
Abstract
Background and aims:
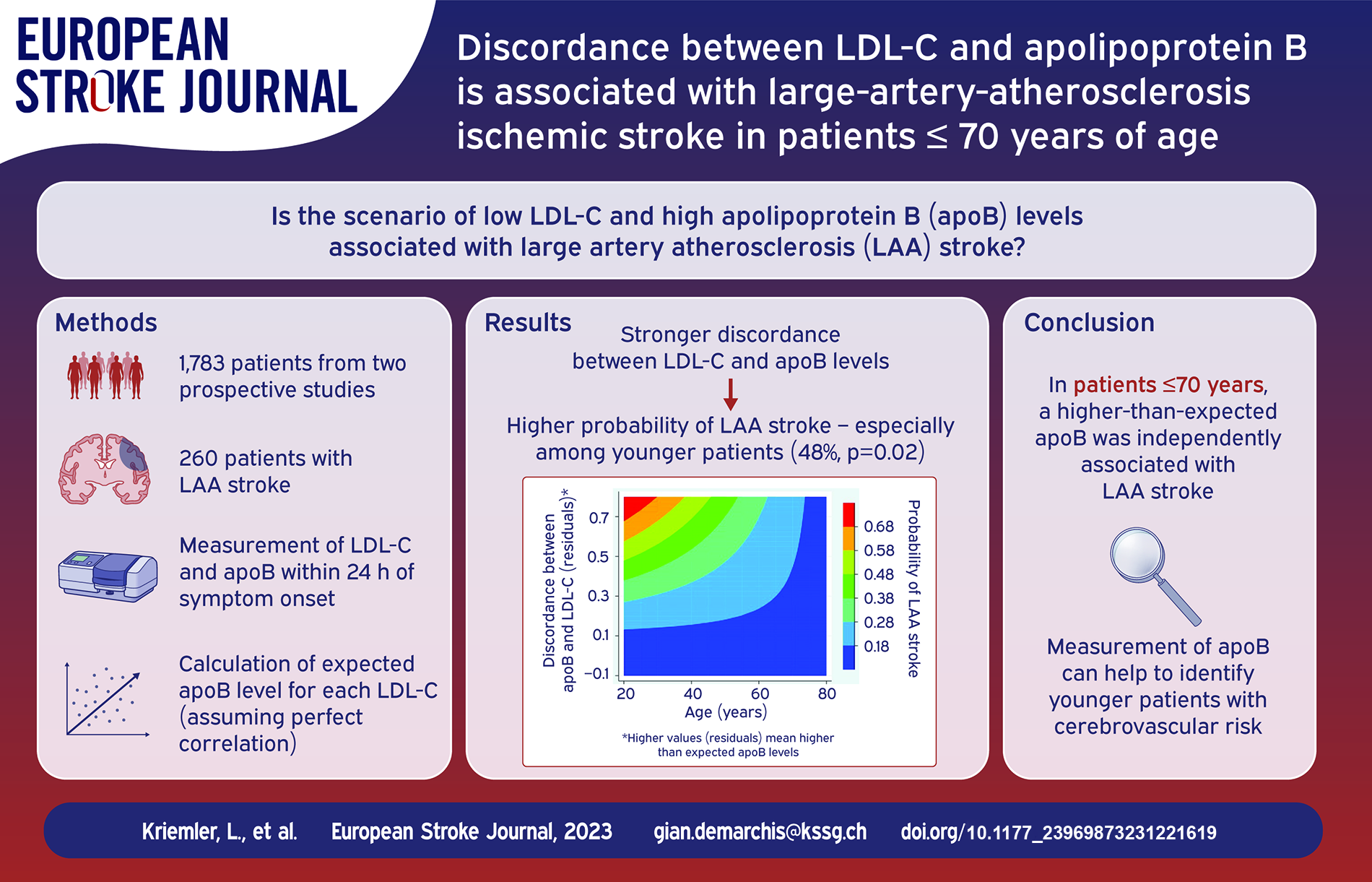
Low density lipoprotein (LDL-C) and other atherogenic lipoproteins are coated by apolipoprotein B100 (apoB). The correlation between LDL-C and apoB is usually thight, but in some cases LDL-C underestimates apoB levels and residual cardiovascular risk. We aimed to assess if a discordance of LDL-C-levels with apoB levels is associated with LAA stroke.
