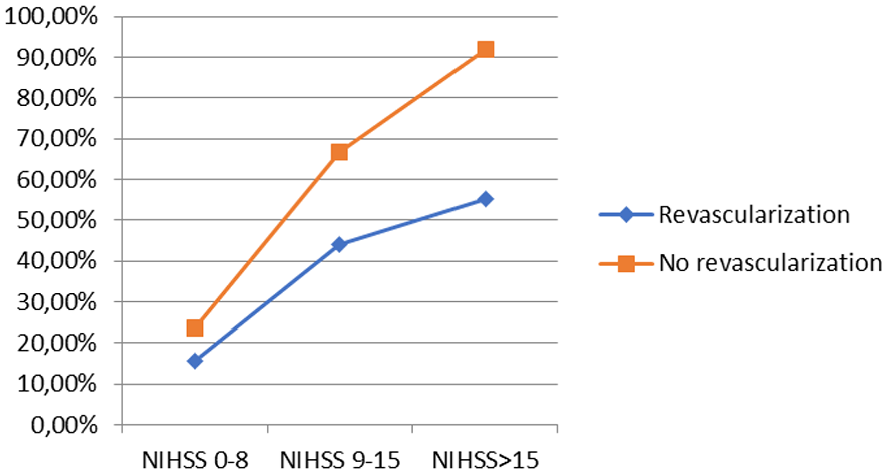
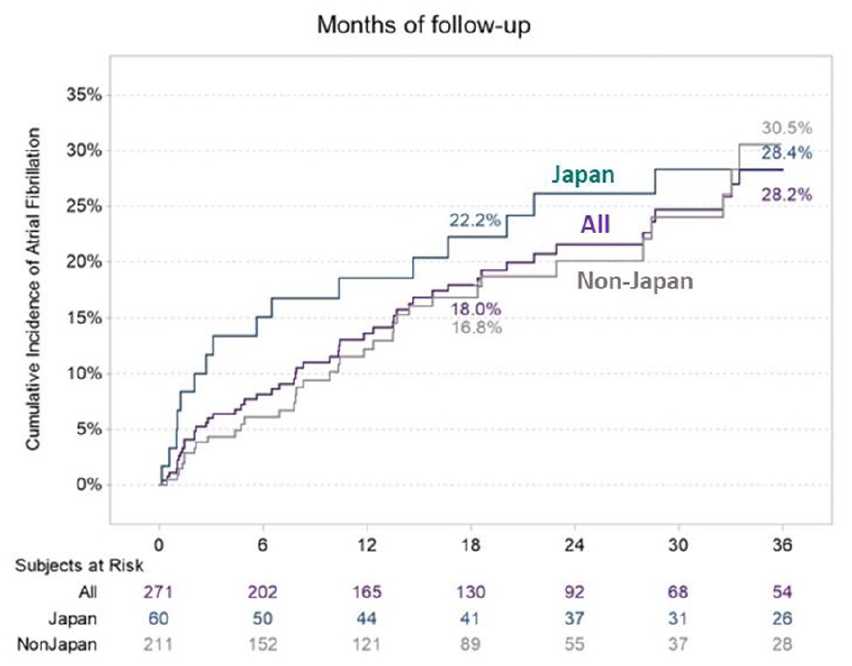
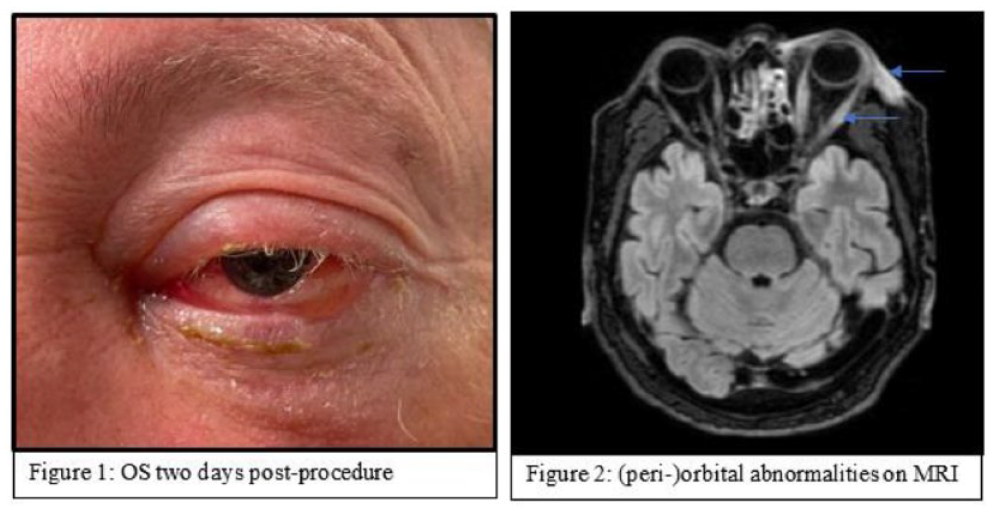
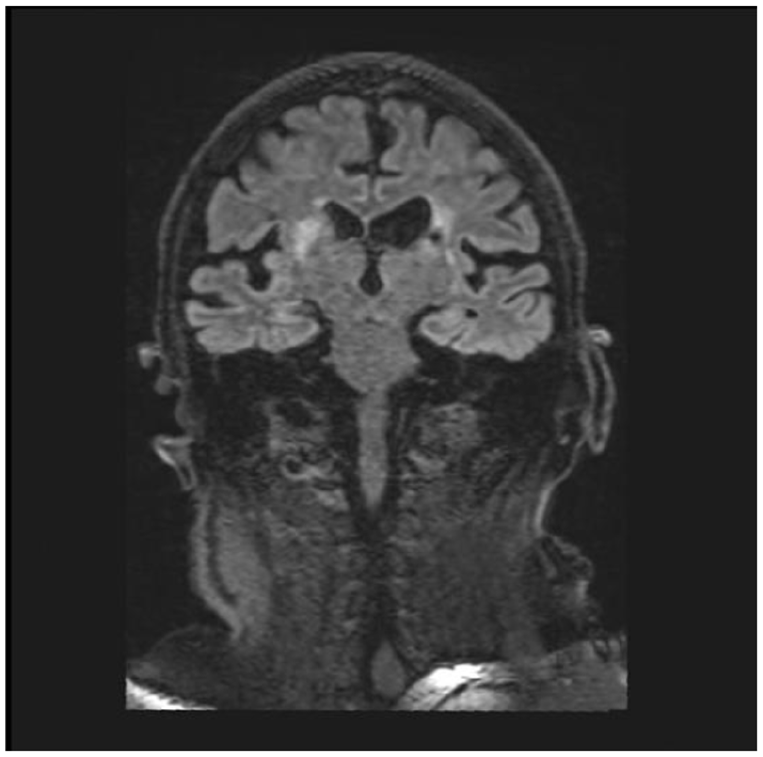
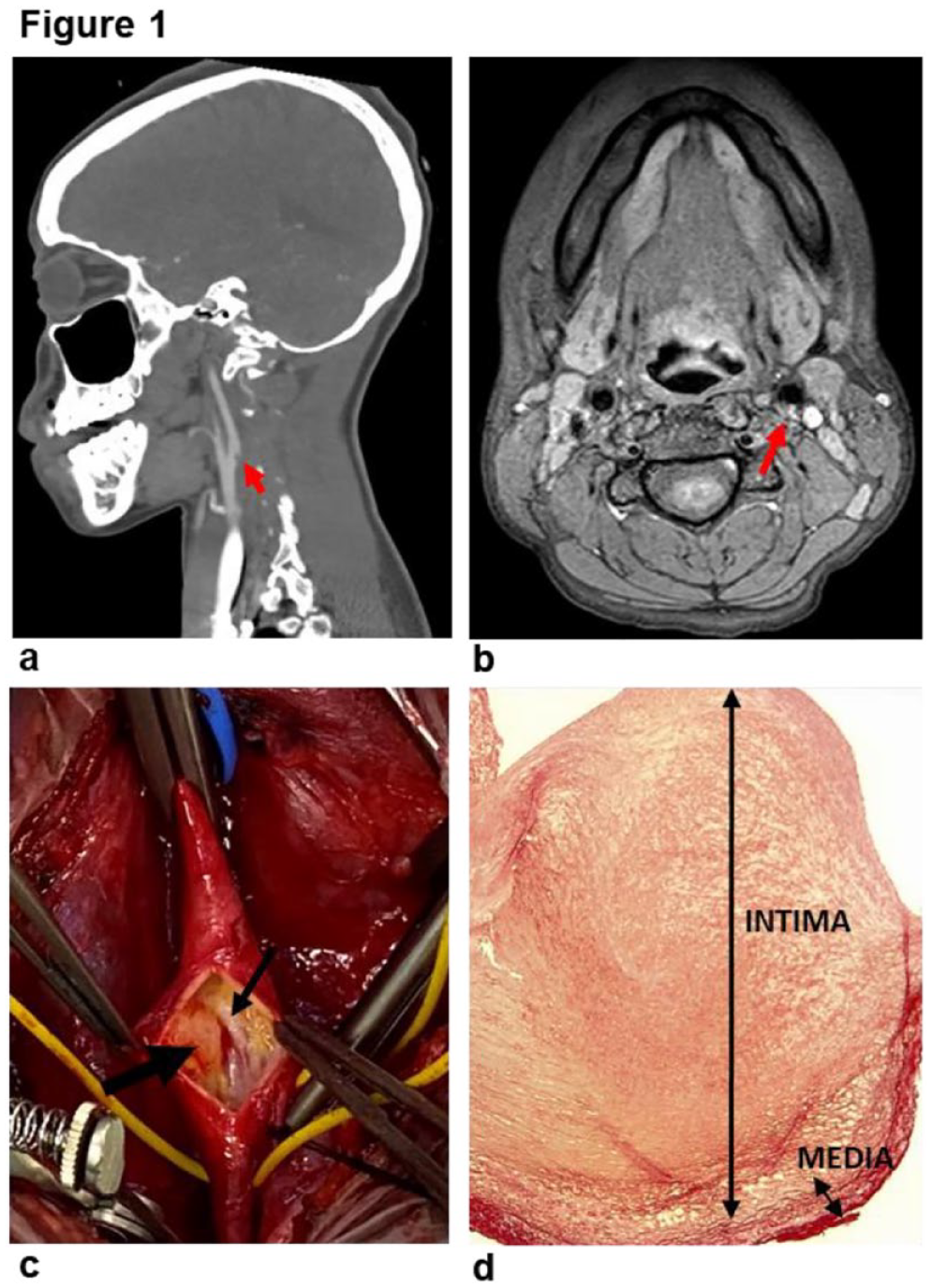
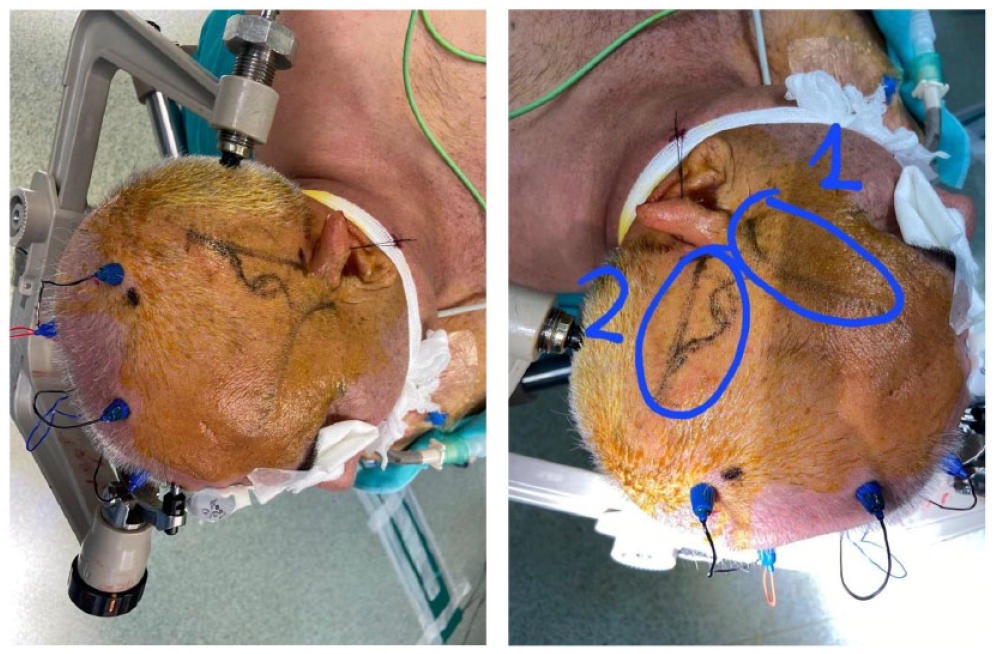
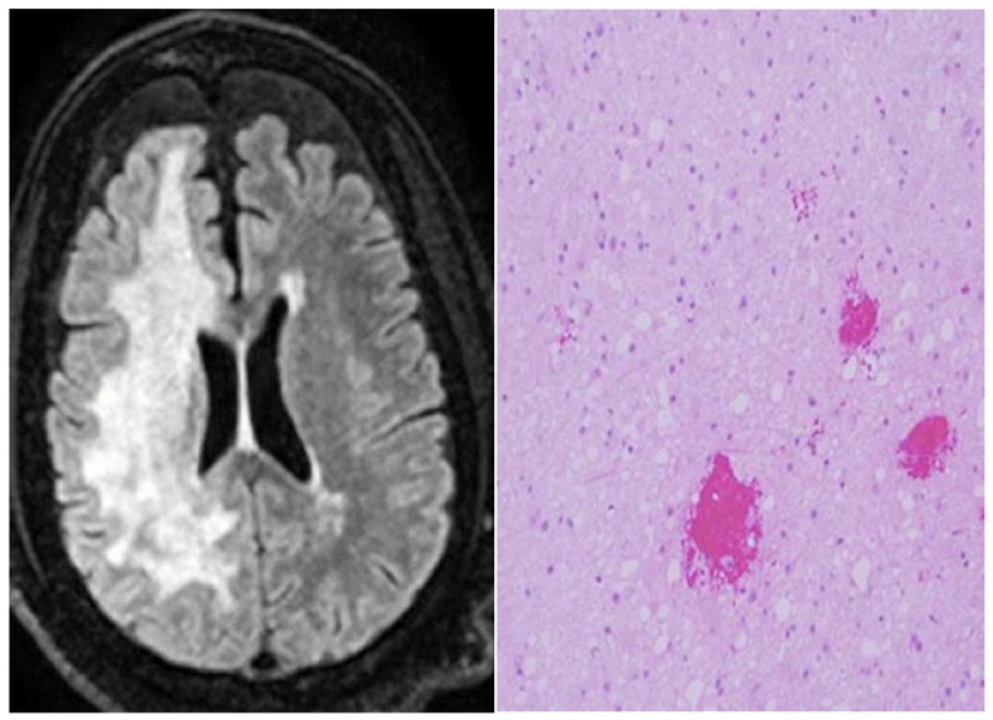
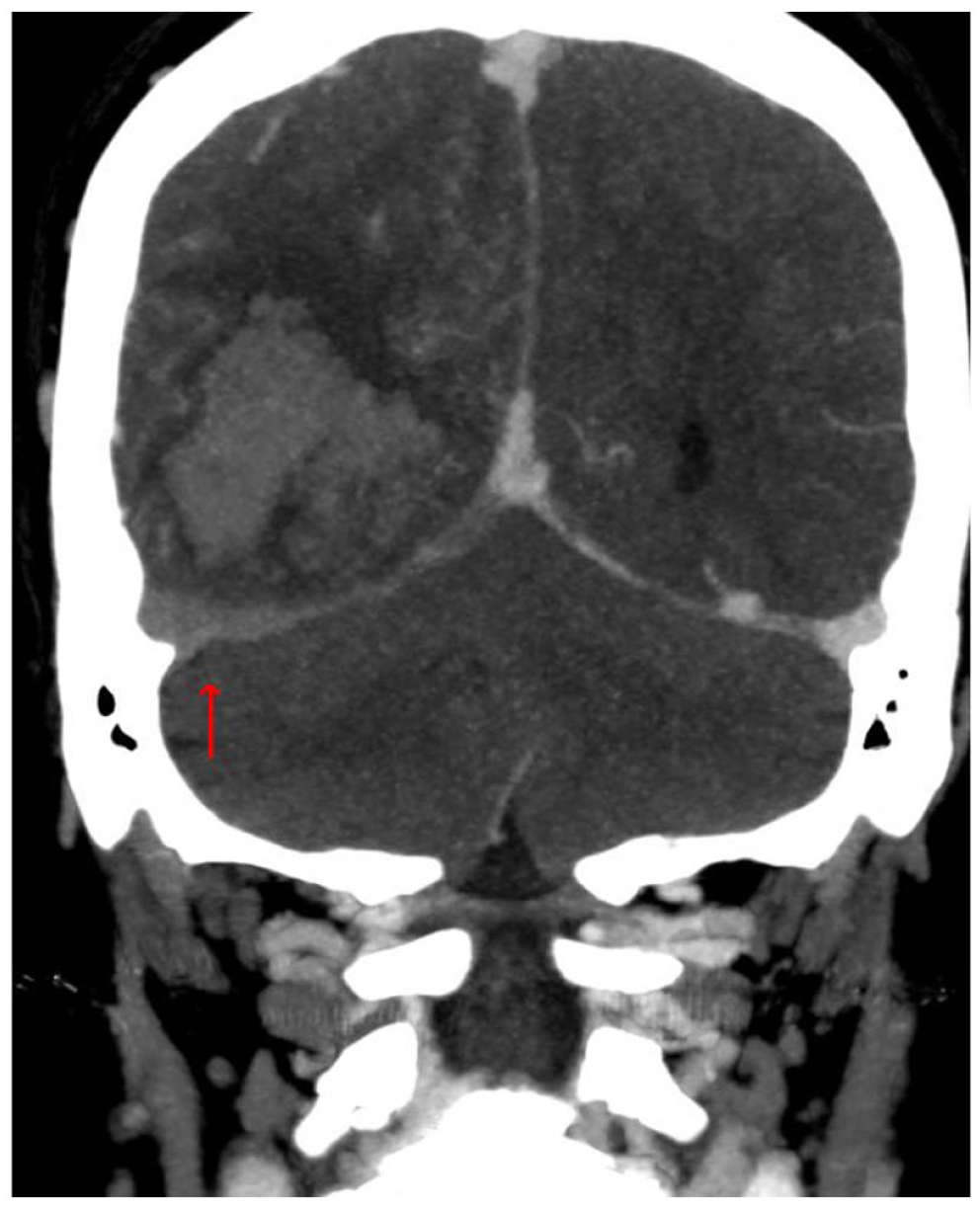
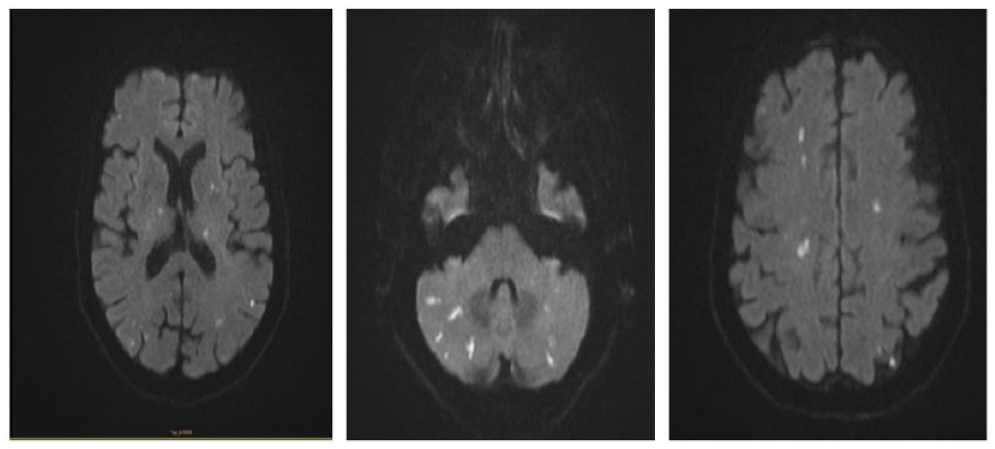
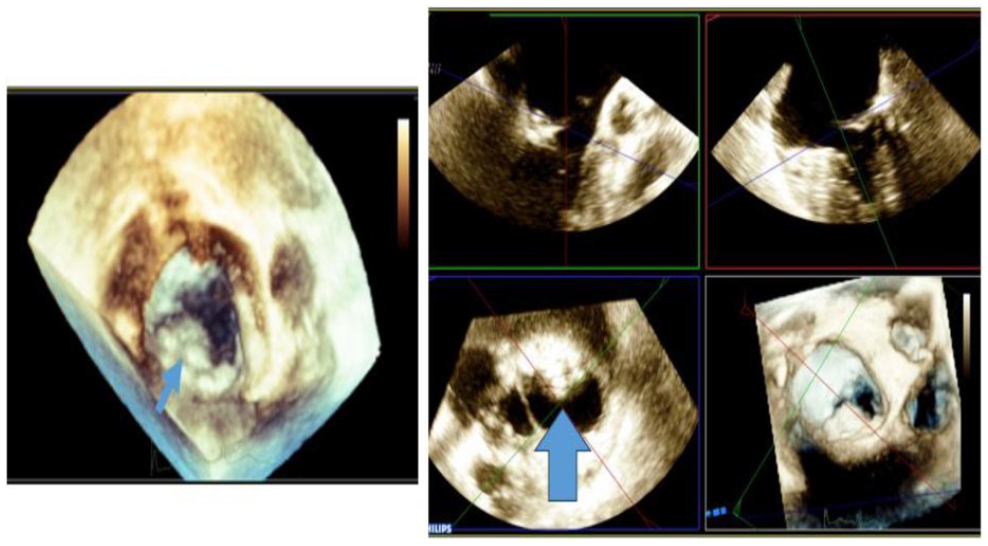
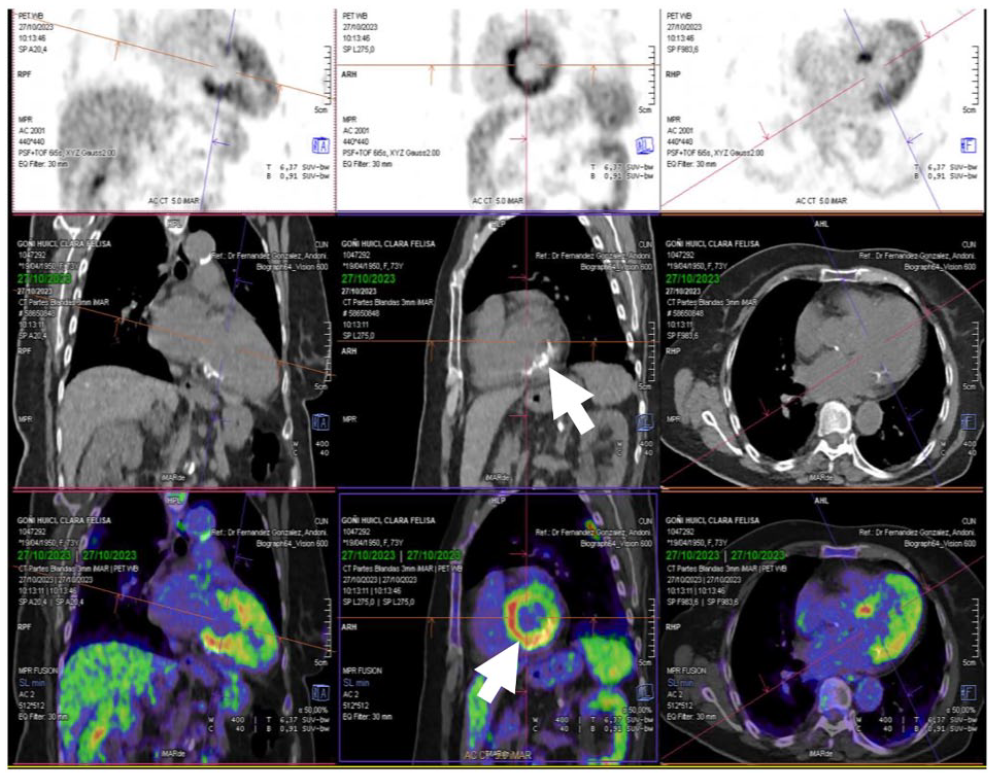
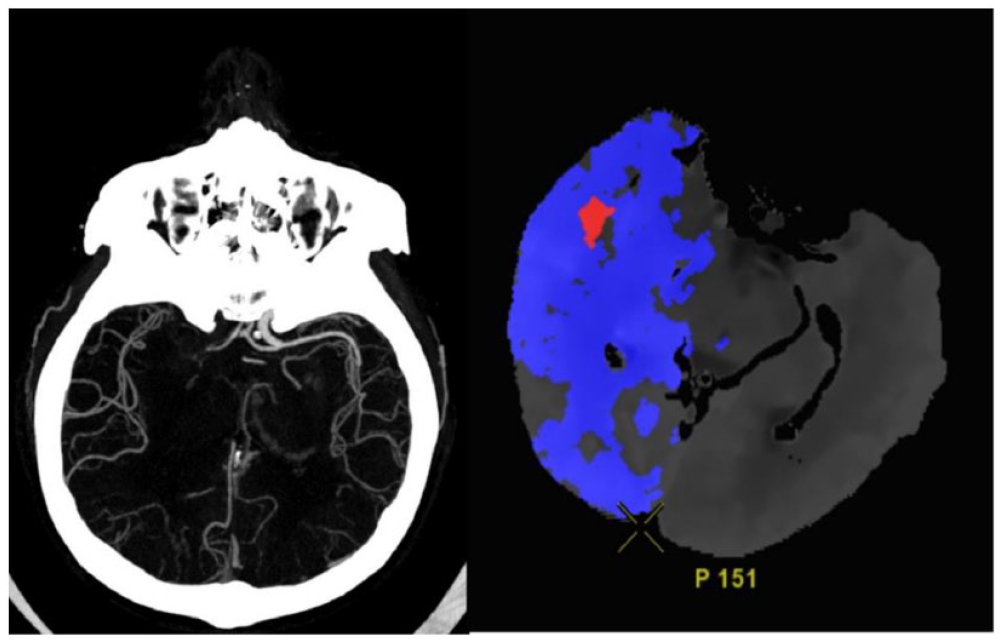
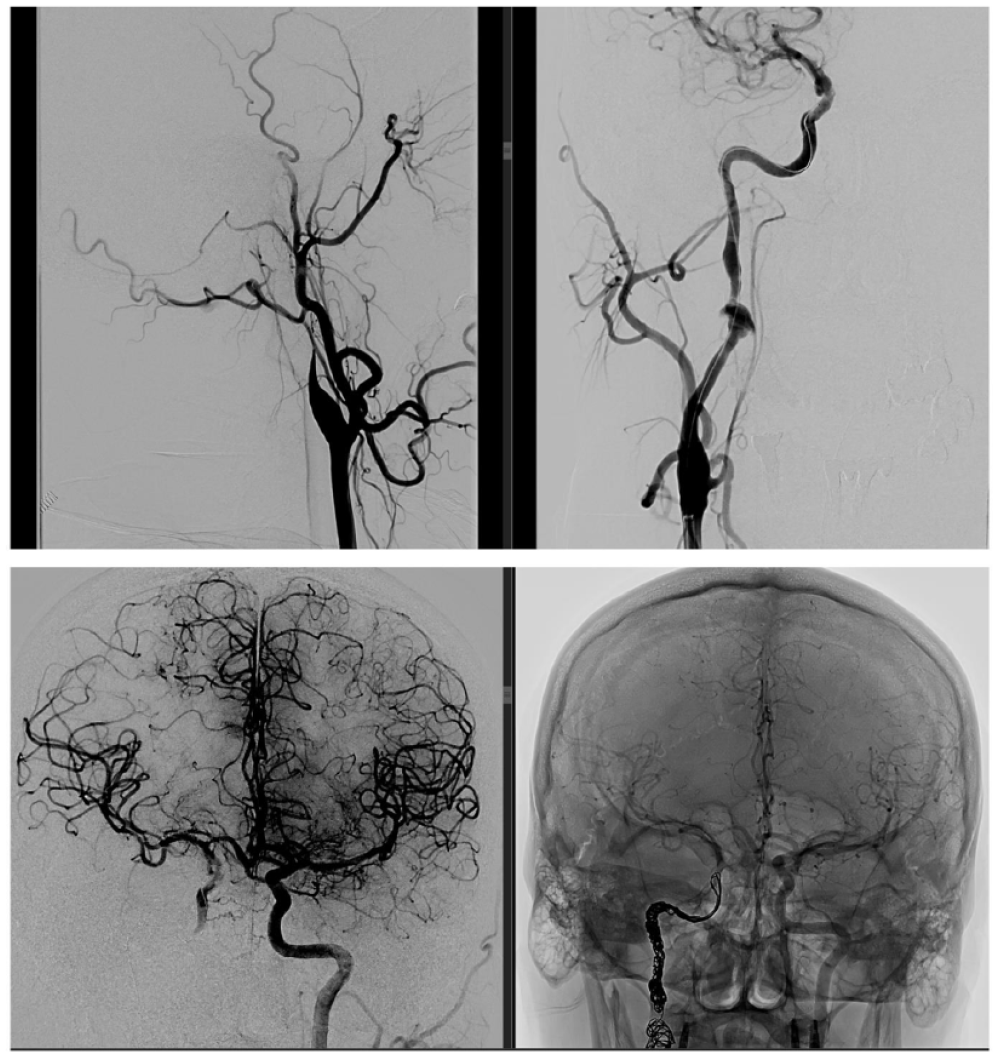
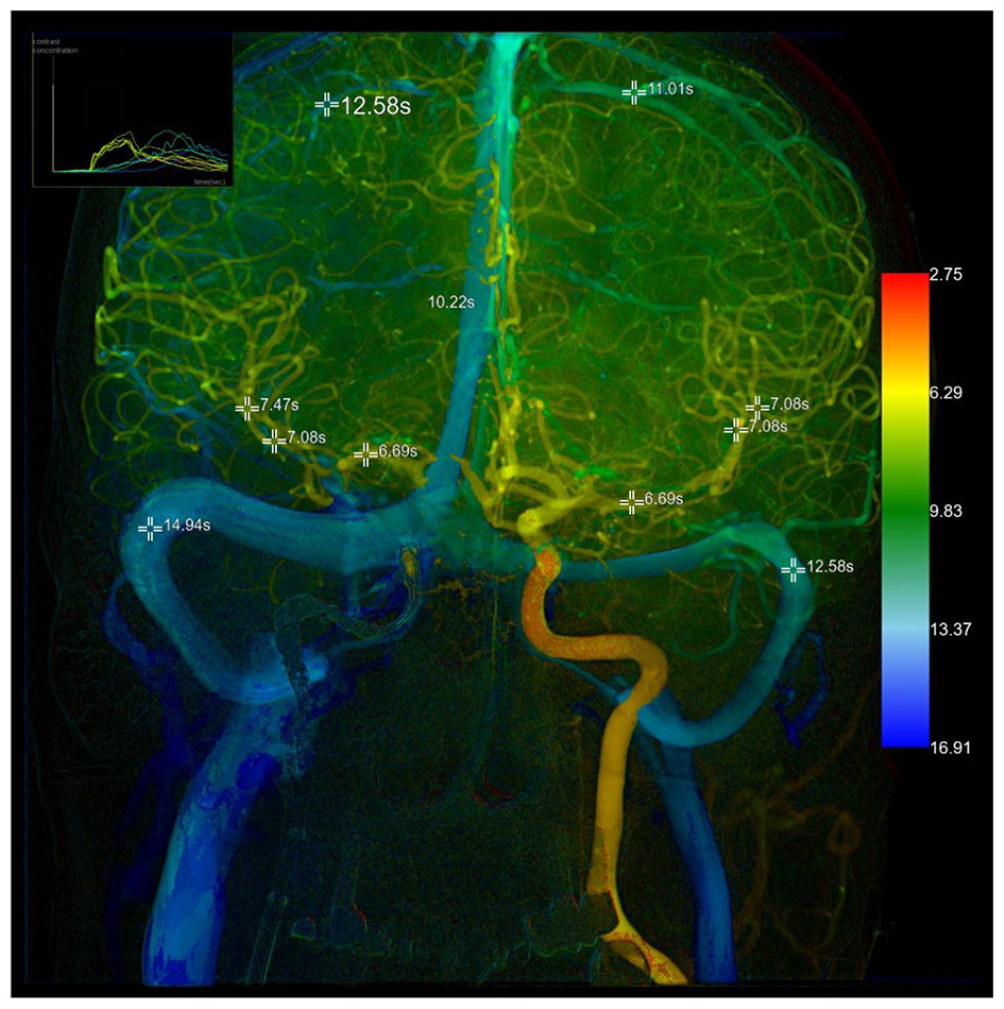
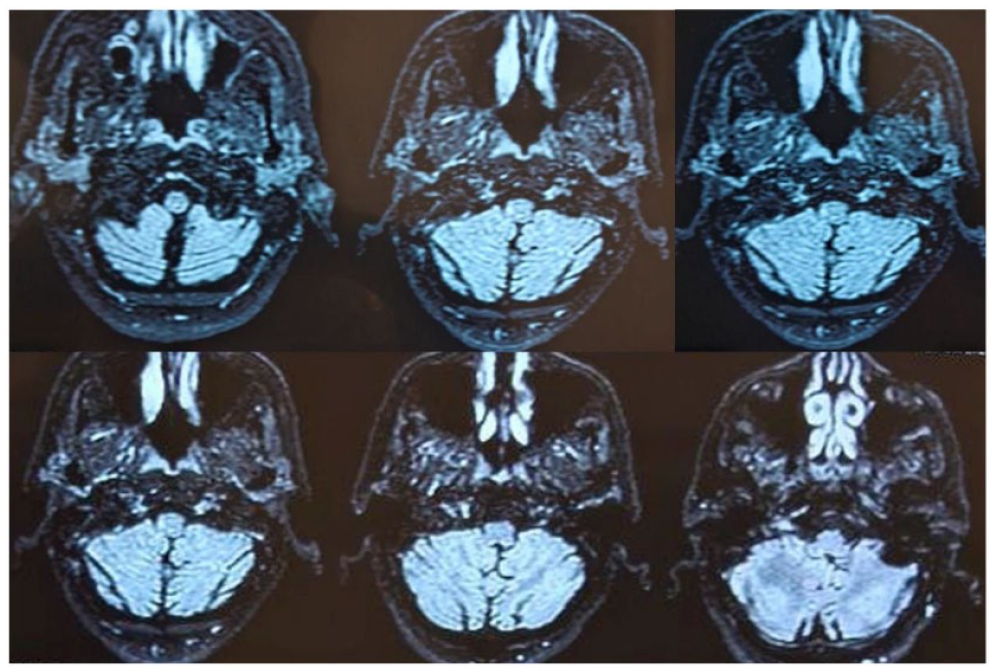
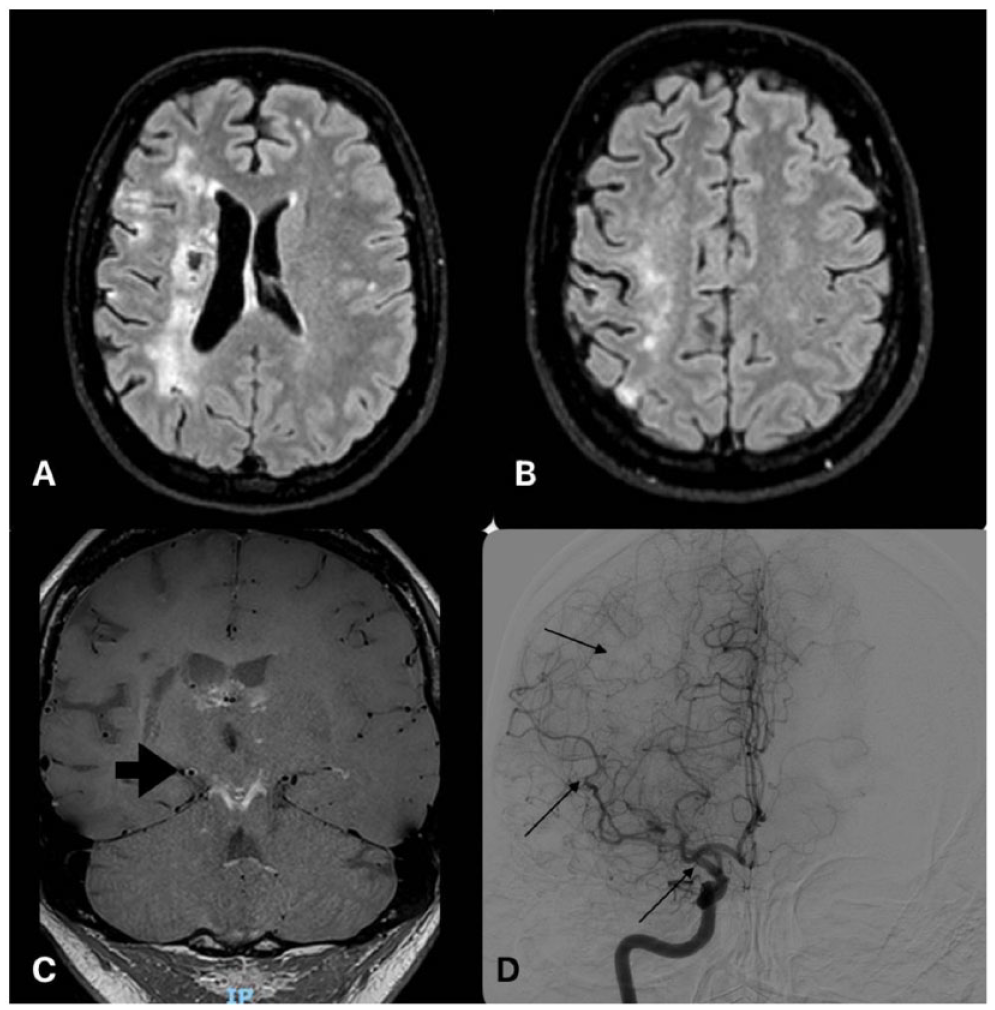
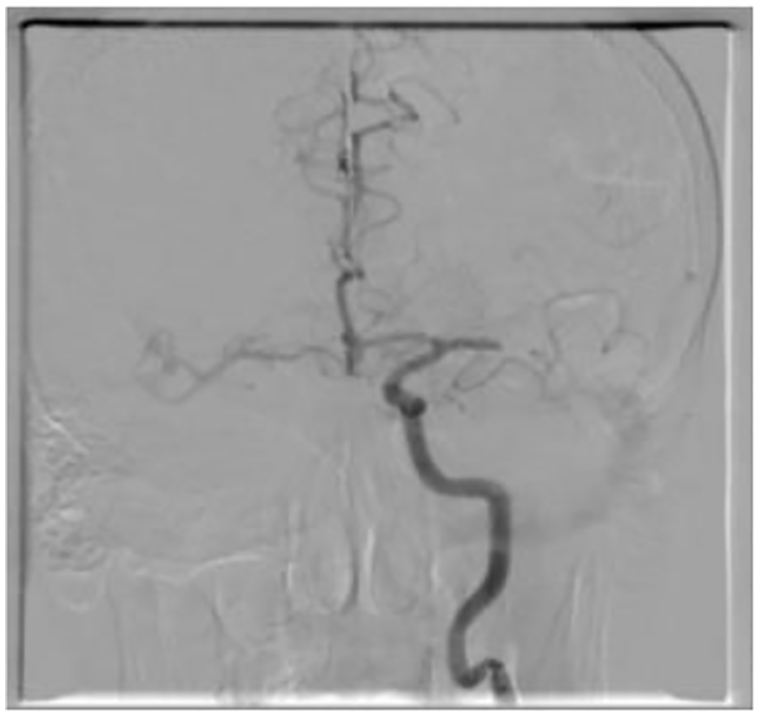
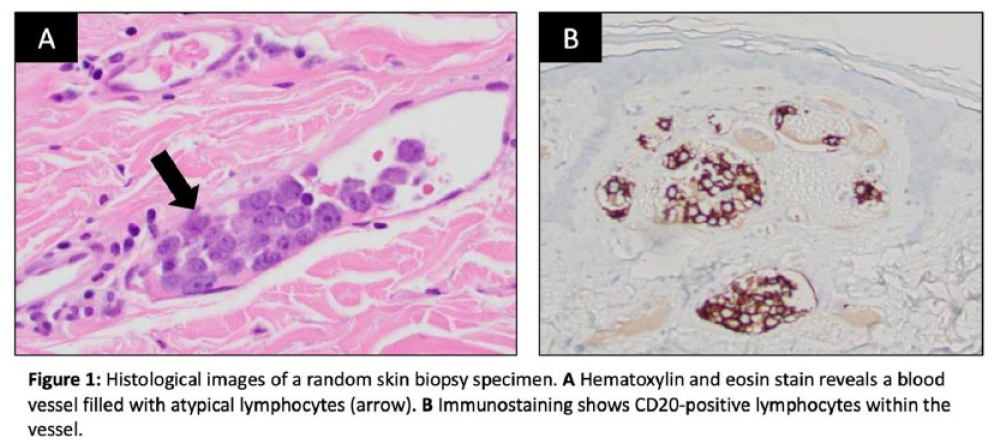
