
Abstract
Introduction:
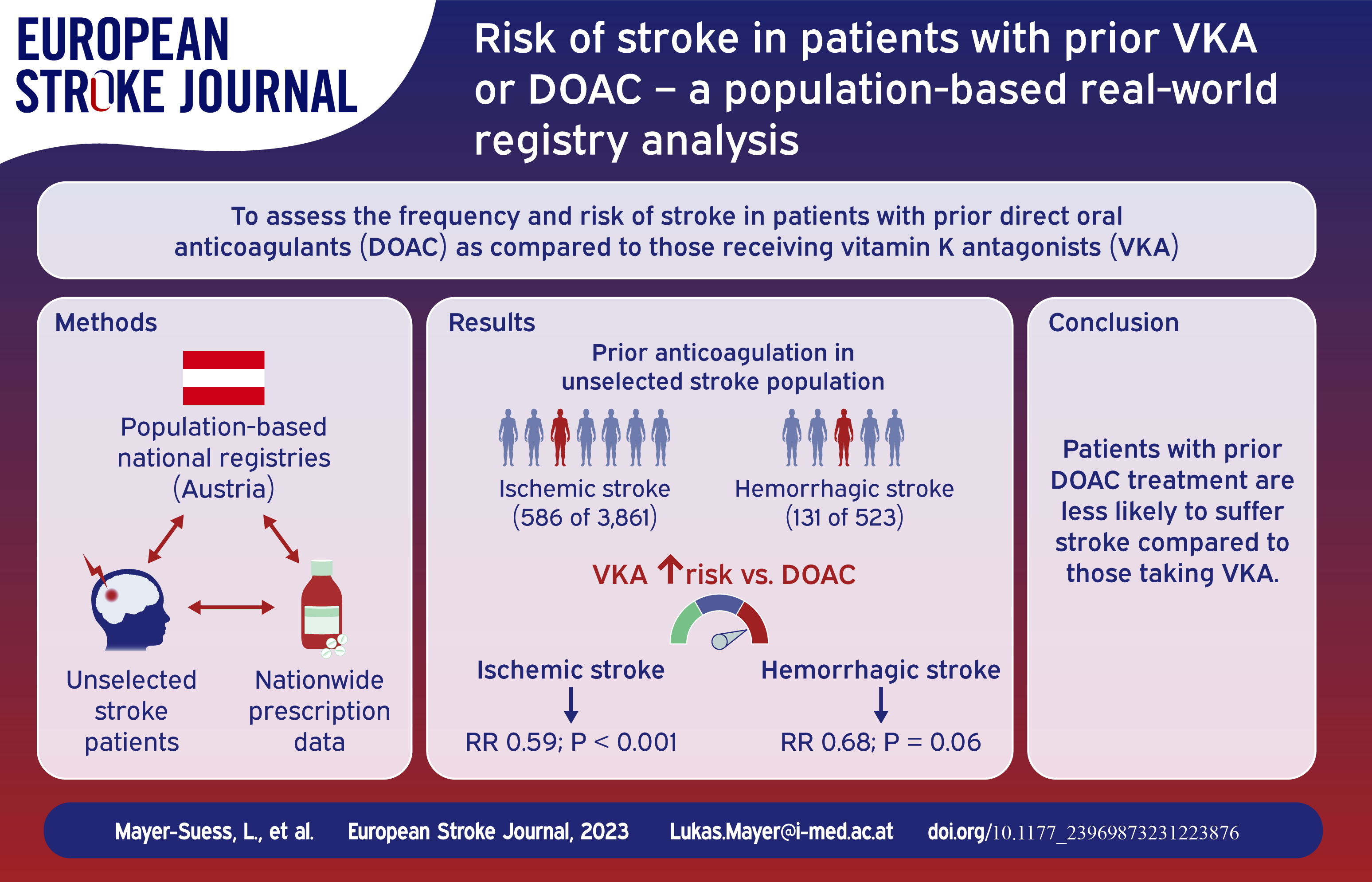
To date, risk assessment of suffering ischemic and hemorrhagic stroke in individuals under oral anticoagulation (OAC) is limited to hospital-based cohorts and patients with atrial fibrillation.
