
Abstract
Introduction:
Stroke in young people shares traditional modifiable risk factors with older groups, and greatly affects quality of life. However, evidence on the effectiveness of educational interventions in young populations, aiming at spreading stroke knowledge and enhancing prevention, is still scarce. We evaluated baseline knowledge of stroke and possible improvements after an educational intervention among Italian high school students, also considering differences related to sex and type of school.
Subjects and methods:
Using a mixed educational strategy, a prospective evaluation of stroke knowledge was performed in five humanities and sciences (lyceums) and five vocational high schools of Tuscany (students of the 12th and 13th grade). A baseline assessment with a structured questionnaire (21 questions) was followed by a standardized oral presentation, using audiovisual materials. After 3 months, the same questionnaire was re-administered to evaluate the long-term impact of the educational intervention.
Results:
Overall, 573 students (50.8% males; age range, 17–19 years) were enrolled; 288 (50.3%) were from lyceums and 285 (49.7%) from vocational schools. Follow-up participation was 97.2%. Baseline performances were comparable between groups for most variables examined. At 3 months, all groups showed a significant improvement from baseline regarding reaction to a stroke event, identification of stroke risk factors, such as smoking (from 62.9% to 83.7%; p < 0.001) and alcohol abuse (from 49.6% to 67.2%; p < 0.001), and symptoms. Knowledge of the existence of stroke units and thrombolysis increased from 25.4% to 60.7% (p < 0.001) and from 35.8% to 84.0% (p < 0.001), respectively.
Conclusions:
Our educational intervention improved stroke awareness in high school students. The effects persisted after 3 months. Improved knowledge in young populations may reduce stroke burden in adult life, increase timely access to therapies, and spread knowledge across families.
Introduction
Worldwide, stroke is a leading cause of death and disability, with approximately 10% of events occurring in people aged 16–55 years.1–4 In the last decades, several time series studies in different countries showed a significant increase in incidence and hospitalization rates for stroke among young adults.5–8 Stroke is a high cost condition, and when it affects younger people, there is a greater overall impact in terms of disability-adjusted life years (DALY) and indirect costs from losses in productivity from premature death and disability. 9
Stroke occurring in adolescent and young adults shares traditional modifiable risk factors and health risk behaviors including hypertension, diabetes, coronary heart disease, obesity and lipid disorders, smoking, alcohol, and illicit drug use.5,6,10–12 These data indicate both the opportunity and the urgency of public health initiatives aiming at reducing the frequency of the disease in this important segment of the population. 13
The role of education is seen as essential to reduce the burden and consequences of stroke at any age, potentially increasing prevention, early recognition of stroke symptoms, timely hospital arrivals and thrombolytic treatments, and also enabling the dissemination of knowledge among the population.14–18 However, evidence on the effectiveness of educational interventions directed to increase knowledge and change behavior toward stroke and stroke risk factors in young populations is still scarce. The aim of this study was to evaluate the effectiveness of a mixed educational intervention targeting Italian high school students, also considering differences related to sex and type of school.
Methods
The Project “Ictus: Comunicazione & Innovazione” (Stroke, Communication & Innovation), funded by Ente Cassa di Risparmio di Firenze, in collaboration with the Stroke Patients Association ALICe Toscana, started in June 2013 aiming to improve education and stroke knowledge among the general population, and to help the development of a stroke network involving different health professionals and authorities from the Tuscany Region of Italy.
As part of these activities, several yearly educational campaigns were promoted among general population of Tuscany, and the first and only Italian stroke app, called “ICTUS3R,” was also developed. 19 The app was designed to improve, at regional and national level, public awareness of stroke and to translate this knowledge into virtuous behavior in terms of prevention and timely access to health services.
The Project also included an educational program involving Tuscany high schools, performed during the third year of activity. The purpose was to evaluate baseline stroke knowledge among students and the effectiveness of a mixed educational intervention aimed to improve stroke awareness in a young population.