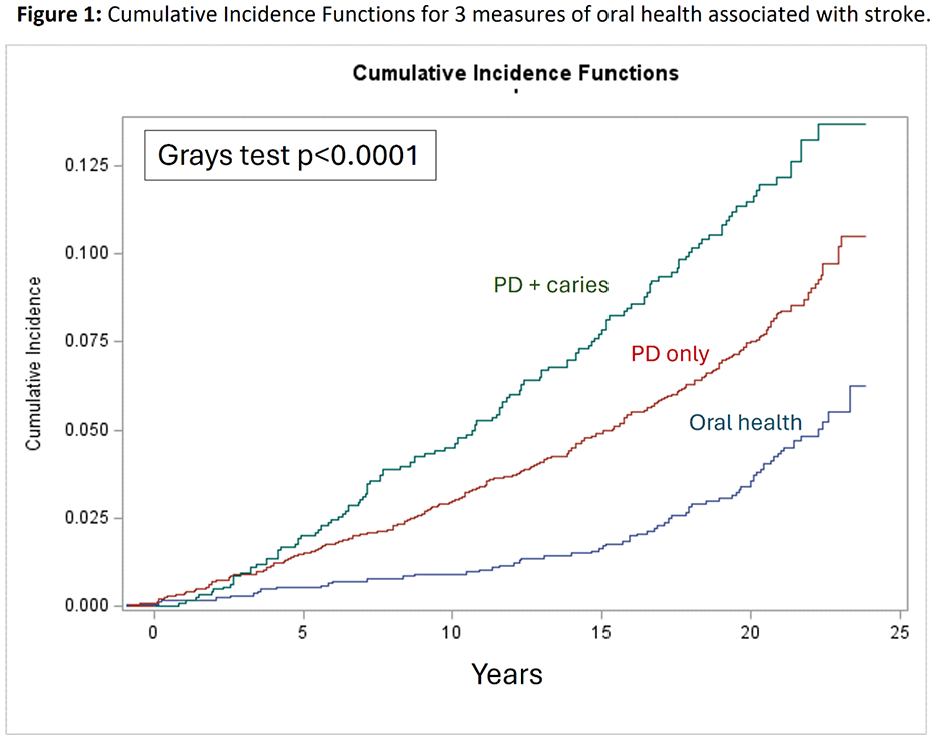
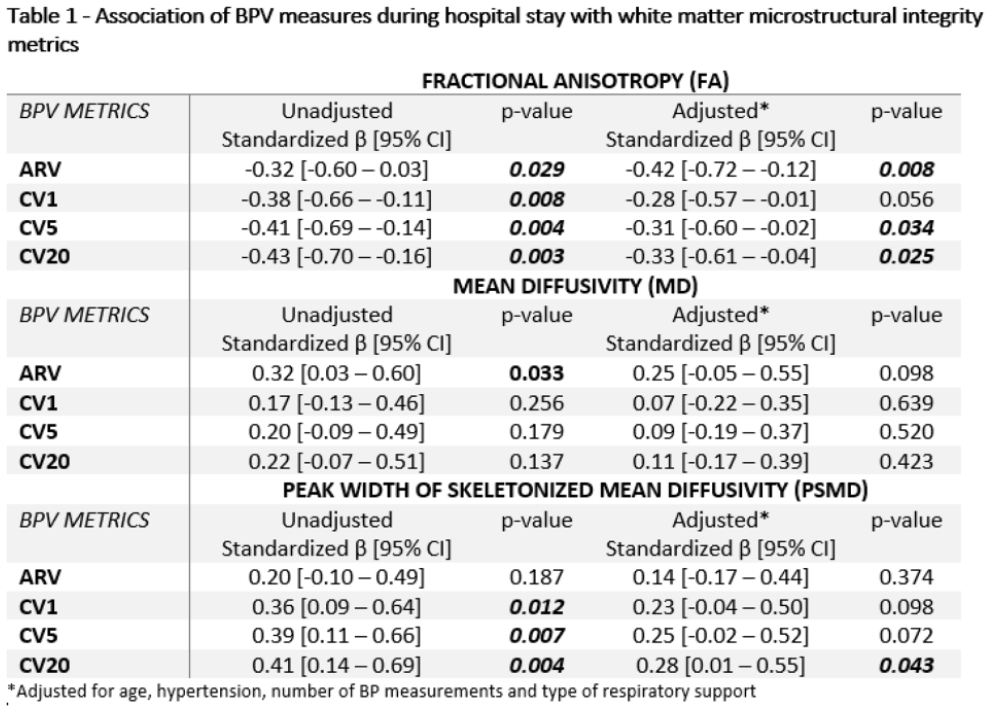
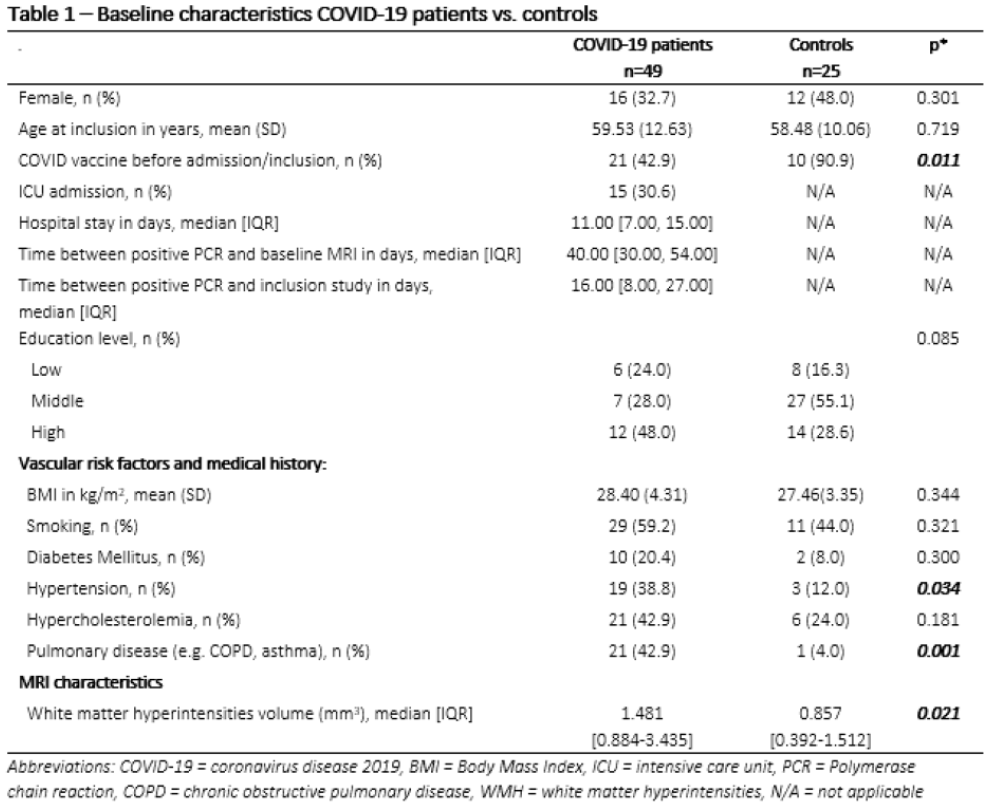
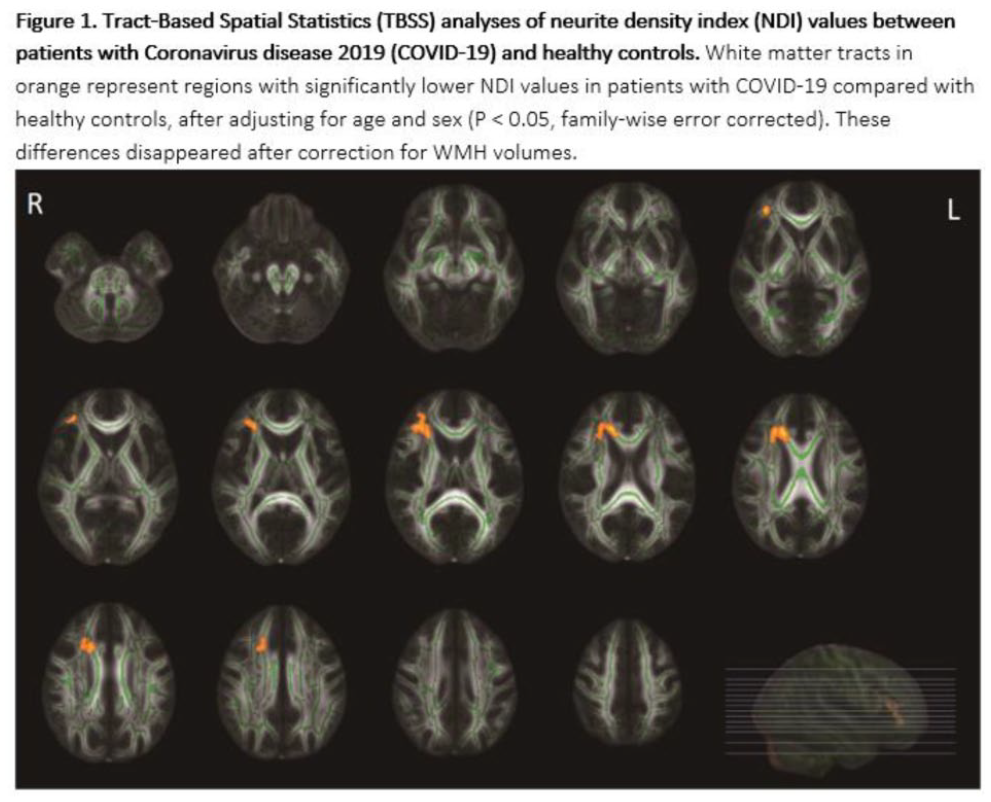
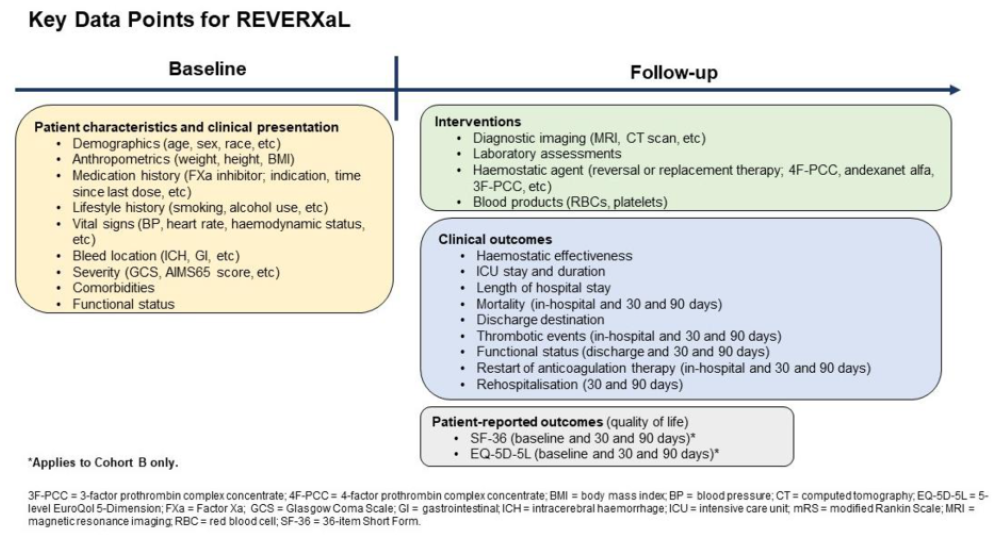
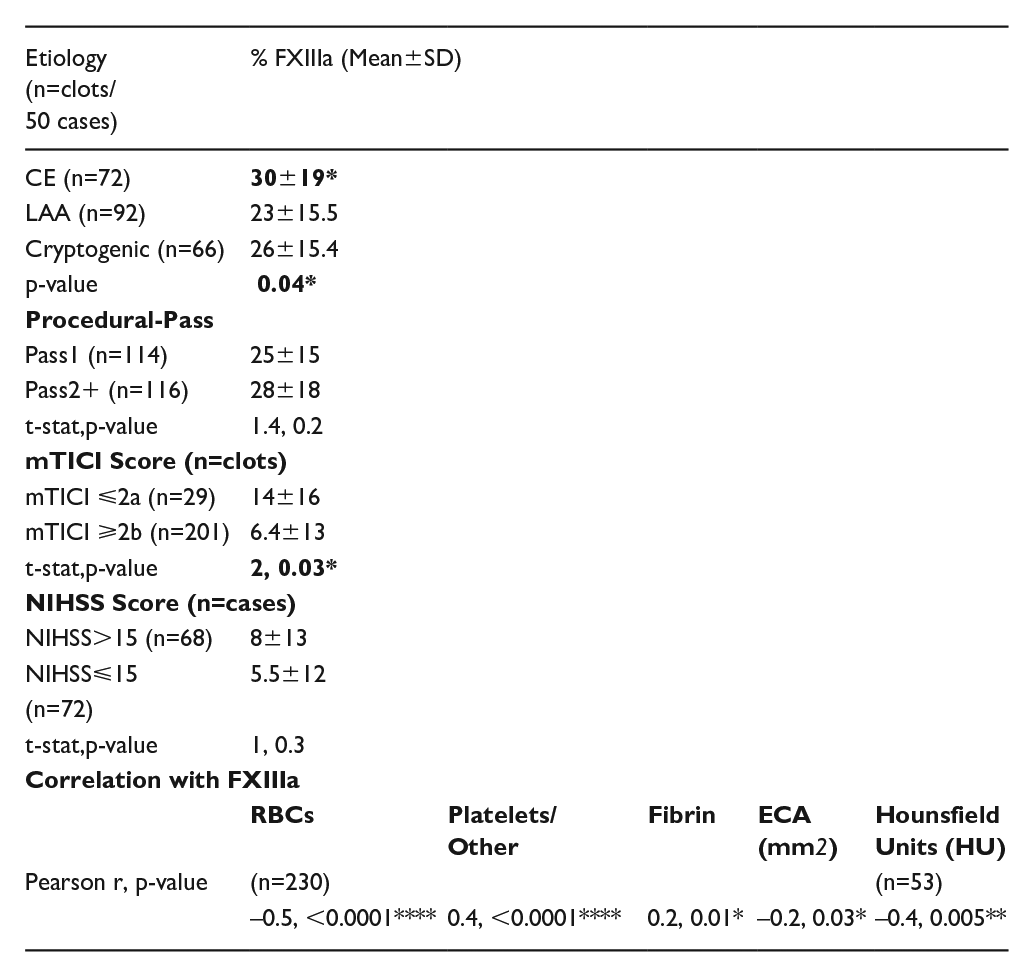
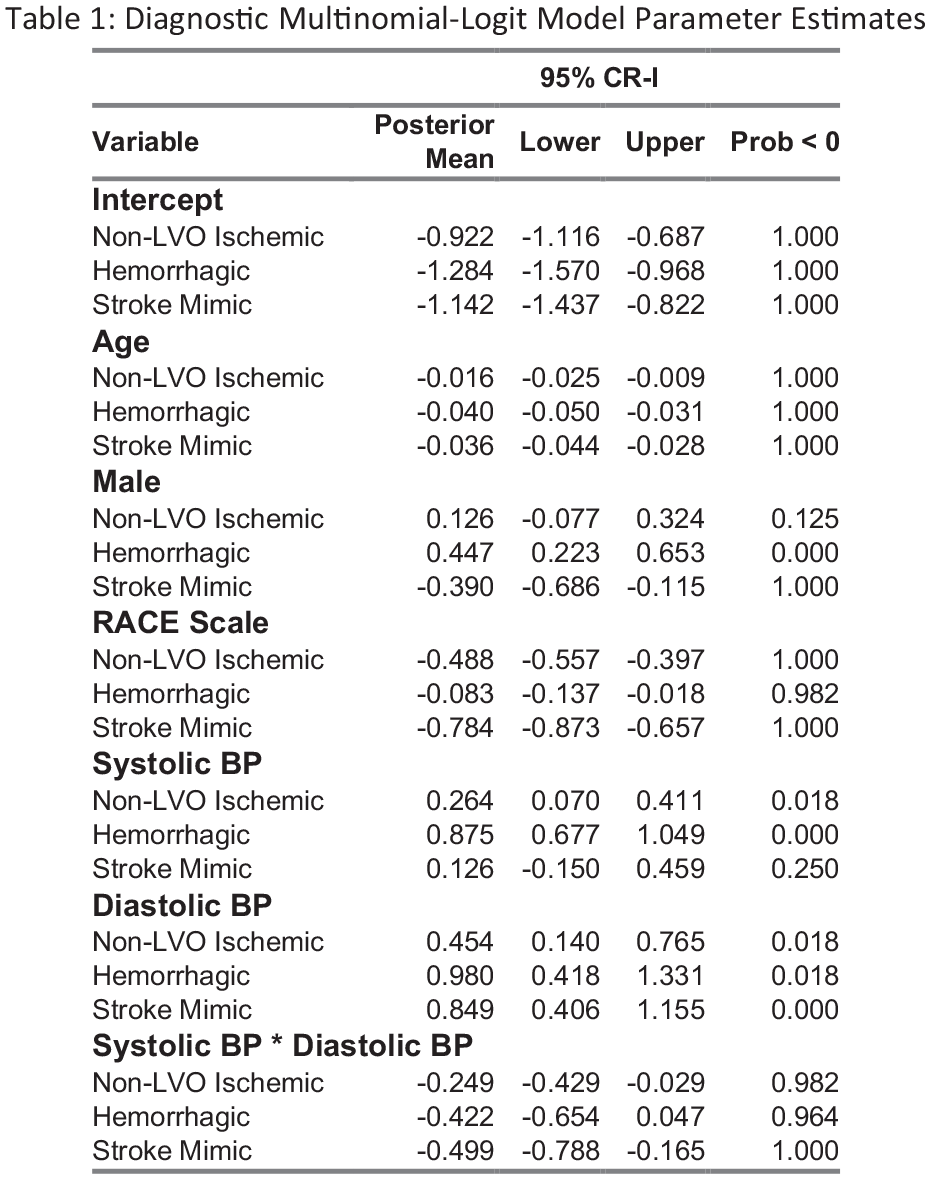
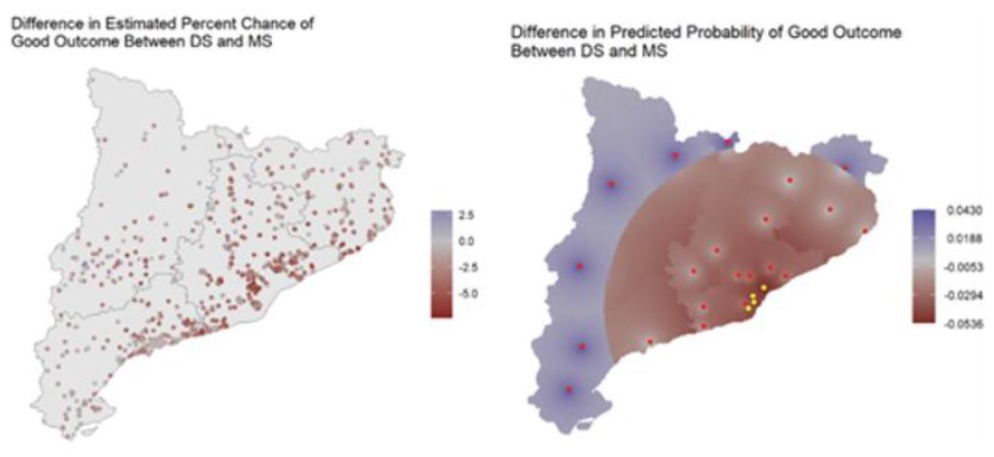
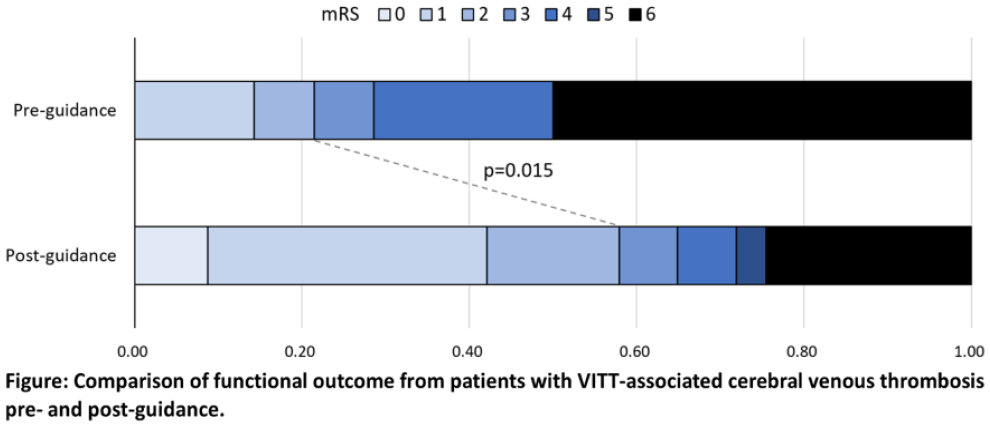
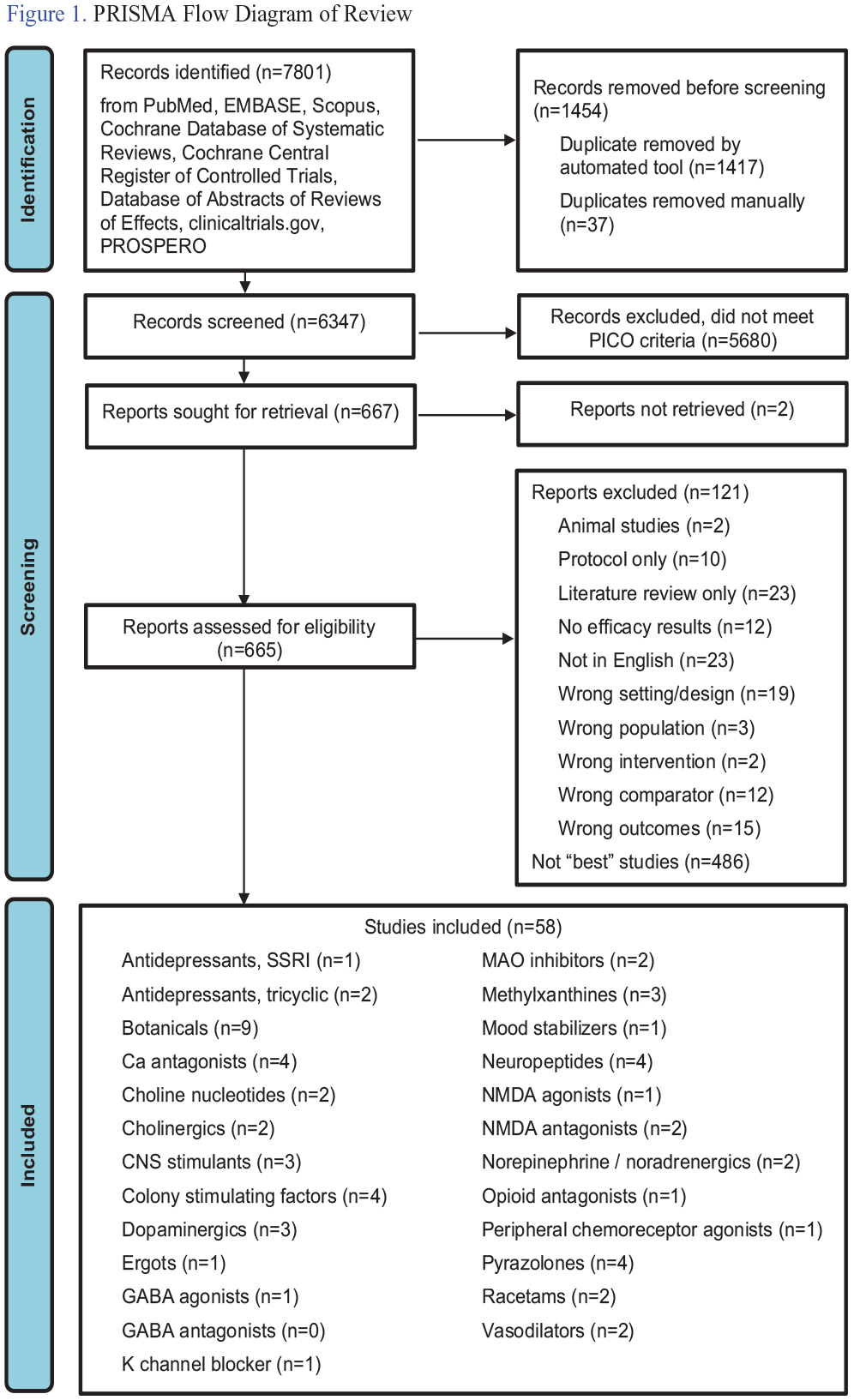
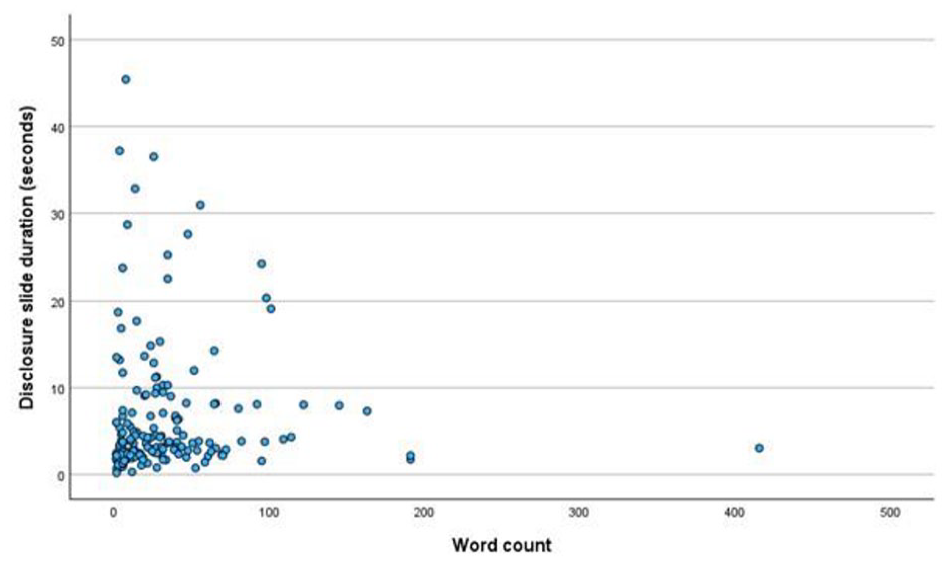
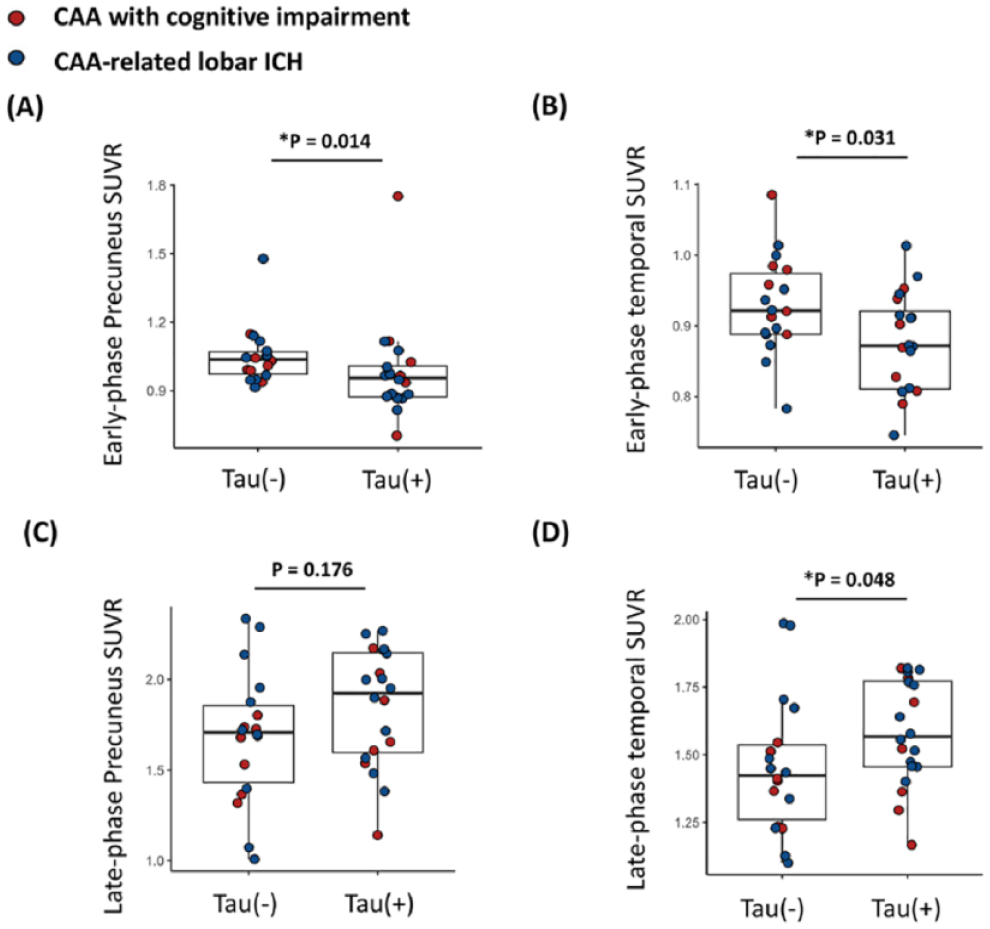
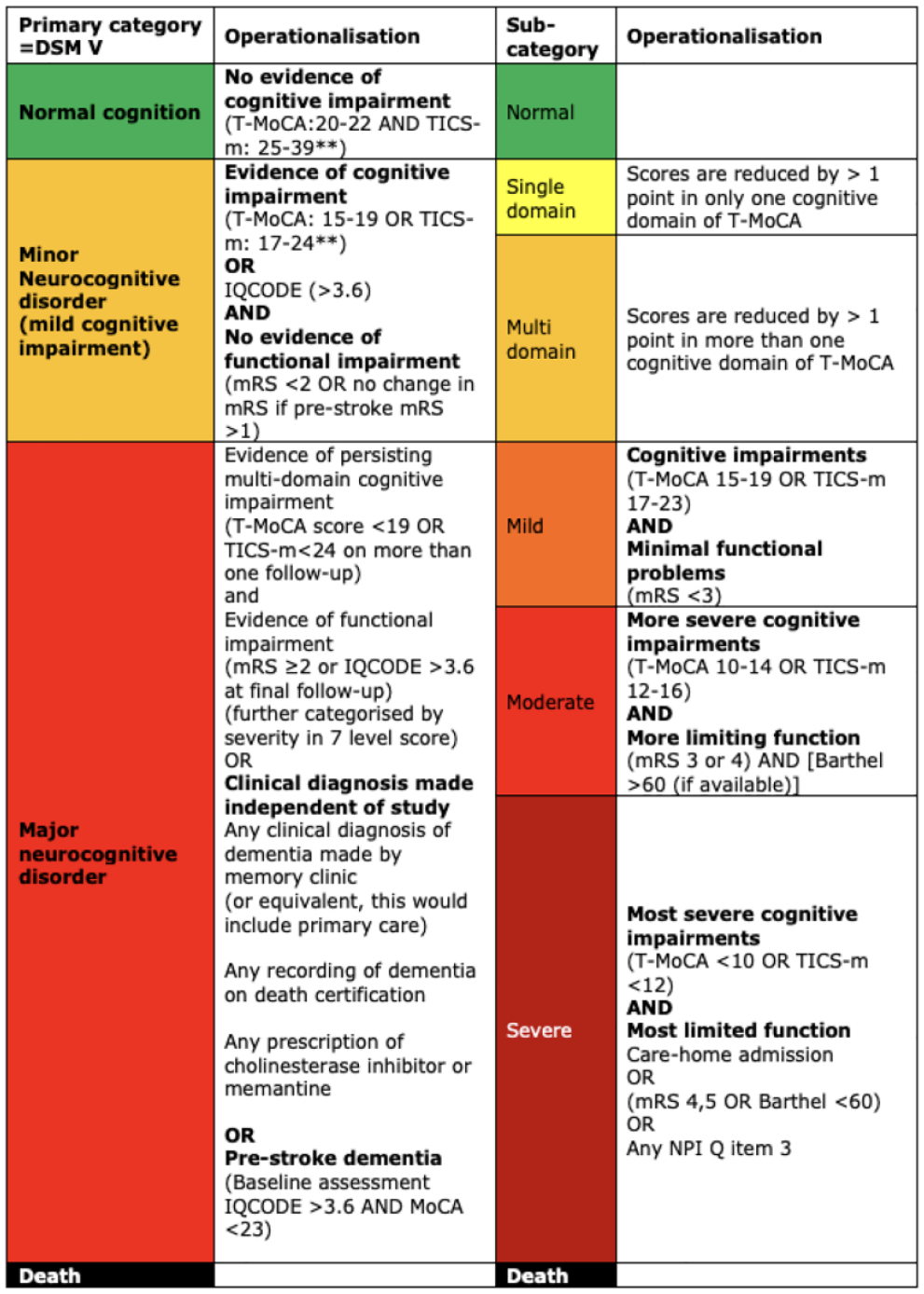
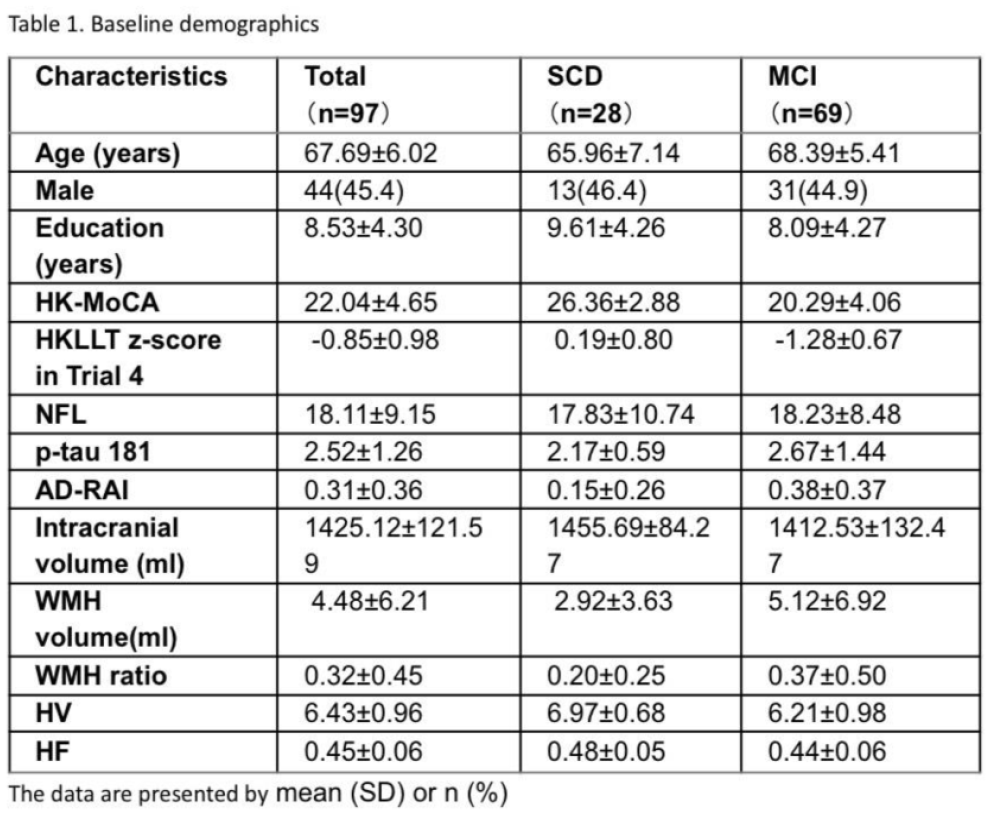
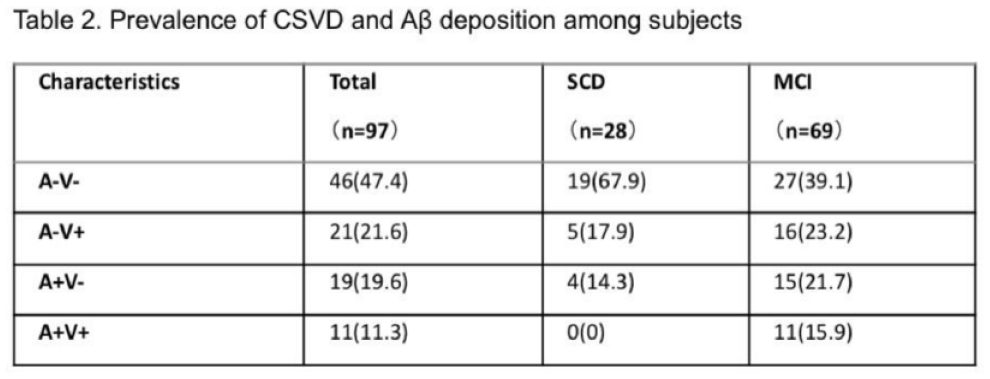
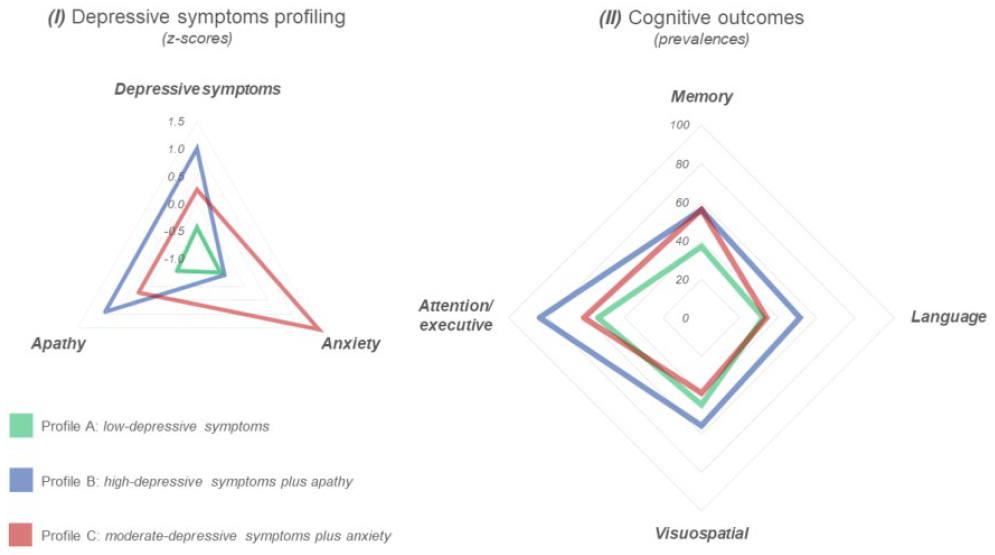
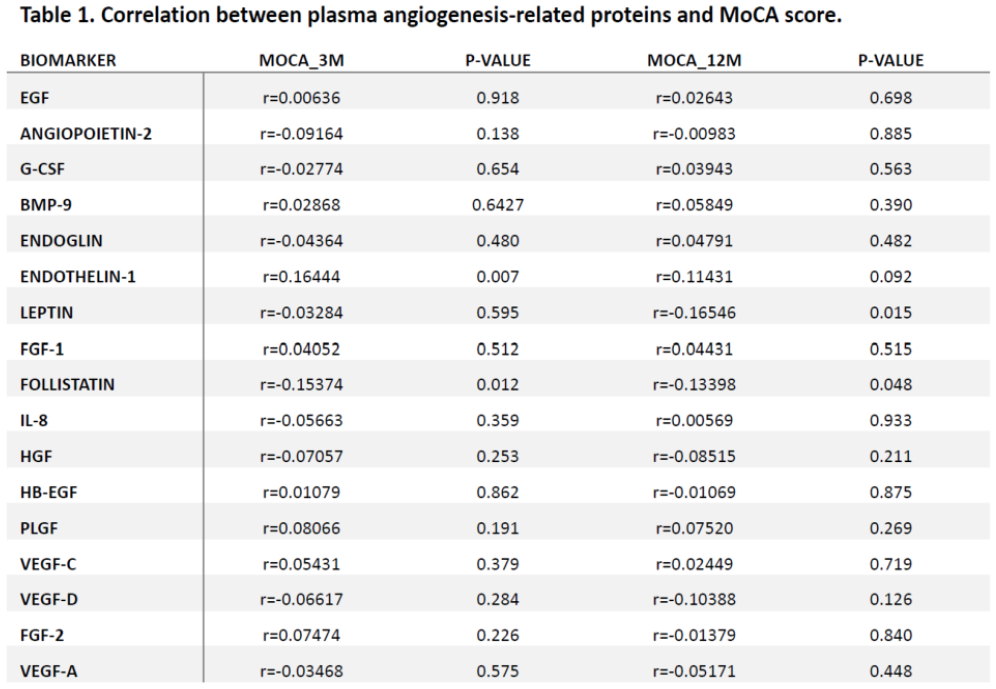
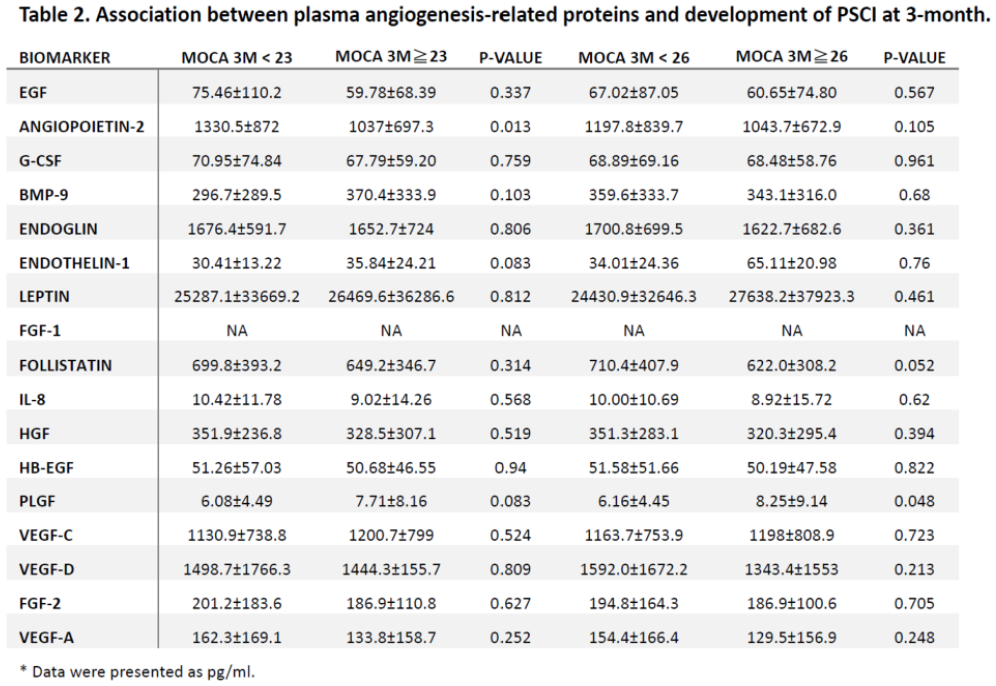
