Plenary Sessions - OFFICIAL WELCOME AND LARGE CLINICAL TRIALS
O300/3103
REMOTE ISCHEMIC CONDITIONING IN PATIENTS WITH ACUTE STROKE: A MULTICENTER RANDOMISED, PATIENT-ASSESSOR BLINDED, SHAM-CONTROLLED STUDY (RESIST)
Rolf Blauenfeldt*1,2, Niels Hjort1,2, Jan Brink Valentin3, Anne-Mette Homburg4, Boris Modrau5, Birgitte Sandal6, Martin Faurholdt Gude7, Kristina Dupont Hougaard1, Dorte Damgaard1, Marika S. Poulsen1, Tove Diedrichsen1, Marie Louise Schmitz1, Paul von Weitzel-Mudersbach1,6, Alex Alban Christensen4, Krystian Figlewski5, Erik Lerkevang Grove2,8, Margrét Katrín Hreiðarsdóttir6, Henning Morthorst Lassesen9, Søren Mikkelsen9, Ulla Væggemose2,7, Palle Juelsgaard7, Hans Kirkegaard10, Martin Rostgaard-Knudsen11, Niels Degn5, Sigrid Breinholt Vestergaard1,2, Andreas Gammelgaard Damsbo1,2, Ane Bull Iversen1, Janne Kærgård Mortensen1,2, Jesper Petersson12,13, Thomas Christensen14,15, Anne Brink Behrndtz1,2, Hans Erik Bøtker16,17, David Gaist18, Marc Fisher19, David Hess20, Søren Paaske Johnsen3, Claus Ziegler Simonsen1,2, Grethe Andersen1,2
1Aarhus University Hospital, Department of Neurology, Aarhus, Denmark, 2Aarhus University, Department of Clinical Medicine, Aarhus, Denmark, 3Department of Clinical Medicine, Aalborg University, Danish Center for Health Services Research, Aalborg, Denmark, 4Odense University Hospital, Department of Neurology, Odense, Denmark, 5Aalborg University Hospital, Department of Neurology, Aalborg, Denmark, 6Regional Hospital Gødstrup, Department of Neurology, Gødstrup, Denmark, 7Prehospital Emergency Medical Services, Central Denmark Region., Department of Research and Development, Aarhus, Denmark, 8Aarhus University Hospital, Department of Cardiology, Aarhus, Denmark, 9Odense University Hospital, Prehospital Research Unit, Region of Southern Denmark, Odense, Denmark, 10Aarhus University Hospital, Aarhus, Denmark, Research Center for Emergency Medicine, Aarhus, Denmark, 11Prehospital Emergency Medical Services, North Denmark Region, Prehospital Emergency Medical Services, Aalborg, Denmark, 12Lund University, Lund, Sweden, Department of Neurology, Lund, Sweden, 13Region Skåne, Malmö, Sweden, Department of Health Care Management, Malmö, Sweden, 14Copenhagen University Hospital, Copenhagen, Denmark, Department of Neurology, Copenhagen, Denmark, 15University of Copenhagen, Copenhagen, Denmark, Department of Clinical Medicine, Copenhagen, Denmark, 16Aarhus University, Aarhus, Denmark., Faculty of Health, Aarhus, Denmark, 17Aarhus University Hospital, Aarhus, Denmark., Department of Cardiology, Aarhus, Denmark, 18Odense University Hospital, Research Unit for Neurology, Department of Neurology, Odense, Denmark, 19Harvard Medical School, Boston, MA, USA, Beth Israel Deaconess Medical Center, Boston, United States, 20Medical College of Georgia, Augusta University, Department of Neurology, Augusta, United States
Background and aims: Remote ischemic conditioning (RIC) with transient cycles of limb ischemia and reperfusion is cerebroprotective in preclinical models and some clinical stroke trials. We investigated whether combined prehospital and in-hospital RIC improves functional outcome in patients with acute stroke.
Methods: We performed a multicenter, prospective, randomized, patient-assessor blinded, sham-controlled study. Eligible patients were adult, independent in activities of daily living, had prehospital stroke symptoms with a duration <4 hours. Patients were randomly assigned to RIC or sham. Treatment was started in the ambulance and continued in-hospital. The primary endpoint was improvement in functional outcome measured as shift across the modified Rankin Scale in the target population with a final diagnosis of ischemic or hemorrhagic stroke.
Results: From March 16, 2018, to November 11, 2022, 1500 patients underwent prehospital randomization. Median age was 71, and 591 (41%) were female. Of these, 149 (10%) patients were diagnosed with transient ischemic attack and 382 (27%) with a stroke mimic. In the remaining 902 patients with a target diagnosis of stroke a total of 436 were treated with RIC and 466 with sham. Treatment with RIC was not associated with a shift towards better functional outcome at 90 days (Odds ratio, 1.05; 95% confidence interval,0.83-1.33, p=0.67). We found no significant effect on key secondary endpoints and no safety concerns.
Conclusions: We did not show improvement on functional outcome of combined prehospital and in-hospital RIC among patients with acute stroke. Half the patients were included within the first hour after stroke onset.
ClinicalTrials.gov:NCT03481777.
Disclosure of interest: No
O301/3094
EFFICACY AND SAFETY OF TENECTEPLASE IN PATIENTS WITH LATE-WINDOW ACUTE ISCHAEMIC STROKE AND EVIDENCE OF SALVAGEABLE TISSUE: RESULTS FROM THE PHASE III TIMELESS TRIAL
Gregory W. Albers*1, Mouhammad Jumaa2, Barbara Purdon3, Syed Zaidi2, Christopher Streib4, Ashfaq Shuaib5, Navdeep Sangha6, Minjee Kim7, Michael T. Froehler8, Danoushka L. Tememe9, Neil Schwartz1, Wayne M. Clark10, Charles Kircher11, Ming Yang3, Lori Massaro3, Xiao-Yu Lu3, Joseph Broderick12, Ken Butcher13, Maarten Lansberg1, David Liebeskind14, Amre Nouh15, Lee Schwamm16, Bruce Campbell17
1Stanford University, Department of Neurology and Neurological Sciences, Palo Alto, United States, 2ProMedica Toledo Hospital, Department of Neurology, Toledo, United States, 3Genentech, US Medical Affairs, South San Francisco, United States, 4University of Minnesota, Department of Neurology, Minneapolis, United States, 5University of Alberta, Department of Medicine, Edmonton, Canada, 6Southern California Permanente Group, Los Angeles Medical Center, Department of Neurology, Los Angeles, United States, 7Northwestern University Feinberg School of Medicine, Department of Neurology, Chicago, United States, 8Vanderbilt University Medical Center, Vanderbilt Cerebrovascular Program, Nashville, United States, 9University of Pittsburgh Medical Center, Department of Neurology, Pittsburgh, United States, 10Oregon Stroke Center at Oregon Health and Science University, Department of Neurology, Portland, United States, 11University of Cincinnati College of Medicine, Department of Emergency Medicine, Cincinnati, United States, 12University of Cincinnati College of Medicine, Department of Neurology and Rehabilitation Medicine, Cincinnati, United States, 13School of Medicine, University of New South Wales, Clinical Neurosciences, Sydney, Australia, 14University of California, Department of Neurology, Los Angeles, United States, 15Cleveland Clinic Florida, Department of Neurology, Weston, United States, 16Massachusetts General Hospital, Harvard Medical School, Department of Neurology, Boston, United States, 17Melbourne Brain Centre at the Royal Melbourne Hospital, Department of Medicine and Neurology, Parkville, Australia
Background and aims: Recent studies have suggested patients with acute ischaemic stroke (AIS) and evidence of salvageable tissue may benefit from intravenous thrombolytic, even when treated >4.5 hours after last-known well time (LKWT). This study investigates whether tenecteplase improves clinical outcomes in patients with AIS due to large vessel occlusion who present >4.5 hours after LKWT.
Methods: TIMELESS (NCT03785678) is a phase III, double-blind, randomised, placebo-controlled trial of tenecteplase in patients with AIS and evidence of salvageable tissue on imaging who present 4.5-24 hours after LKWT with an internal carotid or middle cerebral artery (M1 or M2 segment) occlusion. Patients meeting predefined imaging criteria were randomised 1:1 to receive intravenous tenecteplase (0.25 mg/kg; maximum, 25 mg) or placebo. Endovascular thrombectomy was planned following study drug administration. The study enrolled 458 patients. The primary endpoint is the distribution of modified Rankin Scale (mRS) scores at Day 90. Secondary endpoints include reperfusion/recanalisation 24 hours post randomisation, median NIH stroke scale score at Day 90, and proportions of patients with mRS score of 0-2 at Day 90 and good recovery based on the Glasgow Outcome Scale at Day 90. Key safety outcomes include symptomatic intracranial haemorrhage within 36 hours, parenchymal haematoma within 72-96 hours and mortality up to Days 30 and 90.
Results: To be presented at ESOC 2023.
Conclusions: Results from the TIMELESS trial will provide evidence regarding the efficacy and safety of tenecteplase for patients with AIS and imaging evidence of salvageable tissue in the 4.5- to 24-hour window.
Disclosure of interest: Yes
O303/1449
PREVENTION OF COMPLICATIONS TO IMPROVE OUTCOME IN ELDERLY PATIENTS WITH ACUTE STROKE (PRECIOUS): A RANDOMISED, OPEN, PHASE III, CLINICAL TRIAL WITH BLINDED OUTCOME ASSESSMENT
Jeroen de Jonge1, Wouter Sluis1, Rik Reinink1, Philip Bath2, Lisa Woodhouse2, Berber Zweedijk1, Diederik van de Beek3, Anne Hege Aamodt4, Iris Alpers5, Alfonso Ciccone6, Laszlo Csiba7, Jacques Demotes8, Janika Kõrv9, Iwona Kurkowska-Jastrzebska10, Kennedy R. Lees11, Malcolm Macleod12, George Ntaios13, Gary Randall14, Sven Poli15, Charalampos Milionis16, Stefano Ricci17, Paolo Candelaresi18, Sebastiaan De Bruijn19, Rohan Pathansali20, Kailash Krishnan21, Brian Clarke22, Götz Thomalla23, H. Bart van der Worp*1
1University Medical Center Utrecht, Utrecht University, Department of Neurology and Neurosurgery, Brain Center, Utrecht, Netherlands, 2University of Nottingham, Stroke Trials Unit, Division of Clinical Neuroscience, Nottingham, United Kingdom, 3Amsterdam University Medical Center, Department of Neurology, Amsterdam Neuroscience, Amsterdam, Netherlands, 4Oslo University Hospital, Oslo & Norwegian University of Science and Technology, Department of Neurology, Trondheim, Norway, 5University Medical Center Hamburg-Eppendorf, CTC North GmbH, Hamburg, Germany, 6ASST di Mantova, Department of Neurology and Stroke Unit, Mantua, Italy, 7University of Debrecen, Department of Neurology, Debrecen, Hungary, 8European Clinical Research Infrastructure Network & Institut National de la Santé et de la Recherche Médicale, ECRIN, Paris, France, 9University of Tartu, Department of Neurology and Neurosurgery, Tartu, Estonia, 10Institute of Psychiatry and Neurology, 2nd Department of Neurology, Warsaw, Poland, 11Institute of Cardiovascular and Medical sciences, University of Glasgow, Glasgow, United Kingdom, 12Centre for Clinical Brain Sciences, University of Edinburgh, Edinburgh, United Kingdom, 13Larissa University Hospital, University of Thessaly, Department of Medicine, Larissa, Greece, 14Stroke Alliance for Europe, SAFE, Brussels, Belgium, 15Hertie Institute for Clinical Brain Research, University of Tübingen, Department of Neurology & Stroke, Tübingen, Germany, 16Faculty of Medicine, School of Health Sciences, University of Ioannina, Department of Internal Medicine, Ioannina, Greece, 17Città Di Castello Hospital and Gubbio-Gualdo Tadino Hospital, Stroke Center - Neurology, Città di Castello, Italy, 18AORN Antonio Cardarelli, Neurology and Stroke Unit, Naples, Italy, 19Haga Hospital, Department of Neurology, The Hague, Netherlands, 20King's College Hospital NHS Foundation Trust, Department of Stroke Medicine, London, United Kingdom, 21Nottingham University Hospitals NHS Trust, Stroke, Department of Acute Medicine, Nottingham, United Kingdom, 22St George's University Hospitals NHS Foundation Trust, Department of Neurology, London, United Kingdom, 23Center for Clinical Neurosciences, University Medical Center Hamburg-Eppendorf, Department of Neurology, Hamburg, Germany
Background and aims: Elderly patients are at high risk of complications after stroke, such as infections and fever. The occurrence of these complications has been associated with an increased risk of death or dependency. In the PREvention of Complications to Improve OUtcome in elderly patients with acute Stroke (PRECIOUS) trial, we assessed whether preventive antiemetic, antibiotic or antipyretic therapy improves functional outcome in elderly patients with acute stroke.
Methods: PRECIOUS was a European, 3*2-factorial, randomised, controlled, open-label clinical trial (ISRCTN82217627) with blinded outcome assessment in patients aged 66 years or older with acute ischaemic stroke or intracerebral haemorrhage and an NIHSS score ⩾6. Patients were randomly allocated to any combination of metoclopramide (10mg thrice daily); ceftriaxone (2000mg once daily); paracetamol (1000mg four times daily); or usual care, started within 24 hours after symptom onset and continued for four days or until discharge from hospital, if earlier. The score on the modified Rankin Scale at 90 days was the primary outcome.
Results: Enrolment stopped prematurely because of cessation of funding. From April 2016 through June 2022, 1493 patients from 68 sites in nine European countries were randomised, against a target of 3800 patients. 1471 patients with a mean age of 79.2 years (SD, 7.8) and a median NIHSS of 12 (IQR, 8-17) were included in the intention-to-treat analysis. The main results will be presented at the Conference.
Conclusions: PRECIOUS aims to provide evidence whether prevention of complications reduces the risk of death or dependency in elderly patients with acute stroke.
Disclosure of interest: Yes
O304/3037
Early vs Late Anticoagulation in stroke patients with atrial fibrillatioN
Urs Fischer*1,2, Masatoshi Koga3, Daniel Strbian4, Mattia Branca5, Stefanie Abend1, Sven Trelle5, Maurizio Paciaroni6, Götz Thomalla7, Patrik Michel8, Krassen Nedeltchev1,9, Leo Bonati10, George Ntaios11, Thomas Gattringer12,13, Else Charlotte Sandset14,15, Peter Kelly16, Robin Lemmens17, Pn Sylaja18, Diana Aguiar de Sousa19, Natan Bornstein20, Zuzana Gdovinova21, Takeshi Yoshimoto22, Marjaana Tiainen4, Helen Thomas23, Manju Krishnan24, Gek Shim25, Christoph Gumbinger26, Jochen Vehoff27, Liqun Zhang28, Kosuke Matsuzono29, Espen Saxhaug Kristoffersen30,31, Philippe Desfontaines32, Peter Vanacker33,34,35, Angelika Alonso36, Yusuke Yakushiji37, Caterina Kulyk38, Dimitri Hemelsoet39, Sven Poli40,41, Ana Paiva Nunes42, Nicoletta Giuseppa Caracciolo43, Peter Slade24, Jelle Demeestere17, Alexander Salerno8, Markus Kneihsl12,13, Timo Kahles2,9, Daria Giudici6, Kanta Tanaka3, Silja Räty4, Rea Hidalgo23, David Werring44, Marcel Arnold1, Cecilia Ferrari1, Seraina Beyeler1, Christian Fung45, Bruno Weder46, Turgut Tatlisumak47,48, Sabine Fenzl49, Beata Rezny-Kasprzak49, Arsany Hakim49, Georgia Salanti50, Claudio Bassetti1, Jan Gralla1, David Seiffge1, Thomas Horvath1, Jesse Dawson51
1University Hospital Bern, University of Bern, Department of Neurology, Bern, Switzerland, 2University Hospital Basel, University of Basel, Department of Neurology, Basel, Switzerland, 3National Cerebral and Cardiovascular Center, Department of Cerebrovascular Medicine, Osaka, Japan, 4Helsinki University Hospital, University of Helsinki, Department of Neurology, Helsinki, Finland, 5University of Bern, CTU Bern, Bern, Switzerland, 6Santa Maria della Misericordia Hospital, University of Perugia, Internal, Vascular and Emergency Medicine – Stroke Unit, Perugia, Italy, 7University Medical Center Hamburg-Eppendorf, Department of Neurology, Hamburg, Germany, 8University Hospital Lausanne, University of Lausanne, Department of Neurology, Lausanne, Switzerland, 9Cantonal Hospital Aarau, Department of Neurology, Aarau, Switzerland, 10Reha Rheinfelden, Research Department, Rheinfelden, Switzerland, 11University of Thessaly, Faculty of Medicine, Department of Internal Medicine, Larissa, Greece, 12Medical University of Graz, Department of Neurology, Graz, Austria, 13Medical University of Graz, Department of Radiology, Division of Neuroradiology, Vascular and Interventional Radiology, Graz, Austria, 14Oslo University hospital Ullevål, Department of Neurology, Oslo, Norway, 15The Norwegian Air Ambulance Foundation, Oslo, Norway, 16Dublin Mater Misericordiae University Hospital, Department of Neurology, Dublin, Ireland, 17KU Leuven, University Hospitals Leuven, Department of Neurology, Bruxelles, Belgium, 18Sree Chitra Tirunal Institute for Medical Sciences & Technology, Department of Neurology, Thiruvananthapuram, India, 19Lisbon Central University Hospital, University of Lisbon, Stroke Center, Faculty of Medicine, Lisbon, Portugal, 20Shaare-Zedek Medical Center, Department of Neurology, Jerusalem, Israel, 21University Hospital L. Pasteur Kosice, P.J. Safarik University, Department of Neurology, Faculty of Medicine, Kosice, Slovakia, 22National Cerebral and Cardiovascular Center, Department of Neurology, Osaka, Japan, 23Betsi Cadwaladr University Local Health Board, Glan Clwyd Hospital, Rhyl, United Kingdom, 24Morriston Hospital, Stroke Unit, Swansea, United Kingdom, 25University Hospital of North Durham, Stroke Department, Durham, United Kingdom, 26Heidelberg University Hospital, Department of Neurology, Heidelberg, Germany, 27Cantonal Hospital St. Gallen, Department of Neurology, St. Gallen, Switzerland, 28St George's University Hospital, Neurology Department, London, United Kingdom, 29Jichi Medical University, Department of Medicine, Division of Neurology, Tochigi, Japan, 30Akershus University Hospital, Department of Neurology, Lørenskog, Norway, 31University of Oslo, Department of General Practice, Oslo, Norway, 32CHC MontLégia Hospital, Department of Neurology, Comprehensive Stroke Unit, Liège, Belgium, 33AZ Groeninge Kortrijk, Department of Neurology, Kortrijk, Belgium, 34Antwerp University Hospital, Neurovascular Center and Stroke Unit Antwerp, Antwerp, Belgium, 35University of Antwerp, Faculty of Medicine and Health Sciences, Antwerp, Belgium, 36Medical Faculty Mannheim, Heidelberg University, Department of Neurology, Mannheim, Germany, 37Kansai Medical University, Department of Neurology, Hirakata, Japan, 38Kepler University Hospital, Johannes Kepler University, Department of Neurology 2, Linz, Austria, 39Ghent University Hospital, Department of Neurology, Ghent, Belgium, 40Tübingen University, Department of Neurology & Stroke, Tübingen, Germany, 41Tübingen University, Hertie-Institute for Clinical Brain Research, Tübingen, Germany, 42Lisbon Central University Hospital, Stroke Unit, Lisbon, Portugal, 43University La Sapienza, Department of Human Neurosciences, Rome, Italy, 44University College London, UCL Queen Square Institute of Neurology, Stroke Research Centre, Department of Brain Repair and Rehabilitation, London, United Kingdom, 45University of Freiburg, Medical Center, Department of Neurosurgery, Freiburg, Germany, 46University Hospital Bern, Support Centre for Advanced Neuroimaging, Bern, Switzerland, 47University of Gothenburg, Department of Clinical Neuroscience, Gothenburg, Sweden, 48Sahlgrenska University Hospital, Department of Neurology, Gothenburg, Sweden, 49University Hospital Bern, Institute for Diagnostic and Interventional Neuroradiology, Bern, Switzerland, 50University of Bern, Institute of Social and Preventive Medicine, Bern, Switzerland, 51University of Glasgow, School of Cardiovascular and Metabolic Health, Glasgow, United Kingdom
Background and aims: We aimed to estimate the effect of early compared to late initiation of direct oral anticoagulants (DOACs) in people with acute ischemic stroke related to atrial fibrillation.
Methods: We performed an open-label, multicenter, randomized, two-arm, assessor-blinded trial at 103 sites in 15 countries. Out of 2013 participants, 1006 were randomly assigned to early (within 48 hours of minor/moderate, or day 6–7 following major stroke) and 1007 to late DOAC initiation (day 3–4 following minor, day 6–7 following moderate, or day 12–14 following major stroke). The primary outcome was a composite of symptomatic intracranial hemorrhage, major extracranial bleeding, recurrent ischemic stroke, systemic embolism or vascular death within 30 days. Secondary outcomes included the individual components of the primary outcome at 30 and 90 days.
Results: XXX
Conclusions: XXX
Disclosure of interest: Yes
O305/2079
PRIMARY RESULTS OF THE ATRIAL CARDIOPATHY AND ANTITHROMBOTIC DRUGS IN PREVENTION AFTER CRYPTOGENIC STROKE (ARCADIA) RANDOMIZED TRIAL
Hooman Kamel*1
1Weill Cornell Medicine, Neurology, New York, United States
Background and aims: One-fifth of ischemic strokes lack an identifiable cause. Emerging data suggest an abnormal left atrium may cause thromboembolism in the absence of clinically apparent atrial fibrillation. Some cryptogenic strokes may arise from such atrial cardiopathy, which may respond to anticoagulation given shared pathophysiology with atrial fibrillation. The ARCADIA trial compared apixaban versus aspirin for secondary stroke prevention in patients with evidence of atrial cardiopathy.
Methods: At 185 U.S. and Canadian centers, we enrolled patients with cryptogenic stroke and atrial cardiopathy, defined as P-wave terminal force >5,000 μV*ms in ECG lead V1, serum NT-proBNP >250 pg/mL, or left atrial diameter index ⩾3 cm/m2. Patients were randomly assigned apixaban 5 mg BID versus aspirin 81 mg QD in double-blind fashion. The primary outcome of recurrent stroke was assessed using the intent-to-treat principle in all randomized patients, including crossovers to anticoagulation when AF was detected after randomization.
Results: With 1,015 of the target 1,100 patients enrolled and a mean follow-up of 1.7 years, the trial was halted after a planned interim efficacy/futility analysis, with no safety concerns. Mean age was 68 years; 54% were female, 75% White, 21% Black, 8% Hispanic, 2% Asian. Mean P-wave terminal force was 4,741 μV*ms, NT-proBNP 579 pg/mL, left atrial diameter index 1.9 cm/m2; 46% of patients qualified by NT-proBNP, 38% by ECG, <1% by echocardiogram, and 16% by a combination.
Conclusions: ARCADIA is the first trial of stroke prevention in atrial cardiopathy. The main results will be ready for presentation at ESOC 2023.
Disclosure of interest: Yes
O306/2330
SECRET: Study of rivaroxaban in CeREbral venous Thrombosis
Thalia Field*1,2, Vanessa Dizonno1,2, Fouzi Bala3, Karina Villaluna2, Mohammed Almekhlafi3, Ibrahim Alhabli3, Monica Norena4, Hubert Wong4, Princess King-Azote1,2, Namali Ratnaweera1,2, Laura Wilson1,2, Stephen van Gaal1,2, Brett Graham5, Brian Buck6, Dylan Blacquiere7, Mark Boulos8, Luciano Sposato9, Kanjana Perera10, Céline Odier11, Aleksandra Pikula8, George Medvedev1, Aleksander Tkach12, Jennifer Mandzia9, Oscar Benavente1,2, Dar Dowlatshahi7, Andrew Demchuk13, Sylvain Lanthier14, Deepa Suryanarayan15, Jeffrey Weitz16, Agnes Lee17, Michael Hill13
1University of British Columbia, Neurology, Vancouver, Canada, 2Vancouver Coastal Health, Vancouver Stroke Program, Vancouver, Canada, 3University of Calgary, Neuroradiology, Calgary, Canada, 4Centre for Health Evaluation & Outcome Sciences, Statistics, Vancouver, Canada, 5University of Saskatchewan, Neurology, Vancouver, Canada, 6University of Alberta, Neurology, Edmonton, Canada, 7University of Ottawa, Neurology, Ottawa, Canada, 8University of Toronto, Neurology, Toronto, Canada, 9Western University, Neurology, London, Canada, 10McMaster University, Neurology, Hamilton, Canada, 11Centre Hospitalier Universitaire de Montreal, Neurology, Montreal, Canada, 12Kelowna General Hospital, Neurology, Kelowna, Canada, 13University of Calgary, Neurology, Calgary, Canada, 14Université de Montréal, Neurology, Montreal, Canada, 15University of Calgary, Hematology, Calgary, Canada, 16McMaster University, Hematology, Hamilton, Canada, 17University of British Columbia, Hematology, Vancouver, Canada
Background and aims: Cerebral venous thrombosis (CVT) is an uncommon cause of stroke affecting 10-20/million/year. Vitamin K antagonist (VKA) anticoagulation has been the guideline-recommended therapy. Direct oral anticoagulants (DOACs) have superior safety and comparable efficacy to VKA for peripheral venous thromboembolism (VTE) and may be a reasonable alternative therapy for CVT. In this study comparing DOAC to standard-of-care anticoagulation for CVT, individuals aged >18 with a neuroimaging-confirmed diagnosis of CVT within the last 14 days were randomized 1:1 to receive rivaroxaban 20 mg daily versus VKA or ongoing parenteral anticoagulation.
Methods: Participants received a minimum of 180 days of study medication with optional extension up to 365 days at the treating physician’s discretion. The primary feasibility outcome was recruitment of 50 patients within 12 months of final site initiation. The primary safety outcome was a composite of symptomatic intracranial hemorrhage, major extracranial hemorrhage, and death at day 180. Secondary outcomes included recurrent VTE, recanalization, functional outcome (modified Rankin Scale), cognition (Montreal Cognitive Assessment), mood (PHQ-9), fatigue (fatigue assessment score), headache (HIT-6), and quality of life (EQ-5D) at day 180 and day 365.
Results: From March 2019-October 2022, 53 participants were recruited across 12 Canadian sites, meeting the primary feasibility outcome. Median age was 48 (range 19-86); 66% were female. Baseline NIHSS score was 0 in 66% and 1-4 in 34%. Median time from symptom onset to randomization was 8 days (IQR 5-14).
Conclusions: We will present detailed demographics and outcomes at the 2023 ESOC late-breaking clinical trials session.
Disclosure of interest: Yes
O307/2021
The structured ambulatory post-stroke care program (SANO) - A cluster-randomised interventional trial to enhance outpatient aftercare for stroke patients in Germany
Christopher Schwarzbach*1, Felizitas A Eichner2, Viktoria Rücker2, Anna-Lena Hofmann2, Moritz Keller3, Heinrich Audebert4, Stefan von Bandemer5, Stefan Engelter6, Dieter Geis7, Klaus Gröschel8, Karl Georg Häusler9, Gerhard F Hamann10, Andreas Meisel4, Dirk Sander11, Martha Schutzmeier2, Roland Veltkamp12, Peter Heuschmann2, Armin J Grau1
1Klinikum der Stadt Ludwigshafen a.R., Neurology Department, Ludwigshafen am Rhein, Germany, 2Universität Würzburg, Institute for Clinical Epidemiology and Biometry, Würzburg, Germany, 3Katholisches Klinikum Koblenz – Montabauer, Department of Neurology, Koblenz, Germany, 4Charité – Universitätsmedizin Berlin, Department of Neurology with Experimental Neurology, Berlin, Germany, 5Ruhr Universität Bochum, Institute for Work and Technology, Gelsenkirchen, Germany, 6Universiätsspital Basel, Department of Neurology, Basel, Switzerland, 7Bayrischer Hausärzteverband, Honorary Chairman, München, Germany, 8Universitätsmedizin Mainz, Department of Neurology, Mainz, Germany, 9Universitätsklinikum Würzburg, Department of Neurology, Würzburg, Germany, 10Bezirkskrankenhaus Günzburg, Clinic for Neurology and Neurological Rehabilitation, Günzburg, Germany, 11Benedictus Krankenhaus Tutzing, Department of Neurology, Tutzing, Germany, 12Alfried-Krupp Krankenhaus Rüttenscheid, Department of Neurology, Essen, Germany
Background and aims: SANO aimed to reduce the frequency of recurrent vascular events and death as well as optimise control of cardiovascular risk factors (CVRFs) by a post-stroke care program.
Methods: SANO is a prospective, open-label, blinded-endpoint, parallel-armed, cluster-randomised controlled trial performed in 30 clusters in Germany (drks.de, DRKS00015322). SANO comprises a one-year behavioural, organisational and patient-centred intervention within a cross-sectoral multidisciplinary network. The primary endpoint was the composite of any recurrent stroke, myocardial infarction and death within 12 months after baseline-assessment. Control of predefined CVRFs was defined as secondary endpoint. All patients not withdrawing consent and completing the primary endpoint-assessment were included in the primary analysis (modified intention-to-treat analysis (mITT)).
Results: From Jan 2019 until Dec 2020 1,396 patients were enrolled in the intervention group (Int-Grp) and 1,395 patients in the control group (Con-Grp). 1,203 (86%) patients in the Int-Grp and 1,283 (92%) patients in the Con-Grp were included in the mITT. The primary endpoint was confirmed in 64 (5.3%) patients in the Int-Grp and 80 (6.2%) patients in the Con-Grp. The unadjusted odds ratio (OR) for the primary endpoint was 0.80 (95%-CI 0.49-1.30). After adjustment for pre-specified confounders adjOR was 0.95 (95%-CI 0.54-1.67). Mortality was lower in the Int-Grp in the unadjusted (OR 0.42, 95%-CI 0.20-0.86) but not adjusted analysis (adjOR 0.61, 95%-CI 0.26-1.46). Specific CVRFs were better controlled in the Int-Grp.
Conclusions: SANO did not lead to a reduction of vascular events in ischemic stroke patients after one year, despite positive effects in control of specific CVRFs.
Disclosure of interest: Yes
O308/2395
Ayurvedic Treatment in the Rehabilitation of Ischemic Stroke Patients in India: A Randomized Controlled Trial (RESTORE) study
1Professor and Head, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Comprehensive stroke care program, Department of Neurology, Thiruvananthapuram, India, 2Indian System of Medicine, Government Ayurveda Hospital, Ayur, Kollam, Ayur, Thiruvananthapuram, India, 3Department of Medicine, University of Alberta, Edmonton, Edmonton, Canada, 4Sree Chitra Tirunal Institute for Medical Sciences and Technology, Comprehensive stroke care program, Department of Neurology, Thiruvananthapuram, India, 5Amrita Institute of Medical Sciences, Kochi, Kochi, India, 6JIPMER, Puduchery, Puduchery, Pondicherry, India, 7Sree Chitra Tirunal Institute for Medical Sciences and Technology, Comprehensive stroke care program, Department of Neurology, Ludhiana, India, 8Christian Medical College, Vellore, Vellore, Vellore, India, 9Indian Council of Medical Research, Delhi, Delhi, India, 10Sree Chitra Tirunal Institute for Medical Sciences and Technology, Thiruvananthapuram, Thiruvananthapuram, India, 11Professor and Head, Christan Medical College, Ludhiana, Ludhiana, Ludhiana, India
Background and aims: In patients with ischemic stroke, conventional physiotherapy (CP) is the primary modality of rehabilitation. Ayurveda is an alternative system of medicine that offers unique rehabilitation for post- stroke recovery.
Hypothesis: The Ayurvedic rehabilitative treatment (ART) is superior to CP in improving the sensorimotor recovery in ischemic stroke.
Methods: AyuRvedic TrEatment in the Rehabilitation of Ischemic STrOke Patients (RESTORE) is an investigator-initiated, multi-center, prospective, randomized, controlled, parallel-arm, blinded outcome assessment trial being conducted across the four stroke centers in India. Patients with first acute ischemic stroke, between 1 to 3 months from onset were randomized (1:1) to receive either 1 month of ART or 1 month of CP.
Outcome: The primary outcome measure was Fugl Meyer Assessment-Upper extremity (FMA-UE) for physical performance at 90 days. The secondary outcomes were Barthel Index (BI), Berg Balance scale (BBS) and SF-36 at 90 days.
Results: Of 140 patients, the mean age was 54±10.62 years. At 3 months there was no significant difference in the improvement in the FMA-UE score between the ayurveda and physiotherapy group (7.53±13.24 vs 12.10±14.18; p=0.065). None of the secondary outcomes (BI, BBS and SF-36) showed statistically significant improvement between the two groups. On multiple linear regression analysis, after adjusting for age, stroke severity, risk factors and revascularization therapy, the improvement in the FMA-UE between two groups remained insignificant. There was no difference in serious adverse events between the two groups.
Conclusions: Ayurveda treatment is not superior to physiotherapy in the rehabilitation of patients with ischemic stroke.
Disclosure of interest: No
Plenary Sessions – PRESIDENTIAL SYMPOSIUM AWARDS & LARGE CLINICAL STUDIES
O309/2271
UKPDS trial: the effect of randomisation to tight or less tight blood pressure control, and to intensive or conventional blood glucose control on 44-year incidence of stroke or dementia
William Whiteley*1, Ruth Coleman2, Jose Leal3, Philip Clarke3, Amanda Adler2, Rury Holman2
1University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom, 2Diabetes Trials Unit, University of Oxford, Oxford, United Kingdom, 3Health Economics Research Centre, University of Oxford, Oxford, United Kingdom
Background and aims: Epidemiological data suggest that blood pressure (BP) or glucose lowering in mid-life reduce the incidence dementia through cerebrovascular mechanisms. We tested this hypothesis by following-up the UK Prospective Diabetes Study (UKPDS) cohort.
Methods: Between 1977–1997 participants with type 2 diabetes were randomly allocated for median 10 years to tight or less-tight blood pressure control and, in a factorial design, to intensive glucose control with sulfonylurea or insulin (or metformin if overweight) or to conventional glucose control (primarily with diet). All participants were linked to health and death records held by UK central registers, and outcomes were defined with validated ICD-10 codes. Incidence of stroke or dementia was compared between groups.
Results: 4,209 participants in England, Wales, Northern Ireland and Scotland were followed up (median 18 years, maximum 42 years).
To be presented: (1) baseline characteristics (2) effect on incidence of stroke or dementia of randomisation to: tight or less-tight blood pressure control; intensive or conventional blood glucose control.
Conclusions: UKPDS is one of the few long-term randomised assessments of more intensive BP and glucose control on dementia incidence. Whether neutral, positive, or negative, the results will be a major contribution to our understanding of improved BP and glucose control on dementia in people with type 2 diabetes.
Disclosure of interest: No
O310/3138
VERY EARLY MINIMALLY INVASIVE REMOVAL OF INTRACEREBRAL HEMORRHAGE: THE ENRICH TRIAL
Gustavo Pradilla1, Jonathan Ratcliff2, Alex Hall*2, Benjamin Saville3, Jason Allen4, Michael Frankel5, David Wright2, Daniel Barrow1
1Emory University, Neurosurgery, Atlanta, United States, 2Emory University, Emergency Medicine, Atlanta, United States, 3Berry Consultants, Biostatistics, Austin, United States, 4Emory University, Radiology and Imaging Sciences, Atlanta, United States, 5Emory University, Neurology, Atlanta, United States
Background and aims: Spontaneous supratentorial ICH is common and causes significant morbidity and mortality. Previous RCTs of clot evacuation have not shown definitive benefit. The study aims to determine if a Minimally Invasive trans-sulcal, Parafascicular Surgical (MIPS) ICH clot evacuation improves functional outcome at 180 days compared to MM.
Methods: The ENRICH Trial evaluated the MIPS approach using the BrainPath® and Myriad® devices. This was a two-arm, randomized, Bayesian adaptive comparative-effectiveness study. Patients with ICH, within 24 hours from LKN, were block randomized to MIPS or medical management (MM) by ICH location (anterior basal ganglia [ABG] vs lobar) and GCS. The enrollment scheme (ICH location) could be adapted at pre-specified accrual increments.
Results: Eligible patients were enrolled at 37 US centers over 6 years. Data collection ended February 2023. After 175 subjects were enrolled, the study was adapted and the ABG location was halted. 300 participants were randomized: 92 (30.7%) ABG and 208 (69.3%) lobar. Follow-up was completed in 286 participants (95.3%). Per final DSMB report (n=300) no meaningful baseline differences for age, ICH volume, GCS, NIHSS, or safety were observed between groups. Combined mortality was 21.7% (23.3% MM, 20% MIPS). The database was locked March 22, 2023. Pre-specified analyses are in progress and expected to be complete prior to ESOC 2023.
Conclusions: Currently, no RCT of ICH clot evacuation has demonstrated functional benefit. The ENRICH Trial seeks to determine if MIPS ICH evacuation improves functional outcomes. The ENRICH findings will have implications on care for patients with ICH.
Disclosure of interest: No
O311/1048
THE THIRD INTENSIVE CARE BUNDLE WITH BLOOD PRESSURE REDUCTION IN ACUTE CEREBRAL HAEMORRHAGE TRIAL (INTERACT3): AN INTERNATIONAL STEPPED-WEDGE CLUSTER-RANDOMISED CONTROLLED TRIAL
1The George Institute for Global Health, Global Brain Health, Sydney, Australia, 2The George Institute China, Stroke program, Shanghai, China, 3West China Hospital, Neurosurgery, Chengdu, China
Background and aims: To determine effectiveness of a goal-directed care bundle for early physiological control and anticoagulation reversal in acute intracerebral haemorrhage (ICH).
Methods: Pragmatic, international, multicentre, blinded-endpoint, stepped-wedge (4 phases / 3 steps) cluster-randomised controlled trial (Clinicaltrial.gov NCT03209258) at 121 hospitals in 10 countries during 2017-2022. Adults with ICH (<6 hrs) had central follow-up as hospitals were randomly allocated to progressively cross from ‘usual care’ to implementing a ‘care bundle’ of intensive BP lowering (systolic <140mmHg), glucose control (6.1-7.8mmol/L and 7.8-10.0mmol/L without/with diabetes mellitus) antipyrexia treatment (body temperature ⩽37.5 °C), and anticoagulation reversal (INR <1.5). A sample of 8360 patients from 110 hospitals was estimated to provide 90% power (α 0.05) to detect a 5.6% absolute improvement in the primary outcome (physical function) at 6-months, assessed by shift in mRS scores, according to ITT, and using ordinal logistic regression.
