
Abstract
Introduction:
A previous systematic review of population-based studies from 1973 to 2002 found a decrease in case fatality for spontaneous subarachnoid haemorrhage, but could not find a sufficient number of studies to assess changes in functional outcome. Since then, treatment has advanced distinctly. We assessed whether case fatality has decreased further and whether functional outcome has improved.
Patients and methods:
We searched PubMed and Web of Science for new population-based studies using the same criteria as in our previous systematic review. We assessed changes in case fatality and functional outcome over time using linear regression.
Results:
We included 24 new studies with 827 patients and analysed 9542 patients described in 62 study periods between 1973 and 2017. Case fatality decreased by 0.3% (95% CI: −0.7 to 0.1) per year. In a sensitivity analysis excluding studies that did not provide 1-month outcome and outliers, the age and sex-adjusted decrease was 0.1% per year (95% CI: −0.9 to 0.6). The mean case fatality rate decreased from 47% (95% CI: 31–63) in the 1970s to 35% (95% CI: 30–39) in the 1990s, and remained stable in the 2000s (34%; 95% CI: 27–41) and 2010s (38%; 95% CI: 15–60). In 15 studies, the mean proportion of patients living independently increased by 0.2% per year (95%CI: −0.7 to 1.1) and the mean was 45% (95% CI: 39–50) in six studies that reported outcome after 12 months.
Discussion and conclusion:
From 1973 to 2017, the case-fatality rate of spontaneous subarachnoid haemorrhage declined overall by 13.5%, but remained stable over the last two decades. The data on time trends in functional outcome were inconclusive.

Introduction
Patients with spontaneous subarachnoid haemorrhage (SAH) have a poor prognosis. The majority dies within the initial days to weeks after the haemorrhage or remains dependent on help from others. In a previous meta-analysis of population-based studies on the outcome after spontaneous subarachnoid haemorrhage, the case fatality rate (CFR) decreased between 1973 and 2002 and was lower in Japan than in other regions in the world. 1 There were only a few studies that assessed the functional outcome of patients, which did not permit to determine whether the improved survival rate resulted in more patients becoming dependent on others or regaining their independence.
Since the previous publication of this systematic review, the management of patients with SAH has improved considerably. In 2002 the results of ISAT were published, showing a 7% absolute decrease in risk of poor outcome for coiling versus surgical clipping. 2 The results of this trial led to a steady increase in SAH patients treated by coiling.3,4 Centralisation of care and development of comprehensive stroke centres may also have improved outcome, since large volume centres have better outcomes. 5 This may in part be explained by higher proportions of patients treated endovascularly in such centres. 6 We therefore updated the systematic review to assess whether case fatality rates have declined further and at a higher pace, and whether this concurs with an increased proportion of patients having a good clinical recovery. Further, we were interested to see whether we could find other regional differences in outcome after SAH than in the previous version.
Methods
Search strategy and selection criteria
Using the same literature search methods as in the previous review, 1 we updated the literature search in PubMed from July 2007 onwards up until May 2022. We also expanded our search and included a search in Web of Science for the same time period. We used the following keywords: (‘subarachnoid he[a]morrhage’) and ‘outcome’ or ‘mortality’ or ‘case fatality’ or ‘population’ or ‘epidemiology’) and (‘2007/7/1’; ‘2022/05/01’). Also: (‘stroke’) and ‘outcome’ or ‘mortality’ or ‘case fatality’ or ‘population’ or ‘epidemiology’) and (‘2007/7/1’; ‘2022/05/01’) (Figure 1).
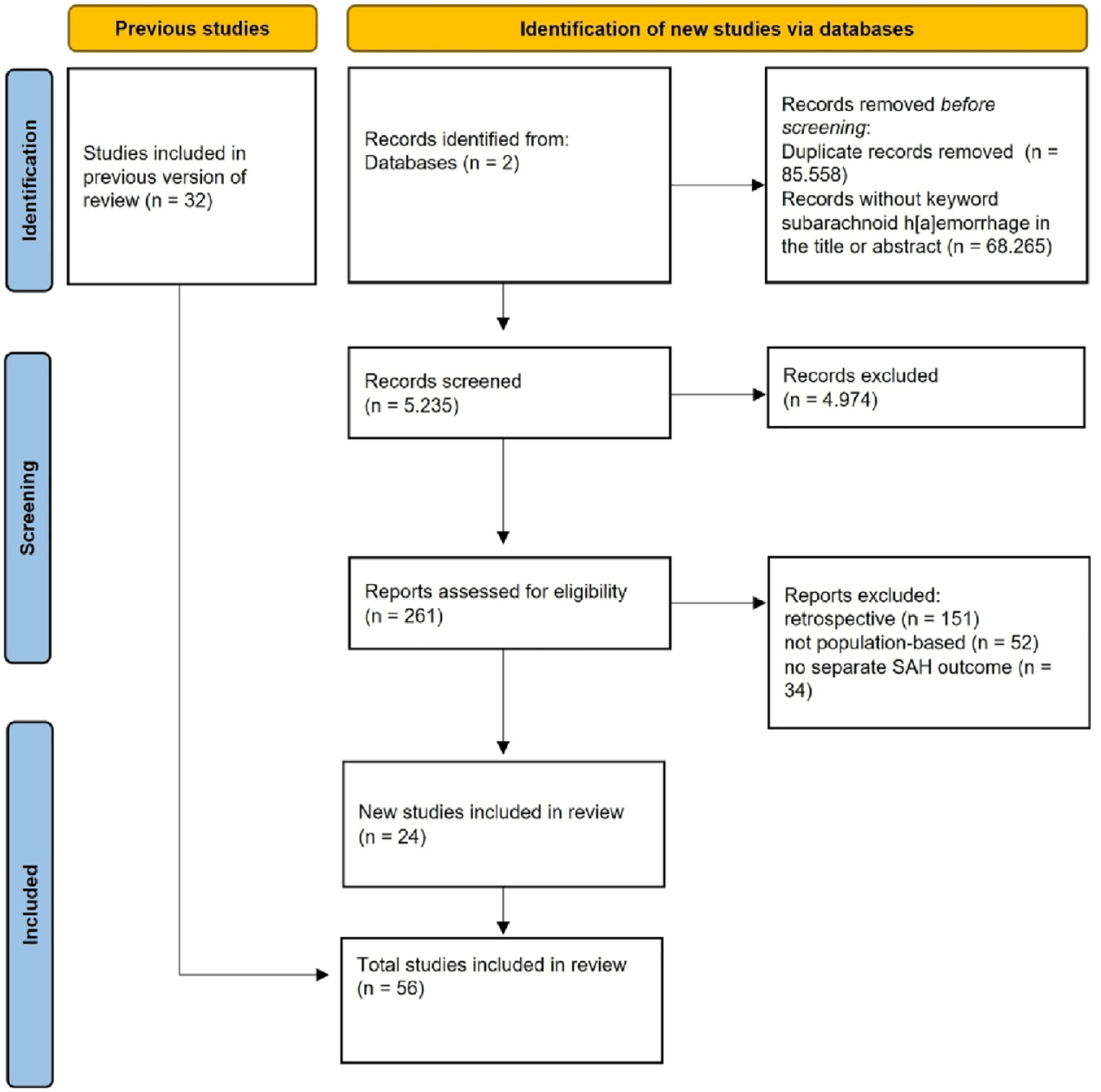
Preferred reporting items for systematic reviews and meta-analyses flow diagram.