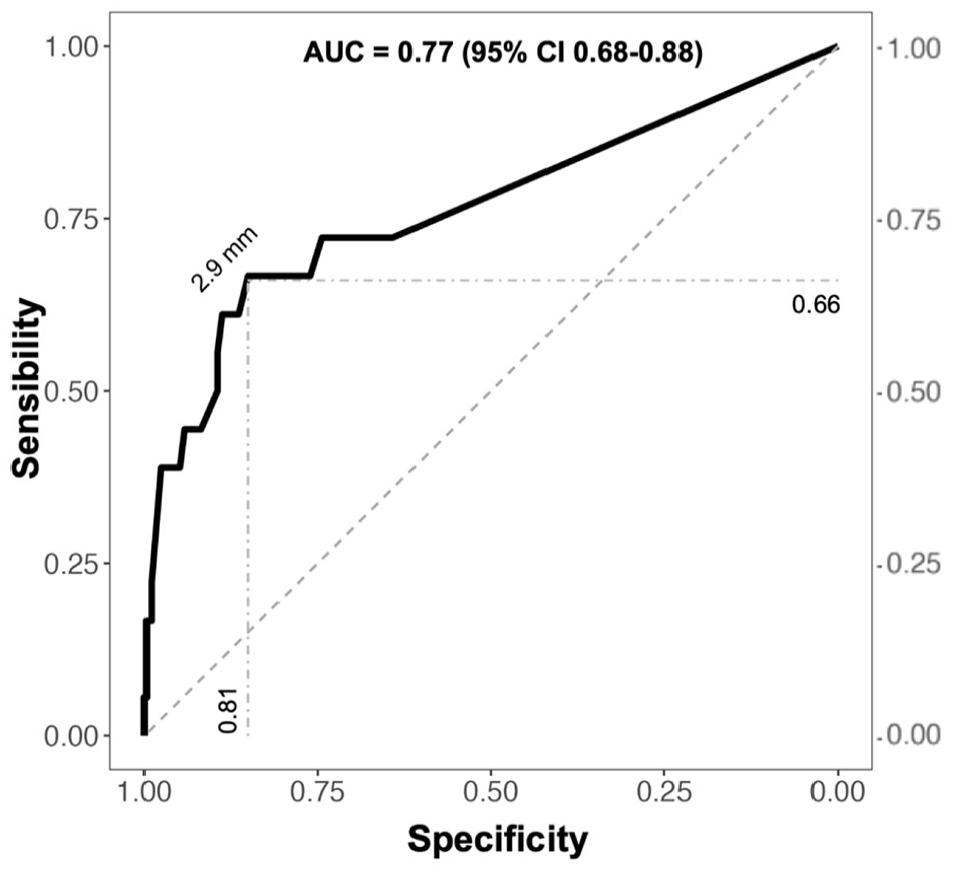
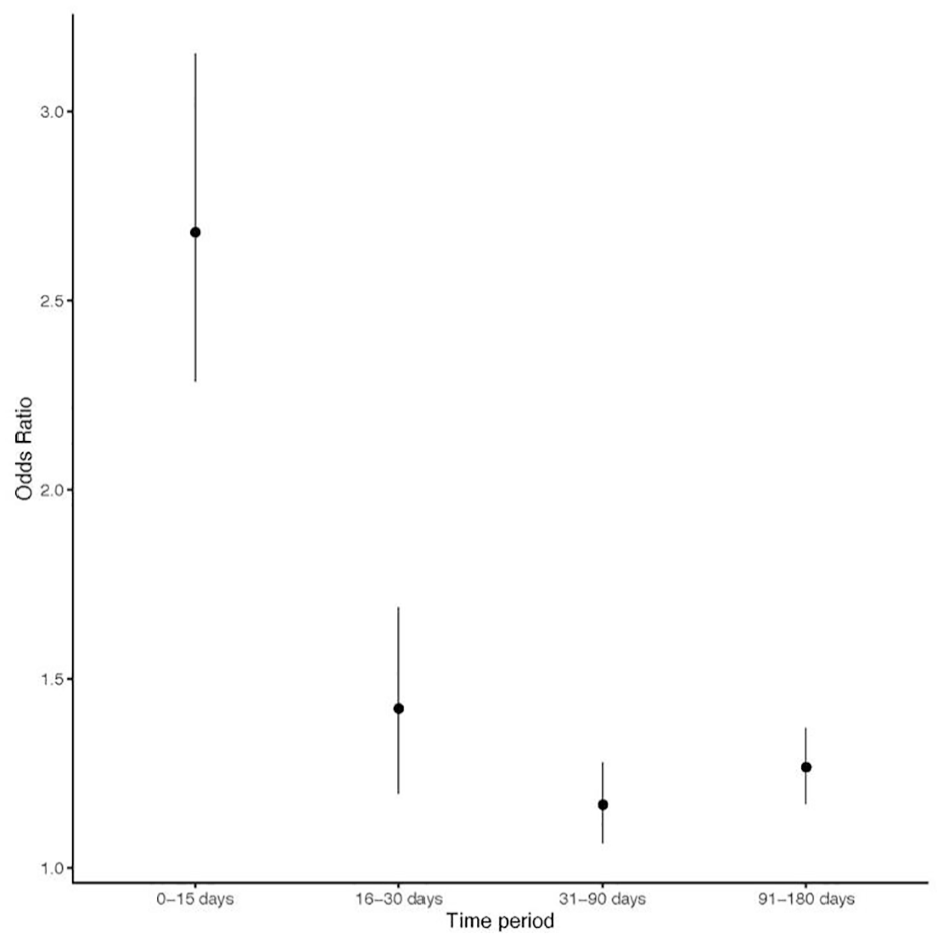
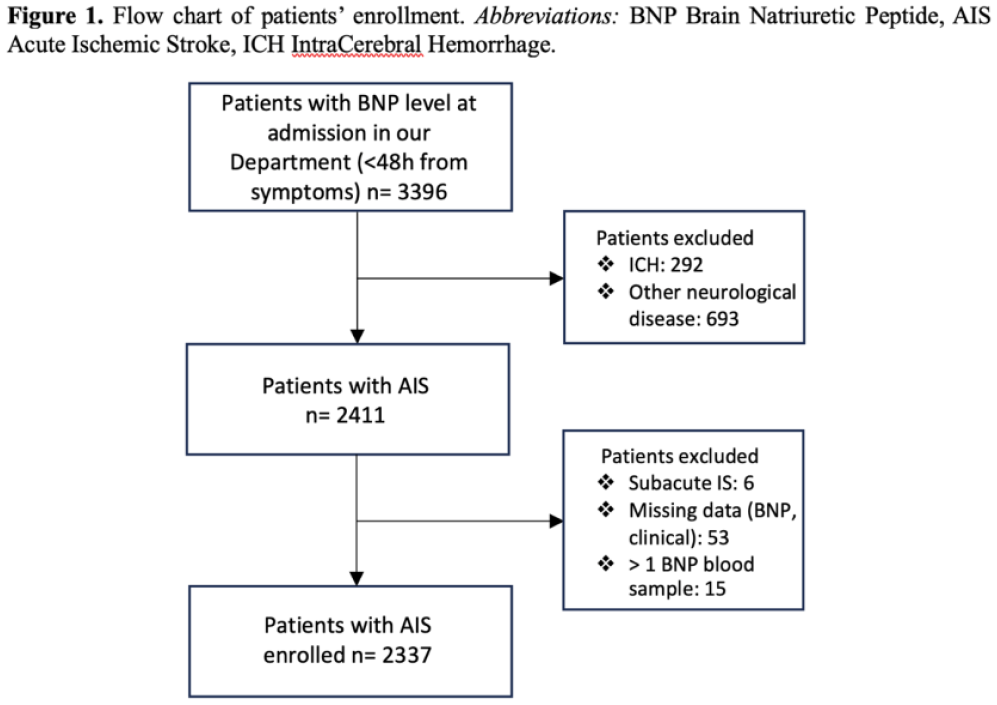
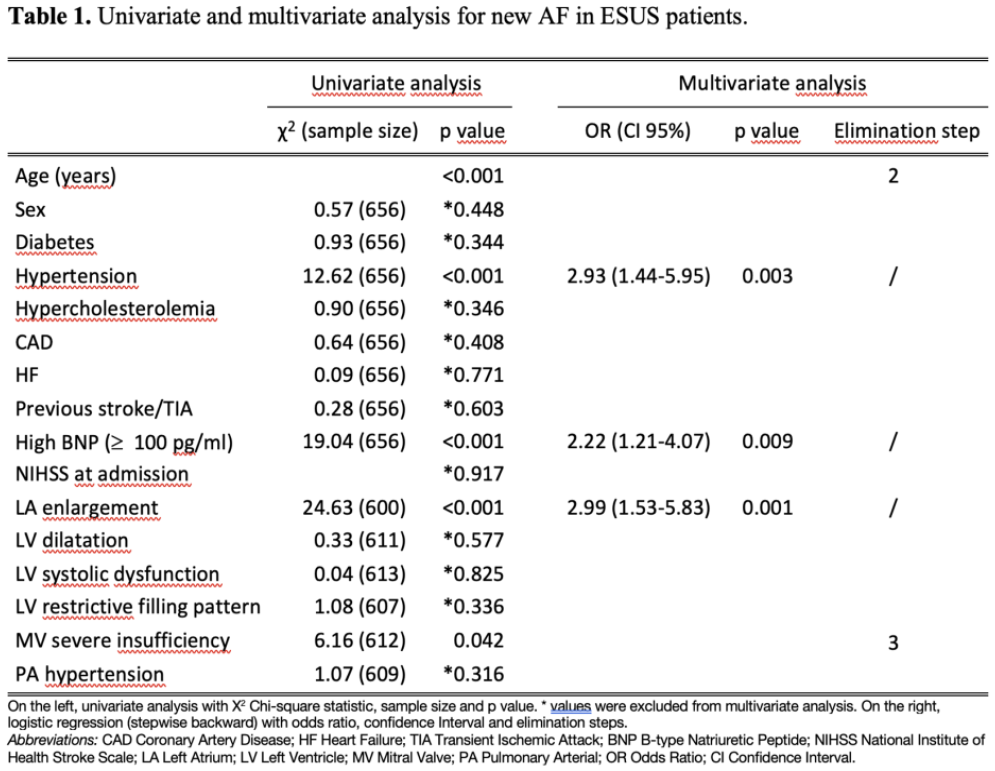
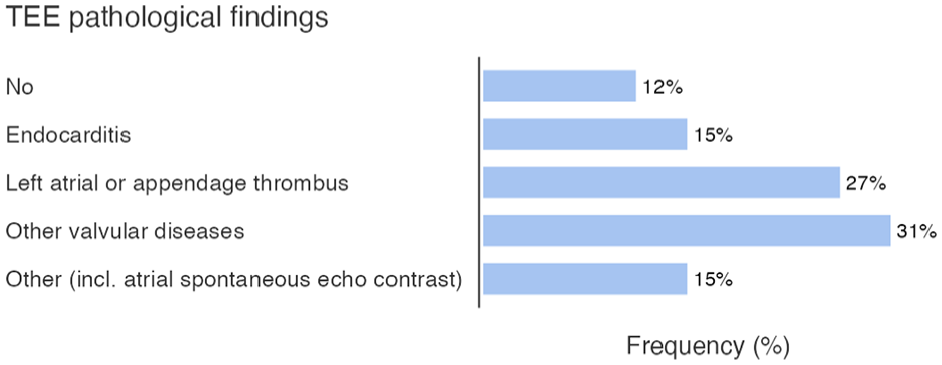
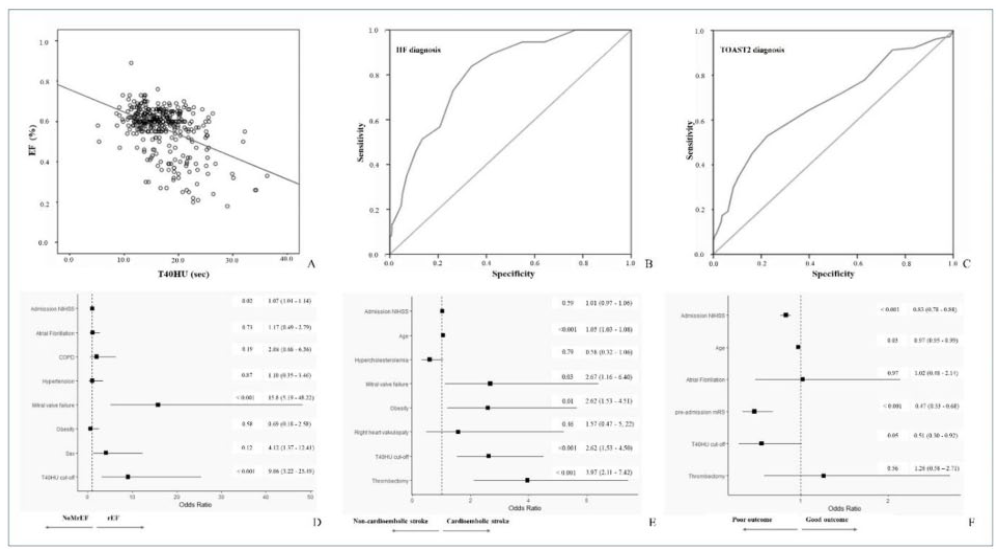
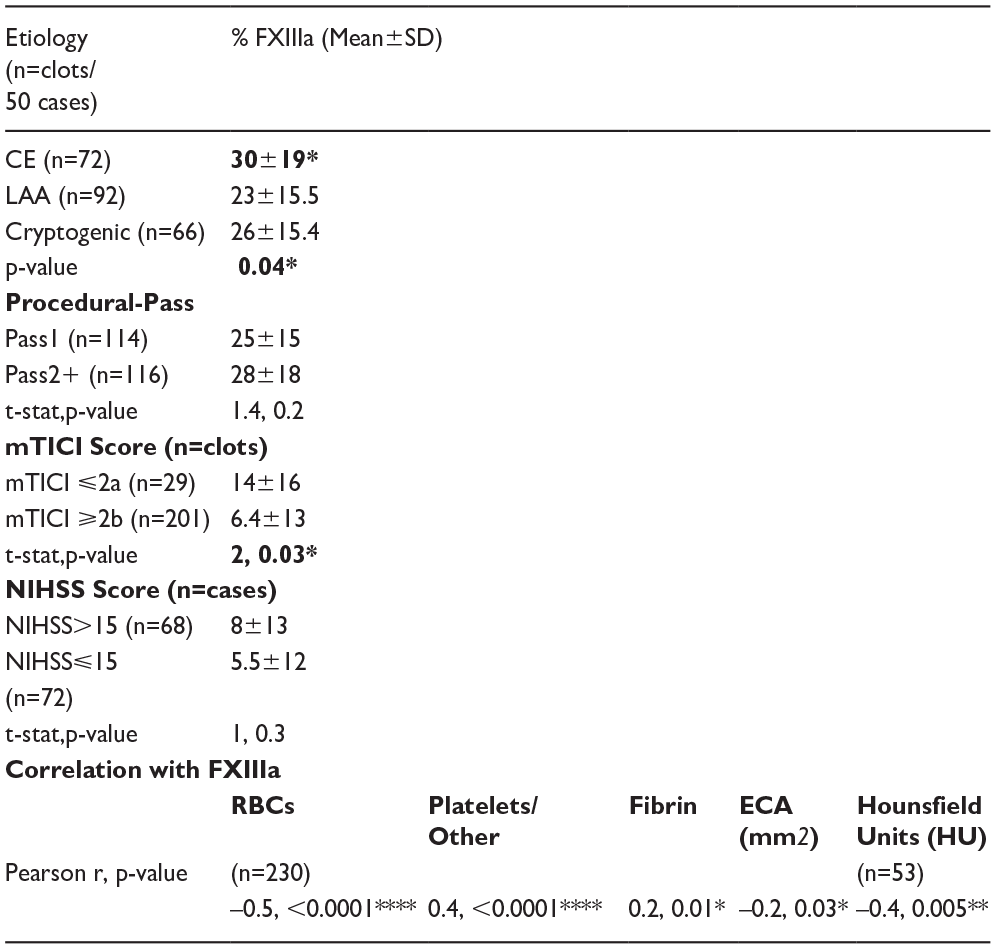
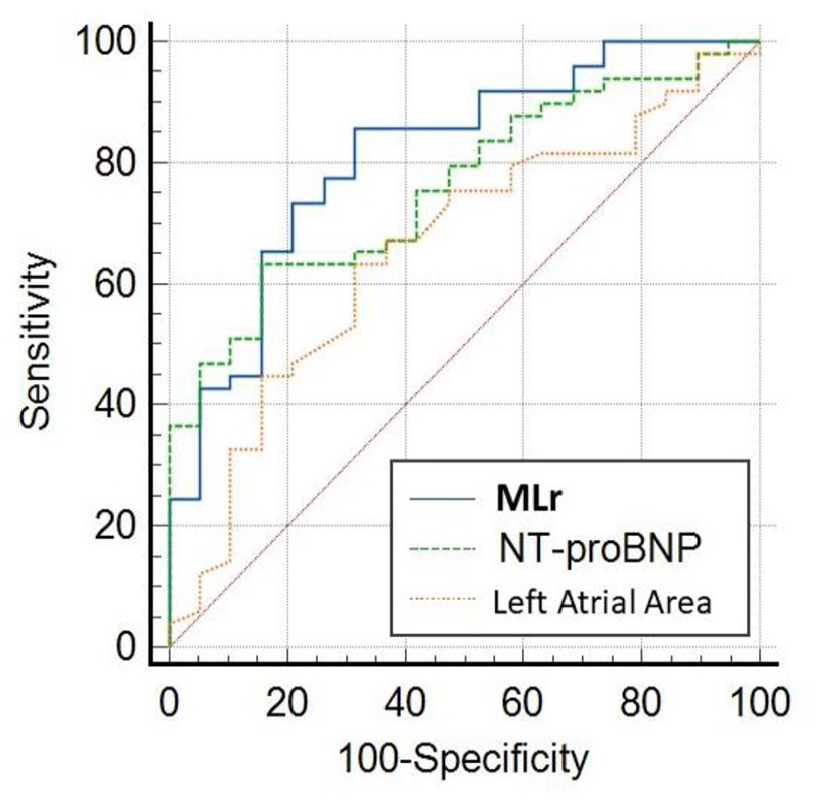
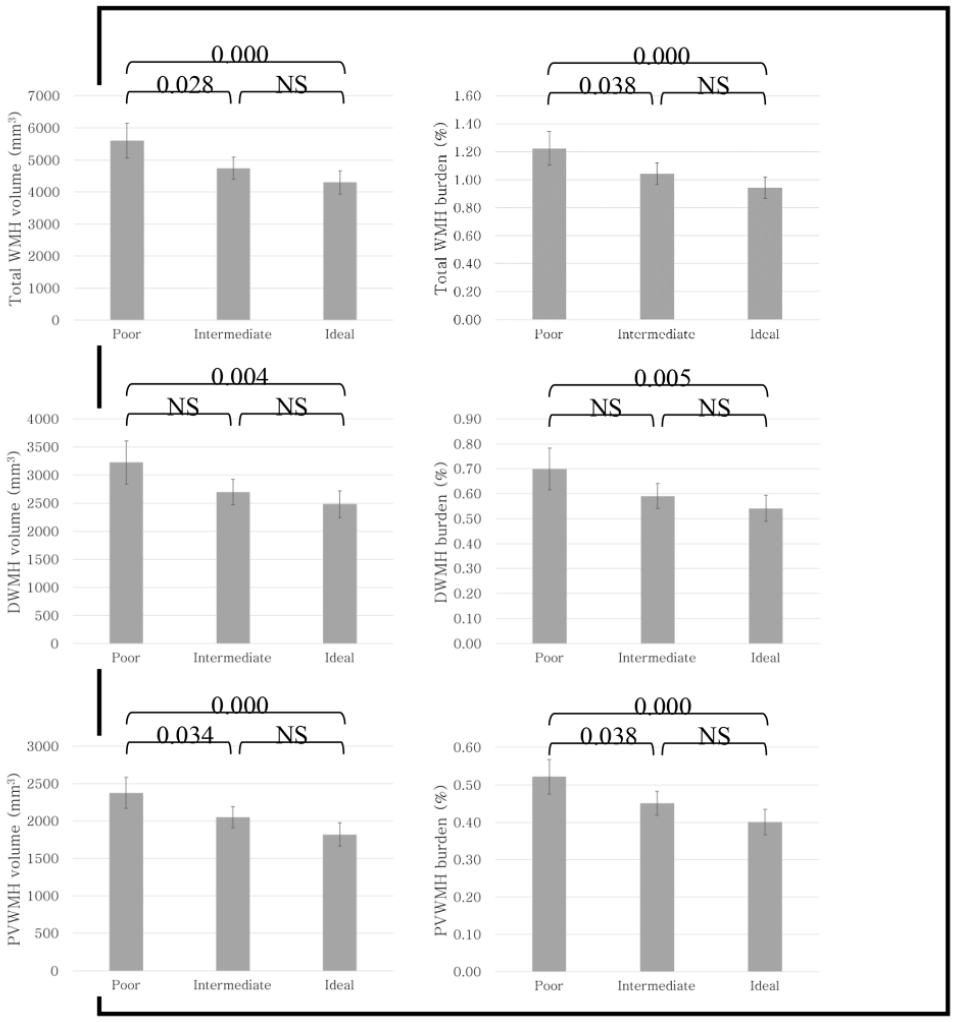
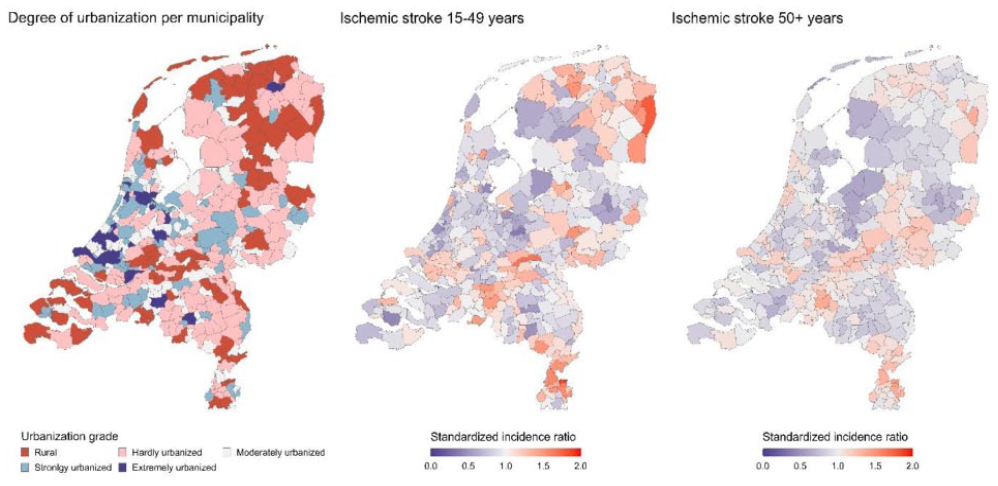
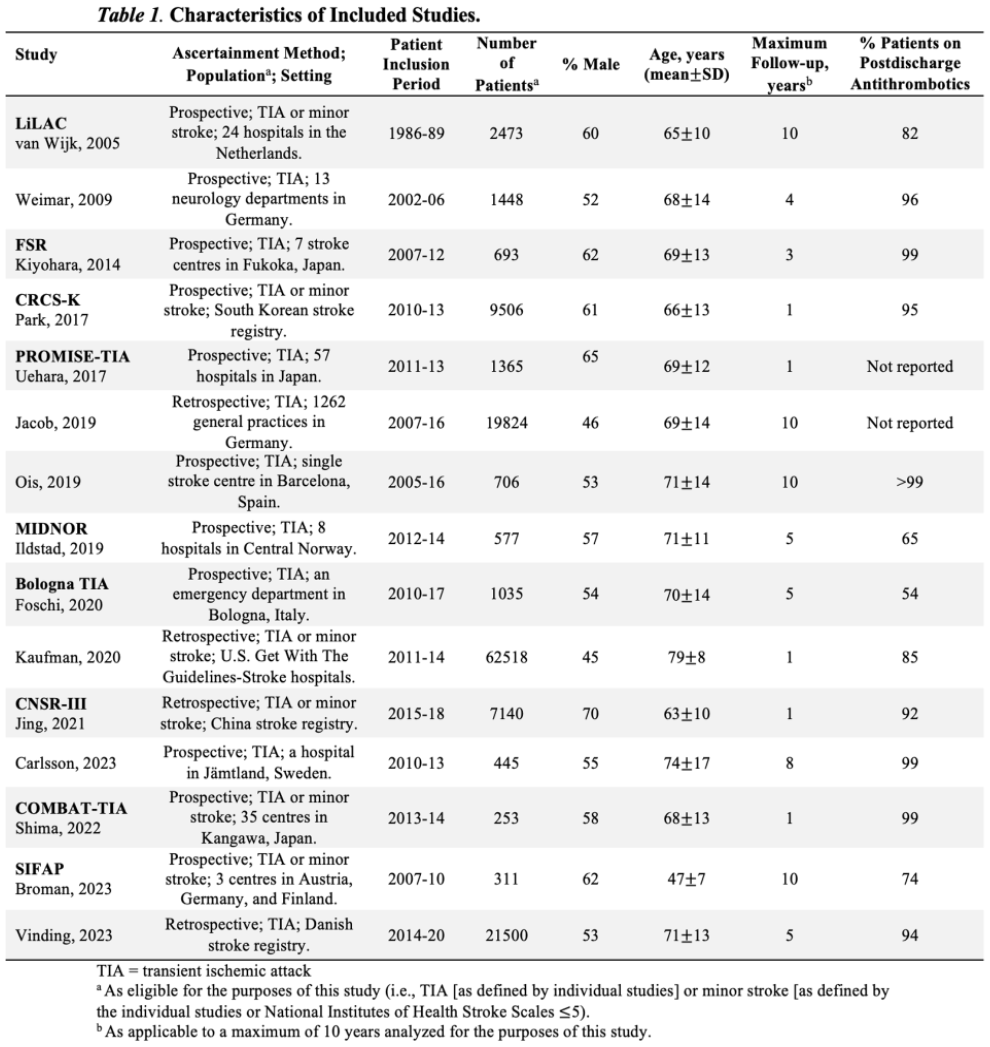
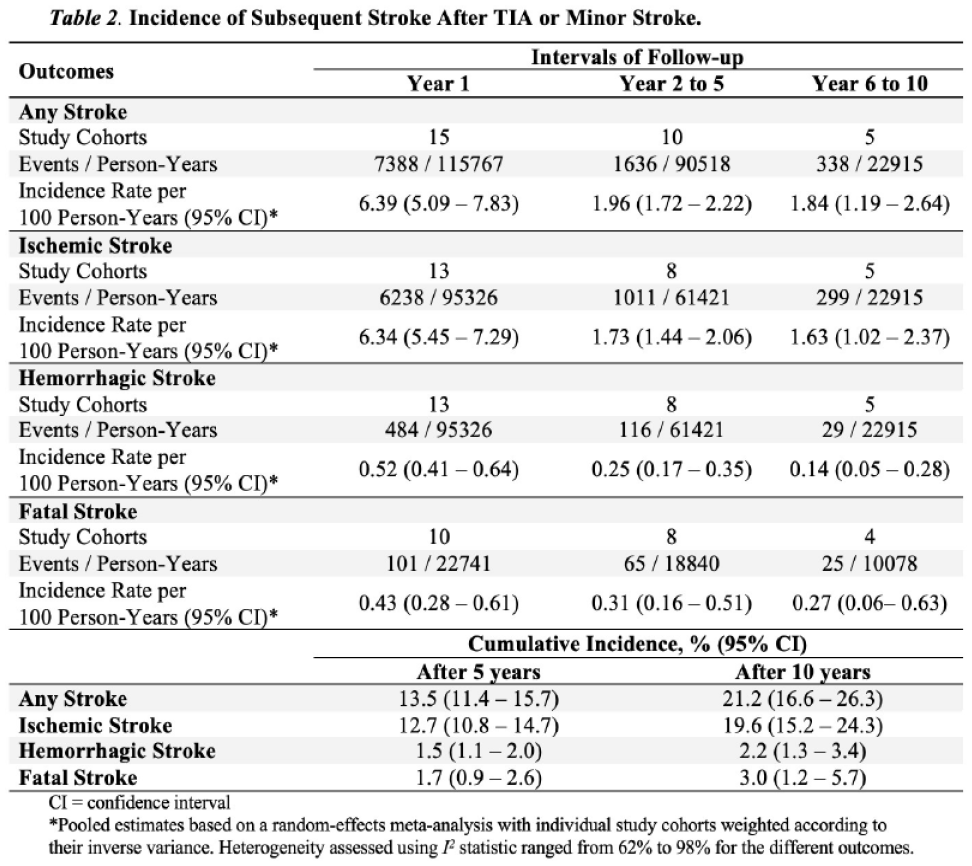
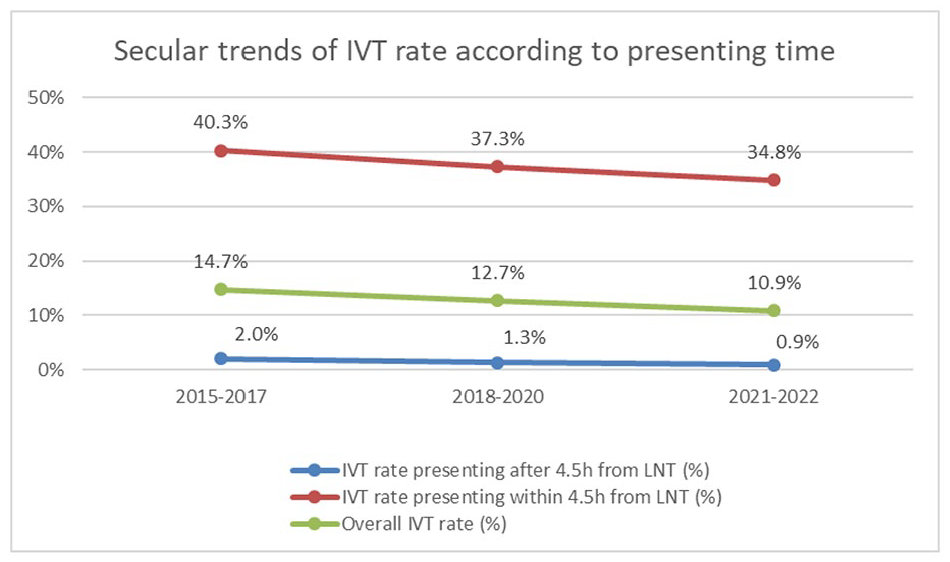
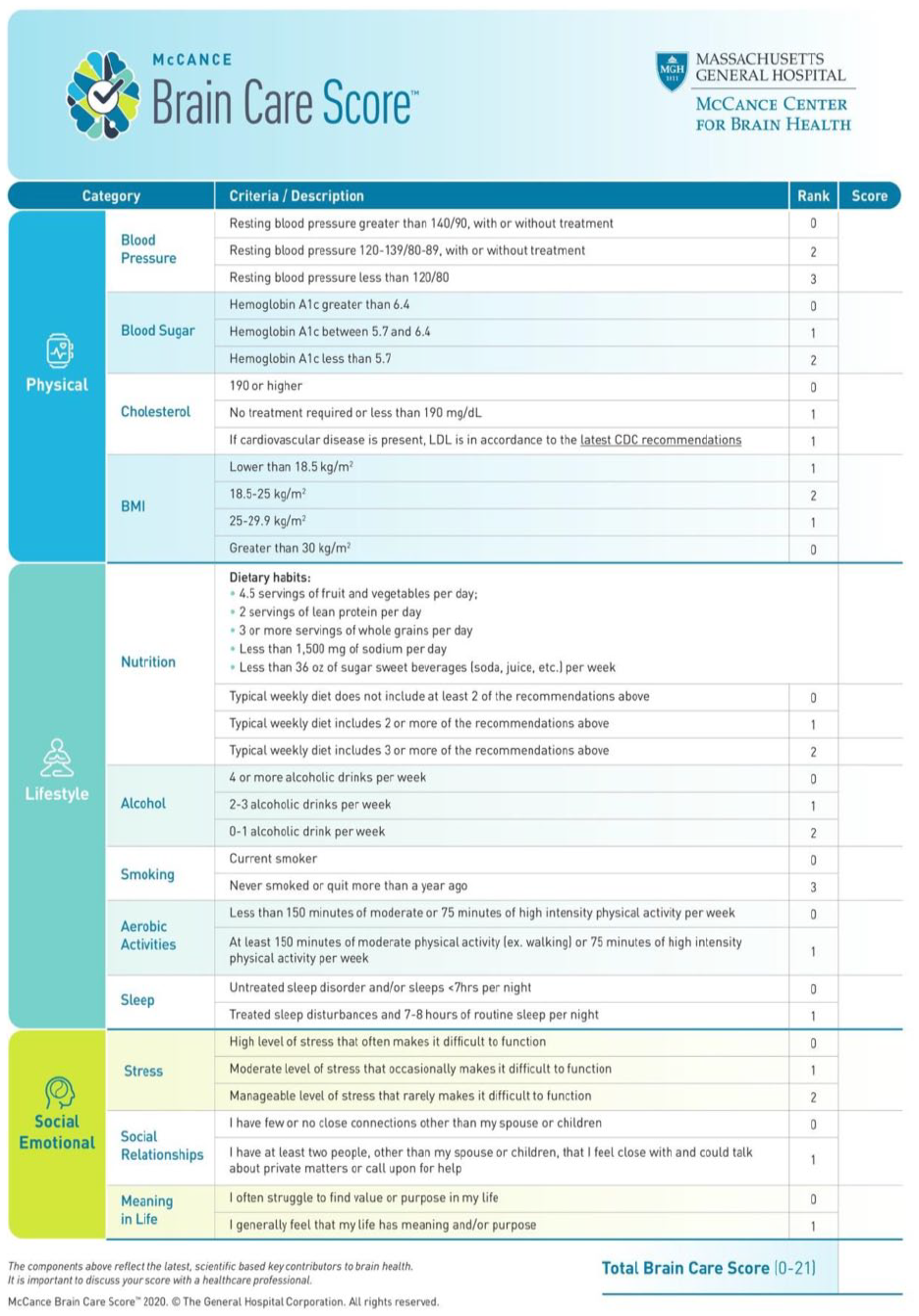
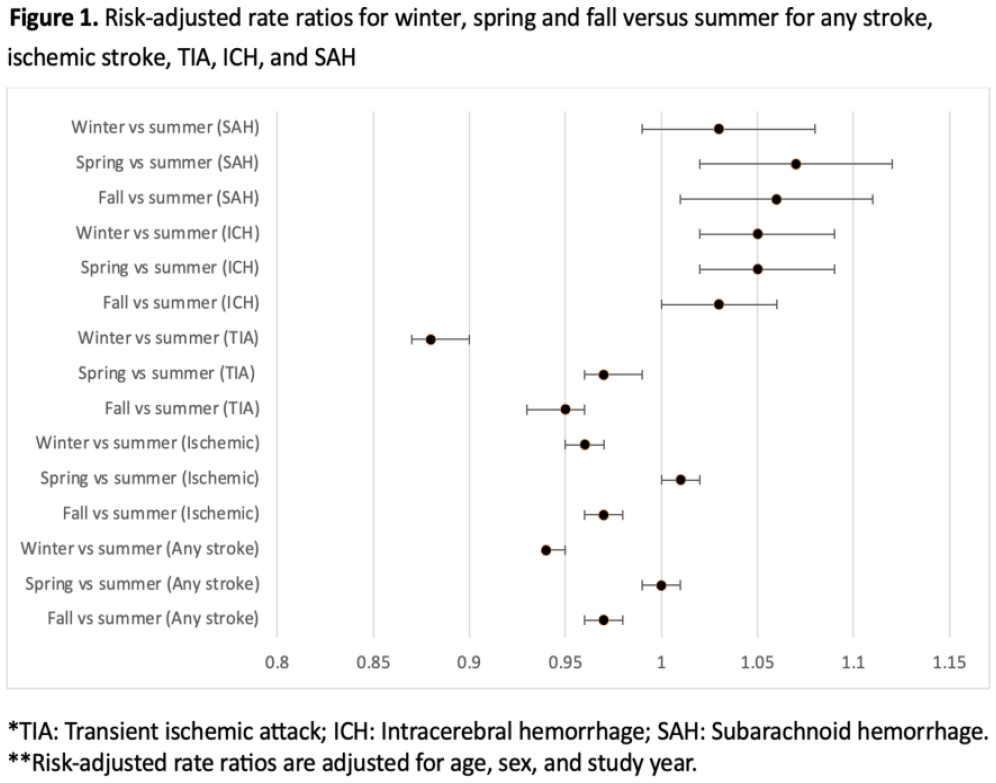
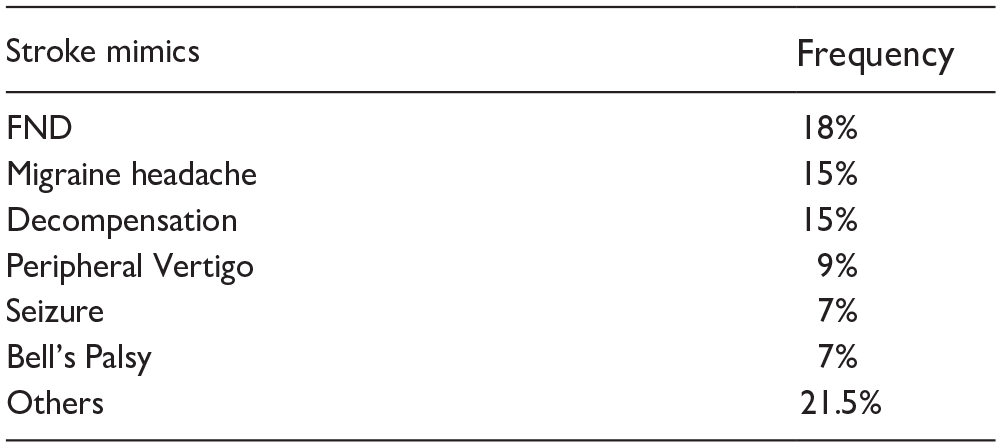
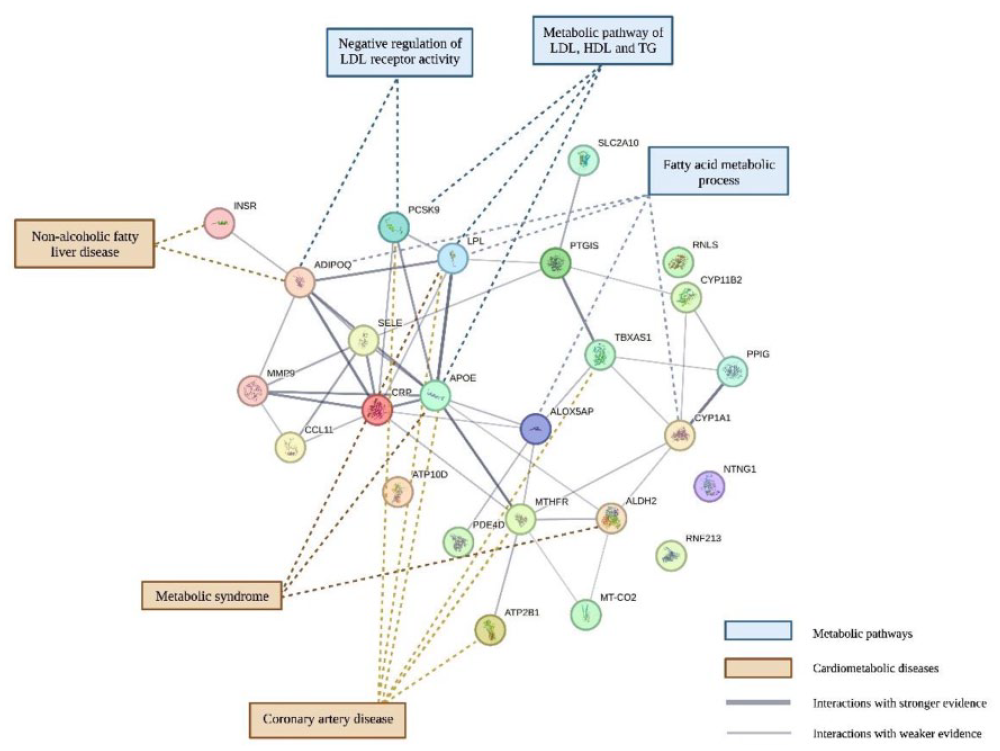
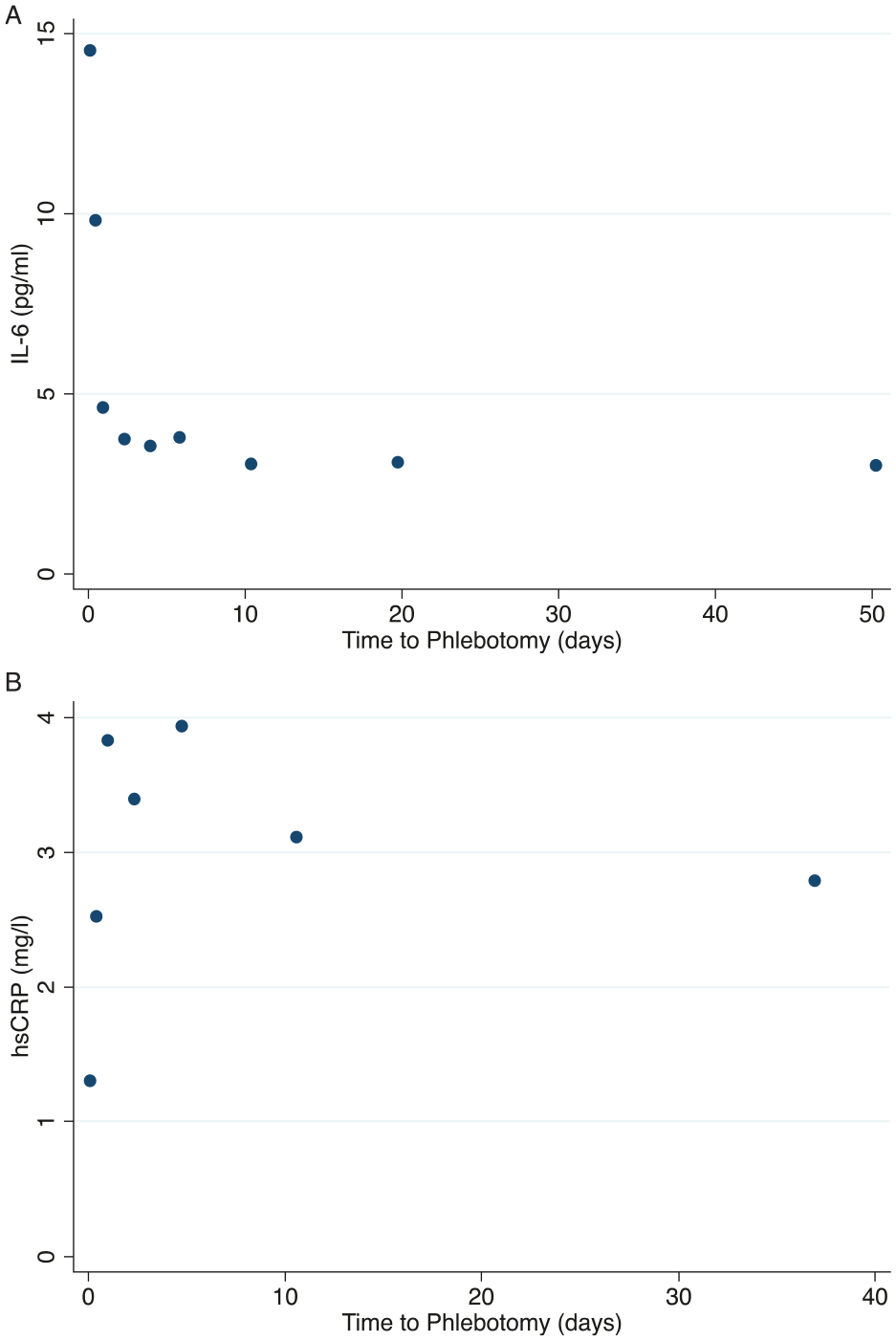