An evaluation of stroke knowledge in students of the fourth and fifth years (corresponding to a 12th and 13th grade) was planned in 10 out of the 159 high schools of Tuscany. The 10 schools were pragmatically selected to represent a cross-section of schools and students selected from 7 out of the 10 provinces in Tuscany. Age of students ranged between 17 and 19 years. To have a representative sample in terms of school location, family and social backgrounds, average income, educational opportunities, and performance of students, we included five humanities and sciences (in Italy, called “lyceums”) and five vocational schools. Traditionally, in Italy, frequency of lyceums, focused on university preparation, is an indicator of higher household income. 20 The survey was completely anonymous. Sex and type of school were the only personal information requested.
The study had a prospective design, and used a mixed educational strategy, including didactic and interactive elements. Baseline information on stroke knowledge was collected through a structured paper questionnaire. Students were asked multiple-choice (n = 3) and close-ended (n = 18) questions, which included the identification of stroke as a brain disease, affecting old as well as young people, and indication (among different choices) of the right thing to do (call an ambulance) if a stroke is suspected. Other questions included sudden onset of symptoms suggesting a stroke (paralysis of arm and leg in one side, difficulty speaking or understanding speech, trouble seeing or visual loss, headache), risk factors (hypertension, diabetes, atrial fibrillation, high cholesterol, obesity, smoking, alcohol abuse, illegal drugs assumption), awareness of the existence of stroke units, specialized in stroke care and providing a better outcome, and of thrombolysis as an important therapy for acute stroke. Among response options there were also false possibilities (e.g. stroke is a disease of heart, affecting only older people; in case of suspected stroke, lie down and wait for the symptoms to disappear, or call the family doctor, are right things to do).
Straight after the questionnaire administration, a standardized 45-min oral presentation was given by stroke neurologists and epidemiologists, using audiovisual materials. The presentation focused mainly on risk factors, stroke symptoms, appropriate reaction to a stroke event, and available treatment opportunities. As part of the interactive teaching methodology, questions related to the information provided during the presentation and personal experiences of the disease among relatives or friends were stimulated from audience. After 3 months, the same questionnaire was re-administered to evaluate the long-term impact of the educational intervention in terms of stroke knowledge (outcome measure). This was possible as the teachers from each school had kept a record of the students that participated in the baseline survey and were able to ask these students to complete the 3-month follow-up survey.
The institutional review board of each participating institution approved the survey, which, anyhow, used an anonymized and completely untraceable dataset. Therefore, no subject consent was required, considering the absence of any identifiable data.
Statistical analysis
The chi-square test was used to compare categorical variables for cross-sectional analyses. Test for the equality of two proportions was used to evaluate the differences in longitudinal comparisons, considering total sample, sex, and type of school. Estimates as well as 95% confidence intervals (95% CI) were provided. All p-values were based on a two-sided test and a significance level of <0.05. Analyses were performed using SAS version 9.4. (SAS Institute, Cary, NC).
Results
Overall, 573 students (50.8% males) were enrolled at baseline; 288 (50.3%) were from lyceums and 285 (49.7%) from vocational schools. At follow-up, the questionnaire was completed again by 557 students (49.9% males), corresponding to 97.2% of the original sample; 287 (51.5%) were from lyceums and 270 (48.5%) from vocational schools. Illness related absences from schools (n = 16; 15 were from vocational schools; 81.2% males) explained the slightly lower response rate at follow-up.
Table 1 shows main results for cross-sectional comparison at baseline and follow-up between sexes and the two type of schools. At both examinations, more than 90% of participants indicated stroke as a brain disease, involving old as well as young people; in case of a suspected stroke, more that 85% indicated “call an ambulance” as the right choice. No significant differences were found between sexes and type of school.
Cross-sectional comparisons of baseline and follow-up performances between males and females, lyceums and vocational schools.