For combinations with the keyword ‘stroke’, the reference list including the abstracts was downloaded. The key words ‘subarachnoid he[a]morrhage’ or ‘SAH’ were then searched in titles and abstracts using the Paperpile reference management software (Google Inc. 2022). Studies without either of these terms in the title or abstract were not considered for further evaluation. There was no language restriction.
Additional studies were identified by cross-checking the reference lists of matching studies. Finally, the available studies were compared with the personal database of one of the authors (GJER). This collection was prospectively built up over the last 25 years by daily searches in PubMed using the key words ‘subarachnoid h[a]emorrhage’, ‘aneurysm’ and ‘arteriovenous malformation’.
The inclusion criteria were as follows: (1) The study was published between 1965 and May 2022. (2) The study period did not exceed 10 years unless separate results were reported for each decade. (3) The study design was prospective and population-based and the study population was representative of the general population. All hospitals that provided care to the study population and all death certificates were reviewed or data on deaths were examined, or data on deaths of patients who were not hospitalised were obtained from the medical examiner. (4) The upper age limit for the study population was no younger than 74 years, and the lower limit was no older than 25 years. (5) In population-based studies of stroke in general, SAH was treated as a separate entity with defined criteria, and the case fatality rate or case morbidity was included or could be calculated. (6) The diagnosis of SAH could be verified for study purposes. (7) The incidence of SAH in the population studied was at least 3 per 100,000.
Studies from the previous review had the same inclusion criteria and were therefore eligible for inclusion (Figure 1). Since we applied the same methods as in the previous versions of the review, we did not pre-register the study protocol.
Statistical analysis
We calculated 95% confidence intervals (CI) for case fatality rates if these were not provided in the parent articles. When studies reported case fatality at multiple time points, 1-month outcome was used for the analysis. Linear regression weighted by the inverse of the standard error was performed. The standard error of the case fatality rate for each study was used to analyse the relationship between the case fatality rate and the mid-calendar year of the study. The results are expressed as the percentage change in the case fatality rate per calendar year with the corresponding 95% CI. In pre-defined sensitivity analyses we excluded studies with strikingly low or high case fatality rates, studies from regions with lower CFR than elsewhere and studies that did not provide case fatality data at 1 month. For those studies that provided data on age and sex, we used linear regression models to adjust for age and sex differences between studies.
Studies were also grouped by continent and the case fatality rates per continent were compared to those of each of the other continents. Linear regression for regional differences was performed and the single-factor analysis of variance was calculated using Scheffè’s post hoc test with correction of the alpha error. We performed a separate analysis for populations wherein case fatality was studied in two or more periods, separated by more than 5 years, updating a previous meta-analysis. 7 We used linear regression analysis and the results are expressed as the absolute percentage change in case fatality per calendar year.
When studies provided data on clinical outcome at several time points, we used the time point that was reported by most studies (12 months), to assess changes in case morbidity over time. We dichotomised functional outcome into being able to live independently for help from others (modified Rankin Scale of <3 or Glasgow Outcome Scale > 3) versus being dependent on help for activities of daily life from others.
The statistical analyses were performed using MedCalc software (version 19.6) and SAS software (version 9.4). The random effect model was used in the meta-analysis. Forest plots were created to visualise the 95% CI results. A p-value of <.05 was considered statistically significant.
Results
We identified 24 new studies, which reported on 827 patients. One study from the previous systematic review was excluded, since an updated version of this study was available (Figure 2). In total, we analysed 56 studies, which reported on 9542 SAH patients described in 62 study periods between 1973 and 2017 (Table 1).8–62 Most studies (n = 34; 57%) were conducted in Europe, and most patients were included (n = 5976) in Asia. A detailed list of studies per region and their main characteristics is provided in Supplemental Table 1. The median mid-calendar year of all studies was 1997.
