
Abstract
Introduction:
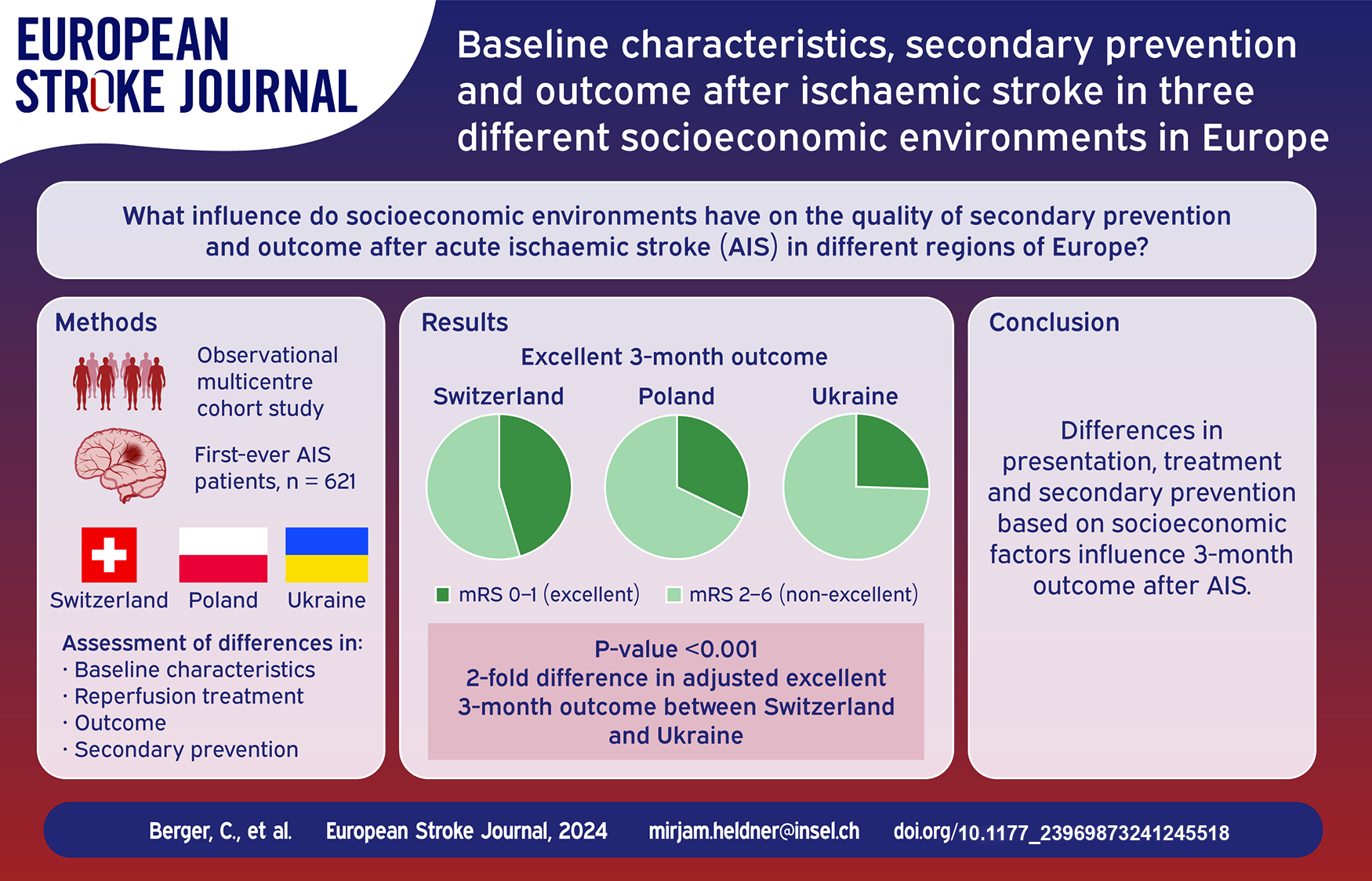
The differences in vascular risk factors’ and stroke burden across Europe are notable, however there is limited understanding of the influence of socioeconomic environment on the quality of secondary prevention and outcome after acute ischemic stroke.
Patients and methods:
In this observational multicenter cohort study, we analyzed baseline characteristics, reperfusion treatment, outcome and secondary prevention in patients with acute ischemic stroke from three tertiary-care teaching hospitals with similar service population size in different socioeconomic environments: Bern/CH/n = 293 (high-income), Gdansk/PL/n = 140 (high-income), and Lutsk/UA/n = 188 (lower-middle-income).
Results:
We analyzed 621 patients (43.2% women, median age = 71.4 years), admitted between 07 and 12/2019. Significant differences were observed in median BMI (CH = 26/PL = 27.7/UA = 27.8), stroke severity [(median NIHSS CH = 4(0-40)/PL = 11(0-33)/UA = 7(1-30)], initial neuroimaging (CT:CH = 21.6%/PL = 50.7%/UA = 71.3%), conservative treatment (CH = 34.1%/PL = 38.6%/UA = 95.2%) (each p < 0.001), in arterial hypertension (CH = 63.8%/PL = 72.6%/UA = 87.2%), atrial fibrillation (CH = 28.3%/PL = 41.4%/UA = 39.4%), hyperlipidemia (CH = 84.9%/PL = 76.4%/UA = 17%) (each p < 0.001) and active smoking (CH = 32.2%/PL = 27.3%/UA = 10.2%) (p < 0.007). Three-months favorable outcome (mRS = 0–2) was seen in CH = 63.1%/PL = 50%/UA = 59% (unadjusted-p = 0.01/adjusted-p CH-PL/CH-UA = 0.601/0.981), excellent outcome (mRS = 0–1) in CH = 48.5%/PL = 32.1%/UA = 27% (unadjusted-p < 0.001/adjusted-p CH-PL/CH-UA = 0.201/0.08 and adjusted-OR CH-UA = 2.09). Three-months mortality was similar between groups (CH = 17.2%/PL = 15.7%/UA = 4.8%) (unadjusted-p = 0.71/adjusted-p CH-PL/CH-UA = 0.087/0.24). Three-months recurrent stroke/TIA occurred in CH = 3.1%/PL = 10.7%/UA = 3.1%, adjusted-p/OR CH-PL = 0.04/0.32). Three-months follow-up medication intake rates were the same for antihypertensives. Statin/OAC intake was lowest in UA = 67.1%/25.5% (CH = 87.3%/39.2%/unadjusted-p < 0.001/adjusted-p CH-UA = 0.02/0.012/adjusted-OR CH-UA = 2.33/2.18). Oral intake of antidiabetics was lowest in CH = 10.8% (PL = 15.7%/UA = 16.1%/unadjusted-p = 0.245/adjusted-p CH-PL/CH-UA = 0.061/0.002/adjusted-OR CH-UA = 0.25). Smoking rates decreased in all groups during follow-up.