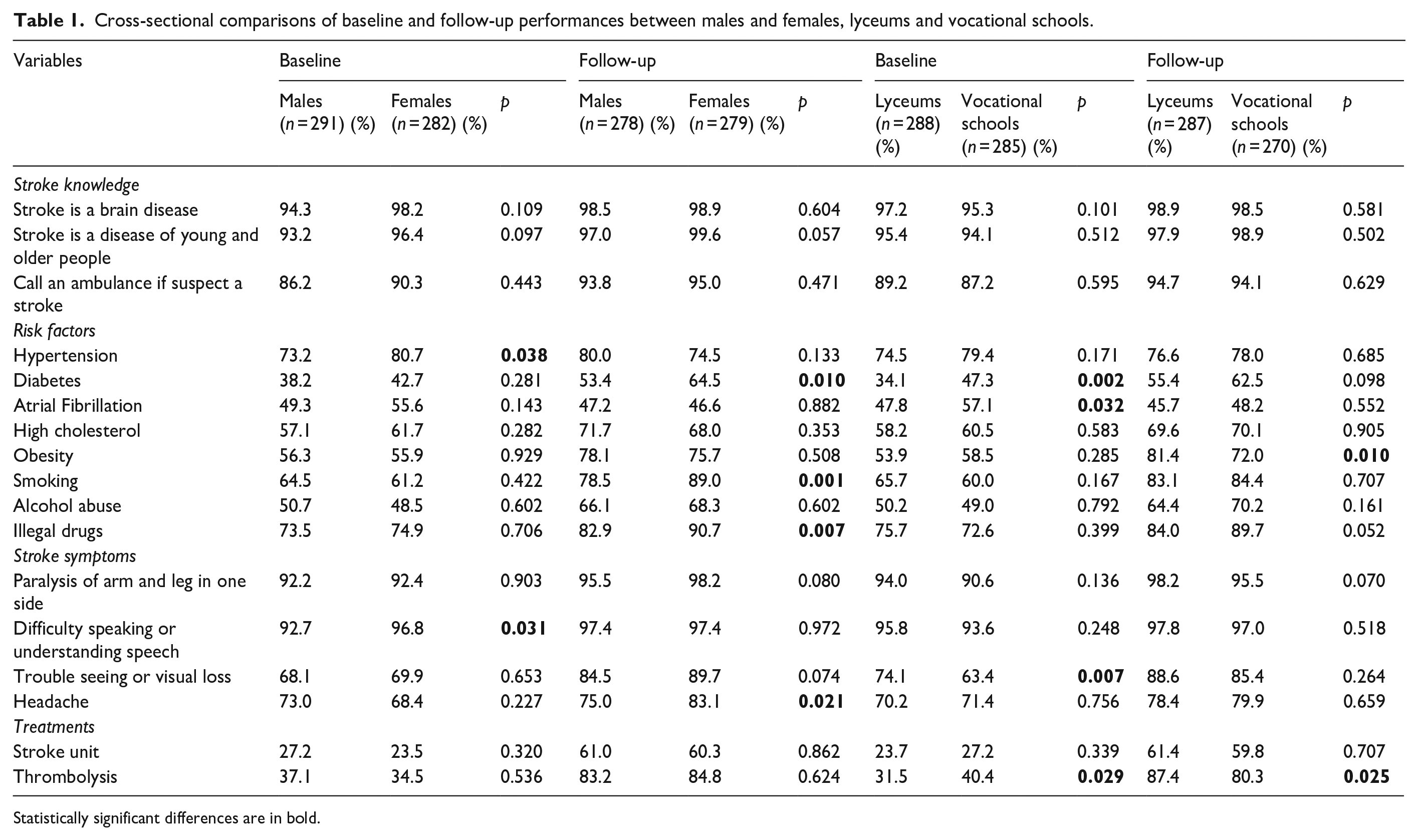
Statistically significant differences are in bold.
At baseline, the survey item with the lowest percentage of correct responses was for knowledge of the existence of stroke units, recognized by 27.2% of males and 23.5% of females. The highest percentages of correct answers were for difficulty speaking or understanding speech (92.7% for males, 96.8% for females), followed by knowledge of paralysis of arm and leg (92.2% for males, 92.4% for females) as symptoms suggesting a stroke. At follow up, these two symptoms remained the variables with the higher percentages of correct answers for both sexes, while atrial fibrillation was the less acknowledged one (47.2% of males and 46.6% of females).
Compared with males, at baseline female students showed higher percentages of correct answers for knowledge of hypertension and difficulty speaking or understanding speech, and at follow-up higher percentages for knowledge of diabetes, smoking, illegal drugs use, and headache.
