
Abstract
Purpose:
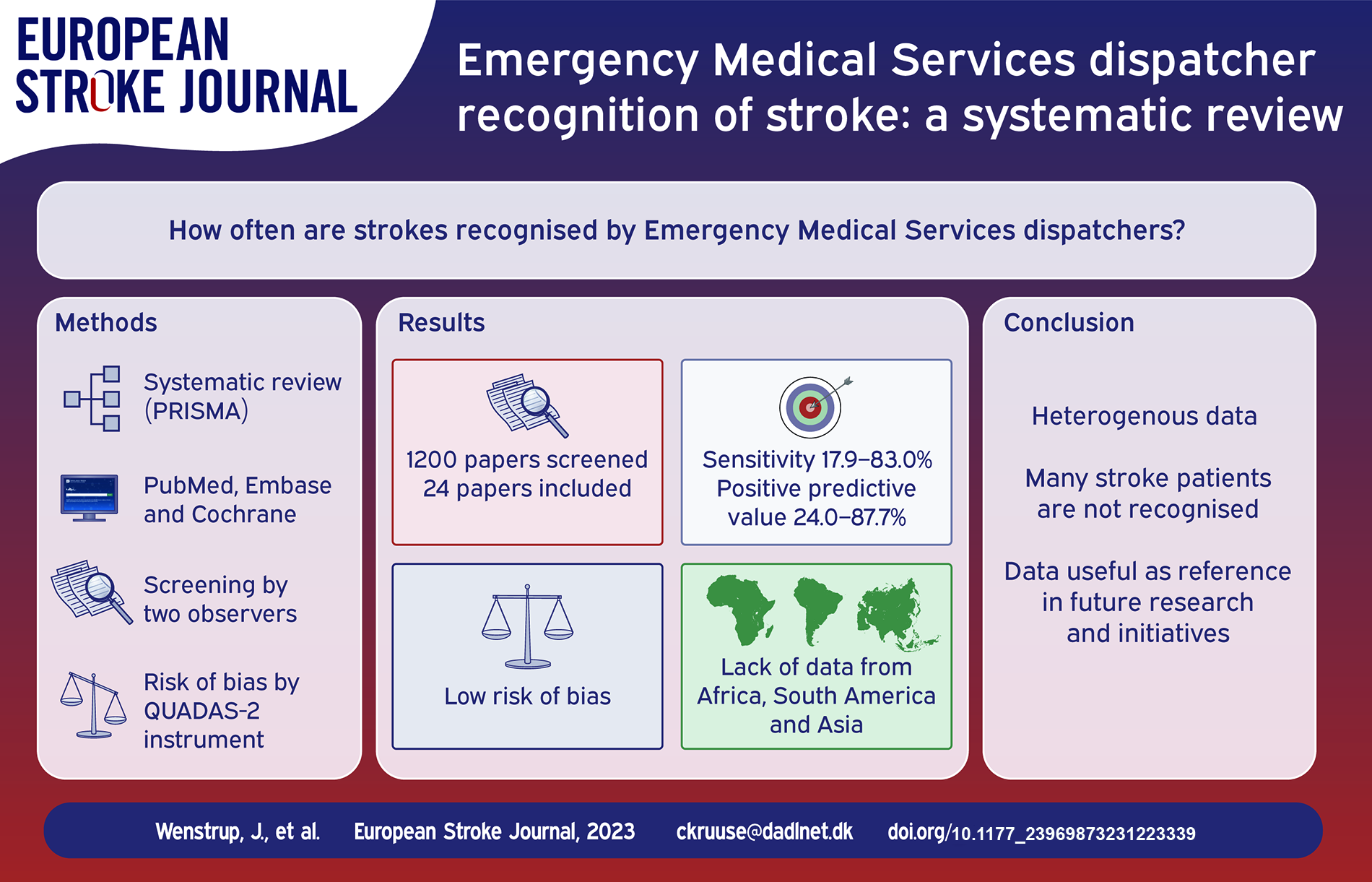
Stroke treatments are time-sensitive, and thus early and correct recognition of stroke by Emergency Medical Services is essential for outcomes. This is particularly important with the adaption of mobile stroke units. In this systematic review, we therefore aimed to provide a comprehensive overview of Emergency Medical Services dispatcher recognition of stroke.
Methods:
The review was registered on PROSPERO and the PRISMA guidelines were applied. We searched PubMed, Embase, and Cochrane Review Library. Screening and data extraction were performed by two observers. Risk of bias was assessed using the QUADAS-2 instrument.
Findings:
Of 1200 papers screened, 24 fulfilled the inclusion criteria. Data on sensitivity was reported in 22 papers and varied from 17.9% to 83.0%. Positive predictive values were reported in 12 papers and ranged from 24.0% to 87.7%. Seven papers reported specificity, which ranged from 20.0% to 99.1%. Six papers reported negative predictive value, ranging from 28.0% to 99.4%. In general, the risk of bias was low.
Discussion:
Stroke recognition by dispatchers varied greatly, but overall many patients with stroke are not recognised, despite the initiatives taken to improve stroke literacy. The available data are of high quality, however Asian, African, and South American populations are underrepresented.
Conclusion:
While the data are heterogenous, this review can serve as a reference for future research in emergency medical dispatcher stroke recognition and initiatives to improve prehospital stroke recognition.