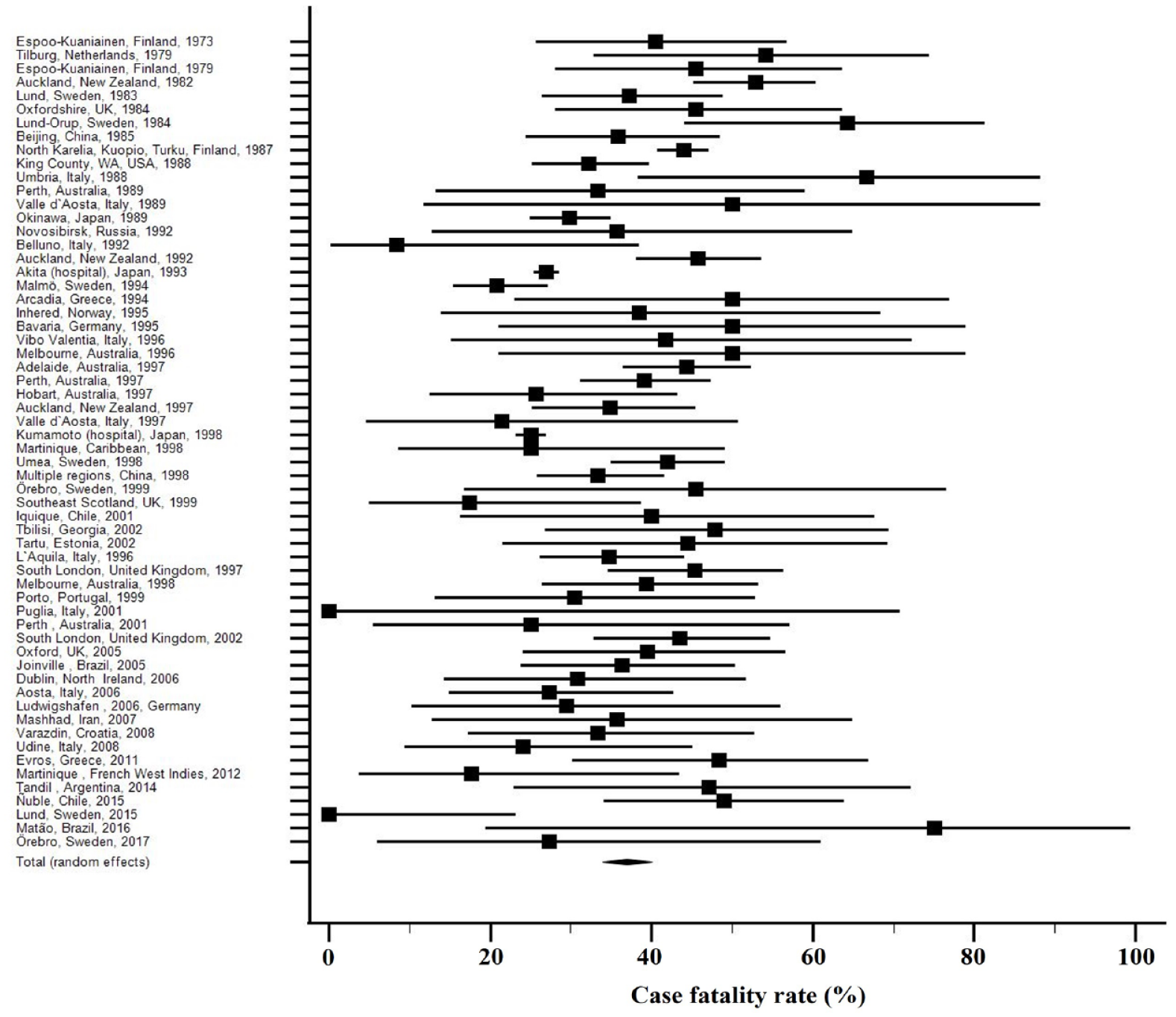
Case fatality rates per study.
Study characteristics.
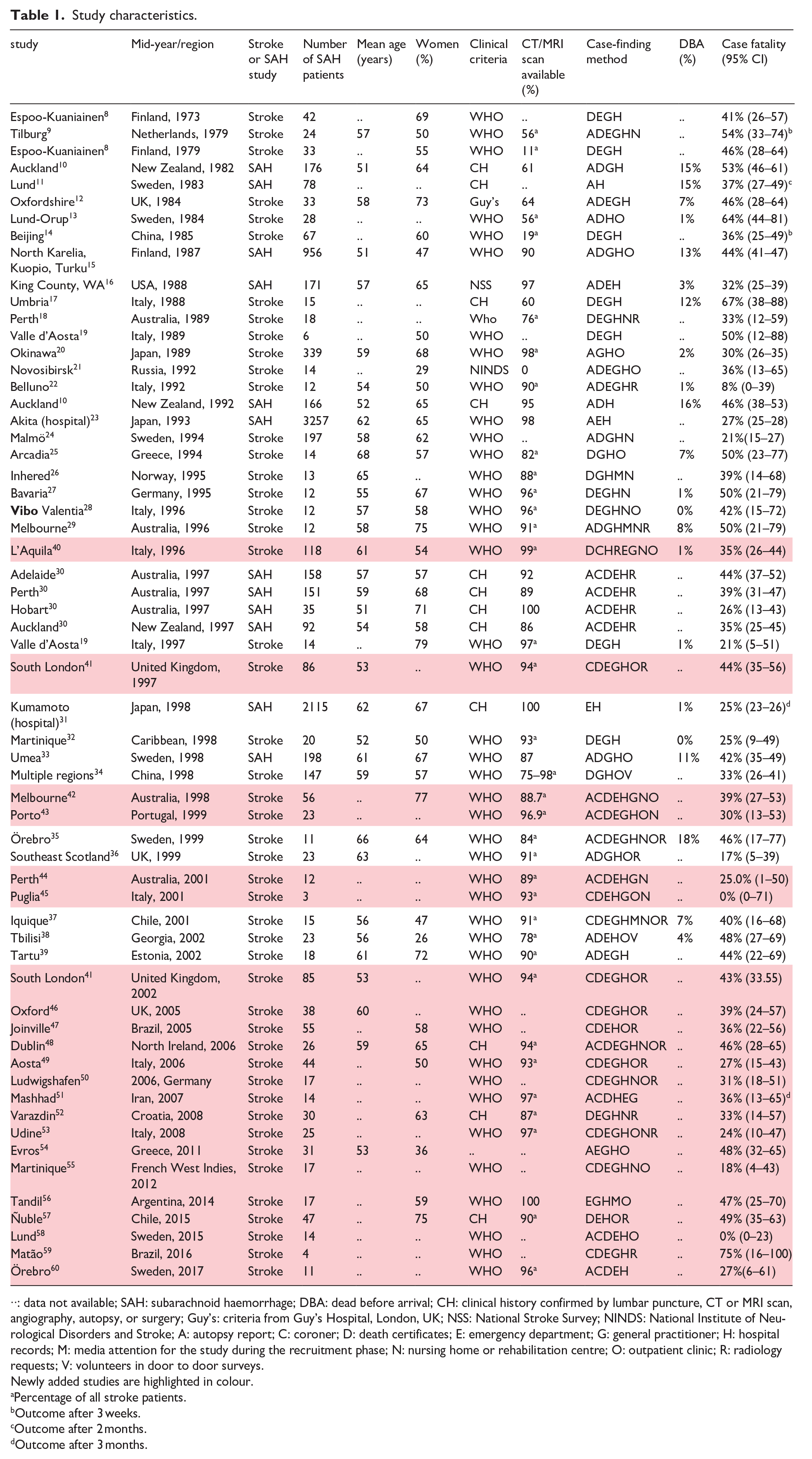
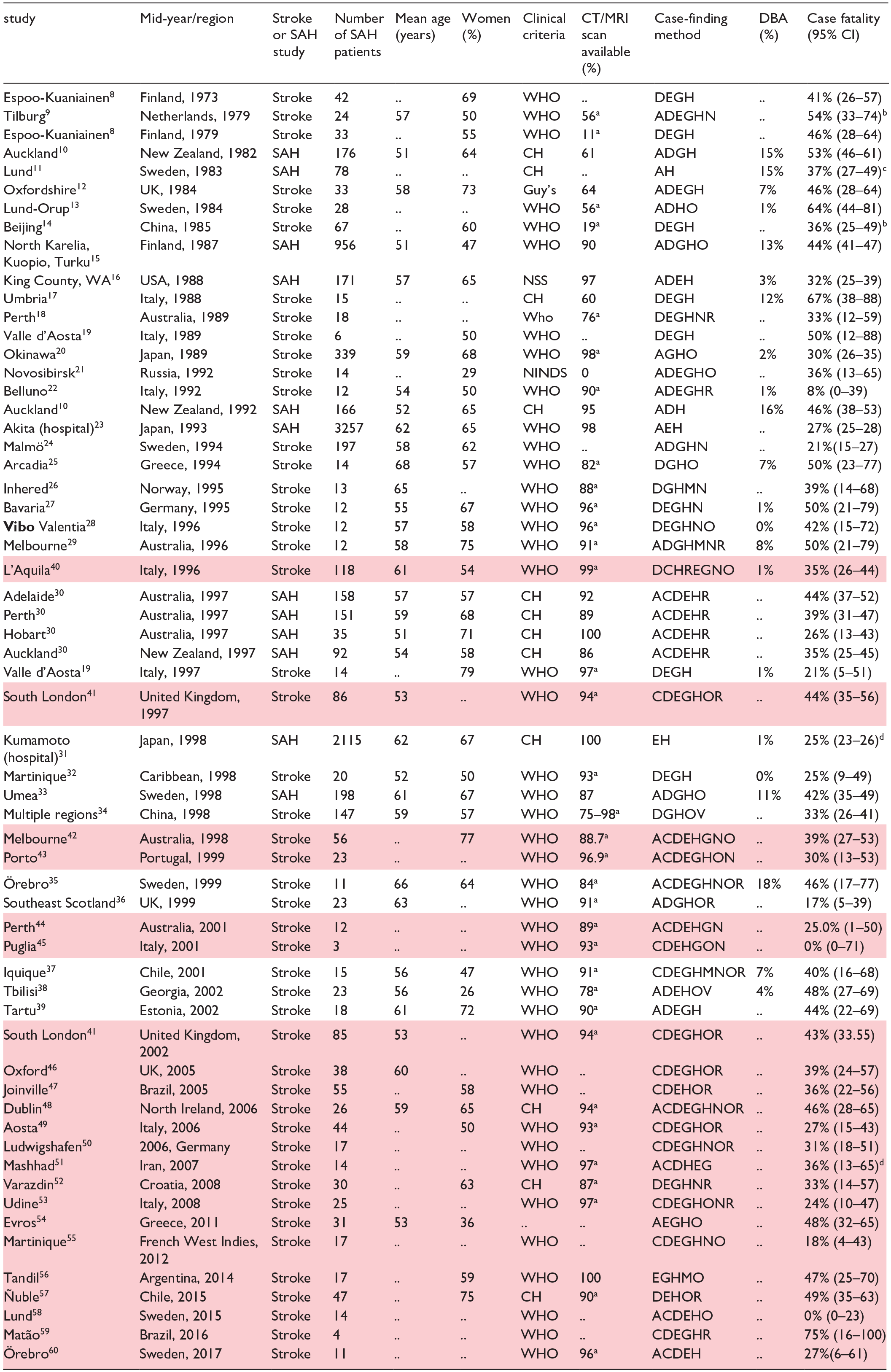
··: data not available; SAH: subarachnoid haemorrhage; DBA: dead before arrival; CH: clinical history confirmed by lumbar puncture, CT or MRI scan, angiography, autopsy, or surgery; Guy’s: criteria from Guy’s Hospital, London, UK; NSS: National Stroke Survey; NINDS: National Institute of Neurological Disorders and Stroke; A: autopsy report; C: coroner; D: death certificates; E: emergency department; G: general practitioner; H: hospital records; M: media attention for the study during the recruitment phase; N: nursing home or rehabilitation centre; O: outpatient clinic; R: radiology requests; V: volunteers in door to door surveys.
Newly added studies are highlighted in colour.
Percentage of all stroke patients.
Outcome after 3 weeks.
Outcome after 2 months.
Outcome after 3 months.
Thirty-two studies reported on the age of the SAH patients. The overall mean age was 58 years (SD ±4.4) and was stable over time (Supplemental Table 2). In the 41 studies that reported on sex, the overall female proportion was 60%. Also the proportion of women was stable over time (Supplemental Table 2). There were no new studies that reported on age for men and women separately. The mean age ranged from 54 to 60 in different regions and the female sex ratio ranged between 56% and 67% over the different regions (Supplemental Table 1). None of the included studies separated patients with a proven aneurysm as a cause of the SAH from those without a proven aneurysm.