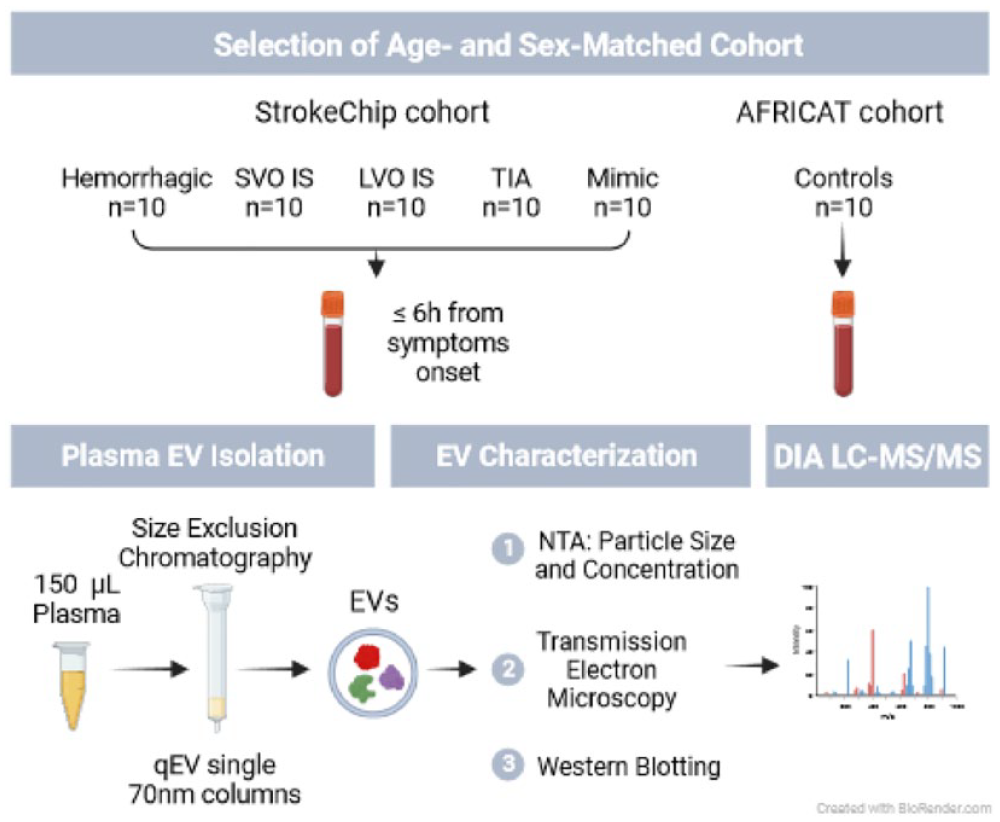
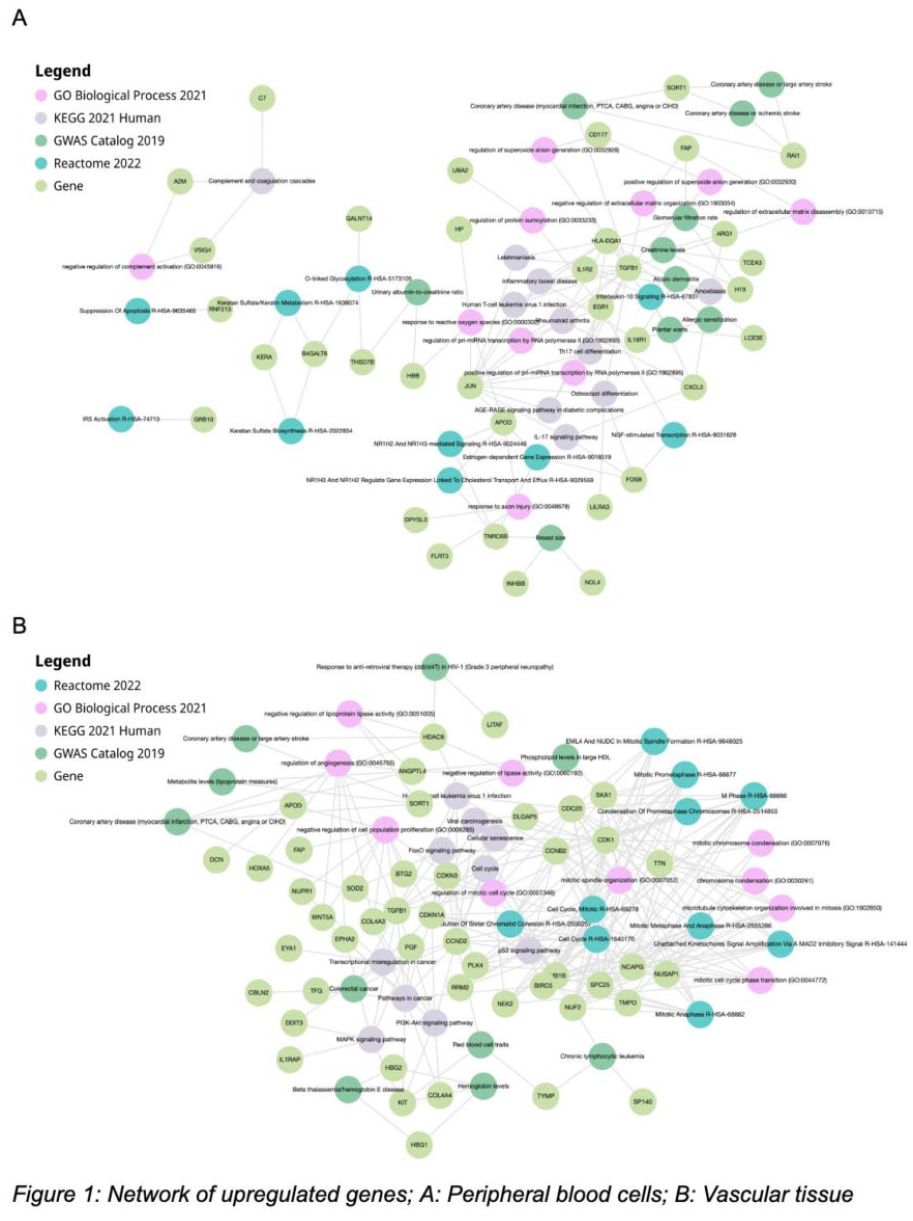
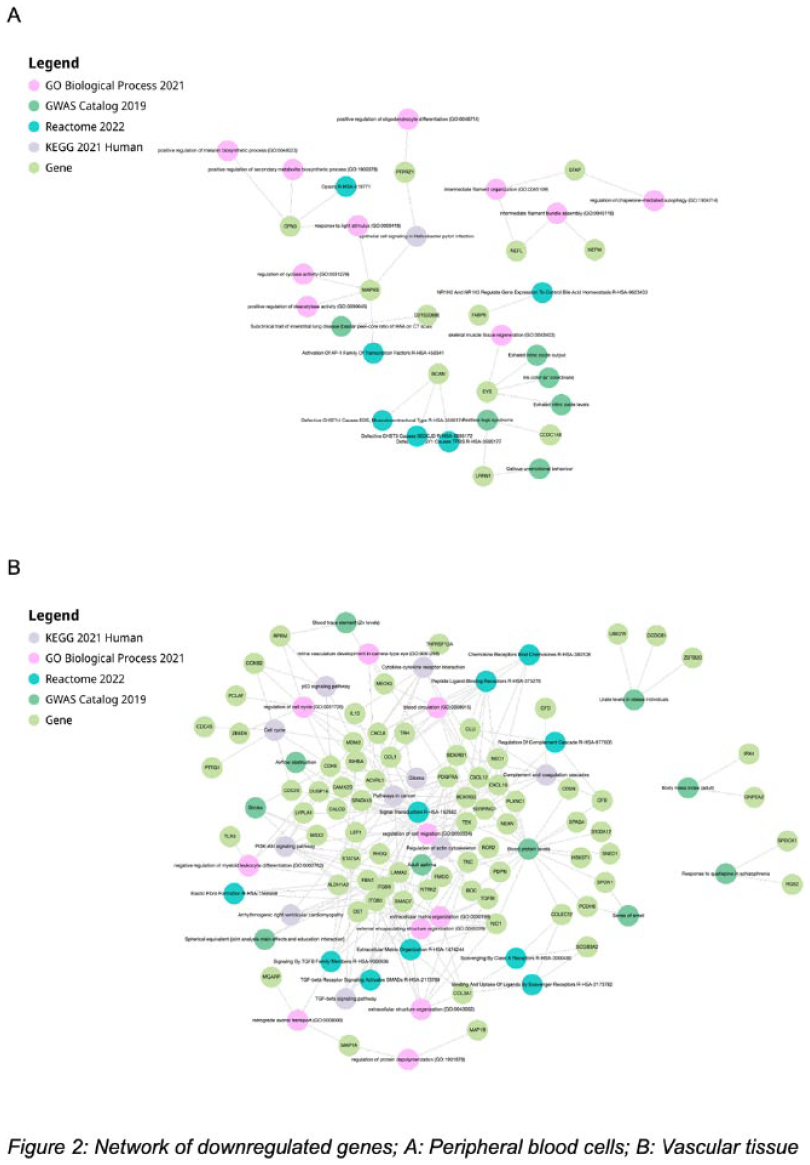
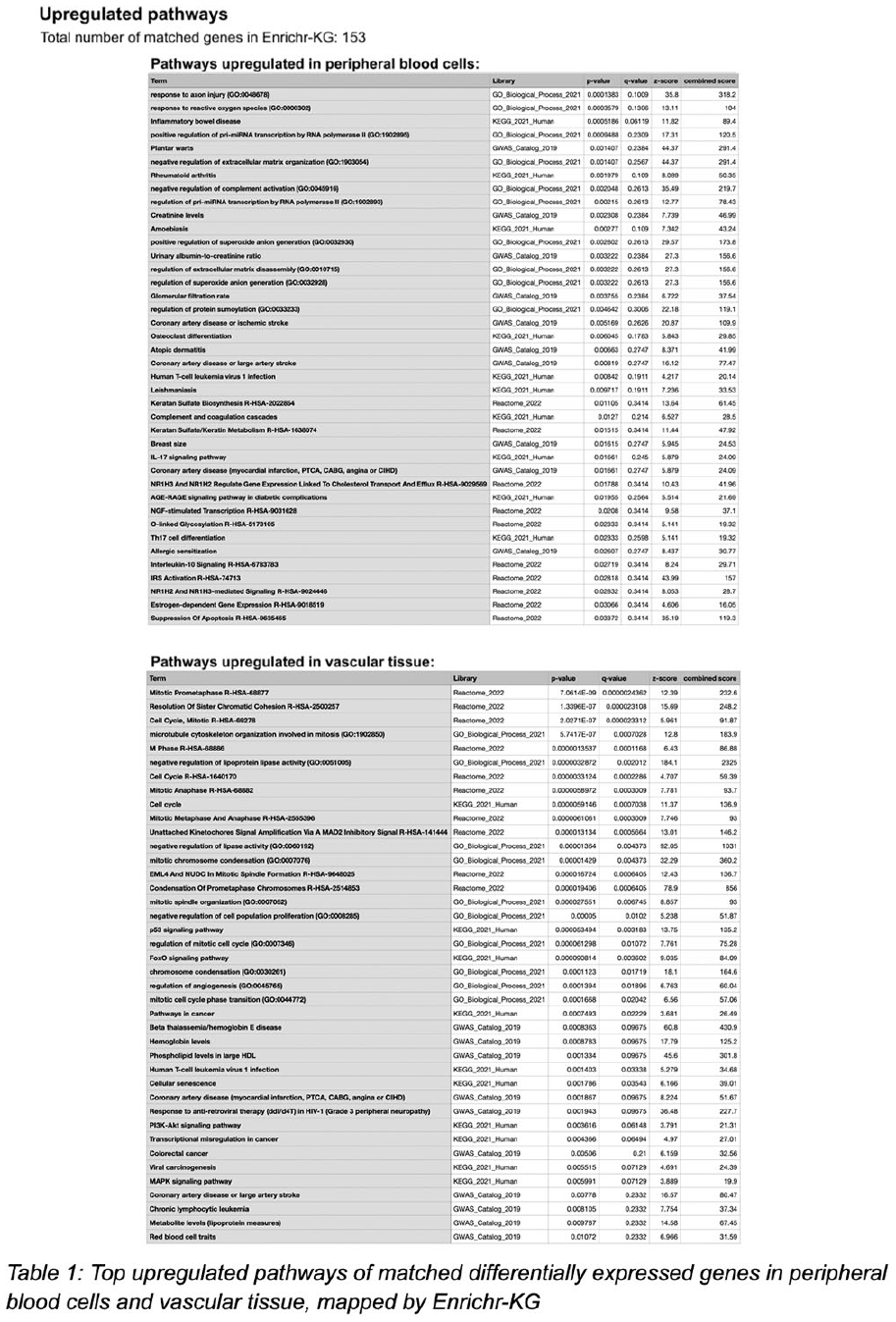
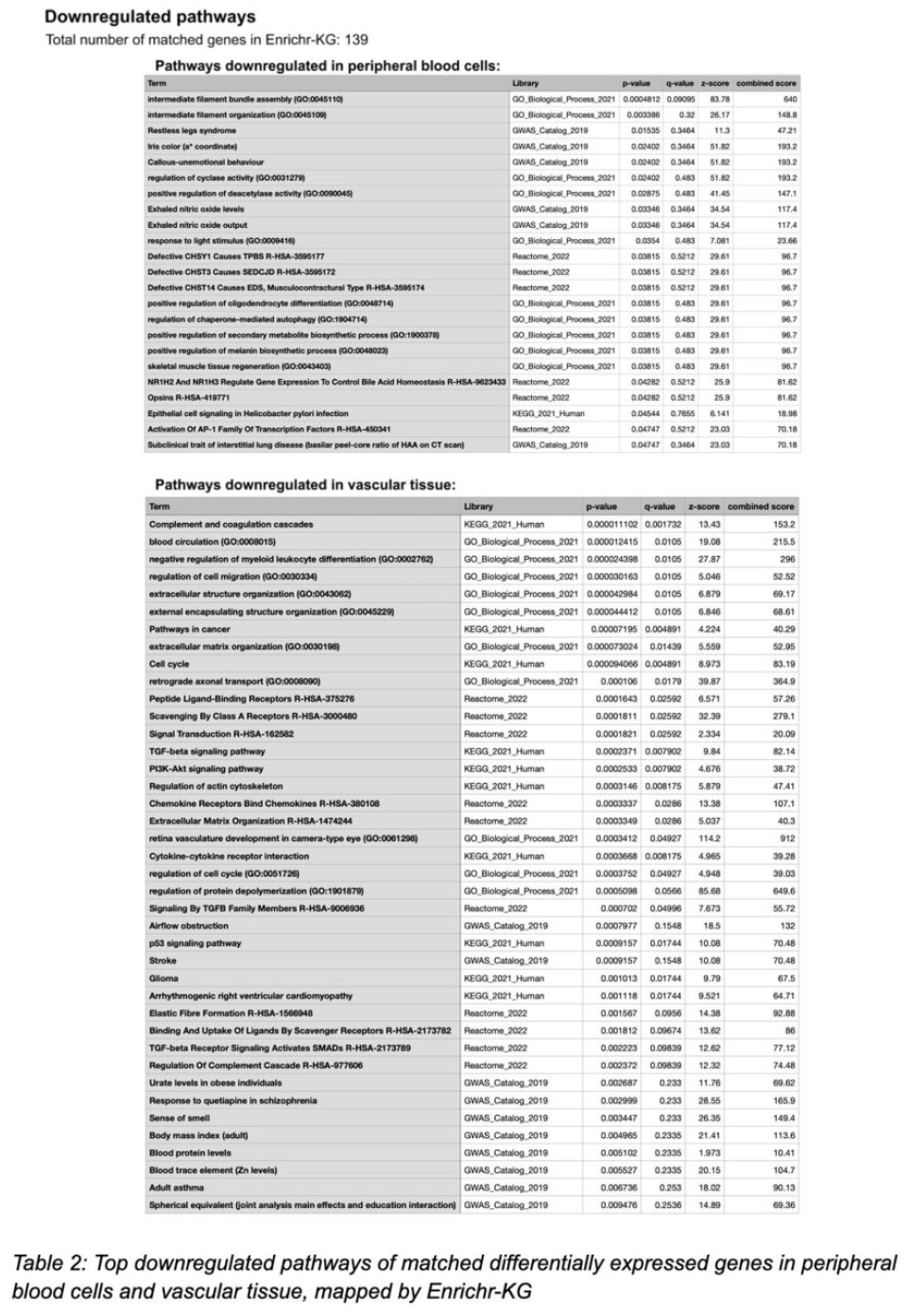
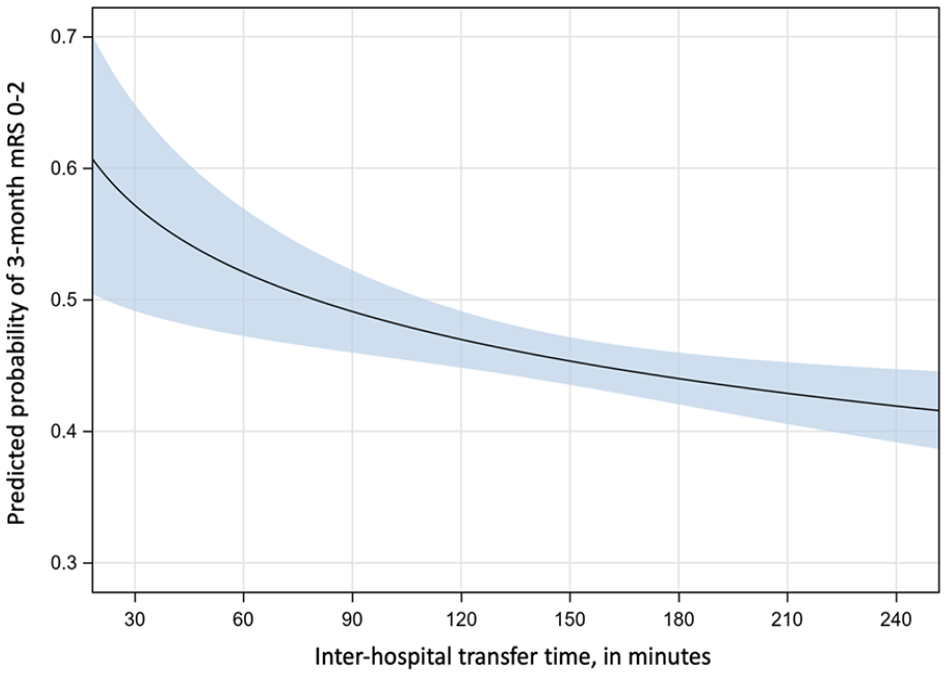
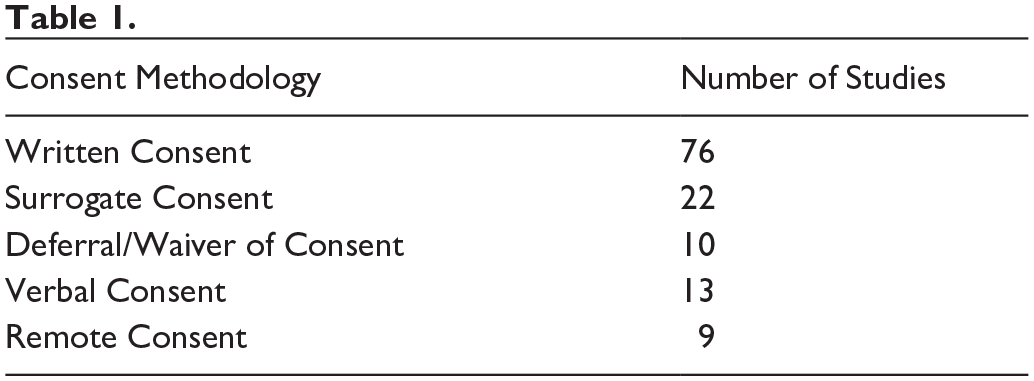
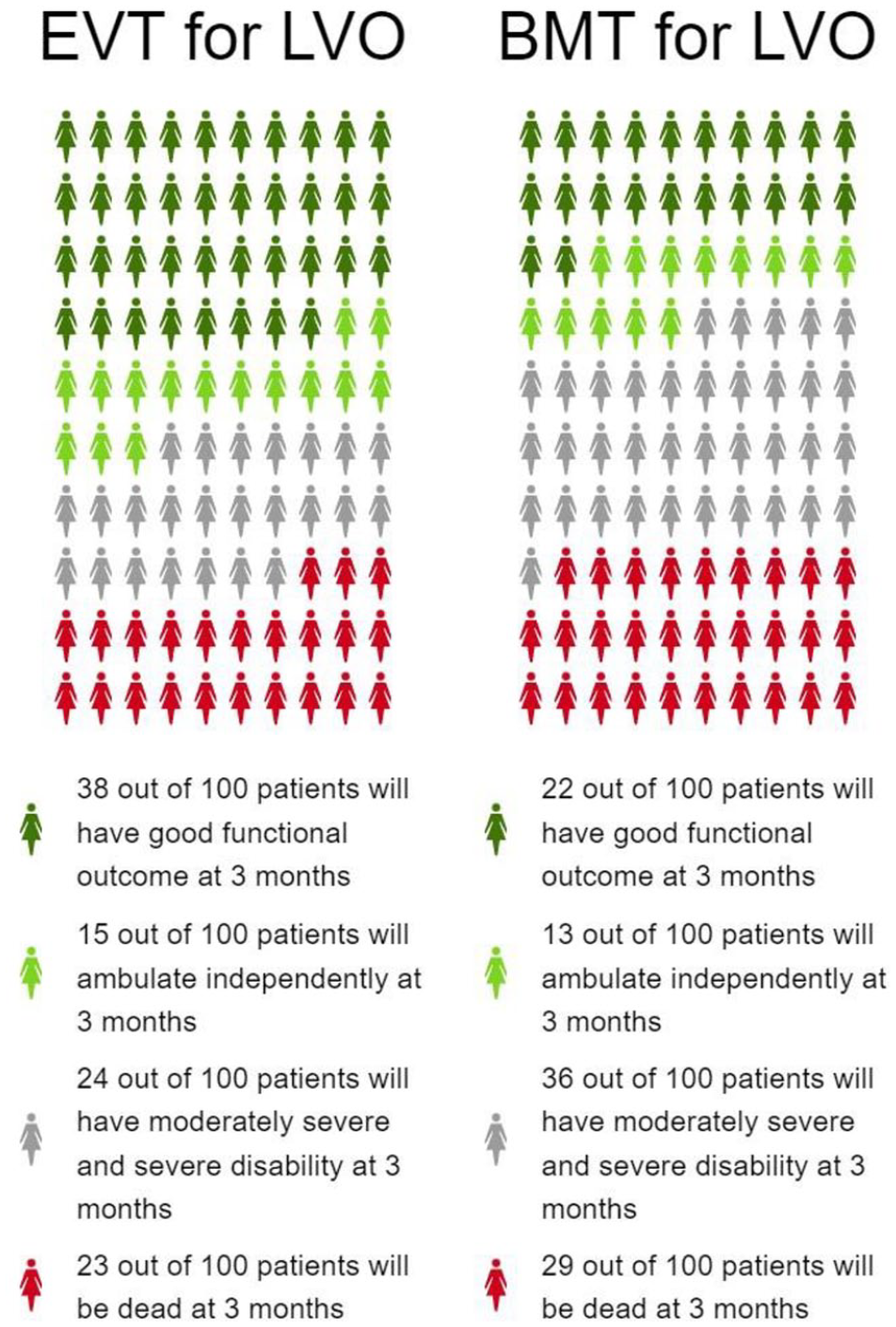
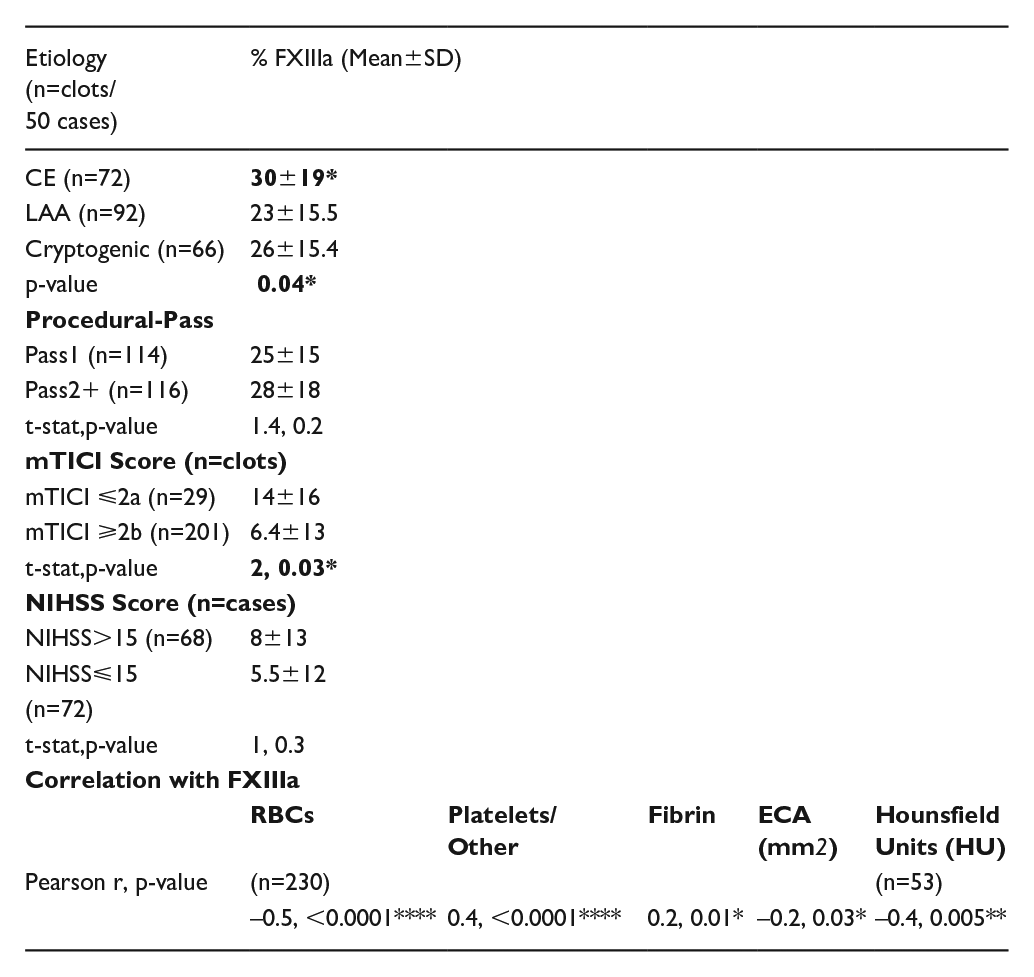
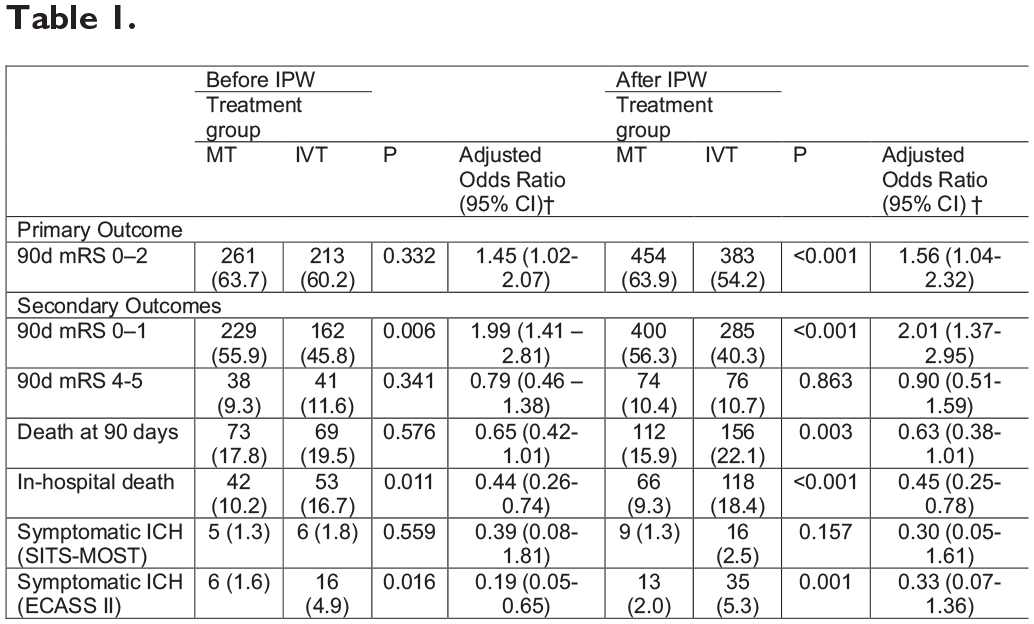
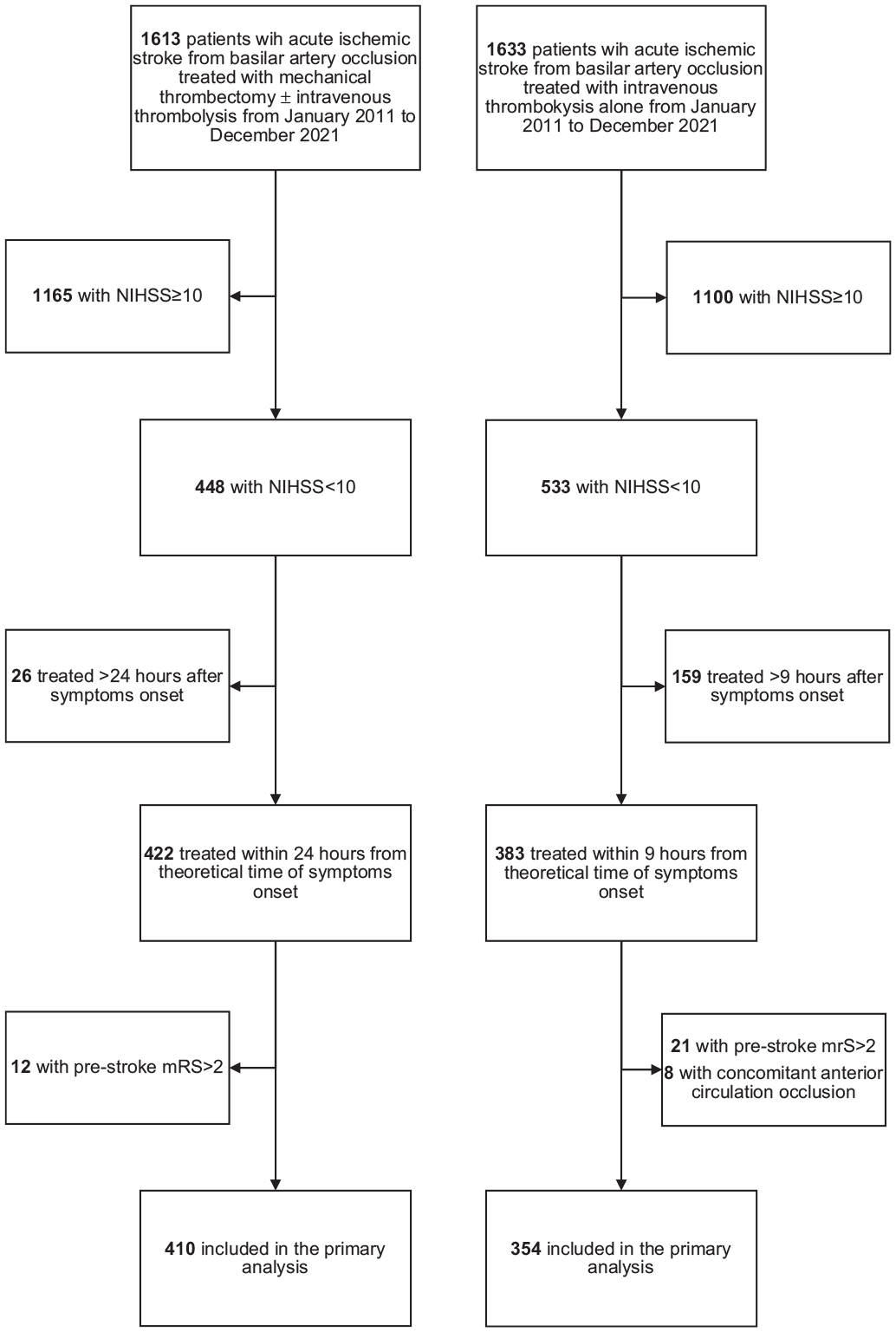
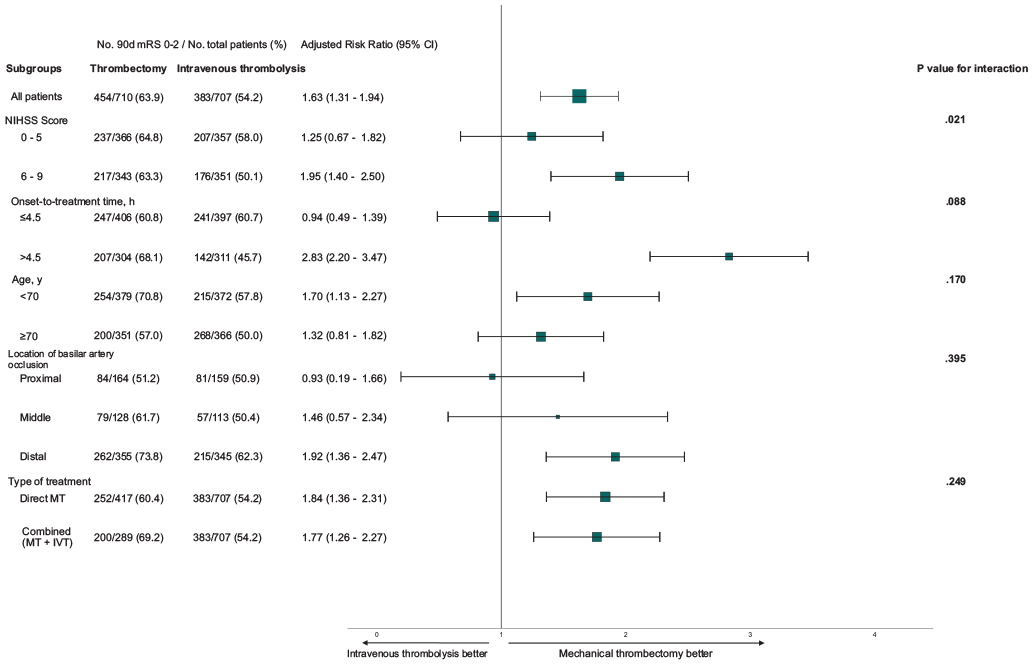
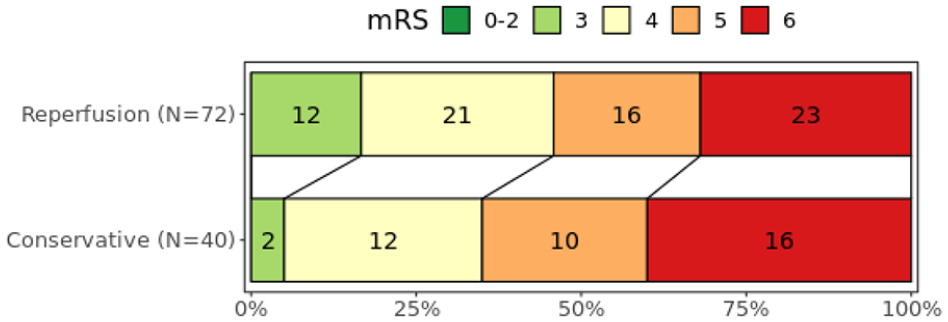
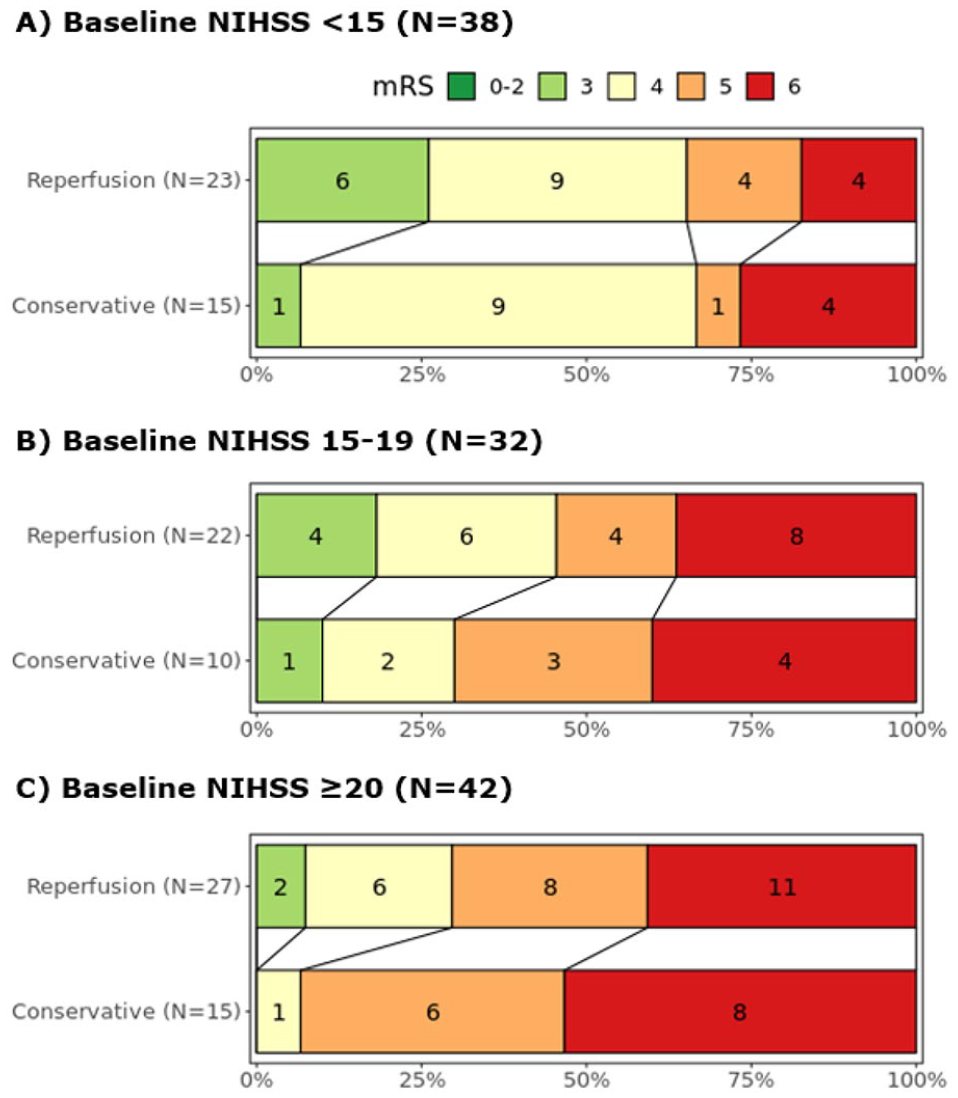
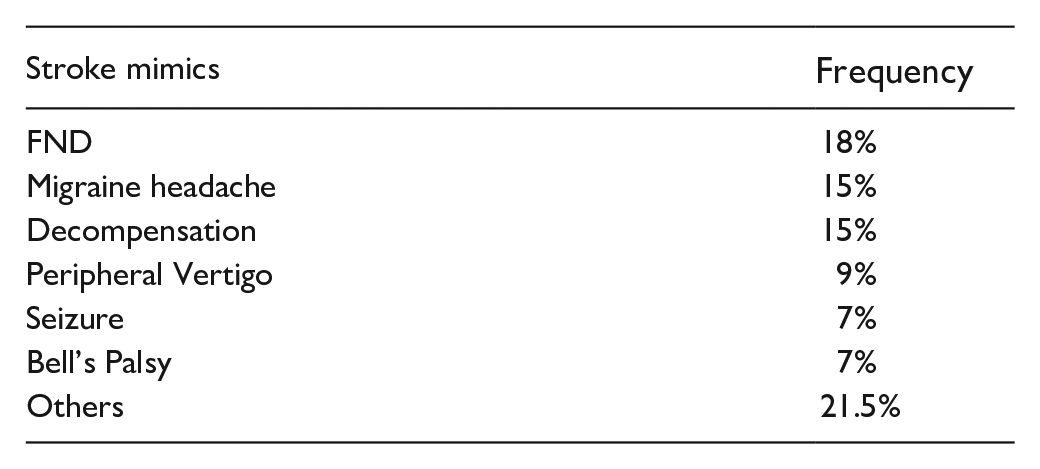
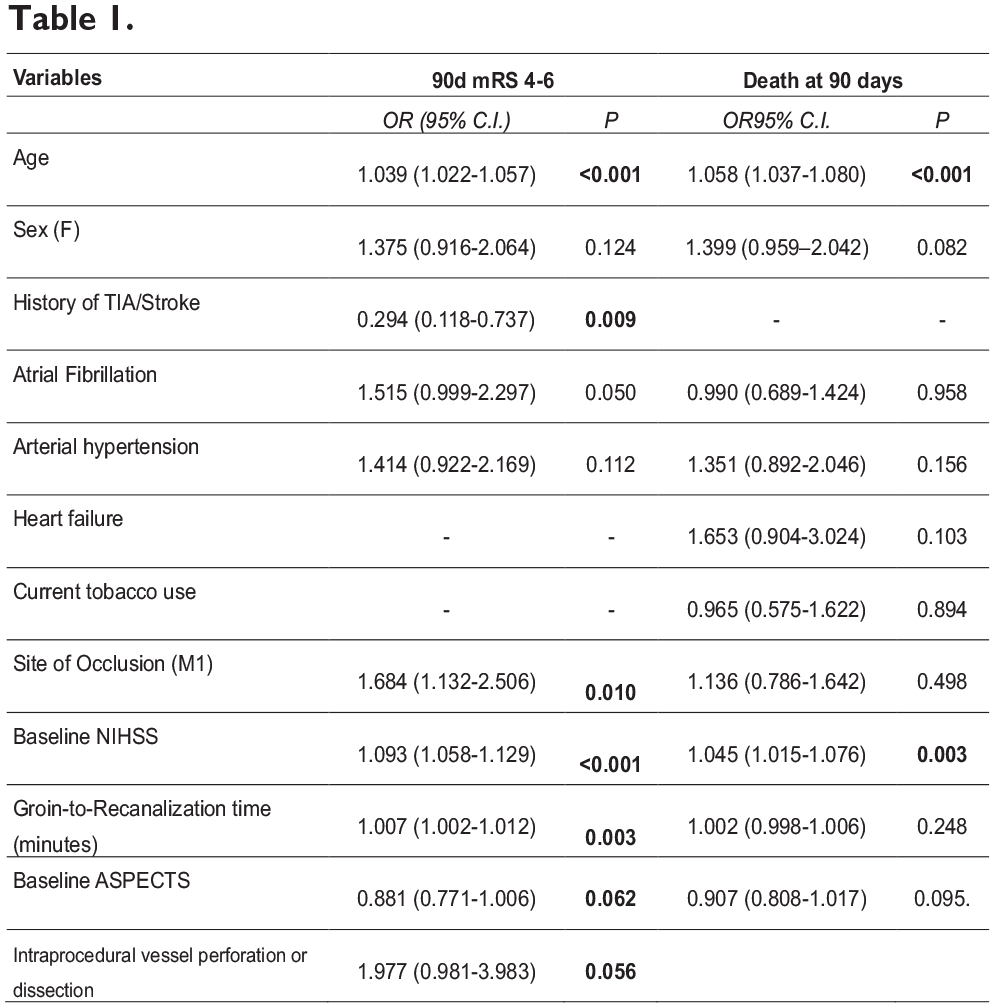
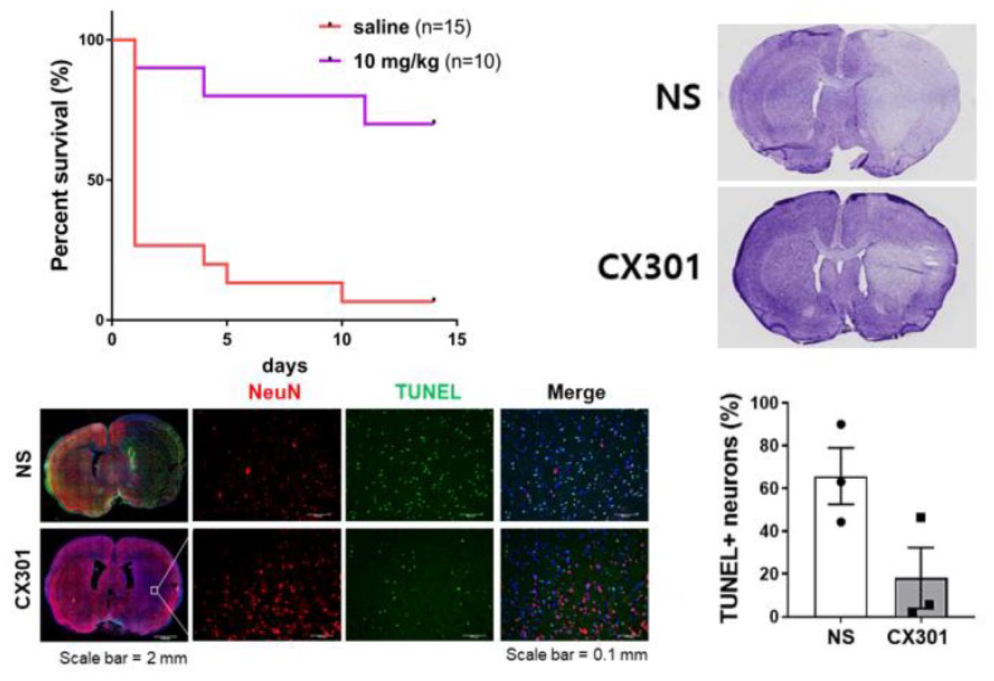