Results: Of 7,036 randomised patients, primary outcome data were available in 6,255 (89%): 3,815 (control) and 3,221 (intervention). Baseline characteristics (mean age 62 yr, male 64%), severity (median NIHSS score 13 [7-22]) and haematoma volume (median 15 [8-30]) were well balanced between groups. The main results will be presented
Conclusions: We provide a reliable assessment of whether a widely applicable protocol improves outcome from ICH
Funding: Joint Global Health Trials funding from the Department of Health and Social Care, the Foreign, Commonwealth & Development Office, the Medical Research Council and Wellcome; the National Health and Medical Research Council of Australia; West China Hospital; Sichuan Credit Pharmaceutic, and Takeda China.
Disclosure of interest: No
O312/658
Prevention of Cerebral Ischaemia in Stent Treatment for Carotid Artery Stenosis - A randomised multi-centre phase II trial comparing Ticagrelor versus Clopidogrel with outcome assessment on MRI (PRECISE-MRI)
Leo Bonati*1,2, Marco Duering3, Gert Jan De Borst4, Trevor Cleveland5, Philippe Lyrer1, Marie-Luise Mono6, Krassen Nedeltchev7, Marcel Arnold8, Pasquale Mordasini9, Isabelle Van Herzeele10, Philip Lerut11, Enrico Cagliari12, Andrea Pacchioni13, Bernd Eckert14, Olav Jansen15, Peter Arthur Ringleb16
1University Hospital Basel, Department of Neurology, Basel, Switzerland, 2Reha Rheinfelden, Department of Research, Rheinfelden, Switzerland, 3University Hospital Basel, Medical Image Analysis Center, Basel, Switzerland, 4University Medical Center Utrecht, Department of Vascular Surgery, Utrecht, Netherlands, 5The Northern General Hospital, Sheffield Vascular Institute, Sheffield, United Kingdom, 6Triemli Hospital Zürich, Neurology, Zürich, Switzerland, 7Kantonsspital Aarau, Department of Neurology, Aarau, Switzerland, 8University Hospital Inselspital Bern, Department of Neurology, Berne, Switzerland, 9University Hospital Inselspital Bern, Institute of Diagnostic and Interventional Neuroradiology, Berne, Switzerland, 10UZ Gent, Department of Vascular Surgery, Gent, Belgium, 11AZ Groeninge, Department of Neuroradiology, Groeninge, Belgium, 12Ospedale dell'Angelo, UOC Neuroradiologia, Mestre, Italy, 13Ospedale Civile di Mirano, Divisione di Cardiologia, Mirano, Italy, 14Asklepios Klinik Altona, Department of Neuroradiology, Hamburg, Germany, 15UKSH Campus Kiel, Department of Neuroradiology, Kiel, Germany, 16Universitätsklinikum Heidelberg, Neurologische Klinik, Heidelberg, Germany
Background and aims: Carotid artery stenting (CAS) is an alternative to surgery for treatment of atherosclerotic carotid stenosis. Dual antiplatelet therapy with clopidogrel and aspirin is given to prevent embolic brain infarcts during the procedure. Ticagrelor, a reversible inhibitor of the platelet adenosine diphosphate receptor P2Y12, was superior to clopidogrel, as add-on therapy to aspirin, in preventing stent thrombosis, cardiovascular outcome events, and death in patients undergoing coronary artery stenting. The aim of the present study was to investigate if antiplatelet therapy consisting of ticagrelor plus aspirin is superior to clopidogrel plus aspirin in preventing ischaemic brain lesions occurring during CAS.
Methods: Randomised, active-control, open, parallel-group, international, multicentre phase II trial with blinded outcome assessment on serial MRI. Patients with symptomatic or asymptomatic atherosclerotic carotid stenosis (⩾50% narrowing of the lumen) undergoing CAS were eligible to participate. The primary efficacy outcome is the presence of at least one new ischaemic brain lesion on the second MRI scan done 1-3 days after CAS or on the third MRI scan done 28-32 days after CAS, which had not been present on the first MRI scan done 1-3 days before CAS. The primary clinical safety outcome was the composite of stroke, myocardial infarction, major bleeding, or cardiovascular death occurring at any time during the study. Enrolment of 370 patients was planned.
Results: The trial was stopped after 210 patients had been randomised due to slow recruitment and lack of further funding.
Conclusions: Full trial results will be presented at the conference.
Disclosure of interest: Yes
O313/2283
Immediate revascularisation versus optimised medical therapy alone in patients with carotid stenosis at low to intermediate risk of stroke: interim results of ECST-2
Paul Nederkoorn*1, Simone Donners2, Twan van Velzen1, Amanda Cheng3, John Gregson4, Gert Jan De Borst2, John M Bamford5, Philippe Lyrer6, Martin Brown3, Leo Bonati6
1Amsterdam UMC, location AMC, Neurology, Amsterdam, Netherlands, 2UMC Utrecht, Department of Vascular Surgery, Utrecht, Netherlands, 3Stroke Research Centre, Institute of Neurology, University College London, Department of Brain Repair and Rehabilitation, London, United Kingdom, 4London School of Hygiene and Tropical Medicine, Department of Medical Statistics, London, United Kingdom, 5Leeds Teaching Hospitals NHS Trust, University of Leeds, Department of Neurology, Leeds, United Kingdom, 6University Hospital Basel, University of Basel, Department of Neurology, Basel, Switzerland
Background and aims: Carotid endarterectomy is currently recommended for patients with recently symptomatic carotid stenosis ⩾50%, based on randomised trials started > 30 years ago. Several factors such as carotid plaque ulceration, age and associated comorbidities might influence the risk-benefit ratio of carotid revascularisation. A model based on these features developed in previous trials that calculates the future risk of ipsilateral stroke when treated with medical therapy alone can be used to stratify patients into low, intermediate or high risk. Since the original trials, medical treatment has improved significantly. Our hypothesis is that patients with carotid stenosis ⩾50% at low to intermediate risk of stroke will not benefit from additional carotid revascularisation when treated with optimised medical therapy (OMT).
Methods: The 2nd European Carotid Surgery Trial (ECST-2) was designed as a multicentre, prospective, randomised, controlled, open, multi-centre, non-inferiority clinical trial with blinded outcome adjudication. Patients were randomised between immediate revascularisation plus OMT versus OMT alone. Suitable patients were those with asymptomatic or symptomatic carotid stenosis ⩾50% with an estimated 5-year risk of stroke of <20%, calculated using the Carotid Artery Risk score. This initial analysis includes outcome events occurring during the first 2 years of follow-up. The primary outcome measure is the combined 2-year rate of any stroke, myocardial infarction or periprocedural death.
Results: On November 1th 2019 recruitment was stopped after inclusion of 428 patients.
Conclusions: Analysis of two-year follow up will be presented at ESOC 2023.
EFFECTS OF AMLODIPINE AND OTHER BLOOD PRESSURE LOWERING AGENTS ON MICROVASCULAR FUNCTION IN SMALL VESSEL DISEASES (TREAT-SVDs): MAIN TRIAL RESULTS
Anna Kopczak*1, Michael Stringer2, Hilde van den Brink3, Danielle Kerkhofs4, Gordon Blair2, Maud van Dinther4, Carmen Arteaga Reyes2, Daniela Jaime Garcia2, Laurien Onkenhout3, Karolina Wartolowska5, Michael Thrippleton2, Marco Düring6, Julie Staals4, Martin Middeke7, Elisabeth André8, Bo G. Norrving9, Marie-Germaine Bousser10, Ulrich Mansmann11, Peter Rothwell5, Fergus Doubal2, Robert van Oostenbrugge4, Geert Jan Biessels3, Alastair Webb5, Joanna Wardlaw2, Martin Dichgans1
1Institute for Stroke and Dementia Research, University Hospital, LMU Munich, Munich, Germany, 2Centre for Clinical Brain Sciences, University of Edinburgh, Edinburgh, United Kingdom, 3Department of Neurology, UMC Utrecht Brain Center, University Medical Center Utrecht, Utrecht, Netherlands, 4Department of Neurology and School for cardiovascular diseases (CARIM), Maastricht University Medical Center+, Maastricht, Netherlands, 5Wolfson Centre for Prevention of Stroke and Dementia, Nuffield Department of Clinical Neurosciences, University of Oxford, Oxford, United Kingdom, 6Medical Image Analysis Center (MIAC AG) and Department of Biomedical Engineering, University of Basel, Basel, Switzerland, 7Hypertoniezentrum München, Excellence Centre of the European Society of Hypertension (ESH), Munich, Germany, 8Münchner Studienzentrum, Faculty of Medicine, Technical University Munich (TUM), Munich, Germany, 9Neurology, Department of Clinical Sciences Lund, Lund University, Lund, Sweden, 10Hôpital Lariboisière, APHP, Université Paris-Cité, Paris, France, 11Institute for Medical Information Processing, Biometry, and Epidemiology, LMU Munich, Munich, Germany
Background and aims: Hypertension is the leading modifiable risk factor for cerebral small vessel diseases (SVDs). Whether antihypertensive drug classes differentially affect cerebral microvascular function is unknown. We addressed this question in patients with symptomatic SVDs.
Methods: TREAT-SVDs (NCT03082014, EU-Horizon2020-funded) was conducted as an investigator-led, multicentre, randomised, open-label, three-period-crossover phase-3 trial with blinded endpoint assessment (PROBE). Eligible participants had symptomatic sporadic SVD (group A) or CADASIL (group B), and an indication for antihypertensive treatment. Participants were randomly assigned (1:1:1) to one of three sequences of antihypertensive treatment: a two-week washout period followed by three four-week periods of amlodipine, losartan, or atenolol. The primary endpoint was change in cerebrovascular reactivity (ΔCVR) between treatment and no treatment as determined by hypercapnic challenge on MRI at the end of each period. Secondary endpoints were change in mean systolic BP and BPv.
Results: 101 participants (75 sporadic, 64.9±9.9years; 26 CADASIL patients, 53.1±7.0years) were included between 02/2018 and 04/2022. ΔCVR was larger with amlodipine (15.7±27.5x10-4%/mmHg; p=0.019; primary study hypothesis) and losartan (19.4±27.9x10-4%/mmHg; p=0.006; secondary study hypothesis) than with atenolol (-23.9±27.5x10-4%/mmHg) in CADASIL patients, but not in the overall group of sporadic patients (Figure). All drugs lowered BP to a similar extent. BPv decreased with amlodipine and increased with atenolol in sporadic patients (poverall<0.001), with a similar pattern in CADASIL patients (poverall=0.108).
Conclusions: CVR was differentially affected by BP lowering agents in CADASIL but not in the overall group of sporadic patients. The results emphasize differential effects of BP lowering classes on microvascular function in SVD.
Disclosure of interest: No
Plenary Sessions – CLOSING CEREMONY & LARGE CLINICAL TRIALS 2
O315/3106
THROMBECTOMY FOR EMERGENT SALVAGE OF LARGE ANTERIOR CIRCULATION ISCHEMIC STORKE PRESENTED BY OSAMA ZAIDAT, MD AND ALBERT YOO, MD
Albert Yoo*1, Osama Zaidat2, Sami Al Kasab3, Sunil Sheth4, Ansaar Rai5, Santiago Ortega-Gutierrez6, Curtis Given7, Syed Zaidi8, Ramesh Grandhi9, Hugo Cuellar10, Maxim Mokin11, Jeffrey M. Katz12, Amer Alshekhlee13, Muhammad Taqi14, Sameer Ansari15, Nobl Barazangi16, Adnan Siddiqui17, Alberto Maud18, Jawad Kirmani19, Rishi Gupta20, Dileep Yavagal21, Jason Tarpley22, Dhruvil Pandya23, Marshall Cress24, Sushrut Dharmadhikari25, Kaiz Asif26, Tareq Kass-Hout27, Ajit S. Puri28, Nazil Janjua29, Aniel Majjhoo30, Aamir Badruddin31, Randall Edgell32, Rakesh Khatri33, Larry Morgan34, Anmar Razak35, Alicia Zha36, Priyank Khandelwal37, Nils Mueller-Kronast38, Dennis Rivet39, Thomas Wolfe40, Brian Snelling41, Ali Sultan Quarraie42, Shao-Pow Lin43, Rajkamal Khangura44, Alejandro Spiotta3, Jazba Soomro1, Sergio Salazar-Marioni4, Eugene Lin2, Abdul Tarabishy5, Edgar Samaniego6, Murali Kolikonda7, Mouhammad Jumaa8, Vivek Reddy9, Pankaj Sharma10, Kristine Below2, Hannah Slight2, Tanner Gray2, Mary Patterson2, Charles Majoie45, Ludo F.M. Beenen45, Bart Emmer45, Wim Van Zwam46, Adriaan van Es47, Pieter Jan Van Doormaal48, Olvert Berkhemer45, Ashutosh Jadhav49, Lucas Elijovich50, Daryl Gress51, Diederik Dippel52, Scott Brown53, Thanh N. Nguyen54, Wade Smith55
1Texas Stroke Institute, Department of Neurointervention, Dallas, United States, 2Mercy Health — St. Vincent Medical Center, Neuroscience Institute, Toledo, United States, 3Medical University of South Carolina, Department of Neurology and Neurosurgery, Charleston, United States, 4UTHealth Houston (The University of Texas Health Science Center at Houston), Department of Neurology, Houston, United States, 5Rockefeller Neuroscience Institute, Department of Neuroradiology, Morgantown, United States, 6The University of Iowa, Department of Neurology, Neurosurgery and Radiology, Iowa City, United States, 7Baptist Health Lexington, Department of Neuroradiology, Lexington, United States, 8ProMedica Toledo Hospital, Neurosciences Center, Toledo, United States, 9University of Utah, Department of Neurology, Salt Lake City, United States, 10LSU Health Shreveport, Department of Radiology, Shreveport, United States, 11University of South Florida, Department of Neurosurgery and Brain Repair, Tampa, United States, 12Northwell Health - Donald and Barbara Zucker School of Medicine, Department of Neurology, Manhasset, United States, 13SSM-DePaul Hospital, Neurosciences Institute, Bridgeton, United States, 14Lost Robles and West Hills Hospitals and Medical Centers, Department of Neurology, Thousand Oaks, United States, 15Northwestern University, Departments of Radiology, Neurology, and Neurlogical Surgery, Chicago, United States, 16Central Pacific Medical Center, Department of Neurology & Neurointervention, San Francisco, United States, 17University at Buffalo, Department of Neurosurgery, Buffalo, United States, 18Texas Tech University - El Paso, Department of Neurology, El Paso, United States, 19JFK New Jersey Neuroscience Institute, Stroke and Neuroendovascular Center, Edison, United States, 20Wellstar Medical Group, Department of Neurosurgery, Marietta, United States, 21University of Miami/Jackson Memorial Hospital, Department of Neurology, Miami, United States, 22Providence Little Company of Mary Medical Center - Torrance, Department of Neurointerventional Surgery, Torrance, United States, 23Northwestern Central Dupage Hospital, Department of Neurointerventional Radiology, Winfield, United States, 24Orlando Health Medical Group, Neurosurgery, Orlando, United States, 25Baptist Health Medical Center, Stroke and Neuroendovascular Surgery, Little Rock, United States, 26Ascension Health and University of Illinois Chicago, Neuroendovascular Surgery, Lisle, United States, 27University of Chicago, Neurology, Chicago, United States, 28University of Massachusetts Memorial Center, Radiology, Neurosurgery and Neurology, Worcester, United States, 29Pomona Valley Hospital Medical Center, Interventional Neurology, Pomona, United States, 30McLaren Health System, Department of Vascular and Interventional Neurology, Macomb, United States, 31Community Care Network Inc., Neurology, Munster, United States, 32St. Louis University School of Medicine, Neurology, St. Louis, United States, 33Lutheran Medical Group, Department of Neurology, Ft. Wayne, United States, 34Bronson Neuroscience Center, Neurology, Kalamazoo, United States, 35Michigan State University, Department of Neurology, East Lansing, United States, 36The Ohio State University Wexner Medical Center, Department of Neurology, Columbus, United States, 37University Hospital Newark, Neurological Surgery and Neurology, Newark, United States, 38Tenet South Florida, Neurology, Delray, United States, 39Virginia Commonwealth University, Department of Neurosurgery, Richmond, United States, 40Aurora St Luke's Medical Center, Department of Neurology, Milwaukee, United States, 41Marcus Neuroscience Intitute, Department of Neurological Surgery, Boca Raton, United States, 42UW Medicine Valley Medical Center, Neurointervention and Neurocritical Care, Renton, United States, 43PIH Health Whittier Hospital, Department of Neurology, Whittier, United States, 44Sutter Institute for Medical Research: Sutter Medical Center, Sacramento, Department of Neurointerventional Radiology, Sacramento, United States, 45Amsterdam University Medical Center, Department of Radiology and Nuclear Medicine, Amsterdam, Netherlands, 46Maastricht University Medical Center, Department of Radiology and Nuclear Medicine, Maastricht, Netherlands, 47Leiden University Medical Center, Department of Radiology, Leiden, Netherlands, 48University Medical Center Rotterdam, Department of Radiology and Nuclear Medicine, Rotterdam, Netherlands, 49Barrow Neurological Institute, Neurosurgery, Phoenix, United States, 50University of Tennessee - Semmes-Murphy Neurologic and Spine Institute, Neurology, Memphis, United States, 51Nebraska Medical Center, Neurology, Omaha, United States, 52Erasmusc University Medical Center, Neurology, Randstad, Netherlands, 53Altair Biostatistics, Biostatistics, St. Louis Park, United States, 54Boston Medical Center, Neurology, Boston, United States, 55University of California San Francisco, Neurovascular, San Francisco, United States
Background and aims: Recent large core randomized clinical trials (RCTs) of intra-arterial therapy (IAT) utilized advanced imaging for patient selection. Currently, there are no large core infarct RCTs comparing MT to standard medical therapy in the population selected based solely on non-contrast computed tomography (NCCT). The aim of the Thrombectomy for Emergent Salvage of Large Anterior Circulation Ischemic Stroke (TESLA) clinical trial is to demonstrate the efficacy (3 months and one year disability post-stroke) and safety of IAT in patients with large volume infarctions assessed on NCCT.
Methods: TESLA is a prospective, multi-center, assessor-blinded RCT with adaptive enrichment design, enrolling up to 300 patients. Anterior circulation ELVO patients with large core infarction based on NCCT Alberta Stroke Program Early CT Score (ASPECTS 2–5) and meeting trial entry criteria are randomized in a 1:1 ratio to undergo IAT plus best medical management (BMM) or BMM alone up to 24 hours from last known well.
Results: The primary endpoint is the difference in the distribution of 90-day utility-weighted mRS scores between the IAT plus BMM and BMM arms. The primary analysis will be based on the intention-to-treat principle and will be based on the Bayesian posterior probability that, adjusted for ASPECTS score, large-core patients with IAT have higher expected utility-weighted mRS than large-core patients with BMM alone. The primary safety outcome is 90-day mortality rate.
Conclusions: Enrollment into the TESLA trial was completed October 17, 2022. Primary efficacy and safety results will be presented at the ESOC meeting in May 2023.
Disclosure of interest: No
O316/3127
MechAnical thrombectomy for larGe braiN infArctions (MAGNA) – An Individual Patient-level Data (IPD) Meta-analysis of SELECT2, RESCUE Japan LIMIT and ANGEL ASPECT Trials
Amrou Sarraj*1,2, Shinichi Yoshimura3, Xiaochuan Huo4, Nobuyuki Sakai5, Zongen Gao6, Ameer Hassan7, Na Xu8, Michael Chen9, Hiroshi Yamagami10, Yaxuan Sun11, Takeshi Morimoro12, Michael Abraham13, Santiago Ortega-Gutierrez14, Kazutaka Uchida15, Dongsheng Ju16, Seigo Shindo17, M Shazam Hussain18, Cunfeng Song19, Jinggang Xuan20, Vitor Mendes Pereira21, Manabu Inoue22, Deep Pujara2, Masataka Takeuchi23, Feng Zhou24, Qing Shi25, Leonid Churilov26, Manabu Sihrakawa15, Yukako Yazawa27, Dapeng Sun28, Scott Kasner29, Naoto Kimura30, Yue-Song Pan31, Marc Ribo32, Keigo Shigeta33, Bruce Campbell34, Zhongrong Miao28
1Case Western Reserve University, Neurology, Cleveland, United States, 2University Hospitals Cleveland Medical Center, Neurology, Cleveland, United States, 3Hyogo Medical University, Department of Neurosurgery, Nishinomiya, Japan, 4Beijing Tiantan Hospital, Capital Medical University, Interventional Neuroradiology, Department of Neurology, Beijing, China, 5Kobe City Medical Center General Hospital, Department of Neurosurgery, Kobe, Japan, 6Shengli Oilfield Central Hospital, Department of Neurology, Dongying, China, 7Valley Baptist Medical Center, Interventional Neurology, Harlingen, United States, 8The Second Affiliated Hospital to Xiamen Medical College, Neurology, Xiamen, China, 9Rush University Medical Center, Interventional Neurology, Chicago, United States, 10NHO Osaka National Hospital, Neurology, Osaka, Japan, 11Shanxi People Hosp-Neurology Dept 3, Neurology, 内, China, 12Hyogo Medical University, Clinical Epidemiology, Nishinomiya, Japan, 13The University Of Kansas Medical Center, Interventional Neurology, Kansas City, United States, 14University of Iowa Hospitals & Clinics, Interventional Neurology, Iowa City, United States, 15Hyogo Medical University, Neurosurgery, Nishinomiya, Japan, 16Songyuan Jilin oil Field Hospital, Neurology, Songyuan, China, 17Japanese Red Cross Kumamoto Hospital, Neurology, Kumamoto, Japan, 18Cleveland Clinic, Cerebrovascular Diseases, Cleveland, United States, 19Liao Cheng the Third People's Hospital, Interventional Neuroradiology, Liaocheng, China, 20Changzhou 1st People's Hospital, Neurology, Tang Shan Shi, China, 21St. Michael's Hospital, Radiology, Toronto, Canada, 22National Cerebral and Cardiovascular, Cerebrovascular Medicine, Suita, Japan, 23Seisho Hospital, Neurosurgery, Odawara, Japan, 24Taiyuan Central Hospital, Neurology, Taiyuan, China, 25Affiliated Jiangmen Traditional Chinese Medicine Hospital of Ji’nan University, Neurology, Jiangmen, China, 26The Royal Melbourne Hospital, Medicine, Parkville, Australia, 27Kohnan Hospital, Neurology, Sendai, Japan, 28Beijing Tiantan Hospital, Interventional Neuroradiology, Beijing, China, 29Hospital of the University of Pennsylvania, Neurology, Philadelphia, United States, 30Iwate Prefectural Central Hospital, Neurosurgery, Morioka, Japan, 31China National Clinical Research Center for Neurological Diseases, Neurology, Beijing, China, 32Vall d'Hebron University Hospital, Interventional Neurology, Barcelona, Spain, 33National Disaster Medical Center, Neurosurgery, Tachikawa, Japan, 34The Royal Melbourne Hospital, Neurology, Parkville, Australia
Background and aims: Endovascular thrombectomy (EVT) efficacy and safety in patients with large ischemic stroke was recently demonstrated in multiple randomized clinical trials. However, no pooled, patient-level meta-analysis has been performed from these trials to date.
Methods: We performed an individual patient-level meta-analysis of randomized controlled trials to explore the evidence for efficacy and safety of EVT in patients with large ischemic core up to 24 hours of last known well in key clinical and imaging subgroups. A systematic search of PubMed and EMBASE was executed on 3/15/2023 to identify all eligible randomized clinical trials that randomized patients with anterior circulation large vessel occlusion (ICA/MCA) and a large ischemic core on non-contrast CT/MRI (ASPECTS 5 or less) and/or CT/MR perfusion/diffusion imaging (ischemic core⩾50 ml) to receive EVT vs medical care only and were published after 3/2018. All identified clinical trials were invited to contribute patient data for a pooled, individual patient-level meta-analysis. The primary efficacy outcome was the distribution of modified Rankin Scale score at 90-day follow-up. Key secondary outcomes included functional independence (mRS 0-2), independent ambulation (mRS 0-3), symptomatic ICH (SITS-MOST definition) and mortality. Additionally, analysis of primary and key secondary outcomes was repeated in pre-specified subgroups based on selected clinical and imaging characteristics.
Results: Three clinical trials (SELECT2, RESCUE Japan LIMIT and ANGEL ASPECT) met inclusion criteria and were included in this meta-analysis. The results will be available for presentation at the European Stroke Organisation Conference.
1University Hospital Nantes, Department of Neuroradiology, nantes, France, 2University Hospital Bordeaux, Department of Neuroradiology, Bordeaux, France, 3University Hospital Nancy, Department of Neuroradiology, Nancy, France, 4Foch Hospital, Department of Neuroradiology, Versailles, France, 5University Hospital of Montpellier, Department of Neuroradiology, Montpellier, France, 6University Hospital of Rennes, Department of Neuroradiology, rennes, France, 7Ste Anne Hospital, Department of Neuroradiology, Paris, France, 8La Pitie-Salpetrière Hospital, Paris, France, Department of Neuroradiology, Paris, France, 9Foch Hospital, Department of Neurology, Versailles, France, 10Fondation Rothschild, Department of Neuroradiology, Paris, France, 11University Hospital of Lyon, Department of Neuroradiology, Lyon, France, 12Regional Hospital of Bayonne, Department of Neurology, BAyonne, France, 13Department of Biostatistics, Department of Biostatistics, Lille, France, 14University Hospital Marseille, Department of Neuroradiology, Marseille, France, 15University Hospital Strasbourg, Department of Neuroradiology, Strasbourg, France, 16University Hospital of Limoges, Department of Neuroradiology, Limoges, France
Background and aims: A correlation between the susceptibility vessel sign (SVS) and red thrombi has been identified in MRI. We hypothesized that the use of stent retriever (SR) allow better recanalization of SVS+ occlusions. The AdaptatiVe Endovascular strategy to the CloT MRI in large intracranial vessel Occlusion (VECTOR) trial is a multicenter, prospective and randomized study designed to compare a first-line strategy combining SR added to contact aspiration (CA) versus CA alone in patients with SVS+ occlusions.
Methods: The primary objective is to show the superiority of first-line combined SR and CA strategy compared to first-line CA alone strategy to increase the near to complete reperfusion (eTICI 2c/3) after ⩽ 3 passes in patients with acute ischemic stroke from anterior circulation and SVS+ intracranial occlusion on MRI (external core lab). Occlusions involving the termination of the internal carotid artery (ICA), the first (M1) or the horizontal second segment of the middle cerebral artery (M2) and a clear SVS facing the occlusion were randomized allocation of treatment options. Patients could be treated previously with intravenous thrombolysis. To ensure a centralized real-time randomization procedure, a web-based randomization will be performed using the electronic case-report form (eCRF) system. Minimization criteria will be the following: neuroradiology center, age (⩽ 80 versus > 80 years), prior use of IV thrombolysis and occlusion site (isolated middle cerebral artery versus middle cerebral artery/internal carotid artery).
263 patients per arm (a total of 526) have been included.
Results:
Conclusions:
Disclosure of interest: No
O318/3079
EFFECT OF INTENSIVE VS CONVENTIONAL BLOOD PRESSURE LOWERING AFTER SUCCESSFUL INTRA-ARTERIAL THROMBECTOMY IN ACUTE ISCHEMIC STROKE: THE OPTIMAL-BP RANDOMIZED CLINICAL TRIAL
Hyo Suk Nam*1, Young Dae Kim1, Joonnyung Heo1, Hyungwoo Lee1, Jaewook Jung1, Jin Kyo Choi1, Il Hyung Lee1, In Hwan Lim1, Soon-Ho Hong1, Minyoul Baik1, Byung Moon Kim2, Dong Joon Kim2, Na-Young Shin2, Bang-Hoon Cho3, Seong Hwan Ahn4, Hyungjong Park5, Sungil Sohn5, Jeong-Ho Hong5, Tae-Jin Song6, Yoonkyung Chang7, Gyu Sik Kim8, Kwon-Duk Seo8, Kijeong Lee8, Jun Young Chang9, Jung Hwa Seo10, Sukyoon Lee10, Jang-Hyun Baek11, Han-Jin Cho12, Dong Hoon Shin13, Jinkwon Kim14, Joonsang Yoo14, Kyung-Yul Lee15, Yo Han Jung15, Yang-Ha Hwang16, Chi Kyung Kim17, Jae Guk Kim18, Chan Joo Lee19, Sungha Park20, Hye Sun Lee21, Sun U Kwon9, Oh Young Bang22, Craig Anderson23, Ji Hoe Heo1
1Yonsei University College of Medicine, Department of Neurology, Seoul, South Korea, 2Yonsei University College of Medicine, Department of Radiology, Seoul, South Korea, 3Korea University Anam Hospital and College of Medicine, Department of Neurology, Seoul, South Korea, 4Chosun University School of Medicine, Department of Neurology, Gwangju, South Korea, 5Brain Research Institute, Keimyung University School of Medicine, Department of Neurology, Daegu, South Korea, 6Seoul Hospital, Ewha Woman’s University, College of Medicine, Department of Neurology, Seoul, South Korea, 7Mokdong Hospital, Ewha Womans University College of Medicine, Department of Neurology, Seoul, South Korea, 8National Health Insurance Service Ilsan Hospital, Department of Neurology, Goyang, South Korea, 9Asan Medical Center, University of Ulsan College of Medicine, Department of Neurology, Seoul, South Korea, 10Busan Paik Hospital, Inje University College of Medicine, Department of Neurology, Busan, South Korea, 11Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Department of Neurology, Seoul, South Korea, 12Pusan National University School of Medicine, Department of Neurology, Busan, South Korea, 13Gachon University Gil Medical Center, Department of Neurology, Incheon, South Korea, 14Yongin Severance Hospital, Yonsei University College of Medicine, Department of Neurology, Yongin, South Korea, 15Gangnam Severance Hospital, Yonsei University College of Medicine, Department of Neurology, Seoul, South Korea, 16Kyungpook National University Hospital, School of Medicine, Kyungpook National University, Department of Neurology, Daegu, South Korea, 17Korea University Guro Hospital and College of Medicine, Department of Neurology, Seoul, South Korea, 18Daejeon Eulji Medical Center, Eulji University School of Medicine, Department of Neurology, Daejeon, South Korea, 19Yonsei University College of Medicine, Division of Cardiology, Department of Internal Medicine, Seoul, South Korea, 20Integrative Research Center for Cerebrovascular and Cardiovascular Diseases, Yonsei University College of Medicine, Division of Cardiology, Seoul, South Korea, 21Biostatistics Collaboration Unit, Yonsei University College of Medicine, Department of Research Affairs, Seoul, South Korea, 22Samsung Medical Center, Sungkyunkwan University School of Medicine, Department of Neurology, Seoul, South Korea, 23University of New South Wales, The George Institute for Global Health, Sydney, Australia
Background and aims: The optimal level of blood pressure (BP) control after successful recanalisation with intra-arterial thrombectomy (IAT) in acute ischaemic stroke is unclear. We investigated whether intensive BP management during the first 24 hours after successful recanalisation leads to better clinical outcomes compared to conventional BP management for patients with large cerebral artery occlusion.
Methods: This multicentre, randomised, open-label, blinded end point evaluation trial included patients with acute ischaemic stroke who were treated with IAT due to large vessel occlusion and who achieved successful recanalisation (a modified Treatment In Cerebral Infarction score of ⩾2b) and elevated systolic BP ⩾140 mmHg within 2 hours of successful recanalisation. Participants received intensive BP management (targeting systolic BP <140 mmHg) or conventional management (targeting systolic BP between 140-180 mmHg) for 24 h after enrolment. The primary outcome was functional independence at 3 months (a modified Rankin Scale score <3).
Results: Of 305 patients included in the primary analysis, mean age was 73.1 ± 11.5 years, and 123 (40.3%) were women. The intensive treatment group had a lower proportion of patients achieving a favourable outcome (39.4%) compared to the conventional group (54.4%) (an adjusted odds ratio of 0.56 [95% CI 0.33 - 0.96], P = 0.034). Symptomatic intracerebral haemorrhage (P = 0.816) and death related to the index stroke (P = 0.307) were similar.
Conclusions: Intensive blood pressure lowering during the first 24 hours after successful recanalisation may be harmful in acute ischaemic stroke patients who have undergone intra-arterial thrombectomy.
Disclosure of interest: No
O319/803
EFFECT OF INDIVIDUALIZED VERSUS STANDARD BLOOD PRESSURE MANAGEMENT DURING ENDOVASCULAR STROKE TREATMENT UNDER PROCEDURAL SEDATION (INDIVIDUATE) ON CLINICAL OUTCOME - A Randomized Clinical Trial
Min Chen1, Jan Meis2, Arne Potreck3, Lukas Sauer2, Meinhard Kieser2, Martin Bendszus3, Wolfgang Wick1, Peter Arthur Ringleb1, Markus Möhlenbruch3, Silvia Schönenberger*1
1University Hospital Heidelberg, Neurology, Heidelberg, Germany, 2Heidelberg University Hospital, Institute of Medical Biometry, Heidelberg, Germany, 3University Hospital Heidelberg, Neuroradiology, Heidelberg, Germany
Background and aims: Optimal blood pressure management during endovascular stroke treatment (EST) is not well established. The aim of this study therefore was to compare an individualized blood pressure management approach in which intraprocedural blood pressure targets were set to preinterventional values to a standardized blood pressure approach regarding functional outcome, safety, and feasibility of those strategies.
Methods:INDIVIDUALIZED BLOOD PRESSURE MANAGEMENT DURING ENDOVASCULAR TREATMENT OF ACUTE ISCHEMIC STROKE UNDER PROCEDURAL SEDATION (INDIVIDUATE) is a randomized clinical trial with a PROBE (Prospective Randomized Open, Blinded End-point) design. Patients suffering from acute ischemic stroke of the anterior circulation with occlusions of the internal carotid artery and/or middle cerebral artery and a National Institutes of Health Stroke Scale (NIHSS) score of ⩾ 8 receiving EST in procedural sedation were screened, from which 250 patients were included in this study.
The main prespecified outcome is favorable functional outcome 90 days after stroke, defined as modified Rankin Scale (mRS) 0-2.
Secondary outcomes include mortality, NIHSS 24h and 72h after stroke onset, measured blood pressure values and predefined safety outcomes like critical hyper or hypotension, symptomatic postprocedural hemorrhage and necessity of vasopressors or vasodepressors.
Results: We will present the final results including primary outcome of the first prospective randomized trial concerning blood pressure management during stroke thrombectomy.
Conclusions: The results will have the potential to influence the prospective blood pressure management of acute ischemic stroke patients with large vessel occlusion undergoing stroke thrombectomy.
Disclosure of interest: No
O320/3137
Performance feedback to improve time to thrombectomy for ischemic stroke: a stepped wedge cluster randomized trial (PERFEQTOS)
Daniël Hansen*1,2, Sanne den Hartog1,2,3, Nikki van Leeuwen1, Frank Eijkenaar4, Laurien S Kuhrij5,6, Lotte Stolze5,6, Paul Nederkoorn6, Hester Lingsma1, Adriaan van Es7, Ido van den Wijngaard8,9, Aad van der Lugt3, Diederik Dippel2, Bob Roozenbeek2,3
1Erasmus MC University Medical Center, Public Health, Rotterdam, Netherlands, 2Erasmus MC University Medical Center, Neurology, Rotterdam, Netherlands, 3Erasmus MC University Medical Center, Radiology and Nuclear Medicine, Rotterdam, Netherlands, 4Erasmus University Rotterdam, Erasmus School of Health Policy & Management, Rotterdam, Netherlands, 5Dutch Institute for Clinical Auditing, Medical Advice, Leiden, Netherlands, 6Amsterdam University Medical Centers, location AMC, Neurology, Amsterdam, Netherlands, 7Leiden University Medical Center, Radiology, Leiden, Netherlands, 8Haaglanden Medical Center, Neurology, the Hague, Netherlands, 9Haaglanden Medical Center, Radiology, the Hague, Netherlands
Background and aims: An efficient care process is crucial to minimize treatment delays and improve outcome after endovascular thrombectomy (EVT) for acute ischemic stroke. The aim of this study was to evaluate the effect of a performance feedback intervention on time to EVT.
Methods: We performed a stepped wedge cluster randomized trial in 13 hospitals in the Netherlands providing EVT for ischemic stroke. The intervention consisted of performance feedback -through computer-dashboards- on patient characteristics and structure, process, and outcome indicators for patients treated with EVT. Feedback was provided to local quality improvement teams that developed performance improvement plans based on the performance feedback. Each 6 months, 3-4 hospitals were randomized to the intervention. The primary outcome was door-to-groin time in minutes. The effect of the intervention was estimated with a multivariable linear mixed model with adjustment for calendar time, hospital and time and patient characteristics and expressed as beta.
Results: Between July 01, 2019 and June 30, 2022, 5606 patients were included of which 2441 were enrolled in the intervention group and 3165 in the control group. Mean age was 72 years and median baseline NIHSS was 14. The intervention reduced the door-to-groin time with almost 5 minutes (beta = 4.69, 95%CI: -9.00 to -0.19, p=0.041), corresponding to 9%.
Conclusions: Performance feedback through a dashboard used by a local quality improvement team reduces time to EVT for ischemic stroke patients, independent of trends in treatment times.
Disclosure of interest: No
O321/1090
SONOLYSIS IN PREVENTION OF BRAIN INFARCTIONS DURING INTERNAL CAROTID ENDARTERECTOMY (SONOBIRDIE): THE RESULTS OF RANDOMIZED CONTROLLED TRIAL
David Skoloudik*1, Tomáš Hrbáč2, Roman Herzig3, Jiří Fiedler4, Vladimír Beneš5,6, Petra Kesnerova7, Martin Kovar8, Milan Vosko9, Vladimir Nosal10, Vladimír Beneš11, Mattia Branca12, Jean-Benoit Rossel12, David Netuka11
1Faculty of Medicine, University of Ostrava, Center for Health Research, Ostrava, Czech Republic, 2University Hospital Ostrava, Neurosurgery, Ostrava, Czech Republic, 3Charles University Faculty of Medicine and University Hospital Hradec Králové, Neurology, Hradec Králové, Czech Republic, 4České Budějovice Hospital, Neurosurgery, České Budějovice, Czech Republic, 52nd Faculty of Medicine, Charles University and University Hospital Motol, Neurosurgery, Prague, Czech Republic, 6Liberec Hospital, Neurosurgery, Liberec, Czech Republic, 72nd Faculty of Medicine, Charles University and University Hospital Motol, Neurology, Prague, Czech Republic, 8Na Homolce Hospital, Neurology, Prague, Czech Republic, 9Kepler University Hospital Linz, Neurology, Linz, Austria, 10University Hospital and Jessenius University of Medicine Martin, Neurology, Martin, Slovakia, 11Military University Hospital Prague, Neurosurgery, Prague, Czech Republic, 12University of Bern, Clinical Trials Unit, Bern, Switzerland
Background and aims: Sonolysis/sonothrombolysis is a novel therapy for arterial recanalization using a transcranial Doppler (TCD) monitoring. SONOBIRDIE Trial is a multi-center, randomized, double-blind, sham-controlled study aimed to demonstrate the safety and effectiveness of sonolysis using 2-MHz diagnostic TCD probe during carotid endarterectomy (CEA) in a reduction of risk of stroke/transient ischemic attack (TIA) and brain infarctions detected using MRI in 14 European centers.