Discussion and conclusion:
Substantial differences in presentation, treatment and secondary prevention measures, are linked to a twofold difference in adjusted 3-months excellent outcome between Switzerland and Ukraine. This underscores the importance of socioeconomic factors that influence stroke outcomes, emphasizing the necessity for targeted interventions to address disparities in treatment and secondary prevention strategies.
Introduction
Stroke is the third-leading cause of death and disability combined in 2019 (measured in disability-adjusted life years (DALYs)), 1 posing a significant global challenge. The aging population contributes to an increased stroke burden,2–4 with a projected 31% increase in disability adjusted life-years by 2050. 3 Despite a decline in age-adjusted stroke incidence rates, particularly in high-income countries,4–7 about 25% of patients experience recurrent ischemic strokes within 5 years, 8 leading to poor rehabilitation outcomes and cognitive impairment. 9 While tailored secondary prevention could reduce stroke recurrence risk by up to 80%, 2 there remains limited data on the quality of secondary prevention and long-term outcome, particularly in less affluent European countries.2,10
Differences in stroke burden across Europe are notable, with Eastern European countries facing higher stroke rates and related deaths,2,4 attributed to socioeconomic factors influencing vascular risk factors and healthcare access and quality.2,4,10,11 Lower-income European countries encounter delays in patient assessment, limited access to interventions, and fewer lifestyle and atrial fibrillation monitoring programs. 10 Despite initiatives like the second Helsingborg declaration having aimed at universal stroke unit access by 2015, significant discrepancies persist, with Eastern European countries lagging behind compared to Western European Countries.2,11 Furthermore, it has been shown that Gross Domestic Product (GDP) per capita affects specialist care accessibility, 10 and income levels impact secondary prevention. 12
The European Stroke Action Plan 2018–2030 13 aims to address these challenges, necessitating a deeper understanding of care variability across European countries with different history, socioeconomic status and vascular risk. Switzerland, Poland and Ukraine exemplify this diversity, differing significantly in terms of GDP per capita, unemployment rates, and insurance coverage. Switzerland, on the one hand, is a representative of a highly developed Western European country. On the other hand, Poland and Ukraine are countries in Eastern Europe with less developed economic resources. It is worth noting that Poland has been a member of the EU since 2004, which distinguishes it from Ukraine, a nation facing greater economic challenges and geopolitical complexity. Both countries were classified as high vascular risk countries.14–16
This study aims to elucidate baseline characteristics, secondary prevention and outcome after first acute ischemic stroke in different socioeconomic environments, that is, Switzerland, Poland, and Ukraine, providing insights into European stroke care.
Methods
We conducted an observational multicenter cohort study of patients who experienced their first acute ischemic stroke between July and December 2019 and received treatment at three tertiary care centers. In this study, we focused on AIS patients, excluding those with ICH. AIS represents the majority of strokes, with distinct pathophysiology and treatment approaches compared to ICH. Our study’s aim was to investigate specific aspects of AIS, limiting our focus to this subtype. However, we recognize the importance of ICH and its impact on outcome. Future research could explore similar topics related to ICH.
Data for 293 patients from Bern, Switzerland (CH), 140 patients in Gdansk, Poland (PL), and 188 patients in Lutsk, Ukraine (UA) were consecutively collected from three prospective stroke registries. We gathered information on demographics, baseline characteristics, and vascular risk factors, including arterial hypertension, atrial fibrillation, diabetes mellitus, hyperlipidemia, smoking status, and history of prior myocardial infarction. Vascular risk factors were defined based on a combination of patient records, raw values and medication intake (see Supplemental Table 2 for further details).
Clinical assessment was performed by a certified neurologist on admission using a standard-ized acute ischemic stroke (AIS) protocol based on the AHA/ASA (American Heart Association/American Stroke Association) 2019 guidelines 17 and included NIHSS (National Institutes of Health Stroke Scale) score in the emergency room and a detailed neurological examination on the ward or in the Stroke Unit. 18 Suspected clinical diagnosis of AIS was confirmed by Magnetic Resonance Imaging (MRI) or Computed Tomography (CT). The diagnosis was made based on the AHA/ASA 2013 definition of ischemic stroke. 19
Information in regard to initial therapy (conservative therapy, thrombolysis treatment, mechanical thrombectomy, decompressive craniectomy) and stroke etiology classification according to TOAST (Trial of ORG 10172 in Acute Stroke Treatment 20 ) was collected from individual patient records. Also, in-hospital treatment duration, in-hospital mortality, disability (measured with modified Rankin scale; mRS 21 ) on discharge, discharge destination and discharge medication was assessed.
The follow-up parameters 3 months post-stroke were collected through clinical examination by a board-certified neurologist, by telephone by a trained study nurse or extracted from external rehabilitation center reports. Data on the primary endpoint, outcome at discharge, were collected. Additionally, data on secondary endpoints, mRS at follow-up, dichotomized into excellent (mRS 0–1), favorable (mRS 0–2) outcome, death, intake of secondary preventive medication and reported information on lifestyle behavior (dietary counseling, regular exercise, smoking status) and recurrence of stroke or TIA at 3 months were documented.
Detailed information on the definitions of variables is listed in Supplemental Table 1.