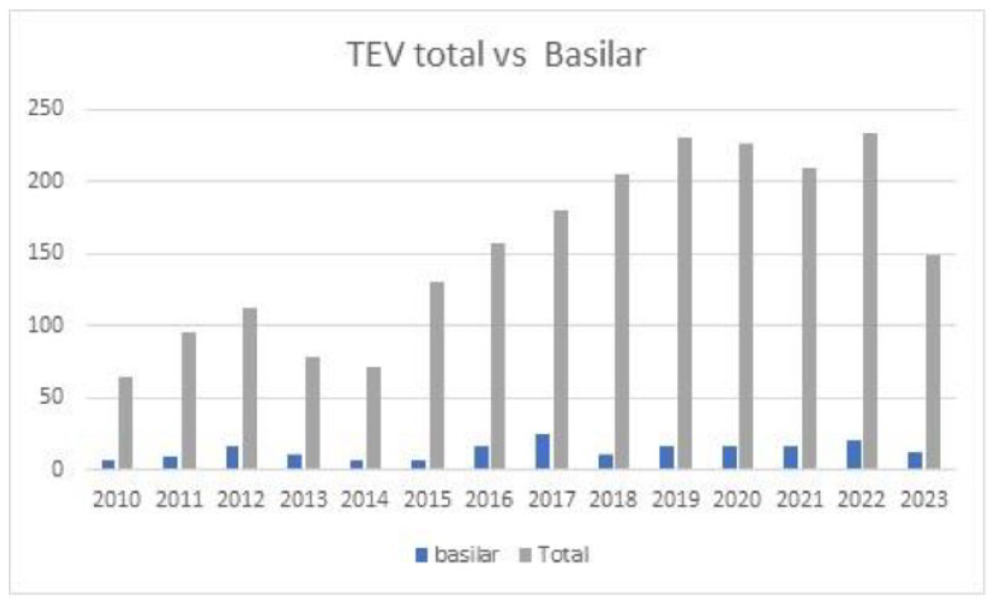
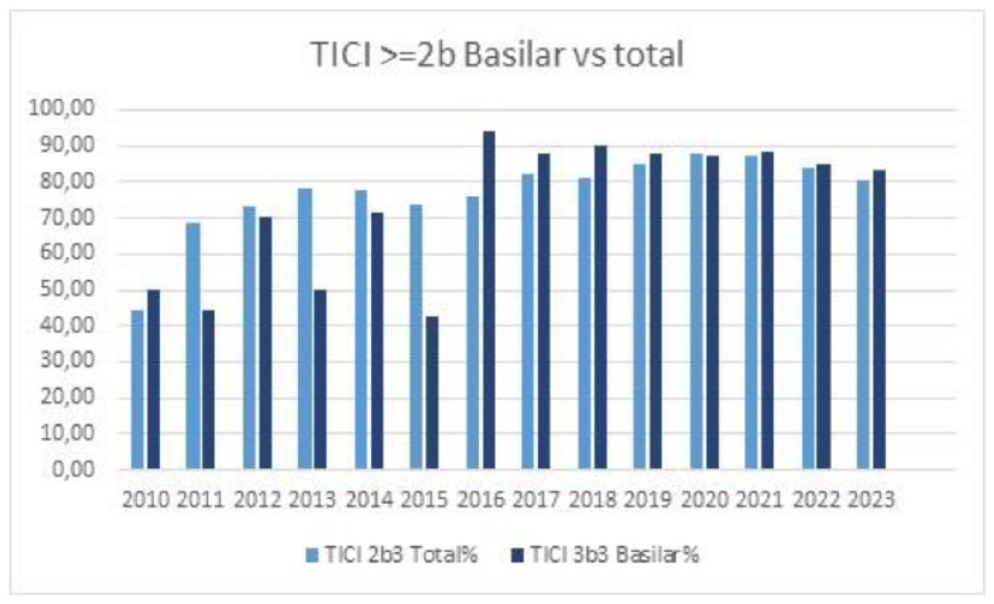
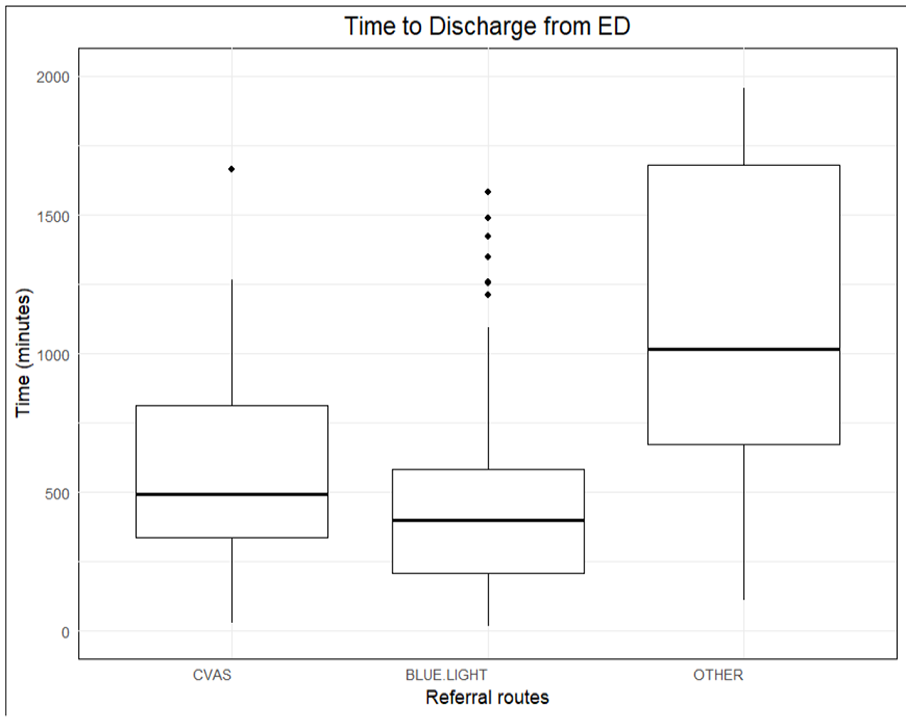
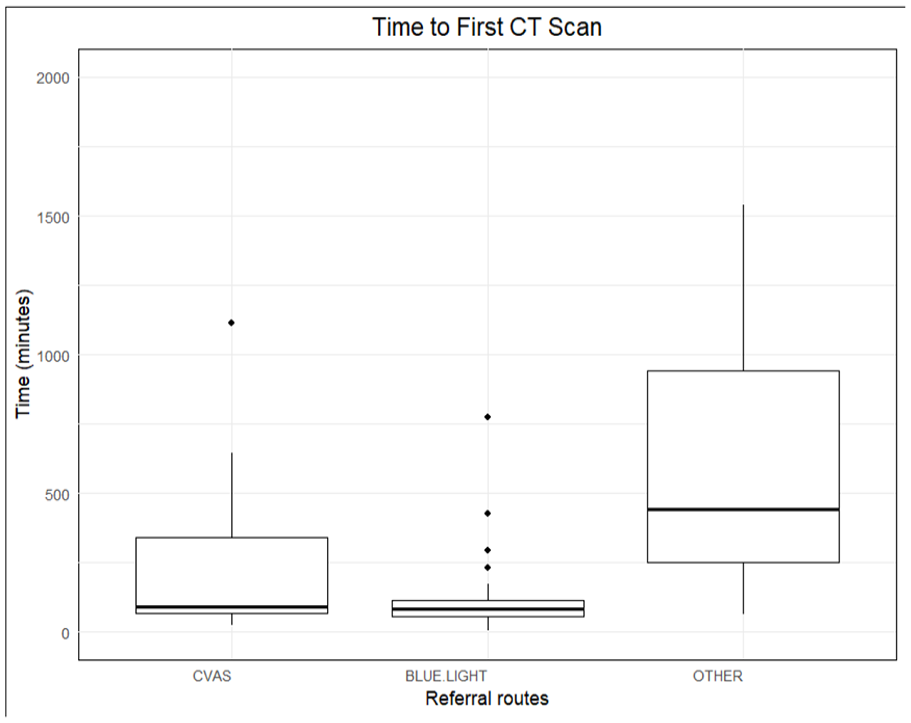
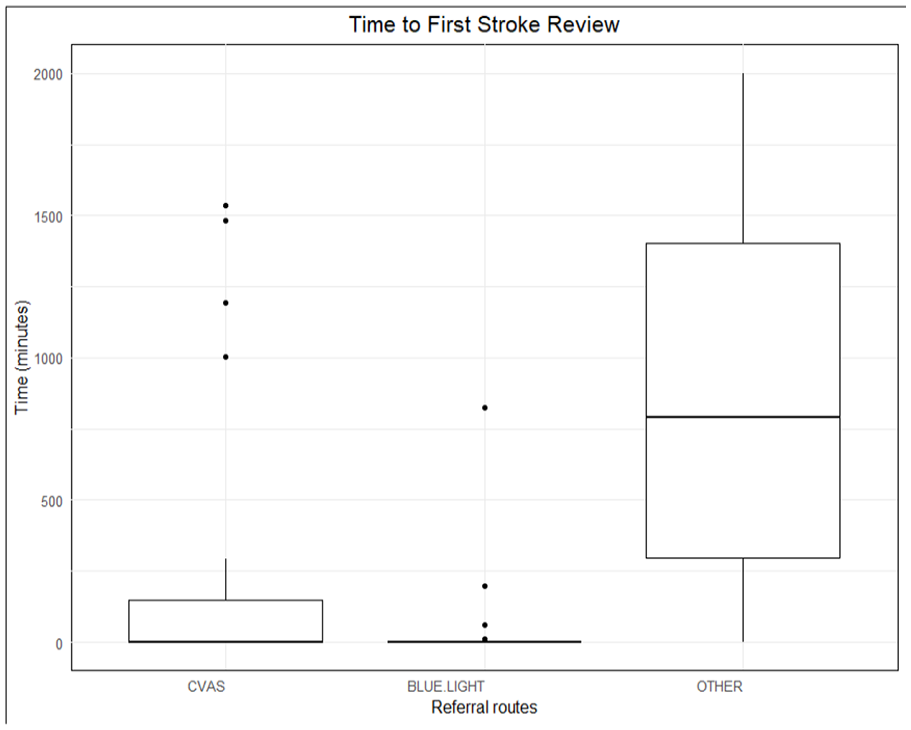
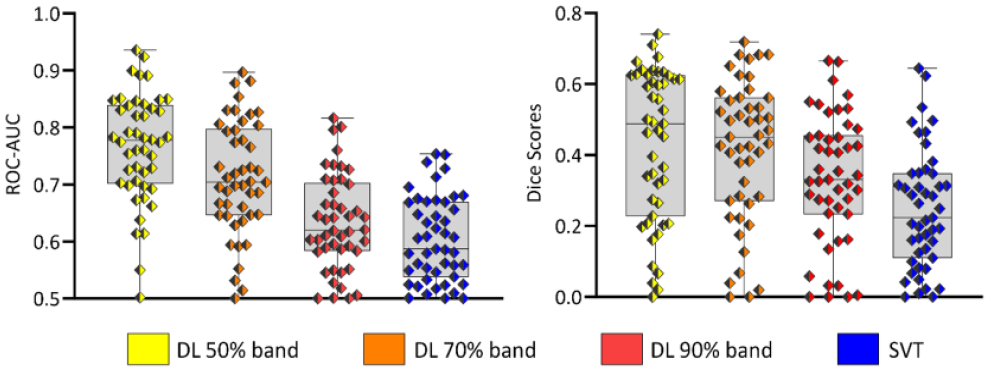
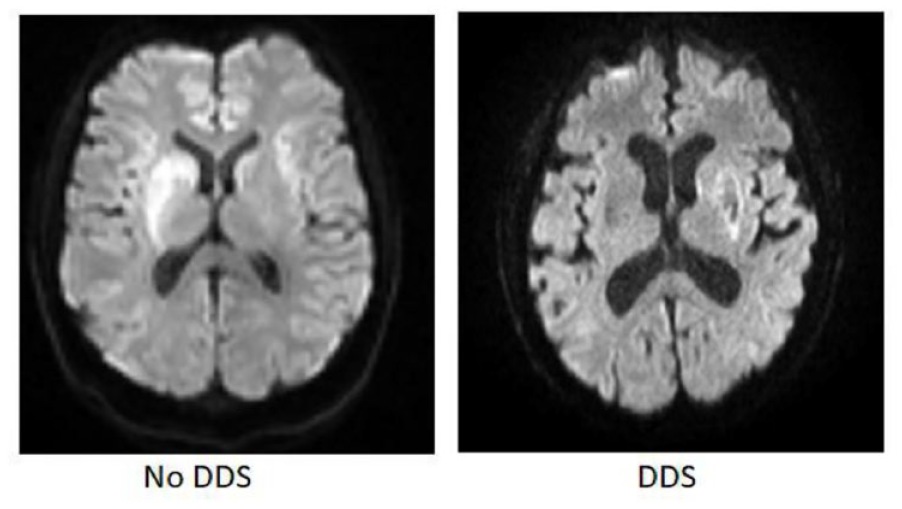
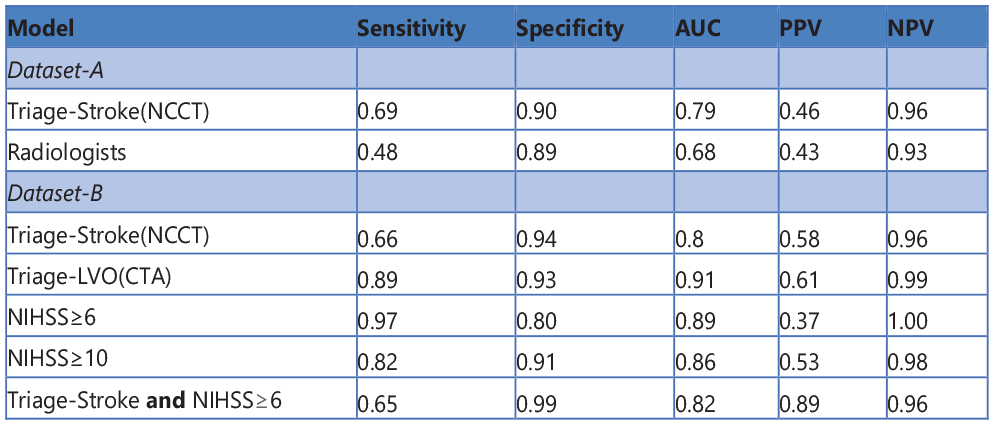
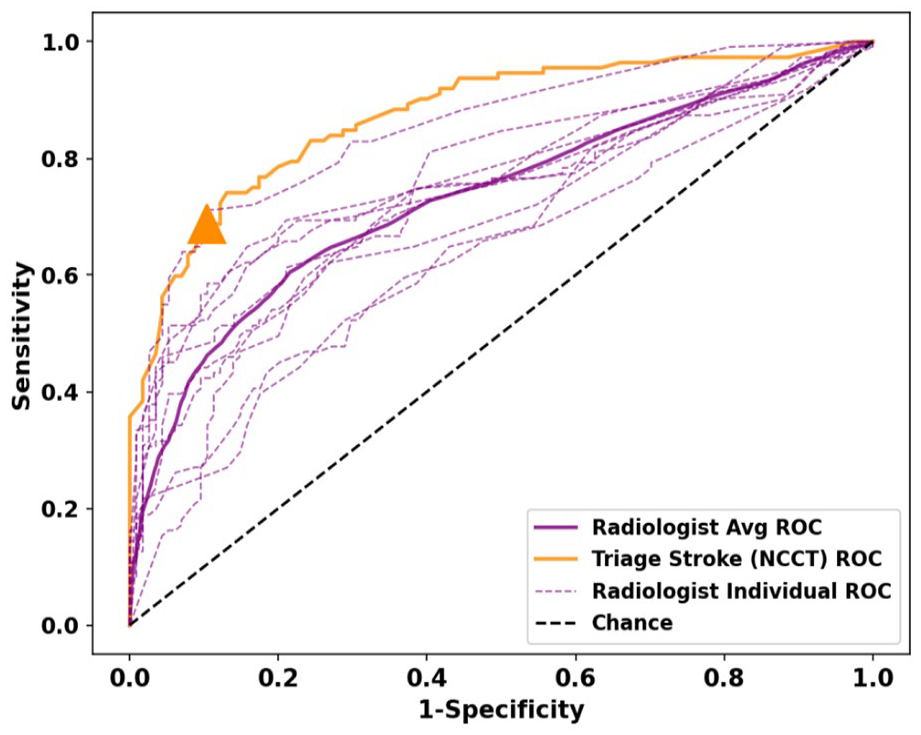
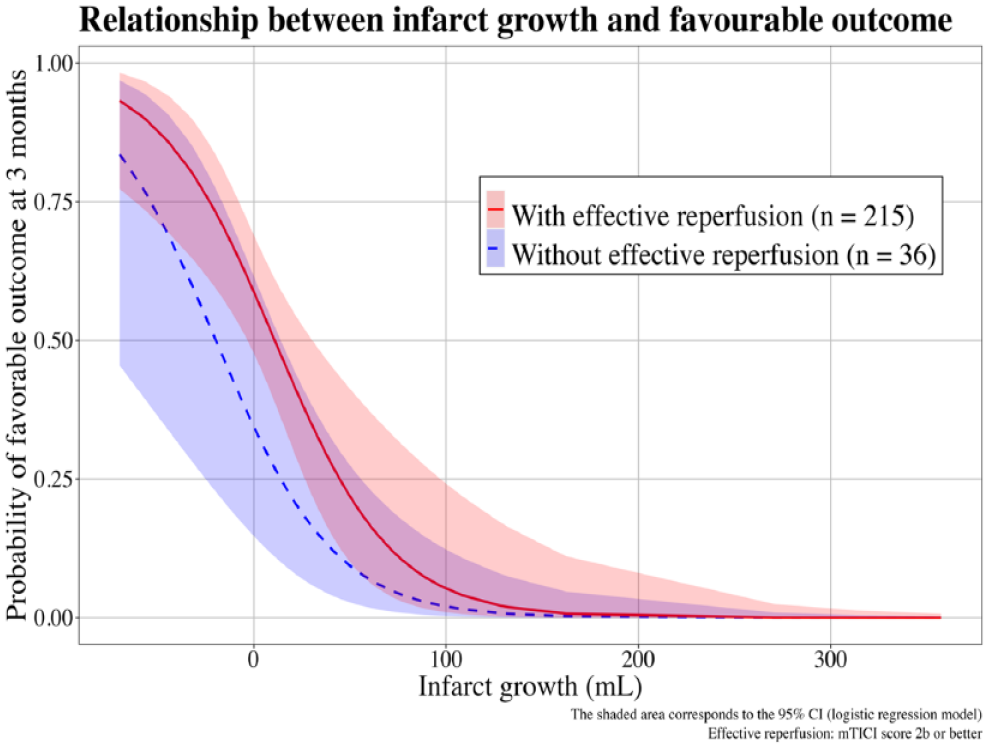
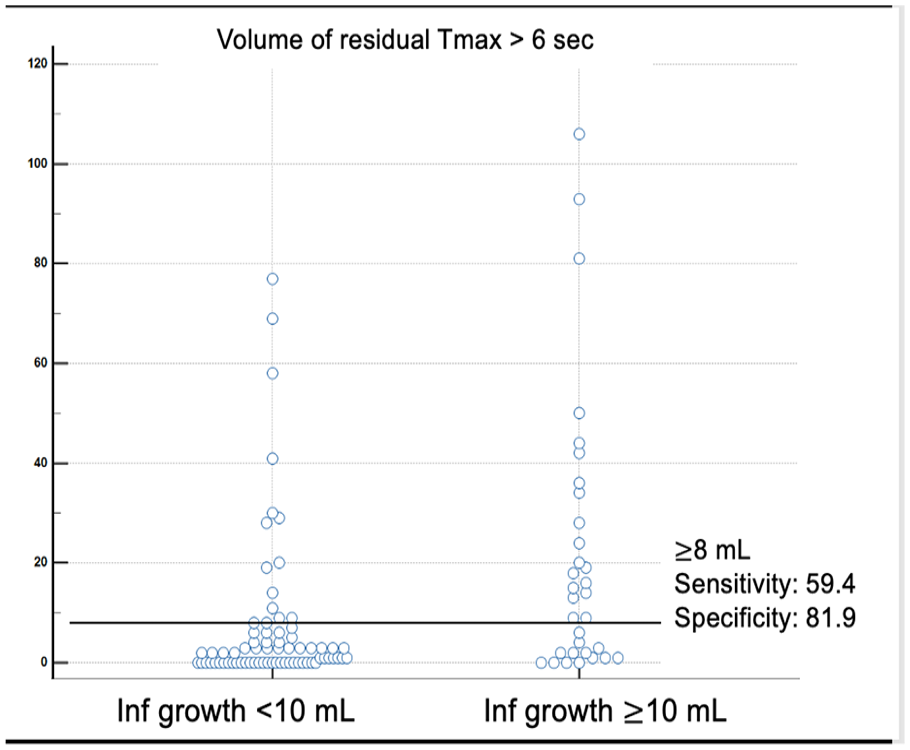
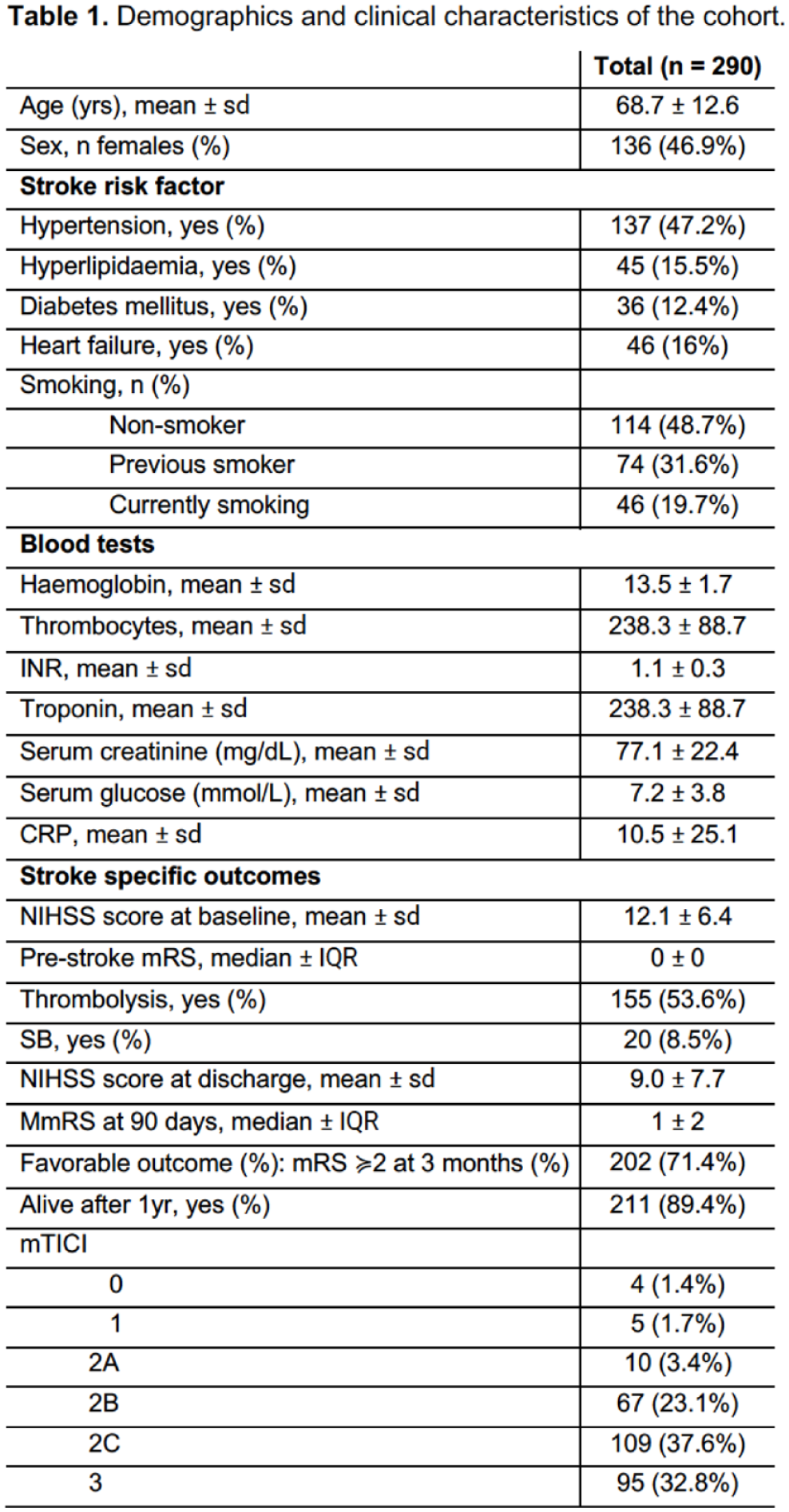
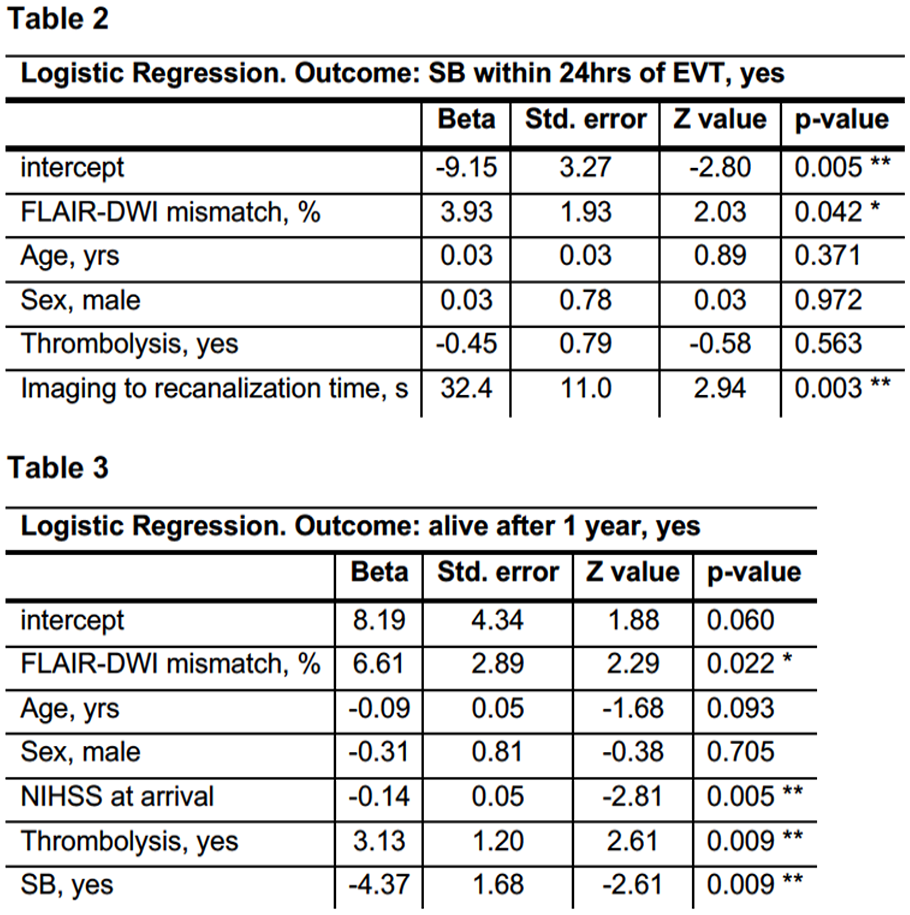
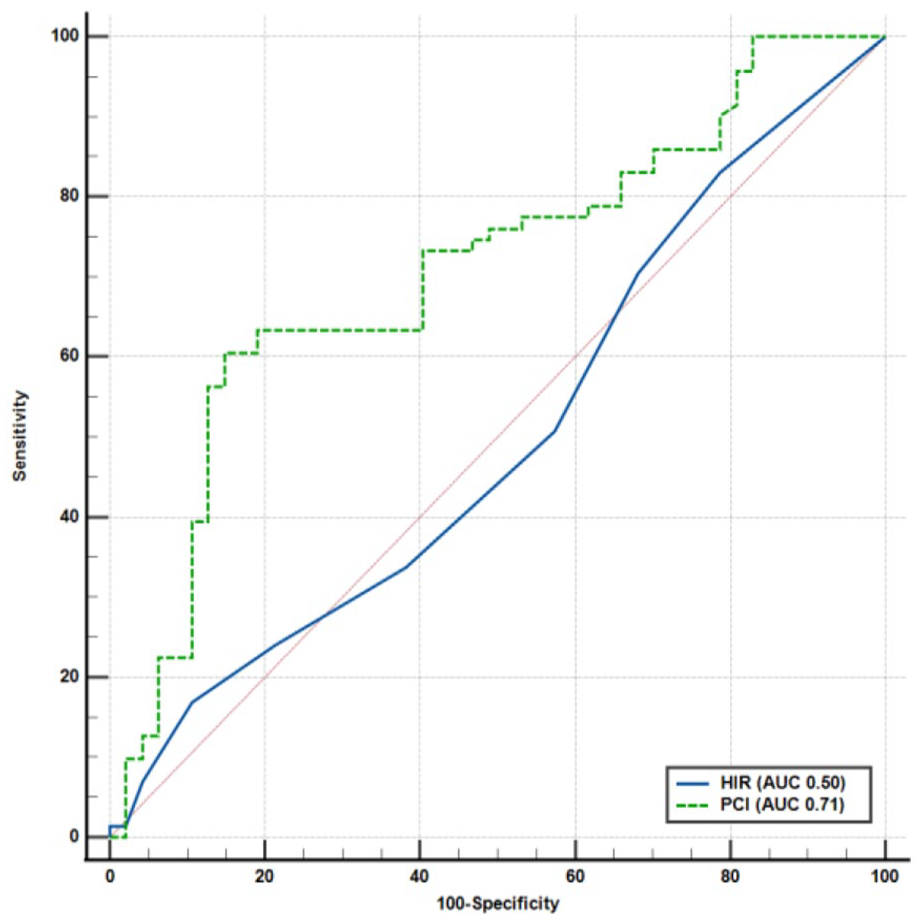
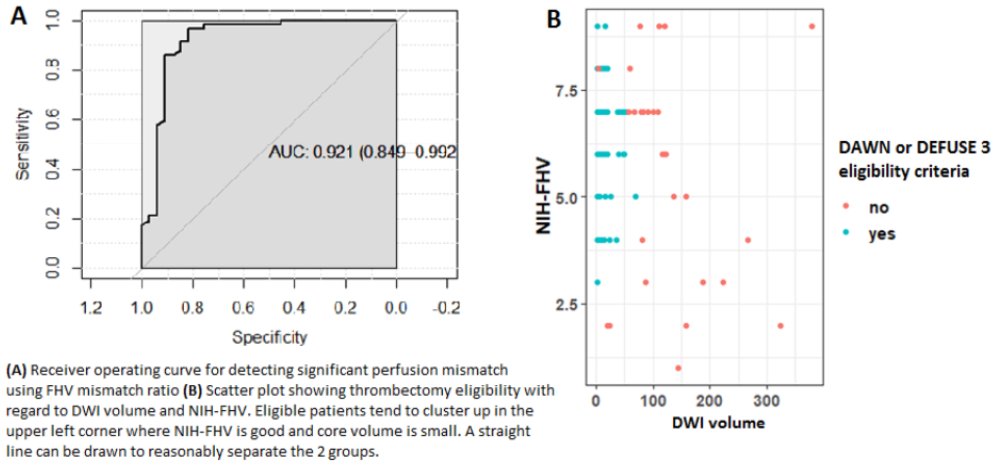
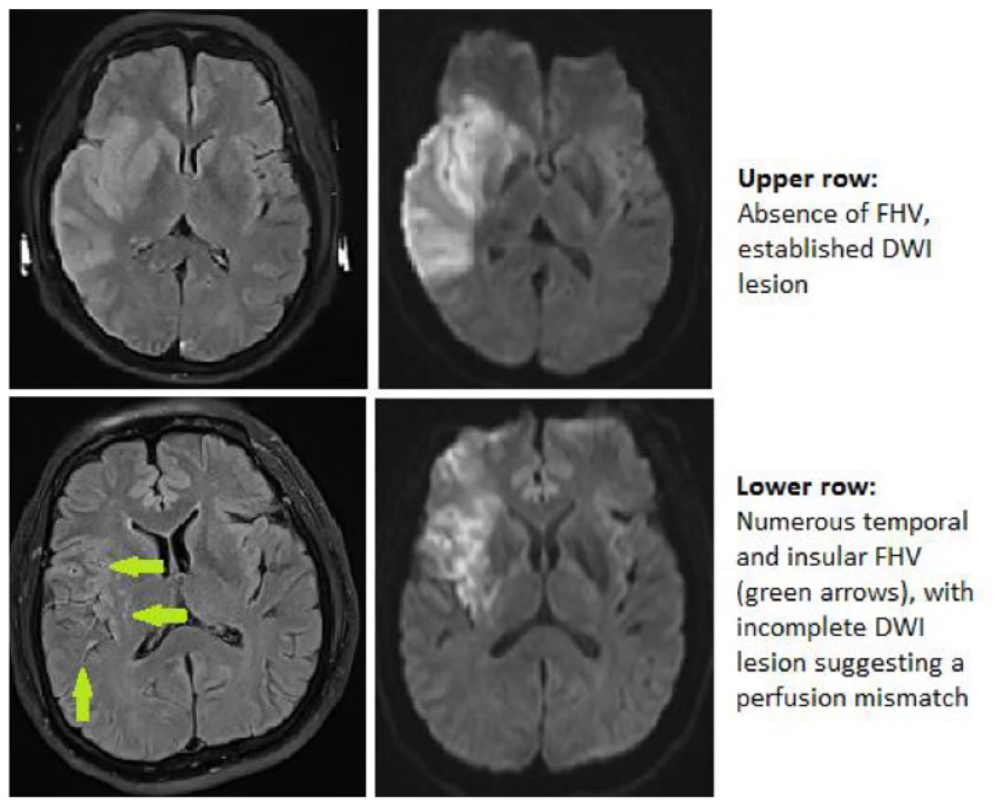
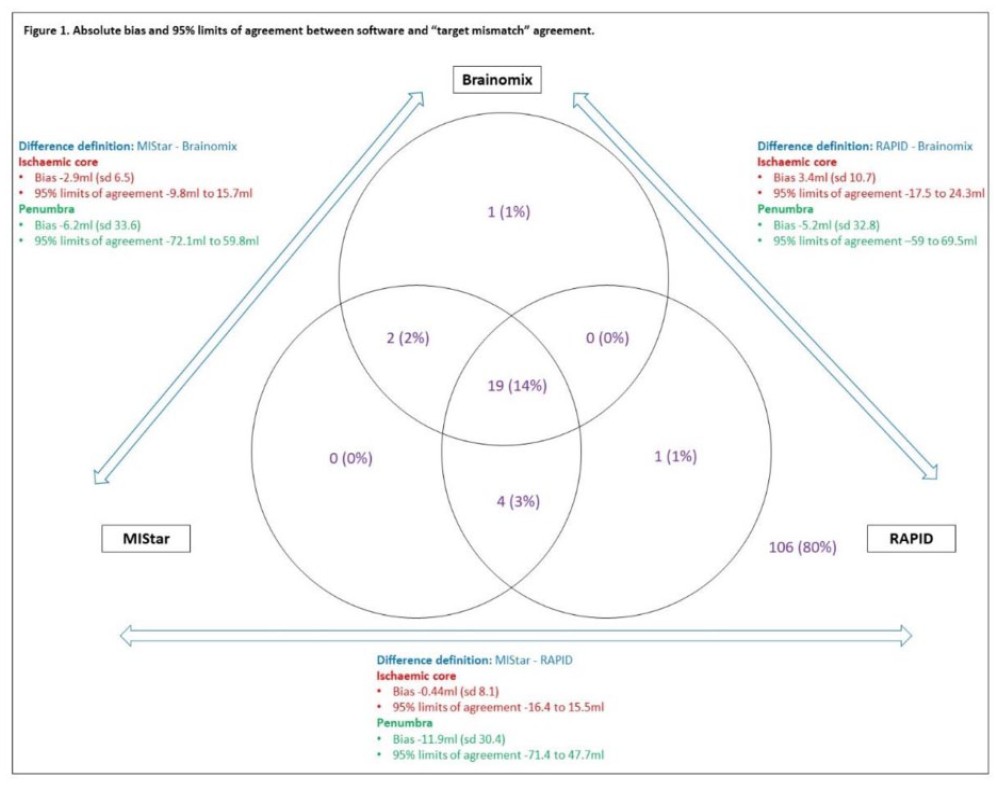

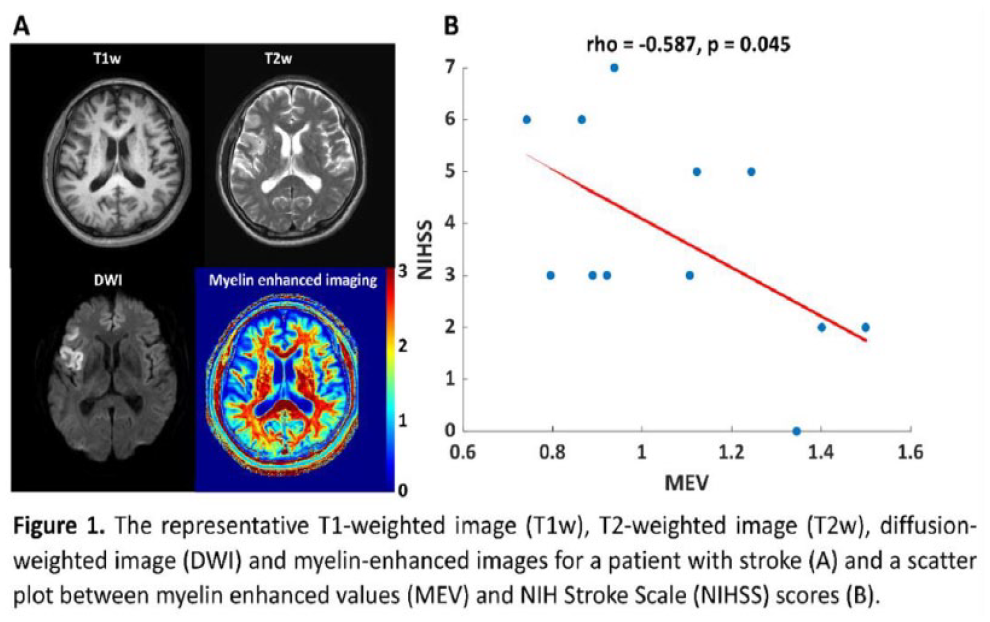