Patients and methods:
Through the combination of three individual datasets, (1) the population-based Tyrolean Stroke Pathway database, prospectively documenting all (unselected) stroke patients in the entire federal state of the Tyrol and (2) nation-wide prescription data, detailing each reimbursed prescription in Austria as well as (3) the Austrian Stroke Unit Registry, a nation-wide registry comprising data on all patients admitted to any of the 38 stroke units in Austria, we assessed risk of stroke in patients with prior oral anticoagulation and compared characteristics of patients taking direct oral anticoagulants and Vitamin-K-Antagonists.
Results:
In Austria, oral anticoagulant prescription reimbursements increased from 292,475 in 2015 to 389,407 in 2021. In the Tyrol, prior oral anticoagulation treatment was evident in 586 of 3861 (15.2%) patients with ischemic and 131 of 523 (25.0%) with hemorrhagic stroke, with 20% and 35% of those stroke patients respectively having prior oral anticoagulation due to other indications than non-valvular atrial fibrillation. Considering prescription rates, treatment with direct oral anticoagulants was associated with a reduced stroke risk compared to Vitamin-K-Antagonists, especially in ischemic (1.05% vs 0.62%; RR 0.59, p < 0.001) but also in hemorrhagic stroke, even if less pronounced (0.21% vs 0.14%; RR 0.68, p = 0.06). In Austria, prior intake of direct oral anticoagulants was associated with lower risk of suffering acute large vessel occlusion stroke (RR 0.79, p = 0.003).
Discussion and conclusions:
One in seven patients suffering ischemic and one in four suffering hemorrhagic stroke had prior oral anticoagulation treatment. Both ischemic and hemorrhagic strokes are less frequent in those with direct oral anticoagulant intake compared to those taking Vitamin-K-Antagonists. Establishment of clear standard operating procedures on how to best care for acute stroke patients with oral anticoagulation is essential.
Introduction
According to the Global burden of disease study, stroke is among the top three leading causes for death and disability globally and its burden has increased substantially within the last three decades. 1 In patients with atrial fibrillation, oral anticoagulants (OAC) are effective in the prevention of ischemic stroke and are associated with reduced ischemic stroke severity. 2 Therefore, stroke and cardiac societies have recommended OAC for primary and secondary prevention of cerebral ischemia in these patients.3,4 Medication incompliance or under-usage in community practice hamper the effectiveness of OAC in ischemia prevention.5,6 In turn, there is a risk of OAC-associated intracerebral hemorrhage (ICH), with hospital-based cohorts reporting a prior OAC intake in 15% of patients with ICH. 7 As frequency of OAC prescription is steadily increasing, safety and effectiveness of VKA and DOAC is of utmost importance. 8 To date, risk assessments of suffering ischemic and hemorrhagic stroke in individuals taking OAC mostly rely on studies of hospital-based cohort studies and are not community- or population-based. Literature offers extensive data on characteristics of ischemic stroke patients with prior atrial fibrillation and oral anticoagulation, but neglects patients taking these drugs for other indications. Our aim was to (1) define the frequency of OAC treatment prior to ischemic stroke or ICH in an unselected population-based cohort and (2) elaborate on the risk of ischemic stroke despite or ICH due to OAC.