Keywords
Introduction
Revascularization, by use of intravascular thrombolysis (IVT) or endovascular thrombectomy (EVT) are both effective treatments for acute ischaemic stroke.1,2 Their use is strongly recommended in current guidelines. 3 However, attempted revascularization is only an option within a specific and narrow time window, which requires that patients with stroke are admitted to stroke units for urgent evaluation. Such admissions are most often mediated by Emergency Medical Services (EMS) 4 and key to the stroke chain of survival (Figure 1). The proportion of patients with stroke who are eligible to undergo revascularization procedures depends greatly on correct EMS dispatcher recognition of stroke symptoms and fast-track admission, 5 and dispatchers making stroke recognition and correct choice of emergency response level a priority is recommended in current guidelines. 3 If dispatchers do not recognise stroke, it could lead to delay in hospitalisation, for example if an ambulance is not dispatched, or is not dispatched with the required urgency. The importance of dispatcher stroke recognition is also evident in the case of mobile stroke units, where dispatcher recognition is essential for the dispatch and effect of the mobile stroke unit.6,7
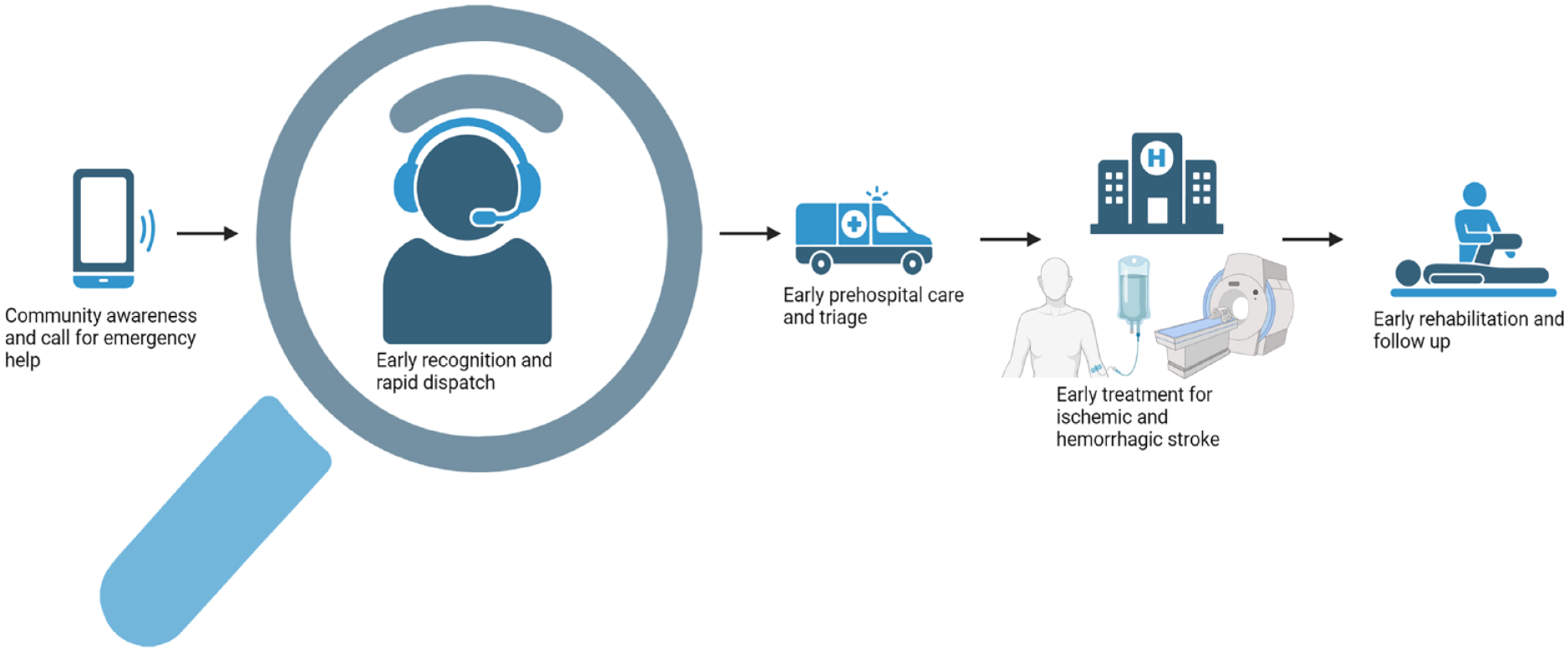
The pre-hospital chain of survival for stroke. Created with Biorender.com.
There are variable approaches to dispatch systems overall and for dispatcher recognition of stroke specifically. Some EMS utilise an overall software based dispatch system, such as the Medical Priority Dispatch System, 8 which is used for triage of all calls. Other systems employ specific stroke screening tools, such as the Cincinnati Stroke Scale, 9 used when stroke is suspected. Some systems rely on unstructured interviews, based on the dispatcher’s personal experience in health care. 10 Combinations of these approaches are also possible.
The two available systematic reviews on EMS dispatcher recognition do not include the most recent studies, 11 or primarily evaluate specific screening instruments. 12
We aimed to systematically evaluate the studies of EMS dispatcher recognition of stroke, to yield an updated and comprehensive summary of current research, which may be used to guide future interventions aimed at improving dispatcher recognition of stroke.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines were applied. 13 The data search, screening, selection, data extraction, and analysis were executed according to a pre-specified study protocol, registered on the International Prospective Register of Systematic reviews (PROSPERO) (registration ID: CRD42022354584).
Search strategies and selection criteria
We searched the PubMed, Embase, and Cochrane Library databases using a search string consisting of the words ‘stroke’, ‘recognition’ and ‘Emergency Medical Services Dispatcher’, as well as a wide variety of synonyms and more specific terms (see Supplemental Material for full search string). The search string was modified to fit each database and subsequently reviewed and approved by an information specialist. For included papers, we evaluated the reference list to identify possible additional papers.
The first search was performed on March 2nd, 2022. To yield an up-to-date search, we repeated the search again for papers from 2022 and 2023 on June 6th, 2023 in PubMed and June 9th 2023 in Embase and Cochrane Library, using the original search string.
Inclusion and exclusion criteria were as stated in the ‘Population, Intervention, Comparison and Outcome (PICO) statement:
The included papers had to be written in English, Danish, Swedish, or Norwegian and not be reviews, case studies, case series, letters to journals, conference abstracts and editorials as well as papers in languages different from those mentioned above.
Data extracted
We extracted data on sensitivity, PPV, specificity, NPV, patient population size, number of patients with stroke, country of origin, year of publication, exclusion, and inclusion criteria. If sensitivity, PPV, specificity and NPV were not available from the text, we extracted data from which it could be calculated.
Extraction process and risk of bias assessment
Initially, two reviewers (JW and MVS) independently screened papers yielded by the search in two steps: Title and abstract screening and full text screening. Due to changes in the research group during the process, the remaining screenings were undertaken by BH instead of MVS. JW and BH extracted data independently and compared the resulting two datasets. A consensus was reached on the final dataset. In cases of disagreement, it was to be settled by one of the the last authors (CK), though no such disagreements occurred.
JW and BH assessed risk of bias and the quality of the papers using the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2) scale, 14 and in the event of disagreement a third researcher (CK) was to have final say, though no such disagreements occurred.
The QUADAS-2 scale is developed for evaluation of diagnostic accuracy. 14 While the scale is primarily developed for paraclinical tests, the instrument is also an appropriate assessment tool for studies on clinical diagnostic accuracy.
When using QUADAS-2 papers are evaluated based on four criteria: Patient selection, index test, reference standard and flow of patients. Except for ‘flow and timing’, all criteria are rated in both ‘risk of bias’ and ‘applicability concerns’. The rating is binary, with either ‘low’ or ‘high’ risk. The rating is based on ‘signalling questions’, which are adapted for each research project with the exclusion or inclusion of specific signalling questions. In our study, two signalling questions were left out, as they did not fit our study design: Index test – Risk of bias – Signalling question 2: ‘If a threshold was used, was it prespecified?’ and Flow and timing – Risk of bias – Signalling question 1: ‘Was there an appropriate interval between the index test and reference standard?’
No overall rating of bias or applicability is made on the papers, as per the QUADAS-2 instructions. 14
Findings
We screened 1200 papers based on title and abstract. This comprised 1100 papers from the initial search and 100 papers from the updated search for 2022 and 2023. A total of 1115 papers were excluded based on title and abstract. We performed full text screening on 85 papers and finally included 24 papers in the review and excluded 61 as they either did not report dispatchers’ recognition numbers, or did not provide data for calculating any of the chosen outcome measures (Figure 2).