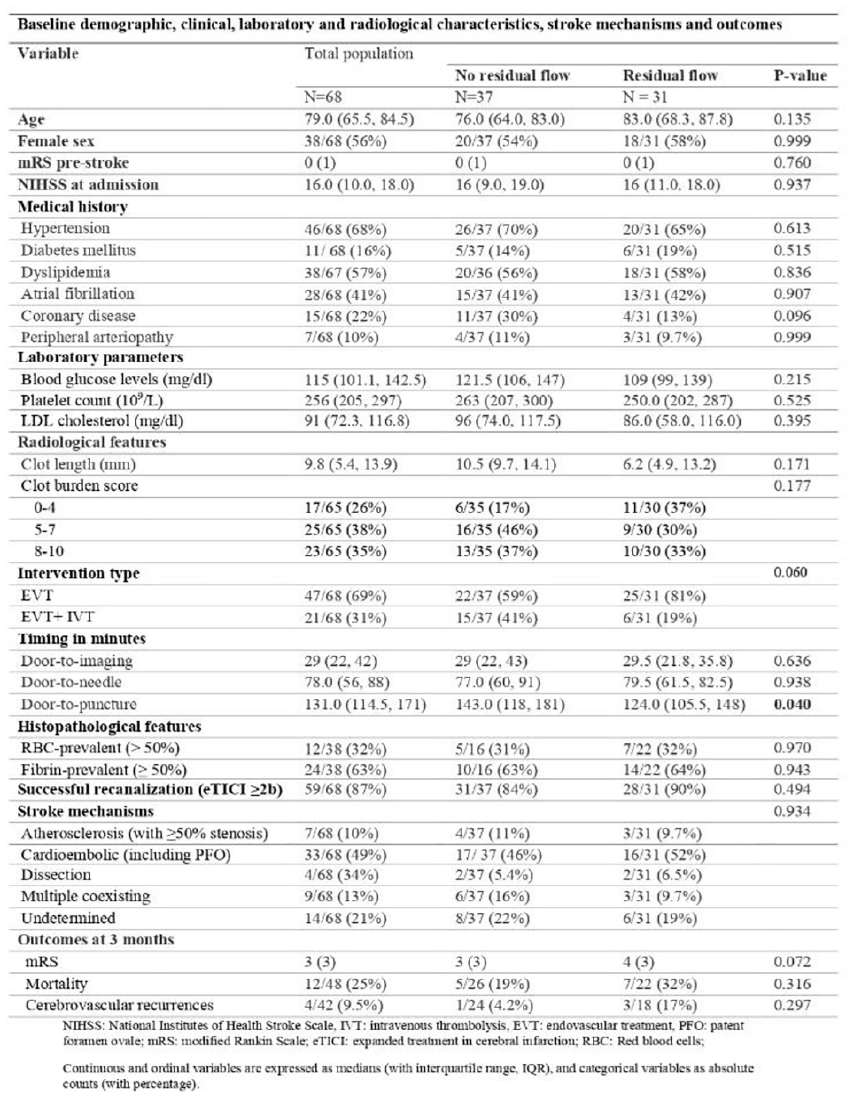
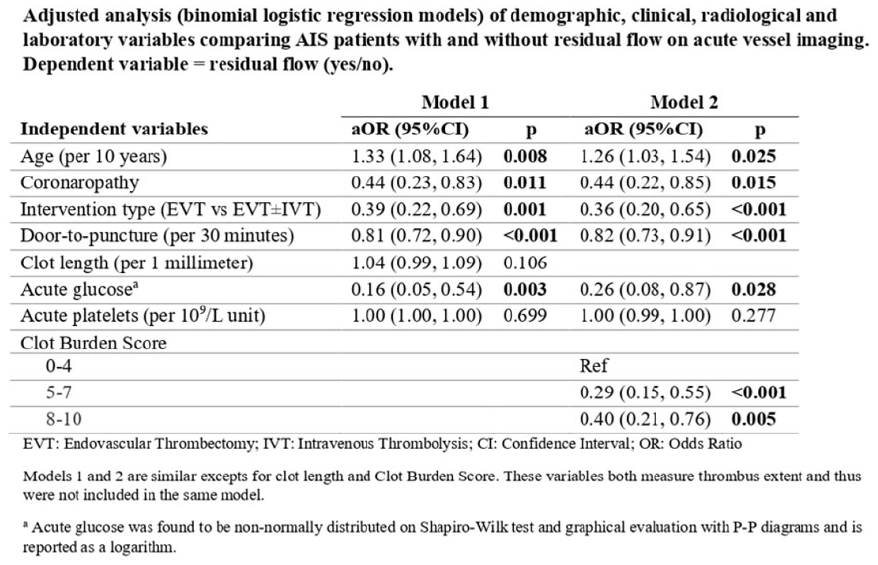
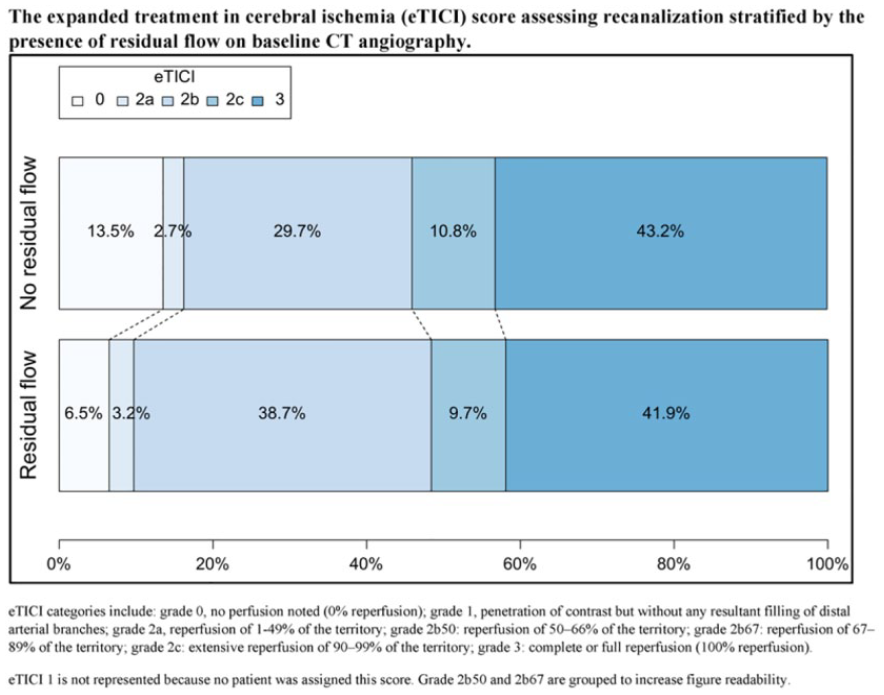
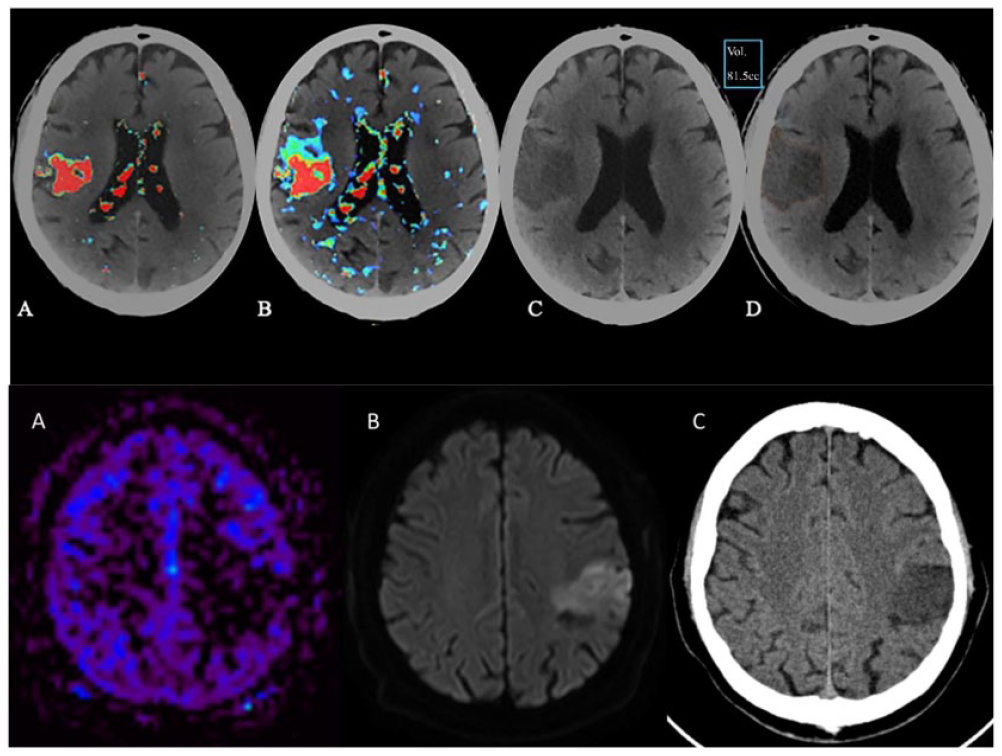
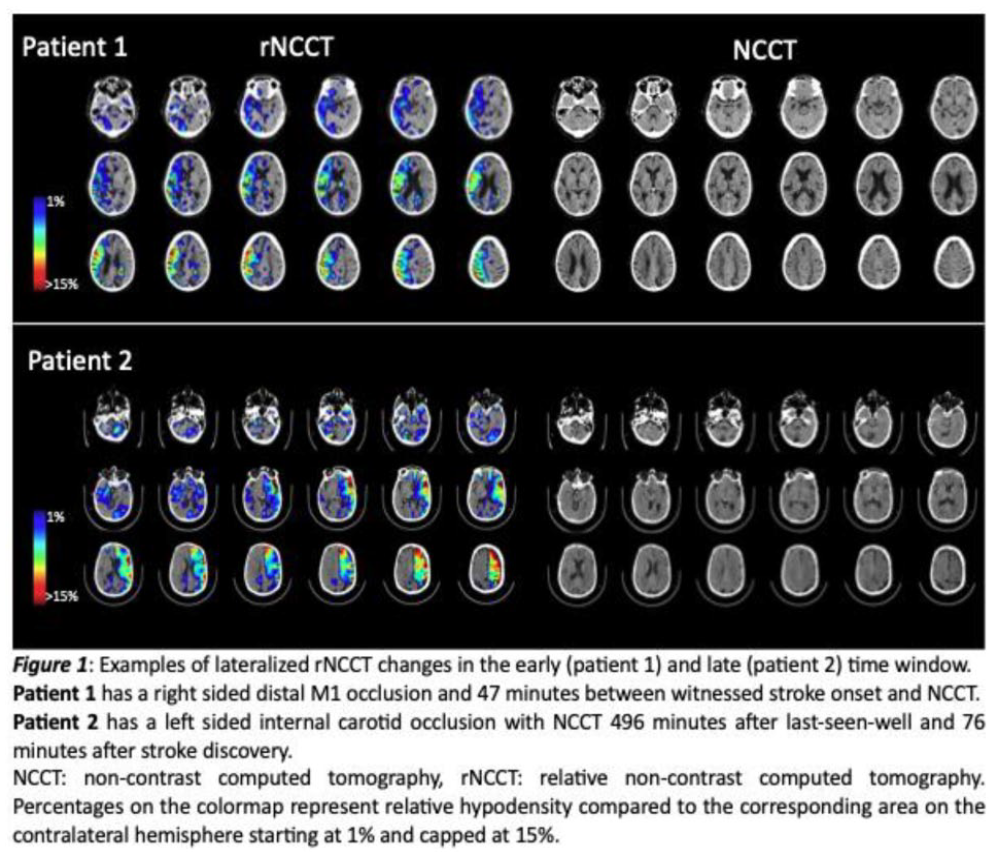
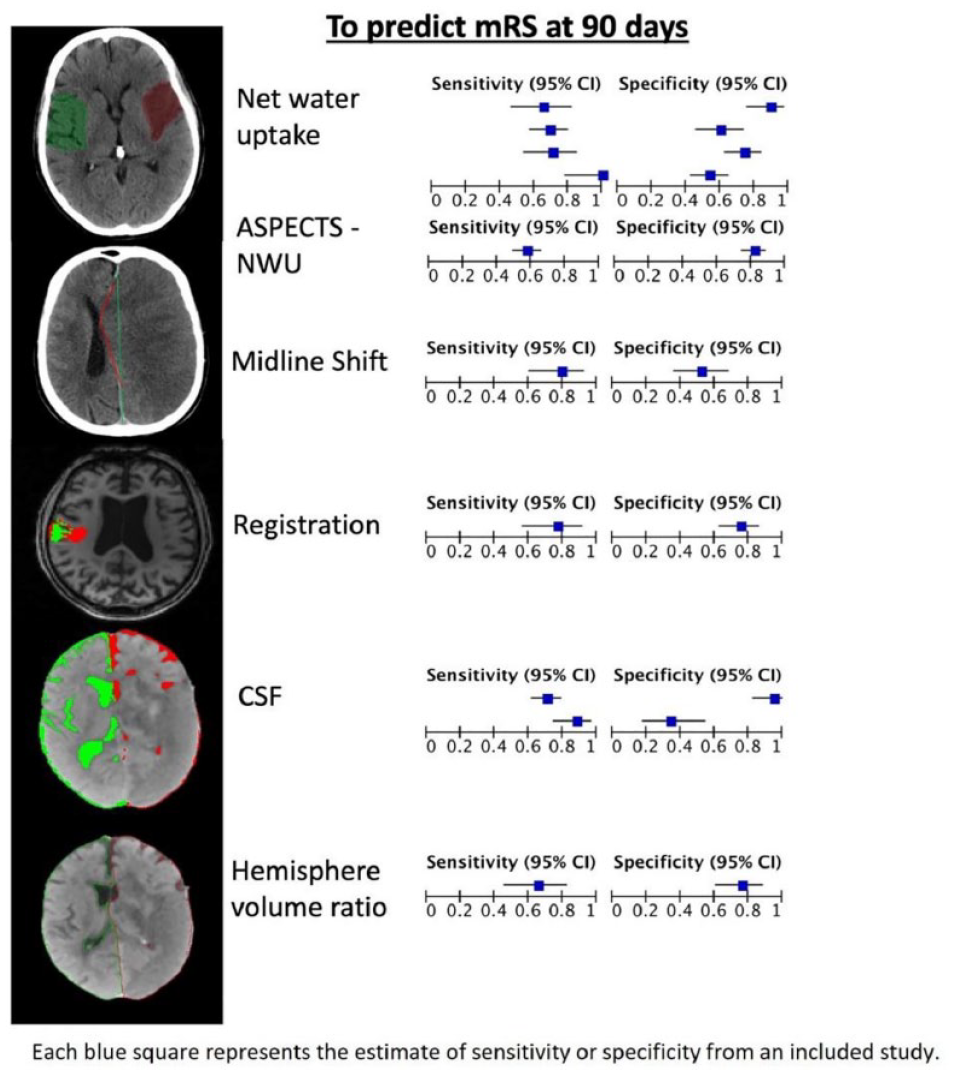
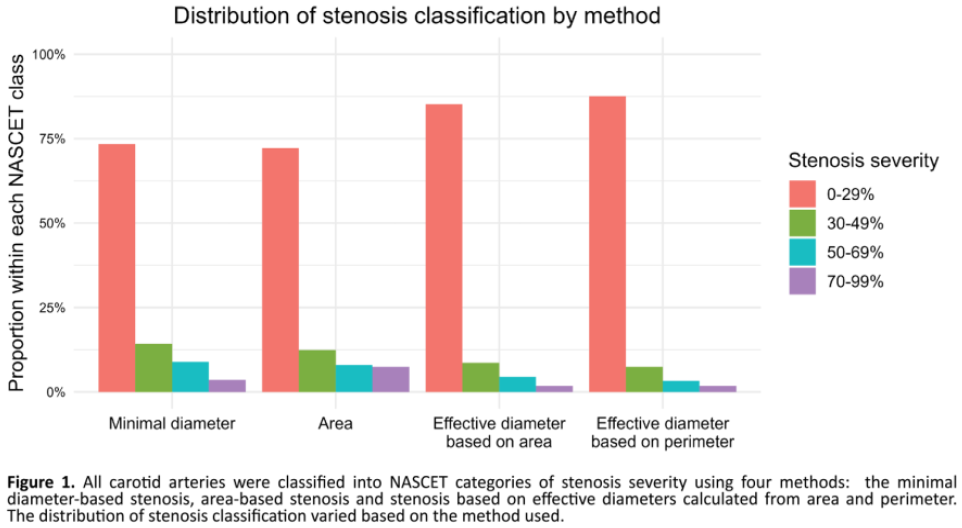
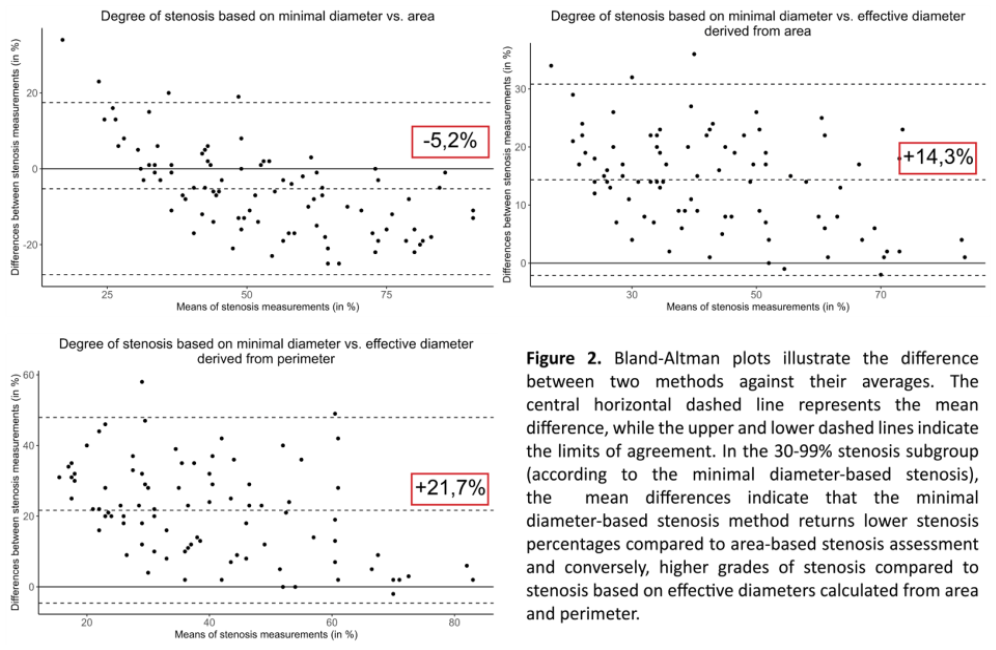
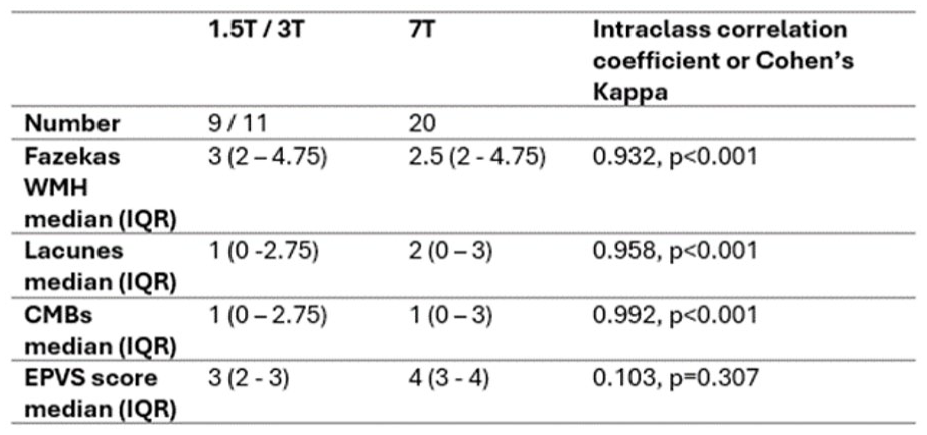
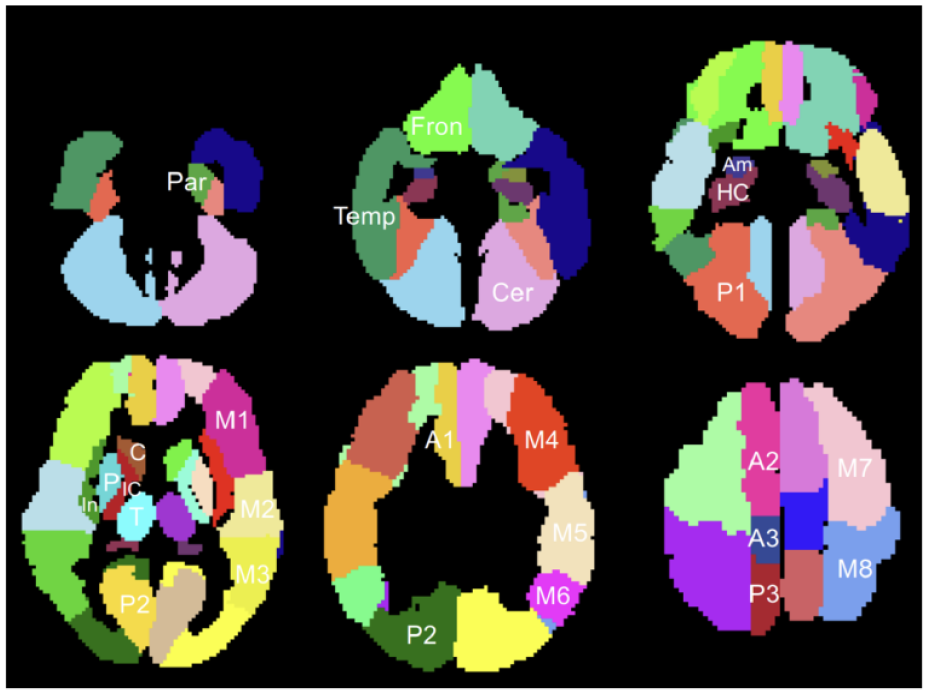
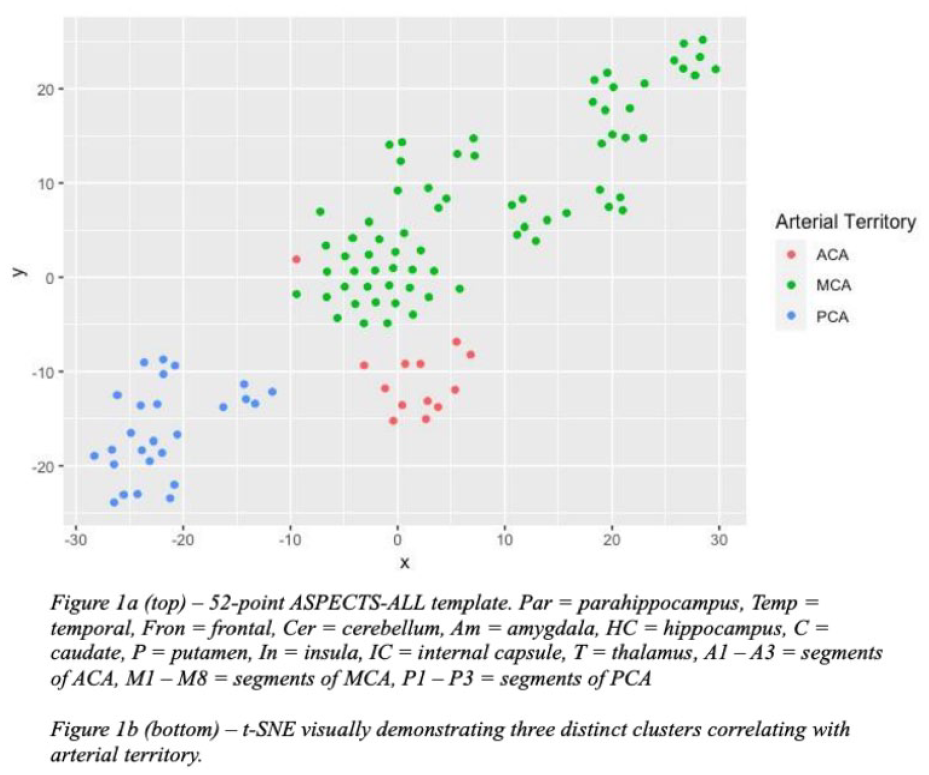
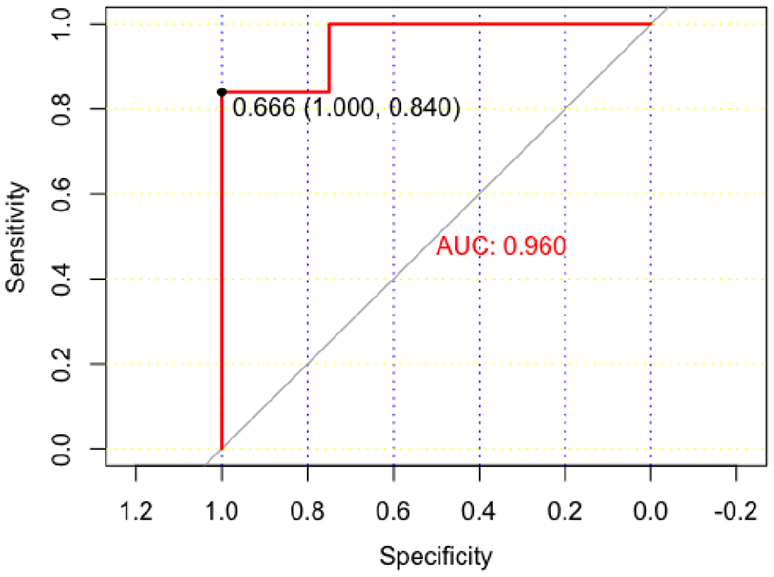
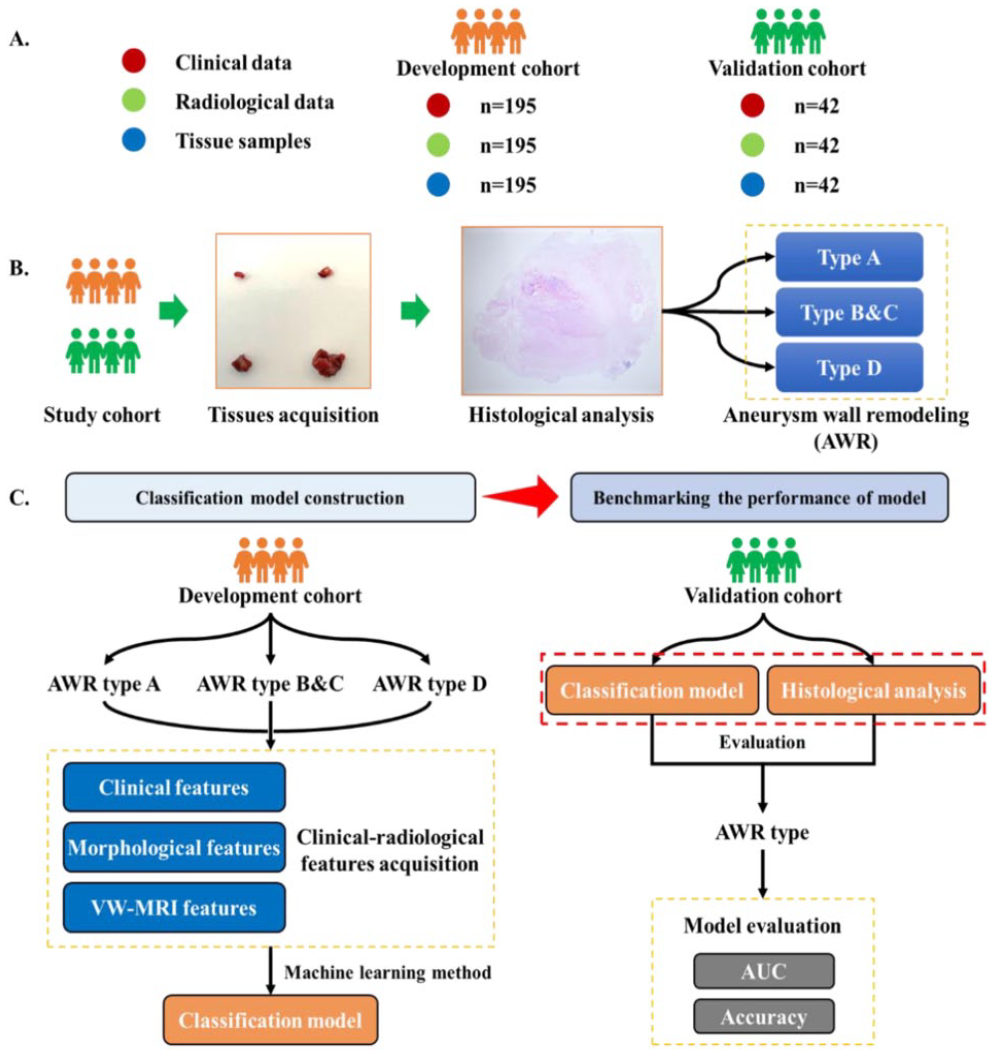
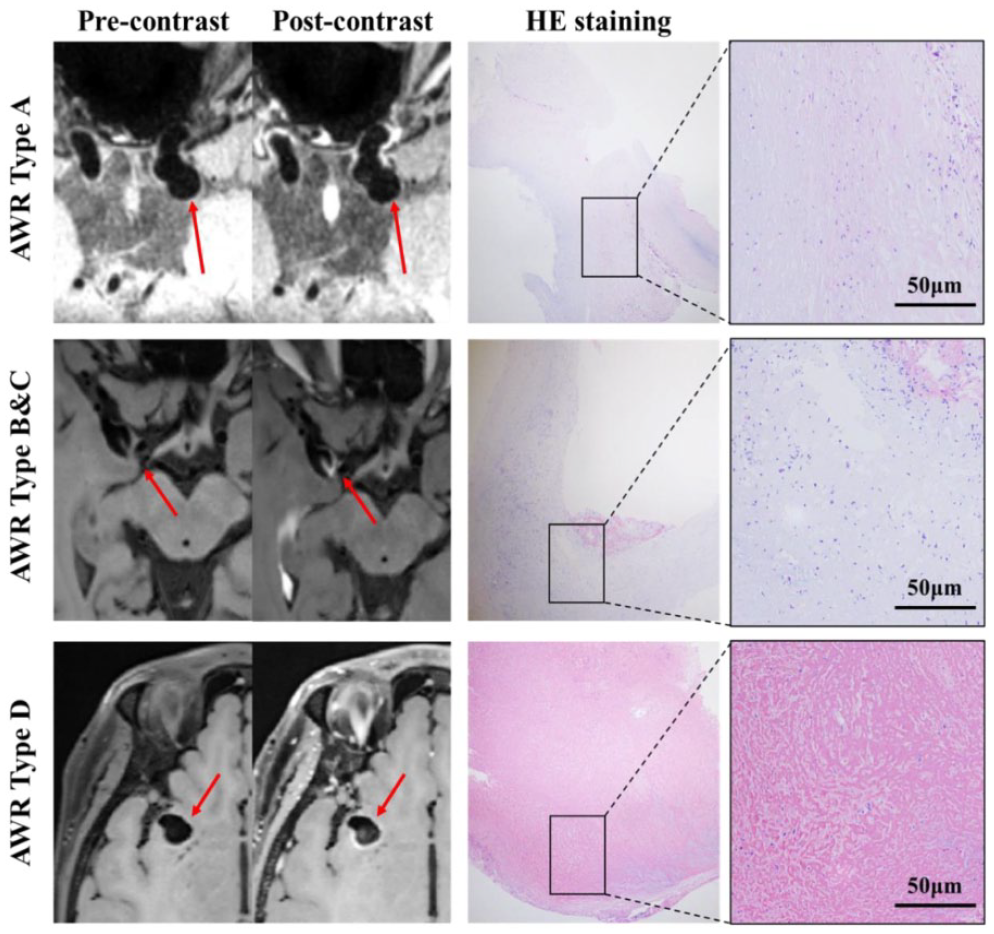
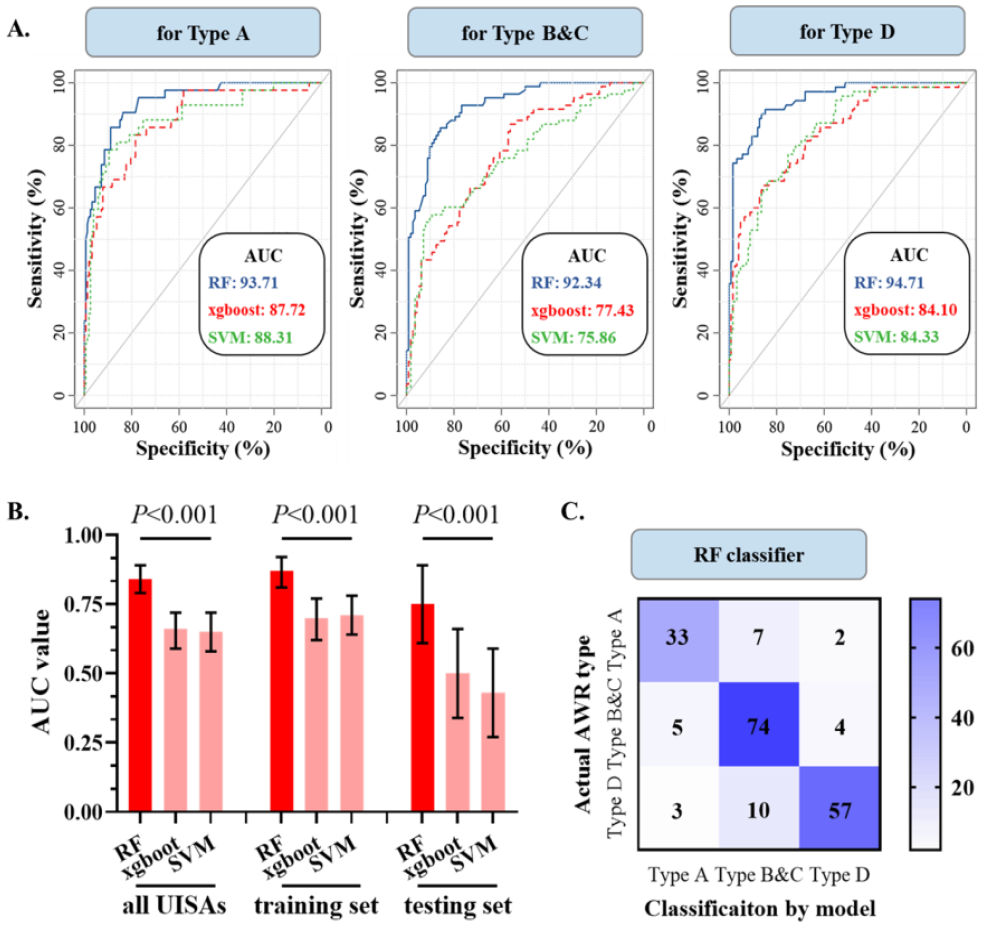
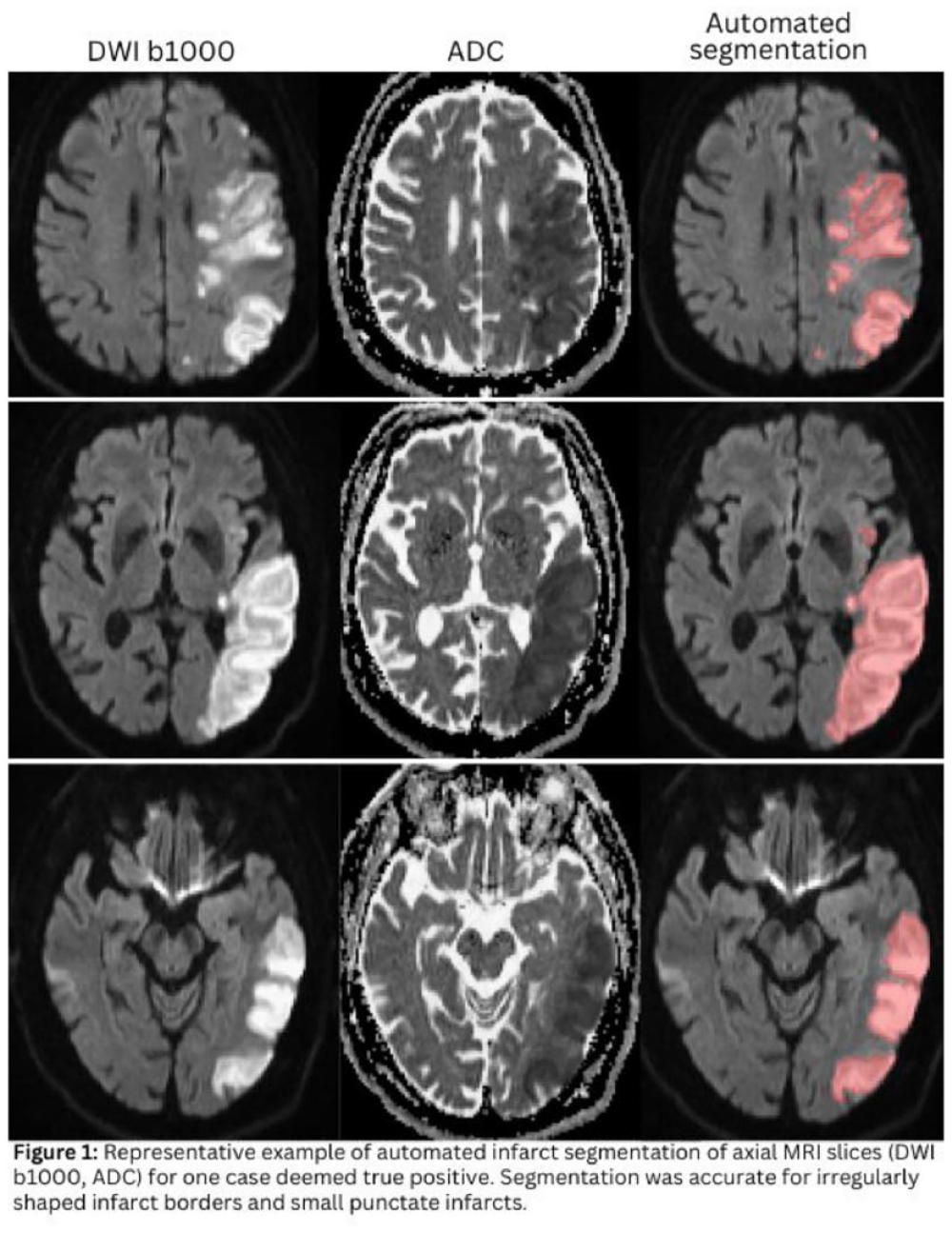
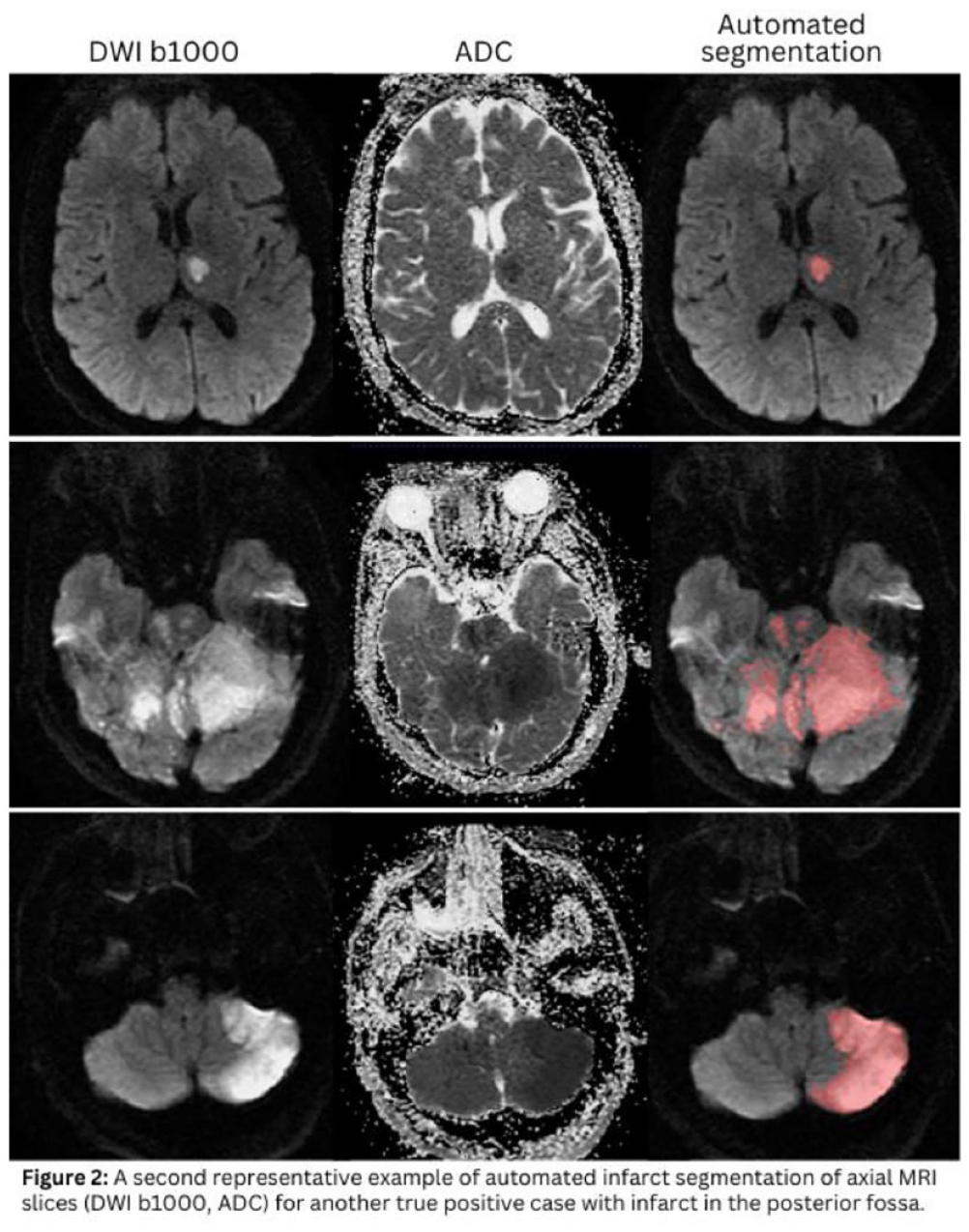
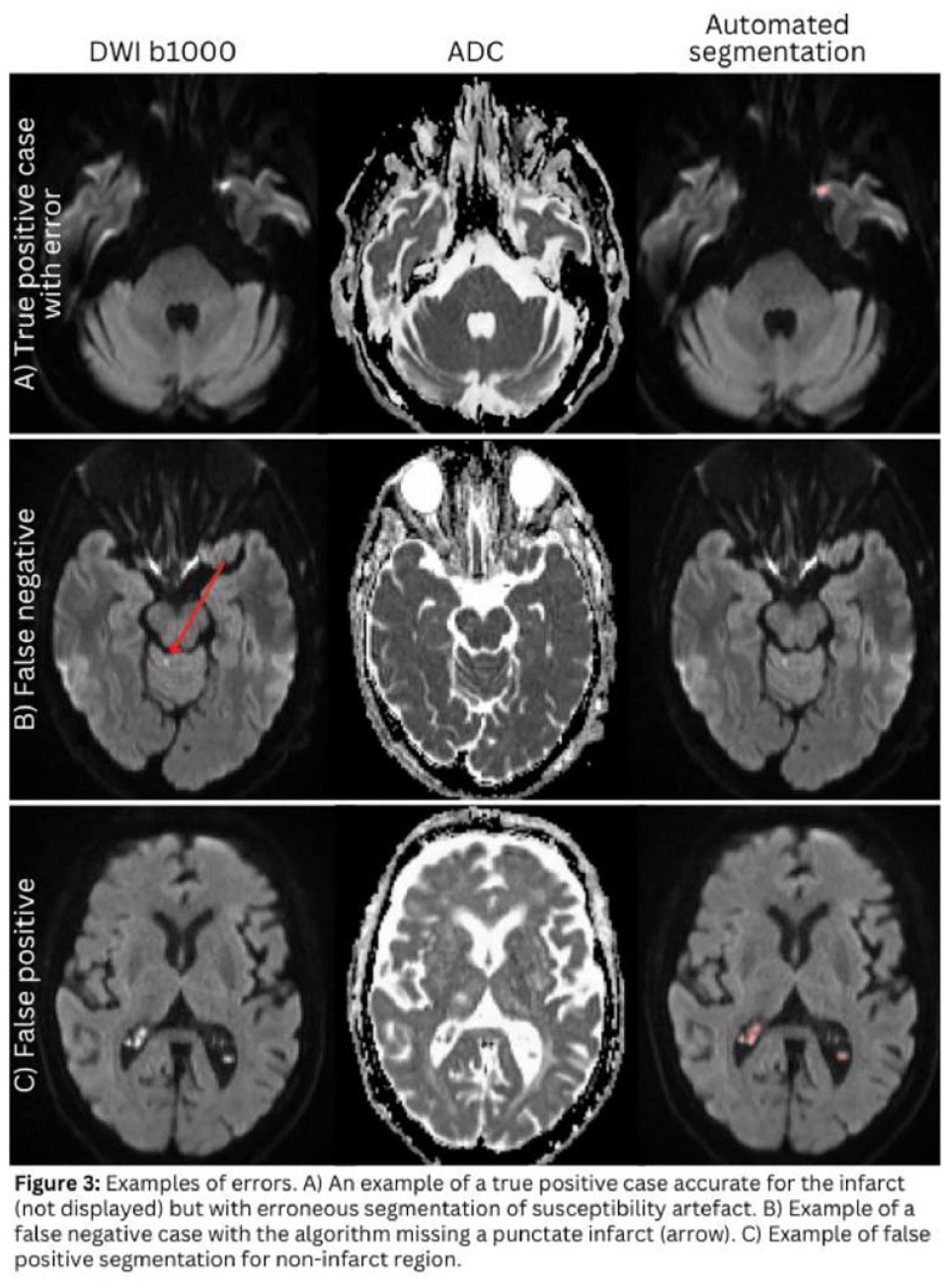