Material and methods
Available databases
Data were gathered using three independent sources. First, the population-based Tyrolean Stroke Pathway database, which was implemented as quality control tool documenting all stroke patients admitted to any hospital or department in the entire federal state of Tyrol from 2009 onward. 9 The Tyrol covers an area of 12,534 km2 in the Austrian Alps, inhabits 771,304 individuals (50.7% women) with a mean age of 43.0 years. The pathway is funded by the Tyrolean Government and health insurance carriers, administered and monitored by the Tyrolean Healthcare Fund based on the Tyrolean Healthcare Fund law (TG §18) and the federal law on health care documentation and the target control health (Art. 15a Bundesverfassungsgesetz – Zielsteuerung Gesundheit). Prospective data entry is mandatory for all patients with any stroke discharge code. For the current analysis, only those with ICD10 codes I61 or I63 at discharge are considered. To limit false entry, codes I62, I64 and G46 are not permitted as the primary diagnosis in the Tyrol. Further, tests of random samples of discharged patients are performed by the data management team to ensure quality. Data entry is done by stroke teams located at each hospital in the Tyrol and, specifically for in-hospital complications, the registry is cross-checked with ICD-10 codes upon discharge during data monitoring. In-hospital deaths are reliably documented through in-house death certificates. We have previously shown that 2.6% of Tyrolean stroke patients are treated outside the Tyrol and that 97.4% of stroke patients are indeed hospitalized, making selection bias negligible. Reasons for non-hospitalization were death (0.2%), denial by the patient (0.9%), on-site medical care (0.7%), and other conditions (0.7%). 9 Data on prior OAC treatment is available from 2019 onward. Second, we utilized the Austrian Stroke Unit registry (ASUR), which collects demographic, baseline and follow-up data on each individual treated on one of the 38 stroke units in Austria. It is a quality control tool with obligatory data entry for all centers. The registry is based on the federal law promoting quality in health care (and administered by the governmental Austrian National Public Health Institute. Data integrity and completeness are legally required and the database is regularly monitored for all components. Data entry is limited to experienced stroke neurologists and scientific analyses are approved and supervised by an academic review board. Overall, more than 70% of ischemic stroke patients in Austria are registered in the ASUR and it harbors data on each endovascular thrombectomy performed nation-wide, which is the basis for our analysis on large vessel occlusion (LVO) in individuals with prior OAC.10,11 Lastly, each prescribed drug in Austria is detailed by a unique pharmaceutical registration number, which is linked to the Anatomical Therapeutic Chemical (ATC) Classification System. Health care insurance funds, providing health care to residents in Austria, collect these data and can deliver information on all reimbursed drug prescriptions. For the current analysis, total reimbursed prescriptions of DOACs and VKA in all of Austria, and individually for the federal state of Tyrol, from 2015 to 2021 were assessed retrospectively using the data provided by insurance carriers.
Variable definitions and statistical methodology
Both our population-based databases (Tyrol Stroke Pathway database and reimbursed prescriptions) were used to depict absolute number of stroke patients and prescription reimbursements to subsequently calculate risk of stroke under OAC. The ASUR was applied to assess the risk for acute intracranial LVO in ischemic stroke patients with prior OAC. All strokes events, including recurrence, were counted independently. Vascular risk factors were evaluated applying current guidelines.3,4 Lastly, severe in-house complication was a composite variable consisting of infections, myocardial infarction, recurrent or progressive stroke, intracranial- or extracranial bleeding, epileptic seizure and deep vein thrombosis or pulmonary embolism. The statistical analysis was performed using R statistical software, version 4.2.2. Comparison between categorical variables were done using the χ2 test or Fisher exact test and Kruskal-Wallis test for continuous variables. Categorical variables are presented as frequencies with percentages and continuous ones as median and interquartile range. Significance was set at p < 0.05. To address potential factors associated with LVO, a multivariate analysis including baseline characteristics that differed in group comparison between LVO and non-LVO patients was done.
Standard protocol approvals, registration, and patient consents
All analyses were approved by the local ethics committee at the Medical University of Innsbruck EK#1059/2023.