Statistical analysis
Statistical analysis was performed using SPSS 25.0 (SPSS Inc., Chicago, Illinois, USA). In univariable analysis, the χ2-test was applied for categorical variables and the ANOVA-test for ordinal and continuous variables to compare baseline characteristics and outcomes between patients from Switzerland (CH), Poland (PL) and Ukraine (UA). A two-tailed p-value <0.05 was considered significant. Binary logistic regression and ordinal and linear regression analysis were performed for outcome analysis where appropriate. Regression analyses got adjusted for the differences in admission NIHSS, and therapy, which differed significantly in comparison of baseline characteristics.
Standard protocol approvals, registrations, patient consent, and reporting
The Bernese stroke registry was approved by the local ethics committee (KEK Bern 2016-01905) for quality control and research. Informed consent for study participation was waived by the ethics committee, and patients were informed about the registry and the potential use of their data for research. In accordance with the Swiss law, patients who refused the use of their data for research were excluded from the analysis. For patients from PL and UA, the study protocol and supporting material were approved by the local ethics committee and each patient signed a consent form for the use of their data for research. This study complied with the Declaration of Helsinki and data analyses followed Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines. 22
Results
We included 293 patients from CH [128 (43.7%) women, median age 74.2 (20–97.4)], 140 from PL [54 (38.8%) women, median age 70 (18–85)], and 188 from UA [86 (45.7%) women, median age 71.4 (18–97.4)]. About 19 Swiss and 6 Ukrainian patients were lost to follow-up, none from PL. Ukrainian and Polish patients had significantly higher median Body Mass Index (BMI) than Swiss patients (p < 0.001). Pre-stroke mRS differed significantly between Polish and Swiss patients (p < 0.001) (no data available for Ukrainian patients, since not routinely assessed) (Table 3). For socioeconomic and hospital characteristics of the three study centers see Tables 1 and 2.
Socioeconomic situation in Bern (Switzerland), Gdansk (Poland), Lutsk (Ukraine) in 2019.
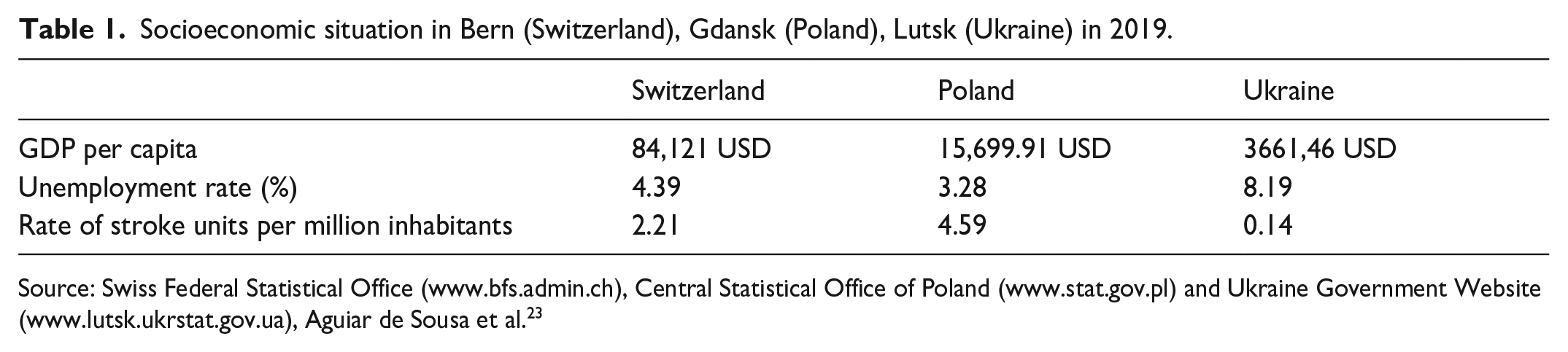
Source: Swiss Federal Statistical Office (www.bfs.admin.ch), Central Statistical Office of Poland (www.stat.gov.pl) and Ukraine Government Website (www.lutsk.ukrstat.gov.ua), Aguiar de Sousa et al. 23
Hospital characteristics and services of three different study centers in Bern (Switzerland), Gdansk (Poland), Lutsk (Ukraine) in 2019.
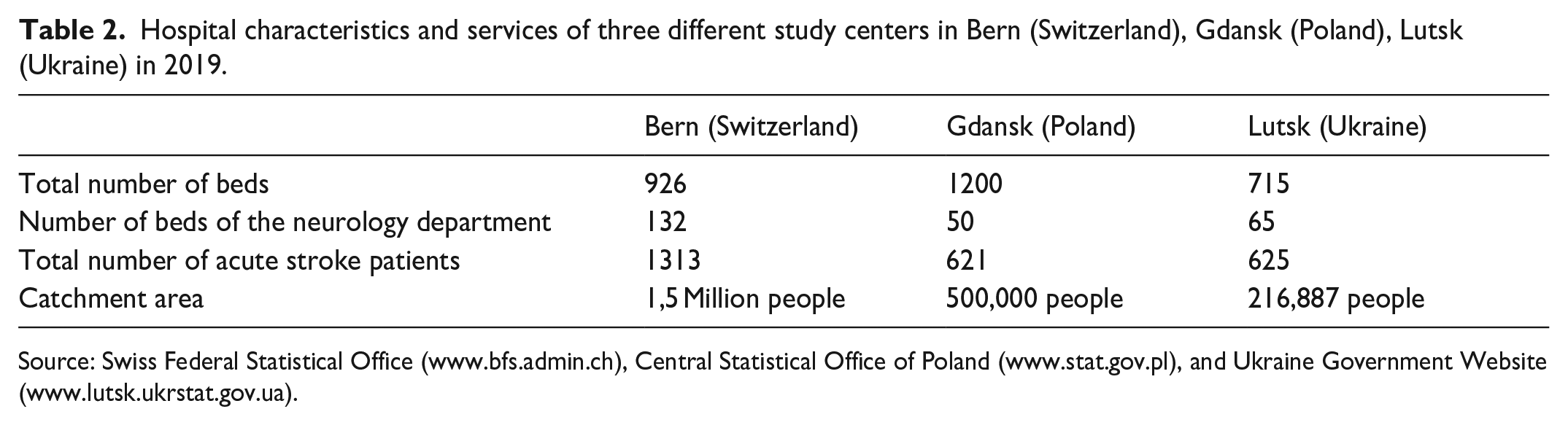
Source: Swiss Federal Statistical Office (www.bfs.admin.ch), Central Statistical Office of Poland (www.stat.gov.pl), and Ukraine Government Website (www.lutsk.ukrstat.gov.ua).