Methods:
We included patients with an acute ischemic stroke from two prospective studies enrolled at the University Hospital Bern, Basel and Zurich, Switzerland. LDL-C and apoB were measured within 24 h of symptom onset. By linear regression, for each LDL-C, we computed the expected apoB level assuming a perfect correlation. Higher-than-expected apoB was defined as apoB level being in the upper residual tertile.
Results:
Overall, we included 1783 patients, of which 260 had a LAA stroke (15%). In the overall cohort, higher-than-expected apoB values were not associated with LAA. However, a significant interaction with age was present. Among the 738 patients ⩽70 years of age, a higher-than-expected apoB was more frequent in patients with LAA- versus non LAA-stroke (48% vs 36%, p = 0.02). In multivariate analysis, a higher-than-expected apoB was associated with LAA stroke (aOR = aOR 2.48, 95%CI 1.14–5.38). Among those aged ⩽70 years and with LAA, 11.7% had higher than guideline-recommended apoB despite LDL-C ⩽ 1.8 mmol/L (<70 mg/dl), compared to 5.9% among patients with other stroke etiologies (p = 0.04). A triglyceride cut-off of ⩾0.95 mmol/L had, in external validation, a sensitivity of 71% and specificity of 52% for apoB ⩾ 0.65 g/L among patients with LDL-C <1.8 mmol/L.
Conclusions:
Among patients aged ⩽70 years, a higher-than-expected apoB was independently associated with LAA stroke. Measuring apoB may help identify younger stroke patients potentially benefiting from intensified lipid-lowering therapy.
Introduction
Low-density-lipoproteins cause atherosclerosis. 1 Increased low-density-lipoprotein cholesterol concentration (LDL-C) represents a risk factor for ischemic stroke, particularly of large-artery atherosclerotic origin (LAA), via arterio-arterial embolism. Lowering LDL-C lowers the risk of ischemic stroke. In the Treat-Stroke-to-Target Trial, lower pharmacological LDL-C targets – 1.8 mmol/L versus 2.6 mmol/L – were associated with a lower risk of recurrent stroke and major adverse cardiovascular events among patients with a recent history of ischemic stroke and atherosclerosis. 2
Even when low LDL-C targets are achieved, substantial cardiovascular risk remains. Compared to LDL-C, a better marker of cardiovascular risk is the serum concentration of apolipoprotein B100 (apoB).3,4 One apoB molecule coats one circulating atherogenic lipoprotein (including LDL-C, lipoprotein(a), and the triglyceride-rich very-low-density lipoproteins). apoB is responsible for lipoprotein docking and trapping on the arterial endothelium and intima, where atherogenic lipoproteins initiate and sustain atherosclerosis. 5
In the Copenhagen population study, the proportion of ischemic stroke attributable to apoB was double that attributable to elevated LDL-C. 6 Because most clinicians are more familiar with LDL-C than apoB, and because LDL-C is highly collinear with apoB, LDL-C is measured more frequently. Exceptions to the collinearity exist. Among people with elevated triglycerides or diabetes mellitus type 2, LDL-C levels tend to be lower than expected from the apoB levels – a scenario called discordant. 5 Guidelines of the European Society of Cardiology recommend routine measuring of apoB for patients with “high triglycerides, diabetes mellitus, obesity or metabolic syndrome, or very low LDL-C.” Target apoB below 0.65 g/L is recommended for patients with very high cardiovascular, risk including those with a history of ischemic stroke. 3
Whether the discordant LDL-C/apoB scenario is associated with LAA stroke is unknown. Also, a triglyceride cut-off above which discordant scenarios become likely are unclear. Since triglyceride levels are routinely measured, they can inform clinicians when to assess apoB on top of LDL-C, thus unmasking LDL-C/apoB discordance. In this prospective cohort study, we aimed to assess whether the discordant scenario is associated with LAA stroke. Moreover we sought to determine the triglyceride level cut-off above which a specific LDL-C/apoB discordant scenario – LDL-C <1.8 mmol/L but apoB above target ⩾0.65 g/L – is likely. The discordant scenario represents a therapeutic opportunity since intensified lipid-lowering therapies can further lower apoB levels and the associated residual cardiovascular risk.