Data availability
Anonymized data not published within this article will be made available to any qualified investigator upon reasonable request after ethics approval and receipt of a signed data transfer agreement. The current manuscript adheres to reporting guidelines of observational cohorts. 12
Results
In Austria, the number of number individuals that reimbursed OAC prescriptions increased from 292,475 in 2015 to 389,407 in 2021 (Figure 1(a)). This increase stems from the upsurge in DOACs as VKA reimbursements decreased each year. Similar trends were observed in the Tyrol (Figure 1(b)). In the unselected cohort of stroke patients in the Tyrol, prior OAC treatment was evident in 586 of 3861 (15.2%) of ischemic and 131 of 523 (25.0%) of hemorrhagic stroke patients (Figure 2). Taking Tyrol’s prescription rates into account, the risk of ischemic stroke was higher in patients with prior VKA compared to those under DOAC treatment (1.05% vs 0.62%; RR 0.59 [CI 0.49–0.71] p < 0.001) and that was also true, though less pronounced, for hemorrhagic stroke (0.21% vs 0.14% respectively; RR 0.68 [CI 0.45–1.02] p = 0.06) (Supplemental Table 1). Table 1 presents the comparison of individuals suffering stroke with prior VKA or DOAC intake.
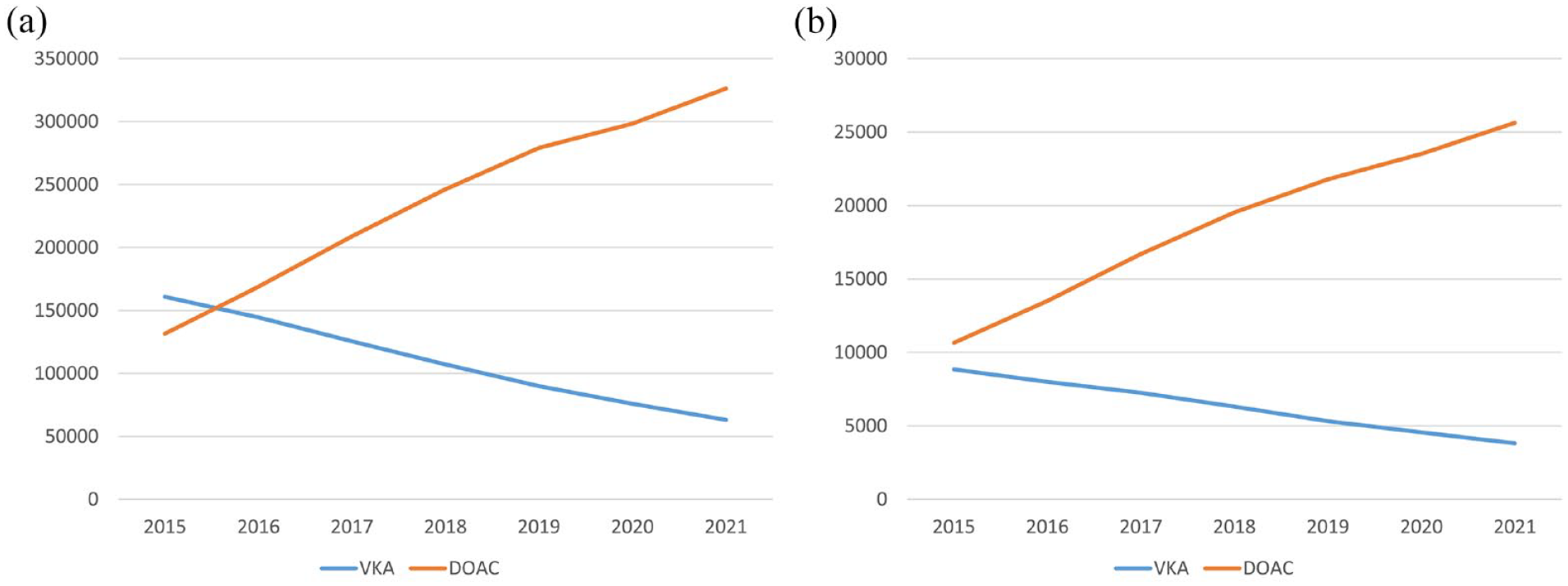
Absolute number of oral anticoagulants reimbursed from 2015 to 2021 ((a) Austria; (b) Tyrol).