Methods: Functionally independent patients with symptomatic/asymptomatic internal carotid artery stenosis ⩾70% indicated for CEA with TCD detectable blood flow in middle cerebral artery and aged 40–85 years were assigned (1:1) to sonolysis or control group. Sonolysis/sham procedure was performed for 40–120 min during CEA. Neurological examination was performed 24±4 h prior to CEA, 24±4 h after CEA, 30±2 and 365±14 days after CEA. Brain MRI including diffusion-weighted images was performed 24±4h prior and 24±4h after CEA. Primary composite outcome was ischemic stroke, TIA or death within 30 days.
Results: In total 1004 consecutive patients (30% women; mean age 68±7.8 years) were enrolled (507 into sonolysis group). In the sonolysis versus control group, the primary endpoint occurred in 2.2% vs. 7.6% (risk difference 5.5%; 95% CI=2.8–8.3%; p<0.001), stroke/TIA in 1.8% vs. 7.5% (p<0.001) and new ischemic lesion on MRI in 8.6% vs. 17.4% of patients (p<0.01), resp.
Conclusions: Sonolysis during CEA seems to be a safe and effective method for prevention of periprocedural stroke, TIA or MRI-detected brain infarctions.
SONOBIRDIE trial was registered (NCT02398734) and funded by the Czech Ministry of Health (16-29148A/NV19-04-00270/NU22-04-00389).
Disclosure of interest: No
O322/1330
ISOSORBIDE MONONITRATE, CILOSTAZOL AND THEIR COMBINATION FOR ONE YEAR: EFFECT ON COGNITIVE OUTCOMES IN PATIENTS WITH SMALL VESSEL STROKE: THE LACUNAR INTERVENTION TRIAL-2 (LACI-2)
Joanna Wardlaw*1, Fergus Doubal1, Vera Cvoro1,2, David Werring3, Tim England4, Ahamad Hassan5, John M Bamford5, Lisa Woodhouse4, Iris Isheanesu Mhlanga4, Christine Roffe6, John O'brien7, Philip Bath4
1University of Edinburgh, Clinical Brain Sciences, Edinburgh, United Kingdom, 2Victoria Hospital NHS Trust, Medicine for the Elderly and Stroke, Kirkcaldy, United Kingdom, 3University College London, Neurology, London, United Kingdom, 4University of Nottingham, Stroke Medicine, Nottingham, United Kingdom, 5Leeds General Infirmary, Neurology, Leeds, United Kingdom, 6Keele University, Stroke Research, Stoke, United Kingdom, 7University of Cambridge, Old Age Psychiatry, Cambridge, United Kingdom
Background and aims: Cognitive impairment is common following lacunar ischaemic stroke, a form of cerebral small vessel disease (SVD), but there is no specific treatment. The LACunar Intervention Trial-2 (LACI-2, ISRCTN14911850) assessed if isosorbide mononitrate (ISMN) and/or cilostazol could improve post-lacunar stroke cognitive outcomes.
Methods: LACI-2 was an investigator-initiated randomised, open-label, blinded-endpoint, 2x2 factorial trial. Participants age >30yrs with clinical lacunar ischaemic stroke, compatible MR/CT brain imaging, and capacity to consent, were randomised to one year of ISMN 25mg bd, cilostazol 100mg bd, both, or neither. At one year, cognitive function was assessed centrally, masked to drug, using telephone Montreal Cognitive Assessment (tMOCA), telephone Interview of Cognitive Status (TICS), animal naming, and mapped to a 7-level ordinal scale reflecting Diagnostic and Statistical Manual of Mental Disorders (DSM-5) neurocognitive categories. All analyses were co-variate adjusted. Data are median [interquartile range], adjusted odds ratio (aOR), mean difference (aMD), 95% confidence interval.
Results: LACI-2 recruited 363 patients at 26 UK hospitals from 05/02/2018-31/05/2021. Baseline characteristics were well balanced: age 64 [56-72] years, female 112 (31%), stroke-to-randomisation 79 [27-244] days. LACI-2 retained 358 (99.0%) participants at one year, 308 (86%) provided data for 7-level cognition, of whom 184 (60%) had mild or worse cognitive impairment. ISMN (aOR 0.55, 0.36-0.86, p=0.008), and ISMN+cilostazol (aOR 0.44, 0.23-0.85, p=0.015) reduced 7-level cognitive impairment. ISMN+cilostazol improved tMOCA scores (aMD 1.14, 0.24-2.04, p=0.013).
Conclusions: LACI-2 suggests that ISMN, alone or with cilostazol, may improve post-lacunar stroke cognition; a definitive phase-3 trial in lacunar stroke (LACI-3) is planned.
Disclosure of interest: No
O323/3116
IMMEDIATE INTENSIVE STATIN VERSUS DELAYED INTENSIVE STATIN FOR PATIENTS WITH ACUTE MILD ISCHEMIC STROKE OR TIA WITH INTRACRANIAL OR EXTRACRANIAL ATHEROSCLEROSIS
Yilong Wang*1
1Beijing Tiantan Hospital, Capital Medical University, Department of Neurology, Beijing, China
Background and aims: Comparisons between immediate and delayed intensive statin in patients with acute ischemic stroke or TIA with intracranial or extracranial atherosclerosis (ICAS/ECAS) have not been well studied for secondary stroke prevention.
Methods: We conducted a randomized, double-blind, placebo-controlled and 2-by-2 factorial trial of 6,100 patients with mild ischemic stroke or high-risk TIA of ICAS/ECAS origin. In one comparison, patients were randomly assigned within 72 hours of onset, in a 1:1 ratio to receive immediate intensive atorvastatin or 3-day delayed intensive atorvastatin. The primary efficacy outcome was new stroke and the primary safety outcomes were hepatotoxicity and muscle toxicity, both within 90 days.
Results: New stroke occurred within 90 days in 245 patients (8.05%) versus 257 patients (8.46%) in the immediate and delayed intensive statin group, respectively (hazard ratio, 0.95; 95% CI, 0.80 to 1.13; P=0.550). Poor functional outcome (mRS score 2-6) occurred in 299 patients (9.81%) in the immediate statin group and 348 patients (11.42%) in the delayed statin group (P=0.041). Hepatotoxicity and muscle toxicity occurred in 39 patients (1.28%) versus 32 patients (1.05%) (P=0.404), and 2 patients (0.07%) versus 1 patient (0.03%) (P=0.571) in the immediate and delayed intensive statin group, respectively.
Conclusions: Among patients with acute mild ischemic stroke or TIA from ICAS/ECAS, immediate intensive statin initiated within 72 hours of onset was not found to reduce the risk of stroke recurrence at 90 days compared to intensive statin with a 3-day delay, but significantly improved the poor functional outcome. (INSPIRES ClinicalTrials.gov number, NCT03635749)
Disclosure of interest: Yes
Scientific Communication SC2 - IV Thrombolysis
O330/1950
Tenecteplase versus Alteplase in acute ischemic stroke due to medium vessel occlusion (MeVO): Results from the AcT trial
Fouzi Bala*1,2, Bijoy Menon1, Nishita Singh1, Brian Buck1, Shelagh Coutts1, Yan Deschaintre1, Houman Khosravani1, Ramana Appireddy1, Francois Moreau1, Stephen Phillips1, Gord Gubitz1, Aleksander Tkach1, Luciana Catanese1, Dar Dowlatshahi1, George Medvedev1, Jennifer Mandzia1, Aleksandra Pikula1, Jai Shankar1, Heather Williams1, Thalia Field1, Herbert Manosalva1, Muzaffar Siddiqui1, Atif Zafar1, Oje Imoukhuede1, Gary Hunter1, Michel Shamy1, Mackenzie Horn1, Ibrahim Alhabli1, Faysal Benali1, Ayoola Ademola1, Michael Hill1, Tolulope Sajobi1, Richard Swartz1, Mohammed Almekhlafi1
1Clinical Neurosciences, Neurology, Calgary, Canada, 2Tours University Hospital, Neuroradiology, Tours, France
Background and aims: The safety and efficacy of tenecteplase in stroke patients with medium vessel occlusion (MeVO)-stroke is still not well studied. We assessed the safety and efficacy of tenecteplase compared to alteplase in the Alteplase compared to Tenecteplase (AcT) trial.
Methods: Patients with baseline M2/M3-MCA, P2/P3-PCA, A2/A3-ACA occlusions were included. Primary outcome was the proportion of 90-day modified Rankin Scale (mRS) 0-1. Secondary outcomes were 90-day mRS 0-2, mortality, and symptomatic intracerebral haemorrhage (ICH). Angiographic outcomes were successful reperfusion (eTICI 2b-3) on first and final angiographic acquisitions. Multivariable analyses were performed to assess the association between thrombolysis treatment type and outcomes. Treatment effect modification by occlusion location was assessed.
Results: Among 1577 patients; 455 (28.8%) had MeVO of which 78.9% (359/455) were M2/M3; 13.6% (62/455) were P2/P3 and 7.5% (34/455) were A2/A3 occlusions. 87/455(19.1%) patients underwent endovascular thrombectomy. The primary outcome was achieved in 37.9% (89) in the tenecteplase versus 34.7% (76) in the alteplase group (p=0.50). Rates of 90-day mRS 0-2 (59.1% versus 54.3%), symptomatic ICH (1.7% versus 2.3%) and mortality (14.1% versus 17.0%) were similar in the tenecteplase and alteplase groups, respectively. No statistical difference was noted in the first (13.0% versus 7.5%) or final successful reperfusion rates (71.7% versus 60.0%) among the 87 patients who underwent endovascular thrombectomy. No treatment effect heterogeneity by occlusion site was observed for any of the assessed outcomes.
Conclusions: Intravenous tenecteplase had comparable safety and functional outcomes compared to alteplase among patients with MeVO in the AcT trial.
Disclosure of interest: No
O331/976
INFLUENCE OF TREATMENT DELAY ON THE EFFECT OF INTRAVENOUS ALTEPLASE BEFORE THROMBECTOMY: AN INDIVIDUAL PARTICIPANT DATA META-ANALYSIS FROM SIX RANDOMIZED CLINICAL TRIALS (IRIS)
Johannes Kaesmacher*1, Leon Rinkel2, Manon Kappelhof2, Fabiano Cavalcante2, Kilian Treurniet2, Urs Fischer3, Charles Majoie2, Jan Gralla1, Jianmin Liu4, Pengfei Yang4, Yongwei Zhang5, Qingwu Yang6, Wenjie Zi6, Raul Nogueira7, Bernard Yan4, Peter Mitchell4, Zhongrong Miao8, Kentaro Suzuki9, Kazumi Kimura9, Yuji Matsumaru10, Yvo Roos2
1Inselspital, Neuroradiology, Bern, Switzerland, 2Amsterdam UMC, Neurology, Amsterdam, Netherlands, 3Universitätsspital Basel, Neurology, Basal, Switzerland, 4Changhai Hospital - Naval Medical University, Neurosurgery, Shanghai, China, 5Naval Medical University Changhai Hospital, Neurology, Shanghai, China, 6Xinqiao Hospital and The Second Affiliated Hospital, Army Medical University (Third Military Medical University), Neurology, Shapingba District, Chongqing, China, 7Marcus Stroke & Neuroscience Center, Grady Memorial Hospital, Emory University School of Medicine, Neurology, Atlanta, United States, 8Beijing Tiantan Hospital, Capital Medical University, Fengtai District, Department of Interventional Neuroradiology, Beijing, China, 9Nippon Medical School, Tokyo, Japan., Neurology, Tokyo, Japan, 10University of Tsukuba, Division of Stroke Prevention and Treatment, Department of Neurosurgery, Faculty of Medicine, Ibaraki, Japan
Background and aims: The clinical efficacy of intravenous alteplase for ischemic stroke decreases with longer time since symptom onset. It is unknown whether this association is also present in patients receiving IVT prior to thrombectomy. We aim to assess treatment effect heterogeneity of intravenous alteplase before thrombectomy with strata of treatment delays.
Methods: We will conduct a pre-specified meta-analysis of individual participant data from six randomized clinical trials comparing intravenous thrombolysis plus thrombectomy versus thrombectomy alone (IRIS collaboration, n=2313). We hypothesize that there is significant treatment effect heterogeneity between intravenous alteplase prior to thrombectomy and treatment delay, in the direction that patients with shorter intervals from onset to randomization will benefit from intravenous alteplase, while patients with longer intervals will not. For this purpose, we will conduct a mixed model regression analysis adjusted for relevant baseline characteristics with 90-day ordinal modified Rankin Score shift as the primary outcome. Primary analysis will be conducted using interaction terms in an as-treated population. Variation of the treatment effect of intravenous alteplase before thrombectomy will be reported as change in the common adjusted Odds Ratio per hour increase in onset-to-randomization time.
Results: The results, together with more detailed sensitivity analyses and dichotomizations reflecting country specific drug authorizations (e.g. 3h treatment delay in the US) will be presented at ESOC 2023.
Conclusions: If the additional value of intravenous alteplase before thrombectomy is considerably time-dependent, this may be taken into consideration for decisions on whether to administer or withhold intravenous alteplase in patients undergoing thrombectomy.
Disclosure of interest: No
SCIENTIFIC COMMUNICATIONS – NEUROINTERVENTION – IMAGING AND REPERFUSION
O332/3111
Key Clinical Characteristics and Their Association with Outcomes and Thrombectomy Treatment Effect in Patients with Large Ischemic Core Strokes: SELECT2 Subgroups Analyses
Amrou Sarraj*1, Michael Abraham2, Michael Chen3, M Shazam Hussain4, Santiago Ortega-Gutierrez5, Vitor Mendes Pereira6, Maarten Lansberg7, Deep Pujara1, Leonid Churilov8, Clark Sitton9, Greg Albers7, Ameer Hassan10, Marc Ribo11, Bruce Campbell8
1University Hospitals Cleveland Medical Center, Neurology, Cleveland, United States, 2The University Of Kansas Medical Center, Neurology, Kansas City, United States, 3Rush University Medical Center, Interventional Neurology, Chicago, United States, 4Cleveland Clinic, Cerebrovascular Diseases, Cleveland, United States, 5University of Iowa Hospitals & Clinics, Interventional Neurology, Iowa City, United States, 6St. Michael's Hospital, Radiology, Toronto, Canada, 7Stanford University, Neurology, Stanford, United States, 8The Royal Melbourne Hospital, Neurology, Parkville, Australia, 9UTHealth Houston (The University of Texas Health Science Center at Houston), Radiology, Houston, United States, 10Valley Baptist Medical Center, Interventional Neurology, Harlingen, United States, 11Vall d'Hebron University Hospital, Interventional Neurology, Barcelona, Spain
Background and aims: SELECT2 trial recently demonstrated efficacy and safety of endovascular thrombectomy (EVT) in patients with large ischemic core on non-contrast CT (ASPECTS 3-5) and/or Perfusion-Diffusion imaging (ischemic core⩾50ml). We aimed to further characterize the treatment effect of EVT in selected subgroups based on key clinical characteristics.
Methods: SELECT2 was an international, multicentre randomized clinical trial, that enrolled 352 patients across 31 centres in US, Canada, Europe, Australia and New Zealand. All patients enrolled in SELECT2 were included in this analysis. Age, NIHSS at presentation, time from last known well to randomization, occlusion location and stroke laterality were pre-specified as characteristics of interest and evaluation of their association with thrombectomy clinical outcomes and treatment effect was performed. The primary outcome was the distribution of modified Rankin Scale score at 90-day follow-up. Key secondary outcomes included functional independence (mRS 0-2), independent ambulation (mRS 0-3), symptomatic ICH (SITS-MOST) and mortality.
Results: Of 352 enrolled patients, 178 were randomized to receive endovascular thrombectomy and 174 to receive standard medical care. Endovascular thrombectomy resulted in higher odds of better functional outcome (GenOR: 1.51, 95% CI: 1.21-1.87, p=0.0004) and functional independence (20% vs 7%, RR: 2.97, 95% CI: 1.60 to 5.51), with no difference in symptomatic ICH (0.6% vs 1.1%, RR: 0.49, 95% CI: 0.04-5.36). Further results for subgroups based on pre-specified clinical characteristics will be available for presentation at European Stroke Organisation Conference 2023.
Ischemic Injury Estimates on Different Imaging Modalities and Their Association with Outcomes and Thrombectomy Treatment Effect in Patients with Large Ischemic Core Stroke: SELECT2 Imaging Analyses
Amrou Sarraj*1, Michael Abraham2, Ameer Hassan3, Santiago Ortega-Gutierrez4, Michael Chen5, M Shazam Hussain6, Deep Pujara1, Leonid Churilov7, Clark Sitton8, Vitor Mendes Pereira9, Maarten Lansberg10, Marc Ribo11, Greg Albers10, Bruce Campbell7
1University Hospitals Cleveland Medical Center, Neurology, Cleveland, United States, 2The University Of Kansas Medical Center, Neurology, Kansas City, United States, 3Valley Baptist Medical Center, Interventional Neurology, Harlingen, United States, 4University of Iowa Hospitals & Clinics, Interventional Neurology, Iowa City, United States, 5Rush University Medical Center, Interventional Neurology, Chicago, United States, 6Cleveland Clinic, Cerebrovascular Diseases, Cleveland, United States, 7The Royal Melbourne Hospital, Neurology, Parkville, Australia, 8UTHealth Houston (The University of Texas Health Science Center at Houston), Radiology, Houston, United States, 9St. Michael's Hospital, Radiology, Toronto, Canada, 10Stanford University, Neurology, Stanford, United States, 11Vall d'Hebron University Hospital, Interventional Neurology, Barcelona, Spain
Background and aims: The SELECT2 trial recently demonstrated efficacy and safety of endovascular thrombectomy (EVT) in patients with large ischemic core on non-contrast CT (ASPECTS 3-5) and/or Perfusion-Diffusion imaging (ischemic core⩾50ml). We aimed to further characterize the treatment effect of EVT in selected subgroups based on key pre-treatment imaging biomarkers of ischemic injury.
Methods: SELECT2 was an international, multicentre randomized clinical trial, that enrolled 352 patients across 31 centres in US, Canada, Europe, Australia and New Zealand. All patients enrolled in SELECT2 trial were included in this analysis. Non-contrast CT ASPECTS, Ischemic core estimates, mismatch volume and ratio were pre-specified as characteristics of interest and evaluation of their association with thrombectomy clinical outcomes and treatment effect was performed. The primary outcome was the distribution of modified Rankin Scale score at 90-day follow-up. Key secondary outcomes included functional independence (mRS 0-2), independent ambulation (mRS 0-3), symptomatic ICH (SITS-MOST) and mortality.
Results: Of 352 enrolled patients, 178 were randomized to receive endovascular thrombectomy and 174 to receive standard medical care. Endovascular thrombectomy resulted in higher odds of better functional outcome (GenOR: 1.51, 95% CI: 1.21-1.87, p=0.0004) and functional independence (20% vs 7%, RR: 2.97, 95% CI: 1.60 to 5.51), with no difference in symptomatic ICH (0.6% vs 1.1%, RR: 0.49, 95% CI: 0.04-5.36). Further results for subgroups based on pre-specified imaging characteristics will be available for presentation at European Stroke Organisation Conference 2023.
PRevention Of Hypertensive Injury to the Brain by Intensive Treatment of blood pressure after IntraCerebral Haemorrhage (PROHIBIT-ICH): 3-month outcomes of a randomised controlled trial of remote-telemetric home BP-monitoring
Iain McGurgan*1, Michelle Wilson1, Josephine Edens1, Jo Hornby2, Maja Dabagh2, Shahena Butt2, Rustam Al-Shahi Salman3, Craig Anderson4, Philip Bath5, Hugh Markus6, Thompson Robinson7, Nikola Sprigg8, Louise Silver1, David Werring2, Peter Rothwell1
1University of Oxford, Wolfson Centre for the Prevention of Stroke and Dementia, Oxford, United Kingdom, 2UCL Queen Square Institute of Neurology, Stroke Research Centre, London, United Kingdom, 3University of Edinburgh, Cerebrovascular Research Group, Edinburgh, United Kingdom, 4The George Institute, Global Brain Health, Sydney, Australia, 5University of Nottingham, Division of Clinical Neuroscience, Nottingham, United Kingdom, 6University of Cambridge, Neurology Unit, Cambridge, United Kingdom, 7University of Leicester, College of Life Sciences, Leicester, United Kingdom, 8University of Nottingham, Faculty of Medicine & Health Sciences, Nottingham, United Kingdom
Background and aims: Intracerebral haemorrhage (ICH) associated with cerebral small vessel disease (SVD) has a high recurrence risk, particularly if BP-control is poor. PROHIBIT-ICH aimed to assess the feasibility, efficacy and safety of centralised BP-management using remote-telemetric home-BP monitoring (RT-HBPM) during post-hospital follow-up after ICH.
Methods: Patients (target=112) with imaging-confirmed SVD-associated ICH and BP>130/80mmHg were recruited from multiple UK hospitals to a parallel-group, open-label, randomised(1:1) trial of 1-3 months of RT-HBPM-guided treatment (calcium channel blocker-based regimen) coordinated centrally from Oxford (target HBPM-BP<120/80mmHg) versus locally-based standard care. The efficacy outcome was the between-group difference in BP-reduction from baseline to 3-month follow-up based on clinic measurements (primary outcome) and on daytime-BP on 24-hour ambulatory BP-monitoring (ABPM).
Results: Recruitment began in 2019, but was suspended repeatedly because of the COVID-19 pandemic, and ended due to funding constraints in January 2022 after inclusion of 86 patients from 16 centres (43 per group; mean/SD age=66.2/12.6; mean/SD baseline SBP=148.5/16.3mmHg). Four patients withdrew before 3-months and two declined 3-month BP assessments. Among 80 (93%) patients with 3-month BP (41 RT-HBPM vs 39 local-care), the mean reduction from baseline in 3-month clinic-BP was greater with RT-HBPM vs local-care (∆SBP=19.4 vs 5.8, p=0.003; ∆DPB=8.6 vs -1.0, p=0.0003), with similar results on ABPM (∆SBP=19.7 vs 2.5, p=0.0007; ∆DBP=8.8 vs -1.1, p=0.0005).
Conclusions: Centralised BP-management using RT-HBPM is feasible after SVD-associated ICH, and resulted in better BP-control at 3-months than standard care. Longer-term BP-control, safety and brain imaging markers will be assessed at one-year follow-up.
Disclosure of interest: No
SCIENTIFIC COMMUNICATIONS – CARDIOEMBOLISM AND HEART-BRAIN INTERACTIONS
O335/2198
Outcomes of ischemic stroke patients with unrecognized myocardial fibrosis detected by cardiovascular MRI – results from an international multicenter collaboration
Simon Hellwig*1,2,3, Ana Catarina Fonseca4, Thomas Meinel5, Santosh Murthy6, Annerose Mengel7, Shadi Yaghi8, Luciano Sposato9, Patrick Krumm10, Eric D. Goldstein8, Helena Stengl1,2,3, Ramanan Ganeshan1, Regina von Rennenberg1,2, Edyta Blaszczyk11, Jochen B. Fiebach2, Matthias Endres2,3,12,13, Simon Greulich14, Jeanette Schulz-Menger11, Alexander Merkler6, Simon Jung5, Christian Nolte1,2,3,13, Karl Georg Häusler15, Jan Scheitz1,2,3,13
1Charité Campus Benjamin Franklin, Department of Neurology, Berlin, Germany, 2Center for Stroke Research Berlin (CSB), Center for Stroke Research Berlin (CSB), Berlin, Germany, 3Berlin Institute of Health (BIH), Berlin Institute of Health (BIH), Berlin, Germany, 4Department of Neurology, Hospital de Santa Maria, Centro Hospitalar Universitário Lisboa Norte, Lisbon, Portugal, 5Department of Neurology, Stroke Research Center Bern, Inselspital, Bern University Hospital, Bern, Switzerland, 6Department of Neurology, Weill Cornell Medicine, New York, United States, 7Department of Neurology and Stroke, University Hospital Tübingen, Tübingen, Germany, 8Alpert Medical School, Brown University, Providence, Rhode Island, United States, 9Department of Clinical Neurological Sciences, Western University, London, Ontario, Canada, 10Department of Radiology, University Hospital Tübingen, Tübingen, Germany, 11Working Group on Cardiovascular Magnetic Resonance, Experimental and Clinical Research Center, Charité - Universitätsmedizin Berlin, Berlin, Germany, 12Department of Neurology, Charité - Universitätsmedizin Berlin, Berlin, Germany, 13German Center for Cardiovascular Research (DZHK), German Center for Cardiovascular Research (DZHK), Berlin, Germany, 14Department of Cardiology and Angiology, University Hospital Tübingen, Tübingen, Germany, 15Julius-Maximilians-Universität Würzburg, Department of Neurology, Würzburg, Germany
Background and aims: Myocardial fibrosis indicating previous myocardial infarction (MI) or other non-ischemic cardiac pathologies can be precisely detected by contrast-enhanced cardiovascular MRI (CE-CMR). The burden and outcomes of unrecognized myocardial fibrosis in patients with recent ischemic stroke (IS) has not been established. We aim to fill this gap of knowledge by creating an ‘International Stroke CMR Collaboration’.
Methods: Following a pre-registered systematic review (PROSPERO, 401666), we collected individual patient data from eligible centers that performed CE-CMR after recent IS. Unrecognized myocardial fibrosis was defined as the presence of late gadolinium enhancement (LGE) on CE-CMR in patients without history of MI. Outcomes of interest were unfavorable functional outcome according to modified Rankin Scale at three months (mRS >2), and one-year mortality.
Results: A total of 832 patients with CE-CMR from seven centers in five countries were analyzed (median age 70 years, 35.7% female). Of these, 765 patients (91.9%) had no history of MI. Myocardial fibrosis was detected in 236 (30.8%) patients. Presence of myocardial fibrosis was associated with unfavorable outcome at three months (25.6% vs. 15.8%, unadjusted OR=1.83, 95%CI 1.25-2.68, adjusted OR=1.93, 95%CI 1.26-2.93; adjustment for age, sex, NIHSS, history of stroke, hypertension, diabetes).
Conclusions: In this international, multicenter study, there was a high burden of unrecognized myocardial fibrosis in patients with recent IS. The strong association with unfavorable functional status at three months suggests that efforts are needed to screen for subclinical heart disease. At ESOC, in-depth analyses of LGE subtypes (ischemic/non-ischemic) and longer-term prognosis will be available.
Disclosure of interest: No
O336/3082
ISCHEMIC STROKE TEMPORALLY ASSOCIATED WITH INCIDENT ATRIAL FIBRILLATION: A POPULATION-BASED REGISTRY-LINKAGE STUDY
Jukka Putaala*1, Konsta Teppo2, Olli Halminen3, Jari Haukka4, Paula Tiili1, Jussi Jaakkola2, Elin Karlsson4, Miika Linna3, Pirjo Mustonen2, Janne Kinnunen1, Juha Hartikainen5, Juhani Airaksinen2, Mika Lehto6
1Helsinki University Hospital and University of Helsinki, Neurology, Helsinki, Finland, 2Heart Center, Turku University Hospital and University of Turku, Finland, Turku, Finland, 3Aalto University, Industrial Engineering and Management, Espoo, Finland, 4University of Helsinki, Public Health, Helsinki, Finland, 5University of Eastern Finland, Heart Center, Kuopio, Finland, 6Jorvi Hospital and Helsinki University Hospital, Espoo, Finland and University of Helsinki, Internal Medicine, Espoo, Finland
Background and aims: We assessed temporal relationship between incident atrial fibrillation (AF) and ischemic stroke and its impact on patients’ clinical characteristics and mortality.
Methods: A population-based registry-linkage database including all patients with incident AF, 2007-2018. Based on distribution, ischemic stroke temporally associated with AF (ISTAF) was defined as an ischemic stroke occurring within ±30 days from AF (Figure 1). Factors associated with ISTAF were studied with adjusted logistic and 90-day survival with Cox regression.
Results: Among 229 565 patients with incident AF (mean age 72.7; 50% female), 204 774 (89.2%) experienced no ischemic stroke, 12 209 (5.3%) had an ischemic stroke >30 days prior AF, and 12 582 (5.8%) had ISTAF. The annual proportion of ISTAF decreased from 6.0% to 4.8% during 2007-2018. Factors associated with ISTAF were older age, lower level of education, alcohol abuse, and absence of vascular disease, heart failure, renal failure, cancer, and psychiatric disorder. Compared with patients without ischemic stroke and those with ischemic stroke >30 days prior AF, ISTAF was associated with approximately 3-fold (adjusted hazard ratio 2.90, 95% confidence interval [CI] 2.76-3.05) and 1.5-fold (1.47, 1.39-1.57) risks of death (Figure 2). 90-day survival probability of ISTAF patients increased from 0.79 (95% CI 0.76-0.81) in 2007 to 0.89 (0.87-0.91) in 2018.
Conclusions: We propose a distinct clinical concept of ISTAF based on the prominent temporal clustering of ischemic strokes around AF. Despite having fewer comorbidities, ISTAF patients have poorer, although improving, survival than patients experiencing stroke never or >30 days prior AF.
Disclosure of interest: Yes
SCIENTIFIC COMMUNICATIONS - DIAGNOSIS / INVESTIGATION OF STROKE ETIOLOGY AND PATHOPHYSIOLOGY
O337/3001
PFO CLOSURE TO AVERT RECURRENT STROKE: THE PASCAL STRATIFICATION SYSTEM DISTINGUISHES PATIENT GROUPS WITH NET BENEFIT AND NET HARM
Orly Termeie1, Jeffrey Saver*2, Scott Kasner3, Jason Nelson4, John D. Carroll5, Gilles Chatellier6, Geneviève Derumeaux7, Anthony J. Furlan8, Howard C. Herrmann9, Peter Jüni10, Jong S. Kim11, Benjamin Koethe4, Pil Hyung Lee12, Benedicte Lefebvre9, Jean-Louis Mas13, Heinrich Mattle14, Bernhard Meier15, Mark Reisman16, Richard W. Smalling17, Lars Søndergaard18, Jae-Kwan Song12, David Thaler19, David Kent4
1Florida Atlantic University, Charles E. Schmidt College of Medicine, Boca Raton, United States, 2University of California, Los Angeles, Comprehensive Stroke Center and Department of Neurology, David Geffen School of Medicine, Los Angeles, United States, 3University of Pennsylvania Medical Center, Comprehensive Stroke Center, Department of Neurology, Philadelphia, United States, 4Tufts Medical Center/Tufts University School of Medicine, Predictive Analytics and Comparative Effectiveness Center, Boston, United States, 5University of Colorado Denver, Division of Cardiology, Department of Medicine, Aurora, United States, 6Hôpital Européen Georges-Pompidou, Assistance Publique-Hôpitaux de Paris, Centre d'Investigations Cliniques, Unité de Recherche Clinique, Paris, France, 7Université Paris-Est Créteil (UPEC), Département de Physiologie, Hôpital Henri Mondor, Assistance Publique-Hôpitaux de Paris, INSERM U955, Créteil, France, 8Case Western Reserve University, Department of Neurology, Cleveland, United States, 9University of Pennsylvania, Division of Cardiovascular Medicine, Perelman School of Medicine, Philadelphia, United States, 10University of Toronto, Applied Health Research Centre, Li Ka Shing Knowledge Institute of St Michael's Hospital, Toronto, Canada, 11University of Ulsan, Department of Neurology, Asan Medical Center, College of Medicine, Seoul, South Korea, 12University of Ulsan, Department of Cardiology, Asan Medical Center, College of Medicine, Seoul, South Korea, 13Université de Paris-Cité, GHU Paris Psychiatrie et Neurosciences, Hôpital Sainte-Anne, Service de Neurologie, Institut de Psychiatrie et Neurosciences de Paris, Paris, France, 14Bern University Hospital, Department of Neurology, Bern, Switzerland, 15University of Bern, Department of Cardiology, Bern, Switzerland, 16Weill Cornell Medical Center, Division of Cardiology, New York, United States, 17UTHealth/McGovern Medical School and The Memorial Hermann Heart and Vascular Institute, Division of Cardiology, Department of Medicine, Houston, United States, 18University of Copenhagen Hospital Rigshospitalet, Department of Cardiology, Copenhagen, Denmark, 19Tufts Medical Center/Tufts University School of Medicine, Department of Neurology, Boston, United States
Background and aims: Patent foramen ovale (PFO) closure decreases recurrent stroke but increases atrial fibrillation (AF), including, early, periprocedural AF (within 45d of closure, generally benign) and late, post-periprocedural AF (>45d after closure, more clinically concerning). We quantified the differential benefit-risk tradeoffs among patient groups with strokes classified by the PASCAL diagnostic system as: Probable (PROB), Possible (POSS), or Unlikely (UNL) PFO-related.
Methods: Analysis of individual participant-level data from all 6 completed randomized trials of PFO closure to derive number-needed-to-treat-to-benefit (NNTB), number-needed-to-harm (NNH), benefit-per-thousand treated patients (BPT), and harm-per-thousand treated-patients (HPT).
Results: The 6 completed randomized trials enrolled 3740 patients (1889 PFO closure, 1851 medical therapy), followed for a median of 57 months. Among these patients PASCAL classified 37.0% as PROB, 48.4% as POSS, and 14.6% as UNL. NNTBs to avert 1 recurrent ischemic stroke over 5 years were: PROB 37; POSS 29; UNL -250. NNHs to cause 1 additional late atrial fibrillation were: PROB 167; POSS 77; UNL 20. Treatment group event rates and BPT and HPT values are shown in Table 1.
Conclusions: These findings prospectively validate the PASCAL classification algorithm for distinguishing, among patients with PFO and otherwise cryptogenic ischemic stroke, the 6 of every 7 patients in the net benefit group (PROB, POSS) and 1 of every 7 patients in the net harm group (UNL) with PFO closure.
BPT and HPT Over 5y among 1000 Treated Patients.
Probable
Possible
Unlikely
Strokes Averted (BPT)
27
34
-4
Late AF Caused (HPT)
6
13
51
Disclosure of interest: Yes
SCIENTIFIC COMMUNICATIONS – HYPERACUTE MANAGEMENT
O338/2012
Impact of the Flying Intervention Team vs Patient Interhospital Transfer for Endovascular Treatment in the Early Time Window
Nikolai Hubert*1, Sophie Herdegen1, Hanni Wiestler1, Lucie Esterl-Pfäffl1, Thomas Witton-Davies2, Heinrich Audebert3, Roman Haberl1, Gordian Hubert1
1Munich Clinic, Academic Teaching Hospital of the Ludwig-Maximilians-University, TEMPiS Telemedical Stroke Center, Munich, Germany, 2Munich Clinic, Department of Diagnostic and Interventional Radiology, Munich, Germany, 3Campus Benjamin Franklin, Charité Universitätsmedizin Berlin, corporate member of Freie Universität Berlin, Humboldt-Universität zu Berlin and Berlin Institute of Health, Department of Neurology, Berlin, Germany
Background and aims: Use of a Flying Intervention Team (FIT) significantly reduces time to endovascular thrombectomy compared to interhospital transfer of patients in nonurban areas. Thrombectomy is most effective when performed early after onset. However, the impact of the FIT model stratified by time of presentation has not been studied so far. We aim to determine whether this new system of care is associated with improved outcome in patients presenting in an early time window.
Methods: Thrombectomy eligible patients included in the FIT study and a subsequent prospective registry between 02-2018 and 01-2022 are included in the analysis. Patients treated by a flying neurointerventional team in the primary stroke center are compared to patients transferred from the primary stroke center to a referral center for rthrombectomy. Patients presenting within the early and late time window are analyzed separately. Primary endpoint is the distribution of the modified Rankin Scale score at three months.
Results: Results will include demographic and baseline variables, time metrics and workflow as well as an adjusted analysis of functional outcome three months after presentation.
Conclusions: The analysis will show whether deployment of FIT is associated with improved functional outcome in patients presenting in the early time window. The findings may have an impact on the consideration of this new system of care in areas where neurointerventional expertise is scarce.
Disclosure of interest: No
SCIENTIFIC COMMUNICATIONS – NEUROINTERVENTION – ORGANISATION AND OUTCOME
O339/3109
Nerinetide Reduces Early Infarct Growth Among Stroke Patients Undergoing EVT Without Thrombolysis
Nathaniel Rex*1,2, Johanna Ospel1, Rosalie Mcdonough1, Nima Kashani3, Leon Rinkel1, Brian Buck4, Jeremy Rempel5, Ryan Mctaggart2, Raul Nogueira6, Alexandre Poppe7, Dar Dowlatshahi8, Brian van Adel9, Richard Swartz10, Ruchir Shah11, Eric Sauvageau12, Andrew Demchuk13, Michael Tymianski14, Michael Hill13, Mayank Goyal1
1University of Calgary, Department of Radiology, Calgary, Canada, 2Brown University, Department of Radiology, Providence, United States, 3Saskatoon City Hospital, Department of Radiology, Saskatoon, Canada, 4University of Alberta, Department of Medicine, Edmonton, Canada, 5University of Alberta, Department of Radiology and Diagnostic Imaging, Edmonton, Canada, 6University of Pittsburgh School of Medicine, Department of Neurology, Pittsburgh, United States, 7CHUM, Neurology Service, Department of Medicine, Montréal, Canada, 8University of Ottawa, Department of Medicine, Ottawa, Canada, 9McMaster University, Division of Neurosurgery, Hamilton, Canada, 10University of Toronto, Department of Medicine (Division of Neurology), Toronto, Canada, 11CHI Memorial Stroke and Neuroscience Center, Neurology, Chattanooga, United States, 12Baptist Health, Department of Neurosurgery, Jacksonville, United States, 13University of Calgary, Department of Clinical Neurosciences, Calgary, Canada, 14University of Toronto, Department of Neurosurgery, Toronto, United States
Background and aims: Nerinetide treatment was associated with better clinical outcomes among stroke patients undergoing EVT that were not treated with concurrent alteplase. We investigated the impact of Nerinetide on early infarct growth.