Methods
Ethics
This study was approved by local ethics committees (Bern and Zurich, Switzerland) and was conducted according to the principles expressed in the Declaration of Helsinki. All patients or their welfare guardians provided written informed consent. The deidentified data supporting the findings of this study are available from the corresponding author on reasonable request. The manuscript adheres to the STROBE Statement checklist, uploaded separately. 7
Study design and patient population
Patients were culled from two prospective multicenter cohort studies with blood banking, the CoRisk Study 8 (n = 698/cohort of the study center at the University Hospital Bern, Switzerland. Enrollment period: March 2009 through April 2011) and the BioSignal Study 9 (n = 1028 and n = 57/cohort of the study center at the University Hospital Zurich and Basel, Switzerland. Enrollment period: October 2014 through October 2017). All patients included had an acute ischemic stroke within the prior 24 h. Ischemic stroke was defined according to the World Health Organization criteria as an acute focal neurological deficit lasting longer than 24 h with no sign of intracranial bleeding on cerebral imaging. Patients were excluded if they had missing LDL-C, apoB levels or informed consent. On admission, we collected demographic variables, vital signs, and vascular risk factors. Dyslipidemia on admission was defined as either use of lipid-lowering therapy or LDL-C on admission >2.6 mmol/L. Clinical stroke severity was assessed by the National Institute of Health Stroke Scale (NIHSS). 10 Stroke etiology was documented according to the TOAST criteria. To define stroke etiology according to the TOAST classification 11 cardiac and neurovascular ultrasound were collected, as well as 24-h ECG.
Biomarker measurement
During the index hospitalization, a non-fasting lipid profile including LDL-C (calculated with the Friedewald-Formula), high-density lipoprotein, and triglycerides was measured and entered in the study database. For biobanking purposes, blood was drawn within 24 h of stroke onset and immediately centrifuged at 3000g for 20 min at room temperature. The samples were aliquoted and frozen at −70°C at each center. ApoB levels were assessed in a batch analysis with the Siemens Atellica® NEPH 630 System/BNII System/BN ProSpec® System (Siemens Healthcare Diagnostics Products GmbH, Marburg, Germany) in the central laboratories of the University Hospital of Basel and Zurich.
Discordance analysis between LDL-C and apoB
The association between each pair of LDL-C and apoB levels was plotted. By linear regression, for each LDL-C, we computed the expected apoB level assuming a perfect correlation. For each patient, we computed the difference between the observed and expected apoB concentration. These values represent the residuals. Residuals were divided in tertiles, reflecting: (1) apoB higher than expected (upper residual tertile); (2) apoB as expected (middle residual tertile); (3) apoB lower than expected (lower residual tertile). A positive or negative residual imply that the risk predicted by apoB is higher or lower than that predicted by LDL-C.
Statistics
Discrete variables were expressed as counts (percentages) and continuous variables as medians (interquartile ranges (IQR)). Baseline characteristics were compared using Fisher’s exact test for categorical and Mann-Whitney U for continuous variables. Multivariate models were built in order to assess the adjusted associations between apoB and discordant scenarios with large-artery stroke. To visualize the interaction between age and apoB/LDL-C discordance, we generated a contour plot. To adjust for confounders linked with large-artery stroke, we developed a logistic multivariate model with for LDL-C, HbA1c, age, gender, arterial hypertension, lipid-lowering therapy on admission, never-smoker status, and coronary heart disease. We used receiver-operating characteristics (ROC) to derive and validate the triglyceride level cut-off above which a specific discordant scenario is likely (apoB ⩾ 0.65 g/L and LDL-C < 1.8 mmol/L). The derivation cohort was the CoRisk cohort, the validation one the BioSignal, as described above (see patient population). The choice of apoB ⩾ 0.65 g/L is the recommended target by the Guidelines of the European Society of Cardiology. 3 The choice of LDL-C < 1.8 mmol/L represents the lower LDL-target in the Treat-Stroke-to-Target Trial, which focussed on secondary prevention in patients with ischemic stroke. 2
Results
Overall, we included 1783 patients with stroke in the prior 24 h, of which 260 had a LAA stroke (15%). Median age was 73 years (IQR 62–81); on admission, median LDL was 2.7 mmol/L (IQR 2.0–3.4 mmol/L), apoB 0.93 g/L (IQR 0.75–1.1 g/L), and triglycerides 1.31 mmol/L (IQR 0.95–1.87). The frequencies of the etiological investigations are reported in the Supplemental Table 1. Among patients with LAA stroke, more cardiovascular risk factors such as hypertension, diabetes mellitus and smoking were recorded; LDL-C and apoB levels were significantly higher compared to patients with stroke etiologies other than LAA (Table 1).