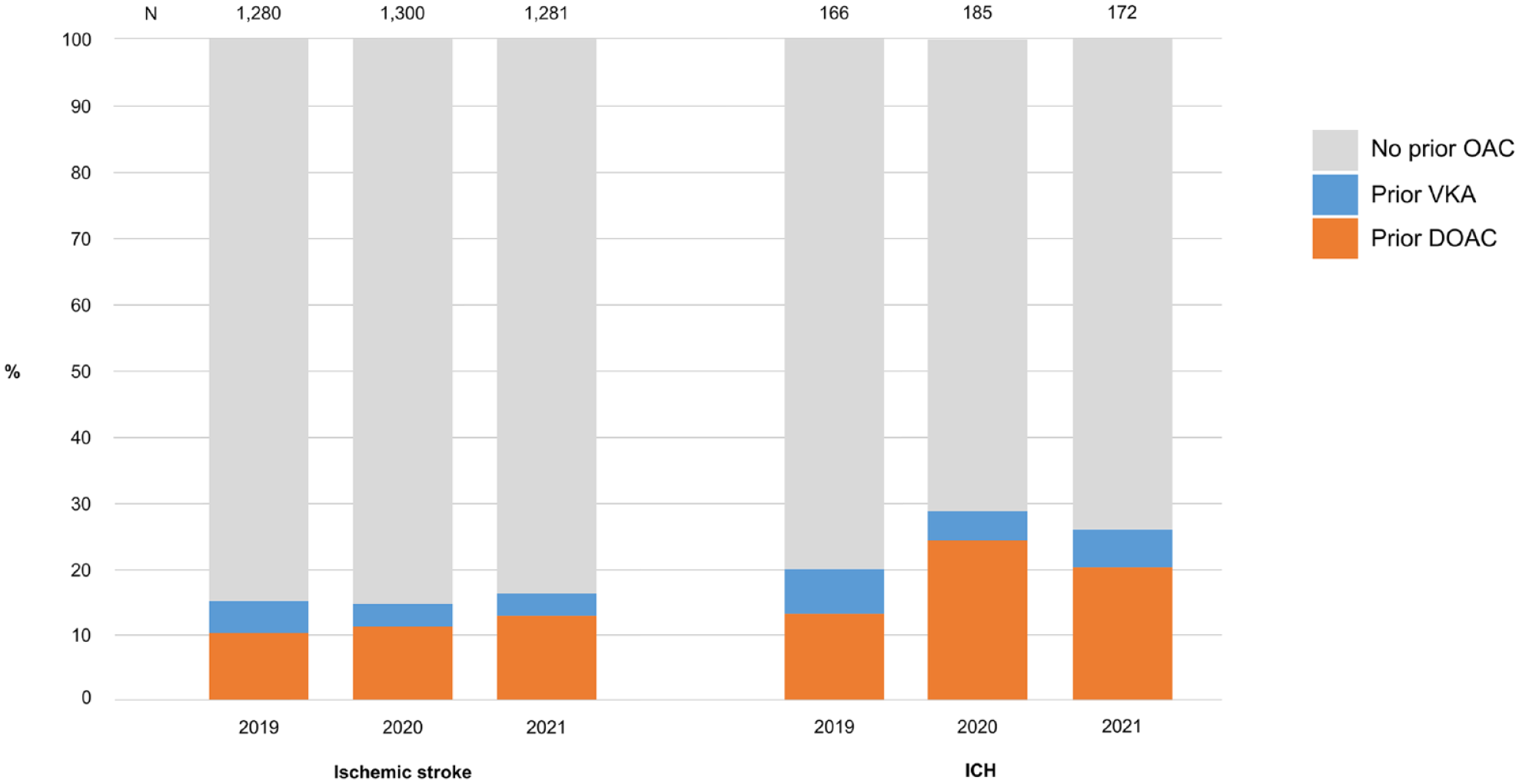
Per year percentage of our unselected patients cohort with VKA or DOAC treatment prior to ischemic stroke or ICH.