Arterial hypertension and atrial fibrillation were found significantly more often in Ukrainian and Polish compared to Swiss patients (p < 0.007). However, hyperlipidemia and active/former versus never smoking was significantly less often found in Ukrainian, compared to Polish and Swiss patients (17% vs 76.4% vs 84.9%, p < 0.001, and 40.1% vs 60.4% vs 56.7%, p < 0.001) (Table 3).
Baseline characteristics, risk factors, diagnostics and reperfusion treatment [n (%)].
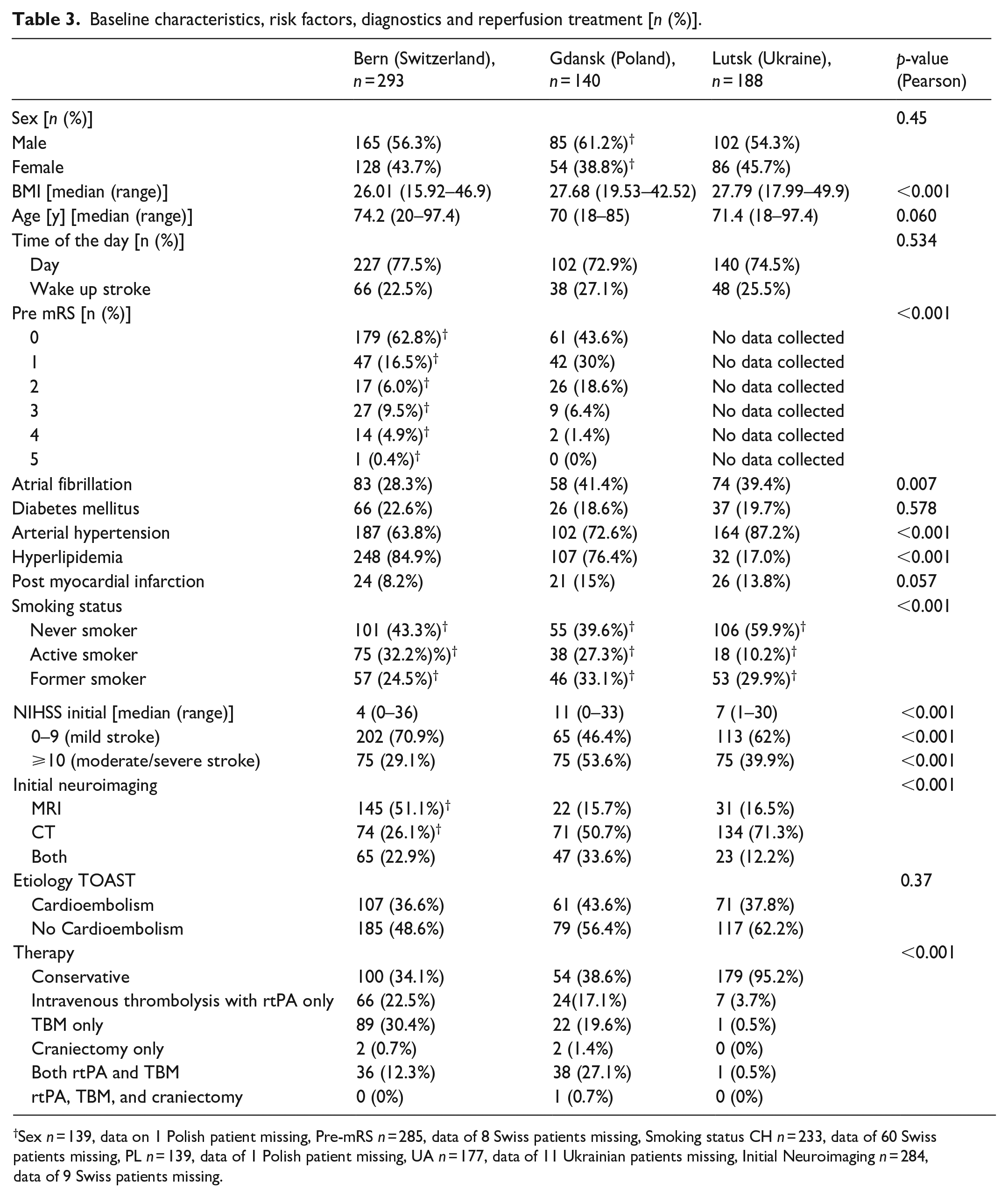
Sex n = 139, data on 1 Polish patient missing, Pre-mRS n = 285, data of 8 Swiss patients missing, Smoking status CH n = 233, data of 60 Swiss patients missing, PL n = 139, data of 1 Polish patient missing, UA n = 177, data of 11 Ukrainian patients missing, Initial Neuroimaging n = 284, data of 9 Swiss patients missing.
Admission stroke severity differed significantly: Swiss patients had a median admission NIHSS of 4 (0–36), Ukrainian 7 (1–30), and Polish patients of 11 (0–33) (p < 0.001). Initial neuroimaging was significantly more often CT versus MRI or both in UA (71.3%) and PL (50.7%) compared to in CH (21.6%) (p < 0.001). Initial conservative versus reperfusion treatment was applied to 95.2% of Ukrainian, compared to 34.1% of Swiss and 38.6% of Polish patients (p < 0.001). Reperfusion treatment was most often mechanical thrombectomy (TBM) compared to intravenous thrombolysis with recombinant tissue Plasminogen Activator (rtPA) and both TBM and rtPA with 30.4% versus 22.5% versus 12.3% in Switzerland, 19.6% versus 17.1% versus 27.1% in Poland, and 0.5% versus 3.7% versus 0.5% in Ukraine (p < 0.001) (Table 3).