Baseline and outcome characteristics,
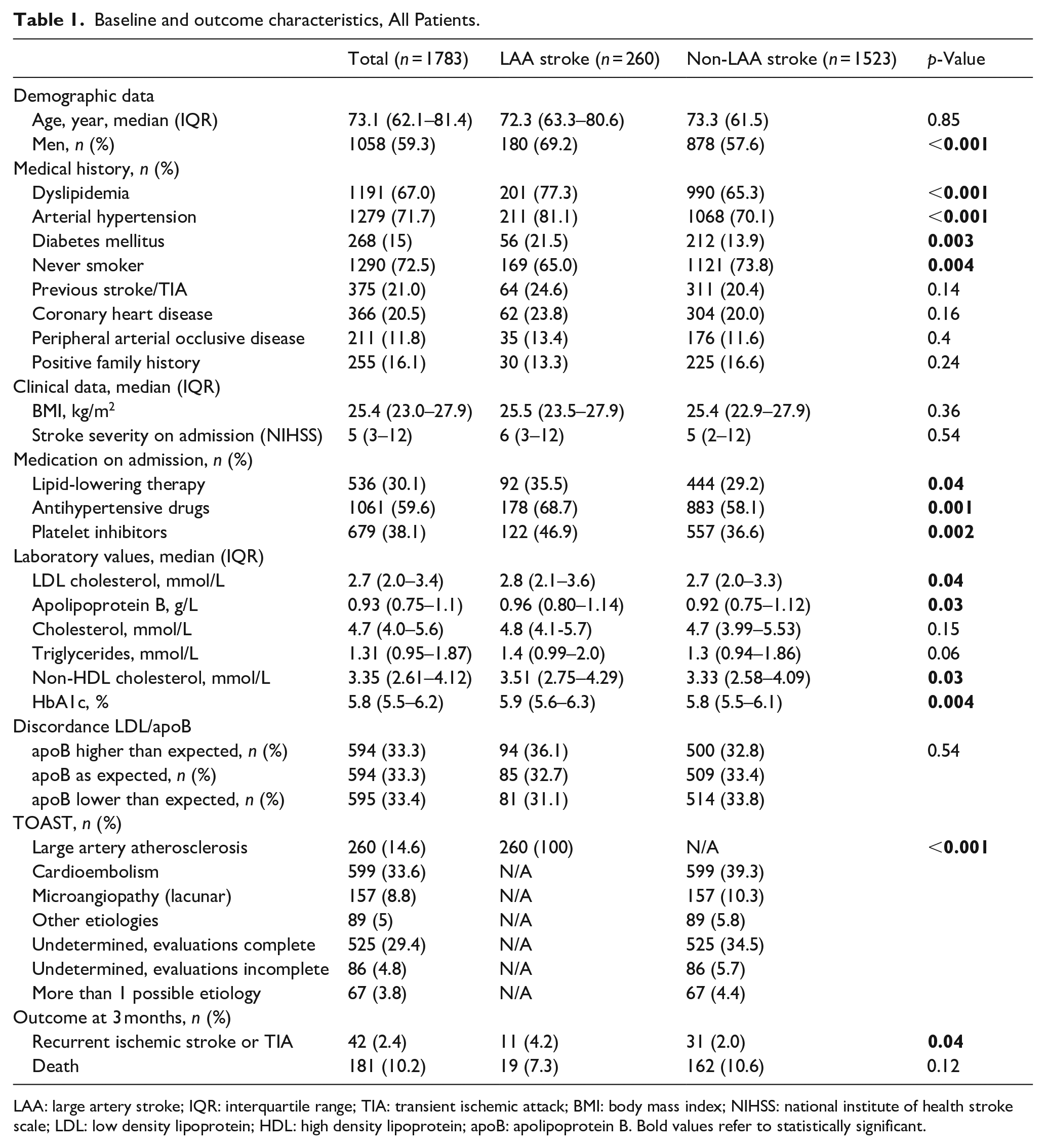
LAA: large artery stroke; IQR: interquartile range; TIA: transient ischemic attack; BMI: body mass index; NIHSS: national institute of health stroke scale; LDL: low density lipoprotein; HDL: high density lipoprotein; apoB: apolipoprotein B. Bold values refer to statistically significant.