Differences between ischemic stroke patients with prior VKA or DOAC in the population based Tyrol cohort.
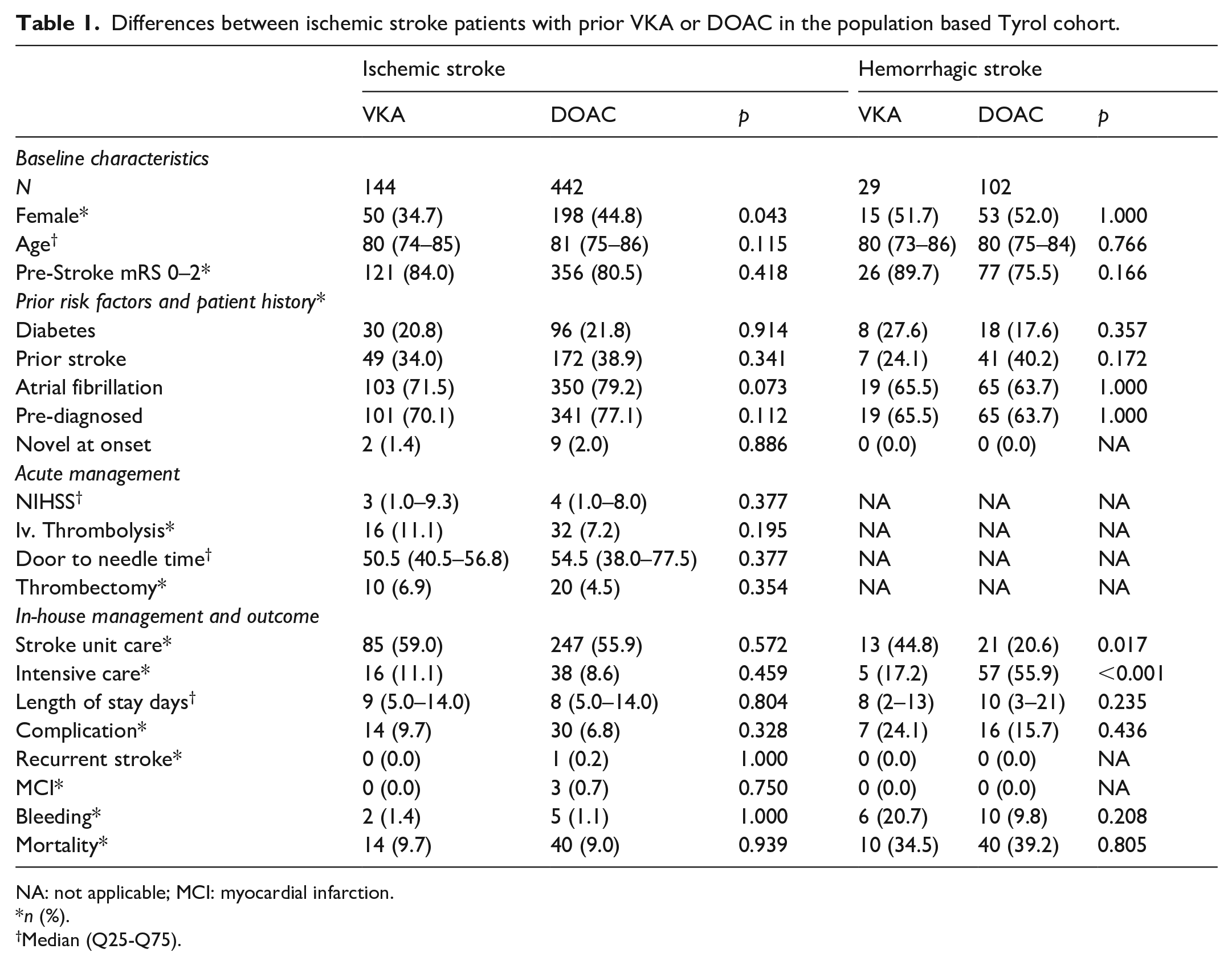
NA: not applicable; MCI: myocardial infarction.
n (%).