Considering the two categories of schools, at baseline vocational schools’ students performed slightly better in knowledge of stroke risk factors, in particular diabetes and atrial fibrillation, and of thrombolysis as a therapy for acute stroke, while trouble seeing or visual loss at baseline was indicated significantly more frequently by lyceums’ students. At follow-up, performances of lyceums’ students were significantly better for knowledge of obesity and of thrombolysis, while illegal drugs use was recognized more frequently by vocational schools’ students, with a difference approaching significance.
Table 2 shows longitudinal comparisons of changes from baseline to follow-up performances for males, females, and total sample. Small but yet significant improvements were seen in the already high percentages of participants indicating stroke as a brain disease (+2.4%; 95% CI, 0.6%–4.3%), involving old as well as young people (+3.6%; 95% CI, 1.4%–5.7%), and “call an ambulance” as the right choice in case of a suspected stroke (+6.2%; 95% CI, 2.9%–9.4%). This was confirmed in total sample and in both sexes. At follow-up, correct identification of stroke risk factors by total sample increased significantly from baseline for diabetes (+18.5%; 95% CI, 12.5%–24.4%), high cholesterol (+10.6%; 95% CI, 4.9%–16.2%), obesity (+20.8%; 95% CI, 15.3%–26.3%), smoking (+20.8%; 95% CI, 15.7%–25.9%), alcohol abuse (+17.6%; 95% CI, 11.8%–23.4%), and illegal drugs use (+12.6%; 95% CI, 7.9%–17.2%). These changes were also confirmed considering changes from baseline to follow-up separately for males and females, apart from high cholesterol in females, whose increase was not significant.