As expected, the correlation between LDL-C and apoB was high, but not complete: LDL-C accounted for 75.6% of the variability in apoB levels (p < 0.001, Supplemental Figure 1). The scenario higher-than-expected apoB was more common among patients with versus without LAA stroke, but the difference was not significant (Table 1). However, a significant interaction between age and higher-than-expected apoB was present (p = 0.046). Among the 738 patients aged ⩽70 years, 48% of those with LAA stroke had higher-than-expected apoB, compared to 36% of those without LAA stroke (p = 0.02, see Supplemental Table 1 for a detailed comparison of patients aged ⩽70 years with and without LAA). Figure 1 depicts that lower patient age and greater discordance are associated with an increased probability of LAA as stroke etiology.
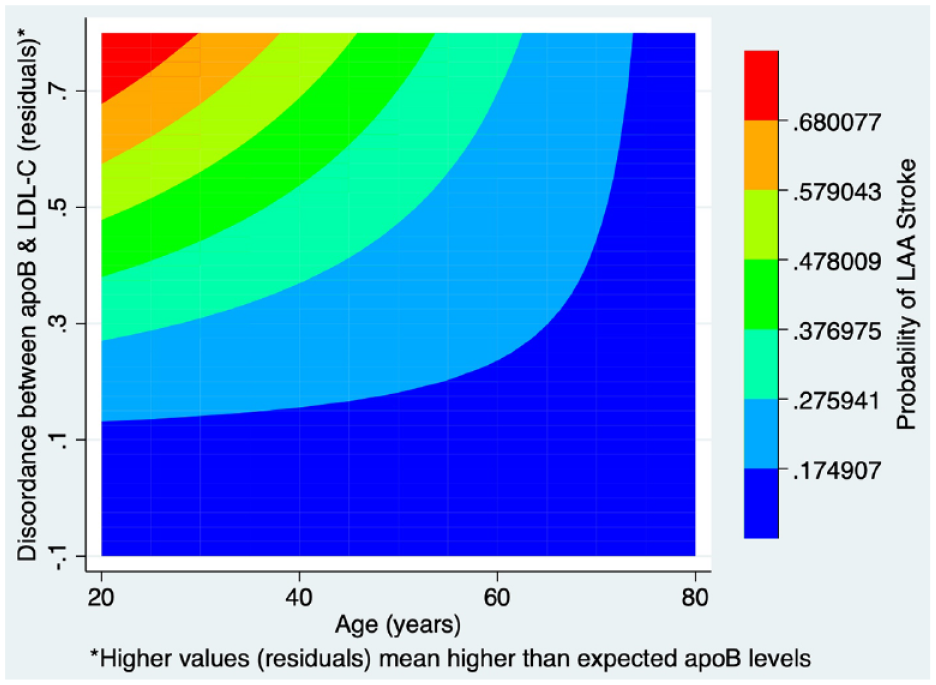
Interaction between patients age and discordance degree on the probability of LAA stroke.
Among patients aged ⩽70 years, those with higher-than-expected apoB had more than twice higher odds of LAA stroke compared to those with lower than-expected apoB levels (Supplemental Table 2). After adjusting for confounders such as lipid-lowering therapy on admission and LDL-C, the association remained significant (aOR 2.48, 95%CI 1.14–5.38, p = 0.02, Table 2). Overall, a specific discordant scenario – apoB above the guideline-recommended target (⩾0.65 g/L) despite LDL-C on target (<1.8 mmol/L) – occurred in 154 patients (8.6%). Among those aged ⩽70 years and with stroke due to LAA, the discordant scenario – apoB above the guideline-recommended target (⩾0.65 g/L) despite LDL-C on target (<1.8 mmol/L) – occurred twice as often compared to patients with stroke due to other etiologies (11.7% vs 5.9%, respectively, p = 0.04).
Multivariate logistic regression model for large-artery atherosclerotic stroke among patients ⩽70 years of age.