At discharge, excellent outcome was found in 47.1% of Swiss, 33.6% of Polish and 11.7% of Ukrainian patients (unadjusted-p < 0.001, adjusted-p CH-PL = 0.913, adjusted-p CH-UA < 0.001, adjusted-OR CH-UA = 6.03). Favorable outcome at discharge was found in 59.9% of Swiss, 51.4% of Polish and 36.7% of Ukrainian patients (unadjusted-p < 0.001, adjusted-p CH-PL = 0.195 and adjusted-p CH-UA = 0.114). Hospital mortality did not differ significantly between groups. Discharge destination was most often home in PL (52.1%) and UA (84.1%) and to another acute care facility in CH (43.5%) (un-/adjusted-p < 0.001). Median duration of hospitalization was 3.63 [0–59] days in CH, 8 [3–98] days in PL, and 10 [1–32] days in UA (un-/adjusted-p < 0.001) (Table 4). Medication prescription at discharge differed as follows: antihypertensive intake was higher in UA than PL and CH (92.6% vs 81.7% vs 65.3%, unadjusted-p < 0.001, adjusted-p CH-PL/CH-UA = 0.378/<0.001, adjusted OR CH-UA = 0.15). Statins were significantly more often used in PL (unadjusted-p = 0.002, adjusted-p CH-PL < 0.001 and adjusted-OR CH-PL = 0.19) (Table 4).
Outcome at discharge and medication at discharge.
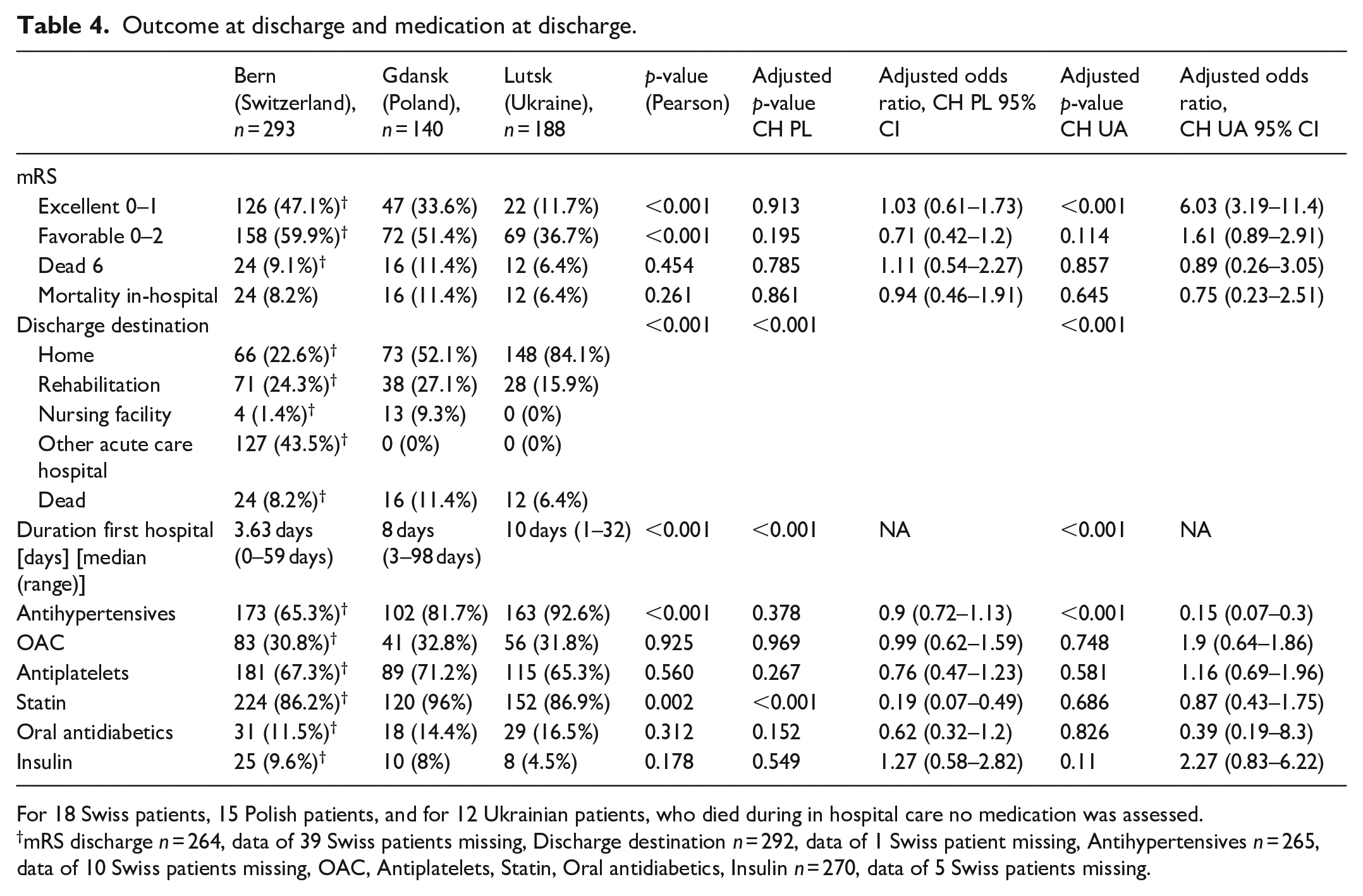
For 18 Swiss patients, 15 Polish patients, and for 12 Ukrainian patients, who died during in hospital care no medication was assessed.
mRS discharge n = 264, data of 39 Swiss patients missing, Discharge destination n = 292, data of 1 Swiss patient missing, Antihypertensives n = 265, data of 10 Swiss patients missing, OAC, Antiplatelets, Statin, Oral antidiabetics, Insulin n = 270, data of 5 Swiss patients missing.
At 3 months follow-up, excellent outcome was seen in 48.5% Swiss, 32.1% Polish, and 27% Ukrainian patients (unadjusted-p < 0.001, adjusted-p CH-PL/CH-UA = 0.201/0.008 and adjusted-OR CH-UA = 2.09). Favorable outcome was seen in 63.1% Swiss, 50% Polish, and 59% Ukrainian patients (unadjusted-p = 0.01, adjusted-p CH-PL/CH-UA = 0.601/0.981). Mortality did not differ significantly between groups.