Longitudinal comparisons of baseline to follow-up performances for males, females, and total sample.
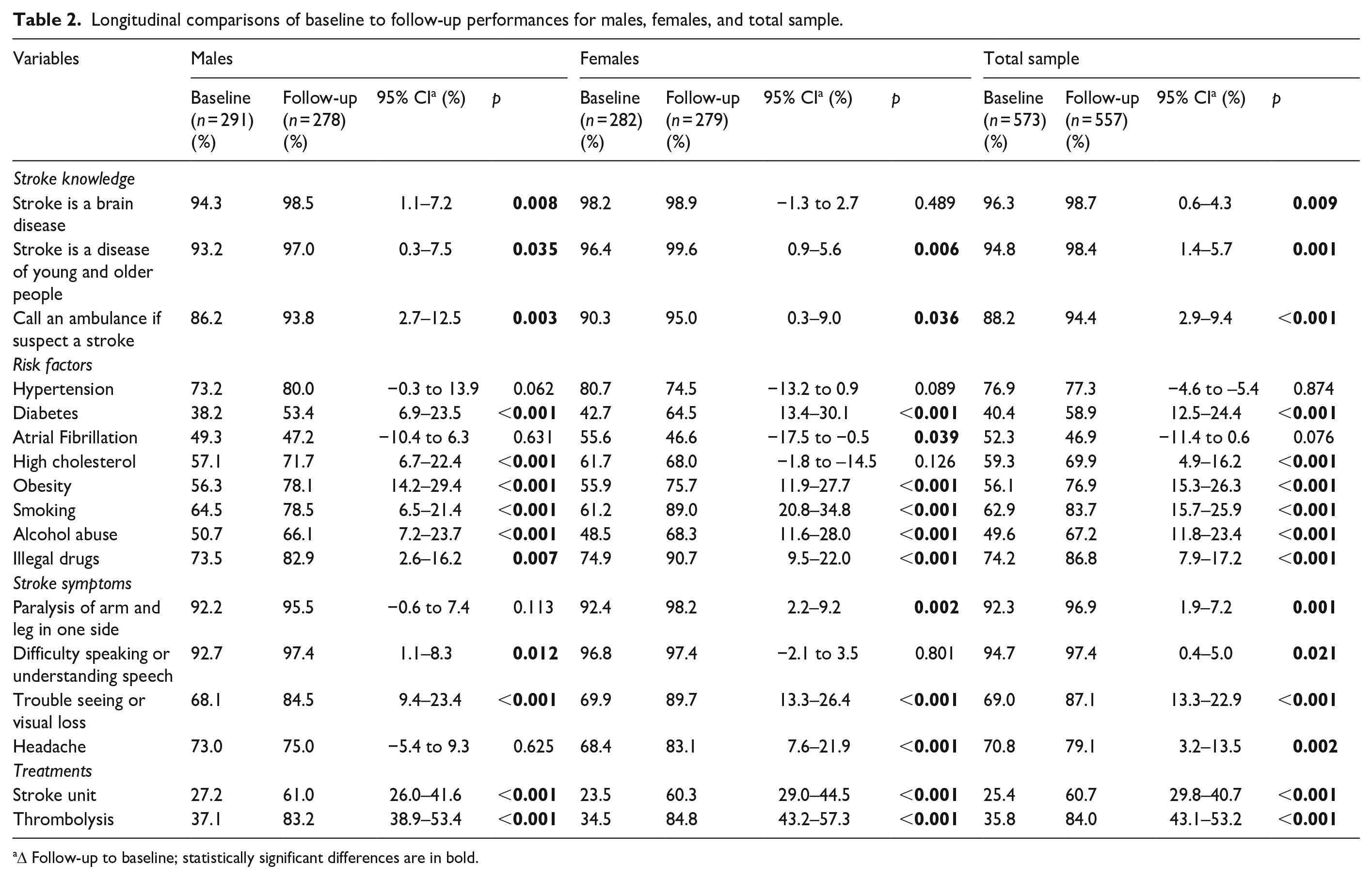
Δ Follow-up to baseline; statistically significant differences are in bold.
Among possible stroke symptoms, more than 90% of students accurately identified paralysis of arm and leg and difficulty speaking or understanding speech at both examinations, with a small but significant improvement at follow-up in total sample. Changes were significant in females for paralysis of arm and leg and in males for difficulty speaking or understanding speech. Correct identification of stroke symptoms increased significantly in total population also for trouble seeing or visual loss (confirmed for both sexes) and headache (improvement significant only in females).
Knowledge of the existence of stroke units and thrombolysis increased significantly at follow-up in total sample from 25.4% to 60.7% and from 35.8% to 84.0%, respectively, and changes from baseline were highly significant for both sexes (p < 0.001).
Table 3 reports longitudinal comparisons of baseline to follow-up performances by type of school. Globally, follow-up results indicated a consistent and significant improvement from baseline in both lyceums and vocational schools. Among small differences, a statistically significant increase was evidenced in vocational schools considering knowledge of stroke as a brain disease and involving old as well as young people, although the final percentage of correct answers was around 98% for both types of schools.