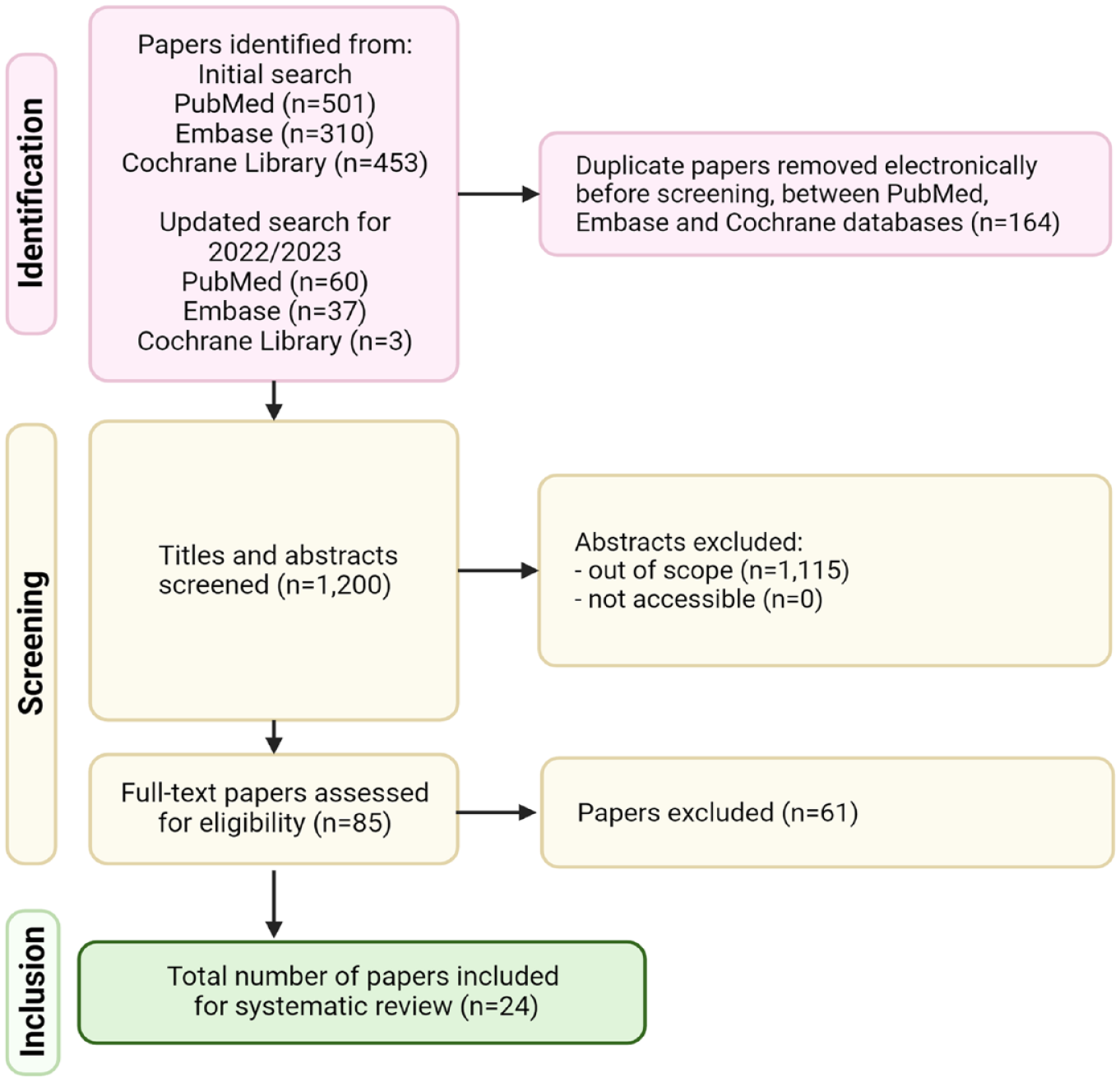
The screening and selection process of included papers.
Twenty-two papers reported either sensitivity or data from which sensitivity could be calculated. Sensitivity varied from 17.9% to 83.0%. Most papers reported sensitivity in the mid-range of 40%–70% (Table 1). PPV was reported in 12 papers and ranged from 24.0% to 87.7%. (Table 1).
Main results.
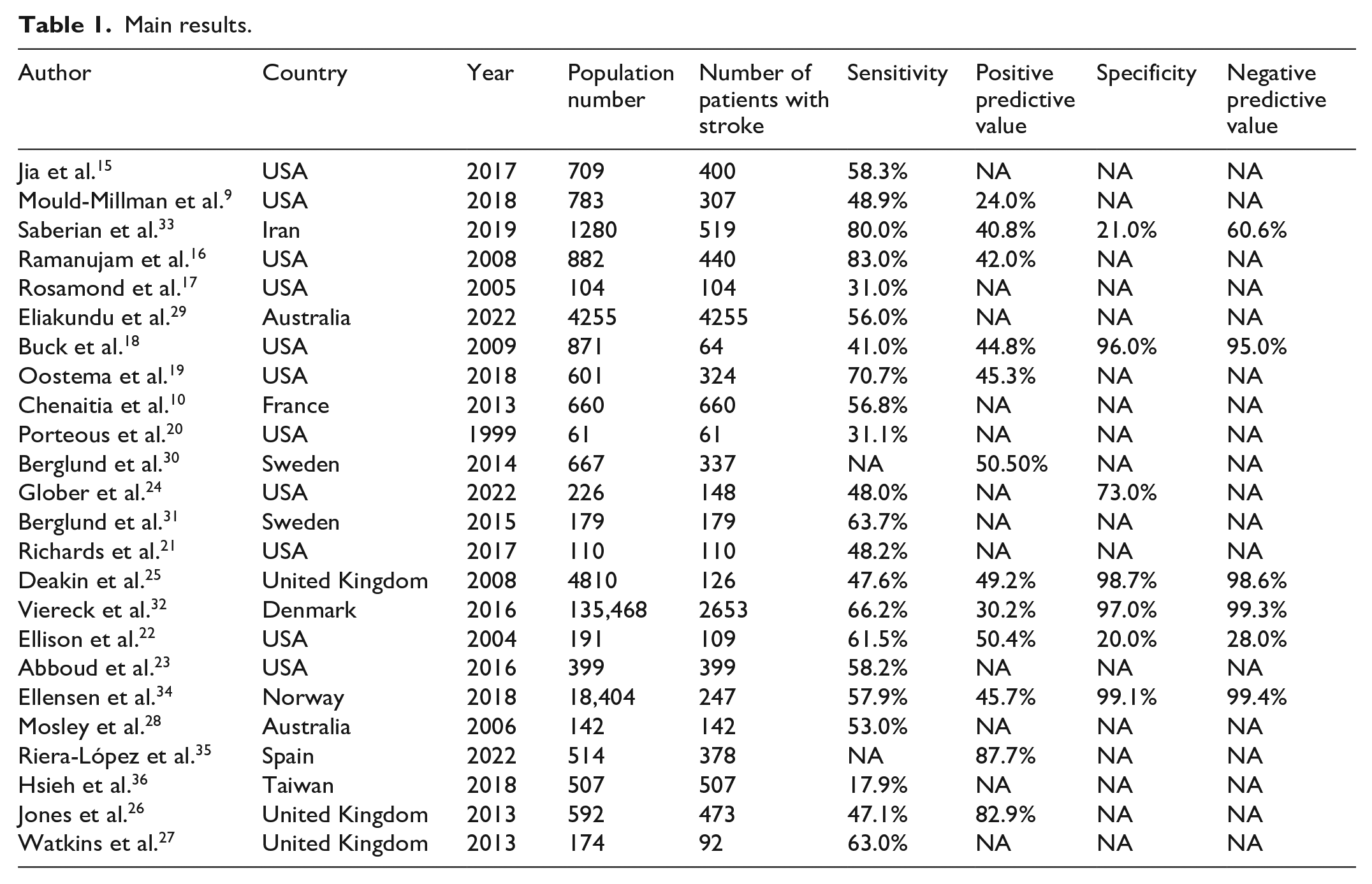
In the seven papers which reported specificity, two reported a low specificity of 20.0% and 21.0%, while the remaining five ranged from 72.7% to 99.1% (Table 1).