Case fatality and time-trends
Case fatality was assessed at 3 weeks in one study, at 1 month in 56 studies, at 2 months in one study and at 3 months in two studies. Case fatality ranged from 0% to 75% (Figure 2). The funnel plot shows three studies that break the symmetry of the plot (Supplemental Figure 1).
The overall reduction in case fatality was 13.5% (95% CI −29.6 to 2.7) between 1973 and 2017. Weighted linear regression analysis of all studies showed that case fatality rate decreased by 0.3% per year (95% CI −0.7 to 0.1). The mean case fatality rate from 1970 to 1979 was 47% (95% CI 31–63), from 1980 to 1989 it was 45% (95% CI 36–53), from 1990 to 1999 it was 35% (95% CI 30–39), from 2000 to 2009 it was 34% (95% CI 27–41) and 38% (95% CI 15–60) from 2010 to 2019 (Figure 3).
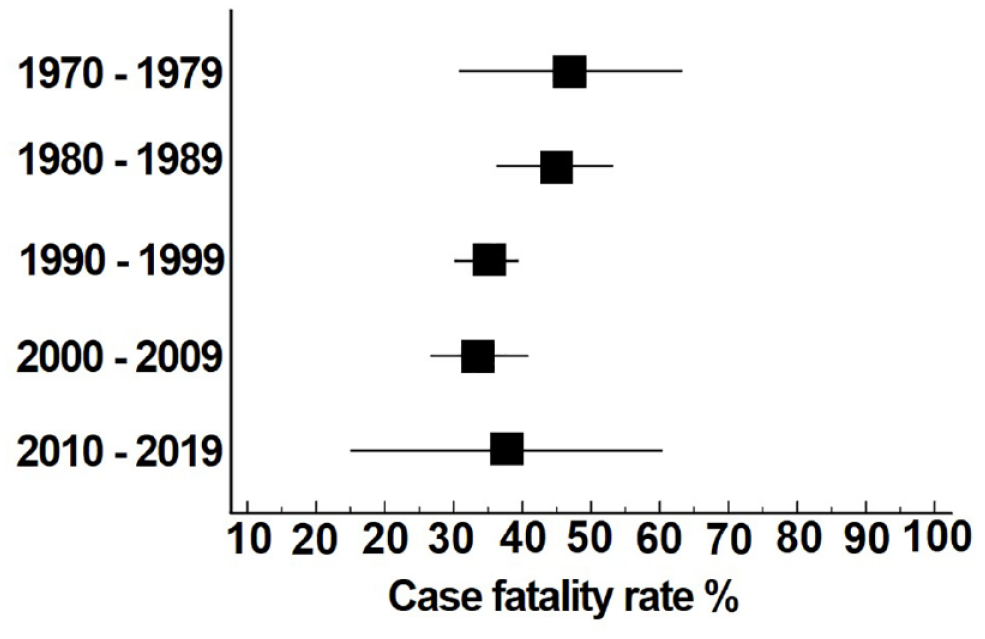
Case fatality rates per decade. Case fatality rates per decade of the studies. Squares are means and bars are 95% CI.
After excluding studies with strikingly low or high case fatality rates (0%, 8.3% and 75%), case fatality ranged from 17% to 67% and decreased by 0.4% per year (95% CI −0.7 to −0.1). Further exclusion of studies that did not provide case fatality data at 1 month did not change the results (case fatality rate decreased by 0.4% per year (95% CI −0.7 to −0.1). Of all 9488 patients, 5711 came from three Japanese studies, which were reported in the previous meta-analysis with a median case fatality of 26.7%. After further excluding these Japanese studies, weighted linear regression analysis showed that the case fatality rate decreased by 0.5% per year (95% CI −0.8 to −0.1). Additional adjustment for age and sex in this subset led to a decrease of 0.3% per year (95% CI −1.1 to 0.4).
The mean case fatality rate without exclusion of specific studies and without adjustment of age and sex was in Europe 37% (95% CI 32–42), in Asia 34% (95% CI 28–40), in Australia and New Zealand 39% (95% CI 32–46), in North America 32% (95% CI n/a) and in Central and South America 41% (95% 24–59). The mean case fatality rate in Asia, excluding all Japanese studies, was 38% (95% CI 31–45). Figure 4 shows separated case fatality rates per continent. Linear regression analysis showed no significant continental differences in the case fatality rates.