Methods: Data are from the non-alteplase stratum of the ESCAPE-NA1 trial. Patients who underwent CT-perfusion (CTP) as part of routine clinical care were included. Admission CTP data were processed using RAPID software. Infarct core at baseline was defined as areas of relative cerebral blood flow (rCBF)<30% on CTP. Final infarct volume was determined via manual segmentation on 24-hour CT or MR diffusion-weighted imaging. We compared infarct growth (defined as 24h infarct volume minus CTP-estimated baseline infarct core) among patients treated with vs. without Nerinetide.
Results: CTP maps were available in 413/1105 patients. We confirmed effect modification between alteplase and Nerinetide in this subgroup (p=0.005). Of these, 179 (43%) were treated without alteplase, and 79 (44%) received Nerinetide, 100 (56%) received saline control. Infarct growth was larger in the control (34.9ml IQR [6.8-127] vs. Nerinetide (19.6ml IQR [1.7-49.1], p=0.008) group. After adjusting for age, sex, baseline infarct volume, expanded thrombolysis in cerebral infarction score, and baseline imaging to reperfusion time, Nerinetide remained significantly associated with reduced infarct growth (beta=-44.5, p=0.002). In patients receiving alteplase (n=234), there was no difference in infarct growth between those that received placebo vs Nerinetide (10.5ml IQR [-1.3, 67.4] vs. 12.8ml IQR [0.35-55.5], p=0.49).
Conclusions: Nerinetide was associated with decreased infarct growth in stroke patients undergoing thrombectomy without concurrent alteplase in the ESCAPE-NA1 trial.
Disclosure of interest: No
O340/318
A CLINICAL PREDICTION MODEL FOR INDIVIDUALIZED TREATMENT BENEFIT OF INTRAVENOUS THROMBOLYSIS PRIOR TO ENDOVASCULAR TREATMENT: RESULTS OF SIX RCTs POOLED IN IRIS
Jasper Daems*1,2, Fabiano Cavalcante3, Manon Kappelhof3, Kilian Treurniet3,4, Esmee Venema2,5, Bob Roozenbeek1, Diederik Dippel1, Yu Zhou6, Lei Zhang6, Kentaro Suzuki7, Kazumi Kimura7, Johannes Kaesmacher8, Thomas Meinel9, Jan Gralla8, Urs Fischer9, Wenjie Zi10, Raul Nogueira11, Bernard Yan12, Peter Mitchell13, Zhongrong Miao14, Yongwei Zhang6, Pengfei Yang6, Yvo Roos15, Charles Majoie3, Jianmin Liu6, Hester Lingsma2
1Erasmus MC University Medical Center, Department of Neurology, Rotterdam, Netherlands, 2Erasmus MC University Medical Center, Department of Public Health, Rotterdam, Netherlands, 3Amsterdam UMC location University of Amsterdam, Department of Radiology and Nuclear Medicine, Amsterdam, Netherlands, 4Haaglanden MC, Department of Radiology, The Hague, Netherlands, 5Erasmus MC University Medical Center, Department of Emergency Medicine, Rotterdam, Netherlands, 6Changhai Hospital, Naval Medical University, Neurovascular Center, Shanghai, China, 7Nippon Medical School, Department of Neurology, Tokyo, Japan, 8Inselspital, Bern University Hospital, University of Bern, University Institute of Diagnostic and Interventional Neuroradiology, Bern, Switzerland, 9Inselspital, Bern University Hospital, University of Bern, Department of Neurology, Bern, Switzerland, 10Xinqiao Hospital and The Second Affiliated Hospital, Army Medical University (Third Military Medical University), Department of Neurology, Chongqing, China, 11Grady Memorial Hospital, Emory University School of Medicine, Department of Neurology, Marcus Stroke & Neuroscience Center, Atlanta, United States, 12The Royal Melbourne Hospital, University of Melbourne, Department of Medicine and Neurology, Melbourne Brain Centre, Parkville, VIC, Australia, 13The Royal Melbourne Hospital, University of Melbourne, Department of Radiology, Parkville, VIC, Australia, 14Beijing Tiantan Hospital, Capital Medical University, Department of Interventional Neuroradiology, Beijing, China, 15Amsterdam UMC location University of Amsterdam, Department of Neurology, Amsterdam, Netherlands
Background and aims: On average intravenous thrombolysis (IVT) prior to endovascular treatment (EVT) for anterior circulation large vessel occlusion (aLVO) stroke is not non-inferior to EVT alone, but the benefit is small. To capture potential between-patient heterogeneity in benefit and support decision making, we aim to develop a clinical prediction model to predict benefit of IVT prior to EVT.
Methods: We used data from an individual participant data meta-analysis of six randomized clinical trials (RCTs) comparing IVT prior to EVT with direct EVT in aLVO stroke patients presenting directly at EVT-capable centres (the IRIS collaboration). We used multivariable penalized ordinal logistic regression, with a fixed effect for study, to predict the 90-day modified Rankin Scale (mRS) with and without IVT with alteplase, prior to EVT. Based on literature review, clinical expertise, and availability we selected 10 predictors and 3 interactions (Table 1). Treatment benefit was defined as the difference in predicted probability of mRS 0-2 between both treatments, derived from the ordinal model. The model was validated with leave-one-study-out cross-validation and performance was assessed with discrimination and calibration.
Results: 2284 patients (median age 71 years) treated with alteplase in the IRIS database are included and ready to be analysed. The model results will be available at the conference.
Conclusions: Our model may identify patients for whom a larger than average benefit of IVT prior to EVT is expected, or patients with no benefit or even harm. The model may support individualized treatment decision making concerning IVT administration prior to EVT.
Disclosure of interest: No
SCIENTIFIC COMMUNICATIONS – IMAGING
O341/3021
MINocyclinE to Reduce inflammation and blood brain barrier leakage in small Vessel diseAse - results of the MINERVA randomised controlled trial
Robin Brown*1, Daniel Tozer1, Laurence Loubiere1, Young Hong1,2, Tim Fryer1,2, Guy Williams1,2, Martin Graves3, Franklin Aigbirhio1,2, John O'brien4, Hugh Markus1
1University of Cambridge, Dept of Clinical Neuroscience, Cambridge, United Kingdom, 2University of Cambridge, Wolfson Brain Imaging Centre, Cambridge, United Kingdom, 3University of Cambridge, Dept of Radiology, Cambridge, United Kingdom, 4University of Cambridge, Dept of Psychiatry, Cambridge, United Kingdom
Background and aims: Cerebral small vessel disease (SVD) is a major cause of cognitive impairment and stroke. Neuroinflammation and blood-brain barrier (BBB) leakage may play a role in pathogenesis, but a causal link has not been definitively established. In a rodent SVD model, minocycline treatment reduced brain lesions, neuroinflammation and BBB permeability. We determined whether these processes can be therapeutically altered in SVD.
Methods: MINERVA is a phase II, double blind, randomised controlled trial of minocycline in moderate-to-severe SVD. Participants with lacunar stroke and confluent white matter hyperintensities underwent simultaneous dynamic contrast-enhanced MRI to quantify BBB permeability and 11C-PK11195 positron emission tomography (PET) to quantify microglial activation (a marker of neuroinflammation). They were randomly allocated to receive either minocycline 100mg bd or placebo for three months, after which PET-MRI was repeated. The co-primary outcomes were volumes of hotspots of increased BBB permeability and microglial signal. A sample size of 44 allowed us to detect a 20% reduction in these metrics (power = 80%, α=0.05).
Results: 44 patients were recruited from September 2019 - June 2022 at median 12.1 (IQR: 4.4–25.5) months after lacunar stroke. Mean age was 70.7±10.5 years and 29/44 (65.9%) were male. 83.8% had a history of hypertension, 75.7% of hypercholesterolaemia and 20% were diabetic. 59.4% were current/former smokers. Participants had mean white matter lesion volume of 36.9±27.9cc and 2.5±1.8 lacunes.
Conclusions: The treatment period concluded in September 2022. We will present the primary outcomes for the first time.
Radiological Phenotypes of Brain Health in a Stroke Population: Primary Results of the Assessing Population-Based Radiological Brain Health in Stroke Epidemiology (APRISE) Study
Achala Vagal*1, Heidi Sucharew2, Vivek Khandwala1, Lily Wang1, Rebecca Cornelius1, Mary Gaskill-Shipley1, Thomas Tomsick1, David Wang3, Shantala Gangatirkar1, Brady Williamson1, Thomas Maloney1, Mary Haverbusch4, Paul Horn5, Janice Carrozzella1, Kathy Alwell4, Dawn O. Kleindorfer6, David Robinson4, Robert Stanton4, Brett Kissela4, Pooja Khatri4
1University of Cincinnati, Radiology, Cincinnati, United States, 2University of Cincinnati, Emergency Medicine, Cincinnati, United States, 3I-MED Radiology Network, Radiology, Melbourne, Australia, 4University of Cincinnati, Neurology, Cincinnati, United States, 5Cincinnati Childrens Hospital, Neurology, Cincinnati, United States, 6University of Michigan, Neurology, Michigan, United States
Background and aims: To date, no population-based study has characterized the full extent of pre-existing small vessel disease (SVD), ischemic large vessel disease, and intracranial hemorrhage in patients presenting with stroke. Our objective was to assess radiological and clinical phenotypes in a biracial stroke/TIA population. We hypothesized that we would identify distinct radiological phenotypes associated with specific clinical factors.
Methods: Clinical imaging was collected from all hospitalized stroke/TIA patients ascertained in a metropolitan population of 1.3 million in 2015 as part of the Greater Cincinnati/Northern Kentucky Stroke Study. Trained central neuroradiologists characterized all CT and MRI neuroimaging including volumetric analyses. We performed a data driven hierarchical cluster and factor analysis to identify relationships among imaging parameters, and then assessed their association with prespecified clinical variables in lasso selected multivariable models.
Results: In 2015, among 3496 stroke/TIA patients, 3486 (99%) patients had available imaging data (mean 70±15 years, 21% Black race, 54% female sex) and 2560 (73%) had MRIs. Three distinct imaging clusters were identified and each cluster was associated with specific set of clinical variables (Figure)
Conclusions: In this first comprehensive characterization of the full spectrum of radiological brain health in stroke patients ascertained at a population level, we identified three distinct clusters of imaging. Notable findings include the lack of clustering of microbleeds with white matter disease, and the confirmed relationship of perivascular spaces with white matter disease, global cortical atrophy, and lacunes. Understanding brain health imaging patterns may help target future interventions.
Disclosure of interest: No
SCIENTIFIC COMMUNICATIONS – GENETICS OMICS AND BIOMARKERS
O343/3130
Genomics of perivascular space burden unravels early mechanisms of cerebral small vessel disease
Marie-Gabrielle Duperron*1,2, Maria J. Knol3, Quentin Le Grand1, Tavia Evans4,5, Aniket Mishra1, Ami Tsuchida6, Fumihiko Matsuda7, Tzourio Christophe1,8, Joanna Wardlaw9,10,11, Sudha Seshadri12,13, Hieab Adams4,5,14, Stéphanie Debette1,2
1University of Bordeaux, Inserm, Bordeaux Population Health Research Center, UMR 1219, Bordeaux, France, 2Institute of Neurodegenerative Diseases, Department of Neurology, Bordeaux, France, 3Erasmus MC University Medical Center, Department of Epidemiology, Rotterdam, Netherlands, 4Erasmus MC University Medical Center, Department of Clinical Genetics, Rotterdam, Netherlands, 5Erasmus MC University Medical Center, Department of Radiology and Nuclear Medicine, Rotterdam, Netherlands, 6University of Bordeaux, CNRS, CEA, Groupe d’Imagerie Neurofonctionelle - Institut des maladies neurodégénératives (GIN-IMN), UMR 5293, Bordeaux, France, 7Kyoto University Graduate School of Medicine, Center for Genomic Medicine, Kyoto, Japan, 8Bordeaux University Hospital, Department of Medical Informatics, Bordeaux, France, 9University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom, 10University of Edinburgh, UK Dementia Research Institute Centre, Edinburgh, United Kingdom, 11University of Edinburgh, Row Fogo Centre for Research into Ageing and the Brain, Edinburgh, United Kingdom, 12Boston University School of Medicine, Department of Neurology, Boston, United States, 13The Framingham Heart Study, NA, Framingham, United States, 14Universidad Adolfo Ibáñez, Latin American Brain Health (BrainLat), Santiago, Chile
Background and aims: Perivascular space burden (PVS) is an emerging, poorly understood, MRI-marker of cerebral small vessel disease (cSVD), a leading cause of stroke and dementia.
Methods: We conducted genome-wide and whole-exome/genome association studies of PVS burden in up to 40,095 participants (18 population-based cohorts, 66.3±8.6 years, 96.9% European ancestry). Genome-wide significant results were followed up in independent samples of young healthy adults and older Japanese community participants. PVS burden was quantified using both visual rating scales and cutting-edge machine-learning approaches. We conducted extensive bioinformatics exploration of identified PVS risk loci.
Results: We identified 24 genome-wide significant PVS risk loci, mainly in the white matter (WM). These showed association with WM-PVS already in 1,748 students aged 22.1±2.3 years and were enriched in genes causing early-onset leukodystrophies and genes expressed in fetal brain endothelial cells, suggesting an important role of early-life factors. 53% of WM-PVS loci showed nominally significant associations (27% after multiple-testing correction) in a Japanese population-based cohort (N=2,868; 68.3±5.3 years). Mendelian randomization analyses supported causal associations of high blood pressure with basal ganglia (BG) and hippocampal (HIP) PVS, and of BG-PVS and HIP-PVS with stroke, accounting for blood pressure. Two-thirds of PVS loci point to novel pathways, involving extracellular matrix, membrane transport, and developmental processes, enriched in targets of existing drugs for vascular/cognitive disorders. We prioritized 12 genes for functional follow-up through transcriptome-wide association studies.
Conclusions: Our findings provide completely novel insight into the biology of PVS across the adult lifespan and its contribution to cSVD pathophysiology.
PRevention Of Hypertensive Injury to the Brain by Intensive Treatment of blood pressure after IntraCerebral Haemorrhage (PROHIBIT-ICH): 3-month outcomes of a randomised controlled trial of remote-telemetric home BP-monitoring
Iain McGurgan*1, Michelle Wilson1, Josephine Edens1, Jo Hornby2, Maja Dabagh2, Shahena Butt2, Rustam Al-Shahi Salman3, Craig Anderson4, Philip Bath5, Hugh Markus6, Thompson Robinson7, Nikola Sprigg8, Louise Silver1, David Werring2, Peter Rothwell1
1University of Oxford, Wolfson Centre for the Prevention of Stroke and Dementia, Oxford, United Kingdom, 2UCL Queen Square Institute of Neurology, Stroke Research Centre, London, United Kingdom, 3University of Edinburgh, Cerebrovascular Research Group, Edinburgh, United Kingdom, 4The George Institute, Global Brain Health, Sydney, Australia, 5University of Nottingham, Division of Clinical Neuroscience, Nottingham, United Kingdom, 6University of Cambridge, Neurology Unit, Cambridge, United Kingdom, 7University of Leicester, College of Life Sciences, Leicester, United Kingdom, 8University of Nottingham, Faculty of Medicine & Health Sciences, Nottingham, United Kingdom
Background and aims: Intracerebral haemorrhage (ICH) associated with cerebral small vessel disease (SVD) has a high recurrence risk, particularly if BP-control is poor. PROHIBIT-ICH aimed to assess the feasibility, efficacy and safety of centralised BP-management using remote-telemetric home-BP monitoring (RT-HBPM) during post-hospital follow-up after ICH.
Methods: Patients (target=112) with imaging-confirmed SVD-associated ICH and BP>130/80mmHg were recruited from multiple UK hospitals to a parallel-group, open-label, randomised(1:1) trial of 1-3 months of RT-HBPM-guided treatment (calcium channel blocker-based regimen) coordinated centrally from Oxford (target HBPM-BP<120/80mmHg) versus locally-based standard care. The efficacy outcome was the between-group difference in BP-reduction from baseline to 3-month follow-up based on clinic measurements (primary outcome) and on daytime-BP on 24-hour ambulatory BP-monitoring (ABPM).
Results: Recruitment began in 2019, but was suspended repeatedly because of the COVID-19 pandemic, and ended due to funding constraints in January 2022 after inclusion of 86 patients from 16 centres (43 per group; mean/SD age=66.2/12.6; mean/SD baseline SBP=148.5/16.3mmHg). Four patients withdrew before 3-months and two declined 3-month BP assessments. Among 80 (93%) patients with 3-month BP (41 RT-HBPM vs 39 local-care), the mean reduction from baseline in 3-month clinic-BP was greater with RT-HBPM vs local-care (∆SBP=19.4 vs 5.8, p=0.003; ∆DPB=8.6 vs -1.0, p=0.0003), with similar results on ABPM (∆SBP=19.7 vs 2.5, p=0.0007; ∆DBP=8.8 vs -1.1, p=0.0005).
Conclusions: Centralised BP-management using RT-HBPM is feasible after SVD-associated ICH, and resulted in better BP-control at 3-months than standard care. Longer-term BP-control, safety and brain imaging markers will be assessed at one-year follow-up.
Disclosure of interest: No
SCIENTIFIC COMMUNICATIONS – SECONDARY PREVENTION
O345/3081
Comprehensive large-scale mapping of routine laboratory tests after stroke identifies pathophysiological junctures and systemic biology as a strong predictor of clinical outcome
Michael Karg1, Mario Abruscato2, Anna Alegiani3, Jörg Berrouschot4, Felix Bode5, Tobias Boeckh-Behrens6, Georg Bohner7, Albrecht Bormann4, Michael Braun8, Franziska Dorn9, Bernd Eckert3, Ulrike Ernemann10, Marielle Sophie Ernst11, Jens Fiehler12, Klaus Gröschel13, Gerhard F Hamann8, Andreas Kastrup14, Keil Fee Christiane15, Lars Kellert16, Jan Liman17, Christian Nolte7, Martina Petersen18, Gabor Petzold5, Sven Poli19, Joachim Röther3, Jan Hendrik Schaefer20, Maximilian Schell21, Eberhard Siebert22, Götz Thomalla21, Johannes Wischmann16, Silke Wunderlich23, Timo Uphaus13, Sarah Zweynert7, Steffen Tiedt*1
1University hospital, LMU Munich, Institute for Stroke and Dementia Research, Munich, Germany, 2Klinikum Hanau, Department of Neurology, Hanau, Germany, 3Asklepios Klinik Altona, Department of Neurology, Hamburg, Germany, 4Klinikum Altenburgerland, Department of Neurology, Altenburg, Germany, 5Universitätsklinik Bonn, Department of Neurology, Bonn, Germany, 6Klinikum Rechts der Isar, Department of Neuroradiology, Munich, Germany, 7Charite, Department of Neurology, Berlin, Germany, 8Klinikum Günzburg, Department of Neurology, Günzburg, Germany, 9Universitätsklinik Bonn, Department of Neuroradiology, Bonn, Germany, 10Universitätsklinik Tübingen, Department of Neuroradiology, Tübingen, Germany, 11Universitätsklinik Göttingen, Department of Neurology, Göttingen, Germany, 12Universitätsklinikum Hamburg-Eppendorf, Department of Neuroradiology, Hamburg, Germany, 13Universitätsklinik Mainz, Department of Neurology, Mainz, Germany, 14Klinikum Bremen Ost, Department of Neurology, Bremen, Germany, 15Universitätsklinikum Frankfurt, Department of Neuroradiology, Frankfurt, Germany, 16University hospital, LMU Munich, Department of Neurology, Munich, Germany, 17Paracelsus klinik Nürnberg, Department of Neurology, Nürnberg, Germany, 18Klinikum Osnabrück, Department of Neurology, Osnabrück, Germany, 19Universitätsklinik Tübingen, Department of Neurology, Tübingen, Germany, 20Universitätsklinikum Frankfurt, Department of Neurology, Frankfurt, Germany, 21Universitätsklinikum Hamburg-Eppendorf, Department of Neurology, Hamburg, Germany, 22Charite, Department of Neuroradiology, Berlin, Germany, 23Klinikum Rechts der Isar, Department of Neurology, Munich, Germany
Background and aims: Lab tests provide an important window into the systemic biology after stroke, but their value to understand stroke pathophysiology and to predict outcome has not been comprehensively analyzed. Here, we aimed to systematically map the extent, course and importance of laboratory changes after stroke.
Methods: We mapped 51 routine lab tests including measures of inflammation, metabolism, and peripheral organ injury over the first week after stroke onset in 5,036 patients (55,380 blood collections) with large-vessel occlusion stroke at 17 sites. We applied sliding time-window analyses and mixed models, adjusted for covariates and multiple testing, to determine changes over time and associations with 90-day functional independence (mRS 0-2).
Results: Of 5,036 patients (age 76 [66-83]; 50.7% women), only four patients showed consistently normal lab tests. The median count of abnormal lab tests upon admission was seven (IQR 4-9) and across the first week 16 (12-21, Fig. 1). The overwhelming majority of lab tests changed at 5 and 31 hours, indicating pathophysiological tipping points, and arrived at a steady state after 48 hours (Fig. 2). Different sets of lab tests significantly improved clinical outcome prediction models over time after stroke with highest value of leukocytes, red cell distribution width, and glucose levels up to 72 hours, and of CRP, urea, sodium, and hemoglobin levels from 72 to 168 hours (Fig. 3).
Conclusions: Our study identifies pathophysiological junctures after stroke and novel time-dependent outcome predictors and might thus help guiding the selection and timing of lab tests after stroke.
Disclosure of interest: No
O346/568
Effect of Factor XIa Inhibition by milvexian on cerebral infarcts in people with acute ischaemic stroke or transient ischaemic attack (TIA) – A secondary analysis of MRI Outcomes in the AXIOMATIC-SSP Trial. Placeholder abstract
Mike Sharma*1, Scott Kasner2, Georgios Tsivgoulis3, Ashfaq Shuaib4, Jesse Dawson5, Carlos Molina6, Kazunori Toyoda7, Daniel Bereczki8, Helmi Lutsep9, George Ntaios10, Anna Czlonkowska11, Pierre Amarenco12, Matthias Endres13, Byung-Woo Yoon14, David Tanne15, Danilo Toni16, Laetitia Yperzeele17, Paul von Weitzel-Mudersbach18, Gisele Sampaio19, Alvaro Avezum20, Daniel Strbian21, Turgut Tatlisumak22, Jens Eckstein23, Sebastian Ameriso24, Joerg R. Weber25, Else Charlotte Sandset26, Nana Goar Pogosova27, Pablo Lavados28, Antonio Arauz Gongora29, Shrikant I. Bangdiwala30, Anja Kahl31, Chahin Pachai31, Danshi LI31, Graeme J. Hankey32
1McMaster University, Population Health Research Institute, Hamilton, Canada, 2University of Pennsylvania, -, Philadelphia, United States, 3Attikon University Hospital, National and Kapodistrian University of Athens, Athens, Greece, 4University of Alberta Hospital, -, Edmonton, Canada, 5College of Medical, Veterinary & Life Sciences, Queen Elizabeth University Hospital, School of Cardiovascular and Metabolic Health, Glasgow, United Kingdom, 6Hospital Universitari Vall d’Hebron, -, Barcelona, Spain, 7National Cerebral and Cardiovascular Center, -, Osaka, Japan, 8Semmelweis University, -, Budapest, Hungary, 9Oregon Health & Science University, -, Portland, United States, 10University of Thessaly, Department of Internal Medicine, Larissa, Greece, 11Institute of Psychiatry and Neurology, 2nd Department of Neurology, Warsaw, Poland, 12Bichat Hospital, University of Paris, Paris, France, 13Charité- Universitätsmedizin Berlin, Dept Neurology and Center for Stroke Research Berlin, Berlin, Germany, 14Eulji University, Uijeongbu Eulji Medical Center, Gyeonggi-do, Korea, Dem. People's Rep. of, 15Rambam Health Care Campus, Stroke and Cognition Institute, Haifa, Israel, 16Sapienza University of Rome, -, Rome, Italy, 17Antwerp University Hospital, Department of Neurology, Edegem, Belgium, 18Aarhus University Hospital, Department of Neurology, Aarhus, Denmark, 19Universidade Federal de São Paulo/UNIFESP and Hospital Israelita Albert Einstein, -, São Paulo, Brazil, 20Hospital Alemão Oswaldo Cruz, Centro Internacional de Pesquisa, São Paulo, Brazil, 21Helsinki University Central Hospital, -, Helsinki, Finland, 22Institute of Neuroscience and Physiology, Sahlgrenska Academy at the University of Gothenburg and Sahlgrenska University Hospital, Department of Clinical Neuroscience/Neurology and Department of Neurology, Gothenburg, Sweden, 23University Hospital Basel, -, Basel, Switzerland, 24FLENI, Servicio de Neurología Vascular, Departamento de Neurología, Buenos Aires, Argentina, 25Klinikum Klagenfurt, Department of Neurology, Klagenfurt, Austria, 26Oslo University Hospital and The Norwegian Air Ambulance Foundation, Department of Neurology, Oslo, Norway, 27National Medical Research Center of Cardiology after E. Chazov, -, Moscow, Russian Federation, 28Unidad de Investigación y Ensayos Clínicos, Clínica Alemana, Universidad del Desarrollo, Departamento de Neurología y Psiquiatría, Santiago, Chile, 29Instituto Nacional de Neurología y Neurocirugía Manuel Velasco Suárez, -, México City, Mexico, 30McMaster University, Population Health Research Institute and Department of Health Research Methods, Evidence, and Impact, Hamilton, Canada, 31Bristol Myers Squibb, -, Princeton, United States, 32The University of Western Australia, Medical School and Perron Institute for Neurological and Translational Science, -, Perth, Australia
Background and aims: In the AXIOMATIC-SSP phase 2b trial, there was no dose response relationship between oral milvexian (FXIa inhibitor) and the primary outcome of symptomatic ischaemic stroke or covert brain infarction. However, milvexian was associated with fewer symptomatic ischaemic strokes at all doses, except 200 mg BID. In this pre-specified secondary analysis, we performed a detailed examination of the number, size and topography of all incident infarcts on MRI by treatment.
Methods: We randomized 2366 participants with non-lacunar ischemic stroke or TIA to double-blind treatment with one of 5 doses of milvexian, ranging from 25 mg QD to 200 mg BID, or matching placebo in addition to standard antiplatelet therapy. A study-specific MRI was obtained at baseline and 90 days. Images were interpreted by 2 neuroradiologists. Incident infarcts on 90-day images were classified by number, size and location.
Results: A baseline MRI brain scan was obtained in 2315 (99.5%). A follow-up MRI at 90 days was acquired in 2100 (90.3%) participants. Incident brain infarcts were identified in 13.3% of 618 participants assigned placebo, and similar proportions assigned milvexian: 13.1% (25 mg QD), 17.2% (25 mg BID), 11.8% (50 mg BID), 12.7% (100 mg BID), and 11.3% (200 mg BID). Detailed characterization of incident infarcts by size and topography by treatment allocation is on-going and will be presented.
Conclusions: Detailed analysis of imaging detected infarcts will improve understanding of their pathogenesis, response to therapy, and validity as a surrogate outcome and help assess the efficacy of this novel drug class.
Disclosure of interest: No
O347/2467
EFFECTS OF SILDENAFIL ON CEREBROVASCULAR FUNCTION IN SMALL VESSEL DISEASE: RESULTS OF THE RANDOMISED, DOUBLE-BLIND, CROSSOVER, PLACEBO-CONTROLLED OXFORD HAEMODYNAMIC ADAPTATION TO REDUCE PULSATILITY (OxHARP) TRIAL
1University of Oxford, Wolfson Centre for Prevention of Stroke and Dementia, Department of Clinical Neurosciences, Oxford, United Kingdom, 2University of Oxford, Centre for Statistics in Medicine, Oxford, United Kingdom
Background and aims: White matter hyperintensities (WMH) are associated with stroke, dementia and late-life functional impairment but have no specific treatment. OxHARP is testing whether sildenafil, a PDE5 inhibitor, improves cerebral pulsatility and cerebrovascular reactivity in mild-moderate WMH versus placebo, with non-inferiority versus cilostazol, a PDE3 inhibitor.
Methods: OxHARP (NCT03855332) was a prospective, double-blind, randomised, placebo-controlled crossover trial. Participants with lacunar or cryptogenic TIA or stroke and mild-moderate WMH received placebo, sildenafil 50mg and cilostazol 100mg, twice daily for 3 weeks each, with at least 1 week washout. The primary endpoint compared effects of sildenafil versus placebo on Gosling’s pulsatility index on TCD (MCA-gPI). Secondary outcomes included effects on mean MCA velocity change during 4-6% CO2 inhalation (CVR). BOLD-MRI white matter reactivity (MRI-CVR) was assessed in a substudy, initially including 30 patients comparing placebo with sildenafil, amended to include all three phases during the trial. Funding: Wellcome-CRCDF:206589_Z_17_Z.
Results: In 75/75 patients (median 70 years, 51-86; 79% male; 60% stroke), 40 had mild WMH (Fazekas score ⩽2) and 35 had at least moderate WMH. 73/75 patients received at least one dose, and 65/73 (89%) had primary outcome data. 43 participants had an MRI-CVR comparison for sildenafil versus placebo, whilst 15 had MRI-CVR during all phases.
Conclusions: This is the first trial to use TCD and MRI to assess cerebrovascular effects of sildenafil in a mild-moderate SVD population, and non-inferiority to cilostazol, to assess its physiological potential to target WMH progression. Primary and secondary outcomes will be presented at the conference.
Disclosure of interest: No
YSPR: YOUNG STROKE PHYSICIANS AND RESEARCHER
O200/1492
THE EFFECTS OF INDUCED BLOOD PRESSURE CHANGES ON CEREBRAL SMALL VESSELS: THE HYPERINTENSE STUDY
Esther Janssen*1, Annemieke Ter Telgte2, Esmée Verburgt1, Joost de Jong3, José P Marques Marques4, Roy Kessels4,5,6, Walter Backes3, Anton Meijer7, Jaap Deinum8, Niels Riksen8, Anil Tuladhar1, Frank-Erik de Leeuw1
1Radboud University Medical Center; Donders Institute for Brain, Cognition and Behaviour, Department of Neurology, Nijmegen, Netherlands, 2VASCage, Research Centre on Vascular Ageing and Stroke, Innsbruck, Austria, 3Maastricht University Medical Center, School for Mental Health & Neuroscience, Maastricht, Netherlands, 4Radboud University, Donders Institute for Brain, Cognition and Behaviour, Centre for Cognitive Neuroimaging, Nijmegen, Netherlands, 5Psychiatry, Vincent van Gogh Institute for Psychiatry, Venray, Netherlands, 6Radboud University Medical Center, Department of Medical Psychology and Radboudumc Alzheimer Center, Nijmegen, Netherlands, 7Radboud University Medical Center, Department of Medical Imaging, Nijmegen, Netherlands, 8Radboud University Medical Center, Department of Internal Medicine, Nijmegen, Netherlands
Background and aims: Hypertension is the most established risk factor for cerebral small vessel disease (SVD), but the pathophysiological changes following hypertension that cause SVD remain poorly understood as studies generally include elderly individuals with already extensive SVD burden. We aim to examine the effects of high blood pressure on cerebral microvasculature in young/middle-aged adults to detect the earliest microvascular changes associated with SVD.
Methods: HYPERINTENSE is a prospective observational cohort study consisting of two non-overlapping substudies. (1) Cross-sectionally, we will assess differences in advanced and conventional MRI markers between hypertensive patients aged 18-40 years (n=100) and age-matched controls. (2) Longitudinally (n=4 serial MRI scans), we will examine the effects of induced blood pressure increase and decrease by antihypertensive medication withdrawal and restart on MRI outcomes in hypertensive patients 18-55 years (n=30). Exclusion criteria comprise pre-existing cerebrovascular disease, MRI contraindications and major risk factors for non-SVD ischemic stroke. MRI outcomes include blood-brain barrier integrity measured with dynamic contrast-enhanced MRI, diffusion properties measured with multi-band diffusion-weighted imaging and intravoxel incoherent motion imaging and SVD MRI markers, assessed on T1, FLAIR and SWI. Furthermore, subjects will undergo a standard cognitive assessment.
Results: Between July 2021-January 2023,11 patients were included in study 1 and 13 in study 2 Although inclusions started slow due to the COVID-19 pandemic, patient recruitment is currently as scheduled and expected to be complete by December 2023.
Conclusions: HYPERINTENSE is unique in its design and therefore expected to provide new insight into the pathophysiological link between hypertension and SVD.
Disclosure of interest: No
O201/2116
APHASIA DUE TO ACUTE STROKE TREATED WITH THE TABLET-BASED SPEECH THERAPY APP NEOLEXON®: A RANDOMIZED CONTROLLED TRIAL
Leanna Brasch1, Johannes Wischmann*1, Julia Franzen1, Franziska Erbert1, Pitt Young2, Oliver Meier3, Katharina Feil4, Lars Kellert1
1University Hospital, Ludwig-Maximilians-University (LMU) Munich, Germany, Department of Neurology, Munich, Germany, 2Medical Park Reithofpark, Specialized Clinic for Therapies in Neurology, Bad Feilnbach, Germany, 3Passauer Wolf, Neurological Rehabilitation, Bad Griesbach, Germany, 4Tübingen University Hospital, Eberhard Karl University of Tübingen, Department of Neurology and Stroke, Tübingen, Germany
Background and aims: Aphasia is a common symptom in acute stroke patients, which has severe impact on both functional independence and quality of life. Current guidelines recommend face-to-face speech therapy as early as possible after stroke onset. Speech therapy smart devices are a promising approach to complement face-to-face logopaedics and are suitable for self-training purposes. We hypothesize, that speech therapy assisted by the tablet-based app Neolexon® is superior to standard logopaedics (NCT04080817).
Methods: We aim to enroll 180 adult German native-speaking patients with aphasia due to acute stroke and ⩽13 points in the Language Aphasia Screening Test (LAST). Probands are dichotomized into three groups based on their LAST scale and randomly assigned (1:1) to receive either standard speech therapy or standard speech therapy and Neolexon®-therapy. Patients will be visited four times within three months during hospital stay and rehabilitation. Study visits comprise both comprehensive neurological and speech therapy examinations. Primary outcome is defined by a 10% mean difference in the change of percentile rank of the Bielefelder Aphasie Screening (BIAS) after three months. Secondary outcomes include quality of life, scale in Becks Depression Inventory and modified Rankin Scale after three months.
Results: From July 2021 up to now we enrolled n=62 patients, of which n=24 completed their last study visit. We aim to present preliminary results of ongoing analysis.
Conclusions: The Neolexon® application could be a beneficial complementary tool in speech therapy. This trial is suitable to provide evidence for computer-supported speech therapy in acute stroke patients with aphasia.
Disclosure of interest: No
O202/3120
SMARTWATCHES FOR DETECTION OF ATRIAL FIBRILLATION IN SECONDARY PREVENTION OF CRYPTOGENIC STROKE – WATCH AFIB
Horst Penkert1, Johanna Härtl*1, Eimo Martens2, Silke Wunderlich1
1Klinikum Rechts der Isar, Neurology, Munich, Germany, 2Klinikum rechts der Isar, Cardiology, Munich, Germany
Background and aims: In the secondary prevention of ischemic stroke, detection of atrial fibrillation (AFib) and subsequent anticoagulation therapy reduce the risk of recurrent stroke by approximately 60%. Prolonged electrocardiogram (ECG) monitoring up to 6 months significantly increases the detection of AFib in cryptogenic stroke. Thus, prolonged ECG monitoring is likely to lead to a reduction of recurrent stroke by prompting adequate anticoagulation therapy.
Hypothesis: We hypothesize that AFib detection via smartwatch in patients suffering from cryptogenic transient ischemic attack (TIA) or ischemic stroke is accurate for AFib detection compared to an implantable event recorder.
Methods: We introduce a prospective, intraindividual-controlled, multicentre clinical study in patients with cryptogenic ischemic stroke or TIA. In addition to an implanted event recorder as indicated by clinical standard, included patients will receive a smartwatch for detection of AFib. The ECG- data of the smartwatch and the event recorder will be continuously monitored by two independent cardiologists. As soon as AFib is confirmed, a doctoral appointment is set to evaluate start of anticoagulation. The follow-up period will be six months. The study consists of four visits: a baseline visit, two phone visits at one and three months, and an end of trial visit at six months (Figure 1).
The study is financially supported by a grant from the Deutsche Forschungsgemeinschaft (DFG).
Primary Objective: To estimate and compare sensitivity and specificity for AFib detection per patient after six months of the smartwatch- based rhythm analysis and the event recorder.
Results: n/a
Conclusions: n/a
Disclosure of interest: No
O203/1545
THE IMPACT OF LESION CHARACTERISTICS FOR INDIVIDUALIZED STROKE REHABILITATION – PROPOSAL FOR THE NESTED ESTREL-IMAGE STUDY
Annaelle Zietz*1,2, Valerian Altersberger1,2, Cristina Granziera3,4, Tim Sinnecker3,4,5, Josefin E. Kaufmann1,2, Nils Peters1,2,6, Christopher Kenan Traenka1,2, Stefan Engelter1,2
1University Hospital Basel and University of Basel, Switzerland, Department of Neurology and Stroke Center, Department of Clinical Research, Basel, Switzerland, 2University Department of Geriatric Medicine FELIX PLATTER, University of Basel, Switzerland, Neurology and Neurorehabilitation, Basel, Switzerland, 3Faculty of Medicine, University Hospital Basel, University of Basel, Basel, Switzerland, 3Translational Imaging in Neurology (ThINK) Basel, Department of Biomedical Engineering, Basel, Switzerland, 4University Hospital Basel, University of Basel, Basel, Switzerland, Neurologic Clinic and Policlinic, MS Center and Research Center for Clinical Neuroimmunology and Neuroscience Basel (RC2NB), Basel, Switzerland, 5University of Basel, Basel, Switzerland, Medical Image Analysis Center (MIAC) and Quantitative Biomedical Imaging Group, Department of Biomedical Engineering, Basel, Switzerland, 6Klinik Hirslanden, Zürich, Switzerland, Stroke Center, Zürich, Switzerland
Background and aims: In stroke, enhancement of recovery processes is a clinically important goal. Such recovery processes are highly heterogeneous. Infarct characteristics including size, number and location of brain lesions are likely to influence the recovery process of individual patients. However, specifics of this influence and its meaning for individual patients are as yet unknown. In particular, it is unclear, whether brain lesion characteristics visible by MR imaging modify the treatment response to levodopa regarding enhanced recovery. ESTREL (Enhancement of STroke REhabilitation with Levodopa) is a large SNF-funded, randomised, placebo-controlled trial to test whether Levodopa in addition to standardized rehabilitative therapies based on the principles of motor learning will led to a patient-relevant improvement of motor function. Our aim in this proposed nested sub-study is to test whether lesion size, number and location modify (i) functional recovery and (ii) levodopa-treatment response for motor recovery in stroke patients.