Six papers reported NPV, ranging from 28.0% to 99.4% (Table 1).
Of the included papers, 11 were from USA9,15–24, three from United Kingdom25–27, two from Australia28,29, two from Sweden30,31, one from Denmark, 32 one from France, 10 one from Iran, 33 one from Norway, 34 one from Spain 35 and one from Taiwan. 36
Though no papers were excluded based on publication year, the earliest paper included was from 1999, 20 and the remaining were published after year 2000, with the majority published after 2010.
Only five studies25,29,32–34 included more than 1000 contacts to EMS, and only two studies29,32 included more than 1000 patients with confirmed stroke. Inclusion of more than 1000 patients with stroke was possible due to comprehensive stroke registries in Denmark and Australia.
Nine studies included exclusively patients with an in-hospital diagnosis of stroke, and no calls from patients without stroke to EMS.10,17,20,21,23,28,29,31,36 There was significant overlap in sensitivity and PPV between papers including EMS calls without stroke, and those including only in-hospital diagnosed stroke patients (Tables 2 and 3).
Inclusion and exclusion criteria of included papers, dispatcher background, dispatch setup and type of study.
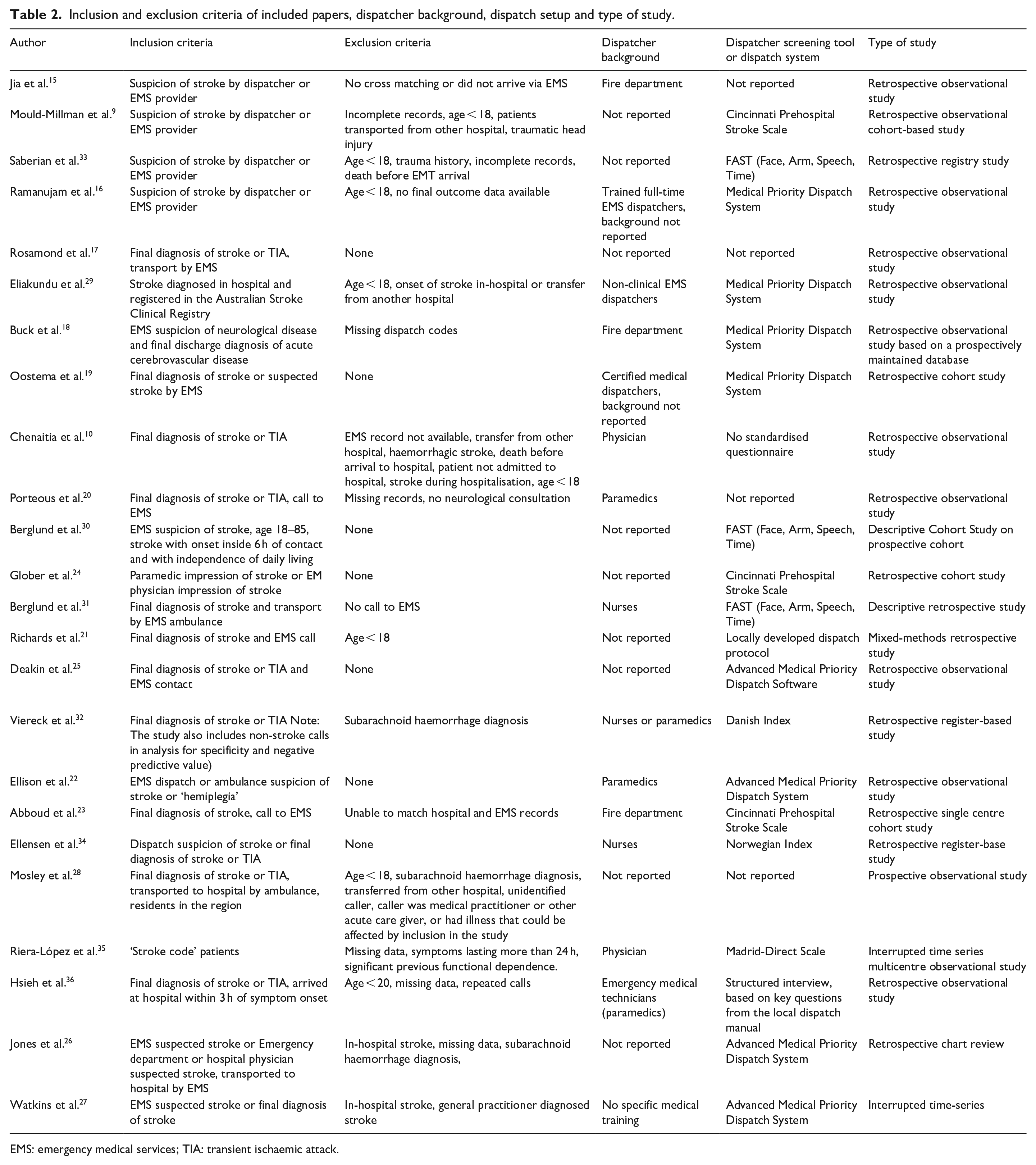
EMS: emergency medical services; TIA: transient ischaemic attack.