Longitudinal comparisons of baseline to follow-up performances for lyceums and vocational schools.
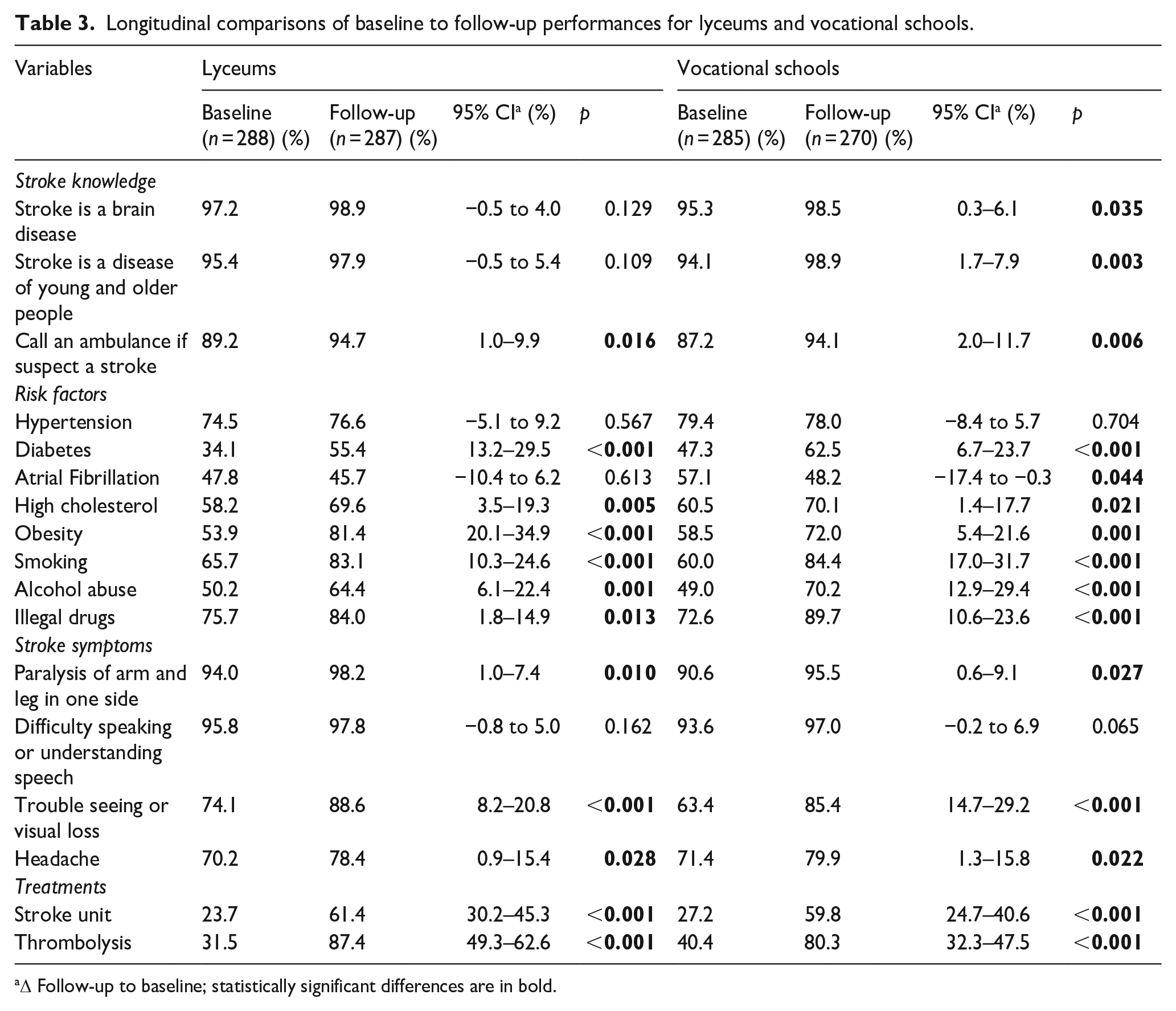
Δ Follow-up to baseline; statistically significant differences are in bold.
Discussion
In a prospective survey involving students from 10 high schools of Tuscany, we evaluated baseline awareness of stroke and the effect of a mixed educational intervention on improving stroke knowledge after a 3-month follow-up. We observed a significant improvement from baseline to follow-up examination in all groups considered, underlining the effectiveness of this educational strategy. Performances were comparable between groups for most of the variables examined. We found only small differences between sexes, all pointing in favor of a better knowledge of stroke risk factors and symptoms among female students. At baseline, vocational schools’ students performed slightly better than lyceums’ students, considering knowledge of some stroke risk factors and the existence of thrombolysis, but at follow-up they did better only on the knowledge of illegal drugs use, while lyceums’ students performed better on knowledge of obesity and thrombolysis. Overall, our data underline the relevance of educational interventions aimed to promote health in these age groups.