Recurrent stroke or TIA occurred in 10.7% of Polish, 5% of Ukrainian and 3.1% of Swiss patients (unadjusted-p = 0.152, adjusted-p CH-PL = 0.038 and adjusted-OR CH-PL/CH-UA = 0.32/0.71). Re-hospitalization for any reason (including causes unrelated to TIA/AIS) occurred in 16.4% of Swiss, 16.1% of Polish, and in 4.3% of Ukrainian patients (unadjusted-p < 0.001, adjusted-p CH-PL/CH-UA = 0.914/<0.001 and adjusted-OR CH-UA = 5.24) (Table 5).
Follow-up at 3 months.
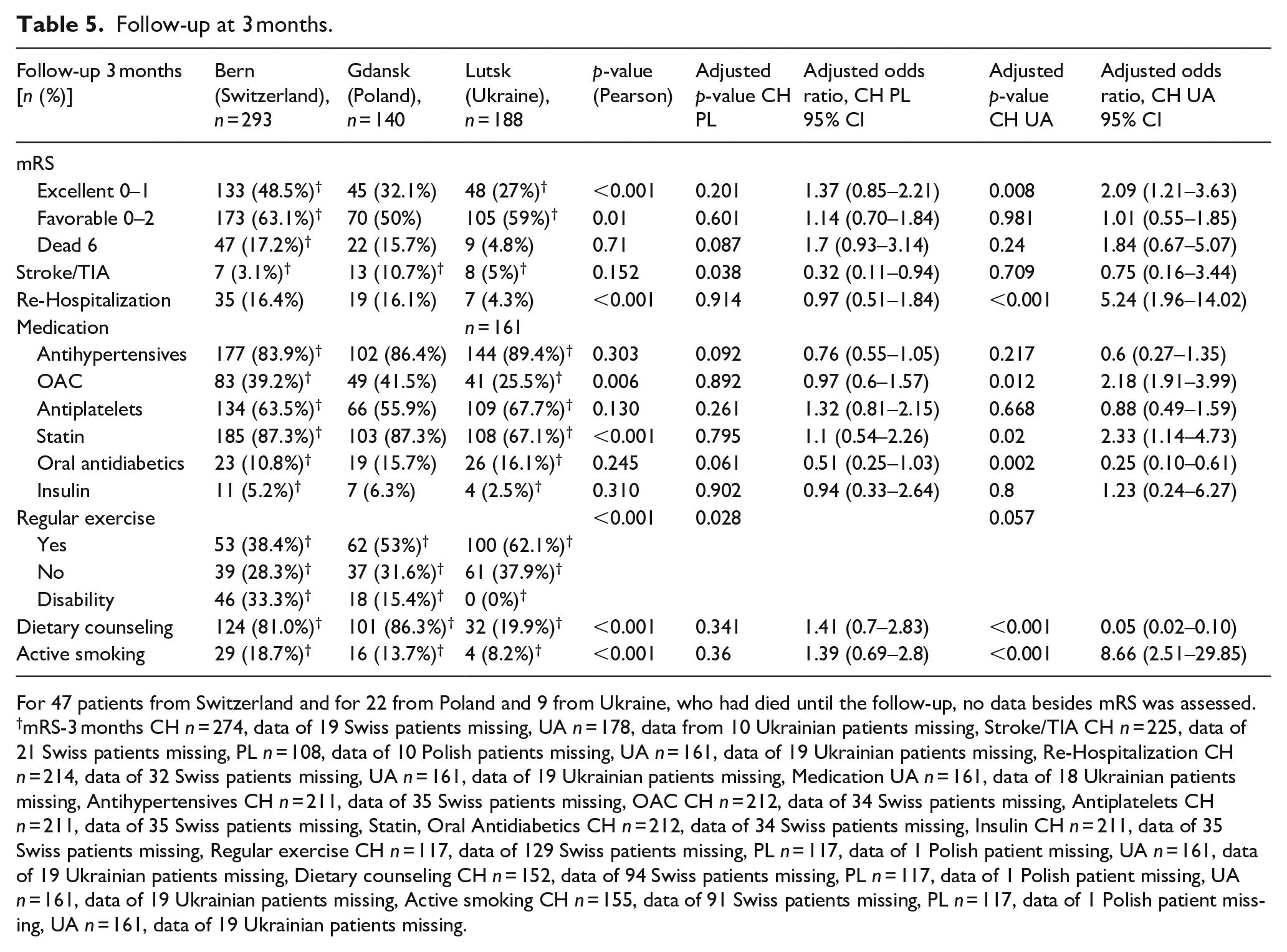
For 47 patients from Switzerland and for 22 from Poland and 9 from Ukraine, who had died until the follow-up, no data besides mRS was assessed.
mRS-3 months CH n = 274, data of 19 Swiss patients missing, UA n = 178, data from 10 Ukrainian patients missing, Stroke/TIA CH n = 225, data of 21 Swiss patients missing, PL n = 108, data of 10 Polish patients missing, UA n = 161, data of 19 Ukrainian patients missing, Re-Hospitalization CH n = 214, data of 32 Swiss patients missing, UA n = 161, data of 19 Ukrainian patients missing, Medication UA n = 161, data of 18 Ukrainian patients missing, Antihypertensives CH n = 211, data of 35 Swiss patients missing, OAC CH n = 212, data of 34 Swiss patients missing, Antiplatelets CH n = 211, data of 35 Swiss patients missing, Statin, Oral Antidiabetics CH n = 212, data of 34 Swiss patients missing, Insulin CH n = 211, data of 35 Swiss patients missing, Regular exercise CH n = 117, data of 129 Swiss patients missing, PL n = 117, data of 1 Polish patient missing, UA n = 161, data of 19 Ukrainian patients missing, Dietary counseling CH n = 152, data of 94 Swiss patients missing, PL n = 117, data of 1 Polish patient missing, UA n = 161, data of 19 Ukrainian patients missing, Active smoking CH n = 155, data of 91 Swiss patients missing, PL n = 117, data of 1 Polish patient missing, UA n = 161, data of 19 Ukrainian patients missing.