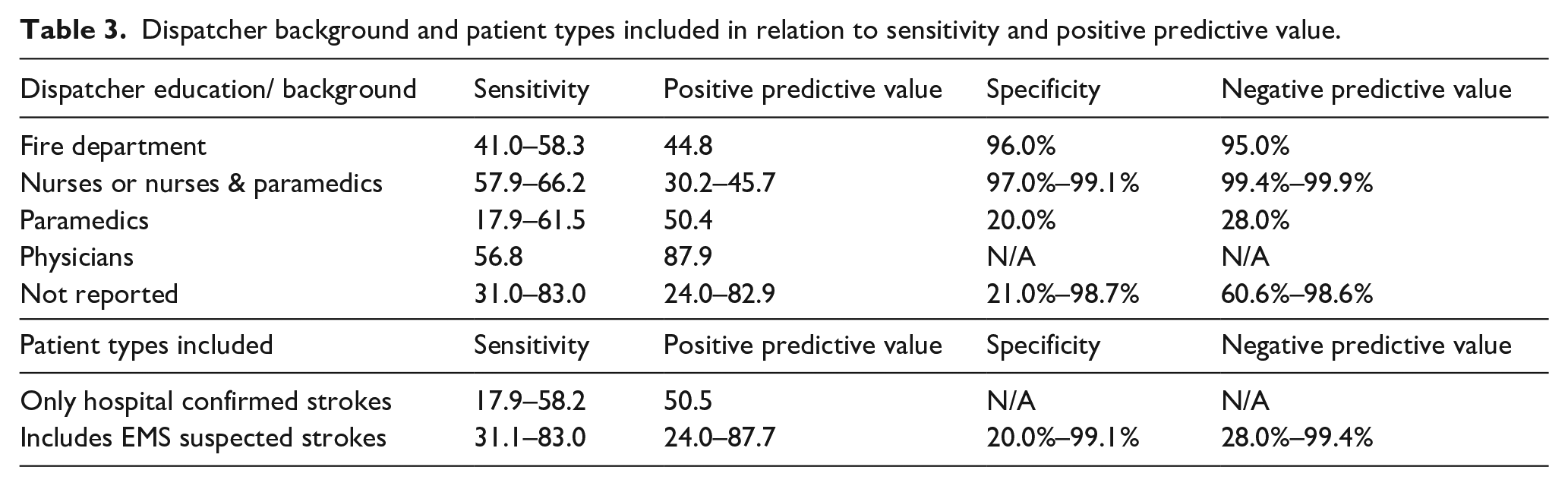
Dispatcher background and patient types included in relation to sensitivity and positive predictive value.
The inclusion and exclusion criteria were generally uniform, except whether studies had a requirement for in-hospital diagnosis of stroke or only of EMS suspicion of stroke (Table 2). In 16 papers there was no inclusion requirement of EMS suspicion of stroke, while eight papers required EMS suspicion of stroke. Most studies excluded patients with age < 18 years and missing data (Table 2). Four studies excluded patients with haemorrhagic stroke10,26,28,32, two studies excluded a fraction of patients with confirmed stroke based on time since symptom onset.30,36
The majority of studies did not report dispatcher background (Table 2). For those studies where dispatcher backgrounds were either not reported or non-clinical, sensitivity and PPV varied greatly (Table 3), with sensitivity ranging from 31.0 to 83.0 and PPV from 24.0 to 82.9. This contrasted with more narrow ranges in data from studies reported dispatcher backgrounds. For dispatcher with backgrounds in fire departments sensitivity ranged from 41.0 to 58.3 and only one reported PPV of 44.8. For dispatchers with background as nurses or combined nurses and paramedics sensitivity ranged from 57.9 to 66.2 and PPV from 30.2 to 45.7. For dispatcher with background as paramedics sensitivity ranged from 17.9 to 61.5 and only one paper reported PPV of 50.4. Finally, for dispatcher with background as physicians, one paper reported sensitivity of 56.8 and one paper reported a PPV of 87.9. Based on the limited data on NPV and specificity, dispatcher background in fire departments or as nurses or nurses and paramedics reported higher specificity and NPV than paramedics. Specificity and NPV varied greatly for unreported background of dispatchers (Table 3).
All but four papers15,17,20,28 reported the system used for triaging stroke patients (Table 2). The most common triage system type, found in 11 papers, was through dispatch systems encompassing the entire emergency triage task. The specific systems included the Advanced Medical Priority Dispatch System, the Medical Priority Dispatch System, the Danish Index and the Norwegian Index. The second most common type of system for triaging stroke patients, reported in seven papers, was application of stroke specific scales, with three using the Cincinnati Stroke Scale, three using Face-Arm-Speech-Time and one using the Madrid-Direct Scale. The remaining two papers reported using a local manual with a structured interview or having no structured questionnaire.
When using an overall dispatch system, the sensitivity ranges from 41.0 to 83.0 and PPV from 30.2 to 82.9. When using a stroke specific scale, the sensitivity range is 48.0–80.0 and PPV is 24.0–87.7. For the local structured interview, no structured interview or not reported, sensitivity was 17.9–58.3 and PPV was not reported.
Twenty papers employed a retrospective design often based on prospectively maintained registries, with only two papers employing prospective designs, and two papers based on interrupted time series designs.
The risk of bias and applicability concerns were generally low, when rated on the QUADAS-2 scale (Table 4), albeit not void of potential issues.
Risk of bias using QUADAS-2 in papers reporting accuracy of dispatchers’ stroke suspicion.