Previous studies evaluated stroke knowledge among students of different age groups. In the Hip Hop Stroke Program, performed among New York City schoolchildren of fourth, fifth, and sixth grade (age, 9–11 years), stroke knowledge was significantly associated with indicators of school performance and measures of socioeconomic status. 21 In another survey among middle and high school students (7th–12th grade) in Grand Rapids, Michigan, most participants were unaware of all the risk factors and symptoms associated with stroke. 22 A Japanese study designed to improve stroke knowledge in junior high schools students (age, 13–15 years), showed a significant increase of recognition of stroke risk factors, signs, symptoms, and reaction to a stroke event, immediately after a lecture supported by multimedia tools. 23
To our knowledge, our study is the first aiming to assess stroke knowledge at baseline and after a 3-month follow-up in high schools’ students from western countries. Six prospective studies in United States, 24 Portugal, 18 Italy, 25 and Japan26–28 showed a significant improvement of stroke knowledge in elementary schoolchildren and in middle school/junior high school students (ages, 9–14 years) 3 months after an educational intervention, or in high school students a few days after the intervention. Overall, these results strengthen the hypothesis of the effectiveness of an educational intervention in the different ages.
Increased awareness of stroke risk factors among young adults is needed to reduce the burden of cerebrovascular disease in adult life, as well as individual and societal health care costs in terms of DALY and loss of quality of life.9,10,12 After the educational intervention, we observed a significant improvement in the knowledge of modifiable stroke risk factors such as smoking, excessive alcohol intake, and illicit drug use, which are among the most prevalent risk factors found in young patients with cerebrovascular events.10–12,29
Fast treatment of stroke with thrombolysis or endovascular thrombectomy is essential for a successful outcome. However, a delayed hospital arrival prevents many patients from receiving those therapies, and inadequate stroke knowledge is among the reasons for pre-hospital delays.16,17 The role of young adults in both recognizing stroke symptoms and spreading knowledge among relatives is relevant to increase the percentage of patients receiving a timely therapy in the acute phase.18,23,27,28 We found a significant increase in recognition of all stroke symptoms from baseline to follow-up. However, stroke recognition is made even more effective by knowing the opportunities provided by a rapid hospitalization, such as the existence of thrombolysis and stroke units. These turned out to be the least known variables by students at baseline, but also those with a more relevant increase, still lasting at 3 months, with percentages that went from 35.8% to 84% for thrombolysis and from 25.4% to 60.7% for stroke units.
The strengths of this study include the prospective design, with a 3-month follow-up examination, the representativeness of different territories from Tuscany, covering both urban and rural areas, and the inclusion of students from lyceums and vocational schools.
Our survey has also some limitations. Our study population may be not representative of all Italian students and schools. However, our sample included different geographical areas and, traditionally, in Italy a census difference between students of lyceums and vocational schools is observed. 20 Second, the educational intervention was performed by expert neurologists and epidemiologists. Trained schoolteachers will be the ideal figures for large campaigns on a national basis. Third, although improvements in stroke knowledge persisted after 3 months, the effectiveness of the intervention should be monitored in real life, for instance by evaluating an increase of ambulance dispatch for stroke, timely arrival to hospital or number of thrombolysis performed. Finally, the retention of information for a longer period of time is uncertain. Furthermore, repeating the survey to assess changes in knowledge, or to gather information on how to improve the education program post the pandemic, may be warranted.
In conclusion, after a mixed educational intervention on stroke awareness in high school students, we observed a significant improvement persisting after a 3-month follow-up, irrespective of sex and type of school. Educational interventions in these age groups may reduce stroke burden in adult life, increase timely access to acute stroke therapies, and spread knowledge across family members.
Footnotes
Acknowledgements
We thank Maria Elena Della Santa (Institute of Neuroscience, Italian National Research Council) for technical support. We express our deepest gratitude to the teachers and students of participating schools. Finally, we acknowledge the support given by the Stroke Patients Association ALICe Toscana, in particular the provincial sections of Firenze, Massa, Pisa, Siena, Pistoia, Arezzo, and Grosseto.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by the Fondazione Ente Cassa di Risparmio di Firenze, Project “ICTUS: Comunicazione & Innovazione,” grant 2012/0373.
Ethical approval
The survey was approved by the institutional review board of each participating institution.
Informed consent
Informed consent was not sought because the survey was completely anonymous, and the dataset anonymized and untraceable. Sex and type of school were the only personal information requested.
Guarantor
DI.
Contributorship
ADC, MB, and DI designed the study. ADC and FB analyzed the data. ADC, DI, and FB wrote the first draft. All authors contributed to the collection of data, reviewed and edited the manuscript, and approved the final version.