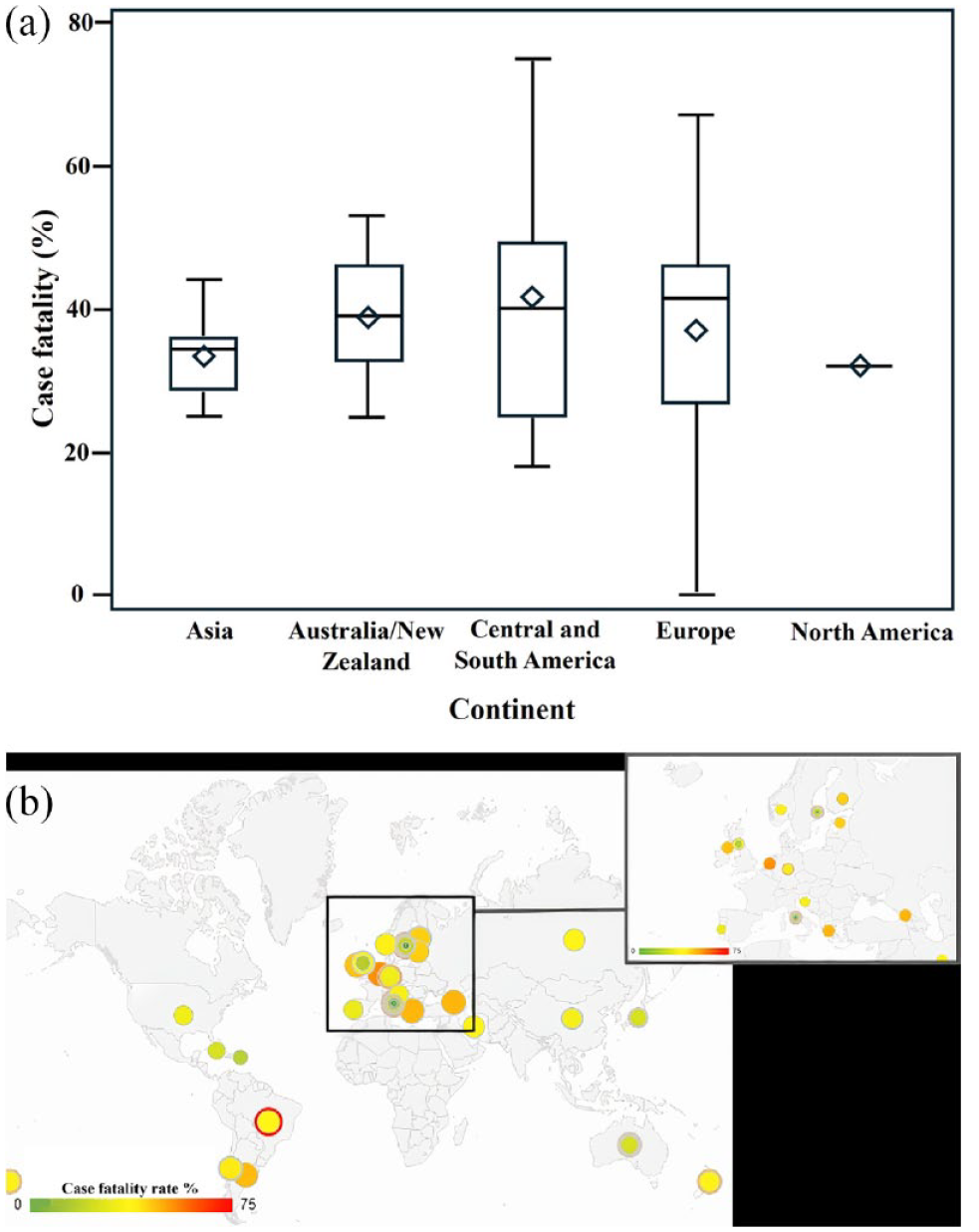
(a) Regional differences in case fatality. Boxes = interquartile range. Lines median. Bars = range. Squares = mean. (b) World heat map showing regional case fatality throughout the study period from 1973 to 2017. Each colour in a circle presents a distinct study or study period.
Two additional studies that assessed case fatality rates within a population at different time points were found since the previous review. 7 The absolute risk reduction per year in Martinique from 1998 until 2012 was 0.5%, in Örebro (Sweden) from 1999 until 2017 it was 1.1%. The overall absolute risk reduction per year of nine studies that assessed case fatality rates at different timepoints within a population included in this systematic review was 0.9% (95% CI 0.4–1.5).
Functional outcome
Two studies reported functional outcome at 1 month, one study at 3 months, three studies at 6 months, four studies at 12 months and one at 44 and 60 months. Two studies reported functional outcomes at multiple time points (one ranging from one to 60 months and another one to 12 months). The total number of articles reporting on functional outcome was 15, which described 15 study periods including 2825 patients (Table 2); 8 new articles with 399 patients reporting on functional outcome were included. One study did not report the proportion of patients remaining dependent but only the combined proportion of death and being dependent, 61 and one other reported only the median modified Rankin Scale without proportions of independent living patients and dependent living patients. 63
Functional outcome.
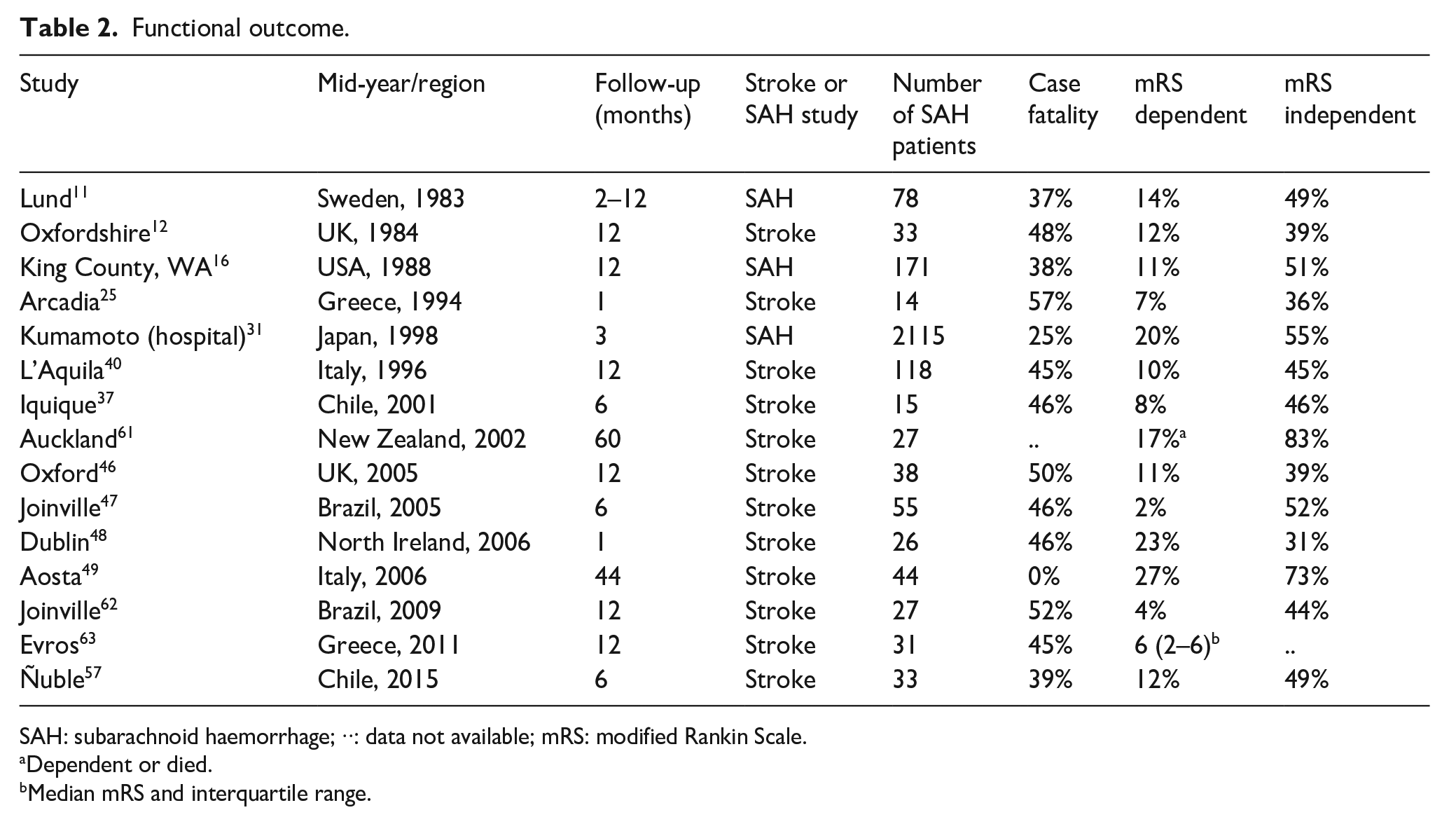
SAH: subarachnoid haemorrhage; ··: data not available; mRS: modified Rankin Scale.