Methods: Proof-of-principle-study implemented as nested study within the ESTREL clinical trial
Results: Baseline MR-images will be retrieved from all ESTREL-centres and analysed centrally regarding brain lesion size, number and location. Sample size n=500. MR-findings will be compared with functional outcomes of the clinical trial taking into account the rehabilitation regimen including levodopa-status, and number of rehabilitation sessions
Conclusions: ESTREL-IMAGE provides a unique opportunity to systemically assess the impact on brain lesions on the effectiveness of stroke recovery regimens of individual patients, including the treatment response to levodopa as pharmacological means to enhance stroke recovery. Thus ESTREL-IMAGE strengths the personalized approach in stroke rehabilitation
Disclosure of interest: No
O204/538
SEROLOGICAL BIOMARKERS OF COMPLICATED CAROTID PLAQUES
Jonathan Andrae*1, Andreas Schindler2, Christoph Strecker1, Ernst Mayerhofer1,3, Karl Winkler4, Christine Contini4, Michael M. Hoffmann4, Hansjörg Mast5, Dominik Obrist6, Pascal Corso6, Ali Mokhtari6, Andreas Harloff1
1Department of Neurology and Neurophysiology, Medical Center-University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg im Breisgau, Germany, 2Department of Neuroradiology, University Hospital, LMU Munich, Munich, Germany, 3Department of Neurology, Massachusetts General Hospital, Harvard Medical School, Boston, MA, United States, 4Institute for Clinical Chemistry and Laboratory Medicine, Medical Center-University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg im Breisgau, Germany, 5Department of Neuroradiology, Medical Center-University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg im Breisgau, Germany, 6ARTORG Center for Biomedical Engineering Research, University of Bern, Bern, Switzerland
Background and aims: Internal carotid artery (ICA) stenoses are responsible for up to 25% of ischemic strokes. Plaque composition is a major risk factor for incident stroke. Especially complicated AHA type VI carotid artery plaques (cCAP) have been associated with cerebrovascular symptoms. Detection of these kind of plaques requires special equipment and MRI-sequences. Thus, we compare the differences in circulating levels of proinflammatory and atherogenic proteins and lipid subfractions between patients with cCAP and those with other plaque types in MRI imaging with the aim to discover new biomarkers that may identify patients at high risk.
Methods: One hundred consecutive individuals with asymptomatic 20-80% ICA stenosis will be prospectively enrolled until May 2023. Plaque type and volume is determined blinded to individuals’ clinical data in a standardized manner from 3 Tesla high-resolution multi-contrast 3D MRI (T1-, T2-, proton density-weighted images, and time-of-flight-angiography). Associations of IL-6, hsCRP, sFlt-1, lipoprotein (a), apolipoprotein B, and Lp-PLA2 with plaque type and plaque volume are assessed.
Results: To date, 60 consecutive patients carrying 80 ICA stenoses of which 20 (25%) had cCAP were included. Results of the whole cohort of one hundred individuals together with the currently pending levels of biomarkers and their associations with AHA-lesion types and volume will be presented at the conference in May 2023.
Conclusions: Novel blood biomarkers associated with cCAP in the carotid artery could lead to more reliable identification of patients at high risk for ischemic stroke and make their application useful in further studies of ischemic stroke prevention.
Disclosure of interest: No
O205/321
ASSOCIATION OF REMOTE VERSUS LOCAL SYMPTOMATIC INTRACRANIAL HEMORRHAGE AFTER INTRAVENOUS THROMBOLYSIS FOR ACUTE ISCHEMIC STROKE WITH CLINICAL OUTCOMES
Lina Palaiodimou*1, Maria Ioanna Stefanou1, Aikaterini Theodorou1, Janika Kõrv2, Ana Paiva Nunes3, Paolo Candelaresi4, Elisa Dall'ora5, Payam Sariaslani6, Leandro Provinciali7, Adriana Conforto8, Alan Alves de Lima Cidrao9, Niaz Ahmed10,11, Georgios Tsivgoulis1,12
1National and Kapodistrian University of Athens, Second Department of Neurology, Athens, Greece, 2University of Tartu, Department of Neurology and Neurosurgery, Faculty of Medicine, Tartu, Estonia, 3University Hospital Lisboa, Stroke Unit, São José Hospital, Lisbon, Portugal, 4AORN "Antonio Cardarelli", Neurology and Stroke Unit, Naples, Italy, 5Bolzano Central Hospital, Stroke Unit, Department of Neurology, Bolzano, Italy, 6Kermanshah University of Medical Sciences, Department of Neurology, School of Medicine, Kermanshah, Iran, 7Marche Polytechnic University, Neurological Clinic, Department of Experimental and Clinical Medicine, Ancona, Italy, 8Universidade de São Paulo, Hospital das Clínicas, Divisão de Neurologia Clínica, São Paulo, Brazil, 9Faculdade de Medicina da UFC, Programa de Pós-graduação em Ciências Cardiovasculares, Fortaleza, Brazil, 10Karolinska University Hospital, Department of Neurology, Stockholm, Sweden, 11Karolinska Institutet, Department of Clinical Neuroscience, Stockholm, Sweden, 12University of Tennessee Health Science Center, Department of Neurology, Memphis, United States
Background and aims: Although remote symptomatic intracranial hemorrhage (rSICH) is a rare complication after intravenous thrombolysis for acute ischemic stroke, patients with rSICH present worse functional outcomes and higher mortality compared to patients without SICH. Whether rSICH compared to local SICH (lSICH) is associated with worse clinical outcomes post-stroke remains currently unknown.
Methods: Prospectively-collected patient-data registered in Safe Implementation of Treatments in Stroke-International Stroke Thrombolysis Register (SITS-ISTR) will be used. Patients who developed SICH according to SITS-Monitoring Study (SITS-MOST) definition will be included in the analysis and will be stratified according to the SICH location in lSICH-group defined as patients with SICH within infarcted area versus rSICH-group defined as patients with SICH outside infarcted brain tissue in addition or not to lSICH. The main outcome of interest will be good functional outcome at 3-months, defined as modified Rankin Scale (mRS) scores of 0-2. Secondary outcomes of interest will be: the distribution of 3-month functional outcomes; favorable functional outcome at 3-months (mRS-scores: 0-1); early mortality; and mortality at 3-months. All outcomes will be assessed before and after propensity score matching to maximize the balance in the distribution of possible confounders between the patient-groups. Additionally, we will perform a systematic review and meta-analysis including randomized-controlled clinical trials and cohort studies that report clinical outcomes post-AIS separately for patients with rSICH versus lSICH. The same outcomes of interest will be assessed using the random-effects model.
Results:Conclusions: This study will provide evidence whether rSICH compared to lSICH is associated with clinical outcomes post-stroke.
Disclosure of interest: No
Moderated Poster - Late Breaking
/148
PROGNOSTIC MARKERS OF POST-STROKE DEPRESSION (PROMoSD): A PROSPECTIVE SINGLE-CENTER OBSERVATIONAL STUDY ON RAPHE HYPOECHOGENICTY AS A PREDICTOR OF POST-STROKE DEPRESSION
Daniel Richter1,2, Ebert Andreas3, Mazul-Wach Lisa1, Ruland Quirin1, Jeyanthan Charles James1, Ralf Gold1, Georgios Tsivgoulis4, Georg Juckel3, Christos Krogias*1,2
1St. Josef-Hospital, Ruhr University Bochum, Neurology, Bochum, Germany, 2EvK Herne, Neurology, Herne, Germany, 3LWL University Hospital, Ruhr-University Bochum, Psychiatry, Psychotherapy and Preventive Medicine, Bochum, Germany, 4National and Kapodistrian University of Athens, Attikon University Hospital, Neurology, Athens, Greece
Background and aims: Post-stroke depression (PSD) is an important and quality-of-live-deteriorating complication after stroke. To date, reliable individual prediction of PSD is not possible. As depressive symptoms have been associated with brainstem raphe (BR) hypoechogenicity in transcranial sonography (TCS), we aimed to explore the association of BR hypoechogenicity and the occurrence of PSD.
Methods: The Prognostic Markers of Post-Stroke Depression (PROMoSD) study is a prospective, observational, single-center, investigator-initiated study that included patients with acute ischemic stroke (AIS) within the past 14 days to investigate the presence of BR hypoechogenicity by TCS early after symptom onset. The primary outcome was the presence of PSD assessed at the three months follow-up investigation and defined according to the fifth version of the Diagnostic and Statistical Manual of Mental Disorders (DSM-V criteria).
Results: From 105 included AIS patients, 99 patients completed the study. AIS patients with a hypoechogenic BR developed a PSD at three months more frequently compared to normoechogenic patients (48.0% versus 4.1%, P<0.001). After adjustment for confounders, a hypoechogenic BR remained independently associated with a substantial increase in the appearance of a PSD (adjusted OR: 6.371, 95%-CI: 1.181 – 34.362)
Conclusions: The results of PROMoSD show that a hypoechogenic BR is a strong and independent predictor of PSD at three months after an AIS. TCS could be a routine tool to assess PSD risk in clinical practice, thereby streamlining diagnostic and therapeutic algorithms. Whether patients with AIS and hypoechogenic BR could benefit from preventive antidepressant therapy should be questioned in future studies.
Disclosure of interest: No
/370
Impact of central blinded outcome adjudication of the modified Rankin Scale with video in a large European randomised stroke trial
Wouter Sluis*1, Jeroen de Jonge1, Rik Reinink1, Alastair Wilson2, Jesse Dawson2, Kennedy R. Lees2, H. Bart van der Worp1
1University Medical Center Utrecht, Neurology and Neurosurgery, Utrecht, Netherlands, 2University of Glasgow, Institute of Cardiovascular and Medical sciences, Glasgow, United Kingdom
Background and aims: ‘Central’ adjudication of the modified Rankin Scale (mRS) by independent investigators based on a video of the mRS interview may be more reliable than adjudication by a local investigator, and improve study power. We assessed the agreement between local and central mRS adjudications and the impact of blinded central adjudication on treatment effect estimates in a multinational, open, acute stroke trial.
Methods: The PREvention of Complications to Improve Outcome in elderly patients with acute Stroke (PRECIOUS) trial was a European, randomised, open, acute stroke trial with blinded outcome assessment. Patients were randomly allocated to any combination of metoclopramide, ceftriaxone, paracetamol or standard care. The score on the mRS was assessed at 90 days after stroke through an interview of a local investigator with the patient or a caregiver, which was recorded on video. The video was assessed ‘centrally’ by three adjudicators who were blinded to treatment allocation. We assessed the agreement between the local and central mRS adjudications, corrected for chance with kappa statistics, and assessed the effect of treatment on local and central mRS scores with multivariable ordinal logistic regression.
Results: Of 1493 patients from 68 sites in nine European countries randomised in PRECIOUS, 1167 (78.2%) were alive at 90 days and could be analysed. For 1118 (95.8%) a video was available. Results will be presented at the Conference.
Conclusions: This study will assess the added value of central mRS adjudication with a video in a multinational acute stroke trial.
Disclosure of interest: Yes
/602
The association between peri-haematomal oedema and functional outcome after spontaneous intracerebral haemorrhage (ICH): individual participant data meta-analysis (IPDMA)
Neshika Samarasekera*1
1Centre for Clinical Brain Sciences, University of Edinburgh, Edinburgh, United Kingdom
Background and aims: Peri-haematomal oedema (PHO) is a therapeutic target after ICH. The strength of its association with outcome and impact of clinical and radiological variables on this association are unclear.
To determine if:
(1-primary analysis) the change in PHO volume between two pre-specified time points in the two weeks after ICH onset is associated with three month functional outcome.
(2) PHO volume measured at a time point in the two weeks after ICH onset is associated with functional outcome.
(3) the association between PHO and functional outcome varies according to the time point of PHO measurement and the timepoints between which change in PHO volume is measured in the first two weeks after ICH onset.
(4) the association between PHO volume and functional outcome (aims 1,2) is affected by clinical or radiological variables.
Methods: IPDMA (PROSPERO CRD42021253263) of 1347 participants (male n= 831 (62%); median age 66 years) from observational studies or randomised controlled trials (USA n=2, Australia n=2, Germany n=1) and the VISTA ICH collaboration.
Results: ICH locations were supratentorial deep (67%), lobar (19%), infratentorial (6%), unknown (8%). The median time interval from onset to first scan was 2.0 hours. The median ICH volume was 11.3 ml. In an unadjusted logistic regression meta-analysis (primary analysis), the odds of a poor outcome increased by 4% per ml increase in absolute PHO volume between baseline and 24 hours (forest plot). Further results to be presented at ESOC.
Conclusions: These results will inform the trial design of an intervention for PHO.
Disclosure of interest: No
/1608
Metoclopramide to prevent pneumonia in stroke patients with a nasogastric tube
Wouter Sluis*1, Jeroen de Jonge1, Rik Reinink1, Lisa Woodhouse2, Willeke Westendorp3, Diederik van de Beek3, Philip Bath2, H. Bart van der Worp1
1University Medical Center Utrecht, Neurology and Neurosurgery, Utrecht, Netherlands, 2University of Nottingham, Stroke Trials Unit, Division of Clinical Neuroscience, Nottingham, United Kingdom, 3Amsterdam University Medical Center, Department of Neurology, Amsterdam, Netherlands
Background and aims: A small randomised clinical trial in the United Kingdom has suggested that in patients with acute stroke who have a nasogastric tube, treatment with metoclopramide reduces the risk of pneumonia. We aimed to validate this finding in the larger PREvention of Complications to Improve OUtcome in elderly patients with acute Stroke (PRECIOUS) trial.
Methods: PRECIOUS was an international, 3*2-factorial, randomised-controlled, open-label clinical trial with blinded outcome assessment (PROBE) in patients aged 66 years or older with acute ischaemic stroke or intracerebral haemorrhage and an NIHSS score ⩾ 6. In the present substudy, we included patients who had a nasogastic tube within 48 hours after stroke onset and had been randomly allocated to metoclopramide (10 mg thrice daily), started within 24 hours after symptom onset and continued for four days or until discharge, if earlier, or to standard care. The primary outcome of this substudy was the occurrence of pneumonia. The score on the modified Rankin Scale was a secondary outcome.
Results: Of 1493 patients from 68 sites in nine European sites randomised in PRECIOUS from April 2016 through June 2022, 355 (24%) had a nasogastric tube and could be analysed. The main results of this analysis will be presented at the Conference.
Conclusions: This post-hoc analysis of PRECIOUS will provide evidence whether treating patients with stroke and a nasogastric tube with metoclopramide reduces the risk of pneumonia.
Disclosure of interest: Yes
/1811
IMPROVED LVO FIRST-PASS EFFECT WITH PRECISE CYCLIC ASPIRATION: EARLY EXPERIENCE WITH THE RAPIDPULSETM SYSTEM
1Univ of Pittsburgh, Neurology, Pittsburgh, United States, 2Odense University Hospital, Neuroradiology, Odense, Denmark, 3General University Hospital of Alicante, Neuroradiology, Alicante, Spain, 4Hospital Geral de Fortaleza (HGF), Neuroradiology, Fortaleza, Brazil, 5Istanbul Aydin University VM Medical Park Florya Hospital, Neuroradiology, Istanbul, Turkey, 6P. Stradins Clinical University Hospital, Neurosurgery, Riga, Latvia, 7Hospital Universitario 12 de Octubre, Neuroradiology, Madrid, Spain
Background and aims: First-pass effect (FPE) is associated with improved clinical outcomes in mechanical thrombectomy (MT) for large vessel occlusion strokes (LVOS). However, FPE is achieved in only 30-40% of patients with the current devices. The RapidPulseTM Cyclic Aspiration System (RP) is a novel technology consisting of a valve box that precisely cycles pressure from full to no vacuum multiple times per second adding kinetic energy to the suction forces. Initial clinical evaluation suggests that the system can achieve FPE rates in the 70% range. We aim to evaluate the RP as a frontline approach in LVOS.
Methods: Prospective, multicenter, open-label, core lab adjudicated, early experience of the RapidPulseTM System. Patients with LVOS involving anterior and/or posterior circulations within 24 hours from stroke onset, without evidence of ICAD and/or tandem occlusions, and amenable to treatment with the Medtronic React-71 aspiration catheter were eligible. The primary outcome was the rate of FPE (mTICI ⩾2c after one pass). Secondary outcomes included frontline technical success (mTICI ⩾2b after final pass with no rescue therapy), and incidence of vessel injury and/or vasospasm. The study will enroll up to 100 participants at 6 centers across Spain, Turkey, Denmark, Latvia and Brazil.
Results: As of December 2022, about two-thirds of the target enrollment has been achieved. Final results will be presented at the ESOC.
Conclusions: RapidPulse TM is a novel cyclic aspiration technology designed to achieve faster and better reperfusion in LVOS while significantly reducing disposable device costs. Additional larger studies are currently underway.
Disclosure of interest: Yes
/2066
Collateral Grade as a Mediator of the Effect of Post-Endovascular Blood Pressure Goals on Outcomes: A Pre-specified Exploratory Analysis of the BEST-2 Randomized Trial
Felipe Ayala*1, Lisa Nobel1, Larry Taylor Davis2, Charles Prestigiacomo3, Shilpi Mittal4, Tapan Mehta5, Pablo Harker1, Neeharika Krothapalli6, Heather Stefek2, Emily Lippincott2, Gregory W. Albers7, Gordon Bernard8, Pooja Khatri1, Eva Mistry1
1University of Cincinnati Medical Center, Department of Neurology & Rehabilitation, Cincinnati, United States, 2Vanderbilt University Medical Center, Department of Radiology, Nashville, United States, 3University of Cincinnati Medical Center, Department of Neurosurgery, Cincinnati, United States, 4Vanderbilt University Medical Center, Department of Neurology, Nashville, United States, 5Hartford HealthCare Medical Group, Department of Neurology, Hartford, United States, 6UConn Health, Department of Neurology, Farmington, United States, 7Stanford Medical Center, Department of Neurology, Stanford, United States, 8Vanderbilt University Medical Center, Department of Medicine, Nashville, United States
Background and aims: Observational studies show high post-endovascular treatment (EVT) systolic blood pressure (SBP) is associated with worse patient outcomes. Randomized trials targeting lower SBP failed to demonstrate benefit due to potential need for individualized approach. We explore whether collateral status affects the relationship between post-EVT SBP and outcomes.
Methods: We conducted a pre-specified, exploratory analysis of the BEST (Blood Pressure After Endovascular Stroke Therapy)-II trial that randomized patients with successful EVT (eTICI ⩾ 2b) for large vessel occlusion to post-EVT SBP target: ⩽ 180 mmHg, <160 mmHg, and <140 mmHg. Pre-EVT collaterals were centrally assessed on initial CTA using modified Tan (mTan) score (0-1= poor collaterals; 2-3= good collaterals). The outcomes were 36(+/-12)h final infarct volume (FIV) and 90(+/-14)d utility-weighted modified Rankin Score (uw-mRS). We used multivariable linear regression models with interaction terms (mTan*SBP) to assess effect of mTan on relationship between SBP and outcomes. Models were adjusted for age, baseline NIHSS, and eTICI (baseline ASPECTs for FIV model; baseline mRS for uw-model).
Results: Among 120 enrolled patients, 108 (90%) had complete data. Mean age was 69(+/-14.5) years and n=60 (55.6%) were female; mean baseline NIHSS was 16 (+/-8) and ASPECT score was 7(+/-2). 37 (34.3%) had poor collaterals. Interaction p value between mTan and SBP was 0.063 for FIV outcome and 0.99 for uw-mRS outcome (Figure 1&2, respectively).
Conclusions: Lowering post-EVT SBP was associated with larger FIV with poor collaterals compared to good collaterals. However, collateral status did not mediate the relationship between post-EVT SBP and 90-day uw-mRS.
Disclosure of interest: Yes
/3006
EX VIVO RESPONSE TO TPA TO GENERATE PLASMIN PREDICTS THE IN VIVO RESPONSE AND THROMBOLYSIS OUTCOME IN PATIENTS WITH ACUTE ISCHAEMIC STROKE
Robert Medcalf*1, Tom Lillicrap2, Stevi Harman1, Jilly Chan1, Charithani Keragala1, Heidi Ho1, Dominik Draxler1, Zikou Liu1, Geoffrey Cloud3, Mark Parsons4, Liz Holliday5, Carlos Garcia-Esperon6, Neil Spratt7, Bruce Campbell8, Philip Choi9, Timothy Kleinig10, Simon Koblar11, Anne Hamilton-Bruce11, Jim Jannes11, John Attia5, Joan Montaner12, Alejandro Bustamante12, Israel Fernandez Cadenas13, Laszlo Csiba14, Rita Kálmándi15, István Szegedi14, Zsuzsa Bagoly15, /Christopher Levi/2
1Melbourne, Australian Centre for Blood Diseases, Clayton, Australia, 2University of Newcastle, School of Medicine, Newcastle, Australia, 3Monash University, Neuroscience, Melbourne, Australia, 4University of New South Wales, Southwestern Sydney Clinical School, Liverpool, Australia, 5University of Newcastle, Centre for Clinical Epidemiology and Biostatistics, Newcastle, Australia, 6University of Newcastle, School of Medicine and Public Health, Newcastle, Australia, 7University of Newcastle, School of Biomedical Sciences and Pharmacy, Newcastle, Australia, 8University of Melbourne, Medicine, Melbourne, Australia, 9Monash University, Eastern Health and Eastern Health Clinical School, Box Hill, Australia, 10Royal Adelaide Hospital, Department of Neurology, Adelaide, Australia, 11University of Adelaide, Stroke Research Program, Adelaide, Australia, 12Vall d'Hebron Institute of Research (VHIR), Neurovascular Research Laboratory, Barcelona, Spain, 13Sant Pau Hospital Institute of Research, Stroke Pharmacogenomics and Genetics Lab, Barcelona, Spain, 14University of Debrecen, Department of Neurology, Debrecen, Hungary, 15University of Debrecen, Division of Clinical Laboratory Sciences, Debrecen, Hungary
Background and aims: Optimal tPA thrombolysis occurs when plasmin is targeted to clot surfaces. We hypothesised that variation in the inherent (systemic) versus fibrin-targeted plasminogen activation following tPA treatment correlates with clinical outcome in patients with acute ischaemic stroke (AIS).
Methods: We evaluated fibrinolytic capacity in pre-thrombolysis plasma from Australian, Hungarian and Spanish (n=218) AIS patients who received tPA within 3 or 4.5h from stroke onset. Ex-vivo formation of plasmin-antiplasmin (PAP) complex after tPA treatment was quantified alone (inherent activation) or with a fibrin cofactor (for maximal activation). Data was compared to in-vivo PAP levels 1h post-thrombolysis. The maximal:inherent response ratio (“fibrin sensitivity ratio”, FSR) was correlated with clinical improvement (decrease in NIHSS⩾8 or NIHSS⩽1 at 24h).
Results: Inducible PAP levels formed ex-vivo significantly correlated with in-vivo levels (r2=0.9343; p<0.0001; n=81) but varied ~100-fold. Patients with higher inherent inducible PAP responses were more likely to have a worse clinical outcome independent of major haemorrhage (p=0.014; n=218). FSR varied widely (range 1.04-59.73, median 4.57). FSR⩽2.17 (lowest quintile) negatively correlated with major clinical improvement (adjusted for atherosclerotic aetiology, major haemorrhage, age, onset-to-lysis time, blood pressure-OR 0.37, 95%CI 0.15-0.93, p=0.035; n=218).
Conclusions: The tPA-inducible PAP test is predictive of plasminogen activation in-vivo yet tPA responsiveness varies substantially (Figure 1). Improved clinical outcome occurs when systemic plasminogen activation is minimal but where maximal potential is maintained. The FSR provides a novel algorithm which may help identify AIS patients in whom thrombolysis is either futile or should be avoided.
Disclosure of interest: No
/3023
Efficacy and Safety of Panax Notoginseng Saponins in the Treatment of Ischemic Stroke: A Randomized Clinical Trial
Longfei Wu*1, Chi Zhang2, Haiqing Song1, Ying Gao2, Xunming Ji3
1Xuanwu Hospital, Department of Neurology, Beijing, 2Dongzhimen Hospital, Institute for Brain Disorders, Beijing, 3Xuanwu Hospital, Department of Neurosurgery, Beijing,
Background and aims: Pre-clinical and clinical studies have suggested the neuroprotective effect of panax notoginseng saponins (Xuesaitong soft capsules). However, robust evidence in patients with ischemic stroke is lacking. We conducted the present study to investigate the efficacy and safety of Xuesaitong soft capsules in patients with ischemic stroke.
Methods: This multicenter, randomized, double-blind, placebo-controlled clinical trial including 3072 patients with ischemic stroke was conducted at 67 centers in China from July 2018 to June 2020. Eligible patients were randomly assigned within 14 days after symptom onset to receive either treatment with Xuesaitong soft capsules or placebo for 3 months. The primary outcome was functional independence at 3 months, defined as a modified Rankin Scale score of 0 to 2.
Results: Among 3072 eligible patients with ischemic stroke who were randomized (median age, 62 [55, 68] years; 2052 male patients [66.8%]), 2966 (96.5%) were included in the modified intention-to-treat cohort. The number with functional independence at 3 months was 1328 (89.3%) in the Xuesaitong group and 1218 (82.4%) in the control group (odds ratio, 1.79; 95% CI: 1.45 to 2.21; P < 0.01). In the safety cohort, the proportion of patients with serious adverse events was 1.0% (15/1488) in the Xuesaitong group and 1.1% (16/1482) in the control group (P = 0.85).
Conclusions: In this randomized clinical trial, Xuesaitong soft capsules significantly increased the likelihood of functional independence at 3 months in patients with ischemic stroke.
Disclosure of interest: No
/3039
Transport strategy in patients with symptoms of acute large-vessel occlusion stroke TRIAGE-STROKE a randomized clinical trial
Anne Behrndtz*1,1,2, Rolf Blauenfeldt1, Søren Paaske Johnsen3, Jan Brink Valentin3, Martin Faurholdt Gude4, Mohammad Ahmad Al-Jazi5, Paul von Weitzel-Mudersbach5, Boris Modrau6, Dorte Damgaard1, Kristina Dupont Hougaard1, Niels Hjort1, Tove Diedrichsen1, Marika S. Poulsen1, Marie Louise Schmitz1, Marc Fisher7, Grethe Andersen1, Claus Ziegler Simonsen1
1Aarhus University Hospital, Neurology, Aarhus, Denmark, 2Aarhus University, Health, Aarhus, Denmark, 3Aalborg University, Department of Clinical Medicine, Aalborg, Denmark, 4Aarhus University Hospital, Prehospital Emergency Medical Services, Aarhus, Denmark, 5Goedstrup Hospital, Neurology, Goedstrup, Denmark, 6Aalborg University Hospital, Neurology, Aalborg, Denmark, 7Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, United States
Background and aims: When patients with acute ischemic stroke (AIS) present with symptoms of a large vessel occlusion (LVO) in the catchment area of a primary stroke center (PSC), benefits of direct transport to a comprehensive stroke center (CSC) have been suggested.
Methods: We conducted a national investigator-driven, multi-center, randomised, assessor-blinded clinical trial. Patients eligible for intravenous thrombolysis (IVT) and with symptoms indicating LVO were randomized for admission to the nearest PSC (prioritizing IVT) or direct CSC admission (prioritizing endovascular therapy). The primary outcome was functional improvement at day 90 for all patients with AIS, measured by the modified Rankin Scale score (mRS).
Results: We enrolled 171 patients of whom 104 had AIS. Baseline characteristics were well balanced. Primary analysis (ordinal logistic regression) revealed an odds ratio (OR) for functional improvement at day 90 in mRS of 1.42 (95% confidence interval (CI): 0.72 to 2.82, P=0.31). OR for becoming ambulatory (mRS score 0-3) in the group admitted first to the CSC was 2.65 (95% CI, 1.06 to 7.13, P=0.034). Onset to groin time for patients with LVO was 35 minutes (P=0.007) longer when patients were transported to a PSC first, whereas onset to needle (IVT) was 30 minutes (P= 0.012) longer for all patients with AIS when they were transported directly to a CSC.
Conclusions: For patients with AIS, significance was not reached in the primary analysis of mRS improvement. However, patients admitted directly to a CSC had significantly better odds of becoming ambulant at day 90.
Disclosure of interest: No
/3043
Impact of Periodontal Treatment on Outcomes in patients with Stroke/TIA: PeRiodontal Treatment to Eliminate Minority Inequality and Rural Disparities in Stroke (PREMIERS) study
Souvik Sen*1, Emma Mason2, Makenzie Logue2, James Curtis3, David Hicklin3, Cynthia Nichols3, David Huang4, Cristiano Susin5, Kevin Moss5, James Beck5
1University of South Carolina, Neurology, Columbia, United States, 1University of South Carolina, Neurology, Columbia, United States, 3Prisma Health Richland Hospital, Dentistry, Columbia, United States, 4University of North Carolina, Neurology, Chapel Hill, United States, 5University of North Carolina, Dentistry, Chapel Hill, United States
Background and aims: Recently we showed lack of superiority of intensive versus standard periodontal disease (PD) treatment in preventing composite vascular outcome in stroke/TIA. The next goal was to investigate the effect of treatment on PD outcome and vascular risk factors, and effect of treatment frequency on composite vascular outcome.
Methods: In PREMIERS (NCT00091949), 280 patients with stroke/TIA and PD were assigned to intensive/standard PD treatment. Secondary outcome included changes in blood pressure (BP), haemoglobin A1C (HbA1C), lipid profile and high-sensitivity C-Reactive protein (HS-CRP). PD outcome included sites with pocket depth ⩾4 mm, bleeding on probing, and clinical attachment loss measured at baseline, 3, 6, 9 and 12 months. The dental-visit numbers were correlated with composite vascular outcome.
Results: Diastolic BP and high-density lipoprotein cholesterol improved in both arms (p<0.05) (Table-1). HbA1C and Median HS-CRP were lower, significant in the standard arm. The PD outcomes were significantly better in the intensive vs. the standard arm (Table-2). Over the study period, 10% attended baseline dental visit only, 25% 2-3 visits, and 65% 4-5 visits. Compared to the first group, those attending 2-3 visits (HR 0.47, 95% CI 0.18-1.26) and 4-5 visits (HR 0.21, 95% CI 0.08-0.54) had lower composite vascular event rates (Figure-1).
Conclusions: We report significant improvements in vascular risk factors in both treatment arms, significant improvements in PD outcomes in the intensive vs. standard arm. The 4-5 dental-visits group reaped the most benefit in secondary prevention. (Sponsored by the National Institute of Minority Health Disparity, Orapharma and Philips)
Disclosure of interest: No
/3053
BLOOD PRESSURE MANAGEMENT IN STROKE FOLLOWING ENDOVASCULAR TREATMENT (DETECT): A FEASIBILITY TRIAL AND META-ANALYSIS OF OUTCOMES
Aristeidis Katsanos*1, Luciana Catanese1, Demetrios J Sahlas1, Abhilekh Srivastava1, Areti Angeliki Veroniki2, Kanjana Perera1, Kelvin Ng1, Raed Joundi1, Brian Van Adel3, Ramiro Larrazabal3, Christine Hawkes4, Aviraj Deshmukh5, Kanchana Ratnayake1, Georgios Tsivgoulis6, Oscar Benavente7, Robert Hart1, Mike Sharma1, Ashkan Shoamanesh1
1McMaster University, Division of Neurology, Hamilton, Canada, 2University of Toronto, Institute of Health Policy Management and Evaluation, Toronto, Canada, 3McMaster University, Division of Neurology, Neurosurgery, and Diagnostic Imaging, Hamilton, Canada, 4University of Toronto, Department of Medicine (Division of Neurology), Toronto, Canada, 5NOSM University, Department of Medicine (Neurology), Greater Sudbury, Canada, 6National and Kapodistrian University of Athens, Second Department of Neurology, Athens, Greece, 7The University of British Columbia, Division of Neurology, Vancouver, Canada
Background and aims: Post procedure blood pressure (BP) correlates with outcome in stroke patients who have had endovascular thrombectomy (EVT). The optimal target is unknown.
Methods: We performed a randomized, open-label, blinded endpoint, trial to establish feasibility of testing intensive (systolic BP target <140 mmHg) vs. standard BP target (systolic BP <180 mmHg) after successful EVT for anterior circulation large vessel occlusion. Eligible individuals with persistently elevated BP after EVT were randomised within one hour to either BP target for 48 hours. Feasibility metrics were enrolment rate and adherence to allocated BP target. Exploratory endpoints included neurological deterioration, functional improvement, intracranial hemorrhage and flow dynamics detected by transcranial Doppler ultrasound. Our data was pooled into an aggregate data meta-analysis of clinical and imaging outcomes from all completed randomized clinical trials to date.
Results: Between 10/23/2020 and 2/4/2023, 221 patients were screened and 30 randomized (14%; average recruitment of 1.2 participants/month). Participants in the intensive BP arm had a mean +/-SD systolic BP of 131±18mmHg over 48 hours (75% of the readings under 140 mmHg), while participants in the standard BP arm had a mean 48-hours systolic BP of 139±18mmHg (48% of the readings between 140 and 180 mmHg). No differences between the two groups were found in any of the predefined exploratory endpoints. The meta-analysis is currently being undertaken and results will be presented.
Conclusions: The natural course of BP normalization following successful recanalization poses a challenge for the conduct of clinical trials evaluating different BP thresholds post EVT (NCT04484350).
Disclosure of interest: No
/3124
IMAGING OUTCOMES IN THE APRIL STUDY: A DOUBLE-BLIND, PLACEBO-CONTROLLED, RANDOMIZED, PHASE IB/IIA CLINICAL STUDY OF APTOLL FOR THE TREATMENT OF ACUTE ISCHEMIC STROKE
Maria Hernandez Perez*1, Adrián Valls Carbó1, Macarena Hernández2, Francisco Abad3, Ian Cotgreave4, Jaime Gallego5, Bernd Jilma6, Alan Alberto Flores7, Tudor Jovin8, Jose Vivancos9, Carlos Molina10, Joan Montaner11, Joaquín Casariego12, Mads Dalsgaard13, David Liebeskind14, Mar Castellanos15, Pere Cardona16, Jaime Masjuan17, Francisco Moniche Alvarez18, Jose Tembl19, Mikel Terceño20, Juan F. Arenillas21, Patrica Calleja22, Lionel Calviere23, Jean Marc Olivot24, Hilde Henon25, Mikael Mazighi26, Marc Ribo Jacobi10
1Germans Trias i Pujol Hospital, Neurosciences, Badalona, Spain, 2Aptatargets SL., Madrid, Spain, 3Hospital Universitario de La Princesa, Clinical Pharmacology Department, Madrid, Spain, 4Karolinska Institute., Solna, Sweden, 5Centro Neurológico de Navarra., Pamplona, Spain, 6Medical University of Vienna, Clinical Pharmacology, Vienna, Austria, 7Hospital Joan XXIII, Stroke Unit, Tarragona, Spain, 8Cooper Neurological Institute., Cherry Hill, NJ, United States, 9Hospital La Princesa, Neurology, Madrid, Spain, 10Vall d'Hebrón Hospital, Neurology, Barcelona, Spain, 11Hospital Macarena, Neurology, Sevilla, Spain, 12Aldebaran Health Intelligence., Madrid, Spain, 13Cureteq AG., Zug, Switzerland, 14UCLA Stroke Center, Neurology, Los Angeles, United States, 15Hospital Universitario de A Coruña, Neurology, La Coruña, Spain, 16Bellvitge Hospital, Neurology, Bellvitge, Spain, 17Ramón y Cajal Hospital, Neurology, Madrid, Spain, 18Virgen del Rocío Hospital, Neurology, Sevilla, Spain, 19La Fe Hospital, Neurology, Valencia, Spain, 20Josep Trueta Hospital, Neurology, Girona, Spain, 21Hospital Clínico Universitario, Neurology, Valladolid, Spain, 22Hospital 12 de Octubre, Neurology, Madrid, Spain, 23Centre Hospitalier Universitaire de Toulouse, Neurology, Toulouse, France, 24Centre Hospitalier Universitaire de Toulouse, Neurology, Toulouse, Spain, 25CHU Lille, LilNCog - Lille Neuroscience & Cognition, Lille, France, 26Fondation Rothschild, Interventional Neuroradiology Department, Paris, France
Background and aims: The APRIL study aimed to assess safety and efficacy of ApTOLL combined with endovascular treatment in patients with acute ischemic stroke. Here we report the effect of ApTOLL on prespecified imaging outcomes
Methods: This multicenter, double-blind, randomized, placebo-controlled, Phase Ib/IIa study included patients with acute large vessel occlusion within a 6h window with a predicted infarct core volume on CT perfusion at arrival 5-70ml. For the present analysis we selected those patients allocated to ApTOLL doses 0.05, 0.2mg/kg and placebo.
An imaging core lab evaluated final infarct volume on DWI at 72h. Cerebral edema (CED) was evaluated on FLAIR (or non-contrast CT if FLAIR not available) at 72h according to the SITS-MOSTS edema scale (ranging from CED1: less severe to CED3: most severe with midline shift).
Results: Out of 139 included patients, we had radiological data of 111 patients at 72h that received placebo (n=43), ApTOLL 0.05mg/kg (n=31) and ApTOLL 0.2mg/Kg (n=37).
At 72h, median final infarct volume was similar with placebo 67.7 [24.2;110]ml and ApTOLL 0.05mg/kg 62.5 [30.0;133]ml but lower with ApTOLL 0.2mg/kg 29.5 [15.2;57.3]ml (ApTOLL 0.2mg/kg vs.placebo, Log-B 0.58, 95%CI [0.35 -0.97]). Rates of CED 3 were similar with placebo 12 (27.9%) and ApTOLL 0.05mg/kg 6 (19.4%) but lower with ApTOLL 0.2mg/Kg 5 (13.5%) (ApTOLL 0.2mg/Kg Vs placebo, cOR 0.33 [0.14-0.78]).
Conclusions: ApTOLL 0.2mg/kg in combination with mechanical thrombectomy significantly reduced lesion volume and cerebral edema at 72h. Further data about the effect of ApTOLL on imaging outcomes will be given at the conference.