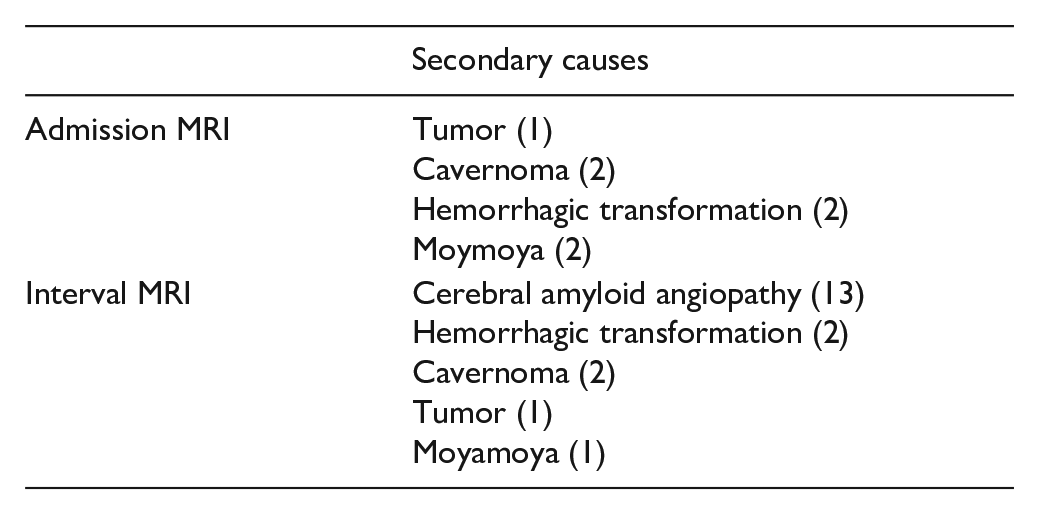
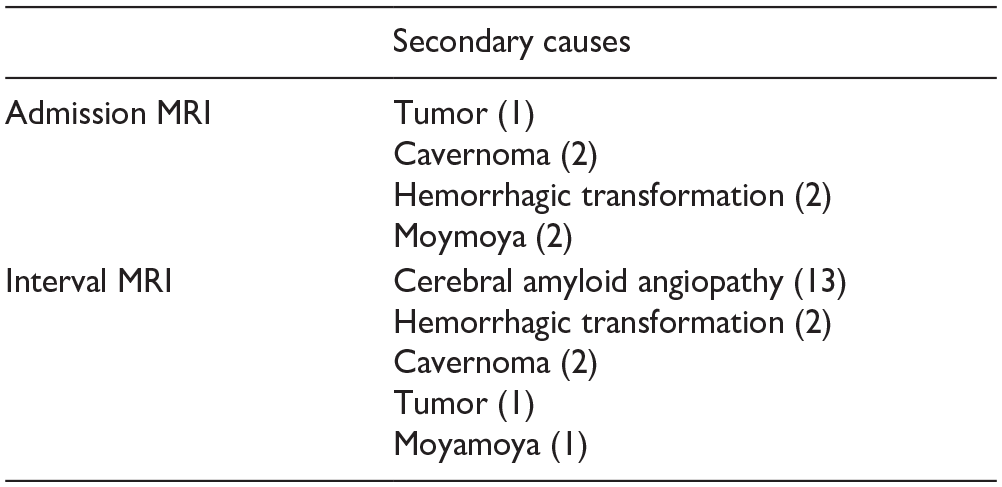
 , Jordan, 3Faculty of Medicine, Al-Azhar University Damietta, Egypt, 4Faculty of Medicine Al-Azhar University Boy's Branch in Cairo, Egypt, 5Misr University for Science & Technology, Egypt, 6Faculty of Medicine_October 6 University, Egypt, 7Faculty of Medicine, Kasr Alainy, Cairo University, Cairo, Egypt, 8Poznan University of Medical Sciences, Poznań, Poland
, Jordan, 3Faculty of Medicine, Al-Azhar University Damietta, Egypt, 4Faculty of Medicine Al-Azhar University Boy's Branch in Cairo, Egypt, 5Misr University for Science & Technology, Egypt, 6Faculty of Medicine_October 6 University, Egypt, 7Faculty of Medicine, Kasr Alainy, Cairo University, Cairo, Egypt, 8Poznan University of Medical Sciences, Poznań, Poland
 , Jordan, 3Faculty of Medicine, Al-Azhar University Damietta, Egypt, 4Faculty of Medicine Al-Azhar University Boy's Branch in Cairo, Egypt, 5
, Jordan, 3Faculty of Medicine, Al-Azhar University Damietta, Egypt, 4Faculty of Medicine Al-Azhar University Boy's Branch in Cairo, Egypt, 5
 , Mouʿtah, Jordan, 6Faculty of Medicine_October 6 University, Egypt, 7Faculty of Medicine, Kasr Alainy, Cairo University, Cairo, Egypt, 8Poznan University of Medical Sciences, Poznań, Poland
, Mouʿtah, Jordan, 6Faculty of Medicine_October 6 University, Egypt, 7Faculty of Medicine, Kasr Alainy, Cairo University, Cairo, Egypt, 8Poznan University of Medical Sciences, Poznań, Poland