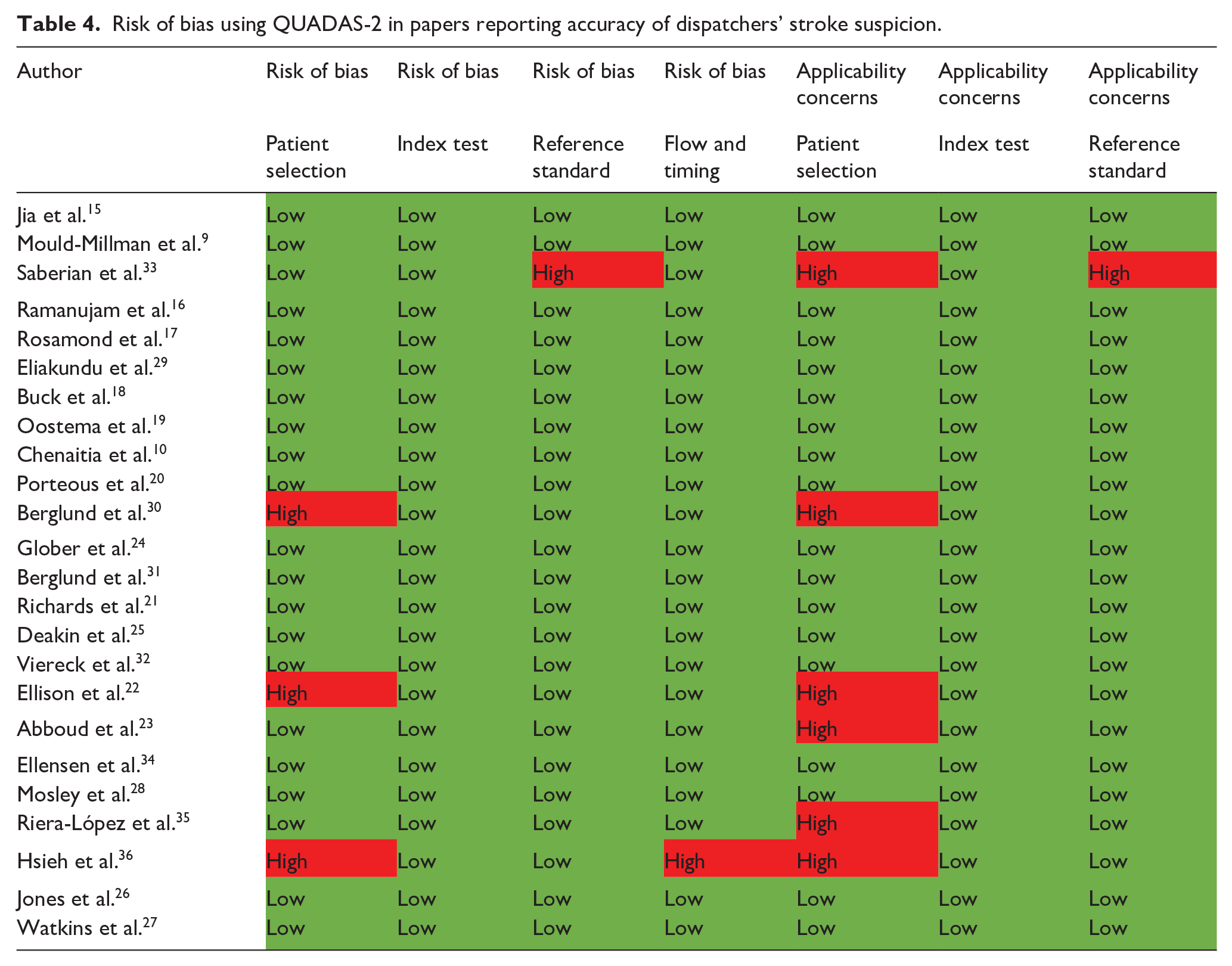
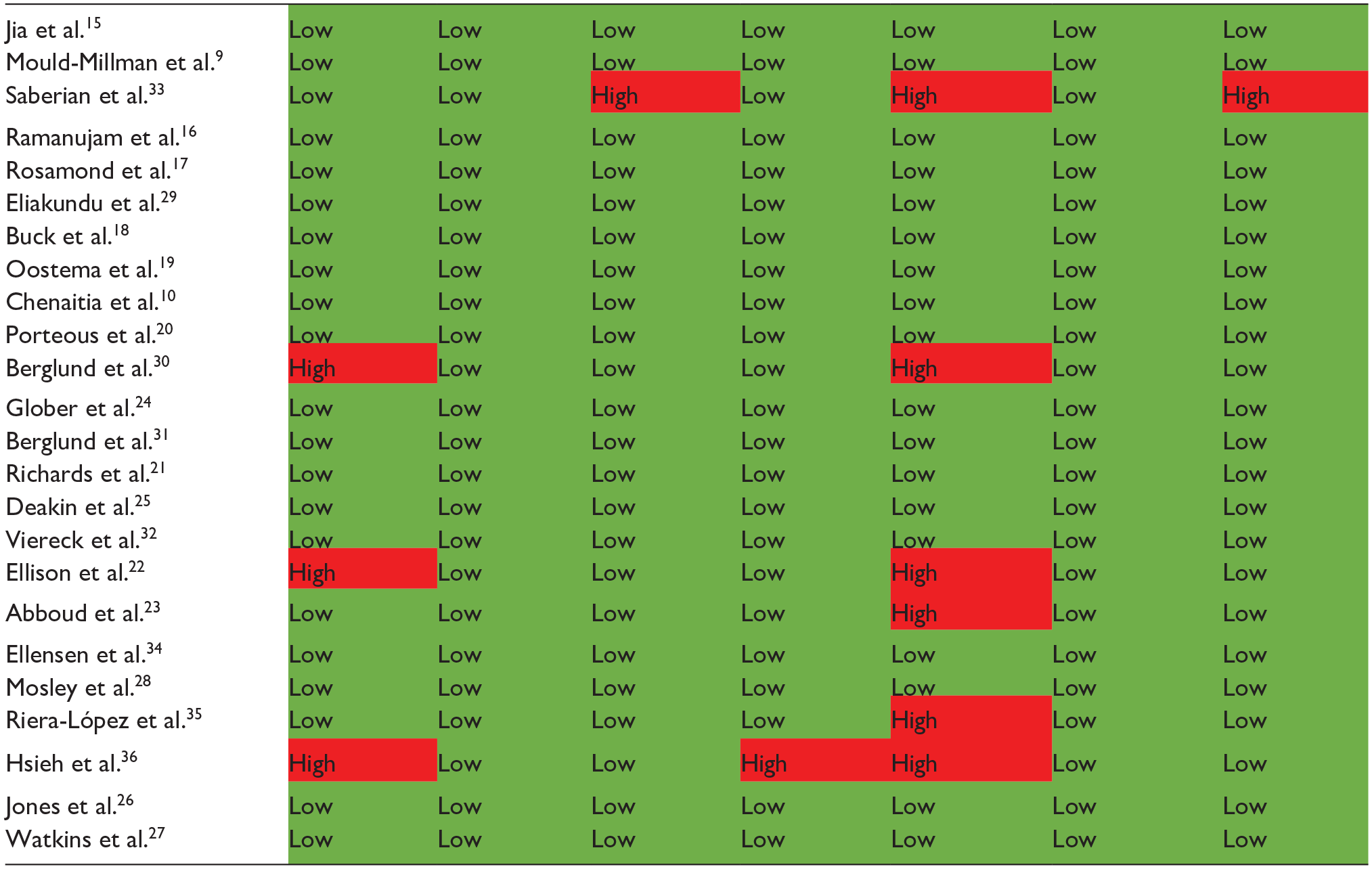
One paper was found at risk of bias and applicability concern on ‘patient selection’ and risk of bias on ‘flow and timing’, as they excluded patients who arrived at hospital later than 3 h from onset, and included only the first call by each patient. 36
Risk of both bias and applicability concern in ‘patient selection’ were found in two papers. One included only patients with suspected stroke while still reporting specificity and NPV (which requires knowledge of how many patients were not suspected of stroke). 22 Another excluded patients with dependence in activities of daily living, patients over 85 years and patients with symptom onset more than 6 h before the call. 30
There were applicability concerns due to ‘patient selection’ and both applicability concerns and risk of bias on ‘reference standard’ in one paper. The cause was researchers only including patients suspected of stroke by EMS and sole use of MRI result without clinical correlation. 33
Two papers were deemed at risk of applicability concerns on ‘patient selection’. The first for exclusion of more than one-third of calls due to data incompleteness. 23 The second for including only patients diagnosed within 24 h of stroke onset and excluding patients without independent functioning. 35
There were no concerns of risks of bias due to the index test in the included papers.