Dependent or died.
Median mRS and interquartile range.
Studies with a follow-up time of 12 months reported a range of the proportion of patients living independently from 39% to 51% and those remaining dependent from 4% to 14%. In the linear regression analysis of all studies from 1983 to 2015, the proportion of patients living independently increased by 0.2% (95% CI −0.7 to 1.1%) per year (Figure 5), and case morbidity did not change (0.0%) (95% CI −0.5% to 0.5%). Age and sex data were not available for functional outcome and therefore we could not adjust analyses on functional outcome for these factors.
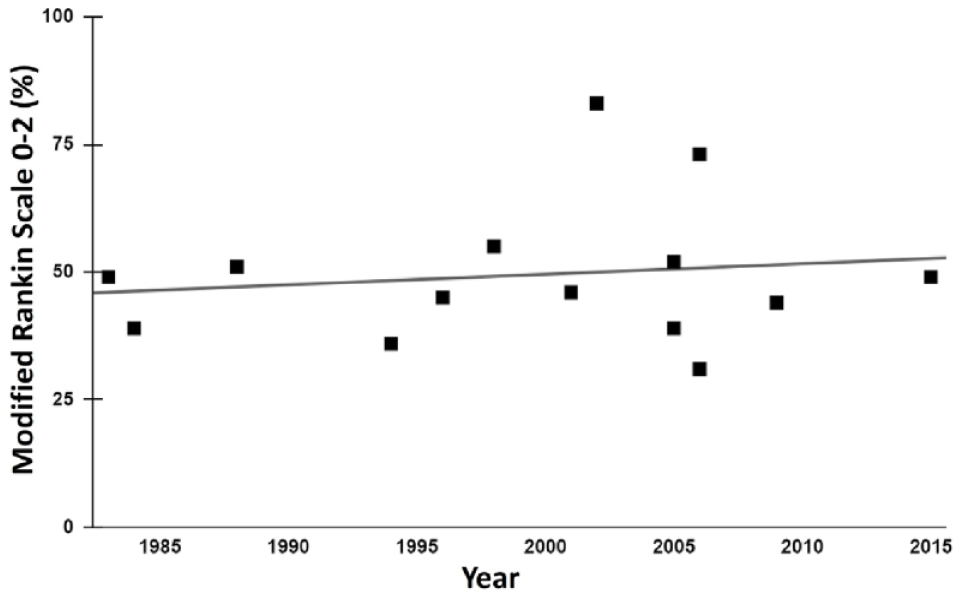
Mid-calendar year and proportions of patients who regained independence for daily life activities for studies reporting on functional outcome after spontaneous subarachnoid haemorrhage. Linear regression demonstrates a trend towards increase in the proportion of patients living independently after subarachnoid haemorrhage by 0.2% per year (95% CI −0.7 to 1.1).
Discussion
This systematic review included 24 new studies and one and a half decades of observations. The overall case fatality decreased but to a lesser extent than in the previous version. The decline in case fatality rate occurred mainly in the last decades of the 20th century, and seems to level off in the last two decades. The number of studies reporting on functional outcomes doubled in comparison with the previous version of the review. There was a trend towards an increase in the proportions of SAH patients who regained independence for activities of daily living, and no sign of increasing proportions of patients who remained dependent, but the data on the functional outcome were overall inconclusive.
In contrast to our finding of a stable case fatality rate over the last two decades, a hospital-based study found a statistically significant decrease in case fatality rates between 1999–2002 and 2009–2012, which was mainly attributed to a decrease in in-hospital rebleeding. 64 This hospital-based study did not include deaths before arrival the hospital. Because these sudden deaths from SAH are responsible for 10% to 15% of overall case fatality in SAH patients, 65 not taking into account these sudden deaths may in part explain the difference between this hospital-based study and population-based studies on case fatality rates over the last decades. A registry-based study in Finland, which captures also a large part of the sudden deaths from SAH, found an overall decrease in case fatality between 1998 and 2017, but when comparing the periods 1998–2000 and 2015–2017, case fatality rates decreased in women but increased in men, in particular in men older than 65 years of age. 66 In this registry-based study the proportion of women gradually increased during the study period, while the CFR decreased merely in women. In this systematic review the proportion of women did not increase and point estimates even suggested a decrease in the last two decades. Thus, the lack of a further decline in the CFR over the last two decades in our review may be partly explained by the stable proportion of women in the parent population-based studies.
In the subset of studies that assessed case fatality rates within one population at different time points we also found an overall decrease in case fatality over time, which strengthens our findings in the entire set of population-based studies. The two new studies with multiple assessments over time both had the first assessment in the 1990s and the newest in the 2010s. In both, the point estimates suggest a decline in case fatality rate over time. Similar findings were done in a recent systematic review on study populations with assessment of case fatality at different endpoints. 67 This study used different inclusion criteria and included 16 populations, 14 of which showed a decline in case fatality rates over time. Comparable to our findings in the overall data set, the decline in this review seemed stronger over the last two decades of the 20th century than over the first two decades of the 21st century.