Disclosure of interest: No
YSPR: Young Stroke Physicians and Researchers – Poster
/355
UNDERSTANDING AND DETECTING INTRACRANIAL ANEURYSM GROWTH USING CELL-TYPE SPECIFIC GENE EXPRESSION - PLANNED RESEARCH
Mark Bakker*1
1University Medical Center Utrecht, Neurology, Utrecht, Netherlands
Background and aims: Growth of an unruptured intracranial aneurysm (IA) is the best surrogate for future aneurysmal subarachnoid haemorrhage (ASAH). Detecting growth allows better decision-making for endovascular or surgical treatment, or monitoring, but prediction methods currently perform poorly. As a result, most ASAH are caused by rupture of an IA assessed with low rupture risk. Genetic predisposition for IA is associated with rupture, but heterogeneity in contribution of vascular cell-types to the pathogenesis of IA has limited our progress in understanding the mechanisms ultimately leading to ASAH.
I aim to identify the genetic mechanisms underlying IA growth in a cell-type specific manner, and identify markers for early detection of IA growth.
Methods: Aim 1: pathogenic mechanisms underlying IA and ASAH
Single-cell RNA sequencing on IA biopsies taken during elective surgical clipping to obtain cell-type specific gene expression data. In combination with genome-wide association summary statistics I can identify cell-type specific pathogenic mechanisms underlying IA and ASAH.
Aim 2: biomarkers for IA growth
Compare cell-type specific gene expression between recently growing IA, and stable IA, thereby identifying genes of which their expression distinguishes between these groups. By validating these findings in blood of patients with growing IAs, detectable biomarkers that predict ASAH can be identified.
Results: Estimated results include a cell-type specific gene expression atlas of the intracranial arteries, understanding of cellular mechanisms underlying IA and ASAH, and biomarkers associated with IA growth.
Conclusions: With this project I ultimately aim to detect IA growth early and reduce the burden of ASAH.
Disclosure of interest: No
/679
Effects of Aerobic Exercise During the Early Rehabilitation After Ischemic Stroke
Frederike Anne Straeten*1, Mailin Hannah Marie Koecke1, Stephanie van Zyl1, Sabine Bruchmann1, Catharina Groß1, Jens Minnerup1, Antje Schmidt-Pogoda1
1University Hospital Muenster, Department of Neurology with Institute of Translational Neurology, Münster, Germany
Background and aims: In animal experiments, running wheel training improves stroke recovery. Translating these findings into the clinic has been challenging for several reasons, e.g., difficulties in controlling exercise intensity and precise assessment of motor skills not reflected by the mRS. Further, effects on cognition and psychological endpoints have not been assessed. We hypothesize that physical exercise will not only improve motor skills, but also counteract post-stroke fatigue, post-stroke depression and post-stroke cognitive impairment.
Methods: 30 stroke patients with mild to moderate stroke symptoms will be included within the first 14 days after the event. For the following 90 days participants in the intervention group are instructed to walk 30-45 minutes 3-5 times weekly. The intensity of walking is heart rate controlled. To overcome difficulties in controlling exercise intensity, participants are equipped with smartwatches. Motor function will be assessed by the fugl-meyer score in combination with an innovative testing by "speedzone", where patients respond to a visual signal. Cognitive functions are evaluated by MoCA and SDMT; extent of fatigue and depression by FSMC, HADS-D and WHODAS. Further, we will perform flow cytometric analyses to characterize exercise effects on the immune system. Structural correlates of functional repair shall be visualized by MRI-DTI.
Results: We have included the first patients in 2022 and are still recruiting. We aim to present results of these first patients.
Conclusions: So far, the study design appears feasible. We aim to identify subgroups of patients who benefit most from exercise.
Disclosure of interest: No
/792
MR-IMAGING CHARACTERISTICS AND THEIR IMPACT ON ISCHEMIC OR HAEMORRHAGIC COMPLICATIONS IN CERVICAL ARTERY DISSECTION PATIENTS RANDOMISED TO EITHER ANTICOAGULATION OR ASPIRIN
Josefin E. Kaufmann*1 2
1University Hospital Basel and University of Basel, Department of Neurology and Stroke Center, Basel, Switzerland, 2University Department of Geriatric Medicine FELIX PLATTER and University of Basel, Neurology and Neurorehabilitation, Basel, Switzerland
Background and aims: Uncertainty remains about whether to prefer anticoagulation or aspirin in cervical artery dissection patients despite two RCTs (CADISS and TREAT-CAD). It is unknown, whether MR-imaging characteristics matter for this decision. The aim of this study is to explore the impact of MR-imaging characteristics in relation to the occurrence of ischemic or haemorrhagic complications in TREAT-CAD-participants randomised and treated with either anticoagulation or aspirin.
Methods: This study is based on the per-protocol-dataset from the TREAT-CAD (NCT02046460) trial. In all 173 participants, MR-imaging was performed at baseline and 14 days (±10 days) after treatment onset. MR-imaging assessments included diffusion-weighted imaging with apparent diffusion coefficient maps, paramagnetic sequences, and contrast-enhanced MR-angiography with fat suppression.
Results: Two independent investigators, unaware of treatment allocations, will examine the MR-imaging and perform a final consensus assessment. MR-imaging assessment will include a detailed characterisation of the dissected artery, and the presence, number, size, and pattern of ischemic brain lesions at baseline. In line with the main study, the primary endpoint is defined as a composite of clinical (stroke, major haemorrhage, death assessed at 90 ± 30 days) and MRI-outcomes (new ischemic or haemorrhagic brain lesions assessed at 14 ± 10 days after commencing treatment). Exploratory analyses will include (i) calculating logistic regression models for each MR-imaging characteristic, (iii) including a test for interaction.
Conclusions: Testing the idea of individualised treatment approaches for cervical artery dissection patients based on MR-imaging characteristics of the dissected artery and the brain.
Disclosure of interest: No
/1064
A DEEP LEARNING EMPOWERED PENUMBRA-BASED PIPELINE FOR PREDICTING RESPONSIVENESS TO THROMBOLYTIC THERAPY IN ACUTE ISCHEMIC STROKE PATIENTS
Huiling SHAO*1, Xiang-Yan Chen1, Heng Du1, Qilin MA2, Zhiyu Shao2, Lawrence Wing Chi Chan1
1The Hong Kong Polytechnic University, Department of Health Technology and Informatics, Hong Kong, Hong Kong, 2The First Affiliated Hospital of Xiamen University, Department of Neurology, Xiamen, China
Background and aims: Considering the importance of prompt penumbra evaluation in predicting clinical outcome of stroke patients, the study aimed to develop an automated pipeline to generate penumbra feature and to evaluate its effectiveness in predicting responsiveness to thrombolysis.
Methods: We included 188 stroke patients undergoing thrombolysis within 4.5-h without endovascular thrombectomy. Penumbra feature was defined using a modified clinical-diffusion mismatch considering that the NIHSS is strongly weighted towards anterior circulation infarct: (Anterior circulation lesion volume + (29/42) * Posterior circulation lesion volume)/Baseline NIHSS. Lesion volume was calculated by our convolutional neural network. The consistency between manual calculation and automated calculation was assessed using dice score coefficient (DSC). Favorable response was defined as a decrease on the NIHSS of at least 8 points or an NIHSS = 0 at 1 week. Favorable outcome was defined as three-month mRS ⩽ 2. The adjusted influence of penumbra feature on responsiveness was evaluated by logistic regression analysis.
Results: 48.40% of patients had favorable response and 67.02% had favorable outcome. Penumbra feature ranged from 0 to 25473.55 with a median of 457.60. The pipeline achieved acceptable performance with a DSC of 80.3% ± 0.05. Logistic regression analysis revealed that a small value of penumbra feature was both independently associated with favorable response (OR = -1.88; 95% CI: -3.84 – 0.07; P = 0.04) and favorable outcome (OR = -2.90; 95% CI: -5.40 – 0.41; P = 0.02).
Conclusions: Our pipeline empowered by deep learning can generate penumbra feature independently associated with favorable responsiveness to thrombolysis therapy.
Disclosure of interest: No
/1087
Sleep disturbances in vascular cognitive impairment
1County Clinic Hospital, Department of Neurology, Brasov, Romania, 2Faculty of Medicine, Transilvania University Brasov, Department of Neurology, Brasov, Romania
Background and aims: Sleep disturbances (SD) are common in elderly people and in those with cognitive disturbances. Prevalence of SD increases with age and comorbidities. SD may occur due to several mechanisms including specific changes for each type of cognitive decline, and high frequency of comorbidities such as pain, depression, anxiety, and medications. The aim of this study was to describe frequency [prevalence?] and characteristics of sleep disturbances in people with vascular cognitive impairment (VCI). We assessed insomnia, excessive daytime sleepiness, sleep-disordered breathing, REM sleep behavior disorder, restless legs syndrome.
Methods: Prospective study on 37 people (59.45% males) with a mean age of 67.25 ± 11.23 years with vascular cognitive impairment and 37 sex- and age-matched controls. We used a standardized battery of comprehensive scales and questionnaires to evaluate sleep and its different components.
Results: In the study group there was a higher prevalence of obstructive sleep apnea (OSA) comparing with the control group (p<0.05), and the prevalence of insomnia was also higher (56.75% vs 21.62%, p<0.05). Compared with normal subjects, patients with VCI showed significantly reduced total sleep time (371.23 ± 156.67 vs 437.34 ± 197.45 minutes), increased waking times, and reduced sleep efficiency.
Conclusions: Sleep disturbances are more frequently encountered in vascular cognitive impairment compared with normal population. Screening for these disturbances and appropriate treatment may improve the outcome of these patients.
Disclosure of interest: No
/1174
RAISED INTRACRANIAL PRESSURE FOLLOWING INTRACEREBRAL HAEMORRHAGE: ASSOCIATION WITH SURVIVAL AND PHYSIOLOGICAL VARIABLES
Meeriam Kadicheeni*1, Ronney Panerai1, Thompson Robinson1, Adrian Parry-Jones2,3, Jatinder Minhas1
1University of Leicester, Cerebral Haemodynamics in Ageing and Stroke Medicine (CHiASM) Research Group, Department of Cardiovascular Sciences, Leicester, United Kingdom, 2University of Manchester, Division of Cardiovascular Sciences, Faculty of Biology, Medicine and Health, Manchester, United Kingdom, 3Manchester Centre for Clinical Neurosciences, Salford Royal NHS Foundation Trust, Salford, United Kingdom
Background and aims: Debate exists regarding blood pressure (BP) lowering and the effects on clinical outcome in acute intracerebral haemorrhage (ICH). There are limited data assessing the effect of BP on cerebral perfusion pressure (CPP), determined by intracranial pressure (ICP) and central venous pressure (CVP). This work is designed to determine if raised ICP is associated with increased mortality in patients with ICH and to examine the relationship between admission BP and BP lowering, and ICP, CVP and CPP. Lastly, to determine if variability in BP in the first 72 hours post ICH correlates with variability in ICP, CVP and CPP.
Methods: Single centre, retrospective, observational study of patients admitted with acute ICH with haemodynamic measurements. Data were collected regarding patients’ baseline characteristics, observations, and mortality. Up to 72 hours of haemodynamic data were collected for each participant including heart rate, BP, mean arterial pressure, CPP, CVP, ICP and end tidal CO2.
Results: 120 patients had haemodynamic data collected, totalling over 7000 hours. Initial descriptive analysis demonstrated that the mean (SD) age was 52.4 years (15.1) with 52.5% males. 113 patients underwent a neurosurgical procedure, which included ventricular drain placement (n=65), shunt (n=4), craniectomy (n=19) and ICH evacuation (n=73).
Conclusions: This study gives an opportunity to gain insight into the interplay between key physiological parameters in acute ICH. Given the high mortality of ICH and limited treatment strategies, understanding these relationships may enable us to target therapeutic options and minimise variation.
Disclosure of interest: No
/1197
IMPACT OF A FULLY ELECTRONIC HEALTH RECORD SYSTEM IMPLEMENTATION ON HEALTHCARE DELIVERY IN A TERTIARY STROKE CARE CENTRE
Background and aims: Electronic health medical records (EMRs) aim to increase the efficiency of health care delivery and improve patient safety by reducing transcription errors. However, published data on the impact of EMR implementation on the different markers of quality of health care delivery are conflicting. Our study aims to assess the impact of EMR implementation on surrogate markers of healthcare delivery in patients admitted to the stroke unit of a tertiary stroke center.
Methods:Study Design and participants: We will review the medical records of consecutive adult patients admitted with a diagnosis of ischemic or hemorrhagic stroke to the stroke unit of the Hamilton General Hospital, Ontario, Canada for a period of one year before and after the implementation of a full EMR system (June 2022).
Data collection: Baseline demographics, acute stroke treatment delivery, medication transcription errors, processing times for laboratory and imaging tests, discharge disposition and length of hospital stay will be captured in a dataset. We will evaluate for potential differences and time-trends between patients admitted before and after the implementation of the full EMR system.
Outcomes: Primary outcome will be the length of hospital stay (in days). Secondary outcomes will include - medication errors rate, the in-hospital mortality rate, door to needle times (in minutes) for patients receiving intravenous thrombolysis, door to groin puncture times (in minutes) for patients receiving endovascular thrombectomy and average time (in hours) between hospital admission and obtaining investigations for stroke work-up.
Results:
Conclusions:
Disclosure of interest: No
/1357
THE PROGNOSTIC ROLE OF IRON DEFICIENCY IN ACUTE ISCHEMIC STROKE PATIENTS
Antonio Ciacciarelli*1, Anne Falcou1, Sabrina Anticoli2, Aldobrando Broccolini3, Marina Diomedi4, Giovanni Frisullo3, Danilo Toni1
1Sapienza University of Rome, Emergency Department, Rome, Italy, 2AO S. Camillo, Stroke Unit, Rome, Italy, 3Università Cattolica del Sacro Cuore, Department of Neurosciences, Rome, Italy, 4University of Rome Tor Vergata, Comprehensive Stroke Center, Rome, Italy
Background and aims: Iron is essential for most of the metabolic processes. Iron deficiency (ID) plays a prognostic role in patients with heart failure and in acute coronary syndrome. In cerebrovascular diseases, the role of iron status is controversial. The aim of this study is to determine the impact of ID to the outcome of patients with acute ischemic stroke.
Methods: This is an observational prospective multicentric cohort study. We will include consecutive acute ischemic stroke patients admitted to the stroke units of the participating centers. We will perform venous blood sample at stroke unit admission to determine the iron status (serum iron, ferritin, transferrin). ID is defined as either a serum ferritin concentration <100 ng/mL or 100–299 ng/mL with transferrin saturation (TSAT) <20%. We will collect data concerning baseline stroke characteristics, routine blood tests, time from onset to venous blood sample, ejection fraction, cardio/cerebrovascular risk factors, home and hospital treatments, days of hospital stay, stroke etiology.
Results: The primary endpoint of the study is the functional outcome at 90 and 180 days measured by the modified Rankin Scale (mRS). Secondary endpoints include the in-hospital mortality, all-cause mortality at 90 and 180 days, hemorrhagic transformation classified by the ECASS-II criteria, stroke recurrence and myocardial infarction at 180 days, early neurological deterioration defined as a worsening of the NIHSS ⩾ 4 points at 24-hours and 7-days.
Conclusions: We aim to determine the role of ID to the functional outcome and to identify new prognostic factors and therapeutic approach.
Disclosure of interest: No
/2015
IDENTIFYING PROTEOMIC AND LIPIDOMIC BIOMARKERS IN PLASMA TO DIFFERENTIATE BETWEEN TRANSIENT ISCHAEMIC ATTACKS (TIAs), MINOR STROKES AND TIA MIMICS
Deeksha Sharma*1, Sushma Rao2, Marten Snel2, Paul Trim2, Austin Milton3, Erik Noschka4, Roman Kostecki5, Stephan Lau6, Suzanne Edwards7, Joshua Mahadevan8, Craig Kurunawai8, Timothy Kleinig8, Jim Jannes8, Simon Koblar1, Anne Hamilton-Bruce8
1University of Adelaide, Medicine, Adelaide, Australia, 2South Australian Health & Medical Research Institute, Proteomics, Lipidomics, Metabolomics and MS-Imaging, Adelaide, Australia, 3Central Adelaide Local Health Network, Cardiology, Adelaide, Australia, 4University of Adelaide, Animal and Veterinary Science, Adelaide, Australia, 5University of Adelaide, Physics, Chemistry and Earth Sciences, Adelaide, Australia, 6University of Adelaide, Computer and Mathematical Sciences, Adelaide, Australia, 7University of Adelaide, Adelaide Health Technology Assessment, Adelaide, Australia, 8Central Adelaide Local Health Network, Neurology, Adelaide, Australia
Background and aims: Ischaemic strokes are a leading cause of death and disability worldwide and are often preceded by a TIA. Accurately diagnosing TIAs can improve subsequent management of ischaemic stroke. This is difficult due to symptomatic overlap with minor strokes and TIA mimics (e.g., migraines, seizures, etc.). We aim to identify proteomic and lipidomic biomarkers in plasma to differentiate between TIAs, minor strokes and TIA mimics to improve clinical management.
Methods: Patients presenting at the Royal Adelaide Hospital (RAH) with TIA-like symptoms are enrolled <48 hours after symptom onset. A 9mL blood sample is collected and processed for proteomic and lipidomic investigation. Proteomic processing is conducted using the DIA-PASEF methodology on a TimsTOF Pro Mass Spectrometer. All proteomic and lipidomic data is analysed using the MetaboAnalyst platform to identify proteins and lipids of interest. Patients are clinically classified retrospectively by 2 vascular neurologists. Methodology for discovery metabolomics in addition to the use of an in vitro oxidative stress (IVOS) biosensor on the samples is in development. All data will be used to train and validate machine learning models.
Results: Fifty patients have been enrolled from the RAH (20 males, 30 females) aged 40-97 years (Median: 75). Proteomic and lipidomic analysis is currently underway.
Conclusions: Identified proteins and lipids are being explored by pathway enrichment analysis, using biomolecule interaction databases. This is an ongoing study with method development underway to establish machine learning modelling, metabolomic and IVOS methodologies to identify potential biomarkers to differentiate TIAs, TIA mimics and minor strokes.
Disclosure of interest: No
/2091
Reporting of Data Collection and Resourcing in National Stroke Audits: A Systematic Review Protocol
Agnes Jonsson*1, Anne Hickey2, David Williams3, Lisa Mellon2
1Royal College of Surgeons in Ireland, Department of Medicine, Dublin, Ireland, 2Royal College of Surgeons in Ireland, Department of Health Psychology, Dublin, Ireland, 1Royal College of Surgeons in Ireland, Department of Medicine, Dublin, Ireland
Background and aims: An ongoing challenge in stroke care, is providing equal access to care for patients in both acute hospitals and rehabilitation. The Irish National Audit of Stroke (INAS) has reported disparities in outcomes across hospitals, and a need for continuous audit to support quality improvement. This systematic review will build on a scoping review of existing audits carried out by the RCSI APA (Applied Partnership Awards) group as part of the ‘Maximising stroke care in Ireland’ HRB-funded project.
The aim of this systematic review is to identify what data collection procedures are used in Stroke audit internationally, and how these audits are resourced.
Methods: An initial scoping review has identified 21 relevant existing national stroke audits. For each of these audits, we will seek to identify documentation concerning their data collection procedures and how these are resourced. We will search the following databases: Medline Ovid; Embase; CINAHL EBSCOHost and search the grey literature for materials pertaining to the previously identified audits. We will include published reports and methodology documents. Resulting documents will undergo selection and review by two researchers to ensure they fulfil inclusion criteria.
Results: A narrative synthesis of the published documents will be conducted charting the data into standardised forms.
Conclusions: This systematic review will help to identify best practice for data collection and resourcing of stroke audit internationally. It will contribute to a larger project and the results will be used to produce a draft implementation guideline for the development of INAS.
Disclosure of interest: No
/2214
DELIRIUM IN ACUTE STROKE PATIENTS: DEVELOPMENT OF A NEW PREDICTION SCORE
Pauline Kremer*1, Johannes Wischmann1, Andrea Becker-Pennrich2,3, Ludwig Hinske2,4, Lars Kellert1
1University Hospital Ludwig-Maximilians-University (LMU) Munich, Department of Neurology, Munich, Germany, 2University Hospital Ludwig-Maximilians-University (LMU) Munich, Department of Anesthesiology, Munich, Germany, 3University Hospital Ludwig-Maximilians-University (LMU) Munich, Institute for Medical Information Processing, Biometry, and Epidemiology, Munich, Germany, 4University Hospital Augsburg, Institute for Digital Medicine, Augsburg, Germany
Background and aims: Delirium is a complication in acute stroke patients occurring in up to 50%, and is associated with increased morbidity and mortality. Thus, there is a need for predictive tools to identify high risk patients for subsequent early preventive measures. We aimed to develop and validate a score for early prediction of delirium in patients admitted to a stroke unit.
Methods: We retrospectively included adult patients (n=106) with confirmed or suspected stroke, admitted to our local stroke unit between December 2020 and April 2021. Medical history, clinical and paraclinical findings were assessed in detail. Subsequently, association of each parameter with delirium was determined, using cross-validated recursive feature elimination and logistic regression models. After internal retrospective validation (n=50), we enrolled n=42 patients for prospective validation up to now.
Results: Out of 106 patients, suspected stroke was confirmed in 53.8% and 50% developed delirium during hospital stay. The score comprises eight features and ranges from 0 to >12 points, with corresponding predicted probability of developing delirium ranging from less than 15% to >90%. Computed accuracy was 0.81 and area under the curve (AUC) was 0.84. Further prospective validation and adaption is subject of ongoing studies.
Conclusions: We herein present preliminary results of a clinical score for early prediction of delirium in stroke unit patients. Incorporating easy assessable parameters, which are available in basic stroke diagnostics, makes it potentially suitable for broad clinical application.
Disclosure of interest: No
/3019
Knowledge, Attitude and Perception of Stroke in the Global South: A Geospatial and Multivariate Statistical Assessment
Obot Akpan IBANGA*1, Edidiong Samuel Akpabio2, Mrs. Veronica Nnenna Victor Enya3
1University of Benin, Geography & Regional Planning, Benin City, Nigeria, 2Trinity University, Political Science, Lagos, Nigeria, 3Nigerian Institute of Medical Research, Innovation and Development, Yaba, Lagos, Nigeria
Background and aims: In the global south, the perils of stroke are likely to escalate and emerge as one of the key drawbacks to sustainable development. This study will explore the capabilities of geospatial technologies (GTs) and multivariate statistical functionalities in assessing the knowledge, attitude and perception (KAP) of stroke in a typical global south urban and rural setting.
Methods: Over 31 KAP indicators of stroke pigeonholed into risk factors (RFs), organ affected (OA), warning signs (WS) and immediate response (IR) will be interrogated in cross-sectional field study of about 1,000 respondents to be chosen randomly from 10 communities in five local government areas (LGAs) of primordial Esan Kingdom (PEK), Edo State, Nigeria between June to August 2023 using structured questionnaires. Data will be analysed using descriptive and multivariate statistics including principal component analysis (PCA) in SPSS 22 and results will be exported to ArcGIS 10.8 software where weighted arithmetic aggregation (WAA) will be executed with map algebraic algorithm utilising weights from PCA-varimax rotated components scores. RFs, OA, WS and IR will be mapped disjointedly and subsequently coalesced to achieve the overall stroke KAP index (OSKI).
Results: The study is expected to unearth the socio-demographic profiles of study respondents in addition to the compilation of five spatial cartographic models depicting RFs, OA, WS and IR as well as OSKI of PEK.
Conclusions: The findings of this study will form the basis for the scaling-up of precise mitigation and adaptation actions to reduce the burden of stroke among the citizenry.
Disclosure of interest: No
/3065
Smartphone-enabled machine learning algorithms for autonomous stroke detection
Radoslav Raychev*1, Jeffrey Saver1, David Liebeskind1, Svetlin Penkov2, Daniel Angelov2, Krasimir Stoev2, Delian Georgiev3, Denislav Dimov3, Ana Koralov3, Filip Alexiev4, Teodora Sakelarova4, Dobrinka Kalpachka4, Rosen Kalpachki4, Emanuela Kostadinova5, Theodora Manolova6, Ivan Milanov7
1University of California, Los Angeles, Neurology, Los Angeles, United States, 2Neuronics Medical, AI, Sofia, Bulgaria, 3Haskovo General Hospital, Neurology, Haskovo, Bulgaria, 4St. Ana University Hospital, Neurology, Sofia, Bulgaria, 5Pulmed University Hospital, Neurology, Plovdiv, Bulgaria, 6University Hospital Prof. Dr. Stoyan Kirkovich, Neurology, Stara Zagora, Bulgaria, 7St. Naum Univeristy Hospital, Neurology, Sofia, Bulgaria
Background and aims: Using the well-established FAST paradigm, we developed an automated smart phone application for detection of acute stroke signs using machine learning (ML) algorithms for recognition of facial asymmetry, arm weakness, and speech changes (Fig. 1)
Methods: We analyzed collected data from patients admitted to 4 major metropolitan stroke centers. Speech and facial data were captured via smartphone video recording and arm data was captured via device sensors.
A. Face. This module extracts standard 68 facial landmark points, passed through a machine learning pipeline consisting of a dimensionality reduction step and an asymmetry classifier. (Fig. 2)
B. Arm. Using data extracted from the 3D accelerometer, gyroscope, and magnetometer, while the smartphone is being held and moved, we designed a grasp agnostic classifier to process motion trajectories and detect arm weakness. (Fig. 3)
C. Speech. We developed a model based on frequency analysis and Mel Frequency Cepstral Coefficients (MFCC) to detect abnormal/slurred speech. (Fig. 4)
All tests were conducted within 72 hours of symptoms onset. ML outputs were correlated with neurologists’ clinical impression and brain imaging results. Characteristics of the studied population are included in table 1.
Results: Results of final analyses of each individual modality for detection of abnormal speech, arm weakness, and facial asymmetry are summarized in Table 2. Confirmed diagnosis of stroke is based on merged data from all 3 modalities.
Conclusions: Our results confirm that smartphone enabled ML-algorithms can reliably identify acute stroke features with high accuracy comparable to neurologists’ clinical impression.
Disclosure of interest: Yes
/3123
DESIGNING A PREHOSPITAL PREDICTION MODEL FOR ACUTE LARGE VESSEL OCCLUSION STROKE BASED ON SWEDISH STROKE REGISTRIES
Hoor Jalo*1, Anna Bakidou1, Mattias Seth1, Ida Häggström1, Minna Pikkarainen2, Bengt Arne Sjoqvist1, Katarina Jood3,4, Stefan Candefjord1
1Chalmers University of Technology, Department of Electrical Engineering, Gothenburg, Sweden, 2Oslo Metropolitan University, Department of Occupational Therapy, Oslo, Norway, 3Gothenburg University, Department of Clinical Neuroscience, Gothenburg, Sweden, 4Sahlgrenska University Hospital, Department of Neurology, Gothenburg, Sweden
Background and aims: Large vessel occlusion (LVO) stroke leads to severe disabilities in over 37% of stroke cases. Studies show that providing endovascular thrombectomy to LVO patients as early as possible after stroke onset can decrease mortality and morbidity rates and improve patient outcomes. Research into prehospital procedures for triaging patients to the most appropriate centers, including bypass algorithms, was urged by the American Heart Association Guidelines in 2019. Although identifying acute LVO patients during prehospital triage is a challenging but essential step to prevent treatment delays. The aim of this study is therefore to build and evaluate a machine learning model to identify acute LVO patients in prehospital settings based on Swedish stroke registries.
Methods: Swedish health registries, such as Väststroke, Riksstroke and the registry for endovascular treatment of stroke, will be used for feature extraction of, for example age, onset time, and the National Institutes of Health Stroke Scale (NIHSS) score. Several machine learning models will be trained and validated to predict acute LVO, including Artificial Neural Network, Support Vector Machine, Random Forest, Logistic Regression and XGBoost.
Results: This is a planned study; there are therefore no results available to show. The results will be based on accuracy metrics, such as Precision-Recall curve and area under the receiver operating characteristic curve to assess the models’ performance.
Conclusions: The findings of this study could potentially have a significant impact on the future of prehospital stroke care, specifically on achieving transport of more LVO patients directly to comprehensive stroke centers.
Disclosure of interest: No
Paper Poster – Late Breaking
/414
EVALUATION OF WEARABLE PATCH MONITOR TECHNOLOGY (ZIO XT) IN A STROKE/TIA POPULATION COMPARED TO HOLTER MONITOR FOR THE DETECTION OF ATRIAL FIBRILLATION
Barbara Madigan*1, Lina Manounah2, Barnes Anna2, Philip Clatworthy1
1North Bristol NHS Trust, Stroke, Bristol, United Kingdom, 2King's College London, King’s Technology Evaluation Centre, London, United Kingdom
Background and aims: Ambulatory ECG is used to investigate for atrial fibrillation following ischaemic stroke or transient ischaemic attack in patients where the cause of stroke/TIA has not been determined. New wearable patch technology has become available providing 14-day continuous recording of heart rate and rhythm and is preferred by patients as well as recommended by NICE MTG56. However, the effect of adopting Zio XT on costs and resource is uncertain because there is not enough evidence about resource use and the long-term clinical consequences, for example, rate of anticoagulation uptake.
Methods: NHS AI lab funded evaluation study using retrospective data collection of 240 stroke/TIA patients in the ZIO XT group versus 240 in the Holter group over a 6 month period.
Results: Primary outcomes: time from prescription to device fitting, diagnosis and treatment decision.
Secondary outcomes: time to ECG report, resource utilisation (number of hospital visits, repeat tests, insertable cardiac monitors), diagnostic yield, patient and clinician experience.
Conclusions: Through this evaluation, it is hoped that uncertainties regarding resource use and some of the long term clinical consequences of using this technology can be reduced and firmer NICE recommendations made.
Disclosure of interest: No
/794
Effects of a digital learning platform on health behaviors in stroke patients from baseline to 6 months after discharge: a randomized controlled study
1Sun Yat-sen University, School of Nursing, Guangzhou, China, 2Guangdong Provincial Hospital of Chinese Medicine, Department of Neurology, Guangzhou, China, 3The Third Affiliated Hospital of Sun Yat-sen University, Department of Neurology, Guangzhou, China
Background and aims: The existing health education interventions requires more human resource. Lack of constructing a low-cost, highly universal and easy-to-use stroke secondary prevention platform based on the existing medical resources.
Methods: This was a randomized controlled trial to test the effects of a digital learning platform on the health knowledge, beliefs and behaviors of stroke patients 6 months after discharge. A total of 90 patients were included: 45 each in the intervention group and the control group. The control group received routine health education while the intervention group received health belief education during hospitalization and used digital learning platform for 6 months after discharge. The health knowledge was assessed by the Stroke Health Knowledge Questionnaire, health beliefs by The Short Form Health Belief Model Scale for Stroke Patients and health behaviors by Stroke Health Behavior Scale for Stroke Patient.
Results: At 6 months at discharge: (1) The health knowledge score of the intervention group was insignificantly higher than that of the control group. (2) The health belief score of the intervention group was significantly higher than that of the control group. (3) The intervention group had higher health behavior scores especially in physical activity than that of the control group. Other health behavior dimensions have non-significant time effect.
Conclusions: The digital learning platform can improve health behaviors of stroke patients 6 months after discharge, especially in physical activity. However, the lack of differences from conventional health education in other health behavior dimensions indicates that the intervention needs more reminders.
Disclosure of interest: No
/1031
EARLY EXPERIENCE OF USING NON-IMMUNOGENIC STAPHYLOKINASE FOR STROKE THROMBOLYSIS IN ROUTINE PRACTICE
Tatiana Kharitonova*1, Igor Vozniuk2
1The National Society of Neurosonology and Cerebral Circulation, Board secretary, Saint-Petersburg, Russian Federation, 2The National Society of Neurosonology and Cerebral Circulation, Board member, Saint-Petersburg, Russian Federation
Background and aims: Recently a new medication, non-immunogenic staphylokinase (NIS), was introduced for stroke thrombolysis. We aimed to assess the safety of NIS in routine clinical practice.
Methods: We retrospectively collected data of patients treated with NIS according to the current stroke thrombolysis guidelines (similarly to alteplase) in 7 dedicated stroke centres in 2021-2022. Safety was assessed via comparison of the proportion of intracerebral haemorrhage (ICH) with the results of the FRIDA trial (the only randomized trial of NIS in acute stroke), and with the outcomes of stroke thrombolysis with alteplase reported in SITS (Safe Implementation of Treatments in Stroke) annual report in 2021. ICHs were classified according to the Heidelberg Bleeding Classification.
Results: We identified 169 patients, 47% (78) females, median age 70 (IQR 60-79), time-to-treatment 180 min (IQR 140-215), baseline NIHSS 10.5 (IQR 6-15). Local hemorrhage occurred in 11% (n=17; haemorrhagic infarction type 1– 4, haemorrhagic infarction type 2– 9, parenchymal haemorrhage type 1 – 2, parenchymal haemorrhage type 2 – 2); remote haemorrhage in 7% (n=11; type 1 remote haemorrhage – 5, type 2 remote haemorrhage – 1, subarachnoid haemorrhage – 4, subdural hematoma - 1). ICH proportion was similar to FRIDA study (31/168 (19%), p>0.05), but tends to exceed that of previously reported after thrombolysis with alteplase (15,8%), especially regarding the rate of remote hemorrhage (7% vs. 2,9%, p>0.05).
Conclusions: Safety of NIS use in acute stroke may raise concerns. More information of NIS use in routine practice is warranted (prospective data collection has already started on Jan 1, 2023).
Disclosure of interest: No
/3013
Improving the Door-To-Needle Time in Patients for Thrombolysis to 60 Minutes or Less through Implementation of MSD Ischemic Stroke Guidelines and Code Drill Simulation Training
Hossam Younis1, Rasha Alsubaie*1, Ruba Baamer1, Ahmed Daabees Dr Ahmed1
1King Fahad Armed Forces Hospital Pharmacy, NEUROSCIENCE, , Saudi Arabia
Background and aims: In eligible patients with acute ischemic stroke(AIS), rapid revascularization is crucial for good outcome. At our treatment center, we identified that the median door-to-needle time is more than 75 minutes. We hypothesized that improvement could be achieved through implementing a revised MSD treatment protocol and implementing a stroke code and in situ simulation-based team training sessions
Methods: All members of the AIS treatment team were surveyed to tailor the interventions to local conditions. Through a review of responses and available literature, including the new MSD Early Management of Patients with AIS guidelines, the improvement team suggested changes to implement the new MSD protocol, activate stroke code protocol and designed in situ simulation-based team training sessions. Implementation of interventions started in November 2019.
Results: A total of 204 consecutive patients, including a 1-year baseline, treated with intravenous thrombolysis were assessed. Median door to needle times were significantly reduced from 75 to less than 60 min.
Conclusions: Implementing a stoke code treatment protocol in combination with in situ simulation based team training sessions for stroke thrombolysis was followed by a considerable reduction in door-to-needle times and improved patient outcomes
Disclosure of interest: No
/3024
Safety and Tolerability of Ischemic Post-conditioning in Acute Ischemic Stroke following Successful Thrombectomy Recanalization (PROTECT)
1Xuanwu Hospital, Capital Medical University, Beijing, 2Tianjin Huanhu Hospital, Tianjin Huanhu Hospital, Tianjin,
Background and aims: Ischemic post-conditioning (IPC) has been found to attenuate ischemia-reperfusion injury in stroke model. This study aimed to investigate the safety and tolerability of IPC in both dogs’ model and patients with acute ischemic stroke (AIS) after successful thrombectomy.
Methods: In dogs’ study, 4 cycles of 5 min ischemia followed by 5 min reperfusion were performed in the anterior spinal artery to induce IPC. A 3+3 dose-escalation clinical trial was conducted in AIS patients after successful thrombectomy recanalization. IPC was performed proximal to the culprit lesion with ischemia and reperfusion durations in progressive increments of 0 to 5 min.
Results: IPC was firstly investigated in four dogs, no vessel perforation or rupture, dissection, or vasospasm was observed, whereas one vessel experienced mild injury between the intima and the internal elastic membrane. Eighteen patients were recruited, median baseline NIHSS was 11.5 (IQR, 10-13), and mean time from stroke onset to successful recanalization was 17.4 ± 5.5 hrs. The ischemia and reperfusion duration of IPC was progressively escalated to 4 cycles of 5-minute of ischemia followed by 5-minute of reperfusion with no major response happened. No patient experienced agitation, discomfort, or other tolerability issues during the procedure. At 3-month follow-up, no patients died and 9 patients (50%) achieved functional independence.
Conclusions: IPC inducing by 4 cycles of 5 minutes ischemia followed by 5 minutes of reperfusion is safe, feasible, and tolerable in AIS patients treated with thrombectomy. Further investigations that determine the preliminary efficacy of IPC are needed.
Disclosure of interest: No
/3068
Prevalence and clinical significance of intracerebral thrombus detected by optical coherence tomography in patients with recent stroke or TIA
Ran Xu*1, Bin Yang1, Liqun Jiao1, Haibo Jia2, Adam Dmytriw3
1China International Neuroscience Institute (China-INI), Department of Neurosurgery, Xuanwu Hospital, Capital Medical University, Beijing, China, 2Second Affiliated Hospital of Harbin Medical University, Department of Cardiology, Harbin, China, 3Brigham and Women’s Hospital and Harvard Medical School, Neuroradiology & Neurointervention Service, Boston, United States
Background and aims: Thrombosis has been recognized as a factor in the development of atherosclerosis and a cause of heart attack and stroke. However, the frequency and clinical associations of thrombosis in intracranial atherosclerotic stenosis (ICAS) remains unclear. The purpose of this study was to determine the prevalence, characteristics and clinical significance of thrombosis in patients ICAS using optical coherence tomography (OCT).
Methods: A prospective study (NCT05550077) was conducted in 135 patients with intracranial arterial stenosis who underwent pre-intervention OCT. The enrolled patients were classified according to the presence of in situ thrombus defined by OCT. Clinical data, OCT characteristics and post-interventional outcome were compared between two groups.
Results: 82 patients were diagnosed as ICAS and finally enrolled. In situ thrombus was identified in 34 patients (41.5%). Patients with atherosclerotic thrombus are prone to have cerebral infarctions rather than TIA (44.1% vs 29.2%, P=0.022). Perioperative cerebral infarction (73.5% vs 43.8%, P=0.013) and in-stent restenosis (67.7% vs 39.6%, P=0.015) was more frequently to be observed in patients with thrombus.
Conclusions: This study achieved in vivo analysis of ICAS and revealed high incidence of in situ thrombosis for the first time. In addition, the in situ thrombus has significant influence on clinical events and outcomes of ICAS. Interventional treatment may produce additional cerebral infarction and higher incidence of in-stent restenosis in ICAS patients with in situ thrombus.