Discussion
With this study, we aimed to provide an updated and comprehensive review of the current literature on dispatcher stroke recognition at EMS. Extracting data from 24 papers on dispatcher stroke recognition of stroke revealed great variations in stroke recognition by dispatchers between EMS settings. Sensitivity was less than 50% in eight of the 22 papers which reported sensitivity, with a gap of 65.1% from the highest to lowest reported sensitivity. Such variations could in part be explained by diversity in methodology and patient populations between studies.
PPV was also reported with large variations in results, with a 63.7% gap between the highest and lowest value. This variation could be a result of diversity in data registration and research methods, in addition to the differences between EMS setups.
Only seven of 24 papers reported either specificity or NPV, and the results were characterised by wide ranges between the highest and lowest values, likely due to differences in data registration. If all EMS calls were sampled, we would expect a high specificity and NPV.18,25,32,34 Some papers only included patients suspected of stroke while still providing specificity and/or NPV,22,24,33 presumably calculated without including all true negatives, which could in part explain the observed variations. To evaluate differences in the stroke populations included in the different papers, especially those reporting NPV and/or specificity, it would be informative to investigate differences in severity, using NIHSS, between patient groups. However, only four papers reported NIHSS score,15,19,23,24 and only one of these reported NPV or specificity, 24 making comparisons between papers with regard to true and false negatives impossible.
Methodological differences did not allow for a direct comparison between studies by way of meta-analysis, and direct comparisons between settings were not possible. This review, however, provides a comprehensive overview of dispatcher performance worldwide, useful in evaluating future research, and emphasising the importance of a structured dispatch system and the use of stroke scales in daily clinical practice.
The large variation seen in both sensitivity and specificity, as well as the association between the two (Table 1), may reflect different approaches and hypotheses regarding the optimal triage. No specific guideline exists for the recommended level of ‘overtriage’, that is, how many false positives are acceptable when working with dispatch stroke recognition. Given the extensive in-hospital workup involved for each suspected stroke patient with the resulting use of system and patient resources, the level of acceptable overtriage needs to be considered when dispatch systems are designed. In high-income countries, it may be an option to prioritise sensitivity over PPV, but in systems with limited resources, the opposite could be a necessity. The necessity of such choice of priority is underscored by no paper reporting a simultaneously high sensitivity and high PPV.
Methodologically advanced comparisons of change in observed outcome measures over time for the EMS setting has little merit, due to the variations in EMS setups and diverse methodology of the included papers. Of note, there was no obvious trend towards improvement over time though acute stroke treatment options and awareness in general has increased within the last decades. The lowest sensitivity reported was 17.9% in 2018, 36 while the second lowest was 31.0% in 2005. 17 Similarly, the highest reported sensitivity was 83.0% in 2008, 16 while the second highest was 80.0% in 2019. 33 This lack of improvement over time was also seen for reported PPV, with the lowest PPV being 24.0% in 2018 9 and the second lowest 30.2% in 2016. 32 The highest reported PPV was 87.1% in 2022 35 and the second highest 82.9% in 2013 26 (Figure 3).
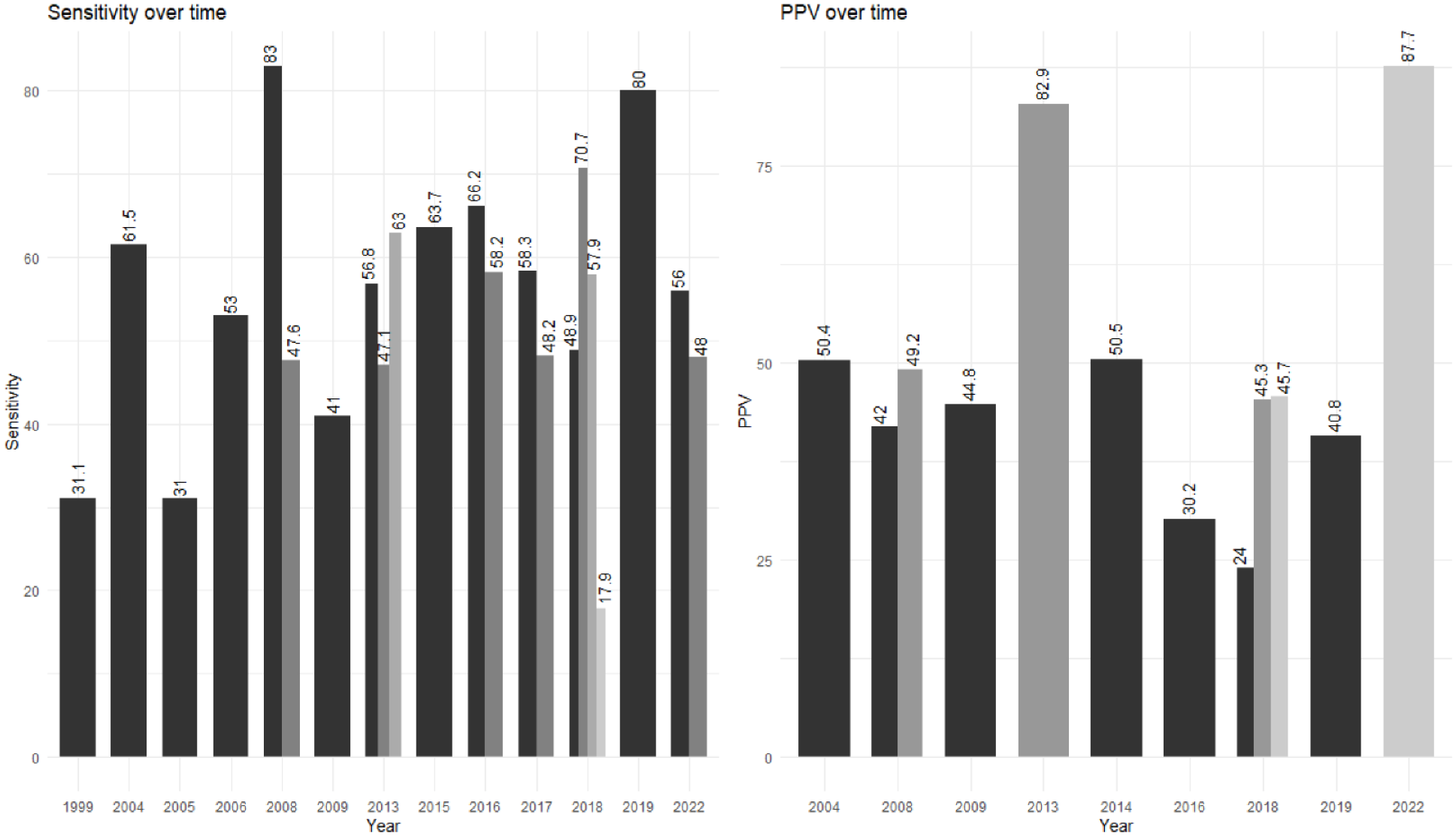
The sensitivity and positive predictive value over time. Different colours denote different papers in the same year.