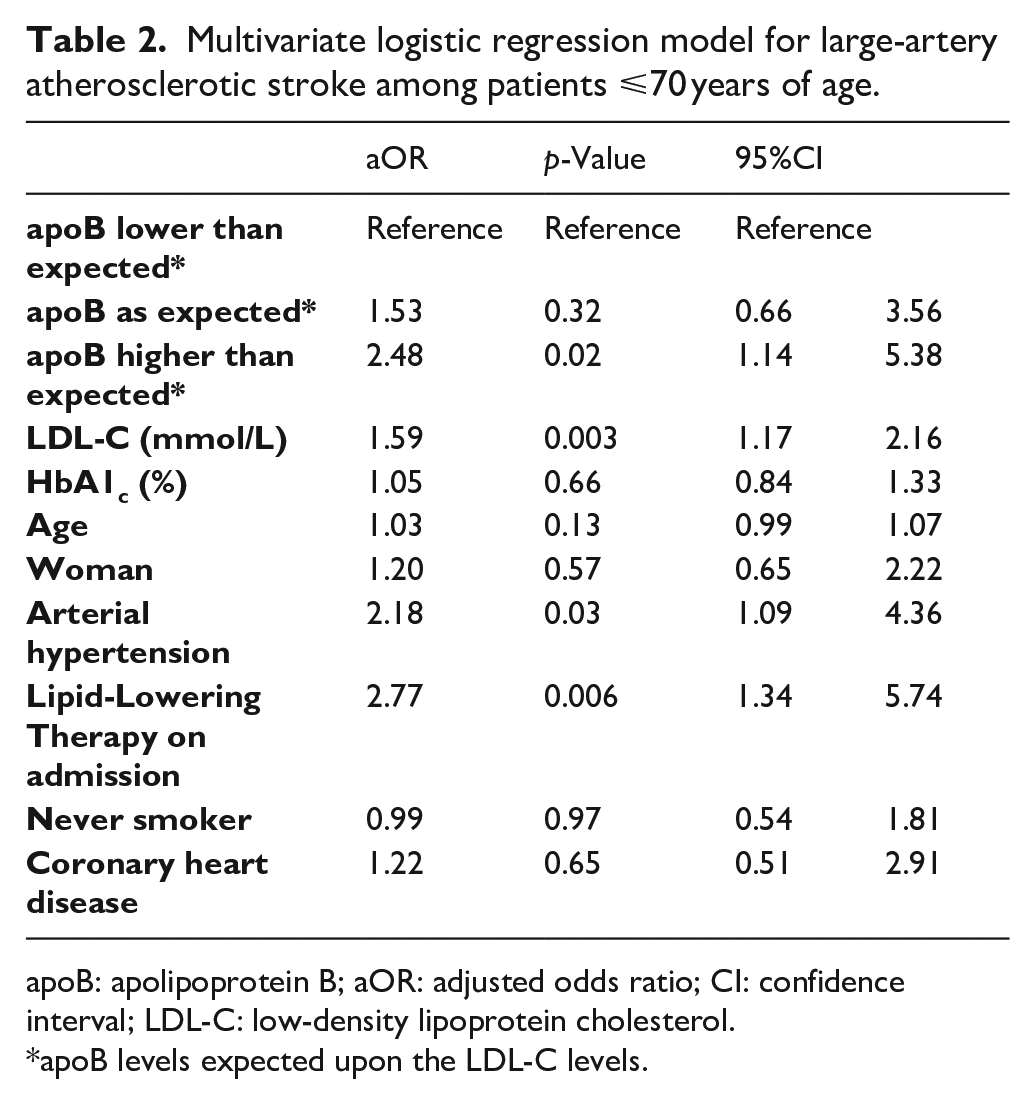
apoB: apolipoprotein B; aOR: adjusted odds ratio; CI: confidence interval; LDL-C: low-density lipoprotein cholesterol.
apoB levels expected upon the LDL-C levels.
The degree of discordance between LDL-C and apoB increased with increasing triglycerides levels (p < 0.001, Figure 2). In the derivation cohort, among patients with LDL-C <1.8 mmol/L, a triglyceride cut-off of ⩾0.95 mmol/L had a sensitivity of 91% and specificity of 48% for apoB⩾0.65 g/L. In the validation cohort, sensitivity was 71% and specificity 52%.