At 3 months, follow-up medication intake rates were the same for antihypertensives in UA, CH and PL (89.4% vs 83.9% vs 86.4%, unadjusted-p = 0.303, adjusted-p CH-PL/CH-UA = 0.092/0.217). However, statin and oral anticoagulants (OAC) intake was lower in UA than in CH and PL (67.1% vs 87.3% vs 87.3%, unadjusted-p < 0.001, adjusted-p CH-PL/CH-UA = 0.795/0.02 and adjusted-OR C-UA = 2.33 and 25.5% vs 39.2% vs 41.5% unadjusted-p = 0.006, adjusted-p CH-PL/CH-UA = 0.892/0.012 and adjusted-OR CH-UA = 2.18). Intake of oral antidiabetics was lowest in CH (10.8% vs PL = 15.7% vs UA = 16.1%, unadjusted-p = 0.245, adjusted-p CH-PL/CH-UA = 0.061/0.002 and adjusted-OR CH-UA = 0.25).
Regular exercise was reported most often in UA at 3 months, but dietary counseling was given to only 19.9% of Ukrainian versus 86.4% of Polish and 81% of Swiss patients (unadjusted-p < 0.001, adjusted-p CH-PL/CH-UA = 0.341/<0.001 and adjusted-OR = 0.05). Smoking rates in comparison to baseline decreased in all groups with 18.7% in CH, 13.7% in PL and 8.2% in UA (unadjusted-p < 0.001, adjusted-p CH-PL/CH-UA = 0.36/<0.001 and adjusted OR CH-UA = 8.66) (Table 5).
Discussion
The main finding of this observational cohort study in 2019 shows a more than twofold difference in adjusted 3-months excellent outcome between the high-income-country Switzerland and the lower-middle-income country Ukraine. Data on acute ischemic stroke patients in three different socioeconomic environments in teaching hospitals in Bern (Switzerland) (high-income), Gdansk (Poland) (high-income), and Lutsk (Ukraine) (lower-middle-income) were collected and analyzed. The world bank classification of countries by GDP per capita defined high-income as GDP per capita of over 12,375$ in 2019. While the per capita GDP in Poland was 15,699.91$ in 2019, GDP per capita in Switzerland was more than five times higher at 84,121.93$. 24
While the hospitals share similarities in carrying capacity, guideline compliance (as demonstrated by the prescription of guideline-based drugs at discharge) and research and teaching engagement, this study identified differences in baseline characteristics, reperfusion treatment, secondary prevention and outcome among the three cohorts.
Baseline characteristics
In our analysis, Polish patients had a higher pre-stroke mRS than Swiss patients. Data for Ukrainian patients were not available. This aligns with previous findings associating lower socioeconomic status (SES) with higher pre-stroke comorbidity rates.25,26
Ukrainian and Polish compared to Swiss patients showed higher BMI, arterial hypertension, and atrial fibrillation prevalence, consistent with higher vascular risk factor burden in Eastern European countries, where these risk factors are often less effectively controlled.2,8,13,26–28 In contrast, our study revealed a lower prevalence of hyperlipidemia among Ukrainians (17%) compared to Swiss (84.9%), and Polish (76.4%) patients, potentially due to differences in screening practices, diagnostic approaches, and disease awareness levels, but also underreporting in Ukraine.2,29 Moreover, we observed a lower smoking prevalence among Ukrainians, particularly in women, possibly attributed to historical smoking patterns and anti-smoking measures implemented in UA since 2006, but also underreporting could have contributed to this observation. 30
Ukrainian patients presented with the highest median NIHSS score on admission, Swiss patients with the lowest. This disparity may be attributed to varying referral practices, as well as a higher prevalence of atrial fibrillation in Polish and Ukrainian patients in our cohorts, potentially contributing to increased stroke severity. 31 Furthermore, a consistent association exists between lower socioeconomic status (SES) and increased stroke severity. 32 Also, this could be due to discrepancies in demographics, healthcare structure and limited access to acute medical care for patients with minor stroke.2,10,33
The initial neuroimaging technique differed significantly, with MRI more often used in CH compared to UA and PL, likely due to factors such as limited accessibility, availability, and the higher cost of MRI compared to CT. 34 Additionally, CT is favored in many places due to its shorter examination time.
Reperfusion treatment
Despite higher stroke severity, Ukrainian patients received intravenous thrombolysis and endovascular treatment less often than Swiss and Polish patients, possibly due to delayed hospital admission.2,30,35 Delayed hospital admission often results from factors such as delayed stroke symptom recognition, organization of emergency services, and care protocol implementation. 30 Unfortunately, we have not registered time delays from last seen well or first seen sick to hospital arrival and treatment in our study.
Additionally, accessibility and availability of treatment may be have been limited in UA. 13
This was evident in 2019 during the reform of the healthcare system in UA. Insufficient funding and limited state provision led to low rates of intravenous thrombolysis (0.9%) and endovascular treatment (0.2%) in patients with acute ischemic stroke. 13 Reimbursement initiatives by the National Health Service of UA in 2020 then resulted in an increase in reperfusion treatment, with intravenous thrombolysis rates increasing to 6.4% and of endovascular treatment to 0.7%. 36 Lutsk City Hospital, which participated in this study, reflected a similar trend, with 21.1% and 7.1% of all acute ischemic stroke patients receiving reperfusion treatment. The substantial changes observed in UA highlight the dependence of stroke reperfusion treatment on SES. Nevertheless, it is still essential to validate the overall effect on mortality and morbidity through comprehensive analyses.