Median (Q25-Q75).
Through our analysis of the ASUR, encapsulating data on 52,585 ischemic stroke patients, those with prior DOAC treatment had a lower risk of LVO (RR 0.79 [CI 0.67–0.92] p = 0.003) compared to those with prior VKA. Differences of our ASUR cohort on patient characteristics of individuals with prior DOAC or VKA as well as those with and without LVO despite prior OAC are presented in the online supplement (Supplemental Table 2–3).
Discussion
We present a representative real-world analysis reporting risk of ischemic stroke despite and ICH associated to OAC. Our data are based on population-based nation-wide OAC prescriptions, as recorded by Austria’s health care insurance funds, and the Tyrolean Stroke Care Pathway, one of the very few population-based, data monitored, registries worldwide that covers information on all stroke patients in the entire federal state. 9 Prescription rates of OAC in Austria and in the Tyrol, mainly driven by DOACs, have greatly increased over time (Figure 1). This development relies on primary prevention and structured disease management programs in secondary prevention. The STROKE-CARD program reported an OAC compliance 1 year after stroke event in more than 90% of patients. 13 The incidence of ischemic stroke, TIA and ICH in Austria and the risk of recurrent stroke declined over the last years parallel to the upwards trend in OAC. 14 As frequency of OAC prescription is steadily increasing, safety and effectiveness of VKA and DOAC as well as clear SOPs on how to best care for acute stroke patients on OAC is essential.15,16 This is emphasized by our analysis of unselected stroke patients, as 15% of ischemic stroke and 25% of ICH patients had prior OAC treatment. In terms of ischemic stroke, this is in line and in ICH is remarkably higher than the previously published data of hospital-based cohort studies.7,15,17 Further, 20% of ischemic stroke and 35% ICH patients had prior OAC intake due to reasons other than non-valvular atrial fibrillation. Concerning ischemic stroke, recent findings put forth the potential for off-label use of iv. thrombolysis in patients with prior DOAC intake, as no excessive risk of ICH in selected individuals could be reported in observational data. 16 This adds to endovascular thrombectomy at least seemingly being safe and effective in ischemic stroke patients with prior OAC and LVO. 18 Investigations on the acute management of stroke patients with prior OAC are crucial and therefore should not be limited to ischemic stroke but expanded to ICH as prior OAC can have a tremendous negative impact on patient outcome, either through the larger initial hematoma volume and increased likelihood of hematoma expansion. 19 Moreover, we report an explicitly reduced risk of stroke as well as a lower risk of LVO in patients with prior DOAC compared to VKA intake. These observational data are in line with prior meta-analyses suggesting a beneficial safety and efficacy profile of DOACS compared to VKA.20,21 An explanation may be medication incompliance or reduced drug efficacy in VKA as a recent analysis of the STROKE-CARD trial reported that a large proportion of patients with prior VKA suffering ischemic stroke had an INR of <1.7 at admission. 22 Still, it is important to mention that all prior studies mentioned investigated a distinctly selected group of patients, being those taking OAC due to non-valvular atrial fibrillation, neglecting a group of patients that significantly differs in key characteristics (Supplemental Table 4).15,17 Even though indications for DOACs have expanded over the years, the use of VKA still remains the gold standard in patients with, for instance, valvular atrial fibrillation, antiphospholipid syndrome or mechanical heart valves. 23 Both in ischemic stroke and ICH, the sheer number of patients suffering stroke under OAC treatment holds the potential for large randomized controlled acute management trials. Further, safety and efficacy of additive secondary prevention strategies, such as atrial appendage occlusion in patients with recurrent ischemic stroke despite OAC treatment, would be fruitful, as an evidence-based pathway for clinicians in such cases has hitherto been lacking. Limitations of our databases have to be acknowledged. First, the absolute numbers of OAC prescriptions are slightly overestimated as over the course of our study OAC-switching within a calendar year was evident in 4.0% of patients and counted toward both drugs separately. Detailed information on OAC indication other than atrial fibrillation in stroke patients and demographic data on the general-public of Austria taking OAC were not available. Lastly, individual patient level data on the general population taking OAC (i.e. those without stroke) was not available, we were not able to perform formal adjustment for co-variables.