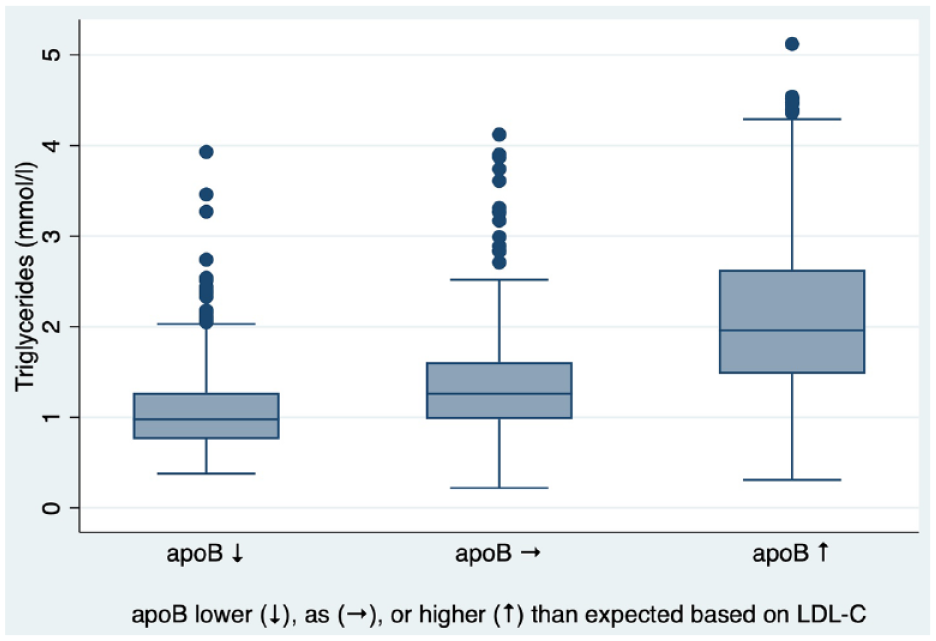
Association between triglycerides and apoB-LDL discordance scenarios.
Discussion
In this prospective cohort study, we made three main observations. First, after adjusting for LDL-C and other confounders, higher-than-expected apoB levels were more than twice as common in patients with LAA stroke aged ⩽70 years rather than other stroke etiologies. Second, one out of nine patients with LAA stroke ⩽70 years of age had admission apoB levels above the guideline-recommended target of 0.65 g/L, despite an LDL-C < 1.8 mmol/L (<70 mg/dl). Third, we extended the observation to stroke patients that higher-than-expected apoB levels are significantly more frequent among patients with elevated triglycerides. A triglyceride cut-off of ⩾0.95 mmol/L had, in external validation, a sensitivity of 71% and specificity of 52% for higher-than-expected apoB levels. As triglycerides are often part of routine lipid panel, the triglyceride cut-off may inform clinicians on when measuring apoB levels is likely to unmask LDL/apoB-discordance.
There are several reasons why apoB is, compared to LDL-C, a more reliable marker of the atherogenic burden. One apoB molecule coats one circulating atherogenic lipoprotein. Higher apoB levels mean that there are more circulating atherogenic lipoproteins. At any given LDL-C, higher apoB levels imply that the cholesterol molecules are distributed into more and smaller atherogenic low-density lipoproteins. In turn, more and smaller atherogenic lipoproteins are more likely to get trapped in the arterial intima, where they initiate and sustain atherosclerosis. 5 The well documented apoB role in atherogenesis substantiates, along with our observation, a causal link between apoB levels and LAA stroke. Since LAA stroke has the highest recurrence risk, the study observations have implications for recurrence prevention. 12 Cardiovascular risk reduction is associated more strongly with the magnitude of pharmacological apoB reduction, rather than that of LDL-C reduction. 13 Thus, identifying patients with above-target apoB despite on-target LDL-C is important. In the overall study population – that is, encompassing all patient ages – higher-than-expected apoB levels were not significantly associated with LAA stroke. Among patients >70 years of age, competing stroke etiologies – cardioembolism in particular – are significantly more common, blunting the association between higher-than-expected apoB levels and LAA stroke. Similarly, in a prior publication from the BIOSIGNAL consortium with 1733 patients with acute stroke, the association between LAA and lipoprotein(a) – that is, an apoB-coated, highly atherogenic lipoprotein – was strongest in patients <60 years. 9
The fact that one in nine patients ⩽70 years and LAA stroke had above the guideline-recommended target of 0.65 g/L, despite an LDL-C<1.8 mmol/L underscore the need to identify patients with LDL-C/apoB discordance. Being aware that routine lipid panel often lacks apoB and leveraging on the association between high triglycerides levels and higher-than-expected apoB, we suggest the triglyceride cut-off of ⩾0.95 mmol/L to request measuring apoB on top of the routine lipid panel. The therapeutic consequence of finding LDL-C/apoB discordance is to intensify the lipid-lowering therapy, to achieve both on-target apoB and LDL-C. We are aware that hypertriglyceridemia should not be used to restrict the measurement of apoB, since cholesterol-depleted apoB lipoproteins have been shown to be present even among patients with low triglycerides. 14 However, since apoB is measured much less than LDL-C, we believe that the cut-off of ⩾0.95 mmol/L can be helpful to give some guidance on increasing the pre-test probability of finding increased apoB levels.