Dispatcher background was only reported in less than half of papers (Table 2), which did not allow for a firm evaluation of the influence of dispatcher background on stroke recognition. Of those papers reporting dispatcher background or education, there were no clear superiority of particular groups in terms of stroke recognition.
There was no clear difference in sensitivity or PPV between using a stroke specific scale and using an overall dispatch system. The approach to have a structured triage system, however, showed higher sensitivity than having either local structured interview, no structured interview or in cases where the dispatch system was not reported (Tables 1 and 2). The heterogeneity in settings, even when using the same type of system, should be considered when interpreting these observations.
Papers including all EMS calls, and papers only including in-hospital diagnosed stroke patients exhibited no clear difference in results, and again, great heterogeneity in results for both groups (Table 3).
Most studies included retrospective data (Table 2), which is part of the conditions for comparing hospital diagnoses and pre-hospital EMS data. Several papers, however used prospectively maintained registries, which may bolster the reliability of their results. Nevertheless, the retrospective nature of most included papers does impact the level of evidence available in this review.
In general, the included papers were of high quality with relatively low risk of bias. The most notable risk of bias was inclusion of selected populations, such as including only patients with stroke within a short time since symptom onset.30,36 Given the current variations in reported findings on dispatcher recognition of stroke, as well as the observed nine papers which only reported on selected populations of hospital confirmed strokes, it should be recommended that future studies include all calls to EMS and all confirmed strokes from the area served by EMS who were treated in hospital to obtain data more directly comparable between countries and EMS settings. Such efforts would require comprehensive epidemiological registries, as also suggested in the Action Plan for stroke initiated by the European Stroke Organisation (ESO). 37
Not all patients with stroke contact the emergency medical call centre at EMS when experiencing symptoms of stroke. Only two included papers quantified this, however, they found that only 29% and 46% of stroke patients, respectively, had the emergency call line as their first point of contact.10,34 Since only a minor part of patients with stroke choose EMS as their first point of contact, data from other sources of contact, such as out-of-hours services, are important to fully establish the void in early stroke recognition. The scarcity of data available for patients not contacting the emergency call line is likely due to lack of registry data, and the further research is needed into this patient subgroup.
This review has limitations. Firstly, the risk of bias assessment tool QUADAS-2 was not specifically designed for use in triage, but for paraclinical tests. Although the index questions were modified as per the QUADAS-2 guidelines, this may have affected the bias assessment. Secondly, we substituted an investigator during the screening procedures, however, neither the screening method nor criteria were altered. Thirdly, nine studies only included patients with a confirmed hospital diagnosis of stroke, which limits the usefulness of those studies in accurately reflecting the dispatcher stroke recognition, due to the selected nature of the populations. Fourthly, as we chose to exclude papers presenting training and/or development of a new interview protocol or diagnostic tools, this may have led to some studies being excluded, which could provide useful data.38,39 This choice of inclusion and exclusion criteria was made to increase the comparability of data included in this review. Finally, though hospital diagnosis is considered the ‘golden standard’, not all stroke patients are recognised in the Emergency Departments, 40 which will affect all estimations of the number of false negatives in regards to dispatcher recognition of stroke.
Conclusion
There was high variability in EMS dispatcher recognition of stroke, with data mainly obtained from the US, Europe, and Australia, leaving Asia, Africa and South America underrepresented. Though data were generally of high quality, the results were nevertheless very heterogenous. The papers were based almost entirely on emergency call lines, with medical helplines and out-of-hours services only studied in one paper. Despite initiatives to improve stroke literacy and stroke action plans, many patients with stroke still go unrecognised by EMS dispatchers, and initiatives are needed to ensure improvement. Additionally, further research on dispatcher recognition of stroke in Asia, Africa and South America is warranted.
Supplemental Material
sj-docx-1-eso-10.1177_23969873231223339 – Supplemental material for Emergency Medical Services dispatcher recognition of stroke: A systematic review
Supplemental material, sj-docx-1-eso-10.1177_23969873231223339 for Emergency Medical Services dispatcher recognition of stroke: A systematic review by Jonathan Wenstrup, Bartal Hofgaard Hestoy, Malini Vendela Sagar, Stig Nikolaj Fasmer Blomberg, Hanne Christensen, Helle Collatz Christensen and Christina Kruuse in European Stroke Journal
Supplemental Material
sj-docx-2-eso-10.1177_23969873231223339 – Supplemental material for Emergency Medical Services dispatcher recognition of stroke: A systematic review
Supplemental material, sj-docx-2-eso-10.1177_23969873231223339 for Emergency Medical Services dispatcher recognition of stroke: A systematic review by Jonathan Wenstrup, Bartal Hofgaard Hestoy, Malini Vendela Sagar, Stig Nikolaj Fasmer Blomberg, Hanne Christensen, Helle Collatz Christensen and Christina Kruuse in European Stroke Journal
Footnotes
Acknowledgements
We would like to thank all the researchers who produced the papers this study is based on.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: HC is Chair of Action Plan for Stroke in Europe Implementation, Co-chair Scientific Stroke Panel, EAN and Senior Guest Editor: AHA Stroke. She has received grants from the Velux foundation, Tværsfonden, Helsefonden, the Hartmann Brothers Foundation, The Lundbeck Foundation, and the Novo Nordic Foundation. HC also co-authored the paper by Viereck et al. included in this review. HC has received honoraria from Bayer and BMS and receives royalties from Gyldendal publishing. CK has received grants from the Novo Nordic Foundation, Lundbeck Foundation and Trygfonden and is Vicechair (since 2023 Chair) of the Danish Resuscitation Council (unpaid) and the Vicechair of Danish Stroke Society (unpaid). JW, BHH, MVS, HCC and SNB have no conflicting interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by grants from Trygfonden, Copenhagen University Hospital - Herlev and Gentofte research grant, Region Zealand Research Fund, Novo Nordisk Fonden (CK), Funders had no other role in the production of this review.
Ethical approval
As this was a systematic review of previously published literature, ethical approval was not necessary.
Informed consent
As this was a systematic review of previously published literature, informed consent was not necessary.
Data availability
All included studies are publicly accessible, though some are behind pay walls of individual journals. Data for this review can be provided upon reasonable request.
Guarantor
CK.
Contributorship
JW, SNB, HC, HCC and CK contributed to the conceptualisation of the study. JW performed the literature search. JW, BHH and MVS screened papers. JW and BHH performed data extraction. JW performed data analysis and wrote the first draft of the manuscript. JW, BHH, MVS, SNB, HC, HCC and CK provided critical revisions to the manuscript. All authors approved the version to be published. JW is the first author. HCC and CK share last authorship.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.