In conclusion, one in seven ischemic stroke and one in four ICH patients reports OAC intake prior to event. Due to the ever-increasing number of OAC prescriptions, a dire need exists for trials to establish evidence for management guidelines for these patients in the future.
Supplemental Material
sj-docx-1-eso-10.1177_23969873231223876 – Supplemental material for Risk of stroke in patients with prior VKA or DOAC: A population-based real-world registry analysis
Supplemental material, sj-docx-1-eso-10.1177_23969873231223876 for Risk of stroke in patients with prior VKA or DOAC: A population-based real-world registry analysis by Lukas Mayer-Suess, Heinrich Rinner, Wilfried Lang, Stefan Greisenegger, Dominika Mikšová, Thomas Gattringer, Christian Enzigner, Marek Sykora, Milan Vosko, Johannes S Mutzenbach, Julia Ferrari, Stefan Kiechl and Michael Knoflach in European Stroke Journal
Supplemental Material
sj-pdf-1-eso-10.1177_23969873231223876 – Supplemental material for Risk of stroke in patients with prior VKA or DOAC: A population-based real-world registry analysis
Supplemental material, sj-pdf-1-eso-10.1177_23969873231223876 for Risk of stroke in patients with prior VKA or DOAC: A population-based real-world registry analysis by Lukas Mayer-Suess, Heinrich Rinner, Wilfried Lang, Stefan Greisenegger, Dominika Mikšová, Thomas Gattringer, Christian Enzigner, Marek Sykora, Milan Vosko, Johannes S Mutzenbach, Julia Ferrari, Stefan Kiechl and Michael Knoflach in European Stroke Journal
Footnotes
Acknowledgements
Non-author Contributions: Tyrolean Stroke Pathway group and the Austrian Stroke Unit Registry Collaborators.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by VASCage – Research Centre on Clinical Stroke Research. VASCage is a COMET Centre within the Competence Centers for Excellent Technologies (COMET) program and funded by the Federal Ministry for Climate Action, Environment, Energy, Mobility, Innovation and Technology, the Federal Ministry of Labour and Economy, and the federal states of Tyrol, Salzburg and Vienna. COMET is managed by the Austrian Research Promotion Agency (Österreichische Forschungsförderungsgesellschaft). FFG Project number: 898252.
Ethical approval and informed consent
All analyses were approved by the local ethics committee at the Medical University of Innsbruck EK#1059/2023.
Trial registration
N/A.
Guarantor
Lukas Mayer-Suess
Contributorship
Data acquisition: Lukas Mayer-Suess, Wilfried Lang, Stefan Greisenegger, Thomas Gattringer, Christian Enzigner, Marek Sykora, Milan Vosko, Johannes S. Mutzenbach, Julia Ferrari, Stefan Kiechl, Michael Knoflach; Data analysis: Lukas Mayer-Suess, Dominika Mikšová, Heinrich Rinner; Drafting of manuscript: Lukas Mayer-Suess; Critical revision of manuscript: Lukas Mayer-Suess, Wilfried Lang, Stefan Greisenegger, Thomas Gattringer, Christian Enzigner, Marek Sykora, Milan Vosko, Johannes S. Mutzenbach, Julia Ferrari, Stefan Kiechl, Michael Knoflach, Dominika Mikšová, Heinrich Rinner; Conceptualization of study: Lukas Mayer-Suess, Stefan Kiechl, Michael Knoflach.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.