The study has strengths and limitations. A strength is the prospective study design and large sample size, that allowed to confirm the association between apoB and LAA among patients with stroke. Since the study population derives from two independent studies (CoRisk 8 and BioSignal 9 ), it was possible to externally validate the triglyceride cut-off of 0.95 mmol/L. Limitations include lack of follow-up lipid levels, so that – after discharge – the proportion of patients with LDL-C ⩽ 1.8 mmol/L but apoB > 0.65 g/L is unclear. Since, however, most clinicians use LDL-C without apoB to guide lipid-lowering therapy, it is reasonable that, even at follow up, the proportion of the higher-than-expected apoB scenario is considerable. Finally, statistical power did not allow to assess if stroke recurrences were more frequent among patients with the higher-than-expected apoB. Longer – even register-based – follow-ups would allow to potentially observe more stroke recurrences and see if they are more frequent with higher-than-expected apoB.
In summary, we believe that the findings are of clinical relevance, as they allow to identify an additional number of patients who may benefit from enhanced lipid-lowering strategies despite having reached the recommended LDL-C target.
Non-standard abbreviations and acronyms
AIS: Acute ischemic stroke
aOR: Adjusted odds ratio
apoB: Apolipoprotein B
BioSignal: Biomarker Signature of Stroke Aetiology
CoRisk: Copeptin for Risk Stratification in Acute Stroke Patients
HDL: High density lipoprotein
IQR: Interquartile range
LAA: Large artery atherosclerosis
LDL-C: Low density lipoprotein cholesterol
NIHSS: National Institute of Health Stroke Scale
ROC: Receiver-operating characteristics
TIA: Transient ischemic attack
Supplemental Material
sj-docx-2-eso-10.1177_23969873231221619 – Supplemental material for Discordance between LDL-C and apolipoprotein B is associated with large-artery-atherosclerosis ischemic stroke in patients ⩽70 years of age
Supplemental material, sj-docx-2-eso-10.1177_23969873231221619 for Discordance between LDL-C and apolipoprotein B is associated with large-artery-atherosclerosis ischemic stroke in patients ⩽70 years of age by Lilian Kriemler, Salome Rudin, Joanna Gawinecka, Felix Gross, Markus Arnold, Juliane Schweizer, Laura Westphal, Corinne Inauen, Thomas Pokorny, Tolga Dittrich, Anna Toebak, Marcel Arnold, Mirjam Christ-Crain, Arnold von Eckardstein, Katharina Rentsch, Mira Katan and Gian Marco De Marchis in European Stroke Journal
Supplemental Material
sj-jpg-1-eso-10.1177_23969873231221619 – Supplemental material for Discordance between LDL-C and apolipoprotein B is associated with large-artery-atherosclerosis ischemic stroke in patients ⩽70 years of age
Supplemental material, sj-jpg-1-eso-10.1177_23969873231221619 for Discordance between LDL-C and apolipoprotein B is associated with large-artery-atherosclerosis ischemic stroke in patients ⩽70 years of age by Lilian Kriemler, Salome Rudin, Joanna Gawinecka, Felix Gross, Markus Arnold, Juliane Schweizer, Laura Westphal, Corinne Inauen, Thomas Pokorny, Tolga Dittrich, Anna Toebak, Marcel Arnold, Mirjam Christ-Crain, Arnold von Eckardstein, Katharina Rentsch, Mira Katan and Gian Marco De Marchis in European Stroke Journal
Footnotes
Acknowledgements
None.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Gian Marco De Marchis reports a grant from Novartis for the study “Atherogenic Lipoproteins in Stroke.” He reports consultant honoraria by Novartis and Daiichi Sankyo. Industry payments are made to the research fund of the University Hospital Basel. All other authors report no disclosures.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Jubiläumsstiftung from SwissLife (01-1285). Swiss National Science Foundation (Grant-Nr 32003B_200573, Grant-Nr 142422, Grant Nr 182267), the Baasch Medicus Foundation and the Swiss Heart Foundation.
Ethical approval
The ethics committee in Bern, Basel and Zurich approved this study.
Informed consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Guarantor
Gian Marco de Marchis
Contributorship
LK and SR researched literature and conceived the study. LK and GMDM wrote the first draft of the manuscript. JG and FG were involved in the laboratory analysis. TD was involved in protocol development and gaining ethical approval. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.