Outcome at discharge and 3 months
Previous studies found poorer functional outcome in patients with lower SES. 33 In our study, functional outcome at discharge showed differences in univariable analysis, but after adjustment for admission NIHSS score and treatment, only excellent outcome remained 6 times more likely in Swiss compared to Ukrainian patients. This could be partly associated with lower vascular risk factor burden in Swiss patients. At 3 months, excellent outcome in CH was around 1.5 times more likely than in PL and almost 1.8 times more likely than in UA, but only the difference between CH and UA was significantly different in the adjusted analysis. Mortality did not differ between groups. Overall, the association with SES and outcome after stroke is to some extent consistent with previous studies.33,37
Also, recurrent stroke/TIA occurred around 70% less likely in Swiss compared to Polish patients, potentially linked to the higher prevalence of atrial fibrillation and comorbidities in the Polish patient cohort. 31 Feigin et al. reported a greater stroke burden in Eastern European countries, yet there is limited evidence concerning the association between SES and stroke recurrence.27,38
In PL and UA, patients were most often discharged home, while in CH, they were transferred to another acute care facility. Some evidence suggests that higher SES serves as a determinant of postacute stroke rehabilitation, potentially explaining this variation. 38 Swiss patients experienced the shortest median first hospital stay, possibly attributed to efficient healthcare systems, streamlined processes, and prompt access to necessary post-acute stroke care services. However, despite a lower vascular risk factor burden, rehospitalization for any reason (including causes unrelated to TIA/AIS) within 3 months was approximately five times more frequent in Swiss patients compared to Ukrainian patients. This increased rate of rehospitalization may have been influenced by factors such as closer post-acute monitoring or a higher threshold for readmission to ensure comprehensive medical care.10,29,33
Secondary prevention
In our study, secondary prevention measures were implemented to a considerable extent across all three groups, with high intake rates of guideline-recommended medications. Statin intake at discharge was 80% less likely in CH than in PL, and antihypertensive intake was 70% less likely in CH than in UA. After 3 months, statin and OAC intake was twice as common, while intake of oral antidiabetics was 75% less likely in CH compared to UA. Some of these differences can only partly be explained by differences in vascular risk factor burden between cohorts. Previous research in UA indicated lower intake until follow-up of statins and OACs after vascular events, potentially influenced by socioeconomic factors such as income per capita, reimbursement, and insurance coverage. 12 Antihypertensive intake rates were high in all cohorts, showing no significant differences between groups.
At 3 months, regular exercise was reported most often in UA. However, dietary counseling was least frequently provided to Ukrainian compared to Polish and Swiss patients. Smoking rates decreased in all groups compared to baseline but remained around 9 times more likely in Swiss compared to Ukrainian patients. These differences could be linked to factors like differences in reporting and wage definition (e.g. of regular exercise), in cultural practices (e.g. of lifestyle), in healthcare infrastructure and in disease awareness levels (e.g. of hyperlipidemia and unhealthy diet).2,39,40
Strengths
This study’s primary strength lies in its type of multicenter data collection, enabling a direct comparison between hospitals with comparable service population and research engagement in three different socioeconomic environments. The comprehensive assessment of numerous parameters allowed not only the evaluation of outcome differences but also an exploration of distinctions between the three cohorts, primarily influenced by socioeconomic factors. Beyond acute clinical practice, this study underscores the significance of such factors for secondary prevention and health outcomes. It aligns with the European Stroke Action Plan 2018–2030s framework for healthcare policy, research, and stroke services development, highlighting the need for a deeper understanding of the current state and diversity across European countries.
Limitations
The study’s main limitation arises from patients not providing consent or being lost to follow-up or from missing variables, particularly regarding incomplete data on secondary prevention measures such as dietary counseling, smoking status and medication at 3 months. In addition, caution is required when extrapolating results from individual hospitals to entire European countries. The stroke centers participating in the study stand out in terms of quality compared to the national average. It can therefore be assumed that the national average for each country might be worse and these differences are likely to be greater the less affluent a country is. Furthermore, socioeconomic factors were not assessed at the individual patient level.
Also, the data collected in 2019 may not reflect current realities given the widespread adoption of therapies and socioeconomic changes due to the Covid-19 pandemic and the war in Ukraine. Future research should compare these data with current data to assess the evolution of stroke care amid these global events.
Conclusion
Substantial differences in presentation, treatment and secondary prevention measures, are linked to a twofold difference in adjusted 3-months excellent outcome between high- and lower-middle-income countries. This underscores the importance of targeted interventions to address treatment and secondary prevention disparities.
The Stroke Alliance for Europe (SAFE) projects a 35% increase in stroke cases by 2035, necessitating comprehensive investment in primary and secondary prevention beyond acute care. The lack of comprehensive data, as seen in Ukrainian patients in our study, 2 underscores the need for standardized pan-European data collection to guide intervention. Addressing these socioeconomic disparities should be central to policy programs aimed at reducing the burden of stroke in Europe and promote a more equitable healthcare system.
Supplemental Material
sj-docx-1-eso-10.1177_23969873241245518 – Supplemental material for Baseline characteristics, reperfusion treatment secondary prevention and outcome after acute ischemic stroke in three different socioeconomic environments in Europe
Supplemental material, sj-docx-1-eso-10.1177_23969873241245518 for Baseline characteristics, reperfusion treatment secondary prevention and outcome after acute ischemic stroke in three different socioeconomic environments in Europe by Charlotte Berger, Helly Hammer, Marino Costa, Pawel Lowiec, Andriy Yagensky, Adrian Scutelnic, Kateryna Antonenko, Olga Biletska, Bartosz Karaszewski, Hakan Sarikaya, Tomasz Zdrojewski, Anastasiia Klymiuk, Claudio LA Bassetti, Natalia Yashchuk, Kamil Chwojnicki, Marcel Arnold, Hugo Saner and Mirjam R Heldner in European Stroke Journal
Footnotes
Acknowledgements
We are grateful to all stroke teams, which contributed to data acquisition for this study.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MRH reports grants from SITEM Research Funds and the. Swiss Heart Foundation, outside the sumbitted work and grants from the Swiss National Science Foundation partly related to the submitted work. KA reports grants from the Swiss National Science Foundation, partly related to the submitted work. All other co-authors report no disclosures directly related to this manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data sharing statement
Raw data of all patients included in this study can be made available upon request to the corresponding author and after clearance by the local ethics committee.
Ethical approval and informed consent
The Bernese stroke registry was approved by the local ethics committee (KEK Bern 2016-01905) for quality control and research. Informed consent for study participation was waived by the ethics committee, and patients were informed about the registry and the potential use of their data for research. In accordance with the Swiss law, patients who refused the use of their data for research were excluded from the analysis. For patients from PL and UA, the study protocol and supporting material were approved by the local ethics committee and each patient signed a consent form for the use of their data for research. This study complied with the Declaration of Helsinki and data analyses followed Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines.
Guarantor
MR Heldner.
Contributorship
MR Heldner had full access to all the data and take responsibility for the integrity of the data and the accuracy of the data analysis.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.