There are several explanations for a lack of further decrease in case fatality on a population-based level over the last two decades. First, while the overall incidence of SAH is declining, the incidence of hospitalised elderly patients increases.68,69 It is a challenge to improve outcomes in older patients, as underlined in the Finnish registry study. 66 Second, we hypothesised that the greater availability of coiling had led to a decrease in case fatality. In a study on 7658 aneurysmal SAH patients from 22 tertiary care hospitals from Europe, USA, and Australia, endovascular coiling did not result in lower 14-days case-fatality rates than neurosurgical clipping. 70 In clinical cohorts from the same study, also 90 days case fatality rates were higher after coiling than after clipping, but the proportion of patients with poor functional outcome were lower after coiling than after clipping. Thus, in clinical practice, that is, outside trials, the advent of coiling may have more impact on clinical outcome than on case fatality. Moreover, it is unclear whether new endovascular treatment options are widely used in all areas represented in this systematic review. Third, treatment in high-volume centres reduces case fatality in SAH patients, 5 but data on (change in) the volume of the treatment centres was not available in the included studies. Lack of regional centralisation may have influenced results. Another explanation is that a plateau has been reached and no further reduction in CFR can be achieved. Still, around 10%–15% of patients with subarachnoid haemorrhage die before reaching the hospital, and even the best medical and surgical treatment cannot change the fate of these patients. The improvement achieved for patients admitted at hospitals may therefore not translate to an improvement of case fatality rates on a population-based level.
The range of patients living independently was very high. This may relate to different definitions of independent living between the studies or to differences between countries when a patient is considered able to live independently. Whatever the cause is, the wide range hampers proper assessment of the change in functional outcomes over time, even though the number of patients included in this analysis has doubled compared to the previous review. We also did not find studies with assessment of functional outcomes at different time points within one population, which further precludes assessment regarding time trends.
Our study has several strengths: We could include a considerable number of new and recent prospective, population-based studies into the meta-analyses, which enabled us to further estimate time trends of the case fatality rate in spontaneous SAH as well as functional outcomes over nearly five decades. Moreover, we used established, robust case-finding methods for the review. Our meta-analysis also has limitations. First, even though the number of new studies is large, the number of patients with SAH included in the new studies are in general smaller than in many studies already included in the previous version of the review. Second, for many confounders such as age, sex, or other potential risk factors for adverse functional outcomes, no additional data were available. Thus, we could not adjust for these factors. Both the relatively small numbers of patients and the lack of ability to adjust for risk factors are in part explained by the fact that most newly identified studies are population-based studies on stroke in general, with SAH as one of the subsets, instead of population-based studies on SAH in general. In the majority of studies on stroke in general, age and sex-specific data were not available for SAH patients separately. In both the previous and current systematic review we could not differentiate between aneurysmal and non-aneurysmal SAH because the underlying studies did not provide specific outcome data. We assume that most cases were of aneurysmal origin, but advocate that future studies report on the proportion of patients with proven aneurysms and separate outcomes for those with and without a proven aneurysm as cause for the SAH, as outcomes may be different. 71
The lack of a further decline in case fatality on a population-based level over the last two decades, despite the overall reduction in case fatality over the last five decades, warrants further study. Although sudden deaths from SAH will prove difficult to eliminate, insight into the care provided and the case fatality per region could facilitate implementing strategies that proved successful in some regions into other regions. If further studies confirm the lack of further decline in case fatality, this would imply that further reduction in case fatality can only be achieved through prevention of aneurysm development and rupture. Future studies should also focus on functional outcome, using established outcome scales to facilitate comparability between the studies.
Supplemental Material
sj-docx-2-eso-10.1177_23969873241232823 – Supplemental material for Case fatality and functional outcome after spontaneous subarachnoid haemorrhage: A systematic review and meta-analysis of time trends and regional variations in population-based studies
Supplemental material, sj-docx-2-eso-10.1177_23969873241232823 for Case fatality and functional outcome after spontaneous subarachnoid haemorrhage: A systematic review and meta-analysis of time trends and regional variations in population-based studies by Andreas Ziebart, Judith Dremel, Svetlana Hetjens, Dennis J Nieuwkamp, Francisca HH Linn, Nima Etminan and Gabriel JE Rinkel in European Stroke Journal
Supplemental Material
sj-docx-3-eso-10.1177_23969873241232823 – Supplemental material for Case fatality and functional outcome after spontaneous subarachnoid haemorrhage: A systematic review and meta-analysis of time trends and regional variations in population-based studies
Supplemental material, sj-docx-3-eso-10.1177_23969873241232823 for Case fatality and functional outcome after spontaneous subarachnoid haemorrhage: A systematic review and meta-analysis of time trends and regional variations in population-based studies by Andreas Ziebart, Judith Dremel, Svetlana Hetjens, Dennis J Nieuwkamp, Francisca HH Linn, Nima Etminan and Gabriel JE Rinkel in European Stroke Journal
Supplemental Material
sj-jpg-1-eso-10.1177_23969873241232823 – Supplemental material for Case fatality and functional outcome after spontaneous subarachnoid haemorrhage: A systematic review and meta-analysis of time trends and regional variations in population-based studies
Supplemental material, sj-jpg-1-eso-10.1177_23969873241232823 for Case fatality and functional outcome after spontaneous subarachnoid haemorrhage: A systematic review and meta-analysis of time trends and regional variations in population-based studies by Andreas Ziebart, Judith Dremel, Svetlana Hetjens, Dennis J Nieuwkamp, Francisca HH Linn, Nima Etminan and Gabriel JE Rinkel in European Stroke Journal
Footnotes
Acknowledgements
None
Author contributions
Drs Rinkel and Ziebart conceptualised and designed the study. Drs Rinkel and Etminan coordinated and supervised the systematic review. Drs Ziebart and Dremel selected the articles, extracted the data. Dr Hetjens performed the data analysis and assessed the risk of bias. Drs Ziebart and Rinkel drafted the initial version of the manuscript. All authors critically reviewed and approved the final manuscript as submitted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Guarantor
Gabriel JE Rinkel
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.