Clinical outcomes in thrombus group and non-thrombus group.
Intracranial atherosclerotic thrombus under OCT and related statistical analysis.
Disclosure of interest: No
/3076
DIRECT ORAL ANTICOAGULANTS FOR THE TREATMENT OF CEREBRAL VENOUS THROMBOSIS (DOAC-CVT)
Anita van de Munckhof*1, Katarzyna Krzywicka1, Mayte Sanchez van Kammen1, Sanjith Aaron2, Diana Aguiar de Sousa3, Florina Antochi4, Antonio Arauz Gongora5, Miguel A. Barboza6, Adriana Conforto7, Francesco Dentali8, Daniel Galdames9, Xunming Ji10, Katarina Jood11, Mirjam Rachel Heldner12, Maria Hernandez Perez13, Wayneho Kam14, Timothy Kleinig15, Espen Saxhaug Kristoffersen16, Ronen R Leker17, Robin Lemmens18, Sven Poli19, Nilufer Yesilot20, Mohammad Wasay21, Teddy Wu22, Saskia Middeldorp23, Lia Lucas-Neto24, Marcel Arnold12, Jukka Putaala25, Turgut Tatlisumak26, Jose Férro27, Jonathan Coutinho1
1Amsterdam UMC, locatie AMC, Neurology, Amsterdam, Netherlands, 2CHRISTIAN MEDICAL COLLEGE, Neurology, Vellore, India, 3Centro Hospitalar Universitário de Lisboa Central, Neurology, Lisbon, Portugal, 4Spitalul Universitar de Urgenţă Bucureşti, Neurology, Bucharest, Romania, 5National Institute of Neurology and Neurosurgery, Neurology, Ciudad de México, Mexico, 6Rafael Angel Calderon Guardia Hospital, Neurology, San José, Costa Rica, 7Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, Neurology, São Paulo, Brazil, 8Asst Sette Laghi, Medical Area Department, Varese, Italy, 9Hospital Clínico de la Univeridad de Chile, Stroke Unit, Santiago, Chile, 10Xuanwu Hospital, Capital Medical University, Neurology, Beijing, China, 11Sahlgrenska University Hospital, Neurology, Gothenborg, Sweden, 12Inselspital, Neurology, Bern, Switzerland, 13Hospital Germans Trias i Pujol, Neurology, Badalona, Spain, 14Duke University Hospital, Neurology, Durham, United States, 15Royal Adelaide Hospital, Neurology, Adelaide, Australia, 16Akershus University Hospital, Neurology, Nordbyhagen, Norway, 17Hadassah - Hebrew University Medical Center, Neurology, Jerusalem, Israel, 18UZ Leuven, Neurology, Leuven, Belgium, 19Tübingen University Hospital, Neurology, Tübingen, Germany, 20Istanbul Tip Fakültesi, Neurology, Istanbul, Turkey, 21Aga Khan University, Neurology, Karachi, Pakistan, 22Canterbury District Health Board, Neurology, Christchurch, New Zealand, 23Radboud University Medical Center, Internal medicine, Nijmegen, Netherlands, 24North Lisbon Medical Center, Neuroradiology Department, Lisbon, Portugal, 25Helsinki University Hospital, Neurology, Helsinki, Finland, 26University of Gothenburg, Neurology, Gothenburg, Sweden, 27Universidade de Lisboa, Neurology, Lisbon, Portugal
Background and aims: Patients with cerebral venous thrombosis (CVT) are generally treated with oral anticoagulants for 3-12 months. Vitamin K antagonists (VKAs) are recommended by most guidelines, but direct oral anticoagulants (DOACs) are increasingly used. An exploratory randomized trial among 120 patients with CVT suggested that the efficacy and safety profile of DOACs is similar to VKAs for the treatment of CVT, but large-scale prospective studies from a real-world setting are lacking.
Methods: DOAC-CVT (ClinicalTrials.gov: NCT04660747) is an international, prospective, comparative cohort study. Patients are eligible if they are 18 years or older, have a radiologically confirmed CVT, and have started oral anticoagulant treatment (DOAC or VKA) within 30 days of CVT diagnosis. Patients with an absolute contra-indication for DOACs, such as pregnancy or severe renal insufficiency, are excluded from the study. We aim to recruit at least 500 patients within the study period. The primary endpoint is a composite of recurrent venous thrombosis and major bleeding at 6 months of follow-up. We will calculate an adjusted odds ratio for the primary endpoint using propensity score inverse probability treatment weighting.
Results: Recruitment is currently ongoing. Per March 23, 2023, 417 patients from 46 centres in 22 countries have been included in the study. We expect to reach 500 inclusions in Q4 of 2023. Researchers who are interested in joining DOAC-CVT may contact the Principal Investigator at j.coutinho@amsterdamumc.nl.
Conclusions: DOAC-CVT will provide real-world data on the comparative efficacy and safety of DOACs versus VKAs for the treatment of CVT.
Disclosure of interest: No
/3078
Transesophageal Echocardiography as Dysphagia Risk in Acute Stroke - Follow-Up Trial
Samra Hamzic*1, Tobias Braun1, Romy Baumgart1, Viola Kirchhoff Da Cruz1, Patrick Schramm1, Hassan Khilan1, Marius Butz2, Martin Jünemann1
1University Hospital Giessen and Marburg, Campus Giessen, Department of Neurology, Giessen, Germany, 2Gesundheitszentrum Wetterau, Department of Geriatrics, Friedberg, Germany
Background and aims: T.E.D.R.A.S. - Trial (Transesophageal Echocardiography -TEE: Dysphagia Risk in the Acute Phase After Stroke; ClinTrial.gov identifier NCT04302883) was the first study of its kind to address the question of the extent to which TEE increases dysphagia risk in acute stroke patients.
Patients with ischemic stroke were randomized to an intervention or control group. The results of the study confirm the hypothesis that dysphagia severity worsens after TEE in the intervention group (Hamzic et al. 2020).
The aim of the present TEDRAS II – follow-up trial is to investigate the limitations of the initial TEDRAS - trial in patients with ischemic stroke.
Methods: In the study, patients with ischemic stroke receive a Flexible Endoscopic Evaluation of Swallowing (FEES) 24 hours before TEE and 4 hours after TEE.
In particular, the following parameters will be examined:
1) The influence of the type and route (intravenous vs. oral) of anesthesia administered during TEE on swallowing in all cohorts studied.
2) The influence of the duration of TEE on swallowing
3) The interrater reliability for the Flexible Endoscopic Evaluation of Swallowing.
Results: Since this is an ongoing trial we will introduce the detailed study design and the preliminary results during the ESOC 2023.
Conclusions:Disclosure of interest: No
/3087
Effect of family participatory health management on health behavior, blood pressure and recurrence of stroke patients at 12 months after discharge: a randomized controlled trail
zhuoran Li*1, Lihong Wan1
1Sun Yat-sen University, School of Nursing, Guangzhou, China
Background and aims: The high recurrence rate of stroke is associated with the poor health behavior of stroke patients. Existing health education lacks a theoretical framework and multidisciplinary teamwork. This study aimed to confirm the impact of a nurse-led multidisciplinary family participatory digital health management on health behavior, blood pressure control, homocysteine (Hcy) and stroke recurrence in stroke patients at 12 months after discharge
Methods: This was a single-blinded randomized controlled trial with 141 participants randomly assigned to the intervention and control groups receiving usual care.The intervention group received the family participatory digital health management, including: receiving health belief education before discharge, and using the family participatory digital health management platform for 12 months after discharge. The Health Behavior Scale for Stroke Patients (HBS-SP) was used to assess health behaviors.
Results: At 3,6 and12 months of discharge, there were significant differences in health behaviors and blood pressure control rate between the two groups.In terms of health behaviors,the intervention main effect, time main effect and the interaction effect of intervention and time all had a statistical effect (P <0.05). Hcy values were significantly lower in the intervention group than in the control group at 6 and 12 months after discharge. At 12 months of discharge, the recurrence rate in the intervention group (4.23%) was significantly lower than that in the control group (17.14%).
Conclusions: Family participatory digital health management can improve the health behavior, Hcy, blood pressure control and recurrence rate of stroke patients after discharge.
Disclosure of interest: No
/3088
ALGORITHM DEVELOPMENT THROUGH ARTIFICIAL INTELLIGENCE FOR THE TRIAGE OF STROKE PATIENTS IN THE AMBULANCE WITH ELECTROENCEPHALOGRAPHY (THE AI-STROKE STUDY)
Eva Groenendijk*1,2, Maritta van Stigt1,2, Monique Theunissen3, Gaby Franschman3, Martin Smeekes4, Arjen Siegers5, Marieke Visser2, Sander van Schaik6, Patricia Halkes7, Charles Majoie8, Yvo Roos2, Hans Koelman1, Miou Koopman8, Henk Marquering8,9, Wouter Potters10, Jonathan Coutinho2
1Amsterdam UMC location University of Amsterdam, Department of Clinical Neurophysiology, Amsterdam, Netherlands, 2Amsterdam UMC location University of Amsterdam, Department of Neurology, Amsterdam, Netherlands, 3Witte Kruis Ambulancezorg, -, Alkmaar, Netherlands, 4Ambulancezorg Nederland, -, Zwolle, Netherlands, 5Ambulance Amsterdam, -, Amsterdam, Netherlands, 6OLVG Hospital location West, Department of Neurology, Amsterdam, Netherlands, 7Noordwest Ziekenhuisgroep location Alkmaar, Department of Neurology, Alkmaar, Netherlands, 8Amsterdam UMC location University of Amsterdam, Department of Radiology and Nuclear Medicine, Amsterdam, Netherlands, 9Amsterdam UMC location University of Amsterdam, Department of Biomedical Engineering and Physics, Amsterdam, Netherlands, 10TrianecT, -, Utrecht, Netherlands
Background and aims: Endovascular thrombectomy (EVT) greatly improves outcome of patients with anterior circulation large vessel occlusion (LVO-a) stroke, but its effect is time-dependent. A prehospital triage instrument would enable direct routing of LVO-a stroke patients to an EVT-capable hospital and hence save time. Electroencephalography (EEG) is a promising technique for prehospital stroke triage. An automatic EEG-based LVO-a detection algorithm will be the key to reliable, simple and fast interpretation of EEG by paramedics. AI-STROKE aims to develop one or more artificial intelligence (AI) algorithms for prehospital LVO-a stroke detection.
Methods: AI-STROKE (ClinicalTrials.gov Identifier: NCT05437237) is a prospective, investigator-initiated, multicenter, diagnostic study. Single dry electrode EEG recordings (8 electrodes) are performed in adult suspected stroke patients in the prehospital and in-hospital setting. The primary aim is to develop EEG-based AI algorithms with maximal diagnostic accuracy to identify patients with LVO-a stroke in a population of patients with suspected stroke. Secondary aims include establishing the diagnostic accuracy of EEG for LVO-a stroke, posterior circulation LVO stroke and intracerebral hemorrhage, and assessing the technical and logistical feasibility of performing EEG recordings in the prehospital stroke setting. We aim to recruit a maximum of 1192 suspected stroke patients.
Results: Recruitment started in June 2022 and is currently ongoing. Per March 30th 2023, 183 patients have been included in the prehospital setting and 8 patients in the in-hospital setting.
Conclusions: The AI-STROKE study will help to determine if EEG can be implemented into routine practice for prehospital stroke triage by ambulance paramedics.
Disclosure of interest: Yes
/3115
Humanized anti-HMGB1 monoclonal antibody therapy for marmoset intracerebral hemorrhage
1Okayama University, Department of Pharmacology, Okayama, Japan, 2Okayama University, Department of Translational Research and Drug Development, Okayama, Japan, 3Evec Inc., Drug Development, Kobe, Japan
Background and aims: Intracerebral hemorrhage (ICH) is recognized as a severe clinical problem lacking effective treatment. High mobility group box-1 (HMGB1) exhibits inflammatory cytokine-like activity once released into the extracellular space from the nuclei. We previously demonstrated that intravenous injection of rat anti-HMGB1 monoclonal antibody (mAb) remarkably ameliorated brain injury in a rat ICH model.
Methods: We developed a humanized anti-HMGB1 mAb (OKY001) for clinical use. The present study examined whether and how the humanized anti-HMGB1 mAb ameliorates ICH injury in common marmosets. The intracerebral hemorrhage was induced by a microinjection of collagenase into striatum. The plasma levels of HMGB1 and 4-HNE were determined by ELISA. The contrast medium-assisted CT and neurological test was done during the course. Histological studies were performed on paraffin embedded sections.
Results: The results show that administration of humanized anti-HMGB1 mAb inhibited HMGB1 release from the brain into plasma, in association with a decrease of 4-HNE accumulation and a decrease in cerebral iron deposition. In addition, humanized anti-HMGB1 mAb treatment resulted in a reduction in brain injury volume at 12 d after ICH induction. Our in vitro experiment showed that recombinant HMGB1 inhibited hemoglobin uptake by macrophages through CD163 in the presence of haptoglobin, suggesting that the release of excess HMGB1 from the brain may induce a delay in hemoglobin scavenging, thereby allowing the toxic effects of hemoglobin, heme and Fe2+ to persist.
Conclusions: Taken together, these results suggest that intravenous injection of humanized anti-HMGB1 mAb has potential as a novel therapeutic strategy for ICH.
Disclosure of interest: Yes
/3118
Swiss trial of decompressive craniectomy versus best medical treatment ofspontaneous supratentorial intracerebral hemorrhage (SWITCH): a randomizedcontrolled trial
Juergen Beck1, Christian Fung1, Daniel Strbian2, Ringel Florian3, Seraina Beyeler4, Andreas Raabe1, Urs Fischer*4,5
1Medical Center - University of Freiburg, Department of Neurosurgery, Freiburg, Germany, 2Helsinki University Central Hospital, Department of Neurology, Helsinki, Finland, 3Medical University, Johannes Gutenberg University Mainz, Department of Neurosurgery, Mainz, Germany, 4Bern University Hospital and University of Bern, Department of Neurology, Bern, Switzerland, 5University Hospital Basel, University of Basel, Basel, Department of Neurology, Basel, Switzerland
Background and aims: Decompressive craniectomy (DC) is beneficial in patients with various diseases including malignant middle cerebral artery infarction. In intracerebral hemorrhage (ICH), DC without hematoma evacuation has only been evaluated in small retrospective studies with a trend towards reduced mortality. However, no randomized trial has ever assessed whether DC is beneficial in patients with ICH. Therefore, the SWITCH trial evaluates whether DC and best medical treatment (BMT) in patients with spontaneous supratentorial ICH will improve outcome compared to BMT alone.
Methods: SWITCH is an international multicenter randomized trial. 300 patients will be randomized (1:1) into either DC and BMT or BMT alone. Main inclusion criteria are spontaneous supratentorial ICH of deep origin, NIHSS⩾10 and ⩽30, GCS>7 and <14 and ICH volume ⩾30 and ⩽100. The primary endpoint is severe disability and mortality, measured with the modified Rankin score 6 months after ictus.
Results: 199 patients have been randomized into the trial in 35 sites (Switzerland, Germany, The Netherlands, Spain, Finland, Austria, France, and Belgium). The Data Safety Monitoring Board reviewed data of the first 150 patients and recommended continuing recruitment with the current protocol. The next interim analysis will take place after randomization of 200 patients.
Conclusions: Currently, 199 patients have been randomized into the SWITCH trial and SWITCH has become the largest trial on DC in stroke ever. Further centers are still highly welcome to help us to answer the clinically relevant question, whether DC improves outcome in patients with supratentorial ICH.
Disclosure of interest: No
/3121
ENDOVASCULAR THROMBECTOMY IN THE MANAGEMENT OF ACUTE ISCHEMIC STROKE WITH LARGE ISCHEMIC CORES IN ELDERLY PATIENTS
Qian Liu*1, Jinghuan Fang1, Xin Jiang1, Muke Zhou1, LI He1
1West China Hospital, Neurology, Chengdu, China
Background and aims: As the combined effects of advanced age and extensive brain infarction can have a greater negative impact on clinical outcomes in the elderly patients with large ischemic cores, it is necessary to fully understand the benefits and risks of endovascular therapy (EVT) for them.
Methods: The study retrospectively analyzed clinical outcomes for elderly stroke patients (age ⩾ 70) with large ischemic cores (Alberta Stroke Program Early CT Score [ASPECTS] < 6 or ischemic cores ⩾ 70 ml) in the anterior circulation using data from our prospective database between June 2018 and January 2022. The effectiveness and risks of EVT in those patients were investigated, with the primary outcome being fair outcome (modified Rankin Scale, mRS ⩽ 3).
Results: Among 182 elderly patients with large ischemic core volume (120 in the EVT group and 62 in the non-EVT group), 20.9% (38/182, 22.5% in the EVT group vs. 17.7% in the non-EVT group) achieved a fair outcome. Meanwhile, 49.5% (90/182, 45.8% in the EVT group vs. 56.5% in the non-EVT group) of them died at 3 months. The benefits of EVT numerically exceeded non-EVT treatment for those aged ⩽ ~85 years or with a mismatch volume ⩾ ~50ml. However, EVT showed increased risk of symptomatic ICH after adjustment (aOR 7.279, 95%CI 1.131-46.845).
Conclusions: This study highlights the significant clinical challenges faced by elderly patients with large infarction, with poor outcomes observed at 3 months. EVT may still offer some benefits, while it also comes with increased risk of ICH.
Disclosure of interest: No
/3122
Safety and Efficacy of intra-arterial Tenecteplase for non-complete reperfusion of intracranial occlusions (TECNO)
Johannes Kaesmacher*1, Adnan Mujanovic1, Seraina Beyeler2, Morin Beyeler2, Daniel Strbian3, Mira Katan4, Pasquale Mordasini1,5, Zsolt Kulcsar6, Marios Psychogios7, Mikael Mazighi8, Götz Thomalla9, Robin Lemmens10, Jan Gralla1, Urs Fischer2,4
1University Hospital Bern Inselspital, Department of Diagnostic and Interventional Neuroradiology, Bern, Switzerland, 2University Hospital Bern Inselspital, Department of Neurology, Bern, Switzerland, 3Helsinki University Hospital, Department of Neurology, Helsinki, Finland, 4University Hospital Basel, Department of Neurology, Basel, Switzerland, 5Cantonal Hospital St. Gallen, Department of Diagnostic and Interventional Neuroradiology, St. Gallen, Switzerland, 6University Hospital Zürich, Department of Neuroradiology, Zürich, Switzerland, 7University Hospital Basel, Department of Neuroradiology, Basel, Switzerland, 8Hospital Lariboisière, Department of Neurology, Paris, France, 9University Medical Center Hamburg-Eppendorf, Department of Neurology, Hamburg, Germany, 10University Hospitals Leuven, Department of Neurology, Leuven, Belgium
Background and aims: Despite recent advances in technical equipment and overall increasing reperfusion quality, still 40% of acute ischemic stroke (AIS) patients show non-complete reperfusion after mechanical thrombectomy (MT). Recent observational reports showed that administration of intra-arterial (IA) thrombolytics may improve final reperfusion grades after incomplete MT. The TECNO trial aims to evaluate the safety and efficacy of IA tenecteplase (TNK) in AIS patients with incomplete reperfusion and residual peripheral occlusions after MT.
Methods: TECNO is an international multicenter clinical trial that will randomize 156 patients to either IA TNK or best medical treatment arm (1:1). Main inclusion criteria is incomplete reperfusion (Thrombolysis in Cerebral Infarction, TICI<3) after MT for initial target occlusions of ICA, M1 or M2. For inclusion, the residual occlusions need to be rated as not mechanically amendable by the treating physician. Primary efficacy outcomes are early and late reperfusion, defined as reperfusion improvement on angiography imaging 25 minutes after randomization and complete reperfusion on the 24h magnet resonance perfusion imaging, respectively.
Results: Recruitment has started in March 2023. Two interim analyses will be conducted when 40 and 80 patients have been enrolled. Over 30 sites in Switzerland, Germany, France, Belgium, Spain and Finland will participate in this randomized clinical trial.
Conclusions: Presently, no evidence on prospective evaluation of IA TNK in patients with incomplete reperfusion is available. This study will provide high-quality evidence on imaging and clinical effects of additional IA TNK in patients with incomplete reperfusion after MT.
ClinicalTrials.gov Identifier: NCT05499832
Disclosure of interest: No
/3139
RANDOMIZED TRIAL OF ANDEXANET ALFA IN INTRACRANIAL HEMORRHAGE PATIENTS RECEIVING AN ORAL FACTOR Xa INHIBITOR: DESIGN OF THE ANNEXa-I TRIAL
Ashkan Shoamanesh*1, Mike Sharma1, Andrew Demchuk2, Truman Milling3, Jan Beyer-Westendorf4, Danilo Toni5, Carlos A. Molina6, David Tanne7, Pierre Amarenco8, Wilfried Lang9, Robin Lemmens10, Jonathan Coutinho11, Thompson Robinson12, Risto Roine13, Hanne Christensen14, Georgios Tsivgoulis15, David Seiffge16, Else Charlotte Sandset17, Anna Czlonkowska18, Robert Mikulik19, Daniel Bereczki20, Vítor Tedim Cruz21, Arne Lindgren22, Anders Himmelmann23, Mikael Knutsson23, Andrew Law24, Ella Ekholm23, Alexander Cohen25, Saskia Middeldorp26, Peter Verhamme27, Roland Veltkamp28, Mark Crowther1, Stuart Connolly1
1McMaster University / Population Health Research Institute, Medicine, Hamilton, Canada, 2Cumming School of Medicine, University of Calgary, Hotchkiss Brain Institute, Calgary, Canada, 3University of Texas, Dell Medical School, Austin, United States, 4University Hospital Dresden, Medicine, Dresden, Germany, 5Sapienza University of Rome, Neurology, Rome, Italy, 6Vall d´Hebron University Hospital, Neurology, Barcelona, Spain, 7Rambam Health Care Campus, Neurology, Haifa, Israel, 8Bichat Claude-Bernard Hospital, Neurology, Paris, France, 9Hospital of St. John of God, Neurology, Vienna, Austria, 10University Hospitals Leuven, Neurology, Leuven, Belgium, 11Amsterdam University Medical Centers, Neurology, Amsterdam, Netherlands, 12Leicester University, Neurology, Leicester, United Kingdom, 13Turku University Hospital, Neurology, Turku, Finland, 14Copenhagen University Hospital, Bispebjerg Hospital, Neurology, Copenhagen, Denmark, 15National and Kapodistrian University of Athens, “Attikon” University Hospital, Second Department of Neurology, Athens, Greece, 16Inselspital, Neurology, Bern, Switzerland, 17Oslo University Hospital, Neurology, Oslo, Norway, 18Institute of Psychiatry and Neurology, Neurology, Warsaw, Poland, 19St. Anne’s University Hospital/Masaryk University, Neurology, Brno, Czech Republic, 20Semmelweis University, Neurology, Budapest, Hungary, 21University of Porto, Neurology, Porto, Portugal, 22Skåne University Hospital, Lund University, Neurology, Lund, Sweden, 23AstraZeneca, Medical Sciences, Gothenburg, Sweden, 24AstraZeneca, Alexion Pharmaceuticals UK Ltd, Uxbridge, United Kingdom, 25Guy's and St Thomas' Hospital, King’s College London, Medicine, London, United Kingdom, 26Radboud University Medical Center, Medicine, Nijmegen, Netherlands, 27University Hospital Leuven, University of Leuven, Medicine, Leuven, Belgium, 28Imperial College, Neurology, London, United Kingdom
Background and aims: FXa inhibitor-related ICH have high rates of hematoma expansion leading to increased risk of death/disability. Andexanet alfa is a modified recombinant FXa decoy that rapidly reverses the anticoagulant effect of FXa inhibitors. ANNEXa-I is an international, prospective, randomized, open-label, blinded end-point trial that is evaluating whether andexanet is superior to usual medical care for achieving hemostasis in acute FXa inhibitor-related ICH.
Methods: Participants aged ⩾18 years with acute ICH within 6 hours from symptom onset, hematoma volume of ⩾0.5 to ⩽60mL, and treatment with an oral FXa inhibitor within 15 hours prior to randomization (or documented anti FXa activity >100 ng/mL) are eligible. Excluded are patients with NIHSS>35, GCS<7, planned hematoma evacuation surgery, or recent history of thromboembolism. Consenting participants are randomized (1:1) to usual medical therapy or one of two dosing regimens of andexanet determined according to the strength and timing of their last FXa inhibitor dose.
Results: The primary outcome is hemostatic efficacy. With a target of 900 patients and an expected hemostatic efficacy rate of 70% in the usual care arm, the study will have 90% power to detect a 10% absolute difference in the rate of hemostatic efficacy with andexanet vs. usual medical therapy. Recruitment has commenced and will continue at a 216 sites in 24 countries.
Conclusions: ANNEXa-I will provide important answers to unresolved questions surrounding the optimal management of acute FXa inhibitor-related ICH.


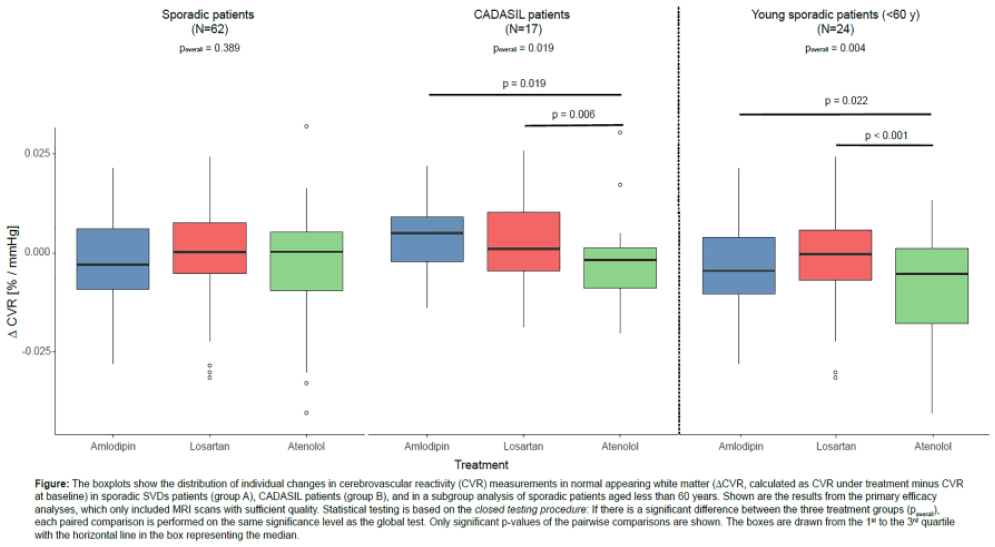
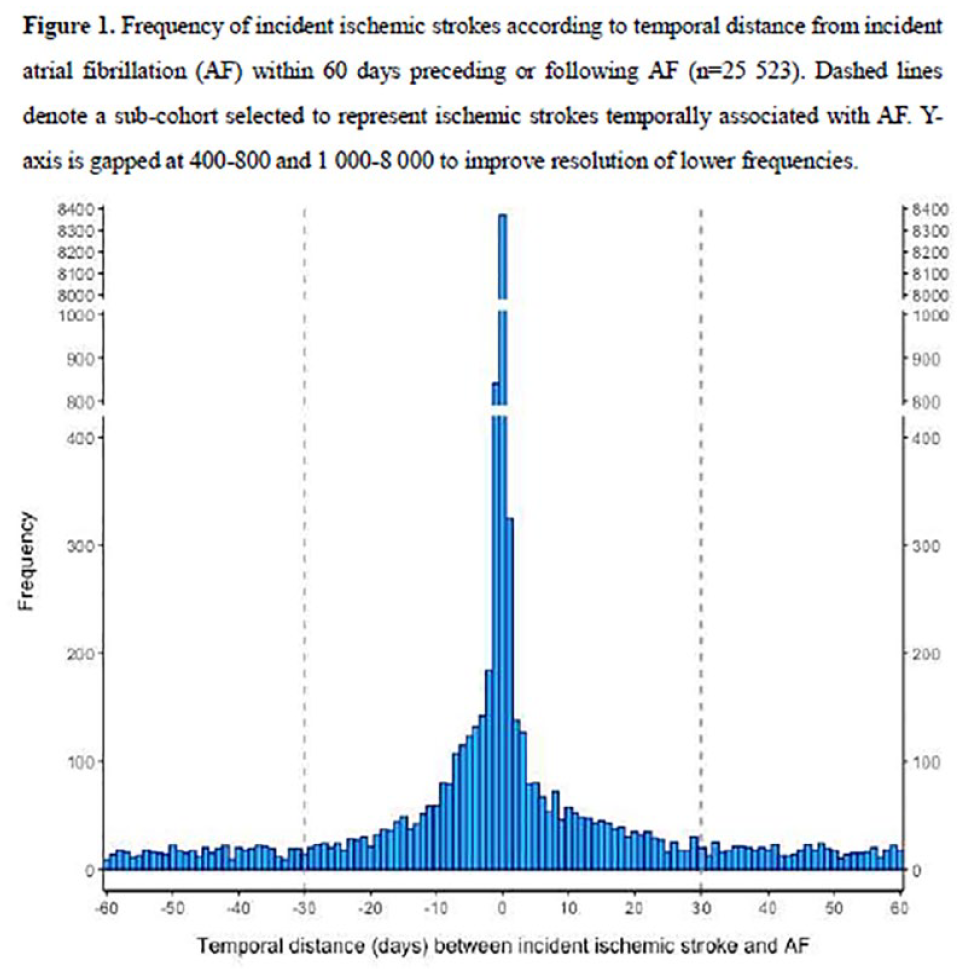
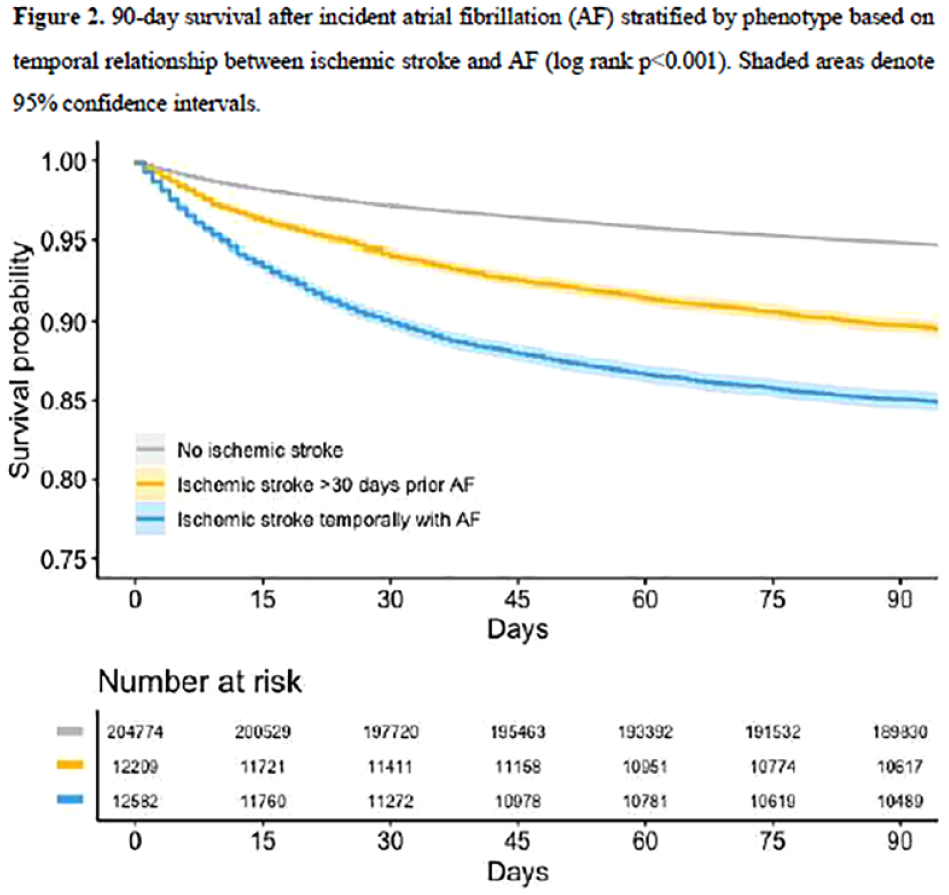
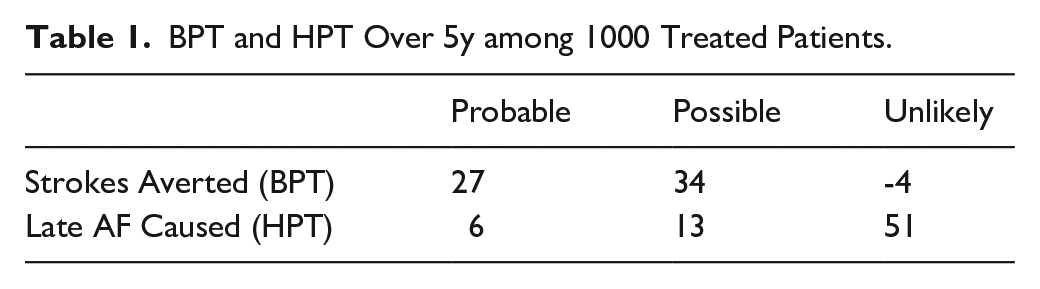
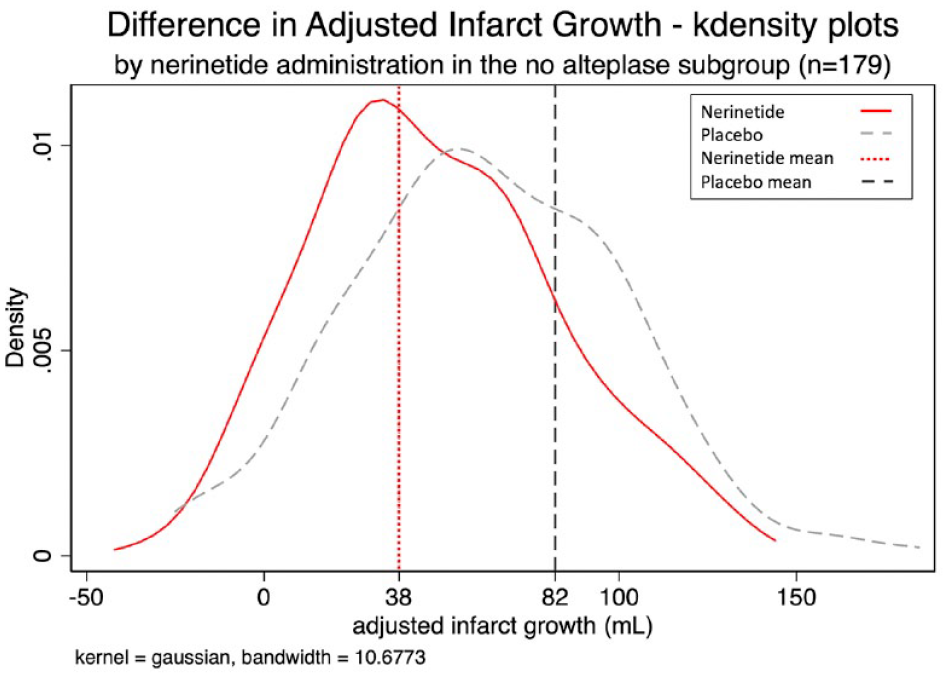
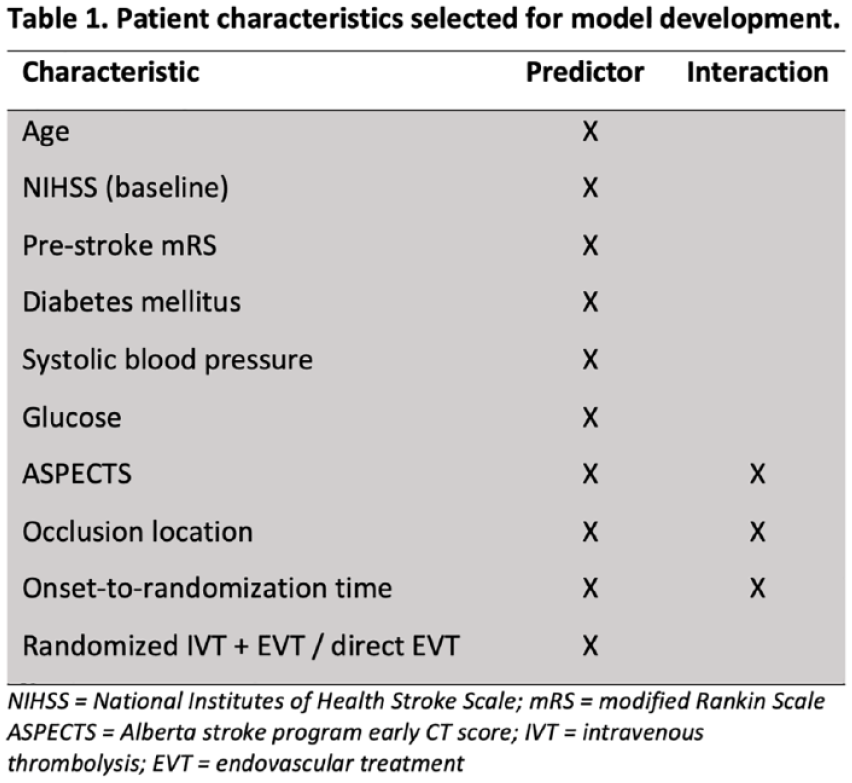
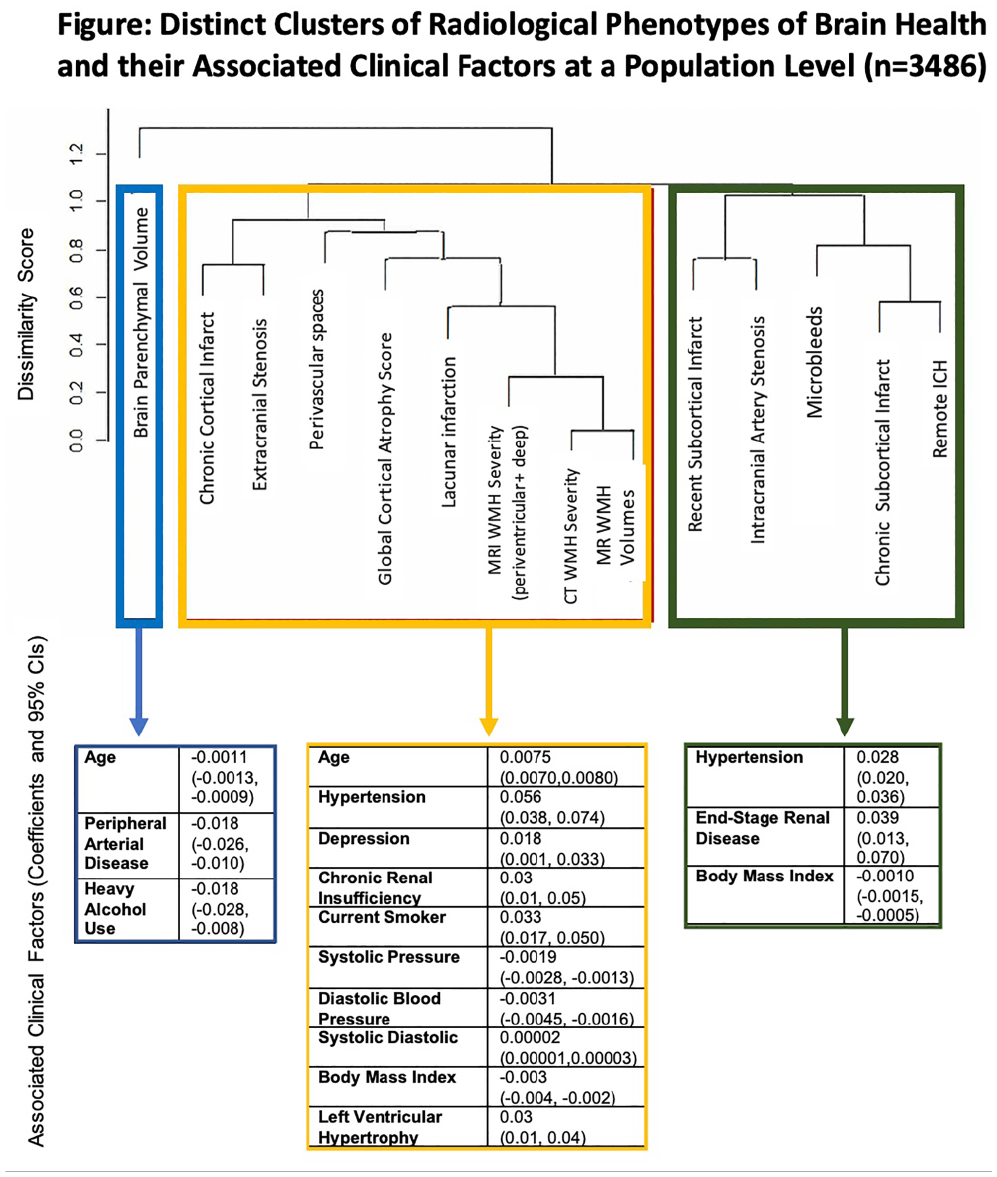
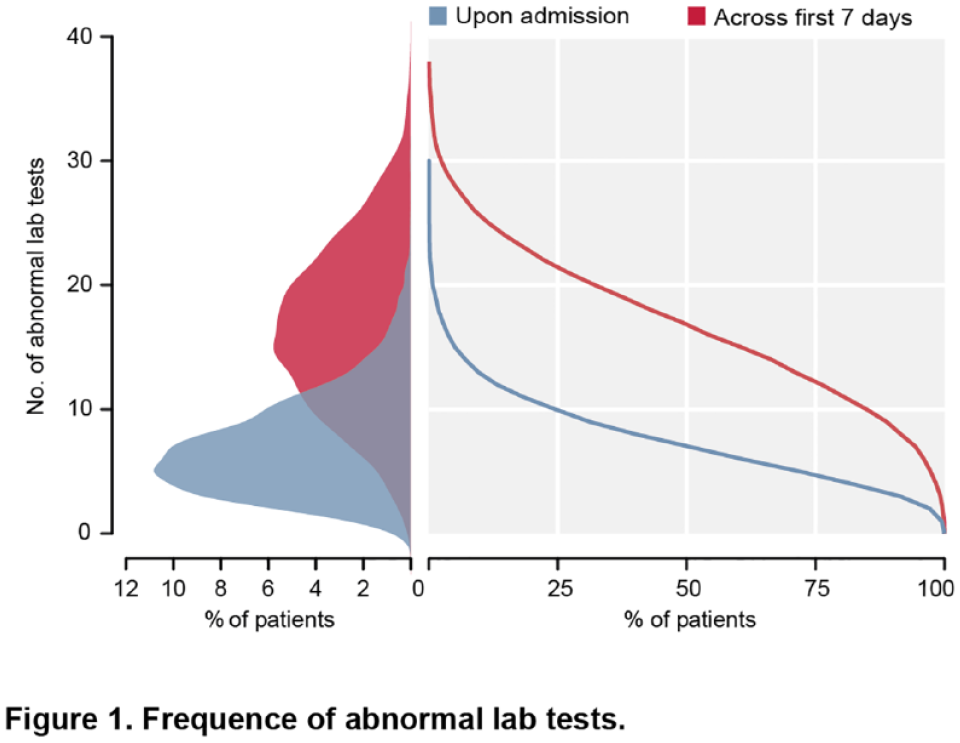
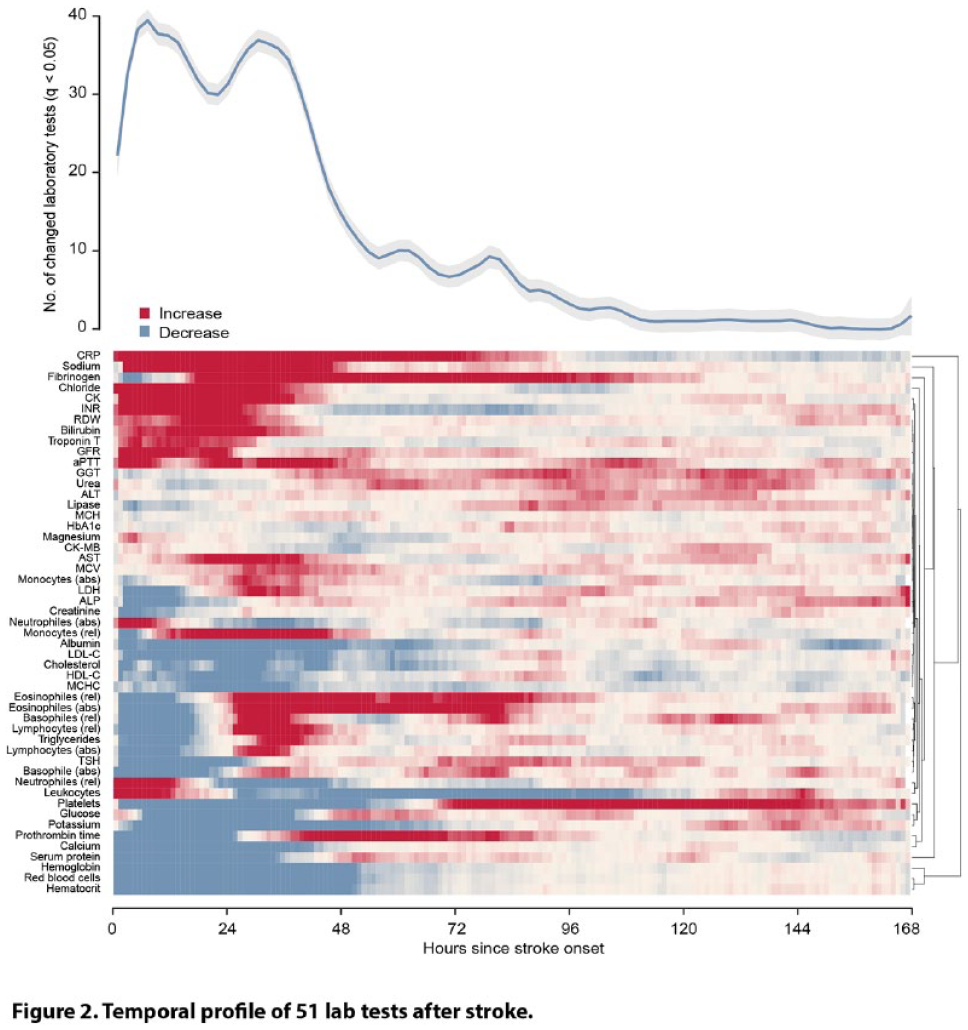
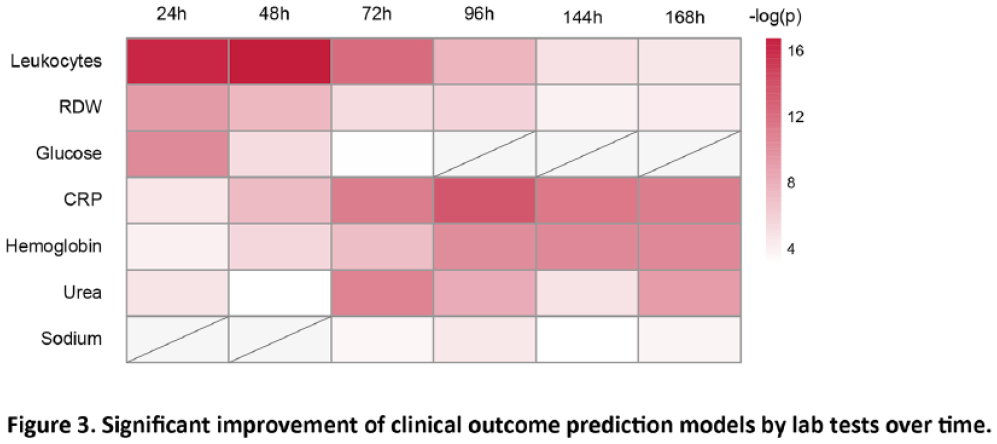
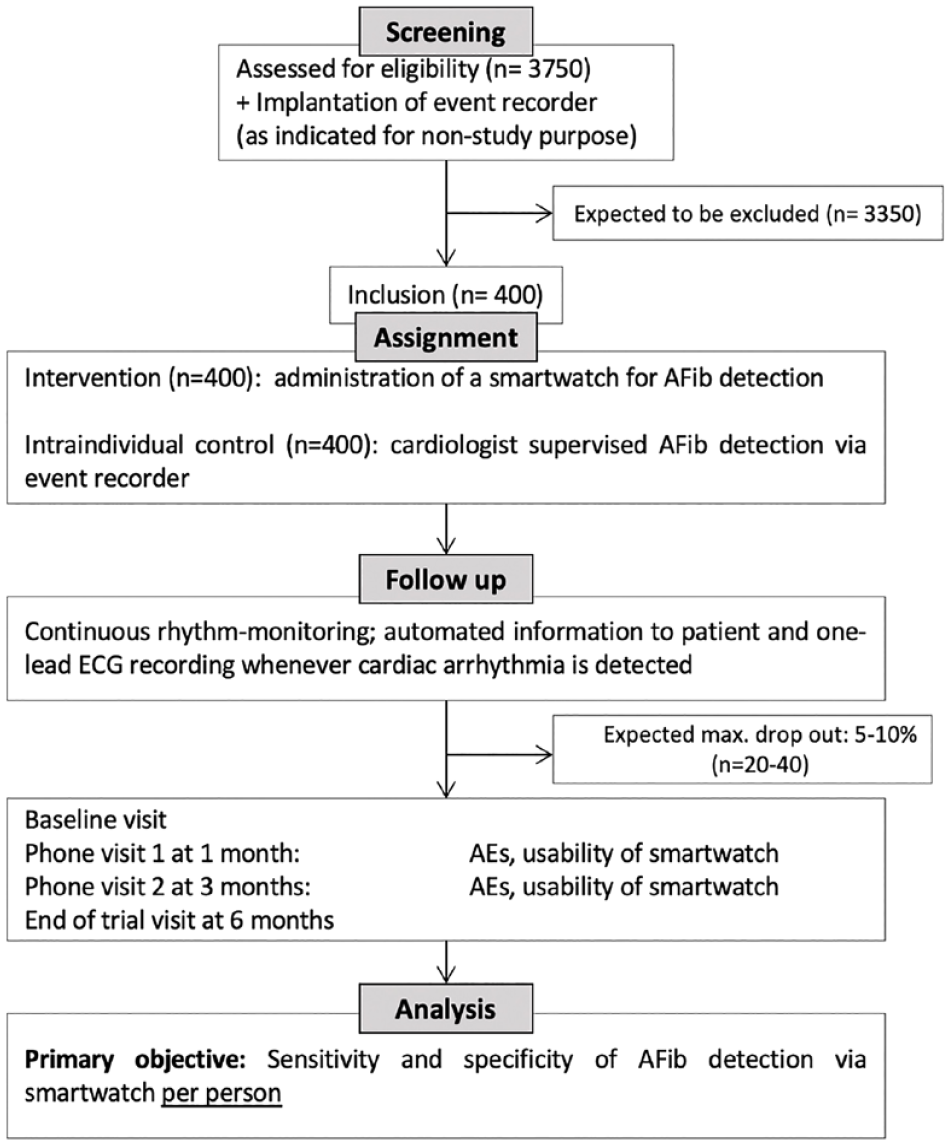
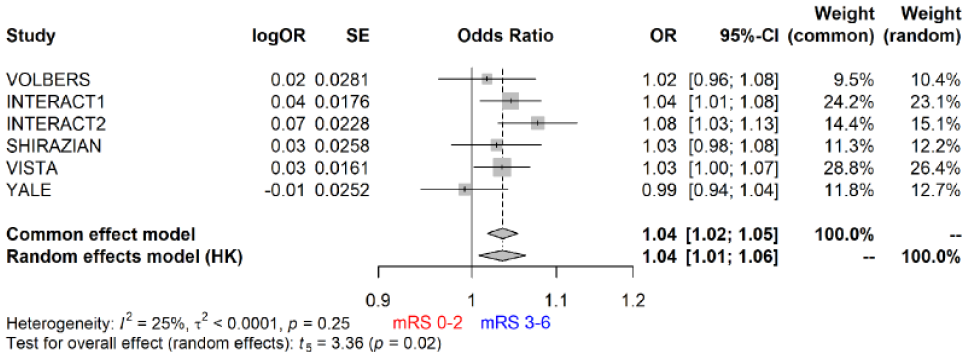
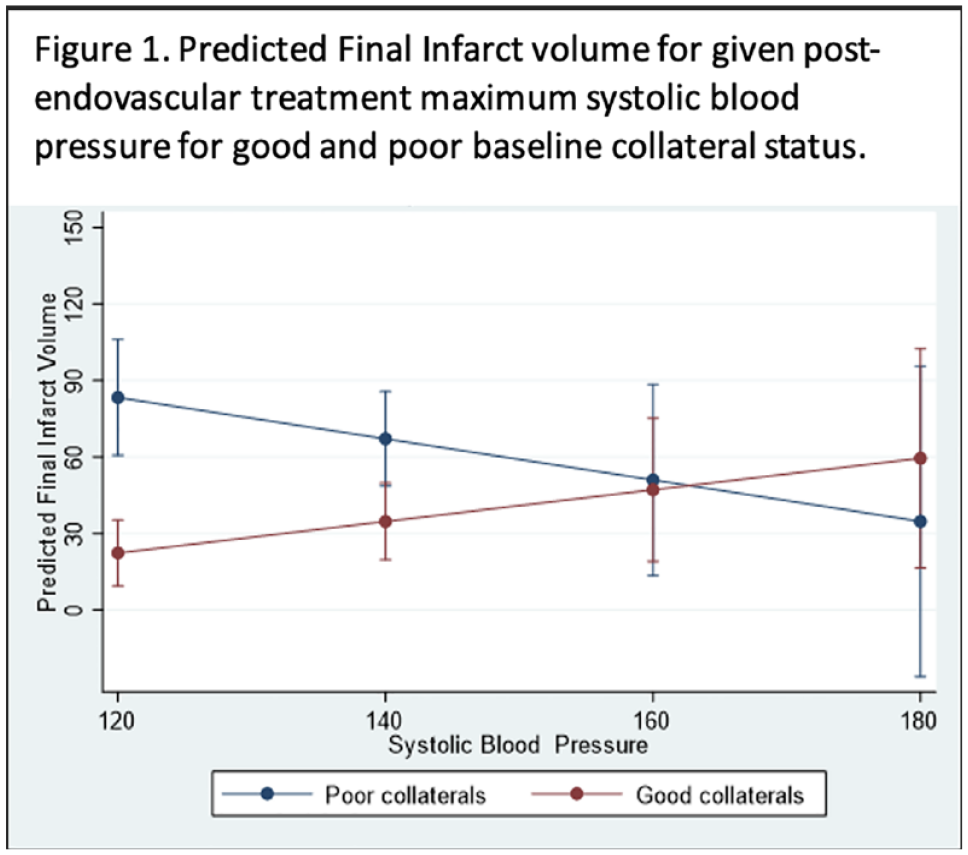
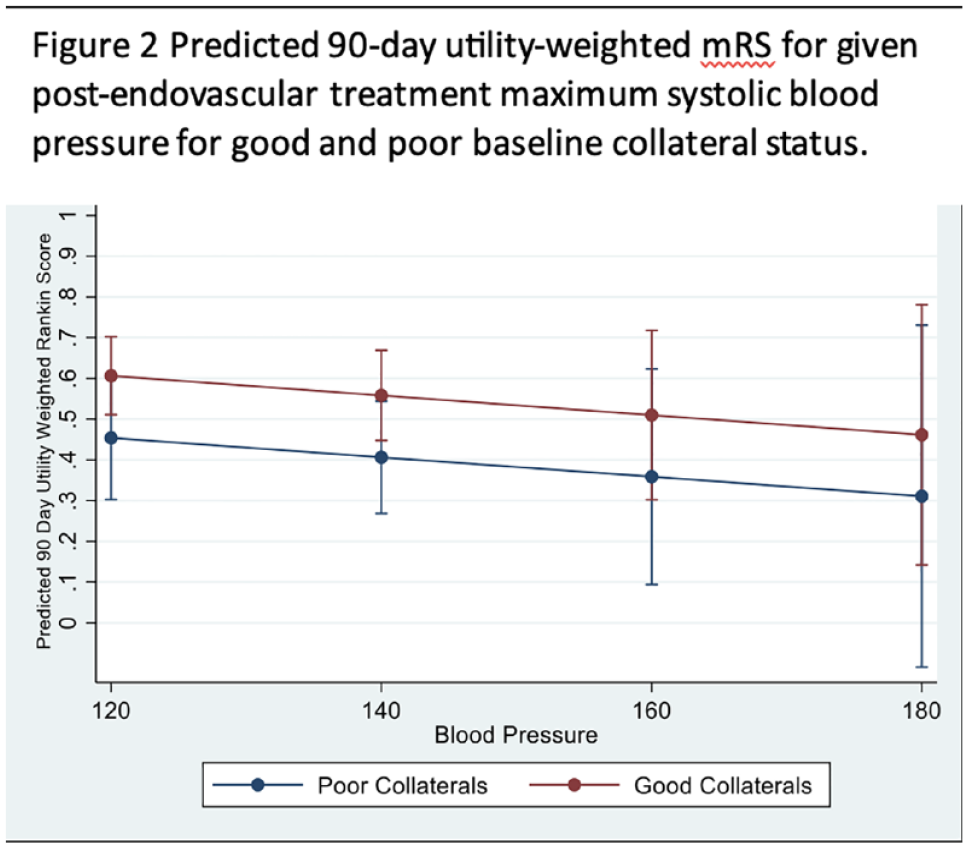

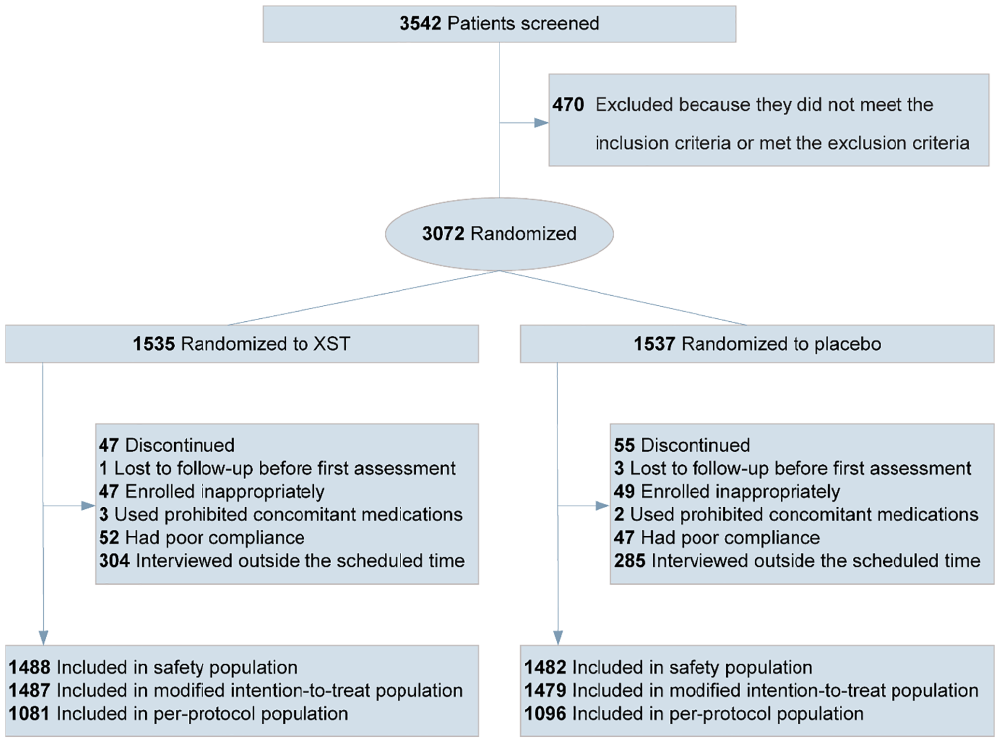
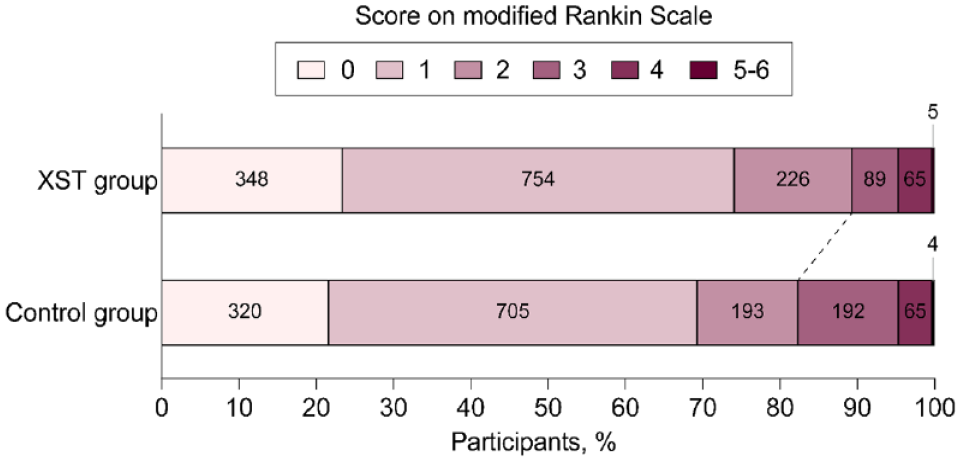
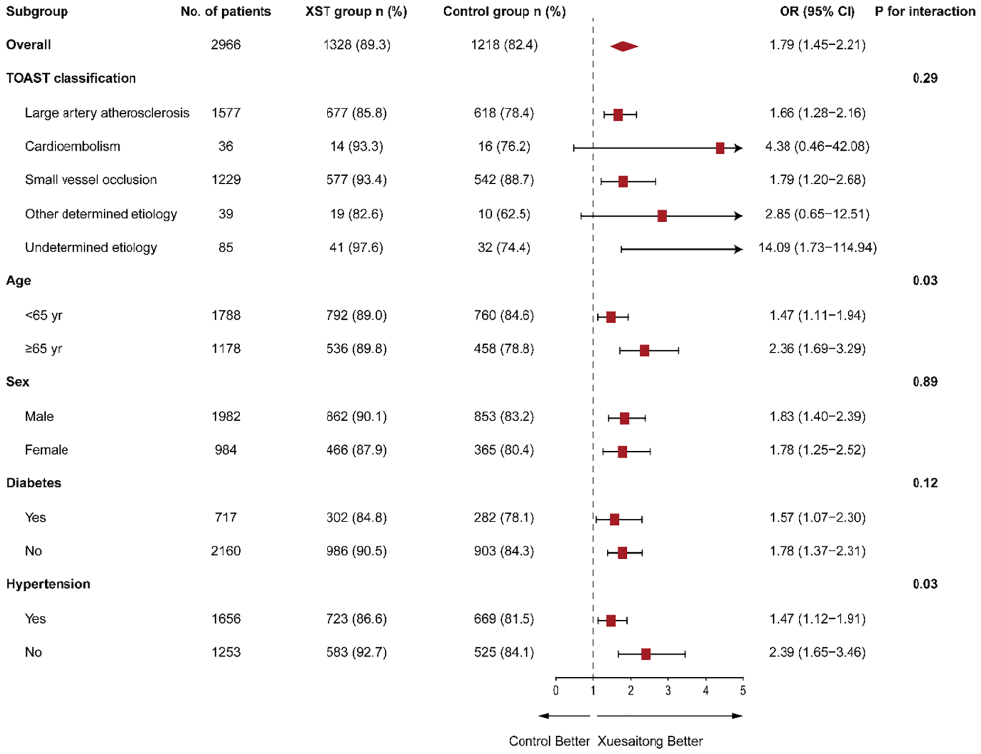
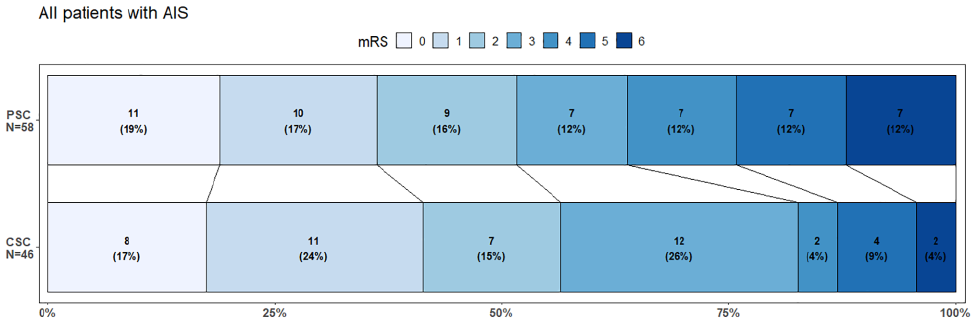
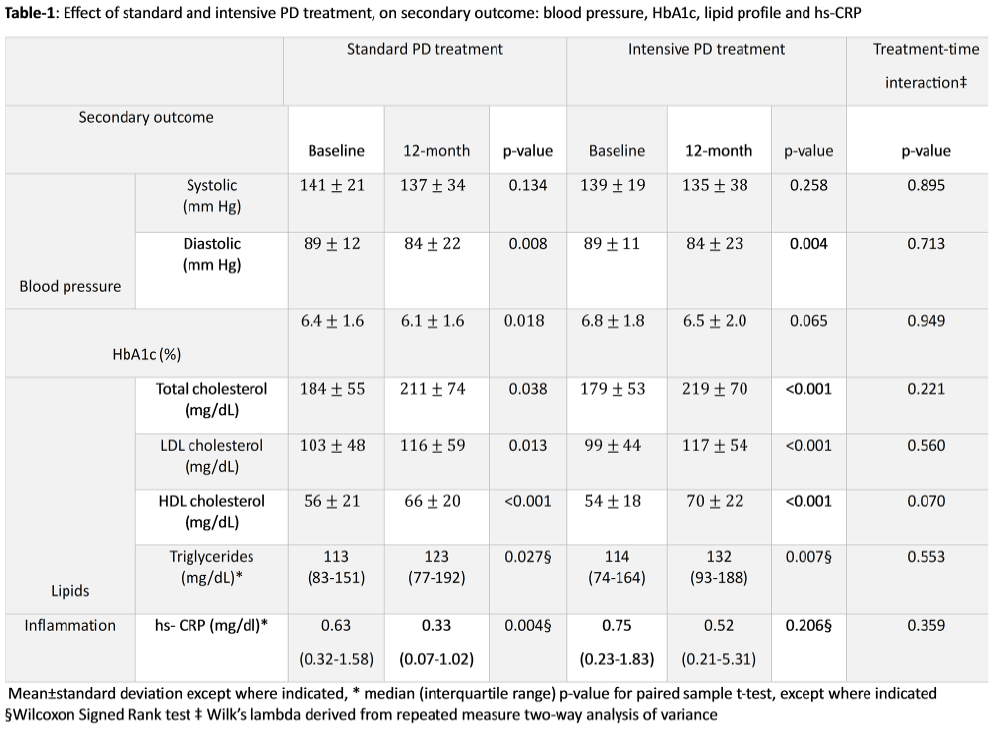
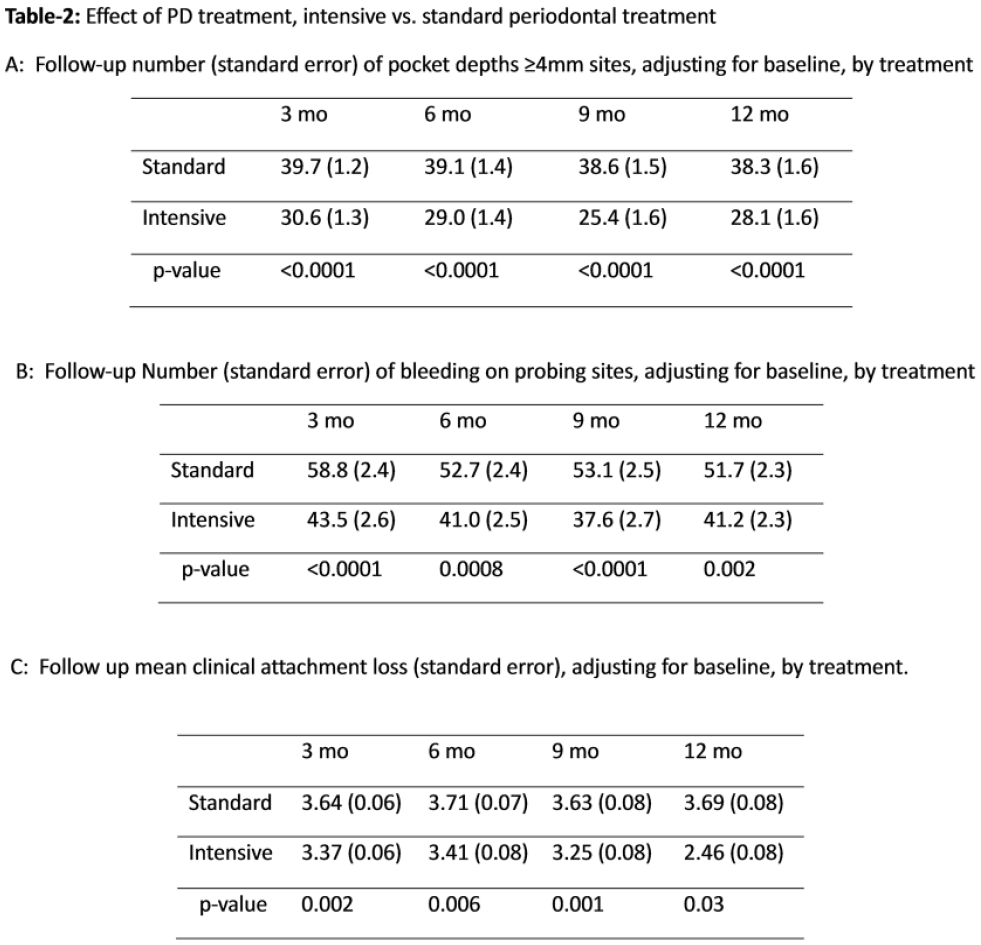
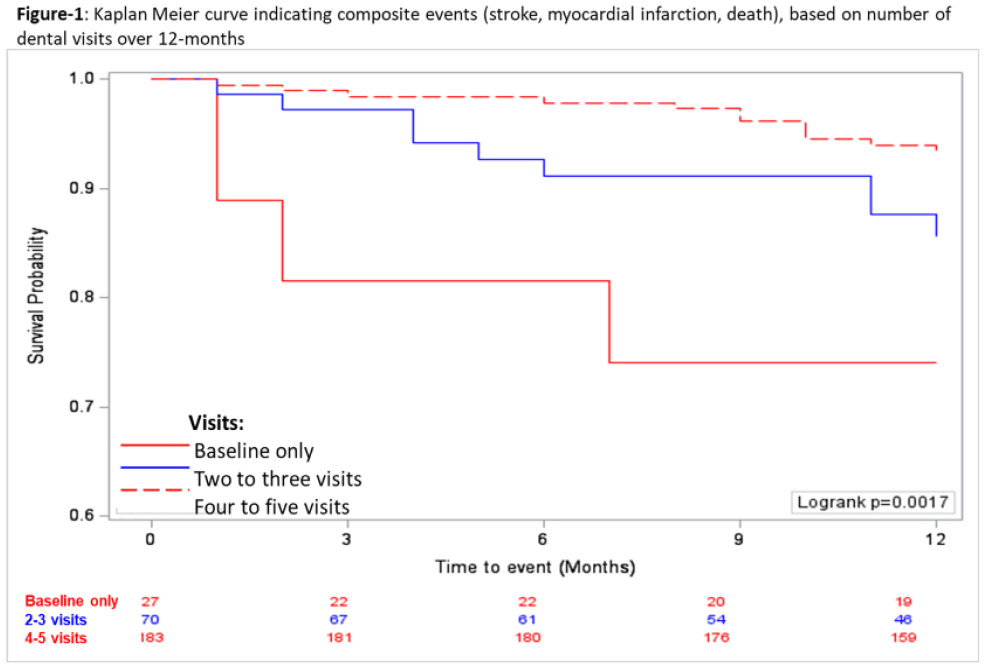
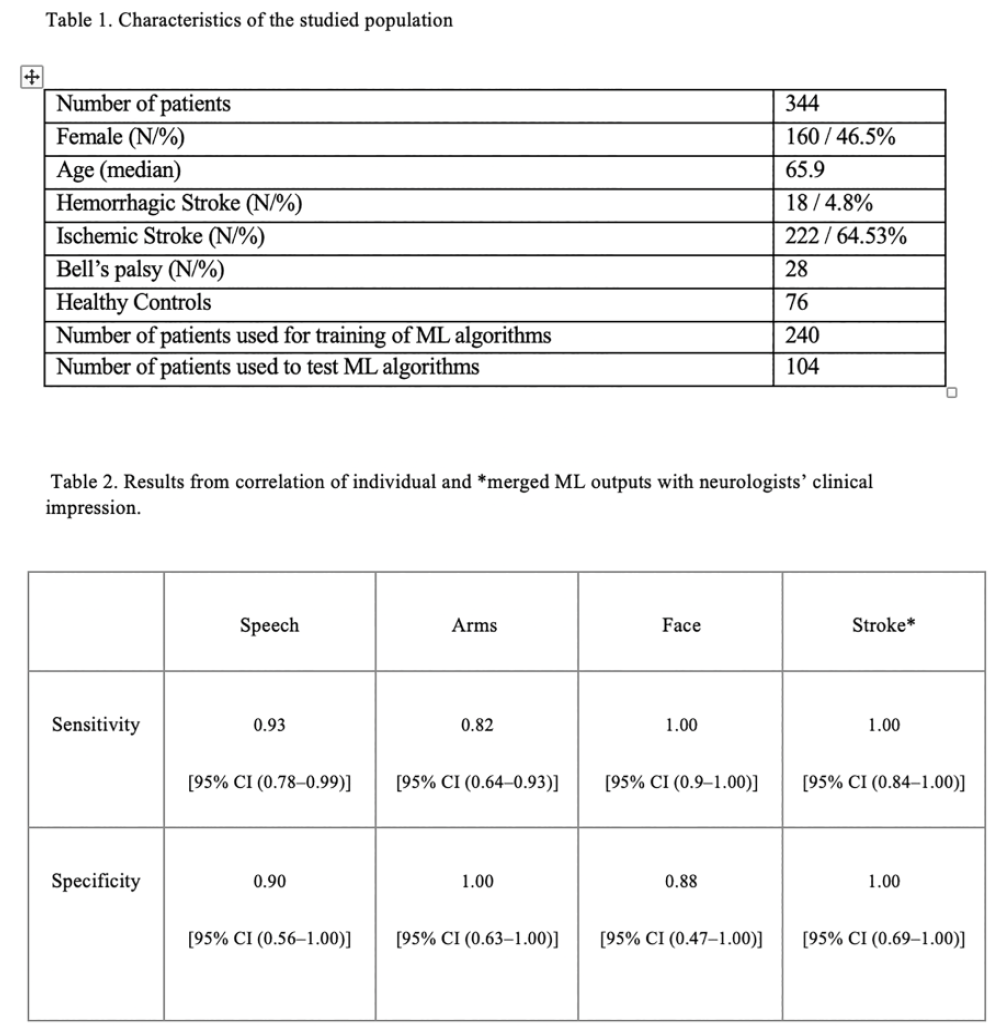
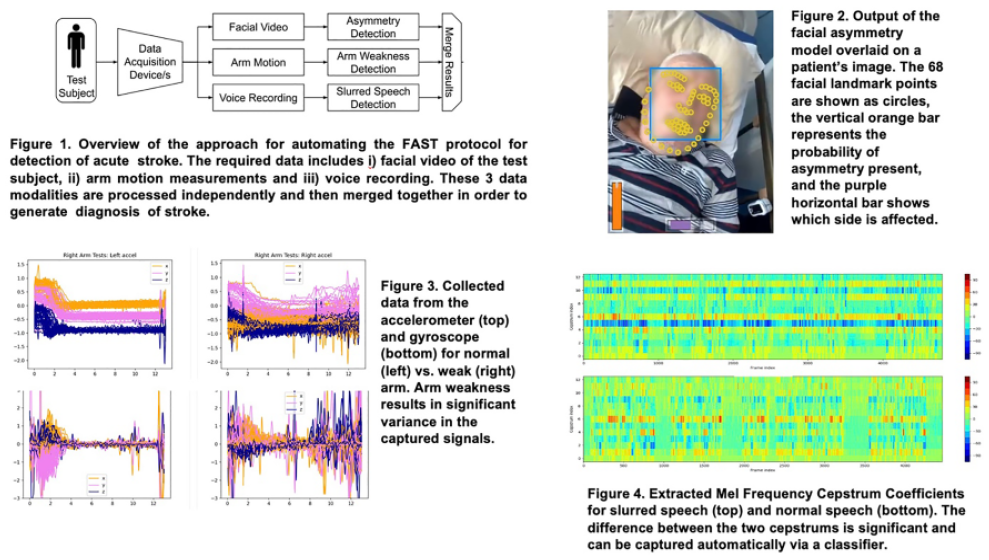
 , Saudi Arabia
, Saudi Arabia